

CAN I SPEAK TO A MANAGER?
As you might have noticed, we live in a world that is increasingly rude and crude. It’s hard to miss. Some may welcome the trend as direct and honest speech, a breath of fresh air, while others are appalled. Either way, the real question is (at least for the Medical Examiner) does it have any connection to health, medicine and wellness? We decided to investigate the science.
What’s happening
First, a bit of historical perspective. Not very long ago in any bedroom scene on TV shows, married couples were always shown in separate beds. Elvis could only be shown from the waist up. When Clark Gable uttered his famous line in Gone With the Wind, audiences gasped at the word “damn.” It was shocking, and many would have walked out of the theater — except that it came at the very end of the movie anyway.
Fast forward to the spring of 2026 and a Georgia gubernatorial candidate tells voters, “I sure as hell didn’t” do this or that. People who hold opposing views are personally attacked as scumbags and sleazeballs. Sexual offenses (including alleged crimes) are defended or dismissed as fake news when not too long ago the very whiff of scandal ended careers. The US Secretary of Defense, in a widely publicized speech to senior military leaders, used the acronym “F.A.F.O.” in a warning to enemies of the United States (IYKYK).
In the advertising world, crude wordplay is a growing trend. An ad starring “Will Shat” fea-
tures a Shih Tzu. A drug ad uses the tagline “Kick pain in the Aspercreme.” A fried chicken restaurant promises a “clucking good time.” Here in Augusta, an orthodontics practice uses “shift happens” as a marketing slogan, and a car dealer offering specials on pickups used “get the truck out” in an ad campaign.” Subtle? Not exactly.
We’re all adults, right?
Actually we aren’t, but even if we were, do things like this really matter within the context of health?
They do indeed, and by way of explanation, let’s address a question you might be pondering at this very moment: is this article an example of bait & switch? After all, the headline makes it seem like
the topic is going to be anger management-related, but so far it isn’t. Well guess what? It’s all related. Crudeness – which broadly defines what we’ve covered so far — breeds rudeness. And rudeness has more negative side effects than this issue — all 16 pages — can contain.
A good place to start is within healthcare. A systematic review and meta-analysis of more than 40 studies encompassing 11,000+ nurses published in 2024 in the Journal of Advanced Nursing came to this conclusion: “Workplace incivility* was associated with a range of [negative] patient safety outcomes including near misses, adverse events, reduced procedural and diagnostic performance, medical error and mortality.” (When they say mortality, they mean death.) And the effect isn’t exactly rare: “Incivility, both witnessed and [personally] experienced, is prevalent in healthcare settings.”

Just how prevalent? The Canadian Medical Association Journal reported in 2024, “More than 75% of health care employees have witnessed uncivil behaviour from physicians, and 31% of physicians report receiving weekly or daily rude, dismissive or aggressive communication from other doctors.”
If incivility in the realm of healthcare of all places can measurably degrade health, then what effect does our widespread and growing cultural incivility — in politics, media, advertising, and public discourse —






* Within the nursing profession, the nature of “incivility” includes wrongfully blaming others for own errors, gossiping, cursing at others, ignoring, yelling, interrupting, or taking credit for someone else’s work.


PARENTHOOD
by Dr. Warren Umansky, PhD
You took a trip to a big city recently a few hours from your home. You loved the tall buildings, all the people walking along the sidewalks, the movement of cars and trucks and bikes and motorcycles. Then, in the midst of that enjoyment, you became aware of the noise. There was so much noise from traffic, emergency vehicles sounding their sirens, loud voices from up and down the street, jets overhead. And at that moment it dawned on you: it gets loud in your house; your kid’s classrooms can be noisy. It seems like it’s too loud everywhere. What do you do?
A. It’s a loud world. It’s best if your children are exposed to it when they are young so they learn to accept and tolerate the noise.
B. Outfit your children with noise-cancelling headphones.
C. Be a role model for your children by speaking quietly and expect that they do the same.
D. Play soft music at home and warn everyone when you are ready to turn on noisy appliances (vacuum cleaners, garbage disposals, for example).
If you answered:
A. Other than those who are particularly sensitive to loud noises, children do adapt to noisy environments. But don’t we want our children to appreciate quiet settings? It is unfortunate that the only “protected” environments these days are libraries and museums. You can make your home one of these quiet settings, as well. Enjoy calm and quiet with your children.
B. Some children need this kind of protection in overstimulating settings. We see this at sports events when parents bring their young children and help them enjoy the event by putting headphones on them to blunt the loud noise. Other adults and children wear headphones, but they are listening to blaring music attacking their ear canals. That’s not so good.
C. You can train your children to be calm and use a quiet voice by modeling that behavior and by correcting your children in a direct and supportive way. Even with several young children, you can de-escalate conflicts with a “divide and conquer” approach that separates the children and encourages using calming words to express wants.
D. Being aware of your home environment is important. If you can make it calmer and more pleasant, you want to do it. Playing soft music is a good way to expose your children to different genres of music. And it certainly demonstrates respect when you let others know that it is about to be noisy.
You may say prayers over food at mealtimes or say prayers at bedtime, times when quiet is expected. You should also teach your children to be quiet when you are on the phone or when you ask for quiet. Appreciating quiet is a privilege in a noisy world. It can start at home.

Dr. Umansky has a behavioral health practice for children in Augusta
THOUGHTS ABOUT THOUGHTS
THOUGHTS
SOMATIC SYMPTOM DISORDER:
“SOMETHING IS SERIOUSLY WRONG WITH ME!”
Editor’s note: Written by local mental healthcare professionals, this series explores how people may think and act when affected by common and lesser-known mental health conditions.
David is a 45-year-old father of two who has been to the emergency room four times in the past six months.
It began with chest pain. His heart tests came back normal, but the discomfort didn’t go away. Then came headaches, stomach issues, and a constant sense of fatigue. Each new symptom felt like confirmation that something had been missed.
He’s seen multiple specialists. He’s had scans, bloodwork, and second opinions — all reassuring. Still, the fear lingers.
His family has started to feel frustrated. “The doctors said you’re fine,” his wife tells him. But to David, the symptoms are real, persistent, and frightening.
David is not making things up. He may be experiencing Somatic Symptom Disorder, a condition where emotional distress manifests as physical symptoms that cause significant disruption in daily life.
What Is Somatic Symptom Disorder?
Somatic Symptom Disorder (SSD) is a mental health condition in which a person experiences one or more physical symptoms that are distressing and interfere with daily functioning, accompanied by excessive thoughts, feelings, or behaviors related to those symptoms.
The symptoms themselves are real — not imagined or fabricated. What distinguishes SSD is the intensity of focus, anxiety, and impairment associated with the symptoms, often disproportionate to medical findings.
SSD can involve any part of the body and often persists even after appropriate medical evaluation has ruled out serious illness.
Signs and Symptoms
Physical Symptoms
• Chronic pain (headaches, back pain, joint pain)
• Gastrointestinal distress (nausea, bloating, abdominal pain)
• Fatigue or weakness
• Shortness of breath or chest discomfort
Emotional Features
• Persistent health-related anxiety
• Fear of serious illness despite reassurance
• Frustration or distress about ongoing symptoms
Cognitive Patterns
• Catastrophic thinking (“This must be something life-threatening”)
• Hyper-focus on bodily sensations
• Difficulty accepting normal test results
Behavioral Patterns
• Frequent doctor visits or “doctor shopping”
• Repeated medical testing
• Excessive health research online
• Avoidance of activities for fear of worsening symptoms
Functional Impact
• Missed work or reduced productivity
• Strained relationships
• Emotional exhaustion
• Increased healthcare utilization
What Causes Somatic Symptom Disorder?
There is no single cause, but several contributing factors are common:
• Heightened sensitivity to physical sensations
• Past trauma or chronic stress
• Anxiety or depressive disorders
• Learned illness behaviors (growing up around illness)
• Difficulty identifying or expressing emotions
The brain and body are deeply connected. In SSD, the nervous system may amplify physical sensations, and the mind interprets them as dangerous — creating a cycle of distress and symptom worsening.
This is not intentional. It is a real and complex interaction between psychological and physical processes.
Common Misconceptions
“It’s all in their head.”
The symptoms are real. The condition reflects how the brain processes and amplifies physical experiences — and are not faked.
“They just want attention.”
Most individuals with SSD are seeking relief, not attention. Many feel embarrassed or misunderstood.
“If tests are normal, nothX X X
Please see THOUGHTS page 3
ing is wrong.”
Normal results rule out certain diseases but do not eliminate the very real experience of pain or discomfort.
“They should just stop thinking about it.”
The focus on symptoms is not easily controlled and often worsens without proper treatment.
Treatment
Somatic Symptom Disorder is treatable, especially with a coordinated approach.
Psychotherapy
• Cognitive Behavioral Therapy (CBT) helps individuals reframe unhelpful thoughts, reduce symptom-focused anxiety, and improve coping strategies
• Mindfulness-based therapies help reduce hyper-awareness of bodily sensations
Medical Management
• Establishing care with a consistent primary provider can reduce unnecessary testing
• Regular, scheduled visits rather than symptom-driven visits are helpful.
Medication
• Antidepressants may help reduce underlying anxiety or depression and improve symptom perception
Lifestyle and Support
• Stress reduction techniques
• Regular physical activity
• Sleep stabilization
• Psychoeducation for both patients and families
Prognosis
With treatment, many individuals experience reduced symptom distress, fewer medical visits, and improved daily functioning.
Recovery does not necessarily mean the complete absence of physical symptoms. Instead, it involves a healthier relationship with those symptoms — where they no longer dominate thoughts, behaviors, and quality of life.
Without treatment, SSD can become chronic, leading to ongoing distress and significant disruption in personal and professional life. Early recognition and compassionate care make a meaningful difference.

WHY DO I
SOMETIMES FEEL MORE TIRED AFTER A NAP?
It doesn’t make sense, does it? You felt sleepy or drowsy so you get some sleep, only to feel even more sleepy when you wake up. But then other times, a nap is completely refreshing. What gives?
Let’s start with quick lesson on how we sleep. There are various sleep stages or cycles that range from barely asleep to practically comatose. It can take 30 minutes or so to descend into the deepest stages of sleep. If a person is in that level of sleep and then the alarm goes off, the result can be fog, disorientation, irritability, and sluggishness.
Sleep experts often say the ideal nap is 20 to 30 minutes long, keeping the brain in lighter stages of sleep. Counterintuitively, perhaps, waking from shorter naps can mean feeling more alert and refreshed than a longer nap.
Understanding that the mind and body are not separate — but deeply interconnected — is key to both treatment and recovery.
About Us
IPS provides inpatient and outpatient mental health services, with or without a referral, to help patients and their families progress through the care journey. To make an appointment, call 706-204-1366 or visit integratedpsych.care.


But not always. Let’s say a person is chronically sleep-deprived. Because of that, their descent into deep sleep may happen quickly. For such a person, even waking up at the 20-minute mark might mean coming up from the deepest depths of sleep to a waiting nap hangover.
There are exceptions to the general shorter-is-better-andlonger-is-worse rule of napping. Naps in the 30 to 60 minute range are most likely to cause problems. Beyond that, say around 90 minutes, can allow a full sleep cycle. Waking up at the end of a cycle can avoid that abrupt and jarring deepsleep shock when an alarm goes off then.
Another factor that can help prevent post-nap grogginess is to cooperate with the body’s natural circadian rhythms. If the afternoon drowsies strike and you’re able, that’s the perfect time to take a short (or long) nap.
Waking up after a whole night of sleep and not feeling refreshed, just like a post-nap scenario, might be because our alarm clock and sleep cycles are not synchronized. Then again, perhaps sleep apnea or another factor might be robbing you of quality sleep. Talk to your doctor.
In the meantime, one of the quickest and simplest nap hangover remedies: splash water on your face. It helps.

Who is this?
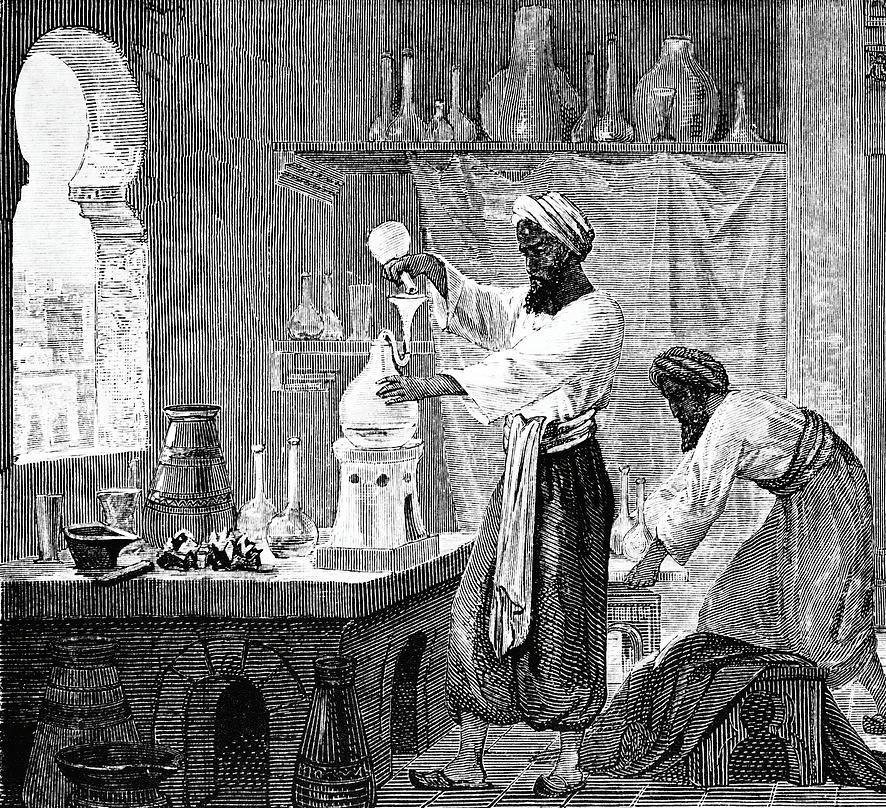
When the year of someone’s birth only has three numbers, it’s hard to find a good photograph of the person. So for the physician above, Muhammad ibn Zakariya al-Razi, we had to settle for an artist’s depiction of him at work.
Sometimes better known as Rhazes, Abu Bakr al-Razi, or just al-Razi, he was born in Persia (now Iran) around 865, and is considered to be one of the most important figures in the history of medicine. That’s saying a lot (and brings to mind the original idea for this column’s title: Important People You’ve Never Heard Of, which was rejected because plenty of people you have heard of would appear in this space).
Why is the work of a man who lived more than ten centuries ago still celebrated today? Among other things, al-Razi basically pioneered pediatrics. His monograph, The Diseases of Children, was the first to recognize its title subject as a distinct, independent field of medicine.
In addition, he was first the first doctor, at least in the Eastern or Persian world, to make medicine available to everyone through his exhaustive guide (36 chapters!) For One Who Has No Physician to Attend Him. He dedicated it to the poor, to travelers, and to ordinary people who could consult it to treat common ailments when a doctor was unavailable. Fittingly, he was said to be compassionate and devoted to the service of his patients, whether rich or poor, and he taught his many students to have the same approach.
A prolific writer and researcher, he also wrote The Comprehensive Book, a massive 20-volume compendium of the collected medical knowledge of Greek, Syrian, and early Arabic culture that anchored medical libraries for centuries.
al-Razi was a pioneer in the fields of pediatrics, obstetrics and ophthalmology, and in plain, simple, practical medical wisdom. In closing, a few of his core principles in his own words:
“A physician should not forget to ask his patient all sorts of questions pertaining to the possible causes of his illness, both internal and external. If a physician can treat a patient through nutrition rather than medicine he has done the best thing. Whoever seeks treatment with too many physicians might suffer the faults of each one of them.”

ADVENTURES IN
Middle Age
BY J.B. COLLUM
I’ve been thinking a lot about people and relationships lately.
As we age, relationships can end because of death. For the ones closest to us, it can feel like we’ve lost a limb—a part of ourselves. We may feel like moving on and continuing to live is somehow a betrayal, but the opposite is true. It would be a betrayal to give up on our lives and the relationships we still have.
We have to be adaptable.
It’s human to grieve. But when loved ones are gone, we have to shift our focus to the ones still here. We have to tend to those living relationships.
We tend to talk about relationships as if they’re fixed things—like a piece of furniture you assemble once and then just… have. But that’s not how they work. Relationships start, they evolve, they strain, they heal, and sometimes they end. They are living things, whether we admit it or not.
And one of the biggest factors shaping them?
Flaws.
Flaws are funny like that. Sometimes they drive people apart. Sometimes they pull people together. And sometimes—strangely enough—they do both at the same time.
If you think about it, flaws can even be comforting. There’s a certain relief in being around someone who shares your imperfections, or at least doesn’t make you feel like yours need to be hidden or fixed. Misery may not exactly love company, but it sure finds it familiar.
But here’s the part that really struck me.
If you try to glue two perfectly smooth, flawless surfaces together, it doesn’t work very well. There’s nothing for the glue to grab onto—no texture, no resistance. So what do you do? You rough them up a bit. You take sandpaper and scratch the surface just enough to give the glue something to hold.
Those tiny imperfections—the very things that make the surface less “perfect”—are what make the bond possible.
Relationships aren’t all that different.
Our flaws—those little scratches and rough edges—can actually give connection something to take hold of. They create places where understanding, patience, and even humor can settle in and do their work.
But—and this is important—the flaws alone aren’t enough.
You still need the glue.

Without it, those rough edges don’t bind anything together. They just grind against each other. And when that happens, instead of holding fast, they wear each other down.
I learned that lesson the hard way.
Several years ago, my parents moved in with us because of my father’s dementia. Up until then, my mother and I had always had a good relationship. Not perfect, but good.
Then life turned up the pressure.
We were suddenly two very flawed people in a very stressful situation, and there wasn’t much room for patience, grace, or understanding—the glue that might have held things together. Instead, we clashed. And when I say we clashed, I mean we had some real, honest-to-goodness doozies of arguments.
After my father passed away, things didn’t magically improve. If anything, the damage lingered. We were both grieving, both raw, and that’s not exactly the best condition for rebuilding anything.
Eventually, we found my mother a place of her own.
And something interesting happened. With a little space between us, the grinding stopped. The wounds had time to heal. The rough edges were still there—but they weren’t constantly scraping against each other anymore.
It didn’t take long.
Within a few months, I found myself missing her. I remembered how much I owed her—and how much I owed my father. Even without him telling me, I know what he would want me to do: take care of his “girlfriend,” as he always called her, my mother.
And what I came to understand is this: sometimes the healthiest version of a relationship isn’t the closest one.
Sometimes what holds people together best is a little space—just enough distance to let the glue do its job without constant friction breaking the bond apart.
We still have our flaws. That hasn’t changed.
But now, instead of grinding, the flaws give us something to hold onto.
And that, it turns out, is enough

J.B. Collum, the author of this column and Special Forces Parenting, is a local novelist, humorist and columnist who wants to be Mark Twain when he grows up. He may be reached at johnbcollum@gmail.com


Special Forces Parenting
When you have a special little one in your life—living in your home—you can’t afford to be too much in love with your furniture, your electronics, the walls, the carpet, or much of anything else, for that matter.
In a previous article, I estimated that she had probably done about $7,000 worth of damage in her first year with us. Thankfully, the rate of destruction has gone down, so the total isn’t now three times that earlier figure, as one might expect nearly three years later. Part of that is because she has stopped going after certain things—like remote controls— once she figured out we needed them to play her Disney movies. The other reason is that we simply haven’t replaced everything she has broken.
Our large dining room table originally came with eight very nice high-top chairs. We are now on our second full set. No, they don’t exactly match, but we decided not to invest too heavily in any more furniture until the coast is clear, so to speak.
The nice sofa and loveseat we bought back in 2016 have been peed on more times than the floor in a gas station bathroom. We’ve bought so much carpet cleaner and fabric cleaner that we probably deserve a vote at the shareholders’ meetings of the companies that make them. All of them.
When we finally do get around to replacing the carpet—which we are in no hurry to do, for obvious reasons—I shudder to think what we’ll find underneath it, despite our best efforts after so many turdnados. I imagine we’ll hire the job out and leave the country for a couple of weeks until they finish and the air fresheners have time to do their work. My Catholic cousin said we might need an exorcism—and that he “knew a guy”—but I politely told him no.
Things aren’t important in the grand scheme of things, but people are. And coping with the stress of children—especially special-needs children—while rewarding in many ways, is not without cost. In this case, I’m not talking about something with a dollar sign in front of it. Our bodies and our minds both pay the toll.
With Freyja, we have to be hyper-vigilant. Many times, Lorie is here at the house alone with her, and she has to keep her head on a swivel like an NFL quarterback playing behind a pee-wee league offensive line.
My wife, Lorie, and I recently took a week-
end away to Myrtle Beach. For this trip, I decided I would not insist on any of the things I usually like to do there. So, for the record, here is my perfect Myrtle Beach trip:
1. Lots of time sitting on the balcony, looking out at the ocean with a delicious ice-cold beverage in my hand—and an air-conditioned condo behind me with more cold drinks and a clean bathroom only steps away.
2. Mini golf.
3. The Player’s Choice retro arcade.
4. A swim in the ocean, if the weather allows. (It did not on this trip.)
5. A walk or two on the beach.
6. Eat at multiple great restaurants, mostly seafood. Sometimes with live music.
7. Walk around Barefoot Landing.
8. Visit Broadway at the Beach—maybe Ripley’s Aquarium, maybe Hard Rock Cafe, but definitely the Margaritaville Sand Bar. For Lorie, the perfect Myrtle Beach trip looks like this:
1. Spend about 80 percent of the daylight hours on the beach.
2. Eat great seafood at restaurants with really good live music—mostly country and classic rock—every single night.
3. Shop the outlet malls, mostly for clothes for the kids and grandkids.
4. Shop for clothes for me at Bass Pro Shop (although now that we have one in Augusta, this is optional).
As you can see, there isn’t a whole lot of overlap.
She did ask me what I wanted to do, and I threw out a small subset of my list. We ended up doing numbers 1, 5, and 6 from my list—and everything on hers. I knew she needed this.
So I didn’t insist on anything I wanted, and I didn’t push back on anything she wanted to do.
What I saw in her after the third night in a row of going to a restaurant with live music made me want to do that every night—despite the fact that loud, crowded places are like kryptonite to me. The smile on her face shone like a lighthouse. She kept telling me she was happy. Of course, a moderate amount of adult beverages helped too. Not me, though—I was the designated driver every night.
But the music was the real tonic.
She danced in her chair, and while I couldn’t quite get her to get up and dance, that was honestly just fine with me.
She opened up to me on that trip—about how she hasn’t been happy in a long time, and how hard it is for her to watch Freyja all by herself for long stretches. She does it anyway, because she loves her. But this trip revealed a lot.
It made my decision about sending our oldest granddaughter to live with her mother feel even more right. It gave me renewed resolve to find ways to lighten Lorie’s load— and to make sure her stressful work at home is punctuated by time away, time with live music, and time to breathe.
It also strengthened my resolve that we have to make a plan—one that allows us to
Please see SPECIAL FORCES page 7
Who is this?
Not everyone in healthcare can be Florence Nightingale, right? Despite the long-running series on page 4, there are clunkers in medicine, and we will examine some of them in this series. Unfortunately, there’s enough material to keep this side of the page going for a while.
The career of this man, Saul Krugman, is a curious one. Look up his name and bio from one source and you’re almost convinced that he could walk on water. Explore his history elsewhere and it feels like you’re reading about a Nazi-era doctor plying his craft at a concentration camp.

The concentration camp analogy is not a stretch by any means. Krugman worked at Willowbrook State School, a ghastly facility in New York built for 4,000 severely developmentally disabled children and adults that housed 6,000 such patients. Senator Robert F. Kennedy made an unannounced visit to Willowbrook in 1965 and described the “cells” where the patients were housed as “less comfortable and cheerful than the cages in which we put animals in a zoo.” He described the institution as a “snake pit.”
That snake pit was Krugman’s laboratory and patient pool. He was on a quest to develop a vaccine for hepatitis, a disease that had killed millions worldwide. At the time, little was known about the disease: back then it was called epidemic jaundice and no one knew there were multiple types. It was Krugman, in fact, who was the first to discover and distinguish between hepatitis A and hepatitis B.
How did he do it?
More than 50 mentally disabled children were deliberately infected with the virus, either through injections or by being fed feces from other infected children.
The program began in 1955 and continued until 1970.
Understandably, a profile about Krugman and his vaccine experiments in Forbes described the program as “hideous.” A report by the Alliance for Human Research Protection described the program as “despicable.” Maurice Hilleman, a medical pioneer featured in this newspaper over on page 4 several years ago called the Willowbrook studies “the most unethical medical experiments ever performed on children in the United States.” Geraldo Rivera aired an exposé in 1972 that prompted a ban on incarcerating “mentally retarded” children in large institutions. And that same year, Krugman became president of the American Pediatric Society. Go figure.
Krugman would answer critics by saying that his studies were sponsored by the Armed Forces Epidemiological Board, the Office of the U.S. Surgeon General, the U.S. Army, and approved by the New York State Department of Mental Hygiene.
Tell that to the kids who were forced to eat excrement to deliberately infect them with hepatitis.
TRAVELING? THINK VACCINES!
Part 3 of a series
by Rebecca Y. Kershner, MSN, WHNP-BC
Traveling to the four corners of the earth? Whether you set foot in Yap, Montserrat, Timbuktu, or worldwide ports in-between, you will want to make sure your vaccines are up-to-date.
When planning a vacation, most people think of packing the appropriate clothing and footwear for
ing, “Oh no, how will I figure all this out?” Don’t worry! We are here to help!
Destination #1: Travel Clinics
To aid travelers in navigating vaccine recommendations, several health departments in the CSRA have Travel Clinics. These clinics are designed to assist you in evaluating your travel plans, including layovers and other
Clinics can also offer routine vaccines if you need to catch-up on your immunizations.
How Soon Before Traveling Should I Get Vaccines?
As soon as a trip is being planned, you should be thinking about vaccines. A wise strategy is to allow 4-6 weeks. You’ll want to give your body plenty of time to build the antibodies or immunity needed to fight disease.


In most cases it takes about three weeks to get the full benefit.
Getting the appropriate vaccine(s) into your system as soon as you know you are traveling is the best strategy. The Health Department Travel Clinics are happy to assist at any stage of your travel planning.
Pack Your Bags
What should you bring to the Travel Clinic? To start off on the right foot, it is important to bring your travel itinerary which includes the countries you’ll be visiting, the dates

of your trip, and the kinds of activities you’ll be engaged in. Take your immunization records or vaccine history card, especially the yellow card so that the provider can learn what vaccines you’ve received and assess whether or not your vaccines are upto-date and what’s needed. Lastly, carry your list of medications and any documentation or a summary of your current health condition that may impact vaccine decision-making.
Currency Exchange
The initial visit to the Travel Clinic is $75 plus the cost of vaccines. Vaccine prices vary depending on which vaccines you’ll get. You’ll also be informed of any costs before you receive any vaccinations. Staff at the Travel Clinics do not typically bill insurance for travel vaccines as insurance companies will not cover vaccines specifically for travel. However, if you need a routine vaccine, even if it is part of the travel recommendation, insurance could be filed on your behalf. Tip: Before you go to the Travel Clinic, check with your health insurance company to deter-
Please see PUBLIC HEALTH page 9







TRYTHISDISH
by Kim Beavers, MS, RDN, CDCES
STEAK & POTATO SALAD
This recipe is great for dinner and then great again for lunch the next day! It is a perfect balance of steak and potatoes + veggies!
The Steak:
• 1 pound Flatiron steak
• 1 Tbs. Worcestershire sauce
• 1 tsp. cider vinegar
• 2 cloves minced garlic
• ½ tsp. coarse salt (kosher salt)
• ½ tsp. coarsely ground black pepper
Trim any extra fat from the flat iron steak and place it in a shallow baking dish. Combine the remaining ingredients in a small bowl and then rub over both sides of the steak.
Allow to marinate for at least 15 minutes. Meanwhile prepare salad and potatoes. To cook the steak, spray a grill pan with vegetable oil cooking spray or lightly oil grill grates of an outdoor grill. Grill steak over medium high heat for 6-8 minutes on each side until the desired degree of doneness has been achieved. Cover loosely with foil and allow meat to rest for 10 minutes. Slice steak across the grain into thin strips and serve on top of salad.
The Potatoes:
• 1 pound Yukon gold potatoes (about 4 medium)
• 1 large onion
• 1 Tbs. olive oil
• 1/8 tsp. coarse black pepper
• 1/8 tsp. coarse salt
• Vegetable oil cooking spray
Preheat the oven to 400°. Cut the potatoes into bite

size pieces (about 1/2 –inch cubes). Cut the onion into slightly larger pieces (onions will cook faster than the potatoes so they need to be cut larger).
Toss vegetables with oil, salt and pepper and place on an aluminum foil lined baking sheet that has been coated with cooking spray. Spread vegetables out single layer and spray the tops with vegetable oil cooking spray. Roast for 15 minutes, turn the vegetables and roast an additional 10 to 15 minutes until the potatoes are tender.
The Salad Base:
• 8 cups Romaine lettuce
• 2 cups quartered cherry
tomatoes
• ¼ cup light Caesar dressing.
Toss salad ingredients together in a bowl. Divide evenly among 4 plates. Top each salad evenly with potatoes and steak (about 1 cup potatoes, 3 ounces sliced steak).
Enjoy!

Yield: 4 servings.
Nutrition Breakdown: Calories 420, Fat 14g (4g saturated, 5g monounsaturated), Cholesterol 65mg, Sodium 530mg, Carbohydrates 35g, Fiber 5g, Protein 37g
Plate Plan: 1 Starch, 3 Vegetables, 4 Lean Meats
beefitswhatsfordinner.com

MEDICALEXAMINER
SPECIAL FORCES
... from page 5
care for Freyja while also giving ourselves a little distance a few days a week. We have some ideas. Now we need to turn those ideas into reality.
I’m not going to let anything stop me from seeing Lorie—my lifetime companion and favorite human—wear that beaming smile that shows not just on her lips and cheeks, but in her eyes.





... from page 1
have in society as a whole?
We all know the answer because we all see the effects every day.
Like seeing an adult go absolutely ballistic and destroy property and attack employees because they ordered large fries and their order had small fries.
Hopefully that’s something we as Examiner readers have seen only on social media posts and on TV.
But anyone whose job requires dealing with the public knows the following is true: a large Swedish study of people who work in retail found they scored worse than average on 32 of 33 indicators for stress, psychological well-being, and overall health.
What’s happening?
We know, we know: we already used that subheading in this article. So sue us! But that first time was about what’s happening in the world around us. This
subheading is introducing what’s happening to each of us on the inside.
Pop quiz: what is inci vility again? The nursing journal had some defini tions we cited on page one, but in the broader context we are talking about rude and crude behavior and disrespect and in all its many variations: belittling others, insulting them and their beliefs or preferences, all the way to physical assault.
care if we did.
The reason?
Like it or not, incivility is a bug, a germ. It’s contagious, and like a literal virus, exposure to it has consequences we can’t control and may not even realize.
For instance, someone who grew up in an era when respectable people didn’t say “hell” or “damn” in polite company might drop such words in conversation all the time now, even in front of their kids. Perhaps most of us wouldn’t even notice, or
Social scientists might call it behavioral contagion. When we see and hear rude and crude behavior — online, on TV, in person — over time it becomes normalized. It’s just the air we breathe. Over time, that normality increases the likelihood that we’ll copy it. The cancer spreads. Maybe in some cases it’s rather benign, but at other times it can be downright lethal. Hence terms like “copycat killer.”
The overall effect
Even for people not bothered in the slightest by the occasional “damn,” the overall trend in society toward more rude and crude conduct and speech is not healthful.
Lest we forget, the study referred to on page one found that 75% of all healthcare workers have experienced uncivil behavior from physicians. Creating that kind of work environment causes everything from low morale, burnout, and absenteeism to poor medical choices, adverse patient outcomes and even death. And we haven’t really even touched on the attendant stress and anxiety.
How sad and ironic that such symptoms should exist in the business of making people healthy, especially since it’s not from the sometimes life & death pressure of the job itself, but from the rude and crude actions
of fellow healthcare workers.
Our society’s lack of manners and civility generates stress and anxiety by the truckload. As unlikely as it might be, no one can be 100% sure that their minor traffic infraction might drive another motorist into a blind rage that ends up sending people to jail, to the hospital, or even to the morgue.
One article we read on this topic made the point that humans require a sense of social safety, whether that circle is the small group at work or the whole country.
When that safety starts to erode and disappear, good things like trust and cooperation fade, replaced by anxiety, depression, and social withdrawal.
It’s not remotely realistic to think the few thousand of us who read this little paper can make a difference by practicing civilized behavior.
But it’s worth a try
S I C K O F W A I T I N G ? S I C K O F W A I T I N G ?

PUBLIC HEALTH... from page 6
mine which vaccines may be covered and if the consultation is a covered benefit.
Travel Clinic Locations

Columbia, Emanuel, McDuffie, and Richmond County Health Departments all have Travel Clinics. Appointments and walk-ins are accepted. To ensure availability, you are encouraged to call the clinic beforehand. Visit the website www.ECPHD.com for more information about Travel Clinics and to learn about the many services public health has to offer.
Travel Health Notices
Keep in mind that the Centers for Disease Control & Prevention (CDC) issues Travel Health Notices (THN) for countries around the globe. THNs inform about health risks due to disease outbreaks, special events or gatherings, and natural disasters. The THN offers cautions and protective steps travelers can take to prevent getting infectious diseases or experiencing adverse health effects. Learn more about Travel Health Notices on the website: cdc.gov/travel/notices.
The CDC’s on-line Yellow Book offers health information for international travelers on a wide range of disease topics including vaccine requirements. The searchable Yellow Book also provides easy to navigate maps: cdc. gov/yellow-book/hcp/maps/index.html.
Happy trails. Bon voyage! Arrivederci!
About the author: Rebecca Y. Kershner, MSN, WHNP-BC, is the District Nursing Director for the East Central Health District 6.
The “What is Public Health?” Series is authored by public health experts at the Georgia Department of Public Health, East Central Health District (ECHD) with administrative offices in Augusta, GA. Learn more about the ECHD at our website: https://ecphd.com
Facebook www.facebook.com/ECPHD Twitter http://twitter.com/eastcentralph



EVERYTHING! EVERYTHING! WE FIX









CRASH COURSE

More Americans have died on US roads since 200 0 than in World Wars I & II combined
From the mid-column quote below and to the right, you might have surmised that this could be an article about motorcycle riding.
If so, you are correct. And what a perfect topic for right now: winter is behind us, Spring Break is here, and months of summer days and summer nights stretch off to the horizon. No wonder millions of people choose the motorcycle option, making this peak season for being a biker, whether hardcore or only occasionally.
As for that second line in the quote, did you take it as an insult directed toward bikers? If so, no such insult was intended.
However...
written knowledge, and road skills). Unfortunately, unlicensed operators are a big problem in both states. In Georgia, for instance, more than half of the bikers involved in a crash did not have a valid ClassM license.
Two wheels: optional Brains: ditto
There is a very real connection between motorcycles and brainless behavior. It’s the kind of conduct that gives the majority of bikers, the ones who are conscientious and safe, a bad name.
As we have noted in a couple of “Operation Zero” articles in past issues (discussing the contention that all or nearly all crashes are preventable), the term “accident” isn’t always accurate. An accident is defined as something that happens “by chance or without apparent or deliberate cause.” That simply does not apply to many collisions. Someone who is speeding, driving drunk, tailgating, etc., and winds up crashing was not in an accident, something “without apparent cause.” They were the cause of their own collision and the headaches that follow.
So how does this all relate to our topic, which is motorcycle safety?
Actually, not as much as you might think. But before we explain that statement, consider the avoidable factors in motorcycle crashes.
• Motorcyclists are twenty-eight times more likely to die per mile driven than car occupants.
• In South Carolina, nearly two-thirds of the riders who died in crashes were not wearing helmets.
• Alcohol was involved in 40% of all fatal motorcycle crashes in South Carolina.
• Motorcycles represent less than 1% of all vehicles on Georgia highways, yet 12% of all driver fatalities.
Both Georgia and South Carolina require a special license before someone can legally operate a motorcycle on the roads. They are called ClassM licenses, and they are issued in connection with various tests (like vision,
In South Carolina, the combination of tourism and the lack of a state helmet law are sometimes a deadly combination. Renting a bike in a cool beach town and being able to feel the wind in your hair while your neighbors back home are shoveling snow is a great experience — until it isn’t. (Note: there are sometimes different laws from one state to the next when it comes to mopeds.)
There is no question that riding a motorcycle is fun and even exhilarating, especially compared to riding in a car. But it is also undeniable that it’s massively more risky than car travel. When something happens, you don’t have a steel cage surrounding you for protection. And while car and truck occupants are expected to buckle up, no such protection is offered on a bike. It’s just hang on. That takes us back to our earlier statement that some aspects of safety — like most “accidents” aren’t really accidents — aren’t as fully relevant to motorcycles as they are to cars. Motorcyclists are much more vulnerable than “cagers” to all kinds of outside factors beyond their control that limit their ability to avoid a collision, and which make the consequences of such collisions worse.
When you’re in a car going through an intersection and someone turns left right in front of you, you slam on the brakes. If a collision happens, you’re protected by a ton of steel surrounding you, kept in place by a harness system, and protected from impact by airbags.
If the same thing happens to a motorcycle rider, he can be seriously injured by the actions he takes to successfully avoid the collision. And if he can’t avoid the crash, the consequences can be extremely dire.
Maybe that’s the other application of the “brains optional” quote above. A biker can do everything right and still be taken out by a brainless, or even just careless, motor vehicle operator.
If you’re traveling on two wheels this summer. please be careful. And please look out for drivers of cars and trucks who aren’t looking out for you.

your most appropriate, clever, or funny caption to the photo shown for a chance to win whatever cool swag we decide to give away someday.










Hey, what’s up? You mean from like 15 years ago?

Wait. What did you ask me again? Huh? All I said was hey, what’s up?

ACROSS
1. Easy stride
5. Short note
9. Breath sounds
14. Part of the eye
15. Saharan
16. Late film critic
17. Almost tailless rodent
18. Home of a noted medical school
19. Robust (Scottish)
20. 1969 bestseller (ending with “-Five”)
23. Character in The Matrix
24. Bottom-row key
25. His donkey spoke
29. A woman, in old movies
31. Just a little drink
34. Unwraps
35. Alpha follower
36. Main ingredient in some casseroles
37. Eye specialist
40. Swing around
41. Threaten, as a crisis
42. Locations
43. Lead-in for 56-D
44. Macon county
45. 2-point football play
46. Tavern
47. There’s a big one in Columbia County
48. Mathematical operation
56. Augusta ________
57. A month of the Jewish calendar
58. Sports award
59. Bladder liquid
60. Sea eagle
61. On the sheltered side
62. Noted apostle
63. No longer living
Monthly expense
1. They can be cyanotic
2. Spoken; verbal
3. Size of type
4. Jacob’s twin
5. He’s in Allstate commercials
6. Muse of lyric poetry
7. 1,760 yards
8. River in central Europe
9. A job for Hakky
10. Approximately 11. Optical device
12. Scottish Gaelic 13. Pigpen
21. Grind teeth together
22. Brightest star in the Aries constellation
25. Uplift
26. Singer Fiona
27. Tiny island west of Kauai
28. Poker stake
29. Send troops home at war’s end (in brief)
30. It comes from a Greek word meaning indivisible
Use the letters
at
by Dan Pearson
Ok, right, yeah. It was a movie in 2009 about an old man, a kid, and a house that flies using balloons.

CAPTION THIS
Check out our new reader contest on p. 10 Write your most appropriate, clever, or funny caption to the photo shown for a chance to win whatever cool swag we eventually decide to give away! Email your entry to Dan@AugustaRx.com
DEADLINE TO ENTER: 5:00 PM FRIDAY, APRIL 10, 2026 Have fun!
31. Connected series of rooms
32. A map within a map
33. Nashville’s Cline
35. Early Steve McQueen movie (with The)
36. Week-ending abbreviation
38. Person used as one’s excuse
39. He founded al-Qaeda
44. Local high school
45. _______ Heart
46. Flying vehicle
47. Princess of Wales, 1981-1996
48. Female horse
49. Single entity
50. Piper adjective
51. Small harplike stringed instrument
52. It can precede gas
53. Small piece of land surrounded by water
54. Nasty type of fracture
55. No to Boris
56. It often follows 43-A
to create words to
the
DIRECTIONS: Every line, vertical and horizontal, and all nine 9-square boxes must each contain the numbers 1 though 9. Solution on page 14.
DIRECTIONS: Recreate a timeless nugget of wisdom by using the letters in each vertical column to fill the boxes above them. Once any letter is used, cross it out in the lower half of the puzzle. Letters may be used only once. Black squares indicate spaces between words, and words may extend onto a second line.
on page 14.
All the listed letters following #1 are the first letters of the various words; the letters following #2 are the second letters of each word, and so on. Try solving words with letter clues or numbers with minimal choices listed. A sample is shown. Solution on page 14


ATHEBESTMEDICINE
ha... ha...
Texan lands in London one evening and takes a cab to his hotel. On the way they pass an impressive building that he asks the driver about.
“That’s Westminster Abbey,” says the cabbie. “Started in 1245 and finished in 1745.”
“Good lord! Back home we could build a place like that in a year,” boasts the Texan. A short time later they pass another grand structure. “What’s that building?”
“That’s what is known as Parliament,” said the cab driver. “Started in 1840 — and you’ll be happy to hear — completed by 1870.”
“In Texas we could have built that in a month!” said the Texan dismissively.
As they drive on, Buckingham Palace comes into view. “What about that one?”
The driver gazes over to where the Texan is pointing, pauses, then says, “I have no idea. It wasn’t there this morning.”
Diner: Waiter, my soup is cold.
Waiter: It’s gazpacho, sir.
Diner: Okay, gazpacho. My soup is cold.
Moe: A person can be vegan without having to tell everyone.
Joe: Not from my experience.
Moe: Dude, I’m living proof. I’m vegan and the only ones who know are my boss and coworkers, neighbors, friends, relatives, and just a few random others here and there.
Moe: I wonder if fish can fall in love.
Joe: That’s beyond weird, but no, fish cannot fall in love.
Moe: What makes you so sure?
Joe: Love is in the air, Einstein.
Moe: So what’s it like being married to a school teacher?
Joe: Very challenging at times.
Moe: Like how?
Joe: Like the other day I came home from work and before I was even halfway through the door she yelled, “You need to do more chores around the house!”
I was exhausted, so all I said was, “Can we please change the subject?” She said, “Sure. More chores around the house need to be done by you.”
Moe: Just when you think vegetables can’t use phones...
Joe: Onion rings.
Moe: I know, right?
Because try as they might, no one can stare at their phone all day. Why subscribe to the

MEDICALEXAMINER?
Staring at my phone all day has certainly had no fffect on ME!

By popular demand we’re making at-cost subscriptions available for the convenience of our readers. If you live beyond the Aiken-Augusta area, or miss issues between doctor’s appointments — don’t you hate it when that happens? — we’ll command your mail carrier to bring every issue to your house!
NAME
ADDRESS
CITY STATE ZIP
Choose six months for $26 ____ or one year for $48 . Mail this completed form with payment to Augusta Medical Examiner, PO Box 397, Augusta GA 30903- 0397

Advice Doctor

Dear Advice Doctor,
I was at a March Madness game last week that was back and forth the entire game. The score must have been tied 50 times. It was a true nail-biter that was literally decided with 2 seconds left on the clock. The crowd noise was off the charts! I realized just how loud it had been when we got outside afterward. Everything was so quiet! I couldn’t hear a thing, and my ears were still ringing when I went to bed hours later. What should I have done differently?
— Playing It By Ear
Dear Playing,
I am always grateful when a reader brings up a personal experience or question whose answer can benefit many others, and that certainly applies here.
In fact, nail biting is one of the most common body-focused compulsive behaviors. Nearly half of all teenagers are nailbiters, making that the peak age for the habit. Estimates are that 20-30% of the general population bite their nails regularly (even when they aren’t attending a tense March Madness game). It may be common but it’s not healthful.
If the pandemic brought one fact to the fore, it is the ease with which bacteria can travel through populations. Each of us probably went through 5 gallons of hand sanitizer a month. Why? Because our hands are one of the main ways bacteria are transmitted from surface to person and person to person. Do we really want to repeatedly put our fingers in our mouth? This habit greatly increases the risk of colds, flu, and worse (like COVID, and even salmonella).
Chronic nail biters also frequently experience infections of the nail bed, and the habit can damage the nail matrix, leading to permanent waves or ridges in the nails as they grow out. The damage nail biting can cause also paves the way for fungal infections, which can result in thickened, yellow, or brittle nails.
And if all of that isn’t enough, some people actually end up with chipped teeth and jaw soreness from chronic nail biting.
I’m glad you enjoyed the game. But please: no nail biting!
I hope this answers your question. Thanks for writing!
Do you have a question for The Advice Doctor about health, life, love, personal relationships, career, raising children, or any other important topic? Send it to Dan@AugustaRx.com. Replies will be provided only in the Examiner.


1.
2.
3.
WORDS
BY NUMBER
An idea isn’t responsible for the people who believe it. — Don Marquis

PROFESSIONAL DIRECTORY
ACUPUNCTURE
Dr. Eric Sherrell, DACM, LAC Augusta Acupuncture Clinic 4141 Columbia Road 706-888-0707 www.AcuClinicGA.com
CHIROPRACTIC

DERMATOLOGY
Evans Chiropractic Health Center

Dr. William M. Rice 108 SRP Drive, Suite A 706-860-4001 www.evanschiro.net

DENTISTRY
Jason H. Lee, DMD 116 Davis Road Augusta 30907
706-860-4048 Floss ‘em or lose ‘em!


Georgia Dermatology & Skin Cancer Center 2283 Wrightsboro Rd. (at Johns Road) Augusta 30904 706-733-3373 www.GaDerm.com


DEVELOPMENTAL PEDIATRICS
Karen L. Carter, MD 1303 D’Antignac St, Suite 2100 Augusta 30901
706-396-0600 www.augustadevelopmentalspecialists.com

Steppingstones to Recovery 2610 Commons Blvd. Augusta 30909 706-733-1935



Home Care Personal Care|Skilled Nursing|Companion 706-426-5967 www.zenahomecare.com

Parks Pharmacy 437 Georgia Ave. N. Augusta 29841 803-279-7450 www.parkspharmacy.com PHARMACY









study
A clinical research study for people who have or are at risk for heart disease or stroke and have high Lp(a) levels

MOVE-Lp(a) is a clinical research study from Eli Lilly and Company. The MOVE-Lp(a) study will test if an investigational medicine safely lowers Lp(a) levels and reduces the risk for heart disease or stroke.
Can I join the study?
Yes, you may be able to join the study if you:
• are at least 18 years of age
• have a high level of Lp(a) in your blood
• already have heart disease or have had a stroke or are at risk for a first heart attack or stroke
information visit https://e.lilly/3FddF4u or scan the QR code

Lipoprotein(a) is also known as Lp(a). Lp(a) is an important risk factor for heart disease and is largely determined by your genes.
Lp(a) carries cholesterol (a type of fat) in the blood. If you have a high level of Lp(a), you may have a higher risk for heart disease or stroke. You may have a high level of Lp(a) even if you have a healthy lifestyle or are taking other medicine for your cholesterol.

CALL
Masters of Clinical Research 1232 Augusta West Parkway Augusta, GA 30909 Tel: (706) 210-8890