
http://www.inosr.net/inosr-experimental-sciences/
Abagye
INOSR Experimental Sciences 11(2):89-107, 2023.
©INOSR PUBLICATIONS
International Network Organization for Scientific Research
ISSN: 2705-1692
Evaluation of the factors that Contributes to Malnutrition, its significances and avoidance in children admitted at Kampala International University Teaching Hospital, Bushenyi District, Uganda.
Abagye, FrankSchoolofNursingScience,KampalaInternationalUniversityWesternCampus
ABSTRACT
Uganda has one of the highest levels of childhood stunting in sub-Saharan Africa. Western Uganda has persistently registered highest levels of childhood malnutrition despite being referred to as “the food basket” of the country. To assess factors contributing to malnutrition, its consequences and prevention among children less than five years of age admitted at Kampala International University Teaching Hospital (KIU-TH) was the aim of this study. A descriptive cross-sectional study design quantitative in nature was used in which96respondentsweregivenquestionnaires.55.2%oftherespondentsagreedthatlack of parental knowledge about infantile and childhood diet could contribute to malnutrition among children under five, 71% the respondents strongly agreed that malnutrition among childrenunderfiveyearsofagecouldcontributetoandperpetuatepovertyduetocostsof treatment and 70.8% of the respondents agreed that effective nutrition programs could help scale down prevalence of malnutrition among children under five years. The researcher concluded that the factors contributing to malnutrition among children under five years of age included; lack of parental knowledge about infantile and childhood diet, improper nutrition and dietary practices and infections. The consequences of malnutrition included; increased mortality, anaemia, poverty and effects on education and intellectual performance of children. Preventive measures of malnutrition identified included; Exclusive breast feeding for the first six-month, effective nutrition programs and promotinggoodhygienepractices.
Keywords:Malnutrition,childhooddiet,nutrition,poverty.
INTRODUCTION
Malnutrition is the cellular imbalance between the supply of nutrients, energy and the body’s demand for them to ensure growth, maintenance and specific functions [1][2][3][4][5][6][8][9][10]. The causes of malnutrition are multi-factorial. Dietary and environmental factors contribute to the risks of malnutrition in children[11][12][13][14][15]16][17][18].
The global number of child deaths under the age of five due to malnutrition recorded in 2008 by United Nations International Children’s Emergency Fund (UNICEF),WHO,United NationsPopulation Division (UNPD) and United Nations Statistics Division (UNSD), was around 10 million. During 2009, UNICEF recorded 9.2 million malnutrition related child
deaths under the age of five, globally [2] [19][20]. Globally, per region, 4.8 million child deaths were recorded in SubSaharan Africa; 900, 000 in East Asia and the Pacific; 3.1 million in South Asia; 400, 000 in the Middle East and North Africa and 300, 000 in Latin America and the Caribbean[21][22][23][24][25][26].
Africa shows rising numbers of stunted children due to population increase and an almoststagnantprevalenceofstunting over the past two decades that accounts for 90% of the global burden of malnutrition. In Africa, the estimated prevalence of under-five overweight increased from 4% in 1990 to 7% in 2011 and this trend is expected to continue [4][7][8][9][10][27][28[29]
http://www.inosr.net/inosr-experimental-sciences/
Despite Uganda’s favorable natural and human resource capacity, malnutrition remains one of the most important health and welfareproblems [5][11].Thecountry has one of the highest levels of stunting in Sub-Sahara Africa [6][12][13][30][31]
The 2008/09 Uganda Demographic and Health Survey (UDHS) showed that stunting was 39%, underweight 23% and wasting 4% among under-five children. The nutritional situation of the children has not significantly changed since the previousDemographicandHealthSurveys of late 1980’s and mid 1990s [7][14][15][32][33][34].
Itisimportanttonotethatmalnutritionis theunderlyingcauseofasmanyas45%of child deaths in Uganda. Children who are malnourished are at greater risk of infections (such as diarrhoea and pneumonia), which in turn increases the risk of malnutrition. Malnourished children also have a greater risk of developing chronic diseases (such as diabetes and heart disease) in adulthood [8][35][36][37][38].
A survey by [9] showed that the prevalence of malnutrition among children under 5 varied significantly by region in Uganda. The prevalence of stunting was highest in Karamoja followed by the Southwest and North, underweight was highest in East Central and the North and wasting was highest in Karamoja,EastCentral,theSouthwestand WestNileregions[10][16][17][18][39][40].
Malnutrition in children is the consequence of much food insecurity, which stems from poor food quality and quantity, severe repeated infections or combinations of all three. These conditions are linked to the standard of livingandwhetherbasicneedscanbemet [11][19][20][21].Thelackofknowledgeon the nutritional needs of children and the benefits of breastfeeding contributes to childhoodmalnutrition[12].Theextentof hunger has also been associated with low energy intake, low micronutrient intake and poor income levels. This affects growth patterns negatively [13]. Malnutrition can cause physical, cognitive and psychological impairment, which
over time causes permanent learning disabilities[14][22][23][24][25].
A study conducted in Kabarole district by [15] found that factors with a significant association with child stunting under two years included education level of caretaker and if the caretaker had receivedinformationonchildfeeding.
Statement of the Problem
The prevalence rate of global stunting is estimated at 39.1%, underweight 22.8% and global wasting 4.1% [16] Protein energy malnutrition is a major cause of morbidity and mortality in children in sub-Saharan Africa. The prevalence of malnutrition is high in Africa, with 38.6% of the children under five years stunted, 28.4% underweight, and 7.2% wasted [17][26][27][28]
Uganda has one of the highest levels of childhood stunting in sub-Saharan Africa. Under nutrition in Uganda remains severe. The Ministry of Health (MoH) indicatesthatundernutritiondirectlyand indirectly contributes up to 60% of child mortality in Uganda, which makes it a great contributor to childhood mortality inthecountry[18][28][29][30].
Meanwhile [19] noted that Western Uganda has persistently registered highest levels of childhood malnutrition despite being referred to as “the food basket” of the country. Almost half (46%) of children below 5 years were stunted, which is comparable to national prevalence of 47.8% for Western Uganda andthisisunacceptablyhigh[39][40][41]. Similarly, at Kampala International University Teaching Hospital (KIU-TH) though no published study has been conducted about contributing factors for malnutrition among children under five years, unpublished statistics indicate a high level of malnutrition of up to 30% in both in and out patients records hence a needtocarryoutthestudy.
Aim of the study
To assess factors contributing to malnutrition, its consequences and prevention among children under five years of age admitted at Kampala International University-Teaching Hospital.
http://www.inosr.net/inosr-experimental-sciences/
Specific objectives
i) To assess factors contributing to malnutrition among children under five years of age admitted at Kampala International University-Teaching Hospital.
ii) To find out consequences of malnutrition among children under five years of age admitted at Kampala International University-Teaching Hospital.
iii) To determine the preventive measures for malnutrition among children under five years of age admitted at Kampala International University-Teaching Hospital.
Research questions
i) What are the factors contributing to malnutrition among children under five years of age at Kampala International University-TeachingHospital?
ii) What are the consequences of malnutrition among children under five years of age at Kampala International University-TeachingHospital?
iii) What are the preventive measures of malnutrition among children under five years of age at Kampala International University-TeachingHospital?
Justification of the study
It is well documented that the nutritional status of young children is one of the most sensitive indicators of sudden changes in health status and food
Study Design and rationale
availability, acting as an indicator of socio-economic development. Uganda is heavily heat by malnutrition and poses heavy burden to the health sector in managing malnourished children and associated complications. The study findingswillthereforebebeneficialto;
The community
The community members will be encouraged to embrace infant and child feeding practices that promote healthy growthanddevelopment.
Nursing research
The study findings will be used as a reference for other researchers with similar interest in assessing factors contributing to malnutrition among childrenunderfiveyears.
Nursing education
The recommendations generated from this study may be integrated into nursing curriculum in order to address malnutrition among children under five yearsofage.
Nursing practice
Before interventions can be planned to the malnourished children, it is necessary to understand the causes, consequences and preventive measures of malnutrition, the findings of this study will therefore help the nurses in the prevention and management of malnutrition among childrenlessthanfiveyearsofage.
METHODOLOGY
This study was conducted through a descriptive cross-sectional study design quantitative in nature. The study design was selected because it aids in rapid data collection and allows a snap short interaction with a small group of respondents at a certain point in time thus allowing conclusions about phenomena across a wide population to be drawn. This method is also relatively inexpensive for the researcher as it takes a little time to conduct. The study design was used to examine mothers and care givers of children under five years of age aboutfactors contributingtomalnutrition amongchildrenunderfiveyearsofage.
Study setting
The study was carried out at Kampala International University-Teaching Hospital opened in January 2007 to help the already compromised health infrastructure in western Uganda. It is located in Ishaka municipality, Bushenyi district. It is approximately 375km by road south west of Kampala, Uganda’s largestcityandcapital.Thehospitalhasa capacity of 500 beds receiving both inpatient and outpatients with ultramodern technology and advanced patient care. It’s comprised of both private and public wing. The hospital is used to enhance learning of nursing and medical students. The hospital receives approximately 400 admissions per month in the paediatrics ward. Of these, 20% of
http://www.inosr.net/inosr-experimental-sciences/
are due to malnutrition and its complications.
Study Population
The study population consisted of mothers and caregivers of children aged 0-5 years who are admitted in the paediatricward.
Sample size determination
Sample size was determined using [20], method in which the sample size is given bytheexpression:
n= Z2pq
d2
n=desiredsamplesize
Z = Standard normal deviation usually set at 1.96 for maximum sample at 95% confidencelevel.
p=50%(constant)or0.5%sincetherewere nomeasuresestimated.
ThereforeP=1-O.5=0.5
q=1-p =1-0.5=0.5and,
d= Degreeofaccuracydesired0.1 0r 10% error acceptance (at 95% confidence level or0.09probabilitylevel)
BySubstitutionweget:
n= 1.962x0.5x0.5 =96 0.1x0.1
n=96. Therefore,thesamplesizewas96.
Sampling procedure and rationale. The researcher used a convenient sampling method which is a non probability sampling method which involves selecting participants that are easily accessible to participate in the research.Convenientsamplingischeapas it facilitates data collection in a short periodoftime.
Selection criteria
Inclusion criteria
The study included all mothers or caregivers of children aged 0-5 years admitted at Kampala International University-Teaching Hospital paediatric ward who were present at the time of the interview and willing to consent for the study.
Exclusion criteria
Respondents who were very sick, mentallyill,thedeaf,those withverysick children and those who did not consent wereexcludedfromthestudy.
Definition of variables Dependent variable
Prevalence of malnutrition among childrenaged0-5years.
Independent variable
Factors contributing to malnutrition among children under five years of age. Consequences of malnutrition among children under five years of age. Preventive measures of malnutrition amongchildrenunderfiveyearsofage.
Research Instruments
A structured questionnaire was used as a tool for gathering information. The structured questionnaire was divided into four sections; The first section was used to collect data about socio-demographic profile, the second section assessed factors contributing to malnutrition among children under five years of age, the third section assessed consequences ofmalnutritionamongchildrenunderfive years of age and the fourth section assessed preventive measures of malnutrition among children under five yearsofage.
Data collection procedure
After the approval of the proposal by the research committee of school of nursing sciences, an introductory letter was issued which the researcher used for seeking permission from Kampala International University-Teaching Hospital. Before sampling process was done, the researcher introduced himself to the prospective participants and read to the individual participant the consent formthatdetailedthetitleandpurposeof the study as well as the rights of the participant. Whenever a participant agreed to be interviewed, he/she was asked to provide written consent by signing or fingerprinting. If they refused to participate the interview would not proceed.
After obtaining the written consent, the researcher entered the questionnaire serial number and date of interview and proceeded from the first up to the last question using a language understood by the participant. The researcher entered responses given by the participant by
http://www.inosr.net/inosr-experimental-sciences/
ticking the appropriate responses and entering the same number in to the coding box. This was done to ensure data quality as the response number ticked was supposed to be the same as the one entered in the coding box. If the numbers were different, it would not be valid response. The researcher reviewed the questionnaires on a daily basis to ensure they were being completed correctly and any errors corrected to avoid being repeated. The process of data collection continued until every effort to contact every study participant in the sample. All completed questionnaires were kept safe bytheresearcheruntiltimeofanalysis.
Data management
Completed questionnaires were checked for accuracy, for any missing data and completeness on a daily basis after data collection at the end of the day. This was followed by coding and entry of the data using Epi info 3.4.1 software for Windows and double entry into Statistical Package for Social Scientists (SPSS) version 16.0 softwareforanalysis.
Data analysis and presentation
Data was analyzed by descriptive statisticsusingSSPSversion16.0software and presented in frequency tables, pie chartsandbargraphs.
Quality control techniques
For reliability and validity, the questionnaires was pretested with a tenth ofthesamplesizeoutsidestudyarea.The questionnaire was then be revised and content adjustments made accordingly. After data collection, questionnaires were checked daily, for completeness, clarity, consistency and uniformity by the researcher.
Ethical consideration.
Aletterofintroductionwasobtainedfrom Kampala International University Western Campus School of Nursing sciences to permit the researcher to carry out the research.
Permission was obtained from the Executive Director of Kampala International University-Teaching Hospital and ward in charge paediatrics ward.
All participating respondents were selected on the basis of informed consent.
The study was on voluntary basis and information was kept private and confidential. Participants' anonymity will be kept by use of codes instead of their names. The study was conducted while upholding the professional cord of conduct in a manner that did not compromise the scientific inclinations of theresearch.
http://www.inosr.net/inosr-experimental-sciences/
RESULTS
Bio demographic data
Table 1: Shows bio demographic data of the respondents (n=96)
More than half of the respondents (51%) were oftheagerangebetween 24-29years while only 4.2% were between 36-41 years. Most of the respondents 76% were female while only 24% were male. Majority of the respondents 92.7% were Banyankole while only 7.3% were Bakiga. Greater proportion of the respondents
(89.6%) were Christians while only 10.4% were Moslems. All the respondents (100%) weremarried.Majorityoftherespondents (79.2%) were unemployed while only 8.3% were employed. About three thirds of the respondents (77.1%) attained primary level of education while only 2.1% attainedtertiarylevelofeducation.
Factors contributing to malnutrition among children under five years Table 2: Shows response on whether lack of parental knowledge about infantile and childhood diet contributes to malnutrition among children under five years of age (n=96).
More than half of the respondents (55.2%) agreed that lack of parental knowledge about infantile and childhood diet could
contribute to malnutrition among children under five years of age while
http://www.inosr.net/inosr-experimental-sciences/
only 9.4% strongly disagreed and 19.8% disagreed.
malnutrition among children under five yearsofagewhileonly3%disagreed.
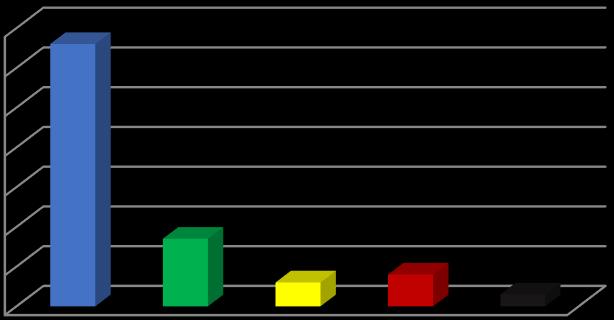
Figure 1: Shows response on whether improper nutrition and dietary practices contributes to malnutrition among children under five years of age (n=96). Most of the respondents (66%) strongly agreed that improper nutrition and dietary practices could contribute to
Table 2: Shows response whether infections and infestations contribute to malnutrition among children under five years of age (n=96).
Most of the respondents (62.5%) strongly agreed that infections and infestations could contribute to malnutrition among
children under five years of age while only8.3%disagreed.

http://www.inosr.net/inosr-experimental-sciences/
More than half of the respondents (58%) strongly agreed that household food insecurity was one of the contributing
factors to malnutrition among children under five years of age while only 7% disagreed.
Table 3: Shows response on whether irresponsible parenting and negligence contributes to malnutrition among children under five years of age (n=96).
Most of the respondents (72.9%) strongly agreed that irresponsible parenting and negligence contributes to malnutrition
among children under five years of age whileonly4.2%disagreed.
Consequences of malnutrition among children under five years.
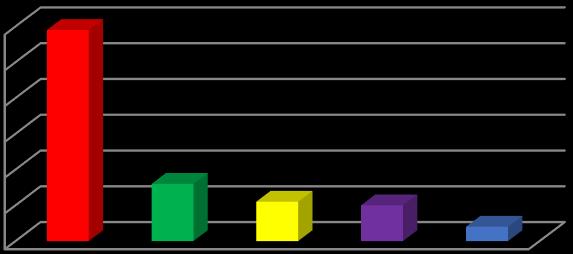
Figure 3: Shows response on whether malnutrition leads to increased mortality among children under five years of age (n=96).
More than half of the respondents (59%) strongly agreed that malnutrition leads to increasedmortalityamongchildren under fiveyearsofagewhileonly4%disagreed.
Table 4: Shows response on whether malnutrition can cause anaemia among children under five years of age (n=96).
Most of the respondents (69.8%) strongly agreed that malnutrition can cause
anaemia among children under five years ofagewhileonly6.3%disagreed.
http://www.inosr.net/inosr-experimental-sciences/
Neither agree nor disagree
Strongly disagree
Figure 4: Shows response on whether malnutrition among children under five years of age can contribute to and perpetuate poverty due to costs of treatment (n=96). Most of the respondents (71%) strongly agreed that malnutrition among children under five years of age can contribute to
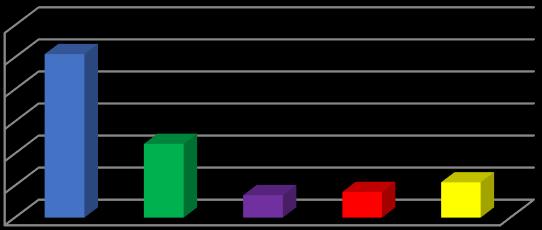
and perpetuate poverty due to costs of treatment while only 2% strongly disagreed.
Table 5: Shows response on whether malnutrition affects education and intellectual performance of children (n=96).
More than half of the respondents (57.3%) strongly agreed that malnutrition could affect education and intellectual
performance of children while only 9.4% disagreed.
Preventive measures of malnutrition among children under five years.
Neither agree nor disagree
Strongly disagree
Disagree
response on whether exclusive breast feeding for the first six month could help prevent malnutrition among children under five years of age (n=96).
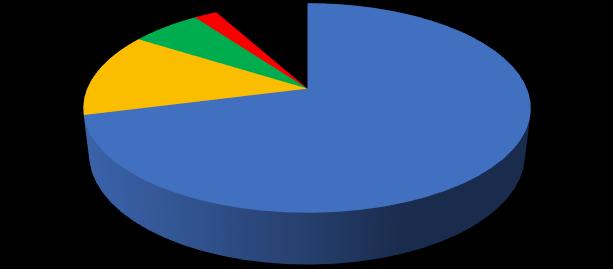
Figure 5:
More than half of the respondents (51%) stated that exclusive breast feeding for
http://www.inosr.net/inosr-experimental-sciences/
the first six month helps in preventing malnutrition among children under five
years of age while only 7% disagreed.
Table 6: Shows response on whether effective nutrition programs could help in scaling down the prevalence of malnutrition among children under five years (n=96).
Greater proportion of the respondents (70.8%) agreed that effective nutrition programs could help in scaling down the
prevalence of malnutrition among children under five years while only 2.1% disagreed.
agree
Neither agree nor disagree
Strongly disagree
Figure 6: Shows response on whether promoting good hygiene practices could help in preventing malnutrition among children under five years of age (n=96). Mostoftherespondents(65%)agreedthat promoting good hygiene practices could help in preventing malnutrition among
children under five years of age while only2%neitheragreednordisagreed.
Table 7: Shows response whether promoting maternal nutrition education and growth monitoring programs could help in the fight against malnutrition among children under five years of age (n=96).
More than half of the respondents (56.3%) agreed that promoting maternal nutrition education and growth monitoring programs could help in the fight against
malnutrition among children under five years of age while only 3.1% and 10.4% disagreed and strongly disagreed respectively.
http://www.inosr.net/inosr-experimental-sciences/
Figure
Biodemographic data
help in preventing malnutrition among children under five years of age while only2%disagreed.
DISCUSSION
More than half of the respondents (51%) were of the age range between 24-29 years whileonly 4.2% werebetween 36-41 years. The age of the parent or caregiver can have influence in the nutritional status of the child due to experience generated over time and it is common for young parents or caregivers to seek guidance from elders though it may not be professional but might benefit them basingonexperience.
Most of the respondents 76% were female while only 24% were male. Although this studydidnotcorrelate betweengenderof the parents and malnutrition in children, it is worth noting that the female gender inAfricansocietiesistheonethatismost of the time in contact with the young childrenandarethereforethefirstpeople to notice any changes in the health status of the child and seek medical interventions while the male genders is concerned with meeting the costs of treatment and managing other family affairstheythereforeonlypayshortvisits to the hospital to see the progress of medical treatment and meet any necessarycosts.
Majority of the respondents 92.7% were Banyankole while only 7.3% were Bakiga. Certain tribes have cultural practices that may encourage malnutrition among children for example tabooing children from consuming certain foods such as eggs.Thesefindings alsosupport the fact that the Banyankole and Bakiga are the
indignant tribes of the study area and are themajority.
Majority of the respondents (89.6%) were Christians while only 10.4% were Moslems. Religion can as well influence the nutritional status of the child and medical interventions for example some religions discourage certain types of food as well medical intervention such as blood transfusion which is very crucial in managing a severe malnourished child withanaemia.
All the respondents (100%) were married. Married couples share collective responsibility of taking care of the child and share costs of treating the child hence better management of childhood infections which also pose a risk for malnutrition.[32][32][33][42][43][44][45]
Majority of the respondents (79.2%) were unemployed while only 8.3% were employed. Employment status of the respondents can influence his ability to afford the cost of feeding the child and meeting the treatment costs in case of any illness therefore they are better preparedforthecare comparedtotheun employed parents or caregivers. This study findings agree with the findings of [13] who linked malnutrition to poor incomelevels.
Majority of the respondents (77.1%) attained primary level of education while only 2.1% attained tertiary level of education. Educational status of the respondent determines his or health seeking behavior in that educated parents
http://www.inosr.net/inosr-experimental-sciences/
or caregivers tend to have better health seeking behavior and take up health messagespositivelyhencearemorelikely to participate in nutritional programs compared to the un educated ones. This study findingsarein line with thefinding in a study conducted in Kabarole district by [15] that revealed that factors with a significant association with child stunting under two years included education level of caretaker and if the caretaker had receivedinformationonchildfeeding. Factors contributing to malnutrition among children under five years
More than half of the respondents (55.2%) agreed that lack of parental knowledge about infantile and childhood diet could contribute to malnutrition among children under five years of age while only 9.4% strongly disagreed. Parental knowledgeaboutmalnutritionisvitalasit influences selection of food choices for the child as well as the frequency of feeding the child, Its further important in that it influences the nutritional status of themotherfromthetimeofpregnancyup to the time of breast feeding which in turn indirectly influences the nutritional status of the infant. The high percentage of 55.2shows that parents had awareness got from health workers. This study findings concur with the findings of [21][34][35][36][46][47][48][49][50] who identifiedparentalfactorsassociatedwith malnutrition in children to include parents’ being unaware of the fact that children’s diet is versatile and if the importance of breast feeding is not fully understood and that mothers suffering from malnutrition give birth to malnourished children and because their breast milk does not contain the important nutrients that the infant needs, malnutritionwillbeexacerbated.
Most of the respondents (66%) strongly agreed that improper nutrition and dietary practices could contribute to malnutrition among children under five years of age while only 3% disagreed. Impropernutritionpracticessuchasearly weaning or delayed weaning, poor dietary choices for children for example feeding them with too much of one food type as well as underfeeding could contribute to
malnutrition [50][51][52][53][54][55]. The higher parental awareness from the findings is as result of increased number of malnourished children being admitted and education talks by health workers. This study findings agree with the findings of [22] who stated that several factors play a role in malnutrition in children which include but not limited to poor dietary practices such as inadequate infant and young child feeding [37][38]39]. The study findings also agree with the findings of [23] who found out that proper nutrition and dietary practices were un even in Uganda, while 98% of children were breastfed for some period of time, only 63% of children less than 6 months were exclusively breastfed and that among all children aged 6-23 months, only 13% were fed with the correctdiet[40][41].
Most of the respondents (62.5%) strongly agreed that infections and infestations could contribute to malnutrition among children under five years of age while only 8.3% disagreed. It is true that infections decrease the child’s appetite and interfere with absorption of nutrients whereas infestations for example hook worm infestations compete with the host for nutrients and as well causing complications like anaemia which make malnutrition worse. This study findings concur with the findings of [8] who mentioned diseases like HIV, measles, diarrhoea and infestations like hookworms among others are the underlying causes of malnutrition among children. More than half of the respondents (58%) strongly agreed that household food insecurity was one of the contributing factors to malnutrition among children under five years of age while only 7% disagreed. Availability is crucial in determining the frequency of feeding and therefore the nutritional status of the child. This study findings agree with the findings of [24] who mentioned food insecurity as one of the second group of the underlying causes of malnutrition among children. The findings also agree with the finding of [14] who stated that the level of food insecurity within the household
http://www.inosr.net/inosr-experimental-sciences/
determines the nutritional status of children and is the immediate cause of malnutrition. The findings further concur with the findings of [25], who stated that seasonality in food production, variable food prices and seasonal earning patterns exacerbate the instability and the poor quality of the diet the household consumes throughout the year and could leadtomalnutritioninchildren[42][43].
Most of the respondents (72.9%) strongly agreed that irresponsible parenting and negligence contributes to malnutrition among children under five years of age while only 4.2% disagreed. Irresponsible parenting such as poor child spacing, in adequateprovisionofbasicneedssuchas food and health care as well having large family sizes could contribute to malnutrition among children. This study findings are in line with the findings of [26] who stated that care related constraints lead to both inadequate dietary intake and a high disease burden in young children all of which are associatedwithmalnutrition[44].
Consequences of malnutrition among children under five years.
More than half of the respondents (59%) strongly agreed that malnutrition leads to increasedmortalityamongchildren under five years of age while only 4% disagreed. It is true malnutrition is associated with complications, some of them can be so severe and acute that if not appropriately intervened in time could lead to mortality. This study findings are in line with the findings of [27] who stated that malnutrition kills many children in Uganda each year and that Low Birth Weight (LBW)isrampantin Ugandadueto maternalmalnutrition.
Most of the respondents (69.8%) strongly agreed that malnutrition could cause anaemia among children under five years ofagewhileonly6.3%disagreed.Anaemia isoneofthemostcommonandimportant cause of mortality among the malnourished if the causes are not corrected in time. This study findings are tandem with the findings of a study in Nigeria by [28] that found that anaemia affected49%ofchildrenwithmalnutrition and that without any intervention, 15,000
children would die of anaemia related causesbetween2006and2015. Most of the respondents (71%) strongly agreed that malnutrition among children under five years of age could contribute to and perpetuate poverty due to costs of treatment while only 2% strongly disagreed. Malnutrition like any disease has a lot of costs in trying to regain the normalstateoffunctioningofthebodyas intreatmentandrehabilitationcosts.This study findings agree with the findings of [29], who stated that malnutrition contributes to poverty for example Uganda loses US$310 million worth of productivity per year due to the high levels of stunting, iodine-deficiency disorders, iron deficiency, and low birth weight.
More than half of the respondents (57.3%) strongly agreed that malnutrition could affect education and intellectual performance of children while only 9.4% disagreed. Malnutrition not only impairs physicaldevelopmentbutalsointellectual development which causes poor performance in both social and academic aspectsoflife.Thisstudyfindingsconcur with the findings of [30] who stated that malnutrition affects the education and intellectual potential of children during school years and that stunting causes children to start school late because they looktoosmallfortheirage.
Preventive measures of malnutrition among children under five years
More than half of the respondents (51%) stated that exclusive breast feeding for the first six month could help prevent malnutrition among children under five years of age while only 7% disagreed. Breastmilkcontainsallthefoodnutrients that the baby requires for proper growth anddevelopmentthereforeinfantsshould be exclusively breastfed for the first six month and then gradually weaned off sincebysixmothofagebreastmilkalone will no longer be sufficient to provide adequate amount of nutrients for infant growth. This study findings are in line with the findings of [1] who stated that exclusive breast feeding for the first six month then continued up to 2 years after weaning is one of the best strategies to
http://www.inosr.net/inosr-experimental-sciences/
minimize malnutrition among children and that during the first six months of breast feeding the infant receives enough nutrients for growth and development and the risk of acquiring infections is reduced due to immune benefits or antibodiescontainedinmilk.
Most of the respondents (70.8%) agreed that effective nutrition programs could help scale down prevalence of malnutrition among children under five years while only 2.1% disagreed. To prevent malnutrition, it is important to deal with the root causes of malnutrition operating locally in the community by designing and implementing appropriate interventions and programs involving the community members ratheronlyfocusing on curative approach. This study findings are in line with the findings of [31] who stated that identifying and implementing cost effective nutrition programme models that are scalable at both district and national levels could help minimize prevalence of malnutrition among children and that such models would involve behaviour change and social marketing, fortification of common staple foods, use of bio-fortified produce, and micronutrient supplementation programs among others. The study findings also agree with the findings of [14] who stated that planning nutrition programs appropriately and whenever possible, the programs should be planned, managed and implemented at community and local government levels in a cross sectoral manner targeting geographic areas where young child and mothers are most vulnerabletomalnutrition.
Mostoftherespondents(65%)agreedthat promoting good hygiene practices could help prevent malnutrition amongchildren under five years of age while only 2% neither agreed nor disagreed. Good hygiene or sanitation practices helps to prevent malnutrition by minimizing the risk of acquiring infections and worm infestations. This study findings are in line with the findings of [8] who stated that promoting good hygiene practices increases community awareness and reduces helminth related diseases and that regular hand washing and promotion
of this through awareness can reduce diarrhoea morbidity which contributes to andcomplicatesmalnutrition.
More than half of the respondents (56.3%) agreed that promoting maternal nutrition education and growth monitoring programs could help in the fight against malnutrition among children under five years of age while only 3.1% disagreed. It is important to note that the more knowledgeable the mother is about nutrition of the child and herself, the more likely that she will translate this knowledge into practice and improve her nutritional status and that of her baby. This study findings are in line with the findings of [7] who urged that promotion of maternal nutrition education programs could be beneficial in reducing childhood malnutrition as the child’s survival is dependent on promoting maternal knowledge on appropriate feeding practices.
Mostoftherespondents(68%)agreedthat community-based programs such as immunization, micronutrient supplementation and deworming could help prevent malnutrition amongchildren under five years of age while only 2% disagreed. In addressing the problem of malnutrition, it is prudent to tailor approach that tackles the causes of malnutrition by designing programs such as mass immunization and deworming of children. This study findings are in line with the findings of [10] who stated that growth monitoring and promotion programs with intent to support families to monitor and address nutrition and health related problems is important in addressing issues to do with malnutrition in children.Thestudyfindingsarealsoin line with the findings of [11] who stated that. Supplementation was beneficial in reducing nutrition-related deficiencies in Ethiopia by 50%. The study findings further agree with the findings of [32] who found out in Kenya that addressing severe child malnutrition in institutions or community settings through community-based programs such as immunization,vitaminAsupplementation and deworming against helminthes showed30%reductioninmalnutrition.
http://www.inosr.net/inosr-experimental-sciences/
The following conclusions were drawn as result of the research work carried out to assess the factors contributing to malnutrition, its consequences and preventive measures among children underfiveyearsofage:
i) The study findings revealed factors contributing to malnutrition among children under five years of age such as; lackofparentalknowledgeaboutinfantile and childhood diet, improper nutrition and dietary practices, infections and infestations, household food insecurity and irresponsible parenting and negligence.
ii) The study findings also revealed consequences of malnutrition such as; increased mortality, anaemia, Poverty and affects education and intellectual performanceofchildren.
iii)Preventive measures of malnutrition identified in the study findings included; Exclusive breast feeding for the first sixmonth, effective nutrition programs, promoting good hygiene practices, promoting maternal nutrition education and growth monitoring programs and community-based programs such as immunization, micronutrient supplementation and deworming
REFERENCES
[1]. Onis, M., Monteiro, C. and Akre J. (2013). The worldwide magnitude of protein energy malnutrition; an overview from the WHO Global Database on Child Growth. Bulletin oftheWorldHealthOrganization. 71 :703-712.
[2]. Venture, A. K., Gromis, J. C. and Gohse, B. (2010). Feeding Practices and Styles Used by a Diverse Sample of Low-income Parents of Preschoolage Children. Journal of Nutrition Education and Behaviour (JNEB), 42(3):98-9.
[3]. Yambi, O. and Belbase, K. (2013). Towards Institutionalization of Community based Actions to ImproveChildNutrition.AReviewof African Experience. Modern Aspects of Nutrition New York: Karger. pp. 111-113.
[4]. Brown,G.A.,Bull,J.andPendlebury, M. (2013). Assessingstudentlearning inhighereducation.Routledge.
[5]. Olwedo, M. A., Mworozi, E., Bachou, H. and Garimoi, O. C. (2009). Factors associated with malnutrition among children in internally displaced person's camps, northern Uganda. Medical education resource Africa,(39),244.
[6]. Jitta,D.J.,Wagenaar,L.J.,Mulder,B. J., Guichelaar, M., Bouman, D. and vanMelle,J.P.(2016).Threecasesof hepatocellular carcinoma in Fontan patients: reviewof the literature and suggestions for hepatic
screening. International Journal of Cardiology, 206,21-26.
[7]. Bryan, N. S., Alexander, D. D., Coughlin, J. R., Milkowski, A. L. and Boffetta, P. (2012). Ingested nitrate and nitrite and stomach cancer risk: an updated review. Food and Chemical Toxicology, 50(10), 36463665.
[8]. Grantham, R., McGregor, S. and Ani, C. (2011). A review of studies on the effectofiron Health. JAMA 270:6005.
[9]. Sebudde,S.andNangendo,F.(2009). Voluntary counselling and testing services: breaking resistance to access and utilization among the youths in Rakai district Uganda. EducResRev, 4,490-7.
[10]. Vella, S., Schwartländer, B., Sow, S. P., Eholie, S. P. and Murphy, R. L. (2012). The history of antiretroviral therapyandofitsimplementationin resource-limited areas of the world. Aids, 26(10),1231-1241.
[11]. Wright, N.D., Lukoschek, P. and Wylie-Rosett, J. (2007). The School Yard Kids: A puppet Show to promoteahealthfullifestyle. Journal ofNutritionEducationandBehaviour (JNEB), 39(5):290-294.
[12]. Walsh, C. and Joubert, G. (2009). Nutritional surveys. Epidemiology. A Research Manual for South Africa. 2ndEdition.OxfordUniversityPress. SouthernAfrica.Chap.24.p11
http://www.inosr.net/inosr-experimental-sciences/
[13]. Labadarios,D.,Swart,T.,Maunder,E. M. W., Kruger, H. S., Gericke, G. J., Kuzwayo,P.M.N.,Ntsie,P.R.,Steyn, N. P., Schloss, I., Dhansay, N. A., Jooste, P. L., Dannhauser, A., Nel, J. H.,Molefe,D.andKotze,T.J.(2008). National Food Consumption Survey: Fortification Baseline (NFCS-FB-1): South African Journal of Clinical Nutrition(SAJCN), 21(3):254-267.
[14]. Pelletier, D., Frangillo, E. J. R. Schroeder, D. G. and Habicht, J. P. (2009). The effects of Malnutrition on child mortality in developing countries. Bulletin of World Health Organization,73(4):443-448.
[15]. Knai, C., Nolte, E. and McKee, M. (2008). Caring for people with chronic conditions–experience in eight countries. Copenhagen: WHO RegionalOfficeforEurope
[16]. Bhutta, Z. A. and Salam, R. A. (2012). Global nutrition epidemiology and trends. Annals of Nutrition and Metabolism, 61(Suppl.1),19-27.
[17]. Zottarelli, L. K., Sunil, T. S. and Rajaram, S. (2007). Influence of parental and socioeconomic factors on stunting in children under 5 years in Egypt. EMHJ-Eastern MediterraneanHealthJournal,13(6), 1330-1342,2007.
[18]. Pitt, M. and Rosenzweig, M. (2009). Estimating the Intra Household Incidence of Illness: Child Health and Gender Inequality in the Allocation of Time. International EconomicReview 31,1139-1156.
[19]. Black,R.E.,Allen,L.H.,Bhutta,Z.A., Caulfield, L. E., De Onis, M., Ezzati, M. and Rivera, J. (2008). Maternal and child undernutrition: global and regional exposures and health consequences. The lancet, 371(9608),243-260.
[20]. Fisher, S. and Groce, S. B. (1990). Accounting practices in medical interviews1. Language in Society, 19(2),225-250.
[21]. Kruger, R. and Gericke, G.J. (2013). A qualitative exploration of rural feeding and weaning Practices, knowledge and attitudes on
nutrition. Public Health and Nutrition, 6(2):217-223,April2003.
[22]. Danton, W., Hill, I., Nishida, C. and James, T. (2014). A life course approach to diet, nutrition and the Prevention of chronic diseases. PublicHealthNutrition 7(1):101-21.
[23]. Horton, S., Alderman, H. and Rivera, A. l. (2008). Copenhagen Consensus 2008 Challenge Paper: Malnutrition and Hunger. Washington, DC: World Bank.
[24]. Brabin, B. J. (2012). Iron deficiency anemia: Reexamining the nature and magnitude of the Deficiency on cognitive development in children. JournalofNutrition 131:649-66.
[25]. Binengank, F. (2012). Monitoring the severity of Iodine Deficiency disorders in Uganda. Journal of AfricanHealthSciences 2(2):63-8.
[26]. Kabubo, M J., Ndenge, G. K. and Kirii, D. M. (2009). Determinants of Children’s Nutritional Status in Kenya: Evidence from Demographic and Health Surveys. Paper Presented attheCentrefortheStudyofAfrican Economies Conference, University of Oxford,March17-21,2008.
[27]. Pitt, M. and Rosenzweig, M. (2011). Estimating the Intra Household Incidence of Illness: Child Health and Gender Inequality in the Allocation of Time. International EconomicReview 31,1139-1156.
[28]. Smith, L. C. and Haddad, L. (2012). Explaining Child Malnutrition in Developing Countries: A CrossCountry Analysis. IFPRI FCND Discussion Paper No. 60, IFPRI, Washington,D.C.USA
[29]. Armar, K., M., Ruel, M. T., Maxwell, D. G., Levin, C. E. and Morris, S. S. (2010). Poor Maternal Schooling is the Main Constraint to Good Childcare Practices in Accra. Journal ofNutrition,130,1597-1607.
[30]. Wamani, H., Nordiehaug, A. and Stefan, P. (2008). Boys are more stunted than girls in Sub-Saharan Africa: a meta-analysis of 16 demographic and health surveys. BMCPaediatrics7;(17):23-31
http://www.inosr.net/inosr-experimental-sciences/
[31]. Klugman, G. (2012). Addressing malnutrition in South Africa. Science in Africa. June 2012. Available at: <http://www.scienceafrica.co.za/20 02/june/food2.htm>. Accessed 20/02/2016.
[32]. Toole, M. J. and Waldman, R. J. (2007). Refugees and displaced persons. War, hunger and public Public health problem. An analysis of anemia and child mortality. JournalofNutrition 131(2):636-648.
[33]. Eze, E. D., Barasa, A., Adams, M. D., Rabiu,K.M.,Ayikobua,E.T.,Ezekiel, I. and Okpanachi, A. O. (2018). Assessingfactorscontributingtothe prevalence of protein–energy malnutrition among children under five years of age attending Kigoma District Hospital, Tanzania. Journal of Food and Nutrition Sciences, 6(5), 123-128.
[34]. Mada, S. B., Bawa, K. D., Saliu, M. A., Garba, A., Abarshi, M. M., Muhammad, A. and Garba, I. (2020). Evidence of Malnutrition and its AssociatedFactorsamongUnder-five Children in Danko-Wasagu Kebbi State, North-western Nigeria. Nigerian Journal of Basic andAppliedSciences, 28(1),56-65.
[35]. Odwee, A., Kasozi, K. I., Acup, C. A., Kyamanywa, P., Ssebuufu, R., Obura, R. and Bamaiyi, P. H. (2020). Malnutrition amongst HIV adult patients in selected hospitals of Bushenyi district in southwestern Uganda. African health sciences, 20(1),122-131.
[36]. Achinewhu,S.C.,Ogbonna,C.C.and Hart, A. D. (1995). Chemical composition of indigenous wild herbs, spices, fruits, nuts and leafy vegetables used as food. Plant Foods forHumanNutrition,48(4),341-348.
[37]. Afiukwa, C. A., Ogah, O., Ugwu, O. P. C.,Oguguo,J.O.,Ali,F.U.andOssai, E. C. (2013). Nutritional and antinutritional characterization of two wild yam species from Abakaliki, Southeast Nigeria. Research Journal of Pharmaceutical, Biological and Chemical Sciences, 4(2),840-848.
[38]. Asomugha, I. C., Uwaegbute, A. C. and Obeagu, E. I. (2017). Food insecurity and nutritional status of mothers in Abia and Imo states, Nigeria. Int. J. Adv. Res. Biol. Sci, 4(10),62-77
[39]. Ibegbu, A. O., Saidu, U., Shuaibu, A., Musa,S.A.,Ibe,U.M.,&Ezemagu,K. U. (2018). Assessment of nutritional status in Hausa infants using some anthropometric variables in Zaria Area of Kaduna State Nigeria. Bionature,240-248.
[40]. Ifeanyi, O. E. (2018). A review on nutritional anaemia. International Journal of Advanced Multidisciplinary Research, 5(4), 1115.
[41]. Kumbakulu, P. K., Ndeezi, G., Egesa, W. I., Nakalema, G., Odoch, S., Kambele, R. L. and Nduwimana, M. (2022). Prevalence, feeding practices, and factors associated with undernutrition among HIVexposed uninfected children aged 6 to 18 months in Bushenyi district, western Uganda: A cross-sectional study. Research Square, Pp 1-22, DOI:https://doi.org/10.21203/rs.3.r s-2079841/v1
[42]. Moses,E.,Ogbanshi,L N.,Ebenyi,M C., Ominyi, B U., Nwali, N E, Ali, F U. and Esther, U. A. (2022). Comparative Evaluation of Nutritional and Toxicological Implication of Consumption of Wild Fishes from Ebonyi River and Fishes Cultured in Concrete Pond with Different Feed Formulations. InternationalJournalofBasicClinical Toxicology,1(2):1-7.
[43]. Olagunju, A., Muhammad, A., Aliyu, S.,Mada,S.B.,Isah,R.,Abdullahi,S., and Nasrin, A. (2013). Nutritional values of powdered milk commercially consumed in West Africa. Int.J.FoodNutr.Saf, 4(2),5561
[44]. Obeagu, E. I., Okwuanaso, C. B., Edoho, S. H. and Obeagu, G. U. (2022). Under-nutrition among HIVexposed Uninfected Children: A Review of African Perspective. Madonna University
http://www.inosr.net/inosr-experimental-sciences/
journal of Medicine and Health Sciences ISSN: 2814-3035, 2(3), 120127.
[45]. Enechi, O.C., Ugwu, Kenneth K., Ugwu Okechukwu P.C. and Omeh YS (2013).Evaluation of the Antinutrient Levels of Ceiba Pentandra Leaves IJRRPAS 3(3),394400
[46]. Afiukwa CA, Oko A, Afiukwa JN, Ugwu OPC, Ali FU and Ossai EC. (2013). Proximate and Mineral Element Compositions of Five Edible Wild Grown Mushroom Species in Abakaliki, Southeast Nigeria Research Journal of Pharmaceutical, Biological and Chemical Sciences, 4(2): 1056-1064
[47]. OfforCE,PCUOkechukwu,UAEsther (2015).Determination of ascorbic acid contents of fruits and vegetables Int.J.Pharm.Med. Sci 5, 1-3
[48]. Afiukwa CA, IO Igwenyi, O Ogah, CE Offor and OO Ugwu (2011).Variations in seed phytic and oxalic acid contents among Nigerian cowpea accessions and their relationship with grain yield. Continental Journal of Food Science andTechnology 5(2),40-48
[49]. Asogwa FC, PCU Okechukwu, UA Esther, OE Chinedu, E Nzubechukwu (2015). Hygienic and sanitary assessmentofstreetfoodvendorsin selected towns of Enugu North District of Nigeria AmericanEurasian Journal of Scientific Research 10(1),22-26
[50]. Enechi, OC., C D Peter, OPC Ugwu, SMC Udeh and Y S Omeh (2013). Evaluation of the nutritional potential of Ceiba pentandra leaves. MintageJournalofPharmaceutical& MedicalSciences 2(3),25-27
[51]. Nassali S. (2023).Evaluation of the impacts of care givers on malnourished children in Ishaka Adventist Hospital. IDOSRJournalof ExperimentalSciences 9(1),11-29.
[52]. Patrick M. (2023).Evaluation of Factors that are influencing quick initiation of Breast Feeding in Post Natal Mothers at Kabale Regional
Referral Hospital. IDOSR Journal of Biology, Chemistry and Pharmacy 8 (1),1-14.
[53]. Awino S. (2023).Factors Associated with under Nutrition in Children under Five Years in Bangaladesh Parish, Namasale sub-County, Amolatar District INOSR Scientific Research 9(1),59-68.
[54]. Teko F. (2023).Factors Related to Malnutrition among Children Below Five Years in Rengen Health Center III, Kotido District INOSR Experimental Sciences 11 (1), 112124
[55]. Ganafa A (2023)Knowledge, Attitude and Practices regarding Exclusive Breastfeeding Among Mothers Attending Maternal Child Health Clinic at Kitagata Hospital, SheemaDistrict,Uganda IAAJournal ofAppliedSciences 9(1),17-26
http://www.inosr.net/inosr-experimental-sciences/
Abagye, Frank (2023). Evaluation of the factors that Contributes to Malnutrition, its significances and avoidance in children admitted at Kampala International University Teaching Hospital, Bushenyi District, Uganda. INOSR Experimental Sciences 11(2):89106.