Living Well with Myeloma: Infection Prevention and Management
Heather Cooper Ortner
Incoming President & CEO International Myeloma Foundation
“I am humbled to serve alongside so many who are making a difference every day for patients and families affected by myeloma, and I look forward to building on the IMF’s legacy of impact”
Thank you to our
sponsors!
Workshop Video Replay & Slides
As follow up to today's workshop, we will have the speaker slides and a video replay available.
These will be provided to you shortly after the workshop concludes and posted to our website under “IMF Videos”
WHY
ARE INFECTIONS SO COMMON IN MYELOMA?
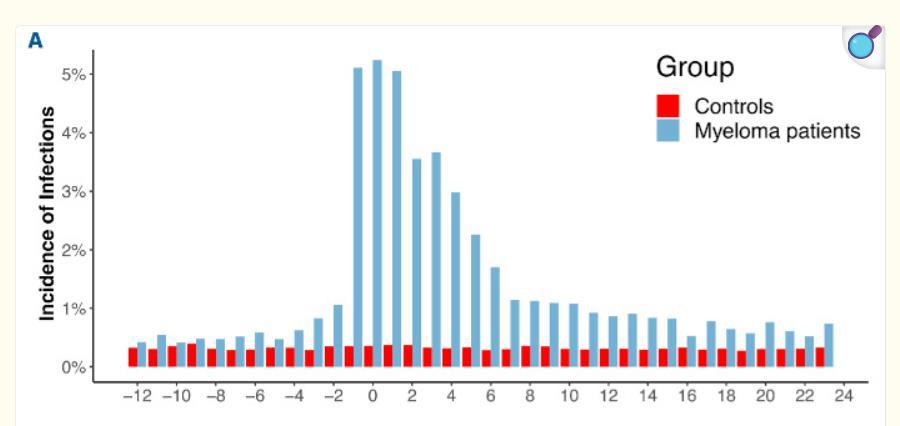
Incidence of infections in myeloma (MM)
1) The incidence of infection in multiple myeloma (MM) patients is high, with a risk up to 5-7x greater than the general population
2) Greatest risk during the first year after diagnosis, with the risk of infections up to 70% and severe infections at 28% in some studies
3) Specific treatments for MM can lead to disease related and immune system deficiencies, which increase susceptibility to infections
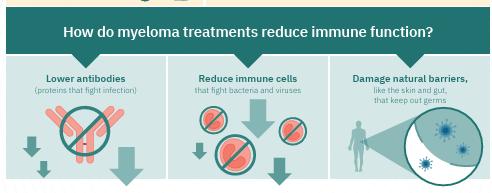
Why infections are common in myeloma (MM)
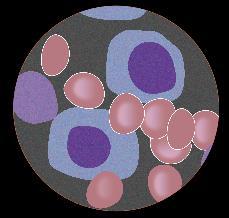
Biology of Disease
MM cells replace healthy plasma cells
Role of Plasma cells
Specialized immune cells that produce and secrete large quantities of antibodies to fight specific infections and foreign substances
Treatment
Side Effects treatments given can lower the number of healthy white cells such as “neutrophils” , further susceptible
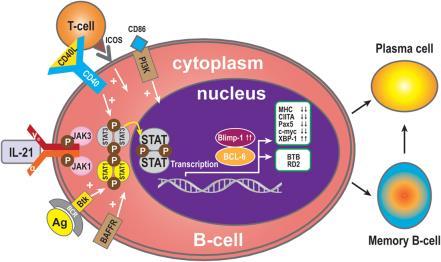
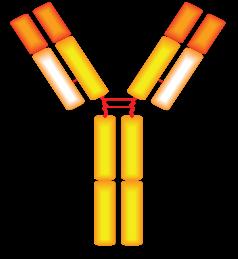
Immunoglobulin (Ig)cells
•Immunoglobulin (Ig) cells are Yshaped proteins produced by plasma cells, recognize and bind to specific foreign substances (“antigens”)
Bone marrow aspirate
Immunoglobulins consist of 2 heavy chains and 2 light chains
•Neutralize and eliminate foreign viruses, bacteria and pathogens once bound, tagged for destruction
•IgG, IgA, IgM, IgD and IgE
•Immune response activation and prevent foreign invaders from entering cells
Ig = immunoglobulin, M = myeloma.
Khouri J, et al. Cleve Clin J Med. 2019;86(1):39-46.
•Immune memory after infection
Plasma cell
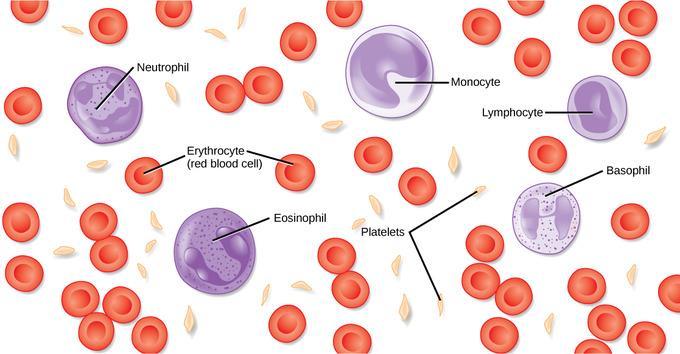
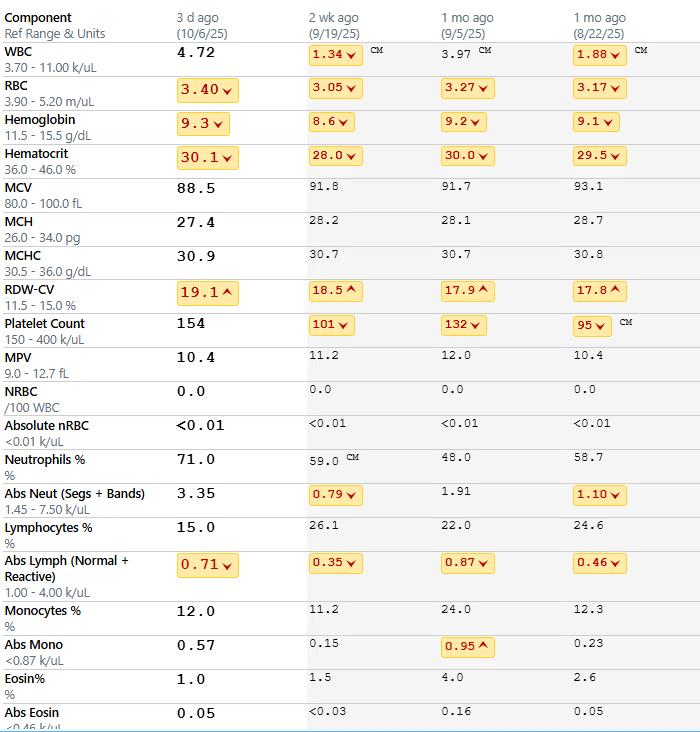
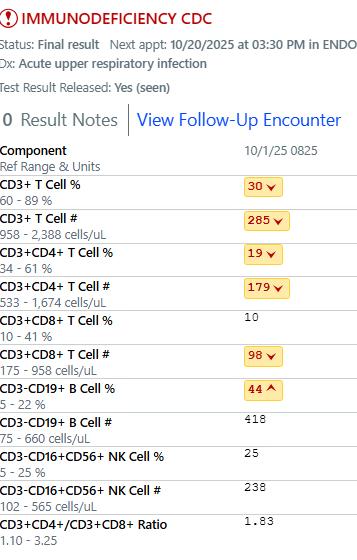
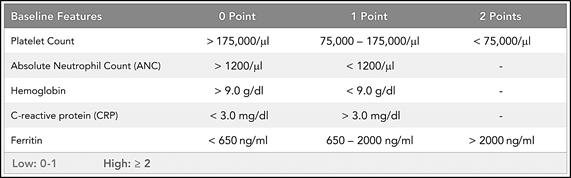
Common Measures of Immune Function: CBC
White Cells fight infection
Hemoglobin carries Oxygen
Platelets Blood clotting
Neutrophils help your immune system fight infections and heal injuries
Lymphocytes fight viral infections
• The CBC test is a window into your body’s ability to make healthy red cells, white cells and platelets, measured in the peripheral blood stream.
• Low white cells can cause a variety of infections, particularly neutrophils
• Low lymphocytes place you at risk for viruses
“Hypogammaglobulinemia”
Low immunoglobulin levels from the disease, treatment places one at risk for infection
Lab values vary slightly amongst institutions and laboratories
⚫ Patients undergoing certain types of transplants, CART-cell therapy, or treatment with bispecific antibodies will have even lower immune systems than with standard treatment
⚫ Tests for hepatitis, cytomegalovirus, or immunodeficiency panels will often be checked by your providers.
⚫ Risk is at any time during therapy
⚫ Earliest in the beginning, then later in the disease
⚫ Age, health concerns, and prior infections increase risk
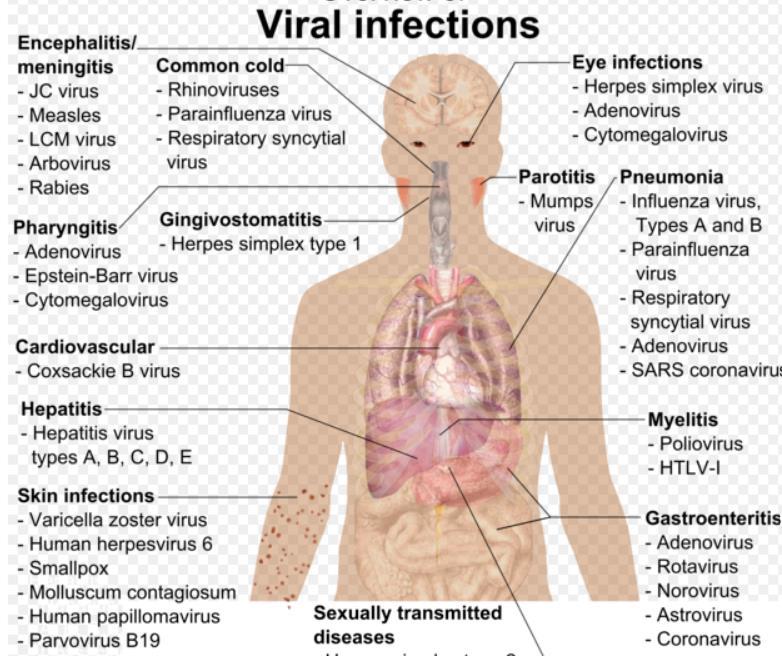
⚫ Types:
⚫ Viral
⚫ Bacterial (Urinary, GI, lung)
⚫ Fungal
Pause for discussion with Dr Shahid
What are your thoughts on why infection is so common in myeloma, and do you see more infections early In the diagnosis (first year) or later in the illness?
RISK FACTORS
Host Factors Associated with Infection Risk
Health conditions
can increase ones’ risk of infection
Diabetes
• Host immune response is lowered; dysfunction of immune cells, chronic inflammation from high blood sugars result
Heart, Kidney and Liver Disease
• Impaired organ function can lead to lower immune response
Rheumatologic disorders
• Altered immune function of cells, medications to treat rheum diseases
Older Age
• Immune senescence (cells stop dividing but remain active) and increase in other illnesses
Some studies suggest starting antibiotics for 3 months (levofloxacin, moxifloxacin)
Protect yourself with good hand washing, vaccinations, healthcare provider recommendations
Highest risk is commonly at first diagnosis and relapse
Lowest risk is commonly during remission or maintenance
Drayson, M.T., et al. (2019). Levofloxacin prophylaxis in patients with newly diagnosed myeloma (TEAMM): a multicentre, double-blind, placebo-controlled, randomised, phase 3 trial. The Lancet Oncology, 20(12), 1760-1772 ; Mohyuddin, et al. (2020).Antibiotic prophylaxis for patients with newly diagnosed multiple myeloma: Systematic review and meta-analysis. European journal of haematology, 104(5), 420–426.
Maintenance Therapy
Low risk on lenalidomide maintenance
Newer studies with combination drugs (such as anti-CD38 monoclonal antibodies), CART and Bispecific antibodies in maintenance may increase one’s risk of infection
Relapsed Multiple Myeloma
“Bi-Modal” distribution of infection risk
The longer one lives with MM, the higher the infection risk with ongoing treatments, bone marrow suppression, t-cell fatigue, types of therapies given
C. H (2025). Risk of infections in multiple myeloma.A populationbased study on 8,672 multiple myeloma patients diagnosed 2008-2021 from the Swedish Myeloma Registry. Haematologica, 110(1), 163–172. https://doi.org/10.3324/haematol.2024.285645
Blimark,
FREQUENTLY ASKED QUESTIONS REGARDING CART AND IMMUNITY
DR. SHAHID
Frequency of infections among CAR-T cell therapy recipients
Santos et al. reported NRM(varying from 5.7%-10.6%) 50% caused by infection
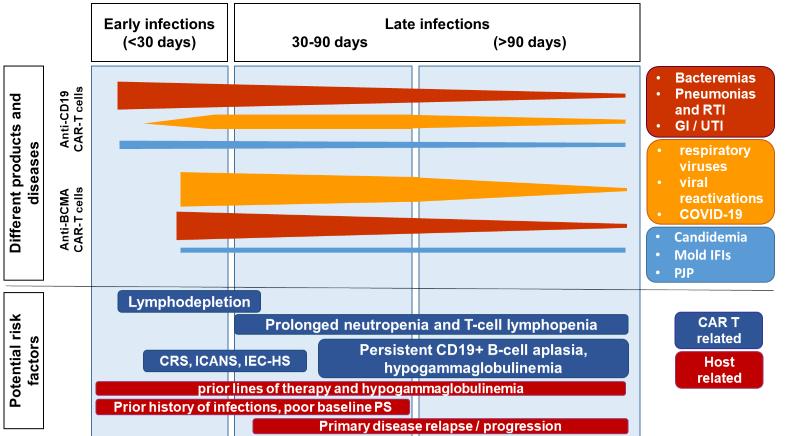
CD19 CART-Cells:
• High infection density (mainly bacterial) before day 30
Dizman et al. Pooled attributable mortality 1.8%)
• Resp. Viral Infections (RVIs) are more common >30 day
• Fungal infections are rare (<6%)
BCMA CAR T-Cells:
• Infection rates are higher 58%-68% but occurred later (median 46-60 days)
• Infection density highest between days 30-100
• RVIs are prevalent before and after day 30
• Viral reactivations have been observed, recent studies highlighting CMV specifically
Epidemiology of infections post CAR T cell therapy
Risk factors for infection after CAR-T cell therapy
Antimicrobial prophylaxis is recommended after CAR-T cell therapy
Antibacterials1
Antivirals
At lymphodepletion therapy until ≥6 m post-CAR-T At lymphodepletion therapy until ≥12 m post-CAR-T Antifungals
with ANC recovery (at least by Day 30 post-CAR-T) therapy until ≥6 m post-
INFECTION PREVENTION AND MANAGEMENT
Ways to protect yourself from infection
Preventing infections is paramount.
Infection remains the leading cause of death in patients with multiple myeloma. Several factors account for this infection risk, including the overall state of immunosuppression from multiple myeloma, treatment, age, and comorbidities (e.g., renal failure and frailty).
IMWG Consensus guidelines and recommendations for infection prevention in multiple myeloma; Lancet Haematol.2022;9(2):143–161.
Infection Prevention Tips
Good personal hygiene (skin, oral)
Report fever of more than 100.4°F, shaking chills even without fever, dizziness, shortness of breath, low blood pressure to HCP as directed.
Environmental control (avoid crowds and sick people; use a high-quality mask when close contact is unavoidable)
As recommended by your healthcare team:
Immunizations:
Flu, COVID, RSV & and pneumococcal vaccinations; avoid live vaccines
CRS/ICANS requiring any dose of steroids Prolonged neutropenia <500 for 14 days
Prolonged lymphopenia <200 for 14 days Recent cellular therapy
To be used in all patients on bispecific therapy and to be continued up to 1 year after last dose
PJP
Fungal
Bactrim 1 DS MWF
Atovaquone 1500 mg daily
Dapsone 100 mg daily
Bacterial
Fluconazole 200-400 mg daily
Posaconazole 300 mg daily*
Voriconazole 200 mg BID*
Not of clear benefit. TBD
Start prophylaxis and consider continuing until therapy complete (approx. 3 months) for patients receiving high dose steroids for 3 days or more Not of clear benefit Not of clear benefit
Not of clear benefit. Not of clear benefit.
Follow standard for cellular therapy
Start Fluconazole until neutropenia resolves. If <500 for more then 3 weeks, consider switching to mold active prophylaxis Not of clear benefit.
Follow standard for cellular therapy
Immunoglobuli
Levofloxacin 500 mg daily
Ciprofloxacin 500 mg BID
Cefpodoxime 200 mg BID
Not of clear benefit. Not of clear benefit.
Start until neutropenia resolves Not of clear benefit. Not of clear benefit.
n replacement therapy IVIG if IgG<400 and patients have evidence of recurrent respiratory infections or a single severe bacterial infection
VACCINATION GUIDANCE
TIMELINE FOR DELAYED TOXICITIES WITH CAR T-CELLS
Fungal Infections (Molds)
Pneumonia
Late Bacterial and Viral Infections
Prolonged Cytopenias
Impaired B-Cell and T-Cell Recovery Late Neurologic and Psychiatric Events
Immune-Related Adverse Events
Malignancies
ASH-ASTCT Guidelines for Revaccination Following CAR T-Cell Therapy
Killed/Inactivated
Pneumococcus‡
Diphtheria, tetanus, and acellular pertussis (DTap)
*For inactivated “dead” virus vaccines, vaccination should be at least 2 months after last dose of IVIG. †If patient is going to receive CAR T-cell therapy during influenza season, administer annual inactivated influenza vaccine after leukapheresis and 2 weeks prior to beginning lymphodepletion chemotherapy (if not previously administered). Subsequent annual vaccinations can resume > 6 months after CAR T-cell therapy. RSV vaccine guidance by ACIP and ASTCT guidelines. ‡Check titers for Streptococcus pneumonia (IgG, 23 serotypes) 1 to 2 months after each PCV20. A positive response to PCV20 is defined as achieving a seroprotective IgG level against Streptococcus pneumonia in 15 out of 20 PCV20 serotypes at 1 to 2 months after vaccination. A positive response requires no further PCV20 vaccination . §Separate component vaccines (shots) may be used instead for DTaP, IPV, and Hib if Pentacel is unavailable. ║Check titers to Hib, tetanus toxoid. ¶If NOT administering hepatitis B series using Heplisav-B, Twinrix can be administered on days when HAV and HBV are given together (Twinrix approved for age ≥ 18 years).#Hepatitis A and B surface antigen IgG. **Hepatitis B vaccination is accomplished preferably with Heplisav-B based on data extrapolated from patients with chronic kidney disease or on hemodialysis for ESRF. Alternatively, double (40 mcg/dose = 2 mL total) doses of Engerix-B maybe given. Patients who do not respond to the primary vaccine series should receive an additional 1 to 3 doses of the same vaccine or, alternatively, repeat series with a different vaccine brand (eg, double doses of Engerix-B if no response to Heplisav-B or single dose of Heplisav-B if no response to Engerix-B). ††Not until 1 year after CAR T-cell therapy, 1 year after transplant, 8 months off all systemic immunosuppressive therapy for chronic GVHD, and absolute CD4 T-cell count > 200/μL.
ACIP Advisory Committee on Immunization Practices; ASH = American Society of Hematology; ASTCT = American Society for Transplantation and Cellular Therapy; CAR = chimeric antigen receptor; DTaP = diphtheria tetanus pertussis; GVHD = graft vs host disease; IPV = HAB = hepatitis; HAV = hepatitis A virus; HBV = hepatitisB virus; Hib = Haemophilus influenzae type b; mo = month; PVC = Pneumococcal conjugate vaccine; Td = tetanus diphtheria; VZV = varicella zoster virus. Shahid Z, et al. Transplant Cell Ther. 2024;30(10):955-969.
Recommendations for re-vaccination after CAR-T therapy?
Eligibility Immunization Response
> 6 months and eligible vaccinate
Seroprotection
Response, no seroprotection
No response
Strep pneum, Tetanus, Hib,
Hep A and B
Eligibility: Starting at 6 months post CART
No preceding IVIG for > 2 mo, B cell depleting agents e.g. rituximab for > 6 months
Vaccines to be considered: RSV, Influenza, COVID-19 at 6 months
Strep pneumoniae (PCV20, PVC 21), HiB &Tdap, Hep A and B, Shingrix, Meningococcal ACWY and B*
* Men ACWY and Meningococcal B isrecommended for patients who are: functionally or anatomically asplenic, college students or military recruits, taking a compliment inhibitor such as eculizumab, HIV positive, traveling to endemicareas, or are part of a population identified to be at risk because of a disease outbreak.
Follow-up
No more vaccine, ? check for durability
Additional Vaccines per schedule
• Defer vaccines until immune reconstitution
• Recheck in 6 months
• Consider IVIG replacement if indicated
Criteria for revaccination:
For GVHD: Less than 1 mg/kg/day of prednisone equivalent
• CD4 > 200 cells/µL
• IgG > 400 mg/L and CD19
• >20 cells/µL
FALL 2025
Getting Ready for Fall
• Discuss antimicrobial prophylaxis with your provider
Get up to date on vaccines
Community surveillance of Respiratory Viruses
Seek medical attention early
Educate your community
FREQUENTLY ASKED QUESTIONS AND
DISCUSSION
Key Takeaways
• Infections are a major risk of morbidity, mortality in multiple myeloma
• Ways to minimize risk: Hand washing, antibiotics, antivirals, IVIg, growth factors
• Immunizations
Discussion, Question and Answer
Thank you!
Q&A
Workshop Video Replay & Slides
As follow up to today's workshop, we will have the speaker slides and a video replay available.
These will be provided to you shortly after the workshop concludes and posted to our website under “IMF Videos”
We Want to Hear From You
Feedback Survey
At the close of the meeting a feedback survey will pop up.
This will also be emailed to you shortly after the workshop.
Please take a moment to complete this survey.
Thank you to our
sponsors!
OUR VISION: A world where every myeloma patient can live life to the fullest, unburdened by the disease.
OUR MISSION:
Improving the quality of life of myeloma patients while working toward prevention and a cure.
IMF Core Values:
These are the core values we bring to accomplishing our mission each day.
Patient Centric
The patient experience is the focus of everything we do. Every interaction is an opportunity to establish a personal connection built on care and compassion which is the basis for continued support.
Respect All
As a team, we value honesty and transparency while creating a culture of mutual respect. We foster a myeloma community built on sincerity, authenticity, and kindness.
Excellence and Innovation
We value accountability, personal responsibility, and a steadfast commitment to excellence. We respect the legacy and reputation of our organization while seeking new solutions and advancements to improve outcomes, quality of life, and access to the best available resources for everyone impacted by myeloma.
Honor differences
We recognize each team member's skills and talents through collaboration and cooperation. Our programs aim to celebrate and support the diversity of our patients and their communities.