


Get the definitive diagnosis for targeted treatment with BakoDx's PCR Test
The Difference with Our Proprietary PCR Technology

629 West Hillsdale St. Lansing, MI 48933 (800) 968-6762 www.MPMA .org
Derek E. Dalling Executive Director derek@kdafirm.com
Jason Wadaga Deputy Executive Director jason@kdafirm.com
Geri Root Director of Events geri@kdafirm.com
Trina Miller Membership Director trina@kdafirm.com
Lauren Concannon Continuing Education Coordinator lauren@kdafirm.com
Melissa Travis Advertising Coordinator melissa@kdafirm.com
Lauren Gass Legislative Assistant lgass@kdafirm.com
Miranda Strunk Financial Administrator miranda@kdafirm.com
Brooklyn Heath Administrative Assistant brooklyn@kdafirm.com

Kathy Schaefer Writer, Editor cr@crmarketing.biz
Joe Ross Writer, Editor cr@crmarketing.biz
Allison Clemons Graphic Designer cr@crmarketing.biz
Spartan Printing & Promotional Products www.printspartan.com

Dr. Andrew Mastay
PRESIDENT
Andrew Mastay, DPM
PRESIDENT ELECT
Joshua Faley, DPM
TREASURER
Bruce Jacob, DPM
SECRETARY
Michele Bertelle, DPM
IMMEDIATE PAST PRESIDENT
Zeeshan Husain, DPM
UPPER PENINSULA
Jake Eisenschink, DPM
MACOMB/OAKLAND
Marc Weiner, DPM
NORTHEAST
Joyce Patouhas, DPM
WESTERN
Vacant
SOUTHEAST
Crystal Holmes, DPM
Randy Kaplan, DPM
SOUTHERN
Mark Hosking, DPM
Colleagues,
As we move into the heart of a Michigan winter, I’m grateful for the strength and steadiness of this Association—and for the work you do every day to protect mobility, preserve limb health, and improve quality of life for patients across our state. This issue of Podiatric Profiles reflects that full scope: clinical excellence, public education, and the advocacy required to keep podiatric physicians practicing to the full extent of our training.
On the advocacy front, MPMA acted quickly when recent changes to Michigan’s educational limited license rules created an unexpected barrier for incoming podiatric residents. Thanks to prompt coordination with LARA and the Board of Licensing and Regulation for Podiatric Surgery, the immediate obstacle was suspended for residents already matched to Michigan programs—and the underlying rules are now under formal review. Protecting a clear, stable licensure pathway is not administrative “busy work.” It is essential for residency continuity, patient access, and parity with MD/DO training models.
This winter edition also highlights how podiatry supports people where Michigan lives—on the ice. From high ankle sprains and skate-related tendon irritation to overuse injuries and stress reactions in figure skating, our specialty plays a key role in accurate diagnosis, return-to-sport planning, and prevention strategies that keep athletes and recreational skaters moving with confidence.
Clinically, you’ll also find timely practice-relevant updates, including how ICD-10-CM interpretations and FY2026 code changes can affect documentation and claims—and a patient safety reminder on cannabis use and wound recovery, particularly for patients with diabetes or chronic wounds.
Finally, I encourage you to stay engaged: join us at the MPMA Great Lakes Conference (February 18–22, 2026), and consider supporting our advocacy efforts through MPAS and APMAPAC. When we invest together, we protect our patients, our practices, and the future of podiatric medicine in Michigan.
With appreciation, Andrew Mastay, DPM President, Michigan Podiatric Medical Association
View & Register for Great Lakes Conference (See pages 6-11)


In 2025, a change in Michigan’s podiatric licensure rules created an unexpected barrier for new podiatric residents—one that could have disrupted an entire class of trainees already matched to residency programs in the state. Through prompt communication and collaboration with state regulators, that immediate issue has now been resolved, and the underlying rules are under formal review.
The Michigan Department of Licensing and Regulatory Affairs (LARA) updated the rules governing educational limited licenses for podiatric physicians. These licenses are required for newly matched DPM graduates to begin practicing within their Michigan residency programs.
A similar situation occurred during the COVID-19 pandemic, when emergency-era adjustments to licensure requirements created uncertainty for podiatric residents. At that time, the MPMA worked with LARA to align DPM resident licensure more closely with the pathways used for MD and DO residents, helping to clarify expectations and maintain parity across physician training programs.
The most recent rule change, however, effectively reverted to the earlier, more restrictive framework that had been used during the pandemic. As written, it would have prevented an entire upcoming year of matched podiatric residents from receiving the licenses they need to practice in Michigan.
If left unaddressed, the change would have meant that residents already matched to Michigan programs might not have been able to obtain the licensure necessary to begin practice. Residency programs would have been forced to manage sudden disruptions in staffing, scheduling, and clinical coverage, at the same time they were expecting a new cohort of trainees to arrive. These disruptions would not only have affected educational continuity for residents, but also could have had a direct impact on patient access to podiatric care in teaching hospitals and clinic
settings across the state. Understandably, program directors and residents raised concerns about the implications for trainees who had already made professional and personal commitments based on their Michigan match.
Once the impact of the new rule language on podiatric residents became clear, MPMA reviewed the changes and communicated its concerns to LARA and the Board of Licensing and Regulation for Podiatric Surgery. Those discussions focused on ensuring that residents already matched to Michigan programs could still obtain educational
A key consideration throughout was maintaining as much alignment as possible with the licensure pathways used for MD and DO residents, to reflect parallel expectations across physician training models. As a result of this engagement, LARA temporarily suspended the problematic rule language as it applies to podiatric residents, allowing affected residents to secure licensure and continue their training on schedule. From the perspective of programs and trainees, the immediate licensure obstacle has been removed.

The 2026 MPMA Great Lakes Conference will be held February 18-22. This year’s conference, offering 40 hours of continuing medical education, will be held virtually on Wednesday, Thursday and Friday and in-person at The Henry Dearborn on Saturday and Sunday, with a welcome reception on Friday evening. Don’t miss Michigan’s largest podiatry event of the year!
Lectures will be delivered virtually on Wednesday, Thursday and Friday and in-person on Saturday and Sunday with two hours of continuing education and a welcome reception on Friday evening. You must attend the live lectures on each day to receive credit. There isn’t an option to attend virtually on the weekend. The lectures are ending earlier on Friday to allow for travel to The Henry.
MPMA Member .........................................................................
MPMA/APMA Senior Member
$475
$250
MPMA/APMA Life Member Complimentary
Resident Member ................................................. Complimentary
Students Complimentary
APMA Member (Other State)
$550
APMA Member (Federal) ....................................................... $550 Non-Member
Registration fees are based on current membership status with APMA. Early registration ends February 10. An additional $75 will be added to all registrations received after February 10, including all complimentary registrations. Registration for residents and students is complimentary if you register by February 10. Beginning February 11, registration for residents and students is $50. Registration is available at mpma.org or scan the QR code.
Complimentary self-parking is available. Valet parking is also available for a fee.
For assistance, contact the MPMA office at mpma.org or 800-968-6762.
The conference will be held live virtually on Wednesday, Thursday, and Friday morning. Approximately 3 days prior to the conference, you will receive an email with login information. Your login is unique to your and will be used to determine the number of continuing education contact hours to be awarded.
Time will be scheduled on Wednesday morning so that you can test your log in, become familiar with the virtual platform and CME sign-in. Prior to the conference, MPMA will send instructions on how to achieve continuing education credits, along with the conference program.
The Henry Fairlane Plaza, 300 Town Center Drive | Dearborn, MI 48126 888-709-8081

The conference will be held in person at The Henry on Saturday and Sunday. The Henry is offering a special rate of $160 for the conference. To make reservations, call 888-709-8081 by January 30 and be sure to mention MPMA Conference to receive this rate. An online reservation link is available on the conference page at mpma.org
The convention will be of interest to podiatric physicians and surgeons. Other healthcare professionals with special interest in the diagnosis and treatment of lower extremity disorders will also benefit from this conference.
The topics and speakers may have changed since this brochure was published. Visit mpma.org for the most upto-date schedule and for lecture descriptions and learning objectives.
This activity has been planned and implemented in accordance with the standards and requirements for approval of providers of continuing education in podiatric medicine through a joint provider agreement between the American Academy of Podiatric Practice Management and the Michigan Podiatric Medical Association. The American Academy of Podiatric Practice Management has approved this activity for a maximum of 40 continuing education contact hours.
Continuing education certificates will be available beginning March 9, 2026. If your license renews before this date, please contact the MPMA office.
A refund, less a $50 processing fee, will be provided for cancellations received in writing by February 6, 2026. No refunds will be provided after February 6. Send notice of cancellation to mpma@kdafirm.com. In lieu of a refund, your paid registration can also be applied to a substitute attendee.
The Michigan Podiatric Medical Association (MPMA) reserves the right to cancel or reschedule this event due to circumstances beyond its reasonable control, including but not limited to acts of God, government regulations, public health emergencies, severe weather, venue issues, or other factors beyond our control. In the event of cancellation by MPMA, registered attendees will be notified as soon as reasonably possible, and any applicable registration fees paid directly to MPMA will be refunded. If the event is rescheduled, registrant will have the choice to attend or receive a refund. MPMA shall not be responsible for any additional costs, losses, or expenses incurred by attendees, including travel or accommodation expenses.
CONFERENCE PURPOSE AND OBJECTIVES
This conference will provide information on the most up-todate diagnostic and treatment methods for lower extremity disorders. Conference objectives include:
• To provide the podiatric physician with a broad range of programs offered in an intensive five-day conference.
• To establish an understanding of developing concepts in the diagnosis, evaluation and treatment of lower extremity disorders and foot conditions.
The objective of the Michigan Podiatric Medical Association shall be to promote the art and science of podiatric medicine and surgery within the state of Michigan, promote the improvement of the practice of podiatric medicine and surgery, and promote the betterment and protection of the public’s podiatric health. This will be accomplished through affiliation with the American Podiatric Medical Association, to cooperate in carrying out the purposes of the Association.
Michigan Podiatric Medical Association’s (MPMA) Policy on Privacy and Confidentiality dictates the Association’s handling of a learner’s personal information. This policy is enforced in all areas of the Association’s business, including online communications, offline communications, direct marketing, and event registration.
MPMA maintains a comprehensive database of information on its learners in accordance with the general needs and expectations of the organization and its learners. This information is intended exclusively for purposes related to official Association business and to facilitate interaction between the Association and its learners. Directory information in the database may include home or work addresses, telephone numbers, fax numbers, e-mail addresses, and activity registrations/online purchases.
MPMA will use personal information to fulfill registrations for events, orders for materials and services made online, and other requested services. For educational meetings (CME activities), MPMA may share a list of registered attendees with the registered sponsors for that event.
WEDNESDAY, FEBRUARY 18
Lectures offered virtually | 9.5 CECH
9:00 a.m.-10:00 a.m.
Coding Updates for 2026 | 1 CECH
Alan Bass, DPM
10:00 a.m.-11:00 a.m.
Medical Ethics | 1 CECH
This lecture qualifies for 1 hour of medical ethics education.
11:00 a.m.-12:00 p.m.
Regenerative Medicine in Foot and Ankle | 1 CECH
Steven Karageanes, DO
12:00 p.m.-12:45 p.m.
Break
12:45 p.m.-1:15 p.m.
CAC Update | 0.5 CECH
Jodie Sengstock, DPM
1:15 p.m.-2:15 p.m.
Chronic Pain and Its Management | 1 CECH
Steven Karageanes, DO
This lecture qualifies for 1 hour of pain and symptom management education.
2:15 p.m.-2:45 p.m.
MRI of the Foot and Ankle: Ligament Review and Pathology | 0.5 CECH
Reza Sazgari, MD
Visit mpma.org for the most current lecture information.
2:45 p.m.-3:15 p.m.
CT: What All Podiatrists Should Know | 0.5 CECH
Rocky Saenz, DO
3:15 p.m.-3:45 p.m.
Ultrasound Applications of the Lower Extremity | 0.5 CECH
Nicole Brouyette, DPM
3:45 p.m.-4:15 p.m.
Advanced Imaging of infection of the Lower Extremity | 0.5 CECH
Daniel Kalabat, MD
4:15 p.m.-5:00 p.m.
Break
5:00 p.m.-6:00 p.m.
AI and Podiatry | 1 CECH
David Schweibish, DPM
6:00 p.m.-7:00 p.m.
Metabolic/Functional
Health | 1 CECH
Sean Cassleman, DO
7:00 p.m.-8:00 p.m.
DREADD: Diabetes-Related Extremity Amputation Depression and Distress | 1 CECH
Brandon Brooks, DPM
Welcome Reception and Resident Poster Session | 2 CECH
Friday, February 20 | 6:00 p.m.-8:00 p.m. | The Henry Hotel
Kick-off the in-person conference by joining colleagues at the Welcome Reception and Resident Poster Session. Connect with peers, faculty, and industry partners while enjoying beverages, appetizers, and engaging conversation. Explore innovative research and clinical insights presented by podiatry residents and help celebrate the next generation of leaders in podiatry.
THURSDAY, FEBRUARY 19
Lectures offered virtually | 11 CECH
7:00 a.m.-8:00 a.m.
CMS and the WISeR Program and Wound Documentation | 1 CECH
Alan Bass, DPM
8:00 a.m.-8:30 a.m.
Consent and Capacity
Considerations | 0.5 CECH
Andrew Mastay, DPM
This lecture qualifies for .5 hours of medical ethics education.
8:30 a.m.-9:00 a.m.
Biomechanical Considerations of the Diabetic Foot | 0.5 CECH
Brennen O’Dell, DPM
9:00 a.m.-9:30 a.m.
Early Identification and Intervention in Lower Extremity Wounds | 0.5 CECH
Alton Johnson, DPM
9:30 a.m.-10:00 a.m.
Surgical and Non-Surgical Management of Osteomyelitis | 0.5 CECH
Brennen O’Dell, DPM
10:00 a.m.-10:15 a.m.
Break
10:15 a.m.-10:45 a.m.
Using Principles of Skin Viscoelasticity for Challenging Wound Closures | 0.5 CECH
Daniel Ladizinsky, MD
10:45 a.m.-11:15 a.m.
Adjunctive Soft Tissue Procedures for Ulcers | 0.5 CECH
Randy Semma, DPM
11:15 a.m.-11:45 a.m.
STSG in Lower Extremity: Indications and Technique | 0.5 CECH
Daniel Ladizinsky, MD
11:45 a.m.-12:15 p.m.
Neuroma | 0.5 CECH
Rachel Height-Kaplan, DPM
12:15 p.m.-12:45 p.m.
Transverse Tibial Transport | 0.5 CECH
Michael Subik, DPM
12:45 p.m.-1:30 p.m.
Break
1:30 p.m.-2:00 p.m.
Management of Plantar Fasciitis | 0.5 CECH
Joshua Rhodenizer, DPM
2:00 p.m.-2:30 p.m.
Reducible, Reliable Foot and Ankle
Surgery | 0.5 CECH
Gage Caudell, DPM
2:30 p.m.-3:00 p.m.
From Footcare to First Response | 1 CECH
Alton Johnson, DPM
3:00 p.m.-4:00 p.m.
Lecture to be Announced | 1 CECH
4:00 p.m.-5:00 p.m.
Peripheral Arterial Disease in Podiatric Practice | 1 CECH
John Evans, DPM
5:00 p.m.-6:00 p.m.
Break
6:00 p.m.-7:00 p.m.
Lymphedema | 1 CECH
John Chuback, MD
7:00 p.m.-8:00 p.m.
From PIMP to Purpose | 1 CECH
Patrick DeHeer, DPM; Andrew Mastay, DPM; and Johanna-Marie Richey, DPM
FRIDAY, FEBRUARY 20
Lectures offered virtually | 5.5 CECH
7:00 a.m.-7:30 a.m.
Bone Grafting and Use of Synthetic Substitutes | 0.5 CECH
Erik Kissel, DPM
7:30 a.m.-8:00 a.m.
Achilles Injuries | 0.5 CECH
Randy Semma, DPM
8:00 a.m.-8:30 a.m.
FHL Tendon Transfer for Achilles
Tendinopathy | 0.5 CECH
Gage Caudell, DPM
8:30 a.m.-9:00 a.m.
Indications and Technique for Zadek | 0.5 CECH
Jason Weslosky, DPM
MPMA Annual Membership Meeting and Breakfast
9:00 a.m.-9:30 a.m.
Syndesmosis Instability and Fixation | 0.5 CECH
Jake Eisenchink, DPM
9:30 a.m.-10:00 a.m.
Arthroscopic Brostrum | 0.5 CECH
Vince Lefler, DPM
10:00 a.m.-10:15 a.m.
Break
10:15 a.m.-11:15 p.m.
Open vs. MIS Ankle Fracture ORIF | 1 CECH
Colin Mizuo, DPM
11:15 p.m.-11:45 a.m.
Isolated Posterior Malleolar Fractures | 0.5 CECH
Gage Caudell, DPM
11:45 a.m.-12:15 p.m.
Geriatric Considerations with Ankle Fractures | 0.5 CECH
Jake Eisenchenk, DPM
12:15 p.m.-12:45 p.m.
Peroneal Pathology | 0.5 CECH
Randy Semma, DPM

Saturday, February 21 8:30 a.m.-10:00 a.m. | The Henry New time for the MPMA Annual Membership Meeting! This year’s Annual Meeting will be held on Saturday, February 21, from 8:30 a.m. to 10:00 a.m. All MPMA members are encouraged to attend. The morning will kick off with a coding lecture from Dr. Alan Bass beginning at 7:30 a.m.
FRIDAY, FEBRUARY 20
Lectures offered in person at The Henry | 2 CECH
5:00 p.m.-8:00 p.m.
Conference Registration
5:00 p.m.-6:00 p.m.
Past Presidents Reception
6:00 p.m.-8:00 p.m.
Welcome Reception and Resident Poster Session | 2 CECH Zeeshan Husain, DPM (Moderator)
Visit mpma.org for the most current lecture information.
SATURDAY, FEBRUARY 21
Lectures offered in person at The Henry | 8 CECH
8:00 a.m.-5:00 p.m. Exhibit Hall Open
6:30 a.m.-6:00 p.m.
Conference Registration
7:30 a.m.-8:30 a.m.
The Difference Between BLA and Non-BLA Skin Substitutes | 1 CECH Alan Bass, DPM
8:30 a.m.-10:00 a.m.
MPMA Annual Membership Meeting and Breakfast
All MPMA members are encouraged to attend. A full breakfast buffet will be available for this event.

8:30 a.m.-10:00 a.m.
Continental Breakfast and Visit Exhibits
10:00 a.m.-12:00 p.m.
Student Recruitment Event
10:00 a.m.-11:00 a.m.
Utilizing Cytology for Lower Extremity Pathology | 0.5 CECH
David Schweibish, DPM
11:00 a.m.-11:30 a.m.
Developments in Preventative Diabetic Care | 0.5 CECH
Gary Rothenberg, DPM
11:30 a.m.-12:00 p.m.
Lecture to be Announced | 0.5 CECH Crystal Holmes, DPM
12:00 p.m.-1:15 p.m. Randy K. Kaplan Advocacy Luncheon
1:30 p.m.-2:00 p.m.
Lesser MPJ Pathology | 0.5 CECH
Greg Sheremeta, DPM
2:00 p.m.-2:30 p.m.
Equinus | 0.5 CECH
Patrick DeHeer, DPM
2:30 p.m.-3:00 p.m.
PCFD | 0.5 CECH
Patrick DeHeer, DPM
3:00 p.m.-3:30 p.m.
Break and Visit Exhibits
3:30 p.m.-4:30 p.m.
Panel Discussion: MIS Complications | 1 CECH
Raquel Sugino, DPM and Karl Dunn, DPM, Joshua Faley, DPM, and Andrew Mastay, DPM (Moderator)
4:30 p.m.-5:00 p.m.
Break and Visit Exhibits
5:00 p.m.-7:30 p.m.
Abstract Competition | 2.5 CECH
Zeeshan Husain, DPM, Moderator
5:00 p.m.-6:00 p.m.
Hands-on Lab: Millimeters Matter -
Surgical Approaches with MIS | 1 CECH
Raquel Sugino, DPM
6:30 p.m.-7:30 p.m.
Hands-on Lab to be Announced | 1 CECH
SUNDAY, FEBRUARY 22
Lectures offered in person at The Henry | 4 CECH
7:00 a.m.-12:00 p.m. Conference Registration
7:00 a.m.-11:00 a.m. Exhibit Hall Open
7:30 a.m.-8:00 a.m.
What Shoes Should I Get? | 0.5 CECH
Anthony Giordano, DPM
8:00 a.m.-8:30 a.m.
Metatarsus Adductus | 0.5 CECH
Anthony Giordano, DPM
Alan Bass, DPM
Brandon Brooks, DPM
Nicole Brouyette, DPM
Sean Cassleman, DO
Gage Caudell, DPM
John Chuback, MD
Patrick DeHeer, DPM
Karl Dunn, DPM
Jake Eisenchink, DPM
John Evans, DPM
Joshua Faley, DPM
Anthony Giordano, DPM
Rachel Height-Kaplan, DPM
Crystal Holmes, DPM
Zeeshan Husain, DPM
Alton Johnson, DPM
Daniel Kalabat, MD
Steven Karageanes, DO
Erik Kissel, DPM
Daniel Ladizinsky, MD
Vince Lefler, DPM
Andrew Mastay, DPM
Jeffrey Miller, MD
Colin Mizuo, DPM
Brennen O’Dell, DPM
Register at mpma.org.
8:30 a.m.-9:15 a.m.
Breakfast and Visit Exhibits
9:15 a.m.-10:30 a.m.
Kaplan-Kanat Memorial Keynote Presentation: Lecture to be Announced | 1 CECH
Lawrence Fallat, DPM
10:30 a.m.-11:30 a.m.
Healthy Veins, Healthy Lives: A Practical Guide to Venous Disease Management | 1 CECH
Jeffrey Miller, MD
11:30 a.m.-12:30 p.m.
Deep Venous Arterialization (DVA) and Why it Matters | 1 CECH
John Evans, DPM
Joshua Rhodenizer, DPM
Johanna-Marie Richey, DPM
Gary Rothenberg, DPM
Rocky Saenz, DO
Reza Sazgari, MD
David Schweibish, DPM
Randy Semma, DPM
Jodie Sengstock, DPM
Greg Sheremeta, DPM
Michael Subik, DPM
Raquel Sugino, DPM
Jason Weslosky, DPM
limited licenses and begin practice as planned, while also preserving continuity of training for existing podiatric residency programs. A key consideration throughout was maintaining as much alignment as possible with the licensure pathways used for MD and DO residents, to reflect parallel expectations across physician training models. As a result of this engagement, LARA temporarily suspended the problematic rule language as it applies to podiatric residents, allowing affected residents to secure licensure and continue their training on schedule. From the perspective of programs and trainees, the immediate licensure obstacle has been removed.
Although the immediate issue has been addressed, the broader rule structure is still being examined. LARA and the Board of Licensing and Regulation for Podiatric Surgery have initiated a review of the podiatric licensure rules, including the provisions that govern educational limited licenses. MPMA is participating in this process with the aim of restoring a stable, transparent licensure pathway for podiatric residents and aligning that pathway with MD/ DO educational licensure standards in a way that reflects podiatry’s role as a physician-level profession.
For residents, the resolution ensures they can begin and continue training without encountering unexpected licensure barriers after matching to a Michigan program. For residency programs, it supports continuity in staffing, education, and patient care, allowing directors to plan their clinical and academic schedules with greater confidence. For patients and communities, preserving a predictable
licensure framework helps maintain access to podiatric medical and surgical care across Michigan.
MPMA will continue to monitor the rulemaking process, provide input where appropriate, and share updates with members as the revisions move forward, helping to ensure that Michigan’s licensure framework supports both high standards of care and a clear pathway for the next generation of podiatric physicians.
Podiatric medicine is practiced using ICD-10-CM (or International Classification of Diseases, Tenth Revision, Clinical Modification) codes. It’s the standardized system for naming and classifying diseases and health conditions. The current ICD is within its 10th revision of that system. Clinical Modification relates to the U.S. clinical version that adds extra detail (more specifically) for medical documentation, billing and health data tracking.
In day-to-day podiatry practices, ICD-10-CM is the diagnosis code set used to describe what the podiatrist is treating, for instance, plantar fasciitis, diabetic foot ulcer, cellulitis, neuropathy , or osteomyelitis - so it can be communicated consistently across providers and payers.
Each year ICD-10-CM gets updated—and for podiatrists, it becomes the “official language” used to document conditions, communicate risk, and support accurate claims. In the U.S., these revisions flow through the federal ICD-10 Coordination and Maintenance (C&M) Committee process, co-chaired by CDC’s National Center for Health
Continues on pg. 14




Statistics (NCHS) and CMS, which hosts public meetings to review proposed diagnosis and procedure code changes. Final decisions are made by the U.S. Department of Health and Human Services (HHS).
Specialty groups like Podiatry submit proposals and provide public comment during the C&M cycle. The American Podiatric Medical Association (APMA) tracks and interprets the annual updates for foot and ankle care: the goal is to make sure the coding system keeps pace with how conditions are actually diagnosed and managed in real clinics.
The most recent changes to ICD-10-CM became effective October 1, 2025 (FY 2026)—including updates that intersect directly with podiatric medicine, such as clearer coding for type 2 diabetes “in remission” and more explicit classification of certain lower-leg ulcer locations. These FY 2026 codes apply to healthcare services provided from October 1, 2025 through September 30, 2026.
APMA flagged several updates that commonly intersect with podiatric documentation and billing:
Type 2 diabetes “in remission” got its own code
• New code: E11.A – Type 2 diabetes mellitus without complications in remission.
• Practical meaning: if “type 2 diabetes in remission” is clinically relevant to the encounter (risk status, history guiding management, ulcer risk, etc.), you now have a more precise way to represent it in diagnosis

coding. APMA ties this to the international consensus definition of remission.
Shin ulcers are now explicitly captured under the “calf” ulcer family
• ICD-10-CM’s L97- family covers non-pressure chronic ulcers of the lower limb.
• Previously there wasn’t a clean way to say “shin ulcer.” Starting Oct 1, 2025, “non-pressure chronic ulcer of shin” becomes an inclusion term under L97.2(the calf category).
• Practical meaning: documentation/coding workflows for lower-leg wounds may shift—shin ulcers should route to L97.2- now (still requiring the usual specificity for laterality/severity where applicable).
A few “adjacent” diagnoses got more granularity
These aren’t “podiatry-only,” but they come up in lowerextremity care and can affect medical necessity/risk documentation:
• Aggressive fibromatosis (desmoid tumor) added as an inclusion term under D48.11.
• Multiple sclerosis: G35 is no longer a complete code; it now requires added characters (new subtypes).
• Financial insecurity (SDOH): Z59.86 is no longer a complete code; it splits into more specific options.
What this means “exactly” for a podiatry practice
• Correct code set by date of service: Use FY 2026 ICD10-CM codes for encounters on/after Oct 1, 2025 (older codes for earlier dates).
• More specificity = fewer avoidable denials: When ICD-10-CM adds specificity (new codes, expanded characters), payers and clearinghouses may reject “old” or incomplete codes for new-date claims. (This is why APMA and CMS publish annual update files and guidance.)
• Documentation needs to match the new options: If your clinicians document “shin ulcer” or “type 2 diabetes in remission,” the coder can now reflect that directly—but only if it’s charted clearly and used in management.
For more information, click the sources below:
Sources:
• www.apma.org/about-apma/news/newsreleases/2025/icd-10-cm-changes-related-to-podiatry
• www.cdc.gov/nchs/icd/icd-10-maintenance/index. html
• www.cms.gov/files/document/fy-2024-icd-10-cmcoding-guidelines-updated-02/01/2024.pdf

As cannabis use becomes more common for both recreation and symptom relief, many people assume it is harmless during recovery from surgery, injuries, or chronic foot problems. Current research indicates a different picture. Across Podiatric literature, as well as other medical journals, cannabis use—especially smoking or vaping—shows consistent signals of worsening, not helping, wound healing, and recovery.
When cannabis is smoked or vaped, the body takes in combustion byproducts like carbon monoxide and airway irritants along with THC. These changes can reduce oxygen
delivery to tissues by lowering the blood’s oxygen-carrying capacity, inflaming the airways, reducing respiratory efficiency, and stressing the heart and blood vessels, thereby affecting circulation.
Healing tissue depends on oxygen to make collagen, build new blood vessels, and support infectionfighting immune cells. Lower oxygen levels and impaired circulation result in slower, less reliable healing.
According to Podiatry Management, physiologic effects of cannabis—particularly smoked forms— raise concerns for cardiovascular stress, changes in pain perception and medication use, and potential interactions with anesthesia and postoperative care.
A 2025 retrospective database review of lower-extremity trauma patients found that those with a diagnosed cannabis use disorder had significantly higher rates of post-operative complications, including problems with bone and soft-tissue healing and increased emergency department use, compared to non-users.
Podiatric authors are increasingly warning about cannabis in the context of foot and ankle surgery and chronic wound care. A 2025 review in Podiatry Management on cannabis and diabetes notes that the physiologic effects of cannabis—particularly smoked forms—raise concerns for cardiovascular stress, changes in pain perception and medication use, and potential interactions with anesthesia and post-operative care.
For podiatric patients, this is not a theoretical issue. Poor oxygenation, higher infection risk, and cardiovascular strain directly threaten the success of procedures such as bunion surgery, ankle fixation, and diabetic foot wound care.
For individuals living with diabetes, cannabis can be particularly problematic. The Podiatry Management review reports that cannabis use among people with diabetes is rising and is associated with:
Even if some patients feel that cannabis helps with pain or sleep, any pattern of use that disrupts glucose monitoring, diet, medication schedules, or follow-up appointments can indirectly worsen wound outcomes. From a foot-health perspective, stable blood sugars and consistent podiatric care are far more important for healing than any perceived benefit from cannabis.
Continues on pg. 24

• Worse glycemic control (higher blood sugars over time)
• Increased risk of diabetic ketoacidosis (DKA), a dangerous metabolic emergency
Poor glucose control and DKA are major drivers of:
• Diabetic foot ulcer formation
• Slow or non-healing wounds
• Higher rates of infection and amputation






Ice skating is a winter staple in Michigan—whether it’s a weekend public session, a youth hockey practice, or year-round figure skating. From a podiatric standpoint, although the skate boot is designed to be stiff, it limits normal ankle motion and concentrates forces through the foot; many injuries occur during falls, rapid edge changes, repetitive jumping, or contact. Large U.S. injury-pattern research also shows that fractures are common in skating-related injuries overall, with injury location varying by skating type.
Michigan podiatric physicians can help shorten recovery and reduce prepeat injuries–regardless of the type of skater.
(AMATEUR TO PRO): TRAUMA, “HIGH ANKLE” SPRAINS, AND SKATE-RELATED PROBLEMS
Hockey adds two major risk multipliers: contact/collisions and direct trauma (pucks, sticks, boards, blades). In U.S. emergency-department reporting on ice hockey injuries, lower leg/ankle/foot injuries account for a meaningful share of visits, alongside common lacerations and contusions.
1. Foot/toe contusions and fractures from pucks and shot-blocking
NCAA injury surveillance data show that in men’s college hockey, the single most common foot/ankle diagnosis is foot and/or toe contusion (bruising), consistent with puck impacts and shot-blocking.
2. High ankle sprains (syndesmotic sprains): a “time-loss” injury
In the same NCAA surveillance study, high ankle sprains account for the most severe time-loss (≥14 days) foot/ankle injuries.
At the professional level, an NHL study reported 105 high ankle sprains over five seasons; among players who missed games, the median time missed was 8 games, and MRI commonly showed injury to the anterior-inferior tibiofibular ligament (AITFL).
Why podiatry matters here: “high ankle” sprains typically require a different protection/ rehab strategy than routine lateral sprains, and return-toplay decisions often depend on pain with cutting/pushing and objective stability.
3. “Lace bite” (skate bite): front-of-ankle tendon irritation
“Lace bite” is commonly described as tibialis anterior tendinopathy/irritation at the front of the ankle, often flaring early in the season with stiff tongues and tight lacing.
Podiatric care can be especially helpful because treatment is frequently a mix of medical management + equipment modification (padding, tongue adjustments, lacing changes), not just “rest and hope.”
Continues on pg. 21

Contact Quantus Solutions TODAY to receive your NEW FREE Smart Chip EMV Terminal
4 SIMPLE STEPS TO ENROLL:
1) GO TO MPMA WEBSITE

2) FIND MPMA’S NEW PARTNER—QUANTUS SOLUTIONS
3) SELECT YOUR PRICING PROGRAM AND EQUIPMENT OPTION
4) APPLY
MPMA ENDORSED BENEFITS INCLUDE:
• Average Savings 38% per practice
• Negotiated MPMA Group Rates for all members
• Free EMV “smart chip” Terminal OR Virtual Terminal OR Mobile Device
• Dedicated Medical Customer Service & Support
• 24 hour Next Day Funding for all members
• HIPAA, PCI, SIGIS Certified Partner

FIGURE SKATING: OVERUSE, TENDON PROBLEMS, AND BONE STRESS INJURIES
Figure skating has its own signature: repetitive practice, boot constraints, and (for many skaters) high-impact jump takeoffs and landings. A major retrospective review of pediatric/adolescent figure skaters found that most injuries were overuse, and the foot/ankle was the most commonly injured region (29.6%).
1. Tendinopathy and chronic ankle/foot pain
Overuse pain in the foot and ankle often reflects tendon overload (Achilles, peroneals, anterior ankle tendons), especially when training volume rises quickly. The figure-skating injury literature also discusses boot-related tendon irritation—another reason podiatric evaluation often includes both the athlete and the skate.
2. Bone stress reactions and stress fractures
In the pediatric/adolescent figure skating review, about 1 in 10 injuries were bone stress reactions/fractures, and a substantial portion occurred in the foot/ ankle.
According to NIH/MedlinePlus, stress fractures are defined as breaks that develop from repeated stress/ overuse, and early recognition matters because continued loading can convert a stress reaction into a true fracture.
Ankle sprains still happen (even in elite skaters) Even though figure skating has a strong overuse profile, ankle sprains remain a leading injury category in reviews and skater-reported studies.
GENERAL PUBLIC SKATING: FALLS, TWISTS, AND FIRST-TIME ANKLE INJURIES
For recreational skaters, the dominant mechanism is straightforward: a fall or sudden twist. While many skating injuries involve the upper extremity, foot and ankle fractures are a leading cause of injury across skating activities.
Foot and ankle injuries you’re most likely to see:
• Ankle sprains (oftern from the blade catching or landing awkwardly after a slip). MedlinePlus notes that sprains are among the most common ankle problems and can take weeks to months to fully heal depending on severity.
• Ankle and foot fractures (especially when someone falls with the foot trapped under them or lands with a twisting load). MedlinePlus summarizes fractures as broken bones that can range widely in severity and management.
Podiatric physicians focus on distinguishing a routine sprain from injuries that look like sprains but behave








Ice skates are intentionally stiff. The rigid boot helps skaters transfer force efficiently into the blade, hold a stable edge during turns and stops, and provide the ankle support needed for highspeed direction changes (and, in hockey, added protection from impacts).
From a podiatric standpoint, that same stiffness matters because it limits normal ankle motion and redistributes load through the foot, which can both protect and provoke: it may reduce certain rollover motions, but it can also contribute to ankle sprains, tendon irritation, pressure injuries (like “lace bite”), and overuse pain when training volume or intensity climbs.
A skate boot isn’t meant to feel like a sneaker. It’s designed to:
• Hold your heel and midfoot stable so your power transfers into the blade (better control, cleaner edges)
• Protect (especially in hockey) from pucks, sticks, and contact
• Limit certain motions that would be unsafe on a blade— but that same stiffness can also create pressure points and tendon irritation if fit or lacing is off
If skates are causing pain—or you’ve had repeated sprains— podiatric physicians can help by:
• Identifying whether pain is from fit/pressure vs. a true injury pattern (tendonitis, stress injury, instability)
• Recommending lacing/padding modifications (often central to lace bite management)
• Using orthotics/boot modifications when mechanics like overpronation contribute to symptoms (AAP specifically mentions orthotics/boot modification in skating contexts).
• Creating a plan for recurrent ankle sprains (bracing/rehab strategies supported in NIH evidence reviews for ankle sprain supports).
differently—such as occult fractures, tendon injuries, or cartilage lesions—then building a plan that restores stability and confidence. A Michigan DPM, or Doctor of Podiatric Medicine) evaluates for worsening pain, swelling, bruising, redness, or difficulty walking after a foot/ankle injury.

PODIATRIC PHYSICIANS HELP SKATERS RECOVER—AND PREVENT REPEAT INJURY
Podiatric physicians and surgeons are trained specifically to diagnose and treat foot and ankle conditions, including sports injuries.
For skaters, care commonly includes: Accurate diagnosis (especially when “it’s just a sprain” isn’t improving)
• Targeted physical exam to identify ligament vs tendon vs joint injury
• Imaging when needed (X-ray for fracture concerns; MRI when recovery is atypical or to evaluate deeper injury patterns), consistent with major clinical guidance on sprains and ankle injuries
Sport-specific treatment plans
• Functional bracing/taping, progressive rehab, and return-to-ice criteria for ankle sprains (early rehab is emphasized in foot/ankle–specific guidance)
• Tendon management (activity modification, rehabilitation, and footwear/skate adjustments)
• Bone stress injury protocols (load reduction, protective immobilization when needed, and staged return— guided by location and risk)
• Equipment guidance (lacing patterns, padding, tongue modifications) for lace bite and pressure injuries
If a skater cannot bear weight on their foot/ankle, consider urgent evaluation from a podiatrist. This includes noticing significant swelling/deformity or pain that worsens after an injury. A Michigan Podiatrist can determine the extent of the injury and create a plan of care.
Sources:
• APMA and FootHealthFacts (ACFAS patient education)
• NCAA ice hockey foot/ankle injury surveillance (Crowley et al.)
• NHL high ankle sprains + MRI patterns and time missed (Mollon et al.)
• Pediatric/adolescent figure skating injuries (Kowalczyk et al.)
• Figure skating injury epidemiology review (Han et al.,


One Step at a Time
Experience the difference with Kerecis, the advanced solution for diabetic foot ulcers (DFUs). Powered by fish skin technology, Kerecis offers superior1 healing by supporting tissue regeneration and reducing complications. Clinical studies show improved closure rates and faster recovery times compared to traditional methods.2

• Smoking or vaping cannabis can slow wound healing and increase complication risk, particularly around surgeries and serious injuries.
• People should tell their podiatrists and other medical personnel about any cannabis use so risks can be managed.
• Those with diabetes or existing foot wounds should be especially cautious; cannabis-related blood sugar problems and inconsistent self-care can seriously impair healing.
The safest approach during recovery is simple: avoid smoking or vaping cannabis, follow proven wound-care instructions, and work closely with podiatrists to support healing.
References:
• Cheema A, Wu S. Implications of cannabis use on diabetes and diabetic foot wound healing. Podiatry Management. 2025.
• Parikh AC, Jeffery CS, Sandhu Z, et al. The effect of cannabinoids on wound healing: a review. Health Sci
Rep. 2024;7:e1908.
• Niyangoda D, et al. Cannabinoids in integumentary wound care: a systematic review. Pharmaceutics. 2024;16(10):1277.
• Veliky C, et al. The association between diagnosed cannabis use disorder and post-operative outcomes in lower-extremity trauma patients: a retrospective database review. J Orthop Exp Innov. 2025.
• OU Researchers. Cannabis and facial wound healing after surgery (research announcement).
Charcot neuroarthropathy (CN) is a challenging complication that occurs in patients who have developed numbness in their limbs from various causes with the most common cause being neuropathy from diabetes mellitus currently. CN is a non-infectious condition resulting in structural collapse of bones and joints resulting in deformities (Figure 1). These deformities result in abnormal pressure points that ulcerate. Due to the loss of protective feeling, these ulcerations can become infected leading to bone infection. Prior to 2000, patients who developed CN underwent primary leg amputation due to complications with conservative and surgical treatments. Poor outcomes were less favorable compared to current times primarily due to delayed diagnosis, limited treatment options (especially surgical), and potentially less effective medical management of the underlying conditions like diabetes mellitus. The risks of progression to severe deformity, ulceration, infection, and amputation were significant. Even after surgical reconstruction, deformities can persist which makes bracing challenging due to irritation from the bracing itself. With significant partial foot and leg amputations, life expectancies are lower.

Based on 2005 data, above- and below-knee amputation mortality rates range from 13-40% in the first year, 35-65% in three years, and 39-80% in five years (1).
Advances in the podiatric profession have been able to make strides to manage complications stemming from CN. Early recognition is paramount in improving outcome results. A red, hot, and swollen foot in a patient with numbness is usually a late-stage clinical finding suggesting the process has already begun. Early intervention involves immobilization and non-weightbearing. Coordinating medical care with their medical doctor to improve diabetes control is also essential. Once medically stabilized, surgical intervention may be considered to help stabilize the fractures and deformities that arise from CN. Previously, stabilization with screws and plates were aggressively used to hold the foot and ankle in straight position so that it could be braced effectively. However, due to the nature of neuropathy, the increased stress from a rigid foot which is normally meant to move cannot accommodate these forces and may result in another Charcot event. We will discuss a newer approach to perform limb salvage on CN
eLearning Portal Features:
• 12 Regulatory-Mandated Training Modules all in one place
• Bloodborne Pathogen, Fraud & Abuse, Medicare Part C & D Managed Care, PCMH, ICD-10, Hazcom, MACRA, Cyber Security and more
• Printable Forms, Documents, & Letters
• Q & A for each Section of Training
• Certificate of Completion for each Initiative
• 24/7 Access
| dprohealthcare.com | skip@dprohealthcare.com | | 248.765.1729 | Administration Support: Benefits:
• Easy to Comply with Regulatory Training Demands
• Progress Monitoring & Analytics
• Progress Results Tracking

• Training within Healthcare is Paramount
• Certify Your Practice to be Compliant
• Fee Schedule Increase are available through Completion of certain Training
• Don’t Allow Your Practice to be at Risk for Non-Compliance

patients to create a more functional foot that may have longer longevity than what has been performed previously.
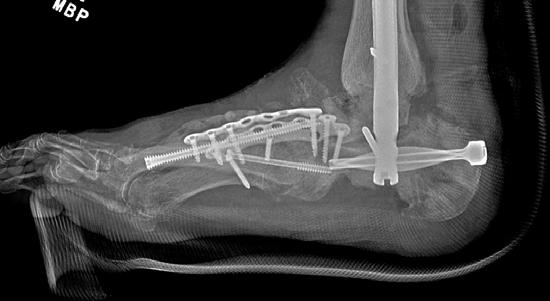
To illustrate the pitfalls of CN treatment, we have presented a 61-year-old male who already underwent midfoot fusion for prior Charcot event (Figure 2). He comes in for a second opinion and declined an ankle fusion and wanted to preserve his motion so that he could drive. The second set of radiographs demonstrate attempted hindfoot fusion that resulted in collapse to the talus bone in the ankle joint (Figure 3). Recent podiatric research shows an alternative treatment option to the traditional rigid fixation. The Charcot flipper foot construct involves fusing the hindfoot while leaving the midfoot mobile to allow for motion to lower risk of further breakdown (2). The final surgery was performed to replacing the dislocated talus with a cadaver bone and fusing the hindfoot with an intramedullary nail all through small incisions for preparation and hardware fixation. The

midfoot screws that were added in his second surgery were removed and an osteotomy was created to allow for the forefoot to move in the sagittal plane (Figure 4).
Charcot neuroarthropathy is a devastating condition with significant risk factors for limb loss. Podiatric surgical advances have been able to improve limb salvage rates and restore function. With the continued evolution of podiatric surgical treatment, patients with this condition have better prognosis and functional status than in the past so that they can be productive members of society.
1. Singh N, Armstrong, DG, Lipsky BA. Preventing foot ulcers in patients with diabetes. JAMA. 2005; 293(2): 21728.
2. Loveland JD. New surgical techniques in the treatment of charcot neuroarthropathy deformities. Clin Podiatr Med Surg. 2025; 42(3): 505-19.

Figure 1. Typical clinical pictures of patients who develop ulcerations from hindfoot and midfoot Charcot deformities due to bony prominences and joint instability (yellow-shaded areas).


Figure 2. Initial presentation of 61-year-old male with new midfoot Charcot neuroarthropathy of the midfoot following previous midfoot surgery six-months previously. Collapse started after going to physical therapy (second Charcot event).

Figure 3. Result after attempted hindfoot fusion to preserve the ankle motion. The talus collapsed and the foot dislocated medially (third Charcot event). The deformity was so severe that the lateral ankle developed a large wound due to breakdown against the walking boot.

Figure 4. Final surgery resulting in plantigrade foot by fusing the entire hindfoot and unlocking the midfoot to allow for active plantarflexion of the forefoot (dotted line). The talus was replaced with a cadaver bone. Previous ulceration on the lateral ankle healed uneventfully.


Last year, the MPAS raised over $12,000 from contributions here in Michigan. The MPMA would like to thank the following members who donated to MPAS in 2025.
This year, MPAS has once again set a goal to raise $20,000 to assist in the MPMA political strategies here in Michigan.
To make your 2026 contribution simply visit: https://www.mpma.org/political-action
All contributions are greatly appreciated!
Anthony Alessi, DPM
William Bennett, DPM
Marc Borovoy, DPM
Norman Brant, DPM
Stephanie Carollo, DPM
Andrew Cohen, DPM
Derek Dalling (Exec. Dir.)
Marie Delewsky, DPM
Judi Ecker, DPM
Joshua Faley, DPM
Jeffrey Frederick, DPM
Arnold Gross, DPM
Neil Hertzberg, DPM
Michael Holland, DPM
Crystal Holmes, DPM
Scott Hughes, DPM
Emily Hurst, DO (MOA President)
Zeeshan Husain, DPM, FACFAS, FASPS
Laura Jamrog, DPM
John Johnson, DPM
Randy Kaplan, DPM
Vincent Lefler, DPM
Jeffrey Levitt, DPM
Don Lutz, DPM
Andrew Mastay, DPM
Patrick Meyer, DPM
John Miller, DPM
Heidi Monaghan, DPM
David Moss, DPM
Joyce Patouhas, DPM
Jessica Patterson, DPM
Craig Pilichowski, DPM
Nicholas Post-Vasold, DPM
Kristin Raleigh, DPM
Angela Robin-Croft, DPM
Lawrence Rubin, DPM
Mark Saffer, DPM
Ali Safiedine, DPM
Peter Schaffer, DPM
David Schweibish, DPM (Florida member)
Jodie Sengstock, DPM
Zoe Simaz, DPM

Jeffrey Solway, DPM
Harold Sterling, DPM
Ingrid Stines, DPM
Rebecca Sundling, DPM
David Taylor, DPM
Elizabeth Tronstein, DPM
Christine Tumele-Vogt, DPM
Gregory Vogt, DPM
Jason Wadaga (Deputy Executive Director)
Marc Weiner, DPM
Laal Zada, DPM
The following MPMA members contributed to the APMAPAC in 2025, and the MPMA would like to recognize them for their outstanding leadership. In all, Michigan contributed almost $20,000 to the APMAPAC in 2025.
Additionally, the MPMA continues to support the APMA PAC as well. Every year, the MPMA is among the leading state associations supporting the advocacy efforts of the profession. In 2025, the MPMA provided $5000 to the APMA PAC.
There is new leadership and renewed sense of energy for the podiatric profession’s advocacy efforts in our nation’s capital. Your contributions to APMAPAC will help get our new legislative team on a solid path.
Platinum Level Supporters
($1,000–$2,499)
Dr. Marc Borovoy
Exec. Dir. Derek Dalling
Dr. Scott Hughes
Dr. Randy K. Kaplan
Dr. Andrew Mastay
Silver Level Supporters
($300–$499)
Dr. Michael Kelley
Dr. Craig Pilichowski
Dr. Mark Saffer
Dr. Harold Sterling
Gold Level Supporters
($500–$999)
Dr. Hatim Burhani
Dr. Zeeshan S. Husain
Dr. John Johnson
Dr. Vincent Lefler
Dr. David Moss
Bronze Level Supporters
($150–$299)
Dr. Marie Delewsky
Dr. John Evans
Dr. Rachel Height-Kaplan
Dr. Crystal Holmes
Dr. Douglas Johnson
Dr. Ali Safiedine
Dr. Jodie N. Sengstock
Dr. Rebecca Sundling
Dr. Donald Lutz
Dr. Hengelberth Montufar
Dr. Joyce Patouhas
Dr. Marc Weiner
Patriot Level Supporters
(Less than $150)
Dr. Michele Bertelle-Semma
Dr. Lawrence Brown
Dr. Joshua Faley
Dr. Arnold Gross
Dr. Thomas Hall
Dr. Alton Johnson

The future of our great profession and your future depends upon your support of APMAPAC.
To make your 2026 contribution to APMA PAC, simply go online and visit: www.apma.org/Donate or scan the QR Above!
Be safe and healthy.
Dr. John Miller
Dr. Brennan O’Dell
Dr. Jessica Patterson
Dr. Steve Sheridan
Dr. Zoe Simaz
Dep. Exec. Dir. Jason Wadaga

RURAL NORTHERN MICHIGAN PRACTICE FOR SALE, OSCODA
Looking either to hire a Podiatrist to work in this office daily or seeking to sell the office. 2600 square foot office. Four treatment rooms, one surgical room with a scrub sink. Patient, employee, and physician bathrooms. Physician’s office area with bathroom. Large waiting room. Front desk area for check-in with window slider. X-ray area with digital x-rays. Break area for the staff in the back. Unfinished full basement. Handicap ramp in the front entrance with employee back entrance and parking spaces for both. Patient volume is between 25-30 patients per day, 4-5 days a week with possible surgery at MyMichigan in Tawas or Alpena. Drawing from 3-4 counties for your patients. Can live either in Oscoda or 20 minutes south in Tawas, Michigan. Corner lot building with extra space for addition or add-ons. Contact: northernfa@hotmail.com
ADRIAN: PRACTICE FOR SALE
Turnkey foot and ankle practice for sale in Adrian, MI, a college town near the Ohio border—just 30 miles from Toledo and 35 miles from Ann Arbor. Well-established with 15+ years in the community, consistent revenue, strong referral base, and 25% overhead. Fully equipped 3500 sq ft office with experienced staff, full hospital privileges, no call, and ample parking. Grossing $550,000 on a 20-hour workweek. No Medicaid or HMO. Owner willing to assist with transition, mentoring, and financing. Asking $450,000. Ideal for a new practitioner or satellite office expansion. Contact: forsalepodiatryclinic@gmail.com.
CHARLEVOIX: PRACTICE FOR SALE
Practice for sale in Northwest Michigan: Charlevoix, “The Beautiful” resort town on Lake Michigan and Lake Charlevoix with a satellite office in Gaylord, “The Alpine Village”. Outstanding opportunity with even greater potential. Doctor is retiring after 44 years of practice serving the Charlevoix and Gaylord communities, including 16 assisted living, extended care, and skilled nursing facilities in 5 Northern Michigan counties. The Charlevoix office has 4 treatment rooms; Gaylord office has 3 treatment rooms For information call: 231-547-4662.
Well-established group practice, encompassing all aspects of foot, ankle and leg health care: multiple office locations, hospital affiliation along with nursing home care. Seeking well-trained energetic associate, PSR-24/36. Candidates must possess a strong medical/surgical knowledge base, with compassionate care towards patients. We offer a favorable compensation package with potential for long term buy-in. Practice locations are in rural Northern Michigan communities with abundant outside activities located on the shores of Lake Huron. Please respond to: 321 Long Rapids Plaza c/o Dr. Craig Pilichowski, Alpena, MI 49707.
ROCHESTER: PRACTICE FOR SALE
Well established 46 year practice for sale across from Crittenton Hospital. 4+Tx, 1 X-ray room, 2000 sq. ft. Great parking and easy car access. Senior bus access. Can make 1000 sq. ft. 2 Tx, 1 X-ray. Immediate availability. Can stay for transition. Contact: SellMyPractice2@gmail.com
PETOSKEY: PRACTICE FOR SALE
Well established 36 year practice for sale in beautiful Petoskey. Two locations with a steady inflow of new patients. Turnkey practice with three well equipped treatment rooms, digital X-rays, certified EHR, and onsite furnished apartment. Office buildings available - purchase or lease. Contact: Upnorthfoot@gmail.com.
PRACTICE SEEKING PART-TIME ASSOCIATE
Part-time associate needed in Macomb County. 2-3 half days per week in office, HC, and NH. Flexible hours. Generous compensation.Contact: lb@innersolegroup.com.
PRACTICE SEEKING ASSOCIATE
Established, full scope modern podiatric practice with 2 locations in South Central Michigan. Will remain with practice during future transition. Can train and help new practitioner with board certification in forefoot, and rear foot and ankle certification. Recommend residency trained individual Contact: thankyourfeet@comcast.net
Page 2 - Bako
Page 13 - Beyond Financial Planning
Page 14 - Miller Vein
Page 15 - ASPMA
Page 17 - PICA
Page 20 - Quantus Solutions
Page 21 - Stryker
Page 23 - Kerecis
Page 25 - DPro Healthcare
Page 26 - Treace Medical Concepts
Page 28 - MPAS
Page 28 - APMA PAC
If podiatry is a target market for your company, the MPMA Corporate Partner Program will give your company heightened visibility to reach Michigan’s podiatrists. MPMA offers five levels of participation, each with corresponding partner benefits. Enrollment in the Corporate Partner Program is for a period of 12 months and is renewable on an annual basis. Connect at a whole new level. Click here to become a 2026 MPMA Corporate Partner.









