Jane Braithwaite responds to a private doctor’s plea for some advice in setting up a group P14
The business journal for doctors in private practice
Broadening the access to digital care
Dr Leah Jones of Bupa analyses where we’re at with digital healthcare P20
A guiding hand in a time of stress
Dr Udvitha Nandasoma of the MDU outlines support available to private doctors suffering from rising stress n Turn to page 28
‘Dog lists’ are barking up the wrong tree
A financial adviser on why you should ignore ‘worst buy’ investment lists P32
Practising privileges reviews to be stricter
By Robin Stride
Consultants’ requirements to gain and maintain practising privileges are being standardised in all private hospitals as part of a drive to beef-up patient safety and improve transparency.
The changes are among several in a new version of the four-yearsold Medical Practitioners Assurance Framework (MPAF) produced by the Independent Healthcare Providers Network (IHPN).
Authors of the 24-page document, designed to enhance the quality of care in the sector, say the content remains consistent with, or has been updated to reflect, relevant new or updated guidance or legislation published since 2019.
The practising privileges section has been updated to ‘better allow for a risk-based approach, directing that a review of practising privileges is undertaken biennially for all medical practitioners and more regularly in circumstances where additional scrutiny is requires’.
A wide range of medical organisations have reacted positively to the ‘refresh’, including the Federation of Independent Practitioner Organisations (FIPO), the Royal
In association with
College of Surgeons of England, the Independent Sector Complaints Adjudication Service and the Patients Association.
FIPO company secretary Rosemary Hittinger said the MPAF refresh demonstrated the sector’s ongoing commitment to rigorous standards and processes of clinical governance. ‘As we move towards a more integrated system, the MPAF will support consultants and providers to enhance and improve patient safety.’
Strengthened areas include giving more prominence to expectations around patient consent and the need for greater transparency around conflict of interest declarations.
New initiatives such as the Learn from Patient Safety Events (LFPSE) service are also reflected, along with the IHPN’s Development Plan which sets out how the network will support providers to continue to implement the MPAF.
The MPAF is also promoted as a way providers can provide assurance to the Care Quality Commission that they are ‘well led’.
Its update takes account of recommendations from the Paterson Inquiry and the Department of
Health and Social Care’s response, and the 2020 ‘First do no harm’ report of the Independent Medicines and Medical Devices Safety Review.
IHPN chief executive David Hare said the document reflected the independent health sector’s commitment to continuously improving safety and quality. Providers had used it to review and update their practices to raise the bar and ensure they adhered to the latest medical governance practices.
It would also enable greater consistency in how clinicians worked across the sector and give confidence to patients that independent healthcare providers were committed to delivering the safest possible care.
The MPAF says although practising privileges policies will vary, sector-wide standardisation of some aspects will provide much needed transparency and set the sector’s expectations of doctors.
It calls for the application for practising privileges to be based on a standard dataset – published as an appendix in the MPAF document – incorporated into all providers’ practising privileges application forms.
Where doctors are employees, ‘then appropriate recruitment and selection processes, together with policies and procedures for monitoring and managing performance, should reflect the dataset’ . Practising privileges should be reviewed biennially for all medical practitioners, and more regularly in circumstances where additional scrutiny is required, while practising privilege reviews should be the same across all independent providers.
The MPAF added: ‘Where the independent provider does not have the required information necessary to make a decision about renewal, practising privileges should be suspended until that information is available.
‘Collection of whole-practice clinical data, co-operation with the appraisal process and sharing of relevant information should be a requirement for maintaining practising privileges.’
Independent providers are told to have robust processes for assessing novel therapies/procedures ‘that protect patients, medical practitioners and the organisation without stifling innovation’. n See page 38
The Consultants Mobile App
Our mobile application puts your practice in the palm of your hand giving you anytime, anywhere access to your business.
Dynamic Diaries
Our comprehensive diary system allows you to view your diary and the diaries of your colleagues side-by-side on the same screen.
Book a demonstration with us today!
iMedDoc is a brand new practice management system designed to manage every aspect of your practice, securely. We simplify your daily tasks so you can focus on your patients.
Electronic Medical Record
At the core of our system is our cloud-based electronic medical record giving you everything you need to manage patient information.
Reporting and Analytics
Build a better business clinically and commercially. Track financial performance interpret medical records across your patient population.
www.imeddoc.com
+44 20 35141393 sales@imeddoc.co.uk
TELL US YOUR NEWS. Contact editorial director Robin Stride
ADVERTISE WITH US. To advertise in the digital journal, on our website or in our business and lifestyle directories, contact Andrew Schofield at Spot On Media. Phone: 0161 408 3912
Email: andrew@spotonmedia.co.uk
GET A SUBSCRIPTION DISCOUNT
£90 independent practitioners. £210 organisations. £90 GPs and practice managers (private & NHS).
Save £15 paying by direct debit: individuals £75 (organisations £180).
TO SUBSCRIBE
Email karen@marketingcentre.co.uk
Or phone 01752 312140.
Chief sub-editor: Vincent Dawe
Head of design: Jonathan Anstee
Publisher: Gillian Nineham
Email: gillian.nineham@gmail.com
Phone: 07767 353897
Follow Independent Practitioner Today on
EDITORIAL
COMMENT
Safety becomes unified
The ‘refresh’ of the Medical Practitioners Assurance Frame work (MPAF), aimed at improving the safety and quality of care independent providers give patients, will be important reading material for established and new private practitioners (see page 1).
Although originally launched by the Independent Healthcare Providers Network (IHPN) only three years ago, there has been quite a bit to add and to update. Its aims to strengthen and build upon the medical governance systems already in place in the sector.
The document has already been widely welcomed, including by the Care Quality Commission (CQC), which now uses the framework’s principles in assessing how well led an independent service is.
The IHPN points out that the framework is a requirement of the NHS’s 2022 23 Standard Contract which all independent
sector providers of NHSfunded care must adhere to.
Among additions to the document are taking account of recommendations from the former Bishop of Norwich’s inquiry into rogue surgeon Ian Paterson, plus Baroness Cumberlege’s Independent Medicines and Medical Devices Safety Review.
Doctors’ representatives in the Federation of Independent Practitioner Organisations and medical royal colleges helped develop the MPAF in a group including the Department of Health, CQC, the GMC, NHS Resolution and the Patients Association.
Royal College of Surgeons’ guidance for surgeons working in the private sector already gives advice on good practice for individual doctors and it is hoped this will be used in conjunction with the IHPN framework.
If you work in a non IHPN member private hospital, then ensure they adopt it too.
Why tax returns need to go in early Minimise your annual tax hassles by dealing with things early and enabling your accountant to help with planning. Julia Burn has some useful tips P12
How do groups go about billing?
Simon Brignall continues last month’s reflection on the challenges groups face with their billing and provides a check list when setting up a group P16
Face up to the risk of being sued
Lawyer Deborah Pyzer has some advice for cosmetic practitioners servicing the quest for supermodel looks from their demanding patients P18
The importance of expert witnesses
Private practitioners acting as a medical expert witness can play a crucial role in improving patient safety, explains Dr Lucy Hanington of the MPS P26
How coroners arrive at conclusions
In the last of a three-part series on how the inquest process works, solicitor Thorrun Govind explains inquest conclusions and what they mean P34
When interpreter is a family member
Dr Ellie Mein of the MDU replies to a query from a doctor worried that his patient with complex comorbities is using a relative to translate P36
PLUS OUR REGULAR COLUMNS
Doctor on the Road: Blast from the past is a blast for today
Dr Tony Rimmer tests the resurrected Alpine A110 sports car and can’t wait to get back in it P40
Start a Private Practice: Keep a tab on your tax dates
Accountant Richard Norbury of Sandison Easson sets out some of the more common tax deadlines P42
Private doctors are on the rise, but still trail pre-Covid era
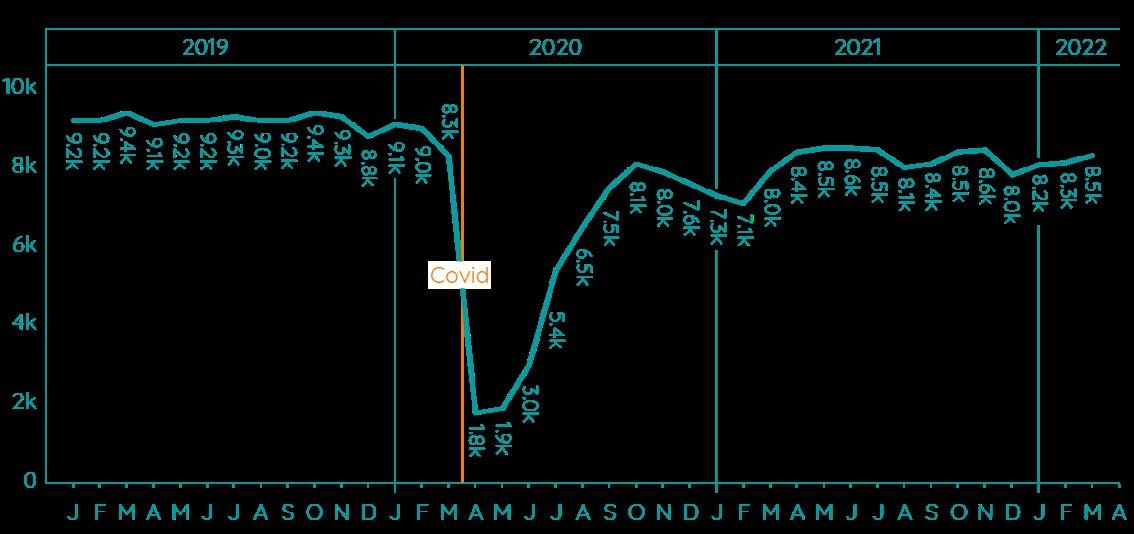
Latest key trends for the private sector show a gradual rise in the number of consultants who are actively working in the independent sector.
A steady increase has been recorded in figures released by the Private Healthcare Information Network (PHIN).
It said: ‘Following a traditional seasonal fall in December, the number of consultants actively treating private patients continued to grow month on month in Q1 2022.
‘March 2022 saw the fourth highest number active since the pandemic began. However, this figure was still 10% below March 2019.’
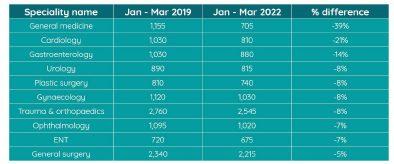
Compared to the largely preCovid first quarter of 2019, the data for the same period this year records a drop of 1,515 consultants in ten top specialties.
PHIN said this was most pronounced for general medicine (down 39%) and cardiology (down 21%). The lowest change was general surgery (down 5%).
ENT replaces medical oncology in the top ten specialities from the previous reporting period.
The data was taken from PHIN’s unique national private dataset describing admitted activity (day case and inpatient).
It said this excluded activity outside of its mandate from the Competition and Markets Authority (CMA), such as outpatient diagnostics and mental health.
Poor pay rates putting off anaesthetists
By Agnes Rose
Poor payment levels are contributing to a fall in the number of consultant anaesthetists wanting to work privately.
The Association of Anaesthetists has reported seeing an increasing number of its specialist members –usually more recently appointed ones – choosing not to take independent practice work.
It said availability of anaesthetists had also been hit by an
increase by the number of specialists retiring.
In a statement to Independent Practitioner Today, the association blamed remuneration as one of many causes for anaesthetists choosing not to put their time into the independent sector.
It said: ‘Fees for anaesthetists have always been very much less than for surgeons, and now the numbers just don’t stack up.
‘This is true for insured patients and is particularly so for NHS work
undertaken in independent hospitals, which can be paid at £50£100/hour.
‘With the current backlog, there are, in most NHS hospitals, plenty of extra lists or initiative lists which are usually better remunerated – i.e. per hour.
‘Do patients want their care in independent hospitals to be provided by the ‘usual team’ or anaesthetist – and in some cases a surgeon – appointed by the hospital? We are not sure they have ever been asked.’
Association president Dr Matt Davies, responding to Government’s financial plans for the NHS announced last month, said:
‘With a 1,400-short anaesthetic workforce, we need to see an increase in efforts to recruit and retain anaesthetists if we are to sustainably clear the surgical backlogs and maintain an acceptable level of patient safety’.
See the Federation of Independent Practitioners Organisations’ opinion on page 9
Volume of consultants by Top Ten specialty
Pension plan dismissed as inadequate tinkering
By Edie Bourne
The medical profession has widely criticised an announcement by the new Health Secretary and Deputy Prime Minister for missing the crucial help needed for doctors’ pensions.
Thérèse Coffey’s ‘plan for patients’ set out a package of measures aimed at tackling the crisis in the NHS and reducing the risk of the service facing extreme winter difficulties.
But many critics say she missed the opportunity to remove the significant tax burdens forcing senior consultants to reduce shifts or retire early.
Patrick Convey, technical director with specialist financial planners Cavendish Medical, said: ‘We know that thousands of doctors are facing substantial tax bills on their deemed pension growth. These extra charges are enough to force them to take early retirement with devastating effects on the NHS workforce.
Association
‘On a positive note, the proposals did address the rules which link the NHS pension to inflation by amending the revaluation date in the scheme – and that NHS trusts would be mandated to offer pension recycling by 2023.
‘Recycling in this sense is where employees have opted out of the
NHS Pension Scheme but the employer may pay any unused employer contributions as additional salary’.
Mr Convey added: ‘Sadly, we are still not seeing much hope of any changes being introduced to stop the detrimental effects of the annual allowance, but the published measures to increase retirement flexibilities for NHS staff will be welcomed.’
The Hospital Consultants and Specialists Association (HCSA) president Dr Naru Narayanan said the Government had delivered ‘a hotchpotch on pensions’ which failed to tackle the fundamental issue.
‘The vow to correct unfair rules around scheme growth due to inflation is positive, as is news that trusts will be required to offer pensions contribution recycling from 2023. But all of this is just tinkering around the edges on pensions tax.
‘The time for a solution has long since passed when everyone from
the Office for Tax Simplification to the NHS Confederation sees that there is a need for radical reform.
‘We need the abolition of the unfair annual allowance in defined benefit schemes like the NHS pension. We also need to see lifetime allowance thresholds uplifted and linked to inflation so that senior staff are not incentivised to retire.’
Prof Philip Banfield, BMA Council chairman, said: ‘The pledges around pensions may provide relief for some doctors and show that the Government is finally starting to sit up and take notice of the threat that absurd taxation rules pose to the sustainability of the NHS and patient care – something the BMA has been warning for years.
‘However, they fall short of the long-term solutions that we have been calling for. Consequently, these measures will not prevent doctors being left with little option but to reduce hours or retire early.’
Pension fix ‘won’t stop early exodus’
The Government’s solutions to the pensions crisis facing large numbers of Independent Practitioner Today readers are only ‘sticking plasters’, according to the BMA pensions committee chairman.
Dr Vishal Sharma warned that rising inflation, plus anomalies in the Finance Act, meant thousands of doctors would incur huge tax bills on ‘false, non-existent’ pension growth and might be forced to retire this financial year.
The BMA has told the Government to fix anomalies directly by urgently amending the Finance Act to prevent doctors being unfairly taxed on pension benefits
they will never receive. But instead, the Government was suggesting amending the NHS pension scheme.
Dr Sharma said: ‘While moving the revaluation date in the scheme rules will, at best, partially mitigate the problem, it does not solve it and for some doctors it may make matters worse.
‘Additionally, doctors who are members of non-NHS schemes may be excluded, hence why a robust solution would be to enact such changes in the Finance Act.
Following public sector pension reforms, most NHS staff are members of two different but connected schemes.
‘The Government must urgently correct the anomaly that negative growth in one scheme can neither be offset against growth in another, nor carried forward or backwards into alternative tax years.’
He said the BMA had long campaigned to ensure those adversely impacted by pension taxation and left with little option but to opt out of the scheme could access the employer’s pension contributions.
Encouragingly, the Government had committed to ensure this was made available, but this had to happen in every employing organisation and represent the full value of the employer’s contributions.
Dr Sharma warned that the Government’s measures would not prevent doctors having to reduce their work or retire early as a result of punitive pension tax charges.
Doctors were simply asking that higher earners in the NHS paid the correct amount of tax on their pension savings.
‘We believe that a tax unregistered scheme, similar to the one the Government introduced to address recruitment and retention problems with senior judges in the judiciary, would provide a long-term and fundamentally fair solution both for taxpayers and for doctors.’
Dr Naru Narayanan, president of the Hospital Consultants and Specialists
Mini-Budget round-up
Specialist medical accountant
Alec James (below) reports on the impact of the ‘mini-Budget’ for Independent Practitioner Today readers and gives some advice for their businesses
JUST 18 DAYS into his new role as Chancellor of Exchequer, Kwasi Kwarteng delivered his first miniBudget.
With tax cuts across the board, while good news for the taxpayer, one does worry of the impact this may have on the British economy.
Individuals
From 6 April 2023, the basic rate of income tax will reduce from 20% down to 19%. This means an extra £375 in most doctors’ pockets.
Kwarteng originally announced at the Budget that the 45% tax band for earnings over £150,000 would be removed from 6 April 2023, reverting back to 40% being the highest rate of income tax.
Since the Budget, the Government has been receiving backlash for the tax cut. It has since been agreed between the Chancellor and the Prime Minister that the decision would be reversed, meaning that the additional rate of 45% will continue.
There are rumours that the ‘Tapering of Personal Allowance’ will also be dispensed with in the near future, but we will have to wait until the new year to see if this transpires.
Kwasi also announced that the 1.25% Health and Social Care Levy will be abolished and the employee, employer and selfemployed National Insurance rates will return to the pre April 2022 levels. This will take effect soon –from 6 November 2022.
The 1.25% reduction will also be applied to dividend tax rates from 6 April 2023, meaning they will revert back to 7.5%, 32.5% and 38.1%, depending on the tax bracket applicable.
All these reductions will lead to some potential tax planning for those independent practitioners with limited companies.
Unless rates are altered, Scotland will still have five rates of tax with the additional rate remaining at 46%.
There may be some realignment of the Scottish rates, as we understand that the reduction in tax for the rest of the UK allows the Treasury to release a higher grant to Scotland.
Companies
The headline announcement for companies was that the proposed increase in corporation tax rate from 1 April 2023 to 25% has now been abandoned. Many of you would have been facing a significant increase in corporation tax before the change.
While corporation tax will now remain at 19% for the foreseeable future, companies still have up to 31 March 2023 to benefit from the ‘super deduction’ on qualifying capital purchases.
The scheme allows 130% of the cost of the asset to be claimed against profits, ultimately saving 25% tax rather than 19%.
Those with companies may therefore look to accelerate any
expenditure to benefit from the scheme.
For those of you that may be considering developing or refurbishing a clinic, the planned reduction in the Annual Investment Allowance, which gives companies 100% tax relief in the year of purchase, has also been cancelled.
The £1m limit will remain for the foreseeable future.
IR35/Off-payroll working
The off payroll working rules introduced for public sector bodies and the private sector in 2017 and 2021 respectively have been reversed back to the rules that came into existence in 2000.
This means that the determination of whether IR35/off payroll working applies is once again the responsibility of the ‘worker’.
This reform means that there may be new opportunities for your limited companies, as there is likely to be less bureaucratic red tape for the organisations engaging with companies.
Stamp Duty
In England and Northern Ireland, the nil rate band for stamp duty has increased from £125,000 to £250,000 with immediate effect.
This saves up to £2,500 of stamp duty on the purchase of residential properties, whether this is your main home or investment properties.
Scotland and Wales have separate and devolved legislation covering land transaction tax.
NHS Pensions change
Prior to the mini Budget, the Government published a document called ‘Our Plan for Patients’. The document outlined a plan for the NHS and social care.
As part of the plan, the Government addressed ongoing retention issues for senior members of the NHS and how the ‘Consumer Price Index (CPI) disconnect’ and resulting annual allowance tax charges are contributing to this issue.
It was hoped that Kwasi would make further announcements in the mini Budget following on from the new Health Secretary Thérèse Coffey’s comment earlier in the week, where she highlighted the impact of CPI and its impact on doctors.
How this will work remains to be seen, but it hopefully will correct the issues caused by significant fluctuations in CPI rates.
Alec James is a partner at Sandison Easson & Co
Chancellor Kwasi Kwarteng
Private income up 38% for Marsden
Compiled by Philip Housden
The Royal Marsden Private Care revenue had strong recovery in 2021-22
Despite the challenges of the ongoing Covid19 pandemic, The Royal Marsden Private Care posted record revenues last year.
The trust’s annual accounts report a return of international patients, particularly over the latter half of the year, and sustained demand from UK patients.
Income of £141.6m for the financial year was 38% up on 202021 (£102.4m) and 4% above the plan for the year.
Shams Maladwala, managing director of private care, said: ‘A major highlight of 2021 22 was the opening of the new researchled diagnostic and treatment facility in Cavendish Square in April 2021.
‘This facility offers patients fast and direct access to worldleading cancer experts and has further enhanced the trust’s care provi
sion. The first year has been very successful, with income being 5% above plan for the year.
‘As a diagnostic centre, the facility was also able to support the treatment of patients during the Covid19 pandemic as part of the trust’s integrated model of care.’
The Royal Marsden retains the dominant spot as number one NHS trust for private care, significantly ahead of Guy’s & St Thomas’, second with £50.6m revenues.
It is also the most private patientdependent. In the 202122 financial year, 34.6% of total trust revenues were from private patient income. Only three other England NHS trusts are likely to report private income in excess of 10%.
London’s private maternity care reviewed
A recent Which? survey of nearly 2,000 parents has found that while most women give birth within the NHS, around 5% opted to give birth privately, many of these in NHS PPUs.
Their main reason for going private was to get ‘more personalised medical care’ and a desire for additional comfort.
Several London NHS trust PPUs provide private maternity care, where private birth costs can vary from £5,900 to over £10,000 for a problemfree pregnancy, a natural delivery and much more for complications.
The following NHS PPUs offer maternity care:
The Westminster Maternity Suite at St Thomas’ Hospital has provided private care for 20 years and more than 400 of the total of more than 7,000 babies delivered in the St Thomas’ maternity unit each year are private;
The Lindo Wing at St Mary’s Hospital;
The Sir Stanley Clayton Ward at Queen Charlotte’s and Chelsea Hospital, Imperial College;
The Kensington Wing at Chelsea and Westminster Hospital;
The Fitzrovia Suite at University College Hospital.
NHS PPU conference
This year’s national conference on NHS PPUs is to be held online on 20 October.
It is returning after a two year absence since the last successful event held in March 2020 at St Thomas’ Hospital. This year the focus is ‘NHS private patient service roadmap: strategise how to get your PPU back to full capacity’.
Sessions will include an insurer forum involving Bupa, AXA and Aviva; case studies from trusts and an export focused talk from Healthcare UK.
Details of how to book can be found at www.sbk healthcare. co.uk/events/nhsprivatepatientserviceroadmap
Philip Housden is director of Housden Group
Call to have more NHS work in private units
Private doctors’ should be offered more NHS work in independent hospitals under Government plans outlined last month by Health and Social Care Secretary Therese Coffey. Now the Independent Healthcare Providers Network (IHPN) is pressing for the policy to be fasttracked.
Responding to the Government’s ‘Our Plan For Patients’ report, published by the Department of Health and Social Care, IHPN chief executive David Hare welcomed her pledge to maximise the use of independent sector capacity and ensure patients can choose the fastest possible treatment.
But with NHS waiting lists at record levels and set to rise even further, he said it was ‘vital’ that this and other commitments in the policy document were quickly implemented.
He added: ‘Recent IHPN research conducted with the Patients Association found that, across England, patients need to travel just 13.2 miles – around 30 minutes by car – to cut over threeandahalf months off their NHS waiting time by choosing an alternative provider.
‘But with almost half of the public unaware of these rights, much more needs to be done to ensure the public are fully aware of the
choices available to them, and we look forward to working with the Government to ensure all blockers to patient choice are removed and that the independent sector can play its full role in the elective recovery.’
Earlier last month, the private healthcare sector was pleased to hear news that patients will be able to use the NHS app to shop around for hospitals with the shortest waiting lists.
Mr Hare said this should ‘urgently be made a reality so that NHS patients aren’t left languishing’.
He was responding to NHS performance figures showing a record
David Hare, the IHPN’s chief executive
6.8m people are waiting for NHS elective care.
Mr Hare said record NHS waiting list underlined the need for the Health and Social Care Secretary to take urgent action to tackle the growing backlog of care and get a grip of the growing crisis in the NHS.
Shams Maladwala, director of Royal Marsden Private Care
New site unveiled by Healthcode
Thousands of independent practitioners’ businesses are set to benefit using a new website from private healthcare sector online solutions provider Healthcode.
The official clearing company for medical invoices says it wants to make it easier for customers to benefit from its innovative technology.
Its new website, with revised branding, has a clear layout which practitioners and their staff are finding much easier to navigate so they can quickly find the section most relevant to them.
Healthcode, specialists in IT products and services for the private healthcare sector, is also making it easier for customers to access help and support with instructional videos on the website and more ways to get in touch.
The site also features clearer, jargon-free information on the company’s wide range of online products and services that connect different parts of the private healthcare sector, from claims management and The PPR (Private Practice Register) to secure messaging and eBooking.
At a launch in London, stakeholders from across the industry saw the new website for the first time and learned more about what Healthcode’s transformation programme means for them.
Managing director Peter Connor
Healthcode’s new website makes is easier for customers to access help
said: ‘Healthcode was founded on the belief that technology can bring about positive transformation.
‘We are constantly looking for better ways for our customers to do business, whether that’s automating time-consuming processes like payment reconciliation and shortfalls or ensuring they have the latest accurate data.
‘At the same time, it’s right for us to look at how we can improve our performance and be the best we can be for our customers and the industry as a whole.
‘That includes investing in our business systems to operate efficiently on a bigger scale and ensur-
ing that we make our customers’ lives easier through our engagement with them.
‘There’s much more to come, but our new website is an important part of that mission, helping us support our customers every step of the way.’
Healthcode now clears around 28,000 invoices daily, worth around £3bn annually for hospitals and independent practitioners. It has also applied its expertise to developing industry solutions that benefit all key stakeholders.
The PPR is Healthcode’s awardwinning online directory of practitioners who offer services in the private healthcare sector.
Surgeons call for more cash to slash record waiting backlog
Surgeons are pressing for health secretary Thérèse Coffey to add Elective recovery and Funding to her ‘ABCD’ mantra, as NHS statistics reported a record 6.84m waiting list in July for planned hospital treatment.
Royal College of Surgeons of England vice-president Mr Tim Mitchell said: ‘I hope Ms Coffey will add an E and F to her alphabet list of priorities. E for elective recovery and F for funding. Without this, the backlog that she wants to tackle will continue to grow.’
Outlining her ‘ABCD’ mantra, Ms Coffey pledged to focus on ‘ambulances, backlogs, care, doctors and dentists’.
The college welcomed her promise ‘to deliver for patients’, but stressed this would depend on continuing to fund the elective recovery.
Mr Mitchell said surgeons had made significant progress reducing very long waits for hospital treatment. Those waiting two years or more dropped from 23,778 in January to 2,885 in July, down to the commitment of surgeons, anaesthetists and nurses supported by additional elective recovery funding.
‘We cannot afford to let this progress slip or the elective recovery could be derailed at a vital juncture. Funding new surgical hubs and investment in staff will be key to the elective recovery in the months ahead,’ he said.
Whistleblowing surgeon unfairly sacked
A surgeon has been successfully supported by the BMA in his whistleblowing case against the Care Quality Commission (CQC) after he was dismissed by the watchdog following his raising of patient safety concerns.
Orthopaedic surgeon Mr Shyam Kumar worked part-time as a special adviser on hospital inspections for the CQC, but between 2015 and
2019 he raised several concerns with senior colleagues there, including around safety at his own trust, Morecombe Bay, Lancashire.
He said that he was expected to simply ‘rubber stamp’ inspections. He was then dismissed by the CQC in 2019.
The Manchester Employment Tribunal found Mr Kumar had been unfairly dismissed, with the
safety issues he raised playing a significant part in this.
BMA council chairman Prof Philip Banfield said: ‘It is absolutely paramount that doctors are able to raise safety concerns without fear of recrimination or backlash from employers.
‘This judgment clearly underlines the fundamental need to protect whistleblowers and is a
significant legal victory that the BMA is proud to have supported.
‘That such a case happened within the very organisation that is meant to safeguard standards within the NHS and social care is incredibly concerning indeed and the CQC must answer serious questions about its culture and the policies that allowed this to happen.’
Doctors eschew private practice
The demand for treatment in the private sector has rebounded.
This has been led largely by the self-pay market – up by around a third on 2019 figures – as patients, frustrated with very long NHS waiting lists, opt to pay for their treatment themselves.
This contrasts with an approximate 16% reduction in the volume of patients using insurance to pay. In terms of regional variations, the biggest increases in self-pay patients have been in Wales and Scotland, 90% and 83% respectively.
London has seen the smallest increase at 20%. This probably reflects the capital’s higher percentage of insured patients.
What is more surprising from figures released by the Private Healthcare Information Network (PHIN) has been the significant reduction in consultants working in the private sector, down by about 12%.
FIPO believes that this is due to a combination of retirements and the failure of young consultants to opt to enter private practice but preferring instead to do NHS waiting list initiative lists. These do not require the start-up
BY MR RICHARD PACKARD, Chairman, Federation of Independent Practitioner Organisations (FIPO)
costs in the independent sector and can be carried out on an ad hoc basis.
Cancelled lists
In particular, a reduction in the number of anaesthetists wishing to carry out private practice is beginning to impact accessibility for patients willing to pay for their treatment.
FIPO has heard of cancelled lists in certain areas of the country due to lack of anaesthetic cover.
Anaesthetist colleagues find NHS Choose and Book lists a more appealing option, as their administrative and regulatory responsibilities are covered and the re-imbursement is a more realistic compensation for their expert professional services
FIPO remains very concerned that the multiple pressures on private practice, such as indemnification costs, reporting requirements, loss of professional autonomy and decreasing re-imbursements from private medical insurers, will indeed result in a reduction of both choice and accessibility.
Distortions in competition
This was foretold by the Competition and Markets Authority (CMA) who said a report: ‘If extensively and rigidly applied, fee-capping consultants could lead to distortions in competition between consultants and to reduced consumer choice.
‘Fee-capping – and derecognition of consultants who do not agree to abide by the insurer’s fee schedule – has the potential to increase the disincentives on consultants from setting fees to reflect their costs, experience, expertise
and the local market conditions.
‘This distortion may potentially be increased, the greater the number of insured patients on policies that require open referrals from GPs, as policyholders are channelled to lower-cost consultants.’
This is an excerpt from the 2014 CMA Report and we all know that, unfortunately, this is the current situation.
Further evidence
However, I believe that by providing further evidence of private medical insurers’ behaviour, we may get a more sympathetic hearing. Please keep telling FIPO about your members’ experiences in this regard.
The effect of private medical insurers’ behaviour as above is a further attempt to deprofessionalise and commoditise medical practitioners and their expertise.
Thus, expertise and experience and personal attention – which is what patients are looking for when they opt for private medicine – are no longer recognised as being as important as the cost of a claims episode. Choice for patients is the casualty.
As we have seen already, consultant numbers in the independent sector are falling. This, combined with the increasing difficulty in guaranteeing anaesthetic cover, do not augur well for the future of the independent sector.
It is currently being propped up by the surge in self-pay patients engendered by the long waiting lists in the NHS. One must assume this will not last forever.
PHIN says its data is boon for patient choice
Publication of new information about patient-reported health improvement following treatments in the independent sector have been described as a ‘hugely positive step in helping patients to make informed choices about their private healthcare’.
Jayne Scott, chairwoman of the Private Healthcare Information Network (PHIN) – which has published the data for cataract surgery – added: ‘It is also important infor-
mation for hospitals, consultants and others within the sector to help identify where improvements can be made in the care they deliver.
‘PHIN will continue to work alongside hospitals to increase future participation and response rates.’
lead to an improvement in their health.
The data publisher said the public could now get a better understanding of how likely it was that their operation would
It has published new information at phin.org. uk for around one-fifth (42) of 227 independent hospitals providing cataract procedures.
PHIN said it received outcome data from 76 hospitals, but the results for 34 of them could not be published due to the small number of
cases involved and the consequent risk of patient re-identification.
The information is also available in a downloadable and analysable format at https:// www.phin.org. uk/data/health-improvementdatasheets.
PHIN has also produced a short guide to Patient Reported Outcome Measures (PROMs) to help members of the public considering which healthcare provider is right for them.
Jayne Scott
A look back through our journal’s archives of a decade ago reveals that although times change, some issues are not so new
A trawl through the archives: what made the news in 2012
Never hype up your ads
A hospital group’s logo row with the advertising watchdog sparked warnings for private doctors to exercise caution when making claims about themselves in publicity material.
BMI was appealing after the Advertising Standards Authority (ASA) upheld an objection that the group’s emblem’s use of the statement ‘The Consultants’ Choice’ misled by implying specialists were more likely to recommend BMI Healthcare than other providers.
The group disagreed and said the wording, which appeared at the top of hundreds of consultants’ marketing leaflets provided by its hospitals, had been in use for five years without complaint until then.
But as BMI prepared its next move, a doctors’ defence expert warned that the case highlighted
the need for practices to regularly review their own electronic and written materials to ensure these were accurate and in line with the GMC’s Good Medical Practice guidance.
A medico-legal adviser at defence body MPS said: ‘The guidance states that any information provided about medical services must be factual and verifiable and must not make unjustifiable claims about the quality or outcomes of services.
‘If patients have skewed expectations because of assertions you have made on your website or brochures, it could damage the doctor-patient relationship and possibly lead to complaints.’
According to the ASA, private doctors’ increased spend on marketing material was likely to lead to more complaints, whether or not there were legitimate wording issues.
Complaints against private docs
Figures on the level of complaints against private doctors were predicted to be available in 2013 because revalidation would make it easier to collect data, according to the GMC.
Complaints about doctors hit a record high the previous year, but the council told Independent Practitioner Today it could not break down the figures to identify private practice numbers.
A BMA leader said increased
complaints against doctors reflected a trend across healthcare and also that the public was more willing to complain than it did in the past.
Surgeons call for ban on baits for beauty ops
The British Association of Aesthetic Plastic Surgeons (BAAPS) had submitted a new, strict advertising code to regulator, the Committee of Advertising Practice (CAP), which set out policies for the Advertising Standards Authority.
Although continuing to call for an outright ban on all forms of cosmetic surgery advertising, it said that outlawing a ‘dirty dozen’ hit list was the bare minimum that would be considered acceptable to help protect the public, particularly the young.
It called for prohibition on all advertising aimed at under-18s, an end to advertising in public places where children could see them and a ban on all forms of discounted offers and financial inducements.
BAAPS also called for a stop to time-limited offers, loyalty cards as an inducement to have multiple or repeat procedures, ‘buy-one-getone-free’ deals, recruitment of patients for cosmetic surgery by agent, refer-a-friend schemes and cosmetic surgery as prizes.
The group’s president Mr Fazel Fatah said it strongly believed
that, in the absence of a complete ban, these and other measures were needed to ensure patients were protected from unethical practices.
College boss warns overconfident surgeons
The Royal College of Surgeons of England president warned wouldbe private practitioners to ensure they worked within their capabilities.
Prof Norman Williams told a joint Medical Protection Society/ Association of Surgeons in Training (ASIT) conference that surgeons ‘time and time again’ went to the private sector and took on work beyond their competence.
He also urged ASIT members to avoid clashes with colleagues.
‘Even if you don’t like a colleague, you’ve got to get on with them –or leave.’
TELL US YOUR NEWS
How about making the news today? Independent Practitioner Today is always keen to hear from doctor entrepreneurs willing to share their stories in private practice – and from independent practitioners embarking on the journey.
Contact our editorial director Robin Stride at robin@ip-today. co.uk
Spending too much time on billing instead of patient care?
Let Medical Billing & Collection do the hard work for you.
With 30 years’ experience helping over 1,500 private consultants, groups, clinics and hospitals.
• Dedicated account manager
• Reduce bad debts to less than 0.5%
• Increase net income by up to 25%
• 24/7 online access to your data
• Faster payments through e-billing for insurers and patients.
Discover more at medbc.co.uk or 01494 763999
ACCOUNTANT’S CLINIC
Why tax returns need to be submitted early
Minimise your annual tax hassles by dealing with things early and enabling your accountant to help with some useful planning. Julia Burn has some tips for the upcoming tax season
IT IS the time of the year again when taxpayers should really start thinking about their personal taxes and their tax submissions.
The last tax year ended on 5 April 2022 and personal tax returns for this year are becoming due by 31 October 2022, if filed on paper, and 31 January 2023, if filed electronically.
Any balancing tax payments for the year must be made by 31 January 2023 and payments on account for the following year 2022-23 by 31 January 2023 and 31 July 2023.
As we continue to emerge from the Covid-19 pandemic, the tax world also returns to normality. In the previous two years, HM Revenue and Customs (HMRC) allowed taxpayers to file returns and pay taxes later to help struggling businesses and individuals. These breaks are no longer available.
Estimating your tax liability
Many taxpayers, including doctors, took advantage of HMRC’s schemes to assist them with paying off their past tax liabilities. For some, part of those liabilities may still be in the process of being repaid to the Exchequer.
With current tax liabilities becoming due on 31 January 2023, this may cause a strain for some taxpayers. HMRC has discretion to allow further payment plans, but that is completely up to its officials.
Any late payments for 2021-22 and payments on account for 2022-23 will incur late payment interest, and balancing payments due post 2 March 2023 will result in automatic 5% penalties if no new payment plans are agreed.
Cash flow planning for your tax bill is important and you may wish to consider submitting your 202122 return early to give yourself
adequate time to plan. Your accountant will be able to calculate how much you should save each month to generate enough funds by 31 January.
If your tax return for 2021-22 is submitted by 30 December 2022, your tax liability is less than £3,000 and you pay tax under PAYE, you will be able to elect for this to be coded out.
This means your liability will be spread out over the tax year and collected with the PAYE tax, so no physical payment will then be required by 31 January 2023.
Inquiry windows
HMRC audits several returns every year to check they have been completed correctly.
As long as all relevant information is provided and no details are omitted, HMRC has 12 months from the date of the submission of
a return to inquire into it – otherwise, it could go back as far as 20 years.
If a return is submitted late, this window for HMRC extends to the anniversary of the end of the quarter following the submission date.
The sooner your return is submitted, the sooner the inquiry window closes.
Pension annual allowance charges
Medical practitioners are often members of defined benefit pension schemes. These schemes are extremely valuable, as the pension payments on retirement are based on their final salaries. While this means attractive future pension benefits, it can result in tax charges for breaching the pension annual allowance.
Taxpayers are allowed to contribute up to 100% of their relevant earnings if their earnings are lower than £3,600 a year. But the
amount contributed should not exceed the annual allowance – and any unused brought forward annual allowances from the previous three tax years.
The standard annual allowance is currently £40,000, but this gets tapered for higher earners who earn in excess of £200,000, with the minimum annual allowance being £4,000. Otherwise, any excess contributions will be subject to a tax charge at your marginal rate of tax.
It is harder to monitor the contributions in a defined benefit scheme, as it is not clear how much your pension fund increases by until NHS Pensions issues your annual statement, usually around October following the end of the tax year. Medical practitioners often exceed their annual allowances without knowing.
NHS Pensions may pay your annual allowance charge as long as an appropriate election is made
by 31 July following the year in which the charge arises. You need to ensure that any annual allowance charges are reported in your tax returns.
HMRC has published a pension annual allowance calculator and you can find this at www.tax. service.gov.uk/pension-annualallowance-calculator/tax-yearselection . On the opening page, you have to select the years you were a member of a registered pension scheme.
Superannuation returns
Once your 2021-22 tax return has been submitted, you may also need to file your superannuation return to report the superannuation contributions made by you and any employer.
The superannuation returns for 2021-22 are due for filing by 28 February 2023. As they can only be filed once your personal tax return for 2021-22 has been final-
ised, you may wish to consider filing your return in good time before the deadline to allow plenty of time for these complex calculations.
These tax rules are complex and we recommend that you speak to your accountant regarding all of the above.
In conclusion, we would recommend that you attend to your personal tax affairs sooner rather than later, as this will allow you and your accountant more time for any tax planning.
And it will reduce the risk of any surprising last-minute tax liabilities.
See ‘Keep a tab on your tax dates’, page 42
Julia Burn (right) is a director at Blick Rothenberg and part of the team that advises medical practitioners
Spire Bushey
TROUBLESHOOTER: GROUPS
The big benefits of banding together
Consultants’ groups may be an increasingly attractive option for those in private practice in the current financial climate. Our Troubleshooter Jane Braithwaite tackles a question on the lips of many.
This month: I have been happy as a solo independent practitioner, but with pressure on costs and other factors, I am thinking of setting up a group. What advice would you give me?
A LOT OF doctors in private practice choose to form groups with like-minded colleagues.
Some decide to go down this path soon after starting independent work, while others transition into it with a large amount of private practice experience.
There are myriad reasons to form a group, ranging from personal to financial. Let’s look at why you might want to form a private practice group and examine some of the important issues you might want to consider.
There are a number of benefits to group formation, which I explain more fully below:
☛ Income benefits
As a solo practitioner, you only have so many hours in a day. You might find that the number of tasks you have to complete seems overwhelming.
Not only do you have to undertake all the clinical tasks that caring for your patients involves, but you are responsible for all the necessary, but not always exciting, activities that a thriving business throws up.
When working by yourself, your income is directly related to the number of patients that you can see and treat. If you want to increase your income, generally speaking, you have to work more.
The number of hours can add up quickly, risking burnout and making it difficult to provide the same high-quality care to each patient.
Additional complications include the expense or lost income related to taking holidays and how to find clinical cover in the event of your absence.
Working as part of a group can negate some of these problems. Clinical work can be evenly distributed and, overall, you can see more patients. You might even be able to take a holiday or two.
☛ Personal and professional benefits
Being a solo practitioner has the potential to be a lonely experience.
Those working in the NHS may be used to large departments with many peers and juniors. Getting a second opinion before making a decision, asking for help or even just socialising with colleagues can be rewarding.
For some, working alone may be isolating. Forming a group has the potential to negate some of these problems and maybe a positive experience.
Having peers who are working towards the same collaborative goal as you can provide a support system.
This can be valuable when things are going well, but essential when there are difficulties. Having a sense of community can be really important when dealing with the trials and tribulations of modern clinical practice.
A group can allow collaboration when working on specific projects that will benefit your clinical service. Together you might be able to provide investigations or treatments that would not be viable, either practically or financially as a solo practitioner.
The colleagues that you bring together to form your group may well have different, but complementary, skill sets. This ability to offer a wider range of treatments will ensure that the pool of patients that you can manage is greatly expanded and that a greater part of each patient’s treatment journey can be spent with the group.
☛ Financial benefits
It is no secret that the costs of practice are increasing. The bills for rooms and premises, secretarial support, indemnity cover, marketing and accountancy are all steadily going up.
The fees paid by medical insurers, like Bupa, are not increasing in step with the rising costs of medical practice.
The self-pay market is becoming more prominent, but patients without insurance are likely to be much more price-sensitive than those using other payment methods.
A group can help offset some of these cost increases by allowing much greater efficiency in the business side of your practice. This can include money invested in advertising your practice, accountancy and book-keeping and medical secretarial costs.
Some insurers may have a preference for dealing with groups rather than solo practitioners, and you might find this reflected in increased patient referrals or ease of dealing with re-imbursement.
Having a sense of community can be really important when dealing with the trials and tribulations of modern clinical practice
The realities of setting up a group
Setting up a group is a significant commitment. As the one who is initiating this, you may find that, naturally, you will act as the leader and manager of your peers.
Running a group requires a different set of skills than managing a solo practice and there can be a steep learning curve.
Before starting, you will need to be prepared for the extra time required to run the group practice, both due to increased administration and also from managing the other people involved in your endeavour.
When starting this new business, it is easy to get carried away with thoughts of all the possibilities, from more patients to better treatments and perhaps even greater profits.
It is easy to focus on the excitement and not to have the difficult but essential conversations and agreements that have to happen right at the beginning.
Everyone needs to be clear about what expectations they have going into this enterprise, both of themselves and of each other. Will everyone commit the same amount of time to the group? How will profits be distributed? Does everyone have an equal say in the running of the group?
All of these questions need to be addressed and agreed upon before the group can start work.
One item that is often not discussed is what will happen if the group is not the success that you
hope. The reasons for this could vary from the costs being too high, not bringing in enough patients or disagreements among members of the group.
Dissolving the group
If you have to make the difficult decision to dissolve the group, how will the financial obligations be dealt with and how will any remaining profit be distributed?
It is important to consider how each member of the group would transition back to independent practice if they wish to leave the group or if the group was to come to an end.
You may find that embedding routine or regular reviews, where you each openly discuss issues within the group and follow up on past decisions, makes sure that everyone feels involved in the management of the business.
These meetings have to allow all partners to freely bring up problems, as having issues fester can cause significant problems down the road.
Your patients come to you for specialist advice and you should do the same when forming your group.
Accountants and legal professionals will be able to steer you in the right direction, be it the requisite contracts with your colleagues, whether your business should be a limited company or a partnership, or how to ensure you are paying the correct taxes.
Forming a new group should be exciting, both professionally and personally. Careful planning at the outset, backed up with expert professional advice, will hopefully lead to your future success.
If you have any specific questions that you would like answered in upcoming editions, please do feel free to get in touch.
See ‘How do groups go about their billing?’, page 16
Jane Braithwaite (right) is MD of Designated Medical, which offers flexible, experienced support for private practice needs.
Its experts offer bespoke support across accountancy, marketing, medical PA, HR, and recruitment
How do groups go about their billing?
Simon Brignall (left) continues last month’s reflection on the challenges groups face with their billing and provides a check list for you to use when considering setting one up
IN LAST month’s article, we discussed the fundamental differences that consultants find about groups, such as the volume of patients being treated as well as the various structures they adopt in their set-up.
Now it is time to get into the specific challenges groups face with their billing and collection and why it is important to ensure you have the correct processes and infrastructure in place.
Billing and pricing
Because a group consists of a variety of consultants, it is required to manage the various pricing policies used by each specialist.
This can arise either by choice, as a reflection of the consultant’s expertise and experience, but more commonly it is because of the individual contractual terms each consultant is subject to with the private medical insurers.
And that has become more prevalent in recent years with newer consultants restricted to set consultation fees with Bupa and AXA and some of the other insurance companies, while older consultants may have their own tariff or higher contracted fees.
Each consultant can also have their own fee schedule for self-pay patients, although some groups choose to employ a consistent
Some consultants require their self-pay fees to be collected
It can be quite common for us to take on groups where we find that payments have not been going to the correct bank account and so the group had been missing out on income for years
choose to practise outside of the group; however, this requires vigilance and co-operation between the group’s administration team and those servicing the consultant’s external activity.
directly from the patient or as part of a fixed-price package and this can vary depending on the hospital or specific procedure.
All this requires the group to maintain accurate records of the price structures and payment pathways used by each consultant. All this is on top of keeping up to date with the ongoing changes that occur within each insurer’s schedule and the changes to the Clinical Coding Schedule and Development Group (CCSD) schedule to ensure the group is invoicing correctly for each doctor.
In our experience, groups find this area challenging and if it is not done correctly, then we have seen groups that have lost tens of thousands of pounds in income. Always remember that incorrectly invoicing insurance companies leads to delays in payments, recoups and, in the worse cases, derecognition.
Bank accounts
Depending on the model the group choses to adopt, there can be different arrangements for payments and bank accounts.
Formalised group structures generally have one pooled bank account or, on rare occasions, individual sub-accounts. It is important to note that insurance billing is normally processed using the individual consultant’s provider number which will pay into a single designated bank account. Some groups have their own provider number that is shared by all members of the group for billing, but this is rarer.
In each of these examples, each payment needs to be identified and allocated to the appropriate consultant so that any subsequent onward payments can be made to them depending on the group’s revenue distribution model. Some consultants may also
As discussed earlier, payments can only be made to one designated bank account associated with the provider number and remittance advice can only be sent to one contact point. This means robust procedures need to be adopted to allow for transfer payments and remittance sharing.
Even in those cases where a second bank account is an option, it is common for payments to be made to the wrong account.
In virtual group structures where consultants act as individual practices, payments are made to each practice. But they still require reporting that allows for the recovery of costs for the running of the group.
It can be quite common for us at Medical Billing & Collection (MBC) to take on groups where we find that payments have not been going to the correct bank account and so the group had been missing out on income for years.
Reporting
It is key to ensure whatever processes you implement that there is good visibility for all stakeholders involved and that reports are both accurate and up to date.
At MBC, we recreate the specific structure the group adopts in our software, which allows for reporting at both the group and the individual consultant level. This provides the group’s management an array of real-time reports at the group level as well as providing each consultant access to their own data.
The trend towards consultants choosing to operate in groups is well established and groups now make up a major share of our activity.
If you are seeking to establish or join a group, this article will act as useful guide to some of the challenges you may face and some of the questions you need to consider. Often the best solution is to seek the advice of a professional medical billing company.
Simon Brignall is director of business development at Medical Billing & Collection
Questions to ask
Here is a simple group check list of questions for you to use if you are considering joining a group. It could also be useful if you are thinking of setting one up:
What group structure have they employed and is this right for me?
What are their costs and how are they allocated?
How are funds distributed to each group member?
Are funds collected centrally?
Are there any specific rules that relate to founding partners and new entrants?
Ensure that you understand whether funds are distributed out of received income and when you can expect these payments to be made once received by the group.
How is the administration of the group managed?
What is the impact to this should the group shrink or expand?
Does the group use practice management software?
If YES, is reporting available to you? How easy is this to do and is the data accurate and up to date?
If NO, then what systems do they have to provide you with the information above?
Are there any issues whichever system they employ?
What is the current state of the group’s finances?
Pay specific attention to any delays in invoicing and the size of the groups aged and bad debts, as this will impact your cash flow.
Does the group accommodate bespoke pricing?
How often are fees and CCSD codes reviewed to ensure any changes that are relevant are applied and opportunities are not missed?
Will the group accommodate all of your private activity?
If not, how will the remaining activity be invoiced?
And what will be the implication of this for payments and the reporting in relation to this activity?
Simon Brignall’s piece in last month’s issue of Independent Practitioner Today
Face up to the real risk of being sued
Lawyer Deborah Pyzer (right) has some advice for cosmetic practitioners servicing the quest for supermodel looks
IN THE post-Zoom era, many of us now spend several hours a day looking at our own reflections in a computer screen during meetings held via video-conferencing as we have moved towards more remote ways of working.
It is therefore unsurprising that, in 2020, there was a 57% increase reported in email and web inquiries for cosmetic treatment.
In a world governed by social media and celebrity culture, with the ready availability of professional airbrushing or quicklyapplied filters, it is no wonder that people want their natural appearance to be aesthetically enhanced to match what they see across social and popular media.
In addition to the risks and complications of treatment set out on the patient consent form, there is one risk that is less widely recognised for the aesthetic/cosmetic practitioner and that is litigation.
The potential for a legal claim arising out of cosmetic treatment has recently shot to the limelight with the news of settlement of supermodel Linda Evangelista’s CoolSculpting* claim.
A question that may be on some practitioners’ minds is ‘what can I do to reduce the chances of a claim being brought against me?’
From our experience of managing complaints and claims arising
out of aesthetic treatment, here is our advice:
1 Trust your instinct and watch out for ‘red flags’ It is important to be aware that not all clients are suitable candidates for procedures.
With hindsight, we often hear practitioners saying that they should have acted on signs that the client was not likely to be happy with the outcome of treatment.
Identifying a client’s reasons for seeking treatment is key. Explore their levels of anxiety around their appearance before offering treatment.
Asymmetry and varying results are recognised risks of aesthetic and cosmetic treatment, and a client that has severe underlying anxiety about their appearance is more likely to be dissatisfied with the outcome of a procedure that is known to have variable effects.
2 Ensure your written consent documentation is clear and comprehensive, and that you provide clients with a thorough explanation of the risks of treatment before proceeding.
A client is less likely to be dissatisfied with treatment if they understand that the complication they
A client that has severe underlying anxiety about their appearance is more likely to be dissatisfied with the outcome of a procedure that is known to have variable effect
We recommend making contact with your insurers before taking these steps: there is a risk of policy coverage being declined due to late notification or payments being made without insurers’ agreement.
When we are instructed by your insurers, we are able to provide documentation to go alongside any offer of a refund to ensure that any payment accepted by the client is in ‘full and final settlement’ of any future claim arising from the same injury and we can provide practitioners with hands-on advice and support with managing tricky clients.
The free digital prescribing platform for all private prescribers.
CloudRx take care of the dispensing, payment and delivery of medicines direct to your patients, wherever in the country they may be, for more convenient access to their medicines.
are experiencing was a recognised risk, which they clearly understood in advance of agreeing to treatment.
In practice, consent forms can become a tick-box exercise or, worse, a client may sign the consent form without having actually read it. It is important to have a face-to-face discussion of the risks with your client and ensure they have sufficient opportunity to digest the risks and ask any questions.
In our experience, consent forms can also be missing some recognised risks of treatment and it is important to review and update your consent forms to ensure they include all relevant risks.
You may wish to compare your consent form with practitioner colleagues or we are happy to provide advice on review of your consent forms.
3
Seek advice sooner rather than later In the event of complications or client complaints, do not delay in notifying your insurers. Seek advice at an early stage to help you to manage your relationship with your client.
The nature of the relationship between an aesthetic or cosmetic practitioner and their client is unique and entirely different to those practising in a traditional medical setting.
There is often a temptation for the practitioner to try to do everything in their power to keep the client happy, whether by offering the patient a refund or offering repeat clinic follow-up appointments to discuss complications.
Deborah Pyzer is a solicitor in the clinical risk department at Bevan Brittan LLP.
She advises both public and private sector clients in a variety of clinical negligence/medical malpractice claims. She has acted for independent practitioners and clinics/practices in claims concerning aesthetic practitioners, cosmetic and ophthalmic surgery and is experienced in managing psychiatric, orthopaedic, dental and obstetric claims
➲ This article was first published on the Bevan Brittan website and is reproduced with permission
THE LINDA EVANGELISTA CASE
*CoolSculpting – a brand name for cryolipolysis – is a nonsurgical fat reduction treatment, using cooling technology to target and remove fat cells in the body.
Supermodel Linda Evangelista underwent CoolSculpting in 2016 but suffered a rare complication, paradoxical adipose hyperplasia (PAH), resulting in overgrowth of fatty tissue. Studies indicate that the risk of PAH as a consequence of CoolSculpting is less than 1%.
Evangelista brought a lawsuit in the US against CoolSculpting’s parent company for $50m in damages in respect of the complication she had suffered. She publicly announced settlement of the CoolSculpting lawsuit in July 2022.
TRANSFORMATIONAL
Order prescriptions at the touch of a button to support all consultations and add a whole new level of convenience for your patients.
SIMPLE, CONVENIENT AND SECURE
Simple and fast digital prescribing.
Legal paperless prescriptions, repeat prescriptions and controlled drugs.
Prescriber fees can be charged to the patient if requested.
INTEGRATED
Our API enables frictionless integration with healthcare brands & clinical software including Heydoc, MidexPRO, eClinic and YouClinic.
“We were struggling to keep up with the admin side of the prescriptions, not to mention storage for medication to cope with a huge increase in prescriptions. CloudRx immediately took away the strain. Since our partnership we have grown by more than 200% in size. We could not have done that without their support.”
– Dr Louise Newson, Newson Health
Broadening the access
Healthcare insurers and providers now need to consider some important issues as part of the digital healthcare revolution if we are to keep up the momentum. Dr Leah Jones (right), head of behavioural insights at Bupa, analyses where we are when it comes to accessing healthcare online
access to digital care
BEFORE COVID-19, the preventative use of fitness and well-being apps was increasing; however, telemedicine had been slow to take off because face-to-face care remained the preferred option.
In January to February 2020, 96% of households in Great Britain had internet access, up from 93% in 2019 and 57% in 2006 when comparable records began.1
Fast forward to when the pandemic struck and overnight patients and healthcare providers were forced to switch their interactions online. Many countries adopted digital-first strategies, remote monitoring and telehealth platforms to enable healthcare provision without the risk of transmitting Covid-19.
In the UK, primary care embraced telehealth at scale and deployed a new digital-first pathway as a route to managing streaming of care to the appropriate place.
Our own Digital GP service saw a 50% increase from just over 8,000 to just under 12,500 appointments a month between February and March 2020.
Internet use became almost necessary for survival rather than a luxury; however, during the pandemic years there were still an estimated 2.6m people who were offline.2
A May 2021 report by McKinsey and Company3 found that 88% of people said that they had used telehealth services at some point since the pandemic began. And furthermore, 83% of clinicians surveyed in 2021 offered virtual services, compared with only 13% in 2019.
With telemedicine the default option, things looked promising for the long-awaited digital healthcare revolution.
In April 2020, use of telehealth was 78 times higher than in February 2020. But that spike in uptake has now stalled at 38 times higher than pre-Covid-19 levels.
A May 2021 report by McKinsey and Company found that 88% of people said that they had used telehealth services at some point since the pandemic began
And while more physicians could offer care via telehealth, they still continue to recommend in-person care when possible again in 2021.3 With 90% of the population in an Ofcom survey having a smartphone,4 we could be forgiven for thinking that people would be keen to continue to use telehealth, as it offers a quick and convenient way to access healthcare. However, there are some hurdles that we need to overcome to ensure greater uptake of digital healthcare:
Data security and privacy
Our health data contains our most private information, so it is understandable that patients would be concerned about its safety and use. Concerns about the privacy and security of electronic health information usually fall into two categories:5
❶Inappropriate releases of information from individual organisations; for example, if an authorised user intentionally or unintentionally shares the information in breach of the organisation’s rules – for example, a data leak – or when outsiders hack into an organisation’s computer system to steal data and hold it ransom with the threat of releasing it.
❷ The systemic flow of information throughout healthcare and related industries and the use of this information in a way ➱ continued on page 22
that may be against the interest of the patient or perceived as invading the patient’s privacy – for example, sharing information which the patient may be embarrassed about.
Even before the introduction of electronic medical records, the healthcare sector took significant steps to protect patients’ health information and maintain its confidentiality.
These same principles – deciding who can access the health information and whose needs for access are legitimate and put policies in place to ensure this – still apply with digital health information.
There are numerous mechanisms that can be used to protect electronic health information. These include both technical measures to improve network and computer security and the kinds of organisational measures mentioned above to make sure that only those who need to can access patients’ information.
Preference for face-to-face care
Analysis of GP practice data carried out by The Health Foundation found that 10% of patient care requests made to GP practices between March and September 2021 indicate a preference for a face-to-face consultation.6
At population level, this still represents a significant number of people who we need to ensure can access healthcare in a way that meets their needs.
A survey by Healthwatch Wandsworth7 found that views and experiences of using digital and phone appointments were mixed, even among different sections of the community.
Although some people praised and preferred phone appoint -
Lack of digital literacy
Financial factors
The key to successful remote consultations is understanding which approach is the right one based on individual patient’s needs and circumstance
ments, particularly for routine checks, others fed back negative experiences including long waiting times to speak to a healthcare professional, rushed calls and feeling that they did not provide the same level of care as face-to-face appointments.
It seems that confidence using technology may be a factor in this.
A study of colorectal cancer patients found that those with experiences of using video calling in daily life seem to choose videos over face-to-face consultations more often.
Patients who were hesitant in choosing a video consultation spoke of feeling insecure about using new technology.
However, 38% of patients in the face-to-face group were willing to try a video consultation in the future, but said they first wanted to get familiar with using video calling in daily life before using it for health purposes.8
The key to successful remote consultations is understanding which approach is the right one based on individual patient’s needs and circumstance.9
Healthwatch Wandsworth has put together a list of tips to help patients and healthcare professionals get the most out of the virtual health and care experience entitled The Doctor Will Zoom You Now.
There are many definitions of digital literacy, but, put simply, it means having the information technology skills needed to search, sort, evaluate and use online information.
Covid-19 highlighted the importance of digital literacy and widening access to online information by helping people to gain the skills they need to navigate and judge whether what they read is true or false.
According to the National Literacy Trust, in the UK 7.1m adults read and write at or below the level of a nine-year-old, and 43% of adults do not understand written health information.
With healthcare services, information and advice increasingly dependent on the internet, navigating digital information adds yet another layer of difficulty for those struggling with literacy who may also lack technological skills.
Health Education England’s National NHS Knowledge and Library Services team is working with the Chartered Institute of Library and Information Professionals to improve health and digital literacy at local level.
Its initiative is aimed at empowering patients, their families and carers by giving them the tools they need to maximise the health information and digital resources available to them.
Fragmentation of provider systems
People want services that are designed around them. At Bupa, we are trying to create a single front door for customers behind which we integrate a range of provider systems.
This requires providers and payers to work together.
According to the UK Consumer Digital Index 2021,2 26% of people who had not used the internet in the previous three months said it was because it was ‘too expensive’. This is backed up by a review by Ofcom4 which found that 11% of fixed broadband households with the lowest incomes (up to £10,399) and the same proportion of those receiving means-tested benefits experienced an affordability issue with this service, which meant they had to modify or cancel their contract.
Furthermore, the UK Consumer Digital Index 2021 2 found that more than a third of UK benefit claimants have very low digital engagement.
The digital engagement score looks at people’s online spending, their interaction with digital services and products, and their use of digital devices and fintech services that use technology to provide automated banking and other financial services.
The average benefit claimant scored zero across many measures – however, 14% of their spend is online, some of it on mobile phones. They tend not to use email or online banking.
Benefit claimants are also more likely to have less digital engagement compared to the rest of the population and there is a greater digital disparity within this group.
Given the inability to leave home during the spring 2020 lockdown, the UK Consumer Digital Index 20212 found that millions of people across the UK struggled to engage with the online services required to access support.
Encouragingly, however, digital engagement has also increased for this population across the board since 2020.
Groups at risk of digital exclusion
When thinking about digital healthcare services, we need to be mindful that certain segments of the population are more likely to be offline than others.
These are:
➲ Older adults: The ability of new telehealth initiatives to reach older people is uncertain, as many do not have smartphones or computers and some have poor or no connectivity due to their location.10
The older a person is, the more likely they are to be digitally excluded, according to the UK Consumer Digital Index 2021.2 This is exacerbated in those who live alone, have a limiting or impacting condition such as hearing or dexterity and are financially vulnerable.
Older people are also less likely to own a PC, laptop, tablet or smartphone, and less time spent online tends to correlate with lower confidence and comfort accessing digital services.
➲ Disabled people: Having a condition that limits or impairs the use of communications services – such as hearing, eyesight, mobility, dexterity, breathing, mental abilities, social behaviour or mental health – is also likely to be a barrier to using digital services.11
Households including someone with a limiting or impacting condition were also more likely than average to experience affordability issues with their broadband service (8%) and to say they had cancelled the service (2%) according to the Ofcom report.11
➲ Minority ethnic groups:
The technology required to implement telehealth consultations may be problematic for some patients from racial/ethnic minorities because of the cost of equipment, limited understanding of the use of equipment and limited digital literacy.12
The financial barrier is demonstrated by the unemployment and income data. From January to March 2022, the UK unemployment rate was 3.1% for people from a white ethnic background compared to more than double
The older a person is, the more likely they are to be digitally excluded, according to the UK Consumer Digital Index 2021
that (7.1%) for people from minority ethnic backgrounds.13
Coupled with the fact that black households (54%) were most likely out of all ethnic groups to have a weekly income of less than £600,14 it is no surprise that one hurdle to accessing digital healthcare is an inability to afford internet connections and the devices required to access telehealth.
This is further exacerbated by the added complication of language proficiency and cultural considerations.
Conclusions
1
Covid-19 has shown us that digital healthcare is a good way to interact with patients, particularly when we adopt a hybrid of digital and face-to-face consultations.
2
Use of Bupa’s Digital GP has continued to climb steadily as the UK returns to normal life again, from almost 12,500 in March 2020 to almost 49,000 in July 2022.
3 While digital healthcare is not clinically appropriate for all circumstances, it is particularly suited to things such as fol -
low-up appointments and the treatment of some ongoing chronic conditions where a physical assessment isn’t necessary.
4
However, in adopting a digital approach, we need to create a way forward that is accessible to all and takes account of patient needs and preferences.
5
We need to bear in mind the challenges faced by groups who tend to be digitally excluded and develop services that help them overcome the barriers to access – for example, by offering options in multiple languages and alternative formats.
References
1. Internet access – households and individuals, Great Britain: 2020, Office for National Statistics, August 2020.
2. UK Consumer Digital Index 2021, Lloyds Bank UK, 2021.
3. Patients love telehealth – physicians are not so sure, McKinsey and Company, May 2021.
4. Communications Market Report 2022 Ofcom, 2022.
5. For the Record, Protecting Electronic Health Information, National Research Council (US) Committee on Maintaining Privacy and Security in Health Care Applications of the National Information Infrastructure, National Academies Press, 1997.
6. Clarke G, Dias A, Wolters A. Access to and delivery of general practice services: a study of patients at practices using digital and online tools. The Health Foundation; 2022.
7. Experiences of digital and telephone appointments, Healthwatch Wandsworth, March 2021.
8. Video consultation during follow-up care: effect on quality of care and patient and provider attitude in patients with colorectal cancer, Esther Z. Barsom, Marilou Jansen, Pieter J. Tanis, Anthony W. H. van de Ven, Marjolein Blussé van Oud Alblas, Christianne J. Buskens, Willem A. Bemelman, Marlies P. Schijven, March 2020.
9. The Dr Will Zoom You Now: getting the most out of the virtual health and care experience: Insight report – Key findings from research June-July 2020, Healthwatch England, National Voices, Traverse, PPL, March 2021.
10. Malcolm Fisk, Anne Livingstone, Sabrina Winona. Telehealth in the Context of COVID-19: Changing Perspectives in Australia, the United
Kingdom and the United States; Journal of Medical Internal Research, 2020.
11. Digital exclusion, A review of Ofcom’s research on digital exclusion among adults in the UK, 30 March 2022.
12. Mandy Truong, Ladan Yeganeh, Olivia Cook, Kimberley Crawford, Pauline Wong, Jacqueline Allen. Using telehealth consultations for healthcare provision to patients from nonIndigenous racial/ethnic minorities: a systematic review; Journal of the American Medical Informatics Association, Volume 29, Issue 5, May 2022.
13. Research briefing: Unemployment by ethnic background, House of Commons Library, July 2022.
14. Household income, Department for Work and Pensions, July 2022.
COMPLAINTS IN THE PRIVATE SECTOR
Helping patients in
Patients in NHS PPUs are not allowed to make complaints through the Parliamentary Health Service Ombudsman. The Independent Sector Complaints Adjudication Service is working to ensure they are aware of the relevant route for private patients to use. Sally Taber explains
A PATIENT IN any healthcare environment who finds it necessary to complain is, unfortunately, unlikely to be well informed about the process to follow.
For patients treated by the NHS, there is a clear path leading to the Parliamentary Health Service Omb udsman (PHSO) and, for patients in the independent sector, to the Independent Sector Complaints Adjudication Service (ISCAS) code.
Confusion arises for private patients treated in NHS hospitals in their private patients units (PPUs). In the environment of an NHS hospital, it might be natural to assume that a complaint would be handled through the NHS system to the PHSO, but this is not, in fact, the case.
PPUs exist as treatment centres financially independent of the NHS and with no call upon Government funds, being the product of local economicallydriven initiative.
For this reason, the Care Quality Commission (CQC) lays down in its inspection framework for PPUs that ‘where . . . the patient is receiving non NHS funded care…
patients do not have access to the PHSO.’ Instead, the CQC points the way to the ISCAS Code for Handling Complaints as a suitable alternative.
According to data from the Private Healthcare Information Network, 277 PPUs currently do not have access to an external review of unresolved complaints.
That leaves many private patients of PPUs in jeopardy, paying for treatment but with no safety net in case of dispute. This is not a good situation.
Defensive system
In the First Do No Harm report published in July 2020, Baroness Cumberlege referred to a defensive healthcare system that does not listen to the concerns of patients.
The NHS website ‘How to complain to the NHS’ is only relevant for NHS funded treatment and refers to escalating complaints to the PHSO. Therefore, this and other information for NHSfunded care should not be provided to private patients treated in the NHS.
ISCAS is provided as a link for complaints about private health
care by the CQC on their website ‘Complain about a hospital, community or mental health service’. This section of the CQC website signposts patients who remain dissatisfied with the response from the provider. The CQC differentiates the point of escalation based on how healthcare has been funded; namely PHSO for NHSfunded treatment and ISCAS for privately funded treatment.
ISCAS is provided as a link for complaints by the PHSO website page on private healthcare.
Pilot schemes
ISCAS, in conjunction with the PHSO, will be carrying out pilot schemes – hopefully with the Great Ormond Street Hospital PPU and the University Hospital Southampton PPU – to provide PPUs with true guidance on the correct route for processing complaints so that their PALS (Patients Advice and Liaison Service) can confidently continue to advise, support and inform PPU patients.
NHS and private patients continue to say they do not understand how to escalate complaints
complaints limbo
in both the NHS and the independent sector.
This was highlighted in the Paterson Inquiry Report published in February 2020, which recommended: ‘Information about the means to escalate a complaint to an independent body is communicated more effectively in both the NHS and independent sector.’
Listening to patients is an important component in any management system, public or private.
In July 2020, the Patients Association facilitated a focus group with patients who had received private and NHS funded health
care and had complained about their treatment.
The focus group concluded: ‘It would not be clear to the person on the street that private patient complaints cannot be escalated to the PHSO. The focus group stated that ‘most patients wouldn’t know where to find it [information] or that it even existed’.
The focus group said that information about how to escalate private patient complaints should be simple information guides in one page if possible and should: ‘Be part of the information sent with the admission letter and then
explained by the consultant at the initial consultation.’
Consist of ‘a pack of information, including how to complain given to the patient at the outset. A leaflet, posters around the hospital, in GP waiting rooms etc.’
Another bureaucratic cost?
No. Listening to users and understanding their point of view is an important link in any management improvement system; economically valuable and therefore worthy of investment.
The lessons from the Paterson Inquiry point out the need for
good complaints handling processes and Baroness Cumberlege states organisations should designate a non executive member of the board to oversee the complainthandling processes and outcomes and ensure that appropriate action is taken.
The NHS invests in the PHSO. PPUs, independent of the NHS, need to invest into ISCAS by subscribing to us to give patients an avenue for complaints.
Sally Taber (right) is director of ISCAS
BOOK YOUR DEMO Are you happy with your current software?
Maybe you're completely happy with the software you use to run your practice. Perhaps you have everything in one place, routine tasks are automated, and reporting is accurate and insightful. If so, stop reading now.
However, if you think the day to day running of your practice could be improved, we'd love the chance to demonstrate e-clinic to you.
The number one choice for private practice
Future-proof your practice and offer everything a modern patient expects:
> iPad compatibility
> Online booking & payments with fully integrated card processing
> Electronic consent & treatment forms
> Integrated drugs database & digital prescribing with direct delivery
> Fast & easy patient communications by email or text
The importance of expert witnesses
Private practitioners acting as a medical expert witness can play a crucial role in improving patient safety and ensuring doctors are not made scapegoats for system failures. Dr Lucy Hanington explains – and calls on more clinicians to get involved in expert work
There is a large body of research to support the notion that patient harm arising from medical error is rarely attributable solely to the actions of a single individual
THE COVID-19 pandemic has placed a huge strain on healthcare systems and those working in them, with staff reporting high levels of fatigue, burnout and mental illness.
Its impact is likely to be felt for years to come as patients suffer the consequences of delayed presentations, the public health effects of lockdown become apparent and the treatment backlog is slow in abating.
There is ongoing disquiet that those who have shouldered much of the burden of caring for patients, while NHS services, systems and resources have been stretched to breaking point, may in due course face the additional pressure of medico-legal disputes.
New ways of working including remote consultations, redeployment, the unknowns of a novel infection and a huge increase in patient numbers will have inevitably contributed to missed diagnoses, medication errors and, sadly, patient deaths.
Despite these difficulties, the legal and regulatory frameworks governing doctors have remained largely unchanged.
Little allowance has been made for extreme circumstances or human factors. Indeed, a ruling of the Supreme Court in November
2020 arguably increased the medico-legal risk faced by doctors; the standard of proof required for a conclusion of unlawful killing at an inquest was lowered from ‘beyond reasonable doubt’ to ‘on the balance of probabilities’.
There is a large body of research to support the notion that patient harm arising from medical error is rarely attributable solely to the actions of a single individual.
Systems issues – including inadequate staffing levels, lack of resources, or faulty IT systems – play a key role in the majority of cases.
Honest communication
When things go wrong, blame –and the fear thereof – helps no one. Patients and families desire honest communication. They want to understand what has happened and seek reassurance that changes will be made to prevent future recurrence.
Identification of all factors contributing to an adverse incident is key in providing such understanding and reassurance, so it is good for patient safety.
It is also good for doctors. While any individual performance concerns must, of course, be addressed, doctors should not be scapegoats for the failings of the settings in which they work.
At Medical Protection, we believe it should be mandatory for all expert reports to consider systems issues when providing an opinion on the standard of care provided by a doctor
How can medical experts
help?
Many private practitioners do medical expert work and find it both challenging and rewarding. Medical expert opinion continues to play a critical role in a range of criminal, civil, coronial and regulatory processes.
Such opinion can determine, for example, whether or not the Crown Prosecution Service pursues a conviction for gross negligence manslaughter (GNM) following an incident or error that leads to the death of a patient.
In the Family Courts, medical opinion is relied upon in relation to decisions where the lives and well-being of children are at stake.
Due to the nature of the instructions received, expert reports often focus on the individual and there may be little, if any, consideration of the broader context in which events occurred.
At Medical Protection, we believe it should be mandatory for all expert reports to consider systems issues when providing an opinion on the standard of care provided by a doctor.
Our recent report, ‘Getting it right when things go wrong: the role of the expert witness’, calls on the GMC to add this requirement into the Good Medical Practice guide to empower doctors acting as experts.
Imperfect environments
Tired and burnt-out doctors are working in increasingly imperfect environments and thought should be given to safeguards that can be implemented to make allowance for this and the additional challenges Covid-19 has brought.
Systems issues and human factors are more relevant than ever when thinking about patient safety and medical error.
Our report also highlights some other worrying issues – in particular, a lack of appropriately qualified doctors willing to undertake expert work .
This leads to delays in the judicial process, with potentially harmful consequences for children and families. Instruction of an expert often relies on word of mouth, and there is no central register.
Two key reviews, commissioned
While any individual performance concerns must, of course, be addressed, doctors should not be scapegoats for the failings of the settings in which they work
in the wake of Dr Bawa-Garba’s conviction for GNM, identify similar concerns and note the absence of a clear governance structure for the expert witness role, with no requirement for specific training.
Sir Norman Williams’s Review into Gross Negligence Manslaughter in Healthcare (June 2018) called for improvements in the training of medical experts, and support for those wishing to undertake the work.
Leslie Hamilton’s 2019 Independent Review of GNM and Culpable Homicide , commissioned by the GMC, echoed these recommendations and set out key elements that should be included within all expert reports.
Notably, both reviews also recommended that medical experts should be in current, relevant, clinical practice.
Ongoing involvement in clinical work helps to ensure that experts are up to date; it also allows for a more realistic assessment of what is ‘reasonable’ as opposed to ‘text-book’ or ‘gold standard’ practice. Those working within a system are best placed to understand its challenges and imperfections.
Given the difficulties experi -
enced by the courts and others in identifying suitably qualified experts, we want to explore how the pool of experts might be increased and diversified.
It could be argued that the majority of consultants and GPs –particularly after an initial period in post – should have the requisite technical knowledge to provide an expert opinion in their field of practice.
However, very few come forward to do the work. While barriers are varied and complex, they include financial considerations, lack of training and support, and fear of criticism.
NHS employers, NHS England, the GMC and the Academy of Medical Royal Colleges all have a role to play in bringing about positive change in this area.
But we as doctors also need to step up.
I hope private practitioners reading this article will consider putting themselves forward to provide expert opinion if they have relevant experience; and ideally while being in current clinical practice.
All doctors who have achieved a Certificate of Completion of Training and who are in the appropriate register should possess the clinical knowledge to act as an expert within their field and should feel empowered to do so.
Dr Lucy Hanington (right) is a medicolegal consultant at Medical Protection
A guiding hand in a time of stress
Independent Practitioner Today’s joint survey with the MDU last month revealed worsening stress and anxiety levels among a high proportion of doctors in private practice.
Dr Udvitha Nandasoma (right) outlines some of the support available and urges consultants and GPs to seek help if they are struggling
IN CONTRAST to the busy and sometimes frenetic environment of an NHS hospital, the world of private healthcare may have the public perception of a serene and controlled environment.
And yet it would be a mistake to think that working in the private healthcare sector is a stress-free experience.
According to a survey of independent practitioners by the Medical Defence Union (MDU) and Independent Practitioner Today – see our September digital issue and website news section – over half (55%) of people working in independent practice feel that their stress and anxiety levels are now worse compared to before the pandemic, while 45% reported feeling stressed and anxious on a weekly basis.
Patients are unlikely to see any deterioration in service quality: 81% of respondents still believe they are making a positive difference to their patients, while 65% and 62% respectively feel supported by colleagues and are able to do their jobs effectively.
However, they may unknowingly encounter more healthcare staff and clinicians who are outwardly calm but inwardly struggling.
The heat is on Every independent practitioner will have personal challenges, from health and career to relationships and family, but there are some commonalities.
Inflationary pressures on practice running costs, for example, are likely to cause financial strain.
Practitioners will have seen their management responsibilities increase, too, as they are expected to collate and submit more information more frequently to different organisations: the Care Quality Commission (CQC), the Private Healthcare Information Network (PHIN) and the hospitals where they hold practising privileges, to name a few.
And despite the pandemic, there has been no remission in medicolegal pressure and scrutiny.
Doctors have had to keep pace with rapidly-evolving professional and clinical guidance as well as respond to patient complaints about pandemic healthcare provision, such as remote consultations, delays and mask-wearing.
We highlighted the results of our joint survey with the MDU on our front page last month
The long-term upward trend in clinical negligence claims is another cause for concern.
Being involved in a clinical negligence case often feels very personal for independent practitioners because they – rather than the hospital – receive the initial solicitor’s letter setting out the allegations and criticising their practice.
And while the MDU closed 85% of claims against our medical members without paying damages in 2021, the civil litigation process can drag on for many years.
This situation is inevitably an anxious time for doctors, even with the support of their defence organisation and family.
Sleepless
nights
Of course, it is the possibility of a GMC complaint which is most likely to cause sleepless nights. Being notified of an investigation can be distressing and the emotional strain is often compounded by a fitness-to-practise process which is unnecessarily prolonged, leaving the practitioner in limbo.
The GMC has rightly introduced measures to support those under investigation and has made efforts to be transparent about the deaths of doctors by suicide while under investigation or monitoring. Its first report on this issue was published in March 2022.
However, it has been constrained by outdated legislation when it comes to making the process faster and fairer and we were dismayed in July, when the Government announced it was
➱ continued on page 30
Create
repeat
mPrescribe® app allows you to prescribe flexibly without a laptop, for same day or next day delivery to your patients nationwide
Secretary Supported Administrator access reduces workload for practitioners.
mPrescribe® facilitates patient entry, status monitoring and preparation of prescriptions for mobile authorisation.
Clinical Governance
Co-founded and co-owned by leading private clinicians, our secure and encrypted technology is compliant with all GPhC, GDPR and e-Prescribing regulations.
GP and Consultant Reviews
“Wonderful, seamless, easy to use service.” Dr Catrin Bevan, London General Practice
“Competitively priced.” Dr Sean White, Consultant in Pain Medicine
“Intuitive and secure.” Dr Tim Wigmore, Consultant Intensivist & Anaesthetist, Schoen Clinic
“Delivered the same day.... Outstanding!” Dr Elisa Astorri, Academic Physician Rheumatologist, Rheumatology
“Go the extra mile.” Dr John O’Donohue, Consultant Gastroenterologist
On the medico-legal side, practitioners should be able to look to their medical defence organisation for advice and support as well as legal representation and indemnity
shelving the necessary GMC reforms until 2024-25.
What support is available for independent practitioners
This could be the toughest period that most independent practitioners will face in their professional lives – but they do not have to deal with this alone.
On the medico-legal side, practitioners should be able to look to their medical defence organisation for advice and support as well as legal representation and indemnity.
In addition to core services, such as our 24-hour advice line and the pastoral care provided by our medico-legal advisers and inhouse legal team, the MDU has launched a number of initiatives to support doctors’ well-being.
For example, we started our Peer Support Network in 2020, which put members who were feeling the strain of a GMC investigation or negligence claim in touch with a fellow member who had been through the same experience and could provide reassurance, practical advice and a shoulder to lean on.
The scheme has been so wellreceived that we extended it to include members involved in complaints or inquests.
We also support external organisations that provide help to struggling doctors and point members to these resources.
Dr Clare Gerada, chairwoman of Doctors in Distress, talked to us about the charity’s work and the issues surrounding doctors’ mental health.
And we were able to donate more than £30,000 to the Doctors Support Network and the Royal Medical Benevolent Fund on behalf of our Foundation Year 1
Last month, we reported in details the results of our joint survey with the Medical Defence Union on stress
members thanks to a scheme where we reduced their subscription from £10 to £5 and they donated the difference. This scheme will continue in 2022.
Seek help if you’re struggling
Our joint survey with Independent Practitioner Today shows that independent practitioners are not shielded from the stress and anxi-
ety caused by the pandemic and a host of other factors.
Sadly, the fact that nearly onethird of respondents said that they often go to work when they do not feel fit or well suggests that many feel they just have to get on with the job, which could have implications for their performance and even patient safety.
The MDU strongly advises any
struggling clinician to seek specialist help, whatever their seniority or healthcare setting. There is no need to face mental health challenges alone and the sooner help is sought, the greater the likelihood of making a full recovery.
Dr Udvitha Nandasoma is head of advisory services at the MDU
CHECK OUT OUR BUSINESS DIRECTORY
Independent Practitioner Today now features an online advertising directory to complement our journal and website.
Split into ‘business’ and ‘lifestyle’ directories, they list the services independent practitioners need to run their practices or spend their well-earned money on.
Free legal advice for Independent Practitioner Today readers
Independent Practitioner Today has joined forces with leading healthcare lawyers Hempsons to offer readers a free legal advice service.
We aim to help you navigate the ever more complex legal and regulatory issues involved in running and developing your private practice – and your lives.
Hempsons’ specialist lawyers have a long track-record of advising doctors – and an unrivalled understanding of the healthcare system as a whole.
Call Hempsons on 020 7839 0278 between 9am and 5pm Monday to Friday for your ten minutes of free legal advice.
Advice is available on:
Business structures (including partnerships)
Commercial contracts
Disputes and litigation
HR/employment
Premises
Regulatory requirements and investigations
‘Dog lists’ are barking
Warning: short-term performance analysis can be dangerous to your wealth. Dr Benjamin Holdsworth explains why disciplined exposure to risk will reap rewards
barking up the wrong tree
SOMETIMES WE read an investment article that causes much frustration. One regular such item is Bestinvest’s ‘Spot the dog – the guide fund managers would love to ban’ report.
This report would be laughable if it did not have such a potentially serious impact on investors’ wealth.
It is often quoted in the Sunday papers and can influence many DIY investors – those who do not seek advice – in their fund buy and sell decisions, despite the caveats that Bestinvest provides.
It can also unsettle sensible long-term investors if they see a fund on the list that their adviser has recommended.
While we have no problem calling out poor value for money in funds – which is far too common – the methodology used to identify ‘dogs’ is blunt to the point of being unhelpful.
In essence, a ‘dog’ fund is one that has underperformed a Bestinvest nominated market benchmark by a cumulative 5% over the past three years.
Market noise
From an investment perspective, three-year performance is riddled with market noise and is too short a time frame to make any decision based on performance.
In fact, you need around 16 years of data to be able to distinguish skill from luck. Most investors have long investment time horizons of, say, ten, 20 or even 30 years or more.
This provides the luxury of being able to take evidencedbased, strategic decisions around which to build portfolios, also known as systematic investment. Systematic investors will base their decisions on empirical evidence which points to higher expected returns that may be captured over the sorts of horizon investors hold.
In its 2021 report – data to December 2020 – Bestinvest included a particular fund as one of the ‘Biggest beasts in the Spot the Dog by fund size’ category.
It may have met its three-year criteria, but this fund does not simply try to track the emerging market index, but holds longterm, strategically-allocated stocks. For the longer-term investor, that can be exceptionally valuable.
When looking at market data at the end of June 2022, 18 months after the report was published, we can check how the fund actually performed against its peer group. In fact, the fund beats the market index and the peer group average.
‘Pedigree’ list
The annual SPIVA Report tracks the performance of actively managed funds in relation to those which are ‘passively’ managed.
In the 2022 edition, it reveals that 93% of all actively managed emerging market funds in the US failed to beat the emerging market benchmark over 20 years to the end of 2021. Not bad for a so-called ‘dog’ fund.
Perhaps ironically, the highly concentrated, growth stock-oriented active investment trust that heads the ‘pedigree’ list for best global equity performers in the 2022 report (data to December 2021) has fallen almost 50% from its high in November 2021.
Remember that going up 100% followed by going down 50% puts you back where you started. This fund has fallen almost 40% since the report was published. In comparison, the global market was down around 11% to the end of June 2022.
Once again, we are reminded that we should ignore the noise of short-term performance and be very wary of buy and sell ‘charts’ that use such data to create fund rankings.
The content of this article is for information only and must not be considered as financial advice. Cavendish Medical always recommends that you seek independent financial advice before making any financial decisions.
Levels, bases of and reliefs from taxation may be subject to change and their value depends on the individual circumstances of the investor. The value of investments and the income from them can fluctuate and investors may get back less than the amount invested.
We should be very wary of buy and sell ‘charts’ that use such data to create fund rankings
Dr Benjamin Holdsworth (right) is a director of Cavendish Medical, specialist financial planners helping consultants in private practice and the NHS
LET US HELP YOU GROW YOUR PRIVATE PRACTICE AT WEEKENDS
LONDON MEDICAL, the award-winning outpatient clinic in the Harley Street Medical Area is expanding its weekend opening hours. We are inviting applications for practicing privileges.
We can offer you:
Fully CQC-registered clinic
Nursing support
Appontment-making
Secretarial support
Billing service
In-house pharmacy
For more details
Contact: david.briggs@londonmedical.co.uk 49 Marylebone High Street, London W1U 5HJ
londonmedical.co.uk
How coroners arrive at their conclusions
In the last of this three-part series explaining how the inquest process relates to independent practitioners, Thorrun Govind explains inquest conclusions and what they mean
Record of Inquest
For simplicity, I will be referring to inquests without a jury in this article. A jury will not be present for the majority of inquests.
The coroner’s final role upon hearing the evidence is to complete the Record of Inquest. This includes:
Box 1 – Name of the deceased;
Box 2 – Medical cause of death;
Box 3 – How, when and where –and for investigations where section 5(2) of the Coroner’s and Justice Act 2009 applies, ‘in what circumstances’ – the deceased came by their death.
Box 4 – Conclusion of the coroner; Box 5 – Further particulars required by the Birth and Deaths Registration Act 1953 to be registered concerning the death; for example, date and place of death, name and surname of the deceased, sex, maiden name for a woman who has married, date and place of
birth, occupation and usual address.
Box 1 and Box 5 – Particulars to the individual
These are often established prior to the inquest and do not require much investigation by the coroner.
Box
2
– Medical cause of death
With consideration to post mortem evidence, if available, or from witness evidence, the coroner will be able to finalise this for the Record of Inquest.
The formulation is based on World Health Organization recommendations:
1 a) Disease or condition leading directly to death;
1 b) Other disease or condition, if any, leading to 1(a);
1 c) Other disease or condition, if any, leading to 1(b);
2 Other significant conditions contributing to death but not related to the disease or condition causing it.
Box 4 – Conclusion of the coroner
This is the stage that requires most coronial input. The Coroner’s Court is a fact finding inquiry reaching a conclusion and not an adversarial trial with a verdict.
Conclusions used to be called verdicts. However, in 2013, coronial law changed this to reflect the non adversarial nature; though they are often still labelled as this incorrectly in the press.
Legal representatives present in court can make submissions about which conclusion(s) the coroner should consider. Coroners are reminded by the Chief Coroner’s Guidance that they should at all times use moderate, neutral and welltempered language, befitting the holder of a judicial office.
The coroner is required, having heard the evidence, and in addition to deciding the medical cause of death, to arrive at a conclusion by way of a threestage process. It is important to remember that it may take some time for the coroner to reach their decision.
1
To make findings of fact based upon the evidence.
The coroner will state the key findings of the evidence that they have heard. In doing so, they work
The Coroner’s Court is a fact-finding inquiry reaching a conclusion and not an adversarial trial with a verdict
to the civil standard of ‘on the balance of probability’.
2
To distil from these findings of fact ‘how’ – in other words, by what means – the deceased came by their death.
This will usually be a description of the mechanism of death such as ‘by drowning while swimming in the open sea’.
3
To distil from the above findings of fact as to ‘how’ the deceased came by their death and to record that briefly in Box 3 of the Record of Inquest.
The coroner will add to the wording at point 2 above, the date and place of death, where known, and, where necessary, a brief description to expand upon how the deceased came by their death.
Conclusion
The conclusion – which is placed in ‘Box 4’ of the Record of Inquest – will either be what is known as a ‘shortform’ conclusion or a narrative conclusion.
Short Form – for example, natural causes, suicide, industrial disease, alcohol/drug related, accident/misadventure, open;
Natural causes – This is considered be the normal progression of a natural disease or illness, where a naturally recurring disease runs its full course without any significant amount of medical care or human intervention;
Suicide – This is defined as a deliberate act by the deceased and that the intended consequence of this act was, at all times, to be death;
Industrial disease – when the
death resulted from a disease caused by work;
Alcohol/drug-related – this can cover an accidental death resulting from abuse of alcohol or drugs or from the result of being addicted to alcohol/drugs;
Accident/misadventure – an unnatural event which was neither unlawful nor intended by the deceased to result in death.
This may therefore be appropriate where medical treatment caused the death. Accident or misadven ture can be used interchangeably;
Open – This is used when none of the other verdicts are appropriate and the evidence does not fully explain the cause and circumstances of death;
Narrative – As an ‘alternative’ to a short form conclusion, the coroner may record a ‘brief narrative conclusion’ which goes into more detail regarding the factual findings.
The coroner also has the ability to return a conclusion which includes a rider of neglect, and the case of R v HM Coroner of North Humberside and Scunthorpe Ex p Jamieson [1995] is the authority.
For this, the court must be satisfied that the deceased was in a dependent position and that legally there is evidence of a gross failure of basic medical care which should obviously have been provided.
There must be a clear and direct causal connection between the gross failure and the death for neglect to be applied; for example, a nurse failing to provide antibiotics to a patient for a day despite them being prescribed.
The patient in this case would be obviously in need and deteriorating and this omission would have to directly cause the death.
For an introduction to the inquest process, see our previous articles in Independent Practitioner Today : ‘When you’re asked to go to an inquest’ and ‘What happens when you’re called to an inquest?’.
Thorrun Govind (right) is a pharmacist and solicitor at Hempsons law firm. For further information, email her at t.govind@ hempsons.co.uk
Dilemma 1
Do I proceed with this interpreter?
QI am working in the private sector and have concerns about a patient who has been added to my list for elective surgery.
When reviewing the patient’s records, I noted that the patient spoke no English and that their daughter had been acting as an interpreter for outpatient appointments and for the consent process so far.
This is concerning to me, as the patient has multiple comorbidities, is at high risk of complications from the procedure and the outcome is uncertain.
Given these various obstacles to successful surgery, I feel that it is important to have clear and open lines of communication when obtaining consent from the patient.
I did mention having an independent translator present rather than relying on a family member, but when I discussed this with a colleague, they stated that this was unnecessary. How should I proceed?
AThe GMC does not specifically comment on the use of relatives as interpreters, but in its guidance Decision-making and consent it states that ‘you should use an interpreter or translation service if they have difficulty understanding spoken English’.
But it says you should also ‘accommodate a patient’s wishes if they would like anyone else – a relative, partner, friend, carer or advocate – to be involved in discus
When interpreter is family member
The importance of interpreters during the consent process are discussed here by Dr Ellie Mein (right)
sions and/or help them make decisions’ with regards to their care.
NHS England does, however, address this specific issue. In Guidance for commissioners: Interpreting and Translation Services in Primary Care (2018), it states: ‘6. Patients should always be offered a registered interpreter. Reliance on family, friends or unqualified interpreters is strongly discouraged and would not be considered good practice.
‘7. If a patient expressly desires a family member or friend to act as their “interpreter”, the patient should give informed consent in their own language, sought from them independently of the family member/ friend. The consent must be noted in the patient’s record.’
Although this guidance is aimed at primary care and is not applicable to the private sector, it is good
practice to use a suitably qualified and independent interpreter rather than a relative.
Without an independent interpreter, there is no assurance of quality and accurate translation of complex medical terminology, and relatives, through no fault of their own, may filter or omit key points to save the patient distress or to steer the patient into making a decision the relative feels is best for them.
Confidentiality issue
Additionally, there is also a confidentiality issue when using relatives and not checking via an independent interpreter what information the patient would want their family member to know.
The patient may subsequently feel uncomfortable asking questions via their relative, especially
for conditions of a sensitive nature.
Finally, you should be aware of the safeguarding aspects of minors being used as interpreters – for example, exposure to inappropriate information and missing school.
It is important to remember that in the event of an adverse outcome or complaint, you would need to be able to justify why you had relied on the relative being a translator if there was time to arrange an alternative, professional option for an elective case.
This question would be particularly pertinent for a patient at high risk of a complications when the need for meaningful dialogue would be even greater to satisfy the requirements for appropriate consent.
Dr Ellie Mein is a medico-legal adviser at the Medical Defence Union
I have been called to an ‘Article 2’ inquest
Dr Kathryn Leask (below) explains what an Article 2 inquest is and how to prepare for one
Dilemma 2
What is involved in this inquest?
QI am a consultant surgeon who has been asked to attend an inquest. The inquest relates to the death of a patient I operated on who was detained under the Mental Health Act.
Concerns have been raised about the delay in the mental health team and social services seeking medical advice when the patient first presented with symptoms.
I have been told by the coroner’s office that it is an Article 2 inquest, but I wasn’t sure what this meant and what the relevance of it was. At this stage, I have been asked to provide a statement and keep certain dates free in case I am asked to attend the inquest.
Can you explain more?
AArticle 2 inquests are enhanced inquests and are held where there is a possibility that the state has failed to protect a person from risk or if there has been a death in custody.
The State has an obligation to take steps to safeguard the life of vulnerable people and the coroner may be interested in what action
by any systemic or institutional failures within the organisation where the patient was detained.
requires legal representation if they are an IP or whether IP status should be requested.
An Article 2 inquest can take place if the deceased was detained in a prison or under the care of social services or healthcare professionals
was taken before medical assistance was sought.
An Article 2 inquest can take place if the deceased was detained in a prison or under the care of social services or healthcare professionals. Where such an enhanced inquest takes place, there is likely to be a jury sitting with the coroner.
Institutional failure
In addition to the usual investigation a coroner would undertake, they will consider the wider circumstances surrounding the death – for example, was the death caused
Once the coroner has all the information they need, they will decide who is required to give oral evidence. This may be as a witness to fact or as an ‘interested person’ (IP). An IP is a person or organisation, such as a hospital trust, who may be of particular interest to the coroner.
The IP will be entitled to copies of all the documents the coroner will be relying on and to be legally represented.
It is important that your report is a factual account of your involvement in the patient’s care based on the medical records and, if appropriate, your recollection of events.
Also it is recommended that doctors seek advice from their medical defence organisation early if they are asked to provide evidence, in writing or verbally, to the coroner and consideration be made as to whether the doctor
Where an unexpected death has occurred and therefore referred to the coroner, it is also important to reflect on the care that was provided to the patient to see whether there are any lessons to learn and whether any action needs to be taken as a result of the death.
Under regulation 28 of The Coroners (Investigations) Regulations 2013, the coroner can issue a ‘Prevention of Future Death’ report if they have heard evidence that further avoidable deaths could happen if preventative action isn’t taken.
Where healthcare professionals have carried out their own review of the care and made changes, if necessary, the coroner may feel that this is not necessary, as any concerns have already been addressed.
Dr Kathryn Leask is a medico-legal adviser at the Medical Defence Union
Ensuring safety is an ungoing task
As we report in our top story this month, doctors in private practice need to be aware of important changes to the Medical Practitioners Assurance Framework. David Hare (right), chief executive of the Independent Healthcare Providers Network (IHPN), sets the scene
AS Independent Practitioner Today readers may be aware, it is now almost three years since the IHPN, together with former NHS England national medical director Sir Bruce Keogh, launched our Medical Practitioners Assurance Framework (MPAF).
While acknowledging the overwhelmingly safe, highquality care delivered in the independent healthcare sector, this framework of
principles – developed with the NHS, regulators and royal colleges – was designed to help foster a more standardised approach to medical governance in the independent sector and drive even further improvements in safety and quality.
Since its launch in 2019, the framework is now firmly embedded in the patient safety and regulatory landscape.
The Care Quality Commission
uses the framework’s principles in assessing how ‘well led’ an independent service is and it is now also part of the NHS Standard Contract – requiring all independent sector providers who deliver NHSfunded care to adhere to it. Moreover, the Government’s response to the former Bishop of Norwich’s inquiry into surgeon Ian Paterson noted the ‘significant work’ undertaken by independent
providers and individual practitioners to fulfil his recommendations, specifically through the implementation of the MPAF. Of course, as those working in the sector will know, the world of healthcare does not stand still and the MPAF was always designed to be a ‘live document’.
Further strengthened
Since it was published, the IHPN has been working with providers, stakeholders and practitioners to look at areas where the framework can be further strengthened to ensure the principles remain in keeping with current best practice around medical governance in the health system.
Last month, we were therefore delighted to launch the ‘refresh’ of the MPAF, which takes a renewed look at the framework and takes account of the many changes in the safety and regulatory landscape over the past few years.
Most notably, this includes:
The Bishop of Norwich’s independent inquiry report into Ian Paterson;
Baroness Cumberlege’s Independent Medicines and Medical Devices Safety (IMMDS) Review;
Their respective Government responses;
New initiatives such as the Learn from Patient Safety Events service and wider regulatory
changes in the 2022 Health and Care Act.
With the support of our External Advisory Group, including the Federation of Independent Practitioner Organisations, the MPAF refresh retains the principlesbased approach of the framework, but strengthens them in key areas. This includes the importance of
patient consent and declaring any conflicts of interest – both of which were key themes in both the Paterson and IMMDS reviews.
Practising privileges
Likewise, the section on reviewing practising privileges has been updated to better allow for a riskbased approach.
Since it was published, the IHPN has been working with providers, stakeholders and practitioners to look at areas where the framework can be further strengthened
It stipulates that a review of practising privileges is undertaken biennially for all medical practitioners and more regularly in the rare circumstances where additional scrutiny or oversight is required.
And it also highlights the need for independent providers to have arrangements in place to better support practitioners returning to practice after an investigation and has more detail on best practice for the management of patient complaints.
In addition, in the ‘Medical
NHS Pensions & Annual Allowance Tax
Get ready in advance of April 2022 when the proposed changes to the NHS Pensions will allow you to reclaim some or all of any Annual Allowance tax you may have suffered in the past.
With our knowledge and in-house calculators, we will be able to predict in advance and check statements produced by NHS Pensions and Scottish Public Pensions Agency for accuracy for any refunds due.
For further information contact us at aa@semail.co.uk or telephone 01625 527351.
Practitioners Responsibilities’ section, doctors are now asked to seek appropriate help if they are experiencing pressures that may lead to an impairment of their practice.
With the health service under scrutiny and many practitioners experiencing system pressures like never before, it is crucial that the MPAF continues to evolve and accurately reflect the latest medical governance practices.
A BIG THANK YOU!
From everyone at IHPN, we would like to thank all practitioners working in the sector for their engagement with the framework.
We look forward to working with you over the coming years to further embed the MPAF and continually improve the safety and quality of care delivered by independent sector providers to both NHS and private patients.
DOCTOR ON THE ROAD: ALPINE A110
Blast from the past is a blast for today
Our motoring correspondent Dr Tony Rimmer (right) reached the height of satisfaction when driving the new Alpine – now he just cannot wait to get back in it
IT IS a very common human trait to find comfort in positive elements of our past lives and then recreate them with modern updates to please us all over again.
As an example, there is something warmly reassuring about listening to a classic 1960s Roberts radio that has modern FM and DAB clarity.
Car manufacturers have tapped into this rich seam of nostalgia to great effect and produced excellent profits. BMW was the first with the new MINI which was launched in 2001 and went on to be – and continues to be – a huge success.
The giant FIAT corporation watched on with interest and, in 2007, replicated BMW’s success with the new 500. These new models are hugely more sophisticated in engineering and safety terms than their predecessors. However, although their physical size may have increased, they have been very successful at retaining the charm of the originals.
The MINI and FIAT 500 are both urban runabouts and, apart from the not-so-successful VW Beetle recreation, are almost alone in the world of modernised old favourites.
Mid-life update
There is one other car that has been reborn in modern form and comes from a very different background: the sports car sector. It is the Alpine, a recreation of the successful French rear-engined rally car of the 1970s.
Still under the umbrella of Renault, the new car was released in 2018 and has recently had a mid-life update. I have been trying these new versions to see just what is on offer.
There are three models to choose from. The entry-level A110 has
252bhp, the A110GT has 300bhp and the A110S has 300bhp and a sportier suspension which would suit the occasional track day outing.
The Alpine was designed as a pure back-to-basics sports car using the Lotus ethos of light weight and relatively small engine. At 1,100kg, it weighs roughly half of most electric cars and big SUVs and although power comes from a modest 1.8litre fourcylinder turbo engine, the powerto-weight ratio is impressive.
Alpine have focused on the driver and have built a chassis to satisfy us petrolheads who appreciate the tactile nature of a well sorted sports car that can be placed accurately on a windy ‘B’-road and dole out plenty of fun while doing so.
Driver-focused environment
Having driven lots of electric cars of late, I approached my drive of the Alpine with barely hidden excitement. I slipped into the low driver’s seat and was presented by, as expected, a very driver-focused environment.
The sports seats are really comfortable and supportive, and the steering wheel and pedals are perfectly placed. Ah yes, the pedals: there are just two because the Alpine is only available with a seven-speed automatic dualclutch gearbox.
Unfortunately, Renault felt that it would be too expensive to develop a bespoke manual box, which is a great shame for enthusiasts such as myself.
The styling looks great. The blend of retro 1970s A110 with a modern twist works brilliantly. I think it looks at its best in classic French blue. This is a strictly twoseater car and, unfortunately, boot space is restricted.
You can pack a couple of large soft bags, but forget conventional
suitcases. The interior trim materials do not feel as premium as you would like and there is switchgear recognisable from lowly Renault models.
The latest revised models have a larger infotainment screen and better connectivity such as Apple CarPlay and Android Auto.
Out on the road, it soon becomes apparent that the chassis set up is as impressive as hoped. There is a suppleness that is allied to playful control that allows all road types to be tackled with gusto.
The steering is sharp and accurate although not quite as communicative as found in the Alpine’s greatest competitor, the Porsche Cayman 718. Performance is super quick even in the 252bhp entry model and the 300bhp A110GT that I tried felt barely quicker.
Sporty sound
Although the 1.8litre engine only has four cylinders, it has a great sporty sound – better than the Cayman’s four-cylinder unit. The Alpine is physically a low and narrow car so is perfectly suited to tackle our narrow UK ‘B’-roads.
It is a car that you just want to jump back into for another blast after arriving at your destination and that is a rare attribute nowadays. The fun factor has been dialed up to eleven.
So, would I recommend the Alpine to the enthusiastic petrol head Medic? Absolutely.
It looks stylish and is a fantastic sports car. As long as its certain limitations are acceptable, it would be a great car to use as a dayto-day commuter and then at weekends for a blast down favourite roads to blow away all the cobwebs of a busy week.
Dr Tony Rimmer is a former NHS GP practising in Guildford, Surrey
The sports seats are really comfortable and supportive, and the steering wheel and pedals are perfectly placed
A PRIVATE PRACTICE – Our series for doctors embarking on the independent journey
Keep a tab on your
Extreme busyness goes with the territory of clinicians when they are occupied with their NHS commitments, private practice and other roles. As their careers progress, it is likely their tax affairs will become more complex and it is easy to miss some vital dates. That can be financially costly as well as increasing the chance of a HM Revenue and Customs (HMRC) inquiry.
Richard Norbury (right) covers some of the more common tax deadlines you will face during your career
Individuals
Most readers will surely be familiar with the tax return deadline of 31 January. In recent years, this has been extended to 28 February due to Covid.
But it is expected that the usual 31 January deadline will now be enforced in future. The majority of consultants and GPs will be required to prepare a tax return by this date.
Here are few of the most common reasons why you might need to submit a personal tax return:
Untaxed income received – for example, self-employed earnings/ dividends/property income/partnership profits;
Taxable earnings in excess of £100,000;
Declaration of annual allowance pension tax charges.
Property income
Income received from properties, both in the UK and abroad, are
subject to tax. Again, allowable costs can be offset to arrive at the taxable profit figure.
If you own the property with other parties, you need to declare your share of the income and expenditure.
If you have a mortgage on the property, you are able to claim some tax relief on the interest payments made during the year, although this is no longer a full deduction against your taxable profits.
From 27 October 2021, if you were to sell an interest in UK residential property that has ever been a rental property, then you have 60 days from the date of conveyance to report your disposal and pay any tax due. You will be subject to late filing penalties and interest if this deadline is missed.
If the residential property is held jointly, each owner is required to submit their own in-year return. The new regime is aimed at the
tax dates
Personal tax liability payment due dates
In recent years, the tax deadline has been extended to 28 February due to Covid. But it is expected that the usual 31 January deadline will now be enforced in future
property owners, not the property itself.
This could also apply to a sale of residential property following a gift, transfer in or out of a trust or a transfer as part of a divorce settlement.
If you sell your own home, then this is likely to be covered by your principal private residence (PPR) waiver and thus would not be caught by these rules.
Tax is payable on or before 31 January each year. If you pay more than 80% of your tax via Pay As You Earn (PAYE) or if the total liability for the year is under £1,000, then this is likely to be the only liability you need to pay.
However, if you do not qualify for either of these exemptions, then you will be required to pay a payment on account by 31 July each year in addition to the 31 January payment.
The payment on account is based on 50% of your previous tax liability. If your profits have reduced significantly, you may be in a position to review these payments on account and reduce them accordingly.
If you delay payments of personal tax, then HMRC will charge pro rata interest at 3.75% at the time of writing this article.
➱ continued on page 44
If you delay your January balancing payment by 28 days, then you will be subject to a 5% surcharge based on the tax outstanding.
Failure to file a personal tax return before the 31 January attracts an automatic penalty of £100 and this rises when three months late.
You can pay your tax liability through your PAYE tax code as long as all of the following apply:
Less than £3,000 is owed on your tax bill;
You already pay tax through PAYE – for example, you’re an employee or you get a company pension;
A paper tax return is submitted by 31 October or your online tax return online by 30 December.
‘Scheme Pays’ election
Many independent practitioners will be subject to pension tax charges based on the annual growth of their pension. This is a complicated area and has been covered in previous articles in Independent Practitioner Today and will be revisited in the future.
If you choose to apply for NHS Pensions to pay the annual allowance tax charge, then the deadline for submitting your scheme pays election is 31 July following the end of the tax year. For example, if you have a tax charge for the year 2021-22, then you have until 31 July 2023 to apply for the scheme to pay the tax.
There is an appeal process available in certain circumstances; for example, a delay or error in the figures from NHS Pensions.
This is a complicated area and a specialist medical accountant can help calculate any tax charge and offer advice.
Limited companies
Company year-ends often do not coincide with the usual 31 March/5 April tax year.
The year-end is usually based on the month the company was originally formed, but it is possible to change the company year end.
The company has four main deadlines each year:
Filing accounts with Companies House;
Filing tax return with HMRC;
Paying corporation tax;
Filing a confirmation statement.
Failure to file your company accounts on time results in a penalty of £150 if filed within one month of the required date, rising to £1,500 for over six months late
now have property portfolios within a limited company.
Some companies will own residential properties. If any of the properties are valued above £500,000, then you may be subject to the Annual Tax for Enveloped Dwellings (ATED).
Normally you need to submit your return:
By 30 April if your property is within the scope of ATED on 1 April;
are now required to file their VAT returns online.
The online filing deadline and payment of VAT are the same date being one calendar month plus seven days.
However, if you are on the annual accounting scheme –essentially you prepare a 12-month VAT return and pay payments on account during the year – then you have two months after the year-end to file the return.
The deadline for filing limited company accounts is usually nine months after the year-end date unless you are preparing your first year of accounts or have altered the year-end at Companies House.
Failure to file your company accounts on time results in a penalty of £150 if filed within one month of the required date, rising to £1,500 for over six months late.
These penalties are doubled if you file late in two successive financial periods.
The company tax return deadline (form CT600) is 12 months following the year-end. If the period of reporting is longer than 12 months, then you may be required to file a CT600 soon after the period end.
Even though you usually have 12 months to file a CT600, the payment of tax is due nine months and one day after your period end. For longer accounting periods, this can lead to two separate payments of tax which may be in quick succession. Interest is charged on late payments.
The company is required to file a confirmation statement confirming details including directorships, registered office address, structure and people with significant control. This is usually due two weeks after the anniversary of the date the company was formed.
Various other deadlines apply to companies, such as you have 14 days to report an appointment of a change in office holders – mainly directors and company secretaries.
It is best practice to inform your accountant of any changes that you are planning to make so they can ensure you meet your reporting requirements.
Properties within companies
With the changes in the allowable mortgage interest and stamp duty in recent years, many companies
Within 30 days of acquisition if your property comes within the scope of ATED after 1 April;
For a newly built property, within 90 days of the earliest of the date your property becomes a dwelling for council tax purposes or when it is first occupied.
Certain exemptions are available, meaning you may not have a tax charge. However, qualifying properties will need to submit a return each year to remain compliant.
Partnerships
It is more common than ever that consultants will be involved in a partnership or limited liability partnership (LLP).
For an LLP, the filing deadlines at companies house apply in much the same way as a company as explained earlier in this article. The subtle change is that, instead of directors and company secretaries, an LLP will have members and designated members.
However, as an LLP is taxed as if it is a traditional partnership, there is a requirement to submit a partnership tax return to HMRC by 31 January each year.
Failure to submit can lead to £100 penalty per partner plus £100 for the partnership tax return.
In addition, assuming the figures were not finalised, then this will prevent you from filing your own personal tax return, so failure to submit can be expensive, especially in large partnerships.
VAT
For those doctors who are VATregistered – which will, in the main, be due to medico-legal work – you will be well aware of the deadlines, as these are much shorter than those imposed on tax returns and accounts.
The vast majority of businesses
Penalties for late payment of VAT are complicated and based on a surcharge system where you enter a ‘probationary period’ for 12 months and if you are late again, you are subject to a charge for a percentage of the VAT liability outstanding.
Making Tax Digital
Many doctors have heard of the Government proposals to introduce Making Tax Digital over the next few years.
HMRC aims to create one account for each taxpayer for all of their individual taxes. This will involve quarterly filing of returns and possibly payments on account for businesses and landlords.
The implementation has been delayed due to the pandemic, but the latest proposed dates are as follows:
VAT – already implemented; Self-employed businesses, including landlords – from April 2024;
Partnerships – from April 2025; Corporation tax – from April 2026.
Some exemptions may be available if your turnover is below £10,000 a year, but these businesses may be introduced to the rules in the future.
Bearing this in mind, it is more important than ever that you have robust systems and accounting software that is fit for purpose. There are many pitfalls that can result in significant financial loss and stress and specialist medical advice can help you to navigate these to ensure you meet the required obligations.
Next month: Don’t miss our update on annual allowance tax charges
Richard Norbury is a partner at Sandison Easson & Co, specialist medical accountants
With you every step
Protection that’s by your side
For over 130 years, we’ve supported our members with discretionary indemnity that covers a wide range of occurrences and claims.
Never feel restricted by your protection again.
Coming in our November issue, published on 15 November:
Are you missing out on the self-pay boom? Medical marketing expert Catherine Harriss shows how to attract self-payers to your practice
Check out an important update on annual allowance tax charges on pensions, by Sandison Easson specialist medical accountant Alec James in our Start A Private Practice series
Having survived the stress of a GMC hearing, a doctor may think they can get on with their life. Not necessarily. See our report from Amie Roadnight of Hempsons Solicitors regulatory and crime team
Catch up on all the news from one of the biggest events of the year –
LaingBuisson’s private acute conference
‘We have been working in a group for two years now and we are starting to experience tensions between us. How do we manage these tensions without breaking up the group?’ We called in our Troubleshooter Jane Braithwaite to help and outline a way forward
In our Business Dilemmas series, Medical Defence Union medico-legal adviser Dr Sissy Frank explains the process for ending professional relationships with a particularly difficult family. And she answers a query from an independent consultant who has been asked to provide medical assistance in an upcoming half marathon event
Doctors working for private providers who have been commissioned to provide services to NHS patients, or undertaking extra work through NHS waiting list initiatives, should check they hold adequate indemnity, warns Dr Sophie Haroon, a medico-legal consultant at Medical Protection
INDEPENDENT PRACTITIONER
Published by The Independent Practitioner Ltd. Independent Practitioner Today is editorially independent and thanks Bupa for its assistance with distribution.
Material is governed by copyright. No part of this publication may be reproduced, stored in a retrieval system or transmitted in any form without permission, unless for the purposes of reference and comment. Editorial layout is the copyright of the publishers. If you wish to use it for promotional purposes on websites or for reprints, we would be happy to discuss licensing the copyright to you.
Over the past two years, we have seen both public and private hospitals being used to fight Covid-19, so the traditional dynamic between the two sectors has become distorted. Only by listening to clinicians and understanding how the two systems need to work together effectively can we begin to manage the scale of the health crisis in the UK, concludes Tim Morris, vice-president of Clinical Solutions at Elsevier Health
Despite the popularity of WhatsApp as a platform to converse with family, friends and colleagues, there is a huge question mark around its confidentiality. Simon Hemingway, healthcare director at technology solutions integrator The Barcode Warehouse, examines the implications of using WhatsApp for communicating in a healthcare environment
Cardiovascular disease is one of the leading causes of death and disability in the UK, but rehabilitation following a cardiac event is often forgotten about, reflects Dr Ajay Jain, a consultant cardiologist at Nuffield Health at St Bartholomew’s Hospital
Complaints in NHS private patient units – a new pilot study about to get underway could be good news for patients. The Independent Sector Complaints Adjudication Service director Sally Taber reports
Plus all the latest news, views and regular features including help with billing issues from Medical Billing & Collection, advice from Cavendish Medical and a report from the Independent Healthcare Providers Network
And don’t forget to check out our additional news updates every week online
ADVERTISERS: The deadline for booking adverts in our November issue is 28 October
Write to Independent Practitioner Today 7 Lindum Terrace, Lincoln LN2 5RP
CHANGING ADDRESS, EMAIL ADDRESS OR SUBSCRIPTION DETAILS?
Phone 01752 312140 or email karen@marketingcentre.co.uk
To advertise in the digital journal, on our website or in our business directory, contact advertising manager Andrew Schofield at Spot On Media. Phone: 0161 408 3912 Email: andrew@spotonmedia.co.uk
Follow Independent Practitioner Today on
GET A SUBSCRIPTION DISCOUNT!
£90 independent practitioners.
£90 GPs and practice managers (private & NHS).
£210 organisations.
Save £15 paying by direct debit: individuals £75 (organisations £180). TO SUBSCRIBE
Email karen@marketingcentre.co.uk or phone 01752 312140
Publisher Gillian Nineham Phone: 07767 353897.
Email: gillian.nineham@gmail.com
SAVE £15 WITH DIRECT DEBIT!
Guarantee delivery of your next copy of Independent Practitioner Today. Take out a subscription and you will get full access to our news, features and previous issues on our website. See details on the left.