ALTIMED 30 Years of Innovation in Medical Manufacturing
For over three decades, Altimed has stood at the forefront of medical device manufacturing in Eastern Europe. Founded in Belarus, the company has consistently demonstrated a commitment to innovation, quality, and biocompatibility—core principles that have allowed it to remain a trusted partner for healthcare professionals and institutions around the world. Since its inception, Altimed has specialized in the development and production of advanced medical solutions aimed at improving patient outcomes and advancing surgical standards. Over the years, the company has grown from
a small-scale workshop into a high-tech manufacturer with its own research, development, and production capabilities. This long-standing experience has given Altimed a unique position in the medical technology sector, combining scientific expertise with practical, real-world applications.
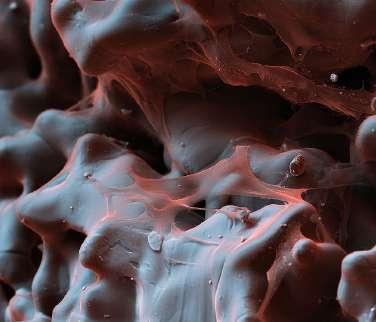
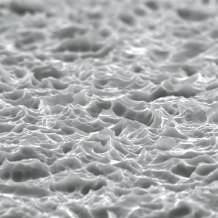
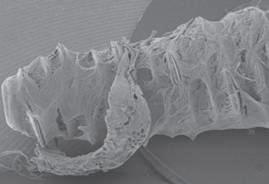
One of the company’s key strengths lies in its proprietary manufacturing technologies. Altimed is renowned for its development and application of biocompatible porous materials that are engineered to integrate seamlessly with the human body. These materials include porous titanium and specialized porous polymers—cutting-edge substances that support tissue ingrowth and long-term biological compatibility.
Porous titanium, in particular, has revolutionized the way implants interact with living tissue. Thanks to its unique microstructure, it encourages osteointegration, meaning it allows bone cells to grow directly into the implant surface. This enhances the stability, longevity, and functionality of medical implants, especially in orthopedic and dental applications. Altimed's
proprietary processes allow them to precisely control the porosity, geometry, and mechanical properties of their titanium structures, ensuring optimal performance in clinical settings.
In addition to titanium-based solutions, the company has developed a range of porous polymer materials tailored for soft tissue applications. These polymers are designed to promote vascularization and reduce the risk of rejection, making them ideal for reconstructive surgeries, wound healing systems, and implantable medical devices.
Altimed’s integrated approach—from material science to finished product— allows for continuous innovation and customization. The company works closely with medical professionals to develop solutions that meet real surgical needs, offering both standard and tailor-made devices. Its facilities comply with international standards for quality and safety, ensuring that every product meets rigorous regulatory requirements.
Today, Altimed exports its products to various international markets while maintaining strong roots in domestic healthcare. With an emphasis on sustainable development, cutting-edge biotechnologies, and close collaboration with surgeons and researchers, Altimed continues to shape the future of biocompatible medical devices.
As the medical industry evolves, Altimed remains committed to its founding vision: creating technologies that integrate with the body to restore health, improve lives, and push the boundaries of modern medicine.
www.altimed.by/en minsk@altimed.by
BIONIKA
MARKET LEADER IN DENTAL IMPLANT
MANUFACTURING IN HUNGARY
Bionika Medline Ltd. was established in 1989 by private individuals as a family-owned Hungarian company. We have more than 35 years of experience in the development, production and trade of medical instruments and implants in dentistry, oral surgery, traumatology, orthopedics and rehabilitation. ln accordance with our goals and approach, we attach great importance to the word „BIONIKA” (Bionics in English), which marks a form of scientific thinking at the boundaries of biology, technology and electronics, which combines these three areas in our research and development activities.
Our company strives to raise wide awareness in Hungary not only about its own products, but also of the state-ofthe-art products of our innovative foreign partners. After the insertion of the implant, BIONIKA assumes the risk of the ossification process, regardless of the cause-andeffect relationship, and provides an exchange guarantee within one year of purchase. ln addition, we provide a long-term, 10-year guarantee for our products.
DENTISTRY ORAL SURGERY
DENTAL IMPLANTS
MEMBRANES
Clinical and technological experiences: We continuously process, integrate and exploit accumulated clinical and technological experience in our development activities. Development: Our products are developed in collaboration with doctors and engineers. We manufacture custom-made components based on provided samples.
Quality: BIONIKA Medline Ltd. operates according to EN ISO 9001 and EN ISO 1348S quality management systems. Our products have CE marking.
Guarantee: Otherwise, we provide a longterm, 10-year guarantee for our products.
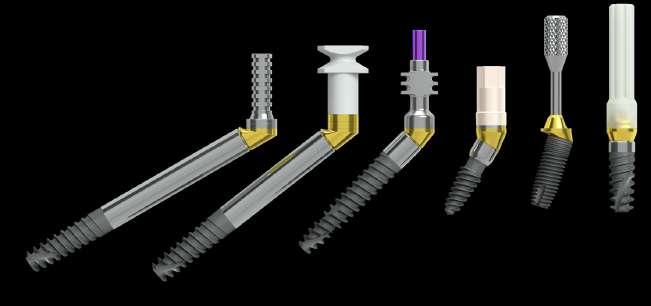
BTK
Iuxta-3D, for ten years the original sub-periostal implant, obviously from Btk Dental
In the ever-evolving landscape of surgical innovation, the company Btk stands out as a pioneer with its groundbreaking Iuxta 3D device. With over a decade of unparalleled expertise, Btk has continuously redefined surgical precision, setting new standards in the field. What sets the Iuxta-3D apart from its competitors is not merely its advanced technology, but the meticulously designed patented features tailored to enhance surgical procedures.
At the core of Btk's innovation lies a commitment to simplifying surgical intricacies. The Iuxta-3D boasts a range of patented products aimed at streamlining surgical processes. Among these are positioning guides meticulously engineered to ensure the precise placement of osteosynthesis screws. This innovative approach not only expedites procedures but also minimizes the margin of error, ultimately enhancing patient outcomes.
Furthermore, Btk's dedication to excellence is evident in the development of osteotomy guides tailored for accurate bone cuts. These precision instruments empower surgeons to execute osteotomies with unparalleled accuracy, enabling long-term functionality of the Iuxta-3D. One of the crowning achievements of the Iuxta-3D device is the integration
of a positioning bar designed for the precise alignment of prosthetics. This revolutionary feature revolutionizes the implantation process, ensuring optimal prosthetic positioning and stability, thereby maximizing patient comfort and longevity.
What truly sets Btk apart is not just the innovative features of the Iuxta 3D, but its longstanding presence as a leader in the industry. With over a decade of proven success, Btk has established itself as a trusted partner for surgeons worldwide, consistently delivering cutting-edge solutions that redefine surgical excellence.
In conclusion, Btk's Iuxta-3D device represents a paradigm shift in surgical precision. With patented features designed to streamline procedures and enhance patient outcomes, Btk continues to lead the way in revolutionizing surgical innovation. As technology advances and boundaries are pushed, Btk remains steadfast in its commitment to empowering surgeons and improving patient care.
For information: www.btk.dental info@btk.dental
Dental Tech Beyond Technology: the human touch in every implant
With over 45 years of experience, Dental Tech is a proudly Italian company specialized in the design, production, and distribution of high-performance dental implant solutions. Every step of the production process is carried out in-house at our facility in Italy, ensuring full control, quality, and consistency—hallmarks of true Made in Italy excellence. From concept to packaging, each implant follows a precise internal workflow:
DESIGN & ENGINEERING
Our R&D department develops high-precision geometries using advanced CAD/CAM systems, aiming to optimize osseointegration.
PRODUCTION
Using state-of-the-art CNC machinery, we manufacture all implant lines and prosthetic components with micrometric tolerances.
SURFACE TREATMENT
Implants undergo sandblasting and acid etching (BWS surface), followed by sequential washing phases to ensure cleanliness and ideal surface roughness. CONTROLLED ENVIRONMENT & STERILITY
In our ISO-certified clean room, implants receive plasma treatment to remove carbon residues. SEM/EDX analysis and 3D surface reconstruction confirm surface quality.
PACKAGING
Implants are sealed in sterile ampoules and plastic blisters, color-coded by type and diameter. Sterilization by gamma rays is the only external phase, after which each implant receives tracking labels and documentation for clinical traceability.
Dental Tech: where every implant tells a story of passion and precision. Craftsmanship, professionalism and quality all come together in the same place.
As the dental patient population ages, both patients and dentists seek efficient treatment solutions that avoid extensive bone augmentation. A standardized approach to implant selection and prosthetic workflows can minimize treatment duration and costs while maintaining high-quality outcomes.
• Case Study
A 70-year-old patient presented with issues in the right mandible affecting an approximately 30-year-old bridge. Assessment revealed a subcoronally damaged tooth 45 under the bridge and pressure sensitivity in tooth 47. Treatment planning considered several key factors:
• Whether tooth 47 needed replacement with a single implant
• The bone width in region 46 and implantation feasibility without augmentation
• The proximity of implant placement in region 45 to the mental foramen
• The patient's expectations, given successful prior implant treatments
The treatment aimed to avoid additional augmentation procedures, using narrow implants (3-3.5 mm in diameter) in atrophied areas. Due to the absence of an antagonist tooth, replacing tooth 47 with an implant was unnecessary. The patient was to receive fixed dentures after healing phase, prioritizing ease of cleaning for potential future manual dexterity decline.
• Clinical Procedure
Teeth 45 and 47 were removed using minimally invasive techniques, preserving the almost complete alveolar walls. After six weeks of healing, a 12 mm long implant with diameter 2.9 mm was placed at site 45, and a 3.5 mm implant at site 46 (BioniQ® Plus, LASAK). Both implants featured a machined collar of 1.7 mm to reduce plaque accumulation in case of future gingival or bone reduction.
A structured approach to implant selection allowed a streamlined procedure with a simplified surgical tray. The implants were inserted with primary stability, and open healing was preferred. Implant stability was confirmed using the Ostell Osseo 100 (NSK), showing values above 70 ISQ for both implants. The impression was taken with an open tray technique. Although treatment could have proceeded after eight weeks, an additional two-month healing period was observed given the patient's age.
• Prosthetic Considerations
Milled all-ceramic restorations were selected over metal-ceramic for cost efficiency. Implant-supported prosthetics were designed to be screwretained, ensuring straightforward maintenance for potential complications, particularly in bruxism cases. The restorations provided sufficient interdental space for effective hygiene.
A radiographic follow-up at 14 months showed stable peri-implant bone levels, with possible bone gain around the 2.9 mm BioniQ Plus implant.
Treatment success was attributed to adequate healing time, regular hygiene monitoring, and a structured prosthetic workflow.
• Conclusion
Modern patients increasingly expect time- and cost-efficient implant solutions. The BioniQ implant system, with its wide range of implants that can accommodate even extremely low bone volume, helps meet these expectations. In this case, narrow BioniQ Plus implants enabled treatment without extensive surgical intervention. Proper implant selection ensured a functional, esthetic, and cost-effective restoration, providing long-term stability and ease of maintenance.
www.lasak.com export@lasak.cz
CONNECTIVE TISSUE ATTACHMENT
Tooth-like tissue growth
BioniQ implants have an implant neck with a bioactive, hydrophilic, moderately rough surface to provide an effective connective tissue attachment. The direct contact of connective tissue with the bioactive, hydrophilic, moderately rough neck significantly reduces marginal bone resorption during biological width restoration.
Looking for distributors Join a partner with over 30 years of expertise
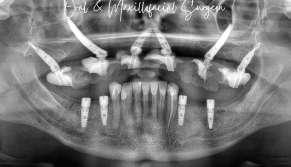
Dental Rehabilitation with Tuff TT and Zygomatic Implants
Following Severe Maxillofacial Trauma & Atrophy Classic Series | TUFF ™
This patient had a severe motor vehicle collision in the past suffering what appears to be a Le Fort 3 fracture and had been edentulous in the maxilla for many years.
He never wore his denture due to being unhappy with it because of his atrophic maxilla. He was also missing his posterior mandibular teeth for many years leading to atrophy in those areas as well. Starting off with the mandible, the ridge was split with a piezo and expanded with Densah burs. Using a pilot guide, Tuff TT implants were placed in the #19, 21, 29, 30 sites.
A veneer graft was then done with allograft.
Going to the maxilla, the anatomy was very scarred
and atrophic from the previous trauma.
Tilted V point Tuff implants to the nasal crest allowed good BIC, massive torque, and avoided the quad zygo.
Pterygoids and bilateral zygomatic implants were placed with very high primary stability.
Buccal fat was advanced and an immediate chairside conversion was performed to put the patient in a screwretained temporary.
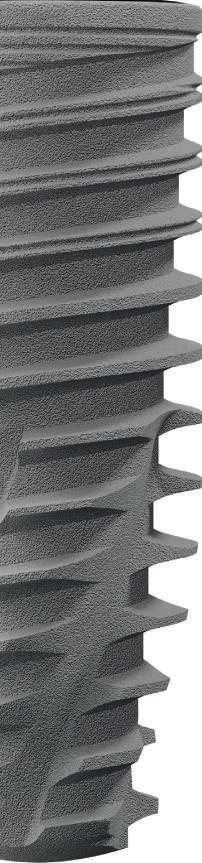
Bone Level Implant, suited for all bone types, with internal hex prosthetics platform.
DESIGN FEATURES:
• Condensing variable threads design
• Apically tapered threads and tapered core body
• Double thread with large step
• Double flutes
CLINICAL BENEFITS:
• Self tapping
• High primary stability
• Minimal drilling
• Fast insertionoptimal for soft bone
• Immediate loadingsuitable for extraction sites
Dr. Alexander Nguyen DDS, OMS
NORIS Medica l Excellence in Execution
Noris Medical provides comprehensive, innovative solutions for all dental implant applications, ensuring you lifelong quality and precision.
Our turnkey approach integrates implant systems, peripheral instrumentation, and professional training, offering all the clinicians a seamless workflow from surgery to restoration.
With a commitment to excellence, service, and quality.
For More Info ContactKasia Radajewska
Phone: +44 779 503 1003
Email: kasiar@norismedical.com
AROUND IMPLANTOLOGY
Discover all ImplantBook editions
Looking for Distributors
Aseptico Inc., the leading US manufacturer of electric motors for dentistry, has introduced the powerful, easy-to-use 1070 Series Implant Motor, expanding its extensive portfolio of implant and surgical systems. This compact, user-friendly device is specifically designed to streamline dental implant procedures without unnecessary complexity. Equipped with a brushless 40,000 RPM motor, the AEU-1070 Series ensures consistent power and precision to handle osteotomies and implant placement, especially when paired with the available Mont Blanc or AHP-85-SS 20:1 reduction handpieces.
The 1070 Series boasts an intuitive, touchscreen display and a multifunction foot control that allows hands-free management of speed, direction, irrigation flow, torque, and presets — enhancing workflow efficiency and infection control. Additionally, its 1:1 setting and optional 1:1 straight handpiece attachment accommodate both surgical and low-speed procedures, making this motor a highly versatile asset for any dental practice.
Dentists will appreciate the eight programmable presets, enabling clinicians to customize motor settings to match their preferred techniques. For added accuracy, an integrated handpiece calibration feature ensures precise speed and torque at the bur. Meanwhile, the motor’s water-resistant chassis design and use of autoclavable irrigation tubing demonstrate Aseptico’s commitment to durability and sustainability.
EU MDR, Health Canada, and US FDA-complaint.
For more details, visit aseptico.com/AEU-1070 or contact SGefter@Aseptico.com
Distributor inquiries are welcome!
exoplan Case Report
Initial Situation
The 72-year-old patient Monique presented with a classic free-end situation from 14 to 17. Her primary request was a quick fixed closure of the esthetically compromising gap (Fig. 1a). Due to an autoimmune disease (Sjögren's syndrome), her saliva production was limited, which reduced the body's natural inhibition of oral bacterial growth and increased the risk of wound healing complications. The patient was aware of this and therefore explicitly requested a minimally invasive surgical procedure that avoided complex augmentation measures.
Fig. 1 and Fig. 1a Initial clinical situation of the patient‘s upper jaw
Fig. 2 The patient wanted fixed teeth on implants, preferably with immediate restoration.
Fig. 3 Intraoral scan of the maxilla (Source: Dr. Jan Erik Jansohn)
Diagnostics and Treatment Options
During the first appointment, the patient was photographed in our photo studio. The 2D images (Fig. 2) were required for prosthetic planning with Smile Creator (exocad). Standard diagnostics with intraoral scan and CBCT (Fig. 3 and Fig. 4) showed reduced bone availability in regions 15 to 17, but sufficient for immediate implant placement. The endodontically restored tooth 13 showed a root filling that clearly extended beyond the apex along with periapical periodontitis. In consultation with the patient, it was decided to remove the tooth. The patient had previously received a treatment proposal from another dentist, which included an external sinus lift and lateral augmentation of the alveolar ridge as part of the implantological restoration of the right maxilla. However, this plan did not meet the patient's desire for a minimally invasive, fixed restoration. A removable prosthetic restoration was not an option for the patient. Together with the patient, we defined the goal of achieving an immediate, although initially long-term temporary restoration of function and esthetics in a single minimally invasive procedure.
Dr. Jan Erik Jansohn, M.Sc., from Düsseldorf (Germany), demonstrates the advantages of digital pre-planning with guided implant placement for minimally invasive immediate restoration concepts using the case study of patient Monique. The patient underwent restoration of a free-end situation in the right maxilla from 13 to 17, using three implants with guided implantation and immediate restoration through a fixed implant-supported long-term provisional bridge.
Planning
The first step was to visualize the final prosthetic outcome using Smile Creator. This allowed the esthetic outcome to be coordinated with the patient at the outset. The digital planning of the optimal 3D implant positions from both a surgical and prosthetic point of view was carried out using the exoplan implant planning software (exocad), based on CBCT and intraoral scan data. The challenge was to plan the immediate implant placement in region 13 alongside two additional implants, ensuring optimal utilization of the available bone in terms of sufficient primary stability for immediate loading by means of a longterm provisional immediate restoration with an implant-supported bridge. One implant (length 10 mm, diameter 3.3 mm) was positioned exactly in front of the sinus at 15 and the second implant (length 8 mm, diameter 4.1 mm) was planned in region 17 (Fig. 6). The software’s warnings and safety distance indications were particularly useful in this process. The canine tooth, deemed non-restorable, was to be extracted and an implant (length 12 mm, width 4.1 mm) inserted immediately at 13. A tooth-supported surgical guide was designed in exoplan / Guide Creator (Fig. 7) to ensure precise implant placement during the surgery. Given the planned immediate implant placement after extraction of tooth 13 and the immediate restoration, conical bone-level implants with an aggressive implant thread design (SL Active, Straumann Group) were chosen to achieve the required high primary stability. Following the planning, the long-term provisional restoration was designed in DentalCAD using Immediate Load (Fig. 8).
Surgical Intervention
The surgical guide and the prefabricated PMMA long-term provisional restoration (Fig. 9) were ready for the surgical appointment.
Fig. 4 CBCT image of the initial situation (Source: Dr. Jan Erik Jansohn)
Fig. 5 Implant planning in exoplan (Source: exocad)
Fig. 6 The available bone is optimally utilized, planned implant positions at 13, 15, and 17 (Source: exocad)
Dr. Jan Erik Jansohn, M.Sc
Fig. 7 The surgical guide design in exoplan / Guide Creator (Source: exocad)
Fig. 8 Design of the provisional bridge for immediate restoration in DentalCAD (Source: exocad)
Fig. 9 The long-term provisional restoration made of a high-performance PMMA-based resin was available at the time of surgery. (Source: Dr. Jan Erik Jansohn)
Under local anesthesia, tooth 13 was first extracted atraumatically (Fig. 10), then the surgical guide was positioned (Fig. 11) and the implant was inserted in region 13 with navigated guidance. The gap to the implant was filled with bone chips obtained during implant bed preparation. This was followed by vestibular soft tissue augmentation with a connective tissue graft from the palate. The two additional implants in the molar region were inserted flaplessly after punching the gingiva. Using the surgical guide, they could be inserted bicortically exactly as digitally planned, ensuring optimal bone utilization (Fig. 12 and Fig. 13) and achieving a high primary stability of 40 Ncm. The surgical procedure itself lasted 30 minutes. The long-term provisional restoration, a milled five-unit bridge made of high-performance PMMA-based resin, was first checked for fit and attached to the implants without the need for individual adjustment (Fig. 14). The precision of the digital workflow was reflected in the exact fit of the provisional restoration. After a total treatment time of around 90 minutes, the patient left the practice pain-free with fixed teeth (Fig. 15). As a prophylactic measure, she was prescribed a painkiller and an antibiotic. She was also advised to favor the left side of the jaw when chewing for the first month after the surgery. However, she was able to use the implant-supported long-term provisional bridge from day one.
Outcome and Patient Satisfaction
The wound healing process was uneventful. Four months after implant placement, intraoral scans were taken and the permanent bridge was designed in DentalCAD based on the scan data using the original design at the start of
Fig. 10 Atraumatic and tissue-preserving extraction of tooth 13 (Source: exocad)
Fig. 11 Mounted and positioned surgical guide with precisely planned drilling channels (Source: Dr. Jan Erik Jansohn)
Fig. 12 Implants directly after insertion (Source: Dr. Jan Erik Jansohn)
treatment. On her fourth visit to the practice, around five months after the surgery, the patient received the permanent bridge. She was highly satisfied with her new teeth, both esthetically and functionally. The zirconium oxide bridge blends in harmoniously with the remaining natural dentition of the patient's upper jaw. The patient was particularly satisfied with the minimally invasive procedure, as she did not experience any pain or swelling at any stage of the treatment.
Conclusion
The use of CBCT images and intraoral scans in conjunction with suitable planning software such as exoplan enables the precise preoperative visualization of the patient's osseous situation and allows for a comparison of the surgically possible options with the patient's wishes. The case exemplifies how a digital approach with virtual implant planning and subsequent guided implant placement can lead to reliable and highly precise outcomes in a minimally invasive procedure for a given indication. In this case, it was only possible to achieve an immediate implantological restoration using a closed procedure without extensive exposure of the bone thanks to the precise virtual pre-planning and implementation using guided implant placement. The minimally invasive approach resulted in a significantly more comfortable postoperative experience for the patient, free from pain and swelling. Two aspects in particular are crucial to the success of cases involving immediate implant placement and restoration: The digital workflow from virtual implant planning and design of the surgical guide to the design of the provisional and permanent prosthetics must be able to be implemented precisely and reliably. This means the interface between surgical and dental planning plays a key role, which is facilitated by software such as exoplan, DentalCAD and Smile Creator. In addition, collaboration with a dental technician who understands the virtual planning of immediate restorations is essential. Overall, the case demonstrates that treatment success in terms of esthetics, function and patient comfort can be achieved predictably, efficiently and safely using virtual 3D-planned guided implantation concepts. You’ll find the video documentation of this case via https://youtu.be/ynzc6eMY1Qs. CAD design and implant planning by Uli Hausschild, Italy. www.exocad.com / info@exocad.com
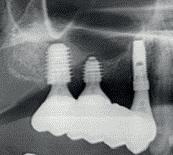
Fig. 13 The X-ray control scan after implant placement shows that all three implants were inserted exactly as planned.
Fig. 14 Upper jaw directly after surgery with screw-retained provisional bridge from 13 to 17
Fig. 15 The happy patient with the permanent bridge. (Source: Dr. Jan Erik Jansohn)
and dentists
NEW LIFE RADIOLOGY Go digital with New Life Radiology:
New Life Radiology, the Italian Leading Manufacturer of Intraoral and Extraoral imaging devices, with more than 35 years experience in this field, is able to to provide its Customers THE BEST DIGITAL EXPERIENCE.
• The smallest focal spot for a periapical x-ray: BEST-X-DC with palmtop TIM-X, a high frequency intraoral x-ray with 0.3mm focal spot, for more detailed images: controlled by a completely touch palmtop (radio-frequency), is also equipped with dosimeter on board.
• High quality CEPH images in only 0.2s exposure time!
OPERA 3D CEPH MULTIFOV (5x5, 6x11, 9x9, 11x11, 14x11) with SINGLE SHOT DR (Digital Radiology), equipped with double CMOS sensors (one dedicated only to Cephalometry) with the unique SINGLE SHOT DR Technology.
• The fastest 3D intraoral scanner in the world in model scanning*
DIGISMILE, 3D intraoral scanner: software free, no subscriptions required, completely Open System “STL FREE” (scanner file output STL/OBJ/PLY), Exocad compatible, accessoried with the exclusive 3D Glasses for DIGISMILE (wireless): Doctors don’t need to watch to the monitor while scanning anymore, for a more digital and accurate workflow.
(*Digital Dentistry University of Budapest test report)
All-on-Six Full-Arch Immediate loading Implant Rehabilitation Following Guided Alveolar Ridge Reduction: A Case Study
Abstract: Dr. Maxym Prytula's (UA) case study illustrates a full-arch implant rehabilitation procedure, using the all-on-six methodology complemented by guided alveolar ridge reduction in an edentulous patient with significant mandibular alveolar ridge atrophy. The integration of advanced digital planning tools, specifically ImplaStation software, facilitated precise pre-surgical planning and execution, demonstrating a successful clinical application in dental implantology.
Patient Background and Pre-Surgical Planning
A comprehensive pre-surgical evaluation was conducted, incorporating Cone Beam Computed Tomography (CBCT) scans, intra-oral scans, photographs, and diagnostic wax-ups. The treatment plan included immediate implantation with immediate loading, utilizing the available bone volume for All-on-6 implementation and addressing the correction of the ridge shape in the frontal area. The gingival biotype and atrophied ridge shape did not guarantee stability for the soft tissue-supported surgical guide, whereas bone support offered precise and reliable positioning for both the surgical guide and implants.
Technical Planning and Challenges
Key technical planning steps:
• Integration of CBCT data and optical jaw scans in a single platform.
• Creation of a Wax-Up project incorporating a temporary prosthetic structure for immediate loading.
• Precise bone surface segmentation from CBCT data.
• Virtual implant and abutment placement planning considering bone anatomy and prosthetic requirements.
• Generation of Stackable Surgical Guide for bone reduction and osteotomy.
• Preparation of a temporary prosthetic structure for accurate positioning on abutments.
The utilization of 3D diagnostic information and digital implant planning has become standard practice. However, in complex cases, certain technical stages demand high expertise, substantial effort, and time investment. Specifically in this case:
• Achieving precise digital segmentation of CBCT data into a surface model
(STL file) for virtual mandibular bone reconstruction is crucial despite potential artifacts.
• Creating stackable surgical guides necessitates proficiency in multiple software tools for implantation planning, surgical guide design, 3D surface editing, and typically spans several days.
The ImplaStation software streamlined the digital segmentation of CBCT data, bone reduction planning, and implant placement, including the creation of Stackable Surgical Guides.
Surgical Phase and Prosthetic Phase
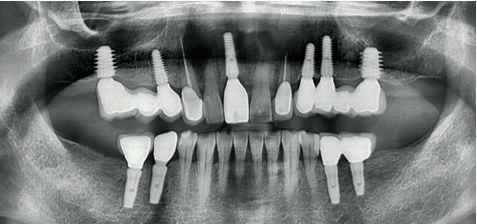
The surgery started with flap reflection and roots extraction, followed by placing and securing a "Stackable Guide Fixation Base" for bone reduction guidance. The prepared alveolar ridge was contoured for implant placement. Six implants were then accurately placed using a Osteotomy Guide attached to the Fixation Base. In the prosthetic phase, a carrier guide aligned the transitional prosthesis accurately over multi-unit abutments (MUAs). Temporary abutments were then secured to the prosthesis, ensuring a precise fit. After adjustments and soft-tissue closure, the prosthesis was immediately loaded, completing the procedure.
The ImplaStation software offered several significant advantages
• All essential modules in one application.
• ImplaStation's Wizard-driven Stackable Guide module creates comprehensive set of guides within a 15-minute timeframe.
• The built-in STL surface editor implements any technical solution without extra apps.
Conclusion
Advanced digital planning tools are an effective solution for complex cases, such as significant atrophy of the alveolar ridge. The use of ImplaStation software in preoperative planning has significantly increased the accuracy and efficiency of both surgical and orthopedic stages, with reasonable time costs, leading to the successful full rehabilitation of the dental arch.
www.implastation.com / info@prodigident.com
ImplantBook is the only global guide about implantology addressed to dealers and dentists.
It helps you search the dental implants and the related items that best fit your needs.
Distributors and dentists love the accessibility of the information and companies the incredible visibility. Please, write to implantbook@infodent.com if you have any suggestions for improvement.
ARE YOU A DEALER?
Read the product highlights and the feature articles.
All the advertisements you see are from companies looking for distributors.
ARE YOU A DENTIST? Download ImplanBook soft copy on its website:
HOW TO GET THE BEST FROM IMPLANTBOOK?
1. READ carefully the articles to select the companies closer to your needs.
2. CONTACT your next manufacturer and express your interest for the product.
Circulation & Distribution
The soft copy is available:
• on implant-book.com
• promoted on Social media
• emailed to 20,000+ worldwide dealers, manufacturers, importers, exporters, wholesalers, agents and trade associations in 189 countries