
the Bionic Man (Second Edition) George K. Hung
Visit to download the full and correct content document: https://ebookmeta.com/product/biomedical-engineering-principles-of-the-bionic-man-s econd-edition-george-k-hung/

of
More products digital (pdf, epub, mobi) instant download maybe you interests ...
Biomedical Device Technology Principles and Design 3rd
Edition Anthony Y K Chan
https://ebookmeta.com/product/biomedical-device-technologyprinciples-and-design-3rd-edition-anthony-y-k-chan/
Biomedical Engineering 1st Edition
https://ebookmeta.com/product/biomedical-engineering-1st-edition/
Food Engineering: Principles and Practices 1st Edition
Sanjaya K. Dash
https://ebookmeta.com/product/food-engineering-principles-andpractices-1st-edition-sanjaya-k-dash/
Multiscale Modelling in Biomedical Engineering (IEEE Press Series on Biomedical Engineering) 1st Edition
Antonis I. Sakellarios
https://ebookmeta.com/product/multiscale-modelling-in-biomedicalengineering-ieee-press-series-on-biomedical-engineering-1stedition-antonis-i-sakellarios/
Principles of Cell Biology Third Edition George Plopper
https://ebookmeta.com/product/principles-of-cell-biology-thirdedition-george-plopper/
Principles of Logo Design 1st Edition George Bokhua
https://ebookmeta.com/product/principles-of-logo-design-1stedition-george-bokhua/
Biomedical Engineering Design 1st Edition Jospeh
Tranquillo
https://ebookmeta.com/product/biomedical-engineering-design-1stedition-jospeh-tranquillo/
Man and Superman George Bernard Shaw
https://ebookmeta.com/product/man-and-superman-george-bernardshaw/
Smolder Anita Blake Vampire Hunter 29 Laurell K
Hamilton
https://ebookmeta.com/product/smolder-anita-blake-vampirehunter-29-laurell-k-hamilton/
SERIES ON BIOENGINEERING AND BIOMEDICAL ENGINEERING
Series Editor: John K-J Li (Department of Biomedical Engineering, Rutgers University, USA)
The aims of the book series are to present a publishing forum for established researchers, educators and professionals in the field of bioengineering and biomedical engineering to promote in-depth documentation of new scientific findings, technological advances, and to provide effective teaching tools of the fundamental aspects of the field. Single or multiple authored or edited books, research monographs, textbooks, lab manuals and specialized conference proceedings are welcome. Topics of interest include biosensors, biomedical devices and instrumentation, physiological modeling and signal processing, medical imaging, drug delivery systems, clinical monitoring, tissue engineering, systems biology and bioinformatics, biomechanics and biomaterials, rehabilitation and prostheses, nano and micro applications to biomedicine, biomedical optics, biofluid mechanics, artificial organs and assist devices.
Published
Vol. 10 Biomedical Engineering Principles of the Bionic Man Second Edition by George K Hung (Rutgers University, USA)
Vol. 9: Dynamics of the Vascular System: Interaction with the Heart Second Edition by John K-J Li (Rutgers University, USA)
Vol. 8: Neuroprosthetics: Theory and Practice Second Edition
edited by Kenneth Horch (University of Utah, USA) and Daryl Kipke (University of Utah, USA)
Vol. 7: Further Understanding of the Human Machine: The Road to Bioengineering edited by Max E Valentinuzzi (National Scientific and Technical Research Council (CONICET), Argentina)
Vol. 6: Cardiac Fibrillation-Defibrillation: Clinical and Engineering Aspects by Max E Valentinuzzi (University of Buenos Aires, Argentina & University of Tucumán, Argentina)
For the complete list of volumes in this series, please visit www.worldscientific.com/series/sbbe

Published by
World Scientific Publishing Co. Pte. Ltd.
5 Toh Tuck Link, Singapore 596224
USA office: 27 Warren Street, Suite 401-402, Hackensack, NJ 07601
UK office: 57 Shelton Street, Covent Garden, London WC2H 9HE
Library of Congress Cataloging-in-Publication Data
Names: Hung, George K., editor.
Title: Biomedical engineering principles of the bionic man / [edited by] George K. Hung, Rutgers University, USA.
Description: Second edition. | New Jersey : World Scientific, [2023] | Series: Series on bioengineering and biomedical engineering, 2010-2909 ; vol. 10 | Includes bibliographical references and index.
Identifiers: LCCN 2022028858 | ISBN 9789811259180 (hardcover) | ISBN 9789811259197 (ebook for institutions) | ISBN 9789811259203 (ebook for individuals)
Subjects: LCSH: Prosthesis. | Biomedical engineering. | Gene therapy. | Tissue engineering.
Classification: LCC RD130 .B565 2023 | DDC 617.9--dc23/eng/20221005
LC record available at https://lccn.loc.gov/2022028858
British Library Cataloguing-in-Publication Data
A catalogue record for this book is available from the British Library.
Copyright © 2023 by World Scientific Publishing Co. Pte. Ltd.
All rights reserved. This book, or parts thereof, may not be reproduced in any form or by any means, electronic or mechanical, including photocopying, recording or any information storage and retrieval system now known or to be invented, without written permission from the publisher.
For photocopying of material in this volume, please pay a copying fee through the Copyright Clearance Center, Inc., 222 Rosewood Drive, Danvers, MA 01923, USA. In this case permission to photocopy is not required from the publisher.
For any available supplementary material, please visit https://www.worldscientific.com/worldscibooks/10.1142/12914#t=suppl
Desk Editors: Nimal Koliyat/Steven Patt
Typeset by Stallion Press
Email: enquiries@stallionpress.com
Printed in Singapore
Tomycloseandlong-timegolfingfriend,MortReinhart,whose numerousmedicalproceduresinspiredthisbookonthebionicman. Hismedicalproceduresincludedintraocularlensimplantsfor cataracts,monovisioncorrection,quadrupleheartbypass, radioactiveseedimplanttreatmentforprostatecancer,andknee surgery.
This page intentionally left blank
c 2023WorldScientificPublishingCompany
https://doi.org/10.1142/9789811259197 fmatter
Foreword
Theinspirationforthisbookismyfather,MortReinhart,whoalso happenstobethegolfpartnerofDr.GeorgeHung,thisbook’s editor.At88,myfatherisstillabletomoveaboutevenwithmultiplereplaced,repaired,andrejuvenatedbodyparts.Hehasocular implants,akneereplacement,andundergonecardiacbypasssurgery; Georgekiddinglyreferstohimas“thebionicman”.
Tomeasanorthopedicsurgeon,myfatherseemstobeafairly typicalpatientwhohasbenefitedgreatlyfromthewonderfulbiomedicaldevicesandtechniqueswidelyutilizedinmanyareasofmedicine. Thistextbookdescribessomeofthesedevicesandconveysasense ofexcitementabouttheopportunityforfurtheradvancesasnew technologiesemergeinBiomedicalEngineering.
GolferslikemyfatherandDr.Hungoftenlooktoinnovations inequipmentdesignandmaterialstoimprovetheirperformance. Thesameprocessworksinmedicinewherephysicians,patients, andresearchershopeforimprovedpersonal“performance”through advancesintechnology.However,whereasingolftheideaisto improvetheexternalequipment,inmedicinetheideaistoimprove theinternalattributesoftheplayer.
Newtechnologyaloneisnotsufficienttodriveinnovationin medicine.Theotherfactorwhichcontinuestopushinnovationis theincreasinglyhighdemandsandexpectationsofpatients.Many individualswithavarietyofmedicalconditionsexpectthattheir problemscanbeaddressedsothattheycancontinuetopursueallof theiractivitiesatahighlevelandoverincreasinglyextendedperiods oftime.Moreandmorethefocusinhelpingpatientisnotsimplyin relievingsymptomsbutintrulyrestoringnear-normalfunction.
vii
This2ndeditionbookpresentsafabulousandfascinatingarray oftechnologieswhicharealreadywelldevelopedorarecurrently underdevelopment.Advancesinmaterials,design,electronics,and biologictechniquesallhavethepotentialtoenablepatientstosense theworldaroundthemandmovethroughtheirdailyactivitieswith greaterenjoymentandease.
InmyspecialtyofOrthopedics,thetraditionalfocushasbeenon repairingorreplacingbrokenpartswithvariousmechanicaldevices. However,inOrthopedicsaswellasinmanyothermedicalspecialtiesasdescribedinthisbook,thefocusisbroadeningfromsimple mechanicalsolutionstobiologicalsolutionsaswell.Variousbiomedicaltechniquesaredescribedthataugmentorassistnormalstructures,thatmonitorandcorrectabnormalconditionsonaninstantaneousbasis,andthatcanstimulateorsubstituteforimpairedbodily symptoms.Thenewfrontiersinbiology,includingtissueengineeringandgenetherapy,offeropportunitiestoregenerateorrecreate healthiersystemsaswell.
Theconceptofa“bionicman”mayonthesurfaceseemtoimply amechanicalorroboticcondition.However,withthesenewtechniques,abionicmanisactuallyacombinationofenhancednatural functionsaswellassubstituteorartificialparts.Thisnewbionicman isactuallymorehumaninthathehasagreaterabilitytoenjoylife notonlyinhisrequiredday-to-dayactivitiesbutalsointhedesired activitieswhichbringhimpleasure.
Thisbookpresentsstudentswithbasicscientificprinciplesand hopefullyalsoprovidestheinspirationtopursuenewandcreative ideasandvisionarythinkingabouthowtocontinuetoimprovethis bionicman.
GlennReinhart,M.D.FreibergOrthopedic&SportsPH:(513)221-55009825
KenwoodRdSte200FX:(513)221-1962 Cincinnati,OH45242EM:gareinhart@zoomtown.com
Dr.Reinhartisaspecialistinsportsmedicineandshouldersurgery andisamemberoftheAmericanAcademyofOrthopedicSurgeons andtheArthroscopyAssociationofNorthAmerica.Hecurrently
viii Foreword
servesasthemedicaldirectoroftheKenwoodSurgeryCenterand hasprovidedcareasaphysicianfornumeroushighschools,collegiate,andprofessionalteams.Inaddition,hehasaspecialinterest inpediatricorthopedicsandshoulderreconstruction.
Foreword ix
This page intentionally left blank
c 2023WorldScientificPublishingCompany
https://doi.org/10.1142/9789811259197 fmatter
Preface
Agingisasinevitableasthechangeofseasons,fromspringtosummer andthenwintertofall.Asweage,mobility,strength,andstamina alldecline.Thesearetheclassicsignsofaging.Theagingprocess iswritteninourgenes.Asthetelomerelengthrecedes,therateof celldivisiondeclines,andthefabricofourbonesandskinlosetheir resilience,leadingtothelossinvitality.
Yet,remarkableprogresshasbeenmadeintheunderstanding oftheagingprocessandinturnhowtoslowitsprogress.Avitally importantarsenalinanti-agingistheminimizationofoxidation,or rusting,ofthebody.Freeradicalsthatresultfromoxidationcan interferewiththenaturalrepairprocessinthecells,leadingtogenetic damagethatincreasestherateofaging.Propernutritionandexercise playsignificantrolesinslowingtheeffectsofaging.Nutrientswith antioxidantpropertiesactatthemicroscopicleveltocounteractthe damagingeffectsoffreeradicalsandinturnmaintaintheintegrityof thestructureofthecellsinthebody.Exerciseactsatthemacroscopic leveltostrengthenmuscles,joints,andbonesaswellasincreasethe functionsofthecardiovascular,respiratory,andhormonalsystems tobettercounteractthephysicalandemotionalstressesofdailylife. Nevertheless,thereisonlysomuchnutritionandexercisecando tostemthetideofaging.Eventually,somebodypartswillbegin tobreakdownovertime.Thebabyboomers,whohavedominated thesocial,economic,andpoliticaldemographicsofthepopulation overthelasthalfcentury,willnowdominatethesearchforelixirs andremediestoholdbacktheravagesoftimeastheyageand theirbodypartsbegintomalfunction.Repairorreplacementofthe bodypartsprovidesameansinasensetoreversetheagingprocess.
xi
xii Preface
Biomedicalengineershavebuiltcomponentsordevicestoassistand revitalizetheaginghumanbody.Indeed,itisnownottooextraordinarytofindseniorpersonswhohavehadsurgeryforcataract, monovision,Lasik,heartbypass,hip,knee,and/orcochlearimplants. Thus,thematuringofthebabyboomersalsoheraldstheageofthe bionicman,whoisliterallycomposedofvariousreplacementorgans orbiomechanicalparts.
Thepurposeofthis2ndeditionbookistoprovideacomprehensiveandup-to-datescientificsourceofbiomedicalengineering principlesof“replacementpartsandassistdevices”forthebionic man.Itcoversbiomechanical,biochemical,rehabilitation,andtissue engineering,aswellasapplicationsincardiovascular,visual,auditory,andneurologicalsystems.Itcontainsupdatedchaptersfrom theoriginalbookaswellasnewchapters,includingTheBionic Pacemaker;BionicAgeHemodynamicMonitoring:Invasive,Noninvasive,Wearable,andWirelessApplications;andfourchapterson KinematicsandPosturalMechanicsinBaseballPitching.Itcanserve asatextorreferenceforstudents,scientists,andlaymeninterested inthefundamentalunderlyingprinciplesofbiomedicaldevicesand procedures,aswellasrecentadvancesintransplant,genetherapy, andstemcellresearch.Thebook’semphasisonfundamentalprinciplesthatarereviewedwithinrelevantchaptersensuresthecontent willremainrelevantandusefulforyearstocome.
c 2023WorldScientificPublishingCompany https://doi.org/10.1142/9789811259197 fmatter
AbouttheEditor

GeorgeK.Hung receivedaB.S.inmechanicalengineering,M.S.inbioengineering,and Ph.D.inphysiologicaloptics,allfromUC Berkeley.Heiscurrentlyaprofessorof BiomedicalEngineeringatRutgersUniversity. Hehaspublishedextensivelyintheareasofeye movementcontrol,nearsightednessdevelopment,andsportsscience,withover110refereed journalpublications.Hehasco-authoredorcoeditedfivebooks,alongwiththepresentvolume:(1) ModelsofOculomotorControl,WorldScientific,2001,(2) ModelsoftheVisual System,KluwerAcademic/PlenumPublishers,2002,(3) Biomedical EngineeringPrinciplesinSports,KluwerAcademic/PlenumPublishers,2004,(4) BiomedicalEngineeringPrinciplesoftheBionicMan, WorldScientific,2010,and(5) BiomechanicalEngineeringPrinciples andApplicationsinSports,Springer,2019.Outsideofacademics,he andhiswife,Joan,areavidlinedancingandsocialballroomdancing enthusiasts.
xiii
This page intentionally left blank
c 2023WorldScientificPublishingCompany
https://doi.org/10.1142/9789811259197 fmatter
Foreword vii
Preface xi
AbouttheEditor xiii
IBrainandRehabilitation 1
1.TechnologiesforRestoringLimbFunction3 WilliamCraelius IIEye 37
2.VisionCorrectionSurgery:RefractiveSurgeryand IntraocularLensImplants39
DanielJ.HuandPeterA.Rapoza
3.ApplicationsofAdvancedTechnologiestoRetinal Prosthesis83 DeanScribnerandLeeJohnson
4.ModelsofMyopiaDevelopment127
AndrewJ.Fiedler,JimoLiu,GeorgeK.Hung, andKennethJ.Ciuffreda
Contents
xv
5.AdvancesintheDesignofHearingAids159 IanC.Bruce
6.RestorationofHearingbyElectricalStimulation oftheHumanCochlea,Brainstem,andMidbrain203 RobertV.Shannon
7.TheBionicPacemaker237 GaryM.Drzewiecki
8.BionicAgeHemodynamicMonitoring:Invasive, Non-invasive,Wearable,andWirelessApplications257 JohnK.-J.Li
9.TissueEngineeringoftheHeart287 MichaelO.Zembala,RicardoA.Bello,and RobertE.Michler
10.GeneTherapyfortheHeart329 ChristianSpiesandGaryL.Schaer
11.StemCellTransplantationTherapyforHeartDisease355 WangdeDaiandRobertA.Kloner
12.TotalKneeReplacement397 W.ThomasGutowski
xvi Contents IIIEar 157
IVHeart 235
VTissueEngineeringandGeneTherapy 285
VIJoints 395
13.MedicalAdvancesinTreatingtheMastersAthlete435 AnthonyLukeandMarcR.Safran
14.BaseballPitchingKinematicsandPostural Metrics:IntroductionandMethodology469
CourtneySemkewycandWilliamCraelius
15.BaseballPitchingKinematicsandPostural Metrics: Velocity 485
CourtneySemkewycandWilliamCraelius
16.BaseballPitchingKinematicsandPostural Metrics: Torque 503
CourtneySemkewycandWilliamCraelius
17.BaseballPitchingKinematicsandPostural Metrics: OptimalAttributesofHighVelocity andLowTorqueinPitching 523
CourtneySemkewycandWilliamCraelius
Contents xvii VIIBionicAthlete 433
AnswerstoReviewQuestions 537 Index 551
This page intentionally left blank
PartI
BrainandRehabilitation
This page intentionally left blank
c 2023WorldScientificPublishingCompany
https://doi.org/10.1142/9789811259197 0001
Chapter1
TechnologiesforRestoring LimbFunction
WilliamCraeliusDepartmentofBiomedicalEngineering, RutgersUniversity,599TaylorRoad, Piscataway,NJ08854,USA billcraelius@gmail.com
1.1Introduction
1.1.1 Needsofthepopulation
Motorimpairmentsofthelimbsaccompanymanyneurologicalor musculoskeletalconditionsandinjuries,includingstroke,cerebral palsy,Parkinson’s,injurytothecentralnervoussystem(CNS), rheumatoidarthritis,andmanyothers.Strokeistheleadingcauseof seriouslong-termdisability,affectingoverhalfofthesurvivorsover 60yearsofage.AccordingtotheU.S.CDC,over795,000peoplein theUnitedStatessufferfromstrokeseachyear,andabout610,000 ofthesearefirstornewstrokes,andthereareover4.8millionstroke survivors,makingittheleadingcauseofparalysisintheU.S.Stroke affectsupto8peopleinevery1,000overtheageof25yearsand 47peopleinevery1,000overtheageof55years.Intheyear2007, theestimatedeconomicimpactofstrokewas$62.7billion.Together, braininjuriesfromaccidentandbraindamagefromstrokeaccount forover10millionpeopleintheUnitedStatesleftwithlong-term disabilities.Incidenceofstrokeislikelytoincrease,asriskfactors forstroke,suchashighbloodpressureandcarotidarterydisease, andagingincrease.Cerebrovasculareventsusuallyaffectprimarily oneside,resultinginhemiplegia.Thisconditionlimitsfundamental
3
W.Craelius
activitiesofdailyliving(ADL),suchaswalking,eating,dressing, drivingacar,writingandtyping,telephoneusage,equipmentoperation,andself-care.Beyondfunctionalloss,peoplecanexperience chronicpainanddistortionintheaffectedlimb,aswellasinexorable musculoskeletaldeteriorationandfurtherneuronalthroughlearned disuse(Platz etal.,2001).
Cerebro-vascularevents(CVEs)generallycausehemiplegia, aweaknessthatprimarilyaffectsonesideofthebody,resultingin asymmetricbodydysfunction.Incaseswherethelocomotiveparts ofthebrainaredestroyed,walkingisdifficultorimpossible.Itisa majorconcernforpeoplesurvivingastrokebecauseitmaynegativelyaffecttheabilitytoperformactivitiesofdailylivingandlimit overallindependence.Asaresult,improvingmobilityisoneofthe maingoalsofstrokerehabilitationandhasrelevancethroughoutthe strokesurvivor’slife.Asecondresultofastrokeisthattherecanbe atleastpartiallossofbodilyawarenessoftheaffectedside.
Someambulatoryabilitycanberestoredbyimmobilizingor assistingtheaffectedanklewithanorthosis,butthisassistance tendstoinhibitneurorehabilitationthatdependsonactiveneuromuscularefforts.Restorationofnormalgaitandlower-limb(LL) functionisthusrareafterhemiplegia.Restorationofupper-limb (UL)functionisevenmoreproblematicdueto(1)itsenormous complexityand(2)thehigherprioritiesgiventorestoringambulation.Furthermore,compensatorystrategies,learnedbythepatient forADL,tendtoinhibitrecovery.Asaresult,manypeoplewithUL paralysisareunlikelytorecovermuchfunctionality.Forexample,a studyofstrokepatientsenteringrehabilitationwithnon-functional armsrevealedthat61%showednoimprovementafter2years (Turton etal.,2002).Manyindividualsthatdorecoversignificant armfunctionexperienceepisodicrelapses,makingitriskyforthem tocarrythings.
Ingeneral,recoveryoutlookaftercentralhemiplegiaispoor,and mostindividualscanexpecttoregainonlypartialmobilityandlimitedULfunctionality.Mountingevidencesuggests,however,that theCNSissufficientlyplastictoeffectmoresignificantreversals fromparalysis,whengiventheproperstimuli(Edgerton etal.,2001; Krebs etal.,2003;Feys etal.,2004;Reinkensmeyer etal.,2004;
4
Bharadwaj etal.,2005;Riener etal.,2005).Itisbelievedthatsensorimotorstimulationprovidedbyrepeatedvoluntaryattemptsto extendmovementsofthelimbs,orevenappliedsensorystimulation, cancausethebraintoreorganizeandre-gaincontrolandcoordination.Restorationofatleastsomefunctionalitymaybepossible throughintensivephysicaltherapyinvolvingrepetitiveexercising, bothpassiveandactive,oftheaffectedlimb.Wecannotpredict, however,thetypes,amount,anddurationofmovements,exercise,or stimulationthatwillbeeffectivenorpredictwhichindividualswill respondtogivenprotocolsandwhethertheoutcomeofsuchdemandingtherapywillbeworthwhile.Moreover,therearefewtoolsavailabletohelptheprocess,andonlyalimitedavailabilityofrehabilitationservices,sincetheyarecostly,constrainedbytime,practicality, traveldistance,andmotivationandarevariablyapplieddepending onindividualproviders.
Tosummarize,bionictechnologiesappliedtopeoplewithhemiplegiaareincreasinglycapableofrestoringsignificantfunctionality topeoplewithstrokeorotherinjuries.
1.1.2 Potentialforfunctionalrestoration
Fortunately,mostindividualswithhemiplegiahaveaccesstophysiotherapydeliveredbydedicatedprofessionals,butthisaccessis necessarilylimitedbytimeandavailabletechnology.Eventherapiesthatemploystate-of-the-artapproachesofferlittleforneural recovery,sincetheyfocusonassistivedevices,encouragingcompensatorystrategiesthroughconstraint-inducedmovementtherapy, oronactivemanipulationofthejointswithroboticdevices.Except forsimpleassistivedevices,theseregimensanddevicesaregenerally impracticalformostindividualswithoutexpertassistanceandlarge expense,andthemoreadvancedapproachesareunlikelytobewidely availablesoon.Asaresult,afterterminationofregularphysiotherapy,neglect-induceddeclinesinfunctionareinevitable,andclients mayincreasinglydependonmedicalandpharmacologicaltreatments forspasticity,sores,andpain.
Neglectingtheaffectedmusclesandjointsiscounter-productive, sincedisusepatternsandassociatedpathologycommencesoonafter
TechnologiesforRestoringLimbFunction 5
W.Craelius
immobilizationoflimbs.Thissituationcouldberemediedifscientificallydesignedtoolswereavailabletoencourageclientstoimplement provensensorimotorprotocolsathome.Thevalueofrelativelyshorttermsensorimotorexercisetraining,withinsupervisedrehabilitation protocols,iswellestablished(Ouellette etal.,2004;Pang etal.,2006; Lam etal.,2008),andtheadditivebenefitsofin-homeexercisecarriedonfor12weeksbeyondthestandardpost-stroketherapyhave beenshowninclinicalstudies(Duncan etal.,2003).Thus,thereis noreasontobelievethatprogresswouldnotcontinueindefinitely withpropertrainingtools.
1.2RehabilitationApproaches
1.2.1 General
Amyriadofstrategies,devices,andprotocolshavebeendevelopedto helprestorefunctiontopeoplewithhemiplegia,eachofwhichmay infactbeefficaciousforneurorehabilitation,butnoneofwhichis apriori superiororindicatedforanygivenclient.Therearetwo assumptionscommonlyheldamongtheemergingandcompeting therapyoptions:(1)theCNSissufficientlyplastictoreorganizeitself andregainsensorimotorcontrolafterinjuryand(2)sustainedand repetitivemovementsoftheaffectedlimbscanpromotere-learning bytheCNS,leadingtosensorimotorrecovery.Beyondthese,thereis insufficienttheoryuponwhichtobuildarationaltreatmentplan,due totheenormouscomplexityofhemiplegiaanditssequelae,involving notonlytheCNSbutalsotheperipheralnervoussystem(PNS), muscles,joints,metabolism,aswellaspsychology.Forthisreason,it hasbeensuggestedthatthemostpromisingtherapyregimensshould beopentoempiricallycombininganarrayoftechnologies(Hogan etal.,2006).
Whileneurorehabilitationstrategiesdifferwidely,andoftenoverlapinmethods,theygenerallycanbecategorizedasthosethatwork on(1)strengtheningorrelaxingindividualmusclesor(2)promoting functionalmovements.Thefirstcategoryincludesstandardphysiotherapeuticexercisesadministeredbyaprofessional.Thesecondcategoryincludestools,suchasconstraint-inducedmovementtherapy,
6
biofeedbackdevices,movementassistivedevices,andelectricalstimulation,thatgenerallyinduceorencouragebothpassiveandactive motions.
Thesecondcategoryisknownas“sensorimotortraining”(SMT), wherebytheclientattemptstomovetheaffectedlimbwhilereceiving sensoryinputregardinghissuccessatnormalmotion.The goalof SMTisthustocoercere-organizationofthedamagedmotorcortex byhelpingtheclientassociatehisvolitionswithsubsequentmovementswiththeirsensoryconsequences,includingproprioceptive,tactile,andvisualmodalities.SMTrequiresactivevolitionbytheclient, whetherornothe/sheisassistedbymechanicalrobots.
1.2.2 TrainingtheaffectedUL
RehabilitativeapproachestoparalysisoftheULcanbecategorizedas(1)standardsupervisedexerciseprotocols,(2)constraintinducedmovements,(3)assistivedevices,(4)activedevices,and (5)biofeedbackofmovementsusingelectromyographic(EMG)and virtualreality.Theseapproachesinvolvesensorimotortrainingto variousdegreesthatencouragesand/orassistsrepetitivemotionsof theaffectedlimbs.
Toapplyappropriatetechnology,therehabilitationengineer shouldhaveanunderstandingofthepotentialuser.Thefollowing tables(Tables1.1and1.2)arenotexhaustivebutaremeanttooutlinespecificproblemsofthetargetpopulationsandtheirpotential forrehabilitation.
Commonstrategiesforrehabilitationfromapplyingrigorousprotocolstoencouragemovementexerciseswithorbyconstrainingthe soundarmforseveralhoursperweekcanforceclientstousetheir affectedlimb,therebyencouragingplasticreorganizationwithinthe CNS.Highlymotivatedclientswhoconstantlyusetheiraffectedarm forseveralmonths,eitherwithexerciseregimenorbyconstraint,have regainedconsiderablefunction(Page etal.,2005;Wolf,2007).Toprovidestructureforpatientsdoingconstraint-inducedtherapy,aworkstationfordirectingandrecordingtaskshasbeendeveloped(Lum etal.,2004).Unsupervisedexerciseandconstrainttherapieshave limitations,however,sincetheymayteachcompensatorystrategies
TechnologiesforRestoringLimbFunction 7
W.Craelius
Table1.1.ProblemsofstrokeandTBIandpotentialsolutions.
ResidualAbilities
“Irrepairable”damage toareasofthebrain thatformerly controlledoneor morelimbs,i.e., strokeandTBI.
Centralnervoussystem plasticity;sensory perceptionintact.
Fixedflexureof affectedarmand generallystiffjoints andco-contraction ofagonistand antagonistduring movement,i.e., “synergy”.
Lossofwristandhand dexterity.Poorforce control.
Usuallycanbe extendedby unaffectedarm. Proprioceptionmay beintactbutpossibly anomalous.
Somemusclesare usuallyactive,even inearlyrecovery.
Re-learningmovements throughproper trainingandsensory feedbacktoreduce conflict.Repetitive tasktrainingand playinginan engaging environment.
Anti-flexionexercise, stretching,and weightbearing.
Stagedprotocolsthat beginwithrestoring reachingabilityand progresstohand grasping.
Source :Corrias etal. (2021). involvingthetrunkandshoulder,withlittleimpactontheunderlying paralysis.
Thetypicalproblemsandresidualabilitiesofpeoplewithstroke arelistedinTable1.1.
AsshowninTable1.1,strokedestroysmanyaspectsofmotor controlneuronsinthebrain,causinglossoflimbfunction.Recovering limbfunctionafterstrokeisdifficult,andrecoveryprospectsdecline withtime.Standardrehabilitationexercisesattempttorecruitsurvivingneuronsforthetaskofrestoringspecificmotorfunctions,however,theseareseldomentirelysuccessful.Successisdependenton manyfactors,includingearlytherapeuticinterventionandoptimal retraining.
8
Table1.2.ProblemsofSCIandpotentialsolutions.
ResidualAbility
C1-C2
Allvegetativeand motorfunctionsare notcontrolled.
C3-C5
Lostallmotor functionsbelowneck.
Braincognitionintact.Brainsignals,either fromEEGorinternal electrodes,can controlcomputerfor communicationwith humanandrobot BCI.
Usuallycanbe extendedby unaffectedarm. Proprioceptionmay beintactbutpossibly anomalous.
C6-C8Somemusclesare usuallyactive,even inearlyrecovery.
Anti-flexionexercise, stretching,and weightbearing. Neuroprosthesesto restorestanding.
Stagedprotocolsthat beginwithrestoring reachingabilityand progresstohand grasping. Neuroprosthesesfor armandlegs.
AnexampleofasimplerehabilitationdeviceisDynawheel. Dynawheeltherapyengagestheuserwithagripchallengegame basedonFitts’paradigm.Theuserispromptedtoexecutevarious handgripswithDynawheelandisscoredbasedonthesuccessofthe user’sgripforcetrackingoftheprompts.Therapycanbeenhanced byAI,whichwilllogandreporttheneurologicalfeatureswhichproduceoptimalperformance,intermsofgripforceanddexterity.This paradigmissimilartothosethatmyresearchgroupandothershave developedforspinalcordstimulation.Thus,theAIsystemrecords themechanicalandelectricalinputsfromtheuserandselectsthose mostefficaciousforgainingoptimalperformance.
EfficacyofDynawheelwasdemonstratedinastudyof6subjects withrightupper-limbparesiscausedbystroke.Agerangewas64–72 years,andtheaveragepost-stroketimewas7.3years.RehabilitationtrainingwithDynawheelconsistedofgripforcedynamometry. Grippingstrengthsandfunctionalityweretestedfollowing6weeks
TechnologiesforRestoringLimbFunction 9
W.Craelius
oftraining.Subjectsshowedmajorgainsinstrengthandcontrolof grip.Thetherapythusrestoredsignificantfunctiontotheaffected upperlimb.Theseresultsareparticularlysignificant,sincefunctional recoveryisseldomsuccessfulwithsubjectswhosestrokeoccurred morethan5yearspreviously.Ourstudieson6ULpatientshaving experiencedstrokeformorethan7yearspreviouslyshowedthat trainingwithDynawheelrestoredsignificantdexterity.Thisstudy wasselectedforspecialmentionbythe JournalofPhysicalTherapy (Kim etal.,2010).
Functionalelectricalstimulation(FES)ofmusclesrepresentsa typeofsensorimotortraining.Theearliestcommercialversionswere developedatCaseWesternReserveUniversity(CWRU),suchasthe FreeHand(Fig.1.1).ThevalueofFESintheacutephaseofstroke wasshowninarandomizedtrialinvolving100patientswhowere givenSMTfor6weeksshortlyfollowingtheevent.Thesepatients outperformedthecontrolsevenafter5years(Feys etal.,2004). ArmandhandfunctioncanberestoredtosomedegreeusingFES. TheFreehandusedimplantedmyoelectrodestostimulatemuscles forgraspingandbendingtheelbow.Theelectrodes,andsubsequent movementsoftheparalyzedUL,wereactivatedbythemovements ofacontralateralarm.
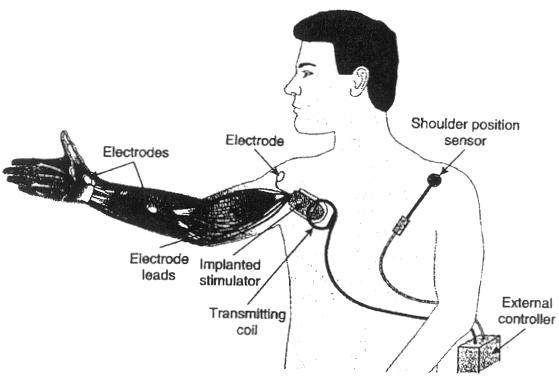
Figure1.1.TheFreehand,showingelectrodesimplantedintothearm,atransmittingcoiltoactivatethem,ashoulderpositionsensortoindicatevolitionto grasp,andanexternalcontroller.
10
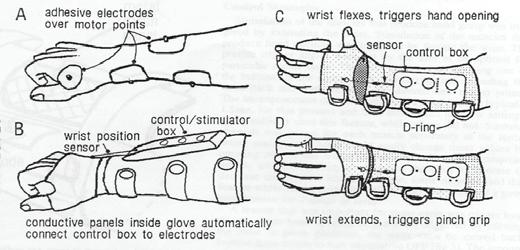
Figure1.2.GraspcontrolwithsurfaceEMGelectrodes.Thewristpositioncontrolsopeningandclosings.
VariationsoftheFreehandincludeastrictlyexternalorthosis thatactivatesthegripmusclesusingnon-invasiveEMGelectrodes, withactivationbybuttons,asshowninFig.1.2.
Amoresophisticatedinterfacetomuscularcontrolisthe BIONSTM ,asshowninFig.1.3.Bionsarethesizeofagrainof riceandcanbeinjectedintomuscles,withoutexternalwires(Micera etal.,2006).Theyareactivatedbyanexternalradiofrequency (RF)coilthatisactivatedbytheuser.ClinicaltrialswithBions haveshowntheirefficacyinreversingshouldersubluxationfollowing stroke,byrestoringtonetoparalyzedshouldermuscles(Salter etal., 2004).Tobettercontrolmuscleactivity,usingclosed-loopfeedback, Bionswillhavemusclesensingability.
AdvancedassistivedevicesuseFES,eitherexternallyappliedor usingBIONSTM .Adepictionofagraspingcontrolsystem,controlling theextrinsicforearmmuscles,isshowninFig.1.4.
1.2.3 SMTandfeedbacktools
Task-orientedsensorimotortraining,sometimesaidedbyconstrainingthesoundarm,iscentraltopromotingneuroplasticrehabilitationoftheupperlimb(Platz,2003;Winstein etal.,2004;Goffredo etal.,2008).Incomparisontoprotocolsforstrengtheningspecific
TechnologiesforRestoringLimbFunction 11