Other documents randomly have different content
(See Chapter XXVI for further reference to the pathology of hydatid cysts.)
—The treatment is purely operative. The contents of the cysts should be evacuated and its walls radically destroyed by caustic, spoon, etc. All sequestra should be removed; in the limbs amputation is sometimes necessitated by the extent of the affection.
—The general character of this parasitic disease has already been considered. (See Chapter VIII.)
The peculiar fungus may be found in the periosteum, in the compact outer layers of the bone, or within its more spongy depths. When the lesion is sufficiently large to be recognizable to the naked eye it assumes, for all practical purposes,
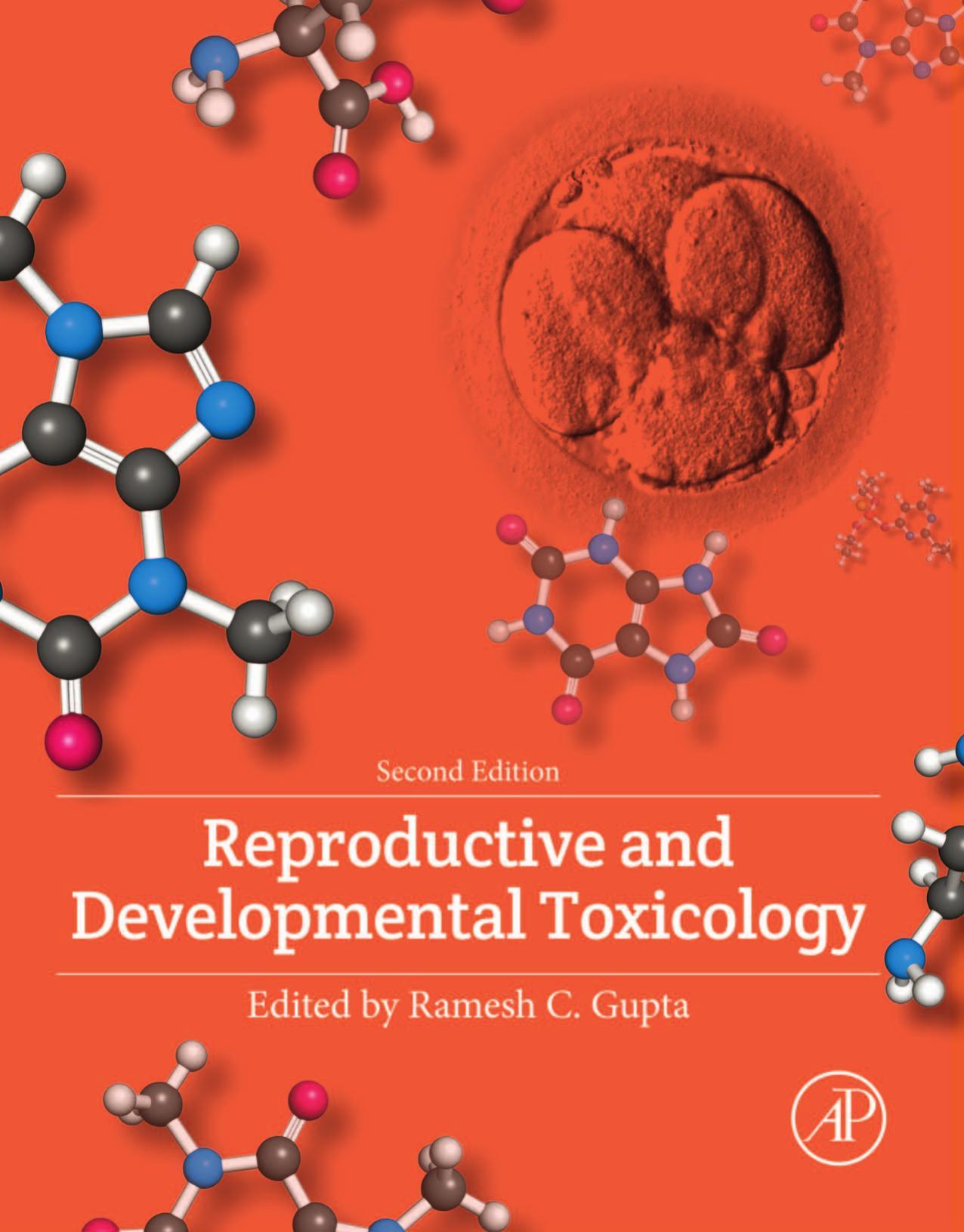
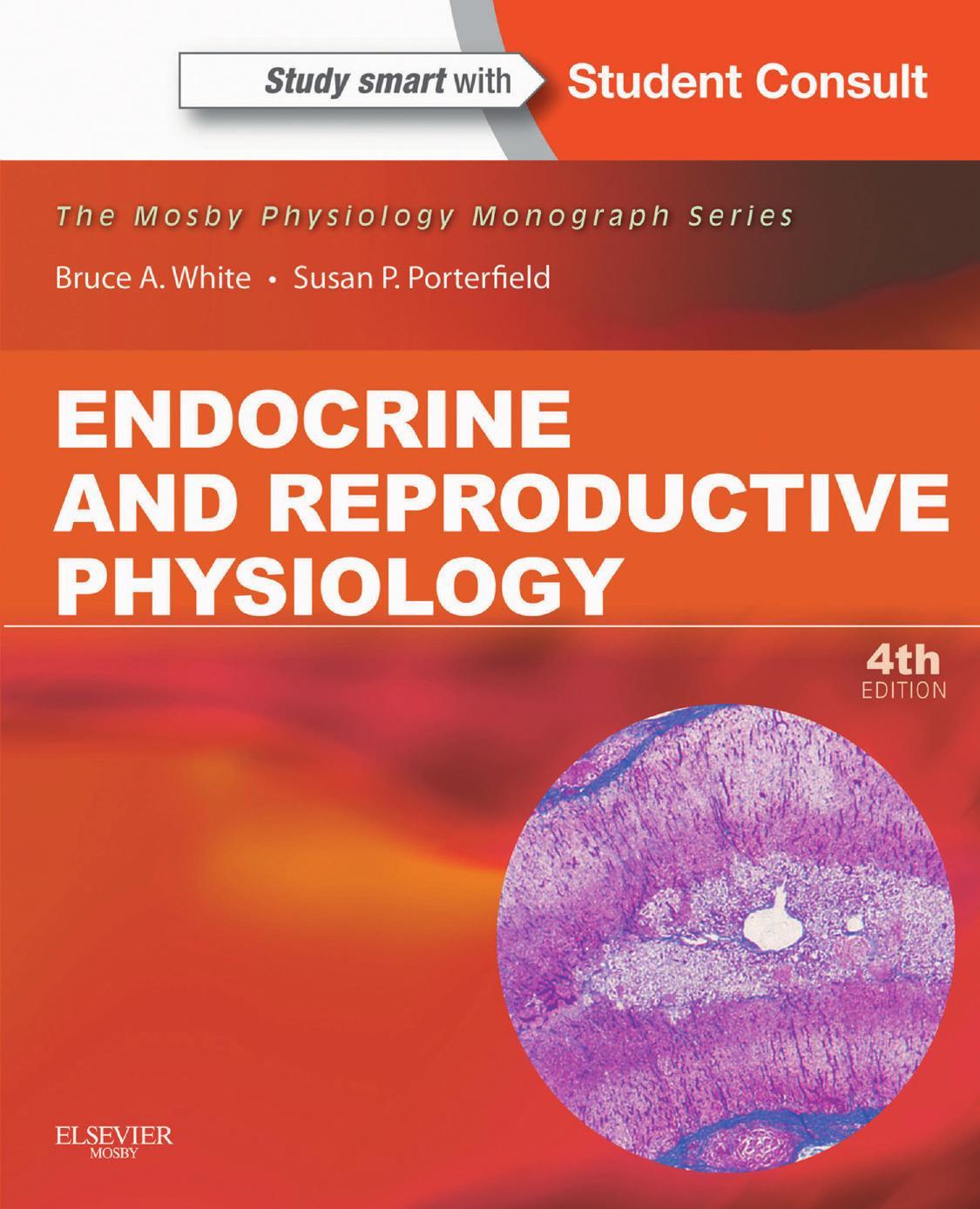
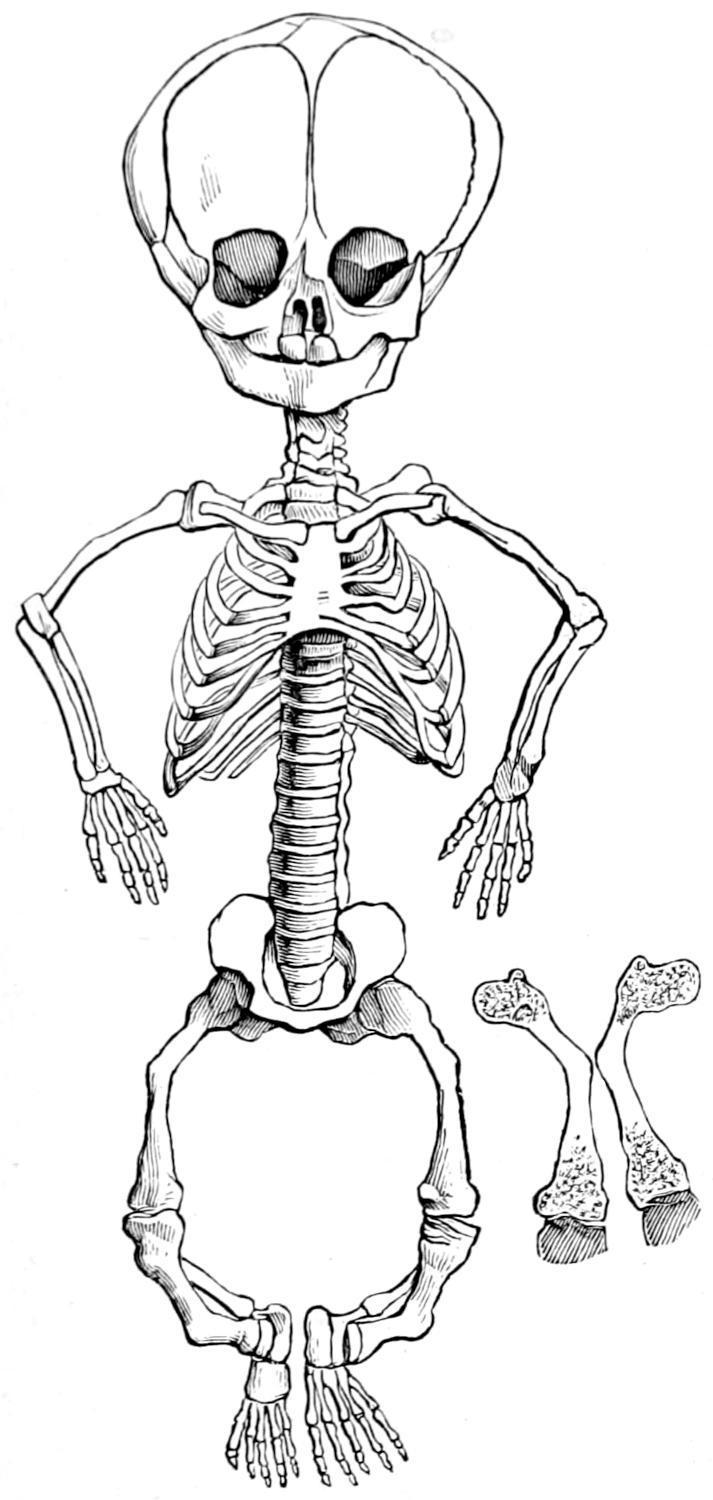
Achondroplasic skeleton. (Porak.)
Hydatid Disease of Bone. Treatment. Actinomycosis.
the appearance of caries, like that due to tuberculous or leprous diseases, while in the pus or debris discharged from the same or contained within the invaded bones the characteristic yellow, cheesy, or calcareous particles will always be recognized. In this disease there never seems to be the slightest tendency to encapsulation nor to protect against further spreading by any process of repair. The diseased area constantly enlarges its dimensions, involving everything as it spreads, it being limited by no membrane or tissue of the body. Occurring in the bones, it is usually a secondary or metastatic infection, and may be found in any part of the body.
The symptoms will be those of osteoperiostitis, first occurring frequently in the jaws, as it nearly always does in cattle, and often in man; this is accompanied by loosening of the teeth and involvement of the submaxillary tissues. The course of the disease is slow, with little or no tendency toward spontaneous recovery.
TROPHONEUROTIC DISEASES OF THE BONES.
Under this heading it is proposed to group a number of diseases whose clinical manifestations are distinct or classic, but whose underlying causes are more or less obscure. —This is a lesion of intra-uterine life which includes a softening of primary cartilaginous structures and curvature or malformation of the bones which should be formed from them. It belongs to that period of fetal life between the third and sixth months. It is sometimes referred to as intra-uterine rickets. Under this name it was first described by Müller, in 1860, and since then under various names, most commonly as fetal rickets. It appears that in this disease the fetal cartilage contains mucus abnormally collected, quite generally, in minute cavities or cells just at its borders. The chondroblasts and osteoblasts are not regularly dispersed, and the development of the growing bone is thereby much interfered with. The periosteum appears to have nothing to do with this condition. In consequence the cartilage does not do its
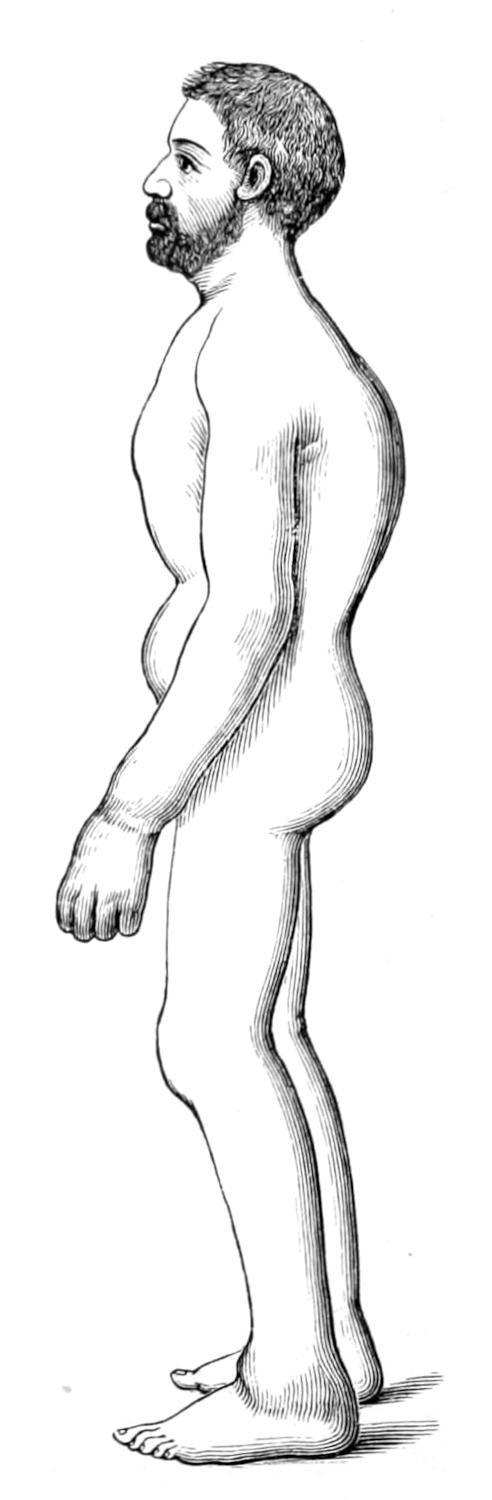
Achondroplasia.
proper duty The long bones fail to attain their proper proportionate length, but become thicker than normal, the periosteum being unaltered. On the other hand, those bones into whose formation cartilage enters but slightly, such as the clavicle and the ribs, retain their normal proportions—the consequence is a peculiar malformation and disproportion of the whole skeleton (Fig. 236).
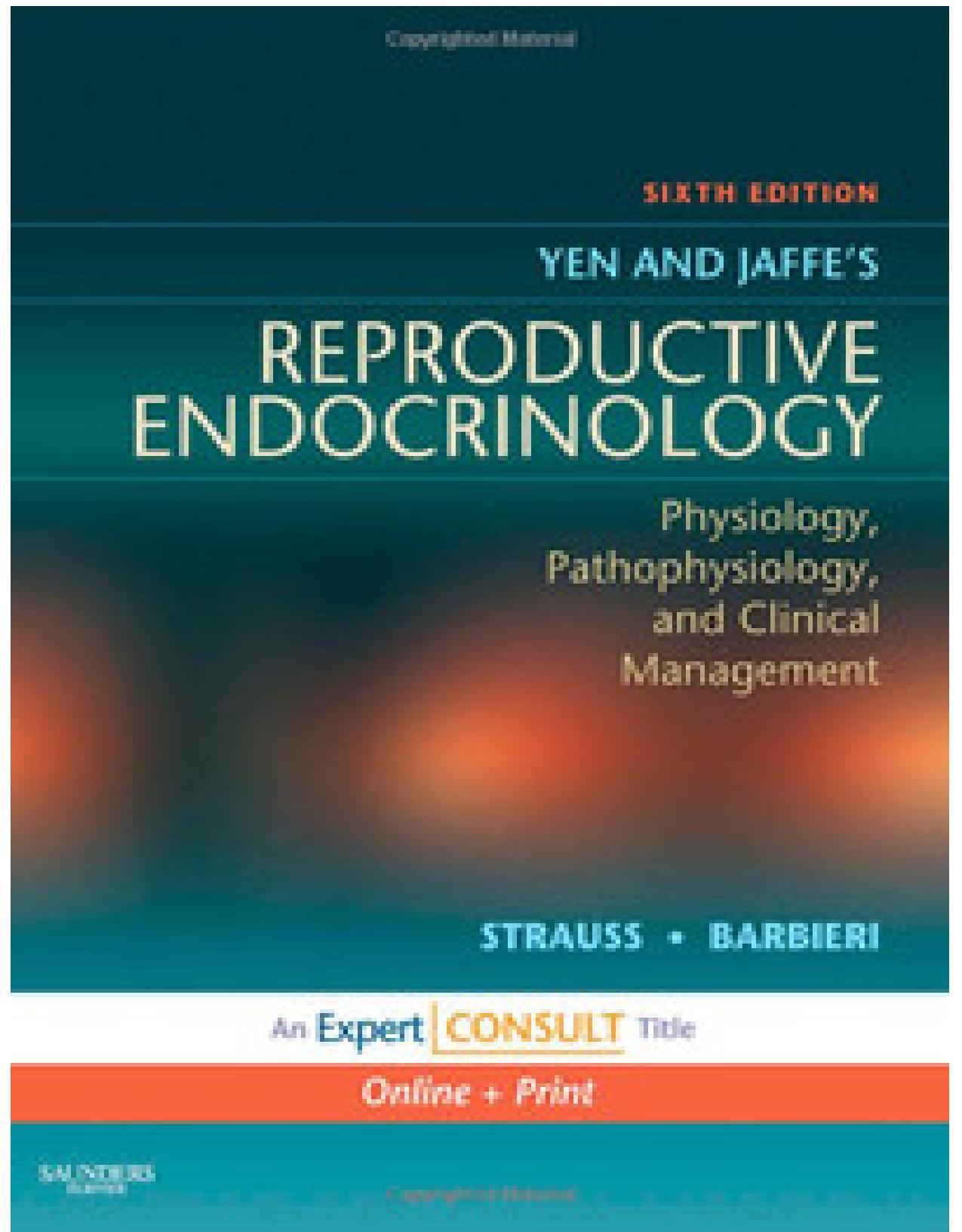
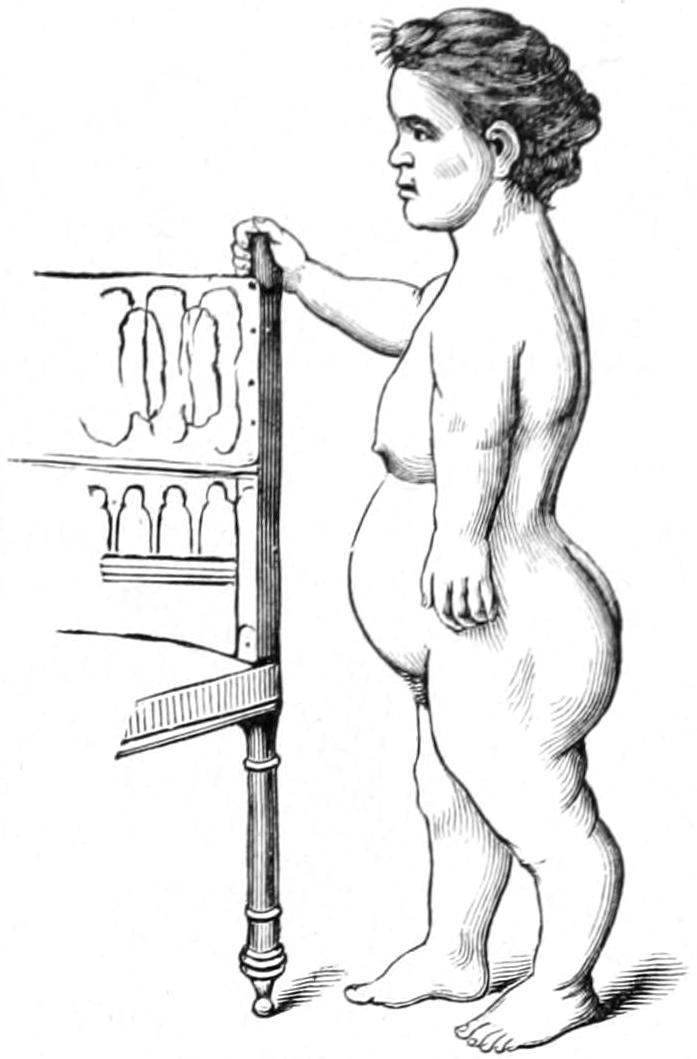
These deformities are symmetrical, and pertain mostly to the bones at the base of the skull and to the long bones of the limbs; therefore the distinctive appearance may be recognized even at the birth of the child. The head is disproportionately large, the spinal column short, the lumbar curvature exaggerated, all of which is rather the reverse of the ordinary rachitic manifestations. The disease is not common (Fig. 237).
Prognosis.
—The prognosis is unfavorable, because it seems impossible to undo the faults of the intra-uterine condition. The disease, however, is not incompatible with a long life.
Rachitis.
—This also is a constitutional condition, and has been described in Chapter XIII. So far as the manifestations in the bones are concerned it is a constitutional dystrophy caused by improper deposition of calcareous material in the softened and somewhat perverted fetal cartilages. It is a condition, however, pertaining rather to postnatal life, and while inconspicuous at birth becomes more and more marked as the child develops. It is essentially a disease of malnutrition, and consequently may be seen in all
Achondroplasia (Lugeol )
walks of life, as well in the bottle-fed babies of the wealthy as in the best-nourished children of the poor. The subject should be studied also in connection with the facts set forth in the chapter on the Status Lymphaticus, which bear on the relation of the ductless glands to tissue growth, and especially to rickets. The lesions are widely distributed. The disease is divided by some writers into three periods: (a) Rarefaction of bone tissue; (b) softening of same; (c) reossification.
The first stage is the intra-uterine part; the second and third stages are postnatal. To fetal rarefaction have been attributed intra-uterine fractures, even by Hippocrates.
The general dyscrasia and visceral alterations of rachitis interest us here less than deformities of the various bones. The head is disproportionately large, the vertex flattened, the frontal and parietal eminences pronounced; the anterior fontanelle closes very late. To the atrophic alterations of the head have been given the name craniotabes. The face is disproportionately small, the lower jaw assuming a polygonal shape. The palatal vault is of the Gothic type, dentition irregular and retarded. In the thorax the clavicular curves are exaggerated, by which the bones are shortened and the shoulders made narrow. The costochondral junctions are enlarged, the result being the so-called rachitic rosary. The sternum projects and gives the peculiar appearance known as pigeon-breast. The pelvis is often deformed, and frequently distorted to such an extent as in after years to make normal delivery impossible. The spinal column may either be distorted early or is likely to undergo alterations of curvature, due to the combined results of pressure and traction upon softened vertebræ. The joint ends of the long bones are enlarged or clubbed, this being true even of the phalanges. Joint movements are often accompanied by crepitation. The axes of the long bones are distorted, and more or less marked deviations and curvatures result, giving rise to such deformities as knock-knee, bow-leg, etc. (See pp. 161 and 162.)
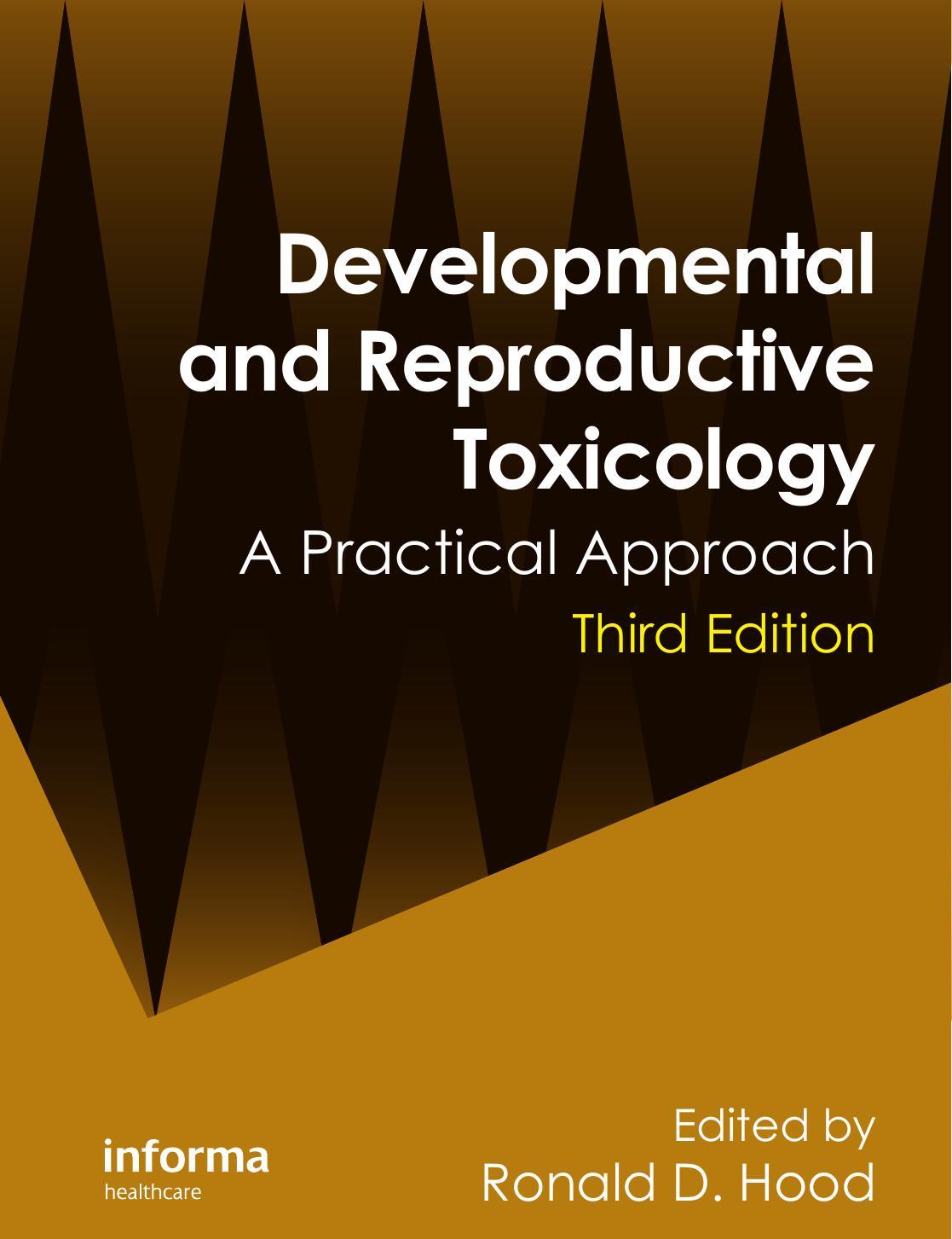
Osteomalacia.
—As rickets is essentially a disease of early childhood, osteomalacia is practically confined to adults. The name implies a peculiar softening of the bones, by which their resistance and rigidity are weakened and deformity permitted.
The disease is common to man and to animals in confinement, and is frequently noted among wild animals dying in zoölogical gardens. It commonly occurs in pregnant women, where it would appear as if the mineral elements needed for the growing fetus were abstracted from the mother’s bones rather than from the food ingested. It is brought about also by starvation, possibly by lactation, especially among those who nurse their children for unusual periods.
F��. 238
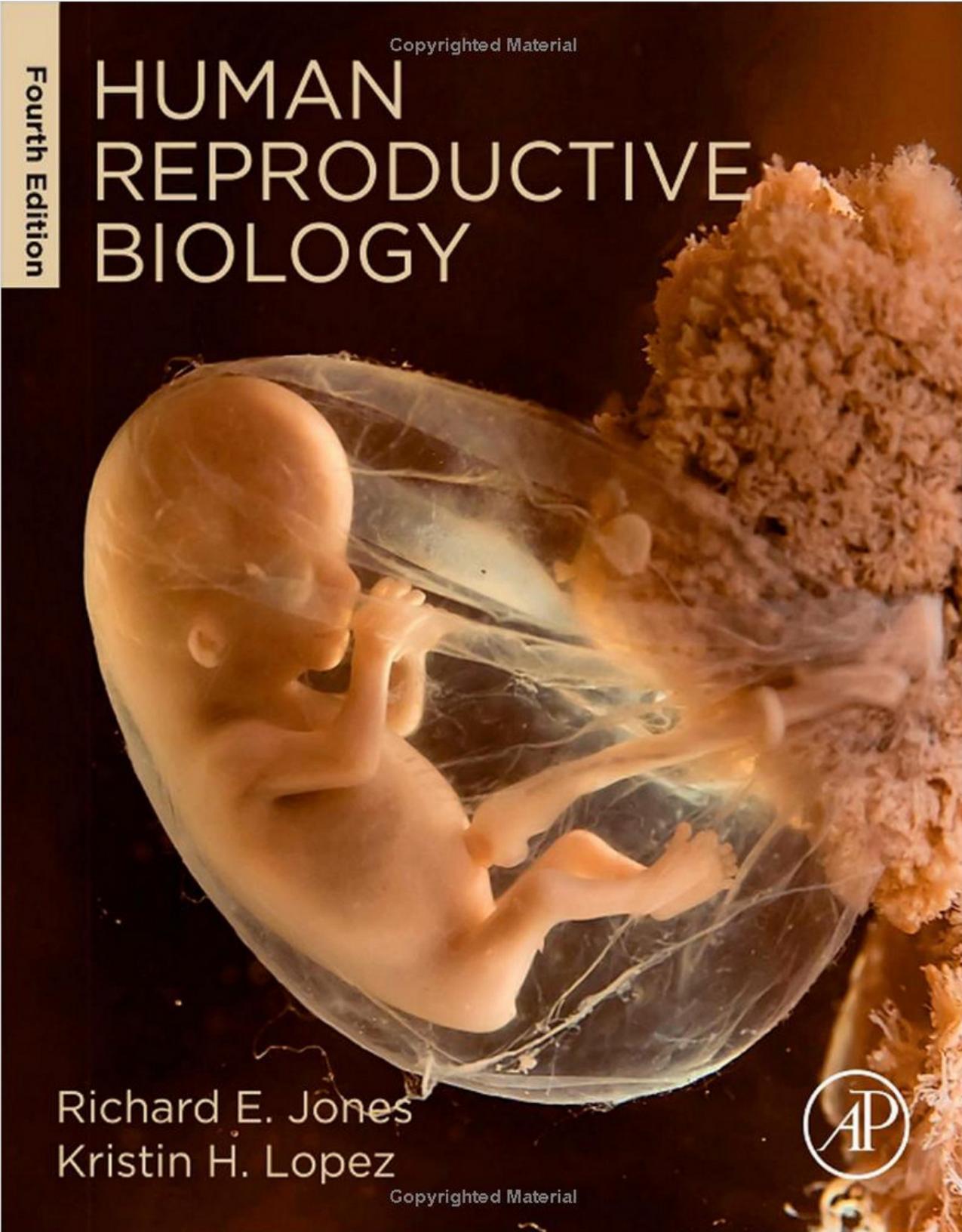
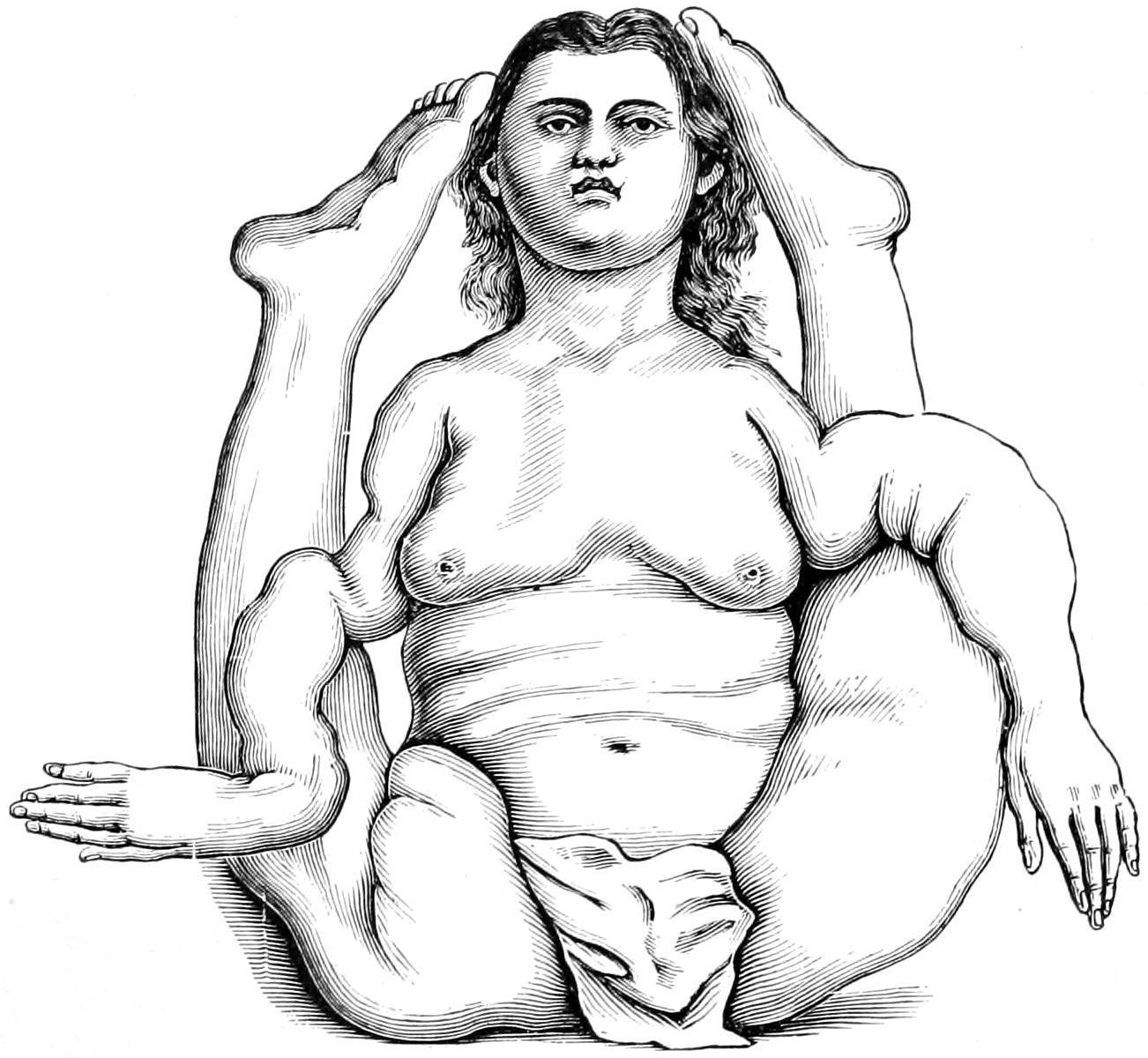
Osteomalacia: celebrated case of Moraud, 1753 (Skeleton now in Musée Dupuytren )
Spontaneous fractures, especially of the long bones, are frequent. These may refuse to unite properly and false joints may result. The urine will under these circumstances contain an excess of mineral salts, carbonates, phosphates, and oxalates, and when these are discovered in the urine of those suffering from fractures it should always be a warning to administer calcium salts and mineral acids, preferably phosphoric, internally, and to carefully watch the excretions. The progress of the disease is slow, yet steady, and often not easily checked, if at all affected, by mineral acids. Occurring in pregnant women, it may be checked after delivery, especially if the child be not allowed to nurse from the mother. In some instances it occurs with each successive confinement in the same patient, and makes distinct advance with each fresh attack.
Prognosis.
—The prognosis is therefore unfavorable, least so in puerperal cases.
An infantile form, as well as a fetal form, have been noted, but it is doubtful whether these forms really come under the same category, and whether they are not manifestations of rickets. A senile form has also been described which affects most frequently the sternum and thorax, which is characterized by excess of nervous excitability and by bone pains, as well as by liability to multiple fracture upon the slightest provocation. This form, however, differs but little from the osteoporosis of advanced years, and scarcely deserves distinct consideration. Certain writers have also mentioned a symptomatic form—cancer, syphilis, scurvy, etc.—which, however, is unnecessary, since the fractures occurring in cases of cancer or syphilis are due to secondary lesions of the same character, while those occurring during scurvy are simply an expression of starvation and weakening, even of the bones. Cases of cancer, for instance, where bones have broken without being previously weakened by secondary growths, are exceedingly rare.
Under the name of osteogenesis imperfecta has been described the “fragilitas ossium” of certain writers. The condition has also been known as congenital fetal rickets. These cases may usually be recognized in infancy, in that the extremities are more or less bent and deformed, and the bones very fragile. Sometimes intra-uterine fractures occur, which may be recent or old, and united with more or
less callus and deformity The spinal column will be soft and friable, with marked divisions, and the ribs are often fractured. The clavicle shows lesions of this kind more frequently than any other single bone. Bones so affected will be found extremely fragile and delicate, and sometimes so thin that they may be crushed between the fingers. They are defective in every respect of structure. But these changes pertain mostly to the shafts of the long bones, and do not concern the cartilages. They are to be distinguished from chondrodystrophia fetalis, in which the extremities are shortened, the skin thickened, and the subcutaneous tissues extremely fatty or edematous.
The condition is to be distinguished from rickets, as there is no enlargement of rib ends or epiphyses and no disturbances of the alimentary or nervous systems. Osteomalacia usually occurs after puberty. Hereditary syphilis, in very rare instances, is a factor, but should give additional evidences in other parts of the body. At present there is no satisfactory explanation as to the cause of the condition.
—The treatment for all these conditions should be removal of the cause if discoverable and the administration of calcium salts in accessible shape, as in cases of rickets, combined with thymus or pituitary extract.
—This is a condition distinct from osteomalacia and is due to trophic nerve disturbance. The condition seems to be hereditary, often extending through several generations. It is characterized by fracture of long bones upon the slightest provocation, and is common to all ages. While apparently congenital in origin, it persists often throughout life, no impression being made upon the condition by medication. It is not characterized by distinctive histological changes, and all theories heretofore advanced toward its cause are disappointing. It is seen, at least in this country, most often in paretics and inmates of insane asylums. The ease with which the bones of such patients are broken has given rise to repeated charges of violence or homicide. From one case in which this charge was made I secured specimens of the ribs, which were so fragile that they could be crumbled between the fingers. Such patients might easily sustain serious fractures when undergoing necessary
Treatment.
restraint, even of the gentlest nature. Allegations of undue violence are frequently made in these cases, which, especially in asylums, may be most unjust and difficult to prove or disprove.
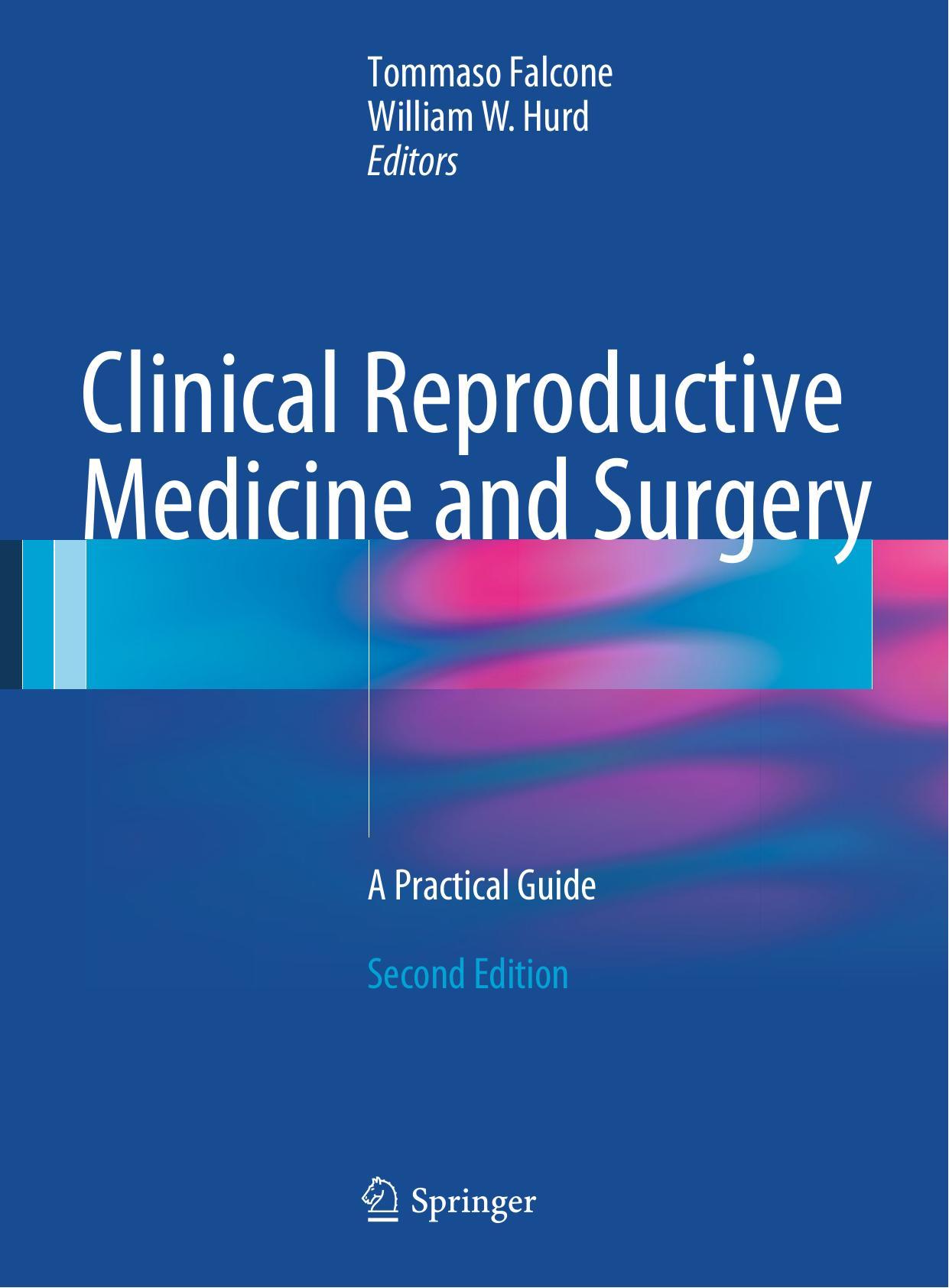
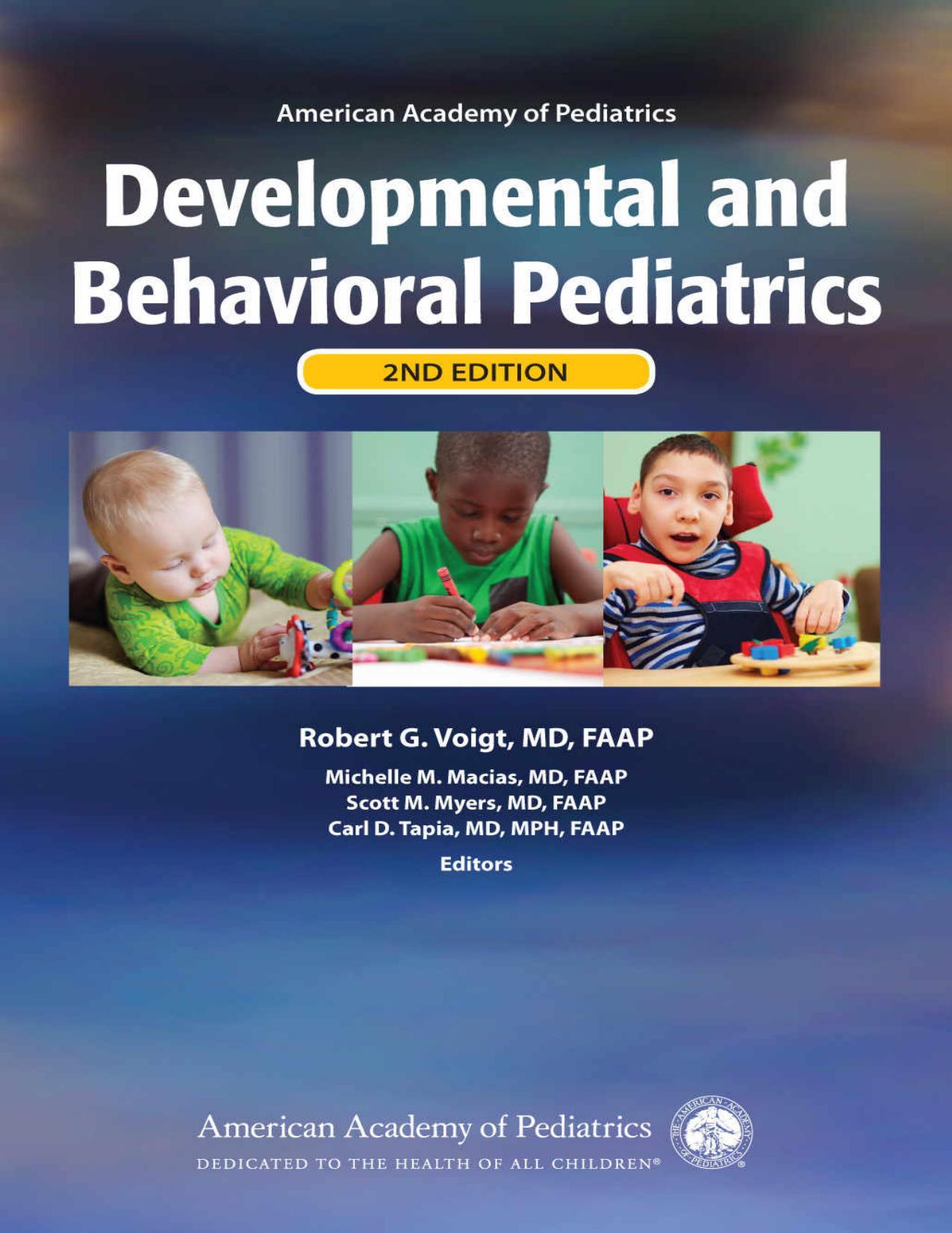
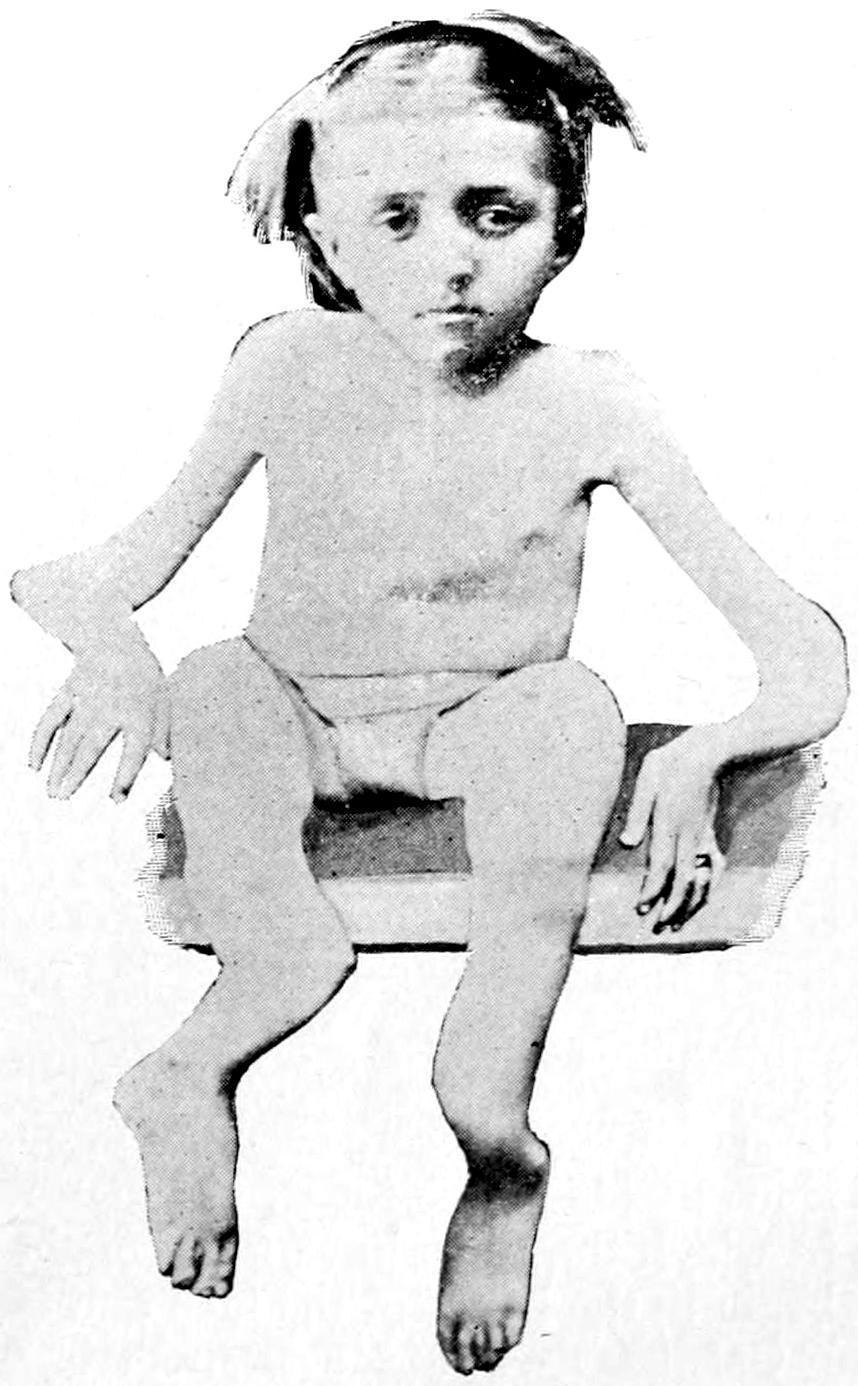
Osteopsathyrosis. (Blanchard’s case.)
Osteopsathyrosis, or Fragility of Bones.
The relationship of osteomalacia to exophthalmic goitre furnishes another illustration of the peculiar and mysterious influences which the thyroid exercises upon nutrition. The conditions have a similar geographical distribution, as well as being coincidental in the same individual. Honicke, who has recently studied the subject, believes the bone condition to be an expression of thyroidal disorder, the more so in that castration does not remedy the disease, thus proving that the genital glands are not at fault.
The peculiar relationship between the bone and the thyroid in these cases is probably one of disturbance of the elaboration of the phosphorus compounds which are necessary for the proper development of bone, these compounds being excreted rather than utilized.
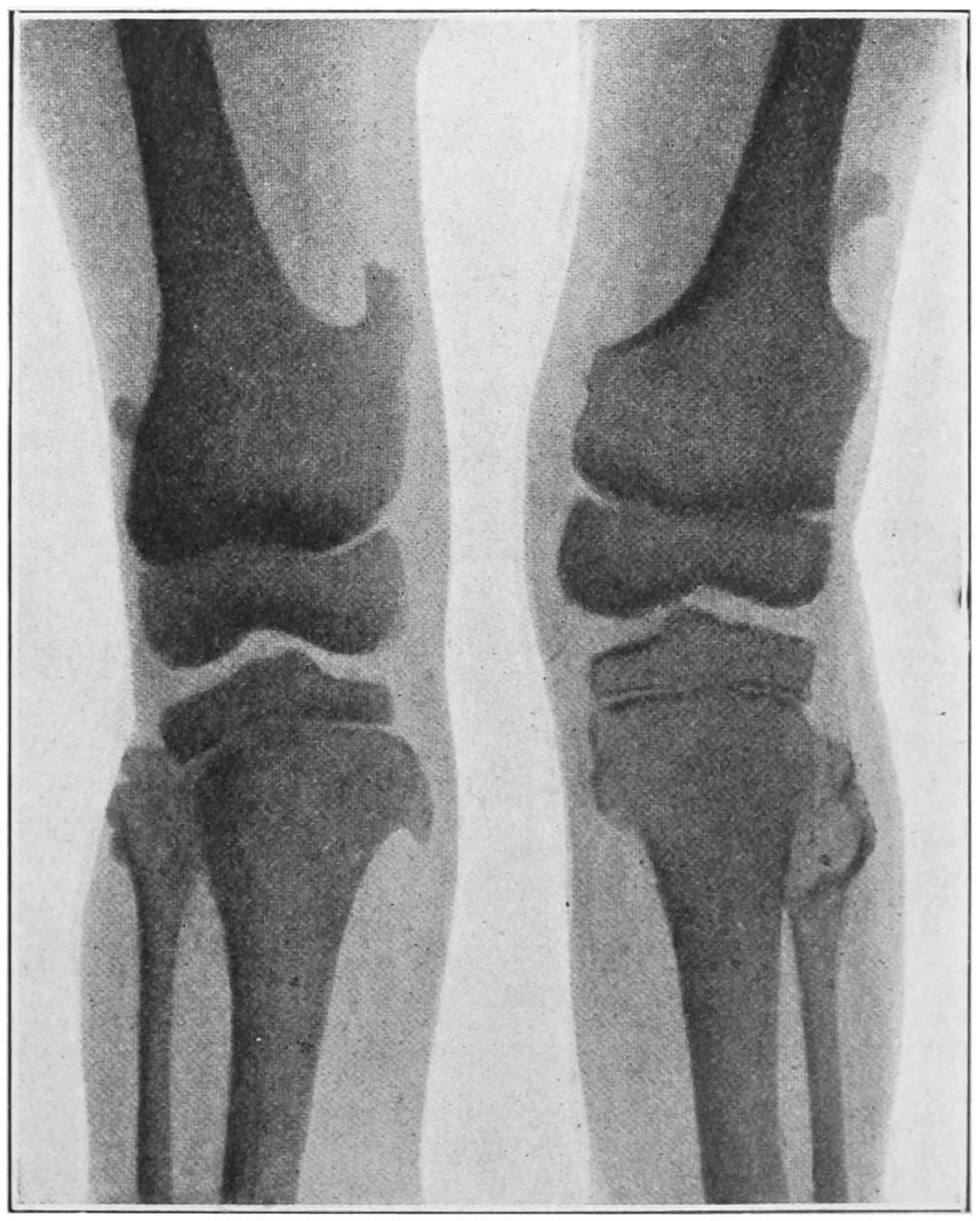
Osteopsathyrosis of this congenital type is perhaps best illustrated by a case reported by Blanchard,[35] of Chicago, in the case of a woman twenty-seven years of age at the time of his report, who up to that time had sustained over one hundred fractures. In her case it was sufficient to merely gently slide from the sofa to the floor to break some bone. Treatment in her case had been of no avail. (See Fig. 239.)
[35] Trans Amer Orthopedic Assoc
Senile Fragility of Bones.
—This means weakening of the bones which is incident to advanced age in either sex, due to and comprised under the term osteoporosis. Added to this, in certain places is a positive change in shape, also characterizing the senile condition—e. g., the neck of the femur. Under these circumstances bones will break with a minimum of violence and without invoking any theory of osteomalacia, osteopsathyrosis, or the like. As bone disappears under these circumstances fat usually takes its place, so that while the volume of the bone may not be particularly diminished, its weight and density are materially altered. (See introductory remarks to this chapter.)
Atrophic Elongation.
—This is a term first applied by Ollier, and refers to a distinct type of alteration in long bones by which their actual volume is relatively diminished, although they increase in length. It is produced largely by lack of pressure, and is seen in many amputated stumps, in which it has much to do with the conicity of the same. It is seen in certain cases of typhoid fever or in forced confinement of the young in bed, where the bones appear to grow at a much more rapid rate than normal. It may also be due to unequal amounts, or defects, of nutritive supply, especially that furnished by the periosteum, and in certain other cases seems to be a purely reflex or trophoneurotic change which is always inexplicable. Frequently accompanying it is muscular wasting, which
is to be explained rather by reflex action through the cord, produced perhaps through the mechanism of the terminal filaments of the articular nerves.
Ostitis Deformans.
—Ostitis deformans is often called Paget’s disease of the bones, and is a condition found alike in long and flat bones, the osseous tissue being condensed in texture and increased in amount, or at other times the osseous tissue becoming quite porous and the spongy tissue rarefied without alteration in the marrow. It is due to the unknown causes which may be summed up in the expression trophoneurotic, a painful and a painless form having been described, the former the more frequent. It produces deformities, disfigurements, and hypertrophies of the long bones. It is distinguished from arthritis deformans, described in the previous chapter, which is a distinct malady.
In the skull it is usually the face bones which are most involved, although the disease often commences in the cranial bones. The skull proper may be thickened even to 3 Cm. The thorax becomes globular or cubic in form, the arms are relatively too long, and there is usually dorsal kyphosis; the pelvis is thickened and distorted; the ribs are augmented in size and the femora irregularly curved; the patellæ enlarged; the tibiæ more massive and their curves exaggerated. The disease is essentially symmetrical, commonly commencing in the cranium and radius. Fractures are rare, because the bones become stronger rather than weaker.
In many instances these changes are accompanied by severe pains, which may be exaggerated by pressure. The malady is usually regarded as rheumatism, but it may be said that even were accurate diagnosis made early it would scarcely avail in treatment, since there is none for it. It may require to be distinguished from hereditary syphilis, in which the tibiæ have more of the saber shape; from acromegaly or leontiasis, which begin in the bones of the face and involve the cranium only secondarily.
Osteoarthropathie Hypertrophiante Pneumique.
—Under this title, which has no exact equivalent in English, was described, in 1890, by Marie, a peculiar affection, often wrongly spoken of in this country as Marie’s disease. This is in large part a pulmonary affection accompanied by
enlargement of the extremities. There is reason to believe that there are present microörganisms, giving rise to products that are absorbed into the general circulation, the result of whose presence is an irritative hypertrophy of certain parts, particularly the joints and ends of the fingers, the elbow-, shoulder-, and knee-joints, and often the wrist. There is also ordinarily dorsolumbar kyphosis, which in acromegaly is usually cervicodorsal. The cranium remains intact; the borders of the jaw are sometimes involved.
Acromegaly.
—Acromegaly is so named from its tendency to increase the volume of the bone extremities or apices. The first case of this disease was published by Marie in 1885. It is characterized by progressive increase in weight, by enlargement of all the extremities, bones and soft tissues alike; but the most characteristic involvement is that of the lower jaw, the upper jaw being little if at all affected. The lower jaw assumes enormous size and projects so that its teeth are far in front of those of the upper. The supra-orbital ridges enlarge, as do also the sternal ends of the clavicles and costal cartilages. As the disease progresses the ribs are widened and the scapulæ enlarged, the vertebræ and the intervertebral cartilages thickened and fused together, causing usually cervicodorsal kyphosis. The long bones of the limbs suffer later, especially at the lowermost joint ends—i. e., hands and feet. The viscera are rarely affected, but there is a peculiar and characteristic enlargement, usually of the thyroid and pituitary bodies. The lower cervical ganglion of the sympathetic is also sclerosed; the mucous membrane of the nose is usually hypertrophied; the uvula is enlarged and the larynx often participates in the changes. Acromegaly is essentially symmetrical, and for each change upon one side of the body is noticed a corresponding alteration upon the other. Particular features are observed in individual cases, but the above are practically common to all.

F��. 240
F��. 241
Osteoarthropathy. (Marie.)
Acromegaly. (Original.)
The underlying pathological condition is as yet undetermined, though most indications point to late alterations along the original craniopharyngeal tract of the young embryo, whose remains are best known in the pituitary body and the thyroid. On this account there is reason for trying the treatment by extract of the pituitary body, or even of the thyroid. The greatest complaint usually is of headache, which is difficult of relief. The disease is steady, progressive, unaffected by treatment, and the prognosis bad, though its course is slow.
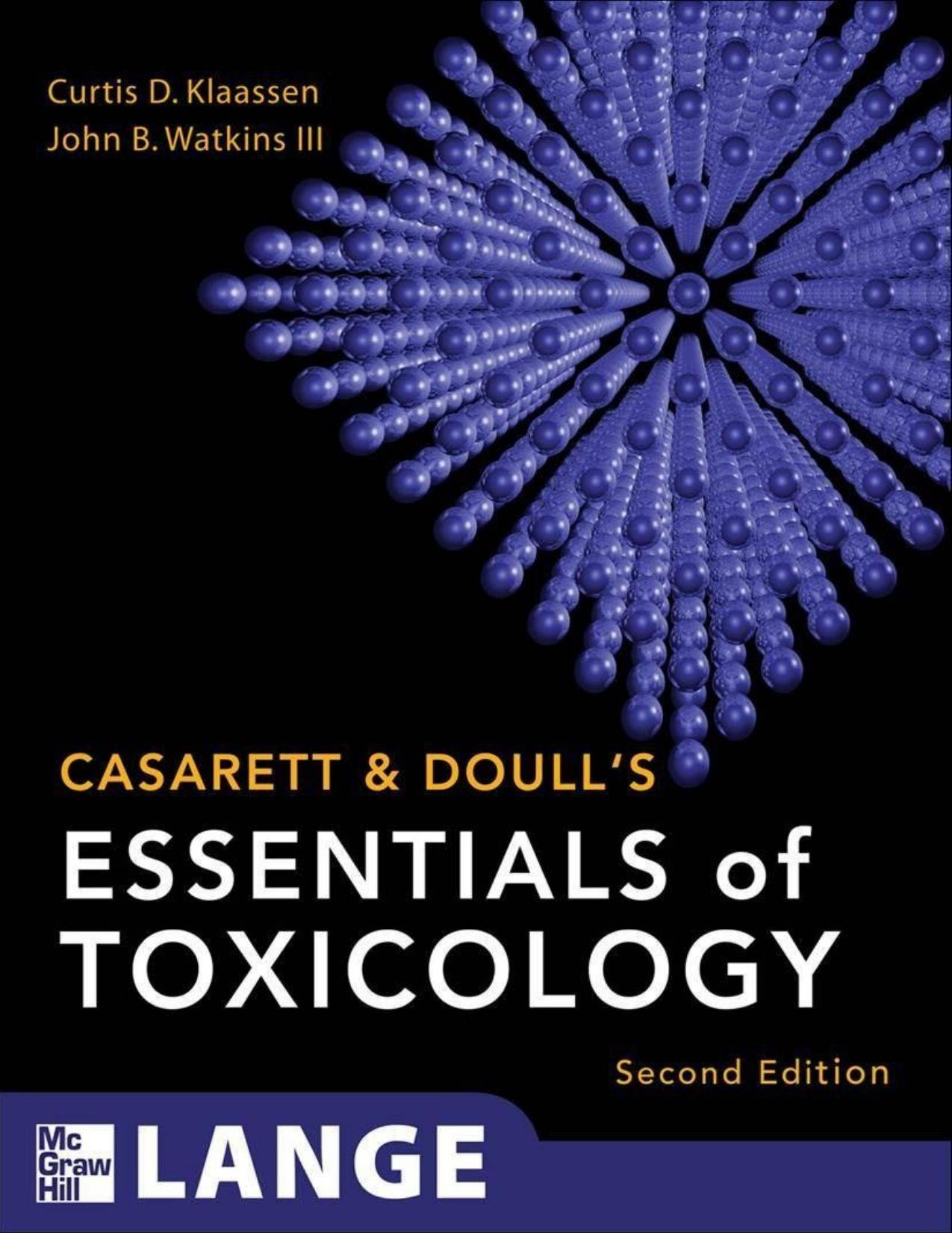
Leontiasis.
—A diffuse bilateral, symmetrical hypertrophy of the bones of the face and later of the cranium, described first by Virchow, the real origin appearing to be in the superior maxillæ, the result being a peculiar leonine appearance of the face, hence the name given to the disease. There is no distinct tumor formation in the bone, but rather the entire structure of the bones involved is affected. As it advances function of the parts is interfered with, mastication becomes impossible, headache and pain are constant. The special senses are disturbed because of involvement of their nerves, and patients die usually from inanition, because no longer able to chew and swallow food. It is distinguished from Paget’s disease, because it shows no tendency to involve the rest of the skeleton; from acromegaly, in which the general shape of the jaw is preserved, though its dimensions are magnified; from tumors of the jaw or face, because of its symmetrical enlargement. Its pathogeny is as obscure as that of the other bone affections mentioned in this list, and its treatment as unsatisfactory.
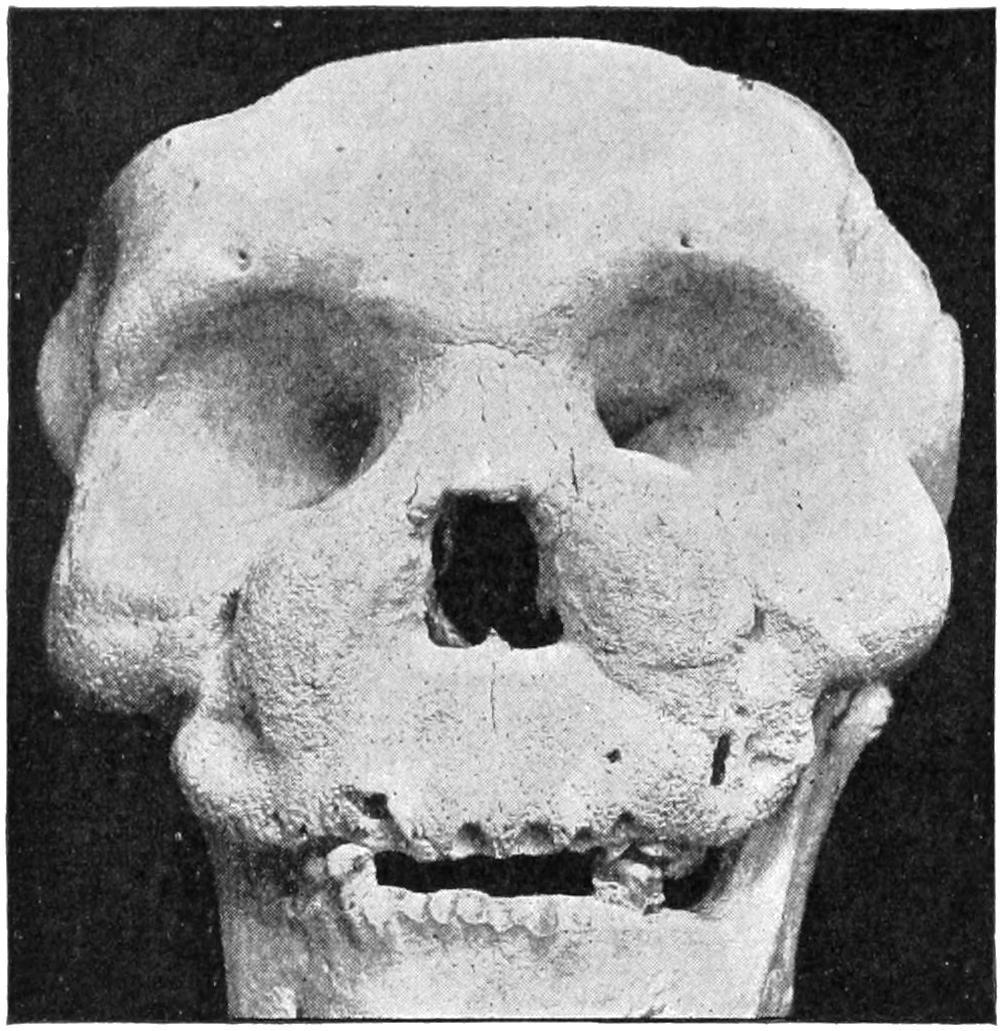
Leontiasis: skull of a Chinese woman (U S A Museum, No 10,620 )
TUMORS OF BONE.
As between the various hypertrophic conditions of the bones above noted should be distinguished the true neoplasms, which answer all the requirements of the definition given in Chapter XXVI.
There are few of the true tumors which may not be met with in bone, including the periosteum.
F��. 243
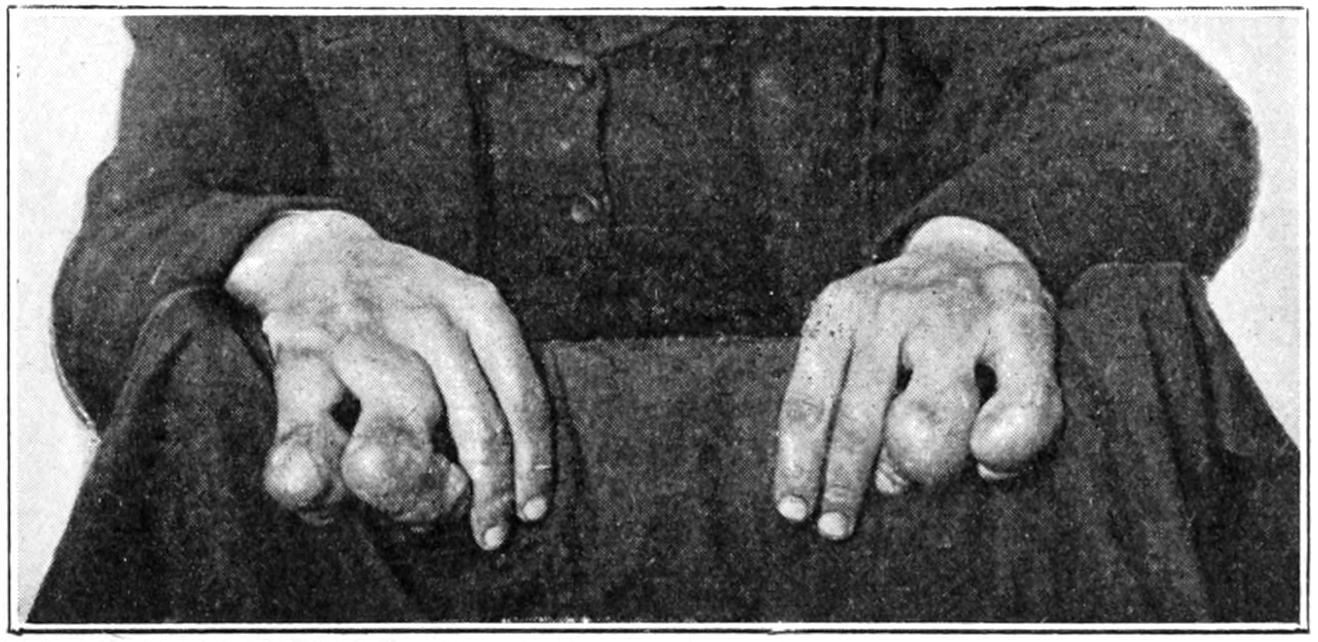
Multiple enchondromas of fingers
Fibromas.
—Fibromas may spring from the periosteum, especially about the jaws and from the base of the skull, from which latter place they may project into the nasopharynx and interfere with the welfare of the patient. Some of these tumors are soft and succulent, as well as extremely vascular, and I have seen death occur upon the table in an endeavor to remove a growth of this kind, hemorrhage being uncontrollable.
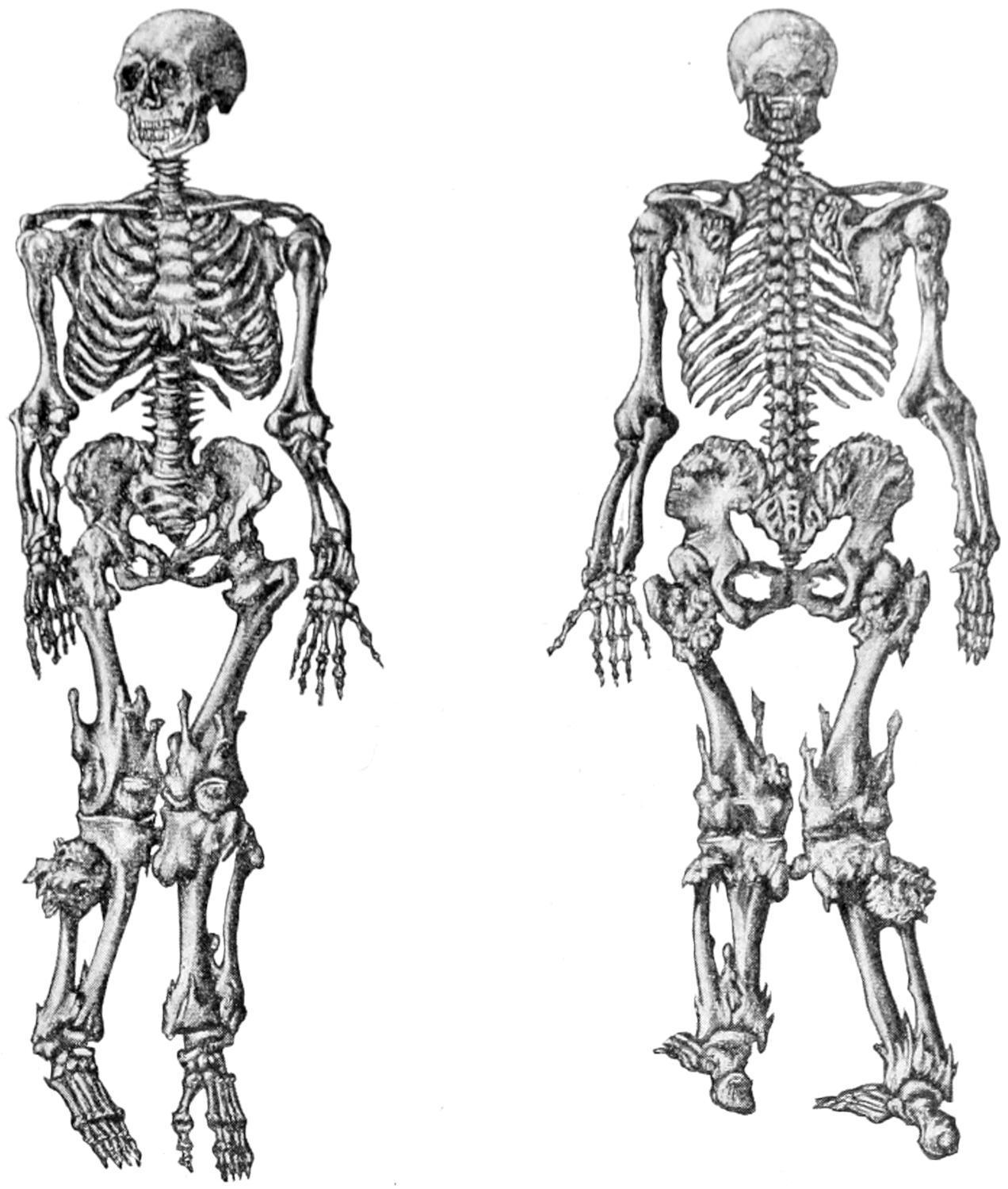
Multiple ecchondroses and exostoses. Skeleton in the museum at Lyons. (Poncet.)
Multiple ecchondroses and exostoses. (Lexer.)
Cancellous osteomas springing from the diploë. (Musée Dupuytren.)
Sarcoma of femur. (Buffalo Clinic.)
Fungating osteosarcoma of cranium. (Pemberton.)
Cartilaginous Tumors.—Cartilaginous tumors, as stated in Chapter XXVI, are not often found outside of the bony skeleton. They may spring from cartilaginous extremities of growing bones, from epiphyseal cartilages, or from the interior of long and short bones, where their origin is probably due to inclusion of cartilaginous elements, as comprehended in Cohnheim’s theory. In young children they are often multiple and involve various parts of
the body Occurring in adults they are less often multiple, but may attain considerable size. (See Fig. 243.) They are found usually about the ribs, sternum, pelvis, and femora. If the entire structure of a given bone be involved in a growth of this kind, its eradication— that is, amputation—will probably be necessary. When otherwise, complete removal with careful cauterization of the base of the growth or surface from which it sprang will usually be sufficient. These cartilaginous tumors tend on one hand to mucoid softening and cystic formation, and on the other to calcification or ossification, by which the original cartilaginous character of the growth may be concealed.
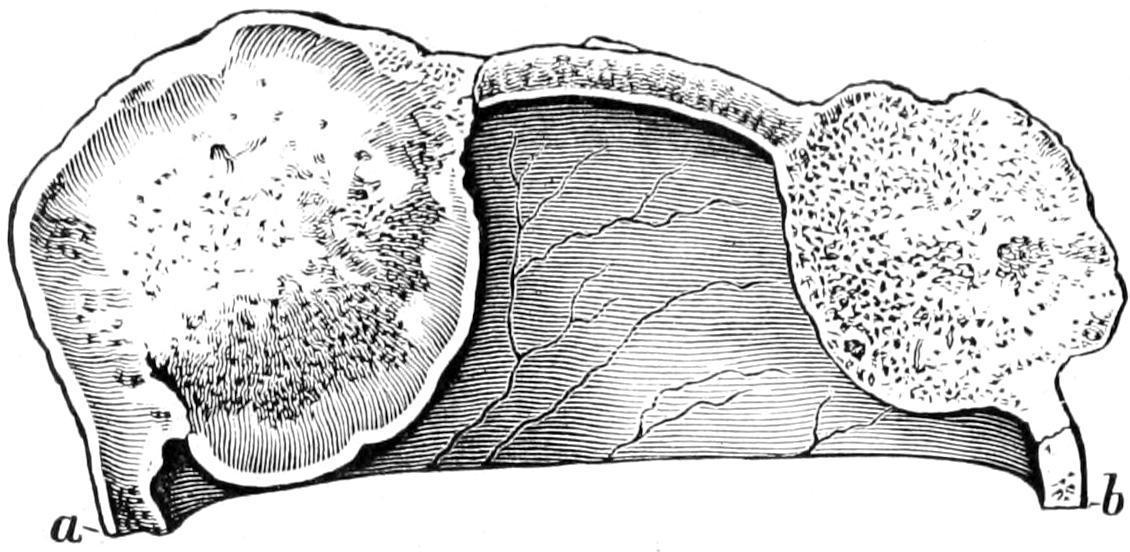
—Osteomas are by some writers made to include exostoses and hyperostoses. In accordance with the system followed in this work only those growths are considered as tumors which are of no physiological usefulness, and it is preferable to maintain a distinction between osteomas and the exostoses or bone hypertrophies, which pertain either to evolutionary relics or to constitutional affections. There is, however, a peculiar form of exostosis which becomes covered by an adventitious bursa, whose walls become in time quite thick, which is called exostosis bursata. In the cavity of this bursa may frequently be found rice-grain or other fibrinous concretions. This lesion is common in the neighborhood of joints, and the new bursa frequently communicates with the joint cavity (Fig. 249).
—Myxomas are rare in bone, and are seen usually only as degenerated forms of cartilaginous bony or malignant growths. They lead to cystic degeneration. A primary growth of this kind has for its origin the bone-marrow.
—As already described, sarcoma of bone should not be confused with osteosarcoma. (See Sarcoma.) The former refers to sarcoma springing from the true osseous tissue or periosteum. When central the bony walls are expanded and form a shell. Osteosarcoma refers to a tumor springing from the original connective tissue which holds the bony elements together, and contains osseous tissue scattered through it. Sarcoma occurs usually in the long bones, although none are exempt; mostly single, it nevertheless may be multiple. It occurs frequently in the young, is seen even at birth, and in these instances is supposed to take its origin usually from epiphyseal structures. No