The business journal for doctors in private practice
In this issue
Succeed at real Monopoly Seven myths that shouldn’t stop you from investing in property P20
No grey areas
How the bold use of colour can help create a great healthcare experience P26
n With thanks to Healthcode for sharing the back page with readers’ addresses
Playing a game of risk
Trying to beat the market?
An expert explains the costly challenges of active investment managment P42
Check your pensions
By Robin Stride
Busy independent practitioners are being urged to schedule space to get their pension position assessed following revised Government plans to ease doctors’ tax burdens.
Specialist medical financial planners warn that, more than ever before, senior medics will need to take some time to carefully plan their likely earnings and contributions for the foreseeable future.
Patrick Convey, technical director of specialist financial planners Cavendish Medical, said: ‘This is an area which requires expert advice and careful modelling of the best options available.
‘This is not a time to make any rash decisions without exploring every opportunity or threat to the financial status quo.’
With annual pensions statements now obtainable from the NHS Pensions Agency, he advised doctors to request their own statement as soon as possible and not wait for it to be sent automatically ‘as there can be errors in the system’.
They should then use this as a basis for detailed discussions to ascertain their position and the resultant tax implications.
Total Reward Statements are also now available from the NHS Pensions Agency, which detail an individual employee’s basic pay,
allowances and pension benefits, but do not include annual allowance liabilities.
Cavendish’s plea came after Prime Minister Boris Johnson signalled that modifying doctors’ pensions was a main priority.
One of his first moves was to scrap a twoweekold consultation outlining a ‘50:50’ flexible pensions plan and replace it with new proposals to allow doctors increased control to scale down pension contributions or take their employer contributions as salary.
Mr Convey said: ‘The NHS Pension Scheme has entered an unprecedented “blinkandyou’llmissit” phase of announcements and aboutturns. No sooner is one consultation launched than another quickly replaces it.
‘This latest attempt at easing the NHS workforce crisis means senior practitioners may be able to adjust their pension contributions in order to change their rate of pension growth.
‘The official line from the Department of Health and Social Care is that NHS scheme members could therefore choose to make contributions in 10% increments while receiving the equivalent accrual rate – possibly building a pension pot at a more gradual rate.
‘While it is good news that the Government is no longer hiding from the very real problems that punitive tax charges are having on
the NHS, on patients and on individual doctors, these plans will undoubtedly add significant extra layers of complexity for busy medics keen to just get on with helping people.’
Meanwhile, some doctors could be compensated for age discrimination following a court ruling favouring firefighters. The Supreme Court upheld an earlier ruling that changes made to firefighters’ pensions in 2015 discriminated against younger workers.
A review of pension related age discrimination will now be conducted across all other public sector schemes.
Under the 2015 changes, those ten years from retirement were protected from reforms which saw
younger workers moved into less generous pension arrangements.
In 2018, the court found that those too far away from retirement, and too young to qualify for ‘transitional protection’, were unfairly discriminated against.
The Treasury has stated that as ‘transitional protection’ was offered to members of all the main public service pension schemes, including the NHS, any firefighters’ remedy must be employed across all public sector retirement plans.
Mr Convey added: ‘This ruling may mean a windfall for affected NHS scheme members who were forced to move to the less generous 2015 pension scheme, but compensation has yet to be established.’
n See page 3
SURGING AHEAD: Consultant Mr David Gateley has sailed away from it all to tackle an epic round-theworld yacht race for charity. But he reckons his operating theatre skills should prove useful during the adventure.
n See page 4
TELL US YOUR NEWS Contact editorial director Robin Stride
Ensure your email marketing flies
Jane Braithwaite explores email marketing strategies, building a contact list and creating great newsletters in tips you can apply to your practice P16
ADVERTISE WITH US Contact advertising manager Margaret Floate at margifloate@btinternet.com Phone: 01483 824094
GET A SUBSCRIPTION DISCOUNT
£90 independent practitioners.
£90 GPs and practice managers (private & NHS).
£210 organisations.
Save £15 paying by direct debit: individuals £75 (organisations £180).
TO SUBSCRIBE – USE SUBSCRIPTION FORM ON PAGE 25
Or email karen@marketingcentre.co.uk Or phone 01752 312140. Or go to the ‘Subscribe’ page of our website www.independent-practitioner-today.co.uk
Chief sub-editor: Vincent Dawe
Head of design: Jonathan Anstee
Publisher: Gillian Nineham at gill@ip-today.co.uk
Phone: 07767 353897
EDITORIAL COMMENT
Next layer of transparency
How many years before the shock waves of the Competition and Markets Authority (CMA) investigation into private healthcare subside?
We reckon there are a good few to go yet.
The roots of the CMA investigation track back seven-and-ahalf years following an initial inquiry by the then Office of Fair Trading (OFT).
There have been a host of hefty changes for consultants since then, some due to the evolving market and others from just what the competition watchdog ordered for doctors.
‘Incentives’ for specialists to work in hospitals, such as free rooms and secretarial support, disappeared and – as our Profits Focus series has demonstrated –ensured it got even more expensive to run a private practice business.
CMA investigators considered there was limited information
on prices and performance for hospitals and consultants and a new age of fee transparency swung underway at the beginning of this year.
Next up, it is performance that is due to feature on the Private Healthcare Information Network (PHIN) website this autumn, starting with infection rates and ‘adverse events’ (see pages 3 and 10).
Patients are, so far, widely unaware of PHIN’s role. But consultants will be eager to see what is displayed about the hospitals where they do private practice. Many have a justified air of foreboding over what could be made of it all, especially when coverage extends to them.
The Federation of Independent Practitioner Organisations has rightly voiced concerns and with ‘much work to be done on the accuracy and completeness of data’, we see a long road ahead.
Boost your CQC score
The Harley Street clinic rose from a ‘good’ CQC rating in 2015 to ‘outstanding’ in 2017. A new report from the commission shows how P29
What you need to pass revalidation
Get it sorted! Experts in the field, Kate Lewis and Darren Wiggins, look at the requirements for successful appraisal and revalidation P32
PLUS
OUR
Stop the online scammers
In the first of our new series, anti-fraud specialist Vin Pandha outlines some danger areas and shows why doctors’ practices are such a big risk P34
What’s up with WhatsApp?
Going app? What doctors should know about using WhatsApp and similar computer applications used at work to communicate with colleagues P35
Be assured when buying and selling Solicitor Justin Cumberlege explains the power of warranties, which are vital when doctors buy and sell a business, as they can inflate or deflate the price P40
REGULAR COLUMNS
Doctor on the Road: Entry level does not mean boring
Dr Tony Rimmer tests an upmarket supermini from a premium brand P48
Start a private practice: Avoid the annual allowance trap
Accountant Ian Tongue looks at ways to mitigate the unfair pension savings annual allowance charge P50
Profits Focus: Self-pay at the heart of it
Our unique benchmarking series looks at the financial fortunes of cardiologists P53
Circulation figures verified by the Audit Bureau of Circulations
Doctors demand pension tax cure
By Edie Bourne
The Federation of Independent Practitioner Organisations (FIPO) has expressed doubts over the Government’s suggested ‘fix’ for the doctors’ pensions tax issue.
It said: ‘It may well be that the only long-term solution to address the adverse impact on the workforce capacity is to scrap the Annual Allowance and the Tapered Annual Allowance in all defined benefit schemes such as the NHS Pension Scheme.’
FIPO said it would like to invite the Government to consider some different action such as enhancing the ‘Scheme Pays’ option and retro-
spective Transitional Protection to all 1995 and 2008 scheme members.
Chairman Mr Richard Packard said FIPO was delighted that the Government had taken medical bodies’ warnings about pension tax effects on doctors and patients seriously.
FIPO said the rise in NHS waiting lists ‘might well be’ due to consultants choosing not to perform extra outpatient clinics and operating lists in order to avoid financial penalties. It argued that the pensions issue, plus medical insurers’ fee restrictions, had influenced consultants not to enter or even continue in private practice.
The Government’s earlier sum -
mer proposal of a 50:50 pension option, rejected by the BMA, the Hospital Consultants and Specialists Association and NHS Providers, provided no acceptable or workable alternative, it added.
The London Consultants Association (LCA) said other options should be considered and it encouraged members to consult financial advisers.
Chairman Dr Mark Vander pump voiced concern on the financial impact and continuation of the punitive annual allowance taper.
He was also concerned at the effect on morale of consultants, considering the time they needed to seek advice, calculate their pen-
Consultants’ warning over adverse events publishing
Plans to publish doctors’ adverse events in the independent sector have brought a strong warning from the organisation representing the professional interests of over 15,000 private consultants.
The Federation of Independent Practitioner Organisations (FIPO), which gives a voice to specialists via their specialty organisations, stressed the importance of advising caution when making quality judgements based on this information. In a statement to Independent Practitioner Today, it said while it welcomed the intention of the Private Healthcare Information Net work (PHIN) to soon publish some adverse events at hospital level, including infection rates for certain procedures, ‘there still remains much work to be done on the accuracy and completeness of data’.
FIPO said: ‘Individual consultants, and especially expert senior consultants, are asked to deal with the most complex problems with
the least straightforward outcomes. Additionally, private sector volumes are low.
‘Despite ongoing work to attain robust and mature information, the significance of any judgements based at individual consultant level would be questionable.
‘How might patients be reasonably expected to interpret and understand raw data presented to them? The implications for expert senior consultants who attract an extremely complex caseload are obvious.’
FIPO said it was supportive of the provision of accurate and relevant information to help to drive safety and quality in private healthcare, hopefully to enable value judgements that allowed patients a meaningful choice.
But it added that it was very easy to draw inaccurate conclusions without adequate context, such as comorbidities, particularly for those not medically qualified.
sion income, then to make a difficult decision over what to do with their NHS pension.
He said: ‘Ultimately, that decision may include the withdrawal of additional NHS session work and may even result in premature retirement at a time where the NHS is under particular workforce pressures.’
The LCA will discuss pensions, and indemnity, at an evening meeting on October 16 at the King’s Fund.
How to avoid the pensions trap, page 50
FIPO continued: ‘While recognising that the private healthcare environment differs from that of the NHS, there is some merit in at least mirroring NHS performance metrics. The Competition and Markets Authority has asked for adverse events to be attributed on an individual basis.
‘This can be misleading, as the hospital and the surgical/medical team are all involved and events of this type are rarely down to just one single person.
‘We know from previous research that healthcare failures are multifactorial, and 96% of the errors that occur within a healthcare environment are due to systems errors; the remaining four per cent being due to human mistakes.
‘However, private hospitals are not homogenous. The range of procedures and clinical support provided at site level differ enormously.’
➱ continued on page 10
SAYING SORRY IS NOT AN ADMISSION OF GUILT
Although an apology cannot prevent a complaint or a legal claim from arising, it is more likely to prevent it than a defensive response.
Read the advice from the MDU in ‘Business Dilemmas’ on page 45
DOCTORS
Make sure the private healthcare industry knows who you are, where you are and what you do. Tell us your story. Contact editorial director Robin Stride at robin@ip-today.co.uk or phone him on 07909 997340
FIPO chairman Mr Richard Packard
Sailing round the world is ‘like surgery’
By a staff reporter
Plastic surgeon Mr David Gateley believes his operating theatre skills will come in handy for the adventure of a lifetime – taking part in a round the world yacht race for charity:
‘As surgeons, we operate on someone in our head, first. We go through each step of the surgery we are going to perform and think about all the possible problems we may encounter on our journey.
‘I feel that sailing is like that, too – you have to meticulously plan each step.
‘Hopefully, my methodical, scrupulous approach will be of benefit to the crew. This is the culmination of more than two years’ planning, intensive training and preparation.’
He hopes his surgical and non-
surgical peers and colleagues will support his challenge and join him in raising funds for children worldwide who have no access to proper medical or surgical treatment.
Mr Gateley, of DRG Plastic Surgery in Harley Street and nakedhealth MEDIASPA in Wimbledon, should by now be over half way through his projected 33 days at sea on a 70-foot ocean racing yacht in the Clipper Round the World Yacht Race.
He started from St Katharine Docks in London on 1 September, joining Team Guy.
This is a crew totalling 60 people aged between 18 and 74. The surgeon is taking part in the first leg of the race – a 7,250-mile passage from the UK to Uruguay.
Mr Gateley, who is posting regu-
Bupa opens new clinic in London
Bupa Cromwell Hospital has launched a new outpatient diagnostic clinic in the City of London, providing a wide range of specialist care and support for patients.
Basinghall Clinic has 16 consulting rooms, two treatment rooms for minor procedures, a gym for physiotherapy and a state-of-theart imaging suite consisting of an MRI, X-ray and fluoroscopy.
Services and treatments include cardiology, complex spinal services, dermatology, musculoskeletal, respiratory and urology. The clinic, open from Monday to
Friday, is near Bank tube station. It was previously a Bupa Health Centre, but due to recent acquisitions and developments, has become part of Bupa Cromwell Hospital to treat outpatients.
People who need more complex diagnostics, day case or inpatient care are referred to Bupa Cromwell Hospital.
Manager Danielle Sharp said: ‘We are delighted to have officially launched Basinghall Clinic as part of Bupa Cromwell Hospital. We have a fantastic range of highly skilled consultants who work
lar updates and video blogs of his journey, is raising money for Unicef UK and Child Action Nepal, which supports an orphanage.
As a CAN trustee, he regularly visits the Nepalese capital, Kathmandu, to teach and work at a specialist hospital. He became involved after he was asked to perform plastic surgery on an orphan called Kalpana, who was badly burned, aged seven.
He brought her to the UK and operated on her at St George’s Hospital, London, covering all the costs and this inspired him to join the board of trustees in 2016.
The Clipper race is an endurance test like no other. Created by Sir Robin Knox-Johnston, the first person to sail solo non-stop around the world, the 40,000-nau-
tical-mile race is now in its 12th edition.
Each of the 11 identical racing yachts have a fully qualified skipper to safely guide the crew, made up of ordinary, everyday people who made it through the rigorous training programme. Most people take part in one of the eight legs, but a small number complete the entire event.
Taking part in the Atlantic Trade Winds leg, Mr Gateley will tackle the first major ocean crossing of the race, sailing via the Canaries towards the equator, through the dreaded Doldrums and on to South America.
➲ Mr Gateley can be sponsored via his JustGiving page: justgiving. com/davidgateley
➲ View his progress at drg-plasticsurgery.co.uk
The outpatients clinic is near Bank tube station in the
closely together to make sure our patients are receiving the best possible care and treatment.’
Patient numbers had risen since opening. Philip Luce, director at the Cromwell, called the development a huge opportunity for the hospital.
City of London
Sailing away in the Clipper race and (inset) surgeon Mr David Gateley
Online booking cuts fee
DISCOUNTS BRING BUSINESS BONUS
Express GP appointments are £60, or £54 with a 10% discount.
A Doctorcall spokesperson told Independent Practitioner Today the thinking behind the discount:
‘Online booking reduces secretarial time, as the patient is inputting their own information. Online booking also requires prepayment, so there is also no need to collect payment after the patient has been seen – this saves both the secretary and the patient time later.
‘It also puts the onus on the patient to let us know if they can’t make the appointment, which is particularly important with new patients who we don’t yet have a relationship with.
‘Doctorcall has decided to pass the saving on to the patient, as everyone benefits in the longer term if people get in the habit of booking online. We also find that the discount makes the services more affordable for patients.’
By Olive Carterton
A private GP service launched by a doctor entrepreneur is offering its London patients discounts on short-notice private appointments with all bookings made online.
The 10% reduction comes with Doctorcall’s acquisition of Dr Kelly & Associates, an established private clinic in central London.
As part of the new partnership, it offers a range of independent healthcare services, including GP consultations, corporate health assessments and health screenings.
Corporate doctor services include an on-site GP facility for corporate clients, giving employees access to regular and one-off consultations while minimising time away from work.
The flexible service allows employees to have fast access to a GP to discuss any health issues and offers a range of services, including travel advice and vaccinations, employee medical assessments and corporate health checks.
This will enable companies to
support their employees’ health and well-being, making sure they have access to the medical care they need quickly and easily, in support of a healthy work environment.
Doctorcall said express GP appointments would cut waiting time for patients and provide an affordable way to be seen by a doctor at a time convenient for them.
Entrepreneur and founder Dr Charles Levinson started the company in 1989 with a Morris Minor to provide a visiting doctor service within London, the first service of its kind in the UK.
He said: ‘Private patients will benefit from an expansion to our service offering, focused on bringing greater convenience, more flexibility and faster access to affordable healthcare.
‘It also presents an opportunity to strengthen our provision for corporate clients, enabling them to champion the well-being of their staff by making sure they have access to medical care when needed, helping to create a healthy and supportive workplace.
Hopes for cannabis clinic
A group of specialist investors were awaiting CQC approval as we went to press to open a centre in Harley Street offering access to medicinal cannabis for all conditions acknowledged to benefit from it.
Sapphire Medical Clinic’s team includes specialists in paediatric and adult neurology, palliative care, psychiatry, gastroenterology, acute general medicine and neuropathic pain.
The clinic aims to operate primarily through GP or consultant referrals.
Its managing director and academic lead is Mr Mikael Sodergren, honorary senior clinical lecturer and consultant hepatobiliary and pancreatic surgeon at Imperial College. He said: ‘We have the expertise to prescribe medicinal cannabis in a way that fits in with
other more conventional treatments as and when we judge that to be in the best interest of the patients.
‘Our service to patients will work on the basis of “we are specialists in your condition, and our aim is to help you get better, which may, or may not, involve medical cannabis, which we have the expertise
to prescribe”, rather than “come to us to try medical cannabis’’.
Other clinics are planned for Birmingham, Manchester and Sheffield. Sapphire said it had also set up the first UK national patient registry for cannabis-based products.
Mr Sodergren said the medical world needed more evidence about medicinal cannabis’s efficacy and its national database would be a major contribution to meet that need.
This would be the first to have meaningful and consistent data of how medicinal cannabis had helped when properly prescribed as part of a full treatment pathway.
He added: ‘Building a reliable database of evidence is critically important in order for medical cannabis to be accepted in the medical mainstream.’
‘We are committed to providing invaluable care to all our patients and are excited for our two brands to be working together to continue providing excellent choice and availability and outstanding medical services to our customers in London and beyond.’
Doctorcall has clinics in Harley Street and Manchester St Ann’s Square, employing 75 staff.
NHS pay rise ‘ignores tax’
A consultants’ leader has criticised a backdated-to-April NHS pay rise for failing to recognise huge additional tax bills generated by the pensions annual allowance.
The BMA’s Dr Rob Harwood said no account was taken of the high rate of pension contributions. He said the Government’s ‘2.5%’ award was only 2.35% in real terms. The pay board had previously willingly cut a pay award because it considered the NHS Pension Scheme was so beneficial.
‘There is no recognition of the fact that’s now not the case. Many senior doctors’ income is being significantly impacted by the punitive pension taxation, so this low pay rise merely adds to the overall position of doctors being undervalued and effectively paying to go to work.’
Dr Charles Levinson, who started the company 30 years ago with a Morris Minor to do visits in London
Clinic director Mr Mikael Sodergren
GMC change ‘will benefit doctors’
By Olive Carterton
Doctors’ defence bodies have welcomed Department of Health plans to reform the GMC’s fitnessto-practise (FTP) procedures.
The MDU’s Dr Michael Devlin said: ‘FTP processes need to be more responsive and proportionate. We agree the GMC should be able to make a decision on a case without a panel hearing, if appropriate.’
He said the process was stressful for doctors and it has been clear for a long time the GMC needed the power to amend the FTP procedures in a more efficient way.
The Government recognises that the current system is bureaucratic and time-consuming and that it can be ‘burdensome and … stressful for patients, their families, registrants and employers’.
Dr Devlin added: ‘We support
the removal of the GMC’s right to appeal decisions to the high court, though this is unlikely to be of any significant relief to doctors, as the Professional Standards Authority (PSA) will still retain the right to appeal decisions.
‘The GMC’s powers will also be modified to exclude reflective notes from FTP procedures. This will help to reassure the profession.
‘The MDU’s experience shows it can be helpful for doctors to offer evidence of their reflections when responding to a GMC investigation; for example, to demonstrate they have learnt from the experience.
‘But the point is, it should be for doctors to offer such evidence and not for the GMC to request it.’
At the MDDUS, Emma Parfitt said: ‘The focus is now on improved regulatory governance
removing GMC rights of appeal rather than redesigning the governance architecture.
‘We very much support UK Government’s acknowledgement of the need to be more responsive to the constantly changing needs of healthcare, being supportive of a flexible workforce while continuing to protect the public.
‘The prioritisation of changes for a modern fitness-to-practise process is also welcome, including the need to see a better process for the professionals involved through quicker decisions and early resolution for all parties.
‘We support members through these difficult issues and we know that this is what will make a difference for everyone involved.’
Further consultation on some challenging secondary legislation is now expected. A clear timetable is awaited.
Patients get help to navigate private care
New resources for patients receiving private treatment are being developed through an initiative from the Patients Association and the Independent Healthcare Providers Network (IHPN).
The patients’ pressure group said
these would be designed to give patients the information they need to make informed decisions about their treatment – from the decision to proceed with receiving private care through to when treatment is no longer required.
Patients attended a summer focus group with the two organisations who wanted to hear from people with both very good experiences and others who thought their could have been improvements.
Preventative clinic
targets executives
Consultants and guests this month are celebrating the opening of the new Mayo Clinic Healthcare in partnership with Oxford University Clinic.
The new preventative healthcare facility at 15 Portland Place, London, said it was committed to delivering ‘a unique approach to patient-centred care’, offering premium screening and diagnostic services.
One promotion from the clinic offers an executive health and wellness plan as ‘a sensible and effective way to enable your executive teams to embrace a healthier way of life and continue to excel and thrive in the workplace’.
Companies are told that offering this plan will give them the edge in attracting and retaining top executives.
IDF chief exec to leave after three years
Independent Doctors Federation (IDF) president chief executive Sue Smith is leaving in November after three years.
Chairman Dr Neil Haughton expressed gratitude for her hard work in raising the IDF’s profile, saying she had constantly focused on the growth of the sector.
Exciting times for Essex consultants
Phoenix Hospital Group (PHG) has predicted exciting opportunities for consultants after buying Baddow Hospital, Chelmsford.
It said it aimed to work collegiately with consultants in Essex to offer ‘the very highest standards of private healthcare in exceptional surroundings’.
The Baddow Hospital, now to be known as Phoenix Hospital Chelmsford, adds to PHG’s portfolio including Weymouth Street
Hospital, 9 Harley Street and 25 Harley Street.
The Chelmsford elective surgery hospital has many of the same specialties carried out at Weymouth Street Hospital.
Phoenix said the hospital had an excellent reputation and loyal consultant base in a range of services, including cosmetic surgery, gynaecology, urology, general surgery, ENT, foot and ankle surgery and pain management.
Essex patients can now access the surgical, diagnostic and outpatient services on offer across the group.
Chief executive Andrew Barker said the Chelmsford area enjoyed a high private medical insurance penetration. There was a strong self-pay market with many of the local population working in London.
He explained: ‘By acquiring Baddow Hospital, we aim to meet
the needs of patients outside the London market, which is part of our wider business strategy.
‘Over the past few months, we have been working hard to engage with consultants in the Chelms ford area to better understand the Essex market and the demand for medical services and believe that there are exciting opportunities for us to work collegiately with consultants in the area.’
Doctor’s suffering is ‘lesson for all’
By Robin Stride
‘If it could happen to him, it could happen to anyone.’
That was the warning to doctors from a leading specialist when introducing a former convict as after-dinner speaker for members of the London Consultants Association (LCA).
Outgoing chairman Prof Neil Tolley was referring to no ordinary prisoner. The guest was surgeon Mr David Sellu, who was wrongly convicted of manslaughter for unlawfully killing a patient.
His two-and-a-half-year prison sentence at The Old Bailey in November 2013 came more than three and a half years after the patient’s death.
Half of it was served behind bars and the remainder out in the community on licence. A long appeal process was launched after the intervention of friends, who teamed up with his family. Finally, his conviction was quashed in November 2016.
The Sierra Leone-born specialist held his audience spellbound as he
told of the extraordinary events leading to his prosecution and a distinguished career cut unfairly short.
He told consultants and their guests that doctors ‘on the coalface’ put a lot of unpaid goodwill into what they did, but what happened to him might influence them otherwise.
There was now much defensive medicine and doctors carried out many tests for no benefit but to protect themselves. Every death in medicine was a reason to apportion blame.
But healthcare had to put away this blame culture. ‘We must have the will to want to do it,’ he said.
Appeal judges criticised the prosecuting barrister, prosecution experts and the trial judge, and said: ‘In the circumstances, we do not believe that Mr Sellu had the benefit of sufficiently detailed directions to the jury in relation to the concept of gross negligence contained within the offence of gross negligence manslaughter.’
Prof Tolley told the LCA event he was ‘staggered’ at the lack of support
Royal Marsden;
Great Ormond Street Hospital;
Imperial;
Royal Brompton and Harefield;
Moorfields;
New record revenues for NHS PPUs
The 2018-19 financial year accounts for private patient units (PPUs) are now mainly published and they show further growth of private patient revenues to a new record.
Total revenues are estimated at £659m, up nearly 6% from £623m in 2017-18, a growth rate in line with annual trends of recent years.
The trend for London NHS trusts to lead the sector is further accelerated. Over half of all NHS trust private patient revenues – £348m – were accounted for by seven central London specialist trusts:
Guy’s and St Thomas’;
Chelsea and Westminster.
Performance remains patchy, even in London, as Barking, Haver ing and Brentwood recorded the most significant fall, down £2.4m due to the closing of a unit previously run by a private provider.
Outside London, the biggest single increase and fastest growth was Basildon and Thurrock University Hospitals, increasing by £3.6m in the year to £6.6m.
Deputy chief executive Tom Abell said: ‘The trust decision to bring back in-house the manage-
Prof Neil Tolley: ‘staggered’ at lack of royal college support for Dr Sellu
the surgeon received from ‘our college’: the Royal College of Surgeons. Suicide had crossed Mr Sellu’s mind in his darkest moments, but the reality was that he’d never been alone – his support group were working in the background to raise money.
As a ‘loved friend and first-rate doctor and surgeon’, Prof Tolley said he would have no hesitation in trusting himself and his family to Mr Sellu’s care.
Don’t miss Independent Practitioner Today next month – David Sellu’s story begins in an adaption from his book Did He Save Lives? A Surgeon’s Story (Sweetcroft Publishing)
ment of our eight-bed cardiac services private patient ward when the contract with a private partner ended has delivered significant surpluses – now reinvested in NHS care – and a wide range of governance and other operational benefits.
‘For these reasons we plan further growth across the Mid and South Essex University Hospitals Group.’
A more detailed summary of the 2018-19 performance will be featured in a future issue, with indepth region-by-region and trust-by-trust analysis through my ongoing series.
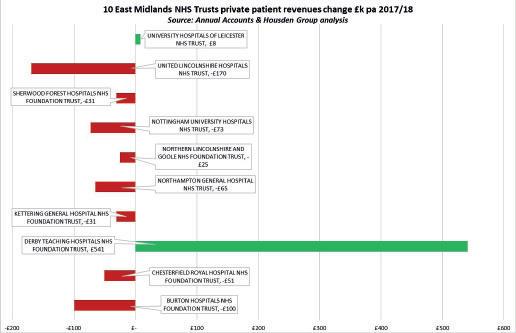
Philip Housden is a director of Housden Group. See his feature article on East Midlands PPUs on page 46
Payments mechanism added to MidexPro
Doctor customers of private practice management software firm MidexPRO are this month being offered a gateway allowing clinics to take payments securely within the package’s Cloud.
Users asked for the facility in response to a survey.
Managing director Gary Parker said: ‘The general thoughts were, providing this option to users would greatly improve the patient experience, increase business cash flow and help to reduce the amount of debt that arises from late payments.
‘By integrating the payment option into MidexPRO, users will have the ability to take payments and record the payments through the individual patient’s page, saving secretaries time.
‘Clinics will also be able to view reconciliations of payments and reduce the costs of having to pay extra for a PDQ machine or credit card machines.’
Mr Parker said the firm was confident this would greatly improve the user experience and help to make the daily workload more efficient.
Compensation rate change is branded useless
Defence bodies the MDU and MDDUS have criticised a rise to -0.25% in the personal injury discount rate for lump sum compensation payments as too little, too late.
The MDU said it still left in place much of the dramatic rises in indemnity costs caused by the discount rate’s reduction over two years ago.
The rate was still far less than the 2.5% it stood at then and the decrease in the rate since March 2017 had caused a grossly inflationary effect on compensation payments.
Compiled by Philip Housden
PPU WATCH
Berkshire beam centre to serve capital Cancer centre wins award for construction
A new proton beam therapy suite in Reading, Berkshire – the first such facility in south-east England – aims to serve patients from London and overseas.
Patients can consult in Harley Street before treatment at The Rutherford Cancer Centre Thames Valley, which opened its doors to patients at the start of September.
Chief medical officer Prof Karol Sikora said: ‘UK cancer care has made major strides over the past year thanks to a complementary mix of private and public facilities, but rising demand for precision radiotherapy
means that there is still some way to go. Based on treatment rates in other advanced European countries, the UK may need approximately 18 proton beam therapy facilities in the years to come.’
The company has two other centres, in Wales and Northumberland, and another being built in Liverpool. Each provides imaging, chemotherapy, radiotherapy, immunotherapy and proton beam therapy as well as a suite of diagnostic services. The fourth centre is currently under construction in Liverpool.
Electronic billing has a record rise
By Leslie Berry
Increased demand from independent practitioners’ practices is pushing electronic billing in the private healthcare sector towards another record year.
Figures from Healthcode, the official clearing organisation for private medical bills, show the volume of private medical insurance bills submitted through its online billing service was higher than average in the first quarter of 2019.
Now it expects to process 6.9m electronic bills this year compared with 6.3m in 2018.
Managing director Peter Connor said: ‘I’m delighted that private practices are making the transition from paper billing in ever greater numbers because everyone benefits.
‘When a bill is submitted through our online system, it is automatically validated according to the private medical insurer’s
own rules and ready to be processed, which saves time and is better for providers’ cash flow.
‘And being encrypted to internet banking standards, this method is more secure than post or email.
‘The adoption of e-billing across the private healthcare sector shows how technology can help us accomplish administrative tasks more efficiently and generate valuable data about trends in the sector.’
He believes this should be taken further in other areas, such as payment transactions, appointment booking and secure information sharing.
But he said this would only be possible if different private healthcare stakeholders were prepared to collaborate and adopt common standards.
Mr Connor added: ‘Healthcode already has the interoperable technology to connect different private healthcare stakeholders on a single
platform and if everyone in the sector commits to a common approach, there is no limit to what we can achieve together.’
Since launching its e-billing service in 2002, volumes have grown year on year and in 2018 the company processed bills worth over £3bn on behalf of private providers, an increase of 15% on 2015 (£2.67bn).
These transactions have enabled it to collect a wealth of valuable anonymised data about market activity within the sector.
Over the last five years, Healthcode has experienced a surge in electronic billing by non-hospital providers, including 22,000 independent practitioners who are registered to use the billing service.
The non-hospital segment submitted 3.4m bills in 2018, overtaking hospital providers (2.9m) for the first time and this rate of increase shows little sign of slowing.
Rutherford Cancer Centre North East, in Northumberland, has been awarded the Building Project of the Year at the Constructing Excellence regional awards. The centre in Bomarsund offers advanced cancer treatments, including proton beam therapy, and is the first of its kind in the region.
Rutherford Estates general manager John McIntosh said: ‘Building an advanced cancer centre, especially one that offers proton beam therapy, presents monumental practical and engineering challenges, but we were able to complete the facility in under two years thanks to the hard work of everyone involved.’
Electronic billing has long been standard practice within hospitals, but it is now clear that it has now been adopted across the whole private sector for insured patients.
There has been a slight rise in electronic billing volumes within the hospital sector after a relatively flat period. Healthcode expects to process more than 2.87m private medical insurance invoices from the hospital sector in 2019, worth approximately £2.3bn.
At the same time, there has been a notable shift towards outpatient care in the last ten years. In 2010, this setting represented 77% of billing volumes and 30% of invoice value, but today it accounts for around 80% of hospital invoice volumes and 39% of invoice value. By contrast, inpatient care represented 8% of invoice volumes and 44% of the value in 2010, but this proportion has shrunk to 5% and 32% respectively in 2019.
Healthcode boss Peter Connor
Rutherford Cancer Centres’ chief medical officer Prof Karol Sikora, centre manager Laura Geer and patient Timon Colegrove
By Douglas Shepherd
Surgeons are pressing for a fiveyear plan to clear a growing NHS patient backlog fuelled by the pensions tax crisis.
As more senior doctors cut their hours due to punitive tax charges on their pensions savings, NHS performance data showed a record 4.4m patients were awaiting consultant-led hospital treatment in June.
The renewed call for action came from the Royal College of Surgeons of England (RCS) after figures showed only 86.3% of patients who were waiting to start planned, consultant-led hospital treatment were seen within 18 weeks – short of the Government’s target of 92%.
More than 600,000 patients were affected – the highest number for over a decade.
Surgeons expressed concern earlier this year when this legal target was quietly dropped from NHS England and NHS Improvement’s accountability framework , which includes the Government’s mandate to NHS England for 2019-20.
The RCS says that while it supports NHS England’s plans to pilot new targets for access to care, it is premature to remove the 18-week target from the mandate when a replacement has not been tested or consulted on widely.
NHS performance statistics revealed 36,971 patients were waiting more than nine months (39
weeks) to start treatment in June 2019, and a further 233,479 waiting longer than six months (26 weeks).
The RCS is also concerned about
19,969 operations being cancelled at the last minute in April to June 2019.
RCS president Prof Derek Alderson said: ‘The number of patients languishing on waiting lists remains at an utterly unacceptable level.’
He said the Government had made welcome moves to cut waiting times by directing more money to hospital infrastructure projects and trying to resolve the pensions issue that had been exacerbating waiting times, but there was ‘still a big job ahead’.
Hospitals needed a clear plan for reducing waiting lists and at least 3,000 more beds, along with the staff and resources to run them, Prof Alderson added.
Call for waiting list plan Clinic offers new therapy for lymphoma
The London Clinic has announced it is offering adult patients with diffuse large B-cell lymphoma the new form of immunotherapy, CAR-T cell therapy.
It is for patients who have no other treatment options, having failed conventional chemotherapy.
The hospital said: ‘A phase 2 clinical trial of 111 patients (www.ncbi.
nlm.nih.gov/pubmed/29226797), has shown positive outcomes, with 52% of patients treated with CAR-T therapy living for 18 months after treatment. Real-world data is at an early stage but consistent with this positive outcome.’
Prof John Gribben, who is leading the treatment, said CAR-T cell therapy was an exciting advancement in the treatment of blood
Private neurologists seek patients for cancer trial
Consultant oncologists and neurologists are being asked to put patients forward to participate in a landmark international clinical trial of a new radiation treatment for people with glioblastoma multiforme, a brain cancer with a high mortality rate.
Prof Keyoumars Ashkan and Mr Ranj Bhangoo, consultant neurosurgeons at the London Neurosurgery Partnership, and oncologist Dr Matt Williams are leading the London Clinic’s participation in an international phase 3 clinical trial of a treatment called intra -
operative radiotherapy (IORT).
Candidates must be aged 18 or older and younger than 80 and must not have had previous cranial radiotherapy.
Clinicians who wish to put people forward for the clinical trial can phone 0203 219 3315 or email enquiries@thelondonclinic.co.uk.
Prof Ashkan said: ‘This approach has been demonstrated to be effective with breast and colorectal cancers and we are optimistic that this new technique can help many people with this aggressive form of brain cancer.’
cancers, offering a new, final treatment option for patients when others haven’t had the result they need from conventional therapy.
‘Diffuse large B-cell lymphoma is an aggressive form of blood cancer. So far, this treatment is showing promising outcomes for many patients, letting them return to normal lives with their families and loved-ones.’
Bluecrest Health Screening, a provider of ‘affordable health checks’, has secured a £17m investment arranged by private equity firm Vespa Capital.
The private healthcare provider launched in 2012 offers ‘comprehensive health screening tests’ and has delivered results to over 250,000 customers across the largest network of mobile clinics in the UK and Ireland.
It claims to offer unrivalled convenience and affordability compared with traditional higherpriced health checks offered by private hospital groups.
RCS president Prof Derek Alderson
Neurosurgeons Prof Keyoumars Ashkan and Mr Ranj Bangoo
Prof John Gribben, haematologist
PHIN to begin safety rate publication next
The Private Healthcare Information Network (PHIN) is mandated by a Competition and Markets Authority (CMA) Order to publish measures to give private patients more transparency over safety, quality and fees.
Safety measures include infections, re-admissions, revisions, mortalities, unplanned transfers, and other ‘adverse events’ agreed with hospitals.
The first, due this autumn, start with surgical site infection and healthcare associated infections, followed by ‘never-events’.
PHIN told Independent Practitioner Today: ‘Our focus is on publishing the first safety measures at hospital level this autumn.
‘Where the Order allows for publication of safety measures at consultant level, we understand there are complexities in doing this in a fair and meaningful way.
‘This will only be considered after extensive engagement with the professional community, associations and royal colleges.
‘Our focus at this time is on publication at hospital level only, and consultants will not be associated with the measures we publish this autumn.’
Adverse events
PHIN describes ‘adverse events’ as a broad and general term, with no fixed definition, for countable events that suggest something might have gone wrong during care.
Near misses might sometimes be included and some measures specifically required by the CMA such as unplanned re-admissions for further treatment.
The NHS uses various categorisations. ‘Never events’, used by England’s NHS Improvement, is a list of 14 harm scenarios considered wholly avoidable. ‘Serious incidents’ and other terms are used. PHIN has primarily focused on CQC definitions in England. Learning from mistakes and
where things go wrong in the NHS helps protect patients from avoidable harm and PHIN says its published safety measures will bring greater transparency, improve patient safety, and give people more informed choices.
The data it collects is called ‘adverse events’, but its website will term these ‘safety measures’ to aid patient understanding and to reflect that they correspond with the CQC’s ‘Safe’ quality of care domain.
Providers of privately funded healthcare have been required to submit data to PHIN, including the ‘adverse events dataset, since September 2016.
Four months ago, it outlined the current state of reporting by providers of private healthcare. It acknowledged that although there was not full coverage in reporting of adverse events by them, there was now a critical mass of providers submitting data which allowed it to move forwards with publishing the first safety measures.
Ground-breaking
Talking of its autumn plans, PHIN said: ‘This is the first time that any measures of the quality of private care have been published systematically by a trusted independent organisation, enabling comparison across hospitals, and potentially with the NHS, across a range of indicators.
‘Previously, some providers have published assessment of their own quality – for example, in annual clinical governance reports – while other assessments using data – for example, by regulators or insurers – are typically narrowly focused and not published.
‘The safety measures we will publish will bring greater transparency to private healthcare, making valuable information available to initiatives to improve patient safety, and helping patients make more informed choices when considering their care provider.’
PHIN considers that, when making decisions, patients would want to know what a hospital’s historical record of events is, and that aligns with the legal requirement laid down by the CMA.
In addition to what the data itself says, PHIN believes patients should pay as much attention to whether hospitals are able to produce effective transparent data on safety
Publication will give patients greater transparency, improved safety and more informed choices, says PHIN
in line with their legal obligations. PHIN stated: ‘We will publish information on: hospitals that have reported a full view of their adverse events and what those events are; hospitals that have confirmed they have no reportable adverse events; and where hospitals have not reported sufficient data on their adverse events in line with their legal obligations.’
More details of hospitals’ intensive care called for
➱ continued from page 3
Federation chairman Mr Richard Packard strongly believes that patients should be supported to choose the provider most suited to their personal medical requirements.
He would like to see the provision of information about each provider site, such as the availability of on-site intensive care, because this would help those with complex conditions.
It considered the capture of this ‘clinically rich and relevant information’ would, in the long term, allow for greater understanding of private healthcare’ complexities and performance.
Mr Packard added: ‘FIPO believes that patients should be able to exercise their informed choice based on accurate, meaningful and relevant information that will allow for a trustworthy and beneficial consultant-patient relationship.’
FIPO said it would encourage all consultants to enter their private patient data onto the appropriate national audits, as proposed by their specialty associations. Providers should be requested to offer support for this.
A look back through our journal’s archives of ten years ago reveals that although times change, some issues are not so new
A trawl through the archives: what made the news in 2009
Revalidation balm
GMC chairman Prof Peter Rubin responded to readers’ worries over revalidation and how it would affect their practices’ future. He promised:
Work was progressing to solve the revalidation dilemmas of doctors in private practice;
Implementation would take on board the private sector’s diversity;
Revalidation would not come to the sector until local systems had been tested and could support it;
Doctors would would be kept up to date on progress and get a chance to have their say.
He told the journal: ‘Doctors in the independent sector have been raising their own questions about implementation. The sector is diverse and there are many who work alone or in small teams who may be worried they do not have the robust clinical governance in place to revalidate. Work is being done to find solutions.’
Revalidation
boost by IDF
Latest revalidation plans would give wholly private doctors access to a responsible officer (RO) through membership of the Independent Doctors Federation, we reported.
With concern about the cost and workload of revalidation mounting, IDF chairman Dr Jack Edmonds welcomed the body’s success in winning empowerment to appoint its own RO.
Data act warning
Thousands of doctors who treated patients privately were risking a criminal conviction and £5,000 Magistrates’ Court fines for failing to register under the Data Protection Act.
The Information Commissioner’s Office (ICO) contacted Independent Practitioner Today to alert private doctors of the need to check they complied with the 1998 law when handling patients’ personal information.
Inquiries suggested well over 50% of independent practitioners were unregistered.
The privacy watchdog’s records showed only 8,799 registrations from ‘private healthcare professionals’, which included many non-doctors such as physiotherapists and homoeopaths.
We warned readers that if they had any medical records on computer then they needed to register – for £35 a year.
The ICO said doctors practising privately were not always covered by the registration of either a hospital they operated from or by an NHS trust.
But a separate registration was required ‘to cover the processing of all personal data relating to any private treatment’.
Doctors are ‘overregulated’
This headline could have been taken from 2019.
A defence body boss warned that doctors were in danger of becoming over-regulated if proposals went ahead to introduce GMC affiliates, responsible officers (ROs) and recorded concerns.
MDU chairman Dr Christopher Evans claimed these innovations were unnecessary, unwelcome and had not been properly considered.
Echoing the concern of many independent practitioner consultants and GPs, he said they could mean countless extra hours of work.
Show you’re different
Independent practitioners needed to toughen up their marketing to show patients the advantages of coming to them rather than the NHS, a major reported recommended.
Key Note’s private healthcare market report 2009 warned that a visibly improved NHS could lead to
less demand for private healthcare, particularly if people increasingly perceived they could get it free.
Flood of job applicants
Independent practitioners were being flooded with high-calibre job applicants for office jobs.
The surge of interest in job adverts was boosted by new graduates who had been unable to find employment.
One consultant’s practice manager in the north of England said that the practice had received more than 90 job applications after advertising the post in a local paper.
School fees rocket
Doctors were paying £5,634 more a year to send each child to private school than they were a decade earlier.
The average cost of sending a child to private school had risen 90% in ten years, from £2,149 a term to £4,027, according to an Independent Schools Council Census.
SUBSCRIBE TODAY
Don’t miss out on what we report and advise in the future. Sign up for a £75 subscription today –consultants, GPs and practice managers can save £15 with a direct debit. See page 24
MEDICAL RISK SERVICES LIMITED
By your side, offering help, experience and expertise
With medical practitioners facing an ever-growing threat of disciplinary complaints and negligence claims, a new service offers them a powerful ally. Peter Anderson explains
A PIONEERING new service for medical professionals is offering a comprehensive package of advice and support for anyone facing the potential risk of legal action by disgruntled patients.
The launch of Healthcare Professional Protection comes as the number of disciplinary complaints and negligence claims against practitioners threatens to skyrocket, fuelled by the growth of no-win, no-fee medical complaints.
The service’s overriding objective is to ensure medical practices are robustly defensible, with high-quality, supportive analysis of each client’s processes and potential risks being carried out by proven experts in the medical and insurance sectors.
Backed by industry-leading indemnity cover, it seeks to offer certainty for healthcare professionals as the future of medical defence organisations (MDOs) remains clouded by the government’s moves to overhaul the traditional system of mutual cover.
Healthcare Professional Protection – available via the new www.hppb.co.uk website – forms part of a broad suite of products launched by Medical Risk Services Limited (MRSL), a prominent provider of support and advice to medical practitioners for the past 15 years.
The new service extends to stand-alone, tailored products that have been launched for specific professionals, such as surgeons, anaesthetists, spinal surgeons, dentists and those offering aesthetic procedures.
According to Roger Houston, MRSL’s co-founder: ‘Potentially huge legal claims can often result from what many would consider to be a very minor grievance.
Our increasingly litigious society – and 1% negligence potentially resulting in a 100% successful legal action – means it’s imperative that medical practices are robustly defensible.
Managing potential risks
‘That’s where Healthcare Professional Protection comes in, offering peace of mind that potential risks are being managed and that any potential complaints can and will be defended robustly.’
The company’s proactive approach to managing risk has won support from countless clients. These include Streamline Surgical, a bariatric surgery specialist working in partnership with NHS and private hospitals in London and the south of England.
Úna Tiernan, Streamline Surgical’s general manager, said: ‘MRSL have been a tremendous help to our business. Their knowledge has not only helped us ensure we have the right cover with an organisation which understands our business, but also warded off any circumstances leading to a claim.
tection Regulation to the ongoing overhaul of MDOs augured by the publication of the ‘Appropriate clinical negligence cover’ consultation document by the UK’s Department of Health and Social Care.
MRSL has been working closely with a range of medical businesses which have been seeking guidance and clarity on the extent of their potential legal liabilities – and the cover required.
These discussions stem frequently from confusion following the creation of partnerships or companies designed to share costs or provide more flexible working practices.
Mr Houston – a former director of operations at the NHS Litigation Authority (now NHS Resolution) – explained: ‘It’s become clear that most doctors understand their potential legal liabilities for the actions of their directly employed staff, or so-called vicarious liability.
‘One of the grey areas for some practitioners has been the extent to which this liability can extend to activities carried out by individuals working in the broader organisation, such as a partner or director or a member of the wider support team.’
ever; example,
MRSL believes that running a defensible and well-documented practice is more vital than ever, for example in ensuring evidence is available that individual patients consented to a procedure only after being made fully aware of the potential risks as well as the benefits.
‘We could not recommend them highly enough.’
Having launched in 2004, MRSL has been able to use its considerable experience and expertise to assist clients on a broad array of issues and potential threats.
Over recent months, these have ranged from the impact of the EU’s new General Data Pro-
However, as Mr Houston outlines, the dangers can cascade even further. ‘Ever-changing working patterns mean the potential fallout from a complaint or grievance can even extend to those working within an external agency or support business, such as administrators or accountants,’ he added.
With the potential for so-called ‘collateral damage’ to be felt by so many individuals, the solution for MRSL is clear. The company stresses the benefits – legally, operationally and financially – of medical professionals taking out insurance that is tailored to the entire business or entity rather than having each doctor sourcing their own indemnity cover.
The company’s discussions with medical practitioners have also alerted clients and potential clients to the very real dangers of liabilities passing from one practitioner to another via much more informal and flexible working arrangements.
These can include cases where much looser agreements see one professional providing support to another in order to share workloads at busy periods or to ensure cover during illness or holidays.
Legal liability in the wake of a patient grievance can also extend Above: The
between these more informal partnerships, with doctors and medical personnel being unwittingly caught out if one of their ‘casual’ business colleagues runs into difficulty.
In MRSL’s view, a sensible way forward can be for informal associates to create more structured partnerships and companies – im-
mediately making them eligible for a range of considerable financial benefits, not least specialist entity-wide indemnity products.
According to MRSL director Christopher Cloke Browne, the rapidly changing work environment – coupled with recent actions both by the UK government and the EU – means the launch
of Healthcare Professional Protection comes at the perfect time for medical practitioners.
Mr Cloke Browne, who joined MRSL following a highly successful career in insurance and financial services, said: ‘The threat of potential negligence claims, or of complaints being lodged with the General Medical Council or General Dental Council, means it’s vital that practitioners have the right support at their side.
‘Through Healthcare Professional Protection, we can offer 24-hour backing and peace of mind, letting medical professionals focus attention on what really matters – the vital clinical work they conduct day in, day out.’
For more information on Healthcare Professional Protection and MRSL’s full suite of products for medical practitioners, visit www.hppb.co.uk, email hppb@mrslenterprise.com or call 0203 058 3733.
This month, it is time for ‘C’ in our A-Z guide of essential matters that consultants and GPs need to consider to run their private practices efficiently. Susan Hutter reports
to of top tips is for cash . . .
TO QUOTE the Dragons’ Den TV programme: ‘Turnover is vanity, profit is sanity, but cash is reality’. This is now more important than ever for all businesses, including medical practices, as it is vital to manage cash flow effectively. Practice owners must constantly look at ways to improve cash flow into the business including:
Speeding up the collection of money from patients/insurance companies. It is vital that the practice’s bookkeeper/personal assistant is always on top of this (See page 37).
Making use of the maximum credit period the practice is offered by its suppliers. But do not upset the landlord!
Using specialist medical fee collection agencies for invoicing and collection. These agencies are particularly useful when it comes to dealing with embassies.
Costs
As well as cash coming into the practice, it is also important to look at what is going out. For example, are there areas of practice expenses that can be reduced, outsourced or generally made more efficient?
This could include:
Renegotiating leases. When you are coming up to a break clause in the practice lease, see if you can negotiate a decrease in rent. Remember that consultants and
Fully-serviced medical rooms for rent
GPs, generally, offer a very good covenant.
Ensure that you are using the discounts available on basic overheads such as stationery, couriers and travel.
Look at the structure of the backoffice staff. Is it possible there is an overlap with certain work? Is there any way you can use the practice accountant to assist with certain processes, thereby reducing, say, one staff member?
Control
Consultants and GPs, like all business owners, must run the business rather than allowing the business to run them. Ensure that you have clear, up-to-date and accurate financial information.
This will not only be a requirement for providers of finance, but will also enable doctors to make sound decisions based on real information rather than on instinct.
Most consultants and GPs do not produce interim accounts. However, it is important to have up-todate, and accurate, lists of monies owed to and by the practice and to ensure that this is reviewed at least on a monthly basis and action taken where necessary.
It is also worth producing a simple cash-flow forecast so that you can cover ‘cash heavy’ times and be prepared for them. This would include paying the tax bill.
The practice accountant will be able to assist you with this.
Children
It is worth consultants and GPs considering employing their children in the business. They must be at least 16 years old and it must be shown that they are carrying out proper work for the practice.
Many doctors enlist their children to assist with IT projects such as setting up and maintaining the practice database or even doing book-keeping work.
In the tax year 2019-20, one can earn up to £719 a month without having to pay tax or National Insurance.
As long as the salary is commensurate with the work carried out, and it can be demonstrated that the work actually is being carried out, the salary for the child will be tax-deductible in the practice accounts.
As always, it is important to take professional advice before proceeding with any of the above suggestions.
Susan Hutter (right) is a partner at Blick Rothenberg and part of the team that advises medical practitioners
PRIVATE PRACTICE GROWTH GUIDE
Make sure your email marketing flies
Jane Braithwaite (right) explores email marketing strategies, building a contact list and creating great newsletters and gives tips you can apply straight to your practice
email
AS YOU may have guessed, email marketing involves constructing and sending a high volume of emails, each one designed with a specific marketing message and a call to action for the recipient.
Recipients of these emails will have provided their email addresses and will have consented to receive marketing emails, but always remember that you are a guest in their inbox.
Chances are high that you will have been the recipient of an email marketing campaign; it is hard to avoid them. Some of us may check our phones in the morning to find four or five emails from companies offering us discounts on products or services, invitations to upcoming events or asking us to rate a recent encounter.
Depending on when you receive these emails, you may view them as unwanted spam, a helpful reminder for an appointment you had forgotten or you may even be grateful to
have something different to read on your morning commute.
The worst kind of marketing email is the one you don’t remember ever asking for and it can’t be stressed enough that you should only ever contact people who have granted permission.
But does it actually work?
Email marketing has been around now for a long time and may seem like a relic when compared to other tools in your digital marketing box.
The secret to its longevity is that it continues to be an effective and lucrative means to contact the widest audience and generate profitable interest. A 2018 study by Statista found that there are three times as many email accounts as there are Facebook and Twitter accounts combined.
That’s around 3.7 billion email accounts! Combine that with a 2017 study by Campaign Monitor, citing a £35 return in profit for
every £1 spent on email marketing, and you can understand why so many companies and service providers continue to invest heavily in email marketing.
Email marketing is only as good as the list of recipients it is based on, however, and quality data is becoming increasingly guarded.
Long gone are the days when companies could bombard email addresses with unsolicited marketing emails and you need to be aware of the various regulations surrounding data permissions before you begin any serious campaigns.
Purchasing lists of email addresses may seem like an enticing way around this, but many email marketeers caution against this, as results are often poor.
Obtaining permission
Someone once said, ‘it’s better to ask forgiveness than permission’, but when it comes to email market
➱ p18
Sending out unsolicited emails is simply bad for business and will frustrate, rather than attract your audience ing, you must always ensure you have obtained consent to use an email address for marketing communication before doing so.
Notwithstanding a multitude of rules under the General Data Protection Regulations that will be broken, sending out unsolicited emails is simply bad for business and will frustrate, rather than attract your audience.
Obtaining contact lists for email campaigns normally involves some quid quo pro, such as offering free content via your website in return for providing an email address and consent to receive marketing emails.
Be clear with your website visitors why you are asking for their email address and avoid using dry language such as ‘provide your email to receive updates’ – it won’t inspire much uptake.
Try instead to incentivise your market by offering free downloads of articles and eBooks, the latest news and titbits from your practice in a daily, weekly or monthly newsletter and details of events or promotions.
Once you have obtained email addresses and marketing permissions, ensure you store this information securely and that you provide the option for people to opt out of receiving your marketing emails in the future.
First
contact
When a visitor from your website or a patient in your practice provides their email address for your list, they are demonstrating a level of intent and interest in your services.
Don’t just sit on an email address until your next scheduled email, such as a monthly newsletter or seasonal campaign, but instead reach out to them as soon as possible with an introductory email.
Several email platforms will allow you to set up an automatic email when a website visitor subscribes, but this can be fiddly and lacks the personal approach.
A short but to the point introductory email that explains who you are and what your practice aims to achieve will be enough.
This is also a great opportunity to provide your availability and contact details, should they wish to make an appointment.
If you plan to send out daily,
weekly or monthly newsletters, let your new subscriber know and manage expectations early on, but ensure you keep to whatever promises you make.
Writing a great newsletter
The most effective email marketing strategies are underpinned by newsletters, which can be either daily, weekly or monthly.
Newsletters provide great opportunities to reach out to potential patients and to place your practice under a spotlight to inform and educate readers.
This is particularly effective for multispeciality practices, as patients who visit you for a specific problem may be unaware that you have colleagues that may be able to help with other conditions they may encounter.
The best newsletters have one thing in common: the content is worth reading. It sounds simple enough, but many healthcare providers struggle to create content that appeals to the general public
and often the balance of promotional content and educational content is wrong.
Effective newsletters will provide 90% free educational information to patients, which may range from tips to avoid injury, common symptoms of the conditions you treat in your practice or helpful thirdparty contacts such as support groups for chronic conditions.
Ten per cent of your newsletter should be promotional, which could take the form of patient testimonials, private practitioner biographies/interviews, service information or guides for patients to book appointments and claim on their insurance.
Whatever content you include in your newsletter, ensure it is unique and highlights what makes you and your practice special. This is a great time to revert to your unique selling point, as discussed in our first article in this series in April.
Be sure to include some eyecatching images and infographics in your newsletter to break up the text and keep your subject lines punchy and memorable when you send out your emails.
Sharing is caring
When you send out a marketing email, you should always include a call to action for your subscribers, such as linking back to a specific page on your website, a number to call to make an appointment or a thirdparty website that may provide unbiased advice about a specific condition or treatment.
Engagement with your marketing emails is an important metric for a successful campaign and you should make it as easy as possible for your readers to do so.
A great way to encourage engagement is to include options for readers to share your newsletter on their social media channels, and you should be sure to share and promote it on your own channels and website.
Many newsletters provide links to social media channels at the bottom of the newsletter, but this relies on your readers scrolling through every article and story you share.
You should instead provide the option to share your newsletter under each section or story, as this will increase the number of
‘shares’ in social media and subsequent engagement.
Encourage your staff members to also comment and ask questions and get a conversation going. People rarely want to be the first person to say something, but are happy to contribute in an active topic.
It’s a marathon, not a sprint Email marketing is a long term commitment and relies on you and your practice building and growing a good contact list of readers.
Social sharing will help you to attract more readers, but consistency is the best tactic to develop your campaigns. Be sure to include a call to action within your marketing emails and to maintain a good balance of educational content and promotional content. Encourage staff and colleagues in your practice to contribute to your newsletter and to engage with your social media posts to foster conversations and engagement. Next month we end our series with a look at analysing the results of your marketing campaigns and how to improve on what has and has not worked well
Jane Braithwaite is managing director of Designated Medical, which offers business services for private consultants, including medical secretary support, book-keeping and digital marketing
Succeed at real Monopoly
Seven myths that shouldn’t stop you from investing in property. Adapted from a new book by Dr Lafina Diamandis
SOME PERCEIVED challenges stop people in their tracks when they first start thinking about investing in property.
Unfortunately for many people I meet at my property courses and events, these challenges plus a fear and a lack of relevant education delay them getting started for many years. This includes me. If only I’d had the necessary knowledge and advice when I was in university. I could have started investing much earlier, quit the part-time jobs I had and taken advantage of other opportunities, instead.
You’re not alone. Forget the past, don’t compare yourself to others and start from where you are without any regret or self-judgment. You can succeed.
I recently heard Jamil Qureshi, a performance psychologist who has trained some of the world’s most successful athletes, speak at a novel property developers’ club of which I’m a member. His talk was centred around how our thoughts translate to feelings which translate to actions and how the internal dialogue we continuously have with ourselves can hugely affect our performance.
Avoiding risk
Many people’s actions may be focused on moving away from negative situations or avoiding risk rather than considering the possibility of success or what would happen if they succeeded.
Jamil told a story of a great footballer who was amazing at taking penalties. Every time he took a penalty, he asked himself the same question repeatedly while he ran up to kick the ball and only answered it just before kicking. Will I run left or right after I score the penalty? Scoring was a given. He had already mentally primed himself into a positive, success mindset. His only question was which way he would run to celebrate his success – quite a different mindset to most people who may find themselves in that position. With property, if you focus on factors you perceive as negative or risky and allow yourself to obsess over them, this could have a serious impact on your feelings and actions. The same goes for listening to negative people who don’t know what they are talking about. A
fear-driven attitude will also affect how others perceive you and what sorts of opportunities come your way – or not.
You shouldn’t ignore risks or the facts of your personal situation. Instead, look at it differently by turning all possibilities and realities into statements, facts or questions. For example:
THOUGHT: I have no funds to invest.
FACT: We need £x funds for this project.
QUESTION: I wonder what funding sources are available for a project like this.
Similarly, when it comes to risk:
THOUGHT: The property market is too risky at the moment.
FACT: There are risks I should be aware of in the property market at the moment.
QUESTION: What exit strategies/plans can I come up with to mitigate the risks or if things don’t go to plan?
It is useful to mentally check in with yourself like this to ensure you are as objective as possible and don’t give up before you even get started.
As medics, we are generally capable at managing risk and most of our perceptions of risk outside of medicine are largely associated with a fear of the unknown.
1I don’t have enough money
You may think you can’t invest in property because you assume you need some, if not a lot, of money to buy your first property. I thought exactly the same before I learned more about property investment.
This is a linear way of thinking and, unfortunately, no one has taught us to think about investment creatively. This assumption is not true for three reasons. It assumes:
The only way to invest in a property is to buy one in the conventional way;
Investing in a property must be with your own money;
You need a lot of money to get started.
The good news is that none of the above are true. If they were, how do you think professional property investors keep their businesses going? How do you think any business ever gets going? Entrepreneurs and start-ups fre -
quently must raise funding for their businesses, and property fundraising is similar. Furthermore, don’t let a lack of experience in doing this put you off. In July 2018, I had the pleasure of hosting the NHS Clinical Entrepreneur programme’s end-of-year event called ‘The Big Pitch’ at Bloomberg HQ in London, where we celebrated the achievements of the entrepreneurs, one of which was that more than £113m of funding has been raised in the first two years. Yes, by doctors. No, not out of their own pockets!
At some point, everyone will run out of funds once they have finished purchasing properties, buildings or land sites and they have to learn to look at alternative funding sources. If you have a good enough business proposition, you’ll find the money required to support it.
2I don’t have any experience
Thinking you don’t have enough experience to get into property or assuming you need to be a ‘professional’ investor is common. Perhaps even more so within the medical profession, as we are accustomed to studying hard for formal qualifications and providing evidence that we are adequately skilled to do something. Developing knowledge and expertise will always be valuable in any field. However, you do not need any prior experience or qualifications to become a property investor. No offence to any investors out there, but, compared to medicine, property investing is pretty straight forward and you can
become a successful property investor in a fraction of the time it takes to become a doctor.
Experience is always beneficial, but it’s not a prerequisite. All you need to do is make sure you invest some time in developing your property knowledge and skills and build a supportive network of people who can help you if you get stuck.
In this regard, it is no different to being a doctor in training or a clinical entrepreneur developing clinical skills and expertise over time. It just happens a bit faster in property-land.
3
I don’t have any time
This is a common reason or excuse. We all have the same 24 hours in a day, so why do some people manage to achieve more within the same time period?
Some of the busiest people I know have achieved incredible things and yet they’re seemingly people who are short of time. As the saying goes, if you want to get something done, give it to a busy person. So how do you do more when resources such as time are finite? This is down to the power of leverage.
Doctors are busy people and when it comes to shift work and the nature of the job itself, it can feel like there is little time or fuel in the tank to do anything other than collapse in front of Netflix at the end of the day.
One way to get around this, if you are really short of time, is to leverage other people’s time and expertise to help you to achieve your mutual goals.
All you need to do is decide why you want to invest in property, what your goals are, how you will achieve them and who you need to help and motivate you along the way.
This might mean using a property sourcer to help you find great deals, setting up searches on property portals, using a lettings agent to manage your properties or doing a joint venture with someone else who has more time than you and can do the majority of the leg work.
I have learnt to be ruthless with my time and realistic about what I can achieve and I’ve chosen to work with great partners, which allows me to keep moving forward. I don’t always get it right with time management, but I’m always continually improving.
You don’t have to do it on your own, either. In fact, you can’t do it alone. In your average property transaction, you’re likely to need
an accountant, solicitor, mortgage broker, builder, estate or lettings agent, handyman, tenant referencing service and more.
You’ll achieve far more and faster by working with others, allowing them to help you and helping them out when you can in return.
There are a number of ingenious ways to get help through employing virtual assistants (VAs) as well as a number of other professionals who can do your admin and any ‘low value’ activities that consume a lot of time, hence giving you your personal time back.
4
Property investing is too risky
There is certainly much anxiety around taking on a large debt, such as a mortgage, but this might be alleviated if you understand the difference between good debt and bad debt.
There is a risk to property invest-
27-30 January 2020
Anaesthesia, Critical Care & Pain Dermatology • Emergency Medicine General Practice • Plastic Surgery Radiology • Trauma & Orthopaedics
• Hands-on workshops
• Multidisciplinary lectures
• Satellite and joint sessions
• Bedside ultrasound course
• Contribution from allied specialities
• Keynote lectures by invited speakers
ing, but, honestly, what isn’t risky? We take on risks every day we go to work, assess patients, write prescriptions and write up medical notes.
Yes, there is a risk to property investment, but you can educate yourself to understand what that risk is – specific to your strategy –and take measures that allow you to mitigate it as far as possible.
For example, always have a contingency plan – ideally, three exit strategy options in case things don’t go to plan – and follow some simple investment rules that will safeguard you against making terrible mistakes in the first place.
The fear of risk seems to stem mainly from a lack of knowledge and understanding about how property investment and the market cycle works.
Contrast the fear of risk in property to the risks we take every day in the profession. There is a great deal of risk involved for the patients we treat as they trust us to treat them or guide them in life-or-death decisions. We are continually treating acute and life-threatening conditions or trying our best to prevent them from occurring.
We also risk our mental health from the responsibility we take on and the stresses, strains and number of emotionally intense situations we experience along the way, such as the death or serious injury of a patient.Pretty serious stuff.
Compare this to the financial risks involved in property. For example, you lose your money, you lose a property through defaulting on payments, you get a bad credit record or – worst-case scenario – you become homeless.
This can be mitigated in the first place, but, if it does happen, it’s far easier to bounce back from something like that than the various disasters related to working in medicine or being investigated by the GMC as a result of a complaint about your clinical practice.
There are many different types of investment. Some investors have an appetite for high-risk –and high-reward – ventures and others prefer to stick to medium- or low-risk ventures, with commensurate low to medium reward. There is no right or wrong as long as you know what the worst thing that could happen is and feel comfortable with taking that risk.
5The market isn’t right
This is one phrase I’ve heard used by many amateur investors of late and with the newspapers reporting the doom and gloom of recession, Brexit, a hung parliament and recent property tax changes, who can blame them?
The problem with taking advice from the newspaper or your nextdoor neighbour is that by the time the news has filtered down to the masses, it’s usually time to do the opposite of what is being reported. As Warren Buffet says: ‘Be fearful when others are greedy and greedy when others are fearful’.
There are two factors here you must be aware of. Firstly, the property market is cyclical, which means it will always move through boom and bust phases.
Secondly, there are different investment strategies that can be used in different phases of the market cycle. It’s not all about buying and selling to produce a profitable investment.
One example is the retirement living sector. This is a billionpound industry that plenty of companies as well as investment funds are moving into. Are they scared off by the state of the current market and Brexit. No. Why?
Successful property investors and developers take a long-term view and consider long-term demographic and societal trends. Therefore, provided you understand the property market cycle and know which part of the cycle you are in, you should be able to invest successfully regardless of what the market is doing.
6
I’m too old – or too young – to start I truly believe you are never too old to start anything. There are some investors within my network who have started out in their 50s and 60s – and , yes, they can still obtain mortgages. Listen up: it’s never too late.
7
The tax rules have changed: it’s not worth it any more Don’t believe everything you read in the papers. Yes, the tax rules have changed. Yes, we are currently in a downward part of the property market cycle with ongoing uncertainty about how Brexit and other factors will affect it.
Does this mean property is no longer a profitable asset class? Of course it doesn’t. Rules change, so you have to learn to be flexible and adapt. Investors who once purchased in their own names are now incorporating.
Investors whose main strategy was flipping (buying to sell) properties for a profit may now be buying houses of multiple occupation and flipping only when the right opportunity comes along or when the market picks up.
I heard one financial adviser tell doctors he wouldn’t touch buy-tolet with a bargepole and they would be better off getting a 5-7% return investing in stocks and shares.
I was perturbed by this, as it gave a one-sided view and I approached him to find out why he had made such a blanket statement. He told me this was due to the recent Section 24 tax changes affecting people who invest in their personal names.
When pressed further, he acknowledged that great profits can be made from property when you know how – most people don’t. The bottom line is that people have their own agendas and will only tell you the story they want you to hear. It’s important to understand the full picture by educating yourself and be able form your own opinion.
Naturally, property is not the only asset to invest in, but given my lack of knowledge about stocks and shares or trading, property is currently lower risk and more accessible to me. It is definitely higher reward – 3% return, for example – than investing in most ISAs and much, much better than leaving your money to depreciate in the bank as inflation erodes its value over time.
I love the fact that property is an asset you can easily understand and control and, as one doctor says, you can ‘scratch and sniff’ it.
You can also make some incredible contacts, provide people in your community with a comfortable home, build a sustainable business and apply your business skills to healthcare, too.
Next month: The big five investment strategies and how to develop yours
Dr Lafina Diamandis is co-founder of Eurekadoc, a start-up helping doctors to realise their full potential through diverse medical education and careers curation and is passionate about helping doctors to become financially independent through property – even with limited time, funds or experience.
She runs the only UK course specialising in property training for doctors, has delivered education and training to over 1,000 doctors and is an advocate for portfolio careers in medicine.
In 2018, Lafina launched the first Learn While Investing crowdfund-
ing project making it possible for doctors to get involved in property projects that are fully transparent and offer an opportunity for education and training.
Lafina and her business partner John Friis made a property development project available to the medical community through Simple Crowdfunding, overfunding it in just seven minutes.
ANNUAL ALLOWANCE
SPECIAL OFFER – £15 direct debit saving
TO RECEIVE OUR TEN ISSUES A YEAR
Dear Reader,
Subscribing to Independent Practitioner Today is the only way you can be sure you will see every issue and have the option of reading us online using our special page-turnable edition. Don’t risk missing out. Our personal subscription for doctors and managers is only £90 a year and £210 for organisations. But you can cut this to just £75 and £180 respectively if you pay by direct debit.
So take advantage of this offer now for our unique business journal dedicated to supporting you in your private practice. We’re confident your subscription will repay itself many times over!
Editorial director
APPLICATION FOR SUBSCRIPTION
Instructions to your Bank or Building Society to pay Direct Debits
Name and full address of your bank/Building Society
To: The Manager Bank/Building Society Address Postcode Ref. No.
Banks and Building Societies may not accept Direct Debit instructions for some types of account
send a copy of your letter to us.
CREATING A GREAT CONSUMER EXPERIENCE: THE POWER OF COLOUR
No grey areas in the good use of colour
Nick Butcher and Dr Nick Hayward follow their last article – on the importance of a strong brand identity – with a look at colour and how this can become a powerful tool in helping to create a great healthcare user experience
MANY PEOPLE find colour a scary subject. We all have our own likes and dislikes; many see it as subjective and difficult to use strongly without offending someone.
Much research has been conducted on colour theory and there are some startling conclusions on how much colour can affect us both physiologically and emotionally. As designers, we can use these findings to great effect.
The psychological effects of colour can be immense. In 2009, blue lighting was fitted at the end of railway platforms in Tokyo in an aim to reduce the incidence of suicide.
It was installed due to claims that blue lighting makes people calmer and less impulsive. As a result, suicide rates fell by 74% at the stations where the lighting had been installed .1
Let us first consider colour as a branding tool. Interestingly, the healthcare industry has traditionally stuck to the green and blue end of the spectrum.
This is probably a natural and appropriate association – words such as safety, nature, tranquillity and calm are associated with these colours, which are often seen throughout hospitals.
At Beyond London, we have worked with some of the best colour theorists, including psychologist Angela Wright. 2 Conventionally, the way we understand colour has been thought to be subjective: our age, gender and social status all playing a part in our unique response to colour.
But, in the 1970s, Angela investigated further how colour can affect our mood and identified objective correlations between colour and human behaviour.
Over the years, as she studied these relationships further, she formed four basic groups that every colour fits into. The colours in these distinct groups each conjure similar emotional responses.
Colours and seasons
Later in the 1990s, Wright’s theory gained weight when she was able to pinpoint mathematical correlations between the colours in each group. These groups can easily be understood as being associated with the seasons.
Take yellow, for instance. This could be a bright primary yellow (group three – winter) or a soft,
warm yellow (group three –autumn). Both are yellow but the primary, winter yellow can be perceived as feeling cold, bold, modern and elitist, while the warm, autumn yellow can be seen as welcoming, reliable and environmentally friendly.
A large number of the ways we are psychologically affected by these colour principles has been proven to be unaffected by age, culture and gender.
Angela described that one cannot just talk about hues when using colour, as this is like describing a table of different cakes as baked goods rather than cream puffs, frangipanes and Victoria sponge.
So, when specifying colour, simply mixing up random colours can lead to dissonance, whereas mix-
Strong colour on reception desks is often used to focus attention where it is needed and to guide people to where they need them
ing colours from the same group creates harmony.
It took a while of working with Angela to really be able to ‘see’ the groups when looking at lots of colour swatches. But once it is grasped, the difference it makes is amazing.
Harmonious effect
Having just one colour from the wrong group in a collection would feel awkward, but as soon as it was swapped to a similar shade from the same group as the others, it would suddenly all look harmonious. Angela shared a story about being contacted by a prison governor who had decided to paint the prison cells yellow as he had heard it might calm the prisoners. Unfortunately, he had chosen a yellow from the wrong group
(winter) and riots ensued. Angela was called in and a new yellow hue was specified, and calm was restored.
Getting colour to work positively in healthcare is important, but precisely how it is used is equally challenging. Within interiors, colour can do many things. It can make spaces feel bigger, it can change the shape of a space, it can highlight things and it can disguise things.
We often use strong colour behind reception desks to focus attention where it is needed and to guide people to where they need them. It always amazes us when people pick out radiators in a different colour to the wall – who wants to draw attention to a radiator?
Linking environmental colour to your brand colour – usually a
toned-down version – can positively link the experience together so the journey feels considered and professional.
Consistent approach
Take ‘One Medical’ from the US, for example. This brand has used a unique green and consistently applied it across all of its communication, ranging from business cards to advertising. You can tell it’s One Medical without even seeing the name.
One has to consider white when discussing about colour. Often seen as a ‘non’ colour, white has some of the most powerful but least understood properties. Firstly, it is often the default option – paint it white, as it won’t offend.
There is nothing wrong with white; in fact, when used with
Words such as safety, nature, tranquillity and calm are associated with green and blue, which are often seen throughout hospitals
other colours, it is the perfect counterfoil. It can reflect colours and take on what is around it so that we rarely see white at all, but more a collection of greys and other subtle reflected tones.
For some, white is about purity, cleanliness and innocence, but for others, it is cold, sterile and stark.
White is important in many cultures for many reasons. In Feng Shui, white is linked to metal to create harmony, while in many Asian cultures, white is associated with mourning.
Speaking as a design agency, white is an excellent surface for colours to be played upon. Coloured lighting can create constantly changing surfaces and white can be brought to life through the juxtaposition of matt and gloss finishes or textures.
Colour can also be one of the biggest and yet cheapest changes to implement in an interior. Simply painting a wall can transform a space from being ordinary to being extraordinary.
This is vital in healthcare because positive environmental interactions can promote psychological wellness among patients and staff, potentially improving healthcare outcomes. For example, simple wall colour changes have been shown to be associated with a shortened duration of hospital stay.3
Few people appreciate blandness and it is colour that can be psychologically supportive through creating uplifting feelings of well-being and joy.
If used with confidence and subtlety, patients and guests will thank you for brightening their
visit and for being confident, assured and even charismatic.
Nick Butcher (below, left) is creative director of Beyond London (www. beyondlondon.com) and Dr Nick Hayward is a neuroscientist and medical technologist with a PhD in neurobiology and medical imaging development
Next month: The use of biophilic design in healthcare
References
1. ‘Does the installation of blue lights on train platforms shift suicide to another station?: Evidence from Japan’ by Tetsuya Matsubayashi, Yasuyuki Sawada and Michiko Ueda. www.sciencedirect.com/science/article/ pii/S0165032714004741
2. The Beginner’s Guide to Colour Psychology by Angela Wright
3. Colour and lighting in hospital design by Hilary Dalke, Jenny Little, Elga Niemann, Nilgun Camgoz, Guillaume Steadman, Sarah Hill and Laura Stott. www.sciencedirect.com/ science/article/pii/S0030399205001283
White is an excellent surface for colours to be played upon
Working with inspectors
The Independent Healthcare Providers Network and the Care Quality Commission have joined forces for ‘outstanding care’. David Hare explains
AS THE trade body representing the independent health sector, the Independent Healthcare Providers Network (IHPN) is mindful of the key role we can play in not only bringing members together to share best practice and learn from each other, but also to act as a single point of contact for regulators to engage with providers on a sectorwide level.
We were therefore delighted to host our first annual IHPN/Care Quality Commission (CQC) joint regulation conference this summer. It was part of a programme of work that IHPN began with the CQC last year to better understand what the regulator considers to be good practice under each of the five key lines of inquiry.
This event looked at what providers need to do to improve on the CQC’s ‘Effective’ domain, following on from an earlier workshop on the ‘Safe and Wellled’ key lines of inquiry.
With more than 80 IHPN members attending from a range of healthcare providers, as well as representative from the Independent Doctors Federation, delegates had the opportunity to take part in a mixture of plenary and breakout sessions.
Sharing best practice
There were keynote speeches, including from CQC chief inspector Prof Ted Baker and Russell Parkinson of the National Freedom to Speak up Guardian’s Office.
IHPN members who have
achieved Outstanding in the ‘Effective’ category gave presentations and question and answer sessions ensured that providers shared their best practice and learnt from each other.
To ensure that providers from all parts of the healthcare sector had the opportunity to engage with the relevant CQC leads on the main issues of the day for each sector, specific sessions were also held for independent hospitals, diagnostic imaging and primary care providers.
Not only did the conference offer practical advice on how to improve the effectiveness of the care they deliver, it also highlighted the clear maturing of the relationship between the CQC and independent providers over the past couple of years.
I saw a much greater focus on mutual co production while, of course, still maintaining the formality required by the regulatorprovider relationship.
As part of this open and constructive approach, we were delighted that the CQC used the joint conference as a platform to launch its Driving Improvement report, which looked at how eight independent acute hospitals have made significant improvements in the quality of care and improved their CQC rating on reinspection (see page opposite).
The case studies draw on interviews with a range of staff from hospitals that have made positive changes to drive improvements for
The conference highlighted the clear maturing of the relationship between the CQC and independent providers
patients, with the key theme of the report focusing on the importance of robust leadership and meaningful engagement with staff.
Room for improvement
IHPN was delighted to have been asked to provide a foreword for what we view as a vital report. While the vast majority of the almost two million patients who are treated in the sector receive very high quality care – with 19 independent acute hospitals rated as outstanding and almost 80% rated as good or outstanding by the CQC – we have always made clear that, as with any system, there should always be room for improvement.
And indeed, the Driving Improvement report demonstrated providers’ determination to imp rove. Made possible by providers’ willingness to be open and reflective both with themselves and with external stakeholders, the report highlights what has been done to improve in both individual hospi
tals as well as between hospitals that are part of a corporate group.
Lodestar to follow
Covering key themes including leadership, culture, communication, learning, staffing and patient and public engagement, it expresses in clear terms the journey that these organisations have gone on and provides a lodestar for others to follow.
It also makes clear the critical importance of CQC’s inspection process and their focus both on providing a thorough assessment of standards of care while also recognising that it has a vital role to play in the provider improvement journey.
Safety and quality of care is ultimately the responsibility of the healthcare provider itself and this report illustrates how central this is to the independent acute sector, with clinical and managerial staff at all levels taking ownership for driving change.
Learning from others and sharing best practice is also vital. And through both documents like this and the joint IHPN/CQC conference, it is clear that being the best is an aspiration for all in the independent sector.
David Hare (right) is chief executive of the Independent Healthcare Providers Network
The CQC used the conference to launch its ‘Driving Improvement’ report
Boost your CQC score
HCA’s The Harley Street Clinic rose from a ‘good’ Care Quality Commission rating in 2015 to ‘outstanding’ in 2017. A new report from the commission shows how
THE LEADERSHIP team and staff at
The Harley Street Clinic were disappointed with the original rating, but saw it as an opportunity to reflect and improve.
Aida Yousefi, its chief executive, says that the first inspection clarified what was expected of a registered manager and chief executive and how she could support her teams.
After the first inspection, the leadership team arranged a meeting with all consultants. Everybody wanted to know what they could do to improve and make things better for patients and staff.
Nurse quality matron Tina Thornton, says: ‘I was part of the
team that got the first draft of the inspection report. We did not know what to expect and were not sure about how CQC had interpreted the evidence that had been shared for the report.’ All staff felt that ‘good was not good enough’ and they wanted to be rated as outstanding.
Acted fast
The leadership team acted fast. They set up monthly governance meetings and arranged for their governance committee to feed into their medical advisory committee to improve communication and information sharing.
Aida also provided regular
updates on her activities as a chief executive. The leadership team also worked to make it easier for patients and staff to share their feedback. This included carrying out leadership rounds and running an independent staff engagement survey to understand any issues.
The Harley Street Clinic also attained the MacMillan accredited association. The accred itation is awarded to providers who show high standards of care and provide a suitable environment for people living with cancer.
Boss Aida says: ‘To continue to attract the best consultants and for
The Harley Street Clinic in Weymouth Street, London, and its chief executive Aida Yousefi (right) ➱ p30
BACKGROUND
The hospital has 103 beds, carries out a range of surgical procedures and provides medical and critical care to adults. It also provides services to children and young people, does outpatient consultations and provides critical care services to children. At the time of the inspection, the hospital was only providing care through insurance and for those who pay themselves.
Lorraine Hughes, HCA
Healthcare UK’s chief nursing executive, says:
‘The corporate HCA UK team’s role is to support all sites to deliver exceptional care. There are dedicated corporate teams that are helping to drive improvements and ensure that facilities maintain their quality marker.
‘Analysis and performance metrics are available on the intranet, so it is available to everyone in the organisation.
‘The team’s activities range from supporting our nurses with information on incidents, risk assessments and patient timelines to leveraging advanced analytical techniques such as natural language processing to extract every improvement opportunity from our patient experience surveys and machine learning to predict outcomes for our patients.’
‘There is so much to come next; it’s exhausting but exciting. We always want to continually improve.’
Stuart James, medical clinical governance lead
the people using our services, we had to find a way to learn from our [CQC] inspections.’
At the time of the first inspection, the leadership team felt evidencing and auditing were key issues. They knew that they provided highquality care, but they did not measure it. The hospital also did not have a fully online auditing system.
This meant that they could not extract all the data effectively – or showcase and evidence the full audit programme. In response to this, HCA Healthcare UK established an online quality system to audit and review the quality of services.
Tina says: ‘We were in the process of making a switch from paper to paperless at the time, so it was difficult to pull data together and share it with CQC. By the next inspection, we had embedded our new system and could show how we measured data.’
Head of clinical services Chris Hague says: ‘We were in the process of learning CQC terminology, so we did not know how to sell ourselves best to show our work to CQC.’ By the second inspection, the leadership team was more embedded, approachable and visible.
Unified approach
Being rated as outstanding in the ‘well led’ category came from focusing on building a strong executive team that spent more time with staff on the wards. The Harley Street Clinic has long standing leaders at all levels, many of whom started their career there. The leadership team now has a unified approach to improvement.
The clinic has also grown its medical engagement by putting in place a now long standing chief medical director and medical governance lead, both of whom have a vital clinical leadership role in setting the standards of what outstanding looks like for the hospital. After being rated as good, The Harley Street Clinic built a culture
that celebrated success and did not blame staff. Now, staff are proud of what they do and are not shy to show this. They feel part of an out standing facility.
The culture of The Harley Street Clinic means that staff are never complacent and are always look ing for improvements.
By the second inspection, the facility had hired established new ‘risk leads’ to make sure that risk management across the facility was aligned and that the hospital investigated all risks and shared learning.
Leadership also implemented a strategy to ‘release nurses back into caring’. Chris added: ‘The cul ture changed and nurses were more empowered. The organisa tional structure is also quite flat, so everyone has a voice now.’
Tina says: ‘Departments used to work in silos, but since the first report, they’ve come together to share learning about what they do well.’
Monette Gomez, clinical nurse manager, says: ‘Staff are being empowered and there is now a cul ture where managers are not fear ful of creating an open forum for staff.’
The hospital has also set up dedi cated weeks where they encourage everyone to share learning around important themes. They include Empowerment Week, Patient First Week, Patient Safety Week, Human Factors Week and Freedom to Speak Up Week.
Despite this activity, the clinic struggled to get patient feedback on areas for improvement. They find it difficult to gather patient views through traditional chan nels because, like many other pri vate hospitals, many of their
Melissa Watson, HCA
Healthcare UK’s director of quality review, says: ‘To make sure that hospitals continue to evidence their quality through being rated as good and outstanding, we have embedded a standardised assurance programme.
This includes using a self-rated assurance platform called HealthAssure that gives visibility and transparency across the group. We also run a peer-review programme.’
The Harley Street Clinic features as one of the case studies in the CQC report
The UK’s medical aesthetic event
Uniting surgical and non-surgical medical aesthetic communities to raise industry standards
What you need to pass revalidation
Get it sorted! Kate Lewis and Darren Wiggins look at the requirements for a successful appraisal and revalidation
AS A LICENSED doctor, it is your responsibility to make sure you read, understand and follow the GMC’s ‘Guidance on supporting information for appraisal and revalidation’, because failure to do so could result in your licence to practise being at risk.
As directors of a revalidation and appraisal service to designated bodies, part of our duty is to contact those doctors who have a prescribed connection through the GMC to remind them when their appraisal is due.
We would say we do this diligently: at least three months before the appraisal date. Some leave it until the second reminder to acknowledge us; some leave it until the third reminder and some ignore us completely.
Often, we get told: ‘I have up to 15 months from the date of my last appraisal to get the next one done’ or ‘I have had three appraisals in this five-year cycle, so I don’t need another before revalidation’.
Unfortunately, this is not the case at all. ‘Annual’ means within every nine to 12 months, unless you have extenuating circumstances that prevent you from completing an appraisal; for example, you may have missed an appraisal due to maternity leave or you have been on long-term sickness leave.
Any mitigating circumstances for missing an appraisal should be approved and confirmed by your Responsible Officer (RO).
The lonely trail to keep up to date
Authors Kate Lewis and Darren Wigins began their series of articles on revalidation in our June issue
What happens If you fail to engage?
Failure to engage with the local processes in your work domain to comply with revalidation requirements, including appraisal, will put your licence to practice at risk. Depending on the circumstances, the GMC may withdraw your licence if, without reasonable excuse, you fail to comply with its guidance and will invite you to make written representations within 28 days explaining why it should not withdraw your licence. Your annual appraisal is the key to revalidation. It should be supportive and is not a pass or fail tickbox exercise.
The appraisal must consider your whole scope of practice and you must declare all the places you have worked and the roles you have fulfilled as a doctor since your last appraisal.
Supporting evidence and information you collect must cover all aspects of your work including voluntary, non-clinical roles and any private as well as NHS work.
Supporting information you must collect to reflect and discuss at your appraisal
The GMC advises that your supporting information should be from practice in the UK. However, your RO may accept supporting information from overseas practice if they are satisfied this meets the required standard. You should check this prior to working overseas while holding a UK licence.
There is no set method for gathering and providing supporting information and there are no hard and fast rules as to how you should
Your annual appraisal is the key to revalidation. It should be supportive and is not a pass or fail tick-box exercise
do this. Many organisations use a MAG4 form, which is an electronic form that you can upload your evidence to.
It may not be used on mobile devices such as phones and tablets; you will need a desktop computer. Other organisations use their own systems on which you may need some guidance and training.
Continuing professional development (CPD)
The most important part of CPD is that you reflect upon it and record what you have learned and how this helps you to maintain or improve upon your quality standards of your practice or influences your behaviour in the workplace. This should be discussed at appraisal.
The GMC does not prescribe exactly how many CPD points you should undertake each year, only that the CPD must relate to your whole scope of practice. Any questions regarding CPD should be discussed with your appraiser or RO.
There seems to be a common misunderstanding that you must do 50 CPD points/hours, but this is not the case.
If, for example, you only have 45 hours’ worth of CPD, then this may become part of your personal development plan (PDP) for the next year. Some medical colleges and professional bodies have requirements and you should check with those if you are a member; otherwise, speak to your appraiser. If you would like a free template for recording your CPD reflection, then please email kate@themlu. org and we will be happy to provide this to you.
Remember, CPD is not just about attending training courses and having certificates. You can also include reading articles/journals relevant to your work and reflecting on them.
We get many questions about what constitutes CPD and what can be used in appraisal on a regular basis. So, if you are confused about CPD, you are not alone. We cannot labour the point enough: Speak to your appraiser – he or she is there to help you.
Quality improvement activity
Like CPD, the purpose of quality improvement activity is to enable you to review the quality of your work and evaluate it. This helps you to identify what in your practice is working well and where you might need to make some changes. It also gives you the opportunity to see if any changes you have made have improved your practice.
At appraisal, your appraiser will want to see that the extent of quality improvement activity you have undertaken is appropriate for the work that you do. If you are unable to yet evaluate the results of any changes you have made or that you plan to make, you can discuss at your appraisal how you intend to do this and include it in your PDP for the next appraisal period.
The faculties and medical royal colleges provide guidance on what would be the most appropriate activity for those doctors working in certain specialities or general practice and you should be advised by their requirements.
Depending on the roles that you perform and your roles and responsibilities, quality improvement activity can take many forms and includes:
➲ Clinical audit – evidence of effective participation in clinical audit or an equivalent quality improvement exercise that measures the care with that an individual doctor has been directly involved.
➲ Reviewing of clinical outcomes – where robust, attributable and validated data are available. This could include morbidity and mortality statistics or complication rates where these are routinely recorded for local or national reports.
➲ Case review or discussion – a documented account of interesting or challenging cases that a doctor has discussed with a peer, another specialist or within a multidisciplinary team. Four case reviews will be required.
➲ Audit and monitoring of the effectiveness of a teaching programme.
➲ Evaluating the impact and effectiveness of a piece of health policy or management practice.
You should demonstrate that you have evaluated and reflected on the results of the activity or audit.
This might be through reflective notes about the implications of the results on your work, discussion of the results at peer-supervision, professional development or team meetings and contribution to your professional development.
You will need to demonstrate that you have taken appropriate action in response to the results.
This might include the development of an action plan based on the results of the activity or audit, any change in practice following participation, and informing colleagues of the findings and any action required.
You should consider if an improvement has occurred or if the activity demonstrated that good practice has been maintained. This should be through the results of a repeat of the activity or re-audit after a period, where possible.
Next month: Significant events, feedback from patients and colleagues, and compliments and complaints
Kate Lewis and Darren Wiggins (below) are from ACI Training and Consult ancy Ltd, specialists in revalidation and appraisal services
NEW SERIES: FIGHTING FRAUD
Stop online scammers
Manage the threat of fraud in private practice. In the first of our new series, anti-fraud expert Vin Pandha (right) outlines some danger areas and shows why doctors’ practices are such a big risk
THE RISK of fraud and cybercrime is growing at an alarming rate with no real signs of any slowdown. Fraudsters are targeting individuals and businesses across the world and across all sectors.
Healthcare is certainly no exception, so it is essential that you know what to look out for when it comes to these risks and, more importantly, what steps you can take to protect yourselves and your practice against fraud.
Criminals successfully stole £1.2bn through fraud and scams in 2018.* This not only has a significant impact on victims of the initial fraud, but the proceeds of these crimes often go on to fund illicit acts which further damage our society such as drug trafficking and terrorism.
Medical practices and GP surgeries can be a favourite target for fraudsters, as the responsibility for managing the finances and organising day-to-day administration often falls on one or two individuals.
They have to perform many functions, whereas larger organisations can call upon more resource and greater funding to protect against fraud attacks.
This also means less opportunity to segregate duties within a practice and if there’s little or no oversight from senior colleagues, preventing insider fraud can be more difficult.
The main objective of fraudsters isn’t always the practice’s money; in some cases, it is to gain access to confidential sensitive data such as patient records.
The criminals then exploit their position, holding organisations to ransom to regain access to the data. Other cyber-attacks can
mean that the cyber criminals are able to disrupt access to devices or, in extreme cases, the whole network.
The internet has, without doubt, driven significant changes in the approach used by fraudsters during recent years. The digital age has relatively quickly offered us so many benefits in both our personal lives and in business and it’s difficult to imagine how we would cope without the internet.
Risks of convenience
We have been very quick to embrace these benefits; however, our appetite to understand the risks that come with this convenience rarely keeps pace.
All too often, we seem to place an inherent trust in what we view on our computer screens and in what we click on when online; a level of trust that would not automatically be present if we were judging a person face to face or a situation live.
Fraudsters have therefore focused
efforts more recently on Authorised Push Payment fraud. In these attacks, their aim is to get a victim themselves to unknowingly authorise a payment to a fraudulent account, but believing they are making a payment to a genuine beneficiary.
Convincing scams
Authorised Push Payment frauds increased significantly in 2018 – up 93% when compared to 2017* –and fraudsters are focusing on these convincing scams at the moment due to the increased chances of a successful attack. These attacks are also usually well researched and well prepared rather than being purely opportunistic.
Malicious software – known as malware – can allow fraudsters to monitor emails without you being aware. Fraudsters can also use phone technology to gather sensitive information about how a practice’s financials are managed when
phoning an unsuspecting member of staff.
This background information helps the fraudster to position a future scam in a totally convincing way.
A 2018 audience poll at a Lloyds Bank Fraud Awareness Seminar in London revealed that over a third of organisations did not undertake any sort of training to help staff spot fraudulent scams.
So it’s important to make sure that fraud awareness is embedded in the culture of your practice and not just for those who have access to the bank accounts but all staff, including someone who may only answer the odd phone call or who purely undertakes administration tasks.
The impact of a fraud attack can often leave long-lasting effects, so preparing to defend your practice against these types of attacks is essential.
We must remember that the impact isn’t always limited to financial aspects. A successful fraud attack can leave long-lasting damage to an organisation’s reputation as well as significant consequences and impacts for those individuals that have unwittingly been tricked by the criminals.
Over the coming months, we will cover the main types of fraud that target practices. We will let you know how they work and what you can do to prevent and detect these scams to ensure your practice doesn’t become a victim.
✱ Source: Fraud The Facts 2019, UK Finance, March 2019. www.ukfinance. org. uk/policy-and-guidance/reports-publications/fraud-facts-2019
Vin Pandha is commercial fraud manager at Lloyds Banking Group
What’s up with WhatsApp?
Going app? Dr Gabrielle Pendlebury (below) reveals what doctors should know about using WhatsApp and similar computer applications used at work to communicate with colleagues
APPS OFFER an efficient, unobtrusive and portable mode of communication for medical staff.
Traditional communication via pagers has proved unreliable and two-way communication is difficult. Using apps on mobile phones to communicate with colleagues is fast, efficient, portable and convenient.
But sharing patient data in this way also raises legal and ethical issues.
A study of 2,107 doctors by the BMJ across five hospital sites found that 98.9% own a smartphone, and just over a third use web-based messaging apps to send clinical information.
The same report also showed that 65% of doctors had texted patient data from their smartphones, 46% had sent pictures such as wounds or X-rays to a colleague and around a third had used an app such as WhatsApp to share confidential information.
WhatsApp allows users to share information quickly, with more than one person if needed, and easily with limited data usage.
End-to-end encryption gives users a sense of security when sharing private information through the platform. As a result of the convenience factor, an increasing number of doctors are turning to WhatsApp to consult with colleagues.
Confidentiality issues
Although WhatsApp and other instant messaging apps offer a fast way of communicating with colleagues, there are serious issues related to the confidentiality of patient information.
Encryption technology prevents the interception of messages between devices, but it is not protected on the actual phone, as anyone with access to that device can see the data. Most clinicians will take precautions by removing any identifying information, but there remains a risk to patient confidentiality.
Former Health Secretary Jeremy Hunt put his support behind a report from The Centre for Policy Studies calling for NHS employees to use communication solutions
that meet required standards for sharing patient information.
But meeting data standards means more than just providing a secure text messaging app to consultants and nurses.
The EU’s General Data Protection Regulations (GDPR) state that patient information can only be used for the purpose to which it was collected and consented for by the patient.
Therefore, it would then be unwise to use these apps for patient information, unless their use has been advised in a privacy notice or consent sought separately.
At Medical Protection, we recommend documenting consent in patient notes when sharing images on mobile phones, so doctors can prove they took the appropriate steps, if they need to.
Measures to protect data
Simple steps may be taken to decrease the risk to patient confidentiality when using mobile phones for communication.
These include obtaining consent from the patient, having pin num-
bers on devices to prevent unauthorised access, removing patient identifiable information and deleting information once it is no longer required.
The future
The increasing development, use and benefits of communication apps need to be balanced against the risk to patient safety and confidentiality.
Developing apps which comply with privacy legislation, protect patient data with encryption and are resistant to cyber-crime may facilitate the use of these apps without risking patient data security. This is a growing area and will, no doubt, raise further ethical and practical questions as the technology develops.
Your indemnifier would be happy to discuss any issues arising to help the individual clinician find communication solutions that fit with their practice.
Dr Gabrielle Pendlebury is a medico-legal consultant at Medical Protection
THE FUTURE OF GENERAL PRACTICE
GPs are going the way of the dodo
What on earth is happening to private consultants’ referrers in the NHS? Legendary healthcare commentator Roy Lilley (right) has big fears for the future of our health service’s GPs
FATHOMING WHAT is happening in the NHS is a mug’s game.
Just as you think you have it figured, something else changes and you start again.
For over 40 years I’ve been in and around the NHS and I’ve lost count of the reorganisations, changes, modernisations and reforms.
No greater are the changes to primary care. From the very start, GPs and their small businesses have been a difficult fit in a nationalised industry.
The problems go back to that fateful July in 1948, when Bevan negotiated the take-over of the existing healthcare infrastructure. GPs had, until then, been free to set up shop wherever they thought they could make a living.
Many doctors resisted the regulatory strictures of a national health service. The BMA ran a campaign claiming doctors would become little more than ‘household servants’ if the scheme went through.
I was born before the NHS and, when it arrived, it lifted off the shoulders of working people the anxiety and worry of accidents, illness and maternity.
Nevertheless, as a toddler, when I became very ill, my parents delayed calling the GP, as they were not convinced that NHS services really were free.
Late at night, things became desperate. My father carried me to the GP’s house. He took us to hospital in his car. The first time anyone in my family had been in a saloon car. He was a wonderful man. He
wore a waistcoat and we wore jumpers. He had cufflinks and we rolled up our sleeves. He had a car and we had bikes. He lived in a big house, we lived in tenements and flats, but he was one of us. He was a family practitioner.
Since those days, each change to the NHS has inched closer to industrialising family practice. GPs no longer have a list; if we are lucky enough and old enough, we might be allocated to a GP with a special interest in geriatric medicine.
Patients displaced
The cost and overheads of running practices is outstripping their ability to create income. Last year, nearly three practices a week closed their doors. Around 367,937 patients were displaced from their current surgery.
Family practice has all but gone. We have primary care, care guides and an invitation to a free Zumba class as a cure for backache or depression.
Family practice is an odd fit in today’s healthcare. To work, it must work at scale. To be effective, it must be personal and intimate. It cannot be both.
Now, more changes. Clinical commissioning groups, which should have put GPs at the heart of commissioning and designing care, have performed poorly. And anyway, they have had no wriggle room in their finances to be innovative or experimental.
GPs who have voluntarily merged with neighbouring prac -
tices into federations to amalgamate their resources and skills are being told they should be in networks and networks are not federations.
If someone knows the difference, I’d be glad to know it.
All this change is standard-stuff restructuring and fiddling. There is a much greater upheaval just around the corner. Modern lifestyles are leading patients to demand video consultations, which are disrupting NHS payment mechanisms and distorting list sizes.
The NHS response has been confused and defensive.
Middle-class families – the Waitrose generation, the Amazon Prime brigade – want it now. The well-pensioned, net-savvy silversurfers won’t wait for weeks to see a GP. They will look after their families, with family practice in their pockets.
Super-surgeries
As long as there are families there should be family doctors. But what if families change, if work changes and the nuclear family, a concept as old as the NHS, morphs into something quite different.
The future is impossible to divine.
Cost pressures will create supersurgeries that will move further away from their communities. Younger doctors are looking to specialise. As specialisms become narrower, the role of the generalist becomes harder to fill.
Family practice has all but gone. We have primary care, care guides and an invitation to a free Zumba class as a cure for backache or depression
ROY LILLEY
In 2003, a Johns Hopkins study found that a health care system with high-quality ‘primary care, particularly family medicine, was associated with better health outcomes’.
I guess we didn’t need a study to tell us that.
I’m concerned for the future. The importance of generalism is easy to overlook. The scope of family practice builds a unique knowledge base. Couple that with a relationship with a family and the vital role is easy to understand.
Sign up for Roy’s free e-letter at https://ihm.org. uk/roy-lilley-nhsmanagers/
Roy Lilley is a health policy analyst, writer, broadcaster and commentator
Self-pay is still on the rise, so don’t ignore it
As the proportion of consultants’ income from self-pay hits a new record, Garry Chapman predicts this trend will continue. Just make sure you have a robust system to collect the money
MANY CONSULTANTS think of private practice as being the insurance market. But it is not that simple.
Our analysis on the invoice values we raised in the past 12 months shows that the private medical insurance market only accounts for 52%.
The percentage has continued to fall every year since 2012 when it accounted for 66% of the total, with the remaining 34% split between other organisations such as embassies, hospitals, solicitors – for medico-legal work – and other commercial organisations.
However, now the lion’s share of this non-private medical insurance invoicing is for self-pay patients, which accounted for an astonishing 33% of the total amount invoiced. This represents a growth from 25% back in 2012 and it is growing year on year at a fast pace.
This figure of 33% is an average across all our consultants and can be significantly more depending upon the specialty, type of practice and the location of the practice.
For almost every client we have, the self-funding patient is either the largest or second largest payment source and, in some practices, they are over 90% self-pay.
There are a variety of reasons why this sector has seen considerable growth and the average of 33% is so high.
The major ones are highlighted below:
➫ NHS
Over 90% of the population do not have private health insurance and the NHS is suffering due to the ever-increasing demands put upon it by the ageing population.
This, coupled with the bad press on the quality of care on the ward and the ever-increasing waiting times, is leading to an increasing number of people seeking an alternative to the NHS.
➫ Insurance policies
To control the costs of the premiums, the insurance policies have ever-increasing elements which are not covered by the policy.
This will be for a variety of rea sons, including benefit limits, patient excess on the policy, coshare policies – where the patient agrees to pay a percentage of each invoice – and certain procedures being excluded.
➫ Overseas patients
If your practice is based in central London, then this has always been
PRACTISING PRIVILEGES NOW AVAILABLE
a part of practice life with patients coming from outside of the UK seeking private healthcare.
➫ Self-pay
There has always been a percentage of people who have sought private healthcare without having an insurance policy and, due to the reasons highlighted above, this has resulted in an increasing number of people in this market, which makes it very buoyant.
On top of this, due to the everincreasing costs of insurance premiums, people are choosing to self-fund.
The reason that this information is so important is that if you do not know what the statistics are in your own practice, you cannot make sure that it gets dealt with correctly from both a billing and collection process.
In our experience, this is rarely dealt with correctly and there is quite often a lack of clarity regard-
ing billing self-pay patients and also collecting the money.
This results in the practice having a huge amount of outstanding debt, which is either chased on a sporadic basis or not chased at all, resulting in debts that amount to a significant sum of money.
The reasons for this debt can be down to many factors, but typically what we see is a lack of a robust system in place to deal with this element of the practice.
What the practice needs to do is have a system in place to deal with each element of the self-pay with the main ones highlighted below.
➲ Overseas patients
When you are going to see a patient who is not a resident of the UK, you need to decide in advance what your charges are going to be, so that it is clear to them exactly what the total cost of the treatment is going to be and then have a discussion about the method of payment.
When we deal with these patients on behalf of our clients, we quite often collect the money in advance, because once the patient has left the UK, then the chances of collecting payment become almost zero.
A common way of encountering an overseas patient is through the hospital. In this instance, the hospital may well agree to collect all money due from the patient.
But unless you get your invoice to the correct department/contact in the hospital in a timely manner, it is likely that your fee will not get collected. This then leaves you with the problems of chasing the patient for payment after they have left the UK.
➲ UK self-pay
The majority of consultants are likely to have an element of patients who are self-pay and therefore they should have a price list and agreed methods of pay-
ment made clear in advance so that the patient is expecting an invoice and is prepared to pay either on the day or shortly afterwards.
When doing this for our clients, we have a variety of methods available to us including taking payment on the day by debit/credit card or, depending upon the requirements of the practice, we can even take money in advance.
When you cannot collect payment on the day, you will need to put in place a system where the patient is chased for payment after an agreed period and then chased on a regular basis until payment is collected.
➲
Insurance shortfalls
Depending upon the specialty and type of practice, this is normally by far the largest volume of the invoices and is also the hardest to collect.
This is because most patients do
not understand their insurance policy and they believe that all costs are going to be met by their insurer, so when they receive an invoice for the consultant’s element of the treatment, it is an invoice they are not expecting.
From our experience, a lot of patients will ignore the invoice, as they are under the misapprehension it is a copy of what has been sent to the insurer; so unless you follow this up with a phone call, it will just be ignored.
Once they are aware that the invoice is correct, then they may contest this with their insurer, as they believe all costs should be met under the terms of their policy.
A large part of what we do on behalf of our clients is liaise between the insurer and the patient to ensure that it is clear who owes the money.
Once the patient accepts that the money is owed by them and depending upon the amount that
they owe, then you need to be able to either take payment immediately or agree payment terms.
The future
I believe that conditions are ripe for continued growth in the selfpay market, so it is likely that the practice will encounter more invoices in this sector. Thus they need to make sure that they have a robust system in place.
The alternative is that you could choose to use a billing company which has the expertise and skillset to remove this burden from your practice.
Garry Chapman (left) is executive chairman of Medical Billing and Collection
Rest assured when buying and selling
When independent practitioners are buying or selling a business, half of the sale agreement will be a schedule of warranties. If you are prepared to answer them before you go to market, your business is likely to be given a higher value, because each warranty you cannot confirm is money off the price.
Justin Cumberlege (below) reports
EVERY BUSINESS has a history and will have entered into many and varied arrangements, and things may have gone wrong which they have patched up and moved on.
It is vital that when you acquire a business, you find out as much about its history as you can, so you know what you are inheriting and what you will be liable for.
Due diligence is a very important part of the process of buying or selling a business and the buyer will ask to look through all the records they would expect the seller to have kept.
Although a buyer trawls through the past accounts, contracts, employee contracts, information
about their premises, claims and reports, these will not tell you everything.
Buyer
beware
The law in England and Wales –and most Anglo Saxon jurisdictions – follows the maxim ‘caveat emptor’ or ‘buyer beware’. This means that the buyer takes the risk on any purchase.
The way to rebut that risk is by requiring the seller to make representations and then, if any of those representations prove to be wrong, the buyer would claim for damages for the losses which resulted. Warranties are those representations.
Warranties are statements of information which you warrant are true. If they prove not to be true, the buyer can claim against the seller for any losses which result. To guard against this, the seller will ‘disclose’ against warranties by making statements which qualify the statement made in the warranty.
The temptation for any seller is to state that the warranty is true ‘so far as it is aware’; but proving awareness can be difficult, so it is important that what is meant by that is defined clearly.
The buyer does expect that the seller makes proper and thorough inquiries and that the seller knows
its business sufficiently well, as opposed to relying on the knowledge of the manager of the operation at the time of the sale.
Disclosure rules
An example of a warranty might be:
‘The seller has maintained licences in respect of all intellectual property deployed by the business.’
In this example, if the seller decided not to renew certain licences – as it thought it would be selling very shortly but was still using the subject matter of the licence – it would have made a misrepresentation.
If the seller didn’t inform the buyer, then the buyer can be expected to make a claim against the seller if a claim was made against the buyer after the acquisition for not having the licence at the time.
If, however, the seller informed the buyer, then the purchase would have been made with the
full knowledge of the situation, and the buyer would have no claim. This can become particularly important where a claim by a member of staff has been made but not disclosed.
Therefore, an important second part of warranties is disclosure. This is the procedure by which the seller informs the buyer that there are issues which mean that the warranty is not totally true and so it is qualified.
Some limitations
To avoid claims for insubstantial amounts as a result of breaches of warranties, there is usually an amount specified below which no claim can be made – unless it is a series of small claims.
Also, the seller may put a maximum amount of claim which is often the purchase price, so no claim can be made which exceeds the purchase price. This limit can be exceeded. For
example, if it is found that the ground had been contaminated by the operations of the seller, the clean-up costs can be very substantial, so you may carve out some losses from the limitations.
The seller may also put a time limit on claims under the warranties, which may be very short: one or maybe three years.
However, certain warranties and indemnities will be excluded, such as tax warranties, as HM Revenue and Customs may make a claim up to four and, in some cases, six years after the end of the relevant tax year.
It is perhaps worth bearing in mind that warranties and indemnities are only as good as the seller giving them. A seller may distribute the sale proceeds very soon after the sale by paying a dividend to all its shareholders.
Unless the shareholders are also party to the sale and purchase agreement, indemnities and war-
ranties may be worthless, however well drafted they are.
But the part they play in allocating risk in a sale should not be underestimated and even the negotiation of warranties and disclosures serve to unearth issues. If the seller is resistant to give a warranty or attempts a broad and general disclosure, then you should look to see what is being hidden.
If you are preparing to sell your private healthcare business, look through some business warranties as far in advance as possible and then attempt to meet the requirements of each statement by the time you put the business on the market.
If you are buying, think ahead of the matters you want to confirm, and make a note of statements of assurance made in negotiations so that they are included in the warranties.
Justin Cumberlege is a partner in the corporate team of Hempsons
Free legal advice for Independent Practitioner Today readers
Independent Practitioner Today has joined forces with leading healthcare lawyers Hempsons to offer readers a free legal advice service.
We aim to help you navigate the ever more complex legal and regulatory issues involved in running and developing your private practice – and your lives.
Hempsons’ specialist lawyers have a long track-record of advising doctors – and an unrivalled understanding of the healthcare system as a whole.
Call Hempsons on 020 7839 0278 between 9am and 5pm Monday to Friday for your ten minutes’ of free legal advice.
Advice is available on:
Business structures (including partnerships)
Commercial contracts
Disputes and litigation
HR/employment
Premises
Regulatory requirements and investigations
Michael Rourke Tania Francis m.rourke@hempsons.co.uk t.francis@hempsons.co.uk
Why managed funds are a game of risk
The odds are stacked against actively beating the market.
Dr Benjamin Holdsworth (below) explains the costly challenges of active investment management
AS YOU will have seen in numerous media reports, Neil Woodford – one of the UK’s best-known fund managers – recently had to suspend trading in the actively-managed Woodford Equity Income Fund.
At its peak, the fund held over £10bn of investments, but, at the time of writing, held less than £4bn.
To summarise very briefly what went wrong, when the performance of the fund did not live up to expectations – Woodford’s previous successes had driven initial enthusiasm – investors began to lose confidence and attempted to remove their money.
The subsequent exodus caused substantial problems because many of the investments could not quickly be turned back into cash.
While the financial future remains uncertain for Woodford’s concerned investors, the key lesson to be learned is that active management adds additional layers of risk to portfolios.
Risks worth taking?
In a world where markets work pretty well and active manager fees are high relative to likely skill, one should question whether these risks are worth taking. The Woodford case provides a useful reminder of the challenges and dangers of doing so.
With actively managed investment funds, a professional fund manager makes all the investment decisions, such as which companies to invest in or when to buy and sell different assets.
The investor, therefore, must pay for the manager looking after their fund and the team researching markets and companies. Note that even during this time of hiatus, Woodford has refused to drop their charges on the locked-in funds and daily fees have been estimated at more than £75,000. Woodford himself enjoyed a 65% stake of a £35m dividend last year. On the other hand, passive or index investment funds are designed to track an index, market or asset class. The funds essentially buy all of the assets in a particular market to give you a return that reflects how the market is performing.
Numerous studies show that a passive approach, using welldiversified portfolios that capture market returns, as Cavendish advocates, makes very good sense. In 2013, Prof Eugene Fama of the University of Chicago was named as a joint winner of the prestigious Nobel Prize for Economics following his 50 years of academic research into financial markets. His lifetime work explains that we are better off letting the market work for us – taking a passive approach – rather than struggling to adopt complex, expensive strategies to ‘beat’ the market.
Fama’s studies show that market prices incorporate all available information. It states that we cannot systematically outperform the market, unless we have information other people do not or can access part of the market others cannot. That does not mean it is impossible to make money – just that returns come from risk rather than stock-picking or market timing. There is much academic debate around the degree to which luck plays a role in investment returns. We know that owning a portfolio
WHY PASSIVE IS BEST
1
Risk and return go hand in hand: if you own an actively managed fund that is quite different to the market, its returns will be too, both on the up and the downside
2 Skill is very rare and luck plays a major role in most active managers’ periods of outperformance. Markets work pretty well, and market-beating performance is likely to come only from taking on higher risks; e.g. owning smaller companies. After costs, the evidence suggests very few active managers deliver skill-based returns sufficient to cover their costs over the sort of horizons that investors require
3
In the same way that noise and luck play a big role in fund managers’ outcomes, so it does when trying to pick active funds. Best-buy lists and advisers’ active fund picks are highly susceptible to this noise
4
Concentrated stock positions, combined with low levels of liquidity, is a dangerously potent cocktail that represents a material risk to investors’ wealth. In our article in the previous issue of Independent Practitioner Today, we discussed the importance of diversification
5 High levels of diversification in liquid, quoted companies, ensuring that no small set of companies dominates outcomes, is essential. That is why the total number of stocks held in Cavendish clients’ portfolio is up in the thousands
6 Gambling on which fund is going to beat the market is an exceptionally low probability strategy. Capturing the market return is a valid and worthy objective
significantly different to the broad market means that there will inevitably be periods of time when the investment thesis will be right – or lucky – and other times when it will be wrong – or unlucky.
Our view is that it is mainly luck and that the evidence suggests that only a handful of managers are skilled enough to deliver returns that exceed their costs and they are hard to identify in advance.
Clear warnings
Despite the hard empirical evidence that active management cannot be relied on to deliver the outperformance it promises, many investors continue to believe that past fund performance is a guide to future activity, despite the clear warnings in place.
Active management certainly has an easier sell – the idea of investing in a ‘best’ fund, rather than an ‘average’ one is much more appealing.
Despite this, there are some important points for investors to remember (see box above).
The Woodford saga reminds us that investing is a tricky game, which can have material costs if you get it wrong. It is hard enough investing in the stock market without the added additional risks of active management.
Instead, we believe that a welldiversified, low-cost approach to investing that avoids active manager, concentration and liquidity risks is the sensible way to go.
Dr Benjamin Holdsworth is director at Cavendish Medical, specialist financial planners helping consultants in private practice and the NHS.
The content of this article is for information only and must not be considered as financial advice. Cavendish Medical always recommends that you seek independent financial advice before making any financial decisions
Levels, bases of and reliefs from taxation may be subject to change and their value depends on the individual circumstances of the investor. The value of investments and the income from them can fluctuate and investors may get back less than the amount invested.
Cavendish Medical Ltd has over 450 consultants as clients and £400m in client assets under administration.
Cavendish Medical operates a transparent investment policy and a fee-based approach allowing independent financial planning advice.
Cavendish Medical Ltd. is authorised and regulated by the Financial Conduct Authority to provide independent financial advice to individuals and businesses. For more information, please visit www.cavendishmedical.com
PROBLEMS WITH THE TAX MAN?
HMRC tax investigations and disputes create difficult and stressful times.
As an award winning firm of tax experts, our highly experienced partners specialise in resolving problems relating to tax investigations and disputes with HMRC.
To find out, in confidence, how we can help call 0800 734 3333.
‘Here to help. Not to judge.’
Patient wants his notes to sue me
Dilemma 1 Must I hand over patient’s notes?
QI am a consultant gastroenterologist in independent practice. A patient with non-specific abdominal pain was recently discharged from my care.
After a thorough investigation, I diagnosed irritable bowel syndrome and I provided the patient with lifestyle advice. He did not appear to be unhappy with this.
However, I have now received a letter from a solicitor with a signed form of authority from the patient requesting a copy of the complete records. They have indicated they are investigating a potential compensation claim against me.
Do I have to comply and do I have to provide all correspondence, such as my letter to the patient’s GP stating I could find nothing wrong and thought the patient’s symptoms might be a result of psychological issues?
AThe solicitor’s letter is a request for records and is accompanied by a signed form of authority from the patient. In effect this is a Subject Access Request (SAR) and its handling is defined by the General Data Protection Regulations which came into effect on 25 May 2018.
This is applicable to all doctors, UK businesses and organisations and is tailored by the Data Protection Act 2018.
Patients have a legal right to access the information you have stored about them and it can be requested for any purpose, including in contemplation of a claim. As a data controller, you cannot charge a patient or their legal representative for reasonable access to their records.
Bear in mind that you cannot exclude information on the basis you think it may be harmful to your position or simply because you think that it might upset the patient.
You should redact information in relation to third parties, such as reference to a relative of a patient who has disclosed information about themselves without the patient being present and asked you not to inform the patient. In situations such as these, it is acceptable to redact only the information in question. In some situations, there may be a public interest in disclosing third party information without the consent of the individual. You should carefully document why you have disclosed in this situation.
Serious harm
It is possible to redact information if you believe it would cause serious harm to the physical or mental health of the patient or another individual.
However, this should be documented and is unlikely to be a common occurrence.
It should not be used as justification to remove information that you think may bother the patient and may make them more likely to pursue a complaint or a claim.
As the solicitors have indicated that the patient wishes to bring a claim for compensation, it is advisable to inform your medical defence organisation.
You only need to provide private records that are within your direct control. There is no obligation to provide other private records or NHS hospital records. These would be for the claimant’s solicitor to seek themselves from the organisations concerned.
As this is a fairly new and occasionally complex area of law, if there is any uncertainty, we would always encourage you to discuss this matter with your medical defence organisation.
Dr
Shabbir
Choudhury advises that a scrip error can be mitigated by an apology
Dilemma 2
Do I say sorry for my scrip error?
QI am a private GP and a patient has written to say he believes I overprescribed lithium which caused him to be admitted to hospital. He is undergoing further tests to assess if there has been longterm damage.
The prescription was started by a consultant psychiatrist the patient had seen privately and the dosage error was made when I prescribed a repeat prescription. Unfortunately, I had not received a letter from the psychiatrist and I wasn’t able to get hold of her to confirm the correct dosage, so I had to rely on the patient’s recollection.
Should I apologise for the error or would I be admitting legal liability for something that I feel wasn’t my fault?
APrescribing errors are fairly common in the MDU’s experience and, unfortunately, the consequences can sometimes be serious as in this instance.
However, you will help to reassure the patient by making a full and frank apology. Not only do you have an ethical duty to apologise if something has gone wrong, explain what happened and what steps will be taken to try to put things right, but it is also the right thing to do.
Remember that an apology is not an admission of liability in law, as specified by Section 2 of the Compensation Act 2006.
Although you may feel that the error wasn’t your fault, it is acceptable to explain your viewpoint while still expressing that you are sorry. An earnest and sincere apology, made in the first person, such as ‘I am sorry I prescribed a higher dose of Lithium than you required’,
Saying sorry is not admission of guilt
may be all the patient wants to hear.
You can then go on to explain why this happened: ‘As I had not received a letter from your psychiatrist and was not able to contact her, we discussed the dose of lithium you were currently taking.
‘I am sorry if I misunderstood what you told me and I am extremely sorry that you were admitted to hospital and that you are undergoing tests to check whether this has caused any longterm harm.’
All organisations registered with Care Quality Commission in England must also comply with the statutory duty of candour. It applies to organisations rather than individual doctors; however, individuals still have an ethical and professional duty to be honest and open with patients when something goes wrong.
It is expected that an organisation’s staff cooperate to meet the statutory duty of candour obligations.
Apologies can be provided in writing or in person, but as the patient has written to you, it would generally be appropriate to write back. If the statutory duty of candour is engaged, a written explanation and apology is mandatory.
You can always offer a meeting to discuss matters and it can be helpful to advise how you will prevent such issues occurring in the future.
Although an apology cannot prevent a complaint or a legal claim from arising, it is more likely to prevent it than a defensive response. You should rest assured that apologising in this way does not mean you are accepting legal responsibility for what occurred.
The MDU finds that a carefully considered genuine apology can prevent further issues down the line.
Dr Shabbir Choudhury is a senior medical claims handler at the MDU
Upright
Positional
• Completely open scanner that is well tolerated by claustrophobic patients
• Weight-bearing scans for spine and joints enable a more precise diagnosis
• Patients who are large or cannot lie down can be accommodated
A carefully considered apology can prevent further issues down the line
PRIVATE PATIENT UNITS
Clear leader shows how it can be done
Our monthly analysis of private patient revenue growth moves to the East Midlands. Philip Housden (right) reports
FIGURES FROM the published annual accounts for this group of trusts shows that total private patient revenues remained flat in 2017-18 as they did in the previous year.
The area covered are the East Midlands counties of Northamptonshire, Leicestershire, Nottinghamshire, Derbyshire and Lincolnshire. There were ten trusts to analyse, but Derby and Burton Hospitals merged in July 2018.
Total revenues remained at £11.8m in 2017-18. This now represents 0.30% of these trusts’ total revenues, essentially a flat figure for the last few years. This is below the combined national average outside of London of 0.5%.
The most active trust for private patient services in the region remains Derby, where the NHS PPU is branded Derby Private Health. It houses 11 ensuite inpatient rooms, five consultation rooms, a private chemotherapy suite and minor procedures room. This unit has delivered growth of 17% in the last year and 76% in the last three, to reach £3.7m.
The trust is ambitious for further growth and is investing £2m to build and equip a new dedicated operating theatre for private patients at the Royal Derby Hospital. It recently hosted the annual NHS PPUs’ managers’ conference.
Merging enables further expansion through incorporation of the private patient activity in Burton, including the Burton Clinic PPU, worth approximately £0.8m last year, down £100k on 2016-17.
This is developing into one of the first NHS PPU ‘chains’ that can lead as centres of excellence to support other trusts who may not have their own local commercial skills to develop private patient services.
Another chain
Northern Lincolnshire and Goole also have their own chain. This is branded Lindsey Private Patients, with a presence in Goole, Grimsby and Scunthorpe. In the past year, the revenues remained flat at £1m and 0.33% of total turnover.
At Goole and District Hospital, the Lindsey Suite provides singleroom accommodation and services offered include those not routinely offered on the NHS, such as cosmetics and some ophthalmic
procedures plus the expected range of fast access to imaging and self-pay admissions.
Nottingham University Hospitals (NUH) is another trust that experienced flat trading in 2017-18. Income from private patients was £1.9m, down £74k (3.7%). The trust does not have a separate PPU, but houses private patients on NHS wards.
It is responsible for the new National Rehabilitation Centre, co-located with the relocated Defence National Rehabilitation Centre near Loughborough, Leicester shire. This new service offers the opportunity for NUH to develop private patient services, particularly in neuro-rehabilitation and musculoskeletal services.
No PPU
University Hospitals of Leicester is a second regional teaching trust in a large catchment but with no dedicated inpatient private patient accommodation. Clinical services remain spread between three main campuses across the city.
Leicester also has a Spire and Nuffield Hospital, both delivering a case mix of higher than average complexity. The trust achieved £2.87m revenues in 2017-18; again, flat on the previous year.
Private patient earnings as a percentage of total turnover is on a longer-term declining trend, down from 0.45% in 2013-14 to 0.35% in 2017-18.
As Leicester and Nottingham can manage the patients the local inde-
Figure 1
pendent hospitals cannot, this patient safety imperative means that a PPU to support most complex patients and treatments is well worth consideration for investment.
Northampton General Hospital is the highest earner of these, earning £845k in 2017-18 and a reported further decline to £719k in 2018-19. This is a fall from 0.35% of total income to 0.31% .
There are four trusts with less than £0.5m a year income from private patients.
Opportunity beckons
United Lincolnshire Hospitals operates from Boston, Lincoln and Grantham; with Pilgrim Hospital, Boston, having a dedicated private patient unit – the Bostonian Wing – with capacity for 18 beds, the largest unit in the region.
Despite this advantage, the trust delivered only £381k revenues from private patients last year, a decline of 31% from £551k in 201617. The long-term trend is down, as earnings were £1.1m in 2011-12.
With neighbouring North Lincs Trust developing their own chain across multiple sites, this looks to be
an opportunity for cross-trust working to help with branding, back office and commercial leadership to re-invigorate Boston’s service.
Kettering General and Chesterfield Royal Hospital Trusts have a negligible level of private patient earnings – less than 0.1% of turnover – at £175k and £80k respectively in the last published annual accounts.
Neither are known to have plans for investment in private patient services. However, at Sherwood Forest Hospitals, plans are being drafted to extend the present limited private patients service at the King’s Mill Hospital near Mansfield. The trust reported revenues of only £88k in 2017-18, down on the £119k earned in 2016-17.
Private patient development in the East Midlands region is essentially grouped into three types:
1. Go-ahead trusts that have developed a brand and are either moving forward quickly – that is Derby and Burton – or have the potential to do so: Northern Lincolnshire and Goole.
To this group could be added United Lincolnshire if they worked
with their neighbours more closely.
2. Leicester and Nottingham are teaching trusts without a dedicated PPU, but with the breadth of clinical services to achieve growth and most probably a significantsized PPU in the future.
3. The remaining trusts do not have a local service and, apart from Sherwood Forest, appear not to have present plans to invest either. All, however, will have the underlying local demand that would
support a minimum-sized six-bed unit due to the inevitable gaps in provision for private patients for the most complex clinical services. The opportunity for growth exists for East Midlands and, to kick-start it, perhaps trusts could initially look to Derby Private Health for advice and support.
Next month: The South-west
Philip Housden is a director of Housden Group
At the heart of medical finance
Figure 2
DOCTOR ON THE ROAD: AUDI A1
Entry level does not mean boring
Dr Tony Rimmer (below) tests an upmarket supermini from a premium brand
ANY INDEPENDENT practitioner knows that the reputation of their practice relies on all aspects of their services, both major and minor, being delivered at the highest level of quality. Attention to detail at all levels is vital.
This is also true for any carmaker. The smallest and cheapest models in the range must uphold the values of the brand as much as the bigger and more expensive models.
The A1 is the entry-level car in Audi’s current range and this allnew and latest iteration has a fivedoor-only body shell sitting on the ubiquitous VW Group floor pan as used for the Volkswagen Polo, among other sister cars.
Being an Audi, it is placed in the premium sector of the car market and is unapologetically taking aim at MINI’s five-door models.
More
adventurous
With this rival in mind, the styling is now more adventurous and there are new bright colour options available, some with a contrasting black roof.
The car is slightly longer than the outgoing model, which allows sharper and sportier lines, particularly enhanced by bodywork addenda on the S-line model.
A nice design touch is the false horizontal vents along the front of the bonnet; reminiscent of the
iconic Sport Quattro Rally cars from the 1980s.
Audi now has a numeric system to identify the available engines based on their power output – no, I don’t know why they have done this either.
The 30 has a 1.0 litre three-cylinder engine producing 115bhp; the 35 has VW’s 1.5 litre four-cylinder engine producing 147bhp and the 40 has a 2.0 litre four-cylinder unit producing 197bhp.
There will be a 20 model next year with a 95bhp version of the 1.0 litre engine and ultimately there will be a powerful supersporty version called the S1. Drive is through the front wheels in all
models and a standard manual gearbox is supplemented by the option of a dual-clutch automatic. The three trim levels start with the SE model, which has 15-inch alloys, LED headlamps and an 8.8-inch touchscreen. Next is the Sport model which adds 16-inch alloys, front sports seats, rear parking sensors and cruise control.
Sweet spot
Top of the range is the S-Line model which adds 17-inch alloys and lower, firmer sports suspension. There is an optional £1,650 Technology Pack that adds a bigger 10.1-inch touchscreen and works well with the digital instruments of the Virtual Cockpit that are standard in all models.
My test car was the 35 TFSI 150PS S-line S-tronic and although this trim level does not represent the best value for money, the 1.5 litre engine probably hits the sweet spot for its combination of performance and economy.
In the flesh, the new car looks smart and modern. Its lines are much sharper and more grown-up that its predecessor. However, it looks best in bright colours and particularly distinctive with a contrasting black roof. The S-line body kit is just a little excessive as Audi tries to chase the cheeky charm of the MINI.
The interior is dominated by the impressive infotainment system. The large central touchscreen and digital dashboard is on par with Mercedes’s latest system as used on the ‘A’ class.
It is easy to use and the choice and control of display is intuitive. But look a little further and the small A1 fails the premium test with its use of hard low-grade plastic on the door trim. This is no better than a VW Polo or SEAT Ibiza.
Generous boot
The driving position is good and the sports seats are comfortable. Oddment space is generous and the rear seats have plenty of room for two average-sized adults; a definite improvement over the outgoing model.
The generous boot benefits from a moveable floor to increase carrying capacity when necessary.
Out on the road, initial impressions are aided by the direct steering and lack of body roll. However this is facilitated by an overly stiff suspension.
The ride, particularly on bigger alloys –18 inches on my test car –and lower-profile tyres is very firm. This is great for the driver but not so good for passengers, especially on longer journeys.
However, the A1 does impress with the quality of its drivetrain.
AUDI A1 SPORTBACK 35 TFSI
150ps s-line contrast edition s-tronic
Body: Five-seater hatchback. Front-wheel drive.
Engine: 1.5 litre four-cylinder turbo-petrol
Power: 147bhp
Top speed: 137mph
Acceleration: 0-62mph in 7.7 seconds
Claimed economy: Combined: 55.4mpg
CO2 emissions: 116g/km
On-the-road price: £26,345
In the flesh, the new car looks smart and modern. Its lines are much sharper and more grownup that its predecessor
The 147bhp 1.5 litre engine in the 35 is lively and eager and the latest version of VW Group’s direct-shift gearbox makes the most of it.
This is no hot hatch, but swift progress can be made. The handling is good but not as controlled or sophisticated as its great rival, the MINI. You wouldn’t go for a drive just for the enjoyment of it, but you might in its adversary.
The latest A1 is a better car than its predecessor. It is smarter, roomier and has great up-to-date tech. But it is not perfect. It is let down by some low-grade interior trim and a firm ride. However, it has a lot to recommend it as an upmarket supermini from a respected brand.
Dr Tony Rimmer is a former NHS GP practising in Guildford, Surrey
A PRIVATE PRACTICE – Our series for doctors considering the independent journey
One of the most difficult aspects is to understand how the pension growth is calculated and your calculations may be very different to a colleague who is older or younger
Avoid the annual allowance
As Independent Practitioner Today has consistently reported, the unfair pensions savings annual allowance charge affects medics particularly badly, even those not carrying out private practice. Ian Tongue (right) takes an accountant’s look at the key concepts and potential ways to mitigate it
THE PENSION annual allowance starts out at £40,000 for everyone, but for those earning more than £110,000, the annual allowance is potentially reduced to as low as £10,000.
This process is known as annual allowance tapering and it came into force for the 2016-17 tax year and remains effective today.
You may have escaped the initial effect of the annual allowance tapering, but with each year that passes, it is more likely you could be affected.
One of the most difficult aspects of the calculations to understand is where the figures come from. It is easy to look at your NHS payslip and add up your contributions paid, concluding in the process that you are well under the £40,000 limit.
But the NHS Pension Scheme is a special type of scheme called a ‘defined benefit’ scheme. Cutting through the jargon, this means that what you get out as a pension is not a product of what you have
put in. There are scheme rules and formulas that determine your actual pay award.
This type of pension scheme is in contrast to the majority of schemes in the UK where the contributions are invested and your pension is based on the value of your fund at the end. This is known as a ‘defined contribution’ scheme.
Some specialists may have both types of scheme if they took out additional pensions earlier in their career, but it is becoming less common to see consultants still paying into these schemes.
The calculations
The first stage of the calculations is to look at your taxable earnings from all sources and this is called your ‘threshold income’. If threshold income is less than £110,000, you will not be exposed to annual tapering no matter what the level of your pension savings are.
You could still have an annual allowance charge, though, if your pension savings exceed £40,000.
allowance trap
For those with threshold income above £110,000, you move on to stage two of the calculations, which is to add on the pension savings for the year. This is called your ‘adjusted earnings’ and if this figure exceeds £150,000, you start to lose the annual allowance: £1 for every £2 above until the allowance reaches £10,000.
An example
If you earned £90,000 from the NHS and £40,000 privately, your threshold income would be £130,000. At this level of combined earnings, annual allowance tapering needs to be considered and the next stage is to calculate adjusted earnings.
NHS Pensions will provide details of your actual pension savings – eventually! – but the figures can usually be estimated in the absence of the statement. If we say that, in this example, the pension savings are £35,000, the adjusted earnings would be £165,000. This is £15,000 over the £150,000
level, resulting in £7,500 of lost annual allowance, i.e. the tapered annual allowance is £32,500.
This individual has exceeded the annual allowance by £2,500 and would most likely have unused tax relief from the three prior years, but if not, they would have an annual allowance charge of £1,000 (40% of £2,500).
Different schemes, different rules
One of the most difficult aspects is to understand how the pension growth is calculated and your calculations may be very different to a colleague who is older or younger. Therefore, you require advice based on your circumstances rather than absorbing advice from others that could be financially detrimental to your circumstances.
The reason for the differences in growth calculations is that there are three NHS schemes that you could be a member of: ➱ p52
Cloud-Based Electronic Patient Records and Patient Portal
eClinicalWorks is a leader among independent, ambulatory practices, covering primary care and more than 50 specialities.
• Integrated Electronic Patient Record (EPR) and Clinic Management
• Comprehensive documentation of patient encounters
• Data analytics to deepen your understanding of your patients
• Streamlined workflows improve the provider and patient experience
Call to arrange a demo to see how we can help meet your needs!
Stuart Tebbutt
07891 217313
1995 scheme;
2008 scheme;
2015 scheme.
The 1995 and 2008 schemes operate as a ‘final salary’ scheme based on your years of service divided by a number – 80 for the 1995 scheme and 60 for the 2008 scheme – multiplied by your wholetime-equivalent final salary on a ‘best of the last three years basis’.
The 2015 scheme is a career average basis, so think of this as a gradual filling up of your pot.
It is important to note that, for those in the 2015 scheme, the calculations for their older pension benefits under the 1995 or 2008 scheme will still be related to their current whole-time-equivalent pay, albeit not accruing any more years of service – in the absence of purchasing added years.
Changes in superannuable pay significantly affect the calculations in the different pension schemes, which is often the reason for a very large annual allowance charge.
The key components of superannuable pay are:
Basic pay – first ten programmed activities;
Local clinical excellence awards (CEAs) – awarded before April 2018, although some older ones still being awarded;
National awards;
On-call supplements;
Any additional responsibilities that may be superannuable.
The earnings trap
Much has been said about earnings traps and how you should not earn £x or £y, but you could make the wrong decision by focusing on an earnings figure.
It is true to say that keeping your earnings below £110,000 guarantees you the full £40,000 allowance, but as we saw in the example on page 51, a person earning £130,000 was barely affected and retained more than three-quarters of their annual allowance.
One of the most common discussions that I am having is around consultants not wanting to perform waiting list initiatives because they will get hit with a massive tax charge and will be paying to work. But is that true?
Let’s add £10,000 additional pay to the example above and consider the effect.
Much has been said about earnings traps and how you should not earn £x or £y, but you could make the wrong decision by focusing on an earnings figure
The person in the example is a 40% taxpayer and will be paying 2% National Insurance on additional earnings. Therefore, tax and NI of £4,200 will be paid through PAYE on the extra income.
The adjusted earnings calculation increases from £165,000 to £175,000 and the pension growth remains the same figure, as the waiting list initiative work is not superannuable.
An additional £10,000 on the adjusted income figure reduces the annual allowance by £5,000 to £27,500. The effect of this is to pay a further £2,000 annual allowance charge.
So the additional £10,000 suffered £4,200 in tax and NI through PAYE and created an additional £2,000 annual allowance charge, an effective tax rate of 62%. Certainly painful and not a great return, but very different to the concept of paying to work or not receiving any additional disposable income.
Where the above looks very different is if the additional income is superannuable. This creates a situation of increasing the adjusted earnings figure from actual earnings and increasing it further again through higher pension growth.
This will happen with pay increments, national awards, CEAs awarded for periods prior to April 2018 and other roles and allowances which may be pensionable.
It is also important to note that if your adjusted earnings – actual earnings plus pension growth –are in excess of £210,000, you are back to the normal tax rates on additional income, as the annual allowance charge reaches a ceiling.
It is also worth noting that things are very different for GPs or perhaps special roles in the NHS where the vast majority of earnings are superannuable.
As always, keep your accountant in the loop regarding your intentions to ensure that you are not heading for a big shock.
Tax planning
We have seen above that the marginal rate of tax increases when you are in the zone of losing your annual allowance.
Many individuals can benefit significantly from considering
Often consultants can significantly mitigate or extinguish the annual allowance charge through tax planning
how their private practice is structured.
In the example above, the individual is self-employed, but using a limited company could reduce the income shown on the personal tax return, particularly if a spouse is paying tax at a lower rate and you involve them or if you do not require all of the money.
At the time of writing, many hospitals are considering the arrangements in place with consultants to carry out waiting list initiatives to allow more flexibility.
This can take the form of using an individual’s company or, more commonly, joining together with colleagues to form a business which undertakes the work and is structured efficiently for tax.
A ‘normal’ year
One important aspect of the calculations is considering a normal year of pension savings for your circumstances and this will vary based on your circumstances. This is important if you are considering restricting earnings, as you need to gauge whether you are affected annually or in a cycle, usually related to pay increments.
Pension savings in the older 1995 and 2008 schemes can be zero, high or anywhere in between, but is it fair to say that if your pay is relatively static, you are likely to have low growth in those schemes as a consultant.
Growth in the new 2015 pension scheme is much more consistent and predictable and increases or reduces based on actual superannuable pay.
No doubt, the pension annual allowance charge will remain the biggest risk area of an unwelcome additional tax charge for a doctor. It is a big issue, but the key message is to consider your circumstances carefully, as often consultants can significantly mitigate or extinguish the annual allowance charge through tax planning.
Discuss your circumstances in detail with your accountant to ensure you are best placed to minimise the effect for you and avoid the annual allowance trap.
Next month: A guide to taxable benefits
Ian Tongue is a partner with Sandison Easson accountants
Self pay at the heart of it
Ticking over nicely. Ray Stanbridge’s financial analysis of specialists’ accounts finds cardiologists’ income and profits are doing well
TWO YEARS ago, I commented that, despite the many changes going on in the marketplace, I anticipated continuing growth in the average private cardiology practice over the next few years. Well, 2016 proved to be a good year and 2017 proved to be an even better one.
It seems the average cardiologist’s gross income from private practice in the UK rose by 6% from £152,000 to £161,000 between 2016 and 2017.
Costs fell slightly by some 2% from £57,000 to £56,000. As a
result, taxable profits rose by 10.5% from £95,000 in 2016 to £105,000 in 2017.
The income growth in 2017 appears to come from self-pay. As reported above, insurance company fees to cardiologists have been under pressure. This growth is in line with other evidence, such as published in LaingBuisson markets reports on London private healthcare.
There have been some very interesting costs developments.
Medical suppliers/assistant fees have fallen slightly. It seems that
AVERAGE INCOME AND EXPENDITURE OF A CONSULTANT CARDIOLOGIST
Expenditure
Year ending 5 April. Figures rounded to nearest
Source: Stanbridge Associates Ltd.
some private hospitals are now providing these services and consultants are no longer having to pay for them themselves.
Staff costs have shown a slight cool, but consulting room costs have increased. There is a correlation here as cardiologists are now subject to the full rigors of the Competition and Markets Authority determinations.
Services provided by private hospitals have to be charged at fair market value, including secretarial. There still seems to be an element of ‘quantity discount’ where a consultant is a major player at a hospital.
Competitive insurance
Subscriptions and indemnity cover remained constant – and this does reflect the fact that some consultants are shopping around in an increasingly competitive marketplace for insurance.
Other costs seem to remain fairly constant, but if anything with a slightly reduced pressure.
What then of the future?
Early evidence from 2018 returns suggests that cardiologists continue to prosper – particularly those with a high self-pay element. Some consultant groups are looking to encourage consultants to form groups themselves and to
Early evidence from 2018 returns suggests that cardiologists continue to prosper –particularly those with a high self-pay element
provide management services for them. In other disciplines, this model seems to have worked quite well.
All in all, it looks as if there is continuing prosperity for consultants in cardiology in private practice.
As previously stated, these headline figures are subject to the usual
caveats and are not, of course, statistically significant.
Significant squeeze
Significant market changes over the years make it difficult to compare like with like. For example, we have seen the effect on income of the growth – and decline in some
instances – in Choose and Book work.
There has been a significant squeeze on newcomer fees by insurers – and fee pressures on more mature consultants.
We have also seen the growth of groups and the possible anomalies and comparison difficulties that arise when consultants incorporate their businesses.
Having said all this, our survey criteria remains as it always has been. Our sample includes those who:
Have had at least five years’ private practice experience;
Have held or hold either a maximum part-time or a new consultant contract in the NHS, so they are not completely private;
Are seriously interested in promoting private practice as a business;
Earn at least £5,000 in the private sector, including Choose and Book work not paid through PAYE;
May or may not have incorporated or be a member of a group.
Next month: ENT surgeons
Ray Stanbridge is a partner with accountancy, finance and tax advisory medical specialists, Stanbridge Associates
HOW ARE YOU DOING?
Use
benchmarks to compare your financial performance with others
Gynaecologists
Ophthalmologists
Years ending 5 April
z
WHAT’S COMING IN OUR OCTOBER ISSUE...
Make sure you don’t miss our next issue, published on 24 October You may not receive every issue if you have not yet subscribed to the journal. Don’t risk missing out on vital topics we tackle next time:
Surgeon Mr David Sellu, wrongly jailed for gross negligence manslaughter after a patient died in his private hospital, begins an adaption from his book Did He Save Lives?
The costs of clinical negligence claims for independent practitioners and upcoming changes that will affect them are reported on by Hempsons’ Niloo Bozorgi
Common invoicing problem issues – and how to stop them
Fighting fraud in your practice: how fraudsters use social engineering techniques as they target potential doctor victims
The amount consultants and GPs draw from their practice is obviously one of the most important issues for them! Accountant
Susan Hutter reports advises on what’s best
Start A Private Practice presents a guide to taxable benefits
Results of a survey of 700 private practitioners about what they want from their practice management system
How biophilic design – a concept increasingly incorporated into stores, offices, homes and healthcare – can boost patients’ satisfaction
The last in our Private Practice Growth Guide series considers how best to learn from successes and failures – and continue to improve outcomes and reduce costs
INDEPENDENT PRACTITIONER
Published by The Independent Practitioner Ltd. Independent Practitioner Today is editorially independent and thanks Bupa for its assistance with distribution. Printed by Pepper Communications Ltd Material is governed by copyright. No part of this publication may be reproduced, stored in a retrieval system or transmitted in any form without permission, unless for the purposes of reference and comment. Editorial layout is the copyright of the publishers. If you wish to use it for promotional purposes on websites or for reprints, we would be happy to discuss licensing the copyright to you.
Registered office: 7 Lindum Terrace, Lincoln LN2 5RP
Write to
PO Box 198, Cranleigh GU6 9BB
TELL US YOUR NEWS
Robin Stride, editorial director
Email: robin@ip-today.co.uk
Phone: 07909 997340
@robinstride
ADVERTISE WITH US
Requirements for successful revalidation looks at significant events, feedback from patients and colleagues, and complaints
In our series on property investing for doctors, Dr Lafina Diamandis sets out the big five investment strategies and how to develop yours
Business Dilemmas advises a consultant who is asked in a solicitor’s letter to provide a written testimonial for a colleague undergoing a disciplinary investigation, and a paediatrician who suspects a child’s injuries might not be accidental as claimed
The NHS Patient Safety Strategy – David Hare examines the implications for independent clinicians
Being asked by a patient to issue an unfit for court certificates is a complex area that can lead to difficulties if unaware of the pitfalls
Timing isn’t everything. Patrick Convey on why political dramas are not a basis for investment success
Our unique benchmarking series takes a look at ENT surgeons
Private patient units in the South-west are featured in our latest regional analysis
Our motoring correspondent gets to grips with the new Porsche 911
Data can be difficult to access in the private healthcare sector, but Healthcode’s Fiona Booth argues that we must all work together to make the most of this asset
ADVERTISERS: The deadline for booking adverts in our October issue is 27 September
Margaret Floate, advertising manager Email: margifloate@btinternet.com Phone: 01483 824094
GET A SUBSCRIPTION DISCOUNT!
£90 independent practitioners. £90 GPs and practice managers (private & NHS). £210 organisations. Save £15 paying by direct debit: individuals £75 (organisations £180).
TO SUBSCRIBE – USE SUBSCRIPTION FORM ON PAGE 25 or EMAIL: karen@marketingcentre.co.uk or phone 01752 312140 or go to the ‘Subscribe’ page of our website www. independent-practitioner-today.co.uk
Publisher Gillian Nineham
Phone: 07767 353897. Email: gill@ip-today.co.uk
SAVE £15 WITH DIRECT DEBIT!
Guarantee delivery of your next copy of Independent Practitioner Today. Take out a subscription and you will get full access to our news, features and previous issues on our website. See details on the left.
BACK ISSUES: £12.50 including post & packaging
business journal for doctors in private practice
Giving voice to the private sector
INDEPENDENT PRACTITIONER
Thanks to Healthcode for helping us to reduce the use of plastic
The new president of the Independent Doctors Federation, private GP Dr Neil Haughton, reveals his plans and hopes for the organisation in the years ahead n See page 18
business journal for doctors in private practice
Make access to self-pay easy
The private healthcare sector needs to do much more to make it easier for patients to access. And clearing up price confusion would be a good place to start, argues Keith Pollard n See page 21
What are you doing to attract patients
ADDRESS LABEL
Jane Braithwaite shows you how to choose the right marketing strategy to attract new patients and grow your practice
n See page 26
If undelivered, please return to: The Marketing Centre, 12 Mary Seacole Road, The Millfields, Plymouth, PL1 3JY
What are you doing sector
Integrated online solutions on one platform built to give customers time efficiency, compliance, robust data security and ability to connect seamlessly
Your financial and practice management on one secure platform
Improve:
• cash flow
• operational efficiency
Peace of mind knowing:
• your data is held securely and backed up
• your data is hosted in the UK
• no additional back office costs
A cost-effective integrated toolkit on one platform that:
• is scalable
return to: The Marketing Centre, 12 Mary Seacole Road, The Millfields, Plymouth, PL1 3JY
• includes key tools to manage both your financial and administrative tasks and processes
• allows you to manage your practice bookings for one or multiple locations
• maintains and manages your patient records and their associated transactions
• gives you the ability to communicate securely with other organisations such as hospitals and insurers
For more information and a demo of the system: ( 01784 263 150