How Circle Group introduced patient-reported outcomes measures at its 53 hospitals P14
The business journal for doctors in private practice
Sustainability is crucial to health of your workforce
Bupa’s Dr Robin Clark explains how developing sustainability initiatives boosts working well-being P18
n See page 24
Avoid those Groundhog Days when billing
The repetitive nature of medical billing issues are set out by
P30
Private practice boom
By Robin Stride
Consultants are gearing up to increase their private practice commitment as independent sector analysts predict a record year for the sector.
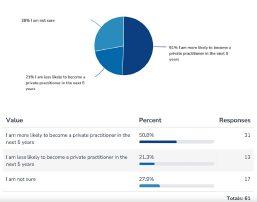
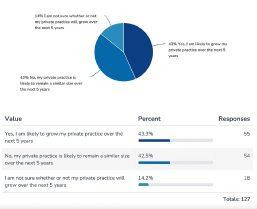
As many as 43% of specialists responding to a joint Independent Practitioner Today/Medical Defence Union (MDU) survey signalled they were likely to grow their business over the next five years.
Another 43% expected their private practice workload to remain the same in the foreseeable future but 14% said they were unsure about what would happen.
Consultants’ numbers in the sector will be boosted by a tranche of doctors who are currently planning to take up private work.
Half of the doctors responding to the survey, who currently only worked in the NHS, thought they were more likely to be in private practice over the next five years, while 28% were unclear.
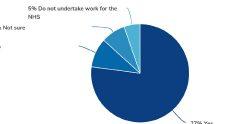
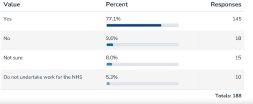
Asked if they still did, or intended to, work for the NHS alongside their private commitment, 77% said yes, 9.6% said no, 8% were unsure and 5% said they were not working for the health service.
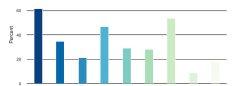
For three-quarters of consultants their biggest motivation to work privately was financial. 43.6% cited greater job satisfaction, 36% considered it gave them a better
work-life balance, while for 34% it represented a new challenge and experience.
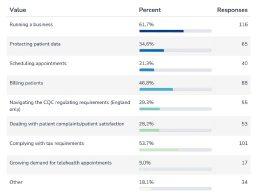
Marketing yourself or your practice was, perhaps unsurprisingly, seen as the biggest challenge to becoming a private practitioner (58%).
This was followed by impact on work-life balance (47%), arranging indemnity for themselves or employees (44%), and managing patient data (41%). Patient satisfaction was an issue for 8%.
Over six in ten placed running a business as their biggest challenge faced or anticipated when in private practice. Complying with tax requirements came in next (54%), billing patients (47%) and protecting patient data (35%).
Nearly a third mentioned their other concerns as navigating the
Our sponsors
Clearly finance is a strong motivator for doctors to do private practice, but job satisfaction is another. The survey shows they have a desire to put their own stamp on the work and to service patients’ needs
MDU medical legal adviser Mr Jerard Ross commented: ‘It has been a record year in the specialty areas you might expect – demand appears to be there. I was slightly surprised more doctors didn’t expect their business to grow, but that might be a lifestyle choice.
‘Clearly finance is a strong motivator for doctors to do private practice, but job satisfaction is another. The survey shows they have a desire to put their own stamp on the work and to service patients’ needs.’
Care Quailty Commission (CQC) regulating requirements and dealing with patient complaints and patient satisfaction issues.
Consultants expressed a huge appetite for learning more to help them with their businesses.
Financial planning, including tax, National Insurance and PAYE came out top (57.2%), with support for marketing and establishing a private practice while maintaining existing NHS commitments were both wanted by 36% of respondents.
These were closely followed by complying with data protection obligations (34%), professional/ corporate indemnity (33.2%), complying with CQC requirements (30%), and ‘how to establish a private practice and ensure it stands out from the crowd’ (28%).
Mr Ross, a former neurosurgeon, was surprised to see that arranging indemnity for consultants or their employees had surfaced as an issue. He told Independent Practitioner Today : ‘There’s a need for us to make positive changes to members’ lives and private practice is not about just providing indemnity.
‘It is about making sure we can help independent practitioners expand their business, run their business well and to make appropriate financial plans.
‘The marketing side is an area we are able to provide advice on and we are rejigging a private practice course and hope to say more soon. This will cover a lot of the issues raised in the survey.’
n See full results and what consultants told us: pages 24-27 n 2023 will be a record year for private healthcare: See page 5
Simon Brignall
Mr Jerard Ross, MDU legal adviser
TELL US YOUR NEWS. Contact editorial director Robin Stride
ADVERTISE WITH US. To advertise in the digital journal, on our website or in our business and lifestyle directories, contact Andrew Schofield at Spot On Media. Phone: 0161 408 3912
Business Dilemmas: Data that may upset a family Medico-legal advice on how you can shield sensitive information when reporting to a coroners court P40
Accountant’s tips: Should I buy a house via a company?
Specialist accountant Richard Norbury explains the tax complexities for consultants investing in homes P46
Doctor on the Road: EV has all the spark expected of a BMW
Our motoring correspondent Dr Tony Rimmer is full of praise for the new electric Beemer – the i4 P50 www.independent-practitioner-today.co.uk
Private group doing it the NHS way
An NHS provider is creating a new market for self-pay patients using salaried doctors. Leslie Berry explains how the Practice Plus Group does it P12
GMC rules updated to reflect society
An update to the GMC’s Good Medical Practice is on its way. The MDU’s Dr Udvitha Nandasoma looks at what it means for private doctors P16
When and what do you tell the police
To report or not to report? Dr Sally Old of the MDU explores when you should and should not disclose patient information to the police P22
Errors harm you as much as patients
Dr Clare Stapleton of Medical Protection discusses the steps you can take to protect yourself against complaints in private practice P28
How to cut down on complaints
The Independent Sector Complaints
Adjudication Service continues to see a rise in gripes against doctors. Here’s what it is doing to reverse the trend P32
Drifting into a contract is perilous
Some key points to consider when entering a contract are outlined here by Justin Cumberlege, a partner at healthcare legal firm Hempsons P34
New retirement option available
Are you considering partial retirement? George Uglow of Cavendish Medical looks at the key points of the new NHS retirement flexibilities P38
Tips on achieving financial health
As costs rise and competition intensifies, Derek Kelly of Medserv unveils key strategies to enhance revenue, profitability and long-term success P44
McCloud latest: what rules will be implemented now?
Consultation outcome published before remedy implementation
By Edie Bourne
Doctors now know how the ‘McCloud remedy’ for pension tax rules will be implemented this month following the publication of the final NHS consultation results.
The outcome of the consultation, which started in the Spring and concluded in June this year, is that some of the technical proposals will be taken forward but others will be amended following critical feedback.
The McCloud remedy aims to recompense NHS scheme members deemed to have suffered age discrimination when the 2015 pension scheme was introduced. They will now be able to receive their original benefits from the 1995 or 2008 scheme for the seven years of the ‘remedy period’ which runs from 2015 when the new pension scheme began to 2022.
It was announced that a new digital service from HMRC, which is yet to be made available at the
time of writing, will allow scheme members to correct their tax payments for the years within the remedy period.
They will also be able to apply for compensation online for any tax overpayments.
Importantly, members will not need to include an annual allowance charge on their tax return for tax year 2022-23 or resubmit a selfassessment tax return for any tax year during the remedy period.
Patrick Convey, technical director at Cavendish Medical, told Independent Practitioner Today: ‘We have waited a long time for the details of McCloud implementation to be presented.
‘The outcome of the consultation is largely advantageous for doctors, but it is still very challenging for the busy medic to unpick the many caveats.
‘The results of the consultation have also been released just a few weeks before the official implementation deadline.
The outcome of the consultation is largely advantageous for doctors, but it is still very challenging for the busy medic to unpick the many caveats PATRICK CONVEY OF CAVENDISH MEDICAL
annual pensions savings statement this autumn as usual, as the NHS Pensions Agency attempts to rework the calculations for every year of the remedy period. But these should instead be provided by 6 October 2024.
‘One of the significant announcements is that if members opted out of the pension scheme within six months of the remedy period starting, they will be able to ‘buy back’ their missing service without having to provide too much evidence that they opted out because of the discrimination.’
It was also announced that scheme members who are affected by McCloud will not receive an
Mr Convey said: ‘We have been talking about McCloud for years now and it is good to finally get the information we need to move things forward. There is a huge amount of work needing to be done – by the NHS Pensions Agency and by the individual medics trying to understand their complex data.
‘For many, calculating their pension input and subsequent annual allowance charges was hard enough the first time, but now reworking those figures is daunting.’
‘We cannot stress enough that you do not need to attempt these sums on your own. Make sure you seek expert help from those who are adept at working with these figures daily.’
Boost your skills at private practice meeting
Independent Practitioner Today columnists and other leading experts are out in force for one of the most useful ‘teach ins’ about the business side of private practice.
They will feature at the BMA’s annual private practice conference on 17 November which aims to cater for established and new consultants and GPs in the sector –
plus others planning to go private.
Topics include:
An overview of private healthcare;
Engaging with private medical insurers;
Medical defence issues and mistakes in private practice;
Practising privileges and engagement with private hospitals;
The interface between primary and secondary care;
Self-pay and private medical insurance patients;
Accounting issues;
Multidisciplinary teams;
The Private Healthcare Information Network (PHIN).
Consultants and private GPs from the BMA’s private practice
committee will present various talks, while Dr Charlie Chan of the Federation of Independent Practitioner Organ isations will advise on ‘planning to succeed in private practice’.
Doctors can also attend online.
Details at www.bma.org.uk/ events/private-practice-conference-2023.
Those new to private practice advised to fill in tax form
Don’t forget to have your selfassessment tax return for the 20222023 tax year completed in time. That’s the message from specialist medical accountants, especially to the many new private doctors.
As Independent Practitioner Today warned in our 26 September news e-alert, doctors who started working privately in the tax year ended 5 April 2023 should have registered with HM Revenue and Customs (HMRC) for self-assessment by 5 October.
Alec James of Sandison Easson specialist medical accountants, reminded senior doctors their latest tax return was due for submis-
sion to HMRC by 31 January 2024. He advised those with complex tax affairs to seek a specialist medical accountant’s advice to ensure they paid the correct amount of tax on their self-employed income.
SECOND SCANNER FOR SPIRE HOSPITAL WILL ALSO SERVE NHS PATIENTS
Users asked to compare NHS vs private
Private patients are being quizzed by university researchers as part of a project exploring what NHS and private hospitals ‘think and know about activities that help to support and improve high standards of care’.
Researchers from the Universities of Manchester, York and Birmingham are inviting patients or carers to take part in a one-hour interview on clinical governance for which they are paid £25.
Participants or an individual they look after must have received care for the same health issue in both a private and NHS hospital in the last three years – excluding mental health services.
They must have had an overnight stay in either or both an NHS and private hospital or may have been transferred from a private hospital to an NHS hospital.
Hybrid hospital is built
By Agnes Rose
Medical skills and facilities on offer at a new £100m West Midlands hospital are tipped to make it a magnet for private patients in the area.
Building work on the longawaited Harborne Hospital, Birmingham, a joint venture between HCA and the NHS, is now completed and specialists are looking forward to working there in early January 2024.
According to Leighton Chumbley, the boss of healthcare property developers Prime, it will be the most technically advanced private hospital constructed outside of London.
Hospital chief executive Claire Smith, vice-president of HCA Healthcare UK NHS Joint Ventures, said: ‘It’s been a huge collaborative effort to get to this milestone moment and I want to thank everybody involved for their dedication to this innovative project.
‘For HCA Healthcare UK, work only continues now and at pace to ensure that, come January, this impressive building is an even more impressive hospital, equipped with the state-of-the-art facilities, with teams of skilled medical professionals and leading consultants that will make the hospital the destination for highquality private care in the region.’
The 50-inpatient bed, four-theatre hospital will also have two floors with 72 NHS inpatient beds through HCA Healthcare UK’s partnership with the University Hospitals Birmingham NHS Foundation Trust.
Julian Miller, the trust’s chief financial officer, said the hospital had ‘world-class facilities’ for the people of Birmingham and Solihull.
Peter Manners-Smith, fund manager at M&G Real Estate, called the project an excellent example of how private sector cap-
The front of the new Harborne Hospital, a joint venture by the NHS and HCA
ital could be used to build exemplar facilities.
He said: ‘By financing the construction through long-term leases, we have also been able to generate sustainable long-term returns for our investors and benefit retirement savers.’
Facilities include: Four theatres, including a hybrid catheterisation laboratory; Two minor operating/endoscopy suites; 44 inpatient beds, Six ITU beds; 16 day-case beds.
Spire St Anthony’s Hospital in Cheam, Surrey, has installed a second £1.4m MRI scanner which will benefit both NHS and private patients. From left: deputy imaging manager Jo Bryan, department assistant Freddie O’Meara, radiographer Aisling Harte, hospital director Jonathan Head and clinical services director Shelia Enright.
Botched beauty ops abroad under fire
The Independent Sector Complaints Adjudication Service (ISCAS) has expressed concerns about adverts in the UK for cosmetic surgery abroad, particularly from Turkey.
This follows Advertising Standards Authority findings that two promotions trivialised the decision to have cosmetic surgery, pressurised consumers and misleadingly omitted information about preconsultations. One advert used the term ‘mommy makeover’.
Many more adverts for cosmetic surgery abroad on Facebook and Instagram were found to have a significant proportion appearing to breach ISCAS’s rules. The problem was highlighted at a meeting of ISCAS’s cosmetic surgery group.
Director Sally Taber said around 30 deaths had occurred due to a variety of problems with the treatment of UK patients abroad while others had required treatment in the NHS when they returned.
Private care growth not all due to self-pay
A rise in the number of patients paying for private care is coming from both self-pay and insurance.
Responding to Private Healthcare Information Network (PHIN) data (see our reports of 19 September), the Independent Healthcare Providers Network (IHPN) said the strong growth in insurance-based admissions in the most recent quarters was a notable factor.
Chief executive David Hare said there were around 70,000 self-pay
Top year forecast for private care
By a staff reporter
A record year for private healthcare in 2023 is forecast by Healthcode, which expects to clear over ten million invoices to insurers on behalf of hospitals, practitioners, practices and clinics.
The official clearing organisation for the private healthcare sector cleared nearly 20% more invoices by the end of July compared with the same point in 2022.
Total invoice value cleared up to July was approximately £2.5bn in funds that have helped private providers grow their businesses and care for their private and NHS patients.
Healthcode managing director Peter Connor said: ‘After achieving great things in 2022, private providers are treating more insured patients than ever and we’re seeing year-on-year growth across every region, care setting and specialty.
‘I’m proud that Healthcode’s technology is helping to power the sector forward on several fronts at a time when health provision is a national priority.’
He said these fronts included:
Rapidly cleared insurer invoices so providers can realise quarterly income of £1bn;
A secure messaging service used by industry professionals to annually send over 350,000 electronic messages, sharing confidential information in support of patient care;
The Private Patient Register (PPR), which now has over 38,000 registered practitioners and has become the sector’s information hub. Mr Connor said this was driving collaboration and streamlining the practising privileges process;
The company’s new ICE (integrated channel exchange), making real-time appointment booking a reality for the private healthcare sector.
Headlines from Healthcode’s latest analysis of insurer invoice activity covering January to July 2023 include the following:
Episode setting
Between January and July 2023, the averaged year-on-year growth in non-hospital billing volumes was 27%, while for hospital billing volumes it was 13%.
The average year-on-year growth was 13% for outpatients and 16% for admitted patients. This reflects the different recovery rate for admitted care which lagged
behind outpatient episodes after the pandemic.
Medical specialties
Orthopaedics and trauma was the largest hospital specialty, with an insured bill volume of £53,000 in July 2023, up 17% on the same month in 2022. Over the seven months to July 2023, the averaged year-on-year increase was 11%.
Radiology was second – £40,000 in July, up by 13% on 2022. The averaged year-on-year increase was 15% over the seven months to July.
Obstetrics and gynaecology saw the largest year-on-year growth in billing volumes in July 2023 (32%) with cardiology only just behind on 31%. Over the seven months to July 2023, both specialties saw averaged year-on-year growth of 23%.
Countries and regions
Hospital billing volumes were up across all UK countries in July 2023 compared with July 2022. Wales achieved year-on-year growth of 26% while the equivalent year-onyear growth in England was 19%.
Scotland and Northern Ireland were 9% and 5% respectively.
All English regions saw growth of more than 15% in July 2023.
admissions every quarter compared to 50,000 in 2019.
‘It’s no surprise that with NHS waiting times at record levels and continuing to climb, patients are choosing to pay to get the care they need.
‘This includes not only significant procedures or surgery, but diagnostics too and GP appointments – providers are also reporting significant growth in those areas.’
OPPORTUNITIES FOR PRIVATE DOCTORS ARE SET TO CARRY ON, EXPERTS SAY
Private work opportunities for independent practitioners are set to increase in the months and years ahead, according to leading sector commentators.
Healthcode’s managing director Peter Connor (right) told a WPA Health Insurance webinar he did not envisage current growth levels declining in any way.
He said the increasingly competitive employment market meant more employers were offering private healthcare while many private medical insurers had made it easier to claim.
Online accessibility options were increasing and insurers were offering more online GP services.
Independent Healthcare Providers Network’s boss David Hare told the same meeting it was ‘inconceivable’ that current growth would not continue.
Many more employers were looking at their options to support the well-being of existing and new staff, he added.
Private hospitals had capacity to see more patients, including evenings and weekends, and people wanted to work in the sector.
Bupa and the London Clinic start prostate special unit
By a staff reporter
A new specialist centre for prostate cancer has been launched by The London Clinic and Bupa UK Insurance to give the insurer’s customers rapid access to diagnostic tests and treatment from leading oncology experts.
For peace of mind, the insurer’s customers worried about symptoms can get an appointment for prostate cancer within two working days.
All initial diagnostic tests and scans can be made in the same appointment and, if necessary,
then the provider said customers would be treated within 31 days of calling Bupa – twice as fast as national targets.
This is the third specialist centre status Bupa has awarded to The London Clinic. The hospital’s breast cancer pathway received this recognition in 2019 and, more recently, its bowel cancer pathway in June 2022.
Al Russell, chief executive at The London Clinic, said: ‘We’re honoured to have received this reputable stamp of approval from Bupa for our prostate cancer care services.
The London Clinic’s cancer wing houses the new prostate centre, the third specialist centre status awarded it by Bupa UK Insurance
‘Our world-leading urologists and pioneering treatment options mean patients being treated for prostate cancer are in the very best of hands.’
Alex Perry, chief executive of Bupa UK Insurance, added: ‘We’re proud to be expanding our specialist centres for cancer even further, providing fast access to tests and treatment for our health insurance customers.
‘This speed and early diagnosis helps many Bupa customers to avoid more invasive treatments in the long term and saves lives.’
Treatments available at The
London Clinic’s dedicated cancer unit, the Duchess of Devonshire Wing, include radical prostatectomies using a da Vinci robot surgical system, allowing surgeons to perform operations with greater accuracy than open surgery. The many benefits for patients include faster recovery.
Cancer Research UK said that although prostate cancer is one of the most common cancers in the UK, improved awareness and early diagnostic testing options meant nearly 80% of people who have it survive the disease for ten years or more.
Royal Marsden appoints new managing director Royal Marsden NHS Trust has announced Mark Hawken has been appointed managing director of The Royal Marsden Private Care. He follows Shams Maladwala who left the role in early 2023 for Dubai.
Mark joins from the London Clinic, where he had been commercial director since 2018. In this role, he was responsible for building private care revenue as well as implementing new services and partnerships with clinicians and other healthcare organisations.
He said: ‘I am delighted to join The Royal Marsden Private Care, a world-class cancer centre with a reputation for pioneering innovative research and providing outstanding care and treatment.
‘I very much look forward to supporting the growth of the organisation’s integrated private service, which provides benefits for patients and staff across the whole hospital.’
After beginning his healthcare career as a pharmacist, Mark has also held senior commercial roles for Bupa and Aspen Healthcare, including responsibility as a turnaround specialist and hospital director for Aspen.
The trust’s published 2022-23 annual accounts show growth in private patient income of £162.2m, up 14.5% and £20.5m on the £141.6m achieved in 202122.
The two-year growth in bounceback from Covid has been 37% and £60m. Royal Marsden Private Care maintains its strong position as the NHS trust with the highest grossing private patient income
and highest percentage of total income from this source. That figure remains over one-third at 34.2% last year.
Central London trusts report private patient growth
Final private patient revenues growth rates in the 2022-23 financial year for the ten central London NHS trusts was 22.8%, in line with the forecast made in last month’s PPU Watch.
Nine of the ten reported growth, the exception being Imperial College which had a small decline of 2.7% and £1m.
King’s College also had a positive year, with growth of 71.5% and £3.9m to reach £9.35m. The full reports are summarised above.
Philip Housden is director of Housden Group commercial healthcare consultancy
Mark Hawken
PPU WATCH
Budget stems exodus from pension scheme
By Charles King
Pension tax reforms in the last Spring Budget have reduced the number of doctors leaving the NHS Pension Scheme (NHSPS) due to issues with the lifetime allowance and annual allowance.
According to Government data, the number has nearly halved since the change was announced, Figures from the NHS Business Services Authority (NHSBSA), which have been analysed by specialist financial mutual Wesleyan, show 46% fewer individuals left the scheme between April and June 2023 because of issues with the allowances than
did so over the same period in 2022.
This compares to a 2% rise in the number of medical professionals citing the lifetime and annual allowances as the reason for withdrawing between April and June 2021 and the same period in 2022.
Wesleyan’s head of medical, Alec Collie, said: ‘These figures are an early indication that the Spring Budget tax changes are alleviating some of the tax pressures that are impacting doctors and dentists.
‘However, this isn’t a magic wand and problems persist. Those who received unexpected tax bills and left the NHSPS won’t all be rushing
to rejoin the scheme unless they see evidence that the new limits aren’t just going to result in the same issues.
‘We are urging anyone now thinking about rejoining the NHSPS or worried about their pension or tax situation to seek professional advice. This is still a very complex area, with different implications for different circumstances.’
Research by Wesleyan last autumn found 29% of 293 doctors quizzed planned to retire this year amid pension taxation issues and workload pressure.
Of those retiring earlier than planned, one in six said it was
King Edward VII’s unit wins joint op laurels
King Edward VII’s Hospital has been celebrating after attaining National Joint Registry (NJR) Quality Data Provider recognition for three years in a row.
The NJR monitors the performance of hip, knee, ankle, elbow and shoulder joint replacement operations to improve clinical outcomes primarily for the benefit of patients, but also to support orthopaedic clinicians and industry manufacturers.
It collects high-quality orthopaedic data in order to provide evidence to support patient safety, standards in quality of care and overall cost-effectiveness in joint replacement surgery.
The ‘NJR Quality Data Provider’ certificate scheme was introduced to offer hospitals a blueprint for reaching high-quality standards
relating to patient safety and to reward those who have met registry targets.
To achieve the award, hospitals are required to meet a series of six ambitious targets during the audit period 2021-22.
One of these is compliance with the NJR’s mandatory national audit aimed at assessing data completeness and quality within the registry.
This compares the number of joint replacement procedures submitted to the registry to the number carried out and recorded in the local hospital patient administration system. The audit ensures that the NJR is collecting and reporting upon the most complete, accurate data possible across all hospitals performing joint replacement operations.
NJR medical director Mr Tim Wilton said: ‘Congratulations to colleagues at King Edward VII’s Hospital.’
He added: ‘The Quality Data Provider Award demonstrates the high standards being met towards ensuring compliance with the NJR and is often a reflection of strong departmental efforts to achieve such status.
‘As well as being a fundamental driver to inform improved quality of care for patients, registry data provides an important source of evidence for regulators, such as the Care Quality Commission, to inform their judgements about services.’
Full details about the NJR’s Quality Data Provider certificate scheme can be found online at www.njrcentre.org.uk.
because they had hit their lifetime allowance. Thirty per cent of medical professionals said they had cut their hours to help manage their tax situation.
In a bid to help address this issue, Chancellor Jeremy Hunt announced in March’s Spring Budget that the annual allowance would increase from £40,000 to £60,000 from the start of the 2023-24 tax year, and that the lifetime allowance would be abolished.
Wesleyan said its analysis of data was received from the NHSBSA through a Freedom of Information request about the number of monthly opt-outs from the NHSPS and the reasons for opting out.
Videos give doctors help to deal with complaints
Consultants and GPs in private practice can now get help with handling complaints via four new training videos from the Independent Sector Complaints Adjudication Service (ISCAS).
The ten-minute videos aim to ‘enhance complaints training and adherence to the ISCAS Code’.
They are:
General Complaint Handling Principles Under the ISCAS Code;
Stage 1: Managing Complaints Under the ISCAS Code;
Stage 2: Managing Complaints Under the ISCAS Code;
Stage 3: Managing Complaints Under the ISCAS Code; ISCAS subscribers have immediate access to them using their subscribers log-in.
See ‘Cut down on complaints by managing expectations’, page 32
Cleveland Clinic wins digital records kudos
By Olive Carterton
Digitalisation innovation at the Cleveland Clinic London has enabled it to become the first UK private hospital to win recognition from an organisation committed to encouraging better use of technology.
It takes its place alongside seven NHS hospitals who have achieved Stage 6 accreditation of the Electronic Medical Record Adoption Model (EMRAM).
This eight stage framework assesses and measures the level of digital maturity and sophistication of healthcare organisations’ electronic medical record (EMR) systems.
The scheme is run by the Healthcare Information and Management Systems Society (HIMSS), a global adviser, thought leader and memberbased society.
HIMSS digital strategist John Rayner paid tribute to the hospital for its ‘remarkable journey towards a near paperless, patient centric healthcare environment’ in only 18 months since its opening.
He said: ‘They are the first hospital in the UK to achieve unitdose dispensing and administration of pharmaceuticals.
‘Their visionary leadership, cutting edge technology and unwavering commitment to excellence
are shaping the future of healthcare.’
Cleveland Clinic London president Dr Rob Lorenz said: ‘This is a fantastic demonstration of what we can achieve when we demonstrate our values of teamwork and innovation.’
Hospital spokesman Raihaan Mughal called the hospital ‘one of the most technologically advanced hospitals in the UK’.
To reach Stage 6 standards, the hospital demonstrated a significant level of digitalisation and integration of EMR into operations.
This led to improved patient care, efficiency, data utilisation and other benefits contributing to the overall quality of services.
Its review noted that leaders were visible and impactful, the culture was strongly committed to improving quality of care and patient safety; and caregivers took ownership and were proud of achievements.
HIMSS praised the hospital’s pharmacy department as being one of the most forwardthinking in the UK.
It was the first private hospital to use a pharmacy barcoding/closed loop medication administration, and a unit dose pharmacy robot that individually wraps and tracks medication by barcode to the patient’s bedside.
THE EMRAM ACHIEVEMENT COMES WITH MANY BENEFITS:
Improved patient care and safety: Hospitals at EMRAM Stage 6 have advanced clinical decision support systems, electronic medication administration records and electronic order sets. This can lead to better-informed medical decisions, reduced medication errors and improved patient outcomes.
Enhanced efficiency: Hospitals operating at this stage have streamlined workflows and reduced reliance on paper-based processes. This can result in faster access to patient information, reduced administrative burdens and improved operational efficiency.
Data availability and analysis: EMRAM Stage 6 hospitals have robust data repositories, making it easier to access and analyse patient data for quality improvement initiatives, research and strategic decision-making.
Interoperability: These hospitals have achieved a high level of data-sharing and exchange among different healthcare systems and providers, leading to better care co-ordination and smoother transitions of care for patients.
Patient engagement: With advanced EMR systems, hospitals can provide patients with online access to their medical records, lab results and other health information, promoting patient engagement and empowerment.
Regulatory compliance: Many healthcare regulations and standards are tied to the use of electronic medical records. Hospitals at EMRAM Stage 6 are likely to be better positioned to meet compliance requirements and data security standards.
Cost savings: While the initial investment in EMR implementation can be significant, hospitals that have reached EMRAM Stage 6 often realise cost savings over time due to streamlined processes, reduced paperwork and improved resource utilisation.
Clinical decision support: Advanced clinical decision support systems can help healthcare providers make more informed decisions by presenting relevant patient data, treatment guidelines and best practices at the point of care.
Preparation for future stages: Achieving EMRAM Stage 6 sets the groundwork for potentially reaching Stage 7, which involves full interoperability and utilisation of EMR data to improve population health.
Cleveland Clinic London’s Stage 6 accreditation for EMRAM will be valid for three years.
MDU hails fee cap in negligence
The Medical Defence Union (MDU) has welcomed a Government announcement that it is to cap legal costs in lower value clinical negligence cases.
But the defence body will campaign for this to be just the start.
Senior medical claim handler Dr Claire Wratten said: ‘The MDU has always believed that for this scheme to have a meaningful impact on ris
ing clinical negligence costs, it should be far more ambitious. Rather than just applying to claims up to £25,000, it should include claims up to £250,000.
‘However, this is an important first step given that disproportionate legal costs are one of several defects in the current litigation system and affect lower value claims.’
In MDU cases last year, the average sum paid in claimants’ legal costs on medical claims settled for up to £10,000 was over £24,000. The average for claims settled between £10,000 and £25,000 was around £46,000.
Dr Wratten added: ‘It cannot be right for legal costs paid to claimants’ lawyers to regularly exceed the damages paid to claimants.’
Dr Claire Wratten of the MDU
Optegra celebrates its 15th birthday with opening of new theatre
After treating more than one million eyes, specialist ophthalmic clinic Optegra marked its 15th anniversary with a visit to its first UK hospital in Guildford, Surrey, from local MP Angela Richardson. It launched a second operating theatre there, which the MP officially
Surgeons’ sexual crimes slammed
By Agnes Rose
The private hospitals’ trade body and the BMA are among organisations expressing horror at survey findings reporting a high percentage of female surgeons say they are being sexually harassed, assaulted and in some cases raped by colleagues.
Dawn Hodgkins, of the Ind ependent Healthcare Providers Network (IHPN), said: ‘It’s not just the appalling severity of the incidents reported, but the frequency and scale of the problem is equally damning. There are clearly massive, endemic issues which need rooting out.
‘This must be a wake up call to make significant and unequivocal changes to the culture which has enabled these behaviours to bed in and become so worryingly normalised.
‘It’s totally unacceptable.’ In a response to research published in the British Journal of Surgery she called on everyone –‘whether that’s professional bodies, employers or colleagues within and around surgical teams – to take a zerotolerance approach to this issue’.
She added: ‘This will include taking urgent steps to ensure that we are supporting colleagues to call out this behaviour, to investigate incidents and to make sure appropriate action is taken, so that female colleagues can begin to feel safe and supported.
‘We will be encouraging members and partners to engage swiftly and fully to make the progress which is so clearly needed.’
The Working Party on Sexual Misconduct in Surgery survey found a third of NHS female surgical staff had been sexually assaulted by colleagues in the past five years.
BMA equality lead Dr Latifa Patel labelled the scale and severity of sexual assault against female surgeons ‘atrocious’.
She said: ‘Doctors who abuse their positions to commit sexual assault have no place in the medical profession. The GMC has to review its outcomes of sexual misconduct cases in order to identify whether institutional sexism is playing a part in how seriously claims are taken.
‘Only then, by working together and being accountable for what has and continues to happen, with the implementation of clearer policies and codes of conduct, can we change the culture that enables sexual harassment in the workplace.’
Dr Patel said the BMA’s ‘Ending Sexism in Medicine Pledge’ had long called for more to be done to require employers to bring in policies that eliminated any form of sexual harassment in the workplace.
‘This survey shows the need more than ever for action to be taken urgently and we will continue to highlight the prevalence of these behaviours being experienced by doctors and the fears around reporting that prevent people from speaking up.
‘It is truly horrifying to continue to hear about the experiences of these women. We encourage them and their colleagues who experience sexual harassment and sexism of any kind to seek support from the BMA. These dreadful actions must be challenged and not be tolerated any longer.’
opened, and now runs 11 hospitals and clinics. These treated around 3,000 NHS cataract patients pre-pandemic, but this shot up to over 35,000 in the past year.
Chief executive Dr Peter Byloos said more clinics would open in the next year following one in York last month.
‘Tell patients their right to pick provider’
New figures from a Care Quality Commission (CQC) study underline the importance of NHS patients being made aware of their rights to choose private providers, according to the Independent Healthcare Providers Network (IHPN).
The organisation was reacting to the CQC’s 2022 adult inpatients survey where fourinten patients reported their health had deteriorated while they waited to be admitted.
IHPN chief executive David Hare said the finding drove home the impact that growing waiting lists were having on patients and their quality of life
He said: ‘With 7.6m people on the growing waiting lists and with winter in full view and the inevitable pressure that it always brings, with more patients likely to be cancelled or postponed, we need to be pulling on every lever at our disposal to bring the waiting lists down.
‘The independent sector stands ready to increase its support of the NHS. There is capacity to deliver more highquality care and we are committed to working with the NHS to get patients the treatment they need as quickly as possible.’
Mr Hare added that many patients were often unclear they had the right to choose a provider to deliver their NHS care.
MP Angela Richardson (centre) cuts the ribbon with Optegra’s Surrey team (L-R) surgeon Mr Alex Shortt, Lorand Berecki, Martina Zillwood-Hunt, Nin Lasham, Jamie Camp, Optegra NHS Director Richard Armitage
Dawn Hodgkins
A look back through our journal’s archives of a decade ago reveals that although times change, some issues are not so new
A trawl through the archives: what made the news in 2013
Pension tax bill horror
Shocked consultants were hit with tax penalties of up to £50k after inadvertently busting pension fund limits.
Many were amazed to find HM Revenue and Customs’ pension contribution calculations based on annual deemed pension growth –bearing little resemblance to what they put in their pot.
Simon Bruce, of financial experts Cavendish Medical, said: ‘We have been helping new clients who received letters showing pension savings in 2011-12, with one as high as £150,000 – much more than the individual actually put in.
‘The doctors may have no “carry forward” allowance available from the previous three years, so as the annual allowance cap is £50k, this particular doctor will have exceeded it by £100,000.
Thousands of doctors risk losing licence
Private doctors who had so far failed to respond to GMC requests to provide information for their revalidation were putting their licence to practise at risk.
The GMC wrote to 54,000 doctors the previous year as part of a campaign asking them to confirm their designated body.
But as many as 7,818 doctors who did not answer received a final notice letter advising them they had 28 days to either confirm their designated body or tell the council they did not have one.
If they failed to respond, the GMC said it would be forced to take steps to scratch their licence to practise.
Innovation pay-off on the way
Consultant innovators were set to be major drivers fuelling a predicted double-digit growth in self-pay over the next few years as the private healthcare sector emerged from the outcome of a Competition Commission investigation.
Authors of an influential industry report, incorporating opinion from 750 clinicians, hospital bosses and
decision-makers, hailed clinical innovation as a trump card in recessionary time.
They said that those who actively promoted self-pay and adhered to the competition watchdog’s call for pricing clarity would be the ones to benefit most by converting marketing into business.
Respondents told the survey they were committed to spending their marketing budget on self-pay and fixed-price surgery because it was proven to be effective.
Healthcare marketing consultant Liz Heath, who revealed details of The Private Healthcare UK Self-Pay Market Study, said getting savvy with social media and having a good online presence would grow in importance.
Her team’s findings revealed huge price variation by region and by procedure.
Coding is set to be enforced
Clinical coding was set to become a requirement for all consultants in the foreseeable future, according to the boss of online solutions company Healthcode.
Peter Connor said that although not widely used now in independent practice, it was essential for the sector to be able to access data about pricing, quality and outcomes to usefully compare with NHS performances.
The Clinical Coding and Specialist Development (CCSD)
group was bringing in a new industry schedule of diagnostic tests to drive further coding standardisation and improve transparency in line with Competition Commission provisional findings in its private healthcare investigation.
Surgeons urge tough action
Fewer than a third of medical professionals in the cosmetic surgery arena believed recommendations in a review of the sector by Sir Bruce Keogh went far enough.
Three-quarters feared there could still be a repeat of a health scandal such as the breast implant crisis.
Don’t throw away records too early
Private doctors were being recommended by defence body the Medical and Dental Defence Union of Scotland to be sure to stick to the retention periods for medical records set out in their local NHS guidelines.
Its advice came after a widower of a London private gynaecologist and obstetrician found numerous boxes of his wife’s private patient records in the attic and wanted to know if they could be dumped or stored instead at a local hospital.
Spending too much time on billing instead of patient care?
Let the UK’s number 1 provider, Civica Medical Billing & Collection do the hard work for you.
• Reduce bad debts to less than 0.5%
• Increase net income by up to 25%
• 24/7 online access to your data
• Enable faster payments through e-billing for insurers and patients
• Focus on your practice whilst our account managers manage it all for you
Private group doing what the NHS used to do
An NHS provider is creating a new market for selfpay patients using salaried doctors. Leslie Berry reports
CHANGE IS in the air for Practice Plus Group – one of the UK’s largest providers of NHS services –under a drive to increase self-pay activity, with a new ‘middle market’ offer to meet the demand resulting from record NHS waiting lists.
The business has recognised that around half of its inquiries are now from people who have never considered private healthcare before and it is intent on ‘removing the complexity, hidden costs and exclusivity typical of the traditional private sector’.
Instead, it says it is offering easy, rapid access to high-quality surgery – at a typically 20-30% lower price point – for those who cannot afford to wait.
A key factor in being able to pass savings onto patients is the group’s employed model, where doctors are employed full-time or part-time, with 150 doctors across Practice Plus Group’s ten hospitals and surgical centres working in this way. It says that by employing its doctors on a salaried basis it can use theatre time very efficiently. Rather than an NHS doctor seeing a handful of patients privately each week, and all the associated costs of running that theatre list, it has a high throughput.
Many benefits
Medical director Dr Marcelle Michail, explains: ‘For our doctors, being salaried has a number of benefits.
‘We are fully committed to supporting their further professional development in the shape of paid study leave, budget for training and courses, and providing the resources they need.
‘We also support with appraisals and revalidation and, of course, offer benefits such as sick leave,
Practice Plus Group’s Barlborough Hospital, near Chesterfield, Derbyshire
The reception area at Practice Plus Group’s Emersons Green Hospital, just outside Bristol
annual leave, pension, a far greater work-life balance than in the NHS and faster pay progression.
‘But more than that, we run consultant-delivered services providing outstanding care and excellent patient outcomes.
‘We are innovators and our doctors can quickly and easily implement ideas to affect change in their service without layers of red tape and bureaucracy.’
Mr Chris Waller is consultant orthopaedic surgeon and medical director at Practice Plus Group Hospital, Southampton. He says: ‘We’re increasingly attracting doctors who are in the prime of their careers and are drawn to our ability to do what the NHS was original set up to do – to do the right operation for the right patient at the right time.
‘Doctors coming to join us observe what we do and comment that this is what they’d imagined the NHS to be.
‘For me personally, I have found a place where I can effect change and implement best practice; where instead of multiple layers of managerial sign-off, if I have an
idea I can knock on a door to speak to colleagues about it and I’ll be listened to.
‘What I’m particularly proud of is that although a lot of our work is high volume, low complexity, within that there are people with challenging circumstances who we can be nimble enough to help; someone with learning disabilities who needs extra time, or a cancer patient fitting in dental treatment around chemotherapy.
‘We have the ability to just slow things down and meet their needs. I’ve also never had to cancel a patient’s operation because there
wasn’t a bed. We see as many patients as we can with the resources we have, safely and to a high quality.’
While Practice Plus Group does not offer practising privileges, it has around 130 doctors who supplement existing substantive or private commitments by working additional ad hoc hours on a selfemployed or personal service company basis.
Consultant specialties include orthopaedic surgeons, ophthalmologists, urologists, gynaecologists, ENT specialists, dentists, general surgeons and radiologists.
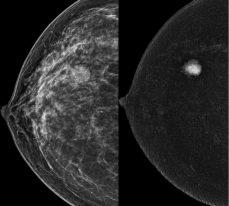
108 Harley Street introduces London's first private HOLOGIC Contrast Enhanced Mammography System, revolutionising breast cancer screening. Mammography has long been the primary method for detecting breast cancer at an early, treatable stage However, with the advent of Contrast Enhanced Mammography (CEM), a specialised and advanced mammography test, breast imaging has reached new levels of precision and detail Our facility now offers this state-of-the-art technology, ensuring patients receive the highest quality breast cancer screening available
CEM goes beyond the capabilities of standard mammography by utilising a special dye (contrast) injected into the patient's arm, enhancing the visibility of breast tissue changes.
CEM is recommended for several patient groups, including those who require assistance in resolving findings detected through conventional breast imaging, individuals needing pre-operative staging of breast cancer, patients with contraindications or intolerance to MRI (e g , pacemakers or claustrophobia), and patients over 40 who have suspected cancer based on ultrasound but normal mammography results Additionally, CEM can be employed as an alternative to MRI for women at an increased risk of developing breast cancer, such as those with dense breasts or a strong family history.
The specialties currently in high demand are ophthalmologists, endoscopists and anaesthetists.
Practice Plus Group rebranded from Care UK in 2020 and is managed by Bridgepoint private equity firm.
Private healthcare now represents 15% of Practice Plus Group’s secondary care revenues, but it expects to see this grow in the next 12 months with a bolder marketing approach.
Its hospitals and surgical centres are mostly concentrated in the South-east: from Ilford, London, to Portsmouth, Southampton, Bristol, Shepton Mallet in Somerset, Devizes in Wiltshire, and Plymouth.
There is a hospital in Barlborough near Chesterfield, Derbyshire, an ophthalmology centre in Rochdale, Greater Manchester, and a new site set to be announced in the coming months.
For more information, phone 07555 147760. Email: abby.samuel@practiceplusgroup.com. Website: https://practiceplusgroup.com
To learn more about CEM or refer a CEM patient please contact our X-Ray
Surgeon Mr Chris Waller
Medical director Dr Marcelle Michail
CRUNCHING THE NUMBERS
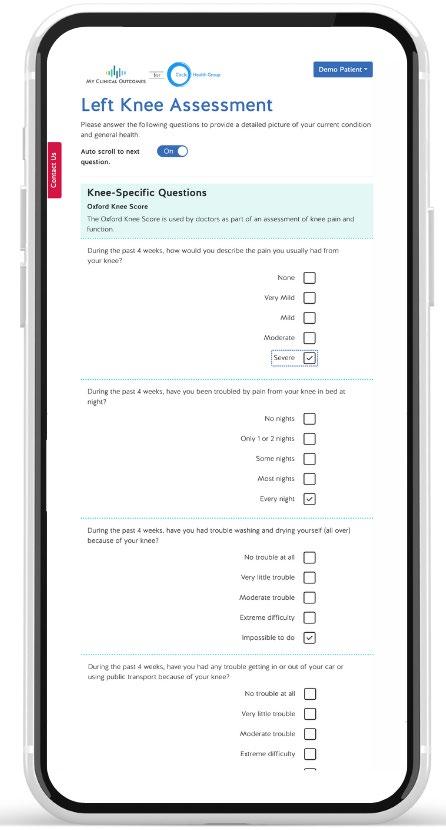
Outcome data key to clinical success
Circle group medical director and consultant orthopaedic surgeon Mr Peter James reports on joining forces with My Clinical Outcomes to introduce its Patient Reported Outcomes Measures platform at each of the provider’s 53 hospitals
Our consultants’ enormous commitment to continuous improvement has also made us the top-rated provider for patient experience, according to PHIN data
CIRCLE WAS founded with a unique ethos of clinician leadership, engagement and empowerment. This has remained a core value as it has grown from a small challenger provider to the largest player in the UK independent hospital sector.
We have always prioritised patient outcomes above every other metric and this is reflected in best-in-class results in the sector.
For example, last year, PROMs were 9% higher than the NHS benchmark and 2% higher than the independent sector average in the hip surgery category.
In the knee category, outcomes were 33% higher than the NHS benchmark and 14% higher than the independent sector average.
Our distinctive model of clinical leadership – with a senior consultant employed as clinical chairman at each of our 53 sites – means consultants are highly engaged in collaborative efforts to improve clinical practice, patient safety, patient experience and patient outcomes.
For example, Circle also leads the field in another key clinical quality metric: JAG* accreditation, where we have the largest number of JAG-accredited facilities in the independent sector. Twenty-five sites are accredited, more than double the second highest performing provider in the sector on this measure.
Our consultants’ enormous commitment to continuous improvement has also made us the top-rated provider for patient experience, according to PHIN data, with 92% rating their experience ‘very good’ versus 85%, 78% and 72% for the next three highest performers respectively.
This unrelenting focus on clinical quality has also been recognised in the hospital regulator’s ratings, with a 13% increase in the proportion of sites rated ‘good’ or ‘outstanding’ by the Care Quality Commission across the portfolio in 2022, and a reduction in the number of sites rated ‘requires improvement’ from 40% to 18% since Circle’s acquisition of BMI Healthcare in 2019.
Clinical audit
Circle is also unique in the sector in its embrace of transparent clinical audit in surgery, with 100% of sites completing the ‘Getting It Right First Time’ best practice surgical initiative – the gold standard of clinical audit in the UK healthcare sector.
However, as anyone who works in the field of quality improvement will know, maintaining standards is not a tick-box that can be completed and then moved on from. Quality can only be maintained through a relentless focus on continuous improvement and marginal gains. As Circle’s founding motto notes, ‘good enough never is’.
That’s why the next step in our continuous improvement journey is joining forces with My Clinical Outcomes to introduce its Patient Reported Outcomes Measures platform at each of Circle’s 53 hospitals.
Founded by doctors in 2011, My Clinical Outcomes is widely recognised as one of the UK’s leading providers in the field of patient outcomes and clinical performance measurement.
It offers one of the most comprehensive platforms available and the organisation’s technology cur-
Mr Peter James of Circle Health Group
Effective management of data and understanding trends in patients is fast becoming key to ensuring the safe operation of a hospital and network
Effective data capture is vital to ensuring the success of a service or treatment pathway offered at a hospital
rently supports more than 150 hospitals with over 1,000 clinicians and 200,000 patients in the UK.
Effective data capture is vital to ensuring the success of a service or treatment pathway offered at a hospital. Increasingly, platforms like the one offered by My Clinical Outcomes are becoming instrumental to helping clinical teams evaluate and inform decisionmaking.
Safe operation
From identifying unwarranted variation in surgical results to automatic data submissions and finally registering group-wide results with registries and regulators, effective management of data and understanding trends in patients is fast becoming key to ensuring the safe operation of a hospital and network.
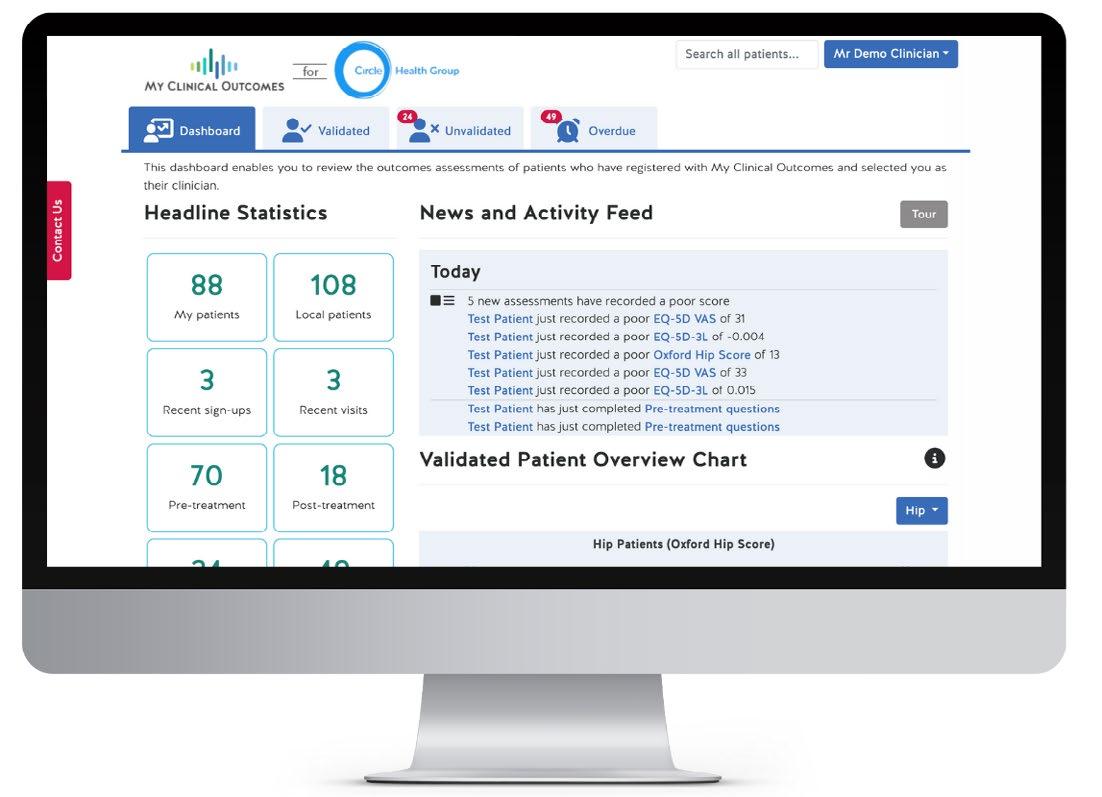
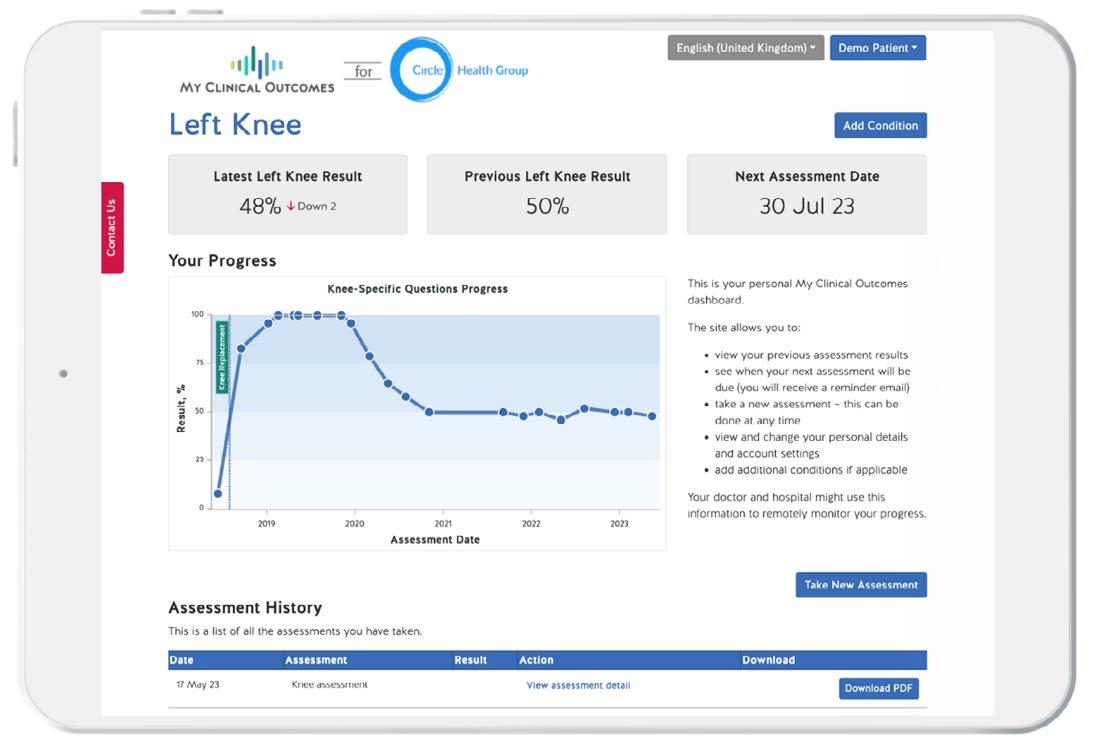
This innovation will support Circle with managing and tracking consultant level data – providing teams at hospital and national level with valuable insight into
COMPREHENSIVE DATA SET: Just some of the screens of information available on My Clinical Outcomes. The top two are different pages of a consultant’s dashboard and the bottom one is a patient’s portal
the performance of consultants in every specialty offered across the UK.
This will make outcomes measurement a routine part of patient care, delivering not only regulatory compliance but rich, actionable outcomes data and analysis.
The partnership with My Clinical Outcomes is another step forward in digital transformation that will revolutionise our ability to track, collect and monitor the performance of our hospitals, and ultimately help us to continue offering outstanding care to the patients we serve.
Circle is enormously proud to have been awarded ‘best hospital group of the year’ for three consecutive years at the landmark Health Investor awards, recognising our sector leading performance.
We put this success squarely down to our unique model of consultant leadership and engagement, and we are determined to continue to excel in this field.
At a time of global and national staff shortages, Circle was a net recruiter of clinical staff throughout 2022. As a result, 12% of UK registered medical consultants now have practising privileges at Circle.
We are committed to supporting all of them to continue to improve and innovate and become leaders in their fields. Together, we believe we can push the boundaries of excellence in patient care in the UK. ‘Good enough’ never is.
* JAG accreditation is the formal recognition that an endoscopy service has demonstrated that it has the competence to deliver against the criteria set out in the Joint Advisory Group on GI Endoscopy standards
A patient’s questionnaire on a smartphone
Guidelines revamped to reflect society CHANGES TO GMC’S ‘GOOD MEDICAL PRACTICE’
The new and updated version of the GMC’s Good Medical Practice comes into effect in January 2024 and will set standards of professional behaviour for many years to come. The MDU’s Dr Udvitha Nandasoma (below) looks at what it means for independent practitioners
SETTING STANDARDS for doctors is one of the GMC’s most important functions, providing a ‘framework for ethical decision-making’ by practitioners and also for fitness-to-practise decisions.
The publication of the new core guidance in August was therefore a significant moment which followed more than 18 months of consultation by the GMC.
In the years ahead, Good Medical Practice 2024 (GMP) will ‘set out the principles, values, standards of care and professional behaviour expected of all medical professionals’.
The GMC stresses that GMP isn’t a set of rules, as the regulator says it will take into account factors like the extent of any departure from professional standards, whether this was premeditated or persistent, or involved abuse of power when assessing the risk posed by a doctor after concerns have been raised.
By familiarising yourself with the contents of the new 28-page edition and understanding how the guidance applies to your own practice you should be able to have
confidence that you understand the GMC’s expectations.
To get you started, the Medical Defence Union has put together this quick guide to some of what’s in there and most relevant for independent practitioners.
Overview
Slightly longer than its predecessor at 101 paragraphs – compared with 80 paragraphs in 2013 – the new GMP addresses changes in medical practice, such as remote consulting, as well as broader social changes.
It covers communication as a professional in greater depth and, for the first time, it focuses on how doctors should respond if they witness sexual harassment, bullying and discrimination in a new section devoted to contributing to a positive working and training environment.
As before, the guidance topics are set out in four domains, although each of these now has a short introduction which summarises the behaviour expected of good medical professionals.
These are different to 2013,
including a completely new domain called ‘colleagues, culture and safety’ which reflects the GMC’s concern with workplace culture and has implications for senior doctors or for those with their own practice or clinic.
DOMAIN 1 – Knowledge, skills and development (paras 1-15)
This section of the guidance focuses on what you should do to maintain your professional knowledge, skills and performance. As well as clinical practice, the GMC says you ‘must be competent in all aspects of your work, including, where applicable, formal leadership or management roles’ (para 1).
To keep professional skills and knowledge up to date, the GMC requires you to ‘take part in systems of quality assurance and quality improvement to promote patient safety across the whole scope of your practice’, such as regular reviews and audits of your work (para 13).
Besides setting out the ingredients for effective clinical care (para 8), this section re-iterates GMC
The updated GMC rulebook addresses changes in medical practice, as well as broader social changes
guidance on remote consultations and the need to offer an alternative if it’s not possible to provide safe and effective care through a particular mode of consultation. (para 9).
DOMAIN 2 – Patients, partnership and
communication (paras 16-47)
Following the Montgomery Judgment of 2015, doctors have had a duty to discuss the material risks of treatment options with patients and support them to make an informed decision. This section looks in detail at your professional relationship with patients and how to work in partnership with them.
Much of this section echoes the content of the GMC’s current
Consent guidance from 2020, such as para 31 which says ‘you should check patients’ understanding of the information they’ve been given and do your best to make sure they have the time and support they need to make informed decisions’.
There’s also more on treating patients fairly, with kindness, courtesy and respect (paras 16-23) which emphasises the significance of communication skills, listening and being aware of body language. Para 23f, for example, refers to ‘being alert to signs of pain and distress’.
While the patient may have been referred to you about a specific problem, the GMC says your role requires you to care ‘for the whole patient’ which includes
Last month, we reported how the MDU fears doctors will be under time pressure to absorb and understand all the new GMC rules
Those in a formal leadership role, such as a practice owner/ employer, are expected to take greater responsibility
We advise independent practitioners to have a disciplinary/ grievance procedure in place and contact their medical defence body or seek advice from an employment lawyer if they have concerns about how to deal with this situation.
asking them about other treatment and guarding against the risks of polypharmacy. Para 40 says: ‘You should consider the overall impact of the patient’s treatments and whether the benefits outweigh any risk of harm’.
Finally, the GMC reiterates the responsibilities set out in its guidance on the professional duty of candour (updated 2022) and makes the important distinction that ‘apologising does not, of itself, mean that you are admitting legal liability for what’s happened’. (para 45b).
DOMAIN 3 – Colleagues, culture and safety (paras 48-80)
The previous version of GMP covered effective teamwork with colleagues, but this time, the GMC has expanded on this to incorporate workplace culture, as well as more familiar aspects like handovers and continuity of care.
The regulator has raised concerns about discrimination recently in the context of NHS workforce shortages and made specific references to it in its most recent training survey.
The GMC gives examples of how doctors can contribute to ‘a positive working and training environment’ by ‘showing respect for and sensitivity towards others’ life experience, cultures and beliefs’ (para 55) or taking action if you witness abuse, discrimination, bullying or harassment (para 58) although it recognises some might find it harder to speak up.
On the other hand, those in a formal leadership role, such as a practice owner/employer, are expected to take greater responsibility. Para 59 says that if you are made aware of this behaviour, ‘you must act’ to ensure the behaviour is adequately addressed, that people are supported and concerns are dealt with/escalated promptly.
Under the heading ‘Keeping patients safe’, the GMC says you should use the risk management structures in ‘any organisation that you work for or are contracted to’ and must help keep patients safe by contributing to processes like confidential inquiries, adverse event reporting and incident reviews.
This point is essentially repeated under para 98 which requires doctors to ‘co-operate with formal enquiries, patient safety investigations and complaints procedures’.
DOMAIN 4 – Trust and professionalism (para 81-101) The final domain covers similar territory to the current guidance (Maintaining trust), concentrating on the need to behave with integrity and avoid conflicts of interest.
Perhaps due to the increased profile of media doctors during the pandemic, the GMC has included guidance on communicating as a medical professional, including social media and instant messaging, and signposting readers to its supplementary guidance on this topic.
Finally, while doctors have always been expected to ensure they have adequate and appropriate indemnity, para 101 goes further by saying this has to cover the full scope of your practice and the level of cover should be kept under regular review.
Good Medical Practice takes effect on 30 January 2024 and although that means there’s still time to get to grips with the GMC’s new guidance, this is in the context of the enormous pressure that many doctors are under.
For our part, the MDU will be doing everything we can to clarify and explain what the new guidance means for members, but, more importantly, we’ll be there to advise and support them with GMC matters in the years ahead.
Dr Udvitha Nandasoma is head of advisory services at the Medical Defence Union
Sustainability is key to health of workforce
The connection between the health of the planet and its people is undisputed. Now we find that involvement in developing sustainability initiatives not only boosts workplace well-being and motivation, but is key to attracting the best young talent, writes Dr Robin Clark (left)
Read his explanation overleaf on page 20 ➱
By reducing the reliance on resource-intensive treatments and interventions, healthcare systems can minimise their ecological footprint and contribute to a more sustainable future
WHEN WE launched the Bupa Wellbeing Index a little over a year ago, our aim was to uncover the state of the UK’s health and wellbeing.
In that time, we’ve seen how our healthcare needs and expectations have evolved, influenced by the changing global and geo-political landscape.
However, it seems that our physical and mental health has somewhat stagnated.
The Bupa Wellbeing Index is a nationally representative sample survey of over 8,000 UK adults.* In 2022, 51% of respondents rated their physical health positively, with 14% reporting very good health and 37% saying their health was somewhat good.
In 2023, the percentage of respondents rating their physical health positively decreased to 49%, the number reporting very good physical health remained at 14% and those rating their physical health as somewhat good also remained similar at 36%.
The same pattern can be seen when it comes to mental health. In 2022, 54% of respondents rated their mental health positively, with 22% saying their mental health was very good and 32% rating it somewhat good.
Shifting towards a proactive approach and prioritising preventive care not only benefits individual well-being, but also yields significant environmental advantages
And encouragingly, an overwhelming 88% of respondents believe that their health and wellbeing is a priority for them in the future.
Key concerns causing anxiety
of respondents rating their mental health positively slightly decreased to 50%, the proportion of respondents reporting very good mental health decreased to 20%, while the percentage of those rating their mental health as somewhat good decreased to 29%
These statistics clearly show that there’s work to be done to support a healthier population.
We know that we’re still seeing the long-term impact of the pandemic on our health and wellbeing, and our focus is now on finding innovative solutions to address this.
We want to encourage people to take action, provide information about where and how they can access it and support them to stay well for
Wellbeing Index respondents reported climate change, social injustice, poverty and mental health as the significant concerns causing them anxiety. Increasing rates of poor mental health caused anxiety for 62% and increasing rates of poor physical health worried 59%.
The survey revealed that 60% of respondents are anxious about the negative impacts of climate change, while unsurprisingly 79% are anxious about the cost of living.
Younger people also feel a significant sense of responsibility for facing up to ecological issuesnearly half of Gen Z (46%) agree they feel the burden of climate change on their shoulders.
The majority of both Millennials and Gen Z (56% and 59% respectively) agree their anxiety about environmental issues will only increase in the future.
The power of
prevention
In healthcare, the importance of pioneering a more sustainable system is paramount – particularly in light of increasing pressure on the system and, as our survey reports, nearly six in ten people (59%) are currently feeling anxious about increasing rates of poor physical health.
A key focus in the months and years ahead must be on recognising the value of prevention in healthcare and its positive implications for the planet.
It’s concerning that fewer than one in ten (9%) people report making any lifestyle changes to contribute to preventive measures in the last three months.
This isn’t just the responsibility of the healthcare sector, employers have a role to play here too.
Respondents reported that initiatives associated with maintain-
ing good health would increase their motivation at work; 53% said free gym memberships, 62% said health insurance and 40% said cycle to work schemes.
Shifting towards a proactive approach and prioritising preventive care not only benefits individual well-being, but also yields significant environmental advantages.
By reducing the reliance on resource-intensive treatments and interventions, healthcare systems can minimise their ecological footprint and contribute to a more sustainable future.
People are aware of the impact that the healthcare system itself has on the environment, and over half (56%) of Wellbeing Index respondents agree the healthcare industry has a responsibility to be more sustainable.
One potential solution to explore is digital services and their role in promoting sustainability. For example, our survey reveals that in the last three months alone, nearly one in ten (9%) of people have attended a remote medical appointment.
And 9% of people – rising to 13% of 16 to 24-year-olds – have used a wearable health tracker, with many capable of remote healthcare monitoring for markers like heart rate, blood pressure and blood sugar.
This digital transformation not only enhances efficiency but also contributes to sustainability efforts. Digital services such as telemedicine and remote monitoring reduce the need to travel, resulting in decreased carbon emissions and a smaller ecological footprint.
Embracing these digital technologies enables healthcare providers to improve patient outcomes while simultaneously reducing their environmental impact.
Sustainability in workplaces
The latest Bupa Wellbeing Index findings also highlight employees’ growing expectations of being actively involved in shaping sustainable practices at work. By embracing employees’ input and buy-in, organisations can unlock the full potential of their sustainability initiatives, ensuring greater success and effectiveness.
By weaving sustainability into the fabric of their operations, organisations can cultivate a culture of shared environmental responsibility while simultaneously nurturing the health and happiness of their workforce
Organisations across the world have recognised the vital importance of sustainability in shaping a better future, supporting the health of their workforce and fulfilling their responsibilities for future generations. This should not merely be an external commitment; it starts from within.
Against the backdrop of an evolving climate crisis, the connection between individual wellbeing and a sustainable planet has become increasingly apparent.
Nearly half of employed respondents (45%) say their motivation at work would increase if they had the opportunity to contribute their sustainable and eco-friendly initiatives to leadership. This rose to 56% among Gen Z respondents.
A similar proportion (44%) say the same about having the chance to recommend sustainable and eco-friendly companies to partner with.
A strong commitment to meeting sustainability targets is also imperative when it comes to attracting new talent. Nearly half of Gen Z workers are willing to leave their jobs if their employer doesn’t demonstrate action on environmental issues.
Alongside this, nearly half (42%) express their willingness to accept a pay cut to work for a more ethical or environmentally friendly organisation.
On average, respondents are willing to accept a 19% reduction in salary to work for a more ethical or environmentally friendly organisation, rising to 23% among Gen Z and Millennials as they continue to become a larger proportion of the workforce.
Across the board, respondents are also more likely than ever to say that if their employer does not take action on social or environmental issues, it will have a negative effect on their mental health and well-being at work – 42% of all workers agree.
Conclusion
While we continue to seek optimum physical and mental wellness, exploring innovative and comprehensive approaches to prevent and treat health issues, we’re becoming increasingly aware of the strong connection between people’s health and well-being, and the health of the planet.
Sustainability has emerged as a pivotal driver of employee engagement, with many people increasingly motivated by meaningful initiatives that make a positive difference.
Involving people in shaping sustainable workplace practices can drive productivity, loyalty and, importantly, talent retention.
Indeed, despite worries about the cost of living, our latest Wellbeing Index research tells us that two-fifths of all respondents (42%) say they’d accept a job on lower pay to work for a more ethical or environmentally friendly organisation.
In recognising this link, it’s clear that organisations must prioritise sustainability to not only preserve our environment but also protect the well-being of their people.
By weaving sustainability into the fabric of their operations, organisations can cultivate a culture of shared environmental responsibility while simultaneously nurturing the health and happiness of their workforce.
This holistic approach not only fuels employee motivation and satisfaction, retention and productivity, but also contributes to the well-being of people and the planet as a whole.
Read more at: ‘Sluggishness in sustainability poses risk of brain drain for businesses’ at Bupa. com.
* Bupa commissioned Censuswide to poll a nationally representative sample of 8,002 UK adults. The data was collected between 09/06/2023 and 16/06/2023. Censuswide abides by and employs members of the Market Research Society and follows the MRS code of conduct which is based on the ESOMAR principles.
Dr Robin Clark is medical director for Bupa Global and UK Insurance
The free and integrated digital prescribing platform for all private prescribers.
CloudRx take care of the dispensing, payment and delivery of medicines direct to your patients, wherever in the country they may be, for more convenient access to their medicines.
TRANSFORMATIONAL
Order prescriptions at the touch of a button to add a whole new level of convenience for your patients.
SIMPLE, CONVENIENT AND SECURE
Simple and fast digital prescribing.
Legal paperless prescriptions, repeat prescriptions and controlled drugs.
Prescriber fees can be charged to the patient if required.
INTEGRATED
Our API enables frictionless integration with healthcare brands & clinical software including Semble, WriteUpp, MidexPRO, eClinic, Pabau and ClinicYou.
“We were struggling to keep up with the admin side of the prescriptions, not to mention storage for medication to cope with a huge increase in prescriptions. CloudRx immediately took away the strain. Since our partnership we have grown by more than 200% in size. We could not have achieved this seamless scalablity without them.”
– Dr Louise Newson, Newson Health
When and what do you tell the police
To report or not to report?
Dr Sally Old explores when you should and should not disclose patient information to the police
CONFIDENTIALITY IS one of the cornerstones of medicine – it is discussed in the Hippocratic oath and emphasised throughout a doctor’s career.
Confidentiality enables patients to trust and confide in their doctors, resulting in the best possible care. However, it is important to remember that confidentiality is not an absolute.
And there are circumstances in which you will be expected to disclose patient information to thirdparty organisations such as the police as covered by the GMC’s Confidentiality: good practice in handling patient information guidance What doctors should disclose to the police, depends on the situation that you – and the patient –find yourself in.
Road traffic accidents
Section 172 of the Road Traffic Act 1988 allows the police, under certain circumstances, to require information from doctors that may lead to the identification of a driver alleged to have committed a road traffic offence.
It is an offence to fail to comply with such a request, but you are only required to give information to enable the identification of the driver and this would not normally involve disclosure of any clinical details.
Court orders
Sometimes the police can require disclosure of information via a court order or a production order. It is wise to seek advice and to ensure the validity of the document before disclosing.
Knife and gunshot wounds
The GMC advises that a gunshot wound or injury sustained from an attack with a knife, blade or sharp instrument must be reported to the police whenever a victim arrives at hospital.
However, accidental injury from, or self-harm with, a knife or blade will not usually require notification.
Either of these scenarios might need an urgent police presence, in which case it may be appropriate to call 999.
The treating doctor will need to ensure the police are contacted, but it may be reasonable to delegate this task to another member of staff while the doctor attends to the patient.
Identifying details such as name and address should usually only be disclosed with the patient’s con-
sent. If the patient refuses, the information may only be disclosed if you consider it is in the public interest or you are required to by court order.
Female genital mutilation
Since 31 October 2015, healthcare professionals in England and Wales who ‘discover’ an act of female genital mutilation (FGM) appears to have been carried out on a child under the age of 18 have a legal duty to notify the police.
‘Discovery’ in this context arises if you are told a patient has been subjected to FGM or if you observe physical signs indicating FGM has taken place, including from surgery not for her physical or mental health nor arising from labour or childbirth.
The Home Office recommends using the 101 non-emergency police number or making a written report. Include your name, contact details, role and place of work, the child’s name, age and address, and why the report is being made.
The police should be made aware of what safeguarding procedures have been put in place and, ideally, this needs to be done by the end of the next working day.
If you are told by a third party that a girl has undergone FGM, the mandatory obligation to report does not apply. You should, however, ensure you follow local safeguarding procedures.
Counter-terrorism
Under section 38B of the Terrorism Act 2000, all doctors –indeed everyone in the UK – must tell the police if they become aware of information that they
The GMC advises that a gunshot wound or injury sustained from an attack with a knife, blade or sharp instrument must be reported to the police whenever a victim arrives at hospital
can be made either to the police or a member of His Majesty’s forces.
The reasons behind the police seeking information about a patient can often be complicated and, as such, it can be difficult to know whether to disclose information or not.
Sometimes, the police may quote data protection legislation which permits disclosure of patient information for the purposes of the detection, prevention, and prosecution of crime.
believe would help prevent a terrorist act, or secure the arrest or prosecution of someone involved in terrorism.
It is a criminal offence not to tell the police ‘as soon as is reasonably practicable’ in these circumstances and conviction could result in a fine or up to five years in prison.
In Northern Ireland, disclosure
But the law does not require it. In such instances, it is worth speaking to your medical defence organisation, which can provide further support and advice on how to proceed and whether to disclose further information.
Dr Sally Old (right) is a medico-legal adviser at the Medical Defence Union (MDU)
All doctors must tell the police if they become aware of information that they believe would help prevent a terrorist act
with a better clinic management platform
• Flexible scheduling
• Patient direct booking
• Online payments
• Pleasure to use EMR
• Accurate voice recognition
• Automated clinic notes
• Video consultations
• ePrescribing
• Deliver physical letters if preferred
• Invoice management …and much more
designed and easy to use
The Road Traffic Act 1988 allows the police to require information from doctors that may lead to the identfiication of a driver alleged to have committed a traffic offence
How do doctors see private practice?
WHAT CONSULTANTS TOLD US ABOUT SETTING UP IN PRIVATE PRACTICE
➲ Understanding how to set up with the various insurance companies and ensure you remain visible at the top of their lists is difficult to navigate.
➲ Having a good secretary with robust billing arrangements is the key.
➲ Having a good PA is essential.
➲ I set up my own website and for one to two years had zero hits, but once I signed up with Nuffield Health, AXA, Bupa etc, I get lots – too many – inquiries
➲ Was involved in a medicolegal practice for over 30 years. Setting this up was relatively easy. I had advice from colleagues.
Advice about taxation and employer regulations with regards to employer employee issues with regards to my receptionist and my secretary would have been very welcome when I started. However, the biggest issue is that there is no advice as to how to close down a medicolegal private practice.
➲ I support the NHS, always have and always will. I didn’t go into medicine for the money, which, frankly, I believe this is the core drive to private practice. I work in a deprived area; patients couldn’t afford private practice and I simply am not of the mindset to take money from my patients.
➲ The ultimate challenge to being a full time private practitioner is being good enough to attract patients to pay their hard earned money for your services.
➲ Work needs to be done to upgrade anaesthetic fees. Significant discrepancy between surgical and anaesthetic fees.
➲ Challenging getting admin support in place.
Having a good secretary with robust billing arrangement is the key
➲ A challenge at the start, but getting the hang of things.
➲ There’s a lot to learn on the finances side: tax, National Insurance, PAYE, the pros and cons of different business structures – sole trade vs limited company.
➲ Difficulties in using my own equipment in a private hospital.
➲ Pharmaceutical medicine is very established as a private speciality. I am exploring expanding my practice to the far east.
➲ I was supported by my NHS trust who have a private practice setup alongside the NHS trust. Therefore, from setting up to advertising was all done by my trust and my private secretary. They even found me a very efficient secretary who helped with initial paperless service.
➲ Would encourage consultants to have their own professional website which is not too ‘corporate’ but tell potential patients about you and your practice.
➲ Conflict of interest by those attempting to practise in private sector and simultaneously working in NHS sector is concerning.
➱ continued on page 26
➲ Difficulties accessing private prescriptions has been major headache. I work in a deprived area; patients couldn’t afford private practice and I simply am not of the mindset to take money from my patients
3. What is the likelihood of you growing your private practice over the next five years?
4. Do you still, or intend to, undertake work for the NHS alongside your private practice work?
5. What was/is your motivation for working in private practice? Tick all that apply
There’s a lot to learn on the finances side: tax, National Insurance, PAYE, the pros and cons of different business structures – sole trade vs limited company
The ultimate challenge to being a full-time private practitioner is being good enough to attract patients to pay their hard-earned money for your services
6. What do you feel are the challenges of becoming a private practitioner? Tick all that apply
Navigating the CQC regulating requirements (England only)
8. What aspects of setting up in private practice would you like to learn more about? Tick
Marketing your practice Professional / corporate indemnity
How to establish a private practice and ensure it stands out from the crowd corporateProfessional/indemnityMarketingyourpracticeEstablishingaprivatepracticewhile maintainingNHSworkHowtoestablishaprivate practice&makesureitstandsout ComplyingwithCQCrequirementsComplyingwithdata protectionobligationsincludingFinancialplanning,tax,NIandPAYE
Establishing a private practice while maintaining existing NHS commitments
Complying with CQC requirements
Complying with data protection obligations
Financial planning, including tax, National Insurance and PAYE
The conflict of interest by those attempting to practice in private sector and simultaneously working in NHS sector is concerning
Errors can harm you as much as a patient
Dr Clare Stapleton (right) discusses the steps you can take to protect yourself against complaints in your private practice
THERE ARE times in a doctor’s career – no matter how competent or experienced you are – when things do not go according to plan or a patient will be in some way dissatisfied with the treatment they receive.
Handling these events effectively can make the difference between a swiftly resolved concern with a good ongoing doctorpatient relationship and the issue escalating into a claim or regulatory investigation.
Complaints, complications and critical incidents can have a significant impact on well-being. This can often be overlooked by doctors and their colleagues.
There are resources available that offer support for doctors facing difficulty, including the Practitioner Health Programme, and our organisation also offers a confidential, independent counselling service as a benefit of membership.
If you or a colleague have been involved in any case with a negative outcome, please do consider the health implications and the support available.
Complaints
The risk of a complaint from a patient exists in the private sector as much as in your NHS practice. However, in private practice a complaint is more likely to come to you directly and you may not have access to the same level of support when responding.
A complaint may not always come in the form of a conventional letter. It is a common error to assume that a complaint made verbally to a colleague or a negative comment on social media, for example, deserves less attention. Any negative description of the treatment a patient has received is a complaint and should be managed as such. We assist many private practitioners with guidance on responding to a complaint to improve the likelihood of a swift and satisfactory resolution and help to maintain your reputation. Our guidance is based on ten key complaints-handling principles –see box above.
It can be difficult for any doctor not to take a complaint personally and this can allow the complaint to adversely affect the doctorpatient relationship.
TEN KEY COMPLAINTSHANDLING PRINCIPLES
1 Be timely
2. Acknowledge the complainant’s concerns
3. Offer an apology, where appropriate
4 Be open
5 Avoid being defensive
6 Reflect on the issues raised
7 Explain, when appropriate, what action will be taken to prevent a recurrence
8 Obtain independent oversight wherever possible
9 Offer a meeting to discuss the concerns
10 Take advice from your medical defence organisation (MDO)
Paragraph 61 of the current Good Medical Practice 2013 states: ‘You must respond promptly, fully and honestly to complaints and apologise, when appropriate. You must not allow a patient’s complaint to adversely affect the care or treatment you provide or arrange.’
While it may be appropriate to offer a second opinion or an alternative clinician in some cases, caution should be exercised before ending a professional relationship with a patient while a complaint is unresolved, unless this is requested by the patient.
It is not uncommon for a third party to complain on a patient’s behalf; for example, a family member. Before responding, it is important to establish that you have appropriate consent in place to avoid the risk of breaching your duty of confidentiality.
Negligence threat
Complainants can use legal terminology such as ‘negligence’ within their correspondence. Fear of litigation may naturally add to the anxiety caused by receiving a complaint.
The use of the word negligence does not necessarily mean that a claim is inevitable; however, it is important to distinguish a clinical negligence claim from a complaint.
There are some indications that a complainant may be considering making a claim, such as a request for their medical records. This request can come from the patient, a representative or a solicitor.
If you are concerned that any
It is a common error to assume that a complaint made verbally to a colleague or a negative comment on social media, for example, deserves less attention
As soon as the clinician is aware that a complication has occurred, it should be discussed openly and honestly with the patient and an apology offered for the fact that it has happened.
An apology is not an admission of liability but a human response that demonstrates empathy toward the patient. This stance can go a long way towards avoiding a complaint or claim.
The GMC has separate guidance on a professional duty of candour, which gives practical advice and explains in more detail a doctor’s obligation to a patient when things go wrong.
Learning opportunity
complaint or incident may result in a claim, then it would be wise to inform your MDO or insurer at an early stage. This is important, as there are strict time limits in which a claim must be acknowledged.
All complaints should be discussed in your appraisal irrespective of whether they arise from your NHS or private practice.
Evidence of reflection on a complaint can certainly improve your position in the unfortunate event that a complaint is escalated by the private provider, your NHS employer or the GMC.
Complications
Complications can arise even from appropriately conducted surgery or medical treatment and can be stressful for the patient and the doctor involved.
The consenting process should include a discussion of all known complications or side-effects of material importance to the patient.
However, even if the complication was discussed pre-operatively, this does not alter the fact that there has been an unwanted outcome. The GMC makes clear a doctor’s obligation in Good Medical Practice paragraph 55:
‘You must be open and honest with patients if things go wrong. If a patient under your care has suffered harm or distress, you should:
A. Put matters right – if that is possible;
B. Offer an apology; C. Explain fully and promptly what has happened and the likely short-term and long-term effects.’
There may be a learning from any complication that has the potential to change your practice and that of your colleagues. System errors and human factors can contribute to any complication as much as the actual conduct of surgery or treatment.
It is wise to consider whether a complication that has occurred meets the threshold for reporting on the private provider’s incident reporting system. Doing so offers the opportunity for learning. It also demonstrates a doctor’s openness and willingness to learn from such incidents.
Failure to do so may risk criticism for not complying with professional or contractual obligations.
If you are not sure whether a complication requires reporting, it would be wise to seek advice from a senior colleague or the patient safety team.
Complications in the private sector and your reflections on them should be discussed in your appraisal, regardless of whether your Responsible Officer is in the NHS or a private organisation.
Complaints and complications can arise for any doctor at any stage of their career. Appropriate action and a considered response can limit the potential for an adverse impact on a doctor’s professional welfare.
It is wise to seek advice from your defence body early and be mindful of your own health during the process.
Dr Clare Stapleton is a medico-legal consultant at Medical Protection
BILLING AND COLLECTION
Avoid those Groundhog Day blues when doing your billing
There are many ways to lose money or suffer from poor cash flow – which is why I continue to have the same “groundhog day” conversations with practices who are struggling
The repetitive nature of the problems private practices experience with their medical billing are revealed by Simon Brignall (below)
THE 1993 film Groundhog Day, starring Bill Murray, depicts Phil Connors as a cynical TV weatherman who visits Punxsutawney in Pennsylvania, US, to cover the annual groundhog festivities.
In the story, he repeats the same day over and over until he learns from the error of his ways.
As director of business development at Civica Medical Billing and Collection for ten years, I’ve had the opportunity to meet hundreds of consultants in private practice and so I’ve been exposed to a wide range of their billing and collection challenges.
Hopefully, my experiences of encountering consultants’ problems means I can pass on what I have learned without you needing to repeat them yourself and experiencing your own groundhog day.
My background is in finance, so when I first started hearing the problems practices were facing, I was constantly surprised at what I came across – and it was soon apparent that these were not isolated cases.
Let me share some of the recurring challenges and, importantly, how you can take steps to mitigate them. As these issues cover a wide range of topics, I will discuss more next month in part two of this article.
Pricing
One of the first things that struck me when I started to meet with consultants was how many of them did not know their fee structure or specific billing arrangements for the range of patient types the practice treated.
This is not surprising when you appreciate how busy most consultants are, quite often running both an NHS and private practice and managing all the demands this entails. In many cases, this means they rely on their secretary for this information.
One common problem is that this data is not always available in a simple format for anyone involved with the practice billing to refer to if required.
A good example is that I still come across practices applying Bupa procedure fees across the full range of their insured patients. Insurance company fees can vary by as much as 100% for the same procedure, so they have often lost out on thousands of pounds.
Fees for consultations and proce-
dures often vary between each private medical insurer and so making sure the correct fee is used when billing is key.
Some insurance companies allow for an extended consultation to be billed at a different rate in specific circumstances.
It is also important to make sure your practice keeps up to date with the changes in Clinical Coding and Schedule Development group (CCSD) codes for your specialty and the approach each insurer has taken to these changes.
These are updated monthly and changes can include:
Rules on which codes can be billed together and those which cannot – commonly referred to as ‘unbundling’;
The narrative against a specific code;
Replacement codes;
Discontinued codes;
New codes.
Most insurers publish a price list detailing what they will pay for each CCSD code. As these vary greatly, you should always check you are billing to the correct tariff.
I have also come across consultants with issues about overbilling the insurers.
This has meant they were either subject to clawbacks, have seen a reduction in the number of patient referrals and, in some extreme cases, have been derecognised by the insurer.
Key person dependency
Key person dependency risk is when one of your employees is solely responsible for something and there is no back-up plan. This means that the subsequent loss of this key individual can have a big impact on your business.
For most practices, the practice manager/medical secretary is the person who manages all the administration.
To expect one person to manage all aspects of the patient’s journey as well as all the billing and collection work is not sustainable, especially as the practice grows. For many busy practices, the first thing to suffer perversely is its finances as patient issues take priority.
Remember, as the practice expands, so does the risk associated with this key individual.
The pandemic highlighted this for many practices, with long-term
secretaries choosing to either retire or reduce their working hours.
Often practices are impacted by maternity leave or absenteeism, which means less experienced staff are brought in and often aren’t up to the task.
Medical secretary
I have many conversations with consultants where the medical secretary who had been with them for many years retires or leaves and all the knowledge around their billing and collection is lost.
There may even have been a handover with the new replacement secretary, but as the practice has then had a series of secretaries, often through no fault of their own, this information is mislaid or is no longer reliable.
This degradation in expertise around the nuances of a practice can cause a downward spiral to its finances and can often coincide with a deterioration in the service quality the patient experiences.
The simplest and most effective way of resolving this issue is to split the billing task from the patient engagement and other practice administration. By outsourcing to a medical billing company, you not only gain functionality and expertise in this key area, but it also means your secretary is able to keep their relationship with the patient focused on their clinical needs free from having to broach those challenging conversations about money.
Invoicing delays
Obviously, it is extremely important to see your work is invoiced in a timely manner. By keeping on top of the invoicing process, this will ensure you have consistent cash flow and you keep debts to a minimum.
There is also the additional benefit that any billing issues are picked up more quickly, which increases the likelihood they can be resolved swiftly. Remember, delays in raising invoices reflects poorly on the professionalism of your practice.
As the raising of an invoice is the first step in the billing process, adherence to this simple rule results in benefits across the whole invoicing and chasing process. I meet with many practices where this is not happening and
they often cite a range of reasons. Here are just a few:
The consultant has responsibility for the billing but no longer has the time due to an increase in the practice size or additional workload;
The practice has fallen behind on its billing and chasing and is now daunted by the size of the problem and is unsure how to tackle it;
Issues related to electronic billing.
There is an increased pressure on consultants due to the adoption of time limits by some insurers. If this is exceeded, it means the invoice is invalid and won’t be paid.
With overseas self-pay patients, it is often preferable to collect payment before treatment or at the very least to have chased for this income before the patient returns home. Once they are abroad, it can be a problem to collect the money. We collect money up front for most of our practices who see overseas patients.
There can also be a requirement to raise and collect payment up front for UK-based self-pay patients for a range of specialties. We collect payments up front for the procedures for all the plastic surgeons that we partner with, as well as for other specialties with large up-front costs, such as clinics and consultants who work in the fertility field.
Summary
As you can see, there are many ways to lose money or suffer from poor cash flow – which is why I continue to have the same ‘groundhog day’ conversations with practices who are struggling.
Next month, I will discuss problems consultants encounter with electronic billing, reconciling and chasing payments and ensuring they have adequate infrastructure. What I would strongly recommend, meanwhile, if you feel your practice is weak in any area I have outlined or that some of the points I have raised struck a chord, then one of the simplest and most effective solutions is to outsource this vital element to a medical billing and collection company.
Simon Brignall is director of business development at Civica Medical Billing and Collection
COMPLAINTS IN THE PRIVATE SECTOR
Cut down on complaints by managing expectations
The Independent Sector Complaints Adjudication Service continues to see an increase in consultant complaints. Its director Sally Taber (right) sets out what it is doing to try and reverse the trend
SOME THREE years ago, Independent Practitioner Today published an article alerting readers that, of all complaints coming to Independent Sector Complaints Adjudication Service (ISCAS), the highest number were about consultants and medical care.
ISCAS, responding to consultants’ need for guidance, analysed information from decided adjudications into seven sections broken down under the headings of:
Consent;
Managing expectations;
Information and advice about procedures;
Record-keeping and documentation;
Communication;
Apologies;
Information about fees.
It then communicated to all its subscribers with suggestions for how their consultants could better relate to patients.
Now, latest data to the end of August 2023 shows that the same problems are still recurring and the number of complaints directed towards consultants is not diminishing.
Independent Practitioner Today is, naturally, asking what subscribers are doing to oversee their consultants’ interaction with patients to reduce this unsatisfactory record.
Two causes are thought to underly the problem:
1
Unrealistic expectations as to outcomes on the part of patients: patients thinking that if they pay, it will always work. Forty-eight per cent of such complaints were not upheld; some more were only partially upheld.
The learning is that, in what may be intense and fast-changing circumstances for the patient, they must be given the best possible prediction of expected outcomes, and this must be recorded.
2
Consultants’ sometimes poor administration of their interface with patients has been further highlighted.
An example of poor practice was consultants not following consultations with a clinical letter, which is required in regulations and a breach of which should raise consequences for continued practising privileges.
In order to help improve the
understanding and guidance to consultants, ISCAS highlights these requirements:
➤ Provide patients with written information about the amount being charged, the associated method of payment prior to outpatient consultations and the commencement of the services.
➤ Be transparent about the costs of any proposed care or treatment.
➤ Explain to patients the reason for any proposed tests or investigations and provide details of any associated costs prior to them being carried out.
➤ Advise patients to check the terms of any insurance policies, where relevant, to enable them to determine their level of cover regarding any proposed tests investigations or procedures;
➤ Where alternative treatments are available but the appropriate treatment can only be identified during surgery, consultants should provide a written estimate
In what may be intense and fastchanging circumstances for the patient, they must be given the best possible prediction of expected outcomes, and this must be recorded
of costs testing out relevant options and associated fees.
ISCAS now invites providers to review how they highlight the learnings to all clinicians and their administrative staff and so help to improve patient satisfaction with their treatment.
To assist with this, we recently prepared four training videos which are relevant and available to both clinicians and their supporting administrative staff.
These are:
General Complaint Handling Principles Under the ISCAS Code
Stage 1: Managing Complaints Under the ISCAS Code Stage 2: Managing Complaints Under the ISCAS Code Stage 3: Managing Complaints Under the ISCAS Code
The series is available from the ISCAS website https://iscas.cedr. com.
The ISCAS Code for Complaints Management, January 2022, cov-
ers complaints about doctors and other healthcare professional staff working in subscribing organisations, even if not directly employed by the organisation but have been provided with practising privileges.
As previously stated, issues identified in complaints about consultants, doctors or medical care include consent, managing expectations, information and advice about procedures, record-keeping and documentation, communication and apologies.
The ISCAS Advisory Board will continue to discuss these issues, with the subscribers’ complaints lead personnel present. The board also always has an adjudicator present to further expand on these issues.
➥ Link to ISCAS videos: https:// www.youtube.com/watch?v=Vi8W1G1gfk
➥ Link ISCAS Code: https://iscas. cedr.com/
BOOK YOUR DEMO Are you happy with your current
software?
Maybe you're completely happy with the software you use to run your practice. Perhaps you have everything in one place, routine tasks are automated, and reporting is accurate and insightful. If so, stop reading now.
However, if you think the day to day running of your practice could be improved, we'd love the chance to demonstrate e-clinic to you.
The number one choice for private practice
Future-proof your practice and offer everything a modern patient expects:
> iPad compatibility
> Online booking & payments with fully integrated card processing
> Electronic consent & treatment forms
> Integrated drugs database & digital prescribing with direct delivery
> Fast & easy patient communications by email or text
Drifting into a contract
contract is perilous
Some key points you should consider when entering a contract are outlined here by Justin Cumberlege, (right) a partner at specialist healthcare legal firm Hempsons
EVERY DAY, we enter into contracts without really knowing about it. For example, when you buy something at a shop, you are entering into a contract to buy the goods.
There are no written terms of that contract – you see what you buy. However, there is now consumer protection legislation which, in effect, imposes written terms on the seller, such as that the goods are fit for purpose.
Those laws do not apply to business-to-business transactions and most contracts in business are more complex, particularly if they involve the provision of services.
So it is important that you are fully aware of when you are entering into a contract and that you are certain of the terms of that contract.
That is why any contract of consequence must be in writing, carefully considered and reviewed before signing.
Here are some areas to consider when entering into a contract.
STANDARD CONTRACTS
It is not unusual for standard terms for a contract to be offered for you to accept. Unlike a consumer, there is little protection for businesses if they enter into an ‘unfair’ contract.
There have been cases where businesses have successfully challenged a contract term because it was particularly unfair and unusual and the party imposing the term was able to use an unfair advantage to impose it and it had also not been flagged up by them.
In addition, if the consequence of a breach is a penalty, such as a payment which is disproportionate to the actual loss, then it may be unenforceable.
However, you should not depend on such a ruling being in your favour and, more importantly, you do not want to find yourself spending the time, costs and resources in litigation.
So, before signing, ensure you fully understand the terms, and you are prepared to accept the terms.
Do not assume that because they are ‘standard’ they are acceptable and fair.
➱ continued on page 36
TERMINATION PROVISIONS
You will, no doubt, agree the commencement date of the contract, but ensure you also check the termination provisions.
If the terms state you must give one month’s notice to terminate the contract, then your worst-case scenario is that you will have to comply with the contract for a month.
But keep in mind that the contracting party has the same right and you should consider whether you would have the ability to find an alternative contractor in such a short time.
Many ‘standard’ terms require long notice periods to terminate, and sometimes come with a catch.
They need to be read carefully. One such example is a contract which had a notice period of 12 months and two days, and the termination date had to be the anniversary date of the commencement of the contract.
By the time we were asked to terminate the contract a year before the termination date for a client, given the notice period of an extra two days and a deemed service period of two days, our client was too late, and had to wait another 12 months before they could terminate.
In addition, many contracts require an initial contractual period which could be several years.
PAYMENT PROVISIONS
You are probably going to be looking at the payment provisions carefully.
You need to check that elsewhere in the contract there are no further provisions regarding, for example, the increase in payments.
Sometimes it is linked to an index and the index may have nothing to do with the actual increases in costs for the provider, but could be at an advantageous rate for the provider.
For example, the retail prices index (RPI) is higher than the consumer prices index (CPI) .
You should also check what interest and other implications are if payments are late.
Many ‘standard’ terms require long notice periods to terminate, and sometimes come with a catch
RESOLUTION OF DISPUTES
Another often overlooked provision is the resolution of disputes. An escalation procedure is useful and needs to be set out in the contract to be a requirement.
The procedure helps the parties agree to seek a resolution of the dispute in a quicker, cheaper and less disruptive manner than going to court – although even the courts expect parties to attempt to settle disputes through mediation first.
To begin with, there may be a requirement for negotiations to take place between the chief executives of each party and then perhaps with a facilitator from a named organisation or professional body. Failing that, you may state that mediation must be attempted before going to arbitration or court.
You may specify that some disputed matters should be referred for an expert determination. Experts are particularly useful if the matter in dispute is well defined, such as remuneration being determined on a formula if certain key performance indicators (KPIs) are met.
An expert will require all the
information to be disclosed to them and then they will determine if, in this example, the KPIs have been met and, as a result, the sum to be paid.
Obtaining that determination should be significantly cheaper than going to court to prove that you were being overcharged or even to find out that, in fact, the charge was correct.
If you were wrong, you are likely to pay not only your own court costs, but those of the counterparty. Also, once you start court or arbitration proceedings, the relationship is likely to irredeemably damaged, so you will also need to find another contractor, if you can terminate the current contract.
It is also worth considering whether to state that disputes will ultimately be determined by arbitration, as opposed by the courtafter an attempt to mediate. This would help to avoid the unpredictability of going to court and not knowing the background, experience and expertise of the judge who will hear the case.
Being able to agree on an arbitrator, perhaps with some expertise in healthcare issues, is a great advantage.
You are able to agree the date when the arbitration will be heard.
An arbitration is also private, so the risk of your reputation being damaged by allegations made in the proceedings being reported is avoided. These factors go a long way in justifying likely slightly greater costs than going to court.
CONDUCT AND PRACTICE
Drifting into a contract can be dangerous and an easy cause of a dispute.
One example of this is asking a supplier to provide a service once and then, seeing that it is good, asking them to provide the service again on several occasions. In this situation you have never had written terms, and the terms of the contract have arisen by this custom and practice.
Consider what happens if they change the service without consulting you. For example, a supplier has always collected specimens on the day and provided test results within three days.
However, on one occasion they do not come and collect the specimen until a day later, and as you do not have the facilities to store the specimen, you have to repeat the test.
Who pays for this additional work? In addition, on this occasion, the supplier provides the results eight days later, so you have to postpone the appointment with the patient.
This causes the patient further distress and additional work for you in moving appointments around.
Even if the delay does not lead to a negligence action, you would like the provider to pay for your additional costs for failing to perform to the contract within the ‘usual’ time.
However, this would mean having to demonstrate that there was an express agreement that they would always collect the specimens on the day of the request and provide the results within three days.
It is very difficult to state that such a term is agreed without having it as a written performance requirement. The supplier would defend such a claim by saying though they may have done that in the past, there was no obligation to respond in that time period.
Therefore, there is no breach of contract and they have no liability for having failed to do so on a particular occasion.
If you have important contracts relying on custom and practice, ensure that they are written down and agreed upon while the relationship is strong and before anything goes wrong.
EMPLOYMENT CONTRACTS
Perhaps the most common business contracts are employment contracts. Section 1 of the Employment Rights Act 1996 requires that certain information is given to an employee before the commencement of their employment.
Some terms may be the same for all your employees, such as sickness leave, pensions or training, and these may be in a staff handbook, together with some other terms not required by Section 1.
It is essential, though, that employment contracts are specific to each employee and contain all the terms which you have agreed on during negotiations, including any requirement that the employee may have to work elsewhere in the future or must attend the premises a certain number of days a week.
Employment tribunals invariably put the onus on the employer to prove their position in the event of a dispute.
INTELLECTUAL PROPERTY RIGHTS
You may have intellectual property rights which you share under the contract. You should ensure those rights are not infringed by the contractor or used elsewhere without you being rewarded. It is important that you grant a licence for the use of the intellectual property rights, setting out
precisely the terms on which they may be used. Even if the intention is that they are used only for your contract, without an express agreement, they may be used elsewhere or even the contractor claims them.
SIGNING THE CONTRACT
When it comes to signing the contract, first check that the other party exists. The contract may state a trading name or the name of a particular department of the contractor, but these are not legal entities and so, if you have a dispute, your initial issue will be proving who your contract is with. You also need to ensure that those signing the contract have got the appropriate authority to sign on behalf of the party, such as a director of the company, whose name you can check at Companies House, or a partner in the firm.
When it comes to signing the contract, first check that the other party exists
TRUST
Contracts are the lifeblood of all businesses, and while businesses should be built on relationships of trust, it depends on others performing at a certain level. If that level is not properly recorded, losses and disputes may arise later. With a written contract, those requirements can be properly negotiated and understood by all. Without a written contract, you may find you are unable to recover the losses and damages which you have incurred as a result.
Advice relating to contracts can be obtained from Hempsons’ commercial healthcare team.
Disclaimer: This article states the position in general terms and does not constitute legal advice. The detail of the legislation or the situation may change the interpretation, and therefore before taking any action, legal advice must be obtained first. No liability is accepted for anyone relying on the contents of this article.
Free legal advice for Independent Practitioner Today readers
Independent Practitioner Today has joined forces with leading healthcare lawyers Hempsons to offer readers a free legal advice service.
We aim to help you navigate the ever more complex legal and regulatory issues involved in running and developing your private practice – and your lives.
Hempsons’ specialist lawyers have a long track-record of advising doctors – and an unrivalled understanding of the healthcare system as a whole.
Call Hempsons on 020 7839 0278 between 9am and 5pm Monday to Friday for your ten minutes of free legal advice.
Advice is available on:
Business structures (including partnerships)
Commercial contracts
Disputes and litigation
HR/employment
Premises
Regulatory requirements and investigations
New retirement option available
Are you considering taking partial retirement? George Uglow (below) looks at the key points of the new NHS retirement flexibilities
FOLLOWING THE consultation earlier this year, some significant changes are being introduced to the retirement options for NHS staff, with the aim of retaining skilled and senior members of the workforce.
‘Retire and Rejoin’ was introduced in April 2023, which allowed doctors to retire, draw their NHS pension benefits and then rejoin the 2015 scheme to accrue further benefits if they planned to continue to work.
This strategy means members of the 1995 pension scheme can enjoy the same facility as those in 2008 section and 2015 scheme.
In contrast, if 1995 benefits were drawn under the ‘Retire and Return’ scheme, you were previously unable to accrue any further NHS pension benefits.
‘Retire and Rejoin’ still requires a short break before returning to employment, but the changes have removed the rule which meant that when returning to work, doctors could not work more than 16 hours per week in the first month after retirement.
Partial retirement
From 1 October, the scheme took this one step further and introduced partial retirement.
This will enable members of the 1995 section of the NHS Pension Scheme to access their pension benefits, continue to work with -
out a break in service and, importantly, continue to accrue benefits within the 2015 section.
This option is already available for those within the 2008 and 2015 sections, but, from this autumn, it will also apply to any 1995 section benefits.
If you are an active member, aged 55 and above, you can choose to take between 20% and 100% of your pension benefits in one or two payments – without having to leave work. However, the main caveat to this is that you must reduce your pensionable pay by at least 10% in the 12 months after drawing 1995 benefits.
In terms of facilitating this reduction, this will need careful planning and discussions with your relevant HR team. These changes are in the process of being implemented, so we have not yet seen a standardised approach across all NHS trusts at the time of writing.
Looking to apply?
NHS Employers has confirmed the criteria needed to be eligible for partial retirement.
A member must:
Have reached their minimum pension age;
Be an active member of the scheme;
Reduce their actual pensionable pay by at least 10 %;
Have a change in their terms and conditions of employment to reflect a reduction in pensionable pay. Other terms remain the same;
Have had the previous level of pensionable pay prior to partial retirement for at least 12 months;
Expect the new level of pensionable pay to last at least 12 months from the point partial retirement is taken;
Not have already claimed partial retirement on two occasions.
Application process
Those applying for partial retirement will need to complete the usual AW8 form, alongside a new supplementary form to accompany their standard retirement application.
It will confirm the arrangements agreed with your employer – how you will reduce pensionable pay –and the percentage of pension you wish to take.
This form has only recently been
Partial retirement will offer substantial opportunities for many senior NHS professionals, particularly in terms of accessing their lump sum payment
published, but NHS Pensions has stated that applications will be managed swiftly, with applications being backdated to 1 October if necessary.
Also available from 1 October is a new online ‘Partial Retirement Calculator’.
This calculator will enable employers and employees to assess how taking different percentages of the pension under partial retirement affects the amount of pension received overall.
Suitability
Partial retirement will offer substantial opportunities for many senior NHS professionals, particularly in terms of accessing their lump sum payment and even more so with the changes to the pension tax lifetime allowance following the March budget.
However, as with all financial matters, it is vital to understand your individual position and how accessing the pension – if at all –can affect this.
If you are working with a financial planner, it is important to discuss this in detail to ensure that any action is suitable and considers your overall financial position.
Some important things to assess when considering partial retirement are deciding what percentage of your pension to take at partial retirement, as this could affect:
1. Your tax position;
2. What order to crystallise benefits – if you have personal pensions outside of the NHS scheme; 3. The impact on future benefit accrual.
You may also need to assess the impact of the ‘McCloud remedy’ on your pension benefits. A new online ‘McCloud Percentage Tool’
was launched in August to allow those affected by the McCloud remedy to see the optimum percentage of pension to take.
Lump sum
Those who do decide to access their 1995 section pension benefits will also be in receipt of a lump sum.
A decision will need to be made with regards to whether you would like to access standard benefits or maximum, which entitles you to a greater lump sum.
Members without any lifetime allowance protection will be able to access 25% of their pension benefits in a tax-free payment – up to a maximum of £268,275.
Those who hold protection schemes, such as Fixed, Individual, Enhanced or Primary, may be entitled to a larger sum.
Upon receipt of the lump sum, there are, of course, many options. You may have long-held plans of how to use this cash; whether that is spending it, paying down debt, investing it for future growth or helping loved ones.
Whatever the ideas, it is important that this is discussed in detail with your adviser.
The lump sum presents a great opportunity, but there can also be some issues to consider when thinking about your broader planning objectives, such as tax and long-term sustainability.
Make sure you have experts on hand to help you navigate the path ahead. After decades of service to the NHS, you deserve to enjoy your retirement, however you choose to spend it.
George Uglow is a chartered financial planner with Cavendish Medical, specialist financial planners helping consultants in private practice and the NHS.
The content of this article is for information only and must not be considered as financial advice. Cavendish Medical always recommends that you seek independent financial advice before making any financial decisions.
Levels, bases of and reliefs from taxation may be subject to change and their value depends on the individual circumstances of the investor. The value of investments and the income from them can fluctuate and investors may get back less than the amount invested.
Dr Kathryn Leask explains what information this doctor should disclose to the coroner following a difficult situation arising from a patient’s death
Dilemma 1 Should I let the coroner know?
QI am a private consultant psychiatrist and have been asked by the coroner to provide a report following the death of a patient.
The patient’s family believe the person took their own life. However, a friend is disputing this and is raising concerns about relationships within the family.
I do have information in the patient’s records about family members, which is likely to be relevant to the coroner but upsetting to those family members concerned. Is it appropriate for me to disclose this in my report?
AYour report is likely to be made available to others who have an interest in the
Data that may upset a family
inquest, including the patient’s family, and could be read out in the coroner’s court.
When writing a report for the coroner, the expectation is that this will contain relevant information about the deceased rather than other third parties.
It is important to co-operate with the coronial process and provide the coroner with any information relevant to the patient’s death. However, you must also consider your duty of confidentiality.
Where you believe information
about another living individual is relevant to the coroner’s inquest, a separate report can be prepared and provided to the coroner highlighting that it contains confidential information about a third party, and you are concerned about it being disclosed at the inquest and the harm or upset this could cause.
This allows the coroner to have the information they need to inform their investigation in addition to allowing them to decide whether any of the information
you have provided should be disclosed at the inquest. It is important to keep a copy of your reports and a copy of any correspondence you have with the coroner so that you can justify your decision making at a later date, if asked.
Dr Kathryn Leask (right) is a medico-legal adviser at the Medical Defence Union (MDU)
Am I covered for Good Samaritan acts?
Your obligations to assist during an outof-hours medical emergency are discussed by Dr Kathryn Leask following an inquiry from a private doctor who provided a ‘Good Samaritan’ act outside her practice
Dilemma 2
What is my duty to provide care?
QI am a private dermatologist working in a building with other healthcare professionals with varying roles, such as physiotherapists and nurses.
Recently, a member of the public came into the building asking for help, as someone was having a seizure on the footpath outside. As I was available, having just finished my clinic and on my way home, I went to help. But a colleague has told me that because the person wasn’t within the building or the grounds and as I had finished for the day, this was a ‘Good Samaritan’ act and I wasn’t legally obliged to assist.
He said he wouldn’t have helped out for fear of litigation if something went wrong.
So I’d like to know what my obligations are so that I am prepared if I find myself in this situation again.
AT he GMC says you must offer help in emergencies whether they arise in a clinical setting or in the community (paragraph 26 of Good Medical Practice).
Although there is no legal obligation in the UK to do so, there is a professional ethical obligation, and a doctor could be criticised if they did not help in an emergency.
You should take into account your own safety and your competence. There may be other people available to assist who are better placed to offer care due to their specific skills and knowledge.
Do make clear the limits of your competence and not act outside them. It is important to keep your skills up to date, such as basic first aid and life support training so that you have the confidence to offer some assistance in the event of a clinical incident while awaiting emergency services.
A Good Samaritan act is one where a doctor or other healthcare professional provides help during an emergency when they’re not on duty.
You need to make sure that you have adequate indemnity in place to cover you for Good Samaritan acts worldwide.
In some European countries, there is a legal obligation to assist in an emergency, as well as your ethical obligation as a doctor.
The risk to doctors being sued after helping in an emergency is very low. Additionally, the Social Action, Responsibility and Heroism Act 2015 provides protection to those acting in an emergency in England and Wales from legal action.
If it is possible, you should obtain consent from the patient as you would during your professional practice and explain your actions and treatment to them. You should also make a detailed record of the incident and your involvement.
SPEAKING UP FOR PATIENT SAFETY
Make it easier for staff to be heard
Creating a speaking-up culture is not easy, but it is essential for patient safety, quality of care and the well-being of staff, says the Independent Healthcare Providers Network’s Dawn Hodgkins (right)
ONE OF the most notable and consistent themes in any significant patient safety failure is that in nearly all cases there were warning signs or concerns.
But, for whatever reason, people who could and perhaps should have raised those concerns didn’t, meaning that issues remained unresolved.
To avoid repeating these failures, providers across the entire healthcare system need to pay attention to and implement the learning from these reports, including the importance of creating a speakingup culture.
In recent years, one of the very welcome developments we have seen has been the introduction and embedding of Freedom To Speak Up (FTSU) guardians.
FTSU guardians support workers to speak up when they feel that they are unable to do so by other ways. They ensure that people who speak up are thanked, that the issues they raise are responded to and make sure that the person speaking up receives feedback on the actions taken.
Independent of management
Guardians also work proactively to support their organisation to tackle barriers to speaking up and, crucially, they are independent from any organisation’s management structure, meaning that they should be able to ‘hold a mirror up’, often supporting anonymous colleagues who have flagged concerns in this way.
There are now more than 1,000 guardians in NHS primary and secondary care and independent sector organisations, national bodies and elsewhere who ensure workers can speak up about anything which has an impact on their ability to do their job or that affects care for patients.
All organisations that provide services under the NHS Standard Contract are required to appoint one or more Freedom To Speak Up Guardians to fulfil the role set out in and otherwise comply with the requirements of National Guardian’s Office Guidance.
This includes, but is not limited to, NHS trusts and private hospitals that provide services to the NHS. However, any organisation can appoint a guardian.
Recent data from the National
Guardian showed a record 25,382 cases raised last year (1 April 2022 to 31 March 2023) – that’s a 25% increase from 2021-22.
Inappropriate attitudes and behaviours
There are some interesting observations to make about the types of cases which are being raised.
While there is a significant number which are related to patient safety and quality specifically (just under 20%), far more cases are being brought forward around bullying or harassment (22%), and in a new category ‘inappropriate attitudes and behaviours’.
This new category has been introduced to broaden the understanding of behavioural cases that do not fall within the bullying or harassment category and it represents 30% – so that’s nearly a third of all cases being raised.
The kinds of behaviours include things like disrespectful attitudes, lack of compassion, micro-aggressions, micromanagement, gossiping, aggressive communication styles, rudeness and unprofessional behaviour; in person and over digital communications.
FTSU guardians also reported initiatives that have been launched to address the issue, such as cultural reviews, civility saves lives training, behaviour charters and the introduction of kindness and respect champions within teams, but it is clear this is a significant issue which will need continued attention.
Sector under-representation
In fact, the latest survey found that independent providers make up 21% of organisations, with 24% of guardians, but are only reporting 3% of cases.
Conversely, NHS trusts, where admittedly this has been introduced for longer, make up 34% of organisations and 39% of guardians, but account for 92% of all cases!
It could be – and I very much hope this is the case – that this is because in some respects the culture in the independent sector is good. I know that many organisations have worked really hard on developing a culture of respect and civility within their teams.
It may also be a factor that the elective services environment is
Far more cases are being brought forward around bullying or harassment (22%), and in a new category ‘inappropriate attitudes and behaviours’
naturally different from the acute and emergency pathways, as well as mental health.
So while it is difficult to compare, it probably also suggests there is some under-representation of speaking-up cases in the independent sector.
This could be due to a number of reasons as noted above, but we need to remain alert to the fact that it could be due to other factors, including a lack of awareness of the Freedom to Speak Up process, a fear of reprisal or a belief that speaking up won’t make a difference.
More to be done
Whatever the reasons, it is clear that more can always be done to create a culture of openness and trust in the independent healthcare sector. This will require a concerted effort from all stakeholders, including leaders, managers, and staff.
I know that different organisations have rightly taken different approaches to FTSU, depending on their unique size, scale, geographical and clinical factors. However, there are some common things that we can all be doing:
Appoint a Freedom to Speak Up Guardian – or guardians. This is an independent and impartial individual who is there to support staff who want to speak up about concerns they have;
Provide training and resources to your staff on speaking up. This will help them to understand their rights and responsibilities and how to raise concerns effectively;
Create a culture where staff feel comfortable raising concerns. This means being open to feedback, listening to concerns and taking action to address them;
Celebrate staff who speak up. This will show that you value their contributions and that you are committed to creating a speaking up culture.
Support essential
It is also important to recognise the challenges facing our guardians. They are often faced with difficult and sensitive issues and they may have to challenge the status quo.
Dealing with distressing cases can affect mental health. The role can be lonely and isolating, with limited support from managers. This can be stressful, and so having the right support to do their job effectively is essential.
Forty-four per cent (44%) of respondents stated that the role had reduced their health and wellbeing, either somewhat or greatly – that’s actually better than last year’s 49%, but it’s still nearly half. However, conversely, it was really encouraging to see that 26% of the respondents reported an improvement in their health and well-being due to the FTSU role –that just shows that, for some, working in this role is a rewarding and positive experience if we can get it right.
So what does good support look like?
➤ Provide them with training and resources. This will help them to understand their role and responsibilities, and how to deal with difficult situations.
➤ Give them access to senior leaders. This will ensure that they have the support they need to raise concerns and make a difference.
➤ Create a culture where they are respected and valued. This will help them to feel confident in their role and to do their job effectively.
➤ Protect their time to carry out the role properly. To perform this role properly takes time – make sure colleagues are supported by carving out proper time to commit to it fully.
Creating a speaking-up culture is not easy, but it is essential for patient safety, quality of care and the well-being of staff. By taking these actions, we can help to ensure that the independent healthcare sector is a safe and supportive place for everyone who works here.
Dawn Hodgkins is director of regulation at the Independent Healthcare Providers Network (IHPN)
Tips on achieving financial health
Maintaining your practice’s financial health is imperative in the rapidly evolving healthcare landscape. As healthcare models shift, costs rise and competition intensifies, Derek Kelly unveils key strategies to enhance revenue, profitability and your business’s long-term success
MEDICAL PRACTICES , like any other businesses, must prioritise financial wellness to thrive and continue providing quality patient care.
In an era of evolving healthcare models, rising costs and increased competition, managing the financial health of your medical practice is essential.
My comprehensive guide here will explore key strategies and best practices to enhance revenue and profitability while ensuring your practice’s sustainability.
1 Evaluate and adjust pricing strategies
Regularly evaluate your fee schedules to ensure they are competitive
while reflecting the quality of care you provide. Consider factors such as payer rates, regional benchmarks and the cost of providing services.
Adjust pricing as needed to strike a balance between affordability for patients and profitability for your practice.
2
Enhance patient collections
Optimise your patient collections process to reduce outstanding balances.
Implement clear and consistent financial policies, including upfront cost estimates and payment plans when necessary. Train your staff to discuss finan-
cial responsibilities with patients in a transparent and empathetic manner. Consider offering online payment options to improve convenience.
3 Negotiate favourable contracts with insurers
Negotiating favourable contracts with insurance payers can significantly impact your practice’s financial health.
Review your existing contracts and explore opportunities for renegotiation.
Advocate for fair re-imbursement rates that reflect the value of your services. Collaborate with medical billing experts to identify negotiation strategies.
4 Implement technology solutions
Leverage technology to streamline financial processes. Invest in practice management systems that integrate seamlessly with billing and revenue cycle management software.
Automation reduces administrative burdens, minimises errors and accelerates claims processing.
5 Monitor key performance indicators (KPIs)
Regularly track and analyse financial KPIs to gain insights into your practice’s financial health.
Key metrics to monitor include accounts receivable turnover, days
in accounts receivable and revenue per patient visit. Use this data to identify trends, make informed decisions and implement strategies for improvement.
6 Control overhead costs
Review your practice’s overhead costs and identify areas where you can cut unnecessary expenses.
Consider renegotiating vendor contracts, exploring group purchasing options or implementing energy-efficient measures in your facility. Small savings in multiple areas can add up to substantial financial benefits.
7 Expand services strategically
Explore opportunities to expand your service offerings strategically. Conduct market research to identify unmet patient needs in your area.
Adding complementary services or specialties can attract a larger patient base and increase revenue. Ensure that any expansion aligns with your practice’s mission and expertise.
8 Cultivate referral relationships
Build strong referral relationships with other healthcare providers in your community.
Collaborate with specialists, primary care physicians and other healthcare professionals. Effective networking can lead to a steady stream of patient referrals, increasing your practice’s patient volume and revenue.
9 Efficient billing and revenue cycle management
Efficient billing and revenue cycle management are at the heart of financial wellness for medical practices. Implement robust billing systems and trained staff to minimise errors and accelerate claims processing.
Regularly review your billing processes and identify common denial reasons to address them promptly. A well-organised revenue cycle ensures consistent cash flow.
10 Plan for contingencies
Financial wellness also involves preparing for unexpected
challenges. Develop a contingency plan for events like economic downturns, natural disasters or sudden changes in healthcare regulations. Maintaining an emergency fund and having access to a line of credit can provide financial stability during tough times.
11
Seek professional financial guidance
Consider engaging financial consultants or advisers who specialise in healthcare practices. These experts can provide valuable insights, financial analysis and recommendations tailored to your practice’s specific needs. Their guidance can help you make informed decisions to improve your financial wellness. Financial wellness is fundamental to the success and sustainability of medical practices. By implementing these strategies and best practices, you can enhance revenue and profitability while ensuring your ability to continue delivering high-quality patient care.
Remember that financial wellness is an ongoing effort that
requires vigilance, adaptability and a commitment to excellence.
As the healthcare landscape evolves, staying financially healthy becomes even more critical. Efficient billing, thoughtful pricing strategies and strong patient relationships can set your practice on a path to financial success.
Continuously monitor your practice’s financial performance, seek professional guidance, when needed, and be proactive in addressing financial challenges.
Ultimately, achieving financial wellness in your medical practice not only benefits your bottom line but it also enables you to provide better care, to invest in your staff and to contribute positively to your community’s healthcare needs.
By prioritising financial wellness, your practice can thrive in an ever-changing healthcare environment.
Derek Kelly (right) is marketing manager at Medserv
Diagnostic Audiology Including Paediatrics • Tinnitus Rehabilitation • Vestibular Testing • PTA & Tympanometry • Speech Audiometry • Speech In Noise Testing• Specialist Tests Including OAE, VEMP & ASSR • Ear Wax Removal • Independent Hearing Aid Provider
A PRIVATE PRACTICE – Our series for doctors embarking on the independent journey
Should I buy a house
house via a company?
Investing in homes? A lot of senior doctors do. But it pays to understand your tax situation and the complexities. Richard Norbury (right) outlines what you need to know
MANY DOCTORS will have, or are thinking about, investing in residential property. This is becoming even more popular as individuals and businesses try and keep pace with higher rates of inflation.
Sometimes individuals will hold an interest in an investment property almost by accident, as properties purchased while in training in a certain city/area or before starting a family are often retained and kept as an investment going forward.
In addition, for those of you who trade via a limited company, you may find cash balances have been kept in the company partly due to a reluctance to vote dividends due to high personal tax rates and to keep under thresholds such as £100,000 (tapering of personal allowances and losing childcare benefits) or £200,000 (tapering of annual allowance for pension).
Property investments are likely to be a medium or longterm investment, so we must consider that tax legislation can change during the ownership period and residential property has definitely seen some significant changes in taxation in recent years.
Once the decision has been made to invest in property, the next decision to make is whether they should own residential property personally or via a company and there are various considerations that need to be taken into account.
COMPANY OWNERSHIP
Corporation tax
One of the big changes recently has been the rise in corporation tax from April 2023. Depending on the level of profits, you could be paying corporation tax at the rate of 19%, 26.5% or 25%.
If a property is let to a connected person – such as a family member – or the property is not let on a commercial basis, then special rules may apply such that the main rate of tax of 25% could be charged. This should be considered by an accountant or tax specialist.
Associated companies
Sometimes investment property is held in a separate company to the trading company. In these circumstances, you need to consider whether the companies are under common control.
If so, the level when higher corporation tax is paid may be lowered and shared between the companies. Professional advice should be taken on a case by case basis to determine the status.
Annual Tax for Enveloped Dwellings (ATED)
This additional tax for residential properties held in companies is applicable to properties worth more than £500,000. The annual charge varies depending on the valuation of the property and starts at £4,150 for 202324.
➱ continued on page 48
Exemptions are available if the property is being commercially let, but annual reporting is necessary to qualify for this.
Stamp Duty Land Tax
Most of you will be familiar with the concept of paying stamp duty land tax when a property is purchased.
As with ATED, there is potentially a higher amount of stamp duty paid by companies if the property is worth over £500,000, although relief may be available. In addition, there is a 3% surcharge on residential properties bought by companies.
Capital Gains Tax
Corporation tax is charged at the relevant rate to the individual company based on the sale proceeds of the property after taking into account the purchase price and any qualifying improvements.
Extraction of funds
If we consider that during the life of the company it may be that a residential investment property was bought, rented out and then sold a number of years later, it is reasonable to assume that there may well be money left in the company – after paying corporation tax – for extraction at a later date.
Therefore, income tax is likely to be due on the final extraction of the funds. Dividends would attract tax of the prevailing rates at the time. If the company has ceased trading, it may be the case that it is wound up as a capital distribution in the future.
If so, different tax rates could apply and this could be treated as a capital distribution or income tax may be charged at the prevailing rate. Obviously, any arrangement should be discussed with an accountant or tax specialist to ensure you are making the right decision.
Mortgage interest
If the company takes out a mortgage to purchase the property, the full amount can be deducted before corporation tax is applied.
However, from a practical point of view, many lenders see property owned within a company as
Many lenders
see property owned within a company as higher risk than owned personally and, as a result, often slightly higher rates of interest are charged
higher risk than owned personally and, as a result, often slightly higher rates of interest are charged compared to properties owned by individuals.
Other considerations
Some companies have the funds available to purchase a property outright. However, for companies that need to apply for a mortgage, many lenders will demand that the company does not have another trade.
This means that separate companies – sometimes referred to as a special purpose vehicle or SPV – may have to be formed to achieve an investment in residential property.
PERSONAL OWNERSHIP
Income Tax
Tax is payable on the profits after deduction for allowable costs in much the same way as the company structure. One large difference is the mortgage interest, which is not a deduction on profits but instead a tax credit of 20% is allowed on any qualifying mortgage interest.
This means higherate taxpayers will not get full relief. The rates of tax are then applied at the relevant prevailing personal tax rates.
Ownership
Residential properties owned outside of a corporate structure are often owned jointly with a spouse or family member. Usually this ownership then dictates which individual the profits are taxed upon.
This can be changed and altered so long as the correct procedures are followed, but careful consideration should be taken, as this could result in capital gains tax implications.
Stamp Duty Land Tax
There is usually a 3% surcharge on top of the prevailing stamp duty land tax rates if buying residential property means you will own more than one property. This is currently the same rate as residential properties owned via a company.
Capital Gains Tax
Income tax is charged at the relevant rate to the individual
There is usually a 3% surcharge on top of the prevailing stamp duty land tax rates if buying residential property
means you will own more than one property
based on the sale proceeds of the property after taking into account the purchase price and any qualifying improvements.
Capital gains tax rates on residential property for individuals is currently charged at 18% for basic rate taxpayers or 28% for higher rate taxpayers.
In addition, each individual has an annual exemption limit of £6,000 (2023 24) reducing to £3,000 (2024 25), meaning this element of the gain is tax free, assuming you have made no other gains in the same tax year to 5 April.
If you have ever lived in the property, you can reduce your exposure to capital gains tax. This allows the gain to be reduced such that you only pay capital gains tax on the period that the property is an investment property and not when it was your principal private residence.
As an added relief, if you have ever lived in the property, you also automatically have an additional nine months of the ownership that is exempt from capital gains tax.
This article looks at residential properties that are making a profit and a capital gain. Properties making losses and/or a capital loss need to be considered separately and as part of your overall affairs and strategy.
You can see from this article, there are many different considerations to make and there is no right or wrong answer to whether you should own property personally or in a company structure.
Ownership through a company often looks like a more taxefficient option, but this can be reversed once the funds are ultimately taken out of the company.
Residential property investment can be a complicated area and taking tailored specialist professional advice specific to your circumstances will help you ensure that you can make an informed decision and be aware of current tax legislation.
Next month: Top tips for private GP practices, by Alec James
Richard Norbury is a partner at Sandison Easson and Co, specialist medical accountants
mPrescribe® app allows you to prescribe flexibly without a laptop, for delivery to your patients nationwide
Download the app and register online www.pharmacierge.com/register
Secretary Supported
GP and Consultant Reviews
Administrator access reduces workload for practitioners. mPrescribe® facilitates patient entry, status monitoring and preparation of prescriptions for mobile authorisation.
Clinical Governance
Co-founded and co-owned by leading private clinicians, our secure and encrypted technology is compliant with all GPhC, GDPR and e-Prescribing regulations.
“Wonderful, seamless, easy to use service.” Dr Catrin Bevan, London General Practice
“Intuitive and secure.” Dr Tim Wigmore, Consultant Anaesthetist and Intensivist
“Delivered the same day.... Outstanding!” Dr Elisa Astorri, Academic Physician Rheumatologist
“Go the extra mile.” Dr John O’Donohue, Consultant Gastroenterologist
“Consistent, efficient , friendly and responsive.” Dr Tim Ladbrooke, Courtfield Private Practice
DOCTOR ON THE ROAD: BMW i4
EV has all the spark expected of a BMW
A practical family car that will not disappoint the keen driver… Independent Practitioner
Today’s motoring correspondent Dr Tony Rimmer is full or praise for this electric Beemer
We are all more comfortable with the familiar. Our patients are most relaxed with a friendly face they know and feel more confident in a clinic or hospital they have been to before.
As practitioners, we work best with a team whom we know and trust. So it is not surprising that it is taking some time for people to embrace unfamiliar electric power and technology when it comes to replacing the family car. Some of us need convincing to make the change.
Car makers have tried to make the switch easier by offering allelectric versions of some of their internal combustion engined (ICE) models to ease the process. Such a car is the BMW i4.
Using underpinnings that are already shared by the regular 3-series and 4-series, it looks iden-
tical to the five-door 4-series Gran Coupé. It carries an 84kWh battery and is available with one or two motors with two- or fourwheel drive.
I have been testing the model that represents the best balance between cost and performance: the eDrive40, which is rear-wheel drive, has 335bhp and would appeal to most medics as a stylish practical family car.
Direct competitors include the Hyundai Ioniq , the Polestar 2 and the Tesla Model Y.
More
aerodynamic
The only external styling feature that might put off loyal BMW buyers is the large plastic blanked off front grille.
Because the i4 is all-electric, it does not need as much cooling as an ICE version and the new look is
more aerodynamic to help economy.
As it has such a large battery, the claimed WLTP range is up to 337 miles, which equates to about 270 miles in the real world.
Unfortunately, the large battery means more weight and the i4 weighs around 500kg more than the equivalent 4-series petrol model.
The interior feels a comfortable and premium place to spend time and all BMW owners will immediately feel at home. The only real clue to electrification is the exclusive blue detailing and the very different information on the driver’s display.
You sit low in the i4, a pleasant change from the raised seating in SUVs and it makes the drive feel sportier.
Rear seating is comfortable but
designed more for two passengers rather than three.
The boot is spacious and the rear hatch improves versatility, so even the family dog won’t get left out. Being a BMW, the i4 really needs to deliver the driving dynamics that are expected of the brand and I was relieved to find that, indeed, it does. The steering is sharp and the body control is excellent despite the extra weight of the batteries.
Dynamic chassis control
This is helped by the optional dynamic chassis control which includes air suspension at the rear. This also helps the ride, which is much less brittle and over-firm as it is in cars like the Tesla Model Y.
Punting the i4 down one of my favourite B-roads was a joy and although it isn’t as agile as a lighter petrol 4-series, I still had fun.
The interior feels a comfortable and premium place to spend time and all BMW owners will immediately feel at home
What is also impressive is the motorway cruising. Well suppressed wind noise combines with the silence of electric travel and the smooth ride to produce a mini-limousine feel and the miles fly by.
Although high speed is the enemy of potential range, a cruise at 70mph is still achieved with an indicated 3.0 miles/kWh economy; a very respectable figure. If you do put your foot down, acceleration is fast and exciting without being too silly.
A 0-62mph time of 5.6 seconds is swift and actually feels faster due to the instant high-torque take-off of electric cars. The i4 is an excellent electric car and succeeds in combining the attributes of electric motoring with the engaging driving experience expected from all BMWs.
It is more conservative in styling than most other EVs, but I see that as appealing to many potential buyers.
It works as a practical family car that will not disappoint the keen driver and I know that, for many of us medics, that is a very important combination. In the world of EVs,
It is more conservative in styling than most other EVs, but I see that as appealing to many potential buyers
only the Porsche Taycan – at much greater cost – does better, so this is high praise indeed.
Dr Tony Rimmer (right) is a former NHS GP practising in Guildford, Surrey
BMW i4 Edrive 40 SPORT
Body: Five-seat hatchback. Rear-wheel drive
Engine: One electric motor. 84kWh battery
Maximum charge rate: 205kW DC
Power: 335bhp
Torque: 430Nm
Top speed: 118mph
Acceleration: 0-62mph in 5.6 seconds
Claimed range: 337 miles
On-the-road price: £59,390
LOUD AND CLEAR?
Make sure you reach your target audience by advertising in Independent Practitioner Today
To discuss your requirements and for details of rates, contact Andrew Schofield at Spot On Media on 0161 408 3912 or email him at andrew@spotonmedia.co.uk
ADVERTISERS: The deadline for booking adverts in our November issue is 27 October
INDEPENDENT PRACTITIONER
TODAY The business journal for doctors in private practice
Published by The Independent Practitioner Ltd. Independent Practitioner Today is editorially independent.
Material is governed by copyright.
No part of this publication may be reproduced, stored in a retrieval system or transmitted in any form without permission, unless for the purposes of reference and comment. Editorial layout is the copyright of the publishers. If you wish to use it for promotional purposes on websites or for reprints, we would be happy to discuss licensing the copyright to you.
Registered office: 7 Lindum Terrace, Lincoln LN2 5RP
Write to Independent Practitioner Today
7 Lindum Terrace, Lincoln LN2 5RP
CHANGING ADDRESS, EMAIL
ADDRESS OR SUBSCRIPTION DETAILS?
Phone 01752 312140 or email karen@marketingcentre.co.uk
TELL US YOUR NEWS
Robin Stride, editorial director
Email: robin@ip-today.co.uk
Phone: 07909 997340 @robinstride
ADVERTISE WITH US
To advertise in the digital journal, on our website or in our business directory, contact advertising manager Andrew Schofield at Spot On Media. Phone: 0161 408 3912
Email: andrew@spotonmedia.co.uk
GET A SUBSCRIPTION DISCOUNT!
£90 independent practitioners.
£90 GPs and practice managers (private & NHS).
£210 organisations.
Save £15 paying by direct debit: individuals £75 (organisations £180).
TO SUBSCRIBE
Email karen@marketingcentre.co.uk or phone 01752 312140
Publisher Gillian Nineham
Phone: 07767 353897.
Email: gillian.nineham@gmail.com Follow Independent Practitioner Today on