There are big picture answers to the “lessons learned” question, and there are small picture responses. In practical terms, there is not a lot individuals can do about big picture changes.
After all, among the big lessons learned is the importance of global monitoring to detect emerging threats to health; the value of international collaboration for sharing information and research about everything from detection to eradication; and improving emergency response capabilities all over the world. And those are just a few of many major needs identified by the pandemic.
What can any of us contribute to those needs in a meaningful way? Realistically, not a lot.
But on a personal and family level, each of us can take actions that show we learned from the experience of enduring a pandemic. Taking lessons to heart may seem unimportant — after all, the pandemic is over — but public health experts always say it’s never a question of if there will be another pandemic. The question isn’t it if; it’s when.
Admittedly, someone might say the next pandemic could be 100 years away. If that was to be the case, what takeaways are there that have value in any situation, whether ordinary times or extremely dire situations?
Health is precious It was amazing how quickly the virus went from a distant and abstract situation, one that seemed at first to be overblown by media coverage, to a genuine threat in our town, our street, maybe even our home.
Health is worth protecting The recommended protective measures were not expensive or com-
HALF
A DECADE HAS GONE BY SINCE THE COVID PANDEMIC ERUPTED
WHAT DID WE LEARN?
plex; they were simple: hand washing, wearing a mask, getting vaccinated. Despite resistance and suspicion surrounding these simple measures, they were largely vindicated as effective.
Family is important Some couples went from seeing each other the barest handful of waking hours per day pre-COVID to being together around the clock for weeks on end. The pandemic tested personal relationships in unexpected ways and demonstrated the importance of making those relationships work.
Change is good The change part of change may or may not be good. It is our personal ability to change as necessary that is good. Adaptability and resilience is essential in life, as the pandemic showed us all (whether we wanted to see it or not).
Be prepared The Boy Scout motto — oops... the Scouting America motto — is true. The pandemic offered a great reminder that we need to save for emergencies; we need to have a grab bag ready to go containing emergency essentials; maybe we need to learn some basic life skills, like how to build a fire or cook without electricity. Stuff happens. We should be prepared for it.
It’s good to meditate For anyone who didn’t learn from COVID that the world can be turned upside down in the blink of an eye, Hurricane Helene offered a refresher course. Knowing that it can disappear so suddenly, it’s good to consciously and actively appreciate what we have while we have it.
These are valuable general guidelines for the days and years ahead.
PETS ARE SALUBRIOUS
ost of us are animal lovers. Nothing is more calming and soothing than being able to pet a soft, furry cat or dog and have it look lovingly into our eyes in return. They do, however, come with certain negatives and because I am a cat person, I’ll tell you about my pet and the wee problem of being a cat Mom.
I’ll call it a tutorial of sorts. The day you have to clean the litter box! You can put it off as long as you can, but the day will come. You know it. Your visitors know it – and maybe even your neighbors.
Certainly Kitty knows it too. I’m sure that she holds it until close to bursting to avoid stepping in the clumps. You watch her carefully lest she selects a very undesirable alternative place to do her business. (That’s an odd phrase, don’t you think? Do her business? Maybe she’s taking dictation or answering the phone in there.)
Sorry I got off track – we were talking about undesirable places. You know, that dark corner near the dining room or upstairs on the new carpet? Instead of emptying the litter box, you watch Kitty very closely as you continue to put off “Cleaning the Cat Box Day.”
She looks at you beseechingly with her big, blue eyes, sometimes uttering a tiny meow of “help.” Oh please, you say. Didn’t I just change the litter? Is it time again? Maybe I should cut down on her kibble and water. Wouldn’t that help?
CAT LOVERS TUTORIAL CAT LOVERS TUTORIAL
Bulging bluish or purple veins visible under the surface of your skin
Painful or achy legs that feel heavy
Muscle cramping in your legs, particularly at night
Itchy legs, especially on your lower legs and ankles
Burning or throbbing sensations in your legs
Swollen feet and ankles at the end of the day
Treatment and Management
Many people with kleptomania do not seek help until they face legal or personal consequences.
However, with the right treatment, it is possible to manage the condition and reduce impulsive urges.
THOUGHTS ABOUT THOUGHTS THOUGHTS
KLEPTOMANIA
Editor’s note: Written by local mental healthcare professionals, this series shares thoughts on how people think and act when affected by common and not-so-common mental health conditions.
Jenna is a 29-year-old accountant with no history of legal trouble—until now.
She was recently stopped by store security for attempting to take a bottle of lotion without paying. The incident left her confused and ashamed. She had no financial need to steal and wasn’t sure why she had done it.
This wasn’t the first time. Over the past year, Jenna had taken various small items from stores—things she didn’t particularly need or even use. Each time, she felt a brief sense of relief, quickly followed by guilt. Despite her best efforts to resist the urge, she found herself repeating the behavior.
Jenna has kleptomania, a mental health disorder that causes an overwhelming, compulsive urge to steal. Unlike theft driven by necessity or personal gain, kleptomania is rooted in impulse control issues.
What Is Kleptomania?
Kleptomania is classified as an impulse control disorder, similar to compulsive gambling or pyromania. It is characterized by the repeated inability to resist the urge to steal, even when the stolen items have little or no value to the individual.
People with kleptomania often experience:
• A mounting sense of tension before stealing
• A temporary feeling of relief or gratification immediately after
• Guilt, shame, or remorse once the act is complete
• Repeated episodes of stealing, despite efforts to stop
Unlike planned shoplifting, kleptomania-driven theft is typically unplanned and impulsive. Those affected do not steal out of financial need, revenge, or thrill-seeking but rather to relieve internal distress.
Who’s at Risk?
Kleptomania is a relatively rare condition, but can affect people from all walks of life. Research suggests that it is more common in women and often first appears in late adolescence or early adulthood.
While the exact cause is unknown, several factors may increase the likelihood of developing kleptomania:
• Family history of mental health disorders, particularly mood disorders and substance use disorders
• Underlying psychiatric conditions, such as anxiety, depression, or obsessive-compulsive disorder (OCD).
• Imbalances in brain chemistry, particularly involving dopamine, a neurotransmitter linked to pleasure and impulse control
Kleptomania is often misunderstood. People may assume that those with the disorder are simply dishonest or lack self-control. In reality, it is a recognized psychiatric condition that requires treatment.
Common treatment approaches include:
• Cognitive Behavioral Therapy (CBT): CBT helps individuals recognize the thought patterns that drive their compulsive stealing and develop healthier coping strategies. For instance, therapists may guide patients through exercises to help them pause and reassess their impulses before acting on them.
• Medication: Selective serotonin reuptake inhibitors (SSRIs) and other medications may help regulate impulse control and reduce the urge to steal. In some cases, mood stabilizers or opioid antagonists (which block the brain’s reward response) are also prescribed.
• Support Groups: Programs such as Kleptomaniacs and Shoplifters Anonymous (KASA) provide a structured support system for individuals seeking recovery.
• Behavioral Strategies: Avoiding high-risk situations, identifying triggers, and using distraction techniques can help prevent impulsive behavior.
Can Kleptomania Be Treated Successfully?
Kleptomania is a chronic condition, but long-term management is possible. Many individuals see significant improvement with therapy, medication, and behavioral strategies. However, relapses can occur, making ongoing support and treatment an important part of recovery.
For those struggling with kleptomania, seeking professional help is a crucial first step. The condition is not about lack of willpower. It’s about addressing an underlying mental health issue to regain control.
Integrated Psych Solutions provides inpatient and outpatient mental health services, with or without a referral, to help patients and their families progress through the care journey. To make an appointment, call 706-204-1366 or visit integratedpsych.care.
WHAT IS DEATH FROM “NATURAL” CAUSES?
Sometimes a death from so-called natural causes seems like the lazy man’s way of saying, “The person was old. What were you expecting? That they would live forever?”
True, deaths described as “natural” often strike older people, but dying of old age is, technically, not natural. At least not in our humble opinion here at Medical Examiner world headquarters. In our view, it falls into the same category as the lazy doctor’s explanation to a patient: “Your knee hurts because you’re 90 years old.” To which the patient replies, “My other knee is also 90 years old, and it doesn’t hurt.”
So plenty of things may happen to us as we age, but none of them are exactly automatic. Or “natural.” True, some dastardly health issue may strike mainly older people. But it doesn’t strike all older people.
Officially, however, a death from “natural” causes means that the death did not result from something that isn’t natural, like a bullet. Or a car crash, suicide, drowning, poisoning, or some other equally unnatural reason. It means that the death was the result of something natural, like an infection, illness, or an internal malfunction of some kind.
Although it might not seem like it should be, dying of a heart attack is considered a perfectly natural death. Ditto for lung cancer (or any other cancer), stroke, Alzheimer’s disease, COPD, diabetes, pneumonia, the flu, kidney failure, and a host of other common life shorteners.
As you may have surmised, then, the vast majority of all deaths fall into the “natural” category. CDC figures for one recent year put the number of natural deaths at close to 93 percent. The unfortunate 7 percent (it’s better to die naturally than unnaturally, right?) succumbed, in order of frequency, to accidental poisoning, vehicular accidents, falls, suicide, murder, drowning, complications of medical care, and fire.
In the U.S. there are only six categories for medical examiners (no relation) to record the manner of death on death certificates: natural, accident, suicide, homicide, undetermined, and pending. Of course, we all want to keep living. That’s natural. +
www.AugustaRx.com
Direct editorial and advertising inquiries to: Daniel R. Pearson, Publisher & Editor E-mail: Dan@AugustaRx.com
AUGUSTA MEDiCAL EXAMINER P.O. Box 397, Augusta, GA 30903-0397 (706) 860-5455
www.AugustaRx.com • E-mail: Dan@AugustaRX.com
www.Facebook.com/AugustaRX
Who is this?
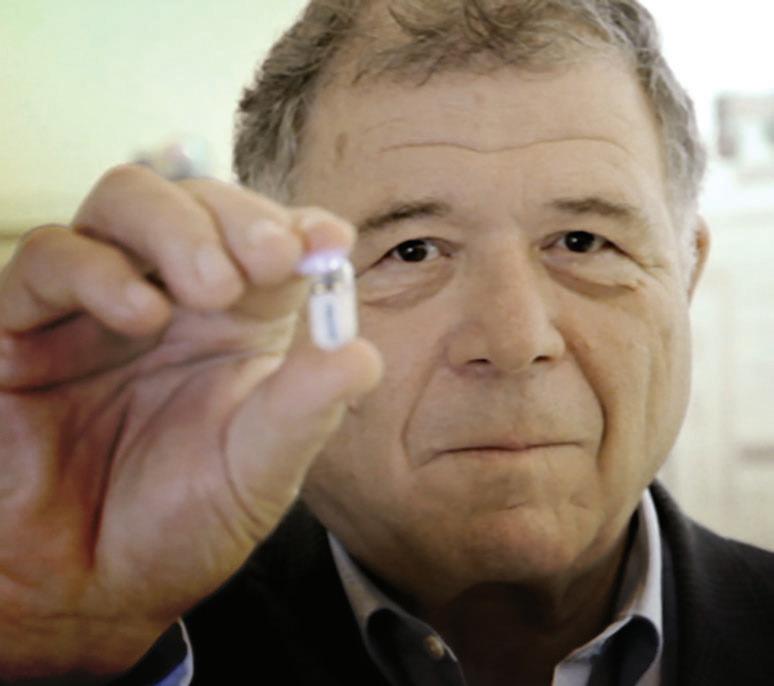
If you read “Who is this?” regularly, you know you’re being whisked from the 1600s in our previous issue all the way to the 21st century for this installment. Medical innovation never rests, as this man’s claim to fame demonstrates.
And “fame” probably isn’t the most accurate word to use. After all, Gavriel Iddan is not exactly a household name. Decades into his career, Las Vegas odds makers would have ranked the chances of him appearing in this particular spot in this particular newspaper at roughly zero. He wasn’t even in the medical field: he worked on guided missile technology for Israel’s Ministry of Defense.
Born on October 1, 1941, Gavriel Iddan’s specific professional focus was developing applications uniting hightech electronics and optics. During the late 1970s, he took a sabbatical during which he lived in Boston. By chance, a neighbor of his was experiencing stomach pains for which doctors had been unable to identify a cause.
Iddan got an idea: what if he could miniaturize a guided missile? Take the basic elements — an on-board camera and remote tracking capability — reduce its size by about a million percent (oh, and remove the warhead) and voila! A lethal device could be transformed into a potentially lifesaving diagnostic tool.
The concept was intriguing, but it was by no means easy to bring it to reality. It took Iddan 20 years to finally develop a prototype that combined a tiny camera, a light source, and a transmitter that would allow the device to continuously send images from the digestive tract to an external receiver. The Food & Drug Administration approved the device in 2001, and capsule endoscopy was born.
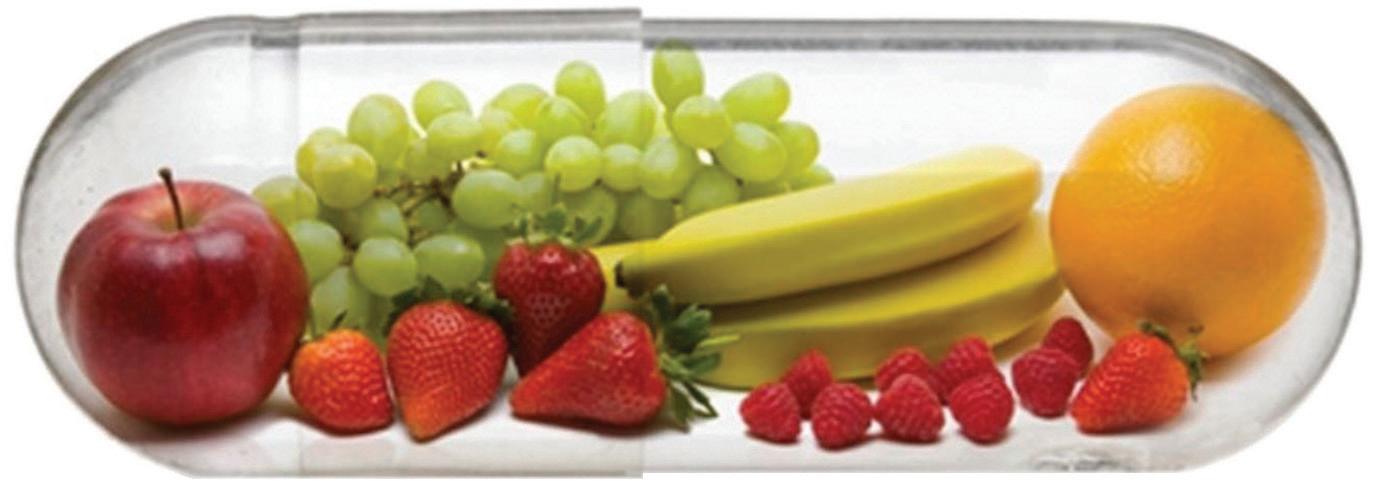
Typically, patients are asked to fast before visiting their doctor to get the procedure started. Some physicians also recommend a bowel prep before the study. The doctor office visit involves getting a small data recorder to wear for the period prescribed, then swallowing the camera, which as you can see (above), is about the size of a large vitamin. Individual doctors and specific situations dictate specific perpatient instructions, but drinking clear liquids and eating a light meal during the procedure is often permitted. Patients return to their doctor as directed (often around 8 hours later) to return the data recorder so images can be downloaded and evaluated by the physician. The camera is disposable, so it makes its way out of the body by the usual means.
The benefits of Gavriel Iddan’s “capsule endoscopy” are many. Aside from the convenience for patients, doctors can see areas and identify problems that previously were unreachable without major surgery. Locating the source of gastrointestinal bleeding, for example, is often like looking for a needle in a haystack. A “pill cam” can identify the source of the problem non-invasively, meaning that major surgery becomes minimally-invasive surgery.
Once upon a time, swallowing a camera would have been viewed as science fiction, and risky sci-fi at that. Over the past two decades, well over a million of Gavriel Iddan’s tiny guided missiles have been safely deployed in gastrointestinal systems all over the world.
Incoming! Outgoing! +
Middle Age
BY J.B. COLLUM
Editor’s note: This column originally appeared in the April 15, 2022 issue of the Medical Examiner
They say that all good things must come to an end. Logically, one would think that the opposite is true as well. So does that mean that all bad things must come to an end? Or should the opposite be, “all good things must have a beginning?” Oh boy, I’m starting to confuse myself again. Be that as it may, in this case, I am talking about the change in our lives that began almost three years ago when we moved my parents in with us after my father’s Alzheimer’s got too advanced for my mother to deal with by herself.
As I write this, she is being moved into her new apartment. It has been seven months since my father passed away, and we knew this moment would eventually arrive. At times it didn’t seem like it would come soon enough for both my mother or me, and probably my wife too. At other times, like now, when it is actually happening, it makes me recall the feeling I had when I realized that Dad couldn’t take care of Mom and couldn’t even take care of himself anymore. I understood that the baton had been passed. I was the patriarch now and I needed to look out for both of them, with a huge heaping dose of help from my wife, without whom I couldn’t have done it. I recall the day my father died, when I knew what he would want me to do, perhaps more than anything else, and that was to take care of his “girlfriend” who, fortunately in this case, is also my mother and his widow. It might have been awkward if it had been someone else.
other benefits to my mother, like having her own kitchen where she can feel comfortable cooking meals her way. All those benefits and numerous others are certainly something we’ve been looking forward to, but it reminds me that even though some miles will separate us geographically, I still am obligated out of love and gratitude — to both my mother and my father — to make sure she is looked after.
{
{ The shirt & tie and pajama bottoms world is disappearing.gradually
I plan to visit regularly, even though the last two years have made me nearly a hermit, as I have worked from home and even attended my Christian meetings online for over two years. Some of that is changing as well. I am now back to getting dressed up fully and attending worship services at a real building in the midst of real people, and not just sitting in front of a computer with my white shirt and tie on and my pajama bottoms on, out of sight of the cameras. Fortunately, I will still be working from home, and I have the pandemic to thank for that, as it forced my company into re-thinking their stance on the subject, and they now allow it and even encourage it for everyone.
As we are packing things up and getting them ferried over to her new home, I see so many of my father’s possessions being boxed up and moved to her new place because she still can’t bear to part with many of them. It brings the full impact home to me. True, it will be nice to have our home to ourselves and not feel like we need to tell someone where we are going and when we’ll likely be back, and it will be nice, for me anyway, to be able to walk around the house without pants and without the fear of giving my mother a heart attack. And there are the
Yes, change is in the air, and it is both thrilling and frightening. I’m a nostalgic person by nature and I tend to miss the old ways, the old places, and especially, the old people that are long gone. I have done a better job of embracing change recently, and I can even get a little bit excited about it at times. So many of us say that we “can’t wait for things to get back to normal.” Someone once told me that things never “get back to normal.” They get back to the “new normal” and we must realize that and accept it so that we can move on and still be happy.
I’m trying to be that person, but it is hard to teach an old dog new tricks.
J.B. Collum is a local novelist, humorist and columnist who wants to be Mark Twain when he grows up. He may be reached at johnbcollum@ gmail.com +
Okay, okay. I’ll do it tomorrow! First I have to make a trip to Wally World to pick up some litter. (As an aside, you cannot use dirt from the yard or potting soil.)
Here I am at the store – lots and lots of selections for litter. There’s scented (lavender?) and non-scented, clumping or non-clumping, light weight or regular, in boxes, bags or plastic containers – most weighing at least 300 pounds (exaggerating only slightly). That would be the best bargain per ounce assuming you could get it home.
At Costco, land of everything big and multiple, you can buy four 10-pound bags that are strapped together. Try getting that off the shelf! Even if I got some hunky guy to put it in my buggy, then what? No bagboys at Costco.
Back to perusing the litter selections. Well, the “lite” might be a good choice. Wonder how they make that and is it absorbent?
BTW, did you know there is litter made from corn? No, not the corn cob thing of outhouse fame, but a ground up product. The bad thing about corn litter is the danger of mold, and it attracts bugs. I’ll pass.
So, I make a selection. Plain old regular, non-scented litter in the twenty pound container. I have learned to put this container in my buggy by swinging it to and fro and on the outward swing, drop it into the buggy. Centrifugal force is my friend. Noisy, but it works.
As an aside (I’m full of asides), I have done some research as to where litter comes from: Wyoming! Yes, clay is strip-mined there to create litter, requiring massive amounts of soil and rock to be removed to get to the clay seam. This leaves a giant hole in the ground that needs to be filled. Then there is habitat loss and soil erosion. Gee whiz, all because of indoor cats! Maybe we
should ship the used litter back to fill in the hole. I’ll have to think about a new state motto for Wyoming.
I have gotten way off from my original tutorial, but I wanted you no-cat people to see what we cat lovers go through. Dog lovers can weigh the difference between taking Doggo out for a walk in the rain, sleet or snow three times a day, or having to clean the box.
So, the day has come, Cleaning the Cat Box Day. You new cat owners are welcome to use my suggestions. Unless you have a tiny kitten, this is best done outdoors. I put on gloves, grab a large plastic bag and carry the offending box outdoors. I place the bag over the end of the box and pour the odorous contents into the bag.
At the same time, I am breathing through my mouth hoping that I am not swallowing miniscule amounts of litter dust. Erk! Okay, the lumpy litter is now in the bag and I carry/drag it to the trashcan. You are not supposed to surreptitiously dump it in your neighbor’s yard – unless there is a deep ditch at the back of their property and they are not home.
Next, grab the hose and use full force water to complete the cleaning.
Back inside, I grab the litter box rug (yes, it effectively collects tracked litter), go outside and shake it.
Whew, nearly done. I replace the rug and clean box and grab the new litter. If it is a new container, I once again do the to and fro thing to fill the box.
Finally, I am done. D-O-N-E. I have a week or so, with occasional sifting of clumps until I have to do it again. Wait! Here comes Kitty straight for the clean box. Noooo. Here we go again.
Not everyone in healthcare can be Florence Nightingale, right? Despite the long-running series on page 4, there are clunkers in medicine, and we will examine some of them in this brief series that should be briefer. Unfortunately, there’s enough material to keep this going for a while.
There is a certain poetic justice to the deadly biography of this woman. For starters there’s her name: Linda Hazzard. Her patients certainly couldn’t say they weren’t warned. Born in Minnesota in 1867, she became the poster girl for quack medicine courtesy of a legal loophole in Washington state which allowed some practitioners of alternative medicine to operate as de facto doctors without a medical degree.
Her specialty was fasting, which she claimed was a panacea for all kinds of maladies, curing diseases and ridding the body of toxins. And, as it turned out in many cases, life itself.
Hazzard opened a sanitarium in Olalla, Washington that she called Wilderness Heights, although townspeople called in Starvation Heights. Her self-promotions included three books about the “science” of fasting: Fasting for the Cure of Disease in 1908, Diet in Disease and Systemic Cleansing (1917), and Scientific Fasting: The Ancient and Modern Key to Health in 1927.
Here’s where it gets a little weird. She was convicted of manslaughter in 1912 for the death of Clair Williamson, a wealthy British woman who was a client of Hazzard at Starvation Wilderness Heights. Williamson weighed less than 50 pounds at the time of her death. As if that wasn’t bad enough, evidence presented at her trial established that Hazzard had stolen most of Williamson’s valuables and forged her will.
Why is that weird? Well, you may be wondering how she managed to publish a book in 1917 describing a regimen that killed one of her patients in 1912. And for which she was convicted by a jury of her peers.
The answer is that her sentence of 2 to 20 years was definitely one of those: 2 (years). The following year, Gov. Ernest Lister gave her a full and complete pardon. Hazzard took her clean slate and her husband to New Zealand, where she practiced medicine as “Doctor” Hazzard and made enough money to return to Olalla and build the sanitarium of her dreams. Because Washington authorities had pulled her previously grandfathered medical license, she called the facility a “school of health.”
Nothing had really changed, however. She continued starving people to death, at least a dozen over her career. Skeletal patients would ocassionally escape from the grounds and stagger into town, begging anyone they encountered for a bite of food.
For all of Linda Hazzard’s deadly and dishonest faults, you have to give her credit for one thing: she was no hypocrite. She practiced what she preached.
At age 70 in the spring of 1938, she wasn’t feeling well, so she embarked on a healing fast. By June she was dead. The official cause of death: starvation.
+
2
The Heart of Hometown Dermatology
Like this newspaper?
MEDICAL MYTHOLOGY
ABOUT FLUORIDE
The polarized climate in which we currently live has spawned two groups of people. Broadly speaking, there are those who think everything that comes out of Washington these days is the very height of idiocy; conversely there are those who think the very same things are almost divinely wise.
One of many Exhibit As in this divide is the emerging debate about fluoride. US Secretary of Health and Human Services Robert F. Kennedy Jr. has called it a “dangerous neurotoxin,” and has expressed strong opposition to fluoridation of public water systems, linking fluoride to a variety of health issues.
His position has generated plenty of controversy. Some states have already announced they are or will be discontinuing water fluoridation; meanwhile the American Dental Association and others have reaffirmed their support for and endorsement of fluoridation as a safe and beneficial component of dental health.
Many people have more or less automatically aligned on one side of the issue or the other.
But what do the facts say?
Rather than saying one side is categorically wrong and the other is categorically right, the facts say this is a topic that needs further study. A recent exhaustive review in the journal Pediatric Research was appropriately entitled, “The evolving science of fluoride:
when new evidence doesn’t conform with existing beliefs.”
Change happens, for which we should all be grateful. Our doctors don’t practice blood-letting anymore, to take an extreme example.
In the case of fluoridation, its launch was hailed as one of the greatest advances in the history of public health.
In the 75 years or so since fluoridation became commonplace, however (over 95% of all water systems in Georgia and 92% in South Carolina are fluoridated), other factors have demonstrated their value. These include increased availability and popularity of fluoride in toothpaste and mouthwash, better access to dental care, and improved knowledge about oral hygiene in general.
As a result, the incidence of teeth that are decayed, missing, or have fillings is uniformly dropping around the world, even in countries like the UK, Japan, Iceland, and Italy (and others), where water is not fluoridated.
Such data allows health researchers to take a fresh look at fluoride safety, knowing that to fluoridate or not to fluoridate doesn’t require a choice between good oral health and poor oral health.
Reexamining fluoride use might confirm its value, benefits and safety. Or it might suggest that it’s time to retire the newest innovation of 1950 and move forward.
Stay tuned. +
TRYTHISDISH
GUACAMOLE POTATO SALAD
a new picnic and party
with this delicious Guacamole Potato Salad made with red potatoes and Fresh California Avocados. With only six ingredients it is surprisingly simple to make and taste good with the added bonus of providing 45% of the Daily Recommended Intake of Vitamin C, while being a low sodium dish (less than 140 mg of sodium per serving).
Ingredients
• 2 pounds small red potatoes, cleaned
• 2 ripe, fresh California Avocados, peeled, seeded, and mashed
• 2 cloves garlic, minced
• 2 green onions, whites only, finely chopped
• 1 large Serrano pepper, seeded and minced
• ½ teaspoon salt or to taste
Instructions
Place potatoes in a microwave-safe bowl. Cover with water and microwave on high for 10 minutes. Test for doneness by piercing one
potato with a fork. The fork should slide in with gentle resistance. Continue cooking if not done, otherwise carefully drain the potatoes and refrigerate them until cold.
Cut potatoes in bite-sized pieces (quarter or dice depending on size of potato). Place in a large bowl. Stir in remaining ingredients, adjust salt to taste and serve immediately.
Sodium 170mg, Carbohydrate 23g, Fiber 5g, Protein 3g.
Serving Suggestion: If made in advance, sprinkle generously with lemon juice and place a layer of plastic wrap right on the surface of the Guacamole Potato Salad and refrigerate. Before serving taste the salad and add additional mashed California Avocado if needed.
Recipe provided by California Avocado Commission. For more information please go to: www. californiaavocado.com
FOODISMEDICINE
Tasty tips from registered dietitians with the Augusta Dietetic District Association
Vitamin B12... Are you getting enough?
by Janice Anglin, MS, RDN, CSG (Certified Specialist in Gerontological Nutrition)
Vitamin B12 is a water-soluble vitamin that is naturally present in some foods, added in others, and available by supplementation. The most common form of vitamin B12 in dietary supplements is cyanocobalamin. Vitamin B12 plays an important role in the central nervous system, red blood cell formation, and DNA synthesis.1,2
Vitamin B12 is bound to protein in food and must be released by a series of processes that naturally occur in the body. If vitamin B12 is added to fortified food and dietary supplements, it is already in free form and does not require additional processes to release it.
Recommended dietary allowance varies by age and sex (see table below).2 Food sources include fish, meat, poultry, eggs, and dairy products. Plant foods do not naturally contain vitamin B12. However, vitamin B12 has been added to fortified breakfast cereal and fortified nutritional yeasts to improve consumption.
Bioavailability is the fraction of a given food that the body can utilize.1 Bioavailability varies by type of food source, but it is three times higher in dairy products than in meat, fish, and poultry. The bioavailability from dietary supplements is about 50% higher than that from food sources.2
Groups at risk of vitamin B12 deficiency include older adults, individuals with pernicious anemia, individuals with gastrointestinal disorders/surgery, vegetarians, and infants born to mothers who follow a vegan diet.
Vitamin B12 is often promoted as an energy enhancer and an athletic performance or endurance booster because of its role in energy metabolism. However, it’s supplementation appears to have no beneficial effect on performance in the absence of nutritional deficit.2
Recommended Dietary Allowances for B12 AGE
Some medications are known to adversely affect vitamin B12 levels. These medications include gastric acid inhibitors (proton pump inhibitors PPI) which are used to treat gastroesophageal reflux disease (GERD) and peptic ulcer disease, as well as Metformin which is used as a first-line treatment for prediabetes and diabetes.2
The federal government’s 2020–2025 Dietary Guidelines for Americans notes that “Because foods provide an array of nutrients and other components that have benefits for health, nutritional needs should be met primarily through foods. In some cases, fortified foods and dietary supplements are useful when it is not possible otherwise to meet needs for one or more nutrients (e.g., during specific life stages such as pregnancy).” 2 You can meet your daily requirement of B12 by choosing food sources first and eating a healthy diet using MyPlate as a guide to better nutrition. 3
Your young child has “meltdowns” regularly through the day. Sometimes, they are triggered by her not getting her way, having to put down her tablet, her brother “bothering” her, or an unexpected change in schedule. She will fall to the floor, scream, flail, throw things, try to destroy objects. You have held her and tried to talk her through it. You have slapped her hand, sprayed water in her face, given her a toy to play with. Nothing has worked. What do you do?
A. Continue to do what seems to be the most effective. Persistence will pay off and eventually her behavior will improve.
B. Yell at her to get her attention, take her face in your hands to get eye contact, and tell her to stop!
C. Ignore her. If the behaviors escalate to aggressiveness and destructiveness, put her in her room with instructions, “You can come out when you’ve settled down. We love you, but you have to behave nicely to be out with us.”
D. Talk to your pediatrician and get a referral to a behavioral specialist who can work you through this.
If you answered:
A. None of what you have done has worked. There’s no reason to believe that continuing an ineffective strategy will change the outcome.
B. If this works, continue. It does no harm. Effectiveness is measured in a decrease in the frequency, intensity, and the duration of the meltdowns. You should see the meltdowns happening less often, become far less intense, and not last as long if you intervene quickly.
C. When children who have difficulty regulating their emotions get attention for their negative behaviors, that attention often reinforces the behaviors. You want to ignore the behaviors when they occur and be sure that others in the environment (grandma, aunt, siblings) ignore the behaviors too. When it is not possible to ignore the behaviors, quickly but calmly move the child to her room with the instructions noted above. She will be in charge of deciding when she can come out of her room. Lock the door from the outside if she continues to come out of her room before she has calmed down. (She is getting attention for negative behaviors when she does that!)
D. Carefully following directions in C should yield improvement in behavior and reduce your frustration if you are consistent. However, if you want additional help, talking to your pediatrician may be helpful and direct you to more excellent resources. Emotional dysregulation in children can be very disruptive at home and is a significant problem in day care, school classrooms, and other public settings. That is why you want to address these behaviors early and effectively. Ignore the behaviors but don’t ignore the problem. With some children who do not respond to behavioral strategies alone, medication may be needed as part of the treatment plan. Above all, always be sure to let your child know that you love her.
Dr. Umansky has a child behavioral health practice in Augusta.
CRASH COURSE
More Americans have died on US roads since 2009 than in World Wars I & II combined
Once upon a time in America’s wild wild west it was said that there was no law west of the Pecos. That is, until Judge Roy Bean (right) came along and appointed himself as the decider and enforcer of the law west of the Pecos River.
Before (and after) assuming that title, Bean was a thief, a serial miscreant, barroom brawler, and killer. He regularly ignored, broke and invented laws as it suited his purposes.
In other words, he was a lot like many of today’s drivers.
As we have explained in this very space before, “accidents” hardly ever happen, and because of that we have largely abandoned that term in this column in favor of the more accurate words like”crash” and “collision.”
Statistically, 94 percent of all traffic collisions in the U.S. can be attributed to driver error. All of us see this demonstrated every single day.
Following are a few driving behaviors that a.) are proven to sharply elevate the risk of a crash, b.) are out of control on area roads, and c) are illegal:
Talking on a cell phone or
texting while driving. Does anyone within the sound of
this newspaper not know it’s against the law to use a device while driving? Answer: nope. But anyone who is even marginally observant while driving can see this law being regularly and blatantly violated by motorists. Perhaps people are being ticketed, but by and large the enforcement effort is not effective. Or visible, for that matter.
Speeding. It is said that speeding is the most commonly broken of all laws. Just about everyone does it. Sometimes it’s about unrealistic speed limits (where it’s safer to go with the flow than constantly risk being rear-ended), but in many cases it’s reckless and aggressive
driving, plain and simple.
Running red lights. How many times have you been sitting at a red light and after it turned green watched not one, not two, but three or more cars sail across the intersection? How many times have you personally gone through an already-red light yourself, and then made that automatic look in the rear view mirror only to see yet another car follow your lead through the intersection? You honestly thought your offense was pretty flagrant, and you were worried enough to look in the rear-view for blue lights, but instead you saw that car 100 feet behind you run the light too.
The list of driving laws people obey only when it’s convenient for them is long. That’s part of the reason why more than 926,000 people have died on U.S. roads just since 2000. Not all of those people were law breakers, though. Some of them were doing everything right when they were creamed by someone who ran a red light, was speeding, or texting, or all three.
Here’s a question all of us should ponder: What am I? A law & order driver? Or a wild, wild west driver? +
Helene, You Lose!
by Leta Paleschic, RN Piedmont Augusta
I headed to work as usual, a nurse I am at night
Not worrying too much about weather, not knowing my future fight.
I watched out the windows as the trees swayed to and fro Worrying about the husband and cats, still not realizing my woe.
The work night ended uneventful but I knew there was doom to face I watched and listened to media as my anxiety began to race.
As staff trickled into work with looks of fear and horror in their eyes My heart sank with fear, as I looked to Him, almighty and wise.
The reports were of major destruction in the city we so love I couldn’t imagine reality, without asking for help from above.
I needed to get home to family, despite warnings to stay there But I set out on my journey, fear and anxiety I chose to bear.
Driving over power lines and downed trees was a feat I was not equipped to try
As I drove cautiously at minimum speed, I began to shake and cry.
My goal was to get to my abode, with no cell service to warn the man.
I found no path into my neighborhood, but I repeated, “yes I can”.
I got within a mile of home, after parking at a local lot. I grabbed my belongings and courage, trudging through horror to get to my own spot.
Brave help moving massive trees was already out en masse. Kind souls with saws and grit, concentrating on the big task.
Although I am over seventy, I dodged massive debris to get home. Wet, muddy, scratched, and tired, my neighborhood was practically gone.
I fell into my precious yard, the man and cats at my side. My mind racing with worry, wondering how many had died.
I watched as EMS removed a body from the rubble. At that moment reality set in, my God, we are all in trouble.
We walked around the property, wondering if it would ever be the same.
We were lucky to have good insurance, and soon the adjuster came.
The estimate was seventy-five thousand, an amount that boggled my mind.
How would we ever live through this, we need patience and time.
One hard thing to see and do, was loss of landscape and things: No food, power, internet, hot water, the thoughts and PTSD still stings.
We gradually began to clean up, and the debris was off the chain . One massive tree crushed the shop, we paid five grand for that crane!
As the landscape began to normalize, and things were looking great We were humbled by the courage of all who accepted their fate.
Not everything is back to normal, and hardships are still around. We will work on hoping for peace, as our courage and strength abound.
So Helene, you came and went, creating havoc in your path. We learned how to handle adversity, across your destructive wrath.
Six months have passed so quickly, as we all endured your sin. Bad news for you Helene, I’m sorry, you lose, WE WIN!
The blog spot
posted by Salim Afshar, MD on April 9, 2025 (edited for space)
There was a time when doctors smoked. No, I’m not advocating for a return to lung cancer. But those smoke breaks? They represented something valuable: time.
Time to pause, to think, to wonder, and to chat with colleagues. Whether in a break room, outside the hospital, or crammed into a poorly ventilated lounge, those moments of informal connection were where the magic happened. People consolidated thoughts, swapped ideas, shared observations and learnings, and occasionally stumbled on breakthroughs. Fast forward to today and those spaces have all but vanished.
SMOKE
Nurses spend more time with paperwork than with patients. And doctors? We’re drowning in a sea of administrative tasks, with little room for reflection or collaboration. We’ve gotten so caught up in making health care more “efficient” that we’ve accidentally squeezed out the humanity.
Let me hit you with some stats, because why not?
Nurses now spend only 31 percent of their time with patients. The rest of their time is sucked up by coordination, paperwork, and, I assume, trying to find a functioning printer. This is insane.
I remember having this aha moment as a surgeon: I asked myself, Why do my patients stay in the hospital after an operation? It’s because they need nursing care—that’s it.
Everything else can be done as an outpatient, so if the backbone of hospitals is nursing, why are we “managing nurses” as a cost center first of all—and why so poorly?
Meanwhile, inefficiencies in health care coordination cost the system over $12 billion a year. And we’re busy trying to figure out how to leverage technology to fix that.
OK, back to smoking.
Those smoke breaks which might have been terrible for our lungs but were oddly beneficial for our collective brains? Long gone. What else is long gone are the spaces that once fostered those meaningful conversations. Hospital libraries? Gone or shoved into some digital corner. Surgeon lounges? A relic of the past.
Technology, as wonderful as it can be, isn’t going to fix this. Sure, we can automate tasks, streamline processes, and slap AI on every problem we can think of. But none of that is going to restore the culture of reflection and connection we’ve lost. Without that, we’re spinning our wheels—more efficient, but also more robotic, less innovative, and, dare I say, less human.
Reflections on AI, health care, and beyond
So, what’s the answer? Do we need more yoga in the break room? No. What we need is real time to connect. Time to have actual conversations—conversations that aren’t squeezed in between tasks or interrupted by a pager. Time to think critically about the work we’re doing, to wrestle with tough questions, and to hash out ideas with colleagues. You know, the kind of stuff that leads to breakthroughs.
Doctors and nurses don’t need to start smoking again. But they do need to reclaim what those smoke breaks represented: a chance to pause, reflect, wonder, and engage with each other in a meaningful way.
If we lose that, well, we might as well hand the whole thing over to the robots and call it a day.
Salim Afshar is a physician executive
You’re saying Junior should do what?
Buy $75,000 worth of lottery tickets.
CROSSWORD
ACROSS
1. Criticize harshly
5. Kid’s play creation
9. Capitol of Vanuatu
13. Pacers’ school
14. ____ Flu
16. Nation east of Iraq
17. Voice of Shrek’s Princess Fiona
18. Synagogue leader
19. Former Dawg Gurley
20. Monetary unit of Thailand
22. Dougherty County seat
24. Speedwagon starter
25. Legendary Brave Sid
26. Inner prefix (med.)
28. Type of talk
29. Macon county
32. Malt beverage
33. Diarist Anais
34. Boston diamond
36. Chop
37. Prostate test abbrev.
38. Letters always associated with “bad”
39. Length of life
40. White of the eye
42. Relaxing anagram of 37-A
43. Take home
44. Bold, for one
45. Lair
46. Thermometer type
48. Containing iodine
50. Synonym of 39-A
51. Johns, artist born in Augusta
53. Actor who died in 2008 from drug intoxication
57. Type of list
58. Pelvic exercise
61. Roof overhang
62. Second-hand 63. Intestinal bacteria
64. Requirement
Instead of going to college? That’s your career advice?
Not to toot my own horn, but it’s a brilliant plan.
65. Pool adjective
66. Throw
67. Makes leather
DOWN
1. Ear _____
2. _______ Minor
3. Command to a cat
4. Certain lights on a car
5. Coen brothers film of 1996
6. Eggs (Latin)
7. ____ eye
8. Short coat (of the Middle Ages)
9. A or C, for example
10. Resolve differences (with “out”)
11. Bug starter
12. Common conjunction
15. World’s longest river
21. Natal start
23. Ancient tower
25. Mr. Hogan
26. Vote for
27. Recently
28. Stroke abbrev.
by Dan Pearson
He’ll have the debt either way, but with my plan he saves 4 years. Please explain.
The Mystery Word for this issue: CAENVCTIA
Simply unscramble the letters, then begin exploring our ads When you find the correctly spelled word HIDDEN in one of our ads — enter at AugustaRx.com
We’ll announce the winner in our next issue!
I N E R S U D O K U
DIRECTIONS: Every line, vertical and horizontal, and all nine 9-square boxes must each contain the numbers 1 though 9. Solution on page 14.
30. Master (in Africa)
31. Ring-shaped bread roll
32. Massage reactions
33. Ft. Eisenhower occupant
34. Fed. med. agency
35. Up until now
37. Before surgery, in short
38. Medical asst.
41. Installment of a TV show
42. Not sweet, in wine terms
45. Type of deposit
46. Metal-bearing mineral
47. ________ Blvd. (near MCG)
49. Former Augusta mayor Copenhaver, to friends
50. Downtown backstreet
51. Joseph (in Juarez)
52. Capital of Yemen
54. Greek goddess of the Earth
55. Uniform
56. Clarets
57. Type of war?
59. Gunk
60. Ernie of the PGA
QUOTATIONPUZZLE
DIRECTIONS: Recreate a timeless nugget of wisdom by using the letters in each vertical column to fill the boxes above them. Once any letter is used, cross it out in the lower half of the puzzle. Letters may be used only once. Black squares indicate spaces between words, and words may extend onto a second line.
Solution on page 14.
INSTRUCTIONS: Use keypad letters to convert numbers into the words suggested by the definitions provided. There is often a theme linking all answers. Sample: 742 (body part) = RIB.
Answers on page 14.
THEBESTMEDICINE
ha... ha...
Moe: My non-binary friend asked if they could borrow my guitar. I said no problem, but they had a minor accident on the way over to my place.
Joe: So it was a gender bender Fender lender fender bender?
Moe: I’m so depressed. The state of the world. My loser job. My miserable marriage.
Joe: Cheer up, Moe. It could be worse. You could be in a deep hole filled with water.
Moe: I know you mean well.
Moe: The other day I had to work over a little, and my wife called and said if I wasn’t home in 15 minutes, she was giving my dinner to the dog.
Joe: Did you make it in time?
Moe: I really love my dog, so yeah, I got home in 10 minutes.
Moe: Why did Jack and Jill go up the hill?
Joe: Probably to get a better signal.
Moe: I keep losing my balance and falling. Think I should go to WebMD and figure out
what’s wrong with me?
Joe: My advice, try Trip Advisor.
Moe: What purpose in nature could possibly be served by goosebumps?
Joe: To slow geese down, Einstein.
Moe: Have you ever thought about being an organ donor?
Joe: No, but to be honest, I really would like to get rid of our piano.
Moe: Customer service is dead!
Joe: You’re just noticing this now?
Moe: No, but today was one more example. Banks have piles of money, but they’re too lazy to stock their ATMs.
Joe: What makes you say that?
Moe: I went to six ATMs today to get some cash, and every one of them said “Insufficient funds.”
Moe: Your spelling is pretty bad.
Joe: We were so poor growing up that we couldn’t even afford alphabet soup.
Moe: And you’re saying that’s why you can’t spell? Seriously?
Joe: I only knew one vowel!
Moe: How is that even possible?
Joe: All we could afford were Spaghetti O’s.
Moe: This will be our first summer not flying to Europe because of sickness in the family.
Joe: Really?
Moe: Yup, first time. Every other summer we didn’t go because we were broke.
Staring at my phone all day has certainly had no Effect on ME!
as they
By popular demand we’re making at-cost subscriptions available for the convenience of our readers. If you live beyond the Aiken-Augusta area, or miss issues between doctor’s appointments — don’t you hate it when that happens? — we’ll command your mail carrier to bring every issue to your house!
NAME
ADDRESS
CITY STATE ZIP
Choose six months for $24 or one year for $42 . Mail this completed form with payment to Augusta Medical Examiner, PO Box 397, Augusta GA 30903- 0397
Dear Advice Doctor,
The Advice Doctor
I’ve always thought that May-December romances could be a little suspect, but December-December romances were okay by me — until last week. Last month we moved my mother into a nursing home, and she is already head over heels for a silver-haired widower down the hall. It has only been a month and they’re already discussing the possibility of marriage. What are your thoughts on this sort of thing?
Dear Not So Sure,
Thank you for bringing up this important topic. I’m sure many families wonder about this issue from time to time.
The way I see it, you should be very grateful for your mother’s situation. It sounds like she’s healthy and active. You don’t mention her exact age, but being old enough to move into a nursing home suggests she is no spring chicken. Her general age group is often prone to issues with balance, falls, and general mobility, but it sounds like that’s not a problem here. Frankly, my concern is with seniors who are in a state opposite of your mother’s: heels over head. That suggests a fall, never a good thing at any age, but especially so as we get older. Your description of your mother’s current state — head over heels — is good. That’s normal. It’s what nature intended.
As long as that’s her state of affairs, well and good. But if she does start having balance and mobility issues — or for anyone else reading this who does or who helps care for someone who does — take all the steps you can to minimize fall hazards: provide clear traffic pathways in your home; remove tripping and slipping risks like throw rugs; add grab bars in the bathroom and porch and stairway handrails if you don’t have them already.
In addition, review medications to make sure none of them are contributing to balance issues. Pharmacists are more than happy to answer questions about such matters, and the information they can provide, valuable though it may be, is free, and available without an appointment.
Of course, her doctor is a key player in situations like this, able to diagnose and hopefully treat — or at the very least to minimize — any issues that could lead to turning tail over teakettle, as the saying goes.
Not to be overlooked is the staff at the very nursing home where she lives. They are right there with her 24 hours a day, all day every day, and should be able to protect her and keep her head over her heels, right where it should be.
— Not So Sure About This +
I hope this answers your question.
Do you have a question for The Advice Doctor about life, love, personal relationships, career, raising children, or any other important topic? Send it to News@AugustaRx.com. Replies will be provided only in the Examiner.
read the Medical Examiner: Reason #41 BEFORE READING AFTER READING
THE MYSTERY SOLVED
The Celebrated MYSTERY WORD CONTEST
...wherein we hide (with fiendish cleverness) a simple word. All you have to do is unscramble the word (found on page 12), then find it concealed within one of our ads. Click in to the contest link at www.AugustaRx.com and enter. If we pick you in our random drawing of correct entries, you’ll score our goodie package!
SEVEN SIMPLE RULES: 1. Unscramble and find the designated word hidden within one of the ads in this issue. 2. Visit the Reader Contests page at www.AugustaRx.com. 3. Tell us what you found and where you found it. 4. If you’re right and you’re the one we pick at random, you win. (Winners within the past six months are ineligible.) 5. Prizes awarded to winners may vary from issue to issue. Limited sizes are available for shirt prize. 6. A photo ID may be required to claim some prizes. 7. Other entrants may win a lesser prize at the sole discretion of the publisher. 8. Deadline to enter is shown on page 12.
PROFESSIONAL DIRECTORY
ACUPUNCTURE
Dr. Eric Sherrell, DACM, LAC Augusta Acupuncture Clinic 4141 Columbia Road
706-888-0707 www.AcuClinicGA.com 3633 Wheeler Rd, Suite 365 Augusta 30909 706-432-6866 www.visitrcp.com
L. Carter, MD 1303 D’Antignac St, Suite 2100 Augusta 30901 706-396-0600 www.augustadevelopmentalspecialists.com
Davis Road
Augusta 30907
706-860-4048 Floss ‘em or lose ‘em!
Life is tough
by Annmarie Morgan
Wouldn’t it be great if we could just pick an age and pause there? When in youth and before all the aches and pains, and life was easier; I never could imagine myself as a senior. I saw others that were physically limited and I thought that is so far into the future that maybe it wouldn’t happen and that Mother Nature would skip over me. Well that is a joke Mother Nature plays upon all of us.
If Mother Nature wasn’t enough, Father Time zips by faster each year. In the early years, health issues weren’t concerning and I thought I was invincible. The words of Roman poet Virgil comes to mind and rings truer than ever, “The greatest wealth is health”.
Then life began to spiral and advance. I took on college and a career, betrothed, and had a family.
As time whisked by, some maladies began to emerge brought on by a handful of illnesses and some came from my mental distress. I had born a severely disabled daughter who was plagued with so much sickness and pain up until her death at the tender age of 32. I was later diagnosed with fibromyalgia, osteoarthritis, digestive disorders along with anxiety and depression.
When seeing different specialist, I learned to be my own health advocate using reputable websites on the internet to research conditions and treatments.
As my own advocate, I sought help from specialist like rheumatologists, orthopedists, neurologists, gastroenterologists, therapists, and psychiatrists. I gave each treatment adequate time, but if I didn’t see results; I would seek other specialist that might have a different avenue for treatment. Being sensitive to medications, I was unable to tolerate an array of medications that were prescribed. Side effects can be brutal and debilitating and actually compound the illness.
I keep a journal of how I am feeling currently and how I feel when beginning a new treatment. I journal daily or at least weekly so that I can ascertain if the treatment is effective. Also it’s good information to keep on hand to ask questions of your health care team.
Above all, I participate in my care and treatment. My quality of life is extremely important to me and I will not give up on my health. I still have fire and a lot to offer the world through my experiences even though my body can’t take the beating it once could. As Jim Rohn once said, “Take care of your body, it’s the only place you have to live.”
I have found that medications can be helpful, but have also discovered that eating small, balanced meals helps my digestive issues and I avoid foods that I have determined that I’m intolerant to. In addition exercise helps me maintain a healthy weight as well as improves my mobility.
Being active helps the pain in my joints and muscles. Simple balance exercises has helped me tremendously in avoiding falls. I also learned not to descend stairs in my socks. That resulted in a few months of recovery. I’ve learned some invaluable lessons the hard way as we all do. I use all the knowledge that I have learned in my walk down this path in order to help protect my health and well being.
E Hugh St., Suite 103 North Augusta, SC 29841 (803) 441-3937