With Harp & Sword: A Doula’s Guide to Providing Trauma-Informed Birth Support
By Kenya M. Fairley

By Kenya M. Fairley
By Kenya M. Fairley
Copyright © 2016 by Kenya M. Fairley. All rights reserved. No part of this publication may be reproduced or transmitted in any form or by any means, electronic or mechanical, including photocopy, recording or any information storage and retrieval system, without prior permission in writing from the author except in the case of brief quotations embodied in critical articles and reviews.
Published in 2016 by Kenya M. Fairley
Brooklyn, NY
United States of America
On the web: www.kenyafairley.com
Please send inquiries to kenyafairley@gmail.com.
Cover, interior design and all enclosed artwork by Erica Keim.
Author photo captured by Heather DeLeon.
I felt capable of writing this book in large part due to the privilege of working alongside a team of amazing people at the National Resource Center on Domestic Violence, led by Anne Menard. I learned so much about articulating a feminist analysis, refining clarity of thought, writing in ways so as to not make the reader cranky, and truly about what it means to be in community with other women. I was by no means perfect but I was able to show up and bring my whole self to the table, and for that I will forever be grateful to Anne, Farzana, Susan, Tonya, Casey, Patty, Ivonne, Annika, Amanda, Ashley, Chelsea, Erica, Dalia, and John.
A million “thank you’s” to my reviewers, who gave me encouragement, critical feedback and meaningful honesty. I appreciate each of you very much. This book is all the better because you read it first!
Michelle Cohen, MTA, RPYT, CBD mom* yoga instructor * birth doula* postpartum doula www.savoritstudios.com
Michele Vigeant, MA, EdM
Licensed Mental Health Counselor Strategic Planning & Program Development Consultant
Nakia D. Hansen, Esq. digital strategist - attorney - party guest extraordinaire www.nakiahansen.com
And to my mother, Joann, whose incredible fortitude, resiliency, compassion and support has bolstered me in so many ways, even when I absolutely did not deserve it. Anytime that I’ve felt lost or confused or in despair like I couldn’t go on, she gave me a moment to cry or be angry about it, to wallow in my self-pity and negativity, and then without fail, she always said, “Ok, you’ve had your little cry. The time for that is over. Now, what are you going to do about it?” That question instilled in me the belief that I was smart, resourceful, and able to solve my own problems.
It is because of her, and many of the strong, fierce women in my family like her, that I am the woman I am today; sending my love out to the women of the Hodge and Fairley families, Grandma Ailey (RIP), Grandma Gussie (RIP), Grandma Mary (RIP), Aunt Sally, Grandma Hazel, Ann, Vickie (RIP), Ammie, Jan, Zanette, Cookie, Delisa, Alfreda, Kelly, Laytoria, Kimberly, Jazmin, Renetta, Rebecca, Amesha, Deidre, Alicia, and Leslie.
Part 1: Experiencing Trauma and Resilience
• Introduction
• Content Notes
• This is My Story
Part 2: Understanding Abuse and Violence
• Guiding Assumptions
• Does This Fall within a Doula’s Scope of Practice?
• How Will I Know If My Client Is or Has Been Abused?
• Impact of Domestic Abuse on Pregnant and Laboring Women
• Impact of Sexual Violence on Pregnant and Laboring Women
• Abuse Related Health Risks for Mom and Baby
Part 3: Strategies and Tactics for Support
• Engaging Survivors and Strategies to Address Trauma Echoes
• Affirmations for Labor and Childbirth
• Helping Clients Heal
• Resources for Survivors
• Doula Self-Care and Rejuvenation
• Resources for Doulas’ Ongoing Education
About the Author
I wrote With Harp & Sword: A Doula’s Guide to Providing Trauma-Informed Birth Support to build a greater understanding of the lifelong impact of interpersonal violence in women’s lives, to discuss trauma-informed care as part of birth support and to offer strategies to enhance the doula practice. This book is meant to be a guide for doulas and other birth workers, whether or not they’ve had formal training or education related to trauma or interpersonal violence, and who are supporting women that may have a current or past history of domestic violence or sexual assault victimization.
Doulas are in a unique position to build genuine, meaningful relationships with survivors of abuse or assault during a time in their lives when they are extremely vulnerable to what’s happening with and to their bodies. Oftentimes, doulas come to share a deep connection with their clients which can decrease isolation and stigma for survivors, attest to the value of their lived experiences and validate that they are worth being cared for. In their role, doulas can enhance survivors’ feelings of safety and control, deepen their sense of agency,1 develop emotional safety plans for support in labor, and strategize ways to manage triggers, or trauma echoes,2 as they arise.
The ultimate goal when supporting survivors of domestic violence and sexual assault in childbirth is to restore their control over their bodies, their birth and their babies.
This is my S.O.S. call to other women who may be struggling with issues related to interpersonal violence or who love someone else who is. This is my S.O.S. call to other doulas and birth workers to see traumainformed care as an integral and necessary part of our practice. Alarming numbers of women experience domestic violence and sexual assault at some point in their lifetimes here in the United States. The 2011 National Intimate Partner and Sexual Violence Survey (NISVS) conducted by the Center for Disease Control and Prevention (CDC) report that:
• 1 in 3 women experience violence from their partners in their lifetime,
• 1 in 5 women are survivors of rape, and
• 1 in 2 women have experienced some form of sexual violence in their lifetimes.3
These are numbers that cannot be ignored as many of the same women are laboring and birthing across the country. In fact, 4-8% of pregnant women experience domestic violence during their pregnancy.4
One study of 3,149 relatively low-risk female patients seeking health care stated that abuse during pregnancy was reported by 5.9% of the women.5
Research reviewed by Prevention and Treatment of Traumatic Childbirth (PATTCh) states that between 25-34% of women report that their births were traumatic.6 Given these numbers, maternity care, labor and childbirth deserve a trauma-informed approach. The Substance Abuse and Mental Health Services Administration (SAMHSA) defines the concept of a trauma-informed approach as a program, organization, or system that:
• Realizes the widespread impact of trauma and understands potential paths for recovery,
• Recognizes the signs and symptoms of trauma in clients, families, staff, and others involved with the system,
• Responds by fully integrating knowledge about trauma into policies, procedures, and practices, and
• Seeks to actively resist re-traumatization.7
This book and the lessons that can be gleaned from my own experience managing trauma echoes (to be described in the section, This is My Story) can be a resource for doulas that are seeking to support and be a vessel to women who may be struggling to manage their own pain as a result of interpersonal violence, whether emotional or physical. I’m referring to the type of pain that can feel so intense when triggered that it’s pulling every ounce of energy and brainpower survivors have into a deep black hole. As doulas, we can be beacons of support to our clients and ensure they are thriving as whole, healthy human beings.
In developing this book, it is not my goal that all doulas become victim advocates or for doulas to become experts on domestic violence and sexual assault. The purpose of this book is to provide doulas and birth workers with:
• Information to recognize the signs of abuse with their clients,
• Trauma-informed strategies to modify service provision and assist clients experiencing anxiety and trauma echoes during labor, childbirth and the postpartum period,
• Guidance to support making warm referrals for clients seeking victim advocacy services,
• Ideas and resources to assist clients in their own healing process,
• Tips for doula self-care, and
• A diverse resource listing for ongoing education and awareness on this topic.
My hope is that this book helps increase your learning and understanding one step further. Please see this book as a resource to begin or enhance your exploration of trauma-informed birth support and as a tool to expand your services as a doula and birth worker. Use this book to have discussions with other birth workers about the continuum of care, to think about how you might want to modify your own practice, and to reflect on how you might have supported past clients had you known better.
In the following pages I share my story of being exposed to domestic violence at a very young age, as well as my experience being sexually assaulted as an adult. I am sharing from my own lived experience, which will be very different from every other survivor out there. What I’ve been through and how I’ve coped with the things that have happened to me may not be applicable to another survivor’s experience or response. I do not have all the answers for how to heal and thrive after being abused or assaulted—truly those answers reside within the women we serve. As doulas we can assist women in unlocking those answers for themselves. The purpose of sharing my personal story is to help bring forth several key points about victimization, the aftermath it has on an individual’s life and to highlight the societal determinants and life-generated factors that impact survivors’ experiences of victimization and disclosure, particularly for readers who may not have considered such factors before.
Social determinants are the conditions in which an individual is born, grows, works, lives, and ages—think of race, gender, socioeconomic status, and access to wealth, power and other resources. Life-generated factors are the cumulative experiences that influence or affect a person’s development over time. Both of these things—social determinants and life-generated factors—make up who we are as unique human beings, how we operate and move about in this world, and who we choose to show up as depending upon the space in which we enter.
When reading my story, themes to consider are listed below.
1. As revealed in the statistics previously referenced, domestic violence and sexual assault are all too common and can happen to anyone—abuse and assault cuts across all races, religions, sexualities, physical abilities and socioeconomic status. There may be survivors in your family, social circle, school, place of employment, and in many other groups with whom you have contact and don’t know about.
2. Survivors disclose their experience when they feel safe to do so, and most likely when experiencing genuine, non-judgmental care and support.
3. We live in a rape culture8 where violence against women thrives and the stigma and judgment associated with being victimized is detrimental to the health and safety of women and girls. The level of victim blaming exhibited within our families, social circles, throughout society and the legal system, among others, contributes to the silencing of victims and the lack of strict, consistent accountability for perpetrators.
4. Memories of the abuse or assault can be triggered within survivors’ minds and bodies based on sights, smells, places, people, similar experiences, and a variety of other factors. These triggers may arise at times when the survivor feels particularly vulnerable or unable to control what is happening, such as in labor and childbirth.
5. Survivors can be extremely resilient and healing is always possible, no matter how soon or how far from the abuse or assault it begins.
We lived down a long, winding dirt path with a little creek that ran through the middle, down in North Carolina, just outside the city limits of Raleigh, in a town called Rolesville. We didn’t have many city roadways established in the area at the time; our address was a route and a box number. I come from the hard dirt of the South. The type of dry, dusty, powder thin dirt that leaves you feeling suffocated and poor of sight as it’s always sifting through the air. We drew water from a well—boiled it for cooking, heated it for cleaning, warmed it for bathing in a metal tub or tin basin. Firewood was chopped for the cook stoves and we kept a bucket in the house for when it was too cold or too creepy at night to venture out down the path at the side of the porch to the outhouse.
I am born of the poor, rural South—ripe with racism, classism and strict gender roles. Although my mother instilled in me that education was the way out, mostly all I knew growing up was living and farming on white people’s land. My grandpa and uncles primed tobacco, tilled soybeans, slaughtered hogs for butchering; eventually they worked in rock quarries and poured concrete or served as foreman at various construction sites. My grandma, aunts and mama picked cucumbers, grew tomatoes, plucked chickens—after ringing their necks and sinking them in hot boiling water to loosen the feathers—and they took shifts driving the town school bus to help make ends meet.
I grew up surrounded by tough love and violence. My mother married my father very young at the age of 16 (he was 19) after having my sister at 14 years old. I was born when she turned 18 (we’re birthday twins). My father was abusive towards my mother while we were growing up. I remember times when my mother would have bruises on her face from being hit. There was constant fighting between them in their on againoff again marriage, all the way until their final divorce in the mid-80’s after we’d moved into the city limits of Raleigh. It took decades for my father and I to repair our relationship.
One of my aunts experienced severe beatings, bruises, broken bones, humiliation and vicious attacks from her long-time boyfriend. As an adult it was traumatizing to hear that he was coming back around the family for Christmas dinner one year, after being released from prison. I was instantly thrust back into memories of seeing my aunt terrorized by this man for years when I was a child and specifically from the memory of hiding out from him one night as he was trying to break into our apartment to get at her. We were crouching together and hiding on the second floor. He was trying to come up the side of the apartment building to come through the second story window. When the police arrived, we were too afraid to open the door until finally we heard my father’s voice.
A different aunt’s best friend had to disappear after suffering years of beatings, both publicly and privately, by her husband. One day she took her kids and fled; my aunt would occasionally get a phone call from her friend letting her know that she was safe and doing okay but the loss of that friendship was devastating.
All of this history comes to mind when I think about who I am and how far I’ve come in 40 years of living—a poor Black girl from the rural South having grown into an educated outspoken, big-mouthed, feminist advocate doula living in New York City. I’ve often felt that my story, my life experiences were not worthy of being told; yet I frequently yearned to tell someone. To have my truth recognized and heard, to be validated and seen. Knowing what it feels like to be silenced, to feel less than, and not wanting that for any other woman lets me know that my story has value. I am born of resilient soil that bears fruit even in the most arid of summers.
No one wants to be the girl in the room who was raped. No one.
While my experience of being raped is not so secret, it’s also not something I’ve talked about very much in a public way. You see, the time my rape occurred I was the primary caregiver for my mother who had recently become paralyzed from the breast down in a car accident, a few months earlier. She needed almost around-the-clock care—it was not the time for me to have my own issues. I had just returned to working partial days after being out for a couple of months to attend to her initial surgery and recovery in rehab. This guy that I had been dating for several months wanted to take me out to celebrate Valentine’s Day and give me a break from caregiving. I thought it was a sweet gesture.
My sister arranged to stay with my mother overnight to ensure her care, and so off we went to dinner and a romantic evening out. I feel sick every time I think of
how he smiled in my mother’s face after meeting her for the first time when he came to pick me up for our date.
We stayed overnight at a hotel in the next city and I felt safe being there because we’d stayed together, overnight, in the same bed many times before, without being intimate. In fact, as two grown adults in our early 30’s seeking a solid relationship, marriage and a family, we were intentionally not having sex so we could focus on developing a stronger relationship—at least that was my understanding of what we were doing.
Later he would describe being overcome by the devil, like being possessed and not in control of himself. What it felt like for me was trying to fend off an attacker who snatched the covers from me in the middle of the night when I was sound asleep, and being faced with the dilemma of being beaten and raped or simply being raped. Those were the choices I felt I had as it became clearer and clearer that I was being overpowered and my struggles were futile. He was at least three times my size and there was nothing I could do to stop what was happening. So I lay there and stared off into space, into a dark void of nothingness as I felt myself breaking into a billion pieces.
He didn’t see my tears. He wasn’t aware of the lifelessness of my body. He took what he wanted and left me there, numb and dead inside as he went back to sleep, satisfied and content. I lay awake the rest of the night, stunned and unsure of what to do next. Even though I was an advocate for victims of domestic violence and sexual assault, I had no clue how to really advocate for myself—a young Black woman who
willingly went with this man that I’d known less than a year to his hotel room to stay overnight. This was in Durham, North Carolina in 2006—in the wake of the Duke Lacrosse Team rape allegations, which were steeped in the complexities of racism, privilege, and Black women being blamed for their own victimization. There’s no way I wanted that vitriol for myself.
The next morning was a blur as I stuffed and stomped my pajamas—stained with sweat, tears and semen— into the trash bin, cried through a shower and dressed to go to work. I confronted my rapist before I left, telling him about what he did to me when he questioned why I was sulking about and unpleasant first thing in the morning. I only wanted to be far away from that place but I also needed him to have some sense that what he did to me was not right, it was not okay. That is when he told me he was possessed by the devil and I should forgive him.
At the office I told one of my colleagues, now one of my best friends, what happened. I couldn’t even say the word, rape. I knew I had been forced to have sex. I knew that I had been taken advantage of and physically overpowered. I felt ill and weak and sick to my stomach. I was in disbelief. She was very empathetic and supportive. She questioned whether I thought being at work was the best thing for me at that moment. I felt guilty because of how much time I’d already taken off with my mother’s accident but she reassured me that our colleagues would understand.
My rapist began texting me Bible verses from 1 Corinthians, “Love is patient, love is kind…. It always protects, always trusts, always hopes, always
perseveres. Love never fails.” For years to come my experience with this man and his newfound faith in the Lord ruined my relationship with God. If this is what new Christians were about, I wanted no part of it. I took a sick day and left the office to go home.
On the way I called and told another close friend what happened to me. She talked more about what she would have done to fight him off and get him off of her than she did about understanding the difficult position I was placed in. She said I should have tried to hit him over the head with the telephone or the lamp from the nightstand; I should have found some way to fight harder because she would never have given up. I felt stupid for not doing more to stop the assault. I felt weak and pitiful. I got home and helped my mother with her care, then told her I didn’t feel well and needed to lie down. I didn’t want to burden her with had happened— she had more than enough to deal with having just become paralyzed and still in recovery. She had just had pieces of her spine fused together with a metal rod and was learning to live life in a wheelchair—I strongly believed that this was not the time for me to have my own issues. I lay down and that was the end of me talking about being raped. But that was not the end of its effects on my life and on me.
From that moment on, I rarely slept fully through the night. No matter where I have lived, I use a nightlight so that I never have to come home and walk into dark spaces. There was a constant pain in my inner thighs that would often wake me during the night if I turned in the wrong position. This reinforced my belief that pain lives in the body, in the memories of our muscles. I stopped wearing cute clothes and high heels, almost
all the color started to drain from my wardrobe. My attire became filled with dark grays, blacks and more modest outfits. I felt a kind of joy slip from me and I just needed to get away; so often I just didn’t feel happy and colorful. I began to have a strong dislike of crowds and crowded spaces where I felt trapped, insecure and out of control of what might happen with my body. Generally I started to feel hypersensitive and uncomfortable around men—my circle of friends became smaller and my time as a social butterfly steadily came to an end. I just couldn’t do it anymore. I was a different person—the need to focus on caring for my mother and her recovery allowed me time to privately cope with now being the girl in the room that had been raped.
Being a victim advocate and not acknowledging my own victimization pushed me into this weird space— very much created in my own mind and not forced upon me by others—but for a very long time I felt unsure of where my experience fit within the spectrum of others’ experiences and within the context of my own life. I knew other survivors whose experiences had been far worse and more devastating than my own. In many respects I felt that I had no right to talk about my experience, but I also wondered when I might have the courage to acknowledge my rape. I felt like I was a coward for not owning my experience while supporting others to find healing and justice in theirs. I felt inadequate and like I was never doing enough. It was all just a little too much.
Later on, I moved from North Carolina to a city in Maryland since my mother was much further along in her recovery and living independently on her own by that time. Moving to another state and becoming immersed in a new job came with its own level of excitement and the thrill of having a fresh start. It felt like an opportunity to leave behind past hurts and toxic relationships to create a new world and a new dynamic for myself. Surprisingly though, given my past trauma, finding a new healthcare provider proved to be a challenge during my relocation. I hadn’t thought much about it other than I wanted a very woman-friendly OB/ GYN—I didn’t need a lot, just my annual well-woman exams and routine preventive care. For some time, I would only have well-woman visits during trips home to North Carolina, but for the long-term that simply wasn’t feasible. I had become accustomed to receiving treatment at a lovely woman-centered practice that had empowering, woman-themed, inspirational quotes painted on the waiting room walls and on the ceilings over the exam table. They had furry purple booties covering the cold metal stirrups, gave you cloth gowns to change into for your exam, offered warm, moist washcloths to freshen up after your exam, and the staff brought their pets into the practice for petting and snuggling if needed. It was absolutely delightful.
But in Maryland, with this one healthcare provider that I was testing out, the experience was drastically different. It was quite horrible and traumatizing. The waiting area and many of the exam rooms left much to be desired and were a bit run down. The physician’s assistant was gruff, curt and rude—she would not even leave the
room to offer me any privacy to undress or dress as she completed her paperwork. Indeed, she dismissed my request for her to leave the room and slightly turned away to keep doing her work. Her vaginal exam was very rough and left me in tears. She had no bedside manner and no awareness of the obvious impact she was having on me. I struggled to get through that forceful, painful vaginal exam and went back to work to tell my colleague who had recommended this practice to me.
What happened to me during that exam was a very clear connection between my memory of being raped, and how being raped directly affected the muscle memory within my body. It was also the first time I had disclosed my rape to another person in years but my friend immediately understood. I was in tears, crying hysterically there in her office and feeling completely devalued after being treated like a piece of meat on that exam room table. My friend was very caring and supportive, yet also surprised because she’d never had that experience with the practice or had seen that particular physician’s assistant.
She encouraged me to write a letter to the practice so that something could be done about it. I left work early that morning and went home to recover but my friend helped me draft that letter a couple of days later. It felt empowering to take some action, even something as simple as writing a letter. Getting it out on paper and letting the practice know that their patient care was unacceptable felt important to me. I couldn’t imagine a young girl or another woman being treated in such a dismissive way and thinking that was how it was for your well-woman care. The practice needed to change
to better meet the needs of women and improve the quality and continuity of care. The provider’s office was very responsive to my letter and called to discuss my concerns. I did not return to that practice but it helped to know that they heard me and were taking steps to address it.
Peace is impossible but we’ll still do it.9
After some time passed since my rape, I met a man that made me feel giddy and happy in love. He helped me regain a sense of body peace and comfort with intimacy, because he gave me all the power and left the decision-making to me when we were intimate. He was an affectionate cuddle monster and taught me that there could be positive physical touch between a man and myself again. He never forced me to do anything that I did not want to do and our lovemaking was amazing, even when we pushed our sexual boundaries together. He gave back much of the joy that had been stolen from me. Yet, as magical and fantastic as that experience was, it also led to a very unhealthy attachment to him for years to come—I just didn’t know it at the time.
What was also wonderful about that man is that he did love me very much. I could have flashbacks, thoughts of self-harm, or relapses in my ability to cope with being raped and he would be right there to hold me as the pieces fell apart. My Love was very protective of me and I always felt safe with him. He was always gentle with me and that’s what I loved so much about him. There was one time when I thought my rapist had been in jail for a few years (for reasons unrelated to my rape) only to randomly see him in a picture on
social media with a friend we had in common. Simply seeing his face and knowing that he was out in the world sent me reeling into a breakdown. I was crying uncontrollably nonstop for hours, curled up in a ball on the couch, unable to move. After a while, and following much self-talk, I forced myself to come back into my life, to be present, to get up and not allow the pain of what happened to me control me. He was out of jail, but he had no access to me. I was in a safe place. I had to practice grounding and centering to gather myself together. I thought of how much healing and growth I had done over the years.
I remembered being in Costa Rica at a yoga retreat and getting some bodywork done to help take the pain away. And it actually worked! I remembered laying there on that massage table and sobbing deeply as one of the healers worked to release the pain of body and womb trauma from my being. I felt several releases during that experience, but it mostly felt cathartic to acknowledge what I’d been through and its impact on my spirit. It felt as if I’d finally embraced the healing process, even though it had been eight years since my rape. The biggest way that I experienced a difference was that the memory of my rape was gone from my inner thighs. I could open my legs wide while laying in the bed and not feel anxious. I could bend my legs with them spread open and not immediately feel tension until I crossed them closed again. It was beautiful, unexpected, and wonderful.
Another great source of healing for me was the practice of becoming a doula. This is one of the greatest loves of my life being in service to women and supporting them as they claim their own agency and birth new
life into this world. What first piqued my interest was seeing the Bravo TV show, Pregnant in Heels, with Rosie Pope. It looked fun and classy and I thought: I can do that! I could go into women’s homes and talk to them about preparing for birth and support their transition into motherhood. Then reading Anita Diamante’s Biblical fiction, The Red Tent, a book about the lived experiences of Dinah, Jacob’s daughter with his wife Leah, and her journey into birth work, was the next inspiration for me. Dinah’s story resonated with me because she grew up in the care of many women just like I did, always surrounded by my grandma, mother, aunts, sisters, cousins. Dinah was in awe of the power of women and she learned to command her own power as a woman. She was a traveler, a healer, and a supporter of laboring and birthing women, just like I aspired to be. I felt inspired by Dinah’s story and saw a new direction and purpose for myself.
Supporting women through labor and childbirth is one of the most fulfilling experiences of a lifetime. I love bearing witness to the power of women, and seeing the spark of their own amazement and discovery of their power is exhilarating. The sum total of these experiences, as well as a few others sprinkled here and there, is what has led me to where I am now, to adding my contribution to the momentum of supporting women’s sense of agency and right to choose the care for their bodies, their births and their babies.
First, which definition of trauma is used as the basis for writing in this book? The Sidran Institute: Traumatic Stress Education and Advocacy defines psychological trauma as:
An event or situation that overwhelms the individual’s ability to cope, and leaves that person fearing death, annihilation, mutilation, or psychosis, including responses to powerful onetime incidents like accidents, natural disasters, crimes, surgeries, deaths, and other violent events as well as responses to chronic or repetitive experiences such as child abuse, neglect, combat, urban violence, concentration camps, battering relationships, and enduring deprivation.10
While traumatic events occur externally, they quickly become incorporated into the person’s mind. Being trauma-informed takes into account both the precipitating event and the subjective aftermath of experiencing the event, such as the person’s response, recovery and coping strategies related to that event. Recovery from traumatic events is usually a years long or life long process.
With regard to trauma as a result of domestic violence or sexual assault victimization, there is an additional layer of stigma, shame, isolation, guilt and self-doubt when being blamed for “causing” the trauma that is often not experienced with other forms of trauma like hurricanes, fires, car accidents, etc. It is highly
important to note that the experience of these types of trauma, and managing the additional layers of stigma often leads survivors to react or engage in ways they typically would not. Consider viewing survivor responses as survival techniques to manage a life or relationship disrupted by violence, oftentimes occurring in an ongoing, cyclical nature.
Second, childbirth is a natural, biological process that is experienced differently by every woman, and women with multiple births will have a different experience each time. Therefore, regardless of experiencing domestic violence or sexual assault, many women may experience trauma in childbirth. The Birth Trauma Association11 describes factors that contribute to these feelings:
• Loss of control, loss of dignity, the hostile or difficult attitudes of the people around them,
• Feelings of not being heard or the absence of informed consent to medical procedures,
• A lengthy labor or very short and painful labor,
• Poor pain relief or induction and high levels of medical intervention,
• Emergency deliveries, lack of information or explanation of procedures,
• Lack of privacy and dignity, and/or
• Stillbirth and/or fear for the baby’s safety.
Practicing with this understanding is key because it recognizes that all women can benefit from traumainformed care, whether they have a trauma history or not and whether you know about it or not.
Third, this book is about supporting women in the choices they make based on what they have determined to be
in the best interests of themselves and their families. Women make a variety of different decisions based on their personal beliefs, faith or cultural practices, individual upbringing, access to medical care, financial resources, family and community support, and many other factors.
In this book, supporting women also means not expressing sentiments or placing judgments regarding women’s birth choices or the care they provide for their newborns, including no mom shaming or birth-shaming about:
• Non-medicated vaginal birth vs. planned use of medication or other interventions
• Breastfeeding vs. bottle feeding
• Breast milk vs. formula
• Working moms vs. stay-at-home moms
Fourth, female pronouns will be used throughout this book when discussing survivors of domestic or sexual violence. This is not to say that men and boys do not experience violence, abuse or sexual assault from their partners, however, given that the focus of this book is on birthing women, it is appropriate to use gendered language.
Lastly, the terms victim and survivor are both used when discussing women’s experience of being abused and/ or assaulted. Victim is most often used in reference to when the abuse is occurring and while the person is still having the experience, whereas survivor is used most frequently to refer to someone who is no longer experiencing abuse or for whom an assault may be in their past. It is always best to use the words that
women use to describe their own personal experience with violence and abuse because they know their own story better than anyone else, and are entitled to name it however they choose.
The matter of whether or not to ask clients about their trauma history is one of the great doula debates. Some think that by asking about it, negative thoughts will be planted or alarm bells will ring for pregnant women who already have enough to manage, while others think that addressing a woman’s trauma history is simply beyond a doula’s scope. Still, many see the inquiry as part of the birth planning process to deliver high quality services. Either way, the debate rages on; let’s delve a little deeper.
First, choosing not to ask about a woman’s trauma history does not negate its existence. Asking about it allows time for the woman to consider whether her past experiences will impact her labor and the birth of her baby, and it gives her time to plan for the type of support she will need to mitigate that impact. Even if you don’t feel very confident in your abilities to provide labor support to a client with a trauma history, you can offer her resources to further her own healing and secure the support services she needs.
Second, within a doula’s scope of practice is advocacy and providing referrals. It is vital that doulas assist their clients in advocating for their needs during labor and childbirth. This includes practicing strategies to effectively communicate those needs to their care
provider, whether or not disclosing their trauma history is part of that communication. Providing referrals to community-based resources on a wide variety of services should be a standard part of every doula’s repertoire.
Warm referrals—defined as a recommendation made to a specific service provider or contact that the referrer has a relationship with and can vouch for their quality of character and service provision—are most effective. Links to national service providers are provided in the Resources sections of this book. Use those links to find statewide and local resources in your area to update your current list of resources and build working relationships. Contact the programs in your area to set time for an appointment to learn about their services and how they serve victims of domestic and sexual violence. You may also attend any of their community outreach events and connect with their volunteer services, training or outreach coordinators to learn about their services in the community.
Including local domestic violence programs and rape crisis centers as part of your standard resource list makes the information accessible to women that may need it, without them having to disclose their abuse or assault. Also, in this way, access to the information will be less likely to raise an eyebrow from the abusive partner if the websites and crisis line phone numbers are discreetly included amongst a wide variety of other community-based resources.
Third, some doulas say they don’t ask about a woman’s trauma or abuse history because having that information would not change their manner and
methods of providing support. Well, to that I say asking about a woman’s trauma history is not about you, as the doula. It is about helping a woman find and strengthen her voice, her sense of agency and her right to have control over her body, her birth and her baby, especially for women birthing in hostile environments and who have a history of being silenced, marginalized and diminished.
As a doula, this is an important question. In very many cases, a doula may not know that their client has a trauma history—and that’s perfectly okay.
All women benefit from receiving trauma-informed care, which reduces the need to know more about our clients than they may feel comfortable disclosing. Those clients that specifically want labor support from a doula due to her trauma history will be very clear about it. For others, they may eventually disclose their experience once they’ve built a trusting relationship with the doula as part of their birth team. Other times a disclosure may happen are noted below.
Observation. In some cases, during prenatal visits, a doula may suspect that abuse is occurring through keen observation of the interactions between a woman and her partner, or based on comments made by the woman or her partner. It is best not to assume but rather to plan a time to speak with the woman privately, when it is safe to do so, and tactfully, politely share your concerns.
Intake. Many doulas will ask about a woman’s trauma history when conducting an intake. It’s best not to lead or start the relationship with these types of questions but as the relationship grows, perhaps during the second prenatal visit, find time for a private moment to thoughtfully raise the question of past experiences with abuse or violence as part of the standard questions asked while planning for the birth experience.
A few examples are listed below.
• Are there any experiences in your past that would be considered traumatic that could affect your experience giving birth at the hospital or birth center now?
• In the past, have you spent any time in the hospital that would cause anxiety for you being in the hospital now?
• It is helpful for women to stay mentally focused on their labor and their baby as its moving down into her pelvis and vagina for birth; have you had any troubling or frightening experiences in the past that may get in the way of your mental focus during labor?
If the response to any of the above listed or similar types of questions is “yes,” respectfully follow-up with more probing, open-ended questions, such as:
• If you feel comfortable, will you please tell me more about what you experienced?
• What helped you the most in healing from your experience?
• When these issues are triggered or resurface for any reason, what do you do to cope?
• How do you think those past experiences will affect your birth experience now?
Be careful not to probe too deeply too soon and be watchful of your clients’ nonverbal clues (e.g., body language) and comfort level with the topic. Now that you have introduced the issue, it’s okay to give your client time to think it over and come back to it later. Depending upon how you’ve organized your intake, you may want to ask your client if she would like to set a time to further discuss if and how her past experiences might impact her birth experience and what that impact may look like. Be sure to follow through with the commitment to discuss these issues in further detail. The follow-up may be an in-person meeting, a phone chat or sending additional information via email—follow your clients’ lead and ask for her preferences.
Be mindful that birth can also be a time of positive transformation and breaking the chains of past trauma experiences as well. Highlight this for your client and identify ways in which to support her in making this healing into a reality.
During Labor. Just as the impact of trauma echoes may be unexpected for survivors in labor, some doulas may not become aware of their client’s past trauma history until labor begins and their client is in distress. Seeing a woman become disengaged from the birth experience, seeing in her eyes that she may be disconnecting or dissociating12 from her body and her baby, hearing in her birth sounds increasing anxiety, hysteria, or wailing, or seeing her physically respond to the triggers in the room or from the labor are good indicators that focused attention and support is needed.
After the Birth. In some instances, a doula may not know until after the birth whether the experience was challenging or transformative for the client, or that the client’s actions were a result of previous trauma. Processing the birth experience during the postpartum period is key to supporting the survivors’ ongoing healing processes. Some clients may disclose the abuse during the postpartum period or the 4th trimester when life with a newborn has altered the family dynamics and their perspective on their family situation may have changed. Continue to provide support and offer warm referrals for access to longer-term care.
What is domestic violence? A pattern of one person exerting power and coercive control over their intimate partner through intimidation, threats, harassment, emotional manipulation, physical force and other forms of abuse, including abuse of children, financial abuse, and sexual violence. In short, there needs to exist three things: 1) a pattern 2) of coercive control 3) between intimate partners. Legally other remedies may exist for various relationships—abuse between family members, abuse of children, abuse of elders— however, for the purposes of this book the focus is on intimate partner relationships.
The Centers for Disease Control (CDC) provides a comprehensive definition of intimate partner violence: http://www.cdc.gov/violenceprevention/ intimatepartnerviolence/definitions.html.
Experiencing relationship abuse is an ongoing traumatic event that is cyclical in nature. Victims of abuse are usually wooed and groomed by their perpetrators in ways that appear caring, loving and devoted—very quickly falling in love and solidifying the relationship, monopolizing the victim’s time, commenting on the victim’s appearance, going above and beyond to do or buy things for the victim, charming the victim’s family and friends. Over time these actions become more and more about what the victim now owes her partner, including emotional debt, leading to the perpetrator’s ability to control and manipulate her.
Often the use of violence escalates in terms of intensity, frequency, and severity of abusive actions by the perpetrator—starting with emotional shame and humiliation, moving to minor incidents of physical harm (pinching, shoving, arm grabbing, physical intimidation), to other forms of control (financial, sexual, etc.), and on to more aggressive physical attacks including punching, kicking, restraining or holding down, strangulation, use of weapons, destruction of property, and manipulation, neglect or abuse of children, among many other damaging acts of violence. By this time the victim feels trapped in an ongoing cycle of abuse that feels overwhelming, inescapable and embarrassing.
Many women can benefit from discussing their options for safety, legal remedies and healing from the abuse with a compassionate, well-trained victim advocate. This is where giving a referral can make the difference in women’s access to helpful resources and lifesaving support. The National Domestic Violence Hotline is a helpful gateway for women seeking services in their community. Domestic Violence Victim Advocates are
skilled at assessing victims’ situations, knowledgeable about national, state and community-based resources, adept at safety planning, and helping survivors discuss the benefits and risks of their particular choices.
1-800-799-7233
Live chat: http://www.thehotline.org/what-is-live-chat/
For survivors in need of legal assistance, identifying the legal options and remedies available is best handled with a legal advocate from a domestic violence program or an experienced attorney with specific training and knowledge in this area. Legal assistance can help survivors assess their legal priorities, explore their options within the civil or criminal legal system, file motions (such as an order of protection,13 which may include remedies related to child custody, eviction of the abuser from the home, possession of the family vehicle, and other options to ensure relief from the abuser), and offer long-term legal guidance as needed.
Survivors may also educate themselves about their legal options. WomensLaw.org, A Project of the National Network to End Domestic Violence14 provides state-by-state legal information and online support specifically to victims of domestic violence and sexual assault.
The Domestic Abuse Intervention Project (DAIP)15 based in Duluth, Minnesota created the Power and Control Wheel16 from focus groups with women who had been
battered as a way to describe battering for victims, offenders, practitioners in the criminal justice system and the general public. The wheel depicts power and control as the core or center of abusive relationships being supported all around by the physical and sexual violence, as depicted on the rim of the wheel. Each spoke of the wheel identifies and describes a variety of tactics used by those who abuse. Some examples have been noted below:
• Exhibits intense emotional extremes and mood swings such as jealousy, anger, control, intimidation and threats
• Isolates their partner from freely communicating or spending quality time with family, friends and loved ones
• Erodes their partner’s self-esteem through gaslighting, belittling, humiliation, name calling and emotional manipulation
• Monitors, stalks and harasses their partner in person, by phone, text, email, and/or through social media, family, friends and co-workers
• Increases frequency and severity of physical violence, use of weapons, abuse of pets, or threats of suicide or homicide
• Coerces sexual intimacy following an assault, forces participation in unwanted sexual acts, commits rape, infidelity, engages in risky sexual behavior
• Tampers with birth control, knowingly passes STIs/STDs, coerces termination of pregnancy or causes miscarriage, coerces victim to carry an unwanted pregnancy to term
• Sabotages employment and/or credit, controls finances, withholds access to essential selfcare items and/or medication
• Exploits vulnerabilities in partner’s age, sexual orientation, disability, immigration status, language access, or HIV status
Some of the tactics listed here and on the Power and Control Wheel may be used, while others may not; in some cases all of the tactics will be used. It is important to follow the victim’s lead in determining whether any of the tactics of abuse, or combination of tactics, constitute abuse and victimization for her. The common thread amongst all of the tactics is isolation of the victim from her support system and the use of violence.
A Safe Passage created an adaptation of the Duluth Model’s power and control wheel, Woman Abuse During the Childbearing Year.17 This variation of the wheel depicts abuser tactics specifically related to the victim’s pregnancy and postpartum period, and is a simple way to communicate the complex nature of experiencing abuse during pregnancy.
The DAIP also has two other wheels that may be of use to doulas in their practice to provide traumainformed birth support. The Equality Wheel18 can give doulas language to talk with their clients about healthy relationships, particularly in planning for the 4th trimester when significant changes occur in the home with a newborn, and possibly other children. This may also be a time when the usual roles and responsibilities in the household shift as the mother needs to attend to her own recovery and her newborn child.
And, the Nurturing Children Wheel19 can be used when helping clients strengthen their relationship with their children and develop healthier family dynamics for parenting their children.
Using Abusive Tactics is Not About Problems with Anger Management. A common misconception is that people abuse out of anger. While the abuser may be angry at times when committing acts of abuse, anger is not the root cause of why a person abuses. Abuse is a choice that the abuser makes. The following table depicts some differences between use of abusive tactics and problems with anger management to help illustrate the point that abusers choose whom, when and where they will abuse.
Anyone may be a target of the aggression or physical attack—family, friends, co-workers, strangers, fellow drivers
Assaults or verbal attacks happen publicly
Marks and bruises are aimed anywhere on the body; no attempt to conceal the attack
Intimidation, aggression and physical attacks are targeted towards one person—their intimate partner
Assaults occur in private and in isolation
Marks and bruises aimed at areas that tend to be covered, e.g., head, stomach, back, thighs
Loses control of emotions Often maintains an eerie calm over emotions
Exhibits anger at any time, including when detrimental to their own interests
Inability to peacefully resolve conflict
Individual issues may be managed with conflict resolution training, therapeutic counseling and/or medication
Exhibits anger when it aids in their control over their partner
Lack of accountability for their actions
Behavior choices may be addressed through legal or social measures such as family, faith or community accountability; batterer intervention programs (psychosocial-educational intervention); financial restitution; other civil or criminal sanctions
Pregnant Survivors. It is important to keep in mind that domestic violence may begin, worsen or halt during pregnancy. There is no one specific indicator of what may happen during pregnancy other than past history of violence towards women, pregnant or not. In addition to the stress and rigor of coping with physical abuse, the health effects of experiencing domestic violence during pregnancy include:
• Potential injury to the fetus
• Miscarriage
• Low birth weight
• Preterm labor
• Placental abruption
• Maternal or fetal hemorrhaging
• Failure to thrive
• Still birth
• Maternal or fetal demise
While a warm referral to a local domestic violence program or shelter is appropriate, it is also vital that doulas continue their care and support to pregnant survivors while they are exploring their options for safety, if they are residing in shelter, or if they access shelter shortly after giving birth. These survivors may express an even greater need for support and resources due to:
• Being in an unknown environment;
• Acclimating into an unfamiliar system;
• Lacking stable long-tern housing, employment, childcare, and other life necessities;
• Managing legal matters and the hardship of navigating the legal system;
• Experiencing pressure from family, friends, their
cultural beliefs or faith community to maintain the family unit;
• Being uncertain about their future; and
• Recovering physically and emotionally from a traumatic relationship during a particularly vulnerable time.
Keep in mind that some women may determine that remaining with a partner that uses abuse is in their best interest at the time, and separation may not be their goal. There are a multitude of reasons why this may be the case, including familial and parenting considerations, cultural and spiritual beliefs, economic circumstance, housing needs, and emotional interests, among many other factors.
As doulas, it is not our role to pressure or shame women for making that decision—we don’t know and are not entitled to know the entirety of their situation. It is best to focus on supporting your client to have a safe and positive birth experience and providing warm referrals as needed or requested.
What is sexual violence? Sexual violence is any unwanted sexual contact or sexual act committed against a person without their freely given consent, including:
• Rape, sodomy, or forced penetration (including oral), whether completed or attempted
• Drug or alcohol facilitated penetration
• Coerced consent or acquiesce through verbal pressure, intimidation, harassment, or misuse of authority or position
The Centers for Disease Control (CDC) provides a comprehensive definition of sexual violence: http://www.cdc.gov/violenceprevention/ sexualviolence/definitions.html.
Forms of Sexual Violence. There are many forms of sexual violence that may impact women throughout their lifetime. One aspect of all forms of sexual violence is that sex is the weapon used to exert power and control over another person. Although the majority of rapists know their victim (the U.S. Department of Justice reports that 47% of rapists are a friend or acquaintance), sexual violence is not about sexual chemistry or compatibility—it is about one person’s need to control the other and using sexual acts to do so, such as:
• Childhood sexual abuse
• Molestation or incest
• Street harassment
• Rape or forced penetration
• Repeated sexual violence
• Rape as a tactic of war or gang-affiliated assaults
• Sexual violence as part of domestic violence relationship
Responding to Sexual Violence. Whether the assault occurred once or multiple times, in all cases the victim’s sense of safety, security, trust and justice in the world are shattered. Initially, survivors experience a complete disruption of their lives following the assault, including the need to recover from any physical injury, infections or disease incurred from the assault (e.g., attending to wounds, bruises, soreness, aches, pains, STIs/ STDs). This may require ongoing medical attention, depending upon the nature and extent of the assault. Many survivors experience pain specific to the areas of the body that were targeted during the assault. In some cases the pain will be psychosomatic yet this type of pain is equally as valid and real as the physical trauma victims experience.
Emotionally, some survivors will openly and outwardly express their reaction to what happened to them. They may appear agitated, angry, talkative, or hysterical, while others may turn inward and bottle-up their emotional reaction to the assault. These survivors may appear withdrawn, numb, detached or calm. There is no “one way” or perfect response to being a victim of sexual assault.
All victims of sexual violence are transformed by their experience and go through a period of redefining what their life will be like moving forward. During this time, survivors will experience sleeping and eating
patterns that are different than their usual routine— some sleeping and eating much more, others sleeping and eating much less—and they may begin to have nightmares or flashbacks. Some even have dreams where they may become strong or violent and reclaim their power over their rapist.
Over time, survivors learn to cope with the impact of the sexual assault on their lives. They develop new routines and practice ongoing coping skills, which may be healthy: participates in therapy or support group, re-establishes healthy eating and sleeping habits, etc., or unhealthy: abuses substances, self-harms, engages in risky sexual behavior, etc. or a combination of both types of coping skills. Factors that influence how a person copes with being sexually assaulted include:
• Their level of resilience and learned methods of coping with life’s challenges
• Whether or not they have an established support system in place or access to an empathetic support system they can join
• How they are treated in response to disclosing the assault, including the reactions of advocates, medical professionals, law enforcement, family, friends and others
• The existence of other life problems or difficulties related to family, relationship status, employment, living situation, etc.
• Prior history of victimization or trauma, which may intensify the experience and make recovery even harder
I believe you. It’s not your fault. Some of the most difficult emotional challenges survivors of sexual assault face are guilt that they were unable to stop what happened, self-blame that they did not keep themselves safe, and fear that others will not believe them about the assault. It is vital that doulas believe their clients and reinforce the belief that what happened to them was not and is not their fault. This understanding is essential to providing trauma-informed birth support. In a blog post titled, For Women & Girls Who Have Experienced Rape, posted on March 31, 2011, I wrote about what victims need:
1. What victims need most is to be believed and not judged or blamed for the actions of someone else, or the decisions they may have made as a result of that experience.
2. Victims of rape need to have their privacy and their choices for healing honored and respected, without blame or pressure.
3. We need safe, compassionate medical attention, healthcare, and accurate information; not just immediately following the incident, but for the remainder of our lives.
4. We need time and space to redefine what safety means in our world—in our personal space, in our homes, at our place of employment, in crowds, in dark spaces, when being intimate, when alone in a room with a man… anywhere and everywhere that we feel the need to redefine what “safe space” means.
5. We need rest, we need light, we need warmth, and positive touch.
6. We need to be reminded that it was not our fault; that we did the best we could with an experience that we did not ask for, that was forced upon us without our consent. It is always okay to remind us that we did not deserve this and that what happened to us does not define who we are.
7. We need access to supportive healing processes and information, however we define that. Whether it is through reading, journaling, seeing a therapist or counselor, reconnecting with our faith, or sharing our story—we need access those avenues for healing.
8. We need ongoing, unconditional love.
Pregnant Survivors. For pregnant survivors, the impact that sexual violence may have on women’s pregnancy and labor can include:
• Disbelief about the pregnancy
• Increasing anxiety related to her ever-changing body
• Unfamiliar sensations in the pelvic and vaginal areas may reactivate trauma
• Emotional disconnection to her growing baby
• Trepidation and fear about the birth experience
• Flashbacks, nightmares, distorted sleep patterns, harmful coping practices
• Delayed access to prenatal and maternal health care
Well-trained advocates and volunteers at rape crisis centers are knowledgeable about a myriad of issues related to sexual violence such as individual or group counseling, medical attention, reporting a crime to law
enforcement, and many national, state and communitybased services. Again, while a warm referral to a local rape crisis center may be appropriate, it is vital that doulas continue their care and support to pregnant survivors. National Sexual Assault Hotline 1-800-656-4673 (HOPE)
Live chat: https://ohl.rainn.org/online/
Doulas must be prepared that some survivors of sexual assault will engage their services very early on in the pregnancy, during the first trimester rather than the third, to allow time for the relationship and trust to develop. For others they may not realize their need for doula support and guidance until very late in their pregnancy when they are nearer to term. In either instance, it is crucial that doulas honor the path towards healing that survivors are on and provide support that makes a positive birth experience part of their recovery. For example, survivors may:
• Request guidance on selecting the birth location (home birth, birth center, hospital) and care provider (unassisted, midwife or OB) that can best give them the outcomes desired,
• Want practical suggestions and assistance with developing a mutually respectful and positive relationship with their care provider,
• Need greater planning to anticipate and cope with trauma echoes that may arise during labor and childbirth, and
• Require ongoing support during the immediate postpartum period, when nursing, and during 4th trimester recovery.
Doulas are not medical professionals and should never act as such—in fact, doing so falls outside the doula’s scope of practice as does offering medical advice, performing clinical tasks, making a diagnosis, or conducting other activities similarly rooted in the practice of medicine. The lists provided below are for informational purposes only. Should a doula observe, suspect or be made aware of any of the health risks noted below, it is best to encourage clients to discuss these issues with their care providers. A doula’s knowledge and experience serving clients with similar challenges can be instrumental in assisting survivors with how to talk about these issues with their OB or Midwife.
• Avoidance or dissociation
• Emotional numbing
• Sleep problems
• Disordered eating
• Appearing to lack motivation
• Thoughts of suicide or self-harm
• Flashbacks, anxiety, panic disorder
• Depression
• Low birth weight
• Low fluids
• Premature birth
• High intervention birth
• Fetal demise or miscarriage
• Stillbirth or death
• Difficulty thriving
Trauma Echoes. Some survivors will experience trauma echoes related to their sexual assault or experience with ongoing domestic abuse. Listed below are examples of trauma echoes specific to pregnancy and childbirth. Doula strategies to mitigate each of these triggers are discussed later in this book.
• Survivors may feel out of control of their body and/or mind
• Intense sensations of the baby moving through the birth passage may cause distress
• Standard positions for birth (on back, legs spread wide apart) may increase vulnerability, exposure and loss of dignity and modesty
• Authoritative, demanding attitudes devalue, dismiss and silence survivors’ needs
• Significant discomfort with fetal monitors, IVs, blood pressure cuffs, and other medical instruments or interventions may lead to survivors feeling held down, trapped or restrained
• Use of dim lighting or closed door, small spaces (like bathrooms or showers) may trigger painful memories
• Frequent exposure and the physical demands of breastfeeding may increase survivors’ feelings of helplessness and powerlessness
Doulas are here to serve and be of service to pregnant and laboring women. When issues of domestic violence or sexual assault come up, a doula should follow their client’s lead and discuss what her priorities are. For some survivors, addressing the violence or trauma history may not be the most immediate priority. Her concerns and attention may be focused on the growing needs of her baby, how she will care for and provide for her baby long-term, and how to maintain a sense of stability and normalcy during the pregnancy. Some questions to ask are:
• What are your three priorities right now and immediately after the birth?
• Which priority would you like to focus on now?
• When these issues have come up in the past, what has helped?
• Are there strategies that weren’t so helpful?
• What would you like to try now?
• How can I support your next steps?
• How can I help you feel safe?
Remember to be honest yet tactful about any concerns you have without overreacting or underreacting to what you may be hearing from your client. Seek to find a balance between being compassionate and maintaining your role and scope as a doula—your primary focus is on providing labor support to help women safely and confidently birth their babies. Maintaining a thoughtful balance will allow your client the time and space to share more as her trust and comfort level grows. One of the effects of abuse is that women’s self-esteem will
deteriorate over time. Help her rebuild her self-esteem and sense of agency by encouraging her to trust her own instincts and decisions to do what’s best for herself, her baby and her family. Offer credible, reliable information through warm referrals but do not make promises about what will happen.
If you observe or are made aware of imminent physical danger to mother or baby, contact the authorities when it is safe to do so. Imminent physical danger is defined as the existence of any threat, series of behaviors or set of circumstances which could reasonably be expected to cause or lead to the serious physical harm or death of another person. For example, this would be hearing a direct threat of harm towards your client by her partner who has the means to carry out the threat or witnessing a physical assault.
This can be a delicate situation to manage as you need to ensure your own safety and support your client in seeking safety as well. Some survivors do not want law enforcement or social services intervention due to prior interaction with law enforcement in their community, disbelief in the legal system, mistrust of social services helping professionals, historical and institutionalized racism, the stigma associated with being a victim and a myriad of other factors. It is important to balance your client’s wishes with what your intuition senses about the severity of the situation and potential risk of harm or injury to your client and/or her baby.
Additional details are outlined in the following pages about how to engage survivors at each stage of the doula-client relationship.
Website & Marketing Materials. Your doula website should display that you offer trauma-informed birth support and make reference to any advanced training, education, or experience you’ve had in this area. This will make it easier for women seeking those services to find you. Using language in your services brochure or one-pager that reflects your ability to provide this unique type of support to women in need will also aid them in finding you. Additionally, this allows women to discreetly seek the support they desire without having to talk about their trauma experience until they decide they are ready to do so.
Client Interviews. During client interviews, be sure to let potential clients know that you provide traumainformed birth support as a standard part of your service delivery—you should say this as part of your introduction and include this in written materials (see the highlighted sections on the previous pages). This gives women the understanding that you can provide specialized support, if needed, while giving them the space to determine if and when they might want to discuss those needs. As you begin to build a trusting relationship through the initial interview, potential clients that need these specific services can assess whether you will be a good fit to support them and meet their needs for trauma-informed birth support.
Prenatal Visits. Prenatal visits are prime times to build trusting relationships with your clients, especially if there is a trauma history that may impact the birth. Focusing on clear communication, validating client concerns, and reducing your client’s fears through education is fundamental. The use of birth education tools and props can be helpful in illustrating what can
be expected during labor and childbirth. Visualizing how the baby will come down through the birth canal may be less scary when a woman can see the mechanics of how the body works through a doll, pelvis, uterus or similar type of educational prop.
Level setting client expectations about the birth experience can also dispel misconceived notions of what happens in labor, particularly related to the specific birth location and care provider. Explaining to women the different philosophies and approaches to managing a birth—between an OB and a midwife—can guide women in first, choosing the care provider and birth location that will best meet their needs, and second, in cultivating a productive relationship with their care provider. Read more about this in Birth Monopoly’s blog post, Why Are We Asking Doctors if Women Should Have Midwives? at: http://birthmonopoly.com/ midwives/#sthash.YCIh4lmQ.dpuf.
An additional handout, Factors to Consider When Selecting a Birth Location, is provided in the Resources section to further assist women in prioritizing their needs for achieving a positive birth experience and identifying the care provider that can best support that outcome.
Prenatal visits are also the best time to discuss and plan for any trauma echoes that may arise later. While survivors may not be able to fully anticipate exactly how their trauma history will impact their labor, they may be able to discuss what has worked well for them in the past when they have been triggered. It can be helpful to talk through known triggers, such as people, smells, sounds, or situations and possible remedies
prior to labor beginning and during non-stressful times. One approach that works well is to discuss who and what the woman does want in her birth space.
Ask her to spend some time with her partner envisioning the birth experience that would leave her the most satisfied and proud of herself. Have her describe that experience in detail by writing in a journal, scribbling a series of notes or by drawing images on a piece of paper. She should consider where she is, who is with her, what items are there in the space, and how she plans to manage the discomfort that comes with labor. Discussing this imagery during one of your prenatal appointments will be key to understanding how to best support your client in achieving the birth experience she wants.
Most literature and pop culture images depict women birthing on their backs with their legs in stirrups and their arms attached to various medical instruments. For many survivors of abuse, birthing in this supine position may lead them to feeling particularly vulnerable and without control over what’s happening. Demonstrating and practicing active positions for labor20 during prenatal visits and writing out a plan for early labor can help survivors feel better prepared for labor to begin.
Active birthing positions increases women’s control over their bodies and their birth because they are powerfully engaged in managing the positioning of their bodies and the sensations of their baby moving down and through the birth passage. In these active positions, survivors can clearly see everything that is happening around them and better anticipate changes they need to make to stay grounded and secure in their birth experience.
Early & Active Labor. Just as you would with clients who do not have a trauma history, in early labor you’ll want your client to engage in activities of distraction, nesting or to just keep doing what they would normally do. This is a good time for your client to enjoy a light snack, a warm cup of tea and snuggle in to rest as labor progresses. You may also encourage your client to journal their thoughts and feelings of anticipation of meeting her new baby for the first time. She can journal her dreams for herself as a mother, her baby’s future and the future of her family. Survivors may use this as a time to plan for their future or to let go of past hurts and continue healing.
As labor begins to become more consistent and intense, you may need to help your client identify her ritual or routine and help her continue cycling through it. This should include a variety of position changes, movement (taking a walk or shaking the apple tree if laboring in bed, pacing the birth space, moving through a yoga sequence, belly dancing, or partner swaying), bathroom breaks, and repeating affirmations to remain grounded and centered.
Flowing through the simple yoga pose (instructions below) can help your client slow down, focus inward, and find her center.
With feet firmly planted about two steps more than shoulder width apart, soles flat against the floor mom should be standing strong and rooted in place. Her arms should hang loosely at her sides with palms facing outward. She should inhale deeply in through the nose and exhale fully through the mouth, releasing all of her breath to empty her lungs.
On the next inhale mom should raise her hands out to her side and bring them above her head, palms closing together and coming down to her heart center as she exhales. Palms should press firmly together, fingers spread open and apart.
Mom should inhale her arms upward once more, circling her arms around to bring her palms together on the exhale. She should step slightly to the side, bend her knees and sink towards the floor into a low squat or goddess pose—depending upon comfort level. When rooted, she should open her hands out to her sides with bent elbows by her waist, palms facing upwards toward the sky, or hold the back of a chair or touch the wall for balance.
In this pose mom’s feet should be firmly planted on the ground and she should be able to sway and move her hips back and forth with the pressure of the contractions as they come. Mom should inhale and exhale deeply with each sway from one side to the other. Her hand can be on her heart and her belly or extending out from her sides in rhythm with her movements. She should move and flow through about 10-12 deep breaths in this way.
To come out of this pose, mom should slowly return to center in her strong goddess pose, exhaling deeply with her arms bent at her waist, palms facing upward towards the sky. Mom should inhale and sink just a bit deeper than she thinks she can, bringing her hands to heart’s center. As she exhales mom should straighten her legs to standing position and extend her hands up above her head, circling around to her sides, ending in mountain pose with her arms resting by her side.
Addressing Trauma Echoes. As labor progresses be alert that trauma echoes may begin to present themselves. A listing of effective strategies and the role of the doula are noted in the following chart to address triggers that may arise. If the decision is made at any time during labor for mom to birth via cesarean (C-section), assist her in advocating for a familycentered or gentle cesarean birth.
Survivors of domestic violence may be anxious or fear how their partners will act during the birth
• Check-in discreetly with mom to be certain the abusive partner’s presence is still wanted; engage the L&D nurses to clear the room for medical procedures if needed to have a conversation in private
• Focus on modeling healthy relationship behaviors and respectful interactions with both mom and baby for the abusive partner
• Keep in mind that witnessing their child’s birth may be a transformative experience and motivation to change for the abusive partner
Affirmation: “You’re braver than you believe. Stronger than you seem. And smarter than you think.” ~Christopher Robin, Pooh’s Grand Adventure
If separated, survivors of domestic violence may fear that her partner will show up unexpectedly at the birth location
• Prior to the birth discuss with mom how to handle this situation if it arises: Will other family or friends be at the birth that can manage her partner if they show up?
• Is there a Protective Order in place that would bar the partner from being at the birth location? Ensure that hospital and L&D security are aware of the order
• If legal restrictions are not in place, consider that during labor mom may decide that she wants her partner there; seek to include them as much as she wants in the birth experience
• If legal restrictions are in place through an order of protection or no contact order, remember that it is the abusive partner that would be violating the order—not the mother—if the abusive partner shows up to the birth; your client should not be made to feel responsible for the actions of the abuser
Affirmation: “Focus on what you can do, then do it with all your heart.” ~Lois Wilson
Labor happens faster than expected
• Provide strong emotional support and physical comfort
• Talk mom through what’s happening and help her remain grounded in the experience
• Help mom focus her breathing to mentally slow down the experience and work with her body as labor progresses
• Offer guidance during the pushing phase to minimize possible tearing (slow pushing, use of warm compresses and oils)
Affirmation: “Birth is powerful, let it empower you.” ~Anonymous
Labor begins to slow down significantly or doesn’t progress
• Pause—take a break from all interventions and actions to speed up the labor
• Make mom as comfortable as possible so that she may rest and recover
• After mom has had proper rest, talk with her about what may be mentally blocking her progress; consider doing a fear release or cleansing ritual to help mom re-center
• Begin the Miles Circuit21 to get mom back into a routine focused on her labor and to ensure baby is in optimal position for birth
Affirmation: “My baby is healthy and innately knows when to begin labor. My body knows how to birth by instinct. My mind has released all fears and trusts birth.” ~Mrs. BWF, January Harshe
Women may feel out of control of their body and/or mind or may appear to disassociate from the experience by staring off into space
• Make direct eye contact and explain to mom where she is and what is happening to bring her back to present
• Maintain a physical connection if allowed: hold hands, place hand on shoulder or back, press cold compress on mom’s forehead or back of her neck
• Use counter pressure if allowed to help mom physically ground herself: pressing forearms on shoulders, press palms down firmly on mom’s knees if in sitting position
• If necessary, give mom clear, firm direction to help her stay in the present
Affirmation: “Nothing in life is to be feared. It is only to be understood.” ~Marie Curie
Intense sensations of the baby moving through the birth passage may cause distress
• Help mom focus her breath to breathe for her baby and stay calm
• Due to the severity of the trauma, some women may choose an epidural or have a planned cesarean to negate these issues; if so, help mom advocate for a family-centered or gentle cesarean
Affirmation: “The power and intensity of your contractions cannot be stronger than you, because it is you.” ~Unknown
Significant discomfort with fetal monitors, IVs, blood pressure cuffs, and other medical instruments may lead to feelings of being trapped or restrained
• Prepare women in advance for the medical use of these instruments; discuss what this may be like for her
• Encourage mom to inquire about the need for each instrument and to request their removal when not necessary
• Mom may request external fetal monitoring with a Doppler or intermittent monitoring to reduce feelings of restriction
Affirmation: “Birth is an opportunity to transcend. To rise above what we are accustomed to, reach deeper inside ourselves than we are familiar with...” ~Marcie Macari
Some body positions for labor (on back, legs spread wide in stirrups) and authoritarian attitudes may create trauma echoes
• Support women to use different positions for labor and birth:
o Side-lying position
o Hands and knees
o Leaning over a birthing ball
o Squatting, possibly with a birth bar
o Sitting up in the throne position
• Prior to the birth, support women in developing a mutually respectful relationship with their care provider based upon open communication and understanding
• Work with L&D nurses as allies to listen to the laboring woman’s voice, validate her needs and respond to her concerns in a respectful, supportive manner
• Encourage women to ask as many questions as needed to ensure clarity regarding medical procedures and their necessity or alternatives
Affirmation: “However much we know about birth in general, we know nothing about a particular birth. We must let it unfold with its own uniqueness.” ~Elizabeth Noble
Use of dim lighting or closed door, small spaces (like bathrooms or showers) may trigger painful memories
• Prior to the birth, ask mom what she prefers, be prepared in case this preference changes once labor begins
• If mom wants to labor in the bathroom, ask if she prefers to keep the door open or for you to stay near the doorway or inside
• To diminish the intensity of fluorescent lights in the birth space while still keeping it lit, use white Christmas lights in the bathroom to illuminate the space and batteryoperated LED candles or tea lights to help light the birthing room
• Keep all of the lights turned on and let the birth team know this is mom’s preference
• Support mom to bring different scents into the room that help her feel safe and secure
Affirmation: “Focus only on the now. One breath, one contraction at a time.” ~Unknown
Frequent body exposure and the physical demands of breastfeeding may increase women’s feelings of vulnerability and powerlessness
• Maintain the woman’s dignity and modesty by being steadfast about helping her redress when needed
• Hold up sheets for added privacy when mom is being checked or having a procedure completed
• Offer breastfeeding support, suggestion use of a lactation consultant and provide warm referrals for skilled lactation specialists and La Leche League leaders in the community
Affirmation: “Giving birth is a transformation and it doesn’t matter whether you’ve had eight babies before. It’s still a transformation…because you are no longer the same woman you were before you had that baby.” ~Penny Handford
Transition. This is one of the most intense times of a woman’s labor as she fully opens and becomes complete to birth her baby. This is also a time when many women feel that they cannot go on. The wellknown and widely used birth affirmation, “the only way out is through,” applies here. During this time, survivors may feel even more so out of control of their bodies than at other times during their labor.
Prior to the birth, prepare your client for this time and talk with her about how she’d like to be supported. Allow her the space to turn inward and find her inner strength. This is a key time that you must work not to become an intervention in the woman’s birth unless she desires additional support. She may vocalize that she can’t do it—remind her of how much she’s accomplished during her labor. Validate that it may be hard but she’ll still do it!
If wanted, hold her or stroke her hair and provide the emotional comfort needed to help her through this time. Be prepared that some survivors may appear in a trance as if they’re outside of their bodies or they may express very intense and raw emotions during this time that their support team may not be able to respond to. As the doula, you are there to be a vessel for her feelings and to guide her through this period to ensure a positive, satisfying birth experience. Help her give in to the birth process—use affirmations and grounding to help her know that she will get through it.
Postpartum Recovery. Now that baby is here, support mom’s connection with her newborn. Some survivors may take to their babies immediately, while others may need more time to process what just happened before
bonding with their baby. Prior to the birth, discuss with mom whether she’s afraid or concerned about potential attachment issues with her baby. Depending upon the past trauma, some survivors may be fearful of repeating the cycle of abuse or of being unable to protect their baby from harm, which could impact their initial bonding. If possible, help mom access the needed counseling and support to mitigate these issues before her baby is born. In any case, model healthy, nurturing, bonding behaviors with the baby until mom is ready.
Breastfeeding & Bottle Feeding. Women choose how to nourish their babies for a variety of different reasons. Your role as the doula is to support your client in her decision and ensure she has the tools and resources needed to be successful. For survivors that desire to breastfeed, additional support and education may be needed to address any feelings of trauma related to their abuse. Nursing is a new experience for both mom and baby. Normalize the need to practice and develop a nursing routine that feels empowering and successful.
Encourage mothers to be patient as they learn this new skill. When needed, help survivors give themselves permission to stop if the trauma echoes are too overwhelming. They may be able to take a short break and begin again or they may decide that they cannot continue for good. Be aware that the survivor’s partner may exhibit extreme jealousy towards her or the baby while breastfeeding and may demand that she stops or increase the abuse to make it difficult for her to continue. Part of the abuser’s aim will be to create distance between mom and baby — continue to be supportive, encouraging and affirming of her efforts. Remember that self-doubt, uncertainty, guilt or fear of
repeating the abuse can increase her anxiety during this time. Alternative feeding options, such as pumping and bottle-feeding or using donated breast milk through community milk sharing and bottle-feeding may be helpful suggestions. Significant issues related to breastfeeding and trauma echoes will be beyond a doula’s scope. Be sure to have reliable warm referrals available for lactation specialists, licensed lactation consultants, experienced La Leche League leaders and others in the community that can assist these women.
Part of the joy of postpartum visits is helping women realize their own strength and power in labor and childbirth. If women express concern over not recalling certain aspects of the birth or if they recall certain events out of order, explain that this is a very common occurrence for many birthing women. Use the time to process the experience with her and focus on her strengths and accomplishments during her labor. Talk with her about any lingering concerns about the impact of her trauma history on her new journey into motherhood. As needed, refer out if there are signs or significant concerns related to postpartum depression, postpartum psychosis or post-traumatic stress disorder.
The ultimate goal when supporting survivors of domestic violence and sexual assault in childbirth is to restore their control over their bodies, their birth and their babies.
Birth affirmations can be an effective tool to help women stay focused on their labor, mentally grounded and emotionally connected to a power source within and beyond them. Many women find comfort being in community with the hundreds of women that have given birth before them and knowing that hundreds of women are birthing at the same time as they are—the universe is full of amazing women birthing their babies!
A few positive birth affirmations are illustrated on the following pages and can be used along with deep, calm breathing techniques to help survivors manage the sensations of labor and childbirth and get into a rhythm for their own experience. Eye contact and partner breathing increases the effectiveness of these affirmations.
• One breath, one contraction at a time
• Inhale peace, exhale joy
• I am a Goddess giving birth, the most beautiful, powerful creation of life.
• Blow it away, let the contraction float away
• Letting go of other people’s birth stories
• My body, my birth, my baby
• I have the power to choose how my birth goes
• Breathe for baby, come down baby
• I am strong, I am capable
• Progress is happening even when you can’t see it


Listed below are suggestions to help survivors find healing, support and advocacy for themselves. This list is not meant to be exhaustive but rather a starting point for doulas to assist their clients in accessing the help they need.
• Survivor Support Group or Individual Counseling: Offered free of charge at local, community-based domestic violence programs and rape crisis centers
• Therapeutic counseling sessions via the client’s insurance
NOTE: Couples counseling is contraindicated
Why is couples counseling not recommended in relationships where there’s violence?
Couples counseling is contraindicated for couples where one partner uses violence and abuse against the other. Couples therapy assumes an equal balance of power in the relationship, which is not the case with intimate partner violence, and it’s often used as another tool for the abusive partner to manipulate the relationship.
The foundation to make couples counseling effective isn’t met when there’s an imbalance of power in which one partner is threatening, emotionally manipulative, coercive and abusive towards the other.
For example, describing an incident as a communication issue where they both share responsibility is concerning if in fact, one partner used violence against the other and has a history of doing so. Partners who abuse make the CHOICE to abuse in their relationships and they alone bear the responsibility for those actions, not their partner.
Further, it should be noted that not all therapists are educated in the dynamics of domestic violence or have experience serving couples with these concerns, which can further isolate and blame the victim as a mutual participant in the violence and abuse. It is best for each individual to engage in therapeutic support prior to coming together to participate in couples counseling if desired.
That being said, it is not the role of the doula to sort these matters out for the family. It is vital that in our role as doula, we do not make assumptions about what may or may not happen in the future of our clients’ relationship. Utilizing the strategies discussed earlier, the doula should take precautions to stay safe, be supportive with the client, provide resources and warm referrals and encourage the survivor to talk with a domestic violence victim advocate to gain another perspective and discuss her concerns. As she’s ready, she’ll reach out to you again if needed.
Healing Through Art
• Coloring, mandalas
• Journaling
• Poetry, song
• Birth affirmations
• Positive birth stories
• Placenta print keepsakes
Healing Through Bodywork
• Reiki
• Polarity Therapy
• Meditation
• Massage
• Yoni steaming
• Placenta encapsulation
Benefits:
• Set time for women to slow down, focus on their breath, their baby and their bodies
• Increases bonding and connection between mother and baby

• Heightens women’s body awareness, understanding of how their body moves and how to shift in response to discomfort during labor
• Women can practice positions for birthing and staying active during labor
• Helps women learn to turn inward, build strength and confidence for birth
• Helps women practice tuning out the sounds and distractions around them
• Increases circulation, improves footholds, balance and allows for continuous exercise and movement during pregnancy
• Builds community with other expectant and soon-to-be birthing women
• Helps calm fears and anxieties
• It’s fun! And can be an emotional release when needed
• A ceremonial, oftentimes spiritual, gathering of women to support, encourage, and promote healing of the expectant mom through pregnancy, birth and motherhood
• Many are held as a cultural celebration and in lieu of a baby shower
Often includes:
• Symbolic offering for the mother
• Smudging, release of negative spirits
• Positive re-focusing of energy
• Loving affirmations and prayers for the birth and motherhood
• Creative activities, henna, music, food
National Domestic Violence Hotline
1-800-799-7233 (SAFE)
Live chat: www.thehotline.org/what-is-live-chat/
National Sexual Assault Hotline
1-800-656-4673 (HOPE)
Live chat: https://ohl.rainn.org/online/
Loveisrespect: Teen Dating Violence Hotline
1-866-331-9474 or text ‘loveis’ to 22522
Live chat at www.loveisrespect.org
Safe Helpline: Sexual Assault Support for the DoD Community
1-877-995-5247
Online Helpline: safehelpline.org/about-dod-safehelpline
Why Does He Do That? Inside the Minds of Angry and Controlling Men by Lundy Bancroft
The Courage to Heal Workbook: A Guide for Women and Men Survivors of Child Sexual Abuse by Laura Davis
Surviving the Silence: Black Women’s Stories of Rape by Charlotte Pierce Baker
Healing The Pain of a Traumatic Birth Experience by Nicola Hogg (eBook) - www.amazon.com/ Healing-Pain-Traumatic-Birth-Experience-ebook/dp/ B00EILWISO
Sacred Cesarean Birth Guide: A Planned Entrance into the World by Kelly Meehan (eBook) - www. birthhealing.com/sacred-cesarean-birth.html
Survivor Moms: Women’s Stories of Birthing, Mothering and Healing after Sexual Abuse by Mickey Sperlich and Julia Seng - www.survivormoms.com/ books/survivormoms.asp
Cut, Stapled, and Mended: When One Woman Reclaimed Her Body and Gave Birth on Her Own Terms After Cesarean by Roanna Rosewoodhttp://www.amazon.com/Roanna-Rosewood/e/ B00B084LWO
Project Unbreakable, a photography project aiming to give a voice to survivors of sexual assault, domestic violence, and child abuse - http://project-unbreakable. org
ImprovingBirth.org, a photo campaign striving to break the silence on abuse and trauma in maternity care, #breakthesilence - http://improvingbirth.org/traumatoolkit/
Birth Without Fear
http://birthwithoutfearblog.com
Blooma Blog
http://blooma.com/blog
Belly Button Bliss: A Small Collection of Happy Birth Stories - http://mamahhh.com/belly-button-bliss/
Labor Day: True Birth Stories by Today’s Best Women Writers - http://www.labordaybook.com
Birth Location Chart
Factors to Consider When Selecting a Birth Locationhttps://kenyafairley.com/book
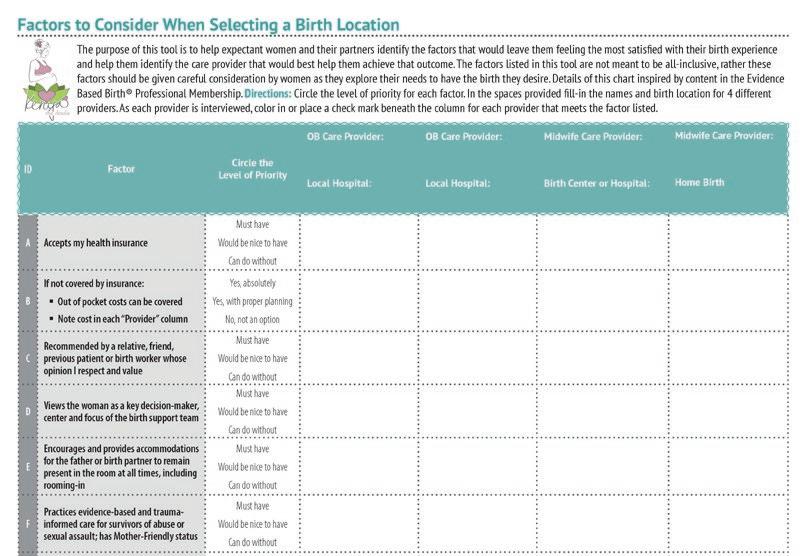
Taking care of self is critical to sustaining a high-quality doula practice. Being a vessel of support for laboring women requires significant physical, mental, and emotional stamina and endurance. Ideas for beginning or expanding doula self-care are provided below.
• Safety plan with loved ones to ensure your own safety
• Trust your instincts and err on the side of caution if you feel uneasy about a particular client, her partner or a situation that occurs when providing services
• Manage the energy you bring into the birth space
• Know your limits—emotionally, physically and mentally
• Pursue ongoing education, training and professional development
• Maintain knowledge of community resources to make warm referrals, including local domestic violence programs, rape crisis centers, breastfeeding/ lactation consultants, and StillBirthday, Hearthside Bereavement Care or similar supports
• Engage your back-up—not only for relief from exhaustion but also for assistance if you begin to experience trauma echoes from your own history or what you witnessed during the birth
• Practice a cleansing or smudging ritual at the end of each birth to clear your mind, your hands and your heart
• Continuously process and debrief with doula mentors and other birth professionals; be sure to maintain client confidentiality and focus on improving your doula skills
• Keep a journal—use after each birth or periodically when the need arises
• Develop a self-care plan and adhere to it to ensure you have proper rest and rejuvenation
Domestic Violence and Sexual Assault Resources
VAWnet.org, A Project of the National Resource Center on Domestic Violence www.vawnet.org
National Network to End Domestic Violence www.nnedv.org
WomensLaw.org, A Project of the National Network to End Domestic Violence www.womenslaw.org
National Sexual Violence Resource Center www.nsvrc.org
National Alliance to End Sexual Violence www.endsexualviolence.org
NO MORE www.nomore.org
Birth Related Resources
Childbirth Connection www.childbirthconnection.org
Evidence Based Birth® www.evidencebasedbirth.com
Improving Birth www.improvingbirth.org
Mama Glow www.mamaglow.com
Le Leche League www.lalecheleague.org
Hearthside Perinatal Bereavement Care www.hearthsidecare.com
When Survivors Give Birth by Penny Simkin (6mins 15secs) - http://youtu.be/YhEVY2k9DWw
toRaise Questions Doula Podcast, hosted by toLabor - Episode 11 - Abuse Survivors, released April 09, 2014 - http://tolabor.memberlodge.org/page-1577947
Books
Survivor Moms: Women’s Stories of Birthing, Mothering and Healing after Sexual Abuse by Mickey Sperlich and Julia Seng - www.survivormoms.com/ books/survivormoms.asp
When Survivors Give Birth: Understanding and Healing the Effects of Early Sexual Abuse in Childbearing Women by Penny Simkin and Phyllis Klaus - www.pennysimkin.com/shop/when-survivorsgive-birth
Handouts:
• Strategies for Specific “Triggers” of Anxiety in Childbirth
• Clinical Challenges in Childbirth Related to Childhood Sexual Abuse
National Intimate Partner and Sexual Violence Survey (NISVS) Report - www.cdc.gov/violenceprevention/ nisvs/
The Facts on Reproductive Health and Partner Abuse - www.futureswithoutviolence.org/userfiles/file/ Children_and_Families/Reproductive.pdf
Coercing Pregnancy by A. Rachel Camp for William & Mary Journal of Women and the Law (2015) - http:// scholarship.law.wm.edu/wmjowl/vol21/iss2/3/
Violence During Pregnancy and the Postpartum Period by Sandra L. Martin, Jennet Arcara, and McLean D. Pollock with contributions from Lonna Davis (December 2012) - http://vawnet.org/Assoc_ Files_VAWnet/AR_DVPregnancyPostpartum.pdf
Groupwork with Men Who Batter: What Research Literature Indicates (February 2012) - http:// www.vawnet.org/Assoc_Files_VAWnet/AR_ GroupworkMenWhoBatter.pdf
Assistance Guidance
How can I support pregnant survivors of abuse? http://www.vawnet.org/news/2014/07/pregnantsurvivors/
Birth Doulas and Shelter Advocates: Creating Partnerships and Building Capacity - http://www. vawnet.org/Assoc_Files_VAWnet/FINAL-April2014DV-DOULAS.pdf
Even the Elephants Know. Elephants in the wild have midwives who surround them in a circle during their labor, protecting the pregnant mother and swaying along with the laboring elephant. (…) In labor, the elephant midwives may stroke the mother and make sounds along with the laboring elephant. Within the circle of birth, the midwives protect the laboring elephant and assist the newborn to be released from the amniotic sac, stand up, and take its first steps.22
1 Agency is defined as awareness of one’s capacity to initiate and exert control over their own thoughts, beliefs, actions, and decisionmaking power within their lives.
2 Trauma echo is defined as a trigger or reminder of experiencing a traumatic event such as sights, sounds, smells, places, people, physical items, or similar circumstances that are reminiscent of the actual event.
3 Available at: www.cdc.gov/violenceprevention/ nisvs/
4 Gazamarian, J.A., Peterson, R., Spitz, A.M., Goodwin, M.M., Saltzman, L.E., Marks, J.S. (2000). Violence and reproductive health: current knowledge and future research directions. Maternal and Child Health Journal, 4(2), 80.
5 Neggers, Y., Goldenberg, R., Cliver, S., Hauth, J. (2004). Effects of domestic violence on preterm birth and low birth weight. Acta Obstetricia et Gynecologica Scandinavica, 83(5), 455-460.
6 Available at: http://pattch.org/resource-guide/ traumatic-births-and-ptsd-definition-andstatistics/
7 Available at: http://www.samhsa.gov/nctic/ trauma-interventions
8 Rape culture is defined by Marshall University Women’s Center as an environment in which rape is prevalent and in which sexual violence against women is normalized and excused in the media and popular culture…. through the use of misogynistic language, the objectification of women’s bodies, and the glamorization of sexual violence, thereby creating a society that disregards women’s rights and safety. Learn more at https://www.marshall.edu/wcenter/ sexual-assault/rape-culture/.
9 Englander, N. (2015, October 14). “Man on the Moon.” Podcast. The Moth Radio Hour. Retrieved from http://themoth.org/posts/stories/ man-on-the-moon
10 Learn more at: http://www.sidran.org/resources/ for-survivors-and-loved-ones/what-ispsychological-trauma/
11 Available at: http://www.birthtraumaassociation. org.uk/what_is_trauma.htm
12 Dissociation is defined as a mental coping strategy of protection by losing connection with one’s thoughts, feelings, and physical experiences of the body; akin to getting lost daydreaming or driving and then realizing you don’t remember the last several minutes or miles or feeling like you’re staring down from afar at one’s own body and what’s happening to it.
13 An Order of Protection may be referred to, depending upon the region and jurisdiction as domestic violence protection orders (DVPO),
protection from abuse orders (PFA), restraining orders or no contact orders.
14 Learn more at: http://womenslaw.org
15 Learn more at: http://www.theduluthmodel.org/ training/wheels.html
16 Available at: http://www.theduluthmodel.org/pdf/ PowerandControl.pdf
17 Available at: http://domesticpeace.ca/images/ uploads/documents/ChildbearingYear_000.pdf
18 Available at: http://www.theduluthmodel.org/pdf/ Equality.pdf
19 Available at: http://www.theduluthmodel.org/cms/ files/Nurturing%20Children.pdf
20 Learn more at: http://exaltbirthservices.com/ empowering-choices/birth-positions/
21 More information at: http://sharonmuza.com/ resources/miles-circuit-positioning-baby/
22 Ananda, K.M. (2014, December 22). Elephants Need Female Elephant Midwives to Give Birth Calmly and Safely. Kara Maria Ananda: Empowering Transformational Leaders to Thrive. Retrieved from http://karamariaananda.com/ blog/elephant-midwives

Kenya M. Fairley is a birth doula with experience, knowledge and education related to childbirth and supporting pregnant survivors of abuse. Building on over 16 years of experience as a strong, compassionate advocate for survivors of domestic violence and sexual assault, Kenya brings an empowering, feminist perspective to her doula practice. In January 2014, Kenya received her birth doula certification from DONA International, Advanced Doula training from Carriage House Birth in 2015 and is currently studying to become a postpartum doula through DTI—Doula Training International. Kenya is a Blooma certified prenatal yoga teacher as well as a bereavement doula and placenta encapsulation specialist.
Utilizing her expertise as a doula, domestic violence victim advocate, shelter director, trainer and national technical assistance (TA) provider, Kenya has co-authored guidance for advocates on building partnerships between doulas and domestic violence shelters; published a TA Question of the Month blog post on supporting pregnant survivors of abuse; conducted training on improving support to pregnant women with a history of trauma; and continues to provide ongoing assistance to doulas and advocates seeking help in this area.
Her ongoing development includes membership to professional organizations such as DONA International and Evidence Based Birth® Professional Membership. Learn more about Kenya and her work at kenyathedoula.com.