Jane Braithwaite shares details of support available for an alternative career P16
The business journal for doctors in private practice
Road map to recovery
Follow these signals to ensure your practice is best placed to benefit from the recovery P26
your career away
Dr Clare Gerada looks at doctors’ unprofessional behaviour
Business Dilemma: When you must confess to GMC Medico-legal advice on when you need to disclose a driving offence to the regulator P32
Doctors quitting private practice
By Robin Stride
The medical director of a leading private hospital has warned of a ‘huge exodus’ of specialists from the independent sector in the wake of Covid-19.
Consultant surgeon Mr Satya Bhattacharya, of The London Clinic, said although large numbers of doctors had suffered heavy falls in their profits during the pandemic, he doubted money was the key factor.
He told this year’s Private Healthcare Summit that large numbers of consultants saw a significant drop in their income in the early part of 2020 and many had to lay off or furlough their employees.
‘But I don’t think that’s the main reason why people are leaving the profession,’ he said.
‘You’re seeing a huge exodus of consultants from the NHS and private sector and I think Covid has been very draining on people, their energy and morale, and a lot of people have just said “That’s it, I’ve had enough, I’m going”. I’m seeing that a lot among colleagues.’
Mr Bhattacharya, who stepped down from the NHS last October, also voiced concern at Covid’s big impact on hospital staff.
Speaking to over 300 attendees of
In
association with
the digital LaingBuisson event, he said: ‘We are seeing fewer colleagues wanting to come and work in the UK, so how we recruit and fill vacancies is going to be a challenge for our HR.’
And he warned that fixing the staff recruitment problem would be a challenge for the whole sector and the whole country.
‘The scale of the problem will probably become more apparent over the coming months because I think a lot of nurses and doctors are taking stock at the moment and wondering what to do next.’
According to David Hare, head of the Independent Healthcare Providers Network, workforce matters have been ‘the biggest issue by a long way’ over the last three months.
There were worries about stability, concerns about getting people in, and domestic supply – and there were no easy answers.
‘It’s something we are going to have to try and tackle in partnership with the public sector and we are going to have to throw the kitchen sink at it because it is an existential challenge to all of us working in healthcare.’
Jenni Wilson, Nuffield Health hospitals commercial director, warned the meeting that staff availability would be the biggest limit-
ing factor in private healthcare’s ability to meet demand.
Dr Mark Vanderpump, chairman of the London Consultants’ Association (LCA), later added his views on why consultants were leaving.
He said: ‘The LCA recognises that younger consultants require considerable support to build a private practice in the current private health market. There are many issues that result in disenchantment with increasing administration and costs of setting up a practice, which can appear prohibitive.
‘The major limiting factor is the behaviour of the private medical insurers towards consultants, including the low consultation fees that have to be accepted by new consultants to enjoy the privilege to be listed as a provider.’
The MDU said it was too early to say what the long-term trend would look like, but it had not seen a significant movement of doctors from private practice.
‘During 2020, although we saw a large number of consultant members doing less private work due to pandemic changes, many are now increasing their levels of work again. This includes doctors who did little or no private work during the crisis period last year.’ n See pages 6 and 7
Insurance sellers say business is on the rise
Consultants in private practice can expect a welcome increase in patients with private medical cover, according to an insurance industry survey.
Nearly 60% of Association of Medical Insurers and Intermediaries members expect to see a rise in demand over the next few months.
Four in ten respondents said they anticipate more patients wanting private healthcare, while 18% expect a significant increase.
When asked about the main opportunities for their business, a third of respondents cited lengthening NHS waiting lists as a driver for increased interest in private health insurance.
Several firms also identified the fact that private healthcare offers their clients access to digital healthcare and to fast treatment.
A further 35% expect an increase in demand from employers, with one in three of these looking at opportunities with small to medium-sized enterprises.
Almost a third highlighted opportunities for organic growth through things like client retention and quality service, an uplift in additional cover and benefits for existing and new clients, account development and referrals, and digital marketing and lead generation.
➱ continued on page 3
TELL US YOUR NEWS. Contact editorial director Robin Stride
ADVERTISE WITH US. To advertise in the journal or our website business and lifestyle directories, contact advertising manager Andrew Schofield at Spot On Media. Phone: 0161 408 3912
Email: andrew@spotonmedia.co.uk
GET A SUBSCRIPTION DISCOUNT
£90 independent practitioners. £210 organisations. £90 GPs and practice managers (private & NHS).
Save £15 paying by direct debit: individuals £75 (organisations £180).
Our combined July/August issue is packed with some smart topical tips from our team of expert writers, so we thought we would draw attention to a few before you delve into the following pages.
Private waiting lists are growing as we emerge from lockdown, but coping with this increased demand from a financial perspective may be a challenge. Ian Tongue shares some great advice on page 38.
Accountant Julia Burn (page 15) warns it will be important to recover trade debtors as quickly as possible after providing a service as well as negotiating favourable payment terms with suppliers.
You may also need to manage payment terms for procedures or treatment plans that span over a long period of time and are classified as work in progress.
This can be done by, maybe, agreeing payment arrangements to ensure clients pay piecemeal
to avoid long waiting time for payment.
‘Invoice as soon as possible’ is the message from billing expert Simon Brignall (page 26), especially as some insurers now put a time limit on this.
And while we are on the subject of fees – this could be a good time to review your rates for consultations and procedures. Some consultants have charged the same prices for years.
If you are a new independent practitioner – welcome! Check out Kirsty Odell’s advice for a smooth private practice purchase (page 40).
And for those doctors contemplating a move, see Jane Braithwaite’s article (page 16) about the support and the organisations available that can offer a route to your alternative career path.
And if you’re planning to refresh your business’s brand, check out what designers Simon Marrett and Michael Sullivan have to say on page 24.
A new type of inspector will call
You and the Care Quality Commission in 2021 and beyond – what does the watchdog’s new strategy mean for independent healthcare providers? P12
How to avoid claims against you Clinical negligence claims against ear, nose and throat surgeons in private practice are explored here by two MDU medico-legal experts P18
The mental health of your staff
Dr Pablo Vandenabeele, clinical director for mental health at Bupa UK Insurance, shows how to make your practice a supportive environment P20
How IT raises your quality of service
Healthcode’s Kingsley Hollis shows how technology can help you offer a high level of service that will attract patients through recommendations P22
Pictures have the greatest impact
The last in our series on branding and marketing for private healthcare takes a closer look at using imagery in your branding and design P24
So you want to buy a practice?
Solicitor Kirsty Odell sets out some of the key stages to buying or selling a practice, which will keep you on the right track for a smooth transition P30
PLUS OUR REGULAR COLUMNS
Accountant’s briefing: Are you ready to take on a surge in work?
Ian Tongue provides some tips on how to get fighting fit for the boom in private work post-Covid P38
Doctor on the Road: The quietest car I have ever driven
Dr Tony Rimmer luxuriates in amazing level of comfort and refinement of the electric Audi e-tron P40
Profits Focus: Better than expected
General surgeons’ earnings have exceeded their accountants’ expectations P45
Pensions tax hike would be disaster
By Edie Bourne
Doctors have been alarmed to hear reports of new pension tax changes being discussed by the Treasury to help pay for the country’s response to the Covid 19 pandemic.
Measures believed to be under consideration include introducing a flat rate of tax relief and lowering the lifetime allowance.
The lifetime allowance was frozen in this year’s Spring Budget at £1,073,100, but a report by The Daily Telegraph suggests this could drop to just £800,000.
The lifetime allowance is the total amount which can be saved into a pension free of tax.
Pension savings above the rate are taxed at 55% if taken out as a lump sum or 25% if paid in any other way.
Patrick Convey, technical direc
tor for specialist financial advisers Cavendish Medical, explained:
‘We need to be cautious because rumours of pension tax changes circulate every year – although normally this happens before a major fiscal review such as the Budget or Autumn Statement.
‘However, if any of these changes are put in place, it will have serious consequences for doctors, particularly those tied into the NHS pension.
‘The lifetime allowance limit was £1.8m in 2011 12 and each time it has been reduced, it has meant more doctors facing harsh tax bills. If this reduction is true, a drop to £800K would be extremely detrimental to many NHS pension savers.’
In addition, increasing the flat rate of tax relief would effectively increase doctors’ net contributions to the pension scheme.
Mr Convey said: ‘Many senior doctors contribute 14.5% of pensionable salary to their NHS pension but get tax relief at 40 or 45%. This results in a net contribution figure of 8.7% for 40% taxpayers or 7.98% for 45% taxpayers.
‘If a flat rate of tax relief was introduced at, for example, 30%, this would result in a net contribution figure of 10.15%, regardless of tax rate. For a doctor with a salary of £120,000 a year, this would cost an extra £1,740 annually as a 40% taxpayer or £2,604 per annum as a 45% taxpayer.
‘The problems caused by the complexities of pension tax are fuelling a workforce crisis among senior medical staff.
‘These changes will undoubtedly cause more concern for those in defined benefit schemes than any other pension and will present substantial problems.
Poll reveals insurers’ optimism
The insurance sales body, AMII, said only 10% of its members expected to see a decrease in demand in 2021.
When asked about the greatest threat facing their business, three in four of those who answered this question cited a challenging postpandemic economy as a major threat.
AMII executive chairman David Middleton said: ‘The pandemic has undoubtably had an immense impact on healthcare in the UK, with disruptions to services, increasing waiting lists and a reduction in GP referrals and screening services.
‘The private health industry is well placed to reduce the burden on the NHS in these challenging times, ensuring people can access the healthcare they need, when they need it.
David Middleton, executive chairman of the Association of Medical Insurers and Intermediaries
‘These findings shed light on the optimism of AMII members for the year ahead and we could indeed start to see more of a shift in how people access healthcare, leading to accelerated growth in our sector.
‘As the voice of the industry, it’s important for AMII to gather and
If these measures go ahead, we will see more senior doctors leaving the profession at a time when the NHS desperately needs its staff
PATRICK CONVEY
share these kinds of insights and we were delighted to work with the team at The Exeter on this research.’
The Exeter head of sales Karen Woodley said: ‘We are encouraged by the level of optimism from the AMII membership.
‘It is important for us to seek feedback from advisers so we can continue to ensure our products and service meet the needs of advisers and their clients.’
Mark Allan, commercial director for Bupa UK Insurance, said: ‘The past year has amplified the importance of health and supporting people with their well being. Insurers, consultants, therapists and healthcare services need to continue to drive innovation to ensure that we support the changing needs of our customers.’
A total of 47 members completed the survey.
‘We await to hear more definite outcomes of this latest pension shake up, but if the measures go ahead, we will see more senior doctors leaving the profession at a time when the NHS desperately needs its staff.’
Fifth of clinic staff aim to stay away
Doctors’ practices with office staff who are still working from home could find many of them never return, a survey suggests.
Nearly one in five healthcare staff who work in medical office jobs and not face to face with patients do not intend to return to the office again after the pandemic.
The study of 258 workers, by corporate transport specialist Kura, found they were reluctant to go back to normal due to ongoing concerns around infection control and social distancing issues on public transport.
They plan to never commute after lockdown – with regional variations from 10.8% in London to 29.1% in Wales.
➱ continued from front page
By Olive Carterton
Complaints about consultants have become the top area of dissatisfaction from patients receiving private practice treatment during Covid19.
These accounted for 18% of the heads of complaint received by the Independent Sector Complaints Adjudication Service (ISCAS) in the year to the end of March 2021. Its annual report said complaints handling received 17% of gripes, accommodation 10%, clinical –nonmedical and nursing 8%, and nursing 7%.
In this reporting period, 109 complainants received a final deci
New clinical director for brain and mind clinic
Re:Cognition Health has appointed the former head of commercial management at Schoen Clinic UK, Dustin Reibe, as director of clinical services. He will develop the company’s private patient and medicolegal business, which is expanding its services for all ages, from young children with autism to the older population with Alzheimer’s. Medicinal cannabis and longCovid clinics are also planned.
Mr Reibe said: ‘Re:Cognition Health’s vision to change the
HCA establishes first paediatric spinal surgery unit Complaints on the rise
Four spinal surgeons – Mr Jonathan Lucas, Mr Mark Harris, Mr Stewart Tucker and Mr Thomas Ember – are leading the UK’s first and only dedicated paediatric and young adult private scoliosis and spinal surgery unit.
Based at HCAs’ The Portland Hospital for Women and Children,
sion from an independent adjudicator. Of these, adjudicators identified 624 heads of complaint, up from 348 the previous year.
ISCAS believes a possible explanation for this increase is the nature and complexity of the complaints received during the previous 12 months.
Some people had ‘unrealistic expectations’ about the possible outcomes of adjudication – seeking a refund, revision surgery and/ or financial compensation.
These customers were signposted to ‘more appropriate’ forums such as Citizen’s Advice Bureau or to seek independent legal advice. However, goodwill payments
future of brain and mind health is inspirational and I am thrilled to be in a unique position at the forefront of innovation in brain and mind services for the future.’
Company founder Dr Emer MacSweeney added: ‘This is an extremely exciting time, worldwide, for new biomarkers and medications for diseases affecting the brain and mind. The rate of change and process in this challenging arena of healthcare has never been more rapid.’
were made in around 83% of completed cases in this reporting period, an increase of around 9% compared to the previous year. The average goodwill payment rose from £605 the previous year to £613.
Of ISCAS’s 200+ subscribers, 34 were new, including five NHS private patient units (NHSPPUs).
ISCAS reported: ‘While it is good to see more NHSPPUs subscribing to ISCAS, the pace of expansion is slow and ISCAS continues to receive complaints from private patients treated in the NHS who have no access to an appropriate body for complaint escalation’.
Adjudicators either ‘uphold’,
‘partially uphold’ or ‘do not uphold’ a particular head of complaint.
58.8% of complaint heads were either upheld or partially upheld, a slight decrease on the previous year.
ISCAS subscribers bear the cost of adjudications, averaging £2,053 which is down from the previous financial year.
A quarter of cases required expert clinical advice, up from 14%, costing an average of £1,653 per case, up from £1,357 per case.
Independent adjudicators have discretion whether to engage the services of an expert, depending on a case’s nature and complexity.
Heart scan service starts
HCA’s The Harley Street Clinic has announced it is the first UK private hospital to offer a revolutionary new prediction technology, called CaRiHeart.
Consultant cardiologist Prof Ronak Rajani said the pioneering scan offered hope and reassurance to potentially thousands of people with heart problems or a family history of heart disease.
He told Independent Practitioner Today : ‘The technology allows patients to understand their risk of having a significant heart attack in the future, far enough in advance for them to put preventative measures in place.’
Prof Rajani said a published study involving approximately 4,000 patients who were followed
up for nine years after their original CT angiogram (CCTA) scan showed that an abnormal Fat Attenuation Index (FAI) was associated with up to a nine fold increase in sustaining a fatal heart attack in the next nine years compared with those with low or normal FAI readings.
‘The study also showed that at least one third of patients who underwent a routine CCTA and were initially considered low risk had a much higher risk after CaRiHeart was applied to their scan.
‘This demonstrates that CaRiHeart is more thorough in determining risk than a CCTA scan alone and as a result, could potentially help save lives.’
A test costs £495.
the new Scoliosis and Spinal Surgery Centre will offer integrated and multidisciplinary non-surgical and surgical care for young patients experiencing the full range of spinal problems. The consultants also work at the Evelina London Children’s Hospital and Great Ormond Street Hospital.
Dustin Reibe
Jonathan Lucas Mark Harris Stewart Tucker Thomas Ember
Bupa hospital boasts ‘top radiotherapy unit in Europe’
Arrival of the MRIdian MR linac at GenesisCare’s Centre for Radiotherapy at Cromwell Hospital, London, makes it ‘the most advanced radiotherapy centre in Europe’, according to the provider’s clinical lead.
Dr John Conibear said the new technology meant patients could receive the best care possible with fewer hospital visits.
A surge of new cancer diagnoses are expected when patients come forward after social distancing for Covid19 eases.
The MRIdian is the only linear accelerator model with automated beam control. If a tumour moves even a few millimetres, the treatment will automatically pause until it returns into position, to avoid missing the target and irradiating healthy tissue unnecessarily.
While conventional radiotherapy can involve up to 37 treatments, patients typically only need from three to eight with the new machine.
New gynae clinic at King
Edward VII unit
Independent charitable hospital King Edward VII’s has launched a Gynaecological Diagnostic Centre offering screening, diagnostic and interventional services to women.
Prof Davor Jurkovic, who leads the consultant team, said the aim was to provide a userfriendly service offering immediate diagnosis and an individualised management plan in a single visit without the need for additional blood tests, imaging such as MRI or diagnostic surgical procedures.
Sick doctors to be judged differently
By Douglas Shepherd
Alarm bells are ringing over health department proposals for the GMC to investigate doctors with health concerns under ‘lack of competence’ grounds.
Defence bodies have strong concerns about the possible axing of ‘health’ as a separate category under which relevant fitness topractise concerns could be investigated.
Dr Rob Hendry, medical director at MPS, warned: ‘Removing “health” grounds and instead categorising doctors with a health concern under “lack of competence” grounds would be extremely demoralising and could exacerbate their health issue.
‘It may also discourage doctors from seeking help at an earlier
stage and this could endanger both patients and the doctor.’
A consultation proposes the GMC has just two grounds for investigating doctors – ‘lack of competence’ and ‘misconduct’.
Dr Hendry said GMC inquiries brought many doctors considerable stress and anguish – as tragically demonstrated by the number of doctors who die by suicide each year while under investigation.
He added: ‘More broadly, we are concerned that even for those who do not have health concerns, the term “lack of competence” is unnecessarily pejorative.
‘There are variables which can affect a doctor’s performance in situations where competence may not be the primary concern – for example, systemic and organisational factors that are outside of the direct
Surgeon taught in robotics entirely by private sector
A surgeon has been trained in robotic surgery entirely in the independent sector for the first time.
Consultant gynaecologist Mr Denis Tsepov, who specialises in complex cases, was trained at HCA’s The Princess Grace Hospital.
The six month programme involved a series of exercises, including virtual simulation training, elearning, facetoface training, lab teaching and supervised patient cases.
He was proctored by Mr Tony
Mr Tsepov said he found robots made surgical work feel much simpler by providing improved visualisation and access ‘and making you feel calmer and more comfortable during surgery’.
HCA plans to expand its robotic training to include general surgery and treatment of colorectal conditions and hernias.Its surgeons performed over 500 robotic ops using the da Vinci Xi System last year.
control of the clinician. We hope to see a more neutral phrase.’
The MPS has urged the Government to ensure it delivers on its 2018 commitment to strip the GMC of its power to appeal fitnesto practise decisions and give it greater discretion in deciding whether and how to investigate a fitnesstopractise concern.
It said this would avoid thousands of doctors going through unnecessary investigations.
Dr John Holden at the MDDUS said: ‘Health cases need to be dealt with more sensitively than other cases.
‘This is of utmost importance with cases involving mental health problems.
‘It is simply not appropriate for health to be placed into the same ground as competency.’
Doctors respond to call-up for data-sharing study
A spokesman said the response showed the sector’s enthusiasm for improving how healthcare data is collected and used.
The pilots are part of The Acute
The Private Healthcare Information Network (PHIN) says it is ‘delighted’ at the number of private hospitals asking to participate in pilot studies for the first comprehensive national dataset of ‘whole practice’ information for doctors and hospitals in England.
Data Alignment Programme (ADAPt) to integrate private healthcare data into NHS systems. The need for this dataset was highlighted by the independent inquiry into rogue breast surgeon Ian Paterson.
Chalhoub – a national leader in robotic gynaecology.
Mr Denis Tsepov
LAINGBUISSON PRIVATE HEALTHCARE SUMMIT
Covid spurred improvements
Reports by Robin Stride
Covid-19 has been a catalyst for a vast range of improvements in private healthcare as consultants, hospitals and their staff were forced to look more closely at aspects of their work which had not previously been high on the management agenda.
Many of these were highlighted as Mr Satya Bhattacharya, a consultant surgeon and medical director at The London Clinic, reflected on the early months of trying to deal with the pandemic – and considered the positive impacts.
He, like many doctors, confessed to feeling an overwhelming pride in how staff and his hospital stood up to the challenge.
It had demonstrated that a public and private partnership can work – and collaboration was achievable in the future.
The private sector seeing complex NHS patients and sharing
Insurer gives back £125m to customers
Leading medical insurer Bupa has paid back millions of pounds to its customers in rebate payments, sparked by the pandemic.
Mark Allan, commercial director at Bupa Insurance, said: ‘We, like a number of insurers, made a commitment very early in the pandemic that we would give back any exceptional financial benefit due to lower claims through that period of disruption.’
He announced that the insurer was in the process of paying £125m back to its customers in rebate payments. The process was
staff and consultants worked very well, he said.
Mr Bhattacharya drew attention to four big lessons learned:
1 The need for swift decisions and brisk implementation, such as was seen with the rapid upscaling of laboratory capacity and the creation of an infection diseases unit;
2 The importance of clear and timely communications;
3 The importance of visible leadership;
4 Not to always look to the NHS for guidance, even on clinical matters.
The private sector had often tried to copy the NHS and, by and large, that was fine, he told the Private Healthcare Summit 2021. But there were times ‘when you had to do your own thing’ and not look to the state service for guidance.
Turning to the many positives of Covid-19, he cited technology,
due for completion by the end of June.
Mr Allan added: ‘It’s been great to see the reaction we’ve had from both the market and our customers.’
During the pandemic he thought people had seen Bupa respond and innovate quickly.
remote monitoring of patients, and the impact of online consultations on patients and doctors’ practices.
Now there was a need to establish long term what makes a ‘good’ virtual consultation and what governance mechanisms are needed.
Incorporation of private hospitals into the Image Exchange Portal was another plus. He had tried to get his hospital into it for a long time, but Covid made it happen.
Free parking from Westminster Council was a bonus and the pandemic made his team look at aspects of their hospital that they did not always think about – such as ventilation in wards, offices and public areas, and how much office space was really needed.
More than 3.2m operations, scans, tests, chemotherapy sessions and consultations were delivered on an ‘at cost’ basis under the contract between the
NHS and independent sector from March 2020-March 2021.
Central London providers were removed from the contract last September, but private hospitals continue to support the NHS through the ‘increasing capacity framework’.
As a central London hospital, The London Clinic had always had a significant volume of embassy work and foreign patients. That market had closed off, but that shortfall had been made up by insured and self-pay patients. Mr Bhattacharya said it would be interesting to see what the longer-term impact on the market will be from Covid. He expects the huge NHS waiting lists now will drive self-pay demand, but whether overseas medical tourism returns to London is something ‘we will have to wait and see’.
Remote consultation to ‘be part of future’
New technology could enable a large proportion of medical consultations and monitoring online.
William Laing, executive chairman of LaingBuisson, said it was possible now to complete ‘30-40% of medical consultations online, without time-consuming followon, but remote monitoring and patient-held devices could see this rise to’ maybe 70%.
Insurers were talking to tech platforms about developing online models for delivering more economical and more convenient services for managing chronic
conditions, for which there was ‘a massive potential market’.
He said winners would include tech platforms for virtual consultations and remote monitoring, particularly those with Care Quality Commission registration to deliver services as well as simply enabling consultations.
‘Consultants will presumably prove powerful enough to defend their interest, though they will need to accept a change in working practices for the potential efficiencies from online consultations to be realised.’
Surgeon Mr Satya Bhattacharya
Mark Allen of Bupa Insurance
LAINGBUISSON PRIVATE HEALTHCARE SUMMIT
Massive differences between the prices charged in private hospitals for the same operations are causing confusion and concern to wouldbe self-pay patients, the conference heard.
According to LaingBuisson’s selfpay pricing analysis, using the example of total hip replacement, the cheapest was £9,025 at three NHS treatment centres.
But patients could pay over £6,000 more at the most expensive venue. The op at the Nuffield Health Cambridge Hosp ital cost £15,625. The average was £11,826.
Self-pay adviser Richard Gregory said the market should not be seeing any more of these huge fluctua-
tions. Prices could differ vastly even among one provider’s units within a few miles of each other.
Much of the differences being seen in prices were historical and he doubted there had been a concerted pricing strategy.
‘In my view, and it’s always been a bugbear of mine, there should be more price convergence. I don’t necessarily feel that there should be one price for a hip across the UK; for example, a national price.
‘I think the emphasis should be more on convergence. So for hospitals to achieve that they probably need to be better at negotiating more common rates for surgical and anaesthetists fees.’
Private sector ‘must fix its poor customer follow-up’
Patients in private healthcare get their treatment, go home and never hear from their surgeon or hospital again.
It is an all-too-common scenario for many patients, including the summit chairman Keith Pollard, a healthcare consultant for LaingBuisson.
He complained of a lack of post-treatment customer service in private healthcare.
purchase and they would be in touch about possibilities for your next car.
If he bought a car, then salesmen would follow up with phone calls to see you were happy with your
Pricing anomalies attacked Research
Research by market analysts
LaingBuisson suggests there is optimism and confidence about the future of self-pay, although there are barriers to growth.
These include reports of growing waits for initial private consultations and treatment, plus consumers not being signposted into
But he said he had gone private for some operations and the only follow-up phone call he got was ‘would you pay your bill?’
A number of speakers agreed the sector could improve its post-op service by showing it was looking after the customer and thinking of the future when, for example, an operation on a second knee might be required.
Liz Heath, author of LaingBuisson’s annual reports on selfpay, said some providers had standardised their pricing across the country, which was helpful for consumers if there were several hospitals run by the same provider within their catchment area.
But she said some big anomalies in pricing still existed and for anyone in an area where there were many local options, then these would be ‘confusing at best and worrying at worst’ .
In some procedures, there was much less price variation across the country where the pathway had been more standardised. But there was work to be done on the
wide variation of prices, although the average price point might not have greatly shifted.
Responding to a question, Nuffield Health hospitals commercial director Jenni Wilson said there was no standard pricing across the charity.
But she said it was important to know if prices were a like-for-like comparison; for example, a physiotherapy service might be included in one locality but not another.
She said she ‘tended’ to agree with Mr Gregory’s comments but felt that as this market continued to grow and mature, there would be fewer outliers.
Credit deals urged to grow self-pay market
Credit and finance payment options for customers have a huge part to play in growing self-pay, an independent consultant to healthcare organisations told the summit.
Richard Gregory said these were expected for all ‘big ticket’ purchases and healthcare should be no different. Pluses included:
A mutual benefit to customers and operators;
Customers can make an instant decision to have private treatment;
They can select a payment option best suiting their financial situation;
Payment options offer more consumer protection;
They increase perceived value by removing uncertainty;
They create more loyalty because the hospital operator is making things easier.
Self-pay sales could also increase through the breaking down of price into a more palatable cost, he said. The processes were easier and operators were paid early in full.
Mr Gregory argued that payment options were an integral part of customer choice, they should be central to any proposition, and they drove better sales and loyalty.
private healthcare choices and options, according to self-pay consultant for the company, Liz Heath. She reported growing recognition that the NHS might be unable to be as responsive and available for planned diagnostic and elective treatment in the future, and the
signs were that many people were able to save during Covid.
Talking of online reviews, she quoted research by Reputation in 2021 in the US showing 80% of health consumers trust online reviews, and ratings are the third most important factor for patients after insurance and location.
Are they patients, customers or consumers?
It is customers every time for selfpay expert Mr Gregory. He said: ‘What is a customer? It is somebody who is seeking to purchase something either for themselves or somebody else and that’s exactly what a self-pay patient is.’
Keith Pollard
Get tough on fake doctors, says MDU
By a staff reporter
Tougher sentences are being urged for fake doctors in a bid to protect the public in the wake of the pandemic.
The Medical Defence Union (MDU) made the call because it is concerned by recent cases of members of the public posing as doctors and exploiting vulnerable patients with fake vaccines and other scams
A Government review is currently looking at the way it regulates doctors, including penalties for those posing as medical professionals.
Section 49 the Medical Act makes it a criminal offence for someone not on the GMC’s medical register to falsely portray themselves as a registered member of the medical profession.
But the maximum sentence for someone found guilty is a fine, putting the offence on the same scale as a TV licence payment evasion.
The MDU wants the offence recategorised so that it can either be tried summarily by magistrates or on indictment before judge and jury at the crown court.
Chief executive Dr Christine Tomkins said: ‘The Government is proposing that the current maximum penalty for the offence in the Medical Act should remain as a fine. We do not believe that is right.
‘A fine does not reflect the seriousness of the offence. We believe the courts should have all sentencing options open for offenders and that is what we have urged the Government to do.
‘This would put the offence on a par with other fraud offences; ensure the offence is prosecuted
and treated with all the seriousness it merits and, crucially, allow the public to see a full and accurate picture of the number of prosecutions that take place.’
Between 2006 and 2017, 12 people were charged under the Medical Act 1983 with pretending to be registered as a doctor, Crown Prosecution Service figures show.
Three years ago, the GMC carried out a review of 3,000 doctors’ qualifications after a person who had dropped out of medical school practised as a psychiatrist for 23 years.
The MDU said it was difficult to get a true picture of how commonly this type of crime occurs. With penalties for the offence so low, it was possible that offenders had been prosecuted under different legislation such as the Fraud Act 2006, where prison sentences are available to the courts for serious offences.
MDU continues its ‘doctor for doctors’ ethos with new chief
The Medical Defence Union (MDU) has appointed Dr Matthew Lee as its new chief executive to take over from Dr Christine Tomkins, who retires in September.
She has been in the role since 2009 and worked for the MDU for more than 36 years.
Dr Lee is currently director of professional services with responsibility for key services MDU members rely on, including 24-hour medico-legal advice, claims handling, legal services and clinical risk management. He joined the MDU in 2000 from a background in paediatrics and anaesthetics in the Wessex region. He initially worked for the company as a medico-legal
adviser and clinical risk manager before taking on broader management responsibilities.
Dr Lee said: ‘During the pandemic, our members have been under tremendous pressure and we know that many challenges lie ahead, such as supporting them with increasing numbers of complaints and claims.’
He said the defence body aimed to broaden its range of benefits and services in line with being a not-for-profit, wholly memberowned company.
Chairman Dr Paul Riordan-Eva said: ‘We are proud to continue our long tradition of being the only UK medical defence organisation with a doctor at the helm.’
Pension policy causing rush to retire early, says union
The Hospital Consultants and Specialists Association (HCSA) has hit out at the Treasury for a ‘misguided, dogmatic attitude’ to NHS pension reform and warned that this must change.
Responding to strong criticism of Treasury reforms by Parliament’s Public Accounts Committee (PAC) in a new report, the union’s pensions lead Dr Sarah Tennant called it is a stinging critique of the department over its mishandling of pension reforms and tax rules.
These had driven much-needed hospital doctors out of the NHS into retirement and directly impacted on patient care.
She said: ‘Even more deplorable is the Treasury’s plan to pass the costs of fixing its failed reforms onto future generations of NHS staff.
‘HCSA, the PAC and many, many others warned ad nauseum of the negative impact of forcing through flawed plans on NHS pensions which have encouraged many highly skilled staff to retire early or reduce their working hours.
‘The very viability of the NHS Pension Scheme is at stake if the Treasury does not alter its misguided, dogmatic attitude and ensure that its future approach is not just based on the breathless pursuit of cost-savings, but fully considers the long-term implications for recruitment, retention and equality.’
Dr Sarah Tennant. pensions lead at the Hospital Consultants and Specialists Association
Dr Christine Tomkins
Dr Matthew Lee
In separate deals, two NHS trusts have expanded their private patient businesses with acquisitions from the independent hospital sector.
The Royal United Hospitals Bath Foundation Trust has bought Circle Bath as part of a deal with the competition regulator relating to Circle’s takeover of BMI Healthcare, as both firms had hospitals in the city.
To be renamed Sulis Hospital Bath – after the Roman name for the town, Aqua Sulis – it currently provides services for private and NHS patients. The trust said the move would ‘increase capacity at the facility for the benefit of all patients – both NHS and private’.
The trust’s private patient income in 2019-20 was £882,000, an increase of 37% from the previous year, and this is set to increase substantially as the trust has undertaken to maintain 30% private patient activity at the site.
Compiled by Philip Housden
It is understood the annual private income of the Circle Hospital is less than £10m.
East Sussex Healthcare Trust (ESHT) has also used NHS capital to buy Spire Sussex Hospital, which is physically linked to the trust’s Conquest Hospital in Hastings. The building has been leased to Spire and operated as a private hospital since 1997.
The trust is planning to use the 22 beds and two operating theatres to expand private patient services following the transfer, which will complete at the end of the present financial year.
ESHT chief executive Joe Chadwick-Bell told a board meeting the deal ‘would enhance the trust’s ability to recruit and retain consultants and would give more choice for patients’.
The trust had an income of £3m a year in 2019-20 from its current private patient service the Michelham Unit at the East bourne
Epson and St Helier is latest NHS trust to go live with Compucare Trusts purchase private hospitals
Epsom and St Helier’s University Hospitals is the latest NHS trust to invest in Streets Heaver’s private patient activity, billing and credit control system Compucare 8. Compucare is a comprehensive and modular hospital management system already used by all the
top ten NHS trusts by private patient income and over 90 private health organisations across the UK.
On going live with Compucare 8, Romi Appanah, head of private patients, said: ‘It is the best software I know of for private patient management. The staff were very
District General Hospital , an increase of £834,000 and 39% on £2.1m the previous year.
These acquisitions follow other recent similar moves by NHS trusts. Mid Cheshire Hospitals Trust completed the purchase from BMI of the South Cheshire Hospital at Crewe on the Leighton Hospital NHS campus in 2020.
The trust now benefits from two additional theatres and 32 beds, but private patient incomes declined in 2019-20 by £300,000 (20%) to £1.2m from the £1.5m revenues achieved in 2018-19.
In Norfolk, the Queen Elizabeth Hospital, King’s Lynn, purchased in September 2019 the onsite BMI Sandringham Hospital, with 30 inpatient beds and two additional operating theatres.
Although income in 2019-20 was relatively low at £125,000, this was up £61,000 and 95% on the previous year.
Is this the start of a wider trend?
On the move...
Several experienced NHS trust private patient managers are on the move.
Following the merger to form University Hospitals Dorset , Mandy Llewellyn has left Royal Bournemouth Hospital’s Bourne mouth Private Clinic , with the combined Bournemouth and Poole service now to be headed up by Jo Clothier, who was an internal trust appointment.
Under Mandy’s leadership, Royal Bournemouth private patient incomes grew in four years by more than £1m a year, including a 14% increase in 2019-20 to reach £3.3m last year.
Poole Hospital’s equivalent income that year was £826,000, down 15% on the year before.
The Royal National Orthopaedic Hospital (RNOH), in Stanmore , Middlesex, has appointed Rick Windas, private patient manager at Cambridge University Hospitals (CUH), to succeed Eileen Scrase who has retired.
RNOH reported private patient income of £7.6m in 2019-20, up 7.4%, in part due to the opening of brand-new dedicated facilities in the Stanmore Building.
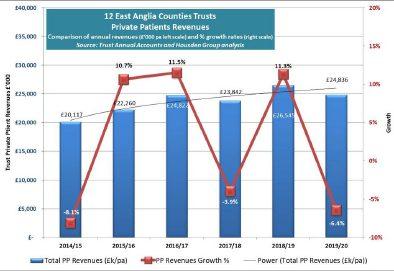
At CUH, Rick has led a 66% improvement in private patient revenues in two years from £6.4m to £10.7m. The trust now ranks 12th by income in England and second outside of London.
helpful and proactive in our implementation of Compucare 8 at The Northey Suite’.
The Northey Suite, the trust’s dedicated private patient unit in Epsom Hospital, delivered revenues of £3.7m in 2019-20, down 24% on £4.8m the previous year.
Paul Goodrich has left his post as managing director private care at Chelsea and Westminster Hospital after four years for an occupational health business. In that time, the trust grew private patient revenues by 20% from £15.8m to £18.9m.
Philip Housden is a director of Housden Group. See his feature article on PPUs in East Anglia on page 34
Doctors urged to review sharps injuries after cases rise
Employer doctors and hospitals are being urged by the British Safety Council (BSC) to review annually their sharps injuries data and prevention policies following a 50% rise in accidents revealed in a Royal College of Nursing survey. 15% of survey respondents said they suffered a sharps injury last year compared to 10% in 2008.
BSC chief executive Mike Robinson said: ‘The onus remains on employers to assess all factors which increase sharps injury risk, including workloads, fatigue,
stress, poorly lit environment, staff shortages, wearing of additional PPE and lack of space, and to put measures in place to reduce the risk of harm.’
A look back through our journal’s archives of a decade ago reveals that although times change, some issues are not so new
A trawl through the archives: what made the news in 2011
Hospitals tell doctors to up their indemnity
Private hospitals are requiring consultants to increase their indemnity limits to retain practising privileges after finding some new policies offered only £1m cover.
The move followed doctors’ switches to new defence firms who were cheaper than the ‘big three’ established bodies.
Hospital bosses said their own insurers would want consultants to have up to £5m cover depending on their specialty.
At least 45 Spire consultants were found to have only £1m cover and had to pay more on their annual defence renewal date to continue with the group.
Patients get strong voice
Patients were set to gain a stronger influence in private practice affairs following the launch of a new national platform.
The Private Patients’ Forum (PPF), set up by a voluntary independent group featuring some well-known private-sector names, planned to help them make the best choices and secure first-rate service from consultants, GPs, insurers and hospitals.
It said independent practitioners
could benefit widely, as its aim was to educate existing and would-be private customers about the sector.
The forum would:
Tell patients they had ultimate responsibility to pay fees –whether or not they got insurance reimbursement;
Urge them to check charges; before agreeing to procedures;
Find out about any insurer shortfalls well in advance.
‘TrueBeam’ arrives in UK
HCA Hospital claimed a UK first by installing the world’s fastest linear accelerator.
The £3mVarian TrueBeam STx was installed at Harley Street at UCH, the group’s joint venture with University College London NHS Trust as part of a joint project with the Fight for Life charity at University College Hospital.
‘Majority’ fill in Bupa’s vetting form
The vast majority of knee consultants were said to be participating in Bupa’s arthroscopy medical review, despite criticism from leaders of bodies who represented them.
The insurer revealed it had already received over 3,000 completed forms and only 10% were not taking part so far.
And it said that percentage was falling as some early refusers were ‘tending to change their minds’.
The one-page form was introduced after Bupa found the arthroscopy rate among its injured customers was more than double that of adjusted NHS comparison groups.
It required completion and approval to confirm funding eligibility.
Twitter ye not . . .
Independent practitioners were sent a ‘think before you tweet’ warning in the wake of recent ‘super-injunctions’ to stop media publication of online allegations of romantic affairs by the rich and famous.
The Medical and Dental Defence Union of Scotland said posting an off-colour remark might not seem the worst thing – but, for doctors, there could be more at stake.
A spokesman said: ‘The two
biggest mistakes doctors risk making when on social networking sites are breaching patient confidentiality and bringing the profession into disrepute.
‘Both could attract the attention of the GMC, which has the power to launch an investigation, suspend the doctor involved and –in the most extreme cases –remove them from the register.’
Enthusiastic GPs clog BMI heart chamber
GPs’ response was anything but faint-hearted when consultant cardiologists invited them to an education meeting.
So many wanted to attend that they were put on a waiting list to hear the specialists from the BMI Healthcare London Independent Hospital.
Eventually more than 240 GPs squeezed in at the hotel venue, making it the biggest turnout in the firm’s history. But some others had to be content with a live video feed.
TELL US YOUR NEWS
Share your experience of what has and has not worked in your private practice. Even if it’s bad news, let us know and we can spread the word to stop others falling into the same pitfalls.
Contact editorial director Robin Stride at robin@ip-today.co.uk
WATCHDOG INSPECTIONS
Soon a new type of inspector will call
You and the Care Quality Commission in 2021 and beyond – what does its new strategy mean for independent healthcare providers? David Hare (right) reports
HEALTHCARE IS an ever-evolving industry and, indeed, the past year alone has led to significant change for all parts of the health system and those who work in it.
As healthcare delivery advances, so must regulation, with last month seeing the publication of the Care Quality Commission’s (CQC’s) new strategy for 2021 and beyond.
The CQC has promised that it will result in its regulation being ‘more relevant to the way care is now delivered, more flexible to manage risk and uncertainty, and will enable us to respond in a quicker and more proportionate way as the health and care environment continues to evolve’.
But what will it mean in practice for independent healthcare and those who work in it?
At the heart of its new strategy is the desire to become a more ‘dynamic regulator’ which can provide an up-to-date and accurate picture of quality in the health system and, importantly, make it easier for services as well as patients to exchange relevant information with them.
From the private sector’s perspective, this is a welcome ambition.
For some time, we at the Independent Healthcare Providers Network (IHPN) have raised concerns that CQC ratings can be based on inspections undertaken several years ago, with providers holding a ‘requires improvement’ rating based on outdated information and little prospect of an inspection to improve the rating.
This not only impacts on providers but also the ability of both patients and commissioners to make meaningful choices based on the best possible information.
And likewise, many independ -
ent providers who have multiple sites across the country are subject to often repetitive requests for information and data.
They could certainly benefit from a much more flexible regime which acknowledges the differences between the NHS and independent sector and works to streamline processes without compromising on quality.
Having up-to-date access to accurate data is, of course, key to the CQC becoming a more ‘responsive and relevant’ regulator.
Complete picture
But the devil will be in the detail and IHPN will closely engage with the CQC about its agenda. While it is positive that the CQC will use data from the Private Healthcare Information Network (PHIN) and the NHS Digital’s Acute Data Alignment Programme (ADAPt), this will not necessarily provide a complete picture. The CQC will also need to get data directly from providers to be able to make an accurate assessment. Greater clarity will be needed about how this additional data and intelligence will be used to support a model of continual assessment for the full range of independent providers.
Linked to this, the CQC’s strategy also focuses on what it can do to help drive and accelerate improvements in safety and quality across the healthcare system. We welcome its proposals to provide more clarity on standards of care, increase engagement around improvement and to increase benchmarking data.
Hopefully, this will lead to:
More opportunities to share best practice about safety and quality;
An ability for providers to ask for advice and guidance without fearing this will affect their rating;
A CQC framework to support providers with a ‘requires improvement’ rating.
In line with the health services’ wider move towards integrated care systems and delivering more joined-up care, the CQC is keen to mirror this approach and work towards assessing healthcare on a systems level.
Definition of safety
System-wide collaboration and a shared definition of safety is vital to sustaining and building safety across the healthcare landscape. With an ageing population and growing numbers of people with multiple chronic conditions accessing a range of services, this is undoubtedly the right way to go.
But this will undoubtedly be the most challenging to achieve.
Key to getting ‘system-wide’
A move away from a one-sizefits-all approach to assessing providers with a systems-level view will be vital
assessment right will be ensuring that the unique attributes of the independent sector, and the ways it participates in the UK’s healthcare system, are recognised and accounted for.
For example, people’s interactions with the independent sector can differ from those with the NHS. A patient may only interact with private healthcare for one test or procedure as part of their pathway.
Awareness of these differences and a move away from a one-sizefits-all approach to assessing pro-
viders with a systems-level view will be vital.
We would welcome the opportunity for the sector to contribute to the CQC’s forthcoming pilot studies to test out this new ‘systemwide’ assessment.
Other CQC ambitions include better engagement with patients and communities and ensuring everyone is empowered to speak up about their healthcare experiences.
Providing feedback
It is a welcome ambition, but it is important the different feedback people may have for private sector and NHS providers is recognised.
While many independent sector providers deliver NHS-funded care, they also serve private insurance and self-pay patients from the UK and overseas who may provide feedback differently than they would to an NHS trust or social care service.
There is much to digest in the
CQC’s new strategy, but the independent sector and its workforce should be prepared for an evolutionary rather than revolutionary approach to regulation.
And with the Department of Health and Social Care working hard on its response to the Paterson inquiry, it is likely that there will be many more recommendations for the CQC and how it regulates all healthcare providers.
The coming months and years will therefore prove an interesting time for healthcare regulation.
Providers and practitioners should be reassured that the IHPN will be working closely with the CQC and other regulators to effectively represent the sector and ensure providers in the sector can continue to deliver ever better care for their patients.
David Hare is the chief executive of the Independent Healthcare Providers Network
Whether you are a GP or a consultant, Doctors’ Indemnity can provide you with appropriate cover for your private practice including, but not limited to:
• A–rated* Lloyd’s underwritten insurance cover: commercial contract-based cover for claims covered under your policy, and not discretionary-based cover
• Indemnity limits to suit the nature of your practice
• 24/7 access to a team of dedicated specialist medico-legal advisors and practising medical malpractice specialist lawyers to assist with any claim or potential claims you might have
• Indemnity for medico-legal work you carry out
• Where appropriate our underwriting partners will be pleased to consider retroactive cover
• 20+ years’ extended reporting period to offer peace of mind when you retire or cease clinical practice
to of top tips
is for working capital
Our A-Z of top tips continues with ‘W’. Julia Burn (below) reports
WORKING CAPITAL, also known as a company’s liquidity or net current assets, is a calculation to show how well a firm can cover its shortterm liabilities as they fall due.
The calculation is current assets, which includes items such as cash and cash equivalents, stock and work in progress, and current assets – trade debtors, other debtors and prepayments and accrued income – less current liabilities such as trade creditors, amounts due to HM Revenune and Customs
for PAYE, National Insurance and corporation tax accruals and deferred income.
For most companies, it is desirable for the net current assets to be positive.
Tight rein
To achieve this, they need to manage their short-term assets and liabilities efficiently. This could be as simple as keeping a tight reign on trade debtors and stock to ensure cash is not tied up for long periods.
It is also good to try, where possible, to match supplier payment terms with the terms given to customers so that the cash flows remain in the same periods.
For a medical practice, managing working capital will mainly revolve around ensuring that stocks of equipment and medicines are kept to a minimal level without compromising the service you provide your clients.
The other important factor, especially in the current post-Covid
environment, is to manage cash. This will include recovering trade debtors as quickly after providing the service as possible as well as negotiating as favourable payment terms as possible with suppliers.
There may also be the need to manage payment terms for procedures or treatment plans that span over a long period of time and are classified as work in progress.
This can be done by, maybe, agreeing payment arrangements to ensure clients pay piecemeal to avoid long waiting time for payments compared with when the treatment is actually delivered.
Government
packages
The pandemic has really squeezed cash flows for businesses and consumers alike, and many businesses and individuals have had to rely on Government support packages to be able to manage their finances.
This may have involved loans, grants, furlough for employees and deferral of tax liabilities, some of which will need to be repaid.
Clients may therefore seek to stretch payment terms or agree payment plans with you and these need to be considered very carefully.
It will inevitably take a long time for the economy to recover, but there does seem to be light at the end of the tunnel.
Timely reporting
The most important part of managing a business’s working capital is timely reporting, especially in the current climate where quick decisions may need to be made.
Updating book-keeping records is a major part of this and most accountants offer an outsourcing solution to assist with this, often taking on the back office for a company so that you can concentrate on what you do best, deliver-
ing outstanding service to your clients.
Preparing budgets and cash flows is also likely to be necessary in the current climate. These need to be as accurate and timely as possible and regularly reviewed and flexed to ensure they are giving as true review of the business as possible. Your accountant should be able to assist with this.
Consideration also needs to be made of the practice’s current circumstances.
If some of your key people are considering moving on, retiring or selling up, they will need the business to look as healthy as possible.
This again could be another reason to ensure that the working capital of the business is as liquid as possible so that current assets significantly cover current liabilities.
Along with the profits of a business, working capital requirements can also be a major
PATIENT CENTRED HEARING CARE
The most important part of managing a business’s working capital is timely reporting, especially in the current climate where quick decisions may need to be made consideration when valuing a business.
The working capital of a business is important and needs to be well managed at all times.
Julia Burn is a director at Blick Rothenberg and part of the team that advises medical practitioners
Exceptional audiological care starts with the right referral. At Pindrop Hearing, we understand each case as unique, and our team of expert Audiologists will work with your patients to find the right solution for them
• Specialists in Diagnostic Audiology including Paediatrics and Tinnitus rehabilitation
• Cutting edge on site facilities, including purpose built sound proof rooms and audiovestibular diagnostic services
• Comprehensive range of diagnostic tests including PTA, tympanometry and specialist tests including OAE's and VEMPS
•A wide range of hearing devices, not available on the NHS
• Outstanding aftercare and patient services
• Fully GDPR compliant
• Medico-Legal Audiology service including gold standard objective Audiological testing using Cortical AEP and ASSR
• Full COVID protection measures in all clinics alongside a dedicated online consultant portal
Opportunities exist outside of the NHS
Planning to leave the NHS? For the huge number of doctors who say they are contemplating a move, Jane Braithwaite (right) shares details of the support available that can offer a route to an alternative career path
THE LAST year has been a struggle for everyone in some respect, but for those working in the NHS the pressure of dealing with Covid-19 has been immense.
We all vividly remember the battle to provide everyone in the health service with adequate PPE, so they felt some level of protection, closely followed by harrowing images of faces battered and bruised by long periods of wearing masks.
Those working in primary care had to adapt to deliver a Covidsafe environment for patients and transform the provision of most services using technology to provide virtual consultations.
As vaccines became available, GP practices and hospitals have worked something close to a miracle to ensure they can be administered throughout the population rapidly.
We have recently seen a new campaign entitled ‘If I die, it will be your fault’, launched by the Institute of General Practice Management to call for an end to abuse from patients following their latest report, which concludes that most GP receptionists face unprecedented levels of abuse at work.
And now the same NHS staff face the challenge of dealing with long waiting lists of patients whose treatment has been delayed by Covid.
Worrying report
A report earlier this summer from the BMA delivers a stark and worrying insight into how doctors are feeling right now, and the evidence is clear that many of them are unhappy and are considering leaving the NHS in the next year. It said: ‘Thousands of exhausted doctors in the UK have told the BMA they are considering leaving the NHS in the next year, as many continue to battle stress and burnout without adequate respite from the exhaustion caused by the demands of the pandemic.’
Responses came from over 4,000 doctors and 31% of them stated they are more likely to take early retirement, which has more than doubled since the survey was done 12 months ago Half of the respondents said they are more likely to work fewer hours and 25% more likely to take a career break.
In looking for alternative careers, opportunities that offer a more manageable workload and a better work-life balance will be hugely appealing
The survey also suggests a strong desire by many to continue to work, but in a different environment. Twenty per cent of respondents are more likely to leave the NHS for another career, with 17% considering working in another country and 14% more likely to work as a locum.
If doctors follow through on these desires to retire, work fewer hours or leave the NHS for another career, huge resource gaps will develop in the NHS.
Support available
Of course, over time, the desire for some doctors to leave the NHS may decline and the NHS pension may be an important factor, but for those who are considering alternative careers, I wanted to investigate and share details of the support and the organisations available that can offer a route to an alternative career path.
Before considering the options, it is also helpful to understand the reasons why there is a desire to leave the NHS, as this gives useful insight into the objectives of doctors when seeking alternative careers.
We often assume, when it comes to career choice, that money is the greatest motivator for most individuals.
But the BMA survey showed that pay was quoted as the main reason for leaving the NHS by 29% of the respondents, while workload and personal well-being drew a much higher response.
Forty-four per cent of respondents looking to leave the NHS said that workload was a factor and 43% highlighted their own personal well-being.
So in looking for alternative careers, opportunities that offer a more manageable workload and a better work-life balance will be hugely appealing.
Of course, finances will be a sig-
nificant factor for many and a great place to look for helpful information is Medics Money (www.medicsmoney.co.uk).
Medics money was founded by Dr Tommy Perkins and Dr Ed Cantelo to help doctors, dentists and other professionals make better financial decisions. Of particular note, Ed is a GP trainee and also a chartered accountant and tax adviser with nine years’ experience at accountancy firm PWC.
On its website, you will find a wealth of resources in the form of articles and eBooks, but its most valuable offering is a series of podcasts in which it covers a huge range of topics of relevance to the profession.
Its latest offering, called ‘Episode 44 – The NHS pensions trap with salary sacrifice’, would be a good listen as would ‘Episode 25 – Using a limited company to save tax and invest to retire early’.
Private practice
One obvious option for doctors looking for a career outside the NHS is, of course, private practice, and with a greater desire for improved well-being and a more manageable workload, this is most definitely an option that may appeal to many.
The aim of Private Practice Pro is to help doctors launch, run and grow their own private medical practice. It is founded by Mr Giles Davies, consultant oncoplastic breast surgeon, and Tom Davies who is a lawyer and former chief investment officer of Seedrs.
Private Practice Pro offers a video-based course for doctors looking to set up in private practice with Giles acting as medical coach and Tom as business coach. (www.privatepracticepro.co.uk).
The course is made up of over 55 on-demand videos complemented by 30 templates and guides and, for interested doctors, Private Practice Pro regularly runs webinars and small-group workshops.
For the more entrepreneurial doctors, Doctorpreneurs is a global community of doctors, medical students and other interested individuals focusing on healthcare innovation and entrepreneurship (www.doctorpreneurs.com).
In its most recent newsletter, it includes an inspiring interview
with the chief executive and founder of Tympa Health, which is a London based start-up that has created the world’s first, all in one, hearing health assessment system. It also includes details of job opportunities across a wide range of sectors. This is a good place to start to understand the type of job opportunities that are currently available and it is an exciting discovery.
It is free to join, and you simply sign up on its website.
Changing career
My final suggestion is Medic Footprints, who provide ‘The world’s biggest gateway to alternative careers for doctors’ (https:// medicfootprints.org).
This is again an organisation led by doctors, providing a wealth of information on their website regarding changing career and connecting doctors with career coaches who can help manage the process.
Their job board presents several exciting opportunities including some overseas roles that will appeal to those doctors interested in working outside the UK.
You can join their community for free on their website or upgrade to their premium package for access to their series of webinars and a free CV review.
In my search for supportive organisations for doctors when looking for a career change, I also discovered that the NHS provides further information on its website.
Back in 2017, NHS England published a paper offering guidance for doctors looking to leave the NHS, which included a selection of organisations including Medic Footprints.
In an ideal world, we would all like doctors to enjoy their career within the NHS and to want to stay, but right now it seems the best approach may be to ensure that the wealth of talent is not lost and is engaged in other rewarding healthcare careers that ultimately benefit the UK population now and in the future.
In my role as MD of Designated Medical, I work with many doctors pursuing either a full- or part-time career in private practice and I would be happy to help anyone who would like to know more about getting started.
CLINICAL NEGLIGENCE: ENT SURGEONS
How you can avoid claims against you
Clinical negligence claims against ear, nose and throat surgeons in private practice are explored here by Dr Gemma Taylor and Greta Barnes – and they offer advice on managing risk in this specialty
A CLAIM FOR clinical negligence can be brought at any time, often without warning and sometimes many years after the incident occurred, which can be extremely distressing for an ear, nose and throat (ENT) surgeon.
Many factors can affect the likelihood of a claim being brought against an ENT specialist, including the extent of their private practice and their individual case mix.
But, broadly, an ENT consultant working privately can anticipate being on the receiving end of a claim about once every ten years.
This article focuses on an analysis of a cohort of more than 100 clinical negligence claims recently brought against ENT surgical members working in independent practice.
In 75% of claims reviewed, the claim was successfully defended
without any payment of damages or claimant legal costs.
Reasons for claims
The reasons for ENT claims range from post-operative pain or scarring to severe complications resulting in significant further treatment, trauma and in some cases, the patient’s death.
The key themes of claims are:
Dissatisfaction with outcome
ENT procedures performed for cosmetic reasons, such as septoplasties and rhinoplasties, can result in claims of dissatisfaction with the final aesthetic result.
Numerous claims arose from patients alleging a lack of improvement or worsening of their symptoms, such as breathing difficulties, snoring, sleep apnoea and sensory
loss affecting taste, smell and hearing.
These claims will usually involve the cost of refunds, second opinions, revision surgeries and psychological therapy.
Consent issues
One third of the cases alleged inadequate consent, with a focus on failure to discuss risks of complications and failure to warn that symptoms may not be improved. A thorough consent process is paramount in order to manage a patient’s expectations of a procedure, including balancing the potential risks and benefits.
Claims can be defended where a thorough and detailed discussion with the patient takes place and is well-recorded in the notes.
Other cases alleged that the treatment provided was unnecessary or incorrect in the circumstances or that more conservative treatment options, including medication or no treatment, should have been tried or reviewed with the patient.
Intra-operative complications
Several claims focused on alleged poor operative technique, during the course of the procedure. Such issues included:
Diathermy burns causing scarring or nerve damage;
Dental damage or loss of teeth;
Perforations such as of the septum or oesophagus; Nerve damage and bone damage such as cracking of the orbital plate;
Severe bleeding and stroke.
Postoperative complications
In 40% of cases, postoperative complications were the reason
MANAGING RISKS
ENT surgeons can take several actions to prevent a future claim. These include:
Manage the patient’s expectations as best as possible in terms of what can realistically be achieved. A thorough consent process is crucial in all ENT procedures, but especially for cosmetic procedures or if the treatment risks may outweigh the potential benefits.
Ensure that patients have detailed information on all treatment options both in writing and verbally and ensure they have appropriate time to make a decision.
Retain detailed records of your discussions with patients, including any phone calls by you or your administrative team and discussions between you and other clinicians such as GPs, out-of-hours’ clinicians and other consultants involved. Be aware that many claims are brought a considerable time after the events in question.
Consider whether all avenues have been exhausted before considering invasive procedures, including more conservative treatment options.
See the patient as a whole not just the isolated issue at hand. This includes consideration of comorbidities and psychological factors.
Remember your professional duty of candour. If something goes wrong, apologise and notify the patient and any necessary parties as soon as possible.
Give appropriate safety-netting advice so the patient knows in what circumstances to return for further advice.
Unfortunately, in recent years the cost of claims has spiralled despite the number of claims remaining steady.
This is not because of a decline in clinical standards but a deteriorating legal environment which the MDU is campaigning to reform. You can learn more at www.themdu.com/faircomp
behind a claim against an ENT surgeon. Some cases involved known complications such as pain, nausea, dizziness, scarring, poor healing, infections and mild to major sensory loss.
Neurological damage was seen in several cases. For example:
Nerve damage causing muscle paralysis and reduced arm function following excision of a neck lesion;
Swallowing and speech difficulties after the laryngeal nerve was damaged during a thyroidectomy;
Subarachnoid haemorrhage following revision sinus surgery;
Stroke after a septoplasty;
Brain infections or meningitis necessitating further procedures and a poor outcome for the patient.
Delayed diagnosis or referral
Allegations of delayed diagnoses or referral were also common. The diagnoses allegedly missed or delayed included:
Brain tumours;
Cholesteatomas;
Sensorineural hearing loss;
Meningitis;
Claims can be defended where a thorough and detailed discussion with the patient takes place and is well-recorded in the notes
Labyrinthitis;
Post-operative infections or hae matomas;
Cleft palate;
Cancers of the tonsil, skin, naso pharynx, oropharynx and larynx;
Mucocele.
Dr Gemma Taylor (below, left) and Greta Barnes (right), are senior claims handlers at the Medical Defence Union
A digital prescription platform to allow convenient prescribing from home
CloudRx is a digital prescription system that allows prescribers to create and send an electronic prescription to our fully licensed pharmacy for fast delivery direct to your patient. It can be used from home by doctors working away from their practices.
No cost to prescribers
Simple and quick prescription creation.
Legal paperless prescriptions, including repeat prescriptions and controlled drugs.
Patients receive text and email requesting secure payment. Alternatively, we can invoice the prescriber or clinic each month.
Prescriber Fees can be added if requested
Medicines are dispensed and dispatched by a variety of delivery options
Fully integrated into MidexPRO
Register for free by visiting cloudrx.co.uk
“We have worked with CloudRX to maintain a cold chain for the medication and direct delivery to patients at home.”
Dr Charlotte Norton, Medical Director of The Slimming Clinic, the UK’s largest chain of private doctor-led weight loss clinics
WORKFORCE WELL-BEING
A survey of Royal College of Physicians’ fellows and members earlier this year revealed that more than onein-four doctors have sought mental health support during the pandemic. Taking care of your own mental health, and those around you, is key to giving patients the best level of care
Ensuring the mental health of your staff
Dr Pablo Vandenabeele (right), clinical director for mental health at Bupa UK Insurance, shows how to make your practice a supportive environment
WHEN WE think about ‘mental health’, we often think about mental health conditions, such as depression or anxiety.
But, like physical health, we all have times when our mental health is good and also times when it affects our overall well-being.
As healthcare professionals, we have a really important role in supporting the well-being of our practice teams and colleagues and being advocates for good mental health in the workplace.
Ways to do this include improving working practices, encouraging your team to speak openly and reassuring them of the support they need. Guidance is available to help you do this correctly.
Mental health challenges
Workplace issues such as uncertainty, lack of control and a demanding role can all lead to changes in mental health and are linked to the development of common mental health conditions.
The new challenges presented by the coronavirus pandemic have added to this, with many people facing added stress and anxiety, both at work and home.
Additional pressures it has created include:
➲ Coping with a significant increase in patients;
➲ The emotional strain of losing patients to Covid-19;
➲ Adjusting to changes in working practices, such a carrying out
video consultations and the resulting lack of human contact;
➲ Fears about the risk of contracting the virus from patients and infecting family members.
It is common knowledge that even in normal circumstances, healthcare professionals experience higher levels of work stress than the general population and the pandemic has exacerbated this.
A BMA survey of 6,550 doctors across the UK last October found that more than two-fifths said that their mental health is now worse than before the pandemic.
They reported they were currently experiencing work-related depression, anxiety, stress, burn -
out, emotional distress and other mental health conditions.
All this may be particularly difficult for those with pre-existing or previous mental health conditions, as well as being a trigger for mental ill health for the first time.
Healthy workforce
We need to take our mental wellbeing and that of our practice teams and colleagues seriously now rather than wait until we reach crisis point.
Aside from the immediate impact on our practice, our ability to cope and to offer our patients safe care, we need a healthy workforce to ensure our healthcare
system functions properly in future.
The benefits of supporting your team’s mental health
☛ Creating a positive environment where employees can talk openly about their mental health reduces the stigma of mental ill health. It leads to more understanding and a greater likelihood that employees will seek support early.
☛ It is much easier to support employees at an earlier stage than waiting until they reach crisis point.
☛ Mental health conditions are the leading cause of long-term sickness absence. Effectively supporting employees experiencing a change in their mental health means you can retain them and help them thrive.
Common mental health conditions
Understanding how mental health conditions manifest themselves is helpful in being able to effectively spot when an employee may need some support.
Here’s a reminder of some common mental health conditions:
Anxiety disorders: Anxiety is a feeling of unease. We all get anxious when faced with stressful situations and it is normal to feel anxious when we face something new or unknown. But if someone has anxiety that has lasted a long time and it is severe, it will affect their everyday activities.
Depression: Everyone has ups and downs. It’s common for people to say that they are ‘depressed’ when they are feeling low. However, if the sadness becomes persistent and a person loses interest in life, affecting how they think or behave, it’s possible they have depression.
Obsessive-compulsive disorder (OCD): Obsessive-compulsive disorder is an anxiety disorder with two key parts: obsessions and compulsions.
Obsessions are intrusive and unwelcome images, urges, thoughts or doubts that repeatedly appear in a person’s mind. Compulsions are activities that they feel they must do to reduce the discomfort caused by the obsessive thoughts. If a person does not act on the compulsions, their anxiety or mental discomfort
We need to take our mental well-being and that of our practice teams and colleagues seriously now rather than wait until we reach crisis point becomes distressing and unmanageable.
Signs to look out for Everyone’s experience of mental health is different and can change at different times. As a leader, it is important to get to know your team and understand what they need and when.
Understanding the signs of poor mental health means you will notice when to check in and start a conversation about how a practice team member or colleague is coping.
Some early signs might be:
Poor concentration;
Being easily distracted;
Worrying more;
Finding it hard to make decisions;
Low mood;
Feeling overwhelmed by things;
Tiredness and lack of energy;
Talking less or a flat, slow way of speaking;
Avoiding social activities;
Talking more or talking very fast, jumping between topics and ideas;
Finding it difficult to control emotions;
Drinking more;
Irritability and short temper;
Aggression.
Sources of support
More information and resources on mental health and well-being for managers are available on Bupa’s website at:
l www.bupa.co.uk/health-information/workplace-mentalhealth;
l www.bupa.co.uk/business/ workplace-wellbeing-hub/managing-wellbeing.
Also see:
l Mind – www.mind.org.uk
l Chartered Institute of Personnel and Development – www.cipd. co.uk.
HOW YOU CAN HELP YOUR PRACTICE TEAM
AND COLLEAGUES
1
Be open in your conversations: Talking about mental health has come a long way in recent years, and it’s important to keep this conversation going. By encouraging people to talk about mental health in the workplace, you can help shape the culture, attitudes and behaviours towards mental health in your organisation. Removing the stigma surrounding mental health will help your team to feel comfortable to approach you should they need to talk.
2
If you think someone is having difficulties, it is important to talk to them about it early on. This can help you understand the situation and work together to agree appropriate adjustments to prevent things from getting worse.
3
If you are working remotely, it might be more difficult to get an idea of how people are coping. You can use video calls to help you see body language and expressions, as well as hear what somebody is saying. This works for formal conversations, as well as for casual chats and virtual coffee breaks.
4
Lead by example: Some people might refrain from speaking up, fearing that it will be seen as a sign of weakness or failure or could jeopardise their prospects at work.
This is particularly true of healthcare professionals, who tend to be reluctant to seek help due to the perceived stigma surrounding mental health issues. (See page 52 of our May issue).
As a manager, you can set an example for those around you by sharing your own experiences and showing that you understand. This helps make it easier for team members to ask for help.
5
Practise empathy: Many of us will have been affected by mental health in some way throughout our lives or know someone who has been, so it’s something we can all relate to. If one of your team is struggling, try to put yourself in their position.
If you and others adopt this approach, you will build an empathetic culture at your practice and they’ll know they’re part of a team that cares about their well-being.
6
Invest in training and education: Early intervention can play an important role in helping someone with poor mental health in their recovery. By teaching your leaders to spot the signs of mental health problems and help, you can help your practice team to get the help they need as soon as possible.
7 Make sure that your policies and procedures are up to date. Things to consider include:
Checking whether stress is included in your health and safety policy. If not, you can get more information from The Health and Safety Executive;
Making sure that you have a separate mental health policy, which includes promoting staff well-being as well as managing mental health problems;
Ensuring you have guidance for managers about managing mental health, mental health-related sickness absence and return to work.
You can find more information about this at: www.bupa.co.uk/healthinformation/workplace-mental-health/workplace-support.
8
Provide support: Supporting your practice team with their mental health is important, through both the highs and lows. Make sure your team members know what’s available to them, both inside and outside of work.
If someone in your team is struggling with their mental health, you may need to make some adjustments for them. Perhaps you need to make some changes to their environment or working hours, ensure they take time off or ease their return to work to help them recover.
INFORMATION TECHNOLOGY
How IT raises your
Lengthening waiting lists for NHS treatment are a ‘push factor’ which should prompt more people to re-evaluate private healthcare, but it is also important to consider the ‘pull factors’ that will lead them to your practice.
Healthcode’s Kingsley Hollis (right) shows how technology can help you offer a high-quality level of service that will exceed the expectations of new patients and attract word-of-mouth recommendations
THE PANDEMIC did much to open our eyes to the significant contribution made by the private healthcare sector to meeting people’s care and treatment needs.
Independent practitioners and hospitals were quick to join the national response to the pandemic and more than three million patients had their NHS procedure carried out, at cost, by private providers in England under landmark national arrangements.
This support will continue as the NHS tries to get back on its feet, but it will take time to address the backlog. With a record number of patients now on the waiting list for
NHS hospital treatment, it is probable that people who might not have previously contemplated going private will think again.
LaingBuisson’s recent report into the UK Self-Pay market ( Independent Practitioner Today, May 2021) found evidence of heightened interest in private treatment across the country.
Attractive reason
At the same time, the private sector cannot simply wait for NHS waiting lists to drive patients in its direction. As LaingBuisson put it: ‘The challenge will be converting this interest to business’, which means
doctors need a compelling and attractive reason for patients to choose them and – more importantly – speak positively about their experience to friends and family.
This is where technology has a key role to play. We all know that the right technology enables practices to operate more efficiently and profitably, but it’s now time to look at how technology can also help you improve access, deliver a high-quality service and exceed expectations.
Listed below are five ways that Healthcode’s technology can make the difference to your patients’ experience of private healthcare:
1
Efficient appointment booking
Your patients should be able to expect a professional and responsive service, whichever way they choose to make an appointment. However, it can be challenging for practices to co-ordinate diaries where several specialists practise across multiple locations.
The appointment functionality within Healthcode’s ePractice system shows which practitioners are active on a specific day across all treatment sites, so when patients make an inquiry, your receptionist can instantly view the available slots and reserve a suitable
quality of service
appointment there and then, rather than having to check and call back.
If nothing is available at the patient’s preferred time, they can be added to a waiting list and there will be an automatic alert if the slot becomes free.
Once an appointment is made, the system can generate confirmation letters, emails or texts with all the information patients need.
And when a patient presents for their appointment, receptionists can change their status on the system to ‘arrived’ so that practitioners are aware they are waiting to be seen.
2 Choice and convenience
For every patient who contacts a practice directly, there are likely to be more who would prefer to have a choice of specialists and hospitals offering private healthcare and book a consultation on their computer or mobile device.
Until recently, online appointment booking on this scale has simply not been possible because there was no way to synchronise the mass of data – providers, services, practitioners and appointment slots – and the many different booking systems.
Healthcode’s online appointment booking service, which will be available later this year, is essentially the hidden engine room that can power the appointment booking process for the whole sector by enabling diverse service providers to connect and exchange information in real time.
Practitioners and other providers will be able to publish their services and synchronise availability through Healthcode’s solution, which makes this information available in real-time to booking websites. This will extend their reach to many more patients.
From a patient perspective, online appointment booking will undoubtedly increase the appeal
of private healthcare by making it more accessible.
For the first time, it will be possible to use a single booking application to search multiple healthcare organisations, using different criteria and filters to find the service that meets patients’ needs and then make an appointment at a convenient time and location.
3
Reassurance about private medical insurance
While the self-pay market is growing, it remains true that most of your patients will have private medical cover, although not all will have their membership details to hand when they contact your practice.
Healthcode’s insurer membership look-up feature enables you to put patients’ minds at rest that they have valid insurance cover by matching their details against participating insurers’ databases.
This simple and secure online check is possible thanks to our interoperable technology which enables different organisations to connect seamlessly via our online platform.
This also eliminates the need for multiple phone calls and also ensures your practice has the correct details on its own system from the outset.
4
Ensuring continuity of care
Whether you are ordering diagnostic services, arranging for a patient to be admitted to hospital for surgery or discussing their case with others in a multidisciplinary team meeting, it is essential that you provide relevant information in a timely and secure way.
The GMC’s leadership and management guidance emphasises the importance of communication with colleagues and says doctors in senior roles ‘must provide necessary and timely information to
From a patient perspective, online appointment booking will undoubtedly increase the appeal of private healthcare by making it more accessible
those you manage so they can carry out their roles effectively’.
The same guidance also says: ‘You must make sure that records you are responsible for are made, stored, transferred and disposed of in line with the data protection law and other relevant legislation.’
Regular email is inherently insecure and should never be used to send identifiable patient information.
By contrast, Healthcode’s secure messaging and file sharing services (healthDrive) are encrypted, enabling you to share sensitive and confidential information with individuals or specifically created contact groups on our global directory of practitioners, private hospitals and private medical insurers (PMIs) without compromising patient privacy.
This enables you to co-ordinate patient treatment effectively and ensure continuity of care when patients transfer to other healthcare settings.
5 Efficient billing
While electronic billing for PMI-funded treatment is the norm thanks to Healthcode’s Clearing Service, the rise in self-funded healthcare means practices also need to consider how best to collect payment from patients.
Finance arrangements are common for some types of cosmetic treatment, but most patients will expect to be billed promptly and have a stress-free way to pay.
In partnership with the patientzone online payment platform, Healthcode offers a secure online patient e-billing and payment service for ePractice users to charge for self-funded care and PMI shortfalls.
Once signed-up with the patientzone service, practices can create bills in ePractice and send them through to patientzone. Patientzone then notifies the patients by email or text that they have received a bill which they can access and pay securely online.
Within 30 minutes, their payment is automatically reconciled – in ePractice plans with payment recording – and the practice also receives notification of payment by email or text.
Online electronic billing for patients through Healthcode and patientzone meets your data protection obligations – unlike insecure email – and is more efficient than sending a paper bill in the post.
It is a more cost-effective way to implement online patient billing and payment, as there is no need to arrange merchant accounts or pay credit card processing fees. Most importantly from a patient perspective, the process is seamless, secure and convenient and they have the reassurance of payment confirmation so they can focus on their recovery.
Private healthcare is likely to become a more realistic and appealing option for patients in the current climate, which gives everyone in the sector a golden opportunity to convert new business.
Patients may be seeking fast access to advanced diagnostic and medical care, but with the help of technology you can show them what else private healthcare has to offer.
Kingsley Hollis is head of business development at Healthcode
MARKETING AND BRANDING: USING IMAGERY
Pictures have the greatest impact
Over the last five issues of Independent Practitioner Today, Simon Marett and Michael Sullivan have covered important aspects of branding, design and marketing for private healthcare practices, including logo and website design, colour and typography.
Their last article in this series takes a closer look at using imagery in your branding and design
‘A PICTURE CAN paint a thousand words’ is a commonly used phrase and that is relevant when it comes to working on your healthcare practice’s brand and design.
Imagery is an area of marketing and design that is often last on the priority list. But out of all the aspects we have covered, it is the one area that can help you engage with your audiences on a deeper, emotional level.
By doing so, it can help you connect with and entice potential customers or patients towards your brand or practice.
So, before you download a folder of free images that you have found on a Google search, take a step back and think about the style of imagery you are using.
A little more time planning can make all the difference to your healthcare brand and business. Here are some of the aspects of imagery you should consider:
1Think about whom are you talking to
We have touched on this point in our previous articles on imagery and colour, but it really is a fundamental rule of marketing and design.
Putting your personal opinions to one side and getting a good understanding of who your patients and potential customers are and the imagery that will appeal to them is a vital step in the process.
For example, if your practice is a high-end men’s health clinic targeting affluent men in London and the South-east, then you need to think about the type of imagery that will appeal to men in their 30s and 40s who are living in that part of the country.
Free ‘stock’ imagery from a website that can be found on half a dozen other health websites might not hit the notes you’re aspiring to. Take a step back, discuss some options with your team or designer and look at some selections of images that will work well.
TOP TIP: Pick two to three images that you think will work and then conduct a quick market survey with a handful of patients to get a
steer on which they prefer. This is a good indicator of what imagery might appeal to future patients and the growth of your practice.
2
‘Stock’ imagery versus bespoke photography
Good use of imagery can often make the difference between having an average and a great healthcare brand and website.
One of the decisions you will
A potential patient doesn’t want to see a snapshot of you on holiday
Illustrations (above) can help humanise your brand, and take care when selecting stock shots that they come from the UK rather than the US
need to make early on is whether you want to use a stock image library like iStock or Shutterstock or whether you want a more bespoke approach and to appoint a professional photographer.
The latter option may be more expensive, but professional photography can be a sound longterm investment if you are positioning your practice in the premium category.
If stock imagery is the route you want to go down, then make sure you spend time researching the types of images you want on your individual website pages and remember to ask a designer to put a colour filter or treatment on the images you’ve selected.
This will help you achieve a consistent, premium feel across your website rather than a mishmash of stock images that are different colours and styles.
TOP TIP: ‘Meet the Team’ and ‘About us’ pages are often the most visited pages on a website. Even if you are not using a professional photographer, take time on these
pages and make sure the team photos are consistent and shot with similar backgrounds and dress codes. A potential patient doesn’t want to see a family snapshot of you on holiday with your sunglasses on.
3
Illustrations can be a good option
One of the most common mistakes we see with healthcare brands and
websites is where the use of imagery just does not work and jars with the brand.
A good example of this is where all the imagery has come from a ‘stock’ website and is American in style rather than from the UK.
In some instances, if you cannot get the imagery to work, it is worth considering using illustrations and animations as an alternative, as they can help humanise your healthcare brand and break down boundaries between your practice and your patients.
You may wish to appoint a professional designer to work for a bespoke style, but there are also many websites available that offer a good range of illustration styles that are easy to navigate and inexpensive.
TOP TIP: Speak to a recommended designer about providing some options on imagery and illustrations before you decide which route to go down. A good designer will always help mock-up some ideas and it can often make the decision easier.
4
Pay attention to file size
In today’s mobile-first world, most websites are now viewed on mobile and tablets and therefore quick download speeds are vital. When you are downloading images to use on your website, pay close attention to the resolution and the file size.
Many image library websites will automatically default to the highest resolution images with large file sizes that aren’t suitable for websites because they’re designed for print.
Most website are now viewed on mobiles, so be careful to select images with file sizes that don’t take ages to download
First impressions count and if the image sizes are too big, it may take several seconds for a potential patient to view your website and they will bounce off and find an alternative healthcare practice.
TOP TIP: When you are using images for a website, make sure you ask for or download the ‘On-screen’ resolution option. This option is designed specifically for websites and will be the desired resolution you need and will help quick download speeds.
To conclude....
To conclude, good use of imagery is essential when you are designing and building your healthcare practice’s brand and website, so dedicate some time for planning before you make any big decisions. As with typography and colour, there is more to effective use of imagery than meets the eye.
Stock image libraries are often the easiest and cheapest route to go down, but they may not necessarily be the right option for your healthcare practice. The quality of stock image libraries also varies wildly, so make sure you do your research and consider illustration as an alternative.
Working with a recommended designer or marketing agency can be also a good option. They will have designed and built many brands and websites before and will be able to provide recommendations based on their experience.
This can help you get the key decisions right and ensure you avoid many of the expensive and time-consuming mistakes that are associated with design, branding and marketing.
Simon Marett (below, left) and Michael Sullivan (right) are managing director and creative director of Ellerton Marketing Ltd, a specialist strategic marketing consultancy for independent healthcare practitioners
BILLING AND COLLECTION
Follow this road map to recovery
Simon Brignall (below) signals the best route to follow to ensure your practice is best placed to benefit from the recovery
THE INDEPENDENT sector continues to benefit from the increased demand from patients wishing to access private healthcare.
At Medical Billing and Collection, we are pleased to see the growth in the activity conducted by the practices we partner with and, judging by the number of inquiries I am receiving, there are plenty of practices keen to benefit from this recovery.
As a result of these conversations, I thought it would be useful to provide some simple directions to follow to ensure your practice is also best positioned to benefit.
Stay in your lane. Make sure you spend as much time as possible focusing on your core skill set.
It seems obvious, but it is important to prioritise seeing and treating patients. If you and your secretary can focus on the medical side of the practice, this will not only benefit your patients but also lead to increases in the revenue for the practice.
Running a private practice is not easy and many tasks do not fall naturally into a consultant’s skill set or even those of their medical secretary. Take stock and consider what elements of your practice could be outsourced, leaving you and your team to prioritise the clinical side of the practice.
Queues likely. Make sure your practice is ready to accommodate the increase in demand for your services resulting from NHS waiting lists.
Headlines about NHS waiting lists have always translated to increases in demand for the services of consultants working in the independent sector.
This typically has meant more self pay patients. It is important that your practice has the full range of functionality a modern practice needs to service these patients. This includes the ability to invoice these patients electronically and take payment on a 24/7 basis.
No parking. Avoid unnecessary delays. Make sure your work is invoiced in a timely fashion.
It is only natural that on seeing this increase in demand for their services, most consultants will try
Late invoices are indicative of poor service to patients. They are a major contributor to their dissatisfaction and often lead to bad debts
to treat as many patients as possible. Not only so they can deliver the urgent care they require, but also to make up for the practice’s lost income.
This work should be invoiced as soon as possible, as this function not only reflects on the professionalism of the practice, but also ensures you obtain the benefit from your activity and are not just storing up problems for the future.
Some major insurers now enforce time limits for submitting invoices and if you miss the deadline, they will not pay. Late invoices are indicative of poor service to patients. They are a major contributor to their dissatisfaction and often lead to bad debts.
Delaying the patient’s awareness of a shortfall means the patient assumes the invoice has been settled, which can lead to disputes over the bill.
Late invoices sent direct to patients may be ignored by them if they think you are not serious about wanting payment.
Review your fees. It is always important to regularly review your fee structure and so if it has been a while since you have done this, this could be a good time to review your rates for consultations and procedures.
I still come across practices who have not reviewed their prices for many years and even decades. If you bill your procedures to insurance guidelines, make sure your price list is up to date, as these constantly change and are not always communicated clearly. This means you may be charging less than you could or more than you should.
I quite often see practices who are still making wrong assumptions that lead to issues with insurance companies, delays in payments and losses in revenue.
Be vigilant. Review the way your work is being billed to ensure you are compliant with the regulations communicated monthly from the Clinical Coding and Schedule Development Group (CCSD).
If you are taking the time to review your fees, this would also be a good opportunity to check that you are abreast of the latest CCSD changes and establish if/how they affect your specialty and possibly your income.
Practices commonly make billing errors through being unaware of the changes and so it is important to establish what rules each insurer adopts, as each insurance company can differ.
Clearly signpost relevant Information. Make sure your price policy is clear and that your patients are notified of it before commencing treatment.
All modern practices should have a clear fee structure and payment terms that are both well documented and communicated to their patients. This is a key requirement of the Competition and Markets Authority (CMA).
Alongside a transparent fee policy, a patient registration form outlining the terms and conditions of the practice can be useful. Having terms and conditions will ensure there is no room for ambiguity by laying out responsibilities and methods available for the payment of your medical invoice. And that leads to fewer delays in getting your money.
When we take on a practice’s backlog of outstanding invoices, there are often patients who have built up debt over years, yet the practice has continued to see them
Dashboard data . Ensure you have key management information on your practice to allow for informed decisionmaking.
I often speak to consultants who have no minimum access to uptodate accurate data on their practice.
Police problem payers by having a robust chasing process in place for outstanding invoices.
The past year has highlighted the need to have strong procedures in place to resolve aged debt. But, for these to be effective, they need to be applied on a consistent and continual basis to ensure invoices are paid in full and cash flow improves.
If you do not do this, you will end up regularly throwing money away by adding to the problem.
The vast majority of calls we have received over the last year have been from practices with issues in this vital area, which is why they continued to run high levels of debt.
Almost every practice which joins us has an outstanding backlog of invoicing going back years.
Debt levels can typically be over 20% of turnover and sometimes have reached 50% of annual turnover. I am pleased to say we achieve bad debts of less than 0.5%.
Visibility around problem payers means you can ensure the patient settles any outstanding invoices before you allow them to make their next appointment.
When we take on a practice’s backlog of outstanding invoices, there are often patients who have built up debt over years, yet the practice has continued to see them.
But every practice should be able to see the number and income derived from the patients they treat. It needs to be broken down by location, payment type – selfpay, private medical insurer – or individual payment company as well as payment information relating to these invoices.
Our consultants can access a market leading reporting dashboard that shows all the key performance indicators (KPIs) for their practice. The dashboard also has as range of reports providing financial information at both the summary and granular level, including aged debt and patient activity.
Without access to any of this key data, it is extremely difficult to understand in which direction your practice is going and so it is very easy to make wrong decisions based on outdated assumptions.
Full speed ahead. Consider whether now is the time to join thousands of other doctors who have outsourced this vital role to a professional billing company.
Most consultants find the billing and collection side of the practice a challenge to manage and this can often result in unnecessary and consistent financial losses.
Outsourcing could be the best decision you make this year to guarantee your practice benefits from the recovery.
Simon Brignall is director of business development at Medical Billing & Collection
INVESTING IN CRYPTOCURRENCIES
Bitcoins are a bit of a flighty flutter
Why the excitement over cryptocurrencies?
Dr Benjamin Holdsworth on why it might be gambling, not investing
WE HUMANS are never lacking in our enthusiasm for crazy ‘investment’ ideas. Around 400 years ago, the Dutch managed to work themselves into a frenzy over tulip bulbs.
At the height of the hysteria, one bulb of Semper Augustus apparently changed hands in exchange for 12 acres of land.
In the 1700s, the South Sea Company Bubble ruined many as the stock price rose almost ten-fold in 1720, largely on the back of false rumours, and then crashed precipitously. Even Sir Isaac Newton himself got burnt, losing almost all his savings:
‘I can predict the movement of heavenly bodies, but not the madness of crowds.’
By all accounts, the madness surrounding equity investments was widespread at the time, with one company supposedly coming to market with the greatest marketing spin ever, describing itself as ‘a company for carrying out an undertaking of great advantage, but nobody to know what it is’.
Shell companies
Today, investors face similar sentiment in certain corners of the investment world, from the rise of Tesla’s stock price – at the time of writing, down -36% from high – to GameStop’s ‘to the moon’ rally, now down -51% from high.
Shell companies – known as SPACs (Special Purpose Acquisition
Companies) – raise cash from investors to buy as yet unidentified companies – sound familiar? – and have multiplied in the past 18 months.
Cryptocurrencies, such as Bitcoin and the spoof Dogecoin, now have ‘market capitalisations’ of US$741bn and US$47bn respectively.
Unfortunately, humans seem programmed to suffer from FOMO (fear of missing out), which might have been an advantage in the days of being a hunter gatherer, but can be especially dangerous when it comes to the world of investing and ‘hot’ markets.
Just because something has gone up spectacularly does not mean
that it is a good investment or even an investment at all. A material risk always exists that latecomers to any speculative game get left holding the hot potato. Knowing what you are getting yourself into is a good place to start.
‘When you have difficulty in finding out what the real fundamentals of an investment are, then what you are doing is not a “real investment”,’ said European Central Bank vice-president Luis de Guindos this year about cryptocurrencies.
Understand money
In attempting to understand cryptocurrencies, a good starting point is defining what money is. In sim-
Kirsty Odell (below) sets out some of the key stages to buying or selling a practice, which will keep you on the right track for a smooth transition from buyer to practice owner
So you want to buy a practice?
BUYING A PRIVATE practice will, no doubt, be an exciting time for you, but it is important to be aware of the steps involved in the purchase and to prepare yourself for the process ahead. The following are the crucial steps involved:
1
Appoint advisers
The market is still buoyant despite Covid-19, with many potential buyers looking to invest in the private medical practice sector.
Most opportunities are often where providers are looking to retire and have no alternative succession plans in place.
So your first step may be to approach specialist sales agents, who will introduce you to sellers of practices that fit your requirements.
An early approach to other inter-
mediaries is also important. This includes your funder, your accountant and your legal advisers.
If you do not have your funding offer ducks in a row, then this will cause transaction delays. The ideal position would be to get an offer ‘in principle’ as early as possible so you are able to make the application without delay as soon as the seller has accepted your offer.
Always instruct specialist lawyers and accountants, as they will have a better understanding of the requirements of a purchase of a medical business and should therefore be able to offer a more efficient approach.
A key question to ask them is the best structure for you to follow for the purchase. This may be dictated to some extent by the seller’s requirements, but you also need to
ensure that it is tax-efficient and structurally sound for you too, now and for the sustainability of the practice in the future.
2 Exercise due diligence
This is perhaps one of the more tedious parts of the transaction and it may cause delays depending on how organised the seller is. Nevertheless, carrying out due diligence may be the difference between buying well or paying for years of problems.
Your legal advisers will raise a whole host of questions about the business and the seller will need to respond to those and provide supporting documentation.
Your lawyer will then provide you with a report on the due diligence received and raise some further follow-up questions. It allows
you and your legal advisers to investigate the business and draw out any possible issues that you need to be aware of.
These include, for example, any patient complaints, compliance issues or employee disciplinary issues or grievances. Being made aware of these things gives you the opportunity to decide whether to address them or look elsewhere.
It may take the seller a little bit of time to collate the documentation requested in the due diligence, which is time for you to ensure that you have satisfactory funding terms and Care Quality Commission (CQC) registration.
3 Register with watchdog
Whether a new CQC registration is required will depend on the structure of the transaction and
whether you are already registered.
So it could simply be a matter of adding a new location to an existing registration or updating the details of registration for a company that you are buying.
If a new registration is required, then you should apply for this as soon as possible. In the first instance, a CQC countersigned check with the Disclosure and Barring Service will be needed. Once that is received, the application for registration can be submitted.
Currently, applications are taking a considerable amount of time to be processed, so it is strongly recommended that you make this a priority at the start of the transaction.
4 Prepare sale documents
Your legal advisers will draft and negotiate the sale documentation with the seller’s legal advisers. The key document will be a busi-
You will need to ensure that you are aware of the terms of the existing staff contracts, as the employees will transfer to you on their existing terms
ness transfer agreement or, in the case of a purchase of shares in a company, a share purchase agreement.
This document should address:
Protections required because of matters arising from the due diligence;
Warranties and indemnities which are intended to protect you from certain liabilities that may arise post-completion;
Restrictive covenants to be imposed on the seller post-completion to seek to protect the good-
will of the practice that you are purchasing;
Funding documents, such as loan agreements, facility letters and debentures.
Depending on the structure of the transaction, there may be several other ancillary documents to agree as part of the process.
These may include, for example, any property documentation to transfer an interest in the premises, employment/associate contracts where the seller is staying on at the practice after completion, and company-related documents if any entity involved in the transaction is a company.
5
Draw up staff contracts
It is most common that the Transfer of Undertakings (Protection of Employment) Regulations (TUPE) will apply where you are buying a practice.
You will need to ensure that you are aware of the terms of the exist-
ing staff contracts, as the employees will transfer to you on their existing terms. You will also need to engage and possibly consult with the employees about your proposed takeover of the business.
Your legal advisers will be able to guide you on this process and your legal requirements under TUPE.
If you are buying a company, then the staff will just continue to be employed by the company you have purchased.
You will also need to consider any self-employed members of staff and negotiate new contracts with them with effect from completion, as their contracts are not subject to TUPE.
This summary provides you with some guidance of the process of buying a private practice. With specialist advisers, you will be guided through the transaction.
Kirsty Odell is an associate at Hempsons
Free legal advice for Independent Practitioner Today readers
Independent Practitioner Today has joined forces with leading healthcare lawyers Hempsons to offer readers a free legal advice service.
We aim to help you navigate the ever more complex legal and regulatory issues involved in running and developing your private practice – and your lives.
Hempsons’ specialist lawyers have a long track-record of advising doctors – and an unrivalled understanding of the healthcare system as a whole.
Call Hempsons on 020 7839 0278 between 9am and 5pm Monday to Friday for your ten minutes of free legal advice.
Advice is available on:
Business structures (including partnerships)
Commercial contracts
Disputes and litigation
HR/employment
Premises Regulatory requirements and investigations
Michael Rourke Tania Francis m.rourke@hempsons.co.uk t.francis@hempsons.co.uk
BUSINESS DILEMMAS
When you must confess to GMC
Dr Kathryn Leask (below) answers a doctor’s query about when you need to disclose a driving offence to the GMC
Dilemma 1
Do I tell GMC I’ve been speeding?
QI have received a fixed penalty notice, having been found to be travelling 49 miles an hour in a 40mph zone in addition to a fixed penalty for leaving litter.
A colleague has advised me that I need to disclose this to the GMC. Apparently, she received a driving conviction and did not declare this.
The GMC was informed of the conviction by the police who then contacted my colleague informing her they had opened an investigation.
This had implications for her private practice, as her practising privileges were suspended while the investigation was ongoing.
I understand that there are a number of other circumstances
which a doctor must declare to the GMC. Please could you confirm whether I need to inform the GMC of this matter?
AThe GMC’s guidance Good Medical Practice does state in paragraph 75 that you must inform the GMC if, anywhere in the world, you have accepted a caution from the police or have been criticised by an official inquiry.
An official inquiry might, for example, include a coroner’s inquest. You must also inform the GMC if you have been charged with or found guilty of a criminal offence or if another professional body has made a finding against your registration as a result of fitness-to-practise procedures.
In its more detailed guidance, Reporting criminal and regulatory proceedings , the GMC goes on to say that you must also inform it if you receive a cannabis warning or are given an anti-social behaviour order.
The guidance also refers to you accepting the option of paying a penalty notice for disorder on the upper penalty tier, where a list of offences can be found on the Home Office and GMC website.
You will note that littering falls under the lower tier and is not something that you need to declare to the GMC.
The guidance also makes reference to payment of a fixed penalty notice for a road traffic offence. Again, you are not required to inform the GMC about this.
More severe sanction
But you would need to inform the GMC if you were convicted, cautioned or found guilty of a road traffic offence, as seems to have been the case with your colleague.
This could, for example, relate to drink or drug driving, driving dangerously or travelling at an excessive speed which would result in a more severe sanction than a fixed penalty notice.
A lack of declaration of a relevant offence would be in breach of the GMC’s guidance and is likely to result in an investigation
If a doctor is ever unsure about the circumstances under which a matter should be reported to the GMC, it is important that they seek advice from their medical defence organisation.
A lack of declaration of a relevant offence would be in breach of the GMC’s guidance and is likely to result in an investigation, not only into the circumstances of the event, but also the reason why it was not declared.
Dr Kathryn Leask medico-legal adviser at the Medical Defence Union
Private doctors have raised a number of queries about conducting remote consultations with their patients who live abroad. Dr Kathryn Leask discusses the implications in answer to a GP’s question
Dilemma 2
Any curbs on a video session?
QI am a private GP and have a number of patients who have moved abroad either temporarily or for the foreseeable future, due to the pandemic.
These patients have asked that I continue to be their GP and consult with them remotely. Like many healthcare professionals, many of my consultations are being held either by phone or video at the moment and this is likely to continue where appropriate.
I am keen to support my patients and know their past medical histories well. Where necessary, I would refer them on to the appropriate specialist in their current country of residence. Are there any restrictions in being able to consult with patients abroad?
AAs you will be aware, the GMC regulates registered medical practitioners in the UK and the GMC can investigate doctors whose fitness to practise is called into question.
Section 35C(3) of the Medical Act 1983 states that this can include allegations that have occurred outside the UK. From this point of view, therefore, it
Treating patients moved overseas
does not matter where the consultation took place or what the location of the doctor or patient is.
The GMC has the jurisdiction to investigate allegations that suggest a doctor’s fitness to practise is impaired.
However, in its guidance on prescribing and managing medicines, the GMC refers to prescribing for patients overseas and the need to consider whether registration with a regulatory body in the country in which the prescribed medicines are being dispensed is also required.
It is important to check, therefore, whether you need to be registered in each country your patients are residing.
Not all countries have the same requirements, with some necessitating registration in the patient’s country of residence and others being satisfied with registration in the doctor’s country of residence.
The GMC’s guidance also makes reference to the need to consider how you or local healthcare professionals will monitor the patient’s condition.
It is also important to take into account differences in the licensed name, indications and recommended dosages of medications and products in the country the patient is residing in.
Potential clinical negligence claims are another consideration. If a claim were brought against you, it would be better for this to be in an English court applying English law and it is likely that an English court would have jurisdiction if you are practising in the UK.
However, the courts located in the country the patient is situated may also accept jurisdiction, applying foreign law.
It is important, therefore, that any healthcare professional intending to consult with patients abroad discusses their indemnity arrangements with their medical defence organisation.
PRIVATE PATIENT UNITS: EAST ANGLIA
Perhaps it’s time to join the chain gang
Philip Housden’s monthly review of PPUs looks at the private patient services in the 12 NHS trusts delivering acute care services across East Anglia, from the counties of Norfolk, Suffolk, Essex and Cambridgeshire
THIS REPORT is based on the information published in the Trust Annual Accounts for 201920, which was partially adversely impacted by the early months of the Covid pandemic
For this group of trusts, the accounts show that total private patient revenues declined by 6.4% from £26.6m to £24.8 m over 2018-19 (Figure 1).
This now represents 0.55% of these trusts’ total revenues, down from 0.65% the previous year, the lowest proportion for at least a decade. However, this is still above the combined national average outside of London of 0.43% (Figure 2).
Top earner
A comparison of performance by trust (Figure 3, opposite, and Figure 4 overleaf) shows that the highest percentage of private revenues and proportion of total trust incomes in the region is delivered by Royal Papworth with private patient income in 2019-20 of £6.7m, down £1.4m and 17.7% on the £8.1m achieved in both the previous two years.
This represents a decline from 5.7% to 4.5% of total trust incomes. This still places the trust at #2 by proportion of total trust revenues outside London and 16th by revenues in the NHS.
As the UK’s largest cardiothoracic hospital, Papworth has a distinctive edge and focus, ensuring that the brand can stand out sufficiently to support private
patient local, regional and international demand. This was reinforced by the move from 1 May 2019 to the new Royal Papworth Hospital located on the Cambridge Biomedical Campus.
The new hospital has five operating theatres, five cardiac catheterisation labs, extensive diagnostic modalities and over 300 beds. Of this total capacity, 12 beds are in the new Varrier-Jones private patient ward, which is a significant
reduction on the previous 32 beds on the old campus.
This loss of dedicated capacity, plus the teething challenges of moving sites and the Covid impact at the end of the financial year all contributed to the year-on-year decline.
Doubled revenues
Cambridge University Hospitals’ private patient revenues grew by £1.25m to reach £10.65m in 2019-
20, a rise of 13.3%. The trust has doubled private patient revenues in the last five years and jumped from 0.88% to 1.32% of total turnover.
The trust is now ranked 12th by revenues in the NHS and second outside of London, only marginally behind the longstanding provincial leader Frimley Health in Camberley, Surrey.
This growth has been achieved in part through improved com -
Figure 1
mercial management systems with strengthened tariffs and a one-off improvement to revenues in 2019-20 from receipt of historic undercharging for private patient activity.
A significant increase in revenues was achieved from fertility services, while cardiology continues to perform well through the Cambridge Heart Clinic. This is a joint venture with Regent’s Park Healthcare operating since 2008, who have access to five inpatient and day-case beds and three consulting rooms.
Looking to the future, in the field of cardiology, it will be interesting to see how Cambridge University and Papworth Hospitals work in such close proximity going forward.
In the longer term, the strategic opportunities for the trust are significant with the new Cancer Hospital (www.cambridgecancer. org.uk ) and the new Cambridge Childrens Hospital (www.cambridgechildrens.org.uk), the UK’s first combined physical and mental health hospital.
Both of these new hospitals will seek to attract increased UK and international private patient income streams.
Basildon’s PPU is also predominantly based on the delivery of cardiac services and is located within the Essex Cardiothoracic Centre, the trust’s eight-bed Brook Suite PPU.
Total private patient incomes in 2019-20 were £5m, down £772,000 and 13.3% on 2018-19. This performance now equates to 1.49% of trust incomes, down from 1.85% the year before.
PPU chain network
From April 2021, the trust merged with both Southend and Mid Essex Healthcare in Chelmsford to form Mid and South Essex NHS Foundation Trust.
Although Basildon’s income declined in 2019-20, Mid Essex grew by 47% to £600,000 from £407,000, at 0.19% of turnover, and Southend also grew by 22.6% from £270,000 to £331,000, reaching 0.1% of total income from private patients.
The trust’s common brand is Nash Private Healthcare and there are opportunities to build on the combined income of £6m to
develop a common service offer, as they now effectively provide one of the few NHS ‘PPU chain’ networks. Further growth can be achieved through investment in expanded capacity based on the regional burns and plastics services at Chelmsford and the regional cancer centre at Southend.
Norfolk and Norwich does not have a dedicated PPU since it closed the ward in 2016, but still reported revenues of £1.97m, up £579,000 and 41.8% on 2018-19 at 0.34% of revenue. This is the highest private patient income the trust has achieved since 2013-14. Since 2016, the trust has been
working more closely with the other two providers in Norfolk and Waveney: The Queen Elizabeth Hospital, King’s Lynn, and James Paget Hospital, Great Yarmouth. Could this closer working be extended to private patient services in the future?
Figure 2
Figure 3
King’s Lynn is located away from big centres of population and experienced a steep decline in private patient revenues in 201718.
Private hospital purchase
Although income in 2019-20 was relatively low at £125,000, this was up £61,000 and 95% on the previous year. This growth has been made possible through the acquisition in September 2019 of the on-site BMI Sandringham Hospital
The purchase provided additional capacity for the trust from 30 inpatient beds and two additional operating theatres and room for private patient services.
James Paget Hospital , Great Yarmouth, has an eight-bed PPU, the Charnwood Suite, and outpatient and ambulatory services through a sub-brand entitled East Point Consulting Rooms and was considering expansion of capacity pre-Covid.
In 2019-20, the trust experienced a marginal decline of 2.4% and £19,000 to a new total income of £762,000.
This equates to 0.37% of total revenues, well down on the 0.60% in 2017-18 when private patient incomes were over £1m for the first time.
Also declining in 2019-20 was North West Anglia, which comprises Peterborough and Hinchinbrook Hospitals. Although there is at present little or no private patient service out of Peterborough, Hinchinbrook did operate seven beds under the brand Mulberry Private Healthcare from 1994 to 2019.
The trust’s private patient revenues were reported as £1.01m, down £719,000 (41%) on 2018-19, due in significant part to the loss of capacity.
In Suffolk, both trusts experienced a dramatic reduction in private patient incomes in 2019-20. At West Suffolk, Bury St Edmonds, income was £1.0m, a reduction of 52.1% and £1.1m from £2.1m the previous year.
This is a decline from 1.0% to 0.42% of turnover. It is a similar story for East Suffolk and North Essex NHS Foundation Trust , created by the merger of
Colchester and Ipswich in July 2018. In 2019-20, the combined trust’s private patient revenues declined by £595,000 (30%) to £1.4 m and were 0.20% of total revenues – down from 0.33%.
Although both main hospital sites are within attractive markets, it is not known whether the trust is considering private patient services growth.
Significant investment
Princess Alexandra , Harlow, Essex, is a smaller single-campus hospital with no PPU. The trust has been awarded significant capital for investment in a new hospital to deal with estates and capacity issues.
The trust had a 22.6% (£61,000) growth in private patient revenues in 2019-20, but this represents only 0.12% of turnover.
Private patient provision in East Anglia is heavily concentrated in the centres of excellence that deliver high-acuity regional services that the independent sector does not provide.
In Cambridge, the two trusts have the potential to link up their
private patient approach to develop a substantial business. For other trusts across the region, the potential for private patient services on campuses that essentially provide a ‘district general’ service range are more limited, but still there.
As the independent hospitals in these catchments are also generally restricted in ability to provide clinically complex care, all trusts therefore do have potential for growth, particularly where it is designed in alongside and aligned with the core NHS site and service strategy.
In mid and south Essex, and potentially across Norfolk too, other joined-up thinking could develop a local ‘chain’ or group approach to the delivery of private patient services.
Next month: East Midlands
Philip Housden (below) is managing director at Housden Group commercial healthcare consultancy
Figure 4
PREPARE FOR GOOD TIMES AFTER COVID
Now is the time to get fighting fit for the boom in private work post-Covid. Ian Tongue (right) provides some excellent tips
Are you ready to take on a surge in work?
THE IMPACT of Covid on the private medical sector will be felt for several years to come as both the NHS and private sector try and cope with a surge in demand and finite resources.
I am hearing from clients of significant private waiting lists and it is encouraging to hear that the capacity in the private hospitals is opening up.
Coping with this increased demand from a financial perspective may be a challenge and it is important that you are prepared for the increased demand on your time. This article looks at some of the key areas that will help ensure that you are able to hit things running.
Availability
One of the key challenges will be the availability of clinical and theatre space to see patients and carry out procedures or operations.
Many of the private hospitals are juggling NHS usage with the private medical sector and often the spaces available are outside of normal clinic times. Therefore, being available and flexible will be key to utilising this available capacity until normal clinics are restored.
Accounting systems
Having a reduction in volume can present an opportunity to change accounting or clinical database systems with less disruption than at busier times. These accounting and clinical database systems can generate significant efficiencies for your private practice and pay for themselves in a very short space of time.
Ensuring that you have robust systems in place should avoid situations of you not being paid for work that is undertaken and will enable you to invest time gaining experience on the higher-level features of those systems for when the volume increases.
Consider your tax structure
Many consultants have had personal factors which have prevented them from changing their trading structure.
Some of these issues can result in the acceleration of tax payable to change from one trading structure to another and can be a significant barrier; for example, a financial
It is likely that the NHS will have to look to the private sector to manage the surge demand that is exacerbated by the increased demand in the public sector
Medico-legal work
During the Covid pandemic, many consultants have diversified into new income streams and the most common of these is medico-legal work.
For those with practices growing in this area, it is important that you are keeping on top of payments for work done and reviewing your payment terms to ensure you are paid within a reasonable time-scale.
ties will arise. So speak with your accountant who can help you with this to avoid any surprises later on from the combination of earnings falling and then restoring.
Consider locations
year that is not the same as the tax year-end.
A reduction in profit may present an opportunity to move a self-employed individual or partnership into a limited company, which may be more tax-efficient.
Conversely, with the proposed changes to corporation tax to increase the rate by 6% from 1 April 2023 and rumblings of changes to capital gains tax, it may be a time for certain practices to formulate a plan to move away from a limited company.
As always in these cases, your individual circumstances will determine the most appropriate structure for you and taking the advice of a medical accountant is extremely important.
Employees
Many employees have been furloughed since the Covid pandemic began and this was a welcome support to businesses.
The furlough scheme is more flexible than it was at the start and therefore you can continue to use the scheme for the hours that are not worked and pay your employee for the hours they do.
This helps you with cash flow as you rebuild your private practice and the scheme is available until the end of September 2021.
Indemnity
Often the most significant expense within your private practice is your medical indemnity/ defence fee.
Given the reduction in activity from Covid, many practices could be paying an incorrect premium, whether too much or too little.
It is important that you set your future anticipated activity level realistically and if this figure is too low, you need to contact your provider to advise them of your circumstances.
It is important you have robust accounting records to ensure you track work done and the date of payment – which can often be many months or even years in some cases.
Where payment does drag on, it is likely that will have to pay taxes in advance of being paid yourself.
Plan for tax
One of the most difficult financial situations consultants have faced from the reduction in activity is not saving enough for tax along the way.
Where taxes are paid out of current income rather than historic income, it can be particularly painful to settle your tax liabilities.
For many, the income tax payable for 2020-21 should have been reviewed to reflect the reduced activity and lower private practice profit. This will have a knock-on effect to the payments that are made in 2022 leading to a catch up in 2023.
It is really important that if you have struggled to meet your tax liabilities in the past that you are on the front foot going forward.
Often, it can be confusing how much to save and when tax liabili-
For those consultants with admitting rights in one hospital, your activity is likely to be restricted for a period, so consider whether there are any other opportunities to practise elsewhere to increase your capacity.
Certain specialties have been hit harder than others and we are likely to see more consultant-led private facilities arising.
These facilities are likely to be available to other consultants outside of the owners and could be an alternative for certain work, particularly if your usual private hospital is unable to offer you the required capacity.
Covid has certainly changed the landscape within the medical profession, both within the NHS and private sector. It is likely that the NHS will have to look to the private sector to manage the surge demand that is exacerbated by the increased demand in the public sector.
There will certainly be bumps in the road managing the two sectors, but private practices will restore, so being prepared for the surge in demand is extremely important.
See our September issue for tips to avoid an inquiry by HM Revenue and Customs
Ian Tongue is a partner with Sandison Easson accountants
DOCTOR ON THE ROAD: AUDI E-TRON SPORTBACK
The quietest car I have ever driven
Doctors after amazing levels of comfort and refinement in a high-quality package should take a close look at this electric offering, recommends our tester Dr Tony Rimmer (below)
WHEN PROVIDING services, independent medical practitioners know that reliable high-quality delivery counts hugely to build up a reputation for excellence.
Once achieved, this position needs to be constantly reviewed and any new patient assessments and/or treatments need to meet these high standards.
In the automotive world, premium brand Audi is well known for producing cars of superior build quality across all its models and it continues to outshine rivals such as BMW and Mercedes in this respect.
So, when it came to launching its first all-electric model, the e-tron, the car had to be right from the start. Being a premium brand, it was logical to launch an electric vehicle to compete with the market leaders, Tesla.
An Audi Q5-sized SUV, the e-tron is available with a 71-kWh battery in the 50 model and a 95-kWh battery in the 55 model. Power outputs are 313bhp and 408bhp respectively.
Both have quattro four-wheel drive and air suspension is standard. There are two slightly different body styles on offer: the standard SUV and the Sportback SUV. The Sportback has a sloping coupé style that slightly reduces the bootspace and the rear headroom by a couple of centimetres.
Mirror stalks
My test car was a Sportback 55 S-line, which retails at £79,185 before options. This may seem expensive, but the Tesla Model X starts from £82,980. As with all German premium cars, it is easy to add a few thousand pounds to the final cost if you delve into the options list too freely.
My test car was £89,470 in total. One expensive option I could not get used to was the £1,250 virtual door mirror package. Small cameras extended on slender stalks from each front door.
They may be aerodynamically efficient, but the position of their images on screens at each end of the dashboard did not feel natural at all.
This is interesting, because a similar set-up I tried while testing the little Honda ‘e’ felt much more intuitive. When you first approach the e-tron it does seem like a big car from the outside; almost RangeRover-sized. In its favour, the Sportback bodyshell is quite stylish and certainly reduces the ‘big and boxy’ SUV look of its sister.
Up-market feel
It does look classy and very much an Audi. Step inside and you are greeted by the familiar high quality of the brand. The seats, interior trim and electronic dashboard have a very up-market feel and you start to understand where all the money has gone. Because the e-tron is not based on a dedicated electric-only platform – like Volkswagen’s iD3, for instance – interior space is not as great as you would expect for a car that is this long and wide. It is good but can only accommodate four or five passengers despite its bulk. The rear headroom compromise in the Sportback will only
affect passengers over 6’2”. The battery is under the floor of the whole car, so boot space is perfectly adequate.
It is the smooth, silent and effortless driving that marks out all electric cars and the e-tron is no exception. Indeed, with its £500 acoustic double-glazed side windows and standard air-suspension, this e-tron offers the most comfortable and quiet limousine-like travel of any car I have ever driven. A journey of any length will leave you fresh and relaxed.
However, you cannot deny the substantial 2.5 tonne weight, so performance is swift rather than Tesla-fast. I am a great fan of regenerative braking and, fortunately, you can dial it up on the e-tron to allow near ‘one-pedal only’ driving level.
Handling, although compro -
mised by the car’s mass, is reasonably controlled by the clever air suspension, but this is no sportscar. We will have to wait for the Porsche Taycan-like e-tron GT to see if an electric Audi can deliver on this front.
Useful feature
As far as charging is concerned, the e-tron can accept fast charging at rates up to 150kW, so a quick ten-minute ‘fill-up’ at a fast charger – if you can find one –could add up to 60 miles of range.
A useful feature are the dual charging points on the front wings so it does not matter which side of the car is parked next to an external charger.
Unfortunately, this large car is generally not that efficient and although Audi quotes a range of up to 277 miles, a real-world range
of around 200–220 miles is more realistic.
So, should the keen electric-convert medic consider the e-tron?
Well, as a well-made premium alternative to the ubiquitous Tesla Models S and X, I would suggest you take a good look.
The e-tron offers amazing levels
A journey of any length will leave you fresh and relaxed
of comfort and refinement in a high-quality Audi package. It is practical and the range is reasonable. Electric vehicles have got a long way to go, but this is not a bad starting point.
Dr Tony Rimmer is a former NHS GP practising in Guildford, Surrey
AUDI E-TRON SPORTBACK 55 quattro s-line
Body: Five seat coupe-hatchback SUV
Engine: Two electric motors. 95kWh battery Power: 408bhp
Torque: 664Nm
Top speed: 124mph
Acceleration: 0-62mph in 6.6 secs
Claimed range: 277 miles
On-the-road price: From £79,185
A ten-minute ‘fill-up’ at a fast charger could add up to 60 miles of range
The interior trim and electronic dashboard have a very up-market feel A useful feature are the dual charging points on both front wings
The e-tron looks classy and very much an Audi
Throwing your career away
With 58% of doctors now suffering from some form of anxiety or depression – and 46% saying their condition has worsened since last March – our final serialisation of a new book edited by Dr Clare Gerada (below) looks at professional and unprofessional behaviour
Independent Practitioner Today readers can save 20% on Routledge.com with discount code BWC21. Offer ends 31 August 2021. Order now: www.bit.ly/Routledge_IPT
THERE ARE now over 30 different sets of guidance for doctors to adhere to in areas relating to clinical, managerial, leadership, medico-legal, research, communication and other areas of our daily professional and even personal lives.
Around 8,000 doctors each year are referred to the GMC and about 200 receive a serious sanction, most commonly suspension, and between 60 and 80 doctors have their licence to practise removed. Because human behaviour itself is complex, it is hardly surprising that the ways in which it can become deviant from normal mores are so diverse. Of the 119 cases in 2015 that resulted in suspension or erasure, 103 cases related to transgressions involving the doctor’s professional life –most often related to dishonesty, clinical issues or inappropriate relationship with patients – and 16 cases that involved their personal life – drink driving, sexual issues. Dishonesty and inappropriate sexual relationships made up nearly one-third receiving these sanctions.
Strict professional codes of conduct and public expectations means that the vast majority of doctors follow the rules, honour the trust given to them by virtue of their status and never break the law for their entire career.
However, occasionally, they do transgress and fall short of these standards, some so seriously that they receive a criminal charge and, on rare occasions, a custodial sentence.
Criminal charges
Criminal sanctions against doctors are rare. GMC data for 20052019 show just over 2,000 doctors in the UK had criminal records –against more than 200,000 on the register.
More than 50% of crimes were for vehicle-related offences such as dangerous driving (speeding, drink- or drug-driving) and motoring offences (driving without insurance or tax).
While it is only speculation, it is likely that many of these are related to alcohol and drug use; this means for treatable mental health problems if the individual had sought help before the criminal incident.
Hopefully, with more accessible, confidential treatment services, doctors in whom health problems have been the underlying issue will come forward for treatment instead of risking their career by suffering in silence.
Other offences occurring much less often involve forgery, fraud, possessing indecent images of children and sexual offences.
Impact on career
Doctors are surprised that an offence committed quite unrelated to work, such as being found guilty of offences against health and safety regulations, can impact on their career. Most regulators expect that doctors’ conduct is of a certain standard, even if they are not at work.
The UK regulator says ‘you must make sure that your conduct justifies your patients’ trust in you and the public’s trust in the profession’. Any conviction or caution received anywhere in the world needs to be disclosed and doctors must follow the GMC guidance about this.
Doctors are surprised that an offence committed quite unrelated to work, such as being found guilty of offences against health and safety regulations, can impact on their career
to doubt a person’s honesty, which is a vital requirement expected from a doctor.
Cheating in exams is one of the most powerful predictors of future dishonest behaviour. Some offences, however, such as using illegal drugs or motoring offences, do not necessarily imply that a person is dishonest, though they suggest the offenders are willing to engage in behaviour that is illegal and harmful to themselves or others.
I have looked at the determinations from the Medical Practitioners Tribunal Service and devised a taxonomy that describes what I suspect was the ‘frame of mind’ the doctor was in when they crossed their professional boundary.
1‘It was only a little lie’. Dishonesty, fraud, probity
A criminal conviction does not automatically disbar a doctor from working, though the more serious crimes such as possession of indecent images of children and sexual offences will almost always lead to erasure.
This seems reasonable given public confidence has been breached when a doctor transgresses so seriously. Also, the most robust predictor of future serious offence – such as violence or sexual assault – is a history of past offence. For less serious crimes, the chances of being able to work are mixed. Many, but not all, minor criminal convictions give reason
Serious questions
Clearly, such offences raise serious questions about possible risks to patients, the possibility of more serious crimes being committed or other unprofessional behaviours.
All these issues are taken into account by a regulator and a proportionate balance made on an individual case-by-case basis.
Most cases brought before a medical tribunal concern probity, fraud and dishonesty, and they tend to lead to the harshest of sanctions. Acting with honesty and integrity is a fundamental tenet of the medical profession.
NHS Pensions & Annual Allowance Tax
Get ready in advance of April 2022 when the proposed changes to the NHS Pensions will allow you to reclaim some or all of any Annual Allowance tax you may have suffered in the past.
With our knowledge and in-house calculators, we will be able to predict in advance and check statements produced by NHS Pensions and Scottish Public Pensions Agency for accuracy for any refunds due.
For further information contact us at aa@semail.co.uk or telephone 01625 527351.
This includes doctors who commit what they might consider to be small deceits, maybe in a genuinely perceived belief that what they are doing is ‘almost true’ and no harm will be done.
They might even believe that it is justifiable, given how busy they are, to take a short cut to obtaining the necessary paperwork or doing the required training.
They might also feel no one will find out and no harm will be done by their ‘little lie’. But it will be found out and harm will be done. The following are examples under this category.
☛ Dishonesty about claiming sick pay while working. A common error is where a doctor regu-
larly works across two sites, maybe a substantive job with the NHS but also a small amount of selfemployed private work elsewhere.
If signed off as unwell and receiving sick pay, it is important to stop all work, including teaching, training, academic, medicolegal, private, media and so on, unless agreement has formally been agreed from the employer issuing the sick pay.
☛ Dishonesty about having done training. A senior doctor amended and uploaded an Advanced Life Support course certificate, adding it to his training portfolio.
Despite a relatively light sanction, he had to still go through 18 months of investigation and shame. His name and what he did will appear on the website for years, and he will have to disclose this misdemeanour whenever he applies for a new job. This is a high price to pay for not doing half a day’s training.
☛ Dishonesty about references. These are not minor errors – which we are all guilty of – but major falsehoods, such as claiming to have obtained degrees. These cases tend to result in harsh sanctions.
As part of a planned move overseas, a doctor submitted two false references with his application. His actions involved the manufacturing of references from start to finish, including false letterhead, false representations, fake personalities from human resources and fake signatures.
He was erased from the medical register, a high price to pay for wanting to speed up an administrative process.
This doctor could easily have obtained the necessary references; there were no reasons why they would not have been provided. Instead, in his haste to emigrate, he forged them and lost his livelihood.
2
What harm can it do?
There are many examples of doctors who fall foul of their professional code or even commit an overt crime by trying to help members of their families or friends.
A doctor wrote prescriptions for patients whose names he took from the hospital computer data-
base and took the prescriptions to the hospital pharmacist who noticed discrepancies in the prescription.
He admitted that he wrote the prescriptions for a friend who lived overseas and was erased from the medical register. It is unusual to get such a harsh sanction, but it shows the risk.
3'I only wanted to be friendly'. Boundary violations
Given the changing nature of medicine, with less formal, more collaborative working and with fuzzy boundaries created by social media, it is becoming harder to maintain clear professional and personal borders between patient and doctor.
Boundary issues involve departures from usual professional practice and can be thought of as being along a spectrum, from ‘crossings’ to ‘violations’.
These are unethical and unprofessional because they exploit the doctor-patient relationship, undermine the trust patients and the community have in us and can cause psychological harm to patients, compromising their ongoing medical care.
The most serious of all boundary violations are those involving sexual contraventions. These cover a range of behaviours including inappropriate contact with staff, colleagues or in unequal relationships, such as with medical students and patients.
Position of trust
Doctors are powerful authoritative figures and in exploiting patients for their own gratification, transgress a position of trust, which can have a similar effect as a parent abusing a child.
It is difficult to know how many doctors have crossed a sexual boundary, as they are unlikely to self-disclose and patients are reluctant to disclose this form of abuse to authorities, due to embarrassment, fear or even misplaced loyalty towards their doctor.
Reviews involving doctors in different countries over a number of years suggest that between 0.2% and 10% of doctors admit to a sexual relationship with a patient and that around 1.6% doctors are sanctioned.
RISKS OF UNPROFESSIONAL BEHAVIOUR
Proportionately, male doctors are four times as likely to be erased or suspended as female doctors
Hospital specialists are erased or suspended at around one-half the rate of GPs and other non-specialist doctors working in hospitals or community settings
Doctors in all career groups are more than twice as likely to be erased or suspended in later life
Doctors who obtained their primary medical qualification overseas are more than twice as likely to be erased or suspended as those trained in the UK
These doctors are more likely to work in general practice, psychiatry and obstetrics and gynaecology, reflecting the greater likelihood of physical contact and/or psychological intimacy.
A striking feature of the literature into sexual boundary violations is the absence of ‘red flags’, meaning that the doctors who perpetrated the violations had no features that could be identified through screening tests.
Except for rape, cases occurred without obvious signs of a personality disorder in the doctor and involved both patients who were particularly vulnerable as well as those who exhibited no special vulnerabilities other than being a patient.
Understanding motives
While the literature is rich in examples of doctors who commit sexual crimes against their patients, there is very little actual data with respect to understanding their motives or any predictive personality characteristics.
I think it is fair to say that currently there is no actual reliable way of predicting which of the many hundreds of thousands of doctors will commit crimes of this nature, given the only reliable discriminant is being male.
It is difficult to assign motives to why doctors conduct themselves in this manner, other than the performance of the sexual act itself. Nevertheless, as with all of life, it’s not always so clear cut.
The daily practice of medicine is filled by opportunities to develop intense emotions between the patient and clinician. These emotions engendered might include hostility, aggression, despair or even love.
Patients can evoke powerful responses in the clinician who
cares for them; these responses are called counter transference. If recognised and understood, they can be a tool in gaining a better understanding of the patient.
If not – as, for example, where the patient evokes feelings of love in the clinician – it can have destructive and damaging sequelae.
Doctors themselves, in a vulnerable position from their own life events, might find themselves in a psychological state where compromising their professionalism is possible.
This might be where the doctor becomes emotionally entangled with a patient, due in part to what has been thrown up by the doctor’s own life experiences during the doctor-patient interaction.
This is why it is so important that we have access to supervision, especially when we are in susceptible psychological states.
Sexual relationships between doctor and patient are often the culmination of a series of ‘boundary crossings’ where the first one might be perceived as entirely innocent; for example, seeing the patient for extended appointments at the end of the day or giving one’s personal phone number.
4
I forgot (dishonest)
This category includes omitting to do things that a doctor is mandated to do. For example, have up-to-date medical indemnity, renewing necessary training – such as Section 12 Approval for conducting assessments under the Mental Health Act – or forgetting to inform the GMC if one obtains a caution or conviction.
Dr Clare Gerada is medical director of the Practitioner Health Programme, London, and a former chairman of the RCGP
FOCUS: GENERAL SURGEONS
Better than expected
General surgeons’ earnings have exceeded their accountants’ expectations. Ray Stanbridge reports
OUR UNIQUE benchmarking survey reveals good news for general surgeons.
It shows that gross incomes from their private practice increased by 6.8% between 2018 and 2019, going up from £147,000 to £157,000.
Costs increased by 6.3% from £63,000 to £67,000. As a result, pre-tax profits went up by 7.1% on average from £84,000 to £90,000. We had been less optimistic about the future for this discipline, but general surgeons proved us wrong and they continued to enjoy a good year in 2019.
So how was the profit increase achieved? Incomes continue to show an upward trend assisted by the growth in self-pay particularly in London.
While some consultants did experience insurance company pressure on fees, it appears that the amount of overseas business, particularly in London, showed a small increase in the year.
As a whole, specialists tended to perform rather better than generalists.
We note that staff costs rose, on average, from £19,000 to £24,000. Some of this may be attributable
AVERAGE INCOME AND EXPENDITURE OF A CONSULTANT
Expenditure
to adjusted salaries of family staff by the national personal allowance figures.
This rise was also partially accounted for by the increased charges imposed by some hospitals for use of secretarial staff and administration services under the Competition and Markets Authority (CMA) rules.
Conversely, some consultants managed to reduce their consultancy room hire costs by working more efficiently or negotiating arrangements with hospitals.
Defence cover
The costs of professional defence cover rose slightly. Most consultants this year accepted the increase and stayed with their chosen provider. The propensity to ‘shop around’ by general surgeons is probably lower than for some other disciplines.
‘Use of home’ costs showed some increase, reflecting the fact that some consultants undertake the bulk of their administrative work from home rather than conduct it in the hospital or clinic from where they consult.
Other costs remained broadly the same in 2019, although we did spot some reduction in marketing expenditure.
What then of the future?
There currently appears to be a large unsatisfied demand for the services of general surgeons. Save for unforeseen Covid or other disasters, 2021 looks to be very promising
Obviously, 2020 results will be affected by the implications of the Covid lockdown. There currently appears to be a large unsatisfied demand for the services of general surgeons. Save for unforeseen Covid or other disasters, 2021 looks to be very promising.
Consultants who are eligible for inclusion in the survey:
Are not in full-time private practice;
Hold either an old- or a newstyle NHS contract. This can seriously distort figures, as some consultants close to retirement can choose to switch to the new contract and wind down their private practice;
May or may not have incorporated their business;
May or may not work in a group;
Have a keen interest in develop-
HOW ARE YOU DOING?
ing a private practice. This requirement essentially excludes medical academics who maintain a very small practice;
Have been engaged in private practice for at least five years;
Earn at least £10,000 a year from private practice. In previous surveys for this specialty, they were included if they earned at least £5,000.
Making realistic year-to-year comparisons has, of course, become harder due to market
changes, which should be noted. General surgeons, like other consultants, now trade in a variety of ways through limited liability companies and limited liability partnerships, in addition to the traditional sole trader model.
Some have decided not to set up a business in private practice but to negotiate a second employment with a private hospital or clinic.
Others have chosen to specialise in a particular area – commonly breast surgery – rather than do a variety of procedures.
The increased specialisation has been encouraged by the process of revalidation and the increasing centralisation of information through organisations such as the Private Healthcare Information Network (PHIN).
Nevertheless, we believe our findings here are a reasonable representation of what an average general surgeon earns and spends in his or her practice. Next time: Cardiologists
Ray Stanbridge is a partner with accountancy, finance and tax advisory medical specialists, Stanbridge Associates Ltd
Ophthalmologists
Years ending 5 April Source:
ONLINE SOLUTIONS
INNOVATIVE ONLINE SOLUTIONS AT THE HEART OF THE HEALTHCARE SECTOR.
Our Online Solutions
Trusted by leading hospitals, independent practitioners and insurers to deliver high quality, secure and cost-effective IT systems. Seamlessly connect key stakeholders to support transparency within the sector and enhance patient safety.
Healthcode is the UK’s official medical bill clearing company and has provided secure and encrypted systems to healthcare professionals since 2000. Pre-pandemic we processed around 27,000 electronic medical bills to insurers daily.
To find out more about our solutions visit our website www.healthcode.co.uk
Our digital page-turn issue will be back on 7 September. But you can stay in touch with news developments on this website and these will be featured in our weekly news email updates to you every Tuesday. Don’t forget to notify us of any change to your email address! Meanwhile, we do hope as many of you as possible are able to take some sort of well-earned break over the next few weeks. Here’s a taster of the September line-up:
All doctors are at risk of this . . . an HM Revenue and Customs inquiry. Don’t miss specialist medical accountant Ian Tongue’s tips to help you avoid being a victim
Expert witness work: Lord Hodge, deputy president of the Supreme Court, shares his views of what makes for a competent expert witness
Time for online appointment booking? Today, the appointment booking process in the private healthcare sector is so fragmented that it is holding us all back. Peter Connor explains why a centralised online booking system is vital to the sector’s prosperity and how Healthcode’s technology is making this a reality with benefits for doctors and patients
Solicitor Kirsty Odell follows her article on five steps to buying a private practice – featured in this July/August issue – with a guide to help sellers prepare for the acquisition process
A private GP asks what to do if a patient requests a letter exempting them from a PCR test before travel. Dr Kathryn Leask, medico-legal adviser at the Medical Defence Union (MDU), has the answer
Ray Stanbridge’s Profits Focus benchmarking series examines the income, expenses and profits of cardiologists
INDEPENDENT PRACTITIONER
TODAY
The business journal for
Published by The Independent Practitioner Ltd. Independent Practitioner Today is editorially independent and thanks Bupa for its assistance with distribution. Material is governed by copyright. No part of this publication may be reproduced, stored in a retrieval system or transmitted in any form without permission, unless for the purposes of reference and comment. Editorial layout is the copyright of the publishers. If you wish to use it for promotional purposes on websites or for reprints, we would be happy to discuss licensing the copyright to you.
Digital messaging apps. Can you guarantee the safety and confidentiality of your patients? Joost Bruggeman, a former surgery resident at Amsterdam University Medical Centre and now chief executive and co-founder of Siilo, gives his opinion; and Philip Luce, chief executive at Cromwell Hospital, London, which started using Siilo as the pandemic took hold last year, gives his verdict
A cardiologist is approached by a high-profile exercise brand to participate in a series of webinars on the benefits of exercise on heart health and future trends in healthcare. But is it appropriate for her to take part? Dr Ellie Mein gives her views in Business Dilemmas
If you are one of the specialists working in an NHS private patient unit in the East Midlands, then check out Philip Housden’s analysis to see how you are contributing towards the profit line
Calling cardiologists! Around a third of doctors in this specialty with the MDU have needed to seek its assistance in the last ten years. Dr Claire Wratten, senior medical claims handler, analyses their clinical negligence claims and provides advice on managing risk.
Our ‘Ten Years Ago’ column looks back at the start of the campaign that eventually brought us the Competition and Markets Authority restrictions that transformed private practice.
Accountant’s Clinic’s A-Z of top tips reaches letter ‘X’ for eXit strategy
Our motoring correspondent Dr Tony Rimmer has a date with the latest version of the Skoda Octavia – based on the Golf Mark 8 platform
Plus all the latest news and views
Don’t forget – you can find more news on our website throughout the month
ADVERTISERS: The deadline for booking adverts in our September issue is 20 August
Write to Independent Practitioner Today 7 Lindum Terrace, Lincoln LN2 5RP
CHANGING ADDRESS, EMAIL ADDRESS OR SUBSCRIPTION DETAILS?
Phone 01752 312140 or email karen@marketingcentre.co.uk
TELL US YOUR NEWS
Robin Stride, editorial director Email: robin@ip-today.co.uk Phone: 07909 997340 @robinstride
ADVERTISE WITH US
To advertise in the journal or our website business and lifestyle directories, contact advertising manager Andrew Schofield at Spot On Media. Phone: 0161 408 3912 Email: andrew@spotonmedia.co.uk
Follow Independent Practitioner Today on
GET A SUBSCRIPTION DISCOUNT!
£90 independent practitioners.
£90 GPs and practice managers (private & NHS).
£210 organisations.
Save £15 paying by direct debit: individuals £75 (organisations £180).
TO SUBSCRIBE
Email karen@marketingcentre.co.uk or phone 01752 312140
Guarantee delivery of your next copy of Independent Practitioner Today. Take out a subscription and you will get full access to our news, features and previous issues on our website. See details on the left.