The business journal for doctors in private practice
In this issue
Careful when contracting others
A recent court case has re-affirmed precedents about vicarious liability, which could be costly for doctors P20
Give them a great initial experience
Delivering a good first impression is key to retaining a patient P28
COMPLETE OUR SURVEY WITH A CHANCE TO WIN A £100 VOUCHER What
n Turn to page 9
You think you’re a whizz at medical billing?
Answer this quiz to find out how you fare in the billing and collection stakes P34
Inflation’s perfect storm
By Robin Stride
Consultants’ representatives have warned that mounting inflation coupled with other business pressures are creating ‘a perfect storm’ threatening private practice.
The London Consultants’ Association (LCA) has expressed ‘growing fears’ about the future of private practice, while the Federation of Independent Practitioner Organisations (FIPO) voiced concerns that hefty expense increases made it ‘increasingly unattractive’.
LCA chairman Dr Mark Vanderpump said: ‘A perfect storm of external pressures and changes in the market has resulted in a situation discouraging to both existing consultants and those who might have been considering entry.
‘The LCA believes that in the longer term this situation represents not only an existential threat to private practice but also threatens the ability of patients to choose the consultant with the expertise most relevant to their needs.’
He reported that the LCA was seeing consultants frustrated at all levels of their careers over significantly increased costs while fees and re imbursements had stayed ‘static’ for many years.
Dr Vanderpump told Independent Practitioner Today : ‘An important issue for all is the attitude of private medical insurers (PMIs) to consult
In association with
ants. Those newly appointed are forced to agree to low professional reimbursements to be “listed”.
‘More established consultants are being delisted for refusing to accept significantly reduced payments. In addition, there is a lack of clarity over which consultants are being selected for patients who book via the open private medical insurance referral pathways.
‘Decisions about patients’ clinical care are made remotely by those who have not examined the patient,’ he added.
He believed the pandemicinduced closure of private hospitals and clinics had exacerbated the mood of the consultant body, which felt its expertise was undervalued.
Dr Vanderpump said a salaried
More established consultants are being delisted [by insurers] for refusing to accept significantly reduced payments
DR MARK VANDERPUMP Chairman of
the London Consultants Association
model might attract some specialties, but could prove restricting long term due to a loss of a key attraction of private practice – professional independence.
He pledged LCA help for consultants in all phases of their private practice, including supporting younger doctors through the difficult early phase of setting up a private practice.
‘We offer newly appointed consultants a support network, including an appraisal service, medicolegal training and access to senior members providing mentorship.’
FIPO predicted many young consultants would be put off entering private practice due to high startup costs and low reimbursements from private medical insurers.
Others would leave as the financial and administrative burden of running a practice became uneconomic.
It said: ‘The latest inflation rate of 9%, which is expected to rise to 11% by the end of the year, when combined with rising indemnity insurance and other costs makes private practice an increasingly unattractive prospect.
‘As more and more consultants leave private practice or do not join, the pool for patients to choose from for their treatment reduces. This is further reduced by some restrictive policies of the PMIs when often only two consultants may be offered to a patient.’
FIPO stated that consultants’ re imbursements had been continually eroded by inflation since the last substantive increase in 1993 and young consultants starting in private practice from 2010 had seen no increase to take account of inflation.
These doctors, who it said were only recognised by the main insurers if they accepted low reimbursement rates, should have had fees raised up until the beginning of this year by an annual 2.36% to keep up with inflation.
Reimbursements had, in effect, remained flat since 1993. ‘Consultation fees have indeed increased, but procedural fees with only a few exceptions have remained static.’
➱ continued on page 3
TELL US YOUR NEWS. Contact editorial director Robin Stride
ADVERTISE WITH US. To advertise in the digital journal, on our website or in our business and lifestyle directories, contact Andrew Schofield at Spot On Media. Phone: 0161 408 3912
Email: andrew@spotonmedia.co.uk
GET A SUBSCRIPTION DISCOUNT
£90 independent practitioners. £210 organisations. £90 GPs and practice managers (private & NHS).
Save £15 paying by direct debit: individuals £75 (organisations £180).
TO SUBSCRIBE
Email karen@marketingcentre.co.uk Or phone 01752 312140.
After the damage done to private doctors’ practices during Covid there is another ugly beast to contend with.
Inflation’s return is ravaging the roots of businesses and threatens growth and, for some, long-term survival.
How bad it can get remains to be seen, but there are increasing concerns among independent practitioners, those who advise them and economists who study the independent sector.
Consultants’ representatives have warned that mounting inflation coupled with other business pressures are creating ‘a perfect storm’ threatening private practice.
As we report on page 1, the London Consultants’ Association has ‘growing fears’ about the future of private practice, while the Federation of Independent Practitioner Organisations fears that big expense hikes make it ‘increasingly unattractive’.
A grim combination of external pressures and market changes is said to be discouraging existing consultants and would-be entrants into private practice.
Severe financial pressures on the business are blamed on the sad demise of the Rutherford Health Group which went into liquidation (see page 6) last month and we suspect other surprises lurk around the corner.
Market analysts LaingBuisson warn (page 5) that high inflation and the economic fall-out from the Ukraine war and sanctions against Russia could hit demand for private medical insurance. There is not much you can do about that nor the lower rewards for your excellence in the NHS (page 3). But with bad debts rising, it’s important to mend any gaps in your self-pay collection. However, it is not all bad news out there and independent practitioners’ vision and drive will see many survive choppy waters.
Why London lags in self-pay boom
Ted Townsend, author of a report on private acute care in central London, looks at whether the self-pay growth seen across the capital is set to last P12
How to help your staff financially
This month, our Troubleshooter Jane Braithwaite tackles what the rocketing cost of living crisis means for doctors as employers and suggests some ideas P16
A barometer of the nation’s health
Bupa’s medical director Dr Robin Clark explains how and why the insurer has launched its Wellbeing Index on the 75th anniversary of its formation P22
The revised Good Medical Practice
The MDU’s Dr Caroline Fryar takes a closer look at one of the domains in the GMC new guidance and highlights a few potential problems P26
Avoid complaints in minor surgery
Minor surgical procedures are usually straightforward, but doctors should be aware of the pitfalls. Dr Clare Devlin of Medical Protection explains P32
Don’t go chasing star performers Dr Ben Holdsworth of Cavendish Medical explains why investors should not run after star funds – because they are usually already past their peak P36
PLUS OUR REGULAR COLUMNS
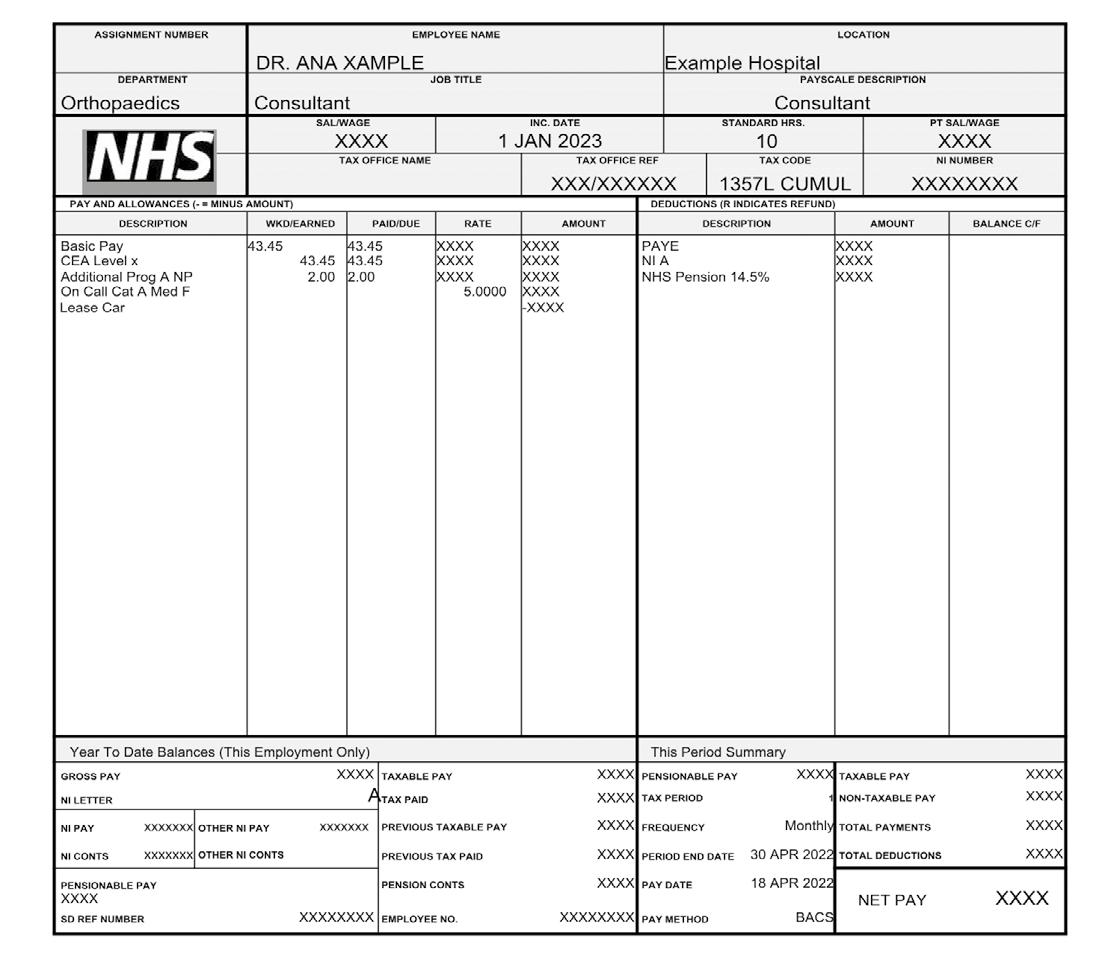
Business Dilemmas: Don’t slip up on your pay
Medical accountant Richard Norbury has some practical tips to help understand your payslip P42
Doctor on the Road: Sensible, yes – but it lacks sparkle
Medical motoring correspondent Dr Tony Rimmer says the VW iD4 impresses but doesn’t stir the blood P46
Profits Focus: Financial fortunes of dermatologists & oncologists
Accountant Ray Stanbridge puts the fiscal performance of these two specialties under the spotlight P48
Clinical Excellence Awards now worth half and no longer pensionable Awards scheme gets new name and rules
By Edie Bourne
Doctors who have been rewarded for going ‘above and beyond’ in the medical profession will find their award for excellence is now worth almost half of what it would have been last year.
In a shake up of the National Clinical Excellence Awards (CEAs), the Government has announced more consultants will be rewarded with bonus payments but the value of individual awards will be worth considerably less.
The awards, now renamed as the National Clinical Impact Awards, will also no longer be pensionable.
The Department of Health and Social Care (DHSC) has revised the national version of the awards to ‘broaden access to the scheme, make the application process fairer
Inflation is set to trigger rise in bad debts
Inflation means independent practitioners will need to be alert to the potential for bad debts to increase.
James Gransby, vice-chairman of the Association of Independent Specialist Medical Accountants, said: ‘Those running a private practice are likely to be accustomed to bad debts cropping up from time to time.
‘With inflation leading to personal finance pressures for patients, then the incidence of bad debts occurring is likely to increase.
‘If this has been an area which has lacked focus in the past, then turning attention to it now may help to prevent bad debts increasing.’
and more inclusive, and to change the application process’.
Patrick Convey, technical director at specialist financial planners Cavendish Medical, explained: ‘The changes have been launched to make the awards more inclusive and accessible, but critics will argue that consultants will be receiving a much smaller bonus for going the extra mile. This comes at a time when many senior doctors are already questioning the value of staying in their roles because of punitive taxation.
‘The fact that the new awards are non-pensionable could be seen as a positive for some because, historically, the payments often triggered annual allowance tax charges. It may be easier going forward to calculate your tax status without considering the CEA pay-
ment, but there could be a substantial loss to pension benefits.’
The 2022 round of the National Clinical Impact Awards was launched in April. Previously the awards in England were worth £36,192, £47,582, £59,477 or £77,320 a year for five years at
Bronze, Silver, Gold and Platinum level. Now the awards will have just three numbered levels and be worth £20,000, £30,000 and £40,000. Wales also has a £10,000 award.
Mr Convey continued: ‘There have been lots of changes to both the national and local CEA schemes in recent years, not helped by the pandemic putting things on hold.
‘These latest substantial changes could have a bearing on your retirement income and, as ever, ascertaining your true financial position as soon as possible is the best starting point to ensure your future security.’
The Clinical Excellence Awards have existed since the inception of the NHS in 1948 but have been in the most recent format since 2004.
BMA’s ban on private units helping NHS is ‘misguided’
A bid by the BMA’s policymaking doctors to prevent consultants treating NHS patients in independent hospital settings has been described as ‘deeply misguided’ by the organisation representing the UK’s private hospitals and clinics.
Doctors at the trade union’s annual representative meeting last month backed a demand for the UK governments to stop the health service using its budget to pay for treatments in the private sector.
One BMA leader complained that money was being poured into expensive independent sector contracts to do NHS work when this would be better spent boosting capacity in the health service itself.
But David Hare, chief executive of
the Independent Healthcare Providers Network (IHPN), responded: ‘Independent healthcare providers have worked hand in hand with the NHS throughout the pandemic and are committed to playing their role in helping clear the growing elective care backlog.
‘Removing the independent sector from the NHS is deeply misguided and would significantly undermine patients’ ability to get the care they need – drastically reducing the capacity available to the NHS at its moment of need, and in turn lengthening waiting times and adding millions to NHS waiting lists.’
Some NHS hospitals are already failing to even discuss private hos-
pital potential. An Independent Practitioner Today website news story last month reported capacity being wasted because NHS hospitals were failing to involve them in planning to ease the elective care backlog in 2022-23.
An IHPN survey of 20 private hospital members found one in four had not been involved in any planning discussions about the elective recovery. Mr Hare has urged the NHS to pull out all the stops to ensure patients can access the care they need. He said most independent providers were being asked to deliver the same or even less NHS activity in 2022-23 than pre-pandemic.
See story on page 6
Patrick Convey of Cavendish Medical
By Douglas Shepherd
Patients’ complaints about fees are on the up Bupa teams up with HCA to take on bowel cancer
Issues over consultants’ fees are a continued increasing trend in the number of formal complaints being made by private patients.
According to the Independent Sector Complaints Adjudication Service (ISCAS) the rising dissatisfaction relates to a lack of transparency about what people will be charged for consultations, tests, investigations and/or surgery. In a new report it is sending for dissemination to consultants at independent hospitals, clinics and other providers, it underlines the need to follow the existing ISCAS Position Statement on Fees.
It highlights these requirements to:
Provide patients with written information about the amount being charged, the associated method of payment prior to outpatient consultations and the commencement of the services;
Be transparent about the costs of any proposed care or treatment;
Explain to patients the reason for any proposed tests or investigations and provide details of any associated costs prior to them being carried out;
Advise patients to check the terms of any insurance policies, where relevant, to enable them to determine their level of cover regarding any proposed tests, investigations or procedures;
Where alternative treatments are available, but the appropriate treatment can only be decided during surgery, to provide a written estimate of costs setting out relevant options and associated fees.
Director Sally Taber said: ‘Over
WHAT THE BUPA-HCA DEAL OFFERS
Key features of the specialist centres for bowel cancer include:
One appointment for all initial diagnostics under one roof within four working days of calling Bupa
Treatment begins within 31 days of first calling Bupa, twice as fast as national targets. Customers can also access clinical trials and genetic testing, if appropriate
Emotional and well-being support from counsellors and nurses, and access to Bupa’s ‘Live Well with Cancer’ and enhanced recovery programmes
recent years, there has been an increase in the number of complaints made about consultants, doctors and the medical care provided, which ISCAS analysed under seven separate headings that range from giving of consent to information about fees.
‘I want to ensure that the learnings are highlighted to all clinicians and thus help to improve patient satisfaction with their treatment.’
ISCAS said its Position Statement on Fees stated at 22.5 that ‘for tests or treatment given on the same day as the consultation, the information may be given orally rather than in writing’.
‘ISCAS seeks to remind consultants that in cases where this information has been given orally, full details of the discussion must be documented in the patient’s clinical records.’
The ISCAS Code covers complaints about doctors and other healthcare professional staff working in subscribing organisations, even if not directly employed by the organisation but have practising privileges.
Other issues identified in complaints about consultants, doctors or medical care include consent, managing expectations, information and advice about procedures, record-keeping and documentation, communication and apologies.
ISCAS said it hoped that following its guidance would lead to a downward trend or reversal in the number of complaints about consultants and their medical care.
A full report will appear in Independent Practitioner Today ’s September issue.
UK Insurance has partnered with HCA Healthcare UK to launch new specialist centres for bowel cancer, giving patients fast access to diagnostic tests and onward care if required.
These offer the health insurer’s customers ‘market-leading speed of access’ from diagnostics to treatment and aim to ensure the patient journey is as smooth as possible by offering all initial cancer tests under one roof.
The first three centres have opened at HCA’s London Bridge Hospital and The Wellington Hospital, and Bupa’s Cromwell Hospital. It is planned to extend the network later this year.
President and chief executive at HCA Healthcare UK, John Reay, said: ‘Partnering with Bupa to launch specialist centres for bowel cancer means that more people will be able to access our rapid diagnostic services – and, if required, the highest standard of person-centred care from our expert multidisciplinary teams, including the latest innovative treatments and, importantly, emotional and physical support therapies.’
and over a third (35%) of adults do not know the warning signs. This is a contributing factor to people being diagnosed with bowel cancer much later when it is harder to treat. A recent study found a third of UK cancer patients are now first diagnosed after going to A&E with severe symptoms.*
To speed access to cancer tests and treatment, Bupa customers who are worried about symptoms can call its Cancer Direct Access service to be referred to the specialist centres for bowel cancer, usually without needing to see a GP.
There they can have all initial diagnostic tests and scans in the same appointment for a diagnosis and if it is not cancer, be given the all-clear on the same day.
If treatment is needed, it will start within 31 days of calling the insurer – twice as fast as national targets.
Bupa UK Insurance chief executive Alex Perry said the insurer’s network of specialist centres for breast cancer launched in 2019 had helped thousands of patients to get the all-clear or a diagnosis and access to quick treatment.
Bowel cancer is the second biggest cause of cancer deaths in the UK, with 43,000 people diagnosed each year.
But findings from the new Bupa Wellbeing Index conducted by Censuswide show there are significant levels of confusion and embarrassment surrounding the disease
Bupa commissioned Censuswide to poll a nationally representative sample of 8,185 UK adults. The data was collected between 18-24 March 2022. (See page 22).
* According to research published in the Lancet Oncology journal, more than a third of British cancer patients are diagnosed in A&E
Bupa
John Reay
FIPO decries inaction by competition watchdog
By Robin Stride
The Federation of Independent Practitioner Organisations (FIPO) aims to continue campaigning to persuade the Competition and Markets Authority (CMA) to investigate private medical insurer practices, which it claims distort competition and limit patients’ choice.
It wrote to the watchdog last month about the issue citing insurers’ threats of delisting if senior consultants’ fees were not reduced and the effects on patients’ ability to choose their specialist.
The CMA replied that FIPO’s information did not provide sufficient grounds for it to carry out a market study at this time.
FIPO called the response disappointing, but said it provided a window to accrue further evidence
from consultants about insurers’ behaviour.
It is asking any consultants who have been treated in a similar way by any insurer to get in touch with it or its sister organisation the London Consultants’ Association (LCA). It said names would be redacted.
The doctors’ body said: ‘Insurers are there to re-imburse on behalf of their clients who pay premiums to defray the costs of private treatment. They, of course, have a maximum amount they will pay for a given service and many consultants choose these amounts for their fees.
‘We believe that the issue now is that many insurers are actually telling consultants what their fees should be. Some even have a so called ‘fee calculator’ available on their website.
‘FIPO finds this surprising since, in 1993, the BMA were told by the then Monopolies and Mergers Commission that suggesting fee levels in their guidelines constituted a complex monopoly.’
Increasing pressure from insurers on consultant re-imbursements meant that a situation the CMA had foreseen had come to pass, FIPO added.
It has been reminding the CMA, which published a Private Healthcare Market Investigation Order in 2014, of its own words: ‘If extensively and rigidly applied, fee-capping consultants could lead to distortions in competition between consultants and to reduced consumer choice.
‘Fee-capping – and derecognition of consultants who do not agree to abide by the insurer’s fee schedule – has the potential to
increase the disincentives on consultants from setting fees to reflect their costs, experience, expertise and the local market conditions.
‘This distortion may potentially be increased, the greater the number of insured patients on policies that require open referrals from GPs, as policyholders are channelled to lower cost consultants.’
FIPO said if patients’ policies were for ‘fee-assured’ doctors only, then their choice would be very limited and generally to those consultants on the lowest re-imbursement rates.
‘Should these patients wish to go to a more experienced consultant or be given a tertiary referral to a non-fee-assured super-specialist by their original consultant, this may well be denied even if the patient wishes to top up.’
War and inflation hit PMI market
High inflation and the economic fall-out from the Ukraine war and sanctions against Russia could hit demand for private medical insurance, market analysts warn.
The financial problems will reduce personal disposable income as well as increase margin pressure on companies, they say. But the positive side for private health interests is seen as the huge backlog the NHS is struggling with as a result of Covid and shortages of qualified healthcare staff, which the Government recognises will take several years to correct.
LaingBuisson’s latest Health Cover UK Market Report, 17th edition states the same economic factors may increase company-paid demand for private medical cover as employers seek to retain staff.
Authors, economist William Laing and former Bupa UK Insurance operations director Riko
Scandelius make no short-term projections of demand but report sector sources indicating there was continued growth last year.
Their report says: ‘The deterioration of NHS waiting times and many other aspects of NHS services during and after Covid should, other things being equal, be a major factor boosting company-paid and individual demand for access to private healthcare through health cover products.
‘But the lessons of recent history highlight the primacy of the state of the economy and consumer confidence rather than state of the NHS.
‘With the UK apparently having entered into a phase of “stagflation” in 2022, albeit temporary, the immediate prospects do not look positive for that element of economic growth and consumer confidence which can support
expansion of mainstream private health cover demand.’
Demand for UK private medical cover, as measured by subscribers to private medical insurance and enrolees in self-insured medical expenses schemes (healthcare
trusts), rose marginally – 0.4% – in 2020, after 2.5% growth in 2019.
Subscriber/enrolee numbers reached an estimated 4.1m at December 2020. Including dependents, 7.1m people had private medical cover – 10.6% of the UK population (12% in the early to mid-2000s). 2021 figures, when available, are expected to confirm further growth.
The authors believe ‘well-being’ is the one element of health cover, funded by employers, that appears to have the potential for transformative expansion in the medium term.
Whether it reaches its full potential depends on the capacity of largely online services to engage their audience and demonstrate real value to both employers and employees, they say. ‘For employers, the “holy grail” would be strong evidence of payoffs in containment of sickness absence.’
By Edie Bourne
Private doctors will have no NHS work to do in private hospitals if policy-making doctors at the BMA get their way.
At the annual meeting of the union in Brighton, a majority of its representatives from all specialties voted in favour of demanding the UK governments block health service cash from being used to pay the independent sector.
They backed a motion from the association’s Islington division calling for the money destined to pay the private sector to do NHS work to be invested instead in expanding NHS capacity.
BMA council deputy chairman Dr David Wrigley said: ‘After the most harrowing two years of their careers, staff are now staring headlong at a further tsunami of work with no back-up. The cavalry is not on the way.
Private care ‘must not get NHS cash’ Rutherford group to be wound up
Covid has contributed to the demise of another victim with the application of The Rutherford Health group, operators of a network of UK cancer and diagnostic centres, to be placed into liquidation.
Since 2015, it built a network of Rutherford Cancer Centres in south Wales, Northumberland, Liverpool and Thames Valley and recently opened the first community diagnostics centre of its kind in England, in Somerset.
The group comprises subsidiary companies including Rutherford Cancer Centres, Rutherford Diagnostics, Rutherford Innovations and Rutherford Estates.
Sean Sullivan, chief restructuring officer and interim CEO, said: ‘Rutherford Health has been committed to providing high-quality care and the past couple of years
‘And we cannot continue pouring money into expensive contracts with the private sector –dealing with its own Covid-related backlog – to do NHS work, when this would be better spent boosting capacity in the health service itself, something the Health Secretary seems to be ruling out.’
The meeting backed motions calling for the Government to urgently put in place an NHS workforce plan to tackle the record backlog in care and also demanded the governments invest money to recruit, train and retain staff, and drop unrealistic targets that put ‘impossible pressures’ on employees.
Dr Wrigley observed: ‘Even before the pandemic the length of time people were waiting for the care they needed was too high. But following the huge disruption and added pressure Covid-19 placed on the UK’s health services, waiting
lists have now gone up to a perilous level.
‘We have a record 6.5m people waiting for treatment in England, as well as the significant “hidden backlog” of people who have still to come forward for care after the worst of the pandemic or whose referrals were cancelled.’
He said: ‘We continue to lose doctors to burnout, punitive pension taxation rules and bureaucratic barriers for colleagues from overseas –all areas the Government can tackle now. If they fail to do so, patients will continue to suffer and the impact on the health of the nation will be devastating.’
Dr Wrigley added: ‘Without knowing how many staff are needed to safely deliver services, now and into the longer term, how on earth can the Govern ment, education and training providers and healthcare leaders plan ahead for the care that patients need?’
The Medical Defence Union has voiced concern that the amount of money earmarked to cover clinical negligence claims against the NHS has risen to an ‘astonishing’ £86bn.
Dr Michael Devlin, its head of standards and liaison, said a Treasury report showed provision for clinical negligence claims in England was worth £3,600 for every household, compared to £700 ten years ago.
He said a House of Commons’ Health and Social Care Select Committee report, which included evidence of a system on the brink of disaster, found the system for compensating injured patients in England was unfit for purpose, being grossly expensive, adversarial and promoting individual blame instead of collective learning.
‘It is vital that the Select Committee’s warning is heeded and that the Government quickly moves ahead with the legal reforms that are necessary.’
has proven to be an extremely challenging time for the business.
‘Covid has been particularly damaging for us, as fewer patients were presenting with side-effects during the lockdowns and, as a result, cancer diagnosis has been delayed and sadly, in many cases, missed. This has meant fewer cancer patients have been presenting to our centres.
‘Added to that, the business had grown rapidly over recent years. It was a very expensive business to set up, with over £240m of capital expenditure to build and develop the cancer centres across the country, but, unfortunately patient numbers have not matched that.’
Mr Sullivan said the company made several offers to the NHS, but the number of contracts secured were insufficient.
This added to severe financial pressures on the business leaving it no option but to place the group into liquidation.
But Rutherford was ‘very proud’ to have been able to serve the community and cancer patients across the country.
Its centres offered an extensive range of advanced cancer treatments including high-energy proton beam therapy, radiotherapy, chemotherapy, immunotherapy, diagnostic imaging and supportive care services.
Arrangements were made to transfer patients to alternative facilities and a small number of locally commissioned NHS patients were returned to their local NHS trust to finish their treatment.
Rutherford said: ‘The group had
invested heavily in building its cancer centre network, one of the most advanced in Europe, and the cost of infrastructure combined with impacted patient flow presented extremely challenging trading conditions.
‘The group made efforts to increase patient flow by offering the NHS a not-for-profit national contract in addition to existing local contracts, but this was not taken up.’
Rutherford Cancer Centre in Cardiff
A defence body has urged for an urgent Government update on when it will strip the GMC’s power to appeal Medical Practitioners Tribunal Service (MPTS) decisions – a commitment it made four years ago.
The Medical Protection Society’s call came after a Freedom of Information request showed the GMC had lodged 23 appeals since June 2018, when the Government accepted recommendations of the Prof Sir Norman Williams review into gross negligence manslaughter.
His review, following the case of Dr Hadiza Bawa-Garba, said removing the GMC’s right of appeal against MPTS decisions would help address doctors’ mistrust of the Council and contribute to cultivating the openness culture needed for improved patient safety.
It also said public protection would still be maintained, with the Profes sional Standards Authority retaining its near identical right to appeal MPTS decisions.
MPS medical director Dr Rob Hendry said: ‘The GMC’s power to appeal decisions made by the MPTS has created distrust between the medical profession and the regulator and contributed to a culture of fear.
‘Fitness-to-practise proceedings are stressful and lengthy enough for doctors, without the added worry that the GMC can seek to override the decision made by the MPTS if it does not agree.
‘This is a concern for all doctors, whether they are working in the NHS or in private practice.’
Thirteen leading healthcare organisations last year joined MPS in calling on the Government to finally see through its commitment on this.
Dr Bawa-Garba was erased from the medical register after the GMC appealed against a tribunal ruling suspending her for 12 months, then reinstated after judges found the original tribunal decision appropriate.
GMC powers ‘causing distrust’ Women surgeons suffer huge amount of abuse
By Agnes Rose
A Europe-wide survey has highlighted struggles of abuse and discrimination faced by female surgeons and is urging healthcare leaders across the globe to act.
Key findings include:
72% of female surgeons surveyed have suffered or witnessed gender abuse;
Over half have been personally attacked or humiliated at work by colleagues;
Just 17% of male surgeons say they have witnessed gender discrimination at work;
44% of both male and female surgeons feel their work institution or employer does not guarantee respect in gender equality, sexual orientation or race diversity.
In response to the study, which interviewed 300 female surgeons, the European Society of Coloproctology (ESCP) has launched its ‘Operation Equal Access’ campaign.
This aims to expose and explore how a range of inequalities across the medical sector are impacting well-being, patient care and career progression.
Female surgeons received ‘widespread discrimination by male col-
leagues while they work’ including abuse and humiliation, according to the study.
Some 72% of female surgeons have witnessed or suffered gender inequality at work. Over half (56%) have endured personal attacks, a toxic work environment or even humiliating comments by colleagues.
Dr Franco Marinello, consultant colorectal surgeon at the Vall d’Hebron University Hospital in Barcelona, called the study a wakeup call.
He said: ‘Discrimination in surgery continues to be an unresolved issue in many countries. We simply cannot accept unfair treatment any longer. We hope this new research highlights the struggles facing female surgeons and urge healthcare leaders across the globe to take action.’
Race and religious discrimination was an issue for one-in-ten (12%) surgeons. And those who have suffered racial or religious discrimination were particularly likely to observe a negative impact on their chances of receiving a promotion (39%) or to develop surgical techniques (27%).
ESCP member Vittoria Bellato added: ‘When speaking to colleagues about measures in place to
A survey revealed that over half of female surgeons have been
work
counter inequality in medicine, we found the measures in place are specific to a single hospital unit, and not representative of a national framework.
‘Our campaign aims to help fill a gap in the data, initiate a proactive conversation among surgeons on this issue and prompt positive change as a result of this exchange of information and ideas.’
Spencer Hospitals recruiting new chief executive
An opportunity has opened for one of the biggest private patient leadership roles outside London now that the longstanding Spencer Private Hospitals’ (SPH) chief executive Di Daw has announced her retirement for later this year.
Spencer Private Hospitals (SPH) is a wholly-owned subsidiary of East Kent Hospitals University Foundation Trust (EKHUFT) which bought Spencer’s parent company shares in 2008. It sold them in 2009 after achieving foundation status, then repurchased them in 2012.
Spencer provides a blend of both NHS PPU-style private patient services, but also delivers NHS waiting list activity and has annual revenues of approximately £14m.
SPH operates from the three main EKHUFT sites at Margate, Ashford and Canterbury, utilising many of the trust’s facilities such as operating theatres, radiology and pharmacy.
This is managed through a contract and service-level agreements with SPH paying a percentage of income for each service to the trust. It employs more than 130 staff across all sites.
Philip Housden is a director of Housden Group
attacked or humiliated at
Compiled by Philip Housden
Dr Rob Hendry
Major ortho clinic opens in Hants
By Olive Carterton
Consultants were on hand to see in the official opening of a new orthopaedic and vision care clinic extending the private practice offering available in Hampshire.
Winchester and Chandlers Ford MP Steve Brine cut the ribbon alongside former international hockey star Alex Danson-Bennett to declare the Healthshare Clinic Winchester in business.
With 15 consultation rooms, it will be the company’s flagship site, with facilities including Hampshire’s only private 3T MRI scanner and aims to offer improved patient choice, helping to support private and NHS patients in the local area.
Mr Brine said: ‘Post-Covid, we
know that there are challenges in tackling the NHS backlog, and so improved patient choice and, of course, relationships between the NHS and independent healthcare providers is vital. We’re very lucky to have this fantastic facility open and available in Winchester.’
The day-case facility has 42 consultants with practising privileges and another 92 are in progress. It also offers private GP and physiotherapy services, with a pre- and post-rehabilitation gym with topof-the-range equipment.
Alex Danson-Bennett, Olympic hockey gold medallist, now retired, said from her perspective as both an athlete and a local resident, the facilities were ‘exceptional’.
‘Being able to see leading con -
(Left) Steve Brine MP and hockey gold medallist Alex Danson-Bennett cut the opening tape
sultants, some of which I have worked with for many years, as well as rapid access to imaging and physiotherapy, provide a fantastic new option for both local sportspeople and the general public.’
Specialties include diagnostics, orthopaedics and vision care.
Partnering with leading specialist consultants, the hospital will offer access to the latest diagnostic technology including a Siemens widebore 3T MRI scanner, X-ray, ultrasound and standing CT, as well as a large outpatients department, two operating theatres and private patient rooms.
Attendees at the opening event in Chilcomb, on the city outskirts, included senior figures from Healthshare Group, staff and members of the local business community.
Hospital executive director Jacqui Dorney said the clinic would provide rapid access to top consultants and technology.
Healthshare is an independent healthcare provider with established roots in muscular-skeletal health and diagnostics, founded by expert NHS clinicians.
Independent charitable hospital King Edward VII’s has added genetics testing to its services.
The new service supports patients by identifying the genetic risks of developing breast cancer.
Spearheading the service are adult and breast cancer genetics specialist Dr Anjana Kulkarni, Prof Marc Tischkowitz, chairman of the UK Cancer Genetics Group, and Dr Vishakha Tripathi, genetic counsellor and chairman of the Genetic Counsellor Registration Board.
Dr Kulkarni said: ‘Genetics are increasingly becoming an essential element of cancer treatment and I’m thrilled to be working with King Edward VII’s to further the UK’s offering in the field.
‘With greater understanding of genetics, though, comes the need for more holistic support for patients, which is such an important element of the hospital’s unique offering. Identifying any mutations through DNA testing is just the first step in the care journey.’
There are plans to use genetics screening for other cancers in the future.
HCA’s Lister Fertility Clinic expands
HCA’s Lister Fertility Clinic has expanded its reach by launching a new fertility centre at The Portland Hospital in central London.
The move comes in response to increased demand for fertility care and treatment.
The clinic, one of the most successful IVF treatment clinics in the UK, has seen more than 20,200 babies born since opening in 1998. It performs around 2,400 fresh cycles of IVF each year.
It said it hoped the new clinic would make it easier for patients living across London and beyond to access world-leading services.
The development enables a continuity of care for patients at HCA’s The Portland Hospital’s offering in maternity, gynaecological and paediatric care.
It will provide the full spectrum of fertility care to patients, with a specific focus on IVF. This will include initial and follow-up fertil-
ity and gynaecology consultations, scans, ovulation induction, cycle monitoring, intra-uterine insemination, frozen embryo transfer cycles and blood tests, as well as performing egg retrieval and embryo transfer.
At the forefront is Mr Rehan Salim, specialist in reproductive medicine, who joins the team after over 20 years’ NHS experience.
He said: ‘There is a growing demand for fertility services
within central London and so the new clinic at The Portland Hospital offers a hugely exciting opportunity to further extend the expertise of Lister Fertility Clinic so that even more patients can benefit from its services.’
Lister Fertility Clinic chief executive Suzy Canham said the centre encompassed every part of the fertility care and treatment process and patients had access to unparalleled IVF expertise.
Dr Anjana Kulkarni
MDU/Independent Practitioner Today 2022 survey IMPACT OF THE PANDEMIC ON PRIVATE PRACTICE
Dear Reader
Independent Practitioner Today is running a survey in partnership with the MDU to find out your views about the impact of the pandemic on private practice.
We’d be very grateful if you could spare the time to take part. In return for completing the survey you can ask to be entered into a draw for a chance to win one of two £100 Amazon vouchers.
Click here to take the survey, whose questions are also repeated below.
Please answer these questions based on your experiences in private practice only – even if you also work in the NHS.
The survey will run until midnight on Sunday 31 July.
Your responses to this survey will remain anonymous. The results of the survey will be shared with the MDU to be used in marketing communications, but no personal information will be passed on.
You can read the prize draw terms and conditions by clicking here
Many thanks for your help.
Best wishes,
Editorial director
Complete our survey for a chance to win a £100 voucher
1. What position best describes your current role?
a) Consultant
b) General practitioner
c) Retired
d) Other (please state)
2. How has your private practice been affected since the pandemic?
a) Activity has increased since the pandemic
b) Activity has decreased since the pandemic
c) Activity is similar to pre-pandemic levels
3. Do you anticipate undertaking more private practice work over the next two years?
a) Yes
b) No
4. Did you provide additional NHS services during the pandemic?
a) Yes, I provided additional NHS services for the duration of the pandemic and continue to do so
b) Yes, I provided additional NHS services but am not currently
c) No, I did not provide any additional NHS services during the pandemic
[If answer yes, go to Q5. If answer no, then jump to Q6]
5. Do you anticipate undertaking more NHS work over the next two years?
a) Yes
b) No
6. In what ways has private practice changed following the pandemic?
(Please tick all that apply)
a) Waiting times for patient initial appointments have increased
b) Waiting times to complete treatments have increased
c) Patients presenting with more advanced pathologies
d) Increased demand for routine screening and tests
e) Increased use of remote consultations/ telemedicine
f) Greater flexibility of appointments for patients
g) Greater flexibility of work for doctors
h) Easier to communicate with patients
i) Harder to communicate with patients
j) Other – please explain
7. How likely are you to undertake employed, rather than self-employed, work in private practice?
a) Highly likely
b) Somewhat likely
c) Neither concerned nor unconcerned
d) Not likely
e) Not at all
f) I am already working in an employed role in private practice
8. To what extent do you agree with the following statement: I am more likely to retire from private practice due to the pandemic?
a) Strongly agree
b) Tend to agree
c) Neither agree nor disagree
d) Tend to disagree
e) Strongly disagree
9. How has working during the pandemic impacted upon your health and well-being? Please rate (agree or disagree)
f) I feel stressed and/or anxious on a weekly basis
g) I often go to work when I do not feel fit or well
h) I am unable to spend adequate time with patients
i) I feel like I am making a positive difference to my patients
j) I feel I am able to do my job effectively
k) I am supported by my colleagues
l) Relationships at work are strained
m) I feel I have a good work/life balance
10. How would you rate your stress and anxiety levels now compared to before the pandemic? (Tick one)
a) Significantly worse
b) A little worse
c) No change
d) A little better
e) Significantly better
11. Do you have any further comments about your experiences of the pandemic or what the MDU could do to help you in your private practice?
A look back through our journal’s archives of a decade ago reveals that although times change, some issues are not so new
A trawl through the archives: what made the news in 2012
Beware the ‘traps’ of groups
Consultants planning to join groups were being urged to beware of a cash trap which could leave them tens of thousands of pounds out of pocket.
Growing numbers of doctors were embarking on ‘big is beautiful’ business structures, but advisers warned they needed to be careful they were not victims of their own success.
Often the amount of financial administration needed was underestimated and, as a result, they found they had less money in the early months than they earned when they were practising solo or with just another partner.
Billing exert Garry Chapman, of Medical Billing & Collection, warned that most groups initially underestimated the level of administrative activity created by working together in the mushrooming ‘centre of excellence’ sector.
The volume of phone calls from patients, private medical insurers, other clinics and hospitals typically resulted in delayed invoicing because the patients took priority, he said.
These holdups then resulted in greater bad debt, as not only were invoices going out late but practices were often running out of time to chase the outstanding bills.
Writing in Independent Practitioner Today, he warned:
‘This situation can then escalate very quickly, as the busier the group practice becomes, the less time is spent on the billing.
‘That results in a backlog of work which has either not been billed or not collected. In many cases, this can actually result in consultants earning less money than they were before they formed or joined a group practice.’
Mr Chapman said it was not unusual for a group practice to seek help after running up a sixfigure backlog.
Get ready for rise in mortgages
Doctors with massive mortgages were being warned they could soon be hit by sharp rises in their repayments.
Some of the biggest mortgage
lenders had just announced increases to repayment rates on their standard variable rate loans.
The move came despite no change to the base rate set by the Bank of England, which had stayed at 0.5% for three years.
With the average senior doctor likely to be considering not just one property but also loans on second homes or university houses for children, they were warned that a significant hike on variable rates could have a substantial effect on income.
Average new mortgages for private doctors were around £400,000 with the top end at £2m.
Pay tax now to avoid a 10% fine
Medical accountants were advising independent practitioners to act immediately to pay their tax bills due to HMRC on 31 July.
A typical average consultant would need to pay over £10,000 and the advice was to ensure this was paid by 27 July so that it was received on time.
18% fail to pass the CQC visit
Nearly oneinfive independent healthcare providers just inspected by the Care Quality Commission (CQC) in England failed to meet all
the essential standards of quality and safety.
It found 82% in the private sector were hitting the targets; a higher performance than in the NHS (77%) and adult social care (72%).
The CQC said it aimed in future to provide more insight into systemic reasons for poor performance.
Martha Walker, an independent adviser on CQC registration to GPs and consultants, said: ‘The key to a successful inspection is to ensure that you understand what evidence is required for each outcome, make sure it is in place, up to date and everyone who should know about it does.’
TELL US YOUR NEWS
How about making the news today? Independent Practitioner Today is always keen to hear from doctor entrepreneurs willing to share their stories in private practice – and from independent practitioners embarking on the journey.
Contact our editorial director Robin Stride at robin@iptoday. co.uk
Martha Walker, adviser on CQC issues
Choose protection with real value
The devil is always in the detail. Compromising quality of protection for price could leave you exposed when you most need support. With Medical Protection, you’re protected for a range of different scenarios by the largest team of medical defence experts in the world.
That’s why it pays to check the hard facts, not the soft claims.
For just £549, consultants working in the NHS can feel safe in the support membership brings. We also offer competitive, tailored prices for consultants working in Private Practice.
GROWTH IN SELF-PAY
London is busy, but lags behind
Ted Townsend, author of LaingBuisson’s eighth edition of its Private Acute Healthcare Central London report, looks at whether the growth being seen across the capital’s private hospitals is set to last
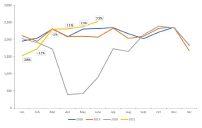
SELF-PAY REVENUES for private hospitals in central London have been slow to come back, although now appear to be booming, according to analysis by LaingBuisson.
Data provided by the Private Healthcare Information Network (PHIN) shows that self-pay volumes in the area for the first half of 2021 were only marginally up on the first six months of the 2019 fiscal year (H1) and, in fact, slightly down on the same period in 2018.
However, during the same period, self-pay volumes were booming in the rest of England, with volumes up an average 25-30%, although this disguises a huge variation within the period.
Broadly, outside central London, the first three months of 2021 were only marginally up on 2019, while for the later months the growth reached up to +42% in April, +44% in May and +55% in June.
However, in central London,
self-pay volumes in the first three months of 2021 actually fell by a total of 39% compared to 2019 before bouncing back more modestly +11% in April, +13% in May and + 23% in June.
Pick-up in activity
Given that self-pay volumes in central London in the first half of 2020 fell by 42% – and in the second half by 19%, or 25% overall –compared to 2019, it appeared that the region was struggling to make
up the deficit of around 7,000 selfpay episodes lost during Covid. (see graph above)
However, HCA’s revenues were up around 2% vs 2019 across calendar 2021, suggesting H2 saw a real pick-up in activity, while anecdotal reports from other private hospitals suggest everyone is ‘busy’. Given that embassy and private insured patients are all at much weaker levels than 2019, the difference must be self-pay.
HCA commercial director
Source: PHIN, number of episodes, percentage changes vs 2019
OLLIE
DAWE
Andrew Coombs says: ‘We’re very confident about self-pay. All the arrows are pointing in the right direction.’ Indeed, ‘patients are arriving sicker’, says Mr Coombs.
And this corresponds to Spire’s self-pay results. About half of its 63% increase in self-pay revenues for 2021 over 2019 was attributed to an increase in volumes, the rest to increases in average revenue per case.
Apart from addressing some of the self-pay backlog, private hospitals are benefiting from the slower return to normal service by the NHS’s private patient units.
How long any of this will last is an open question.
Regional shift
Indeed, the relative boom in noncentral London self-pay suggests there has been a regional shift out of London, at least until more employees start coming back into the city on a regular basis.
If this shift was happening in the private medical insurance (PMI) market – and there is some evidence it is –then ‘I’d be loving it,’ said one insurer privately.
The main structural reason is that central London hospitals are broadly set up to treat more complex albeit still elective patients. This means they are more focused on attracting PMI and well-paying international or embassy patients.
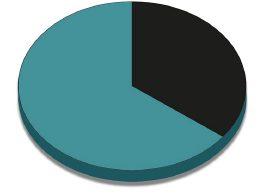
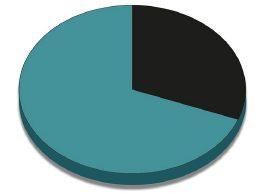
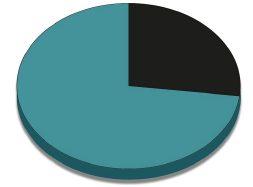
Looking only at the two payer groups, PMI and self-pay, the latter has increased its share of activity from 18% to 21% over the past three and a half years, according to the PHIN data, or a +3% share gain in Central London.
However, in the rest of England, the same figure has gone from 29% to 37%, or +8%, on a much higher base.
CENTRAL LONDON SELF-PAY ACTIVITY BY MAIN CONSULTANT SPECIALTY
Note: the top ten specialties account for c. 85% of total activity in central London;
Source: PHIN 12 months from July 2020 to June 2021
Given self-pay often comes third in most central London hospitals’ list of priorities – depending on how good a year it is for embassy patients – logistically it is often difficult for them to convert initial inquiries into actual procedures in theatre.
Prospective patients
I constantly hear stories about who is going to answer the call, and whose job is it to follow up with the prospective patient.
Some of the smaller hospitals, where call-handlers know the different consultants and their specialties and can book initial consultations on the hospital’s internal software while the patient is still on the line seem to do better than the bigger groups where inquiries are managed through centralised systems.
This applies to benefit both PMI
2018-2021
Central London hospitals have a different mix of activity compared to the rest of the UK
and self-pay patients, as it happens. (See graph below left).
This analysis is supported by evidence, again from PHIN, that central London hospitals have a different mix of activity compared to the rest of the UK.
For example, while specialties like ophthalmology, general and plastic surgery are roughly the same in relative importance for an in-London or out-of-London hospital, specialties like gynaecology, gastroenterology and medical oncology are much more important to central London hospitals.
Teaching hospitals
The reasons for this are varied but in part depend on the expertise of the central London teaching hospitals compared to the rest of the UK, as well as the predominance of super-specialisations in those hospitals that can be transferred to the private sector.
their list of ‘big-hitter’ consultants who bring with them their whole practice of PMI, self-pay and international patients, generally at the more complex end of the scale.
Financially, these consultants often do not need to chase selfpay work by lowering prices or agreeing to package deals just to get volumes up, so it seems much harder for inquiries generated by the hospital to convert into actual treatments in theatre simply because the consultant is not interested.
There’s probably a little bit more interest in self-pay at the moment because PMI and international patients have been slow to come back and, indeed, some of these volumes are in fact still down on 2019, so it is not yet clear if this increase in self-pay activity is sustainable.
All of these more complex cases leave less room for the bread-andbutter of self-pay – hip and knee surgery – in the capital.
Whereas outside London this is between a quarter and a third of private hospital activity – generally more on revenue – trauma and orthopaedics represents only 10-15% of patient volumes in London, depending on the hospital. (See table at top of page).
Another factor, though harder to quantify, is that central London hospitals have fought to build up SPLIT OF ACTIVITY BY PAYER –
Anecdotally, there is also, of course, a lot for these consultants to get on with in their NHS practices as well, so sometimes they have less time for private work overall.
We sometimes forget in private healthcare that often it is the consultant that is the brand and that drives activity. That means it can be hard for a hospital to ‘move the dial’ on self-pay without the other’s full engagement, at least in central London.
This article first appeared in Healthcare Markets and is used with their kind permission
Benefits of annual accounts
YEAR-END ACCOUNTS for a business are often just seen as a necessary process that needs to be completed for submission to Companies House and used for the preparation of the annual tax return – whether corporate tax or self-assessment for a partnership or sole trader.
In my opinion, it is far more valuable for a business to view this as an opportunity to assess how they are performing and plan their future strategy.
Annual accounts meetings often occur after the accounts have been prepared, with the agenda being mainly focused on finalising the accounts and associated tax return.
But it is of far greater value to arrange a meeting with your accountant before the accounting year-end.
This way, the meetings will be pro-active rather than reactive. You can work with your account-
ant to ensure that the business is being as tax-efficient as possible, and any identified issues or potential benefits are addressed on a timely basis.
There are often tax-efficient measures to be implemented; for example, how staff are remunerated.
You can also ensure that, for pensions to be an allowable deduction for tax purposes, they are fully paid within the accounting year.
Plan for eventualities
And it is a good opportunity for business owners to ask the ‘what if’ questions and plan scenarios for various eventualities.
These questions can be:
What if I bought a car?
What if I refitted the surgery?
What if I developed an online diagnostic tool?
What if I want to exit the business?
The economy and all businesses
in general have had to adapt and change focus over the last couple of years and, with the increased cost of living, it is even more important to have timely management accounts, budgets and forecasts to ensure the businesses remain on the desired targets.
Budgets and forecasts should not be seen as a one-off annual exercise but should be revisited and revised or updated on a regular basis.
Your accountants are able to do far more than just prepare and submit your annual accounts and tax returns. They should be an integral part of your planning process to assist you with the smooth running of your business.
Julia Burn (right) is a director at Blick Rothenberg and part of the team advising medical practitioners
Do you specialise in treating varicose veins or venous conditions?
We are looking for new consultants
The Whiteley Clinic is expanding and we’re looking for full and part-time Surgeons and Interventional Radiologists who want to specialise in treating varicose veins and other venous conditions.
Why join our award award-winning team?
Receive full training in The Whiteley Protocol
Ongoing support & training and Back-Office services will be provided
Become a member of The College of Phlebology
Access to the Venous Registry
Excellent results and patient satisfaction
Positions available current clinic locations plus new locations to be announced.
Please contact us for more information at jobs@thewhiteleyclinic.co.uk
TROUBLESHOOTER: THE COST OF LIVING CRISIS
How to help your staff
Our Troubleshooter Jane Braithwaite answers independent practitioners’ frequently asked questions on business matters. This month, she tackles what the rocketing cost of living crisis means for doctors as employers – and suggests what can be done
staff financially
FOR THE last few months, one of the top news stories each day relates to the increasing cost of living in the UK.
The headline as I write is that inflation has hit the highest rate in 40 years and reached 9% in April 2022. Maybe by the time you read this it has gone even higher.
Energy prices are increasing drastically as well as the cost of food, clothing and many other household items. As a result of the increase in inflation, the Bank of England raised the base rate of interest for the first time in many years, putting more pressure on home-owners with higher mortgage payments.
With the additional increase in National Insurance, this is all putting a significant number of people in the UK under financial pressure.
I think it is safe to assume that most employees would like a pay rise in their current job or they will start to look for a new role with a higher salary. As employers, there is a risk that we will lose staff if we do not take action to support our current employees.
Pay demand
Most employees will be demanding a pay increase at least in line with inflation so that they feel they are at least standing still in terms of their financial well-being. But for most employers, the prospect of giving every individual within their company an inflation-based increase is simply not a possibility.
Offering every employee a pay rise in line with inflation is not only difficult for most employers to deliver, but economists would warn us against doing so for other reasons.
Now, I am no expert when it comes to economics, but my understanding is that economists caution us against increasing salaries across the board, as it would
allow spending to continue at current levels, which will cause inflation to continue to rise resulting in a vicious circle.
I am happy for anyone to question this, of course, as many readers of Independent Practitioner Today will have a far deeper understanding of the issue than I can claim to have.
Research shows us that one of the most common causes of stress for individuals is their financial well-being and this is going to become a major concern for many more in the coming months and potentially years.
Extreme stress
As employers, we also appreciate that if our teams are feeling stressed in their personal lives, they are not going to be able to perform to the best of their abilities in the workplace and extreme stress can also lead to a higher absence rate from work due to ill health.
So, what do we do to support our employees through this difficult time? If increasing salaries in line with inflation is not possible and not advisable, then what do we do as employers?
Maybe the answer is to increase salaries where possible by a margin not in keeping with inflation but enough to try to alleviate the situation for individuals, especially for those on lower salaries. There may be other ways in which employers can help by thinking beyond the immediate issue of salaries.
Several schemes may be relevant to our employees, including season ticket loan schemes which aim to help employees where the cost of commuting is a major budget item.
Research by the company Employee Benefits confirms that this is one of the most common benefits offered by employers, with 59% of employers doing so.
The season ticket loan is an interest-free loan for employees to cover the cost of traveling to and from the workplace via modes such as tram, rail or bus. Some schemes can also be used to cover parking costs too. The loan repayments are paid monthly through the employee’s net pay over a set period.
For keen cyclists, the cycle to work scheme* could be an attractive possibility. It allows employees to save 26 to 40% on their bikes and accessories. The employee has no up-front payment and the monthly payments are taken taxefficiently from the employee’s salary by their employer.
Tax breaks
During the Covid pandemic, when we were all advised to work from home if possible, the Government introduced tax breaks to help alleviate high energy bills.
From April 2022, this tax break has been tightened and while some employees can claim, for many this is no longer possible.
Without a doubt, heating costs are higher for those working from home and next winter this will become more of an issue. If the Government is not going to provide support for home workers, then employers may need to step up.
For companies who have introduced a working-from-home strategy, there will be cost benefits associated with reducing the need for office space and a proportion of this saving could be passed on to employees to help with higher energy costs.
A different type of approach would be to offer an Employee Discount Scheme to help employees save money on their purchases. These schemes offer employees discounts for products and services that they are likely to buy regularly. For example, one com-
pany called PerkBox offers discounts at Sainsbury’s and M&S.
The final suggestion is to help employees manage their finances more effectively by offering access to support services and financial training.
There are lots of organisations and training providers offering such support and these could prove to be very helpful to some employees. But this type of approach needs to be handled with extreme care to avoid any suggestion that employees are being judged or criticised.
Tone deaf
Over recent times, we have seen numerous politicians slated for their comments regarding individuals being unable to budget and unable to cook.
It was even suggested that individuals solve the issue by taking on extra hours or an extra job. All of these comments appear tonedeaf to people who are working hard just to keep their heads above water.
Everything I hear and read suggests that the cost-of-living crisis is going to be a long-term issue and so, as employers, we must do what we can to support our employees.
One obvious solution for our employees will be to move to a better-paid job and so, if we do not take action, our biggest issue will be a recruitment crisis, which is time-consuming and expensive.
Retaining our employees by supporting them will prove to be the best option for both employer and employee.
If you have any specific questions that you would like answered in coming editions, please do get in touch.
* www.gov.uk/government/ publications/cycle-to-work-schemeimplementation-guidance Companies a doctor can use to implant the scheme include: www.bike2workscheme.co.uk www.cyclescheme.co.uk
Jane Braithwaite (right) is managing director of Designated Medical, which offers flexible, experienced support for doctors’ private practice needs
Good advice on managing staff
Being a successful manager does not come easy to many doctors. Jane Braithwaite (right) reviews a book that sets out to help
The Successful Manager: Practical Approaches for Building and Leading HighPerformance Teams, James Potter and Mike Kavanagh, ISBN-13: 979-8557682312 Available from Amazon.com
MANAGING PEOPLE can be one of the most rewarding jobs. Just ask someone to describe their best manager and you will hear very clearly the impact that a good manager can have on an individual.
But managing teams is challenging and requires a new set of techniques, expertise and processes.
For most people, the journey into a management role goes something like this.
You master your job role and your company recognises you as a valued employee who delivers great work. Your company offers you a promotion into the role of team manager so that you can lead a team of individuals, some of whom were your peers, and ensure they all, in turn, do good work and become a valuable asset to the company.
Difficult adventure
Whether you are a doctor, an accountant or a nurse, this typical journey is very common. Very few organisations offer management training at the right time and so, as new managers, we find ourselves embarking on an important and difficult new adventure with limited knowledge and guidance.
I love managing people and while I have been doing it for many years now, I still enjoy learning more about leadership and management from others with more experience by reading books and listening to podcasts.
So when I was asked to review this book by James Potter and Mike Kavanaugh I was very happy to take on the task.
The Successful Manager is a book
that promises to deliver practical approaches for building and leading high-performance teams, and it does not disappoint. The authors have drawn on their vast experience within their organisations and their work with other organisations to produce the book.
James Potter is the chief operating officer at Dunes Point Capital. Before this, he was the senior managing director and Global Practice Leader at Blue Ridge Partners, a global management consulting firm that focuses exclusively on accelerating profitable revenue growth.
He has helped more than 100 organisations and their leadership teams. The measure of his success is the results he drives for his clients and their organisations.
Mike Kavanagh is an entrepreneur, author, speaker, consultant and educator in the areas of leadership, performance and personal development. He is the founder of Self-Mastery for Leaders, a business that arms individuals with the tools to maximise well-being, reclaim their time and freedom, and become world-class leaders.
Greater performance
The book is an excellent read for those moving into management for the first time and I would highly recommend it to all new managers. But it also helps more experienced managers to reflect on their management style and enhance their working methods to achieve greater performance.
Managing is incredibly challenging especially in the first year as you establish yourself as a leader
and manager. An important part of being a great manager is being very clear on your style, standards and expectations, so, initially, there is a process of clarifying this for yourself before you can communicate your ethos to your team.
In Chapter 2, the authors share their opinions on the seven characteristics of great managers by way of the acronym TEACHER. The seven elements of TEACHER are a great support tool for both new and experienced managers, providing some clear pointers on what characteristics are important to be a good manager.
For example, ‘T’ represents ‘transparency’ and the importance of being open and honest to develop trust. Your team needs to trust you and you need to trust them. To build this trust, the manager must be honest, even when the news being shared is not positive. Being courageous enough to share difficult information with your team develops an environment where your team knows that honesty is paramount. They will also recognise your integrity which in turn develops loyalty.
Relax control
One of the greatest challenges for managers is delegation, as it requires us to relax our control and trust others to deliver to our high expectations. There are numerous helpful tips on prioritisation, delegation and time management in Chapter 4.
For most managers, but especially for new managers, there is a desire to control the work that their team is doing and importantly how they do it.
This desire for control is understandable, as we want to ensure that the work is delivered to our high standards, but, in the longer term, too much control will always prove to be unproductive. Eventually, to become a good manager, there is a need to release control and to empower team members to do their work in the manner that suits them best, which may well be a better way. Learning how to delegate effectively is a vital skill for all managers for the very basic reason of productivity. One person simply cannot be involved in everything. And, for team morale, there is nothing worse than microman -
agement, as it makes the team feel that they are not trusted and develops a negative culture.
As this is such a recent book, there is a chapter dedicated to managing remote and distributed teams and the effects the pandemic has made on the growth of this type of team.
Working with remote individuals does require an adapted approach and this is well described by the authors. To lead a successful remote workforce, managers have to stop focusing on what the authors describe as ‘face time’ or presenteeism but on the outcomes that are being delivered and this can be a big change for many.
Walking around
Another very strong example of how managers need to adapt is the practice of managing by walking around. When the whole team is office-based, a regular walk of the office informs a manager about how his/ her team members are doing. (See ‘How to hang onto your staff’ in our June issue).
The general demeanour and body language of staff will give useful insights into their motivation levels and identify any individuals who may need additional support. When team members are remote, a manager has to work harder to get these insights, by holding regular catch-up calls and asking the right questions.
If I was asked how the book might be improved, I would suggest that some tasks were set for the reader at the end of each chapter. This would encourage the reader to reflect on what they have read and their behaviours and agree and document some actions for change, making the book more of a workbook.
In my experience, taking the time to undertake exercises like this helps to embed what has been read and makes it much more likely that the learning will be put into practice.
I would highly recommend taking the time to read it and embrace many of the authors’ welldescribed suggestions.
Jane Braithwaite is managing director of Designated Medical, which offers bespoke support across accountancy, marketing, medical PA, HR and recruitment
The free digital prescribing platform for all private prescribers.
CloudRx take care of the dispensing, payment and delivery of medicines direct to your patients, wherever in the country they may be, for more convenient access to their medicines.
TRANSFORMATIONAL
Order prescriptions at the touch of a button to support all consultations and add a whole new level of convenience for your patients.
SIMPLE, CONVENIENT AND SECURE
Simple and fast digital prescribing.
Legal paperless prescriptions, repeat prescriptions and controlled drugs.
Prescriber fees can be charged to the patient if requested.
INTEGRATED
Our API enables frictionless integration with healthcare brands & clinical software including Heydoc, MidexPRO, eClinic and YouClinic.
“We were struggling to keep up with the admin side of the prescriptions, not to mention storage for medication to cope with a huge increase in prescriptions. CloudRx immediately took away the strain. Since our partnership we have grown by more than 200% in size. We could not have done that without their support.”
– Dr Louise Newson, Newson Health
Careful when you contract others
A recent court case has re-affirmed legal precedents which could prove costly for some independent practitioners. Elena Goodfellow (below) explains what it means and suggests action they can take
The case of Hughes v Rattan
This was a Court of Appeal decision from February 2022 concerning the issues of vicarious liability and non-delegable duty of care.
It involved a patient, Mrs Hughes, who had undergone dental treatment at a practice owned by the primary defendant Dr Rattan by other dentists who were self-employed associates who held independent contracts with the practice for their work.
So what does vicarious liability and non-delegable duty of care mean in medical malpractice claims?
In a nutshell, vicarious liability is the concept that one individual or business entity can have responsibility – i.e. liability – for another’s care of a patient.
A non-delegable duty of care is the concept that an individual/ entity who has a duty of care towards a patient is unable to pass on or delegate that duty of care to
another in situations where they have delegated the actual provision of care of the patient.
What did Hughes v Rattan decide?
The Court of Appeal decided that Dr Rattan was not vicariously liable for the negligent treatment provided by independently contracted dentists.
This decision followed other court decisions made in recent years on the issue by looking at the relationship between Dr Rattan and the associate dentists and considering how similar this relationship was to the relationship between an employer and an employee.
As the associate dentists were free to work as much as they liked, were responsible for their own tax, National Insurance, professional clothing and development and they had to hold their own liability insurance for their work, the
court found that the relationship was not ‘sufficiently akin to employment’ so as to make Dr Rattan vicariously liable.
The court did, however, find that Dr Rattan owed a non-delegable duty of care to the claimant. The law on this is found in a 2013 case called Woodland v Essex County Council.
This sad case concerned the brain injury of a young child suffered during a swimming lesson provided by an independent contractor. The claim was against the school who arranged the lesson. The principles considered in this case are manifold and require a separate article in itself, but, in summary, concern the relationship between the claimant and the primary defendant, how vulnerable the claimant was and how much control the claimant had over how the primary defendant performed their obligations to the claimant – such as Dr Rattan arranging treatment with another dentist.
Implications for those who use independently contracted practitioners
Most businesses who use independently contracted practitioners will have secured, as part of the contract, an agreement that the practitioner is responsible (liable) for their own actions, negligence and any claims arising from their care.
However, claimants suing for personal injury can pursue whomever they chose and it is for the defendant to then establish that they are not the correct defendant. In my experience, it is fairly common for claimants to sue both the practitioner who actually pro-
vided their care and also the entity – be it a clinic, practice or other company – who arranged it.
This can be for a variety of reasons: the independent practitioner may no longer be traceable or even in the UK, may not be solvent or have adequate/correct insurance or the claimant may simply do this to ‘cover all the bases’, leaving the defendants to work out between them who has responsibility for the claim, which can take time and incur legal costs.
To limit exposure in these situations, various steps can be considered.
First, entities should look to the agreements they hold with both their contracted practitioners and their patients. Is the practitioner’s contract so restricting that it is close to a contract of employment? How much control over care does the agreement with the patient allow for?
Second, organisations should
ensure that they have appropriate provisions for indemnity insurance in their contracts and mechanisms to ensure their practitioners comply with this.
They should also ensure that they also have suitable insurance cover for themselves.
What does Hughes v Rattan mean for independent practitioners?
While in this case Dr Rattan was found to be responsible for the claim because of a non-delegable duty of care, meaning Mrs Hughes was able to recover compensation for her injuries from him, this does not mean the dental associates would necessarily have escaped liability.
This is because:
1Mrs Hughes would also have had a valid claim against them (we are not told in this decision if she was suing both Dr Rattan and the associates) ;
Cases involving multiple defendants can become drawnout and expensive, and it may sometimes be that the independent practitioner ends up paying not only their own legal costs but also those of the entity they are contracted to
2Their contracts with Dr Rattan probably contained provisions that they were liable to him for any claims against him, arising out of their care.
Cases involving multiple defendants – especially where the defendants themselves need to sort out who is responsible – can become drawn-out and expensive, and it may sometimes be that the independent practitioner ends up
paying not only their own legal costs but also those of the entity they are contracted to.
So independent practitioners should make sure that they:
Hold appropriate defence cover, taking care to ensure their policy covers claims brought years after the treatment occurred or that they purchase ‘run-off’ insurance; Can afford any excess on their policy should they be subject to multiple claims;
Report any potential or threatened claims to their defence bodies/insurers as soon as possible.
Elena Goodfellow is an associate solicitor in the clinical disk department at Bevan Brittan LLP. She advises both public and private sector clients in a variety of clinical negligence/medical malpractice claims. She has acted for both independent practitioners and clinics/practices in claims concerning cosmetic, ophthalmic and orthopaedic surgery
BOOK YOUR DEMO
Are you happy with your current software?
Maybe you're completely happy with the software you use to run your practice. Perhaps you have everything in one place, routine tasks are automated, and reporting is accurate and insightful. If so, stop reading now.
However, if you think the day to day running of your practice could be improved, we'd love the chance to demonstrate e-clinic to you.
The number one choice for private practice
Future-proof your practice and offer everything a modern patient expects:
> iPad compatibility
> Online booking & payments with fully integrated card processing
> Electronic consent & treatment forms
> Integrated drugs database & digital prescribing with direct delivery
> Fast & easy patient communications by email or text
YOUR FREE 30 MINUTE
Bupa’s WELLBEING INDEX
When Bupa was founded in 1947, no one could have anticipated just how much the healthcare landscape would evolve by the time it reached its 75th anniversary this year.
But, just as in the post-war period when the insurer was created, clinicians once again face the challenge of finding ways to improve the nation’s health.
Dr Robin Clark (below), medical director for Bupa Global and UK, explains how Bupa is embarking on the first step towards this with the launch of its new Wellbeing Index
It’s a barometer the nation’s health
of health
AGEING POPULATIONS , huge leaps in science, digital technologies, not to mention consumerism and national mobility, have had a dramatic impact on our health and well-being.
Then came the biggest global health and societal challenge of a generation – the Covid-19 pandemic – which has dominated the lives of countries and communities around the world for the past two years, changing the way we live, interact and decide our priorities.
While it now appears that the most intensive phase of the pandemic may now be behind us, its profound and ongoing impact on our mental and physical health, as well as how we view healthcare, will influence our way of life for many years to come.
Much may have changed since 1947; however, this new post-pandemic era has many parallels with the period when Bupa was founded. In 1947, the nation was also scarred – both physically and mentally – from the after-effects of World War II.
However, this created a renewed focus on the importance of providing good healthcare and finding ways to improve the nation’s health, which led to the creation of both the NHS and Bupa.
THE BUPA WELLBEING INDEX
From the beginning, Bupa has been driven by a passion to pioneer, promote and improve healthcare. So as we emerge from seismic changes to our industry, we are launching the Bupa Wellbeing Index, which will prove a useful tool for all of us working in the healthcare sector.
Carried out by Censuswide, this rolling dataset will track five key health and well-being metrics for 8,000 UK adults each quarter, capturing a range of health, wellbeing, lifestyle and behaviour datapoints to help us and our healthcare partners understand more about the nation’s health.
As the Bupa Wellbeing Index builds quarter by quarter, it will create an in-depth data driven barometer of health and wellbeing in the UK, exploring how the pandemic has impacted us and shifted our expectations of healthcare.
The survey population is split by
It’s important that we take stock of the current landscape so that we know the challenges we are facing and where there are opportunities for improvement
demographics, including sex, age and geographic location, which enables us to explore key trends and spotlight where there are potential issues, so that we can continue to design and deliver healthcare in the most impactful way.
It’s important that we take stock of the current landscape so that we know the challenges we are facing and where there are opportunities for improvement.
So our first Wellbeing Index explores the pandemic’s impact on the nation’s health, as well as looking at how attitudes and expectations towards health and well-being are changing, what this means for the future and the steps individuals are taking for more ownership of their health.
Benchmarking the barometer baselines
PHYSICAL HEALTH
Lockdowns during the pandemic meant many people in the UK had to adjust to homebound lifestyles, the abrupt disappearance of their commutes and a drastic increase in time spent sitting.
For some people, Covid-19 was a wake-up call to improve their diet and fitness; they became more active and cut back on alcohol. Others experienced the opposite effect: a shift to a more sedentary lifestyle led them to struggle with weight gain or become more dependent on alcohol.
Compared to 2019, for instance, there has been a 20% increase in alcohol-related deaths and a 21% increase in deaths from alcoholic liver disease.1
The impact of the Covid-19 pan-
demic is clear from our Wellbeing Index data, which was collected between 18 and 24 March 2022. Only 51% of respondents rated their physical health positively, with 14% reporting very good health and 37% saying their health was ‘somewhat’ good.
As you would expect, these scores decline with age. People aged 16 to 24 were the most likely to say they enjoyed very good health (18%) and the over-65s were the least likely (11%).
When asked what worried them most about their personal health and well-being, respondents reported that their weight was the biggest worry (33%), followed by mental health problems (24%); back pain, joint problems and other musculoskeletal issues (23%) and fitness levels generally (21%).
While people were unwilling or unable to access healthcare during the pandemic, the research found that 54% of those surveyed had interacted with a healthcare provider in the three months before taking part in the survey.
Missed appointments
Dental treatment or advice was most commonly accessed (13%), but it’s unlikely this had much impact on the backlog of people needing treatment. Our data suggests the effects of missed appointments may already be emerging, as 6% reported a dental emergency and 7% had undergone an extraction.
One-in-ten women (10%) also sought medical help for femalespecific issues around menopause, endometriosis and menstruation, yet despite the challenges around menopause, which every woman will experience, uptake was relatively uniformly spread.
With increased awareness over the last few years following a number of high-profile campaigns, menopause issues are gaining visibility. To help boost support for women’s well-being, last year we launched the Menopause Healthline, a helpline for customers and employees. It offers access to menopause-trained nurses for advice and guidance on managing symptoms.
Our Health Clinics offer a Menopause Plan (www.bupa.co. uk/health/payg/menopauseplan), which gives women access
➱ continued on page 24
to primary care for symptoms through specially trained GPs.
And our Women’s Health Hub at www.bupa.co.uk/womens-health gives all women access to advice and guidance from resident health experts on topics spanning menopause and endometriosis to periods and fertility, whether or not they are Bupa customers.
The mental health impact
The Bupa Wellbeing Index found that people’s perceptions of their mental health were more positive, with almost a quarter (22%) saying their psychological health was very good, and a third (32%) rating it somewhat good.
However the correlation with age is reversed for this metric –older adults were far more positive, with 38% of over-65s reporting very good mental health, more than twice the number of 16- to 24-year-olds (14%).
It’s clear the pandemic had a more severe impact on the mental health of younger adults and women, a demographic who were already more likely to be struggling.2
Only 48% of women gave positive scores for their mental health, compared to 61% of men, and 28% of men describe their mental health as very good, almost twice the number of women (15%).
Family and caring responsibilities, as well as social factors, may have played a role in this. The Index found that women were more likely to be managing housework and childcare during the lockdown than men and there is evidence of an association between these adjustments and psychological distress.3
This is echoed by a poll of 1,030 UK mothers with children between the ages of 0 and 16 years carried out for us by Censuswide in January 2022. It found that 63% of the mums surveyed said that they have driven themselves to exhaustion with the pressure to be a ‘supermum’: one who successfully manages a home and raises children while working full time.
Driven by a fear of judgement and people seeing their imperfections, 31% of mums said it made them put on a facade of coping to appear infallible and 43% agree they struggle to ask even their partner for support.
Although 29% of the mums sur-
tively identify when a patient may need some support, not least because people may be reticent about raising mental health issues. At Bupa we offer a range of support and our health information is available for both customers and non-customers. Visit: www.bupa. co.uk/health-information/mental-health.
The good news
While the findings of our first Wellbeing Index paint a mixed picture in terms of the pandemic’s impact on the nation’s health, we know that many diseases can be preventable if patients follow optimal health behaviours.
The good news is that our data shows people are taking a more proactive approach to their health – 11% of those surveyed had undergone a health assessment, and this climbed to 15% in the 16 to 24-year-old age group.
veyed said they have sought help from a medical professional for mental health concerns, they kept it a secret from their loved ones. Similarly, only 37% of 16- to 24-year-olds and 49% of 25- to 34-year-olds assessed their mental health as very or somewhat good, while three out of five (59%) 55- to 64-year-olds and almost threequarters of over-65s (73%) were upbeat about their mental health.
Most robust
Over-65s reported the most robust mental health (38% stating very good), followed by 55- to 64-yearolds (26% stating very good) while Gen Z and the Sandwich Generation, who are juggling caring for parents and children, were the least likely to say their mental health was very good (14%).
Overall, 6% had begun counselling for a mental health condition, but there is a sharp gender divide, with 8% of women having started taking therapy sessions compared to 4% of men. This was mirrored in the statistics for those starting a prescription for a mental health condition.
Understanding how mental health conditions manifest themselves is key in being able to effec-
A further 10% had started a new prescription for a health condition – and, unexpectedly, this was also slightly more common in the younger age groups.
There are a number of reasons why this might be: The prescriptions might be preventative and already improving respondents’ mental or physical health. For
FITNESS AND WELL-BEING
Lockdowns, lethargy, gym closures and general uncertainty made it difficult for many people to manage their personal well-being and maintain a consistent exercise regime during the pandemic.
Although general well-being saw the highest overall score, with 16% of people surveyed reporting this was very good and 40% rating it somewhat good, a deeper dive into the data reveals a U-shaped curve to these scores.
The youngest and oldest demographics report the best general well-being; 17% and 18% respectively, and 35- to 44-year-olds giving the lowest score (13%).
And it looks like this struggle to stay active has persisted post-pandemic for many –fitness was a major red flag in our data. Only 10% of respondents said their fitness was very good and 29% thought it was somewhat good.
This is worrying because of the huge body of evidence showing that physical fitness not only reduces people’s risk of many preventable health problems including cardiovascular disease, diabetes and many cancers, but it can also help prevent and relieve mental health problems.
The World Health Organization has identified exercise and physical activity as one of four lifestyle habits – alongside a healthy diet, avoiding harmful use of alcohol and not smoking – which will dramatically reduce the risk of many preventable diseases, including cardiovascular disease and diabetes.4
Many different factors affect our overall health and well-being. Apart from our genetic inheritance and lifestyle choices, there are multiple socio-economic drivers that influence our physical and emotional well-being.
For this reason, it’s perhaps no surprise that 50% of those surveyed put a high priority on financial stability as well as their personal health and well-being.
However, much of our concern is outward-facing. The data reveals people are far more likely to prioritise their family’s health and well-being than their personal well-being: 65% compared to 50%. The fact that only 19% of adults now put a high priority on their career also points to a renewed focus on the importance of work-life balance.
The good news is that our data shows people are taking a more proactive approach to their health
example, effective medication may lead someone to rate their mental health highly. Even the act of taking steps to improve health by getting a prescription could account for this.
Younger respondents might also be including prescriptions for skin conditions, allergies or contraception in their responses, all of these don’t necessarily mean ill physical health.
And finally, they will be more likely to have started a new prescription, as older respondents will likely already be on a repeat prescription.
We now need to build on this to reach those most at need of intervention. In these cases, it will be key for healthcare providers to embrace behaviour change techniques to encourage patients to make the healthier choices necessary to improve their overall quality of life and future health outcomes.
In our next issue, Dr Clark digs deeper into what this means for the future and the challenge for healthcare professionals trying to turn around the impact of the pandemic.
As the GMC’s consultation on a new version of Good Medical Practice continues, the Medical Defence Union’s Dr Caroline Fryar (below) takes a closer look at one of the four domains in the guidance and highlights some of the potential problems with what is proposed
their patients, and the GMC
WHEN I SET out on my medical career, my primary motivation was crystal clear: I wanted to care for patients. My aim was not unique. Indeed, I believe it is the motivation of the overwhelming majority of my medical colleagues.
So, in studying Domain 2 of the GMC’s proposed new edition of Good Medical Practice, I am immediately struck by its title – Working with patients. Surely, given how central this is to the very essence of what it means to be a doctor, this should be Domain 1, rather than number two?
That overarching point aside, there are many paragraphs in Domain 2 that give the MDU cause for concern. Let’s look at some examples:
☛ Paragraph 22: You must treat patients with kindness, courtesy and respect.
A common theme across many of the concerns we have about this revised guidance is the significant expansion of the use of subjective terms.
‘Courtesy’ and ‘respect’ are subjective terms, but ‘kindness’ is especially so. While most doctors undoubtedly set out in the morning to be kind – what does that word ‘kindness’ mean?
It, of course, means something different to everyone: patients and doctors. The question I pose is a simple one: does the word ‘kindness’ need to be included in this paragraph and in the guidance at all?
‘Courtesy’ and ‘respect’ are well understood in terms of what is meant by them in a professional setting with patients, but the same simply isn’t true of ‘kindness’.
scribed when the doctor is ‘satisfied that the drugs or treatment serve the patient’s needs’. Plainly put, we do not believe this reflects the realities of medicine.
In medicine, there are many situations where a number of seemingly appropriate drugs may be available, and doctors have to begin by prescribing one to see if it works. It will only be then they can be satisfied that it serves the patient’s needs.
There are times when a doctor needs to prescribe without being sure it will serve the patient’s needs, so we believe the GMC needs to change the wording of this paragraph.
We increasingly see GMC guidance quoted back at doctors in complaints and we are concerned that reference to kindness could be used against doctors in an unreasonable way.
We are also concerned that, in some cases, doctors seeking to demonstrate that they are complying with the GMC’s edict to be kind may inadvertently find themselves close to – or over –the line of the doctor-patient relationship.
A duty to treat patients with courtesy and respect would seem amply sufficient.
☛ Paragraph 37a: In providing clinical care, you must propose, provide or prescribe drugs or treatment (including repeat prescriptions) only when you have adequate knowledge of the patient’s health and are satisfied that the drugs or treatment serve the patient’s needs.
Overriding duty
The use of the words ‘you must’ is highly significant in Good Medical Practice . The GMC defines the statement as ‘an overriding duty or principle that will usually apply’.
Alternatively, the statement ‘you should’ is used. This is in part defined by the GMC as an instance ‘where the duty or principle will not apply to all situations or circumstances’.
We believe this paragraph is a prime example of where the guidance needs to read ‘you should’ rather than ‘you must’.
Why is that? Paragraph 37a says that drugs ‘must’ only be pre -
☛ Paragraph 44: You must not unreasonably deny a patient access to treatment or care that meets their needs….
The following scenario is not an unheard-of occurrence. A patient arrives for a consultation with a clear view of what course of action will meet their needs. Yet, the patient’s perception of what meets their needs differs considerably from what the doctor considers clinically appropriate.
Doctors are, of course, obliged to not stray beyond such realms. So, this paragraph would benefit from a small but consequential addition. We believe the word ‘appropriate’ should be added, so it reads ‘access to appropriate treatment or care that meets their needs’.
This is the first substantial edit of Good Medical Practice since 2013. We can therefore expect the endproduct of this consultation exercise to carry the profession through into the 2030s. The GMC must get this right.
We at the MDU are continuing to formulate a comprehensive and robust response to this consultation and we are committed to working with the GMC so that this guidance delivers for the profession.
This is a rare opportunity to actively shape a fundamental piece of guidance from the GMC. Independent practitioners can go to www.themdu.com/press-centre/contact-the-press-office to share their views with the MDU. The GMC’s consultation deadline is 20 July.
Dr Caroline Fryar is head of advisory services at the MDU
Give them a great initial experience
Following his article last month about the process of ‘onboarding’ new patients, Simon Marett (below) goes a stage further and zeros in on the importance of delivering an excellent first-time experience. And he shows why mapping patient journeys is a crucial exercise in delighting your patients and driving positive word-of-mouth recommendations
IT COSTS seven times more to acquire a new patient than retain one.
That is a widely used marketing statistic and it highlights the importance of keeping your current patients happy.
After all the time, effort and budget you have put into acquiring and onboarding a new patient, the hard work has been done. So it is vital that independent practitioners do not undo that by falling at the final hurdle by delivering a mediocre patient experience.
What is more, your current patients can be your best mar keting tool by recommending you to other patients and driving word-ofmouth endorsement, which can result in you spending less marketing budget on patient acquisition.
But delighting your patients is not a one-person job. It requires a team effort and for all departments and people involved to pull together in the same direction.
There is nothing worse than a patient calling after responding to an advert or promotion and your clinic team not being aware there was one
ing and requesting prior to the consultation and when are your reminders (SMS and email) being scheduled? This is a critical part of the patient journey and can make or break a first-time patient experience before the consultation has even taken place.
During the consultation:
Think about the whole package
It is of no use for the marketing team to deliver a great looking website with a clear value proposition and pricing only for the operations team and practitioners in the clinic not to be fully informed when a patient phones or visits the practice.
This can only lead to a poor experience that fails to live up to expectations and can result in complaints.
Breaking down the patient journeys
Patient journeys can be complex and there are often multiple journeys to map, so it is important to break them down into different sections.
Typically, we advise our clients to look at three different aspects of the journey/pathway: pre-consultation, during the consultation and post consultation.
By breaking it down into more manageable sections, you can dig deeper into the detail of what happens at each stage and understand where the issues may lie.
At each of these stages you will need to take the time to look at the processes, technology and people behind every touchpoint with the patient.
Pre-consultation: Communication is key
The initial stage of the patient journey is vital, as this is where you will communicate key information about your clinic including your proposition, credentials, pricing and what the patient can expect if they proceed.
This sets the expectation from the start and so it is vital the administrative operations are aligned to deliver on the marketing promise.
The starting point is always where a patient first hears about you and where they have started from.
For example, if you are running a patient acquisition campaign on Google Ads or Facebook, pay close attention to the wording and make sure your clinic team and doctors are aware of any promotions or price changes that have recently been introduced. There is nothing worse than a patient calling after responding to an advert or promotion and your clinic team not being aware there was one.
Also, you need to get into the detail of every touchpoint a patient will have with the clinic in the run-up to an appointment.
What information are you send-
Equally important is the journey and experience during the day of the consultation with the healthcare professional. Whether you are delivering an online video consultation or seeing a patient face to face, getting ‘granular’ and breaking down the journey into bite-sized segments is a very useful exercise.
Details matter and paying attention to directions, car parking, how the patient is greeted on arrival and how they leave your clinic are all incredibly important.
The patient may have had an excellent consultation and be happy with their treatment plan with a doctor, but if the experience around that consultation is poor, then that is often what the patient remembers.
Post-consultation:
Finish on a positive note
Post-consultation communication is often the aspect of the patient journey that gets forgotten about, but it can make the difference between a patient recommending your clinic to a friend or colleague or leaving a negative review online.
Paying close attention to detail is important here and touchpoints to consider include summary letters/emails from the practitioner, courtesy follow-up calls, requests for patient feedback alongside clear communication about further tests or examinations that need to happen.
Post-consultation is the stage of the patient journey where you can make the big gains, exceed expectations and drive patient loyalty and advocacy.
Summary
Delivering an excellent patient experience is fundamental for any successful private healthcare clinic, but success does not come
without hard work and paying close attention to detail.
Mapping the patient experience can be a time-consuming but worthwhile process and it is one that should involve the entire clinic team, not just the marketing team. It is critical that practitioners, clinic employees and management work together on this and cover every touchpoint with the patient.
Retaining patients and driving positive word-of-mouth recommendations can be an incredibly cost-effective way of driving new patients and save valuable marketing budget that be allocated elsewhere in the business.
Patient reviews are becoming more and more important and a growing percentage of patients are now doing their research before deciding which clinic or practitioner they want to go with.
Mapping patient journeys is an exercise that can be done internally. but it is worthwhile speaking to an experienced consultant or specialist for advice before you start. They will have tried and tested methodology and will be able to offer valuable advice and guidance, helping you avoid the pitfalls and common mistakes. If you think your clinic could benefit from some advice relating to attracting or onboarding new patients, do get in touch with me. In my September marketing feature, I take a closer look at the importance of retaining patients and discuss some ideas and initiatives to help you drive loyalty and advocacy.
Simon Marett is founder and director at Ellerton Marketing
GET A FREE BUSINESS ‘HEALTH CHECK’
Ellerton Marketing is providing a free 60-minute business ‘health check’ for Independent Practitioner Today readers and can help guide you through some of the key steps you should be thinking about when it comes to marketing your clinic and delivering a first-class experience.
A joined-up drive on safety
The Independent Healthcare Providers Network recently held a conference on safety. David Hare (right) reports on what changes in regulation the private sector is facing, including a new system of inspection by the Care Quality Commission
Independent Practitioner Today readers are increasingly aware that the healthcare world is in a period of transition.
We are moving away from Covid ways of working and back to more ‘normal’ practices and at the same time there is a need to respond to the new changes in the world of healthcare regulation and patient safety.
Not only is the Care Quality Commission (CQC) implementing a new strategy, the last two years have also seen the publication of numerous reviews into patient safety incidents: from Paterson to Cumberlege to Ockenden. These contain important learnings for providers and practitioners across the healthcare system.
So we at the Independent Healthcare Providers Network (IHPN) were pleased recently to host a joint patient safety conference alongside the CQC – attended by over 100 members – to ensure independent providers and practitioners are fully up to speed with this changing landscape.
We had a particular focus on how the sector can achieve ‘wellled for safer care’.
Kicking off the conference, CQC directors Victoria Vallance and Fiona Allinson gave an overview of the regulatory changes and set out their reflections on what those working in the independent sector should expect in terms of the healthcare watchdog’s new approach.
While the changes are still in the process of being developed, some of the key areas independent healthcare providers and practitioners should be aware of include:
1 Moving away from the CQC’s current three frameworks of registration, health and adult social care to a ‘single assessment framework’ that will be used for assessments of all sectors, service types and at all levels.
These will be applied from the point of registration through to the ongoing assessment and rating of providers – reducing much of the current duplication.
2
Introducing new ‘I statements’ to help encapsulate the views and expectations of patients and the public and make this a clear focus for health and social care providers.
Likewise, providers will have new ‘we statements’ to help to make clear the expectations on services; for example, ‘we understand our duty to collaborate and work in partnership, so our services work seamlessly for people’.
3
Moving away from a separate ‘monitor’, ‘inspect’ and ‘rate’ process and instead making greater use of data and information to analyse and assess providers more frequently.
The information will come from multiple sources and not just through inspection, with the establishment of a dashboard to help the CQC make better decisions.
Similarly, CQC reports will be shorter and more accessible to support patients in making the best choices about their care.
Looking more broadly than the CQC, we were delighted to hold several interactive sessions at the conference, including hearing from the new National Guardian for Freedom to Speak Up, Dr Jayne ChidgeyClark.
While there are almost 200 Freedom to Speak up Guardians in the independent sector, not all providers have appointed a guardian and there is significant variation about whether they sit at site level, board level or for clinical vs nonclinical staff.
Open cultures
Jayne had some fantastic reflections on how those working in the sector can better foster more open cultures in healthcare, including having a clear organisational route for speaking up and for practitioners, to really interrogating the data collected from your guardians.
This includes looking at whether your organisations have high levels of anonymous ‘speaking up’ cases and what this might be saying – particularly on equality and diversity issues – and ensuring there is a real openness in reporting and discussing the data.
The event was also an opportu
CQC reports will be shorter and more accessible to support patients in making the best choices about their care
nity to hear from IHPN members themselves, who deliver both acute and community care, reflecting on their journey to achieving CQC ‘outstanding’ in ‘well led’.
There is no onesizefitsall model on this, but key themes cropping up again and again included:
Organisations meaningfully engaging with you as practitioners at all levels;
Empowering you to voice any concerns;
How services can be improved;
Making sure providers have the systems and processes that permit practitioners to be proactive, not reactive, when it comes to safety; Having a growth mindset where everyone feels able to question things and explore ‘how might we do this better?’
Improve safety
We had some fantastic speakers including from the GMC, NHS Resolution, Patient Safety Learning, the Healthcare Safety Investigation Branch, the Private Healthcare Information Network and CQC, which really helped inform the work we are doing to refresh the IHPN’s Medical Practitioners Assurance Framework and help further improve the safety and quality of care independent providers and practitioners deliver to patients.
We finished the day with a sobering session about how we can better engage with patients and staff to improve services.
Whether it is the Paterson inquiry, Cumberlege report or the recent Ockenden report, too often it is down to patients or relatives themselves to ring the alarm bell when it comes to poor care, with lessons for both providers, practitioners and regulators on how to better engage with patients and families in a more proactive way. It was fantastic to see so many IHPN members and practitioners working on the ground at the event and it gave both attendees and us much food for thought. Perhaps most importantly, however, it signalled just how ambitious and committed all those working in the sector are in striving towards safer care through wellled organisations and all parts of the healthcare system working together to make this happen.
David Hare is the chief executive of the Independent Healthcare Providers Network (IHPN)
CHECK OUT OUR BUSINESS DIRECTORY
Independent Practitioner Today now features an online advertising directory to complement our journal and website.
Split into ‘business’ and ‘lifestyle’ directories, they list the services independent practitioners need to run their practices or spend their well-earned money on.
Avoid complaints by consent in
Minor surgical procedures are usually straightforward, but practitioners should be aware of some common pitfalls. Dr Clare Devlin (right) explains more
PATIENTS VALUE the speed and convenience of having minor surgical procedures undertaken privately, but there are inherent risks that practitioners should be aware of and minimise to avoid claims.
A common feature in many clinical negligence claims relating to minor surgery is a problem with consent.
Shortcomings in the consent process can occur even with the most experienced doctors and sometimes make the difference between a successful defence and settlement.
When the doctor and patient discuss the treatment options available, this must include alternatives such as non-surgical management or no treatment at all – and when fully informed, the patient then agrees to a particular course of action.
On top of the expected benefits of treatment, patients need to understand the risks and potential complications.
KEY POINTS
Following the 2015 Supreme Court judgment in Montgomery v Lanarkshire, 1 it is important for doctors to have an individualised discussion with a patient, so that the ‘material’ risks – the significant risks that may matter to the patient – are identified and addressed.
Material risks
The Supreme Court ruling explains what it considered to be a ‘material’ risk: ‘The doctor is therefore under a duty to take reasonable care to ensure that the patient is aware of any material risks involved in any recommended treatment, and of any reasonable alternative or variant treatments.
‘The test of materiality is whether, in the circumstances of the particular case, a reasonable person in the patient’s position would be likely to attach significance to the risk, or the doctor is or should reasonably be aware that the particular patient would be likely to attach significance to it.’
The importance of documenting the consent process cannot be overemphasised
The presence of consent should be recorded, as well as the date and whether it was written or verbal
Clinicians should document a list of the alternatives discussed, as well as the treatment proposed.
Any technical aspects of the treatment discussed should be recorded, such as the type of incision or site of procedure
The risks discussed should be outlined, as well as the fact that the patient was asked if they had any specific concerns and, if so, what was discussed
Always recognise and work within the limits of your competence when considering minor surgical procedures
GMC guidance ‘Decision Making and Consent’ provides practical, detailed guidance, written in accordance with the current legal view of consent, including specific guidance on the approach to consent in a number of challenging scenarios which arise in clinical practice3
by getting in surgery
A way to open this individualised consenting discussion can be to ask a patient if there is anything in particular that they are concerned about or anything in particular that would make them decide against treatment.
The Montgomery judgment emphasises the expectation of discussion taking place between patient and doctor: ‘The doctor’s advisory role involves dialogue, the aim of which is to ensure that the patient understands the seriousness of her condition, and the anticipated benefits and risks of the proposed treatment and any reasonable alternatives, so that she is then in a position to make an informed decision.
‘This role will only be performed effectively if the information provided is comprehensible. The doctor’s duty is not therefore fulfilled by bombarding the patient with technical information which she cannot reasonably be expected to grasp, let alone by routinely demanding her signature on a consent form.’
Record-keeping in the consent process
An important feature of the consenting process is documenting the issues that were discussed with the patient during the process, as well as taking the patient’s signature on a consent form when consent is written.
In the absence of documentation of the issues discussed, it is possible to give an account of your usual practice when consenting a patient for the procedure in question.
But if the patient brings a claim and disputes that certain points were discussed, it is important to
COMMON PROBLEMS IN MINOR PROCEDURES
CRYOTHERAPY
Cryotherapy can be complicated by scarring that can lead to cosmetic concerns in certain patients. They may then seek dermatology review and further dermatological management of the scarring.
In some cases, their scarring may ultimately need to be addressed with camouflage make-up.
Following the 2015 Supreme Court judgment in Montgomery v Lanarkshire, it is important for doctors to have an individualised discussion with a patient, so that the ‘material’ risks are identified and addressed have a contemporaneous record of the consenting discussion to support your account.
It can also be helpful to record that the patient was asked if they had any particular concerns or any particular issues that were important to them.
Working within your competence
The GMC guidance Good Medical Practice sets out clearly that ‘You must recognise and work within the limits of your competence’.2
When doing minor surgery, it is important to be mindful of securing appropriate training and assistance, where required, and being prepared for how you will manage any complications encountered.
References
1. Montgomery v Lanarkshire Health Board (Scotland) – The Supreme Court
Dr Clare Devlin is a medico-legal consultant at Medical Protection
It is also possible for burns from cryotherapy to be deep and even require skin grafting or undergo protracted healing by secondary intention.
Discussion of possible scarring will therefore be important in the consenting process and a documented consenting discussion could enable minor scarring to be defended in the context of a claim.
IMPLANON CONTRACEPTIVE IMPLANT
A number of different complications can be seen with the contraceptive implant.
It is possible, if interrupted or distracted during the insertion procedure, to lose one’s place in the procedure and to believe the procedure has been completed when the implant is in fact still in the introducer.
This risk can be avoided by always palpating the implant after insertion. Using a check list can also prevent steps being forgotten when you are busy and experiencing distractions.
Alternatively, the implant may be wrongly sited or can appear to migrate from an initially correct and palpated site of insertion.
It can lead to symptoms such as pain or tingling and, in some cases, may require referral to secondary care for removal if it is not possible to locate and remove the implant in the clinic.
So it is important to document the anatomical site of Implanon insertion within the patient’s medical record.
INTRA-UTERINE CONTRACEPTIVE DEVICE
It can happen that an intrauterine device (IUCD) is inserted without the previous one having been removed. This can be avoided by taking a clear history from the patient of the removal of their previous IUCD and looking for corroboration of the patient’s account in the medical records.
Another complication that we see in IUCD clinical negligence claims is uterine perforation, leading in some cases to chronic pelvic pain or unplanned pregnancy.
Clear documentation of the discussion in the consenting process and the steps taken in the insertion procedure itself can be of assistance in defending such claims, by demonstrating that the practitioner had a reasonable insertion technique.
We can also make use of an account of the practitioner’s training and experience in IUCD insertion, together with a detailed statement of their usual practice.
INGROWN TOENAIL SURGERY
Toenail procedures can lead to claims about pain, bleeding and infection, which can even progress in some cases to osteomyelitis, requiring prolonged antibiotic treatment or further surgery.
A detailed record of the consenting process, including discussion of all options available to the patient, will assist in defending these claims.
BILLING AND COLLECTION
You think you’re a billing
Give your private practice a financial health check-up. Simon Brignall poses ten questions relating to the medical billing and collection task in your business. Once you have answered the questions, total up your score to obtain your prognosis
1
Are you up to date on the medical billing for your practice?
A. I honestly don’t know.
B. I think we are up to date on the billing, but the chasing is where we have an issue.
C. We have strong procedures that ensure we routinely raise and chase outstanding invoices.
D. We haven’t raised an invoice in months.
2 Do you know how much money is outstanding in relation to unpaid invoices for the practice?
A. I have access to a live aged debt report that breaks down outstanding invoices by a range of criteria.
B. I have no visibility whatsoever.
C. I get a report every month, but it’s difficult to see what is outstanding.
D. I only get something if I ask my PA and then I often end up waiting for days/weeks for the answer.
3 What is your chase process regarding outstanding payments?
A. As we are a busy practice, the chasing is always the first task that gets set aside.
B. We have a robust chase procedure that we routinely follow to ensure the practice’s aged debt is kept to a minimum and cash flow is optimised.
C. As we don’t have visibility on what is outstanding, my patients are rarely contacted about the money they owe.
D. We have a blitz once or twice a year when it starts to mount up.
4 Do you write off much debt in your practice?
A. We write off anything that is outstanding after a year rather than chase it.
B. We struggle to work out what is outstanding. I think we have tens of thousands of pounds owed going back years.
C. Due to our robust chase process
that includes debt collection, bad debts are minimised to less than 0.5%.
D. I am not sure what is the difference between aged and bad debt?
5 Do you review your fee structure regularly?
A. I looked at it a few years back, but I can’t remember when.
B. I didn’t know it was something I should regularly review. I haven’t looked at this since I started in private practice.
C. I have been meaning to do this, but I wasn’t sure where to start.
D. I review my fees every year so they are up to date and, where possible, ensure they reflect my experience and other factors.
6 Does the person in charge of your medical billing have other responsibilities within your practice?
A. My personal assistant (PA) does everything for the practice. She/he
SCORES
billing whizz?
is great with patients, and while they are on top of the invoicing, chasing debt is an area where she/ he struggles.
B. My PA does this for the practice; however, I often feel that the billing role could be handled better.
C. As I partner with a medical billing company, this role is carried out by experienced professionals. This allows my PA to focus on the clinical journey for the patient.
D. I do the billing myself. It’s probably not the best use of my time.
7 Are you aware of any changes to either the Clinical Coding Schedule and Development group (CCSD) schedule or the private medical insurance (PMI) companies’ fees schedule that may impact your practice?
A. I wasn’t aware that these changed.
B. We just invoice to Bupa fees for everything.
C. We review the monthly changes to the CCSD schedule to see what is applicable and we always ensure we bill to the relevant PMI tariff - following their specific coding formula when multiple codes are used.
D. We try and look at this every couple of years.
8 Do you make it easy for patients to pay your invoices?
A. Patients can make card payments if they can get through to my PA during work hours.
B. Patients can make payments into my bank account, but as a practice we struggle to reconcile these payments against the relevant invoices.
C. We try and collect payment on the day, but often patients leave without paying.
D. We offer patients a range of payments options to meet their needs – including the ability to make online payments 24/7.
Your
score
100. You are a medical billing superstar. Can we employ any members from your team?
75-95. Your practice is in fair shape, but there is still room to improve. It’s the small changes and the desire to constantly improve that differentiate at this level.
50-75. Your practice could do with a health check. Time to conduct a full review to tighten up on processes and reporting as well as add functionality. Of course, the easiest option would be to partner with a medical billing company that is an expert in this area.
25-50. Your practice is in poor financial health. While not critical, it is time to implement radical change to ensure it is on the road to recovery.
0-25. Your practice is on life support. Time to bring in the experts to resuscitate before you flatline.
We have a pay invoice button on our website and we have the option for patients to settle all outstanding invoices at the same time.
9 What happens at the end of each financial year when your accountant is submitting your reporting to HM Revenue and Customs?
A. As we have access to accurate up-to-date reporting on the practice financials, we can send my accountant a simple report with all the data they need.
B. We struggle to provide the data needed and it often creates more questions than answers.
C. Both my accountant and I are often tearing our hair out, as we can’t find the relevant figures.
D. My PA provides me with a report every year, but I really worry that it does not always reflect the true financial position of the practice.
10
Is the cost of your current medical billing solution reflective of performance in this area?
A. I just pay my PA a flat salary.
B. I pay my PA an hourly fee based on the work carried out, but I don’t know where their time goes as we still have lots of money outstanding.
C. As my PA has been with me for ages and patients like her/him, I don’t like to push.
D. I have a fee structure that is based on received income which ensures we both share the same objective.
Simon Brignall (below) is director of business development at Medical Billing & Collection
Don’t go chasing star performers
It is evident that most investors failed to capture the strong upswing, piling in at the top and suffering the subsequent calamitous downturn
the urge to jump on the runaway train of rampant performance despite the warning signs that flash as they clatter down the track.
We know too, from experience, that often funds that outperform over the shorter term are riding an investment style train, such as technology companies or growth stocks, that happens to be in favour.
2021, just as performance peaked. Assets gathered from investors in 2020 and 2021 represented around 90% of all net inflows since the fund’s inception in 2015. Bad timing is never good news.
Calamitous downturn
‘Live by performance, die by performance’.
Dr Benjamin Holdsworth explains why investors should not run after star funds
Markets make managers. This is combined with the recency bias gremlin that also lurks in our psyche, which places more weight on more recent experiences than on those that occurred further in the past.
Train wreck
This is then exacerbated by the fact that most investors get excited and invest only after much of the stellar performance has been delivered – one can spot the coming train wreck.
The harsh reality is that past performance does not tend to persist. This is clearly demonstrated by data and research going back decades.
It is evident that most investors failed to capture the strong upswing, piling in at the top and suffering the subsequent calamitous downturn. The average investor’s return is likely to be materially worse than the fund’s return, on account of this poor timing, although no exact data is yet available.
Investing is a hard enough emotional challenge at the best of times. Chasing performance just adds to the complexity and stress involved and may well put longterm investment goals at risk. Taking specific risk on such a fund is simply a gamble.
ON ANY piece of investment literature the warning ‘past performance is not a guide to future performance’ is always prominent, in bold, and generally glossed over by most readers.
Yet all actively managed funds are sold specifically on their ‘great’ past performance, usually by comparison to a ranking against their peers or a market benchmark. Funds that perform poorly never get to see the light of day in adverts or best-buy lists.
Many investors would be well advised to take heed of this warning. Those investing in a systematic way, seeking to capture market returns for market risks taken on, certainly do.
Little demon Deep down in the investor’s psyche lurks a little demon that wants to get rich quick, suffers terrible pangs of FOMO (fear of missing out) and becomes blinded by
Examining one of the funds that hit the headlines in 2020-21 with its stellar performance provides a sobering insight into the dangers of chasing performance. ARK Innovation – a highly concentrated, high-risk, ‘disruptive innovation’ technology fund – had a stellar rise of over 214% from the start of 2020, in US dollar terms, to its peak on 12 February 2021.
Its chief executive Cathy Woods was a regular on US business TV shows, spawning an almost cultlike following. It hit a unit price high of $157 – up from US$50 on 1 Jan 2020 – but has since then plummeted to US$37, losing 76 % of its value (to 12 May 2022).
ARK’s return is now almost exactly in line with the broad US equity market for those invested over the entire period.
As the saying goes, ‘if you live by performance, you die by performance’. It is worth remembering that the worst fall ever in the UK equity market since 1900 was of a comparable magnitude to ARK’s (-73%) in 1973-4.
Unfortunately, performancechasing investors tend to come to the game late. Net flows into the ARK fund peaked at the start of
Next time you see an advert for a fund in the paper, avoid the siren calls of stellar performance and take a moment to reflect on the free, sensible and seemingly boring advice it is obliged to provide: ‘Past performance is not a guide to future performance’.
Dr Benjamin Holdsworth (below) is a director of Cavendish Medical, specialist financial planners helping consultants in private practice and the NHS
The content of this article is for information only and must not be considered as financial advice. Cavendish Medical always recommends that you seek independent financial advice before making any financial decisions. Levels, bases of and reliefs from taxation may be subject to change and their value depends on the individual circumstances of the investor. The value of investments and the income from them can fluctuate and investors may get back less than the amount invested.
A private GP asks for advice about a patient who wishes to make an advance decision to refuse medical treatment. Dr Sally Old (left) responds
Asked to assist with a living will
Dilemma 1
Must I help her with a living will?
QI am a private GP and have been asked by one of my long-term patients to help her set up a ‘living will’.
Both of her parents spent a considerable amount of time in hospital during their last illnesses.
She was very distressed about this and does not want this to happen to her. Although she has no medical problems at the moment and is generally fit and well, she wants it on record that she would not want hospital treatment if she was terminally ill and could not make decisions for herself.
I feel uncomfortable about this, as she is currently well. Do I have an obligation to assist her?
ASince the introduction of the Mental Capacity Act 2005 in England and Wales –although other UK jurisdictions have similar legislation in place –the concept of a living will has been replaced by the ‘advance decision’ to refuse treatment.
The law allows for a person to specify that, in future, if they have then lost capacity to make the decision for themselves, certain treatments should not be carried out or continued.
A valid and applicable advance decision to refuse treatment in this way is legally binding.
Advance decision
A patient facing an illness likely to limit their life and/or ability to make decisions might foresee what lies ahead for them and write an advance decision about the treatments that they would not want in those circumstances.
Indeed, the GMC advises doc -
The law allows for a person to specify that, in future, if they have then lost capacity to make the decision for themselves, certain treatments should not be carried out or continued
in a situation that was not anticipated at the time they signed the advance directive, then it may not be effective. This may result in them receiving treatments that they would not have wanted.
The patient may wish to consider the alternative of arranging a lasting power of attorney (LPA) for their personal welfare, which would include medical treatment. By appointing someone they trust, the patient could ensure that the attorney is updated regarding any changes in their health and wishes over time.
tors to anticipate this and encourages such patients to plan their future care.
The difficulty for this patient, as you have identified, is in producing a valid and applicable advance decision when the nature of any future illness is unknown.
If they were to later lose capacity
The personal welfare LPA would only apply once the patient had lost the capacity to make decisions for themselves. The attorney can then make decisions on behalf of the patient in the patient’s best interests.
If the patient wants the attorney to make decisions about life-sustaining treatment, then this must be specified in the LPA.
When a chaperone is declined
Dr Sally Old discusses how
to
proceed when a patient does not want a chaperone
present during an intimate examination
Dilemma 2
Should I refuse to treat my patient?
QI am due to see a patient in the coming weeks for a check-up which will include an intimate examination, namely of the breast area.
When I offered a chaperone to facilitate this, the patient refused, citing it as unnecessary. I believe chaperones are a good idea in these types of examinations to safeguard both the patient and the doctor; however, I want to respect my patient’s wishes.
What should I do? Should I refuse to treat the patient?
AIn the first instance, make sure the patient knows that a chaperone is there for them. Their function is to reassure them if they experience distress, protect their dignity and confidentiality, and offer support throughout the examination.
They can also facilitate communication, especially if there is a language barrier. A secondary function of the chaperone is to discourage unfounded allegations of improper behaviour, as they are present during the examination as a witness.
Current GMC guidance makes it clear that a patient’s opinion and a doctor’s opinion of what constitutes an intimate examination can be different.
As you have done, doctors should use their professional judg-
ment and offer the patient the option of a chaperone wherever possible before conducting an intimate examination.
The chaperone should usually be a trained health professional. However, it may be worth asking whether the patient would be more comfortable with a family member or friend present as well. As long as this is a ‘reasonable request’, you should comply with it.
Patients do have a right to refuse a chaperone, and if this is still the case after they have been fully informed, this decision should be respected.
Try to avoid putting pressure on the patient either way. If you are unwilling to conduct the examination, you should explain why to the patient, making your reasons clear.
You may need to offer an alternative appointment or an alternative doctor. However, if the examination is needed, and no suitable alternative arrangements can be made, then you will need to proceed without a chaperone.
It is a good idea to publicise your chaperone policy; for example, by way of posters in the waiting room and clinical areas. This can help manage expectations and encourage patients to make their wishes known as soon as possible.
If you do go ahead with the examination without a chaperone, make sure you record that you offered one, but the patient declined.
Dr Sally Old is a medico-legal adviser at the Medical Defence Union (MDU)
When you’re asked
In the first of a new three-part inquest series, Thorrun Govind explains the inquest process and what happens if you are called to attend – with additional material from James Down
Now open on weekends
LET US HELP YOU GROW YOUR PRIVATE PRACTICE AT WEEKENDS
LONDON MEDICAL, the award-winning outpatient clinic in the Harley Street Medical Area is expanding its weekend opening hours. We are inviting applications for practicing privileges.
We can offer you:
Fully CQC-registered clinic
Nursing support
Appontment-making
Secretarial support
Billing service
In-house pharmacy
For more details
Contact: david.briggs@londonmedical.co.uk
49 Marylebone High Street, London W1U 5HJ
londonmedical.co.uk
AS FRONT-LINE healthcare professionals – and I write this as a pharmacist myself – we are very much focused on the care we are providing and working in the challenging environments that we do.
Legal correspondence can therefore feel like an unnecessary distraction from the day job and feel very far removed from our role caring for patients. However, our work can have life and death implications.
The prospect of engaging with court proceedings is very daunting, no matter how long you have been qualified. Here at Hempsons solicitors, we have supported
numerous clinicians through the coronial process.
We have a duty of candour. As registered persons, we must act in an open and transparent way with relevant people in relation to care and treatment provided to service users in carrying on a regulated activity.
Seek answers
Our engagement with the coronial process is therefore an important part of helping the bereaved seek answers and closure. It is as much a component of our role as keeping up to date with the latest NICE guidelines or making sure a patient
Thorrun Govind James Down
to go to an inquest
is fully informed about their latest immunisation.
Inquests are coroner-led legal proceedings with the family at centre of process. They are nonadversarial, in that there are no ‘sides’ and all those involved in the case work together to assist the coroner to establish the facts.
In simple terms, it is an inquisitorial fact-finding investigation with the aim of answering four questions: Who died? Where did they die? When did they die? And how did they come by their death?
Coroners are independent judicial officers appointed by the local authority who have a statutory
The coroner’s court also plays an important part in preventing future deaths and the coroner may ask you about your current practices and ways of working
well as communications with other healthcare professionals and internal policies.
If you do not have the documentation requested, it is better to be honest and up-front as soon as possible, rather than delaying the coronial process. You also have a duty to provide ‘full and frank’ disclosure, which includes documents that are not helpful to your position, but relevant to the investigation.
to prepare for attending the coroner’s court as a witness. This includes the formalities of addressing the coroner as ‘Sir’ or ‘Ma’am’. It is important to give a good impression, so smart clothes are a must and do not forget to have your mobile phone on silent, with your notes, statements and documentation easily accessible.
Attend remotely
duty to establish who the deceased was, as well as how, when and where they died when the cause is unknown or where there is reason to suspect the death may not have been due to natural causes.
Duty to assist
Inquests are prompted by concerns raised by family, clinicians, pathologists, circumstances that give rise to concerns and for deaths in custody, such as in prison or a secure mental health unit.
When you are initially contacted to assist the coroner, it is likely that you will be corresponding with the coroner’s officers, rather than the coroner themselves.
You have a duty to assist the court and should let your defence or insurance providers and legal team know you have been contacted so they can guide you through the process.
You may be asked to provide information or to write a statement, and the time spent gathering this will depend on what exactly has been requested. Do not be tempted to put it off.
The coronial process begins with information-gathering to narrow down the issues for the coroner to consider and to set the scope of the inquest. You could be asked to provide patient medical records as
Coroners have been sympathetic to the pressures on healthcare professionals during the pandemic; however, a simple unwillingness to engage is not acceptable. They also have a wide discretion to require evidence to be given or produced.
This can include the power to require witnesses to attend court and in certain situations they can impose criminal sanctions –including a fine or imprisonment.
Provide clarity
Once the coroner has received all the relevant information, they will decide who will be called to give oral evidence live in court and what parts of the evidence can simply be read into the court record. This is usually reserved for uncontroversial elements.
Providing a clear detailed statement can therefore prevent the requirement to attend court to give oral evidence and if your legal team are asking you to provide clarity, you would do well to heed this advice.
At the inquest, if you are called to provide evidence, you will do so under oath: a reminder that your duty is to the court and not to the parties. The coroner and other parties – formally recognised and known as Properly Interested Persons (PIPs), such as the deceased’s family – will have the opportunity to ask you questions.
While doctors and healthcare professionals are well-versed in talking to patients, it is important
Courts are increasingly allowing witnesses to attend remotely and you should consider your location as an extension of the court room. Legal support will make the process less daunting.
The coroner’s court also plays an important part in preventing future deaths and the coroner may ask you about your current practices and ways of working.
The coroner must make a Prevention of Future Deaths report where the investigation they have been conducting reveals something which gives rise to a concern that there is a risk of deaths in the future. The coroner will suggest that action should be taken to eliminate or reduce that risk, although coroners cannot recommend what that action should be.
You may have wondered how the coroner’s courts have dealt with Covid. As it is a naturally occurring disease, it is therefore capable of being a natural cause of death and therefore Covid does not automatically prompt an inquest.
There may, of course, be additional factors around the death which mean a report of death to the coroner and subsequent inquest is necessary – for example, where the cause is not clear.
Thorrun Govind is a pharmacist and solicitor at Hempsons law firm, where James Down is Head of Inquests and expert in inquests and coronial law. For further information, contact t.govind@hempsons.co.uk or j.down@hempsons.co.uk
Most Independent Practitioner Today readers have some form of employment income in addition to their private practice. For many, this will be the NHS – and the health service’s payslip can be complex.
Although this complexity makes understanding your payslip more difficult, this does mean we can gather a significant amount of information from a single payslip. Richard Norbury (right) has some practical tips to aid understanding of the payslip and highlights some common pitfalls
Don’t slip up on your
pay
Tax code
Your tax code reflects the tax-free amount being applied to your salary.
It is made up of a number of elements, but for medics will primarily relate to personal allowance, tax relief on employment expenses and adjustments for unpaid tax in previous years.
The tax code is usually a number with a prefix or suffix letter. The number dictates the tax-free amount divided by ten.
For a lot of people, the tax code will just be the personal allowance, currently £12,570 for 2022-23.
The tax-free personal allowance can be reduced when an individual earns over £100,000 of taxable income. Then it reduces by £1 for every £2 over the threshold.
This means when you reach £125,140 you have none of the original £12,570 left. The effect of losing your personal allowance in full is additional tax payable of £5,028.
Your tax code may also include any professional subscriptions paid so that the tax relief is spread during the year. The code may also incorporate regular charitable donations under Gift Aid.
It may be that you have underpaid tax in previous years. If you are not ordinarily submitting a tax return or if you opted to pay any shortfall of tax via your tax code, your tax code may include the collection of underpayments.
The loss of personal allowance can lead to an underpayment of PAYE. Understandably, HM Revenue and Customs (HMRC) struggles to accurately calculate tax codes in these circumstances, especially if the salary goes up during the year.
If your taxable income was under £100,000 in the preceding tax year, then HMRC will have no reason to reduce your tax code in the next financial year. HMRC should send you a copy
The boxes at the top of an NHS payslip give us accountants information that we can use to check that you are being paid correctly
of your tax code calculation. It is possible to have the tax code amended if required.
Additional roles
Often additional roles such as bank work, waiting list initiatives or second employments are not included on your usual payslips, even if this is paid by the same trust.
If you have multiple employments, a separate tax code should be applied. A common error is that your main tax code is applied to
this post as well as the main substantive post, which again can cause an underpayment of PAYE. This is often easily rectified by changing the code with HMRC but needs to be done ‘in year’, so being aware of this is key.
Payslip
The boxes at the top of an NHS payslip give us accountants information that we can use to check that you are being paid correctly.
The following boxes are important:
Sal/wage – This should be reflective of the pay scale that you are currently on as a ten-programmed activity equivalent.
You should review if this is in line with the current pay scales to ensure you are receiving the correct salary.
INC. date – This should be the date that you will move on to the next pay scale.
continued on page 44
Free legal advice for Independent Practitioner Today readers
Independent Practitioner Today has joined forces with leading healthcare lawyers Hempsons to offer readers a free legal advice service.
We aim to help you navigate the ever more complex legal and regulatory issues involved in running and developing your private practice – and your lives.
Hempsons’ specialist lawyers have a long track-record of advising doctors – and an unrivalled understanding of the healthcare system as a whole.
Call Hempsons on 020 7839 0278 between 9am and 5pm Monday to Friday for your ten minutes of free legal advice.
Advice is available on:
Business structures (including partnerships)
Commercial contracts
Disputes and litigation HR/employment
Premises
Regulatory requirements and investigations
Michael Rourke Tania Francis m.rourke@hempsons.co.uk
Standard hrs – Often not your actual hours but the amount of programmed activity that you work.
Within the body of the payslip are more terms and abbreviations that can be confusing:
Basic Pay – this is the pensionable amount of your basic pay;
Additional Prog A NP – this is the non-pensionable amount of your basic pay;
On Call – this is a percentage of your basic pay and is pensionable. Usually the ‘rate’ applied relates to the percentage paid.
Only the first ten programmed activities are pensionable. Therefore, on the payslip, the NHS will split the basic pay and additional programmed activity.
For example, if you work a job with 12 programmed activities, then the additional two will show as the non-pensionable amount. This can be checked back to your salary/wage figure and it is important to check regularly and especially if you have recently altered your job plan.
In addition, you may have a clinical director role or similar post. Depending on the role and the arrangement with the NHS trust, some of these roles are pensionable and some are not. These need reviewing on a case-by-case basis.
Clinical excellence awards
Local awards can be both pensionable and non-pensionable depending on when the award was achieved.
➲ If a local clinical excellence award was already being paid prior to April 2018, that same award remains pensionable after April 2018.
➲ If a current local award increases as a result of a points increase – i.e. from level 6 to level 7 – the increased amount is not pensionable.
➲ Any new local awards made from April 2018 are non-pensionable.
This can have the impact of local awards appearing as two separate headings on the payslip: one element being pensionable and one not pensionable. Understanding this will help when planning and preparing for annual allowance tax charges.
National awards have recently changed from the National Clinical Excellence Award (NCEA)
An example of an anonymised NHS payslip
scheme to the National Clinical Impact Award (NCIA) scheme. The new awards will be non-pensionable and there will be no formal renewal process.
To maintain the awards, a new application will need to be made. Awards paid to individuals working less than part-time will no longer be paid pro rata.
The value of the awards has also altered from:
Platinum: £77,320;
Gold : £59,477;
Silver: £47,582;
Bronze: £36,192; to:
N3: £40,000;
N2: £30,000;
N1: £20,000;
N0: £10,000 – only in Wales.
If you hold an existing pensionable NCEA, then you should be invited to renew this at the relevant renewal date. If you are successful, then the previous (higher) amount should be honoured and the total value will remain pensionable.
If your pensionable pay falls due to changes to clinical excellence awards, your 1995/2008 pension can be reduced. So it is important to take professional advice in this area if you anticipate a reduction to your pensionable pay.
Salary sacrifice
Salary sacrifice schemes offered by the trust can come in various forms, but arguably the most common in recent times would be for a
Pension – tiered rates
The NHS pension has fixed tiered employee rates based on a member’s pensionable earnings. Unlike the tax rates, the rate is applied to all pensionable earnings rather than a stepped deduction being applied.
Most consultants will be paying either 13.5% or 14.5% pension contributions based on the scale of seven different tiered rates. This scale is changing from 1 October 2022 and then again from 1 October 2023.
The likelihood is that many consultants will pay pension contributions at a maximum rate of 13.5% from October 2022, dropping to 12.5% from October 2023.
Remember that tax relief on pension contributions is given at source, so please bear this in mind – your taxable pay will increase.
vehicle lease under the NHS fleet scheme.
A salary sacrifice for a car is usually only tax-efficient if you are considering an electric or long-range hybrid car due to the way these cars are taxed on you personally.
Salary sacrifice schemes work by reducing your taxable and pensionable pay by the cost of the vehicle lease. You are then subject to a ‘benefit in kind’ tax.
The benefit in kind on cars is taken by multiplying the list price of the car by a percentage based on the CO2 emissions of the vehicle. Currently, electric cars and longrange hybrids have low percentages, which can make the scheme tax-efficient.
Doctors who have their own limited companies for private practice may be posed with the choice of a salary sacrifice or to use the limited company funds.
An initial thought process may be to think that the tax and superannuation savings would outweigh corporation tax savings. But it is important to consider the effects on your NHS pension and potentially annual allowance issues when you return the vehicle after the lease.
If you are considering an electric car and the NHS fleet scheme, you can obtain an example of how the salary sacrifice would impact your overall take-home pay and it is worth discussing the short- and long-term implications with a professional adviser.
Underpayments of salary
Often, we encounter issues where a backdated underpayment based on a change in job plan or perhaps a delay in processing the jump in a pay scale has not been paid. This leads to a lump sum payment that can fall in a different tax year to the year it was earned.
HMRC treatment is to tax you in the period that the payment falls, regardless of which period it relates.
However, for pension purposes, the pensionable pay should be allocated according to the year the money was earned, which is in contrast to HMRC treatment. If you have received backdated pay, then it is worth consulting a specialist accountant to ensure you have not been adversely affected.
You may be entitled to apply for some form of compensation, particularly if this has caused you to lose part of your tax-free allowance.
It is good practice to review your payslips regularly to ensure you have been paid correctly and so that no unexpected tax liabilities arise. Specialist medical accountancy advice can help to clarify these issues.
In our September article: Choosing the right team
Richard Norbury is a partner at Sandison Easson & Co, specialist medical accountants
Spending too much time on billing instead of patient care?
Let Medical Billing & Collection do the hard work for you.
With 30 years’ experience helping over 1,500 private consultants, groups, clinics and hospitals.
• Dedicated account manager
• Reduce bad debts to less than 0.5%
• Increase net income by up to 25%
• 24/7 online access to your data
• Faster payments through e-billing for insurers and patients.
Discover more at medbc.co.uk or 01494 763999
DOCTOR ON THE ROAD: VOLKSWAGEN iD4
Sensible, yes –but lacks sparkle
VW’s new offering ticks all the boxes needed to satisfy the medic family in need of all-electric transport. But is that enough? Independent Practitioner Today’s motoring correspondent Dr Tony Rimmer (right) finds out
MOST OF us tend to be cautious when it comes to investing in new technology. We usually trust brands that have served us well over the years.
And this applies to the cars we choose as much as it does the medical equipment we buy to benefit our patients. So when Volkswagen launched its new all-electric iD range, it was logical that it launched the Golf-sized iD3 first.
The Golf has been its most successful model after the Beetle and it was a way to introduce its future all-electric models without alienating a loyal customer base.
However, although the Golf was a default choice for families over many years, the current trend is for buyers to go for a larger SUV sized vehicle.
This is probably driven by the increased size of all the necessary child-carrying paraphernalia that comes with modern parenting. So, meet the iD4, a bigger and roomier SUV based on the same VW MEB platform as the iD3.
The range starts with the £34,995 148bhp Life Pure with a 52kWh battery and tops out with the Tesla-priced £49,025 299bhp four-wheel drive GTX with a 77kWh battery.
I have been driving the version that will have most appeal to most medics with growing families – the £43,500 204bhp Life Pro Performance with the 77kWh battery.
You could not call the iD4 a good-looking car. It is not overtly ugly, but the large body has a certain bloated appearance.
Direct competitors such as Hyundai Ioniq 5 and the Mustang Mach-E look smarter and more characterful. The iD3 is a betterlooking Volkswagen. The bonnet area is particularly bulbous, which seems unnecessary, as there is no
The interior is light and roomy and the driving position is excellent
engine and it does not even offer any extra luggage space.
Step inside, though, and you can forgive the bland external styling. The interior is light and roomy. The driving position is excellent and the driver’s controls are basically the same as the iD3.
That means that the central touch screen controls most features and there are useful steering wheel buttons too. But, unfortunately, the confusing temperature sliding control bar as used on the iD3 and Golf 8 is retained.
Impressive room
Rear passenger room is particularly impressive. Families will have no problem fitting large rear-facing baby seats and there is excellent head- and leg-room for adult occupants.
Large door-bins and seat-back pockets will be appreciated by owners too. The rear hatchback door may not be electrically operated, but it opens up an impressive 543 litres of space in the boot; enough for most needs. There is a useful under-floor compartment to house the charging cables too.
Driving the iD4 is really easy and relaxing. The acceleration is not as dramatic as in other electric cars, but it is still quick enough.
The tall SUV driving position and smooth brakes are complemented by light steering and a really impressive tight turning circle.
Refined progress
It is a doddle to drive in urban traffic and just what a busy medic parent needs to keep young occupants comfortable and quiet. On faster roads and motorways, progress is also refined due to minimal wind and road noise.
Handling on the twisty bits is as you would expect from any twotonne electric car; the chassis is tuned for smoothness and ease of use rather than any sportiness.
Having said that, the ride is a great compromise between firmness and comfort – Volkswagen has done well here.
As my test car had the larger 77kWh battery, the real-world range was a useful 250 miles or so. This means that long journeys are perfectly possible in this iD4 and you will be able to complete many urban trips without frequent topups.
So, the iD4 ticks all the boxes needed to satisfy the medic family in need of all-electric transport. It is a very good and reasonably priced electric SUV and would be a sensible purchase.
However, it somehow lacks sparkle and character in the way it looks and the way it goes about its business. Competitors from Ford, Hyundai and Kia have offerings that feel a bit more, well, special. In such an increasingly crowded and competitive marketplace, Volkswagen probably need to up its game for future iD models.
Dr Tony Rimmer is a former NHS GP practising in Guildford, Surrey
VW iD4 LIFE 77kwh PRO PERFORMANCE 204ps
Acceleration is not as dramatic as in other electric cars, but it is still quick enough
Body: Five-seat SUV rear-wheel drive
Engine: Single electric motor Power: 204bhp
Torque: 310Nm
Top speed: 99mph
Acceleration: 0-62mph in 8.5 seconds
Claimed range: WLTP 322 miles
CO2 emissions: 0g/km
On-the-road price: £43,500
PROFITS FOCUS: DERMATOLOGISTS
Good job in cutting costs
The dermatology and oncology markets were both seen as growth areas back in their high point of 2017. Here specialist medical accountant Ray Stanbridge examines how they have been doing since
WE ESTIMATE that average gross earnings for a consultant dermatologist in private practice in 2020 was £152,000. This showed no change from 2019.
Average costs fell by £7,000 – or 13% – from £54,000 to £47,000 between 2019 and 2020. As a result, gross margins rose by £7,000 – or 7.1% – from £98,000 to £105,000.
There are some cost changes to report, notably the apparent reduction of staff costs from £18,000 to £11,000.
These reductions, although arithmetically correct in our sample, seem high and we are doing further work as to why there appears to be a distortion.
Consulting room costs fell slightly between 2019 and 2020, as more consultants used their home offices for teleconsultations. In
the first months of the Covid pandemic, a number of consultants implemented teleconsultation for the first time.
Motor and travel costs show a slight increase, perhaps reflecting dermatologists’ pattern of work. However, they are not very significant.
Other costs remain broadly similar to 2019.
Online
consultations
We now know dermatologists generally did quite well in the first full year of Covid-19 from online consultations and we expect to see reasonable performance for 2021.
The self-pay market in dermatology is also rising and from what we can see most dermatologists who are seriously interested in private practice can expect a good financial outcome.
HOW ARE YOU DOING?
Pandemic causes a surge in income
AT FIRST sight, there appears to have been a large growth in the average incomes of oncologists in private practice between 2019 and 2020. Income growth, according to our survey, rose by over 20% between 2019 and 2020 to £170,000.
Costs went up by £3,000, or 8.6%, from £35,000 to £38,000. As a result, gross margins grew between 2019 and 2020 by £38,000, or 40%, from £94,000 to £132,000.
There seems to have been a significant growth between 2019 and 2020 with many patients switching from the NHS to the private sector to ensure ongoing treatment. However, this growth in income was at the very highest of our expectations and we are still reviewing figures for any distortions.
Costs look remarkably similar to 2019 levels. There is some increase in use of home costs between 2019 and 2020, reflecting an increasing trend from consultants to work from home.
There was also a slight growth in travelling costs, reflected in the growth of activity. A similar trend was noted with respect of professional fees.
Incomes to stabilise
But we do not expect the exceptional growth in average incomes apparently recorded between 2019 and 2020 to continue, even though the private oncology market is showing good growth.
We expect incomes to stabilise; this not least, because insurers may turn their attention on oncologists’ fees and on margins for drugs oncologists prescribe. As we have previously reported, our survey is not statistically significant. Rather it is an attempt to show what the average consultant oncologist and dermatologist is earning and spending.
The criteria for membership of our survey has been well documented in previous articles and is not repeated here, save to remind readers that the minimum income figure from private practice for inclusion in the survey has been increased from £5,000 to £10,000.
As we have reported in previous articles, consultant dermatologists and oncologists now trade in a wide range of legal entities notably sole traders, partnerships, limited
liability companies and limited liability partnerships.
Those trading through a group generally, but not always, report higher earnings. The trend for collective working is continuing and the number of consultants working ‘solitaire’ seems to be in decline.
Next time: General surgeons
Ray Stanbridge is a partner with specialist medical accountancy firm, Stanbridge Associates
Use these benchmarks to compare your financial performance with others
HOW DERMATOLOGISTS AND ONCOLOGISTS STACK UP
AND EXPENDITURE OF
Year ending 5 April. Figures rounded to nearest £1,000 (percentage is also rounded up)
Source: Stanbridge Associates Ltd.
Year ending 5 April. Figures rounded to nearest £1,000 (percentage is also rounded up)
Source: Stanbridge Associates Ltd.
NHS Pensions & Annual Allowance Tax
Get ready in advance of April 2022 when the proposed changes to the NHS Pensions will allow you to reclaim some or all of any Annual Allowance tax you may have suffered in the past.
With our knowledge and in-house calculators, we will be able to predict in advance and check statements produced by NHS Pensions and Scottish Public Pensions Agency for accuracy for any refunds due.
For further information contact us at aa@semail.co.uk or telephone 01625 527351.
Coming in our September issue, published on 6 September.
We present some learning points and an analysis of private patients’ complaints about consultants and private hospitals, made to the Independent Sector Complaints Adjudication Service (ISCAS)
How to go ESG in your practice – commercial lawyer Jamie Foster, a specialist in the health and life sciences sectors at Hill Dickinson, shares his thoughts on environmental, social and governance issues
Following this month’s article on the Bupa Wellbeing Index, Bupa Global and UK medical director Dr Robin Clark digs deeper into what this means for the future and the challenge for healthcare professionals
Growth in the fertility business: gynaecologist Mr Rehan Salim – who heads the new Lister Fertility Clinic at The Portland Hospital – gives his perspective on the boom of fertility treatments and what is driving the expansion of private clinics
In our Business Dilemmas series, Dr Kathryn Leask of the Medical Defence Union discusses what to do if asked to complete a medical form for an introductory SCUBA course and responds to a query about whether a new healthcare assistant can carry out cervical screenings
Inquests: How to write your statement and give your evidence. Our three-part series from Hempsons’ legal experts continues with Clementine Robertshaw explaining how to prepare for giving evidence in writing and if called to attend
Private practice troubleshooter Jane Braithwaite looks at how much should you be spending on marketing. We know that doctors are anxious about spending money on marketing and many of them would appreciate guidance on what would be a sensible investment and how to measure the success of that investment
INDEPENDENT PRACTITIONER
Published by The Independent Practitioner Ltd. Independent Practitioner Today is editorially independent and thanks Bupa for its assistance with distribution. Material is governed by copyright. No part of this publication may be reproduced, stored in a retrieval system or transmitted in any form without permission, unless for the purposes of reference and comment. Editorial layout is the copyright of the publishers. If you wish to use it for promotional purposes on websites or for reprints, we would be happy to discuss licensing the copyright to you.
Indemnity surrounding data and confidentiality breaches can be complex, but by taking steps to understand it and ensure appropriate protection is in place, doctors can potentially avoid a costly claim. Medical Protection’s Dr Dawn McGuire looks at some cases and explains more
Our Profits Focus financial benchmarking series examines the income, expenses and profits of general surgeons
Making sure you choose the right team to support you as your private practice grows is vital because who you pick can impact the success of your business and can have different financial implications. Read the advice of Alec James of Sandison Easson accountants
Patient retention: Simon Marett, of Ellerton Marketing, discusses tips and techniques you can implement to ensure patients return, recommend you and become advocates for your clinic
More analysis from the Medical Defence Union on the GMC’s proposed new fitness-to-practise guidance
Plus all the latest news and views and more articles to help your private practice from Medical Billing & Collection, Cavendish Medical, and the Independent Healthcare Providers Network
And don’t forget to check out our additional news updates every week online
ADVERTISERS: The deadline for booking adverts in our September issue is 19 August
Write to Independent Practitioner Today 7 Lindum Terrace, Lincoln LN2 5RP
CHANGING ADDRESS, EMAIL ADDRESS OR SUBSCRIPTION DETAILS?
Phone 01752 312140 or email karen@marketingcentre.co.uk
TELL US YOUR NEWS
Robin Stride, editorial director Email: robin@ip-today.co.uk Phone: 07909 997340 @robinstride
ADVERTISE WITH US
To advertise in the digital journal, on our website or in our business directory, contact advertising manager Andrew Schofield at Spot On Media. Phone: 0161 408 3912 Email: andrew@spotonmedia.co.uk
Follow Independent Practitioner Today on
GET A SUBSCRIPTION DISCOUNT!
£90 independent practitioners.
£90 GPs and practice managers (private & NHS).
£210 organisations.
Save £15 paying by direct debit: individuals £75 (organisations £180).
TO SUBSCRIBE
Email karen@marketingcentre.co.uk or phone 01752 312140
Publisher Gillian Nineham Phone: 07767 353897.
Email: gillian.nineham@gmail.com
SAVE £15 WITH DIRECT DEBIT!
Guarantee delivery of your next copy of Independent Practitioner Today. Take out a subscription and you will get full access to our news, features and previous issues on our website. See details on the left.