Day after day, life gets heavier. Professional duties expand, emails multiply. Family coordination intensifies and life demands more. My calendar feels like a game of Jenga – each new obligation is another piece added to a delicate stack, always hoping the next load doesn’t send it all crumbling down.
And then there’s the question so many professional organizations like MPA hear all too often: “Does this even matter?”
And yet, here I am in my eighth year on the executive board and an active MPA member since 2010, when I was a P3 student.
In the earlier years, I came back for the conversation that unexpectedly shifted my thinking. For the person I met at a committee meeting who became a mentor
I didn’t know I needed. For the quiet moment when someone said, “I’ve struggled with that too,” and I knew I was not alone.
As I grew into my professional self, I came back because I realized something happens when people show up not just for themselves, but for something larger. We don’t talk about that enough – how rare it is to have a space where people genuinely care about building something together.
It’s not always glamorous. It’s not always efficient. But it’s real.
Now, years later, I’ve watched ideas go from half-formed
thoughts in a hallway to actual initiatives that made people’s lives better. I’ve seen professionals who never thought they belonged at the table become the ones shaping it. And yes, I’ve seen the frustration too – slowmoving decisions, disagreements and burnout.
But even in the mess, there's meaning.
The truth is, MPA isn’t perfect. It’s a living, breathing thing. It grows with us, stumbles with us and gets better because of us. That’s what keeps me coming back.
Some loyalty, a little bit of habit – but mostly, hope. Hope that showing up still matters. Hope that voices – even the quiet ones – can shift the direction of something bigger. Hope that if we keep building, more people will see themselves here – and stay, lead and lift others up, so that MPA can lift our profession up.
So yes, I’ll be there at the next meeting. Probably a little tired. Probably juggling a hundred other things, as we all are these days. But I’ll be there.
Involvement in MPA isn’t just another block added to the teetering tower of life’s responsibilities. It’s one of the foundational pieces anchoring the whole structure. It’s the block that absorbs the weight of our profession’s biggest challenges so the rest of us can keep standing strong. Why do I keep coming back? Because I’ve learned that involvement in MPA isn’t just another obligation. It’s what helps hold everything else up.
"The truth is, MPA isn’t perfect. It’s a living, breathing thing. It grows with us, stumbles with us and gets better because of us. That’s what keeps me coming back."
ENERGIZED BY YOUR ENGAGEMENT
ENERGIZED
BY MARK GLASPER, chief executive officer, Michigan Pharmacists Association
We always talk in association circles about how important membership engagement is to the overall health of the organization. It’s essential we have an engaged Executive Board that oversees the welfare of MPA. Our sections, local associations, regional societies and committees drive the organization forward year after year.
But it’s also the individual member – pharmacist, pharmacy technician, student pharmacist – whose engagement motivates and energizes your MPA staff, myself included. We work with such members every day and it’s rewarding to see them find their niche as an association volunteer where their work makes a difference for the profession.
It’s impossible to name all the members who inspire us, but I want to take this opportunity to highlight a few from just the last few months.
Advocacy Unites Members
There’s no greater cause for association members to rally around than advocacy. It’s no different with MPA. That’s why we have 24 members on the Government Affairs Committee, 124 members participating in the Legal & Regulatory Special Interest Group (SIG) and 54 members on the new Independent Pharmacy Council, formerly Independents SIG. Those are impressive numbers of individual members advocating on behalf of pharmacy in Michigan.
Then we have members who advocate for a special cause; we saw that earlier this year with the signing of House Bill 5436, our signature hormonal contraceptive legislation. Many thanks to Mary Beth O’Connell, Lisa Bade and David Bright for their leadership in advocating for this issue over the years.
We also have individual members who have an interest in advocating at the national level. The annual National Community Pharmacists Association Congressional Flyin presents the opportunity for members to meet with our members of Congress and their staff to advocate for pharmacy benefit manager reform. Big thanks to Jordan Marchetti, Amar Sappidi, John Gross, Chris Munden, Nash Algumaei and Arun Tandon for taking pharmacy issues directly to our Michigan members of Congress in Washington, D.C.
MPA Delegates Serve APhA, ASHP, NCPA
We’re all familiar with MPA’s House of Delegates and the work that members do to affect MPA policy here in Michigan. At the national level, we have members who enjoy doing likewise, serving as delegates in the House of Delegates for the American Pharmacists Association, American Society of Health-System Pharmacists and NCPA. I am always impressed with our members who step up to the microphones to articulate their views in these settings.
Delegates at the APhA HoD in March in Nashville included MPA President Ryan Greenley, Ashley Blanchette, Mark Bomia and Tonino Michienzi. Jesse Hogue led the ASHP HoD as Speaker of the House in June in Charlotte, North Carolina, with MPA delegates Rox Gatia, Lama Hsaiky, Amber Lanae Martirosov and Becky Maynard participating. David Zimmerman, Joshua Gross, John Gross and Anthony Codrean all served as delegates at the NCPA HoD in Columbus, Ohio, last October. Thanks to all these members for serving the pharmacy profession at the national level!
Mark Glasper, David Zimmerman, Joshua Gross, John Gross and Anthony Codrean attend the NCPA House of Delegates in October.
ENERGIZED
Student Engagement Key to Future
Many paths to engagement in MPA are available to our student pharmacists while pursuing their education. The Student Michigan Pharmacists Association is an affiliated chapter of MPA, representing students at Michigan’s three colleges of pharmacy, while the Student Pharmacist Executive Council (SPEC) communicates actions of the Association to students at each college of pharmacy. There are so many students who are engaged in these activities, but one – Rania Bardage – rises to the top for serving as the SPEC representative on the MPA Executive Board. Engaged student pharmacists are on full display at every MPA Annual Convention & Exposition during the National Alliance of State Pharmacy Associations Self-Care Challenge. Teams of students from each of the three colleges of pharmacy in Michigan compete mightily for bragging rights and a trophy. Competing at ACE in 2025 were Ferris State University’s Adam Anderson, Madison Briggs, Tan Vo and Mackenzie Parish; Justin Xu, Emma Silverman, Aaron Paul and Payton Gilmore from the University of Michigan; and Shannon Habba, Justin Zimmerman, Alexis Brecht and Marisa Marcath from Wayne State University. While the team from Wayne State University won the event, we celebrate the engagement of all these students.
Academic engagement is critical to the success of our student pharmacists and that’s why I enjoy attending commencement events at our three colleges of pharmacy each year. That’s when I have the privilege of presenting awards on behalf of MPA and MSHP to deserving students. This year’s winners include:
MPA Dean’s Professionalism Award
Hannah Bronz, Ferris State University
Jessica Chioma Orizu, University of Michigan
David Frond, Wayne State University
MSHP Student Recognition Award
Noelle Strzelecki, Ferris State University
Calise Wang, University of Michigan
Bryce Van Horn, Wayne State University
I always tell our graduating student pharmacists to stay engaged with a state pharmacy association wherever they may practice and not to forget the national pharmacy associations either, because I know for a fact that one will become a future President of MPA or even one of the nationals.
Thanks to all our members who are actively involved in MPA. We are so appreciative of your time and support. And for those who are not engaged, I invite you to take your career to the next level and get involved with MPA. The result could be engaging!
Mark Glasper, Ryan Greenley, Ashley Blanchette, Tonino Michienzi and Mark Bomia attend the APhA House of Delegates in Nashville.
Gov. Gretchen Whitmer signs HB 5436 into law. Representing MPA at the signing were CEO Mark Glasper, MSCP Chair David Bright, MPA Executive Board member Lisa Bade, Mary Beth O’Connell, MPA Director of Government Affairs Eric Roath and Chief Pharmacy Officer Farah Jalloul-Rizk.
Rox Gatia, Lama Hsaiky, Amber Lanae Martirosov and Becky Maynard represented MPA at the ASHP HoD in Charlotte, North Carolina.
Mark Glasper, Jordan Marchetti, Amar Sappidi, John Gross, Chris Munden, Nashwan Algumaei and Eric Roath flew to Washington at the end of April to bring issues directly to federal legislators. MPA member Arun Tandon (not pictured) also made the trip.
Ferris State awardees: Noelle Strzelecki, above left, and Hannah Bronz, above right, with Mark Glasper and FSU College of Pharmacy Dean Stephen Durst.
U-M awardees: Jessica Chioma Orizu, above left, and Calise Wang, above right, with Mark Glasper and U-M College of Pharmacy Dean Vicki Ellingrod.
WSU awardees: David Frond, above left, and Bryce Van Horn, above right, with Mark Glasper.
EVENTS CALENDAR
MPA events, as well as health observances, are included below. For the most up-to-date information, please visit our online calendar at MichiganPharmacists.org/events
JULY 2025
4
14 -15
15
24
Friday, July 4 Independence Day Nationwide
Monday, July 14-Tuesday, July 15
MPA Strategic Planning Retreat
MPA Headquarters, Lansing
Tuesday, July 15
MPA Executive Board Meeting
MPA Headquarters, Lansing
Thursday, July 24
CSPM Board of Directors Virtual
AUGUST 2025
1-31
8
21
Friday, Aug. 1Sunday, Aug. 31 National Immunization Awareness Month Nationwide
Friday, Aug. 8 MSPT Board of Directors Virtual
Thursday, Aug. 21
MPF Board of Trustees Virtual
Please note: Some board and committee meetings may be subject to a change in format to virtual or in-person at the discretion of the members. Please check the online calendar or contact MPA@MichiganPharmacists.org for more information.
SEPTEMBER 2025
1-30
1
4
10-12
18
Monday, Sept. 1Tuesday, Sept. 30 Ovarian Cancer Awareness Month Nationwide
Monday, Sept. 1 Labor Day Nationwide
Thursday, Sept. 4
MSHP Planning Retreat and Board of Directors
MPA Headquarters, Lansing
Wednesday, Sept. 10-Friday, Sept. 12 NABP District 4 Meeting Fort Wayne, Indiana
Thursday, Sept. 18 Pharmacy Day at the Capitol
Michigan Capitol Building, Lansing
18
18
23
Thursday, Sept. 18 MPA Executive Board Meeting
MPA Headquarters, Lansing
Thursday, Sept. 18 MSHP Social High Kaliber Carting, Okemos
Tuesday, Sept. 23 MSCP Board of Directors Virtual
25 Thursday, Sept. 25 MSHP Board of Directors Virtual
WEDNESDAY, AUG. 13
Pharmacy Technician Immunization Administration
Mixed format: Self study and live webinar training.
Live session registration: https://www.lecturepanda. com/v2/announcement/ag1zfnJ4Y2V0cmFja2VychMLEgZDRVVzZXIYgICAsLaLigoM/ag1zfnJ4Y2V0cmFja2VycicLEgZDRVVzZXIYgICAsLaLigoMCxIHTGVjdHVyZRiAgJCe16-YCQw
Home study registration: https://www.lecturepanda. com/v2/announcement/ag1zfnJ4Y2V0cmFja2VychMLEgZDRVVzZXIYgICAsLaLigoM/ag1zfnJ4Y2V0cmFja2VycicLEgZDRVVzZXIYgICAsLaLigoMCxIHTGVjdHVyZRiAgODWkprvCww
The 2025 Outpatient Antimicrobial Stewardship Innovations Symposium, sponsored by the Michigan Society of Health-System Pharmacists and the Ferris State University College of Pharmacy, is a 4.5-hour educational meeting that will have both in-person and virtual options for attendees.
TUESDAY, SEPT. 9, 9 a.m.-5 p.m.
APhA Pharmacy-based Immunization Training
Mixed format: Self study and live webinar training https://fs27.formsite.com/7jFRIO/rvvtjkxxie/index
FRIDAY, OCT. 24, 7:30 a.m.-4:45 p.m.
MSHP Annual Meeting
Hilton Doubletree-Dearborn, 5801 Southfield Freeway, Detroit
The MSHP Annual Meeting offers continuing education for pharmacists, pharmacy residents, student pharmacists and pharmacy technicians, along with a chance for exhibitors and sponsors to showcase products and network with MSHP members. Registration will be available beginning Aug. 1.
SATURDAY, OCT. 25, 8 a.m.-5 p.m.
MPA Upper Peninsula Division Fall Conference
Northern Center, 1401 Presque Isle Ave, Marquette
Join MPA and its Upper Peninsula Division for the annual UP Fall Conference.
*Registration and hotel booking for OASIS, MSHP Annual and the UP Fall Conference will be available soon, so please check the MPA Events Calendar for updates frequently.
QUESTIONS
If you have any questions about any of these MPA education events, please email MPA@MichiganPharmacists.org
Michigan Pharmacists Association (MPA) is accredited by the Accreditation Council for Pharmacy Education (ACPE) as a provider of continuing pharmacy education.
INTRODUCING MPA’S 2025-26 EXECUTIVE
FELLOW:
LEANG MEY TAO
Pharmacy has always stood out to me as the true backbone of health care. It’s not just about dispensing medications. Pharmacists are critical decision makers who contribute deeply to treatment, disease monitoring and continuity of care. We are experts not only in pharmacology, but also in navigating complex insurance systems, ensuring regulatory compliance and offering frontline patient care. This multifaceted role is what drew me to pharmacy. It’s a profession that blends clinical expertise, business acumen, legal understanding and public health impact.
Despite their extensive knowledge and responsibilities, pharmacists are often overlooked. This is why my journey in pharmacy has been focused on advocacy – raising awareness of our value, developing innovative models of practice and pushing for reforms, particularly around the role of pharmacy benefit managers, and the broader financial systems that limit both provider autonomy and patient access. I believe pharmacists should be both empowered and properly compensated for the care they provide and I want to help make that happen.
With a background in public health, I see my new role as the Executive Fellow with the Michigan Pharmacists Association as a pivotal platform to take action. My hope is that the experience will give me the tools, connections and experience to advocate for change at the policy level while learning how to lead with impact. I am excited to work alongside others who are just as committed to moving the profession forward and protecting the integrity of pharmacy practice in our communities.
Long term, I aspire to become a pharmacy-based business owner with a mission greater than profit. My goal is to create generational wealth and use it to establish a foundation for high school students from low-income backgrounds who want to pursue a career in pharmacy and need guidance and resources along the way.
As the first in my family to reach this level of education, I know firsthand what it’s like to pursue opportunity against the odds. I want to build pathways for others to follow as well as to leave the profession stronger and more inclusive than I found it.
ANTHONY CODREAN NAMED NEW PRESIDENT OF SAV-MOR PHARMACY SERVICES
MPA Member Chosen to Lead Southfield-Based Company
Sav-Mor Pharmacy Services has a new president in MPA member Anthony Codrean, who took over the position June 1.
Codrean replaces Yvonne Gallagher as president of the Southfield-based company. Gallagher retired after nearly 30 years with Sav-Mor.
“(She) helped me grow and taught me a lot in terms of the retail side and the administrative side of pharmacy,” Codrean said of his predecessor.
Codrean began his pharmacy career 14 years ago as a certified pharmacy technician at Henry Ford Macomb Hospital. Initially he aspired to become a pharmacist, but didn’t know if he wanted to see it through.
“Still, I knew I wanted to be involved in pharmacy and at the same time the door opened here at Sav-Mor, where I can get involved in the back side of things on the retail side and more administratively,” he said.
His interest in pharmacy began with his mother, who is a pharmacy technician and a 25-year veteran at Royal Oak Beaumont. A native of the Dearborn and Lake Orion area, he graduated from Troy Athens High School and earned a degree in biology from Rochester College (now known as Rochester Christian University). He currently lives in Lake Orion with his wife, Bethany, and children Luca and Levi.
This fourth of July marked his 10th
BY RYAN WEISS, MPA marketing and communications manager
anniversary with Sav-Mor, where he held several different roles over the past decade before becoming president, including vice president and director of pharmacy services.
The significance of a pharmacy technician being named president was not lost on him.
“I've worked with a number of technicians who have opened up their own pharmacy, where they just started as a tech,” he said. “It’s all dependent on aspirations of the individual. There are certain techs who can prioritize and take a lot of the burden off the pharmacist, where maybe their focus was just on becoming a pharmacist and not so much the business side of things.”
Codrean laid out several goals as he takes over as president. His first priority is working with Sav-Mor’s member pharmacies so they can get the best pricing possible from wholesalers.
“What we can effectively do is help pharmacies buy better. We try to skim any fat from these deals that are offered in the marketplace to put it all back in the financial side for the pharmacies,” he said. “Sav-Mor’s sole focus is doing that, whether it's through our buying group, our PSAO, or our services that we offer; we try to do it effectively as best as we can at a low cost and put money back in the pocket of these pharmacies.”
Codrean noted the tough landscape of
pharmacy, particularly for independents. He is currently working on advocating for independent pharmacies – whether they are members of Sav-Mor or not. He is collaborating with MPA’s Government Affairs Committee and its Independent Pharmacy Council on advocacy issues.
“We want to save the occupation and see the business grow for pharmacies, because there's definitely a value in it in everyone's community,” he said.
Codrean said he’s also focused on getting more involved, be it politically with advocacy or with industry partners and vendors. He has been an MPA member since 2018 and emphasized the value of being an active participant in the association.
“It's important to just stay on top of it, in terms of what's happening at the state level, especially for our members,” he said. “As the president of the organization we want to make sure that we have a seat at the table to share our members’ voice as well as relay back any information that the association provides – at the same time providing our support to (the Michigan Pharmacy Foundation) through some financial means that we have allotted to provide back to associations.”
MEMBER SPOTLIGHT
Calvin J. Ice
PharmD, BCPS, BCCCP, FASHP
Pharmacy Manager, Training & Education
New MPA members
(Apr. 1-June 30)
Hussein Al-Mansori
Ohod Alabsi
Rama Aleech
Mohamed Ali
Yusra Alraeai
Bassam Alsubari
Ashely Alvardo
Alexis Anthony
Laura Atherton
Salah Bazzi
Tara Berry
Jessica Boonstra
Adam Brady
Veronica Bryant
Phern Cain
Matthew Carrier
Lori Childs
Nure Chowdhury
Azira Cinac
Lauren Csurgo
Mary Lynn Cudejko
Debora Curry
Vivian Davis
Employer: Corewell Health
Member Since: 2015
Describe Your Role/Day in the Life: In my role, I support our teams of pharmacy preceptors, supervisors and coordinators in designing and conducting pharmacy technician student, pharmacy student, pharmacy intern and pharmacy residency training programs at Corewell Health. I help schedule and facilitate educational events for our pharmacy team throughout the health system and my team engages new team members in orientation to our pharmacy department. I currently serve as the PGY1 pharmacy residency program director at Corewell Health Grand Rapids Hospitals, and I still practice clinically in the Surgical-Trauma ICU at Butterworth Hospital.
Why You’re an MPA Member: I am a member of MPA and MSHP to engage and network with peers across the state while supporting advancement of our profession. I appreciate MPA’s commitment to advocacy and the meaningful opportunities provided to members to engage in committee work.
Recent Accomplishments: I was recently named a Fellow of the American Society of Health-System Pharmacists and was honored at the ASHP Pharmacy Futures Meeting in Charlotte, North Carolina. Additionally, in June my sixth and final class of PGY1 pharmacy residents completed residency as I transitioned out of a residency program director role. I feel accomplished having served as the residency program director for 42 PGY1 pharmacy residents and seeing them reach the next steps in their careers.
How MPA Has Helped You Achieve Any Accomplishments: Involvement in MSHP and its committees has been very meaningful to me in my professional development. The networking and leadership skills this engagement have helped foster has greatly supplemented the skills I have built through engagement in ASHP over the past decade.
Lizbeth De La Cruz
Victoria Derry
Hunter Dewitt
Zeinab Elhourani
Fatima Fazal
Elayna Fick
Allison Folin
Amanda Hart
Aline Hatoum
Abigail Hayes
Megan Hill
Sarah Hollander
Theresa Hoover
Patricia Huey
Rhonda Hunter
Jessica Jacks
Sanjana Jarin
Tammy Jarvis
Dawn Johnson
Amanda Jones
Zahraa Kansou
Mahbuba Khanom
Patrick King
Josiah Knewtson
Kourtney Kraftchick
John Kurian
Todd Lacksonen
Hoi Man Leung
William Londo
Robert Louwers
Lina Lsdesai
Mark Luea
Emily Mackler
Isaac Madura
Ashley Malburg
Connor Mcwain
Samuel Migala
Keith Misiak
Nour Mohanna
Kristen Monarch-Mocek
Haylee Moser
Brittnie Mroueh
Stephanie Murphy
Rudy Najm
Abdulsattar Nasser
Paul Newman
Hugh Nguyen
Jenna Nordin
Katie Norris
Rawan Noureddine
Claire Nowicki
Heather Obrien
Gunnar Olson
Kavita Parikh
Snehal Patel
Tyler Phillips
Hugh Quinn
Maci-Lynn Quisenberry
Haitham Rababeh
Janice Richardson
Chelsea Rios
Caitlyn Robbins
Clystia Robbins
Demi Rodriguez
Brianne Rogers
Jennifer Rudd
Renee Russell-Schaub
Erna Saric
Madeline Schneider
Aissatou Seck
Graham Selegean
Hector Serrato
Austin Seymour
Hadil Shalan
Nicole Slain
Amanda Smith
Laurie Snellenberger
Devin Stephens
Timothy Stiff
Celina Stumpp
Glen Tanner
Pasha Tanveer
Leang Tao
Shelia Taurianen
Matthew Taylor
Sandra Taylor
Amy Thompson
Robyn Thompson
Tanya Timiney
Minh Tong
Safwan Uddin
Maci Walters
Jasmin Wang
Amanda Watson
Glenn Watson
Samantha Watson
Jessica West
Brody Wiederhold
MJ Williams
Shatila Zaman
Viva Zaya
BY RICK DRABEK, executive director, Michigan Pharmacy Foundation
G LF CLASSIC
I would like to extend my sincerest appreciation to all who supported the Michigan Pharmacy Foundation (MPF) Golf Classic that was held June 12 at Timber Trace Golf Club in Pinckney.
This year’s event was a great success, and it wouldn’t have been possible without your support. For all who were sponsors, golfed and volunteered, your support enabled the Foundation to have a wonderfully successful event and provided funding for our mission: “To Foster the Future of Pharmacy.”
For that, I am tremendously grateful! The Foundation’s mission is more than just a slogan to us, it's a commitment to make a difference in the lives of the individuals and communities who depend on the pharmacy profession.
Supporting the MPF Golf Classic is not just about playing a round of golf; it's about helping to shape the future of pharmacy. The funds we raise through this event are a vital source of support for student pharmacist scholarships, enable us to provide leadership development training for pharmacy professionals and fund pharmacy-focused grant opportunities for underserved communities in Michigan.
Your participation and support in the Golf Classic allows us to make a real difference and helps us continue to fund Foundation initiatives. If you were unable to join us at the Golf Classic this year and would like to learn more about MPF, please visit our website at MichiganPharmacyFoundation.org or help to support MPF’s programs by making a donation at donate2MPF.org
June 17, 2026,
MPF Executive Director Rick Drabek addresses golfers before they begin play.
MPF Vice Chair James Vander Linde hits a tee shot during the outing.
The winning team of Chris Wolfinger, Matt Simons, Kevin Bucci and Bryce Lund with MPF Chairman John Brubaker.
Tom Tomaski reacts after sinking the winning putt in the putting contest.
MPA President-Elect Michelle Kelly participates in the putting contest.
MPF Chairman John Brubaker addresses attendees before the awards ceremony.
MPF Trustee Doug Samojedny speaks to golfers at the awards ceremony.
RYAN
STEVE
1967-2025
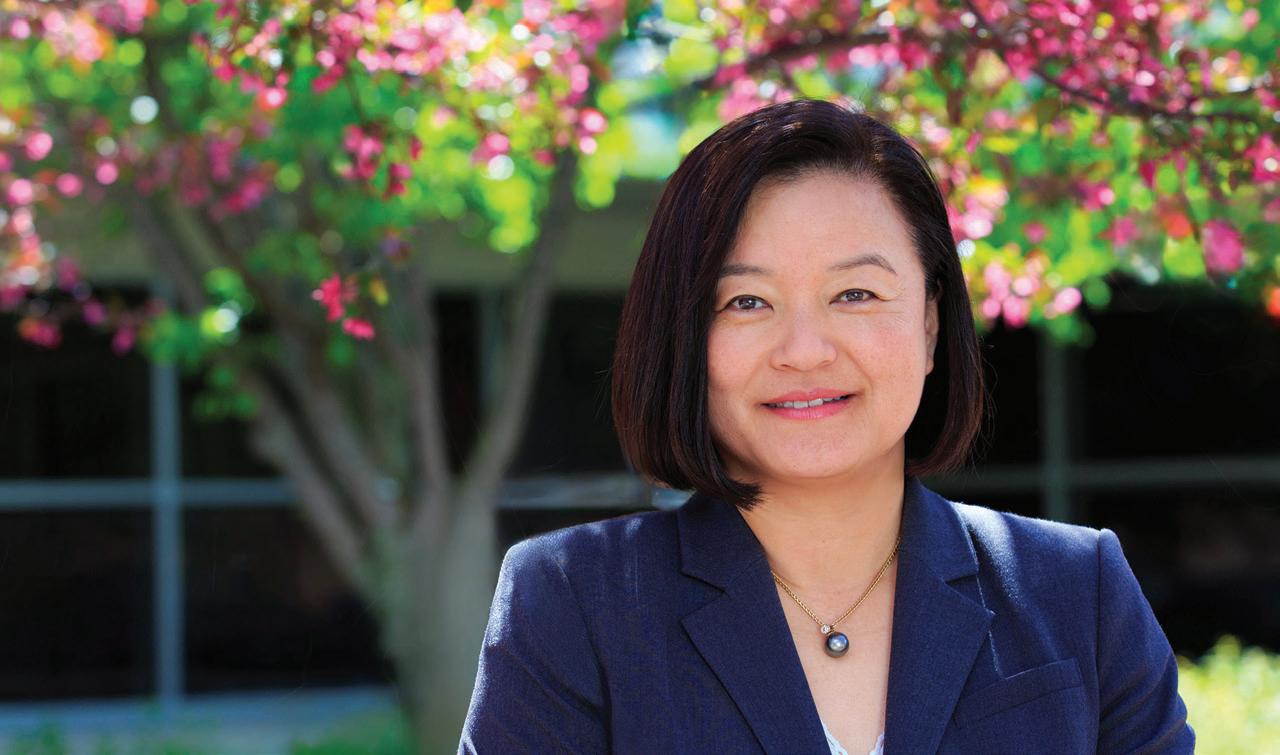
HAE MI CHOE, PHARM.D.
A VISIONARY LEADER, INNOVATOR, AND ADVOCATE FOR PATIENTS AND PHARMACY
A pioneer in the field of ambulatory pharmacy practice, Dr. Hae Mi Choe’s career was defined by transformative leadership, relentless innovation and a strong commitment to improving patient care.
Throughout her career, Dr. Choe served in numerous leadership roles, including associate dean for pharmacy innovations and partnerships at the University of Michigan College of Pharmacy; chief population health officer at Michigan Medicine; and executive director of the Michigan Institute for Care Management and Transformation with Blue Cross Blue Shield of Michigan. She earned her Pharm.D. from the University of California, San Francisco, and began her career by establishing ambulatory pharmacy services at Samsung Medical Center in Seoul, South Korea, before joining the University of Michigan in 1999.
A champion of team-based care, Dr. Choe revolutionized ambulatory practice with the integration of pharmacists into primary care and specialty care areas across Michigan Medicine and our state. Dr. Choe’s influence extended across clinical practice, research, education and health policy. She was a widely-respected scholar in chronic disease management, medication optimization and pharmacogenomics. She received numerous accolades, including the ASHP Board of Directors Distinguished Leadership Award; the American Association of Colleges of
Pharmacy Crystal APPLE Award; the Pinnacle Award from the American Pharmacists Association Foundation; the Michigan Society of Health System Pharmacists President’s Award; and was a two-time winner of the Michigan Pharmacists Association Innovative Pharmacy Practice Award (now known as the Excellence in Innovation Award).
Beyond her professional achievements, Hae Mi was a remarkable human being. She was graceful, generous and deeply committed to those around her. Even in the face of personal adversity, she led with purpose and empathy, always thinking about how to make the health system more just and accessible. In her final days, she continued advocating for patients, telling those close to her: “We need to make this easier for patients. Help me, help others.”
Hae Mi brought people together, bridged vision into action and elevated the role of pharmacy in health care in ways that will continue to resonate for generations. Her legacy lives on in the programs she built, the people she mentored and the lives she touched.
She is survived by her beloved husband, Yong, and their two children, Allison and Chris.
Hae Mi will be dearly missed, but never forgotten.
Details regarding memorials for Hae Mi will be announced at a later date. MPA extends its deepest sympathies to Hae Mi's family, friends, colleagues and all who had the privilege of knowing her for their tremendous loss.
SCOPE OF PRACTICE: THE LONG WAIT FOR CRITICAL REFORMS
BY ERIC ROATH, Pharm.D., MBA; MPA director of government affairs
In 2023, the Michigan Legislature passed for the first time legislation that gave prescriptive authority to pharmacists for immunizations, point-of-care tests and antiviral medications for influenza and COVID-19. This was followed by the governor signing legislation that granted pharmacists prescriptive authority for hormonal contraceptives. While pharmacy professionals in Michigan should take a well-deserved victory lap, the question remains, “When can we start?”
Unfortunately, that answer is… complicated.
In order for both laws to go into effect, the Michigan Board of Pharmacy needs to promulgate rules that, at a minimum, identify the nature of the training requirements for pharmacists to provide these services. The timing for the 2023 bill was rather unfortunate given this requirement as the ruleset that needed to be updated was already going through the tail-end of the promulgation process. We had to wait for the previous set of rules to finish the process before the Board of Pharmacy could even begin to craft the newly required rules.
The timing for the passage of the hormonal contraceptive package was far more fortuitous and MPA advocated that the Board include the required rules for this practice among the revisions it was already working on. Now those rules have received their initial approval from the Board and are progressing through the process.
The Rule Promulgation Process
The process by which rules are promulgated differs significantly from the legislative process we tend to be more familiar with. Here is a brief summary of the process.
• Request for Rulemaking
o A department submits a Request for Rulemaking (RFR) to the Michigan Office of Administrative Hearings and Rules (MOAHR)
o MOAHR reviews and approves the RFR and notifies the Joint Committee on Administrative Rules (JCAR)
• Draft Rules
o Rules are drafted and submitted to MOAHR to review for legal authority.
• This draft is made by the Rules Workgroup and approved by the Board of Pharmacy
o MOAHR approves draft rules and notifies JCAR.
o MOAHR sends the draft to the Legislative Service Bureau (LSB) for informal editing. (NOTE: This is where we are currently in the process for the Pharmacy – General Rules)
• Public Hearing
o A Regulatory Impact Statement (RIS) is prepared by the agency and sent to MOAHR for approval 28 days prior to the public hearing. MOAHR notifies JCAR.
o A Notice of Public Hearing is published online and in three newspapers, including one in the Upper Peninsula, not less than 10 days after but not more than 60 days prior to the hearing.
o Public comment is accepted by the agency (in our case, LARA) from the notice date up through the public hearing date.
• JCAR Report
o The agency submits the final draft of the rules and the JCAR Report to MOAHR.
o MOAHR submits the final draft to LSB to formally certify the rules.
o MOAHR legally certifies the rules and sends the JCAR Report (which includes the rules, certifications, RFR and RIS) to JCAR.
• JCAR
o The JCAR Report must be submitted to JCAR within one year after the public hearing.
o The JCAR Report summarizes the purpose of the draft rules and any comments made at the public hearing or submitted in writing.
o The rules must be before JCAR for 15 session days, unless JCAR grants a waiver of the remaining days.
o During those 15 days, JCAR may object to the rules, but then must introduce legislation within another 15 session days to stop or delay the rules.
• Great Seal
o After 15 session days, MOAHR can file the rules with the Office of the Great Seal (or after a waiver is granted).
o The agency director confirms the intent to adopt the rules by submitting a Certificate of Adoption to MOAHR.
o The rules may become effective immediately upon filing with the Office of the Great Seal, or at a later date specified by the agency in the rules.
What are the proposed changes?
As you can see, we still have a ways to go in the process. The next stage is the “public comment period,” where health care stakeholders have the opportunity to weigh in on all the proposed changes. Listed below are the changes proposed related to scope of practice.
• Draft Immunization Rules (paraphrased)
o Before ordering and administering a qualified immunizing agent, “a pharmacist shall successfully complete a training course on the administration of vaccines that is provided by an entity accredited by the ACPE.”
• Draft Test-to-Treat Rules (paraphrased)
o “Before ordering and administering a qualified laboratory test and dispensing, without a prescription, a drug based on the test results” a pharmacist “shall complete a training program requiring the pharmacist to”:
• Demonstrate sufficient knowledge of how to administer and interpret each laboratory test.
• Demonstrate sufficient knowledge of each illness, condition, or disease for which the pharmacist provides treatment based on the results of the laboratory test.
o Any of the following is acceptable to meet this requirement:
• Employer-based training.
• Training completed as part of a professional degree from a school of pharmacy accredited by the ACPE.
• A certificate program.
• Draft Hormonal Contraceptive Rules: Training (paraphrased)
o Before issuing a prescription for a contraceptive, a pharmacist shall “successfully complete a training course on prescribing and dispensing contraceptives that is provided by an entity accredited by the ACPE.”
• Draft Hormonal Contraceptive Rules: Standard Procedure (paraphrased)
o Before issuing a prescription for a contraceptive, a pharmacist shall:
• Require the patient to complete the self-screening risk assessment tool.
• Review the patient’s completed self-screening risk assessment tool before issuing a prescription.
o Upon issuing a prescription for a contraceptive, a pharmacist shall:
• Refer the patient to their primary care provider or another appropriate health professional.
• Refer the patient for a physical examination if the patient has not had one in 12 months.
• Provide the patient with a written record of the prescribed contraceptive and advise they consult with a physician or other licensed health professional.
• Dispense the prescribed contraceptive or transfer the prescription to the pharmacy of the patient’s choosing.
o If the pharmacist does not issue a prescription to the patient, the pharmacist shall refer the patient to another appropriate provider. The rules also contain an appendix which specifies the minimum requirements for the self-screening risk assessment tool that must be used by the pharmacist as part of the hormonal contraceptive prescribing service.
What is the timeline?
Unfortunately, this is hard to say for sure. For reference, the last time the Board of Pharmacy – General Rules were modified, the RFR was filed on March 9, 2022. The rules were not filed and effective until Feb. 29, 2024. That made for a roughly two-year process and the most recent RFR for the same ruleset was filed on May 9, 2025. A number of complicated factors prolonged the previous rule promulgation process, but an 18- to 24-month time horizon for implementation is not unreasonable.
SUMMER EDUCATION UPDATE
BY ASHLEY BUILTA, Pharm.D., director of professional development and education
Thank you all so much for the amazing turnout in Traverse City for the 2025 Annual Convention & Exposition! MPA is pleased to report that we had more than 700 attendees at the Grand Traverse Resort and Spa. We have received tremendous positive feedback on the location, continuing education offerings and food.
We are looking forward to reviewing the data from 2025 to see what suggestions for improvement you all had and how we can make 2026 even better! Looking forward to seeing you all in Lansing!
MPA is also working on the MSHP Annual Meeting and the Upper Peninsula Division Fall Conference in October. The MSHP Annual Meeting will be held Oct. 24 at the Hilton Doubletree-Dearborn, while the UP Fall Conference will take place Oct. 25 at the Northern Center in Marquette.
Registration and agenda information for these events will be available soon, so stay tuned!
MPA takes over Michigan’s Capital City in 2026
MPA’s Annual Convention & Exposition (ACE) will be on the move again, taking over the Lansing Center for three years beginning in 2026! Registration will open in fall 2025, but for now, block off your calendars for April 17-19, 2026 and join us at the Lansing Center!
EMPOWERING PHARMACY TECHNICIANS: A VITAL STEP TOWARD ADVANCING HEALTH CARE
BY STACY BROUSSEAU, Pharm.D., BCPS; MSHP president; emergency medicine clinical pharmacist, Bronson Methodist Hospital
As we look toward the future of pharmacy practice, it's clear that empowering pharmacy technicians is essential for enhancing patient care, improving health care outcomes and creating a stronger, more resilient health care system. This year, the Michigan Society of Health-System Pharmacists’ presidential theme, "Empower, Engage, Enact" encapsulates the powerful role pharmacy technicians play in the health care landscape. By empowering technicians, engaging them in meaningful roles and enacting policies that support their development, we pave the way for a more effective, efficient and patientcentered pharmacy practice.
actively contribute to decision-making processes in the workplace. This engagement is essential for fostering a sense of ownership and pride in their work, which ultimately leads to better job satisfaction, retention and patient care.
"Pharmacy technicians are the backbone of the pharmacy profession. They are responsible for a wide range of tasks which directly impact the quality of care provided to patients."
Pharmacy technicians are the backbone of the pharmacy profession. They are responsible for a wide range of tasks which directly impact the quality of care provided to patients. However, despite their critical contributions, technicians have often been underrecognized and undervalued in comparison to other health care professionals. This is starting to change, thanks in part to organizations like the American Society of Health-System Pharmacists and The Pharmacy Technician Society (TPTS), which has made tremendous strides in advocating for the recognition and advancement of technicians.
The first pillar of this year’s MSHP’s theme (empower) resonates deeply with the work being done by ASHP and TPTS to elevate the role of pharmacy technicians.
In 2023, ASHP launched The Pharmacy Technician Society to provide a professional home for technicians and act as a catalyst for their career advancement and education. The vision for this society is not only to support the growth of individual technicians, but ensure the profession is more recognized and respected within the health care community.
ASHP CEO Paul Abramowitz recently wrote that “when pharmacy technicians thrive, everyone benefits.”
This statement highlights the significant impact that empowered technicians can have on patient care. As technicians gain more recognition and responsibility, they can contribute more fully to the health care team. They are better equipped to support pharmacists and other clinicians, creating a more collaborative and efficient work environment. When technicians are empowered with the tools, education and resources they need to succeed, the entire health care enterprise – and, most importantly, the patients – benefit.
The second pillar (engage) calls for actively involving technicians in every aspect of pharmacy practice. One of the key goals of TPTS is to provide technicians with opportunities to take on greater responsibilities and to
Engaging pharmacy technicians also involves providing them with professional development opportunities and creating clear career paths. Abramowitz also points out that many technicians are seeking opportunities for growth, specialization and advancement. TPTS has recognized this need and is working to standardize education and training programs to ensure technicians have access to consistent skill development. By creating pathways for career advancement, we not only empower technicians but also foster a workforce that is wellprepared to meet the evolving demands of health care. The final pillar (enact) focuses on the importance of enacting policies and practices that support the advancement of pharmacy technicians. TPTS is working closely with ASHP to advocate for legislative changes that will improve working conditions and compensation for technicians. ASHP and TPTS are pushing for greater recognition of technicians in the policy arena, including advocating for pharmacy technician representatives on state boards of pharmacy. These efforts are crucial for ensuring that the contributions of pharmacy technicians are fully acknowledged and their roles continue to evolve to meet the needs of modern health care.
The work of ASHP and TPTS is already having a significant impact. With the release of TPTS’s first strategic plan, the foundation has been laid for even greater strides in technician empowerment, engagement and advocacy. This strategic plan emphasizes the importance of fostering an inclusive environment, supporting career development and advocating for the professional recognition of pharmacy technicians. As the pharmacy workforce continues to evolve, the advocacy and policy work being done by ASHP and TPTS will be essential for ensuring that technicians are given the resources, training and recognition they deserve.
As we move further into 2025, “Empower, Engage, Enact” serves as a reminder of the important role pharmacy technicians play in the health care system. By empowering technicians, engaging them in meaningful work and enacting policies that support their growth, we are not only improving the lives of technicians but also enhancing the quality of care we provide to our patients.
With continued advocacy, education and support, we can ensure that pharmacy technicians thrive and continue to make a positive impact on the health care landscape.
EXPAND OUTPATIENT ANTIMICROBIAL STEWARDSHIP PROGRAMS BY OPTIMIZING RESOURCES WITH CHARM
BY MICHAEL KLEPSER, Pharm.D., FCCP, FIDP; MINJI SOHN, Pharm.D.; BENJAMIN PONTEFRACT, Pharm.D., BCPS; KAYLEE CANIFF, Pharm.D., BCIDP; and KUSHAL DAHAL, MS; Ferris State University
The Collaboration to Harmonize Antimicrobial Registry Measures (CHARM) is an initiative launched at the Ferris State University College of Pharmacy in 2015. The idea for CHARM came from the need to fill a gap surrounding the use of antimicrobials in the outpatient setting.
At the time, such data were only available from sources that charged significant fees and the reports produced generally had an appreciable time lag and failed to provide the level of detail needed to support antimicrobial stewardship initiatives. As a result, we began to explore means to utilize the data existing at our practice site in the electronic medical records system. We knew the data we wanted were there, but rather than only gathering summary data, we desired data that would also provide insight into patterns of antimicrobial use at the diagnosis, prescriber and patient levels.
It was determined no validated methods existed that could provide the data we wanted – so, we decided to develop our own methodology. Minji Sohn was enlisted to collect, clean, analyze, validate and share information. Each step of the way we learned from and listened to stakeholders to produce our first reports.1
Soon afterwards, we shared our project with members of the Surveillance for Healthcare-Associated & Resistant Pathogens (SHARP) Unit at the Michigan Department of Health and Human Services. We discussed the steps that had been taken and the time we had spent to develop and validate CHARM and decided that health systems across the state could benefit. In addition to providing MDHHS insight into outpatient antimicrobial usage patterns in the state, members of the SHARP Unit hoped that we could provide CHARM at no cost to health systems so they could use their resources to develop and implement stewardship activities rather than re-create a tool.
With that, we set upon a quest to partner with as many health systems and other prescriber networks as possible to integrate CHARM into their outpatient antimicrobial stewardship programs.
College of Pharmacy
Serendipitously, in January 2020 the Joint Commission released Standard MM.09.01.03 for antimicrobial stewardship in ambulatory care.2 These standards listed five performance measures related to outpatient antimicrobial stewardship:
EP 1: The organization identifies an individual(s) responsible for developing, implementing and monitoring activities to promote appropriate antimicrobial medication prescribing practices.
EP 2: The organization sets at least one annual antimicrobial stewardship goal. Note: Examples of antimicrobial stewardship goals may include decreasing the use of antibiotics to treat viral infections or addressing overuse of a specific medication.
EP 3: The organization uses evidence-based practice guidelines related to its annual antimicrobial stewardship goal(s). Note: Guidelines may include diagnostic criteria and treatment recommendations to use when prescribing antimicrobial medications.
EP 4: The organization provides all clinical staff and licensed independent practitioners with educational resources related to its antimicrobial stewardship goal(s) and strategies that promote appropriate antimicrobial medication prescribing practices.
EP 5: The organization collects, analyzes and reports data pertaining to the antimicrobial stewardship goal(s) to organizational leadership and prescribers. Note: Data may include antimicrobial medication prescribing patterns, antimicrobial resistance patterns, or an evaluation of the antimicrobial stewardship activities implemented.
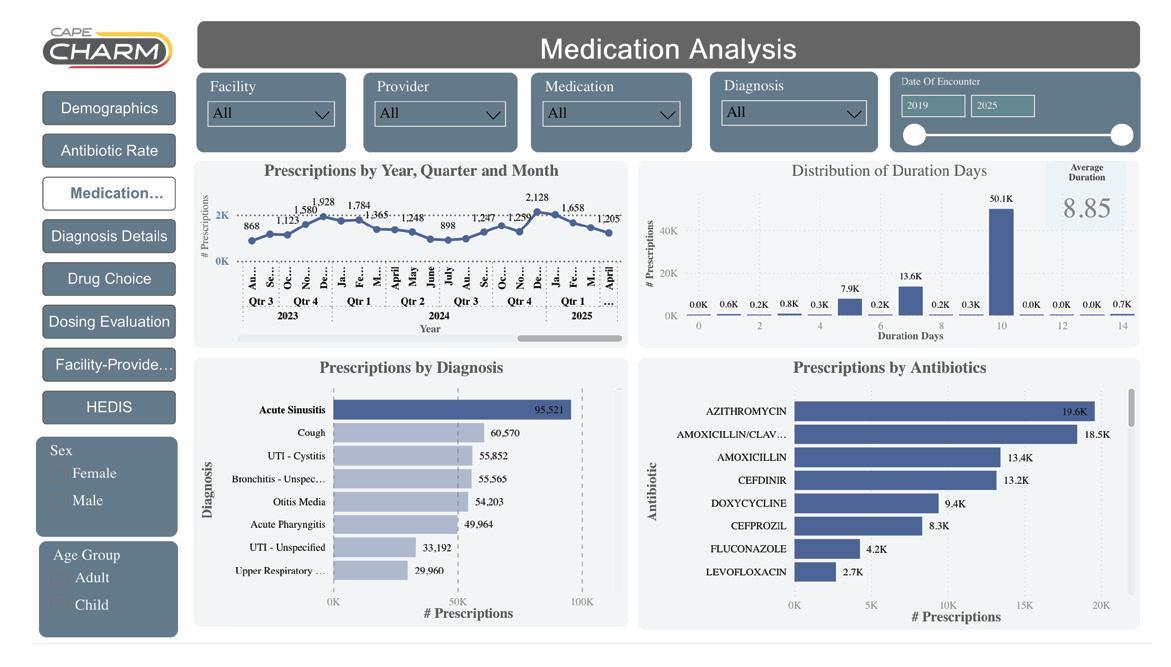
We believed that CHARM could help support all of these performance measures and be extremely valuable to health systems. Additionally, we noted that CHARM had the potential to be used by health systems to track progress towards meeting Healthcare Effectiveness Data and Information Set (HEDIS) measures related to antimicrobial use. Since these data could directly impact Star Ratings and reimbursement levels, we worked with Blue Cross Blue Shield of Michigan to develop and validate a process that allows us to provide an estimate of HEDIS measure performance for avoidance of antibiotic treatment for acute bronchitis/bronchiolitis (AAB) and appropriate treatment for upper respiratory infection (URI).
Figure 1
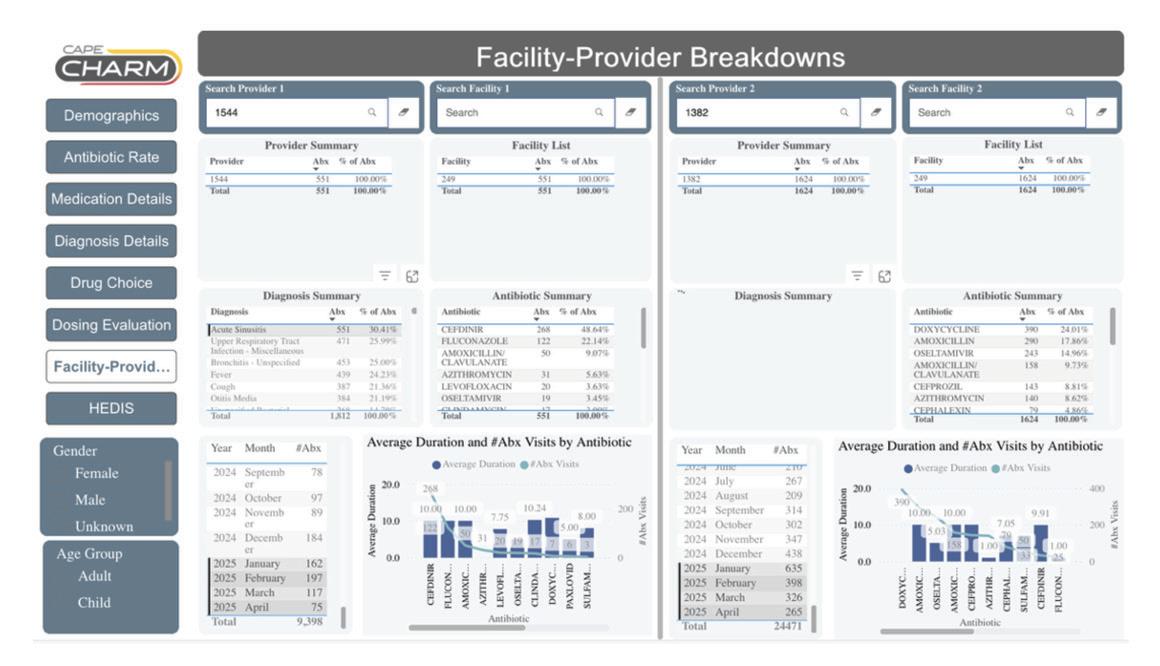
“One of the newest features of CHARM is a function that allows users to generate peer-to-peer, prescriber-to-clinic, prescriber-to-health system, or prescriber-tobenchmarking reports. This function will hopefully allow CHARM to serve an even greater role in supporting outpatient antimicrobial stewardship programs.”
Currently, CHARM is funded by grants through the MDHHS and the Illinois Department of Public Health. This support has allowed us to partner with 31 health systems across eight states. These include large academic health systems, small community hospitals, federally-qualified health centers and an Indian nation. We have been able to expand our efforts into dental practice through collaborations with Ohio State University, the Connecticut Department of Health, and the University of Connecticut School of Dental Medicine. Additionally, we have sought to provide a "One Health" perspective to CHARM by partnering with the Michigan State University School of Veterinary Medicine to track and report antimicrobial usage patterns in veterinary hospitals and clinics. We provide all partners with an individualized, interactive dashboard that allows them to track and assess concordance of antimicrobial use within their systems with highly granular reports. (Figure 1)
One of the newest features of CHARM is a function that allows users to generate peer-to-peer, prescriber-to-clinic, prescriber-to-health system, or prescriber-to-benchmarking reports. This function will hopefully allow CHARM to serve an even greater role in supporting outpatient antimicrobial stewardship programs. (Figure 2)
The mission of CHARM is to “provide near real-time guidance and direction to clinicians and health systems to optimize antibiotic use.” We seek to provide the tools clinicians need to establish, justify and support outpatient antimicrobial stewardship programs. Our goal is to provide these services at low or minimal cost to partners, and our desire is in doing so, they would be able to direct their limited resources towards improving patient care. In this way, we hope to allow our partners to do more with less.
If you have questions or would like to participate with CHARM, please email Michael Klepser at michaelklepser@ferris.edu.
REFERENCES:
1. Sohn M, Chung D, Winterholler JE, Hammershaimb B, Leist C, Kucera M, Trombley M, Tracey J, Dregansky G, Schauer M, Rauch H, Woodwyk A, VanLoo D, Warner A, Klepser ME Assessment of antibiotic use and concordance with practice guidelines within three diverse ambulatory clinic systems. JAPhA. 2020;60:930-6.
2. Antimicrobial Stewardship in Ambulatory Health Care. R3 Report. Issue 23, June 20, 2019 (https://www.jointcommission.org/-/media/tjc/documents/standards/r3-reports/r3_23_ antimicrobial_stewardship_amb_6_14_19_final2.pdf)
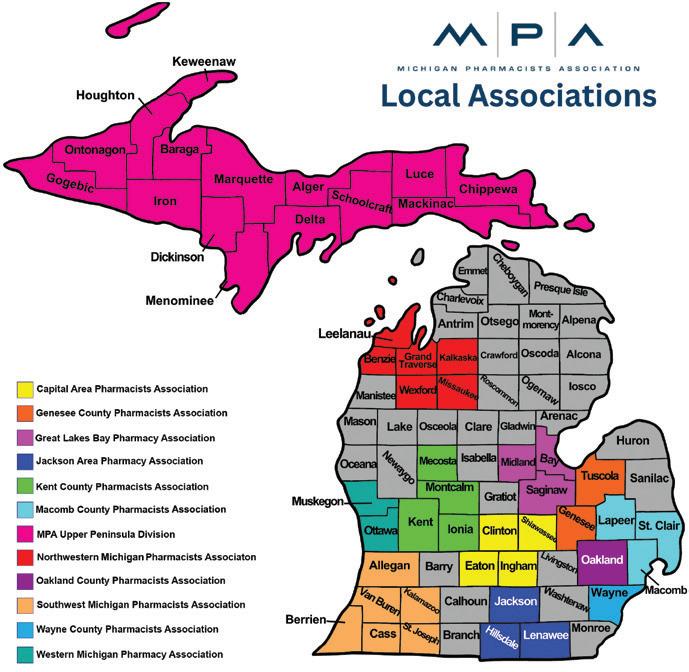
Capital Area Pharmacists Association: capapharm@gmail.com; website: capapharm.org
Genesee County Pharmacists Association: geneseepharmacists@gmail.com; website: geneseepharmacists.org
Great Lakes Bay Pharmacy Association: greatlakesbaypharmacy@gmail.com; website: sites.google.com/a/glbpa. com/great-lakes-bay-pharmacy-association/home
Jackson Area Pharmacists Association: Kyle Kronemeyer, president, kylerph@comcast.net
Kent County Pharmacists Association: kcpapharmacists@gmail.com
Macomb County Pharmacists Association: mcpa586@gmail.com
Wayne County Pharmacists Association: waynepharmacists@gmail.com
Western Michigan Pharmacists Association: Neal Miller, chair, pillbox81.nm@gmail.com
RARE DISEASE REVIEW:
BY ANDREW BRITTON, Pharm.D., MBA
Phenylketonuria (PKU) is a rare, inherited metabolic disorder that exemplifies the crucial importance of early detection and appropriate management of genetic diseases. Primarily, PKU is caused by mutations in the PAH gene, which encodes phenylalanine hydroxylase (PAH).1,2 Phenylalanine hydroxylase is an enzyme involved in the process of converting the amino acid phenylalanine into tyrosine. When PAH is deficient or dysfunctional and left untreated, phenylalanine can accumulate to toxic levels. The build-up of phenylalanine, particularly in the brain, can potentially lead to various neurological, developmental and physical issues. Though some of the more serious clinical manifestations of PKU can be avoided with prompt, early treatment, patients with PKU still often show differences in executive functioning, such as planning or sustained attention, when compared to healthy patients.1,2
“Domestically, PKU has an
incidence
of
approximately 1 in
10,000
live births.The prevalence of PKU varies worldwide. PKU ranges from 1 in 850 births in the KarachayCherkess Republic (a republic of Russia located in the North Caucasus region) to merely 1 in 112,000 births in Finland.”
A Look at Phenylketonuria (PKU), its Diagnosis and Appropriate Treatment
From a pathophysiological standpoint, the disease mechanism involves impaired hydroxylation of phenylalanine leading to hyperphenylalaninemia. In addition, a portion of accumulated phenylalanine is converted into other, non-tyrosine metabolites (e.g., phenylacetate, phenylpyruvate), which are neurotoxic.1,3
Notably, also phenylalanine competes with other large neutral amino acids for transport across the blood-brain barrier. Hyperphenylalaninemia reduces cerebral levels of tyrosine and tryptophan, which are precursors for neurotransmitters dopamine and serotonin, respectively.4 Furthermore, PAH participates in the synthesis of tyrosine itself and therefore, a deficiency in this enzyme results in significantly reduced levels of tyrosine , further compounding the issue with
transport across the blood-brain barrier.1
Epidemiology and the Classification of PKU as a Rare Disease
Individuals must inherit two copies of the mutated gene, one from each parent, to develop PKU.1 Globally, PKU has an estimated prevalence of 1 in 23,930 live births; however, it varies considerably among ethnic groups and geographic regions.5
Domestically, PKU has an incidence of approximately 1 in 10,000 live births.5 It ranges from 1 in 850 births in the KarachayCherkess Republic (a republic of Russia located in the North Caucasus region) to 1 in 112,000 in Finland.5 Generally, the prevalence of PKU is lower in Asia, particularly in Japan,
Philippines and Singapore.
Conversely, PKU rates are significantly higher in the Middle East. The highest are in Iran and Jordan, which are both reported as 1 in 5,000.6
A contributing factor in this region is the frequency of decent from a common ancestor. Marriage between close relatives, particularly first cousins, increases the likelihood of both parents carrying the recessive mutation.7
Currently, there is not a single universally agreed upon international definition of a rare disease. As such, a particular disease could be classified as rare in one region but not in another due to differences in these definitions. This is further confounded by diseases for which the prevalence and incidence rates can vary between geographic regions or ethnic groups, such as PKU.
The Food and Drug Administration defines a rare disease as a condition affecting fewer than 200,000 individuals.8 PKU clearly falls under this definition, with current estimates indicating fewer than 20,000 individuals have PKU.5
The European Union classifies rare diseases as those affecting fewer than 1 in 2,000 people.9 This classification is not merely academic; it grants access to orphan drug incentives and increased funding for research and therapeutic development.8,9
Newborn Screening and the Inclusion of PKU
Pioneered by Dr. Robert Guthrie in the 1960s, PKU was the first condition identified through newborn screening.10 His development of the bacterial inhibition assay allowed for detection of elevated phenylalanine levels on dried blood spots.11 Starting in the 1990s, more quantitative and efficient methods have replaced the Guthrie test in many places.12
Today, PKU is a core condition on the United States Recommended Uniform Screening Panel and is included in newborn screening programs in most developed countries.13 Screening typically occurs 24-48 hours after birth and after the newborn has had some protein in their diet. This process involves obtaining a blood sample (i.e., newborn blood spot screening). The blood is obtained from the baby’s heel and placed on a filter paper card, which is promptly sent to a centralized laboratory for analysis.14
Before newborn screening, PKU was often diagnosed after the development of symptoms (such as intellectual disability and behavioral problems). By this time, the elevated levels of phenylalanine have caused irreversible damage to brain tissue.15 Universal screening has dramatically reduced the incidence of intellectual disability associated with PKU, as early treatment (initiated within the first few weeks of life) prevents neurotoxicity.16
Symptomatology and Diagnosis
In untreated individuals, symptoms typically emerge within the first months of life and include the following: severe intellectual disability, seizures, eczema-like skin rash and behavioral disturbances (such as hyperactivity and aggression).1,2
Because tyrosine is essential for melanin synthesis, patients with PKU experience significant loss of pigmentation in hair, skin and iris. Additionally, the deficiency in phenylalanine metabolism leads to the abnormal production of phenylacetate. Subsequently, phenylacetate is excreted in the urine and contributes to the musty odor that is characteristic to PKU patients.1,2
Furthermore, maternal PKU (i.e., a pregnant woman with uncontrolled phenylalanine levels) may disrupt normal fetal brain development, would could lead to issues such as to microcephaly (a condition in which the baby’s head is considerably smaller than normal), low birth weight and heart defects.17 With early intervention, most symptoms can be prevented.16 Unfortunately, some individuals may still exhibit subtle neurocognitive deficits, especially if blood phenylalanine levels are not tightly monitored throughout their life.18
Following detection of PKU through newborn screening, the diagnosis of PKU is confirmed through elevated plasma phenylalanine levels (greater than 360 µmol/L).19 Additionally, clinicians may suggest genetic testing to identify specific PAH mutations.
Other important biomarkers and tests include:
• Phenylalanine to tyrosine ratio: Elevated ratios (exceeding 3:1) are abnormal and indicative of PKU.20
• Urinary phenylketones: Often positive in “classic” PKU (a complete or near-complete deficiency of phenylalanine hydroxylase).1,6
• Genetic sequencing of PAH gene: Helps stratify patients based on residual enzyme activity and guides treatment decisions.21
• Tetrahydrobiopterin (BH4) loading test: Used to identify BH4-responsive forms of PKU, which can be treated with pharmacotherapy.22 Notably, BH4 is an important cofactor that helps to stabilize phenylalanine hydroxylase and potentially enhance enzyme activity.
Therapeutic Interventions
The cornerstone of PKU management is lifelong dietary restriction of phenylalanine, primarily achieved through a low-protein diet, phenylalanine-free medical formula (amino acid mixtures) and special low-protein foods.6,16,19
To prevent long-term complications, blood
phenylalanine levels should be maintained between 120-360 µmol/L for children under 12 years of age. Furthermore, the treatment target for those 12 years and older is 120600 µmol/L.23 To minimize the risk of birth defects, (such as neurological deficits and microcephaly), the recommended treatment range for women who are trying to conceive or are pregnant is 120-360 µmol/L.23 The American College of Medical Genetics and Genomics recommends that all PKU patients should have a lifelong maintenance goal of 360 µmol/L or lower.19
The frequency of monitoring depends on the patient’s age and clinical status. During the first year of life, phenylalanine levels should be checked once weekly.24 The recommended monitoring schedule for those 1 to 12 years of age is twice a month, followed by a decrease to monthly after 12 years of age. Due to the importance of maintaining tight control of phenylalanine levels, pregnant women with PKU should have bloodwork performed at least twice weekly.24
Other monitoring parameters should include tyrosine levels, which must be supplemented, as well as the patient’s nutritional status to prevent deficiencies in vitamins, minerals and essential fatty acids.1,6,25
Pharmacists play a key role in the management of PKU patients. When counseling these patients, they should emphasize strict dietary compliance and stress the importance of monitoring for nutritional deficiencies.16 Due to the significance of following a phenylalaninerestricted diet, pharmacists should educate PKU patients on reading food and drink labels, as well as the labeling for over-the-counter medications. Many sugar-free OTC products contain aspartame, which is metabolized into phenylalanine.26
Finally, pharmacists can assist PKU patients in obtaining and understanding insurance coverage for medical foods.27
Sapropterin (Kuvan), which is a synthetic form of BH4, acts as a cofactor for the PAH enzyme.28 In responsive individuals (reduction of 30% or more in phenylalanine blood levels), it enhances residual enzyme activity, allowing for higher phenylalanine tolerance.16,28 Sapropterin is indicted for use in adults and children (1 month of age and older) and is commercially available as tablets and a powder for oral solution.29 Importantly, sapropterin has been shown to be effective and well-tolerated during pregnancy.30
Sapropterin, which is to be used in combination with a phenylalaninerestricted diet, is FDA-approved to decrease phenylalanine concentrations in those with HPA associated with BH4-responsive PKU.29 For individuals 1 month to 6 years old, the manufacturer recommends a starting dose of 10 mg/kg taken by mouth once a day. Patients 7 and older should be prescribed a starting dose of 10 to 20 mg/kg once a day. If the patient has an appropriate biochemical response (i.e., reduction in phenylalanine concentrations), the patient may be adjusted to a maintenance dose of 5 to 20 mg/kg daily. For those that do not exhibit an appropriate biochemical response after one month of treatment), therapy with sapropterin should be discontinued.29
Sapropterin was the first pharmacologic treatment for PKU. The efficacy and safety of sapropterin was established in multiple clinical trials involving PKU patients.26 The manufacturer cites the Phase 3 randomized, controlled trial conducted by Levy and associates as pivotal in proving the efficacy of sapropterin.31, 32
The double-blind, multi-center study involved 88 PKU patients deemed BH4-responsive. The researchers used a primary endpoint of mean change of phenylalanine levels from baseline. At the end of the six-week trial, patients treated with sapropterin experienced a reduction in mean phenylalanine levels of 236 (257) µmol/L, while those given placebo had an increase of 3 (240) µmol/L from baseline (p<0.0001). Furthermore, 18 of 41 participants (44%) in the treatment group (95% confidence interval, 28-60%) had a 30% or greater decline in blood phenylalanine levels. Conversely, only four of 47 patients (9%) in the control group (95% CI, 2-20%) experienced a similar reduction from baseline. The study's authors noted in some instances the use of sapropterin in patients with BH4-responsive PKU might even replace dietary restrictions.32
Following the drug’s approval, the Phenylketonuria Demographics, Outcomes, and Safety (PKUDOS) registry was designed to obtain and analyze data on the sustained efficacy and tolerability of sapropterin.33 The PKUDOS registry consisted of 1,189 patients with PKU who were treated with sapropterin; 504 patients remained on continuous therapy, while 211 patients had short-term exposure.
After five years of uninterrupted treatment, continuous users experienced a mean 34% reduction in blood phenylalanine levels,
dropping from an average of 591 μmol/L at baseline to 392 μmol/L (p = 0.0009). Importantly, this metabolic improvement was accompanied by a notable increase in dietary phenylalanine tolerance, rising from 1,000 mg/ day at baseline to 1,539 mg/day after six years.33
Only 6% of continuous users reported drug-related adverse events, which were predominantly non-serious (e.g., gastrointestinal, respiratory, or nervous system complaints). Additionally, serious drugrelated adverse events occurred in less than 1% of registry participants. Markedly, these encouraging safety and efficacy outcomes were observed across age groups, including children younger than 4 years of age.33
The “real-world” data from the PKUDOS registry shows that long-term use of sapropterin is well-tolerated, sustains significant reductions in phenylalanine concentrations and increases dietary phenylalanine tolerance. Importantly, the clinical evidence obtained from the registry reinforces the value of sapropterin in personalized PKU management.33
To determine responsiveness to sapropterin therapy, a seven-to-28-day BH4 challenge is often used in the U.S., while a 48-hour challenge is more common in Europe.34 Genotyping, which is often performed following confirmation of the patient’s diagnosis, can help predict responsiveness to sapropterin.28 Notably, if genotyping was performed and the patient was deemed to possess two null (no response) mutations, the sapropterin response test should not be conducted, as these patients are not likely to exhibit an appropriate biochemical response.34
In the responsiveness test, patients typically receive an initial daily dose of 20 mg/kg and are frequently monitored throughout the challenge.34 The seven-to-28-day duration is used to detect late responders (i.e., PKU patients who may not show an appropriate response within the first 48 hours) and to confirm the long-term impact on dietary considerations.
Sapropterin is generally considered welltolerated with the most common adverse reactions (occurring in 4% or more of users) being headache, rhinorrhea, pharyngolaryngeal pain, vomiting, cough and nasal congestion.29 It is important to counsel patients on important warnings and precautions, such as hyperactivity (restlessness, fidgeting, or excessive
talking) and upper gastrointestinal mucosal inflammation (e.g., esophagitis, gastritis).29
Pharmacists should counsel patients and their caregivers on the importance of frequent blood draws for phenylalanine monitoring. Additionally, patients should be instructed on the proper administration of sapropterin (i.e., take with a meal, ideally at the same time each day).29 Finally, pharmacists should advise users that the powder formulation of sapropterin should be dissolved in water or apple juice, or stirred in a small amount of soft food such as apple sauce or pudding. Tablets may be swallowed whole, dissolved in liquid, or crushed and mixed with soft foods.29
Approved in 2018, pegvaliase-pqpz (Palynziq) is an enzyme substitution therapy that metabolizes phenylalanine to non-toxic metabolites.35 Pegvaliase-pqpz is FDAapproved to decrease phenylalanine concentrations in adults with uncontrolled PKU (blood phenylalanine levels over 600 µmol/L) despite dietary therapy. Pegvaliasepqpz is commercially available as singledose prefilled syringes and is intended for subcutaneous administration.36
The recommended starting dose of pegvaliase is 2.5 mg injected once weekly for four weeks. Based on the patient’s tolerability, the dose should be increased, in a step-wise manner over a minimum of five weeks, to a maintenance dose of 20 mg once daily.36 In those who have administered 20 mg/ day continuously for 24 weeks and have not achieved appropriate phenylalanine concentrations, pegvaliase may be increased to 40 mg/day. Subsequently, clinicians may consider an increase to 60 mg/day (maximum dose for pegvaliase) if the patient did not achieve an appropriate biochemical response after 16 weeks of continuous administration of 40 mg once daily.36
Due to the substantial risk of anaphylaxis, the initial dose of pegvaliase should be administered under the close supervision of a clinician equipped to address an anaphylactic reaction. Following the injection of pegvaliase, the patient should be closely observed for a minimum of 60 minutes. Notably, health care providers should consider premedication (i.e., H1-receptor blocker, H2-receptor blocker, and/ or antipyretic) for hypersensitivity reactions.36
Safety and efficacy data obtained from the Pegvaliase Risk Investigation of Systemic Manifestations 3 (PRISM-3) program was pivotal in the FDA-approval of pegvaliasepqpz. The PRISM clinical trial program
enrolled adults with uncontrolled PKU (blood Phe levels over 600 µmol/L) and consisted of PRISM-1 and PRISM-2.37-38
PRISM-1 was a Phase 3, open-label, multicenter study; participants were randomized (1:1) to receive a maintenance dose of either 20 mg/day or 40 mg/day. Study participants reached their maintenance dosing regimen after an induction phase and titration phase, which were used to improve patient tolerability and mitigate the risk of hypersensitivity reactions. The purpose of the PRISM-1 study was to evaluate the efficacy and safety of pegvaliase in pegvaliase-naïve (i.e., no prior treatment with pegvaliase) adults with uncontrolled PKU.37
In addition to serving as the foundational phase 3 study of the PRISM clinical program (i.e., establishment of dose titration protocol, identification of key adverse effects, and development of risk management strategies) PRISM-1 independently demonstrated the ability of pegvaliase to significantly decrease blood phenylalanine levels in adults with uncontrolled PKU. Furthermore, many patients in PRISM-1 self-reported neurocognitive improvements, such as better mood and enhanced attentiveness.37
PRISM-2, which was a four-part clinical trial, aimed to further evaluate the safety and efficacy of pegvaliase in adult PKU patients. Part 1 was an open-label continuation of PRISM-1, with participants continuing their prescribed maintenance dose of pegvaliase (either 20 mg/day or 40-mg/day). Part 2 was a randomized discontinuation trial ; participants were randomized (2:1) to either continue their maintenance dose (either 20 mg/day or 40 mg/day) or switch to placebo for eight weeks. In part 3, patients who received placebo (i.e., randomized to receive placebo in part 2) returned to treatment with pegvaliase. Researchers used data obtained in part 3 to analyze the drug’s pharmacodynamic and pharmacokinetic properties. Part 4 was an open-label extension study to assess long-term outcomes. Participants in part 4 received pegvaliase doses from 5 mg/day to 60 mg/day, which was based on investigatordetermined tolerability and efficacy parameters.38
Results from PRISM-2 demonstrated that treatment with pegvaliase lead to clinically meaningful and sustained reductions in blood phenylalanine levels. Additionally, data obtained from part 2, which was the only placebo-controlled portion of the PRISM-3
program, was essential for the FDA efficacy review. From the start of part 2 to week eight, the pooled pegvaliase group showed a mean change of 26.5 µmol/L versus 949.8 µmol/L and 664.8 µmol/L for the 20 mg/day and 40 mg/day placebo groups, respectively (p< 0.0001).38
In a combined analysis of PRISM-1 and PRISM-2 (i.e., results from the overall PRISM-3 program), investigators noted that pegvaliase allowed for a higher protein intake versus other treatment options. Additionally, within 24 months, the researchers noted significant reductions in phenylalanine concentrations; 68.4% of patients attained blood phenylalanine levels of 600 µmol/L or less, and 60.7% of patients reached blood phenylalaninelevels of 360 µmol/L or less. A substantial percentage of patients (51.2%) achieved blood phenylalanine levels of 120 µmol/L (the upper limit of normal for healthy, non-PKU patients) or less.37,38 The blood phenylalanine levels achieved by most patients were consistent with target treatment ranges (i.e., below the upper limit recommended in treatment guidelines).19,23 Furthermore, the researchers documented sustained improvements in cognitive dysfunction, memory impairment, behavioral problems, and psychiatric disorders such as anxiety and depression).37,38
In study 165-304 (an open-label extension study), researchers continued to evaluate the safety and efficacy of elevated doses of pegvaliase (doses greater than 40-60 mg/ day). Study 165-304 featured eligible patients from PRISM-2 who were receiving over 40 mg/day of pegvaliase. Researchers noted that pegvaliase, despite being administered at higher doses, continued to provide long-term, clinically significant reductions in phenylalanine concentrations. Notably, the drug’s safety profile improved over the duration of the induction and titration phases. Moreover, the adverse effects associated with pegvaliase were deemed manageable for most patients; however, as with all pharmaceuticals, individual results vary.39
Unfortunately, the use of pegvaliase was associated with serious immune-mediated adverse effects. These events are believed to stem from the immune system’s response to the foreign enzyme, a non-human protein. Notably, the most significant safety concern related to the drug’s immunogenicity, is anaphylaxis, which occurred in approximately 9% of patients during clinical trials.40,41
Due to the risk of anaphylaxis, the FDA mandated a Risk Evaluation and Mitigation Strategy program for prescribing and dispensing purposes. The REMS program requires prescriber and pharmacy certification, as well as patient educational enrollment. Importantly, patients must be instructed on the recognition and management of anaphylaxis. Because anaphylaxis may occur while undergoing treatment with pegvaliase, patients must always carry auto-injectable epinephrine. The REMS program aims to ensure the safe use of pegvaliase while allowing access to a potentially life-changing therapy for adults with poorly-controlled PKU.36
According to the manufacturer’s package insert, the most common adverse effects (occurrence of 20% or more in the treatment phase) include the following: injection site reactions (redness, pain, swelling etc.) wwww; arthralgia; hypersensitivity reactions; headache; generalized skin reactions lasting two weeks or more; gastrointestinal effects (nausea, vomiting, diarrhea, abdominal pain); cough; oropharyngeal pain; pruritus; nasal congestion; fatigue; dizziness; and anxiety. To emphasize the magnitude of the drug’s risk of anaphylaxis, the package insert featured a boxed warning, which highlights key prescribing points, such as the availability of pegvaliase only through its REMS program.36
Besides counseling patients on the importance and appropriate use of autoinjectable epinephrine, pharmacists should also instruct patients on proper storage and administration of pegvaliase. Pegvaliase should be stored under refrigeration (36 to 46 degrees Fahrenheit) in its original carton to protect from light. To help reduce the sting or discomfort of the injection, users may store pegvaliase in the original carton at controlled room temperature (68 to 77 degrees) for up to 30 days. The recommended injection areas for pegvaliase are front middle of the thighs and the abdomen at least 2 inches away from the navel). As with many other injectable medications, patients should rotate injection sites. Health care providers should also demonstrate and ensure the patient’s ability to perform proper injection techniques (i.e., gentle pinching of the skin, slow injection of the drug at 45-degree to 90-degree angle, etc.).36
Finally, patients should be instructed on the importance of obtaining recommended labwork, primarily phenylalanine concentrations. Until a maintenance dose is established, blood phenylalaninelevels should be obtained
every four weeks. During maintenance therapy, blood phenylalanine levels should be monitored periodically. Furthermore, health care providers should confirm the patient’s understanding of dietary restrictions (i.e., monitoring and adjusting dietary protein and phenylalanine intake, etc.).36
Health care Disparities in PKU
Despite the success of newborn screening in high-income countries, individuals with PKU continue to face pronounced disparities in access to care and treatment. Unfortunately, not every state covers medical foods under their newborn screening program.27 In a study by the New York State Department of Health, nearly 50% of private insurers denied coverage for essential PKU dietary formulas, while Medicaid covered only 10% of requests for special foods.42
Generally, providing care for PKU patients has a substantial financial burden. According to data collected from a detailed cost and utilization survey, the yearly out-of-pocket cost for low-protein foods was $1,651 for children and $967 for adults.43
Another survey found uncovered spending (out-of-pocket costs for products not covered or only partially covered by medical insurance) was reported by 59% of families requiring modified low-protein foods.27
Food insecurity, which is the limited or uncertain availability of nutritionally adequate and safe foods, affects millions of Americans. Due to the importance of dietary management, food insecurity can have a profoundly negative impact on PKU patients. In a 2020 study, authors noted that women with PKU reported considerably higher rates of food insecurity (40%) compared to the U.S. general population (11.1%).44 Moreover, the prevalence of food insecurity for adolescents
was greater than adult PKU patients (44% vs. 36%). Furthermore, food-insecure patients tend to consume more phenylalanine and less medical food, potentially leading to cognitive impairments and behavioral issues.44,45
The coverage gaps and financial inadequacies contribute to poor dietary adherence and elevated blood phenylalanine levels.46 In a California survey, 27.6% of families had difficulty obtaining formula, and 34.7% struggled to access low-protein foods. Furthermore, 57.1% of families noted resultant spikes in blood phenylalanine levels along with 44.9% reporting declines in their children’s school performance.47
Pharmacologic treatments like sapropterin and pegvaliase are scientific breakthroughs in the management of rare diseases; they serve as safe and effective treatment modalities for PKU patients. However, the excessive cost, specialty pharmacy distribution and variable insurer requirements create barriers, especially for underinsured patients.43,46 Moreover, limited inclusion of non-white populations in clinical trials raises concerns about treatment generalizability.48
Addressing health care disparities requires robust policy action: passing and enforcing comprehensive legislation, such as the Medical Nutrition Equity Act to ensure universal coverage for required medical foods (i.e., medically necessary forms of nutrition).49 Other strategies to mitigate health care disparities include expanding access via telehealth and regional metabolic networks, reducing socioeconomic and racial gaps in pharmacotherapy access, and implementing food-insecurity screening and support services in routine PKU care.44,46,50
Cultural and linguistic barriers may further hinder care.51 Dietetic counseling is a cornerstone of PKU management; however,
minority patients may have trouble in following dietary plans that are not tailored to their cultural food preferences.52 For example, Hispanic families may struggle to reconcile traditional staple foods like beans, rice and tortillas (typically made with corn) with the protein restrictions inherent in the PKU diet.53
Pharmacists, especially those embedded in community settings, can play a vital role in reducing disparities by offering medication counseling, assisting with insurance navigation, and promoting adherence to pharmacologic therapies. Culturally competent communication and proactive screening for social determinants of health, such as food insecurity or transportation barriers, can help pharmacists identify and mitigate barriers to care.46,54 Moreover, pharmacists involved in specialty pharmacy services can advocate for coverage of medical foods and coordinate with dietitians to ensure continuity of care across racial and socioeconomic lines.55
Conclusion
PKU, though rare, represents a powerful model for the triumph of early diagnosis and targeted treatment in genetic disease. From its historical role as the first disorder in newborn screening to its innovative therapies like pegvaliase, PKU management continues to evolve. However, significant gaps remain, especially in ensuring equitable access to care and lifelong support.
Pharmacists play a pivotal role in education, monitoring and advocating for patients with PKU. Continued research, policy reform and collaboration among health care providers are essential to close the disparity gap and optimize outcomes.
References available on request
2026 PRESIDENT-ELECT CANDIDATES
RYAN BICKEL, PHARM.D.,
MHA, FASHP, recently transitioned from regional director of pharmacy at Ascension Borgess in Kalamazoo to Beacon Health System, based out of South Bend, Indiana. He has 25 years of pharmacy experience, mostly in health-system pharmacy. Bickel earned a bachelor’s degree in biomedical sciences from Western Michigan University, a Doctor of Pharmacy from Ferris State University and Master of Health Administration from Simmons College. He completed a pharmacy practice residency at Spectrum Health in Grand Rapids and is a diplomate of the American Society of Health-System Pharmacists Pharmacy Leadership Academy.
In his current role, Bickel oversees a pharmacy enterprise, which includes hospital, community and infusion pharmacies. His primary focus areas include patient safety, quality, pharmacy and hospital leadership. He also enjoys precepting residents and pharmacy students. Bickel has been professionally active in ASHP, the Michigan Pharmacists Association and the Michigan Society of Health-System Pharmacists. He is a past MSHP board member and president, a past Michigan Pharmacy Foundation trustee and chair, and a past Michigan delegate to the ASHP House of Delegates.
Bickel resides in Kalamazoo and is currently in his third year on the MPA Executive Board.
List what you consider MPA’s priority projects or programs should be – reflecting either an expansion of current activities or entirely new services: Over the past several years, the MPA Board and staff has worked hard to achieve a balanced budget. One of my priorities will be to continue to maintain financial growth through stewardship of resources and pursuing new business opportunities that align with MPA’s members and mission. This will allow us to replenish some of our long-term investments, protect our future, better support our members and fulfill our mission. Some topics which particularly interest me are continued PBM reform, protection of the 340B drug pricing for hospitals, advancing pharmacy technicians and gaining provider status for pharmacists.
That said, the priorities are not to be chosen by me, but by the members. In July, MPA board members, staff and representatives from the various sections met to revise our strategic plan. This plan will serve as a guide for us for the next several years. If elected, I will support advancing the priorities chosen during the planning retreat.
What will be your top priority as president of MPA? Why do you believe this issue is important? I believe the top priority for pharmacists is gaining provider status at both a state and federal level. While we have made some recent strides in expanding pharmacists’ scope of practice at a state level, we are still challenged with getting government and private insurance payers to reimburse us for these services. It has been a primary focus of the Government Affairs Committee and MPA has been tirelessly advocating for pharmacists to be recognized as providers. They have attempted to
engage the MPA membership in advocating for this through writing and/ or meeting with their local governmental representatives, both at state and federal level.
I will continue to support these efforts and attempt to recruit additional members to participate in grassroots activities. We need as many pharmacists and pharmacy technicians as possible involved in education and advocacy efforts.
Why do you think it is important for MPA members to be actively involved in the association? One thing that makes MPA somewhat unique as a state pharmacy association is that it represents most practice settings (community, health-system, consulting and specialty) and pharmacists, student pharmacists and pharmacy technicians. This means there is a place for everyone!
It has been stated that “an organization is only as strong as its weakest link.” If we wish for MPA to remain as the preeminent pharmacy association in Michigan, all members need to be actively engaged. Active members are what creates our strength and relevance. The more members are involved, the easier it is to fulfill our mission of uniting and empowering us to optimize care and pursue health equality.
Beyond strengthening the organization, I believe that being actively engaged benefits members individually. Some of the benefits are concrete, such as educational offerings, pharmacy news and law updates, professional publications, and insurance offerings. Some benefits are equally meaningful, but more difficult to measure. This includes opportunities to lead, mentor and network.
The Michigan Pharmacists Association (MPA) recently held elections for the 2026 MPA Executive Board and its practice sections. Ryan Bickel of Kalamazoo and Maria Young of Canton were both on the ballot this year for president-elect. MPA will announce the winner of this year's elections later this summer.
MARIA YOUNG doesn’t just practice pharmacy, she lives it. After earning her bachelor’s degree in pharmacy from St. John’s University in 1996, she relocated from New York to Michigan following the CVS acquisition of Arbor Drugs. In 2008, she opened University Pharmacy, where she realized pharmacists weren’t considered providers and set out to redefine it. Her pioneering efforts during the H1N1 pandemic introduced immunizations, diabetes self-management education, medication therapy management and point-of-care testing, proving pharmacists are essential frontline healthcare providers.
As the regulatory and compliance pharmacist for outpatient pharmacies at Henry Ford Health and Pharmacy Advantage, Young takes a respectful approach to regulations, ensuring pharmacies uphold ethical and legal standards.
A recognized leader in the industry, she has held key positions at the local, state and national levels, including vice chair of the Michigan Board of Pharmacy and NABP District IV executive committee. She currently serves on the executive boards of the Wayne County Pharmacists Association and the Michigan Pharmacists Association, actively contributing to NCPDP, NABP, NCPA and ADCES.
Her impact has earned prestigious honors such as MSCP Pharmacist of the Year, WSU Preceptor of the Year, MPA Excellence in Innovation Award, WCPA Roland T. Lakey Award and APhA Immunization Champion Award.
Beyond leadership, Maria drives innovation through pharmacist-led immunization clinics, hypertension programs and POCT initiatives. Holding multiple state licenses and certifications, she remains committed to shaping the future of pharmacy through mentorship, research and advocacy.
List what you consider MPA’s priority projects or programs should be – reflecting either an expansion of current activities or entirely new services. The Michigan Pharmacists Association must pursue an ambitious vision – one that not only acknowledges pharmacists as essential health care providers, but also secures reimbursement for the vital services they provide daily. Since opening University Pharmacy and pioneering pharmacy innovation during the H1N1 pandemic, I’ve seen firsthand how patients, providers and regulators underestimate pharmacists’ expertise. Pharmacists and pharmacy technicians interact with patients more frequently than many health care providers, positioning them to be indispensable to patient care. Beyond dispensing, pharmacists serve as problem-solvers, addressing health care challenges with their expertise and accessibility. I believe pharmacy is the missing link for increasing outcomes and decreasing cost within the health care system.
Despite being among the most highly regulated and disciplined health care professions, policies fail to reflect the training and capabilities of pharmacists. MPA must advocate relentlessly for provider status and equitable reimbursement, ensuring pharmacists practice to the full extent of their education – just like other health care providers. Regulatory reform should emphasize professional growth over punitive measures, establishing accountability systems that enhance patient safety and satisfaction. In demanding, understaffed environments, pharmacists and pharmacy technicians skillfully navigate complex corporate and regulatory policies while remaining vital to highquality care. Strengthening legislative advocacy will secure proper
reimbursement for pharmacy services, allowing pharmacists to continue making a meaningful impact in health care.
With my daughter now enrolled in a direct-entry pharmacy program, I’m more committed than ever to shaping a future where pharmacists receive the respect and compensation they deserve. MPA must invest in leadership development and mentorship, equipping new graduates to lead and innovate the evolving pharmacy landscape.
A pharmacist is a pharmacist, regardless of their setting or title. By securing legislative and payer reimbursement, we can break down silos within the profession, promoting unity and advancement. MPA must lead decisively – because the future of pharmacy depends on it.
What will be your top priority as president of MPA?
Why do you believe this issue is important? As president of the Michigan Pharmacists Association, my top priority will be driving statutory change to officially recognize pharmacists as health care providers. I will advocate for the removal of outdated, restrictive regulations, ensuring pharmacists can exercise their clinical judgment within a legal framework – just as physicians, nurse practitioners and physician assistants do. Modernizing pharmacy statutes will enable the Social Security Act to allow insurance reimbursements for pharmacistprovided services. Empowering pharmacists to fully utilize their expertise, expanding patient access to essential care, and strengthening the health care system are critical steps towards addressing today’s health care crisis. I believe pharmacy holds the key to solving many of these challenges and I am committed to making that vision a reality. This isn’t about less oversight – it’s about implementing smarter
oversight that trusts licensed professionals to apply their training effectively. It’s about giving pharmacists the flexibility to innovate while maintaining accountability and patient safety.
With my background in independent community and health system pharmacy and a career marked by pushing boundaries in public health, I know firsthand the impact we can make when we're empowered to act. I want every future pharmacist to enter a profession that’s dynamic, respected and fully integrated into the health care team.
This change demands bold advocacy, collaboration and persistence – but it’s time. Michigan can’t afford to wait any longer. The future of pharmacy depends on it.
Why do you think it is important for MPA members to be actively involved in the association? Active involvement in the Michigan Pharmacists Association isn’t just beneficial, it’s essential for every pharmacy professional. Regardless of practice setting, pharmacists must unite to drive meaningful change.
MPA is our collective platform for advocacy – whether it’s securing provider status, expanding our scope of practice or protecting essential services. When pharmacists, technicians and students engage, we
strengthen our profession from within. Every voice adds value to the conversation. To solve challenges effectively, we must understand our history and how we arrived at this point. Retiring pharmacists possess invaluable knowledge that should be passed down to future generations. By learning from their experiences, we can avoid repeating past mistakes and ensure the continued growth and advancement of pharmacy.
Beyond advocacy, MPA fosters a strong professional community. It connects pharmacy professionals across different practice settings, sparking innovation, cultivating leadership and supporting mentorship. These relationships aren’t just professional – they’re personal, and they sustain us through the highs and lows of our careers.
With my daughter now enrolled in a direct-entry pharmacy program, my commitment to pharmacy has never been greater. Bold leadership is essential, but broad participation is just as critical. MPA isn’t just for a select few – it’s for all of us.
Your voice, your experience and your energy matter in shaping the future of pharmacy in Michigan. Together, we can advance our profession, advocate for our patients and build a health care system that truly recognizes pharmacy’s impact.
IN 2025,
THE STAKES ARE HIGH
Join fellow pharmacy professionals across the state in the Michigan Pharmacy PAC
Challenge and help us make a powerful impact on the profession of pharmacy
Legislators need to hear from us — the pharmacists, pharmacy technicians and student pharmacists who keep Michigan citizens healthy every single day.
TWO WAYS TO CONTRIBUTE
Community Support
• Providing valuable health services to the community like: vaccinations, medication therapy management, point of care services, and drug take back.
• Collected over 45 tons of unused and expired medication last year in our drug take back program.
• Generated and donated more than $9M to food banks in 2023 in addition to over 11M pounds of food donated to Feeding America to help our neighbors in need.
Investing in You
• Great Place to Work 2024.
• Benefit package with over 40 offerings!
• Meijer invests in our technicians offering training programs that lead to state board certification, national certification, and training in advanced clinical services.
• Through partnership with ACPE-accredited colleges of pharmacy and pharmaceutical industry, Meijer offers 2 community-based PGY1 residencies.
Pet Prescriptions Nutrition by Meijer mPerks Rewards
FILLING PRESCRIPTIONS WITH TWO NDCS –WHAT YOU NEED TO CONSIDER
BY TRENTON THIEDE, Pharm.D., MBA, president,
PAAS National®, expert third-party audit assistance and FWA/HIPAA compliance
We’ve all been in the sticky situation of having a few straggling pills left associated with one NDC that would be ideal to get off the shelf and free up some space. Maybe this NDC used to be the preferred product and now it has changed, or the manufacturer was bought out by another company. What is the proper way to bill and dispense two different NDCs on the same fill? It’s important to take both physical dispensing and claim processing into consideration to avoid the additional risk of this situation.
It should be clear to the patient that they are receiving two NDCs when dispensing. Some pharmacies prefer to place both products in the same vial (separated with clean cotton) and include an auxiliary sticker that notifies the patient that ‘This is the same medication you have been getting. Color, size, or shape may appear different’. Note that dispensing two products in one vial could lead to misbranding the product dispensed, as there is likely only going to be only one NDC with the manufacturer and item description listed on the label. To avoid unintended allergic responses, do not use recycled cotton from manufacturer stock bottles (e.g., sulfasalazine, penicillin, etc.). Pharmacies may want to consider using two separate vials, each labeled with the correct NDC, manufacturer, and item description accurately reflecting its contents. While this method does not require cotton, it should still include an auxiliary sticker to inform the patient.
Processing the claim appropriately can be a complex endeavor. The data logged in the pharmacy dispensing software and submitted to the third-party payors has important downstream purposes. Incorrect data reflecting the claim can cause problems with FDA recalls and PBM audits.
Let’s consider an example where the pharmacy is dispensing #30 atorvastatin 20 mg tablets and only has #20 tablets of old manufacturer NDC ‘A’ and needs #10 tablets of new manufacturer NDC ‘B’ to complete the fill. Many pharmacies would process a single claim transaction with only one of the NDCs being filled. In this example, NDC ‘A’ would likely be billed as this NDC represents most of the fill. This can cause many problems including the following:
• If there is ever an FDA recall on NDC ‘B’ that requires a claim utilization report for the pharmacy to find impacted patients, you may not be able to find this claim. Recalls may be rare, but patient safety can be at risk
• The claim may be considered in violation of PBM contracts – identification and enforcement by PBMs may be difficult
• The pharmacy may have an inventory shortage on a future PBM invoice audit
The best practice to avoid these issues would be to process two separate claim transactions. This way each NDC is appropriately accounted for in your pharmacy software and adjudicated to the PBM. This may require the utilization of the Submission Clarification Code (SCC) value of 62. In Section 3.1.12 Submission Clarification Code (SCC) of the NCPDP Telecommunication FAQ document1 defines this value as being,
“Shortened Days Supply of Same Drug, Strength and Dosage Form with Multiple NDCs Dispensed. Used to request an override to plan limitations and/or copay benefits when there are multiple claim billing transactions for same drug and strength due to NDC change(s)”
This will tie the claims together to help align with the plan benefit parameters. When using this override on a plan that recognizes the code, the pharmacy should receive Approved Message Code (548-6F) value 023, “Prorated copayment applied based on days supply. Plan has prorated the copayment based on days supply,” according to the NCPDP Telecommunication FAQ document linked above.
PAAS Tips:
• Pharmacies may need to contact PBM helpdesks if they do not recognize SCC-62 to resolve an early refill and/or duplicate copays
• Pharmacies will need to assess their own risk tolerance and practicality of using SCC-62