Simon Brignall advises on how to get the money in from medico-legal work P28
The business journal for doctors in private practice
When patients say ‘no’ Medico-legal experts discuss how to deal with a patient who changes their mind and refuses the recommended treatment P32
Give us your views on setting up in private practice
Win a £100 Amazon e-gift card
Take part in our survey: See details on page 26
Avoid falling out with partners
Hempsons’ solicitor Ross Clark looks at partnership disputes and how to avoid them P38
Tough new GMC rules
By Robin Stride
Doctors fear workload pressures could expose them to falling foul of new GMC ethical standards guidance due to the time needed to prepare.
They voiced concerns about digesting and implementing new standards setting out what it means to be a good doctor in a survey by the Medical Defence Union (MDU).
As reported on Independent Practitioner Today ’s news section, a major revision of the Council’s core guidance Good Medical Practice has been published following a consultation last year.
But it has emerged that, based on the draft guidance, only 15% were confident the new standards could be delivered in their work environment.
Seven-in-ten doctors (68%) said they were unsure about this and nearly one in five (17%) felt this could not be done.
The MDU said: ‘Crucially, only half (49%) were confident they would have time to fully absorb the new standards before they are implemented, with seven in ten (69%) saying they would have to read the guidance in their own time outside of work.’
Its survey of 610 doctors, mostly consultants and GPs, found 96% had made use of the current standards and 62% found them helpful in knowing what was expected of
them. The new guidance takes effect from 30 January 2024.
Dr Udvitha Nandasoma, head of MDU advisory services, said:
‘Being a doctor is a challenging career and, too often, the challenges facing independent practitioners can be underestimated.
‘That’s why we have been strongly calling for the maximum amount of time to be given so doctors can digest this guidance and consider what impact it may have on their practice. We are pleased the GMC has listened, and given five months.’
But the MDU warned doctors would still be challenged to read and absorb the revised standards over the busy winter months on top of their daily duties and responsibilities to patients.
Director of medical services Dr Caroline Fryar said: ‘Doctors know how important the guidance is and need time to understand and
Our sponsors
familiarise themselves with the changes being made.
‘The standards have been substantially revised for the first time in a decade. We are calling on employers to ensure they give medical professionals time to digest it and the GMC to do all they can to make sure doctors can easily understand the main changes.
‘Doctors shouldn’t be getting homework at a time when they are already working incredibly hard, around the clock, to deliver safe and effective patient care.’
She added: ‘There is much at stake for doctors, as failing to follow the standards could lead to a fitness-to-practise investigation, something nearly half of those responding to our survey (43%) were concerned about.
‘For our part, we are doing everything we can to make sure doctors are aware of what this means for them and for patients. We have an
extensive educational programme to support understanding of GMC guidance and will be focusing on Good Medical Practice.’
A bespoke webinar series is planned for coming months.
The top issues doctors consult Good Medical Practice about are:
1. Patient consent or capacity to make a decision – 49%;
2. Reflecting on a complaint, claim or incident – 40%;
3. Whether to protect confidential information or disclose it in the public interest – 39%;
4. Raising concerns about a colleague, system or resource – 31%;
5. Prescribing – 15%.
Mr Tim Mitchell, president of the Royal College of Surgeons of England, welcomed specific Good Medical Practice guidance on preventing bullying and sexual harassment.
He said: ‘There is no place for these abhorrent behaviours in UK medicine and they bring shame to the profession. We need to be creating a work environment where every person feels welcome, safe and protected. The GMC’s new standards send a strong message to the profession that these behaviours will not be tolerated.’
The college is reviewing its own core standards document Good Surgical Practice to reflect changes to the GMC’s guidelines.
Good Medical Practice is available on the GMC's website.
Dr Udvitha Nandasoma
TELL US YOUR NEWS. Contact editorial director Robin Stride
ADVERTISE WITH US. To advertise in the digital journal, on our website or in our business and lifestyle directories, contact Andrew Schofield at Spot On Media. Phone: 0161 408 3912
Our medico-legal series looks at what you have to do when retiring and how to cope with service dogs P46
Accountant’s tips: Taking the unfairness out of pension taxation
Alec James of accountants Sandison Easson explains the McCloud remedy for anomalies in pension schemes P48
Doctor on the Road: A good-looker with an Achilles heel
Dr Tony Rimmer says experience of driving the Alfa Romeo Tonale doesn’t match its good design P52
A general practice as they used to be Harley Street GP Dr Tony Banerjee relates a moving story from his own experience which influences the setting up of his new private practice P16
How insurance salesmen can help David Middleton, executive chairman of the Association of Medical Insurers and Intermediaries, explains why doctors could benefit from its expertise P18
Psychiatry claims in the spotlight
Negligence claims pursued against MDU private psychiatrist member are analysed by medico-legal experts, who offer tips on managing risks P20
Saving the planet and boosting care
Digital solutions can create sustainable healthcare systems while ensuring efficient and accessible patient care, says Dr Robin Clark of Bupa P23
Prepare to be investigated
Private doctors’ experience of the CQC can be daunting. Solicitor Paul Ridout relates some experience he has come across and gives some advice P30
Innovators improve care & efficiency
In our July-August issue, Rob McGough highlighted the move to value-based healthcare. Here he gives examples of this approach in private healthcare P36
Remember to stay in balance
Balanced portfolios are far from dead. Dr Benjamin Holdsworth of Cavendish Medical on why they remain a valuable protector against inflation P42
Boon of co-operation
A long-awaited Government report from its ‘elective recovery taskforce’ has set the ball rollling on new partnerships between private sector and NHS P44
New details on flexible NHS retirement options
More doctors to be able to take pension benefit while working
By Edie Bourne
Doctors who are members of the 1995 Section of the NHS Pension Scheme will be able to take their pension benefits while retaining their current NHS role from this October.
New details on the application process and the criteria needed to apply have just been released –although some of the key tools have been delayed.
The partial retirement option is already possible for pension benefits earned in the 2008 Section and 2015 Scheme, but from this autumn it will apply to 1995 Section benefits too.
Doctors aged 55 and above can choose to take between 20% and 100% of their pension benefits in one or two payments – without having to leave work.
However, those choosing this option must reduce their pensionable pay by at least 10% in the 12 months after drawdown.
In order to proceed with an
application, doctors must complete a new document called a ‘Partial Retirement Supplementary Form’, which was published in July.
There is also a new online ‘Partial Retirement Calculator’ to help members plan their next steps, but this will not be available to use until 1 October at the earliest.
Patrick Convey, technical director at retirement management specialists Cavendish Medical, explained: ‘As with all NHS finance matters, the devil is in the detail and yet we are only just receiving some of the most important information on these flexibilities now.
‘The new application form has only just been published, which means it might be difficult for NHS Pensions to process in time for those wishing to start their flexible retirement in October.
‘NHS Pensions has vowed to make quick progress with applications but standard retirement
Convey, technical director of Cavendish Medical
forms can take at least three months. The online tool designed to facilitate easier decisionmaking will also not be ready until after the launch date of the scheme, but benefits will be backdated to 1 October if there are delays.
‘If you are considering taking this opportunity, you should discuss your options with your financial adviser. The “McCloud remedy” legislation is also due to
be published in October and may have an impact on your decisions.’
The McCloud remedy, which seeks to redress the age discrimination caused by moving some members to the 2015 scheme, confirms that those impacted will be given a choice between taking their benefits for the remedy period from the 1995 2008 Section or the 2015 Scheme instead.
Pensionable service for the remedy period will be automatically put back into the 1995/2008 Section until it is time for the member to make a choice. Those applying for partial retirement will be contacted by NHS Pensions within 12 months of taking pension benefits to ask for the decision.
Further online assistance has been available via the new ‘McCloud Percentage Tool’ available since 1 August. It allows those affected by McCloud to conduct various modelling to help plan their remedy choice.
What private patients gripe about Healthcare is a healthy investment
Private patients’ grievances against consultants and medical care accounted for the most heads of complaint received by the Indep endent Sector Complaints Adjudication Service (ISCAS) last year.
ISCAS’s annual report to March 2023 says the complaints about doctors concerned information about fees, consent, managing expectations, information and advice about procedures, recordkeeping/documentation and apologies.
Complaints against consultants accounted for 29% of the total, with complaints handling coming
in second at 27%, clinical/nonmedical and nursing (10%), accommodation 9% and discharge 6%.
A total of 550 complainants contacted ISCAS with a concern, down from 672 the previous year.
The independent complaints service, subscribed to by the majority of large private healthcare providers, says some complainants had unrealistic expectations about the possible outcomes of adjudication – seeking a refund, revision surgery and/ or financial compensation.
Most (71%) complaint heads were either ‘upheld’ or ‘partially
upheld’ by adjudicators – a significant increase from the 57% reported the previous year.
Individual ISCAS subscribers paid an average £1,687 for adjudications, a 9% decrease from £1,856 in the previous financial year.
A total of 12% of cases required expert clinical advice, a decrease from 16% the year before.
Total costs associated with expert clinical advice came to £21,200 – an average of £1,927 a case.
These were down from £27,633 and £1,973.
Goodwill payment awards rose from £38,776 to £53,910.
The healthcare sector ranks third among the best sectors for investment, according to a new study. It comes in after the IT sector, with an average return of investment of 18.1% and the consumer discretionary sector with 15.3%, according toInvestinGoal.com.
Average return in the healthcare sector, including businesses providing medical services, producing devices or medicines, offering medical insurance or aiding in the overall delivery of healthcare, is 13.4%.
Patrick
PHIN anxiety at units using fake reviews
By a staff reporter
The Private Healthcare Information Network (PHIN) has voiced its concerns over BBC reports of fake Google reviews being used by medical clinics.
Chief executive Dr Ian Gargan said transparency in healthcare was so important and that is why this BBC report about fake reviews was worrying.
‘Planning for an operation can be a stressful time and people need to be able to trust their hospitals and consultants. They should be able to rely on the reviews of other patients when looking into who should treat them,’ he said.
PHIN is an independent, notforprofit, Governmentmandated service and the information pub
lished on its website is supplied and verified by the private hospitals and consultants it works with.
Dr Gargan said: ‘We do not edit or amend patient feedback in any way, nor do we charge for profiles or have any advertising on our site.
‘Our main role is to help people to make a more informed choice when considering which hospital and consultant is right for them.
‘We publish information about quality, safety and costs for all hospital based private healthcare in the UK, including private services in NHS hospitals. You can search for services in your area from our homepage.’
The BBC reported that five people who had rated a clinic highly also posted negative comments on a local competitor.
Surgeons excited at arrival of Mako robot
Consultant orthopaedic surgeons at Nuffield Health Warwickshire Hospital have taken delivery of a Mako robot, enabling more precise knee and hip replacements and faster recovery.
One of them, Mr Andrew Shepherd (pictured far right), said: ‘I have been replacing joints for 20 years and this is the most exciting new development in surgery I have seen.’
Spire unit performs first open heart op
A new cardiac service for NHS and private patients in Manchester has seen its first patient for open heart surgery.
With hundreds of people currently waiting for cardiac surgery in the northwest of England, Spire Healthcare has invested £2.3m in new equipment and facilities for the service.
It expects to care for up to 200 people annually and has announced a recruitment programme with opportunities for more cardiac consultants, cardiac scrub nurses, cardiac nurses, critical care nurses and operating department practitioners.
Hospital director Lesley Lock said: ‘We are in conversations with local NHS trusts to see how we can start supporting them with their cardiac patients. Every patient treated at Spire Healthcare is one
less person on an NHS waiting list.
‘Driving clinical excellence, investing in new technologies and training colleagues encapsulates everything that is great about this new cardiac unit.
‘The newly formed cardiac team will bring relief to people in northwest England who need fast access to complicated lifesaving surgical procedures.’
The first patient received a double coronary artery bypass.
Consultant cardiac surgeon Mr Paul Modi said: ‘We have a fantastic cardiac team here at Spire Manchester Hospital – their dedication and attention to detail is secondtonone.
‘Our months of planning and practising different scenarios from before and after surgery to the postoperative stages have paid off.’
Spire expands it nursing apprenticeship scheme
Spire Healthcare is expanding its nursing apprenticeship programme with 25 new roles across 16 hospitals from December.
Colleague Mr Jon Waite added: ‘The Mako robotic system has already been shown to reduce soft-tissue damage during surgery, resulting in less pain and bleeding postoperatively, thus making rapid recovery easier.’
Mako robots are also at Nuffield Health’s Bournemouth, Bristol, Glasgow, Leeds, Cambridge, Exeter, Cardiff & Vale and Woking hospitals.
Its fouryear programme leads to a BSc in adult nursing.
Participants earn while learning, with a £21,000 starting salary depending on previous experience.
The group is training and supporting 500 apprentices across a wide range of clinical and nonclinical specialties.
Prof Lisa Grant, Spire group clinical director and chief nurse, said: ‘While national shortages in
healthcare professionals are still a concern for all healthcare providers in England, continued investment in our nursing apprenticeship programme – one of the largest of a single organisation in England – is aimed at building a talent pipeline for our business and the broader healthcare sector.
‘Importantly, this programme contributes to the sustainability of the whole healthcare sector in the UK, because many of our graduates will go on to careers in the NHS and elsewhere – something we encourage as a net contributor to society.’
Spire Manchester Hospital in Barlow Moor Road
Cost puts patients off cosmetic work
Cleveland performs augmented reality op
By Agnes Rose
Cost is the numberone factor preventing people from undergoing cosmetic procedures.
Too expensive fee levels were cited by 50% of 500 men and women who took part in a survey looking at why people who have considered cosmetic treatments did not go ahead.
This is closely followed by fears of possible complications (46%); looking unnatural – for example, over inflated lips, frozen expressions – with 41% quoting this as the cause; and ‘horror stories in the media’ at 32%.
Other highlights include:
Nearly a quarter (22%) don’t know how to find a reputable practitioner;
28% are scared of suffering pain during the treatment;
One in five (21%) decided they want to ‘grow old gracefully/ accept their flaws’ – yet there is a considerable age discrepancy, with older people less likely to accept their fate;
16% fear being judged by friends and family. The older the respondent, the less likely they were to care;
14% are worried their partner wouldn’t like it.
The research was conducted by independent survey company
OnePoll on behalf of SafeAP (https://safeap.co.uk), a marketplace app that helps people find qualified practitioners, founded by two doctors.
Maxillofacial surgeon Miss Sieuming Ng, along with Dr Subha Punj, pioneered the app to ensure nonsurgical aesthetic procedures are delivered by qualified healthcare professionals in a safe environment.
She said: ‘It’s always interesting to get an overview of human behaviour in times of social change, such as during the current cost of living crisis and a postpandemic world.
‘Unsurprisingly in this climate,
cost is still the overriding factor for many people considering undergoing an aesthetic treatment.
‘However, the survey did throw up some interesting results with, for example, few over65yearolds cite a fear of pain as an issue, compared to almost 60% of 18 to 24yearolds.
‘This may simply mean that with age comes less worry when compared to the benefits of achieving a rejuvenating look.
‘Gender differences were also notable – perhaps men feel less of a societal stigma and therefore are less fearful about possible complications or looking “unnatural”.’
The survey found a considerable gender divide in certain factors, such as the worry about complications – over half (53%) of women cite that as a concern, compared to just over a third (36%) of men.
Women are also more likely to be put off by horror stories in the media, with half (49%) scared of having treatments thanks to frightening headlines.
Men care considerably less, with just over a quarter (27%) being concerned about what they see or read in the news – although it is thought possible women are simply more exposed to negative
stories in femalefocused publications.
Genders are aligned when it comes to growing old gracefully, with equal numbers (21%) saying they are resigned with what they see in the mirror and will accept their flaws.
More men than women are concerned about what partners will think, with around 15% of men reporting that as a factor, compared to about 13% of women.
Interestingly, more than twice the amount of men (21%) than women (9%) admit to having already had a negative experience with a cosmetic procedure.
SafeAP also released the results of a companion survey, which polled 500 women only. The results were largely the same, although it further revealed that 80% of women in Northern Ireland are concerned they would appear unnatural, superseding all other concerns.
The Safe Aesthetic Practitioner (SafeAP) is an app for both practitioners and customers. It offers qualified practitioners business management tools, including a platform to outline their qualifications, while offering customers a portal where they can connect with registered professionals.
Cleveland Clinic London has announced it is the first hospital in the city to successfully perform a total knee replacement procedure with the assistance of an augmented reality based surgical platform designed with artificial intelligence and machine learning.
Consultant orthopaedic hip and knee surgeon
Mr Panagiotis
Gikas ( right ) led the surgical team during the procedure to treat knee pain caused by osteoarthritis.
He said: ‘Augmented reality gives a visualisation of the joint that is more dynamic as it is 3D.
‘The advanced technology helps with planning the procedure and allows for the best positioning of the implant for each patient during the procedure. The end result is tailored to the unique anatomy and specific needs of each patient.’
Cleveland Clinic has used augmented reality technology in joint replacement procedures at its main campus in Ohio, US.
Fees rise for complaints adjudication
A 13.3% rise has been announced in the adjudicators’ daily fee rate charged to Independent Sector Complaints Adjudication Service (ISCAS) members – representing a majority of private providers. It increases from £600 to £680 from 1 October 2023. ISCAS said all other charges would remain unchanged.
The fee is for eight hours of the adjudicator’s time to review and assess a private patient’s complaint about a doctor, clinic or hospital.
Maxillofacial surgeon Miss Sieuming Ng and Dr Subha Punj
Plight of autistic doctors revealed
A quarter of autistic doctors have attempted suicide, more than three-quarters (77%) have considered it and nearly half (49%) have also self-harmed.
These are the findings of a new study by Brighton and Sussex Medical School (BSMS), Thomas Jefferson University and Autistic Doctors International (ADI) – published in Frontiers in Psychiatry.
Lead author Dr Sebastian Shaw, lecturer in medical education at BSMS and ADI research lead, called it ‘deeply concerning’ to see the extent to which his fellow autistic doctors have struggled with their mental health.
But he felt perhaps this was unsurprising considering the many barriers and challenges faced by autistic people working in the healthcare sector.
‘We also found that those who considered autism to be a “disorder”, rather than a difference or disability, were more likely to have attempted suicide. This may reflect a degree of internalised shame from being trained to understand autism as a disorder through their medical practice.
‘This association would seem to support a neurodiversity-affirmative view of autism. Fostering more acceptance of autism as a difference may potentially improve the well-being of autistic health-
care professionals and patients alike.’
He told Independent Practitioner
Today the study gathered no specific data about private practice because of the international/ worldwide context, where the distinction of private practice would not always have held similar meaning in each country.
He added: ‘I suppose it may be possible though that any autistic doctors who may be forced out of NHS roles due to their differences may find some refuge in private practice, where there is typically more independence, albeit with its own sets of unique challenges, I’m sure.’
The study also found many autistic doctors did not disclose their diagnosis in the workplace, with 29% not having told anyone at work, 32% having disclosed being autistic to their supervisor and 30% to their colleagues.
Linked to this appears to be a sense of isolation. Although fourfifths reported having worked with another doctor they suspected was autistic, only one-fifth reported having worked with another doctor they knew was autistic.
Those having never worked with any suspected autistic colleagues were also more likely to have considered suicide.
As awareness and diagnosis of autism grow, more medical students and doctors are discovering they are autistic; the study showed an average age of formal diagnosis of 36.
Some were diagnosed following difficulties in stressful clinical environments or highly demanding career paths – and found that support from employers was inconsistent, with some colleagues refusing to believe a qualified doctor could be autistic.
Dr Shaw said: ‘Key to improving the experience of autistic doctors is ensuring that neurodivergence is viewed in a positive light. Workplaces need to provide better support and improve awareness of autistic healthcare professionals.
‘Employing a well-supported and neurodiverse medical workforce will mean that the diversity of the public is reflected in their medical providers, with likely improved experiences and outcomes for neurodivergent patients.’
Despite these striking findings, overall, three-quarters usually enjoyed their work as doctors (74%) and three-quarters (73%) felt being autistic was helpful in their role as doctors.
Dr Mary Doherty, senior author and founder of ADI, commented: ‘Autistic doctors are a hidden minority in the medical work-
Fostering more acceptance of autism as a difference may potentially improve the wellbeing of autistic healthcare professionals and patients alike
Dr Sebastian Shaw (pictured)
force, and the range of specialties in ADI challenges autistic stereotypes. General practitioners are the largest subgroup, followed by psychiatrists.’
Dr Wendy Ross, director of the Jefferson Center for Autism and Neurodiversity, added: ‘This study is a call to action for the entire medical field to meet the needs of autistic medical talent as well as patients.’
The cross-sectional study, the first to gauge the experience of autistic doctors, modified a preexisting survey of autistic school staff, with 225 members of the organisation ADI taking part in the study.
☛ The full study is published at www.frontiersin.org/ articles/10.3389/fpsyt. 2023.1160994/full
Eye clinic’s new laser offers a quicker recovery time
Independent eye surgery provider OCL Vision reports that it is the first in the UK to introduce SmartSight, a new procedure to speed up recovery time for patients having laser surgery at its New Cavendish Street Clinic in Marylebone, central London.
The clinic recommends SmartSight for patients with prescriptions higher than -3 dioptres with or without astigmatism.
It said the procedure was known to significantly reduce the risk of developing dry eye following surgery, which may be particularly
welcome in those suffering from intolerance of contact lenses.
SmartSight has also proved popular among those doing contact sports, as it allows for a rapid return to the activity.
Ophthalmic surgeon and company co-founder Mr Allon Barsam said: ‘People are becoming more concerned about recovery time and want faster results so that they don’t have to take as much time out from their busy lives. This procedure goes some way towards making the process more efficient and ensuring smooth aftercare.’
London PPUs return to record earnings
Compiled by Philip Housden
Many NHS trusts have now published their 2022-23 annual reports and accounts and although gaps remain, it is clear that private patient incomes have largely returned to pre-pandemic levels and may be at a record high.
Seven of the top ten central London trusts have released their accounts and these show a forecast revenue of £444m, representing an average growth rate of 32%.
However, the final underlying rate may be closer to the 20-25% range when Royal Marsden, Moorfields and King’s College publish their own results.
Highest growth achieved was at Great Ormond Street which reports private patient income of £54.8m in the last financial year.
This is up £17.4m and 120% on 2021-22 and places it as the third highest grossing trust after Royal Marsden (yet to publish) and Guy’s and St Thomas’, where income is now £62.7m – up £12.1m and 24% year on year.
A more detailed review of the overall NHS trust private patient performance will feature in PPU Watch in forthcoming issues.
UCLH Private Healthcare expands private neurophysiotherapy service
UCLH Private Healthcare is expanding its neuro-physiotherapy service at the Private Consulting Rooms 23 Queen Square, situated next door to the National Hospital for Neurology and Neurosurgery, London.
MDU expands its help for doctors in trouble
A service to help doctors suffering a GMC investigation has been extended to include other medico-legal matters such as inquests, complex complaints and claims.
The Medical Defence Union (MDU), which launched the support in 2020, said its wider support package would come to the aid of more healthcare professionals in distress.
Its peer support programme connects members struggling over a complex medico-legal matter with a colleague who has been through a similar process. The colleagues offer personal support, guidance and reassurance.
Chief executive Dr Matthew Lee said: ‘Members have told us time and again that dealing with inci-
dents can impact both their professional and personal lives – and that having a conversation with a colleague who has been through something similar and come out of the other side can be a huge comfort.
‘For example, one member told us: “As well as legal advice, it would be good to have access to practical support, be that peer support or a counsellor.”
We are delighted to be able to extend the peer support programme so that more members will have someone to talk to at a difficult time.’
The revamped service came as the MDU’s 2022 report disclosed:
MDU solicitors representing medical members in Medical Pract itioner Tribunal service (MPTS) cases between 2017-21
The team is now offering both outpatient physiotherapy and domiciliary physiotherapy sessions for patients living in central London who require therapy related to neurological conditions. Online sessions are to be provided for patients living outside of this catchment.
UCLH reported private patient income of £8.3m in the just published 2022-23 annual accounts.
This is an increase of £950,000 and 12.9% on the previous year – a growth rate below the average for trusts in central London – and still well below the £20m a year achieved pre-Covid.
Philip Housden is director of Housden Group commercial healthcare consultancy
achieved no finding of impairment in over 40% of cases. The equivalent MPTS figure for outcomes overall is 25%.
During 2022, it closed 82% of medical claims without a payment of damages. In total, where cases came to trial, it had a success rate of 60%.
99% of calls to its medico- and dento-legal advice lines were answered within 20 seconds.
Orthopod celebrates a century of robot ops
A consultant orthopaedic surgeon has celebrated the completion of his 100th Mako robotic-assisted joint replacement operation.
Robotic hip and knee surgeon Mr Nadim Aslam performed the operation at Spire South Bank Hospital in Worcester.
He said: ‘This has been an incredible journey, from our very first procedure in January to now, marking my 100th procedure in just seven months. The feedback from patients has been nothing short of astounding.
‘They have reported exceptional outcomes, remarkably fast return to work or being able to do the things they love, and unmatched levels of satisfaction.’
Ms Hilary Fowler who received a robotic-assisted knee replacement, said: ‘I had previously undergone a successful operation by Mr Aslam many years ago, so I had no hesitation in entrusting him with my robotic knee replacement.
‘Moreover, several of my friends have been his patients before, making it an obvious choice.’
Hospital director Dawn Pickrell said the hospital was seeing record levels of interest from people wanting robotic over the traditional hip and knee replacement techniques.
Mr Nadim Aslam with knee replacement patient Hilary Fowler
MDU head Dr Matthew Lee
Joint appointments can reduce costs
By Douglas Shepherd
Shared medical appointments could reduce costs for private care and be the key to solving global healthcare shortages, according to researchers.
New research from the European School of Management and Technology (ESMT) Berlin found shared medical appointments improve patient satisfaction, learning and medication compliance without compromising follow-up rates or clinical outcomes. Researchers wanted to understand the impact of shared medical appointments (SMAs) on patient experience – knowledge gained and satisfaction – and on behaviour such as follow-up rates and medication compliance rates.
In SMAs, patients with the same medical condition meet with the physician in a group, with each patient receiving attention in turn.
The physician shares information customised to a patient’s specific needs as well as standardised information relevant to other patients with the same condition.
SMAs have been touted as a potentially effective way to meet healthcare demand worldwide, especially in countries facing significant strain on their healthcare systems.
But the limited adoption of SMAs in the healthcare sector has been attributed to patient concerns about loss of privacy, which may impede open discussion of sensitive medical issues and
Up to the challenge
Consultants from Spire Hull and East Riding Hospital walked the Yorkshire Three Peaks of Pen-y-Ghent, Ingleborough and Whernside with colleagues. They covered a total of 711.36km during Spire Healthcare’s 2023 charity focus week – all in aid of the charity PAUL for Brain Recovery.
Consultants and colleagues at Spire Healthcare’s hospitals and clinics across England, Scotland and Wales have raised over £40,000 after walking, cycling and running nearly 43,000 kilometres during their hospital group’s 2023 charity focus week.
The ambition was for them to collectively cover 40,000km – the equivalent of circling the globe once – with all the money raised going to a range of local and national charities.
Individual hospitals managed their own fundraising events, including sponsored static bike challenges, walks, runs, sports days and traditional fundraising activities such as bake sales, raffles and quizzes.
dampen learning, satisfaction, and engagement.
ESMT Berlin researchers conducted a randomised controlled trial at the Aravind Eye Hospital, India.
One thousand patients with primary glaucoma were randomly assigned to either attend one-onone appointments or SMAs with five total patients in four successive routine follow-up visits scheduled four months apart.
After each appointment, patients were surveyed to assess their satisfaction with the appointment, their knowledge about glaucoma and their intention to return for a follow-up appointment. Patients were also tracked for their medication compliance rates.
Researcher Nazlı Sönmez, from
ESMT Berlin, said: ‘The demand for healthcare worldwide is soaring and exceeds supply. In underdeveloped countries, especially, the patient-to-doctor ratio is staggering and patients face high barriers to receiving care.
‘We must use innovative solutions, like shared medical appointments, to meet this demand. Failure to do so would deprive a huge number of people of their fundamental human right to healthcare access.’
According to the researchers, SMAs could expand access to public healthcare, lower costs for private care and significantly improve medical outcomes for various conditions, particularly for Type 2 diabetes, in both primary and secondary care settings.
They report that the innovative utilisation of SMAs could ensure more patients receive access to healthcare faster, facilitating healthcare for all.
This research was published in PLOS Global Public Health. The full research paper is at https:// journals.plos.org/globalpublichealth/article?id=10.1371/journal. pgph.0001648.
Patient was so impressed she took a job at the clinic
A woman diagnosed with a sightthreatening condition was so impressed by the surgeons who saved her vision that she got a job at the clinic.
Tracey Coyle was only 32 when she was diagnosed with cataracts. She went back to work as a healthcare assistant at Newmedica in Newcastle and is now going to university to train as a nurse.
She said the surgery had enabled her to train for her dream job and help other people.
Clinic operational director Amanda Bargewell said Tracey’s personal experience of cataract surgery gave her an invaluable insight she could pass on to patients.
‘We’re very lucky to have her. She’s wonderful with our patients – comforting those who are nervous and explaining the procedure in a way that patients find helpful.’
Healthcare assistant Tracey Coyle
Newmedica Newcastle is run by Amanda and a team of four consultants: Mr Mustafa Kadhim, Mr Gerard Ainsworth, Mr Ayad Shafiq and Mr Nicholas Wride.
Robot surgery gets boost in tie-up with manufacturer
A robotic-assisted surgery (RAS) company has developed its support for the Royal College of Surgeons of England (RCS England) by supporting a new multi-professional network expected to shape the future national development of using robots.
The three-year collaboration aims to accelerate the safe integration of RAS into healthcare nationally and help surgeons at all levels of training and experience to become RAS proficient.
RCS England and Intuitive see RAS as one of the key changes in how surgery is delivered across healthcare in the next ten years.
The collaboration will help the college’s work to review and develop the evidence base for using robotics and ensure training in using them enables improved patient outcomes.
Surgeons believe Intuitive’s support will enable RCS England to strengthen the programme man-
agement infrastructure and resources available to support a multiprofessional network of experts.
The multiprofessional expert network team will regularly convene to:
Drive future research into RAS;
Facilitate improved access to training in robotic techniques;
Improve the quality of national data available about RAS;
Raise public, patient and policy awareness.
Since publishing its Future of Surgery report in December 2018, the RCS England Robotics programme has helped secure funding to drive research in surgical data science and qualitative assessment of RAS’s introduction in the NHS.
The college has developed guidance on the safe and structured introduction of RAS which aims to support fruitful collaboration between surgeons, hospitals and industry.
PROF
NEIL MORTENSEN,
ROYAL COLLEGE OF SURGEONS’ IMMEDIATE PAST-PRESIDENT:
WHAT THEY SAY Applications to work in Australia are on the rise
‘Robotics is here to stay and we need to leverage this technology and increase take-up where this supports the best quality patient care.
‘When I have spoken to surgeons across the country, I have heard how RAS can help reduce the physical strain of their work. The college wants to be a driving force in the safe integration of RAS into healthcare nationally, a crucial move in recruiting and retaining surgeons.
‘Robotic-assisted surgery is not part of the future of surgery; this shift is already occurring. It is the here and now and, when used appropriately, can help surgeons to conduct procedures more precisely and enable patients to recover quicker.
‘The college is committed to supporting the safe introduction and development of RAS across all platforms and welcomes the close and constructive dialogue between the profession and all RAS industry stakeholders in the interest of better care for patients. Our collaboration with Intuitive is one major step in this process.’
DAVID MARANTE, INTUITIVE UK AND IRELAND REGIONAL DIRECTOR:
‘The Royal College of Surgeons of England has set a clear vision for the future of surgery and the role of RAS in evolving surgical training and care for patients. The future is now – which is why it is a privilege to support the college’s efforts as it drives forward this important work.
‘I’m confident that over the course of this three-year collaboration, the college and Intuitive can work together to continue demonstrating the clinical, operational and strategic value of RAS, enabling current and future generations of surgeons and care teams to continue to have access to our da Vinci RAS technology and ensure they are able to deliver the best outcomes for patients.’
Australian medical clinics and recruiters are reporting a significant rise in applications and inquiries from UK GPs hoping to move down under.
Health Recruitment Australia
managing director Gemma Gough said while pay was a big issue, the doctors her agency was talking to were also prioritising lifestyle.
‘It is very hard for the UK to compete with Australia on that.
Having made the move myself, there is no denying that there are challenges moving across the world, but there are absolutely no regrets – Australia is a great place to build a career, grow a family and create a life worth living.’
Ms Gough said while it was disappointing to see the challenges facing the UK health system, Australian clinics and hospitals were eager to satisfy their own urgent needs for qualified doctors.
‘Australia also has a huge shortage of doctors and the reality is that clinics and hospitals have to search overseas for GPs to meet the growing demand of their local communities.’
Benefits of filing tax return early
With many doctors still reeling after their latest tax payments, HM Revenue and Customs (HMRC) is highlighting the advantages for self-assessment customers in filing their next tax return early.
The self-assessment deadline for the 2022 to 2023 tax year is not until 31 January 2024, but tax officials say early filers have more control over their financial affairs and beat the January rush.
Tax officials say they will get an early sight of what they owe, be able to budget better, and check if they are due a refund using the HMRC app.
Robot manufacturer Intuitive’s surgery proctor team mentoring trainees
Our Tuesday news e-alerts have been busy with some important stories during the holiday period since our last digital issue. So here and on the next two pages is a round-up for readers who may have missed out while they were away
Competition watchdog gets tough on fee data
Published on 25 July
The competition watchdog this week warned private consultants could end up in court if they drag their feet over the supply of fee transparency data.
In an open letter spelling out enforcement action to doctors and independent hospitals, the Competition and Markets Authority (CMA) said all the most active consultants had submitted the information required under the Private Healthcare Market Investigation Order 2014 to the Private Healthcare Information Network (PHIN). These are specialists who have
reported at least 100 admissions a year to the data-gathering and publishing body.
David Stewart, CMA executive director of markets, remedies and regulation, wrote: ‘As with hospitals, this work is ongoing and we are now engaging with consultants that carry out fewer than 100 episodes per year.
‘While it is reassuring that on receiving contact from the CMA, many hospitals and consultants are remedying these breaches, both groups are well aware of the legal responsibility to comply with the Order.
‘It remains a concern that these
businesses and individuals do not comply with their legal requirements in the absence of a specific threat of public enforcement. The CMA expects all hospitals and consultants that are not compliant to take immediate action to end breaches of the Order by logging in to the PHIN Portal or speaking to PHIN on 020 7307 2862.
‘The CMA is committed to seeing full compliance across the sector. Working with PHIN we are stepping up our enforcement action. Those in breach will now be escalated more swiftly to the CMA’s formal enforcement tools.
‘This will deliver greater compli-
BMA sceptical of plans to divert care to private sector
Published on 7 August
Current pressures on private doctors means there is no guarantee that diverting more patients to the independent sector will cut NHS backlogs, according to the BMA.
It warned that planned expansion of independently run community diagnostic centres was no substitute for investment in the NHS workforce.
The association claimed any expansion of community diagnostics centres needed careful implementation to ensure it does not just shift the problem – resulting in longer waiting times for private patients needing treatment and still not making a significant difference to the NHS backlog.
Its comments came in response to the Government’s announcement of further investment into the expansion of community diagnostic centres in the independent sector to tackle NHS waiting lists in England.
BMA workforce lead Dr Latifa Patel agreed more should be done to help those on waiting lists with whatever capacity was available, but she voiced concerns over how plans for the expansion of the use of the independent sector to cut diagnostic waiting lists would work.
‘We do not have enough staff working in the NHS or the private sector. Doctors working in the private sector are also under pressure, so there is no guarantee that
diverting more patients to the independent sector will cut NHS backlogs.
‘Any expansion of community diagnostics centres needs to be carefully implemented to ensure that it does not just shift the problem – resulting in longer waiting times for private patients needing treatment and still not making a significant difference to the NHS backlog.’
She added that the Government’s goal should ultimately be long-term investment in the NHS to ensure the best possible value for public money and a sustainable healthcare system that avoided an overreliance on the independent sector.
‘We currently have a situation
ance across the sector more quickly and give a level playing field, preventing hospitals and individuals gaining from not complying with the Order in full.
‘Hospitals and consultants should be aware that, as well as publishing the names of hospitals and consultants, the CMA has the power to issue legally binding Directions against them, which are enforceable in court.’
PHIN boss Dr Ian Gargan welcomed the CMA letter, saying it recognised great work many were doing to meet the requirements of the Order and help patients make more informed choices.
where both consultants and junior doctors are taking industrial action over years of pay erosion. It makes little sense to invest more into the independent sector but ignore the major crisis facing the current NHS workforce who can actually care for these patients and help to cut waiting lists.’
Dr Patel said diagnostics was just one part of the problem, and even with an earlier diagnosis, there was still the issue of how patients referred for treatment would be seen.
Dr Latifa Patel of the BMA
Matching scheme to allocate NHS patients to private hospitals
Published on 15 August
Doctors are being urged by private hospitals to get behind a new online ‘matching’ platform aiming to quickly allocate NHS patients to hospitals who can take on their care.
An ‘easy-to-use tool’ announced by NHS England (NHSE) allows NHS staff to view and add available surgery slots in hospitals across the country, including independent providers.
The development was welcomed by the Independent Healthcare Providers Network (IHPN), which hailed it as a good example of how the private sector and NHS could work together to cut waiting times and get patients seen faster.
David Furness, its director of policy and delivery, said: ‘We encourage trusts and clinicians to fully explore this new option, sharing intelligence and information so that the right providers can be offered to provide the right care.’
Clinical teams can upload details of patients on their waiting list who are willing to travel, with other NHS and independent sector providers able to log on and ‘match’ people up to treatment.
Initially introduced for patients needing a hospital admission, the platform will now expand to include cancer, diagnostic checks, and outpatient appointments. Around four-in-five patients on an NHS waiting list won’t need a hospital admission.
Since its launch in January, more than 1,700 offers of support have been made with thousands of patients set to benefit as the platform grows, the NHSE reported.
The system includes patient information – how far the patient is willing to travel, illness severity, BMI, and how long they have been waiting for care – to help organisations decide if they can pick up a case.
If more than one provider offers treatment, the options are put to the patient who can choose based
Cromwell Hospital’s bid to attract top clinicians
Published on 15 August
A major expansion at London’s Cromwell Hospital is tipped to help it attract more world-class consultants.
It has announced it will enlarge into the adjoining Lexham Gardens building and increase capacity to treat more patients. The adjacent and connecting site has been designed to provide an enhanced patient experience through comfortable and spacious outpatient facilities, state-of-the art radiology and therapies departments.
Redevelopment delivers a new
theatre, the hospital’s third MRI scanner and new staff welfare facilities.
Chief executive officer Philip Luce said: ‘This is an exciting opportunity for the hospital and we’re looking forward to being able to offer more services to patients, providing them with high-quality care and treatment.
‘The expansion will also help us to attract more world-class consultants to the hospital, to continue providing leading innovative treatments for our patients.’
New technologies and improved efficiency will seek to reduce carbon emissions, while the building
on factors including how far they would have to travel.
Gynaecology, colorectal and trauma and orthopaedics are the top three specialties to have benefited so far, but hundreds of different treatments or appointments can be uploaded.
Patients Association chief executive Rachel Power said: ‘We welcome the expansion of the hospital matching platform and think it will make it even easier for patients and the healthcare professional to make a decision together about where to have treatment or a test.
‘Patient choice has been a right for over decade, but not all patients are aware they have the right and it isn’t always offered to them. Hopefully, making it easy for health professionals to easily see the choices of where patients can be treated will increase the number of patients who can take advantage of mutual aid within the NHS.’
The NHSE said the new platform was just one example of how the
NHS was maximising all available health sector capacity to support elective recovery. Use of the independent sector had risen by over a third since 2021 – from 65,000 appointments and procedures a week to more than 90,000 a week now.
The IHPN and the Patients Association research last year showed that people were prepared to travel if it meant faster treatment.
73% of patients said they would be happy to travel more than 30 minutes to get treatment more quickly. The IHPN said weeks of months could be knocked off potential waits by travelling further.
The NHSE announcement follows another earlier in August, from the Government’s elective recovery task force, about the importance of patient choice and closer partnership working between private healthcare and the NHS in cutting waiting times.
has already been rated as ‘excellent’ by BREEAM, the leading science-based validation and certification for sustainable built environments.
Sarah Melia, general manager for Bupa Health Services, said: ‘This hospital expansion is part of our long-term transformation and growth strategy. We want to keep growing our hospital services to provide world-class treatment for our
patients and this expansion demonstrates this continued commitment.
‘We’re expecting to open the hospital extension in 2024 and are looking forward to welcoming patients to our new facilities.’
The new development supports the Bupa owners’ ambition to be net zero by 2040. The 33,000 square feet site was formerly the Mercure Kensington Hotel. Building work starts this month. ➱ More on page 12
Our Tuesday news e-alerts have been busy with some important stories during the holiday period since our last digital issue. So here’s a round-up for readers who may have missed out while they were away
GMC stamps down on sexual harassment
Published on 22 August
New professional standards for all doctors are demanding ‘zero tolerance’ towards sexual harassment.
They are contained in a major update of the GMC’s Good medical practice, published today.
Zero tolerance of sexual harassment includes:
Clear definitions of what constitutes it;
An expectation that doctors who see such behaviour will act.
An addition, in the first major update to the guidance in a decade, explicitly covers sexual harassment of colleagues.
Guidance says doctors ‘must not act in a sexual way towards colleagues with the effect or purpose
of causing offence, embarrassment, humiliation or distress’.
The standards make clear this includes:
Verbal or written comments;
Displaying or sharing images;
Physical contact.
This adds to existing guidance that doctors must not act in a sexual way towards patients or use their professional position to ‘pursue a sexual or improper emotional relationship’.
Udvitha Nandasoma, head of advisory services at the Medical Defence Union, told Independent Practitioner Today : ‘This is a substantially revised piece of guidance from the GMC.
‘It applies to every doctor registered in the UK, including those in
the private practice. This really is the core piece of guidance for the profession.’
The regulator also sets out for the first time what doctors should do if they witness bullying or harassment.
GMC chairwoman Prof Dame Carrie MacEwen, said: ‘Sexual harassment, bullying and discrimination are entirely unacceptable. Where workplace cultures of this kind of behaviour go unchecked, they are detrimental to wellbeing, performance and patient safety.
‘Doctors are increasingly, and bravely, speaking out about it, and as a regulator, it is important we leave no doubt that such behaviour has no place in our health services.
Consultants praised as Phoenix agrees to buy One hospitals
Published on 22 August
Independent provider Phoenix Hospital Group has reached agreement to acquire One Healthcare, the operator of both One Ashford Hospital, Kent, and One Hatfield Hospital, Hertfordshire.
It says the acquisition, subject to a ‘small number’ of formalities, provides excellent opportunities for collaboration and growth.
Phoenix works with 800 consultants in private practice and runs two London outpatient centres at 9 Harley Street and 25 Harley Street, and two hospitals: Weymouth Street Hospital (London) and Phoenix Hospital Chelmsford, Essex.
One Healthcare will continue operating through the transaction with no changes to its hospitals’ activities or staffing.
Phoenix chief executive Andrew Barker called One Healthcare an ‘outstanding provider of care’ which had established strong collegiate partnerships with consultants, the NHS, and local partners.
‘Phoenix has always enjoyed strong partnerships and adopted a collegiate approach to working with consultants. We very much look forward to building on all the relationships already established at One Ashford and One Hatfield, which are both excellent hospitals.
‘Ultimately, our hospitals are only as good as the consultants providing the care and we wish to ensure that all Phoenix locations are welcoming, engaged and joined up with our consultants with all parties having a voice in everything that we do.
‘We believe a strong GP presence can only enhance care and we are keen to work with local pri-
‘Those who experience harassment or discrimination must feel supported to speak out, by employers, peers, managers and leaders. We heard from thousands of doctors, patients and members of the public during this consultation.
‘We hope that by addressing this issue so clearly in the standards, this will spark discussion on making meaningful cultural change throughout medicine.’
The updated Good Medical Practice includes an entire section devoted to ‘contributing to a positive working and training environment’.
See full story on our website
vate GPs to build successful partnerships, increase patient numbers and provide outstanding primary care.’
He said his team had been ‘incredibly impressed’ by the One Healthcare staff, consultants and management team and looked forward to welcoming them into Phoenix Hospital Group.
‘This is an exciting opportunity to bring together two successful and complementary hospital groups both delivering outstanding care. Phoenix already has a strong and successful approach focused on central London and Essex. One Healthcare is a natural fit with a strong range of services and impressive patient demand.
‘It has been our intention to grow by acquisition and we are delighted to be able to take One Healthcare forward as part of our larger group, further expanding our geographic reach.’
See full story on our website
One Hatfield Hospital,Hertfordshire
A look back through our journal’s archives of a decade ago reveals that although times change, some issues are not so new
A trawl through the archives: what made the news in 2013
Huge rise in self-pay set to go on
Independent practitioners were being exhorted to gear up for a double-digit self-pay bonus on the back of a raft of changes affecting private practice.
Ongoing research into the opinions of 750 private healthcare market leaders and shapers revealed unprecedented opportunity for self-pay growth.
Researcher Liz Heath said consultants should now be talking to their private hospitals and asking them what they could do together to take advantage of the potential.
She told Independent Practitioner Today: ‘The message for consultants is self-pay has not only revived since the recession but is continuing to grow year on
year in excess of private medical insurance growth.
‘Some commentators are saying they anticipate anything between 20-25% of income to come from self-pay over the next three years – which suggests the current growth will be more than sustained.’
Competition report is ‘a golden chance’
We reported that no private doctor’s business could expect to escape the outcome of the (then) Competition Commission’s ongoing investigation into the private healthcare market (and how right we were – Ed).
Provisional findings from the competition watchdog were forcing specialists to consider a raft of possibilities likely to affect their future incomes and working environment.
We said incentives from private hospitals would be banned, practitioners would be forced to give patients a written list of proposed charges before treatment and fees would have to be displayed on websites.
‘Potentially thousands of consultants could face upheaval as their private hospitals changed ownership and information about the results of their work would be accessible for patient to compare.’
According to one observer, all this added up to ‘the most
important potential reform to the UK’s private healthcare market in decades.
Cosmetic adverts censured
The Independent Healthcare Advisory Services pledged to maintain its watchdog role on unacceptable advertising by cosmetic surgery providers.
It warned that it would not hesitate to take further complaints about clinics’ advertising to the Advertising Standards Authority if their advertisements did not meet current standards.
Private mixup warning
Would-be private GPs were blasted by a defence body for failing to clearly separate between NHS and private treatments.
The organisation intervened after finding:
Doctors billing for private treatments when patients thought they were being seen on the NHS;
A surge in inquiries from doctors asking if they could see their NHS patients privately;
GPs increasingly asking if they could prescribe privately for their NHS patients.
An adviser for the Medical and Dental Defence Union of Scotland said: ‘Doctors should keep a clear separation between NHS and
private treatment and must act openly and honestly to ensure there can be no perceived conflict of interest…
‘If the doctor believes a private assessment or treatment is required, then they are obliged to refer the patient and cannot make any financial gain from the patient – either directly or indirectly.’
NHS curbs mean more go private
The number of NHS GPs encouraging their patient to use private medical insurance – if they had it – was at record levels.
A Spire Healthcare survey found more than twice as many GPs doing so than two years previously.
The percentage had risen from 30% in 2011 to 63%.
Doctors’ plans to retire hit by interest rate
Senior doctors with substantial savings were facing new blows to their retirement projections following far-reaching decisions on interest rates.
Financial advisers warned those who were near to claiming their pensions to avoid making any hasty decisions.
Spending too much time on billing instead of patient care?
Let the UK’s number 1 provider, Civica Medical Billing & Collection do the hard work for you.
• Reduce bad debts to less than 0.5%
• Increase net income by up to 25%
• 24/7 online access to your data
• Enable faster payments through e-billing for insurers and patients
• Focus on your practice whilst our account managers manage it all for you
PROFILE OF A NOVEL PRIVATE PRACTICE
A general practice as they used to be
Harley Street GP
Dr Tony Banerjee (below) relates a heart-moving story about the setting up of his new private practice
WE ARE very excited about my new venture, HarleyDoc. We’ve had lots of great feedback and interest in what we’ve achieved so far.
I’m originally from Yorkshire, studying medicine in Leicester and have been based in London for over a decade now.
I’ve been in medicine for 25 years and a GP for 17 years. During this time, I’ve worked in every level of general practice in locum, salaried and partnership roles, both for the NHS and in private practice, as well as holding managerial roles throughout, such as chairman of a regional NHS Clinical Commissioning Group.
This gave me a solid understanding of how general practice works from the top down, as well as its strengths and inefficiencies.
I was diagnosed with advanced bowel cancer aged 23 while work-
ing as a junior doctor, so I have also experienced healthcare at its most acute and invasive as a patient as well as a doctor.
First-hand experience
This has given me a really good insight into the patient experience and journey, and I believe that, as a clinician, there is little more powerful than being able to sit with a patient at their most vulnerable and be able to share that you have also been sat where they are, experiencing what they’re going through.
Working in central London near Westminster, I started to build a private list of patients including MPs, dignitaries, sportspersons and business people.
Many of them use London as a base but have multiple residences. They often spend times in the Mediterranean or the Middle East,
and are unable to access the standard of healthcare they require.
I realised that the landscape of healthcare and our patient offering needed to adapt accordingly.
I started the building blocks of HarleyDoc pre-Covid, but, with lockdown, opportunities for advancing it were restricted. And besides that, it was all hands on deck at the NHS practices.
During the pandemic, I worked on the front line throughout in general practice and urgent care, and am proud to have worked with my primary care colleagues to help patients at this critical time.
I felt there was a real opportunity to re-invent NHS primary care at this stage, and that we reverted to type as lockdown was lifted. In an already-stretched system, I was unable to spend the time that my patients required and that their problems warranted.
We want our private clients to be able to access the same doctor every time that they need us, who already knows their history before they’ve contacted us
We reported on Dr Tony Banerjee’s HarleyDoc enterprise in July
Patients were complaining that there was a four-week waiting list to see me routinely and this was a system that was clearly not serving its clientele adequately.
My father is a retired GP and during his career, and certainly for the first few years of mine in general practice, patients had excellent access to their GP and they had the familiarity of seeing the same doctor who knew their history every time they accessed them.
This, in my opinion, has been lost in the primary care of recent years, with patients lucky to see the same doctor twice, which means often starting from scratch every time they attended the clinic.
This is where HarleyDoc is looking to disrupt the system. We want our private clients to be able to access the same doctor every time that they need us, who already knows their history before they’ve contacted us.
We offer phone consultations, video consultations, face-to-face consultations and home visits. Our pledge is that the client will be
contacted within three hours of their query reaching us, following an immediate acknowledgement.
We want this same level of individualised bespoke healthcare to follow our clients wherever they travel in the world and we source local pharmacies and specialists as required like a concierge medical service - the first of its kind in the world, to our knowledge.
Grow organically
I recognised that we needed to have a presence in the Mediterranean and the Middle East, and so set up businesses in Dubai and Monaco with consultation rooms available when we require them for our clients who live there or find themselves there for business or leisure.
We are looking to expand towards Asia, as there is a large demand from our clients for our services to cater for them in that region. We are taking our time to grow organically rather than rushing the process and losing the quality of the service.
Now we have got so many clinicians from multiple countries
interested in working with us – it is great to see other colleagues believing in and sharing our vision.
We have NHS and fully private hospital consultants in several specialties working with us already and I like to think of us as a ‘huband-spoke’ service with the hub being the patient’s named doctor, and the spokes being the specialists who we can call upon readily when necessary to offer their expertise.
Currently, we are also working on an education and training arm to the business, catering for developing clinical skills both locally in the UK but also remotely to developing nations looking to modernise their healthcare systems.
We are rapidly progressing as a company and look forward to modernising healthcare for our clients. We welcome clients joining HarleyDoc on a membership or ad hoc basis, and are busily building our database of generalists and specialists whose care our clients can access - almost becoming like a marketplace for health services.
BOOK YOUR DEMO
Are you happy with your current
software?
Maybe you're completely happy with the software you use to run your practice. Perhaps you have everything in one place, routine tasks are automated, and reporting is accurate and insightful. If so, stop reading now.
However, if you think the day to day running of your practice could be improved, we'd love the chance to demonstrate e-clinic to you.
The number one choice for private practice
Future-proof your practice and offer everything a modern patient expects:
> iPad compatibility
> Online booking & payments with fully integrated card processing
> Electronic consent & treatment forms
> Integrated drugs database & digital prescribing with direct delivery
> Fast & easy patient communications by email or text
BOOK YOUR FREE 30 MINUTE DEMO
PRIVATE MEDICAL INSURANCE ADVISERS
How insurance salesman
The Association of Medical Insurers and Intermediaries (amii) was established in 1998 as a trade association for independent medical insurance advisers and it now has over 135 members. Executive chairman David Middleton (right) explains more about the organisation and why consultants could benefit from its expertise
SINCE OUR association was founded 25 years ago, the landscape of amii has developed significantly. Our members are now made up of intermediaries, health and well-being organisations and insurers.
They provide advice on private medical insurance, health cash plans, group risk and protection products and general health and well-being matters, including occupational health services and employee assistance programmes.
We have been working in recent years to broaden the range of organisations we work with.
Since the Covid pandemic, patients have faced immense challenges when trying to access NHS diagnostic services and treatments, and this problem looks set to persist for some time to come.
Wealth of information
With record numbers of people stuck on NHS waiting lists and little prospect of accessing treatment such as hip and knee replacement surgery, the number of people joining private medical health insurance schemes and paying privately for the procedures they need has been on the rise.
There has also been an increase in companies recognising the benefits of offering health and wellbeing for their employees. This includes a growing recognition of the need to incorporate mental health care provisions and to recognise the health needs of women in the workplace.
We recently revamped the amii
website to improve the wealth of information available to consumers, companies and members and non-members of amii alike.
And we have also launched the amii Talking Health & Wellbeing podcast series, where I chat with leading figures in the healthcare industry who have an interesting story to tell or can provide guidance on tackling some of the current challenges society faces.
The feedback on this has been outstanding and we have some fascinating guests lined up for future episodes.
Changing landscape
As an association, we recognise that the health and well-being landscape is changing and we are committed to the importance of actively managing wellness before people fall ill, as well as the treatment of those with acute and chronic illness.
That is why we made the decision to expand our support for the health and well-being industry and look to recruit more new members operating in the field.
We recently welcomed organisations like HCA Healthcare to the amii family. HCA is the largest private healthcare provider in the world and one of the leading providers in the UK. The organisation is also the largest provider of robotic surgery in the independent sector, with a world-class network of over 30 facilities in London and Manchester.
It is great to see an internationally recognised healthcare pro -
salesman can help
vider join and, in doing so, recognise that the breadth and depth of amii now reaches far beyond health insurance.
HCA’s vice president of corporate sales, Soraya Chamberlain, praised amii’s ‘strong voice in our industry’ and believes the company has a valuable and influential
role to play in supporting intermediaries, insurers and corporates. So we are excited to work with it as members in the months ahead.
Attracting member organisations of the size and scale of HCA is a big coup for us and forms part of our vision to be the voice of the health and well-being industry.
Benefits of membership
Our membership now comprises of over 135 intermediary, health and well-being and insurer organisations, and it is this wide pool of expertise that has made the association the leading body for the health insurance industry.
amii is the only association which has 16 insurer members and all the organisations we support are reputable insurers.
We promote and maintain high standards of professional and ethical conduct among our members. All amii members are authorised and regulated by either the Prudential Regulatory Authority (PRA) or Financial Conduct Authority (FCA) to sell general insurance products.
We support initiatives to improve customer experience. For instance, we recently established a data transfer group, which enables the process of a patient or company transferring from one provider to another to be much more efficient.
By working with amii, consultants can increase their awareness of funding options for patients, enabling them to better advise those who come to them seeking treatment.
HOW CAN KNOWING ABOUT AMII HELP CONSULTANTS?
Some consultants are not aware of how patients fund their consultations or treatments.
While most treatments will be funded by an insurer, they do have to be pre-authorised by the insurer and it is important to know that this can be required at each stage of the process if the treatment/ investigation pathway changes.
There may even be cases where a self-funded patient has underestimated the cost of the treatment they have agreed to.
Consultants have a duty of care to protect patients in this process to ensure they avoid falling victim to hidden charges imposed on them either by their insurer or by underestimating the self-funded costs.
ANALYSIS OF MEDICO-LEGAL CLAIMS
Psychiatry claims under the spotlight
Clinical negligence claims pursued against MDU private psychiatrist members are analysed here by Dr Claire Wratten and Lee Lewis, who also offer tips on managing common risks
ACCORDING TO Mind, the mental health charity, approximately one-in-four people in the UK have mental health difficulties.
The Medical Defence Union (MDU) supports members with issues such as complaints, performance concerns, inquests and GMC investigations.
We also support members working in private practice who find themselves facing a clinical negligence claim.
A data analysis of MDU claims over a ten-year period showed that the most common reason for a patient bringing a claim against a psychiatrist related to prescribed medication, and the most implicated drugs were lithium, benzodiazepines, and antipsychotics.
Allegations from patients prescribed lithium often related to development of impaired renal function.
Claims arising from prescriptions of benzodiazepines related
either to addiction or problems with rapid detoxification.
The main other problems arising from prescribed drugs were sideeffects, including neuroleptic malignant syndrome.
Another common cause for a claim related to deliberate selfharm and suicide. Several allegations also focused on a failure to
recognise the patient was at risk of suicide or deliberate self-harm or that the patient was inadequately managed, often following multiple consultations.
Several high-value psychiatric claims involved patients attempting deliberate self-harm resulting in a significant brain injury and the requirement for lifetime care
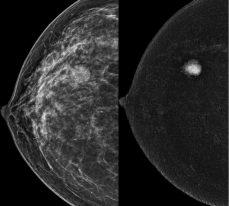
108 Harley Street introduces London's first private HOLOGIC Contrast Enhanced Mammography System, revolutionising breast cancer screening Mammography has long been the primary method for detecting breast cancer at an early, treatable stage However, with the advent of Contrast Enhanced Mammography (CEM), a specialised and advanced mammography test, breast imaging has reached new levels of precision and detail Our facility now offers this state-of-the-art technology, ensuring patients receive the highest quality breast cancer screening available
CEM goes beyond the capabilities of standard mammography by utilising a special dye (contrast) injected into the patient's arm, enhancing the visibility of breast tissue changes
CEM is recommended for several patient groups, including those who require assistance in resolving findings detected through conventional breast imaging, individuals needing pre-operative staging of breast cancer, patients with contraindications or intolerance to MRI (e g , pacemakers or claustrophobia), and patients over 40 who have suspected cancer based on ultrasound but normal mammography results Additionally, CEM can be employed as an alternative to MRI for women at an increased risk of developing breast cancer, such as those with dense breasts or a strong family history
To learn more about CEM or refer a CEM patient
provisions and associated expenses.
There can be a great number of factors which lead a patient to attempt to take their own life, therefore it can be difficult for the claimant to prove causation – in other words, to demonstrate that but for the alleged negligent act by
REASONS FOR A CLAIM
Following
the doctor, the patient would not have self-harmed or died by suicide.
In several cases, it was alleged the patient had been inappropriately detained in hospital for treatment.
Although all but two of these cases were successfully defended, it is important to ensure that all appropriate alternatives are considered and that there is appropriate input from all involved parties and that the reasons and discussions are thoroughly documented.
This is a complex area of the law, and it is always worth getting specialist advice if there is any doubt about detaining a patient.
Alleged misdiagnosis
In general, claims following an alleged misdiagnosis or inadequate assessment arose when it was alleged that a physical condition was misdiagnosed as a mental health issue, including subarachnoid haemorrhage, stroke disease and obstructive sleep apnoea.
The MDU also received claims where third parties were injured by the patient in the period following a section 12 assessment under the Mental Health Act.
Several claims concerned patient information being inappropriately passed to third parties or incorrect information being referred to in medico-legal reports. Examples included information being divulged about the patient to a family member without their consent and inaccurate statements being made in a medico-legal report which affected the court case for which the report was prepared.
Claims were also brought for alleged defamation following comments made, for example, in referral letters and reports.
Outcome of the cases
It can, of course, be very distressing to find out a patient is bringing a claim against you. If you face a claim from your private practice, you can be assured that the MDU’s expert claims handlers understand how stressful this is and the importance of mounting a robust defence of your position.
The MDU will defend claims whenever possible and we involve members in the conduct of their cases and will always seek your consent to settle a case.
If you face a claim from your private practice, you can be assured that the MDU’s expert claims handlers understand how stressful this is and the importance of mounting a robust defence of your position
A clinical negligence claim can either be settled by the defendant, with a payment of compensation being made to the claimant; or it can be discontinued, become statute barred (out of time) or a case can be won at trial by either party.
The vast majority of cases brought against psychiatrists were successfully defended, with damages payments only being made in under 10% of claims in this analysis.
However, even when a claim is successfully defended, considerable costs can be incurred by the MDU on behalf of the member in that defence process.
The purpose of compensation is to put the patient back in the position they would have been in had it not been for the problems caused by negligence.
Two claims settled over the period of analysis had damages paid of well over £1m and both
MANAGING RISKS
Claims involving psychiatrists are very diverse. But there are some common risk factors, which, if managed appropriately, can help to reduce risks.
These include:
Ensure that where there is a significant risk of suicide or self-harm, both the patient and the medication prescribed are appropriately reviewed.
Be aware of the current available guidance on the prescription of medications that you prescribe, including the British National Formulary and the National Institute for Health and Care Excellence (NICE).
If a patient’s care is being managed by several professionals, there should be clear agreement on the responsibility for the monitoring and treatment of that patient. Explain this to the patient and, where appropriate and with consent, share with families and carers.
Be prepared to refer patients for specialist treatment when necessary. This is in line with GMC requirements to ‘recognise and work within the limits of your competence’ (paragraph 14, Good Medical Practice). You should ensure that you have the appropriate qualifications, skills and experience for the care you are providing.
Have a system in place to review patients on long-term medication, and for ensuring any necessary monitoring is occurring.
Get specialist advice if there is any doubt about whether a patient’s detention is appropriate and lawful.
Clearly document your discussions with patients and family members.
If things go wrong, be open and honest with the patient by providing an apology, an explanation of what has happened and the short- and long-term effects of this. Get advice from the MDU if you believe the incident triggers the organisation’s duty of candour requirements.
related to prescription of benzodiazepines.
Limitation
A competent adult claimant can bring a claim for alleged medical negligence for up to three years from the date of the incident or the date of their knowledge of the alleged harm.
However, there is no time limit for a claimant who lacks capacity, and for children, the three-year time limit doesn’t commence until they reach 18. In Scotland, it’s 16.
In addition, the claimant may occasionally not be aware of the injury for some time after the events in question – for example, it can be many years following initiation of lithium therapy before renal impairment develops.
This means that a claim can arise may years after the psychiatrist was caring for the patient and this underlines the importance of
keeping detailed notes regarding clinical decision-making and advice given to patients.
Dr Claire Wratten is claims team manager and Lee Lewis is high-value claims handler at the MDU
Saving the planet and boosting care
Digital solutions, such as electronic health records and virtual consultations, offer promising avenues for creating sustainable healthcare systems while ensuring efficient and accessible patient care. Dr Robin Clark (right) reports
WHEN THE UK entered Covid-19 lockdown in March 2020, the demand for video consultations sky-rocketed almost overnight.
This is a really striking example of how the pandemic catalysed the already emerging trend towards digital health services and permanently changed people’s attitudes towards their healthcare access.
Digital health infrastructure has huge potential to enhance the patient experience and improve both population health and the work life of healthcare professionals.
Virtual care can reach more people than face-to-face care and is widely seen as more convenient.1 Many benefits of digitising healthcare, such as reducing the need for patient travel and electronically storing health records, are also reducing our impact on the planet.
Our health is directly linked to the health of our planet. It is impacted by:
Climate changes, such as heatwaves and floods;
Pollution, in the form of air, plastic, light and noise;
Natural habitats, which impact our well-being and vulnerability to infectious diseases.
Digital healthcare and planet health are seemingly then in a positive feedback loop, where using health technologies is reducing our environmental
➱ continued on page 24
impact, which is improving the health of the planet, which is enhancing people’s health.
Digitalisation and telehealth play a key role in our ambition to be a net zero, resilient health system and, more broadly, are important parts of our corporate strategy to transform our business.
Bupa is embracing digital solutions across its businesses – from dental practices to outpatient clinics and hospitals – connecting patients and healthcare professionals effectively and efficiently to provide the highest-quality sustainable care.
Digital platform
Bupa’s digital platform, Blua, was launched by our business in Spain and is now available for our UK customers.
The app can be used by our Spanish customers to remotely monitor their heart disease, obesity and to monitor pregnancy, reducing the need for patients to travel to hospitals and clinics.
Users can also access a digital prevention programme and record live tracking of their vital signs such as heart rate, breathing rates and blood pressure using their mobile phone camera, as well as having same-day access to virtual consultations with doctors. We’re exploring how we can introduce similar features for our UK customers.
Enhancing access to care and leveraging digital solutions that support prevention and wellbeing are widely regarded as helping to reduce healthcare resource consumption.
This data-led digital approach to healthcare is also allowing clinicians to diagnose and treat patients with real-time information, making for a precise and personalised experience that can further reduce the environmental impacts of healthcare by eradicating ineffective interventions.
In developing Blua, our Spanish business hasn’t underestimated the importance of bringing customers along on our sustainability journey. So now when a patient in Spain attends a video consultation – or downloads a medical report to the Blua app instead of visiting a clinic to collect results – an estimation of the avoided emissions is shared with the patient via the Bupa app.
3,662,352 medical reports digitally.
The Carbon Trust helped with this calculation of avoided emissions, which involved adding together the carbon savings associated with patient travel and document printing, while subtracting the emissions from video-conferencing.
Electronic health records
We hope to offer this function to our UK customers in time.
Shared learnings from our colleagues in our Spanish business, Sanitas, have shown that, in 2022, Bupa patients avoided over 8,000 net tonnes of CO2 – equivalent to powering 1,008 homes for a year2 – as a result of 771,002 video con sultations and downloading
Alongside digitising patient records, consent forms and health insurance policies in Blua in Spain, we’ve been piloting electronic medication administration records (eMAR) across care homes in the UK.
eMARs are electronic patient records that are used to document information about medications, often used on hand-held devices such as smartphones, rather than using a paper form.
At the moment, six Bupa care homes and one retirement village are using eMAR, and the current plan is to deliver eMAR across all care homes and villages before May 2024.
Alongside the reduction in our printing and paper use, eMAR will significantly reduce the time it takes to provide safe medication administration to residents, helping to improve their clinical outcomes.
Further afield, Bupa’s medical provision in Hong Kong, Quality HealthCare, is replacing physical films for X-ray, CT, MRI and PET scans with digital versions at all western medicine and diagnostics and imaging centres.
This operational change will save around ten tonnes of plastic films a year, the equivalent of around 400,000 plastic bottles.
Bupa’s digital platform, Blua, was launched by our business in Spain and is now available for our UK customers
Further digitalisation of health services is helping Bupa continue to reduce the impact on the planet, while also offering convenient, efficient and effective care to patients
Intra-oral scanners
In the UK and Spain, Bupa dental clinics have introduced intra-oral scanners to increase precision, efficiency and convenience.
These digital scanners produce none of the clinical waste of traditional dental impressions, which use plastic trays, alginate powder and the ‘forever chemical’ polyvinyl siloxane (PVS), which never breaks down and may have hormone-disrupting properties.
Patients are also saved from unnecessary travel when adjustments or recreations of moulds are required, reducing our emissions associated with travel.
Remote care
Bupa is offering a remote skin assessment service using a smartphone app that allows customers to send images of concerning moles and skin lesions for assessment by a qualified dermatologist.
Results are given within two working days, which compares very favourably to a traditional face-to-face care journey.
So far in 2023, our advisers have helped nearly 3,000 customers who have received a fast and convenient diagnosis by their clinician.
Because the patient can use the app without leaving their home, the environmental impact of their care is reduced by eliminating the need for travel and clinical resource consumption – such as electricity or personal protective equipment.
Looking to the future
Further digitalisation of health services is helping Bupa and other UK organisations, such as the NHS 3 and Ramsay Health Care, 4 continue to reduce the impact on the planet, while also offering convenient, efficient and effective care to patients.
Download the app and register online www.pharmacierge.com/register
mPrescribe® app allows you to prescribe flexibly without a laptop, for delivery to your patients nationwide
Decision-making on the role of digital solutions should always be clinically led and based on individual care needs, preferences and sustainability considerations. Ultimately, we see digital services as supporting, but not altogether replacing, the traditional, in-person provision of quality healthcare.
References
1. Advantages and limitations of virtual online consultations in a NHS acute trust: the VOCAL mixed-methods study. Southampton (UK): NIHR Journals Library; Jun 2018.
2. Greenhouse Gas Equivalencies Calculator. United States Environmental Protection Agency. June 2023.
3. Delivering a net zero NHS. Greener NHS. July 2023.
4. Impact Report 2022. Ramsay Health Care. July 2022.
Dr Robin Clark is medical director for Bupa Global and UK Insurance
Secretary Supported
and Consultant Reviews
Administrator access reduces workload for practitioners. mPrescribe® facilitates patient entry, status monitoring and preparation of prescriptions for mobile authorisation.
Clinical Governance
Co-founded and co-owned by leading private clinicians, our secure and encrypted technology is compliant with all GPhC, GDPR and e-Prescribing regulations.
“Wonderful, seamless, easy to use service.” Dr Catrin Bevan, London General Practice
“Intuitive and secure.” Dr Tim Wigmore, Consultant Anaesthetist and Intensivist
“Delivered the same day.... Outstanding!” Dr Elisa Astorri, Academic Physician Rheumatologist
“Go the extra mile.” Dr John O’Donohue, Consultant Gastroenterologist
“Consistent, efficient , friendly and responsive.” Dr Tim Ladbrooke, Courtfield Private Practice
Your views on setting
Independent Practitioner Today is running a survey with the Medical Defence Union to get consultants’ views on setting up or growing their private practice.
We would value hearing from readers currently undertaking both private and/or NHS work. If you could spare 5-10 minutes, we’d appreciate your answers to this survey.
In return, you can choose to enter a prize draw to win a £100 Amazon e-gift card.
Responses will be anonymised and the results of the survey published by Independent Practitioner Today, but no personal information will be passed on.
Thank you for your time completing this survey.
up in private practice
1. What position best describes your current role?
A) Consultant currently working in private practice. (Go to Q3).
B) Consultant looking to establish a private practice. (Go to Q2).
C) Other (please state).
2. What is the likelihood of you becoming a private practitioner in the next five years?
A) I am more likely to become one in the next five years.
B) I am less likely to become one in the next five years.
C) I am not sure whether I will become one or not.
3. What is the likelihood of you growing your private practice in the next 5 years?
A) Yes, I am likely to grow my private practice in the next five years.
B) No, my private practice is likely to remain a similar size over the next five years.
C) I am not sure whether or not my practice will grow over the next five years.
4. Do you still/intend to still undertake work for the NHS alongside your private practice work?
A) Yes.
B) No.
C) Not sure.
D) Do not undertake work for the NHS.
5. What was/is the motivation for undertaking private practice work? (Tick all that apply)
A) Better work/life balance.
B) A new challenge/experience.
C) Financial compensation.
D) Greater job satisfaction.
E) Desire to focus on a particular clinical area/further develop a specialist interest.
F) Other (please explain).
6. What do you feel are the challenges of becoming a private practitioner? (Tick all that apply)
A) Marketing yourself/your practice.
B) Lack of employee benefits due
to being self-employed – for example, sick pay, maternity/paternity pay etc.
C) Arranging indemnity cover for yourself/employees.
D) Managing patient data.
E) Patient satisfaction.
F) Growing demand for telemedicine appointments
G) Impact on work-life balance.
H) Other (please explain).
7. What challenges have you faced/anticipate when running a private practice? (Tick all that apply)
A) Running a business.
B) Protecting patient data.
C) Scheduling appointments.
D) Billing patients.
E) Navigating the Care Quality Commission (CQC) regulation requirements – in England only.
F) Dealing with patient complaints.
G) Complying with tax requirements.
H) Patient satisfaction.
I) Growing demand for telehealth appointments.
J) Other challenges (please explain).
8. What aspect of setting up in private practice would you like to learn more about? (Tick all that apply)
A) Professional/corporate indemnity.
B) Marketing your practice.
C) How to establish a private practice and ensure it stands out from the crowd.
D) Establishing a private practice while maintaining any existing NHS commitments .
F) Complying with CQC requirements.
G) Complying with the data protection obligations.
H) Financial planning, including tax, National Insurance and PAYE. I) Other (please explain).
9. Do you have any further comments about your experiences of setting up in private practice generally that you would like to share? [USE BOX BELOW]
If you would like to be entered into a prize draw for a chance to win one of two £100 Amazon vouchers, please leave your details here:
BILLING AND COLLECTION: MEDICO-LEGAL WORK
Medico-legal reports can be a valuable revenue stream if you manage the billing effectively. Simon Brignall (below) discusses some of the problems you may face with this work, including the importance of ensuring you devise terms and conditions
The devil is in the detail
THE COMPOSITION of revenue streams in a typical private practice can be varied and may change over time.
When they start out in private practice, many consultants opt for a clinical-based practice treating predominantly self-pay and insured patients.
The practice could also include embassy or NHS patients in a private hospital – often referred to as choose and book – depending on where it is located.
Diversification of revenue is beneficial to any business, as it helps mitigate any fluctuation in demand from one source just as a mixed portfolio of investments can help manage risk.
This portfolio approach can be accomplished in many ways and often may be as simple as adding a new practice location with a different patient demographic. For example, adding a central London location will likely increase your exposure to international self-pay and embassy patients.
Medico-legal work
One option consultants choose is medico-legal activity, but they can be put off because they often find the medical billing and credit control challenging.
So I thought it would help to focus on this sector this month, explaining what you need to know from a billing perspective if you are thinking of expanding into this area.
The medico-legal sector is extremely fragmented with thousands of solicitors working in this field either independently or as part of a group alongside the work coming from the medico-legal agencies.
This wide range of potential clients means you often need to manage a multitude of commercial relationships, so it is important to be able to standardise these where possible.
Terms and conditions
The most effective way of doing this is to have detailed terms and conditions (Ts&Cs) in place before any work is carried out. Your Ts&Cs should include your fee structure and payment terms.
Practices that do not have these in place can find the case they have been working on turns out to be on a ‘no win, no fee basis’,
which can mean they end up waiting years for their money.
Remember, problems around delayed/deferred payments will negatively impact the cash flow of the practice and will only become more of an issue if they are inadequately addressed.
It is important to note that when you raise an invoice, you create a tax liability, which means that until you collect the money owed, you are effectively paying to carry out this activity.
For larger medico-legal practices, which are required to charge VAT, the situation is even worse, as you would have had to pay the VAT to His Majesty’s Revenue and Customs every quarter – which just exacerbates the problem.
Ensure you have clear terms and conditions that are agreed by your client when they engage you. These should cover the following specific areas.
Fees
☛ How much do you want to charge for your standard medicolegal report? This should be based upon the length of time taken to review medical records, include any interview or examination of the client, including any dictation and preparation of documents.
You may prefer to quote an additional cost per hour to provide some flexibility for cases that take longer to review, particularly where there are a large amount of medical records or where the case is very complex.
☛ For court cases where you are required to attend, you should have a fee schedule per day. Please note that your fee should be for a minimum charge and not related to the amount of time you have to appear.
This is due to the impact on your schedule and your availability to do other work. You should also outline your fees for travelling expenses as well as any other costs you may incur.
☛ Supplementary work should also be quoted using an hourly rate. This is to cover any further reviews and additional work relating to the case. This work can then be invoiced using your hourly rate, and typically can be broken down into 15-minute increments.
☛ You need to outline your ‘did not attend’ (DNA) rules. These
Practices that do not have terms and conditions in place can find the case they have been working on turns out to be on a ‘no win, no fee basis’, which can mean they end up waiting years for their money
Access to up-to-date and accurate information about your aged debt is key, as this will allow you to police your problem payers.
Where there are issues with collecting payment from a particular solicitor/agency, then you can decide whether to take on other cases from the same company or you could end up making the problem worse.
cover cases where the patient does not attend without prior cancellation within a set time-frame or where your court appearance is cancelled within a given notice period.
Decide what your charges will be in these instances and make sure they are clear and transparent. Some legal practices have different time stipulations that may result in your fee being invoiced either in full or a percentage thereof, depending on what notice was provided.
Payments rules
You will need to decide what your standard payment terms are going to be for your medico-legal reports. These will need to be tailored to the sector that you are operating in and reflect what you are prepared to enforce. They can include penalty clauses for late payment. You should have different payment terms for any court appearance and these should also be applicable to any charges you enforce under your DNA policy.
Credit control
As in all aspects of medical billing, it is important to ensure you have a robust system to reconcile and chase outstanding invoices.
The most important step is to always make sure your fees and terms and conditions are accepted up front before taking on any case.
Once you have raised the invoice and it has been sent to your counterparty, then it needs to be followed up with a phone call to ensure it has been accepted and has been put on the solicitors/ agency system with the correct payment terms.
Your practice will need to ensure it has an effective system to routinely chase outstanding invoices to ensure payment is made in a timely manner.
You may ask them to settle any invoices in full before you take on any new business from them. At Civica Medical Billing and Collection, our comprehensive reporting dashboard provides you with access to an array of reporting tools to analyse your data and tailor your approach accordingly.
As your reputation and workload increases, you may choose to consider how you prioritise your availability and whom you work with based on many factors which will often include how quickly they pay.
Chasing outstanding money owed is time-consuming and is the hardest part of the administrative process. Many practices do not have adequate processes or infrastructure to do this effectively and can find the task intimidating. It is only through the routine application of a rigorous chase process that aged debt and bad debts are kept to a minimum and cash flow is optimised. Our tried and tested chase process ensures we have a bad debt rate of less than 0.5%.
Practices taking on medico-legal work often do not have time to effectively carry out this task or they find they lack the specific skill set. This is especially the case when medico-legal work is just one component of the many tasks managed by the practice team.
For most practices the best option is to use a professional billing company who have years of experience in this field. Ideally, this will be before you start doing medico-legal work. But if you have been in the sector for some time, have experienced some of the problems I have related here and feel you want to gain control over the situation, we would be happy to hear from you.
Simon Brignall is director of business development at Civica Medical Billing and Collection
WATCHDOG INSPECTIONS
investigated Prepare to be
The independent practitioner’s experience of the Care Quality Commission can be daunting. Solicitor Paul Ridout relates some experiences he has come across and gives useful advice to doctors who find themselves in the firing line
THE CARE Quality Commission (CQC) has the powers to inspect without warning or notice. It is courteous but not friendly.
It is entitled to view all books and records. Its inspectors must be given access to computers and patient information – doctors can use patient confidentiality as an excuse to refuse access.
The CQC will see its role as public protection. It is entitled to have access, to probe and to challenge.
It does not have to make appointments.
One practitioner was surprised to arrive at work to:
Find inspectors in his rooms;
Have postponement of the visit declined;
Be challenged to justify his business and medical practice.
We advised full co-operation –the CQC is entitled to behave in this way. Be careful and make notes and records of what transpires.
Another practitioner found their prescribing practice under challenge, stating ‘But that is my professional judgment; that is none of your business’.
Not so. The CQC is entitled to seek justification. If not satisfied, it may take enforcement action.
De-registration/enforcement
The CQC has a range of powers. It operates on relevant information; for example, patient complaints, staff whistle-blowing, concerns from pharmacists and GPs – particularly NHS GPs.
A senior and experienced consultant surgeon was surprised and infuriated to be asked to justify surgical intervention decisions.
This demand was by a CQC team without relevant experience. They act on their advice as to direct clinical judgements. The CQC expected detailed justifications in diagnosis procedures and aftercare.
Such challenges are rigorous. However intimidating, unpleasant and time-consuming this may be, the only safe response is careful and reflective explanation.
The CQC will scrutinise patient notes and criticise shortcomings. The privacy of the practitioner is not recognised.
Failure to co-operate; failure to justify a challenge to an inspector’s competence – these can all
A senior and experienced consultant surgeon was surprised and infuriated to be asked to justify surgical intervention decisions
lead to deregistration and the destruction of the practice.
Be careful! Do not ignore push back. And, where appropriate, recognise mistakes. Show the ability to reflect and learn, however irritating.
Conclusion
The CQC is an important force in medical practice. The law gives it an important role in public health care protection.
Be careful, recognise the role and work with the CQC, not against them.
Paul Ridout (below) is a solicitor and founder of Ridouts Professional Services Ltd, a law firm acting for health and social care providers, including doctors, and advises on regulatory matters affecting their business, including CQC inspection and enforcement
HOW THE CQC AFFECTS HOW YOU PRACTISE
The CQC regulates all medical practice –independent or NHS. It does not directly address the licence to practise, but it is a systems regulator of operations.
It works closely with the GMC, and adverse enforcement by the CQC will usually lead to fitnessto-practise concerns from the council.
Medical practice without CQC registration is a criminal offence. Before achieving registration, the CQC will expect applicants to demonstrate fitness to operate. This must be done by delivery or policies of business and professional management. Simply being licensed by the GMC is not sufficient.
Applicants must prepare policies. Those must detail every part of the proposed practice. They must be relevant to the individual practice.
The applicant must know and understand the policies. There will be an interview. The applicant must be prepared and demonstrate business competence.
Applicants have found this challenging because it is an extra level of compliance.
When patients say
A patient changes their mind and refuses the recommended treatment. Medicolegal experts Dr Lucy Gibberd (right, top) and Dr Emma Green (right) discuss some important points on dealing with the situation
Providing the patient is found to have capacity and fully understands the proposed treatment options, they can refuse to be treated and are free make what a medical professional may consider to be an unwise decision in relation to their treatment
said he did not want to go ahead unless the surgeon could guarantee he would ‘get it all out’.
The surgeon explained he could not make that guarantee and so the patient declined to go ahead with the surgery and opted for ‘close observation’ as an alternative.
When the cancer later became locally invasive and required majorly disfiguring surgery, the patient complained that his refusal of treatment was not fully informed, as he had not been aware of the possible consequences of refusing surgery.
World-class Diagnostics with rapid results
DOCTORS MAY think that when a patient has refused to undergo an operation or a treatment, their obligations finish there, but this is not the case.
We see complaints every year which arise after patients refused treatment.
The right to refuse treatment is fundamental in the ethics of modern medicine and in England and Wales the Mental Capacity Act 2005 is the legal basis on which a patient should be assessed as to their ability to decide.
Providing the patient is found to have capacity and fully understands the proposed treatment options, they can refuse to be treated and are free make what a medical professional may consider to be an unwise decision in relation to their treatment.
If the clinician considers that the patient may be lacking in capacity, then this must be clarified. If the patient lacks capacity, other options for consent to treatment may need to be considered.
Case study
Let us consider this case where a patient withdrew consent:
Mr A was a 72-year-old man on immunosuppressive treatment following transplant surgery.
He presented with a biopsyproven, histologically aggressive, squamous cell carcinoma near the bridge of his nose. When he presented for a wide excision, the lesion was not visible to the naked eye, as it had been largely removed by the biopsy.
This patient questioned why further surgery was necessary and
The issue in this case is that the patient had initially agreed to the wide excision and only refused to proceed during a discussion in the pre-operative area on the day of surgery.
He was having other skin surgeries that day and the other surgeries went ahead. Because the discussion occurred in the pre-op area, it was not well documented and there was nothing in the notes recording that the patient had been told about the possible consequences of not going ahead with surgery.
The surgeon in this case clearly could not proceed with the recommended surgery, in the face of the patient’s withdrawal of consent –but what could he have done to avoid a subsequent complaint?
Poorly documented
It is not uncommon for conversations that occur in the pre-op area to be poorly documented. Often the patient is being seen in between cases in the theatre, there may be no facilities to dictate or record a file note, and it may not be obvious where such conversations should be recorded.
There may also be concerns about the patient’s competence to make a reasoned decision in this situation, particularly if they have been given a premed.
If a patient refuses treatment in this situation, it is probably better to arrange to meet with them later and have a full, documented discussion about the possible consequences of declining the treatment.
If the patient does not wish to agree to or attend such a follow-up meeting, then a letter to the patient and GP recording the ➱ continued on page 34
Based in the heart of Marylebone, King Edward VII’s Hospital Diagnostic & Imaging Centre is equipped with the most advanced technology, equipment and a wealth of expertise. Our specialist team of radiologists and radiographers are all multi-trained in all modalities and experts in their fields, supported by a highly-qualified technical, administrative and support team.
We pride ourselves in making the patient journey as smooth and hassle-free as possible.
Imaging services includes:
• 3T MRI Siemens Vida Scanner
• 1.5T MRI Siemens Magnatom
• Aquilion One Prisom Canon CT with Cardiac CT
• Siemens Somatom Definition AS CT Scanner
For more information, to request referral forms or to make an appointment call 020 7467 4317, email imagingsecretary@kingedwardvii.co.uk or visit kingedwardvii.co.uk
When a patient is refusing a recommended treatment, it is even more important that the conversation is carefully documented
discussion, the matters set out below and the offer of a follow-up consultation should be sent.
The GMC guidance Decision Making and Consent is clear on the information that should be shared with a patient as part of the dialogue to enable them to decide. It is also clear with regards to the non-disclosure of information.
‘You should not withhold information a patient needs to decide for any other reason, including if someone close to the patient asks you to. In very exceptional circumstances, you may feel that sharing information with a patient would cause them serious harm and, if so, it may be appropriate to withhold it.
Limited exception
‘In this context, “serious harm” means more than that the patient might become upset, decide to refuse treatment or choose an alternative. This is a limited exception and you should seek legal advice if you are considering withholding information from a patient.’
Doctors should familiarise themselves with the case of Montgomery v Lanarkshire Health Board [2015] and understand that the consent process should be patient-centred and focus on information relevant to that individual.
Increasingly, doctors are now aware that when they are obtaining consent from a patient to have a procedure or treatment, they must carefully record the possible complications which have been explained to the patient.
However, when a patient is refusing a recommended treatment, it is even more important that the conversation is carefully documented.
If you are facing the dilemma regarding a patient refusing treatment, contact your medical defence organisation as soon as possible for advice and support.
See the box on the right for the key points to remember in this situation.
Dr Lucy Gibberd and Dr Emma Green are medico-legal consultants at Medical Protection
KEY POINTS TO REMEMBER
1
There should be clear written documentation that the patient has been offered a treatment but has declined it.
2 It should be documented that the possible consequences of declining the treatment have been explained to the patient, including the worst possible outcome.
3 Alternative treatments should be discussed, and the pros and cons of these treatments should be discussed and documented.
4 A follow-up appointment should be arranged to give the patient a chance to reconsider and to again discuss other treatment options.
5 If possible, it is helpful if a relative or support person accompanies the patient to the follow-up appointment, both to support the patient, but also so the family is aware of the choices the patient has been offered.
6
There is no legal requirement for the patient to sign a document saying they have refused treatment. In fact, good contemporaneous notes, where it is clear the patient has been warned of the possible outcome of declining treatment, are probably better than a signed document where this detail has not been clearly laid out.
7 It should be made clear to the patient that, if they were to change their mind in the future and wish to undertake the treatment, whether that may be possible and, if so, what pathway the patient would follow to achieve this.
8 Giving the patient written information about the proposed treatment is always helpful and exactly what has been provided should be documented in the notes.
9 If there are any concerns that the patient may not be competent to consent or decline treatment, a formal competence assessment may be advisable.
...aaand breathe
Choose protection that goes above and beyond
Relax. Our experts are always there, ready to provide you with support when you need us.
From medicolegal experts to case handlers, everything you need to help to protect your career, your reputation, and your finances is under one roof. This all-inclusive support helps take the stress away.
For just £549, consultants working in the NHS can feel safe in the support membership brings. We also offer competitive, tailored prices for consultants working in Private Practice.
Innovators improve care and efficiency
In our July-August digital issue, Rob McGough (right) highlighted the move to value-based healthcare. Here he gives examples of the adoption of this approach in the private healthcare sector
The Cleveland Clinic, London. The 2008 transformation programme of the US-based hospital group re-organised its structure around patient groups/ disease areas, rather than tradition medical disciplines
THE ADOPTION of value-based healthcare (VBH) by independent doctors can offer numerous advantages. However, its adoption, in the UK certainly and to an extent internationally also, is currently patchy.
I have set out below examples from a broad geographic spectrum which include elements of valuebased approaches.
They demonstrate through a range of initiatives, both with private and public-sector practitioners, that advantages can flow from the development of valuebased healthcare:
➲The Martini Klinik in Hamburg, Germany , specialises in treating patients with prostate cancer. It stands out as a prime example of an organisation that has successfully embraced the principles of value-based healthcare, prioritising patient outcomes and clinical excellence while effectively managing costs.
A key aspect that distinguishes the Martini Klinik is its patientcentred approach. By focusing on outcomes that matter most to patients, such as quality of life and functional improvement, they align care with patients’ goals and preferences.
This approach not only enhances patient satisfaction but also contributes to better clinical outcomes. Through clear measurement and monitoring of patientreported outcomes, the hospital can also continually evaluate and improve its performance, ensuring that resources are allocated to interventions that yield the greatest benefit.
Optimise cost-effectiveness
The Martini Klinik has made substantial efforts to optimise cost-effectiveness without compromising on quality.
By implementing evidencebased practices and fostering a culture of innovation, the hospital has taken steps to streamline processes, reduce unnecessary tests or procedures and minimise waste. This judicious resource allocation, coupled with a focus on prevention and early intervention, has resulted in improved patient outcomes and reduced healthcare costs.
It has also embraced greater col-
laboration and co-ordination among its multidisciplinary teams, fostering shared decisionmaking and interdisciplinary care.
This integrated approach promotes seamless transitions between different phases of care, reducing fragmentation and improving efficiency.
➲
The US-based Cleveland Clinic has a reputation as an organisation that embraces valuebased healthcare to deliver patient outcomes and clinical excellence in a cost-effective manner.
Its 2008 transformation programme re-organised its structure around patient groups/disease areas, rather than traditional medical disciplines.
Doing so enabled a more patient-centred approach, taking a more holistic view of their treatment and the costs involved in each element of this.
The Cleveland Clinic has now expanded into the UK, having opened in London, where it has a number of areas which focus on value-based principles such as:
A multidisciplinary approach;
Standardised care protocols;
Measurement of patient outcomes to optimise resource utilisation and enhance overall quality of care.
➲ Santeon Group, in the Netherlands , is a consortium of seven independent hospitals which formed a co-operative to work together on quality improvements.
These focused on achieving better outcomes for patients, reporting transparently between them on what was being achieved and, in time, expanding the programme to 16 improvement programs.
It adopted an approach consisting of four elements:
1 A multidisciplinary team to define the right metrics to improve outcomes;
2
To share and learn internally, and then initiate a strict and simultaneous cadence of improvement cycles within the member hospitals;
3
After a few internal cycles to validate and stabilise the process and data, share results externally to accelerate improvements;
By implementing evidence-based practices and fostering a culture of innovation, the hospital has taken steps to streamline processes, reduce unnecessary tests or procedures and minimise waste
Rob McGough explained the benefits of value-based healthcare in our previous issue
WHAT VBH CAN ACHIEVE
The evidence from the adoption of value-based healthcare approaches within the UK and internationally is that it can provide significant advantages for independent practitioners focused on delivering better patient outcomes.
By embracing patient-centric care, enhancing care co-ordination, emphasising prevention and wellness, aligning with value-based reimbursement, leveraging datadriven decision-making and improving professional satisfaction, independent practitioners can drive positive changes to the healthcare system while providing highquality care to their patients
4
Engage with patients and payers to move toward value-based contracting.
Through the focus on value and transparency as its strategy, Santeon achieved reductions of nearly 30% in unnecessary inpatient stays and up to 74% in the rate of re-operation due to complications in breast cancer patients in a year and a half.
➲ Lambeth, London. A contractual alliance was formed between mental health and local public health/council providers and payers – both NHS and independent – across a borough in London.
The aim was to focus on patientcentred outcomes and value-based rewards and move away from an activity-based remuneration system.
This solution included gamechanging performance incentives for where providers innovated and improved the outcomes from the services in a new and significant way.
➲ London Medical employs a multidisciplinary approach to providing tailored personal care to meet patients’ requirements, ensuring quality care through incorporating the most up-to-date clinical practices and techniques.
➲ OneWelbeck brought together US and UK specialists to provide truly patient-centred care in one place, through situating all specialists in one place and ensuring a seamless patient experience, with consultants collaborating closely together and ensuring the application of global best practice.
And there are generally more, quality registries – clinician-led organisations which collect comprehensive data on health outcomes in patient populations experiencing the same conditions or who have had the same procedures.
These registries, used optimally, both track outcomes and serve as a basis for clinicians to work together to drive improvements and innovation in clinical practice.
Rob McGough is a partner at Hill Dickinson LLP
Avoid falling out with
Partnerships in private practice – be it through groups of consultants or GPs – have been growing over the last 15 years. And with them has come a rise in disputes.
Partnership dispute expert Ross Clark (right) looks at the main causes of disagreements, the importance of a good partnership deed, the three principal expulsion provisions and expulsion process, and what can be done to safeguard your partnership and avoid a dispute escalating
with your partners
PARTNERSHIP DISPUTES are often sensitive, time-consuming, complex and and costly. They are stressful and destabilising for those involved because those people have often been in close professional relationships for many years.
It’s best to avoid a dispute by taking pro-active steps where possible. Partnership disputes can arise for many reasons, but the most common I deal with in turn below.
Performance issues
If a partner only committed a clear and substantial breach of his or her duties, expulsion would be easy. But this is rarely the case and, instead, it is usually a feeling that is hard to define that leads partners to decide they no longer wish to continue with a colleague.
We often hear opaque phrases such as ‘their heart is not in the practice anymore’ and ‘they’re not pulling their weight’.
In the absence of a binding ‘without cause’ expulsion provision – explained below – finding grounds to expel can be difficult. However, failing to address these concerns early results in a slow and painful escalation of the issues and associated stress and frustration.
Behavioural issues
As in life, members of a partnership are diverse individuals whose differences can manifest in attitudes or behaviours that the other partners find increasingly difficult to accept. This can be enhanced where a partner has a condition, such as autism, that leads to certain behaviours that can be misunderstood.
That can be difficult to navigate, as there is a distinction between behaviours and personalities that simply clash with others and behaviours which affect performance and cause problems with patients and staff.
The stress of running a practice while a partner is absent for a long period, and the difficulty of addressing the sensitive issue of retiring an ill partner, is one of the most common causes of disputes
Addiction
We have seen a marked increase in disputes based on addiction, principally alcohol and drugs, in the past few years. Addiction can affect a partner’s personality, –though some hide it well – as well as their ability to perform their duties.
Surprisingly, the addiction itself is not usually the issue. We acted for a partnership in the expulsion of a partner who, when pressed to explain his erratic and unusual behaviour, confessed he had been taking cocaine for over two years.
The addiction itself was not the reason the partners lost faith and wanted to expel him, but that he had hidden it despite their repeated expressions of concern.
It was this breach of trust and confidence that led them to their decision, and had he disclosed his addiction earlier, they would have supported him in his recovery and continued the partnership.
Long-term absence
Long-term illness is perhaps a surprising basis for a dispute and one that usually causes real distress and difficulty, as partners are inherently altruistic and want to support each other in difficult times.
However, the stress associated with running a practice while a partner is absent for a long period, and the difficulty of addressing ➱ continued on page 40
HOW CAN YOU AVOID A DISPUTE?
So how can independent practitioners in a partnership avoid or mitigate the effects of a dispute?
The best defence is an up-todate and binding partnership deed that includes:
A mechanism to address the main causes of disputes and to try and resolve them early. This could include processes to address performance or behavioural issues, such as regular performance reviews and actionable improvements; progress reports; and a clear escalation and disciplinary process.
’With cause’ compulsory retirement provisions that link to the performance review and disciplinary procedures, giving an ultimate right of expulsion if the issues are not resolved.
‘Without cause’ expulsion provisions. However, if a performance review procedure is in place and being followed, partners can be accused of not acting in good faith if they expel under the ‘without cause’ provision.
the sensitive issue of retiring an ill partner, is one of the most common causes of disputes.
The importance of a partnership deed
The Partnership Act 1890 lays down key principles that will apply to a partnership, except to the extent that the partners agree otherwise. These include:
All partners are entitled to share equally in capital and profits;
No person can be introduced as a partner without the consent of all partners;
Matters are to be determined by a simple majority decision;
Any partner may terminate the partnership at any time simply by giving notice to the other partners;
A partner cannot be expelled from the partnership. Instead, the partnership must be wound up.
The last two of these are particularly concerning, as where there is a ‘partnership at will’ – that is to say, there is no partnership deed in place – any partner can dissolve the partnership upon giving notice, which can be served and take effect immediately.
Given that the other partners have no right to expel them, the partner in a dispute has a significant negotiating leverage.
However, a partnership deed can replace these provisions. Accordingly, it is vital that partnerships of independent practitioners have a robust partnership deed in place, ensuring it includes provisions to address disputes.
Importantly, a new deed – or a deed of adherence – should be signed by all partners each time a new partner is admitted, effectively creating a new partnership.
Without this, the existing terms may not apply and though it can be argued they were adopted by implication, this is fertile ground for dispute.
The three main expulsion provisions
A well drafted partnership deed contains three separate clauses to permit the compulsory retirement or expulsion of a partner if a dispute cannot be resolved:
1
Long-term sickness
This enables the partners to compulsorily retire a partner who has been on long-term sickness. Typically, this applies when a partner has been absent for a significant period; for example, a period of 12 consecutive months or a cumulative absence of 12 months in any 36-month period.
2
With cause expulsion
This permits the immediate expulsion of a partner due to a material breach of the partnership deed, a criminal conviction, misconduct seriously and adversely affecting the practice, being struck off by the GMC or breaches of the ethics of the medical profession, and the like.
However, many of these clauses are subjective and can therefore be contested. For example, what counts as ‘misconduct seriously and adversely affecting the practice’? Have they been found guilty? If so, by whom and how was that judgment made? And so on.
The burden of proof lies with the expelling partners and they need to establish clear evidence to substantiate the basis for the expulsion.
3
Without cause – or ‘green socks’ – expulsion
This happens when the other partners simply decide they no longer wish to continue in partnership with the relevant partner.
So there is no need to establish a cause for the expulsion, which makes it difficult to contest, subject to the duty of good faith and following the correct process – see below.
The simplicity of this clause can be concerning, but we always recommend including it in contrast with the difficulty and burden of a ‘with cause’ expulsion.
It is commonly referred to as a ‘green socks clause’ due to a popular myth that a partner was expelled for no other reason than he always wore fluorescent green socks to work and this drove his partners mad!
The duty of good faith
Partners are also subject to several fiduciary duties, the principal one being that each partner must always act in the utmost good faith to his or her partners. This applies in every dealing between partners, but particularly where there is a dispute. It does not prevent addressing issues with or expelling a partner, but ensures a fair process.
The expulsion process
It is vital to comply with any dispute resolution or expulsion processes set out in the partnership deed.
Expulsion provisions usually allow the partner concerned to make his case before a final decision is made. The other partners must take care not to appear to
prejudge their decision, as any evidence to this effect can cause the process to be contested for a breach of the duty of good faith.
We dealt with a good example of this recently. A partner had been arrested by the police, but not charged, for misfeasance in a public office – a misuse or abuse of power or authority – on the basis that he had had a relationship with a (possibly vulnerable) patient at a previous practice.
Though he expressed his innocence to his partners, they expelled him from the practice.
During our review of the partnership agreement, we found good grounds for expulsion, should the allegation be substantiated, as such a relationship is clearly prohibited by the GMC’s Good Medical Practice guidance.
However, we were able to challenge the expulsion on these following grounds:
The partners had prejudged his guilt and had not awaited the outcome of the police investigation. The police subsequently confirmed that the allegation had been withdrawn and no further action would be taken.
They handled the expulsion process without legal advice and failed to comply with their partnership deed. They stated loss of trust and confidence as their reasons for expulsion, but these were not specific grounds for expulsion in the ‘with cause’ provisions of the deed.
The deed also required a right to appeal before final judgment, but they gave him notice of the appeal meeting at the same time they served notice of expulsion on him.
We obtained a significant settlement for our client because of his wrongful expulsion. But the partners could have avoided this had they followed the correct process.
Ross Clark is a partner and specialist in independent practitioner work at Hempsons solicitors and specialises in partnership dispute work
RETAIN THESE KEY CONSIDERATIONS
Remember the risk of being a ‘partnership at will’, as this gives a partner the power to dissolve a partnership without notice if a dispute arises.
Whatever you do, don’t ignore the underlying causes of a concern or hope that it will simply disappear or resolve itself in time. Even with a binding partnership agreement, ensure you get legal advice as soon as the possibility of a dispute arises.
Our primary care law experts can advise you on the key issues and best approach to resolve the dispute as quickly and painlessly as possible in the circumstances.
Even if the result is a partner leaving the partnership on agreed terms, avoiding the need for a forced exit, this is significantly easier, cheaper and less stressful for everyone.
Free legal advice for Independent Practitioner Today readers
Independent Practitioner Today has joined forces with leading healthcare lawyers Hempsons to offer readers a free legal advice service.
We aim to help you navigate the ever more complex legal and regulatory issues involved in running and developing your private practice – and your lives.
Hempsons’ specialist lawyers have a long track-record of advising doctors – and an unrivalled understanding of the healthcare system as a whole.
Call Hempsons on 020 7839 0278 between 9am and 5pm Monday to Friday for your ten minutes of free legal advice.
Advice is available on:
Business structures (including partnerships) Commercial contracts
Disputes and litigation
HR/employment Premises
Regulatory requirements and investigations
Remember to stay in balance
Balanced portfolios are far from dead. Dr Benjamin Holdsworth on why they remain a valuable protector against inflation
LEGEND HAS it that, in 1895 while in London, the novelist Mark Twain, who had been feeling a little poorly, discovered that a journalist had written his obituary and quipped: ‘The reports of my death are greatly exaggerated’.
In the past few years, obituaries for a traditional ‘balanced’ portfolio of, say, 60% equity, 40% bonds have been written by several journalists and fund managers. We think that such a portfolio continues to be alive and kicking.
Good investing is grounded in three things:
1
Using investment logic to think clearly about what one puts into a portfolio;
2
Using empirical insights to inform us of general longerterm characteristics of assets and how they work together in a portfolio – and the shorter-term exceptions to these generalities;
3
The fortitude to stick with a sensible portfolio strategy through these shorter-term, trying periods. A portfolio mix of bonds and equities balances the potentially severe downside falls in equity markets by owning far less volatile, good-quality bonds that will not fall as far, if they do fall at all. There is a general expectation that at times of severe equity market trauma, what is known as
‘scared money’ – that is to say, those who are risk-averse – will move into high-quality bond, pushing yields down and bond prices up.
There is a see-saw effect between yields and prices. That is often but not always the case as 2022 and 1994 demonstrated.
It is certainly fair to say that the past five-year period has been tough for 60/40 balanced portfolios, given that it included the global pandemic, the war in Ukraine, a rapid end to the era of low nominal and negative real interest rates, the highest inflation in 40 years in the UK and a downturn in global equity markets in 2022.
Even so, it delivered a return that more or less matched inflation over this period, which should be regarded as a good outcome.
Delivered growth
Having the patience to stick with an investment strategy over the longer term is really important
Data shows us that this structure has delivered growth of purchasing power in the vast majority of five-year horizons and beyond. The longer one holds, the more consistent returns become.
Compare this to the 1970s, which saw a decade of rampant inflation – up an alarming 240% cumulatively from 1970 to 1979.
Five-year, after-inflation returns for a 60/40 balanced portfolio from 1970 to 1975 were, perhaps not surprisingly, negative. Yet investors who stuck with it during this very difficult period ended up with positive real returns after 15 years, increasing purchasing power by around 50%.
Over the same period, holders of cash would have turned £100 into £85 of purchasing power. More proof if we needed it that investing is a long-term game.
From 1970 to 2022, the 60/40 balanced structure doubled an investor’s purchasing power every 15 years, on average.
Recency bias
Press articles are often influenced by recency bias, which encourages investors to make portfolio decisions based on recent events.
For example, the spectacular return of commodity futures in 2021-2022 hides their material underperformance compared to global equity assets over the longer-term.
Yet to include them in a portfolio, after a bout of strong shortterm performance, fails the investment logic and empirical evidence tests.
Useful balance
Investment logic still suggests that shorter-dated, high-quality bonds will remain a useful balance to extreme equity markets, if and when they occur, providing strong downside protection.
At market extremes, scared money will still flow to these assets. Bonds are now yielding substantially higher yields today than 18 months ago, providing more return and a greater buffer against any future yield rises.
Empirical evidence suggests that bonds are often, but not always, negatively correlated to equities –that is to say, they move in the opposite direction.
It also suggests that markets work pretty well and trying to guess which asset class will do well this or next year is well-nigh impossible.
As such, having the patience to stick with an investment strategy over the longer term is really important.
The last five years may not have been spectacular, but protecting an investor’s purchasing power from inflation over this difficult and inflationary period suggests that balanced portfolios are alive and well, despite the headwinds faced.
Dr Benjamin Holdsworth (right) is a director of Cavendish Medical, specialist financial planners helping consultants in private practice and the NHS
The content of this article is for information only and must not be considered as financial advice. Cavendish Medical always recommends that you seek independent financial advice before making any financial decisions.
Levels, bases of and reliefs from taxation may be subject to change and their value depends on the individual circumstances of the investor. The value of investments and the income from them can fluctuate and investors may get back less than the amount invested.
Boon of co-operation
A long-awaited Government report from its ‘elective recovery taskforce’ has set the ball rolling on new partnerships between the private healthcare sector and NHS. Taskforce member David Hare reports
INDEPENDENT PRACTITIONER
Today readers will know that establishing co-operation between the NHS and the private sector has been a rather long-running project, but let’s recap how we got here and then talk about some of the implications.
The ‘elective recovery taskforce’ first convened at the end of last year and I, along with colleagues from the independent sector, the NHS, Government and a large range of other stakeholders including patient groups were involved as members.
Our objective was to try and establish a programme of shared ambitions and alight on ways we could do more to harness the capital, capacity and capability of the independent sector to tackle the growing NHS waiting lists.
Some content of the taskforce report and its recommendations will undoubtedly be familiar to those blessed with a longer mem-
ory going back to the Blair reforms of the 2000s and some of the announcements and commitments made earlier this year.
An interesting point about how this work has unfolded over the past few months has been that rather than save all the big announcements to the end, the process has been more iterative –for example, the Prime Minister’s announcement on patient choice at the end of May, of which more below.
When we first embarked on this process, there were four strategic issues we saw as key priorities. They either needed to be further embedded, firmed up or highlighted for attention, both inside and outside the taskforce process:
1 Payment by results. We felt there needed to be a return to a method of payment by elective activity – both for NHS and independent providers – to ensure the NHS and independent sector
were being incentivised appropriately to treat as many patients as possible, as quickly as possible.
2 Patient choice. We and patient groups knew that patients were simply not aware of their rights to choose how and where they could receive their NHS care and there were concerns that signposting to the independent sector was not effective or not happening.
3
Procurement/the marketplace. How could the procurement landscape be improved to ensure that the playing field is level, that independent providers can access the market and that decision-making is transparent and fair?
4
Diagnostic capability and capacity. How could we boost utilisation of the significant opportunities presented by the private sector to deliver additional diagnostic capacity?
The taskforce had its last formal
meeting in March and, with a draft report and recommendations in place, it was clear on a number of key areas. In the intervening months, we have seen some encouraging progress.
So how are we progressing in those key areas?
1 Payment by results
Following conversations we held along with NHS England (NHSE) and the Department of Health and Social Care, the NHS Payment Scheme for 2023-24 saw the re-introduction of payment by results for elective activity for both the independent sector and NHS providers.
We feel this is definite progress in terms of reducing financial blockers to the movement of elective activity between providers –including independent providers.
2
Patient choice
At the end of May, Prime Minister Rishi Sunak personally fronted a significant announcement saying he wanted to make it much easier for patients to choose where they receive their NHS care and that improvements to the NHS app would be made, along with a public awareness campaign. This in itself is significant – to have the Premier’s personal commitment in such a clear and explicit way was, I think, both welcome and unusual.
He was clear in his support, saying: ‘Currently, just one-in-ten patients make a choice about where they receive care. We want to change that by helping the NHS to offer patients a real choice while also giving patients the information they need to decide.’
The PM added: ‘Our aim is to create an NHS built around patients, where everyone has more control over the care they receive, wherever they live or whatever their health needs are.’
The idea is that patients should, either via the NHS or via their
referring clinician – usually the GP – be receiving a minimum of five choices of options where they can receive their care, including those in the independent sector.
3
Procurement/Provider Selection Regime
A few weeks ago, following a consultation we responded to, the Government announced the Provider Selection Regime.This is an important set of rules to support fair play.
It now sets out an approach we think is positive for all concerned and certainly much better than the initial consultative proposals.
One of the most significant changes we believe is the move to establish independent oversight to resolve complaints, which will help bring transparency and consistency to decision-making.
There will be two independent panels – one relating to choice issues and one for procurement issues – but operating as one. This is a positive step because, by ensuring transparency and consistency in decision-making, it will help give patients and taxpayers maxi-
mum confidence about the decisions made on their behalf. There is more for us to do to ensure guidance is issued and that providers are well equipped to work constructively with the NHS under the new rules, and that there is a good wider understanding of how this will all work in practice. But, again, we see this as a very positive step.
4
Diagnostic capability and capacity
As part of the announcement around the report, we were pleased to see the commitment to opening further independent sector-led community diagnostic centres (CDCs). However, we believe this really can and should be dialled up significantly.
CDCs are undoubtedly a key piece of the jigsaw. We know millions of people await diagnostic appointments, tests and scans. The principle of providing easily accessible capacity, in convenient locations and, crucially, away from hospital sites to shield this activity from the urgent and emergency pathway, seems spot-on.
We feel this is still an area of huge untapped potential and makes big financial sense. Why would we not want to lever in private sector capital to actually build the facilities, rather than fund them from NHS budgets?
It is also really important that we are seeing CDCs as the route to additional capacity, not just moving around activity which would already have been undertaken.
We have made some great progress. The idea of a taskforce, set up directly by the Prime Minister with the explicit purpose of finding ways to maximise the contribution of the independent sector in tackling NHS backlogs, would have seemed out of the question not too long ago.
Lots of the work done in the past few months has definitely been steps in the right direction. It is always easy to say we could do more, go further, move faster.
But reflecting on the historically polarised and often hysterical debate that usually surrounds private healthcare’s role in the NHS, it is no mean feat to be in a place where both Conservatives and
Labour leaderships can see the value of the independent sector. From a private healthcare perspective, the more that patients get exposure, familiarity and experience of the independent sector, it can only be a good thing.
Our research at the Independent Healthcare Providers Network shows that many patients, once they have experienced the quality and safety of independent sector care, feel favourably about it. This may lead to longer-term choices about going private in the future.
People feel that the independent sector can help them and we could be seeing the beginning of a significant behavioural shift, with people feeling it is perfectly normal and sensible to use private healthcare when they need it in addition to, or separate from, their NHS care.
David Hare (right) is chief executive of the Independent Healthcare Providers Network (IHPN)
When the time comes to retire and perhaps close your private practice, there are some important issues to consider. Dr Kathryn Leask (right) highlights what to be aware of
Dilemma 1
What must I do on retirement?
QI am a private consultant who is looking to retire and close my private practice. What issues should I consider as I begin this process?
AYour primary concern is to your patients, who will need to know your plans as soon as possible to discuss their ongoing care.
For these patients, you will need to discuss the options with them and involve them in any decisionmaking.
This may include referring them on to another colleague in private practice. In Delegation and Referral
Duties on closing up shop
(2013), the GMC says you should explain to the patient that you plan to transfer their care and pass on the relevant information about their condition and history.
Make sure the patient knows who will be responsible for their future care or treatment. The patient will also need to know that, in referring them on, you will be disclosing confidential information and that without that disclosure, referral on is not possible.
As a private practitioner, you will collect and hold information about patients and will therefore need to be registered as a data controller with the Information Commissioner’s Office. This is a statutory duty.
Even after closing the practice, as long as you hold information, you will need to be able to fulfil your duties as a data controller.
These duties include responding to a Subject Access Request – that is a request for access to the notes you hold about a patient. The request could be made for a number of reasons, including clinical negligence claims.
Legal responsibility
You will therefore need to safely retain your patients’ records. This is a legal responsibility under Principle 7 of the Date Protection Act. The Department of Health publishes an NHS Code of Practice for Records Management, part 2 of which lists the retention schedules.
Although, as a private practitioner, you are working outside the NHS and are therefore technically exempt, the GMC’s Confidentiality guidance states that everybody should follow guidance on how long health records should be
Even after closing the practice, as long as you hold information, you will need to be able to fulfil your duties as a data controller
kept, even if you do not work in the NHS
The retention schedules detail the minimum retention period for each type of health record. The starting point for calculating retention is the beginning of the year after the last entry in the record.
Finally, you need to consider any employees who remain at your practice at the time it closes, as some may be made redundant. Redundancies are never an easy option because it means the termination of employment through no fault of their own. It is essential that you keep staff informed of what is going on and seek specialist employment advice if necessary.
Dr Kathryn Leask is a medico-legal adviser at the Medical Defence Union
Coping with an unruly guide dog
Dilemma 2
Can we stop dog from coming in?
QA patient recently brought their assistance dog, which was a large, boisterous dog. During his visit, it jumped up at a nurse who was frightened of dogs.
Obviously, I do not want my staff to be frightened at work and am wondering whether we can refuse entry to the animal because of hygiene or patient safety?
AAssistance dogs are often thought of as guide or hearing dogs for blind or deaf people, but they can also refer to service dogs for those with disabilities not related to vision or hearing.
While many of these dogs receive specific training, it should be noted that assistance dogs can be owner-selected and trained.
Medical facilities should be accommodating of service dogs as outlined in the Equality Act 2010, and the Disability Discrimination Act (DDA) 1995 in Northern Ireland. The law sets out a duty to make reasonable adjustments to enable disabled users to access services.
The Equality and Human Rights Commission has produced a guide for businesses on assistance dogs.
This advises that you can expect that assistance dogs will be highly trained, that they will not wander freely around the premises, they should sit or lie quietly on the floor next to their owner and are unlikely to foul in a public place.
Most will wear a harness or collar identifying them as an assistance dog, though there is no requirement for this.
Disability discrimination
It is the responsibility of the practice to take reasonable steps to minimise the exposure of staff who have a phobia or are allergic to dogs.
However, neither are valid reasons for denying an assistance dog entry to the practice.
Refusing entry to an assistance dog could result in a complaint or a claim of disability discrimination which could involve financial compensation.
The law requires reasonable adjustments to be made. This is an objective test, and the courts will consider the facts of each specific case – for example, if it were obvious that the dog was poorly trained.
In this case, given the incident with a nurse, it would seem reasonable to ask the patient to try to ensure the dog is well behaved when on the premises.
Dr Sally Old is a medico-legal adviser at the Medical Defence Union (MDU)
Refusing entry to an assistance dog could result in a complaint or a claim of disability discrimination, which could involve financial compensation
THE McCLOUD REMEDY
Taking the unfairness out of pension taxation
Recent announcements have been made about the actions doctors will need to take as part of the long talked about ‘McCloud remedy’ to solve anomalies in different pension tax schemes. Alec James explains
unfairness taxation
READING THIS article will be crucial if you have been required to pay annual pension saving tax charges in the past or retired from the NHS Pension Scheme with both a 1995/2008 – now referred to as the legacy schemes – and 2015 pension.
Sit back in a comfy chair with a cuppa as Alec James looks at the McCloud remedy complexities and gives a roadmap of the years ahead.
On 1 April 2015, new pension schemes were created for public sector workers. For the NHS, this was aptly named the 2015 scheme. It brought a significant change to the way the pension was calculated for hospital doctors.
The 2015 scheme is not based on your pensionable pay on the years leading up to your retirement like the legacy schemes were. Instead it is calculated using your ‘Career Average Revalued Earnings’ or CARE.
In layman’s terms, each year a percentage of your career earnings contributed to the 2015 scheme. So that the earnings are not time eroded by inflation, each year the historic earnings are uplifted by the Consumer Price Index (CPI) + 1.5%.
Unlike when the 2008 scheme was introduced, members were not given a choice as to whether to transition from the legacy schemes to the 2015 scheme. Instead, they were transitioned to the new scheme based on their age.
Those closer to retirement were either given full protection to remain in their legacy scheme or had a deferred transition date.
Those who were not eligible for any form of protection were transferred to the 2015 scheme on 1 April 2015.
In 2018, the Court of Appeal found that offering levels of protection to those closer to retirement was discriminatory to other members and so we now have the McCloud remedy, which looks to put right the age discrimination.
To do this, from 1 April 2022 all members of the NHS Pension Scheme are now contributing to the 2015 scheme. The period of 1 April 2015 – or whatever date you transitioned to the 2015 scheme –
➱ continued on page 50
The free and integrated digital prescribing platform for all private prescribers.
CloudRx take care of the dispensing, payment and delivery of medicines direct to your patients, wherever in the country they may be, for more convenient access to their medicines.
TRANSFORMATIONAL
Order prescriptions at the touch of a button to add a whole new level of convenience for your patients.
SIMPLE, CONVENIENT AND SECURE
Simple and fast digital prescribing.
Legal paperless prescriptions, repeat prescriptions and controlled drugs.
Prescriber fees can be charged to the patient if required.
INTEGRATED
Our API enables frictionless integration with healthcare brands & clinical software including Semble, WriteUpp, MidexPRO, eClinic, Pabau and ClinicYou.
“We were struggling to keep up with the admin side of the prescriptions, not to mention storage for medication to cope with a huge increase in prescriptions. CloudRx immediately took away the strain. Since our partnership we have grown by more than 200% in size. We could not have achieved this seamless scalablity without them.”
– Dr Louise Newson, Newson Health
to 31 March 2022 is called the reform period.
For pension purposes, you will be given the choice as to which pension scheme you would like the reform period to be included in. This decision does not need to be made until you are retiring.
However, for annual allowance purposes, the reform period will be recalculated as if the 2015 scheme never existed.
Annual allowance tax charges
Many of you will have received the dreaded envelopes over the last few years. In these envelopes, you would have received two statements from NHS Pensions, one showing the growth figures from your 1995/2008 pension scheme(s) and the other showing the growth from your 2015 scheme.
The two growth figures are then totalled and compared to your annual pension savings allowance in the tax year. For tax years up to 2022-23, the pension savings allowance was £40,000, but it is reduced if the following limits are exceeded:
If your threshold income is more than £200,000;
If your threshold income together with your pension savings are more than £240,000 –referred to as adjusted income.
Your threshold income is effectively your total taxable income from all sources in the year and is not limited to your NHS income.
It is only if you exceed both limits that you will be subject to tapering of the annual allowance.
The effect of this is similar to those of losing your personal allowance. For every £2 your adjusted income goes over £240,000, your pension savings annual allowance for the tax year reduces by £1 to a minimum allowance of £4,000 for some years.
If you exceeded the annual allowance in a tax year and it gave rise to a tax charge, then this would need to be declared on your personal tax return form.
The tax due would either be paid personally or you could opt to use ‘scheme pay elections’ whereby the pension pays the tax and your pension when you come to retire is reduced to reflect the liabilities paid on your behalf.
The appointment of an accountant with specialist knowledge of the NHS pension will be invaluable in calculating an estimated annual allowance growth figure
McCloud remedy actions
As mentioned earlier, the reform period will be recalculated with the growth being attributed to your legacy schemes rather than the 2015 scheme.
This requires NHS Pensions to update all its members’ records.
NHS Pensions had initially said that the recalculations for members would be available by October 2023 and therefore this article would be more specific about the actions that would be required.
However, earlier this year, this was extended until 6 October 2024 for the active and deferred NHS pension members.
For those of you already receiving your NHS pension and who are affected by the McCloud remedy, it is expected you will be provided with the information in October 2023.
Once the information has been released, it will be entered, together with the original annual allowance information, into a new HM Revenue and Customs (HMRC) calculator.
Details of the calculator will be released shortly before October 2023, but the calculator will look at your annual allowance position before and after the McCloud remedy.
It will then calculate any annual allowance tax adjustments, splitting these into ‘in scope’ and ‘out of scope’ adjustments. Here, we are talking about HMRC’s rules in respect of amending tax returns.
‘In scope’ years are where HMRC will accept a revision to your tax position and any refunds or additional tax due will be recovered from or paid to HMRC.
Any corrections outside of this period becomes ‘outside the scope’ and therefore is no longer the responsibility of HMRC.
If you are due a refund from the
‘outside the scope’ years, you will have suffered a taxation loss that you cannot recover from HMRC.
As the tax paid was due to the move to the 2015 scheme, as part of the McCloud remedy, you will be able to recover the tax refund via the NHS pension compensation scheme.
Compensation scheme applications will need to be made to the scheme manager together with evidence of the taxation losses incurred.
The scheme manager will then be able to make either direct compensation to you – if you paid any annual allowance tax personally –or indirect compensation by way of increased annual pension benefits if you opted for scheme pays elections.
NHS Pensions has confirmed that it will not seek to recover any additional tax that would be due on any ‘out of scope’ years which would have ordinarily been due to HMRC – good news for the taxpayer.
If you are already in receipt of your NHS pension and retired
with both a legacy scheme and 2015 scheme, you will be able to make elections to receive all the pension based on your legacy scheme.
The information regarding this should be available in October 2023.
For those members who opted out of the NHS Pension Scheme between 1 April 2015 and 31 March 2022 as a result of the changes to the scheme, you will be able to reinstate your pension for those years if you apply before 1 October 2023.
To do this you must confirm that your original decision to opt of the scheme would have been different had it not been for the age discrimination impact of the 2015 scheme transitions.
If you choose to do this, the pension contributions due on the amounts will become payable again. You should always seek the advice of specialist medical independent financial advisors and accountants before making any decisions regarding this.
Looking into the future…
2022-23 annual allowance position
With the McCloud remedy statements not being issued until October 2024, many doctors will be considering what they need to do for their 2022-23 tax returns.
As the McCloud remedy work will not have been completed, NHS Pensions will be unable to provide statements for 2022-23.
While you may breathe a sigh of relief that you do not need to make entries on this year’s return, unfortunately it is not quite that simple.
To help minimise any interest and surcharges that could be imposed by HMRC, you should include an estimate of your annual allowance position for 2022-23.
This can then be updated once the annual allowance statements are available from NHS Pensions in October 2024. The appointment of
an accountant with specialist knowledge of the NHS pension will be invaluable in calculating an estimated annual allowance growth figure.
Post-Budget changes
In spring 2023, three key announcements were made about NHS pensions:
1
The annual pensions savings allowance was increased to £60,000 for 2023-24;
2 Lifetime allowance tax would not be charged for 2023-24 – providing certain criteria are met – and will be abolished from 6 April 2024
3
Alignment of the CPI figures used by NHS Pensions and HMRC (2015 scheme) and allowing in-year negative pension input amounts incurred on the legacy schemes to be offset against
If you are already in receipt of your NHS pension and retired with both a legacy scheme and 2015 scheme, you will be able to make elections to receive all the pension based on your legacy scheme
growth on the 2015 – which has previously not been allowed.
The £60,000 annual pension savings allowance should help many doctors avoid hefty tax charges on their NHS pension. This also helps alleviate the pressure of annual allowance tapering, because the adjusted income has been increased to £260,000. The minimum allowance has also been increased from £4,000 to £10,000. CPI alignment was a pressing issue which was addressed outside
of the Budget. As mentioned earlier, the 2015 scheme is a Career Average Revalued Earnings scheme. This means that each year, the NHS revalued historic earnings by CPI + 1.5%.
Historically, this was done on 1 April each year using the September prior figure. HMRC allows for such increases; however, it uses the CPI figure prior to the start of the tax year and there has always been a disparity between the two rates used.
Many Independent Practitioner
Today readers will have seen the impact of this on their 2021-22 annual allowance statement when the 2015 scheme growth was considerably more than it has been in previous years, despite doctors’ circumstances remaining similar. This was likely to be a result of the CPI uplift.
From 2022-23, NHS Pensions will now revalue on the 6 April, meaning that the CPI rates used by
both NHS Pensions and HMRC will be aligned.
Therefore, the only inflationary increase which will be included in the calculation against your annual pension savings allowance will be the 1.5% given each year.
Common misconception
Finally, in the past, many of you will have received a 1995/2008 statement which show nil growth in a particular tax year. There is a common misconception that this means your pension has not grown within the tax year.
But what this actually means is that your pension grew by less than the allowable inflationary amount applied by HMRC. In some cases, this may have been a negative figure. Rather than showing the negative figure, this was historically shown as a zero.
This meant that the taxpayer was missing out on relief that could be offset against the growth
seen on the 2015 scheme. In the Spring Budget it was announced that, from April 2023, members of the NHS pension will be able to offset these in-year negative figures from their legacy schemes against the 2015 growth figures.
The McCloud remedy and pension annual allowance matters in general is a very complex area and ensuring you make the correct disclosures will be imperative.
You should seek the advice of a medical specialist accountant to ensure you have declared the correct annual allowance tax charges. In October’s issue: Richard Norbury warns about the tax implications of investing in property
Alec James (right) is a partner at Sandison Easson and Co, specialist medical accountants
Diagnostic Audiology Including Paediatrics • Tinnitus Rehabilitation • Vestibular Testing • PTA & Tympanometry • Speech Audiometry • Speech In Noise Testing• Specialist Tests Including OAE, VEMP & ASSR • Ear Wax Removal • Independent Hearing Aid Provider
DOCTOR ON THE ROAD: ALFA ROMEO TONALE
Good-looker with an Achilles heel
The manufacturer says it is the ‘beginning of a new Alfa Romeo era’. Our motoring correspondent Dr Tony Rimmer (right) gives his view
Parent company FIAT knew that it had to do something special to rejuvenate the sporty image. In 2016, it launched the latest Giulia and this was a car that could truly compete with arch-rival BMW.
However, the Giulia and the related Stelvio SUV have not been big sellers. So, six years later, in 2022, the manufacturer announced ‘the beginning of a new Alfa Romeo era’ with the launch of a compact SUV: the Tonale.
The adaptive dampers, standard on my Veloce test car, change the ride quality significantly. In Comfort mode, most bumps are smoothed out, but the Sport mode is too firm for our poor British road surfaces.
Disappointing drivetrain
WE COME across the influences of brand image on an almost daily basis in our medical world.
The big medical insurers work hard and spend lots of money on promoting their positive attributes to both us doctors and our general public clients.
Some have been around longer than others and they all use event sponsorship to increase general awareness and so hopefully their market share. A well recognised and respected brand has a great advantage in a competitive world.
Alfa Romeo is a car brand with a fantastic image created on the back of an impressive sporting heritage. The Alfa racing team was very successful in the 1930s and was run by a certain Enzo Ferrari before he set up his eponymous team in competition.
Real charm
Even the Alfa Romeo badge has real charm – the cross of the municipality of Milan and a mythical serpent swallowing a warrior.
When Alfa started building road cars in large quantities in the 1960s, they were all designed to be sporty in nature and drove really well.
I have fond memories of one of my first cars, an Alfasud, that performed better than most small saloons and was great fun to drive down a twisty ‘B’-road. Unfortunately, it rusted very badly and very few survive to this day.
The brand then went through a few difficult decades producing cars that had bland styling and were not particularly special to drive.
It hopes to sell more of this new model in the UK than the Giulia and Stelvio sales combined. With a starting price of £38,620 – my test Veloce model is £42,520 – the Tonale competes directly with the Volvo XC40 and the Range Rover Evoque, both from alternative and well-respected brands.
Cuts a dash
The chassis is based on that of the Jeep Compass, which is an older FIAT platform. Fortunately, Alfa has pulled out the stops for the styling.
In a world of anonymous and anodyne small SUVs, the Tonale cuts a real dash. It looks smart and sporty with design references to Alfa sports cars of the past.
The interior continues the positive theme and it is a pleasant environment for both driver and passengers.
Rear legroom and headroom is adequate and the boot is of average size for the class.
Alfa Romeos should be all about the driving experience and, as far as the handling is concerned, the Tonale gives a pretty good account of itself.
The steering is sharp and the chassis control is better than I expected from a relatively old design base.
But now we come to the Tonale’s Achilles heel – the disappointing drivetrain. Powered by a four-cylinder 1.5litre mild hybrid engine that produces 158bhp, acceleration is leisurely.
It is made worse with a full complement of passengers and luggage, when it can feel quite strained at times, particularly on uphill stretches.
Compounding the problem is the automatic gearbox, which has an unnerving delay and seems to get confused as to what ratio it should select for the appropriate situation.
This is at its worst around town when stop-start motoring should be smooth and predictable. Perhaps the alternative, but £10,000 more expensive, plug-in hybrid version will be better in this respect, but I am yet to drive it.
So the Alfa Tonale is a great looking car that, in this version, is let down by its driving experience. It is a good small SUV package and the brand has great appeal, but I would recommend any medic with it on their short list goes for a good test drive first.
What I would really like Alfa Romeo to do is to produce an allelectric car that is fun to drive and would consolidate the brand’s sporty image for a new generation of car buyers.
Dr Tony Rimmer is a former NHS GP practising in Guildford, Surrey
The interior is a pleasant environment for both driver and passengers
anodyne small SUVs, the Tonale cuts a real dash
TAKE PART IN OUR SURVEY
Your views on setting up in private practice
Independent Practitioner Today is running a survey with the Medical Defence Union to get consultants’ views on setting up or growing their private practice –see page 26 of this issue.
We would value hearing from readers currently undertaking both private and/or NHS work. If you could spare 5-10 minutes, we’d appreciate your answers to this survey.
In return, you can choose to enter a prize draw to win a £100 Amazon e-gift card.
Responses will be anonymised and the results of the survey published by Independent Practitioner Today, but no personal information will be passed on.
ADVERTISERS: The deadline for booking adverts in our October issue is 22 September
INDEPENDENT PRACTITIONER
TODAY The business journal for doctors in private practice
Published by The Independent Practitioner Ltd. Independent Practitioner Today is editorially independent.
Material is governed by copyright.
No part of this publication may be reproduced, stored in a retrieval system or transmitted in any form without permission, unless for the purposes of reference and comment. Editorial layout is the copyright of the publishers. If you wish to use it for promotional purposes on websites or for reprints, we would be happy to discuss licensing the copyright to you.
Registered office: 7 Lindum Terrace, Lincoln LN2 5RP
Write to Independent Practitioner Today 7 Lindum Terrace, Lincoln LN2 5RP
CHANGING ADDRESS, EMAIL
ADDRESS OR SUBSCRIPTION DETAILS?
Phone 01752 312140 or email karen@marketingcentre.co.uk
TELL US YOUR NEWS
Robin Stride, editorial director
Email: robin@ip-today.co.uk
Phone: 07909 997340 @robinstride
ADVERTISE WITH US
To advertise in the digital journal, on our website or in our business directory, contact advertising manager Andrew Schofield at Spot On Media. Phone: 0161 408 3912
Email: andrew@spotonmedia.co.uk
GET A SUBSCRIPTION DISCOUNT!
£90 independent practitioners.
£90 GPs and practice managers (private & NHS).
£210 organisations.
Save £15 paying by direct debit: individuals £75 (organisations £180).
TO SUBSCRIBE
Email karen@marketingcentre.co.uk or phone 01752 312140