Discover a plug-in hybrid SUV that’s powerful and stylish – combining the benefits of an electric vehicle with the flexibility of a combustion engine. Plus, with standard xDrive, BMW’s intelligent all-wheel drive system, your plug-in hybrid SUV automatically shifts power between its wheels – so you can drive confidently under any condition.
Visit BMW of Murray or BMW of Pleasant Grove today to learn more.
BMW of Murray 4735 S. State Street
Murray, Utah
801-262-2479
bmwofmurray.com
BMW of Pleasant Grove 2111 West Grove Parkway Pleasant Grove, Utah 801-443-2000
bmwofpg.com
ADA
Dr Len Aste
Sang Woo Bae
Dr Randall Capener
Dr Erin Elliott
Dr Laura Kadillak
Dr Erinne Kennedy
Dr Brett Kessler
Dr Scott L Morrison
Sonia Ramirez
Dr Ben Russell
Gary Salmon
Dr Rodney Thornell
Tracy Thorup
Becky S. Waters
Dinosaurland – Sheep Creek & Spire
Tom
The Utah Dental Association holds itself wholly free from responsibility for the opinions, theories or criticisms herein expressed, except as otherwise declared by formal resolution adopted by the association. The UDA reserves the right to decline, withdraw or edit copy at its discretion.
UDA Action is published bi-monthly. Annual subscriptions rates are complimentary to all UDA members as a direct benefit of membership. Non-members $30.
UDA Action is published by Mills Publishing, Inc. 801-467-9419; 772 East 3300 South, Suite 200,
Utah 84106.
BELIEVING IN OUR OWN POTENTIAL
Sometimes, our biggest obstacle isn’t the challenges we face—it’s our own selfdoubt.
I was reminded of this recently while celebrating my son’s 16th birthday in New York. We went to see Hadestown on Broadway, a retelling of the Orpheus and Eurydice myth. If you’re not familiar, Orpheus embarks on a journey to rescue Eurydice from the underworld. Hades agrees to let them leave—on one condition: Orpheus must lead the way without looking back. He has to trust that she’s behind him. But just before they reach the exit, doubt creeps in. He turns around, and in that moment, he loses her forever.
It’s a powerful reminder of how doubt can derail us. And as dentists, we sometimes fall into the same trap—we hesitate, question our own abilities, and underestimate the power we have to shape our profession and our future.
I recently spoke with a dentist who was debating whether to renew his ADA membership. At first, his frustration was about a new piece of legislation. But as we talked, it became clear that
his real concern was something deeper: the struggle to maintain a skilled team while dealing with rising costs and stagnant insurance reimbursements.
Here’s the irony—the very legislation he was unsure about is actually designed to help dentists like him. It expands the scope of auxiliary team members, increases efficiency, and creates a more sustainable, fulfilling work environment. In other words, it’s meant to strengthen the dental team, not weaken it.
But beyond legislation, there’s a bigger conversation to be had: profitability. The reality is, our financial health as practitioners depends on the choices we make. While the ADA and UDA advocate on our behalf, their influence on fee negotiations is strongest before we sign contracts. Once you’re locked into an in-network agreement, your flexibility is limited.
So, what can you do? You have options. You can invest in education to offer high-value procedures, negotiate better insurance contracts, adjust your hours, charge for non-covered services, or even consider going out-of-network. What you can’t do is stand still and assume the system is working against you.
I decided to go out of network with insurance—a choice that, at the time, felt like a huge risk. I doubted whether I was good enough or talented enough to make it work. I feared that patients wouldn’t stay, and that this decision might even put me out of business.
But the frustration of accepting low reimbursements and feeling like I had no control over my own practice became greater than my fear of failure. So, I took the leap.
Looking back, it was one of the most important decisions of my life. It hasn’t just transformed my practice—it’s had a positive impact on every aspect of my life.
Success starts with recognizing your own worth even if doubt persists, and having the confidence to take control of your career. My hope is that you see your potential clearly and trust in your ability to build the practice and life you want. Don’t let doubt hold you back— move forward knowing you are capable and deserving of success.
Rodney Thornell, DMD UDA President
PRACTICE
THE BRITISH ARE COMING AND THE SEVEN YEAR ITCH
When you hear the name Paul Revere, you probably think of his “midnight ride” to warn of the movement of the British army toward Lexington, but there’s more to his story. By trade, Revere was a skilled silversmith. His ability to create small items out of silver and produce fine engravings served him well. He made various items, such as surgical equipment; however, he became known for producing objects, such as tea sets, that were—and still are—highly valued. But that wasn’t all—he was also an amateur dentist!
In the early 1760s, an English “dental surgeon” named John Baker arrived in the colonies. Recognizing an opportunity, Revere eagerly studied under Baker, who taught him how to create and insert false teeth.
His work as a silversmith prepared him well for working in the small space of a client’s mouth or carving a false tooth. He used his talents to fabricate dentures made of walrus ivory or animal teeth, which he wired into his patients’ mouths.
In 1768, the silversmith ran an advertisement in the Boston Gazette to promote his fledgling dentistry practice, which was followed by a second ad in 1770. The latter boasted, “Paul Revere… can fix [teeth] as well as any surgeon dentist who ever came from London; he fixes them in such a manner that they are not only an ornament but of real use in speaking and eating.”
One of Revere’s patients was Dr. Joseph Warren, a close friend who shared his revolutionary affiliations and connections. Warren told Revere that the British were probably coming to capture Sam Adams and John Hancock, sending him off on his famous midnight ride. The British shot and killed Warren during the Battle of Bunker Hill and buried him in a mass grave without his uniform or identification.
Nine months later, after the British evacuated Boston in March 1776, Revere, some friends, and Warren’s brothers went to the battlefield to look for Warren’s body. After searching for a while, they found a grave with two unrecognizable bodies. Revere was able to identify the body of his fallen friend, Joseph Warren, by recognizing the walrus tooth and the wire he had used to replace a missing tooth. Identifying his friend through his dental records led him to become the first person to practice forensic dentistry in the United States—although it wasn’t intentional.
Fast forward to 2008, when a man came into my dental practice in Manti, Utah, for an exam and a toothache. His name was Lance Leeroy Arellano, from a neighboring town. I performed an exam, took four bitewing X-rays, and one periapical of tooth #19, the tooth that was causing him trouble. He wanted the tooth extracted that day, which we did, and I informed him that he should return for a cleaning and several fillings. He didn’t make another appointment, and we never heard from him again.
On November 19, 2010, Utah State Park Ranger Brody Young was going about his routine checks in the canyon near Moab in Utah’s Dead Horse State Park when he saw a vehicle parked in an otherwise empty parking lot in a restricted camping site. Officer Young noticed a man sleeping inside the car. He woke him up and told him he would need to move on. As a matter of routine, Officer Young asked him for his identification. The man supplied fake details, and Officer Young turned back to his patrol car to check them. That’s when the shooting began.
Officer Young had been shot nine times. Although his bulletproof vest stopped two of the bullets, he sustained gunshot wounds to his lung, heart, shoulder, back, hip, and groin. In spite of his serious injuries, Young was able to return fire. The other man, thought to be 40-year-old Lance Leeroy Arellano based on the 1999 silver Pontiac found parked in the bushes several miles south of the scene, simply vanished into the park’s maze of towering red rocks.
Despite a weeks-long manhunt that filled the canyon with dozens of investigators and search planes, the trail went cold. Either Arellano was dead, or he’d somehow slipped past the swarms of officers. The FBI put out a notice of a $30,000 reward for information about the missing man.
Five years later, brothers Caleb and Jarom Shumway, a pair of aspiring Hardy Boys from nearby Moab, Utah, who dedicated their Christmas break to searching the canyon where Arellano disappeared, uncovered remains thought to belong to the shooter. Shortly thereafter, I received a call from the Utah State Medical Examiner’s Office asking me if I had a patient named Lance Leeroy Arellano and if I had any of his dental records. If so, they requested them as part of an investigation. It had been almost seven years to the date that I saw him in my office, and thankfully, I still had his records. I sent them off to their office, and shortly thereafter, the Medical Examiner informed the police and the public that they used dental records to positively identify the remains as those of Lance Leeroy Arellano. The Shumway boys claimed their reward, and that became my first case of forensic dentistry—although it wasn’t intentional.
The State of Utah requires that dental records be retained for seven years. Utah Admin. Code 432-600-21(7) Medical records shall be retained for at least seven years after the last date of patient care. Records of minors shall be retained until the minor reaches age 18 or the age of majority plus an additional two years. In no case shall the record be retained for less than seven years.
With electronic records, it shouldn’t be hard to maintain records indefinitely, so if you get the itch to destroy old dental records, just remember—you too could become a forensic dentist— although unintentionally.
Len Aste, DDS UDA Past President
HOW THE ADA AND UDA ACTUALLY WORK: WHAT DO WE EVEN DO?
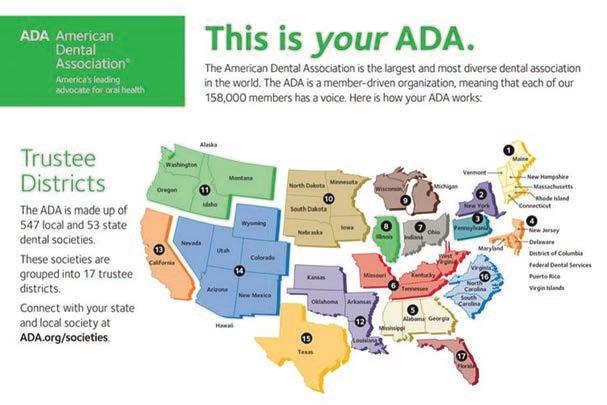
The American Dental Association has been a longstanding organization, founded in 1859, with a mission focused on the success of dentists and the promotion of public health. As with any professional group, challenges emerge with the development of modern times. Policies, goals, and actions must be constantly evaluated to align with the evolution of the profession. I have witnessed on many online platforms where there is no shortage of dissatisfied grievances against the ADA, whether in the form of valid frustrations from members or unfounded claims in social media forums. While many of these complaints stem from deeper problems within our profession, I have seen many that come from a widespread misunderstanding of how the organization works, both on a national and regional level.
What does the ADA even do? What are they capable, and not capable, of achieving? I think if members took the time to understand how our organization works, then they may see more value in the impacts that we can all make together, from local up to national scales. The ADA is not a faceless entity with their own motives; it is purely composed of dental professionals, like you and me, that are united in our desires to succeed in our careers while expanding oral health care of the public.
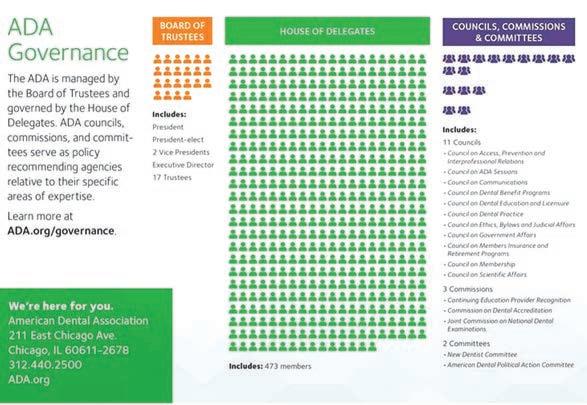
On a national level, the ADA is composed of 53 state dental societies (which include Federal Services, Puerto Rico, and US Virgin Islands) which are broken up into 17 Trustee Districts. Utah is part of District 14, which includes our neighboring states of Wyoming, Colorado, New Mexico, Arizona, and Nevada, in addition to Hawaii. Each of the 17 Districts has a Trustee, chosen by the states’ representatives to lead and oversee their District. These 17 Trustees, in addition to the ADA President, President-elect, 2 Vice Presidents, and Executive
Director, comprise the Board of Trustees, which manages the national component. The Board of Trustees conducts the business of the ADA, and helps carry out any resolutions or actions put forth by the House of Delegates. The President, Vice Presidents, and Executive Director manage national activities on a daily basis, aided by action and support of the Board, similar to how our own UDA Board operates. The ADA is governed by the House of Delegates, akin to Congress, which is made up of 473 members elected by each state.
The House of Delegates meets every year at the annual ADA Convention, and votes on every resolution put forward by its members, in addition to selecting the next President and Vice Presidents to serve. The resolutions are the directives that create ADA policy and action for future years. Having involved delegates who represent each state’s members is essential for the House of Delegates to be able to vote according to the wishes of the members in their state. These delegates also often serve on committees, or councils, which review specific resolutions and policy. These 10 councils range over multiple topics, such as the Council on Government Affairs or the Council on Dental Practice, and serve to recommend input on policies. We have Utah representatives on some of these councils, helping to communicate the important issues from the ADA that have national impacts.
Most of the workings of the ADA include governing and managing the organization from a very broad, national perspective. When dentists complain about issues that are specific, such as “why doesn’t the ADA help with my state’s issue?”, there is often a major disconnect in their understanding of how resources are allocated. If the ADA spent all their resources combatting issues in just one state, how would the other states manage? Especially now, when membership is dwindling nationwide. This is why our state membership is imperative to help advocate for our local issues. Donating to our national lobby group, ADPAC, is the most effective way we can make national changes in law. Advocating, supporting, and opposing national legislation is not the only focus of the ADA, which is why ADPAC donations are the most important resource in this realm. In addition, the ADA is made up of ALL dentists, and represents dentists in every capacity. When someone complains in general about DSOs, for example, they need to understand that DSOs include other dentists, especially young career dentists, who are also part of the ADA. We must accept the fact that those dentists need support, just as dentists in small private businesses need support.
Our state level organization, the UDA, has a much more visible impact to our daily activities. The UDA Board consists of our President, President-elect, Secretary, Treasurer, Past President, Executive Director, and 4 ADA Delegates. We also recently have included an Alternate ADA Delegate, after losing one of our ADA Delegate spots, which is based on percentage of state membership. In order to have more of a voice in the national House of Delegates, we need to increase our state membership to be allotted a fifth representative. This is why our state membership is crucial, so Utah can continue to play an integral role in policy and changes that occur, especially in law. Our Utah House of Delegates meets at our UDA Convention every year, and includes one representative for every 15 members. These representatives will elect the officers for the next year, in addition to discussing state policies and resolutions.
This year, we have seen a lot of action regarding dental legislation. One of the most notable bills to affect Utah is the fluoride bill, HB081, which bans fluoride in our drinking water statewide. The UDA vehemently opposed this bill, but we were unsuccessful in convincing our legislators to vote it down. At the public hearings for this bill, the anti-fluoride group was the overwhelming majority present. The voices of the dentists were drowned out. This is a problem we need to address within our own state, by promoting and encouraging our members to be more vocal and advocate for public health, in addition to protecting our profession. The more members we have that can talk to their representatives and senators, the more likely we are able to convince lawmakers to listen to our voices.
Our UDA leadership was successful in working with legislators for other bills, such as the Dental Practice Act, but organized dentistry is only as strong as the community behind it. Much of what the UDA does includes efforts toward making sure bad policy is NOT enacted, which is just as important as the good policies that are passed. If the dentists in our state are apathetic or abandon our organization whenever results are unfavorable, it makes any future advocacy efforts much harder to achieve. Without the support from our members at a local level, the
UDA Officers
ADA and UDA (continued from page 7)
Weber
Wasatch Back
Uintah Basin
Tooele
South Salt Lake
South Davis
Provo
North Salt Lake
North Davis
Dixie
Cedar Breaks
Central
Carbon-Emery
Canyonlands
Cache
Box Elder
UDA is destined for being less effective over time.
Our local leadership is invaluable for the future of our organization. The UDA is comprised of 16 districts, each with leadership of President, President-elect, and a Secretary and/or Treasurer position. These members are essential for voicing the opinion of local dentists in their district at the annual UDA House of Delegates. They are also instrumental in local events, such as CE, social events, and community service opportunities. These local leaders are really where the UDA can stay connected, and make meaningful impacts on a community level. In a world where politics and policy are changing radically, it is important to ensure our members have the input and representation they deserve. The best way to achieve this is through more communication with district leadership, and encouraging advocacy that supports state and local level goals.
If every member could contribute time, money, skills, or connections with key players, our dental society will increase our effectiveness in achieving our goals. It is about time that we recognize who the UDA and ADA really are: YOU! The entities of organized dentistry are only as good as its members make it. My response to the nay-sayers and internet criticism is usually along the same lines: “get involved”. If you are upset with a policy, get involved to help change it! If you are passionate about making a new law, introduce it! Recently, some UDA members have introduced and successfully passed a bill fighting unfair dental insurance policies. You can make an impact by reaching out to your district and state leadership with your feedback and ideas. There are multiple local and statewide committees that need help and volunteers. With more members and support, the easier it is to enact meaningful changes. The UDA and ADA are only the vehicles through which we organize ourselves, so it’s time to invoke the old cliché – ask not what the UDA can do for you, but what YOU can do for dentistry in Utah.
Laura Kadillak, DDS ADA Delegate
Dr. Laura Kadillak is searching for volunteers with the new Legislative and Advocacy Committee. If you are interested in joining, please contact her via e-mail at laura.stewart.dds@ gmail.com or Dr. Ben Russell at benrussel@gmail.com.
ASSOCIATION
ENTERING THE ARENA
One of my favorite quotes is by Teddy Roosevelt:
“It is not the critic who counts: not the man who points out how the strong man stumbles or where the doer of deeds could have done better. The credit belongs to the man who is actually in the arena, whose face is marred by dust and sweat and blood, who strives valiantly, who errs and comes up short again and again, because there is no effort without error or shortcoming, but who knows the great enthusiasms, the great devotions, who spends himself in a worthy cause; who, at the best, knows, in the end, the triumph of high achievement, and who, at the worst, if he fails, at least he fails while daring greatly, so that his place shall never be with those cold and timid souls who knew neither victory nor defeat.”
—Theodore Roosevelt Speech at the Sorbonne, Paris, April 23, 1910
This past year, I’ve had the amazing opportunity to serve on the UDA Board. And what a learning opportunity it’s been to see brave, selfless folks dedicate time, energy, and talent to the betterment of our shared profession…to choose to “enter the arena”!
I’ve seen the tireless efforts that are spent to strengthen the profession that has given so much to me, and that brings me a deep sense of purpose and reward; physically, emotionally, financially, and mentally.
I’ve had the opportunity to attend UDA Board meetings, see the daily efforts of Val, Becky and Dotty, learn about pertinent legislative bills at a deep, “reading line by monotonous line even on a Saturday” level, attend the House of Delegates meetings at both national and local levels, attend our district caucus meetings at a district level, attend local district Wellness meetings, and speak about local advocacy at UDA Lobby Day in the State Capitol Rotunda (boy, did I ever feel imposter syndrome wearing a tie and standing in THAT fancy building!!) where I was invited by local State Representative Tom Peterson (thanks again, Tom!) to sit on the House floor and be introduced to my local elected officials who have the power to vote on our behalf in this wonderful republic! I can’t overstate what an honor it was to see the inner machinations of the legislative process that affects each and every one of us whether we’re consciously aware of it or not!
Over the past few years, as I’ve confessed in a previous UDA Action article, I found myself falling into a bit of a dental funk. I feel that I spent years and years of blood, sweat, and tears working so incredibly hard. I felt that I owed it to my patients, my employees, and my family to give my best attempt at
perfection “all”. After all of these efforts, I often saw the practice do little more than break even month after month and year after year. I noticed that the very last thing I wanted to think about after-hours or on weekends was dentistry. Weekend emergencies and possible CE courses were the LAST thing I would/could focus on. The demands of so many things were weighing heavily indeed. I recognized that this was a dangerous and unhealthy place to remain. So…on the recommendation of a local colleague, I made the decision to hire professional practice management help (thanks, Rob and Tracy!!), dropped a couple of illogical, irrational, bordering-on-criminal, arbitrary, unintelligible, idiotic insurance plans (yes, those ARE the best words to describe those specific plans), and drew a few personal and professional boundaries (thanks for the book recommendations, Jaren!). After making these adjustments, I found myself again really, really enjoying my personal interactions with patients and employees, my physical health improved, and I found that dentistry was once again the profession that I found so much joy in, because it was allowing me to DO something I love, FOR people I love, WITH people I love!
With some of this new-found (or re-found) energy, I felt it my “civic dental duty” to dedicate some of my energies and resources to organized dentistry (not just the UDA, btw) and I’m grateful for having been afforded the opportunity to do so by serving on the UDA board. In the past, I’ve just flitted around the periphery of the UDA (kinda like the old Atari 2600 video game Yars’ Revenge…remember that one, old timers?), dipping my toe in here and there, getting a small taste of what the UDA was about without having to commit much to it, often researching with the mentality of “what’s in it for me?” Upon more intimate and careful, closer inspection, I’ve realized that there are an awful lot of awfully giving, intelligent, energetic, compassionate, generous people that are working hard to maintain the strength of our profession. I feel awfully awful that I didn’t see that before! (Apologies to Mr. Goldsberry, my high school English teacher for the superfluous use of “awful” in those past couple of sentences. But, hey, it was better than asking “CAN I have the hall pass to go to the restroom?” His reply, “No, but you MAY” still rings in my ears 36 years later).
I am reminded over and again that “our” UDA is in good hands, but it will only remain so as we keep empowering it with our committed membership. The forces out there that try to limit the strength, power, and autonomy of our profession are very real. Our profession of dentistry requires safeguarding and, although our ADA and UDA are certainly not perfect, they are incredibly and favorably positioned and staffed to protect our professional interests and the oral health of our patients. I appreciate that our organizations are only as strong as the people who commit to them. We are living in an age where more and more of us are becoming individually isolated in our fractious society. We have so much information at our fingertips, but run the risk of enjoying less enduring “meaning”. We are tempted to live wider, but shallower.
I am often reminded that I possess no extra special talents or qualifications that have set me apart to serve on the UDA board. Not trying to be overly and depressingly self-deprecating, but anyone willing could perform the duties I’m asked to perform…and most likely perform them SO MUCH BETTER! Ultimately, I think that’s super cool. Anyone can throw their hat in the ring. Anyone can choose to “enter the arena”. So, I recommend you do so. Whether you get involved just by informally reaching out and taking a fellow dentist to lunch, new or old, or volunteer to get involved in your next local district activity, or run for ADA president (ok, maybe don’t start THERE. That might be a little overwhelming and bad strategy), I promise you’ll see positivity and deepened relationships.
I recently ran across the African proverb that states:
If you want to go fast, go alone.
If you want to go far, go together.
Let’s go further together! (Or is it “farther”? Again, sorry, Mr. Goldsberry!)
Randall Capener, DDS UDA Treasurer
MOVING FORWARD WITH FLUORIDE
During the 2025 legislative session HB 81 (Fluoride Amendments) was introduced which would ban communities from adding fluoride to their community drinking water.
The Utah Dental Association worked with the Utah Oral Health Coalition as well as others to lobby against this bill. These efforts included 3 UDA dentists testifying at the House Natural Resources, Agriculture and Environment Committee. Also, representatives from the Oral Health Coalition and the Utah Medical Association spoke out at this committee hearing against this bill.
During the Senate Natural Resources, Agriculture and Environment Committee 5 UDA dentists spoke against the bill, 2 medical doctors, the Oral Health Coalition and the Utah Medical Association.
The Utah Dental Association sent out multiple Call to Action requests, to contact your Representative and Senator, and finally
to ask Governor Cox to veto this bill. Thank you for contacting your legislators.
Even with the efforts of the ADA, UDA, Oral Health Coalition and others the bill passed and was signed, going into effect May 7.
So now we pivot our approach and work to educate the public on ways to obtain fluoride supplements and the importance of fluoride in preventing decay.
A fluoride toolkit with naturally occurring fluoride levels in water districts, along with dosing information is currently available on the UDA website.
Watch for more information from the UDA with resources for you and your practice coming soon.
Becky S. Waters, RDH Assistant Director Utah Dental Association
LEGISLATIVE
BIG WINS FOR UTAH DENTAL
TEAMS: HOW UTAH’S NEW LAWS ARE MAKING LIFE EASIER AT THE OFFICE
Let’s be real—working in a dental office isn’t exactly a spa day. It’s a fast-paced mix of ringing phones, back-to-back patients, last-minute cancellations, and deciphering EOBs that might as well be written in hieroglyphics. And just when things settle down, someone walks in asking if “a quick cleaning” can be squeezed in during their lunch break—without an appointment. That’s why at My Practice My Business (MPMB), Dr. Rob Thorup and I made it our mission to bring real, practical change to the hard-working professionals who keep dental offices running smoothly.
We’ve always believed in empowering dental teams—not just through education, but through real, boots-on-the-ground action. Together, with Representative Jim Dunnigan (Taylorsville) we took that mission to the Utah Legislature. The result? Two groundbreaking bills—HB 495 and HB 23—that are already creating a ripple effect of positive change across the state.
Let’s dive into five specific wins and what they mean for your daily workflow, your bottom line, and your peace of mind.
1. Say Goodbye to Surprise Virtual-Credit Cards: No More Auto Re-enrollment
You know the drill. A payment comes in, but it’s not a direct deposit or a check—it’s a virtual credit card (VCC). That sounds fine until you realize that:
• You didn’t ask for it.
• It comes with hidden processing fees.
• Your team makes the effort to “opt out” only to be re-enrolled shortly after.
• It adds yet another step for your front office team, when we already have so much to do.
HB 495 makes it illegal for third-party payers to automatically re-enroll your office in VCC programs after you “opt out” without your expressed consent. When I sat down with Representative Dunnigan to show him the process of “opting out” and how frustrating it was to “play the game” to get a different form of payment, he realized how important this law really was. Finally, you get to choose how you want to be paid—no sneaky re-enrollments, no extra credit card fees, and no hours lost trying to change payments over and over again.
Front office teams everywhere, rejoice. This one’s a game-changer.
2. Dispensing Medications In-Office: Now It’s Officially Legal
Let’s be honest—many dental offices have already been
dispensing things like prescription toothpaste, mouth rinses, and post-op medications for years. Why? Because it makes sense. It’s better for patient compliance, saves them a trip to the pharmacy, and ensures they leave with exactly what they need.
What HB 495 does is remove the gray area. Dental offices in Utah are now explicitly allowed to dispense certain medications in-office—legally.
Here’s what that means for your team:
• You can confidently provide prescribed items like fluoride toothpaste or chlorhexidine rinse without worrying about regulatory ambiguity.
• You’re staying compliant while continuing to deliver top-tier care.
• Patients leave with clear instructions and the products they need—no follow-up pharmacy run required.
• The law allows for a 30-day or less supply of those specific medications to be sold from the dental office. The patient must come back for an exam for another refill or you can simply call in a prescription.
• Fluoride tablets are allowed for more than 30 days without an exam.
ATTENTION
SEPT 9 - CACHE DISTRICT
SEPT 23 - WEBER DISTRICT
SEPT 25 - CENTRAL DISTRICT
OCT 7 - WASATCH BACK DISTRICT
OCT 9 - CARBON-EMERY DISTRICT
OCT 10 - CANYONLANDS DISTRICT
OCT 14 - NORTH DAVIS DISTRICT
OCT 16 - CEDAR BREAKS DISTRICT OCT 16 - DIXIE DISTRICT OCT 21 - PROVO DISTRICT OCT 30 - TOOELE DISTRICT NOV 11 - SALT LAKE NORTH SALT LAKE SOUTH DISTRICT
ADD YOUR DISTRICTS TO YOUR CALENDAR TODAY
It’s one of those changes that simply makes sense: you’ve been doing it to help your patients, and now the law recognizes and supports that.
Clarity for the office. Continuity of care for the patient. A win all around.
3. No More Forced Write-Offs for Services Rendered
Here’s one of the most misunderstood issues in dental billing: insurance companies have long claimed they could force you to write off services rendered. They started by stating that “non-covered” services had to be reduced or written off, and Utah combatted that with SB44 in 2017, known as Utah’s “non-covered” law. The insurance companies pivoted by stating that services were covered, yet were “inclusive and not billable” when done on the same day as another service. MPMB fought back in 2021 with HB 359, also known as Utah’s “Network Leasing, Down-coding, and Bundling Protections” law.
Last year, we observed insurance companies pivot yet again by changing their requirements for coverage and forcing write-offs when services rendered did not meet their requirements. An example was noticed by several third-party payers stating that scaling and root planing would only be covered if the pocket depth was at least 6mm, and if those requirements were not met, the services rendered were not covered and not billable to the patient. The dental office was then faced with an impossible decision: do the needed service for free at its early stages of infection, or wait until the infection got “severe” and risk a malpractice lawsuit. That stops now.
Under HB 495, third-party payers can no longer require write-offs for services rendered especially if you’re in-network. Of course, there are “generally accepted practice standards” that regulate the dentist and their teams to ensure that services are being done ethically. Thankfully, those “generally accepted practice standards” are being regulated by over 600 dentists independently surveyed in the state of Utah by My Practice My Business, and we continue to send updated results to the state insurance commissioner every time we get an additional survey results. This protects dental offices from unfair payment reductions on both covered and non-covered services and adds a new level of transparency and respect to the reimbursement process.
What this means for your team:
• If a procedure isn’t paid for by the third-party payer, you can bill the patient your full fee for “non-covered” services or the agreed-upon fee if the service is “covered” under their dental plan.
• No more second-guessing EOBs or arguing with reps about whether a service “should be” written off. Dental teams deserve to be paid fairly for the services they provide.
It’s about honoring the work you do—and ensuring insurers don’t manipulate the system to underpay for legitimate care, or force dental businesses to do “free dentistry” at will.
4. Automatic Recoupment? Not Anymore
Raise your hand if you’ve ever checked your remittance report and thought, “Wait… where did that money go?”
Previously, insurance companies could claw back “over-paid” funds—sometimes months after a claim was paid—without even giving you a heads-up. The burden was always on you to figure out what happened and whether it was even valid.
With HB 495, insurance companies can no longer automatically recoup overpayments without first:
• Notifying the provider in writing of the overpayment.
• Giving the provider 60 days from the date of the notice letter to send a refund
No more mystery subtractions. Just fairness and transparency.
This provision alone can save your office thousands of dollars and countless hours spent chasing down missing money. It gives your billing team the ability to catch and contest errors before the funds disappear. Please note that this portion of the law will be effective January 1, 2026.
*Side note: we highly recommend certifying the letter/refund check so that you can track the refund payment and prove that it was received by the third-party payer.
5. More Time, Less Stress: Timely Filing Deadline Extended to 6 Months
Last but certainly not least—HB 23 increases the timely filing deadline from 90 days to six full months
If you’ve ever had a perfect “claim” get denied because it was filed one day too late, this one’s for you. Whether you’re buried under end-of-month reconciliations, navigating system updates, or just trying to take a lunch break, you now have more time to file clean claims without penalty.
More time = fewer denied claims = fewer appeals = happier team.
Quick Note on Coverage
As with any legislation, there are some limitations to be aware of. The changes enacted by HB 495 and HB 23 apply specifically to insurance plans that are regulated within the state of Utah, which makes up the majority of the plans Utah Dentists take. This includes fully insured plans written in Utah—but not federally regulated plans such as:
• ERISA plans,
• Self-funded employer plans, and
• Federal programs like Medicare or Medicaid.
While these new laws are a major step forward, they don’t yet apply to all insurance types. That said—this legislation lays the foundation for future reform, and the more we work together, the more impact we can have on a broader scale.
A Personal Note—and a Call to Action
It’s been humbling and energizing to see our incredible MPMB
clients rally behind these efforts. Let’s be clear—these wins didn’t happen by accident. They happened because Dr. Rob Thorup and I rolled up our sleeves, partnered directly with legislators, and refused to sit back while third-party payers chipped away at the rights of dental professionals, let alone our profit margins with every-day dentistry.
We’re incredibly grateful for the support we did receive from Dr. Val Radmall and Dr. Randell Capener at the Utah Dental Association. Their encouragement was meaningful and helped shine a light on how collaboration can lead to change.
However, imagine what we could accomplish if that support extended further.
Imagine what could happen if more leaders within the Utah Dental Association stepped forward and joined forces with us.
Together, we could create an unstoppable alliance—fighting not just for fair policies, but for meaningful, lasting improvements in how dental teams operate, get paid, and provide care. Or as we call it at My Practice My Business: the clinical business of dentistry.
And here’s the bigger picture: Utah is now setting a standard for the nation to follow. These aren’t just feel-good reforms— they’re financially relevant, practice-protecting laws that directly impact the day-to-day operations of dental offices. We’re leading by example, and the rest of the country is watching.
We’re stronger when we advocate together. These victories are proof that positive change and profitability with Third-Party Payers is possible—and just the beginning of what’s to come. We believe it’s time for dental associations to stop saying, “you signed a PPO contract and there’s nothing we can do to help”, or that dropping dental insurance is the “only” answer to battling third-party payers. IT IS possible to work with dental insurance plans, retain those wonderful patients you’ve been caring for over the years, and obtain procedural profitability. It’s what we’ve taught for years here at My Practice My Business, and we invite everyone to experience how “real” guaranteed dental business training will positively change the lives of dentists, their teams, and the patients they serve.
Tracy Thorup, MBA CEO, My Practice My Business
Got questions? Want to know how to implement these changes in your practice? Reach out to us at My Practice My Business at 801-226-4420.
Interested in Dental Business Training? A portion of your training fee goes directly towards passing dental laws to protect Utah dental offices and is appreciated! Visit our website at www.mypracticemybusiness.com or email tracy@mypracticemybusiness.com. We’re here to help, and we look forward to you joining the MPMB family.
Practice Transition Specialists
“I have used the advice and services of Randon Jensen and CTC over many years. First, to form a partnership, and more recently to move out of complete ownership of the practice I started 43 years ago. I have the highest regard for Randon and his honesty and integrity. His knowledge and skill has made all the difference. I give him my highest recommendation and would surely encourage you to trust him with your practice transition.”
–Roger L. Farley, DDS
randon jensen
marie chatterley
TOP 3 WAYS HACKERS BREACH DENTAL PRACTICES (AND HOW TO PROTECT YOURSELF)
Cybersecurity might not be the first thing you think of when running a dental practice, but hackers know your office is a treasure trove of sensitive patient information. From insurance details to Social Security numbers, to driver’s licenses, to highly regulated data controlled by New York State and Federal laws, dental practices are prime targets. Understanding how hackers breach networks—and how to prevent these breaches—can protect your practice from financial, legal and reputational damage. Patient data is highly regulated under New York State and Federal Law (think HIPAA). In more than 90% of ransomware attacks, hackers will steal some or all your patient data regardless of whether you are using the Cloud or your own server. The hacker’s modus operandi includes stealing your data, destroying backups, and encrypting all computers and data…basically “bringing you to your knees.”
Here are the top three ways hackers gain access to dental practice networks and simple steps to reduce the risk.
1. Human Risk: Clicking Links, Attachments, or Giving Up Credentials
Hackers frequently exploit human error. Phishing emails are one of their favorite tools—posing as legitimate messages, they trick employees and doctors into clicking malicious links, opening infected attachments, or providing login credentials. For example, you might receive an email that looks like it’s from a supplier asking you to update payment details, but in reality, it’s a trap. These emails are now being crafted by leveraging Artificial Intelligence…so the days of improperly worded emails are gone.
Preventative Measures
• Train Your Team: Cybersecurity awareness training is essential AND required under HIPAA. Utilize Cloud-based dental specific training platforms to educate your entire team on the various forms of threats and scams.
• Implement Multi-Factor Authentication (MFA): Even if credentials are stolen, MFA adds an extra layer of security, requiring verification via a code sent to a phone or email.
• Use a Password Manager: Encourage staff to use strong, unique passwords stored securely in a password management tool.
• Phish Your Team: Leverage platforms that create and send simulated phishing emails to test your team on their knowledge and readiness to identify a malicious email, phone call or text message.
2. Vulnerability Exploitation of Computers and Firewalls
Hackers exploit outdated software, vulnerable technology and poorly configured firewalls to break into systems. Many dental practices unknowingly leave their networks exposed because they don’t regularly update software, perform daily vulnerability scans or replace aging technology. They are simply relying on anti-virus software to detect and stop threats. Unfortunately, most anti-virus software can be defeated by advanced hacking groups. Detecting and eliminating vulnerabilities often thwarts a hacker’s ability to get into your network.
Preventative Measures
• Regular Software Updates: Ensure operating systems, dental practice management software, and all devices are updated with the latest patches. Outdated software is like leaving the front door unlocked. Use real-time vulnerability scanning technology to detect these vulnerabilities AND automatically fix them. Scanning quarterly or annually is not effective.
• Secure Your Firewall: A properly configured firewall acts as a digital gatekeeper, monitoring and blocking unauthorized access. Have a cybersecurity company “pressure” test your firewall to determine if it is vulnerable to a hacker.
• Conduct Vulnerability Scans: Daily vulnerability scans and penetration testing conducted by a cybersecurity company can identify and fix weaknesses before hackers exploit them. Hackers are targeting you hundreds of times per day.
• Have Full Visibility into Cyber Risk: Ultimately, you are responsible for your security. Leverage third-party platforms that identify, mitigate and report all cyber risk so you have clear transparency into your cyber risk…you can’t simply trust that your IT company is doing this. These platforms should provide a cyber risk score, show you key performance indicators, and help you understand your overall security posture so you can make educated decisions, based on real data, for your practice.
3. Third-Party Breaches
Hackers also target the third-party vendors you work with— such as billing companies, practice management software vendors, insurance providers, or even IT service providers—to gain access to your network. If these vendors are compromised, your practice could be collateral damage.
Preventative Measures
• Vet Vendors Thoroughly: Ensure third-party vendors
follow robust cybersecurity protocols. Ask about their data protection measures and request regular security audits.
• Limit Vendor Access: Provide vendors with only the data they absolutely need and nothing more. Always understand where your data is located and who has access to it. Make sure you sign a Business Associates Agreement with all vendors that have access to or store your data.
• Use a Cybersecurity Partner: A cybersecurity company can evaluate third-party risks and set up safeguards to minimize exposure.
Why You Need Both an IT Company and a Cybersecurity Company
While IT companies focus on keeping your technology running smoothly—managing hardware, software, and day-to-day troubleshooting—cybersecurity companies specialize in protecting your network from threats. Think of your IT company as the builders of your digital office and your cybersecurity provider as the security team guarding it.
Having both ensures your practice is well-equipped to stay productive and secure. IT companies typically lack the advanced tools and expertise needed for cybersecurity, such as vulnerability scans, threat detection, credentialed security experts, and real-time monitoring. By partnering with both, you cover all bases: reliable operations and robust protection.
The risk of a cybersecurity breach in dental practices is real, but it’s manageable with the right precautions. By addressing human error, patching vulnerabilities, and mitigating third-party risks, you can protect your practice and your patients. Engaging both an IT company and a cybersecurity company ensures your systems are both functional and secure—giving you peace of mind to focus on delivering excellent patient care.
Don’t wait for a breach to happen—invest in your practice’s cybersecurity today. Your patients, reputation, and bottom line depend on it.
Gary Salmon Black Talon Security
SLEEP APNEA
It’s another gorgeous day in North Idaho, and my schedule is packed with restorative dentistry and hygiene checks. On today’s schedule is one of my favorite patients, Shawn. I usually see him every six months and am always prepared to exchange jokes with him. I have a good one for this visit, but thankfully, I’m not seeing his daughters today.
I usually have to do a really bad cartwheel for them in the waiting room. All three are amazing gymnasts, and after I told them that I got kicked out of gymnastics because I couldn’t figure out how to do a cartwheel, they made me prove it by showing them my “cartwheel” but only if they didn’t have any cavities. In addition to his three teenage daughters, Shawn has a wonderful wife and a great job. He travels often, but he’s wondering why he feels more and more rundown. When I checked Shawn during his routine six-month visit I asked about his girls, wife, job, how he was feeling and finally how his teeth were. Of course, he said they were fine; they’re always fine. Shawn is a healthy, middle-aged male with a clean health history. Certainly he has no problems. Does that sound familiar?
Ever since I finished my training to treat sleep apnea and now screening and treating it for the past 15 years, I’ve been looking at teeth, tongues, and throats entirely differently. What I noticed about Shawn that I hadn’t before was that his canines had bruxing wear, which we had discussed at one time, but I had dismissed my concern; he had a large scalloped tongue and a constricted mandible. But he was thin and tall with a small neck, not a stereotypical sleep apnea patient. I figured there was no way he had sleep apnea. His medical doctors didn’t mention it. Certainly there was nothing to pursue. Or was there? My mission is to spread the message that SLEEP APNEA IS NOT AN OLD FAT MAN’s DISEASE!
Shawn saw that I had a poster about snoring and sleep apnea in my waiting room, so he mentioned that he’d been having trouble feeling rested and rundown. Also, he falls asleep immediately when the plane takes off on his business trips. Shawn was wondering if it was because he snored at night. However, he’s getting older, works hard and has teenage daughters. Why wouldn’t he be getting tired? We think there’s no problem; he’s just getting older.
I contemplated all this a bit further. His wife says his snoring is getting worse, that he complains about fatigue and I find signs in his oral cavity that suggest sleep apnea. I recommend that he get a sleep study done. An oral appliance is a dental solution for sleep apnea, but sleep apnea is a medical problem that requires a medical diagnosis. Oral appliances help open a closing airway (and serendipitously help snoring) which is called obstructive sleep apnea. Some with sleep apnea have breathing disorders that are unable to be treated by an oral appliance. In addition, with the advent of wearables that track sleep, many can get a false sense of security as it can provide a
false negative, just as a pulse ox screener can do. A sleep test is the ONLY way to screen for Obstructive Sleep Apnea.
We see many patients in my office, and we have almost the same routine for every exam. We’re supposed to check medical history, the throat and jaw soft tissue abnormalities, the tongue and cheeks for oral cancer, and finally, the bone levels, gums and teeth. What about the airway? We’re most certainly right there looking at it, but do we ever pause and wonder? If we do, we may discover one of the 400+ undiagnosed sleep apnea patients currently in our practice. There are approximately 2,000 patients in a modest dental practice, and about 20% or more of those have sleep apnea or sleep-disordered breathing and approximately 80-90% of those patients go undiagnosed. These patients go undiagnosed because like Shawn, we don’t believe there can be a problem.
There are some hurdles. The uneducated patient may resist a sleep study and may tell you to “just treat my snoring.” Or even worse is, when I hear “my family snores, everyone I know snores, I’m fine.” I’m still trying to determine why such resistance and denial exist. I digress. Without a sleep study to know exactly what is going on, we may be creating a “silent apneic,” which is a patient that does not snore a night. Still, his or her oxygen levels are dangerously low and obstructions continue untreated. Fortunately, we have sleep studies to address these unknowns and home sleep studies are becoming more common, and this helps address patient follow through issues.
Thankfully, Shawn accepted my recommendation and had a home sleep study performed that was read and diagnosed by a sleep physician. I was anxious to see his results because I’m rarely wrong in identifying sleep apneics in my patients. What were his results? Shawn was, in fact, one of the 20% or more of the undiagnosed sleep apneics in my practice. In fact he had moderate sleep apnea in which he stopped breathing for 10 seconds or more 99 times a night and subconsciously tried to wake himself up to breathe better 57 times a night. No wonder he was tired!
After receiving his oral appliance, Shawn returned for his oneweek-follow-up with his wife. Almost immediately, she said, “I can sleep with him in the same room again!” Shawn proclaimed, “I’ve stopped falling asleep on the plane when I travel for my job. I’m so much more productive.” Shawn couldn’t stop thanking me, and his wife and kids couldn’t stop thanking me. I love changing lives!
There are potentially 400 or more undiagnosed people in your practice. Dentists are the front line. The medical doctors need us. They are farther downstream than we are. Shawn admitted he never would have gone to the doctor for his complaint, and he goes to the doctor only when he is sick. Even at his bian-
(continued on next page)
PRACTICE
BEATING ANTIMICROBIAL RESISTANCE TAKES ALL OF US
For the past few decades, dental care professionals have been trying to change how we prescribe antibiotics. However, data suggest that although we have antibiotic steward champions, their collective contribution is not enough for the substantial change we need against the rapid increase in antimicrobial resistance. As Drs. Laurie Hicks and Debbie Goff, national antimicrobial resistance experts said at the 2024 Organization for Safety, Asepsis and Prevention Antibiotic Stewardship Conference, “Antibiotic resistance anywhere, is antibiotic resistance everywhere.”1
This observation is a call to arms for all of us, particularly in dentistry.
According to the Centers for Disease Control and Prevention (CDC),2 antibiotic resistance is an urgent national public health threat and the leading cause of death globally, killing approximately 5 million people per year. The 2019 antibiotic resistance report, published by the CDC, estimated that there are more than 2.8 million antimicrobial-resistant infections (ARIs) in the United States annually, and more than 35,000 people die as a result.2 Although there are collaborative efforts to improve this, the CDC reported a 20% increase in ARIs after the COVID-19 pandemic, 100% of ARI threats categorized as urgent increased from 2019 through 2022, and 75% of ARI threats categorized as serious increased during this same time.3
In 2017, researchers evaluated outpatient antibiotic claims data in dentistry for the 2015 calendar year.4 General dentists and other dental care provider types were ranked third among health care professional groups in antibiotic prescribing, ac counting for approximately 13% of all prescriptions during this 1-year period. Antibiotic courses were typically from 7 through 10 days, broad-spectrum antibiotics were used often, and clindamycin contributed to 15% of all antibiotic prescriptions.4 These prescribing patterns among dentists in the United States are risk factors for patients developing ARI. It takes all of us changing our prescribing pat terns to reduce the average course of antibiotics and reduce our patients’ risk of ARI. It takes all of us changing our prescribing patterns to reduce the average course of antibiotics and reduce our patients’ risk of antibiotic-resistent infections.
Clostridioides difficile is a bacterium that results in one of many urgent ARI threats that we are facing as a society. In the United States, C difficile resulted in 223,900 cases among hospitalized patients and claimed at least 12,800 lives annually.2 Researchers have found that a single dose of clindamycin results in disruption of the microbiome for up to 1 year, or sometimes longer, and can put the patient at risk of developing C difficile infection.5 Historically, dentists are top prescribers of clin damycin and are more likely to prescribe clindamycin inappropriately as well.6 It takes all of us to stop prescribing
clindamycin to reduce the risk of our patients developing an ARI. Clinical practice guidelines have updated previous treatment practices and have been published for patients who may require prophylaxis, such as patients with total joint replacements (2015),7 heart conditions (2007, 2014, 2021),8–10 and for treating infections in patients with tooth pain and swelling (2019).11 Despite the updated evidence-based guidance, preliminary data suggest that there has been minimal or no change in prescribing patterns, a consequence that increases the danger of ARIs for patients.12 It takes all of us implementing the guidelines in practice to decrease this danger.
How can dental care professionals win this battle? First, we must fight together.
● Join me in becoming an antibiotic steward; identify 1 champion in your practice who will help team members prescribe more safely n
● thinking twice before prescribing and using the guidelines to prescribe more safely
● reducing or eliminating the use of clindamycin in dentistry
● asking your patients about their risk of ARIs and history of C difficile risk factors in their medical history
● using a shorter duration of antibiotics when it is necessary to prescribe them
● bringing antibiotic stewardship into your study club, dental society, or state continuing education course schedule
● encouraging each state to adopt an antibiotic stewardship policy, toolkit, and mandatory continuing education training for dentists in fighting antimicrobial resistance and saving lives.
With all of us together, united in our fight against antimicrobial resistance, we finally can win the war.
Erinne
JADA
Kennedy, DMD, MPH, MMSc
Sleep Apnea (continued)
nual checkup, the doctor didn’t ask him about his sleep, and I bet he didn’t tell a joke, either. Because we know and see our patients and their families often, we can help them breathe better by asking ourselves and our patients a few simple questions. Sleep apnea was subtle to catch in Shawn, but he’s just the tip of the iceberg.
Dr Erin Elliott
ADA WINS IN 2024 ASSOCIATION
Together, we accomplished so much in 2024, from advancing legislation and scientific research to delivering new resources and benefits to help you thrive. Here’s a look back at some of our favorite moments.
ADVOCACY
• Introduced or advocated more than 150 bills or regulations during the second session of the 118th Congress. Some notable accomplishments in 2024 include efforts to expand the oral health care workforce, enhance access to care for underserved populations including veterans, and improve the dental insurance landscape.
• Issued more than $4.25 million in State Public Affairs grants to state dental societies to support insurance reform, bolster workforce development and champion improvements to Medicaid.
• From 2018 to 2024, state societies successfully advocated for 164 new insurance reform laws, tackling key issues like network leasing, non-covered services and dental loss ratio.
• Since 2023, 22 states have introduced dental loss ratio bills that prioritize patient care over profits. Eleven states have enacted medical loss ratio laws that adopt transparency or require insurers to spend a minimum amount of money on dental care.
• Secured long-sought student loan reforms to the Public Service Loan Forgiveness program and the Indian Health Service Loan Repayment Program.
• Held our largest Lobby Day ever with more than 1,200 students and dentists advocating on Capitol Hill. We were joined by 700 students from 55 schools, and nearly all dental specialty organizations were represented. We also had the largest turnout of new dentists in Lobby Day history.
WORKFORCE
• Boosted the dental workforce and improved access to care by providing more than $700,000 in grants
• The Dentist and Dental Hygienist Compact legislation expanded the number of states which enacted the law to include 10 states, enabling more professionals to serve the communities that need their care.
ORAL AND COMMUNITY HEALTH
• The first-ever “Dentistry’s Role in Complete Health” symposium welcomed a standing-room only crowd of dental and medical professionals who gathered to explore oral-systemic health and its implications for the health care community. The symposium was the ADA’s most-attended live CE event prior to SmileCon® and it returns to Chicago in 2025.
• Partnered with The Children’s Oral Health Institute to fight childhood tooth decay by sponsoring 20,000 lunch boxes as part of the Lessons in a Lunch Box program, which brings oral health literacy to life for 2nd and 3rd graders nationwide.
• I n 2024, the ADA Foundation’s Give Kids A Smile® program provided more than $14.7 million in donated dental care to 310,000 children at approximately 1,300 events held nationwide. This impact was made possible by the generous volunteerism of 4,500 dentists and 18,500 dental team members, and the invaluable support and product donations from corporate sponsors, Colgate and Henry Schein.
• The ADA Foundation’s Give Veterans A Smile (GVAS), a new initiative to help address veterans’ unmet oral health needs, launched at SmileCon 2024.
SCIENTIFIC AND CLINICAL EXCELLENCE
• Updated radiation safety guidelines removing the need for abdominal and thyroid shielding became JADA’s most downloaded paper, spurring national media conversations and coverage by major outlets.
• The first clinical practice guidelines on acute oral pain management for adults and adolescents, published in JADA (Feb 2024), marked a breakthrough in combatting opioid misuse. Endorsed by 5 medical and dental associations, they were the result of collaboration between the ADA and two dental schools.
• The ADA Forsyth Institute (AFI) received a $6.2 million grant from NIDCR to develop smart materials using AI, marking one of the first applications of this technology to advance basic research in oral health.
• Leaders from research, industry, academia and more gathered at the sold-out ADA Forsyth dentech 2024 to drive global health innovation. The event featured panel discussions, networking and crowned two winners in the Tech Showcase.
CONNECTING THE DENTAL COMMUNITY
• More than 111 interviews were arranged with ADA spokespersons covering topics that range from healthy hygiene habits to new recommendations around clinical care and oral health issues on Capitol Hill.
• ADA Dental Sound Bites™ podcast won 4 national awards, surpassed 180,000 downloads and continues to bring you real talk on the biggest issues facing dentists today.
• On social media, engaged more than 6,500 viewers in expert-led Instagram Live events and partnered with rising dentist and dental student influencers with a reach of over 935,000 followers. We kept the dental community informed with 179 real-time news updates through ADANow and ICYMI social media updates, resulting in 314,000 video views and reaching 841,000 people. Like, love, share or DM us on Facebook, Instagram, LinkedIn, TikTok and YouTube.
• Connected 8,000+ dentists and dental professionals at SmileCon 2024 with 300+ CE offerings, wellness sessions, speakers and networking opportunities. Advocates, professors and rising stars in organized dentistry were among 2024’s winners
Connecting the Dental Community
• More than 111 interviews were arranged with ADA spokespersons covering topics that range from healthy hygiene habits to new recommendations around clinical care and oral health issues on Capitol Hill.
• ADA Dental Sound Bites™ podcast won 4 national awards, surpassed 180,000 downloads and continues to bring you real talk the biggest issues facing dentists today.
of the ADA 10 Under 10 Awards, who were recognized during SmileCon’s first Changemakers Celebration.
WELLNESS
• On social media, engaged more than 6,500 viewers in expert-led Instagram Live events and partnered with rising dentist and dental student influencers with a reach of over 935,000 followers. We kept the dental community informed with 179 real-time news updates through ADANow and ICYMI social media updates, resulting in 314,000 video views and reaching 841,000 people. Like, love, share or DM us on Facebook, Instagram, LinkedIn, TikTok and YouTube.
• Connected 8,000+ dentists and dental professionals at SmileCon 2024 with 300+ CE offerings, wellness sessions, speakers and networking opportunities. Advocates, professors and rising stars in organized dentistry were among 2024’s winners of the ADA 10 Under 10 Awards, who were recognized during SmileCon’s first Changemakers Celebration.
• Members and students can now get a personalized mental health assessment in just one minute using the Dental Well-Being Index. This validated and anonymous tool from the Mayo Clinic allows users to track their well-being journeys over time.
Wellness
annually) interest rate discount on any dental practice loan and $0 origination fees on any dental practice loan ($3,570 value). Total ADA member value is projected at more than $15,000+ over the lifetime of the loan.*
• 120 ADA dentists completed their free 30-minute student loan repayment consultation from Laurel Road Student Loan specialists at GradFin.**
• Members and students can now get a personalized mental health assessment in just one minute using the Dental Well-Being Index. This validated and anonymous tool from the Mayo Clinic allows users to track their well-being journeys over time.
• Worked to eliminate stigmatizing mental health questions from licensure applications. States like Texas, Virginia, Iowa, Minnesota and Oregon have already made important changes, and more are on the way.
• Worked to eliminate stigmatizing mental health questions from licensure applications. States like Texas, Virginia, Iowa, Minnesota and Oregon have already made important changes, and more are on the way.
• Expanded wellness resources on the ADA Member App and at ADA.org/wellness, including exclusive guided stretches that improve your day-to-day ergonomics in and out of the operatory.
Member Benefits
• Expanded wellness resources on the ADA Member App and at ADA.org/wellness, including exclusive guided stretches that improve your day-to-day ergonomics in and out of the operatory.
MEMBER BENEFITS
• Launched new endorsement for Practice Financing with Panacea Financial offering ADA members a 0.25%
interest rate discount on any dental practice loan and $0 origination fees on any dental
* Panacea Financial is a division of Primis, Member FDIC. 0.25% rate discount for Panacea Financial Practice Loans: Terms and conditions apply. Offer good for practice financing customers only and subject to lender approval. To receive the offer, you must meet Panacea Financial underwriting criteria and be an ADA member. Offer good for new customers only. Offer cannot be combined with any other offers, except any discount for making automatic payments. Offer subject to change. Lifetime benefit calculation estimation based on a loan size of $750,000 over a 10-year term with a 0.25% interest rate discount and zero origination fees. A borrower’s actual savings could be higher or lower depending on the size and term of their practice loan.
member value is projected at more than $15,000+ over the lifetime of the loan.*
** GradFin and Laurel Road are brands of KeyBank N.A.
• 120 ADA dentists completed their free 30-minute student loan repayment consultation from Laurel Road
• Launched new endorsement for Practice Financing with Panacea Financial offering ADA members a 0.25% ($1,750
SERVICE
GIVE AND YOU SHALL RECEIVE
These days, nearly everyone is focused on value; value for dollars expended and return on investment. At the American Dental Association, the Board of Trustees is continually analyzing the use of membership dues and non-dues revenues to maximize the impact of dollars expended and benefits to member dentists.
I feel as though our society, and in many ways our membership, is focused on only answering the question “What’s in it for me”? I can still recall a famous inaugural address of a short term United States president stating, “Ask not what your country can do for you, ask what you can do for your country”. The importance of that kind of civic action and public service has, I am sorry to say, faded. That being said, membership in organized dentistry is not solely about what you get but is it also about what you have to opportunity to give.
So, how can we give?
Give through your continued membership, and encourage other dentists to join. Give by offering your time and talents to serve in an advisory or leadership position, and work with others to enhance the purpose and outreach of your local dental society, state dental association, and the American Dental Association (ADA). Give by supporting humanitarian efforts such as Give Kids a Smile, Dental Lifetime, Mission of Mercy, Remote Area Medical and now, Give Veterans a Smile.
Envisioned to address the dental health care needs of veterans who do not currently qualify for dental services through the Veterans Administration System, Give Veterans a Smile will kick off during Smile Con 2024. The initial kick-off and fund-raising event will be held at the World War II Museum in New Orleans, a museum that offers an absolutely fabulous tribute to the operations of the European and Pacific theaters of the war.
Finally consider providing dental care to a military veteran in need. Dental Lifeline is an organization that works to match individuals in need of dental treatment with providers who are willing to volunteer their services. The difference you can make in the life of a disabled veteran is undoubtedly priceless.
Giving back to the community and to the dental profession is a personal decision; a decision that only you can make. I just want each of you to know that there is a place for every one of us to give back whether it be related to dental health education, legislative advocacy, wellness, or governance. Think about how you might be interested in giving back, and ask how you might help your local community, your local dental society, your state dental association and the ADA.
Dr Scott L Morrison District 10 Trustee
THE BREATH OF LIFE A True Story in Which Help Was Given, and Also Received
The interesting thing about trauma is that sometimes you don’t know you even went through it. As dentists we spend so much time helping others that we often internalize our own needs and experiences. This happened to me last fall and I needed help –but didn’t realize it until weeks/months later.
I went swimming with three friends in Hawaii. It was great to be on the big island again. I raced at the Ironman World Championship there in 2018 and 2019 – two of the best days of my life. I was so excited to swim in those hallowed waters again and to share it with three friends who hadn’t swam there before.
The conditions were a little rough, but nothing I haven’t been in dozens of times before. All of us were strong swimmers, with varied levels of experience in open water. We swam in a group for safety reasons, and we had bright-colored swim buoys that we dragged behind us so we could be seen by boats and have them as flotation devices if needed.
As we went out, one of the swimmers started to become labored and out of breath. He and I stayed back while the others decided to go forward. We made our way to a small buoy and treaded water for a few minutes to catch our breath. After a few minutes, he was gasping for air. He looked scared.
I went into strategy mode. How can I help calm him down? I started to share some stories from past adventures to try to distract him. If it didn’t calm him down, I hoped that he would be so sick of me talking he would be able to push through and get back to shore.
Suddenly, with a panicked look, he said, “Brett, I need help. I can’t catch my breath. I need to be rescued.”
Swimming in open water is unpredictable and potentially danger for anyone -even experienced swimmers. I started to access my water rescue training from my years as a triathlon coach.
Thoughts instantaneously started going through my head: How far away is the pier? One-third of a mile away? Can we breast stroke there together? Is the shore a little closer? But with that sea wall, would rescue be nearly impossible?
I began yelling and waving to try to attract attention from the shore, the dock and the other two swimmers in our group. Suddenly, with a desperate look on his face, he said to me, “I need help, I can’t breathe, I can’t catch my breath, help me!”
I swam closer to him as his eyes rolled up into the back of his head. Within seconds, his lips turned blue as he lost consciousness. I got under his seemingly lifeless body and did my best to keep his head above water. The two other swimmers appeared. I yelled in an urgent voice that we needed to be rescued. They quickly swam toward the pier and attracted the attention of a boat. The boat fired up its engine and quickly made it out to us.
There were two people on the boat. I pushed my friend up so they could grab him but he was too big for the two of them to pull him up, so I climbed aboard, and we got his limp body on the back deck.
I started to give CPR. I desperately pumped his chest. Water exited his trachea with every pump. How did he ingest so much water and never exhibit a protective choking reflex? Come on, BREATHE!
He had been unconscious for several minutes. I moved enough water out of his lungs and he began breathing on his own. I turned him to his side and watched his chest move up and down while we waited for the EMTs to arrive. He was still unconscious, but he continued to breathe.
He was rushed to the hospital. His chest xray showed 70% of his lungs were filled with seawater. He spent the next few days in the ICU.
I am grateful to say he is alive and well. No brain damage, his body recovered and he is back to normal. Thank goodness!
When he was sent home from the hospital, the four of us got together to celebrate his survival and share our recollections of the near tragedy. I don’t remember a lot. My only explanation was that I was in hyperfocus mode to do whatever was necessary to save our friend. I blacked out a lot of events during that period.
As we collectively shared recollections and put together a timeline of what happened, we all recognized the presence of something much larger than ourselves that helped us all play a part in his rescue. A bond that was strong before this even now is indelibly etched in ways that only survivors can understand. We all witnessed the power of the universe and how fragile life can be.
As the days moved forward, I found myself somewhat disconnected and emotionally flat. I became filled with guilt. My thoughts drifted to blaming myself for being irresponsible, as we shouldn’t have been swimming in rough water. It was hard for me to focus as this event consumed my thoughts. I didn’t know what to think. And more importantly, I didn’t know what to do.
I have been involved with tragedies twice before. The first was in 2009. I was running along the beach at sunrise, and I saw what I thought was a seal that was resting near the shore. I ran towards it and noticed it was the body of a deceased female. I helped pull her out of the water onto the shore. There was no saving her. Her body was cold and bloated from the water.
The second was a few years ago. I was driving to work, and traffic was unexpectedly backed up. People were getting out of their cars and walking toward the intersection. I put the car in
(continued on page 22)
LEGISLATIVE UPDATE ON A FEDERAL LEVEL
The ADA recently had their annual Lobby Day in Washington D.C. and we wanted to provide you an update on what is happening on a federal level and what the ADA is doing for you as dentists on Capitol Hill in Washington D.C.
Combining together with over 1500 current dental students and over 500 practicing dentists during the course of 3 days they were able to meet with Senators and Representatives from each of their respective states. They were able to personally and individually converse with them and make the legislators aware of some of the issues facing dentistry and ask them to help sponsor some of the specific bills that are currently before congress that the ADA has helped produce. The following are some of the bills that the ADA is currently sponsoring and ones that were discussed with our Legislators.
The first one is the DOC Access Act. This is the bill that would fix the Employee Retirement Income Security Act (ERISA) loophole many insurance companies use to avoid following insurance laws that states have put in place. This specific bill would make it so in the 43 states that have passed legislation insurance companies would not be able dictate fees for services that they do not cover. Nor would they be able to dictate fees for services that they only pay a nominal fees towards.
The second one is the REDI Act. This bill would essentially pause the accrual of interest and required payments required on federal student loans for both medical and dental residents during a residency training program.
The third one is an appropriations request that the ADA is asking for federal dollars to be spent by the National Institute of Health to create and perform a study to evaluate and confirm the efficiency and safety of fluoride in community water systems at the proper levels (.7 mg/L).
Finally the UDA has a legislative advocacy committee to help advocate for our profession and take a more proactive approach going forward. We hope to send out regular updates to keep our membership informed. If you or someone you know would like to be involved in the Advocacy Committee, please contact Ben Russell at benrussel@gmail.com or Laura Kadillak at lkadillak@roseman.edu.
Dr Ben Russell Advocacy Committee Co-chair
(continued on next page)
Attending ADA Lobby Day as a third-year dental student from Utah was a transformative experience that deepened my understanding of dentistry beyond the clinical scope. It was incredibly empowering to engage with our elected officials—Rep. Celeste Maloy, Rep. Blake Moore, and Sen. Mike Lee—and advocate for issues critical to the future of oral health and the dental profession. I had the opportunity to speak about the REDI Act, sharing how the burden of student debt, with average balances over $300,000, weighs heavily on students pursuing additional training. I expressed how the Act’s interest-free deferment during residency would provide not just financial relief but peace of mind, allowing us to focus on becoming better healthcare providers and encourage more dental students and dentists to specialize without the worries of thousands of extra dollars. Overall, my experience in Washinton D.C not only was exciting but helped trained me to be better prepared to work with Congress and advancing public health in my local community. Additionally, Dr. Fisher was amazing to work with and treated us with respect. He made sure that we were prepared, and I want to thank him for his hard work and support.
Sang Woo Bae
University of Utah D3 Student
As a first-year dental student, I never imagined how soon I’d be standing on Capitol Hill, advocating for the future of oral health care. But here we all were, surrounded by dental professionals and decision-makers, representing the ADA during Lobby Day—an experience that would shape my understanding of advocacy and cement my commitment to policy-driven change. Lobby Day was a weekend spent advocating for equitable, evidence-based oral health care, student wellness, and provider satisfaction—the foundation for long-term improvements in health care. More than just meetings, it was an opportunity to tell the story of why oral health matters.
The day began with nerves, but I wasn’t alone. I had the incredible guidance of Dr. Fisher, Dr. Russell, and Dr. Chamberlain to guide me through the process, which helped me grow more confident as I began to find my voice. Their experience and poise in answering tough questions from representatives and staffers were inspiring. They didn’t just speak about the issues; they shared personal stories and practical insights from their years of practice. That made me realize advocacy isn’t just about presenting facts but it’s about presence, experience, and genuine connection.
What struck me the most was how brief our interactions were with each representative. In just a few minutes, we had to make our case, offer solutions, and connect on a human level. Many didn’t ask follow-up questions, but they jotted down notes when something resonated. That moment was a powerful lesson in the importance of being clear, concise, and intentional. When it comes to advocacy, every word counts.
More than anything, I left Lobby Day with a deep sense of gratitude. I’m here today, pursuing a career in dentistry, because others before me advocated for students to have these opportunities. Their efforts opened doors that I now have the chance to walk through. This experience reminded me that advocacy is a long, often slow-moving process, but it’s one we must commit to daily. It’s not just a one-day event but a responsibility we carry forward. I can’t wait to return to Lobby Day year after year, growing, learning, and continuing to make a difference for both my peers and future patients
Sonia Ramirez
University of Utah D1 Student
The Breath of Life (continued)
park and followed the other drivers to see what the holdup was. In the intersection was a cyclist on the ground gasping for air in a pool of his own blood. One of the Samaritans cradled him as he was gasping for air. He was hit by a car, whose driver left the scene of the accident. He passed away a few hours later at the hospital.
These two tragedies that I witnessed and buried came back to the forefront of my thought in a recollection so vivid it was as if they had just happened. I could no longer stuff down my emotions. Even though my friend survived and was thriving. I didn’t know what to do with my thoughts.
I needed help. And I sought help.
The Colorado Dental Association has a program available to members and our household members that grants us five free counseling sessions for any event (and per life event) that could derail us emotionally.
I used this program for my counseling. I went online and filled out some forms. Within a day, they sent me a list of three licensed therapists who were deemed a good match. I called each of them and chose the one I felt the most comfortable with.
The counseling helped me process these traumas. Within a few sessions, I was able to gain insight into how my brain processed these events.
I learned that my “blackout” was a protective measure that my brain used to protect me in the moment. But these protective coping mechanisms can come back in deleterious ways. I will never forget these events.
I had my five free telehealth sessions where I gained inside on how my brain processed these traumas while I picked up tools to use as I navigated forward.
I continue to work with this licensed counselor on my own to help me in other areas of my life productively. I am grateful for the CDA for these resources to help me when I needed it most. I’m a big advocate for seeking help, but I personally never expected to use this benefit.
Tomorrow is probable but not guaranteed. Therefore, we must live our best lives today (and every day)!
Dr Brett Kessler ADA President (Reprinted with permission)
At
When it’s time to sell, expert planning and strategic guidance are essential for a successful transition.
Don’t go it alone. Scan the QR code to learn more about the value of using a Transition Professional.
Matt Hamblin with DDSmatch did an amazing job helping my partner and I complete our partnership.
He worked with us for over a year preparing us for a successful transition, and his insight, knowledge, and people skills made everything go smoothly.
We both feel like we are ready to start the newest phase of our practice lives in a great spot and are excited for the future.