An aesthetics doctor warns of times when it’s best to turn down earning opportunities P18
The business journal for doctors in private practice
Would a mobile app boost your practice?
A plastic surgeon explains how his app for patients improves care P34
We begin a new series this month with a regular look back at events over our last decade n See page 11
Can we afford to live ever longer?
With life expectancy increasing, an expert gives advice on preparing for a 40-year retirement P50
Alarm bells on self-pay
By Robin Stride
Consultants are often missing out on the self-pay boom because their private hospitals have not geared themselves up to make the most of it.
Researchers report a string of failures, including:
n Complex websites that make it hard for customers to access cost information;
n Unclear pricing structures;
n ‘Huge’ variations in charges;
n Phone inquiries not being answered;
n Recorded messages not being returned.
Findings of a study for BMI Healthcare show how some operators fail to fully exploit the business opportunities available from the non-cosmetic self-pay market, valued at £700m this year.
They demonstrate how wouldbe patients who are researching hospital websites must often make multiple clicks to even find a price for procedures – and when they do, they are confronted with huge prices differences.
In one example shown at The Private Healthcare Summit 2018 by the group’s director of market engagement Richard Gregory, potential customers trying to navigate their way around information on hip treatments were having to make six mouse clicks to see prices. Some figures were fixed-price,
Marketing specialist Richard Gregory
but others were just a ‘guide’ and varied from between £9,500 as a set figure to £12,500 as a guideline cost.
Mr Gregory argued that private healthcare customers in 2018 expected to be able to easily access information and services, when they wanted and through the medium of their choice, just as in the retail world.
But they were also being let down when they tried to get information from private hospitals on the phone.
BMI’s researchers phoned hospitals from different operators over an eight-week period at set times each week.
Of 160 calls: n 106 were answered, but 54 were not; n 50 calls went to voicemail, but only 19 of these messages were returned. One hospital returned none;
n Only 100 calls were answered within 30 seconds.
And when callers did manage to speak to somebody, researchers considered some of the voices at the other end were unfriendly and not informative enough.
Empathy was judged extremely poor by some callers. In one hospital, only two callers, from 14 phone calls answered, considered the person they spoke to was empathetic.
Mr Gregory described call backs as ‘a lottery’. Customers expected a personalised, quality service including the ‘soft’ elements –knowledge, reassurance, empathy, and trust. They wanted to be guided through the complexity of healthcare and a ‘wow’ factor like this was the loyalty creator for those who really wanted to grow their business.
He said the opportunity to build the self-pay sector had been aided by a fall in private medical insurance coverage and a 53% rise in the last five years in NHS treatment waiting lists. Waiting lists were growing 50% faster than the population.
But he warned the privatehealthcare.co.uk conference in London that if customers could not even access an operator, then they were effectively being turned away.
He told Independent Practitioner Today: ‘I think a growth rate in the vicinity of 10% a year in self-pay is modest.
‘I would encourage consultants wanting to grow their private practice to be a little bit more consumer-savvy and look at their processes that happen before they see the patient.
‘If they are not getting the telephone service they expect, then they are going to lose out.’
In BMI’s research, ‘friendliness’ was based on the tone of voice and use of names and a welcome; informativeness on the confidence and accuracy of answers given to set questions; and empathy was judged on a subjective view of the extent of unprompted interest shown in the caller.
n See pages 4 and 5
A BMI Healthcare survey found phone inquiries went unanswered
In this issue
July-August 2018
You don’t need a diploma to run a practice
jane Braithwaite starts a new series on practice management, giving helpful tips on all aspects you need to master to have a perfectly-run practice P12
Keep on the right side of taxman accountant susan Hutter explains how to keep on the right side of the taxman and, in the event of an inquiry, gives advice on how this should be handled P16
How to handle your lawyer solicitor lynne abbess shows you how you can, with careful planning, get the best advice and keep your legal bills down to a minimum P23
editorial comment
Think like supermarkets
A sign of the times at this year’s Private Healthcare Summit was that speakers talked more of ‘customers’ than patients.
But what would it mean to treat patients as customers? The question was asked by specialist healthcare marketing agency managing director Ed Hudson, of Create Health.
He took everyone on a little shopping trip, with the audience being asked to look at the Morrisons supermarket chain for an answer.
Customers going to its website receive a prompt to set up an account, followed by a ‘welcome’ and continued communications.
Morrisons’ website also flags up ‘BIG offers’ to attract customers again.
In the health world, people might hope not to have to go back to have another knee done, but they might be enticed back for a physio,
healthcare checks or elective treatments.
Or maybe their friends and family would need a treatment from that provider?
Mr Hudson questioned how many hospitals reached out after appointments, like the supermarket does.
The supermarket also has a ‘Tell us what you think’ section, informing customers that their opinion is valued.
This enables personalised marketing. The marketing boss rightly suggested customer satisfaction is not being used in private healthcare to build real competitive advantage.
His message to providers is worth taking on board for independent practitioners. Mr Hudson told them they needed to ‘innovate or die’, because the market and culture had changed and new entrants are sweeping in with innovative models.
that’s the way the money goes... the Mdu’s senior medical claims handler demonstrates why multimillion-pound compensation payments are more common now and what doctors can do to protect themselves from the risk of litigation P30
Screen time with doctors the founder of top doctors explains the rationale behind the development of the online service and how it fits into the current landscape of medical search engines P36
the low-down on insurance
Bupa’s dr tim Woodman explains why the insurer has published guidance for new independent practitioners on how to handle insured patients and understand insurance policies P44
PlUS oUr regUlar colUmnS
Start a private practice: taxman treats big costs differently accountant ian tongue explores some of the concepts and factors to consider around capital allowances P52 doctor on the road: mixed reception our motoring correspondent dr tony rimmer takes a look at the Volvo s90 hybrid P54
Profits focus: a very stable picture our unique benchmarking series looks at the financial fortunes of general surgeons P56
tell US YoUr newS Editorial director Robin Stride at robin@ip-today.co.uk Phone: 07909 997340 @robinstride to advertiSe Contact advertising manager Margaret Floate at margifloate@btinternet.com Phone: 01483 824094
SUbScriPtion rateS
£90 independent practitioners.
£90 GPs and practice managers (private & NHS). £210 organisations. Save £15 paying by direct debit: individuals £75 (organisations £180). to SUbScribe – USe SUbScriPtion form on Page 24 or email: lisa@marketingcentre.co.uk Or phone 01752 312140 Or go to the ‘Subscribe’ page of our website www.independent-practitioner-today.co.uk chief sub-editor: Vincent Dawe Head of design: Jonathan Anstee Publisher: Gillian Nineham at gill@ip-today.co.uk Phone: 07767 353897
Risks enlarged by pension freedom
by edie bourne
Many private doctors have welcomed the pension freedoms introduced in 2015, but – without proper guidance – this can leave them ‘at risk of harm’, warns a new report from the financial watchdog.
The Financial Conduct Authority (FCA) study found that savers who take their pension pots as cash do not fully understand pension drawdown – taking money from the pension flexibly – with some receiving 37% less income from their pot every year by investing in cash rather than a mix of assets.
Now, after a twoyear investigation, the FCA has warned that some pension firms are overcharging savers who are accessing their money via expensive arrangements. It found customers are not clear on fees and that charges were complex and hard to compare.
Independent Pract itioner Today columnist and specialist financial planner Dr Benjamin Holdsworth, of Cavendish Medical, said: ‘The FCA investigation has confirmed what we knew to be the case –some pension companies are not being clear on costs.
‘Some of the most expensive
deals are around four times the norm. The charges can be so opaque that many savers would not realise they are being overcharged.’
Pension freedoms came into force so that savers were no longer forced to buy a guaranteed income for life in the form of an annuity, but could instead use their pension like a bank account. Drawdown pensions mean savers can invest in the stock market while still taking an income.
Dr Holdsworth added: ‘With the right guidance, pension drawdown can be very successful, giv
cavendish medical’s dr benjamin Holdsworth said the study confirmed that pension firms were overcharging
ing retirees the flexibility to spend their money as they wish.
‘However, it involves complex investment decisions on an ongoing basis, meaning that the support of experienced financial advice is imperative.
‘If considering your own options, make sure you are in the best position to make important choices.’
The FCA is proposing a range of measures to help consumers decide what to do with their pension pot, including ‘wake up’ packs which summarise their savings and current risks.
Check private data before publication
Private consultants are being asked to check data on the number of procedures they do and typical lengths of stay before it is published on an official public website.
The information compiled by the Private Healthcare Information Network (PHIN) is the first step in it publishing a range of performance measures to help patients make informed choices, as required by the Competition and Markets Authority following its private healthcare inquiry.
Consultants admitting private patients can preview and approve their performance measures through PHIN’s online portal in advance of publication.
PHIN is hopeful that at least 1,000 consultants will approve their data for an initial launch anticipated for the end of this month (July).
Chief executive Matt James said: ‘We want to launch this service for patients with a strong representation of the leading consultants in the country. The response from the professions so far has been superb, with the
main specialty organisations giving us great input and support to prepare the data and communicate with their members.’
At the last count, just 4,500 consultants had logged in to PHIN’s portal to start checking data provided by private hospitals, to cor
rect errors and give feedback to improve the process.
But PHIN eventually needs to publish performance data for all the estimated 14,000 consultants admitting patients privately, with measures ranging from patient satisfaction and reported out
ScHeme to align nHS and Private data
a new initiative aims to ensure data in private healthcare and the nHS in england is recorded in the same way so as to improve consistency across the system. the acute data alignment Programme (adaPt) will address concerns about the lack of visibility of quality in private care and will promote the completeness of patient records, where some care has been received privately. the programme is being jointly led by nHS digital and the Private Healthcare information network in partnership with government bodies and the care Quality commission.
Phase 1 will see co-operation between all parties to accelerate
publication of information mandated by the cma Phase 2 will aim to redirect the flow of data for approximately 750,000 privately-funded hospital episodes each year from PHin to nHS digital, alongside nHS data. a public consultation on the scope and objectives is due to start later this year.
nHS digital’s tom denwood said: ‘integrating data from private suppliers with data from the nHS presents a great opportunity to build a complete picture across the healthcare sector that will give us insight into patient outcomes in the private sector and how they compare to the nHS.’
comes through to adverse event rates.
Fee information for an even wider group of consultants, including those who see only outpatients, will be published in 2019.
Royal College of Surgeons president Prof Derek Alderson said: ‘This is a major opportunity for the private healthcare sector to rally behind transparency and demonstrate genuine commitment to improving patient safety and reducing risk.
‘We encourage all of our members to get behind this opportunity to review and approve performance data and take a lead on safety and transparency.’
PHIN chairman Dr Andrew VallanceOwen said: ‘The publication of consultant level private healthcare performance information is an important step in the journey towards greater transparency for private healthcare.
‘Approving their measures will enable consultants to demonstrate the scope of their care to patients, contribute to public understanding of clinical quality, and drive service improvements.’
‘Putting the customer first – exceeding the expectations of patients, doctors and payers’ was the theme for this year’s Private Healthcare Summit. Robin Stride reports
Cash in on self-payers
With self-pay the only proven growth area in private healthcare, providers were challenged as to why they did not ‘throw everything at it’.
LaingBuisson consultant and self-pay expert Liz Heath said the sector had a ‘rare opportunity’ to grow the self-pay market.
But, referring to the issue of poor performance from hospitals – covered in our front-page story this month – she warned that everyone had to get the phoneanswering right if they were to build future business from the first episode of care.
Ms Heath surprised her audience by telling them that 37 years ago the percentage of self-pay in the UK private healthcare market was as high as 28.6%.
It was currently 18.6%, but she said some providers were now getting more than a quarter of their business from people who paid for their own treatment.
Figures from market analysts LaingBuisson, given at the conference run by privatehealthcare. co.uk at the QEII Centre, West -
Great leader who knew the value of customers
BMI Healthcare marketing expert Richard Gregory quoted Mahatma Gandhi to a standing room-only audience of operators, doctors and independent sector firms:
‘A customer is the most important visitor on our premises, he is not dependent on us. We are dependent on him.
‘He is not an interruption in our work. He is the purpose of it.
minster, illustrated just why consultants and private hospitals should want to get their fair share of the self-pay boom.
The market for acute medical care in independent hospitals and clinics, including NHS private patient units, was worth an estimated £5.78bn in 2017.
This was equivalent to growth of just 0.6% from £5.75bn in 2016, representing a contraction in the market in real terms, given CPI inflation running at 2.7%.
But 2017 self-pay spending on private acute medical care grew strongly for the fourth year in succession – up around 38% over a four-year period.
‘He is not an outsider in our business. He is part of it. We are not doing him a favour by serving him. He is doing us a favour by giving us an opportunity to do so.’
Ms Heath reported that self-pay for Spire grew 9.6% in 2017, Nuffield rose 14% in 2016, in BMI it grew 9.6% in 2016 and for Ramsay, although not reported, it was thought to be over 5% growth.
She said customers were now making considered purchases and providers should not worry so much about affordability. Most operators had partnerships with finance companies.
Dr Andrew Jones, chief executive at Ramsay Health Care UK, identified four main drivers of self-pay: longer NHS waiting times, NHS rationing, high costs of private health insurance, and better marketing, customer service and packages from independent providers.
Fleur Hicks, managing director at onefourzero digital diligence and research strategists, recommended that consumers were targeted online, as 72% of patients researched common medical conditions and treatments available on the web. She urged providers to keep up with the digital revolution.
Although some operators might
fear competitors would see the details, people did not want to be shocked about prices and they were looking for fee transparency.
And she said people were willing to travel further for services offering a good price, availability and quality.
Presenting her summary, she said: ‘It’s clear from our data that patients’ appetite for private health/technology is increasing, with more and more turning to online providers for consultations, prescriptions and help managing long-term conditions.
‘With this demand showing no signs of slowing down, the question for providers operating in this space is how they can ensure they offer the best possible service for patients without compromising on patient safety and best practice.
‘In a sector as sensitive as health tech, gaining and sustaining trust among users is vital to building brand value. For companies that successfully do so, the market evidently exists.’
see feature on how to bill self-payers correctly, page 40
Factors that lead to rise in self-pay
Seven big factors have influenced the number of self-pay admissions over the last 12 months.
Market analysis figures from a survey presented by LaingBuisson consultant Liz Heath, in descending order:
1. NHS waiting times;
2. A local marketing campaign;
3. CCG demand management;
4. A national marketing campaign;
5. Availability of in-house finance;
6. The economic situation;
7. Increased local competition.
But when providers were asked what proportion of their marketing budget they intended to allocate to the promotion of self-pay surgery (excluding cosmetic surgery) as many as 34.69% said they would spend under 5%.
16.33% aimed to spend between 5-10%; 8.16% to spend 10-15%, and 8.16% to spend 15-20%. 12.24% said they would spend 20-30%, while only 20.41% confided they would spend more than 30%.
Self-pay expert Liz Heath
The privaTe healThcare summiT 2018
EnSuRE tHat it SuitS patiEntS
the chief executive of a concierge service warned that the days are gone when the private healthcare sector can just tell a customer to come and see a doctor at a time set by the operator or clinician.
according to annabelle neame, of Lexihealth, patients want to be seen at a time of their choosing.
She appealed for the private sector to build partnerships in the uK and abroad, and collaborate to promote medical tourism as part of a wider London experience.
Mrs neame said a unified message was needed to sing the uK’s praises and proclaim it could offer what self-pay customers from abroad were looking for. they did not just want healthcare but the whole package that went with it.
Bupa boss’s recipe for boosting private market
The private sector provides a great service to its customers, but needs to do more to ensure it consistently meets the highest standards expected by consumers and regulators, a health insurance boss said.
James Sherwood, director of health and benefits management at Bupa UK, made the plea while taking part in a panel discussion on how the sector could give insurance customers what they want.
All customers were looking for affordable private healthcare and
expect services to meet the highest standards of quality and safety, he said, but transparency and the sharing of data needed to be improved.
He told Independent Practitioner Today later: ‘We’ve made a start through the Private Healthcare Information Network, but need to go further and faster. The NHS is running the ‘Getting It Right First Time’ campaign and is showing how important it is to measure, understand and, where necessary, tackle variation in care.
Choosy patients ‘will drive care advances’
Private providers will need to diverge and adopt new models of working to survive in the next 12 months, according to the boss of a private hospital group.
Ramsay Health Care UK’s chief executive Dr Andrew Jones forecast that consumerisation would drive up standards and that increasing patient expectations would lead to improvements in care.
People were demanding better outcomes, they wanted more transparency and more information about their care, and they were getting more value conscious, Dr Jones said.
The former GP said market con-
solidation and global models of working would deliver value and improve quality.
Dr Jones believed political factors might change the long-term funding solution, while an early general election could drive system improvements.
He said healthcare digitalisation would change the way care was delivered and redefine care packages and pathways, including proactive prevention and rapid access to services.
The market would also see increasing use of artificial intelligence, gene therapy and robotics in surgery to improve outcomes and patient experience.
‘The private sector should be embracing a similar level of transparency in care to create the conditions for continuous improvement but crucially to show the value we offer to our customers.
‘We also need to tackle excess capacity. This is major contributing factor to the prices charged to customers but also makes establishing the level of oversight and governance expected by the regulators difficult to achieve.’
Good food gives hospitals a lot to chew over
Food in hospitals punches above its weight when it comes to creating patient satisfaction.
Although meals account for 5% of the business budget, they can deliver as much as 40% of the positive perceptions of the hospital, according to a food expert.
Kevin Hall, marketing director at catering and support services provider Compass Group, told hospital operators if they could build up a ‘stand-out’ food service, then this was an important point of differentiation.
Food could drive the business and had the power to significantly influence patient satisfaction.
Test your knowledge of the private sector
Delegates were tested on their knowledge of aspects of the sector – with some surprising results for some:
1
In 2009, 7.6m people were covered by private medical insurance. How many were covered in 2017? Choose from: 5.2m, 6.9m, 7.8m, 8.5m.
2
What is the average price for a self-pay hip replacement package in the UK? Choose from: £8,750, £10,200; £11,155, £15,410.
3 According to the ONS, how many UK citizens travelled abroad for treatment in 2017? Choose from: 15,000, 55,000, 105,000, 145,000.
4 What proportion of private hospital revenue came from the NHS in 2017? Choose from: 10%, 20%, 30%, 40%.
5 206 independent hospitals have been inspected by CQC. What proportion were deemed to need improvement? Choose from: 10%, 20%, 30%, 40%.
Quizmaster: Keith Pollard, executive chairman, LaingBuisson
IT fix helps with data privacy law
By Edie Bourne
Private doctors are using private healthcare IT experts’ help to meet their obligations under the General Data Protection Regulation (GDPR).
Produced in partnership with specialist corporate and technology lawyers, Healthcode says its GDPR Toolkit is a cost-effective and comprehensive resource for independent practices using the ePractice system.
The toolkit gives a guide to the practicalities, as well as a number of templates and tools for private practices to implement.
These include:
A Template Privacy Policy – this template will guide practitioners on the essential information to include in their privacy policy under GDPR;
Subject Access Request Procedure – guidance on best practice with dealing with a subject access request;
Subject Access Request Register – to document subject access requests from patients;
Information Asset Register – to
record what data is held by the practitioner and where it can be accessed;
Subject Access Export – enabling Healthcode’s ePractice users to extract information held on a patient, such as notes, alerts and correspondence, so they can respond to a subject access request quickly and easily.
Managing director Peter Connor said the company was concerned to find many independent practices were unprepared for the GDPR, particularly in view of the more severe financial penalties for failures to comply since 25 May.
Healthcode ePractice customers can buy the GDPR Toolkit when they log onto their account. It costs £149.99 for a single specialist and £374.99 for a practice (excluding VAT).
Surgeons attack beauty op ads during TV’s ‘Love Island’
The British Association of Aesthetic Plastic Surgeons (BAAPS) has hit out at the screening of cosmetic surgery procedure adverts during ITV2’s Love Island Its comments came after NHS boss Simon Stevens criticised breast enlargement adverts during the hit TV programme, saying they were fuelling a crisis in young people’s mental health.
Consultant plastic surgeon and former BAAPS president Mr Rajiv Grover said: ‘We are seeing the damaging effects of this cultural phenomenon on an increasingly vulnerable population, whereby the decision to seek out treatment is trivialised while individuals face intense psychological pressure to conform.
‘By advertising cosmetic surgery alongside this type of programming – and in some instances, even using the stars of the show –unscrupulous clinics are targeting young people in a way that commodifies surgery as a quick fix and endangers patients.
strating that young people are suffering from negative body image issues.
‘It is worth noting that many of these clinics have a history of targeting young people using influencers to promote surgery, for which they have received public criticism, but which has not halted this aggressive and unethical marketing tactic.’
BAAPS urged the Government to ban cosmetic surgery advertising in 2012 citing studies demon-
Bupa begins accreditation for groups
A consultant group accreditation scheme has been launched by Bupa following talks with 25 groups over the last 16 months.
Bupa-recognised members of the group will be promoted as ‘Accredited’ on www.finder.bupa. co.uk, the insurer’s private healthcare directory, which gets over 70,000 weekly visits from customers, doctors and the public.
Dan Howcroft, provider management medical director, said: ‘It’s still early days for us, so groups becoming accredited now will have a key role in shaping how we work with consultant groups in future.
‘We’re taking a phased approach, writing out to individual consultants to let them know that if they are part of a group, that group could now become accredited.
‘We’ve just contacted ENT and will be getting in touch with obstetrics and gynaecology, trauma and orthopaedics, urology, cardiothoracic and general surgery over the next two months.’
The criteria for accreditation focus on: structure, level of subspecialist coverage, clinical governance, complaints management, cross-cover arrangements and collection of outcomes information.
Safe messages
Mr Grover added: ‘We recognise that in a more image-conscious society than ever, the pressure to conform to unrealistic standards of beauty is even greater.
‘In the absence of a complete ban, BAAPS also proposed measures necessary to ensure that patients are protected from unethical practices, and urges the Government to implement legislation that will help protect the young and vulnerable from the unhealthy body image ideals which have become so prevalent in society.’
Instant messaging app Hospify has seen a surge in sign-ups from private practice teams looking for a GDPR-compliant alternative to WhatsApp since featuring in our journal last month.
Doctors, staff and patients can download the app and send secure messages and images without the need to anonymise health information, thanks to pin-code login and end-to-end encryption. The app, from entrepreneur consultant vascular and endovascular surgeon Mr Neville Dastur, even automatically removes messages after 30 days to ensure patient data is handled in line with the new GDPR regulations.
The Hospify app is available free to download in the Apple and Android app stores.
Healthcode boss Peter Connor
Mr Rajiv Grover, former BAAPs head
Urgent care unit opens
By Robin Stride
HCA Healthcare UK has opened a new Urgent Care Centre at London Bridge Hospital in response to increased demand from locals and commuters.
London Bridge Hospital Urgent Care Centre, at 29 Tooley Street, aims to be a rapid-access alternative to A&E – providing diagnosis and treatment for patients with non-life-threatening injuries and health concerns.
Walk-in appointments cost £100, with average waiting times of 11 minutes to see a nurse, and shortly thereafter a GP.
HCA said most blood work and other diagnostic tests would be turned around within an hour,
Dr Helen Mitakidis: on the lookout for more doctors for HCA’s urgent care centres and for primary care
with urgent access to imaging available at the London Bridge Hospital campus – at The Shard or in the main hospital building.
Breast unit offers one-stop service
The Platinum Medical Centre Breast Care Unit at London’s Wellington Hospital, re-opened after refurbishment, is providing a one-stop service which aims to investigate and diagnose breast conditions in a single visit. Consultant-led workshops were provided for local GPs and healthcare professionals at the relaunch, which is part of a £15m investment in services at the HCA Healthcare UK hospital.
Miss Joanna Franks, consultant breast and oncoplastic surgeon, said she was delighted to offer a one-stop service at the Platinum Medical Centre Breast Unit to
ensure women are assessed by a breast consultant and appropriately imaged using state-of-the-art equipment.
‘Patients are then able to discuss their results with the team all in one visit. We know women feel frightened if they notice a new change in their breast.
‘Getting a complete personalised assessment in one visit makes all the difference to their experience.’
Hospital deputy chief executive Jane Whitney-Smith said: ‘The relaunch of this centre is part of significant investment which has been made into The Wellington
The Wellington Hospital has introduced Selective Internal Radiation Therapy (SIRT), used to treat and control liver cancers that cannot be removed with surgery.
The treatment allows strong doses of radiotherapy to be delivered directly to a tumour, without impacting the surrounding healthy liver tissue – which can be affected in traditional liver cancer radiotherapy treatment.
Prof Ricky Sharma, consultant in clinical
Services offered across the London Bridge campus, including operating theatres, physiotherapy and pharmacy, will support the unit with referrals to consultants organised immediately.
Treatments will be provided for:
Traumatic injuries, sprains, fractures and sports injuries;
Respiratory and chest complaints, including upper and lower respiratory tract infections;
General ear, nose and throat conditions;
Stomach, bowel and bladder problems, including acute appendicitis and food poisoning;
Minor neck injuries and whiplash;
Wounds, minor burns and general aches and pains;
Other conditions on a ‘see and treat’ basis.
Hospital chief executive Janene Madden said: ‘Unlike other private urgent care services, we will be able to provide our patients with direct access to further investigatory procedures, consultants, inpatient care, MRI scanning and much more.’
Dr Helen Mitakidis, HCA’s urgent care physician group lead, said: ‘We are always on the lookout for more doctors and nurses to work across our urgent care centres and also more broadly across the HCA Healthcare UK primary care services. Doctors should contact Cecily Parkes at Cecily.Parkes@hcahealthcare. co.uk.’
Sky Sports news presenter and former Olympic gymnast Jacquie Beltrao (centre) opens the unit with consultant breast and oncoplastic surgeon
Miss Joanna Franks (left) and Wellington Hospital’s deputy chief executive Jane Whitney-Smith
Hospital to ensure the quality of the service we provide is at the forefront of private healthcare and meets all the needs of the community.
oncology, said: ‘There are many people in the UK who have been diagnosed with liver cancer and before SIRT was introduced, we would have to treat the tumour using chemotherapy.
‘SIRT allows us to treat patients with really high doses of radiation directly to the tumour, safeguarding the healthy tissue.
‘I have conducted many clinical trials looking into the efficacy of SIRT and the studies I published last year treating over 1,100 patients
‘We have many exciting plans to develop and expand the hospital’s offering in 2018, and this new dedicated centre forms a major part of this.’
in over 14 countries showed real optimism that this treatment can successfully treat liver tumours better than chemotherapy on its own.’
Chief executive John Reay said: ‘We pride ourselves on being at the forefront of private healthcare and the introduction of SIRT reinforces this position.’
SIRT is also available at HCA’s The Harley Street Clinic and The Christie Private Care in Manchester.
Soon-to-be-opened Schoen Clinic London has announced some of the specialist spinal and orthopaedic consultants who are joining the payroll.
They are consultant spinal surgeons Mr Colin Natali, Mr Ramesh Nadarajah, Mr Rohit Shetty and Mr David Cumming, plus consultant orthopaedic surgeons Mr Sam Rajaratnam and Mr Hugh Apthorp.
Unique within UK private healthcare, the hospital offers a new model for employing consultants on a full-time or part-time basis. But it said it would also welcome consultants wanting to practice on an independent basis.
The spinal and orthopaedic hospital said the approach had worked well across its 23 German locations.
Executive director Andreas Ludowig said: ‘In Germany, we believe that when you have a dedicated team that is part of your organisation, it becomes much easier to provide better quality – everyone signs up fully into the processes and the entire organisation.
‘It also enables us to organise our specialists to work as multidisciplinary teams for the discussion of complex cases and decisions on the best treatment for any individual.’
The first six names announced will all be employed part-time at the hospital at 66 Wigmore Street.
They follow the announcement back in March of medical director Dr Tim Wigmore, who is now in post.
The hospital said further names would be released as soon as contractually possible.
London surgeon Mr Natali, well known for his non-surgical treatment of back pain using innovative spinal strengthening, will head up the Spine Department.
The Hip and Knee Department will be led by Mr Rajaratnam and Mr Apthorp.
Schoen said: ‘Mr Rajaratnam is currently the leading knee surgeon on the UK National Joint Registry, performing the highest number of successful knee replacement operations each year, while
Mr Apthorp pioneered rapid recovery in the UK, setting up the first Rapid Recovery Programme for joint replacements in 2004.’
London adult and paediatric spinal surgeon Mr Nadarajah will work alongside his NHS posts at Royal London Hospital NHS Trust and Great Ormond Street Hospital for Children.
Mr Cumming will practise privately for the first time, believing Schoen Clinic London offers the unique private opportunity for multidisciplinary working, specialist care and outcome measurement that he has been waiting for.
Completing the line-up is Mr Shetty whose experience includes being the education lead for the British Association of Spine Surgeons and London Regional Representative for the British Spine Registry Steering Group.
Schoen Clinic London said it would offer rapid assessment, diagnostic imaging, evidencebased treatments, inpatient care and technical rehabilitation for adult private patients.
Bid to curb GMC powers Recruits for salaried hospital
By a staff reporter
A defence body is pushing for swift legislation enabling the removal of the GMC’s power to appeal Medical Practitioners Tribunal Service (MPTS) decisions.
The Medical Protection Society (MPS) wants the Government to set out a clear time-frame for change.
Removing the GMC’s right of appeal was one of many recommendations made by Sir Norman Williams as part of a rapid review into how gross negligence manslaughter is applied in healthcare, and was accepted by the Secretary of State for Health and Social Care last month (June).
This review followed concerns around the case involving Dr
Bawa-Garba, where the GMC appealed the MPTS’ decision to suspend her from the medical register for two years and sought agreement from the High Court to instead erase her.
The decision to strip the GMC of its power to appeal MPTS rulings was welcomed by MPS, which has – since the power was granted in 2015 – warned that it is an unjust and unnecessary duplication of powers for both the Professional Standards Authority (PSA) and GMC to have a right of appeal.
The GMC is the only professional healthcare regulator with this power.
But MPS medical director Rob Hendry said the legislative process required to enable the change –repealing section 40A of the 1983 Medical Act 1983 – could be
lengthy and urged the Government to bring legislation forward swiftly.
Speaking at a Westminster Health Forum event he said: ‘I am delighted that the Government has accepted the need to remove the GMC’s power to appeal decisions by the MPTS.
‘We have consistently argued that the GMC should not have this power.
‘The PSA has a near identical power, and regardless of whether the GMC uses its power of appeal correctly or not, in an era where we are looking to make the allocation of regulatory powers more efficient, such duplication is highly unsatisfactory.
‘The impact on the doctor at the centre of a case is significant. The regulatory process is complex,
lengthy and extremely stressful, and doctors face the prospect of a prolonged period of stress and uncertainty.
‘It also creates an unwelcome perception for many in the profession, that the MPTS is too closely linked to the GMC, or in some ways beholden to it.
‘One of the driving rationales in creating the MPTS in the first place was to separate out the investigation and adjudication elements of the Fitness to Practise process’.
He said when the GMC no longer had the power of appeal, doctors appearing before the MPTS would have greater confidence that the tribunal and the GMC were moving further towards being separate, independent entities.
(Left to right, from top) Colin Natali, Ramesh Nadarajah, Rohit Shetty, David Cumming, Sam Rajaratnam and Hugh Apthorp
Bupa guide to speed up bill payment
Compiled by Philip Housden
CMA consultation on private patient unit review process
The Competition and Markets Authority (CMA) conducted a short consultation last month on the approach to reviewing PPU arrangements brought in following its investigation into the private healthcare market in 2014.
At that time, the CMA found that because PPUs benefit from onsite NHS 24/7 infrastructure and support facilities, partnering with a trust to manage a PPU can provide low-risk market entry for independent hospitals.
The regulator’s concerns are that any such commercial arrangements should not lessen competition and so are unlikely to be supported where an independent hospital operator with weak competitive constraints in an area was seeking to enter into a partnership with their local trust.
The CMA’s new draft guidance considers whether there is a realis-
By Olive Carterton
Answers to many health insurance questions commonly asked by doctors can be found in a new guide from Bupa.
Important points about your Bupa patients’ cover aims to make health insurance more transparent by explaining the things that policies do and don’t cover.
The guide is designed to give doctors and their medical secretaries an overview of the standard features and benefits of health insurance policies, as well as some helpful tips to make working with the insurer easier.
Dr Tim Woodman, Bupa medical director for healthcare payments, said: ‘We hope that doctors will find the guide really useful. We developed it based upon the questions they commonly ask us, and have organised it so they can dip in and out as they need information.’
Bupa said it created the guide following a review of the reasons why doctors tend to get in touch. The insurer found that billing delays are among the top reasons for calling and many of these can be attributed to confusion about what is covered by health insurance.
tic prospect of finding that the relevant private hospital operator faces weak competitive constraints in the relevant local area.
It is unclear on the impact this will make, but potentially the revised guidance might be making it easier for new market entrants to manage PPUs, while also could be a spur to NHS trusts linking up in ‘chains’.
NHS PPUs offer ‘win-win’ for NHS and private sector
‘Build and they will come’ was the message on NHS PPUs at the Private Healthcare Summit 2018.
I told delegates at the conference organised by privatehealthcare.co.uk that PPUs offered a ‘win-win’ for all stakeholders in the healthcare sector.
They achieved this by:
Delivering more beds; Aiding patient throughput; Reducing demand and acting as an enabler to system improvement through commercial skills.
Research carried out by Housden Group also shows that PPUs are consistently supported by the
It covers some of the main features of health insurance policies such as excesses, choice of hospitals and outpatient limits.
There are definitions of some common insurance terms, such as chronic conditions, as well as an explanation of the steps involved when a patient authorises their treatment and the information Bupa might need to do this.
majority of consultants, who see them as offering a convenient route to private practice, fees growth and reduced risk for patients.
I told delegates that patient safety was driving change on a daily basis as consultants and anaesthetists increasingly took a precautionary principle to complex cases and sought to manage the risk of private patients with co-morbidities.
I said: ‘As these patients are generally more difficult to treat in private hospitals, the demand is driving new solutions.’
PPUs provide access to the best staff, equipment and multi-skilled teams on a 24/7 basis.
There are significant opportunities, both for NHS trusts and, potentially, their private sector partners, to develop the market.
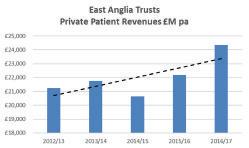
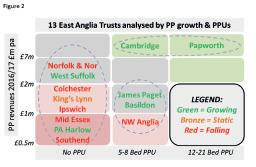
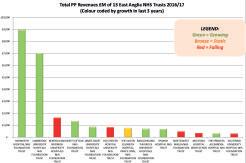
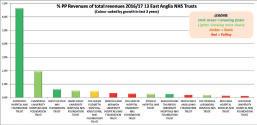
A majority of NHS trusts still have little or no private patient activity and, even in London, a third of trusts have virtually no private patient earnings.
NHS PPUs could also join together and create chains, with
A similar guide, called Important points about your cover, is also available on Bupa’s website for its insurance customers: www.bupa. co.uk/important-points-aboutyour-cover.
You can download Important points about your Bupa patients’ cover from www.bupa.co.uk/ healthcare-professionals/for-yourrole/consultants.
See page 44
the potential for a single NHS private patient brand to help explain the private choice within the wider health service.
The future of NHS PPUs, I believe, has something for everyone. For insurers, they offer a more open and comprehensive service and network coverage.
For hospital providers, this doesn’t have to mean more competition, but instead a mutual growing of the market and partnership opportunities.
For consultants, this is about convenience, 24/7 support and fees growth.
For trusts, they mean a virtuous circle of reduced costs and extended capacity.
And for the NHS leadership, if they are listening, this is one key to open up a systemic change, where the place of PPUs should be openly included in all forward plans as a joint priority for commissioners and providers.
Philip Housden is a director of Housden Group. Read his feature article on page 46
PPU WAtCH
Private hospitals want safety incidents involving privately-funded patients to be investigated by the forthcoming Health Service Safety Investigations Body (HSSIB).
The NHS Partners Network, now representing independent healthcare providers as well as those in the health service, has asked the Government to ensure the body acts on all patient safety incidents.
The umbrella body said: ‘Patient safety is the number-one priority for independent healthcare providers and the sector welcomes any efforts to improve patient safety, including investigating incidents properly when things go wrong’.
A draft Parliamentary bill says the proposed Health Service Safety Investigations Body (HSSIB) will
only cover NHS-commissioned services in England.
NHSPN said it was vital that independent providers were fully able to contribute to the HSSIB and that there was comprehensive coverage so as to best protect patients.
NHSPN clinical director Dr Howard Freeman said: ‘Safety is the number-one priority for the
independent healthcare sector and it is clear even at this early stage that the HSSIB is going to be critically important in driving up safety standards across the system.’
Including privately-funded as well as NHS-funded care would enable the learning and best practice from any safety investigations to be shared, he said.
Salaried service ‘is only way to go’ Safety body omits private care
By Leslie Berry
Many private doctors will find it uneconomic to continue unless they opt for a salaried service, according to one of the UK’s most experienced independent hospital bosses.
Keith Hague, who controversially pioneered the concept of wholly-employed doctors in UK private hospitals, predicted the ‘employed’ model would spread across the country.
He said: ‘Indeed already, despite their initial scepticism, we see some of the other providers actively considering and preparing for this.
‘Without wholly-employed status, many doctors will be forced out of business by uneconomic levels of professional indemnity costs, a trend we can already see in some disciplines elsewhere in the world.’
His comments came as he announced he had handed over the reins at the Cleveland Clinic hospital project in London.
He joined the team in 2014 and later became chief operating officer, with responsibility for preparing for and overseeing the initial stages of building a new hospital and separate outpatient facilities.
His first task was to see whether
Cleveland’s salaried doctor model would be acceptable to the UK private sector. Without that, the US group would not have come to London.
Enough doctors welcomed the concept, as they were increasingly faced with prohibitively high indemnity costs and the withdrawal of cover for some major procedures. And private medical insurers also gave the concept the thumbs-up.
The 200-bed hospital in Grosvenor Square is due to open in 2021 and an outpatient facility in Knightsbridge the year before.
Former chief executive at The Wellington Hospital, Mr Hague
said: ‘Many of us had been concerned about the pressures on the medical profession for some time and it was clear to me that the old system of private independent practitioners was gradually becoming “not fit for purpose”.
‘We now have a terrific team of senior managers at The Cleveland along with the first tranche of senior consultants – or, as they are known, Institute Chairs.’
Mr Hague also heads Worldwide Health care Associates and will stay as a special adviser to the Cleveland ‘for the time being’.
He is replaced by orthopaedic foot and ankle surgeon Mr Brian Donley.
Contact editorial director Robin Stride at robin@ip-today.co.uk TeLL US yOUR STORy
So what has been going on in your private practice? Independent Practitioner Today invites all those entrepreneurial consultants and private GPs out there to tell us their story. Let us share your achievements and good news.
Keith Hague (left) is handing over the reins of the nascent Cleveland Hospital in London’s Grosvenor Square to US surgeon Mr Brian Donley (above)
Women’s clinic teams up with eye specialists
Phoenix Hospital Group, buyers of the 25 Harley Street women’s clinic last winter, has joined forces with London Eye Diagnostic Centre (LEDC).
LEDC will deliver a range of ophthalmic diagnostic and clinical services at the site to complement existing facilities, including optical coherence tomography, fundus photography and laser treatments.
Phoenix Hospital Group chief executive Andrew Barker said their approach had always been to build their services around the very best consultants to ensure they offered patients the highest standards of care.
‘We are delighted to be working with LEDC, who are leaders in their field and believe this initiative will enable us to meet the growing need for ophthalmic diagnostics,’ he said.
Mr Ananth Viswanathan, a consultant ophthalmic surgeon and LEDC director, said coupling with Phoenix’s ‘excellent and comprehensive’ facilities would make a superb combination under one roof.
LEDC consultants include:
Prof Ted Garway-Heath, who, in addition to his role as a senior surgeon and academic specialising in glaucoma and cataracts, is president of the European Glaucoma Society;
Mr Jonathan Clarke;
Mr Ananth Viswanathan, chief scientific adviser to the Government on vision and driving;
Miss Narciss Okhravi.
The partnership is one of several initiatives from Phoenix including the development of its Women’s Health Services and Health Screening programme.
It said more leading specialists were joining the team. Patients can now get fertility issue advice from consultant Mr Rehan Salim. Gynaecologists Mr Angus McIndoe and Mr Jeffrey Braithwaite are also now based at 25 Harley Street.
IPT
A trawl through the archives: what made the news in 2008
A look back through our journal’s archives of ten years ago reveals that although times change, some issues are not so new
The power of co-operation
‘The future is in groups’, ran one prophetic headline, as we reported on the falling profits of anaesthetists. It was a message for many specialties in the years to come.
We advised: ‘Any consultant who is not in any form of grouping should reconsider the lone route. At worst, groups protect incomes and, in some cases, significantly enhance them.
‘There are also the first signs that anaesthetist groups are able to negotiate concessional packages –for example, with indemnity and private medical insurance. We expect activity here to increase significantly in future years.’
Recognition policy slated
A decade ago, AXA PPP was being attacked for suspending registration of new consultants during a tough review of specialist recognition and fee structure.
The insurer had suspended applications for several months while it revised its criteria. Terms and conditions were clarified, meaning that registration with AXA became discretionary and doctors could be denied registration.
Recognition was conditional upon agreeing to its fee schedule –published for the first time.
The BMA private practice committee called the approach ‘high-handed’ and long-winded.
Working for competitors
Consultants were warned of trouble ahead for those working in the NHS while also providing non-clinical work for private companies.
The BMA said some NHS trusts were developing policies to address potential conflict of interest issues where consultants were working for private companies that might be competing for business with their NHS employers.
Our forecast came true
Our editorial comment proved prophetic: ‘…we see a greater blurring at the edges of the two sectors. Specialists who work in both can expect increasing pressure on their private work from business-minded NHS trusts.’
Doctors face 25k car tax
Car expenses were the new battleground between consultants and the taxman, we warned.
Specialist medical accountant Ray Stanbridge wrote: ‘If the attack on motor expense claims intensifies, then it could be very serious for many doctors in private practice if they are found to have underpaid tax on car expenses.
‘Assuming a typical motor expense claim of £1,500 a year, retrospective re-assessments from the taxman and then penalty and
interest, then it could mean one-off tax bills of up to £25,000 per consultant.’
Charges for urgent care
A new emergency care centre set up at BMI’s Clementine Churchill Hospital, Harrow, north London, was charging £47 for an initial 20-minutes consultation with either a doctor or nurse.
Seniors’ NHS pay in 2008
Consultants’ public-sector pay rose an average 3.2% in the last year. The average new NHS-contract senior earned £115,000. The average consultant salary was £85,900 with a median of just £80,800.
Big growth in beauty work
The cosmetic surgery market was said to be growing at a rate of 35% a year.
SubScribe today don’t miss out on what we report and advise in the future. Sign up for a £75 subscription today – consultants, GPs and practice managers can save £15 with a direct debit.
See page 22
You don’t need a
diploma to run a practice
Managing your own practice is a huge challenge, with so many variables to control. In a new series of practice management articles for Independent Practitioner Today, Jane Braithwaite (right) covers all the aspects that you need to master to have a perfectly-run practice
Do you have an MBA? Perhaps a Diploma in Business Management? If not, you’re in the same boat as the vast majority of doctors who decide to start their own private medical practice, which is, in fact, a complex business like any other.
But don’t worry. In this series, I will
be looking at managing complaints, business development, systems and processes and more.
These are all important aspects of practice management, but the two areas you absolutely must get right at the very start are: planning and people. So here is what you should start doing:
Strategic planning
Being clear on goals and ambitions for your practice will help you achieve them. Allowing regular time in the calendar to step back and look at the bigger picture will keep your business on the right track.
There are four steps to successful strategic planning:
Manage performance;
Determine your position;
Develop a strategy;
Build your plan.
1. Manage performance
Taking this approach means you won’t miss any gaps. Ideally, garner input from anyone who contributes to the success of the practice and ensure that all your stakeholders are aware of your plan.
2. Determine your position
Like any other business, the leader of a medical practice needs busi-
We know your time is valuable, so we’ve put our support services together in one convenient website – just what you’d expect from one of the world’s leading suppliers of vaccines.
Visit www.sanofipasteur-portal.co.uk to explore our range of services and see how they could help you with your surgery’s vaccine management.
ness intelligence to survive. As the one in charge, it’s critical that you have access to executive information which shows analytics, forecasting tools and reports.
I’ve written about this previously in this journal with some suggestions on how to create a dashboard which shows the ‘big view’ of your business. I would strongly suggest you allocate time to setting this up so that you will easily be able to access trends.
For example, you should be able to see at a glance the split between self-pay patients and those with insurance over the last six months and how it compares to the previous six months.
You should also look at what changes are coming in business or medicine. If your practice is dependent on international patients, is there a downwards drift for certain countries?
The more insight into strategic issues you can gather, the better your planning will be. Combine all the data you’ve pulled together and document it.
There are many business planning methods and tools that you can use, and each has its pros and cons. The format is that important; the key is to have a short statement that you can refer to and change over time.
3. Develop a strategy
This is something you probably did when you first set up your practice, but you need to keep repeating the process to ensure your practice continues to grow in the direction you want it to grow.
We are often asked to have a five-year plan, and while it is difficult to have clearly defined goals for five years, it is possible and valuable to have goals and objectives for the coming two years.
When thinking about the longer term, a business mentor advised me to think of ‘the view from the beach’. Imagine yourself in five years’ time relaxing on the beach and envisage what you would like to have achieved by that point.
How will your practice look? How will the finances look? This becomes your longer-term goals and allows you to focus very clearly on the next two years and what you need to do now to ensure your reach ‘that view from the beach’.
You may already have a longterm plan, but when did you last review it? Does it need amending?
Can you distill your practice ambitions into four to six longterm objectives? Is your financial forecast still accurate? Try to add as much clarity as possible so your goals and priorities are accurate.
4. Build your plan
This is the nitty-gritty – an operational plan that ensures your practice achieves what you want it to. It’s important that you work with your team to come up with achievable goals and that they have an opportunity to feedback on plans.
Depending on the size of your practice, you might choose to allocate goals to specific areas; for example, the administration team answers 85% of calls each week. What does success mean? An increase in patients or a decrease in patient complaints?
No matter the goal(s), make it as easy as possible to measure progress and keep on track by defining what success looks like and sharing it with the team.
Manage performance
It’s essential to communicate your plans, objectives, decisions, and results to everyone working for the practice.
Not only will the team feel pride in being a part of the practice, they will feel as though they are working towards something meaningful. That’s an incredibly motivating factor.
Managing staff
The principles of managing a happy and productive team apply whether they number five or 50. Employees value an open and supportive culture with clear line management.
A Harvard Business Review article I read recently had some interesting things to say about what makes people happy at work. As a leader of a team of over 50, I have found much of this to be true.
Let people be themselves
Getting the best out of individuals means valuing them for their skills and embracing differences in perspective, dress and habits. This allows for diversity and shows another side to the much-
Make it as easy as possible to measure progress and keep on track by defining what success looks like and sharing it with the team
Top Tips
Write down your plan including clear objectives. You might only need one piece of paper, but record your plan and then book time in your diary to review it regularly, perhaps every three months.
share the vision: Have you shared your long-term goals with the rest of your team? if they don’t know what you’re working towards, they can’t help you get there.
Consider your long-term vision: Take a quiet moment over a cup of coffee to contemplate your ‘view from the beach’.
Create a dashboard: Can you make use of the systems you already have in place to put together a dashboard? Excel combined with data from your practice management software might be more than enough.
Avoid jargon: No ‘key performance indicators’! You don’t have to use business language if it doesn’t fit with your practice. Reword internal documents and patient information if a more relaxed approach suits – e.g. ‘We will know we’re successful when...’ Look it up: The BMA provides a wealth of free information to support those working in private practice.
Attend events that will remind you to take a broader look at your practice and your longer-term goals. Make a date: put dates in the calendar to review progress so you keep on track.
vaunted flexible working which is so prevalent in business today.
I have found that the more flexible I am with my employees, the more commitment I have from them. Does one of your team harbour a secret talent with Excel?
Can your medical secretary turn her hand to graphic design?
Snap up the opportunity to expand the practice knowledgebase at the same time as helping develop your employees’ careers.
Show how the work makes sense
This is when business intelligence and good systems can combine to energise your team. Patients are at the heart of any practice and sharing positive outcomes helps
everyone in your team see that their efforts make a difference. Not only will they feel pride in working for your practice, they will feel that their work is meaningful. Find a simple way to share patient reviews and feedback with everyone who helped make it happen.
Achieving (near) perfection in practice management takes an enormous amount of hard work. But all that hard work must be directed towards the right goals, or it’s pointless. With proper planning and dedicated staff, you will ensure that there are no gaps –just triumphs.
Jane Braithwaite is managing director at Designated Medical
Keep on the right side of the taxman
Along with many other businesses, a number of consultants have been involved in HM Revenue and Customs tax inquiries in recent years.
Susan Hutter (below) explains how to keep on the right side of the taxman, and, in the event of an inquiry, gives some tips on how this should be handled
It Is obviously far better to prevent a tax inquiry wherever possible. so to ensure you keep on the right side of HM Revenue and Customs (HMRC), you should observe the following rules:
☛ File your personal tax returns and business returns on time . Personal tax returns for the tax year ended on 5 April 2018 must be filed by 31 January 2019. It is best to get all the information together as soon as possible, if you have not already done so, so you do not have a last minute scramble. t here is no point in bringing yourself to the attention of HMRC for wrong reasons, such as filing late.
☛ Similarly, it is best to ensure that personal and practice tax is paid on time Practice tax will be included in your personal tax if you trade as a sole trader or a partnership. But if you trade as a limited company, the practice tax will be subject to corporation tax. HMRC expects all taxpayers to put money aside to pay their tax on time. If you fail to do so, HMRC may consider giving you time to pay. You will need a good reason and HMRC will usually expect everything to be paid within six months of the due date. Regular defaulters tend to get short shrift from the taxman. s o try not to make a habit of this.
☛ Ensure that you and your accountants make best use of the ‘white space’, which is on your tax return to explain fully any unusual entries. For example, you could use this space to explain why a source of income is materially different from the previous year; for example, if you have come into an inheritance or if your expense claim is unusually high. Using the white space may prevent HMRC asking the question in the first place.
Although HMRC can make random inquiries, these represent only a very small proportion. Most these days are ‘risk-based’ selections. Matters we have seen coming to the fore recently are:
➤ Income from investment properties – both rental income and also gains on investment property sales.
Most of this information can be obtained quite easily by HMRC from the Land Registry and it will be able to spot if there appears to be a gap in your tax return; for instance, where it knows you have held a property which is not your home but never reported any income from it or any gains on sale.
We have come across doctors who thought that, as they do not make a profit from the rental income – where all the expenses including mortgage interest is more or less the same as the income – they do not have to report it.
similarly, if they make a loss on sale, they thought they did not need to report it. these assumptions are incorrect.
➤ the practice expense claim is materially higher than in previ-
ous years, whether you trade in your own name or via a company.
➤ You have come into an inheritance that you have invested, giving rise to different forms of income compared to what you have had in the past.
You can see where the ‘white space’ note explained above can come in handy here.
Take out insurance
All independent practitioners should consider taking out ‘fee protection insurance’. Most accountants offer this via a thirdparty insurance company. this is insurance against professional fees that will be necessary to deal with an inquiry on your behalf.
s elf-employed individuals, which includes nearly all doctors who have private practice income, are at higher risk than those who only have a salary whereby all tax is deducted at source. the protection does not prevent an inquiry,
but it does ensure that the costs of having one are covered.
HMRC has one year from the date of the tax return filing deadline to delve into your tax return. therefore for 2017-18, where the deadline for filing is 31 January 2019, HMRC has up to 31 January 2020 to raise the inquiry.
If an inquiry is raised, do not panic, but ensure that you have an experienced professional to help you to deal with the inquiry. When HMRC raises the inquiry, it normally gives a deadline by which you should reply to its letter. the deadline is normally 30 days later. It is sensible to comply with the deadline if at all possible. But if you know at the outset that you cannot comply due to reasons beyond your control – because it will take you a long time to get the information or you will be on holiday for part of the time – contact HMRC immediately to extend the deadline. tax officers are quite
amenable as long as it is a reasonable time period.
HMRC will sometimes ask for a meeting with the taxpayer. this sounds scary, but is often a good idea, as it can bring the inquiry to a close more speedily than protracted correspondence.
It is not recommended to have a meeting without your accountant present, and they will advise you whether or not they think a meeting is a good idea in the first place.
You will need to prepare for the meeting and your accountants will guide you on this. In all cases co-operation with HMRC at all stages of the inquiry will ensure that you have the best outcome possible.
Next issue: Make an early start on a tax return – plus some important considerations
Susan Hutter is a partner at Blick Rothenberg and part of the team that advises medical practitioners
Practitioners use us because we offer the very best people and technology to deliver the most efficient and satisfying experience for patients. Discover how we will make your practice even more successful. Talk to us today.
When to say No!
‘I’m ready to pay you, so why won’t you treat me?’ Have you ever struggled to know when to refuse a client treatment?
Dr Sharan Uppal (below), aesthetic clinician, shares her thoughts and experiences
‘Why W on’t you treat me?’ I had this question put to me by a client when I advised him that I would unfortunately not be able to treat him with dermal filler. I knew the treatment would not make him happy or deliver the outcome he was looking for.
he looked at me as though I was insane: doing myself out of business and handing that business to my competitors down the road. yet, I felt a sense of pride that I knew ethically I had made the right call.
Being a people-pleaser, saying ‘no’ has never been something I’ve found easy to do. h owever, reflecting on this case and similar cases, I’ve been able to create a mental check-list, which has really helped me say ‘no’ with more confidence. here it is:
➽ Abide by the fundamental principles
Although there is no formal regulatory body in aesthetics, all medical professionals are answerable to their professional regulatory body, whether that’s the GMC, the General Dental Council or nursing and Midwifery Council. We need to keep the fundamental principles set by our regulatory bodies at the forefront of our mind.
My background is general practice and, like all doctors in the UK, I am regulated by the GMC and its ethical handbook Good Medical Practice this document explains the code of conduct expected of doctors towards patients and the wider society.
It is there to protect patients by ensuring confidentiality of care and non-maleficence, which essentially means that the doctor should do no harm or the least harm possible to reach a beneficial outcome. It requires a doctor to work in their patients’ best interests, within the limits of their competence and maintain life-long learning to stay up to date with current practices.
All good doctors live and breathe this ethos and not doing so can have serious consequences, including the loss of a licence to practise medicine.
Although aesthetic treatments may be seen as part of the beauty industry, the treatments all carry possible side-effects and risks.
Having appropriate training in procedures and achieving competence is essential before treating clients ➱ p20
When these treatments are performed by medical practitioners, we should still abide by the same code of conduct that we do with our nhS work. hence, any time we risk breaching this code of conduct, we should be saying ‘no’ to treating our client.
Some questions we should ask ourselves before deciding upon treating a client are:
is the treatment in the clients’ best interest? this isn’t always easy to ascertain in aesthetic practice, as treatments are not a necessity, but more a want, usually underpinned by a psychological need that the client desires to meet. We should remember that meeting psychological needs are usually in the client’s best interest.
Am i competent to perform the treatment? h aving appropriate training in procedures and achieving competence is essential before treating clients to ensure techniques are safe and cause the least possible harm.
The consultation – are all the jigsaw pieces in place? A great consultation is key in achieving a positive outcome for both client and practitioner. It will also highlight any possible red flags as to when not to proceed with treatment.
I view the consultation like a jigsaw puzzle, the pieces being:
➽ What the client wants the consultation provides the client with an opportunity to express what they hope to achieve from treatment. t his may be something specific, such as reducing the appearance of their frown lines or something more general along the lines of wanting to look more beautiful.
More often than not, what the client wants can be achieved by some means. however, in the rare instances that a doctor thinks it is simply not possible, a refusal to treat may come at this early stage.
➽ Why the client wants it It is the practitioner’s role to elicit from the client why he/ she wishes to achieve the result. he or she may feel their frown
If we simply cannot see what our client views to be a concern, treatment should not be undertaken
lines make them look worried or unapproachable. t hey may feel self-conscious of their lines and find that it impacts their self-confidence, which can hinder them in many aspects of life.
It is a skill to get clients to open up to the underlying reason they are seeking treatment and the process becomes much easier once a positive connection has formed and there is trust in the professional relationship.
Many of the instances when I have refused to treat a client have been when ‘the what’ and ‘the why’ do not correlate from an objective perspective.
For example, the client may have hyperpigmentation in their undereye region and request a tear trough dermal filler procedure.
t heir ‘why’ being that it will lighten the area, but objectively you may not see any tear trough deformity to treat or, despite there being a treatable tear trough, you may feel that it will not lighten the area to any significant degree. Providing your professional opinion that the treatment will not meet expectations is important to prevent dissatisfaction later.
It can be at the stage of eliciting the ‘why’ that occasionally other suspected conditions may become apparent, such as body dysmor-
phia. t hose with body dysmorphia are excessively distressed by their appearance.
We need to be able to see what our client does in order to help them attain their goals. If we simply cannot see what our client views to be a concern, treatment should not be undertaken.
Morally, I think it is important that we direct our clients to other avenues to get further support if we feel there is an underlying mental health issue.
We may also find ourselves in a scenario where we can see our client’s concern, but our instincts tell us that the ‘flaw’ is very much magnified in the client’s eyes. In such cases, we need to take a considered approach.
Being honest, while displaying empathy, is an approach I personally find helpful in these circumstances.
➽ can i deliver the desired result?
It is only once the practitioner knows what the client wants and why that an assessment can be made as to whether he/she can practically deliver the outcome desired by the client.
there may be cases where it is simply not possible to achieve the desired outcome by non-surgical means and it is imperative that we give honest information and refuse to do treatments that we know are not going to meet the client’s goals.
Self-awareness of our competency in the required treatment and a willingness to refer to aesthetic colleagues should further expertise be required makes for responsible practice.
➽ should i deliver the desired result?
We must not forget ourselves in this process and we need to protect ourselves from providing treatments that leave us feeling uncomfortable.
the easiest scenario for one to picture is the client who already has very full lips and requests a further lip enhancement, because she feels it will enhance her beauty.
We know we can deliver the result, but some of us may feel uncomfortable with the request. Personally, I know I feel uneasy when I am aware that the result
will go against the scientific principles of beauty, the very principles that I work hard to achieve. Each medical professional will have their own comfort zone with how far they personally feel able to venture away from conventional beauty rules. the key is to have that self-awareness and be confident to explain why you do not wish to proceed with further enhancement.
If this is done with genuine care, the client often respects you more for your honesty. She may still seek that enhancement with another practitioner, but you have respected your autonomy.
➽ capacity and informed consent
t he client needs a good understanding of the benefits, sideeffects and risks of the procedure to give informed consent to treatment. Without this, we should not treat.
➽ Are there any contraindications to treatment?
Pregnancy and breastfeeding are common contra-indications with many injectable aesthetic treatments. A detailed medical history should always be undertaken to ascertain any other contraindications or relative contraindications.
Seek advice from aesthetic colleagues or the client’s relevant specialist where necessary. there will always be cases where the refusal to treat does not go down well, even with the best worded delivery. however, if we can demonstrate logical reasoning to our clients, by dint of crossreferring with the above check-list, then it is a pill that is easier for them to swallow.
In many of the instances when I have delivered a caring refusal, I have actually gained a great deal of respect from my client for not simply provided a vending machine service.
As medical aesthetic practitioners we should aim for happy outcomes, without compromising our ethics along the way.
Dr Sharan Uppal is medical director of Pegi Day Aesthetics, Huddersfield, and senior aesthetic clinician and trainer at SkinViva, Manchester
The bespoke pathology service for your practice
WHEN A DOCTOR needs confirmation of a diagnosis or a measure of the progress of a treatment or condition, he or she needs to be 100% certain that the sample they have sent off will be assessed and reported on accurately and quickly.
Every doctor needs that certainty, that trust, every single time they send a sample to the pathology lab.
Most patients arrive at the clinic or consulting room feeling anxious, unwell and needing advice, reassurance and often, some measure of certainty. The patient, frequently unsure and slightly disoriented, particularly if it is the first time they have been referred to a specialist, puts his or her trust in their doctor. So the faster the test is reported, the earlier the treatment can begin.
Because of our experience over the years, when we set up Cellular Pathology Services (CPS) we wanted to provide a higher level of
service, a more accessible, agile, and more direct service, where for example, we could offer every doctor personal contact with the consultant pathologist whenever it was needed. We wanted to become an extension of their practice.
It is why we prefer to work as a close partner and collaborator, helping our clients to provide a world class standard of care for every patient. It’s part of our culture at CPS.
We are here for our clients whenever required; we are there at MDTs, we are available on the phone or in person. We are always available.
Working with practice or nurse managers, we strive to take away any process hassles to provide a seamless and timely service. Our own team of drivers get to know the special needs of each customer and make sure we receive samples without delay. At every level, we try constantly to make doing business with us very easy!
Every member of our team is focused on the needs of our clients; everyone is passionate about their work. Every member of the team is at the top of their game and the esprit of our team is palpable. We like to think this is unique in our sector!
As a result, our customers tell us they enjoy more than just a cold, standard business relationship with CPS.
And that’s how we build our reputation. By getting to know each client and adapting our services to match its particular requirements and ensuring access to our team, whenever that’s required.
Perhaps it is why much of our new business comes by recommendation and why we continue to grow to meet customer demand.
So, if you are looking for a pathology service that can be structured specifically for your practice, then call me, Scott Hague on 07741 855 550.
Histopathology, Diagnostic Cytology, Gynaecologic Cytology, Mohs Surgery, Frozen Section are just some of our services.
Dear Reader,
Subscribing to Independent Practitioner Today is the only way you can be sure you will see every issue and have the option of reading us online using our special page-turnable edition. Don’t risk missing out. Our personal subscription for doctors and managers is only £90 a year and £210 for organisations. But you can cut this to just £75 and £180 respectively if you pay by direct debit. So take advantage of this offer now for our unique business journal dedicated to supporting you in your private practice. We’re confident your subscription will repay itself many times over!
Editorial director
ApplicATion FoR sUbscRipTion
i enclose a cheque for £ ........... made payable to the independent practitioner
please debit my Mastercard/Visa/amex/diners
Please debit my Mastercard/Visa/ Amex/Diners Card
i would like to pay by direct debit (please complete all details in box below). don’t forget, it’s £15 cheaper to pay by direct debit; £30 less for
Instructions to your Bank or Building Society to pay Direct Debits
Name and full address of your bank/Building Society
To:
Banks and Building societies may not accept direct debit instructions for some types of account
post your application (no postage required – uK only) to: independent practitioner today subscriptions department, Freepost, po Box 36, plymouth, pl1 1Br
Banks and Building Societies may not accept Direct Debit instructions for some types of account
phone: 01752 312140 Fax: 01752 313162 email: lisa@marketingcentre.co.uk or subscribe online at www.independent-practitioner-today.co.uk if you want to pay by
by writing to your Bank or Building Society. Please also send a copy of your letter to us.
How to handle your lawyer
With careful planning, you can get the best advice –and keep your legal bills down to a minimum. Lynne Abbess shows how
EvEry businEss, no matter how large or how small, leaves a ‘legal footprint’ – so if you operate without any legal advice at all, you do so at your peril.
i t is no coincidence that it is those who claim to be able to function without legal advice who often end up with the biggest problems.
And while there might be a perception that lawyers should be avoided at all cost, as they are simply too expensive, with careful planning it is perfectly possible to achieve the best of both worlds – receiving the best advice
while keeping costs to a minimum. s o how can this be achieved? Here are my top tips to assist you in achieving this objective.
➲ Always appoint an expert
Healthcare is a very specialised area of law and not one which is on the radar of the vast majority of lawyers. your personal solicitor is highly unlikely to know anything about it – and so to receive appropriate advice, you need to source an expert.
While costs are always high up on the radar, it is a false economy to appoint a non-specialist. not only are they likely to take more time to produce an answer to your inquiry – but it might not be the right answer.
And your costs may well increase on account of the additional research or referrals that need to be made. you certainly don’t want to be a ‘guinea-pig’ –and there is no substitute for experience.
Make sure the individual expert you select is part of a business with the back-up resources to provide the wider advice you’re likely to require.
b e aware that, just like clinicians, lawyers practise within an area of specialty – and a real estate lawyer will not personally be best placed to advise you on, for example, an employment law issue. your business will be best served by appointing a firm which has specialisms covering a broad range of healthcare law to enable you to benefit from ‘joined-up thinking’, meaning – hopefully –nothing will fall between the cracks.
While a well intentioned colleague might be keen to make a recommendation, they might not be best placed to judge whether their advice was the most appropriate or not on the basis that ‘you don’t know what you don’t know!’
independent research therefore is usually the safer way forward and the legal directories (Chambers and Legal 500) can be very useful, as they provide an independent ‘peer-assessed’ review of specialists in the field.
And once you have established some names through this route, any practical experience a colleague has to offer of dealing with that particular expert could provide a useful back-up.
➲ don’t leave it to the last minute
Don’t risk small incidents blowing up into a crisis by failing to take advice at an early stage.
And even in a non-dispute situation, be aware that the legal process may not follow what you assume to be a logical or ‘common-sense’ path.
There are many hidden traps
Just like clinicians, lawyers practise within an area of specialty
which will not be apparent from the surface, which, if you have not resolved them in advance, you will be living with for many years ahead.
it is a wise precaution to have an on-going account with your lawyer, which will enable you to pick up the phone and seek advice at a moment’s notice, thereby allowing you to run decisions pass them at an early stage.
This will also enable your lawyer to have a better understanding of new developments within the context of your business overall.
An early approach, therefore, will put you in the best position to structure your case in the most appropriate way – even if it results in you being advised to come back later.
➲ Understand the terms of engagement before providing any advice, your lawyer is required to send you a Client Care Letter which clearly sets out their terms of engagement. This should identify the personnel dealing with your case – by name and job description/ status.
Do not always expect to deal with a partner, as the more work that can be undertaken at a more junior level, the lower your costs should be.
The letter should also set out the extent of the advice to be provided. you shouldn’t assume the advice will cover anything more than specified – unless you specifically agree this later.
s o, for example, if the terms provide for advice on your acquisition of a business, do not assume this will automatically extend to employment law advice concerning your intention to subsequently change the contractual employment terms of the staff.
➲ Fees
you should also be provided with not only the hourly charge out rate of the individuals concerned, but also with an estimate of the overall time/cost that may be spent on your case. if you are unclear about anything, don’t be afraid to ask.
if a ‘fixed fee’ is proposed, clarify whether this is ‘fixed’ as an absolute figure – even if the case
if you try to screw your fees down to a bare minimum, it is bound to impact upon the level of advice provided
does not proceed all the way – or whether it is ‘capped’. And if it is fixed and the case is indeed concluded, check whether there is any prospect of an additional charge being levied if it has taken longer than expected.
While it is natural for a consumer to want to secure a ‘good deal’, if you try to screw your fees down to a bare minimum, it is bound to impact upon the level of advice provided.
in fact, you should be wary of a ‘fixed’ fee which is absolute, as it is human nature that once the ‘budgeted’ figure has been reached, there may be a natural tendency for those involved to want to ‘wrap it up’ as quickly as possible thereafter, even though it might not be in your best interests to do so.
➲be organised
The more of your lawyer’s time you can save by careful preparation, the quicker you will receive the advice required – and the more cost-effective it is likely to be.
b efore receiving any advice, every client has to undergo antimoney laundering and ‘conflict’ checks. Make sure the originals of your passport and two utility bills bearing your name and current home address are readily available. And if you have moved recently, inquire what else would be acceptable as evidence of your identity.
your lawyer may ask you to transfer funds as ‘cost on account’, so have the funds available to do so.
Prepare a resume of the nature of your case with as much supporting documentation as possible – and present it in a coherent order.
Failure to provide your lawyer with the material required in a timely fashion is bound to have an adverse impact upon you, whether this results in additional costs – or even the collapse of your case entirely.
There may be time limits that are imposed by third parties which impact upon your dealings and cannot be moved.
be aware that anything legal is likely to generate a wealth of paperwork – or digital attachments.
Of course, your lawyer will
retain a copy, but the more organised you can be as your case progresses, the less likelihood there will be of misunderstandings or missed opportunities arising.
➲ communication
Don’t expect your lawyer to be a mind-reader. Make sure you let them have every piece of information available to you, as something which may appear to be of minor significance to you may be of major importance to your case. Allow your lawyer to filter what is relevant and what is less so.
When you communicate with your lawyer, try to prepare what you need to say in advance – and avoid ‘ping-pong’ emails, not least as they will add to the cost.
And while we all live in an electronic age, sometimes there is simply no substitute for a face-toface meeting – albeit this may take place by s kype rather than sitting in the same room.
such meetings can often be more cost-effective than a lengthy series of email exchanges – and very often points arise during the course of discussion which would not surface in an electronic exchange.
➲ be commercial b e aware that you, rather than your lawyer, are the decisionmaker, although you are likely to base this upon the advice you receive. you should not expect your lawyer to make the decision for you – or criticise them for failing to do so.
And try not to allow emotion to influence the decision you take. r emember that the law is based on a history of legislation and case law rather than emotion – and if your lawyer advises you to let something go, there is, no doubt, a very good reason behind it.
And if the advice you receive is not what you want to hear – don’t shoot the messenger.
➲ Annual health check
Have an annual health check. you expect to meet with your accountants at least once a year and inevitably your discussion will range beyond the scope of your accounts and into the realms of your business planning.
i f you adopt a similar policy with your lawyer, not only will this enable your plans to be achieved in a more timely fashion, but you are more likely to avoid the pitfalls that could otherwise arise.
Lynne Abbess (right) is consultant solicitor at Hempsons
independent practitioner Today has joined forces with leading healthcare lawyers Hempsons to offer readers a free legal advice service.
We aim to help you navigate the ever more complex legal and regulatory issues involved in running and developing your private practice – and your lives.
Hempsons’ specialist lawyers have a long track-record of advising doctors – and an unrivalled understanding of the healthcare system as a whole.
call Hempsons on 020 7839 0278 between 9am and 5pm Monday to Friday for your ten minutes’ of free legal advice.
Don’t be afraid to have an ongoing relationship with your lawyer. until you know them better, your reaction might be to regard all lawyers as sharks – but they won’t bite – honestly!
Free legal advice for independent practitioner Today readers
Advice is available on: business structures (including partnerships) commercial contracts disputes and litigation HR/employment premises Regulatory requirements and investigations
Jamie Foster
Tania Francis
Keeping up to date has been clarified
Doctors now have new GMC guidance on supporting information for appraisal. Mr Ian Mackay (below), Responsible Officer for the Independent Doctors Federation, runs through
what you need to know
Following Sir Keith Pearson’s report Taking Revalidation Forward, published at the beginning of last year, the g MC set up a r evalidation oversight group (rog) to replace the revalidation Advisory Board.
rog was tasked with tackling the issues raised by Sir Keith’s report and is due to be completed by September. Part of its work involved reviewing the g MC’s guidance on supporting information for appraisal and revalidation.
Although there have been no changes to information type or frequency, the overarching principles have been stated more explic
itly: quality not quantity, focus on reflection and learning, and whole scope of practice.
clarification
on requirements for revalidation
How does the new clarification fit with the guidance doctors may receive in the relevant specialties or in the workplace?
The g MC’s position on local appraisal requirements is now clear. Doctors must collect, reflect on and discuss supporting information generated from a doctor’s whole UK practice.
There is also clearer guidance on doctors working overseas. r esp
onsible officers (ros) may decide to accept supporting information drawn from overseas practice if they are satisfied it meets the same standards as those expected in the UK and is relevant to the doctor’s UK practice and therefore gives assurance about their continued fitness to practise.
Doctors are reminded that it is important to speak to their ro as soon as they know that they intend to practise overseas while holding a UK licence to practise.
o nly in exceptional circumstances would a doctor with supporting information drawn from practice wholly or significantly
overseas be able to maintain their UK licence to practise.
The Academy of Medical royal Colleges, individual colleges, faculties and specialty specific organisations provide additional guidance about appraisal and revalidation for doctors working in different specialties. This is because the range of supporting information expected depends on their scope of practice.
The organisation where doctors work may set other appraisal or contractual requirements as part of a doctor’s employment – for example, completion of health ➱ p28
and safety training. That is a matter for employers and they are not gMC requirements.
Failure to meet local appraisal or contractual requirements may be discussed at a doctor’s appraisal but should not influence the revalidation recommendation.
Whole scope of practice
i t is particularly important for independentsector doctors, who may have a portfolio career, to know they must declare all the places they have worked and the roles they have carried out as a doctor since their last appraisal.
Supporting information must cover clinical – including voluntary work – and nonclinical roles in the n HS and private sector, including academic ones.
n ew guidance has also been given on the balance between the quality and quantity of supporting information so that doctors don’t feel pressured to gather too much evidence.
Doctors will be reassured to hear that it is the quality and not the quantity of supporting information that is required. The gMC does not set a minimum or maximum quantity of supporting information doctors must collect, but it should be of high quality and support the full scope of the doctor’s work.
importance of reflection
Appraisal provides the opportunity to reflect on a doctor’s professional practice. r eflecting on supporting information and what it says about a doctor’s practice is intended to help doctors improve the quality of patient care.
But there has been much discussion about the role of reflection at appraisal, particularly following the case of Dr Bawagarba. new guidance for doctors on reflective practice is to be produced jointly by the g MC, the Academy of Medical royal Colleges, the Conference of Postgraduate Medical Deans and the Medical Schools Council later this year.
collecting feedback from colleagues
At least once in a revalidation cycle, normally every five years, doctors must collect, reflect on and discuss feedback from colleagues at their annual appraisal.
There is a view that patient feedback should – and often already is – undertaken on a more frequent basis
The colleagues who are asked to give feedback must be chosen from across the doctor’s whole scope of practice and must include people from a range of different roles who may not be doctors. Doctors must now explain the basis of their selection for colleague feedback, must choose colleagues impartially and be able to explain to their appraiser why they have chosen the colleagues and, importantly, must reflect on what the feedback means for their current and future practice.
in addition, unless a doctor has no contact with patients, they
We reported on the new guidance on revalidation last month (left)
must collect feedback from patients. it is clear that it is easier for some groups of doctors than for others. i f a doctor believes they can’t collect such feedback, then they must agree with their ro why they do not need to.
The timeframe for the gMC to consider ongoing requirements for patient feedback has now been extended to Spring 2019.
There is a view that patient feedback should – and often already is – undertaken on a more frequent basis. Many doctors do this either on a less formal routine annual basis for their own information or as part of ongoing feedback for other bodies, such as the Care Quality Commission, or it may be collected by employers. where patient feedback is collected, this information should be included with a doctor’s supporting information for discussion with their appraiser.
Pragmatic recommendations
Sir Keith concluded his report with the following statement: ‘i believe my recommendations are pragmatic and can be largely delivered within the next five years.
‘in particular, i would expect to see early action to strengthen revalidation processes for locum doctors, remove unnecessary burdens for doctors and increase public understanding of the purpose and impact of revalidation.’
Having represented the independent sector on the r evalidation o versight g roup, i have been impressed by the fact that there is a genuine desire to remove unnecessary burdens for doctors, to encourage supporting information to be of high quality rather than excessive quantity and to clarify existing requirements rather than introducing new ones.
There was also a genuine desire on the part of the gMC to listen to members of the group, who were representing a wide range of stakeholders, including the independent sector.
You can read the whole updated g MC Guidance for Supporting Information document at: www. gmcuk.org//media/documents/ rt supportinginformationforappraisal and revalidationdc5485_pdf55024594.pdf
Could flawed assumptions let you fall foul of the law?
Doctors and medical businesses are facing potential legal dangers due to confusion over vicarious liability, medico-legal work and the demands of GDPR. Peter Anderson reports
MANY MEDICAL businesses are leaving themselves vulnerable to potentially crippling costs because of confusion over the extent of their insurance cover.
Recent legal developments, coupled with doctors’ ever-changing work patterns, mean practitioners and their teams could find they are not covered following a claim.
There are concerns that some medical professionals face an additional threat because their recent efforts to comply with the EU’s new General Data Protection Regulation (GDPR) still leave them vulnerable to legal action.
The warnings come from Medical Risk Services Limited (MRSL), a prominent provider of insurance, advice and services to medical practitioners. The company, which was established in 2004, specialises in helping doctors and medical businesses mitigate and manage their risks and reduce their indemnity costs.
Administrators facing threat
MRSL’s Co-Founder Roger Houston said: ‘Medical businesses – including doctors, their nursing staff but also support teams ranging from administrators to accountants – could potentially fall foul of the law simply by assuming they’re covered when they’re not.’
According to Roger, one of the greatest risks is posed by doctors having formed partnerships or companies to share costs or provide more flexible services. ‘Our experiences show that doctors typically understand they can
be liable legally for the actions of their directly employed staff – or so-called vicarious liability,’ he said.
‘What many don’t appreciate is that liability could result from the actions of any partner, director or person working within the group. The broad scope of vicarious liability means this is no longer just about employers and employees.’
He continued: ‘There are also justifiable fears that lawyers could prove more successful in pursuing action when they don’t need to prove negligence or malpractice on the part of a single, named individual.
‘An individual is exposed to the “collateral damage” following the errors or omissions in relation to all aspects of the activities of co-directors or partners. The implications being that if a liability threatens the business it will affect all involved which can, in turn, affect an individual’s ability to hold directorships or create partnerships in the future.’
He added: ‘MRSL’s solution is for medical professionals to take out insurance tailored to the entire business or entity rather than each doctor carrying their own indemnity.’
Another potential threat has emerged for doctors acting as expert witnesses or conducting medico-legal work – and when their medical indemnity policy may not apply or may offer only limited cover.
Roger explained: ‘There’s a huge legal distinction between doctors providing their day-to-day
surgical or consultancy services to a patient and doctors giving medico-legal advice or providing comment on a patient to a third party.
‘In this latter case, a doctor needs to ensure they have professional indemnity rather than medical indemnity – and also that the limit is sufficiently high. Recent developments have also removed certain aspects of expert witnesses’ legal immunity.’
Specialist advice is essential Roger, who has a 30-year career in insurance claims, urged doctors to seek specialist advice, with the team at MRSL experienced in handling the complexities of the cover required.
The company also operates a highly effective risk-profiling approach that enables risks to be accurately scored and for insurance to be targeted and cost effective.
Meanwhile, doctors and medical entities have been warned not to be complacent following the
introduction in late May of the EU’s new GDPR rules on handling data.
With human error identified as the largest cause of data breaches, MRSL offers advice and services that include email encryption, document transfer facilities and accurate recording of email delivery.
The company has also signed up to the #StopAttachments campaign, which enables clients to transfer data via centralised single-source documents or via a secure document-sharing platform.
‘GDPR goes way beyond shredding old documents and publishing a privacy policy,’ Roger Houston explained. ‘At MRSL we’re able to help with everything from password protection to foiling would-be hackers by encrypting storage.’
For further information on MRSL and its services, please telephone 0203 058 3733, email enquiries@mrslenterprise.com or visit www.mrslenterprise.com
That’s the way the money goes. . .
Unpicking a multimillion-pound compensation claim
As compensation claim costs against private doctors hit record levels, Independent Practitioner Today asked the MDU’s senior medical claims handler Dr John Dale-Skinner (right) to show why huge compensation payments are more common now – and what doctors can do protect themselves from the risk
A lot h A s changed in the medico-legal landscape since the MDU was founded to defend doctors more than 130 years ago.
In the 1880s, negligence claims were pretty much unheard of and even some 50 years later in 1932, the MDU paid out just over £3,000 in total for medical negligence claims against its members. today, individual settlements can be in excess of £20m.
Claims inflation has been rising at 10% a year for several years and a recent change to the legal formula for calculating compensation payouts – the personal injury discount rate – has added to the problem by doubling the size of some awards.
the aim of compensation is to put the injured party into the same position as he or she would have been but for the injury.
this is known as the full compensation principle. Damages are assessed on the basis of meeting the injured party’s reasonable needs and, as the law currently stands, the cost to defendants is not taken into account.
to illustrate the size and complexity of a compensation payment, let us examine the details of a payment of £11.5m (see box on opposite page ➱).
For example, an MDU case in which a patient had tetraplegia following spinal surgery and 45 years’ life expectancy could receive a compensation payment of £9.2m under the previous discount rate and £17.4m under the new rate.
t he costs of care have also increased as medical advances improve the life expectancy of patients with severe injuries.
this is a fictional case, based on those paid by the MDU and involves a 29-year-old man who sustained a brain injury after suffering a cardiac arrest following knee arthroscopy during a private day-case procedure.
Future care
It is not uncommon, as in this case, for the majority of compensation to be due to the cost of future care.
the right of an injured party to ➱ p32
DiSSecting a claim
CPS Your pathology partners
At CPS we tailor our service to your practice. Our highly experienced team work with you to give you the highest quality reports, delivered on time, every time. And when you need it, you’ll have access to consultant pathologists and not just in office hours. Our integrated and personal service helps to give your patients the finest care possible. It is also why we are one of the most respected and preferred labs in the UK.
To find out more on how we can partner with you Call Scott Hague on 07741 855 550 or email scott.hague@cellpathservices.co.uk www.cellularpathologyservices.co.uk @cpshisto
seek damages on a private basis has been confirmed by legal precedent. For example, in the case of Peters v East Midlands s trategic h ealth Authority (2009), the Court of Appeal ruled that an injured party is entitled to opt to claim damages for care and accommodation on a private basis and is not required to rely upon local authority provision.
At the MDU, we have been campaigning for a change in the law to allow defendants such as the MDU to buy Nhs and social care packages to meet patient needs.
Currently, s ection s 2(4)of the l aw Reform (Personal Injuries) Act 1948 requires all personal injury defendants to disregard the availability of N hs care when paying compensation. this should be repealed, boosting Nhs funds for the benefit of all patients, including those whose need for long-term care is not due to negligence.
in 2017, almost a quarter of all consultant claims were from members who had been in practice for over 20 years and never before faced a private practice claim
You can find out more about how to support our campaign at www.themdu.com/faircomp.
Avoiding litigation risk sadly, the chances of being sued has increased in recent years, but the good news is that so has the MDU’s rate of successfully defending cases. latest figures show no compensation payment being made in over 80% of medical claims against our members.
Nonetheless, in 2017, almost a quarter of all consultant claims were from members who had been in practice for over 20 years and never before faced a private practice claim.
Although the risk of being sued is always present to a degree, there are some considerations for clinicians to bear in mind in day-today practice that may stand them in good stead if a case is brought against them. these are:
➤ Accurate record-keeping remains paramount and the MDU has long emphasised its importance. Clin icians are often surprised at the level of scrutiny applied to records when a clinical negligence claim is pursued.
It is important to avoid ambiguity in medical abbreviations and also in the general content of your clinical note.
Read it back – could it be interpreted in more than one way? t his is particularly relevant to safety-netting advice, which is often the subject of disagreement during litigation.
➤ legibility is important. Illegible records may be used to infer a careless or rushed approach.
➤ to avoid discrepancies in the sequence of events, ensure that you date and time your clinical records carefully.
Consultation software may do this automatically, but if this is not the case, clinicians may need to do this manually. Review your clinical note. Can you tell when, where and with whom the consultation took place?
➤ It is helpful to keep records of phone conversations and email exchanges about consultations and appointment histories. this can assist in dispelling any false recollections, should a claim be pursued at a later date.
➤ Involve the MDU or your med-
ical defence organisation as soon as possible if you receive a request for records under the clinical negligence pre-action protocol. this is usually a solicitor’s letter which sets out the allegations and includes the patient’s signed consent to release their records. the civil litigation process runs to a strict timetable and our claims handling experts will guide you through the process and fully involve you in decisions about whether to defend or settle a case if the case proceeds – and many do not.
Although claims numbers and costs are outside the control of doctors, the risk of being sued is ever present.
Providing first class medical consulting and therapy rooms at prime locations in Central London and Liverpool
London
www.tenharleystreet.co.uk 020 7467 8300
Liverpool
www.eightyeightrodneystreet.co.uk 0151 709 7066
FOR SALE
Established practice with high interior specifications
consultant-based aesthetic and implant/oral surgery centre in a southern Bedfordshire market town, 30 minutes to euston by train (Waitrose and costa coffee within walking distance of practice). accredited by private medical insurance companies. the practice consists of:
One dental surgery;
One oral surgery/sedation suite;
One non-surgical treatment room;
a further room plumbed and ready for a dental surgery installation;
an additional treatment room;
cone beam ct & orthopantomogram imaging room.
additional rooms are installed and used for meetings and consulting.
the sterilising room is off the oral surgery suite and a lift allows access from the sedation floor to the ground floor.
the three-floor facility is fully air-conditioned and has cat 5 connectivity.
Valued at 620k inclusive of freehold and car parking spaces. call 0330 088 11 56 for details
Mr David Floyd (right) provides an app for his patients. Here he discusses how it improves the quality of information and care at his practice
Why did you decide to create an app?
It came about after I looked into the statistics of my website and found that more than half of those visiting it were doing so using an iPhone.
There has been a quantum shift over the past ten years in the way patients find you. When I started private practice as a consultant, I had a phone and a secretary – you wouldn’t find me unless you knew somebody that had my phone number.
I’ve now had a website for six years and today when patients come to see me, they seem to know everything about me and, having already done their research online, have decided that I’m the right person.
At the CCR Expo trade exhibition and conference last year, I met the team from Patient Journey who asked if I might be interested in having my own app. I had been thinking of redesigning my website
to be more compatible with a smartphone, but realised that this app was an even better solution.
What does your app do exactly?
The app is designed to guide the patient through every step of their treatment. Firstly, it shows you what to expect during your first consultation and how to book your treatment.
Once the treatment is booked, the app informs the patient of everything they need to do to prepare for surgery. For example, when to stop taking the contraceptive pill or when you should stop taking aspirin and other blood-thinning medications.
It notifies you when to plan time off work and when you should arrange a lift to get to the hospital, what to do the night before surgery and what you should take with you in your bag to the hospital.
It means the patient doesn’t
How Mr David Floyd’s app appears on a smartphone screen
have to worry about remembering everything in the run-up to surgery. Instead, they get notified by a text delivered automatically to their phone, with all the information they need, exactly when they need it.
in what ways does it help your patients?
I now consider the app to be an essential part of the patient’s preparation for surgery. I ask all patients to download the app and, so far, the feedback has been very positive. I spoke to a patient recently about the app who said: ‘It’s amazing. It’s all the sorts of information that I kind of knew about, but it’s presenting it to me exactly when it’s time to think about it.’
The app is a fantastic way of communicating with patients, and acts as another layer of information to make sure that we’ve not forgotten anything.
My responsibility as the surgeon
is to ensure that every patient is fully prepared for surgery. Important issues are always discussed with the patient, but they cannot be expected to remember everything.
Occasionally, a patient will turn up for surgery still taking a medication they were asked to stop. This can result in the surgery being postponed, which is very inconvenient.
Now with the app, the patient sees a notification and is reminded to stop the medication and if they are unsure, they can call my secretary for confirmation. This is exactly what I want, as it engages the patient in preparing for surgery and gives them easy access to all steps of the treatment pathway.
how has the app improved your clinical service?
The app has allowed our patients to feel much more engaged in their treatment. We now have this all-
encompassing interactive tool that takes the patient from thinking about their first consultation, through their run-up to surgery, the post-operative recovery phase right until to the point of discharge.
What features do you particularly like in the app?
The app is very intuitive and customisable. I have added general information about myself and my clinic together with ‘before and after’ galleries and videos to help inform patients as much as possible. It is also possible to include questionnaires in the app, which are quick and easy to complete. This provides a powerful automated tool for data collection.
It means we can easily capture outcome data, including patient satisfaction, which will help us refine and improve the service we provide.
I wonder when was the last time other Independent Practitioner Today
readers sent a questionnaire to their patients to ask what they thought of their service.
Another feature we are hoping to add is encrypted two-way communication with the patient through the app. The patient would be able to send me a photo of their wound after surgery so I can reassure them all is well.
Do you envision that technology will play an important role in shaping the future of patient care?
I think it is already happening. Just this week, a GP service is launching an online consultation app where you can Facetime with a GP instead of going to a consultation. They’re starting to diagnose over Skype now too. We are definitely moving into that domain.
see ‘screen time with doctors’, page 36
www.patientjourneyapp.com
Screen time with doctors
Alberto Porciani (right), founder and chief executive of Top Doctors, explains the rationale behind the development of the service and how it fits into the current landscape
‘Siri, my stomach hurts. What’s wrong with me?’
‘OK, Google, how can I tell if I have diabetes?’
‘Alexa, why can’t I lose weight?’
IT MIgHT sound far-fetched, but these can be questions the digitally-savvy patient poses to their smartphone in their hour of medical need.
in the digital age, online presence is everything
The internet has made it possible for us to access most everyday services at the simple click of a button or through taking just two minutes to install the latest app.
Order your taxi, do your weekly shop, find that ideal fitness class, study Chinese in your coffee break – our lives are indeed simpler and we wouldn’t dream of turning back the clock now. When everything we do becomes a search term on google, the only thing to do is embrace change and adapt.
Why should finding a doctor be any different?
Top Doctors was founded in 2013 with a simple concept in mind: to effectively and efficiently bring patients and doctors together through technology.
The aim was to help patients connect with expert doctors when they experience a health problem and to help doctors manage their online presence.
Digital health is a revolution and nobody wants to get left behind. We have observed the direct shift in patient-doctor interaction from the early days of the internet, and this shows no sign of slowing down.
In this digital era, patients google symptoms, ask questions, and look for their doctor online –something we noticed they were not finding in their searches. A technology gap was what came between the specialist and the patient.
Until relatively recently, many of those in the medical profession did not particularly see the need to rely on external factors such as the internet to secure their reputation as a leading expert.
In the UK, patients strongly
relied on their gP to recommend the ideal specialist, along with word of mouth, family recommendation or proximity.
Nowadays, however, the internet has made the world a different place and word of mouth alone is not enough. Everything is searchable and, to this end, we knew it was important that doctors had online visibility and that we could be the ones to provide them with the tools to make this possible.
When patients search for medical professionals online, they do not want to find any doctor – they want to find the best.
Top Doctors finally gave patients access to leading medical experts globally, where they could search for the best medical specialists in each and every specialty and find relevant information they would need to choose the right doctor for them, 24 hours a day, 365 days a year.
Set apart
We believe what sets Top Doctors apart is our unique, rigorous selection process for becoming a member, modelled on the screening program of our business partner, Castle Connolly: America’s Top Doctors.
This system has been implemented in the US for over 25 years, providing patients with an invaluable source of information to allow them to identify leading physicians who are just a click or a phone call away.
We consider our selection process the most rigorous of its kind in the world, with only one in ten doctors passing the process and being extended an invitation to become a part of Top Doctors.
We regularly ask thousands of doctors to nominate which specialists they would go to when faced with a disease or illness of their own or that of a relative.
Independent medical experts, Adecco Medical & Science, work alongside Top Doctors to audit every nomination against 15 demanding criteria to verify that the nominated doctor is a professional of the highest standard. The Top Doctors’ professional team then concludes the audit with a personal interview.
Since our inception in Spain in 2013, we have successfully launched in countries around the
We will be launching the app in the UK, along with our online telemedicine platform, giving patients the chance to speak to a leading specialist on their computer, wherever they are in the world
Being listed on the Top Doctors platform allows specialists to publish medical articles targeted at the public, increase awareness of pathologies they treat or procedures they perform, produce video content and gain exposure on social media. We are currently the second largest eHealth platform of our kind on social networks in the UK.
where technology moves fast and creates so many opportunities.
After European success in Spain and Italy, we launched in the UK in 2017, initially concentrating on London where we now have over 600 high-level specialists registered on our platform and more than 20 of London’s most respected clinics.
world, including Italy, Mexico, Colombia and Chile, and in 2017 we launched in the UK.
We currently have 60,000 of the world’s leading doctors as members covering more than 80 different specialties and millions of patients have contacted us so far to obtain doctor recommendations.
When the business started in 2013, we were no more than two sole founders – myself and my wife Lorena. Since then, our workforce has grown, now standing at more than 160 employees representing over 20 different nationalities, with 100 staff at our European headquarters and 60 at our Mexican counterpart.
From the beginning, we were clear that we did not want to be a platform which only allowed patients to search for a doctor.
latest medical information
We wanted our portal to be the go-to place for patients to find all the information they required, both for the right specialist and for reliable advice regarding their pathology or medical procedure.
We seek to provide the patient with the latest medical information, straight from the mouths of our doctors, meaning patients know they can trust the advice they read.
We have collaborated with our specialists on over 8,000 articles and 3,000 videos, with information across our website reaching more than six million viewers.
Our mission has always been to enable patients to be in control of their own healthcare while increasing doctors’ visibility in the digital world, allowing them to stay up to date with the latest technologies.
Early this year, we were excited to launch the Top Doctors app in Spain which, among other features, gives access to an interactive tool which pre-analyses the user’s symptoms and evaluates their state of health.
The app is the first of its kind, in which a patient can use the intuitive tool to assess their symptoms, allowing them to receive a reliable ‘pre-diagnosis’.
The app then gives recommendations, which can include the option of speaking to a specialist through private messaging or video conference or suggesting an appointment with relevant experts with the option of booking online, all completely secure through our data encryption process.
With this system, we aim to diffuse the influx of consultations which could be resolved quickly and remotely.
This year we will be launching the app in the UK, along with our online telemedicine platform, giving patients the chance to speak to a leading specialist on their computer, wherever they are in the world.
Bringing this app to the UK opens new doors for both patients and doctors alike, in a world
We are now expanding our services into the Home Counties and other cities across the UK: Birmingham, Liverpool, Manchester and Leeds.
After our impressive reception in the capital, we are excited about what the future holds for the UK and what more we can make available to doctors through our in-depth knowledge of the eHealth market.
The medicine of the future is here – personalised healthcare has arrived and it allows so many possibilities.
At Top Doctors, we believe that access to the best healthcare should be within everyone’s reach. Technology is a huge part of our daily lives, and the only barrier it now faces is resistance to change.
KnOW A tOP dOc?
do you know somebody who should be a top doctor? nominate them on www. topdoctors.co.uk/nominations. the nominee will be audited and, if successful, will be contacted.
top doctors does not represent GPs, but is looking to expand into this in the future.
Are you protected against lawsuits?
Under the terms of the GMC’s Good Medical Practice 2013, every practising doctor must have adequate indemnity for the full scope
of their practice. Dr Karen Ellison (right) discusses some common misunderstandings and how to ensure you have adequate protection for both your professional and clinical practice
Indemn I ty can be defined as ‘security or protection against a loss or other financial burden’, ‘security against or exemption from legal responsibility for one’s actions’.
Independent practitioners who do not adequately indemnify themselves could have to personally foot the bill for a clinical negligence claim as a consequence.
But this is just the tip of the iceberg, as there are potentially significant legal costs resulting from other problems arising from professional practice.
For instance, n HS indemnity may cover the costs associated with a claim relating to a n HS patient, but it would not cover legal expenses arising from a subsequent referral to the General medical council.
nHS indemnity
all doctors employed by the nHS will be covered by n HS indemnity, also known as the clinical n egligence Scheme for trusts ( cn S t ), in the event of a claim arising from treatment of a nHS patient.
this scheme is managed by nHS Resolution and funded by n HS trusts. the claim would actually be against the trust.
you must ensure that if you are seeing or operating on n HS patients as part of nHS choices or the Waiting List Initiative, in the private sector, that you have documentary proof of who would be indemnifying you in the event of a claim.
If it is part of n HS c hoices or the Waiting List Initiative, it would usually be the n HS, but this may not be the case in other situations that appear similar.
Scope of practice
you must have adequate indemnity or insurance for all work carried out in the private sector and covering the full scope of your practice.
When applying for indemnity with a defence body, you may be asked for details about what your clinical role entails. For instance, whether, as a radiologist, you do interventional procedures.
If you take on a new or novel treatment or procedure, you should tell your medical defence organisation without delay to ensure you hold adequate indemnity.
d o not be tempted to treat a condition outside of your indemnified scope of practice, except in exceptional circumstances such as
an emergency or life-threatening situation.
We regularly encounter situations where members have not updated us about changes in their scope of practice, professional status or private earnings.
a nd there are cases of people returning to practising after a period in deferred membership, such that they find themselves not in benefit of membership when needing to request assistance because a claim has arisen.
WHat to Do NoW
Check your indemnity arrangements for both your NHS and private practice work
Do not rely on state indemnity for all your NHS work
Reactivate your membership after a period in deferred membership, such as a career break
Ensure adequate protection for the whole scope of your practice
tell your defence body immediately if you change your scope of practice
Keep it abreast of changes in your private earnings
Beyond claims
From our experience, many of the problems our members face are not related to clinical negligence claims; but other areas of professional practice, including:
complaints;
Inquests;
disciplinary proceedings;
Gmc referrals;
criminal investigations.
the cnSt does not offer protection for these problems. Similarly, some private providers of medical indemnity will only cover claims. It is important that you are able to request support, advice and legal assistance with these issues even if they occur within the nHS.
Legal costs for Gmc investigations, for example, can run into several thousand pounds and occasionally more.
Dr Karen Ellison is a medico-legal adviser at Medical Protection
NHS indemnity may cover the costs associated with a claim relating to a NHS patient, but it would not cover legal expenses arising from a subsequent referral to the GMC
CaSE StuDy 1
a consultant surgeon had been operating on patients in a private hospital which had a contract with the local clinical commisioning group. a claim was brought against the hospital and the consultant, who was a named defendant.
the consultant was able to provide a contract from the private provider which showed that this cohort of patients was covered by the Clinical Negligence Scheme for trusts. the consultant’s medical defence organisation wrote back to the solicitor and directed all correspondence to the hospital’s legal team, as, in this case, indemnity lay with the NHS.
CaSE StuDy 2
a newly qualified consultant began working in a private clinic which had a contract with the local NHS trust to treat their patients. She had only been seeing these patients.
a couple of months after starting, she received a complaint from a patient who threatened legal action and she contacted her defence body for advice.
She had been paying membership fees as a consultant working in the NHS. Given that the treatment was carried out in a private clinic, she was asked if she had signed an agreement or clause within her contract dealing with indemnity. But she did not recall if she had and was directed to the clinic legal team to clarify whether she was covered by them. It transpired that the clinic had expected her to obtain her own professional indemnity for this work.
WELCOME TO THE NEW PINDROP HEARING CLINIC
Offering state-of-the art facilities at 41 Harley Street. After 11 successful years we have moved to a beautiful new purpose-built clinic, designed to deliver the most advanced Audiology services for your patients.
Refer your patients today
• NEW paediatric testing, including visual reinforcement audiometry (VRA) and Oto-acoustic emissions (OAEs)
• NEW specialist-led tinnitus rehabilitation service, equipped for complex cases
• 2 purpose-built Sound Lounges complete with sound field and speech-in-noise audiometry facilities
• Evidence-based hearing aid fittings, using the latest technology not currently available on the NHS
• Full suite of audio-vestibular diagnostic services
• Outstanding aftercare and patient service
Billing And
Managing self-payers correctly?
Self-pay patients account for nearly 50% of our billing now due to the shift to patients using private healthcare as a ‘pay-a-you-go service’ – and sparking a rise in consultants’ shortfalls. Findlay Fyfe shows you how to deal with it
The big swing to self-pay continues and consultants need to be on top of the game to ensure they get fully paid for the increased amount of work they are doing for their patients.
Private medical insurance work now accounts for less than half of our billing total. The largest second sector is the self-pay market.
nHS
With the growing pressures on N h S waiting times and some of the concerns raised in the media regarding quality of care, many patients are turning to private healthcare for specific treatments.
Self-pay
• Completely open scanner that is well tolerated by claustrophobic patients
• Weight-bearing scans for spine and joints enable a more precise diagnosis
• Patients who are large or cannot lie down can be accommodated
The figure is an average across our consultants and can vary dependent on specialty, although in many cases it is significantly more.
The reasons for the growth in self-pay is down to a number of factors. Let’s deal with the main ones in turn:
insurance policies
To try to control premiums, insurance companies have areas that are not covered by the policy.
Also, for more long-standing consultants, a larger proportion of the patient’s invoice is now shortfalled as a self-pay invoice.
overseas patients
For practices based in central London, this has always been a part of any practice with non-UK patients seeking high-quality private healthcare.
There has always been a number of patients who have sought out private healthcare without an insurance policy. g iven the changes in private medical insurance payment structures and people taking a tighter control of their finances, this area is the fastest growing area of patient referral.
The reason all this information is important is if you do not know the statistics of your own practice, you cannot make sure that it gets dealt with correctly for the billing and collection process.
i n our 26 years of experience, this is rarely dealt with in the proper way. On so many occasions, there is a lack of clarity regarding the billing and collection for selfpay patients. This can result in a slowly increasing spiral of debt for the practice.
The reasons for the debt can be down to a number of factors. but, typically, what we see is a lack of a
robust process to collect the debt. The practice needs to have a system to deal with each and every self-pay patient.
overseas patients
When you are seeing a patient from outside the UK, you will need to be clear what your charges will be so they can be advised in advance of the full costs of treatment. And you will also need to be clear on their payment method.
When we deal with these patients, we often collect payment in advance, as once the patient has left the UK, there may be difficulties chasing the debt. A common way of taking on an overseas patient is through the hospital. in many cases, the hospital will agree to recover your fees from the patient. however, unless you invoice the correct contact in the hospital in a timely manner, your fee will not be collected.
UK self-pay
The majority of consultants have a growing element of patients who are self-pay. Therefore, they should be provided with a price list and have agreed payment methods made clear in advance. This way, the patient is aware of the figure they will be invoiced, avoiding a later dispute on costs.
While taking payment, we have a variety of methods available, including taking payment on the day or in advance. Our payment portal is always open for credit card or debit card payments. if you cannot take payment on the day, then you will need a robust system where the patient is politely reminded after an agreed time then chased on a regular basis until payment is collected.
insured shortfalls
Depending on your specialty and how long you have been in private practice, you may have a level of shortfall on all or some of your self-pay invoices.
This is the hardest to collect, as many patients do not fully understand their policy and wrongly assume that all costs are covered (see page 44).
The result can be they are surprised to see the shortfall invoice and choose to ignore it, as they assume that it should have gone to the insurer. if these invoices are not called and chased, they invariably remain unpaid.
Once many patients are aware of the invoices following a call, they dispute it with their insurer. i n fact, a large amount of our work is liaising between patient and insurer to ensure the patient is made aware it is their liability.
Once the patient accepts liability, then you can discuss payment of the invoice.
Economic pressure
The continuing economic pressure has decreased incomes in real terms over the last years for many people. This means a robust system as described in this article should be in place.
if you don’t have one, then the debt will become older and increasingly difficult to chase. The alternative is to chose to use a billing and collection company with the expertise and processes in place to manage this for you.
This, in turn, allows you to concentrate on the medical side of your practice without the burden of dealing with debt.
Findlay Fyfe is managing director at Medical Billing and Collection
PROBLEMS WITH THE TAX MAN?
HMRC tax investigations and disputes create difficult and stressful times.
As an award winning firm of tax experts, our highly experienced partners specialise in resolving problems relating to tax investigations and disputes with HMRC.
To find out, in confidence, how we can help call 0800 734 3333.
‘Here to help. Not to judge.’
Quelling quackery
Suzie Grogan (right) ends her series tracing the development of the medical profession with an examination of the battle for the pennies of the poor
A doctor administers ‘a gentle emetic’
☛ Adapted from Death Disease & Dissection – the life of a surgeon apothecary 1750-1850, by Suzie Grogan. Pen & Sword Books Ltd, ISBN 1473823536, Price £12.99
SpeciAl offer!
independent practitioner
Today readers can get 25% off, plus free UK p&p. Quote ipT25. phone 01226 734555
John Corry was the author of The Detector of Quackery, published in 1802, and determined to expose fraud, not just in the medical profession, but across a wide range of the arts and science.
An Irish-born writer and journalist, Corry wrote the ‘detector’ as a ‘well-intended satire [to] rouse the public to just indignation against the quacks and their abettors’.
h e said that ‘Quack doctors’, some of whom he mentions by name, ‘practise their fraudulent arts with most success in a wealthy commercial country like England, especially in the busy populous and luxurious capital, where the multitude have neither leisure or inclination to detect imposture’.
Corry was determined, by such satirical exposure, to alert the population to the dangers inherent in a number of medicines, available directly from a sales person or via newspaper advertisements, and given credence or support by legal patent.
The medical profession was, in this period, still riven by disagreement as to its structure and the relative value of titles given to medical men within it.
Degrees in medicine could be ‘bought’ from colleges only interested in the payment of fees and Corry considered that many were being duped into using these men instead of the ‘regular’ trained and experienced doctor, whether physician, surgeon or apothecary.
As the decades passed, he was joined by other zealous voices calling for the outlawing of those who traded in and benefited financially from, the misery and ill health of others, knowing how little their treatments might help.
Little did he know when he wrote his pamphlets and pursued his campaign that the medicines he so despised would still be sold and relied upon, particularly by the poor and the working class, well into the 20th century.
Some medicines, and those who sold them, were obviously fraudulent; at best useless and at worst positively dangerous.
Attacks upon the community of ‘irregular’ practitioners – those midwives, chemists nurses and ‘horse-doctors’ who had practised healing in their local areas for many years – began in earnest at the end of the 18th century, and continued well into the 19th.
When the attack was on traditional providers of medical care, rancour was often stirred up by the medical profession itself, under threat from above by increased political pressure to reorganise, reform and regulate, and from below by the many they perceived to be unqualified and untrained.
Guarding privilege
At the top of the profession there were the ‘elite’ practitioners, closely guarding their privilege, and the fortunes that privilege brought with it.
In the middle were the ‘regulars’ – those working in small towns and villages, trained as surgeons or apothecaries – who performed the function of GP to the areas they served, often at the expense of their own health and for only a modest, if not lowly, remuneration.
At the bottom were the ‘irregulars’ and these were the ones most easily labelled as ‘quacks’ by those higher up the structure of the medical profession.
For example, in the John Johnson Collection, held at the Bodleian Library, is an advert placed around 1780, by ‘J. Dalton, chemist and druggist, (from London,) King Street, richmond, Surrey’. Wearing his London credentials proudly, he wishes to inform ‘the nobility, gentry, and public’, ‘that he prepares and sells every article in the medical line, on the same terms as in London’. Typically, Mr Dalton then pro-
ceeds to recommend his ‘horse medicines, which are kept ready prepared, agreeable to the recipes of the most eminent Farriers…’ his products include ‘diuretic or urine balls’, ‘purging balls with rhubarb’ and ‘pectoral balls for coughs, or asthmatic and thickwinded horses’. These over-thecounter remedies required no prescription from any doctor, however well qualified, and it was therefore not surprising that many who had undertaken a lengthy period as apprentice felt threatened in what was an already over-crowded market.
Power of advertising
Medical schools oversupplied. They competed with one another and with the glut of qualified men it became a ‘patient’s market’, and there were dedicated doctors worn out by the constant need to secure a viable list of the sick – who were also often poor.
‘Dr’ Solomon of Liverpool made his fortune making and selling the ‘Cordial Balm of Gilead.’ h is genius was in advertising and he said he could spend £100 on adverts to bring in £2,000 of profit. But he was not alone.
The Lancet, under the control of surgeon Thomas Wakley, was at the forefront of the campaign against the continued success of the ‘irregular’ in the 1820s. h e acted as coroner in a number of cases where death appeared to have been directly caused by an over-the-counter, proprietary medicine.
These cases infuriated him into print, where he highlighted the
Between the devil and the deep blue sea: a cholera patient with his ‘cure’
tragedies caused by, in his words, a ‘satanic system of quackery’. In many ways, he was right to focus on the ‘sharp’ end of the market, where manufacturers and purveyors of patent medicines were well aware that they were offering false hopes and taking money by deception.
Excessive claims
Traditional ‘irregulars’ often genuinely believed they could help and were horrified if it seemed they were the cause of a tragedy.
Many of those who peddled the ‘nostrums’ were more businessman, or occasionally, woman, than doctor. It was their sales technique and their sheer bravura in making excessive claims about the effectiveness of their potions that distinguished them from the country herbalist or horse doctor.
Wakley, in The Lancet, published the ingredients of many of the most popular brands. For example, ‘Spilsbury’s Antiscorbutic Drops’, advertised widely as a treatment for scrofula – a disease associated with tuberculosis – was exposed as made up almost entirely of antimony, a substance generally used as a purgative.
‘Daffy’s Elixir’, marketed as a curative for flatulence and colic, might have the same effect, composed as it was of senna leaves.
Wakley, in true tabloid style, went into battle with those supplying the useless and potentially dangerous remedies. he called to those living in even the smallest towns to expose local quacks to try and put them out of business.
r oy Porter in Health for Sale
details the case of Dr r eynolds Fowler of Wiltshire, who sold his treatment for worms via newspaper adverts and stalls in local markets, where the local, seemingly worm-ridden, populous queued to take advantage of whatever properties the doctor’s concoction claimed.
It is to be hoped it was not in any way similar to Ching’s Patent Worm Lozenges. A three-year-old boy given them by his parents saw him deteriorate in the following most horrible way very soon afterwards: ‘…the mouth ulcerated, the teeth dropped out, the hands contracted and a complaint was made of a pricking pain in them and the feet, the body became flushed and spotted, and, at last, black convulsions succeeded, attended with a slight delirium; and a mortification destroyed the face, which proceeding to the brain, put a period (after indescribable torments) to the life of the little sufferer, on Sunday…28 days after he had taken the poisonous lozenges.’
The lozenges were sold by travelling agents who were instructed to reassure those buying them that they contained ‘not a single particle of mercury’. But these symptoms included classic indicators of mercury poisoning and the coroner concluded the boy had indeed been ‘poisoned by Ching’s Worm Lozenges’.
Depraved condition
The Evening Standard of 12 n ovember 1845 reported on another case involving a child, Matthew Muir, whose death was caused by the effects of ‘sugar of lead’ which had caused ‘paralysis of the involuntary muscles, general emaciation and depraved condition of the blood’.
The mixture had been prepared by a Mr Gibbons of Shoreditch ‘who sold it to the poor to treat whooping-cough’. Analysis at The London hospital had shown the mixture contained enough to poison the five-year-old.
Poor Matthew has been dosed on this medicine for about six weeks, and despite the fact that Gibbons had given instructions on the label that a laxative should be administered at the same time, most, including castor oil, would have had no effect.
The parents were exonerated, and the court concluded that a verdict of manslaughter would be difficult to prove.
other people came forward to say how beneficial they had found Gibbons’ medicine to be, and the jury found it hard to come to a verdict, with some considering the medicine so dangerous it should be withdrawn, and others thinking that Gibbons simply needed to make the instructions on the bottle clearer – despite this being at a time when many of the poor could still not read.
The coroner stated that if another case should come before him, Gibbons would be held responsible, but held that Matthew’s death was ‘natural’. Gibbons withdrew his medicine.
A year previously, a case came before the Westminster Coroner’s Court where the coroner heard the tragic tale of an unnamed nine-week-old child who had died, seemingly due to the ingestion of a ‘Godfrey’s Cordial’, administered by its desperate father.
The cordial was a quack medicine ‘composed of laudanum and treacle’, apparently used by mothers who had no idea it was dangerous to infants. The coroner observed that ‘he scarcely knew any medicine which had so large a sale; he knew of one man alone who sold gallons of it in a single week and realised a handsome fortune in a short space of time’.
Entrepreneurial salespeople existed in, and treated, even the most aristocratic circles and ‘quack’ medicines were used to treat patients by some of the most famous doctors in the biggest London hospitals. It was unsurprising that they were still so popular with such open endorsement.
In the 1830s, Thomas Wakley established the ‘Anti-medical Quackery Society’ to ‘educate the public and to ensure the total suppression of the sale of stamped patent and secret medicines’. roy Porter describes Wakley as ‘at times messianic’ in his zeal and determination to end quackery in ‘high places’.
But his campaign was always to be frustrated by the simple fact that even the most famous of doctors were endorsing products that were of no proven worth.
The low-down on insurance
With 6.9m people – over 10% of the UK population –covered,* private medical insurance is a strong source of income for most consultants in private practice. Knowing the standard features of policies is vital for new independent practitioners wanting to make it work for them, says Dr Tim Woodman (above)
Understanding health
insur ance can be a complicated business, particularly for those new to private practice, not least because the UK’s health insurers offer a multitude of policies catering to their customers’ different needs and budgets.
But there are some features that many of the policies have in common.
Recognition
Patients wanting to claim for treatment on their health insurance policy usually need to see a consultant recognised by their insurer at a hospital also recognised by their insurer.
recognition means the consultant or hospital has met specific criteria set by the insurer and that it has agreed to include them in their recognised networks.
h ospitals will need to have agreed prices for the services offered with the insurer.
Excesses
at its most basic level, the higher the excess the customer chooses, the lower their premium will be. the customer pays the excess up to the amount they have chosen once each policy year, no matter how many claims they make during that year.
Where their treatment spans their policy renewal date, in most cases they will need to pay the excess again. g enerally, health insurance customers pay the excess straight to the consultant after the insurer has reviewed the consultant’s invoice.
this is not to be confused with co-insurance – sometimes referred to as co-pay – where the customer pays a set percentage of each claim
for treatment up to a maximum amount in a policy year. a gain, the health insurance customer would usually pay this sum straight to their consultant.
hospital networks to cater for different budgets, insurers tend to offer customers a selection of hospital networks to choose from.
For example, customers with a larger budget may choose a network with a more comprehensive list of hospitals which might include central london hospitals, where treatment is usually more expensive.
outpatient treatment
another option that people buying health insurance can choose if they want to reduce their premiums is an outpatient limit or allowance.
this is a pot of money intended to cover all their outpatient consultations, minor diagnostic tests such as X-rays and blood tests and outpatient treatments and therapies, such as physiotherapy, for their policy year.
i f they use up this allowance, they will need to pay for any outpatient claims beyond this point.
what is covered at its most basic, health insurance is designed to give people fast access to private treatment for acute conditions.
an acute condition is a disease, illness or injury that is expected to respond quickly to treatment which aims to return the patient to their previous state of health.
Policies cover the cost of medically necessary, planned private consultations, tests and treatment for acute conditions.
Exclusions and pre-existing conditions
things which are not usually covered by health insurance policies are known as general exclusions. examples include:
t he maintenance of chronic conditions;
the natural ageing process;
treatment of allergies;
Cosmetic surgery;
Pregnancy.
a s well as these general exclusions, health insurance does not usually cover people for conditions they experienced before they took out their health insurance; these are known as pre-existing conditions or special conditions. if you are not sure whether tests or treatment you are proposing for an insured patient fall into any of these categories, i recommend you ask the patient to contact their insurer to check before you begin.
chronic conditions
Most health insurance does not cover the treatment of chronic conditions. Chronic or long-term illnesses can often require recurring consultations over a long period, checks on medication, and/or long-term therapy or treatment usually needed to keep a condition or its symptoms under control.
Bupa uses the a ssociation of British insurers (aBi’s) definition of chronic conditions, which is: a disease, illness or injury which has one or more of the following characteristics:
it needs ongoing or long-term monitoring through consultations, examinations, check-ups and/or tests;
it requires rehabilitation or for
you to be specially trained to cope with it;
it needs ongoing or long-term control or relief of symptoms;
it continues indefinitely;
i t comes back or is likely to come back.
What this means in practice is that, although health insurance policies differ, they generally cover specialist consultations until policyholders are diagnosed with a chronic condition.
Chronic conditions often need consultations over a long period, checks on medication, long-term therapy or treatment which usually keep a condition or its symptoms under control.
When this happens, treatment for the ongoing management of the condition is not covered by health insurance because the symptoms are part of its natural progression.
With Bupa, if a patient experiences a sudden unexpected dete-
rioration in their condition, also known as an acute flare-up, we will usually pay for a short course of treatment to restore them back to their state of health immediately before suffering the flare-up provided it is covered by the patient’s policy.
Authorisation
if someone with health insurance wants to use their policy to pay for their tests or treatment, they will usually need to call their insurer to check it is covered by their policy before they begin. this is known as authorisation or pre-authorisation.
Pre-authorisation lets the patient, and you, know that the test or treatment the patient needs is covered by their health insurance policy and, if so, whether there may be any shortfall the patient needs to pay.
While this might sound like common sense, sometimes the
patient might have an exclusion on their policy which is specific to them – for example, if they have a pre-existing condition that their insurer is unable to cover, so treatment may not be covered when you or they would expect it to be.
Once the test or treatment is authorised, the insurer will give the patient a pre-authorisation number, which you should use when invoicing for that test or treatment.
For more information about health insurance, see Bupa’s guide, Important Points About Your Bupa Patients’ Cover, which is available to download for free from: www. bupa.co.uk/important-pointsabout-your-bupa-patients-cover.
✱ LaingBuisson health cover
UK Market Report 14th edition
Dr Tim Woodman is Bupa medical director for healthcare payments
Bupa’s advice on insurance cover is available to download from its website
PRivATE PATiEnT UniTs
NHS units could form regional PPU brand
Our series by Philip Housden (right) reviewing the NHS private patient unit (PPU) sector continues with a study of the private patient services in the 13 NHS trusts delivering acute care services to the East Anglia counties of Norfolk, Suffolk, Essex and Cambridgeshire
Figures F rom the published annual accounts for this group of trusts show that total private patient revenues have started to bounce back to growth in the past two years, rising 18% from £20.6m to £24.3m between 201415 and 2016-17 (Figure 1).
This now represents 0.72% of these trusts’ total revenues, which is a return to the 2013-14 levels. The combined national average outside of London is 0.5%.
These 13 acute trusts can be divided into three groups based on analysis of private patient facilities and capacity, and revenue size and growth (Figure 2):
Trusts with private patient beds and growing: Two trusts have revenues of more than £7m a year, putting both in the top ten trusts for private patient incomes outside of London.
Both have grown by more than 19% in the past three years and private patient revenues in these trusts now account for around 2% or more of total trust revenues. These are Papworth and Cambridge university Hospitals.
Smaller trusts with a PPU: Three trusts have an entry-level private patient unit – eight beds or less – and, of these, two are growing (Basildon and James Paget in great Yarmouth) and one declining (North West Anglia).
No dedicated private patient beds: The final group of eight trusts are those that have no dedicated private patient capacity. of these, two – West s uffolk and Harlow – are growing, albeit from a low base, and the rest are at best holding their own or declining.
Top of the regional tree is royal Papworth with private patient revenues in 2016-17 of £9m, representing 6.63% of total trust incomes and placing it top of the PPus outside London.
As the u K’s largest cardiothoracic hospital, Papworth has a distinctive edge and focus, ensuring that the brand can stand out sufficiently to support private patient local, regional and international demand.
The trust now manages the Papworth Clinic in-house, including the 32-bed Varrier-Jones Ward, one of the largest PP u wards in the NH s , having sourced operational support from s pire for a period a few years ago.
The planned move into a new hospital on the Cambridge Biomedical campus looks set to support further expansion of private patient services in the coming years, building on the 31.7% growth of the past three years.
Cambridge university Hospitals is also performing strongly versus the peer group of regional teaching hospitals with respect to private patient earnings. The trust has grown these revenues by £1.1m in the 2015-16 financial year to reach 1.95% of total turnover.
A significant part of this relates to the Cambridge Heart Clinic, a joint venture with regent’s Park Healthcare operating since 2008. The trust’s plans for a new on-site 82-bed, five-theatre private hospital run by r amsay, called The Forum, are now on long-term hold.
smaller trusts
Turning to the smaller trusts with PPus, the first, Basildon, continues the cardiac services link. The home of the essex Cardiothoracic Centre, the trust’s eight-bed PPu was, until last autumn, managed by ramsay Healthcare. Following a rebrand as Nash Private Healthcare and through in-house operational management, the trust is now understood to be benefiting from a significant improvement in revenues of more than £4m a year and is now working to develop non-cardiac private patient services also.
James Paget Hospital, g reat Yarmouth, has a seven-bed PPu, the Charnwood s uite, which delivers £0.9m a year, 0.5% of trust revenues. The trust delivers outpatient and ambulatory services through its sub-brand east Point and is understood to be considering expansion of its capacity to boost this total.
The third smaller PP u in this group is North West Anglia, comprising Peterborough and Hinchinbrook Hospitals. There is little to no present private patient service out of Peterborough, but, since 1994, Hinchinbrook has operated the seven-bed mulberry suite, now recently refurbished. The trust reported private patient income of only £478k in 2016-17, 20% down in the past three years and only 0.2% of total trust incomes.
o f the eight trusts without a PPu, the largest two by revenue are
Norfolk & Norwich and West s uffolk. The former’s private patient revenues appear to be on long-term decline, down from £2.7m in 2011-12 – 0.7% of total income – to only £1.6m in 201516, a fall to 0.34% of trust revenues. i n o ctober 2016, the trust turned the 21-bed Cringleford private patient ward into a day-case facility and so a further reduction can be expected in the 2016-17 accounts when published.
West suffolk, the ‘outstanding’rated NHs trust, delivers £1.35m revenues at 0.6% of turnover without a PPu
King’s Lynn is another smaller to medium-sized NHs trust with a turnover of £166m in 2016-17, of which £780k was from private patients, a slowly declining contribution.
Both have a Bmi Hospital either on campus or within walking distance and this offers call-off capacity advantage to the trust, but largely hinders in-house PP u development of inpatient activity.
Colchester and i pswich, two s uffolk trusts working towards merger, have a similar profile at present. Around 0.3% of total trust income is from private patients, being £836k and £687k respectively in 2016-17, with both reasonably flat in cash terms but declining in percentage of turnover.
Attractive markets
i t is understood that private patient opportunities have begun to be considered as part of the merger site and service strategic thinking, without any particular routes to market being identified at this early stage.
Both sit in potentially attractive markets and with a combined turnover of around £600m, there is likely to be enough complex activity to support an entry level PPu to meet the needs that the local private hospitals cannot fulfil.
The final three trusts are all in south essex. Princess Alexandra, Harlow, is another smaller singlecampus hospital with no PPu its location at the edge of London means that a high proportion of the local insured population commute and are able to access a range of strong central and east London healthcare providers, both NH s and private.
The trust has reviewed PP u opportunities in recent years without this leading to a development and the main opportunity remains the low volume, but higher acuity and revenues, that result from the level-three critical care backing that the trust offers and local private hospitals do not. This may be enough to enable a future ‘entry-level’ PP u to be introduced.
Finally, mid essex – Broomfield Hospital in Chelmsford – and southend are presently at the lowest point on the scale at 0.1% of turnover, around £300k a year each and falling. The two trusts are working towards merger with Basildon following on from the essex success regime.
it is understood that the newly established joint executive team has already recognised the potential from the thriving PP u at Basildon and the Nash Private Healthcare branding.
so the three trusts are starting to move to leverage the skills of the back office and private patient services leadership team to create a network or ‘PPu chain’ that will invest in expanded capacity.
The regional burns and plastics services at Chelmsford and the regional cancer centre at southend balance the cardiac services hub at Basildon and it is therefore possible to see how private patient growth could support the wider joint trust site and NH s service reconfiguration strategy over coming years.
This innovative approach is possible because of the bringing inhouse of the ongoing PPu business last year. (Figures 3 and 4).
east Anglia may not be the largest NHs PPu market, but growth is being delivered and there remain several trusts, presently not delivering a private patient service, that have the potential market which may well support investment in additional capacity.
s hould such action be taken, this may well be the geographical area that sees the first NH s PP u combined brand, or ‘chain’, emerge with the potential to take on the incumbent independent hospital groups.
next month: East Midlands
Philip Housden is a director of Housden Group
Figure 4
Figure 3
Figure 1
Figure 2
A consultant seeks help when there is a clash between a patient’s religious beliefs and treatment. Dr Kathryn Leask gives her view
Patient can’t give consent
Dilemma 1 Should we delay this operation?
QI am an anaesthetist working in private practice. I have just reviewed the records of the first patient on the orthopaedic theatre list and noted that the records stated ‘Jehovah’s Witness – no blood’.
The person who carried out the pre-operative assessment has not noticed this. The patient has early onset dementia and I don’t believe he would be able to give informed consent to the use of blood products.
I have alerted the theatre team, but the consultant surgeon wants to proceed and give blood products if required. I’m unsure what to do. The procedure is non-urgent.
There does not appear to be an advance decision to refuse treatment in place nor a relevant power of attorney. The patient’s granddaughter is on route to the hospital and will be here within the next couple of hours and she is his only relative.
AIf a procedure is non-urgent and can safely be postponed, then this should be considered in line with the Mental Capacity Act 2005 and an alternative plan considered. This will allow the doctors to obtain further information.
A doctor should always start with the assumption that a patient has capacity, even if they do have a condition such a dementia.
From there, an assessment can be made as to whether the patient does, in fact, lack capacity to make a decision. In this case, the anaesthetist had established that the patient lacked capacity to accept or refuse blood products.
And it had also been confirmed that there was no advance deci -
sion to refuse treatment in place or a relevant power of attorney. If contact can be made with a family member and if the procedure is not urgent, a doctor should consider whether it would be appropriate to delay the procedure until after a conversation can take place with the family member and confirm whether the patient was indeed a Jehovah’s Witness and whether they would have refused blood products. If the family member is unaware of what the patient would have wanted, then the clinical team should reach a ‘best interests’ decision. To do this, they would need to try and establish what they could about the patient’s previously expressed views on the matter, as well as the views of family members and carers. All discussions regarding capacity, as well as views of relevant family members, carers and the medical team should be documented in the patient’s records. Guidelines offered by the Joint UK Blood Transfusion Service Joint Professional Advisory Committee (JPAC) state that many Jehovah’s Witnesses will accept the transfusion of derivatives of primary blood components (www.transfusionguidelines.org/transfusionhandbook/12-management-ofpatients-who-do-not-accepttransfusion/12-2-jehovah-s-witnesses-and-blood-transfusion), and there is usually no objection to intraoperative cell salvage or to recombinant products.
The anaesthetist was happy to discuss with the surgeon whether any of these options could be used in this case.
The GMC’s guidance on personal beliefs and medical practice (www. gmc-uk.org/ethical-guidance/ethical-guidance-for-doctors/personalbeliefs-and-medical-practice) makes clear that the doctor’s words and actions must not imply judgement of the patient’s beliefs and values.
tody, in the first instance you may wish to ask the police officer to obtain consent from the patient for the disclosure of information. If the patient provides consent, the relevant information from their medical records can be disclosed to the police officer.
When police ask for patient’s data
The police pose problems for a doctor when they come looking for a patient’s details. Dr Kathryn Leask (right) advises an independent practitioner on how to respond
Dilemma 2
Is my refusal to aid police right?
QI work as a private physician and today I received a visit from a detective constable who was investigating what he described as ‘a serious crime’. He did not give any details about what the crime was, but asked for details of a patient’s medical history and said it was imperative that I gave it to him, as it was to help his investigations.
The patient is currently in custody. I told him that I could not give him this information there and then and that I would have to speak to my defence organisation first of all. He said this was unnecessary and asked again for the information, but I refused. What should I do?
ADoctors have a professional ethical duty of confidentiality to patients which must be considered before making any disclosures of confidential patient data.
In certain circumstances, it may be appropriate for a doctor to disclose confidential patient information and the GMC has produced GMC guidance on disclosures in
the public interest (www.gmc-uk. org/ethical-guidance/ethical-guidance-for-doctors/confidentiality/ disclosures-for-the-protection-ofpatients-and-others), which may be helpful.
The GMC has recently updated its guidance on confidentiality to reflect the requirements of the General Data Protection Regulations and Data Protection Act 2018.
In circumstances where you have already decided that disclosure in the public interest is justified, you may not need to ask for consent from the patient, but should let them know of the disclosure if it is appropriate to do so.
One justification for disclosing information may be for the detection or prevention of a serious crime. However, as the police officer has failed to provide you with any information about the crime, it will be difficult to justify the disclosure without consent.
Where a patient is in police custody, it’s unlikely that they will be a risk to the public and therefore consent should be sought wherever possible. If consent is not available, the doctor needs to be able to justify their decision to disclose information and should clearly document their reasons for doing so.
As the patient is in police cus-
If the patient refuses to provide consent, then you will need to consider whether or not you have enough information to justify making the disclosure. This would depend upon the information you are provided by the police.
If you do not think the crime is serious enough for disclosure to be made in the public interest and the police still want the information from the patient’s medical records, then they may decide to obtain an order from the court, which will order the GP to disclose the information.
Dr Kathryn Leask is a medico-legal adviser with the MDU
Can we really afford to live ever longer?
Could you predict your life expectancy? Dr Benjamin Holdsworth gives advice on preparing for a 40-year retirement
According to Aubrey de grey, a biomedical gerontologist – or life extension expert – the first person to live to be 1,000 years old is alive today.
r eading this statement two years ago prompted d r d avid goldhill, former head of icU at the r oyal London, to write his new book ‘ Longevity: why we are living longer than ever and the discoveries that may allow us to live to 1,000’.
d avid looks at the time that each of us has been allotted and how life, thanks to the complex and dynamic human body, may eventually be extended into the hundreds – even if such a feat sounds far-fetched now.
As doctors, our first thought might be how the nHS could sustain the pressures of supporting post-centenarian clients, as well as how far back our retirement age would be pushed to cope. Would the 85-year-old consultant or surgeon become the norm?
Even without this brave-newworld way of thinking, doctors retiring today could look forward to a three- or four-decade retirement. clearly, an important consideration of living to a ripe old age will be financial – how you fund 40 years of free time should be an important consideration.
Significantly underestimating recent research from the institute for Fiscal Studies compared individuals’ reported expectations of survival with official figures from the office for national Statistics. i t found many people were significantly misjudging their chances of surviving through their fifties, sixties and seventies. i n underestimating how long
they might survive, they were prone to saving less during their working life and spending more in the earlier years of retirement than was appropriate.
t hose in their 50s and 60s underestimated their chances of reaching age 75 by some 20%.
Men interviewed at age 65 believed they had a 65% chance of making it to 75. t he official estimate is 83%. Women believed they had a 65% chance of survival, but the real figure was 89%.
Widows and widowers were even more pessimistic, which could lead to exhausting their retirement income early. At age 60, their official chances of surviving to age 80 were 77% and 67% respectively, yet they believed they only had a 49% and 39% chance respectively of becoming an octogenarian.
t he reverse can also be true.
o verestimating likely mortality can lead to a reluctance to spend
According to an expert, the first person to live to be 1,000 years old is alive today
wealth or enduring a lower standard of living than necessary.
c areful planning and a thorough review of all outcomes will give a clear picture of your own financial status. certainly in our office, we have persuaded many clients that after a lifetime of hard work and a strong financial strategy, they are in a position to book the dream trip or switch to travelling business class.
Being financially independent and having the freedom to choose
when and if to work in your later years is a luxury not afforded to many, but medical professionals prepared to consider their realistic options in good time will be in the best position to do so.
However, the finances should not come first. Understanding what you and your family would like to achieve is the first step. What type of lifestyle would you like to enjoy? What are the key goals that would ensure your happy retirement and are they realistic? From there, a good financial planner will help you make well-considered decisions and plot the essential stages to make the right things happen.
Your increased longevity should be a blessing, not a curse.
Dr Benjamin Holdsworth (right) is director of Cavendish Medical, specialist financial planners helping consultants in private practice and the NHS
The content of this article is for information only and must not be considered as financial advice.
Cavendish Medical always recommends that you seek independent financial advice before making any financial decisions.
Levels, bases of and reliefs from taxation may be subject to change and their value depends on the individual circumstances of the investor. The value of investments and the income from them can fluctuate and investors may get back less than the amount invested.
A PRivATE PRACTiCE: CAPiTAl AlloWANCES
Taxman treats big costs differently
Ian Tongue (right) explores some of the concepts and factors to consider around capital allowances
When incurring expenses for running your private practice, some costs will derive benefits over many years and these costs are generally referred to as capital expenditure.
c apital expenditure is not deducted directly against your private practice income for accounting purposes and is given special treatment for tax.
What is capital expenditure? capital expenditure can be a wide term, but for the majority of independent practitioners carrying out private work, it will relate to the purchase of either medical, computer or office equipment used in carrying out their private practice.
Within accountancy there are rules around how an expense is shown in your private practice accounts and these rules can be different to the taxman’s. capital expenditure is one such example of a different treatment for accountancy and tax.
As an example, if you were to buy a piece of medical equipment for £20,000 and expect it to last four years, within your private practice accounts you would normally show a cost of £5,000 a year for four years until the cost has been written off against profit fully.
This is known as your depreciation policy and if the tax treatment followed the accounting treatment, it would clearly be an area that large businesses would use to manipulate profits. So hM revenue and customs has its own version of depreciation which is called capital allowances.
Rates
For capital allowances, expenditure has to be classified by type and the rates vary, but the most common ones for a consultant carrying out private work are:
Plant and machinery 18%
integral fixtures -8%
cars
100%, 18% or 8% depending on emissions.
Over the years, the government has used capital allowances to stimulate economic growth by offering incentives to invest in your business.
One of the more commonly used incentives is the annual investment allowance which allows you to deduct from your profit up to £200,000 of qualifying capital expenditure and receive all of the tax relief up front.
For most independent practitioners, this allows them to deduct the entire cost of their qualifying capital expenditure against their accounting profit thereby generating a lower taxa-
ble profit when compared to accounting profit.
Another commonly used incentive is the first-year allowance, which allows you to deduct the full cost of the expenditure without capping how much the asset is. The effect is the same as discussed above but with the total cost being deducted when calculating taxable profits.
The expenditure that qualifies for the first-year allowance is restricted, with a lot of environmentally-friendly costs qualifying, including low-emission cars; more on that below.
Different pools
expenditure is placed in different ‘pots’ or pools, as they are known, to track their value for tax purposes.
Over time, most assets are written off, but unlike the common accounting treatment of writing the asset off in equal amounts over its life, the tax treatment can spread the tax relief over a longer period if the annual allowance was used up.
Smoke and mirrors?
i t is all about timing when it comes to the annual allowance, as it is an acceleration of tax relief rather than necessarily giving you something extra. it can, however,
be very useful from a cash flow point of view, as some of the cash saved up for tax can be used to help fund the new expenditure.
Cars
A common question is whether it is tax-efficient to buy a car through your business. The answer will be ‘it depends’, but one quirk of the system can be very attractive for the selfemployed or those in partnership, assuming that there is a reasonable level of business use.
This relates to the ‘pools’ previously mentioned and how a privately-owned asset such as a car is given special treatment for the self-employed.
For those considering a company car, it is rare that anything other than a low-emission or fully electric car make sense. This is due to the individual being taxed for the benefit of being provided with a car effectively as a substitute for salary.
however, with the onset of pension annual allowance tax charges, we have seen an increase in those taking a salary sacrifice through the nhS for a company car. Advice from a financial adviser should be sought if you are considering this option, as your final pension can be affected by this.
however, for the self-employed let’s compare things for two popular cars at perhaps different ends of the ‘eco’ spectrum: an electric Tesla and a petrol Porsche. Assume that both cost £90,000, there is 30% business use and both have a residual value of £50,000 after four years.
i n year one, the Tesla would attract a 100% first-year allowance, but this would be restricted for 60% private use. This results in the actual initial outlay to buy the car being £73,800.
in year one, the Porsche would only receive an 8% allowance and this would be restricted for 60% private use. On the face of it, the Tesla is far more tax-efficient, but let’s roll things on to years two, three and four.
in years two and three, the Tesla gets no further tax relief, as you had it up front in year one. The Porsche, on the other hand, continues to get drip fed the tax relief at 8% of the written-down value restricted for 60% private use.
Year four is where the sting in the tail lies and it is down to the tax written-down value at the time. The Tesla has a tax writtendown value of £0 and the Porsche £70,082. At disposal, the Tesla has a value of £50,000, so you have to effectively repay £9,000 of the tax relief received in year one.
The Porsche has a further allowance called a balancing allowance on the difference between the actual value and tax value.
The result of this is that both cars receive tax relief on £40,000 of expenditure at their business use of 30%. That is to say, you can only ever get tax relief on what it actually cost you, which is £40,000 in both cases.
Of course, the example is simplistic and doesn’t factor in changing attitudes to the internal combustion engine and savings on fuel and car taxes, but it does highlight how you could make a decision thinking that you are getting a lot of tax relief and it reverses later on.
r esiduals is the other key unknown, with both facing their own challenges ahead. The moral of that example is that you should buy the car that suits you best rather than being driven by perceived tax benefits that may not be there in the long run.
Buildings
Buildings are a special class of asset and it is relatively uncommon for consultants to buy business premises nowadays.
For those that do or perhaps convert buildings into consulting rooms, there are special rules for claiming the capital expenditure incurred.
This is a specialist area with companies available who can apply surveying principles to categorise expenditure into expenses that qualify for capital allowances. This type of exercise can be particularly effective in identifying additional capital allowances that can be claimed.
The availability of capital allowances and in particular the annual investment allowance can be a very effective way of funding capital items.
Always discuss your proposed spending with your accountant, as they will be able to confirm the amount of tax relief available and when this can be claimed.
Next month: Planning steps ahead of Making Tax Digital
Ian Tongue is a partner with Sandison Easson accountants
docToR on ThE RoAd: volvo S90 hybRid
Mixed reception
City-based independent practitioners are best-placed for this smart looker, says our motoring correspondent Dr Tony Rimmer (below)
WHEn THE writing is on the wall, we all do well to take notice. In private practice, when certain interventions or procedures become superseded by more modern practice, we stop offering them and focus on the new.
Also, independent medical practice is not immune to trends and fashions. If clients stop asking for a particular service and there is greater demand for others, we will, if clinical indications still apply, tailor our offerings accordingly.
In the world of cars, the current trend is to focus on petrol power instead of diesel, as the environment issues associated with diesel particulates has frightened away most buyers. Green issues have become fashionable, so more and more people, including us medics, are looking at electrified cars.
Pure electric vehicles like the Renault Zöe, nissan Leaf and Tesla are still sold in relatively small numbers, as problems with bat -
tery range and access to charging persist.
A half-way house is the petrol/ electric hybrid like the Toyota Prius and these are made even more attractive if they can be plugged into an external electricity source for charging. However, the electric-only range for a plugin hybrid is typically limited to 20-30 miles.
Plug-in hybrid
Chinese-owned Volvo made front-page headlines in the media last year by claiming to make only electric cars by 2019.
What it actually said was that all models will be either fully electric or hybrids so it will continue to sell petrol and diesel cars well into the 2020s, albeit with an electric power component.
Currently, it does not sell a pure electric vehicle and the closest they get are the plug-in hybrid ‘Twin Engine’ T8 variants of the
S90 saloon, V90 estate and the XC60 and XC90 SUVs.
It is the S90 T8 saloon that I have been driving recently and I was interested to find out whether living day to day with a plug-in hybrid makes sense. The S90 is a big saloon that competes directly with the BMW 5 series and Mercedes E class.
The Twin Engine moniker is slightly misleading, as it refers to the main powerplant, a 320bhp four-cylinder two-litre petrol engine driving the front wheels, being supplemented by an 80bhp electric motor driving the rear wheels. A 10.4kWh battery sits centrally in the car, so does not interfere with boot space.
The S90 is a smart-looking saloon. The frontal appearance, enhanced by the signature ‘Thor’s hammer’ running lights, is elegant and modern.
The styling of the rear is not so successful and, as is often the
case, is not as good-looking as the V90 estate version.
The interior, benefiting from Inscription Pro trim, is a really pleasant place to be. The soft leather seats are supremely comfortable both front and rear and the fascia and trim is beautifully designed and appointed.
A clear centre-dash display is intuitive and easy to use and is backed up by a large 12.3-inch digital display directly in front of the driver that, like Audi’s Virtual Cockpit, displays the sat-nav too.
The boot may have a narrow opening but it is huge and, if you take advantage of the fold-down rear seats, can accommodate long loads: I transported a set of stepladders without a problem.
It also has a neat feature that
should be copied by other manufacturers; a one-touch close and lock button for the powered lid in addition to the usual close button.
I took advantage of the car’s electric capability by fully charging the battery overnight from a household plug. The next day, I set off to see just how far the S90 would go on electric power alone.
Silent progress
Volvo claims a range of 31 miles, so I set the controls to Pure mode and headed into London. The overall experience using electric power is very similar to driving a Tesla. Silent progress and instant acceleration works really well for stress-free urban motoring. However, push the accelerator a bit harder or push the speed up on
a dual-carriageway and the petrol engine cuts in to help. The transition is quiet and incredibly smooth, but it feels a bit like cheating. It does encourage steadier driving though.
Electric range? Well, it was a real-world 22 miles.
Another Tesla-like feature is Volvo’s Pilot Assist system which, with adaptive cruise control, delivers semi-autonomous assistance with the steering and looks after acceleration and braking to keep the S90 within lane markings at the desired cruising speed.
It works up to 80mph. The system works well but the steering can be a bit disconcerting when the wheel is moving in your hands with robotic power.
The styling of the rear is not as successful as the smart front
The benefits of the electric hybrid element only works if your daily commute is less than 20-30 miles and you can charge the battery at home
The S90 is a large, comfortable limousine-like saloon. It is at its best on long journeys and can take on a Mercedes S-class for passenger comfort. The T8 model has great performance but the benefits of the electric hybrid element only work if your daily commute is less than 20-30 miles and you can charge the battery at home.
It is also an expensive car at £57,705 before extras. If most of your journeys are longer, then stick to the cheaper petrol or diesel models. For City-based practitioners though; it is worth consideration.
Dr Tony Rimmer is a former NHS GP practising in Guildford, Surrey
volvo s90 T8
Body: Five-seat saloon with fourwheel drive
Engine: 2.0 litre four-cylinder supercharged turbo petrol and electric motor with 10.4kWh battery
The fascia and trim is beautifully designed and appointed
All you need to know about accountancy for private practitioners
A very stable picture
General surgeons have managed to keep the lid on expenses – resulting in a small profits rise, according to our latest benchmarking survey. But, effectively, they are still having to work harder to stand still. Ray Stanbridge reports
Aver A ge privA te practice income of consultant general surgeons increased by 3% between 2015 and 2016, going up from £133,000 to £137,000.
p erhaps surprisingly, average costs remained unchanged. As a result, taxable profits rose by about 3.5% from £75,000 to £79,000.
t hese are small changes and seem to confirm the headlines in our report last year ( Independent Practitioner Today , July-August
2017 – ‘Hard work to stand still’).
As we said in our 2017 report, average per unit costs for many procedures have fallen following the Bupa ‘open referral’ system some years ago.
Costs unchanged in addition, average per unit costs have continued to fall for those with a significant Choose and Book component for their practices.
general surgeons are certainly
aveRage INCOMe aND eXPeNDITURe OF a CONSULTaNT geNeRaL SURgeON WITH aN eSTaBLISHeD PRIvaTe PRaCTICe
having to work harder to stand still.
As we have said above, costs have shown no change on average in the year – a very rare occurrence.
We would have expected some increase in room hire and secretarial costs following the implementation of the Competition and Markets Authority order, but this does not seem to have happened.
insurance premiums also seem to have remained static. We have become used to a steady rise in premiums from the established providers over recent years.
Costs have shown no change on average in the year – a very rare occurrence
Expenditure
However, the market has become far more competitive and those who choose to ‘shop around’ have been rewarded with lower premiums in many cases. Whether or not this provides as comprehensive a cover remains to be seen.
Marketing costs
We note a small cut in phone costs – but we cannot find any particular explanation for this.
‘Other costs’ have shown a modest increase – of £1,000 on average. this includes marketing and promotional costs for many
and reflects the increasing interest by some consultants in trying to differentiate their services from others.
All in all, it is a pretty stable picture.
What then of the future? As we have previously reported, the traditional general surgeon is a dying breed. t here are a lot more specialists around who would expect a continuing growth in income for those specialising in gastroenterology.
Many other general surgeons specialise in breast surgery and we note that this area of activity is probably in decline as other methods of treatment become available.
However, as far as we can see, the future of general surgeons is ‘steady as she goes’.
Note that, with increasing spe-
Year ending 5 April. Figures rounded to nearest
Source: Stanbridge Associates Ltd.
The UK’s largest medical aesthetic event
n Connect with over 4,000 key industry buyers
n Showcase your products and launch new innovations
n A cost effective platform to present your brand to the industry
n Network with your professional peers
n Demonstrate your innovations and technologies live at our theatres
EXPERT ADVICE YOU CAN TRUST
EXPERT ADVICE YOU CAN TRUST
EXPERT ADVICE YOU CAN TRUST
Since
Since starting in the mid 1970’s Sandison Easson has continued to grow and is one of the largest independent medical specialist accountants in the UK.
Since starting in the mid 1970’s Sandison Easson has continued to grow and is one of the largest independent medical specialist accountants in the UK.
Sandison Easson
Sandison Easson acts for medical professionals throughout all stages of their career and has clients in almost every town in England, Scotland and Wales.
Sandison Easson acts for medical professionals throughout all stages of their career and has clients in almost every town in England, Scotland and Wales.
We provide the usual services you would expect from an accountant such as preparation of your accounts and tax declarations but offer so much more including advice
We provide the usual services you would expect from an accountant such as preparation of your accounts and tax declarations but offer so much more including advice on:
We provide the usual services you would expect from an accountant such as preparation of your accounts and tax declarations but offer so much more including advice on:
• Setting up in Private Practice
• Setting up in Private Practice
• Developing your Private Practice
• Developing your Private Practice
• Setting up in Private Practice • Developing your
• Tapering of the Annual Allowance
• Tapering of the Annual Allowance
• Lifetime Allowance planning
• Personal Allowance planning
• Expenses that you can claim and those you cannot
• Minimising your tax bills
• Reviewing your PAYE Coding Notices
•
cialisation in the NHS and elsewhere, it is becoming increasingly difficult to define a ‘general surgeon’. there are now a significant number of subspecialties.
And we have the data compari-
son problems arising from the development of the open referral system, Choose and Book, incidents in individual practices and the method a consultant chooses to trade: sole trader, partnership,
limited liability partnerships or limited liability companies.
We have, of course, reported before that our survey is not straightforwardly significant; rather that it represents a report on what is happening to a typical sample of general surgeons.
Having recited all the macro problems, we can confirm that membership criteria for our sample remains consistent. Our survey includes those surgeons who:
Are not in full-time practice;
Hold either an old- or a newstyle NHS contract;
May or may not have incorporated their business;
May or may not work in a group;
Have a keen interest in private practice;
Have been engaged in private practice for at least five years;
earn at least £5,000 a year from private practice.
next time: Cardiologists
Ray Stanbridge is a partner with accountancy, finance and tax advisory specialists, Stanbridge Associates
geNeRaL SURgeONS’ PROFITS ROSe SLIgHTLy aS COSTS ReMaIN THe SaMe
what’s coMing in our septeMBer issue
Make sure you don’t miss our next issue, published on 20 September. you may not receive every issue if you have not yet subscribed to the journal. Don’t risk missing out on vital topics we tackle next time:
So what is your ideal retirement age? Dr Benjamin Holdsworth, a practising doctor and director of specialist financial planners Cavendish Medical, on planning the right time to leave
Doctors are doin’ it for themselves!
The desire for doctors to engage in consultant equity participation schemes is growing, although still resisted by some. Dr Tony Lopez (right), founder and chief executive of Incorporated Health, reviews the position and offers advice
all patient care in the Uk should be measured in exactly the same way – whether NHS or private, says HCa Healthcare Uk’s chief medical officer Dr Cliff Bucknall
are your patients really understanding your terms of business? With the requirement for greater transparency of fees and the advent of the new gDPR legislation, it is time to review your terms
Complaints are an almost inevitable part of medical practice and can be stressful and time-consuming. But an expedient response to a complaint which addresses the concerns can help to resolve the matter. Medical Protection writers dispel the myths surrounding complaints
eDITORIaL INqUIRIeS
Robin Stride, editorial director
The business journal for doctors in
Published by The Independent Practitioner Ltd. Independent Practitioner Today is editorially independent and thanks Bupa for its assistance with distribution. Printed by Pepper Communications Ltd Material is governed by copyright. No part of this publication may be reproduced, stored in a retrieval system or transmitted in any form without permission, unless for the purposes of reference and comment. Editorial layout is the copyright of the publishers. If you wish to use it for promotional purposes on websites or for reprints, we would be happy to discuss licensing the copyright to you.
Registered office: 7 Lindum Terrace, Lincoln LN2 5RP
Write to Independent Practitioner Today PO Box 198, Cranleigh GU6 9BB
Email: robin@ip-today.co.uk Phone: 07909 997340
@robinstride
Worst website sins. grant Brookes of thewebsurgery.com shows where people go wrong and why it’s important to update your website
Catch up on some recent employment law changes and developments relevant to employers managing negotiations with departing employees and the financial entitlements of such staff
Transparency isn’t an ambition; it’s a reality that will drive consistency in patient-reported outcome measures and quality of care for patients. a viewpoint from Prof Carl Philpott, honorary secretary of eNT-Uk and honorary consultant rhinologist and eNT surgeon
Profits Focus examines cardiologists’ income and expenses
Business Dilemmas looks at anonymising cases for publication and a private doctor in a quandary after being asked to treat an animal
Filing your tax return for 2017-18 may not be due until January, but the sooner you get this done, the better, says accountant Susan Hutter
Our PPU series by Philip Housden takes a look at what’s going on in the east Midlands
The Mercedes Benz brand is a favourite of private doctors. But how will the 2018 a-Class go down with our motoring correspondent?
What was making the news in our journal ten years ago
Plus all the latest news and views
aDveRTISeRS: The deadline for booking adverts in our September issue is 24 august
aDveRTISINg INqUIRIeS
Margaret Floate, advertising manager Email: margifloate@btinternet.com Phone: 01483 824094
SUBSCRIPTION RaTeS
£90 independent practitioners. £90 GPs and practice managers (private & NHS). £210 organisations. Save £15 paying by direct debit: individuals £75 (organisations £180).
TO SUBSCRIBe – USe SUBSCRIPTION FORM ON Page 22 or eMaIL: lisa@marketingcentre.co.uk or phone 01752 312140 or go to the ‘Subscribe’ page of our website www. independent-practitioner-today.co.uk
guarantee delivery of your next copy of Independent Practitioner Today. Take out a subscription and you will get full access to our news, features and previous issues on our website. See details on the left.
BaCk ISSUeS: £12.50 including post & packaging CHaNgINg aDDReSS OR SUBSCRIPTION DeTaILS?
Phone 01752 312140 or email lisa@marketingcentre.co.uk
Circulation figures verified by the Audit Bureau of Circulations
private practice
Full Practice Management System
Complimentary ePractice App
Free support with 24/7 data back-up and recovery
No software installation required
Free multiple users - access anywhere, any time
Secure and encrypted system
Advanced reporting features and payment tracking
Faster payments with pre-populated invoices
Real-time online checks for patient demographic details
Manage your diary and send appointment letters
Automated prompts to avoid payment shortfalls
YOUR CASH FLOW Take advantage of this limited time offer*. Benefit by subscribing to ePractice manager today and book your free demo online.
* Condition of offer: Single Specialists Only. Valid for new Healthcode customers subscribing to ePractice manager only and is valid until 31st July 2018