

2025 IMF REGIONAL COMMUNITY WORKSHOP
ATLANTA, GA

APRIL 5, 2025

Thank you to our speakers & our sponsors!








Welcome & Introductions
Robin Tuohy
Vice President, Patient Support
International Myeloma Foundation
Understanding Myeloma Basics
Nisha Joseph, MD
Winship Cancer Institute of Emory University, Atlanta, GA
IMF REGIONAL COMMUNITY WORKSHOP
ATLANTA MORNING AGENDA

(Video) Closing the Gap: Health Disparities in Myeloma
Joseph Mikhael, MD, MEd, FRCPC, FACP, FASCO,
Chief Medical Officer, International Myeloma Foundation
Advancing Treatment Options Through Clinical Trials
Manisha Bhutani, MD
Atrium Health Levine Cancer Institute, Charlotte, NC
Q&A with Panel
Coffee Break
Breakout: Frontline or Relapsed Treatment Approaches
-NDMM: Getting Started with Myeloma Management
Dr. Nisha Joseph
-RRMM: Continuing the Myeloma Treatment Journey
Dr. Manisha Bhutani
Housekeeping Items
Presentation Slides: Are available by scanning the QR code.
Program Evaluations: Please be sure to complete your program evaluation and return your evaluations at the end of today.
Restrooms: Restrooms are located outside across from the elevators
Parking: Please see Meghan at the registration desk to receive your parking voucher.
We greatly appreciate your time and feedback!
The IMF Support Group Team is Here For

Atlanta Area Multiple Myeloma Support Group
Meets virtually on the 1st Saturday of each month at 11AM

Atlanta Multiple Myeloma Men Only Support Group
Meets virtually on the 4th Tuesday of each month at 6PM

Southside Atlanta Multiple Myeloma Support Group
Meets virtually on the 4th Saturday of each month at 10AM
Myeloma Voices at ASH


Myeloma Voices 10 In Person / 5
Virtual

Myeloma Voices #1 tweeters out of ASH

#FaMMily

IMF InfoLine
Connecting Patients to Resources…
Shortening “Time to Hope” for Over 1,000 First-Time Callers Each Year
Assistance with understanding lab results, terminology and disease state
Preparing for medical visits
Access to medical providers
Access to medications
Financial resources
“Thank you so much for the informative conversation and all the time you spent listening and helping me decipher the MM lingo. What an amazing service!”

“Thank you for your response and excellent question suggestions for my hematology team.”



Myelo:
The first generative AI Assistant designed specifically for multiple myeloma.
Written Education
Understanding Booklets
Tip Cards
Myeloma Minute Weekly Updates
Myeloma Today Quarterly News









Live Patient Education




2025 Live Patient Education
Patient & Family Seminars
• Boca Raton, FL – March 14 – 15
• Philadelphia, PA – May 2 – 3
• Los Angeles, CA – August 15 – 16
• Chicago, IL – October 3 – 4

Myeloma Community Workshops
• Virtual - March 4
• San Francisco, CA - March 29
• Atlanta, GA - April 5
• Edina, MN - April 26
• Denver, CO - June 21
• Virtual – July 29
• Seattle, WA - August 9
• Waltham, MA - September 27
• Raleigh-Durham, NC - November 15
• Virtual – November 18
Scan for Upcoming Events!






Understanding Myeloma Basics
Nisha Joseph, MD
Winship Cancer Institute of Emory University ,
Atlanta, GA
Review the basics of blood and cancer
OBJECTIVES
Define multiple myeloma and its key features
Discuss the staging and classification of myeloma
Outline the approach to therapy of myeloma


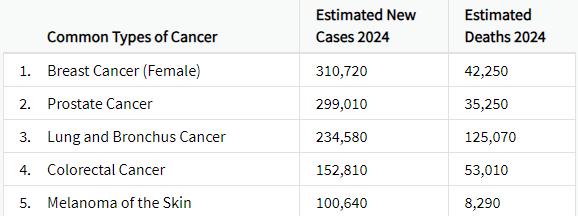
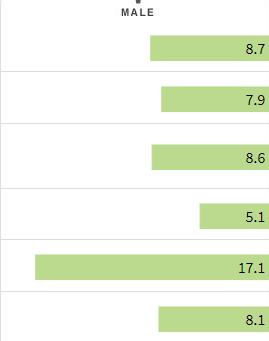
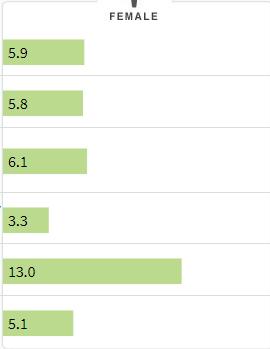
How common is Myeloma in the US?




What Causes Myeloma? How/Why Did
I Get This?
Environmental Factors:
• Exposure to some chemicals
• Radiation exposure
Examples:
Agent Orange
Burn pits
Pesticides, Herbicides
Firefighter/First Responder exposures
Individual Factors:
• Age
• Family History of related disorders
• Personal History of MGUS or SMM
• Obesity
VA Study Documents Health Risks for Burn Pit Exposu
res
Leukemia and Multiple Myeloma Set to Be Added to List of Conditions Linked to Burn Pits
In most cases, the honest truth
WE DON’T KNOW

Multiple Myeloma Diagnosis Can Be Challenging



Kyle RA. Mayo Clin Proc. 2003;78:21-33.


What is the Connection Between Bone Marrow & Myeloma ?
Hematopoietic stem cell
Red Blood Cells Carry Oxygen White Blood cell Fight Infection Platelets Prevent Bleeding



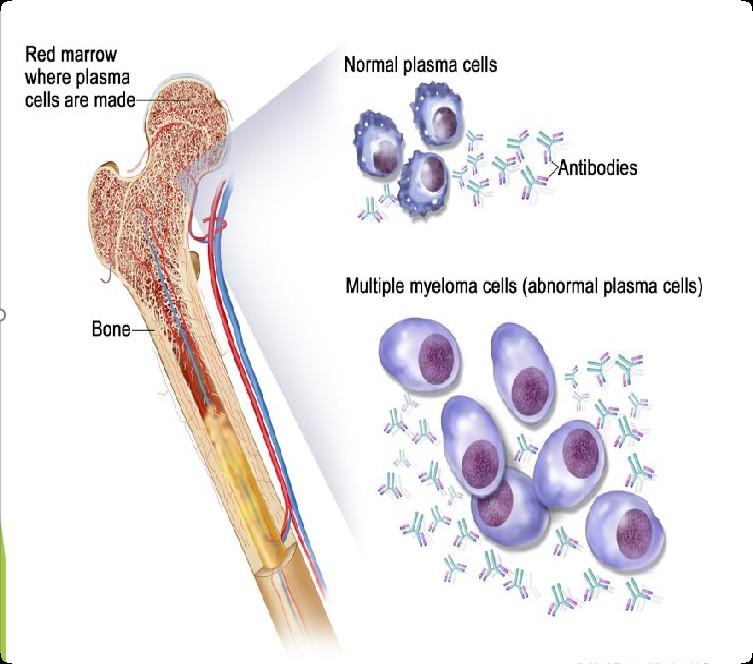
Photo Credit
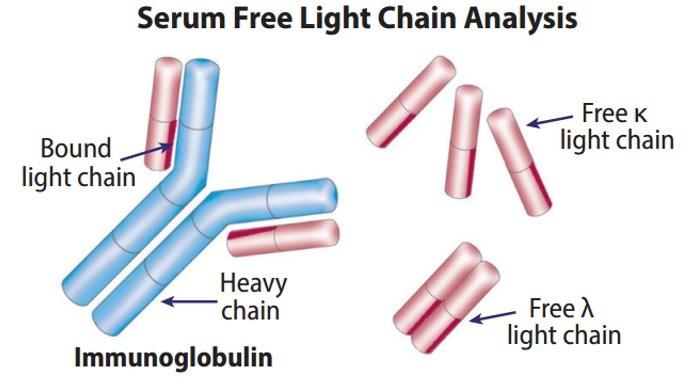
Understanding (Mono)clonal Plasma Cells

Heavy Chain: G, A, M, D, E

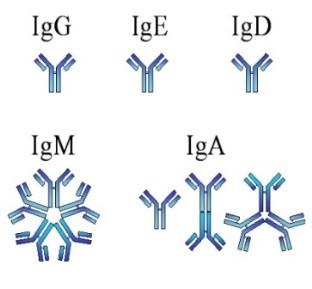
Chain = M-Spike

65% IgG – most common
20% IgA – associated with AL Amyloid
5%
Less common: IgD, IgE, IgM

• AL-Amyloid
Is Myeloma the Only Protein Disorder?
• POEMS
• Light or Heavy Chain Deposition Disease
• MGCS = Clinical
• MGRS = Renal
• MGNS = Neuro
Condition
MGUS1-4
(Monoclonal Gammopathy of Undetermined Significance)
SMM1-5,8 (Smoldering Multiple Myeloma) Active Multiple Myeloma6-8
Clonal plasma cells in bone marrow
Presence of Myeloma Defining Events
Likelihood
* In clinical trial
Multiple Myeloma and
Myeloma Defining Events

Testing For Myeloma: Blood & Urine
Test Name
CBC + differential
Complete metabolic panel
What it means

Hemoglobin, WBC, Platelets
Creatinine, Calcium,
Albumin, Liver function
Beta-2 Microglobulin (B2M)
Lactate Dehydrogenase (LDH) Part of staging and risk stratification
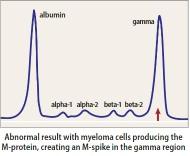
Serum Immunofixation and
Protein electrophoresis (SPEP+IFE)
Immunoglobulins (G, A, M, D, E)
Free light chain assay with kappa/lambda ratio
Urine immunofixation & protein electrophoresis (UPEP+IFE)

Measures the level of normal and clonal protein Identifies the type of clonal protein

Measures the level of normal and clonal protein
Identifies the type of
This Photo by Unknown Author is licensed under CC BY-SA-NC
Testing For Myeloma: Imaging
Imaging:
– Skeletal survey: Series of X-rays; less sensitive than other techniques
– Whole body low dose (CTWB-LD CT )
– Positron Emission Tomography (PET/CT)
– Magnetic Resonance Imaging (MRI)
Healthy bone versus myeloma bone disease

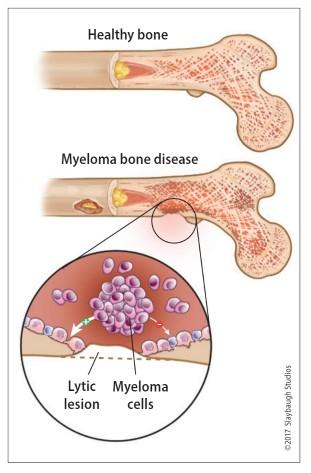
This Photo by Unknown Author is licensed under CC BY-NC-ND
Testing For Myeloma: Bone Marrow

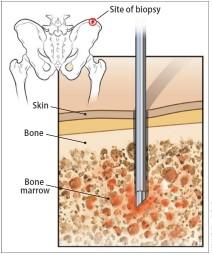
Bone marrow genetics
• Cytogenetics
• Fluorescence in situ hybridization (FISH)
• Next generation sequencing (NGS)

What is (the importance of) Myeloma Staging & Risk Stratification?
Putting It Together

• Updated as new information becomes available
• Helps to guide therapy and measure response to treatment
• Provides some prognostic value
• Standardizes terminology in medical practice


What is the Myeloma Treatment Landscape?
Initial Therapy (a.k.a. Frontline, Induction)
Quad Therapy (ex. CD38+ MoAb + VRd)
HD-Melphalan + Stem Cell
Transplant (ASCT)
Treatment for Relapse
Supportive Care and Living Well
Drug Class Overview
(thalidomide)
(lenalidomide)
(pomalidomide)
Drug Class Overview
Peptide Drug Conjugate*
BCMA Targeted Antibody Drug
Conjugate (ADC)*
Bispecific Antibodies
(Melphalan
Blenrep (belantamab mafodotin-blmf)
Abecma (idecabtagene vicleucel)
Carvykti (ciltacabtagene vicleucel)
Tecvayli (teclistimab)
Talvey (Talquetamab)
Elrexfio (Elranatamab)
Cevostamab, Iberdomide, Mezigdomide, Venetoclax Linvoseltamab, LCAR-B38M, ABBV-383 ……………………………
Measuring Disease Response: IMWG Response Criteria









Negative by next generation flow (NGF) (minimum sensitivity 1 in 10-5 nucleated cells or higher)*
mCR AND normal Free Light Chain ratio, Bone Marrow negative by flow, 2 measures
CR AND negative PCR
Complete Response: Negative immunofixation (IFE); no more than 5% plasma cells in BM; 2 measures
Very Good Partial Response: 90% reduction in myeloma protein
Partial Response: at least 50% reduction in myeloma protein
Minimal Response
Stable Disease: Not meeting above criteria
Progressive Disease: At least 25% increase in identified myeloma protein from lowest level
MRD = Minimal Residual Disease
sCR = Stringent Complete Response; BM = Bone Marrow
When Do I Need A New Treatment?
• Not every relapse requires immediate therapy
• Each case is different
Asymptomatic high-risk disease or rapid doubling time or extensive marrow involvement
Symptomatic or extramedullary disease
Initiate Treatment
Asymptomatic biochemical relapse on 2 consecutive assessments
Consider Observation Monitor Carefully Consider Treatment
Patient-/Disease-Specific Monitor Carefully
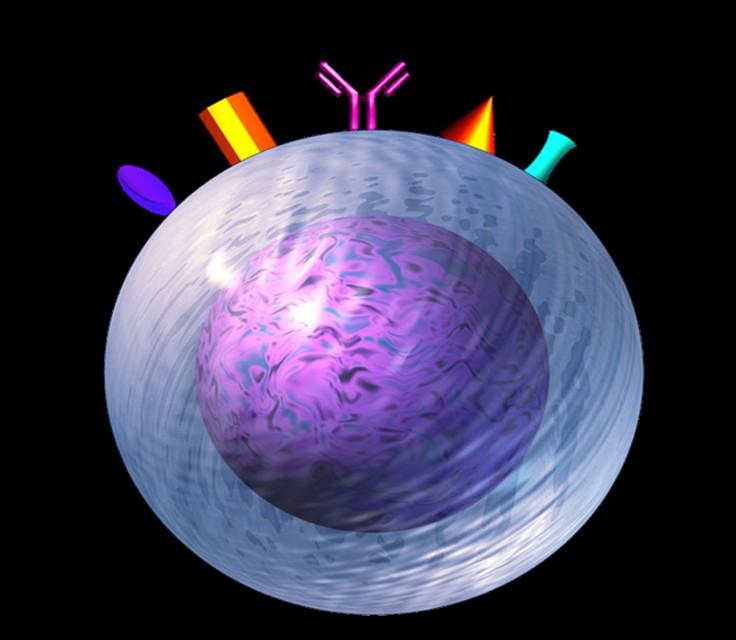
Targets on the Myeloma Cell Surface and Therapeutic Antibodies

Bi-Specific Antibodies
Talvey (Talquetamab) CAR-T


Antibody Drug
Empliciti (Elotuzumab)
Bi-Specific Antibodies
Bi-Specific Antibodies CAR-T

Monoclonal Antibodies
Daratumumab and Darzalex Faspro
Sarclisa (Isatuximab)
TAK-079 MOR202
Immune Therapies
Abecma (Ide-cel CAR-T)
Carvykti (Cilta-cel CAR-T)
Tecvayli (Teclistamab)
Elrexfio (Elranatamab)

Other CAR-Ts
Other Bi-Specific Antibodies
Antibody Drug Conjugates
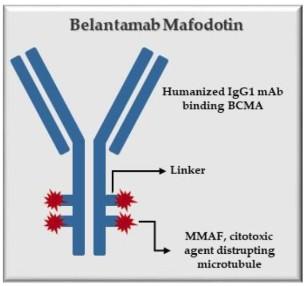
How it works:
An antibody directed at a target (BCMA) combined with a cytotoxic agent (chemotherapy)
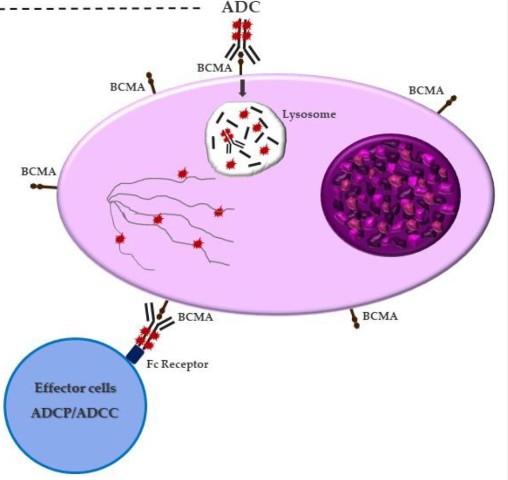
ADC = Antibody-Drug Conjugate
BCMA = B-Cell Maturation Antigen
ADCP/ADCC = Antibody-Dependent Cellular Cytotoxicity & Phagocytosis
Image Credit: https://creativecommons.org/licenses/by-nc/3.0/
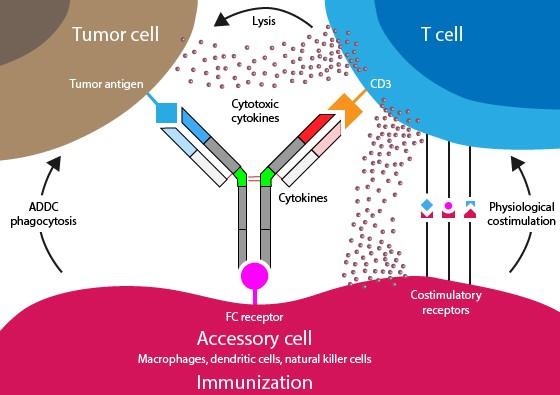
Bispecific Antibodies: Mechanism of Action
• Incorporates 2 antibody fragments to target and bind both tumor cells and T cells
• Brings target-expressing MM cells and T cells into close proximity, enabling T cells to induce tumor-cell death
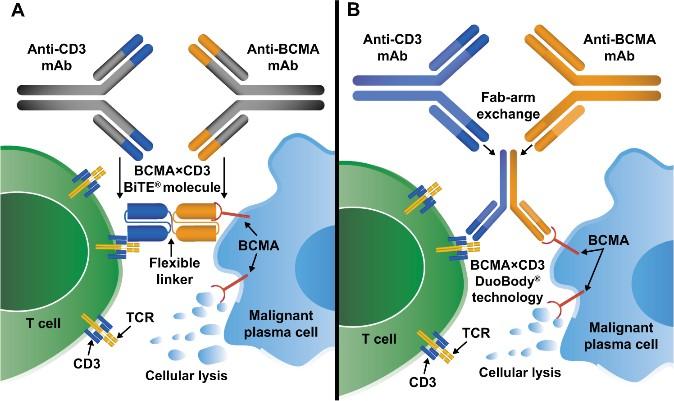

Targets of Bispecific Molecule Vary
“Off the Shelf” Advantage
• No manufacturing process, unlike CAR T-cell therapy (but like ADC/belantamab therapy)
• Thus, no delay between decision to treat and administration of drug
ADC = Antibody-Drug Conjugate; BCMA = B-Cell Maturation Antigen; CD3 = Cluster of Differentiation 3; FcRH5 = Fc receptor-homolog 5; GPRC5D = G-protein coupled receptor family C group 5 member D
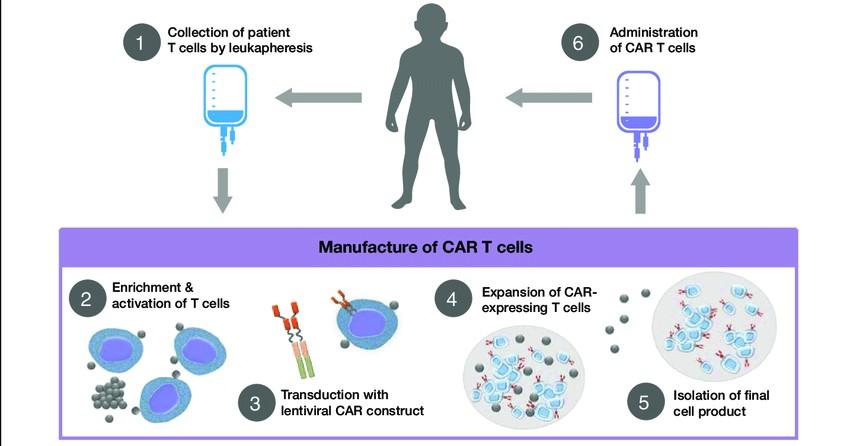
The Process of CAR T Cell Therapy








The Evolution of Myeloma Therapy
VD
Rev/Dex
CyBorD
VTD
VRD
KRD
D-VMP
DRD
ASCT
Tandem ASCT (?)
Nothing
Thalidomide?
Bortezomib
Ixazomib
Lenalidomide
Combinations
Bortezomib
Lenalidomide
Carfilzomib
Pomalidomide
Selinexor
Panobinostat
Daratumumab
Ixazomib
Elotuzumab
Isatuximab
Belantamab mafodotin*
Melphalan flufenamide*
Idecabtagene autoleucel
Ciltacabtagene autoleucel
Teclistamab, Talquetamab
Elranatamab
D-VRD
Isa-VRD
D-KRD
Isa-VRD “More” induction?
Daratumumab?
Carfilzomib?
Lenalidomide + PI
ASCT, autologous stem cell transplant; CAR, chimeric antigen receptor; Cy, cyclophosphamide; d- daratumumab; D/dex, dexamethasone; isa, isatuximab; K, carfilzomib; M, melphalan; PD-L1, programmed death ligand-1; PI, proteasome inhibitor; Rev, lenalidomide; V, bortezomib.
Speaker’s own opinions.
CAR T Cell Therapy
Bispecific/Tri-specific
Antibodies
Cell Modifying Agents
Venetoclax
PD/PDL-1 Inhibition?
Small Molecules
* These agents are currently off the market but available through special programs
Anito-cel
Cevostomab
Linvoseltamab
Iberdomide, Mezigdomide
Sonrotoclax
Second/Expert Opinion
• You have the right to get a second opinion. Insurance providers may require second opinions.
• A second opinion can help you:
– Confirm your diagnosis
– Give you more information about options
– Talk to other experts
– Introduce you to clinical trials
– Help you learn

which health care team you’d like to work with, and which facility



Closing the Gap: Health Disparities in Myeloma (Video)
Joseph Mikhael, MD, MEd, FRCPC, FACP, FASCO Chief Medical Officer, International Myeloma Foundation
Advancing Treatment Options Through Clinical Trials
Manisha Bhutani, MD
Atrium Health Levine Cancer Institute, Charlotte, NC
Advancing Treatment Options Through Clinical Trials
Manisha Bhutani, MD
Atrium Health Levine Cancer Institute
Charlotte, NC

Clinical Trials - Overview
Some Of The Important Principles Of Clinical Trials:
The drive of research has brought us to where we are
No one is expected to be a “guinea pig” with no potential benefit to them
Research is under very tight supervision and standards
Open, clear communication between the physician and the patient is fundamental Driving research forward!



Types of Clinical Trials
Observational Interventional Treatment Prevention Screening
Diagnostic Quality of Life

Clinical Trials: Myths versus Facts
MYTH: If I participate in a clinical trial, I might get a placebo, not active treatment
MYTH: If I participate in a clinical trial, I can’t change my mind
• Phase 1 and 2, everyone gets active treatment
• Phase 3 standard of care vs new regimen: often standard regimen with/without additional agent in MM trials
• Patients can withdraw their consent for clinical trial participation at any time

MYTH: Clinical trials are dangerous because they have new medicines and practices
• Some risk is involved with every treatment, but medicines are used in clinical trials with people only after they have gone through testing to indicate that the drug is likely to be safe and effective for human use

MYTH: Clinical trials are expensive and not covered by insurance
• Research costs are typically covered by the sponsoring company
• Standard patient care costs are typically covered by insurance
• Check with clinical trial team/insurers; costs such as transportation, hotel, etc may not be reimbursed and are paid by patient
PhRMA website. Accessed March 25, 2024. https://phrma.org/-/media/Project/PhRMA/PhRMA-Org/PhRMA-Org/PDF/A-C/CLINICAL-TRIALS-MYTH-FACT-PRINT.pdf?hsCtaTracking=f6689b95-1626-40d9-8c87-c6b 8d31600a4%7C35221aa8-d487-4db3-9416-b9c3c35e3bac
.
Overview of New Drug Development

Identify a target for therapy in the laboratory
Confirm the anticancer activity in laboratory and animal studies
Clinical trials (human studies) to determine safety, dosing and effectiveness
The whole process costs millions of dollars and years of effort!
Preclinical
Clinical Trial Phases
ANIMAL STUDIES: Examine safety and potential for efficacy
PHASE 1
PHASE 2
FIRST INTRODUCTION OF AN INVESTIGATIONAL DRUG INTO HUMANS
• Determine metabolism and PK/PD actions, MTD, and DLT
• Identify AEs
• Gain early evidence of efficacy, studied in many conditions; typically, 20 to 80 patients; everyone gets agent
EVALUATION OF EFFECTIVENESS IN A CERTAIN TUMOR TYPE
• Determine short-term AEs and risks; closely monitored
• Includes up to 100 patients, typically
PHASE 3
GATHER ADDITIONAL EFFECTIVENESS AND SAFETY
PHASE 4
INFORMATION COMPARED TO STANDARD OF CARE
• Placebo may be involved if no standard of care exists; hundreds to several thousand patients
• Often multiple institutions; single or double blind; sometimes open label
APPROVED AGENTS IN NEW POPULATIONS OR NEW DOSE

Clinical Trials – Why Me??
Every patient is unique and must be viewed that way
Benefits of trials are numerous and include:
Early access to “new” therapy
Delay use of standard therapy
Contribution to myeloma world – present and future
Financial access to certain agents
Must be balanced with potential risks
“Toxicity” of side effects
Possibility of lack of efficacy
Why Do So Few Cancer Patients Participate in Trials?
Patients may:
• Be unaware of clinical trials
• Lack access to trials
• Fear, distrust, or be suspicious of research
• Have practical or personal obstacles
• Face insurance or cost problems

• Be unwilling to go against their physicians’ wishes
• Not have physicians who offer them trials
• Have a disconnect with their healthcare team
Importance of Clinical Trial Participation by Diverse Populations
[P]eople from racial and ethnic minorities and other diverse groups are underrepresented in clinical research. This is a concern because people of different ages, races, and ethnicities may react differently to certain medical products.
– FDA

Leadership and commitment


Community engagement practices
Investigator hiring, training, and mentoring practices


Patient engagement practices

US Cancer Centers of Excellence: Strategies for Increased Inclusion of Racial and Ethnic Minorities in Clinical Trials
FDA = US Food and Drug Administration. Regnante JM, et al. J Oncol Pract. 2019;15(4):e289-e299. FDA website. Clinical Trial Diversity. Accessed March 27, 2024. https://www.fda.gov/consumers/minority-health-and-health-equity/clinical-trial-diversity.
Is A Clinical Trial Right For Me?
Discuss with your physician if you are eligible for a clinical trial
Work with your physician to determine the best trial for you
Meet with the clinical research nurse or trials coordinator to discuss the trial
Carefully review the provided “Informed Consent” Describes the study and any potential safety concerns related to the experimental medication


Commonly Asked Questions
How does the study work? How often will I need to see my doctor or visit the cancer center?

Will I need to undergo additional tests?
What is currently known about the new drug or combination?
What benefits can I expect?
What side effects should I expect? Who should I notify if I have side effects?
Can I take my vitamins or other medications?
Can I get the treatment with my local doctor?

Will my insurance pay for my participation in the clinical trial?
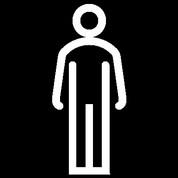
Clinicaltrials.gov https://clinicaltrials.gov/


ncreasing-diversity-in-cancer-clinical-research
Q&A WITH PANEL
Housekeeping Items
Presentation Slides: Are available by scanning the QR code.
Program Evaluations: Please be sure to complete your program evaluation and return your evaluations at the end of today.
Restrooms: Restrooms are located outside across from the elevators
Parking: Please see Meghan at the registration desk to receive your parking voucher.
Badge Holders: Please return and we can recycle them
We greatly appreciate your time and feedback!
BREAK
WHEN YOU RETURN FROM BREAK
PLEASE HEAD TO YOUR SELECTED BREAKOUT SESSION:
BREAKOUT A: NDMM - GETTING STARTED WITH MYELOMA
MANAGEMENT
Please move to Galleria Room
BREAKOUT B: RRMM - CONTINUING THE MYELOMA TREATMENT JOURNEY
Please remain in this room
Thank you to our speakers & our sponsors!
IMF REGIONAL COMMUNITY WORKSHOP: NDMM
Nisha S. Joseph, MD
Associate Professor
Winship Cancer Institute, Emory University
Atlanta, GA, USA




MM TREATMENT PARADIGM
COMBINATIONS CAN ACHIEVE BETTER DEPTH OF RESPONSE, BUT DURATION IS LINKED TO MAINTENANCE


APPROACH TO NDMM: HOW DO WE OPTIMIZE DEPTH AND DURATION OF RESPONSE?
Induction (4-6 cycles)
HDT/ASCT
Risk-stratified maintenance
Goal: Maximize depth of response with minimal overlapping toxicities
Risk status
Comorbidities
Tumor Burden
Revlimid (Lenalidomide)
Velcade (Bortezomib)
Dexamethasone
RVD
Daratumumab (Darzalex)
Revlimid (Lenalidomide)
Velcade (Bortezomib)
Dexamethasone
EMORY: RVD 1000
(months)
Median OS for the entire cohort was ~11 years
Parikh et al Abstract # 8061, ASCO 2022; Joseph et al JCO 2020
GRIFFIN STUDY: ADDING DARATUMUMAB TO INDUCTION
• Median Follow Up: 49.6 months • 4-year PFS rate: 87% vs 70% • 55% risk reduction for PD/death
Take Home Message:
There is a benefit of adding Daratumumab to the RVD backbone
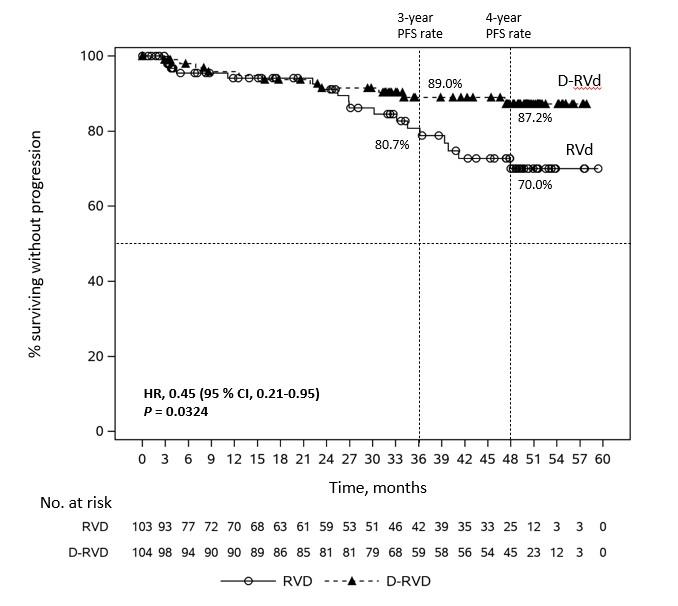
Sborov et al, IMS 2022
PERSEUS: STUDY DESIGN
eligibility criteria
• Transplanteligible NDMM
• Age 18-70 years
• ECOG PS ≤2
Induction
Consolidation
Maintenance
: 40 mg PO/IV Days 1-4, 9-12
VRd administered as in the VRd group
Primary endpoint: PFSc
Key secondary endpoints: Overall CR rate,c overall MRD-negativity rate,d
Discontinue DARA therapy only after 24 months of D-R maintenance for patients with CR and 12 months of sustained MRD negativity
Restart DARA therapy upon confirmed loss of CR without PD or recurrence of MRD
ECOG PS, Eastern Cooperative Oncology Group performance status; V, bortezomib; SC, subcutaneous; PO, oral; d, dexamethasone; IV, intravenous; QW, weekly; Q2W, every 2 weeks; PD, progressive disease; Q4W, every 4 weeks; MRD, minimal residual disease; OS, overall survival; ISS, International Staging System; rHuPH20, recombinant human hyaluronidase PH20; IMWG, International Myeloma Working Group;
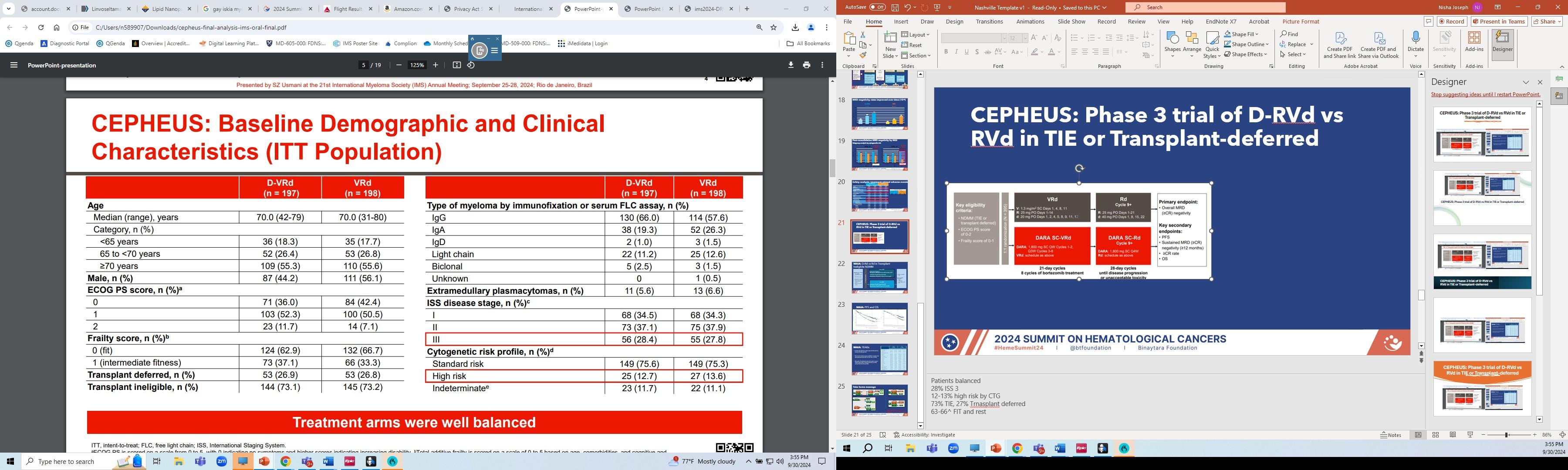
PERSEUS: BASELINE DEMOGRAPHIC AND CLINICAL CHARACTERISTICS
• D-VRd and
PERSEUS: STEM CELL COLLECTION AND TRANSPLANTATION
Stem cell mobilization and collection were feasible with D-VRd
D-VRd did not impact the ability to receive transplant or engraftment
aAmong patients who proceeded to stem cell mobilization (D-VRd, n = 335; VRd, n = 317). bAmong patients who had stem cells collected (D-VRd, n = 326; VRd, n = 314). cIn the safety population (D-VRd, n = 351; VRd, n = 347). dAmong patients who proceeded to transplant (D-VRd, n = 315; VRd, n = 302). eNumber of days from the transplant date, excluding patients whose counts did not nadir below the set threshold. The date of engraftment post-ASCT was defined as the latest date of absolute neutrophil count ≥0.5 × 109/L and platelet count ≥20 × 109/L. Patients with hematopoietic reconstitution were included (D-VRd, n = 314; VRd, n = 300).


PERSEUS PRIMARY ANALYSIS: CONCLUSIONS
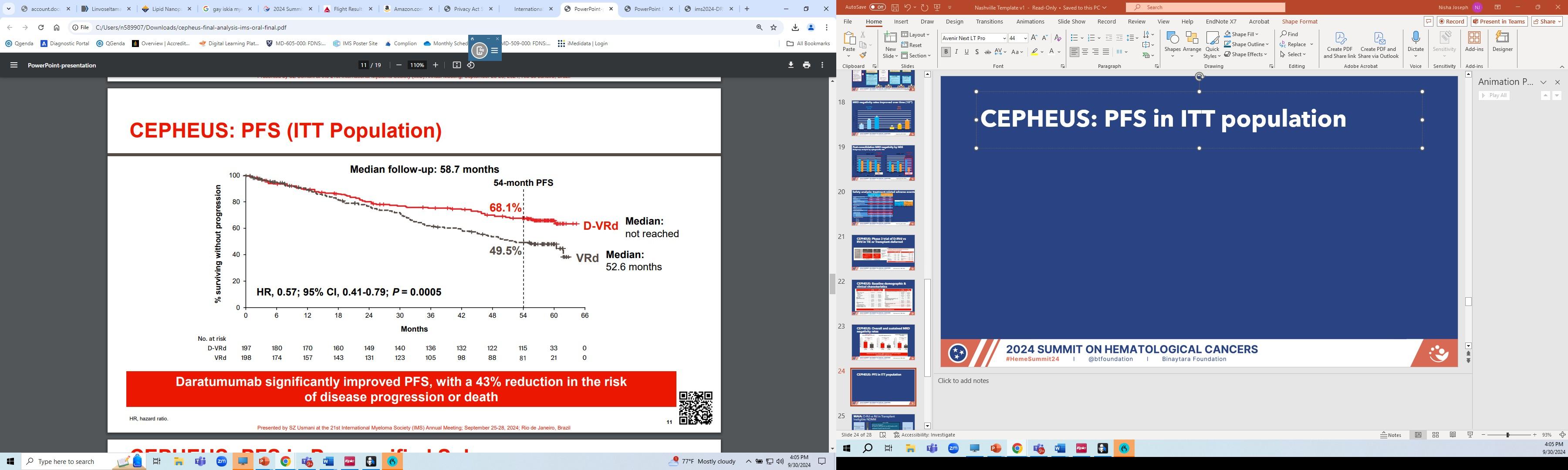
• D-VRd induction followed by ASCT, D-VRd consolidation, and D-R maintenance significantly improved PFS in transplant-eligible patients with NDMM (HR, 0.42; P <0.0001)
48-month PFS rates: 84.3% versus 67.7%
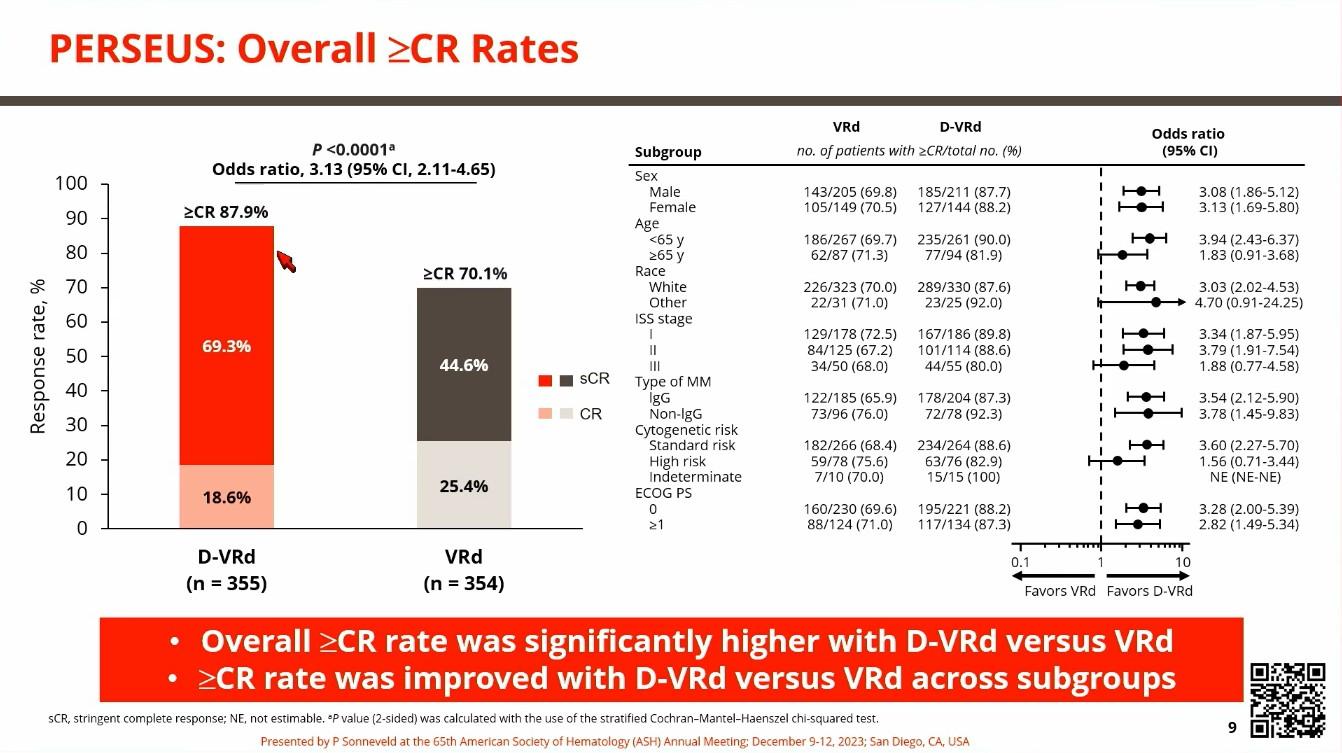
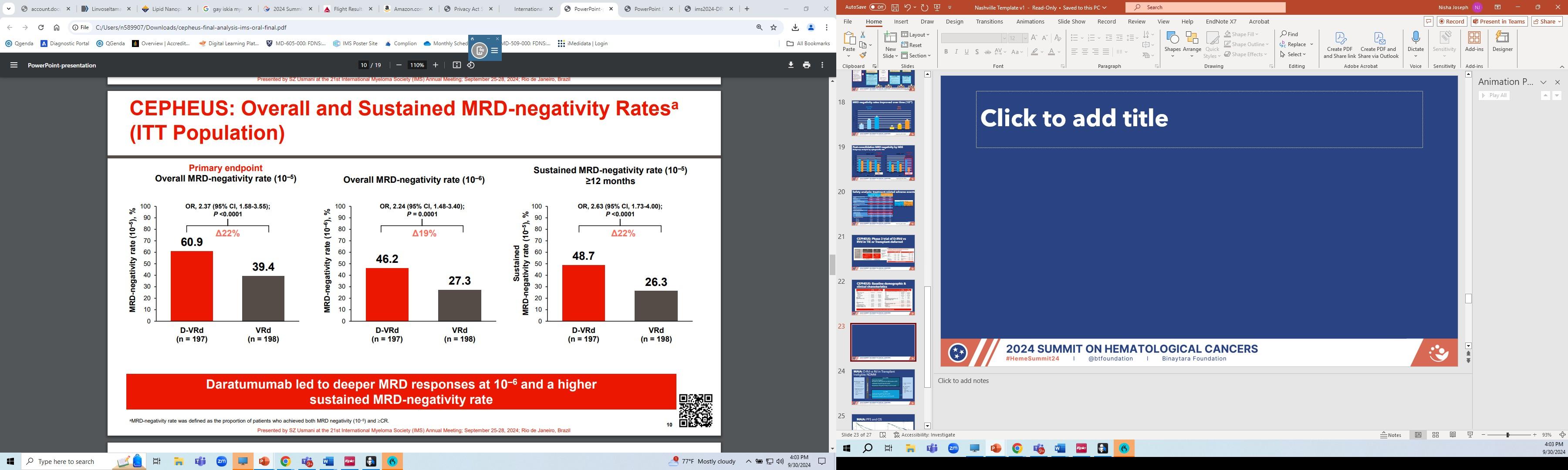
• D-VRd regimen significantly improved depth of response versus VRd regimen
Overall CR rates: 87.9% versus 70.1%
Overall MRD-negativity rates: 75.2% versus 47.5%
64% of patients receiving D-R maintenance for at least 2 years were able to stop DARA after achieving sustained MRD negativity
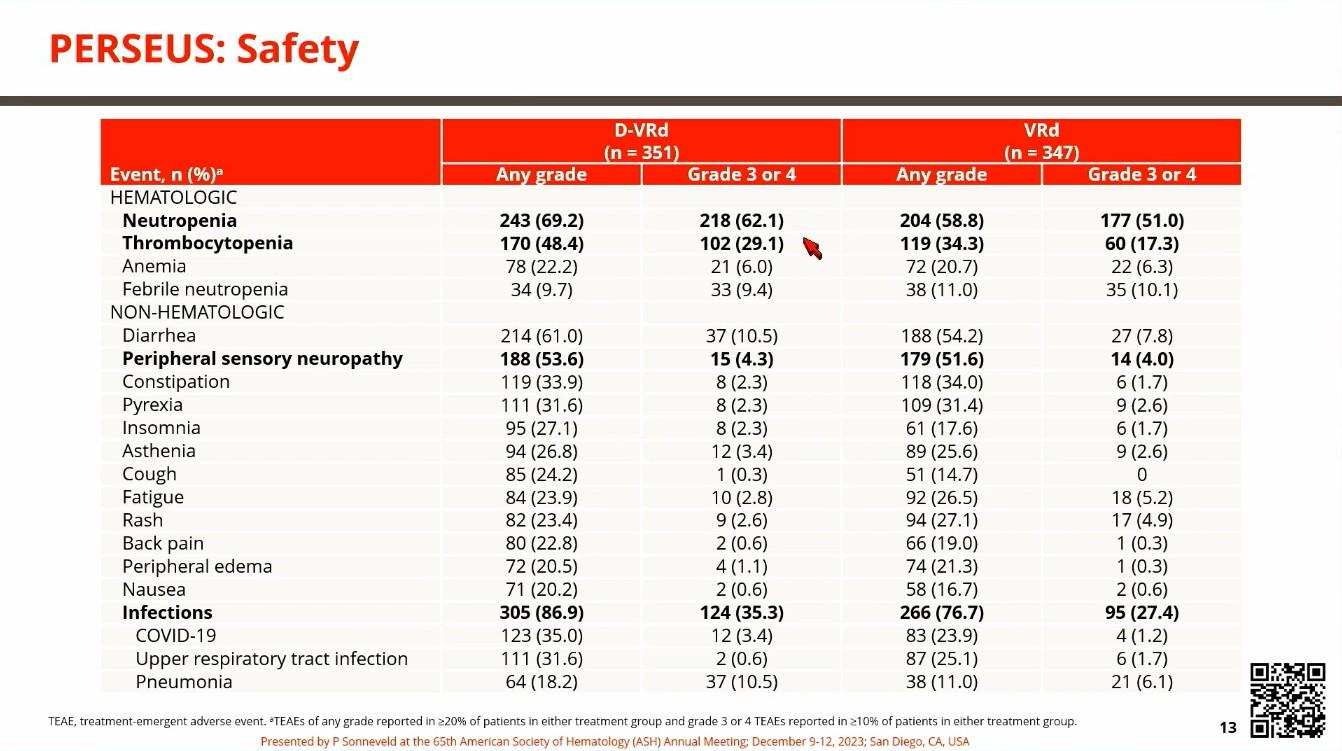
• Observed safety profile was consistent with the known safety profiles for DARA SC and VRd
• These randomized phase 3 results support D-VRd followed by D-R maintenance as a new standard of care for transplant-eligible patients with NDMM
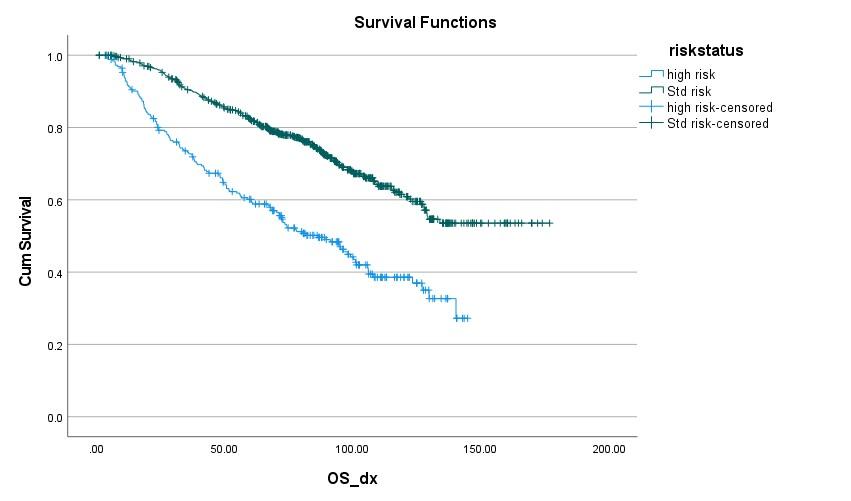
EMORY RVD VS D-RVD
STUDY DESIGN
No consolidation
Risk-stratified maintenance approach No Dara-based maintenance
RVd
Key eligibility criteria:
• Transplant-eligible newly diagnosed standard risk or high- risk multiple myeloma
• Received either RVd or D-RVd induction
• Eligible to receive maintenance treatment
• Len: 25 mg on days 114/21 days
• Bort: 1.3 mg/m2 on days 1,4,8,11/21 days
• Dexamethasone (oral) days 1,8,15/21 days
D-RVd
• Dara: IV or SQ on days 1,8,15/21 days for C1-4 and day 1 only if C5-6 given
• Len: 25 mg on days 114/21 days
• Bort: 1.3 mg/m2 on days 1,4,8,11/21 days
• Dexamethasone (oral) days 1,8,15/28 days
ASCT
Standard-risk: Lenalidomide maintenance until PD
High-risk1: PI/IMiD maintenance x 3 years or PD
Primary end-point:
• ≥Complete Response Rate (≥CR rate)
Secondary endpoints:
• ORR
• ≥VGPR
• PFS
• OS
1. High risk defined as presence of del(17p), t(4;14), t(14;16) or complex karyotype at diagnosis RVd: lenalidomide, bortezomib, dexamethasone; D-RVd: daratumumab, lenalidomide, bortezomib, dexamethasone; ASCT: Autologous Stem Cell Transplant; PFS: Progression Free Survival; ≥VGPR: Greater than Very Good Partial Response; CR: Complete Response, ORR: overall response rate;OS: overall Survival, Dara: daratumumab, Len: lenalidomide; Bort: bortezomib; Dex: Dexamethasone; IV: intravenous; SQ: subcutaneous; PD: disease progression
Ajay K. Nooka MD MPH
PATIENT
CHARACTERISTICS: D-RVD VS RVD
RESPONSE RATES DEEPENED OVER TIME: RVD V DRVD
Assessment in progress
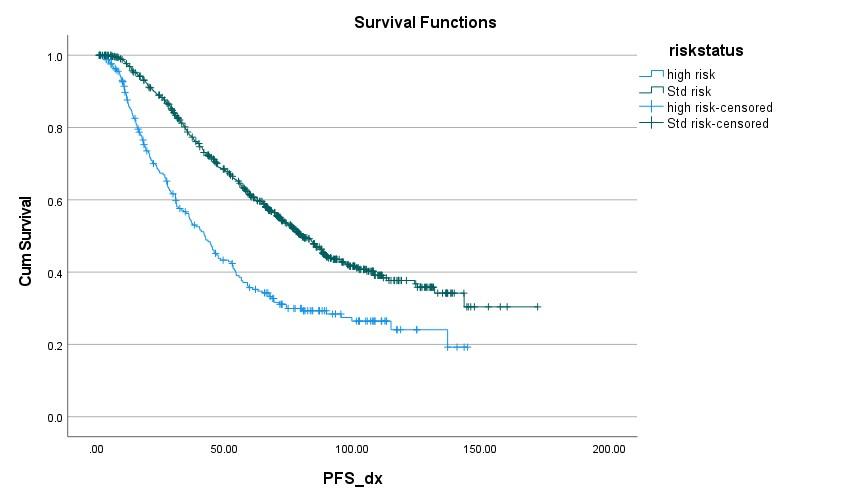
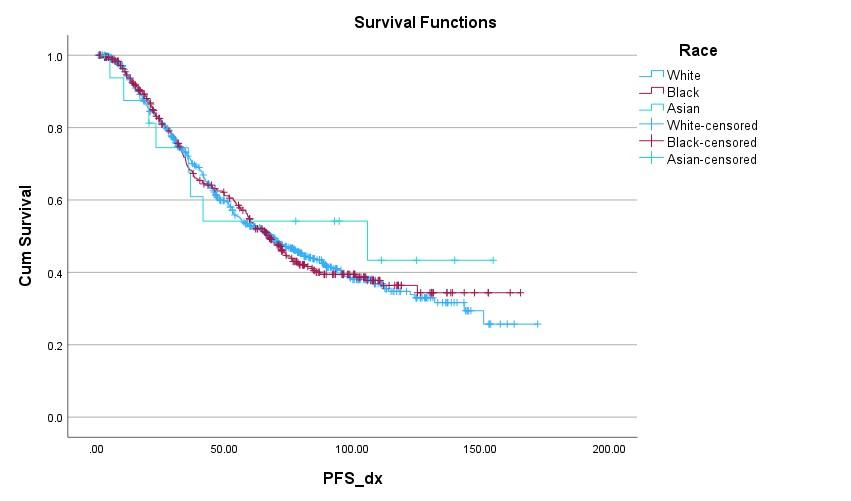
SURVIVAL OUTCOMES: OVERALL COHORT

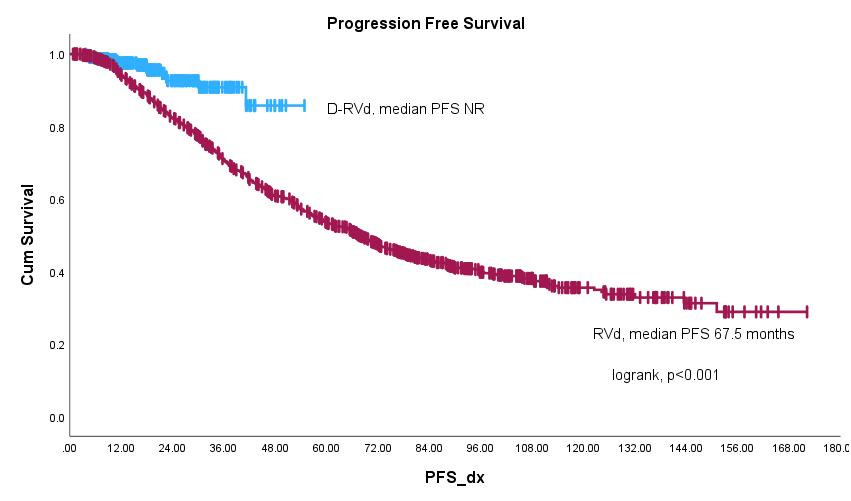
D-RVd mPFS NR
RVd mPFS 67.5 months p <0.001 Time (months)
1-year PFS, D-RVd vs RVd: 98% vs 93%
2-year PFS, D-RVd vs RVd: 93% vs 82%
Median follow up DRVd: 18 months, RVd: 87 months
= 0.034
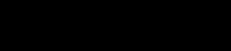
D-RVd mOS NR
(months)
1-year OS, D-RVd vs RVd: 99% vs 97%
2-year OS, D-RVd vs RVd: 94% vs 91%
Median follow up DRVd: 18 months, RVD: 96 months
(months)
D-RVd
White mPFS NR Black mPFS NR)
Asian mPFS NR
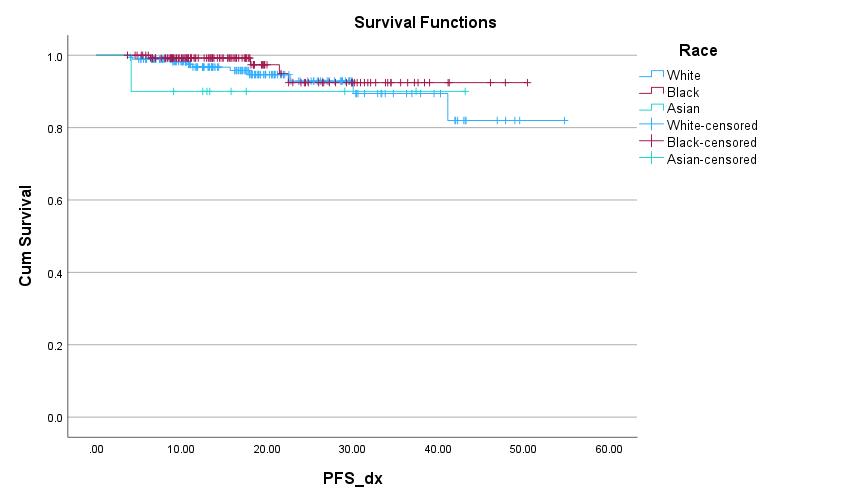

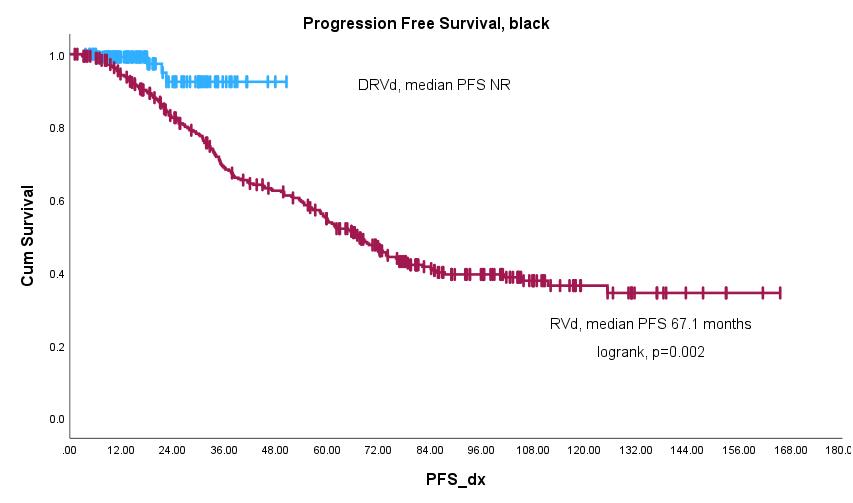
BLACK PATIENTS: D-RVd
vs RVd
TAKE HOME MESSAGES
• What we select for frontline therapy matters: First remission tends to be the longest remission
• Goal of induction therapy: Achieve deepest response with manageable toxicity
• Transplant Eligible patients:
• Standard of care induction regimen: Dara + RVD (PERSEUS trial)
• Upfront transplant remains standard of care
• Deferred transplant reasonable for select patients
• Maintenance therapy until progression
IsKia EMN24 Study Design
Induction
Key eligibility criteria:
TE NDMM patients aged <70 years
Stratification: - Centralized FISH (standard risk/missing vs. high risk defined as del(17p) and/or t(4;14) and/or t(14;16); - ISS (I vs. II and III)
Four 28-day cycles Post-ASCT consolidation
MOBILIZATION
Cy: 2-3 g/m2 followed by G-CSF for stem-cell collection and MEL200-ASCT MEL: 200 mg/m2 followed by ASCT
Twelve 28-day cycles Light consolidation
POST-CONSOLIDATION MRD NEGATIVITY
(ITT ANALYSIS)
≥VGPR after consolidation was 94% in both arms; ≥CR 74% vs 72% and sCR 64% vs 67% in the IsaKRd vs KRd arms.
High MRD compliance and sample quality (97-100% of sample evaluable at 10-5 and 10-6 cut off.
Consistent MRD results were detected by next-generation flow
In the logistic regression analysis, ORs, 95% CIs, and p-values were adjusted for stratification factor.
MRD NEGATIVITY RATES IMPROVED OVER
Isa-KRd (N=151)
(N=151)
MRD NEGATIVITY RATES IMPROVED OVER
Isa-KRd (N=151) KRd (N=151)
POST-CONSOLIDATION MRD NEGATIVITY BY NGS
SUBGROUP ANALYSIS BY CYTOGENETIC RISK

1 HRCA was defined as the presence of one of the following high-risk cytogenetic abnormalities: del(17p13.1), t(4;14) (p16.3;q32.3), t(14;16) (q32.3;q23), gain(1q21), or amp(1q21); 2+ HRCA was defined as the presence of at least two high-risk cytogenetic abnormalities.
SAFETY ANALYSIS: TREATMENT-RELATED ADVERSE EVENTS
TAKE HOME MESSAGES
• IsKia study also looking at the addition of a monoclonal anti-CD38 Ab to induction with a different backbone (KRD instead of RVD)
• High rates of MRD negativity even in ultra high risk patients
• Limited follow up – do not know the impact on PFS/OS as yet
• Higher rates of carfilzomib-associated toxicity
TRANSPLANT-INELIGIBLE/FRAIL PATIENTS
MM TREATMENT PARADIGM
HOW DO WE DEFINE TRANSPLANT-INELIGIBLE
• Not a specific age cut-off
• Performance status
• Comorbidities
• Cardiac function
• Pulmonary function
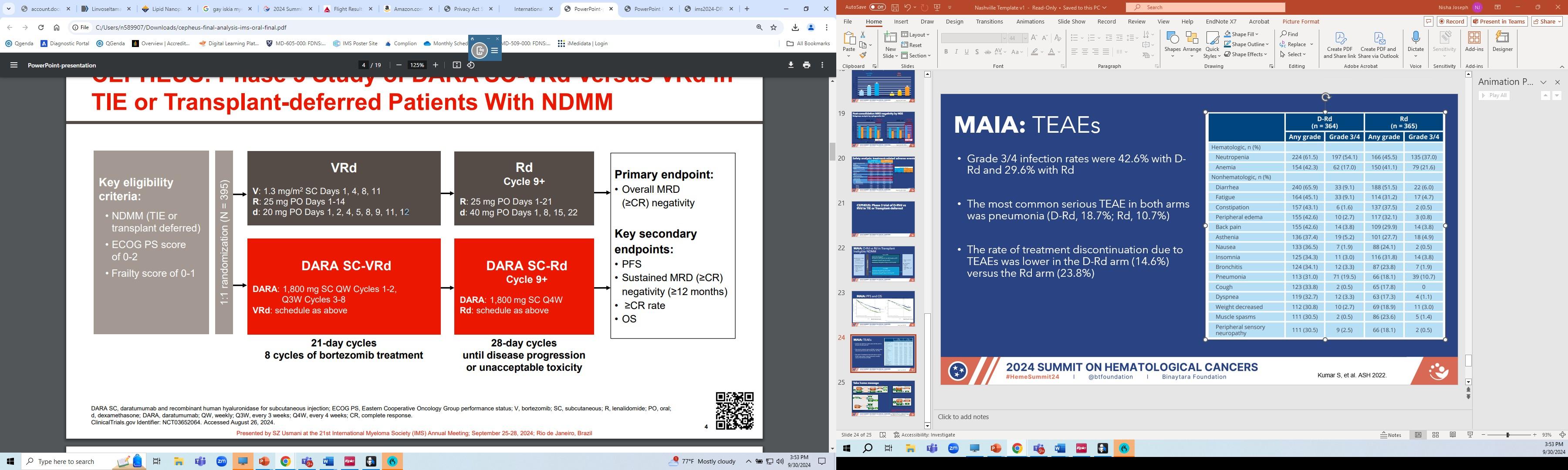

MAIA: D-RD VS RD IN TRANSPLANT INELIGIBLE NDMM
Key eligibility criteria
• TIE NDMM
• ECOG PS score 02
• CrCl ≥30 mL/min
Stratification Factors
• ISS (I vs II vs III)
• Region (NA vs other)
• Age (<75 vs ≥75 years)
D-Rd (n=369)
Daratumumab: 16 mg/kg IV
QW Cycles 1-2, Q2W Cycles 3-6, then Q4W thereafter until PD
Lenalidomide: 25 mg PO, Days 1-21 until PD
Dexamethasone: 40 mg PO or IV, Days 1, 8, 15, 22 until PD
Rd (n=368)
Lenalidomide: 25 mg PO, Days 1-21 until PD
Dexamethasone: 40 mg PO, Days 1, 8, 15, 22 until PD
Cycle: 28 Days
Primary Endpoint:
• PFS Key Secondary Endpoints:
• ORR
• ≥CR rate
• MRD (NGS; 10-5)
• OS
MAIA: PFS AND OS
PFS with D-Rd and Rd in the ITT population
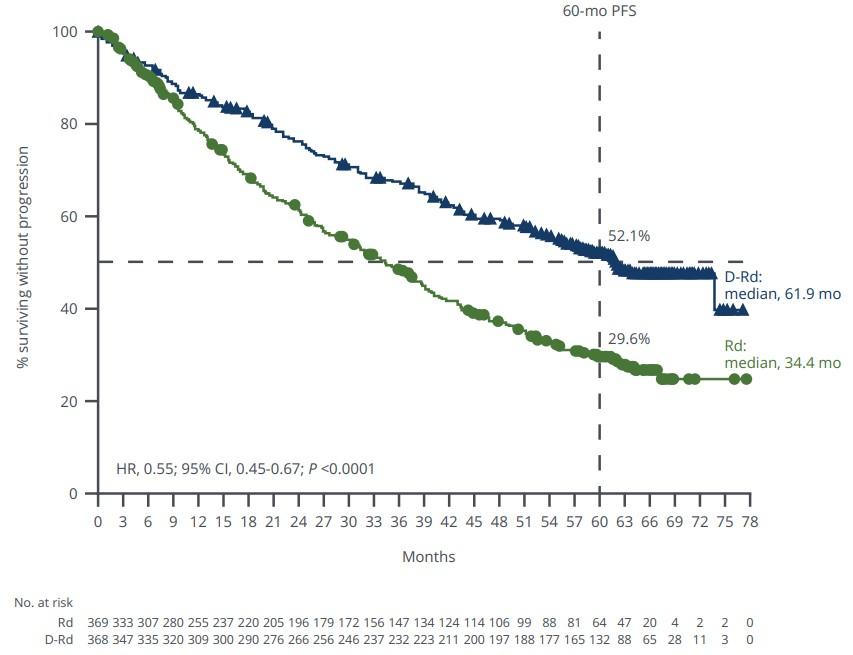
Median Follow-Up, 49.6 months
OS with D-Rd and Rd in the ITT population

Median Follow-Up, 73.6 months
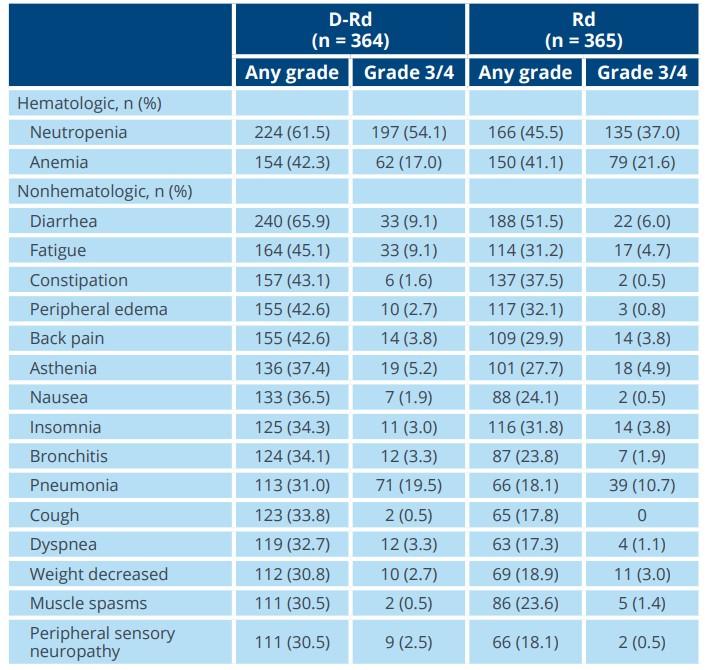
MAIA: TEAES
Grade 3/4 infection rates were 42.6% with D-Rd and 29.6% with Rd
The most common serious TEAE in both arms was pneumonia (D-Rd, 18.7%; Rd, 10.7%)
The rate of treatment discontinuation due to TEAEs was lower in the D-Rd arm (14.6%) versus the Rd arm (23.8%)
Breakout B (Main Room)
RRMM: Continuing the Myeloma Treatment Journey
Manisha Bhutani, MD
Atrium Health Levine Cancer Institute, Charlotte, NC
Relapsed Multiple Myeloma: Continuing the Treatment Journey
Manisha Bhutani, MD
Charlotte, NC
Atrium Health Levine Cancer Institute
Discuss an approach to treating relapsed myeloma based on patient, disease and treatment characteristics
OBJECTIVES
Review the important trend of using an aggressive approach in early treatment of myeloma
Discuss the approach to late relapse and the use of novel therapies such as CAR T and bispecific antibodies
Definitions:
What is relapsed/refractory disease and a line of therapy?
• Relapsed: recurrence (reappearance of disease) after a response to therapy
• Refractory: progression despite ongoing therapy
• Progression: change in M protein/light chain values
• Line of therapy: change in treatment due to either progression of disease or unmanageable side effects
• Note: initial (or induction) therapy + stem cell transplant + consolidation/ maintenance therapy = 1 line of


Therapy Selection Considerations
Disease-Related
• Nature of the relapse
– Biochemical vs symptomatic
• Risk stratification
– High-risk chromosomal abnormalities: del(17p), t(4;14), t(14;16)
• Disease burden
Therapy-Related
• Previous therapies
• Prior treatmentrelated adverse event
• Regimen-related toxicity
• Depth and duration of previous response
• Cost to patient
Patient-Related
• Renal insufficiency
• Hepatic impairment
• Comorbidities
• Preferences
• Social factors
– Support system
– Accessibility to treatment center
– Insurance coverage
An Approach to Relapsed MM
• It is not a simple algorithm of treatment #1 then 2 then 3…
• Leverage the benefit of multiple mechanisms of action in combination therapy
Categories
• Earlier relapse (typically first or second relapse or 1-3 prior lines)
• Later Relapse (3rd or 4th relapse and beyond)
• Triple Class Refractory: Refractory to PI, IMiD and MoAb
Principles
1. Depth of Response matters…likely incorporate MRD soon
2. High risk vs standard risk…more aggressive Rx in high risk
3. Balance efficacy and toxicity…initially and constantly assess
4. Overcome drug resistance…change mechanism of action when possible
Multiple Myeloma is Not One Disease!
RVD+ASCT+Lenalidomide Maintenance
Relapse 2
Relapse 1
Time: Years! D i s e a s e A c t i v i t y
Relapse 1
Relapse 2
Relapse 3
Relapse 1
Pillars of Myeloma therapy
Emerging immunotherapies in multiple myeloma


Modified from: Shah A, Mailankody S. BMJ 2020; 370
Carvykti
Talquetamab (CPRC5D)
Cevostamab (FcRH5)
Naked antibodies
Examples:
Cancer cell
1. Daratumumab (Darzalex) — recognizes CD38
2. Isatuximab (Sarclisa) — recognizes CD38
3. Elotuzumab (Empliciti) — recognizes SLAMF7
Antibody drug conjugate
linker

Examples:
1. Belantamab mafodotin (Blenrep) — recognizes BCMA
BISPECIFIC ANTIBODY
Bispecific MM target Brand name
Teclistamab BCMA Tecvayli
Talquetamab GPRC5D Talvey
Elranatamab BCMA Elrexfio
Cevostamab FcRH5
Livoseltamab BCMA
Etentamig (ABBV383) BCMA
Bispecific antibody
Plasma cell aka myeloma cell T-cell • Cytokine release • T cell activation • Perforin/Granzymes
Fc domain
CAR-T CELLS
Cilta-cel CARVYKTI (BCMA)
Early Relapse
General Principles
Use mechanisms of action not previously used
Do not continue to use lenalidomide if progressing on len maintenance
Triplets are preferred over doublets
In real practice - most patients receiving VRD (Bortezomib-LenalidomideDex) like regimens, 1st relapse is typically
Daratumumab + Pomalidomide + Dex (APOLLO)
Isatuximab + Pomalidomide + Dex (ICARIA)
Daratumumab + Carfilzomib + Dex (CANDOR)
Isatuximab + Carfilzomib + Dex. (IKEMA)
Selinexor + Bortezomib + Dex (BOSTON)
Important Update – CAR T cell therapies can be used as early as first relapse!
First or Second Relapse (Options after Considering Clinical (Modified from mSMART But Added New CAR-T Approvals)
Not refractory to Lenalidomide and standard risk or long 1st remission
Refractory to Lenalidomide
KPd or PVd or PCd or EloPd Or CAR-T (Cilta-cel If 1+ prior LOT, Ide-cel if 2+ LOT) DRd
Not Refractory to Anti-CD38 Refractory to Anti-CD38 and Len DPd or IsaPd Or DVd
Favor CAR-T Cilta-cel (1+ prior LOT) Or Ide-cel (2+ prior LOT)
Others to the left if not candidate for CAR-T
Standard Risk and >23 years remission <2 years of remission and/or HRCA > 2-3 year remission and standard risk < 2 year remission or HRCA Cilta-cel CAR T or Anti-CD38 + Kd
Dingli D, et al. Mayo Clin Proc. 2017;92(4):578-59. Updated 2024.
Abecma (CAR T) vs Standard of Care: 2-4 prior lines of therapy
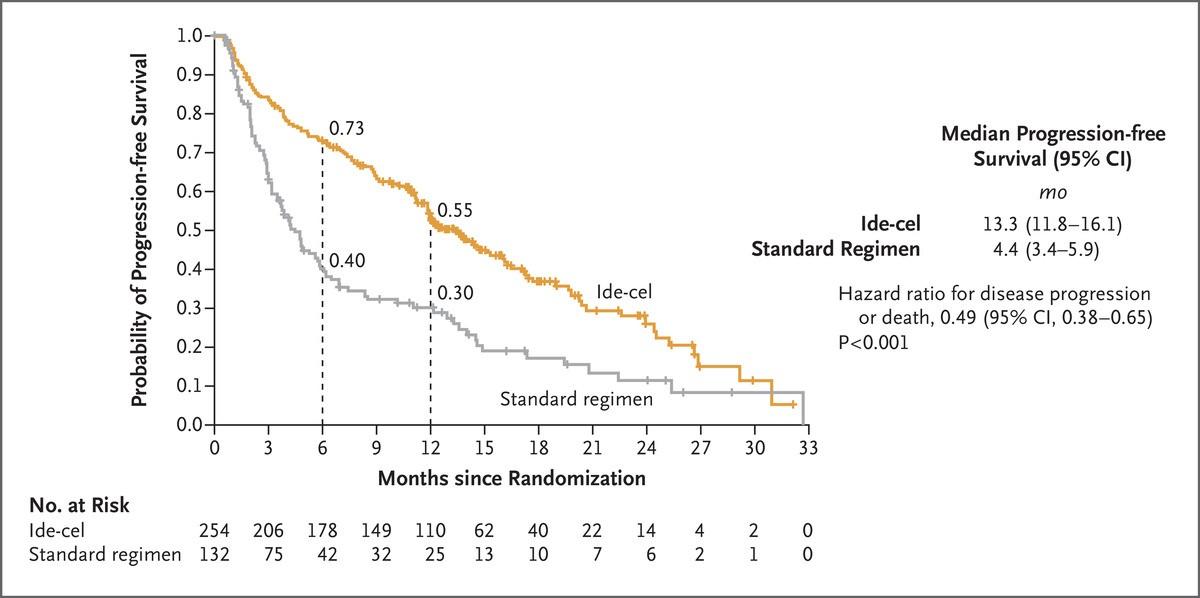
Carvykti (CAR T) vs Standard of Care: 1-3 prior lines of therapy

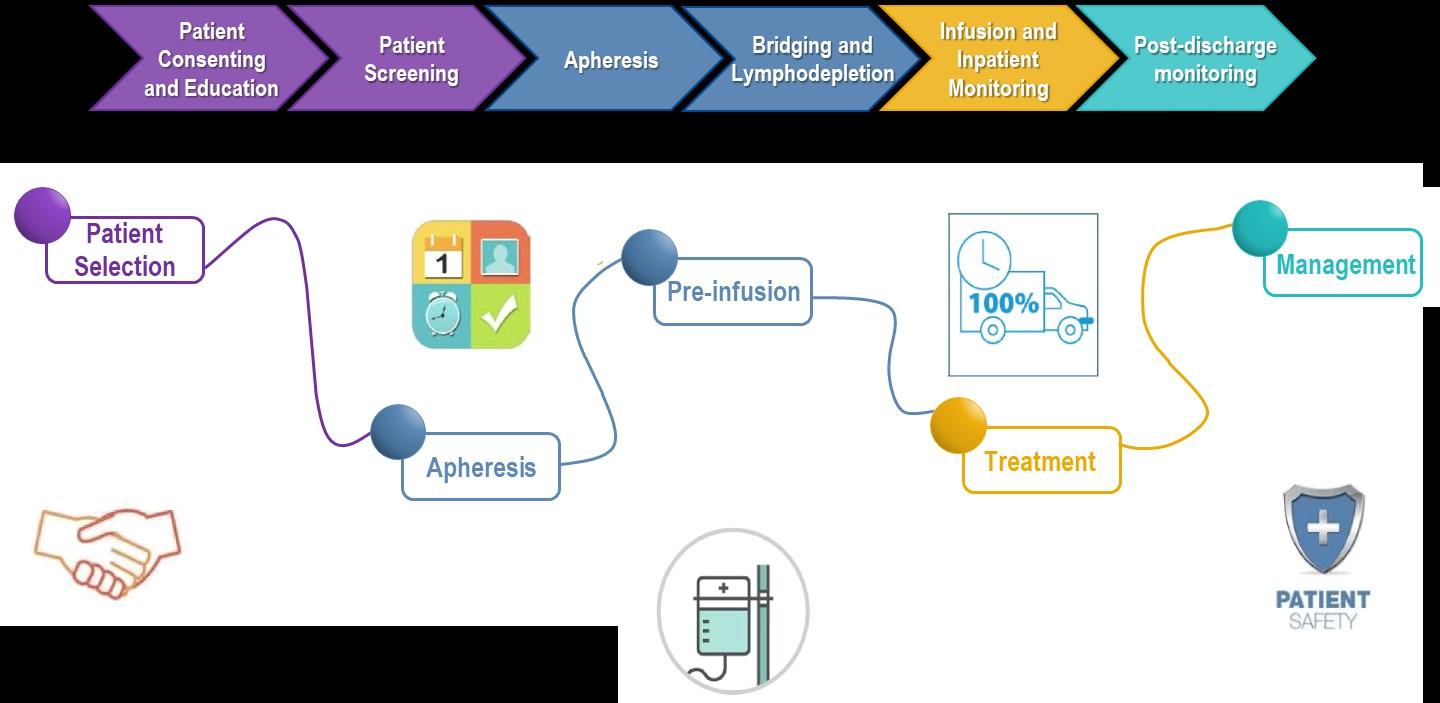
CAR T-Cell Therapy Patient Journey

Immune cells from the patient are collected

Standard of care therapy is permitted until CAR T cells are ready for infusion
Fludarabine and Cytoxan are used to create “immunologic space” to CAR T cells to expand

CAR T: Expected Toxicities

Cytokine release syndrome Neurotoxicity (ICANS)


Cytopenias Infections
CRS ICANS
Onset 1 9 days after CAR Tcell infusion 2 9 days after CAR Tcell infusion
Duration 511 days 317 days
Symptom
s
Managem
ent
• Fever
• Difficulty breathing
• Dizziness
• Nausea
• Headache
• Rapid heartbeat
• Low blood pressure
• Actemra (tocilizumab)
• Corticosteroids
• Supportive care
• Headache
• Confusion
• Language disturbance
• Seizures
• Delirium
• Cerebral edema
• Antiseizure medications
• Corticosteroids
*Based on the ASTCT consensus; †Based on vasopressor; ‡For adults and children >12 years; §For children ≤12 years; ‖Only when concurrent with CRS
Bispecific and Trispecific Antibodies
There are currently 3 approved bispecific antibodies:
Teclistamab (Tecvayli)
Talquetamab (Talvey)
Elranatamab (Elrexfio)
Bispecific
Antibodies: Expected Toxicities
• Cytokine release syndrome (CRS)
• Neurotoxicity (ICANS)
• Usually occurs within first 1–2 weeks
• Frequency (all grade and grade 3–5) higher with CAR T
• Cytopenias
• Target unique
• For example, rash, taste disturbance seen with GPRC5D, but not with BCMA
• Infections
• Incidence for bispecifics at RP2D not yet known
• Viruses: CMV, EBV
• PCP/PJP
• Ongoing discussions regarding prophylactic measures
IVIG
Anti-infectives
Similarities and Differences Between CAR T-Cell
Therapy and Bispecific Antibodies
Approved product Abecma, Carvykti Tecvayli
Key Points – CAR T and Bispecifics
CAR T and bispecific antibodies are very active even in heavily pretreated patients.
Side effects of CAR T cells and bispecific antibodies include cytokine release syndrome, confusion, and low blood counts, all of which are treatable.
Abecma and Carvykti are only the first-generation CAR T cells and target the same protein. Different CAR Ts and different targets are on the way.
Bispecific antibodies represent an “off-the-shelf” immunotherapy; Tecvayli was approved in October 2022, and now Talvey and Elrexfio in August 2023
Several additional bispecific antibodies are under clinical evaluation.
Emerging Therapies for
Relapsed/Refractory Multiple Myeloma
Bispecific antibodies
• Cevostamab, Alnuctamab, ABBV383, and others
• Target BCMA, GPRC5D, or FcRH5 on myeloma cells and CD3 on T cells
• Redirects T cells to myeloma cells
Cereblon E3 ligase modulators (CELMoDs)
• Iberdomide, Mezigdomide
• Targets cereblon
• Enhances tumoricidal and immune-stimulatory effects compared with immunomodulatory agents
Small molecule inhibitors
• Venetoclax, Sonrotoclax
• Targets Bcl-2
• Induces multiple myeloma cell apoptosis
LUNCH
Please move to the Vinings Room
Engage and Partner with the IMF
Sylvia Dsouza
Vice President, Development, International Myeloma
Foundation
IMF REGIONAL COMMUNITY WORKSHOP
ATLANTA
AFTERNOON AGENDA
Managing Side Effects and Living Well with Myeloma
Kevin Brigle, PhD, NP
Massey Comprehensive Cancer Center
Virginia Commonwealth University, Richmond, VA
Living the Myeloma Life: Local Patient & Care Partner
Pat Conley (Patient Advocate & Care Partner) &
Mike Conley (Patient Advocate & Care Partner)
Beyond Myeloma Therapy: How to Optimize and Protect your Immune System: A Nutrition Approach
Stephanie Boyea, MS, RD, CSO, LD
Winship Cancer Institute of Emory University
Q&A with Panel
Closing Remarks
Robin Tuohy
Vice President, Support Groups, International Myeloma Foundation
Engage and Partner with the IMF
Sylvia Dsouza, Vice President, Development
International Myeloma Foundation
Engage & Partner with the IMF
Sylvia Dsouza, Vice President, Development
WHO AM I
WHAT DO I DO?

Vice President of Development for the IMF
Securing philanthropic support and resources for the IMF through diverse mechanisms
Oversee a team of passionate and determined fundraising professionals who are committed to advancing the mission of the IMF
Have the incredible honor of working with dedicated volunteers from the US and across the globe.
3 Ways to Engage
Philanthropy
Make a philanthropic gift to support research, education, advocacy or patient support programs.
Volunteer
Join your local support group/become a Support Group Leader
Join our grassroots patient Advocacy program
Volunteer your time at local races organized by the IMF to engage the community
Engage on social media to connect with others affected by myeloma and spread awareness and empower patients with knowledge and resources.
Intellectual capacity
Offer your expertise as a speaker or panelist at events.
Be a beta tester for various new tools and products and provide reviews and feedback


Philanthropy Fuels Our Mission
Peer-to-Peer Fundraising
Peer-to-Peer Fundraisers are created from YOUR ideas. Starting a Fundraiser is easy and fun. They also make a world of difference in the myeloma community.
Join a IMF P2P event or start your own and engage your family, friends, co-workers, your network who honor your journey with myeloma and want to support you. Let them show you that you are not alone.
Ex: Hole in One Golf Tournament, Iceland Cycling Expedition, Miracles for Myeloma 5K Run/Walks (hybrid)
Join the HOPE Society (Recurring Monthly & Annual Giving Program)
Help us cultivate the future by joining the International Myeloma Foundation's Hope Society.
Monthly and annual gifts support IMF core programs, including educational events, publications, the toll-free InfoLine, and more.
Start with a monthly contribution and when ready turn it into a yearly commitment. You will be a part of likeminded individuals united in the quest to find a cure for myeloma and a better quaity of life for all myeloma patients.
Transformative Gifts (Major Giving and Principal Giving)
Gifts can be designated toward a specific program, project or initiative .
Is there something specific that resonates deeply with you and you want to see change happening?
Gifts can also be unrestricted, expendable and/or an endowment
Major Giving -
Designate Your Gift
• Research: The IMF is dedicated to finding a cure for multiple myeloma.
• Education: The IMF provides education for patients and caregivers.
• Support: The IMF provides support for patients and caregivers through inperson and virtual support groups.
• Advocacy: The IMF advocates for better access to care and more affordable options for myeloma patients.
Research
The Black Swan Research Initiative was funded by a Board member/donor who was a visionary and saw the need for the IMF to launch this initiative
The IMF's Black Swan Research Initiative serves as a conductor of sorts to this orchestra of collaborating experts in the field of myeloma.
The BSRI sponsors more than 50 projects around the world aimed at curing multiple myeloma. Among them:
SPAIN: The CESAR trial uses the combination of Kyprolis, Revlimid, and dexamethasone plus autologous stem-cell transplant to treat high-risk smoldering multiple myeloma. It applies: precise mininal residual disease (MRD) testing using next-generation flow cytometry (NGF) and Blood testing for routine monitoring
USA: The ASCENT 1.0 trial tests early intervention in high-risk smoldering multiple myeloma.
ICELAND: Launched in 2016, the iStopMM project identifies and treats multiple myeloma at the earliest signs of disease.
GERMANY: Studies are exploring long-term survival and hereditary risk factors in multiple myeloma.
AUSTRALIA: Identifying mechanisms of the progression of multiple myeloma and t esting DNA mutations in the blood.
SINGAPORE: Hub for the clinical trials network in Asia led for the IMF’s Asian Myeloma Network (AMN) program by Prof Wee Joo Chng. A collaboration of eight countries (or regions), the AMN is unique in providing access to novel agents in a clinical trial setting throughout Asia. In addition, research projects appropriate for the region are conducted in an effort to improve outcomes and achieve a cure.

Brian D. Novis Grants
• The Brian D. Novis Grants award Senior and Junior investigators in the myeloma field with critical funding to elevate their ideas, work, and efforts in finding a cure for myeloma.
• Helps support novel research ideas that can be a breakthrough
• Historically, the IMF has awarded 46 Senior Grants and 109 Junior Grants. (157 grants for $8M+ since inception)

IMF's Scientific Advisory Board
The Scientific Advisory Board (SAB) of the International Myeloma Foundation (IMF) is a group of world-renowned experts in the field of myeloma research. The SAB provides guidance and expertise to the IMF on scientific and medical matters, including research priorities, clinical trials, and patient care.

Education
Patient and Family Seminars: 4 in-person events across the United States
Regional Community Workshops: 6 in-person and 4 virtual
M-Power Initiative:
M-Power Community workshops and we have covered Atlanta, Detroit, Baltimore, New York, Richmond, Charlotte, and Tampa in the last couple of years with goals to expand to more cities in the U.S.
The Health Equity Scholars is a mentoring program that pairs 12 students and 12 myeloma experts to conduct projects that address myeloma research on health disparities. This program educates individuals from minority communities about myeloma, engages communities at the earliest level on training to share a deeper understanding of the disease, and improves sensitivities towards myeloma diagnosis.
Open Global Advocacy
The IMF is the voice of the myeloma community in Washington, DC.
Our objective is to inform and influence the critical healthcare policy decisions impacting the myeloma community.
Danielle Doheny
U.S. Policy & Advocacy
Michael Riotto
U.S. Grassroots Advocacy
We believe in the value of working to improve healthcare laws to ensure there are no barriers to care as patients navigate their myeloma journey.
What Do We Advocate For?
The following policy principles are the foundation on which we prioritize our advocacy work.
1. Ensure Access to Care: We advocate for policies that ensure all myeloma patients have equitable, comprehensive, patientcentered care without insurance barriers that limit options or delay treatment initiation.
2. Eliminate Financial Barriers: We advocate for policies that allow myeloma patients access to treatments and supportive care interventions without facing financial hardships.
3. Advance Myeloma Research: We advocate for annual appropriations funding for myeloma research and the advancement of clinical trial eligibility and research protocols that ensure representation from diverse populations.

Grassroots Advocacy at the IMF


Grassroots Advocacy is the critical component to influencing policy decisions
The IMF brings advocates to Capitol Hill to share their experience with lawmakers.
Together, we champion legislative priorities that directly impact the lives of millions of patients and elevate the voices of of the myeloma community.
The IMF Grassroots Advocacy Program is multi-faceted and growing
• Advocacy Training & Leadership Development
• Policy and Legislative Education
• Grassroots Campaign Planning
• Health Policy Forums & Roundtables
• Advocacy Resource Development
• Storytelling and Personal Narratives
Summit:

Support Group Team Report – November 2024
MYELOMA VOICES AT ASH 2024 TEAM
We were excited to celebrate the 25th Anniversary Support Group Leaders Summit with 98 Support Group Leaders representing 74 Support Groups with 32 first-time attendees and 66 returning leaders

LINK TO Myeloma Voices Webpage 2024
The IMF brings myeloma support group leaders and patients to ASH to learn and share their voices. This information and hope is heard globally and locally from their perspective utilizing social media, blogs, vlogs, and interviews to offer their personal insights.
The IMF is committed to fostering interaction between the patient community and the myeloma experts.
“In the last 20 years, 19 myeloma treatments have been approved by the FDA. With so many combination therapies and clinical trials, we have a better chance than ever before of providing the patient with excellent treatment. Be your own best advocate!” Jack Aiello



P2P
Laughs 4 Life (Hattiesburg, MI, comedy celebration)-- 8 years, $483,850!
Peer-to-Peer (P2P) and Monthly & Annual Giving
Miracles for Myeloma(Clark, New Jersey, 5K run/walk) -- 12 years, $804,422!
Iceland Cycling Expedition raised close to $250K
Hole In One (Golf Tournament, Jackson, New Jersey)– Inaugural golf tournament that has raised $73K
Monthly & Annual Giving – HOPE Society
Join our flagship monthly and annual giving program, the HOPE Society.
Get invited to Regional Salon Dinners in your area with IMF leadership and KOLs.
Receive exclusive updates on research and trials fresh off the press.
Play a pivotal role in supporting our four pillars.
Support long-term initiatives that make a lasting difference.



Upcoming Peer-to-Peer Fundraising Events in 2025
• 7th Annual Schleicher's Hikers 5K
• Mission for Matt
• Jack's Education and Experience Grant
• San Fernando Valley Support Group Fundraiser
• Raging for Ray
• Czerkies Memorial Golf Outing
• Hole in One Golf Tournament
• Inland Empire Walk
• Walkathon & BBQ To End Multiple Myeloma
• Row for a Cure






IMF's Miracles for Myeloma Virtual/In-Person 5K Run/Walk Series
The IMF will lead five Virtual/In-Person 5K Run/Walks across the United States in the following regions (Goal: $100K net from each event)
• Miracles for Myeloma Virtual/In-Person 5K Run/Walk in Boca Raton, FL (03-15-2025)
• Miracles for Myeloma Virtual/In-Person 5K Run/Walk in Los Angeles, CA (04-12-2025)
• Miracles for Myeloma Virtual/In-Person 5K Run/Walk in Philadelphia, PA (05-03-2025)
• Miracles for Myeloma Virtual/In-Person 5K Run/Walk in Clark, NJ (09-13-2025)
• Miracles for Myeloma Virtual/In-Person 5K Run/Walk in Chicago, IL (10-04-2025)
Iceland Cycling Expedition 2025
• The 2025 Iceland Cycling Expedition will take place from Wednesday, August 27, 2025 through Tuesday, September 2, 2025.
• The Iceland Cycling Expedition is a 6-day/7-night fundraising cycling challenge in the High Mountains of Iceland.
• 20 Participants including industry sponsor slots
• Applications for in-person participation now closed but you can participate and support virtually! More information coming soon.






International Myeloma Foundation’s Signature Marquee Annual Endurance
Click here to look back to where i t all started in 2024!



Three goals:
1. Raising awareness and visibility for multiple myeloma and a patient/care-partners journey to and through it (humanizing the disease)
2. Raising awareness and visibility for the International Myeloma Foundation
3. Raising critical funding to help accelerate research to find a cure for myeloma
Additional outcome that organically emerged – building a strong, interconnected myeloma community where all myeloma patients and their loved ones see hope, resilience and determination as part of the journey and feel empowered

Ashley Dieks (Patient) Garson, Ontario

ICE 2025 Participants

Dr. Saad Usmani (Myeloma Clinician and Researcher) Memorial Sloan Kettering, NY

Jered Haddad (Patient) Germantown, TN

Dr. Douglas Sborov (Myeloma Clinician and Researcher) Huntsman Cancer Institute at the University of UT
Richard Pampe (Patient) Jackson, WY
Dr. Jeffrey Zonder (Myeloma Clinician and Researcher) Department of Oncology at Wayne State University, MI

Tatum Byhre (Care Partner) Minneapolis, MN


Christian Hoff (Patient) Pittsboro, NC

Benjamin Freund (Patient) East Canaan, CT

Troy Fischer (Care Partner) Bloomington, IL

Katherine Podgorski (Patient) Toronto, Canada

Dr. Cristina Gasparetto (Myeloma Clinician and Researcher) Duke Cancer Institute, NC
Iceland Cycling Expedition 2024
Phare International
Malibu Film Festival
Beverly Hills Film Festival
Tribeca Festival
Atlanta Film Festival
Palm Springs International Film Festival
Miami Film Festival
Flicker's Rhode Island International Film Festival
LA Shorts
11. Holly Shorts Film Festival Portland Film Festival

Leave a Lasting Legacy
Planned Giving
Join the Brian D. Novis Legacy Society and make a planned gift!
Gain immediate tax benefits
Potentially increase your income during your lifetime.
Continue to fund our core programs and four pillars.
Make a bequest (a gift from your estate)
Include a provision in your will or living trust.
Designated us as a beneficiary of a life insurance policy, or retirement plan (IRA, 401(k), or 403(b).
Leave us in your will is one of the most profound ways to support the people and causes important to you.
Corporate and Foundation Gifts
Your organization can contribute a corporate gift or foundation grant
Provide seed funding that is necessary to accelerate the path to a cure.

Reach Out to the IMF Development Team
We welcome you to continue to learn more about our programs, projects, and initiatives at the IMF and find alignment with your own philanthropic passion and as well as ways to deepen and strengthen your engagement with us. Reach out to the IMF Development Team to start a conversation on how you can make a difference in the lives of the people impacted by myeloma.
Sylvia Dsouza- Vice President of Development sdsouza@myeloma.org or (310)947-4126
Simona Grace- Director of Development, Major Gifts sgrace@myeloma.org or (818)487-7455 x 307
Kimberly Francis- Assistant Director of Development Peer-to-Peer Fundraising kfrancis@myeloma.org or (818)487-7455 x 304
Managing Side Effects and Living Well with Myeloma
Kevin Brigle, PhD, NP
Massey Comprehensive Cancer Center
Virginia Commonwealth University, Richmond, VA
Seasons of Multiple Myeloma
Kevin Brigle, PhD, NP
Oncology Nurse Practitioner
VCU Massey Comprehensive Cancer Center

Wintery Mix of Treatment Options Spring into Managing Side Effects
Summer of Success




Wintery Mix of Treatment Options

Diverse and Complex Treatment Combinations





Myeloma Treatment Common Combinations
Velcade® (bortezomib)
Lenalidomide
DVRd, VRd, Vd
DVRd, VRd, Rd
Kyprolis® (carfilzomib) KRd, Kd, DKd, Isa-Kd
Pomalyst® (pomalidomide) Pd, DPd, EPd, PCd, Isa-Pd
Darzalex® (daratumumab)
DVRd, DRd, DVd, DPd, DVMP, DKd
Ninlaro®(ixazomib) IRd
Empliciti® (elotuzumab) ERd, EPd
Xpovio® (Selinexor) XVd, XPd, XKd
Sarclisa® (Isatuximab) Isa-Kd, Isa-Pd
Blenrep® (Belantamab mafodotin) Bela-d
Abecma® (Idecabtagene Vicleucel) --
Carvykti™ (ciltacabtagene autoleucel)
Elrexfio™ (elranatamab)
Tecvayli® (teclistamab) --
Talvey™ (talquetamab) --
Venclexta® (venetoclax) Vd + ven
New agents or regimens in clinical trials are possible options
ASCT = autologous stem cell transplant; Bela = belantamab; C = cyclophosphamide; D = daratumumab; d = dexamethasone; E = elotuzumab; Isa = isatuximab; I = ixazomib; K = carfilzomib; M = melphalan; P = pomalidomide; R = lenalidomide; V = bortezomib; ven = venetoclax.

Stem Cell Transplant
ELIGIBILITY
Measuring Treatment Response
Determining Transplant Eligibility
Insurance Authorization Collecting Stem Cells

TRANSPLANT
High Dose Chemotherapy
Stem Cell Infusion
Supportive Care Engraftment
Duration: Approximately 2 weeks
Location: Transplant Center
Duration: Approximately 3-4 weeks
Location: Transplant Center
POST-TRANSPLANT
P H A S E 1 P H A S E 2 P H A S E 3
Restrengthening
Appetite recovery
“Day 100” assessment
Begin maintenance therapy
Duration: Approximately 10-12 weeks
Location: HOME
CAR T: Another Treatment Approach
Ask for a referral to CAR Tcell center as soon as it is possible as next treatment option (ie, before relapse)
Manufacturing takes
≈ 4 to 6 weeks
Bridging therapy may be needed
T-Cell Collection
No driving for 8 weeks
“One & Done” with continued monitoring
• Away from home
• Often some hospital stay
• Care Partner needed
• Side effect management
• CRS, ICANS
• Low blood counts
• Fatigue and fever
• Some patients need ongoing transfusion support
Bispecific Antibodies
• Different bispecific antibodies have differences in efficacy, side effects
– Available after 4 prior lines of therapy (or clinical trial)
– About 7 in 10 patients respond
– Off-the-shelf treatment; no waiting for engineering cells
– CRS and neurotoxicity
– Risk of infection
• BCMA target: greater potential for infection
– Tecvayli® (teclistamab)
– Elrexfio™ (elranatamab)
BISPECIFIC ANTIBODIES
• GPRC5D target: potential for skin and nail side effects, GI issues of taste change, anorexia and weight loss
– Talvey™ (talquetamab)




CAR T and Bispecific Antibodies: Unique Side Effects


CRS is a common but often mild & manageable side effect
CAR = chimeric antigen receptor; CRS = cytokine release syndrome. Oluwole OO, Davila ML. J Leukoc Biol. 2016;100:1265-1272. June CH, et al. Science. 2018;359:1361-1365. Brudno JN, Kochenderfer JN. Blood. 2016;127(26):3321-3330. Brudno JN, Kochenderfer JN. Blood Rev. 2019:34:45-55. Shimabukuro-Vornhagen, et al. J Immunother Cancer. 2018;6:56. Lee DW, et al. Biol Blood Marrow Transplant. 2019;25:625-638.
CAR T and Bispecific Antibodies: Unique Side Effects

Spring Into Managing Side Effects

The Early Bird Gets the Worm: Communicate Proactively with Your Healthcare Team
Your team may be able to help, but only if they know how you feel.
Unmanaged Myeloma can cause:
• Calcium elevation
• Renal dysfunction
• Low blood counts
• Infection Risk
• Blood clots
• Bone pain
• Neuropathy
• Fatigue

Side Effects of Treatment can
cause:
• GI symptoms
• Renal dysfunction
• Low blood counts
• Infection Risk
Tip: proactively discuss common side effects and what to do if they occur

How You Feel
• Blood clots
• Neuropathy
• Fatigue


Tip: Keep a Symptom Diary and bring it to appointments



Steroids enhance the effectiveness of other myeloma therapies
Your provider may adjust your dose. Do not stop or alter your dose of steroids without discussing it with your provider
Managing Steroid Side Effects
• Consistent schedule (AM vs. PM)
• Take with food
• Stomach discomfort: Over-the-counter or prescription medications
• Medications to prevent shingles, thrush, or other infections
Are Steroids Messing With Your Sunny Disposition?
Steroid Side Effects
• Irritability, mood swings, depression
• Difficulty sleeping (insomnia), fatigue
• Blurred vision, cataracts
• Flushing/sweating
• Increased risk of infections, heart disease
• Muscle weakness, cramping
• Increased blood pressure, water retention
• Stomach bloating, hiccups, heartburn, ulcers, or gas
• Weight gain, hair thinning/loss, skin rashes
• Increased blood sugar levels, diabetes
Infection Can Be Serious for People With Myeloma
Preventing infections is paramount.
Infection remains the leading cause of death in patients with multiple myeloma. Several factors account for this infection risk, including the overall state of immunosuppression from multiple myeloma, treatment, age, and comorbidities (e.g., renal failure and frailty).
IMWG Consensus guidelines and recommendations for infection prevention in multiple myeloma; Lancet Haematol.2022;9(2):143–161.
Infection Prevention Tips
Good personal hygiene (skin, oral)
Environmental control (avoid crowds and sick people; use a high-quality mask when close contact is unavoidable)
Report fever of more than 100.4°F, shaking chills even without fever, dizziness, shortness of breath, low blood pressure to HCP as directed.
As recommended by your healthcare team:
Immunizations:
Flu, COVID, RSV & and pneumococcal vaccinations; avoid live vaccines


Preventative and/or supportive medications (next slide)
Medications Can Reduce Infection Risk
Type of Infection Risk
Viral: Herpes Simplex (HSV/VZV); CMV
Medication Recommendation(s) for Healthcare Team Consideration
Acyclovir prophylaxis
Bacterial: blood, pneumonia, and urinary tract infection Consider prophylaxis with levofloxacin
PJP (P. jirovecii pneumonia)
Fungal infections
COVID-19 and Influenza
IgG < 400 mg/dL (general infection risk)
ANC < 1000 cells/μL (general infection risk)
Consider prophylaxis with trimethoprim-sulfamethoxazole
Consider prophylaxis with fluconazole
Antiviral therapy if exposed or positive for covid per institution recommendations
IVIg recommended
Consider GCSF 2 or 3 times/wk (or as frequently as needed) to maintain
ANC > 1000 cells/μL and maintain treatment dose intensity
GI Symptoms: Prevention & Management
Fluid intake can help with both diarrhea and constipation and helps kidney function
Constipation is more common in the induction phase
• Opioid pain relievers, antidepressants, heart or blood pressure medications (check with provider, pharmacist)
• Supplements: Calcium, Iron, vitamin D (rarely), vitamin B-12 deficiency Increase fiber
• Stay well hydrated
• Fruits, vegetables, high fiber whole grain foods
• Fiber binding agents – Metamucil® , Citrucel®, Benefiber®
Anorexia, the inability to eat, is common during transplant and resolves with time.
• Hydration is most important
• Small, frequent meals with a focus on protein intake
• You will work closely with a dietician to help monitor your calorie intake
Diarrhea is common during transplant and long-term maintenance therapy. Other medications and supplements
• Hydration is very important
• Electrolyte replacement is common
• Good skin care will help prevent irritation
• Stool exam may be needed to rule-out infection
• If no infection, anti-diarrheal medication may be prescribed

Discuss GI issues with healthcare providers to identify causes and make adjustments to medications and supplements
Management of Oral Side Effects
OTC dry mouth rinse, gel, spray are recommended. Advise patients to avoid hot beverages. Initiate anti-fungal therapy for oral thrush
Dexamethasone oral solutions “swish and spit” have been tried but with no proven benefit yet. Sour citrus or candies before meals are also recommended. Taste Changes
Dietary modifications with small bites, eating upright, and sips with food can help manage symptoms.
Some medications lead to weight gain, others to weight loss.
Dry mouth leads to taste changes which can lead to anorexia. Meet

Dry Mouth
Dysphagia
Catamero D, Purcell K, Ray C, et al. Presented at the 20th
Myeloma Society (IMS) Annual Meeting Nurse
September 27–30, 2023; Athens, Greece.
Skin and Nail Side Effects
Possible side effect to some treatments and supportive care medications

Skin Rash:
• Prevent dry skin; apply lotion
• Report changes to your care team
• Medication interruption or alternative, as needed
• Steroids:
– Topical for grades 1-2,
– Systemic and topical for Grade 3
• Antihistamines, as needed


Nail Changes:

• Keep your nails short and clean. Watch for “catching and tearing”
• Apply a heavy moisturizer like Vaseline or salve. Wear cotton hand coverings to bed
• A nail hardener may help with thinning
• Tell the team if you have signs of a fungal infection, like thickened or discolored nails
Photos: Mount Sinai Hospital, NY, NY
Feel Like a Spring Chicken: Prevent and Manage Pain
Pain can significantly compromise quality of life
Sources of pain include bone disease, neuropathy and medical procedures
• Management
– Prevent pain when possible
• Bone strengtheners to decrease fracture risk
• Antiviral to prevent shingles
• Sedation before procedures
– Interventions depend on source of pain
• May include medications, activity, surgical intervention, radiation therapy, etc
• Complementary therapies (Mind-body, medication, yoga, supplements, acupuncture, etc)
• Scrambler therapy for neuropathy


Tell your healthcare provider about any new bone or chronic pain that is not adequately controlled
Peripheral Neuropathy Management
Peripheral neuropathy happens when there is damage to nerves in the extremities (hands, feet, limbs). Damage can be the result of myeloma, treatment or unrelated conditions (i.e. diabetes).
Symptoms:
• Numbness
• Tingling
• Prickling sensations
• Sensitivity to touch
• Burning and/or cold sensation
• Muscle weakness
Prevention / management:
• Bortezomib once-weekly and/or subcutaneous administration
• Massage area with cocoa butter regularly
• Neuroprotective Supplements:
– B-complex vitamins (B1, B6, B12)
– Green tea
• Safe environment: rugs, furnishings, shoes
If neuropathy worsens, your provider may:
• Adjust your treatment plan
• Prescribe oral or topical pain medication
• Suggest physical therapy
Report symptoms of peripheral neuropathy early to your healthcare provider; nerve damage from neuropathy can be permanent if unaddressed

Understanding Changes to Kidney Function
• Risk Factors
– Active multiple myeloma (light chains, high calcium)
– Other medical issues (ex: Diabetes, dehydration, infection)
– Medications (MM treatment, antibiotics, contrast dye)
– Poor Nutrition
• Prevention
– Stay hydrated – drink water
– Avoid certain medications when possible (eg, NSAIDs), dose adjust as needed
• Treatment
– Treatment for myeloma
– Hydration
– Dialysis

Many myeloma patients will experience kidney issues at some point; protecting your kidney function early and over time is important
Additional Supportive Care
Faiman B, et al. CJON. 2017;21(5)suppl:19-36. Dimopoulous M, et al. Leukemia. 2009;23(9):1545-56. Brigle K, et al. CJON. 2017;21(5)suppl:60-76. Faiman B, et al. CJON. 2017;21(5)suppl:19-36.
Faiman B, et al. CJON. 2011;15suppl:66-76. Miceli TS, et al. CJON. 2011;15(4)suppl:9-23.

Summer of Success
Let the Sun Shine In
Fatigue
Fatigue is the most reported symptom.
Sources include anemia, pain, reduced activity, insomnia, treatment toxicity, bone marrow suppression 98.8%
Often, people do not share these symptoms with their providers. Talk to your provider about symptoms that are not well controlled or if you have thoughts of self-harm.


>35% of patients
of patients

Bee an Empowered Patient
Ask
questions
– What are my treatment options?
– What are the pros and cons of the different options?
– How will we know if treatment is working?
– What do the different labs mean?
– Who will be monitoring my labs?
– How can I access my test results (eg, patient portal)?
– What will we do if my treatment doesn’t work or quits working?
Participate in decisions
– Share your priorities and preferences
– Include care partner(s) in your discussion

Speak up if something seems different or unusual
– Normally 4 vials of blood but only drawing 3?
– Normally specialty pharmacy confirms delivery but haven’t heard from them this month?
Live in the sunshine, swim the sea, drink the wild air.
– When is my next appointment?
Communicate with your healthcare team
– Understand the roles of each team member
– Who to contact for your needs (eg, side effects, insurance issues, other)
Develop a support network
– Learn from others: IMF has many support groups or you can start one (IMF’s can help)
– Ralph Waldo Emerson
Care Partners Are Vital for Success
If you want to go fast, go alone, if you want to go far, go together
• Care partners may help with medical appointments, managing medication, daily living, physical assistance, emotional support, myeloma knowledge, healthy lifestyle, patient advocacy, financial decisions
• Care partners can be a spouse, close relative, a network of people (family, friends, neighbors, church members, etc)




African Proverb
• Caring for the Care Partner
– Recognize that caregiving is difficult/stressful
– Encourage care partners to maintain their health, interests, and friendships
– The IMF has information and resources to help care partners


Cultivate A Care Network
If you want to go fast, go alone, if you want to go far, go together
• Multiple studies demonstrate that strong social ties are associated with longevity, improved adherence to medical treatment and overall improved health outcomes
• Care partners can be a spouse, close relative, a network of people (family, friends, neighbors, church members, etc)
• Care partners may help with medical appointments, managing medication, daily living, physical assistance, emotional support, myeloma knowledge, healthy lifestyle, patient advocacy, financial decisions
• Caring for the Care Partner
– Recognize that caregiving is difficult/stressful
– Encourage care partners to maintain their health, interests, and friendships
– The IMF has information and resources to help care partners

Martino J, et al. Am J of Lifestyle Med. 2015;11(6):466-475. Yang YC, et al. Proc Natl Acad Sci U S A. 2016;113(3):578-583. Pinquart M and Duberstein PR. Crit Rev Oncol Hematol. 2010; 75(2):122–137.
African Proverb
IMF Care Giver Tip Cards

Enjoy Life’s Bounty

Harvest Good Health
Have a Primary Care Provider & Have Recommended Health Screenings
• Blood pressure
• Cholesterol
• Cardiovascular disease
• Diabetes
• Colonoscopy
• Women specific: mammography, pap smear
• Men specific: prostate
• Vision
• Hearing
• Dermatologic evaluation
• Dental checkups & cleaning
Develop & maintain healthy behaviors
• Good nutrition
• Regular activity
• Quit tobacco use
• Sufficient Sleep (next slide)
An ounce of prevention is worth a pound of cure. Benjamin
Franklin

Faiman B, et al. CJON. 2017;21(5)suppl:19-36. Dimopoulous M, et al. Leukemia. 2009;23(9):1545-56. Brigle K, et al. CJON. 2017;21(5)suppl:60-76. Faiman B, et al. CJON. 2017;21(5)suppl:19-36. Faiman B, et al. CJON. 2011;15suppl:66-76. Miceli TS, et al. CJON. 2011;15(4)suppl:9-23.



Living the Myeloma Life: Local Patient & Care Partner
Pat Conley (Patient Advocate & Care Partner) &
Mike Conley (Patient Advocate & Care Partner)
Pat and Mike Conley Before Myeloma

Pat and Mike with Family My Care Partners

Atlanta Support Group Leaders
Pat with Doris Morgan and Nancy Bruno
Beyond Myeloma Therapy:
How to Optimize and Protect your Immune System: A Nutrition Approach
Stephanie Boyea, MS, RD, CSO, LD
Winship Cancer Institute of Emory University, Atlanta, GA

OPTIMIZING & PROTECTING THE IMMUNE SYSTEM:A NUTRITION APPROACH

2025 IMF Regional Community Workshop
CLINICAL ONCOLOGY DIETITIAN
MALIGNANT HEMATOLOGY & BONE MARROW TRANSPLANT
WINSHIP CANCER INSTITUTE OF EMORY UNIVERSITY
STEPHANIE BOYEA, MS, RD, CSO, LD

Today’s Objectives:
• Review the Immune System
• Nutrition’s key role
• Identify if/when supplements have a role
• Recommended resources
WHAT IS THE IMMUNE SYSTEM?
A complex network of immune cells, proteins, receptors, antibodies, and organs1
Acts as the body's law enforcement, providing lines of defense:
• Innate Immune System (General) – “Standard Police Force” - Rapid, non-specific response to any threats.
• Surface Barriers: skin, mucus membranes, tears, secretions
• Neutrophils: like street patrol
• Adaptive Immune System (Special Forces/Detectives): Slower but highly targeted response.
• lymphocytes, antibodies
Works to defend, prevent & limit infection
Immune system’s response naturally produces inflammation
IMMUNE SYSTEM & INFLAMMATION
• Immune system’s inflammatory response 2
• In response to dietary & environmental toxins, body produces free radicals
• Immune cells also produce free radicals as a way to fight infections
• Free radicals are NORMAL.
• BUT High levels of free radicals
inflammation
more free radicals, adding to increased oxidative stress and inflammation
MULTIPLE MYELOMA & THE IMMUNE SYSTEM
DISEASE’S IMPACT: 3,4
• Decrease white blood cell count
• Reduced antibody production
• Increased inflammatory cytokines
TREATMENTS’ ROLE:4
• Chemotherapies (melphalan, cyclophosphamide, etc.) and stem cell transplant process toxic effect on bone marrow
• Proteasome inhibitors and immunomodulatory drugs (IMiDs) decrease white blood cell count (WBC), esp. neutrophils
• Steroids: Slow down or stop WBCs from moving to area of inflammation/infection
CAN NUTRITION INFLUENCE IMMUNE FUNCTION?
• YES!
• Just like gas for your car, diet provides the “fuel” your immune system needs to perform1

NUTRITION’S ROLE IN IMMUNE SUPPORT
5, 6, 7
You CAN fuel your immune system with an adequate amount of the “right” diet for your body
• Adequate energy intake
• Adequate protein intake
• Adequate micronutrient intake
• Supporting the gut microbiome
• Hydration
• Minimize inflammation through lifestyle
The Western Diet 5
DIET AND IMMUNITY
• High in: sugar, trans fats, saturated fats
• Low in: complex carbohydrates, fiber, micronutrients, bioactive molecules (polyphenols – anti-inflammatory), omega-3s
• Risk factor for “metabolism-induced inflammation”
• High saturated fat intakes Chronic activation of innate immune system + suppression of adaptive immune system

Reduces Inflammation

IMPACT OF A PLANT-BASED DIET AND IMMUNITY
Supports Immune Surveillance
Lowers Oxidative Stress
Supports Gut Health
PLANT-BASED DIET IN MULTIPLE MYELOMA
Reduced Risk:
A whole foods, plant-based diet has been associated with a decreased risk of multiple myeloma 17,18
Support gut microbiome: which has been correlated with sustained minimal residual disease (MRD) negativity in MM 17
NUTRIVENTION Study: A 12-week plant-based dietary intervention in those with precursor conditions
Results: improved metabolic and microbiome profiles, with some having a favorable shift in disease progression 19

DO SUPPLEMENTS HAVE A ROLE IN IMMUNE SUPPORT IN MM?
FISH OIL CURCUMIN
CO-Q10 MUSHROOMS
ASTRAGALUS
VITAMIN C GREEN TEA
POPULAR SUPPLEMENTS FOR IMMUNE SUPPORT
GLUCOSAMINE ECHINACEA
VITAMIN D GARLIC


ZINC
SUPPLEMENTS FOR IMMUNE SUPPORT: VITAMIN D
• Crucial for bone & immune health 8, 9
• Sources: Cod liver oil, fish, egg yolk, some mushrooms exposed to UV light, fortified milk
• Sunlight: 5-30 minutes sun between 10AM – 3PM twice a week
• Role in MM:
• Affects bone health, osteoclast activity, and decreases pro-inflammatory cytokines
• Higher rate of deficiency in MM: up to 24% may be deficient & 87% may have insufficient levels
• Vitamin D deficiency may be a predictor for poor overall survival in white patients with MM but not African American patients with MM 9
• Key Takeaways:
• Everyone request a Vitamin D level!!
• If normal, supplement with RDA (600 IU for adults </= 70 and 800 IU for adults > 70)
• If deficient, speak with your provider
• Warnings: Long-term intakes of > 4,000 IUs per day can lead to hypercalcemia
SUPPLEMENTS FOR IMMUNITY IN MM: VITAMIN C
• Role in immune cell growth and function, including antibody production
• Dietary intake linked to reduced cancer risk, but supplements do not appear to lower cancer risk10
• Food sources: citrus fruits, tomatoes, potatoes, peppers (1/2 cup = 100% DV), etc.
• RDA = 90mg for men; 75mg for women
• At risk for deficiency: poor quality diet, smoking, dialysis
• Caution with supplements:
• High-dose oral vitamin C (10 grams daily) does not improve survival or decrease disease progression11
• IV vitamin C may offer benefits on survival rate in some patients, however, these were poorly designed studies
• Use caution if: undergoing radiation, on proteosome inhibitors (bortezomib or ixazomib), have G6PD deficiency, excessive iron, or history of recurrent kidney stones.
SUPPLEMENTS FOR IMMUNITY IN MM: ZINC
• Supports immune response, wound healing
• Mild deficiency has been associated with defects in immune response
• Symptoms: decreased appetite, taste changes, and infections
• Found in red meat, poultry, whole grains, beans, nuts, oysters,
• Decreased levels found in stage 1 MM patients 12
• Excess supplementation can cause a copper deficiency
• Safe dose/Upper Limit: 40mg per day
SUPPLEMENTS FOR IMMUNITY IN MM: CURCUMIN
• Yellow pigment of turmeric plant used in Indian traditional herbal medicines 13
• Antioxidant, antiinflammatory, and cytotoxicity (cell ‐‐death) to numerous cancer cell types including myeloma
• One study found it may have synergistic effect when used in combination with an IMiD or PI (Ramakrishna, 2020, very small study of 15 patients)
• Consume with fat and piperine for improved absorption (poorly absorbed)
• WARNING: piperine may increase absorption of other drugs as well!
• Contraindications:
• Blood thinners (patients on Revlimid)
• History of Liver or Bile duct problems
• ALWAYS discuss supplements of interest with your care team
SUPPLEMENT RESPONSIBLY
• Physician (Oncologist AND Internal Medicine/Primary Care), Pharmacist, & Registered Dietitian
• Be open and honest with your care team
• Don’t hesitate to ask questions
BOTTOM LINE…
• There is no clear evidence that you can “boost” your immune system to work beyond its design with a supplement or any particular food
• BUT you can SUPPORT an optimally functioning immune system:
• Adequate energy & protein & fluid intakes
• Balanced diet with variety of vegetables, fruits, whole grains
• Limit intakes of sugar, alcohol, & saturated fats
• Request aVitamin D level & supplement appropriately
• If at risk for deficiency, request aVitamin C Level
• Other key strategies:
• Food Safety, Hand washing, Physical activity, Sleep, & Stress Management
REFERENCES:
(1) Collins, K. Can Your Diet Boost Your Immune System and Provide Better Protection Against COVID-19? AICR.org.April, 15, 2020.
(2) Upham, B. Explained: How Your Immune System Fights Off Coronavirus (and Other Germs). Everyday Health. March 12, 2020.
(3) Blimark C, Holmberg E, Mellqvist UH, et al. Multiple myeloma and infections: a population-based study on 9253 multiple myeloma patients. Haematologica. 2015;100(1):107. Epub 2014 Oct 24.
(4)Nucci M, Anaissie E. Infections with multiple myeloma. In: UpToDate.” Editor: Bow E. (Accessed April 1, 2025.)
(5) Childs CE, Calder PC, Miles EA. Diet and Immune Function. Nutrients. 2019;11(8):1933. Published 2019 Aug 16. doi:10.3390/nu11081933
(6) Malone,A.The role of hydration in the acute inflammatory process & recovery. Abbott Nutrition Health Institute.
REFERENCES:
(7) Li P,Yin YL, Li D, Kim SW,Wu G.Amino acids and immune function. Br J Nutr. 2007;98(2):237-252. doi:10.1017/S000711450769936X
(8).AR, Jolliffe DA, Hooper RL, et al.Vitamin D supplementation to prevent acute respiratory tract infections: systematic review and meta-analysis of individual participant data. BMJ. 2017;356:i6583
(9). Sarvari V.Yellapragada,Vitamin D deficiency predicts for poor overall survival in white but not African American patients with multiple myeloma. Blood Adv (2020 4 (8) 1643-1646
(10) Byers T, Guerrero N. Epidemiologic evidence for vitamin C and vitamin E in cancer prevention.Am J Clin Nutr 1995;62:1385S92S.
(11) Moertel CG, Fleming TR, Creagan ET, et al. High-dose vitamin C versus placebo in the treatment of patients with advanced cancer who have had no prior chemotherapy.A randomized double-blind comparison. N Engl J Med 1985;312:137-41
REFERENCES
(12) Khadem-Ansari MH,Asoudeh M, Gheshlaghi HFK, et al. Copper and zinc in stage I multiple myeloma: relation with ceruloplasmin, lipid peroxidation, and superoxide dismutase activity. Horm Mol Biol Clin Investig. 2018;37(3):/j/hmbci.2019.37.issue-3/hmbci-2018-0055/hmbci-20180055.xml. Published 2018 Oct 26. doi:10.1515/hmbci-2018-0055
(13) Ramakrishna, R, Diamond,TH,Alexander,W, Manoharan,A, Golombick,T. Use of Curcumin in Multiple Myeloma patients intolerant of steroid therapy. Clin Case Rep. 2020; 8: 739– 744. https://doi.org/10.1002/ccr3.2735
(14) Calder PC, Carr AC, Gombart AF, Eggersdorfer M. Optimal Nutritional Status for a Well-Functioning Immune System Is an Important Factor to Protect against Viral Infections. Nutrients 2020, 12(4), 1181; https://doi.org/10.3390/nu12041181
(15) FDA.gov
(16) Foodsafety.gov
REFERENCES
(17) Shah UA, Maclachlan KH, Derkach A, Salcedo M, et al. Sustained Minimal Residual Disease Negativity in Multiple Myeloma is Associated with Stool Butyrate and Healthier Plant-Based Diets. Clin Cancer Res. 2022 Dec 1;28(23):5149-5155. doi: 10.1158/1078-0432.CCR-22-0723. PMID: 36170461; PMCID: PMC9722533.
(18) Castro F, Parikh R, Eustaquio JC, Derkach A, et al.. Pre-Diagnosis Dietary Patterns and Risk of Multiple Myeloma in the NIHAARP Diet and Health Study. medRxiv [Preprint]. 2023 Sep 23:2023.09.20.23295639.
(19) Urvi A. Shah, MD1,2, Laura Lucia Cogrossi, MS3,4*,Andriy Derkach, PhD5*, Francesca Castro, MS, et al. Oral Abstract:A HighFiber Dietary Intervention (NUTRIVENTION) in Precursor Plasma Cell Disorders Improves Biomarkers of Disease and May Delay Progression to Myeloma.ASH. Dec 8 2024.
Q&A WITH PANEL
Closing Remarks
Robin Tuohy, Vice President, Patient Support International
Myeloma Foundation
Housekeeping Items
Presentation Slides: Are available by scanning the QR code.
Program Evaluations: Please be sure to complete your program evaluation and return your evaluations at the end of today.
Restrooms: Restrooms are located …
Parking: Please see Meghan at the registration desk to receive your parking voucher.
We greatly appreciate your time and feedback!
Thank you to our speakers & our sponsors!
OUR VISION:
A world where every myeloma patient can live life to the fullest, unburdened by the disease.
OUR MISSION:
Improving the quality of life of myeloma patients while working toward prevention and a cure.
IMF Core Values:
These are the core values we bring to accomplishing our mission each day.
Patient Centric
The patient experience is the focus of everything we do. Every interaction is an opportunity to establish a personal connection built on care and compassion which is the basis for continued support.
Respect All
As a team, we value honesty and transparency while creating a culture of mutual respect. We foster a myeloma community built on sincerity, authenticity, and kindness.
Excellence and Innovation
We value accountability, personal responsibility, and a steadfast commitment to excellence. We respect the legacy and reputation of our organization while seeking new solutions and advancements to improve outcomes, quality of life, and access to the best available resources for everyone impacted by myeloma.
Honor differences
We recognize each team member's skills and talents through collaboration and cooperation. Our programs aim to celebrate and support the diversity of our patients and their communities.
