Why being clinically excellent alone is no longer enough to grow your practice P16
The business journal for doctors in private practice
If only I had known that at the time
A medical director shares the advice he wishes he had been given when starting out P22
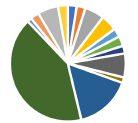
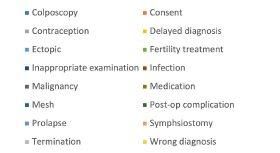
An examination of the clinical negligence claims notified by gynaecologists n Page 26
Harassment isn’t just an NHS matter
Private sector providers are promoting a culture where colleagues can speak out against bullying P38
Bittersweet for private GPs
By Robin Stride
New figures showing a boom in the UK’s private GP market have sparked mixed emotions among independent doctors.
Market analysts LaingBuisson estimates as many as 13% of GP consultations are now private, up from just 3% two decades ago, while the sector is worth around £1.6bn.
But the Independent Doctors Federation (IDF) GP committee, which helps doctors in the specialty set up and manage their clinics, warned that the reason for this increase was due to patients’ difficulties obtaining appointments to see their NHS GP and long health service waiting times.
Dr Shaima Villait, its chair, said: ‘Although this is a boost for the private healthcare industry and we are here to reduce the burden on the NHS, it is a bittersweet boost knowing our NHS colleagues are suffering with limited funds trying to meet the increased patient needs.
‘Rapid access for patients is priority, and although we are here to support our NHS colleagues, more needs to be done to improve NHS primary care ensuring patients are not forced to seek private treatments but have the option to do so if they wish.’
LaingBuisson’s Primary Care UK Market Landscape Report (first edition) says the private pay GP market is growing to meet demand. At
Our sponsors
mid-2024, there were over 550 services registered with the Care Quality Commission offering private GP consultations, 447 of them in private ‘clinics’ and 103 in independent hospitals.
The analysts’ executive chairman and report author William Laing believes attitudes towards paying for GP appointments are changing with people more receptive to buying care than they have been in generations, while employers are attracting top talent with benefits like private GP services.
His report notes that providers of group health cover and protection products, ranging from private medical insurance to health cash plans, critical illness and life insurance, have vigorously taken up the opportunity offered by web technology to add value to their products with low-cost online GP consultations as an add-on.
Although this is a boost for the private healthcare industry . . . it is a bittersweet boost knowing our NHS colleagues are suffering with limited funds trying to meet the increased patient needs.
DR SHAIMA VILLAIT, Chair of the
Independent Doctors Federation's GP committee
Employers for their part, have bought into the offer enthusiastically as a low-cost benefit which is not only valued by employees but can also reduce time off work.
Mr Laing said: ‘People are willing to pay for quick access, ease of booking and the choice of appointment delivery – getting to choose between virtual or face-to-face appointments is not always available in the public sector. This attitude shift is clearly a response to long waiting times in the NHS and other problems in primary care.’
His 116-page analysis highlights how NHS GP practices are under growing strain, covering a huge majority of the population with a small proportion of the overall NHS budget. They have capacity issues, financial pressures, workforce stresses and an increasingly complex patient workload.
Earlier this month, Royal College
of GPs’ (RCGP) chair Prof Kamila Hawthorne told 1,500 delegates at its annual conference in Liverpool that when she became an NHS GP it was normal to have a list size of between 1,600-1,800 patients.
But latest figures revealed the average is now 2,300. There were fewer qualified GPs and they were delivering 14% more appointments than five years ago.
She called on the new Government to take urgent action to review all general practice funding streams to channel more spending to areas of greatest need.
And she urged for a much greater share of NHS funding plus robust initiatives to recruit new GPs and encourage existing GPs to remain on the front line.
The college’s most recent ‘GP Voice’ survey of its members revealed more than 40% of GPs said they were planning to leave general practice within five years. Retirement was one reason for planning to quit, but the two biggest causes were work-life balance and stress.
Nearly 20% of GPs reported that most days they felt stressed and feared they could not cope – over 40% said they felt like that at least once or twice a week.
Only 10% of survey participants were contracted to work 40 hours or more, but 40% were putting in those hours regularly.
n Bupa launches new GP subscription service, page 4 What
TELL US YOUR NEWS.
Contact editorial director Robin Stride (right)
Email: robin@ip-today.co.uk
Harley St landlords hatch bold plans
Howard de Walden’s chief executive
Mark Kildea explains why his business’s biennal healthcare conference ties in with plans for the Harley St area P10
Phone: 07909 997340 @robinstride
ADVERTISE WITH US.
To advertise in the digital journal, on our website or in our business and lifestyle directories, contact Andrew Schofield at Spot On Media. Phone: 0161 408 3912
Email: andrew@spotonmedia.co.uk
Chief sub-editor: Vincent Dawe
Head of design: Jonathan Anstee
Follow Independent Practitioner Today on OUR REGULAR COLUMNS
Business Dilemmas: Court report may harm patient
Why don’t we expand PPUs?
Investment made by the NHS in staff ends up benefiting the private sector, so why don’t NHS trusts try to get some return on that investment? P18
Tips for gettting practising rights
A medical advisory committee chairman gives advice to new independent practititioners on how to get practising privileges at a private hospital P20
Stats show private care continues up
Latest data from the PHIN reveals that records for private admissions and growth in medical insurance continue to be broken P30
The MDU’s Dr Kathy Leask advises a GP worried about writing a court report for a domestic abuse victim P48
Start a private practice: Understanding your accounts
Accountant Alec James continues his lesson on making accounts clearer to new private doctors P50
Doctor on the Road: Novel approach to boost affordability
Our motoring correspondent Dr Tony Rimmer says the MG3 is good value for money and fun to drive P52
www.independent-practitioner-today.co.uk
Tech is transforming women’s health
Dr Rebecca Rohrer, a Bupa medical director, shows how the integration of digital technology into healthcare is transforming women’s health P34
When patients ask to alter records
Can you amend medical records?
Hannah Egan, a case manager at Medical Protection, discusses some different scenarios P36
You must treat disabled favourably
A recent Employment Appeal Tribunal ruling affects private doctors who have employees. Solicitor Rachel Levine explains what they need to know P40
When bonds come bouncing back Samuel Kirton of financial planners
Cavendish Medical explains why shorterdated high-quality bonds are still in favour despite recent volatility P46
Brown envelopes bring revised tax calculations
Pension annual allowance statements now being issued
By Douglas Shepherd
Doctors waiting to see how their previous tax payments on pensions savings have been impacted by the ‘McCloud’ remedy should soon be receiving their annual allowance statements.
Every year these statements are issued to show a member’s pension input for the tax year. This then determines whether the member has breached the annual allowance, which is the maximum amount of tax-free growth an individual’s pension can grow by in one year.
Last year, no annual allowance statements were issued as NHS Pensions worked through revised figures for members because of McCloud.
Now the 2022-23 and 2023-24 documents will be issued together and will show the recalculations of pension growth and therefore annual allowance positions across the seven years known as the ‘remedy period’.
To recap, the McCloud remedy
aims to recompense NHS scheme members deemed to have suffered age discrimination when the 2015 pension scheme was introduced.
Those members now have the option to receive their original benefits from the 1995 or 2008 scheme for the ‘remedy period’ which runs from 2015 when the new pension scheme began to 2022.
Guy Beck, senior financial planner with Cavendish Medical, told Independent Practitioner Today : ‘Everything to do with McCloud has always been complex and this stage is no different.
‘The first step when receiving these documents is to check that any recalculations are indeed correct.’
He explained that with the vast volume of statements being created and the sums involved, doctors would need to verify the data presented by NHS Pensions very carefully.
‘You should have specialist advisers working with you to check these numbers – small
Guy Beck of Cavendish Medical
errors can often lead to much bigger problems if not spotted by advisers well versed in looking at these types of figures.
‘Many members will find that their annual allowance position has been reduced over the years, which would lead to a rebate, plus interest, on any erroneous tax paid to HMRC.
‘For others, the new figures could establish that tax has been underpaid on pension growth –and the treatment of this is not straightforward.
‘You will also need your figures checked and verified to be able to complete your tax return by the usual January deadline.’
The NHS has launched a ‘cost claim back scheme’ to allow members impacted by McCloud to reclaim some of the cost of using professional advisers to assist with the complex decisions associated with the judgement.
Mr Beck continued: ‘It is a positive step that the Government is giving some financial assistance to pension scheme members to help cover the cost of understanding what McCloud means.
‘The claims scheme covers not only professional advice such as financial advisers and accountants but also direct financial losses or tax losses incurred because of the remedy. A good adviser will also help you to apply for this scheme.’
The NHS Cost Claim Back Scheme limits claims for using an accountant are £1,000 including VAT and for using a financial adviser, £500 including VAT.
More younger people now going private
Younger patients are increasingly looking to private doctors for their healthcare, new figures reveal.
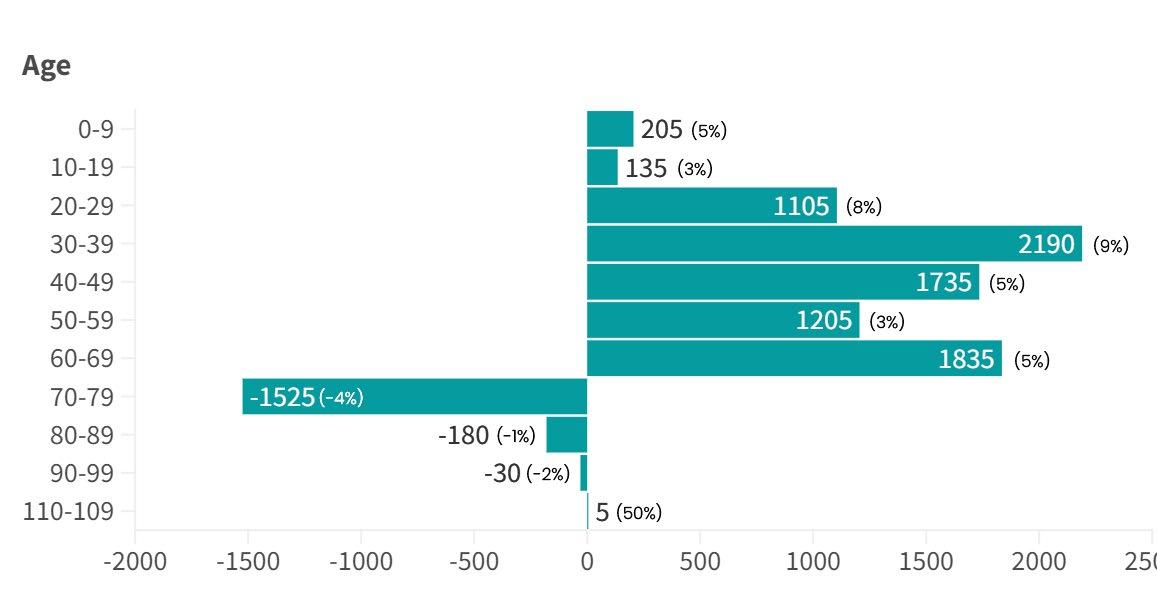
Record levels of people are turning to the independent sector’s consultants and private GPs, but the biggest increases are in the 20-29 and 30- to 39-year-old age groups, which were both up by 13%.
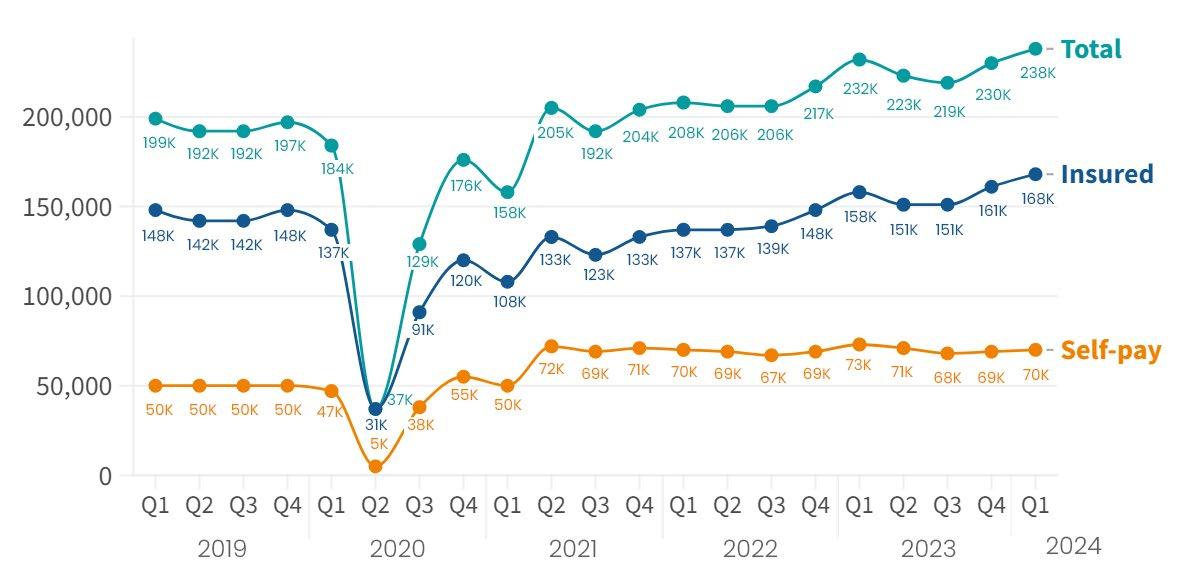
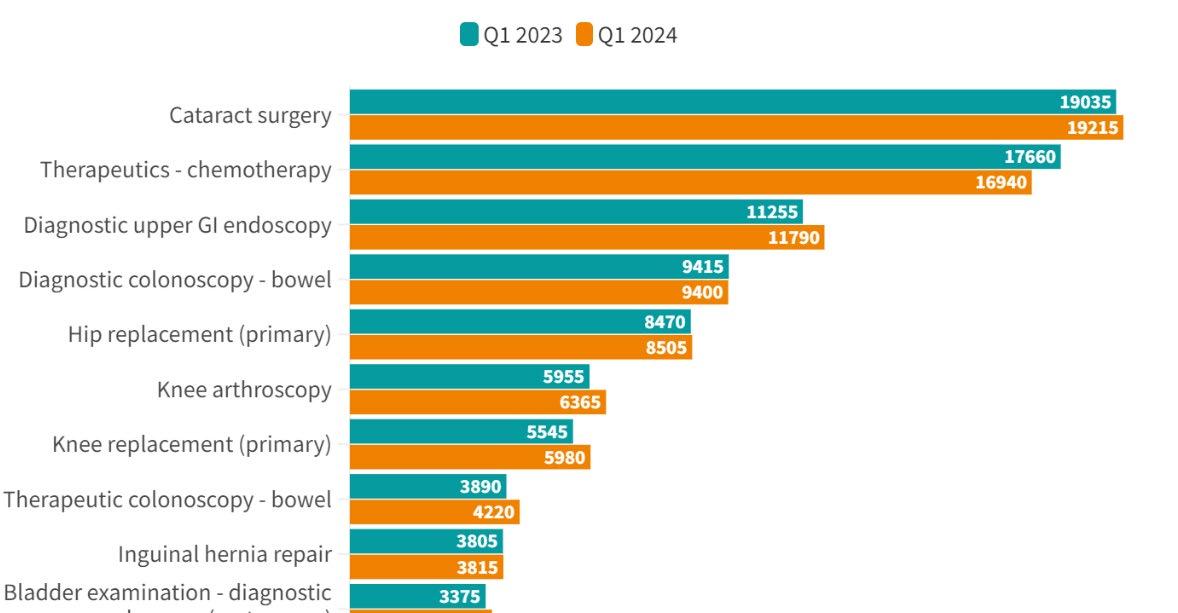
Data from the Private Healthcare Information Network (PHIN) shows in Q1 2024 there were more private hospital admissions –238,000 – than in any previous quarter on record.
An unprecedented number of these were paid for using private medical insurance, rather than self-pay.
The data body found an increased number of patients in every age group, except 70- to 79year-olds, used insurance to pay for their procedure, compared to the same quarter in 2023.
PHIN’s healthcare informatics director Richard Wells said: ‘Traditionally, the biggest users of private healthcare are those in the 50-59 age group and that hasn’t changed.
‘However, these latest figures suggest that younger generations are also giving more thought to their health and taking out private medical insurance to fund the elective procedures they might require.
‘This may be because of an increase in the number of employers offering insurance as an incentive, insurers marketing their products in different ways or due to worries about NHS waiting lists and how long it may take to be seen.’
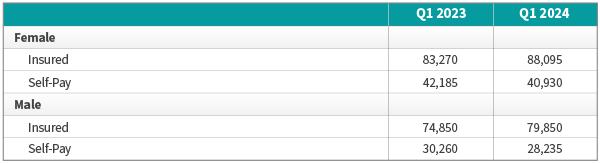
PHIN reports a slightly bigger
increase in male patients (7%) using insurance than females (6%) in Q1 2024 compared to Q1 2023, but women continued to be the primary users of private healthcare and insurance.
Mr Wells added: ‘It’s quite a small difference between the sexes, but it would be good to think that men are also considering their health and the plans they need to make, as often men’s health can be something of an afterthought.’
See PHIN’s latest quarterly market update starting on page 30
Private GP service launched by Bupa
By a staff reporter
A new GP subscription service from Bupa is charging from under £20 per month.
The insurer’s healthcare subscription service provides patients with same-day GP appointments and a 24/7 nurse-led HealthLine to improve speed of access to care.
Two subscription options are available. The first is a remote GP subscription for £16.66 a month –just short of £200 a year – where patients can discuss health concerns with a doctor over the phone or by video call.
Bupa said they can book an appointment on the same day they initiate the subscription, at a time of their convenience through the day.
A remote and in-centre GP subscription cost £21.66 a month – an annual £260 – for those who want to see a doctor face to face.
Customers are offered an appointment by phone, video call or an in-person appointment at
one of the Bupa Health Clinics across the UK.
Both services include free prescription delivery to either a home or nearby pharmacy and access to the Anytime HealthLine, where nurses are available at any time of day or night, every day of the year.
The easy-access service comes as research conducted for Bupa found a third of Brits find it difficult to get a GP appointment and a further 22% say they wait on average between three to seven days to see a GP.
When surveyed, respondents said a healthcare subscription service appealed to them due to the ease of getting an appointment (30%) and better access to healthcare services (29%).
Other reasons included a greater focus on personal health and wellbeing (23%), feeling reassured by having on-demand support available if needed (18%) and being able to have remote appointments from the comfort of their own homes (18%).
This is similar to other ‘one-tap’
A ton up for robot surgeons at Nuffield Health Warwickshire
A surgical team at Nuffield Health Warwickshire in Leamington Spa is celebrating a century of joint replacement surgeries using a robot.
The Stryker Mako robotic-armassisted technology enables precise hip and knee replacements, with patients likely to experience less pain and faster recovery.
Consultant orthopaedic surgeon Mr Andrew Shepherd said: ‘It’s rewarding to see how robotic-armassisted surgery has changed the lives of so many of our patients.
‘Taking patients out of pain and aiding their journey to recovery is inspiring. I look forward to being one of the surgeons involved in performing the next 100 cases.’
services, like gym memberships, supplement and other wellness subscriptions.
The research also revealed that 32% of people say they would value a GP or dental subscription service more than their TV streaming subscription.
Carlos Jaureguizar, chief executive for Bupa Global, India and UK, said: ‘We know that being able to see a GP when needed, gives people peace of mind.
‘Our new GP subscription service will provide more support, giving them face-to-face access to GPs in our 54 health clinics, as well as remotely.
‘Our new on-demand service aims to offer people fast and easy access to healthcare professionals and treatment, as and when they need it, for all their healthcare needs.’
The research was conducted by Censuswide, among a sample of 2,001 UK adults over the age of 16. The data was collected in August 2024.
GensisCare appoints a second doc to its board
A second doctor director has been appointed to private cancer care provider GenesisCare UK’s board.
Consultant oncologist Dr Simon Russell, who has a private practice in Cambridge and works for the city’s University Hospitals NHS Foundation Trust, specialises in providing radiation and systemic therapy to patients with breast and urological cancers.
Board chair Evelyn Bourke said: ‘Simon and GenesisCare have worked closely together over
New chief executive for Bupa Insurance
Bupa Insurance has gone ‘down under’ to recruit its new chief executive, who starts work in January 2025, subject to regulatory approval.
Chris Carroll (right) joins from the firm’s health insurance business in Australia, where he has been managing director since March 2022.
The company said he had worked ‘to transform the customer experience in Australia’ with a focus on creating value for customers and delivering a range of new insurance products.
A spokesperson said: ‘With more than 25 years’ commercial experience across health insurance, media and telecommunications in Australia and Europe, Chris has an unwavering customer focus and a proven track-record in growing Bupa’s business to deliver simpler, more personalised and relevant products to customers.’
recent years and his breadth of expertise combined with experience in developing joint venture models with clinicians provides us another strong clinical advocate at board level.’
Dr Russell said: ‘I look forward to being able to support the board and represent the voice of the clinical community as we continue to focus on improving access to highquality oncology services across the UK.’
Oncologist Dr Simon Russell
Rise in beauty ops that needed fixing
By Robin Stride
Rising numbers of patients being treated for complications caused by other practitioners are only the tip of the iceberg, warn aesthetic doctors.
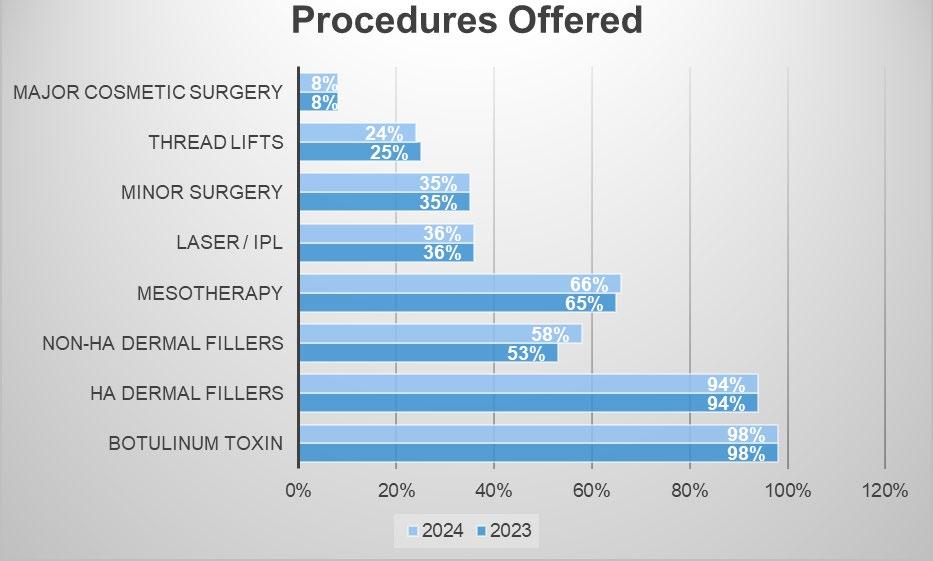
Members of the British College of Aesthetic Medicine (BCAM) provided treatment to correct 3,547 complications resulting from aesthetic procedures carried out by other practitioners last year – up from 3,523 in 2022-23.
But, in a new report, they ‘conservatively estimate’ the number of patients suffering harm due to poorly performed aesthetic treatments by inadequately trained and experienced practitioners can be numbered in the tens of thousands each year.
Due to a lack of regulation and no mechanism for recording complication rates in patients who present directly to secondary care, they warn it is impossible to accurately measure the scale of this risk to patient and public safety.
The BCAM’s annual clinical survey 2023-24, covering experiences of the specialty’s doctor and dentist members, says a significant proportion of patients treated for complications caused by others (60%) were reported to have been carried out by beauticians.
Fake brands
Complications included soft tissue infections, necrosis and scarring. Many required specialist, longterm and often costly treatment to correct and high volumes of patients were referred to the NHS for ongoing care as a result.
The college also expressed concern that patients suffering from botched procedures were victims of fake brands.
It says: ‘A number of BCAM members reported atypical complications resulting from botulinum toxin treatments performed by beauticians, including localised ery-
Dr Aggie Zatonska, report author
Procedures offered
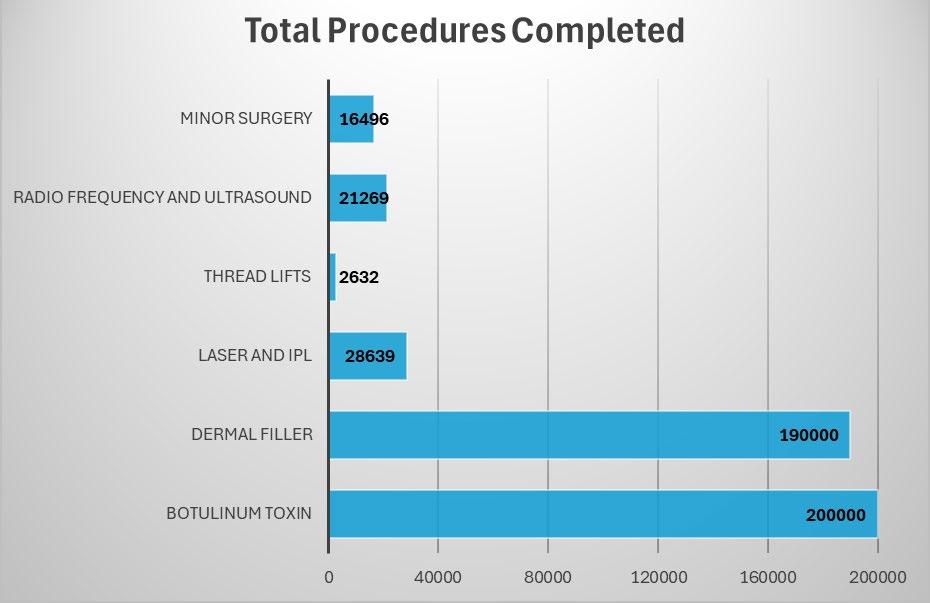
Total procedures completed
thema, followed by blistering and eventually scarring. It is the expert clinical opinion of these members that such atypical reactions suggest the use of counterfeit products.’
Report author Dr Aggie Zatonska said: ‘Lack of appropriate regulation that facilitates patient safety is frequently raised by BCAM members as an area that needs to be addressed urgently.
Counterfeit products
‘Notably, our members have reported unusual complications suggesting use of counterfeit products. This data will help BCAM to campaign for better regulations and improvement of patient safety.’
She stressed in the report that college members always discuss
the risks during consultations, including their likelihood and potential impact, to ensure patients are able to give informed consent to treatment.
Members reported ‘extremely low’ complication rates, experiencing 1,913 complications across all procedures, with the significant majority being minor complications including bruising or patient dissatisfaction with overall aesthetic results.
The report says: ‘Severe complications with BCAM members are extremely rare; for example, the risk of soft tissue infection is as low as 0.003% in injectable treatments.’
As many as 30% of members reported requests for treatment from children under 18 years of age.
They received 62 requests to correct botched injectable treatments with botulinum toxin or dermal fillers, a treatment which has been a criminal offence to administer to a child under 18 in England since 1 October 2021.
Due to a lack of regulation, the BCAM says it is impossible to accurately measure the number of children being illegally treated with injectable, prescription-only, aesthetic medicine each year.
Dr Catherine Fairris, its president, said BCAM was proud that its members had low complication rates and prioritise patient safety.
‘Our data shows a continued rising trend in complications caused by unqualified lay injectors, and we urge the Government to take action and bring forward robust legislation that will put patient safety at its core.
‘We are hopeful that the new Labour Government will take this matter seriously, we will of course be sharing our data with them.’
The college said it continued to work with partners from across the specialty, to reinforce its assertion that there is a clear and urgent need for regulation in the aesthetic medical specialty across the UK, and in line with European standards, for the protection of particularly young and potentially vulnerable patients and in the public interest.
Specialty trends
58% of all patients treated were aged between 35 and 60, with only 7% being younger patients (1824);
16% of all patients treated identified as male. These proportions are largely consistent with previous years;
28% of respondents reported that at least 20% of their time is dedicated to consultations only. The BCAM said this indicated patients were effectively and appropriately counselled before embarking on aesthetic treatments.
Don’t use AI to write reply to complaints
By Agnes Rose
Doctors are being alerted by a defence body against using artificial intelligence (AI) technology to draft medical complaint responses.
In the latest issue of the MDU journal, the Medical Defence Union explains some doctors are turning to AI programs to help draft complaint responses for them.
But it warns that doing so increases the risk of a response being inaccurate or being perceived as insincere. Using AI in this way also raises issues of confidentiality and data protection.
The union’s medico-legal adviser and Independent Practitioner Today columnist Dr Ellie Mein said: ‘In the face of increased complaints and immense pressure on the
Dr Ellie Mein of the MDU
health service, it’s only natural for healthcare professionals to want to find ways to work smarter.
‘There are many ways in which AI technology is being used to improve the quality of patient care, such as in health screening. But when responding to patient concerns, there is no substitute for the human touch.
FIVE BIG RISKS OF AI-GENERATED REPLIES
The MDU has identified five big risks involved in using AI to draft a complaint response:
1. INACCURACY
AI-drafted responses may sound plausible, but can contain inaccurate information or use language or law from their country of origin – often the US – rather than the UK. An example is the use of the word plaintiff rather than claimant.
2. CONFIDENTIALITY
The medical history set out in a complaint response is likely to be unique to that patient and such confidential information cannot be disclosed as a prompt. Patients need to know how their data will be processed and data protection laws may prevent transfer of data outside the UK.
3. FALSE APOLOGIES
Generalised wording in responses which AI can often generate like ‘I am sorry you feel your care was poor’ is unlikely to address a patient’s concerns and may inflame the situation. Apologies need to be specific and genuine.
4. OMITTING KEY INFORMATION
This can include the offer of a meeting or the complainant’s right to refer the matter to the Ombudsman.
5. INABILITY TO REFLECT
Reflection on concerns raised is a necessary part of a complaint response, so outsourcing it to AI defeats that purpose.
‘That’s not to say that AI can’t act as a prompt to get you started, but it’s vital that patient complaints are responded to in a suitably authentic and reflective manner.
‘There have been cases where recipients who were suspicious of the wording in a complaint response were able to reproduce
the same text by asking AI to draft a similar letter.
‘Would you feel comfortable in this scenario and would the patient feel you had taken their complaint seriously?’
Read the full MDU journal at https://mdujournal.themdu. com/issue-archive/summer-2024.
Doctors split over using AI in medicine
Doctors in the UK are split over whether to use generative AI to treat their patients.
Around half (47%) of UK doctors would not, while a similar proportion (48%) would consider using the technology for this purpose.
New research from Medscape UK into attitudes towards AI among UK doctors revealed the vast majority of the 745 physicians surveyed (86%) expressed concern that patients using generative AI for medical advice could receive misinformation.
Eighty-two per cent were concerned that patients trying to selfdiagnose could take AI more seriously than their doctor.
In the Medscape UK Doctors and AI 2024 report, concerns about unfettered use of AI in healthcare
settings were highlighted by 83% of doctors who agreed there should be government and/or medical association oversight of its use.
A third of those surveyed (33%) said they were not confident that either government or medical associations will be able to ensure patient confidentiality in the context of AI use.
The company’s editorial director
Nadia El-Awady said: ‘What these results are telling us is that doctors have the same concerns that we all have about AI in relation to privacy, misinformation and the need for regulation.
‘Our research showed that half of those surveyed felt the use of AI could reduce the risk of medical error and can also be a useful information source for physicians themselves, both of which present significant benefits to patients.’
Most doctors surveyed (57%) were enthusiastic about the use of AI in supplementing their own expertise with diagnostic or treatment option information. In particular, over half (55%) were positive about the use of AI for scan interpretation.
Ms El-Awady added: ‘We have
seen some exciting advances in the use of AI in healthcare, particularly in the interpretation of scans for earlier diagnosis of conditions like cancer, so it’s encouraging to see that UK physicians are seeing its potential benefits.’
Doctors reported that AI could save them time, particularly on administrative tasks, with 75% reporting a positive attitude towards this.
Around one-in-ten doctors are already using AI to research conditions (14%), office administration (13%) and for staff and patient scheduling (10%).
One doctor said: ‘AI is coming whether we like it or not, we just have to find a way to work with it.’
www.medscape.com/doctors_ and_ai_uk_2024
PPU WATCH
Compiled by Philip Housden
Trusts grow private care income
NHS trusts are experiencing significant growth in private patient incomes, as reported in PPU Watch last month.
Many more trusts have now published 2023-24 annual accounts and approximately twothirds are in the public domain.
Analysis of these accounts confirms a run-rate of a 23% average increase in income from private patients, with the projected NHS England-wide total now £794m, up from £643m in 2022-23.
It should be noted that some of the leading hospital PPUs in the total private patient income stakes are yet to publish their accounts at the time of writing.
Housden Group has again contacted trusts to assess 2024-25 inyear private patient activity.
The findings of this report, the NHS PPU Barometer, were shared at the national PPU conference held on 27 September in Birmingham and provide an up-to-date snapshot of performance and valuable insights into the changing sector.
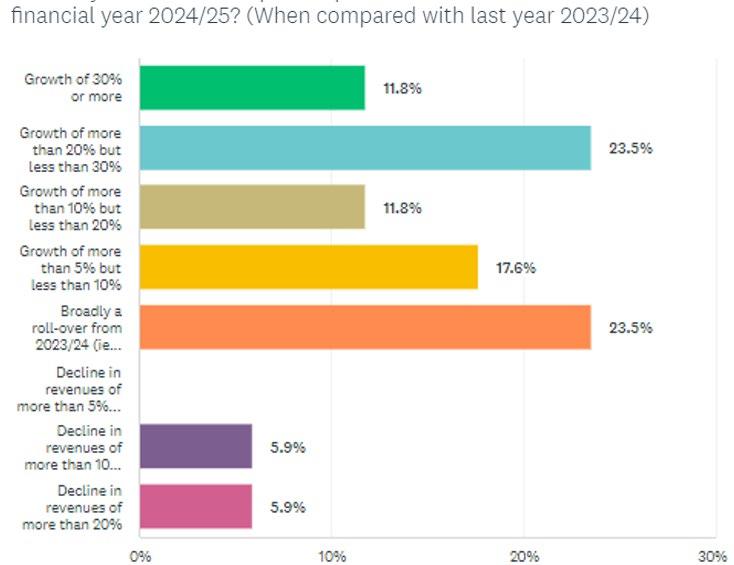
The NHS PPU Barometer, completed by 18 trusts representing 14% of total England revenues and 28% outside London, suggests that 2024-25 is turning into another growth year for private patient income in the NHS.
What is your forecast for private patient services revenues for the full financial year 2024-25? (When compared with last year 2023-24)
Growth of 30% or more
Growth of more than 20% but less than 30%
Growth of more than 10% but less than 20%
Growth of more than 5% but less than 10%
Broadly a roll-over from 2023-24 Decline in revenues of more than 5% Decline in revenues of more than 10%
Responses received ranged from 12% reporting likely growth of over 30% and a similar number expecting a decline.
taking the projected total to £875m in 2024-25 – a new record – with £1bn likely in 2025-26.
The average settles at a little over a 10% anticipated increase, which, if realised, will deliver total private patient revenues growth of c£80m,
A fuller report on the NHS PPU Barometer findings and the conference will be included in next month’s column.
healthcare consultancy
MDU offers help with death certificates
Doctors are being reminded by the Medical Defence Union about new rules governing death certification, which took effect from 9 September in England and Wales. The changes mean a wider pool of doctors will be able to certify deaths, reducing delays in death certificates being issued. All deaths will now be subject to scrutiny either by a medical examiner, or by a coroner, including deaths in the community. The aim is to improve the experience of bereaved people, allowing them to
ask questions and raise any concerns.
The MDU regularly supports doctors when their patients raise complaints or queries about death certificates. Over the past five years, nearly 200 cases have been opened, with the majority being raised by GPs and primary care staff.
Dr Udvitha Nandasoma, head of advisory services at the MDU, said: ‘Doctors play a vital role in certifying deaths and issuing death certificates. It’s important they are aware of the changes to the rules and that they complete the new
medical certificate of cause of death (MCCD) accurately.
‘We do see complaints alleging inaccuracies in death certificates or that there was an undue delay in issuing a certificate. We hope the new system will help to avoid such complaints.
‘One major change is that any doctor who attended the deceased during their lifetime will be able to complete the MCCD. Before, this was restricted to those doctors who had attended the patient during their last illness.
‘Doctors in England and Wales who are notified of a patient death will need to work closely with medical examiners to allow them to independently scrutinise deaths not referred to a coroner. This will include sharing records of deceased patients.’
The MDU has produced guidance for doctors on the changes to the system and members with queries about certifying deaths or the role of medical examiners are welcome to contact the MDU for further advice.
Philip Housden (right) is director of Housden Group commercial
Mid Leicestershire MP Peter Bedford gets an eye test at the clinic’s opening
Eye clinic in Leicester to work on NHS cataracts
A new Optegra Eye Clinic in Leicester is dedicated purely to providing NHS cataract surgery for patients across Leicestershire and the East Midlands.
Mid Leicestershire MP Peter Bedford visited the Meridian Business Park clinic to cut the ribbon for the official opening.
Richard Armitage, NHS director for Optegra Eye Health Care, said: ‘Over the past couple of years, we have been expanding our NHS cataract treatments by opening a series of new clinics around the country. Our leading surgeons are supported with eye care specialists to provide excellent outcomes.’
The clinic, committed to treatment within four-six weeks of referral, said cataract patients simply needed to ask their optician or GP to refer them.
Consultant ophthalmologist Dr Magdalena Edington has joined the Leicester clinic to lead on all NHS cataract surgeries.
Consultant surgeon Ms Lana Faraj will be leading cataract surgery for NHS patients at the new Optegra Eye Clinic Nottingham, officially opened by Rushcliffe MP James Naish, pictured below at the clinic’s opening with healthcare technician Abi Nicholls
Eye surgeon’s clinic joins Optegra stable
An entrepreneurial consultant ophthalmologist’s clinic has joined the Optegra Eye Health Care portfolio. Custom Vision Clinic in Bramham, Wetherby, Yorkshire, is seen by the bigger company as ‘a premium, boutique-style hospital’.
Housed in the impressive setting of Bowcliffe Hall, it was established by ophthalmic consultant surgeon Mr James Ball, who previously worked at Optegra. Now he has returned as one of the company’s
‘ambassador’ surgeons and will continue to lead the treatments for the company in Wetherby.
Mr Ball will maintain all his staff, including fellow surgeon Mr Jack Gormley, and his team of 11 colleagues including clinical and administrative employees.
The Optegra total portfolio is now 25 UK hospital and clinics. It recently launched 11 full new NHS clinics and six diagnostic clinics.
AI ‘will transform care for patients’
By Agnes Rose
The AI healthcare market is valued globally at $26.7bn today and is expected to surge to $614bn by 2034, according to market analysts.
In a new report, they say AI is an exciting area of growth for healthcare with this technology being hailed as a solution for multifaceted problems worldwide.
‘AI in Private Healthcare: Driving Commercial, Operational and Clinical Excellence’ consolidates insights from over 60 hospitals across 26 countries, examining AI’s current and future applications in the healthcare sector.
The report, developed by LaingBuisson in partnership with sector experts Curzon Consulting, provides a global overview of AI adoption, identifies key trends and challenges and offers strategic recommendations to guide healthcare providers in maximising AI’s value.
Tim Read, LaingBuisson’s director of research and content, said: ‘Ever since it first emerged, the potential for AI to drive a radical
reshaping of healthcare delivery has been clear.
‘However, for a long time it seemed to remain as exactly this –potential. What our latest report makes clear is that these possibilities are now in the present.
‘Over the next ten years, we expect AI solutions to become an integrated part of a successful healthcare provider and, as a result, we project the global AI healthcare market to grow by a staggering 36% annually to reach $614bn by 2034.’
As much as 60% of AI investment in healthcare is currently directed towards alleviating administrative burdens rather than direct patient care activities.
Private and public sector partnerships with technology companies around the world are delivering observable improvements for providers and patients in clinical support, administration, maintenance and discharge procedures, monitoring and postoperative follow up.
Chetan Trivedi, co-report author
and partner of healthcare at Curzon Consulting, said: ‘The integration of AI in private healthcare offers transformative potential, especially in elective care.
‘By automating critical processes, AI can greatly enhance operational efficiency, enabling healthcare providers to offer more precise and personalised care.
He forecasts AI’s role in diagnostics, treatment planning and operational management promises significant improvements in patient outcomes, from faster diagnoses to more effective treatments.
But he added that realising AI’s full potential depended on overcoming barriers such as data integration, workforce readiness and regulatory compliance.
‘AI is not just a tool for operational efficiency; it is set to enable us to transform and re-invent how we approach patient care.
‘The future will see AI facilitating greater patient autonomy, supporting healthcare professionals in decision-making and improving the overall patient experience.’
Mr James Ball and the clinic in Wetherby
GMC guide to deal with impropriety
By Olive Carterton
What to do if you think you have been subject to sexual misconduct by a doctor is a new GMC resource aimed at patients, doctors and other staff who may have been victims of unacceptable behaviour within or outside of the workplace. It covers what constitutes sexual misconduct, how to raise a concern, what to expect from an investigation and lists organisations who can give support.
The regulator has also published information for employers and responsible officers (ROs) to help them prevent, identify and respond to sexual misconduct cases.
This covers how the problem can manifest in the workplace and how employers can create cultures where behaviours are safely challenged.
Welcoming the documents, cofounder of campaign group
Surviving in Scrubs, Dr Becky Cox, said: ‘The resource for survivors is informative and will be valuable for individuals affected and who may be considering raising a concern.
‘Guidance for employers and responsible officers provides clear information on sexual misconduct and processes which will help ensure the correct actions are taken when a concern is raised. We would encourage all doctors, managers and responsible officers to read these documents.’
The resources were developed after GMC work with victim and survivor advocacy groups, patient organisations, doctor representatives and other regulators.
Further clarity on the ‘five-year rule’ has been given to its staff who look into sexual misconduct cases.
It said: ‘Currently, due to existing legislation, the regulator is unable to consider complaints outside this time-frame unless cer-
tain criteria are met. It has now been made clearer that victims and survivors may only feel in a position to report what happened many years later, and so this should be considered when deciding if the rule should be waived.’
GMC chief executive Charlie Massey said: ‘Much has changed for the better in recent years. But it’s important for us to acknowledge the scope for improvements to the way we handle complaints about sexual abuse and misconduct.’
The new resource for victims and survivors is at https://tinyurl. com/44k9crwd, the information for employers and ROs is at www. gmc-uk.org/responsible-officerhub, and a full report on the GMC’s work to improve handling of sexual misconduct cases is available to read at www.gmc-uk.org/ about/how-we-work/corporatestrategy-and-plans/our-responsesto-reviews -and-inquiries.
Minor ops suite benefits NHS patients
A £2.6m new minor operations suite at Spire Claremont Hospital is benefiting NHS and private patients in the Sheffield area. Treatments for orthopaedic, spinal, ophthalmic, dermatological, cosmetic and ENT conditions performed there will free up space so doctors and their teams in the main surgical theatres can do an estimated 800 more complex procedures every year.
Eight recovery bays also help release more ward space for patients requiring longer stays. The hospital said its investment aimed to increase the number of NHS and private patients by 50%.
Patients now get a smoother and more efficient journey from checkin to their procedure, through to recovery and discharge.
The unit has significantly short-
ened waiting times for people needing complex surgery, and more patients with minor conditions are being seen faster.
Hospital director Tim Smith said: ‘By increasing our capacity to deliver more minor and complex procedures, we will be reducing waiting times and improving the overall patient experience.
‘Our investment into this new
Medical director for fertility unit
Consultant Dr Babbur Vijayalakshmi has been appointed medical director at Euston’s Bridge Clinic for fertility services, launched last year.
She brings extensive experience in general fertility and assisted conception to the team, with a particular interest in complicated cases and management of gynaecological disorders such as polycystic ovarian syndrome, endometriosis, premature ovarian failure and menopause.
Clinic managing director James Barr said: ‘Her addition to the clinical team will strengthen our ability to help patients across London and the country get closer to achieving their dream to start or grow their family.’
STARTING OUT IN PRIVATE PRACTICE?
Spire Claremont Hospital, Sheffield
If so, don’t miss Independent Practitioner Today’s trio of useful articles to help you in this issue:
➲ Tips for getting practising privileges and keeping them – page 20
facility will not only benefit our private patients, but also support the NHS by alleviating pressure on local healthcare services.’
Members of the hospital’s theatre team were joined by Spire’s chief operating officer John Forrest, chief financial officer Harbant Samra and chief commercial officer Peter Corfield at the official opening.
➲ If only I’d known that then … Dr Peter James, group medical director at Circle Health Group, shares the advice he wishes he had been given when starting his private practice journey – page 22
➲ Understanding accounts – page 50
Harley St landlords hatch bold plans
Harley Street Health District’s major landlord, Howard de Walden, is set to host its biennial Healthcare Conference on 31 October at the Royal Society of Medicine.
The event will gather leading experts, innovators and policymakers to explore the theme of advancing healthcare through technology and innovation, exploring the challenges and opportunities.
Howard de Walden’s chief executive Mark Kildea (right) speaks to Independent Practitioner Today about why the conference is so relevant in today’s increasingly tech-focused healthcare environment
THIS IS the third conference we have organised to address key challenges and developments in healthcare, and we are excited to be focusing on health technology and innovation.
With clear challenges such as a shortage of healthcare workers, both in independent practices and the public sector, technology is becoming increasingly essential.
Despite the incredible potential that innovation brings, it is no secret that the adoption of innovation in healthcare can sometimes be painfully slow and this is a key issue we aim to discuss.
Harley Street Health District is the perfect backdrop for this discussion. We are in a very fortunate position being close to large hospitals, both public and private.
The area is uniquely situated, with proximity to major NHS trusts, leading academic institutions and the life sciences-focused Knowledge Quarter at King’s Cross.
Rich environment
Its location means Harley Street offers a rich environment for innovation, helping to bridge the gap between traditional healthcare and the digital future. Technology is being harnessed in remarkable ways, in healthcare and beyond. This conference is particularly relevant for those wishing to stay ahead of the curve and learning how innovation and technology are set to shape the future of healthcare.
We will in particular be exploring the obstacles to innovation adoption, ways of overcoming these barriers and how innovation
➱ continued on page 12
CloudRx take care of the dispensing, payment and delivery of medicines direct to your patients for more convenient access their medicines.
Prescribe within your chosen clinical system via our frictionless integration with Semble, WriteUpp, MidexPRO, eClinic, Pabau, Jelly Software, and ClinicYou. Alternatively, simply register for free and prescribe directly at www.cloudrx.co.uk.
Repeat prescriptions and controlled drugs.
Prescriber fees can be charged if desired.
Easy access to medicines not normally stocked by most pharmacies at great prices.
“We were struggling to keep up with the admin side of the prescriptions, not to mention storage for medication to cope with a huge increase in prescriptions. CloudRx immediately took away the strain. Since our partnership we have grown by over 200% in size. We could not have done that without their support. It has allowed for seamless scalability...”
– Dr Louise Newson, Newson Health
can be embedded into healthcare businesses to improve the patient journey.
The theme of this year’s conference reflects the significant shift we are seeing towards preventative care and remote monitoring of patients. But it is important to remember the focus is not solely on technology.
Healthcare will always need a human touch. The real challenge is integrating new technologies successfully into existing clinical settings.
What we believe is that Harley Street offers a unique environment where innovators can trial their products in both clinical and remote settings, ensuring their solutions work effectively in realworld scenarios.
Clinicians here can collaborate with innovators, offer feedback, and even invest in new but proven solutions, creating a dynamic cycle of improvement and innovation.
Active role
We could easily be just another landlord focused on managing buildings and property, but our approach goes far beyond that. We are increasingly focused on understanding the clinicians who occupy these buildings, their business models and what success looks like for them.
And we take an active role in supporting these businesses, by collaborating and curating talks, exhibitions and events.
Our goal is to provide the right environment for collaboration and, by bringing together the best and brightest, our ambition is to
make this cluster the most connected health community worldwide.
We are also working to create a hub for health tech entrepreneurs and innovators on our estate.
This conference will highlight not only the opportunities within the area but also emphasise our commitment to helping our community make those valuable connections, which are so important for driving progress and collaboration in healthcare.
We want people to see that if they’re looking for an area with excitement about healthcare innovation and are looking to be part of a dynamic environment, Marylebone is that place.
‘Whole health’
The area is evolving and we are broadening our message around healthcare. We are moving towards a more inclusive concept of health – often referred to as ‘whole health’.
This approach encompasses not just specialist hospitals and complex surgeries, but also outstanding ambulatory and outpatient facilities.
Preventative care and wellness is becoming increasingly significant as people are more proactive about achieving a healthy lifestyle, embracing physical and mental well-being, and even financial health.
We are also exploring the introduction of rehab facilities, which we have not had in the Harley Street area before. Expanding the breadth of healthcare and the range of services available is crucial to us.
The 31 October conference is being held at the Royal Society of Medicine
This is an exciting shift as we work to integrate health innovators and new technologies with existing clinics and new healthcare operators in Harley Street. This represents a significant opportunity to enhance the services and care available in the area.
The NHS has reported the need to transition from an analogue world to a digital one. There is a certain perception that Harley Street is a place for high-priced consultants and outdated practices.
Pioneering hub
That is at odds with the reality and our vision for ‘whole health’. Our goal is to position Harley Street as a hub for pioneering healthcare, where patients can confidently seek out the best, most advanced care available, and where clinicians and businesses feel supported in their pursuit of innovation.
We are committed to making sure Harley Street healthcare is a leader
Our goal is to provide the right environment for collaboration and, by bringing together the best and brightest, our ambition is to make this cluster the most connected health community worldwide
the last 20 years – and want to ensure Harley Street keeps pace with these developments. We aim to encourage our existing hospitals and clinics to integrate new technologies, because our goal is to see them succeed in this rapidly changing landscape.
Attract global business
in technological adoption. This means actively embracing change and integrating the most effective technologies into our facilities.
For instance, we have already introduced occupiers with stateof-the-art equipment like MRI scanners and the latest diagnostics for radiotherapy to enhance the quality of care and the best outcomes for patients.
We recognise that technology is evolving rapidly – faster than in
Our focus is on bringing together top healthcare operators who lead in health technology and the best outcomes for surgical experience. We want Harley Street to be known for these strengths. We aim to attract global businesses that fit this vision and we endeavour to help them succeed here.
Looking ahead, we envision the area will become a more integrated healthcare hub than it is today. We anticipate a shift towards more comprehensive care, including rehab and prehab services that improve surgical outcomes and emphasise preventative healthcare.
Technology in healthcare has been slower from creation to adoption compared to other sectors, but this is changing rapidly. Demand for healthcare is rising, but the number of providers is not keeping pace.
So technology will play a much bigger role in addressing this gap than it has in the past. By promoting innovation and collaboration, we aim to keep Harley Street at the forefront of healthcare excellence.
Our 2024 Healthcare Conference is an exciting opportunity for anyone eager to understand how technology is shaping the future of healthcare. If you are passionate about staying ahead in the industry, we warmly invite you to join us, learn from our excellent speakers and be part of the conversation on the future of healthcare.
For more information including registration details and a full schedule of events, visit www.hdwe. co.uk/healthcare-conference.
A look back through our journal’s archives of a decade ago reveals that although times change, some issues are not so new
A trawl through the archives: what made the news in 2014
Surgeons: ‘Stop the stitch-ups’
Many independent practitioners faced intensified verbal grilling from both patients and the press following the launch of a campaign to get the public to probe the true value of new product claims and procedures.
Surgeons themselves called in national journalists to their annual scientific meeting in London to brief them on what they and their readers should look for to try and ensure treatment transparency.
The British Association of Aesthetic Plastic Surgeons (BAAPS) also warned of possible financial conflicts of interest among those involved in some clinical businesses.
Consultant plastic surgeon and incoming BAAPs president Mr Michael Cadier said new so-called
‘clinically proven’ treatments promising unbelievable results were launched almost daily.
‘We believe that asking the right questions, doing a bit of research and engaging in a dose of scepticism is the healthiest approach for the public.’
Outgoing president Mr Rajiv Grover described a huge rise in media reporting of aesthetic treatments, but he urged the press and patients to ‘cut into bombastic claims – even from surgeons’.
He said consumer press journalists had their work cut out keeping pace with many issues in the sector. ‘I don’t envy the challenges of reporting credible developments from such a murky field, but that doesn’t mean the cosmetic surgery sector should be allowed to stitch people up.’
Watchdog rules on publishing prices
The Competition and Markets Authority’s (CMA) final order following its private healthcare market investigation brought into force some required changes.
These included a crackdown on benefits and incentive schemes provided to referring clinicians by private hospital operators, and better information for patients, from April 2015.
The CMA’s full plans to increase information to patients on consultant fees were subject to
the findings of an appeal hearing at the Competition Appeal Tribunal the following January.
CMA plans, aimed to kick in by 1 December 2016, required consultants to publish:
Outpatient consultation fees, expressed as either a fixed fee or an hourly rate;
The standard procedure fee for the 50 types of procedure most frequently undertaken by the consultant;
Standard terms and conditions, plus any exclusions or caveats, expressed in a standard form.
Call to alter compensation
The Medical Defence Union (MDU) was calling for the repeal of a 1948 law which meant compensation must be calculated to pay for private, rather than NHS care.
In a renewed attack on the spiralling costs of compensation awards against doctors, it warned everyone would suffer if nothing was done to reform the system where huge damages payments were common.
Chief executive Dr Christine Tomkins said damages awards in England were now higher than most countries, even many US states.
With compensation inflation rising 10% a year, the MDU wanted caps on the level of damages for future care and damages for loss of earnings to be
capped at three times the national average salary per year to ‘reduce large awards for lost future earnings which can run into millions of pounds’.
Tough inspections for private clinics
Doctors were facing beefed-up scrutiny by Care Quality Commission (CQC) inspectors in private facilities where they worked. These would include unannounced visits at nights and weekends when the watchdog claimed people could experience poor care.
Cutting costs
Specialists were advised by a private healthcare commentator to help make the independent sector more affordable by delegating care to nurses.
Keith Pollard pointed to some NHS services moving to nurse practitioner delivery, adding: ‘“Old school” consultants may see these changes as a major threat to their autonomy, but the new consultants coming into private practice may be more open-minded and view such changes as an opportunity to grow their private practice income quickly.’
Practice management made simple.
Make the work... flow.
Effectively manage and grow your private practice with iMedDoc.
Mobile app
Cloud based
Patient por tal
Integrated billing
Integrated digital dictation
I am very happy with iMedDoc! The app is amazing, I don’t need to print anything for my clinic. All the information I need is there and it helps with confidentiality and GDPR compliance. The support service is also excellent.
–
Mr. Sidha Jayabalan C onsultant Orthopaedic Surgeon
TROUBLESHOOTERS: GROWING YOUR PRACTICE
It’s the extras that
Being clinically excellent alone is no longer enough to grow your practice or facility.
Our troubleshooters Sue O’Gorman and Hannah Browning
explain why
QAs a stand-alone practitioner who considers themself to be clinically excellent, what can I do in an increasingly competitive environment of employed consultants and groups to differentiate myself and maintain my market share of patients?
ABeing clinically excellent is undoubtedly a critical factor in healthcare, ensuring high-quality patient care and positive health outcomes.
But in a competitive market, clinical excellence alone is not always sufficient to grow market share for several reasons, which we outline below.
PATIENT EXPERIENCE AND SATISFACTION – The friends and family test
While clinical outcomes are important, the overall patient experience – the interactions that patients have with you – and patient satisfaction – a patient’s evaluation of the care received relative to their expectations – significantly influences their choices.
This includes factors like
Ease of booking an appointment;
How your team communicates with the patient;
How quickly can they be seen;
The environment of the clinic or facility.
Patients are more likely to choose and remain loyal to a provider who offers not only excellent clinical care but also a positive, supportive and efficient overall experience.
BRAND AWARENESS AND REPUTATION – Why your digital footprint matters
In a competitive market, patients often choose healthcare providers based on reputation and brand awareness.
A facility may be clinically excellent, but if it lacks visibility or a strong reputation in the community, potential patients might not even consider it.
With an increasing deluge of information available across multiple channels, effective marketing efforts are essential to building and maintaining a strong brand identity and reputation.
ACCESSIBILITY AND CONVENIENCE – How easy are you to do business with?
Convenience also plays a crucial role in patient decision-making.
Factors like location, parking, availability of multiple specialties under one roof, telemedicine options and flexible appointments can make a significant difference.
Answering the phone and responding to inquiries promptly will give the patient reassurance that you care. Don’t leave the patient to chase you for an appointment.
Even if a practitioner or facility offers superior clinical care, it may lose out to competitors that provide more convenient and efficient options for patients.
AFFORDABILITY, ACCESSIBILITY AND AFFABILITY – The triple ‘A’ concept Healthcare costs and insurance
coverage are major considerations for patients.
Even a highly skilled provider may struggle to attract patients if their services are perceived as too expensive or not covered by major insurance policies.
Patients often prioritise providers that offer affordable care and accept a wide range of insurance options.
Think about accessibility, not only in terms of how quickly can a patient be seen, but also in relation to meeting the needs of communities. They may, for example, require an interpreter or have reduced mobility, so navigating stairs within the clinic might be challenging.
Your environment is equally as important as your clinical ability.
AFFABILITY – does my patient like me?
Never to be underestimated, compassion and empathy are critical for establishing trust with your patient to improve patient satisfaction, regardless of your specialty.
Patients are more likely to engage with their treatment plan when they feel heard and understood.
THE BACK OFFICE FUNCTION –
There’s no ‘I’ in ‘team’
The interactions patients have with non-clinical staff, such as receptionists, billing and the selfpay team or other support staff who may not typically be clientfacing, can significantly impact their perception of the healthcare provider.
Friendly, helpful and efficient customer service can enhance patient satisfaction and retention.
ADOPT A PATIENT-CENTRED, VALUE-BASED CARE MODEL
Value-based care emphasises providing the best possible outcomes at a reasonable cost.
This approach not only improves patient satisfaction but also distinguishes your practice as one that prioritises patient welfare over profit. Referring doctors and patients themselves are more likely to choose and recommend surgeons who offer high-quality care at fair prices.
In addition, patients are increasingly looking for more than just clinical outcomes; they want to feel cared for and understood.
A patient-centred approach builds trust, improves patient satisfaction and often leads to better health outcomes. Happy and wellinformed patients are more likely to recommend your services to others.
This not only sets you apart in a crowded market but also aligns your practice with the evolving expectations of patients and referrers.
By prioritising patient outcomes, transparent pricing and comprehensive care, you build trust and loyalty.
This reputation for high-quality, compassionate care becomes a powerful driver for referrals, as both patients and other healthcare providers seek out reliable, distinguished practitioners who consistently deliver excellent results.
that really matter
FOCUS ON CONTINUOUS IMPROVEMENT AND FEEDBACK
Demonstrating a commitment to continuous improvement shows that you value patient input and are dedicated to providing the best possible care. This responsiveness builds a positive reputation, leading to word-of-mouth referrals. Have a robust mechanism in place to gather patient questionnaires, online reviews and testimonials. Be accountable and share success stories. But also consider how you address and resolve issues and be open about areas for development.
Sue O’Gorman is director of Medici Healthcare Consultancy. Website:
Hannah Browning is director of Beyond Excellence Healthcare Consultancy. Website: www.beyondexcellenceconsultancy.co.uk. Email: info@beyondexcellenceconsultancy. co.uk.
Sue O’Gorman & Hannah Browning
Happy and well-informed patients are more likely to recommend your services to others
EMBRACE TECHNOLOGY AND INNOVATION
➤ Stay at the forefront of clinical or surgical advancements, such as minimally invasive techniques, robotic surgery or cutting-edge diagnostic tools.
➤ Highlight your expertise in these areas through patient education and marketing channels.
➤ Implementation of advancements in digital tools and technology such as patient portals for easy access to medical records, secure messaging systems and virtual follow-up appointments will help boost your overall patient experience.
➤ In summary, while clinical excellence remains a fundamental requirement, it must be complemented by a broader strategy that includes excellent patient experience, strong marketing, convenience, and a comprehensive approach to care.
➤ By focusing on these additional factors, healthcare providers can better differentiate themselves in a competitive market and attract a larger share of patients.
NHS PRIVATE PATIENT UNITS
Why don’t we expand PPUs?
Investment made by the NHS in staff ends up benefiting the private sector – so why don’t NHS trusts at last try to get some return on that investment?
Andrew Robertson (right) argues the case for change
WHEN I WAS working for some of the major private healthcare companies, it was always said that the biggest threat to the business was if the NHS got its act together in delivering private patient services.
At the time, I was grateful that most trusts made little or no attempt to step into the private patient arena.
But having been director of private care at Moorfields Eye Hospital NHS Foundation Trust for the last almost five years, I cannot understand the reluctance of many trusts to grasp what is surely a significant opportunity to generate much-needed money for the benefit of all patients.
There are some excellent examples of private patient units (PPUs), mainly in London: The Royal Marsden Hospital, Great Ormond Street Hospital, Royal National Orthopaedic Hospital and Moorfields Eye Hospital being some of the larger ones.
These PPUs contribute millions of pounds towards the treatment of NHS patients, as well as to education and research. But the development of PPUs outside London is variable and, in many cases, nonexistent.
With little or no central directive or guidance, it is left to local management of trusts as to whether they treat private patients.
And as experience of private healthcare is limited within NHS senior management, there is either no appetite for private patient services or little understanding as to how to capitalise on the opportunity. The latter is reflected in the variable investment in staffing and facilities.
No choice
In an era when ‘choice’ has been the watchword of the NHS, it is confusing why patients who wish to follow a private patient pathway are not given that choice in many NHS trusts.
The choice they have is to find their local private hospital or be treated on the NHS. It is ironic that, over the last 25 years, the private hospitals have made much money by treating patients funded by the NHS, yet in many parts of the country trusts are reluctant to treat private patients.
In a number of private hospitals,
over 50% of their patients will be NHS-funded and around half of all NHS patient hip and knee replacements are carried out in private hospitals.
We have choice in most walks of life. We can choose to stay in a five-star hotel or pay less and stay in a three-star hotel; we can pay for Sky TV or settle for the choice of terrestrial channels.
But when it comes to healthcare, the NHS seems nervous about offering that choice as though differentiating in healthcare is wrong.
But let’s be clear, we are not talking about differentiating treatment; we are talking about the experience.
It’s a bit like getting on an aeroplane. One can choose to pay more and turn left or pay the standard price and turn right. All passengers achieve the same objective of arriving at their chosen destination, but they enjoy a different experience along the way.
About 12% of the population choose to be treated privately. If they didn’t, there would be an increased burden on an already strained NHS.
Slice of the cake
The results of not offering private patient services in NHS trusts is that the money generated by private patients ends up in the private sector.
While it is important that private companies flourish in order to support the healthcare economy, it feels almost irresponsible not to take at least a slice of the cake.
After all, who trains the doctors, nurses and other healthcare professionals who end up working in the private sector – the NHS does. The investment made by the NHS in staff ends up benefiting the private sector, so why not try to get some return on that investment?
So why is it that many NHS trusts do not include private patient services as part of their strategy or are so cautious in their investment in them to capitalise on the opportunity?
One reason already mentioned is unfamiliarity with how private patient services work and need to be set up. But that can and is addressed by many by buying in
The results of not offering private patient services in NHS trusts is that the money generated by private patients ends up in the private sector
expertise. But the main reasons appear to be more to do with how it looks.
At a time when elective care waiting lists are at record highs and the NHS is struggling to cope with the backlog, trusts are understandably worried about what it looks like if they turn attention to providing private patient services that many will think will compromise NHS patient care.
If private patients are to be accommodated, surely that will take up valuable capacity needed for NHS patients? I can see the argument, but it really doesn’t have to be that way.
The trusts that do have successful PPUs perform no less well against their NHS targets than other trusts. They separate NHS and private patient care by either investing in separate facilities or they use NHS facilities at times when they are not being used, mainly in the evenings and at weekends.
More attractive
I have heard it said that NHS facilities should not be used for private patients. But private patients treated in NHS trusts are trust patients, they just happen to choose to pay for a different experience.
The quality and range of equipment actually makes being treated in the NHS as a private patient more attractive to both patient and consultant, as the equipment is often more up to date and technically advanced than in many private hospitals.
I have heard it said many times that trust management are concerned about ‘the Daily Mail test’; that is, what would journalists say about the NHS treating private
patients when there are such long NHS waiting lists.
In my five years at Moorfields, I never heard any adverse press about our private patient services and I am sure other successful PPUs have not either.
However, it is important to be clear and transparent about private patient services and not treat them like some kind of dirty secret. If challenged, it should be straightforward to defend having a comprehensive private patient service. I would have no hesitation in stating that:
Treating private patients in NHS trusts does not compromise NHS patient care;
Private patients are seen and treated outside of NHS clinic and operating times or in separate facilities;
vices encourages consultants to generate private patient income for the trust rather than for other private providers;
Income from private patients contributes to staffing, training, equipment, education and research for the benefit of all patients;
Treating private patients helps to reduce NHS waiting lists.
NHS PPUs are not only an important and acceptable source of income but also play their part in the overall healthcare provision. Trusts should not ignore the opportunity to pick this lowhanging fruit.
Andrew Robertson has spent his career managing private hospitals. For the last five years, he was director of private care at Moorfields Eye Hospital. He is now looking to support the development of other private patient units. He can be contacted at andrew@pripatconsulting.co.uk
START A PRIVATE PRACTICE 1
Tips for getting practising rights
Private medicine is rewarding on many different levels and consultants will enjoy an environment that provides control over their practice.
There will still be pressure, but working with a responsive local management team can make things easier.
Many doctors will work with an independent healthcare provider, often dictated by the proximity of the hospital or clinic rooms for convenience.
But to gain practising privileges at an independent hospital or clinic, a successful application process with a continuing commitment to governance is expected.
Mr Adrian Chojnowski (left) gives some thoughts on that journey from his perspective as a consultant orthopaedic surgeon and chair of the Medical Advisory Committee at Spire Norwich Hospital
1
Engagement and networking
The local hospital director is responsible for the safety of patients and will ultimately decide whether to grant practising privileges. So arranging a meeting will be the most important first step.
You will need to gauge the local need for your specialty/practice intent and if it can be safely supported by that hospital or clinic through, for example, equipment needs or staff training.
Consideration must be given to any colleagues who work in your area of expertise, not least to arrange for cross-cover.
Reasonable colleagues will be supportive of your start-up – they all had to do this once themselves, so start networking.
A supportive group of doctors who can help each other with advice or in a clinical emergency, is without doubt a safer proposition than a lone clinician.
2
Admission pack
Spire Healthcare publishes a Consultants Handbook , which should be read thoroughly and outlines your responsibilities alongside those of the hospital to support your patients.
It will form part of an admissions pack that will need to be completed with, for example, suitable medical defence cover in place.
The hospital director will consider the formal application and may take advice from the medical society – consultants who practise at the hospital – such as specialty representatives and the medical advisory committee (MAC) via its chair at the hospital. All being well, you are now a member of the society.
3 Practice set-up
Communication is key and you will need to engage with several hospital teams.
If you require access to theatres, then flexibility at the start, reliability and forward planning are essential.
Managing your lists well by booking suitable surgical times for your cases and clear instruction on equipment needs helps build a good relationship and establish regular slots.
Similarly, working with clinic and invoicing staff helps your practice grow smoothly.
4 Good governance
Good governance is paramount for the independent provider, your practice and your patients. For every consultant seeking practising privileges at a Spire hospital or clinic, they must be listed on the GMC medical register and undergo a thorough vetting process.
You will be expected to work to guidelines set out in the Medical Practitioners Assurance Framework (2022 refresh). While you are responsible for clinical decision-
making and the quality of the care you deliver to your patients, the hospital is responsible to ensure systems of monitoring and oversight are in place and adhered to.
This is designed to ensure that all consultants practise in accordance with Spire/hospital policy, and in line with their practising privileges.
All consultants must maintain adequate minimum levels of medical malpractice indemnity cover, in keeping with GMC guidance, and comply with Spire/hospital checks to ensure that indemnity certificates are in place.
There is an expectation that medical practitioners share their activity and outcomes data with independent providers through the annual appraisal process. You will need to put your cases on any national registries to help provide data on quality.
5 Maintain probity
Defined as ‘honesty and decency’, you must aspire to the highest standards in keeping with the GMC’s Good Medical Practice As well as complying with Good Medical Practice , there are other obligations about openness with patients to comply with, such as the Competition and Markets Auth ority requiring fees to be transparent to patients.
Set your rates, but be clear in advance with patients what these are and what they will receive in return. Fees must be communicated to The Private Healthcare Information Network (PHIN).
Coding your cases must be transparent and honest. Patients are under the care of the private provider, so any equipment you use must be agreed or provided through the hospital which will help maintain the highest standards.
6
Build your service
Build your service with the hospital by talking to your business development manager about advertising or GP education sessions.
Never criticise staff if you do not have the right drugs or equipment – what did you do to plan your service and discuss equipment in advance?
If the hospital is at fault, do the best you can before providing constructive feedback, which any
member of the senior management team should respond to so that the issue is not repeated.
7 Practice review
Expect your practice to be reviewed at least every two years alongside details of the range of procedures you carry out. The hospital director and specialty lead from the MAC conduct this and, for most consultants, it is a straightforward process.
8 Deal with complaints
Sadly, these do happen. For example, a self-pay patient reasonably wants to feel they have had value for their new patient consultation fee.
A simple diagnosis and plan delivered in a few minutes will leave a patient feeling let down, so spend the time of the consultation with them to ensure a good understanding of the problem. If complaints are received, many will be made to your hospital, so early and constructive engagement with your hospital team is important. You are in it together.
9 Prepare to serve
Consider stepping up to join the governance or medical advisory committee at your hospital, which you will find rewarding. These should be suitably resourced and you will feel that your advice is taken and acted upon, helping maintain a safe environment for patients and staff.
10 Enjoy
The above may all sound quite a lot, but once you are up and running, it is worth reflecting on the time you can spend with your patients and the high quality of care being delivered and the positive impact it is making to their lives.
It is in your hospital’s interest for your private practice to operate well and, as an engaged, reflective consultant who is easy to communicate with, you should be easy to support.
Spire Healthcare works in partnership with over 8,600 experienced consultants. The group delivered tailored, personalised care to over one million inpatients, outpatients and day-case patients and occupational health programme clients in 2023
If only I had known that at the time . . .
Consultant orthopaedic surgeon Mr Peter James (left), group medical director at Circle Health Group, shares the advice he wishes he had been given when starting his private practice journey
IT CAN be daunting for clinicians to contemplate private practice for the first time, but once you are established, it quickly becomes one of the best decisions you ever made.
After decades in private practice, and many years of supporting colleagues as the biggest private operator’s medical director, here is the advice I wish I’d had when I began my private practice.
The most important things to strive for are the three ‘A’s: affordability, availability and affability. These will be the mainstays of
Developing a team you know and trust is paramount in every industry, but it is mission-critical in high-risk fields such as surgery in healthcare
your success and you have real autonomy to deliver all three.
In the independent sector, you have a rare opportunity to be ‘master of your fate and captain of your soul’ in the words of the poem Invictus. But the corollary of this is that you must be mindful of the fact there is no middle-grade support and the buck stops with you.
As such, the first and most practical piece of advice I can give to new joiners is to start simple. Select straightforward cases with predictable outcomes to enable you to establish a track record; avoid complexity and risk until you are secure and well-established in your specialty.
Develop a team
It is crucial to remember that being autonomous does not mean being isolationist. Developing a team you know and trust is paramount in every industry, but it is mission-critical in high-risk fields such as surgery in healthcare.
Finding a regular anaesthetist you can partner with will help you to grow in confidence and skill, and taking the time out of your busy schedule to get to know theatre and ward staff personally will prove invaluable in the long term.
You should make a point of getting to know the resident medical officer (RMO) or resident doctor well: you will need to have each other’s back and work collaboratively and flexibly to make your practice a success.
In an independent sector setting, the RMO is your principal support, colleague and back-up, so invest in that relationship.
You will also need to invest in a network of colleagues and nurture those relationships. As in many industries, networking can bring beneficial, new contacts to help you along your way.
➱ continued on page 24
From holiday cover to advice on complications, to informal referrals, your colleagues can be incredible sources of support, so do not allow the daily juggle to prevent you from investing in those relationships.
The caricature of surgeons with a ‘God complex’ is rarely true in practice, but it can be the case that highly educated and specialised professionals are sometimes reluctant to ask for help.
Avoid this mistake at all costs. Study after study has shown that the most effective organisations in healthcare have flat, non-hierarchical structures that prioritise learning lessons when things go wrong.
‘Stop the line’
There is simply no escaping the fact that the most effective way to minimise errors is to tap into the skills and observations of every single person in a team.
That is why Virginia Mason – a US hospital renowned for its trailblazing work on patient safety –instituted a ‘stop the line’ approach borrowed from Toyota production lines.
In its factories, every single worker on the production line has the right to bring the factory floor to a halt if they spot a defect.
The same approach in operating theatres can dramatically improve patient safety, with every member of the surgical team encouraged and empowered to speak up if they spot a mistake.
Of course, as a consultant you are in a leadership role. But as intensive care consultant George Findlay, a well respected NHS leader, puts it: we must be leaders with ‘big eyes, big ears and a small mouth’.
Know your hospital
One thing that I wish someone had told me earlier is the importance of getting to know your hospital well. Find out:
What services and acuity of services are offered?
What central support services does it offer? From procurement to PR, there are a wealth of central services who are willing and able to support you;
Crucially, what are its clinical governance policies and processes? This can seem like red tape,
In the independent sector, the RMO is your principal support, colleague and back-up, so invest in that relationship
but it is actually about protecting you and your patients, so take the time to read up, ask questions and become fluent.
Clinical governance
Our robust clinical governance processes at Circle have led to some of the best clinical outcomes and patient satisfaction stats in the sector – recognised when we were awarded LaingBuisson’s Private Hospital Group of the Year for four consecutive years.
Embracing clinical governance procedures diligently can help boost your clinical outcomes and reputation among colleagues and patients.
From a personal perspective, the importance of maintaining appropriate levels of indemnity cover
and being honest at all times with declarations will protect you from regulatory and financial challenge.
Less is more
Another top tip is to limit the number of hospitals you work at in order to become established in one place rather than spreading yourself thinly over two.
Contrary to popular belief, working at two hospitals does not make you twice as busy; it often just means you spend more time commuting and are less well known in both organisations. When I decided to commit to one hospital in Nottingham earlier in my career rather than split my time between two, my practice took off and I found myself much busier than before.
AND ANOTHER THING…
In this digital age, no one can afford to ignore marketing. Word-ofmouth recommendations are still invaluable, but it is now rare to meet a patient who has not first looked their doctor up online.
Seek out the hospital marketing manager and ally your efforts to promote your services with their work to pitch the hospital.
You do not have to dance on TikTok to get noticed, but you will need to become familiar with search engine optimisation (SEO) and put consistent effort into your own personal web presence.
Nothing is more powerful for your practice than a large number of positive patient reviews, so be diligent in requesting these and uploading them promptly across a range of platforms.
Working at two hospitals does not make you twice as busy; it often just means you spend more time commuting and are less well known in both organisations
Remember the importance of the personal touch in every interaction: patients paying for healthcare want to feel seen and heard, so spending extended time connecting with your patients in outpatients is critical when starting out.
Finally, hindsight is a wonderful thing, but I would advise my younger self not to rush when starting out.
Concentrate on quality above all else; never cut corners. Aim for consistency, excellence and organic growth, accepting that anything worth having in life requires patience, persistence and sheer grit.
Next month: Mr James will be back with some brilliant tips to help independent practitioners as they contemplate another giant leap – retirement from private practice
When I was told I was being excluded from work following complaints of rough treatment from two of my urology patients, it was like being punched.
Medical Protection immediately assigned me a medicolegal consultant, who was able to downgrade the exclusion to a restriction while the situation was under investigation.
He negotiated a meaningful action plan and consistently moved things forward. Eventually, after two long years, the complaints were found to be based on a misunderstanding and I was fully back in my role. It was a hard lesson on the need to explain everything to patients, especially uncomfortable procedures.
There is no way I could have got through it without Medical Protection. They know their stuff inside-out and are exceptionally skilled at dealing with difficult working relationships. They really are, as they say, always there for you.
MEDICO-LEGAL: NEGLIGENCE CLAIMS AGAINST GYNAECOLOGISTS
What we can learn from these errors
The most common reason for a claim brought against a gynaecologist was due to postoperative complications
THE MDU supports members working privately as gynaecologists who have been notified of a clinical negligence claim against them.
Managing known risks linked to clinical negligence claims is important both to protect patients and to reduce the chance of a claim being brought.
There were a wide range of different reasons for potential claims being brought against them, perhaps reflecting the variety of work carried out by gynaecologists.
POSTOPERATIVE COMPLICATIONS
The most common reason for claims was postoperative complications. These ranged from minor instances of pain, infection or bleeding to very severe consequences, necessitating extensive remedial treatment and in some cases leaving permanent damage or resulting in death.
Over 60% of these cases were successfully defended, including six claims that were won at trial.
In many cases, the complications necessitated additional procedures, either because the original one had not achieved the expected outcome or to repair damage; for example, of organ perforation, recurrent prolapse or incisional hernia.
Damage caused during a procedure was the most common reason for postoperative complications, with the majority of such damage being perforation of the bowel or ureteric injury. There were also several claims involving vascular damage, nerve damage, thermal burns and damage to the bladder and uterus.
In a number of instances, the clinician also allegedly failed to note the damage caused and to take immediate action, which could have meant remedial surgery was less complex and the recuperation period shorter.
One settled claim involved damage to the bowel during a hysterectomy, resulting in the need to remove the bowel and the claimant required a colostomy.
In another settled case, thermal burns were caused to the uterus and small bowel during a hysterectomy and laparoscopic thermoablation of endometriosis, resulting in perforation, resection
of the bowel, ileostomy and infection.
A further case, which was successfully defended, involved perforation of the iliac artery during a diagnostic laparoscopy resulting in a prolonged period in intensive care with serious infection, acute respiratory distress syndrome and consequent psychological damage.
In a few instances, claimants suffered postoperative deep vein thrombosis and consequent pulmonary embolism. In another case, a patient sadly died after experiencing massive haemorrhage following the hysteroscopic resection of a fibroid.
Some claims involved items unintentionally left in situ following surgery such as swabs, needles, misplaced sutures or retention of tissue.
These usually necessitated surgical removal. There were also two cases of wrong site surgery involv-
ing removal of the wrong fallopian tube or ovary. These claims were all settled on behalf of the MDU members involved.
A handful of claims were brought regarding the development of a fistula, incisional hernia or prolapse after a procedure. In many of these, the claimant experienced permanent consequences, the most common of which being bowel and/or bladder dysfunction. Settlement of such claims took into account the impact of these problems on the claimant’s day-today function and quality of life, as
➱ continued on page 28
Dr Claire Wratten Greta Barnes
COMPENSATION COSTS
This analysis is based on over 330 claims brought against gynaecologist MDU members working in the independent sector. Approximately 70% of these claims were successfully defended, with no payment made to the claimant or their solicitor.
The aim of a compensation payment is to restore the claimant and/or their dependents to the position they would have been in had the negligence not occurred.
When large payments are made, much of the settlement is comprised of funding the future care of seriously injured patients or to compensate them and/or their dependants for loss of earnings and/or pension.
The overall average damages payment made was over £100,000. As set out in this article, the most common reason for a claim brought against a gynaecologist was due to postoperative complications.
Damages paid to the claimants in these cases varied widely; from just over £2,000 for a retained foreign body following a laparoscopic hysterectomy necessitating further surgery, to £760,000 in a claim regarding alleged negligent management of pelvic pain resulting in hysterectomy, bilateral salpingo-oophroectomy and perforation of the bowel.
When a compensation payment is made, the paying party is also responsible for settlement of the costs incurred by the claimant’s solicitor in bringing the claim. The amount sought for claimant costs increases with the length and complexity of a claim.
However, even in a relatively straightforward claim, these costs can be considerable and can exceed the amount of damages paid to the claimant.
In 30% of cases analysed, the claimant’s legal costs paid exceeded £100,000. The largest payment made was over £680,000 in a case where the damages settled for a considerably lower sum of £275,000, in a case concerning complications after a laparoscopy for endometriosis.
The MDU incurs costs investigating and negotiating settlement of those claims that do settle, but in addition, costs can be incurred in the successful defence of a claim.
Costs are incurred on, for example, instruction of independent experts, and solicitors and barristers on behalf of the MDU member. The defence costs spent ranged from under £100 up to £110,000 in claims that were successfully defended, and up to £162,000 in claims that required settlement.
These figures demonstrate the need for gynaecologists to have appropriate indemnity arrangements in place, as even lower-value claims can result in payment of a total sum for damages and legal costs that is considerable.
Quite apart from the financial implications, it can also be very distressing to find out that a patient is bringing a claim against you. If you face a claim, you can rest assured that the MDU’s expert claims handlers and medico-legal advisers are there to support you. They understand how stressful the claims process can be and the importance of mounting a robust defence of your position. The MDU will defend claims whenever possible and we involve members in the conduct of their cases throughout.
If a case requires settlement, we will always obtain your express consent to do so.
Even in a relatively straightforward claim, legal costs can be considerable and can exceed the amount of damages paid to the claimant
well as the required past and future treatment and management and, in some cases, care.
VAGINAL MESH
The second most common reason for a claim being brought against a gynaecologist related to vaginal mesh.
Claims concerned mesh used for both pelvic organ prolapse and stress urinary incontinence, and the allegations generally focused on consent for the procedure in question, with some claims including allegations about operative technique as well.
In terms of the difficulties suffered by the claimants, these included mesh erosion, voiding difficulties, nerve damage, dyspareunia and chronic pain.
Over 70% of the claims were, however, successfully defended. For the claims that were settled, there was a large range of damages payments agreed, ranging from £16,000 up to high six-figure sums to patients suffering severe chronic pain or nerve damage.
Following the surgical mesh pause in 2018, gynaecologists are carrying out far fewer, if any, of these procedures.
However, claims following insertion of mesh are often notified many years after the index operation, and this is based on a date of knowledge argument – that the claimant did not appreciate that they had difficulties due to having mesh or problems did not arise until a considerable time after it was put in.
This can mean that the parties to the claim are hampered in their investigations into the case because the medical records, and contemporaneous patient information leaflets, have been destroyed due to the passage of time.
It has also meant that claims may be notified some time after the gynaecologist has retired.
DELAYED DIAGNOSIS
Seven per cent of claims arose following an alleged delayed diagno-
REASON FOR THE CLAIM
sis of malignancy. The underlying malignancy was gynaecological in all but one case, with almost equal proportions of cervical and uterine tumours and a smaller number of ovarian tumours representing the underlying diagnosis.
Almost 70% of these claims were successfully defended. However, settlement of claims following a delayed diagnosis of malignancy resulted in payment of a six-figure sum in half of the cases settled.
The reason for this is that the delayed diagnosis resulted in metastatic spread of disease. As a result, in some cases additional adjunctive treatment was necessary that would have been avoided but for the delay, causing unpleasant and sometimes permanent side-effects such as neurological damage.
In some cases, the delay also meant that the patient would die of their malignancy, whereas earlier diagnosis would have meant curative treatment was possible. If a patient has died, and but for the allegedly negligent delayed diagnosis they would have survived, compensation is payable for earnings and/or care that they would have provided had they lived.
Just over 4% of claims followed an alleged delayed diagnosis of a benign condition, most often endometriosis.
However, other conditions in which it was alleged the diagnosis was delayed included premature menopause, pelvic infection and fibroids. Almost all of these cases were successfully defended.
Just over 2% of claims followed an alleged delayed diagnosis of ectopic pregnancy.
It was generally alleged that but for the delay, salpingectomy would have been avoided. Threequarters of the claims were successfully defended.
CONSENT
Concerns about the consent process featured in a lot of claims where postoperative complications were suffered and in the majority of claims concerning vaginal mesh.
But, in some cases, consent issues were the main reason for the claim and those cases proved very difficult to defend, with three-
quarters of them being settled on behalf of the MDU member.
All the compensation payments to the claimants were under £60,000. The main issue in common with the cases was surgical procedures being performed which, it was alleged, were unnecessary and that with appropriate advice, the claimant would have elected for conservative treatment.
CONTRACEPTION
Over 5% of claims against gynaecologists concerned contraception. The issues concerned migration of IUCDs outside the uterus resulting in the need for surgical removal or pregnancy, failed sterilisation and problems with contraceptive implants – particularly pain and migration of the implant.
The majority of claims were successfully defended and, in the few that were settled, compensation paid was relatively modest.
TERMINATION OF PREGNANCY
Almost 6% of claims followed termination of pregnancy, with three main issues arising – failed termination resulting in either the need for a second procedure or continuation of the pregnancy, retained products of conception or uterine perforation.
Almost 40% of these claims required settlement, even though these are all recognised risks of termination of pregnancy.
All claims are managed by the MDU based on the unique circumstances of the case, but the fact that these cases could not always be successfully defended underlines the importance of robust preprocedure processes, detailed discussions with the patient about the procedure and potential risks, and prompt treatment of any complications that do arise.
FERTILITY TREATMENT
Nearly 3% of claims concerned fertility treatment, none of which were settled by the MDU.
Allegations generally centred around unsuccessful IVF treatment, although the alleged reasons for this varied and included a failure to diagnose endometriosis, incorrect diagnosis of polycystic ovary syndrome and a failure to treat intra-uterine adhesions.
Settlement of claims following a delayed diagnosis of malignancy resulted in payment of a six-figure sum in half of the cases settled
MANAGING RISKS
Before undertaking any procedure, it is important to ensure that the patient is aware of the risks, benefits and complications of the proposed procedure as well as other therapeutic options including conservative treatment – if appropriate. These should be carefully documented.
Refer to the GMC’s guidance on consent and other relevant guidelines such as those from NICE.
Provision of supporting written information and an opportunity to discuss questions before the day of surgery will also help ensure patients are fully informed of the reasons for their procedure and the potential risks. Provision of written information should be documented in the medical records.
Consent should be obtained by an appropriate member of the team and, ideally, by the gynaecologist doing the procedure.
A claim may follow a recognised complication of a procedure. Again, the chance of a claim can be minimised by ensuring a thorough consenting process and documenting this.
Consider the patient’s past medical history, medication history and allergies before administering medication.
Ensure procedures are in place to offer a chaperone to patients and ensure familiarity with the GMC’s recently published guidance on chaperones and intimate examinations.
If things go wrong, be open and honest with the patient by providing an explanation of what has happened and the likely short- and long-term effects of this.
Say sorry and get advice from your medical defence organisation. Consider whether the incident triggers the organisation’s duty of candour requirements.
MEDICATION RELATED
There were only a handful of claims related to medication issues, but these included administration of a penicillin-based antibiotic to a patient with a known allergy and problems with postoperative analgesia.
In one case, settlement was agreed at over £180,000 because the claimant developed a functional neurological disorder as a result of the complications from the prescription error.
INAPPROPRIATE BEHAVIOUR
There were a few claims notified to the MDU that concerned alleged inappropriate behaviour by the treating gynaecologist – with the suggestion from the patient being
that examinations were sexually motivated. Particularly concerning in this type of case is the potential for police involvement. Given the nature of examinations that gynaecologists need to perform, it is essential to ensure that there are arrangements in place for chaperones to be present and the GMC has produced recent guidance on intimate examinations and chaperones.
SYMPHYSIOTOMY
A handful of claims were brought against gynaecologists practising in the Republic of Ireland, alleging that symphysiotomy procedures, performed several decades before, had been inappropriate.
PRIVATE SECTOR MARKET DATA
Stats show private care continues up
Latest data from the Private Healthcare Information Network (PHIN) reveals that records for private admissions and growth in medical insurance continue to be broken
LATEST
OFFICIAL figures show the number of active consultants in Q1 2024 was the highest Q1 figure since before the Covid pandemic.
And according to the Private Healthcare Information Network (PHIN), the number is the joint second highest of any quarter since thousands of doctors in private practice were hit during the lockdowns.
Consultants actively working in private healthcare rose by 280 (2.7%) from Q1 2023 to Q1 2024, although the data body points out numbers regularly fluctuate.
Rise in ophthalmologists
PHIN’s private healthcare market update, issued last month, found the biggest rise in active consultants in the top ten procedure groups was in ophthalmology with an extra 32 consultants (3.9%).
Clinical oncology had the second largest increase in volume –an extra 26 consultants – and the largest percentage increase (14%).
A loss of consultants was recorded in gastroenterology (-6), plastic surgery (-17) and ENT (-7) and general surgery (-10).
The latest quarterly update uses PHIN’s unique, national dataset to look at the key trends in the independent healthcare sector up to and including Q1 2024.
Data covers private healthcare inpatient/day-case market activity, insured cases, self-pay, plus national/regional and procedural breakdowns and demographic information.
ACTIVE CONSULTANTS IN PRIVATE HEALTHCARE
Quarterly comparison of active consultants for the top ten PHIN specialties Q1 2023 v Q1 2024
Q1 2024 AT A GLANCE
Private admissions were at their highest ever level for a quarter in the UK.
Private medical insurance growth continued with a second consecutive record quarter. It was up 6% on the same quarter last year.
Self-pay remains ‘steady’ but dropped 4% on the same quarter in 2023.
RECORD INDEPENDENT
HEALTHCARE INPATIENT ADMISSIONS IN Q1 2024
PHIN said: ‘There were 238,000 admissions in Q1 2024, a 3% increase on the former highest quarter (Q1 2023) and a 4% increase from the previous quarter (Q4 2023).
‘This was the second quarter increase in a row following a slight dip in Q2 and Q3 2023.
‘There were nearly 100,000 more admissions paid for by private medical insurance than by those self-paying. This is the biggest gap in the payment methods since before the Covid pandemic (Q4 2019). Self-pay has consistently been more popular than it was before the pandemic.’
* Figures are rounded to the nearest 1,000. The total may not add, as this is calculated using the actual figure then rounded
AND SELF-PAY CHANGE (%) BY NATION (Q1 2023 V Q1 2024)
Based on non-rounded figures
INSURED ADMISSIONS
Admissions funded by private medical insurance rose in all English regions when comparing Q1 2024 to Q1 2023. The Northeast had the fewest insured admissions (2,000) in these quarters.
London continued to have the most insured admissions – rising from 56,000 to 61,000 – followed by the South-east – 30,000 rising to 31,000. Insured admissions also rose in each devolved nation.
SELF-PAY ADMISSIONS
There were fewer self-payers in all regions except London – up 1,000 to 15,000 admissions – when comparing the quarters.
Self-pay admissions also rose in Northern Ireland and Wales but dropped in Scotland.
➱ continued on page 32
ADMISSION CHANGE (%) BY NATION
Private medical insurance admissions continue to grow as self-pay remains steady
INSURED
PHIN reported an increased number of episodes in eight of the top ten procedures by volume when comparing Q1 2023 and Q1 2024. Only ‘Therapeutics –Chemotherapy’ and ‘Diagnostic colonoscopy – bowel’ had fewer admissions.
Outside the Top Ten, ‘Diagnostics – blood test’ had the biggest increase in admissions by percentage (192%) and was only just behind ‘Peripheral nerve block’ in terms of volume increase.
‘Spinal injection (facet joint injection or paravertebral block)’ had the largest decrease in episodes outside the Top Ten procedures at -585 (-42%).
PATIENT DEMOGRAPHICS
Volume of admissions by sex and payment method (Q1 2023 v Q1 2024)
The data organisation added: ‘There was an increased number of insured admissions and reduction in self-paid admissions for both sexes compared to the same quarter in 2023.
‘The growth in insured admissions for males was 5,000 (7%) compared to 4,825 (6% for females.
The drop in self-pay was also more pronounced for male admissions at 2,025 (-7%) compared to 1,255 (down 3%) for females.
Admissions for females continue to be higher than for males across both payment methods.
CHANGE IN VOLUME OF ADMISSIONS BY AGE
Admissions in all age groups up to and including 60- to 69-year-olds increased when comparing Q1 2023 and Q1 2024, PHIN reported.
The largest increase by volume and percentage was in the 30- to 39-year-old age group, but this age group was still only the fifth highest for admissions with the most being in the 50-59 group.
Three age groups (70-79, 80-89 and 90-99) had a decrease, but there were five more 100- to 109year-olds treated.
PHIN added: ‘Comparing Q1 2023 and Q1 2024, the use of insurance to pay for admissions was up in every age group except 70- to 79-year olds.
TOP TEN PROCEDURES (Q1 2023 V Q1 2024)
Cataract surgery
Therapeutics – chemotherapy
Diagnostic upper GI endoscopy
The largest increase by volume was in the 30- to 39-year-old group. The largest percentage PURCHASER TYPE AND SEX (Q1 2023 V Q1 2024)
There was an increased number of insured admissions and reduction in self-paid admissions for both sexes compared to the same quarter in 2023
increase (13%) was shared by the 20-29 and 30- to 39-year-olds.
‘In contrast, the use of self-pay reduced in every age group except 0-9 and 100-109 year-olds where there was a slight increase. The largest decrease by volume came in the 70-79 year-old group (1,020) and the largest percentage decrease was for 90- to 99-yearolds (10%).’
All data above is taken from PHIN’s unique, national private dataset describing discharge activity (day case and inpatient). This excludes activity outside of PHIN’s mandate from the Competition and Markets Authority (CMA) such as outpatient diagnostics and mental health.
There is a time lag between collecting, validating and processing the data received from hospitals before publication. This can be up to six
months after treatment has been completed to ensure a fair process and accurate data.
Activity numbers are rounded to the nearest five, with percentage based on the unrounded figures.
Diagnostic Audiology Including Paediatrics • Tinnitus Rehabilitation • Vestibular Testing • PTA & Tympanometry • Speech Audiometry • Speech In Noise Testing• Specialist Tests Including OAE, VEMP & ASSR • Ear Wax Removal • Independent Hearing Aid Provider
Tech is transforming
The integration of digital technology into healthcare has been transformative and this is particularly true in women’s health. Dr Rebecca Rohrer (right) reports
Blua gives customers access to an online doctor, nurse, pharmacist, physiotherapist or mental health nurse – by video or audio call – day or night
transforming women’s health
THE HEALTHCARE sector continues to face complex and everevolving global challenges, including clinical workforce shortages, aging populations and access to care, for which there is no panacea.
However, just as digital has transformed the world of entertainment and leisure, where we can now stream films and TV series 24/7 or book a holiday at the click of a mouse, similar digital innovation is revolutionising how women access care and manage their health.
This enables them to better manage their health and enjoy a great customer experience.
Innovations including prescriptions ordered through a smartphone and delivered to your door, and AI-powered physiotherapy sessions that are enabling people to access healthcare when and where is convenient for them.
They are also helping clinicians to make more informed decisions and making healthcare more preventative, accessible and personalised.
We are seeing widespread adoption of digital healthcare across all age groups at Bupa and have more than six million people using our digital health service, Blua, across ten countries.
Online access
Blua gives customers access to an online doctor, nurse, pharmacist, physiotherapist or mental health nurse – by video or audio call – day or night, including weekends and bank holidays.
And one demographic which has embraced digital healthcare is women, with recent Bupa research (www.ipsos.com/en-uk/attitudestowards-digital-healthcare) showing that three-quarters (73%) of women are open to using technology to improve their health and wellbeing.
In addition, our own data from Blua shows that, earlier this year,
We are seeing widespread adoption of digital healthcare across all age groups at Bupa and have more than six million people using our digital health service, Blua, across ten countries
they can use this device to perform these tests under the doctor’s guidance.
This reduces any potential stress and the costs associated with travelling for in-person visits, ensuring prompt and convenient care for expecting mothers.
Digital healthcare is not just about convenience; it’s about providing timely, personalised and preventative care that meets the health needs for women.
sleep patterns and tackle it in the early stages.
One interesting area of development is the progress being made in using AI to detect anxiety and depression from listening to people’s voices. One of the biggest blockers for people managing their mental health better is acknowledging they might be unwell, so this could help them get support sooner.
20% of GP appointments at Bupa across the UK, Australia, Spain and Poland were virtual consultations, and 65% of those were for female patients.
Access to virtual consultations means people are better able to fit appointments around their busy lives and prioritise their health, resulting in earlier diagnoses and better health outcomes.
This is particularly true for women who may be juggling a career with caring responsibilities.
Our own Wellbeing Index (Chapter Seven, www.bupa.co.uk/ wellbeing-index) found that women (38%) are more likely to look after the family than men (30%). And women dedicate (36%) more time to looking after loved ones; on average, five hours and 26 minutes more per week.
Maternal health
Digital healthcare offers substantial benefits for women’s health in areas such as maternal health. Throughout pregnancy, and in the first few years after birth, women need to attend more medical appointments.
Now there are companies like Tytocare (www.tytocare.com) which offer a digital medical examination for pregnant women, from the comfort of their own home.
The customer receives a device that allows them to examine their ears, lungs, throat, skin, abdomen and temperature from home. During a virtual consultation,
The old saying about ‘prevention being better than cure’ may pre-date digital healthcare, but illness prevention is an area where it really has a role to play. Helping people to avoid being unwell in the first place is the most effective form of healthcare.
Wearable technology
Wearable technology and remote monitoring devices enable continuous health tracking, allowing for early detection and effective management of a range of conditions.
We are harnessing this in Blua’s health features which can sync with wearable devices to produce extensive health data.
For example, in Spain, a ‘Monitor your Health’ programme is available for customers with chronic illnesses like arrhythmias or high blood pressure. It connects real-time health data to a professional team of doctors, psychologists, nutritionists, personal trainers and physiotherapists.
Similarly, AI-powered solutions have the potential to be transformative for mental health management. Evidence suggests that women are more prone than men to experience anxiety, depression, and somatic complaints and there have been several developments in this space.
For example, in Spain, Blua’s ‘Take care of your Mind’ feature aims to spot a potential health episode from the earliest symptoms such as changes in customers’
Real-time insights
As a healthcare provider, analysing customer data from digital healthcare services not only helps us to measure how we’re doing, it can help us make changes to existing pathways and develop new strategies to ensure engagement and adherence to health programmes.
More precise data means we can harness real-time insights and more accurate diagnoses to make care more personalised and proactive. This not only improves outcomes for customers, but also eases the burden on healthcare systems by preventing complications and reducing hospital admissions, as well as increasing access to care.
Despite the widespread challenges facing the global healthcare industry, digital health developments are revolutionising patient care. The full effects of these advancements may not yet be fully realised; however, it’s encouraging to see that women in particular are embracing digital solutions to make healthcare work for them.
Digital health services are breaking down barriers to care. Virtual consultations and remote monitoring devices allow women to fit healthcare into their busy lives, leading to earlier diagnoses and better health outcomes.
Dr Rebecca Rohrer is medical director, healthcare management, Bupa UK Insurance
NOTES
When patients ask to alter their records
Can you amend medical records? Hannah Egan discusses some different scenarios
IT IS important for a patient to give an honest account of their concerns and medical history during a clinical consultation.
And it is equally important for a clinician to document in the medical record an accurate summary of the information conveyed so this can be reviewed and considered as part of the patient’s medical history in the future.
But what happens when a patient later learns about the extent of the information written in their records and requests amendments to reflect their interpretation of the consultation?
There are a number of reasons why a patient may request a doctor amends their medical record – for example:
To dispute a diagnosis;
To request that the record of a provisional diagnosis is removed and replaced with the confirmative diagnosis which was later made;
To dispute the relevance of an entry.
The question facing the inde -
pendent practitioner, who is the data controller for the information stored, is: can I amend the medical record?
UK General Data Protection Regulation
Under the UK General Data Protection Regulation (GDPR), individuals are afforded the right for inaccurate information which is held about them to be amended. The Information Commissioner’s Office (ICO) has discussed this further in its guidance on the right to rectification:
‘Under Article 16 of the UK GDPR, individuals have the right to have inaccurate personal data rectified. An individual may also be able to have incomplete personal data completed – although this will depend on the purposes for the processing. This may involve providing a supplementary statement to the incomplete data.’
In a similar vein, UK GDPR also provides individuals with the right to have personal data erased – which is also known as the right to be forgotten.
However, it is important to highlight that while individuals generally have a right for inaccurate information which is held about them to be amended, it does not provide a patient with the right for factually accurate information within a medical record to be amended.
Nor does it afford a patient with the right to request that an entry which reflects medical opinion is amended.
Factual inaccuracies
When an independent clinician receives a request from a patient for their medical record to be amended, or for certain information to be removed, it is important that they, as the data controller, consider the request carefully to determine whether the contended information is factually accurate.
As an example, consider a situation where a patient has attended a consultation about a recently sustained left-sided fracture; for example, left radius. But the clinician accidently notes the record to detail that the patient has suffered a right-sided fracture.
Given the apparent and unquestionable lack of ambiguity, the cli-
While individuals generally have a right for inaccurate information which is held about them to be amended, it does not provide a patient with the right for factually accurate information within a medical record to be amended
Outdated diagnosis
There may also be circumstances where a patient approaches a doctor to request that a medical opinion detailed within the record is amended because it reflects a perceived outdated diagnosis.
During an initial consultation to discuss a health issue, it is often not possible to confirm with certainty the specific condition a patient is suffering from, as further investigations may be required.
It would be important to consider if the information bares clinical relevance and, if so, this should not be removed from the record.
These sorts of entries may naturally be subjective in reflecting the clinician’s perspective and opinion and it would be inappropriate to amend a record that accurately reflects a medical opinion or a record and is not clearly and undisputedly inaccurate.
nician may reasonably conclude that an honest error has been made in the documented entry. Because the information detailed is inaccurate, the clinician feels justified in amending the medical record accordingly.
Here, the clinician must ensure that an audit trail would be able to clearly confirm why the amendment within the record has been made. Crucially, in this scenario, the disputed entry is unequivocally inaccurate.
Now consider a scenario where a patient asserts that they disclosed suffering from knee pain for a number of months during a consultation, whereas the records reflect that the pain had been felt for several weeks.
In this instance, it is far more challenging to conclude with any certainty that there is a factual inaccuracy within the records given that the patient is disputing, and is solely relying upon, a conversation which took place in private between two individuals.
The patient’s perspective
Therefore, the clinician in this instance may conclude they cannot be certain a factual inaccuracy has been included within the records and reject the request for the entry to be amended.
This does not mean an addition cannot be added to the records to reflect the patient’s perspective.
When a clinician feels it would be inappropriate to make the requested amendments, then it is possible to add an addendum to the record reflecting the date the supplementary note is included.
The benefit of an addendum is that it allows a patient’s opinion of an entry to be reflected, while ensuring the content of the original entry is not amended.
Therefore, a clinician may document a provisional diagnosis within the records while investigations are ongoing. If the results of the investigations return to confirm a differing diagnosis to one which the clinician was initially considering, this does not mean the provisional diagnosis documented in the records is inaccurate.
Rather, the entry reflects the clinician’s medical opinion based on the information available to them at the time.
It is, of course, possible that a patient may contend the importance of maintaining reference to a provisional diagnosis, when they have later received a confirmative diagnosis.
But there is an undisputed benefit of continuing to include this information because it allows clinicians who are involved in the patient’s care in the future to be aware of all possible diagnoses considered previously.
In turn, this will assist the treating clinician in determining whether previous diagnoses considered are of any relevance to the clinical care they then provide to the patient moving forwards.
Relevance
A further avenue a patient may explore relating to amending their medical record is to dispute the clinical relevance of the information which has been recorded.
There may be instances where a clinician makes reference to the appearance of a patient when they present for a consultation, or provides comment on a patient’s living environment, for example.
When a patient learns this information has been entered into their records, they may understandably have questions and concerns about the reason.
This would not prevent a clinician from explaining to a patient why they recorded such detail and it is possible that explaining the rationale for the information recorded may assist in a dispute about the entry in any event.
It is essential for a clinician to ensure a patient’s medical record only contains information justifiably relevant to the person’s future clinical care. Any other information should be stored separately to the medical record.
An example of this could be a subject access request, given that this may not be information relevant to the patient’s care. But the decision of clinical relevance is something for a clinician to consider and justify on an individual basis.
UK GDPR affords individuals the right for inaccurate information held about them to be amended and also provides individuals with the right to have personal data erased.
But this does not extend to information contained in a medical record which is factually accurate and reflects clinical opinion.
As data controllers, independent practitioners should always consider a medical record’s factual accuracy, as it would be inappropriate to amend any information which is not clearly and undoubtedly factually inaccurate.
If in doubt, always contact your defence organisation for advice.
Hannah Egan (below) is case manager at Medical Protection
Harassment is not just ‘an NHS issue’
There’s no place for bullying and harassment in the healthcare sector. David Hare appeals for everyone to join the growing campaign to foster a culture where colleagues can speak out when they have experienced or witnessed these behaviours
WHILE MY columns typically focus on the importance of keeping patients safe, this month I want to talk about the often overlooked role of keeping our workforce safe, and particularly our female colleagues.
In recent years, there have been growing evidence of the bullying and harassment of women working all across the health sector.
The NHS Staff Survey, published earlier this year, found almost 9% of all NHS staff, and 18% of medical and dental staff in training, have been the target of unwanted sexual behaviour in the NHS from patients, service users, their relatives or other members of the public.
Overall, 58,000 staff reported unwarranted sexual approaches from patients or other members of the public last year – that is one in every 12 NHS workers.
One in 26 reported experiencing similar harassment from work colleagues.
Likewise, the BMA’s Sexism in Medicine report found that 91% of female respondents had experienced sexism, with:
61% feeling they were discouraged to work in a particular specialty;
70% of women respondents believing their clinical ability had been doubted or undervalued;
44% of women saying they have had fewer training opportunities compared to men.
Moreover, 56% of women and 28% of men respondents reported receiving unwanted verbal conduct, and 31% of women and 23% of men respondents experienced unwanted physical conduct.
Problem in surgery
Looking more specifically at certain specialties in healthcare, the problem is even more acute.
Research from the University of Exeter and University of Surrey, published in the British Journal of Surgery , analysed anonymous online survey responses from over half of the surgical workforce.
It found almost two-thirds of women (63.3%) had been the target of sexual harassment from colleagues, along with almost a quarter of men (23.7%).
The majority of participants (89.5% of women, 81% of men) said they have witnessed some
The prevalence of harassment and misconduct that has been found means this issue absolutely cannot be seen as an ‘NHS only’ problem, but one that affects all healthcare providers
petrators working unchallenged within the healthcare environment –‘I was informed that he was known for this behaviour, that he’d got away with so much before and he was capable of ruining careers.’
Such behaviour is utterly unacceptable in any setting, let alone one where patients come to receive treatment and care during what can often be a vulnerable experience in their lives.
Thanks to the work of organisations like Surviving In Scrubs who campaign on this issue, some progress has been made in this area.
The evidence is unfortunately clear that too many people, largely women, are being subject to unacceptable levels of harassment and misconduct by their peers
form of sexual misconduct by colleagues, but just 16% of those impacted by sexual misconduct made a formal report.
These figures are quite simply shocking and, above all, unacceptable.
And while some of this research relates to the NHS, the prevalence of harassment and misconduct that has been found means this issue absolutely cannot be seen as an ‘NHS only’ problem, but one that affects all healthcare providers.
At the Independent Healthcare Providers Network (IHPN) we are taking this issue very seriously.
This summer, we were pleased to hold a ‘Sexual Safety’ session with our members to look at this issue in more detail and discuss what independent providers can do to support their staff and ensure there is an absolutely zero tolerance approach to bullying, harassment and sexual misconduct of any kind in their facilities.
First-hand experience
As part of the session, we were pleased to be joined by the organisation ‘Surviving In Scrubs’, who spoke of the first-hand experiences of women in the health service.
This includes:
How women were objectified during their ward rounds with their senior registrar gesturing to patients and saying ‘don’t we have a pretty female doctor with us today’;
GP trainees being told almost every week ‘we don’t employ women of child-bearing age’;
Multiple stories of known per-
The GMC’s Good Medical Practice now explicitly makes clear that doctors ‘must not act in a sexual way towards colleagues with the effect or purpose of causing offence, embarrassment, humiliation or distress’, as well as guidance on active bystander behaviour.
Equally the Royal College of Surgeons of England – who also spoke at our event – is reviewing its own policies, including its Good Surgical Practice guidance, to make sure it reflects the need to tackle sexual misconduct.
Zero-tolerance approach
The NHS has also established a sexual safety in healthcare charter. This calls on signatories to commit to a zero-tolerance approach to any unwanted, inappropriate and/ or harmful sexual behaviours towards their workforce.
It covers ensuring appropriate, specific and clear policies are in place, including appropriate and timely action against alleged perpetrators, as well as ‘ensuring appropriate reporting mechanisms are in place for those experiencing these behaviours, with the capturing and sharing of data on prevalence and staff experience transparently’.
So far almost 90% of IHPN’s Strategic Council members – our governing body – plus over half of our members, have signed up to the charter, but we are striving to ensure that 100% of our members are signatories.
Here at IHPN, we have specifically developed a ‘Sexual Safety’ managers toolkit for members, with six steps for well-led organisations to consider for tackling this issue.
We will also be establishing a Community of Practice, where members will be able to come together and share learning on this issue, including looking at specific anonymised cases, thinking about what worked well and identifying improvement areas. Through this, we hope to bring together different professional perspectives and broaden understanding of the issue and provide peer support.
Of course, the vast majority of staff working in the independent and wider healthcare sector behave with the utmost integrity and professionalism towards other colleagues.
But the evidence is unfortunately clear that too many people, largely women, are being subject to unacceptable levels of harassment and misconduct by their peers.
We know the culture of learning and the striving for continuous improvement that exists in the sector.
As part of this, we hope both providers and practitioners will equally work to foster a culture where healthcare colleagues who have experienced or witnessed these offences are empowered to speak up, report and call out this behaviour.
David Hare (right) is chief executive of the
Independent Healthcare Providers Network (IHPN)
You must treat the disabled favourably
A
recent Employment Appeal Tribunal (EAT) ruling affects independent healthcare providers who have employees. Employment solicitor Rachel Levine explains what they need to know
THE OBLIGATION to make reasonable adjustments for disabled employees is well known, but the parameters are often very difficult for employers to confidently identify.
Trial periods in new roles are often useful in this regard and can be evidence that an employer has looked to address a disadvantage.
But, in the new case of Rentokil v Miller, the Employment Appeal Tribunal (EAT) has considered whether offering a claimant a trial period in a new role can and should be considered a reasonable adjustment in and of itself.
The claimant (Mr Miller), a fieldbased pest controller, was diagnosed with multiple sclerosis and gradually became unable to undertake his physically demanding role. He applied for another role with the same organisation, a service administrator role.
Following the standard interview and written test, the claimant was unsuccessful. He went on to be dismissed on the grounds of capability on the basis that there were no adjustments that could be made to his pest controller role to enable him to continue in it and no suitable alternative roles could be identified.
The claimant brought claims of:
1 Failure to make reasonable adjustments;
2 Discrimination arising from disability;
3 Unfair dismissal.
The Employment Tribunal found the employer had failed to make reasonable adjustments: specifically, it had failed to offer the claimant a trial period in the service administrator role.
This finding had a very significant impact on the outcome of the case. The tribunal went on to uphold the complaint of discrimination arising from disability –because the dismissal was not justifiable if there had been a failure to make reasonable adjustments – and also found the dismissal itself to be unfair, because of the outcome of the reasonable adjustment claim.
The employer’s failure to make a reasonable adjustment was central to the success of the claimant’s case in all regards, and a financial remedy was awarded.
It appealed to the Employment Appeal Tribunal, which considered the case in detail before rejecting the appeal and agreeing with the Employment Tribunal.
The case contains commentary which will be very useful to employers when considering their obligations to make reasonable adjustments in relation to disabled employees.
1There is no reason why being given a trial period in a new role cannot, of itself, be a reasonable adjustment, nor is there a requirement that it must be certain that the employee would be successful in a trial.
This point has been discussed by the EAT before. In Environment Agency v Rowan, the EAT considered trial periods to be akin to a consultation and not a reasonable adjustment in its own right. Those comments were made obiter, meaning that they are not binding. This case contradicts this view, and the comments are not obiter. The EAT here found that because putting an employee into a new role on a trial period involves a change to their substantive terms, conditions or arrangements, it is not akin to a consultation. There is therefore no reason why a trial period in itself cannot be a reasonable adjustment.
The EAT also considered the limits of this potential adjustment. It held that a tribunal will not be bound in every case where an employee is facing dismissal to
The Employment Tribunal found the employer had failed to make reasonable adjustments: specifically, it had failed to offer the claimant a trial period in the service administrator role
find that the employer ought to have given them a trial period in another role.
Whether a trial period is appropriate as a reasonable adjustment will depend on the circumstances, including the suitability of the role and the prospects of the employee succeeding at the role and passing the trial.
In Rentokil, the tribunal had found that the trial period would have a real prospect (50%) of avoiding the dismissal of the employee and, as such, the trial period would have been an appropriate reasonable adjustment.
2WHAT THE CASE MEANS FOR INDEPENDENT HEALTHCARE PROVIDERS WHO HAVE EMPLOYEES
This case has highlighted the significant complexities faced by employers considering reasonable adjustments for employees.
What can appear to be a relatively simple decision should be considered carefully.
Employers should consider in particular:
That disabled employees are entitled to be treated more favourably than other candidates when considering redeployment
Whether a trial period in a role should be offered as a separate reasonable adjustment
What the appropriate selection criteria for a role should be, considering the very specific purpose of the trial period in these cases
Whether there is an objective justification for not making the adjustment of offering a trial period, even if there appears to be an objective justification for not making a permanent redeployment
The question of whether the claimant should be put into a role is an objective question for the tribunal to make, and the tribunal is not bound to follow the reasoning of either the employee or employer when coming to a decision.
The claimant had not passed the interview and standard written test required for the role. The employer argued in the EAT that by finding that a trial period was a reasonable adjustment, the tribunal was asking the employer to disapply its essential criteria for the role by disregarding these results.
The EAT considered this point in detail and found that the question of whether a particular employee should have been put into a particular role is an objective question and the tribunal is not required to take the side of either the employee or employer on this point.
In answering the question, the tribunal will usually consider whether the employee met the essential requirements of the role, but the matter for the tribunal is whether this employer ought reasonably to have put this employee into this role – on trial or not. This is the question that should therefore be asked by employers when considering the matter.
It is also not enough generally for an employer to show that the employee did not meet the standards that would be expected in a normal competitive exercise. The question is whether it would be reasonable for the employee to be put in the role, at least on a trial basis, for the purposes of a reasonable adjustment.
In the Rentokil case, the tribunal
Although the employee’s poor performance on the written tests may have reasonably raised some concerns for the employer, those concerns could have been met by offering the employee a trial period
had found that although the employee’s poor performance on the written tests may have reasonably raised some concerns for the employer, those concerns could have been met by offering the employee a trial period.
3
If the employee shows that there is a PCP (provision, criterion or practice), that they have been placed at substantial disadvantage, that there was knowledge, and identifies a role that the tribunal finds could potentially have been considered appropriate and suitable, it will be down to the employer to show that it was not reasonable to have (a) put the employee into that role, or (b) have done so at least on a trial basis.
Once the burden passes, while it is open to the employee to provide further evidence to support their claim, they are not required to do so.
The responsibility is then on the employer to show why it was not reasonable for the employer to make the identified adjustment.
This point highlights the need for thorough, considered reasoning, and the recording of that reasoning, when deliberating potential reasonable adjustments and whether they are suitable within the workplace and according to the specific needs of a business.
Rachel Levine (right) is a solicitor at specialist healthcare law firm Hempsons. If you would like more information, please email her at R.Levine@hempsons.co.uk
Take insurer excess payments up front
The importance of billing for and collecting medical insurance excess payments cannot be underestimated. Yet more and more independent practitioners are seeking help to recover huge outstanding amounts they have never asked for because they just accept what the insurer pays them. Derek Kelly (below) outlines the problem and shows what can be done
INDEPENDENT PRACTITIONERS face numerous challenges to maintain their financial stability and ensure consistent cash flow.
One crucial, yet frequently overlooked, aspect of revenue management is the effective billing and collection of medical insurance excess payments.
If you can ensure these payments are billed and collected, then it not only prevents revenue leakage but also significantly enhances your practice’s financial health.
➱ continued on page 44
EXPERT TAX AND ACCOUNTANCY ADVICE YOU CAN TRUST
Sandison Easson is a firm of truly specialist medical accountants who provide personal and tailored advice to clients.
We act for medical professionals throughout all stages of their career with clients in almost every town in England, Scotland and Wales.
We cut through the complicated jargon and deliver practical, easy to understand advice.
Call us today to organise your FREE no obligation consultation.
Sandison Easson: Specialist Medical Accountants helping you build a successful future
WE PROVIDE THE USUAL SERVICES YOU WOULD EXPECT FROM AN ACCOUNTANT SUCH AS PREPARATION OF YOUR ACCOUNTS AND TAX DECLARATIONS BUT OFFER SO MUCH MORE INCLUDING ADVICE ON:
• SETTING UP A NEW PRIVATE PRACTICE
• BUILDING AN EXISTING PRIVATE PRACTICE
• BUSINESS STRUCTURES TO PROTECT WEALTH
• BUSINESS STRUCTURES TO MAXIMISE TAX EFFICIENCY
• CLAIMING TAX REFUNDS INCLUDING OVERPAID ANNUAL ALLOWANCE TAX
• REMUNERATION PLANNING FOR YOU AND YOUR FAMILY
• UNDERSTAND ANNUAL ALLOWANCE TAX
• MAXIMISING LEGITIMATE EXPENSE CLAIMS
Free legal advice for Independent Practitioner Today readers
Independent Practitioner Today has joined forces with leading healthcare lawyers Hempsons to offer readers a free legal advice service.
We aim to help you navigate the ever more complex legal and regulatory issues involved in running and developing your private practice – and your lives.
Hempsons’ specialist lawyers have a long track-record of advising doctors – and an unrivalled understanding of the healthcare system as a whole.
Call Hempsons on 020 7839 0278 between 9am and 5pm Monday to Friday for your ten minutes of free legal advice.
and
COLLECT EXCESS UP FRONT
Benefits of effective excess collection include:
Improved cash flow: Regularly collecting excess payments ensures a steady cash flow, allowing practices to manage expenses and invest in growth opportunities.
Increased revenue: Capturing all owed amounts means practices can significantly boost their income, enhancing financial stability.
Cutting the administrative burden: Outsourcing excess collections to a specialised company frees up staff time, allowing them to focus on patient care and other critical tasks.
A better patient experience: Clear communication and professional handling of excess collections can improve the overall patient experience, fostering trust and satisfaction.
Educate patients about their insurance policies and excess obligations during the initial consultation. Clear communication can prevent misunderstandings and ensure patients are aware of their financial responsibilities
patients are aware of their financial responsibilities.
2. Upfront collection: Whenever possible, collect excess payments at the time of service. This reduces the need for followup and ensures immediate revenue.
3. Regular follow-up:
Understanding medical insurance excesses
Medical insurance excesses are the amounts patients must pay out of pocket before their insurance policy begins to cover medical expenses. These excesses can be applied on a per-claim, per-condition or per-policy period basis.
For instance, if a patient has an excess of £200 and incurs medical costs amounting to £1,000, they are responsible for the first £200, while their insurance provider covers the remaining £800.
Patients are aware of the excess charge on their policy and are notified of this by their insurer. The money is for work the practitioner has done and is entitled to and should be paid in its entirety.
But, much of the time, patients are awaiting a bill for this. If that does not come, then a large portion of them do not make a payment or even look to do so.
Practical steps for effective excess collection
1. Patient education:
Educate patients about their insurance policies and excess obligations during the initial consultation. Clear communication can prevent misunderstandings and ensure
Implement a structured follow-up process for unpaid excess amounts. Timely reminders and follow-up calls can significantly improve collection rates.
4. Utilise technology: Invest in billing software that can track and manage excess payments. Automated reminders and integrated payment systems can streamline the collection process.
5. Partner with experts: Consider partnering with a medical billing company such as Medserv to manage excess collections. Their expertise and resources can enhance efficiency and ensure maximum revenue capture.
The financial impact of uncollected excesses
Failing to bill and collect excess payments can result in significant revenue losses for medical practices.
The potential for uncollected excess payments has increased due to a growing trend of patients opting for insurance policies with higher excesses to lower their premiums..
This issue is exacerbated by the administrative complexities involved in tracking and collecting these payments, often leading
to lapses in the collection process. Uncollected excess payments can quickly accumulate, creating a substantial financial burden.
Practices may face cash flow issues, hindering their ability to cover operational costs, invest in new technologies, or expand services. And unpaid excesses can result in increased bad debt, further straining a doctor’s financial resources.
The role of medical billing companies
Engaging a professional medical billing company can be a gamechanger in managing excess payments effectively. They specialise in handling the intricacies of medical billing and revenue cycle management, ensuring excess payments are accurately billed and efficiently collected.
Here are some ways a medical billing company can benefit your practice:
➲ Comprehensive billing services: They manage the entire billing process, from claim submission to payment collection, ensuring all patient excesses are correctly identified and billed.
➲ Efficient collection processes: Robust follow-up procedures and patient communication strategies are used to collect excess payments promptly, reducing the likelihood of bad debt.
➲ Technology: They use billing software to track and manage excess payments, providing realtime data about outstanding amounts and collection progress.
➲ Regulatory compliance: Medical billing companies stay updated with the latest regulatory changes and insurance policies, ensuring all billing practices are compliant and that excess collections are handled correctly.
By handling the often-sensitive task of collecting payments, medical billing companies allow consultants and other healthcare professionals to maintain positive patient relationships. Practitioners can focus on delivering quality care without the strain of financial conversations.
Every pound counts – more than ever. Do not let uncollected excesses drain your practice’s resources but take proactive steps today to secure your financial future.
The potential for uncollected excess payments has increased due to a growing trend of patients opting for insurance policies with higher excesses to lower their premiums
World-class Diagnostics with rapid results
King Edward VII’s Hospital Diagnostic & Imaging Centre brings together the most advanced diagnostic technology & equipment, with a highly skilled team of radiologists and radiographers to ensure your patients receive a quick and seamless service.
Results within 24 – 48 hours using PACs System Biotronics 3D
New for Spring 2024
Derek Kelly is marketing manager at Medserv
When bonds come bouncing back
Samuel Kirton explains why shorterdated highquality bonds are still in favour despite recent volatility
MOST INVESTORS would probably like to forget the poor performance of both bonds and equities in 2022 and early 2023.
For many of them, it was their first real experience of bonds falling in value, particularly at the same time as equities.
Different investors would have experienced different outcomes in 2022 and subsequently, depending on the type of bonds that they held. It is worth revisiting what has happened since then.
Bonds are issued by companies or governments in order to raise money. Investors buy the bonds, giving a loan to the organisation and they agree to pay it back on a specific date (maturity), with interest payments along the way.
Unlike equities, bonds do not offer ownership rights, but the market value of them can change along with their popularity to potential buyers.
Going back to first principles, we can remind ourselves of several characteristics that apply to bonds.
Bond prices move in the opposite direction to bond yields – the return or interest the investor expects to receive each year.
So when bond yields rise, bond prices fall. The prices of bonds with maturities further into the future are more sensitive to changes in yields than shortermaturity bonds, making their prices more volatile.
The lower the quality of the borrower issuing the bonds, the more like equities they behave. And, finally, bond markets do not like inflation, generally driving up yields in the face of rising inflation.
Inflation threat
With the growing threat of high inflation following Russia’s invasion of Ukraine in 2022, exacerbated by the instability of the unfunded tax promises of the Conservative government under Liz Truss, bond yields rose dramatically and substantially.
The bond see-saw moved violently, with those owning longerdated bonds suffering material
JellyPx
It is evident that shorter-dated bonds have recovered far more quickly than longer-dated bonds
and painful falls in value. Those who owned shorter-dated bonds fared better, but even so delivered falls in value.
Yet, bond owners from that point on began to benefit from the higher yields that their bonds now delivered, recouping some of those falls in value.
If we look at data showing how far bonds fell for different maturities and what the return has been in cumulative terms in the last two years, we can see a big bond
bounce-back for shorter-dated bonds has occurred.
In fact, they are back to where they started. Meanwhile, longerdated bonds still sit deeply underwater.
It is evident that shorter-dated bonds have recovered far more quickly than longer-dated bonds as the prices of the former fell less far, and the consequent higher yields have helped to recoup these falls, at least in nominal, pre-inflation terms.
At their worst, shorter-dated global bonds were down around -7% in 2022. However, they delivered just over plus 5% in 2023, and around 1% to the end of June this year following small yield rises across major markets.
We have always tended to favour shorter-dated bonds for this reason, believing that the small premium available in lending for longer is outweighed by the downside protection that comes from
owning shorter-dated bonds alongside their bounce-backability.
Samuel Kirton (right) is a financial planner with Cavendish Medical, specialist financial planners helping consultants in private practice and the NHS
The content of this article is for information only and must not be considered as financial advice. Cavendish Medical always recommends that you seek independent financial advice before making any financial decisions. Levels, bases of and reliefs from taxation may be subject to change and their value depends on the individual circumstances of the investor. The value of investments and the income from them can fluctuate and investors may get back less than the amount invested.
Founded in 2010, we bring 14 years of expertise in providing clinical software.
Our cutting-edge clinical solution enhances care across a wide range of specialties, from neurodiversity to comprehensive medical services.
It runs efficiently without bottlenecks in tasks like patient management, appointment scheduling or billing.
Facilitates clinics and clinicians operating across many locations.
Design your own specialist forms for use by patients and users.
Templated notes, documents, diagrams, auto-generation of GP letters are available.
Handles complex billing requirements for self-funders, families or insured patients.
Online booking and patient portal included.
BUSINESS DILEMMAS
Useful tips on how to respond to a complaint following the submission of a medical report to the courts are given here by Dr Kathryn Leask (right)
Dilemma 1 Will I breach confidentiality?
QI am a private GP and a patient has asked me to provide her with a medical report for the court in relation to domestic violence.
She told me she was the victim of abuse by her husband. I provided a report, with her consent, detailing the information she had given me about the cause of her injuries and my findings on examination.
But I had not appreciated this report would not only be seen by the court but would also be in the documents disclosed to the husband’s legal team.
I have now received a complaint from the patient’s husband about the information I gave to the court. I am concerned that responding to the complaint will result in me breaching confidentiality about my patient or putting her at risk.
Court report may harm my patient
AIt is important when writing a medical report to ensure it is written to a named person or someone in a specific role/ organisation rather than ‘To whom it may concern’.
And it is helpful to state at the beginning what the purpose of the report is and who requested it. This prevents misunderstandings and ensures the report is only used for the purpose you intended.
It is also important to state that the report is based on the relevant clinical records and, if appropriate, your recollection.
Duty of confidentiality
Where a patient has told you something has happened, but you are not able to confirm or verify this, you should make clear in your report that this is based on information from the patient and not a matter of fact.
While a complaint should be
While a complaint should be responded to, you should not disclose information about a third party
responded to, you should not disclose information about a third party.
Your duty of confidentiality to all your patients should be explained in the complaint response and that this will inevitably limit your ability to respond.
You can respond in general terms, to explain your usual process when receiving these types of
requests. For example, that the records are reviewed and a report prepared to the best of your knowledge and belief, based on the patient’s self-reported history. This information will have been recorded in the notes in good faith as part of the trust between patient and doctor.
If your practice has a second stage to its complaints procedure, you should make the complainant aware of this. For example, if you are a member of the Independent Sector Complaints Adjudication Service (ISCAS).
It is important that all complaints are handled carefully, no matter how minor they may originally seem. If you need advice, your medical defence organisation will be able to help you.
Dr Kathryn Leask is medico-legal adviser at the Medical Defence Union (MDU)
A
private
consultant
gastroenterologist has a problem with being
asked to provide a testimonial for a former colleague. Dr Kathryn Leask responds
Dilemma 2
What happens if I write reference?
QI have been asked to provide a testimonial for a colleague whom I used to work with in the NHS a year ago. I understand they are subject to a GMC fitness-to-practise investigation and they have contacted me for a reference.
The thing is, I do have some concerns about my former colleague’s behaviour and attitude towards other members of staff when I worked with them, but no concerns about their clinical decision-making at that time.
What are the implications for me if I agree to provide a reference?
AFor you to provide a testimonial, you will need to have adequate information about the reason for its request.
As your colleague is subject to a GMC fitness-to-practise investigation, you will need to understand what the allegations and concerns are so that you can specifically address these.
You may find that the investigation is not about your colleague’s clinical care of patients but relates to their behaviour towards other people.
If this is the case, the fact that you have concerns about this is relevant and, if you decide to provide the testimonial, you will have to include it.
You should make clear your relationship with your colleague and how long you had known and
Writing reference for a colleague
worked with them and provide the dates, so the GMC knows you have not worked with them recently. This is important, as you may not have been working with them at the time the concerns were raised.
Be honest
In its guidance on writing references, the GMC says you must be honest and objective when writing them.
References must include all information which is relevant to your colleague’s competence, performance and conduct. It goes on to say that you must not deliberately leave out relevant information.
If your colleague’s fitness-to practise investigation leads to a hearing at the Medical Practitioner’s Tribunal Service (MPTS), you could be called as a witness to give oral evidence. You could be asked to justify your comments in your reference.
Rather than your colleague request a testimonial directly from you, it would be better for the request to be from the solicitor that is representing them. The solicitor can provide you with a formal request and give guidance on the type of information to include based on the allegations that have been made.
You do not have to provide a testimonial and, where you do, the solicitor and your colleague can choose not to use it.
If you need further advice, your medical defence organisation will be able to help you.
Next month: Dr Kathryn Leask responds to a private cardiologist’s query as to whether he should report himself to the GMC after a coroner at an inquest was critical of the care the cardiologist had provided to a patient who died. And she replies to a private GP to advise on what to do if a parent requests access to their child’s clinical records
ACCOUNTANTS
WE UNDERSTAND YOUR PAIN
As a health consultant you’re probably facing these concerns:
• Higher tax bills as a result of the reform of the tax basis period.
• Delays in getting accounts and tax returns prepared.
Sound familiar...?
If your accountant hasn’t already spoken to you about these concerns, then our dedicated healthcare accounting team are ready and waiting to help you right now.
Contact us for a complimentary review of your accounting requirements.
Scan this QR code to watch a recording of our webinar: ‘Tax Basis Period Reform: Is Your Healthcare Practice Prepared?’
Email: healthcare@robson-laidler.co.uk
Tel: 0191 281 8191
www.robson-laidler.co.uk/healthcare
Ensure you understand
Unless your private income is only a very modest amount, then you should receive a set of financial statements – accounts – each year summarising the financial activity of your business over a period of time. These statements usually cover a 12-month period but can be longer or shorter.
But the figures and terminology used within the accounts can make them difficult to understand when you first come across them.
Alec James (right) follows up his first article last month by explaining some more key parts of the accounts to help make things clearer
understand your accounts
BALANCE SHEET/STATEMENT OF FINANCIAL POSITION
It is always best practice to prepare a balance sheet as part of the annual accounts.
Companies and limited liability partnerships (LLPs) are required to prepare and submit one as part of the statutory accounts.
The balance sheet reconciles the assets and liabilities of the business and balances them to the share capital (for companies only) and reserves – or undrawn profits – of the business.
While preparing a balance sheet, certain reconciliations take place such as agreeing the bank account balances to the statements.
A reconciliation will also be performed between the fee income declared and comparing these to the receipts received during the financial year.
A healthy business will have a positive balance sheet. Having a negative one, where the liabilities exceed the company’s assets, can mean the business is insolvent.
That could see the business owners out of pocket, particularly if they have loaned money to their business. A negative balance sheet can also make obtaining any further finance difficult.
Having a balance sheet drawn up as part of your accounts generally costs more for your accountant to prepare but it gives you comfort that the fees have been declared correctly.
It can often be a false economy to ask your accountant to only prepare a profit and loss account, as this is more likely to raise an inquiry from HM Revenue and Customers (HMRC).
KEY BALANCE SHEET TERMINOLOGY
There are a number of different headings included within the balance sheet which can be a little confusing to understand. So listed below is a summary of
the most commonly appearing headings used in medical business accounts:
➤ FIXED ASSETS
Fixed assets are usually shown as the original cost less any associated depreciation and impairment – an additional reduction in the value of the asset for things like damage to the asset. For most businesses, this is equipment they have purchased.
If your business has other fixed assets such as investments or property, depending on its size, your business may be required to prepare accounts on a ‘fair value basis’.
This is where the business is required to obtain valuations of the affected fixed assets each year and the movement in value is recorded.
It can be a very complex area. You should speak to your accountant to ensure you understand what information is required from you each year.
➤ DEBTORS
Debtors are one of the most important numbers within the balance sheet. This shows the amount of money your business is owed from your customers, whether this is patients, insurers or other businesses such as solicitors.
IT’S YOUR RESPONSIBILITY
Each year you are required to have prepared and signed off your agreement to the accounts prepared.
The accounts are usually prepared by an accountant, but they do so based on the information provided. The ultimate responsibility of the figures contained within the accounts falls to the taxpayer.
So do ensure you fully understand the figures before signing. Having an accountant who is au fait with the complexities of doctors working privately can be extremely helpful in ensuring you are comfortable when doing so.
You should regularly review the debtors of your business to ensure you are being paid for all work done. There is usually a delay between generating the income and physically receiving the payment. However, clinical practices should not have much more than six to eight weeks of income outstanding at any time.
If your business has more than this, then you will need to review the balances to see if there are any older fees which require investigations.
Your secretary should regularly review the older balances and chase payment. If you find you have large numbers of older balances, you may wish to consider outsourcing your invoicing to a third party.
Your fee for medico-legal work can often take much longer to be
received. When working in the medico-legal sector, you need to consider the time taken to receive payments within the rates you charge.
There may be instances where you receive payment before work is done and so your business has no debtors. It is important to record payments received in advance of a service being provided.
You should always provide your accountant with details of invoices which have not been paid as at the end of your financial year. These should include balances that arose from the start of the financial year but also any remaining unpaid from previous years. Most software providers can supply this data.
➤ CREDITORS
Creditors are liabilities of your business. There can be a range of different creditors such as trade creditors – money owed to your suppliers at the end of the financial year – tax liabilities or loans. Most doctors’ private practices do not usually have large liabilities other than resulting tax liabilities. But if your business has large liabilities, then you should review and plan for them to be settled to ensure your cash flow is not adversely affected.
Alec James is a partner at Sandison Easson & Co, specialist medical accountants
DOCTOR ON THE ROAD: MG3
Novel approach to boost affordability
This impressive offering is fun to drive and gives excellent fuel economy for doctors and their families looking for good value, says Independent Practitioner Today’s motoring correspondent Dr Tony Rimmer (right)
ONE OF the great positives to working in medicine is that the tools we use to help and treat our patients are constantly evolving and improving.
This is true whether it be in therapeutics, psychology or the physical tools and techniques of surgery. There is always something interesting and exciting on the horizon to look forward to embracing and master.
Efficiency of cost, better use of natural resources and improved outcomes for our patients are constant drivers of change.
In the world of cars, it has been the current drive towards a low CO2 emission world using electric power that has propelled some very interesting new developments.
Battery weight
We all know that fully electric EVs are the cleanest way forward, but they are hampered by two main issues: battery weight and cost.
These factors are less important in expensive premium cars like the BMW iX or Porsche Taycan, but
they have a huge hampering effect when manufacturers try to advance the small-car class.
In fact, Ford has ceased production of the Fiesta supermini after 47 years, as it feels that producing an electric version would not be cost-effective, so there is a place to fill for small fuel-efficient, preferably hybrid cars.
Most small hybrids like the Toyota Yaris or Renault Clio use small electric motors with small batteries to boost the mainly petrol-powered propulsion particularly when starting from rest.
Novel powertrain
Now, Chinese-owned MG has entered the market with a radically updated MG3 that has a novel powertrain.
Its big electric motor powers the front wheels directly and a 1.5litre four-cylinder petrol engine kicks in to top up the battery or, when extra performance is needed, adds drive to the front axle.
It has a three-speed automatic gearbox to smooth out power delivery.
Styling, particularly at the front, has been modernised and brings a stylish up-to-date look shared by its bigger MG4 and MG5 siblings.
This third-generation MG3 has a completely new chassis and the interior has also been vastly updated.
Its dashboard design is almost identical to MG’s impressive allelectric MG4 stablemate with user-friendly infotainment screens and a multifunction steering wheel.
The body is VW Polo-sized and has plenty of room for four adults or five, at a push. Comfortable seats and nicely textured trim raise
the perceived quality out of the budget market class; a definite improvement over the previous generation car.
Aggressive pricing means the well-equipped SE base car is only £18,495 and my test car, the Trophy model, is only £20,495.
£10,000 cheaper
The Trophy adds LED headlights, keyless entry, a 360-degree parking camera, heated seats and a heated steering wheel.
This is more than £10,000 cheaper than equivalent fullyelectric cars; very significant for any of us on a budget.
Fuel economy is a claimed 64.2mpg, which would be around 55mpg in the real world – pretty impressive.
It is out on the road that the new car impresses. The MG3 drives like a pure EV around town with all the benefits of instant torque and gocart nippiness.
The petrol engine cuts in smoothly and when you need some real power on ‘A’-roads, it joins the 134bhp electric motor and gives the car an almost hothatch combined 192bhp total.
Although the MG3 is not a plug-in hybrid, which would make it a lot more expensive, it is an impressive piece of kit
Its automatic gearbox works smoothly but allows a little hesitation to creep in at low parking speeds – you soon get used to this though.
The steering is direct and the handling is sporty – this is a much lighter car than any pure EV. The ride is comfortable too and is aided by relatively small 16-inch wheels.
So, although the MG3 is not a plug-in hybrid, which would make it a lot more expensive, it is an impressive piece of kit.
It is cheaper than direct rivals such as the Suzuki Swift and Renault Clio and now has the build quality to challenge them directly.
The cheaper SE model with standard sat-nav, advanced driving aids and a rear camera is all you really need.
I had some fun driving this MG around and feel that it would suit any medic who is looking for an excellent value urban run around. It would make an ideal second car in a family household too.
Dr Tony Rimmer is a former NHS GP practising in Guildford, Surrey
MG3 HYBRID + TROPHY
Body: Five-seat hatchback
Engine: Single electric motor plus 1.5litre four-cylinder petrol engine. Front-wheel drive
Power: 191bhp
Torque: 425Nm
Top speed: 106mph
Acceleration: 0-62mph in 8.0 seconds
Claimed fuel consumption (WLTP combined): 64.2mpg
CO2 emissions: 100g/km
On-the-road price: £20,495
The dashboard design is almost identical to MG’s all-electric MG4 stablemate with user-friendly infotainment screens and a multifunction steering wheel
CHECK OUT OUR BUSINESS DIRECTORY
Independent Practitioner Today features an online advertising directory to complement our
and
Split into ‘business’ and ‘lifestyle’ directories, they list the services private doctors need to run their practices or spend their well-earned money on.
ADVERTISERS: The deadline for booking adverts in our November issue is 1 November
or for reprints, we would be happy to discuss licensing the copyright to you.
Published by The Independent Practitioner Ltd. Independent Practitioner Today is editorially independent.
Material is governed by copyright.
No part of this publication may be reproduced, stored in a retrieval system or transmitted in any form without permission, unless for the purposes of reference and comment. Editorial layout is the copyright of the publishers. If you wish to use it for promotional purposes on websites
Robin Stride, editorial director Email: robin@ip-today.co.uk Phone: 07909 997340 @robinstride
ADVERTISE WITH US
To advertise in the digital journal, on our website or in our business directory, contact advertising manager Andrew Schofield at Spot On Media. Phone: 0161 408 3912