The business journal for doctors in private practice
In this issue
Workplace well-being
Mark Allan of Bupa discusses the lessons the pandemic has for our businesses P20
What will digital tax returns entail?
Vanessa Sanders explains the changes involved in Making Tax Digital P24
See page 16
They’re lying if they say they can see the future
Dr Benjamin Holdsworth warns of the futility of trying to beat the market P36
New tax to cost private doctors £250+ a month
By Robin Stride
Typical independent practitioners will have to pay a projected average of £250 a month each as their contribution to the Government’s new ‘third’ tax being introduced from next April.
Prime Minister Boris Johnson expects the health and social care levy of 1.25% to provide £36bn to bolster health and social care over the next three years.
The rise in National Insurance and on dividends will mean an additional tax bill of around £3,000 for a consultant with an NHS salary of £115,000 and £100,000 a year from self-employed practice.
Specialist medical accountant
James Gransby warned: ‘Those that use limited companies don’t escape the new levy, because it has been added to dividend extraction.
‘Those that retain profits in their company would not incur the levy as those profits build up, but they would do if they took them out as a dividend at a later date.
‘But if those retained profits were extracted as capital at the end of the company’s life, then this would not trigger the 1.25% levy, as it is only payable on income and dividends.
In association with
‘Directors could make a big dividends payment now early. If they wanted to declare a dividend before April next year, then they can get it out before the levy comes into force. They don’t need to draw it from the company; it can sit there as a loan to the director.’
Their levy costs would typically be around the same as for the selfemployed doctor in the example above.
For top-earning doctors in private practice, the health and social care levy could cost them up to £1,000 or more extra a month.
Yet another tax
But Mr Gransby, of RSM UK, drew attention to another previously announced tax grab on the way for many independent practitioners in 18-months’ time.
‘Corporation tax is going up anyway in 2023 for companies from 19% to an effective rate of 26.5% for company profits between £50,000 and £250,000, so that’s a big hit to watch out for too.’
Vanessa Sanders, of Stanbridge Associates accountants, warned: ‘Doctors running a private practice will find they suffer an increase on all fronts: as employees of the NHS, as self-employed, as emp loyers in
their own practices, and on dividends distributed from their limited companies.
‘This is a significant blow to those businesses recovering from the financial effects of the pandemic.
‘It is particularly stinging given that their directors were proffered no help themselves, as the Government grants were directed towards employees or the selfemployed.’
She believed pay rises were likely to be reduced to accommodate the tax hike.
From 1 April 2022, there will be a temporary 1.25% increase in class 1 (employee) and class 4 (selfemployed) National Insurance contributions (NIC) paid by workers, in addition to a 1.25% increase in class 1 secondary NIC paid by employers.
The increase will apply to employed – including those deemed as employees under the IR35 legislation – and self-employed individuals and partners earning above £9,568 in 2021-22.
Employers will pay the additional 1.25% for employees earning above the class 1 secondary threshold: £8,840 in 2021-22.
From 2023-24, it will be collected
through the PAYE system and shown separately on pay slips.
Rate will increase
But already there are fears the 1.25% level will not raise enough and will increase, as has VAT. One consultant, now a healthcare strategy adviser, warned a LaingBuisson webinar ( see page 4 ): ‘It’s clearly going to go up over time.’
Independent Practitioner Today columnist Julia Burn of Blick Rothenburg, writing in this issue (page 14), advises it will be crucial for doctors to assess how the levy will affect their business before it is implemented.
She says: ‘By ensuring the financial reporting of your business is regularly updated, you will be able to manage cash flows easier.’
The levy was announced last month as research for our Profits Focus column revealed the alarming early effects of the first two months of the pandemic on the average orthopaedic surgeon’s private income.
Covid-19 resulted in a fall in income, for the first time, dropping 5.9%. Consultants’ costs fell by 10.3% and their profits were down by 3.7%.
n See the full story in our feature next month
TELL US YOUR NEWS. Contact editorial director Robin Stride
‘The measure of intelligence is the ability to change,’ said Albert Einstein – and change is certainly happening in big measures for independent practitioners right now.
We draw attention in this edition of Independent Practitioner Today to some big issues to get to grips with.
Making Tax Digital (MTD) preparations for many readers need reconsidering following a date tweak ( page 24 ) and the impact of the new health and social care levy on National Insurance and dividends (page 1) will see some extra work for doctors’ tax advisers.
Key policy and regulatory changes are on their way for independent practitioners in the coming months and Dawn Hodgkins of the Independent Healthcare Providers Network (IHPN) outlines four big ones (page 12). Independent practitioners will have to grapple with the matter
of possible mandatory Covid vaccination for the health and care workforce. She warns this will raise complex employment, legal, ethical and practical questions for all healthcare providers with no easy answers.
The CQC’s requirements are heading for a shakeup, too, and it is good to see the IHPN will work with members to ensure the watchdog has the right data and insight to make accurate assessments of providers.
We also report on the GMC’s upcoming review of Good Medical Practice (page 9), which is likely to have some hefty updates for doctors to get their head round.
Also coming soon, we are told, is the longawaited Government response to the Paterson inquiry.
And on 27 October, Chancellor Rishi Sunak will present his second Budget of the year. Check us out online to see any arising advice on areas that will affect independent practitioners.
Don’t exaggerate when marketing Doctors must be careful how they present their services to the public to ensure they comply with the rules, says Dr Clare Devlin of the MPS P11
Pushing the private sector’s view Key regulatory changes are on their way in the coming months. Dawn Hodgkins of the Independent Healthcare Providers Network reports P12
Don’t get caught in eye of the storm Dr Shabbir Choudhury of the MDU looks at clinical negligence claims against ophthalmology and offers advice on managing risk P28
Keeping your data secure Raj Patel considers how you can protect your practice against the surge of online scams aiming to steal personal information and money P30
How to get your money in Simon Brignall continues to explore the common themes arising from consultants wanting to address their issues around billing and collection P33
One slip gets you into a lot of trouble Lawyer Dr Tania Francis explains the many sets of proceedings a doctor may face out of just one incident and gives tips on how to avoid them P38
PLUS OUR REGULAR COLUMNS
Doctor on the Road: Electric car ideal for the school run
‘Why buy a car with a massive electric range if you don’t kneed to?’ asks our reviewer Dr Tony Rimmer P42
Starting a private practice: Systems are vital for maximising income
Ian Tongue looks at accounting systems and how to get the most from them to help run your practice P44
Profits Focus:
Breaking through a £200k barrier
ENT surgeons have enjoyed a 15%+ profits rise in our latest and unique benchmark survey P49
Pension remedy does not mean ignore tax
Doctors advised not to get complacent because of the
By Edie Bourne
Independent practitioners have been warned not to ignore their annual pension statements from the NHS because they wrongly believe the McCloud ‘remedy’ has negated their tax issues.
Specialist financial advisers Cavendish Medical has been forced to remind doctors that the McCloud judgment – which will recompense those who have suffered age discrimination by moving to the 2015 NHS pension scheme – will not be implemented for some time yet.
Meanwhile, doctors should continue to address their pension savings tax issues, it says.
Annual pension statements for 202021 are now available from the NHS Pensions Agency and are essential to help doctors establish whether they are likely to be paying substantial tax charges on their pension savings.
The ‘annual allowance’ limits the amount of tax free pension savings which can be accrued each year to £40,000. For higher earners, the ‘tapered’ annual allowance applies and can be as low as just £4,000.
In early 2021, the McCloud consultation was concluded and set out how the deemed age discrimination caused by moving members to the 2015 pension scheme would be corrected.
The ruling was that affected doc
tors have the right to choose which remedy benefits to take – the pension benefits from their previous 1995/2008 pension scheme or those from the 2015 scheme – at retirement.
But although the Government has confirmed that new legislation to help deliver the remedy benefits is being drafted, it will not be in place for several years.
Patrick Convey, technical director at Cavendish Medical, told Independent Practitioner Today: ‘We have been approached by several new clients utterly confused by what the impact of the McCloud remedy has on their current position and it’s easy to see why. As ever, nothing associated with NHS pensions is simple.
Get organised
‘NHS Employers has confirmed that the legislation needed to implement the McCloud remedy will not be ready until October 2023 at least. It is therefore imperative that you continue to assess your tax position now and pay all necessary tax payments. Your tax position will then be corrected at a later date.
‘If you intend to retire before the new legislation has been introduced, you should be contacted and asked to make your McCloud choice retrospectively. Payments will then be backdated to the time when benefits became payable.
‘I can’t stress enough how impor
McCloud pension remedy
tant it is to get organised. You should request your annual statement if you have not yet received it. Please get the statement checked because errors are common and they can cause significant problems.’
Those breaching the annual allowance can apply for the NHS to pay the tax charge under Scheme Pays in exchange for reduced future benefits. The application for Scheme Pays is normally 31 July each year but for the 201920 tax year, this has been extended to 31 March 2022.
No announcements have been made about the deadline for 202021 which currently remains as 31 July 2022. There are also other payments options which should be considered.
Mr Convey added: ‘Doctors are working long hours and about to go into another extra busy winter.
It is imperative that you continue to assess your tax position now and pay all necessary tax payments. Your tax position will then be corrected at a later date
They do not often have the time to keep up to date with the latest regulations.
‘Next year is going to be even more confusing, as NHS Employers has confirmed that, from 1 April 2022, all members of former NHS pensions such as 1995 and 2008 will be moved to the new 2015 scheme, regardless of their age, and the old schemes will subsequently be closed.
‘If you are a member of one of the legacy schemes, you will keep any service that you earned up until 1 April 2022 and be able to access your benefits normally. Going forward, any benefits you earn after this date will be in the 2015 scheme.
‘Now is not the time to bury your head in the sand or believe that it is easy to “go it alone”. We are here to help and hope we can make things much simpler for you.’
Beauty clinic fined for not showing CQC score
A cosmetic surgery provider was ordered to pay £5,070 after failing to display its Care Quality Commission (CQC) performance ratings, which is in breach of the watchdog’s regulation 20A.
The Pemberdeen Laser Cosmetic Surgery Clinic Limited, which runs The Belvedere Private Hospital in Knee Hill, near Abbey Wood, London, was fined £500 by Bromley magistrates and ordered to pay £4,520 costs and a £50 surcharge.
could be found, but this was not displayed conspicuously.
CQC inspector Dr Nigel Acheson called it ‘an egregious breach’. The hospital had a CQC website link where the latest inspection report
A mock inspection report displayed different, more positive ratings than those awarded by the CQC.
PATRICK CONVEY
Patrick Convey of Cavendish Medical
By Robin Stride
A surge in private medical insurance sales during Covid is expected to be confirmed in figures from market analysts.
According to economist William Laing, chief executive at LaingBuisson, figures show last year sparked a large increase in subscription numbers as an annual downward trend was reversed.
Former ophthalmic surgeon Dr Victor Chua, a senior partner with healthcare strategy consultants Mansfield Advisors, confirmed the ‘incredibly resilient’ market was increasing.
A London private charitable hospital has adopted a range of safety quality measures in reaction to Care Quality Commission (CQC) criticism which saw its surgical services rating drop from ‘good’ to ‘requires improvement’.
An unannounced inspection of The London Clinic was made in June after the watchdog received ‘information of concern about the safety and quality of the service’.
According to the CQC, concerns arose after four never events between January and September last year involving surgical items left in the body after surgery and, in one case, wrong tooth extraction.
Following action, a hospital spokesperson told Independent Practitioner Today last month: ‘We are confident that our newly-integrated clinical governance framework has been given fresh impetus under new leadership and has delivered an enhanced safety culture.’
Inspectors rated the surgical service ‘inadequate’ for being well-
A representative survey of 106 small, medium and large firms by his company last July found 70.7% anticipated there would be no change to their private medical insurance policy plans for employees this year, while 9.8% aimed to increase the number of policies.
Speaking at a LaingBuisson webinar, he said 7.3% of firms were undecided while 12.2% had expected to reduce their number of policies.
The biggest reasons for cutting back were because employers thought they would have fewer staff due to the pandemic and they considered Covid had reduced the
value of insurance because less private treatment was available.
Dr Chua predicted ‘good news for private hospitals’ as NHS waiting lists were projected to grow rapidly and could hit 13m in England.
He highlighted a strong rise in orthopaedic volumes across private hospitals south of London at the start of 2021. He predicted the upward trend would continue but perhaps not at the same rate seen earlier this year.
Asked how bad waiting lists could get he replied: ‘I think really it depends on what the Government will do to bring it down and frankly with the new health and social care
levy, it depends on us as voters to decide how much we are willing to put our hands in our pockets to get those waiting lists down.
‘Does anyone really think the health and social care levy will stay at one per cent? VAT started at 5%, right, and now its 20%. It’s clearly going to go up over time and I think it will depend on the political hue of the Government.’
He added: ‘I think we are going to have to get used to quite long waiting times in the public sector for some time, and this is probably good news for private hospital operators for this parliament and probably the next as well.’
led, ‘requires improvement’ for being safe, effective and responsive and ‘good’ for being caring.
The clinic’s overall rating is good and it is rated good for being safe, effective, caring and responsive, but requires improvement for being well-led.
Nicola Wise, CQC head of hospital inspection for London, said the provider told the watchdog that the Covid-19 pandemic had put additional pressures on the
department because, in addition to the usual private work, they were also working with the NHS.
This meant that their theatre activity had significantly increased, resulting in higher volumes of more complex work and working with teams that were new to the organisation.
Mrs Wise added: ‘Although we understand the pressures that healthcare providers have faced and continue to face as a result of the pandemic, never events are precisely that – they should never occur.
‘If they do, it is important that they are thoroughly investigated to ensure that they do not happen again. In this case, each incident was fully investigated and learning was shared with all staff.
‘However, while leaders told us that they were committed to continuous learning, improvement and innovation, we did not see clear evidence of this during our inspection.’
The London Clinic added: ‘The report itself recognised a number of positives in the delivery of surgi-
cal care and patient outcomes, which is corroborated in a review by the Royal College of Surgeons, whom we had invited to independently assess our processes earlier this year following the incidents last year during the pandemic.
‘However, the CQC did identify shortcomings in our supporting governance and assurance framework; in particular, how we apply lessons learned. We accept this feedback.
‘We saw that these processes were disrupted at the height of the Covid pandemic, and it should be noted that a quality improvement programme was already underway at the time of the CQC visit and, three months on, these are now well advanced.
‘In this time, we have made several improvements, including enhanced quality huddles and a quality buddies system; commenced a new ‘good governance’ training programme; realigned the clinical governance responsibility and improved the complaints handling procedures.’
The London Clinic in Devonshire Place
William Laing of LaingBuisson
By Olive Carterton
The quality of senior doctors’ feedback supervision and mentoring of resident medical officers (RMOs) in private hospitals has come in for criticism in a survey for the GMC.
Many RMOs feel they are saddled with too much responsibility and find being the only doctor on site causes difficulties and negatively impacts their well-being.
RMOs told the online and phone survey they would like protected hours for rest introduced into their shifts, more support with managing their workloads, and more than one of them on shift at a time.
IFF Research, which ran the survey of 138 of the 650 doctors believed to be RMOs, reported that many had unmet support needs and suggested the GMC considers improvements.
It said: ‘For some RMOs, the
GOOD FEEDBACK: But RMOs say it is often poor
working pattern of an extended shift followed by extended time off was a reason for taking on the role, as the time off provides opportunities for other priorities such as studying or being with family.
‘However, being the only doctor on-site can at times be difficult and have a negative impact on RMO well-being. In addition, the
fact that senior colleagues are not always available to provide advice can leave RMOs feeling that too much responsibility falls on their shoulders.
‘While RMOs generally feel supported and sufficiently trained, feedback, supervision and mentoring from senior colleagues is an area for improvement.’
It said RMOs mostly felt they received sufficient support, were given training opportunities and felt confident they knew what to do if they had a concern personally or about a patient.
‘However, the quality of supervision and mentoring is viewed to be poor by too many and feedback from senior colleagues is infrequent for many.
‘Because of the often transitional nature of the role, RMOs would benefit from more frequent feedback. It’s likely a yearly appraisal would not provide much time for RMOs to implement feed-
Bupa links with Circle to boost integration RMOs say they get too little support from consultants
Bupa UK Insurance and Circle Health Group, Britain’s largest private hospital network, have announced a deal for a new threeyear contract through to January 2024.
They said this would offer customers a quality healthcare experience at Circle and BMI-branded facilities and would deliver longterm value through ‘sustainable pricing’.
The partners have agreed upon several areas to explore the development, innovation and improvement of services.
This includes enhancing the customer journey through streamlined consultant booking processes,
out key Bupa specialist care centres for oncology and exploring pathway management for musculo-skeletal, cardiology and skin cancer patients.
Circle, with over 50 hospitals in the UK, said it was committed to a faster, digital-first booking experience through integration with Bupa systems and to innovate by creating new digital technologies and experiences to help patients.
Bupa UK Insurance chief executive Alex Perry said: ‘We’re delighted to extend our contract with Circle. Our priority is ensuring our customers have convenient access to quality, affordable healthcare services and that they
KEY FINDINGS
RMOs are mostly younger male doctors who completed medical training outside the UK
86% practised medicine overseas immediately before starting in the role. Many saw the job as a pathway into other UK doctor posts
Only a fifth expect to still be in the role one year on
Some face high workloads, isolation from other doctors, an inability to reach senior colleagues for face-to-face support with treatment for patients, lack of time for training and high levels of responsibility.
RMOs asked for more in-person contact with senior doctors via regularly scheduled meetings.
Source: Understanding the role of resident medical officers – final research
back received before moving on to another role.
‘RMOs would value more regularly scheduled meetings with senior doctors to provide the opportunity for ongoing feedback.’
The GMC said it was keen to further develop its understanding of medical practice in the independent sector and ensure its regulatory approach was relevant and appropriate for doctors in private work.
have a great experience when using their health insurance.
‘This new chapter in Circle and Bupa’s relationship will help further these priorities and is a great example of insurer and hospital
provider working together to deliver the best for our customers.’
Circle Health Group chief executive Paolo Pieri said: ‘We are proud to be extending our valued partnership with Bupa. After our recent purchase of BMI Healthcare, we’re committed to becoming the most technology-enabled healthcare provider in the country.
‘This year alone, we are investing £100m in the latest equipment, technology and infrastructure and to ensure we continue to give patients the best possible hospital experience, with the highest quality and best technology at the core of our offerings.’
rolling
Paolo Pieri, chief executive of Circle Health, said his firm was investing £100m this year in latest equipment
Gripes template is hailed as example
Independent practitioners, clinics and private hospitals who subscribe to the Independent Sector Complaints Adjudication Service (ISCAS) are being encouraged to look at how they are signposting patients to the service.
It has held up the message below, from St Hugh’s Hospital, Grimsby, as a ‘best practice example’.
HOW WE HANDLE COMPLAINTS
We will always:
l Listen to every complaint in full;
l Be open, honest and thorough in dealing with complaints;
l Respond promptly;
l Deal with everyone concerned, fairly and objectively;
l Seek to resolve any issues amicably;
l Use the experience to improve what we do.
RAISING A COMPLAINT
In the first instance, if you wish to raise a complaint or concern please email xxxxx making sure to provide the following details:
Your name and address;
The name and address of the patient (if different);
Patient’s date of birth;
Patient’s hospital number (if known);
Complainant’s contact details including phone and email address;
A full description of all issues about which you wish to complain, including relevant dates and times.
OUR THREE-STAGE COMPLAINT PROCESS
You can download a copy of our complaints procedure here.
LOCAL RESOLUTION
If your complaint cannot be resolved by a member of staff, please write to the hospital director (address provided) or e-mail xxxx. Your complaint will be investigated and a full response will be sent to you within 20 working days, unless the investigation is still ongoing.
INTERNAL APPEAL
If you are not satisfied with the outcome/response to your complaint, you can appeal to the Executive Director, Healthcare Management Trust, 14 Queen Anne’s Gate, London, SW1H 9AA, within six months.
EXTERNAL APPEAL
If you are dissatisfied with the internal appeal outcome, you have the right to refer the matter to Independent Healthcare Sector Complaints Adjudication Service (ISCAS) within six months of the final decision of the hospital’s internal review. ISCAS will then raise the complaint with the hospital within ten working days of receipt. You can find a copy of ISCAS’s complaints procedure here.
COMPLIMENTS
When we get it right, please let us know. Your positive comments are greatly appreciated by our staff and help to ensure good practice is shared.
All service users are encouraged to complete the patient survey leaflet that is available on the ward or in the outpatients area or you can email your feedback to info@ hmtsthughs.org.
HOW WE HANDLE YOUR PERSONAL INFORMATION
You can find out how we handle your personal information in our privacy policy here.
Medical defence body the MDDUS has urged members not to suffer in silence and instead make use of its new, confidential and free wellbeing support service.
The organisation’s Support into Pandemic Recovery programme additionally includes specialist advice on how to handle complaints about care delivered during Covid-19, support for doctors moving into blended remote and face-to-face consulting, and strategies for dealing with challenging patient encounters
New MDDUS chairman Prof Iain Cameron, professor of obstetrics and gynaecology and former dean of the Faculty of Medicine at the University of Southampton, said: ‘As we move into recovery from the pandemic, it has never been more important for clinicians to have resources and support in place to look after themselves as they care for others.’
Members can access help by phoning 0330 175 7043 or going to the website https://healthcare-rm. com/yourhalo/mddus/
Bowel op device is a first for a private unit
King Edward VII’s hospital, London has added LumenEye to its colorectal service – technology designed to improve diagnosis and prognosis.
The device is a new digital alternative to the conventional sigmoidoscope but can be operated by a single doctor and comfortably used without anaesthesia, sedation or full bowel preparation.
It was been shown in a recent study to obtain satisfactory diagnoses in 96% of patients.
It supports accurate diagnosis of bowel conditions as well as detecting polyps and conducting biopsies, using a full-high-definition camera to create images and video of the lower gastrointestinal tract.
It can also be offered as a less invasive alternative to bowel surveillance in patients following bowel surgery and cancer treatments.
Consultant colorectal surgeon
Mr James Kinross said: ‘There has long been a need to re-design cancer pathways and modernise point-of-care diagnostics, so we’re proud to be able to offer this tech-
The King Edward VII Hospital’s colorectral surgeons Mr Danilo Miscovic, Mr Charles Evans , Mr Alex von Roon, and Mr James Kinross
nology at our practice at King Edward VII’s – the first private hospital to do so.
‘The LumenEye device is a really important upgrade to a 200-yearold instrument. It’s also an important teaching tool, as it improves accuracy of information collected and makes it easier to share this information with others.
‘This aids us in driving innovation safely forward, as well as helping to standardise best practice and improving patient outcomes.’
Doctors still fear admitting errors
By a staff reporter
Doctors are overwhelmingly aware of and comply with their duty to be open and honest with patients when something goes wrong – but nearly a third fear the consequences of admitting errors.
An MDU survey of 418 doctors found:
98% were familiar with the statutory duty of candour, which requires organisations to be open and honest with patients if they experience at least moderate harm after an incident;
99% also reported responding to an incident in line with their legal and professional duties by apologising to patients, providing an explanation and putting things right if possible;
71% of doctors had no concerns about always being open and honest after an incident;
29% said they sometimes felt unable to do so because they were
worried about the patient’s reaction, being blamed or that they could face a claim for negligence;
The most common incidents involving the legal duty of candour were medication errors (45%), surgical problems (30%) and delayed diagnosis or referral (28%).
The union urged legislators and policymakers to ensure no obstacles were put in the way of the open exchange of information after something goes wrong.
Dr Michael Devlin, the defence body’s head of professional standards and liaison, said apologising meaningfully and explaining fully and promptly what had happened was vital for everyone involved in an incident, and was not an admission of legal liability.
But much work was needed to ensure an open and learning culture became the new norm.
The legal duty of candour has been in place in England for six years and in Scotland for three. A
Eye group opens new clinic
Eye hospital group Optegra has opened a new eye clinic in Gateshead, Tyne and Wear, specialising in NHS cataract treatment and promising to see patients within weeks. Mr Javad Moayedi, ophthalmic consultant and NHS medical director for the company, said: ‘Throughout the pandemic, Optegra has supported various NHS trusts around the country to be able to perform cataract surgery, which has been an honour. It is wonderful to see the transformation this procedure can make in people’s lives.’
similar duty will come into force in Wales in 2022.
Northern Ireland’s government is consulting on proposals to introduce a duty of candour under which individuals and organisations breaching the duty could be guilty of a criminal office.
Dr Devlin said this could be counterproductive, explaining: ‘If the proposals are fully adopted, Northern Ireland will be unique as the only UK country where the statutory duty applies to individuals as well as organisations, and where breach of the duty could attract criminal sanctions for clinicians.
‘History has taught us that criminalising medical errors of judgement does not make patient care safer. We believe it would have a chilling effect on the profession and be counterproductive to achieving the open and honest culture needed to put patient safety at the front and centre of everything we do.’
Consultants refuse to deal with pay body
Consultants’ representatives in the BMA have pulled out of the Doctors’ and Dentists’ Review Body process after over 80% of members told a survey this year’s 3% NHS pay award was inadequate or completely unacceptable.
Association estimates say a series of Government-imposed pay freezes and pay caps mean estimated take-home pay of the average consultant has fallen by more than 28% in real terms since 2008.
BMA consultants committee chairman Dr Vishal Sharma said: ‘This survey shows that our members no longer have any confidence in this Government to recognise the incredible efforts they have made and will continue to make, including the hours and days spent on Covid wards, putting their lives at risk, away from their families.
‘Consultants have lost all trust in the review body, their decisions and the Government’s management of a process that is no longing offering evidence-based, independent pay recommendations.’
UCLH Private Healthcare plans a further phase of investment in upgraded facilities. Its private maternity ward at University College Hospital, London – The Fitzrovia Suite – will be undergoing total refurbishment.
Work is due to be completed by the end of the year and so the private ward will be closed until 2022.
The project will include refurbishment of the private postnatal rooms, including new en-suite bathrooms, and a new reception and waiting area.
The trust is creating two dedicated private birthing suites to enable the offer a private natural delivery service from next year,
UCLH Private Healthcare director Kerensa Heffron said: ‘We are thrilled we are going to offer such an attractive environment for our new parents, alongside the worldclass care we already provide.’
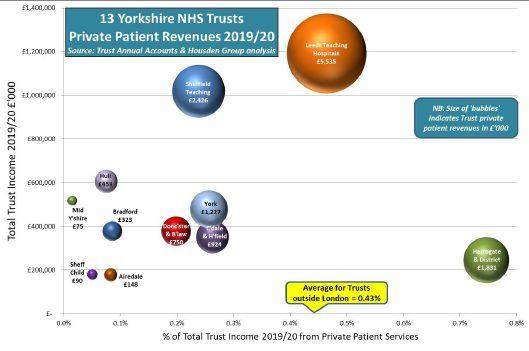
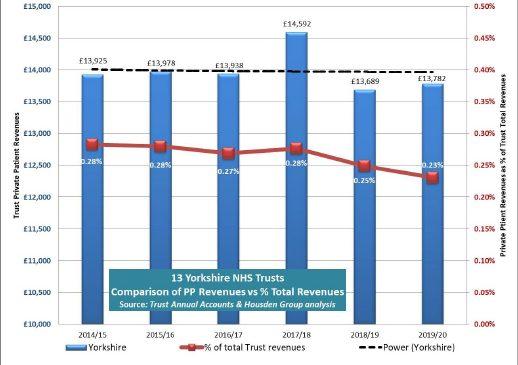
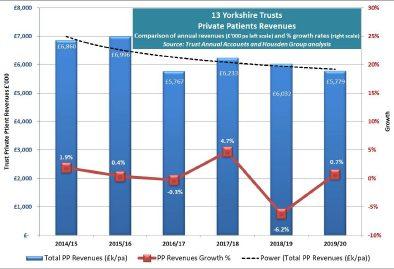
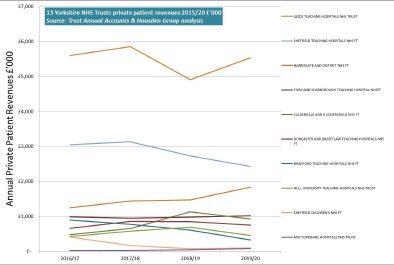
Latest NHS PPU Barometer
A total of 28 trusts took part in the third annual Housden Group NHS PPU Barometer survey, which provides a snapshot of current trading performance and an end-of-year forecast.
Trusts completing the Barometer represented 50% of the NHS’s total private patient revenues.
Are you practising in a PPU? Don’t miss my exclusive report in the next issue.
Philip Housden is director of Housden Group. See his feature article on PPUs in the Yorkshire region on page 46
Compiled by Philip Housden
PPU WATCH
Beware change in beauty op law
By Leslie Berry
A change in the law from this month means cosmetic clinics who fail to verify their customers are 18 or over before administering Botox or dermal fillers will face prosecution.
Speaking while health minister before last month’s Cabinet reshuffle, Nadine Dorries said a central aim was to protect children from pressures to achieve ‘utterly unrealistic’ body images.
It has been reported there were over 41,000 procedures including lip enhancements last year performed on under-18s, with many influenced by TV shows such as Love Island
Age restrictions already apply to body modifications such as tattoos, teeth-whitening and using sunbeds.
A rise in the number of children seeking treatments coincided with Covid-19, according to London
cosmetic surgeon Mr Olivier Amar, of the Cadogan Clinic in Sloane Street.
He said: ‘Since the beginning of the pandemic, practitioners and surgeons in the cosmetic industry have noticed a spike in patient demand for treatments. However, what is concerning to hear is the number of young people seeking treatment under the age of 18.
‘Having any cosmetic treatment or procedure administered is a big
Sports clinic for kids
Orthopaedic Specialists (OS) is expanding its paediatric services with the launch of a weekend trauma and sports medicine clinic for children and adolescents.
The clinic is operating in partnership with London’s Cromwell Hospital.
OS provides a comprehensive range of services for children daily across various hospitals including the Harley Street Specialist Hospital (HSSH).
It said its new clinic was a welcome addition allowing consultants to assist the same day with sports-related injuries and trauma.
OS medical director Mr Ali Noorani said: ‘We are delighted to be offering a dedicated service for young people tailored to their needs and offering the absolute best in orthopaedic exper-
tise, treatment and patient service.
‘This is a clinic that puts the child at the forefront and a place where we can make important decisions at the right time to make a lasting positive impact on the child’s health and well-being.’
OS includes oral and maxillofacial, pain management and rheumatology consultants as well as all orthopaedic subspecialties.
decision which should always be carefully considered.
‘It is known that young people can be particularly influenced by Instagram and other social media platforms – especially when it comes to models and influencers who may publicly discuss their own treatments.’
Mr Amar is chief medical officer at Uvence, a cosmetic treatment business that utilises people’s own cells to rejuvenate the skin.
Research for the company found 31% of 18- to 24-year-olds in Britain said using photo filters had warped their own perception of what they look like, to the point where it shocked them when they saw images of their unfiltered face.
He said while it was obviously good to see attempts were being made to protect the industry and patients, care was needed to prevent bans from making treatments less safe, rather than stopping them happening.
Bupa agrees deal with the Mayo Clinic
and Mayo Clinic Healthcare in London have struck a two-year agreement to deliver care to the insurer’s customers enabling them to access consultations, diagnostics, endoscopy, MRI and CT services.
Mayo Clinic Healthcare at Portland Place also provides a secondary clinical review for Bupa customers who may benefit from pioneering CAR-T cell therapy.
Bupa Insurance chief Alex Perry said: ‘Mayo Clinic Healthcare’s reputation speaks for itself, so its new London clinic is a great addition to the portfolio of hospitals and clinics where our customers can receive treatment and care.’
One-stop breast care clinic opens in the City
Basinghall Clinic, Cromwell Hospital’s outpatient diagnostic clinic in the City of London, has launched a new breast care service offering a one-stop shop for consultations and tests.
The clinic enables patients to see a consultant, undergo scans and a biopsy, if needed, on the same day with fast access to the hospital for a range of treatments.
Research by Breast Cancer Now found that almost 1.2m women in the UK have missed a vital breast screening due to the Covid-19 pandemic.
The hospital’s director of breast surgery Mr Giles Davies said: ‘The location of the clinic is convenient for people returning to the City and back to the office after Covid19 restrictions have been lifted; they can pop in before or after work.’
Basinghall Clinic is open five days a week 8am-6pm. People do not need health insurance or a GP referral to get an appointment.
Research into private care usage begins
The Patients Association is launching a focus group to help produce information for people looking into using private providers to help the group better understand how private healthcare works.
Advice will include how to get a referral to a private provider, what the options are for paying for treatment and how patients can ‘mix and match’ private and NHS care.
The project, funded by the Independent Healthcare Providers Network, follows research by the charity Engage Britain which found one-in-five people had used private healthcare because of difficulty accessing treatment in the NHS.
Bupa
Cosmetic surgeon Mr Olivier Amar
Orthopaedic surgeon Mr Ali Noorani
By Douglas Shepherd
The GMC’s core guidance Good Medical Practice is to be reviewed by an advisory forum of doctors and others including a representative of the Independent Healthcare Providers Network (IHPN).
Every element of the guidance is set to be looked at to assess where changes and updates are needed.
The team will also consider how Good Medical Practice will apply to physician associates and anaesthesia associates when they come into its regulation in future.
Good Medical Practice, outlining the professional values, knowledge and behaviours expected of doctors working in the UK, was last updated in 2013.
But Prof Colin Melville, the GMC’s medical director and director of education and standards, said the healthcare landscape had changed dramatically since then and would continue to do so.
‘It’s vital we update our guidance so doctors and other medical professionals can face the challenges of future practice with confidence.
‘The advisory forum will help us to do that. Its members will provide us with insight, expertise and
Good Medical Practice is the GMC’s rulebook for doctors
a range of knowledge and experience that will be invaluable as we proceed with this complex piece of work.’
Private healthcare sector input will come from Dawn Hodgkins, the IHPN’s director of regulation. She said she would help ensure GMC guidance supports doctors and other medical professionals across the whole healthcare system.
Prof Emma Cave, who is chairing the forum, said it would act as a
critical friend to the GMC throughout the process.
Other members are:
➤ Mikaela Carey, physician associate in urology at St George’s University Hospital NHS Foundation Trust;
➤ Dr Josie Cheetham, GP trainee in south Wales;
➤ Dr Henrietta Hughes, GP in London and the NHS National Freedom to Speak Up Guardian;
➤ Prof Pali Hungin, lead of the Changing Face of Medicine commission at the Academy of Medical Royal Colleges;
➤ Eileen McEneaney, Nursing and Midwifery Council;
➤ Prof Geeta Menon, consultant ophthalmic surgeon in Frimley, Surrey, and a postgraduate dean for Health Education England;
➤ Lucy Mulvagh, Health and Social Care Alliance Scotland;
➤ John Randall, Association of Anaesthesia Associates;
➤ Joan Saddler, NHS Confederation;
➤ Neil Tester, The Richmond Group of Charities.
Find out more about the review of Good Medical Practice, and how to get involved, by signing up at www. smartsurvey.co.uk/s/GMPreview
Spire buys Sheffield hospital with help from its consultants GMC ‘bible’ to get private care input
Consultants are taking a 13% stake in Aspen Healthcare’s Claremont Private Hospital in Sheffield.
The investment is linked to Spire Healthcare Group agreeing a deal to buy 87% of the operating asset for £15.7m.
Subject to the conclusion of final contracts, the hospital will become a Spire Healthcare hospital around the end of October or early November. Claremont Hospital, with 46 beds and three operating theatres,
works with 144 consultants and specialises in orthopaedics, general surgery and neurosurgery, seeing nearly 10,000 private and NHS patients admitted annually. It will become the 40th hospital in the Spire portfolio.
and consultant partners to the group.
Chief executive Justin Ash said: ‘We’re delighted that Claremont Hospital is joining Spire Healthcare and look forward to welcoming our new colleagues
Private care want long plan to cut waiting lists
The Independent Healthcare Providers Network (IHPN) has appealed to the Government to urgently set out a clear long-term plan on how the care backlog will be cleared.
It said that, with a record 5.6m people on NHS waiting lists, tackling this would require an important role for independent sector providers who were committed to playing their full part in the recovery of the health service postCovid.
Spire Health to go green, starting with electricity
Spire Healthcare this month began procuring all its electricity from renewable sources as part of its commitment to go carbon-neutral by the end of 2030.
It believes it is the first provider in the sector to do so and anticipates this will result in a 40% reduction in its carbon emissions.
A range of other initiatives include:
Replacing gas-powered boilers with more efficient equipment powered by electricity;
Replacing older lighting with LED lights which are between 50 and 60% more energy-efficient;
Installing photo-voltaic solar panels on the roof at Spire Cardiff, with similar projects to follow at other Spire hospitals;
‘Claremont is a highly complementary addition to Spire Healthcare’s portfolio. We share a commitment to providing the highest-quality patient care, working in partnership with world-class consultants. Claremont expands our presence into South Yorkshire, an area with a sizeable population where we currently have no hospitals.’
Use of electric vehicles as part of its fleet;
Improved insulation in its buildings.
The group has also appointed and trained a colleague from each of its 39 hospitals to become a carbon champion with the aim of developing and promoting local initiatives for reducing carbon consumption.
Justin Ash
A look back through our journal’s archives of a decade ago reveals that although times change, some issues are not so new
A trawl through the archives: what made the news in 2011
NHS private units are set to roll
Private practice opportunities in the NHS were set to rise as hospital managers in the health service showed mounting interest in harnessing the incomegenerating potential of private patient units (PPUs).
Hospital representatives were out in force to hear business experts at a seminar in London advise them about different models for maximising income.
Just over half the 130 NHS trusts had a PPU. Nine of the 72 units were managed by the private sector.
But with increasing NHS budget pressures, a lifting of the NHS private patients’ cap and competition being placed at the heart of Government reform, experts stressed that the possible
financial contribution of a PPU could not be ignored.
Adrian Stevensen, then chief executive of Independent Care –creators of 40 private healthcare facilities in the UK – said the annual PPU revenue ranged from £25,000 to £50m, although it rarely rose above £2m.
See how PPUs in Yorkshire are faring now in Philp Housden’s analysis on page 44
Costly cover ‘bar to trade’
Rocketing indemnity costs were forcing consultants to give up practice and hampering younger specialists from going private.
Results of a survey by the Federation of Independent Practitioner Organisations (FIPO) claimed chaos in the medical protection market.
Most consultant respondents did not understand:
Their indemnification’s terms and conditions;
The limit of their indemnity;
What to ask an insurer.
A spokesman told Independent Practitioner Today that young consultants were finding it extremely difficult to enter independent practice because of the cost of medical indemnity.
But at the other end of the spectrum, established consultants in high-risk specialties such as obstetrics and neurosurgery were finding indemnification costs so high that some were being forced out of practice.
FIPO said new entrants to the medical indemnity market had
offered products on a selective basis, often at reduced premiums, and were challenging the traditional defence bodies.
But this raised questions for consultants who should be aware of the ‘nuances’ of the indemnification.
‘Do not compete with NHS’
Private doctors who seek to collaborate rather than compete with the NHS are the ones whose businesses are likely to do the best, according to a healthcare banker.
Paul Birley, head of healthcare at Barclays Corporate, said: ‘Competition doesn’t seem to be the right approach. If you can collaborate and provide services that are not a threat and enhance the patient experience, then that seems to be the right way of doing things.’
Accountants can beat taxman’s faults’
Criticism of HM Revenue and Customs’ (HMRC) service to taxpayers sparked advice to private doctors to find the best accountant they could afford to deal with their tax affairs.
The Association of Independent Specialist Medical Accountants’
message followed a Commons’ Treasury Committee report expressing considerable dissatisfaction with the tax service.
Red tape ties up private doctors
A private GP hit out at the increasing burden placed on independent practitioners by the rising number of regulatory bodies.
Dr Martin Scurr, a former Independent Doctors Federation chairman, said the web of regulatory bodies that private doctors had to answer to was now ‘extraordinary.’
Writing in his weekly Daily Mail column, he complained that many of the bodies required a vast bundle of paperwork to be completed regularly – with considerable duplication – and also demanded annual fees. They were creating ‘inordinate amounts of paperwork and administrative hurdles, taking up time and energy that could be spent on patient care’.
TELL US YOUR NEWS
Share your experience of what has and has not worked in your private practice. Even if it’s bad news, let us know and we can spread the word to stop others falling into the same pitfalls.
Contact editorial director Robin Stride at robin@ip-today.co.uk
MEDICO-LEGAL GUIDANCE
Don’t hype up your practice
PRIVATE PRACTITIONERS are increasingly innovative and are seeking new, effective ways to promote their clinic and stay ahead of the competition.
In its Good Medical Practice guidance, the GMC sets out that when advertising your services, you must make sure the information you publish is factual, can be checked and does not exploit patients’ vulnerability or lack of medical knowledge.
Members of the public seeking advice on medical services either for themselves or their families may be particularly vulnerable to persuasive influence and it is important that they are protected from coercive advertising, such as special offers on treatment plans.
In essence, promotional tactics must not be used in a way that could encourage people to make poorly considered decisions. In particular, it would not be appropriate for medical services to be offered as ‘a prize’.
Undermine trust
The over-commercialisation of medical services may undermine public trust in the profession and could eventually also diminish the standard of medical care itself.
The GMC provides further practical guidance about advertising in specific guidance for doctors carrying out cosmetic interventions.
Practitioners are reminded of the necessity of following the Committee of Advertising Practice’s regulatory codes and guidelines, and of taking a responsible approach to marketing their services.
In practical terms, this means that the risks of interventions being carried out within your clinic must be accurately represented and must not be minimised or trivialised in any way.
Private practitioners should be mindful of how they present themselves and their services to the public. Dr Clare Devlin (right) reports
As there are risks associated with even the most minor treatments, doctors are advised to include information about any associated risks, and not to claim that interventions are risk-free.
While positive feedback from patients is usually welcome, it is important to ensure new patients are not misled about the likely results of a procedure and that particular care is taken not to falsely
claim or imply that certain results are a guaranteed outcome of a procedure.
It is also wise to be cautious about using exaggerated claims as testimonials, even if they are written by a patient.
Posting ‘before and after’ photographs of patients is best avoided where they are recognisable or potentially vulnerable, especially with regards to their mental
USING SOCIAL MEDIA IN YOUR PRACTICE
Ms P attended Dr R for cosmetic treatment, including Botox injections to her forehead and perioral dermal fillers.
Delighted with the result, she posted ‘before and after’ photographs on Twitter, recommending Dr R to her numerous followers and stating that he was the ‘leading doctor in his field’.
Dr R’s receptionist saw this and retweeted it, adding
MY TOP TIPS IN THIS SCENARIO
Familiarise yourself fully with the GMC’s guidance which addresses the use of social media
Be vigilant about your social media presence and that of your staff members. Provide training to staff members about the risks of social media and the importance of patient confidentiality and consent
Always consider the potential impact of social media posts on colleagues, patients and the public.
health. If your clinic does publish patient photographs, it must only be done with their fully informed consent, bearing in mind that they can withdraw their consent at any stage.
If you are aware your clinic’s services are being advertised by others, you will be expected to ensure they are not misrepresenting you or offering your services in a way that conflicts with GMC expectations. While market competitiveness is understandable, your fees should be set according to a fair payment for the service, with the BMA providing detailed advice on business and contractual considerations in private practice.
Before the consultation and treatment, you should inform the patient of all likely costs, including any fees for medical assessments, follow-up or for treating any unexpected complications.
Dr Clare Devlin is medico-legal consultant at Medical Protection
that Dr R was ‘the best doctor’ she had ever met. Other clinic staff agreed, and the tweet was shared several times, including from the clinic’s official Twitter account. A complaint was subsequently made to the regulator by a patient, Mrs O, who had become aware of the Twitter activity. She had not had such a good result from her cosmetic treatment with Dr R and felt that the claims in the tweets were unrealistic and unfounded.
Ensure that any information published about your services is accurate and does not make any unsustainable claims
Keep personal and professional use of social media separate, avoiding communication with patients through personal social networking sites
Do not share images of patients online without the patient’s expressed and fully informed consent
REGULATORY CHANGES
Pushing the private sector’s viewpoint
Key policy and regulatory changes are on their way for independent practitioners in the coming months.
PROVIDERS AND practitioners across the whole healthcare system are continuing to adapt to living in a world with Covid, in addition to tackling the longstanding quality, safety and workforce challenges facing the health and care services.
Mandatory Covid jabs
While the Covid vaccine rollout has been an undoubted success of 2021, there remains a significant proportion of people who are not exempt yet choose to remain unvaccinated.
Dawn Hodgkins (left) looks at what is on the horizon
In response to this, the healthcare policy and regulatory landscape is also evolving to meet the needs of the system, with significant implications for those working in the independent healthcare sector.
Below are just a few of the issues that independent practitioners will need to grapple with in the coming months.
And with pandemic rates remaining high, the Government is proposing to make it a legal requirement for health and care workers to have two doses of a Covid-19 vaccine, unless they have a medical exemption, as a way of keeping staff, patients, and vulnerable groups safe.
This approach is already in legislation which comes into force on 11 November 2021 for the care home sector.
From this date, care home managers will be responsible for ensuring that staff deployed to work within the home are either vaccinated or exempt. A consultation published in September aimed at extending this to healthcare providers.
The impact that mandatory vaccination will have on the healthcare sector is not yet clear. However, within NHS services, the number of staff who have had both Covid-19 vaccinations is reported to be around 85-95% in most areas, although this drops to around 75% in others. We anticipate that this picture will be broadly similar in the private healthcare sector.
The Care Quality Commission plans to be more transparent about the evidence that is used and is proposing to use six evidence categories to determine the key pieces of evidence needed to make a judgement on each quality statement
The types of workers that the mandatory requirement might apply to could also have a significant impact on both the staff and service delivery. Currently, the proposals just affect front-line clinical staff, but the Government is seeking views on broadening it out to administrative employees, for example.
Of course, making Covid vaccination mandatory for the healthcare workforce raises significant and complex employment, legal, ethical and practical questions for all healthcare providers with no easy answers.
The Independent Healthcare Providers Network (IHPN) is therefore continuing to work with law firm Bevan Brittan to help ensure our members and their workforce fully understand the issues at hand and, critically, that we can learn from the experiences of those working in social care where such legislation is already in place.
Health watchdog’s evolving assessment approach
Away from Covid-19, the Care Quality Commission (CQC) is continuing to develop its approach to regulation in response to its consultations published in July this year.
While its five ‘key lines of inquiry’ are expected to stay, it is proposing to develop new I/we ‘quality statements’ to support
people using services to understand the assessment framework and to set expectations about what good care looks like from their perspective.
The CQC plans to be more transparent about the evidence that is used and is proposing to use six evidence categories to determine the key pieces of evidence needed to make a judgement on each quality statement.
These are:
1. People’s experiences;
2. What do staff and leaders tell them;
3. What have they heard from their partners;
4. What the CQC itself has observed;
5. What do they know from the organisation’s systems, policies and records;
6. What can they learn from outcomes and performance data. They plan to allocate a score to each pillar of evidence that will ultimately ‘drive’ the service rating.
Clearly, there is much work to do to ensure these new changes work for both patients and providers.
IHPN will therefore be engaging closely with members and the CQC in the coming months. We need to ensure the watchdog has the right data and insight to make accurate assessments of providers, while also ensuring organisations are clear on what they need to do to improve their rating and ulti -
mately the care they deliver for patients.
GMC review of Good Medical Practice guidance
The CQC is not the only regulator looking to reform the way it works.
The GMC has also announced that it will be reviewing its core Good Medical Practice guidance, last updated in 2013, which outlines the professional values, knowledge and behaviours expected of doctors working in the UK.
I am delighted to have been asked to join the GMC’s advisory forum, which will help steer the review and act as a sounding board for key decisions and developments. (See news story on page 9).
It is early days in terms of the review, but a key priority for me in the coming months will be ensuring the revised version is fit for the future and recognises the key role independent providers play in the patient pathway.
I will also want to see that it supports good care and fairness for patients and doctors alike.
Government response to Paterson inquiry
The end of this year will also see the much-anticipated Government response to the independent inquiry into rogue surgeon Ian Paterson.
Wide-ranging recommendations include improving communica -
tion with patients, strengthening patient consent processes, ensuring effective multidisciplinary team-working is in place, and implementing more comprehensive data collection on consultants working across both the NHS and independent sector.
So there will be much to consider and act upon for all those working in the independent sector.
IHPN has been playing a key role in the Department of Health’s Programme Board and task and finish groups to help feed into the development of the Government’s response.
And once published, we will be working closely with members to ensure recommendations are successfully implemented and help the sector deliver the safest possible care for patients.
These are just a few of the policy and regulatory issues that will be impacting independent healthcare providers and practitioners in the coming months.
Independent Practitioner Today readers should be reassured that IHPN is fully plugged into all these changes, ensuring that the sector is factored into the new ways of working in the health system and is fully equipped to deliver the best possible care for patients in future.
Dawn Hodgkins is director of regulation at the Independent Healthcare Providers Network (IHPN)
The end of this year will also see the much-anticipated Government response to the independent inquiry into rogue surgeon Ian Paterson
ACCOUNTANT’S CLINIC: THE BUILDING BLOCKS OF ACCOUNTANCY
to of top tips
Julia Burn continues with her A to Z of top tips. This month she turns to the letter ‘Y’
is for Your financial health check
AS WE approach the end of the calendar year, it seems a good time to review and assess your financial affairs to ensure everything is in order.
There have been so many changes in the economy over the last two years, from Brexit to the fall-out from the Covid-19 pandemic, that now seems like a good time to take a step back and review the financial position of your practice.
Preparation of forecasts and budgets are always a tricky process, as although you know how you would expect your income and expenditure to be, you cannot anticipate external factors which will be beyond your control.
These may have a significant impact on your financial position, such as the cost implications that businesses have had to endure through the pandemic.
Support measures
As mentioned in my previous articles for Independent Practitioner Today, the Government gave businesses a variety of different support measures during the pandemic. But these have now all come to an end, so businesses need to try and adapt and return to some form of normality, albeit slightly different to how they ran before the pandemic.
Forecasts and budgets therefore need to be revisited and updated regularly so that any issues can be identified and tackled early to prevent any unwanted surprises.
Many businesses who have implemented a vast amount of investment into IT to enable them to work from home during the lockdowns are very likely to continue this in some form, whether exclusively working from home or a hybrid of working from home and in the office.
Working remotely
Lots of patients may previously have worked nearby and popped out in a break for a doctor’s appointment, but this may not be as easy to arrange where they are working remotely from home, which could be a significant distance away.
Where the practice itself has been utilising technology to offer virtual appointments rather than facetoface ones, it may be a good time to assess your need for premises.
For some independent practitioners, it may be appropriate to
consider downsizing or changing the way in which their space is used to better accommodate the current hybrid working models.
Rising taxes
During the last Budget, the Government stated that corporation tax for businesses generating profits before tax of £250,000 or more a year, would be increasing from 19% to 25% with effect from April 2023.
Companies generating profits before tax of less than £50,000 will continue to pay corporation tax at 19% and those companies generating between £50,000 and £250,000 will require a calculation because they will receive an element of taper relief as they are between the two rates.
Where companies have generated losses up to £2m during the pandemic, these losses will be available for carry back against profits of the previous three years
rather than the usual one year carryback.
The Government also announced a super deduction for investment in innovation of 130% of expenditure. This may be accessible for medical practitioners involved in clinical research or planning significant capital expenditure.
Business relief
During the Budget, there were no changes to Business Asset Disposal Relief – previously known as Entrepreneurs’ Relief – which currently has a lifetime allowance of £1m. But this change was anticipated, so we will need to watch this space for changes in the future.
Last month, the Government announced its plan to increase National Insurance by 1.25% from April 2022.
This will not only affect all employees by reducing their disposable income, but will also affect businesses because the cost
PATIENT CENTRED HEARING CARE
of employer’s National Insurance will also rise. It will be important to assess how this will affect your business before it is implemented (see news story on page 1).
The Government also announced an increase in tax on dividends of 1.25%. This will affect all those consultants who receive income this way from owning shares in their companies.
It stated that it could not rule out more tax increases, so we will all have to keep abreast of any changes to anticipate how these are going to affect businesses and individuals. By ensuring the fin ancial reporting of your business is regularly updated, you will be able to manage cash flows more easily.
Julia Burn (right) is a director at Blick Rothenberg and part of the team that advises medical practitioners
Exceptional audiological care starts with the right referral. At Pindrop Hearing, we understand each case as unique, and our team of expert Audiologists will work with your patients to find the right solution for them
• Specialists in Diagnostic Audiology including Paediatrics and Tinnitus rehabilitation
• Cutting edge on site facilities, including purpose built sound proof rooms and audiovestibular diagnostic services
• Comprehensive range of diagnostic tests including PTA, tympanometry and specialist tests including OAE's and VEMPS
•A wide range of hearing devices, not available on the NHS
• Outstanding aftercare and patient services
• Fully GDPR compliant
• Medico-Legal Audiology service including gold standard objective Audiological testing using Cortical AEP and ASSR
• Full COVID protection measures in all clinics alongside a dedicated online consultant portal
THE BIRTH COMPANY
Preparing a practice for commercial sale requires a lot of reviewing of its structures and systems.
In the sale process, there is a requirement for professional advice on several levels: commercial, legal, finance and particularly accounting.
Dr Donald Gibb (below) tells Independent Practitioner Today of his long-term project to diversify his business and develop it for a commercial sale
The secrets of gestating a sellable clinic
Kate Richardson, specialist sonographer and managing director of The Birth Company, performs an ultrasound scan
TO CAPITALISE a practice, it is important to diversify and depersonalise it. In our case, this was done in the first instance in 2000 by registering it as a limited company with a catchy name as a vehicle for my personal practice.
In addition to the tax advantages, it had already occurred to me that this could make the company saleable at an exit. The Birth Company was to become a brand. This was a key move for future success.
It is better to have a commercially descriptive name rather than, say, James Smith Ltd. This was the era of the start of the internet and we embraced this enthusiastically.
It is also important for a website to have an identity other than by personal name. You want to attract clients who do not already know your name. It should describe your activity.
I became clinically busy personally with a peak in 2010. I was already 60 years old and my thinking turned to my exit and legacy. Being quieter freed up space in my clinic for sonographer activity: we made some structural changes to accommodate this.
Crucial recruitment
We recruited high-quality sonographers who were well led and trained in all aspects of obstetric and gynaecology ultrasound. This was crucial.
Activity was generated on the internet by investment in seachengine optimisation (SEO): the vast majority of our cases were and are self-referral and self-pay. There was an investment in equipment, staff training and recruitment. We focused on early pregnancy ultrasound scans and fertility scans. The early preg -
We first reported on the success of The Birth Company in July 2013
The ability to immediately record and transmit images electronically by Tricefy to the patient, relatives and other professionals has been a hugely important innovation
nancy scans generated ongoing scans and sometimes births from happy clients.
We linked with reputable overseas fertility clinics providing scans and blood tests. Our sonographers were all qualified and experienced in 12-week pregnancy scans and, in late 2012, the era of non-invasive prenatal testing began. We were the second clinic in Britain to offer NIPTs: a great opportunity. We have now performed more than 10,000 of them.
We also adopted innovative technology. The Viewpoint 6 ultrasound software from Health Net Connections, which we adopted early, was of enormous benefit and an important investment.
The ability to immediately record and transmit images electronically by Tricefy – a cloudbased communication platform – to the patient, relatives and other professionals has been a hugely important innovation.
While still in the ultrasound room, the patient receives a ping of receipt of the images/video on their phone. The grandparents in Australia or elsewhere receive them at the same time!
This is often cited in our Google reviews, now more than 200, as a unique selling proposition of our service. This is also immensely helpful for IVF clinics or consultants waiting to make decisions on results.
I recognised the value and potential of the business in expanding outside London. In 2017, I had more time after ceasing inpatient clinical work and we opened a new clinic in Alderley Edge, Cheshire. This was a strategic location having considered population density, transport links, affluent communities and a known name.
This has proved to be a good choice and demonstrated to buyers the opportunity to expand outside London. We have been able to integrate the support systems for both clinics. The database and diaries can be accessed from either clinic and the phone lines are integrated. Staff are in constant communication.
Booking system
At this time, we developed an online booking system, which we encourage clients to use. We are confident that our website is educational and they can find answers to their questions there.
We find that clients appreciate the convenience of online booking, 24 hours a day. They pay online when booking and beneficial consequences are that we rarely have a non-attender and we have no bad debts. This is great business. Of course, some may want to cancel if they miscarry before an early pregnancy scan, but we have
p18
a very efficient cancellation and re-imbursement system though email.
What is a practice worth?
The answer to this is whatever someone is prepared to pay for it. It is not just based on previous performance but more on future potential. The accounts for the years before need to be scrutinised and therefore need to be complete, tidy and understandable. A good accounting software package and a diligent accountant are important. Net profit is more important than turnover. A calculation of EDITDA (Earnings before Interest, Taxes, Depreciation and Amortisation) should be made.
The advisers of the seller and the buyer will both consider this in determining the worth of the business by using a multiple, which is usually x 4-6 in small medical businesses. It should also be remembered that the value is greater with more potential buyers.
Selling a smaller personal practice is more of a challenge. The benefit for the buyer may be room rental security and a digressive profit share of 30%, 20% and 10% over a few years. This may be a personal arrangement between a senior consultant retiring and a junior consultant stepping up to private practice. There is only a limited legal framework for such a sale. This may be fraught with difficulties
It is important to realise that selling a business costs money, some of it up front in instalments linked to progress
and damaging to personal relationships unless done correctly. Patients cannot be sold as an asset because, if they do not like a successor, they will go elsewhere.
The process of selling
Our company had become very visible. I received occasional emails from businesses involved in the process of buying and selling businesses.
I responded to one based in Oxford who hosted a ‘How it is done’ session at Blenheim Palace: a nice day out. For a small but significant payment, I registered with it and signed a contract.
It is important to realise that selling a business costs money, some
of it up front in instalments linked to progress. Specialist advisers, lawyers in the later stages and a good accountant may remove 10% of the share of the final cake: the consideration. It sounds a lot, but it is worth it, assuming a good consideration.
The advisers usually have a minimum fee. They advise on the structures of the business and go out electronically to seek possible buyers. I did not have to do any of this myself.
They drew up lists, discussing with me inclusion and exclusion. It is important to have more than one buyer to stimulate interest and push the price up through competition. One advantage was that
The entrance to The Birth Company in Harley Street, London, (left) and some of its interiors (below)
there were only two shareholders: myself and a member of my family. This simplified discussion and negotiations.
We reviewed all our systems led by our managing director Kate Richardson, who was also director of ultrasound. This was a matter of trying to get our house in order and this provided an important foundation for what was to become due diligence during the sale process.
We focused on quality care and reduced costs when possible. We did not carry any debt, which was an advantage. We made sure our Companies House registration, insurance policies and other paperwork were up to date.
Possible buyers
It was the autumn of 2020 when the advisers had produced a short list of eight possible buyers. We also had interest from two private equity companies, but opted not to continue with them. Non-disclosure agreements were signed with the interested parties, as we had supplied them with commercially sensitive information.
The Covid crisis presented a serious challenge. The sale process had to proceed on a remote basis on Zoom. Meetings were conducted with the eight possible buyers. We made a 12-minute PowerPoint presentation promoting The Birth Company.
Four of the possible buyers already had a significant presence in the private medical sector in the UK.
By the end of the year, we were able to agree exclusivity with one strong buyer and granted them exclusivity, discontinuing contact with other interested parties. At this stage, the lawyers became involved and in February 2021 we signed the heads of terms agreement to proceed to the next stage of due diligence and negotiation.
We opted for a share sale rather than a trade and assets sale which might have been simpler. During this time, confidentiality had to be observed. Only myself and my managing director were privy to the evolving situation on our side.
This was very important in our approach because of the need not to have public discussions of what was going on. This was hard but necessary.
In the final two months, we started to have operational meetings with The Portland Hospital, which was very encouraging. The due diligence was long and detailed, but resulted in the share and purchase agreement, shareholders’ agreement, articles of association, management agreement and my own employment contract.
We realised that we had outgrown our management systems, such as human resources, accounting, marketing, governance and Care Quality Commission prepa-
rooms at the Birth Company’s Harley Street clinic
Confidentiality was very important in our approach because of the need not to have public discussions of what was going on. This was hard but necessary
ration. We think it will benefit our business to be part of the management systems of The Portland Hospital.
I have become a part-time employee, but am able to advise and consult in the business. I have a minority shareholding which will end after three years. I look forward to helping The Birth Company move forward with HCA Healthcare UK and The Portland Hospital
Ultimately, the sale has guaranteed the future of The Birth Company. Having nurtured it for 20 years, this is very satisfying.
I am also pleased we have secured the jobs of the staff after my retiral in three years’ time.
Acknowledgements and thanks None of this would have been possible without the help of:
➧ Kate Richardson and team at The Birth Company Ltd;
➧ Lawrence Price and team at Rockworth Ltd, www.rockworth.co.uk;
➧ Will Axtell and team at Penningtons, Manches, Cooper LLP, www.penningtonslaw.com;
➧ Lee Manning, Mehul Thaker and team at Raffingers LLP, www.raffingers.co.uk;
➧ Selvavinayagam Vireswer and team at HCA Healthcare UK.
One of the ultrasound
What Covid has taught us about workplace
well-being
The Covid-19 pandemic has set in train many changes, particularly in workplace health and well-being. Bupa UK Insurance commercial director Mark Allan (right) discusses some of these and the lessons from business that consultants can use in their practices
The most striking finding of the census is that a record number of employees have reported good mental health at work over the last year – 78% in fact
The most striking finding is that a record number of employees have reported good mental health at work over the last year – 78% in fact.
LIVING THROUGH a global pandemic over the last 18 months has acted as something of a wake-up call for many of us.
As we emerge from the other side of it, the impact that the workplace – and journeys to and from it – can have on health is more important than ever.
It has also been a reminder to many businesses that keeping their workforce healthy, both physically and mentally, is absolutely central to their success.
Changes to working practices have also shown them that just because businesses have always worked in a certain way, it doesn’t mean change isn’t possible.
More than that, it has shown that changes to how businesses work can deliver both greater productivity and improved health and well-being.
While some of these changes aren’t available to everyone in the healthcare sector, many lessons can also be applied to your practice to improve the wellbeing of your team and those you work with.
Well-being census
Workplace well-being relates to all aspects of working life, from the quality and safety of the workplace, to how employees feel about their work.
Our 2021 Workplace Wellbeing Census involved more than 4,000 employees across 13 key sectors. It looked at changes to working practices over the last year and the impact these changes have had on employee health and well-being.
We’re sharing insights from these organisations to help consultants stay informed as they move their practices to new and different post-Covid ways of working.
Across the board, employees cited a number of well-being gains, with changes to commutes, home working and availability of flexible working being those most likely to have had a positive impact on employee well-being.
More flexibility
The census also shows that some groups have found changes to working patterns particularly beneficial.
Eight out of ten working parents, for example, report that changes over the last year have given them more flexibility, which has been particularly important given the added responsibilities of childcare and home-schooling.
Women have responded particularly well to new ways of working, and employees with disabilities have also seen big improvements. Two-thirds of those with a disability say home-working has removed accessibility issues they previously faced.
And these gains aren’t purely circumstantial. UK organisations have made marked efforts to safeguard the well-being of their workforces over the past 12 months, including nearly half strengthening their well-being services.
Businesses in many – though not all – sectors have also demonstrated a greater understanding of mental health. In financial services, for example, more than half of employees in the sector report finding their employer showed more empathy now.
Not all of the findings are positive, however. Remote working and a lack of employee visibility have increased the strain and the workloads on employees in a number of sectors. It has also allowed incidents of bullying and discrimination to go unnoticed in some cases.
LESSONS FROM THE PANDEMIC
FOUR BUSINESS WELL-BEING LESSONS YOU CAN TAKE INTO YOUR PRACTICE
1 FAVOUR FLEXIBILITY FOR YOUR PRACTICE TEAMS, WHERE POSSIBLE
The majority of us have experienced a change in our working life as a result of the pandemic. Whether it’s a change to how we work – including a greater use of digital technology – the end of our commuting lives or changes to job roles.
The employees in our census perceived some of these changes as positive. The availability of remote working, the opportunity not to have to travel to the workplace and flexible working patterns were all well-being gains that were considered an incentive.
For your practice, as well as for the businesses we spoke to, the challenge is to make sure that these well-being gains brought about by Covid-19 remain. This will enable more people to work in a way that makes them feel comfortable and empowered to put as much into their work as possible.
Businesses are starting to think about the longer term, including alternative ways to structure work communication and hours, as well as physical presence. And what many are converging on is different models of hybrid working.
At its core, hybrid working is an arrangement in which an individual employee, team or organisation work part of their time at the workplace and part remotely. It gives people the best of both worlds: structure and sociability on one hand, and independence and flexibility on the other.
Of course, this won’t suit everyone and isn’t available to everyone in the healthcare sector.
The pandemic has also drawn attention to disparities among those able to work remotely, including the varying quality of internet access, the demands of parenting and caring, and the luxury of roomy homes that make working from home comfortable.
Some roles, such as those that are patient-facing, won’t allow for home-working. There’s also the question of personality.
People who appreciate a fixed routine, for example, may find it difficult to switch between working at home and in a workplace setting.
For your practice, you may wish to look at the needs of both the team generally and the individual members within it – being as flexible and adaptable as they have been during the pandemic.
If hybrid working isn’t an option for some practice team members, perhaps greater flexibility around working hours may offer them the opportunity to improve their well-being.
For example, later starts or changing clinic times to enable school drop-offs or longer lunch breaks to allow for personal activities such as participation in exercise classes. You may also be able to identify elements of work which could be done remotely or asynchronously.
2
PUT MENTAL HEALTH AT THE TOP OF YOUR PRACTICE AGENDA
The mental health impact of the pandemic has been enormous, not just in a work setting, but for people experiencing isolation, bereavement or health anxiety.
Promisingly, mental health is an area which has improved since the pandemic, with many businesses appreciating the stresses and strains of living and working in an uncertain and often worrying time.
As a result, 36% of workers in
our census believe that their employer is more understanding of mental health issues postCovid than they were before the outbreak.
In business, initiatives such as line manager training, teaching resilience and appointing mental health first aiders was making a significant impact on managing mental health in the physical workplace pre-Covid.
Now we have the opportunity to rethink the way that we manage mental health to accommodate the new ways of working brought about by the pandemic. As we transition into post-Covid ways of working, we need to keep the mental health of our teams front of mind.
➲ Encourage your practice team to work sensible hours, take full lunch breaks, and take part in well-being activities. They will be more productive in the long run.
➲ Prioritise regular one-toone meetings and catchups with your team and use this time to check how they are and talk through any difficulties at home or work. Knowing your team’s ‘normal’ outlook and activities will help you spot changes earlier, and will make conversations easier if problems do arise.
➲ Add well-being as a standing item on your agenda at practice meetings so your team has the opportunity to talk about how they have been doing and anything that might be affecting their well-being. Don’t forget to ask them for feedback about your management and any additional support you could provide.
➲ Help team members manage their workloads and feel confident to work effectively. It may not be possible to offer them complete control over their workload and hours. But you can work with them to find areas where they could make their own decisions and manage their own
time. Make sure they’re properly trained to do their jobs, and look for development opportunities.
➲ Show you appreciate your team’s efforts. Employees who don’t feel properly rewarded for their efforts are more at risk of common mental health problems and increased stress.
➲ Deal with bullying and conflict. Workplace bullying and conflict can increase symptoms of depression, anxiety and stress-related problems. The Advisory, Conciliation and Arbitration Service, which works to improve workplace relationships, offers more information on dealing with bullying, harassment and conflict in the workplace.
➲ Ensure there is an area separate from the work zone where employees can get some respite and consider the impacts of light, noise and so on in the workplace. Do what you can to make it a pleasant environment to be in.
3 MAKING HEALTH AND WELL-BEING ACCESSIBLE IS KEY
We’ve seen a marked increase in the number of health and wellbeing services offered by businesses over the last year, and our census recognises that employees are generally pleased to be offered them, even if they haven’t had to use them yet. Most say that their employer has introduced some form of initiative in response to the Covid-19 pandemic and many hope these changes will become permanent.
Good workplace well-being ensures employees are happy, healthy and engaged at work –and need not be costly. One way to start is by creating a wellbeing strategy.
It’s a long-term strategy, so it is better to start with smaller changes and build over time.
Some of the most effective changes you can make are cultural and effectively free to implement and maintain. It just requires a shift in thinking.
Taking a health-first approach to people management and ensuring that your practice team has access to help for both mental and physical health concerns will mean greater productivity, reduced staff turnover and less sick absence, which all makes for a more successful working environment.
You can find more information about creating a well-being strategy at: www.bupa.co.uk/ business/workplace-wellbeinghub/wellbeing-strategy
4 CULTURE, DIVERSITY AND INCLUSION
Organisations with diverse and inclusive workplaces boast a number of benefits: not only does it make for happier working conditions for employees, it also opens them up to new ideas, innovation and greater understanding of the world they serve.
Many organisations are increasingly putting diversity at the top of their agenda. Our census found that some ground has been made over the last year.
One-in-seven employers (14%) has introduced policies to ensure diversity and inclusion in the past 12 months. For the vast majority (68%) of workers who have a disability, working from home removed some of the accessibility issues they face when going to a physical workplace.
But there’s still ground to make up here. More than a quarter of employees (28%) have personally experienced discrimination at work. This rises to 35% of women and 40% of disabled employees.
There are also some specific areas where discrimination is still on the increase – 22% of workers claim that age discrimination has worsened over the last year. And a similar
number (18%) have seen an increase in gender re-assignment discrimination.
Many businesses find that achieving buy-in from the top is key to boosting inclusivity, and those that are most successful write inclusivity into their core business values. You can mirror this in your practice by prioritising inclusivity and promoting it in your team.
Even while operating remotely, the most inclusive businesses encourage a culture of frequent check-ins – opening a dialogue that allows employees to honestly express their needs and discuss challenges they may experience in the workplace –particularly those of a sensitive nature.
As an employer, you can make a difference by providing an inclusive and comfortable environment for your practice team.
Think about trying to find ways to understand more. Every individual’s experience is different, and by educating yourself, you put yourself in a better position to listen to and support your team.
Consider taking time to also think about your policies and how you put these into practice. Assess the facilities you provide, such as toilets or changing rooms, and your practice’s dress code too. Try and find ways to make them more inclusive.
Other simple steps such as encouraging your team to add pronouns to their email signatures and usernames or by inviting them to reserve time for prayer and other personal needs by blocking it out on the calendar help ensure everyone feels comfortable at work. They may find diversity and inclusion training helpful.
Find more resources to support you and your practice at www.bupa.co.uk/business/ workplace-wellbeing-hub
A digital prescription platform to allow convenient prescribing from home
CloudRx is a digital prescription system that allows prescribers to create and send an electronic prescription to our fully licensed pharmacy for fast delivery direct to your patient. It can be used from home by doctors working away from their practices.
No cost to prescribers
Simple and quick prescription creation.
Legal paperless prescriptions, including repeat prescriptions and controlled drugs.
Patients receive text and email requesting secure payment. Alternatively, we can invoice the prescriber or clinic each month.
Prescriber Fees can be added if requested
Medicines are dispensed and dispatched by a variety of delivery options
Fully integrated into MidexPRO
“We have worked with CloudRX to maintain a cold chain for the medication and direct delivery to patients at home.”
Dr Charlotte Norton, Medical Director of The Slimming Clinic, the UK’s largest chain of private doctor-led weight loss clinics
What will digital tax returns entail?
Making Tax Digital is here already, but when do you need to comply? Following our lead story last month, Vanessa Sanders (right) takes you through the changes
DOCTORS’ EYES often glaze over and their minds wander when the rudiments of tax and accounting are discussed, but attention must be paid to Making Tax Digital (MTD).
This is a fundamental change to the UK tax system affecting how businesses and individuals communicate their accounting and tax records to HM Revenue and Customs (HMRC).
MTD compliance is being introduced through a series of changes that have already started for some independent practitioners.
Since April 2019, VAT-registered businesses with a taxable turnover in excess of £85,000 have been keeping their accounting records and submitting VAT returns digitally. From April 2022, all VATregistered businesses, irrespective of turnover, will be forced into digitisation.
Now the digitisation date has arrived for the self-employed, including individual members in limited liability partnerships and landlords – those individuals and partnerships renting property.
The date is 6 April 2024. Those
to assess their business’s technical abilities to know what software, staffing and training requirements need to be implemented for this milestone change to tax filing.
Price sensitivity and the continuous struggle to keep costs under control means doctors should be investigating comprehensive packages which offer added benefits, such as business planning advice, augmented by partnering with others, such as financial advisers, to ensure personal financial objectives guide actions.
Problem for landlords
A stumbling block for landlords generating gross rental receipts over £10,000 is that many do not separate their rental business from their private affairs.
As live bank feeds will be required to link into the MTD software, separate accounts will become a necessity, unless doctors want HMRC to see their spending patterns – which is one of the ways they build a financial picture for inquiry purposes.
MTD forces change
With the introduction of MTD for income tax from April 2024 (MTD ITSA), the reporting of accounting data is to be aligned exactly with the tax year.
The Finance Bill 2022 will contain legislation to abolish basis periods for businesses, meaning that, regardless of the year-end, MTD will apply to the fiscal year (FY) ending 5 April.
The law will not require businesses to alter their accounting period if it is not in alignment; however, from a practical perspective, this is likely to be the action taken.
Without change to reporting periods, taxpayers with several sources of income would need to file MTD reports for differing quarterly periods in the tax year, which would be impracticable to manage – up to 13 returns if VAT is included.
The law will deem accounting periods ending on dates between 31 March to 4 April as ending on the tax year-end: 5 April. Any income/expenses arising after the end of the accounting period will fall into the next tax year. This will apply to both trading and property businesses.
The efficiency gains for private practice are not to be underestimated, although it will be a hard and concentrated slog
Businesses which already draw up accounts to 31 March or 5 April will see no practical difference from 2023-24, the transition year.
Property-letting businesses already have to report to the tax year, but, in practice, many draw up their accounts to 31 March, which, by concession, is treated as a period ending on 5 April.
Under the tax-year basis, the self-employed will file MTD reports for all their sources of income by the same date each quarter, with a possible deviation for VAT if their VAT returns do not align with the normal quarter dates: March, June, September and December.
If you are VAT-registered as a sole trader or partnership, you may wish to change your VAT periods to align to these dates.
The estimated tax liabilities, based on those quarterly MTD reports should make more sense, as the income reported in the quarter will be what drives the tax due for the year instead of being behind and confused with the ‘payments on account’ system.
HMRC has recently consulted on accelerating tax payment dates for both companies and unincorporated businesses, which means that while tax payment dates remain as they are currently, advancing closer to the earnings’ time-frame in the future would clearly only be a small step.
Transitional relief
Businesses with a 30 April yearend will be particularly hit in the transition year (2024), as they will have to report profits for the period from 1 May 2022 to 5 April 2024 in FY 2024.
There will be a transitional relief to spread the extra income falling in FY 2024 over five years to FY 2028, but this bringing into real time could push people into
higher tax bands for those years. This is worrying with rates of tax being increased through the new levies announced
Where businesses are carrying overlap relief arising from when trading commenced because a period was taxed twice, that overlap relief will be offset against profits in FY 2023.
Digital record-keeping
Taxpayers must provide HMRC with returns of their income and expenditure every three months. Separate reports will be required for each type of property business; for example, furnished holiday lets, long-term lets and overseas property businesses.
Four reports in respect of each business will need to be made within one month of each business quarter-end; plus an end-ofperiod statement at the end of the accounting period or tax year. These may not be the same if you choose not to alter the year end to 31 March-5 April.
HMRC has wide powers to choose what financial information is relevant to calculating profits, losses or income of the business, including information about receipts and expenses.
This means actions will need to be decided in real time for inclusion in the appropriate return periods.
For companies, this will need some consideration about budgeting for spending habits in terms of when dividends are declared and paid to shareholders, but there is time yet to form good habits, as MTD for corporation tax is not scheduled until April 2026.
The regulations will set out the account categories for each type of business including adjustments for ‘private use’ and to claim any relief available. HMRC will require summarised totals of each account to be submitted in the periodic updates.
Conclusion
The success of MTD is critical to the Government, especially given the pandemic and our decision as the UK to leave the EU. MTD will not fail.
For everyone, the road ahead is long and likely to be bumpy. The message is: do not procrastinate. The efficiency gains for private practice are not to be underestimated, although it will be a hard and concentrated slog. Ultimately, going digital will help doctors operating in the private sector, when a better understanding of business will be vital to its survival.
Vanessa Sanders is a partner at Stanbridge Associates, specialist medical accountants
Don’t get caught in the eye of a storm
Dr Shabbir Choudhury looks at clinical negligence claims against ophthalmology and offers advice on managing risk in this specialty
EVERY YEAR, the MDU advises or assists hundreds of ophthalmology members facing issues ranging from regulatory investigations, service complaints, performance concerns, inquests and tricky medico-legal or ethical scenarios. Almost every week of the year, the MDU expects to see one or more new ophthalmology clinical negligence claims notified to our claims-handling team and this article focuses on the factors driving litigation in the specialty.
Over a ten-year period, nearly 80% of ophthalmology claims were successfully defended with no payment of compensation or claimant costs.
Claims can result from a number of causes, not always related to surgical error. Informed consent, dissatisfaction with the outcome and delayed diagnosis were a feature of many cases in our study of ophthalmology claims. Managing such risks is important in avoiding future claims.
Reasons for claims
Cataract
surgery
By far the commonest procedure which led to claims was cataract surgery, which accounted for over a third of cases.
Common reasons for cataract claims were intra-operative and postoperative complications, resulting in deterioration of vision or the need for further corrective procedures.
Postoperative infection was also a common factor, as was rupture of the posterior capsule. Other claims involved equipment failure during surgery, incorrect medication provided post-surgery and claims for insertion of the incorrect lens.
Laser refractive surgery
The reasons for claims in this area ranged from inadequate consent and failure of treatment, to dissatisfaction with the results and post-operative complications.
This highlights the importance of a stringent consent process and a realistic discussion of the risks and likely benefits of such procedures.
Consent
Allegations in relation to consent were directly involved in a number of cases, but inadequate consent was also a common allegation in many other claims.
In most cases, the informed consent related to allegations that, had the surgeon adequately explained the risk of the procedure, the claimant would not have chosen to undergo the treatment or may have done so at a later time.
Glaucoma
Failure to diagnose, delayed diagnosis and inadequate treatment of glaucoma all resulted in claims.
Often, cases arose following cataract surgery or were related to
allegations of mismanagement and treatment of glaucoma.
Delay or incorrect diagnosis
Around half of allegations of a delay or incorrect diagnosis were about a missed tumour. This highlights the importance of ensuring that the examination of the eyes is considered holistically and that impairment of visual fields and acuity should be considered in light of pathology outside the eye.
While claims numbers have remained steady in recent years, the cost of claims has spiralled. This is not due to clinical standards but to a deteriorating legal environment which the MDU is campaigning to reform. Learn more at www. themdu.com/faircomp.
Dr Shabbir Choudhury (right) is medico-legal adviser and former senior medical claims handler at the Medical Defence Union (MDU)
Claims can result from a number of causes, not always related to surgical error
MANAGING RISKS
Claims involving ophthalmologists are made for a wide variety of reasons. But there are some common risk factors, which can help to reduce risks if managed appropriately. Risks can be mitigated by:
Providing written information leaflets, if possible, as this may help the patient to remember what was said in a consultation so they can reflect on it later in their own time
Ensuring patients understand the potential risks and benefits of the procedure to give their consent
Documenting discussions with patients and the consent process clearly
Being aware of relevant guidance – for example, from the GMC and NICE
Ensuring you have the appropriate training and experience to carry out a procedure. Consider referral to a specialist in those cases which fall outside your skill set or knowledge
If things go wrong, be transparent with the patient by providing an explanation of what has happened and the likely short- and long-term effects of this. Get further advice from your medical defence organisation if you believe the incident triggers the organisations’ ‘duty of candour’ requirements
NHS Pensions & Annual Allowance Tax
Get ready in advance of April 2022 when the proposed changes to the NHS Pensions will allow you to reclaim some or all of any Annual Allowance tax you may have suffered in the past.
With our knowledge and in-house calculators, we will be able to predict in advance and check statements produced by NHS Pensions and Scottish Public Pensions Agency for accuracy for any refunds due.
For further information contact us at aa@semail.co.uk or telephone 01625 527351.
CYBER SECURITY
The online scams industry has boomed over the last 18 months as criminals take advantage of the pandemic to steal people’s personal information and their money. Raj Patel (right) looks at how you can protect your practice and explains the measures Healthcode takes to keep its customers safe
Keeping your data secure
WHILE ROBBERIES , thefts and homicides in England and Wales fell during the pandemic, computer crime bucked the trend as we spent far more of our work and leisure time online.
According to the latest crime survey from the Office for National Statistics, there were an estimated 1.7m computer misuse offences in the year ending March 2021, up by 85% from the year ending March 2019.
In particular, cases of unauthorised access to personal information such as hacking – which included large-scale data breaches – rose by 162%.
Meanwhile the Government’s latest annual cyber security breaches survey published in March 2021 revealed that 39% of businesses and 26% of charities report having cyber security breaches or attacks in the previous 12 months, most commonly phishing attacks.
Of these, one in five ended up
As the pandemic has created the ideal conditions for cyber criminals, that should also prompt us all to reassess our data protection measures
losing money, data or other assets while many more experienced serious disruption.
Although this was lower than 2020, the survey found that Covid-19 seems to have made cyber security harder for organisations.
For example, it notes that fewer businesses are now deploying security-monitoring tools or undertaking any form of user monitoring, which ‘possibly sug-
gests that they are simply less aware than before of the breaches and attacks their staff are facing’.
Tempting target
This should concern independent practitioners because healthcare presents a tempting target for cyber criminals.
According to the cyber security breaches survey, 58% of private businesses hold personal data about customers, but this rises to 80% in the health, social work and social care sector and 82% in the finance and insurance sector.
However, healthcare organisations consistently report the highest number of data protection breaches to the Information Commissioner’s Office (ICO).
The latest statistics from the ICO for 1 April-30 June 2021 show there were 607 data security incidents in the healthcare sector –including 108 cyber security incidents – compared with 180 for finance, insurance and credit,
including 53 cyber security incidents.
And last year, Independent Practitioner Today reported a study, showing that as many as 67% of healthcare organisations had experienced a cyber security incident in the 12 months to February 2020.
These included the introduction of viruses or malware from thirdparty devices, staff sharing information with unauthorised recipients and malicious links in emails and on social media (28%).
What can you do?
As the pandemic has created the ideal conditions for cyber criminals, that should also prompt us all to reassess our data protection measures.
Even if you have been the victim of a crime, few patients are likely to be sympathetic when they hear that their sensitive data has been stolen.
And in addition to the potential disruption and embarrassment, the ICO could also hit your business with a financial penalty if it finds that you have breached the Data Protection Act.
In July 2021 for example, the transgender charity Mermaids was fined £25,000 for failing to keep users’ sensitive personal data secure.
The following cyber security tips should help steer your practice in the right direction:
1 Protect your systems
Invest in security software to protect your practice systems from malware such as viruses, trojans and ransomware. The software should be set to automatically scan files and webpages and whole system scans should be carried out frequently.
2 Keep up to date
Don’t use old operating systems, software, internet browsers and apps which are no longer supported by the provider, as they will be inherently less secure.
3 Maintain a data protection policy
This written document is a set of principles, rules and guidelines that ensures your practice complies with data protection law. Ensure that everyone is aware of the policy and trained in how to carry out their data protection responsibilities.
4 Have a practice IT security policy
This should cover aspects of security such as internet and email use, passwords and the safe use of mobile devices – encryption.
There should be regular training in cyber security for staff to make them aware of the latest threats, such as suspicious emails. Noncompliance with the policy should be a disciplinary matter.
5 Follow good password practice
Individuals should have their own username and password that controls their level of access, and user credentials should never be shared.
The same password should not be used for multiple accounts and should be regularly changed.
Don’t use old operating systems, software, internet browsers and apps which are no longer supported by the provider, as they will be inherently less secure
HOW DOES HEALTHCODE PROTECT YOUR DATA?
As a provider of online services for more than 20 years, Healthcode processes vast amounts of sensitive health and financial data for independent practitioners and healthcare organisations.
We know that the reputation of our business stands or falls on our ability to do this efficiently and safely, so information security has always been our priority.
Here are some of the measures we take to ensure our systems and procedures are watertight and present the maximum deterrent for cyber criminals:
Encryption – our systems are secured following internet banking conventions, using 2048-bit certificates for full end-to-end encryption.
Enterprise quality – our system infrastructure is designed to contain no single point of failure and is physically located in the UK.
Data protection by design – we have embedded these ICO principles into all our system and product development projects, from ePractice and The PPR to online appointment booking. Access to services is secured by user credentials and role-based controls.
Commitment to IT security standards – Healthcode’s internal policies, procedures and controls comply with ISO/IEC 27001:2013. We first achieved the relevant ISO/IEC accreditation in 2009.
We are also certified under the Cyber Esentials scheme after demonstrating best practice across all aspects of cyber security, including configuring systems to minimise vulnerability to cyber-attack and equipping all applications.
Resilience testing – we regularly review our security measures to identify potential weaknesses and ensure systems remain fit for purpose as technology advances. For example, during lockdown, we migrated to a new infrastructure, hosted by a leader in Cloud infrastructure, which was better able to support our technology in terms of reliability, scalability and security.
Disaster recovery – we take a daily back-up copy of data, which is securely stored in a separate UK facility.
Products and services – Healthcode provides encrypted services specifically to help independent practitioners and healthcare organisations share information securely rather than using unencrypted email, from electronic clearing to secure messaging and file sharing.
6
Encrypt the sensitive information you send or share
Standard unencrypted email is inherently insecure and should never be used to communicate confidential information.
7 Keep track of data
If you don’t know how data is processed and stored, how will you know if there has been a breach?
The sooner you are aware of a security breach, the sooner you can act.
8 Monitor access
Staff should have a valid reason to access personal data as part of their work. Ensure all access is logged for security and audit purposes.
9 Maximise your resilience
Back up your systems so that you can restore your data and get back up and running quickly; for example, in the event of a cyberattack.
10
Know how to respond to an attack
Report serious cyber-security incidents to the National Cyber Security Centre (NCSC) which also has advice on how to manage incidents.
You are legally obliged to report any personal data breaches to the ICO within 72 hours of becoming aware of them, unless you can show that the breach is unlikely to pose a risk to individuals’ rights and freedoms.
For healthcare organisations, reporting is advisable.
11 Seek specialist advice
Talk to an IT security professional about your IT security measures. The NCSC has guidance and resources for small businesses or you could sign up to the Government’s Cyber Essentials scheme which should help you guard against cyber-attacks.
You can find best practice information for healthcare organisations
on the ICO website and NHS Digital – important if you have access to NHS patient data and systems.
12 Check the security credentials of your suppliers
Ask service providers about the measures they have in place to protect your data. You might comply with data protection law but do they?
Cybercrime is not the only potential threat to your data. Many incidents reported to the ICO are caused by human error, such as a misdirected email.
But as malicious attacks become more numerous and more sophisticated, everyone in the independent healthcare sector has a responsibility to shield patients’ and practice data from attack and this is a responsibility that Healthcode is happy to share.
Raj Patel is data protection officer at Healthcode
A crash course in getting your money in
Simon Brignall continues to explore the common themes arising from consultants wanting to address their issues around medical billing and collection
THE ISSUES covered in last month’s article revolved around how to ensure you have set up the practice effectively so you can carry out the medical billing and collection function simply, securely and efficiently.
Now I will address the operational aspects of this vital area.
1 Invoicing
The raising of the invoice is the first step in the revenue cycle process, which is why in my last article I stressed the reasons why you need to bill promptly.
It never fails to surprise me to see how many practices fail to follow this golden rule, as it is not uncommon for me to find practices running many weeks or even months behind.
The invoicing task requires accuracy as well as speed, which is why it is important that there is a checking process.
This is to make sure that the invoice is accurate and contains all
the relevant information before it is sent to the relevant payment company or patient.
Mistakes made on invoices not only reflect badly on the practice, but they can also lead to losses in income through undercharging or delays in payment if the invoice does not contain all the correct information.
Raising invoices to the private medical insurance (PMI) companies needs to be done quickly so that there is the best chance of it being settled in full or even at all.
Insurers
In recent years, some of the main UK PMIs have introduced rules providing fixed time periods following the treatment date in which they need to have received the invoice.
Where the practice fails to invoice in line with these requirements, the insurance company will deny payment and the practice will not have the option
Over the past few years, there has been a major push by insurers to send invoices electronically
to seek recompense from the patient.
If there is a delay in sending the invoice, there is also the risk that the policy benefit limit is exhausted by claims from other consultants. This means the amount becomes the liability of the patient, which creates more administrative work for the practice and that the outstanding amount is often harder to collect. Over the past few years, there has been a major push by insurers to send invoices electronically. This benefits the insurance companies by providing a standard automated pathway, but there is also a huge benefit to the practice, as it means the invoice should be assessed and paid quicker.
Self-pay
As Independent Practitioner Today has reported, the self-pay area has grown considerably over the past ten years and is now either the
The first part of Simon Brignall’s advice was published last month
largest or second largest area of revenue for many practices and it continues to grow. The impact of the pandemic on NHS waiting lists will only support this trend.
The raising of self-pay invoices to patients should always be a priority in a practice, as this area has the greatest risk of bad debts.
Under this heading, I also include invoices raised for shortfalls that are caused by the terms of the insurance policy, such as patient excesses, benefit limits or co-payments.
There are times when a practice should also consider requesting
payment in advance, particularly when treating patients who do not reside in the UK, the invoice amount is considerable or where the practice undertakes a very large element of self-pay.
It is important that a practice has the full range of invoicing and payment options required to best service these patients. At Medical Billing and Collection (MBC) we offer our clients a range of payment pathways including the ability to:
Invoice patients electronically;
Collect payments 24/7 via our payment portal;
Raise invoices and collect monies in advance, on the day and post-treatment depending on their specific needs.
2 Reconciliation
Reconciliation is another area we find continually causes problems; often the practice is way behind with the reconciliation process or the remittances not reconciled correctly against the invoices raised.
Even practices who manage to send out the initial invoice on time find this can be where the process starts to unravel.
A regular complaint from consultants can be that they are unsure what the true picture of their outstanding debt is or whether an invoice has been paid or not. Lack of access to accurate data at this key stage means that is impossible to have an effective chase process.
Each insurer should send a remittance to the practice when it makes payment, which is typically done electronically direct to the practice bank account.
The problem is that it is common for the practice to not receive a remittance or that it is mislaid and so unless the practice is chasing
the insurer or reconciling the bank account regularly, these invoices remain outstanding.
When this happens, it can then lead to further problems, as the remittance which has been missed and so not reconciled may have led to a shortfall being identified which should have been invoiced to the patient. This means practice cash flow suffers and also can increase its bad debts.
Reluctant to pay
Even when the issue is finally discovered, invoicing patients months after the event is never a good thing, as it can lead to complaints and often means people are more reluctant to pay.
At Medical Billing and Collection, we are well versed in this problem, as when we chase a backlog of outstanding invoices for a practice, we encounter these issues all the time.
The way to rectify this is to make sure remittances are reconciled the day they are received, identify any outstanding ones and ensure these are chased regularly with the insurers.
This will ensure you keep on top of outstanding invoices and know at the earliest opportunity if you must invoice a shortfall to the patient.
3 Chasing
This is the area we find gives most practices the biggest operational problem and is a task that is often deferred for a range of reasons such as:
Practice workload;
Lack of transparency around aged debt;
Staff who feel uncomfortable with the credit control role. Few practices find it easy to deal with the patient on both a medical and financial level, as it can lead to many issues on both sides.
Every invoice potentially needs chasing, including invoices sent to the insurers. Reasons for a delay in processing the invoice can be:
Non receipt of the invoice due to EDI (Electronic Data Interchange) issues or postal problems;
Non-preauthorisation of treatment by the patient;
Incorrect membership number or lapsed policy details provided by the patient.
For a robust chase process to be
effective, it must be clearly defined and routinely applied. There needs to be clear understanding of who is responsible for this role so that there can be accountability for its execution.
Once the chasing process has begun, it needs to be followed up or the patient will think you are not being serious. It will reflect on the professionalism of the practice and will often give the patient permission to withhold payment.
The process should allow for a mixture of communication methods used to contact the patient as well as the sending of formal letters. All this needs to be recorded with a log of any action taken.
4 Debt decisions
Once all the avenues in the chasing process have been exhausted, the practice needs to decide whether to send the patient to debt collection.
What you do will typically depend upon the patient, the circumstances and the associated costs.
If you decide not to send the patient to the debt collectors, then the practice should consider writing the amount off as bad debt, as it is unlikely the patient will choose to pay the outstanding amount in the future.
You may choose to consult your accountant, as they would know the individual circumstance of the practice and will be in the best position to offer the correct advice.
5 Tax reports
Finally, the practice needs to be able to raise financial reports from both a business and tax perspective. HM Revenue and Customs (HMRC) takes the view that you are responsible for your own tax affairs and it does not consider ignorance or negligence as a reasonable defence.
You should be able to run reports which show the number of invoices raised, payments received and outstanding invoices monthly to ensure all financial aspects of your practice are in order.
Having access to accurate and up-to-date financial data on your practice ensures you can identify any issues and act to address these quickly.
In my experience, most people underestimate the importance of the medical billing and collection side of the practice
Historically, HMRC has looked upon the private medical sector as being a prime area where the financial affairs are not as robust as they should be. This has resulted in a higher percentage of investigations compared to other business sectors.
We provide our clients with 24/7 access to their data via our reporting dashboard, which has an array of reports to analyse the practice and our account managers are happy to field any request for tax information from their practice’s accountant.
In my experience, most people underestimate the importance of the medical billing and collection side of the practice. I can assure you that it is not easy and, with the demands on a modern practice, it is getting harder and harder to do it internally.
If you decide to continue to carry out this process in-house, then I hope the areas covered over these two articles provide a useful guide.
If you do not want to invest the time and effort to do this internally any more or if any of the problems I have identified strike a chord, then you should consider outsourcing this crucial area to a medical billing and collection company and let the professionals do this for you.
Simon Brignall (right) is director of business development at Medical Billing and Collection
They’re lying if they say they can see into. . .
Luck is not a good investment strategy. Dr Benjamin Holdsworth (right) warns of the futility of trying to beat the market
THE SIMPLE maths of trying to beat the market guarantees that –after costs – the majority of investors, including professional fund managers, will fail to achieve the return that the market offers. Trading stocks or bonds is a zerosum game.
In other words, every winning trade relative to the market must be funded by the losses on the other side of the trade. Not everyone can win.
This can be surprising to some. Surely highly paid, intelligent, hardworking, ambitious fund managers with vast resources available to them should be able to outsmart other investors?
With the advent and popularity of market-tracking index funds, however, weaker investors –including professionals – will have exited the game, leaving the now higher quality pool of survivors competing among themselves for winning trades.
Picking winners
The bar has been raised significantly. Surely there must be a few great managers out there? Maybe, but identifying them is extremely challenging, contrary to popular belief.
Some investors may be tempted to think that they, or their adviser, are able to avoid the losers and pick winning funds.
Without the benefit of 20/20 hindsight, or a large dose of luck, finding a winning manager is wellnigh impossible, as a vast body of empirical research suggests.
As Jack Bogle, the legendary
investor and founder of low-cost investment company Vanguard, used to say:
‘Don’t look for the needle in the haystack. Just buy the haystack [ie the market].’
Many studies show that shortterm performance rarely persists. In other words, funds that perform best in one period rarely carry on this ‘good’ performance, at least with no greater frequency than we would expect simply from by luck.
Most attempts at fund picking by individuals – or the advisers they pay to do this on their behalf
– use three-to-five-year performance data, which means it is almost statistically impossible to tell skilled managers from the noise of the markets. Luck will largely drive outcomes, good or bad.
Even if a fund manager beats the market over a longer time-frame, it does not automatically mean that
Even if a fund manager beats the market over a longer time-frame, it does not automatically mean that they are skilled
they are skilled. To separate skill from luck, studies have shown we need at least 16 years of data to be 95% sure that we are looking at the former rather than the latter.
Not very many fund management firms can provide a historical track record that is representative of the team and process currently in place.
That raises several pertinent questions investors should ask themselves, such as:
Is it really possible to extrapolate past success into the future?
On what basis would one take this risk?
Will the current manager be around in the future?
Without a crystal ball, the odds of picking a skilled, market-beating fund manager for the years ahead is pretty low. There may be some out there, but identifying them today is a real challenge, with a potentially costly downside.
Fund selection based on luck is not a good investment strategy. Play the odds in your favour and pick up the market returns you deserve.
Dr Benjamin Holdsworth is a director of Cavendish Medical, specialist financial planners helping consultants in private practice and the NHS
The content of this article is for information only and must not be considered as financial advice. Cavendish Medical always recommends that you seek independent financial advice before making any financial decisions.
Levels, bases of and reliefs from taxation may be subject to change and their value depends on the individual circumstances of the investor. The value of investments and the income from them can fluctuate and investors may get back less than the amount invested.
Free legal advice for Independent Practitioner Today readers
Independent Practitioner Today has joined forces with leading healthcare lawyers Hempsons to offer readers a free legal advice service.
We aim to help you navigate the ever more complex legal and regulatory issues involved in running and developing your private practice – and your lives.
Hempsons’ specialist lawyers have a long track-record of advising doctors – and an unrivalled understanding of the healthcare system as a whole.
Call Hempsons on 020 7839 0278 between 9am and 5pm Monday to Friday for your ten minutes of free legal advice.
Advice is available on:
Business structures (including partnerships)
Commercial contracts
Disputes and litigation
HR/employment
Premises
Regulatory requirements and investigations
Michael Rourke
Tania Francis m.rourke@hempsons.co.uk t.francis@hempsons.co.uk
One slip gets you in a lot of trouble
If you work in a partnership, your partnership agreement may allow your partners to take action. Your practising privileges may be suspended
YOU MAY have examined a patient without a chaperone because a chaperone wasn’t required – but the patient may allege that an intimate examination took place.
Or you may be accused of fraud because you did some private work while on sick leave from the NHS. You may be involved in the care of a patient who sadly dies in circumstances in which your treatment decisions are criticised. What could happen next?
1
A police investigation. You may be invited to attend an interview under caution. In more serious cases, you may be arrested and taken to the police station, and your home and electronic devices searched. If the Crown Prosecution Services decides to prosecute, you will face a criminal trial.
2
We all know that we live in an increasingly regulated world and particularly so in the healthcare sector. But have you ever thought about just how many sets of proceedings a doctor may face out of one incident? Dr Tania Francis (right) runs through them and gives tips to avoid them
In the meantime, you will be referred to the GMC –probably by the police –and you are under an obligation to selfreport if you are charged. The GMC may put its investigation on hold until the criminal investigation has concluded, but in the meantime, you may be referred to a Medical Practitioners Tribunal hearing and subject to interim conditions or even suspension.
3
Your employer, if you have one, may take disciplinary action. If you are a GP, NHS England may take action under the Performers List regulations. If you work in a partnership, your partnership agreement may allow your partners to take action. Your practising privileges may be suspended.
4
If you are a provider of healthcare, the Care Quality Commission may also take an interest.
5
6
If the allegations relate to the death of a patient, there may be an inquest.
And in addition to all of the above, the patient/ relatives may bring a civil claim for damages.
All of these different jurisdictions are separate and the fact that one does not proceed may not prevent the others from going ahead.
Even if a doctor is acquitted at a criminal trial, the GMC may investigate and proceed with a hearing, because its remit is different, as well as its standard of proof.
Similarly, even if the GMC proceedings do not result in any action, a claim for damages can be made, because a finding that a doctor’s fitness to practise is not impaired does not mean that they were not negligent.
Tania Francis is a solicitor and a partner at Hempsons, a specialist healthcare law firm. She is also a qualified doctor. She advises doctors, dentists and other healthcare practitioners and providers, specialising in regulatory law and clinical negligence litigation, including cases where there are related criminal proceedings
How to avoid trouble
How can you avoid these nightmare scenarios? Sometimes you can’t. But listed below are things you can do to reduce the chance of trouble:
☛ Have a very low threshold for asking for a chaperone. It might make your clinic over-run, but that is a price worth paying. Document the fact that a chaperone was present and their name. Ideally, they should countersign your records. The fact that your patient is the same gender as you does not remove the need for a chaperone.
☛ Keep good records. Document the reason for an examination and the nature of the examination carried out. Document the fact that you have explained both to the patient.
☛ In difficult or serious cases, take care to document the rationale for your treatment decisions. Discuss them with others and document that you have done so.
☛ Communicate well with everyone – patients, relatives, other doctors, nurses and other healthcare staff, managers.
☛ Take professional advice the moment you become aware of a complaint –call your indemnity provider; they are usually a great source of advice.
☛ Make sure that your insurance/indemnity cover is up to date. Put the renewal on direct debit so that you don’t inadvertently forget to pay and lose cover.
☛ Remember to tell them if you move house or your scope of practice or income changes. Be careful when changing providers: think about run-off cover.
☛ Make sure that your cover includes all of the above jurisdictions. The nightmare of a complaint is made far worse if you have to pay for legal advice out of your own pocket.
I hope that you never have to face any of these issues. If you do – take advice and take care of yourself.
Even if a doctor is acquitted at a criminal trial, the GMC may investigate and proceed with a hearing 1 2 3 4 5 6
Patient doesn’t want visitors
Dr Kathryn Leask (right) discusses how to remotely manage a patient’s lithium prescription
Dilemma 1 Should I refuse to prescribe?
QI am a private GP and have been conducting appointments remotely during the pandemic. I am now seeing more patients face to face; however, some patients have found the remote consultations more convenient.
I have one patient who is on lithium. He has social anxiety and does not like people coming into his home. He also has other health problems and has spent much of the pandemic shielding.
Fortunately, he is able to work from home and I have no concerns about his capacity. He hasn’t had his lithium level checked for some time and I am concerned about continuing to prescribe for him, with no recent result.
I have had phone consultations with him where I have asked about signs or symptoms that could be suggestive of lithium toxicity.
Should I refuse to prescribe until he has had his level
checked? I have mentioned to him that I may have to stop prescribing for him, but he has said he will obtain the medication he needs from the internet.
AThere are several important points to consider when bearing in mind the GMC’s updated guidance on prescribing.
Firstly, is whether the mode of a consultation meets the individual needs of the patient and supports safe prescribing.
Usually different options will exist, but if it is not possible to have a face-to-face consultation with this patient, a phone or video consultation is the only option.
As you aren’t able to see the patient, it may be a good idea to consider more regular consultations, done remotely, than you would normally have for this patient if he was being seen for reviews face to face.
This will allow you to assess any
It is important that the patient understands the reasons why monitoring is so important
He also needs to be advised of any signs to look out for that might suggest he is not taking the right amount and how to seek appropriate advice, particularly in an emergency.
With the patient’s permission, it would also be helpful to speak to a friend or relative who can also look out for any potential problems and seek assistance on the patient’s behalf if he is unable to do so himself.
When deciding whether to continue prescribing, it is important to weigh up the risks and benefits to the patient. Will the patient be at more risk if you continue to prescribe without monitoring or would he be at more risk if you stopped the medication?
Talk to others
risk and establish whether he has any signs or symptoms of under treatment or toxicity at an early opportunity.
While the patient is uncomfortable with people going to his home, it is worth seeing if he will compromise and allow a district nurse to visit him to take blood, given that this will probably only be every three months at the most.
Two-way dialogue
If he prefers, you could suggest that a friend or family member whom he trusts could accompany him when the nurse attends.
The GMC’s updated guidance emphasises the importance of a two-way dialogue with patients when prescribing medications.
It is important that the patient understands the reasons why monitoring is so important and the risk he is placing himself at if he does not have his lithium level checked.
You also need to take into account the risks associated with the patient obtaining medication from the internet and the fact that you won’t know whether this is, in fact, lithium or what dose he might be taking.
Whichever decision you make, it is important to be able to justify this and you may, therefore, wish to discuss the situation with a colleague or a mental health professional, particularly if there is one already involved in the patient’s care. It is important to document your discussions with the patient in detail, noting what information he has been given about the risks and his reasons for not agreeing to monitoring.
If you do decide to continue to prescribe, it should also be made clear to the patient that he can contact the practice at any time if he has any concerns or should he change his mind and want to have his blood test done.
Dr Kathryn Leask is medico-legal adviser at the Medical Defence Union
A challenge to your expertise
Dr Ellie Mein (right) explains how to respond to a solicitor’s request for assistance
Dilemma 2 Have I exceeded my expertise?
QI am a private GP who recently received a letter from a patient’s solicitor. The letter, which was sent with the patient’s consent, asked for a letter to confirm that the patient would not be fit to attend court. I responded by writing a brief letter detailing the patient’s mental health problems with the conclusion that these would render the patient not fit to attend a court case.
Following this, the patient’s solicitor forwarded correspondence from the solicitor for the other party which asked what experience I had in assessing individuals as being fit for giving evidence.
They also requested a copy of my CV to clarify my experience of what attending court would entail.
In hindsight, I feel that I may have strayed into giving an opinion in an area that I lacked sufficient knowledge in. What should I do?
AParagraph 74 of the GMC’s Good Medical Practice (2013)
You must explain that your opinion was given in the capacity as the patient’s private GP rather than as a specialist with knowledge of legal proceedings
states that: ‘You must make clear the limits of your competence and knowledge when giving evidence or acting as a witness.’
In these circumstances, it would be advisable to write a letter to the patient’s solicitor explaining that:
1. You had given your opinion based on the numerous medical conditions as listed in the original letter;
2. The patient confirms that they would find giving evidence in court extremely stressful to the detriment of their mental health;
3. Your opinion was given in the capacity as the patient’s private GP rather than as a specialist with knowledge of legal proceedings and their impact on an individual’s mental health.
Dr Ellie Mein is medico-legal adviser at the Medical Defence Union
DOCTOR ON THE ROAD: MAZDA MX-30
Electric car ideal for the school run
Why buy a car with a massive electric range if you don’t need to? Our motoring correspondent Dr Tony Rimmer (right) finds this new offering a perfect second car for a young family with children
MAZDA MX-30
Body: Five-door hatchback. Front-wheel drive
Engine: Single electric motor. 35.5Kh battery
Power: 145bhp
Top speed: 87mph Range: 124 miles
Acceleration: 0-62mph in 9.7 secs
CO2 emissions: 0g/km
On-the-road price: £28,545
Mazda justifies the small battery by suggesting that the average commute is 26 miles and most people, for most of the time, only travel up to 120 miles in a day
The controls are clear and easy to use and the boot can carry a surprising amount of luggage
IN THE motoring world, Mazda is a car manufacturer with a reputation for thinking and acting outside of the box.
Over the years, it has experimented with alternative internal combustion engines such as the Wankel rotary engine in its RX models and is at the forefront of petrol engine technology with the clever Skyactiv-X system, which improves fuel efficiency by up to 20%.
However, to stay competitive, Mazda is having to embrace the powerful movement towards electrification of our everyday cars.
It is therefore no surprise that Mazda is joining the party with a car that represents a slightly quirky left-field approach.
The MX-30 has a coupé/crossover style, a battery size of only 35.5kWh and a range of 124miles.
Reasonable cost
Priced from £28,545, it is at the reasonable cost end of the EV scale. It has seating for four adults and unusual rear ‘suicide’ doors that open from the rear and only when the front doors are open. This is a nod to the same set up used in their classic RX-8 sports car.
Mazda justifies the small battery by suggesting that the average commute is 26 miles and most people, for most of the time, only travel up to 120 miles in a day.
A smaller battery means lighter weight and a more dynamic drive. The MX-30 therefore competes with the MINI electric and the Honda ‘e’ and would suit a city/ urban environment with regular home-charging availability.
In fact, a typical 7kW home charger can replenish the battery in six hours and, when out and about, a 50kW rapid-charger – if you can find one – can provide a 0-80% re-charge in 30 to 40 minutes.
Eco-friendly materials
The interior is stylish and modern and uses eco-friendly materials. The seats are covered in a fabric made from re-cycled plastic bottles and the centre console has a cork covering – Mazda’s first business was as a cork producer.
Standard equipment is generous, and the controls are clear and easy to use – no fiddly touchscreenonly controls like those found in the Golf Mk 8.
Rear passengers have adequate leg- and headroom once ensconced, but the narrow rear doors make entry and exit a bit of a challenge. Also, it is a bit claustrophobic in the back with small non-opening windows. The boot is big, though (366 litres), and a surprising amount of luggage can be carried.
Mazdas have always been good
to drive, so I was interested to see if my MX-30 test car followed in the same tradition. A claimed 0-62mph time of 9.7 seconds does not sound fast, but the instant electric torque makes it feel quicker.
The steering is nice and sharp, and the chassis feels nimble compared to most electric vehicles (EVs); the light battery helps a lot.
Braking regeneration can be controlled by paddles behind the steering wheel and can be set strongly enough to allow for almost one-pedal driving.
Class of its own
For the keen driver, it is similar in nature to the Honda ‘e’ but not quite as much fun as the electric MINI. The ride is nicely compliant as well. Despite trying different driving styles, I found the predicted range of 124 miles from a full charge to be pretty accurate –welcome when planning trips.
So, what are we to make of this new electric Mazda? It seems that the MX-30 has positioned itself in a class all of its own.
Its design and style mark it out as smart and unique. It is bigger and roomier than the city EVs such as the MINI, Honda ‘e’ and Fiat 500, but cannot compete with range abilities of the family hatchbacks such as the VW iD3 and Nissan Leaf.
What kind of medic family would find the Mazda appealing? Well, I see it as a perfect second car for a young family with children. Its space and limited range are ideal for the school run followed by an urban commute and trips to the supermarket.
Why buy a car with a massive electric range if you don’t need to? It makes more sense and is kinder to the planet. I think that Mazda’s lateral thinking might just pay off.
Dr Rimmer is a former NHS GP practising in Guildford, Surrey
The Mazda’s design and style mark it out as smart and unique
A
PRIVATE PRACTICE – Our series for doctors embarking on the independent journey
Systems are vital for maximising income
In private practice, it can be common to think that your accounting system is just to record your activity to ensure an accurate computation of taxes – but it contains a wealth of useful information to help run your business. Ian Tongue looks at accounting systems and how to get the most from them
What is an accounting system?
Systems can vary between businesses, but the key thing is that it records the financial activity of the business and that the transactions are complete and accurate.
From this source, your accountant can extract the information they require to prepare year-end accounts and tax. But there is plenty of useful information available real time to ensure you run your business as efficiently and profitably as possible.
Systems can range from simple spreadsheets to sophisticated computerised accounting packages. Often, consultants use a clinical management software package to run their business and many of those have accounting functions built in, although these would not be of the same functionality as a full-blown accounting software package.
Usually a full accounting package is not required and the necessary information will be available from the spreadsheets or clinical management system.
The basics
When running any business, you are required to keep ‘adequate’ accounting records by HM Revenue and Customs (HMRC).
It is not defined what this is, but the key requirements are for your system to report your income and expenses in a manner that provides a complete and accurate record of your financial activity. If you are a VAT-registered business, the burden on record-keeping is higher and HMRC expects you to use an electronic system as a minimum and favours the mainstream accounting packages, but this is not mandatory.
It is important that you have a chronological record of your fee income and that you are able to identify when you were paid for the work and whether this was in full or if there is any outstanding amount.
The system should be able to provide a list of income earned by accounting period, which is a record of sales activity and you should be able to extract at any time the money owed to you. This is pretty much the most important part of the system.
There should be a record of
expenses by reference to when they were paid. But there can be costs that you are liable to pay that are outstanding and it is important to provide your accountant with anything of this nature, as these can be included within your accounts, or ‘accrued’ as we accountants call it. This ensures you receive tax relief on these costs at the earliest opportunity.
The ‘accruals’ concept basically means you declare your income when earned and not when you have received payment and you can claim costs when you have incurred the liability rather than paid for the cost.
For smaller businesses, you may be able to account to HMRC on a ‘cash’ basis, but often this is short lived for private practices so it is usually easier to account for things on an accruals basis from the start.
Debtors
A regular review is essential to running any business. You should review the list of fee income recorded in your financial records and compare this to work done to ensure all work carried out is billed to the insurer, patient, solicitor or hospital.
It can often be surprising how many times we come across a client saying they – or their secretary – did not bill something and they lose out. If this element of your system is not working effectively, you could end up working for free.
Recording income and its makeup between different types of work is also extremely important for the payment of the correct medical
due to the value, but in practice getting paid is often problematic and many embassies do not expect to pay on a timely basis or to pay full price.
Expenses
Recording all expenses is very important to ensure you are maximising your expense claims and thereby minimising your taxable profit.
It can be common for costs to be paid through the business account as well as personally, particularly if you have transitioned from one trading structure to another – for example, from a sole trader to a limited company.
defence premiums and you should be able to split the work between clinical and medico-legal as well as any NHS-indemnified work. Not having this split could result in paying the incorrect premium.
Reviewing receipts and matching them to your fee listing is essential because errors can arise on the payment received or the patient may have an excess to pay. Make patients aware of any excess payable to you and chase it. It may seem a small amount of money initially but it soon adds up for a busy private practice.
For consultants carrying out medico-legal work, it is important to review your debtors regularly and chase debts vigorously as payment terms can be long.
It is essential for your accounting system to be able to report any outstanding fees from earlier years as well as the current year, because the figures in your accounts are a cumulative record of financial activity.
Bad debts
For a clinical or medico-legal practice, bad debts should be minimal, but often this is not the case. The most common culprit is the patient excess, but medico-legal work with onerous payment terms – for example, on settlement of the case – can also result in bad debts. Having a bad debt means you providing your work for nothing or less than you expected, so spend time reviewing any old debts and ensure payment terms are reasonable before doing any work. Approach embassy work with caution. This work can turn heads
Your accounting records need to include all expenses, and for those not incurred through the business bank account, make sure these are recorded separately so your accountant can incorporate the appropriate claim within the accounts.
Having a robust accounting system is essential for the smooth and profitable running of your private practice.
Don’t see the system as just for sending to your accountant annually, as the information contained within the system will ensure that you maximise the return on your hard efforts.
Ensuring that all fees are recorded and collected together with maximising your expense claims ensures that you pay as little tax as possible. If in doubt about the quality of your accounting system, ask your accountant for some feedback on your systems.
Next month: Proposed tax and National Insurance changes – time for a review?
Ian Tongue (below) is a partner with Sandison Easson accountants
PRIVATE PATIENT UNITS: YORKSHIRE
Only the hot spots show real growth
Our regional round-up of PPU progress continues with Philip Housden’s (right) report featuring Yorkshire PPUs where he analyses private patient revenue growth for 13 NHS acute trusts across the county
THIS REVIEW is based on the information published in the Trust Annual Accounts for 2019-20, which was partially adversely impacted by the early months of the Covid pandemic.
For this group of trusts, the 2019-
20 accounts show that total private patient revenues rose slightly by 0.7% after a year of decline in 201819.
Total revenues are estimated at £13.8m, up £93,000 from £13.7m. This level of income represents
0.23% of these trusts’ total revenues, down from 0.25%. This remains below the combined national average outside of London of 0.43%.
The regional top earner remains Leeds Teaching Hospital Trust (LTHT) at £5.53m, a rise of £628,000 (12.8%) from £4.90m. This is a slight increase to 0.46% from 0.45% of trust revenues.
It holds a partnership with Nova Healthcare, part of Aspen Healthcare, located within St James’s
Institute of Oncology in the Leeds Cancer Centre in Bexley Wing.
The service offers the full range of cancer treatment including radiotherapy, gamma knife and robotic surgery and chemotherapy. There is also access to private beds within the Bexley Wing for patients requiring inpatient admission.
Increasing competition
In response to increasing competition in the city, including a new competitor provider, abc ivf, LTHT is seeking to explore and test the market for opportunities to grow and sustain the in-house PPU brand Leeds Fertility IVF service. The facility currently performs around 1,300 IVF/ICSI treatments and 700 frozen embryo transfers each year.
In the last ten years, there has been an increasing trend nationally towards privately run fertility clinics, often in chains operated by large commercial organisations. In the south of England, almost all NHS and private fertility work is
undertaken in these private clinics. However, in the north, it is common for large NHS teaching hospitals to run fertility clinics, but for private clinics to set up in competition, undertaking private and NHS work.
A trust briefing paper explains:
‘To mitigate the risk to the fertility services provided by Leeds Fertility, LTHT proposes to tender the Leeds Fertility IVF service for a contract period of ten years.’
Sheffield Teaching Hospitals has the second highest revenues in the region, totalling £2.42m in 2019-20. Incomes have fallen back for the second year after a period of growth, dropping £300,000 or 11.0% in 2019-20 to 0.24% of turnover – down from 0.29%.
The trust has no specific private patient services, but instead offers a range of treatments privately across their five hospitals.
Private hot spot
Harrogate and District has a dedicated private patient unit, the tenbed Harlow Suite, branded the
In the north, it is common for large NHS teaching hospitals to run fertility clinics, but for private clinics to set up in competition, undertaking private and NHS work
Harrogate Harlow Private Healthcare Service. It is located in a relative regional hot spot for private medical insurance take-up.
The trust reported growth of 24.6% in 2019-20, with revenues up £361,000 to £1.83m. The unit has access to dedicated space within endoscopy in addition to the ward.
Harrogate achieves 0.75% of trust turnover as private income, the highest in the region and the only one in Yorkshire ahead of the out-of-London national average.
York Hospitals offers private patient services at York, Bridlington and also at Scarborough.
These are for a range of surgical, ambulatory and diagnostic services. The group service is not collectively branded and this could be an opportunity to develop for the trust. Revenues were up 21.5% and £217,000 in 2019-20 to reach £1.23m and now 0.26% of turnover.
Calderdale and Huddersfield is ranked fifth within Yorkshire by private patient revenues and these totalled £924,000, down £202,000 and 17.9% in 2019-20. This is still double the revenues of 2016-17 and growth may have continued without the impact of Covid. Income is 0.26% of total trust revenues.
Doncaster and Bassetlaw’s annual report did not include the full trust annual accounts and so
York and Scarborough Teaching Hospitals also has a private patient unit and is similarly located within an attractive private medical insurance catchment.
Across the Yorkshire region, some trends can be discerned with the trusts prepared to invest and market their private patient services showing significant growth while the others are falling back
an estimate has been made of private patient revenues in 2019-20 taking into account the typical detrimental impact of Covid-19 on the latter part of the financial year.
It is estimated that revenues were c£750k, down around 11.6% and £98,000 on the 2018-9 total of £848,000, representing 0.20% of turnover. The trust does not have dedicated private patient facilities.
Hull University Teaching Hospitals experienced a 33.6% decline in private patient revenues in 2019-20, down £229,000 to total £453,000.
Disappointing drop
Bradford also has an inpatient PPU, the 12-bed The York Suite located on Level 4 of the Duke of York Wing at the Bradford Royal Infirmary.
This offers a range of medical care and surgical interventions from outpatient consultations, diagnostic scanning, minor daycase treatments to complex surgery.
The trust reported a disappointing 46.5% drop in private patient incomes from £604,000 to £323,000, which is now the sixth consecutive year of decline from a high point from £1.34m in 201314.
Airedale Hospital has a PPU, with Ward 19 having 11 bedrooms and two private consulting rooms. Last year, the trust’s private patient revenues declined £53,000 and 26.4% from £201,000 to £148,000 which is only 0.08% of total trust incomes.
Sheffield Children’s Trust is one of only four such specialist trusts in the NHS; the others being Great Ormond Street, Birmingham Childrens and Alder Hey.
The trust grew private patient
revenues 32.4% in 2019-20 from a modest £68,000 to £90,000, which is only 0.05% of turnover. As with the other specialist paediatric hospitals, the trust has the opportunity to develop private overseas patients.
Of the other three trusts, Mid Yorkshire reported income of £75,000 at 0.01% of turnover and
Rotherham and Barnsley both reported nil private patient revenues in 2019-20.
Across the Yorkshire region, some trends can be discerned with the trusts prepared to invest and market their private patient services – principally Leeds, Harrogate and York –showing significant growth while the others are falling back.
Next month: We take a break from our regional reviews to assess the findings from Housden Group’s third Annual NHS Barometer.
Philip Housden is managing director, Housden Group commercial healthcare consultancy
FOCUS: ENT SURGEONS
Through a £200k barrier
ENT surgeons have enjoyed a 15%+ profits rise in our latest and unique benchmark survey. Ray Stanbridge reports
IT IS good to report an encouraging outcome for this specialty in the run-up to the first financial year affected by Covid-19.
Things were not looking so good for them as a result of the pandemic, but our study for 2018-19 has revealed that the average gross private practice income for those who also have NHS jobs was a rise of 14.7%, increasing from £183,000 to £210,00.
Much of this growth has been in self-pay.
Costs rose by about 13.4%, going up from £67,000 to £76,000.
As a result, gross margins rose by
about 15.5% from £116,000 to £134,000.
Expenses
Medical supply costs/assistants’ fees increased slightly as a result of increased activity.
Staff costs rose by about £4,000 from £18,000 to £22,000. To some extent, this is influenced by the growth in personal allowances where family members are employed in the practice.
More generally, however, the result reflects inflationary pressure on secretarial costs, particularly in central London.
AVERAGE INCOME AND EXPENDITURE OF A
Expenditure
Subscriptions/professional indemnity costs again rose, linked we believe to growth in turnover. We would comment that there are always lags and further increases might be expected to reflect ongoing growth in turnover.
Home costs showed a small increase, reflecting a rise in use of their home by an increasing number of consultants, particularly to undertake administration work. Other costs have been broadly similar to 2018 levels or have shown small inflationary upward pressures.
There was a continuing decline in ‘other costs’. As we have mentioned in previous reports, most consultants had by 2019 incurred expenditure on their websites and marketing material, having often spent heavily on this area.
Prospects for 2019-20
An initial review of the data suggests that ENT surgeons generally continued to do well in 2019-20 until about March last year, as might be expected, when the first lockdown began.
It looks as if many ENT surgeons suffered badly through these first few months of lockdown, although, of course, we have still not had the chance to review all the data.
In our report in Independent Practitioner Today last year on ENT surgeons, we commented that we believed they had continued to do well in 2019. Our forecast proved to be totally correct
In our report in Independent Practitioner Today last year on ENT surgeons, we commented that we believed they had continued to do well in 2019. Our forecast proved to be totally correct.
As we have previously reported, our survey is not statistically significant. Rather it tries to give a reasonable picture as to what is happening in the market each year for a particular discipline.
An established reader will know that our sample includes those who:
Have had at least a five-year private practice experience; Hold either a maximum part-
time or a new consultant NHS contract;
Are seriously interested in pursuing private practice as a business;
Are earning at least £10,000 a
year in the private sector – an increase from £5,000 in 2018; May or may not have incorporated or be a member of a group. The elimination of small prac -
tices from our survey has probably resulted in upward pressure on our average results.
As we stated in 2018: ‘Readers will also know that during the period we have been reporting our survey there have been many structural changes in the industry.
‘There has, for example, been a growth in the number of consultants incorporating, a growth in groups – which tend to generate income enhancement – ongoing pressure from insurance companies, a growth in self-pay and perhaps some unforeseen effects of some of the Competition and Markets Authority rulings on how consultants conduct their practices.
‘All these factors, and others, have affected our results and may lead to distortions. This is despite the fact that we have tried to smooth figures.’
Next month: Orthopaedic surgeons
Ray Stanbridge is a partner with accountancy, finance and tax advisory medical specialists, Stanbridge Associates
HOW ARE YOU DOING?
ONLINE SOLUTIONS
INNOVATIVE ONLINE SOLUTIONS AT THE HEART OF THE HEALTHCARE SECTOR.
Our Online Solutions
Trusted by leading hospitals, independent practitioners and insurers to deliver high quality, secure and cost-effective IT systems. Seamlessly connect key stakeholders to support transparency within the sector and enhance patient safety.
Healthcode is the UK’s official medical bill clearing company and has provided secure and encrypted systems to healthcare professionals since 2000. Pre-pandemic we processed around 27,000 electronic medical bills to insurers daily.
To find out more about our solutions visit our website www.healthcode.co.uk
Coming in our November issue, published on 16 November.
How technology can help you make your practice profitable. With the Government keen for firms to get back on track after the pandemic, Healthcode explains how technology can help independent practitioners manage their financial operations and achieve long-term profitability
Orthopaedic surgeons’ plunging profits. Ray Stanbridge’s Profits Focus series reveals how the first few months of Covid-19 took its toll
For consultants looking to start a private practice, one of the most obvious steps is to gain practising privileges with a service provider either at a private hospital, clinic or within independent practice accommodation. The process is often viewed as time-consuming and bureaucratic, but there is a lot more to think about than simply filling in a set of forms. Jane Braithwaite reports
Embassy work has taken a hit in the pandemic. So, as it returns, make sure you get paid. Medical Billing and Collection’s Simon Brignall gives some useful advice
Exploring private GP files: Dr Sarah Jarvis, medico-legal adviser at the MDU, analyses medico-legal files involving private GPs and advises on how to manage risk
The statutory duty of candour. In our Business Dilemmas column, Dr Ellie Mein answers a consultant ophthalmologist’s concerns after a mishap during cataract surgery. A colleague believes the incident is notifiable under the statutory duty of candour because the patient required additional treatment to prevent sensory impairment: ‘He says the hospital could be fined if we don’t comply. Is this correct?’
INDEPENDENT PRACTITIONER TODAY
Published by The Independent Practitioner Ltd. Independent Practitioner Today is editorially independent and thanks Bupa for its assistance with distribution.
Material is governed by copyright. No part of this publication may be reproduced, stored in a retrieval system or transmitted in any form without permission, unless for the purposes of reference and comment. Editorial layout is the copyright of the publishers. If you wish to use it for promotional purposes on websites or for reprints, we would be happy to discuss licensing the copyright to you.
When is it appropriate for expert witnesses to amend their reports? Advice following a spike in requests for help from private doctors who are being asked to edit what they have written. Some are legitimate and appropriate – but others are not
Philip Housden presents his annual NHS PPU Barometer – a snapshot of performance of these private units – and provides valuable insights into the impact of Covid-19 on the sector
Investment preferences and their trade-offs: a younger generation of investors are starting to demand more bespoke investment portfolios to reflect their strong preferences. But at what cost to their portfolio performance? Cavendish Medical reports
The quality of senior doctors’ feedback supervision and mentoring of resident medical officers (RMOs) in private hospitals has come in for criticism in a survey for the GMC, as reported on page 5 of this, our October, issue. Dr Stephen Drotske and Justyn Tollyfield, of RMO training and support company NES Healthcare, give their response
Our motoring correspondent Dr Tony Rimmer reviews the Toyota Yaris Cross
Proposed tax and National Insurance changes. It’s time for a review in your practice, says accountant Ian Tongue
Plus all the latest news and views
And don’t forget to check out our additional news updates every week online
ADVERTISERS: The deadline for booking adverts in our November issue is 29 October
Write to Independent Practitioner Today 7 Lindum Terrace, Lincoln LN2 5RP
CHANGING ADDRESS, EMAIL ADDRESS OR SUBSCRIPTION DETAILS?
Phone 01752 312140 or email karen@marketingcentre.co.uk
TELL US YOUR NEWS
Robin Stride, editorial director Email: robin@ip-today.co.uk Phone: 07909 997340 @robinstride
ADVERTISE WITH US
To advertise in the journal or our website business and lifestyle directories, contact advertising manager Andrew Schofield at Spot On Media. Phone: 0161 408 3912 Email: andrew@spotonmedia.co.uk
GET A SUBSCRIPTION DISCOUNT!
£90 independent practitioners.
£90 GPs and practice managers (private & NHS).
£210 organisations.
Save £15 paying by direct debit: individuals £75 (organisations £180).
TO SUBSCRIBE
Email karen@marketingcentre.co.uk or phone 01752 312140
Publisher Gillian Nineham Phone: 07767 353897.
Email: gillian.nineham@gmail.com SAVE £15 WITH DIRECT DEBIT!
Guarantee delivery of your next copy of Independent Practitioner Today. Take out a subscription and you will get full access to our news, features and previous issues on our website. See details on the left.