FINANCIAL & OPERATIONAL CONTROLLING FROM FINANCIAL PLANNING TO EXECUTION

HOW TO IMPROVE FINANCIAL RESULT AND CARE FOR PATIENT AND HOW TO MANAGE COST IN HEALTHCARE

HOW TO IMPROVE FINANCIAL RESULT AND CARE FOR PATIENT AND HOW TO MANAGE COST IN HEALTHCARE

Leading Central and Eastern Europe private equity fund
Acquired:
Investment: 2007
Business / Middle market brand
Second largest private healthcare provider in Poland
280k subscribers/patients 15 own clinics
Investment: 2007
Economy market brand
Largest private company servicing NHF contracts
350k subscribers/patients 18 own clinics

Leading Central and Eastern Europe private equity fund
Acquired:

Investment: 2008 Premium brand
Third largest private healthcare provider in Poland
230k subscribers/patients 15 own clinics
Investment: 2008 Economy market brand
Good quality, affordable price, operating in South-Western Poland
70k subscribers/patients 10 own clinics


• 94 own clinics
• Ca 1.400 subcontractors across Poland
• More than 1 million subscribers/patients
• 7.5 million medical procedures per year
• More than 3 thousands doctors CURRENTLY





• Four different General Ledger systems
• Different controlling philosophies
• One common controlling system – MS Excel TO BE TRANSFERRED INTO
• One General Ledger and Chart of Accounts
• One controlling philosophy
• One controlling system – dedicated software / not MS Excel
• Developed controlling functions
• From Financial Reporting to Operational and Medical Controlling
FINANCIAL Controlling via dedicated software
‚Stone Age’ controlling history
• MS Excel files
• MS Outlook distribution
• limited understanding what's behind figures

• MS Excel acting as controlling system
• Almost manual preparation of P&L reporting to all Budget Holders, The Board and Investors
• Controlling focused on proper preparation of files and integrity of data
• Limited understanding of what is the story behind figures since only high level KPIs available
• Minimum OPERATIONAL Controlling functions
• Web based system – allowing user to access profiled data and drill them down to singe booking level
• Auto download of data from General Ledger System
• Focusing on understanding the data instead of checking their integrity
• Linking financial data with basic KPIs and analyzing their variances and impact on financials
• Financial controlling and Operational controlling using one, common, joint and synchronized tool acting as ‚single source of data’
• Operational data allowing deep understanding of financials
• THROUGH the SET OF KPIs WE DO UNDERSTAND WHY OUR FINANCIALS ARE IN THE WAY THEY ARE
• Deep understanding of Operational KPIs
• History of data allowing to predict what will happen in the near future
• Active management via operational stimulation
• WE ARE TRYING TO CHANGE THE FINANCIALS BY MANAGING KPIs
• Auto screening of doctor activities and analysis of medical records
• While individual check if the activities are coherent with internationally accepted standards – if we are acting safely for patient
• Standarization of medical process, doctors profiles
Operational
Operation („Production”)
Medical („Technology”)
Managing process efficiency and productivity, managing clinic itself
Chief Operational Director
Operational and financial data
Managing medical processes
Chief Medical Director
Medical history, operational data
Company and client profitability
Chief
Director Financial data
Unit cost, utilization
Return rate, referral rate
P&L and clients profitability
Forecasted utilization depending on number of clients
Frequency ratio
Accessibility, Doctor utilization, Room utilization, Doctor Balanced Score Card
No show, Return rate, Free slots, Referral rate, Inherit rate
Medical costs, Clinic cost
Doctor cost
Referrals costs
Products profitability Services profitability Client profitability
Mystery shopper
Profitable medical company … Is it ethical? Is medical company ethically entitled to bring the profit to the owner? … Is it required?
What makes medical procedure different than any other good or service sold on market? … Is visit in a clinics different than at beautician?
Higher quality = higher costs = lower profits ?
Better accessibility = high medical wages
Better parking and site = high rental
Better equipment = higher CapEx and Depreciation
Better personnel = higher training costs = higher extra profits
Is this the only way ? NO, WHAT ABOUT NO-SHOW
When patient comes back?
How often patient comes back?
How to diminish visit’s frequency?
Have patient received referral?
Does patient come to doctor (no show)?
When patient wants to come to doctor?
Should patient come to doctor?
How patient books a visit?
Medical standards and patient healthcare have superior role
over: Financial, Operational and Medical Controlling
‚Client First’ doctrine have an extra meaning in healthcare
Lux Med employs more than 3k doctors. Only individual doctor management is a successful healthcare process. Therefore Lux Med developed physician scorecard which shows individual doctor performance indicators:
Number of services, number of working hours, unit cost, remuneration, return rate, utilization ration, referral rate, now show, fee for service
Today we will talk about three PI:
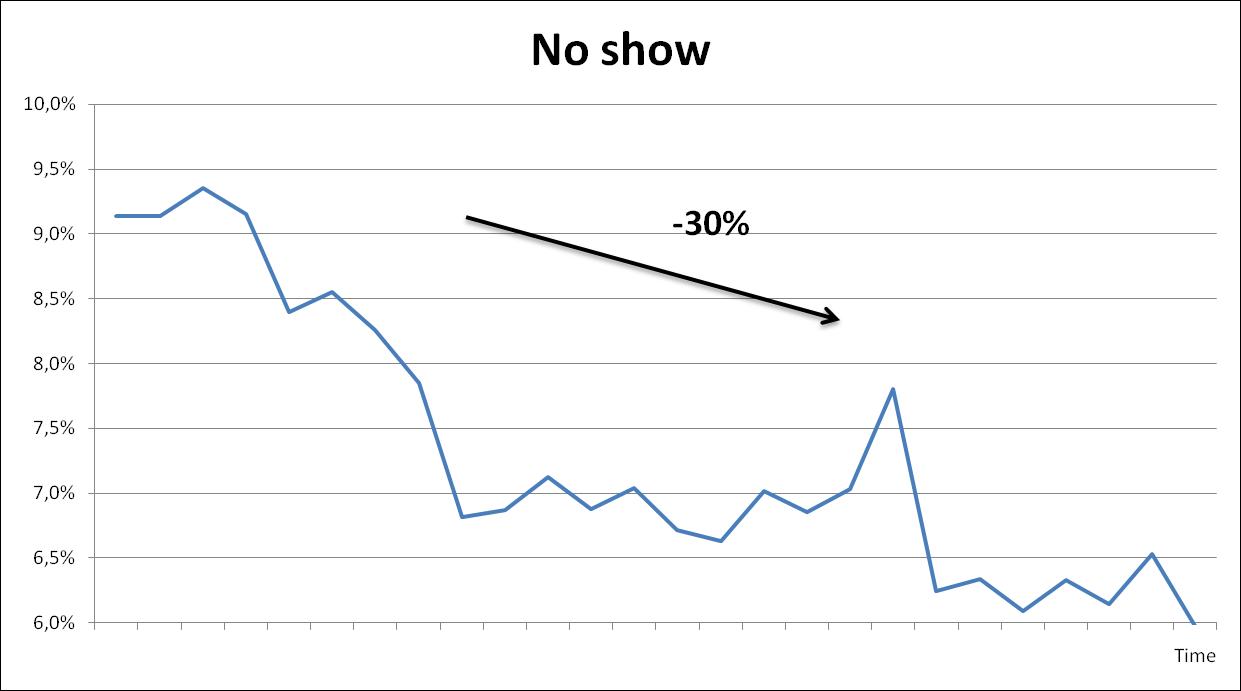
• No show
• Frequency ratio
• Unit cost
No show rate=
Action
Number of consultations when patient did not come
Number of consultations when patient did not come +
Number of consultations executed
• Enabling patient to easily cancel visit via SMS, telephone, email, www
• Informing patient about visit in advance by SMS, mail. Confirming most fragile specialization by phone
• Sending SMS to patient which has not canceled visit to„do it next time”
• Audit of physicians‘ schedules which show area where time is wasted (e.g.: age limit, blockades, doctors’ delays, schedules duplication)
• Introduction of payment for no show visits when rate is very high
• Co-payment product where client pay smaller amount per month and small addition at every visit. Patients do not come to a doctor when it’s not necessary
• Reviewing slot time – checking when doctor utilization (number of visits per working hour) is small and patient safety allows
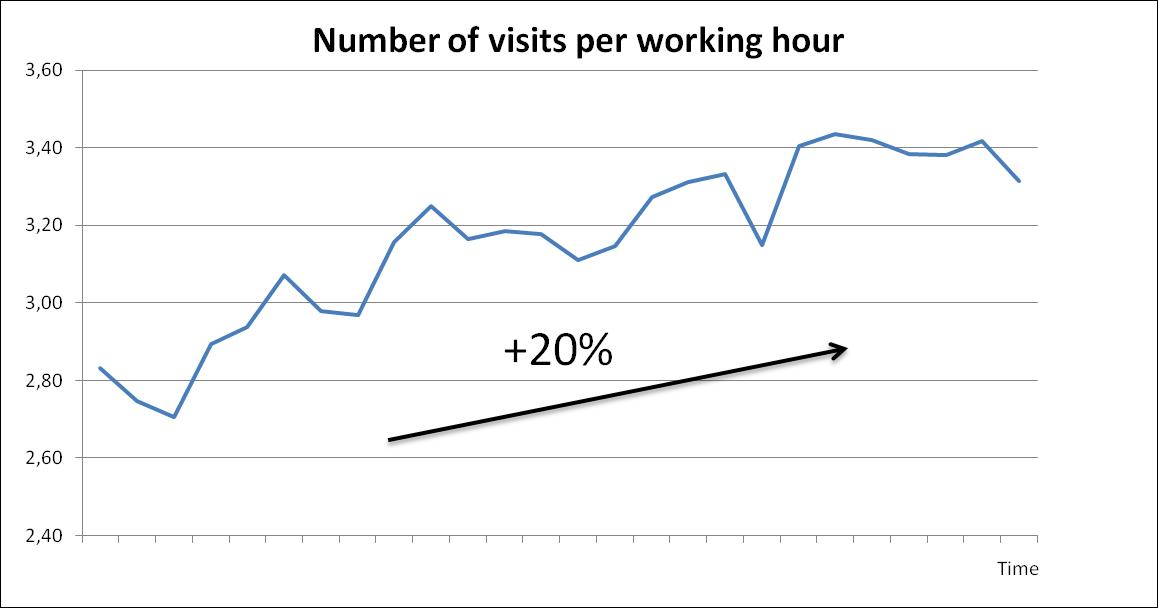
Frequency ratio=
Number of consultations
Number of patients
Actions
• Selection of patient with highest frequency and offering them individual health care scheme
• Introduction of doctors emergency where doctor admit patient without booked visit. It is especially important in pediatric and internist
• Offering slots in time most convenient to patient but not offering when it is not medically justified e.g.: you cannot book visit 2 months ahead, you cannot book 3 visits of the same type
• Estimation of demand for doctors working hours / slots and adjusting supply of slots to predicted demand so that patient can book visit in agreed time (standard) but we do not have doctors which waits for patient
• Variable salary – introduction of physician salary where doctor is remunerated base on number of executed procedures


Operation
s
Accessibility of services
Salary schemes
Medical
Finance
Return control
Referral control
Profitability control
Sales
Co-payment
Exclusions
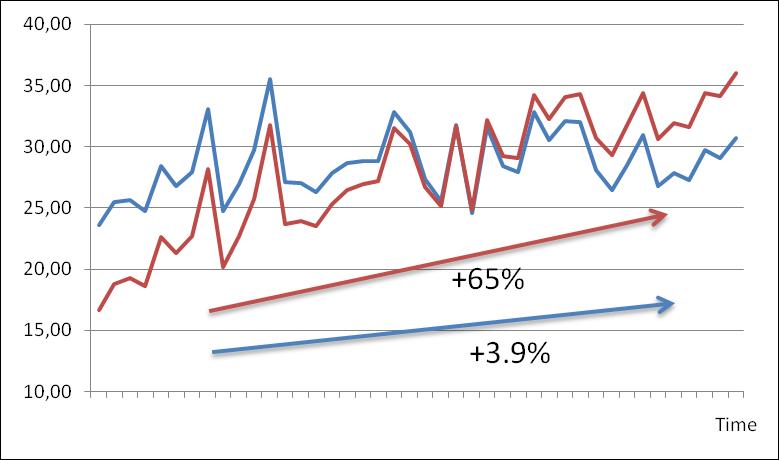
● During last 5 years medical salaries increased to cover gap on salaries between Polish and EU CAGR inflation amounting to 17%
● Moderate growth in ARPU
● Change from salary per hour to hybrid model (now FTEs have 68% salary somehow variable)
● Improvement on schedule management: (moving blockades, no show management, standardization and adjustment of slots time)
● Flexible management of working hours for off peak seasons