10 minute read
Lumbar Muscle Health

Importance in Spine Surgery
Skeletal muscle plays an important role in movement, perfusion, nutrient storage, and stability.[1] Additionally, muscle health has been indicated as a potential marker of how fitness increases the quality of life, including better surgical outcomes and recovery.[2,3] Postoperatively, skeletal muscle plays an important role in bone healing by promoting revascularization with the provision of stem cells.[4] Like other skeletal muscles, lumbar muscle groups play an important role in movement, stability, perfusion, and nutrient storage.[1] Additionally, good muscle health, when coupled with regular resistance training and exercise, is generally associated with reduced injury and better overall health.[5-7] Hence, it is crucial to explore and understand the role of lumbar muscle health in patients undergoing spine surgery.
Lumbar Muscle Groups: Functional Anatomy
The lumbar spine is surrounded by numerous muscles that are typically grouped based on position and function.[8,9] The major functional muscle groups consist of the extensors, flexors, lateral flexors, and rotators.[10] The extensors are posterior to the lumbar spine, which consists of the erector spinae and multifidus muscles.[8,9] The flexors arise from the anterolateral aspect of the lumbar spine, and this includes the psoas major and the abdominal muscles (internal/external oblique, transversus abdominis).[9,11] Coordination by several muscles, including the quadratus lumborum, psoas major, multifidi, and the abdominal musculature, create trunk rotation and lateral flexion and provide support for the low back.[10,12,13]
Radiological Assessment and Validation
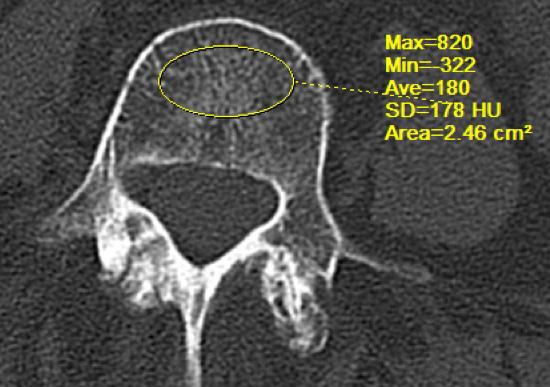
Recent evidence suggests that evaluating the psoas and paralumbar muscles provides a comprehensive understanding of muscle health and is supported by 2 validated methods: the Goutallier classification (qualitative assessment) and the total cross-sectional area (TCSA; quantitative assessment), with or without considering the fat infiltration.14-16 The Goutallier classification based on the qualitative assessment of fatty degeneration is defined as follows: 0 = no intramuscular fat, 1 = minimal to no fatty streaks, 2 = fat evident but less than muscle tissue, 3 = equal amounts of fat and muscle, and 4 = higher quantity of fat than muscle.[17,18] On the other hand, TCSA is commonly measured on a magnetic resonance imaging slice at the upper endplate level of L4 vertebrae quantitatively, which has shown higher reliability compared to measuring at the other levels.[19,20] It is taken as an average of left and right muscles, measured meticulously by manually outlining the innermost fascial border surrounding them.[16,17,18] The literature suggests that fat infiltration (FI) is associated with axial back pain and disability.[16,21]
For the assessment of the psoas muscle, the Goutallier classification is indicated for the qualitative assessment of the muscle mass. Additionally, for the qualitative measurement, the normalized total psoas area (NTPA), is calculated as TCSA divided by the square of patient height as defined in the literature.[17,19] On the other hand, the paralumbar muscle assessment consists of Goutallier grading for the qualitative measurement along with the normalized muscle area defined as TCSA divided by the body mass index (quantitative assessment).[16-18,22] Furthermore, the volumetric analysis of the paralumbar muscles is performed using the lumbar indentation value, which is defined as the minimum distance between the coordinates connecting the bilateral paralumbar muscle bulges and the top of the spinous process.[17,18]
From Bench to Bedside Importance in Lumbar Decompression Surgery
The relationship between lumbar muscle health and the outcomes of decompression surgeries has been the subject of several studies. Song et al conducted a study to evaluate the impact of muscle health on the outcomes of lumbar microdiscectomy. The study included 163 patients, and the results indicated that patients with poorer muscle health took longer to achieve minimal clinically important differences, although they eventually achieved them at similar rates. The study also found that a lower psoas TCSA normalized by height was weakly correlated with greater improvements in pain scores, while the paralumbar TCSA normalized by body mass index positively correlated with changes in physical function. These findings suggest that preoperative lumbar muscle health may influence the recovery and time to achieve functional improvements after lumbar microdiscectomy.[17] In another study by Zotti et al, it was discovered that a reduced cross-sectional area of the lumbar multifidus muscle and muscle atrophy was associated with less favorable outcomes after lumbar spinal decompression surgery.[23] However, not all studies have found a significant relationship between preoperative muscle health and surgical outcomes. Chen et al explored gene expression profiles in paralumbar tissues from patients with lumbar disc herniation who underwent microdiscectomy surgery. The study revealed that patients with poor surgical outcomes had a lower expression of brain-derived neurotrophic factor in the deep multifidus muscle and higher expression of interleukin-1β in subcutaneous fat. These findings suggest a potential relationship between impaired muscle regeneration and inflammatory dysregulation in subcutaneous fat with poor surgical outcomes following microdiscectomy for lumbar disc herniation.[24]
Importance in Lumbar Fusion Surgery
Recent advances have explored the effect of lumbar muscle health on functional outcomes in patients undergoing spinal fusion procedures. Urakawa et al conducted a retrospective study on a group of patients undergoing posterior lumbar surgery with transforaminal lumbar interbody fusion and posterolateral fusion. In a total of 212 patients, it was found that a low NTPA was associated with worse postoperative clinical outcomes. In addition, low NTPA was reported as an independent predictor of failure to reach minimal clinically important differences in the Oswestry Disability Index and visual analog scale for leg pain.[19] In another study, Bokshan et al investigated a subset of patients undergoing thoracolumbar fusion surgery and reported that patients with a low psoas cross-sectional area at the L4 vertebrae have a significantly increased risk of longer length of stay, in-hospital complications, referral to rehabilitation facilities, and mortality.[25] Akin to this, Zakaria et al demonstrated psoas muscle size to be a sensitive predictor for postoperative complications in patients undergoing posterior lumbar surgeries, including fusions. On the other hand, the paralumbar muscle group was not found to predict postoperative morbidity in patients undergoing fusion surgeries.[20]
However, not all studies have found a significant association between lumbar muscle health and postoperative outcomes. Wang et al investigated the association between preoperative paralumbar muscle degeneration and the development of adjacent segment disease (ASD) following posterior decompression and instrumented fusion for degenerative lumbar disorders. They did not identify preoperative paralumbar muscle degeneration as a statistically significant risk factor for ASD. These findings suggest that while poor lumbar muscle health may impact certain outcomes, it may not play a significant role in the development of ASD following decompression surgery.[26]
Barile et al conducted a study in a cohort of 308 patients undergoing posterior spinal fusion surgery and compared the influence of osteopenia and sarcopenia on the postoperative infection rate. It was found that osteopenia (MRI-based M-score) rather than sarcopenia (validated psoas to lumbar vertebral index) was an independent risk factor for postoperative surgical site infection in patients after spinal fusion surgeries.[27] Additionally, in older patients undergoing elective lumbar spine surgeries, sarcopenia (as measured by NTPA) was not found to be a reliable predictor of acute perioperative complications.[28]
Summary
The existing research suggests that there is a positive relationship between lumbar muscle health and postoperative outcomes in certain contexts. Poor muscle health, characterized by reduced cross-sectional area, muscle atrophy, and altered gene expression, may lead to slower recovery, delayed achievement of functional improvements, and less favorable outcomes following lumbar decompression
Patient Fitness
and fusion surgeries. However, the impact of muscle health on specific outcomes may vary, and more research is needed to further elucidate the complex relationship between bench (preoperative muscle health) and bedside (postoperative outcomes) in the context of lumbar muscle health and spine surgery.
References
1. McCuller C, Jessu R, Callahan AL. Physiology, skeletal muscle. StatPearls https://www.ncbi.nlm.nih.gov/books/ NBK537139/. Published April 28, 2023. Accessed June 28, 2023.
2. Sui SX, Williams LJ, Holloway-Kew KL, Hyde NK, Pasco JA. Skeletal muscle health and cognitive function: a narrative review. Int J Mol Sci. 2020;22(1):255.
3. Myers JN, Fonda H. The impact of fitness on surgical outcomes. Curr Sports Med Rep. 2016;15(4):282-289.
4. Shah K, Majeed Z, Jonason J, O’Keefe RJ. The role of muscle in bone repair: the cells, signals, and tissue responses to injury. Curr Osteoporos Rep. 2013;11(2):130-135.
5. Burtscher J, Strasser B, D’Antona G, Millet GP, Burtscher M. How much resistance exercise is beneficial for healthy aging and longevity? J Sport Health Sci. 2023;12(3):284-286.
6. Walters BK, Read CR, Estes AR. The effects of resistance training, overtraining, and early specialization on youth athlete injury and development. J Sports Med Phys Fitness . 2018;58(9).
7. Gabbett TJ. The training—injury prevention paradox: should athletes be training smarter and harder? Br J Sports Med. 2016;50(5):273-280.
8. Gilchrist RV, Frey ME, Nadler SF. Muscular control of the lumbar spine. Pain Physician. 2003;6(3):361-368.
9. Hansen L, de Zee M, Rasmussen J, Andersen TB, Wong C, Simonsen EB. Anatomy and biomechanics of the back muscles in the lumbar spine with reference to biomechanical modeling. Spine . 2006;31(17):1888-1899.
10. Sassack B, Carrier JD. Anatomy, back, lumbar spine. StatPearls StatPearls Publishing; 2023.
11. Bogduk N. Clinical Anatomy of the Lumbar Spine and Sacrum. Elsevier Health Sciences; 2005.
12. Andersson EA, Grundström H, Thorstensson A. Diverging intramuscular activity patterns in back and abdominal muscles during trunk rotation. Spine . 2002;27(6):E152-E160.
13. Akuthota V, Nadler SF. Core strengthening. Arch Phys Med Rehabil 2004;85(3 Suppl 1):86-92.
14. Touban BM, Pavlesen S, Smoak JB, et al. Decreased lean psoas cross-sectional area is associated with increased 1-year all-cause mortality in male elderly orthopaedic trauma patients. J Orthop Trauma. 2019;33(1):e1-e7.
15. Morrell GR, Ikizler TA, Chen X, et al. Psoas muscle cross-sectional area as a measure of whole-body lean muscle mass in maintenance hemodialysis patients. J Ren Nutr. 2016;26(4):258-264.
16. Gibbons D, McDonnell JM, Ahern DP, et al. The relationship between radiological paralumbar lumbar measures and clinical measures of sarcopenia in older patients with chronic lower back pain. J Frailty Sarcopenia Falls. 2022;07(02):52-59.
17. Song J, Araghi K, Dupont MM, et al. Association between muscle health and patient-reported outcomes after lumbar microdiscectomy: early results. Spine J. 2022;22(10):1677-1686.
18. Tamai K, Chen J, Stone M, et al. The evaluation of lumbar paralumbar muscle quantity and quality using the Goutallier classification and lumbar indentation value. Eur Spine J. 2018;27(5):1005-1012.
19. Urakawa H, Sato K, Vaishnav AS, et al. Preoperative cross-sectional area of psoas muscle correlates with short-term functional outcomes after posterior lumbar surgery. Eur Spine J. 2023;32(7):2326-2335.
20. Zakaria HM, Schultz L, Mossa-Basha F, Griffith B, Chang V. Morphometrics as a predictor of perioperative morbidity after lumbar spine surgery. Neurosurg Focus. 2015;39(4):E5.
21. Teichtahl AJ, Urquhart DM, Wang Y, et al. Fat infiltration of paralumbar muscles is associated with low back pain, disability, and structural abnormalities in community-based adults. Spine J. 2015;15(7):1593-1601.
22. Virk S, Wright-Chisem J, Sandhu M, et al. A novel magnetic resonance imaging-based lumbar muscle grade to predict health-related quality of life scores among patients requiring surgery. Spine. 2020;46(4):259-267.
23. Zotti MGT, Boas FV, Clifton T, Piche M, Yoon WW, Freeman BJC. Does pre-operative magnetic resonance imaging of the lumbar multifidus muscle predict clinical outcomes following lumbar spinal decompression for symptomatic spinal stenosis? Eur Spine J. 2017;26(10):2589-2597.
24. Chen X, Hodges PW, James G, Diwan AD. Do markers of inflammation and/or muscle regeneration in lumbar multifidus muscle and fat differ between individuals with good or poor outcome following microdiscectomy for lumbar disc herniation? Spine. 2020;46(10):678-686.
25. Bokshan SL, Han AL, DePasse JM, et al. Effect of sarcopenia on postoperative morbidity and mortality after thoracolumbar spine surgery. Orthopedics. 2016;39(6).
26. Wang H, Ma L, Yang D, et al. Incidence and risk factors of adjacent segment disease following posterior decompression and instrumented fusion for degenerative lumbar disorders. Medicine. 2017;96(5):e6032.
27. Barile F, Ruffilli A, Fiore M, et al. Is sarcopenia a risk factor for postoperative surgical site infection after posterior lumbar spinal fusion? Int J Spine Surg. 2022;16(4):735-739.
28. Charest-Morin R, Street J, Zhang H, et al. Frailty and sarcopenia do not predict adverse events in an elderly population undergoing non-complex primary elective surgery for degenerative conditions of the lumbar spine. Spine J. 2018;18(2):245-254.
AUTHORS
Nishtha Singh, MBBS
Amy Z. Lu, BS
Kasra Araghi, BS
Maximilian K. Korsun, BS
Tomoyuki Asada, MD
Sheeraz A. Qureshi, MD, MBA
From the Hospital for Special Surgery in New York, New York (all authors), and from the University of Tsukuba, Institute of Medicine, Department of Orthopedic Sugery in Tsukuba, Japan (Dr Asada).