The business journal for doctors in private practice
It’s not all plane sailing Treating patients either going or returning from treatment abroad has its medico-legal implications P14 Follow our new series to stop you losing money
n Turn to page 23
To or not to tweet?
Some sound advice on whether or not to use Twitter to promote your private practice P16
Things to get right when starting out How to negotiate the minefield when setting up in practice P38
By Robin Stride
Consultants have hit out at NHS England proposals to try and force them to reveal their private practice earnings, warning the idea is pointless, unworkable and ludicrous.
Doctors’ bodies, including the Independent Doctors Federation (IDF), the Hospital Consultants and Specialists Association (HCSA) and the Federation of Independent Practitioner Organisations (FIPO), all expressed strong criticism.
Accountants also joined the protest against the plan which would require declaration of gross incomes within three suggested bands: under £50,000, £50,000£100,000 and over £100,000.
Independent Practitioner Today columnist Ray Stanbridge, of Stanbridge Associates, called the bands illogical. He said gross earnings were irrelevant since tax was paid on net profit. And it would be ‘impossible’ to file figures from the ‘previous 12 months’, as proposed. He added: ‘The main problems from an accounting viewpoint is that the proposals have not identified what is “private practice”. Until a uniform definition is agreed, any figure will be subject to major error.’
Parties have until 31 October to
respond to the NHS England’s report Managing Conflicts of Interest in the NHS: A Consultation
It claimed the proposals aimed to ensure the existence of private duties is well known ‘in keeping with wider moves towards transparency, and so that conflicts can be either managed or avoided’.
Doctors would also be asked where they practise, when, in which specialty and what major procedures they perform.
Specialists’ organisations say they support transparency, openness and honesty, but the IDF said it ‘shared the views of most of our medical colleagues’ that there was nothing to be achieved by requiring doctors to publish private practice earnings.
Its specialists committee chairman Dr Brian O’Connor said: ‘The vast majority of NHS consultants work well beyond their contractual obligations.
‘Despite this, they are subjected to rigorous annual appraisal, close scrutiny of their NHS commitments at annual appraisal and, of course, as laid down by managers within the NHS implementing specific job plans.
‘It is now a requirement that all doctors declare their time spent in private practice and, indeed pro -
vide additional details as to location, scope of practice and procedures undertaken.
‘The publication of gross income accrued from private practice, which is done outside of NHS contracted hours and in the doctor’s own time is not of any specific interest to anybody and is unworkable.’
If mandatory for doctors, then all individuals with influence on NHS patient care, such as trust board members and managers, should be obliged to declare all their income too.
He added that full disclosure of all private and public sector income by those involved in key NHS decision-making would allay any public anxieties about conflicts of interest.
‘It would seem ludicrous to single out consultants, a small minority of the NHS workforce, for such transparency,’ Dr O’Connor said.
The Federation of Independent Practitioners Organisations (FIPO) said provided consultants worked appropriately within NHS contracts and job descriptions, then private practice arrangements outside and within their own time should not be subject to this type of analysis.
Chairman Mr Geoffrey Glazer said it was difficult to see exactly what benefit there would be be in
asking consultants to declare fee income.
BMA consultants’ leader Dr Keith Brent said the vast majority of consultants already gave beyond their contracted hours. If wishing to do private work, they first had to offer extra NHS time. They made an annual declaration of substantial conflicts of interest in accordance with legislation.
LONDON BRIDGE EXTENDS
HCA is expanding its London Bridge Hospital campus into a new cancer centre (middle foreground). n Read the full story on page 4
Photo: Morley von Sternberg
In this issue
Stay on target in Brexit confusion our accountant shows how to protect your practice against economic uncertainty P12
Your tax is going digital
What private practitioners will have to do when they get an online tax account P18
don’t leave it too late a check list of things to do to make sure your billing and collection is efficient P21
Higher education, even higher costs as school and education costs spiral up, some advice on how to save for them P28
When expenses can be expensive
How your employment status can have an impact on what you claim back on tax P36
enjoy your third age
Learn from the big mistakes other doctors have made in planning their pension P40
PlUS oUr regUlar colUmnS Business
editorial comment
Pay idea doesn’t add up
We’ve seen some mad ideas in our time, but NHS England’s report proposing that consultants should publicise their private practice income is bonkers (see p1 and our story opposite).
Private practice. Now what is that exactly? Does it include Choose and Book, medico-legal work or locum consultancy not treated for tax purposes as PAYE? What about honoraria? PPUs?
If ‘private work’ paid for by the NHS is excluded, then the earnings data risks being distorted against those doing conventional private practice.
The vast majority of consultants view NHS contracts as a pri-
ority and many do much more. We doubt they will be recorded!
Private work is done in consultants’ own time when they are not contracted to the NHS.
Private hospitals have details of consultants working at their premises, so this is very clear.
Hospital and doctors’ websites also state where they practise, when and what they do.
The whole thing has been badly thought through. Targeting consultants as proposed will only encourage more senior ones to leave the NHS, increasing its pressures and having exactly the opposite effect to what is intended.
tell US YoUr neWS Editorial director Robin Stride at robin@ip-today.co.uk Phone: 07909 997340 @robinstride to adVertiSe Contact advertising manager Margaret Floate at margifloate@btinternet.com Phone: 01483 824094 to SUBScriBe lisa@marketingcentre.co.uk Phone 01752 312140
Publisher: Gillian Nineham at gill@ip-today.co.uk Phone: 07767 353897
Head of design: Jonathan Anstee chief sub-editor: Vincent Dawe Circulation figures verified by the Audit Bureau of Circulations
Study shows private value to economy
By edie Bourne
Hip and knee replacements in the independent health sector contribute an estimated £540-£692m annually to the UK economy, a new report reveals.
Around 198,000 hip and knee operations were delivered by the independent sector for NHS and non-NHS patients in 2014-15.
That equates to a third of all hip and knee operations across the UK and includes approximately 83,000 hip and knee replacements.
Consultants in the independent sector carried out approximately 21% of NHS-funded hip replacements and 23% of NHS-funded knee replacements at a cost set by the NHS.
The report, commissioned by The Association of Independent Healthcare Organisations (AIHO) and produced by healthcare information specialists Monmouth Partners, says this helped alleviate NHS capacity demands and gave NHS-funded patients more choice.
It is the first single analysis of all hip and knee joint replacement activity to identify the independent sector’s economic contribution.
The study takes into account productivity gains through reduced employee sick days and knock-on business productivity, welfare and benefits savings, and savings to the NHS as a result of patients choosing to receive treatment by private insurance or selfpay.
The value of non-NHS-funded independent sector provision of hip and knee replacements is estimated at £285m.
AIHO chief executive Fiona Booth said: ‘Not only does the independent sector help to ease the peaks and troughs in service demand experienced by the NHS,
it also treats tens of thousands of privately-insured and self-pay hip and knee patients who would otherwise require treatment via the NHS.
‘The independent sector is providing patients with greater choice, which patients are clearly taking advantage of, which in turn benefits the wider economy.
‘This choice means more people are getting back to work sooner, welfare costs are avoided and there is less demand placed on the NHS.
‘At a time when NHS pressures are continuing to grow with rising demand, chronic conditions and waiting lists, this model of care is an opportunity for the health sector to reduce waiting times for patients and improve patient choice.’
The independent sector has high patient satisfaction, with 99% of NHS-funded patients who received treatment saying they would recommend the service to friends and families.
NHS-funded patients also have shorter waiting times when receiving treatment from private providers.
The report estimates hip and knee replacements have risen by about 50% and about 43% respectively over the past ten years.
Ms Booth added: ‘Demand for hip and knee replacements will continue to grow as our population increases and ages.
‘Independent healthcare provision and a system of care free at the point of need can and do coexist well. In fact, it’s a relationship that is fundamental to the future of healthcare.’
AIHO’s report: Joint Working: Exploring the social and economic contribution of the independent sector for elective hip and knee surgery in the UK
Doctors are polled over bid to reveal private pay
➱ continued from front page
Members of the Hospital Consultants and Specialists Association (HCSA) are being quizzed for their views on NHS England’s plans to force independent practitioners to publish their private earnings.
The consultation was launched after the union questioned the motive for the planned fee disclosure requirement against the backdrop of negotiations on a new contract.
A spokesman told Independent Practitioner Today : ‘We are now asking all members affected by this proposal to offer their view as part of our detailed response to this consultation.’
Time running out to shield pension
By leslie Berry
Senior doctors have only a few more months to apply for a Government scheme aimed at protecting the value of their pension from huge tax charges.
The warning comes as HM Revenue and Customs (HMRC) released data showing it had clawed an extra £126m in tax from individuals caught out by the reduced tax-free pension saving allowance limits in 2015-16 – a 62% rise from the previous year.
breached the allowance when it was set at £1.25m last year. Financial advisers say many more will breach the limit now it has been reduced further.
The Government introduced a protection scheme, Individual Protection 2014 (IP14), two years ago, which allows savers to restore the value of their lifetime allowance back to £1.5m provided certain criteria are met.
allowance limit has changed considerably in recent years.
‘It is very difficult for the busy consultant or doctor to keep up to date with this specialist area and all too easy to breach the savings limits without having pension protection in place. It is an area where many people come unstuck.’
If your pension was valued in excess of £1.25m as at 5 April 2014, you may be eligible to apply for IP14 allowing you to protect up to £1.5m.
eddie Saville, HcSa chief executive
HCSA chief executive Eddie Saville said: ‘Frankly, we’re a bit bemused about the timing of this statement, given that the large majority of NHS hospital doctors do not carry out private work and the many other pressing issues facing our health service, mainly related to insufficient budgets.
‘Doctors work hard, often way beyond their contracted hours, for the NHS and this is just the latest misrepresentation of the entire profession where a few individual examples are used to suggest that all hospital doctors are somehow in it for personal gain.
‘Where NHS hospital doctors do carry out private work, this will have been formally agreed with their trusts as part of their job plan.
‘The real problems facing our hospitals are related to underfunding in the face of rising demand. What’s clear is this measure will do nothing to address growing patient numbers, low morale, recruitment freezes and staff shortages.’
On 6 April 2016, the lifetime allowance for pension savings –the total amount that can be built up and taken from pensions without triggering an additional tax charge – was reduced to £1m.
Any doctors saving over this limit – and even middle-earners could breach the threshold if accumulating NHS benefits for many years – will face tax charges of up to a staggering 55%.
HMRC collected extra tax from 1,539 individuals who had
Sadly, many doctors will miss this valuable opportunity because they are unaware that the deadline for applications closes on 5 April 2017.
Patrick Convey, technical director with specialist financial planners Cavendish Medical, explained: ‘Pensions are already complex, particularly the NHS pension, and then these protection schemes are added into the mix.
‘There are several different schemes and all of them vary in terms of who can apply and what type of financial protection they offer. In addition, the lifetime
the boss of cleveland clinic has said the US group’s plans for a 205-bed hospital in london do not aim to increase competition.
President and chief executive dr toby cosgrove said: ‘london offers a unique combination of worldleading medical research and some of the best and most respected healthcare professionals. our goal is to complement – not compete – with medical offerings available in the london market.’
He was speaking after cleveland clinic, as widely expected, submitted plans to Westminster city council to operate the facility near Buckingham Palace at the building it leased last year (independent Practitioner today, november 2015).
Specialty services will focus on general surgery, cardiology and neurology. the application includes eight operating rooms in the six-story, 198,000ft2 office building at 33 grosvenor Place. a new training programme for ‘physicians in the london area’ is also promised.
Remember that the lifetime allowance limit applies to the sum of your NHS pension value plus any private pensions you hold.
Mr Convey concluded: ‘You will need to move quickly to get your application in place by April, as there are a number of valuations to be obtained first, which can take several months. Don’t delay if this does apply to you – you should act now to defend your future benefits against unnecessary tax charges.’
cleveland clinic runs a 165-acre main campus near downtown cleveland, ohio, nine regional hospitals throughout north-east ohio and facilities in Weston, Florida; las Vegas, nevada; toronto, ontario, canada; and abu dhabi, United arab emirates.
HCA buys into cancer centre
By Robin Stride
HCA’s London Bridge Hospital is to open four floors at the new £160m Guy’s Cancer Centre, unveiled last month.
The group, which has invested £38.2m into the project under a 25-year lease, aims for a Spring 2017 launch as its specialist cancer campus at London Bridge Hospital expands to the new stateof-the-art facility.
John Reay, former chief executive at London Bridge Hospital and now HCA president of operations, said: ‘We are proud to be part of this exciting new development in which London Bridge Hospital at Guy’s will offer worldclass facilities for those with signs and symptoms of cancer.’
The first outpatient clinics were held in the new building last month with chemotherapy treat-
ment following this month and radiotherapy treatments due to start in November.
Dr Majid Kazmi, clinical director of cancer services at Guy’s and St Thomas’, said the opening was the culmination of over ten years of planning and working in partnership with patients to create a building to transform cancer care.
The Centre brings together most treatment under one roof. Previously, cancer care was provided in 13 different locations in eight different buildings on the St Thomas’ and Guy’s sites.
It is the first cancer centre in Europe to provide radiotherapy treatment above ground. Patients said this would make a huge difference to them.
Diana Crawshaw, chairwoman of the Patient Reference Group which has shaped the new Cancer
Centre, said: ‘Patients have been consulted at every stage and no decision has been made without us. Our views have been welcomed, listened to and acted on.’
The Centre also brings together treatment and research in an Innovation Hub.
Prof Peter Parker, head of the Division of Cancer Studies at King’s College London, said: ‘Expanding our experimental
IVF clinic now in The Shard
The UK’s largest private IVF unit, The Lister Fertility Clinic, has been moved by HCA Healthcare UK into the iconic Shard building.
The Lister Fertility Clinic at The Shard will provide initial appointments with senior fertility consultants who will arrange a personalised treatment plan and any necessary treatments or investigations.
Dr Alison Taylor, consultant gynaecologist and specialist in reproductive medicine, said: ‘We recognise that dealing with fertility issues can be stressful and timeconsuming – particularly for prospective parents working in high-pressured jobs in central London, the City of London and at Canary Wharf.
‘We’re always trying to find ways to make the process more convenient and relaxed for patients and we believe this ethos contributes to our success rates.
‘Along with the rest of the Lister Fertility Clinic team, we look forward to welcoming patients to our brand-new facility and starting them on their journey towards completing their family.’
Patients will normally have an ultrasound scan and results discussion on the day of consultation.
They will also benefit from a dedicated nursing team, available to perform cycle monitoring, scans and blood tests as needed, making it quicker and easier to check on progress and giving couples and individuals the best chance of conceiving.
More involved treatments such as egg collection, embryo transfer and intrauterine insemination (IUI) will be carried out by the specialist team at The Lister Fertility Clinic in Chelsea, one of the most successful fertility units in the country with success rates consistently above the national average.
As well as benefiting from consultations and treatments in a convenient location close to transport links and a discreet private entrance, patients will also be able to access wider health services available at HCA at The Shard, including physiotherapy, nutrition and dietetic support, gynaecology and paediatrics.
The Shard also hosts a one-stop breast clinic, which can rapidly diagnose and treat patients with breast-related problems, providing diagnosis and personalised treatment plans in a matter of hours.
John Reay, newly-appointed HCA president of operations, said: ‘We have made this move with our patients’ needs front of mind and hope that, by bringing our services closer to our patients, they will feel safe in the knowledge that they are getting the best care possible, when and where they need it.’
medicine programme will enable us to grow our capabilities in designing and conducting clinical trials for new treatments.
‘Our vision is for the Innovation Hub to cross-fertilise ideas between researchers and clinicians so that potentially impactful discoveries can be advanced rapidly and successful approaches for one cancer type can be tested quickly in others.’
Nightingale ups capacity
A 20% rise in demand for services over the past five years has led to the opening of a new ward at Nightingale Hospital, London, bringing its capacity to 73 beds.
Recent reports suggest one in four adults in England have been diagnosed with a mental health condition.
The new ward features 14 contemporary en-suite bedrooms, occupational therapy spaces, three group therapy rooms and large, open-plan communal areas and a kitchen.
A carefrully selected colour scheme has been chosen to create an atmosphere which the hospital says supports recovery and aids well-being.
The ward will initially best serve general psychiatry patients, who will be offered tailor-made treatment programmes, including individual and group therapy sessions.
The busy reception area at the Guy’s and St Thomas’ Cancer Centre
CQC unveils handbook
By Martha Walker Director of CQC Consultancy
The long-awaited Care Quality Commission (CQC) handbook for independent doctors will be launched at the end of October – a month later than expected.
It will act as tool for doctors in preparing for and undergoing future compliance inspections.
The handbook, and its appendix of Key Lines of Enquiry (KLOEs), will explain the inspection preparation and process that the watchdog devised after consultation with various stake-holders.
These include the Independent Doctors Federation (IDF) and a series of pilot inspections of 40 independent health care providers earlier this year.
The IDF has greeted the new handbook positively. Dr Neil Haughton, chairman of its GP committee, said: ‘The IDF was initially sceptical about the CQC’s willingness to accommodate the private sector.
‘But they have risen to the challenge, which they are legislated to carry out, and have been receptive to the advice given by the IDF and we have been consulted all the way on requirements set out in the new handbook.’
There will be two types of inspection: comprehensive and focused. Independent doctors will welcome the new four-week
➭ Focused: Unannounced, where there may be cause for concern
Provider information request. This is information the CQC requests prior to the compliance visit and typically consists of questions such as:
➭ How many doctors currently work/have practising privileges in your practice?
➭ Who are they and what are the dates of last appraisal and revalidation, who is their designated body?
➭ Do you operate a dispensary?
➭ How many near misses have you had in the last 12 months and what lessons were learnt from them?
➭ How do you manage out-of-hours patient care?
Four weeks’ notice for comprehensive inspections
Use of external bodies such as GMC and iSCAS to gather information
More emphasis on duty of candour and fit and proper persons as directors
notice period that will be given to them before a comprehensive – or scheduled – inspection.
During that period, the doctor will be asked to complete and submit to the CQC a Provider Information Request*. This is intended to assist the inspector in information gathering for the visit.
The CQC may also seek information about the practice from the GMC, Healthwatch, The Independent Healthcare Sector Complaints Adjudication Service (ISCAS) and other bodies.
Emphasis will be on how the doctor provides a service that is
safe, effective, caring, responsive and well-led.
The CQC has devised a set of KLOEs to assess each of the five domains. The KLOEs will expect evidence of systems, processes and pathways, such as demonstrating there are procedures in place, including:
Managing test results and letters;
Identifying near misses and clinical errors;
Providing evidence of clear clinical care pathways and protocols that help standardise and ensure evidence-based care is provided
Dr neil Haughton, chairman of the iDF’s GP committee
and staff follow care pathways and protocols.
Dr Haughton added: ‘The KLOEs are quite standard and can be adjusted over time. Obviously, there may well be teething problems and the message may not necessarily get down to the inspectors at first, but hopefully with experience on both sides, we should be treated fairly at least.’
Part of the inspection process will include the opportunity for the practice to make a 30-minute presentation highlighting all that is good within it.
The number in the CQC inspection team will depend on the complexity and size of the practice.
Independent doctors will not be rated at this time, but the CQC says they may well be in the future.
The inspections using the handbook and its appendix of KLOEs will commence in 2017.
Private proton beams to fill big gap
A leading specialist has forecast that the UK will need as many as 18 proton beam therapy machines to meet rising demand for this more targeted form of cancer treatment.
Prof Karol Sikora, chief medical officer of Proton Partners International, said: ‘The NHS estimates that just 1.5% of cancer patients require proton beam therapy, whereas in the US it is believed 20% of patients would benefit from the treatment and European studies indicate an estimate of 10-15%.
‘In the UK, we should work with the 10% figure. The estimated demand for proton machines is based on a capacity per unit of 500 patients every year, and therefore we can calculate that the machine requirement for the UK is around 18 machines.’
Speaking at The Proton Congress in London, he said this was far more than the two currently planned by the NHS, which would simply not meet rising demand. To help address this gap in pro-
ton beam therapy, his company is in the process of building three centres in the UK: in Newport in Gwent, Northumberland and the third location is still to be announced.
Prof Sikora said: ‘The machines that deliver proton beam therapy are generally very large and expensive. In the last decade, however, we have seen a gradual improvement in these machines and the introduction of more compact models onto the market means
that the treatment is becoming more accessible and affordable.
‘Over a thousand clinical studies are in progress and it’s likely further data on long-term toxicity will support a major expansion in this area.’
He added that there was a huge need in the UK to upgrade the routine radiotherapy machines, as many were over a decade old. But capital was short. Imaginative new ways were needed to fund state-of-the-art cancer care in the UK and abroad.
Taxman warns of failing to disclose
By leslie Berry
A new online disclosure facility gives tax evaders a last chance to come forward and settle tax on wealth hidden offshore ahead of new data-sharing arrangements and tougher penalties.
HM Revenue and Customs (HMRC) said this was the final chance for a few still dragging their feet to put things right with any outstanding tax on undeclared offshore money or assets.
But there are no special terms: those who come forward will pay the tax in full, with interest on top, plus a minimum penalty of 30% of the tax due – and they could still face criminal prosecution.
The quality of the information disclosed will be taken into consideration and it is always advisable to come forward and ensure any outstanding tax liabilities are in order as soon as possible.
HMRC will, from now on, also consider how long it has taken for someone to put their tax affairs in order when calculating penalties. This means those who have delayed disclosing or ignored past opportunities will no longer get a reduction for disclosure.
This last chance comes before HMRC starts receiving an unprecedented amount of data on offshore accounts and tax-evaders get hit by tougher sanctions.
Jennie Granger, HMRC’s director general of enforcement and
compliance, said international co-operation was making it easier to catch evaders because more information was being received about financial assets which people had hoped would remain hidden.
‘Our message couldn’t be clearer: there are no safe havens left for tax evaders and no one should be in any doubt that the days of hiding money offshore with impunity are gone.’
Those who do not come forward will face the new Requirement To Correct (RTC) penalties being consulted on.
One option being considered is a minimum 100% penalty – significantly higher than the current minimums.
London hospital installs extra intensive care pods
More people recovering from serious trauma and major operations can now receive specialist critical care at BMI The Clementine Churchill Hospital, Harrow, following the installation of two additional intensive care ‘pods’.
There are now six selfcontained, climate and air pressure-controlled bedroom units at the north London hospital –bringing the number of critical care pods up to four and the number of total critical care beds to six.
Hospital executive director Claire Armstrong said: ‘Before, we would not have been able to place a critical care patient recovering from surgery next to a critical care patient recovering from an infection, because of the risk of crossinfection.
‘But now we can look after both of these types of patients in the same area, as they are in different
pods with different airflows. It just gives us so much more flexibility in the management of patients that we didn’t have before.’
Consultant intensivist Dr Gary Wares said: ‘The “pods” have transformed the way we look after patients on the critical care unit.
‘Not only do they promote personal space and privacy for our
patients, but they also ensure that infection control and cross-infection risks are minimised due to the physical barriers between patients.
‘Our patients have commented on the lack of noise pollution between bed spaces, which helps promote sleep, which is important for patients recovering from major surgery or life-threatening illnesses.’
BMI healthcare has appointed Kevin Thomson as head of healthfirst, the firm’s UK corporate healthcare division, which offers advice, treatment and support for firms investing in their employees’ wellbeing. he said: ‘The evidence is compelling that, within organisations that continually focus on developing a culture of health where the employee is considered as important as the customers, employees tend to be more creative, more loyal and perform better in terms of customer satisfaction.’
healthfirst will use BMI healthcare’s established network of 59 UK hospitals to provide a range of services including private Gp appointments, health assessments, physiotherapy, imaging, pathology and occupational health.
Prostate premier
Two prostate cancer patients at The London Clinic are said to be the first in the UK treated with new high-tech SpaceOAR hydrogel to protect from radiotherapy treatment side-effects such as rectal damage.
Consultant clinical oncologist Dr Simon Hughes said with existing state-of-the-art radiotherapy techniques there was still a small chance of significant rectum damage due to the anatomy of the region.
He said: ‘The gel acts as a spacer, moving the rectum away from the prostate gland. This enables us to deliver radical treatment to the prostate while minimising the radiation dose received by the rectum – reducing the side-effects of treatment.’
MRI in Newcastle
Nuffield Health has bought a £1m+ Siemens Magnetom Aera MRI scanner for its Newcastleupon-Tyne hospital.
It said this will provide improved image quality for diagnosis and a more open and comfortable experience for patients, especially claustrophobia sufferers.
The hospital’s MRI unit and diagnostic suite are undergoing a complete refurbishment at the same time.
Bupa’s new MD
David Hynam, former general manager of Bupa’s UK Care Services business, has taken over as Bupa UK managing director to replace Richard Bowden, who becomes leader of the insurer’s Australia and New Zealand business.
The Midex pro
Practice management software producers Avebury Computing has appointed a new operations director, Caroline Corrigan, to establish a full training programme for users across the UK. The company recently invested in the development of the software to allow its users to access their data via a new online solution, allowing use on Macs and tablets for the first time.
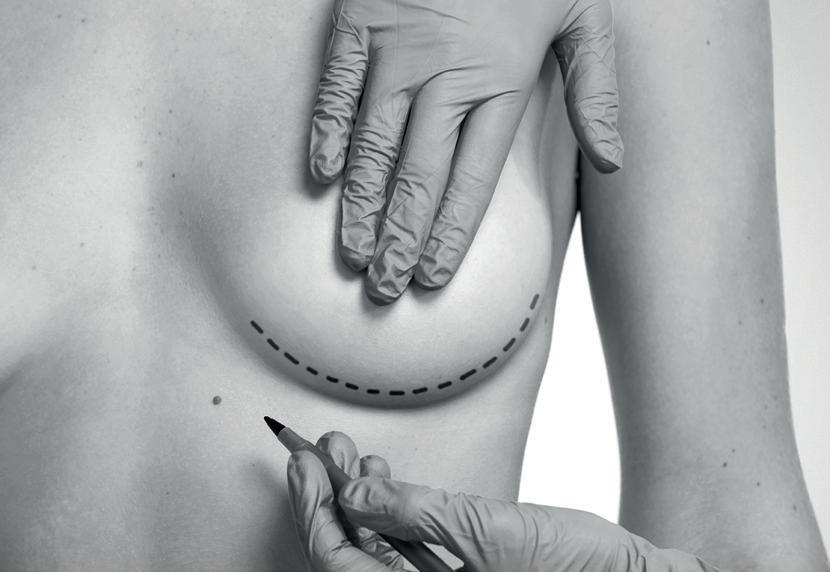
Public decries beauty ops
By Charles King
As many as 57% of patients have a poor view of cosmetic surgery, according to a poll, with as many as 16% giving a wholly negative reaction. Despite this, half have had a treatment or considered it.
The survey, commissioned by sister companies Fitzroy Surgery and MYA Cosmetic Surgery, found people’s biggest cosmetic surgery worries are:
Complications after surgery (60%);
Complications during surgery (49%);
Health scares such as the 2012 PIP scandal (45%);
Botched surgery media stories (42%).
Just over half felt uninformed about cosmetic surgery and thought there was insufficient reliable information available in the UK to make an informed decision.
Sally Taber, director of the Independent Healthcare Sector Complaints Adjudication Service (ISCAS), commented: ‘The lack of unbiased, informed, standardised information coming from the industry to the consumer has always been a real problem.
‘In the first instance, this means that when the patient is trying to
choose a surgeon, they have nowhere to turn and often end up choosing on price or locality.
‘Secondly, this lack of education means consumers often have an unrealistic view of surgery and what it entails. So when the patient discovers it isn’t a walk-in, walkout procedure or it can’t give them the body of a celebrity, they are more likely to perceive the procedure as a failure, which adds to the poor reputation of the industry.’
The poll coincides with the launch of a new report called Cosmetic Surgery – The Road To Reform: working together to restore patient trust.
This takes an independent overview of the industry, charting its meteoric rise in popularity as well as analysing the impact of historical issues such as the PIP breast implant scandal and the current regulations and governance.
Cosmetic surgery procedures in the UK have more than doubled in the last decade to 51,000 last year. The report explores some of the reasons behind this rise and considers factors influencing people’s decisions to have surgery.
The poll of 1,008 UK adults found the main reason for considering cosmetic surgery was to increase body confidence and self-esteem (women 33%, men
16%). Thirty per cent said they trusted their GP to give them information on cosmetic surgery.
While the report finds many examples of best practice, with excellent surgeons and providers, it claims there is a need for greater scrutiny and continued reform to restore patient confidence.
Simon McMillan, managing director at Fitzroy Surgery and MYA Cosmetic Surgery, said the PIP scandal highlighted the urgent need for industry reform, better services for patients and greater assurances on patient safety.
‘Making sure that we pull together as an industry to make that happen is now our greatest responsibility and our biggest challenge.’
The reporT Calls for:
➲ More transparency of data on surgical procedure results so patients understand what a good outcome is and therefore make an informed decision when choosing a cosmetic surgery provider and procedure.
➲ Tougher minimum requirements to become certified as a specialist cosmetic surgeon
➲ The establishment of a wholly independent body to regulate, monitor and standardise the industry and provide one ‘port of call’ as an unbiased source of information for patients
New clinic opens in Peterborough
An independent, consultant-led private group practice featuring a range of specialties opens this Autumn in Peterborough.
The Avicenna Clinic was founded after specialists identified an opportunity in the local Cambridge shire market to offer patients a consultant-led imaging and minimally invasive surgery facility.
A multispecialty business model with a focus on day surgery procedures was chosen.
The right building was found in the city centre offering good transport links from and to the rest of
the UK and making the clinic easily accessible for patients.
Leading the group practice is medical director Dr Hany Elmadbouh (pictured right ). Consultants on the advisory board are Dr Tuba Hussain, Mr George Settas, Mr Richard Hartley, Mr Amer Durrani, Mr Farrukh Bajwa, Mr Sion Lewis, Ms Claudine Horrocks and Mr Harneck Rai. Jacquie Moon is practice manager.
and image-guided intervention techniques.
‘Being the first clinic in the region to have an open MRI scanner is just one example of the way we will be using the latest technology to provide the highest level of patient care here at the clinic.’
Radiologist Dr Elmadbouh said: ‘Avicenna Clinic will be a centre of excellence, specialising in minimally invasive surgery, imaging
The North Street clinic is located in a period building, recently renovated to accommodate a medical practice over three floors. There are X-ray and ultrasound suites, consulting rooms and relaxing patient spaces with easy access.
COSMETIC SURGERY: THE ROAD TO REFORM
WORKING TOGETHER TO RESTORE PATIENT TRUST Authored by Isla Whitcroft, Health Media Expert, on behalf of Fitzroy Surgery and MYA Cosmetic Surgery.
The scanner is craned into the clinic
simon McMillan of fitzroy surgery and MYa Cosmetic surgery, who commissioned the study
Compensation needs total reform
THeresa May, no doubt, has an overflowing in-tray since becoming Prime Minister, not least dealing with the changes resulting from the eU referendum vote.
How health issues will fare remains to be seen, but there are several burning medico-legal issues that have serious implications for doctors in independent practice and for the public purse.
Here are the MDU’s policy priorities for this Parliament:
1A fairer, more sustainable system of compensating patients
Tackling the spiralling cost of compensation claims should be sitting at the top of the Government’s ‘to do’ list.
Claims inflation has been increasing steadily at 10% in recent years. The steep increase is reflected in the indemnity costs of independent consultants.
However, while consultants have to bear the costs for a problem which they cannot control, they are not to blame. The drivers on claims inflation are largely a result of economic and legal factors and the only way to address them satisfactorily is through urgent legal reform.
although not directly linked to independent practice, the most recent annual report of the NHs Litigation a uthority (NH s L a ), which pays negligence claims on behalf of english NHs bodies, is sitting on a time-bomb of legal claims.
The 2015-16 NH s L a report explains that estimated liabilities for hospital clinical negligence claims rose to a staggering £56.4bn. This is double the previous year’s figure, though that is partly down to a one-off Treasury adjustment.
If these liabilities were all realised, it would cost each e nglish taxpayer more than £2,000 each, and that is just for claims against NHs bodies.
The NHsLa’s experience is mirrored in the independent sector, where some of the MDU’s largest compensation payments have been made on behalf of consultant members.
By Dr MIcHAeL DevLIN, Head of professional standards and liaison at the MDU
Legal fees often greatly exceed damages awards in lower-value claims. In one case, the MDU paid £4,200 in compensation while the claimants’ lawyers’ fees were £70,000
The 2015-16 NHSLA report explains that estimated liabilities for hospital clinical negligence claims rose to a staggering £56.4bn. This is double the previous year’s figure
For example, our highest payment to date was £9.2m-plus legal costs to compensate a patient rendered tetraplegic following spinal surgery.
a nd in another case, we paid £6.2m in damages with £3m in legal costs on behalf of a member to a female patient who had nerve damage after plastic surgery.
outdated legal system
soaring compensation awards are not a reflection of clinical care standards, which remain high, but the consequence of an outdated legal system. a mong the essential changes advocated by the MDU is the repeal of s 2(4) of the Law r eform (Personal Injuries) act 1948, which obliges defendants to disregard NHs care and fund private sector care packages.
We are also seeking:
n Caps on the level of damages awarded for future care;
n Damages for loss of earnings capped at three times the national average salary per year.
Patients who are damaged by negligence must be compensated fairly, but the current system is unsustainable. We need urgent legal reform so that clinical negligence awards can become proportionate, sustainable and fair for all parties.
2End disproportionately high legal costs another factor affecting indemnity subscriptions is the disproportion in the amounts charged by claimants’ solicitors.
Legal fees often greatly exceed damages awards in lower-value claims. In one case, the MDU paid £4,200 in compensation while the claimants’ lawyers’ fees were £70,000.
We have many other examples of alarming disparity where the lawyers’ fees far outstrip what their clients receive. Of course, lawyers must take on some cases they won’t win in order to ensure access to justice for their clients, but the MDU’s figures for cases that we defend without a payment have risen recently from 70 to 80%.
Things must change and lawyers need to be more realistic about their fees and about the cases they advise their clients to pursue. Fixing legal costs for lowvalue claims should achieve both these aims if it is done properly, and the Government needs to deliver on its promise.
Introducing a fixed-cost structure for legal costs should result in legal fees becoming more affordable and proportionate, while still providing access to justice for patients alleging negligence.
3A faster, fairer fitnessto-practise (FTp) system
We have long advocated changes to speed up the stressful GMC investigation process for doctors, without compromising patient protection.
We support initiatives such as the GMC’s provisional inquiries scheme, whereby it identifies cases at an early stage that are not likely to amount to impaired fitness to practise, even if the allegations were proven.
By conducting early investigations on such cases, the GMC has managed to close an average of 230 cases a year at this stage. The scheme was also expanded in July so that cases arising from a single clinical incident will be added to the criteria for a provisional inquiry.
We expect this should further increase the number of cases closed early. Without the GMC compromising its primary duty to protect patients, it should also be possible
to relieve even greater numbers of doctors of the stress of an unnecessary GMC investigation.
However, more needs to be done. In 2014, there were 9,624 complaints to the GMC, yet only 218 were referred to an FTP panel that year.
Additional powers
The GMC recognises the need for further change, but in order to make any real difference, it needs additional legal powers to enable it to deal with cases more efficiently and proportionately.
The MDU has warned for several years about the dangers
We urge the Government to give the GMC greater autonomy over its FTP procedures. If the GMC has identified a way to improve the investigation procedure in order to lessen the impact on doctors, and has the agreement of bodies like the MDU, it should be in a position where it can introduce such reforms rapidly, without the need for a lengthy parliamentary process that can take two to three years.
We hope the Government will appreciate the need to make progress in all these important areas.
In some cases, the good work has already been started and the MDU continues to campaign tirelessly on doctors’ behalf to maintain momentum. n
references
1. General Practice Forward View, NHS England, April 2016. See www.england. nhs.uk/wp-content/uploads/2016/04/ gpfv.pdf
Information is power
All consultants’ and hospitals’ performance data for treating privately-funded patients in the UK will begin to be published by The Private Healthcare Information Network (PHIN) from next April.
In the run-up, it has been giving consultants the chance to check their data to ensure the performance measures are fair and robust.
Over the last six months, PHIN has been piloting its system for collecting and displaying data, working with a selection of consultants and hospitals.
From next month, it will start to roll out its system across the sector. Consultants will be contacted for their sign-off in a phased approach as data appears about them on the system.
So what will this process feel like?
Independent Practitioner Today spoke to Dr Voi Shim Wong (right), a consultant gastro-enterologist, one of the specialists who has been involved in PHIN’s pilot study
How have you found being involved in the PHIN pilot?
It has been very useful to see data about all my private practice collected together in one place.
I haven’t had to do very much, as the data is all sent to PHIN electronically by the various hospitals I work with. I just need to log in and check that it’s all there and point out any errors.
There are some inaccuracies in my data at the moment. I’ve been reporting those errors through the system, but getting the data corrected is slow progress, as it’s up to the hospitals and that has felt quite frustrating.
There’s bound to be a few glitches at this early stage, though. And PHIN has been clear that none of this will be published until it’s right.
Even though the system isn’t yet showing the full range of data that will be collected, it’s already very powerful.
I can see my activity, number of patients, length of stay and so on. So far, it has been easy to spot information that’s incorrect, and I can see how it will make it easier to pick up potential safety issues.
Because I can compare data with my peers, I can also see for the first time – just like I can with my NHS work – how my work compares with that of private colleagues.
Why is data so important to you in your practice?
I’m a real believer in the power of data to help us improve the care we provide. That’s why I was interested in being part of this pilot.
Having access to accurate data about my own practice is useful on all kinds of levels: from improving quality to ensuring safety and patient satisfaction. It’s helpful to be able to review my activity over the year.
Of course, having all of this information at your fingertips is also really helpful for appraisal and revalidation.
We have to present all our NHS and private work and it would be very difficult for me to collect this information myself from all the different hospitals I work with.
One big plus is that now I can just click a button and see all of it laid out clearly in front of me.
I can also see how this data will have huge potential from a research point of view. At organisation and also specialty level, we’ll have a picture of what kinds of patients and procedures we’re seeing in the private sector, and about quality and safety. Private healthcare is bound to have processes that NHS can learn from and vice versa.
What’s your big message to colleagues about the changes they can expect over the coming year?
PHIN is coming. My advice is to embrace the process and all the opportunities it offers. Like it or not, it’s regulation now anyway. We’d have to collect this information one way or another. Why not let PHIN do it for us?
Ultimately, once all these glitches with the system have been ironed out, collecting information in this way will help improve clinical quality and it will improve patient information. It’s going to be so powerful in the future to be able to say to my patients: ‘Look, here’s a link to PHIN’s website giving all the data about my practice. I see X many people a year, no complications, I have a 90% patient satisfaction rate...’
This kind of transparency is going to give confidence to GPs when they are making referrals, and to patients and families when they are making choices.
I would say embrace the change and make it work for you.
Dr Voi Shim Wong is a consultant gastro-enterologist at Highgate Hospital, London
Stay on target in Brexit confusion
So how can consultants protect their practices against the current economic uncertainty? Susan Hutter (below) has some timely advice
It I s still early days after the Brexit vote and therefore the uncertainty surrounding exactly what will happen next has not subsided.
All of us in business will need to get used to this, as it will be at least two years before we have a better picture and, even then, we may not have complete clarity.
Nevertheless, the medical profession is largely protected from any post-Brexit fall-out. But recessions are cyclical and we may be in line for a mild recession or at least a downturn in business.
Recent economic indicators certainly suggest this to be the case. t his could affect consultants in
private practice inasmuch as a downturn could cause job losses generally, which will have a knock-on effect on private medical insurance.
Also, if Brexit does have an effect on the City of London, whereby many employees in the financial sector either leave the UK or are unemployed, this could also mean that less people are turning to private medicine in central London.
so what can consultants do to protect their practices in these circumstances?
Protection against downturn
Business practices in the medical profession are changing and have been for some time.
t hey already operate in a far more business-like way than in the old days, which in itself offers protection from a downturn. the sole practitioners, although they still exist, are dwindling in numbers as consultants in similar specialties, or the same specialties, team up to provide an all-round service and also to benefit from certain synergies.
For consultants who have not yet explored the possibilities of ‘merging’, now might be quite a good time to do so, as there is a lot of activity going on.
For all businesses, cash is king and even without a downturn, it is essential that consultants have strong internal procedures to make sure that all their work is invoiced and debts are collected on a timely basis.
Many consultants who provide services to embassies, and large organisations in general, are finding that it is extremely difficult
and time-consuming to get their money in.
some consultants have a debtor list that has been outstanding for a year or even more. By this time, the person who engaged the work may have left the embassy/company and so consultants are having to write off old debts for no other reason than they have hit a brick wall in collection.
If consultants are not going to get paid, there is really no point in them doing the work in the first place.
However, there is a lot consultants can do to protect their position and it is vital that they set up the relationship with the correct personnel at the beginning. If the relationship is ongoing, but not working from a financial point of view, either stop work or go and see the person who can make decisions. A face-to-face meeting usually solves a problem far more quickly than resorting to lengthy emails.
Collecting debt
Many consultants use specialist companies who not only provide invoicing services but also collect debts. In fact, there are companies who specialise in collecting debts from embassies.
If consultants do not have a strong back office, it is recommended that they look at these services. If not, they will have to form the relationship themselves and familiarise themselves with the chain of command within the organisation – for instance, whom
Make or break: Our lead story in July revealed the results of accountants’ analysis of the Brexit vote fall-out
to send the invoice to and whom to chase for debts.
As far as insurance companies are concerned, it is often quite frustrating collecting money from them, although generally they do tend to pay up as long as all their procedures have been complied with.
Once again, it is important for consultants to have a good team behind them to ensure that everything is being done properly.
Another question consultants must ask themselves is: are they earning money from all possible avenues; that is to say, not just seeing patients and carrying out procedures?
Consultants are advised to look at their agreements with others –for example, imaging providers –to see if some sort of ‘referral fee’ can be negotiated. t he whole medical profession is becoming much more business-like nowadays and these providers will not be surprised at such overtures.
In all circumstances, it is important to have robust financial procedures. For consultants who are unsure whether or not their procedures are up to scratch, it is worth taking the advice of the practice accountant who can stand back and take an independent view. there is no doubt that interesting challenges are ahead, not only for the medical profession, but for all businesses and therefore consultants should stay abreast of all developments.
Susan Hutter is a specialist accountant for the medical profession and a partner at Shelley Stock Hutter
It’s not all plane
Independent practitioners may be consulted by patients either considering or returning from treatment abroad and by patients from overseas seeking treatment in the UK. Dr Helen Hartley explains the medico-legal risks involved
There can be many benefits for patients who seek treatment in different countries, such as more cost-effective treatments and the opportunity to combine a holiday with a medical procedure.
requests from patients for referrals for treatment abroad will need to be assessed in the usual way and you should advise whether you believe referral is medically justified in the circumstances.
The referral should be supported by relevant clinical information and you should explain to the patient that their confidential information will need to be shared, with whom and in what way.
You may also need to be prepared for dealing with unexpected requests from the healthcare provider abroad for additional information – for example, in an emergency if a problem arises during treatment.
If you are sending confidential patient information overseas, you should ensure you are registered as a data controller with the Information c ommissioner and comply with the requirements of the Data Protection act 1998 to ensure adequate protection of their personal data.
Adequate protection
If you are transferring data outside the european economic area (eea), you should be aware of the stringent test, which requires the country or territory to ensure an adequate level of protection for the rights and freedoms of data subjects in relation to the processing of personal data.
If your patient has queries relating to possible eligibility for nhS funding for treatment abroad, you should advise them to con -
tact nhS england or its equivalent before embarking on treatment.
You should also advise your patient of the follow-up and aftercare you can provide, and how you would like to be communicated with by the doctor or medical staff who are providing the treatment abroad, such as to exchange medical records.
If you are asked to continue treatment initiated elsewhere which you do not feel comforta-
sailing
tion in which the treatment was provided and are therefore subject to the civil law procedures in that country.
This could present practical difficulties for a potential claimant, so you may want to advise patients who have requested a referral for treatment abroad that they should check that the clinic or doctor providing the treatment holds appropriate indemnity/ insurance to cover such eventualities.
Treating visitors to the Uk
One of the most important aspects of healthcare is communication and, if not done effectively, it could trigger a complaint even if there has been no fault in the patient’s care.
Language can be a particular issue when treating overseas visitors; for example, what language will the prescription or medical record be written in?
Does the patient fully understand the risks of treatment to be able to provide you with informed consent?
Case sCenario
a 22-year-old woman travels to Poland for rhinoplasty surgery, which proceeds uneventfully and she returns to the UK five days later.
However, several weeks later, she is unhappy with the cosmetic result and consults you privately seeking revision surgery. Your clinical assessment reveals some nasal asymmetry which you advise would be amenable to further surgery.
But, on reviewing the discharge letter explaining the treatment given abroad, though written in english, it is brief and does not contain detailed information about the procedure undertaken.
You obtain the patient’s consent to contact the Polish clinic seeking a copy of her records, including the operation note. These require translation from Polish at the patient’s expense. now with sufficient information about her previous surgical care, you proceed to discuss her surgical options.
Necessary assessment as you are unlikely to have access to the patient’s medical records or be familiar with their full medical history, it is important to undertake the necessary assessment –including appropriate history and examination – and other steps to ensure the right medication is prescribed.
You may want to get in touch with the patient’s doctor abroad if you have any doubts and also send them a letter detailing the treatment you provided.
You should, however, make sure that you are satisfied you have the correct contact details. a lternatively, you could give the letter to the patient, who can then give it to their doctor.
ble with, you should seek advice from your medical defence organisation.
Quality of care
The standard and quality of care a patient can expect is the responsibility of the country in which treatment is provided. c omplaints will be dealt with under the system, if any, in operation in the country of treatment. Similarly, negligence claims are usually brought in the jurisdic -
a nd does the patient fully understand the risks of treatment to be able to provide you with informed consent? It may be that they require access to an interpreter along with a written treatment plan and information sheets in their first language.
a common issue is where someone has forgotten their medication or needs a repeat prescription of ‘this little white tablet’ or a medication with an unfamiliar foreign name.
any patient returning to the UK with emergency complications arising after treatment abroad would be eligible for nh S treatment.
We advise doctors who have any patient safety concerns regarding treating patients from overseas or consulting with patients returning from treatment abroad to consult with a colleague or to contact their medical defence organisation for further advice and assistance.
Dr Helen Hartley (right) is a medicolegal adviser at Medical Protection
MARkETing viA sOCiAl MEdiA
To tweet or not to tweet?
Independent Practitioner Today’s new series by Jane Braithwaite continues with advice for all those still wondering whether they should join the ranks of the twitterati
TwiTTer is a global instant communication phenomenon. with 500m tweets taking place every day, should you be allocating professional time to this activity?
while its detractors dismiss the service as a narcissistic aberration, it is universally used by academics, economists and politicians as well as celebrities.
Cristiano r onaldo has 44.3m followers and the Queen made her first tweet in October 2014 to an audience of 724,000. Katy Perry is the most followed celebrity with 85m followers.
we have looked into the relevance of Twitter for a private doctor in London and set out our findings below.
Background
Twitter has been going for ten years, which makes it one of the oldest social media platforms. in 2015, there were 13m UK Twitter users and that number is set to increase to over 17m by 2018. Twitter’s current value is estimated at $10bn dollars; the service employs 4,000 people.
Twitter Users
Some relevant facts:
User profile is 50% male and 50% female;
45% of users are aged 18-29; 40% of users have a degree; The country with the highest percentage of Twitter users is saudi Arabia;
41.5% of all Tweets come from the Us;
9.7% of all Tweets come from the UK.
Twitter Usage:
News: 63% of users say they view it as a source of news;
sport: The UK’s top live topic is sport;
Mothers on Twitter: 69% log in every day;
12 world leaders have had a Tweet retweeted 20,000 + times.
Conclusions for doctors
Twitter should be viewed as part of your marketing strategy. Unlike most forms of marketing, it is free. However, it requires planning and can be time-consuming.
Twitter is a valid way of communicating with your patients, and enhancing your image while marketing your practice.
Your tweets can convey a potent message, creating a brand to attract new patients to your website, eliciting their interest and facilitating new bookings.
Twitter can be used to communicate with the wider medical community, including suppliers and associated clinics. By linking your brand with theirs, you will attract more followers.
The majority of larger medical associations use Twitter and tend to be very active.
sir robert winston has 35,500 followers and Dr Hilary Jones has 25,000. They both tweet on a daily basis. The Bupa Cromwell Hospital has, as i write, 1,422 followers discussing a vast range of subjects, from Vitamin D through to care in old age. They advertise job opportunities as well as announcing senior management appointments.
i t is vital to monitor tweets if they are being written on your behalf. Your image is being represented. Tweets can be detrimental if not used judiciously. if you outsource this activity, it is wise to ensure the service is carried out by someone who understands the complexities of the medical world.
Medical marketing is different from other industries; you need a collaborator who understands this distinction.
Celebrity endorsements may be viable in the fashion industry, but
a doctor’s patients generally prefer discretion and anonymity. remember, patient confidentiality is crucial.
i n the U s , incidences have occurred of patient appointment reminders being tweeted, resulting in legal actions against doctors. This has been a particular issue for cosmetic surgeons in the Us
Twitter is especially relevant if your patient demographic is aged from 18 to 30. Active Twitter usage could also enable you to reach an audience in the Us and the Middle east.
Twitter use is not yet widespread among the UK’s medical community and that offers great potential to lead the way in this field.
Our top tips on how to tweet
Photos and images work well;
Avoid tweeting hypertext links; Use hashtags to improve search ability: #Doctor #health #medical;
The ideal text length is 100 characters;
The best time to tweet is between midday and 1pm; Be authentic.
The future
seeking predictions in relation to digital marketing is like asking a banker about the UK’s future economy.
The phenomenal growth of Facebook, instagram and Twitter was unprecedented. Facebook was explosively embraced and subsequently discarded by the younger generation, who replaced the service with s napchat and instagram; Facebook is now predominantly used by an older demographic. is Twitter worth your time and effort? we have concluded that it is a potent, free marketing tool enabling instant global communication.
Astute usage can enable you to communicate your ethos in a professional and authentic manner –this can only be a good thing for your practice.
Jane Braithwaite (right) is managing director at Designated PA
incomE TAx REvolUTion
Your tax is going
‘Making tax digital’ is a Government initiative to be implemented by 2020. Vanessa Sanders (left) shows what it will mean for those doctors who complete a tax return for themselves or their business
Ev E ryon E curr E ntly has some access to their tax information held by HM r evenue and c ustoms (HM rc ), but this is neither exhaustive nor held in one place.
But new Government proposals mean every individual and small business will, in future, have full access to a digital account so they can check records and manage tax details.
Agents and advisers are considering a practical response to what this will mean for doctors and their business.
It is anticipated that, by 2020, the information provided to HMrc will also need to be up to date rather than by the current
deadline of nine or ten months after the year-end.
t he effect of all this on you is that your records will need to be maintained in real time (rt).
Tightening up
t hat means tightening up on a range of things from recording invoices after clinics, to raising invoices and detailing payments received from patients and insurers. All your records will need to be updated, probably at least monthly.
HMrc will require this information to be uploaded digitally and an assessment of liabilities to be recorded.
In its view, this will ease and speed up tax collection. Effectively,
Some adVantageS of making tax digital
WHat’S HaPPening WHen
end of 2016 authorised agents’ access to digital tax accounts mid 2017 online billing system begins end of 2017 digital tax accounts give taxpayers an overview of their liabilities in one place
end of 2018 Uploading information quarterly for income tax and national insurance via approved software
2020 Uploading quarterly information for corporation tax obligations
you and your business will be paying tax as you do on your employment income – in rt
HMrc has stated this does not mean you will be completing a full tax return every quarter, but updating as you go along. o bviously, this remains to be tested, but it is inevitable.
Sharing data online your adviser will be thinking about how best to organise your record-keeping to comply. For many doctors, this will involve frequent sharing of information across a cloud-based system where access is granted to both you and your adviser.
the manipulation of your core data to comply with the reporting will probably be monthly to ensure that any errors or issues are sorted prior to the online sharing with HMrc
For many doctors, this will be a
access to information held by HmRC will be in real time and can be adjusted via digital access
Under/over payments of tax can be managed more effectively
tax liabilities will be known and monitored more frequently
You will see your business performance emerging, including profits in addition to income
You and your adviser can manage, monitor and advise your business more efficiently online with access at your fingertips – literally
the risk of unnecessary penalties and fines is removed, as deadlines will be clear. Prompts for information will be frequent and easy to handle, as bureaucratic filling of forms is outmoded
positive move, once the painful implementation is over, because it will force effective management of your business.
For example, chasing debtors is often delayed and this allows people who owe you money to build up arrears, causing significant cash flow concerns. reviewing these debts monthly will ensure you or your adviser take appropriate action.
If you are not paid within 90 days, the chance of bad debt is significantly increased, so having to organise your records monthly will alleviate this onerous task. these changes will undoubtedly increase record-keeping and the need for tools to assist in this. these tools will create an up-todate accurate reflection of business data, highlighting and prompting for missing or inaccurate information. As ever, your adviser is there to help and keep you compliant and up to date.
Vanessa Sanders is a partner at specialist medical accountants Stanbridge Associates
for full information, go to www. gov.uk/government/uploads/ system/uploads/attachment_ data/file/494821/making_tax_ digital_-_myth-buster.Pdf
Intelligently precise.
new
The seca 287 ultrasonic measuring station –defining the essence of technical practicality.
From the fully automated ultrasonic height measurement to the voice guidance system for self-sufficient measurement – the intelligent measurement technology of the seca 287 measuring station makes your everyday work more efficient. All measured data can be comfortably transmitted into an EMR system or printed out using seca 360° wireless technology.
www.seca.com
Free legal advice for independent Practitioner Today readers
independent Practitioner Today has joined forces with leading niche healthcare lawyers Hempsons to offer readers a free legal advice service.
We aim to help you navigate the ever more complex legal and regulatory issues involved in running and developing your private practice – and your lives.
Hempsons’ specialist lawyers have a long track-record of advising doctors – and an unrivalled understanding of the healthcare system as a whole.
call Hempsons on 020 7839 0278 between 9am and 5pm Monday to Friday for your ten minutes’ of free legal advice.
Advice is available on: Business structures: commercial contracts: ian Hempseed Faisal Dhalla
Subscribing to Independent Practitioner Today is the only way you can be sure you will see every issue and have the option of reading us online using our special page-turnable edition. Don’t risk missing out. Our personal subscription for doctors and managers is only £90 a year and £210 for organisations. But you can cut this to just £75 and £180 respectively if you pay by direct debit. So take advantage of this offer now for our unique business journal dedicated to supporting you in your private practice. We’re confident your subscription will repay itself many times over!
Editorial director
(See rates listed above)
a cheque for
I encose a cheque made payable to The Independent Practitioner Ltd
Please debit my Mastercard/Visa/
r * indicates this item must be filled in Doctors, please give GMC No.
Instructions to your Bank or Building Society to pay Direct Debits
the Manager
of
Name(s) of account holders
Name and full address of your bank/Building Society Banks and Building Societies may not accept Direct Debit instructions for some types of account
post your application (no postage required – UK only) to: independent practitioner today Subscriptions department, FreepoSt, po box 36, plymouth, pL1 1br
Please post to: Proact Ltd Subscriptions Dept., 12 Mary Seacole Road, The Millfields, PLYMOUTH PL1 3JY Or email to: jackie@marketingcentre.co.uk Or
banks and building Societies may not accept direct debit instructions for some types of account Signature(s) date ___________ phone: 01752 312140 Fax: 01752 313162 email: lisa@marketingcentre.co.uk
to your Bank or Building Society to pay Direct Debits Name and full address of your bank/Building Society Banks and Building Societies may not accept Direct Debit instructions for some types of account To: The Manager Bank/Building Society Address Postcode Ref. No. (Do not complete)
Or subscribe online at www.independent-practitioner-today.co.uk if you want to pay by card
refund from your branch of the amount paid. You can cancel a Direct Debit at any time, by
Don’t leave it too late
The billing and collection side of running the private practice business needs to be well organised to ensure good cash flow – and good cash flow determines the success of most businesses.
Follow Gary Nials’s check list of things to do to make sure the practice’s billing and collection is efficient. If any of these are not followed in your practice, then there is a good chance your cash flow will be hit
£Send out the invoice promptly
There is nothing new in highlighting the fact that people often delay paying invoices for as long as possible.
Logic therefore follows that the sooner you get the invoice in the patient’s hand, the sooner it is likely to be paid.
This should be done on the day of treatment or, by the latest, in the days following treatment.
This way, there is a much greater chance of it being paid quickly and if there is any issue, you will know sooner rather than later.
£check invoices before sending
Having correct information on the invoices is crucial. You do not want to give the person you are sending the invoice to, whether they are the patient, an embassy or an insurance company, any excuse to ignore your invoice or query it.
Also, inaccurate data on invoices reflects badly on the practice.
£ Offer a range of payment options
It is good to offer different payment options to patients. Most will use credit and debit
Property Finance for the Independent Healthcare Sector
cards, some will favour cash and, increasingly, others will use internet banking. Interestingly, at Medical Billing and Collection, we process nearly 60% of payments from patients at weekends. This means having the ability to settle invoices out of normal working hours is important and convenient for patients and should lead to bills being settled quicker.
£code insured work correctly
If you are new to private practice, you will often want to both register with private medical insurers such as Bupa and AXA PPP and also familiarise yourself with Clinical Coding and Schedule Development group (CCSD) codes.
These are the codes commonly used by insurance companies to both define and price what treatment has been carried out. It is important to code the treatment correctly, as insurance com
panies are very particular about this. CCSD codes also change monthly and, as there are over 2,000 codes, it is a good idea to regularly check your coding is up to date and accurate. Don’t miss our new series Code Buster! in every issue of Independent Practitioner Today (see opposite).
£include letters of guarantee and/or medical reports
In London, embassy work is big business with some 50 embassies across the city. You often need to allow more time when seeing these patients due to the complexity of their cases and the common need for an interpreter.
Before seeing the patient, it is absolutely crucial that you obtain a LOG, which stands for a letter of guarantee. This document will authorise treatment for the patient and must be in your name. Without this document, it is
UK Top 20 accountants specialising in the healthcare sector
• National firm of the Year 2013
• AISMA member (Maidstone and Leicester offices)
• 12 offices including London City
• Tax Structures for Hospital Consultants - dispelling myths Surgeon groups and consortia GP Practices including mergers and federations
• Solvent liquidations (for companies at the end of their lives)
For more information please contact: South East
James Gransby FCA
E: james.gransby@mhllp.co.uk
T: +44 (0)1622 754033
M: +44 (0)7712321899 East Midlands
Robert Nelson DChA FCA
E: robert.nelson@mhllp.co.uk
T: +44 (0)1162 894289
M: +44 (0)7814009160
General email: healthcare@mhllp.co.uk www.macintyrehudson.co.uk
unlikely you will get paid. It is also crucial to have the invoice match details on the LOG for facts such as treatment date and doctor’s name.
£Make time to invoice patients for insurance excesses and shortfalls
Private medical insurance (PMI) policies may not always cover treatment in full due to the terms of the policy.
This will also often be a surprise to patients who may not be familiar with the policy terms, especially if their private medical insurance is through their work. This will result in either an excess needing to be paid by the patient or a shortfall.
An excess occurs from the specific terms of each individual policy and a shortfall is when a patient’s policy only covers a proportion of the consultant’s fee.
In either case, a new invoice needs to be raised to the patient for the balance. These co payments need to be identified, invoiced and chased in a timely fashion otherwise they quickly mount up and become a problem.
£chase unpaid invoices regularly
It is important to chase unpaid invoices regularly. This should involve both reissuing invoices as well as making phone calls. But you might want to vary the regularity of chasing invoices based on the type of private work you do; for example, self pay, PMI, embassy and medicolegal.
with simple issues like demand for your services. It is important to keep up to date with insurance pricing for specific procedures, as these vary across each insurer and are also subject to review along with their coding rules previously mentioned. It is also important that you remain not only up to date but also competitive.
£ Adequately resource your
billing department
As practices grow, so do their needs for administration support. This will vary from a consultant starting out in private practice managing everything on their own, to then needing a parttime/ full time secretary, to perhaps joining a group or a clinic with a practice manager and team.
All these changes need to be adequately resourced. Often we find consultants coming to us in various states of disarray, where bad debts have accumulated and often it will be because they have not invested in sufficient administration support.
£
Make necessary changes in a timely fashion
Speaking to a patient about an unpaid invoice should also be prioritised, as it will let you know if there is any dispute, which is important, especially if you plan to see the patient in the future.
Whatever system/procedures you decide upon, it is vital that you follow up unpaid invoices systematically and consistently or, before too long, you can find unpaid invoices mounting up. This is often a major issue in big and busy practices.
Regularly review what
There is a big difference between understanding the theory and putting it into practice. It is all well and good knowing what you should be doing, but change is often difficult, annoying and a hassle and therefore can be put off. All we would suggest here is, if you spot an issue arising, especially if it comes to your billing and collection and thus affecting the all important cash flow of your practice, take action. It is much better in the long term.
So when you next get a spare moment, we suggest reviewing your own practice against the list above or discussing it with your practice manager/secretary if you have not done so recently.
Once you have done this and identified any changes necessary, make sure you implement them and ensure they are adhered to.
Of course, it may make more sense to turn to experts in this field and get some professional help from a billing and collection company.
Gary Nials is the managing director of Medical Billing and Collection
Break the code – not your firm
SO lET code buster! kEEP yOu IN ThE kNOW
Every month, the Clinical Coding and Schedule Development Group (CCSD) reviews its 2,000 plus procedure codes, and more than 3,000-plus diagnostic codes, that form the basis of private medical insurance. It is crucial for independent practitioners and their practices to know these codes, so they bill correctly. If they don’t, then it could cost them money
chaNGes to Note this moNth Specialties recently affected include vascular (Code T & L), spine (Code V), ENT (Code E), radiology (Code X), urology (Code M & N); haematology (Code U); hepatology (Code J) and obstetrics and gynaecology (Code Q).
XR122 – Bilateral image guided vacuumassisted excision of breast lesion (with biopsy).
There are five narrative changes: E0230, V4280, E2500, XR121 and M3411; one unacceptable combination, also known as unbundling: Q0790 with Q2230 ; and two declined/withdrawn requests
Of special note is code E2500, relevant to ENT surgeons. This code replaces the previous E3680 – endoscopic nasolaryngopharyngoscopy as a sole outpatient procedure.
The reinstatement of this code E3680 was requested and declined.
However, as a result, the narrative for E2500 was modified from ‘diagnostic endoscopic examination of pharynx/larynx +/ stroboscopy (including biopsy) (as sole procedure)’ to ‘diagnostic nasolaryngopharyngoscopy (including biopsy) (as sole procedure)’.
no automatic agreement
Please remember that codes are not mandatory by insurers. In other words, the inclusion of procedure codes within the CCSD schedule does not indicate the automatic agreement of individual insurers to provide benefit for this procedure.
You need to contact each insurer directly to find out whether benefit is provided.
HisTORy OF MEdiciNE
A MOMENT OF TRUTH, BATH, 1781
Doctors who specialise in diseases of the rich learn early in their careers that a sound private practice needs an adequate supply of regular patients.
Medical emergencies and exotica may provide for luxury – the Bentley, the opera, the Caribbean winter holiday – but a sufficiency of regular patients protects practitioners from the relentless tyranny of household bills.
In the golden age of private practice, before the coming of the NHS, a ‘regular patient’ was one who figured on the ‘regular visiting list’ and was visited at the same time each week, each fortnight or each month.
Most were lonely women, often widows, who yearned for someone to talk to. They didn’t need, indeed often resented, any form of clinical examination, other than the doctor holding their wrists in pulse-taking mode while they told long, rambling, self-centred stories.
The excuse for the regular visit was the ‘agreed illness’. The ideal agreed illness was not too incapacitating to interfere with the
medical tales
TV doctor and full-time writer Dr Michael O’Donnell, draws from his new book, Medicine’s Strangest Cases, to show how early private practitioners had to ‘own’ their patients
That’s why private practitioners grew not so much protective as possessive of their regular patients. Possession was ninetenths of the income
pleasures of a well-upholstered life, yet serious enough to need regular attention and to allow for occasional spectacular ‘attacks’ that demanded dramatic medical intervention and sympathetic clucking from friends.
Quite baffled
The agreed illness also had to be specific both to patient and doctor. Patients talking to impressionable friends needed to be able to say: ‘My liver (kidney/womb/ metabolism) is unique, you know. Every doctor – and I’ve seen the very best, my dear – has been quite baffled by my X-rays.’
But unless they could add, ‘Indeed, they’re so complicated that only dear Dr Handholder can understand them,’ dual specificity
had not been established and patients could, after a minor tiff, take their profitable illnesses elsewhere.
That’s why private practitioners grew not so much protective as possessive of their regular patients. Possession was nine-tenths of the income.
Sir Walter Farquhar (1738-1819) earned his citation in medical history when one of his regular patients decided to take the waters at Bath.
When she expressed concern at the idea of being separated from the only physician who really understood her, Farquhar assured her he had a ‘wholly reliable’ colleague in Bath and gave her a letter of introduction setting out the details of her case.
During her journey, the woman realised that, though Sir Walter had been her doctor for many years and had assured her that her condition was one of the most complicated with which he had ever had to deal, he had never told her exactly what it was.
The answer clearly lay in the letter. Overcome with curiosity, and despite the protests of her travelling companion, she steamed it open.
It read: ‘Dear Davis, Keep the old lady for three weeks, then send her back.’
Medicine’s Strangest Cases, recommended price £7.99, ISBN 9781910232941. Published by Portico, an imprint of Pavilion Books
It’s all a question
Philip Housden (below) continues his journey following a year in the life of a NHS private patient unit (PPU). This month: your relationship with the trust management
I belIeve In PPUs
Following my 2014 Independent Practitioner Today series on PPUs, I have continued to work with many nHS trusts to help develop and grow profitable private patient services.
This has enabled a real insight into the day-to-day challenges of delivering a private service within a public sector environment.
I am passionate about how PPUs can be part of the answer to the strategic and financial challenges that the nHS faces and so, in these articles, I plan to share learned, practical insights and also comment on how PPUs can best respond to changing policy issues and healthcare current affairs.
Last month , I shared some examples of how nhs private patient units can and should respond to commercial opportunities for growth in their local competitive market. Were any such local opportunities grasped by your PPU?
one-off issues, such as a temporary theatre closure by the competitor private hospital, can obviously be a good prompt to make renewed contact between the PPU and its key customers: consultant users.
t his would mean that, this summer, some consultants used their PPU for the first time or returned after a period of non-use.
other new users may have been newly appointed consultants just considering private practice, for which the PPU is a safe and easy choice.
this month, I want to explore the most crucial of relationships in a PPU. these are those between
the trust – specifically trust management – on the one hand and the consultant as practitioner on the other.
Getting this relationship right is fundamental – but often misunderstood in a trust.
Seeds of discord
Get it right and it lays a strong foundation for mutual commercial success. Getting it wrong stunts growth and lays seeds of discord that can impact adversely on the wider trust performance.
It is important enough for the success of a PPU that I’m minded to make the point by paraphrasing a U s presidential campaign slogan: ‘It’s the consultant economy, stupid!’
In a nhs trust PPU, the relationship with consultants can easily be mishandled. Consultants are the key customers; that much everyone pretty much agrees.
But, of course, consultants are
also employees of the trust, and their nhs activities, delivered under job plans and contracts, take up the large majority of their time.
We also know that consultants prize their independence, which in itself is a driver towards wanting to do private practice in the first place.
Consultants will rightly guard this independence jealously and so, when working in a PPU, the same consultant is not an employee but now an independent practitioner, able to choose when and where to take his/her patients.
so how should these challenges be best managed by a trust and the PPU? the umbrella for getting this right is governance. and the principle for PPU governance is respecting the different relationship with consultants while also protecting the interests of the trust – both directed to
of trust
ensure patient safety and best clinical outcomes of course. how does governance, and consultant relationships more widely, at your PPU measure up compared to your local private hospital? t here are some key building blocks that can help to get PPU governance right and protect the mutual interests of trusts and consultants.
presumption of trust the following list does not need to be onerous, but the structures do need to be in place and clearly ‘owned’; working best in practice, in my view, when there is a presumption of trust in place. so, is there a PPU medical society for all those that practise privately in the trust? It might be that consultants only need to ‘opt-in’ – rather than apply – as their contractual status with the trust delivers automatic eligibility, provided appropriate indemnity cover details are shared, of course.
Does the trust PPU have a clear document setting out the rights and responsibilities of an admitting practitioner in the PPU and how things are different from the nhs, although remaining part of it?
Does this make clear the principles on which this is based and does it look like a partnership approach?
and do consultants read it?
Is there a medical advisory committee with representation from key specialties?
Do colleagues know who the chairman of their PPU maC is?
Does this body act as an effective channel for two-way communication with trust management?
are the maC and chairman able to act at sufficiently armslength from line management, while also being ‘plugged into’ the medical director and the best of the trust’s infrastructure?
Good governance starts with transparency, and good governance is a prerequisite for commercial success in the healthcare market
I mention all these points because although they are good practice per se, they are also entirely consistent with the approach and requirements of the Competition and markets authority’s private healthcare market investigation and subsequent report findings.
While that report was wideranging and went well beyond the hospital provider/consultant relationship, it nevertheless did have something to say about how to increase transparency.
t his is relevant because good governance starts with transparency, and good governance is a prerequisite for commercial success in the healthcare market.
there is a business success winwin here by getting governance right, founded on the nhs trust’s recognition of consultants as independent practitioners in PPUs.
so, from a consultant’s perspective, your local private patient unit’s success really does start with U.
Next month, I will share some thoughts on how PPUs can best create a symbiotic relationship with the rest of the trust that delivers a real win-win for NHS services, including providing support during the to-beexpected winter bed pressures.
Philip Housden is a director of Housden Group, a management consultancy specialising in commercial support in the healthcare sector
Boutique recruitment.
Highly qualified admin staff for doctors & private clinics in London.
Helping doctors nd optimal candidates to complement their teams, from reception sta through to medical secretaries & practice managers.
Having worked in the medical sector 15+ years, we fully understand our clients’ requirements.
Focusing on establishing long term relationships with clients to ensure continuity
Located in the vicinity of Harley Street, enabling us to meet our clients in person to discuss their speci c requirements.
For further information contact our team.
Higher education, even higher costs
Ouch! University and school fees have left many parents in the red this month. With just one-in-five doctors currently saving towards private school fees, Michael Copeland (right) outlines what you need to know about saving for your children’s future, what the new fee rises could mean and how you can make the most of compound interest to help you save
HigHer education costs have soared in recent years and a debate in the House of commons earlier this year has left many predicting that student debts will rise further in the near future.
More than a decade ago, the total cost of university fees in e ngland for a three-year course was £3,000. t hen, in 2006, the average annual university fee in england jumped to £3,000 a year before fees tripled again in 2012 to £9,000 a year for the vast majority of universities.
it’s now believed these annual fees will rise even further for students starting next year.
a Higher education Bill is currently being debated among MPs, with supporters arguing that the quality of teaching should be distinguished and reflect any increase in fees for certain universities.
While any change to make this a reality may be some time away, several universities have already announced an increase above the £9,000 limit per year in their 2017 prospectuses.
u niversity fees already total £27,000 for the average three-year ➱ p30
An independent firm offering one to one meetings anywhere in the UK giving advice and help with:
• how to start in private practice
• how to maximise private practice income
• computer software
• tax and financial advice re: car purchases
• how to start in private practice
• ways to reduce tax payments
• computer software
• how to maximise private practice income
• setting up in Chambers/Groups
• ways to reduce tax payments
• limited companies and LLP’s
• setting up in Chambers/Groups
• financial planning
• record keeping
• limited companies and LLP’s
• tax and financial advice re: car purchases
• pensions: NHS, personal and employee schemes
• pensions: NHS, personal and employee schemes
• purchase of consulting rooms and surgeries
• inheritance tax and capital gains tax planning
• VAT
• purchase of consulting rooms and surgeries
• inheritance tax and capital gains tax planning
• VAT
For more information please contact us by: Wilmslow
Harley Street
For more information please contact us by:
Phone: 01625 527351
Wilmslow
Fax: 01625 539315
Phone: 01625 527351
An independent firm offering one to one meetings anywhere in the UK giving advice and help with: Specialist Medical Accountants
Phone: 020 7307 8759
Harley Street
Fax: 01625 539315
Phone: 020 7307 8759
Email: info@sandisoneasson.co.uk
Fax: 01625 539315
Fax: 01625 539315
Website: www.sandisoneasson.co.uk
Email: info@sandisoneasson.co.uk
Website: www.sandisoneasson.co.uk
undergraduate course, and £45,000 for those who study for up to five years.
With today’s students owing an average £44,500 when they graduate from a three-year course –accounting for living costs and expenses, according to the Sutton trust’s Degrees of Debt report – it is understandable that many parents want to help.
t he message to parents who want to contribute is simple – the earlier they start saving, the more affordable it will be.
how parents want to help o ur research has found parents would like to ease their child’s student debts by contributing, on average, two-thirds (67%) of the university costs.1
on the basis of an average debt of £44,500, it means that parents will need to find £29,815 if they want to make this level of contribution – with parents of those studying for more than three years needing to save even more. that’s a large sum of money to save, and that’s just for one child.
Why saving early matters
Wesleyan calculated that if parents put away just £95 a month from their child’s birth until their graduation at 21, they could cover their anticipated contribution.2
to put this in perspective, if they put off saving until their child starts primary school aged five, they will need to save £132 a month – forcing them to find an additional £1,400 before graduation to make up for lost interest.
Waiting until their child begins secondary school at 11 will mean
having to save £224 a month –and £2,940 extra.
if they wait until their child has taken their gc S e s aged 16, the amount parents will need to save more than doubles to £472 a month – forcing them to put aside a total of £4,380 more than had they started saving at birth.
the additional cost of delaying saving is even greater if parents plan to cover the full cost of their children’s university debts –saving either £142 a month from their child’s birth until graduation, £197 from the age of five, £335 from 11 or £705 from 16.
Saving early also means there is more investment growth over the years. a parent saving £95 a month from their child’s birth until their graduation to raise the £29,815 they want to contribute will actually only have put away £23,940 –with the other £5,875 coming from the investment return.
ideas how to save over time
So the first lesson for parents is to start saving early – even if they can’t afford to put aside the full amount they need to.
the next step is to ensure they have the right long-term savings plans in place. taking advantage of a range of savings products that allow them to build compound interest, make the most of taxefficient savings products and utilise the full i S a allowance will help them reach their target.
i f saving for a goal that is 21 years away, they can afford to save into products that prevent savers from accessing the funds in the short term, in return for a potentially higher return.
Tax adviCe and Planning for doCTorS
• Tax consultancy
• Self-employed and company accounts
• Property investment structuring
• Payroll and vaT services
Contact: nick Brecker. Tel: 020 7253 0030
Email: nbrecker@caldwellandbraham.co.uk
Web: www.caldwellandbraham.co.uk
But what products are available that can help achieve this?
With today’s students owing an average £44,500 when they graduate from a threeyear course, it’s understandable that many parents want to help
one of the easiest ways to achieve this is with an individual Savings a ccount ( i S a ), which allows money to grow free of capital gains and income tax. Because of the tax-efficient nature, there are limits to how much can be saved into an iSa each year. For the tax year 2016-17, this is £15,240.
i t is possible to save the full amount in cash, stocks and shares or the new i nnovative Finance i S a or any combination of the three, provided the limit is not exceeded.
Some providers also have the added flexibility of allowing savers to make withdrawals from their iSa and put it back in later, without losing any of their taxfree allowance, provided the money is put back in within the same tax year.
a dditionally, parents should review any existing savings, investments or assets they already have, as these may provide returns that could contribute towards the fees.
it’s also important to remember who else can help. grandparents may want to help and they too can make tax-efficient contributions towards education costs while potentially reducing any inheritance tax liability on their own estates.
However, reducing inheritance tax liabilities is a complex area, so it is important that expert advice is taken when considering this.
Finally, it may also be worthwhile to explore whether the universities on the wish list have any bursaries, grants or scholarships available to help with the cost. these details should be available from the schools themselves or the local education authority.
Saving for SChool feeS
Parents who want to give their children the best start in life and send their children to private school need to adopt a similar approach.
Yet this can be a very big financial commitment for families, even those with higher incomes. d ata from the i ndependent Schools council shows an increasing number of families are choosing to put their children through private education, with the current numbers at the highest level since records began.
However, with school fees increasing by 25% over the past five years to total more than £200,000 from ages five to 18, if parents do decide to take this option, they will need to plan their finances carefully for it to remain an affordable option.
t he average cost of private school fees for day students is £13,418 a year. if prices continue to rise at the same rate as over the past year, that will amount to at least £218,928 over the course of their education, for children starting school at five this year and finishing at 18.3
the annual fees leap to £32,065, or more than half a million pounds over the course of their education (£519,915), if the children board.4
We again calculated that if parents save £11,248 per year from when their child is born –equivalent to £937 a month – in a savings deposit account paying interest at 2.5% a year, they would build up enough money to cover the cost of day school private education.
While this will still remain a big financial commitment, the interest earned over the years could amount to the equivalent
of one year’s average fees, providing another reason to start saving as early as possible. t he interest accumulated over those 18 years (£16,468) would save them the equivalent of more than the first year’s school fees.
But the research found just one in five (18%) doctors, dentists and lawyers are currently saving towards private school fees.5
While parents who want their child to board would need to save more than double – £26,720 a year or £2,227 per month – the interest earned over 18 years (£38,948) would still equate to saving more than the cost of the first year’s boarding school fee.3
Teaching good habits o ur research showed that many parents did not want to pay for all their children’s higher education costs, meaning children will still leave university in debt.
With this in mind, parents should also help instil good financial habits in their children from a young age to help them cope with their student debt and ongoing money matters once they have graduated.
referenCeS
1. Survey of 388 doctors, lawyers, dentists and teachers by Censuswide, Feb/March, 2015.
2. The monthly savings calculation uses an annual growth rate for illustration based on typically investing over the longer term (more than five years) using a mid rate of 2.5% growth that is considered average. This does not include any product charges, so any personal illustrations from a Wesleyan financial consultant will differ from those shown above. For more, go to
The interest earned over the years could amount to the equivalent of one year’s average fees, providing another reason to start saving as early as possible Get online for faster invoice payment and quicker cash collection! Forget billing and collection agencies, forget phone payments and forget cheques! JAY WEB MEDICAL SERVICES will build you your own secure online payment website where patients can settle their account using just their invoice number and a major credit or debit card
3. Day fee, day school. Calculation based on current average annual fee for day fee day schools (2015-16) of £13,418 with an annual inflation in fees of 3.7% applied for the life of the child’s education up to and including ‘A’-levels. 3.7% is the average rate of fee increase reported by the Independent Schools Council (ISC) for day fee day schools in its annual census, based on a survey conducted in January 2016.
Eighteen annual savings of £11,248 required or £937 per month. Total interest generated from 18 annual instalments of £11,248 = £16,468.
4. Boarding school. Calculation based on current average annual fee for boarding schools (2015-16) of £32,065 as estimated by the Independent Schools Council, with an annual inflation in fees of 3.6% applied for the life of the child’s education up to and including ‘A’-levels. 3.6% is the average rate of fee increase reported by the Independent Schools Council (ISC) for boarding in its annual census, based on a survey conducted in January 2016.
Eighteen annual savings of £26,720 required, equivalent to £2,227 per month. Total interest generated from 18 annual instalments of £26,720 = £38,948.
5. Survey of 290 doctors, dentists and lawyers by Censuswide, February/March 2015.
Please note that past performance is not a reliable guide to future performance and the value of your investment can go down as well as up, so you could get back less than you have invested. Tax treatment depends on individual circumstances and can change in the future.
Michael Copeland is Wesleyan northern area manager for doctors
Your own personalised website 100% of funds in your bank account in 4 working days Receipt emailed to the patient and doctor upon successful transaction Log in to your website for a full report of payments
Contact us now to for a free no obligation consultation www.jaywebservices.co.uk info@jaywebservices.co.uk
You can’t get it write first time
A well-written and carefully considered report takes a great deal of time and effort to produce – but, from the solicitor’s point of view, it’s probably worth every penny of your fee. In our ongoing series, Michael R. Young gives his tips for editing and redrafting
When you have completed the first draft of a report, do not believe it is ready to send to the solicitor. This is only the first draft and there is still a great deal of work to do before it should be submitted.
The purpose of editing is to correct, hopefully shorten and definitely improve the report. everyone has their own method of editing and redrafting their written work. The following one works for me.
I prefer to work on hard copy, but if you prefer to work on screen, then the same principles apply.
use a red pen, if you are working on a paper copy when proofreading, for the obvious reason that red stands out more.
Read the whole report through, checking its appearance, general layout and spacing and for any obvious spelling mistakes and errors of syntax.
Key words
Check factual information, such as names, dates and so forth, and check they are spelled correctly.
Go back to the beginning of the draft and write a key word or words in the margin alongside each paragraph so that you can
follow your train of thoughts from beginning to end.
Ask: Does it flow? have I missed anything out? Do my conclusions follow from what I have previously argued? This is an important stage in report writing.
If necessary, cut and paste and move sentences or whole paragraphs so that the argument flows better, or amalgamate or delete them altogether.
your first draft should have been deliberately sparsely punctuated, so check punctuation next, only adding commas, semicolons, colons and so forth where absolutely necessary.
Print out a new copy and repeat the whole process at least a further three times.
Don’t be tempted to try to save paper by only printing out those pages on which alterations have been made. Adding or removing a sentence or changing the spacing between a couple of paragraphs, can mean that some text moves back to the previous page or forward on to the next page, so always print out the whole report again. Although a report is about the correct use of the written word, if, after several attempts, describing something is causing a problem, then consider using a diagram.
o nly when the report is finalised, the very last thing to do is to check the page numbering and create a contents list, which forms part of the introduction.
Retain all draft copies until you have finished editing and redrafting, because there may be an express or a particular sentence or paragraph that later might be apposite.
Checked by outsider
Whether or not you get someone else to read and check your reports depends on the answer to the following questions:
Does the person have sufficient knowledge and understanding of the subject or subjects?
Does the person have the right level of analytical skills?
Is the person able to read critically?
Is the person’s english of a high standard?
And then there is the question
of confidentiality when having an outsider read the report. e dit and redraft until you are happy with the report, and only sign and date it when you are completely happy with it. Keep a hard copy of the report in your copy of the client’s file for completeness. employ a rigorous editing and redrafting regimen and your final report will nearly always be shorter than the first draft. Solicitors don’t have the time to look for the answer to their question in a long-winded report.
If they can’t find the answers in the report, they will only come back to you with questions and it is unlikely that you will be paid for answering them. A well-written and carefully considered report takes a great deal of time and effort to produce, but, from the solicitor’s point of view, it is probably worth every penny of the fee. however, it is a universal truth that no matter how many times the author of a document reads and re-reads his or her work,
special offeR! BuY the Book and save £20
the book costs £60, but independent practitioner today has secured discount of a third off for readers, so you pay only £40. listen to the audio content which accompanies the book at this website: www.otmoorpublishing.com/audio. for more information and to order, email stephen.bonner@ otmoorpublishing.com, quoting reference ‘Young/ipt’.
errors can go unnoticed. When you read something over and over again you become word-blind. When the report is finished, there are a few things to check before posting it to the solicitor.
✎ Are the pages in the correct order?
✎ Are the contents and the page numbering as set out in the contents list correct?
✎ Is the report dated?
✎ has it been signed?
✎ have you included an up-todate CV in the appendix/ces?
✎ Are any references you have used correct?
✎ Is the invoice/fee note included? Send the report by recorded delivery and check on the Royal Mail website www.royalmail.com to confirm it has been delivered.
Adapted from The Effective and Efficient Clinical Negligence Expert Witness , by Michael R. young, price £60 from otmoor Publishing
Your staff’s rights after
EU legislation and case law has had a huge impact upon UK employment law – so it is very likely BREXIT will have an impact on employee protection and employee rights. But how much of a change are we likely to see? Andrew Davidson and Helen Baxter (pictured right) report
Nothi N g is going to happen very quickly. Even if the government intended to remove all EUgenerated employment legislation, it would take a long time to achieve this.
EU legislation and case law runs like a thread through nearly every aspect of UK employment law. it would not be as straightforward as simply repealing a few acts and regulations, and it seems government lawyers would be busy for quite a while.
Also, it is unlikely that any UK g overnment would be keen to remove all of the protec tion granted by European legislation.
• Completely open scanner that is well tolerated by claustrophobic patients
• Weight-bearing scans for spine and joints enable a more precise diagnosis
• Patients who are large or cannot lie down can be accommodated Upright Positional MRI
For more information go online at: www.mri-london.com or call 020 7370 6003 Medserena Upright MRI Centre 114a Cromwell Road, Kensington, London, SW7 4ES
t his g overnment, and the Coalition one before it, has made certain changes to employment rights, such as Employment tribunal fees, increasing unfair dismissal service requirement to two years, but they have left the bulk of employee protection in place. it should also be borne in mind that not all employment protection comes from EU Directives. Whistleblowing protection under the Public interest Disclosure Act arose purely from the UK legislature, although other EU countries have similar protections.
on the other hand, some protections such as equal pay were introduced when the UK joined the EU.
So where are changes likely? the likely areas for change are:
Transfer of Undertakings, (Protection of Employment) Regulations (TUPE) – in principle, it could be removed in its entirety, but we anticipate that it will remain, albeit with some modification.
We would expect the government to relax the prohibition on posttermination harmonisation of terms and conditions. it might also relax the consultation obligations.
Agency Worker Regulations –giving agency workers rights after
A Private Members’ Bill was introduced to Parliament on 12 July proposing to grant EU citizens the right to stay in the UK following the UK’s withdrawal from membership of the EU
after
12 weeks appears to be unpopular with employers and is unlikely to be strongly defended by the unions, so this protection could be removed.
it’s unlikely the EU protections on working time will be removed, but we would expect the government to modify the provisions. the ghost of the Bear scotland case – a case concerning holiday pay – could be put to rest with the g overnment clarifying that a week’s pay is limited to basic salary only.
i t could also make changes to the way sick pay accrues during a period of sickness absence. For example, it could limit it further – or remove it altogether – on the basis that workers do not need a break from working time if they are off sick.
Discrimination – t here are unlikely to be any significant changes, but there is the possibility of the government introducing a cap on discrimination awards as there is already for unfair dismissal awards.
Collective Redundancy Consul tation Obligation – t his is unlikely to be removed entirely, but the parameters could change. For instance, it could be required only when there is a proposal to dismiss 100 or more employees at one establishment within a period of 90 days or less.
Rights to Remain – there is no certainty that existing EU nationals living and working in the UK will be able to stay or in relation to what the entry require
ments for those people and new EU migrants might be postBrexit.
But the g overnment issued a statement on 11 July to reassure EU nationals living in the UK, which stated: ‘When we do leave the EU, we fully expect that the legal status of EU nationals living in the UK, and that of UK nationals in EU member states, will be properly protected.
‘ t he g overnment recognises and values the important contribution made by EU and other nonUK citizens who work, study and live in the UK.’
A Private Members’ Bill was introduced to Parl iament on 12 July proposing to grant EU citizens the right to stay in the UK following the UK’s withdrawal from membership of the EU. on a more general note, there is great uncertainty about how Brexit will impact on the UK economy. if the economy is adversely affected, there may be more willingness from the government to cut employment protection to make the UK more competitive, but it is too early to tell.
David Davis is now confirmed as the new Minister for Brexit in the challenging position of negotiating Britain’s exit from the EU.
We anticipate a lot more discussion on potential changes to employment law in the months to come and we will keep you updated on developments.
Andrew Davidson is a partner and Helen Baxter is an associate at Hempsons Solicitors
PROBLEMS WITH THE TAX MAN?
HMRC tax investigations and disputes create difficult and stressful times.
As an award winning firm of tax experts, our highly experienced partners specialise in resolving problems relating to tax investigations and disputes with HMRC.
To find out, in confidence, how we can help call 0800 734 3333.
‘Here to help. Not to judge.’
When expenses can
Knowing which expenses can be claimed against your taxable income can be a minefield. The type of expenses and reason for incurring them will be relevant, but so is your status, because the rules can be different for an employee, self-employed or doctors trading through a limited company.
Ian Tongue (right) looks at the more common types of expenses and how your status can make a difference when claiming tax relief
Employees
This is the most restrictive status when it comes to claiming expenses.
For a cost to be tax-deductible, it has to be incurred ‘wholly, exclusively and necessarily’ in the performance of your duties.
This is a rather narrow definition and, in practice, it usually means that it has to be a contractual obligation to incur the expense as part of performing the duties of the job.
For those with no private practice or in training, it can be frustrating and seem unfair to incur costs that are not deductible.
In most other professions, these costs are suffered by the employer and would more than likely be tax-deductible for them – which again makes the system unfair.
A significant ‘win’ for training doctors was achieved in 2010 when Dr Piu Banerjee decided to take HM Revenue and Customs’ (HMRC) interpretation of training costs through the appeal system.
HMRC did not want to allow Dr Banerjee’s training costs to be taxdeductible against her NHS salary.
The outcome was successful for Dr Banerjee, with it being accepted that Dr Banerjee’s training contract gave her a contractual obli-
gation to incur these costs and, crucially, she was still doing the duties of her job while taking her exams.
HMRC came out fighting from this ruling, but with the BMA circularising its members to claim these costs, HMRC now generally waves these costs through without too much resistance.
Other costs that are typically deductible for an employee are:
Professional subscriptions;
Professional indemnity cover;
Business mileage;
Certain medical equipment not provided by the employer;
Laundry of uniforms.
Claiming these costs can sometimes be confusing, as you may not be at the stage where a tax return is actually required.
For costs in excess of £2,500, or if you normally prepare a tax return, you are required to submit a tax return to claim your expenses.
For costs less than £2,500, you can submit form P87 which is completed online via HMRC’s own website.
If you have multiple year claims, it is probably best to have an accountant deal with this for you and review the position before the claims are made.
can be expensive
Self-employment
For doctors who are self-employed, the rules are similar. But in the previous definition of what is allowable, the ‘necessarily’ part is dropped to leave a cost needing to be incurred ‘wholly and exclusively for the purposes of trade’. This is a much wider scope for claiming expenses.
Costs usually fall into those that are incurred directly in performing your private practice. These are more of an overhead nature or perhaps part-business use and partprivate, such as motor expenses.
Typical direct costs are:
Indemnity cover;
Professional subscriptions;
Secretarial costs;
Room rental;
Medical supplies;
Assistants’ fees;
Wages and salaries;
Professional fees.
Other costs include:
Motor and travel;
Use of home as office;
Printing, postage and stationery;
Phone and internet use;
Certain training costs.
Limited company
For those trading as company, all of the above typical expenses would be allowable as a taxdeductible expense.
Despite the fact that you may not be drawing a salary, you are still undertaking your work as an employee of the company.
This does give some scope for costs, such as training, to be paid on behalf of the employee as part of their training package, provided that it can be argued they are in connection with the trade of the company or part of the requirements for continuing professional development for that employee’s job.
Care has to be taken with certain costs, as they can form a ‘benefit in kind’, which is effectively deemed to be extra earnings and you
would suffer income tax on them. A good example of this is being provided with a company car.
Many consultants ask the question about having a company car and usually the numbers do not stack up to do this through your own personal company.
Your accountant will be able to provide you with the real cost of going down this route.
An alternative can be to look at the NHS Fleet scheme which allows you to sacrifice salary for a fully maintained vehicle. Cars at the low-emission end of the spectrum fare better in the calculations.
Again, your accountant should be able to provide you with the ‘real’ cost to you, including on your pension.
It is worth pointing out that, under the new 2015 NHS Pension Scheme, taking any salary sacrifice from your superannuable income will result in a lower pension upon retirement – unlike the 1995 or 2008 pension scheme, which looked at your earnings towards the end of your career and how many years of service you had.
Entertaining
Entertaining can be a prickly subject, as many businesses rely on networking to keep the flow of work and referrals, and a private practice is no exception.
The rules are relatively complicated here, but, generally speaking, the following applies:
l Entertaining employees – taxdeductible expense up to £150 per head per year. This can be more than one event.
l Client/customer entertaining – not usually tax-deductible. The expense can be paid through the business but the cost is added back when calculating taxable profits.
l Personal entertainment – usually this forms a benefit in kind for you and tax is payable on the amount paid.
Care has to be taken with certain costs, as they can form a ‘benefit in kind’, which is effectively deemed to be extra earnings and you would suffer income tax on them
Motor and travel
As with training costs, it took an oft-quoted case to be taken through the tax courts to establish some principles for what constitutes business related use of a vehicle.
Dr Samad Samadian was the taxpayer in question and he had a variety of different working locations and patterns, and his case set some new principles and reinforced some existing ones.
While your home may be a location where private work may be undertaken, such as reading notes or admin, it was successfully argued by HMRC that this was incidental to the main location where the work is performed, which would be a clinic or private hospital.
So routine journeys to and from the private hospital or clinic, whether the origin or destination is home or your NHS base, are not regarded as business journeys and are not a tax-deductible business expense.
The case effectively reduced business travel to travelling between two private hospital/clinic locations and emergency call-outs. This has significantly reduced the claims by most medics.
The Samadian case looked at a self-employed individual rather than an employee relationship and so it remains to be seen whether those who are trading as a company will be able to claim more.
In practice, most consultants trading through companies are applying the same principles to their business travel.
The rules around what can be claimed as a tax-deductible expense can be confusing and, in some cases, unfair. Make sure you are keeping good records and discuss with your accountant any items which could be contentious.
Read ‘Ten things to think about when setting up’, page 38
Next month: Pension protection explained
Ian Tongue is a partner with Sandison Easson Chartered Accountants
Things to get right when starting out
WhERE cAn i hold my pATiEnTs’ consUlTATions?
Think about whether you would prefer to have your own consulting rooms or practise from a hospital. Hospitals will also rent consulting rooms for a fee, so check out the options and costs before deciding.
Setting out in private practice can be a minefield to the uninitiated, especially for doctors beginning their career. Dr Steve Iley shares his tips
WhERE Will i TREAT my pATiEnTs?
Contact your local private hospital to find out how to secure admitting rights, also known as practising privileges. You will need to meet the standards set by the hospital’s medical advisory committee (MAC), which is made up of consultants from a range of subspecialties.
Even if you meet its criteria, this is no guarantee that you will be granted admitting rights, as they are not awarded by right.
Don’t forget to find out what services the hospital offers consultants and the charges they make for them.
WhERE Will my pATiEnTs comE FRom?
Think about the market in the area where you practise and your network. Meet with local GPs to let them know you are in private practice, and also with colleagues in other specialties who may refer patients to you.
Think about what differentiates you from colleagues in the same specialty and highlight this on your website. Use keywords to maximise your position on web searches.
You can also use social media, such as LinkedIn, to promote your expertise and also network in your local area. Don’t forget to make sure that all your details are listed on online directories, such as Google Maps.
Look for opportunities to demonstrate your expertise online. If you’re Bupa-recognised, don’t forget to make the most of your profile on Finder (www.finder. bupa.co.uk), the online directory of Bupa-recognised consultants, therapists and facilities across the UK. It’s a powerful marketing tool to promote you and your practice.
WhAT do i nEEd To knoW AboUT dATA pRoTEcTion And sEcURiTy?
You will need to register with the Information Commissioner’s Office (ICO): all individuals who process personal information are required to by the Data Protection Act 1998. Find out more at https://ico.org.uk/for-organisations/register. Familiarise yourself with how the hospital(s) where you practise and the insurer(s) you work with manage information governance.
The Disclosure and Barring Service (DBS) is the new name for
the Criminal Records Bureau and you will need to have one of its checks to show to hospitals and insurers. Make sure you get a ‘DBS passport’, as you can use this for all the hospitals and insurers that you apply to.
WhAT TEchnology do i nEEd To RUn my bUsinEss? Aside from standard office equipment – a computer with word processing software, phone, shredder and so on – you should consider practice management software. Most health insurers are moving to e-billing now, so you may find one of the many practice management software systems useful in helping you to manage your finances. Alternatively, you may prefer to outsource to a billing service company, who will invoice and collect payment on your behalf. Or use the health insurers’ own practice management websites, such as Bupa’s Providers Online (www. bupa.co.uk/providers-online), to invoice for the care that you provide to their patients.
do i nEEd A sEcRETARy?
You may find a full-time private secretary isn’t affordable when you’re building your practice. The best bet is to ask colleagues about the services that they use. Some hospitals provide secretarial services for a fee or you could consider a medical secretary service to take care of all your secretarial needs.
WhAT ElsE do i nEEd bEFoRE i sTART To pRAcTisE?
Your NHS indemnity won’t cover you for treating private patients, so it’s essential that you’re a mem-
ber of a medical defence organisation or have some other form of appropriate defence cover.
Ensure you have an appropriate level of indemnity cover before you start practising, because a lack of protection can lead to professional and financial ruin. It’s worth checking with providers what the premium costs for your first few years of practice are likely to be.
Familiarise yourself with how things work at the hospital where you practise and let them know how you prefer to work. Arrange inductions with the hospital medical directors and the resident medical officers. If you’re a surgeon, make sure you find out how anaesthetic cover works.
WhAT do i nEEd To do To bE AblE To TREAT hEAlTh insURAncE pATiEnTs?
You’ll need to become ‘recognised’ with each insurer so that
you can be paid for treating their customers.
Most insurers now manage their recognition process online, so take a look at their websites and find out what documents you will need to demonstrate that you’re suitably qualified to provide care to their patients – typically, these are details of your qualifications, posts you have held and your GMC number.
WhAT shoUld i knoW AboUT WoRking WiTh insURERs?
While all private health insurers use the standard coding for procedures set by the Clinical Coding and Schedule Development Group (CCSD), not all of them will cover all the diagnostic tests and procedures.
It’s important to familiarise yourself with their schedule of procedures. You can find Bupa’s at http:// codes.bupa.co.uk (see page 23).
Ensure you have an appropriate level of indemnity cover before you start practising, because a lack of protection can lead to professional and financial ruin
And it’s also important to check that patients have pre-authorised their tests or treatment before you go ahead.
This means that they’ve confirmed it is covered by their health insurance, and their health insurer will have let them know about any policy excess or limits that may apply.
You will need the pre-authorisation number that they are given for your invoices, so if the patient doesn’t have one, please encourage them to call their insurer.
Many health insurance policies tend to come with an excess and limited benefit for outpatient treatment, typically £1,000 at Bupa.
Insurers will usually expect consultants to collect these payments from the patient and, where this is necessary, will let consultants know. At Bupa, we do this on consultants’ statements.
WhAT AboUT TAx?
Don’t forget that you will need to pay tax on the money you have earned through your private practice. It’s worth setting up a dedicated bank account, as most insurers will pay you by BACS, and you will find it easier when you come to submit your tax returns.
Take advice from an accountant with experience in private medical practice. They can give you guidance on tax and expenses, and the fee that they charge for work relating to your private medical practice is a tax-deductible expense.
Dr Steve Iley (left) is medical director for health insurance at Bupa UK
Enjoy your third age
Retirement? Learn from the top ten mistakes other independent practitioners have made. Is your path to retirement clearly marked or are you putting off the crucial planning until tomorrow? Simon Bruce (below) highlights the top ten mistakes every senior consultant should avoid
The bes T way to deal with the current economic uncertainty is to ensure the financial affairs closer to home are in order. but managing your finances in a low interest rate environment is more complex than ever. senior consultants can easily make key errors at a time when their finances most need stability. here’s a round-up of the issues we encounter when helping new clients.
1
Failing to check your pay scale progression. Frequently, consultants are on the wrong pay threshold or have not received contractual pay rises when they were due. Are you being paid what you are contractually entitled to?
2
Unwittingly exceeding the pension lifetime allowance (LTA). The lifetime allowance is the total amount which can be built up in a pension without causing an extra tax charge. breaching the allowance can trigger tax of up to 55%. h ave you checked where you stand?
3
Not protecting the value of your pension. The taxation of pension benefits is a particularly complex area where more senior doctors are coming unstuck through poor advice. each time the Government has cut the lifetime allowance, it has introduced a range of transitional protections to help those individuals affected. each one differs in terms of qualification rules, what can be protected and which benefits can be accrued subsequently. After a long wait, online applications for Individual Protection 2016 (IP2016) are now available for those that had pension savings in excess of £1m as at 5 April. Do you have the right protection in place?
4
exceeding the annual allowance. The maximum amount of tax-relievable pension contri-
butions you can make each year is £40K. b e wary of any N hs pay rises received through increments, new management positions, clinical excellence awards or by any other means. Immediate tax charges of up to 45% can be avoided with planning.
The new ‘tapered’ annual allowance, introduced in April this year, reduces the cap by £1 for every £2 of income for individuals with ‘adjusted income’ of over £150,000, with a maximum reduction of £30,000 for those earning £210,000 or more.
Adjusted income includes not only salary but bonuses, benefits in kind and pension contributions, which adds to the complexity of the earnings calculation.
A doctor with total earnings of £145,000 may be able to contribute £40,000 into their pension each year tax-free, but those earning £210,000 can only save £10,000 for their future.
In the Autumn, the Nhs Pensions Agency issues letters notifying those who have saved more than the annual allowance for the last tax year. hM Revenue and Customs (hMRC) bases calculations for pensions’ contributions on the deemed growth of the pension in the year, so the figures used bear little resemblance to the amount you have actually paid into your pot.
Check the sums carefully – many have been wrong due to the Pensions Agency allocating a backdated award to the wrong tax year.
And if you need to contact the Nhs Pensions Agency for crucial information to help with your allowance planning, you might be surprised that it is now charging fees for many requests –despite a poor service record in terms of giving the correct data in an acceptable time-frame.
5
Drawing pensions in the wrong order. Taking N hs benefits before drawing private pensions could have significant financial disadvantages for some individuals, including being unable to draw any tax-free lump sums from private pensions.
6
Not making the most of inter-generational planning. The introduction of pension freedoms now gives universal access to pension funds from age 55.
This, combined with the ability to pass on pensions tax-efficiently on death to family members and other beneficiaries, makes pension funding attractive – particularly for some spouses of senior consultants or where the lifetime allowance and annual allowances are less of a concern.
Who will receive your pension fund benefits when you die? Would your pension funds be more useful if passed to your children and grandchildren? Are you making the most of savings allowances for each generation of your family?
7 Not taking advantage of your available allowances every year such as I s As, capital gains and gift allowances, or maximising tax reliefs through annual pension allowances to minimise the duty owed to h MRC. This includes your spouse and family.
Individuals have an annual capital gains allowance of £11,100. This provides great scope to harvest investment gains every year free of tax. With proper steward ship, you can both build a goodsized portfolio before you need to worry about capital gains tax.
8
Attempting to go it alone. Online fund groups are adept at attracting the ‘DIY inves tor’ with exciting non-stop com pany information and investment experts dedicated to telling us what will happen in the future. The result is often too much capital directed at an investment which turns out to be hard work for the busy consultant and disappointingly average.
The taxation of pension benefits is a particularly complex area where more senior doctors are coming unstuck through poor advice
‘typical’ saver with ‘average’ luck will receive over a year. Many will receive less. The number of premium bonds prizes has also been cut – the number of monthly £100,000 prizes will fall from five to two and £50,000 from 12 to just five.
Are you sure you will qualify for entrepreneur’s Relief? banking on being able to draw all of your corporate cash under a beneficial tax rate at retirement is a risk. have you explored all of the options for profit extraction and diversification?
10
Not considering mortality. Unexpected events can highlight the fragility of life and the need to ensure that your affairs are in order. This means drafting a will and registering Lasting Powers of Attorney.
Simon Bruce is managing director of Cavendish Medical, specialist financial planners helping senior consultants in private practice and the NHS
The content of this article is for information only and must not be considered as financial advice. Cavendish Medical always recommends that you seek independent financial advice before making any financial decisions.
Levels, bases of and reliefs from taxation may be subject to change and their value depends on the individual circumstances of the investor.
The value of investments and the income from them can fluctuate and investors may get back less than the amount invested.
Practice Management
9 holding too much personal cash or in your limited company over the medium term is an issue. After tax on interest and inflation, there is no refuge for higher-rate taxpayers, as cash is losing real value. Changing multiple deposit accounts and cash IsAs every year is time-consuming.
The Financial services Compensation scheme for individuals covers the first £75K only or £150K if an account is held in joint names. Are your cash-based savings tied into poor yields? In June, National s avings & Investments reduced the prize fund rate of its ever-popular premium bonds from 1.35% to 1.25%. This is the amount a
Recognised as a leading provider of outstanding private practice management. KMS have a proven track record of growing practices, both new and established, giving you a competitive edge and maximising your profitability.
bUsinEss DilEmmAs
Your medico-legal queries answered
Independent Practitioner Today readers’ defence questions are answered here by Dr Emma Doherty (right)
Dilemma 1 Can I let school students sit in?
QI work as a private GP. My nephew, a sixth-form student, is considering studying medicine at university and has asked if he could have a week’s work experience at my private GP practice in the school holiday.
I would really like to help my nephew by giving him experience of his possible chosen career path, but I am unsure if it would be allowed.
AWork placements can be hugely beneficial to students. Not only can they help them to identify if their dream career is right for them, but it can also look good on any university application to show they have taken time to gain some experience.
You are right to consider any potential risks of hosting a young person in your practice, especially if they have contact with patients.
There is no reason why you should not host a student, but it is important to consider any requests on a case by case basis.
Each student will display different levels of maturity and professionalism and it is important that they understand what is expected of them in the workplace and act appropriately.
Confidentiality is key, not just for doctors but for anyone working with you who comes into contact with patients.
You should emphasise this to the student and ask them to sign a confidentiality agreement which stipulates that anything they hear
in the practice is not to be shared or discussed with anyone else.
Patients should be informed that there is a work experience student on the premises. You may wish to display a notice explaining this in a position where it can be seen by patients.
If the student is observing consultations, it is important to get consent from each patient and allow them the opportunity to decline if they don’t feel comfortable.
You may wish to raise the issue first when the patient calls to book their appointment. The patient then has plenty of time to fully consider how they feel about having a student present.
When obtaining consent, explain who the student is and their level of study. The patient should be able to make a fully informed decision about whether they are happy for the student to be present.
You should also make it clear to the patient that they can withdraw their consent at any time and that if they do, it will not in any way affect their care.
Consent should be confirmed when a patient registers at reception on the day of their appointment and the doctor should check again before the patient enters the consulting room. It is advisable to note on the patient’s record that the student was present and that consent was obtained from the patient.
There may be consultations that you feel are inappropriate for the student to sit in on; for example, those where the patient is close in age to the student or those where a patient is particularly vulnerable. In those circumstances, you may wish to ask the student to step outside if you do not feel that their presence is appropriate.
Each year, there is a charity cycle event which passes through my town. I have been asked if I would like to volunteer to provide medical support on the day of the event
Dilemma 2
Am I covered for aiding bike race?
QAs well as my day job as an independent physician, I am a keen cyclist in my spare time. Each year, there is a charity cycle event which passes through my town.
I have been asked if I would like to volunteer to provide medical support on the day of the event. I would love to help out, as the event is for a really good local cause. Would I be indemnified to help out like this?
AIt is important to check your indemnity arrangements whenever taking on additional clinical duties, whether those duties are voluntary or paid. Doctors have an ethical requirement to ensure they have adequate insurance or indemnity in place (GMC, Good Medical Practice [2013], paragraph 63).
In its publication Insurance and Indemnity: Guidance for Doctors , the GMC advises doctors who wish to volunteer to provide medical assistance at an event:
‘Doctors who perform such acts are providing professional services irrespective of whether they are paid or unpaid. If indemnity is not provided by the organisation for which you are providing this service, you will need to make your own arrangements to ensure you are adequately indemnified against any claims that might arise from this work.
‘You should contact your medical defence organisation to advise them of your role and to discuss whether you have or need suitable professional indemnity or insurance cover. In order to enable them to make this judgement, you must provide them with accurate and up-to-date information about the scope and nature of the work.’
Before agreeing to provide assistance, it is important to check whether or not the event organisers will be providing indemnity for doctors acting in a professional capacity.
If they do not have indemnity arrangements in place, you must contact your own defence organisation to make sure your current membership will indemnify you for the voluntary work you plan to do.
It is important to check your indemnity arrangements whenever taking on additional clinical duties, whether those duties are voluntary or paid
Regardless of indemnity arrangements, it is important that if you plan to volunteer at an event, you have the appropriate skills and experience, and do not practise outside of your area of expertise.
The GMC states that you must recognise and work within the limits of your competency (GMC, Good Medical Practice [2013], paragraph 14). As with any care you provide, you should keep detailed records. It is also important to make sure that you have adequate equipment and support to perform your duties.
Dr Emma Doherty is a medico-legal adviser at the MDU
CLINIC SOFTWARE THAT BREAKS THE MOULD...
Trusted by clinics across the UK and Ireland and approved by NHS to help you manage your business. Jelly Clinic management software has everything you need including clinical notes, patient forms and billing.
All inclusive price with no contract or upfront fees. Free training to get started, 500 texts every month. Unlimited diaries with remote access included. Medical records, reports, communication and invoicing. Supports regulatory compliance. £99/Month inc. VAT.
For more information please visit
DocToR on ThE RoAD: REnAUlT mEgAnE gT
Still plenty of va va voom
Our tester Dr Tony Rimmer (right) finds the new Renault Megane GT is a competitor to that long-time doctors’ favourite – the Golf GTI
We medics have always liked our cars. i n the early years after qualifying, if we didn’t aspire to a two-seater sports car, the next best thing was a hot hatchback.
The car to have was the Golf GTi, the pinnacle of understated quality, practicality and great performance.
Offerings from other manufacturers all seemed a bit cruder. Fast Fords like the e scort XR3i and subsequently the Focus Rs were a bit brash. French offerings from Peugeot and Renault were fast but flimsy.
The current mark 7 Golf GTi is still the benchmark hot hatchback, but competitors have become progressively more sophisticated, better made and offer better value for money.
Peugeot and Renault have raised their game significantly over recent years, so it was with great interest that i approached
the launch of the all-new Renault megane in Golf GTi-challenging form: the megane GT 205.
The new megane represents the fourth generation of this mediumsized hatchback that has been around for 20 years.
Advanced tech
it is made in spain alongside the recently-tested Kadjar crossover and is packed full of interesting and advanced tech.
The whole range stretches from the entry petrol model in basic trim at £16,600 through various frugal diesel models and increasing levels of trim up to the rangetopping petrol GT Nav 205 model at £25,500.
Knowing that we independent practitioners like a bit of performance and we also like our tech, i concentrated on this top end model at the megane’s UK launch in Yorkshire.
Peugeot and Renault have raised their game significantly over recent years
RenaulT
megane
GT NAV 205
Body: Five-door hatchback
engine: 1.6 litre four-cylinder
turbo petrol
Power: 205bhp
Torque: 280nm
Top speed: 143mph
acceleration: 0-62mph in 7.2 secs
Claimed economy – combined: 47.1mpg
On-the-road price: £25,500
With fantastic and sparsely trafficked driving roads across the beautiful Yorkshire dales, it was a great opportunity to see if this new French pretender could challenge the mighty Golf.
s adly, safety regulations have compromised the shape of all hatchbacks, so the days of a megane with a boot that spawned the famous ‘ s hakin’ that ass’ advert are gone forever.
To give it some character and identity, Renault has concentrated on distinctive front and rear lighting signatures with permanently-lit Led units together with a bold, swooping grille design surrounding their large diamond logo.
The GT model has lowered suspension and 18-inch diamondcut alloys to complete the sporty look.
i ts interior design is modern and fresh. The materials used are
of higher quality than Renaults of old and although not at the level of premium brands like Audi and B m W, are equal to Volkswagen products.
The centre console is dominated by a large clear 8.7-inch portrait display that allows control of the huge amount of impressive tech on offer. Like getting used to the latest medical equipment, it is worth spending some time considering what is on offer and how to access it all.
Personalised settings
Renault’s m ULT i - se N se system allows a choice of four pre-set modes controlling steering effort, engine responsiveness and chassis control. A fifth mode can be personalised.
The 4 c ONTROL four-wheel steering system allows the rear wheels to turn slightly in the
opposite direction to the front wheels at speeds below 50mph and in the same direction above 50mph.
Traffic-sign recognition, handsfree parking, blind-spot warning, adaptive cruise control, automatic high/low beam headlights, lane departure warning and active emergency braking system completes the impressive tech list. so, how does this all translate to the general driving experience and does it enhance or retract?
The Yorkshire dales revealed all.
Powered by a 1.6 litre turbocharged 205bhp four-cylinder petrol engine with a seven-speed dual clutch gearbox, the megane GT has plenty of get up and go. The ride is firm but supple and the steering really sharpens up when you select the m ULT iseNse sport mode. The car really flowed along the fast open roads
of the dales and i could certainly feel the 4 c ONTROL system at work in the tighter corners.
However, it would take a little getting used to, as the initial feeling is not unlike the rear wheels stepping out with deliberately induced oversteer in a normal car. The usual opposite lock correction would be the wrong solution.
Driver involvement despite this, my overall impression is of an impressive hot hatch that can cover cross-country distances swiftly and safely with enough driver involvement to keep the enthusiast happy.
The Golf GTi is still a better car to drive and its chassis is better sorted, but i am sure that subsequent Renault s port versions of the new megane will address this issue more directly.
As a car to live with on a daily
basis, the Renault makes an ideal partner. Plenty of luggage space and room for five makes it just as capable of taking the family on holiday as it would be getting you to your clinic on time.
modern Renaults have a quality feel that will be a surprise to any of you who haven’t driven one recently and the m egane is no exception. Although the GT is not as well-rounded as the Golf GTi as a hot-hatch, it feels more modern, is £6,000 cheaper like-for-like and can boast some clever tech.
Also, Renault dealers have made great strides in customer service and the brand now tops the wellrespected Auto e xpress d river Power dealer chart for 2016; another reason to give the megane your consideration.
Dr Tony Rimmer is a former NHS GP practising in Guildford, Surrey
Renault has concentrated on distinctive front and rear lighting signatures together with a bold, swooping grille design surrounding their large diamond logo
Gifts with a sting
With Christmas party planning now underway, accountant Vanessa Sanders gives a reminder of the tax treatment of seasonal gifts and benefits to employees and other helpful business contacts
A
social function for the entertainment of employees
There is a tax exemption for employee entertaining to allow the employer to receive a tax deduction for the cost and for the employees to have the benefit tax-free.
The relief only applies to ‘annual parties’ available to all staff and is set at £150 per head of those attending the function. The cost must include VAT.
If the cost of qualifying parties is in excess of £150 per head, then all the costs – not just those above £150 per head – are taxable as a benefit in kind on the individual employees enjoying the party.
It is important to note that the cost is the entire cost of the event, including taxis, overnight accommodation, free bar and anything else on offer. Everything for the event has to be included in the calculation.
If the limit is exceeded, the benefit must be reported on each employee’s P11D. If this seems churlish, then the company can pay the tax over to HMRC on a grossed-up basis using a PAYE settlement approach.
This could mean that a total
cost per head increases to £300 instead of £150, so it is worth considering careful planning.
It is important to note that the amount of £150 per head applies to all those attending the party and not just the employees. So it may be worth considering allowing employees to bring guests.
A word of warning: the guests should not be clients – this would turn the overall function into client entertainment, which is never tax-deductible as an expense.
Tax on business profits
Generally, client entertaining is not allowable for corporation tax purposes. However, the cost of employee entertaining, provided it is not incidental to the entertainment of others, is allowed to be deducted.
If you invite clients and customers to your party, it is important to consider how to apportion the costs for corporation tax purposes.
You should also consider if this is truly entertainment or if it is, in fact, a business meeting with agenda, action plans and outcomes with lunch just thrown in.
A business meeting would be an allowable deduction, but do not
A business meeting would be an allowable deduction, but do not forget, there is not usually much business done if there is too much alcohol consumed
forget, there is not usually much business done if there is too much alcohol consumed.
Gifts to employees
Christmas presents paid in cash to employees are always taxable in the same way as other earnings. The same treatment also extends to vouchers, which can be attributed at money’s worth. So, for example, a £25 Marks and Spencer voucher to be spent at the employee’s behest would be taxable as part of their salary.
The employee has to pay tax on the full value of the voucher. However, they will pay tax on the face value not on a grossed up basis, which means that a voucher
of £100 might attract tax at the basic rate of £20 as opposed to grossing up and paying £25 to receive £100 net.
If employees are given a seasonal present, such as a turkey, an ordinary bottle of wine or a box of chocolates, provided the cost is reasonable, HM Revenue and Customs (HMRC) will not seek to tax it.
Unfortunately, we are given little guidance as to what the limit of reasonable may be, but experience would say that a gift costing less than £50 could be argued as reasonable. A Hermes scarf, however, is not.
If the value of the gift is more than this, it will be taxable and should be included on the employee’s form P11D, or the tax settled on a grossed-up basis. This would apply even if you did not want a tax deduction for the amount if the reason for the gift is because of the employee/ employer relationship.
Gifts from third parties
It is worth noting that gifts can also often be received by your employees from third parties due to contact they may have had
with them throughout the year as a result of their employment. Such circumstances would be, for example, sending flowers, wine or chocolates for theatre staff who assist with operations. Provided such gifts do not exceed £25 in cost, it will not be taxable for the employee receiving the gift.
VAT
Input tax on entertaining is not recoverable. However, tax on employee entertaining is recoverable.
The definition of employees for VAT purposes does not include partners of existing staff or former employees. Therefore, if your party includes
guests, you will need to apportion the relevant costs appropriately for VAT if you intend to make a reclaim.
Where entertainment is provided only for directors, partners or sole proprietors, HMRC does not accept that the input tax has been incurred for a business purpose.
It is, of course, possible for directors to attend parties at the same time as other staff members. In this case, the VAT on the cost of their attendance is not blocked from recovery.
Vanessa Sanders is a partner at Stanbridge Associates, specialist medical accountants
Confounded predictions
Indpendent
Practitioner
Today’s earnings survey of ENT surgeons last year was cautious about the growth rate possibilities of their private incomes. But consultants – happily –
proved us wrong, reports Ray Stanbridge
Our latest financial analysis for this benchmarking series shows average gross incomes of eNt surgeons rose by as much as 8% between 2013 and 2014. t hey rose from £138,000 to £149,000. Costs rose by about 7% from £56,000 to £60,000 on average. as a result, taxable profits increased by about 8.5% over the year, from £82,000 to £89,000. Gross margins were fairly constant at just under 6%.
there are a variety of reasons for the increase in incomes. In a
number of cases, there has been a significant growth in Choose and Book activity.
t here has also been, in some areas, a growth in waiting list initiative work undertaken privately.
Rise in self-pay
Insurance company fee pressure has continued in the year but the figures here reflect a growth in self-pay activity, which has been widely predicted in this journal.
It seems that an increasing number of patients are paying for
aveRage INCOMe aND eXPeNDITURe OF a CONSULTaNT
Expenditure
their treatment privately, often using funds they have accumulated in I sa s. a nd this trend is continuing.
looking in more details at costs, wages and salary expenses have risen. a s previously reported, there is a correlation between growth of such costs and the taxfree personal allowance, particularly if family members are employed.
Office costs have shown a modest increase, for no particular reason. Motor and travel costs have increased slightly as some consultants broaden the bases at which they work.
s ome have incurred increased conference fee costs. Following the impact of the recession, more exotic venues for courses and conferences are coming into vogue.
Finally, ‘other’ costs have shown a modest increase. again this represents increased expenditure on marketing and promotion activity, a feature of many successful practices.
But some costs have actually reduced during the year (see table on the left).
For many consultants, defence indemnity costs seem to have stabilised. We have noticed that there is an increasing tendency
for consultants with a good claim record to look away from the conventional providers and seek l loyds market – or similar –indemnity insurance cover. Whether this trend is short or long term remains to be seen, but there is some evidence that a short-term savings potential has been taken advantage of. Other costs seem to have been relatively stable.
Effect of choose and Book
What then of the future? We were wrong in 2015 in that we forecast a fairly stable income market. But we see no reason to change this view for 2016. If Choose and Book activity is a regular feature of the market, then average eNt private practice income will continue to be firm. If this work falls, then we would expect to see some correction.
Insurance company pressures on fees continue, with some consultants being subject to particularly heavy treatment. However, there is a significant growth in the self-pay market, which seems historically to have offset this trend. a t the very least, we see a ‘steady as she goes’ environment. Or for some – even better.
Year ending 5 April. Figures rounded to nearest £1,000 (percentage is also rounded up)
Source: Stanbridge Associates Ltd.
Would you like to remove the administrative stress of medical billing and collections? Have you an amount of bad debt owed?
Would you like to raise the profile of your practice and attract more patients?
Medical Billing Direct is a dynamic, progressive company with a dedicated team that o ers over 25 years’ experience in successfully providing streamlined billing, collection and marketing services
Look no further for the right help to drive your practice forward. Please feel free to get in touch.
The seca mBCA 525 sets a new standard in bioimpedance measurement.
The will to exceed technical feasibility drove the development of the seca mBCA 525. At work behind the compact touch-screen is software developed for a substantiated analysis of body composition and validated by several medical studies*. The phase-sensitive electronics deliver precise and reproducible measurements while the extensive data storage provides long-term, expert therapy monitoring. Mobile convenience is guaranteed by wireless communication with printers and PCs via a pre-configured Wi-Fi. Experience progress in BIA measurement at: mbca.seca.com
When studying the figures here, remember that our last review of this specialty ( Independent Practitioner Today , s eptember 2015), reported there were increasing problems in trying to present an effective time series comparison of incomes and net profits generated by e N t consultants in private practice.
t his problem continues again
this year. Firstly, many consultants have incorporated and this has made a propper comparison difficult.
Fewer costs
secondly, there has been a significant growth in Choose and Book work in recent years. s ome consultant practices almost exclusively consist of such work.
as a result, these consultants do not carry indemnity insurance, secretarial and room hire costs that have been imposed on their colleagues with a similar-sized conventional private practice.
thirdly, the growth of eNt has distorted figures.
Generally, our experience is that those working in groups earn at a faster rate than those who continue in the traditional sole trader route.
Our survey is not statistically significant but rather it represents a range of typical incomes/expenditures earned by a sample of eNt consultants working through the four countries.
as in previous years, our sample consists of those who:
Have had at least five years’ private practice experience;
Hold either a maximum parttime or new consultant NHs contract;
are seriously interested in pursuing private practice as a business;
a re earning at least £5,000 a year in the private sector;
May or may not have incorporated or be a member of a group.
Ray Stanbridge is a partner with accountancy, finance and tax advisory medical specialists Stanbridge Associates
How ARE YoU doing?
Use
compare your
performance with others
ending
what’S coMing in oUr noveMber iSSUe
Make sure you don’t miss our next issue, published on 24 November. you may not receive every issue if you have not yet subscribed to the journal. Don’t risk missing out on vital topics we tackle next time, including:
Shortfalls: a sign of financial virility or financial folly? Ray Stanbridge reports on one of the biggest practical problems facing consultants in private practice
New series: an introduction to the many new legal pitfalls for doctor entrepreneurs
key person dependency – is your practice at risk? For all the financial benefits of running your own private practice business, there is one big potential risk that you could be exposed to. and that is the business’s dependence on you or another member of staff such a practice manager or secretary as the main cog in the wheel
Top tips for busy doctors – Jane Braithwaite gives advice on managing your profile
Modern customer expectations and how to meet them
a consultant surgeon gives his tips on growing your practice through networking
The promise of absolute returns on your investments is easy to make but hard to keep. Patrick Convey explains why all is not what it seems with such a strategy
INDePeNDeNt PraCtItIONer
Published by The Independent Practitioner Ltd. Independent Practitioner Today is editorially independent and thanks Bupa for its assistance with distribution.
Printed by Pepper Communications Ltd
Material is governed by copyright. No part of this publication may be reproduced, stored in a retrieval system or transmitted in any form without permission, unless for the purposes of reference and comment. Editorial layout is the copyright of the publishers. If you wish to use it for promotional purposes on websites or for reprints, we would be happy to discuss licensing the copyright to you.
Registered office: 7 Lindum Terrace, Lincoln LN2 5RP
Write to Independent Practitioner Today PO Box 198, Cranleigh GU6 9BB
eDITORIaL INqUIRIeS
What should I do? Dr Nicola Lennard, MDU medico-legal adviser, responds to a consultant who has serious concerns about a colleague
Medicine’s Strangest Cases: the private surgeon who hated operating
Building on relationships to ensure your private patient unit delivers commercial and service gains for the trust
Cleveland Clinic’s plans for a major new private hospital in London
Big issues in private acute healthcare – reports from a major LaingBuisson conference
electrifying! Our motoring correspondent Dr Tony Rimmer tests the golf gTe plug-in electric/petrol hybrid
Our monthly ‘Starting a Private Practice’ continues as Ian Tongue casts an accountant’s eye on the pension protection issue
HCa Healthcare Uk sets out its network approach on integrated oncology, palliative care and support services, recently recognised and accredited by the european Society of Medical Oncology (eSMO)
accountant’s Clinic
Breaking into medico-legal work
Plus all the latest news and views
aDveRTISeRS: The deadline for booking advertising for our November issue falls on 28 October
£90 GPs and practice managers (private & NHS). £210 organisations.
But if you pay by direct debit, individuals pay only £75, and organisations £180 Call Proact Ltd on 01752 312140
Email: lisa@marketingcentre.co.uk
To guarantee your copy of Independent Practitioner Today by taking out a subscription (at the rates shown on the left), phone 01752 312140 or send off a subscription form on page 20 or email lisa@marketingcentre.co.uk or go to the ‘about’ page of our website www.independent-practitioner-today.co.uk
If you pay by direct debit, individuals pay only £75 for a subscription. Just fill in the form on page 20 and send it to the Freepost address shown at the bottom of the form.
BaCk ISSUeS: £12.50 including post & packaging CHaNgINg aDDReSS OR SUBSCRIPTION DeTaILS?
Phone 01752 312140 or email lisa@marketingcentre.co.uk
Robin Stride, editorial director
Circulation figures verified by the Audit Bureau of Circulations
I’d be in serious trouble without the diary management feature on ePractice manager! It means I can focus on treating patients while my PA is able to coordinate my appointments remotely across the three practice locations.
Ernest Barlow-Kearsley, Total Footcare Solutions
Securely manage your
patient appointments
Healthcode’s ePractice solution provides independent practitioners the ability to manage their clinics online from multiple locations. The appointments solution is designed for both individuals and group practices to ensure efficient organisation for appointments within your practice.
Using ePractice to manage your patient appointments, you can:
• Easily manage and track your appointments
• Access patient appointments from multiple treatment sites
• Generate appointment reports for clinic and theatre lists
• Set up recurring clinic sessions
• Auto-prompt to raise invoice on completion of appointment
Healthcode’s ePractice solution offers:
Patient Billing
Patient Management
Payment Tracking & Financial Reporting
Appointments
Membership Enquiry
Complimentary ePractice App
Experts in Online Solutions for Smarter Healthcare... ‘code for success.