
http://www.inosr.net/inosr-scientific-research/ Turyasingura
INOSR Scientific Research 9(1):50-58, 2023.
©INOSR PUBLICATIONS
International Network Organization for Scientific Research
ISSN: 2705-1706
Evaluation of the Urinary Retention in Matured Male Patients at Kampala International University Teaching Hospital in Bushenyi District Western Uganda
Turyasingura, Enos
Department of Clinical Medicine Kampala International University Western Campus Uganda.
ABSTRACT
A comprehensive assessment of urinary retention in adult male patients who attended Kampala International University Teaching Hospital (KIU-TH) was conducted. To determine the number of adult male patients diagnosed with Urinary Retention (UR) to determine the risk factors of urinary retention among adult males who were diagnosed with urinary retention, to establish the management of urinary retention among adult males diagnosed with urinary retention at KIU-TH between august 2015 to august 2017. A retrospective and a descriptive study design was used, involving quantitative methods of data collection. Purposeful sampling technique was employed, where all adult males who attended KIU-TH between august 2015 and august 2017 were recruited in the study. From results out of 136 samples of adult male patients with UR, 63 (46.3%) had no UR and 73 (53.7%) had UR. Out of the 73 (53.7%) adult male patients, 52 (71.2%) with presented with AUR then 21 (28.8 %) of thepeoplehadCUR.Furthermore,of73(53.7%)oftheadultmalepatientswithUR,19(26.1%) was in 2015 from August to December, and 32 (43.8%) adult male patients were in 2016 Januaryto December,and22(30.1%)adultmalepatients in 2017betweenJanuaryto August. This was found more in elderly men between the age 60 to 89 years by 53 (72.6%) followed by, 40 to 60 years by 14 (19.2%), then 23 to 40 years by 6 (8.2%) patients.The risk factors UR were BPH, prostate cancer, urinary stricture, and others that included bladder tumors, and urethral traumas where BPH was the leading cause of UR with 45 (61.6%) patients, followed by 10 (13.7%) followed by urethral stricture and 5(6.8%) was due to other causes such as bladder tumors urethral trauma and paraphimosis. 26 (35.6%) people had UR were managed by urethral catheterization, 17 (23.3%) had UR managed by supra pubic catheterization, 23 (31.5%) had UR managed by surgery and 7 (9.6%) were managed by other measures like medication circumcision. In conclusion Results portrayed that although the management measures were available such urethral catheterization and surgery which were the most practice at KIU-TH, there remained high prevalence of UR which was more in the elderly adults commonest cause was BPH. All males above 60 years need to be assed and examined to rule out the causes of urinary retention for early management. It is also necessary to necessary that all males above forty years to be encouraged for BPH and early treatment of urinary tract infections to prevent outlet obstruction ant formation strictures respectively.
Keywords: Urinary retention, adult males, Patients, Bladder tumor, Urethral catheterization
INTRODUCTION
Urinary retention (UR) defined as the inability to completely empty the bladder despite it being full is rare condition amongyoungmencomparedtotheelderly where in their 70s, they become five times more prone to the condition [1, 2, 3, 4]. UR had been commonly an under diagnosed condition with complications that resulted in patient discomfort and possible permanent damage to the lower urinary tract [5, 6, 7]. UR was acute or chronic [1,
8, 9, 10]. In the acute form there was a sudden inability to pass urine despite an urge to pass urine which was usually associated with suprapubic pain. Chronic urinary retention (CUR) was an inability to empty the bladder completely during voiding which usually was not associated with suprapubic pain [11, 12, 13, 14, 15, 16]. There could sometimes be an acute urinaryretention(AUR)onabackgroundof chronic urinary retention (acute-on-
http://www.inosr.net/inosr-scientific-research/ Turyasingura
INOSR Scientific Research 9(1):50-58, 2023.
chronic urinary retention) and was one of the common urologic emergencies worldwide [1, 17, 18, 19, 20]. The causes of UR were categorized as obstructive and non-obstructive [3, 21]. The obstruction of the lower urinary tract at or distal to the bladderneckwhichcouldbeintrinsicsuch as prostatic enlargement, bladder stones, and urethral stricture with the most common obstructive cause being benign prostatichyperplasia(BPH)causingbladder neck obstruction through two mechanisms: prostate enlargement and constriction of the prostatic urethra [3] Furthermore, infection and inflammation were the most common causes of infectious AUR especially acute prostatitis usually caused by gram-negative microorganisms, such as Escherichia coli and Proteus species, and resulted in swelling of the urethra due to a urinary tract infection (UTI) or sexually transmitted infection [3]. Medications with anticholinergic properties, such as tricyclic, antidepressants, caused urinary retention by decreasing bladder detrusor muscle contraction, neurological [3]. Normal functioning of the bladder and lower urinary tract depend on a complex interaction between the brain, autonomic nervous system, and somatic nerves supplying the bladder and urethra so any interruption of these nerves lead to UR [3]. However, when all the above causes of UR were compared BPH was the leading cause (51.8%) followed by urethral stricture (20%), cancer of the prostate (7.3%), urethral injury (7.3%) and bladder tumor (6.4%). More than half of the adult male patients (53.4%) usually presented with AUR, 30.5% presented with CUR,and 16.1% being diagnosed to have acute-on-chronic urinary retention [3]. Although UR was a burden to adult males globally, there were measures to manage it using various ways of management such as use of indwelling urethralcatheterization(IUC),supra-pubic catheterization (SPC) and intermittent urethral catheterization (IC) in low developed countries [4]. Furthermore, in a world survey on the management UR among adult males aged 70 years and above, prostate size of 50gwith severe lower urinary tract symptoms, drained
urine at catheterization of 1000 ml and spontaneous AUR favored trail without cauterization (TWOC). The same study indicated that Catheterization above 3 days did not influence TWOC success but was associated with increased morbidity and prolonged hospitalization for adverse events where in the case of TWOC failed, BPH surgery was done [5]. Globally, the overall prevalence of UR for both AUR and CURwasnotknown[4].Mostofthereports on prevalence of UR were from studies conducted on AUR,in patients with benign prostatic hyperplasia (BPH) and prostate cancer however it had been estimated that by2018thatboththeprevalenceofURand wouldincrease by 20%, withAfricaand the Asian countries experiencing the steepest increase [4]. Previous studies had put the prevalence of UR between 2.7% and 42% in men who underwent prostatectomy in North America and Britain [4], United States with the rate of AUR at 4.5 per 1000 person-years based on 82 cases (1.34%) in 6,100 men included from health professionals follow up study [4]. A recent population – based study of 950 men in west Africa found the prevalence of BPH, was a common cause of UR among adult males in Ghana [6] with 19.9% of men experiencing UR than the United States of America [7; 6] In Africa UR has been on an increase in the ageing males of the population especially of sub-Saharan Africa with a prevalence of 19.9 per 1000 men [8], Ghana with a prevalence BPH among 50 -74years old were 35- 62%With 19.9% of men experiencing UR which was similar to a study made in Sierra Leone with 19.9 per 1000 men [7]. Burkina Faso in the study at Bobo - diousso University Teaching Hospital among adult men out of 155 patients, 104 (67.1%) had AUR aged between 23 and 89 years, patients who were over 60 years formed the majority at 77.8% [9]. In a study made in Nigeria the prevalence of acute urinary retention was 39.3% of patients aged 65-74 years, 33.3% above 75 years, 27.4% were below 65 years [3]. In Uganda however there was no clear report about UR in elderly man due to a generalrecordproblem[4].Therewashigh prevalence of this condition in men older than 50 years of age of BPH [10] however
Turyasingura
INOSR Scientific Research 9(1):50-58, 2023.
the prevalence of the disease is not known but according to the study from Mulago hospital Urology Unit showing that symptomatic BPH was the leading cause of admissions of UR with 177 cases of BPH outof742(24%)ofadmissionsontheward between January 2005 and June 2006 [11] There was barely any study that had been conducted in KIU-TH in Bushenyi district in western Uganda.
Statement of Problem
Though no clear record in Uganda about the prevalence of UR in elderly men due to generalrecordproblembutthefewstudies showed that there was high prevalence of this condition in men older than 50 years of age due to BPH [4; 10]. BPH was the leadingcauseofadmissionsofURnotonly elsewhere in the world but also in Uganda with 177 cases of BPH out of 742 (24%) adult males admitted in Mulago hospital among other causes [11] However, there was barely any information about the prevalence of UR among adult male patients who attended Kampala International University Teaching Hospital (KIU-TH) in Busheny-Ishaka municipality, Bushenyi district. The current study seeks toconductacomprehensiveassessmentof UR among the adult male patients who attended KIU-TH where it included the number of patients diagnosed with UR causes and ways of management.
Aim of the study
To conduct a comprehensive assessment of urinary retention in adult male patients who attended KIU-TH.
Specific objectives
To determine the number of adult male patients diagnosed with UR among adult males who have attended KIU-TH between august, 2015 to august 2017.
To determine the risk factors of urinary retention among adult
males who were diagnosed with urinary retention at KIU-TH Between August 2015 to August 2017.
To establish the management of urinary retention among adult males diagnosed with urinary retentionatKIU-THBetweenAugust 2015 to august 2017.
Research questions
What was the number of adult male patients diagnosed with urinary retentionamongadultmalesatKIUTH Between August 2015 to August 2017?
What were the risk factors of urinary retention among adult males diagnosed with urinary retention at KIU-TH between august 2015 to august 2017?
What were the different management measures of urinary retentionamongadultmalesatKIUTH between august2015 to august 2017?
Justification of the study
This study was to raise the level of awareness to the community about the prevalence and the associated risk factors and the management methods of urine retention among the adult males and health workers of KIU-TH. This would update the available information concerning UR, which could serve as baseline for further intervention in prevention and treatment of urinary retention in western Uganda and worldwide. Results obtained in this study were important to the ministry of health for better planning on how to reach the community and lay necessary health policies aimed at combat ion UR and its associated risk factors among adult males in Uganda.
METHODOLOGY Study Design
A retrospective and a descriptive study design was used, involving quantitative methods of data collection.
Area of Study
The study was conducted at KIU-TH located in Ishaka - Bushenyi Municipality, Bushenyi District in the South Western
region of Uganda as to appendix v. It’s located approximately 65kms by road fromMbarara town, the largest town in the region and 360kms from Kampala the Capital City of Uganda, KIU-TH was alongside Kasese –Mbarara road according to (Appendices III and IV). The main language spoken in Bushenyi district was
http://www.inosr.net/inosr-scientific-research/
Turyasingura
INOSR Scientific Research 9(1):50-58, 2023.
Runyankole as Banyankole people are the main occupants of this area. KIU-TH was a non-government health facility serving in Bushenyi district population of 234,443 People, 114,207 males according to National Population and Housing Census 2014. That area was purposely chosen because of the high population density of 282 people per square kilometer.
Study Population
The study was involved cross examining therecordsofadultmalesofagegroup23-
89 years which was similar to the age of a study by [9]. In patients who attended KIUTH between months of august 2015 to august 2017.
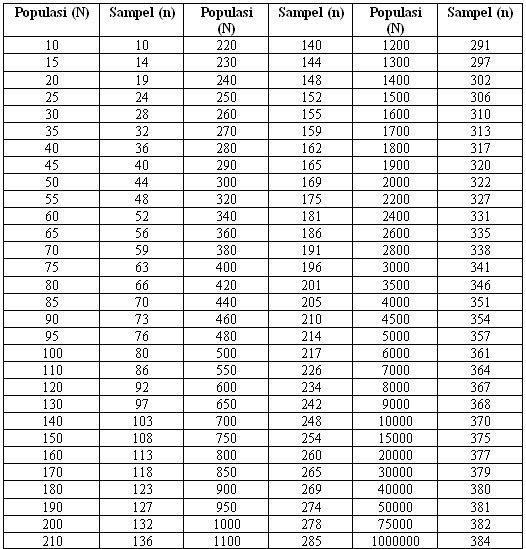
Sample Size Determination and Rationale
All adult male patients aged between 23years to 89years attended KIU-TH were selected according to [12] (Appendix III), for a population (N) of 210 adult male patients on average, the sample size for the given population (S) was 136 respondents.
Sampling Procedure and rationale
Purposeful sampling technique was employed, where all adult males who attended KIU-TH between august 2015 and august 2017 were recruited in the study.
Inclusion criteria
All adult males within the age group (23 to 89 years) who attended KIU-TH both diagnosed with and without between
august 2015 and august 2017 were included in the study.
Exclusion Criteria
Adultmaleswhohadpartialinformationin therecordbookssuchasage,tribe,marital status, sex, address, and people below 23 years and those above 89 years were not included in the study.
http://www.inosr.net/inosr-scientific-research/
Turyasingura
INOSR Scientific Research 9(1):50-58, 2023.
Research instruments
A data collection sheet was used to collect data from KIU-TH hospital patients’ records.
Data collection procedure
After getting approval letter from the school of allied health sciences, the required data of adult males who meet the criteria was recorded in the pre-designed data collection sheet (Appendices I and II).
Data analysis and presentation
Data was presented in chats, figures and table and statistically analyzed using
computer software including MS-Excel 2010 and SPSS.
Ethical considerations
The approval letter was obtained from School of Allied Health after the approval of the proposal which was forwarded toinstitutional research and ethical committee(IREC)ofKIU–THforacceptance and permission to access the patients’ records in KIU-TH.
RESULTS
Prevalence of urinary retention among adult male patients who attended KIU-TH The results indicated that of 136 adult male patients considered in the study period from august 2015, 2016, to august 2017; showed that there was generally a high percentage of adult male patients diagnosed with UR being 73 (53.7%) which was significantly higher (p < 0.05) than 63 (46.3%) who had no UR. Out of 73 (53.7%) of the adult male patients diagnosed with UR, 19 (26.1%), 32 (43.8%), 22 (30.1%) were found to be in 2015, 2016 and 2017 respectively. However, the percentage of adult males diagnosed with UR in 2016 (43.8%) was significantly higher (p < 0.05) than the cases of UR in 2015 and 2017. In addition, of the 73 (53.7%) adult male
patients, 52 (71.2%) were diagnosed with AURwhichwassignificantlyhigh(p<0.05) than21 (28.8 %) of the people had CUR. adult male patients in Whereby out of the 52 (71.2%), 19 (26.1%) who were in 2017; 15 (78.9%) patients had AUR and 4 (21.1%) patients had CUR, and the 32 (43.8%) patients in 2016; 23(71.9%) hadAUR and9 (39.1%) had CUR while 22 patients who were in 2017;14 (63.6%)had AUR and 8 (36.6%)were having CUR. This prevalence of UR was found more in elderly men between the age 60 to 89 years by 53 (72.6%) which significantly higher (p < 0.05) than the adult male patients in the age of 40 to 60 years by 14 (19.2%), and23 to 40 years by 6 (8.2%) patients as seen in the table 2 below.
http://www.inosr.net/inosr-scientific-research/ Turyasingura
INOSR Scientific Research 9(1):50-58, 2023.
UR : Urinary rentetion.
AUR : acute urinary rentetion.
CUR : Chronic urinary rentetion. Risk factors of Urinary retention
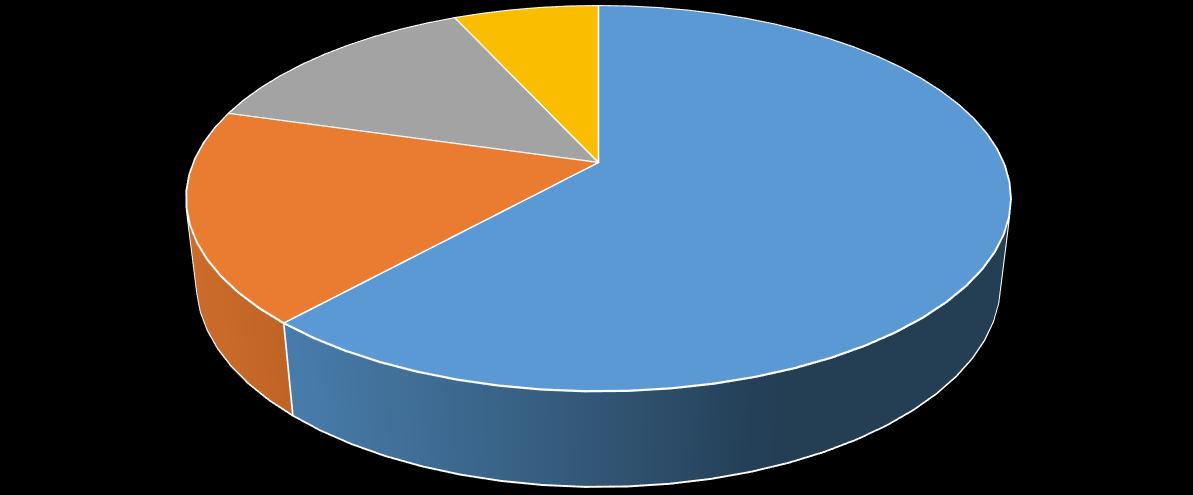
The risk factors were benign prostate hyperplasia, prostate cancer, urethral stricture, and others like trauma of the urethra and age. Results portrayed that 45 (61.6%) patients with UR was due BPH
which was significantly higher (p <0.05) followed by 13 (17.8%) due to Ca p, 10(13.7%) due to urethral stricture and 5(6.8%) that was due to other causes as seen in the figure below;
http://www.inosr.net/inosr-scientific-research/
Turyasingura

INOSR Scientific Research 9(1):50-58, 2023.
Management of urinary retention among adult male patients who attended KIU-TH Results showed that there were various management measures of UR which were urethral catheterization with 26 (35.6%) peoplehadURwhowerebeingmanagedby it, 17 (23.3%) had UR managed by suprapubiccatheterization,23(31.5%) had UR managed by surgery and 7 (9.6%) were
managed by other means like medication. The results portrayed that the percentage of the management of UR by urethral catheterization with (35.6%) and surgery (31.5%) were significantly higher (p < 0.05) than suprapubic catheterization (23.3%) and other measures like medication with (9.6%) as seen in the graph below;
DISCUSSION
The high prevalence of ur73 (53.7%) whereby out of the 73 (53.7%) adult male patients, 52 (71.2%) with presented with AUR and 21 (28.8 %) of the people hadCUR the study results portrayed the percentage of AUR was significantly higher (p < 0.05) than CUR21 (28.8 %), this was in line with the study conducted at the Urology and Accident and Emergency Units of Komfo Anokye Teaching Hospital, Kumasi, Ghana [13].The prevalence washighin theadults of 60 years and above which was also in line with the study at Bobo - diousso University Teaching Hospital in Burkina Faso adult [9] and this was thought to happen with increase in age which increases the growth the prostate. Following the study results regarding risk factors of UR, it was found out that BPH, prostate cancer, urinary stricture, and others that included bladder tumors, and
urethraltraumasleadtoURwhereBPHwas the major risk factor of UR with 45 (61.6%) patients whose percentage was significantly high (p < 0.05) followed by 10(13.7%) followed by urethral stricture and 5(6.8%) was due to other causes such as bladder tumors urethral trauma and paraphimosis. This study was in contrast with the study by [3] which was thought to be due to the increase in size of the prostate with age. Study results portrayed thatURwasmanagedwithmeasureswhich was found that urethral catheterization was commonly practiced to patient with UR 26 (35.6%), followed by surgery 23 (31.5%), followed supra pubic catheterization 17 (23.3%) and other methods 7 (9.6%) by methods of management, in addition the percentages of urethral catheterization and surgery (35.6%), (31.5%) significantly higher (p <
http://www.inosr.net/inosr-scientific-research/ Turyasingura
INOSR Scientific Research 9(1):50-58, 2023.
0.05) than supra pubic catheterization 17 (23.3%) and other method 7 (9.6%) this studywasitlinewiththestudyby[4].This was thought that urethral catheterization was high because it was cheap to afford
other methods and surgery was high because it was a permanent method of managinginvolvedremovaloftheprostate that was obstructing urine flow.
CONCLUSION
Results portrayed that although the managementmeasureswereavailablesuch urethralcatheterizationandsurgerywhich were the most practice at KIU-TH, there remainedhighprevalenceofUR whichwas more in the elderly adults commonest cause was BPH. Therefore, the following recommendations should be done
Recommendations
All males above 60yearsneedto be assed and examined to rule out the causes of urinary retention for early management.
REFERENCES
[1]. Kalejaiye, O. and Speakman, M. J. (2009). Management of Acute and Chronic Retention in Men. European Urology,Supplements, 8(6), 523–529.
[2]. World health statistics (2017). monitoring health for the SDGs, Sustainable Development Goals. Geneva: World Health Organization; 2017. Licence: CC BY-NC-SA 3.0 IGO.
[3]. Abdullahi, M., Yunusa, B.,Mashi, S.A. and Aji, S. A. (2016). Urinary Retention in Adults Male Patients: Causes and Complications among Patients Managed in a Teaching Hospital in North Western Nigeria, (July), 114–121.
[4]. Ugare, U. G., Bassey, I.-A., Udosen, E. J., Essiet, A. and Bassey, O. O. (2014). Management of Lower Urinary Retention in a Limited Resource Setting. Ethiopian Journal of Health Sciences, 24(4), 329–336.
[5]. Fitzpatrick, J. M., Desgrandchamps, F.,Adjali,K.,Guerra,L.G.,Hong,S.J., El Khalid, S. and Ratana-Olarn, K. (2012). Management of acute urinary retention: A worldwide survey of 6074 men with benign prostatic hyperplasia. BJU International, 109(1), 88–95. Foo, K. T. (2017). Pathophysiology of clinical benign prostatic hyperplasia. Asian Journal of Urology, 4(3), 152–157.
[6]. DeNavas-Walt, C. and Proctor, B.
It is also necessary to necessary that all males above forty years to be encouraged for BPH and early treatment of urinary tract infections to prevent outlet obstruction ant formation strictures respectively.
More recommendation goes to the government and ministry of health to make management measures more accessible and affordable to all adult male patients with urinary retention.
(2015). Income and Poverty in the United States: 2014.https://www.census.gov/conte nt/dam/Census/library/publications /2015/demo/p60-252.pdf
[7]. Patel,H.D.,Kamara,T.B.,Kushner,A. L.,Groen,R.S. and Allaf,M.E.(2014). Gross hematuria and urinary retention among men from a nationally representative survey in sierra leone. Urology, 83(6), 1273–1278.
[8]. Campain, N. J., MacDonagh, R. P., Mteta, K. A. and McGrath, J. S. (2015). Global surgery - How much of the burden is urological? BJU International, 116(3), 314–316. Cooney, M. M., Okuku, F., & Orem, J. (2016). Prostate Cancer Burden at the Uganda Cancer Institute, 2(4), 1–5.
[9]. Cyprien, Z., Timothée, K., Adama, O., Karim, P. A., Delphine, Y. O., Lazard, B. B. and Drissa, B. (2015). Acute Urinary Retention among Adult Men at Bobo-Dioulasso University Teaching Hospital: Epidemiology , Aetiologies and Initial Management, (June), 91–96.
[10]. Mahabeer, Y., Chang, C.C., Naidu, D., Dorasamy, A., Lewin, S. R., Ndung’u, T.,Moosa,M.S.,French,M.A.,Mlisana, K.P. and Coovadia, Y. M. (2014). ComparisonofEtestsandVitek2®to broth microdilution for the
http://www.inosr.net/inosr-scientific-research/ Turyasingura
INOSR Scientific Research 9(1):50-58, 2023.
susceptibility testing of Cryptococcus neoformans. Diagnosticmicrobiology andinfectiousdisease,804, 294-8.
[11]. Benfield, N , Young-Lin, N , Kimona, C , Kalisya, L M. and Kisindja, R M (2015).Fistulaafterattendeddelivery and the challenge of obstetric care capacity in the eastern Democratic Republic of Congo. Int J Gynecol Obstet. 2015; 130(2):157–60.
[12]. Krejcie, R. V. and Morgan, D. W. (1970). Determining Sample Size for Research Activities. Educational and Psychological Measurement. SmallSample Techniques (1960). The NEA Research Bulletin, Vol. 38.
[13]. Yenli, E. M. T., Aboah, K., GyasiSarpong, C. K., Azorliade, R. and Arhin,A.A.(2015).Acuteandchronic urine retention among adults at the urology section of the Accident and Emergency Unit of Komfo Anokye Teaching Hospital, Kumasi, Ghana. African Journal of Urology, 21(2), 129
136.
[14]. Gloria, N., A. O. Yamile and E Agwu (2022).Prevalence patterns of bacterial urinary tract infections among febrile children under-five years of age at Kampala International University Teaching Hospital. IDOSR Journal of Biology, Chemistry and Pharmacy 7 (1), 41-55.
[15]. Petrus,B.,E.NzabandoraandE.Agwu (2022).Factors associated with Pelvic Inflammatory Disease among Women Attending the Gynecology Clinic at Kampala International University Teaching Hospital, Uganda. IDOSR Journal of Biochemistry, Biotechnology andAlliedFields 7 (1), 48-63.
[16]. Ikuomola, E. O., O. S. Akinsonmisoye, R. O. Owolabi, and M. B Okon (2022).Assessment of Toxicity
Potential of Secnidazole on Reproductive System of Male Wistar Rats INOSR Applied Sciences 8 (1), 120-133.
[17]. Ikuomola, E. O., O. S. Akinsonmisoye, R. O. Owolabi and M. B. Okon (2022). Evaluation of the effect of secnidazole on the histology of the testes and epididymis of male Wistar rats. INOSR Experimental Sciences 8 (1), 84-94.
[18]. Dalton, K. M., A. C. Fardous and M. G. M. Lazaro (2022). Clinical presentation of Diabetic Peripheral Neuropathy among adults with Diabetes Mellitus attending Kampala International University Teaching Hospital. IDOSR Journal of Biochemistry, Biotechnology and AlliedFields 7 (1), 23-34
[19]. Petrus, B., N. Emmanuel and A. Ezera (2022). Bacteriology of Pelvic Inflammatory Disease among Women Attending the Gynecology Clinic at Kampala International University Teaching Hospital, Uganda. IDOSR JournalofExperimentalSciences 8(1), 1-14
[20]. Gloria, N., A. O. Yamile and E. Agwu (2022). Predictors Patterns of Bacterial Urinary Tract Infections among Febrile Children Under-Five YearsofAgeatKampalaInternational University Teaching Hospital. IAA Journal of Biological Sciences 9 (1), 39-60.
[21]. Gloria, N., A. O. Yamile and E. Agwu (2022). Susceptibility patterns of bacterial urinary tract infections among febrile children under-five years of age at Kampala International University Teaching Hospital. IAA Journal of Biological Sciences 9 (1), 61-79.