The business journal for doctors in private practice
How to avoid the taxman
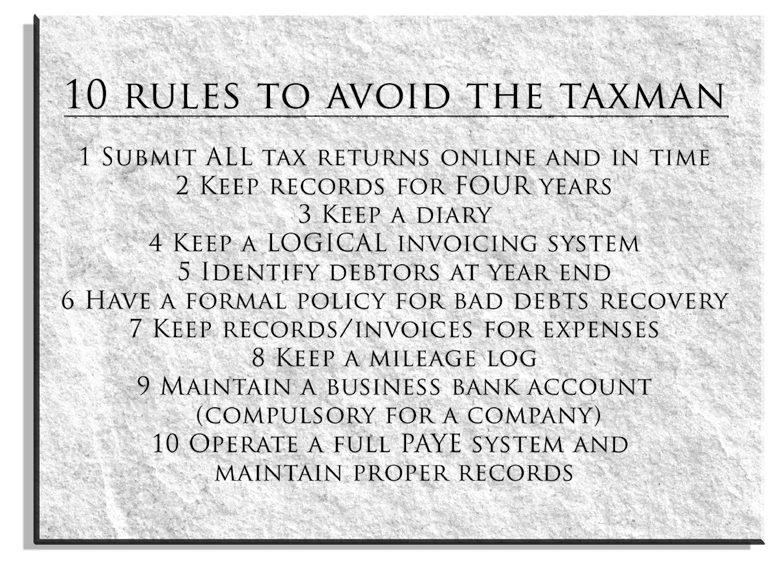
A leading accountant sets out the ten rules to avoid a probe by HM Revenue and Customs n See page 10
Work out a plan to follow Why doctors entering the cosmetic field must have a promotion plan P14
Remember the goldfish Humans have shorter attention spans than they do, so your marketing must stand out P18
What a waste
Tips to help private practices avoid common mistakes when disposing of clinical waste P30
Prepare for self-pay rush
By Robin Stride
Independent practitioners are being advised to scrub up for a self-pay patient bonanza bringing up to 20% growth a year.
New research found nearly half of hospitals and clinics predicting a 10-15% rise by 2018 at the expense of personal and corporate private medical insurance (PMI) policies
It forecast big regional disparities in self-pay growth, with consultants in London taking the largest share with a fifth more self-payers annually, largely driven by patients from overseas.
The study, compiled from an online survey and one-to-one interviews with over 70 leading figures in the UK provider market, was published by medical publishers Intuition Communication.
It said providers and commentators had consistently reported dou-
ble-digit growth in self-pay, as predicted in its first report two years ago.
But a key difference now was a much narrower range of prices, which it said suggested competition was having an effect. Prices were more transparent ‘as healthcare providers invest in the only part of the market that is showing sustainable growth’.
Intuition Communication chief executive Keith Pollard claimed that the Private Healthcare UK SelfPay Market Study 2015 should be a wake-up call for insurers.
He said: ‘If this report tells us one thing, it’s that the traditional models of PMI are simply not going to be sustainable in the future – either for corporate or personally-paid policies. Insurers have yet to demonstrate real innovation in a way that delivers better value for consumers.’
Healthcare providers’ positivity about the current state and future potential of the self-pay market was ‘very encouraging’.
But Bupa UK general manager Alex Perry denied the rise in self-pay was responsible for the fall in PMI. He said: ‘The consumer market for PMI has been in decline since 1997 since the removal of tax relief.
‘Seventy-five per cent of lives covered through PMI are currently employer-paid, while the self-pay market is predominately purchased by individuals who value the benefits of private healthcare on a payas-you-go basis.’
He welcomed the growth in the self-pay market where, he said, the insurer was playing an active role through Bupa on Demand. ‘It demonstrates the increasing demand for private healthcare and that people want to use private services.’
Researcher Liz Heath said price did not appear to be the most influential factor in decision-making. Choice and reputation of consultants, local access and customer service were mainly valued more highly by patients.
GPs still had an important role to play in guiding patients and this figured strongly in the survey as an area providers aimed to invest in. She believed clinicians and providers needed to widen their appeal and make their services and organisations more accessible and welcoming.
Key FindingS
n double-digit rise year on year in the self-pay surgery sector. All agree self-pay market is in a growth period
n Main factors influencing self-pay market growth:
1. Rising PMi premiums
2. Reduced confidence in nHS
3. Less access to nHS services
4. Changing demographics
n Older patients abandoning their PMi in favour of either self-paying or waiting for nHS-funded care n growth in self-pay treatment, particularly cardiology, interventional radiology, dermatology and gastroenterology
n Widely publicised restrictions on nHS funding for cancer drugs likely to be fuelling growth in selfpay oncology.
Source: Intuition Communication
They had to ensure the patient experience was of the highest standard so that patients chose private treatment again and recommend it to friends and family.
n Turn to pages 3, 4 and 5
☞ Save £100! Healthcare companies can buy a full report online at www.privatehealth.co. uk/selfpay/ for £575, but independent Practitioner Today readers are being offered a discounted price of £475.
in the beginning is the word
How to get the best out of your dictation service and avoid annoying errors P12
always remember the goldfish goldfish have longer attention spans than us, so your marketing must stand out P18
no great secret to successful Pr the start of a new series advising how to use the media to boost your business P22
surgeon with an eye on the prize
Mr ahmed el-amir describes his experience in launching an eye clinic in Harley st P26
Property in Portugal our property expert takes a look at why portugal is a good place to invest in P40
informed consent is tailor-make
Medico-legal questions about consent and risk management are answered P42
Practising independent doctors were largely missing from the Private Healthcare Summit 2015 – nobody pays them to go – but the clear message they would have taken from proceedings is that consumerism in the sector will only increase.
How they prepare for it, encourage it and react to it is crucial and, as one speaker said, providers ignore it at their peril.
Doctors can expect more proactive approaches from a more demanding public and a greater expectation of partnerships in decision-making.
The private sector overall must respond faster to consum-
erism than it has been. Some parts of the NHS are way ahead.
Do we know enough about what users and potential users of private healthcare think? No, we don’t, says pressure group Private Patients Forum.
There is a big opportunity for private treatment to start selling itself more strongly and the work of the Private Healthcare Information Network will help.
In our next issue, we will report on one survey about what patients do think. It provides some useful food for thought for anybody wanting to improve the patient experience. See page 4 and 5
Tell us your news Editorial director Robin Stride at robin@ip-today.co.uk Phone: 07909 997340 @robinstride
To adverTise Contact advertising manager Margaret Floate at margifloate@btinternet.com Phone: 01483 824094
To subscribe lisa@marketingcentre.co.uk Phone 01752 312140
Publisher: Gillian Nineham at gill@ip-today.co.uk Phone: 07767
Review your financial plan due to Budget
by leslie berry
Independent practitioners are being urged to revise their financial plans following income-hitting Budget measures.
Successful specialists face a tax hit onslaught, many have a fouryear NHS pay freeze, and insured patient numbers could drop due to an insurance premium tax rise from 6% to 9.5%.
Simon Bruce, of specialist financial planners Cavendish Medical, said with no top tax rate cut, higher tax on corporate dividends, lower annual allowance limits and other imminent pension changes, it was an ideal time to re-evaluate financial plans.
Doctors with buy-to-let properties will also see cuts in tax relief they can claim on mortgage interest.
Mr Bruce warned that practitioners who pay themselves dividends from their company profits could be significantly affected
from next April’s new £5,000 taxfree allowance.
For dividend income above this allowance, basic-rate taxpayers must pay 7.5% tax, higher-rate taxpayers will pay 32.5% and those on the 45% rate will face 38.1% – on top of the 20% paid by their company.
From April 2016, the amount which can be paid annually into a pension free of tax will gradually fall from £40,000 to £10,000 for those with annual income between £150,000 and £210,000.
Accountant Susan Hutter said a corporation tax cut was good news for doctors trading as a company. A business with a £200,000 profit will save £4,000 when the tax is cut to 18% in 2020.
The Association of Medical Insurers and Intermediaries warned the higher tax on PMI would make it less attractive and cause the NHS extra strain.
See page 38
Doctor investors told to keep calm amid Greek fiscal crisis
Senior doctors have been advised not to be unduly concerned by the impact on their investments of a Greek default on its loans.
Specialist medical financial plan ners Cavendish Medical issued the advice after being contacted by independent practitioners keen to establish what the current situation in Greece could mean for financial markets.
Managing director Simon Bruce explained: ‘We have seen heightened volatility in financial markets during this period of uncertainty over the situation in Greece.
‘It is natural, when faced with a possible “Grexit”, to worry about the subsequent impact on per -
sonal finances. While the situation in Greece is important geo-politically, it is of equal importance to keep the effects of the debt crisis in perspective.’
He said pervasively negative 24-hour news coverage encouraged natural instinct to delay decisions, react emotionally or attempt to pre-empt events.
But doctor investors with a solid investment portfolio should recognise these human biases and continue to act long term.
Mr Bruce added: ‘If you have a genuine concern about the riskiness of your portfolio, then you should have this reviewed immediately.
Doctors’ data fear eased
by a staff reporter
Consultants’ watchdogs on the new private practice data body have spoken out to try and reassure specialists with concerns about what it will publish about them.
The trio, just appointed as nonexecutive directors of the Private Healthcare Information Network (PHIN), give their early thoughts
on key issues, and how these might be addressed, in this issue of Independent Practitioner Today (see page 28).
Former Royal College of Surgeons of England president Prof Sir Norman Williams said: ‘We must ensure that each consultant sees their data before publication and has time and the means to validate and correct the data as necessary.’
PHIN had to present whole prac-
tice data, giving a full and fair view of each person’s practice, he said.
Federation of Independent Practitioner Organisations (FIPO) nominee Dr Gerard Panting said many consultants’ questions needed addressing, but he had been reassured by his first few PHIN board meetings.
Prof Sir Cyril Chantler, former chairman of the GMC’s Standards Committee, said: ‘Ultimately,
Private hospitals respond to growth in consumerism
More private healthcare providers are set to consolidate a presence in the self-pay market to boost their business.
According to the lead researcher for Intuition Communication’s self-pay report (see front page), many have been doing extensive consumer research and investing in their customer-facing infrastructure – including their online presence.
Liz Heath told Independent Practitioner Today: ‘The changing demographic of the self-pay market means clinicians and providers need to widen their appeal and make their services and organisations more accessible and welcoming.
‘For example, increasingly restricted funding for routine NHS procedures such as hernia repair,
cataract surgery, arthroscopy and even joint replacement is leading to individuals choosing to “go private” for the first time.’
Clinicians and providers recognised that working together more closely to a common purpose in the self-pay market would become increasingly important, she said.
But this behaviour was still patchy. ‘Clinicians need to push harder to engage with providers to develop products, services and pathways that genuinely have consumer appeal; and providers need to respond positively to this opportunity.’
Some consultants were using a range of media and opportunities to promote their specialty, individual service and performance –including surgical outcomes.
‘We believe that this behaviour needs to be more widely adopted and better disseminated to provide consumers with information to support their decision making.’
Mrs Heath said providers recognised the need to invest further in developing the self-pay marketing – not only in marketing and promotion but also in delivering improved customer service.
‘They recognise that adding value to the self-pay experience across a wider patient pathway is important in influencing consumer decision-making and that such added value may not add noticeably to overall costs.’
Her study showed much improved access to information for the consumer, compared to her last report two years ago. This
patients will not have confidence in PHIN’s information unless their professional advisers have confidence in it – GPs and consultants.
‘However good the data is, it can only provide material for a patient to consider, not give them the answer. We should aim to inform the conversations between patients and clinicians, not to replace or undermine them.’
liz Heath, the report’s researcher
included guide prices for procedures, consultant fees, terms and conditions and signposting to either online or telephone help.
But this still needed further development. ‘The wider dissemination of quality and outcome measures in the private sector will help equip the consumer with a far greater range of decision making tools and clinicians and providers need to ensure they are ready to manage this shift.’
NHS beats private care in survey
The private healthcare sector has much work to do if it wants to better ‘sell’ its merits to many doctors and patients, a report suggests.
Findings from the British Health Report 2015, commissioned by a personal injury and negligence firm, reveal that more than half (58%) of NHS medical professionals claim to have treated patients whose private treatment ‘has resulted in a poor outcome’.
The Your Legal Friend study found 49% of medical professionals believed patients got no better care in private facilities than in the NHS.
And 59% of medical professionals said they would personally choose to receive emergency care from the NHS. This view was most strongly held by consultants (68%) and GPs (60%).
Seventy-nine per cent of the general public said they would prefer to be treated in the NHS for serious or life-threatening illnesses rather than a private hospital.
Fifty-six per cent of the public would choose private treatment over the NHS for plastic surgery, facial surgery (52%) and laser eye surgery (51%).
Laura Morgan, director of medical negligence at Your Legal Friend, claimed the report demonstrated that ‘the public clearly values NHS services over private facilities, particularly for serious illnesses and emergencies’.
She said the results were ‘a clear sign of public confidence in the NHS’s ability to deliver emergency, intensive and acute care for the UK public’.
The study involved an online survey of 400 doctors and 1,300 patients conducted by an independent research agency.
Call for industry to unite
The Private Healthcare Summit, organised by Intuition Communication, brought together key figures in the industry for debates about the sector’s future. Robin Stride reports
The head of the Association of Independent Healthcare Organisations (AIHO) has called on the private healthcare sector to work together and make a stronger case for independent treatment.
Chief executive Fiona Booth said that in the wake of the general election result, the industry should be promoted as a driver of workplace productivity, patient choice and economic growth.
She said the industry might welcome the Tory victory, as it meant many of the last Government’s policies would not be revised.
But public service funding would be cut again and this meant downward pressure on the tariff paid to healthcare businesses providing services to NHS patients.
She warned: ‘Longer waiting times and tighter availability of treatments might lead to more self-paying and insured patients. But it might also mean that the industry is portrayed by our opponents as a privilege for the rich, the fortunate
and people who don’t have a choice but to pay.’
Sector urged to form central booking plan
An IT expert is calling for investment for a private patient central appointment booking system to match the new NHS E-referral service.
Healthcode managing director Peter Connor urged providers and insurers to collaborate in developing the technology, which he said should play a vital part in helping the private health sector grow and prosper.
He warned that the private healthcare sector was currently lagging behind where it should be.
Mr Connor said: ‘Consumers now expect to find what they want, when it is most convenient for them, because a world of different services are now available online, from buying an airline ticket to booking a tuktuk in Bangalore.
‘This shows it’s not just wealthy western corporates who can organise and deliver these online solutions. Every organisation that understands its market is moving in the same direction, including the NHS, which provides a range
of digital health services for patients.’
Mr Connor argued technology could enhance patient experience and make the sector more efficient. In the NHS, England’s National Director for Patients and Information had forecast that the use of technology and data could help plug its £22bn funding gap by cutting out unnecessary paperwork.
He said: ‘There is every reason to think that private providers can streamline their administrative processes and cut costs, but we should think big and benefit from the economies of scale.
‘That means working together to agree information standards and a common technology platform for a central referrals and appointment booking solutions for patients.’
He complained some providers and insurers were trying to implement their own online booking services instead of pooling resources to create a viable equivalent of the NHS central system.
Ms Booth appealed for the industry to speak with one voice whenever it could. ‘There will always be issues on which we disagree, but we should make no mistake that the external environment is still politicised and sometimes tough.’
She hoped there could now be an ongoing dialogue to ensure the sector was represented positively to politicians,
Private care has to fix its manpower ‘timebomb’
A private hospital group boss has voiced concerns over a possible doctor and nurse manpower shortage in private practice in the next decade.
Spire Healthcare commercial director Peter Kahn forecast there
the media, regulators, patient groups and others.
The industry had gone through a challenging period with the Competition and Markets Authority’s investigation and it was time to move forward together in the interests of the patient.
Ms Booth added: ‘Each of us needs to consider what factors drive people to pay for their care, either through insurance or directly to a hospital. We have to ensure that, as an industry, we identify those factors and capitalise on them.’
could be ‘a huge outflow of consultants’ in ten years’ time. Meanwhile, the age profile of nurses was a concern because their average age was now up to 50.
Talking on ‘the shape of things to come’, he said another worry was private healthcare’s dependence on orthopaedics. He hoped the sector would be able to broaden its offering.
And he said the sector had to find a way of being more efficient. It could take a whole day to sort out whether, for instance, a private patient was going into a private hospital or not.
Future is rosy despite price drop prediction
The private healthcare sector is going to have to settle for a lower price in future but from a larger market, a hospital group’s chief medical officer warned.
Dr Chris Streather, of HCA, said he believed the future was ‘pretty bright’ but predicted that prices would drop.
He forecast growing demand particularly for elective care in
non-cancer specialties and for private insurance from companies.
Dr Streather said the sector needed to now think more imaginatively about well-being and ‘getting in’ at an early stage. He described doctors as the ‘biggest asset’ for private hospitals and told managers they should look after them as they were the ones who brought patients in.
ThE prIvaTE hEalThCarE SummIT 2015
AIHO’s Fiona Booth
Bupa’s recipe to grow the market
Bupa UK’s general manager has called for concerted action from all in the private healthcare market to improve patient experience, affordability – and demonstrate quality.
He warned that the need for fundamental reform of the privatepaid sector was more pressing than ever after a year of continued market decline in private medical insurance (PMI).
A brighter future was possible, argued Mr Alex Perry, but he stressed the whole sector needed to work hard together to realise this. He said although the UK economy was improving and population growth was at a record high and employment was up, the private healthcare sector was in no better place than in 2014.
Current market changes to improve information and transparency were ‘heartening’ but more needed doing quickly ‘because customers are losing out’.
Bupa’s long-term agreement with Spire hospitals showed how a better way forward was possible and the insurer aimed to work
similarly with its other providers, he said. ‘Some may be less willing to collaborate, but we will continue to push hard for better value for our customers. There is no alternative if our sector is to survive.’
Mr Perry said the following work was needed on a shared agenda:
1Improving value
‘We know people do want private healthcare and are willing to pay for it. But quite rightly they are demanding for us to control the costs of their premium.
‘It’s a harsh reality that we simply cannot expect customers to continue paying increasingly higher prices, without explaining what they are getting for their money. If we get this right, the prize for us as a sector is clear.’
Bupa last year had, on average, delivered the lowest premium increase for insurance customers since 2011, he said.
For renewing corporate customers, over half had their premiums either cut or held, leading some major corporates to extend PMI
Plea for co-operation to attract self-payers
The self-pay option is not as widely known as it should be, according to Don Grocott, director of the Private Patients’ Forum.
He said there had not been any significant promotion of the selfpay option across the private sector.
Mr Grocott hoped private healthcare could co-operate to grow the business, but he
warned the sector did not know enough about what users and potential users of private healthcare thought.
Responding to comments about the need for closer working between the various interests in the private healthcare sector, he said it was ‘in a pretty bad state’ when it came to cooperation.
across the whole workforce, representing tens of thousands of new lives covered.
He believed customers were entitled to ask why their premiums should rise at all.
Mr Perry warned people were reaching the tipping point for the amount they were prepared to spend on private healthcare and the consumer market would enter free-fall ‘at some point in the next five to ten years’.
2Being customer–focused
Value for money was not just about price. He argued it was also about winning the trust of existing and potential customers. But the sector did not make it easy.
‘I don’t think it’s an exaggeration to say that we’re one of the last industries to realise that improving the customer’s experience should be our driving force for change.’
3
Changing the market context
Mr Perry called for the sector to cut through all the accusations
and myths surrounding private healthcare.
It collectively needed to positively promote the impact it brought to people’s health and lives, the quality of care delivered to patients, and its contribution to the UK healthcare system and the economy.
He hoped hospitals, doctors, insurers and intermediaries would increasingly work together to get PMI up from 10% to 20% in the next three years.
Dr Brian O’Connor, specialists’ committee chairman of the Independent Doctors Federation, agreed doctors did need to engage with the insurers and not be at loggerheads. Doctors were in a prime position to help them cut costs, he said.
TEll US yOUR STORy
Share your experience of what has and has not worked in your private practice.
Even if it’s bad news, let us know and we can spread the word to prevent other independent practitioners falling into the same pitfalls.
Contact editorial director Robin Stride at robin@ip-today.co.uk or phone him on 07909 997340
Take out a subscription for Independent Practitioner Today to keep yourself abreast of all developments in private healthcare. Our feature articles will also show you how to boost your income.
See page 20 for all our subscription rates or contact our subscription department on 01752 312140 or email jackie@marketingcentre.co.uk
Bupa UK general manager Alex Perry
Patients’ rep Don Grocott
Cap for negligence fees
By Edie Bourne
Doctors’ defence bodies have welcomed Government plans to cap excessive legal fees in clinical negligence cases.
The proposals for England aim to set a limit for claims up to £100,000 – around 80% of all cases.
Currently, there is no limit on legal fees, even if the compensation claim is for a small amount.
Dr Matthew Lee, professional services director at the MDU, said: ‘Even with the 2013 reforms, high legal costs charged by claimant
solicitors continue to be a major part of the cost of clinical negligence claims.
‘We still see hourly charging rates of over £400, meaning that these costs often far exceed the underlying compensation claim. This cannot be right and we support any proposals aimed at limiting these disproportionate charges.’
He said patients often had to meet part or all of these costs themselves, but the system should provide access to justice where patients had been negligently harmed. Legal fees therefore had
to be affordable and proportionate.
Emma Hallinan, director of claims and litigation at the MPS, described the move as ‘fantastic’.
She said fixed costs for smallvalue claims would ensure that legal costs did not dwarf compensation payments.
MDDUS chief executive Chris Kenny said: ‘Medical negligence awards are made for the benefit of harmed patients, not the profitability of the legal services industry.
‘We welcome the Government’s determination to cap wasteful costs and hope that their autumn proposals take the form of a practi-
Tummy reductions catching up with breast enlargement
Abdominoplasty is the fastest emerging trend in plastic surgery procedures, according to half-year figures.
Inquiries for the procedure, typically costing £5,330, rose 264% in six months, the private healthcare search engine WhatClinic. com reported.
It said tummies were clearly a top priority for Brits, with lipoabdominoplasty inquiries – average cost £6,321 – also up 172% in the same period.
Arm lift (brachioplasty) is the
second-fastest growing surgical cosmetic procedure, with inquiries rising by 239% over the past six months.
Breast implants received the highest number of inquiries across all treatments in 2014, and so far in 2015.
WhatClinic.com director Emily Ross said: ‘Despite the fact that the range of non-surgical alternatives available to UK consumers has broadened considerably, full surgical procedures for cosmetic purposes are more popular than ever.
‘Breast augmentation is by far the most common plastic surgery treatment being sought by UK patients, though we are also seeing more men seeking treatment for male breast reduction.
‘With demand so high, it is crucial that patients have access to up-to-date information about the credentials and qualifications of their chosen practitioner, which, even in the UK, can be confusing at the best of times.’
Breaking into the aesthetics business – turn to page 14
Data based on the number of inquiries to UK clinics made through WhatClinic.com in the past 12 months, compared to the same period last year.
cal, comprehensive action plan, capable of early implementation.’
The proposal will be open to public consultation in the autumn.
Health Minister Ben Gummer said some lawyers had been unscrupulous. In one case, a lawyer reportedly charged £175,000 while the patient received just £11,800 in damages.
In another, the legal bill was more than £80,000 while the patient only received £1,000. The legal bill was later reduced to less than £5,000 by the courts after a successful challenge.
INquIRIEs INTO non-surgical cosmetic treatments have shot up by 55% in the last half year.
WhatClinic.com found dermal fillers remain top of the list, with the highest number of inquiries across all treatments in 2014 and so far in 2015.
The firm reported a significant boost in non-surgical alternatives availability and warned patients to research their practitioner. It told patients: ‘A sensible question to ask your practitioner is how many patients they have performed this particular treatment on and how many they do per week, as, ideally, you want them to be well-rehearsed in carrying out the procedure.
‘Make sure you have realistic expectations of the results and read patient reviews on websites to get independent opinions.’
* Sample prices from local clinics
The London Sleep Centre on Harley Street has added a dental sleep medicine service led by Dr Karina Patel, a consultant in the specialty and director of the TMJ & Sleep Therapy Centre of London.
Clinical lead Prof Adrian J. Williams said: ‘We have for the first time in the UK and EU, a service offering the full range of diagnostic and treatment services for patients with sleep disordered breathing, temporomandibular
dysfunction (TMD) and craniofacial pain.
‘Dental sleep medicine interventions including custom mandibular orthotics and MLS laser therapy for cranio-facial pain should now be considered essential elements of sleep centres and clinics.’
Medical director Dr Irshaad Ebrahim said the expansion marked a new benchmark for standards of care for patients with sleep disorders.
Doctors exhausted
By Charles King
Consultants are suffering from mounting fatigue and burnout, according to a senior doctors’ leader.
BMA consultants’ committee chairman Dr Paul Flynn told the association’s annual representative meeting in Liverpool that sleep deprivation could impair doctors’ vital judgement and decision-making skills.
He warned the policy-setting convention: ‘Studies have shown it can have similar effects to drinking. We would never allow a consultant under the influence of alcohol to treat patients, but con-
tinue to turn a blind eye to doctors who are sleep-deprived.’
Dr Flynn’s comments came as a
BMA survey found as many as 30% of doctors in the NHS considered themselves to be suffering from, or previously suffering from,
burnout. Four in ten believed they were at high risk of burnout in the near future.
The association said the results revealed the extent doctors were being affected by growing NHS pressures.
Dr Flynn called for the NHS consultant contract to continue to protect against the acute fatigue that risked doctor burnout.
He said: ‘With workloads rising and moves to deliver more services out of hours, the Govern ment must make safe working a priority.’
The BMA survey of 847 consultants found 71% never had access to rest time after a night spent on call. Only 11% did.
Cosmetic op rules to change Awake to opportunity
Final GMC guidance for doctors who carry out cosmetic procedures is due early next year following its current consultation ( Independent Practitioner Today , June 2015).
Safety proposals will require doctors to:
Market services responsibly;
Make no unjustifiable claims about results they can achieve, and not use promotions that encourage ill-considered decisions – such as giving procedures as a prize;
Not target people under 18 in their marketing;
Seek a patient’s consent themselves, not delegate it;
Be open and honest with patients and not trivialise risks;
Allow cool-off time before people decide on a cosmetic procedure;
Check how patients have been affected by a procedure and if they are satisfied with the outcome.
GMC chairman Prof Terence Stephenson described cosmetic practice as a huge and expanding area of medicine where some patients needed better protection than now.
The council is working with the Royal College of Surgeons of England and others to publish information about which surgeons
have the right skills to carry out cosmetic surgery.
This would allow patients to check doctors’ qualifications on the GMC’s medical register. Prof Stephenson said: ‘It is vital patients should be able to tell whether a doctor is competent to carry out these interventions and we have called for new legal powers to enable us to do this.’
The consultation runs until 1 September. Either answer questions on its website, email cosmeticpracticeproject@gmc-uk.org or write to: Standards and Ethics team, GMC, Regents Place, 350 Euston Road, London, NW1 3JN.
New investors in hospital group Spire say they believe the UK healthcare sector has ‘strong market growth prospects’.
Remgro, a major shareholder in South Africa, Switzerland and United Arab Emirates hospital group Mediclinic, has agreed to acquire a 29.9% stake from Cinven for 360p a share, totalling £432m.
Mediclinic, with 70 hospitals and specialist care facilities, then aims to take it on ‘in the near future’.
Spire chief executive Rob Roger said the group expected significant growth in the medium to long term.
Mediclinic and Remgro said they had ‘no current intention’ of making an offer for the whole of Spire.
Boost for Spire from investors Videos plug careers in private care
Videos aimed at boosting independent sector recruitment have been launched by The Association of Independent Healthcare Organisations (AIHO).
Films showcase the wide variety of training and professional development options available for staff within independent hospitals.
They explore the career and educational opportunities for nurses, healthcare assistants, allied health professionals and managers.
Films also demonstrate the significant investment made by the independent sector into training. This includes funding diplomas, degrees and masters’ courses.
AIHO said they would be a useful tool for hospitals and recruiters to showcase the possibilities and dynamism of a career in the independent sector.
See http://aiho.org.uk/recruitment-into-independent-hospitals
Dr Irshaad Ebrahim Prof Adrian Williams
Dr Paul Flynn
Dr Karina Patel
ACCOUNTANT’S CLINIC: OpTIONS FOR gROwTh
How solo doctors can build up their practice
Are you happy being a ‘business singleton’ or are you keen to build up your practice and start employing others? Depending on your future plans and business acumen, there are a number of options for growth. Susan Hutter explores the various avenues open to you
Staying solo or building up the practice?
Not so long ago virtually all consultants traded as sole practitioners with perhaps one or two administrative assistants.
This is a simple model and can still work well, especially so if the consultant is combining a private practice with a busy NHS appointment.
Many consultants remain happy for their private practice income to supplement their NHS salary.
But what about those who want more from their private practice or indeed where the momentum is taking them towards expansion? What are the options for growth?
Organic growth
This is the way that most businesses grow, by recruiting and training ‘junior’ staff in the same or complementary specialism to where they are operating.
It is not always easy for newly qualified consultants to begin on the private practice ladder and many are quite keen to team up with a more experienced specialist with a view to a partnership or something similar.
Many consultants employ others in complementary practices; for example, orthopaedic consultants and physiotherapists. This way, they are in a position to offer their patients a wider service and also someone else can step in if
It is not always easy for newly qualified consultants to begin on the private practice ladder and many are quite keen to team up with a more experienced specialist with a view to a partnership or something similar
they are either fully booked or on holiday.
If patients have confidence in the consultant, they are also likely to have confidence in the ‘alternative’ that is recommended. From a work load point of view, this helps share the burden.
Merger/acquisition
For consultants looking to work with others at a similar level to them, then they could consider merging with/or acquiring a similar practice to their own.
Perhaps a consultant has a surgery or office space to spare or would like to expand the practice to more than one location in order to grow ‘geographically’. Some practitioners are ‘buying out’ others as part of a retirement plan with a view to taking over their practice in, say, three to five years’ time.
In this scenario, professional advisers – lawyers and accountants – should be brought in to help value the practice being bought. Many practitioners are already taking this route and building up ‘centres of excellence’ for their particular specialty.
Disadvantages of growth
As with most business decisions, there is often a downside that needs to be considered.
For many who are doing well as a sole practitioner with a solid private practice, there seems little
point in making life more complicated. In order to expand, one has to take on more staff and/or associates and, with this, comes legal responsibilities.
The practice overheads will necessarily increase and so there is more pressure on you to cover the costs.
A larger turnover does not necessarily mean a larger profit.
However, the business of medicine has been changing quite rapidly and if you are still in the earlier period of your career, it may be wise to look at expansion in order to stay competitive with the rest of the industry.
Trading vehicle
Another area that needs to be addressed is the method of trading. Most consultants start out their private practice as sole practitioners, but when they expand, find they need to either trade as partnerships, including limited
If a practice is earning enough to retain money in the business, which could be used for expansion, there are tax advantages of incorporation
liability partnerships, or as limited companies.
The more complex the structure, the more costs are involved. However, beyond a certain income level, limited companies are often advantageous.
The level depends on the specific needs and also whether or
not one has income outside of private practice.
If a practice is earning enough to retain money in the business, which could be used for expansion, there are tax advantages of incorporation.
The funds that remain within a company are only taxed at corporation tax rates, which at the time of writing are 20%. Compare that with the highest rate of income tax, which for those earning above £150,000 is 45%.
It is quite widely accepted by the profession that the days of con sultants carrying on as ‘singletons’ are numbered. They are now becoming like any other business that needs to look at all the options.
As always, it is crucial that advice is taken at each stage.
Susan Hutter is a partner at specialist medical accountants Shelley Stock Hutter
HM Revenue and Customs seem to think consultants’ incomes should rise 10% a year. If not, then you can get looked at. To help protect Independent Practitioner Today readers, Ray Stanbridge (right) presents his...
If you don’t obey the RuleS, hM Revenue and CuStoMS Can:
1. fine you up to 100% tax lost, plus penalties (5% or £300 every six months)
2. name and shame you
3. fine you £100, plus £10 per day (90 day maximum)
4. Charge a penalty for late payment of tax (5% of outstanding balance if 30 days late and 5% again at 6 months and 12 months later)
5. Charge interest at statutory rate
6. Charge you:
£3,000 for not keeping records;
£300 for not producing records;
£60 a day until you produce records.
note: fines are constantly increasing and company fines are even higher
Ray Stanbridge is a director of Stanbridge Associates, specialist medical accountants
Free legal advice for independent practitioner Today readers IPT
independent practitioner Today has joined forces with leading niche healthcare lawyers Hempsons to offer readers a free legal advice service.
We aim to help you navigate the ever more complex legal and regulatory issues involved in running and developing your private practice – and your lives.
Hempsons’ specialist lawyers have a long track-record of advising doctors –and an unrivalled understanding of the healthcare system as a whole.
Advice is available on:
call Hempsons on 020 7839 0278 between 9am and 5pm Monday to Friday for your ten minutes’ of free legal advice
ian Hempseed Faisal dhalla
Lindsay draffan Hilary King
Fiona McLellan Lynne Abbess
In the beginning is
Do your dictated letters take what feels like forever to be transcribed? When you eventually receive them, are there numerous unnecessary, repetitive and annoying errors requiring correction often late at night? Ilani Aucamp shares how to get the most from your dictation service
There are three key areas to consider when dictating if you want to minimise your frustration and reduce the turnaround time on your letters.
as dictating is arguably the fastest and most effective method to record patient records, it is imperative to get this right.
Let’s look at each area in turn to identify opportunities for improvement:
• Weight-bearing scans and variable patient positioning enables a more precise diagnosis
• Truly open system is a solution for claustrophobic patients without compromise in image quality
1 Equipment
If you are still making use of old dictation machines with tapes – get rid of them. Their overall quality is poor compared to modern digital recorders.
Bear in mind that you should be wary of calling them Dictaphones, as this is a trade-marked name protected by law.
If you own a smartphone, you already own a dictatation device. By implementing modern technology and applications (apps), your smartphone could become a fully functional dictation machine, allowing you to dictate whenever and wherever you desire.
Smartphones deliver good-quality audio dictation in most environments except when there is interference from high levels of background noise – for instance, traffic and operating theatres.
Purposebuilt dictation devices possess more advanced high-level noise reduction specifications.
Therefore, when dictating in the presence of high levels of background noise using a smartphone, the best results will be obtained when the microphone is held in close proximity to the mouth or by making use of headphones with a built-in microphone.
2
instant and secure file sharing
By integrating your smartphone with a secure mobile file-sharing service, you will be able to send your audio files directly and instantaneously to be transcribed, which could reduce your turnaround time quite significantly.
This is achieved by firstly purchasing and installing an audio dictation application on your android or iOS Smartphone from the relevant app store.
You need to ensure that the audio dictation application is able to integrate with your chosen filesharing service – see below.
These applications – for example, Dictamus or h/T recorder –retail for approximately £10.00
the word
and have been found to deliver high-quality sound and a userfriendly interface.
The next step is to install the secure file-sharing service application. When deciding on a suitable file-sharing service provider, your main consideration should be patient confidentiality.
Security features that would assist in maintaining patient confidentiality are access control, including two-step login verification – where an access code is sent to your smartphone when logging into your account as an addi -
tional safety measure – encryption and, thirdly, a back-up and restore functionality.
The final step is to integrate the dictation application with the chosen file-sharing service provider.
Making use of secure file-sharing services also enables you to review your transcribed letters on your smartphone as well as adding comments or any corrections.
3 Style and instructions
Identify yourself at the beginning of your dictation. It may sound obvious, but most consultants omit this crucial piece of information.
State what kind of dictation you are doing; that is to say, clinic letters, operation notes, referrals, and the date you want shown in the reports. also state the date of the patient examination, the date of your dictation or the date the transcriptionist is actually transcribing the work. always dictate as much patient information as possible; for instance, patient first name and surname, date of birth, hospital number, address, GP details or referrer’s details.
Be consistent in the way you approach similar reports or letters. Make sure you use the same headings whenever possible; for instance, reason for referral, diagnosis, investigations and medication.
Use your own set of standard phrases. For example: ‘On physical examination today, he appeared comfortable at rest with no jaundice, anaemia or lymphadenopathy.’ This makes it easier for the transcriber and will limit the number of errors.
a lways include punctuation, especially when starting a new paragraph.
Use instruction terms such as
‘new line’ or ‘new paragraph’, ‘period’ or ‘full stop’ and include ‘open’ and ‘close’ quotation or bracket instructions.
It is also important to say ‘end of dictation’. This informs the transcriptionist that there is no further dictation on the recording.
Speak clearly and at a regular pace, with inflection in your voice. Monotonal voices tend to put transcribers to sleep. Spell words not commonly used; for example, for new treatments or medications.
Try not to laugh, cry, yawn, burp, slurp, cough, eat, drink, chew gum or fall asleep when you dictate.
Yes, this really happens and we hear everything! and these noises lead to confusion for the transcriber and waste valuable time.
Dictate your specific preferences – for instance, ‘one’ as an integer as opposed to ‘one’ spelled out in words.
Give feedback and send corrections. a s transcribers, we try to improve the level of service we provide. By knowing your exact preferences and receiving corrections, your transcriber can continually improve their accuracy.
It is a well known fact that physicians have one of the busiest occupations in the world. By modifying the way you dictate, you most definitely will improve your time management, which will not only benefit your practice but also make life easier.
Ilani Aucamp (right) is director of Typing On Demand
Work out a plan to
In the fourth of her essential series for doctors in the aesthetics world, Pam Underdown shows why you must have a marketing plan
to follow
One Of the most vital aspects of any business is the marketing plan, but it’s sad that many businesses don’t have one.
But what is even sadder is that in a high proportion of those businesses which are destined to fail in their first year – now as high as one in two – the lack of a plan is cited as one of the main reasons for failure.
Truthfully, marketing is one of the single most important places you can focus your attention on, particularly if you hope to create a successful business. Marketing equals the ability to attract and retain enough patients, which ultimately means profits when it is done well.
You can’t make bread without flour; however, most business owners don’t put nearly enough time, focus, attention and investment into their marketing as they should do to get hold of the flour.
A business’s purpose
e xactly how much time should you spend on your marketing? Before I answer, I have a question for you: what is the purpose of a business?
It’s a trick question that catches out most people. Most would say that the purpose of a business is to make a profit, but, in fact, the real purpose of a business is to create and keep a customer.
You can have the finest products and services in the world, but if you don’t have a customer, there is a high chance that you won’t have a business very soon. A business cannot really get off the ground until they sell something and ultimately create a customer. And that is what marketing is all about.
If marketing is how sales are made, then a marketing plan is about figuring out how the sales
will be made. no plan equals no sales and no sales equals no profit and ultimately no business.
So the purpose of an aesthetic business is to acquire and keep a patient, and if you do this enough in a cost-effective way, using strategies you have tested and continuously improved, then a profit will be the result.
Out of the many aesthetic business owners I have interviewed over the years, I’ve discovered that every profitable business owner makes the time to acquire and keep enough of their ideal patients, while also ensuring they have a thorough understanding of exactly what is happening and why.
When you look at those struggling businesses, you will find owners who complain they hardly have any time to master the marketing side of their business.
Poor planning
I have also spoken to many business owners who feel out of control, because they haven’t given themselves the time or the space to stop, take a step back and really plan and structure their business properly.
Often business owners are inadvertently planning their way into a crisis because they are simply not aware of what is happening. When the business is going well, the lack of controls probably didn’t matter too much.
But when a crisis hits, the deadly error of ignoring issues such as consistent marketing, competition, facts and figures and a drop in profits means that the need to then change is then instantly born.
every successful business owner knows they can’t afford to stand still if they want to still be in busi-
➱ p16
...cuts into lost fees!
“MidexPro thinks like a doctor, not a computer exper t”
All you need to run your private practice including document management, diary, clinical data, even test ordering and lab reports from TDL.
From paper billing (incl VAT) to electronic billing (EDI) to management of bulk purchase contracts.
Grow seamlessly from a small solo practice through to a large group practice, remote access network system
MidexPro is the cost effective practice management system with support second to none.
Free download of the full working package (30 day limited) from www.midexpro.com or call for a CD.
Try it for yourself with no sales pressure.
“MidexPro
has revolutionised our lives; it is just so easy”
ness next year. They know that what works today may not work tomorrow. They are constantly asking themselves what can be improved.
How can they improve their patient experience? How can they improve their marketing results? What else can be improved? They listen to their teams, they encourage open communication and, more importantly, they listen and really hear their patients.
They understand that if their patients are not at the heart of everything they do, they won’t have a business next year.
A marketing plan, the way I help my clients build them, is for internal use within your business, and serves as a map to help you and your team get to the destination you’ve chosen for your business.
It will prepare your business to be proactive and enables you to monitor exactly what works and what doesn’t work. Without one, you are simply reacting to the marketplace and to your competition, which means you are always a step behind those who are already prepared.
A marketing plan will also ensure you are ready to deal with the peaks and troughs of the aesthetic market. It’s always better to anticipate and plan for changes ahead of time rather than find out about it later on. You need to be in the leading edge and not the following edge.
Who are your patients?
Before you start, it is best to get a better understanding of why you are in business for yourself. All businesses understand ‘how’ they do what they do – their treatments and services – they talk about everything they sell and provide, they become product- or technology-obsessed, but many never really understand ‘what’ their patients intimately want and what motivates their patients to buy.
Ask yourself: who are your patients? What are they really buying and how will you use your marketing to really connect with them? Who are your competition? You need to understand what they do well and what they don’t do that well, because you can be sure that they know you.
It is essential to have a picture of what you want to ultimately create and cultivate: a realistic working blueprint
Many businesses never really understand what their patients intimately want and what motivates their patients to buy
What are you going to offer that is different to your competitors and what will you offer that no one else does? Ultimately, what will make you stand out from the crowd in a way that matters to the patients?
And how will you put your treatments and services into the hands of your potential patients? What’s the most effective marketing strategies to do so?
It is essential to have a picture of what you want to ultimately create and cultivate: a realistic working blueprint. Any investors or banks will need to see that you have a clear vision of where you want to go and how you are going to get there.
Do your research
They will also want to be sure that you have done your research thorough ly and have carefully thought about the way you will hit your forecasts in year one, with turnover sustaining enough income to keep cash flow strong and allow for re-investment. Remember, it may not be that you see a profit until year two, depending on your overheads. A well planned plan means nothing, though, if it’s not well executed. We will be discussing more of the ‘how to’ in next month’s article. Ultimately, if you want to succeed, then you must make the time now to master the marketing yourself. focus on no more than three strategies at a time to see what works, what needs to be improved and what doesn’t work. Spend small, test small and fail small.
Overall, if you have a good marketing plan in place, you will have a business that is in control of itself. When you’re in control, you can steer it towards profits.
Measurable milestones will let you know if you are on track and a good plan will tell you exactly what to expect to see and when to see those results.
What happens if you don’t have a workable plan? Quite simply, there will be lots of activity and very little productivity.
You’ll end up bouncing from task to task, probably never completing any to the level that you want. Additionally, you can be absolutely certain that, as a result, you will have missed a number of potentially lucrative opportunities.
Most successful business owners say they have learnt more from their mistakes than they ever have from their successes
The bottom line is that without a plan, you can get hopelessly lost and never reach your destination and if the worst does happen, you may just end up going back to your day job.
Learn from your mistakes It goes without saying that you will make mistakes along the way, however well you plan in advance. These mistakes form the essential learning curve that will help you to develop and grow your business.
Most successful business owners say they have learnt more from their mistakes that they ever have from their successes. Also, don’t forget that having unrealistic expectations can be a huge demotivating factor.
Any sense of failure can give you an emotional setback, knocking your confidence and pride, but also denting your enthusiasm. The key is to expect that things will go wrong, but that you will learn from them, adapt and move on. Cultivating the ability to pick yourself up and dust yourself off is one of the best business skills you can develop.
Next time, I will be focusing on exactly how to build your marketing plan and will give all readers a free template to download, as well as discounted access to my live online marketing training programme – The 6D Patient Attraction System
Pam Underdown (pictured left) is chief executive at Aesthetic Business Transformations
Celebrating our 22nd year in Business
www.medbc.co.uk
Come and join the hundreds of other consultants who use MBC and experience the following benefits:
• Bad debts of less than 0.5%
• Increase in net income by up to 25%
• Freedom for the consultant and secretary to focus on the medical side of the practice
• 24/7 online access to both your financial and practice management data
• Having a service tailored to your needs with your own Account Manager
• Our fees are only charged on the money that we collect for the practice and NOT on what we invoice which means we share the same objectives
Special offer:
To celebrate our 22nd year in business we are for a limited period of time offering all new clients an introductory discount of 20%*
Further information:
Please visit www.medbc.co.uk for more detailed information or phone 01494 763999 and speak to Garry Chapman to establish how we may assist your practice.
*Terms and conditions apply MBC – More than just a billing company
Always remember the goldfish
The average human attention span is now thought to be less than that of a goldfish – so make sure your marketing STANDS OUT, says surgeon Mr Dev Lall
Independent p ract I t I oner t oday is the news and features journal dedicated to providing information of interest to the consultant in private practice. It publishes a lot of practical information about how to grow your business.
Now, the chances are that you have been reading us regularly since we launched over seven years ago, but I’d bet that many consultants have still to put a lot of this useful stuff into action.
Why do so many of us behave this way? It’s not because we don’t want to grow our private practices, because clearly we do.
My guess is that the main elements are fear of trying something unfamiliar and apathy.
But the private practice landscape is changing; if not daily then certainly monthly.
New consultants are being
appointed, hungry for private practice success. These are consultants with few of the hang-ups of their more senior colleagues, who tend to look down in disdain at marketing, thinking that it is somehow beneath them.
And the private practice landscape, of course, is very fluid too.
For example, there are:
Changing demands from the public – BRCA gene testing, prostate health and the various screening and ‘wellness’ fads, for instance;
Shifts in public opinion both for and against private practice;
Ever-present efforts by the insurance companies to drive down their costs and the procedure fees paid to consultants;
Limitations and restrictions on care in the NHS, such as varicose vein surgery, hernia surgery, ‘lumps and bumps’.
But in the midst of this dynamic and occasionally depressing environment, there lies opportunity. Because the vast majority of consultants make little, if any, effort to promote their practice beyond holding interminable GP educational meetings and a website presence on the page of the local private hospital, occasionally supplemented by a website of their own.
Which means that, for the consultant willing to embrace the future and promote themselves and their expertise, the field is wide open.
You see, one of the big problems in marketing is getting your message heard. And there are two reasons for that. Reason number one: People are now officially worse than goldfish. It has long been a standing joke
that goldfish have an attention span of around nine seconds. I’ve no idea on where this figure came from or how accurate it is, but it’s fun, so let’s just accept it for the moment and swim with it.
Falling attention span
Because research by Microsoft has shown that whereas the human attention span was 12 seconds in the year 2000, it has now dropped to eight seconds in 2015.
That’s right. The average human attention span in the western world is now thought to be less than that of a goldfish.
Which is a problem if you’re trying to get or hold people’s attention – which, of course, is precisely what you are trying to do in all your marketing: in print, online when people visit your website, everywhere.
Which again brings me to the reason why most consultants’ websites fail to generate patients.
People flit from website to website, looking for content that grabs their attention. And if they don’t find it within a few seconds, they’re gone; often never to return.
So if you have a website and wonder why you get so few patients from it, the likely answer is simply that it is boring. It’s called surfing for a reason.
So the lesson is that the only way your marketing can work is if it stands out. It has to stand out, because if it doesn’t, it won’t be noticed. And if it’s not noticed, it can’t be read. And if it’s not read, it can’t be acted upon.
Secondly, even if it is noticed, your problems don’t end there. Because if it is dull and boring in the mind of the reader, it will rapidly be discounted and ignored, and the viewer will look elsewhere for something more interesting.
Each of us is exposed to the marketing messages and advertis➱ p21
subscribe by Direct Debit anD save £15
Dear Reader,
Subscribing to Independent Practitioner Today is the only way you can be sure you will see every issue. Don’t risk missing out. Our personal subscription for doctors and managers is only £85 a year and £200 for organisations. But you can cut this to just £70 and £175 respectively if you pay by direct debit.
So take advantage of this offer now for our unique business journal dedicated to supporting you in your private practice. We’re confident your subscription will repay itself many times over!
Editorial director
Please debit my Mastercard/Visa/ Amex/Diners Card No
Expiry
Instructions to your Bank or Building Society to pay Direct Debits
Society
Banks and Building societies may not accept direct debit instructions for some types of
Name and full address of your bank/Building Society Banks and Building Societies may not accept Direct Debit instructions for some types of account To: The Manager
post your application (no postage required – uK only) to: independent practitioner today subscriptions department, Freepost, po Box 36, plymouth, pl1 1Br
subscribe online at www.independent-practitioner-today.co.uk
ing of thousands of companies every day, from a myriad of sources: TV, radio, billboards, newspapers, magazines, email inboxes, the internet. Thousands upon thousands of messages every day, all crying out for our attention.
And cutting through the noise and clamour of hundreds of other competitors to get your message heard by your target market is tough, because everyone out there in your industry is trying to do the same thing.
Except, perhaps in medicine. In the US, advertising and marketing by doctors is very much the norm, so getting your message heard can be tough.
But in the UK, the opposite is true. In fact, many doctors frown upon it and see it as both unnecessary and unprofessional, neither of which is true.
So the great advantage you have is that because so few of your colleagues are actually putting themselves out there and marketing themselves and their practices, it is far easier to be heard by your potential patients – by your target market.
And that means opportunity for those brave enough, curious enough and hungry enough to give it a try.
Exploiting the opportunity
The thing with opportunities, of course, is that they don’t last forever. And not only that, those in at the beginning get a head start on everyone else – an advantage that can be difficult for others to overcome. Ask any new consultant having to compete against a more established colleague.
But to be clear, the purpose of marketing is to grow your practice. So we’re not talking about an opportunity to market yourself so much as an opportunity to increase your private income.
Which brings us back to the beginning: the reasons why doctors don’t market themselves. Fear and apathy.
overcoming fear and apathy
Consultants are anxious, I think, firstly because of concern at what colleagues might think, and secondly of looking unprofessional.
And while I can’t magically take that away, what I can say is that
Many doctors frown upon advertising and see it as both unnecessary and unprofessional, neither of which is true
the final arbiter of all your marketing efforts is you. It’s up to you what you say and do in your marketing.
So it’ll only make you look unprofessional if you let it. I shudder at the story of an orthopaedic surgeon who used to drive around the place with his private practice contact details on the side of his car and a giant plastic femur on top.
positive feedback
But perhaps one thing I can do to encourage the doubters out there is to say that positive feedback is really quite magical in overcoming both fear and apathy.
And seeing the numbers of patients rise in your clinic, and therefore your income climb, as a result of a successful marketing campaign works wonders at banishing both of these and so encouraging future marketing efforts.
So my advice is to choose something low-risk, and have a little fun.
Start with either getting on the phone to the local paper or put
Make sure to put up lots of information, pictures, testimonials and patient case stories on your website
together a press release, with a view to getting some PR. This is easy, quick, free and it’s always fun to see yourself in the paper – as long as it’s for the right reasons, naturally. And no matter what your specialty, it is likely the exposure will generate some patients for you. It will also mean you can further capitalise on your press exposure by publishing a link on your website.
interest the reader
The other thing I would do is to make sure your website has decent landing pages on the conditions you want to treat. Make sure to put up lots of information, pictures, testimonials and patient case stories on there. And, above all, make sure it is engaging and interesting to the reader.
Then try driving some paid traffic to those pages, either through Facebook advertising or Google Adwords, depending upon the conditions you are targeting. This will cost a few hundred pounds, but as long as you track things properly – so you know if the campaign has worked – and target clinical conditions that are worth a reasonable amount of money, then it’s a good place to start.
But two words of caution. Firstly, sorting out your landing pages is a necessary pre-requisite. You absolutely must do this before driving paid traffic to the page.
Secondly, either spend a decent chunk of time to learn how to run your Facebook or Adwords campaigns properly or pay someone with appropriate skills to do it for you.
People have lost large amounts of money on poorly set-up payper-click campaigns – we’re talking tens and even hundreds of thousands of pounds. So while it’s not difficult, you really do need to know what you are doing.
Growing your private practice isn’t hard and there are many reasons to believe you have a huge opportunity if you act now. But that opportunity won’t last forever. And you really won’t know until you try.
Mr dev Lall is an upper-GI surgeon and runs a specialist private practice consultancy www. p rivate p ractice expert.co.uk
No great secret to successful PR
Guess what: They’re called ‘newspapers’ for a reason! Tingy Simoes (right) kicks off a new series for independent practitioners who want to use the media to increase their business
With close to two decades of healthcare PR under my belt, a published book and an industry award, i’ve learnt a fair share of lessons in what works and what doesn’t in regards to achieving media coverage for in the surgical sector.
i’ve worked with organisations of all shapes and sizes: from professional associations, charities and august educational institutions, to hospitals, medical devices and individual private practices.
i ’ve launched into the market optical, breast and dental implants both in the UK and internationally. if you’ve seen it in the news and there’s a scalpel involved, it’s likely i was behind it – the story, not the scalpel!
throughout this time i’ve also been uniquely positioned to appreciate up close this awkward, somewhat stilted dance between
uneasy partners who have sometimes directly opposing perspectives: clinicians and mainstream journalists.
i have witnessed awful – and occasionally hilarious – missteps from both sides, as well as fantastic results that benefit everyone, when harmony in communication is achieved.
Unique relationships
the recent anniversary – lucky 13 – of my agency inspired me to propose a short series of articles based on the intricacies of this unique relationship.
My experience has led me to conclude that these medical relationships are different from any other PR arena, so i wanted to share with you some of its quirks, anecdotes and hopefully useful tips when you navigate the ‘big bad world’ of media relations, both traditional and online.
in general terms, clinicians fall roughly into two camps: those who despise dealing with the press and those who enjoy it or, at least, tolerate the process.
But those of you who may look down your nose at PR and social media need to understand one thing: the compromise that you may find unpalatable, is simply Not a compromise.
here’s why. Perhaps you don’t read The Sun or the tabloids or watch the morning t V chat shows, but i can guarantee the people you treat or operate on do.
And an attitude in which you look down or patronise your ‘customers’ – yes, we know they’re called patients; just humour me here – will prevent you from growing a practice.
if you want to engage with an audience, you need to learn their language. You’re not going to magically change the way the vast
majority of the public thinks and acts, just because you don’t think and act like them. Not everyone decides to train at a career for 30+ years. trust me, Y o U are in the minority.
t here is nothing wrong or shameful about wanting new business, but don’t expect to achieve it if you’re not prepared to think like, or engage with, your prospects.
Understand your patients
Don’t miss out on a potential opportunity to speak to them because, in your eyes, it’s somehow a compromise of your principles or dignity.
Understand them first, then make the conscious choice to opt in or opt out. But don’t expect to cash cheques from an audience that you ridicule, condescend to, or don’t understand. Feel free to ➱ p24
Would you like to remove the administrative stress of medical billing and collections?
Have you an amount of bad debt owed?
Would you like to raise the profile of your practice and attract more patients?
sit on the sidelines and sneer at your colleagues, but don’t complain when patients go to them instead of you, because they think ‘that there guy – or gal – speaks in a way i understand’.
t hat’s the biggest lesson i can ever impart. Now, if you’re still with me, in this piece i will offer a little insight into what reporters, producers and editors are after, followed by (less stern, i promise!) upcoming pieces exploring other themes such as:
What makes a story;
the surgeon as a ‘celeb’;
how to market effectively using different media channels, including the web;
how to find the right support to achieve this.
ironically, PR has a bit of an image problem. some of it is down to easy
– if undeniably funny – stereotyping on tV such as frazzled edina from Ab Fab , ruthless Malcolm tucker in The Thick of It , ditzy
siobhan sharpe of ‘Perfect curve’ PR agency in BBc’s mockumentaries Twenty Twelve and W1A. But some of it is down to the real pressures publicists operate under.
i f the client has very little understanding of what counts as news and the publicist or social media manager has very little understanding of what the client does, it can only be a marriage made in hell.
Total howlers
it’s the type of PR that results in total howlers – press releases or pitches that journalists sometimes forward to me, saying ‘ c an you even BelieVe this?’
i’ve read emails where the editor is magnanimously ‘granted the opportunity to interview this famous surgeon about their views liposuction/lens implants/‘tech neck’. h old the front page, i ’m sure.
Remember, they are called
UK Top 20 accountants specialising in the healthcare sector
• National firm of the Year 2013 AISMA member (Maidstone and Leicester offices)
• 12 offices including London City
Tax Structures for Hospital Consultants - dispelling myths
• Surgeon groups and consortia GP Practices including mergers and federations Solvent liquidations (for companies at the end of their lives)
For more information please contact: South East
James Gransby FCA
E: james.gransby@mhllp.co.uk
T: +44 (0)1622 754033
M: +44 (0)7712321899
East Midlands General email: healthcare@mhllp.co.uk www.macintyrehudson.co.uk
Robert Nelson DChA FCA
E: robert.nelson@mhllp.co.uk
T: +44 (0)1162 894289
M: +44 (0)7814009160
newspapers for a reason. the clue is in the name. this, which seems so obvious, seems to go over many clinicians’ heads. The Evening Standard and Metro are not there to let commuters know that you have been invited to lecture at a cleft palate conference in Moscow. seriously, only your mum cares about this. they are not there to educate, inform, protect or somehow elevate the public’s consciousness to a higher plane. t hey are selling newspapers, magazines and trying to get their reader/viewer/listener figures up.
it’s a dogeatdog world in the media right now and they need news to survive. And preferably interesting news their audience can’t find anywhere else.
i remember an editor telling me once: ‘i want stories that people later talk about at the pub’.
i’m only going to say this once because i don’t want it going to
my clients’ heads, which are, ahem, sizable enough already: i adore what they do. i respect their work and the gloriously gruesome history that lay the foundations of today’s refined, lifesaving and lifeenhancing techniques. i find the science fascinating. they’re helping people walk or move better, feel good about themselves, rectify disfigurements, fractures and defects, not die of internal bleeding or strokes, have a nicer smile, fill out a bra, recover their eyesight and live longer, happier lives.
Lack of understanding
And if i, a relatively normal person – o K, just a layperson; let’s forget normal – find it so interesting, surely others will? A recent MoRi poll proved that health stories are still one of the top reasons people read newspapers. Where the bottleneck begins to develop is the lack of comprehen
sion of what news outlets are after. Private practitioners may want – or at least understand the value of –having their name become familiar to the public, but they fail to grasp what the editors and producers need to secure that place.
t hey think it’s just sensationalism and celebrities and vapid features, requiring shameless selfpromotion (how unBritish!) and catering to the lowest common denominator.
And if they try and fail to get stories in the press or the coverage doesn’t result in an immediate upsurge in business, they inevitably think ‘PR doesn’t work’. it’s true that there has to be an element of novelty – the word ‘news’, just like the French ‘nouvelle’, evolved from the concept of, duh, ‘N e W’. And it helps if there’s something topical to peg it to. But i can guarantee you one thing: the surgical sector isn’t lacking in news.
Definitely stuff that would be talked about at the pub, like fancy training simulators or an eye implant inspired by NA s A. But you have to know where to look – it’s not always where you expect – and, crucially, you have to know how to translate it to your audience’s language. t hat does not automatically mean ‘dumbing down’.
good pR works
one thing i can assure you is that good PR does work; i wouldn’t have a successful 18 year career otherwise. the results of good PR are undisputable.
But bad PR that doesn’t respect and elevate the material will not help you or present the profession in a positive light.
You have to listen to the right experts. You might not think dealing with the media is very cerebral, but surely you trust your accountant, independent finan
you’re as qualified to create and dictate pr or social media campaigns as i am to perform a hip replacement, cataract surgery or rhinoplasty
cial adviser and solicitor in their areas of expertise?
You’re as qualified to create and dictate PR or social media campaigns as i am to perform a hip replacement, cataract surgery or rhinoplasty – although i’ve been to so many surgical congresses i might have enough continuing professional development points by now.
in my next article, i will delve deeper into where to find, and how to craft, different types of story to achieve a range of objectives with concrete, reallife examples. there is a wealth of content all around you – and it’s free. the question is, are you ready to dance ‘with the devil’?
Tingy Simoes is owner/managing director of Wavelength Marketing Communications and author of the first-ever PR Manual for doctors and surgeons How to Cut it in the Media by CRC Press
An easy to use software system, which fully supports the clinician and office staff and makes the whole process of running a busy Practice a lot easier.
Call now for a chat and ask about a free, no obligation demonstration of our comprehensive system that has been designed to save your Practice time and money.
Surgeon with an eye on the prize
Ophthalmic surgeon Mr Ahmed El-Amir describes his experiences and the thinking behind his decision to start up a new multidisciplinary eye clinic in Harley Street
Why W ould anyone want to take on the challenge of starting an eye clinic in harley Street?
Trust me; this is a question I’ve asked myself quite a few times in the last six months.
I’ve been deeply interested –some of my family might say obsessed – with the human eye for several years. It all started when I was a student at the Charing Cross hospital Medical School.
We were taught little ophthalmology, but the small amount we did learn fascinated me. Chancing my arm a bit – after all, I was still a student, not a qualified doctor – I started to follow the eminent eye
surgeon, Prof Alan Bird, on his weekly rounds at Moorfields.
Prof Bird was quite surprised that I was there at such an early stage, but I persisted and the kind professor eventually became my mentor. I will always be very grateful to him.
I became a consultant ophthalmic surgeon when I was 32.
Rapid change
I was fortunate to enter a field which was on the threshold of exciting technological developments. I’m now 37 and have to pinch myself sometimes at the rapid pace of change in my profession. We are now helping patients with procedures which we could only dream of ten years ago. But I’m running ahead of myself here.
After I completed my registrar job and the Royal College of ophthalmologists’ advanced training at the oxford deanery School of ophthalmology, I was appointed in 2010 to run a joint vitreoretinal service with the teams at the Royal Berkshire h ospital, Reading, and King Edward VII hospital, Windsor. I also consult at the Princess Margaret hospital, Windsor, and the Spire dunedin hospital in Reading.
I do not intend to give up my NhS work, but I became increasingly conscious that, to stay abreast of developments, I would also have to work in private practice.
This was really brought home to me when I became the first sur
The Harley Street Eye Clinic’s opening party in March
geon in Europe to implant the uS company VisionCare ophthalmic Technologies’ Centrasight miniature telescope, the only one approved by both E u and F d A regulatory authorities.
The lenses for this telescope have to be handmade. Not surprisingly, the procedure is very expensive. o ne eye costs about £15,000.
With N h S budgets under increasing pressure, it is unrealistic to expect this procedure to be widely available in the NhS until unit costs come down. And this will only happen once the procedure becomes standard in private practice.
So, it seemed to me that the rationale for starting my own private practice was obvious.
But where should I start my practice? And what type should it be? Who would be my patients?
Start acting
After mulling over these questions for some time, I resolved in early 2014 that I had to stop thinking and start acting.
I had already started seeing private practice patients in Reading and Windsor, but I had a vision in the back of my mind for something that was more holistic. Something that could provide patients seamlessly with stateofthe art technology and procedures in ophthalmology and optometry, and perhaps related services in due course.
My thinking led me to the conclusion that I should start a clinic. Given the increasing international nature of ophthalmology, I thought I should also offer the clinic’s services to overseas patients.
h arley Street beckoned as london’s focal point for international medicine. yes, I knew that the established competition would be tough. My research told me that there were about 3,000 people working in the medical field in the harley Street area and there were private hospitals offering ophthalmology.
I had used some of them. I realised my nascent clinic would have to offer something different.
I was determined to emphasise a personalised, caring and compassionate service for all eye conditions. Worldclass ophthalmic
treatment and outstanding patient care summed up my thoughts of what I wanted to offer.
h aving settled on a h arley Street clinic, would I be able to find somewhere? h arley Street forms part of the 850acre howard de Walden family estate which strictly guards its prestigious reputation.
Maybe I was lucky: at one of my early meetings with the estate managers, it transpired that a lease was coming up on two floors of No.86. Was I interested? o f course I was.
Spreading the word Premises secured, I then needed to secure access to the latest equipment. Would the suppliers be willing to support me? It seemed they would.
What should I call my clinic? I must admit I was surprised to discover that nobody had already used the name of The h arley Street Eye Clinic.
I now had the foundations of a clinic: name, location and equipment. It was time to start spreading the word and generating referrals.
I managed to recruit a capable
Allow a reasonable amount of time to produce and implement your marketing plan. And then double it
business development manager from a hospital with whom I had previously worked. She assembled a team to design and write the material for our website and brochures and advise on public relations.
My advice to anyone thinking to start up a practice is to allow a reasonable amount of time to produce and implement your marketing plan. And then double it.
I also recruited an able practice manager and secretary to manage my practice and handle what I hoped would be a reasonable number of inquiries.
And then the time came, much quicker than I thought it would, for an official launch. Friends and colleagues gathered to toast to The h arley Street Eye Clinic’s success.
We got off to a flying start, helped by some good media coverage, and our team had to work hard to bed in the administration procedures.
has it been plain sailing? No. As with all startups, it’s been more of a roller coaster ride, but I’m sure that I will always remember my pride when I first entered No.86 harley Street and saw our clinic’s brass plate.
The Harley Street Eye Clinic team: (left to right) Mr James McAllister, consultant ophthalmologist; Nicola Wood, lead optometrist; Mr Ahmed El-Amir, senior consultant ophthalmic surgeon/director; Mr Raj DasBhaumik, consultant ophthalmologist and ophthalmic plastic surgeon
Ensuring consultants’ outcome data adds up
Senior doctors are out to make sure the new performance measures are fair and helpful for consultants in private practice
The Private Healthcare Information Network (PHIN) has recently appointed a number of new non-executive directors to its board after taking up its role as the Competition and Markets Authority’s (CMA’s) approved ‘information organisation’ for private healthcare in April.
Independent Practitioner Today asked three of them – who will be well known to many of our readership – for their early thoughts on some of the key issues of concern for consultants and how they might be addressed.
There will be a number of questions in the minds of consultants that need to be addressed:
what are the practical implications of this process?
how will it help me?
Are there any restrictions on access to my data or will anyone be able to see it?
how will the data be quality-assured?
what if it is wrong?
Does my data have to be published?
what if several surgeons are involved in treatment of a patient?
how will admissions unrelated to recent procedures be distinguished from genuine re-admissions?
how often will my dashboard be updated?
how far back will the data go?
w hat will my personal dashboard look like? (See Independent Practitioner Today, June 2015, page 24).
Personally, i have been reassured by my first few PhiN board meetings and can see that a plan and process is emerging for addressing these questions. This is an ambitious and challenging project dependent upon accurate data as well as a robust iT platform.
As directors, we have been well briefed and we are aware of the magnitude of the task. There is a healthy debate, suggesting that PhiN will listen to all views and take a balanced approach to delivering its remit.
And that’s not just listening to the views from within its own board, but from the whole healthcare sector including FiPO. There is a clear desire to work with all individual specialties and their professional associations. Although there are only two years to implement the CMA’s remedies, PhiN is taking the time to engage with stakeholders, and the approach is measured. it is taking time to ask the difficult questions, so that the final product delivers for patients, their doctors and providers.
Dr Gerard Panting was nominated to PHIN’s board by the Federation of Independent Practitioner Organisations (FIPO) as somebody trusted by consultants to understand and articulate their needs and concerns. He has over 25 years’ experience in medical law, regulation and indemnity, notably with the Medical Protection Society.
Prof Sir Cyril Chantler, a retired paediatric nephrologist, was until recently chairman of UCL Partners Academic Health Science Centre and was formerly chairman of the Standards Committee of the GMC. He has great experience of overseeing the production of trusted, impartial information and of how it might be used.
Prof Sir Norman Williams, a specialist in bowel surgery, was president of the Royal College of Surgeons of England when NHS England first published consultant outcomes from the national audits and registries. As such, he brings direct experience of helping to find the balance between fairness and transparency.
CONSulTANTS will need to have confidence that we will be rigorous in how we measure and report outcomes. The hospitals producing the data will need to be equally rigorous in how they collect and use the information.
The use of proper clinical coding to enable risk adjustment will provide the foundation, but we will also need to find and test appropriate methodologies at every stage and for each specialty. while patients’ safety has to be the overriding concern, we must also consider the outcomes that matter to patients: clinical outcome measures, patient-reported outcome measures (PrOMs) and patient-reported experience measures. Any used must be validated and appropriately adjusted.
ultimately, patients will not have confidence in PhiN’s information unless their professional advisers have confidence in it – gPs and consultants.
however good the data is, it can only provide material for a patient to consider, not give them the answer. we should aim to inform the conversations between patients and clinicians, not to replace or undermine them.
i Agree AbSOluTely with Cyril’s remarks (see left), and would like to spell out some specifics:
1
we must ensure that each consultant sees their data before publication and has time and the means to validate and correct the data as necessary. Of particular concern to me is the N h S h ospital e pisode Statistics data, which is widely believed to be quite flawed. i hope that those fears will prove exaggerated, but any issues must be addressed.
2
PhiN must do its best to ensure that the data are risk-stratified. however, this is no easy matter. it will take time and the involvement of a great deal of expertise to get this right.
3
4
P hi N should utilise, wherever possible, the data from national audits and liaise with the appropriate specialist associations.
PhiN must present whole-practice data, giving a full and fair view of each person’s practice.
Currently, about half of the surgeons who do the work covered by the national audits have had their NhS outcome data published. This process should come as no surprise to them. but what about the other half?
The CMA’s Order requires the publication of outcomes for individual surgeons. This will prove extremely challenging, not least against a background of increasing understanding of the role of teams rather than individuals in the NhS.
it is probably fair, however, to note that things work a little differently in private practice, where a single consultant generally has clear responsibility.
Do you have concerns about how the information project will affect you and your practice? Tell independent practitioner Today by emailing robin@ip-today.co.uk
What a waste
Independent practitioners and their staff are under increasing pressure to understand and adhere to clinical waste regulations. Proper management of clinical waste is vital and there are strict laws to prevent harm being caused to the environment and to human health. But mistakes are still being made. Rebecca Allen outlines the ten big ones and says what should happen
1 incorrect colour coding
Disposing of waste in the wrong colour-coded, rigid and soft container bins is a common problem.
It is essential to segregate clinical waste correctly at the point of production following the ‘Safe Management of Healthcare Waste’ guidance issued by the Department of Health. By using the national colour coding system, which means using coloured bins that segregate your waste by type, you can help to drive waste minimisation and best practice:
Yellow – infectious waste for disposal by incineration
Orange – infectious waste for disposal by treatment or incineration
Yellow/Black (Tiger) –Offensive/hygiene waste for disposal by deep landfill
Blue – medicinal waste for disposal by incineration
Purple – Containing cytotoxic or cytostatic waste for disposal by incineration
Red – Anatomical waste for disposal by incineration.
Proper segregation of different types of waste is critical to safe management. The mixing of waste streams is prohibited by law in Eng-
land and Wales, and best practice in Scotland and Northern Ireland.
2
not understanding that, as the producer of the waste, the practice holds full responsibility for it
It is important to remember with clinical waste that the cradle-tograve rule applies. This means that as the producer of the waste, you are responsible for its correct disposal.
This is due to the Waste (England and Wales) Regulations 2011 and duty of care principles. The regulations state that it is the responsibility of the producer of any controlled waste to ensure the correct and proper management of the controlled waste their business produces.
The main principles of duty of care cover documenting the transfer of waste and ensuring it is handled correctly by waste carriers. As a business producing clini-
cal waste, are you using a registered carrier of waste? Are they taking waste to suitably licensed/permitted sites?
It is worth remembering that failure to comply with the regulations and principles of duty of care could leave your business subject to fines or even the closing down of your premises.
3 incorrect storage of clinical waste bins
Waste bags are quite often found outside of dedicated or secured locations. To comply with legislation, waste bags must be kept in a secure environment, such as a locked area or cupboard.
This is to prevent anyone from accessing the waste that could possibly cause harm to themselves, others or the environment. This falls under the Waste (England and Wales) Regulations 2011 and is something the Care Quality Commission is very firm about.
4
incorrect disposal of sharps
Despite the introduction of the Health & Safety (Sharps instruments in Healthcare) Regulations 2013, not all independent practitioners and/or their staff are disposing of sharps in the correct manner.
Under the new regulations, healthcare facilities need to assess the risk of exposure to bloodborne infections from sharps injuries, identify how to eliminate this and where exposure cannot be eliminated, put into place extensive prevention methods.
The new legislation also requires a framework for the occurrence of a sharps injury. The directive is supported by a local, national and European-wide reporting system and employers need to revise their reporting procedures with health and safety representatives.
Key tips to make sure you comply with the new regulations:
Implement safe procedures for using and disposing of sharp medical instruments and contaminated waste;
Eliminate the unnecessary use of sharps by implementing changes in practice and through providing medical devices incorporating safety-engineered protection mechanisms;
Provide sharps disposal equipment as close as possible to the assessed areas where sharps are being used or found;
Ban the practice of recapping;
Use personal protective equipment;
Train your practice staff on the correct use of sharps devices and the disposal of sharps waste.
5 waste bags not being correctly sealed or contained
Waste bags must be correctly sealed before they are transported. They are often found not tied properly, which can cause spillage.
To seal a waste bag, either tie the top or use a bag tie. Again, this falls under the Waste (England and Wales) Regulations 2011 and principles of duty of care.
Waste that spills out of incorrectly sealed bags could cause harm to people or the environment. It must be safely stored and contained. This means any waste that may pierce the bag must be disposed of in the appropriate ridged waste container to prevent this occurring.
6lack of understanding about clinical waste management contracts and providers
Many independent practitioners do not understand what to look for in a clinical waste management provider or what their contracts should or should not entail.
The first and most important thing to check is that you are using a Registered Waste Carrier. You can do this by asking to see a copy of their licences.
The top ten things you need to look out for are:
Is the waste carrier licensed to take away the types of waste you are producing?
Are the service technicians that will be collecting your waste ADRlicensed (European Agreement Concerning the Carriage of Dangerous Goods by Road)? This is essential when transporting dangerous goods such as clinical waste;
Will you receive all the compulsory waste documentation to cover your waste transfers?
Will your waste be fully traceable from point of product through to end disposal?
Do all the products supplied to you meet legal requirements, such as UN approval for your sharps containers?
Will the supply of products be free of charge or are they an additional cost?
Will your waste be fully segregated on site and during transportation to meet the current regulations?
Can the clinical waste management company guarantee your service delivery will happen on time, every time?
Has the service been tailored to your requirements?
Are there any hidden charges?
7not understanding the importance of consignment notes and paperwork
Practices are sometimes unaware of the documentation that needs to be provided alongside clinical waste. Below is an outline of what is required.
waste transfer notes:
For all transfers of waste – that is to say, waste being taken from the premises to be disposed of –appropriate documentation must be provided.
For non-hazardous waste, such as general domestic waste, this is usually in the form of a waste transfer note.
You will be provided with an annual waste transfer note by your clinical waste management provider, covering all transfers of non-hazardous waste for the previous 12-month period.
This will state what items have been removed from your practice. When you receive this documentation, you must check this for accuracy purposes and the return slip must be given to your clinical waste management provider.
Hazardous (England & wales) or special (scotland) waste Consignment note: All consignments of hazardous (special) waste must be accompanied by a hazardous or special waste consignment note. This would be given to you by your clinical waste management provider.
waste pre-acceptance:
The Environment Agency has imposed a legal requirement, which means Environmental Permits are required for disposal sites to ensure that producers of waste carry out audits of their waste
before it can be legally accepted and disposed of. These are known as ‘pre-acceptance audits’. This is something your clinical waste management provider would also take care of for you.
To ensure your waste is suitable for any chosen method of disposal, all your waste streams must be audited, documented and this information relayed to your final disposal site.
Failure to do this may leave you in breach of your ‘duty of care’ responsibilities, which can lead to prosecution and unlimited fines.
8
General waste
being put in clinical waste bins
When our firm, Initial Medical, collects clinical waste, we often find the waste bins have some items of general waste in them. The most common breach is staff putting uncontaminated packaging containers and other nonclinical type waste into clinical waste bags.
It is important that your employees are trained to put items in the right bins.
The reason for this is that it costs more to dispose of clinical waste in the right manner, so it is only adding additional costs to your practice if general waste is disposed of in the same way that clinical waste is.
9 not using Un-approved containers
Waste containers must all be United Nations-approved. We have witnessed sharps in bags, dental waste stored in glass jars and the use of ordinary plastic containers to store hazardous waste.
UN-approved containers need to be used and transported under the EU ADR regulations. The correct containers ensure there are no leakages and waste is contained safely up to the point of final disposal.
10 not disposing of medicines correctly
Unfortunately, some medicines are still not being disposed of in the correct colour-coded bins. It is imperative they are disposed of correctly to ensure they are broken down properly and are kept away from animals or young children.
Denaturing, where controlled drugs are rendered unusable, is an option for ensuring they are disposed of correctly.
Denaturing normally involves mixing the controlled drugs with a binding matrix to make the material physically irretrievable in the waste chain. The final material is then classified, described and disposed of as a waste medicine.
The Environment Agency guidance states: ‘The Environmental Permitting (England and Wales) Regulations 2010 provide an exemption (T28) for the denaturing of controlled drugs at the premises of production. Furthermore, the Department of Health (DoH) Safe management of healthcare waste guidance states: ‘Denatured controlled drugs should be disposed of as waste medicines of the appropriate type.’
Therefore, denatured drugs cannot be disposed of as non-hazardous waste, in spite of denaturing, which is solely for prevention of drug misuse.
Further DoH guidance in the ‘Controlled Drugs (Supervision of Management and Use) Regulations 2013: Information about the Regulations’ states:
‘Controlled Drugs (CDs) are essential modern clinical care. They include drugs such as diamorphine that are used in a wide variety of clinical treatments; for example, for the relief of acute and chronic pain, end-oflife treatments or as part of the treatment of substance misuse. Other medicines such as anxiolytics, sleeping pills, steroids and growth hormones are also designated as CDs, albeit these are subject to less stringent controls under the Home Office’s Misuse of Drugs legislation.’
More information can be found at www.gov.uk/government/publications/denaturing-of-controlled-drugs.
See www.followthecolourcode.co.uk
Rebecca Allen (right) is category manager for Initial Medical, which is an expert in health care waste management
No more ‘freebies’
A flurry of activity in spring this year saw private hospitals adjusting to the reality of the Competition and Markets Authority’s Private Healthcare Market Investigation Order.
As a result, consultants have been approached and asked to sign new agreements with the hospitals. And the end result for many practitioners is an arrangement which looks quite different from what they have been used to over the years. Lindsay Draffan (right) explains the changes and the need for compliance
The long-running saga of the Competition and Market Authority’s (CMA) investigation into private healthcare continues with appeal and counter-appeal by the affected parties.
Wider press attention has focused on the Draconian requirement by the CMA that h CA should sell some of its l ondon hospitals, while private practice has understandably focused on the publication of consultants’ fees and performance data.
Currently, the CMA is picking its way once again through insured pricing data with provisional findings due in August or September and a final report in January next year.
These appeals have somewhat detracted from the planned entry into force of the prohibition on clinician incentives.
The order was published back in october 2014, but the part relating to ‘referring Clinicians’ (Part 3) had a delayed entry into force until April 2015 to allow clinicians and hospital operators to make the necessary changes to their commercial arrangements.
Ban on incentives
The prohibition makes unlawful any scheme or arrangement which is, or could be reasonably regarded as, an incentive between
a referring clinician and a private hospital operator (Pho) to induce a clinician to refer a patient for treatment or tests at a facility within the Pho group.
The prohibition applies both to the clinician and the Pho, so the legal obligation to comply is on both sides.
it is widely drafted so as to catch any arrangement, whether legally enforceable or not, which might be seen to affect the choices consultants make – or suggest to their patients – about further treatment, including diagnostic tests.
This is notwithstanding compli-
ance with ethical and other professional standards as set by the gMC.
An obvious example is a payment made by a Pho to a consultant in relation to the number of patients referred to a hospital –but an allocation of shares in a P ho or a ‘contract for medical services’ between the two might not be so apparent.
Two types of services
e ven parking spaces for senior consultants raise difficulties if they are not also made available to all staff working at the hospital generally.
The competition watchdog has banned doctors from signing contracts with hospitals that offer subsidised rooms and secretarial service
The CMA does, however, distinguish between two types of service provided to a clinician. ‘highervalue services’ are allowed, provided these are at ‘fair market value’.
These include:
Secretarial and administrative support;
use of consulting rooms;
Contributions to professional indemnity insurance.
For many consultants, the biggest impact so far is the requirement to pay for the use of consulting rooms and secretarial services (see Independent Practitioner Today,
June 2015, page 1), which were previously free or at a discounted rate and therefore fall foul of the ‘fair market value’ test.
‘
l ower-value services’ are permitted. These include:
i n-house training on clinical safety;
operational matters relating to patient admission;
Administration and billing;
general marketing;
Corporate hospitality, within reason.
The cost of higher- and lowervalue services must be published on the hospital’s website, although not the identity of the consultant.
Equity participation in hospital groups
Part 3 of the order also prohibits a clinician from having directly or indirectly a share or financial interest of over 5% in a Pho or in a facility owned or operated by a P ho ; or in any partnership or
The biggest impact so far is the requirement to pay for the use of consulting rooms and secretarial services, which were previously free or at a discounted rate
venture with a Pho to offer private healthcare services; or in diagnostic equipment or equipment for treating patients.
Again, that wide definition can cover a number of scenarios and an ‘indirect interest’ includes interests held by members of a consultant’s immediate family or through a trust.
Enforcement
So to what extent do consultants need to comply?
Put bluntly, the order is law –competition law, to be more precise – and breach of the prohibition could result in enforcement action by the CMA, such as financial penalties and injunctions, as well as other regulatory issues.
Private individuals are also permitted to bring proceedings if they believe they have been disadvantaged or otherwise adversely affected, suffering loss or damage.
i t is essential that consultants
are as well-informed about the need for compliance as the large hospital groups, particularly with continued attention on the independent sector by the competition authorities until at least the beginning of next year.
Competition law is a relatively complex area of law. But the importance of gut reactions cannot be underestimated. A good rule of thumb is how an arrangement might appear to the outside world and how comfortable you would be to publicise it.
Gmc guidance
The gMC has produced Q&A guidance on the order. it also intends to bring attention to the restrictions in the order by writing to all licensed clinicians in the uK.
Lindsay Draffan is an associate specialising in Competition Law in Hempsons Corporate Commercial Team
Free legal advice for independent practitioner Today readers iPT
independent practitioner Today has joined forces with leading niche healthcare lawyers hempsons to offer readers a free legal advice service.
We aim to help you navigate the ever more complex legal and regulatory issues involved in running and developing your private practice – and your lives.
Hempsons’ specialist lawyers have a long track-record of advising doctors – and an unrivalled understanding of the healthcare system as a whole.
call hempsons on 020 7839 0278 between 9am and 5pm Monday to Friday for your ten minutes’ of free legal advice.
Get on the case of your time management
Whether your work comes in as a trickle or as a torrent, planning how you are going to manage your time as an expert witness is important. Michael R. young shows what to consider
It Is best to get into good habits earlier rather than later, when time might be more pressing.
You won’t often have the luxury of setting your own timetables. the court will invariably do that for you. But you will have to manage your time within the time constraints imposed on you. some cases can take years from start to finish, especially if they go to trial. When you accept instructions, you are making a long-term commitment.
You may write a report and then hear nothing more from the solicitor for months. However, expert work can be very time-consuming, especially towards the end of a case when you have to work to tight deadlines, all of which are set by the court.
t he majority of your time is going to be spent writing reports, and predicting how long it is going to take to complete a particular report is never easy.
But however long you decide it is going to take, always allow yourself sufficient time to do the job properly, and never leave it until the last minute.
t here are two aspects of time management to consider. First, the management of each individual case; second, the management of all the cases you might have on the go at any one time.
How many cases you take on at any one time is very much up to you. But, as a general rule, you
Week beginning Task
1 January
8 January
Read case file 1 and make notes
Read case file 2 and make notes
15 January begin writing report
22 January Write report
29 January Write report
5 February Have first draft ready; edit and revise
12 February Half-term holiday 19 February Finish report
should beware that each one is probably going to take you twice as long as you think it is and that once you start a case, it is not easy to withdraw. t here is also the danger that if you take on too much work, you will burn yourself out, physically and mentally.
I never handled more than five or six cases at any one time, and that was only when I was able to commit to at least one full working day a week to my expert work.
Dividing up the time
the essence of the time management process is the division of a piece of work into a series of com-
start reading the case file when I was writing the report of the first case, and so on.
ponent parts or stages. In report writing you cannot, for example, begin writing until you have read and analysed all of the records; one stage naturally follows on to the next.
Always ask the solicitor for a copy of the case file before you give an estimate of your fee, because you have to estimate how long you think it is going to take you to read through the file, make notes, write the report and then edit and redraft. You can’t do that until you have seen the size of the file.
Get into the habit of setting your time plan out on a chart (see box).
For an additional case, I would
special oFFeR! buy THe book and save £20
The book costs £60, but independent practitioner Today has secured discount of a third off for readers, so you pay only £40. listen to the audio content which accompanies the book at this website: www.otmoorpublishing.com/audio. For more information and to order, email stephen.bonner@ otmoorpublishing.com, quoting reference ‘young/ipT’.
It is better to overestimate and to allow for such things as illness, problems at work or family matters. In the example shown on the left, tell the solicitor that the report will be completed by 26 February, but actually plan to finish it the week before. Delivering ahead of time is always preferable to delivering late.
Planning one case is relatively straightforward, but as your caseload increases, so time management becomes more complex and even more important.
You will need to keep an accurate and honest record of all the time you spend on each case.
Record this information in two places: first in the relevant case file, so that if you are charging for time spent you know how much to charge.
s econd, record all of the time you spend on all of your cases, so that you can see how much of your working time your expert work is actually taking up.
I used to use a notebook to record this, but there are software packages that can do this for you electronically.
n Next month: Terms of business
n Adapted from The Effective and Efficient Clinical Negligence Expert Witness , by Michael R. Young, price £60 from Otmoor Publishing
PUZZLE
Crossword
Garry Chapman of Medical Billing and Collection has
ACROSS
1. The leading billing company in the UK (7,7): plus 73 across (3) and 7 down (10)
8. Another word for teeming (6)
9. Someone who specialises in detecting disease through investigative techniques (11)
10. Plantar fasciitis causes pain under this part of the body (4)
13. You would put this on parts of the body to reduce swelling (3)
17. This person would assist you with your tax affairs (10)
19. Intolerance of this is a common digestive problem (7)
22. A clump of earth and grass (3)
23. Exclamation of greeting (2)
24. The act of balancing your bank account (14)
30. See 1 down
32. Concerning America’s Big Apple (4)
33. Medical specialty dealing with pregnancy and birth (10)
35. Something that happens in rugby (5)
36. External egg masses of fish (3)
37. A text message acronym for being happy (3)
38. Famous medical road in London (6) and 51 down (6)
39. Rhinoplasty is a procedure carried out on this part of the body (4)
41. Small growth of horn at the site of a normal horn in cattle and unattached to skull (4)
42. A popular Greek fast food served on a skewer (8)
44. Expressing location or arrival in a particular place, position or time (2)
45. A former government organisation that sets the rules regarding the amount of tax that an individual or company should pay (6,7)
49. A specialist doctor who is an integral part of the team treating patients for operations and procedures (12)
55. Dismissed as inadequate or unacceptable (6)
56. This is a shortcut to a task you do repeatedly (5)
57. The market leader in smartphones (5)
58. A masculine personal pronoun (2)
59. Without these, private healthcare would not exist (8)
62. Something of value is called this (5)
63. Slang for ‘Thank you’ (2)
64. Short for incorporated (3)
65. A form of public transport (3)
67. An idea, belief, or pattern of behaviour that spreads from person to person within a culture (4)
68. An acronym for the application of computers and telecommunications (2)
69. To exist is to ... (2)
70. Shortened form of America (2)
71. A liquid food (4)
72. A meeting with a patient typically carried out in an outpatient clinic (12)
73. See 1 across (3)
DOWN
1. A singular version of the leading ophthalmic unit in the UK (8), plus 30 across (3), plus 38 down (8)
2. A drawing made while a person’s attention is otherwise occupied (6)
3. Orthopaedic surgeons would operate on this part of the body (5)
4. A swelling or outward curve (5)
5. Reluctant or unwilling (5)
6. A person trained to care for the sick or infirm (5)
7. See 1 across
11. Very long periods of time (4)
12. Something a surgeon would do in theatre (4)
14. There is a famous such park in London (3)
15. ‘Aeonian’ means eternal or everlasting, rearrange these letters to complete this clue (7)
16. A unit of coin or currency formerly used in Italy and Sicily (5)
18. To sound a horn in short blasts (4)
20. The provision of what is necessary for the health of someone (4)
21. An item of footwear (4)
25. A well known hospital in west London (8)
26. A robotic non-invasive alternative to surgery for the treatment of both cancerous and non-cancerous tumours (10)
27. Somethings that a consultant would typically dictate (7)
28. See 58 down
29. A person’s specific, unique way of speaking (8)
31. West Indian evergreen tree with medium to long leaves (5)
34. Conjoined inflammation of the choroid and the sclerotic coat of the eye (6, 11)
38. See 1 down
40. Multiple intelligence gathering in a covert way (6)
41. Retail method of reducing the price of goods (4)
43. By way of (3)
46. The initials of a Birmingham NHS facility focused on one specialty (3)
47. Something you would have to charge when doing medico-legal work after exceeding a certain turnover (3)
48. Small North American birds (7)
50. The second largest private medical insurer in the UK (6)
51. See 38 across
52. The number of players in one team on a soccer field (6)
53. A level of care required if the patient is very ill (9)
54. The action or process of puffing or swelling (11)
57. A form of chemistry and speculative philosophy practised in the middle ages (8)
58. A serious medical emergency in which the supply of blood to the heart is suddenly blocked (5), plus 28 down (6)
60. Something that a consultant would do to determine the condition of a patient (6)
61. The application of computers and telecommunications equipment to store, retrieve, transmit and manipulate data (2)
65. The largest private medical insurer in UK (4)
66. The objective case of ‘we’, used as a direct or indirect object (2)
68. Feeling like this is one of the reason you go to see your GP (3)
69. The only mammal that truly flies (3)
71. Possibly the most overused adverb in the English language (2)
Whether you are organising an industry-leading conference, holding a regular training day or looking to fill a job vacancy, Independent Practitioner Today is the place to reach your target audience.
To discuss all your advertising requirements and find out what we can do to help you, contact our advertising manager Margaret Floate
Phone: 01483 824094
Email: margifloate@btinternet.com
“I believe it is important to use this opportunity to bring together board members, doctors, nurses, managers, pharmacists and all those who are seeking to deliver improved safety outcomes for their patients”
DrMikeDurkin,NHSEngland Network with peers. Learn from experts. Implement change.
•
•
• Extensive
more information visit
Education grants are being distributed from May. For more information email d.earl@closerstillmedia.com
Uniting both the Surgical and Non-Surgical Communities
Over 200 world renowned exhibitors
4,000 high level medical healthcare professionals
Over 100 expert faculty
FREE World-class speakers with CPD certified content
FREE conference programme, workshop theatres and live demonstrations
To register and find out more please visit www.ccr-expo.com
What does a Tory election victory mean for the personal finances of senior doctors? Satisfac-tory or nuga-tory? Simon Bruce (right) highlights the key issues to consider
The ConservaT ives’ majority win for a second term in power surprised many voters – and indeed the pollsters whose predictions fell considerably wide of the mark.
so what election promises could have an impact on your finances?
Should i still be contributing to my nHS pension?
Doctors currently enjoying 45% tax relief on their pensions contributions have been spared the introduction of a flat rate of tax relief of around 30%, pledged by
both Labour and the Liberal Democrats.
h owever, the Conservatives’ manifesto declared that those earning over £150,000 will be limited as to how much they can contribute to their pensions.
For every £1 of earnings over £150,000, the annual allowance would reduce by 50p, so that those earning £210,000 and above would have an allowance of just £10,000 rather than the current £40,000.
This means being wary of any nhs pay rises received through
increments, management positions, clinical excellence awards or by any other means. immediate tax charges of up to 50% can be avoided with careful planning.
The pre-election proposal to cut the Lifetime allowance – the total amount which can be saved into your pension free of tax – to £1m from april 2016 will now go ahead. new hM revenue and Customs (hMrC) pension protections will be introduced, so make sure to confirm which apply to you.
if you have not already engaged an adviser to confirm your current
position and pension protection options, then you should not delay.
There are very few circumstances now where a consultant can avoid a Lifetime a llowance reduction to pension savings, particularly if you already have a self-invested pension ( si PP) or personal pension.
Bear in mind that the nhs pension is still very valuable, with guaranteed index-linked benefits in retirement and provision for spouses and dependents.
You may still receive a higher pension after Lifetime allowance charges than if you opt out of the nhs Pension scheme. The ‘new’ consultant contract (2003) has staged incremental increases to pensionable pay that apply to your pension after 12 months. if you opt out, you will not receive this benefit.
The end of pension savings? a reduced Lifetime a llowance does not mean the demise of pension saving. You should be looking to maximise your partner’s, children’s and grandchildren’s allowances, where these are available.
even for those with no taxable earnings, tax relief is available on pension contributions up to £3,600 every year.
More substantial savings can be made for those who operate private practice as a partnership or limited company. Pension contributions have a beneficial effect in reducing corporation tax and higher and additional income tax liabilities for the individual.
can i really pass on my SiPP to my children?
Yes, as of april 2015, you can leave
your entire personal pension to your children or any other beneficiary/ies you choose. With a new Conservative Government, this legislation looks set to remain in force.
Prior to a pril 2015, punitive taxes were applied to pension funds on death after age 75 and any residual fund could fall back into your partner’s estate, leaving an increased inheritance tax bill. This is a step-change in the way we think about pension savings accumulated to date. rather than consider the fund as useful in your lifetime, you can leave it in place for future generations to benefit from, completely free from inheritance tax.
all that is required is a change to the death benefit nomination recorded by your pension provider.
Mansion tax
Consultants concerned by the
contentious ‘mansion tax’ for properties worth over £2m will be relieved that it is no longer on the cards, for five years at least. is this the end of reforms to property taxation following the recent stamp duty changes?
inheritance tax and ‘the family home’
The new Government will introduce a new Family home allowance to increase the inher itance Tax threshold for couples where a family home is included.
From april 2017, married couples and civil partners will enjoy a new £175,000 per person transferable allowance when their main residence is passed down to children or grandchildren on death. This would mean that combined with the existing £325,000 nil-rate band each person has on death, parents would be able to pass on property worth up to £1m free of inheritance tax.
income tax and the personal allowance
The threshold at which the 40% rate of income tax applies will be increased from its current £42,385 to £43,000 for 2016-17.
The £10,600 annual tax-free personal allowance will increase to £11,000 for 2016-17.
What other important rates and reliefs are under scrutiny?
While the Conservatives pledged to eliminate the current budget deficit by 2017-18, they also promised to freeze income tax, vaT and national insurance rates for the term of the next parliament.
Critics argue that this raises the question as to what other measures will be taken to meet fiscal targets.
a fter a decade of pension reforms, the industry desperately requires a period of stability. Unfortunately, the pension sav -
ings of the successful professional often prove to be an easy target. as always when political tinkering is imminent, the best course of action is to take control of your own financial destiny, ensuring your long-term plan is achievable, steadfast and fit for purpose.
Simon Bruce is managing director of Cavendish Medical, specialist financial planners helping senior consultants in private practice and the NHS
The content of this article is for information only and must not be considered as financial advice. Cavendish Medical always recommends that you seek independent financial advice before making any financial decisions.
Levels, bases of and reliefs from taxation may be subject to change and their value depends on the individual circumstances of the investor. The value of investments and the income from them can fluctuate and investors may get back less than the amount invested.
An independent firm offering one to one meetings anywhere in the UK giving advice and help with:
• how to start in private practice
• how to maximise private practice income
• ways to reduce tax payments
• setting up in Chambers/Groups
• limited companies and LLP’s
• financial planning
• record keeping
• computer software
• tax and financial advice re: car purchases
• pensions: NHS, personal and employee schemes
• purchase of consulting rooms and surgeries
• inheritance tax and capital gains tax planning
• VAT
For more information please contact us by:
Wilmslow
Phone: 01625 527351
Fax: 01625 539315
Harley Street
Phone: 020 7307 8759
Fax: 01625 539315
Email: info@sandisoneasson.co.uk
Website: www.sandisoneasson.co.uk
INVEsTINg IN PRoPERTy AbRoAd
Have you considered Portugal for that house you plan to invest in? This could be the time to take a closer look. Dylan Mitchell reports
Portugal Property in
Portugal has often been overlooked by holidaymakers and property investors, but that is starting to change.
From the algarve, with its beautiful sandy beaches, warm climate and fantastic golf courses, to the warm and attractive city of lisbon, with its relaxed café culture and steeped in history, Portugal is finally starting to get
noticed. and let’s not forget the pleasures of the wine-growing region of the river Douro and Porto at its head.
a s the country emerges from the global recession, it has taken drastic steps to attract investors and wealthy immigrants that will help to build a stronger Portuguese economy than this fantastic country has seen in generations.
● The silver Coast ● an hour’s drive north of lisbon is an area known as the silver Coast, so named because the sun seems to paint the sea a shiny silver colour on certain days of the year.
Known as a surfing and golf destination, the coastline is dotted with old fishing ports, and inland you will discover vineyards, fruit orchards and forests.
Property prices here are cheaper than further south, but it is just as attractive as other parts of Portugal.
● Lisbon ● set on the northern bank of the tagus river and overlooked by são Jorge Castle, the old town of lisbon is a combination of palaces, churches and lovely architecture.
First-time visitors are often blown away by the fun café culture and cosmopolitan lifestyle in this ancient capital city.
With a warm climate all year round, sandy beaches and fantas-
tic restaurants and nightlife, l isbon is a city where you can literally live, work and play. With property prices the lowest they have been in years, it is now a hotspot for international investors. this is especially the case in the €500,000 price range, which is the price required for a ‘golden Visa’.
● Tróia Peninsula ● Just south of lisbon on the opposite side of the tagus r iver, the tróia peninsula has been largely developed over the past 20 years and has a more modern feel than the capital. If you’re looking for a relaxed beach culture, then tróia’s surf shops, sandy beaches, golf courses and lively nightlife might be just what you’re looking for.
● Alentejo ●
the area south of the tróia peninsula and north of the a lgarve is the alentejo region. If you prefer a more rustic experience and want to embrace the ‘real’ Portugal, then alentejo is worth a visit. t he area is a largely undevel -
PoRTUgUEsE PRoPERTy HoTsPoTs
oped and has been overlooked by foreign buyers in favour of lisbon and the algarve.
the coastline is peppered with small fishing villages that have not changed much in hundreds of years. as you venture inland, you will discover a beautiful countryside of vineyards and farms, which is why this area is known as the ‘bread basket’ of Portugal. as this area attracts less tourists, some restaurants and bars will only be open in the high season. Property prices in a lentejo are cheaper than many other parts.
● The Algarve ● Portugal’s southernmost region, bordering s pain, has long been popular with holidaymakers all year round as well as property investors. From lagos to Faro, the climate is warm and similar to the Mediterranean, with sandy picturesque beaches and world-class golf resorts.
You are never far away from a small fishing village with great seafood restaurants, and a port to moor your yacht. a quintessential property on the a lgarve is a white-washed villa, overlooking a beautiful golf course or a sandy bay with turquoise water. Faro airport is well connected to the u K and other parts of Europe and the world, making the algarve easy to access.
h ere are a few key points to show why property in Portugal may be a good investment.
Quantative Easing (QE)
t his is when the central banks increase the money supply in a country. When this happens, the excess money has to go somewhere and it ends up in assets like the stock market and property market. the uK and us have been doing QE for a few years now and that is one of the reasons that both countries’ property and stock markets are doing so well. t he European Central Bank started a QE programme in January, which means that money is only starting to reach the property markets.
Low mortgage interest rates
With rates as low as 2.5%, the cost of buying a property in Portugal has not been this low in decades. Property investors are taking advantage of low mortgage rates
and property prices to secure some incredible long-term investments.
New visa programmes
the Portuguese government has been very proactive and creative in finding ways to bring the country out of recession and ensure a prosperous future.
one of the methods it has used is to try and attract wealthy people from within Europe and around the world to both invest into real estate, but also come and live in Portugal. the two schemes created for this are:
1
Non-regular tax regime for non-regular residents
this is a scheme to attract Europeans to become tax resident in Portugal. the scheme is especially aimed at business owners and what is seen as key occupations such as doctors and dentists.
a s a Portuguese tax resident under this scheme, you would be exempt from income tax for ten years, which is very attractive.
If you were considering cashing in your uK pension scheme, the proceeds of which would be liable to income tax, then it may be worth considering this scheme.
2 Portuguese golden Visas
these are aimed at attracting foreign investors from non-European countries by offering a Portuguese residency permit. t here are a number of countries offering golden Visas, but the structure of the Portuguese Visa has made it by far the most successful, attracting over €1.5bn of investment into Portugal.
Both of these schemes are successfully attracting people and capital back to Portugal, which has started to re-ignite the property markets in lisbon and along the algarve.
Planning permission in Portugal has always been tightly controlled, which is why Portugal didn’t experience the construction boom that was seen in many parts of spain. generally, building standards and quality are higher than found in s pain and the coastline is a lot less developed.
Next month: How to buy property in Portugal
Dylan Mitchell is director of PortugalPropertyCo.com
PROBLEMS WITH THE TAX MAN?
HMRC tax investigations and disputes create difficult and stressful times.
As an award winning firm of tax experts, our highly experienced partners specialise in resolving problems relating to tax investigations and disputes with HMRC.
To find out, in confidence, how we can help call 0800 734 3333.
‘Here to help. Not to judge.’
Informed consent is tailor-made
Dilemma 1 What info should I give this carer?
QI was recently visited by a patient who had been referred to my vascular outpatient clinic for consideration for a carotid endarterectomy, after suffering a middle cerebral artery territory transient ischaemic attack.
A carotid duplex scan has shown the relevant carotid artery to be 90% occluded. The patient has a past history of a radiotherapy to the neck for a toxic goitre, but this was 20 years ago.
She is the main carer for her husband, who has Parkinson’s disease, and she is a regular member of the local church choir. What information should I provide to ensure informed consent?
AThe GMC’s guidance
Consent: Patients and doctors making decisions together encourages doctors to consider patients on an individual basis and provide the patient with information that is relevant to them.
This approach has been reinforced by the recent Supreme Court ruling in the judgment of Montgomery v Lanarkshire Health
Independent practitioners’ questions about risk management and consent are answered here by Dr Nicola Lennard (right)
Board (2015 UKSC 11) [see our June issue, page 28].
When discussing the benefits and risks of treatment options with a patient, the ruling requires doctors to consider whether a reasonable person in the patient’s position would be likely to attach significance to the risk or whether the doctor is – or should reasonably be – aware that the particular patient would be likely to do so.
In this case, the patient’s recent transient ischaemic attack is a predictor of a future stroke, but the operation itself carries a risk of stroke as well.
Identify complications
Although the amount of information discussed with the patient will depend on various circumstances, including their condition, general health and individual
Check that the patient has understood your explanation and what it means for her
wishes, it is important to identify complications which the patient would view as having the potential to impact significantly on her life.
Any person undergoing such a procedure should be informed about the potential benefits and risks of the operation and, in particular, the risk of major stroke. However, as the main carer for her husband, the patient could be
affected by even a minor stroke that may also impact on her ability to care.
She might also be worried about the very small but genuine risk of nerve injury affecting her voice. Although the percentage possibility of this risk arising is small, the significance of the complication to the patient has to be discussed. When going through the treatment options, it would be important to explore all the opportunities with the patient. In this case, you should discuss the options open to her, including radiological treatments or maximal medical therapy without surgical intervention, for example. It is commonplace to provide patients with written information when discussing surgery to assist them and their families in absorbing the specifics of the treatment. Such information provides details on the generic risks to patients and is not personalised for the individual, but will still be helpful and will continue to form part of the consent process. It will, however, be important to clearly document that the additional information was given to the patient.
Dilemma 2
What do I tell her about bowel op?
QI am currently treating a 57 year old female who has a twoday history of abdominal pain, vomiting and not opening her bowels. There is no previous history of surgical intervention. She is otherwise well and enjoys swimming and rambling.
On examination her abdomen was distended and generally tender, with tinkling bowel sounds. A rectal examination revealed an empty rectum and no palpable masses, while Xrays showed the presence of a dilated small and large bowel, with no gas visible in the rectum.
I have diagnosed a large bowel obstruction. The patient will need surgery and I want to ensure she has given appropriate consent. What should I discuss with the patient when gaining consent?
AWhen obtaining consent before surgery, the patient should be informed of their diagnosis and the associated prognosis of their condition.
The diagnosis here is one of large bowel obstruction, but the cause of the obstruction will not be clear until the time of surgery.
You should make her aware that you may not be able to provide a definitive diagnosis and prognosis until histology results have been received, which could be some days after surgery.
A clear explanation of the proposed surgery should be given, but you should also check that the patient has understood your explanation and what it means for her.
Evidence of obstruction
You should tell her why the procedure is considered necessary and if there are any alternatives to surgery. In this case, there is clear evidence of obstruction which, without intervention, is likely to progress and the patient is at risk of perforation, leading to peritonitis, septicaemia and ultimately multi-organ failure.
Although there are less invasive methods of relieving the obstruction, these would not remove the underlying pathology, which may impact the prognosis. As with any surgery, the patient should be given information regarding the potential risks and complications as well as the perceived benefits.
When discussing complications, it is important to include those that would be considered significant by the individual patient.
The GMC makes it clear that you must explore the options with the patient, listen to their concerns, ask for and respect their views and encourage them to ask questions.
In this situation, it is highly likely that the patient may require the formation of a stoma and this should be discussed in depth with her.
In particular, you should give her information as to why it might be necessary, whether there will be the prospect of reversing it in future, what factors may affect this and what support she would be given in managing the stoma.
You should also explain what
the effect will be if a stoma is not formed and the potential risk of complications following surgery.
The patient may want to know what impact the stoma may have on her day-to-day life, including her ability to go swimming. If the patient has concerns about how she will manage, and if time allows, you might wish to involve a stoma nurse in the discussions.
You should explain the expected time-frame for recovery, including the potential need for high-dependency care.
Any possible need for additional interventions or treatment following the procedure should also be discussed, including any objections that she may have to these. The patient may wish to explore additional treatment that might be required if the underlying disease is found to be malignant.
If you are carrying out the procedure, then you should be the one to obtain consent. If this is
not practical, you can delegate to a colleague, providing they are suitably trained and have sufficient knowledge to understand the risks involved in the procedure.
If you do delegate this process, you are still responsible for making sure that the patient has been given sufficient information to make an informed decision.
The risks and benefits that you discuss with the patient should be clearly documented in their medical notes, along with any specific concerns or requests that she has raised during the dialogue.
Finally, you may wish to clarify with the patient if she is happy for you to discuss matters with her family members should they request additional information. Again, this should be clearly marked in the medical notes.
Dr Nicola Lennard is a medico-legal adviser at the MDU
On a roll – help in
Ian Tongue shows what you need to know about a payroll scheme if you are employing staff
Many consultants use the services of a secretary or spouse in their business and often there is a formal employee/employer relationship.
It can be daunting to be an employer and you certainly have to take on new obligations, but it should not be too onerous if operated correctly.
The PAYE system all consultants will, no doubt, be familiar with the Pay as you Earn (PayE) system, having paid tax on their employment earnings as a trainee.
the PayE system is designed to be straightforward and collect the right amount of tax from an employee over a 12-month period. For most employees, the system works perfectly well and for the levels of salary that you are likely to pay as an employer, it is likely that the payroll will operate without error.
For the majority of consultants, if you are employing staff, your accountant will maintain the PayE scheme.
Real Time Information (RTI) system
a relatively new change to the PayE system is Real time Information or R t I. t his requires the payroll data to be submitted to HM Revenue and c ustoms (HMR c ) monthly rather than annually.
a gain, for most, this has not been too much of an issue, but if your staff are paid bonuses or commission, you will need to agree the pay period to ensure that your accountant receives the relevant information in good time.
For example, if your employees are paid overtime, it is common for it to paid in the following month.
paying your staff
Key facTors To consIder for a docTor deTermInIng The sTaTus of a worKer
does the individual work for anyone else?
can they turn down the work or are they obliged to work for you?
who decides and controls how the work is done?
can they send someone else suitably qualified in their place at their discretion?
do they supply their own equipment; for example, computer?
who takes on the financial risk?
are there any benefits associated with the engagement?
do they receive holiday pay or sick pay?
It can be easy to get caught out thinking that just because a person provides you with an invoice, they must be selfemployed and you have no obligation to employ them
When is a person an employee or self-employed?
t his is a common query that often has no direct answer. It can be easy to get caught out thinking that just because a person provides you with an invoice, they must be self-employed and you have no obligation to employ them.
this is incorrect and the status of the person in question will be determined by the contract in place in combination with the facts.
It is important to determine who is responsible for paying over the income tax and what national Insurance contributions are paid. If the correct status is not applied, it can result in penalties and financial loss for both parties.
an employee operates under a ‘contract of services’, whereas a self-employed individual operates under ‘contract for services’. It may sound like a subtle difference, but it is key in determining status.
the list of key factors for determining the status of an individual (see box above) is not exhaustive, but they are most likely to represent the key questions for a consultant. a s always, if you are in
If your spouse is not working, it is a good idea to get them involved in the business to at least the extent of paying them a salary to utilise their personal tax allowance
doubt, you should discuss matters with your accountant who will assist you in determining an individual’s status.
Should I employ my spouse?
For many consultants, their spouse is inevitably involved in some way with the private practice.
Where this is the case, it is appropriate to pay them a salary and this can be tax-efficient for you as a couple if your spouse is not working or is a low earner.
the amount paid should be representative of the work performed at an arms-length rate of pay. the figure determines if a P ay E scheme is required and the current level to require a scheme to be in place is approximately £485 a month.
a ny pay in excess of this amount will require a P ay E scheme to be in place.
If your spouse is not working, it is a good idea to get them involved in the business to at least the extent of paying them a salary to utilise their personal tax allowance.
the current personal allowance is £10,600 a year and therefore no income tax is paid until this level is reached.
But it is worth noting that the income tax and n ational Insurance level is not aligned and therefore a small amount of national Insurance is payable at this level.
Due to a current initiative to encourage small businesses to employ staff, you would not pay any employer national Insurance for the first £2,000 of contributions.
Provided that the work performed will justify the salary ‘package’, you could also consider pension contributions for your spouse.
Auto-enrolment
auto-enrolment is a new scheme introduced by the Government to force employers to provide a workplace pension for their staff.
For any employer, you must categorise your staff in order to determine whether they are required to be put into a pension scheme (auto-enrolled) or whether they do not meet the criteria for auto-enrolment but may have rights to join a pension scheme.
Either way, it is unavoidable that some work on auto-enrolment will be required for anyone operating a Pay E scheme and many accountants can assist you with an auto-enrolment solution. Where a pension is required and an employee does not opt out, contributions by both the employee and employer are required. the employee rate starts at 1% and rises to 5% by 1 october 2018 and the employer rate also starts at 1% and rises to 3% from 1 october 2018.
With many of the larger insurance companies not looking to provide small employers with a scheme, there are a small number of pension schemes, including a government-backed scheme, that are available. a n independent financial adviser or your accountant should be able to assist you in this area.
o perating a payroll scheme is an inevitable part of most businesses. With the right help and support from your accountant, it should be a painless process.
Next issue:
Strength in numbers – a guide to working in a group
Ian Tongue (right) is a partner with accountants Sandison Easson and Co
docToR on ThE RoAd: poRSchE cAyEnnE hyBRid
With lots of pep
It’s nice ‘n’ spicey and comes in enough versions to suit a wide range of doctors’ tastes and budgets. Dr Tony Rimmer has been testing all versions of the Porsche Cayenne and opts for the amazing S E-Hybrid
If you look at thriving and successful practices, you can guarantee that they only got to where they are by taking risks and thinking ‘outside of the box’.
No business can stand still and even when drastic changes need to take place, the organisations that encourage flexibility and read their client market pragmatically are the ones that succeed.
Looking from the outside, certain changes may seem to flow against the prevailing current that made the business successful in the first place.
This is what happened behind the closed boardroom doors of the iconic sports car-maker Porsche at the turn of the millenium.
The German manufacturer was in trouble and was having great difficulty making a profit from its performance vehicles.
Motoring journalists loved the
911 and Boxster, but the prevailing global economic situation brought few buyers with ready cash. People were buying practical cars that could function in the real world and the sports utility (SuV) sector was gaining popularity.
Bold gamble
So Porsche made a really bold decision and commissioned a new model that was to break the mould of all previous vehicles it had made over the previous 50 years.
It took a gamble that people would like and, more importantly, buy a sporty five-seat, five-door Porsche. This was like a successful surgical clinic suddenly offering cardiology services.
The new model was the Cayenne and following its release in 2002, despite upsetting Porsche purists, it went on to exceed all sales expectations and saved the
Despite upsetting Porsche purists, the Cayenne went on to exceed all sales expectations and saved the company from very stormy financial seas
company from very stormy financial seas.
There is no doubt that without the success of the Cayenne, we would not still be able to enjoy the constantly updated 911, Cayman and Boxster models that currently still head their respective sports car sectors.
We medics tend to like our cars and a sporting driving prowess certainly appeals. f ew of us can justify a two-seater Porsche, but plenty of us could consider a more practical and useful alternative boasting the same DNA.
The second-generation Cayenne appeared in 2010 and now, in 2015, an updated and face-lifted version has been launched.
I have been driving all variants of the new model and have had an extended test of the new cutting-edge rechargeable electric hybrid version, the E-Hybrid.
The runaway success of the Cayenne had nothing to do with its looks and, if anything, the original car was quite ugly, particularly from the rear aspect. f ortunately, styling upgrades made the second generation car more attractive and now some final aesthetic tweaks have given it a handsome and purposeful look. you would be quite happy to be seen stepping into the current car in your clinic car park.
Six versions
With six versions to choose from, there is a model for all tastes and all budgets.
The £50,252 base model has a three-litre V6 262bhp turbodiesel and the £93,783 top model ‘Turbo’ has a 4.8 litre V8 bi-turbo producing 520bhp.
In between are the S diesel with a 385bhp 4.2 litre V8 turbodiesel, the S with a 420bhp 3.6 litre petrol bi-turbo and the interesting S E-Hybrid with rechargable electric drive and a three-litre V6 petrol engine with 416bhp combined system output.
Having been so impressed by the all-electric TESLA that I tested for Independent Practitioner Today (May 2015), the appeal of a rechargeable sporty but useful SuV is a very attractive proposition. Able to travel up to 22 miles and up to 78mph on electric power alone, many of you urban or citybased independent practitioners could easily justify this S E-Hybrid model.
Charge it up overnight and you only have to use the petrol engine
on weekend trips. What a great way to wear green eco credentials.
Inside the Cayenne, you are greeted by the recognisable Porsche dashboard with a cluster of five dials and a sports steering wheel that could be straight out of the £800,000 918 Spyder supercar.
Solid interior materials
Interior materials of solid quality and comfortable leather seats grip you in all the right places. Rear seats have plenty of headroom and legroom for five passengers. They recline and even slide back and forth to increase boot space if necessary.
PoRsChe Cayenne S E-Hybrid
Body: Five-seat, five-door sports utility vehicle (sUV) engine: one electric motor and a 3 litre V6 petrol engine
Power: 320bhp (petrol) 96bhp (electric)
Torque: 600nm acceleration: 0-60mph in 5.4 secs overall economy: 83.1mpg
Max range electric alone: 22 miles on-the-road price: £61,474
If you have teenage children or transport five adults regularly, the Cayenne trumps the smaller Macan model every time.
o n the road, the excellent straight-line pace combines with the impressive grip, composure and direct steering to convince you that you are indeed driving a proper Porsche.
Silky smooth
The eight-speed automatic gearbox changes with silky smoothness and the ride is almost as relaxed and refined as the rival Range Rover Sport, particularly if fitted with the optional air suspension.
Remember that the Cayenne also performs really well off-road too. Although not up to Land Rover standards, it will do anything you could reasonably ask of it on the rough stuff.
The latest Cayenne is a great leap forward for the model and would really suit the typical successful independent practitioner.
Competitors include the BMW X5, the Mercedes ML and the Audi Q5, but its strongest rival is the superb Range Rover Sport. However, none of these rivals currently offer a state-of-the-art rechargeable hybrid model.
The lack of a seven-seat option may lose some sales, but nothing else proudly and appropriately wears the iconic and famous Porsche badge. And that counts for a lot.
Dr Tony Rimmer (right) is a GP practising in Guildford, Surrey
Interior materials of solid quality and comfortable leather seats grip you in all the right places. Rear seats have plenty of legroom for five passengers
PRoFiTs FocUs: gENERAl sURgEoNs
DO yOU FIND OUR PROFITS FOCUS SeRIeS USeFUL?
Please let us know if it helps you or not. and if it doesn’t, what other data would you like to see presented?
email robin@ip-today.co.uk
Pain from watchdog bite
Latest income figures for general surgeons are showing a 6% drop in profits. Ray Stanbridge identifies a myriad of reasons. Additional material from Martin Murray
It’s gettIng much tougher out there.
We reported in the July-August 2014 edition of Independent Practitioner Today of the difficulties we were facing in analysing income and expenditure trends in this specialty.
t hese included the increasing trend towards subspecialisation among general surgeons. the various alternative means of trading – through groups and limited liability companies, for example –were all creating comparison problems. there was also a growth
in nHs Choose and Book income.
t his time around, we have started to observe a new trend which will also distort results, and reduce the reliability of any comparisons.
Newer breed
Age has now caught up with some of the older players whose private practice was largely conducted in a more benign era.
And it is clear that some of the newer consultants are preferring a different work-home life balance than their predecessors.
It is clear that some of the newer consultants are preferring a different work-home life balance than their predecessors
there is also a growth in ‘parttime’ consultants, which will have the effect of diminishing average incomes.
Having made all these caveats, we have preserved our definitions of our survey members as best we can.
Our general surgeons include those who:
Hold either an old- or a newstyle nHs contract;
May, or may not, have incorporated their businesses;
May, or may not, work with a group;
Have a keen interest in private practice;
Have been involved in the private sector for at least five years;
e arn a private practice gross income in excess of £5,000pa. suffice to say, our income survey is not statistically significant. All it does is to give some indication of what is happening in the real market.
Introduction
Year ending 5 April. Figures rounded to nearest £1,000 (percentage is also rounded up)
Source: Stanbridge Associates Ltd. Additional information: Sandison Easson and Co
Between 2012 and 2013, general surgeons’ gross private practice incomes fell by about 5%
Welcome to the BVRLA – I’m delighted that you’ve decided to join the trade association that provides a face for the vehicle rental and leasing industry, communicating its messages to customers, the media and government.
The BVRLA’s corporate identity, particularly its logo, forms part of that message.
But what our survey does show is that between 2012 and 2013, general surgeons’ gross private practice incomes fell by about 5% from £135,000 to £128,000. Costs have fallen by about 3.5% from £57,000 to £55,000. As a result, taxable profits have, on average, fallen by about 6% from £78,000 to £73,000.
The BVRLA has three categories of membership, each with a logo that members are entitled to use (and, in some situations, are obliged to use). Appropriate use of our logo tells your customers, your suppliers, and the rest of the world that you adhere to the high standards that come with BVRLA membership.
This brief guide explains how we expect our logos to be displayed – and how they should not be displayed. These are not hard-and-fast rules, and we sometimes depart from them ourselves, but we do expect our members to respect them and to gain our prior approval before using our logo in any way other than described here.
If you need a copy of our logo, for use on your printed marketing material, or to go on a page of your website, please contact our communications team, who will be happy to send you an EPS or JPEG version appropriate for your purposes.
If you have any queries about use of the BVRLA logo that are not addressed in this guide, they will also be able to help
Using the BVRLA Logo
Crossword answers
so why not turn to the experts in the field to help you find the vehicle that suits your needs?
anthony K associates are vehicle leasing brokers specialising in providing vehicle contracts for doctors and all associated professions in the medical sector.
testimonials from our very many happy customers are proof of our attention to customer service and our practised ability to help clients get the vehicle
What are the reasons for the income fall?
Firstly, we are now seeing the full impact of the Bupa open referral system and other insurers’ feereduction schemes.
s econdly, the volume of n H s Choose and Book work, at often lower per unit prices than insured work, is rising.
And thirdly, with the growth of more ‘part-time’ private practice consultants, there is a natural tendency for gross income to fall. We would expect these trends to continue.
t here have been a number of changes in costs.
t here seems to have been a slight increase in assistants’ fees/ medical supplies. We cannot identify any particular reason for this.
t here seems to have been a slight decrease in staff costs. Again, there appears to be no clear reason for this.
Room costs rise
Consulting room hire costs seem to have shown a slight decrease. this perhaps represented the calm before the storm.
Certainly, from April 2015, we have noticed that room costs/secretarial costs have increased for many general surgeons, following rulings from the October 2014 Competition and Markets Authority banning ‘inducements’.
t here seems to have been a slight reduction in indemnity costs, on average. A number of consultants in our sample have taken a cheaper policy. It is not known whether or not, in the longer term, these will save money. But, in the short term, they seem to have done.
there seems to have been some growth in ‘other’ costs. As with other specialties, general surgeons are spending more on marketing and promotion.
What of the future? As we have indicated above, the days of the traditional ‘general surgeons’ are almost over. subspecialism is now the norm.
We would expect to see some further income squeeze in future, as a result of the changing pattern of work and ongoing pressures on fees from both insurers and, we suspect, the nHs.
Next issue: ENT surgeons
Ray Stanbridge runs an accountancy, finance and tax advisory service specialising in the medical profession. Martin Murray is a partner at Sandison Easson and Co, specialist medical accountants
geNeRaL SURgeONS’ eXPeNSeS FeLL, BUT THeIR INCOMe DIPPeD
what’s coMing in our septeMBer edition
Make sure you don’t miss our next issue, published on 17 September. Only subscribers to the journal are guaranteed to receive every copy and we don’t think anybody who is serious about continuing private practice in the future, when there is so much happening that will affect them, can afford to miss any issue.
Coming up next month:
Doctors v Fraudsters! It’s a growing problem. So how do you stop them getting their hands on the funds held in your medical practice? Ian Crompton shows how to protect yourself from an increasing number of threats
Ten qualities that consultants look for in a top-class private hospital nurse
Patients expect voice and choice – but our report shows this is not always happening and when expectations are not met, this makes for a disappointing experience
Strength in numbers – Ian Tongue’s guide to working in a group
along with many other businesses, more independent practitioners have been involved in HMRC tax investigations in recent years. Susan Hutter summarises the main types of investigation you are likely to be involved in and shows how these should be handled for the best outcome
New to private practice or about to start out? Surgeon Dev Lall gives his unique take on how to surmount the challenges
eDITORIaL INqUIRIeS
Our ‘Breaking Into The aesthetics Business’ series from Pam Underdown sets out how to build a marketing plan and will give a free template to download, as well as discounted access to her live online marketing training programme
How the statutory duty of candour will apply to independent practitioners. Dr Mike Devlin of the MDU explains
Profits Focus puts the microscope on the earnings of eNT surgeons
Doctor On The Road tester Dr Tony Rimmer goes for a spin in the latest Caterham Seven
Business Dilemmas answers more of your questions
Our property expert Dylan Mitchell shows how to go about buying a property in Portugal
Why is some news covered and other news not? and why are some organisations always in the press – what do they know that you don’t?
Tingy Simoes provides a more practical way of understanding the elements that make a good story, with tips and examples
Plus all the latest news
aDveRTISeRS: The deadline for booking advertising for our September issue falls on 21 august
Robin Stride, editorial director
Email: robin@ip-today.co.uk Tel: 07909 997340
aDveRTISINg INqUIRIeS
Margaret Floate, advertising manager
Published by The Independent Practitioner Ltd. Independent Practitioner
Today is editorially independent and thanks Bupa for its assistance with distribution.
Printed by Pepper Communications Ltd
Material is governed by copyright. No part of this publication may be reproduced, stored in a retrieval system or transmitted in any form without permission, unless for the purposes of reference and comment. Editorial layout is the copyright of the publishers. If you wish to use it for promotional purposes on websites or for reprints, we would be happy to discuss licensing the copyright to you.
£85 GPs and practice managers (private & NHS). £200 organisations. But if you pay by direct debit, individuals pay only £70, and organisations £175. Call Proact Ltd on 01752 312140
Email: lisa@marketingcentre.co.uk
Robin Stride, editorial director @robinstride
IPt
gUaRaNTee yOUR COPy
To guarantee your copy of Independent Practitioner Today by taking out a subscription (at the rates shown on the left), phone 01752 312140 or send off a subscription form on page 20 or email lisa@marketingcentre.co.uk or go to the ‘about’ page of our website www.independent-practitioner-today.co.uk
If you pay by direct debit, individuals pay only £70 for a subscription. Just fill in the form on page 20 and send it to the Freepost address shown at the bottom of the form.
BaCk ISSUeS: £12.50 including post & packaging CHaNgINg aDDReSS OR
Phone 01752 312140 or email lisa@marketingcentre.co.uk
The professional’s choice for practice management
Client management and financial control is the lifeblood of any enterprise. The latest Healthcode online ePractice management tool is the professional’s choice for practice management, giving you the control you need wherever you are. Our ePractice management solution meets the needs of a range of healthcare providers, from independent practitioners to large enterprise organisations. Our different service levels means that ePractice will grow with your practice.
Take Direct Control
Access your patient details, appointments, bills and financial status from anywhere, any time.
What the professional’s say...
Protect Your Practice
The diary management feature on ePractice manager means I can focus on treating patients, while my PA is able to coordinate my appointments remotely.
Mr Barlow-Kearsley, Founder, Total Footcare Solutions
Long Term Partner
I’m delighted to say that we have never looked back. The system is really intuitive which has made it quick and easy to learn and yet it provides all the functionality we need. Most importantly, our consultants tell us it is working well for them too.
Catherine Goodsell, PA to the Hospital Director, Spire Sussex Hospital
Call us today to arrange a demo and to discuss your requirements on 01784 263 150 quoting: IPT. For further information visit: www.healthcode.co.uk/ipt