The business journal for doctors in private practice
In this issue
Marketing and development
Our Troubleshooters explain the differences between marketing and business development P14
Virtual but not distant
Tips on how to ensure vital and effective collaboration between doctors and your virtual secretarial team P32
Keeping it simple is key to better health
n Bupa has made all its written communications with patients clearer. See page 24
Thinking
Hempsons lawyers give advice for doctors thinking of opening a practice in a high street unit P36
MDT meetings boost
By Robin Stride
Consultants in private practice are being recommended to supercharge their multidisciplinary team (MDT) meetings using a new toolkit from the Independent Healthcare Providers Network (IHPN).
Designed with the help of senior doctors, hospital group medical directors and others, it aims to assist independent providers to further improve MDT working.
The resource sets out the latest best practice and innovations from across the healthcare system and has received strong backing from independent providers, insurers, patients’ charities, royal colleges, the Care Quality Commission (CQC) and NHS England.
IHPN clinical director Dr Howard Freeman described MDT working as a fundamental part of delivering safe, high-quality patient care, adding: ‘We hope this new resource supports clinicians to fully utilise all the expertise of the teams they work within, ensuring the delivery of evidence-based patient-centred treatment.’
He told Independent Practitioner Today: ‘It provides both clinicians and healthcare providers with the key principles for successful MDT working, including identifying when MDT meetings should be carried out in the best interests of patients and what clinicians and
Our sponsors
providers should consider when setting up and running MDT meetings.
‘It also sets out best practice examples of where clinicians and providers from across the independent sector and wider health service are already leading the way, from MDT working for highly specialised and complex care, running effective virtual and/or hybrid MDT meetings and engaging patients in the MDT process.’
The IHPN said the 14-page toolkit can be used by independent providers of all types, sizes and structures, and looks to support the use of MDTs beyond cancer care to a broader range of medical settings.
Providers are given key principles to support them in identifying when MDT meetings should happen in the best interests of patients and what clinicians and providers should consider when setting up and running these events.
Best practice examples are set out from across the independent sector and NHS ‘to stimulate and to support independent providers to further strengthen the governance around their MDTs and develop innovative new approaches’.
Dr Freeman said the toolkit was part of the IHPN’s ongoing programme aimed at supporting the private healthcare sector to deliver the highest quality of patient care.
The Patients Association is
among many organisations giving a thumbs-up to the toolkit. Chief executive Rachel Power said by promoting patient-centred multidisciplinary meetings, the resource was making a valuable contribution towards effective, personalised care.
‘It offers guidance to independent providers to deliver co-ordinated, comprehensive care tailored to individual patient needs. We welcome this collaborative approach to improving outcomes and ensuring patients receive the highest-quality care and support throughout their treatment journey.’
Stella Williams, senior specialist in secondary and specialist care at the CQC, said effective MDT working involving clinical expertise in
the round was a fundamental part of delivering safe, high-quality care and it can significantly optimise both patient safety and patient outcomes.
‘The toolkit sets out best practice examples and guidance on how providers can strengthen the governance around their MDTs and aims to help improve the impact and consistency of MDT approaches in a range of independent healthcare settings. We hope it will be a valuable resource to the sector,’ she said.
‘We look at MDT working when we assess services, and we will continue to use our single assessment framework to check that people receive care, treatment and support which is evidence-based and in line with good practice standards.’
Dr Fiona Donald, president of the Royal College of Anaesthetists, said the resource would help ensure more patients benefited from effective team-working between the different healthcare professionals involved in their care.
‘It addresses common questions and scenarios through examples of best practice, which hopefully will serve to drive quality and consistency.’
n A copy of the Multidisciplinary Working toolkit can be found at www.ihpn.org.uk/report/multidisciplinary-team-working.
TELL US YOUR NEWS.
Contact editorial director Robin Stride (right)
Email: robin@ip-today.co.uk
What made the news in June 2014
A look back through our journal’s archives of a decade ago reveals that although times change, some issues are not so new P10
Phone: 07909 997340 @robinstride
ADVERTISE WITH US. To advertise in the digital journal, on our website or in our business and lifestyle directories, contact Andrew Schofield at Spot On Media. Phone: 0161 408 3912
A medico-legal expert explains the importance of marketing and advertising your practice in an ethical way when designing your website P12
What to do to protect patient data
When it comes to data breaches, healthcare is the leading offender. Solicitor Richard Forrest advises on the importance of security protocols P16
Learn from errors and don’t cover up David Hare, head of the Independent Healthcare Providers Network, reflects on its joint patient safety conference with the Care Quality Commission P18
When patients want a second opinion Dr Sabira Hughes of Medical Protection gives some practical steps to consider in light of Martha’s Rule, which has been implemented in 100 NHS trusts P20
OUR REGULAR COLUMNS
Business Dilemmas: Getting rid of a bullying patient
The MDU’s Dr Sissy Franks advises on what to do if you wish to remove a patient from your practice P38
Start a private practice: Making Tax Digital
Accountant Richard Norbury on the plans to reform the payment of tax to make it reflect real time P40
Doctor on the Road:
This EV sounds like a petrol hot hatch
Dr Tony Rimmer loves Hyundai’s gimmick for turning an electric vehicle into a petrol head’s joy P46 www.independent-practitioner-today.co.uk
Record number of patients treated Statistics gathered by the Private Healthcare Information Network (PHIN) show that private healthcare is riding high P26
Beware the fickle allure of cash
What impact does inflation have on your wealth? Cavendish Medical’s Samuel Kirton explains why investing can deliver inflation-busting returns P34
The experts do it better
Partnering with a medical billing firm can significantly reduce administrative burdens, ensure regulatory compliance and enhance overall profitability P36
Senior doctors relieved at pension tax U-turn
Labour will not re-introduce the lifetime pension allowance
By Edie Bourne
Senior doctors have declared relief at the news that the new Labour Government will no longer reintroduce the Lifetime Allowance on pensions.
The party had originally declared it would reverse the decision to abolish the pension savings tax once in power.
Originally the claims were made in March 2023 following the then Chancellor Jeremy Hunt’s shock announcement in the Budget to remove the tax altogether. However, the move was absent
from Labour’s official election manifesto.
Patrick Convey, technical director of specialist financial advisers
Cavendish Medical, said his team had spoken to many senior doctors who had shared concerns that the lifetime allowance would be reintroduced.
The uncertainty caused by a year’s worth of discussion on this has added to the constant confusion surrounding pensions and the tax on them.
But he warned: ‘Of course, this does not mean that there will not be other changes to pension taxa-
tion in the short-term. It is possible that the lifetime allowance is being left alone because other pension taxes may be amended.
‘We will have to wait to see what might happen but there has been over a decade of change to pensions tax and it would be nice to think we might keep the current regulations in place to make retirement planning easier. Trying to make concrete plans for the future while the goal posts are moving is challenging.’
The lifetime allowance limited the total value of an individual’s pensions before harsher tax rates
Collaboration forms theme of BMA’s private practice meeting
Consultants are to be given advice to help them work collaboratively with private hospitals at this year’s BMA Private Practice Conference.
Circle’s group medical director Mr Peter James will be presenting the hospital perspective while gastroenterologist Dr Marcus Harbord will give the clinician’s views.
They are among a large team of expert speakers, many of whom write regularly for Independent Practitioner Today , at the event designed to cater for experienced and would-be private consultants and GPs.
Doctor speakers at the event on 1 November at BMA House in London include BMA Professional Fees Committee chair Dr Peter Holden; sport and exercise medicine consultant Dr Leon Creaney, and Private Healthcare Information Network chief executive Dr Ian Gargan.
A separate session for private GPs will be led by Dr Shaima
Villait of Chelsea Medics and chair of the Independent Doctors Federation’s GP Committee.
The challenge for increasing numbers of GPs working in private general practice alongside NHS general practice will be tackled Dr Tom Black, former chair of the BMA’s Northern Ireland General Practice Committee.
In the same session, Independent Practitioner Today columnist Alec James, of Sandison Easson, will speak on accounting in private general practice and there will be advice on marketing your practice.
The changing landscape and future of private practice will come under the scrutiny of David Hare, chief executive of the Independent Healthcare Providers Network, and attendees will hear from LaingBuisson analyst Liz Heath about private medical insurance and the self-pay market trends.
Facts and figures to influence
consultants’ secondary care private practice model will be presented by Vanessa Sanders of accountants Stanbridge Associates. Advice on setting up independently will feature Mr Vivek Sivarajan, medical director of the Elanic Group, and a Care Quality Commission speaker will give tips on registration.
Dr Jennifer Yell, chair of the BMA Private Practice Committee, said: ‘Independent practitioners or those thinking of becoming one, should attend this conference to hear how the private sector works and get top tips and advice on how to run one’s own practice.’
The day ends with an informal networking reception where speakers and session facilitators are available for questions.
Delegates can attend remotely as well as in person. Full details, fees and more information available at www.bma.org.uk/events/privatepractice-conference-2024.
were applied. Before it was abolished, the lifetime allowance was £1,073,000.
Cavendish Medical’s Patrick Convey
Dr Jennifer Yell of the BMA
Mr Peter James of Circle Group
GOOD NEWS ON GROWTH 1
A record year for entry to hospital
By Olive Carterton
Predictions of a record year for private healthcare sector inpatient admissions have been confirmed by the latest official figures – and now under a new Government the sector says it stands ready to help the NHS deal with its ever-rising waiting list.
Independent hospitals still have spare capacity and have told the Private Healthcare Information Network (PHIN) they can still help more to ease the pressure on patients and stop people suffering unnecessarily.
PHIN’s chief executive Dr Ian Gargan said: ‘With the majority of the private sector carrying out the more easily arranged and most
common procedures, such as cataract surgery, hip replacements and knee replacements, waiting lists can be reduced.
‘The NHS can then concentrate
Healthcode dealt with 1m invoices in May
Healthcode processed over 1m invoices to insurers in a single month for the first time in May as a record number of patients received investigations and treatment.
Based on current trends, the UK’s online clearing service projects that providers will submit 11.5m invoices in 2024, compared with 10.2m in 2023.
Overall, invoice volumes were up by just under 15% compared with May 2023 with both hospital and non-hospital settings showing similar growth levels.
May is traditionally a busy month for the private healthcare sector, but 2024 saw a significant increase in insurer-funded activity with monthly volumes of more
than 900,000 since the year began.
Healthcode says its invoice data is an important measure of market activity because private hospitals and more than 70% of practitioners, practices and clinics submit invoices to all the major insurers through its secure Clearing Service.
Automated validation ensures each invoice complies with the relevant insurer’s requirements optimising accuracy and efficiency for the businesses involved.
Healthcode managing director
Peter Connor said: ‘The number of invoices is another measure of the strength of the private healthcare sector in 2024 with activity across all regions, settings and hospital specialties exceeding previous years.’
on the more complex conditions and chronically ill patients.’
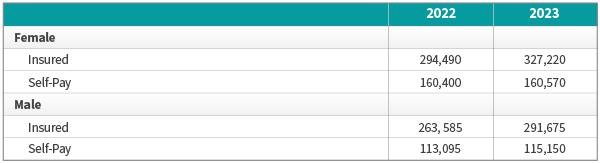
Figures from the data body released last month (June) show new records with more private inpatient admissions in 2023 than any year since recording began, beating the previous high in 2022. There are more insured and selfpay admissions than ever.
The total NHS England waiting list for procedures and appointments increased to 7.57m in April, up from 7.54m in March.
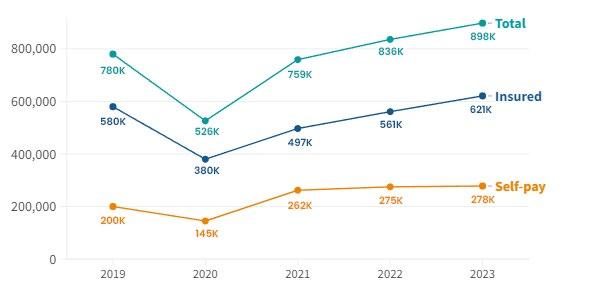
PHIN said there were nearly 900,000 admissions to private hospitals in the UK in 2023.
Admissions funded by private medical insurance rose above prepandemic figures for the first time.
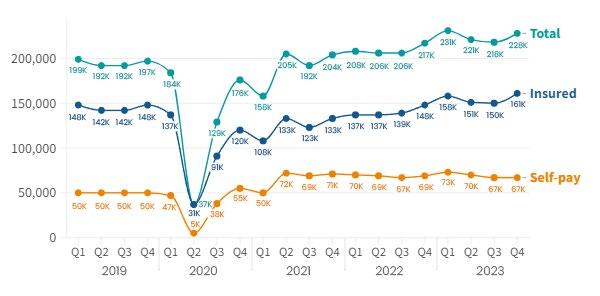
The largest peak came in the final
three months of 2023 when 161,000 private hospital admissions were funded this way. Insured admissions were 7% higher in 2023 than in 2019.
Self-pay admissions peaked in the first three months of last year (73,000 admissions) before reducing slightly but staying well above (39%) pre-pandemic levels.
Dr Gargan said the record figures showed the important role the private sector plays in the nation’s health, something acknowledged by the major political parties.
‘With NHS waiting lists at record levels, a growing number of people are looking for alternatives and choosing to use the private sector rather than risk prolonged waits and potentially seeing their health deteriorate.
‘The number of people using private medical insurance, or opting to self-pay for their procedure, has increased despite the difficult economic conditions over the past few years, demonstrating the importance people place on their health.’
See the full figures, starting on page 26
HEALTHCODE’S INVOICE ACTIVITY IN MAY SPECIALTY
Orthopaedics and trauma was the hospital specialty with the largest volume of invoices (63,000) which represented a year-on-year increase of 10%. Radiology was next with 49,000
The largest year-on-year increase was in oncology (31%) although the specialty was the 7th largest in terms of actual numbers (19,000). Radiology was second, up 27% year on year
The top ten hospital specialties posted year-on-growth of 6% (cardiology) or above
TREATMENT SETTING
Most invoices were from non-hospital settings, but both achieved year-on-year growth of 15% in May. Volumes for the year were 1.73m for hospitals and 3m for non-hospitals.
In hospitals, there was a 16% year-on-year increase for outpatient invoices and 9% for admitted patients.
COUNTRIES AND REGIONS
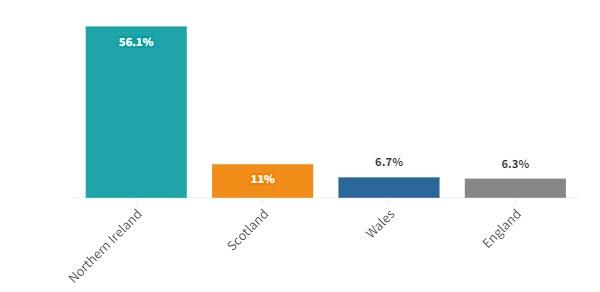
Hospital invoice volumes were up across all UK countries with yearon-year growth of 14% in England, 61% in Northern Ireland, 18% in Scotland and 15% in Wales
London saw the highest year-on-year growth (22%), but all the English regions saw average growth of more with 12% compared with May 2023
GOOD NEWS ON GROWTH 2
PHIN chief executive Dr Ian Gargan
Spire is first to get special CPR award
By Agnes Rose
Commitment to excellence in high-quality cardiopulmonary resuscitation training for thousands of its clinicians has earned Spire Healthcare an internationally recognised resuscitation quality improvement excellence award. It is the first UK and European healthcare provider, and only the third globally, to be recognised for the achievement.
The Resuscitation Quality Improvement (RQI) Excellence Award was presented by its Laerdal and RQI partner organisations.
Spire Healthcare partnered with Laerdal Medical four years ago to standardise basic life support resuscitation training across its 39 hospital and over 50 clinical sites in England, Wales and Scotland.
Two years later, it moved to a central resuscitation service with a new standardised strategy, which is nurse- and operating department practitioner-led. This approach enabled the standardisation and comparison of competence levels across all of Spire’s hospitals.
After a successful pilot of the RQI programme at Spire Cheshire
HCA
starts service for heart health
Consultant cardiologists at HCA UK have launched a new service to give patients a complete picture and better understanding of their cardiovascular health.
The HCA UK Heart Health Check, available at any of the hospital group’s diagnostic centres across London, includes all tests, scans and analysis and costs £995 with a consultant fee of £250-£300. It has been designed to give
Hospital, the e-learning cardiac arrest simulation training was extended across all the group’s hospital sites.
The RQI initiative has been taken up and completed by 6,268 clinicians, including consultants, and now offers the potential for expansion of training to all 16,800 of Spire’s clinicians.
All Spire clinical colleagues have 24/7 access to the online learning simulation sessions through quarterly, rather than annual, training cycles. The current compliance rate
patients peace of mind by identifying and then supporting them to lower their risk of serious conditions.
The service provides a comprehensive, personalised review of the patient’s heart health including over 30 speciality blood tests, imaging and heart rhythm analysis, and consultation time with a cardiologist.
Patients also receive an echocardiogram heart scan, an ECG to check for an abnormal heart rhythm and a score to access their future heart and stroke risk based on age, sex, blood pressure, cholesterol and smoking status. They are given a personalised plan for improving heart health.
SIMULATION-BASED LEARNING
Prof Lisa Grant, the group’s clinical director and chief nursing officer, said: ‘Laerdal Medical is a world leader in resuscitation initiatives and we are proud to be partnering to develop this innovative quality improvement programme that is improving patient safety outcomes for both our NHS and private patients alike.
‘Using a simulation-based learning platform that incorporates human factor training, ‘little and often’ training sessions measure and verify competence, helping colleagues retain those critical life-saving skills.
is 94% with an achievement of 98% competence in chest compressions and airway management.
The provider says this demonstrates extremely high clinical skill levels, leading to improved patient safety: ‘Nationally published inhospital cardiac arrest data reports cardiorespiratory occurrence rates are currently 1 to 1.5 per 1,000 hospital admissions.
‘Spire Healthcare’s comparative data is currently approximately 0.003 occurrences per 1,000 treatment care episodes, which is con-
‘This is a truly innovative QI programme for high-quality cardiopulmonary resuscitation. Spire’s central resuscitation team and our multidisciplinary hospital teams should be proud of their achievements and for helping to share their skills and knowledge with NHS colleagues.’
siderably lower than the national average.’
Spire’s central resuscitation team is also supporting and advising NHS trusts about the programme. Safety data generated during the programme is shared with other healthcare providers to help improve their own patient safety outcomes.
New BMA consultant chiefs carry on fight for better pay
Improving consultants’ pay in their NHS jobs is a major aim of the BMA’s consultants committee new co-chairs, anaesthetist Dr Helen Neary and psychiatrist Dr Shanu Datta, who take over in September from Dr Vishal Sharma.
Dr Datta said work to restore consultants’ pay and value was ‘far from over’ and both of them were committed to improving the way consultants were represented by the BMA in their workplaces.
‘This means promoting tools like the Consultants Charter to ensure
consultants have the best conditions locally and channelling the momentum we saw during industrial action into more local activism.’
Dr Neary added: ‘Vish has done an amazing job in the role over the last three years, leading consultants in England through successful industrial action to secure a pay deal this year and he hands over a strong foundation for us to now take the baton forwards on the path for pay restoration in England.’
Spire’s Prof Lisa Grant receives the Resuscitation Quality Improvement award from Laerdal’s Marco Grit (right) and James Buchanan
Spire to open new unit in Yorkshire
By Douglas Shepherd
Eighty consultants are looking forward to taking up new private practice privileges at a £13m development in North Yorkshire.
And the hunt is on for other doctors to join them at the new Spire Healthcare Harrogate Clinic where building work has commenced to transform office space in the town’s Hornbeam Park.
Specialists will be providing diagnostic services and local anaesthetic treatments for dermatological, ophthalmic, gynaecological and urology conditions, plus minor orthopaedic procedures such as hand, foot and ankle surgery, and general practice services.
The development will create 30 new jobs and is promising people across North Yorkshire faster access to GPs, to X-ray, ultrasound and MRI scans and to surgery not requiring an overnight stay.
A spokesperson told Independent Practitioner Today: ‘We have had a high level of interest from consult-
ants wishing to join the Harrogate clinic.
‘We are particularly interested to hear from consultants who practise in dermatology and gynaecology specialities and they can get in touch with Beverley.Macauley@ spirehealthcare.com who is leading consultant recruitment.’
GPs are also required.
It is planned to open the clinic’s doors in late 2024 and deliver up to 1,500 surgical procedures a year.
Helen Atkinson, Spire Healthcare’s clinics director, said the development was part of a network of ten new Spire clinics being developed in community areas across Britain.
‘Providing medical care in the community leaves our hospital colleagues at the nearby Spire Leeds, Elland and Methley Park Hospitals with the capacity to continue delivering more complex treatment for patients.’
New player eyes an
opportunity in London
The expansion of private ophthalmic clinics continues with the opening of global laser eye surgery provider EuroEyes in London’s Knightsbridge.
A clinical team led by Dr Fadi Kherdaji will also specialise in treatments to help patients suffering with myopia, presbyopia and cataracts.
EuroEyes International Eye Group has additional affiliate groups worldwide, including Hamburg, Berlin, Beijing, Copenhagen, Frankfurt, Hong Kong, Munich and Shanghai.
Nuffield Leicester’s super-accurate breast biopsy
Consultant breast and oncoplastic surgeons and their teams are singing the praises of recently introduced advanced technology to help them remove breast cancer tumours with precision accuracy.
Specialists at Nuffield Health Leicester Hospital are now using the Sentimag system which allows them to localise suspicious tumours for further analysis and also stage cancer.
It works in tandem with two types of cancer markers – the Magseed and the Magtrace lymphatic tracer.
The Magseed, a small metal seed about the size of a grain of rice, is placed into nonpalpable cancerous tissue to pinpoint the location of the cancer.
Previously, the standard of care for this procedure was called a guidewire, which can be
uncomfortable for patients and can also extend the time they spend in hospital.
The Magtrace lymphatic tracer, an iron-oxidebased liquid designed to assess the potential
spread of cancer to the lymph nodes, is injected into the breast any time up to a month ahead of surgery for sentinel lymph node biopsies.
This tracer liquid travels to lymph nodes that are most likely to be affected by cancer and marks those nodes for surgical removal. Once the node has been removed, it will then be analysed to assess if further treatment is needed.
The Sentimag system has been described as working like a metal detector on the skin’s surface to help locate the target tissue, marked by either the Magseed or Magtrace.
Mr Jaroslaw Krupa, consultant breast and oncoplastic surgeon, said: ‘The Sentimag system offers more precision and less invasive procedures which will benefit our patients and improve their quality of life after cancer surgery.’
An artist’s impression of the new Spire hospital in Harrogate, Yorkshire
Theatre manager Kerry Tannahill and clinical leader John Clements with the Sentimag system
Cheap beats efficacy when buying devices
By a staff reporter
Price is more important than longterm effectiveness when purchasing medical devices.
That is the finding of research from Bath University School of Management, Finland’s Aalto University School of Business and Erasmus University Rotterdam.
Researchers presented over 1,300 medical professionals, purchasing managers and general managers in the UK with a hypothetical choice between two pacemakers to bulk-buy: a cheaper basic model and a more expensive model with infection-reducing qualities.
In the experiment, participants were given a scenario in which they gained a personal bonus on cost savings if the cheaper device was chosen.
In this hypothetical situation, the researchers found purchasing managers chose the cheaper option without the increased
PPU WATCH
Compiled by Philip Housden
More private surgery in Surrey?
Consultants could have a new private practice opportunity with the opening of a new elective surgery centre at Ashford and St Peter’s Hospitals in Surrey.
The Surrey Heartlands Elective Centre, based at Ashford Hospital, fully opening this summer, includes a dedicated eye unit and facilities for orthopaedic procedures including hip and knee replacement surgery.
Ashford and St Peter’s Hospitals NHS Foundation Trust Board is considering using the unit to develop a competitive private practice option for the self-pay market.
effectiveness, while medical professionals did not.
Researchers have expressed concern by this finding because healthcare procurement in Europe is increasingly the responsibility of purchasing managers.
Aalto’s Prof Katri Kauppi, a coauthor of the study, said: ‘The results show it is important to align internal incentives for purchasing managers and medical
A board meeting report said any such private patient service ‘would be positioned in an ethical way, delivering a more affordable route to private treatment’.
A trust spokesperson told BBC Radio Surrey: ‘Any details on numbers and pricing have not been developed at this stage and any future development would be positioned in line with our ethical values and enable re-investment in our core NHS services.’
The spokesperson added that private operating is ‘an added tool for recruiting and retaining clinical talent’ and it may offer an opportunity to build a capability to re-invest in improvement across its full range of services and facilities across elective and emergency care.
In 2022-23, Ashford and St Peter’s reported private patient
professionals with the incentives of suppliers in a way that makes everyone strive towards healthcare effectiveness.’
Katie Kenny, another co-author and a doctoral researcher at Aalto University, added: ‘While not every purchasing decision is a matter of life and death, looking at price in procurement decisions has a human cost and indirect economic effects.’
income of £1.8m, a decline of £0.2m from £2.0m and -10.1% on the previous year, representing just 0.45% of total trust income.
On the move
Marcus Taylor, private care director at Buckinghamshire Private Healthcare Ltd – a wholly owned subsidiary of Buckinghamshire Healthcare NHS Trust – is leaving to be private care managing director at the Royal National Orthopaedic Hospital (RNOH), Stanmore.
He headed the Buckinghamshire service for two years, leading the transformation of private care services for consultants and supporting the trust to revitalise a strategic, income-generating and customer-centric service.
Mr Taylor said: ‘We have enjoyed many successes along the way, launching a fantastic brand, pro-
The researchers also found risksharing agreements influenced purchasing decisions.
In another hypothetical scenario, purchasers were offered the opportunity to share post-operation treatment costs with the manufacturer of the more expensive pacemakers if infections still occurred.
This made medical professionals more likely to choose the more effective device, but purchasing managers’ choices were unaffected.
Juri Matinheikki, a co-author at Aalto University, and chief specialist to the Ministry of Finance in Finland said: ‘Health benefits, including their economic importance in terms of labour inputs and tax revenues, should be better valued so they can be taken into account in procurement alongside short-term price savings.’
This research was published in the International Journal of Operations & Production Management
fessionalising our service provision and offering a convenient and responsive service for our consultants and growing our income by over 60% in the past year.
‘Bucks has a fantastic proposition for its patients and a development agenda that will take it to its full potential over the coming few years and is well on course for 2024.’
He added: ‘I am very excited about this new opportunity and how I can utilise my 20 years’ private healthcare experience and local market knowledge to deliver significant benefits for RNOH.’
Philip Housden (right) is director of Housden Group commercial healthcare consultancy
Eye group looks to expand further
A visionary consultants’ group set up by surgeon entrepreneurs has announced plans to partner with independent practitioners as it extends its brand to new sites beyond its South-east heartland Consultants behind the fastgrowing independent eye surgery provider OCL Vision have appointed a chief executive to lead a strategic expansion.
Mr Nik Rudge (pictured below) brings extensive leadership experience to the business gained from his experience running a series of global businesses in the international events industry.
The surgeon-owned company invested £5m in cutting-edge ophthalmic technology in 2023 and grew patient numbers by 45% at its Elstree clinic, Hertfordshire, and 32% at its Kensington clinic in the past year alone
Now Mr Rudge aims to use his experience, and the objectivity and clarity of an outsider’s perspective, to continue to drive operational and service excellence as well as technical innovation.
He explains: ‘I questioned
whether my work outside of healthcare would be transferable to what we do at OCL Vision; however, I now see the similarities.
‘At the heart of the business is the focus on delivering a seamless experience, ensuring we have a team that is clear on what we are trying to achieve and the importance of their role in achieving it and, above all, listening to our patients’ feedback to ensure they have the best possible outcomes.
‘As a newcomer to the UK healthcare sector, I am able to ask questions and challenge assumptions that an industry veteran might not and we are already seeing this impact positively for our patients, our team members and our shareholders.
‘OCL Vision’s 80-strong team are peerless at what they do – the 128% growth achieved in the company’s first five years and 2,500 positive patient reviews are testament to that – but even the best businesses can make further gains by questioning the status quo.
‘Clinical excellence and fantastic patient outcomes are the corner-
stones of what we do, and my first priority is to deploy more of the people and processes that make the entire patient experience seamless from first contact to surgery and aftercare.’
Launched in December 2018, OCL Vision bills itself as the only surgeon-owned, comprehensive private eye care group in England.
Last year, it held 12,000 patient appointments at its three purposedesigned clinics in London and Hertfordshire, with its Elstree clinic recording 45% year-on-year growth and its Kensington site growing patient numbers by 32%.
Almost 20,000 eye surgical procedures have been completed at OCL Vision to date.
In 2023 alone, the company invested £5m in medical technology and capital assets, giving its ten consultant surgeons access to ‘the latest and most advanced treatment options in the UK.’
In April it became one of the first clinics in the UK to perform a revolutionary new corneal replacement surgery called EndoArt.
In addition to corneal work, OCL
Boss experiences care at first hand
Vision offers a range of treatment options including laser, lens, retinal, glaucoma and oculoplastic procedures.
Mr Rudge sees the company’s goal as becoming ‘the number-one provider of personalised eye care in the UK’.
‘All our patients see a consultant surgeon who is a leader in their field right at the start of their journey, allowing them to choose a pathway that’s perfectly tailored to their needs.
‘We want them to feel confident in the exceptional care they will receive.
‘Looking to the future, we would like to offer the same exceptional care, and the transformative power of better vision, to more people.
‘We’ll be doing this in a number of ways: growing our existing clinics and expanding our footprint to new sites across the UK, as well as partnering with independent practitioners and helping develop a new generation of ophthalmic surgeons who share our values and aspirations.’
OCL Vision surgeon Ms Laura de Benito (left, inset) made her new chief executive a very happy man after giving him successful lens replacement surgery in June.
After 42 years of wearing glasses, the procedure gave him perfect vision for the first time in four decades.
Mr Nik Rudge says: ‘I had spent most of my life wearing glasses and was resigned to the idea that this is how it would always be. Now, for the first time, I can see clearly on my own; and my quality of life has been transformed.
‘The gift of sight is immeasurably precious and I feel privileged to be able to work every day with a team dedicated to offering it to more people.
‘I want to do all that I can to grow OCL Vision and to give as many patients as possible the opportunity to get the same benefits that I have experienced first-hand.’
Share views on training complaints handlers
Private healthcare providers who subscribe to the Independent Sector Complaints Adjudication Service (ISCAS) are being invited to give their views about how the organisation trains them.
Feedback is invited by email to the review project manager, John Munton, director of dispute resolution services at CEDR, the parent company of ISCAS, jmunton@ cedr.com.
OCL’s new chief executive Nik Rudge before ‘losing’ his glasses
HCA opens centre in the Docklands
Seventy consultants and GPs in private practice are among a team who will work at the newly opened £18m HCA Healthcare UK Canary Wharf.
The 20,000sq ft outpatient centre aims to meet the growing demand for high-quality private healthcare in convenient locations.
This is largely being driven by corporate workplace health schemes and the growth in private medical insurance paid for by employers.
Specialists will provide care across a range of medical special ties including health screens, cancer, cardiac, orthopaedics and women’s health.
Specialist fertility expertise is also being offered, because it is an area of growing demand as more employers look to incorporate fertility care into their health and wellbeing schemes
HCA Healthcare UK president and chief executive John Reay said: ‘The opening of this outpa-
tient centre reflects our confidence in Canary Wharf as a hub for businesses and we anticipate providing over 50,000 patient appointments in our first year alone.’
The company said services offered reflected a focus on preventative health and early detection in the corporate health sphere, with the availability of
same-day and in-person GP appointments alongside a full range of health screens designed to pick up health issues at the earliest opportunity.
HCA’s new centre is its third multi-million-pound opening this year following The Harborne Hospital, Birmingham, in January and announcements of women’s health centres in May.
Nuffield gets unique CT scanner
Patients with specialist health conditions are being scanned faster and more safely with two new innovative CT scanners at Nuffield Health’s Parkside Wimbledon and Cancer Centre London hospitals.
The Revolution Apex Elite CT scanner at Parkside Hospital can capture an entire image of the heart within just one heartbeat, meaning CT scans are safer for people with serious cardiac conditions and diagnosis is likely to be faster. It is the first installed at an independent hospital in the UK and only the second installed in England.
At Cancer Centre London, the SPECT CT scanner delivers a scan using a lower radiation dose, enabling people undergoing cancer
care or who have an underlying serious health condition to be diagnosed faster and more safely. It also includes a new generation Gamma Camera, which increases the detail of a scan.
Kate Farrow, health systems
Doctor calls for ban on unlicensed providers
A doctor specialising in anti-ageing and longevity is urging the Government to prioritise a ban on unlicensed cosmetic treatment providers.
Dr Dimitri Vichas (Dr Dimi), who runs the Nottingham-based Clinic Eudai, urged swift action as the number of treatments and unqualified practitioners soar.
He called it ‘a Wild West situation’ with no set training for beauty therapists and other nonprofessionals. ‘That elevates the risk from both an efficacy of treatment and safety perspective.
‘This isn’t about creating a monopoly. It is about ensuring the safety of patients – the doctor’s first priority.’
The SPECT CT scanner at Nuffield’s Cancer Centre London, with its radiography team and Kate Farrow, the hospital’s health systems director on the right
director at the hospitals, said: ‘Both CT scanners offer flexibility to clinicians and they enable us to treat and care for more patients from local communities, which demonstrates our purpose of building a healthier nation.’
PERFECT PITCH: Cleveland Clinic London is the new official healthcare provider of Middlesex County Cricket Club for 2024-25.
Dr Phil Batty, consultant in sports and exercise medicine, will provide medical support for home matches at Lord’s as part of the agreement.
The Independent Doctors Federation president is the club’s medical director and was head of sports medicine at Manchester City Football Club in 2011-2012, and senior team doctor for the England Rugby Team from 2012-2014.
Dr Dimitri Vichas
The reception at HCA Healthcare’s Canary Wharf outpatients centre
Your website has to obey the law
Independent Practitioner Today has run a host of articles from experts who help private doctors with marketing their business, especially on websites. But you need to tread carefully.
Here, medico-legal expert Dr Udvitha Nandasoma tackles the subject from a defence perspective and explains the importance of marketing and advertising your practice in an ethical and lawful way when designing a personal/practice website
Your website acts like a shop window, enabling people to see how your practice can meet their needs
THERE ARE a myriad of ways to promote your private practice; from the traditional word-ofmouth through to using online channels to communicate with both existing and potentially new patients.
An advantage of using online or digital marketing tools is that rather than pushing your message out where it may or may not be noticed, you can ‘pull in’ your target audience with high-quality content.
Your website acts like a shop window, enabling people to see how your practice can meet their needs.
What sort of content should I include?
Your practice website should have the right content and keywords. This will help your content to be found by search engines and mean that they move higher up in their list of results.
In turn, this makes the website more visible to patients searching for information or advice about a particular treatment.
If all you have is a simple ‘landing page’ with your name and a profile, patients are unlikely to find your site easily.
The exact content and structure you need to have will depend on the nature of your services and what is practical for your business, but here are a few tips to make your site patient and search-engine friendly.
➲
Be helpful. Think about the questions your patients typically have during appoint ments and try to answer them.
A ‘frequently asked questions’ section works well.
➲
Write in language they can understand and avoid jargon.
➲
Break up text into readable chunks , as a page of densely written copy is unlikely to be read.
➲ Highlight your unique selling points , like location, specific treatments or procedures offered by your practice, your experience and qualifications.
➲ Watch your image sizes. Slow page loading is frustrating for users and can hamper search engine rankings.
➲ Consider different types of content: articles, blogs, Q&As and videos will help broaden your appeal.
➲ What keywords are the most relevant search terms and phrases for your target audience? What will they be searching for? If you decide to do any paid advertising, you will need to list these keywords.
➲ Provide clear menus and links to other pages on your site to help with navigation.
➲ Make sure the site is mobile-friendly and test this during the build phase.
Other relevant information to include
It’s vital that websites include information about any updated procedures, what relevant changes have been introduced, and what to expect when patients contact you.
This information should be provided in a clear and easily understood way and should also be updated regularly to ensure it is current and accurate.
Your website should also include the following policies and information:
➤ A privacy policy in line with data protection law, setting out what personal data you collect, the lawful basis for collection, how data is processed and stored and patients’ rights;
➤ A cookie policy explaining what cookies you use and what they do. You must get consent before you place cookies unless they are strictly necessary for the site to work;
➤ Terms and conditions covering visitors’ use of the site – copyright notices,
disclaimers for third-party links and so on;
➤ Details of the practice complaints policy;
➤ Your professional qualification and the country from which it was derived;
➤ Your GMC number;
➤ The date the website was last updated.
Using patient photographs and testimonials
As the GMC’s Making and using visual and audio recordings of patients notes explains, ‘patients may avoid seeking medical help, or may under-report symptoms if they think their personal information will be disclosed by doctors without consent’.
Consequently, consent for the use of confidential patient information such as photographs or testimonials in marketing material should be contemporaneous and specific.
Patients need to understand precisely what information will be retained, displayed or published, where and when, who will see it and the likely consequences.
Even if the patient cannot be identified, their consent must still be sought.
The patient should not be identifiable unless absolutely necessary, even if the patient consents to the use of patient identifiable material.
The patient must know that they can withdraw their consent at any time and know how they can do so.
Should a patient withdraw their consent, you should have a system in place that allows you to change your website or promotional material in a timely manner.
Adherence to this requires that the practice maintains control of the information and, for that reason, particular care should be taken with online material, where this may be more difficult to monitor and enforce.
Complying with ethical and legal standards
You will be responsible for any marketing and advertising activity such as promotional information or patient communication.
There is detailed GMC guidance
Consent for the use of confidential patient information such as photographs or testimonials in marketing material should be contemporaneous and specific
– especially paragraphs 47-54 – on communicating information about your services, which places strong emphasis on providing accurate and realistic information to patients in a manner that does not risk exploiting a patient’s vulnerability or lack of medical knowledge.
In addition to this regulatory guidance and data protection law, you must also follow the standards and code of practice as published by the Advertising Standards Authority (ASA) and Committee of Advertising Practice (CAP).
For example, ASA requirements state that all advertisements must be legal, decent, honest and truthful. They must not mislead, harm or offend.
The ASA has the power to remove any advert that it feels is unsuitable and refer persistent offenders who advertise inappropriately to other bodies, such as Trading Standards.
Particular care must be taken with prescription-only medicines (PoM). Even simply referring to a specific medication in promotional material or even in a hashtag might risk that being considered an unlawful promotion of a PoM by the ASA. Take care to refer to the service –for example, weight management – as opposed to a particular medicine that might or might not be appropriate for a given patient. We advise our members to assess promotional material against the current guidance and standards and, if in any doubt, to contact MDU for specific advice.
See ‘Troubleshooters’ overleaf
Dr Udvitha Nandasoma (right) is head of advisory services at the Medical Defence Union
GROWING YOUR PRACTICE: MARKETING AND BUSINESS DEVELOPMENT
Marketing and development go hand in hand
Our troubleshooters Sue O’Gorman and Hannah Browning reply to private doctors’ questions
QI set up in private practice a few years ago and I am looking to develop the services at my practice but unsure as to what support I need to do this. I have heard colleagues refer to marketing their practice and others who talk about business development. What are the differences between the two and how could they help my practice flourish?
AAs a private practitioner in the current competitive environment, it is vital to understand how investing in marketing and business develop
ment can support your practice and what each of the disciplines offers.
So let’s break this down by demystifying their benefits and key differences.
Marketing
By definition, marketing largely focuses on promotion and advertising your services to attract new patients, build brand awareness and build a positive reputation in the community.
It should help you understand patient needs and how to best communicate the value of the service you offer to meet those needs.
Key activities
☛ Social media. Managing social media profiles to engage with your audience and share relevant content.
☛ Content marketing. Creating blogs, videos and electronic newsletters to provide valuable information and attract potential patients.
☛ Search engine optimisation (SEO). Enhancing your practice’s website to rank higher in search engine results.
☛ Branding. Developing a strong brand identity through logos, tone of language, values, service and visual design.
The level of marketing support you invest will, of course, depend upon your budget and all of the private hospitals will have inhouse teams who can guide you so long as you are prepared to do some ground work yourself and support them with delivering content ideas.
Provide any copy required in a timely manner and set aside time to update them of any new services you offer. The marketing teams will have hundreds of consultants to support and those who make the greatest effort will reap the rewards.
But marketing is not a ‘one hit
By leveraging marketing and business development simultaneously, you will create a sustainable and effective roadmap for continued success
Business development focuses on identifying, creating and pursuing new and strategic opportun ities for growth, cultivating commercial partnerships and identifying new markets for products and services.
It generally involves a broader scope of activities aimed at achieving long term sustainability and profitability.
Key activities will include:
➲ Market research. Looking at market trends, patient needs and the competitive landscape will inform your strategic decisionmaking.
➲ Service expansion. Identify and develop new services, territories or specialties that the practice can offer.
➲ Partnerships. Cultivate alliances with other entities to expand referral networks and service offerings. This could be hospitals, other independent practitioners or groups that add value to your existing service.
➲ Networking. Build solid and trusted relationships with other providers to attract referrals.
and thereby reduce any dependency upon a single revenue stream.
☛ Market positioning. Effective business development strategies will help to position the practice favourably within the industry and will enhance your competitive advantage.
☛ Long-term sustainability. By identifying growth opportunities and adapting to market changes, your business will remain viable and profitable.
So, to summarise: THE FOCUS
Marketing is patientcentric and aims to attract and retain patients through a range of promotional activities.
Business development focuses on opportunities for growth and expansion.
THE ACTIVITIES
Marketing includes advertising, content creation and online visibility.
explore new services and partnerships, ensuing sustained growth and diversification.
wonder’ and should be a continuous process of evolution whose benefits, when done well, include:
➤ Increased visibility. By raising awareness of your practice with key customer groups and making you more accessible to potential patients.
➤ Patient engagement. Helps to foster stronger relationships and can encourage loyalty.
➤ Patient acquisition. By highlighting your services and expertise, you will attract new patients.
➤ Reputation-building. Trust and credibility is of utmost importance to patients, and consistent and positive marketing efforts will help to build this.
Marketing and business development work best hand in hand. They need each other to succeed and a question we often get asked is: ‘What exactly do business development people do?’
To re iterate, when combined with robust marketing efforts, here are some of the key benefits a business development strategy will bring to your practice:
☛ Revenue growth. The Holy Grail! Business development activities can lead to increased patient volume and higher revenues through new partnerships and services.
It is important to note that this can take time and unlike the transactional process of sales, business development is a strategic process, identifying the most effective ways to grow your business and build partnerships for sustainable growth.
There is no magic wand, onesize fitsall approach and should be viewed as a longer term commitment.
☛ Diversification. Expanding your range of services can attract a new and wider range of patients
Business development includes service diversification, market research, commercialisation, networking and partnerships. It may also explore operational and financial elements of the business.
THE TIME-FRAME
Marketing usually yields more immediate results in terms of patient engagement and acquisition.
Business development typically involves longerterm strategies that gradually but solidly build the practice’s reach and capabilities.
What will combining a marketing plan with a business development strategy offer your practice?
Initial growth: Marketing may quickly bring in new patients and increase your visibility and provide a steady stream of patient volume.
Strategic expansion: Business development activities will then build upon these foundations to
Patient retention: Ongoing marketing efforts will help to maintain communication and relationships with your patients, while business development opportunities will keep your practice relevant and competitive. So, in summary, while both marketing and business development present distinct benefits and advantages for practice growth, by leveraging the two simultaneously, you will create a sustainable and effective roadmap for continued success.
Sue O’Gorman is director of Medici Healthcare Consultancy. Website: www.medicihealthcareconsultancy. co.uk. Email: sue@medicihealthcareconsultancy.co.uk.
Hannah Browning is director of Beyond Excellence Healthcare Consultancy. Website: www.beyondexcellenceconsultancy.co.uk. Email: info@beyondexcellenceconsultancy. co.uk.
Sue O’Gorman & Hannah Browning
DATA BREACHES
What to do to protect patient data
Recent findings from leading UK data breach law firm Hayes Connor – see Independent Practitioner Today last month – have put the spotlight on the healthcare industry, which has been the leading offender in terms of data breach incidents.
Solicitor Richard Forrest emphasises the importance of robust security protocols to protect against both cyber threats and human error within the health sector
Doctors and healthcare professionals are particularly susceptible to data breaches due to the nature of the information they handle
ANALYSIS OF the Information Commissioners Office’s (ICO’s) 2023 data showed that the health sector accounted for a staggering 17.42% of all data breaches in 2023, making it the most frequent violator of all sectors.
This is particularly alarming, as it indicates a consistent trend, with health data breaches making up approximately one in every five reported incidents annually since 2019.
In 2023, basic personal identifiable information was the most common data type compromised, comprising 73.21% of breaches in the health sector. Exposed health data, unsurprisingly, followed closely at 61.66%.
Concerningly, almost one-infive total breaches involved children’s data, with 142 specific cases in the health sector in 2023, raising significant concerns about the safeguarding of vulnerable groups.
The primary cause of breaches was unauthorised access, constituting 18.70% of health sector incidents, followed by emails being sent to the wrong recipient, at 16.22%.
Under the General Data Protection Regulations (GDPR), which came into effect in 2018, organisations are required to report data breaches within 72 hours. Failure to comply not only results in hefty fines –potentially up to £17.5m or 4% of global turnover – but also damages trust and credibility.
It is concerning that 43.88% of health sector breaches were reported beyond this critical timeframe in 2023.
Significant repercussions
they manage and protect personal data against emerging cyber threats and human error.
Doctors and healthcare professionals are particularly susceptible to data breaches due to the nature of the information they handle.
Healthcare records are densely packed with sensitive personal, medical and financial data, increasing the risk of both accidental and malicious breaches.
The healthcare environment also presents unique challenges, such as high workloads and stress, which can lead to errors in data handling. Lack of understanding surrounding the importance of data protection and the myriad ways data can be breached is also a key factor.
Additionally, healthcare systems often involve complex technologies that might not be user-friendly or fully secure, particularly if they are outdated.
The frequent necessity to share patient information among various stakeholders – doctors, specialists, insurers – multiplies the risk of a data breach occurring.
While healthcare workers are highly trained medically, they might lack thorough training in data security, further elevating the risk of mishaps.
Here are some practical tips for independent practitioners looking to safeguard their practices.
Employee training
You should conduct regular training sessions to ensure that all staff are aware of data protection principles and know how to handle sensitive information securely.
Regular audits and updates
Keep security systems up to date and conduct regular audits to identify and address vulnerabilities.
Appoint a data protection officer
Depending on the scale of data processing activities within a practice, it may be advisable to appoint a data protection officer (DPO). This person would be responsible for overseeing data protection strategies and compliance with GDPR requirements.
Design an incident detection and response plan
Establish and maintain an effective breach detection, investigation and internal reporting procedure.
This is critical for ensuring that any data breaches are identified swiftly and that necessary notifications are made to both the supervisory authority and the affected individuals within the required 72-hour time-frame.
Data minimisation
Only collect and retain the minimal amount of personal data necessary for your operations. This not only complies with GDPR principles but also reduces the impact of a potential breach.
The continuous high rate of data breaches in the health sector underscores an urgent need for enhanced vigilance and improved compliance strategies.
The recent ICO trends portray a continuous need for vigilance and updated compliance strategies from businesses, especially in how they manage and protect personal data against emerging cyber threats and human error
Since 2019, the ICO data shows how organisations across all sectors are still failing to implement effective security protocols, leaving personal data vulnerable to breaches, which have significant legal and financial repercussions for the entities involved.
Despite regulatory advancements and the introduction of stricter compliance mechanisms, the rate of data breaches remains a serious concern.
The recent ICO trends portray a continuous need for vigilance and updated compliance strategies from businesses, especially in how
This includes understanding the rights of data subjects, the importance of data security and the procedures for identifying and reporting data breaches.
Access controls
Implement strict access controls and user authentication to minimise the risk of unauthorised access. Regularly review who has access to sensitive data and adjust permissions as necessary.
Secure communication channels
Utilise secure systems for communicating sensitive information. Avoid using unencrypted email for transmitting personal data.
By adopting stronger data protection practices and fostering a culture of security, healthcare providers can better protect their patients’ information and avoid the severe consequences of data breaches.
Independent practitioners must take pro-active steps to ensure that they are not only compliant with legal standards, but are also doing their utmost to protect the personal data entrusted to them.
Richard Forrest is legal director at data breach experts Hayes Connor
Learn from errors and don’t cover up
Listening, leading and learning. David Hare (right) reflects on the Independent Healthcare Providers Network’s joint Patient Safety Conference with the Care Quality Commission
AS THE representative body for independent healthcare providers, it is a real highlight in IHPN’s calendar to host our annual joint conference with the Care Quality Commission (CQC) looking at all things patient safety and quality.
The theme for this year’s event was the ‘Culture of Care: Listening, Leading, Learning’.
More than 120 chief medical and nursing officers and safety and quality experts from the sector had the pleasure of hearing from a wide range of speakers from across the patient safety landscape, from clinicians and regulators to researchers and patients.
We kicked off the day with the director of secondary and specialist care at the CQC, Nicola Wise, who talked through the watchdog’s progress in implementing its new single assessment framework.
Five key questions
Like its predecessor, this is based on the five key questions and ratings system and will be supported by improved technology. This means that physical site visits by the CQC will now be used for specific purposes such as observing care, understanding how staff interact and what the environ -
ment is like, to name just a few, rather than being the default. It is not without controversy, and we have heard from members and those that work in the sector about some of their challenges around this – particularly through the provider portal and the removal of the relationship manager role.
However, there was a welcome reassurance from Nicola that sorting these issues is a priority and that the CQC will continue to work with the independent healthcare sector through the IHPN to ensure private providers and practitioners are confident of the new approach.
Later on in the day, the CQC’s chief executive Ian Trenholm gave his reflections on the CQC’s wider strategy and some of the complexities of regulating health and care services in such a challenging operational environment.
How do you assess a facility that is providing excellent care but, due to rising waiting lists, the ability of patients to actually access it is poor?
And how do you balance the role of a regulator as a judge versus a coach – acknowledging their role in spreading best practice and scaling up innovation but equally understanding they are ‘not in the management consultant business’ and cannot directly implement change.
Also, how can tackling health inequalities be assessed when you cannot inspect an outcome.
Surgical mesh victim support
While understanding the regulatory environment that we operate in is obviously important, healthcare, of course, begins and ends with the patient.
We were therefore so pleased to be joined by Paula Goss, who is a campaigner for people who have been injured by surgical mesh and is the founder of Rectopexy mesh victims support.
You could hear a pin drop in the room as Paula spoke of her experiences of being injured by surgical mesh. She talked not just about the physical impacts, but the psychological and financial ones as well.
Communication with patients is so important – both in terms of practitioners ensuring there is
How do you assess a facility that is providing excellent care but, due to rising waiting lists, the ability of patients to actually access it is poor?
informed consent, with patients well equipped to ask the right questions, as well as the need to not just listen to patients but really hear them and ensure their concerns are acted upon.
Paula’s remarks really set the tone for the rest of the day.
Following her session, members had the opportunity to hear from the Patient Safety Commissioner Dr Henrietta Hughes, who talked through her key priorities in the coming year.
These include implementing Martha’s Rule* across the health system, and the importance of working with other patient safety bodies to ensure there is a joinedup approach in what can seem like a very crowed safety landscape.
Private sector and the HSSIB
Indeed, a new player in the patient safety world is the Health Service Safety Investigations Body (HSSIB) whose role is to investigate incidents where there are implications for the safety of patients. Its remit has expanded to investigate all healthcare services in England, including the private sector.
Interim chief executive Rosie Benneyworth talked through the key investigations the organisation is currently undertaking including ‘Workforce and patient safety – temporary staff, the digital environment, primary and community care co-ordination’ and safety management systems.
The aim is to understand how a wide range of sectors tackle these issues and share insights and information across the whole healthcare system.
In the afternoon sessions, we took a look at the vital role of healthcare staff themselves in fostering a culture of safety and learning.
National Freedom to Speak up guardian Jayne Chidgey Clark looked at the importance of having open cultures so staff can feel they can speak up not just about safety issues, but equally about issues of improvement.
A fascinating discussion with members also took place about how it feels for leaders to be on the receiving end of ‘speaking up’ and the importance of ‘listening with fascination’ and not taking the defensive stance.
Spire’s Erica Bowen built on this theme and outlined how the hospital group had fostered a ‘ward to board’ approach to speaking up with the need for all parts of the organisation to be ‘clinically curious’ and not ‘comfort seek’ when it comes to safety matters.
The importance of the ‘top of the office’ embracing the speaking up agenda was also highlighted and the need to be explicit about what action has been taken in response to staff concerns.
We then ended the day with some brilliant academic insights from the brains of the industry.
What patients can tell us
Prof Jane O’Hara from The Healthcare Improvement Studies (THIS) Institute at Cambridge University showcased her research on ‘What can patients and families tell us about safety, and why should we care?’
All too often, there are cases of patients and families not being sufficiently involved in investigations despite, in fact, being the only people there across the journey.
Not only are you therefore missing the opportunity to fact check and gain new insights, but also the opportunity is lost for those involved to ‘heal’ and understand what went wrong.
Jane has worked on some fantastic resources on how to meaningfully engage with patients and families, which I would recommend all those in the sector to look at.
Another brain from the sector was HSSIB’s senior safety investigator Saskia Fursland who presented the case on ‘Learning from errors and mistakes – retained swabs following invasive procedures’.
While this took place in the
A new player in the patient safety world is the Health Service Safety Investigations Body whose role is to investigate incidents where there are implications for the safety of patients
NHS, there were key take-aways for all parts of the health system. These included the often overreliance on serious incident reports in making predominantly ‘peoplefocused’ recommendations – such as surgical check-lists.
They have a limited application of a systems-based approach to investigation which look at the more complex and interrelated system factors at play in avoiding future incidents.
We finished the day with our sponsor, legal services company Bevan Brittan. While looking specifically at how healthcare providers can use incidents and inquests as an opportunity for pro-active learning and improvement, the presentation really summed up the day nicely around how to develop the right ‘culture of care’. This included being as open and inclusive as possible in any investigation and really getting people’s buy-in to the process. This often involves something as simple as a ‘thank you’, asking open questions ‘with curiosity’ and always seeing incidents as learning opportunities where patient care can be improved, rather than failures.
There was so much for both practitioners and providers to take away from the day, with a clear steer to listen with fascination, don’t comfort seek and ask questions with curiosity.
And remember that patients are unique – they are you, me, our families and friends. Keep this in mind as a practitioner and you can’t go too wrong.
* Martha’s Rule – see the implications for independent practitioners on page 20
David Hare is chief executive of the Independent Healthcare Providers Network (IHPN)
When patients want a second opinion
There are some practical steps private practitioners may wish to consider in light of Martha’s Rule, which was implemented in around 100 NHS trusts in England in April this year. Dr Sabira Hughes (below) reports
IN AUGUST 2021, 13-year-old Martha Mills presented to King’s College Hospital in London following a bicycle handlebar injury to her abdomen.
She was admitted to a paediatric ward and was initially treated for her pancreatic injury. She developed infective symptoms and her condition deteriorated over ten days. Martha died of sepsis on 31 August 2021.
It is reported that Martha’s parents watched Martha deteriorate; that they felt powerless to challenge the treating team who did not escalate her care to HDU/ITU at critical points; and that their concerns were dismissed by treating clinicians.
Further, it is reported that their fears over lack of close monitoring of Martha’s condition were magnified – and borne out – by reduced staff arrangements over the August bank holiday and that they felt powerless to ask for an independent review or second opinion. Above all, they will have to live with the trauma of having watched their child die of sepsis, coupled with the devastating evidence obtained as part of the inquest that, had those critical points of referral and treatment been made, her death would have probably been avoided.
Martha’s Rule
In April 2024, the culmination of Martha’s parents’ and patient safety organisations’ campaigning was implemented as ‘Martha’s Rule’.
It is a patient safety initiative which has invited at least 100 NHS trusts to support patients, families and NHS staff to have access to a rapid review from an independent critical care team 24 hours a day where they have concerns about a patient’s condition.
It will be implemented in some acute NHS sites in England that already have critical care provision. The aim is to minimise avoidable deaths and to change a culture of reluctance to speak up or respond to concerns about an acutely ill patient.
Martha’s Rule has three elements:
1All staff in NHS trusts must have 24/7 access to a rapid review from a critical care outreach
team whom they can contact if they have concerns about a patient.
2
Patients, families, carers and patient advocates must also have access to the same rapid review. Martha’s Rule will be advertised and reviews will be independent from treating clinicians.
3
There should be a daily structured and documented approach to noting information from patients and their families about the patient’s condition.
Potential impact on private practitioners
There is no obligation for private providers to implement any changes arising from Martha’s Rule. However, there could be implications for private organisations and practitioners.
If Martha’s Rule has the effect in the NHS that is hoped for, there could be a positive culture change surrounding raising concerns.
That could affect your work in the private sector: the expectation may be that private treatment should be even safer than in the NHS and one may see a more assertive stance taken by patients, family members or other staff members in raising patient safety concerns.
Generally, private practitioners and organisations are risk-averse. One could say that there is less concern about escalating for a further review in the context of a closely monitored private patient.
However, critical care support may be less readily available in the private sector. The general approach is that, if a private organisation
KEY POINTS
Adopting the principles of Martha’s Rule could play a role in influencing patients’ decision regarding their choice of provider
does not have acute or critical care facilities and a patient deteriorates, there is a transfer to the NHS setting for emergency or urgent treatment.
That is an independent second opinion by default, as the NHS team provides a fresh independent review and takes over care. In that case, what will Martha’s Rule change for private patients, and why raise the issue?
Patients are likely to choose private care based on cost, timing of care and high-quality care, but also re-assurance about a positive culture of patient safety. Adopting the principles of Martha’s Rule could play a role in influencing the decision regarding their choice of provider.
However, the escalation plan may need to be modified depending on the organisational set up and consideration will need to be given to the messaging for patients, so as not to be misleading.
Perhaps the most important consideration for the individual practitioner is to listen when concerns are raised, particularly if they are raised more than once.
Stop and re-assess the situation and consider whether anything is
➱ continued on page 22
☛ As of April 2024, Martha’s Rule is being implemented in some acute NHS settings. Private patients may now expect the same or better patient safety messaging within the private sector.
☛ There may be more questions raised about your care of a private patient – from patients, family members and colleagues also. Alternatively, you may have real concerns about a colleague’s private patient. The GMC’s Good Medical Practice supports you in deciding what action to take in these scenarios, and if in doubt, speak to your medical defence organisation.
☛ Work with your organisation and colleagues in the private sector –ensure you are all aware of the organisational position regarding Martha’s Rule and how it may impact your practice in private sector.
being missed. Taking the extra time and approaching with an open mind may save a life.
PRACTICAL CONSIDERATIONS
Pre-treatment discussions:
As part of your early pre-treatment advice, explain your usual process if patients or their families have any concerns, including:
Written contact information in the case of emergencies;
Clear red flag advice;
Clear handover and delegation to other clinicians;
Demonstrate that you understand that raising concerns will not be viewed as a criticism of your care and that it is something you also encourage to ensure patient safety;
Arrangements for accessing a second opinion – or transfer –where one is requested or is considered a prudent step in the ongoing care delivered;
Fee arrangements: This should be clarified with both the patient and the private provider as to the cost implications, if any, on requesting an urgent/emergency or routine second opinion in the context of concerns about treatment raised by a patient, their family or another colleague within your organisation.
Organisational clarity
Work with your private organisation, where relevant, and your colleagues within the private sector to adopt a position on Martha’s Rule, as it may impact on your organisation or private practice. Start discussions now about how to best promote encouraging patients, their family members or colleagues within the organisation to request a second opinion or independent review in the face of any patient safety concerns.
This may not be straightforward, but it is important that there is organisational thinking about it now. This will minimise the risk of difficulties in the future, if – as it is hoped – that Martha’s Rule becomes culturally embedded within the NHS.
Patient safety advice
Your medical defence organisation (MDO) can advise you on the GMC’s Good Medical Practice 2024 (GMP) requirements to support patient safety in your clinical work
and the GMC’s standards for raising concerns.
Your MDO can support you in responding to any medico-legal processes arising from your clinical work.
It is difficult to find an aspect of GMP 2024 that does not apply to the Martha’s Rule principles: providing good clinical care; treating patients with kindness, courtesy and respect; communicating with those close to a patient; contributing to a positive working environment, to name a few.
But the two key elements that are fundamental to Martha’s Rule are:
1
The patient’s right to a second opinion
GMP guidance in Decision Making and Consent at paragraph 13e explains the information that clinicians should give their patients.
It states that information that might be relevant should be shared with patients, including their right to seek a second opinion.
2 Raising concerns
It is essential that clinicians are familiar with how to raise concerns effectively by communicating concerns in a professional
Stop and re-assess the situation and consider whether anything is being missed. Taking the extra time and approaching with an open mind may save a life
tone and escalating, if necessary, in a step-wise manner within an organisation.
As in Martha’s case, it can be a tragedy when people stay silent in the face of patient safety concerns. It is a part of your professional obligation to raise concerns and your organisation should support you in doing so, however difficult this may be.
Dr Sabira Hughes is a medico-legal consultant at Medical Protection
IT APPLIES TO DOCTORS TOO
The two key elements that are fundamental to Martha’s Rule are:
1. THE PATIENT’S RIGHT TO A SECOND OPINION
The GMC’s Good Medical Practice guidance in Decision Making and Consent at paragraph 13e explains the information that clinicians should give their patients. It states that information that might be relevant should be shared with patients, including their right to seek a second opinion.
2. DOCTORS RAISING CONCERNS
It is essential that clinicians are familiar with how to raise concerns effectively by communicating concerns in a professional tone and escalating, if necessary, in a step-wise manner within an organisation. As in Martha’s case, it can be a tragedy when people stay silent in the face of patient safety concerns. It is a part of your professional obligation to raise concerns and your organisation should support you in doing so, however difficult this may be.
Perhaps the most important consideration for the individual practitioner is to listen when concerns are raised
Practice management made simple.
Make the work... flow.
Effectively manage and grow your private practice with iMedDoc.
Mobile app
Cloud based
Patient por tal
Integrated billing
Integrated digital dictation
I ’ ve been using iMedDoc for nearly 10 years and in that time I have been thoroughly impressed with every aspect of the plat form . The functionality is great . I couldn’ t ask for more!
–
Mr. Subhasis h Sengupta C onsultant G as troenterologis t
Keeping it simple is key to better health
WHEN THE GMC’s latest Good Medical Practice guidance 1 came into effect earlier this year, it incorporated updates to the section on ‘Promoting patient-centred care’, which included:
➲ ‘You must listen to patients and encourage an open dialogue about their health, asking questions to
allow them to express what matters to them’ (paragraph 29)
➲ ‘You should check patients’ understanding of the information they’ve been given, and do your best to make sure they have the time and support they need to make informed decisions if they are able to’ (paragraph 31).
Making sure patients understand the information that we give them is key to an effective doctor-patient partnership and achieving the health outcomes that matter most to them.
At Bupa, we often find that the root cause of patients’ comments in our hospital inpatient survey
Good communication between doctors and patients is vitally important. However, writing well for patients does not always come easily, particularly as it is so different to writing for clinical purposes, explains Dr Ravi Lukha (right)
can be traced back to how they are communicated with and not feeling sufficiently involved in decisions about their care.
This can be a challenge because, according to NHS Workforce, training and education, 2 7.1m adults read and write at or below the level of a nine-year-old in the UK and, critically, 43% of adults do not understand written health information.
So, we need to make sure that we pitch our information at the right level for patients.
Research from the Government Digital Service 3 also supports a simpler approach. It found that people with higher literacy prefer plain English because it allows them to understand information more quickly – they often have more to read and in less time.
Clear communication
In July 2023, the Financial Conduct Authority’s new Consumer Duty regulation came into effect. This sets higher and clearer standards of consumer protection across financial services.
It requires companies to put their customers’ needs first and make sure they receive clear, transparent communications. This helps customers make informed decision about financial products and services and ensures good outcomes.
As part of preparing for the introduction of Consumer Duty, Bupa reviewed, rewrote and updated thousands of customer communications.
We tested our customer communications – another requirement of Consumer Duty – and used feedback to improve them. We also worked with external partners to help us communicate more clearly.
For example, through our partnership with Plain Numbers, an organisation which helps businesses display numbers more clearly, we recently became the first health insurer to achieve Plain Numbers certification on key customer communications.
Certification means a communication has been assessed by Plain Numbers and has reached a high standard of clarity in the way numbers are communicated to customers.
We also worked with the Plain
The way we talk to people changes the way they feel about us. Keeping our language simple, confident and warm means people are more likely to respond positively to us
approachable, while addressing their concerns and it means they’re less likely to need to contact us again.
Speak human
Economist and Nobel laureate Richard Thaler once said ‘If you want to get people to do something, make it easy. Remove the obstacles.’
This is especially true when we are communicating with patients who may be anxious and struggle to take in everything we say.
Healthcare is full of jargon and medical terms which may be meaningless to patients. We can show empathy by using language that we know people will understand
English Campaign to achieve Crystal Mark accreditations for several key customer communications, including our health insurance policy guide.
This is a seal of approval that a communication has reached a high standard of clarity regarding language and layout.
So, what did we learn along the way to achieving these accreditations? Here are some simple steps that can be easily implemented to make sure communications are as clear as possible.
Think about tone of voice
The way we talk to people changes the way they feel about us. Keeping our language simple, confident and warm means people are more likely to respond positively to us. Language is especially important when we are writing, as our intended audience can’t see our faces or hear our voices.
For example, instead of this formal, cold and transactional apology:
‘Please accept my apologies for any inconvenience caused by the alteration to your appointment time. As a gesture of goodwill, if you can send me your receipts, your travel costs will be refunded.’
We can express the same thing using a warmer tone that gets straight to the point:
‘I’m sorry we didn’t let you know about the last-minute change to your appointment time. We’ll pay for your additional travel costs. Send us your receipts and we’ll refund you right away.’
When we use this approach with our patients, it gives them information and shows we are listening and understand. It demonstrates that we care and makes us more
By using everyday words and verbs rather than nouns, we sound more approachable and authentic. We can also help achieve this using inclusive language – such as ‘we’re’ instead of ‘the hospital is’.
Healthcare is full of jargon and medical terms which may be meaningless to patients. We can show empathy by using language that we know people will understand.
For example, instead of using the medical term ‘knee arthroplasty’ use ‘knee replacement’, as this is the term everyone understands.
Or instead of using the medical terms of body parts, use the everyday terms that we know people will understand.
Keep it short
Too much information can get in the way of action, so keep it short and to the point. That does not mean leaving out important information; it means saying everything your audience needs to know, and no more.
In written communication, keep your longest sentences to no more than 20 words and balance them with shorter sentences, as this makes it easier to read.
Use verbs instead of abstract nouns; for example, ‘as we discussed’ rather than ‘following our discussion’.
Help patients navigate through written communications by putting your most important point first, as this is more likely to be remembered, and repeat it at the end, especially for long documents.
And make sure your writing follows a logical order. Plan what you want to say and think about it in the most sensible order that makes things easy for the patient.
Don’t forget about numbers
As with words, do not use more numbers than you need to, so make sure all those you include really matter.
Think about the order in which numbers appear. What does the customer want to know first? Then create a story to explain it; for example, ‘Your check-up costs £x for x and y tests’.
Use the actual figures rather than percentage; for example, ‘You’ll need to pay £15’ instead of ‘You’ll need to pay 8% of the total’. Find ways to replace numbers; for example, two million or 2m instead of 2,000,000; or 7 April 2022 instead of 07.04.22 in dates.
Conclusion
With some simple changes, we can make our communications more accessible to all our patients, irrespective of their literacy level. The benefits of effective writing skills extend far beyond the obvious. For example, by considering the patient’s perspective, we understand more about them, enhancing empathy and offering greater opportunities to more effectively support them.
References
1. Good Medical Practice 2024 (www. gmc-uk.org/professional-standards/ good-medical-practice-2024/get-toknow-good-medical-practice-2024), GMC.
2. Improving health literacy. NHS England, Workforce, training and education (hee.nhs.uk).
3. Writing well for specialists (www. gov.uk/guidance/content-design/ writing-for-gov-uk#writing-specialists), Government Digital Service.
Dr Ravi Lukha is medical director at Bupa UK Insurance
Record number of patients treated
Statistics gathered by the Private Healthcare Information Network (PHIN) show private healthcare is riding high
CONSULTANTS PROVIDING private healthcare have, as expected, helped set new records for the number of patients being treated.
There were more private inpatient admissions in 2023 than any year since records began, beating previous record high in 2022.
And the Private Healthcare Information Network’s (PHIN’s) figures in its latest market update also confirm insured and self-pay admissions are at their highest levels ever.
The number of consultants active in private practice is at its highest level since the pandemic.
Here are the key trends compiled and provided by PHIN.
PRIVATE HEALTHCARE SECTOR MARKET ACTIVITY
AT A GLANCE 2023 v 2022:
Private admissions up 7% across the UK;
Self-pay admissions up 1% and at highest level ever;
Private medical insurance admissions up 11% and at record levels;
Second year in a row with admissions at above pre-pandemic levels;
2022 had previously been a record year.
2023 v 2019 (pre-pandemic)
Private admissions up 15% across the UK.
Self-pay up 39%.
Insured admissions up 7%.
Record independent healthcare inpatient admissions in 2023
The total number of admissions in 2023 was 898,000 (7% above 2022), meaning the private sector had more admissions than in any previous year on record.
Although Q4 2023 reflected the annual pattern and was 5% above the equivalent quarter in 2022, with insured admissions up 9%, self-pay admissions were down slightly (2%).
For the year as a whole, the number of admissions rose in Northern Ireland by 56%, the highest increase by far of any nation. Wales (7%), Scotland (11%) and England (6%) all grew at similar levels.
➱ continued on page 28
The free and integrated digital prescribing platform for all private prescribers.
CloudRx take care of the dispensing, payment and delivery of medicines direct to your patients, wherever in the country they may be, for more convenient access to their medicines.
TRANSFORMATIONAL
Order prescriptions at the touch of a button to add a whole new level of convenience for your patients.
SIMPLE, CONVENIENT AND SECURE
Simple and fast digital prescribing.
Legal paperless prescriptions, repeat prescriptions and controlled drugs.
Prescriber fees can be charged to the patient if required.
INTEGRATED
Our API enables frictionless integration with healthcare brands & clinical software including Semble, WriteUpp, MidexPRO, eClinic, Pabau and ClinicYou
“We were struggling to keep up with the admin side of the prescriptions, not to mention storage for medication to cope with a huge increase in prescriptions. CloudRx immediately took away the strain. Since our partnership we have grown by more than 200% in size. We could not have achieved this seamless scalablity without them.”
– Dr Louise Newson, Newson Health
PRIVATE MEDICAL INSURANCE AND
SELF-PAY ADMISSIONS AT RECORD ANNUAL LEVELS
Insured admissions
The number of admissions paid for with private medical insurance was at the highest level ever in Q4 2023, contributing to the record annual figure.
There were 13,000 more insured admissions than in the same period in 2022 (9% up) and across the year there were 60,000 more insured admissions than in 2022 (11% increase).
Compared to 2022, the number of admissions using private medical insurance rose in every English region – 11% for the whole of England. They also rose in Scotland (13%), Wales (1%) and Northern Ireland (17%).
The biggest rises for insured admissions in England came in the East Midlands (14%) and London (12%). The largest rises by volume were in London (23,800) and the South-east (8,600) followed by the East of England (6,700).
Self-pay admissions
Self-pay admissions dropped by 2,000 (-2%) in Q4 2023 compared to Q4 in 2022. This small decline by quarter was not reflected in the annual total, which was higher than 2022, largely thanks to the record levels in Q1 2023. Overall, self-pay admissions were up by 3,000 (1%) across the year.
In 2023, admissions financed by self-pay fell in every English region compared to 2022 levels, except the East of England (4%) and the North-east (5%).
The biggest percentage fall in England came in the East Midlands (-7%) and the North West (-7%). London and the North-west had the largest fall by volume.
Self-pay continued to grow in the devolved nations in 2023: Northern Ireland (+144%), Scotland (+8%) and Wales (+11%) were all above 2022 figures.
The number of admissions paid for with private medical insurance was at the highest level ever in Q4 2023, contributing to the record annual figure
Top ten procedures UK (2022 v 2023)
The biggest increases by volume in admissions in the top ten procedures were for diagnostic upper-GI endoscopies.
These increased by 3,595 (9%). The next biggest volume increase was in ‘diagnostic colonoscopy –bowel’ at 2,955 (9%).
The biggest decrease was in cataract surgery which was -5,615 (7%). Therapeutics – chemotherapy were also down (5.5%).
MARKET TRENDS FROM 2022 TO 2023
When looking beyond just the top ten procedures, there was a 99% increase in peripheral nerve blocks – a type of regional anaesthetic –but a fall (-25%) in spinal injections.
Three types of cosmetic surgeries – rhinoplasty (-16%), septorhinoplasty (-11%) and breast enlarge ment (-11%) – were also down. Cosmetic surgery is nearly always paid for by self-pay and so the fall in these could be related to the cost-of-living crisis, PHIN suggests.
Active consultants in private healthcare by year
The number of consultants active in private healthcare regularly fluctuates and in 2023 was at the highest level since the pandemic.
The largest increase in active consultants in the top ten procedure ➱ continued on page 30
Private hospital admissions by year 2019-2023
Figures are rounded to the nearest 1,000. The total may not add as this is calculated using the actual figure then rounded.
Figures are rounded to the nearest 1,000. The total may not add as this is calculated using the actual figure then rounded.
Percentage change from 2022 to 2023 by nation
by English region by payment method (rounded figures)
I faced a GMC investigation following criticism of a handover
I’d performed a hip replacement on a 73-year-old patient with multiple co-morbidities. Due to illness, my handover to the weekend team was rushed. Tragically, after developing sepsis, the patient died.
Then I got the call. The coroner had named me an Interested Person for the inquest.
Medical Protection were there for me throughout. The inquest concluded with a Report to Prevent Future Deaths, and I faced a formal GMC investigation. My medicolegal consultant and solicitor advised me on the appropriate post-event analysis and CPD, and thankfully the GMC recognised my reflective practice and closed the matter with no further action.
The experience taught me the vital importance of the handover. I also learned the value of my Medical Protection membership. The team got me through, and saved me a lot of sleepless nights.
Always there for you
There were more insured admissions and self-pay admissions for both sexes in 2023 compared to 2022
groups was in gastroenterology with an extra 59 consultants (7%).
Clinical oncology had the largest percentage increase (12%). Three procedures – general surgery (-2%), plastic surgery (-1%) and medical oncology (-2%) – had fewer active consultants than in 2022.
PATIENT DEMOGRAPHICS
Volume of admissions by sex and payment method
There were more insured admissions and self-pay admissions for both sexes in 2023 compared to 2022.
Insured admissions were up equally for both sexes at 10% compared to 2022.
Self-pay grew slightly (2%) for male admissions but remained the same for female admissions in 2023.
Volume of admissions by age
There was an increase in admissions in all age groups in 2023 compared to the previous year. The largest percentage increases were in the 100-109 (80%) and 30-39 (10%) age groups.
The most common age group for private admissions was 50-59 –14,105 more admissions than 2022.
Important notes
All data described above taken from PHIN’s unique, national private dataset describing discharge activity (day case and inpatient). This excludes activity outside of PHIN’s mandate from the Competition and Markets Auth ority, such as outpatient diagnostics, physiotherapy and mental health services.
There is a time lag between collecting, validating and processing the data we receive from hospitals before we can publish it. This can be up to six months after treatment has been completed, to ensure a fair process and accurate data.
Activity numbers have been rounded to the nearest five, with percentage based on the unrounded figures. (Q1 = Jan –Mar; Q2 = Apr – Jun; Q3 = Jul – Sep; Q4 Oct – Dec).
Effective collaboration between healthcare professionals and your virtual secretarial team is vital. In the first of a two-part article, Stacey Burrows gives some tips
THE TRANSITION from an inhouse secretary to a virtual secretarial team can generate doubts and uncertainties, especially for healthcare professionals accustomed to physical interaction. But virtual secretaries have proven to be invaluable allies, bringing multiple benefits by streamlining workflow and maximising outcomes in medical practices.
This collaboration between healthcare professionals and virtual secretaries can be a resounding success, especially if a strong and effective relationship is established, creating a positive experience for all.
In this article, there are five practical tips that healthcare professionals can implement to establish a good working dynamic with vir-
tual secretaries, ranging from communication and roles to administrative tasks.
TIP 1: Develop detailed handbooks for smooth collaboration
The first step in effective collaboration with virtual secretaries is to clearly define the responsibilities and goals of each party.
The development of detailed handbooks is an essential tool, as it will help to set clear expectations and avoid misunderstandings.
These manuals should be comprehensive and cover all relevant aspects of the job and agreed responsibilities, including:
➲ Detailed description of the tasks and responsibilities of each role: Specify what is expected of each person in each situation.
➲ Step-by-step procedures for key tasks: Define how the most important tasks are to be performed, including screenshots or diagrams, if necessary.
➲ Policies and protocols: These set out the rules and standards to be followed in the medical practice, including protocols for patient care, handling confidential information and appointment management.
➲ Resources and tools: Provide a list of resources and tools available for each role, including software, templates and documentation.
How
to create effective handbooks
➲ Involve both parties: Doctors and virtual secretaries should be actively involved in the development of the manuals, contributing their knowledge and experience.
➲ Use clear and concise language: Manuals should be easy to read and understand for all involved.
➲ Update manuals regularly: Review and update manuals regularly to reflect changes in practices or technology.
TIP 2: Establish channels for clear & timely communication
Effective communication is fundamental to any working relationship and even more so between doctors and virtual secretaries. It is essential to establish clear communication channels and define how information will be shared between the team and healthcare professional. This will allow for smooth, efficient and safe collaboration, ensuring that patients receive the best possible care.
There are several channels of communication that you can consider, also taking into account the situation. For example, email can be a great medium for more formal communications where you need to send important documents.
On the other hand, an instant messaging app that utilises endto-end encryption like WhatsApp is perfect for day-to-day issues or urgent queries that require faster or more urgent communication and action.
For more complex discussions or those requiring a detailed interaction, video calls are a fantastic option.
TIP 3: Hold regular meetings
Regular meetings between doctors and virtual secretaries are essential to keep not only an overview of the patient situation, but also to discuss the overall performance of the practice, evaluate the efficiency of administrative processes, workflow and compliance with established objectives. It is also a great opportunity to
Virtual secretaries have proven to be invaluable allies, bringing multiple benefits by streamlining workflow and maximising outcomes in medical practices
detect areas for improvement, share innovative proposals, implement new technologies, optimise patient management and even to celebrate the team’s achievements.
When conducting these meetings, it is important to:
Involve the whole team, allowing everyone the opportunity to participate;
Create a safe environment;
Use techniques to stimulate inclusion, such as surveys, brainstorming or diagrams;
JellyPx
Define the steps to be taken after each meeting, assign responsibilities and set deadlines for implementation.
TIP 4: Provide virtual secretaries with all the information at their fingertips
To provide exceptional patient care, it is essential that the virtual secretarial team have the tools and knowledge necessary to respond to queries accurately, completely and in a timely manner.
This means being aware of medical specialties, available treatments, appointment availability information and details of posttreatment care.
Doctors are advised to:
☛ Provide virtual secretaries with comprehensive training on the medical specialties offered in the practice, available treatments, patient care protocols and administrative procedures.
☛ Develop guides, manuals and reference documents that virtual secretaries can quickly refer to for accurate information on patient consultations.
☛ Encourage open communication so that they can resolve doubts, clarify information and obtain guidance when necessary.
TIP 5: Provide clear billing instructions for accurate medical billing and timely money collections
Virtual secretaries play a crucial role by ensuring that bills are sent accurately, completely and on time. This not only facilitates collection from self-pay patients, but also meets the payment deadlines set by most major insurance companies.
Virtual secretaries should be clear about tasks such as:
➤ Ensuring that patient information, such as name, address, date of birth, contact details and insur-
Comprehensive diary management.
ance policy numbers, are accurate and up to date;
➤ Confirm that procedure and diagnosis codes are correct and match the services provided to the patient;
➤ Follow up weekly on outstanding invoices to pro-actively identify and resolve any problems;
➤ Keep up to date with billing regulations and fee updates to avoid errors and compliance issues;
➤ Send weekly financial reports to the consultant, providing current facts on the practice finances, including what has been paid and also what is outstanding due for payment.
Look out for our September issue when Stacey will be bringing you five more top tips to ease your transition
Stacey Burrows is manager at Virtual Medsec Direct. Website: www. virtualmedsecdirect.co.uk. Email: sales@virtualmedsecdirect.co.uk
Automation reduces the admin of onboarding and your routine communications.
Patient data from your web site can generate actions in Jelly.
Online booking with portals for your patients and consultants.
A full range of clinical information can be collected on patients.
Integrates with SignatureRx, CloudRx for digital prescriptions, Viva Health labs, TDL for pathology, Healthcode for insurer billing, Stripe, Opayo for card payments, Zoom for telehealth, Xero for accounting.
Image library to track progress and upload images from any remote device.
Design your own specialist forms for use by patients and users.
Templated notes, documents, diagrams, auto generation of GP letters are available.
Handles complex billing requirements for self-funders, families or insured patients.
Beware the fickle allure of cash
ACCOUNTANTS
WE UNDERSTAND YOUR PAIN
As a health consultant you’re probably facing these concerns:
• Higher tax bills as a result of the reform of the tax basis period.
• Delays in getting accounts and tax returns prepared. Sound familiar...?
If your accountant hasn’t already spoken to you about these concerns, then our dedicated healthcare accounting team are ready and waiting to help you right now.
Contact us for a complimentary review of your accounting requirements.
Scan this QR code to watch a recording of our webinar: ‘Tax Basis Period Reform: Is Your Healthcare Practice Prepared?’
impact does inflation have on your wealth? Samuel Kirton (right) explains why investing can deliver inflation-busting returns
MOST OF us are all too aware of the challenge of inflation when we get to the supermarket checkout or when paying our energy bills.
Inflation does not only affect the spending power of our income today, but also the real value of our assets – for example, investment portfolio assets – that will deliver future spending power, perhaps in retirement.
While most people understand the nature of this hidden tax, it may surprise many just how big the impact of the inflation headwind has been over the past few years.
If we look at the impact of inflation on the spending power of £100 over the past 20 years, we can see that even when inflation was relatively low, it silently whittled it away.
On average over the last 20 years, inflation has been around 2.8% a year, which does not sound too bad. In fact, this means more than 40% of our spending power has disappeared.
The £100 from 2003 would be worth around £58 in 2023, according to the Office for National Statistics (ONS).
What is to be done?
For those doctors building a pot for retirement, protecting your wealth from inflation – and hopefully growing its real, after-inflation value – is very important.
The first thing to do is to become an investor, not a saver. For some, elevated deposit rates returning above-inflation interest may look appealing. Unfortunately, cash has had a very poor track record of holding its real value.
On the other hand, global equities (‘stocks and shares’) have managed to provide positive real returns for investors over the past 20 years, which includes the equity market turmoil in 2007-09 during the global financial crisis, and 2022.
That £100 in 2003 might have been worth £384 in 2023, with a period high of £413 in 2021.
Owners of equities, however, require staying power, as these positive inflation-beating returns do not come in straight lines.
Data from that same 20-year period shows us that the longer an investor is able to hold their equity
investments for, the greater the chance that they will receive positive, after-inflation returns.
Things to remember
➲
The allure of cash is clearest during times of market turmoil when it can continue to deliver a positive return even when the value of other assets is falling.
➲ But it has a hidden, dark side, in that it does not protect investors from the erosive power of inflation over the longer term.
➲ A carefully constructed portfolio of other assets, such as equities, bonds and commercial property, is more likely to deliver your long-term financial goals.
Inflation is a risk that all investors must have in their sights and it is not an easy one to mitigate in the short-term.
Over the longer-term, equity assets can help to deliver inflationplus returns to protect and grow wealth.
The key is to mitigate this risk as far a possible by owning, and sticking with, a well-diversified investment portfolio.
Cash may have a role to play in everyone’s overall portfolio of assets. It offers essential liquidity to cover short-term expenses and can provide a buffer for unanticipated life events and emergencies.
If investors are tempted by the relative security of cash, they would do well to remember that there is no market timing bell and there is no knowing what markets will do next.
Trying to second-guess the market is a challenging sport with few winners.
Samuel Kirton is a financial planner with Cavendish Medical, specialist financial planners helping consultants in private practice and the NHS.
The content of this article is for information only and must not be considered as financial advice. Cavendish Medical always recommends that you seek independent financial advice before making any financial decisions.
Levels, bases of and reliefs from taxation may be subject to change and their value depends on the individual circumstances of the investor. The value of investments and the income from them can fluctuate and investors may get back less than the amount invested.
BILLING AND COLLECTION
The experts do it better
Managing administrative tasks in private healthcare can overwhelm even the most efficient practices. Partnering with a medical billing company can significantly reduce these burdens, streamline operations, ensure regulatory compliance and enhance overall profitability, says Derek Kelly
(right)
CONSULTANTS IN private practice are often overwhelmed by administrative tasks – with medical billing being one of the most time-consuming and complex. Efficient management of billing and revenue is increasingly crucial for the sustainability of any private practice. So let’s see how medical billing companies can significantly reduce administrative burdens and allow healthcare professionals to focus more on patient care and less on the paperwork.
THE ADMIN BURDEN IN PRIVATE PRACTICE
➤ Time-consuming processes
Billing involves multiple steps, from patient registration and verification of insurance details to claim submission and follow-up. Each step is time-consuming and requires meticulous attention to detail.
➤ Complex regulations
Navigating through the maze of coding requirements, insurance policies and regulatory compliance is challenging. Mistakes can lead to claim denials, delays and even legal issues.
➤ Resource intensive
Maintaining an in-house billing department requires a significant investment in training, technology, and human resources. But this diverts funds and focus away from core medical services.
HOW MEDICAL BILLING COMPANIES EASE THE BURDENS
➤ Expert handling of billing processes
Medical billing companies employ specialists trained in the latest billing codes, regulations and best practices. Their expertise ensures accurate and efficient handling of all billing-related tasks, from claim submission to payment collection.
➤ Regulatory compliance
Keeping up with the ever-changing healthcare regulations is a daunting task. Billing companies stay updated with all regulatory changes and ensure your practice complies with all legal requirements, minimising the risk of non-compliance.
➤ Enhanced cash flow
The ideal partner should offer tailored solutions that fit the unique needs of your practice, ensuring seamless integration with your existing systems
➤ Advanced technology integration
These companies use state-of-theart software to streamline the billing process. This includes electronic health record (EHR) integration, automated claim submissions and real-time tracking, reducing errors and speeding up the re-imbursement cycle.
➤ Resource optimisation
By outsourcing billing, practices can re-allocate resources towards enhancing patient care. This means more time for consultations, improved patient relationships and a better overall patient experience.
Professional billing services ensure timely submission and follow-up of claims, leading to faster re-imbursements and a steady cash flow.
This financial stability allows practices to re-invest in their services and infrastructure.
CHOOSING THE RIGHT MEDICAL BILLING COMPANY
Look for a company with a proven track record and positive client testimonials. Experience in handling billing for your specific specialty is a plus.
➤ Compliance and security
Ensure the company adheres to industry standards and has robust data security measures in place to protect patient information.
➤ Transparency and communication
Opt for a company that offers transparent reporting and maintains open lines of communication. Regular updates on billing status and performance metrics are essential.
REAL-WORLD IMPACTS
UROLOGY PRACTICE, MANCHESTER
Before outsourcing, this practice faced frequent claim denials and a backlog of unpaid invoices.
After partnering with Medserv, its claim approval rate increased by 20% and it saw a 30% improvement in cash flow. This enabled it to hire additional medical staff and reduce patient waiting times.
DERMATOLOGY CLINIC, LONDON
This practice decided to outsource its billing operations after finding it was struggling with the administrative load.
The move resulted in a significant cut in administrative hours spent on billing tasks, freeing up time for patient care and practice growth.
And the practice also reported higher patient satisfaction due to more efficient appointment scheduling and follow-up processes.
➤ Customised solutions
The ideal partner should offer tailored solutions that fit the unique needs of your practice, ensuring seamless integration with your existing systems.
Reducing administrative burdens is essential for the success and growth of private medical practices. By partnering with a medical billing company, practices can alleviate the stress of complex billing processes, ensure compliance,
EXPERT TAX AND ACCOUNTANCY ADVICE YOU CAN TRUST
Sandison Easson is a firm of truly specialist medical accountants who provide personal and tailored advice to clients.
We act for medical professionals throughout all stages of their career with clients in almost every town in England, Scotland and Wales.
We cut through the complicated jargon and deliver practical, easy to understand advice. Call us today to organise your FREE no obligation consultation.
optimise resources and enhance cash flow.
This allows medical consultants to focus on their primary mission – providing exceptional patient care. It is worth considering the benefits of outsourcing your billing operations and take the first step towards a more efficient and profitable practice.
Derek Kelly is marketing manager at Medserv
WE PROVIDE THE USUAL SERVICES YOU WOULD EXPECT FROM AN ACCOUNTANT SUCH AS PREPARATION OF YOUR ACCOUNTS AND TAX DECLARATIONS BUT OFFER SO MUCH MORE INCLUDING ADVICE ON:
• SETTING UP A NEW PRIVATE PRACTICE
• BUILDING AN EXISTING PRIVATE PRACTICE
• BUSINESS STRUCTURES TO PROTECT WEALTH
• BUSINESS STRUCTURES TO MAXIMISE TAX EFFICIENCY
• CLAIMING TAX REFUNDS INCLUDING OVERPAID ANNUAL ALLOWANCE TAX
• REMUNERATION PLANNING FOR YOU AND YOUR FAMILY
• UNDERSTAND ANNUAL ALLOWANCE
• MAXIMISING LEGITIMATE
BUSINESS DILEMMAS
What do you do if you wish to remove a patient from your practice? Dr Sissy Frank (below) gives her advice
Dilemma
1 How do I remove violent patient?
QI have a patient who, over the last few months, has been increasingly difficult to deal with.
He is intimidating, rude, aggressive and told one of my reception staff that ‘if you treat me badly, you are going to get a reaction’.
His expectations are unrealistic and he makes unreasonable requests at reception.
I am considering ending my professional relationship with him due to the ongoing problems we are having.
Can you suggest the best way to go about this?
AThankfully, the need to remove a patient from the practice is rare but is sometimes appropriate given the circumstances.
Getting rid of a bullying patient
However, the removal of a patient can lead to the individual making a complaint or contacting the media and/or posting comments on social media.
It could also lead to criticism by the GMC. It is essential that you can justify the decision to no longer see a patient.
Firstly, it is imperative that the practice has a zero-tolerance behaviour policy that protects you and your staff and clearly states what behaviours are acceptable and outlines what will happen if patients behave unacceptably.
Grounds for removal
It is worth regularly reviewing the policy for dealing with challenging patients and ensuring staff receive up-to-date training on this topic.
When removing a patient, you must be confident that the reason for ending the relationship is fair and does not discriminate against the patient.
Justifiable grounds for removing a patient might include:
Violence or aggressive behaviour;
Discriminatory abuse;
Sexual advances;
Theft from the practice, staff or other patients;
Repeated unreasonable or inconsiderate actions.
This seems to be in line with the comments you describe above. However, it may be more difficult to justify removing a patient from the practice if:
They have complained – but no other reasons for removal apply;
Their behaviour is caused by their condition;
They are related to a patient who is being removed – and no other reasons for removal apply;
You are concerned about the resource implications of their care;
Their medical condition puts you at risk.
Before removing a patient, you need to inform them of your decision and explain the reasons, in writing if possible, and be clear that they will not be left without medical care. Remember to make a
When removing a patient, you must be confident that the reason for ending the relationship is fair and does not discriminate against the patient
record of your decision and the reasons for it.
The GMC also says you should ‘make sure arrangements are in place for the continuing care of the patient if they are unable to make arrangements for themselves’ and ensure ‘that information recorded in the patient’s records is factual and objective and does not include anything that could unfairly prejudice the patient’s future treatment.’
You must also transfer the patient’s records to their new practice as soon as possible.
However, if a patient has been violent or has behaved in a threatening way that leaves you or your staff in fear, they can be removed immediately.
In this situation, you should report the incident to the police and get an incident number. Only give the police the minimum information needed to allow for proper investigation. The patient’s medical details should not usually be required.
Finally, contact your medical defence organisation if you have any concerns or for further advice and guidance.
Dr Sissy Frank is a medico-legal adviser at the Medical Defence Union (MDU)
if you wish to volunteer at a local sporting event
Dilemma 2
Am I covered for charity fun runs?
QIn my spare time, I enjoy participating in local charity fun runs. Now I’ve been asked by the event organisers of one such event whether I would be able to provide medical assistance in case of an emergency during an event.
I would like to get more involved and support the group, but am not sure if I am indemnified for this type of work. Can you advise?
ADoctors are frequently asked to provide medical cover for amateur sporting events, but there’s a few things to consider before you agree to provide medical assistance.
Firstly, volunteering at an event like this is known as acting as ‘a good neighbour’. This is different from a ‘Good Samaritan’ event,
Volunteers need indemnity cover
which is when a doctor is unexpectedly asked to provide medical care in an emergency.
Next, remember there is an ethical duty and a statutory requirement to ensure you have adequate indemnity or insurance before you agree to help.
have some expertise in areas such as cardiopulmonary resuscitation, airway maintenance and spinal fracture immobilisation if you were to volunteer in a medical capacity for an event such as a charity fun run.
Dr Sissy Frank is a medico-legal adviser at the Medical Defence Union (MDU) Summer sports are all around. Dr Sissy Frank discusses what to do
Some organisations may provide indemnity for doctors acting in a professional capacity (voluntary or paid), and you should check this before the event.
Check indemnity
If the organisers can’t provide you with indemnity, it is important to contact your medical defence organisation in advance of the event to check whether your current membership will indemnify you for this.
Furthermore, the GMC’s Good Medical Practice (2024) guidance states that ‘you must be competent in all aspects of your work’ and, as such, you need to have the required skills, experience, equipment and support.
For example, you may need to
If you are unsure what experience or training you might need, check with the event organiser or relevant sporting organisation and if a medical problem occurs during the event, your ethical
responsibilities, such as the need to obtain consent and maintain confidentiality, remain the same as in your regular medical practice. Finally, keep detailed notes of any incidents that arise and the medical care you provided in case you are later asked about the treatment you gave.
Accountant Richard Norbury (right) gives a comprehensive round-up of the last Government’s plans to reform the payment of tax in an attempt to make it reflect real time
MAKING TAX Digital (MTD) is a term that has been used for a number of years, but due to a mixture of reasons, including the Covid-19 pandemic, has been delayed.
The last Tory Government believed that there was a so called ‘tax gap’ and that failure to take reasonable care accounts for the largest proportion of the tax gap, followed by error as the second largest factor.
MTD has been a key part of its ten-year strategy to build a trusted, modern tax administration system – so they said!
Overview
MTD requirements for businesses and individuals include:
Keeping digital records;
Using software compatible with Making Tax Digital;
Submitting updates every quarter, bringing the tax system closer to real time.
The aim is that these measures
The aim is that these measures will make it easier for individuals and businesses to calculate their tax correctly and reduce the amount of tax lost due to avoidable errors
will make it easier for individuals and businesses to calculate their tax correctly and reduce the amount of tax lost due to avoidable errors and the new system will replace the more traditional methods of filing an annual tax return.
VAT-registered businesses
Those of you with medico-legal practices will be well aware that MTD VAT was introduced in April 2019 for some businesses and was extended to all VAT-registered businesses from April 2022.
Self-employed and rental income
MTD will be mandatory from April 2026 for the self-employed and those with income from property with gross income of more than £50,000 a year. Then one year later, from April 2027, the selfemployed and income from property over £30,000 a year will join the scheme.
The limits are measured by comparing your sole-trader and property income previously reported.
For example, if you exceeded £50,000 in the tax year 2024-25, then you would be required to start MTD from April 2026 and if you exceeded £30,000 in the tax year 2025-26, you would be required to start MTD from April 2027.
It is important to plan ahead and file your tax returns in plenty of time to allow registration to the system and ensure that you have the relevant software and systems to be able to meet the demands. It is likely that financial penalties will be imposed for missed deadlines.
Corporation tax
For those of you who trade via a limited company, HM Revenue and Customs (HMRC) has stated that MTD for corporation tax will
➱ continued on page 42
Diagnostic Audiology Including Paediatrics • Tinnitus Rehabilitation • Vestibular Testing • PTA & Tympanometry • Speech Audiometry • Speech In Noise Testing• Specialist Tests Including OAE, VEMP & ASSR • Ear Wax Removal • Independent Hearing Aid Provider
not be mandated before April 2026.
Partnerships
No timetable has yet been introduced for partnerships.
Exemptions
Certain businesses may be able to apply to HMRC to be exempt from MTD and will be considered on a case by case basis.
The only VAT-registered businesses who can apply for exemption are those businesses who cannot reasonably or practically use computers, software or the internet, which may be due to:
Age;
A disability;
Running a business from a remote location;
You object to using computers on religious grounds;
Another reason why it is not reasonable or practical.
Planning
But the reality for most businesses is that MTD will be an administration and financial burden, so careful planning should be considered.
This may be planning to ensure that adequate systems and software are in place for you to meet the requirements or alternative measures such as bringing in family members to your business or property.
Cash basis
The cash basis is a method that eligible businesses can use to calculate trading profits for income tax purposes, as an alternative to using traditional ‘accruals’ accounting.
The traditional method of accounting will take into account fees invoiced as at the year-end but not paid at the year-end, amounts owing to creditors but not paid at the year-end and other balance sheet items.
It is worth noting that limited companies, partnerships with a corporate member or limited liability partnerships (LLP) cannot use the cash method.
HMRC believes that this method is a simplified regime that reduces the complexity of reporting income while still providing an appropriate measure of trading profits for many businesses.
Currently, a business has to elect
HMRC believes that the ‘cash basis’ method is a simplified regime that reduces the complexity of reporting income while still providing an appropriate measure of trading profits for many businesses
attempting to make changes to the tax system, including basis period reform, which are designed to make the move towards MTD more streamlined.
If you have a sole trader or partnership business, it may be the case that your accounts are drawn up to a year-end that is not 31 March or 5 April.
to use the cash basis, usually through notifying HMRC as part of the tax return.
The accruals basis is the default method of calculating profits, and the cash basis is an ‘opt-in’ regime.
Default method
But, from the tax year 2024-25, the cash basis will be the default method of calculating trading profits and an election will no longer be required to use the cash basis, and businesses will calculate their trading profits using the cash basis unless they make an election to use the accruals basis.
Presently, businesses are only able to join the cash basis if their cash basis turnover is less than £150,000, and are forced to leave in certain circumstances where their turnover exceeds £300,000.
The new legislation removes this turnover restriction entirely, meaning eligible businesses of any size will be able to use the cash basis, allowing them to continue using the cash basis as they grow.
Other previous restrictions to the cash basis will also be relaxed including the ability to claim interest costs and loss relief.
This method of accounting may well be attractive to those of you with medico-legal practices due to the amount of time you have to wait before you are paid.
This method is not likely to suit large practices that may rely on a set of traditional-style accounts for finance from a lender or partnerships. In addition, it is very important that you continue to track your fees to ensure that you are paid for the work that you have performed.
Basis period reform
While not directly linked to Making Tax Digital, HMRC is
In the year 2023-24, these businesses will undergo a transition whereby the ‘current year basis of assessment’ will be changed to a fiscal year basis – 31 March or 5 April.
The financial year-end of accounts can still be retained, if so desired, but adjustments made to tax profits on a fiscal year basis.
In these cases, it is likely that you were taxed twice on the same period of profit in the second year of private practice. This creates a figure known as overlap profit which normally will have been carried forward to the year that you retire or leave the business. Sometimes this creates additional profit to bring into taxation. If this is the case, and you continue to trade in the business, then HMRC has allowed any additional profits to be taxed over a maximum period of five tax years from 2023-24 to 2027-28.
Any additional tax would have been payable on retirement from a partnership or cessation of private practice. There is also the option of bringing forward some profits and, in certain circumstances, accelerating the taxable profits may prove to be beneficial.
It is thought that the cash basis and basis period reform measures are designed to make the tax system simpler so that the reporting requirements can be achieved.
It has also been suggested that, once the system is up and running, HMRC may well use the quarterly reporting system to ask for more regular tax payments throughout the year.
Any decision on changing the method that you report your taxes should be a decision made after careful consideration and consultation from an accountant.
Next time: Alec James looks at understanding accounts
Richard Norbury is a partner at Sandison Easson & Co, specialist medical accountants
Thinking
Location, location, location is not only an important mantra for finding one’s home, it is equally, if not more important, for any independent doctor looking to open a surgery or clinic.
While many private practitioners have traditionally operated from converted houses or office spaces, there is a growing trend towards moving into the high street.
OUR COMMERCIAL real estate team has seen an increase in inquiries over recent months from practitioners looking to either move their practice from an existing property or open a new one in a commercial space.
This shift is driven both by the increase in availability of competitively priced units since 2020, when the pandemic forced businesses to close, and the improved accessibility and modern clinical aesthetics that these units provide.
There are several factors and potential challenges to consider when finding a suitable location for your practice and it is important to seek independent advice from legal advisers, architects and surveyors when considering your options.
Commercial law experts Bryn Morgan and Robert McCartney explain the key considerations for practitioners thinking of opening a practice in a high street unit Advice is available on:
When working with our clients, we advise that they consider the following factors to make sure their relocation or expansion runs smoothly:
Agreeing lease terms
While you may be able to consider purchasing premises for your use, most start-up businesses will be looking to lease space.
It is sensible to engage a specialist valuation surveyor to help you identify options and negotiate terms with prospective landlords. You will need to consider various premises expenses including rent, service charges, business rates and utilities. And you will need to be comfortable with the length of the lease, which may be a sizeable commitment.
Even if you intend to trade through a limited company as the tenant, it is not unusual for the landlord to require personal guarantees and/or a rent deposit.
Planning permission
For planning purposes, clinical services fall under Use Class E, which also includes retail units, restaurants and nurseries. This
Free legal advice for Independent Practitioner Today readers
Independent Practitioner Today has joined forces with leading healthcare lawyers Hempsons to offer readers a free legal advice service.
We aim to help you navigate the ever more complex legal and regulatory issues involved in running and developing your private practice – and your lives.
Hempsons’ specialist lawyers have a long track-record of advising doctors – and an unrivalled understanding of the healthcare system as a whole.
Call Hempsons on 020 7839 0278 between 9am and 5pm Monday to Friday for your ten minutes of free legal advice.
Business structures (including partnerships)
Commercial contracts
Disputes and litigation
Premises
Regulatory requirements and investigations
means many retail units will no longer need planning permission to change their use to medical.
That said, it is important to check existing planning permissions for conditions that restrict changes of uses or other operational matters such as opening hours.
If planning permission is required, an application to the local council will be needed, which can take several months.
There may be local planning objectives and requirements which could hinder the application and it is important to engage with the local planning team to understand this.
Further complications can arise if the unit is listed, which is sensible to check at an early stage.
Facilities and building regulations
Once the unit is identified, you must consider the fit-out of the premises. Retail units are often provided as empty shells, which
allows you to design the ideal solution.
However, sometimes they have existing infrastructure which may need to be removed or altered to meet your requirements. Often you will be able to negotiate a rentfree period to give you a window of time to complete the fit-out before commencing trade.
The fit-out may include significant work to convert the premises to clinical space with consulting rooms and a reception area.
It is particularly important to ensure that the premises meet the appropriate healthcare standards and are compliant with Care Quality Commission rules – for instance, in respect of soundproofing and infection control.
The greater the level of complexity or specialty of the service provided, the more important it becomes to ensure these standards are met.
You will need to ensure that the works comply with building regu-
Often you will be able to negotiate a rent-free period to give you a window of time to complete the fit-out before commencing trade
lations. You are likely to need permission from the landlord, which would usually be governed by a licence for alterations that would need to be agreed as part of your lease negotiations.
Contracts with builders should also be reviewed carefully.
Repair and re-instatement obligations
Leases of retail units will usually include repair obligations. As a tenant, you may be responsible for the whole building if the unit is stand-alone or you may be responsible for structural and external repairs via a service charge.
It is important to understand and, where possible, limit these obligations and to schedule maintenance works and budget appropriate fees.
Leases often require the premises to be re-instated to their previous condition at the end of the term. This could be a significant cost and requirement that needs to be factored into the planning stage.
It is particularly important if you have growth plans and anticipate moving the service in a relatively short period of time. It may be possible to negotiate variations, but it
must be discussed early in the process.
Accessibility
This can be easily overlooked, but it is important to identify whether there are any restrictions which may prevent access to the site.
It is common for retail areas to have fixed open and closing times or for local parking facilities to be closed at certain times. Opening times may also be restricted by the existing planning permission.
This is particularly important if the unit is inside a large retail centre and may not be something the landlord can vary if they are subject to restrictions.
Additional costs such as security and maintenance fees could be affected by this issue.
All these factors are likely to impact on the proposed budget for the business and they will certainly impact on the time-frame for implementing the change.
If you are looking at opening a service in a retail unit or any other innovative location, please contact Hempsons to discuss this further.
Bryn Morgan (right) is a partner and Robert McCartney (below) is an associate at leading healthcare law firm Hempsons. They can be contacted by email at b.morgan@ hempsons.co.uk and R.McCartney@hempsons.co.uk
DOCTOR ON THE ROAD: HYUNDAI IONIQ 5N
This EV sounds like a petrol hot hatch
HYUNDAI IONIQ 5N
Body: Five-seat hatchback Engine: Two electric motors.
Wow! Some clever surgery makes this EV feel like you are driving a very fast petrol-engine hot hatch and will melt the cynicism of any petrol head sceptic. Our motoring correspondent Dr Tony Rimmer (right) loved it
LET US think for a moment of the humble stethoscope. We have all used one in our work and it represents a universal indicator of medical expertise and services.
Pragmatically, in hospital practice at least, it has been overtaken by modern technological diagnostic aids, but is unlikely to disappear any time soon.
We, and perhaps our patients, feel more comfortable and trusting when its initial assessment capabilities are used by us practitioners.
When new technology comes along, we feel less threatened by hanging on to certain analogue elements of replaced equipment.
Think of the bell-ringing sound most of us use to indicate a call on our mobile phones or the use of mechanical clock faces to tell the time on our digital watches. This is called skeuomorphism.
In the world of cars, there is resistance among drivers, particularly keen petrol-heads, to enter the world of electric cars.
Although electric vehicles (EVs) are fast, certainly in a straight line, they lack the nimbleness of handling and directness of steering that makes petrol-engined sports cars so enjoyable to drive.
They also lack an important feature: the drama of the use of a proper gearbox and the associated sound of a sporty engine and exhaust. What if we could reproduce all these features in a pure EV? Would it work?
The South Korean maker Hyundai, who are at the forefront of electric car design and development, has done just this as a feature in its new performance
variant of the Ioniq 5 – the 5N –and I have driven it to assess the effectiveness of the changes made.
The normal Ioniq 5 is an excellent family-friendly five-door EV that has good performance, decent range and is reasonable value. However, it is nothing special to drive. There is nothing to excite the keen driver.
So Hyundai’s N division got hold of the car and, using all the knowledge gained from its World Rally Team, has made significant changes to the chassis and powertrain under the skin.
The body has been stiffened and the suspension redesigned. There is now one motor to power each axle to provide four-wheel drive and their combined power output is a huge 641bhp with 740Nm of torque.
Cosmetic changes
The external bodywork has had some cosmetic changes to distinguish it from the standard model, but they are pretty subtle.
Its interior has gained front sports seats and a thicker steering wheel, but all the space and practicality of the standard model remains.
An excellent and intuitive infotainment system also remains, but there are additional sports submenus and there are physical buttons on the steering wheel to access them.
Among the sporty features is a mode that simulates an eightspeed paddle-shift gearbox with associated petrol engine sounds.
Moving off in normal mode is as easy, smooth and silent as in the regular Ioniq 5 and you could drive around all day taking the kids to
school and shopping at the supermarket without drama or fuss.
You will notice that the steering is sharper and the ride is firmer but not in any way to cause discomfort. But if you get out of town and put your foot down, you know you are in something special.
With acceleration in supercar territory, I was worried that the handling through the bends may disappoint, but was amazed at how controlled and agile this 2.2 tonne EV actually is.
Astounding grip
I had a swift drive along one of my favorite B-roads and found myself having a lot of unexpected fun. Grip is astounding and there is no body roll to speak of. There are few cars of any sort who could keep up on a cross-country journey.
The pièce de résistance, however, is the paddle gearbox mode that sounds like a corny idea but works brilliantly.
It allows you to drive the 5N on a simulated revcounter display up to
the red line in each virtual gear with all the physical characteristics and noise of a sporty petrol engine.
The car hesitates when you hit the rev-limiter forcing you to change up and there is engine braking in abundance with associated pops and crackles from the virtual exhaust.
It truly feels as if you are driving a very fast petrol engine hot hatch and will melt the cynicism of any petrolhead EV sceptic. I loved it.
So, this is a car that has all the green credentials and ease of use that any EV delivers, but can change character at, literally, the touch of a button to satisfy the keenest medic petrol head.
What is more exciting is that the Ioniq 5N is likely to be the first of many new EVs designed to keep motoring interesting and fun. I congratulate Hyundai for being the trailblazer.
Dr Tony Rimmer is a former NHS GP practising in Guildford, Surrey
Hyundai’s N division got hold of the car and, using knowledge gained from its World Rally Team, has made significant changes to the chassis and powertrain
There is an excellent and intuitive infotainment system
CHECK OUT OUR BUSINESS DIRECTORY
Independent Practitioner Today features an online advertising directory to complement our journal and website.
Split into ‘business’ and ‘lifestyle’ directories, they list the services private doctors need to run their practices or spend their well-earned money on.
ADVERTISERS: The deadline for booking adverts in our September issue is 23 August
or for reprints, we would be happy to discuss licensing the copyright to you.
Published by The Independent Practitioner Ltd. Independent Practitioner Today is editorially independent.
Material is governed by copyright.
No part of this publication may be reproduced, stored in a retrieval system or transmitted in any form without permission, unless for the purposes of reference and comment. Editorial layout is the copyright of the publishers. If you wish to use it for promotional purposes on websites
Our sponsors
WRITE TO Independent Practitioner Today 7 Lindum Terrace, Lincoln LN2 5RP
TELL US YOUR NEWS Robin Stride, editorial director Email: robin@ip-today.co.uk Phone: 07909 997340 @robinstride
ADVERTISE WITH US
To advertise in the digital journal, on our website or in our business directory, contact advertising manager Andrew Schofield at Spot On Media. Phone: 0161 408 3912 Email: andrew@spotonmedia.co.uk Follow Independent Practitioner Today on