INDEPENDENT PRACTITIONER TODAY The business journal for doctors in private practice
In this issue
Use your content to grow your practice
What is content marketing and how to use it P20
Make money, not white noise
How to make best use of your data so that it becomes a valuable resource and not meaningless ditigal white noise P30 IS YOUR BRAND WORKING FOR YOU?
Conflict of interests?
By Robin Stride
Consultants’ business relationships with private hospitals are being questioned in a new report voicing concerns about the possible influences on patients’ treatment.
The Centre for Health and the Public Interest (CHPI) think-tank claims those receiving fees for use of equipment they own in the independent sector is ‘problematic’ from the perspective of patient care, as it has the potential to corrupt a specialist’s clinical decision-making.
Its report, ‘Pounds for Patients? How private hospitals use financial incentives to win the business of medical consultants’, states: ‘Put simply, in the worst-case scenario, a patient could be given treatment which is unnecessary or even harmful because the consultant gains financially.’
Doctors’ shares in private hospitals are also put under the microscope. The CHPI cites US research showing ‘that where consultants own shares in the facilities in which they treat patients, the number of healthcare procedures carried out on patients in them is higher than in hospitals where consultants do not own shares.
‘This is also the case when consultants own the equipment which is used to treat or diagnose patients –when consultants own equipment it is used more often on patients than when they are not owned by consultants.’
The report, authored by CHPI director David Rowland, warns if NHS consultants have shares in private hospitals, this has the potential to influence decisions about where patients, possibly unaware of a doctor’s financial interests, are treated.
Some consultants who refer patients to private hospitals have received non-monetary gifts from the operators worth over £1,000 and this ‘might be considered to be likely calculated to induce patient referrals to private hospitals’.
While the Competition and Markets Authority (CMA) 2014 private healthcare order permits ‘proportionate and reasonable’ hospitality, the CHPI questions if £1,226 rugby match tickets given to ten referring consultants, for instance, might be seen as an inducement to refer.
The think-tank claims evidence shows that both the CMA’s and NHS England’s regulations to prevent financial incentives distorting patient care are ineffective.
n See page 26
How to win at billing Ten simple rules to follow to ensure that your practice stays ahead of the pack P32
IMAGE OF OPPORTUNITY: These consultant investors are launching a new PET CT scanner. They are stakeholders in The Imaging Clinic, which created the chance for the oncologists to invest with
Essapen, Dr Anthony Neal, Dr Veni Ezhil, Dr Tony Dhillon, Prof Hardev Pandha and Dr Katie Wood. Directors Dr Tony Lopez and Catherine Lopez are on the far right. n See full story on page 6
The CHPI recommends the Depar tment of Health should take the lead in this issue, as the CMA is ‘not mandated or competent to act to address the potential harm caused to patients as a result of over-treatment or the wasteful use of scarce public healthcare resources’ and
‘Privately
should not be responsible for the law governing financial incentives. It wants fines and, in extreme cases, custodial sentences for legal breaches and a US-type system prohibiting conflicts of interest rather than attempting to manage them.
continued on page 10
funded
healthcare services’
A CMA investigation, titled as above, was this month launched into suspected anti-competitive arrangements relating to the private healthcare sector ‘which may infringe’ the Competition Act 1998. This is unconnected to our ‘Conflict of interests?’ story .
After reviewing parties’ responses, it will decide in October whether to proceed with a case. The CMA said:
‘No assumption should be made at this stage that the Competition Act has been infringed.
‘The CMA has not reached a view as to whether there is sufficient evidence of an infringement of competition law for it to issue a statement of objections to any of the parties under investigation.
‘Not all cases result in the CMA issuing a statement of objections.’
BMI Healthcare in Guildford, Surrey. Pictured from left are Prof Stephen Langley, Dr Steve Whittaker, Dr Sharadah
TELL US YOUR NEWS Contact editorial director Robin Stride
Email: robin@ip-today.co.uk Phone: 07909 997340
@robinstride
ADVERTISE WITH US Contact advertising manager Margaret Floate at margifloate@btinternet.com Phone: 01483 824094
GET A SUBSCRIPTION DISCOUNT
£90 independent practitioners.
£90 GPs and practice managers (private & NHS).
£210 organisations.
Save £15 paying by direct debit: individuals £75 (organisations £180).
TO SUBSCRIBE – USE SUBSCRIPTION FORM ON PAGE 25
Or email karen@marketingcentre.co.uk Or phone 01752 312140. Or go to the ‘Subscribe’ page of our website www.independent-practitioner-today.co.uk
Chief sub-editor: Vincent Dawe
Head of design: Jonathan Anstee
Publisher: Gillian Nineham at gill@ip-today.co.uk Phone: 07767 353897
EDITORIAL COMMENT
Register your interests
In the current climate of increased transparency in private practice, a report such as we feature on our front page was to be expected sooner rather than later.
The Centre for Health and the Public Interest (CHPI) document ‘Pounds for Patients? How private hospitals use financial incentives to win the business of medical consultants’ flags up more of what is to come.
With many consultants’ private fees now published for all to see on the Private Healthcare Information Network, it was only a matter of time before the focus shifted to other payments made to specialists in the independent sector.
The spotlight is now on NHS consultants with private practices who have shares in independent hospitals where they work or/and have also invested in equipment used by them.
We can expect more media
Get the most out of your accountant
Susan Hutter’s A-Z guide to accountancy turns its attention to the letter ‘B’ and gives advice on ‘book-keeping’ and ‘breaking up’ partnerships P16
Making devices safer
Independent healthcare providers argue that to improve the safety of health devices there has to be more involvement of the private sector P18
Hard work goes into doing nothing
Why a set-and-forget investment approach is never just that. Your financial adviser should be doing a lot of behind-the scenes work P34
‘Don’t tell me the risks’
When it comes to getting informed consent, how can you best manage a scenario where a patient doesn’t want to know the risks? P36
publicity on these topics in the months to come and, no doubt, tables will be published showing who earns the most from investments they have had the courage and gumption to provide to improve health services in their local community.
Be prepared for a greater push for private hospitals to publish this sort of information more clearly on their websites and for NHS trusts to make it easier for patients to find data about their specialists’ involvement in the independent sector.
If the CHPI is correct, then NHS England’s conflict of interest guidance to make publicly available information on consultants’ share ownership is still not happening in scores of cases. So if you haven’t made yourself transparent and declared your interests in other businesses, do so now.
Give private healthcare’s critics no beef to bite.
Patients’ DIY justice
The additional challenges of defending a claim when the patient is not legally represented are explored by solicitor Niloo Bozorgi P38
Dating
an ex-patient
Our ‘Business Dilemmas’ series looks at the ethics of a potential relationship between a doctor and their former patient P43
PLUS OUR REGULAR COLUMNS
Start a private practice: Investments giving tax relief
Accountant Ian Tongue looks at the Government-backed schemes for investing your hard-earned cash P44
Doctor on the Road: Converted to this brutal convertible
The all-new BMW 8 Series convertible will have you beaming, says our road-tester Dr Tony Rimmer P46
Profits Focus: Generalists fading away
Our unique benchmarking series looks at the financial fortunes of general surgeons P48
Circulation figures verified by the Audit Bureau of Circulations
Bid to fix pension crisis ‘won’t work’
By Edie Bourne
Doctors who are choosing to cut their NHS hours or retire early due to punitive tax charges on their pension savings have given the thumbs-down to Government proposals to introduce a ‘50:50’ savings option.
Already in use for staff pensions in local government, the scheme allows members to contribute half the normal level of input in exchange for half the accrual.
The idea is part of a wider consultation to ease the current pressures on the NHS workforce – but critics say it does not go far enough.
Patrick Convey, technical director of specialist financial planners Cavendish Medical, backed doctors’ criticism. He observed that a 50:50 option might give some pension savings flexibility, but doctors would receive similarly reduced eventual benefits. It would also create an extra level
of complexity to the challenges already established by the introduction of the tapered annual allowance in 2016, he warned.
‘At present, it is very difficult for doctors to plan their tax situation alone because the taper is based on the current year’s income but working hours may be ad hoc.
‘In addition, extra hours are not pensionable but the increased income will impact the figures used to calculate the tapered annual allowance. This means that some senior doctors will face higher tax bills simply by working extra shifts. It is easy to see why many are unwilling to take on supplementary duties at present.’
Cavendish Medical assumes the Government will discuss the 50:50 option as part of wider consultation. But it pointed out there are other possibilities such as an ‘enhanced opt-out’ option used by the Universities Superannuation Scheme which means members can cease accruing new pension rights but retain death-in-service benefits.
Mr Convey told Independent Practitioner Today: ‘However, doctors and their financial advisers will be hoping that the harsh tapered annual allowance is abandoned completely.’
Teamwork, not isolation, is route to better outcomes
Private practice must move away from a ‘siloed’ mentality with doctors working as individuals and instead gain critical mass to enable outcomes to be more appropriately measured, according to a leading specialist.
Mr David Sweetnam, a consultant orthopaedic and trauma surgeon at Schoen Clinic London, said that during his childhood and subsequent 30 years in the NHS there had been a move away from the firm (team) structure of great teaching hospital units towards individualised practice.
But he told LaingBuisson’s Private Healthcare Summit in London he believed the sector was
now at a crossroads and teamwork was being reborn.
Speaking later to Independent Practitioner Today he said: ‘It is my impression that only by working, once again together as teams in dedicated hospitals specialising in given fields, such as The Schoen Clinic with orthopaedics, that we can start to collate the data and produce meaningful outcomes about the effects of what we do.
‘Increasingly, the private medical insurance companies are going to be looking at us, looking for answers as to who is providing good value for money, and only by being able to demonstrate very clearly, exactly the effects of our
A new report by NHS Employers on the impact of pensions tax on the workforce shows doctors are being hit with average extra tax bills of around £22,000, with many facing charges of over £50,000.
Mr Convey continued: ‘The report highlights a lack of information on the complicated tax positions of doctors and that many are struggling to navigate a clear path through the confusion.
‘There are also many misconceptions being circulated in terms of the best route forward, with some doctors believing their only option is to quit the scheme altogether.
‘We would urge anyone with concerns to seek assistance before making rash decisions that could impact their future finances and that of their loved ones.’
treatments on our patients will we be in a position to prove this to them.
‘It is for that reason that I think we are witnessing the end of standalone practice and the rebirth of the teamwork that was so successful in the “glory days” of the health service.’
He said the NHS had traditionally exemplified to him the very best of clinical practice with a hospital displaying not only a very distinct ethos but also a certain way of doing things. ‘There was clear leadership and one was proud of being a member of a successful team.’
See reports from the Private Healthcare Summit – pages 8-9
Patrick Convey of Cavendish Medical
Orthopod Mr David Sweetnam
Surgical unit for diabetes opens
By a staff reporter
HCA has launched The London Bridge Hospital Metabolic and Bariatric Centre to surgically treat patients with type 2 diabetes (T2D) and obesity.
It is billed as the first of its kind to open within the UK private health sector.
Under the leadership of consultant bariatric and metabolic surgeon Prof Francesco Rubino, the hospital will offer the latest in pioneering surgical treatment for T2D and obesity and related diabetes services.
His research was the first to uncover the anti diabetic sideeffects of weight loss surgery, revolutionising understanding of the diagnosis and management of T2D, and resulting in the introduction of metabolic surgery to treat the disease.
He said: ‘Clinical trials have proven that metabolic surgery is able to treat T2D more effectively than medication and lifestyle management, and for longer.
‘In many patients, blood sugar levels return to normal within weeks of surgery, 80 90% of patients see a dramatic improve
ment in their glycaemic control, and 50% of patients enjoy long term remission – which is lifechanging.
‘London Bridge Hospital is truly visionary as the first private hospital in the country to create a multidisciplinary approach to treating diabetes surgically. I am honoured to be overseeing the new service, alongside a leading team of diabetologists, dieticians, endocrinologists, type 2 diabetes clinical nurse specialists and fellow surgeons.’
London Bridge Hospital chief executive Janene Madden said it was hoped the centre at 27 Tooley Street London SE1 will offer patients nationwide and internationally a more permanent solution for type 2 diabetes treatment.
Prof Rubino is also the chairman of metabolic and bariatric surgery at King’s College London.
MPs criticise NHS plans to introduce a
‘monopoly’
Private hospitals have welcomed the proindependent sector tone of Parliament’s Health Committee’s report on NHS proposals for legal changes.
David Hare, chief executive of the Independent Healthcare Providers Network (IHPN), said the committee had once again made clear that a diverse provider market including the independent sector could contribute to more integrated services for patients. The IHPN was pleased with the com mittee’s endorsement of many of the points the network made itself in written and oral evidence, including safeguards against price competition resulting from changes to the national tariff Mr Hare added: ‘The committee is clear that, without further development, the legislative proposals risk introducing unintended consequences and could even lead to the NHS becoming a “protectionist monopoly provider”.’
New head of consultants’ association
The new chairman of the London Consultants’ Association (LCA) hopes specialists who feel somewhat isolated in the independent sector will reap the benefits of activities being planned by the organisation.
Consultant endocrinologist Dr Mark Vanderpump said private practice can be a very lonely place for doctors.
So he was pleased that the diverse range of activities that the LCA was planning would go some way towards supporting and encouraging specialists.
Dr Vanderpump said: ‘We will also continue our active involvement with the Federation of Independent Practitioner Organisations (FIPO), which represents these views at all levels in the sector and more widely.’
He has taken over from Prof Neil
Tolley, consultant in ENT and thyroid surgery.
The LCA comprises leading consultants in the capital and beyond who work part time or wholly in the independent sector.
Formed in 1998, the association aims to support consultants in private practice, providing individual advice and through a close
working relationship with FIPO, with whom it shares the same Wimpole Street address.
The LCA hosts topical evening meetings with members of the medical and legal profession throughout the year, alongside dinners with distinguished speakers such as Jeremy Hunt, Andrew Lansley and Stephen Dorrell.
It also has a medicolegal expert witness group, which holds training sessions working with leading solicitors Hempsons* and QCs. These are complemented by breakfast meetings.
A spokesperson said: ‘The LCA ethos is one of professional integrity and independence and the maintenance of the high professional standards of the GMC, royal colleges and Governmentregistered organisations.
‘Its principal objective is to
maintain the rights of the patient and doctor as well as the freedom of referral and clinical practice in the face of ever growing constraints.’
Prof Tolley, who did a threeyear tenure, believes the whole tenet of private healthcare is changing under a ‘perfect storm’ of increasing regulation, changes to consultant working practices and employment status in the sector, and pressure on referral paths.
He and Dr Vanderpump agree there is a need to encourage new young consultants into the sector in order that future generations of patients can exercise choice in accessing expert care appropriate to their requirements.
✱ Independent Practitioner Today readers qualify for free legal advice from Hempsons. See page 39 Gear up for digital – and other changes – see page 8
Prof Francesco Rubino, consultant bariatric and metabolic surgeon
LCA chairman Dr Mark Vanderpump
Revamp urged for arraigning doctors
By Leslie Berry
Doctors’ organisations have welcomed a raft of recommendations from an independent review of gross negligence manslaughter and culpable homicide in medical practice.
The review was commissioned by the GMC following the Dr Hadiza BawaGarba case.
Her prosecution and conviction for gross negligence manslaughter after the tragic death in 2011 of sixyearold Jack Adcock sparked a nationwide doctor outcry.
Their trust in the regulator was hugely undermined after it successfully appealed a Medical Practitioner Tribunal Service decision not to erase her name from the medical register.
Responding to the review, Royal College of Surgeons of England president Prof Derek Alderson, said its recommendations should help ensure greater consistency around how gross negligence manslaughter (GNM) cases were initiated and investigated.
‘Our health and legal systems must protect patients from avoidable and unnecessary harm, while also providing clarity about the difference between gross negligence manslaughter and basic human error in medical practice.
‘Currently, there appears to be wide variation over which suspected GNM cases are referred to the police for investigation. We therefore support the recommendation that if a coroner feels that a
doctor’s conduct might reach the threshold for GNM, they should discuss this with the Chief Coroner’s Office before the police are notified.’
He also supported a recommendation that where a doctor is being investigated for GNM or culpable homicide, the system the person worked in should be scrutinised. If the doctor is a trainee, this should include the education and training environment.
The review said the GMC should make transparent its processes for recruitment and quality assurance of those doctors providing expert reports, again welcomed by the college. It also supports a register for expert witnesses in criminal cases if it is fully funded and properly scoped.
Prof Jackie Taylor, president of the Royal College of Physicians and Surgeons of Glasgow, called for urgent action by government and NHS bodies to ensure doctors
have faith that justice will be served after tragic mistakes.
She said it would not be easy to rebuild doctors’ damaged relationships with the GMC, but it was vital that action was taken to build on positive progress begun over the past year. ‘Doctors must have confidence that the system is not loaded against them when mistakes are made.’
Her college agreed with the review that the GMC’s processes had been shown to be inadequate and it welcomed calls to urgently update underpinning legislation.
Prof Taylor said the criminal threshold for the charge of gross negligence manslaughter in England and Wales was lower than the equivalent charge of culpable homicide in Scotland.
English and Welsh systems could learn from the Scottish experience in developing a legal framework which encouraged transparency and commanded greater respect from victims, families, and healthcare workers.
The BMA welcomed a recommendation that all healthcare providers should be consistent when conducting local investigations and in line with the relevant national frameworks. This would alleviate issues of too much variation in who carries out investigations into serious clinical incidents, it said.
BMA Council chairman Dr Chaand Nagpaul expressed relief that the review, led by Leslie Hamilton, said the GMC should lose its right to appeal fitnessto
Doctors must have confidence that the system is not loaded against them when mistakes are made
practise decisions made by its own tribunal service.
The association urged the Government, the GMC, healthcare providers and other relevant bodies to urgently monitor, evaluate and regularly report on the implementation of the recommendations.
Prof Russell Viner, president of the Royal College of Paediatrics and Child Health (RCPCH), said: ‘We support the recommendation that, when there is significant criminal investigation into an individual, the systems around them must also be investigated.
‘This is not about shifting blame or accountability, but recognising that individuals operate within a wider environment and should not become scapegoats – and failings of the system at large need to be addressed.’
GMC says it’s making progress on gross negligence
GMC chief executive Charlie Massey said: ‘We share this report’s desire for a just culture in healthcare and acknowledge that we have a crucial role in making that happen.
‘We are already making progress. Work is underway to address some of the key issues raised in this report, but there is plenty more for us to do.’
He said greater consistency was needed in the response to an unexpected death. ‘Support for, and involvement of, patients’ families must be a priority before, during and even after an investigation into an unexpected death. Doctors need to feel they are part of a just culture when things go wrong.’
Mr Massey added: ‘The report also recognises
that GMC processes are constrained by outdated legislation and calls on the Government to reform the Medical Act to give us more discretion over which cases require investigation. We echo that call.
‘The recommendations in this report will help us move towards the just culture that we all want and that will benefit healthcare.’
Prof Jackie Taylor, President of the Royal College of Physicians & Surgeons of Glasgow
Prof Derek Alderson, Royal College of Surgeons of England’s president
Doctor partners pay for scannner
By a staff reporter
The UK’s first private PET CT scanner in an independent hospital outside London has been opened in Surrey through a unique partnership between 11 consultant investors, BMI Healthcare and Incorporated Health.
The Guildford scanner is facilitated by consultant interventional radiologist Dr Tony Lopez, director of The Imaging Clinic Ltd.
The company says it facilitates engagement by consultant users in a way compliant with the Competition and Markets Auth ority (CMA) – which banned inducements – and balances financial risk and reward, while making the installation of such expensive and rarely-available equipment a reality.
All the consultants are oncologists at The Royal Surrey County Hospital, Guildford, and initially operated a mobile PET CT scanner to prove and grow the business to create the revenue necessary to install the Siemens Biograph scanner during building work at the BMI Mount Alvernia Hospital.
Dr Lopez, who has worked in partnership with BMI Healthcare since 2007, said: ‘I am honoured that my consultant colleagues and our partner hospital have shown such faith in my business plan, each using significant capital in this increasingly challenging financial environment.
‘It is timely that the Centre for Health and the Public Interest has just published its report on the business of consultants. The local NHS trust where all the consultants work, as well as all stakeholders including staff and patients, will be reassured that all
requirements of the CMA Final Order (2014) are being adhered to, including full disclosure on the local NHS trust register and on the front page of the BMI Healthcare hospital website.’
The company has a similar joint venture with Aspen Healthcare at its Cancer Centre London facility at Parkside (Wimbledon), where the installation of another fixed facility by its new owners NMC Healthcare is expected to replace its current weekly mobile service.
It also has several other imaging joint ventures pending, and always with local consultants.
Breast unit allows self-referrers
A new ‘one-stop’ breast unit at HCA’s Chiswick Medical Centre, London, has announced it will be the first in the area to provide patients with fast access to diagnosis and for the option to self-refer.
It will offer the full spectrum of breast assessment, the diagnosis and treatment of benign and malignant breast diseases, as well as breast reconstruction options.
A spokesperson said: ‘By allowing qualifying patients to self-refer, the Breast Unit offers access to a triple assessment breast care service without the need to see a GP.
‘For the almost one-in-five London women who report diffi-
culties accessing medical help for breast concerns – much higher than the national average of one in seven – earlier access to testing may improve their outcomes and survival rates.’
Research commissioned by HCA Healthcare UK* found that if faced with a symptom, more than twoin-five (42%) women would delay visiting a doctor for medical help, with 23% saying they would wait for up to two weeks and one in ten waiting for up to a month.
Just under a third of those polled (29%) in London stated that they would be more inclined to seek help for a breast-related concern if
Guidance on improving CQC scores
A new Care Quality Commission (CQC) report explores how independent acute hospitals have been able to make significant improvements in the quality of care and improve their rating on reinspection.
‘Driving improvement: Case studies from eight independent hospitals’ draws on interviews with a range of staff from eight hospitals. Each made positive improvements for patients.
The CQC said their stories shared some common themes. ‘They show that one of the biggest aspects to supporting improvement across all hospitals was robust leadership. Another is meaningful engagement with staff.
‘Leaders became more visible. They made an effort to listen to staff and bring them into discussions about changes and improvements. Strengthened governance processes supported learning from incidents and complaints, helping to identify and address risks.
‘Alongside this, we heard how efforts were made to adopt a “whole hospital” approach. Staff in different departments worked more closely together. And they could see their part in the wider system.’
In some cases, lessons learned as part of the improvement process were shared across hospitals in the same group. Corporate support provided extra people and finances to back up local teams.
waiting times for appointments and results were shorter.
Mr Richard Sainsbury, consultant breast and oncoplastic surgeon, said: ‘The Chiswick Breast Unit will allow patients to receive a fast diagnosis with results shared swiftly after their appointment. This new state-of-the-art service will offer patients personalised care through every stage of their journey.’
✱ Research conducted by Opinium Research between 11-14 January 2019 among 2002 UK women aged 18+, including 518 women in London and 264 women in Manchester.
CQC inspection reports also helped hospitals to prioritise actions. This helped them make quality improvement a fundamental part of what they do.
Prof Ted Baker, CQC’s chief inspector of hospitals, said: ‘These case studies show just how important it is to have open, honest and visible leadership that engages and empowers staff across all departments to contribute to improving patient care.
‘I hope their stories will encourage and inspire other independent hospitals in their own improvement work and help drive up safety and quality across the sector.’
The new PET CT scanner at the BMI Mount Alvernia Hospital, Guildford
Competition set to soar
By Olive Carterton
Private doctors – be they consultants or GPs – could see a surge in competition if findings from a new report are realised.
It reveals that, with the increasing dissatisfaction with pay and workload pressures in the NHS, as many as 28% of doctors in the UK are considering taking on private work.
Findings from a new Doctor’s Salary report from Medscape reveal that private work is a more popular option with men (30%) rather than women (23%).
Over a third (34%) of GPs are considering exploring the independent route alongside 27% of specialists.
Medscape’s Dr Rob Hicks told Independent Practitioner Today : ‘I know of a number of GPs who have moved to private general practice. Some of them combine a reduced NHS general practice commitment with part-time private practice, others have moved to only practice privately, full-time or part-time.
‘A common theme is trying to achieve a good work-life balance, something that with the everincreasing pressures on NHS general practice is becoming much harder to do.’
Despite last year’s 2% pay rise, more than two thirds of GPs (67%) and 59% of specialists still consider their pay unfair.
This year’s report provides an up-
to-date picture of GPs and specialists’ satisfaction with their jobs, as well as a variety of factors which have an impact on the current recruitment and retention crisis.
Nearly a third (31%) of UK doctors are considering leaving the UK to practise in another country
Almost 40% would choose another profession if they were starting their career again.
Under half (43%) would recommend a medical career to their children. NHS staffing levels or workload are the biggest contributors to making the job difficult (cited by 50%), followed by the high burden of NHS rules and regulations (cited by 20%).
Paperwork and admin alone take up more than 15 hours per week for
Call for NHS to use private care to solve its long waits
Private healthcare providers have called on the Government to heed MPs’ warnings and set out a clear plan for improving speed of access to NHS care, including by using the spare independent sector capacity.
The Independent Healthcare Providers Network (IHPN) warned that a Commons’ Public Accounts Committee report on NHS waiting times had shone a much-needed light on the worrying decline in NHS patients’ access to vital treatments such as hip replacements, cataracts and cancer care.
The IHPNs chief executive David Hare said: ‘Despite a clear legal commit ment in the NHS Constitution, the 18-week target for elective care has not been met in over three years, leaving hundreds of thousands of NHS patients waiting in pain and discomfort for months on end.
‘Having swift access to highquality care is a top priority for the public, but the simple truth is that patients are waiting ever longer for NHS treatment while having no
idea when vital legally binding targets will again be met.’
BMA Council chairman Dr Chaand Nagpaul said: ‘It is particularly worrying that alongside increasing overall waiting lists, cancer treatment services continue to plunge further into crisis, with six out of ten trusts failing to ensure patients are seen within the 62-day standard – a pledge set out in the NHS constitution’s handbook.
‘This is a vital part of the health service which should be providing fast, effective and caring treatment
at an early stage for what can be a life-threatening condition. It is unacceptable that patients and their families should have to endure the added stress of having to wait weeks and weeks for further care, well beyond recommended limits.’
He urged the Government to address ‘this mounting crisis’ and listen to the BMA’s call for increased, immediate funding to frontline services.
This should include a long-term plan to address workload and workforce pressures that were damaging patient care.
Siva Anandaciva, chief analyst at The King’s Fund, said: ‘The NHS is currently reviewing its waiting times targets. But changing waiting time targets alone will not solve the underlying pressures that have led us to this point.
‘Without an effective workforce strategy and increased investment in diagnostics equipment, staff training and social care, the NHS will have little hope of meeting current or new performance targets.’
almost half of respondents (48%). That is in addition to the 31 hours a week on average that UK doctors spend with their patients
The most rewarding aspects of practising medicine for respondents were age-old: being good at their job by finding answers and making diagnoses (36%) and patient gratitude and relationships (22%).
The number of respondents who cited ‘making the world a better place’ (21%) nearly doubled since two years ago.
Medscape’s second UK-specific doctors’ income survey involved over 1,000 full-time practising GPs and specialists, who are Medscape members, between January and February 2019.
Vascular surgeon Prof Mark Whiteley, of The Whiteley Clinic, Guildford, has launched Sonovein in the UK, the first non-invasive treatment for varicose veins using high-precision echotherapy.
He called it a medical breakthrough which would completely alter the way specialists treat varicose veins and venous issues while transforming treatment experience and recovery times for patients.
No catheters, chemical injections or incisions are required, meaning patients are left with no scars or risk of infection and can return immediately to their normal daily activities, and it was more cost-effective.
The clinic now offers echotherapy treatment to all suitable patients.
BMA chairman Dr Chaand Nagpaul
Sector too slow in exploiting its data
By Robin Stride
A leading expert on the private healthcare market has challenged the private healthcare sector to break out of its ‘island mentality’ for the benefit of patients.
Healthcode managing director Peter Connor said the NHS had recognised that data was one of its most precious resources and was basing its digital strategy on building common information standards. But the independent sector lagged behind.
He told the LaingBuisson Private Healthcare Summit: ‘I am concerned that standards and sharing are two words that are rather alien within our sector.
‘I often encounter resistance to sharing on data protection grounds and I also believe we are often hampered by the “island mentality” from organisations that says “we’ve built our own system and if you want to do business you have to do so on our terms”.
‘We need to start thinking about the needs of patients and accept they are unlikely to stay with the same provider or private medical insurer for life.
‘We have to recognise that our data only has a value if it can be shared appropriately, securely and in the interests of patients. And we can only achieve this if we trust each other enough to embrace
common standards and collaborate.’
Speaking on the theme of ‘connecting the sector with technology’, he warned that technology could only deliver value if the sector was willing to embrace common standards and change its attitude to data sharing and collaboration
Mr Connor said Health Secretary Matthew Hancock had acknowledged that the migration towards standards would quickly increase the NHS’s ability to share data across the system and drive insights from the huge amount of data it held.
This was not just rhetoric – NHS England was now actively advocating the benefits of information standards and data sharing across all stakeholders: patients, providers and commissioners.
He went on: ‘Although it’s one thing to advocate standards and data sharing in the public sector, we have also seen how this approach can work in the commercial world, notably in the travel and hospitality sector where different services are linked through a network called a Global Distribution System.
‘Service providers benefit from exposure to vast new markets and, as consumers, it’s much easier and more convenient to access these services. All this interoperability is
only possible because of information standards.’
Mr Connor urged private healthcare organisations to collaborate and think about the needs of patients.
He recognised there has been some successes in developing standards within the private healthcare sector, such as the Private Healthcare Information Network and Healthcode’s own work in billing.
There were also signs of progress in areas such as practitioner data through initiatives such as the Private Practice Register and new consultant oversight framework, but there was still plenty of work to do in booking and patient records.
Cut private cover costs using health promotion
The private medical insurance industry is beginning to wake up to the fact that new models of care are needed to address the rising cost of healthcare and changing consumer expectations.
Andrew Scott, director at insurer Vitality, said the introduction of new technology such as virtual consultations was one solution. He said: ‘Although we have been a very static PMI market for the last ten years, there’s a lot of movement in the space: the rise of wearables, preventative programmes… a wide proliferation of technology and the rise of virtual consultation services.
‘The question for us as an industry is: Are we truly meeting society’s expectations with the products and services that we are delivering?’
Mr Scott said that in Vitality’s experience, the introduction of virtual GP consultations to its customers in 2015 had been one of the most significant developments and that primary care was proving to be a new direction for insurance products.
‘The challenge is that health promotion is ever more significant to PMI and we need to find ways of doing even more and making it even more relevant for consumers.
‘There’s a huge amount of new technology. Some of it will go, some of it will stay. I think the challenge here is not be faddish and not just latch onto anything that comes up, but to systematically integrate it into the PMI offering,’ he said.
He acknowledged that affordability remained a problem in the private healthcare sector and that private insurance was an expensive proposition for most individuals. However, he insisted that could change if providers could effectively integrate new models into their product offering.
Peter Connor, Healthcode boss
The theme of this year’s LaingBuisson private healthcare conference was ‘Healthcare innovation: exploiting new technologies to benefit patients, doctors, providers and payers’
NHS implored to include private healthcare more
Guest writer Maria Davies gives a round-up of key themes from this year’s
LaingBuisson Private Healthcare Summit
The private healthcare sector needs to embrace new digital technology and new models of care delivery to secure future growth, delegates heard.
Almost 200 guests attended the annual event at London’s QEII centre, which this year was dominated by the challenges and opportunities presented by advancing technology and changing patient and payor expectations.
In his keynote address, former Health Secretary and chairman of the European Movement, Stephen Dorrell, said that as health commissioning became more outcomes based, the NHS would need to take a more flexible approach and develop new relationships with alternative providers, including those in the private sector.
Although he warned that there were still considerable risks to the private healthcare sector from the UK’s withdrawal from the EU, particularly in terms of supply chain issues and staffing pressures, he
said the sector needed to be making the case for more partnership working.
He said: ‘I do think within the healthcare sector generally, and the private healthcare sector in particular, we need to think about what the political debate in our country will look like when finally the public policy space has some bandwidth to think about something other than Brexit.’
The private healthcare world needed to think about how it
Former Health Secretary Stephen Dorrell said the state should commission more healthcare from alternative providers
hospitals and more on health outcomes.
‘There’s a lazy habit of thought in this country that thinks of the NHS as state provided. It’s absolutely not true. It never has been,’ he said.
‘The person who invented the private contractor delivery model in the National Health Service was [Health Secretary] Aneurin Bevan. He didn’t choose to do it, he didn’t do it voluntarily, he did it in negotiation with the BMA.
played into the broader healthcare sector and the wider institute of public policy and public services and to how that argument would be made in the political domain beyond the Brexit drama.
Mr Dorrell told delegates there was a ‘real opportunity’ to make the case for a more flexible system in the UK that allows people access to a broader range of services and recognises that the core activity of the public sector should be less focused on the management of
‘But the private contractor model is the model by which primary care has been delivered in the NHS since the date it was founded.
‘And remember, when people think of the NHS as a state monopoly, actually the real question is which profession in the NHS sees more patients every day than all the other healthcare professions put together? The answer is community pharmacists. Not a single one of whom is a state employee.’
Prevention is key to making care affordable
The independent sector needs to embrace new models of care that emphasise prevention.
This was the plea from Michelle Martin, commercial and category development director at Nuffield Health, who echoed Mr Dorrell’s points about the focus on outcomes.
‘We cannot afford some of the trends that we are seeing unless we give prevention the time and care that it deserves,’ she said.
The charity, which itself has remodelled over the last decade to
become a health and fitness provider as well as a hospital group, is operating a number of preventative health programmes in the community aimed at encouraging healthier lifestyles among children, older people and people with longterm conditions.
Ms Martin said that along with an ageing population and increased incidences of multiple and longterm conditions, people were increasingly willing to take responsibility for their own health
and well being, more willing to spend on prevention and increasingly likely to use digital channels.
Combined with an overstretched NHS, she said this would present opportunities for the independent sector and big firms to take more responsibility for the nation’s health.
However, she told the conference that the sector had to change to ensure its relevance in the future of healthcare delivery.
‘For us in the independent sector, elements that we need to give
increasing attention to is the concept of accessibility and affordability. It’s been one of the biggest challenges for the longest time about private healthcare being unaffordable.
‘So how do we expand our networks and make sure that people can access private healthcare in an affordable, accessible way? We need to consider our price points, we need to work with partners, with the supply chain to make it a more affordable and more efficient model.’
Maria Davies is editor of Healthcare Marketing
Membership club for doctors set up
By Olive Carterton
A new membership organisation for doctors, The Doctors Club, has been launched for consultants and health professionals in the UK.
Over the summer, it has started running regular relaxed and informal events for members where they get a chance to network with colleagues and build their referral network.
Through a member-only website (www.thedoctorsclub.co.uk) doctors can access a range of products and services secured exclusively for the club.
There are luxury goods and services from providers such as Harrods, BMW and Scabal.
The website also offers a business services section with businesses especially selected because of their specific experience of dealing with healthcare clients.
The club has been set up by Philip Archbold who has a long history of providing digital services in the private healthcare market.
He said: ‘So many of the events we attended were dominated by long presentations from paying sponsors or from the organisers trying to raise their own profile or standing in the industry.
‘We recognised that the doctors just wanted the opportunity to meet with colleagues and build their referral network without all
the usual flim-flam... the doctors are surprised when they come and there is no sales pitch.’
He said the club aimed to use group buying power to get members big discounts on a range of products from cars, villas in Tuscany, sexy lingerie and Savile Row suits.
The next evening gatherings are on:
15 August, in Maidenhead, Kent, with watchmaker Christopher Ward Watches;
15 September, a networking event at Bang and Olufsen, in London’s Knightsbridge.
Details are available by emailing membership@thedoctorsclub. co.uk or phoning 01494 431258.
Doctors defend investing in kit
Consultant joint ventures facilitator Dr Tony Lopez, chief executive of Incorporated Health, responded: ‘It’s perfectly reasonable for NHS and private consultants to co-fund essential services, equipment and even hospitals and clinics.
‘There is simply too much reliance by the UK healthcare market on foreign investment, including some of the largest established private net-
work groups and new entrants.
Many consultants are well-funded or can access suitable investment capital and vehicles and have a useful intimate knowledge of the market.’
He said the CMA’s 2014 order had safeguards to materially limit equity and ensure ‘related party’ declarations on NHS trust registers and hospital/facility websites.
The Federation of Independent Practitioner Organisations expressed
surprise at some CHPI assumptions, saying the GMC required doctor transparency about interests they had in facilities treating patients.
‘FIPO upholds the premise that the only contractual relationship that matters is that between the treating consultants and the patient in front of them for whom they have a duty of care. It is difficult to understand how the assertions of “overtreatment” have been quantified.’
Psychiatrist pushes to get insurers to raise fees
A private psychiatrist is pressing for higher insurance fees in his specialty to recognise the length of time it takes to see patients.
Dr Stephen Davies, who works in south Wales, said leaving the NHS had been very positive for him; longer appointments with patients making his work more rewarding and effective.
But it could be complicated and his typical appointment slot for a new patient lasts 60-75 minutes, with a follow-up taking 30 minutes.
He told Independent Practitioner Today : ‘I know orthopaedic surgeons and dermatologists who see up to 20 patients in an afternoon, and it’s not a problem.
‘If psychiatrists did even half this for our patients, we’d be jeopardising quality and safety. Without this higher rate per consultation we won’t bring new psychiatrists with fresh ideas into the private sector.’
Dr Davies welcomed an ‘overdue’ uplift in fees recently from AXA-PPP for its fee-approved psychiatry consultants. From April 2019 the insurer has paid psychiatrists £250 for a new patient consultation and £170 for a follow-up.
He said: ‘The insurer said that the step was to recognise the work being undertaken in this speciality, and it sets the bar higher than the rates paid by any other major insurer.’
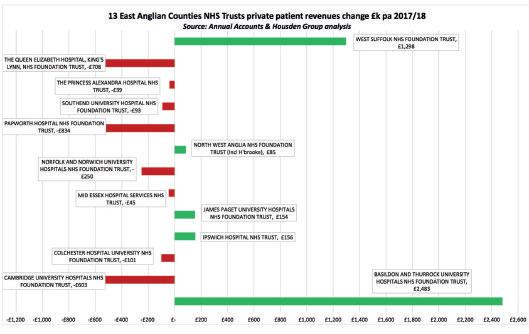
PPUs are big income generators
The income-generation potential of integrated private patient units within the NHS was the focus at a national Trust Commercial Director Network Meeting in London. This NHS Improvement-hosted event was aimed at trusts sharing best practice to maximise the benefits of developing private patient services as a normal part of care delivery. Key messages from the day were:
1. There are tangible benefits when providers work together to share best practice and learn from each other to strengthen local business models.
2. There was a clear commitment to develop a more networked approach to allow peer support and align practice.
This will enable a common approach and a combined voice to support negotiation with insurers to ensure all contracts are mutually beneficial and tariffs are above national tariff, meet reference costs and are at market value.
3. Good support for the creation of an NHS PPU brand to support consistency and transparency, particularly to demonstrate the value of providing private complex care in NHS settings.
It is clear that the benefits of PPU developments to the NHS and to private patients exist nationwide, and that partnerships between trusts may be the way to stimulate the sector.
Philip Housden is a director of Housden Group. See his feature article on East Anglian PPUs on page 40
Now he is hoping other insurers will raise their fees too. ‘For any psychiatrist who has joined Bupa as a provider since 2010, they pay less than £200 for a new patient and £120 for a follow-up.’
Bupa launched improved mental health cover for corporate customers last year and recently extended this to individual customers and their families.
A spokesperson said: ‘We expect use of mental health services to continue to rise, so we regularly review our network capacity and consultants’ and therapists’ fees to ensure customers have fast and convenient access to services.’
Compiled by Philip Housden
➱ continued from front page
Private and NHS GP service barred on the same site
New guidance from NHS England poses ‘cliff-edge threat’ to some GP businesses
By a staff reporter
Private GPs’ hopes of launching their services in NHS GP practices have suffered a serious setback.
Lawyers warn that new NHS England guidance on the GMS contract for GPs outlines a blanket ban on GPs advertising and hosting private GP services from within their surgery premises. They say the changes mark a sea change and are potentially a major threat to some existing practice business models.
According to Hempsons, regulations and directions governing all types of GP contracts have never included specific contractual restrictions on offering private GP services.
In a newsflash on the company’s website last month, partners Bryn Morgan and Michael Rourke said GPs would, of course, need to ensure that any private services did not conflict with their contractual obligations to the NHS and their registered patients.
But, beyond this, and so long as the contract was being performed, practices had relative freedom to design their businesses to include a private GP element if they so wished, the lawyers say.
Zero-tolerance approach
But they warn: ‘Following the publication of the guidance, it seems we are now moving towards a zerotolerance approach, where -by any housing of private GP services in the same building as the NHS practice would amount to a breach of the contract itself.’
The rationale and broad principles of the changes are set out in
section 3.3 of the guidance, which states: ‘To safeguard the model of comprehensive NHS primary medical care, from 2019 it will no longer be possible for any GP provider either directly or via proxy to advertise or host private paid-for GP services that fall within the scope of NHS funded primary medical services.’
The ban is to be qualified to the extent that: ‘This policy will not prevent individual GPs from offering purely private GP services to non-registered patients outside of times they are contracted by an NHS provider of primary medical services and on alternative premises which are not NHS-funded.’
Alternative premises
This seems to leave the door ajar for practices to offer private GP services outside their contracted hours.
But the solicitors say, crucially, it appears that these services must be provided on alternative premises – not on the surgery premises. They say it is unclear whether private GP services will be permit-
It seems we are now moving towards a zero-tolerance approach, whereby any housing of private GP services in the same building as the NHS practice would amount to a breach of the contract itself
services, as those providers could not offer private GP services either physically or digitally.
However, this implies that a practice will not be permitted to either use themselves or rent out part of the premises for private GP services.
Mr Morgan and Mr Rourke conclude that the guidance perhaps poses more questions than it answers and further clarity is unlikely until new regulations are published later this year.
ted in other parts of the practice premises that do not qualify for NHS premises funding – perhaps because they are vacant, let to someone else or just simply underutilised so as not to qualify for NHS funding.
The guidance offers the following commentary on how the ban will apply. A practice will not be able to house an NHS and private GP service in the same building as this would amount to hosting a private GP service.
Only exception
The only exception mentioned concerns leased premises where it recognises the leaseholder – i.e. the practice – has no influence over how the landlord chooses to use other parts of the building.
However, where the GPs own the building, they will clearly have influence and control over all parts, not just the NHS funded part.
A practice may rent out parts of the practice premises to, for example, a pharmacist, optician or dentist who provide some private
They say the key point that has to be addressed is whether the ban is to apply to only those parts of the practice premises for which NHS premises funding is provided or each and every part of the practice premises regardless.
‘Clearly, those offering private GP services will be hoping the first scenario applies.
‘The second is perhaps harder to rationalise, as it would restrict the use of premises which presumably have already been deemed to be surplus to the needs of the NHS service.
‘It also seems difficult to justify why it should be permissible for a practice to occupy two adjoining buildings, providing NHS services from one and private services from the other, but not for a practice to divide its building horizontally with the offerings separated, perhaps between the ground and first floor and accessed by separate entrances.’
They called the ban a potential ‘cliff edge threat’ to a number of existing business models and said those practices affected will need to watch this space carefully and plan as best they can.
Solicitor Bryn Morgan of Hempsons
Hempsons solicitor Michael Rourke
You’ve nothing to fear in revealing your fees
THE PRIVATE Healthcare Information Network (PHIN) began publishing the fees of over 4,500 UK consultants on its website nearly four months ago.
It was another important step towards increasing price transparency in the private healthcare sector.
All consultants with a private practice in the UK are required by Article 22 from the 2014 Competition and Markets Auth ority order to provide their consultation and procedure fees to PHIN.
What surprises me as I compile this article is that there are around 10,000 practising consultants in the UK who are still yet to submit fee information to the organisation.
Changed climate
Well, I understand that there is a natural reticence to say what you charge when it can be compared with all your local and national competitors. Financial matters have traditionally been private. But we do need to acknowledge the changed climate.
In my experience, patients are
Information is good, as patients appreciate transparency in all aspects of their care
The process was simple and easy and assistance can always be found in PHIN’s engagement team
more likely to choose a consultant whose information is readily available. They will prefer the peace of mind of no cost surprises, and so a breakdown of your costs is important information you can provide a patient.
OK, so my initial experience with submitting data to the PHIN portal was not a positive one.
It was impossible for me to submit my fees due to faults in the system. I spoke to the team and let them know I was having difficulties and was assured that I would be able to update my fees soon.
Help available
A few weeks later, I tried again. This time, I was able to access my profile and add my fees to the PHIN website.
The process was simple and easy, and assistance can always be found in PHIN’s engagement team, who are very vigilant.
My favourite feature of the sys
Our front-page story in February reported on the start of specialists’ publication of fees
tem was the ability to submit only one set of fees that could be applied to all the hospitals I work at without any extra labour. What PHIN is doing can only be a positive step forward for the private healthcare sector. Information is good, as patients appreciate transparency in all aspects of their care.
PHIN’s publication of doctors’ fees is only the first step in this journey towards far greater pricing transparency in private healthcare. It is also asking hospitals to provide information about their package prices, giving patients a much better sense of the likely cost of treatment.
Consultants can submit their fee information to PHIN on the PHIN online portal: https://portal.phin. org.uk.
See ‘Better get clear on transparency’, Independent Practitioner Today, April, page 32
PROF FRANK CHINEGWUNDOH, Consultant urological surgeon at Barts Health NHS Trust and Harley Street, London
A look back through our journal’s archives of ten years ago reveals that although times change, some issues are not so new
A trawl through the archives: what made the news in 2009
Revalidamnation!!
Independent practitioners expressed fear that revalidation plans could jeopardise their practices’ future and leave them without the necessary support.
Doctors expressed alarm and dismay as a confusing picture emerged at a packed meeting to explain how the imminent compulsory five-yearly relicensing and recertification process would work for them.
Many, especially private GPs, feared they were at risk, as they would have to provide credentials ‘alien to their professional lives’ and would slip through the gaps in a system originally designed exclusively for the NHS.
Specialists on the floor of the Independent Doctors Federation meeting interjected with cries of ‘absolute farce’ and ‘ridiculous’ as a Department of Health speaker tried to explain how private doctors might work with the stillmysterious Responsible Officers.
The official seemed to think private doctors were employed by private hospitals and had no firm answers on how some could ever access a Responsible Officer.
One 58-year-old disgruntled doctor told the meeting he was thinking of retiring early due to the expected revalidation workload.
Doctors fail to insure
Many doctors’ companies were risking costly claims because they only had cover for clinical liabilities, a defence body warned.
A Medical Defence Union official said: ‘There’s no doubt they are at risk in terms of their corporate exposure. They will have individual indemnity, but the corporate body could be sued or pursued in the event of wrongdoing and this could put share-holders at risk.’
HMRC rigid on car tax
A legal test case was looking to clarify a dispute over whether consultants‘ mileage claims between NHS and private hospitals should be allowed.
Doctors had been furious to find a more rigid treatment of their claims – revealed in our first issue the previous June – meant they could face hefty back-payments of tax.
According to the Hospital Consultants and Specialists Association, the bill for some doctors amounted to over £35,000.
Note-taking lags behind state sector
The quality of doctors’ medical note-taking in the private sector was lagging behind that of the NHS, according to a defence body boss.
Dr George Fernie (right), head of the Medical and Dental Defence Union of Scotland’s medical division, said that although there had been improvements, medical records in private care had tended not to be as detailed as in NHS practice.
‘Often, particularly in the secondary-care sector, you will get notes that are just copies of the letters they have sent back to the GP,’ Dr Fernie said.
‘There are private healthcare providers that have improved things in recent years, but it is still not generally as good as the NHS. Even private GPs are not as good, as a general rule.’
Warning on ‘filler’ perils
Surgeons launched their campaign for women to see properly qualified professionals if they wanted cosmetic fillers – or face the risks.
A British Association of Aesthetic Plastic Surgeons’ (BAAPS) survey
found 38.5% of surgeons had seen one to three patients in the past year with complications from permanent facial fillers.
Nearly a quarter had patients who needed surgery to correct the problems. 81% of surgeons reported no serious complications stemming from temporary fillers. BAAPS warned of unqualified practitioners administering fillers incorrectly, patients being unaware of the risks and side-effects, and lack of regulation allowing UK use of unproven substances.
BMA eases on e-billing
The BMA was being described as ‘positive’ about electronic billing and the role it played in helping consultants run more efficient private practices.
Electronic bill-clearing company Healthcode was asked by the union to draw up a list of practice software vendors that offered consultants the electronic billing option.
The BMA was planning to review its guidance which had recently advised doctors they risked losing control of private practice if handing over billing to third parties.
SUBSCRIBE TODAY
Don’t miss out on what we report and advise in the future. Sign up for a £75 subscription today –consultants, GPs and practice managers can save £15 with a direct debit.
See page 24
ACCOUNTANT’S CLINIC: THE BUILDING BLOCKS OF ACCOUNTANCY
Susan Hutter continues with her A-Z of top tips
to of is for book-keeping top tips
THERE IS a tendency for many consultants and GPs to put the record-keeping on the back burner and only deal with it later, either themselves or using their personal assistants.
And even then this is only once a year when their accountants nag them for the information so that the annual practice accounts can be prepared.
Needless to say, this is not the best method of dealing with the record-keeping. Apart from any thing else, it is very time-consum ing if the records are dealt with only once a year. It becomes diffi cult to remember what some of the transactions relate to and, as a result, this means more work for your accountant, which will be reflected in the fees.
It is a good idea to use a book keeper, who can often be provided by your accountant, to attend at your surgery on a regular basis; for example, monthly or quarterly, depending on the size of your practice.
Apart from anything else, this will make it easier for you/your PA to check and collect outstanding debts both from uninsured patients and also insurance firms.
You can, of course, use someone to do the book-keeping who has no formal book-keeping training. This is not ideal, but can work as long as they understand how to reconcile all of the entries to the practice bank account and that
is for buying a business and buying into a business
Most book-keepers should be able to write up the records and reconcile the bank accounts
sale of consultants’ businesses, and also junior consultants buying into an established consultant’s practice.
Whether you are buying the whole business or just a percentage of it, you will need to look at financial information such as:
The latest finalised year-end accounts together with two previous years;
Up-to-date figures if the latest finalised accounts are more than three months old;
A breakdown of the balance sheet items and any exceptional items in the profit and loss account;
You will also need to be aware of legal issues regarding taking over a lease and also employees. There are strict regulations, particularly regarding the latter;
If you are buying a percentage of the practice, take care if either you do not have control and/or you end up in a 50/50 situation.
Susan Hutter (above) is a partner at Blick Rothenberg and part of the team that advises medical practitioners
Most book-keepers should be able to write up the records and reconcile the bank accounts. Also agree the PAYE figures and calculate what monies are due by and to the practice at the year-end.
Private practices are now becoming more sophisticated and many of them run on the lines of a small or medium-sized business as opposed to the ‘traditional’ sole practitioner.
This has led to the purchase and
Sometimes this is unavoidable. However, in these circumstances, a stalemate can arise in the event of a conflict, making it difficult to resolve.
It is sensible to put a shareholders’ or partnership agreement in place to cover as many potential problems as possible.
is also for breaking up
B is for breaking up
If one of the practice business partners decides to leave, it is important to ensure that the break-up goes as smoothly as possible.
As more consultants begin to work in groups – for example, partnerships, limited liability partnerships (LLPs) and limited companies – practice breakups have become more prevalent.
The main areas that the formal agreement should cover are:
Profit-sharing arrangements;
Expense sharing;
Capital contributions;
What happens to the ‘patients’ if one of the principals leaves;
What happens to the ‘goodwill’ of the retiring principal;
The notice-period.
You never need an agreement until you have a disagreement; so, bearing this in mind, it is vital to have a legal agreement in place
You never need an agreement until you have a disagreement; so, bearing this in mind, it is vital to have a legal agreement in place.
If the agreement is drawn up when everyone is in harmony, it is usually fairly straightforward.
Not all break-ups are acrimonious. Often, they occur because one or more of the partners are retiring from the profession or moving onto something new.
In the case of a principal who is leaving to either join another practice or set up on their own, the way that this is handled will very much depend on the agreement and the circumstances of the retirement.
Realistically, one cannot really force patients to stay with a doctor that they do not want to be with. Overall, practicalities must be considered.
One of the main issues is what a
retiring partner will be entitled to financially on leaving the practice.
In this case, the question that often arises is how to value the practice and whether the outgoing partner is entitled to be paid for their goodwill.
Due to this anomaly, many practices include a clause in their agreement that, on retirement for whatever reason, the retiree would only be entitled to undrawn profits and nothing further.
This is the simplest way of dealing with this situation and at least everyone knows where they stand.
As always, planning is key. Do take advice from financial and legal professionals who will assist you in trying to pre-empt any problems.
DRIVE TO IMPROVE SAFETY
Making safer devices
Not leaving the private healthcare sector to its own devices, the Independent Healthcare Providers Network has been giving evidence to the Government’s Medicines and Medical Devices Review. David Hare (right) reports
THE INDEPENDENT Healthcare Providers Network (IHPN) firmly believe that a ‘whole systems approach’, which fully incorporates the independent healthcare sector, is vital to improve patient safety.
So we were delighted to be invited to contribute when Health Secretary Jeremy Hunt announced a review last year into how England’s healthcare system responds to reports from patients about harmful side-effects from medicines and medical devices.
This followed the controversy around the use of pelvic mesh for urogynecologic procedures, where hundreds of women brought legal action after suffering severe pain and complications.
The review, chaired by Baroness Julia Cumberlege, is not seeking to re-do the work done by other reviews and expert working groups into pelvic mesh, Primodos and sodium valproate.
Rather, it is looking more widely at the healthcare system’s response to patients’ safety concerns raised over time.
Identify sooner
This includes seeing what could be done in the future to identify and acknowledge problems with medicines and devices more quickly and effectively, and how to ensure those concerns are acted upon in a more co-ordinated fashion.
The IHPN and a small number of operators from the sector were
Interestingly, Brexit has created a real impetus around the medicines and medical devices agenda.
It is vital that there is greater co-ordination between the many organisations that work on patient safety issues, with the independent sector being brought into the mix in a structured way
invited to give evidence to the review.
As expected, given the broad nature of the inquiry, the review panel’s questions covered a wide range of areas.
These have included :
Information-sharing in private and public sectors;
Data collection;
Management of complaints;
Adverse event reporting for both privately- and NHS-funded patients.
A video of the evidence session can be found on the inquiry’s website.
Communication fundamental
As with other patient safety issues, IHPN made clear in its evidence that communication across both the NHS and independent sectors is fundamental.
This can be as simple as ensuring, for example, that NHS Improvement uses registered managers and nominated individuals across the whole of the health system as the point of contact for key safety issues, with these details being regularly updated to ensure accuracy.
Equally, using common terminology across the independent sector to highlight concerns, and better aligning escalation processes with the NHS, will go a long way in helping to quickly draw out where there are safety issues across the health system.
Linked to this is having greater consistency in how healthcare providers catalogue and record interventions; something which would be helped by resolving the longstanding issue of interoperability of digital reporting systems across the two sectors.
It has led to much greater communication between the Department of Health and Social Care and the Medicines and Healthcare products Regulatory Agency (MHRA) with the sector as part of Brexit preparations. It is a level of engagement we would welcome continuing.
Likewise, there is more that can be done about ensuring better coordination across the NHS and the private sector around dealing with patients’ complaints.
This does not have to be about having the same mechanism.
A more holistic way
However, the lack of uniform rights for patients receiving private versus NHS care, the lack of a privately-funded advocacy service and published data on complaints management in the sector can make it more difficult to look at patient complaints in a more holistic way across the health system.
Ultimately, a whole-systems approach is needed around this issue. Increasing numbers of implantable devices are being used in modern medicine and more patients use both NHS and private healthcare.
So it is vital that there is greater co-ordination between the many organisations that work on patient safety issues, with the independent sector being brought into the mix in a structured way.
Here at IHPN, we are playing our part in encouraging independentsector providers to learn from each other through highlighting good practice on safety issues.
For example, we have been working with the Care Quality Commission to host workshops and conferences to help members understand what ‘safe’ is and how it can be improved.
Healthcare is complex and while simplifying and standardising systems is not always as easy as it seems, the approach in the independent sector – ‘everyone needs to own patient safety’ – is one that will pay dividends.
David
Hare is chief executive of the Independent Healthcare Providers Network
PRIVATE PRACTICE GROWTH GUIDE
Use your content to grow your practice
Content marketing: Jane Braithwaite (right) shows what it is and why you need it
THE PRIVATE PRACTICE GROWTH GUIDE IS DESIGNED TO GIVE INDEPENDENT PRACTITIONERS THE KNOWLEDGE AND TOOLS THEY NEED TO DEVELOP THEIR PRIVATE PRACTICE.
WHETHER YOU ARE AN EXPERIENCED PRIVATE DOCTOR OR FINDING YOUR FEET, THIS SERIES WILL SERVE AS A HELPFUL GUIDE TO THE EXCITING, AND SOMETIMES CONFUSING, WORLD OF HEALTHCARE MARKETING.
IF YOU have been reading our previous articles in The Private Practice Growth Guide series –these are available online to subscribers if you have not – you will be familiar with traditional marketing techniques and will have a firm grasp on digital marketing strategies.
Content marketing is a very different beast and varies from other marketing strategies. You are not seeking to push your product on your audience, but instead you need to connect with potential patients.
Invest some hours to help, support and educate them, and wait for them to seek out your services at their time of need and when they are ready to book.
It may at first seem counterproductive; after all, if the audience needs you, why haven’t they already found you? Haven’t you been told to be proactive and chase leads?
The answer is deceptively simple: you are sowing the seeds
that will eventually bloom into a dedicated audience who will actively seek out your services and fill your clinics.
Content marketing is a marathon and requires resources, consistency and devotion, but yields high rewards to the faithful. Content marketing has existed for hundreds of years, although the terms and methods have undoubtedly changed, and we will look at an historic example to help illustrate exactly what it is and how to use it.
Jan van der Heyden’s patented fire hose, 1672 ‘Fire, fire!’ they called as men and women gathered in rows with buckets full of water to tackle the blaze. This would have been a common sight in the period; effective but inefficient and requiring swathes of manpower, not to mention lots of buckets.
That is until a very clever chap,
Jan van der Heyden, worked with his brother to invent and patent a suction hose that could connect to water pumps and provide a targeted solution, not all too dissimilar to modern firefighting techniques.
You might think that such an invention would be an instant success, but it was decades before the fire hose was rolled out across the Netherlands.
Fortunately, Jan van der Heyden wasn’t just a brilliant engineer, he was a revolutionary marketeer and devised and implemented a content marketing strategy to help raise awareness of his invention. He combined the following methods to roll out his content marketing strategy:
The White Paper – Issued in 1677, van der Heyden published a paper that compared his fire hose to previous systems and demonstrated its functionality, citing practical applications.
You are sowing the seeds that will eventually bloom into a dedicated audience who will actively seek out your services and fill your clinics
The book – Published in 1690, van der Heyden’s Description of the newly invented and patented firehouse was to be the first book ever written about the fire brigade.
Far from just a treatise on his firehose, the book explored common causes of fires as well as the history of the formation and organisation of the Dutch fire brigade.
The visuals – As a talented artist, van der Heyden created countless artworks and prints to accompany his text and achieve a higher level of understanding of his firehose, its uses and applications. His artworks were reused well into the 18th century.
The social influencer – van der Heyden dedicated his book to Nicolaes Witsen, who served as Mayor of Amsterdam an astonishing 13 times between 1682 to 1706.
This clever ploy would lead to Mayor Witsen commissioning van der Heyden’s firehose across Amsterdam’s 60 districts.
The demos – van der Heyden set out on a tour to demonstrate the use of his firehouse across a multitude of public spaces across the Netherlands, literally bringing the product to his audience.
The results – The commercial success of van der Heyden’s firehose was unprecedented. It was the iPod of its day and when public shares in van der Heyden’s company were listed, it became the largest multinational in the world.
Tsar Peter the Great even paid a visit to van der Heyden in an ➱ p22
CHENIES MEWS IMAGING CENTRE
SPECIALIST MRI IN THE HEART OF LONDON
• Advanced Cardiac MRI
• 3T Neuro MRI
• MRI for patients with cardiac pacemakers
T: 0203 887 0566
E: referrals@cheniesmews.com
W: www.cheniesmews.com
attempt to lure him to organise the Russian fire brigade.
Perhaps without ever knowing it, van der Heyden hit the mark with his content marketing strategy and helped define its very intention: to attract and assist.
Compare that with traditional marketing and advertorials, which are designed to interrupt, disrupt and distract, and you will come to understand just how content marketing differs from other strategies.
But how can you, as an independent practitioner, apply this strategy to your practice and grow your patient numbers?
Applying content marketing to your practice
Jan van der Heyden’s belts and braces approach to marketing provided a multi-channel strategy with a shared message that addressed a problem and provided a solution.
Content marketing today utilises a range of digital technologies that
are far easier to produce and less costly and we can apply these to his strategy in a way that you can emulate in your practice.
The White Paper – Many independent practitioners are actively engaged in research and routinely write journal publications that can be shared online.
If you are not currently doing so, and lack the time to hit the books, your ‘white paper’ could instead be a simple blog article or even just engaging in a discussion with peers on LinkedIn while you commute home.
The book – Once you write your short pieces, you can collate these into an e-Book and make it available online. It’s a great way to recycle content and make the most of the time you invest in your writing. It is common practice that websites prompt users to provide their name and email address in
return for free downloads of e-Books, which can be used to create marketing lists for the future, though this is by no means essential.
If you do request this information, make sure you’re familiar with General Data Protection Regulations on obtaining and storing personal information.
The visuals – You don’t need to be an artist to produce eye-catching infographics and engaging videos to promote your practice.
We all learn in different ways and your audience might get more from a 30-second video of you talking about a condition or treatment than they could from reading an article or book.
There are many options for resourcing visuals and video content, or you could simply record a clip from your phone. If you do create a video, take the time to add subtitles. This won’t just help the audibly impaired but will enable
people to watch your clips on their devices even if they don’t have headphones.
The social influencer – Physiotherapists, nutritionists and cosmetic surgeons were some of the earliest adopters of social media within the medical field and many have attracted tens of thousands of followers.
Engage with them and see if you can mutually benefit from cobranded content that complements your individual services. Start by identifying and engaging social influencers with smaller audiences and grow exponentially. Celebrity endorsements are also powerful but apply the same logic here. Robert Downey Jr is unlikely to endorse your clinic – although ‘I am iron-deficient’ would be a great campaign – but you may gain traction with digital radio hosts, yoga and well-being coaches, as well as other bloggers. Start small, grow big.
Independent Practitioner Today
The demos – Social media has connected many people with a shared experience of medical problems and has helped them to foster communities where they can provide advice and make un biased recommendations for medical practitioners and centres. If you can demonstrate to these communities that you provide understanding, help and support, they will do your marketing for you. Consider inviting an influential member, such as a group moderator, into your clinic and show them what you do best or invite them to participate in a video or blog to help convey a meaningful message. The possibilities are endless!
The results – Traditional marketing strategies of assembling target lists, approaching targets with a direct message and monitoring the rate of return allow for quantifiable results.
For example, you target 50 GPs
and tell them about your treatment and then count how many of those GPs referred patients to that service.
Measuring the results of a content marketing campaign can be less straightforward, but can be measured in terms of social media followers, likes and shares of posts, as well as engagement with your content such as comments and questions.
In our next article, we will look at email marketing and how you can build an effective campaign without breaking the bank. Take a mental note over the next few weeks of the emails you found eyecatching and engaging, and which ones went straight to your trash.
Cloud-Based Electronic Patient Records and Patient Portal
ESSENTIAL TIPS FOR A SUCCESSFUL CONTENT MARKETING CAMPAIGN
➣ However you apply content marketing to your practice, it is of vital importance that you be consistent as to when you post your content and that you spend time promoting your content.
➣ It is advisable to apply the 80:20 rule to your promotions and content writing, so if you spent half an hour writing a blog post, spend two hours promoting and sharing the content online.
➣ It might seem like a lot, but it’s an effective way to ensure your content reaches your target audience and doesn’t get lost among a sea of content.
➣ Plan your content marketing campaign carefully and also ensure that your infrastructure is in place to respond to inquiries and make appointments before you start posting content.
➣ Above all, remember that it takes time to build and retain an audience. Be patient and don’t be disheartened if you struggle to grow your number of followers in the first few weeks or months.
➣ Take note of what works well and what doesn’t make much impact and keep this well in mind when you create your next piece of content.
Jane Braithwaite is managing director of Designated Medical, which offers business services for private consultants, including medical secretary support, book-keeping and digital marketing Call to arrange a demo to see how we can help meet your needs! Stuart Tebbutt 07891 217313
eClinicalWorks is a leader among independent, ambulatory practices, covering primary care and more than 50 specialities.
• Integrated Electronic Patient Record (EPR) and Clinic Management
• Comprehensive documentation of patient encounters
• Data analytics to deepen your understanding of your patients
• Streamlined workflows improve the provider and patient experience
SPECIAL OFFER – £15 direct debit saving
TO RECEIVE OUR TEN ISSUES A YEAR
Dear Reader,
Subscribing to Independent Practitioner Today is the only way you can be sure you will see every issue and have the option of reading us online using our special page-turnable edition. Don’t risk missing out. Our personal subscription for doctors and managers is only £90 a year and £210 for organisations. But you can cut this to just £75 and £180 respectively if you pay by direct debit.
So take advantage of this offer now for our unique business journal dedicated to supporting you in your private practice. We’re confident your subscription will repay itself many times over!
Editorial director
APPLICATION FOR SUBSCRIPTION
Instructions to your Bank or Building Society to pay Direct Debits
Name and full address of your bank/Building Society
To: The Manager Bank/Building Society
Address Postcode
Banks and Building Societies may not accept Direct Debit instructions for some types of account
Please also send a copy of your letter to us.
Shops have lessons
Part
1: Is your working for you?
Our new series by Nick Butcher and Dr Nick Hayward considers the role of design in healthcare environments and how it can be used to positively affect user experiences, create loyalty and ultimately improve organisational and patient outcomes
DEVELOPMENTS IN science, technology and design over the past decade have shaped the way we live our lives and, more importantly, our expectations.
Whether we are out shopping, visiting an entertainment centre or attending a GP appointment, the level of customer experience that we now expect is on the rise.
And it is not just retailers that have to work harder to meet and exceed these expectations. The healthcare sector is growingly under the same spotlight.
Medical advances may be better than ever, but GPs, hospitals, den-
tal clinics and cosmetic surgeries are holding themselves back by far too often failing to offer a sufficiently clear, enjoyable experience for patients and visitors.
In the last 20 years, we have seen an extraordinary level of change in retail at Beyond London, our branding and design agency working primarily in retail and consumer environments.
Connecting with customers
The industry has become extremely sophisticated and has had to evolve at a pace to keep up with the ever more demanding con -
Nick Butcher
Dr Nick Hayward
for private practice
sumer expectations. Technology has driven new ways of connecting with customers and those organisations that have failed to change have been lost.
Those that are succeeding – and there are more of them than the media portrays – have embraced new channels and are offering their customers a level of physical experience never previously imagined.
Many of the learnings from the retail industry equally apply to the healthcare sector. Although very different, the benefits of affecting visitor behaviour can be the same.
Design can help to reassure and soothe people. It can guide them through a calm, comfortable and even relaxing environment.
Careful design can also be exciting and stimulating. It can be used to inform and engage patient and service users with your brand and help you to build a trusting relationship.
These concerns significantly affect the ongoing success and sustainability of healthcare activities.
This series of articles will look at some of the design tools we use in more detail and can hopefully be used to help provide the high levels of service that patients and visitors expect and thus drive loyalty, satisfaction and even speedier recoveries.
Good branding
Branding is often misunderstood as being just a name or logotype, but it is so much more.
Good branding will help communicate everything your organisation believes in. Trust, devotion, reassurance and recognition are all driven by clear and consistent branding.
Good brand communication is often a subconscious understanding.
When a series of well-branded communications, environments and signage come together, then
people perceive a professionalism that is reassuring and trustworthy. These are important values when someone is placing their health in your hands.
A good brand will have many layers to it. One way of representing these layers is with a brand pyramid.
At the base of the pyramid are the tangible attributes and services that you or your brand offer.
Next are the functional benefits to the user, then there are the emotional benefits, then the personality of your brand
And finally at the top is ‘the essence’, which is a short and succinct summary of what the brand is about.
Emotionally supported
As a healthcare example, a hospital website will detail the various services and professionals within, through pictures and prose. Then captions and weblinks for related services may help patients and visitors to feel emotionally and psychologically supported.
The hospital ethos is often then communicated with personality through logos, slogans and pictures that share the caregiver’s values of the whole organisation.
These may include images of a diverse staff group with happy patients in modern facilities as ways of illustrating empathy, trust and technical capacity respectively.
Finally, the home page may state the key values and objectives of the hospital and its staff overall – the essence – to present a welcoming and engaging summary.
If these building blocks can be defined and agreed internally, then they can be manifested through design.
This may well start with a logo which should reflect all these attributes, but the building blocks can equally be reflected in many other ways.
The brand pyramid: a good brand will have many layers to it
These ways include the manner of the interactions between staff and service users on arrival, well written and designed patient information media or how areas such as the toilets and car parks are accessed.
These are all user touchpoints and while some are very physical, many can go consciously unnoticed by a visitor, but subconsciously they still create
experiences that could be great or less so.
Even if subconscious, it is the positive understanding that can really benefit people in healthcare environments.
If the experience in a wellbranded journey is simple, clear, professional, well considered, thoughtful and beautiful, patients and staff will feel a lot better than
➱ p28
The Accountancy Solutions
A dedicated accountancy firm established for over a decade, we understand the individual needs of medical professionals and work closely with them to develop a personal plan. You are never just a number to us, and we pride ourselves on our bespoke services that make us stand out from the crowd. Contact us for free advice and no-obligation quote.
when they conversely experience poorly branded healthcare interactions that are confusing, stressful, ill-considered, cluttered and ugly.
An article in the Harvard Business Review called ‘When the customer is stressed’ 1 researched highlyemotive services that elicited intense feelings.
A focus group was held with breast cancer survivors who were
PRACTISING PRIVILEGES NOW AVAILABLE
asked how they would design the centre at Bellin Health Systems in Green Bay, Wisconsin, US, if money was no object.
The overwhelming result from many was that the centre should not be located in the main hospital but as a stand-alone unit. They found the main hospital ‘complex, scary and inconvenient’.
Stress burden
If patients have to deal with unclear signage and complex floor layouts, then their stress burden within already difficult emotional circumstances can have a major negative health impact.
The tools for good branding can
Carefully designed and consist-
Clever use of colour;
A good tone of voice for communication;
Environmental use of colours and finishes that complement the brand colours.
Even sound and acoustics play a key part in building an experience that is consistently ‘on brand’.
A brand logo is essentially a way of summarising your brand into an easily recognisable and hopefully memorable marque. There are many globally-known logos and they tend to be simple. Think Nike and its ‘swoosh’ tick.
Good branding can be as important for internal use as it is for visitors and service users. All members of an organisation need to understand who they are working for, what they stand for and know how their activities should be communicated to the outside world.
The ethos of an organisation can be manifested through design that, if done coherently, can enhance the experience of patients, staff and visitors
Clarifying an internal understanding of these concepts can be a major achievement and will pay dividends in the long term.
Michael Lee Stallard, author of Connection Culture: The Competitive Advantage of Shared Identity, Empathy and Under standing at Work, 2 found that when employees feel connected to the place and people they work with, their body works more harmoniously, allowing them to physically work at a higher rate and become more productive.
Differentiate services
On the flip side, when employees feel disconnected from colleagues or the organisation, there are often many implications for their mental and physical well-being.
Good branding is about stand -
ing out from the competition and as the health industry evolves over the next decade, there will be an ever greater need to differentiate services and to clearly communicate why your healthcare offering will be the one to choose.
Service users may have a limited attention span when using the internet, so conveying the right impression quickly and succinctly is a good pay-off from good branding.
As a design agency, Beyond works with both small and large organisations and while the issues for these are often the same, making branding changes is much quicker and easier for smaller projects.
An initial design audit of branding and its applications can reveal where improvements can be made and this can then create a priority
list of areas to focus on and potentially redesign.
Branding may include healthcare websites, printed brochures, entrance signage, welcome desks, uniforms, seating areas, corridors, toilets, treatment rooms, staff activities and many other key visitor touchpoints.
All are important and if all are communicating the same high level of design and consideration, then the experience should be a great one.
Our experience from auditing shopping centres is that it only takes one bad experience – often the car park or toilets – to influence how users remember their visit and their decision to go elsewhere next time.
A strong healthcare brand is thus healthy for us all.
It only takes one bad experience –often the car park or toilets – to influence how users remember their visit and their decision to go elsewhere next time
Nick Butcher is creative director of Beyond London. Website: www. beyondlondon.com
Dr Nick Hayward is a neuroscientist and medical technologist with a PhD in neurobiology and medical imaging development. He also works clinically as an NHS registrar/resident doctor in anaesthesia
References
1. When the Customer is Stressed, by Leonards L. Berry, Scott W. Davis and Jody Wilmet. https://hbr.org/2015/10/ when-the-customer-is-stressed
2. Connection Culture: The Competitive Advantage of Shared Identity, Empathy, and Understanding at Work by Michael Lee Stallard
Next issue: The healing power of colour
The tools for good branding can be simple: carefully designed and consistent fonts, clever use of colour and a good tone of voice for communication
Make money, not noise
The challenge for independent practitioners is how to make the best use of their data so that it becomes a valuable resource and not meaningless digital ‘white noise’.
Information needs turning into your biggest asset, says Kingsley Hollis
WE ARE now all so used to going online for answers that it is astonishing to think how recently we were using reference books, paper records and making phone calls to access the information we need.
And yet none of this would have been possible before 1989 when CERN scientist Sir Tim Berners-Lee submitted his treatise ‘Information Management: A Proposal out of frustration at the difficulty of sharing the experimental data held on different computers’.
His idea for a system of connected information that users could access and search developed into the World Wide Web and was an essential prerequisite in the development of the digital economy.
As we celebrate the web’s 30th anniversary this year, it is worth reflecting on how developments have transformed independent practice.
One significant change is the dramatic increase in the amount of data that we now produce.
According to one estimate, there was an eight-fold increase in the global volume of data in the five years between 2010 and 2015 and this is forecast to grow exponentially in the years ahead.1
The challenge for practitioners is how to make the best use of their data so that it becomes a valuable resource and not meaningless digital ‘white noise’.
In my view, information can
only be a practice asset if it meets the following five criteria:
1 Accurate
Data errors are often timeconsuming to identify and fix and frequently costly. For example, invoices with incorrect patient details could be rejected or queried by the private medical insurer, which will delay payment and harm cash flow.
In line with the GIGO principle (‘garbage in, garbage out’), problems typically begin when new details are added to the patient database, so it is important to have a robust system in place to ensure this information is checked at the outset.
Users of Healthcode’s practice management service can validate patients’ insurance and demographic details online against the database of participating insurers to ensure they get it right first time.
2 Complete
There are few things more frustrating than starting a task and then realising you don’t have everything you need.
For instance, when applying for insurer recognition, consultants are typically required to submit a range of supporting documentation, from details of current NHS posts, references and proof of indemnity.
If you are one of the 13,000 practitioners who have a profile on The Private Practice Register, you already have all this information in one place.
This eliminates duplication of effort because you can apply to multiple insurers simultaneously and it makes it easier to keep your credentials up to date, ensuring that hospitals and insurers can view accurate information about you, in line with point 1 above.
3 Timely
Communications technology has accelerated the pace of life and can put us under pressure to act quickly, but that is challenging if we aren’t in a position to make an informed decision.
When it comes to financial decisions in particular, assessments based on outdated information can be costly. That is why one of the most important features of any practice management system is the ability to produce a wide range of reports in real time on key performance indicators such as chargeable activity, payments received, outstanding debtors and patient accounts.
4 Secure
Following the Data Protection Act 2018, practices are legally obliged to have appropriate processes and technology in place to protect data, such as encrypting devices and only working with companies that provide sufficient guarantees about security measures.
Users of Healthcode’s billing and practice management soft -
ware can be confident that we have the necessary controls in place to protect their sensitive patient-identifiable data.
Our systems are secured in accordance with internet banking conventions, housed in a secure UK location and only accessible via encrypted network connections.
We achieved ISO/IEC 27001: 2005 accreditation in 2009 and have maintained it since and we are also certified by the national Cyber Essentials scheme.
5
Shareable
As Sir Tim Berners-Lee pointed out, effective collaboration means sharing information, but incompatible systems and security concerns make it difficult to collaborate in this way and are an obstacle to workflow efficiency.
By contrast, Healthcode has always championed an interoperable approach, developing a secure online platform on which practitioners can manage their data and connect seamlessly with other private sector stakeholders.
For example, our Secure Messaging application allows practices to securely share sensitive and confidential files with individuals or specifically created contact groups on a global directory of private hospitals, insurers and other providers.
Whether you are just starting out or trying to grow your private practice, the way you manage information holds the key to success.
Technology gives us access to a mass of unstructured data but we have to have the tools in place to ensure that we can make sense of it and use it in the right way.
Reference
1. The economic value of data: discussion paper, HM Treasury, August 2018. www.gov.uk/government/ publications/the-economic-value-ofdata-discussion-paper
Kingsley Hollis is head of business development (ePractice) at Healthcode
GUIDE TO GETTING PAID
How to win at billing
In today’s ever more competitive environment, it is important to continually review and improve your practice. Simon Brignall shares ten simple rules to follow to ensure that your practice stays ahead of the pack
1
Regularly review the way your practice is billing your work. This is to ensure you remain compliant with the ever-changing rules and regulations from private medical insurers and that you understand the implications that these could have on your income. A good example of this is that a lot more insurance companies are enforcing the six-month deadline for submitting your invoices. This means you could miss out on income if you fall behind on your billing.
2 Make sure your practice keeps up to date with the latest changes to Clinical Coding and Schedule Development group (CCSD) codes for your specialty and how the insurers have chosen to deal with these.
3
Take the time to review your fees on a regular basis.
This is particularly important if you bill to insurance guidelines, as these are changing all the time.
The current trend towards consolidation in the private medical insurance sector has meant that the price list of the insurance company that acquires the medical insurance business of another company are often introduced to replace their existing arrangements.
4
Make sure that your work is invoiced in a timely manner.
This will ensure you have consistent cash flow and will assist with your debt reduction. There is also the additional benefit that any billing issues are picked up more quickly.
Remember that the invoicing process is a reflection of the professionalism of your practice.
5 Ensure that your fee structure is transparent.
Whatever pricing structure is in place for your practice, check that it is clear and that your patients are made aware of it before commencing treatment.
This is very important in the current climate with the drive to more transparency around fees. There is also a benefit from a billing perspective, as there is no room for ambiguity when it comes to settling the bill.
6
Implement a robust process for chasing outstanding invoices on a consistent basis and make sure it is adhered to.
Designate someone to take ownership of this task so that you can be confident that it is being carried out in a routine and timely manner. In our experience, this is the only way to ensure that your invoices are paid in full and to make sure that you manage both your aged and bad debt.
7
The practice should have good visibility around its aged debt. You should be aware of who the problem payers are so that you can decide if you want to continue treating them while they still have outstanding invoices, as this could potentially be making the problem worse.
8
Check that you have access to good management informa-
tion on the practice and take the time to review it.
This should include data on where your patients are referred from, as well as what percentage of your new patients come from each private medical insurer, self-pay, embassies, solicitors and other payees.
This will allow you to make informed decisions about your practice for the future. Practices are evolving all the time and it easy to make the wrong decisions based on out-of-date data or incorrect assumptions.
9
Consider time and task management. Has your practice grown beyond your current arrangements?
Are you spending too much time on tasks that can be or should be
Remember that the invoicing process is a reflection of the professionalism of your practice
PROBLEMS WITH THE TAX MAN?
done by someone else? Successful consultants spend as much time as possible focusing on their core skill set – which is treating and looking after patients – to maximise their income.
10
If you feel that your practice is weak in any of the areas that I have outlined, then you need to decide what action to take and consider if you should outsource this crucial element of your practice to a professional billing company instead.
Simon Brignall (right) is director of business development at Medical Billing and Collection
HMRC tax investigations and disputes create difficult and stressful times.
As an award winning firm of tax experts, our highly experienced partners specialise in resolving problems relating to tax investigations and disputes with HMRC.
To find out, in confidence, how we can help call 0800 734 3333.
‘Here to help. Not to judge.’
Why hard work goes into doing nothing
Why a ‘set-and-forget’ investment approach is never just that. Dr Benjamin Holdsworth on the behind-the-scenes work your adviser should be doing
IN MOST walks of life when you employ a professional or craftsman, you expect a little bit of action for your money. However, this generality does not always apply.
Take the case of a GP, for example, where a patient comes into the surgery with a sore throat and flu-like symptoms.
Many GPs feel under increasing pressure from patients to come up with some ‘scientific’ solution –such as the prescription of antibiotics – to their ailments, and some patients feel cheated when the advice they receive is simply to swallow a couple of paracetamol tablets and to take it easy for a day or two.
Do we doubt the training, experience and wisdom of the GP because of the advice we receive? Hopefully not; after all, science confirms that antibiotics will not work on viruses.
Evidence-based investing
The same pressures apply to advisers when it comes to investing. Adopting an evidence-driven, systematic approach to investing can seem as if a portfolio, once set up, is left to roll on in a ‘set-and-forget’ manner.
If correctly created at the outset, your portfolio is likely to look largely unchanged when you look at your valuation statement in terms of its structure and the products through which the investment strategy is implemented in practice.
If one of these products catches your eye, as it has not done as well
as the others, or the portfolio as a whole is down, it might be tempting to ask: ‘What are you going to do about it?’
The answer is probably going to be ‘nothing!’
At Cavendish, our clients are familiar with us telling them that:
They should stay calm at times of market jitters;
We will rebalance their portfolio on a regular basis;
Returns come from the markets not humans;
Costs really matter;
A sensible long-term, diversified portfolio structure is key;
They should avoid looking at their portfolio too often.
We advise all of these things because this is what the evidence tells us will give them the greatest chance of experiencing a good investment outcome.
Challenging the status quo
The seeming lack of investment activity on a portfolio from one period to the next belies the considerable time, effort, discipline and fortitude that goes into achieving this for our clients.
The firm’s Investment Committee sits at the heart of this effort and one central question drives its efforts: does the investment approach adopted still represent
best practice, based on the latest evidence and theory available to us?
The Investment Committee will be making sure that client portfolios remain robustly structured and the long-term strategy is executed using best-in-class products. The ongoing oversight is both regular and robust. Risks and opportunities on the horizon are keenly observed.
The fortitude and discipline to deliver ‘not much needs to be done to your portfolio except for rebalancing’ advice, comes from a rigorous process of ongoing challenge to the status quo.
Investment theory, academic research and empirical evidence, robust primary thinking and a good dose of common sense provide the foundations required to run a long-term, strategic and systematic approach to investing.
Without this deep certainty and quiet confidence, the noise,
It is sometimes hard to do nothing, but it is usually the right thing to do
excitement and sometimes pain faced by investors can result in too much action, much of it inevitably of the knee-jerk, emotional variety. It is sometimes hard to do nothing, but it is usually the right thing to do.
Staying calm
It takes strength to stay calm at times of market crisis, to remain invested and to rebalance the portfolio, if necessary.
It takes discipline not to:
Chase ‘hot’ parts of the markets
– bitcoin, gold, tech stocks, China
– or ‘hot’ managers;
Restructure the portfolio to take advantage of or avoid short-term opportunities and challenges –Brexit, China trade wars, low yields on high-quality bonds;
Give up on certain parts of the diversified portfolio that happen to be suffering at present – value stocks and emerging markets.
If you have chosen the right financial planning partner, you should feel reassured that when you open your latest valuation report, despite the lack of activity on the surface, the Investment Committee continues to paddle furiously behind the scenes.
In the immortal words of the investment legend and author Charles Ellis: ‘In investing, activity is almost always in surplus.’
Perhaps we should amend this to: ‘In investing, activity is – except
for the Investment Committee –almost always in surplus.’
Dr Benjamin Holdsworth (right) is director at Cavendish Medical, specialist financial planners helping consultants in private practice and the NHS
The content of this article is for information only and must not be considered as financial advice.
Cavendish Medical always recommends that you seek independent financial advice before making any financial decisions.
Levels, bases of and reliefs from taxation may be subject to change and their value depends on the individual circumstances of the investor. The value of investments and the income from them can fluctuate and investors may get back less than the amount invested.
EXPERT ADVICE YOU CAN TRUST
EXPERT ADVICE YOU CAN TRUST
SPECIALIST
SPECIALIST MEDICAL ACCOUNTANTS
Since starting in the mid 1970’s Sandison Easson has continued to grow and is one of the largest independent medical specialist accountants in the UK.
Since starting in the mid 1970’s Sandison Easson has continued to grow and is one of the largest independent medical specialist accountants in the UK.
Since starting in the mid 1970’s Sandison Easson has continued to grow and is one of the largest independent medical specialist accountants in the UK.
Sandison Easson acts for medical professionals throughout all stages of their career and has clients in almost every town in England, Scotland and Wales.
Sandison Easson acts for medical professionals throughout all stages of their career and has clients in almost every town in England, Scotland and Wales.
Sandison Easson acts for medical professionals throughout all stages of their career and has clients in almost every town in England, Scotland and Wales.
We provide the usual services you would expect from an accountant such as preparation of your accounts and tax declarations but offer so much more including advice on:
We provide the usual services you would expect from an accountant such as preparation of your accounts and tax declarations but offer so much more including advice on:
We provide the usual services you would expect from an accountant such as preparation of your accounts and tax declarations but offer so much more including advice on:
• Setting up in Private Practice
• Setting up in Private Practice
• Setting up in Private Practice
• Developing your Private Practice
• Developing your Private Practice
• Developing your Private Practice
• Tapering of the Annual Allowance
• Tapering of the Annual Allowance
• Tapering of the Annual Allowance
• Lifetime Allowance planning
• Lifetime Allowance planning
• Lifetime Allowance planning
• Personal Allowance planning
• Personal Allowance planning
• Personal Allowance planning
• Reviewing your PAYE Coding Notices SPECIALIST MEDICAL ACCOUNTANTS
• Expenses that you can claim and those you cannot
• Expenses that you can claim and those you cannot
• Expenses that you can claim and those you cannot
• Minimising your tax bills
• Minimising your tax bills
• Minimising your tax bills
• Reviewing your PAYE Coding Notices
• Reviewing your PAYE Coding Notices
ACCOUNTANTS T 01625 527 351 E info@sandisoneasson.co.uk
‘Don’t tell me the risks’
Getting informed consent is at the forefront of doctors’ minds –but how can you best manage a scenario where a patient doesn’t want to know the risks? Dr Gabrielle Pendlebury advises
CONSENT HAS evolved in the last decade due to some high-profile and costly cases. Doctors need to make sure they gain informed consent and provide patients with the relevant information so they can make an informed decision.
Gaining informed consent also allows the doctor to protect their professional welfare, should they need to.
But what happens when a patient puts their full faith in their treating doctor and feels they don’t need to know the risks? When, if ever, is there scope to ignore consent?
Previously, medical paternalism trumped any notion of patient autonomy. In Moyes v Lothian Health Board in 1990, Lord Caplan
gave a summary of how the law believed the doctor knows best:
‘When the patient entrusts himself to the doctor, he expects, and is entitled, to be kept fully informed about decisions which are to be taken and which may concern his welfare, but the paramount expectation is that the doctor will do what is best to care for the patient’s health ...
All changed ‘The doctor, with his own clinical experience and the benefit of the experience of other practitioners, is best able to form a judgement as to what the patient can safely be told in the exercise of medical care.’
Montgomery v Lanarkshire Health Board in 2015 changed all of this, of course. The Supreme Court appeal held that an adult person of sound mind is entitled to decide which, if any, of the available forms of treatment to undergo, and his or her consent must be obtained before treatment interfering with his or her bodily integrity is undertaken.
The doctor is therefore under a duty to ensure that the patient is aware of any material risks involved in any recommended treatment and of any reasonable alternative or variant treatments. The test of materiality is whether, in the circumstances of the particular case, a reasonable person in
PRACTICAL TIPS
1
Two-way dialogue
Whether at a consultation, a GP appointment or in the mix of a surgical procedure, practitioners will need to engage in a two-way dialogue. Decisions should be made on a collaborative basis.
2
Adequate time set aside
In order for the consent process to be meaningful, more time will need to be found, perhaps over more than one consultation, to explore why the patient does not wish to know risks and give the patient time to digest the information.
3
Clear explanation of risks and alternatives
Not all doctors are eloquent and can clearly explain, but this is of paramount importance. The risks of the proposed procedure need to be spelt out clearly. The reasonable alternatives must also be explained, including the option of having no treatment at all. Again, the risks of the alternatives must be explained.
4
Tailored to individual patient, who is key
Medical records – any relevant medical conditions?
Any increased risk factors?
What about the psychological state of the individual?
Family circumstances?
Has the patient understood?
5
Make full notes:
Document clearly and comprehensibly, as you may need to justify your decision and actions at a later date
Specifically record the consent process – consent, advice and patient’s responses
Record both sides of the conversation.
Following the above tips will protect your professional welfare. However, emotions can intervene in issues of this nature and, in those cases, it is always helpful to discuss the matter with your indemnifier, as they can assist in developing a constructive plan that will meet the patient’s needs.
the patient’s position would be likely to attach significance to the risk, or the doctor is, or should reasonably be, aware that the particular patient would be likely to attach significance to it.
There are some exceptions to this test:
➲ The doctor is entitled to withhold from the patient information as to a risk if he or she reasonably considers that its disclosure would be seriously detrimental to the patient’s health.
This exception should not be abused and the court will be slow to find that a doctor was entitled to withhold information except in exceptional circumstances. This is known as the therapeutic exception.
➲ Where a patient requires treatment urgently, but is unable to make a decision, as they are, for example, unconscious, consent need not be obtained.
In certain circumstances, a patient may feel anxious about the proposed treatment and may decline to hear about the risks. This can place the clinician in a difficult position, as in order for an individual to provide valid consent for a treatment, he or she must be informed.
As noted above, the clinician is required to provide:
Information about the nature of the treatment;
Expected benefits;
Material risks and material sideeffects;
Alternative courses of action;
The likely consequences of not having the treatment.
If the patient refuses to hear about the risks, the decision will not be informed and their consent may not be valid.
The GMC’s guidance on ‘Consent’ gives a number of reasons for not sharing information with patients:
‘If a patient asks you to make decisions on their behalf or wants to leave decisions to a relative, partner, friend, carer or another person close to them, you should explain that it is still important that they understand the options open to them and what the treatment will involve. If they do not want this information, you should try to find out why.
‘You must give [patients] the information they need in order to
give their consent to a proposed investigation or treatment.
‘If a patient insists that they do not want even this basic information, you must explain the potential consequences of them not having it, particularly if it might mean that their consent is not valid. You must record the fact that the patient has declined this information. You must also make it clear that they can change their mind and have more information at any time.
‘You should not withhold information necessary for making decisions for any other reason, including when a relative, partner, friend or carer asks you to, unless you believe that giving it would cause the patient serious harm. In this context, “serious harm” means more than that the patient might become upset or decide to refuse treatment.
‘If you withhold information from the patient, you must record
your reason for doing so in the patient’s medical records, and you must be prepared to explain and justify your decision. You should regularly review your decision, and consider whether you could give information to the patient later, without causing them serious harm.’
The GMC’s 2013 guidance included that a doctor should ‘work in partnership with patients. Listen to, and respond to, their concerns and preferences. Give patient information they want or need in a way they can understand. Respect patients’ rights to reach decisions with you about their treatment and care’. Note the reference there to ‘with you’. This is a collaborative process.
Dr Gabrielle Pendlebury (right) is a medico-legal consultant at Medical Protection
CONSULTING ROOMS AVAILABLE
l Modern clinic over 3 floors open Monday – Friday
l CQC-registered
l Multi-specialty outpatient services
l State-of-the-art ophthalmic equipment and lasers
l Diagnostic Endocrine & Cardiac procedures
l Mini theatre for Dermatology & Ophthalmology
l Pharmacy
KEEP IT LEGAL: LITIGANTS IN PERSON
Patients’ DIY justice
The additional challenges of defending a claim when the patient is not legally represented are explored here by Niloo Bozorgi (left). She hopes the courts may becoming a little less lenient towards such litigants
A CLAIM IS always distressing to face and time-consuming to deal with.
Your insurer or medical indemnity provider will assist you or instruct lawyers to advise you. But you will have to provide them with input:
An explanation of the medical records;
Your recollection of what happened;
Your opinion of the allegations made against you.
At various stages throughout the process of defending or settling the claim, you will find this time-consuming; and even more so if the claimant – your patient – is not legally represented.
A litigant in person (LiP) is the term used to describe an individual who represents themselves in legal proceedings.
This is not a new phenomenon in civil law. However, since the cuts to public funding for legal costs and the increase in the jurisdiction of the ‘small claims’ court, there has been a sharp rise in the number of LiPs.
This applies to clinical negligence claims too, in which we are increasingly finding claimants/ patients bringing claims without the benefit of legal representation.
This has a number of disadvantages.
Nearly all cases brought in clinical negligence in which the claim-
ant is represented by a solicitor are funded by a conditional fee agreement (CFA), commonly known as a ‘no win, no fee’ agreement.
Before entering into such an agreement, the solicitor will evaluate whether the case is strong enough to justify taking it forward. This is in their own interests, as they will not be able to recover their costs should the case be without merit.
There is no such analysis when claims are brought by LiPs, and therefore there is a greater chance of an unmeritorious case being pursued.
Heightened emotion
This is only one of the difficulties with claims brought by LiPs. There are others.
Without a solicitor acting for the patient to act as an additional buffer, there is often a heightened degree of emotion in the process and a greater likelihood of personal comments against the defendant doctor in correspondence, which can be distressing.
The LiP must identify the correct medical expert in the right clinical area of expertise who undertakes medico-legal reporting and then instruct the expert to report on all relevant issues and interpret their findings so that they can bring a claim without any specialised knowledge or previous experience.
There is no analysis [by a lawyer] when claims are brought by litigants in person and therefore there is a greater chance of an unmeritorious case being pursued
This is very difficult and, as a result, claims brought by LiPs are often poorly drafted and therefore the defence is put in the position of responding to a case in which the allegations are not at all clear. This leads to greater uncertainty about the likely outcome of a case.
Access to justice
The principle of fair access to justice dictates that a just and fair outcome should be achieved regardless of whether a party is legally represented.
Guidance issued in March 2018 by the Judicial College cautions judges against viewing LiPs as an unwelcome problem for the courts.
Indeed, in order to ensure justice and fair outcomes, the courts have historically shown a degree of leniency to LiPs that has not been granted to represented parties.
In one memorable case, the majority in the Court of Appeal
felt that it was too draconian to deprive a LiP of his right to trial even though he was unable to formulate his cause of action for the judge and the defendant, despite being given repeated opportunities to do so.
Often LiPs attend hearings having failed to comply with procedural rules governing litigation or a court direction and the courts have nevertheless attempted to plough on with the case – something that would not be countenanced if the claimant was legally represented.
One of the consequences of this is that the legally represented party in effect subsidises the LiP by bearing the cost of preparing bundles, drafting additional court documents and dealing with what can be an abundance of informal and unfocused emails from the LiP. At the end of this process, even if the clinician is successful and is awarded costs – rare enough these
days – there is the risk that the LiP may not be able to pay the costs. In the case of medical practitioners with the benefit of insurance or indemnity, there will be no immediate financial cost to the doctor, but there are non-financial costs of dealing with a claim brought by a LiP too. This is because the case may take longer to resolve and the way in which it progresses will be less predictable – because the LiP does not know the rules – and therefore more stressful.
Shift in attitudes
However, there has recently been a shift in judicial attitudes and a series of recent cases have shown that increasingly the courts will have less tolerance for non-compliance with the rules, even by LiPs.
Perhaps most significant of these is the judgment of the Supreme Court in Barton v Wright Hassall LLP [2018], which acknowledged that the restrictions in Legal Aid
and conditional fee agreements mean that, currently, pursuing a claim as a litigant in person is ‘not always a matter of choice’.
However, the court was clear that there was no justification for applying a lower standard of compliance with rules or orders made by the court to LiPs.
This trend has continued and most recently in Al-Hasani v Nettler & Ors [2019] the court held that it should strike out the LiP’s statement of case for various failures to comply with a rule, practice direction or court order.
Those of us who represent defendant doctors hope this will come to be the accepted approach in dealing with LiPs who fail to comply with the procedural rules and/or court orders by dint of having no experience or understanding of the rules governing litigation.
Niloo Bozorgi is a trainee solicitor at Hempsons
Free legal advice for Independent Practitioner Today readers
Independent Practitioner Today has joined forces with leading healthcare lawyers Hempsons to offer readers a free legal advice service.
We aim to help you navigate the ever more complex legal and regulatory issues involved in running and developing your private practice – and your lives.
Hempsons’ specialist lawyers have a long track-record of advising doctors – and an unrivalled understanding of the healthcare system as a whole.
Call Hempsons on 020 7839 0278 between 9am and 5pm Monday to Friday for your ten minutes’ of free legal advice.
Advice is available on:
Business structures (including partnerships)
Commercial contracts
Disputes and litigation
HR/employment
Premises
Regulatory requirements and investigations
PRIVATE PATIENT UNITS
PPU recovery is the heart of the matter
Private patient services in the 13 NHS trusts delivering acute care across East Anglia come under Philip Housden’s spotlight this month
FIGURES FROM the 2017-18 published annual accounts for this group of trusts show that total private patient revenues grew by 5.9% from £25.3m to £26.8m over the previous year.
This now represents 0.7% of these trusts’ total revenues, which is a return to the 2013-14 levels. The combined national average outside of London is 0.48%.
Leading the region by revenues is Royal Papworth, near Cambridge, with private patient income in 2017-18 of £8.15m, down £834,000 on the £8.98m achieved in 2016-17 and representing a small decline from 6.63% to 6.07% of total trust incomes.
As the UK’s largest cardiothoracic hospital, Papworth has a distinctive edge and focus, ensuring that the brand can stand out sufficiently to support local, regional and international demand for private patients.
The trust moved from 1 May 2019 to the new Royal Papworth Hospital located on the Cambridge Biomedical Campus. The £200m facility houses:
Five operating theatres;
Five cardiac catheterisation labs;
Extensive diagnostic modalities;
More than 300 beds, 12 of which are located in the new VarrierJones Ward for private patients.
This is an apparent significant reduction on the previous designated capacity, which was 32 beds on the old campus. However, it is to be anticipated that the apparent shortfall will be made up from
flexible use of other inpatient, ambulatory and diagnostic capacity.
Two cardiac units
Cambridge University Hospitals private patient revenues also fell back in 2017-18, by £603k (8.8%).
The trust achieved revenues of £6.4m in 2016-17 at 0.97% of total turnover.
A significant part of this relates to the Cambridge Heart Clinic, a joint venture with Regent’s Park Healthcare operating since 2008, who have access to five inpatient
and day-case beds and three consulting rooms.
It will be interesting to see how the two Cambridge trusts and their cardiac private patient services work in such close proximity in the future.
Essex trusts
Basildon’s PPU is also predominantly based on the delivery of cardiac services. Within the Essex Cardiothoracic Centre, the trust’s eight-bed PPU – branded Nash Private Healthcare – has delivered significant growth in revenue for
the trust, rising to £2.9m in 201718 from £479k when the unit was managed externally.
This performance now equates to 1.01% of trust incomes. Further growth to well over £5m is expected to be reported in 2018-19 annual accounts.
The trust is due to merge with Southend and Mid Essex (Chelmsford) in 2021 and is already working to a joint executive management structure.
The three trusts are working to share back-office and private patient leadership to develop a
Figure 1
network or ‘PPU chain’ that is able to invest in expanded capacity based on the regional burns and plastics services at Chelmsford and the regional cancer centre at Southend.
Considering expansion
James Paget Hospital, Great Yarmouth, Norfolk, has an eight-bed PPU – the Charnwood Suite – and outpatient and ambulatory services through a sub-brand called East Point Consulting Rooms and is understood to be considering expansion of their capacity to boost this total.
In 2017-18, the trust grew income from £874,000 to £1.03m (17.6%) which equates to 0.6% of total revenues up from 0.51% in the previous year.
The third smaller PPU in this group is North West Anglia, comprising Peterborough and Hinchingbrooke Hospitals, Huntington. There is little to no present private patient service out of Peterborough, but since 1994, Hinchin gbrooke has operated seven beds under the brand Mulberry Private Healthcare. The trust’s private patient reve-
nues were reported as £1.75m, up £85,000 (5%) on 2016-17.
Of the eight trusts without a PPU, the largest two by revenue are Norfolk & Norwich and West Suffolk. Norfolk & Norwich private patient revenues dropped in 201718 from £1.63m to £1.38m (15%), which is a decline to 0.28% of total income from 0.34% the year before.
In 2016, the trust turned a 21-bed private patient ward into an NHS day-case facility and does not now have separate private patient facilities.
Significant growth
West Suffolk, the ‘Outstanding’rated NHS trust, delivered significant private growth of £1.3m in 2017-18, almost doubling revenues to £2.65m; all achieved without a designated inpatient PPU.
This embues the trust with the second-highest ratio of private patient revenues in the region at 1.23% of turnover.
King’s Lynn is a small- to medium-sized NHS trust, located away from big centres of population and has experienced a steep decline in private patient reve -
nues. Income was £780,000 in 2016-17, but this fell to only £72,000 in 2017-18 (91%).
Although the trust has a BMI Hospital very conveniently sited nearby, which has hindered inhouse PPU development in inpatient activity, this does not on its own explain the decline, which is much more likely to be related to NHS access and winter capacity pressures.
Colchester and Ipswich merged in July 2018 to form East Suffolk and North Essex NHS Foundation Trust. In 2017-18, Colchester’s private patient revenues declined by £101k (12%) while Ipswich’s grew by £156k (23%).
It is understood that the new trust is considering private patient services growth, but without any particular new routes to market being identified at this stage.
Both main hospital sites are within attractive markets, which suggest that there is likely to be enough complex activity to support an entry-level PPU to meet the service gaps that the local private hospitals cannot fulfil.
Princess Alexandra, Harlow,
Essex, is another smaller singlecampus hospital with no PPU. The trust is considering a strategy of relocation and rebuild to manage estates and capacity issues.
The trust had a 12% (£39,000) reduction in private patient revenues in 2017-18, but essentially is ‘stuck’ on low earnings representing 0.15% of turnover.
The local NHS sustainability and transformation partnership area links Harlow with Hertfordshire and the potential for private patient growth may stimulate changed services across the trusts in the group.
East Anglia is building private patient revenues principally through cardiac services growth at the trusts hosting the regional centres. There remains the potential for further growth in other clinically complex specialties to add to dedicated capacity for private patients.
Next time: East Midlands
Philip Housden (right) is a director of Housden Group
Storing notes after you retire
Dilemma 1 How long must I retain my notes?
QI am a consultant urologist who works in private practice and am hoping to retire later this year. I am unsure what to do with the patient records for my work. In particular, I am unsure how long I should retain records.
Can you advise?
AUpright Positional
• Completely open scanner that is well tolerated by claustrophobic patients
• Weight-bearing scans for spine and joints enable a more precise diagnosis
• Patients who are large or cannot lie down can be accommodated
Clinical records should be retained for at least the minimum periods recommended in national guidance or required by statute.
At present, there is no definitive guidance relating to the retention of private clinical records. The regulations which did cover this in the past – Schedule Three of The Private and Voluntary Health Care England Regulations 2001 – were repealed and not replaced in 2010 and are so are no longer in force.
Despite this, it would be appropriate to follow the guidance outlined by the Information Governance Alliance’s Records and Management Code of Practice for Health and Social Care 2016.
This document states that different retention periods apply to different types of records and provides a detailed schedule setting out how long different types of records should be retained.
It is important to note that the recommended retention periods contained in the guidance are the minimum periods of time which records should be retained. For patients where you are aware of an adverse incident or a complaint, or in a particularly serious or conten
tious case, it may be appropriate for records to be retained for longer than the minimum period. The MDU regularly receives requests for assistance many years after the event in question has taken place and an absence of records can it make it significantly harder to mount an effective defence against any allegations. However, it is also important to bear in mind that retention of records should also comply with the requirements of the EU’s General Data Protection Regulation (GDPR) which says that data should not be retained for longer than necessary.
Secure storage
There are also the practical considerations such as the availability of secure storage space in relation to the retention of private records that may influence the decision to retain records beyond the minimum retention period. A record should be kept of the decisions taken to destroy or retain records. It is important to use appropriate measures when disposing of records. These include cross cut shredding, incineration or hiring a commercial company to manage the records on your behalf. If you opt for the latter, do make sure that the company holds the necessary British Standard or International Organization for Standardisation (ISO) accreditations to effectively dispose of records.
Finally, although I hope you have a long and happy retirement, you should also be aware that if any records remain in your possession at the time of your death, the executor of your estate may need to seek further advice on how best to store or dispose of these.
Dating an ex-patient
The ethics of a potential relationship between a doctor and their former patient is explored by Dr Kathryn Leask
Dilemma 2 Shall I meet with former patient?
QA former patient whom I had treated for a minor skin disorder asked me to sponsor her to take part in a charity trek to raise money for cancer research.
I was happy to oblige because when I treated her a few years ago, she had been badly affected by the recent death of her younger brother and I knew it was a cause that meant a lot to her.
After completing the challenge, she contacted me again to say thanks for the generous donation and suggested we meet for coffee so she can tell me about her adventures.
I would like to take up this invitation and I admit I am attracted to her but I am worried about the ethical implications. What would you advise or am I reading too much into this?
AYour former patient may only be interested in a platonic friendship, but her intentions are unclear so it is a good time to consider the potential
repercussions of a meeting before it is too late.
While you might be attracted to her, romantic relationships between doctors and former patients are fraught with ethical problems.
In its guidance on maintaining professional boundaries, the GMC is clear that doctors must not use their professional position to pursue a sexual or improper emotional relationship with a patient.
It warns that relationships with former patients may also be inappropriate depending on factors such as the length of time since you treated them, the duration and nature of the professional relationship, the vulnerability of the patient – then and now – and whether you will still be treating other members of their family.
You have also suggested that the ex p atient was very upset by the death of her brother and she may still be feeling emotionally vulnerable. If you believe this to be the case, the GMC warns that you should not begin a personal relationship.
Even if you are sure that the patient is no longer vulnerable, the GMC1 says you should be satisfied that her decisions and actions are ‘not influenced by the previous relationship between you’ and
that ‘you are not – and could not be seen to be – abusing your professional position’.
You may wish to speak to your medical colleagues or your defence body about your intentions and obtain their views without breaching patient confidentiality.
While everything could seem fine initially, there is also a risk that the circumstances in which your relationship began could come back to haunt you if things eventually turn sour.
Reference
1. GMC: Maintaining a professional boundary between you and your patient. www.gmc-uk.org/ethicalguidance/ethical-guidance-for-doctors/ maintaining-a-professional-boundarybetween-you-andyour-patient
Dr Kathryn Leask (right) is a medicolegal adviser with the MDU
A PRIVATE PRACTICE – Our series for doctors considering the independent journey
Investments giving
Independent practitioners use various Government-supported schemes and incentives to get tax relief for investing their hard-earned cash. Ian Tongue gives a specialist medical accountant’s view
THERE ARE four commonly available venture capital schemes of special interest to many high-earning doctors.
And that is in addition to taxefficient savings schemes such as ISAs, familiar to most people.
The information below is not exhaustive and does not represent investment advice. Before considering any investments, you should discuss your individual circumstances with an independent financial adviser.
What are tax-incentivised investments?
There have been many over the years, but the most common ones nowadays are:
Enterprise Investment Scheme (EIS);
Seed Enterprise Investment Scheme (SEIS);
Venture Capital Trusts (VCTs);
Social Investment Tax Relief (SITR).
Many people will, no doubt, have ISAs, which could be regarded as capital and income shielded from future tax rather than the above schemes, where you are provided with a reduction in your income tax liability from the act of investing money.
The main reason for offering income tax relief for investing is to stimulate the economy and allow businesses to grow by raising capital.
Companies may be established or at an embryonic stage, depending on the investment type, which does need to be considered, as you are putting your capital at risk.
Enterprise Investment Scheme (EIS)
The EIS scheme has been around for some time and encourages external investment into smaller companies that are often higher risk.
There are various criteria that the company and investor must meet to offer new shares under the EIS scheme, but provided that they are met, you should qualify for the tax relief.
Under this scheme, you receive
new shares in a company in exchange for investing money in it.
The offer to invest is documented in a prospectus to explain the company and what it intends to use the funds for.
Assuming all criteria are met by the investor and company, the following main tax benefits arise:
30% tax relief available up to £1m invested per year – £2m for knowledge-intensive companies;
Tax relief available in the current or preceding financial year;
Exemption from capital gains tax upon subsequent sale;
Loss relief if the shares are sold at a loss later on.
There are restrictions on raising
tax relief
amount that can be invested is restricted to £100,000.
The same benefits for loss relief as with the two ‘enterprise’ schemes are available, provided that all of the criteria are met by the company and investor.
However, the capital gains tax relief is restricted to 50% of the initial investment. The effect of the additional tax relief of 20% on the initial investment further reduces the capital at risk.
Referring back to the example above, if £20,000 was invested under SEIS and the investment failed, you would have the initial £10,000 tax relief and a further £4,500 (as a 45% taxpayer) and therefore the capital at risk reduces to £5,500.
Venture Capital Trust VCT)
A VCT is a business that will be listed on the stock exchange, which, in turn, uses the money raised to invest in businesses, often young entrepreneurial private businesses.
This has been a long-running scheme and the tax relief available on the initial investment is 30% up to a maximum investment of £200,000 per year.
Again, there are restrictions on what the VCT can do with the money and on the investor.
Social Investment Tax Relief
This type of investment was introduced to primarily help community companies or charities raise money.
Due to its nature, the criteria to use the scheme is more narrowed and it is less common to see this type of investment, which can be either buying new shares or lending money. If you are considering this type of investment, you should speak with your financial adviser.
Venture capital schemes can be an effective way or lowering your tax liability and potentially building wealth for the future. There are several schemes that can reduce the amount of tax payable and provide a longer-term shield from tax.
But I repeat, when considering such schemes, it is vital that you take professional advice to understand the risks and well as the tax benefits.
Speaking to an independent financial adviser is essential before committing your hard-earned money to any venture capital scheme.
Next time: ways to avoid the pensions tax trap – it can be done!
The main reason for offering income tax relief for investing is to stimulate the economy and allow businesses to grow by raising capital
capital using the above scheme if you are connected to the company and therefore this scheme would not usually be available to raise funds for your own private practice.
Given the nature of the businesses in question, there will inevitably be a number of businesses that fail, resulting in you losing your investment. As mentioned above, a further loss relief is available under these circumstances to provide you with income tax relief on the loss.
As an example, a £20,000 investment less tax relief of 30% results in a net cost of £14,000.
Should the investment fail and all of the money is lost, further tax
relief would be available at the taxpayer’s marginal rate of tax.
As a 45% taxpayer, you would receive tax relief of 45% on the £14,000 loss, resulting in a true loss of capital of £7,700.
Seed Enterprise Investment Scheme (SEIS)
The SEIS scheme operates in a similar way as EIS, but the companies raising capital in this way should be starting their trade and are therefore in their infancy.
These businesses are therefore regarded as higher risk often due to a lack of history.
The tax relief available to the investor is higher at 50% of the investment, but the maximum
One of the main differences with a VCT is that any income from dividends is not subject to income tax unlike EIS and SEIS, where income tax is payable.
In relation to capital gains tax, any gains made are not subject to capital gains, but the loss relief against income is not available for a VCT investment if it fails.
Ian Tongue (below) is a partner with Sandison Easson accountants
DOCTOR ON THE ROAD: BMW 8 SERIES CONVERTIBLE
Converted to this brutal convertible
You only live once, so if you are highly successful and love quality then the all-new BMW 8 Series convertible will have you beaming, says Dr Tony Rimmer (below)
IF YOU are a successful independent practitioner and you like cars, then there are a few obvious candidates for the premium brand that you are likely to buy yourself as a treat for all your hard work.
The German makes of BMW, Audi and Mercedes fit the bill, as they all offer models of various types and at different price-points. If you are particularly successful, then you might well be looking at the more expensive sporty models and BMW has just released its latest contender to whet your appetites.
The all-new 8 Series convertible joins the coupé to complete the top level of BMW’s sporty range. With prices starting from £83,295,
this four-seat drop-top GT competes with the Mercedes S-Class convertible and Bentley’s albeit pricier Continental CTC.
Costing £7,000 more than the coupé equivalents, it is initially available with two engine options; a 3.0litre straight-six diesel producing 320bhp in the 840d and a 4.4litre V8 producing a meaty 530bhp in the M850i.
Extra rigidity
The 8 Series platform has needed only a few modifications to provide the extra rigidity required to accommodate a folding roof and the multi-layered fabric top can be lowered and raised in 15 seconds while travelling up to 31mph.
The styling, like the coupé, is dominated by BMW’s new larger trademark kidney-shaped grille. It looks wide, sleek and purposeful and the convertible top retains the coupé’s flowing lines when closed. It is, however, a big car, so parking in the UK will always be a bit of a challenge in tight car parks.
The interior is classic BMW, with all the extra luxury trim and accoutrements expected in its top model. Its latest version of the iDrive system to control the infotainment and sat-nav remains one of the best in the business. Additional touch and gesturecontrol makes it one of the easiest, too. Apple CarPlay is standard,
but, strangely, Android Auto is not.
The driver and front-seat passenger are really-well catered for by very comfortable soft leather sports seats that include scarfheating outlets – useful when driving top-down in cold weather. Rear passengers do not fare quite so well. Such are the head- and legroom restrictions that they are really suited only for children up to teenage years.
Wind deflector
At least when travelling two up you can benefit from the standard foldable wind deflector which does a fine job reducing the drafts when the hood is down.
The boot is quite large – 350 litres with the hood raised – but it
has quite a narrow opening and it is naturally compromised when the roof is stowed away.
But out on the road, the BMW delivers everything you would expect from a manufacturer with a thorough understanding of chassis technology.
The standard four-wheel drive X-drive system is rear-biased and rear-wheel steering that is operational at lower speeds gives real confidence when guiding this large GT along challenging roads.
Adaptive dampers alter the ride depending on the selected mode but, even when ‘comfort’ is selected, cannot compete with the standard air-suspension set-up of the Mercedes S Class convertible. The 8 Series works best on smooth sweeping A-roads and motorways.
Out on the road, the BMW delivers everything you would expect from a manufacturer with a thorough understanding of chassis technology
BMW 8 SERIES CONVERTIBLE 840d xdrive and M850i xdrive
Engine: 3.0 litre six-cylinder turbo-diesel or 4.4 litre V8 turbo-petrol
Power: 320bhp or 530bhp
Torgue: 700Nm or 750Nm
Top speed: 155mph (limited) for both
Acceleration: 0-62mph in 5.2 seconds or 3.9 seconds
Claimed economy: Combined: 39.2mpg or 26.6mpg
CO2 emissions: 161g/km or 25g/km
On the road price: £83,295 or £107,100
It is a real car for crossing continents.
If you do plan to drive that far, you might want to stick with the diesel 840d. It has a claimed economy of up to 39mpg, whereas the petrol M850i only claims 26.6mpg.
Brutal acceleration
However, as far as sporty character and performance goes, the keen driver will go for the wonderful 4.4litre V8. Brutal acceleration of 0-62mph in 3.9 seconds is accompanied by a glorious soundtrack from the exhausts.
The eight-speed automatic gearbox swaps ratios smoothly and quickly, responding to manual paddle changes in an instant.
The M850i feels almost like a completely different car to the
840d; more like the Aston DB11 Volante. A sportier suspension setup completes the picture and the whole package goes some way to justifying the much higher list price of £107,100.
So, will this new car satisfy us medics with a love for driving and quality products? Well, the 8 Series convertible offers a good combination of luxury with above-average dynamics and driver appeal.
The V8-engined M850i is terrific fun but thirsty. The cheaper and more frugal 840d will be the sensible choice for most buyers. However, as we all know, you only live once.
Dr Tony Rimmer is a former NHS GP practising in Guildford, Surrey
The M850i feels more like the Aston DB11 Volante. Brutal acceleration of 0-62mph in 3.9 seconds is accompanied by a glorious soundtrack from the exhausts
The interior is classic BMW, with all the extra luxury trim and accoutrements
All you need to know about accountancy for private practitioners
PROFITS FOCUS: GENERAL SURGEONS
Generalists fading away
General surgeons’ profits have taken a tumble in our latest benchmarking survey. Ray Stanbridge reports
ON THE surface, it does not seem that it has been a great year for general surgeons.
Our unique benchmarking survey shows that between 2016 and 2017, gross fees actually fell by 2.9%, from £137,000 to £133,000.
Costs on the other hand have shown an increase of 5.2% , going up from £58,000 to £61,000.
As a result, pre-tax profits have fallen by £7,000 (or 8.9%) from £79,000 to £72,000. Margins fell by six per cent, from 57.6% to 54.1%.
It is somewhat difficult to
explain the drop in gross income. This could be down to data problems, which we have not yet fully grasped, or that insurance company work – and possibly self-payhave been devoted to other specialists who are reviewed elsewhere in this series.
A dying breed
Alternatively, it may be that general surgeons are becoming a dying breed and, as with all other professions, are becoming more specialist.
Looking at costs, the biggest
AVERAGE INCOME AND EXPENDITURE OF A CONSULTANT GENERAL
It may be that general surgeons are becoming a dying breed and, as with all other professions, are becoming more specialist
change seems to be an increase in consulting room hire, increasing from £4,000 to £9,000. Some providers offer substantial services in their deals and this may explain why there has been a small fall in staff costs.
The reason for such a big rise in room hire is surely the full impact of the Comp etition and Markets Authority (CMA) ruling, whereby general surgeons are now charged facilities at market rate.
Shopping around
There has been some fall in profes sional indemnity costs, which may come as a surprise to some. But this is almost certainly due to consultants shopping around among the relatively new insur ance companies and negotiating cheaper rates.
Motor and travel and account ing/legal costs have risen slightly – probably as a result of inflation.
Expenditure
‘Other’ costs have dropped, on average from £8,000 to £6,000. I think some of this is because, in the previous year, many general surgeon consultants spent money setting up websites and getting marketing support, which they have not yet had to repeat.
In future, we will probably need to have to completely review our
Uniting surgical and non-surgical medical aesthetic communities to raise industry standards
GENERAL SURGEONS’ INCOME DROPPED WHILE EXPENSES ROSE
definition of general surgeons and it may be that this could become a redundant category in this series in due course.
We would expect to see further pressure on general surgeons’ fees,
however – not the least so because we understand the volume of breast surgery is on decline.
Coming up with the averages shown here is increasingly difficult, as general surgeons work in so
many ways, trading as sole traders, groups and limited liability companies. Some have taken an employment option. Some general surgeons have also specialised and this has affected the consistency of data collection.
Nevertheless, we hope the figures here are a reasonable representation of what an average general surgeon earns and spends.
Note that our survey does not cover those who are full-time in private practice. We include those who:
Hold either an old or a new style NHS contract;
May or may not have incorporated their business;
May or may not work in a group;
Have a keen interest in private practice as a business;
Have been engaged in private practice for at least five years;
Earn at least £5,000 a year from private practice.
Next time: Cardiologists
Ray Stanbridge is a partner with accountancy, finance and tax advisory medical specialists, Stanbridge Associates Ltd
HOW ARE YOU DOING?
WHAT’S COMING IN OUR SEPTEMBER ISSUE...
Make sure you don’t miss our next issue, published on 19 September. You may not receive every issue if you have not yet subscribed to the journal. Don’t risk missing out on vital topics we tackle next time:
New series: The risk of fraud and cybercrime is growing at an alarming rate with no real signs of any slowdown. Fraudsters are targeting individuals and businesses across the world and across all sectors. Healthcare is certainly no exception so it is essential that you know what steps you can take to protect yourselves
New Series: Property investing for doctors. Dr Lafina Diamandis explodes seven myths that shouldn’t stop you from investing in property
Avoiding the annual allowance pitfalls: Much has been written about the unfair annual allowance charge on pensions and how this can affect medics particularly badly, even those not carrying out private practice. We look at the key concepts and potential ways to mitigate or extinguish the pension savings annual allowance charge.
The importance of warranties: When independent practitioners are buying or selling a business, half of the agreement for the sale will be a schedule of warranties. If you are prepared to answer them before you go to market, the higher the value your business is likely to be, because each warranty you cannot confirm is money off the price
INDEPENDENT PRACTITIONER
TELL US YOUR NEWS
Robin Stride, editorial director
Email: robin@ip-today.co.uk
Phone: 07909 997340
Published by The Independent Practitioner Ltd. Independent Practitioner Today is editorially independent and thanks Bupa for its assistance with distribution. Printed by Pepper Communications Ltd Material is governed by copyright. No part of this publication may be reproduced, stored in a retrieval system or transmitted in any form without permission, unless for the purposes of reference and comment. Editorial layout is the copyright of the publishers. If you wish to use it for promotional purposes on websites or for reprints, we would be happy to discuss licensing the copyright to you.
Registered office: 7 Lindum Terrace, Lincoln LN2 5RP
Write to Independent Practitioner Today PO Box 198, Cranleigh GU6 9BB
Requirements for a successful appraisal and revalidation
What doctors should know about using whatsapp and similar apps at work to communicate with colleagues
Our Private Practice Growth Guide shows how to effectively promote your practice through email marketing
As the proportion of consultants’ income from self-pay hits a new record, Medical Billing and Collection’s Garry Chapman predicts this trend will continue. Just make sure you have a robust system to collect the money
The odds are stacked against actively beating the market. Cavendish Medical’s Dr Benjamin Holdsworth on the real and costly challenges of active investment management
Business Dilemmas answers a reader’s query on whether he should disclose records he has been asked for
PPUs in the spotlight – our attention turns to East Midlands PPUs
Accountant’s Clinic – this month we reach C in our A-Z of business things you need to know about: cash, costs control and children
Profits Focus puts the financial microscope on cardiologists
Doctor On The Road gets to grips with the new Audi A1
Plus all the latest news and views
ADVERTISERS: The deadline for booking adverts in our September issue is 23 August
ADVERTISE WITH US
Margaret Floate, advertising manager Email: margifloate@btinternet.com Phone: 01483 824094
GET A SUBSCRIPTION DISCOUNT! £90 independent practitioners. £90 GPs and practice managers (private & NHS). £210 organisations. Save £15 paying by direct debit: individuals £75 (organisations £180).
TO SUBSCRIBE – USE SUBSCRIPTION FORM ON PAGE 25 or EMAIL: karen@marketingcentre.co.uk or phone 01752 312140 or go to the ‘Subscribe’ page of our website www. independent-practitioner-today.co.uk
Guarantee delivery of your next copy of Independent Practitioner Today. Take out a subscription and you will get full access to our news, features and previous issues on our website. See details on the left.