H. Lee Moffitt Cancer Center and Research Institute, Tampa, FL
Closing the Gap: Health Disparities in Myeloma
Joseph Mikhael, MD, MEd, FRCPC, FACP, FASCO, Chief Medical Officer, International Myeloma Foundation
Breakout Sessions #2: Patients and Care Partners
Breakout A: Patients Only – Lessons Learned Michael Tuohy, 25-year Myeloma Patient, Support Group Leader
Breakout B: Care Partners Only
Robin Tuohy, Vice President - Patient Support International Myeloma Foundation & 25-year care partner
RETURN TO MAIN SESSION
Grab-and-Go Refreshments
Controversies in Myeloma: Moderated by Dr. Joseph Mikhael
Joshua Richter, MD, FACP
Mount Sinai, New York, NY
Krina Patel, MD, MSc
The University of Texas MD Anderson Cancer Center, Houston, TX
Ask – the – Experts w/ Guest Faculty
Closing Remarks & Evaluation
Program Evaluations
Please be sure to complete your program evaluation today, and turn it in at the end of the program.
We greatly appreciate your time and feedback!
The IMF Support Group Team is Here For
Melbourne Multiple Myeloma Support Group
Meets in-person on the 4th Monday of each month at 10:30AM
Maitland Multiple Myeloma Support Group
Meets in-person on the 2nd Monday of each month at 6:30pm
Palm Beach County Multiple Myeloma Support Group
Meets in a hybrid format on the 1st non-holiday Monday of each month at 6:30PM
Fort Myers Multiple Myeloma Support Group
Meets in-person on the 3rd Tuesday of each month at 6pm
Hollywood Multiple Myeloma Support Group
Ocala Multiple Myeloma Support Group
Meets in-person on the 3rd Saturday of each month at 11AM
Sarasota Multiple Myeloma Network & Education Group
Meets in-person on the 4th Friday of each month at 11AM
Meets virtually on the 2nd Tuesday of each month at 6PM
Jacksonville Multiple Myeloma Support Group
Meets in a hybrid format on the 2nd Wednesday of each month at 6PM
Palm Coast Multiple Myeloma Support Group
Meets in-person on the 2nd Thursday of each month at 3:30PM
Brooksville / Nature
Coast Multiple Myeloma Support Group
Meets virtually on the 3rd Wednesday of each month at 6PM
The Villages Multiple Myeloma Support Group
Meets in-person on the 1st Tuesday of each month at 1PM
North Tampa Multiple Myeloma Support Group
Meets hybrid on the 3rd Saturday of each month at 10:30AM
Tampa Bay/St Petersburg Multiple Myeloma Educational Group
Meets virtually on the 1st Saturday of each month at 10:30AM
Tampa Central-Multiple Reasons Support Group
Meets virtually on the 2nd Thursday of each month at 11AM
Panama City Multiple Myeloma Support Group
Meets in-person on the 2nd Saturday of each month at 10AM
Naples Multiple Myeloma Support Group
Meets hybrid on the 3rd Thursday of each month at 12pm
Sebring Multiple Myeloma Support Group
Meets virtually on the 3rd Thursday of each month at 6pm
Tallahassee Multiple Myeloma Support Group
Meets in-person on the 4th Monday of each month at 5:30PM
Myeloma Voices at ASH
Myeloma Voices 10 In Person / 5
Virtual
Myeloma Voices #1 tweeters out of ASH
#FaMMily
IMF InfoLine
Connecting Patients to Resources…
Shortening “Time to Hope” for Over 1,000 First-Time Callers Each Year
Assistance with understanding lab results, terminology and disease state
Preparing for medical visits
Access to medical providers
Access to medications
Financial resources
“Thank you so much for the informative conversation and all the time you spent listening and helping me decipher the MM lingo. What an amazing service!”
“Thank you for your response and excellent question suggestions for my hematology team.”
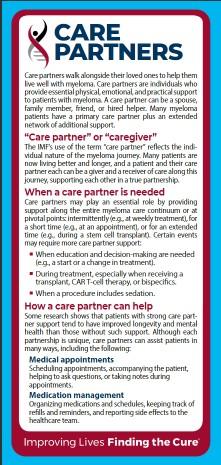
Written Education
Understanding Booklets
Tip Cards
Myeloma Minute Weekly Updates
Myeloma Today Quarterly News
many others!
Live Patient Education
local myeloma experts
2025 Live Patient Education
Patient & Family Seminars
• Boca Raton, FL – March 14 – 15
• Philadelphia, PA – May 2 – 3
• Los Angeles, CA – August 15 – 16
• Chicago, IL – October 3 – 4
Myeloma Community
Workshops
• Virtual - March 4
• San Francisco, CA - March 29
• Atlanta, GA - April 5
• Edina, MN - April 26
• Denver, CO - June 21
• Virtual – July 29
• Seattle, WA - August 9
• Waltham, MA - September 27
• Raleigh-Durham, NC - November 15
• Virtual – November 18
Scan for Upcoming Events!
Diane Moran, RN, MA, EdM Chief Executive Officer
Sr VP
Strategic Planning
with the IMF since April 2006
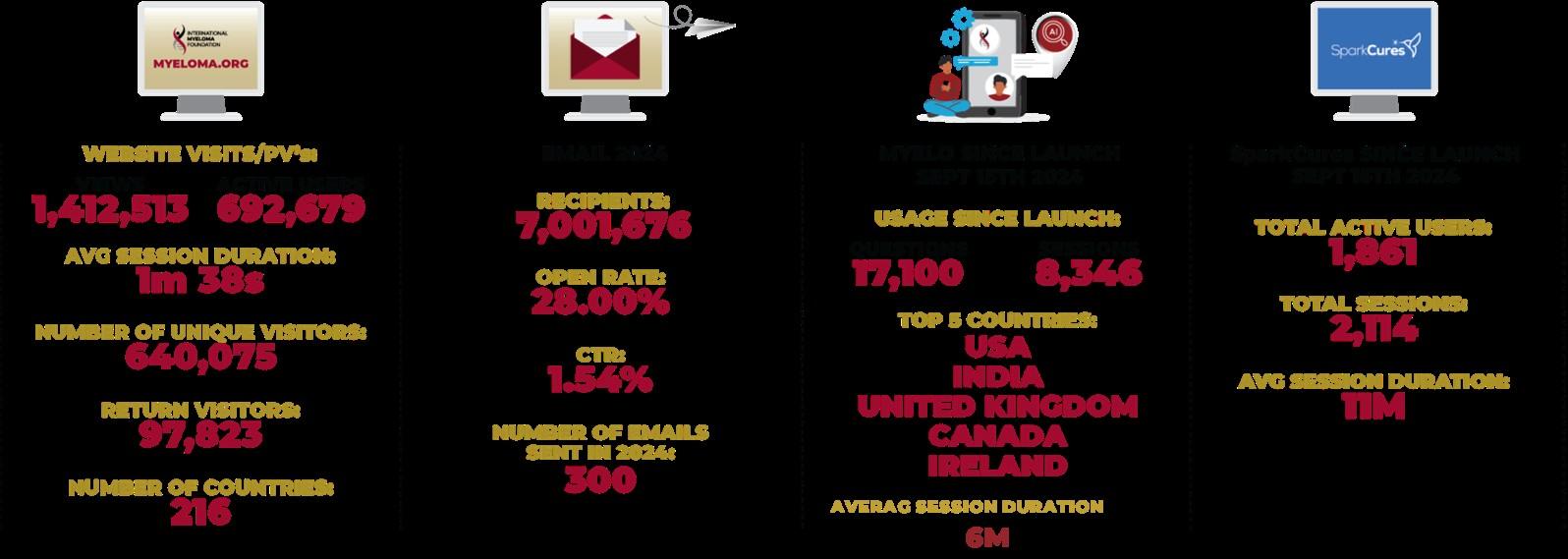
900,000 + views
2024 Highlights
• Support Groups
• InfoLine
• PFS
• RCW
3600 Nurses serving 23,000 patients with MM
• Nurse Leadership Board
• ONS Symposium
• Myeloma University
InfoLine Support groups GMAN Members IMWG Members
A world where every myeloma patient can live life to the unburdened by the disease.
Fireside Chat: What is the Future of Myeloma?
With Q&A
Joseph Mikhael, MD, MEd, FRCPC, FACP, FASCO, Chief Medical Officer ,International Myeloma Foundation
Rafat Abonour, MD
Indiana University, Indianapolis, IN
Thank you to our sponsors!
Breakout B: Managing Relapsed Myeloma
Krina Patel, MD, MSc
The University of Texas MD Anderson Cancer Center, Houston, TX
Managing Relapsed Myeloma
Krina Patel MD MSc
Associate Professor
Multiple Myeloma Section Chief
UT MD Anderson Cancer Center
Houston, Texas
Outline
• General approach to RRMM
• Non t cell redirecting therapies
• T cell redirecting therapies
• Prophylaxis and toxicities
General Approach to RRMM
Patho-physiology
• Myeloma is a blood cancer that develops in the bone marrow[1]
• It is a cancer of the plasma cells
• Normally plasma cells produce immunoglobulins (antibodies) as part of an immune response[1]
• Myeloma results in an excess secretion of one type of dysfunctional antibody (immunoglobulin) known as the monoclonal (M) protein or paraprotein[1,3]
1. Munshi NC et al. In: DeVita VT Jr et al, eds. Cancer: Principles & Practice of Oncology. Vol 2. 8th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2008:2305-2342. 2. SEER stat fact sheet: myeloma. 2020. 3. Kyle RA et al. Leukemia. 2009;23(1):3-9
What is relapsed disease?
• Clinical versus biochemical
• Clinical relapse requires one or more of:
• Direct indicators of increasing disease and/or end organ dysfunction (CRAB features).
• Development of new soft tissue plasmacytomas or bone lesions
• Definite increase in the size of existing plasmacytomas or bone lesions. A definite increase is defined as a 50% (and at least 1 cm) increase as measured serially by the sum of the products of the cross-diameters of the measurable lesion
• Hypercalcemia (> 11.5 mg/dL) [2.65 mmol/L]
• Decrease in hemoglobin of > 2 g/dL [1.25 mmol/L]
• Rise in serum creatinine by 2 mg/dL or more [177 mmol/L or more]
What is a biochemical progression?
• Increase of > 25% from lowest response value in any one or more of the following:
• Serum M-component and/or (the absolute increase must be > 0.5 g/dL)
• Urine M-component and/or (the absolute increase must be > 200 mg/24 h)
• Only in patients without measurable serum and urine M-protein levels; the difference between involved and uninvolved FLC levels. The absolute increase must be > 10 mg/dL
What is refractory disease?
• Disease that is nonresponsive while on primary or salvage therapy, or progresses within 60 days of last therapy. Nonresponsive disease is defined as either failure to achieve minimal response or development of progressive disease (PD) while on therapy.
• relapsed-and-refractory myeloma
• primary refractory myeloma
• What does triple-refractory mean?
• Resistant to all three classes of standard myeloma therapies, which include: Proteasome inhibitors. Immunomodulatory agents. Monoclonal antibodies
• What does penta-refractory mean?
• Disease that is resistant (or relapsed on) 5 standard myeloma therapies – bortezomib, lenalidomide, carfilzomib, pomalidomide and a CD38 monoclonal antibody
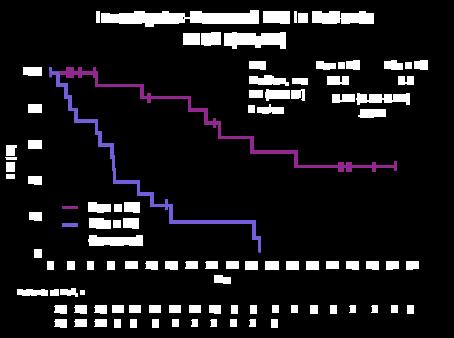
2-4+ years
Not Every Relapse Requires Immediate Therapy
Asymptomatic biochemical relapse on 2 consecutive assessments
Asymptomatic high-risk disease or rapid doubling time
Symptomatic or extramedullary disease
Why it’s not an algorithm:
Many of these variables change over time!
Patient-Related
• Age/frailty
• Performance status
• Drug metabolism
• Compliance/adherence
• Renal insufficiency
• Comorbidities
• Social Support:
• Preference/lifestyle
• Caregiver support
• Financial access
• Logistical access
Disease-Related
• R-ISS
• Rate of growth
• Marrow burden
• CRAB symptoms (hypercalcemia, renal failure, anemia, bone disease)
• Extramedullary dz
• Molecular cytogenetics/ genomics
Treatment-Related
• Response to prior therapy
• Time to relapse
• Clinical trial availability
• Route of administration
• Adverse events/toxicity
• Single agent vs combination
Logistics of Treatment
• Timing
• Cycle = 3-4 weeks
• Number of cycles prior to maintenance= 4-8
• Route of administration: Injections, infusions, or pills?
• Velcade = subq injection, carfilzomib = IV infusion, daratumumab = subq or infusion, lenalidomide = pills, steroids = IV infusion or pill
• Adjunctive treatments:
• Bisphosphonate therapy to strengthen bones (dental clearance before initiating)
• Anti-viral medications for varicella prophylaxis
• Aspirin or another blood thinner to prevent blood clots
• Anti acid reflux medications as steroids/oral chemo can cause gastritis/ulcers
• Anti-bacterial coverage (for frail patients with high risk of infections)
Upfront Rx and Fitness Affects Subsequent
Rx
Non-T cell redirecting therapies
Randomized Studies with Pom Dex or Car Dex as Control Arms
Randomized Studies With BortezomibDexamethasone Control Arms
PFS benefit can translate into OS benefit with adequate follow up (though drug access at relapse confounding issue).
credit: Ajai Chari MD
PI + IMID + Dex (Triplet) Efficacy in Relapsed MM
PI + IMID + Dex triplets result in superior efficacy relative to doublets.
Pineda-Roman M et al. Leukemia. 2008;22:1419; Richardson PG et al. Blood. 2014;123:1461; Richardson PG et al. Leukemia. 2017;31:2695; Paludo J et al. Blood. 2017;130:1198; Wang M et al. Blood. 2013;122:3122; Shah JJ et al. Blood. 2015;126:2284.
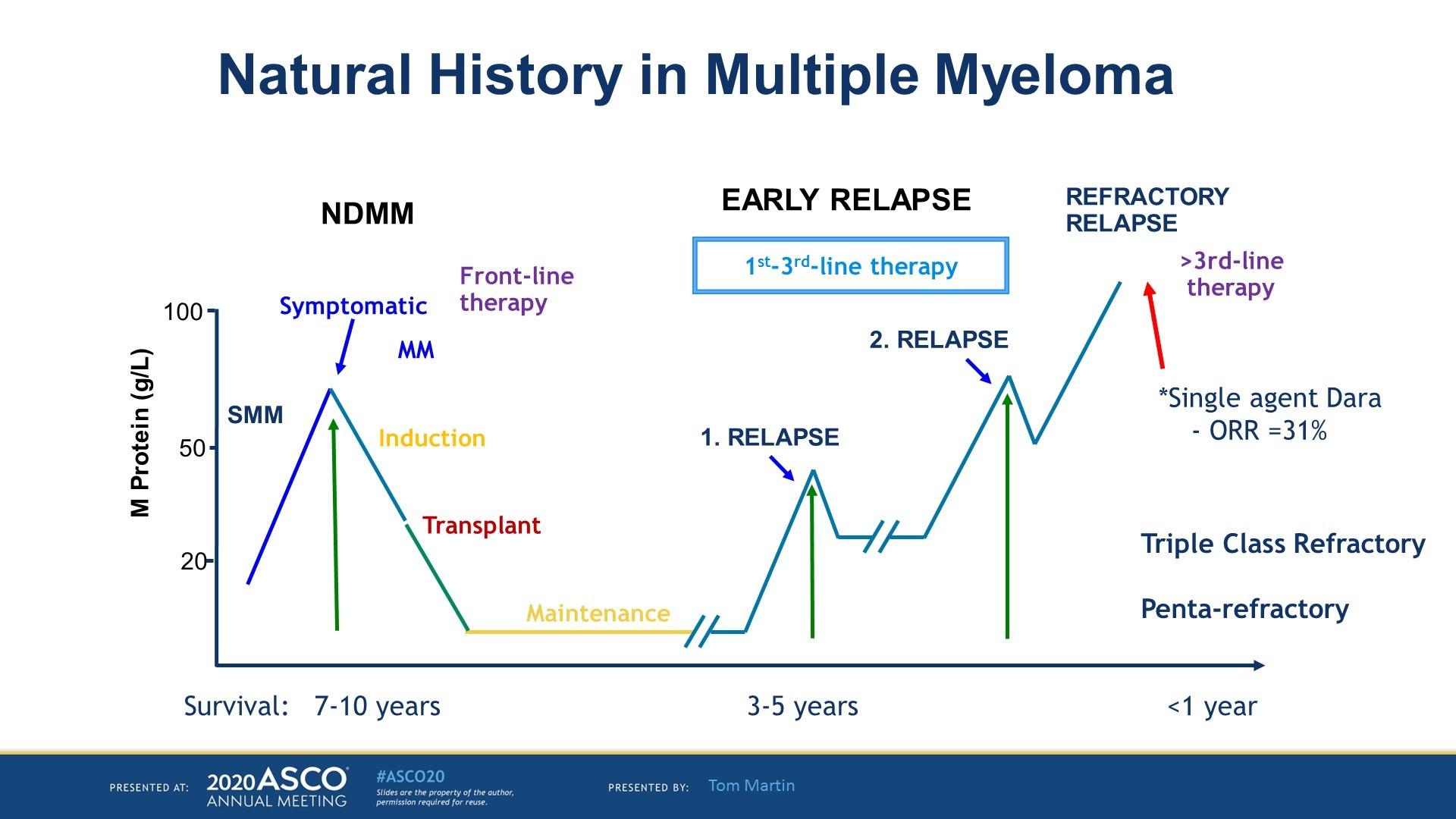
BOSTON: Bortezomib/Selinexor/Dexamethasone
• Grosicki S, et al. Lancet. 2020;396:1563-1573.
Venetoclax for t(11;14)
T cell redirecting therapies
Early Line trials – different patient populations
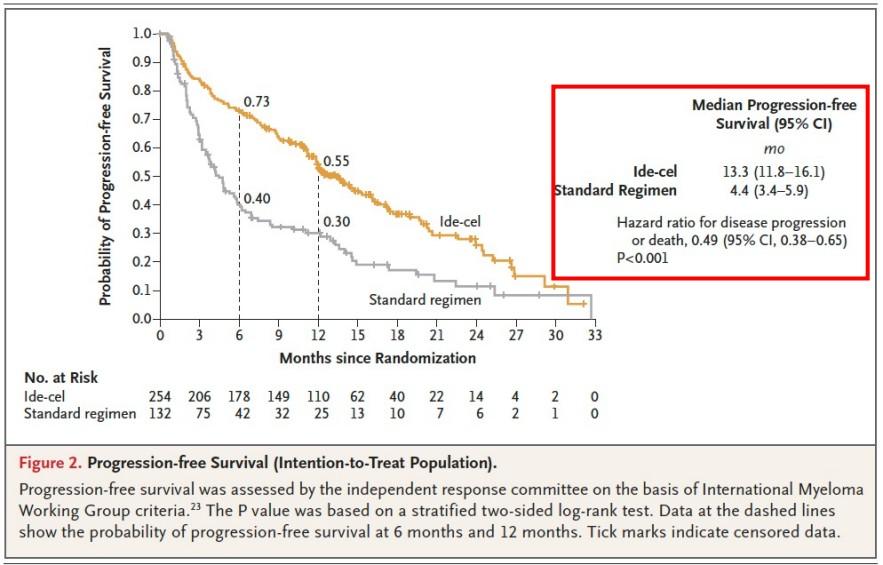
KarMMa 3
Rodriguez-Otero P, et al. NEJM 2023
• KarMMa 3: TCE, lines 3-5, vs DPD/DVD//KD/EPD/IRD
• KarMMa 2
• 2a: (second line in early relapse post ASCT)
• 2c: (consolidation less than VGPR post ASCT)
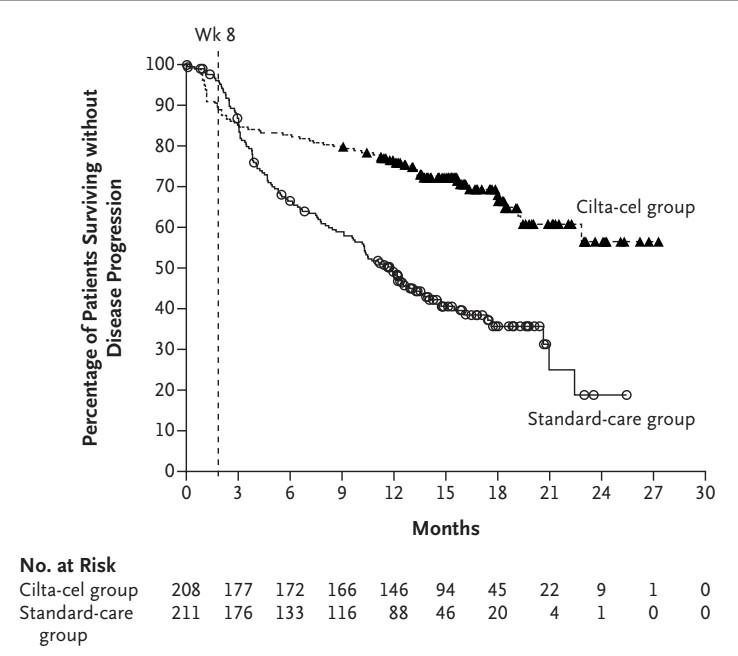
• CARTITUDE 4: lenalidomide refractory, lines 2-4, vs DPD/PVD
• CARTITUDE 2
• 2b: second line in early relapse post induction (+/ASCT)
• 2c: prior anti BCMA Rx
San Miguel J, et al.
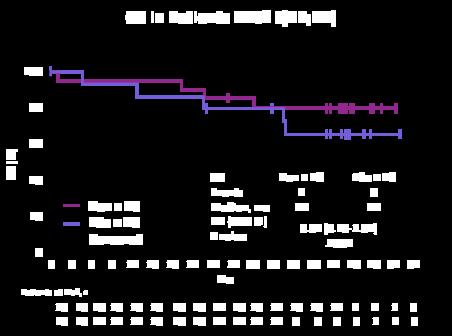
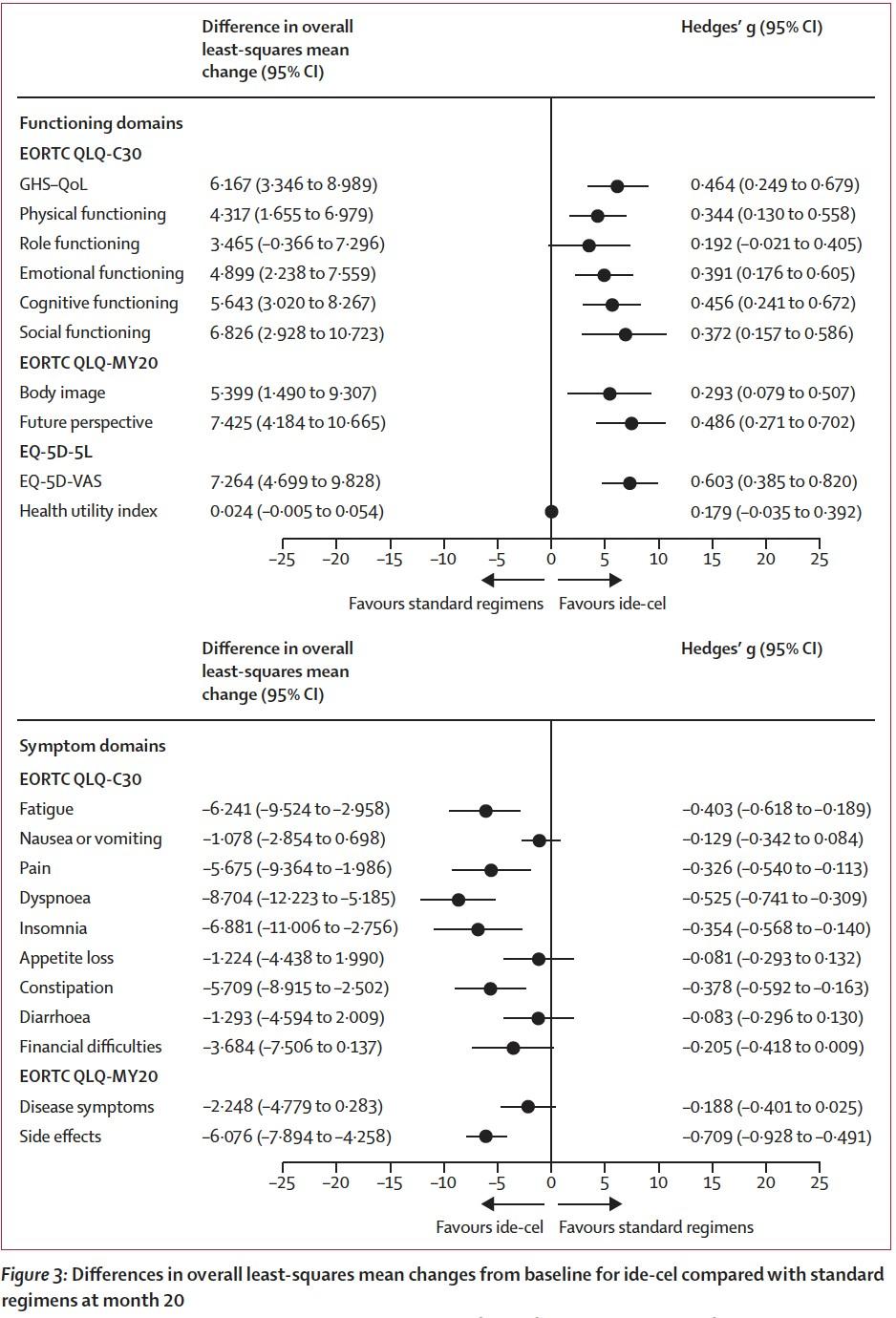
KarMMa 3 HRQoL
”In this study, patients receiving ide-cel demonstrated statistically significant and clinically meaningful improvements across most domains, including fatigue, pain, and physical functioning.” [compared to SOC regimens]
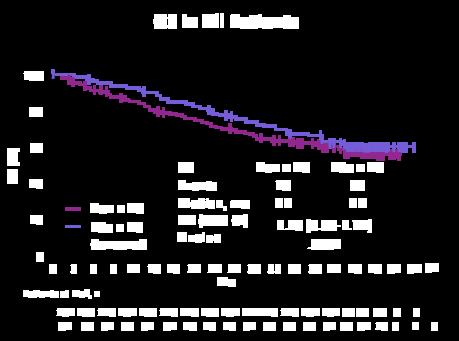
CARTITUDE-4: Effect of Cilta-Cel Single Infusion on QoL
Patients With Lenalidomide-Refractory MM Who Had 1-3 Prior Lines of Therapy
Demonstrated Clinically Meaningful Improvements in Health-Related QoL 1
• Meaningful reductions in disease-specific symptoms on multiple PRO endpoints
• Improvements in healthrelated QoL were numerically greater with cilta-cel than with continuously administered SOC treatments across all scales
EORTC QLQ-C30, mean change (95% CI)
Global health status/QoL
Global health status
Functional scales
Cognitive functioning
Emotional functioning
Physical functioning
Role functioning
Social functioning
Symptom scales/items
Fatigue
Nausea and vomiting
Pain score 10.1 (7.0-13.1) 0.5 (-2.4 to 3.5) 9.5 (6.6-12.5) 6.5 (3.8-9.1) 7.7 (3.7-11.7) 6.1 (2.1-10.0) -9.1 (-12.4 to -5.8) -1.2 (-3.1 to 0.7)
EQ-5D-5L, mean change (95% CI)
(-14.0 to -6.5)
(-5.3 to 2.3)
(-11.2 to -3.9) 2.2 (-1.3 to 5.7) -2.1 (-5.0 to 0.7) -1.7 (-6.3 to 2.9) -0.1 (-4.2 to 4.0) 2.8 (-1.4 to 7.0) 0.6 (-1.4 to 2.7) -3.9 (-7.9 to 0.2)
Visual analogue scale 8 (5.2-10.7) 1.4 (-1.9 to 4.7)
MySlm-Q, mean change (95% CI)
Total symptom subscale
Total impact subscale -0.18 (-0.27 to0.10)
-0.41 (-0.53 to0.29) 0.17 (0.06-0.27) 0.01 (-0.13 to 0.14)
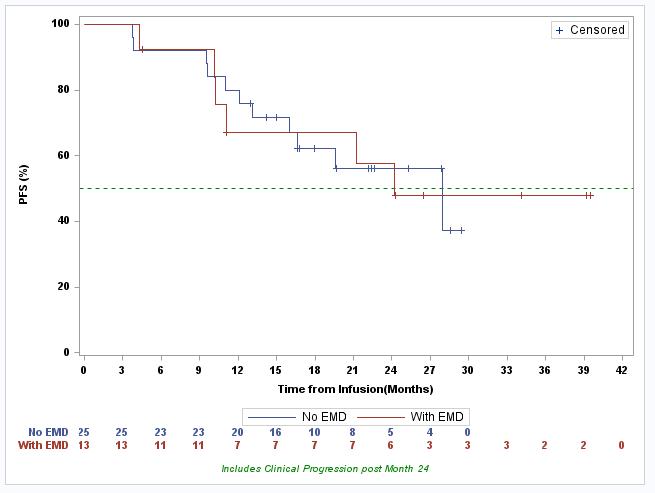
Anito-cel Phase 1 Results: EMD, Non-EMD Patients
Median Follow-Up: EMD Patients ~33-mo. [14-44]; Non-EMD Patients ~25-mo. [15-40]
Note: Data cut-off October 15, 2023
How I treat myeloma patients with CAR T
• I offer it as soon as possible in terms of LOT/refractoriness, 2nd line for high risk, 3rd line for standard risk.
• Less manufacturing failure risk, more likely to respond to bridging, which then leads to less toxicity and better response in my experience
• Currently I avoid alkylators and BCMA therapies right before apheresis, but will use if needed during bridging.
• Goals prior to apheresis: have the highest ALC possible, hopeful best quality too (may need to hold therapy for 2-3 weeks prior for lymphopenic patients (but myeloma has to be stable).
• Goals prior to LD chemo: decrease myeloma tumor burden if possible, but do not increase risk of toxicity (i.e. infections) significantly
• If a patient has comorbidities (i.e. renal insufficiency, cardiomyopathy, etc) we have other consultant services evaluate patient prior to, during and after treatment as needed to optimize those conditions
• Aggressive infection prophylaxis. At MD Anderson, we check CMV PCRs prior to LD and then weekly for first 30 days. If positive, we consult ID and if increasing or CMV disease evident, we treat.
FDA-approved BCMA and GPRC5D Bispecifics
Bispecific antibody
Structure/ function
Teclistamab1
Elranatamab2
AEs, all (Gr 3+)
Infections
Neutropenia
Anemia
Thrombocytop enia
Neurotoxicity
Deaths
Talquetamab3
Phase 1/2 MonumenTAL-1 Study: GPRC x CD3
(64%)
(37%)
(21%) 15% (0.1)
Hypogamma/ IVIg 72% (0.6%) 76% (45%)
49% (37%)
31% (24%)
NR/NR
68 (41 due to PD) 75%/39% 58% (0%) 70% (40%) 49% (49%)
1. Moreau P, et al. N Engl J Med. 2022;387:495-505; 2. Lesohkin AM, et al. Nat Med. 2023;29:2259-2267; 3. Data provided by Lonial S.
Prophylaxis
and Toxicities
Prevention & Management of Complications
• Infections:
• Antiviral & PJP prophylaxis (steroids, bispecifics, CAR Ts)
• Yearly influenza vaccination
• Pneumococcal vaccine
• Consider prophylactic antibiotics during the first months of induction for frail pts/high risk
• IVIG for select patients (bispecifics, CAR Ts, sometimes CD38 monoclonal antibodies)
• These patients have a hard time with encapsulated bacteria & gram-negative organisms education to report & urgent visits/treatment if infection suspected
Prevention & Management of Complications
• Skeletal Lesions & Bone Health
• Prevention: bone-modifying therapy with osteoclast inhibitors (bisphosphonates) or RANK ligand inhibitor (denosumab)
• Spinal Cord Compression: true emergency ER
• Pathologic & impending fractures: long bones may require stabilization. Vertebral fractures may benefit from kyphoplasty or vertebroplasty
• Pain: can usually be controlled with a combinations of analgesics & active myeloma therapy
• Palliative XRT: ~40% of patients will require RT to control disease
• Pain, SCC, plasmacytoma, local control
• Notify provider for new bone pain or jaw pain
• Hold bone-modifying therapy for ~3 months prior to dental work
• Those who don’t have access to appropriate health care or clinical trials
• High risk disease/plasma cell leukemia
• Relapsed refractory with aggressive disease
• Renal failure
• CNS involvement
• Frail Patients/Increased Co-Morbidities
Take Home Points
• Triplets are better than doublets.
• Relapses occur differently for patients; goal should be to treat before clinical decline occurs.
• There are multiple options to choose from; however, patient-, disease-, and treatment-related factors should help narrow down appropriate choices that will provide the best survival, safety, and quality of life.
• Bispecific therapies have impressive response rates and PFS/DOR. Strategies around toxicity management (i.e. infections) will help optimize outcomes
• CAR T therapy response and PFS data is something we’ve never seen for RRMM. Real world data shows similar incredible results.
• ADCs are a good option for those who cannot get bispecifics and/or CAR T therapies or after these therapies; combinations with other anti-myeloma therapy (pomalidomide or bortezomib) are better.
• New targets for myeloma are creating exponential hope and combination/sequencing options we need to figure out.
Thank you: U.S. Multiple Myeloma Immunotherapy Consortium Sites
Neeraj Saini
Christine Ye
Mahmoud Gaballa
Oren
LUNCH
Please Move To Veranda
Partnering with the IMF
Sylvia Dsouza, Vice President, Development
International Myeloma Foundation
WHO AM I
WHAT DO I DO?
Vice President of Development for the IMF
Securing philanthropic support and resources for the IMF through diverse mechanisms
Oversee a team of passionate and determined fundraising professionals who are committed to advancing the mission of the IMF
Have the incredible honor of working with dedicated volunteers from the US and across the globe.
3 Ways to Engage
Philanthropy
Make a philanthropic gift to support research, education, advocacy or patient support programs.
Volunteer
Join your local support group/become a Support Group Leader
Join our grassroots patient Advocacy program
Volunteer your time at local races organized by the IMF to engage the community
Engage on social media to connect with others affected by myeloma and spread awareness and empower patients with knowledge and resources.
Intellectual capacity
Offer your expertise as a speaker or panelist at events.
Be a beta tester for various new tools and products and provide reviews and feedback
Philanthropy Fuels Our Mission
Peer-to-Peer Fundraising
Peer-to-Peer Fundraisers are created from YOUR ideas. Starting a Fundraiser is easy and fun. They also make a world of difference in the myeloma community.
Join a IMF P2P event or start your own and engage your family, friends, co-workers, your network who honor your journey with myeloma and want to support you. Let them show you that you are not alone.
Ex: Hole in One Golf Tournament, Iceland Cycling Expedition, Miracles for Myeloma 5K Run/Walks (hybrid)
Join the HOPE Society (Recurring Monthly & Annual Giving Program)
Help us cultivate the future by joining the International Myeloma Foundation's Hope Society.
Monthly and annual gifts support IMF core programs, including educational events, publications, the toll-free InfoLine, and more.
Start with a monthly contribution and when ready turn it into a yearly commitment. You will be a part of likeminded individuals united in the quest to find a cure for myeloma and a better quaity of life for all myeloma patients.
Transformative Gifts (Major Giving and Principal Giving)
Gifts can be designated toward a specific program, project or initiative .
Is there something specific that resonates deeply with you and you want to see change happening?
Gifts can also be unrestricted, expendable and/or an endowment
Major Giving -
Designate Your Gift
• Research: The IMF is dedicated to finding a cure for multiple myeloma.
• Education: The IMF provides education for patients and caregivers.
• Support: The IMF provides support for patients and caregivers through inperson and virtual support groups.
• Advocacy: The IMF advocates for better access to care and more affordable options for myeloma patients.
Research
The Black Swan Research Initiative was funded by a Board member/donor who was a visionary and saw the need for the IMF to launch this initiative
The IMF's Black Swan Research Initiative serves as a conductor of sorts to this orchestra of collaborating experts in the field of myeloma.
The BSRI sponsors more than 50 projects around the world aimed at curing multiple myeloma. Among them:
SPAIN: The CESAR trial uses the combination of Kyprolis, Revlimid, and dexamethasone plus autologous stem-cell transplant to treat high-risk smoldering multiple myeloma. It applies precise minimal residual disease (MRD) testing using next-generation flow cytometry (NGF) and Blood testing for routine monitoring
USA: The ASCENT 1.0 trial tests early intervention in high-risk smoldering multiple myeloma.
ICELAND: Launched in 2016, the iStopMM project identifies and treats multiple myeloma at the earliest signs of disease.
GERMANY: Studies are exploring long-term survival and hereditary risk factors in multiple myeloma.
AUSTRALIA: Identifying mechanisms of the progression of multiple myeloma and testing DNA mutations in the blood.
SINGAPORE: Hub for the clinical trials network in Asia led for the IMF’s Asian Myeloma Network (AMN) program by Prof Wee Joo Chng. A collaboration of eight countries (or regions), the AMN is unique in providing access to novel agents in a clinical trial setting throughout Asia. In addition, research projects appropriate for the region are conducted in an effort to improve outcomes and achieve a cure.
Brian D. Novis Grants
• The Brian D. Novis Grants award Senior and Junior investigators in the myeloma field with critical funding to elevate their ideas, work, and efforts in finding a cure for myeloma.
• Helps support novel research ideas that can be a breakthrough
• Historically, the IMF has awarded 46 Senior Grants and 109 Junior Grants. (157 grants for $8M+ since inception)
IMF's Scientific Advisory Board
The Scientific Advisory Board (SAB) of the International Myeloma Foundation (IMF) is a group of world-renowned experts in the field of myeloma research. The SAB provides guidance and expertise to the IMF on scientific and medical matters, including research priorities, clinical trials, and patient care.
Education
Patient and Family Seminars: 4 in-person events across the United States
Regional Community Workshops: 6 in-person and 4 virtual
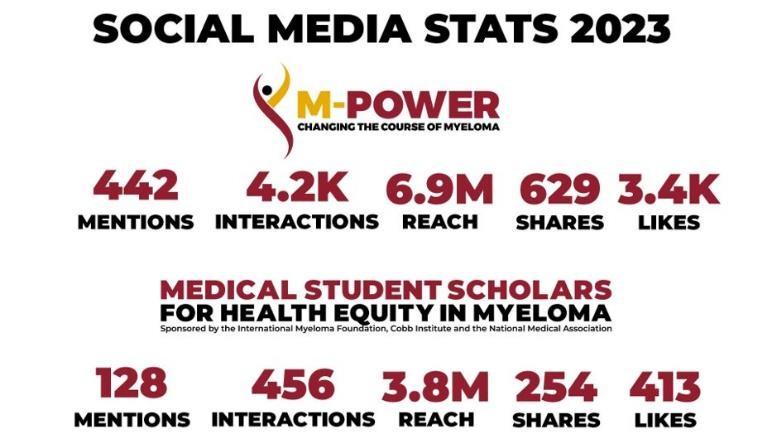
M-Power Initiative:
M-Power Community workshops and we have covered Atlanta, Detroit, Baltimore, New York, Richmond, Charlotte, and Tampa in the last couple of years with goals to expand to more cities in the U.S.
The Health Equity Scholars is a mentoring program that pairs 12 students and 12 myeloma experts to conduct projects that address myeloma research on health disparities. This program educates individuals from minority communities about myeloma, engages communities at the earliest level on training to share a deeper understanding of the disease, and improves sensitivities towards myeloma diagnosis.
Advocacy
Danielle Doheny
U.S. Policy & Advocacy
Michael Riotto
U.S. Grassroots Advocacy
We believe in the value of working to improve healthcare laws to ensure there are no barriers to care as patients navigate their myeloma journey. The IMF is the voice of the myeloma community in Washington, DC. Our objective is to inform and influence the critical healthcare policy decisions impacting the myeloma community.
What Do We Advocate For?
The following policy principles are the foundation on which we prioritize our advocacy work.
1. Ensure Access to Care: We advocate for policies that ensure all myeloma patients have equitable, comprehensive, patientcentered care without insurance barriers that limit options or delay treatment initiation.
2. Eliminate Financial Barriers: We advocate for policies that allow myeloma patients access to treatments and supportive care interventions without facing financial hardships.
3. Advance Myeloma Research: We advocate for annual appropriations funding for myeloma research and the advancement of clinical trial eligibility and research protocols that ensure representation from diverse populations.
Grassroots Advocacy at the IMF
Grassroots Advocacy is the critical component to influencing policy decisions
The IMF brings advocates to Capitol Hill to share their experience with lawmakers.
Together, we champion legislative priorities that directly impact the lives of millions of patients and elevate the voices of of the myeloma community.
The IMF Grassroots Advocacy Program is multi-faceted and growing
• Advocacy Training & Leadership Development
• Policy and Legislative Education
• Grassroots Campaign Planning
• Health Policy Forums & Roundtables
• Advocacy Resource Development
• Storytelling and Personal Narratives
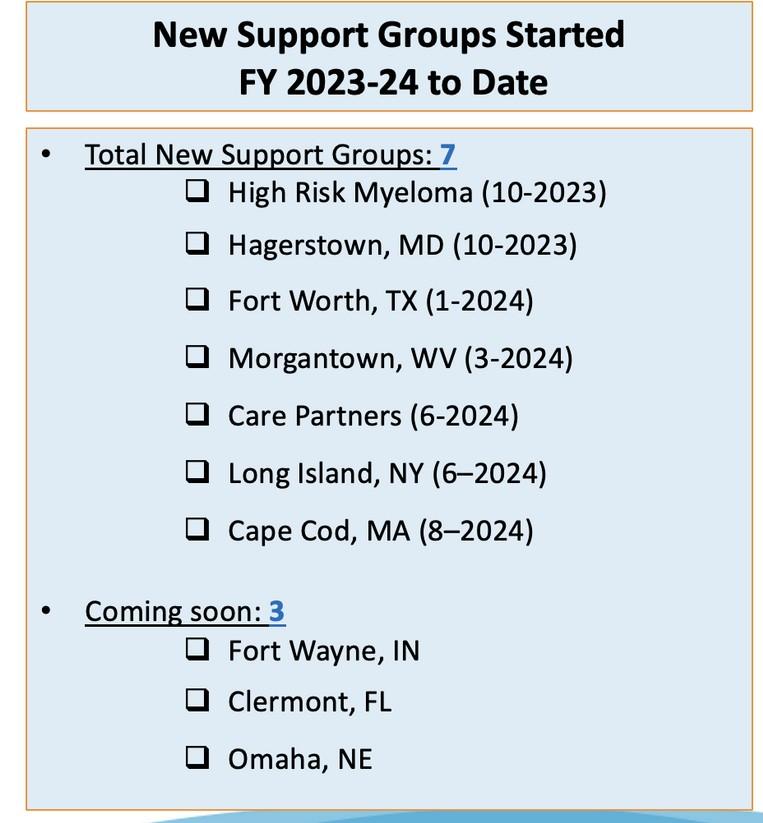
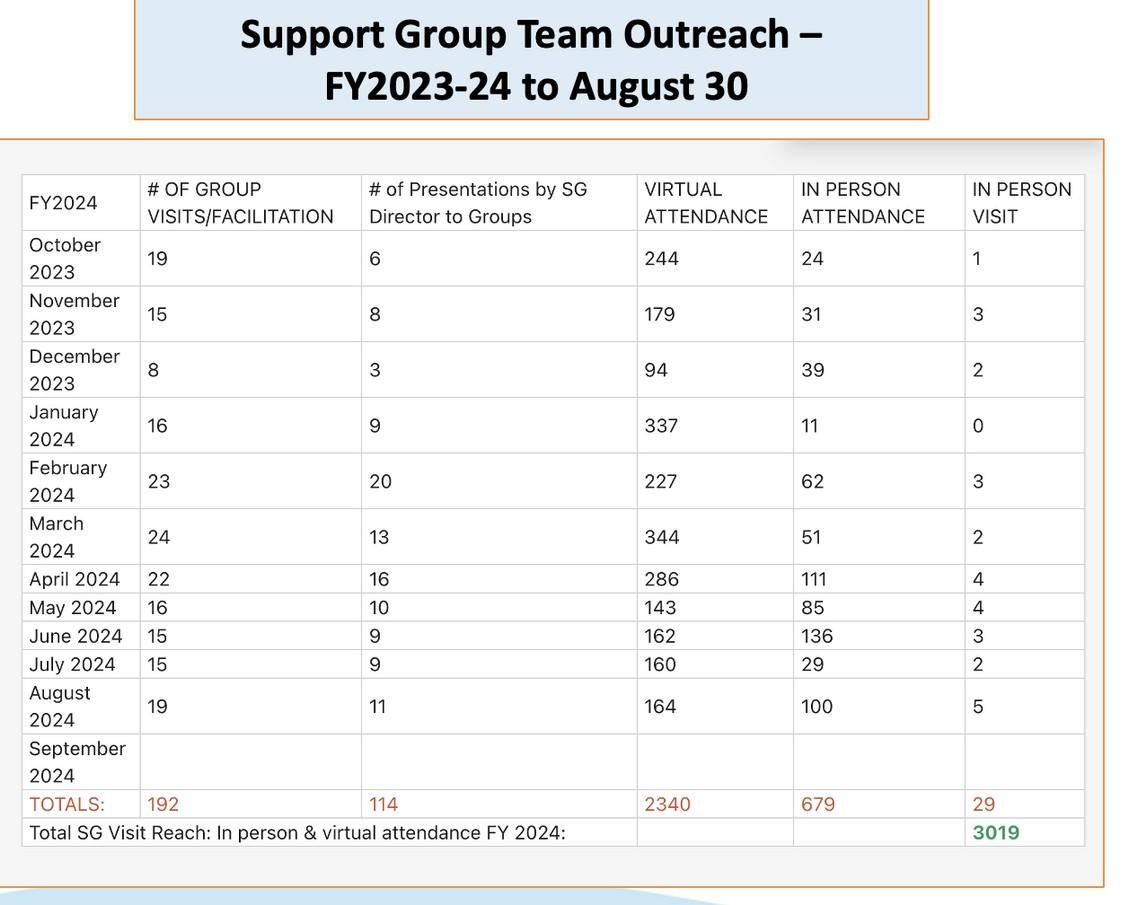
Summit:
Support Group Team Report – November 2024
MYELOMA VOICES AT ASH 2024 TEAM
We were excited to celebrate the 25th Anniversary Support Group Leaders Summit with 98 Support Group Leaders representing 74 Support Groups with 32 first-time attendees and 66 returning leaders
LINK TO Myeloma Voices Webpage 2024
The IMF brings myeloma support group leaders and patients to ASH to learn and share their voices. This information and hope is heard globally and locally from their perspective utilizing social media, blogs, vlogs, and interviews to offer their personal insights.
The IMF is committed to fostering interaction between the patient community and the myeloma experts.
“In the last 20 years, 19 myeloma treatments have been approved by the FDA. With so many combination therapies and clinical trials, we have a better chance than ever before of providing the patient with excellent treatment. Be your own best advocate!” Jack Aiello
P2P
Laughs 4 Life (Hattiesburg, MI, comedy celebration)-- 8 years, $483,850!
Peer-to-Peer (P2P) and Monthly & Annual Giving
Miracles for Myeloma(Clark, New Jersey, 5K run/walk) -- 12 years, $804,422!
Iceland Cycling Expedition raised close to $250K
Hole In One (Golf Tournament, Jackson, New Jersey)– Inaugural golf tournament that has raised $73K
Monthly & Annual Giving – HOPE Society
Join our flagship monthly and annual giving program, the HOPE Society.
Get invited to Regional Salon Dinners in your area with IMF leadership and KOLs.
Receive exclusive updates on research and trials fresh off the press.
Play a pivotal role in supporting our four pillars.
Support long-term initiatives that make a lasting difference.
Upcoming Peer-to-Peer Fundraising Events in 2025
• 7th Annual Schleicher's Hikers 5K
• Mission for Matt
• Jack's Education and Experience Grant
• San Fernando Valley Support Group Fundraiser
• Raging for Ray
• Czerkies Memorial Golf Outing
• Hole in One Golf Tournament
• Inland Empire Walk
• Walkathon & BBQ To End Multiple Myeloma
• Row for a Cure
IMF's Miracles for Myeloma Virtual/In-Person 5K Run/Walk Series
The IMF will lead five Virtual/In-Person 5K Run/Walks across the United States in the following regions (Goal: $100K net from each event)
• Miracles for Myeloma Virtual/In-Person 5K Run/Walk in Boca Raton, FL (03-15-2025)
• Miracles for Myeloma Virtual/In-Person 5K Run/Walk in Los Angeles, CA (04-12-2025)
• Miracles for Myeloma Virtual/In-Person 5K Run/Walk in Philadelphia, PA (05-03-2025)
• Miracles for Myeloma Virtual/In-Person 5K Run/Walk in Clark, NJ (09-13-2025)
• Miracles for Myeloma Virtual/In-Person 5K Run/Walk in Chicago, IL (10-04-2025)
Iceland Cycling Expedition 2025
• The 2025 Iceland Cycling Expedition will take place from Wednesday, August 27, 2025 through Tuesday, September 2, 2025.
• The Iceland Cycling Expedition is a 6-day/7-night fundraising cycling challenge in the High Mountains of Iceland.
• 20 Participants including industry sponsor slots
• Applications for in-person participation now closed but you can participate and support virtually! More information coming soon.
International Myeloma Foundation’s Signature Marquee Annual Endurance
Click here to look back to where i t all started in 2024!
Three goals:
1. Raising awareness and visibility for multiple myeloma and a patient/care-partners journey to and through it (humanizing the disease)
2. Raising awareness and visibility for the International Myeloma Foundation
3. Raising critical funding to help accelerate research to find a cure for myeloma
Additional outcome that organically emerged – building a strong, interconnected myeloma community where all myeloma patients and their loved ones see hope, resilience and determination as part of the journey and feel empowered
Ashley Dieks (Patient) Garson, Ontario
ICE 2025 Participants
Dr. Saad Usmani (Myeloma Clinician and Researcher) Memorial Sloan Kettering, NY
Jered Haddad (Patient) Germantown, TN
Dr. Douglas Sborov (Myeloma Clinician and Researcher) Huntsman Cancer Institute at the University of UT
Richard Pampe (Patient) Jackson, WY
Dr. Jeffrey Zonder (Myeloma Clinician and Researcher) Department of Oncology at Wayne State University, MI
Tatum Byhre (Care Partner) Minneapolis, MN
Christian Hoff (Patient) Pittsboro, NC
Benjamin Freund (Patient) East Canaan, CT
Troy Fischer (Care Partner) Bloomington, IL
Katherine Podgorski (Patient) Toronto, Canada
Dr. Cristina Gasparetto (Myeloma Clinician and Researcher) Duke Cancer Institute, NC
Iceland Cycling Expedition 2024
Phare International
Malibu Film Festival
Beverly Hills Film Festival
Tribeca Festival
Atlanta Film Festival
Palm Springs International Film Festival
Miami Film Festival
Flicker's Rhode Island International Film Festival
LA Shorts
11. Holly Shorts Film Festival Portland Film Festival
Leave a Lasting Legacy
Planned Giving
Join the Brian D. Novis Legacy Society and make a planned gift!
Gain immediate tax benefits
Potentially increase your income during your lifetime.
Continue to fund our core programs and four pillars.
Make a bequest (a gift from your estate)
Include a provision in your will or living trust.
Designated us as a beneficiary of a life insurance policy, or retirement plan (IRA, 401(k), or 403(b).
Leave us in your will is one of the most profound ways to support the people and causes important to you.
Corporate and Foundation Gifts
Your organization can contribute a corporate gift or foundation grant
Provide seed funding that is necessary to accelerate the path to a cure.
Reach Out to the IMF Development Team
We welcome you to continue to learn more about our programs, projects, and initiatives at the IMF and find alignment with your own philanthropic passion and as well as ways to deepen and strengthen your engagement with us. Reach out to the IMF Development Team to start a conversation on how you can make a difference in the lives of the people impacted by myeloma.
Sylvia Dsouza- Vice President of Development sdsouza@myeloma.org or (310)947-4126
Simona Grace- Director of Development, Major Gifts sgrace@myeloma.org or (818)487-7455 x 307
Kimberly Francis- Assistant Director of Development Peer-to-Peer Fundraising kfrancis@myeloma.org or (818)487-7455 x 304
H. Lee Moffitt Cancer Center and Research Institute, Tampa,
FL
Myeloma: Putting the Pieces of the Puzzle Together
Beth Finley Oliver, MSN, ARNP,
AGNP-BC
Moffitt Cancer Center, Tampa, Florida
A presentation from the IMF’s Nurse Leadership Board
Myeloma: Putting The Pieces of the Puzzle
Focus on Managin g Sympto ms
Myeloma: Putting The Pieces of the Puzzle
Myeloma Is a Cancer of the Plasma Cells
Plasma Cells come from white blood cells produced in the bone marrow and make many different antibodies to help fight infection (polyclonal).
In Multiple Myeloma, one plasma cell mutates, making many identical plasma cells (monoclonal).
Bone marrow
Bone marrow
Myeloma Causes Cell Dysfunction &
Anxiety
Stress
Depression
Decreased red blood cells
Anemia & Fatigue
Decreased white blood cells
Myeloma protein in blood and urine
Changes in bone remodeling
Clonal myeloma plasma cells can cause many symptoms
– Crowd out normal bone marrow cells
– Produce myeloma protein
– Can cause kidney dysfunction
– Affect bone cells (balance of osteoclasts & osteoblasts)
Immune Dysfunction & Infection
Renal Dysfunction
Infections Are Serious for People with Myeloma
Preventing infections is paramount.
Infection remains the leading cause of death in patients with multiple myeloma. Several factors account for this infection risk, including the overall state of immunosuppression from multiple myeloma, treatment, age, and comorbidities (e.g., renal failure and frailty).
IMWG Consensus guidelines and recommendations for infection prevention in multiple myeloma; Lancet Haematol.2022;9(2):143–161.
Infection Prevention Tips
Good personal hygiene (skin, oral)
Environmental control (avoid crowds and sick people; use a high-quality mask when close contact is unavoidable)
Report fever of more than 100.4°F, shaking chills even without fever, dizziness, shortness of breath, low blood pressure to HCP as directed.
As recommended by your healthcare team:
Immunizations:
Flu, COVID, RSV & and pneumococcal vaccinations; avoid live vaccines
Treatment of Newly Diagnosed Multiple Myeloma (NDMM)
Induction
Consolidation
Initial treatments aimed at reducing the amount of myeloma cells
Intensification of treatment to deepen response. Either additional cycles of induction or autologous stem cell transplant (in eligible patients)
Prolonged lower-intensity treatment designed to sustain remission
Induction Standard of Care
Induction
Quadruplet therapy is preferred for nearly all patients with newly diagnosed myeloma
Anti-CD38 monoclonal antibody (mAb)
• Darzalex (daratumumab)
• Sarclisa (isatuximab)
Proteosome
Inhibitor (PI)
• Velcade (bortezomib)
• Kyprolis (carfilzomib)
At infusion clinic: subcutaneous injection or infusion
Supportive medication:
Immunomodulator
y drug (IMiD)
• Revlimid (lenalidomide)
• Pomalyst (pomalidomide)
Steroid
• Decadron (dexamethasone)
• Prednisone
Oral medication taken at home
• Antiviral prophylaxis (i.e., acyclovir or valacyclovir) to prevent viral infections particularly shingles.
• Antibacterial agents (i.e., Bactrim, levofloxacin) to prevent bacterial infections.
• Aspirin or other anticoagulant therapy to reduce the risk of blood clots from IMiDs.
• Bone-strengthening agents (i.e., zoledronic acid, denosumab) to strengthen bones and protect against fractures.
Steroids: An Important Piece Of The Treatment Plan
Steroids enhance the effectiveness of other myeloma therapies
Your provider may decrease or discontinue the dose as myeloma responds to therapy.
Do not stop or alter your dose of steroids without discussing it with your provider
Steroid Side Effects
• Irritability, mood swings, depression
• Blurred vision, cataracts
• Increased risk of infections, heart disease
• Muscle weakness, cramping
• Increased blood pressure, water retention
• Difficulty sleeping (insomnia), fatigue
Managing Steroid Side Effects
• Flushing/sweating
• Stomach bloating, hiccups, heartburn, ulcers, or gas
• Weight gain, hair thinning/loss, skin rashes
• Increased blood sugar levels, diabetes
Consistent schedule (AM vs. PM)
Take with food
Stomach discomfort: Over-thecounter or prescription medications
Medications to prevent shingles, thrush, or other infections
Rajkumar SV, et al. Lancet Oncol 11(1):29–37. King T, Faiman B. Clin J Oncol Nurs. 2017;21(2):240-249. Banerjee,R. et al. Blood 9.25.24
Peripheral Neuropathy
Peripheral neuropathy happens when there is damage to nerves in the extremities (hands, feet, limbs). Damage can be the result of myeloma, treatment or unrelated conditions (i.e., diabetes).
New agents or regimens in clinical trials are always an option
Many treatment options are available.
More therapies are being studied
Clinical trials may be an option
a2 or more prior therapies. bOff-label; not currently FDA-approved. C = cyclophosphamide; d = dexamethasone; Dara = daratumumab; FDA = US Food and Drug Administration; E = elotuzumab; Isa = isatuximab; I = ixazomib; K = carfilzomib; M = melphalan; p = prednisone; P = pomalidomide; R = lenalidomide; SQ = subcutaneous; V = bortezomib; X = selinexor.
Rajkumar SV. 2024 Myeloma Algorithm. https://clinicaloptions.com/CE-CME/oncology/2024-mm-algorithm/18440-26989. Accessed 12.14.24. NCCN Guidelines®. Multiple Myeloma. V3.2024. Accessed March 15, 2024. Noonan K, et al. J Adv Pract Oncol. 2022;13(suppl 4):15-21. Steinbach M, et al. J Adv Pract Oncol. 2022;13(suppl 4):23-30. Moreau P, et al. Lancet Oncol. 2021;22(3):e105-e118. O’Donnell EK, et al. Br J Haematol. 2018;182(2):222-230. Mo CC, et al. EJHaem. 2023;4(3):792-810. Chang D. et al., Blood 2024, Abstract 2287.
CAR T Cell Therapy
BCMA target
• Abecma (Ide-Cel)
• Carvykti (Cilta-Cel)
1
Relapsed MM with 1-2 prior LOT Bridging therapy, if needed; Lymphodepleting therapy when CAR T cells are ready T Cell Infusion Close monitoring and Management of side effects
T-Cell Engager (TCE) Therapies
Relapsed MM after 4 prior LOT (or clinical trials)
TCE are innovative immunotherapies used in the treatment of relapsed multiple myeloma. These therapies work by redirecting the patient's own T-cells to recognize and attack myeloma cells.
3
2 a 2 b 4 5 HOME ! Apheresis to Collect T Cells T Cell Manufacturi ng
Bispecific antibodies
• About 7 in 10 patients respond
• Off-the-shelf treatment; no waiting for engineering cells
BCMA target: greater potential for infection
• Tecvayli® (teclistamab)
• Elrexfio™ (elranatamab)
Bispecific antibody
GPRC5D target: potential for skin and nail side effects, GI issues of taste change, anorexia and weight loss
• Talvey™ (talquetamab)
BCMA = B-cell maturation antigen; CAR = chimeric antigen receptor; GPRC5D = G protein–coupled receptor, class C, group 5, member D; MM = multiple myeloma; scFV = single chain fragment variable.
CAR T= Chimeric Antigen Receptor T Cell; LOT = Lines of
Hucks G, Rheingold SR. Blood Cancer J. 2019;doi:10.1038/s41408-018-0164-6.
Shah N, et al. Leukemia. 2020;34(4):985-1005. Yu B, et al. J Hematol Oncol. 2020;13:125.
CAR T and Bispecific Antibodies: Known Side Effects
CYTOKINE RELEASE
SYNDROME
• Fever
• Fatigue & Weakness
• Headache
• Nausea/Vomiting/Diarrhea
• Chills
• Low blood pressure
• Rapid heart rate
CRS is a common but often mild & managea ble side effect
Neurotoxicity is a rare but a serious side effect
• Difficulty breathing PREVENTION AND MANAGEMENT
• Disease management to reduce tumor burden
• Bispecific Step-Up Dosing (SUD)
• Tocilizumab
• Steroids
• Anti-Seizure medications
• Intravenous Immunoglobulin (IVIG)
• Close monitoring
ICANS AND NEUROTOXICITY
• Headache
• Difficulty concentrating
• Lethargy
• Agitation
• Hallucinations
• Tremors
• Aphasia (difficulty with speech, reading, writing, or understanding language)
• Confusion
• Memory loss
• Personality change
• Delayed Neurotoxicity can include Parkinsonism, Cranial Nerve Palsies and Peripheral Neuropathy/Guillan Barré syndrome (GBS)
CAR = chimeric antigen receptor. ICANS = Immune Effector Cell-Associated Neurotoxicity Syndrome Brudno JN, Kochenderfer JN. Blood. 2016;127(26):3321-3330. Lee DW, et al. Biol Blood Marrow Transplant. 2019;25:625-638. Kumar, et al. Blood (2024) 144 (Supplement 1): 4758.
Infection: Medications Can Mitigate Risk
Type of Infection Risk
Medication Recommendation(s) for Healthcare Team Consideration
Consider GCSF 2 or 3 times/wk (or as frequently as needed) to maintain ANC > 1000 cells/μL and maintain treatment dose intensity
Weight, GI Symptoms & The Drugs That Affect Them: Prevention
& Management
Anorexia (difficulty eating) Weight loss
• ASCT
• GPRC5D therapy
Steroids Weight gain, fluid retention
Excess hunger ASCT
GPRC5Ddirected therapy Opioids
Weight Loss
Weight Gain
Weight Management
• Monitor weight for significant loss or gain
• Adjust diet (reduce calories or add supplements )
• Work with a dietician
Smith LC, et al. Clin J Oncol Nurs. 2008;12(3)suppl:37-52. Faiman B. Clin J Oncol Nurs. 2016;20(4):E100-E105.
Management of Oral Side Effects
Xerostom
ia
OTC dry mouth rinse, gel, spray are recommended. Avoid hot beverages. Anti-fungal therapy for oral thrush.
Dysgeusi a
Dysphagi a
=Dry Mouth =Difficulty Swallowing =Taste Change
Dexamethasone oral solutions “swish and spit” may provide benefit. Sour citrus or candies before meals are also recommended.
Dental
Care
Attention to oral hygiene.
Regular dental cleaning and evaluation. Close monitoring for ONJ, oral cancer and dental caries
Dietary modifications with small bites, eating upright, and sips with food can help manage symptoms
Weight Monitorin g
Some medications lead to weight gain, others to weight loss. Meet with a Nutritionist
Consider diet changes, supplements
Work closely with your entire health care team to manage oral side effects.
Skin and Nail Side Effects
Possible side effect to some treatments and supportive care medications
Skin Rash:
Prevent dry skin; apply lotion
Report changes to your care team
Medication interruption or alternative, as needed
Steroids:
• Topical for grades 1-2,
• Systemic and topical for Grade 3
Antihistamines, as needed
Nail Changes:
Keep your nails short and clean.
Watch for “catching and tearing”
Apply a heavy moisturizer like Vaseline or salve. Wear cotton hand coverings to bed
A nail hardener may help with thinning
Tell the team if you have signs of a fungal infection, like thickened or discolored nails
Myeloma: Putting The Pieces of the Puzzle
Fatigue, Anxiety and Depression
Fatigue Depression Anxiety
Fatigue is the most reported symptom. Sources include anemia, pain, reduced activity, insomnia, treatment toxicity, bone marrow suppression. Symptoms can improve with continued physical activity.
Symptoms are under-reported:
“I mentioned it before. Nothing can be done.” “I don’t want to be put on another medication.”
>35% of patients ≈25% of patients
More Pieces to the Big Picture
Adopt Healthy Behaviors
• Mental health / social engagement
• Stress reduction; relaxation
• Sufficient Sleep
• Maintain a healthy weight; eat nutritiously
• Activity / exercise / prevent falls, injury
• Stop smoking Sexual health / intimacy
• Have a PCP for general check ups, preventative care, health screenings, vaccinations
Complementary or alternative therapy
• Have specialists for dental care, eye exams/screening, skin cancer screening
Recommended Health Screenings
• Blood pressure
• Cholesterol
• Cardiovascular disease
• Colonoscopy
• Dental checkups & cleaning
• Dermatologic evaluation
• Diabetes
• Hepatitis
• Hearing
• Vision
• Women specific: mammography, pap smear
Faiman B, et al. CJON. 2017;21(5)suppl:19-36. Dimopoulous M, et al. Leukemia. 2009;23(9):1545-56.
• Men specific: prostate
Brigle K, et al. CJON. 2017;21(5)suppl:60-76. Faiman B, et al. CJON. 2017;21(5)suppl:19-36. Faiman B, et al. CJON. 2011;15suppl:66-76. Miceli TS, et al. CJON. 2011;15(4)suppl:9-23.
Care Partners: Essential Pieces of the Puzzle
Multiple studies demonstrate that strong social ties are associated with
• Increased longevity including people with cancer
• Improved adherence to medical treatment leading to improved health outcomes
• Lower risk of cardiovascular diseases
• Increased sense of purpose & life satisfaction
• Improved mood and happiness
• Reduced stress and anxiety
• Enhanced resilience
Care partners may help with medical appointments, managing medication, daily living, physical assistance, emotional support, myeloma knowledge, healthy lifestyle, patient advocacy, financial decisions
Care partners can be a spouse, close relative, a network of people (family, friends, neighbors, church members, etc)
Caring for the Care Partner
• Recognize that caregiving is difficult/stressful
• Encourage care partners to maintain their health, interests, and friendships
• The IMF has information and resources to help care partners
“Thank You!”
From the NLB and the IMF
Closing the Gap: Health Disparities in Myeloma
Joseph Mikhael, MD, MEd, FRCPC, FACP, FASCO, Chief Medical Officer, International Myeloma Foundation
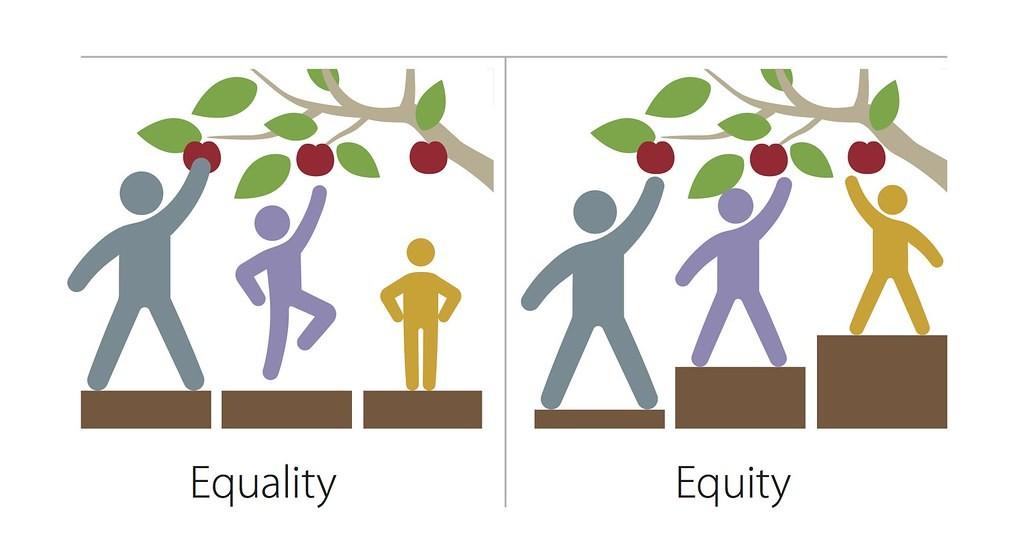
What are Health Disparities?
•Health disparities are preventable differences in the burden of disease, injury, violence, or opportunities to achieve optimal health that are experienced by socially disadvantaged populations
- Centers for Disease Control (CDC)
•Health equity generally refers to individuals achieving their highest level of health through the elimination of disparities in health and health care
This Photo by Unknown Author is licensed under CC BY-NC
What
A Call to Action Facts About Disparities in Myeloma
M-Power = Myeloma Power
The core vision of this initiative is to improve the short- and long-term outcomes for African American patients with myeloma.
We want to empower patients and communities to change the course of myeloma…
Enhance access to optimal care by educating myeloma providers about the disparity and how to reduce it
Engage the community to increase awareness and provide support
Shorten the time to diagnosis by educating primary care providers to recognize the disease and order the right tests
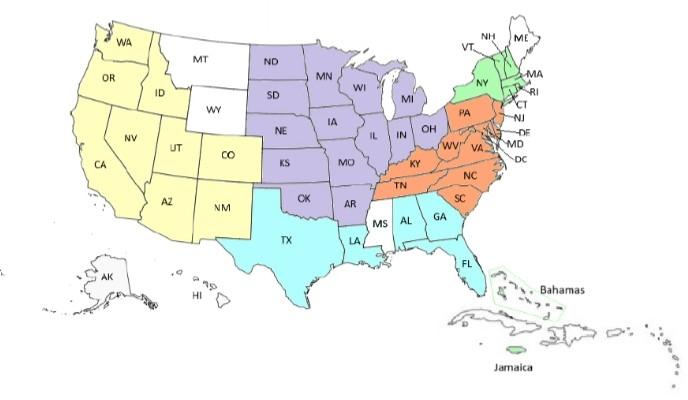
M-Power Is Both a National and Local Movement
2024 M-Power Community Workshops
April 2024
Multiple cities in Indiana
Annual Indiana Black Barbershop Health Initiative
• Health screenings for Black men on the 1st and 2nd Saturdays in April
• Shared materials on myeloma and M-Power for distribution in 18 barbershops in Evansville, Elkhart, and South Bend
June 20, 2024
New York, New York
50+ attended
76% African American
• 86% planned to share something they learned with their family, friend or healthcare provider
• 100% of attendees rated the program as excellent to very good
September 5, 2024
Charlotte, North Carolina
October 10, 2024
Richmond, Virginia
Primary Care Physician Dinner Meeting
• Presenting on multiple myeloma to the diverse community of healthcare professionals during the quarterly meeting of the Charlotte Medical Dental Pharmaceutical Society
40+ Attended
81% African American
• 88% plan to share something they learned with their family, friend, or healthcare provider
• 100% of attendees rated the program as excellent to very good
Juneteenth 2024: Abyssinian Church, Harlem, NYC
M-Power Community Workshop: Richmond, VA
Facebook Live
Education of Primary Care Providers
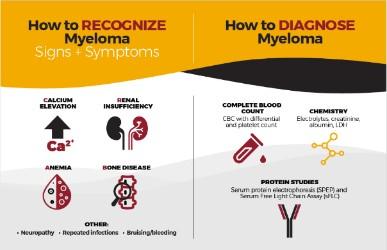
Our goal is to reduce DELAYS in diagnosis among African Americans by educating the primary care community with a focus on:
• Recognizing the signs and symptoms of myeloma
• Discriminating myeloma from other diagnoses such as diabetes
• Capturing an accurate diagnosis through proper use of testing
• Providing referral guidelines for Hematology and Oncology
• Grand Rounds
8,000
• Postcards mailed to 6,000+ PCPs in target cities
• Free PCP CME course “Don’t Miss Myeloma”
• Cobb Institute talk
• Talk at NMA Annual Meeting Dinner Meetings Articles and pending publications
Learners
Annual Meeting of the National Medical Association
• 12 1st – 3rd year medical students from all over the country met on August 5th in NYC at the NMA Annual Convention and Scientific Assembly
• Presented their posters, they worked on with a multiple myeloma experts immediately following the Jane Cooke Wright Symposium; which was dedicated to Dr. Edith Mitchell
Over 400,000 visits to M-Power site!
M-Power Website
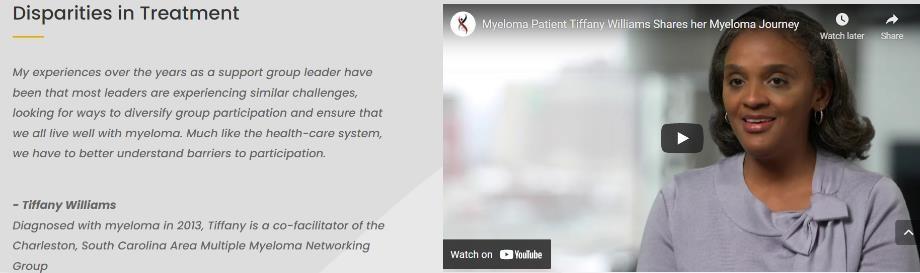
Patient Interview On Local News
M-Power Connections
M-Power Website:
•Web Stats: Over 40k Page views across main, city sites & myeloma.org
•Google PPC targeted web traffic
Email Stats:
•Total Sent: 18 emails
•Total Audience: 38k*
•Open Rate Avg: 31%*
*Note: We have continued to refine lists, contributing to a more engaged audience as evidenced in the Open Rates (The industry standard high-mark is 21%).
M-Minute Promotion Stats:
•Total Sent: 19 emails
•Total Audience: 323k
•Open Rate Avg: 38.91%
M-Power Related Video Stats:
• Total Views: Over 50k
…And Growing!
2025 and Beyond
Engage
• 2025 Juneteenth Workshop, NYC
• M-Power Community Workshop in Miami and Philly
• Expand online and social media strategy
Educate
• Primary care program in Charlotte
• Lab based education
• Electronic Medical Record Initiative
Enhance
• Diversity in Clinical Trial Academy as part of the Diversity in Clinical Trials initiative
• Nurse equity decision tool
What Can I Do??
•Be more conscious of the topics of health equity
•Evaluate the opportunities in your experience to reduce disparities
•Support the M-Power movement!
BREAKOUT SESSION 2
PLEASE HEAD TO YOUR SELECTED BREAKOUT SESSION:
BREAKOUT A: PATIENTS ONLY – LESSONS LEARNED
Please remain in this room
BREAKOUT B: CARE PARTNERS ONLY
Please move to Royal Palm
Breakout Session: Patients Only –Lessons Learned
Controversies in Myeloma: Moderated by Dr.
Joseph Mikhael
Joshua Richter, MD, FACP
Mount Sinai, New York, NY
Krina Patel, MD, MSc
The University of Texas MD Anderson Cancer Center, Houston, TX
Ask – the – Experts w/ Guest Faculty
Closing Remarks & Evaluation
Program Evaluations
Please be sure to complete your program evaluation today and turn it in at the end of the program.
We greatly appreciate your time and feedback!
Thank you to our sponsors!
OUR VISION:
A world where every myeloma patient can live life to the fullest, unburdened by the disease.
OUR MISSION:
Improving the quality of life of myeloma patients while working toward prevention and a cure.
IMF Core Values:
These are the core values we bring to accomplishing our mission each day.
Patient Centric
The patient experience is the focus of everything we do. Every interaction is an opportunity to establish a personal connection built on care and compassion which is the basis for continued support.
Respect All
As a team, we value honesty and transparency while creating a culture of mutual respect. We foster a myeloma community built on sincerity, authenticity, and kindness.
Excellence and Innovation
We value accountability, personal responsibility, and a steadfast commitment to excellence. We respect the legacy and reputation of our organization while seeking new solutions and advancements to improve outcomes, quality of life, and access to the best available resources for everyone impacted by myeloma.
Honor differences
We recognize each team member's skills and talents through collaboration and cooperation. Our programs aim to celebrate and support the diversity of our patients and their communities.