SITE SELECTION CRITERIA
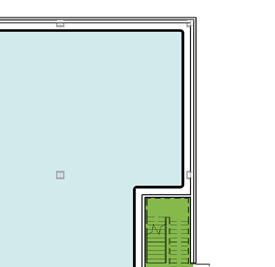
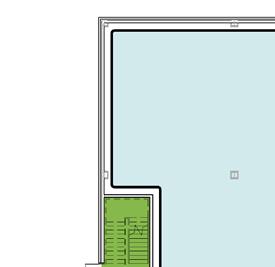
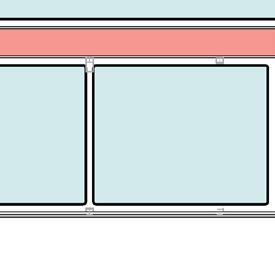
Site Parameters | Figure A
A building’s site will have a major impact on its orientation, form, circulation, and other design decisions. Carefully consider the following elements regarding site selection:
• proposed building type
• land use information
• site and building entry (pedestrian and vehicular)
• current and future parking requirements
• accommodations for mobile services
• relationship to existing buildings (hospital or MOB’s)
• physical or visual connection to other buildings
• potential expansion to medical campus
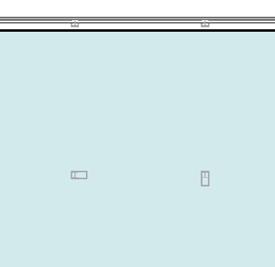
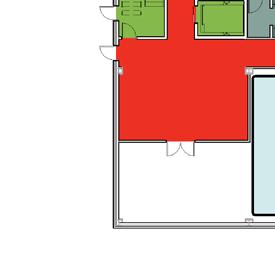
Travel Distances | Figure B
Travel burden is a key element in conceptualizing geographic access to healthcare. A better understanding of distances and mode of travel for individuals seeking healthcare is particularly important.
The average distance traveled for medical/dental care was 10.2 miles, slightly less than the average trip to work at 12.4 miles in 2015.
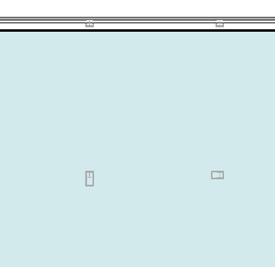
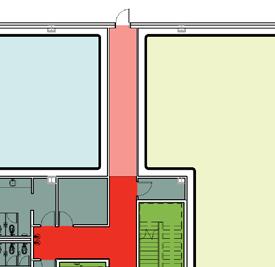
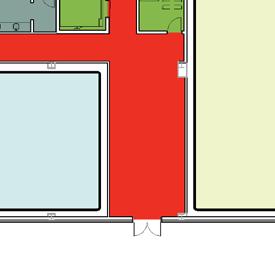
Visibility | Figure C
Access to the site is critical for providing adequate care to individuals. Equally important is the visibility and street presence an MOB can play within the community. Creating a billboard that states a particular brand identity can provide with a competitive advantage.
6
7 1 2 3
Figure A
Figure B
Figure C
PLANNING CONSIDERATIONS
During the earliest stages of programming and conceptual design, a number of important issues will need to be addressed:
• site parameters and traffic flow
• medical practice types and supporting clinical services
• staff and patient flow
• functional organization of primary program elements
• check-in & check-out relationships
• practitioner/exam room ratios
The efficiency of the medical practice is largely influenced by staff, patient, and supply flow. Diagramming the users’ needs at the beginning of a project will help eliminate inefficient or wasted space.

Administration
Patient / Public
Exam Pods
Clinical Support
Building Support
Grouping compatible Medical Practices can provide efficiencies of scale. Shared space for Waiting, Reception/ Check-in, and Scheduling/ Check-out can save space and reduce staffing for long term operational cost savings.
Co-locating Clinical services that support the Medical Practices enhances the care model and provides convenience resulting in high customer satisfaction.
Health System based physician and outpatient services can create efficiencies by consolidating and sharing Billing, Scheduling, and Administrative support. Operational costs can be further reduced by locating these services in a more cost effective location.
9
BUILDING ORGANIZATION
A building’s form and layout will affect its efficiency and economy. Different strategies will perform better for different scenarios.
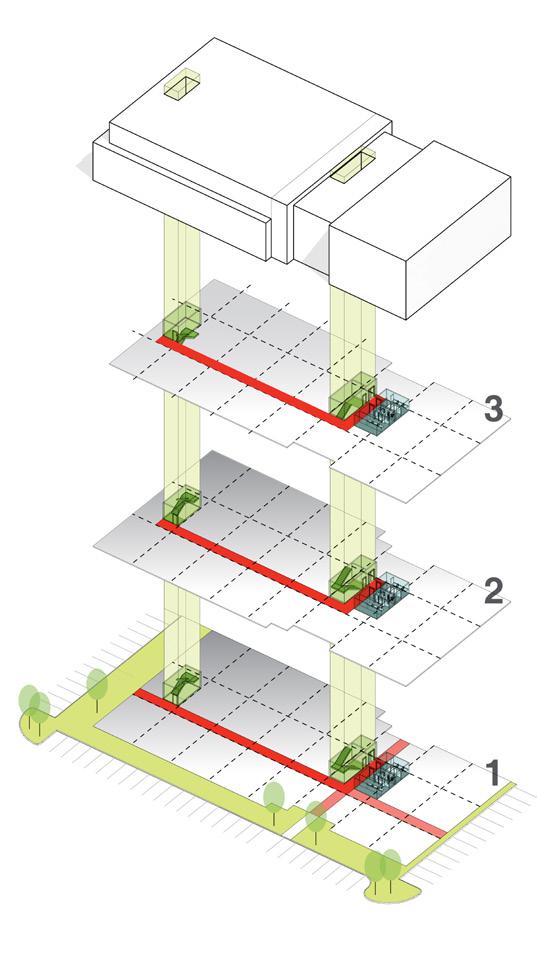
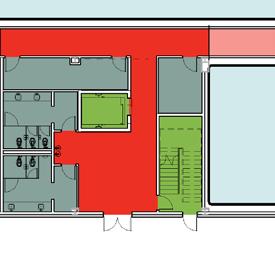
Core Design & Stair Placement
The overall layout will need to accommodate ample space for core functions and stairs with required separation distance. Determining whether public restrooms will be included should come early in the planning process; MOB’s often have minimal public toilets per floor, since build-out of suites will satisfy code requirements. Also, carefully consider exiting requirements for various suite sizes. Possible configurations include:
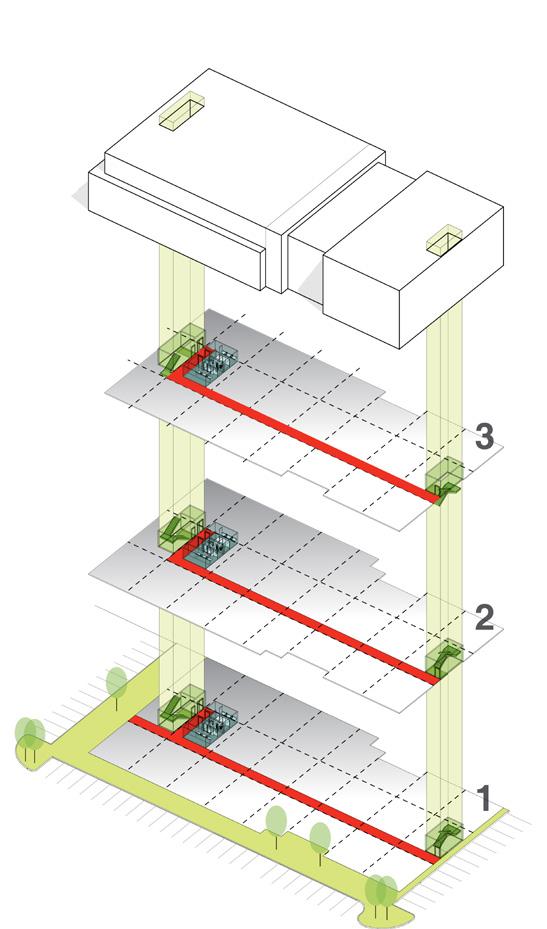
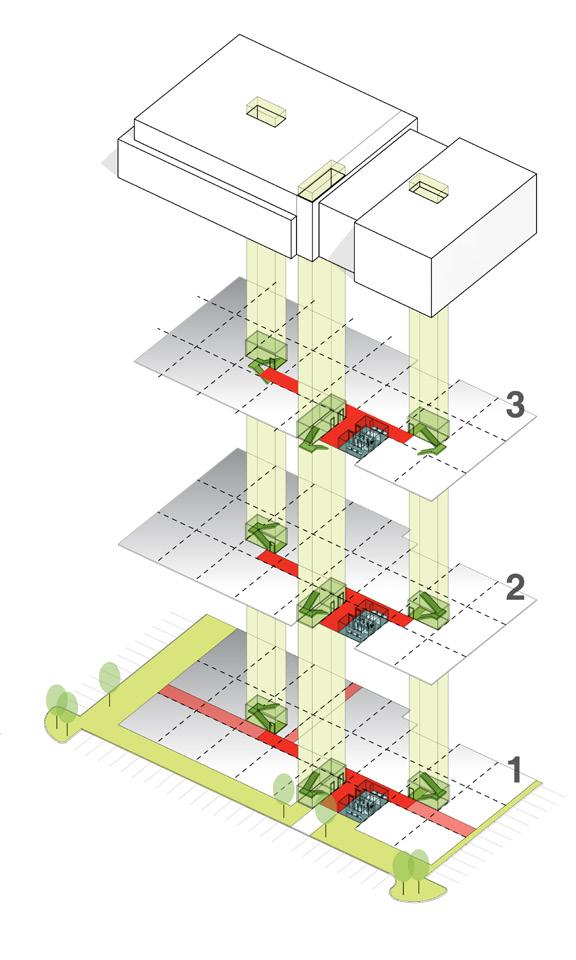
• Central core w/lease area wrapped around
• Double loaded corridor w/ stairs @ ends
• Double loaded corridor w/stairs at ends and additional central stair to allow flexibility for larger tenant occupying a half or full floor
10

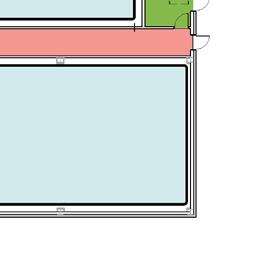
CORE RATIOS
Efficiency Factors
Typical desirable shell and core ratios include 1.12, 1.15, and 1.20.
Building Depths + Floor Plates
100’-0” or 120’-0” x 200’-0” are typical floor plates that work well for an estimated 20,000 square foot MOB. Two-toThree-story MOB’s are most common but there are many MOB’s that flex up or down from this statistic depending on hospital relationships, developer requirements, and tenant needs.
Leasing Depths
Asymmetrical corridor locations provide more flexibility in tenant suite sizes. Common bay depths include:

• 28’-0” bay depth for smaller tenants of 550 - 1,000 SF
• 32’-0” bay depth for smaller tenants of 1,200 - 3,000 SF
• 44’-0” bay depth for medium tenants of 1,800 - 4,000SF
• 60’-0” bay depth for larger tenants of 4,000 - 10,000SF
20% 15% 12%
Medical Practices

Eliminate public corridor to accommodate a larger tenant
Extension corridors may be required for small suites
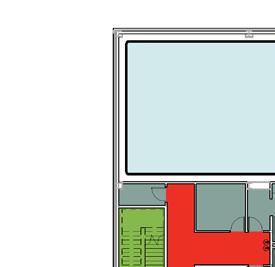
Large Tenants
Asymmetrical
corridor locations provide more flexibility in tenant
Supporting Clinical Service
Central core provides a functional separation between medical offices and clinical support suites.
13
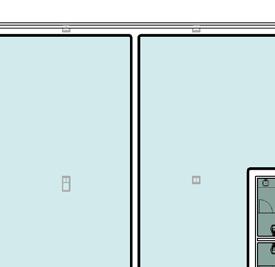
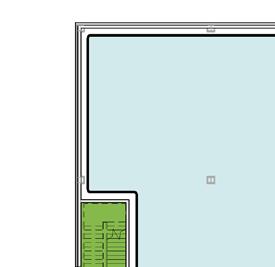
Small Tenants 2/3 1/3
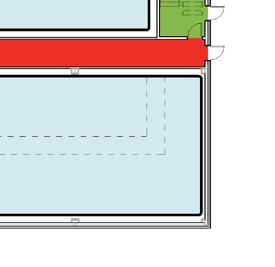
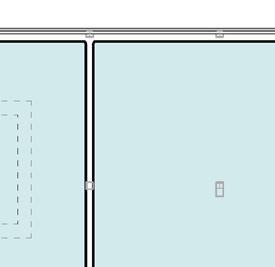
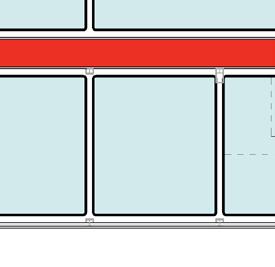
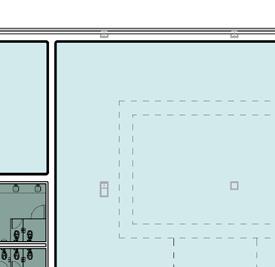
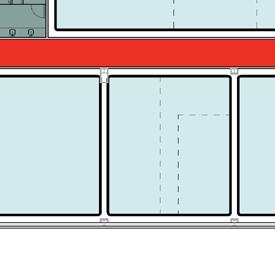
STANDARDIZATION, FLEXIBILITY & EXPANDABILITY
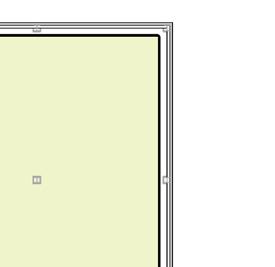
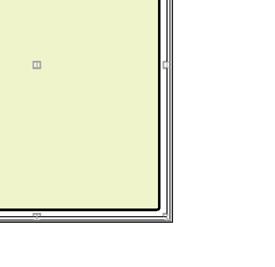
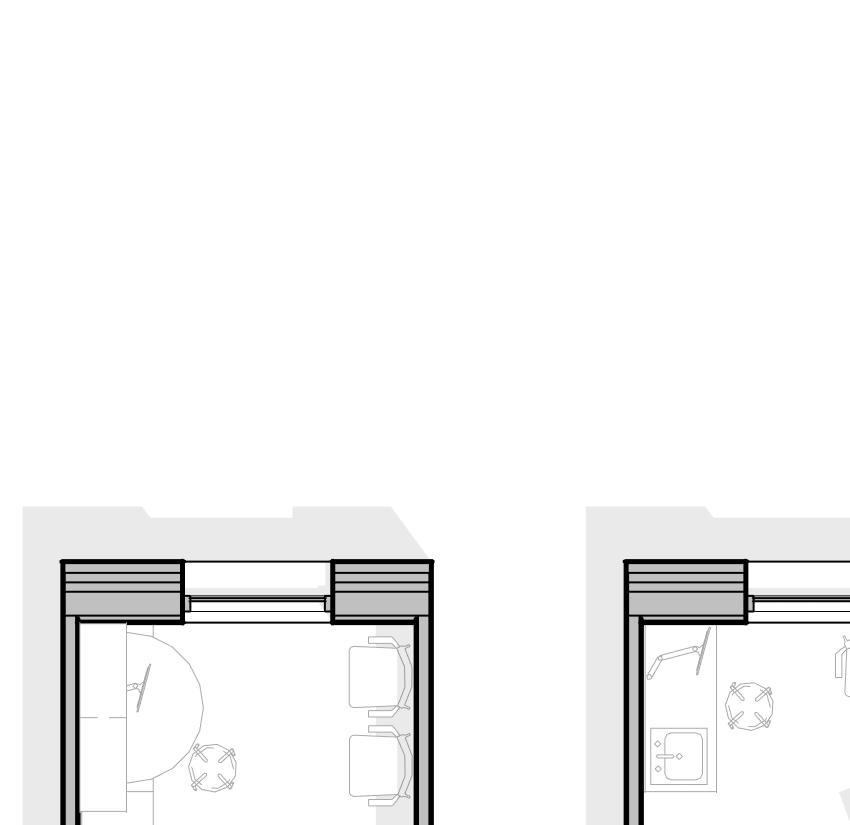
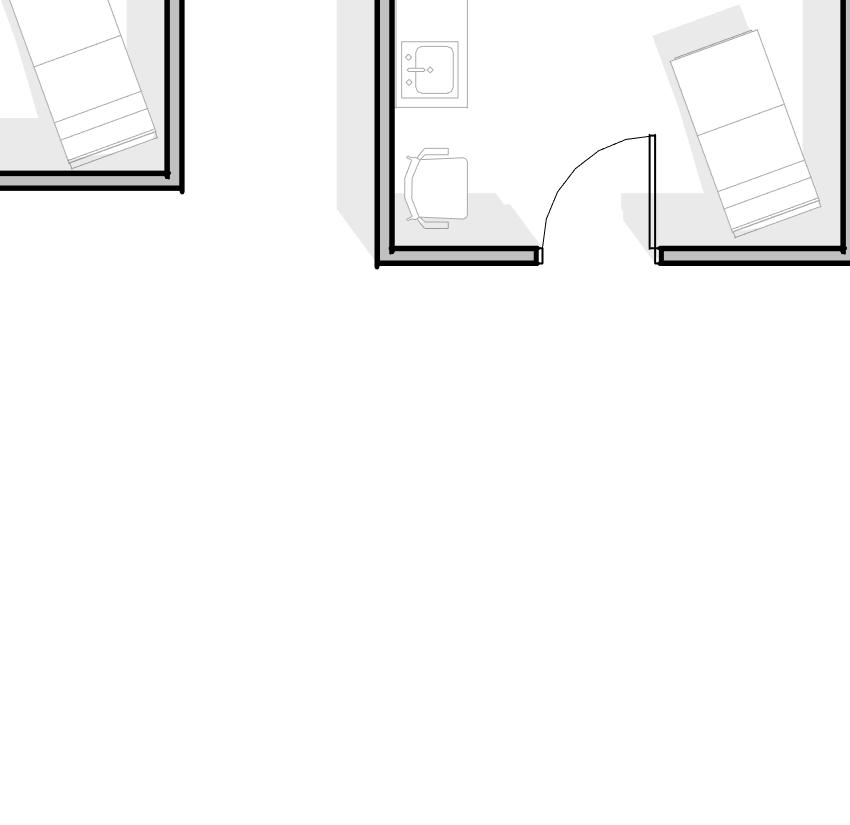
Several “tried-and-true” planning modules have been proven to work effectively within the needs of most MOB tenant suites. Planning modules can be laid out such that each module footprint can be used for a variety of functions. For example, a 3-bay exam room pod may be transformed into a 2-bay exam room with a physician office or 1 exam room and one larger procedure room which include a toilet room. Same handed exam rooms provide standardization, a benefit in suites shared by multiple providers. Attention must be paid to the window placement and mullion placement within curtain walls to accommodate these flexible tenant modules.

The same exam room spacing layout can easily be modified to accommodate offices


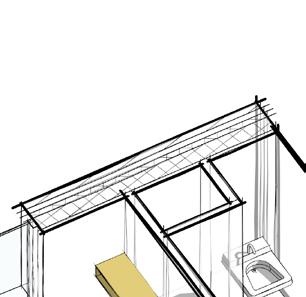














The same exam room spacing layout can easily be modified to accommodate procedure rooms and toilet rooms
15 10 ’ -0” 10 ’ -0” 10 ’ -0”
3-Bay Exam Room Pod



16 9'-0" 12 '0 " 10'-0" 10 '0 " 12 '0 " 12'-0" 9 x 12 10 x 10 12 x 12
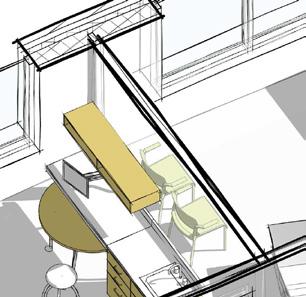
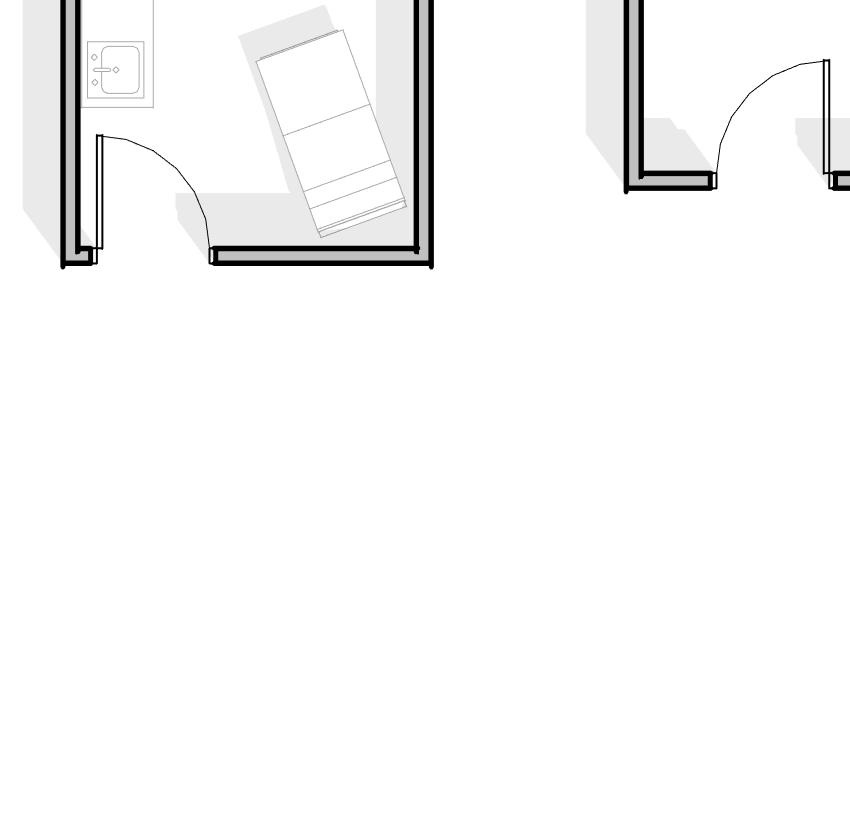
PLANNING MODULES
Planning Modules
Consider exam width in planning modules. A 9’-0” x 12’-0” clear exam room allows for a tight exam module. A 10’-0” x 10’-0” module provides an opportunity for the door to swing in towards the exam table, providing privacy for the patient. A 12’-0” x 12’-0” module allows for ample family waiting or a consultation table.

17
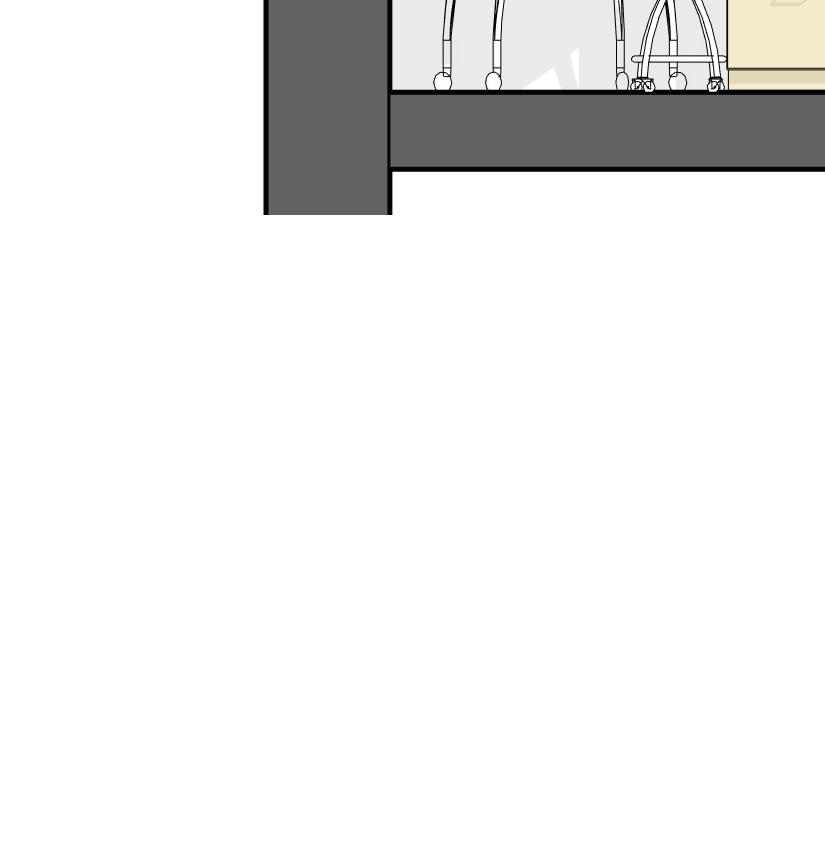
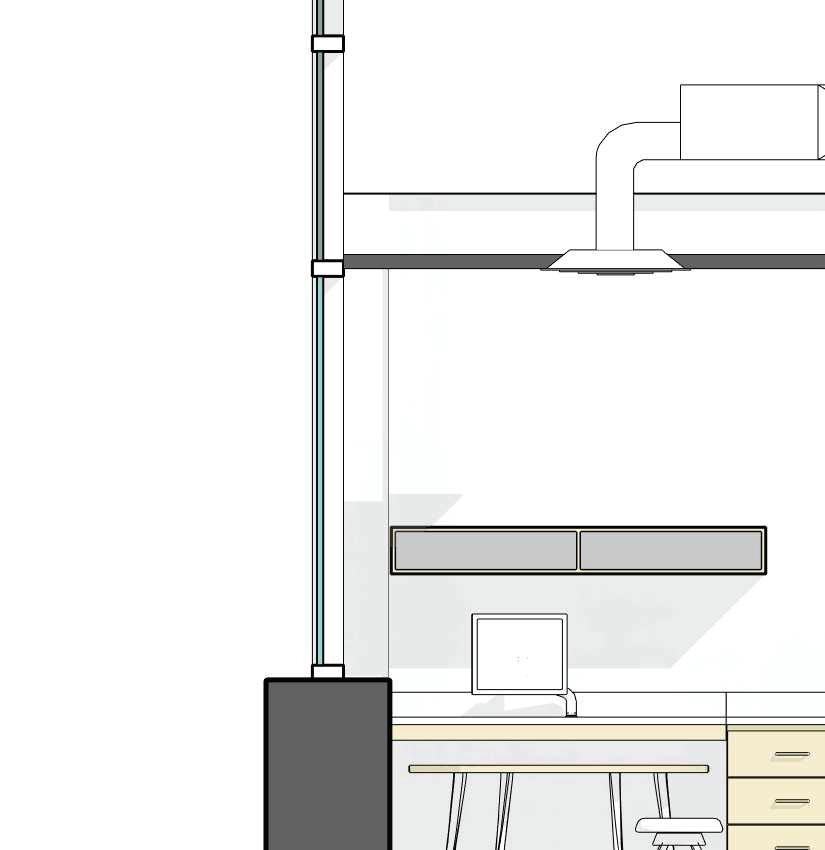

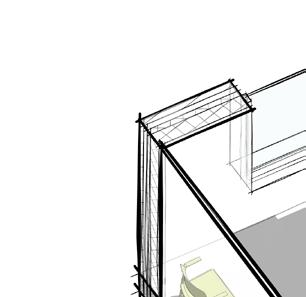
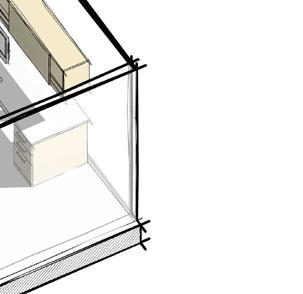
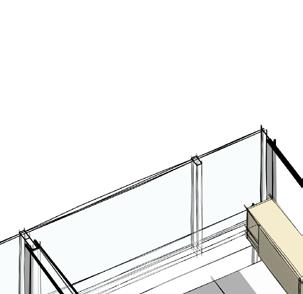
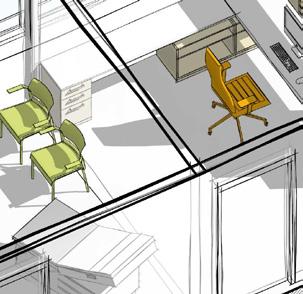
18 14 '0 " 4 '0 " 9 '0 " 4 " 2 '1 0 " or 3’-0” 3 '6 " A FF
Floor to Floor Heights
MOB’s can have extensive above-ceiling requirements for structure, ductwork, piping, lighting, equipment supports, and data cabling. A larger-than-average floor-to-floor height is recommended.
• 14’-0” floor-to-floor is the minimum, higher is better for future flexibility
• 9’-0” ceiling heights are typical for exam rooms
• 9’-0” to 10’-0” ceiling heights are needed for specialty spaces such as Radiology, Ambulatory Surgery, Physical Therapy, etc.
• Additional height is helpful in corridors & lobby/waiting areas for ceiling features such as soffits over reception counters and nurses’ stations which create good wayfinding features
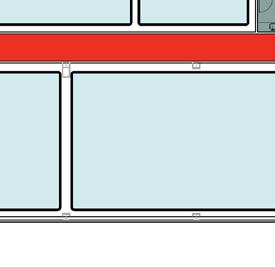
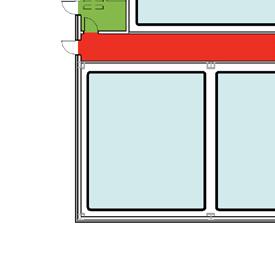
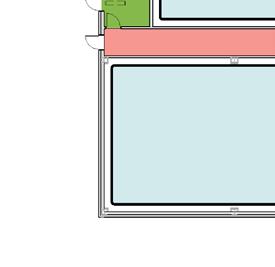
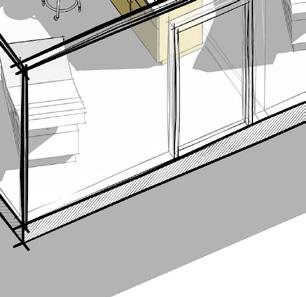
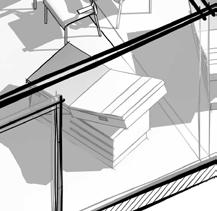
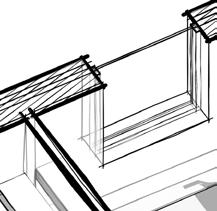
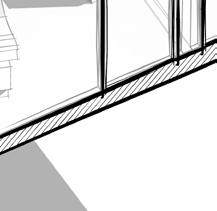
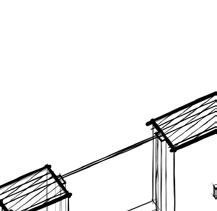
Window Height + Spacing
Planning modules sizes will also affect the window placement or mullion placement locations.
• Window sills +/- 42” above finished floor: maintains privacy and allows cabinetry to pass beneath windows
• Multiple vertical mullions in larger openingsprovides flexibility in partition placement
19
Building Information Modeling (BIM) allows integration between architectural, engineering, and construction teams providing consistent, coordinated, and more accurate buildings before they are built

MECHANICAL / ELECTRICAL / PLUMBING / SYSTEMS
MEP systems are important in any facility; in MOB’s, these systems can be critical to patient safety. The following design elements must be addressed.
Mechanical Considerations
Rooftop packages with VAV units are preferred within suites. Each floor must provide adequate space for mechanical needs. Often, mechanical shafts are located at column locations and at the building core to allow flexibility within the suites to accommodate multiple tenant needs. Mechanical shafts should be sized early in the design process. Certain specialty rooms require additional cooling to offset the equipment heating loads. Liebert units are often used for CT Scan and MRI rooms to offset the special heat loads. Plan for adequate ventilation and exhaust in restrooms, dark rooms, cast rooms, and other special areas with equipment such as laboratory, pharmacy, procedure and surgical rooms.
The COVID-19 Pandemic has proven that special considerations must be made for safe air floor and filtering for building occupants: patients, staff, and visitors. In both new and renovated spaces, even in MOBs, adjustable negative airflow and Merv 13 (and above) filtration should be considered for higher risk spaces, namely exam and procedure rooms. HVAC approaches such as this should be designed in concert with architectural designs that promote social distancing in waiting areas, corridors, and/or other gathering spaces, such as conference rooms.
Plumbing Considerations
Available water quality and pressure impact HVAC, plumbing and fire protection systems design. Wet column locations, water metering and toilet locations affect cost and flexibility.
Electrical Considerations
Metering provisions requirements will vary according to building-wide vs. individual tenants. Additionally, careful consideration for standard lighting requirements for the general public and administrative areas vs. specialty areas must be taken into account. If the MOB requires emergency power an emergency generator may be necessary.
System Considerations
Individual data closets are often required within tenant suites. A building data closet should also be provided. Nurse call and patient tracking may be required within suites. Security considerations must be taken into account building wide as well as within each tenant suite.
21
COMPONENTS FOR CONSIDERATION
Furniture, Fixtures & Equipment
• Lobby furnishings, reception desk, check-in kiosks, vending machines, artwork and window treatments
• Tenant furnishings, demountable partitions, exam room equipment, charting stations, lockers and marker boards.
Medical Equipment & Communication Systems
• Data/telecommunication wiring and equipment
• Telephone equipment
• Security system for tenant spaces (beyond base building system)
• Computer equipment (health information system)
• Location for imaging equipment and structural implications
Special Mechanical & Electrical Systems
• Supplemental cooling for computer rooms
• Mechanical humidification during heating cycles
• Distribution or hook-up of tenant equipment
• Tenant power in excess of 6.5 watts/SF (power and lighting)
• UPS for computers and/or selected outlets
• Computer panels and/or equipment
• Exhaust fans for lab and pharmacy equipment.
• Pandemic ready airflow and filtering adjustability
Building Shell, Miscellaneous
• Window washing equipment
• Manned security station
• Roof top access criteria
• Food service equipment
• Monumental signs
• Removal of unsuitable soil
• Removal of underground obstructions man made or natural
• Options for acoustical privacy
• Different clinic modules
• Construction methodology
• Tilt-up
• Traditional
22
23

24
CASE STUDY
NEW HANOVER REGIONAL MEDICAL CENTER CARDIOLOGY CENTER

The new Cardiology Center for NHRMC consolidates multiple offices and departments to provide improved outpatient services. This 3-story, 63,000 SF medical office building is sited on hospital-owned land near the main NHRMC campus. The new location is more convenient for users and helps decrease congestion on the main campus. The ground floor of the new facility consolidates three existing medical practice facilities into one clinical space. Upper floors provide space for cardiac imaging (stress testing, nuclear imaging, etc.), a pacemaker lab, office space, and a full cardiac rehab area with walking track, education counseling rooms, central registration, and education spaces.

25

CASE STUDY
MUSC CHILDREN’S R. KEITH SUMMEY MEDICAL PAVILION
The concept of patient-centered care drove the entire design process for this 98,000 SF pediatric ambulatory center, informing decisions from site selection through the final finishes. This bright, welcoming facility reduces the stress associated with a clinical visit while paving the way for new models of healthcare delivery.

LS3P led the administration and various user groups through an extensive programming and conceptual design process. Flexible, multifunctional spaces were a primary design goal. Strategies included induction rooms outside of the operating room to maximize through-put while reducing stress for patients by allowing families to bypass the gowning and gloving process to stay together until the procedure begins. An orthopedic clinic transitions to an urgent care in the evening, while standardized exam pods allow rotating teams of specialists to rotate through the clinic for flexible scheduling.

27

CASE STUDY
DUKE HEALTH PRIVATE DIAGNOSTIC CLINIC MOB AT CROOKED CREEK
This 5-story, 125,000 SF medical office building houses diverse practices for one of the largest physician’s practice groups in the country. Located on a highvisibility site with easy access to the interstate, this new facility serves as a marquee building for its owners.

The design focuses on a welcoming patient experience, with parking deck, covered walkway to the entry, carefully considered circulation, and a rear entrance for ambulances and staff.

29

CASE STUDY
UNC HEALTHCARE FUQUAY-VARINA URGENT CARE CLINIC

This new medical facility for the Fuquay-Varina community will provide a supportive, reassuring experience for patients and families close to home. The prototype design for UNC Healthcare includes an urgent care clinic and family medicine practice under the same roof. The patient-centered design for the family medicine practice includes 24 exam rooms, a point-of-care lab test area, and a phlebotomy lab; staff work areas are separated from patient corridors, allowing staff to work and collaborate in care team work areas. The compact, efficient floor plan for the urgent care is designed for operational efficiency and serves patient needs with five exam rooms, x-ray, and point-of-care lab testing. showroom provides a space to highlight student work and emerging technologies.

31

CASE STUDY
WAKEMED MEDICAL PARK OF CARY MEDICAL OFFICE BUILDING
This project includes master planning and design for an outpatient health campus consisting of two medical office buildings supported by a common parking deck. The core and shell design was completed via Design-Bid-Build with Healthcare Trust of America. The Phase I, 5-story, 133,900 GSF Medical Office Building includes 470 parking spaces in a parking deck that is designed for phased construction to allow flexibility of implementation of the overall master plan program. Tenant fit-ups are being completed for WakeMed for various clinics including Cardiology, Imaging, Pharmacy, General Surgery, Vascular, Thoracic, Urology, Uro-GYN, OBGYN, Maternal Fetal Medicine, and an Ambulatory Surgery Center.


33

CASE STUDY
UNC HEALTH CARE PANTHER CREEK MOB & AMBULATORY SURGERY CENTER

LS3P provided master planning, architectural, interior design and engineering services for this multispecialty 99,900 SF medical office building and orthopedic surgery center. The facility provides clinical space for family medicine, pediatrics, OB/ GYN, orthopedics, internal medicine, nuclear medicine, neurology, digestive health, and heart and vascular care. Clinics on the upper floors provide services in a collaborative model with centralized patient check-in and staff support spaces. Clinic layouts are based on Lean design principles, with dual-entry exam rooms and care team work areas separated from patient areas. The facility also includes an imaging center which offers CT, MRI, mammography, ultrasound, bone densitometry, and X-ray.
The Orthopedic Surgery Center of Panther Creek, a joint venture between a large hospital system and a leading private orthopedic practice group, includes one operating room and two procedure rooms, 13 universal prep/recovery rooms, and a dedicated sterile processing department in a footprint designed to accommodate expansion.
This complex project was completed within a 16-month construction period using concrete tilt-up construction.

35

36
MISSION
LS3P is a dedicated, talented, knowledgeable, and passionate team of professionals working toward a common vision to create something special for every client. We customize each project process to meet its specific vision and desired outcomes. Our role is to lead and inform that process to achieve a specific, more holistic result. Expertise, creativity, understanding, empathy, integrity, and trust provide the foundation for bringing success to our clients and their projects.

37
38
Charleston Jacksonville Columbia Greenville Myrtle Beach Wilmington Raleigh Greensboro Charlotte Asheville Atlanta
Savannah
ENGAGE
We are passionate about the process of discovery, from the earliest stages of design through project delivery. We engage with our clients in order to address the unique needs, constraints, and opportunities of each project. We observe, listen, and ask questions. We want to understand your work flow, user groups, project goals, budget, and business model. We want you to enjoy the process.
WILLY SCHLEIN AIA, NCARB, LEED AP HEALTHCARE PRACTICE LEADER

willyschlein@ls3p.com
864.272.1250 (DIR)
864.361.1420 (CELL)
DESIGN
We respond to the discovery process by using our tool kit of strategies to generate design options. We use evidencebased design. Our extensive hands-on knowledge of effective solutions, a series of simulations, and state-of-the-art technology to create the best design for your needs.
TRANSFORM
We want to streamline your operational and functional capacities, improve your bottom line, and allow you to see more patients per hour. We want to provide spaces which facilitate healing, and support physicians, staff, patients and visitors on the path to recovery and wellness. We want to help transform your practice.
39
.COM HEALTHCARE BY DESIGN MEDICAL OFFICE BUILDINGS




