The mornings are getting lighter, the days are getting longer and flowers are starting to blossom – spring is finally here and herein lies a brilliant collection of pieces to draw us out of hibernation and energised into action. Thanks to everyone who has contributed.
How do we nurture, encourage and empower CYP while protecting them from the world's potential and rapidly evolving harms? This is indeed a hard balance, not only as a paediatrician but also as a parent.
While something is to be said for allowing children and young people to be just that, this issue highlights that this is often beyond our control. Libby Henstridge reminds us of the power and bravery of our young carers and the Groovy Tuesdays piece highlights the power we have to provide glimmers of normal childhood experiences for those CYP with lifechanging diagnoses.
The centrepiece of this issue is screen time. Friend or foe? How do we maintain CYP rights to access media and information while safeguarding them from the harms highlighted in this piece? The College archived its 2019 screen time guidance as the evidence on which the recommendations were based had become out of date. With concerns around screen time pivoting from time spent on screens to accessing harmful online content, the College will continue working with its policy committees to monitor the landscape surrounding this topic.
It's time for me to swap my phone for pen and paper to write my shopping list for Ash’s delicious lemon poppy seed muffins. Perhaps you’d like to take out your pen to write for us? If so, please get in touch or say hello in person in Glasgow, as we would love to hear your ideas!
Dr Sharna Shanmugavadivel PEM Registrar
Leicester Children's Emergency Department Contact
We’d love to hear from you – get in touch at milestones@ rcpch.ac.uk
and screens How can we best support children?
Reflections on retirement Dr Julian Eason prepares for a (slightly) slower pace
A disco demonstrating the importance of play in hospital settings
The vital work of the British Paediatric Surveillance Unit
changemakers
doctors' experiences of travel through the Churchill Fellowship
responsibilities would like us to know
Update News, views, diary dates and more
RCPCH &Us
What do you know about children's rights?
Courses, reviews and a delicious muffin recipe
Dr Camilo Stargardter's two roles, in A&E and as a trainee psychotherapist
Copyright of the Royal College of Paediatrics and Child Health. All rights reserved; no part of this publication may be reproduced, stored in a retrieval system, or transmitted in any form by any means – electronic, mechanical, photocopying, recording, or otherwise – without prior permission of the publishers. The views, opinions and policies expressed in Milestones do not necessarily reflect those of the College. While all reasonable efforts have been made to ensure the accuracy of the contents of this publication, no responsibility can be accepted for any error, inconsistency or omission. Products and services advertised in Milestones are also not recommended or endorsed by the College. Readers should exercise their own discretion and, where necessary, obtain appropriate independent advice about their suitability. Royal College of Paediatrics and Child Health is a registered charity in England and Wales (1057744) and in Scotland (SC038299). Registered address: 5-11 Theobalds Road, Holborn, London WC1X 8SH. Design Manager: Christina Richmond Senior Editor: Lizzie Hufton Publisher: James Houston. Milestones is published four times per year on behalf of the Royal College of Paediatrics and Child Health by James Pembroke Media, 90 Walcot Street, Bath, BA1 5BG. T: 01225 337777. Advertising: Alex Brown, Head of
The latest news and views
President’s update
Professor Steve Turner RCPCH President
I hope that 2025 has been good for you so far. The College conference is only days away. Taking place this year in Glasgow, we already have more than 1,300 members registered to attend and it promises to be a really memorable event. And now that we are live-streaming two and sometimes three sessions concurrently, remote attendance can be almost as busy as in-person attendance.
Your College Council met on 4 February and among many items discussed, we had an update on the number of members. Membership has been rising by 1,000 per year for a decade. We currently have 24,477 members, including 5,580 international members. The proportion of international members remains constant at approximately 20%. Putting this into historical context, the British Paediatric Association (BPA) had 18 members in 1928 and the BPA council discussed in 1964 whether membership of more than 400 was sustainable!
A growing membership is clearly good news for any membership organisation, including RCPCH. But it comes with some challenges. First, it can be di cult to represent the views of all members on an issue. I was at a meeting recently where I was asked: “Is it time for the College to get more political?” The
“There is a tricky balance between carrot and stick when seeking to influence decision-makers”
College is very engaged with politicians and NHS organisations across the UK, and I think the question was really asking if we should ru e more feathers. Fair challenge. There is a tricky balance between carrot and stick when seeking to influence decision-makers.
Evidence that we have the balance roughly right can be seen in the Darzi Review reflecting our blueprint recommendations, and many UK government documents are now specifically mentioning children’s services. A second challenge is that our membership infrastructure has needed upgrading and more sta appointing, and this is currently underway. A further
challenge is that we need more members to become actively involved in our College, for example as examiners, ambassadors and committee members.
The expansion of medical student places, which began in 2018, is expected to drive up UK Medical College membership numbers, including RCPCH. And the prestige of passing our MRCPCH examination will attract more international members. I have no idea how long this year-on-year rise in membership will be sustained for, but I know it will need you to consider getting involved at some stage in your career. Please give it a thought and search for ‘RCPCH, get involved’ to find out more. Many thanks.
With more than 1,300 members registered to attend, Conference promises to be a memorable event
Sta spotlight
Suma Surendranath Education and Professional Development Manager
Healthcare has always been the focus of my work. I qualified as a physiotherapist, and my career took me from leading the physiotherapy input in a multidisciplinary chronic pain service to working at Arsenal Football Club’s Youth Academy. Along the way, I realised my true passion was education, so I took a masters in adult learning and professional development and never looked back.
I joined the Education and Professional team in 2017 and can summarise my role as supporting you to do your job better. I manage the safeguarding and exam preparation education programmes – two very different areas, but that variety is what I enjoy about it.
A priority with safeguarding has been raising awareness of less considered areas, such as how to support children and young people with neurodevelopmental disorders and/or neurodisability through the child protection process. In exam preparation, I’m leading the effort to grow our support offer to include more resources, such as managing your wellbeing when preparing for exams and creating a game plan for revision.
As a College, we’re keen to provide the education and professional development opportunities you need in ways that are accessible to you. The pandemic changed everything for us, necessitating a move of our
catalogue of courses and workshops online, which has led to greater participation. Our current priority is creating more on-demand learning opportunities that work with your schedules, such as podcasts and micro-learning. I recently completed a diploma in digital learning design, so I’m better equipped to develop these.
Outside of work, my focus (and energy) is very much on my two young children. So, as a parent, a big thank you for
everything you do! However, I am also the secretary for our tenants’ and residents’ association, so often organise events such as a recent repair shop party – my 30-year-old Tottenham Hotspur hamster mascot can now sing and wave his flag again!
To find out more about the College’s education and professional development offer, go to RCPCH Learning: learning.rcpch.ac.uk
Journal: ADC update
Nick Brown Archives of Disease in Childhood Editor-in-Chief
@ADC_BMJ
Meandering thought for this quarter: why is the beauty of hesitation (and this is the right word, to me) so underrated? Let me explain.
Early on in (for the want of a better expression) learning careers, syllabi are packed with active ‘what to do and when’ information. At medical school and
the immediate postgraduate years, very little (arguably, appropriately at this stage) takes a ‘what not to do’ stance.
But, as time goes by and foundation jobs become specialist training jobs and then consultant posts, there’s an almost osmotic effect in terms of learning when not to intervene. When to give time and a natural trajectory the opportunity and the space to ‘do their jobs’. I’d go so far as to say this is a (tacit) part of training and one that evolves gradually.
Without meandering off-piste
Journal: BMJ Paediatrics Open update
Shanti Raman BMJ Paediatrics Open Editor-inChief
@BMJ_PO
The past year was one of substantial growth for BMJPO, with 719 submissions in 2024 (a 29% increase over 2023) and 283 papers published, more than double the number in the previous year.
Some of this growth is thanks to the topic collections we are committed to.
The ‘Health and Wellbeing of Street and Working Children’ collection call closed last year, and we have 15 papers published already. Topic collections open for submission are ‘Disability and Development in Early Childhood’ and ‘Preventing and Mitigating the Impact of the Climate Crisis on Child Health’. Some terrific recent publications from these include: Mobile health van as an intervention to provide clinical support and health promotion to street children and marginalised populations in the National Capital Region of Delhi: a mixedmethods evaluation (7 January 2025); Exceeding the limits of
paediatric heat stress tolerance: the risk of losing a generation to climate inaction (21 January 2025) and Building relational wellbeing: empowering street-connected young people to transition from precarity to security through youth associations (8 January 2025).
Our Young Voices section is buzzy and active, having recently published Fuelling our passions with the Health Hackathon by young people from a Sydney high school. In terms of political advocacy, the Advertising and child health viewpoint by Prof Imti Choonara says it all.
I encourage you to sign up for e-alerts, and remember, as RCPCH members you benefit from a 25% APC discount when you submit to BMJPO. Reviewers also receive a 25% discount if they submit a paper within 12 months of reviewing for the journal. We always need reviewers, particularly in neonatology, general paediatrics and community paediatrics, so please put yourself forward. And if you have an idea for a thought-provoking viewpoint, a clinical or public health review or an opinion as a young person, reach out to me as the EiC and I will respond with alacrity!
any further, I’d like to flag just a few papers and series in Archives that take this philosophical angle: papers on end-of-life care, a mouth-watering WHOcommissioned series on acute asthma interventions, case law and many more. Do check these out for yourselves.
So, though we instinctively want to act, don’t forget that non-acting is a powerful intervention – a really (often underrated) powerful action in its own right. Thanks, as always, for joining me off the main highway…
Safety eBulletin
Enhance patient safety with the new RCPCH Safety eBulletin
Dr Emma Vittery RCPCH QI
Fellow Great North Children’s Hospital
We heard you in the last members survey –education and CPD are top priorities, but you’re busy and need succinct and timely updates that can fit into daily practice. Building on existing resources like the Patient Safety Portal and the RCPCH Safety Podcast Series, we’re now delivering concise, impactful safety updates – every two months, directly to your inbox.
Curated by a dedicated editorial team
in liaison with College committees, the RCPCH Safety eBulletin o ers information relevant to all UK nations with transferable learning internationally.
Each edition features a spotlight blog by guest editors, exploring a key safety topic. Did you catch our December issue reflecting on the HSJ Patient Safety Congress, or the February issue on what Martha’s Rule means for children and young people?
Beyond the blog, there are updates on:
Medication safety
National safety alerts
Relevant research
College and national safety news
Educational opportunities
Collaborating for child health globally
Dr Rebecca Rhodes
Paediatric Resident in Neurodisability
Nottingham University Hospitals
ICHG Deputy Convenor
A special interest group of the RCPCH, the International Child Health Group (ICHG) values justice, equity and diversity as we partner with a global network of professionals and other institutions (CHIFA, ISSOP, Students for Global Health, RCPCH Global) to promote a child-focused approach to global health issues. Comprising more than 420 child health professionals from 28 countries, we realise that we can learn from each other and are inclusive and respectful while encouraging good practice, advocacy and research. The group strives to inspire and equip students and health professionals with the skills and knowledge to engage with issues in global child health while upholding the core principle of decolonising the global health discipline.
ICHG’s work centres on advocacy, education and research. Dedicated subgroups support each area and all members with an interest are encouraged to participate. Each subgroup hosts annual grants awarded to members with great project proposals for improving global child health.
In 2024, ICHG’s work included: Publishing position statements on critical issues (eg the effect of conflicts in Ukraine, Gaza and Sudan on child health; UK government proposed [now defunct] Rwanda Bill for asylum seekers; cuts to international aid funding by UK government) in collaboration with RCPCH and ISSOP
Writing academic articles to raise awareness and share reliable insights (eg BMJ Article on Gaza, armed conflict and child health)
Contributing to the development of Good Practice Delivery Standards for children seeking asylum or refugee status in the UK (see www.rcpch.ac.uk/
The eBulletin is available to all members who opt into College and professional updates. We welcome feedback and contributions, including from Specialty Groups and Special Interest Groups, via qips@rcpch.ac.uk
Don’t miss out!
To receive the Safety eBulletin, log in to your RCPCH account and click ‘my account’. Then ‘edit your contact preferences’ and ensure the box is ticked next to ‘College updates/professional updates’. Please see safety.rcpch.ac.uk/ safety-ebulletin for previous issues and access for non-members.
asylum-refugee-guidance-ichg)
Hosting webinars focusing on children in conflict and climate change, neonatal medicine, child development, malnutrition and infectious diseases and more
Delivering webinars to enhance transferable academic skills, such as pitching research grant ideas and writing academic abstracts
Hosting the Global Health Lives podcast and the ICHG Mentorship scheme
Hosting our yearly international conference, featuring a day of inspiring talks about sustainable development goals and child health globally
ICHG has many exciting opportunities for 2025, including our session at the RCPCH Annual Conference focusing on innovations impacting global child health – we hope to see you there!
Go to X @intchildhealth and visit internationalchildhealthgroup.org for more information
Diary dates
Events are online unless otherwise stated. We will add to this list over the coming months, so keep an eye on our website
Mentoring skills: Introductory and refresher course (23 April)
How to Manage: Paediatric Allergic Training (PAT 2) (25 April)
Effective Educational Supervision (29 April)
How to Manage: Child mental health (7 May)
Effective educational supervision (2 June)
Expert witness in child protection (Level 3+/4/5) (3-4 June)
How to Manage: Paediatric Allergy Training (PAT 3) (19 June)
How to Manage: Refugee and asylum-seeking children and young people (9 July)
Read more
Find more dates at www.rcpch.ac.uk/courses www.rcpch.ac.uk/events
We celebrate 10 years of RCPCH &Us this April! Discover how we ensure CYP voices are heard at www.rcpch.ac.uk/work-we-do/rcpch-and-us and look out for a special RCPCH &Us takeover of Milestones this winter
RCPCH Learning
RCPCH webinar: Don’t forget rheumatic fever!
Dr Tom Parks and the panel discuss the BPSU study and provide a refresher on Strep A disease and post-infectious disease at a time when UK children are at increased risk.
RCPCH webinar: Understanding childhood poverty
Ailbhe Cashman – Poverty Proofing Coordinator at Children North East – discusses the barriers to health that families experiencing poverty may face and provides information on what you as an individual or as a service can do to help.
Thrive Paediatrics Resource Hub
Discover evidence, good practice examples and stories from
paediatricians’ lived experiences. We all learn differently, so you’ll find tools in different formats – from articles to books, and podcasts to videos: learning.rcpch.ac.uk/thrive/
Talking to patients about air pollution – simulated conversations
In collaboration with Great Ormond Street and Camden Council, we’ve developed a module of four short video simulations where child health professionals incorporate air pollution into their conversations: www.rcpch.ac.uk/air-pollutionsimulation-videos
learning.rcpch.ac.uk
RCPCH Learning user survey
Please share your thoughts about your experience with the RCPCH Learning site. Your feedback will help us enhance the platform and provide the best possible experience for you and other users: https://bit.ly/rcpch-learning-user-survey-2025
What do you know about children’s rights?
Toby, age 19
Nathaniel, age 13
Xai, age 14
The UN Convention on the Rights of the Child is a set of 54 articles (or ‘rules’) universally agreed on by more than 195 countries as important in upholding the rights of children and young people (CYP). Upheld in law, the rules ensure CYP can thrive – including how they should be able to rest, relax and play, receive an education, and be kept safe from harm.
All of the work of RCPCH &Us takes a rights-based approach. We urge other professionals to do the same. Here are the rights that are most important to us.
Article 24: the right to access the best possible healthcare
To us, this means not only having access to the best possible services but also to the best-trained healthcare professionals. We have seen patient feedback forms used to great e ect, enabling our clinicians to develop new knowledge and skills. We believe that paediatric training for doctors, nurses and other roles should have input from CYP to make sure it is patient-led and to ensure young people’s voices are included in the care they receive.
Article 12: the right to give our opinions on matters that affect us
This includes healthcare settings, but is not limited to them – if a young person is passionate about any issue, they should be free to voice their views on it. The most important part of this article to us, however, is that children have the right to be listened to and taken seriously. We’re sure many examples come to mind of when CYP have been dismissed, whether due to a perceived lack of experience, knowledge or something else. Younger voices must be heard. We are the ones who will be most a ected by changes being made today.
Article 17: the right to access information from the media
This article is important – as is receiving that information when it’s relevant to our age and the stage we are at. It should be provided in schools, by the government and through books, TV and the internet. It should be in a language we can understand
“Children have the right to be listened to and taken seriously”
RCPCH &Us: The Children and Young People’s Engagement Team delivers projects and programmes across the UK to support patients, siblings, families and under 25s, and gives them a voice in shaping services, health policy and practice. RCPCH &Us is a network of young voices who work with the College, providing information and advice on children’s rights and engagement.
and in a format that can be shared by the people who are looking after us, when the time is right. Some services already do this, such as the BBC, which has CBeebies and CBBC for younger viewers. However, other services could be improved by having a section that’s aimed at younger audiences.
Article 4: governments must do all they can to ensure every child can enjoy their rights
This is so important because it’s what makes children’s rights real. It’s a government promise that says: ‘We’re not just going to talk about rights; we’re going to make them happen.’
It’s the part that says: If a child needs education, healthcare or a safe place to grow up, governments will make sure they get it. Imagine a child who can’t go to school because their family is struggling, or they’re sick but there’s no doctor nearby. Without this article, those children might be left to fend for themselves. It’s a way of saying that every single child matters and that their wellbeing should be a top priority. Without it, children’s rights are just words on a page; with it, those rights become actions – a chance for every child to have the life they deserve.
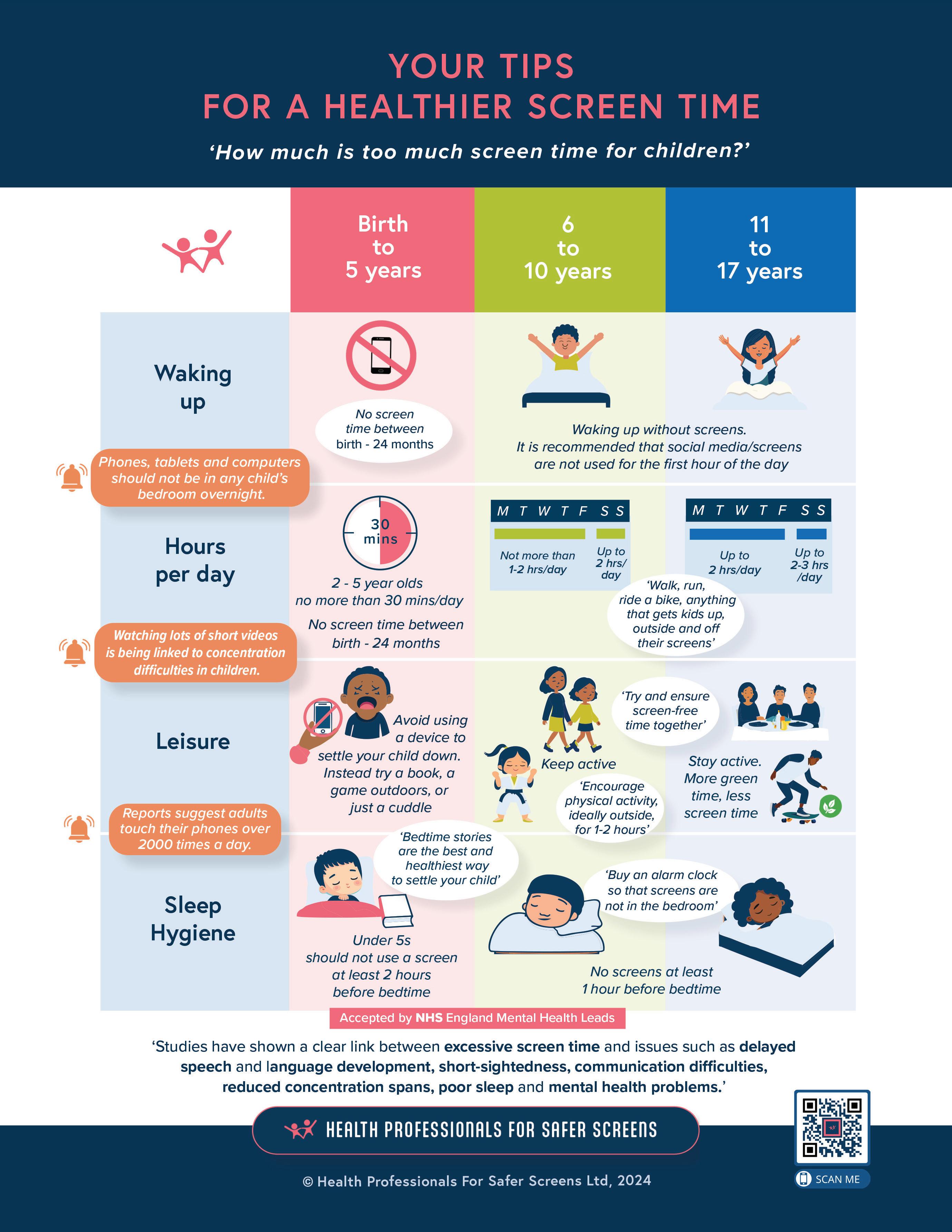
Kids and screens: what’s all the fuss?
Dr Louise Milne and Dr Kelly Brown ask whether we are sleepwalking into a societal norm that is harming children
As we talk to more people about screen use, we realise what strong emotions and debate it sparks in people, especially those with children. This article may inspire you to challenge your own decisions around device use. This is a healthy reflection, but we need to clarify how we, as professionals, view the debate.
More children than ever have social media accounts, which are accessed via smartphones that are within grabbing distance 24/7. The average amount of time a 12-year-old spends on a smartphone is 29 hours a week; they
receive an average of 250 notifications a day. Smartphones are mini-supercomputers and making a telephone call is the least used function. The dependence is clear: 30% of parents have cried over their child’s smartphone use and one in five 16- to 18-yearolds have reported feeling that life is not worth living due to social media.
How can we help these families and mitigate the medical impact in a world where smartphones are an expected norm and, as a result, parents are placed in a seemingly impossible position?
Dr Louise Milne Paediatric Consultant
Queen Alexandra Hospital, Portsmouth Hospitals University
NHS Trust
Dr Kelly Brown Consultant Neonatologist University Hospital Southampton
NHSFT
A paediatrician’s view
Dr Louise Milne
We’re all aware that there is now a child mental health crisis. Sapien Labs’ Mental State of the World Report 2023 demonstrated a strong correlation between the age at which an 18- to 24-year-old receives their first smartphone or tablet and their mental health status in young adulthood. The Millennium Cohort Study (MCS) also demonstrated a correlation between increased hours on social media and an increased chance of clinically significant depression.
Features such as the ‘like’ button, the ability to retweet and front-facing cameras have made social media and smartphones more engaging and compel children to
compare their real selves to curated online personas. In addition, apps are designed to maximise user attention – another factor that’s contributed to their addictive nature, especially for young people. The correlations cited above will be one part of a multifactorial picture, but can we have some influence on this? Is this an ‘easily’ modifiable risk factor?
If the headline cases of children who have had social media linked to their deaths are felt to be isolated tragic accidents, then we need to educate ourselves on what children are seeing on their smartphones. It’s been revealed that 51% of 11- to 13-year-olds have seen hardcore and often violent pornography, 75% of 15-year-olds
“You can’t go back and change the beginning, but you can start where you are and change the ending”
CS Lewis
questioned by the Children’s Commissioner had been sent a beheading video, and 90% of girls and 50% of boys have been sent unwanted sexually explicit material. It doesn’t matter if you think your child is sensible enough to control their smartphone use, they can still be exposed to content that, as a parent, you would not want them to see. Once seen it cannot be unseen and the impact of normalising this content on developing minds is changing childhood.
‘Social’ media is a misnomer – 16- to 24-year-olds are the loneliest group in our population. As the rate of self-harm has increased by 93% in the past 10 years, the number of outdoor accidents involving children has dropped by 70%. Three-quarters of UK children spend less time outside than prison inmates. Smartphone use has also been linked to sleep disturbance, increased myopia and neck pain – ‘tech neck’. The knock-on health effects and relevance to our patient group are obvious.
A neonatologist’s view Dr Kelly Brown
You may think, as a neonatologist, that I wouldn’t have as much interest in protecting my patients from social media and smartphones, but this problem is not limited to older children. Poor screen habits develop early in life. The neonatal unit has a population that has a high chance of ongoing health problems including poor metabolic state, obesity risk, developmental delay, ASD and behavioural issues. These risks are impacted further by unhealthy screen habits.
There is an increasing population of children with speech and language difficulties. Children who spend a higher
“We have a duty of care to promote healthier screen times. Parents need to be able to make an informed decision”
amount of time on screens are less ready for school and a link between screen time and ADHD/ASD has also been documented. The Kindred Squared School Readiness Survey 2024 shows 28% of reception children don’t know how to use a book and are tapping and swiping them. Children who have high screen use from early on are seen to have a lower ability to self-regulate.
Smartphones are great for recording photo and video memories, which is much needed in the neonatal unit. However, their addictive nature means that I witness parents sitting by the cot, endlessly scrolling which, at a time of great anxiety in their lives, will only have negative impacts on their mental health. If this distraction by screens continues for
parents, it can lead to babies not receiving appropriate social interaction and language skill development in the vital first year of life.
What can we do?
Most importantly, we need to keep talking about kids and their screens. All too often, we encounter the response that smartphones and the internet are part of modern life. Yes, they are, but there is enough information to justify applying the precautionary principle. We have a duty of care to give health promotion about safer screen time. Parents need to be able to make an informed decision.
With the safety features tech companies and governments have mooted not yet available, delaying children’s access to smartphones is the clearest approach. We do not want to forget the children who already have smartphones – it’s never too late to implement changes. Apps can be deleted and rules adapted. In fact, young people respond well to the challenge to prove they are not controlled by their phones and enjoy the additional time they gain from reducing their smartphone use. Families
Thank you
We would like to thank Health Professionals for Safer Screens, PAPAYA and Smartphone Free Childhood for their continued hard work to share for free their resources and time. References for this article can be found on the websites below. We encourage all health professionals to join Health Professionals for Safer Screens.
can work together to challenge themselves with smartphone-free days, taking a walk without a phone, using focus-promoting apps (eg Forest) and weekly ‘whoever has the lowest screen time wins’ competitions. Where a smartphone forms part of a child’s medical care, we need to be even more mindful of our moral obligation to promote safer screen use. We also need to consider our increasing mental health and eating disorder inpatients – how do we navigate safeguarding this vulnerable group of children on our wards?
This is a societal issue that needs a collective response, but as ever we cannot shy away from the important role we have in advocating for children. The RCPCH screen time advice from 2019 is no longer available. National paediatric groups around the world are standing up for children and asking why we are not proving screens are safe instead of waiting for evidence they do not cause harm. We call on the RCPCH to lead the way and issue UK guidance. While we await this, we hope you find the information from Health Professionals for Safer Screens, which encompasses all screen time, useful.
Further resources:
● www.healthprofessionals forsaferscreens.org
● www.smartphonefreechildhood. co.uk
● www.papayaparents.com
● RCPsych use of digital media for CYP: https://bit.ly/41JKEG9
Reflections on retirement
After a full and varied career, winding down gradually through part-time work helped prepare Dr Julian Eason for a (slightly) slower pace
Dr Julian Eason
Consultant
Neonatologist
University Hospitals
Plymouth NHS Trust
University of Plymouth
School of Nursing and Midwifery
So here I am, still trying to retire at 63, but it’s di cult as I love my work and will miss the camaraderie. I qualified in 1986 from London’s Middlesex Hospital Medical School. It was di erent in those days. Having chosen our house jobs, we could apply anywhere in the country to gain experience. My dream was to be a paediatrician and, with no such thing as a GRID, you just applied. I spent nine months working in A&E waiting for a paediatric position to become available because it was so popular.
Travelling far and wide I eventually started as a SHO, followed by registrar and senior registrar jobs that took me from my hometown of Plymouth
Julian’s career has included being educational lead for a Level 1 Neonatology course (above) and training doctors with an NGO in Vietnam (opposite, centre) as well as co-authoring a book (opposite, right). One of his proudest moments was flying neonatal medevacs with his paramedic son (opposite, left)
to Oxford, Great Ormond Street, Brighton and Guy’s. During that time, I switched mainly to neonates but, after about nine years, I wasn’t ready to settle down as a jobbing neonatologist, so I went to Vancouver for a neonatal fellowship. It was an eye-opener compared to the UK – I loved it so much that I stayed for three years, obtaining my Canadian fellowship as well as a masters in healthcare and epidemiolo and a wealth of new ideas.
My love of flying babies in Canada took me to Jersey – after a stop-gap in Poole and the Royal Free – to develop the SCBU and air transfer service, but when my neonatal training needed a bigger challenge, I moved to Norwich where I helped lead and develop a NICU in a new hospital at the University of East Anglia and develop the
East of England Ambulance Service that we based in Cambridge.
Family reasons led me back to Plymouth in 2007 where I joined a team to help develop amazing transitional care and transport services. However, soon becoming the Clinical Director of Maternity and GU services, and managing 14 PAs clinically with a £45m budget, took its toll. It was probably the lowest point in my life and I lost over one-and-ahalf stone in weight due to stress despite the accolade of being named an exemplar directorate.
In 2012, I moved to the Middle East as chair of a neonatal department – often with up to 100 babies – which I grew along with my obstetric and fetalmedicine colleagues. I consider it the highlight of my achievements. At the time, we became the only quaternary neonatal centre in the region with many firsts in neonatal care, training and education –producing the first-ever neonatal fellows to qualify in the UAE.
Transitioning
to part-time work
In 2017, it was time to return to the UK and, at 56 years old and after a lifetime of long hours and night work, I prioritised work-life balance and went part-time. I joined an NGO in Vietnam and became the educational lead for a level 1 neonatology course. Of course, COVID-19 interfered so we taught online, however, hospital shifts in Plymouth were never-ending and I worked far more than I’d planned.
Post-COVID, I wound down my shifts to enjoy various social activities, housebuilding and family time. I’ve not always
“I aim to make my ward rounds fun and educational. A smile, kind words or a ‘thank you’ goes a long way”
been the greatest parent as the NHS took my life but, in retrospect, my only regret is the difficulty I had being able to say ‘no’. But getting to fly medevacs with my paramedic son when he worked in neonatal transport made me very proud. I’ve found it hard to stop working. Being part-time with no paperwork, mentoring responsibilities or routine admin allows me to work the clinical shifts I’m extremely well trained for. But now my family and social life come first and I have a great non-medical life – I love gardening, rowing gig boats, playing guitar in a band, riding my bike, travelling and catching up with my twin boys.
When I told colleagues at the NICU I was leaving, many laughed, as I’ve been saying something similar for a couple of years. But I think I mean it this time, although I can be on standby for urgent shifts!
My new life outside of medicine is more than enough to keep me busy and I’ve found the part-time transition extremely helpful in winding down mentally. I still teach overseas doctors online and nurses on the local ANNP courses, but it’s not onerous and keeps me reading. We all like to feel wanted and I still get called in to intubate, place central lines, undertake ECHOs or even place a
cannula, but the current training and skill level of the junior doctors (and even some consultants) are not my problem anymore, though it does worry me.
What I’ve learnt along the way I aim to make my ward rounds fun and educational. A smile, kind words or a ‘thank you’ goes a long way. I love to enthuse about what we do at every opportunity. The small things we do are the most rewarding as I don’t feel we can influence too much, even when I was a clinical director. You don’t have to be a consultant for life in one place if it doesn’t suit you. You can travel and see how the same tasks and treatments can be done differently. My advice is to spread your wings if you can. Take opportunities to enrich your learning in another part of the country or another part of the world. I would do the same again with very few changes.
I’ll feel a loss when it’s all gone, but I’m very proud of my achievements and the letters after my name that remind me of all the work I did to pass those exams. There are so many sad stories of consultants’ retirement being short-lived before serious illness or death intervenes. I look at my health now, probably for the first time, and it’s not perfect. Rugby has taken a toll on my joints, but I’m ready to stop clinical work as I have so much else I want to do. I feel good going into full retirement, so it’s probably time to get rid of all those journals in my library and make way for my love of history, Lego and – of course – my amazing wife and boys. Fingers crossed…
Groovy Tuesdays
Exploring how music – preferably accompanied by a disco ball! –can give a vital injection of playfulness to the hospital environment
Dr Paulina PérezDuarte Mendiola
Consultant
Paediatrician
PEDAL research centre, Faculty of Education, University of Cambridge and ORCHID research centre, Great Ormond Street Hospital @paediatricianw1
It was nearly four o’clock. I entered the oncolo ward, notebook in hand and ready to take some notes when a smiling three-yearold boy pointed at me and screamed: “I’m coming to the disco! See you there!” After five weeks of attending this popular event, most patients recognised me. Children, parents and sta knew that my role in the hospital was to ‘write stories’ so adults could learn how children play, dance and have fun while hospitalised.
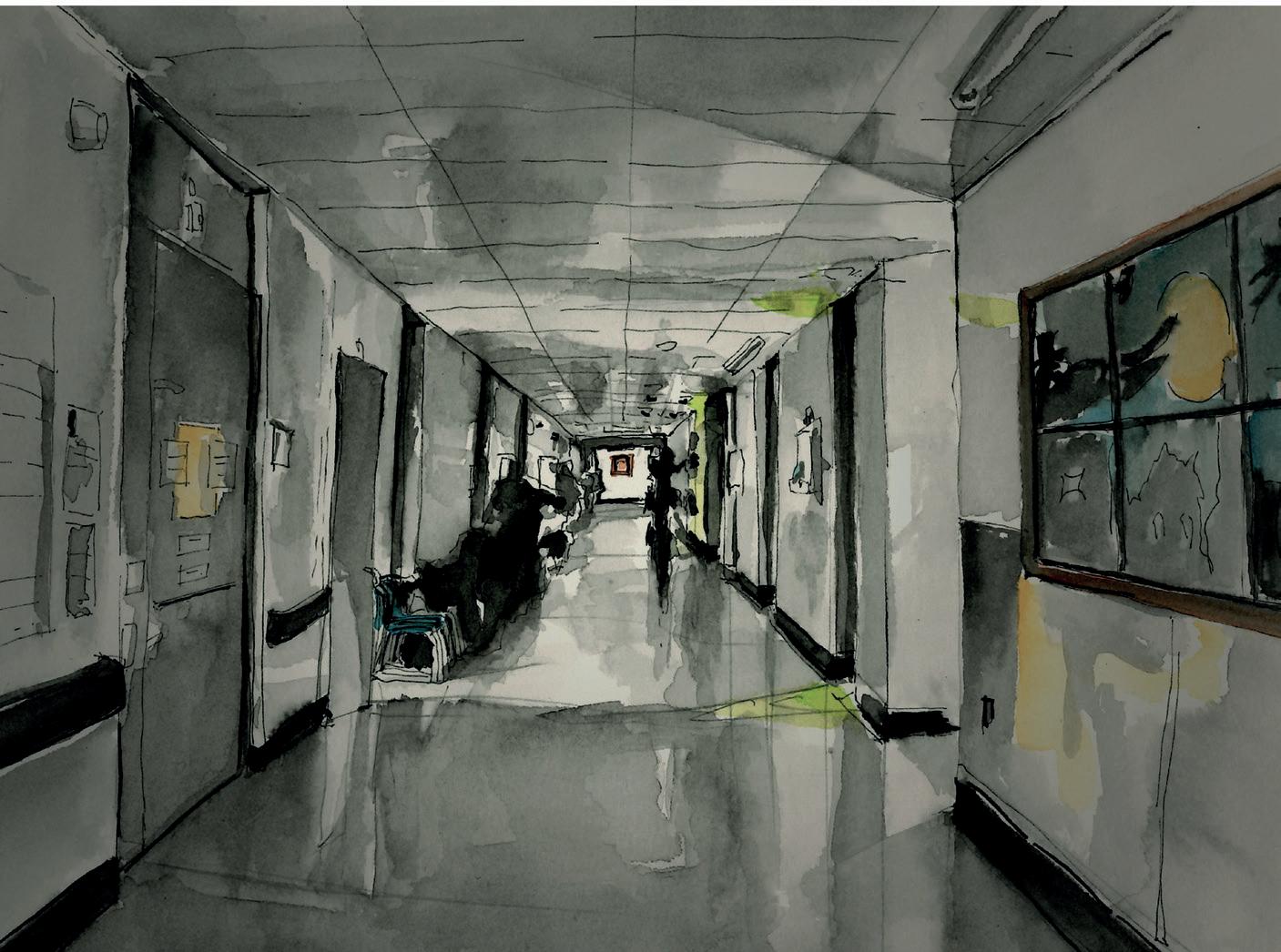
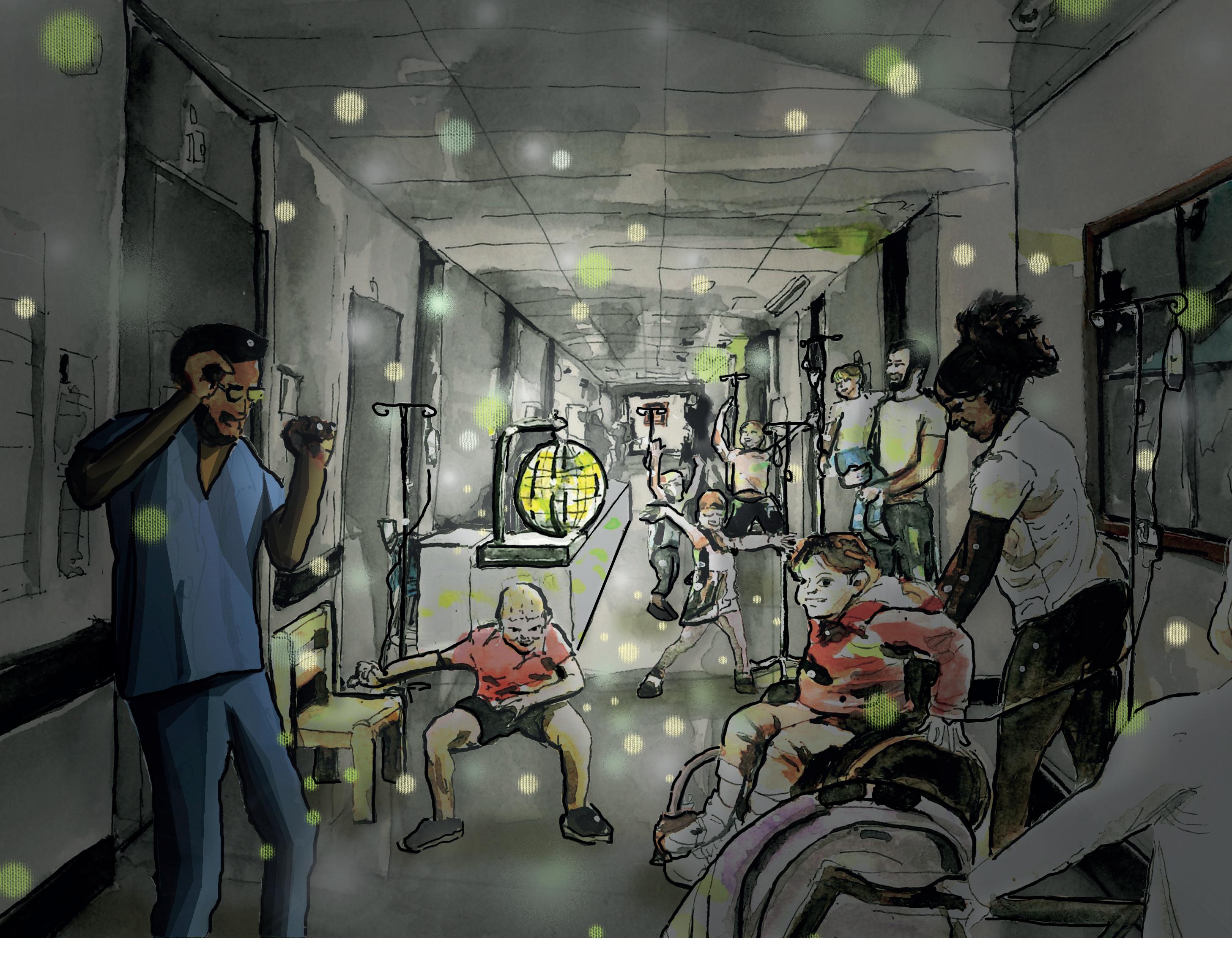
Imagine a hospital ward. White walls, beeping machines, a nurse’s station and a hallway with various doors leading to rooms. Now add loud music, colourful lights, semi-darkness and the sight of young oncolo patients, family members and sta boo ing in the hallway. Crazy, right? This is Groovy Tuesdays!
During my doctoral research on the impact of play in hospitals, I focused on the perspectives of children and young people. Part of my fieldwork involved shadowing play team sta for several months. One day, a health play specialist introduced me to a dancer and movement artist who led therapeutic movement sessions for hospitalised children. She worked for the hospital’s arts team – promoting improvisation and imagination to improve the inpatient experience – and collaborated
with the hospital’s physiotherapists, who aim to make physiotherapy more playful and fun. She explained that dancing and movement o ered therapeutic e ects in the unpredictable hospital environment, emphasising: “It’s all about agency over their bodies.”
I was invited to their weekly event, which I was lucky to join five times during my fieldwork. It was joyous and overwhelming – so much ener , so many emotions. The hallway felt charged, but not in a heavy way. Instead, it felt like taking a mouthful of air after being underwater for a long time. In my research journal, I wrote: “The whole event is emotionally charged, but […] I allowed myself to dance,
o the bright lights in the hallway. As the music blasted at high volume, gradually,
“The songs the children chose reflected themes of overcoming adversity, with the lyrics ‘never gonna give you up’ echoing down the hall”
doors opened and children emerged from their rooms, followed by parents pushing IV trolleys.
Flashing Shoes – a two-year-old with light-up trainers – used her right foot to smash the floor and follow the beat.
The disco ball had the ceiling shining with bright, sparkly pink and blue lights, while her shoes added colour to the floor.
A nurse opened the door of another patient, who was in bed, wearing soundcancelling headphones and looking out the door. Minutes later, the nurse shut the door, mouthing: “He wants this closed.” A 10-year-old boy sat in his doorway, looking down, with no energy to join in. His mum, however, was fully immersed and moving her entire body to the music.
A boy with limited mobility assumed
the role of DJ, as he had done in the past. He was there at 4pm sharp, ready to choose a song.
“Don’t you know that I’m still standing better than I ever did
Looking like a true survivor, feeling like a little kid
And I’m still standing after all this time…”
I’m Still Standing – Elton John
The dancer announced, “We’re taking orders!” and the songs the children chose reflected themes of resilience and overcoming adversity, with the lyrics “never gonna give you up” echoing along the hall. Through it all, they expressed their excitement – laughing, moving and
enjoying a carefree ‘silly’ moment. Some parents bounced up and down with their little ones rolled up like cuddly balls on their chests.
Four physiotherapists joined in, following choreographies, each other or the children’s lead. A dietician and two nursing students danced beside me. A nurse managed to change the IV solutions and program the drip pump of a three-year-old boy while he was still rocking his moves. A superhero-themed zippy cup hung from his IV stand and I recognised him as the boy who said he’d see me at the disco.
A nurse walked past, evidently not enjoying the party. She muttered loudly enough for us to hear “So dark!” in a tone of complete annoyance. Another nurse was more enthusiastic, jumping and saying:
“I witnessed the powerful impact that small, creative efforts can have on children’s hospital experiences”
“This is my weekly exercise!” A couple of dancing doctors remarked, “What a great way to end the day!” and “I’m supposed to be working.”
The busy hospital flow continued. Staff came and went, some danced around for a bit before returning to their duties. A doctor crossing the hallway did a couple of moves through the middle of the dance floor, causing numerous smiles.
Some children sat on chairs to take breaks between songs. Violet, a smiling nine-year-old, spun around in her wheelchair while her sequinned shirt reflected the bright disco lights, her mum filming her. Another nine-year-old girl arrived – an outpatient who knew it was ‘Groovy Tuesday’ and had waited to attend – and was soon jumping and spinning.
I went to check on Heidi, a five-yearold who had surgery that day. She was sitting on her bed looking at her tablet. Meanwhile, a four-year-old boy was doing some robot dancing, while a father, standing behind the group, quietly wiped a tear from his eye.
As the DJ played the penultimate song, Flashing Shoes continued to dance, jump,
run and sparkle. Heidi, followed by her mum, ventured out of her room. She timidly explored what was happening. She watched the children dancing and the sparkling lights on the ceiling. She was invited to join, but she shook her head. Her decision was respected – staff members are aware that hospitalised children can simply say ‘no’ to playful opportunities such as this.
After 30 minutes of dancing, the dancer lowered the speed with a slow song and brought everything to a close. The boy with the zippy cup turned to his dad and said: “That was a LOT of dancing!” Patients, parents and staff walked away repeating, “Same place, same time!”
Groovy Tuesdays and the children taught me some valuable lessons. As little Zippy Cup explained: if you don’t have a disco ball, it’s not a disco, only music! More importantly, I witnessed the powerful impact that small, creative efforts can have on children’s hospital experiences. A childhood cancer diagnosis is devastating for children and their families. The ward can hold difficult memories, from the moment of diagnosis to frequent painful procedures and all the side effects of gruelling treatment. However, when done sensitively and embedded into the culture, the hospital – from the perspective of children – can be momentarily transformed into a time and space of joy, agency and self-expression. When the music stopped, I heard Flashing Shoes say, “I hope I’m here on a Tuesday!”
A pro-play mindset
Throughout my career, I’ve focused on improving the holistic outcomes of children’s health and, when I moved from Mexico City to London to study for my MSc in medical anthropology (and later a PhD in education), I came across a group of unsung heroes: health play specialists. Like the one who helped kickstart this initiative.
Groovy Tuesdays is part of an ethnographic research project conducted in paediatric wards in a UK hospital, comprising 274 hours of participant observation and 14 play-based interviews with children and young people. Some of the lessons drawn emphasise that play is a fundamental aspect of paediatric healthcare.
As a result, child healthcare professionals should be encouraged and trained to acquire a ‘pro-play mindset’ that respects and advocates for: (1) play and the multiple benefits it brings to healthcare settings; (2) health play specialists and play workers, their training and the work they do.
Groovy Tuesdays intended to make physical therapy more entertaining – as one physiotherapist said: “We want children to be doing their physio, without realising that it is physio.” However, plans for the initiative to continue weren’t sustainable due to a lack of funding and volunteers on the ward – highlighting the need for paediatricians and those in leadership positions to promote playful initiatives.
If you want to share the experience and listen to the music collected during fieldwork, search for Groovy Tuesdays at a Paediatric Hospital! on Spotify or use this QR code.
Supporting children and families with rare diseases
Why the work of the British Paediatric Surveillance Unit (BPSU) Scientific Committee is so important
Dr Peter Davis Consultant
Paediatric
Intensivist
Bristol Royal Hospital for Children
Chair of BPSU Scientific Committee
February 28 each year (or February 29 in a leap year) is a date of note for the BPSU as it marks World Rare Disease Day. This is an opportunity for us to meet with others who work in the field, whether that be researchers, advocates and fundraisers for charities, or families a ected by a rare disease. But why should paediatricians take an interest in this area?
The fact is that the majority of rare diseases (75%) occur in children and over 25% of all deaths in children under five years of age are linked to rare diseases. And although you might think that these conditions are only of consequence to extremely specialist paediatric sub-specialists, the reality is that much of the workload of a general or a community paediatrician involves children with a rare disease.
The definition of a rare disease is one that a ects less than 1 in 2,000 people, which is roughly the incidence of cystic fibrosis. I’m not sure that this is what most paediatricians would think of as a rare disease, but it meets the criteria. Many rare diseases or conditions in
“The majority of rare diseases occur in children and over 25% of deaths in children under five years of age are linked to rare diseases”
children will have far lower incidences than this, but will still be familiar to many, such as Rett’s Disease, which has an incidence of around 1 in 8,500. The tendency among paediatricians is to only think of the ultra-rare as ‘rare’ when that’s absolutely not the case.
Beyond the diagnosis
However, that is not to say that there are individual children for whom the development of SWAN (Syndrome Without A Name) Clinics will not be extremely helpful, both to them and their families, especially if a diagnosis can be finally found.
Much of the news you might see around rare diseases focuses on the application of genomics and how this new way of genetic testing can provide quicker diagnoses for patients. Clearly, as noted above, a diagnosis can be extremely important, but this in itself may not provide families with what they need to understand what the future might hold for their child.
This is where surveillance studies, such as those run through the BPSU, can come into their own. However, such studies depend on having a robust reporting system and maintaining response rates.
Since the start of the COVID-19 pandemic, along with other paediatric surveillance units around the world, the BPSU has faced greater challenges maintaining response rates for our studies. Firstly, there has been an increased turnover in consultant sta ng, with both retirements and new appointments. Secondly, we use email for our monthly reporting system and there have been widespread changes in email addresses across the UK. As a result, we undertook a process of contacting (via post) those on our lists who were not
responding to the monthly emails and have subsequently been able to update our contact list. Finally, we are in the process of trying to recruit recently appointed consultant paediatricians.
How you can help
Participating in research that may benefit patients and improve the health of the population is one of the duties of medical professionals as per the latest Good Medical Practice guidance from the GMC. And, for paediatric consultants, this would include responding and contributing to the BPSU reporting system. So if you are a consultant paediatrician who is not currently receiving the monthly reporting emails, here is the link for signing up: www.rcpch.ac.uk/form/ bpsu-sign-up-ereporting
The future can feel uncertain for patients with rare diseases
Meet the changemakers
Funding from the Churchill Fellowship enabled Dr Lynn Snow and Dr Michelle Cutland to travel overseas and learn how other nations are tackling issues that affect the UK
In 2023, we were privileged to be awarded a Churchill Fellowship. It was daunting to have to live up to the expectations of being a changemaker, but exciting to have the opportunity to travel and meet others working in similar fields. It also made us smile, as we got two additional letters – CF – after our names.
Each year, the Churchill Fellowship awards grants to individuals (professionals and those with lived experience) in a range of subject areas to investigate how other countries have found solutions to an issue a ecting the UK. The idea is that we bring back learning and implement change.
If you’re feeling inspired, we encourage you to apply and join a community of changemakers: www.churchillfellowship.org
Dr Lynn Snow Designated doctor for Looked After
Children Leicester Partnership Lead RCPCH Looked After Children Lead
I investigated post-adoption depression (PAD) As an adoption medical advisor for many years, I was aware of PAD but had not seen active engagement with it as part of the adoption assessment process. The emotional health and wellbeing of adopters is a ected by having to adapt to parenting a child who has often su ered emotional trauma and may have a variety of complexities. The research suggests PAD can occur in about 8-15% of adoptions, which is very close to the incidence of postnatal depression. We know that the mental health of a carer has an impact on the outcome for the child. Through adoption disruption and safeguarding practice reviews, it was clear that the emotional impact on adopters needed to be addressed more e ectively with a multiagency and multimodal approach.
I travelled for six weeks in Europe and the US
The literature regarding PAD initially came out of the US, beginning in 1985. I attended 40 virtual meetings and travelled for six weeks in Europe (Denmark and Sweden) and the US, visiting six US states and various agencies and professionals working in adoption. I also attedended two conferences.
I learnt the importance of considering language
When crossing cultures we need to be very conscious about language. Adoption processes in other countries are quite di erent to those in the UK and I couldn’t assume that others would understand what I was looking for. I learnt the need for cultural awareness when talking about emotional and mental health, and found that practices varied between agencies. There were some very good practices at di erent stages in the adoption process, but very few agencies were working proactively to identify and manage PAD. I heard adopters voicing strong opinions that they felt the need for more direct support.
I want to increase the connection between health professionals and adoptive families
“When crossing cultures we need to be very conscious about language. Adoption processes in other countries are quite different to those in the UK and I couldn’t assume that others would understand what I was looking for”
Dr Lynn Snow visited six US states, including Arizona, to learn more about the adoption process there and the impact of postadoption depression (PAD)
I am seeking to change the adoption pathway and hope to create a public nurse health visitor pathway to assess the emotional health and wellbeing of adoptive parents. With a clear set of care packages and referral pathways, the assessment will closely align with the perinatal mental health pathway (postnatal depression) and therefore address the inequality faced by adoptive parents who do not receive this support. I want to see training for health practitioners in understanding the di erences in adoptive parenting, and the creation of a toolkit to improve psychosocial education for adopters and to support the emotional health and wellbeing challenges they face. I know this will be no small task but Churchill encourages us to think big!
Dr Michelle Cutland
Consultant Paediatrician
Clinical
Director Bristol Children’s SARC University Hospitals Bristol NHS Foundation Trust
I visited sexual assault referral centres
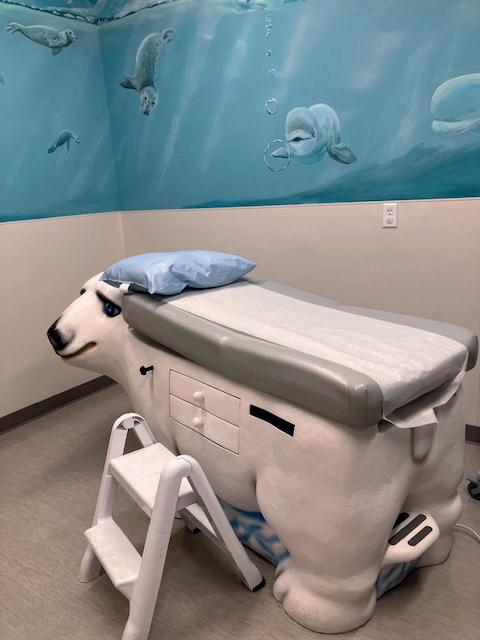
I work in the NHS as a consultant paediatrician and clinical lead for the paediatric service within a regional sexual assault referral centre (SARC). The intention of my fellowship was to visit other highincome countries with similar SARC models to see how they engage with historically marginalised communities, and in particular indigenous communities, to explore what works and what approaches and learning may be applicable in the UK. This fellowship took me to Canada and the US (Alaska) over seven weeks – with 2,000 miles of land, water and train travel!
I came across the practice of ‘cultural humility’
The first key finding was how well Canada and Alaska frame their engagement with marginalised indigenous/native Alaskan people within the historical context of colonialism and related harms. There were many examples of this grounding in the historical context that transcended practice, processes and policy.
The second key finding was the practice of ‘cultural humility’ across services. This included a curiosity and willingness to learn about and listen to cultural di erences, and an acknowledgement that people are individuals and made of ‘intersecting
“Cultural humility as a concept was not something I had come across before”
parts of a whole’. There was also courage and humility in the recognition that often these services do not hold the expertise, and should instead relinquish the role of ‘expert’ to the community they seek to support. There were numerous examples of these findings across agencies and from individuals. Cultural humility as a concept and approach was not something I had come across before, but I feel passionately that this is a core approach in health, especially in trauma-informed care.
What change do I hope to instigate?
On a personal level, I am working hard to be culturally humble! On a wider level, I have used my experiences to reflect and encourage conversation within SARC and allied services about how we better engage with historically marginalised groups that do (and often don’t) access our services. This has led to me presenting in a range of local and national forums over the past year.
Above: Denali National Park, and (left) a paediatric examination room in Anchorage, Alaska
Wellbeing Training survival tips
Dr Jessica Green shares the eight things she wished someone had told her when she started paediatric training
1 Prioritise annual leave
Dr Jessica Green Paediatric ST4 in Merseyside Ormskirk Hospital
This may sound obvious, but many people leave it late to book leave and then it becomes stressful. Chase rota sta for sending out late rotas – you should receive your rota six weeks before your placement. And remember, our contract states that employers must allow leave for a lifechanging event (for example, getting married or moving home) provided that the doctor has given adequate notice.
2 Plan active recovery on rest days
We all need time to do nothing and chill out in front of the TV after a run of long shifts. But over time I’ve found that it’s better for my wellbeing to also incorporate some activity into my downtime, whether that’s going for co ee with a friend, getting
“Over time I’ve found that it’s better for my wellbeing to also incorporate some activity into my downtime”
outside in nature for a walk or going to an exercise class.
3 Reduce financial stress
This means claiming tax deductible expenses and using your study leave budget. Exams, medical indemnity fees, Royal College memberships, GMC fees, training courses, travel/mileage, equipment (eg stethoscopes/scrubs), parking and even allowances for food are included in this. Expenses can be backdated for four years, according to HMRC. You can do this yourself or use a medical accountant who will walk you through it step-by-step. It’s worth noting that the College o ers concessions on membership fees; find out more: www.rcpch.ac.uk/membership/ renewals#concessions
4 Have a mentor
We all have formal supervisors, but a mentor is someone, usually a more experienced paediatric trainee, who has recently walked in your shoes. It tends to be a more relaxed, informal relationship than you would have with a supervisor. I have had mentors to help me with confidence in transitioning to registrar level, work-life balance and careers advice. There are a number of mentoring schemes in training regions, such as the North West Paediatric Mentoring Scheme for Mersey and Manchester.
5 Stop the ‘revenge bedtime procrastination’
This is the phenomenon I know too well: putting o going to bed to make up for lost time in the day. Have you ever got in from a long, busy shift and felt that your mind is still active? You’re scrolling on your phone and you end up going to bed too late. It’s our brain’s way of gaining back some free time but it’s not good for our sleep health. Try to create a structured bedtime routine and keep away from screens as much as possible. See the Sleep Foundation for more information.
6
Take care of your needs
Eat proper meals. Drink plenty of water.
Go to the toilet. I have been guilty of ignoring these, but it’s so important to take time out during the work day for a proper break and to eat some nutritious food. Emergencies cannot be avoided, but often things are just busy and no one thinks about your breaks, so you need to look after yourself. You’ll be a better doctor for it. Having even a few short breaks in the day can also give your mind some muchneeded downtime.
7 Engage in regular mindfulness
Some of you might already be rolling your eyes and thinking this means you need to meditate for 20 minutes a day. You don’t. Mindfulness is about being in the present, and it has been shown to reduce stress
“Often things are just busy and no one thinks about your breaks, so you need to look after yourself. You’ll be a better doctor for it”
when practised regularly. Examples may include sitting quietly for a minute to count your breaths, writing down three things you’re grateful for or focusing on an everyday task without distraction – such as cooking. There are plenty of apps to help with mindfulness. Headspace is free for NHS workers and I’ve found it useful during stressful times.
8
Set boundaries
Mute those WhatsApp groups when you’re not in work, don’t check work emails when you’re on annual leave and don’t feel pressured to engage in workrelated activities if you’re not on study leave or a CPD day. We know that being a doctor is a vocation, and we all care about our patients, but remember there is 24hour cover and we have to hand over to our amazing colleagues.
I also want to give an honourable mention to having a good support system. This will help with every one of the points listed above. It’s so important that we take time for people we love and allow them to take care of us, because we spend so much of our time looking after others.
An insight into life as a young carer
Libby Henstridge urges health professionals to treat young carers and their families with the respect they deserve
Libby Henstridge
Age 15 at time of writing
Did you know, around a million young carers are registered in the UK? Yes, a million people under the age of 18 dedicate their time, care and support to a family member who has a disability or misuses alcohol or drugs. This means a million young people potentially face the day-to-day stigma attached to caring and the mental toll that can come with it. This article aims to help break those stigmas.
Despite being unaware to begin with, I have been registered as a young carer with Barnardo’s – the charity that supports children and young people – since I was five. Over time, as my responsibilities grew, I realised the heart-wrenching truth that my childhood wasn’t like that of other kids my age.
My dad had a car accident
It was a couple of years before I was born and he slipped two discs in his back. The discs lodged into his sciatic nerve, and when the doctors tried to remove them they tore the nerve, so he woke up in more pain than when he went under anaesthetic.
As I grew older, Dad grew worse. He was no longer able to pick me up on his shoulders, chase me up the stairs or even drive me to school. Instead, it was me holding him up without his crutches, following him around in case he fell and pushing him to appointments in his wheelchair. As many as one in five children in the UK have similar roles and might feel isolated from their peers and even be jealous of the life they think
“Young carers’ paths are already lit by the brightness of their bravery”
their peers may have. This is the negative side of being a young carer – 38% of us develop mental health issues due to the strain. The pressure that being a carer can apply to the delicate shoulders of children is like carrying the weight of a world that’s against you. When I was growing up, I remember feeling so sick, so gut-stabbed, when I could see my dad struggling just to make me happy. He would try to do a silly dance or prove that he could lift me.
On the outside, I would have to give him the satisfaction he was desperate for, so I’d
smile or giggle. But on the inside, I’d wish and I’d wish and I’d wish that I could take away the pain even for just five minutes so I could enjoy a laugh with him.
Navigating disability
Gradually, the pain became worse and Dad lost the ability to control his legs or his lower half, so he now has a colostomy bag and a wheelchair. But can’t he walk? I hear you ask. Well, yes, he can. My friends don’t usually see him in his wheelchair due to his embarrassment. Due to the stigmas around disabilities, my dad would rather struggle than be shown sympathy and would rather be in bed recovering for a few days than spend a couple of hours in a wheelchair.
Society suggests that being disabled makes someone less valid, less important
Libby has been registered as a young carer for her dad, Lee, since the age of five and her responsibilities have grown over the years
and less human. It assumes being disabled is a weakness – and in some aspects, like sustaining employment, it is – but in most cases it makes my dad an inspiration. For example, despite the pain, he never fails to make people laugh, never fails to support me when I need it and always motivates me to make the most of life no matter how hard it gets. My dad is a role model, a true hero to those who may not have an easy life –and to those who do.
Don’t you wish you had a normal life?
People ask me this question, and the answer depends on how you define normal. My normal is coming home, checking on Dad, ensuring he’s had his medication, making dinner, doing the washing up… but I wouldn’t change it for the world. I still have time to see my friends, plus the satisfaction that he’s okay and that I’ve fulfilled my role.
“You might consider being a young carer a burden, yet to me, it’s a window to gain the ability to combat the burden of life itself”
Although some young carers don’t realise it, we have skills that prepare us for life. You might consider being a young carer a burden, yet to me, it’s a window to gain the ability to combat the burden of life itself. In particular, the challenges life throws at you and the pathways you have to discover to navigate new experiences and unexpected challenges. Young carers’ paths are already lit by the brightness of their bravery.
As young carers, we need to not only accept our role but love our role – which is to give our family members the best
care possible. If you switched shoes with my dad, would you want sympathy when what you really want is to show your daughter that you’re strong? Or, if you switched roles with me, could you imagine feeling so helpless when your beloved dad is in absolute agony due to society’s belief that asking for help is a sign of weakness?
People assume our relationship as a family is like walking on eggshells, whereas in reality we are the chicks trying to break the shell of the stigmas that young carers and their families face. So, the next time you see a young carer and their disabled family member, don’t think of them as disabled. Think of them as abled di erently. See them as abled with perseverance, bravery and conscientiousness. Treat them with the respect they deserve as a human not as a victim of their disability. Don’t feel sorry for the young carer, feel proud that some of this generation still cares. See their bravery, not the ‘burden’.
Lee rarely uses a wheelchair, preferring to hide his struggles from other people
The latest member news and views
Creative writing
Dr Helen Chitty Consultant Neonatologist
The James Cook University Hospital, Middlesbrough Paediatric Training Programme
Director for NHSE North East
I love creative writing and use it as a means of integrating creativity into my experiences at work. This piece was inspired by the joy I have in seeing our remarkable little patients in neonatal follow-up clinic. It’s a privilege to do a job that combines such wonderful humanity with medical assessment and I hope that is reflected in this piece.
You beam a beautiful smile as your father carries you across the waiting room. “Hello little one. Look at you now.” Twice the size. Radiating life. “Come on through. We’re in the room at the end of the corridor. Have a seat. Thank you for coming.”
Perched upright on your father’s knee, you observe me carefully as we take each other in. With a poker straight back, you hold your moon-shaped head high, no wobbling. You listen to me talk, fascinated for a minute or two before shifting your gaze to the ophthalmoscope on the wall, the blood pressure machine on the cabinet, the sink, the mirror. Like many of my little patients, you become enthralled by the ceiling’s fluorescent strips of electric lights.
I marvel at your development, your change from newborn to six-month-old infant. You are still dependent on the adoring parents who orbit around you but you are now able to communicate your needs, sit up, grab hold, play with your feet. Everything goes into your mouth, your current method of exploring
KEEP IN TOUCH
We’d love to hear from you, get in touch through our channels X @RCPCHTweets Facebook @RCPCH Instagram @RCPCH milestones@rcpch.ac.uk
the world and giving it meaning. You trace a large red Lego block with your fi ngers, creating neural pathways that will become embedded, enabling the future you to build towers, connect pieces, judge sizes, perceive outcomes.
Do you remember me? I doubt it but I will never know. Do you recall the prodding and poking, the holding and checking, the pressing and needling? I like to think that you don’t as you probably wouldn’t be smiling at me right now if you did.
I talk to your parents and learn about the ups and downs, the trials and tribulations, the tears and the triumphs. I attempt to examine you but you do not want me to. You look anxiously at your parents, quickly moving from fretful watching to moaning restlessness. No examination today, thank you doctor.
Despite this, you have shown me almost
everything I need to know and your parents have fi lled in the gaps. You are healthy and developing well. A quite remarkable feat given the challenging start you had. My team and I helped you through those early days but the rest of it, the real hard work of recovery, growth and transformation has been done by you and your parents.
You beam at me again as we say our goodbyes. “Credit goes to you all. She’s doing so well. I don’t need to see her for another six months. Bye bye.” You are not quite done. One more thing to tell me. You fi x me with your gaze and whisper “Bah bah. Bah bah.” Barely a sound. A hushed vocalisation, but a defi nite intention to form your lips, tongue and throat into coordinated movements to say goodbye.
Until next time.
Dr Ashish Patel
Consultant
Paediatric
Nephrologist
Leeds Children’s Hospital
@DrKidneyAsh
Lemon poppy seed muffins
Celebrate spring with a citrus-flavoured bake
Spring is here! I’m so glad the days are becoming longer and brighter. This time of year is a struggle for many – it’s also arguably the busiest time at work, so keep an eye on your colleagues and loved ones and check in with them regularly. Maintaining your wellbeing is also very important and what better way than through the medium of baking?
This quarter I have turned to my favourite flavour – lemon! You can’t go wrong with a lemon bake. The poppy seeds add a bit of nutty flavour to cut through the citrus. A wonderful pick-meup with your late-morning co ee!
Ingredients
• 375g plain flour
• 125g granulated sugar
• 30g poppy seeds
• 1 tbsp baking powder
• ½ tsp bicarbonate of soda
• ½ tsp salt
• 190g plain yoghurt
• juice of 2 lemons
• grated zest of 2 lemons
• 2 large eggs
• 120g unsalted butter (melted)
For the glaze
• 30g granulated sugar
• 30g lemon juice
• sugar, for sprinkling
Instructions
1. Preheat your oven to 180ºC (fan-assisted). Line a mu n tray with 12 mu n cases or just grease the mu n tray without cases.
History taking: In the end, we are all fruit
Dr Richard Daniels
Paediatric registrar
St Mary’s Hospital
@DrRDaniels
In 2002, I went on a date. Probably one of my first and it didn’t really have legs. However, we went to see a film that was to become a cult favourite, My Big Fat Greek Wedding, and it was patriarch Gus Portokalos – in my opinion the true hero of the story –who came to mind when I was asked to ruminate
on the origins of the word ‘paediatrics’.
If you’re one of the eight people who have yet to see this cinematic masterpiece, loveable Gus relates everything to the Hellenes. So while writing this, I had the ghost of Gus and the Ancient Greeks on my shoulder. Here’s the summary: ‘paed’ is derived from ‘pais’ – Greek for child; ‘iatrics’ comes from ‘iatros’ – Greek for doctor or healer. So the word simply means ‘healer of children’.
2. Mix the dry ingredients (flour, sugar, poppy seeds, baking powder, bicarbonate of soda and salt) in a large mixing bowl.
3. In a separate bowl, whisk together the yoghurt, lemon juice, lemon zest and eggs until smooth.
4. Combine the wet and dry ingredients and fold together. Add the melted butter and fold until combined – don’t overmix!
5. Divide the batter equally between the 12 mu n cases. Bake in the oven for 20-25 minutes until golden brown and a toothpick comes out clean.
6. Simmer the sugar and lemon juice together on the hob to make the lemon syrup glaze. Brush the glaze over the mu ns and finish each one with a sprinkle of sugar.
However, paediatrics as a concept also dates from antiquity. Hippocrates, Galen and many others from across the ancient world discussed the need for a separate approach to treating children. Medieval European textbooks exist on the topic – a future column may look at this. However, the term ‘paediatrics’ as a medical specialty, like much in the way of nomenclature, dates from the 19th century.
German-Jewish physician
Abraham Jacobi, a friend of Marx and Engels, moved to New York where he advocated for child health and was appointed to a professorship in 1861. Here, he coined the term ‘paediatrics’, riding the zeitgeist, although ironically, his successors in the US now use ‘pediatrics’. Heathens. That should be the limit of Mr Portokalos’ influence on your practice, though. Please check BNFC for the appropriate dose of Windex.
Can you recognise and respond to possible child abuse or neglect?
Dr Ruth Skelton Consultant Paediatrician
Designated doctor for Child Protection
Bradford Teaching Hospitals NHS Foundation Trust
Children must be protected from possible child abuse and neglect, which is why child protection training is essential to the ongoing career of a paediatrician.
Advanced Life Support Group (ALSG) provides the internationally recognised Child Protection: Recognition and Response (CPRR) course, which has been developed for doctors in training ST1-ST3. It teaches clinicians to recognise indicators of possible abuse and neglect and how to respond, including talking to carers and professionals.
This internationally recognised course teaches clinicians to recognise signs and symptoms of the possible range of abuse and neglect in children of all ages. It also trains candidates to respond competently and confidently via role play and interactive face-to-face training to help them use their knowledge.
Candidates appreciate the safe space the course provides, in which they can discuss how they feel about this potentially
di cult subject. It also ensures candidates understand the referral process around safeguarding through practical examples as well as the importance of follow-up to a child’s health and developmental outcome. Apply to become a CPRR centre and once your new centre form has been processed and approved, you’ll be contacted by ALSG with the details of your ALSG centre account and the practical next steps to running a course.
At this point, you’ll be given access to all
Book
review: Dexter Procter by Adam Kay
Aged 11
This story is about a 10-year-old boy who is a doctor. When he was at school aged two, he was criticised because of his young age but managed to make two friends – and an enemy. When he qualified as a doctor, he met his greatest enemy, Dr Edwin Drake. He got fired and went back to school but all the teachers had caught a serious illness. Whoever figured out the cause would get whatever they wanted. Dexter was desperate to get his job back, so disguised himself as Dr Pluto but was caught out, so his plan failed. At a school football game,
the resources you need to approve and run your child protection course – while we o er support around the administration involved in getting your course set up. ALSG courses must be approved at least two months before they begin, so it’s essential to plan and prepare in advance.
Book a course: https://bit.ly/Book_CP
Apply to become a CPRR centre: https://bit.ly/CPRRCentre
he discovered the illness was caused by a teacher who made cakes on someone’s birthday, because he never washed his hands (because of allergies). Dexter got his job back.
Dexter Procter is an amazing book with a funny twist of events. It’s also relatable, emotional and gross. It has an amazing and inspirational main character (Dexter), and his friends (Otto and Rupi) and his two enemies (Dr Drake and his nephew) also make this a great read. The moral of the story is that it’s good to be unique and different.
Oscar Gray
Starter for ten
We put 10 questions to a consultant paediatrician and their paediatric trainee
Dr Emily Sivers
Consultant General Paediatrician with an interest in metabolic medicine
University Hospitals Leicester @DrEm_Siv
1. Describe your job in three words Challenging, rewarding, busy.
2. After a hard day at work, what’s your guilty pleasure? Playing family games on our Xbox – PlateUp! is our favourite at the moment.
3. What’s the best part of your working day? Moments of great team-working, whether in helping an acutely unwell child or coming together as an MDT towards a common goal. I love how each person I work with brings their unique input.
4. The best advice you received as a trainee? That sometimes we don’t know the answers straight away and that’s OK! Take time to let things marinate, especially if it’s your ward week and by the end of the week you’ll often see breakthroughs.
5. Who’s the best fictional character of all time – why? Han Solo. He didn’t have the Force, but was courageous and brave… with attitude!
6. Name 3 medications you would want if marooned on a desert island filled with paediatric patients Calpol, co-amoxiclav and gaviscon. Tough question!
Dr Louise Ingram
ST8 Paediatric Registrar, Adolescent SPIN
University Hospitals Leicester @drlouiseingram
1. Describe your job in three words Fascinating, satisfying, exhausting!
2. After a hard day at work, what’s your guilty pleasure?
Knitting while watching TV with my husband.
3. What’s the best part of your working day? Hearing a family out – letting them tell me their worries and helping them to understand what’s going on with their child.
4. The best advice you received as a trainee?
Some people like to have lots of things going on at once, your life and your to-do list don’t have to look like everyone else’s.
5. Who’s the best fictional character of all time – why? I can’t answer this! I adore reading, I read more than 100 books last year and it’s like you’re asking me to choose between my children! Maybe Louise Penny’s Inspector Armand Gamache, he listens and pays attention and tries to always act with kindness and integrity.
6. Name 3 medications you would want if marooned on a desert island filled with paediatric patients Paracetamol, salbutamol and co-amox.
7. Choose a superpower – what would it be and why? Can I pick wizardry? So much potential in magical powers!
8. Any advice you’d give yourself as a medical student? That sometimes opportunities need to be sought, but they can be found. Not everything will present itself to you.
9. What do you do to ensure you can Thrive at work? Work-life balance is so important. Doctors who rest well come back ready to be engaged and excited for what impact they can make.
10. How can you and your colleagues inspire the next generation of paediatricians? By sharing the joy that our patients bring us. Where else can you change someone’s journey in hospital by pretending to be Elsa and playing with dinosaurs? Or go from being with a brand-new human, to discussing the meaning of life with a year 11?
7. Choose a superpower – what would it be and why? Endless ener ! I have so much to do every day that some good things have to get left undone.
8. Any advice you’d give yourself as a medical student? There isn’t one way to go through training and work as a doctor. Training paths and careers have so many options and detours can be the most interesting parts!
9. What do you do to ensure you can Thrive at work? I have really clear red lines about what I will and won’t do outside of work. That gives me time to rest and enjoy the rest of my life, which in turn makes me a better doctor.
10. How can you and your colleagues inspire the next generation of paediatricians? Learn about them and help them to find their unique contribution to the field of paediatrics.
A day in the life
“For too long we have concentrated on physical health”
Dr Camilo Stargardter
Senior Paediatric Clinical Fellow in Children’s A&E, University College London Hospitals SPIN Mental Health
Trainee Psychodynamic Psychotherapist for children, young people and families
In much the same way that it’s hard to describe a ‘typical’ paediatric patient, it’s also hard to pin down a ‘typical’ work day. There’s such variation in terms of what each day may bring in general paediatrics – that’s what probably draws many of us to it! But there must be some common denominators. For me, that’s starting each morning with a coffee while listening to Today on Radio 4, before cycling through the streets of central London to work.
For the past two years, I have been undertaking a masters in child psychotherapy. This involves one day a week studying in person, as well as seeing clinical cases for weekly psychotherapy. Mornings are spent in A&E. I’m lucky to work in a great and supportive department where extracurricular interests are supported. I could spend the shift leading calls in resuscitation, stitching a child’s head or supporting junior staff members with their cases. One of the exciting things about working in A&E is that ‘anything and everything’ can walk through the door. We also have multidisciplinary team meetings, such as the weekly emergency department safeguarding meeting, where all psychosocial cases are discussed.
After my A&E shift, I assume my other role as a trainee psychotherapist. My clients are paediatric and adolescent patients who have been offered psychotherapy to help process the difficulties of living with a medical condition. Some I see weekly for up to a
When I finish work
A recent film recommendation is Inside Out 2 (and the original, for that matter). Anyone who wants to see a beautifully creative depiction of mental health and the mind should look no further.
year, others for just a few weeks.
Retraining in a new discipline can be challenging. As paediatricians, we tend to interact with patients and parents in a didactic and performative manner. We seek to promptly ascertain objective facts about their illness through a succinct history and brief examination. We then relay our findings and impressions with authority. The practice of psychotherapy is different. There are relatively few certainties in matters of the mind and the therapist must work with this uncertainty
and actively engage the unconscious part of the patient’s mind.
Through sessions with patients and supervision, we make theories about the patient’s unconscious processes, then tailor our communication to help them understand their minds better. It is theoretically complex, practically challenging and anxiety-inducing. But the benefits are many. The deep connection made in therapy and the feeling of care and empathy for the client is more than any I have experienced in paediatrics. Indeed, many of the skills are directly applicable to paediatrics. Paediatricians frequently have to reassure parents of relatively well children. What is reassurance if not a therapeutic intervention, aimed to reframe the way parents perceive their child’s health? However, the greatest impact psychotherapy training has had on my career is my communication with children.
Paediatricians see many young people with mental health problems. For too long we have concentrated on physical health, subcontracting their mental health to CAMHS or Crisis team nurses. We cannulate and prescribe N-acetylcysteine (NAC), but the real pathology in their life is left untreated. However, we see these young people when they present in a mental health emergency, and this interaction is a therapeutic opportunity. Gaining the skills, experience and confidence to have the right conversation at the right time to help these young people should be a focus of all paediatricians.