

2025 IMF REGIONAL COMMUNITY WORKSHOP
EDINA, MN

APRIL 26, 2025

Thank you to our speakers & our sponsors!








Welcome & Introductions
Robin Tuohy
Vice President, Patient Support
International Myeloma Foundation
Understanding Myeloma Basics
Joselle Cook, MD
Mayo Clinic, Rochester, MN
IMF REGIONAL COMMUNITY WORKSHOP
EDINA MORNING AGENDA

(Video) Closing the Gap: Health Disparities in Myeloma
Joseph Mikhael, MD, MEd, FRCPC, FACP, FASCO,
Chief Medical Officer, International Myeloma Foundation
Advancing Treatment Options Through Clinical Trials
Douglas Sborov, MD, MS
Huntsman Cancer Institute, University of Utah
Q&A with Panel
Coffee Break
Breakout: Frontline or Relapsed Treatment Approaches
-NDMM: Getting Started with Myeloma Management
Joselle Cook, MD
-RRMM: Continuing the Myeloma Treatment Journey
Douglas Sborov, MD, MS
Housekeeping Items
Presentation Slides: Are available by scanning the QR code, Instructions are on the QR code handout on each table. Program Evaluations: evaluations at the end of today.
Restrooms: Restrooms are located outside the ballroom to your right Badge Holders: Please return your badge holders and we can recycle them.

We greatly appreciate your time and feedback!

The IMF Support Group Team is Here For You!










Special Interest Groups
Special interest groups are designed as a supplemental support for specific populations of patients, in addition to their local Support Groups
Las Voces de Mieloma-founded in 2022
Designed for Spanish speaking patients only
Living Solo & Strong with Myelomafounded in 2022
Designed for patients without a care partner

High Risk Multiple Myeloma-founded in 2023
Designed to address the needs of the high-risk MM population
Care Partners Onlyfounded in 2024
Designed to address the needs and concerns of care partners
Veterans SIG-founded in 2025
For those who served our country
Smolder Bolder-founded in 2023
Created for people living with Smoldering Multiple Myeloma
MM Families-founded in 2021
For patients/care partners with young children
Multiple Myeloma Sharing Sessions
Meets virtually on the 3rd Saturday of each month at 10AM Central
Local Support Groups
Twin Cities Multiple Myeloma Education & Networking Group
Meets hybrid on the 2nd Saturday of each month at 10AM Central
Central MN Multiple Myeloma Support Group
Meets in-person on the 2nd Saturday of each month at 10AM Central
Sioux Falls, SD Multiple Myeloma Support Group
Meets hybrid on the 2nd Tuesday of each month at 6PM Central

Eau Claire, WI Multiple Myeloma Support Group
Meets hybrid on the 2nd Monday of each month at 3PM Central
IMF InfoLine
Connecting Patients to Resources…
Shortening “Time to Hope” for Over 1,000 First-Time Callers Each Year
Assistance with understanding lab results, terminology and disease state
Preparing for medical visits
Resource Information:
• Financial & Emotional Support
• Expert Myeloma Referrals
“Thank you so much for the informative conversation and all the time you spent listening and helping me decipher the MM lingo. What an amazing service!”


“Thank you for your response and excellent question suggestions for my hematology team.”







Written Education
Understanding Booklets
Tip Cards
Myeloma Minute Weekly Updates
Myeloma Today Quarterly News







































Live Patient Education
4 PATIENT & FAMILY
including world-renowned experts 10 MYELOMA COMMUNITY WORKSHOPS including local myeloma experts

Locations



2025 Live Patient Education
Patient & Family Seminars
• Boca Raton, FL – March 14 – 15
• Philadelphia, PA – May 2 – 3
• Los Angeles, CA – August 15 – 16
• Chicago, IL – October 3 – 4

Myeloma Community Workshops
• Virtual - March 4
• San Francisco, CA - March 29
• Atlanta, GA - April 5
• Edina, MN - April 26
• Denver, CO - June 21
• Virtual – July 29
• Seattle, WA - August 9
• Waltham, MA - September 27
• Raleigh-Durham, NC - November 15
• Virtual – November 18
Scan for Upcoming Events!






Understanding Myeloma Basics
Joselle Cook, MD
Mayo Clinic – Rochester, Rochester, MN

Joselle Cook MD Mayo Clinic
Terminology
• Plasma cell
• Monoclonal protein
• Serum Protein Electrophoresis
• Immunofixation
• M-Spike
• Light chains
• FISH
• PFS
• OS
What is a plasma cell
• Plasma cells are specialized immune cells found in the bone marrow
Not the same as blood plasma!
• Their job: Produce antibodies /immunoglobulins to help fight infections

• In a healthy immune system, plasma cells make a wide variety of antibodies
What is an antibody
Antibodies are built from two parts:
• �� Heavy chains
These are the bigger building blocks They come in types like IgG, IgA, or IgM
• �� Light chains
These are the smaller connectors They come in two types: kappa (κ) or lambda (λ)

• Together, they form a complete antibody, like two puzzle pieces that snap together
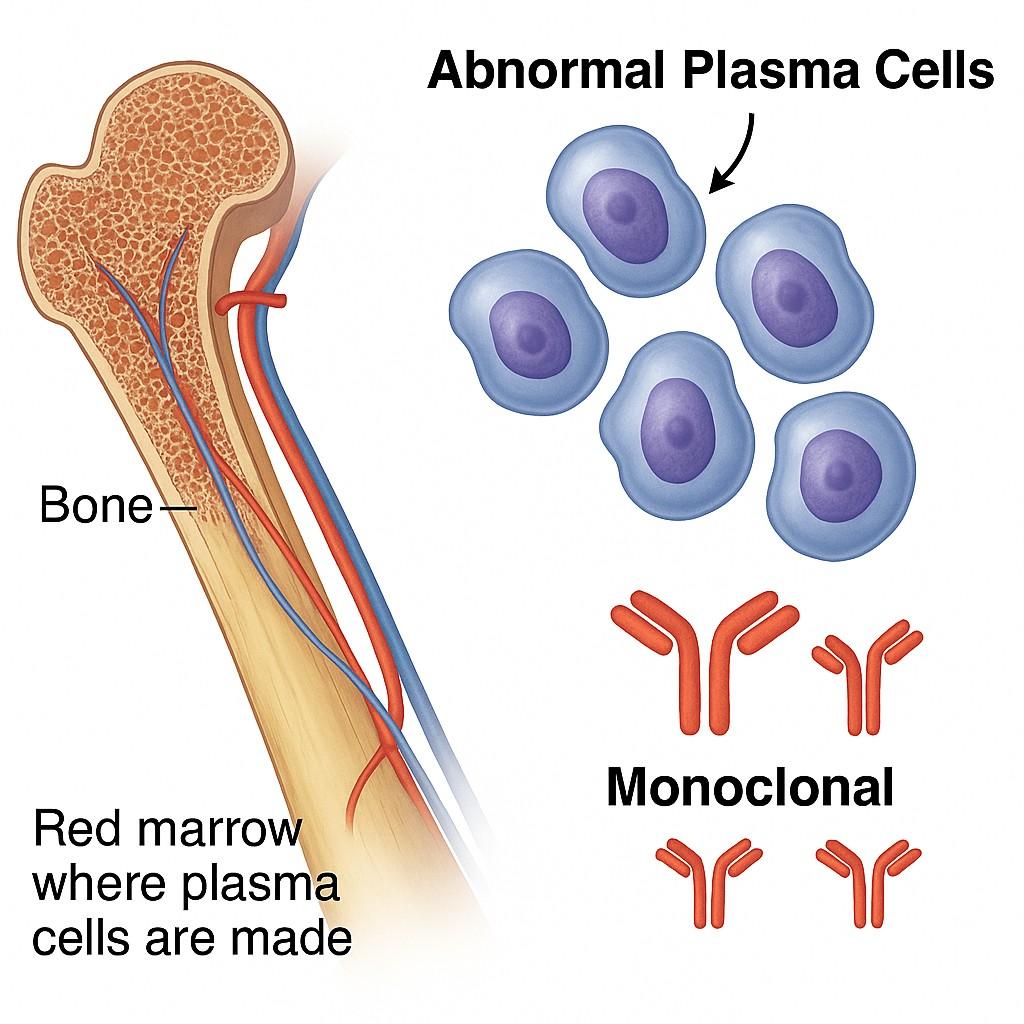
What is a monoclonal protein
• In monoclonal gammopathies, a group of plasma cells (clone) acquires a genetic abnormality (mutation)
• This group of cells (clone) makes only one type of antibody –monoclonal (M) protein.

What are the stages of this disorder
The
plasma cell clone begins making copies of itself
and crowding out healthy marrow




MGUS Smoldering Myeloma

Multiple Myeloma monoclonal gammopathy of undetermined significance




Active
Multiple MyelomaSymptoms

• Determines when myeloma is active and requires treatment.
• Represents organ damage caused by clonal plasma cells
• Actionable signs that myeloma is affecting the body.
CRAB symptoms for Multiple Myeloma
C – Calcium (Hypercalcemia)
• What it is: Myeloma breaks down bone, releasing calcium into the blood.
• Why it matters: Elevated calcium can cause fatigue, confusion, constipation, and kidney injury.
• Threshold: Calcium >11 mg/dL (corrected)
R – Renal Dysfunction
• What it is: Light chains and M-protein can clog the kidneys, leading to damage.
• Why it matters: Impaired kidney function can affect medication clearance and long-term outcomes.
• Threshold: Creatinine >2 mg/dL or eGFR <40
CRAB symptoms for Multiple Myeloma
A – Anemia
• What it is: Myeloma crowds out normal bone marrow, reducing red blood cell production.
• Why it matters: Anemia causes fatigue, shortness of breath, and reduced quality of life.
• Threshold: Hemoglobin <10 g/dL or 2 g below normal
B – Bone Lesions
• What it is: Myeloma activates osteoclasts and suppresses osteoblasts → lytic lesions and fractures.
• Why it matters: Pain, fractures, spinal cord compression, and loss of mobility.
• Threshold: ≥1 lytic lesion on skeletal survey, PET-CT, or MRI
Other Common Symptoms of Myeloma



Fatigue
Often the first and most disabling symptom
Recurrent infections
Suppression of normal immunoglobulins from dysfunctional plasma cells.
Numbness or tingling
Spinal cord compression from collapsed vertebrae or spinal cord compression
Weight loss or night sweats uncommon, but possible
Who is at risk for Multiple Myeloma
• Age: The risk increases significantly with age, Most over 65
• Race/Ethnicity: Black individuals> White or Asian people Also often diagnosed at a younger age.
• Family History: Having a family history of multiple myeloma or MGUS increases the risk.
• Environmental Factors: Agricultural or woodworking chemicals Radiation 9/11 exposure

My uncle, diagnosed with Multiple Myeloma in 2019. Presented with Back
Tests for multiple myeloma

SPEP = Serum Protein
Electrophoresis
• A blood test that determines how much of the abnormal antibody the myeloma cells are making
• Determines the MSPIKE
Immunofixation
• identifies the exact type of abnormal antibody (Mprotein)
• It tells us the heavy chain (IgG, IgA, IgM) and light chain (kappa or lambda)
Free Light Chains (Kappa / Lambda Ratio)
Clone of plasma cells produces extra light chains that float around freely in the blood
What it indicates
Abnormal activity from plasma cells.

• Normal ratio: Around 0.26 to 1.65
• Too high or too low? That means the disease may be active or relapsing.
�� Your ratio is the red flag — not just the number itself.
Lab Test What It Tells You
Hemoglobin Measures red blood cells / oxygen-carrying capacity
Why It Matters Quick Takeaway
Myeloma can suppress marrow → anemia → fatigue �� Low = fatigue; ↑ means marrow is recovering
Creatinine Kidney function
Myeloma light chains can damage kidneys �� Watch for rises; hydration helps
Calcium Bone turnover or breakdown
Myeloma can erode bones → releases calcium �� High = bone activity; watch for bone pain
Beta-2
Microglobulin &
LDH Risk/staging markers
High levels = more aggressive myeloma; part of ISS/R-ISS staging �� You won’t feel it, but we track it closely
Bone marrow
• Confirms the Diagnosis
It shows how many cancerous plasma cells are in your bone marrow.
10% of bone marrow or more
• Genetic tests helps stratify MM Risks
• FISH

FISH (Fluorescence In Situ Hybridization)
• FISH zooms in on the chromosomes inside the myeloma cell to show genetic errors
• FISH helps define Diagnosis, Prognosis, Treatment planning


MRI – Gold standard

Imaging



CT Skeletal survey assesses for for holes (lytic lesions) and even lesions in the bone marrow


PET scan:
Helps find where myeloma is active in the body, and can spot disease outside the bones.
Beyond CRAB: Additional “Myeloma Defining Events”
(MDEs)
Modern criteria (IMWG) also recognize early markers of high-risk disease that warrant treatment before CRAB develops: Feature
What It Means
≥60% clonal plasma cells in marrow Very high tumor burden – almost always progresses Involved/uninvolved FLC ratio ≥100 Light chain disease with high progression risk
≥2 focal bone lesions on MRI Disease is already spreading in bone, even without symptoms
Response criteria

Complete response and absence of clonal cells in bone marrow by traditional techniques
MRD Minimal Residual Disease
This test looks for even the tiniest number of myeloma cells left in the bone marrow after treatment
MRD negative status:
• 59% reduction in disease progression
• 43% reduction in risk of death
• Longer survival
Am J Hematol. 2025 Mar;100(3):427-438. doi: 10.1002/ajh.27582. Epub 2025 Jan 9. PMID: 39784302
Survival
⏳ Progression-Free Survival (PFS)
How long you live without the cancer getting worse
Means the treatment is working
�� Overall Survival (OS)
How long people live after diagnosis or starting treatment, regardless of what happens with the disease.
tracks total survival, regardless of relapse or additional therapies.
Median survival
• The point in time when half of patients are still alive, and half have passed away
• A way to describe what happens for the "typical" patient
Survival depends on multiple factors
FISH risk • Disease biology• Stage (Revised International Stage)•Patient related
Thank you • Questions

Closing the Gap: Health Disparities in Myeloma (Video)
Joseph Mikhael, MD, MEd, FRCPC, FACP, FASCO Chief Medical Officer, International Myeloma Foundation
Advancing Treatment Options Through Clinical Trials
Douglas Sborov, MD, MS
Huntsman Cancer Institute, University of Utah

Clinical Trials - Overview
Some Of The Important Principles Of Clinical Trials:
The drive of research has brought us to where we are
No one is expected to be a “guinea pig” with no potential benefit to them
Research is under very tight supervision and standards
Open, clear communication between the physician and the patient is fundamental Driving research forward!





MYTH: If I participate in a clinical trial, I might get a placebo, not active treatment
MYTH: If I participate in a clinical trial, I can’t change my mind
Clinical Trials: Myths
• Phase 1 and 2, everyone gets active treatment
• Phase 3 standard of care vs new regimen: often standard regimen with/without additional agent in MM trials
• Patients can withdraw their consent for clinical trial participation at any time

MYTH: Clinical trials are dangerous because they have new medicines and practices
• Some risk is involved with every treatment, but medicines are used in clinical trials with people only after they have gone through testing to indicate that the drug is likely to be safe and effective for human use

MYTH: Clinical trials are expensive and not covered by insurance
• Research costs are typically covered by the sponsoring company
• Standard patient care costs are typically covered by insurance
• Check with clinical trial team/insurers; costs such as transportation, hotel, etc may not be reimbursed and are paid by patient
PhRMA website. Accessed March 25, 2024. https://phrma.org/-/media/Project/PhRMA/PhRMA-Org/PhRMA-Org/PDF/A-C/CLINICAL-TRIALS-MYTH-FACT-PRINT.pdf?hsCtaTracking=f6689b95-1626-40d9-8c87-c6b 8d31600a4%7C35221aa8-d487-4db3-9416-b9c3c35e3bac
.
Overview of New Drug Development

Identify a target for therapy in the laboratory
Confirm the anticancer activity in laboratory and animal studies
Clinical trials (human studies) to determine safety, dosing and effectiveness
The whole process costs millions of dollars and years of effort!
Preclinical
Clinical Trial Phases
ANIMAL STUDIES: Examine safety and potential for efficacy
PHASE 1
PHASE 2
FIRST INTRODUCTION OF AN INVESTIGATIONAL DRUG INTO HUMANS
• Determine metabolism and PK/PD actions, MTD, and DLT
• Identify AEs
• Gain early evidence of efficacy, studied in many conditions; typically, 20 to 80 patients; everyone gets agent
EVALUATION OF EFFECTIVENESS IN A CERTAIN TUMOR TYPE
• Determine short-term AEs and risks; closely monitored
• Includes up to 100 patients, typically
PHASE 3
GATHER ADDITIONAL EFFECTIVENESS AND SAFETY
PHASE 4
INFORMATION COMPARED TO STANDARD OF CARE
• Placebo may be involved if no standard of care exists; hundreds to several thousand patients
• Often multiple institutions; single or double blind; sometimes open label
APPROVED AGENTS IN NEW POPULATIONS OR NEW DOSE

Clinical Trials – Why Me??
Every patient is unique and must be viewed that way
Benefits of trials are numerous and include:
Early access to “new” therapy
Delay use of standard therapy
Contribution to myeloma world – present and future
Financial access to certain agents
Must be balanced with potential risks
“Toxicity” of side effects
Possibility of lack of efficacy
Why Do So Few Cancer Patients Participate in Trials?
Patients may:
• Be unaware of clinical trials
• Lack access to trials
• Fear, distrust, or be suspicious of research
• Have practical or personal obstacles
• Face insurance or cost problems

• Be unwilling to go against their physicians’ wishes
• Not have physicians who offer them trials
• Have a disconnect with their healthcare team
Importance of Clinical Trial Participation by Diverse Populations
[P]eople from racial and ethnic minorities and other diverse groups are underrepresented in clinical research. This is a concern because people of different ages, races, and ethnicities may react differently to certain medical products.
– FDA

Leadership and commitment


Community engagement practices
Investigator hiring, training, and mentoring practices



Patient engagement practices

US Cancer Centers of Excellence: Strategies for Increased Inclusion of Racial and Ethnic Minorities in Clinical Trials
FDA = US Food and Drug Administration. Regnante JM, et al. J Oncol Pract. 2019;15(4):e289-e299. FDA website. Clinical Trial Diversity. Accessed March 27, 2024. https://www.fda.gov/consumers/minority-health-and-health-equity/clinical-trial-diversity.
Is A Clinical Trial Right For Me?
Discuss with your physician if you are eligible for a clinical trial
Work with your physician to determine the best trial for you
Meet with the clinical research nurse or trials coordinator to discuss the trial
Carefully review the provided “Informed Consent” Describes the study and any potential safety concerns related to the experimental medication


Commonly Asked Questions
How does the study work? How often will I need to see my doctor or visit the cancer center?

Will I need to undergo additional tests?
What is currently known about the new drug or combination?
What benefits can I expect?
What side effects should I expect? Who should I notify if I have side effects?
Can I take my vitamins or other medications?
Can I get the treatment with my local doctor?

Will my insurance pay for my participation in the clinical trial?

Clinicaltrials.gov https://clinicaltrials.gov/




ncreasing-diversity-in-cancer-clinical-research

Q&A WITH PANEL
Housekeeping Items
Presentation Slides: Are available by scanning the QR code, Instructions are on the QR code handout on each table. Program Evaluations: evaluations at the end of today.
Restrooms: Restrooms are located outside the ballroom to your right Badge Holders: Please return your badge holders and we can recycle them.
We greatly appreciate your time and feedback!
BREAK
WHEN YOU RETURN FROM BREAK
PLEASE HEAD TO YOUR SELECTED BREAKOUT SESSION:
BREAKOUT A: NDMM - GETTING STARTED WITH MYELOMA
MANAGEMENT
Dr. Joselle Cook, MD
Please move to Cahill Ballroom B
BREAKOUT B: RRMM - CONTINUING THE MYELOMA TREATMENT JOURNEY
Dr. Douglas Sborov, MD MS
Please remain in this room
Thank you to our speakers & our sponsors!
Breakout B
RRMM: Continuing the Myeloma Treatment Journey
Douglas Sborov, MD, MS
Huntsman Cancer Institute, University of Utah
Relapsed Multiple Myeloma: Continuing the Treatment Journey
Douglas Sborov, MD, MS Huntsman Cancer Institute, University of Utah

Discuss an approach to treating relapsed myeloma based on patient, disease and treatment characteristics
OBJECTIVES
Review the important trend of using an aggressive approach in early treatment of myeloma
Outline the key results from recent trials in early relapse
Discuss the approach to late relapse and the use of novel therapies such as CAR T and bispecific antibodies




Carfilzomib
Daratumumab
An Approach to Relapsed MM
• It is not a simple algorithm of treatment #1 then 2 then 3…
• Leverage the benefit of multiple mechanisms of action in combination therapy
Categories:
• 1-3 prior lines
• Later Relapse
• Refractory to PI, IMiD and MoAb = Triple Class Refractory
Definitions:
What is relapsed/refractory disease and a line of therapy?
• Relapsed: recurrence (reappearance of disease) after a response to therapy
• Refractory: progression despite ongoing therapy
• Progression: change in M protein/light chain values
• Line of therapy: change in treatment due to either progression of disease or unmanageable side effects
• Note: initial (or induction) therapy + stem cell transplant + consolidation/ maintenance therapy = 1 line of


Therapy Selection Considerations
Disease-Related
• Nature of the relapse
– Biochemical vs symptomatic
• Risk stratification
– High-risk chromosomal abnormalities: del(17p), t(4;14), t(14;16)
• Disease burden
Therapy-Related
• Previous therapies
• Prior treatmentrelated adverse event
• Regimen-related toxicity
• Depth and duration of previous response
• Cost to patient
Patient-Related
• Renal insufficiency
• Hepatic impairment
• Comorbidities
• Preferences
• Social factors
– Support system
– Accessibility to treatment center
– Insurance coverage
Multiple Myeloma is Not One Disease!
RVD+ASCT+Lenalidomide Maintenance
Relapse 2
Relapse 1
Time: Years! D i s e a s e A c t i v i t y
Relapse 1
Relapse 2
Relapse 3
Relapse 1
1. Therapies change over time— clinical trials make this possible 2. Outcomes (e.g. survival) changes over time, as new therapies emerge
GENERAL PRINCIPLES
3. If one therapy did not work well, it doesn’t mean another won’t
4. Terms like “overall survival” and “progression free survival” typically refer to statistical probabilities for GROUPS of people and do not seal the fate of an INDIVIDUAL
5. At a given point in time, there may not be a known “right answer;” hence many opinions
Pillars of Myeloma Therapy
Emerging immunotherapies in multiple myeloma


Carvykti
Talquetamab (CPRC5D)
Cevostamab (FcRH5)
Naked antibodies
Examples:
Cancer cell
1. Daratumumab (Darzalex) — recognizes CD38
2. Isatuximab (Sarclisa) — recognizes CD38
3. Elotuzumab (Empliciti) — recognizes SLAMF7
Antibody drug conjugate
linker

Examples:
1. Belantamab mafodotin (Blenrep) — recognizes BCMA
IS BLENREP (BELANTAMAB) COMING
BACK?
DREAMM 7: Velcade-Dex with
Belantamab or daratumumab

Progression free Survival Overall Survival

Hungria V. NEJM; 391(5): 393-407.
DREAMM 8: POM-DEX WITH BELANTAMAB OR VELCADE

Progression free Survival
Overall Survival Blenrep(belantamabmafodotin)combinations

Dimopoulos MA. NEJM 2024; 391(5): 408-421.
BISPECIFIC ANTIBODY
Bispecific MM target Brand name
Teclistamab BCMA Tecvayli
Talquetamab GPRC5D Talvey
Elranatamab BCMA Elrexfio
Cevostamab FcRH5
Livoseltamab BCMA
Bispecific antibody
Plasma cell aka myeloma cell T-cell • Cytokine release • T cell activation • Perforin/Granzymes
Fc domain
CAR-T CELLS
Cilta-cel CARVYKTI (BCMA)
Early Relapse
General Principles
Use mechanisms of action not previously used
Do not continue to use lenalidomide if progressing on len maintenance
Triplets are preferred over doublets
In real practice - most patients receiving VRD (Bortezomib-LenalidomideDex) like regimens, 1st relapse is typically
Daratumumab + Pomalidomide + Dex (APOLLO)
Isatuximab + Pomalidomide + Dex (ICARIA)
Daratumumab + Carfilzomib + Dex (CANDOR)
Isatuximab + Carfilzomib + Dex. (IKEMA)
Selinexor + Bortezomib + Dex (BOSTON)
Important Update – CAR T cell therapies can be used as early as first relapse!
First or Second Relapse (Options after Considering Clinical Trials) (Modified from mSMART But Added New CAR-T Approvals)
Not refractory to Lenalidomide and standard risk or long 1st remission Refractory to Lenalidomide
KPd or PVd or PCd or EloPd Or CAR-T (Cilta-cel If 1+ prior LOT, Ide-cel if 2+ LOT) DRd
Not Refractory to Anti-CD38 Refractory to Anti-CD38 and Len DPd or IsaPd Or DVd
Favor CAR-T Cilta-cel (1+ prior LOT) Or Ide-cel (2+ prior LOT)
Others to the left if not candidate for CAR-T
Standard Risk and >23 years remission <2 years of remission and/or HRCA > 2-3 year remission and standard risk < 2 year remission or HRCA Cilta-cel CAR T or Anti-CD38 + Kd
Dingli D, et al. Mayo Clin Proc. 2017;92(4):578-59. Updated 2024.
Abecma (CAR T) vs Standard of Care: 2-4 prior lines of therapy

Carvykti (CAR T) vs Standard of Care: 1-3 prior lines of therapy

OVERALL RESPONSE RATE AND PFS OF RECENTLY APPROVED THERAPIES IN RRMM
Richardson Blood 2014; 123:1826-32
Siegel Blood 2012; 120:2817-25
Lonial Lancet 2016; 387:1551-60
Rasche EHA 2024, P915
Van de Donk ASCO 2023; abs 8011
Lesohkin Nat Med 2023; 29:2259-67
Munshi NEJM 2021; 384:705-16
Munshi EHA 2023; S202
Huang ASCO 2024; 7511
CAR T-Cell Therapy Patient Journey
Immune cells from the patient are collected

Standard of care therapy is permitted until CAR T cells are ready for infusion
Fludarabine and Cytoxan are used to create “immunologic space” to CAR T cells to expand

CAR T: Expected Toxicities


Cytokine release syndrome Neurotoxicity (ICANS)


Cytopenias Infections
CRS ICANS
Onset 1 9 days after CAR Tcell infusion 2 9 days after CAR Tcell infusion
Duration 511 days 317 days
Symptom
s
Managem ent
• Fever
• Difficulty breathing
• Dizziness
• Nausea
• Headache
• Rapid heartbeat
• Low blood pressure
• Actemra (tocilizumab)
• Corticosteroids
• Supportive care
• Headache
• Confusion
• Language disturbance
• Seizures
• Delirium
• Cerebral edema
• Antiseizure medications
• Corticosteroids
*Based on the ASTCT consensus; †Based on vasopressor; ‡For adults and children >12 years; §For children ≤12 years; ‖Only when concurrent with CRS
Bi-specific and Tri-specific Antibodies
There are currently 3 approved bispecific antibodies:
Teclistamab (Tecvayli)
Talquetamab (Talvey)
Elranatamab (Elrexfio)

Bispecific Antibodies
Bispecific antibodies are also referred to as dual specific antibodies, bifunctional antibodies, or T-cell engaging antibodies
Bispecific antibodies can target two cell surface molecules at the same time (one on the myeloma cell and one on a T cell)
Many different bispecific antibodies are in clinical development; none are approved for use in myeloma
Availability is off-the-shelf, allowing for immediate treatment

Cohen A et al. Clin Cancer Res. 2020;26:1541.


BCMA, GPRC5D, or FcRH5
Examples:
• Elranatamab
• Teclistamab
• TNB-303B (ABBV-383)
• REGN5458
• Cevostamab
• Talquetamab
Bi-specific Antibodies: Expected
Toxicities
• Cytokine release syndrome (CRS)
• Neurotoxicity (ICANS)
• Usually occurs within first 1–2 weeks
• Frequency (all grade and grade 3–5) higher with CAR T
• Cytopenias
• Target unique
• For example, rash, taste disturbance seen with GPRC5D, but not with BCMA
• Infections
• Incidence for bi-specifics at RP2D not yet known
• Viruses: CMV, EBV
• PCP/PJP
• Ongoing discussions regarding prophylactic measures
IVIG
Anti-infectives
Similarities and Differences Between CAR T-Cell
Therapy and Bispecific Antibodies
Approved product Abecma, Carvykti Tecvayli
Key Points – CAR T and Bispecifics
CAR T and bispecific antibodies are very active even in heavily pretreated patients.
Side effects of CAR T cells and bispecific antibodies include cytokine release syndrome, confusion, and low blood counts, all of which are treatable.
Abecma and Carvykti are only the first-generation CAR T cells and target the same protein. Different CAR Ts and different targets are on the way.
Bispecific antibodies represent an “off-the-shelf” immunotherapy; Tecvayli was approved in October 2022, and now Talvey and Elrexfio in August 2023
Several additional bispecific antibodies are under clinical evaluation.
Emerging Therapies for
Relapsed/Refractory Multiple Myeloma
Bispecific antibodies
• Cevostamab, Alnuctamab, ABBV383, and others
• Target BCMA, GPRC5D, or FcRH5 on myeloma cells and CD3 on T cells
• Redirects T cells to myeloma cells
Cereblon E3 ligase modulators (CELMoDs)
• Iberdomide
• Targets cereblon
• Enhances tumoricidal and immune-stimulatory effects compared with immunomodulatory agents
Small molecule inhibitors
• Venetoclax
• Targets Bcl-2
• Induces multiple myeloma cell apoptosis
The Evolution of Myeloma Therapy
VD
Rev/Dex
CyBorD
VTD
VRD
KRD
D-VMP
DRD
ASCT
Tandem ASCT (?)
Nothing
Thalidomide?
Bortezomib
Ixazomib
Lenalidomide
Combinations
Bortezomib
Lenalidomide
Carfilzomib
Pomalidomide
Selinexor
Panobinostat
Daratumumab
Ixazomib
Elotuzumab
Isatuximab
Belantamab mafodotin*
Melphalan flufenamide*
Idecabtagene autoleucel
Ciltacabtagene autoleucel
Teclistamab, Talquetamab
Elranatamab
D-VRD
Isa-VRD
D-KRD
Isa-VRD “More” induction?
Daratumumab?
Carfilzomib?
Lenalidomide + PI
ASCT, autologous stem cell transplant; CAR, chimeric antigen receptor; Cy, cyclophosphamide; d- daratumumab; D/dex, dexamethasone; isa, isatuximab; K, carfilzomib; M, melphalan; PD-L1, programmed death ligand-1; PI, proteasome inhibitor; Rev, lenalidomide; V, bortezomib.
Speaker’s own opinions.
CAR T Cell Therapy
Bispecific/Tri-specific
Antibodies
Venetoclax
PD/PDL-1?
Small Molecules
* These agents are currently off the market but available through special programs
Anito-cel
Cevostomab
Linvoseltamab
Iberdomide, Mezigdomide
Sonrotoclax

LUNCH
Please move to the Baird Ballroom Pre-function
Engage and Partner with the IMF
Sylvia Dsouza
Vice President, Development, International Myeloma Foundation
IMF REGIONAL COMMUNITY WORKSHOP
EDINA
AFTERNOON AGENDA
Myeloma: Putting the Pieces of the Puzzle Together
Teresa Miceli, RN, BSN, OCN, InfoLine Advisor, Nurse Leadership Board
Mayo Clinic – Rochester, MN
Living the Myeloma Life: Local Patient & Care Partner
Steve Ellingboe (Patient) and Sheila Ellingboe (Care Partner)
Beyond Myeloma Therapy: Exploring Financial and Legal Issues in Cancer Care
Erin Hartung Cancer Legal Care
Q&A with Panel
Closing Remarks
Robin Tuohy
Vice President, Support Groups, International Myeloma Foundation
Engage and Partner with the IMF
Sylvia Dsouza, Vice President, Development
International Myeloma Foundation
Engage & Partner with the IMF
Sylvia Dsouza, Vice President, Development
WHO AM I
WHAT DO I DO?

Vice President of Development for the IMF
Securing philanthropic support and resources for the IMF through diverse mechanisms
Oversee a team of passionate and determined fundraising professionals who are committed to advancing the mission of the IMF
Have the incredible honor of working with dedicated volunteers from the US and across the globe.
3 Ways to Engage
Philanthropy
Make a philanthropic gift to support research, education, advocacy or patient support programs.
Volunteer
Join your local support group/become a Support Group Leader
Join our grassroots patient Advocacy program
Volunteer your time at local races organized by the IMF to engage the community
Engage on social media to connect with others affected by myeloma and spread awareness and empower patients with knowledge and resources.
Intellectual capacity
Offer your expertise as a speaker or panelist at events.
Be a beta tester for various new tools and products and provide reviews and feedback


Want to Make an Impact: Designate Your Gift
• Research: The IMF is dedicated to finding a cure for multiple myeloma.
• Education: The IMF provides education for patients and caregivers.
• Support: The IMF provides support for patients and caregivers through inperson and virtual support groups.
• Advocacy: The IMF advocates for better access to care and more affordable options for myeloma patients.
Philanthropy Fuels Our Mission
Peer-to-Peer Fundraising
Peer-to-Peer Fundraisers are created from YOUR ideas. Starting a Fundraiser is easy and fun. They also make a world of difference in the myeloma community.
Join a IMF P2P event or start your own and engage your family, friends, co-workers, your network who honor your journey with myeloma and want to support you. Let them show you that you are not alone.
Ex: Hole in One Golf Tournament, Iceland Cycling Expedition, Miracles for Myeloma 5K Run/Walks (hybrid)
Join the HOPE Society (Recurring Monthly & Annual Giving Program)
Help us cultivate the future by joining the International Myeloma Foundation's Hope Society.
Monthly and annual gifts support IMF core programs, including educational events, publications, the toll-free InfoLine, and more.
Start with a monthly contribution and when ready turn it into a yearly commitment. You will be a part of likeminded individuals united in the quest to find a cure for myeloma and a better quaity of life for all myeloma patients.
Transformative Gifts (Major Giving and Principal Giving)
Gifts can be designated toward a specific program, project or initiative .
Is there something specific that resonates deeply with you and you want to see change happening?
Gifts can also be unrestricted, expendable and/or an endowment
P2P
Laughs 4 Life (Hattiesburg, MI, comedy celebration)-- 8 years, $483,850!
Peer-to-Peer (P2P) and Monthly & Annual Giving
Miracles for Myeloma(Clark, New Jersey, 5K run/walk) -- 12 years, >$1M
Iceland Cycling Expedition raised close to $1M in less than a year
Hole In One (Golf Tournament, Jackson, New Jersey)– Inaugural golf tournament that has raised $75K
Monthly & Annual Giving – HOPE Society
Join our flagship monthly and annual giving program, the HOPE Society.
Get invited to Regional Salon Dinners in your area with IMF leadership and KOLs.
Receive exclusive updates on research and trials fresh off the press.
Play a pivotal role in supporting our four pillars.
Support long-term initiatives that make a lasting difference.



IMF's Miracles for Myeloma Virtual/In-Person 5K Run/Walk Series
The IMF will lead five Virtual/In-Person 5K Run/Walks across the United States in the following regions (Goal: $100K net from each event)
• Miracles for Myeloma Virtual/In-Person 5K Run/Walk in Boca Raton, FL (03-15-2025)
• Miracles for Myeloma Virtual/In-Person 5K Run/Walk in Los Angeles, CA (04-12-2025)
• Miracles for Myeloma Virtual/In-Person 5K Run/Walk in Philadelphia, PA (05-03-2025)
• Miracles for Myeloma Virtual/In-Person 5K Run/Walk in Clark, NJ (09-13-2025)
• Miracles for Myeloma Virtual/In-Person 5K Run/Walk in Chicago, IL (10-04-2025)
Upcoming Peer-to-Peer Fundraising Events in 2025
• 7th Annual Schleicher's Hikers 5K
• Mission for Matt (Dinner, and Dancing)
• Jack's Education and Experience Grant
• San Fernando Valley Support Group Fundraiser
• Czerkies Memorial Golf Outing
• Hole in One Golf Tournament
• Inland Empire Walk/Run
• Walkathon & BBQ To End Multiple Myeloma
• Row for a Cure









International Myeloma Foundation’s Signature Marquee Annual Endurance



Three goals:
1. Raising awareness and visibility for multiple myeloma and a patient/care-partners journey to and through it (humanizing the disease)
2. Raising awareness and visibility for the International Myeloma Foundation
3. Raising critical funding to help accelerate research to find a cure for myeloma
Additional outcome that organically emerged – building a strong, interconnected myeloma community where all myeloma patients and their loved ones see hope, resilience and determination as part of the journey and feel empowered
• The 2025 Iceland Cycling Expedition will take place from Wednesday, August 27, 2025 through Tuesday, September 2, 2025.
• This signature marque event is a 6-day/7-night fundraising cycling challenge in the High Mountains of Iceland.
• 21 Participants (patients, care-partners, myeloma clinicians, sponsors)
• Applications for 2026 will open in October 2025. Follow us on Icelandcyclingexpedition.com and/or myeloma.org/ice2025




Ashley Dieks (Patient) Garson, Ontario

ICE 2025 Participants

Dr. Saad Usmani (Myeloma Clinician and Researcher) Memorial Sloan Kettering, NY

Jered Haddad (Patient) Germantown, TN

Dr. Douglas Sborov (Myeloma Clinician and Researcher) Huntsman Cancer Institute at the University of UT
Richard Pampe (Patient) Jackson, WY

Dr. Jeffrey Zonder (Myeloma Clinician and Researcher) Department of Oncology at Wayne State University, MI

Tatum Byhre (Care Partner) Minneapolis, MN


Christian Hoff (Patient) Pittsboro, NC

Benjamin Freund (Patient) East Canaan, CT

Troy Fischer (Care Partner) Bloomington, IL

Katherine Podgorski (Patient) Toronto, Canada

Dr. Cristina Gasparetto (Myeloma Clinician and Researcher) Duke Cancer Institute, NC
Iceland Cycling Expedition 2024
Phare
Santa
Malibu Film Festival
Beverly Hills Film Festival
Tribeca Festival
Atlanta Film Festival
Palm Springs International Film Festival
Miami Film Festival
Flicker's Rhode Island International Film Festival
LA Shorts International Film Festival
11. Holly Shorts Film Festival Portland Film Festival

Leave a Lasting Legacy
Planned Giving
Join the Brian D. Novis Legacy Society and make a planned gift!
Gain immediate tax benefits
Potentially increase your income during your lifetime.
Continue to fund our core programs and four pillars.
Make a bequest (a gift from your estate)
Include a provision in your will or living trust.
Designated us as a beneficiary of a life insurance policy, or retirement plan (IRA, 401(k), or 403(b).

Leave us in your will is one of the most profound ways to support the people and causes important to you.
Corporate and Foundation Gifts
Your organization can contribute a corporate gift or foundation grant
Provide seed funding that is necessary to accelerate the path to a cure.

Reach Out to the IMF Development Team
We welcome you to continue to learn more about our programs, projects, and initiatives at the IMF and find alignment with your own philanthropic passion and as well as ways to deepen and strengthen your engagement with us. Reach out to the IMF Development Team to start a conversation on how you can make a difference in the lives of the people impacted by myeloma.
Sylvia Dsouza- Vice President of Development sdsouza@myeloma.org or (310)947-4126
Simona Grace- Director of Development, Major Gifts sgrace@myeloma.org or (818)487-7455 x 307
Kimberly Francis- Assistant Director of Development Peer-to-Peer Fundraising kfrancis@myeloma.org or (818)487-7455 x 304
Myeloma: Putting the Pieces of the Puzzle Together
Teresa Miceli, RN, BSN, OCN, InfoLine Advisor,
Nurse Leadership Board
Mayo Clinic – Rochester, MN


Myeloma: Putting the Pieces of the Puzzle Together
Teresa Miceli, RN, BSN, OCN
Mayo Clinic – Rochester Rochester, Minnesota
A presentation from the IMF’s Nurse Leadership Board
Myeloma: Putting The Pieces of the Puzzle



Focus on Managin g Sympto ms

Myeloma: Putting The Pieces of the Puzzle

Myeloma Is a Cancer of the Plasma Cells
Plasma Cells come from white blood cells produced in the bone marrow and make many different antibodies to help fight infection (polyclonal).


In Multiple Myeloma, one plasma cell mutates, making many identical plasma cells (monoclonal).








Bone marrow
Bone marrow
Myeloma Causes Cell Dysfunction &




Anxiety
Stress
Depression
Decreased red blood cells



Anemia & Fatigue

Decreased white blood cells

Myeloma protein in blood and urine
Changes in bone remodeling
Clonal myeloma plasma cells can cause many symptoms
– Crowd out normal bone marrow cells
– Produce myeloma protein
– Can cause kidney dysfunction
– Affect bone cells (balance of osteoclasts & osteoblasts)
Immune Dysfunction & Infection


Renal Dysfunction






Infections Are Serious for People with Myeloma
Preventing infections is paramount.
Infection remains the leading cause of death in patients with multiple myeloma. Several factors account for this infection risk, including the overall state of immunosuppression from multiple myeloma, treatment, age, and comorbidities (e.g., renal failure and frailty).
IMWG Consensus guidelines and recommendations for infection prevention in multiple myeloma; Lancet Haematol.2022;9(2):143–161.
Infection Prevention Tips
Good personal hygiene (skin, oral)
Environmental control (avoid crowds and sick people; use a high-quality mask when close contact is unavoidable)

Report fever of more than 100.4°F, shaking chills even without fever, dizziness, shortness of breath, low blood pressure to HCP as directed.
As recommended by your healthcare team:
Immunizations:
Flu, COVID, RSV & and pneumococcal vaccinations; avoid live vaccines
Preventative and/or supportive medications
Kidney and Bone Health

Protect Kidney Function
Myeloma Treatment
Stay hydrated--drink water
Avoid certain medications
• IV contrast dyes

• NSAIDs like Advil (ibuprofen), Aleve (naproxen)
Be alert: symptoms of kidney dysfunction
• Fatigue and weakness
• Nausea and vomiting
• Foamy or dark urine
• Swelling in feet, ankles, or face
• Shortness of breath
• Persistent itching
• Loss of appetite
• Muscle cramps
• High blood pressure

Protect Bone Health
Myeloma Treatment
Nutrition
Vitamin D
Calcium (if approved by doctor)
Weight-bearing activity (i.e., walking, standing, climbing stairs, stretching, dancing)
Bone-strengthening agents (prescribed by your healthcare team)
Report any new or worsening bone pain to your healthcare provider
Pain Management
Pain can significantly compromise quality of life and add to distress
Prevention
Sources of pain include bone disease, neuropathy and medical procedures.
Decrease fracture risk through myeloma treatment, bone strengthening agents, physical activity, preventative surgery
Prevent Nerve Damage: prevent shingles, manage diabetes, myeloma medication dosing and route of administration
Combine scheduled medical procedures, when possible (Ex. blood draw, biopsy), use sedation if available

Treatment
Interventions depend on source of pain, may include
Medications, Surgery, Radiation therapy, etc.
Physical therapy & continued activity, complementary therapies (Mind-body, meditation, yoga, supplements, acupuncture, etc.)
Scrambler therapy for neuropathy


Myeloma: Putting The Pieces of the Puzzle
Managin g Sympto ms


Treatment of Newly Diagnosed Multiple Myeloma (NDMM)

Induction
Consolidation
Initial treatments aimed at reducing the amount of myeloma cells
Intensification of treatment to deepen response. Either additional cycles of induction or autologous stem cell transplant (in eligible patients)
Prolonged lower-intensity treatment designed to sustain remission
Induction Standard of Care
Induction

Quadruplet therapy is preferred for nearly all patients with newly diagnosed myeloma

Anti-CD38 monoclonal antibody (mAb)
• Darzalex (daratumumab)
• Sarclisa (isatuximab)
Proteosome
Inhibitor (PI)
• Velcade (bortezomib)
• Kyprolis (carfilzomib)
Immunomodulator
y drug (IMiD)
• Revlimid (lenalidomide)
• Pomalyst (pomalidomide)
Steroid
• Decadron (dexamethasone)
• Prednisone
At infusion clinic: subcutaneous injection or infusion
Oral medication taken at home Supportive medication:
• Antiviral prophylaxis (i.e., acyclovir or valacyclovir) to prevent viral infections particularly shingles.
• Antibacterial agents (i.e., Bactrim, levofloxacin) to prevent bacterial infections.
• Aspirin or other anticoagulant therapy to reduce the risk of blood clots from IMiDs.
• Bone-strengthening agents (i.e., zoledronic acid, denosumab) to strengthen bones and protect against fractures.
Steroids: An Important Piece Of The Treatment Plan
Steroids enhance the effectiveness of other myeloma therapies

Your provider may decrease or discontinue the dose as myeloma responds to therapy.
Do not stop or alter your dose of steroids without discussing it with your provider
Steroid Side Effects
• Irritability, mood swings, depression
• Blurred vision, cataracts
• Increased risk of infections, heart disease
• Muscle weakness, cramping
• Increased blood pressure, water retention
• Difficulty sleeping (insomnia), fatigue
Managing Steroid Side Effects
• Flushing/sweating
• Stomach bloating, hiccups, heartburn, ulcers, or gas
• Weight gain, hair thinning/loss, skin rashes
• Increased blood sugar levels, diabetes
Consistent schedule (AM vs. PM)
Take with food
Stomach discomfort: Over-thecounter or prescription medications
Medications to prevent shingles, thrush, or other infections
Rajkumar SV, et al. Lancet Oncol 11(1):29–37. King T, Faiman B. Clin J Oncol Nurs. 2017;21(2):240-249. Banerjee,R. et al. Blood 9.25.24
Peripheral Neuropathy
Peripheral neuropathy happens when there is damage to nerves in the extremities (hands, feet, limbs). Damage can be the result of myeloma, treatment or unrelated conditions (i.e., diabetes).
Symptoms: Numbness
Tingling
Prickling sensations
Sensitivity to touch
Burning and/or cold
sensation
Muscle weakness

Prevention / management:
Bortezomib once-weekly and/or subcutaneous administration
Massage area with cocoa butter regularly
Neuroprotective Supplements
• i.e., B-complex vitamins (B1, B6, B12)
Safe environment: rugs, furnishings, shoes
If neuropathy worsens, your provider may:
Adjust your treatment plan
Prescribe oral or topical pain medication
Suggest physical therapy
Nerve damage from neuropathy can be permanent.
Early reporting of symptoms may prevent worsening symptoms.
Faiman B, et al. CJON. 2017;21(5)suppl:19-36. Tariman, et al. CJON.2008;12(3)suppl:29-36. Zhao T, et al. Molecules. 2022;27(12):3909.

Blood Clots: Managing DVT and PE Risk

Blood clots can cause swelling, pain, discoloration (DVT), shortness of breath, chest pain, sense of doom (PE). Blood clots
► HCPs may manage DVT/PE risk by
• Adjusting medications and schedules
• Prescribing blood-thinning medications according to assessed risk (DOAC, aspirin, warfarin, heparin)
• Balancing the risk of DVT and PE with that of bleeding with low platelets
► Additional strategies to reduce risk of clots:
• Anti-embolism stockings (elastic stockings)
• Exercise regimen
• Moving frequently when sitting long periods
• Travel precautions (foot/leg exercises, walking, aspirin if not already on blood thinner)
DVT=Deep Vein Thrombosis; PE=Pulmonary
Embolism
are serious and can be life threatening.



Family History
Obesity
Immobility
Smoking
Surgery
Rome, S, et al. Clin J Oncol Nurs. 2008;12(3)suppl:37-52. Faiman B. Clin J Oncol Nurs. 2016;20(4):E100-E105. De Stefano, et al. Hematologica, 2022
Stem Cell Transplant
ELIGIBILITY

P H A S E 1

Measuring treatment response
Testing for Eligibility
Insurance authorization
Collecting stem cells

Duration: Approximately 2 weeks
Location: Transplant Center
A S E 2 TRANSPLANT
P H
HD-Melphalan
Stem cell infusion
Supportive Care
• GI Management
• Transfusions
• Antibiotics
Hair Loss
Engraftment
Duration:
Approx. 3-4 weeks

Location:
Transplant Center

P H A S E 3
POSTTRANSPLA NT
Restrengthening
Appetite recovery “Day 100” assessment
Begin maintenance therapy

Duration: Approximatel y 10-12 weeks
Location: HOME

stem cell transplant remains the standard of care for
Miceli T and Steinbach, M. Multiple Myeloma:
Multiple Myeloma. V1.2025.
GI Symptoms: Prevention & Management
Fluid intake can help with both diarrhea and constipation and helps kidney function
Constipation is more common in the induction phase
Opioid pain relievers, antidepressants, heart or blood pressure medications (check with provider, pharmacist)
Supplements: Calcium, Iron, vitamin D (rarely), vitamin B-12 deficiency
Anorexia, the inability to eat, is common during transplant and resolves with time.
• Hydration is most important
• Small, frequent meals with a focus on protein intake
• You will work closely with a dietician to help monitor your calorie intake
Diarrhea is common during transplant and long-term maintenance therapy.
Other medications and supplements can cause GI issues.
Hydration is very important
Electrolyte replacement is common
Good skin care will help prevent irritation
Stool exam may be needed to rule-out infection
Increase fiber
Stay well hydrated
Fruits, vegetables, high fiber whole grain foods
Fiber binding agents – Metamucil® ,
Citrucel®, Benefiber®
If no infection, anti-diarrheal medication may be prescribed

Discuss GI issues with healthcare providers to identify causes and adjust medications and supplements
Smith LC, et al. Clin J Oncol Nurs. 2008;12(3)suppl:37-52. Faiman B. Clin J Oncol Nurs. 2016;20(4):E100-E105.
Myeloma: Putting The Pieces of the Puzzle
Relapsing Nature of Myeloma
=
Adapted from Durie B. Keats JJ, et al. Blood. 2012;120(5):1067-1076.
Many Treatment Options at Relapse
Myeloma Therapies Common Combinations
Belantamab mafodotinb Bela, BVd, BPd, BKRd
Bortezomib (SQ admin)
VRd, Vd, VCd
Carfilzomib KRd, Kd, Dara-Kd, Isa-Kd
Ciltacabtagene Autoleucel Cilta-Cel
Daratumumab Dara-Rd, Dara-Vd, Dara-Pd, Dara-VMp, Dara-Kd
Elotuzumab ERd, EPda
Idecabtagene Vicleucela Ide-Cel
Isatuximab Isa-Pda, Isa-Kd
Ixazomib IRd
Lenalidomide
VRd, Rd, KRd, Dara-Rd, ERd, IRd
Pomalidomidea Pda, Dara-Pd, EPda, PCdb
Selinexor Xd, XVd, XKdb, Dara-Xdb
New agents or regimens in clinical trials are always an option

Many treatment options are available.
More therapies are being studied
Clinical trials may be an option


a2 or more prior therapies. bOff-label; not currently FDA-approved. C = cyclophosphamide; d = dexamethasone; Dara = daratumumab; FDA = US Food and Drug Administration; E = elotuzumab; Isa = isatuximab; I = ixazomib; K = carfilzomib; M = melphalan; p = prednisone; P = pomalidomide; R = lenalidomide; SQ = subcutaneous; V = bortezomib; X = selinexor.
Rajkumar SV. 2024 Myeloma Algorithm. https://clinicaloptions.com/CE-CME/oncology/2024-mm-algorithm/18440-26989. Accessed 12.14.24. NCCN Guidelines®. Multiple Myeloma. V3.2024. Accessed March 15, 2024. Noonan K, et al. J Adv Pract Oncol. 2022;13(suppl 4):15-21. Steinbach M, et al. J Adv Pract Oncol. 2022;13(suppl 4):23-30. Moreau P, et al. Lancet Oncol. 2021;22(3):e105-e118. O’Donnell EK, et al. Br J Haematol. 2018;182(2):222-230. Mo CC, et al. EJHaem. 2023;4(3):792-810. Chang D. et al., Blood 2024, Abstract 2287.
CAR T Cell Therapy

BCMA target
• Abecma (Ide-Cel)
• Carvykti (Cilta-Cel)

1
Relapsed MM with 1-2 prior LOT Bridging therapy, if needed; Lymphodepleting therapy when CAR T cells are ready T Cell Infusion Close monitoring and Management of side effects
T-Cell Engager (TCE) Therapies
Relapsed MM after 4 prior LOT (or clinical trials)

TCE are innovative immunotherapies used in the treatment of relapsed multiple myeloma. These therapies work by redirecting the patient's own T-cells to recognize and attack myeloma cells.


3


2 a 2 b 4 5 HOME ! Apheresis to Collect T Cells T Cell Manufacturi ng
Bispecific antibodies
• About 7 in 10 patients respond
• Off-the-shelf treatment; no waiting for engineering cells

BCMA target: greater potential for infection
• Tecvayli® (teclistamab)
• Elrexfio™ (elranatamab)



Bispecific antibody


GPRC5D target: potential for skin and nail side effects, GI issues of taste change, anorexia and weight loss

• Talvey™ (talquetamab)
BCMA = B-cell maturation antigen; CAR = chimeric antigen receptor; GPRC5D = G protein–coupled receptor, class C, group 5, member D; MM = multiple myeloma; scFV = single chain fragment variable.

CAR T= Chimeric Antigen Receptor T Cell; LOT = Lines of
Hucks G, Rheingold SR. Blood Cancer J. 2019;doi:10.1038/s41408-018-0164-6.

Shah N, et al. Leukemia. 2020;34(4):985-1005. Yu B, et al. J Hematol Oncol. 2020;13:125.
CAR T and Bispecific Antibodies: Known Side Effects
CYTOKINE RELEASE
SYNDROME
• Fever
• Fatigue & Weakness
• Headache
• Nausea/Vomiting/Diarrhea
• Chills
• Low blood pressure
• Rapid heart rate

CRS is a common but often mild & managea ble side effect

Neurotoxicity is a rare but a serious side effect
• Difficulty breathing PREVENTION AND MANAGEMENT
• Disease management to reduce tumor burden
• Bispecific Step-Up Dosing (SUD)
• Tocilizumab
• Steroids
• Anti-Seizure medications
• Intravenous Immunoglobulin (IVIG)
• Close monitoring

ICANS AND NEUROTOXICITY
• Headache
• Difficulty concentrating
• Lethargy
• Agitation
• Hallucinations
• Tremors
• Aphasia (difficulty with speech, reading, writing, or understanding language)
• Confusion
• Memory loss
• Personality change
• Delayed Neurotoxicity can include Parkinsonism, Cranial Nerve Palsies and Peripheral Neuropathy/Guillan Barré syndrome (GBS)
CAR = chimeric antigen receptor. ICANS = Immune Effector Cell-Associated Neurotoxicity Syndrome Brudno JN, Kochenderfer JN. Blood. 2016;127(26):3321-3330. Lee DW, et al. Biol Blood Marrow Transplant. 2019;25:625-638. Kumar, et al. Blood (2024) 144 (Supplement 1): 4758.
Infection: Medications Can Mitigate Risk
Type of Infection Risk
Medication Recommendation(s) for Healthcare Team Consideration
Viral: Herpes Simplex (HSV/VZV); CMV Acyclovir prophylaxis
Bacterial: blood, pneumonia, and urinary tract infection
PJP (P. jirovecii pneumonia)
Fungal infections
COVID-19 and Influenza
Consider prophylaxis with levofloxacin
Consider prophylaxis with trimethoprimsulfamethoxazole
Consider prophylaxis with fluconazole
Antiviral therapy if exposed or positive for covid per institution recommendations
IgG < 400 mg/dL (general infection risk) IVIg recommended
ANC < 1000 cells/μL (general infection risk)

Consider GCSF 2 or 3 times/wk (or as frequently as needed) to maintain ANC > 1000 cells/μL and maintain treatment dose intensity
Weight, GI Symptoms & The Drugs That Affect Them: Prevention
& Management
Anorexia (difficulty eating) Weight loss
• ASCT
• GPRC5D therapy
Steroids Weight gain, fluid retention
Excess hunger ASCT
GPRC5Ddirected therapy Opioids

Weight Loss
Weight Gain
Weight Management
• Monitor weight for significant loss or gain
• Adjust diet (reduce calories or add supplements )
• Work with a dietician
Smith LC, et al. Clin J Oncol Nurs. 2008;12(3)suppl:37-52. Faiman B. Clin J Oncol Nurs. 2016;20(4):E100-E105.
Management of Oral Side Effects
Xerostom
ia
OTC dry mouth rinse, gel, spray are recommended. Avoid hot beverages. Anti-fungal therapy for oral thrush.


Dysgeusi a
Dysphagi a


=Dry Mouth =Difficulty Swallowing =Taste Change
Dexamethasone oral solutions “swish and spit” may provide benefit. Sour citrus or candies before meals are also recommended.
Dental
Care
Attention to oral hygiene.
Regular dental cleaning and evaluation. Close monitoring for ONJ, oral cancer and dental caries
Dietary modifications with small bites, eating upright, and sips with food can help manage symptoms
Weight Monitorin g
Some medications lead to weight gain, others to weight loss. Meet with a Nutritionist
Consider diet changes, supplements


Work closely with your entire health care team to manage oral side effects.
Skin and Nail Side Effects
Possible side effect to some treatments and supportive care medications


Skin Rash:
Prevent dry skin; apply lotion
Report changes to your care team
Medication interruption or alternative, as needed
Steroids:
• Topical for grades 1-2,
• Systemic and topical for Grade 3
Antihistamines, as needed


Nail Changes:


Keep your nails short and clean.
Watch for “catching and tearing”
Apply a heavy moisturizer like Vaseline or salve. Wear cotton hand coverings to bed
A nail hardener may help with thinning
Tell the team if you have signs of a fungal infection, like thickened or discolored nails
Myeloma: Putting The Pieces of the Puzzle





Fatigue, Anxiety and Depression
Fatigue Depression Anxiety
Fatigue is the most reported symptom. Sources include anemia, pain, reduced activity, insomnia, treatment toxicity, bone marrow suppression. Symptoms can improve with continued physical activity.
Symptoms are under-reported:
“I mentioned it before. Nothing can be done.” “I don’t want to be put on another medication.”

>35% of patients ≈25% of patients
More Pieces to the Big Picture
Adopt Healthy Behaviors

• Mental health / social engagement
• Stress reduction; relaxation
• Sufficient Sleep
• Maintain a healthy weight; eat nutritiously
• Activity / exercise / prevent falls, injury
• Stop smoking Complementary or alternative therapy
• Have a PCP for general check ups, preventative care, health screenings, vaccinations
• Have specialists for dental care, eye exams/screening, skin cancer screening


Recommended Health
Screenings
• Blood pressure
• Cholesterol
• Cardiovascular disease
• Colonoscopy
• Dental checkups & cleaning
• Dermatologic evaluation
• Diabetes
• Hepatitis
• Hearing
• Vision
• Women specific: mammography, pap smear
Faiman B, et al. CJON. 2017;21(5)suppl:19-36. Dimopoulous M, et al. Leukemia. 2009;23(9):1545-56.
• Men specific: prostate
Brigle K, et al. CJON. 2017;21(5)suppl:60-76. Faiman B, et al. CJON. 2017;21(5)suppl:19-36. Faiman B, et al. CJON. 2011;15suppl:66-76. Miceli TS, et al. CJON. 2011;15(4)suppl:9-23.

Care Partners: Essential Pieces of the Puzzle
Multiple studies demonstrate that strong social ties are associated with
• Increased longevity including people with cancer
• Improved adherence to medical treatment leading to improved health outcomes
• Lower risk of cardiovascular diseases
• Increased sense of purpose & life satisfaction
• Improved mood and happiness
• Reduced stress and anxiety
• Enhanced resilience
Care partners may help with medical appointments, managing medication, daily living, physical assistance, emotional support, myeloma knowledge, healthy lifestyle, patient advocacy, financial decisions
Care partners can be a spouse, close relative, a network of people (family, friends, neighbors, church members, etc)
Caring for the Care Partner
• Recognize that caregiving is difficult/stressful
• Encourage care partners to maintain their health, interests, and friendships
• The IMF has information and resources to help care partners
































































“Thank You!”
From the NLB and the IMF



Living the Myeloma Life: Local Patient & Care Partner
Steve Ellingboe (Patient Advocate) &
Ellingboe (Care Partner)
Sheila
Steve and Sheila Ellingboe





Beyond Myeloma Therapy:
Exploring Financial and Legal Issues in Cancer Care
Erin
Hartung Cancer Legal Care

Erin Hartung, Director of Legal Services

BEYOND MYELOMA THERAPY: EXPLORING FINANCIAL AND LEGAL ISSUES IN CANCER CARE
WHAT IS CANCER LEGAL CARE?


A non-profit organization providing assistance for cancer-related legal issues to all Minnesotans affected by cancer.
The only organization providing this assistance in the Upper Midwest.
Services are open to anyone in need, regardless of cancer type, prognosis, county, age, or income.
Services are always free and confidential.
Staff of 9 (6 of whom are lawyers), a board (doctors, lawyers, social workers, community members) and over 80 volunteer lawyers, all of whom:

Have a personal connection to cancer, and Realize people need legal care to be well.
We are funded by private donations, foundation grants, and government contracts.

Our mission is to engage the law to resolve the complex challenges facing people and communities affected by cancer. We do this by providing free legal care and education to Minnesotans affected by cancer, for the legal issues they face that directly impact their health and quality of life.
WHO WE SERVE
Any person (patient, survivor, caregiver) affected by
Any cancer
Anytime (from diagnosis onward)
Anywhere in Minnesota
Any income (certain programs have income/asset eligibility requirements)

Q: Why would a patient need a lawyer on their cancer treatment team?
Social Determinants of Health

Source: Healthy People 2030, U.S. Department of Health and Human Services, Office of Disease Prevention and Health Promotion.
Retrieved, January 26, 2025, from https://odphp.health.gov/healthypeople/objectives-and-data/socialdeterminants-health
Financial Toxicity

Financial toxicity is the detrimental effects of the excess financial strain caused by the diagnosis of cancer on the well-being of patients, their families, and society.
Signs of Financial Toxicity

Legal Services to Address Financial Toxicity
Legal Services
Employment – Preserving Income and Benefits

Family Medical Leave Act (FMLA)
MN Paid Leave (2026)
Earned Safe and Sick Time (ESST)
Americans with Disabilities Act (ADA)
Discrimination
Employment Benefits
Legal Services
Disability Benefits – Replacing Employment Income
Social Security Disability Insurance (SSDI)
Supplemental Security Income (SSI)
Short Term Disability
Long Term Disability
Legal Services
Health (and other) Insurance & Medical Billing, Debt –
Avoiding Financial Drain
Health (and other) insurance denials & coverage issues
• No Surprises Act
Provider billing issues
Medical debt
• Minnesota Debt Fairness Act
• Financial assistance requirements
Legal Services
Asset Management and Protection – Estate Planning
Power of Attorney (POA)
Account beneficiaries
Transfer on Death Deed
Wills Healthcare Directive (HCD)
Q: Why would a patient need a lawyer on their cancer treatment team?
A:
Addressing
the legal issues that affect a patient’s financial wellbeing is integral to reducing cancer’s financial toxicity



Q&A WITH PANEL
Closing Remarks
Robin Tuohy, Vice President, Patient Support International Myeloma
Foundation
Housekeeping Items
Presentation Slides: Are available by scanning the QR code, Instructions are on the QR code handout on each table. Program Evaluations: evaluations at the end of today.
Restrooms: Restrooms are located outside the ballroom to your right Badge Holders: Please return your badge holders and we can recycle them.
We greatly appreciate your time and feedback!
Thank you to our speakers & our sponsors!
OUR VISION:
A world where every myeloma patient can live life to the fullest, unburdened by the disease.
OUR MISSION:
Improving the quality of life of myeloma patients while working toward prevention and a cure.
IMF Core Values:
These are the core values we bring to accomplishing our mission each day.
Patient Centric
The patient experience is the focus of everything we do. Every interaction is an opportunity to establish a personal connection built on care and compassion which is the basis for continued support.
Respect All
As a team, we value honesty and transparency while creating a culture of mutual respect. We foster a myeloma community built on sincerity, authenticity, and kindness.
Excellence and Innovation
We value accountability, personal responsibility, and a steadfast commitment to excellence. We respect the legacy and reputation of our organization while seeking new solutions and advancements to improve outcomes, quality of life, and access to the best available resources for everyone impacted by myeloma.
Honor differences
We recognize each team member's skills and talents through collaboration and cooperation. Our programs aim to celebrate and support the diversity of our patients and their communities.

