Our Troubleshooters tackle this increasingly common question from private doctors P12
The business journal for doctors in private practice
Paying by results becomes a reality
Dr Ravi Lukha on Bupa’s mission to introduce valuebased healthcare P20
Do you know how to protect data?
n See page 14 to read the advice from the Information Commissioner’s Office
Death is going through change
Lawyer Liz Hackett explains the advent of medical examiners, who come into force this autumn P36
Data breach threats
By Robin Stride
Private healthcare providers have been warned to wake up to escalating data breach threats from organised criminals using a vast range of tactics on the unwary.
Cyber-attacks are only one method fraudsters try to access confidential information, the audience at market analyst LaingBuisson’s Private Healthcare Summit 2024 heard.
Criminologist Dr Nicola Harding’s message to independent health sector businesses was stark: ‘We have to consider that this isn’t an “if”, this is now a “when”.
‘You are all a target. You have to plan as though it is going to happen because if you’re not planning, the outcomes for organisations that haven’t got a plan are far more dire.’
Her warnings came after a law firm’s report labelled the health sector as a frequent violator and top spot for data breaches in 2023, accounting for around one-in-five reported data breach cases (see story page 10).
Cyber-security expert Dr Harding, chief executive of We Fight Fraud, said: ‘Criminals are the creative human beings that are using their creativity to circumvent your systems and processes. What we need to get better at doing is planning and ensuring that our
Our sponsors
humans on our side are just as sharp and just as switched on as they are.’
Data was attractive to criminals because it could be used to compromise, exploit and access further revenue. ‘But we need to get away from this idea that the worst thing that can happen to us is a cyberattack. Actually, the worst thing that can happen to you guys on the whole is a data leak.
‘And a data leakage can happen in different ways. A cyber- attack is one of them, but data leakage happens with poor GDPR [General Data Protection Regulations] practices; it happens when you don’t shred documents and they end up in the wrong hands; it happens when people have conversations that should be happening in private – on the train, on the way to work – about a patient.
‘It happens when you open your laptop and you’ve got your records for the day because you’ve maybe got to travel from London up north and that’s three hours on the train when you want to get some work done. But the person next to you is looking over your shoulder at everything you’re doing.’
She added: ‘You don’t know who’s watching; you have to treat every potential piece of data like it’s the royal family’s data.’
Dr Harding said the data compromise cycle was necessary for organ-
ised crime to work and the consequences included terrorist finance, serious child sexual abuse and wars. ‘This isn’t a simple small “Oh, I forgot to shred those documents”. The consequences of it down the line can be extremely dire.’
While technology could do amazing things to prevent data breaches, her work showed it was humans who created compromise.
Staff training was vital and companies should ensure they had instant response plans not just for a cyber security breach but for anything relating to data compromise. These should include their PR response, how they would talk to the public about it and regulatory expectations about what was likely to happen when people’s data was lost.
You are all a target. You have to plan as though it is going to happen, because if you are not planning, the outcomes from organisations that haven’t got a plan are far more dire.
DR NICOLA HARDING (left), Chief executive of We Fight Fraud
Delegates heard from an IBM 2023 report that US organisations with high levels of instant response planning and testing saved $1.49m compared to those with low levels. Only one-in-three data breaches were identified in-house. ‘Sixtyseven per cent of breaches in 2023 were reported by a benign third party or by the attackers themselves. When attackers disclosed a breach, it cost organisations nearly $1m more compared to internal detection.’
Dr Harding warned that data breaches could arise from someone walking up to their reception desk, through a phone call to staff or when someone identified their workplace because they left their lanyard on in the pub after work. n Conference reports, page 4-5
TELL US YOUR NEWS.
Contact editorial director Robin Stride (right)
Email: robin@ip-today.co.uk
Relations with patients & colleagues
The GMC has updated its supplementary guidance to Good Medical Practice. Dr Catherine Wills analyses its advice on keeping professional boundaries P16
Phone: 07909 997340 @robinstride
ADVERTISE WITH US. To advertise in the digital journal, on our website or in our business and lifestyle directories, contact Andrew Schofield at Spot On Media. Phone: 0161 408 3912
A look back through our journal’s archives of a decade ago reveals that although times change, some issues are not so new P22
What we can learn if it goes wrong
The learnings from medical negligence claims from general surgery in private practice are shared by Dr Sarah Townley of Medical Protection P24
Data analytics can bring in the cash Derek Kelly of Medserv shows how data anlaytics can identify revenue opportunities and enhance financial performance in doctors’ billing P26
Fertility parents hate making a fuss
Patient complaints-handling expert
Sally Taber outlines what fertility doctors treating private patients should be aware of P28
OUR REGULAR COLUMNS
Business Dilemmas: When police ask about your patient
The MDU’s Dr Kathryn Leask explains how to respond to a request for information from the police P40
Start a private practice: How you can hit top profits
Specialist medical accountant Alec James gives his top ten tips for maximising your rewards P42
Doctor on the Road: VW’s glad tidings of comfort and joy
Volkswagen’s latest Tiguan offering is a great allrounder, reports Dr Tony Rimmer P44 www.independent-practitioner-today.co.uk
Celebrating becoming sweet 16 June is our birthday month and we are celebrating 16 years of bringing doctors in private practice news, advice and tips to ease their business life P30
Looking to the future is a bit hazy
Do recent returns give investors FOMO? Simuel Kirton of Cavendish Medical on why investors should gain comfort by holding a broad market exposure P34
Maintaining safety of staff & patients
David Hare, head of the Independent Healthcare Providers Network, gives a heads-up on some recent developments in healthcare regulations P38
Thousands of doctors missing pension pay
Doctors unaware of pension rule changes
By Edie Bourne
Many senior doctors are still unaware that working beyond the normal retirement age of 60 if they have benefits in the 1995 Section of the NHS Pension may mean missing substantial payments.
New retirement flexibilities last year were brought into the NHS Pension Scheme, which mean doctors could claim retirement benefits from the 1995 section while continuing to work.
But many pension scheme savers have not claimed these payments, which are not backdated. If they are not taken, they are lost.
Samuel Kirton, financial adviser with specialists Cavendish Medical, told Independent Practitioner Today: ‘In 2022, the 1995 Section was closed and all active members moved to the new 2015 Scheme. At the time, doctors could retain their benefits in the legacy scheme, but not accrue any further benefits.
‘When the new retirement flexibilities were introduced last year in a bid to retain more senior medics, this rule was changed. Now, members can claim benefits from their old pension scheme while continuing to build benefits in the new 2015 pension.’
He explained that the doctors impacted were likely to be in their
50s and 60s. The normal retirement age for the 1995 Section is 60, but some roles with specialist status can retire at 55.
‘Of course, like many things
The capital’s private healthcare business boom set to continue
The business boom reported this month in the London private acute healthcare sector is set to continue, according to independent healthcare market analysts.
LaingBuisson says it expects impressive growth reported by www.independent-practitionertoday.co.uk earlier this month to carry on – albeit at a slower rate.
Revenues for 2023 are reckoned to be around 10% up on 2022 –leading to a potential central London market value of £2.2bn in 2023.
And growth of 9.7% is forecasted for 2024.
The market intelligence specialists reported strong continuing demand for private healthcare as the central London private acute market surged to more than £2bn for the first time.
Its director of research and con-
tent, Tim Read, said: ‘London’s private healthcare ecosystem is not comparable to the rest of the country due to higher levels of PMIs coverage and high earners willing to pay for ultra-premium services.
‘Meanwhile, revenues from inter national travellers and the high concentration of top-tier NHS private patient units (PPUs) ensures that the London private market remains less exposed to political headwinds derived from exposure to a higher-NHS-funded revenue base and instead reflects confidence in the pure private pay market.’
LaingBuisson said its Private Acute Healthcare Central London Market Report (10th edition) presents the first complete picture of the health of the London market as it transitions away from a period
focused on adapting to the challenges of the pandemic.
A rise of over 20% in consumers’ incomes drove revenue from the private patient segment to over £1.5 billion, meaning that overall revenue growth reached £2 billion in central London and nearly £400m across Greater London independent hospitals.
Private health insurance continues to account for the largest share of revenues, but the reports says growth of self-pay in recent years is significant. It is now the secondlargest source of revenue for the London market – growing nearly 19% year-on-year in 2022.
Income from foreign embassies has begun to grow again after falling during the pandemic – reaching £337m in 2022. But it is still £48m below its pre-pandemic peak.
within the NHS Pension Scheme, it is not entirely simple to navigate claiming the benefits. Doctors can either take partial retirement, which means reducing their pensionable pay by 10%, or use “retire and rejoin” which involves leaving the workforce temporarily.
‘Both options require a significant amount of paperwork and, crucially, agreement from the employing trust, which is not always straightforward.’
Mr Kirton advised doctors to always seek expert guidance when planning their retirement to ensure they were making the most of all opportunities and not missing out of any financial benefits.
Bupa to open five health centres with
Five new health centres are being opened by Bupa Health Clinics within private medical and dental provider MyHealthcare sites in Balham, Swiss Cottage (open) and Chiswick, in London, and in Edgbaston, Birmingham, and Peterborough, Cambridgeshire, (opening soon).
The new partnership sites will offer access to Bupa’s private GPs and other primary care services.
MyHealthcare clinics also offer specialist services including paediatrics, gynaecology, dermatology and ultrasound scans. Dr Akash Patel, medical director of MyHealthcare
Samuel Kirton of Cavendish Medical
Competion body to pester doctors
Reports by Robin Stride
Consultants and hospitals have again been warned they face legal action if they continually fail to comply with requirements of the Private Healthcare Market Order, which requires them to provide data to the Private Healthcare Information Network (PHIN).
Andrew Land, senior director at the Competition and Markets Authority (CMA), said they should not wait to be contacted but ‘take action now’.
He told the conference: ‘PHIN are here to help you become compliant. It is the law; we will enforce it, we will enforce against people who fail to comply.’
Ten thousand consultants are said to be compliant with the competition law so far, but many are not and, between February and
March 2024, enforcement action was taken against 40 larger hospital providers. They have delivered action plans and all must be compliant by 3 July.
The CMA wants providers to provide the required data on a routine basis and while many are
making the effort, others were not – and that was unfair on patients, said Mr Land.
Providers who fail to comply after chivvying face being named and shamed and ultimately taken to court.
He said that better information:
Drove consultants and hospital owners to deliver higher-quality treatment, increased choice, innovation and lower prices;
More informed and engaged patients supported choice between hospitals and among consultants;
Consultants and hospitals benefited from greater user awareness of their services and how to get them, and consumers became more confident in using private healthcare;
Compliance lead to quicker identification of and action on outlying poor performance.
‘Starter for ten’ drives conference quiz batty
Independent Practitioner Today helped get things buzzing as over 200 delegates talked about every front page featured in all our monthly issues over the last year.
Conference director Elizabeth Boultbee’s icebreaker quiz presented four options as possible answers to questions she set based on information in our splash news stories.
The biggest surprise came when the audience was asked to name the president of the Independent Doctors Federation (IDF).
Instead of correctly choosing Dr Phil Batty, 43% clicked on the option of David Hare, who is chief executive of the Independent Healthcare Providers Network.
Danger of going in and out of private care
Issues around patients wishing to ‘mix and match’ private and NHS services are likely to bring increasing challenges in healthcare beyond the coming general election.
This is the view of the chief executive of the Independent Healthcare Providers Network (IHPN), David Hare.
Mr Hare said one inevitable consequence of ever-growing numbers of people going privately was the join between the two systems. Providers were seeing a lot of patients wanting to ‘mix and match’ and growing challenges as ever more people went privately for diagnostics.
A routine scan could show up something urgent and then there might be a real challenge in trying
to get back into the NHS for treatment. This area would be something the IHPN would monitor.
He welcomed political parties’ positive signalling about private practice, saying: ‘We very much do now have – for the first time in about 15 years – cross-party politi-
cal consensus on the value of the private healthcare sector can bring.’
The big interest, whoever won the election, would be the position of the NHS and what was happening there. This would affect both private providers delivering NHS services and those in the private market.
But Mr Hare said it seemed inevitable that the ever-growing numbers of patients choosing to pay privately for admissions, outpatients, scans or private general practice was likely to continue.
The general election looked likely for the autumn, but with the imminent winter pressures soon to follow he did not expect to see any miraculous changes straight away.
To laughter, he added: ‘Wes
Streeting has said his ambition is to make the NHS so nobody needs to pay privately at all. I wouldn’t worry hugely in the market about that becoming a reality anytime soon.’
He predicted that with the private sector doing more work both privately and for the NHS, the issue of training in the independent sector would receive a bigger focus.
There was a need to increase the training of doctors, especially where there was difficulty finding enough opportunity for this within the health service, and he felt the private sector could increasingly offer some good training opportunities. This issue was what the new government would expect the sector to respond to.
David Hare, IHPN chief executive
Elizabeth Boultbee
Health insurance boom to continue
Surging demand for health cover is continuing and consultants can expect no let-up in demand for 2024.
According to clearing service Healthcode, private medical insurance claims surged past the 10m milestone to 10.2m last year, which was worth more than £4bn worth of independent healthcare activity.
The company’s Fiona Booth told the conference: ‘That’s up 20% on 2022, which represents the biggest year-on-year rises since 2015, if we exclude the anomaly of 2021 when we were effectively catching up after the pandemic.
‘It’s too soon to tell whether 2024 will be another record year, but, as we’ll see, it’s already shaping up that way and the mood music concerning private healthcare is more harmonic than discordant.’
KEY FACTS
Insured claims volumes broke through the 10m barrier in 2023, 20% higher than 2022.
2024 claims for Q1 suggest another record year
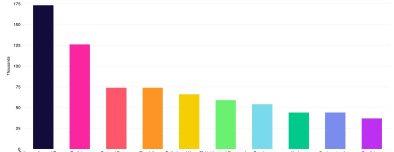
Claims in the top ten specialties (hospital and non-hospital) rose in 2023. Orthopaedics remains number one in hospital settings; physiotherapy is the top non-hospital specialty
Unique patient numbers are still increasing
Healthcode processed claims valued at over £4bn in 2023 and monthly average claims value exceeded 2022 by £6m
The surge is largely being driven by non-hospital episodes of care
Data suggests three important growth areas for insured claims in 2023: physiotherapy, mental health and respiratory care. Some of this relates to the long-term consequences of the Covid pandemic
Claims volumes in January, February and April this year were at an all time high.
Her announcement follows LaingBuisson figures reported by
Independent Practitioner Today last month signalling a boom in work for thousands of doctors in private practice from insured patients.
Top ten claim volume by specialty Non-hospital Q1 2024
I guess working from your sofa should probably come with a health warning
Fiona Booth, Head of external affair and stakeholder management, Healthcode
The number of patients using their private medical insurance for the first time in 2023 was well up on 2021 and 2022.
And the overall rise in claims volumes was largely driven by non-hospital care, including consultations and diagnostic procedures.
Ms Booth, Healthcode’s head of external affairs and stakeholder management, suggested significant growth in physiotherapy claims in hospital and non-hospital settings in 2022 and 2023 could have resulted from the growing prevalence of musculo-skeletal problems among an aging population and – according to a Guardian newspaper comment, due tp ‘changing work practices during the pandemic’.
She said: ‘I guess working from your sofa should probably come with a health warning.’
A significant rise in activity is respiratory care, which was 40% higher in 2023 than in 2022, attributed to long-term damage caused by Covid.
All specialities saw a rise in 2023 volumes. Physiotherapy and ortho paedics remained the top two, but three climbers were radiology, psychology and psychotherapy.
Find-a-doctor app as easy as Airbnb
By Leslie Berry
A consultant’s business helping specialists with their practice management has launched a rescue operation for prospective selfpay private patients who are bewildered by price variations and complexities.
The Get Well Soon app allows them to compare prices between hospitals for 20 of the most common elective procedures.
They can also use the web app to research doctors and hospitals, see a consultant’s availability in real time, book an initial consultation and make payments.
GetWellSoon.co.uk comes from Midlands-based practice management and billing service Medmin Group, headed by marketeer and chief executive Keith Duddy and colorectal surgeon Mr Simon Radley, who began the firm in 2018.
GetWellSoon.co.uk has been designed as a platform to connect patients, clinicians and the facilities in which they are treated, helping patients to feel more confident about the choices they make if paying for surgery.
For uninsured patients, who are already assisted by Medmin to find the treatment they need, the company hopes the launch will prove to be a milestone.
The GetWellSoon app gives doctors’ prices and availability to self-payers
The Get Well Soon team say they have made booking surgery ‘akin to booking an Airbnb – a revolutionary step forward for the sector’.
Mr Duddy said: ‘Self-pay patients now make up a significant part of the market for private surgery but have not been served particularly well by the sector.
‘Patients were finding it difficult to get accurate prices from hospitals, with call-centre agents reluctant to offer a definitive price.
‘There has been a lot of discussion around the fees that consultants charge, but, in actual fact, the clinician’s fees are usually only a small part of the total cost, with
more than 70% of the cost of a procedure in many cases going to the hospital.
‘Prices can wildly vary between hospitals, sometimes when they are only miles apart.
‘At GetWellSoon.co.uk, consultants are paid a fixed fee for an initial consultation as well as a specific surgical fee per procedure, regardless of where the surgery is performed.
Transparent process
‘The difference in prices that a patient can see on the Get Well Soon web app represents the difference in hospital fees. We set out to make the process more transparent while ensuring clinicians were paid a fair rate for their work.
‘We also want to maintain the incredibly high standards of healthcare set by the UK’s medical professionals, and that’s why all the clinicians we invite to join our platform must have been referred or ratified by a clinician already on the platform.’
The site also features in-depth profiles of the featured clinicians including patient testimonials, peer endorsements and direct booking tools.
Clinical director Mr Radley explains: ‘There have been many attempts at consultant directories
in the past, but these have often been expensive subscription models, charging as much as £2,500 a year. We were determined that no one should pay to be on our platform, whether doctor or hospital.
‘We list the information we do to help patients make an informed choice and, unlike traditional price comparison sites, there is no financial incentive for us to recommend any one hospital or clinician over another – we are completely independent.
Doctor’s own page
‘The clinician’s own page will, in addition to listing their qualifications and achievements, also list the hospitals where they practise, show availability and allow booking straight off the page.
‘Patient testimonials and peer endorsements will also feature, allowing patients to do thorough, necessary research when choosing a consultant to see.’
The business operates out of Birmingham and is using the region – which is touted as one of the UK’s most exciting start-up hubs – as a testbed for its innovation before rolling it out country-wide.
West Midlands practitioners will therefore have the chance to be some of the first in the UK to have access to the platform. Fifty surgeons quickly signed up.
Backed by the West Midlands Co-Investment Fund, GetWellSoon.co.uk has ambitious plans to expand its service across the UK over the next 12-18 months.
Mr Duddy added: ‘Our experience in managing the businesses of almost 60 consultants in private practice has given us a unique insight into both the patient and clinician’s perspective.
‘We are determined to provide a more accessible approach to elective surgery for some of the 6.5m people on the waiting list, offering a simpler and more transparent approach to private healthcare.
‘However, we know the launch is only the beginning. We’re proud to be debuting our platform in the Midlands, but we have our sights set on changing the norm across the country, bringing a new way of thinking to the world of private healthcare as we strive to change the industry for the better.’
To find out more, visit https:// getwellsoon.co.uk.
GetWellSoon boss Keith Duddy and clinical director Mr Simon Radley
Birmingham unit has a new owner
The Edgbaston Hospital, part of Circle Health Group and known locally as The BMI Hospital, is under new ownership following a deal with the UK’s largest independent provider of NHS services, Practice Plus Group.
With its ten hospitals mostly in the south of England, this is the company’s first move into the West Midlands where it aims to help reduce NHS waiting lists and offer its Wellsoon ‘more affordable private option compared with traditional private hospitals in the area’.
Chief executive Jim Easton said: ‘People who live in Birmingham and the surrounding areas have suffered particularly long waiting lists for planned treatments in the wake of the pandemic, with many people waiting a long time for hip and knee replacements and eye surgery.
‘We specialise in these operations and have a fantastic reputation for the quality of our surgery.
‘We are looking forward to partnering with the NHS locally to
PPU WATCH
Compiled by Philip Housden
Return of NHS PPUs’ national conference
The national conference for NHS private patient services returns to a face-to-face event this year after being online in 2022 and 2023. It will be held on Friday 27 September in Birmingham.
This is the only in-person event designed to benefit PPUs directly and delegates will be able to hear case studies from leading NHS PPU services, sessions with the major private medical health insurers and a review of the market.
Vanessa Pearce, senior producer and sponsorship sales manager of organisers SBK Healthcare, said
The Practice Plus Group Hospital, Birmingham, is due to open in September after extensive renovation and reconfiguration
unlock access to excellent healthcare for as many people as possible.
‘We also know from the calls we have received that there is demand in the area for our high-quality, affordable private option for those people who want to pay or use their insurance for fast access to high clinical quality treatment.’
The building is a four-floor T-shaped facility with 55 bed -
PPUs would network and share new ideas.
‘No matter the size of the service, like-minded colleagues will be able to strategise through a flexible mix of presentations, group benchmarking and panel discussions.
‘Ask your burning questions to insurance providers and share creative strategies to generate new income.’
For details, see Face-to-face Conference – NHS Private Patients (sbk-healthcare.co.uk) or email enquiries@sbk-healthcare.co.uk.
Private practice in Jersey looks to expand Jersey may prove an attractive proposition to consultants as the island health department aims to double private patient income
Number of private GP clinics triple in Scotland
Private GP clinics in Scotland have more than tripled since the pandemic as patients have struggled to get NHS appointments.
Figures obtained by The Herald in Scotland from Healthcare Improvement Scotland (HIS) – the regulator responsible for inspecting private clinics – show there were three private GP surgeries registered in 2019.
But it reported there are now 11 – mainly located in the Edinburgh and Glasgow areas, with one each in Stirling and Falkirk.
rooms, three theatres, an endoscopy suite, outpatient facilities including ten consulting rooms, an imaging department, physio area and staff and patient parking.
Core services are orthopaedics, ophthalmology, diagnostic services and endoscopy.
Renamed Practice Plus Group Hospital, Birmingham, it opens in September after extensive renovation and reconfiguration.
over the next five years to generate money ‘to support capacity and upgraded facilities for patients’.
It plans to boost this revenue to £18.8m before 2027 and £24m before 2029. Private patient services contributed £12.2m to health in 2023.
Two main untapped income sources have been identified: an estimated £5.3m from insured patients who are receiving statefunded care and up to £12.8m from insured customers who go elsewhere for private treatment.
Health minister Tom Binet said: ‘This strategy signals a commitment to expand the choice of service provision to islanders by enhancing the private healthcare offer, attracting skilled professionals to Jersey and increasing income to be used for the benefit of all islanders.
It said many private GPs also worked in mixed clinics alongside other healthcare professionals –such as physiotherapists or psychotherapists – but HIS said the cost of extracting this data from annual returns would exceed the £600 threshold for responding to a Freedom of Information request.
The report stated there was also a reluctance among independent healthcare companies to disclose any potentially market-sensitive intelligence on the number of GPs currently contracted with them.
‘Our society is diverse and encouraging private patients’ services can support a better balance of healthcare spending and prioritisation towards those who depend most on state-funded care.’
The island will look for local and wider partnerships with solo consultants and consultant groups, private medical insurers and employers.
Private patient income is seen as crucial to help fund services for residents though state health insurance.
Philip Housden (right) is director of Housden Group commercial healthcare consultancy
Bosses ‘victimise whistleblowers’
By Agnes Rose
Consultants who speak out about safety concerns in their NHS hospitals are targeted by a systematic employer ‘playbook’ designed to silence or remove them.
That was the warning from doctors’ union the Hospital Consultants and Specialists Association (HCSA) as it launched a new briefing for doctors on the tactics used by bad employers, ranging from ostracising them to mounting fishing expeditions to support trumped-up disciplinary charges.
Its leaders said the document was based on intensive HCSA research among hospital doctors who have blown the whistle on safety – in line with their professional obligations – but then faced an employer backlash and even dismissal.
This revealed a strikingly consistent ‘playbook’ being deployed against doctors who are often left completely unaware they are being targeted.
The guide details the tactics used and offers advice to doctors on how they can spot the signs and what to do if things go wrong.
A key message is to contact their union before raising safety concerns for advice on how to minimise the risks of management victimisation.
The publication was prompted by earlier findings of an HCSA survey which revealed widespread victimisation of doctors, with 70% of respondents saying it was not possible to raise patient safety concerns without career detriment.
It painted a picture of unaccountable managers who are failing to address safety-critical concerns raised by staff on the ground.
The HCSA is calling for changes to culture and the law for doctors being targeted with disciplinary measures and other damage to their careers simply for speaking up.
Its president Dr Naru Narayanan confessed he was shocked how the research showed the same patterns
emerging again and again nationwide when a doctor was targeted after speaking up about safety.
He said hospital doctors had a professional obligation to raise concerns, but too often found themselves on the receiving end of co-ordinated efforts to silence, ostracise or force them out altogether.
‘We hope this guide will help people to spot the signs and seek help to head off the worst before it happens. But it shouldn’t have to be this way. The current limited protections for whistleblowers and lack of consequences for bad employers creates a completely uneven playing field.
‘That’s why HCSA is calling for a criminal law against victimising whistleblowers and other additional protections for NHS staff, including a new independent body to track and guard against the treatment we see all too often.
‘Our message to those who have safety concerns is to raise them but get informed first and be ready to contact your trade union.’
Cromwell offers new prostate therapy
Cromwell Hospital has launched Aquablation therapy, the minimally invasive procedure that uses a robotically controlled waterjet to treat a symptomatic enlarged prostate.
Consultant urological surgeon Mr Neil Barber, who introduced the procedure to the UK in 2016, said patients had received many benefits, including speed and accuracy of the procedure as well as a faster return to normal activities.
The Aquablation team at the Cromwell Hospital, including urological surgeon Mr Neil Barber (centre) after their first use of it
MRI breast screening service starts in Oxford
GenesisCare, the specialist cancer care provider with 14 UK outpatient centres, has officially opened a new MRI screening service in Oxford and Windsor for patients with dense breast tissue.
Dr Fleur Kilburn-Toppin, consultant radiologist and specialist advisor at the company, said around half of women in their 40s would have dense breasts.
‘An MRI scan is a more sensitive screening test than a standard mammogram and is significantly better at detecting breast cancer in women with dense breasts.’
Breast MRI scans are not widely available as standard screening unless people have a very high risk of breast cancer.
First winners of Spire’s new awards
Three nurses, two healthcare assistants and a mammographer have become the first winners of Spire Healthcare’s recognition awards for ‘outstanding patient care’.
‘It is also less likely to cause damage to surrounding healthy tissues, because it offers greater precision than other treatments for an enlarged prostate.
‘Many patients are often worried about the consequences of treatment on their sexual function.
Aquablation therapy offers a lower rate of irreversible complications, such as incontinence, ejaculatory and erectile dysfunction, which is a real benefit to them.’
Nominations were made for 85 people and a cross-departmental panel selected six winners. The scheme will run four times a year.
DAISY awards recognise extraordinary registered nurses and nursing associates who go above and beyond, while IRIS (Inclusive Recognition of Inspirational Staff) awards are designed to complement that scheme to recognise clinical colleagues.
Dr Fleur Kilburn-Toppin
App manages your clinic on the move
By a staff reporter
Independent healthcare sector software provider Clanwilliam has launched a cloud-based, mobilecentric ‘practice management solution’ for private practice in the UK.
The company, which supplies its DGL Practice Manager to more than 3,000 large private practices, hospitals and clinicians, has added iMedDoc to its portfolio of practice management solutions to give customers more flexibility.
It said offering a lighter and cloudbased solution meant doctors and their practices would be able to adopt the workflow that best mirrors their desired way of working.
Clanwilliam Ireland managing director Eileen Byrne said: ‘Private healthcare is developing rapidly in the UK as patients look for a faster, more personalised service than an under-pressure NHS can deliver.
‘We saw a requirement for a different kind of IT system to support
the clinics and specialists that are looking to deliver that service, and iMedDoc fulfils that requirement. ‘It brings the mobile technology that we have all adopted in our daily lives to bear on practice management tasks so clinicians can save time and focus on what really matters to them – their patients.’
iMedDoc, developed in Ireland by an orthopaedic surgeon who wanted to support his own practice, has evolved over 25 years into a modular system to handle the patient journey from booking to billing.
It operates over a browser from anywhere with internet access or
can be downloaded as an app from Apple or Android app stores.
Ms Byrne added: ‘iMedDoc is used by over 700 consultants in Ireland, so we know it can enable specialists to build an effective private practice.
‘Its features work together to create effective workflows for clinicians of all kinds, whether they are already established or taking their first steps into the fast-moving world of private practice.’
iMedDoc also comes with a patient app, so patients can manage their own booking, complete questionnaires and hold consultations by video link.
To cut the administration associated with billing, its accounts module integrates commercial accounts systems with Billink, a remote payment solution for healthcare that makes it easy for patients to settle bills by phone or text.
Clanwilliam said it had invested around £500,000 in adapting iMedDoc for the UK market, making sure that it meets the specific requirements, including integration with the clearing system Healthcode.
An aesthetics module is scheduled for launch this winter. Among other features, the module will enable clinicians to annotate images, so they can safely deliver cosmetic treatments.
Optegra manager wants consultants’ input
A former nurse who developed a taste for business has won a new role as clinical services director for specialist eye clinic group Optegra. Chris Chisholm told Independent Practitioner Today he would be working directly with the company’s consultant ophthalmic surgeons from the start of their career with the provider.
‘Part of my role is responsibility for their recruitment – working closely with our medical directors – and also planning the induction of consultants.
‘We also have a structure of NHS regional leads among our consultants and I work closely with our consultants to help select the most suitable in each region.
‘I have found that my experience in various roles throughout healthcare establishments allows
me to have very clear knowledge of how our consultants can best support not only patients but also their clinical teams.
‘As part of the UK leadership team, it also means I can support all our consultants to share their opinions at the highest level, and ensure their opinions are shared and influence decisions we make.’
Chris Chisholm:
‘I can support all our consultants to share their opinions at the highest level and ensure their opinions are shared and influence decisions we make’
He started his career in 1999 as an NHS healthcare assistant, soon qualified as a nurse and rapidly moved his way up to charge nurse and then management roles within Newcastle hospitals. Later he joined Fresenius Medical Care as a clinical nurse specialist and then lead nurse.
But eight years ago he decided
on a career change and moved into a sales role, from regional business manager, to sales manager and then director of clinical services and operations.
Mr Chisholm said: ‘This variety of experience spanning clinical and commercial management roles means I can really directly support my team here at Optegra and give clinical services a voice at leadership team level.’
His immediate priorities include an evaluation of services, a patient review and working with regional clinical heads and governance leads. Staff satisfaction is another priority.
Optegra UK managing director Mat Pickering said: ‘It is rare to find a colleague with the combined level of nursing and business acumen which Chris has.’
Eileen Byrne of Clanwilliam
Healthcare worst data leak offender Bupa boss takes over at Nuffield Health
New findings by data breach experts reveal ongoing compliance challenges within the health sector, highlighting the continual need for businesses to train their staff on basic data handling practices.
Data breach solicitors Hayes Connor delved into data breaches, which have been tracked by the Information Commissioner’s Office (ICO) since 2019, to find which sectors experienced the most data breaches last year and beyond.
It found the health sector are frequent violators, coming in first place for data breaches in 2023 (see the top ten offenders in the box on the right).
Hayes Connor’s study found the health sector made up around one-in-five reported data breach cases last year. On average across the five-year span, the health sector remains at the top of the list year on year, at almost one-in-five cases from 2019 to 2023.
Lawyers found basic personal identifiable data was the most common type of data being breached within health sector data breaches last year, making up 73.21% of data breaches. The second highest form of data breaches involved health data, at 61.66%.
Nearly a fifth of total data breaches in 2023 involved children’s data. This is considered particularly sensitive due to the fact children are less aware of the safeguards, consequences and risks regarding personal data processing.
In the health sector last year, 142 cases involved children’s data, making up 7.36% of health incidents.
THE TOP TEN OFFENDERS
1. Health
2.
The findings also showed the different incident types behind the data breaches. The number one reason behind data breaches within the health sector was through unauthorised access, which made up 18.70% of the health data breach cases in 2023.
Data emailed to the wrong recipient showed up as the second most common incident type for this sector, at 16.22%.
Hayes Connor said this demonstrates how human error plays a huge role in many data breach cases in the UK, and therefore the importance of internal business training.
It added: ‘It is important to bear in mind that part of the 2018 General Data Protection Regulations require businesses to report a data breach within 72 hours. Failure to notify a breach when required to do so can result in a significant fine of up to £18m or 4% of your global turnover.
‘Concerningly, in the health sector, it’s taking over 72 hours to report 43.88% of their data breaches. This is leaving the sector vulnerable to large fines.’
Hayes Connor legal director Richard Forrest said: ‘Another year, another representation of how many organisations across all sectors are still failing to implement effective security protocols, leaving personal data vulnerable to breaches which have significant legal and financial repercussions for the entities involved.
‘Despite regulatory advancements and the introduction of stricter compliance mechanisms, the rate of data breaches remains a serious concern.
‘The recent ICO trends portray a continuous need for vigilance and updated compliance strategies from businesses, especially in how they manage and protect personal data against emerging cyber threats and human error.’
Parents can’t afford cover to care for kids
Over half (52%) of all working parents in the UK have no form of financial protection policy in place should they have to take time off work to care for their child if they were unwell or had an accident.
According to new research from
protection and employee benefits provider MetLife UK, among those without protection, well over half (56%) are self-employed and almost two in three (65%) work part-time.
Researchers found the main
deterrents of having any financial protection in place included affordability concerns (44%), a lack of awareness of these type of products (20%), and general disinterest in taking out insurance policies (9%).
Bupa UK Insurance chief executive Alex Perry is leaving the company this month to take over from Nuffield Health chief executive Steve Gray, who is retiring after nine years.
Mr Gray’s Nuffield Health tenure has seen it expand its reach and services by growing its network of fitness and well-being centres and establishing a network of hospitals in London to deliver its connected health ambitions.
Natalie-Jane Macdonald, chair of the charity’s board of governors, said: ‘Steve has led the organisation with integrity and passion and successfully championed our purpose to support people and communities across the UK, including those with the greatest health needs.
‘Under Steve’s leadership, the charity has doubled the number of people we support every year through our health and well-being services.’
Mr Perry said the charity’s mission had never been more important. ‘We have a huge opportunity to help more people lead healthier and happier lives through building on Nuffield Health’s range of services and track record of exceptional quality care.’
At Bupa, Mr Perry led record growth in customers to more than–three million and a significant increase in market share.
Richard Washington, general manager for Bupa UK Insurance’s Consumer division, has been appointed Bupa UK Insurance general manager on an interim basis, subject to regulatory approval.
Alex Perry
Steve Gray
Practice management but simpler. Make
the work... flow.
Effectively manage and grow your private practice with iMedDoc. A trusted solution in Ireland for 25 years, iMedDoc is now live in the UK.
Mobile app
Cloud based
Patient portal
Integrated billing
Integrated digital dictation
“
I’ve been using iMedDoc for nearly 10 years and in that time I have been thoroughly impressed with every aspect of the platform. The functionality is great. I couldn’t ask for more!
–
Mr. Subhasish Sengupta Consultant Gastroenterologist
From £85 per month, sign up before 1st July and get 3 months for free.
How do I find the right PA?
QI am new to private practice and need to get some secretarial support. What do I need to consider and how do I find the right person to support me?
AA practice manager or medical secretary is a highly skilled role. They are critical to your practice and, if you choose the right person or people, they can help your business to grow, keep you compliant and help gain a position reputation with patients and providers.
The decision on choosing your secretarial support should not be rushed. The investment in time in getting it right will hold you in good stead for years to come.
Consideration number 1: The type of support you require It is important to understand what you would like your support function to incorporate. There are a variety of models as every consultant has differing requests and needs.
The primary areas that would fall under your support function are: Phone answering, appointment booking and diary management; Patient and hospital communication and liaison; Typing; Billing; Marketing and website; Accounts.
This is a very high-level list with multiple functions falling under each category. Each of these functions could be provided by a separate company or you may choose to have them all within one place or as a hybrid.
Consideration number 2: Who to provide the support
The main opportunities that consultants have for accessing support are:
NHS secretary; Family member; Doing it yourself; Hospital provision; Employ directly; Group or consortium; Hybrid model.
NHS secretary
This, for many consultants, may feel like a safe option to start off your private practice. Your NHS secretary will have an excellent knowledge of the procedures you
Sue O’Gorman and Hannah Browning
offer and understand how you work.
They are often lower cost, as the hours will be flexed around their NHS commitments.
However, your secretary should not be taking your private calls while at work in the NHS. This automatically puts you at a disadvantage, because those initial opportunities and patient calls will not be captured in a timely manner and may be lost.
It is also much harder for hospitals to liaise with a secretary out of hours when their main office hours will be 8am-5pm.
Family member
Having a family member to look after your practice may appear attractive from a financial perspective. However, there are also other, more important considerations:
Do they have any experience in managing and running a private practice?
Are they able to give it their full attention and be able to take calls/ deal with queries throughout the day?
What happens if you both go away together?
Ensuring you get a break from your practice can be harder if you have a home-based support system.
Do it
yourself
There may be some of the support functions that you would like to do yourself and this would be an
THINGS TO NOTE
option to reduce costs until your practice builds.
But there does need to be an understanding that you are the expert in treating patients and there are others that make it their business to be experts in supporting you.
The balance of your time should also be taken into consideration, as there will come a point where you would be better placed seeing and treating patients that spending time doing your admin.
Hospital provision
Most hospitals will have an inhouse secretarial support function. These teams can often offer flexible time packages while ensuring you still have coverage of the phones.
They also have the advantage of being integrated into the infrastructure of the hospital and therefore the pathways for accessing inquiries, theatre slots and so on should be easier.
This model gets more complex if you would like to work out of more than one location with different providers. Having a secretary in each location is an option, but you would need to understand the flow of inquiries from your marketing and how these will be handled.
Employ directly
For a new consultant, this will feel like a big step because you will be taking on the responsibility of a
When setting up your practice, you will need to get a patient administration system.
➤ There are many on the market and your choice will be impacted by the secretarial support that you choose. If you have a specific system you would like to use, this may narrow your options.
➤ When you are looking to commit to a secretarial service, understand what their terms of business are. If things do not work out, do you own the licence for the patient administration software or do they?
➤ If you are going to employ a secretary, make sure you seek HR advice to get a proper legal contract in place and set up your employee indemnity. You will also need to be clear on your processes to ensure you are compliant with General Data Protection Regulations.
➤ If a secretarial service does not work for you, then change it. The negative impact of a bad service can be long lasting and will be detrimental to the growth of your practice.
Having a company to answer your phones and book appointments will ensure you capture all opportunities while your secretary can look after your administration
practice remit, including marketing and accountancy.
Groups have the advantage of offering cover not only for the phones during the day but also for any holidays and sickness. They consist of teams that have their own areas of expertise, all brought together in a single monthly fee.
The types of packages can be flexible enabling you to add hours as your practice grows.
person’s salary and the associated legal requirements.
You may also not have the funds to cover a full-time post, but still need the phone coverage.
Employing a secretary can often work together as a hybrid model until you can commit fully.
Having a company to answer your phones and book appointments will ensure you capture all opportunities while your secretary can look after your administration.
It may be that you can join with another consultant to spread the cost of employing a secretary. This will give you both phone cover but without the full expense.
Group or consortium
There are a growing number of support function groups available to consultants. They can specialise purely in administration support right through to the full private
The cost for using a group may be higher than other options; however, you get the added benefit of convenience with all the specialists in one place.
Hybrid model
There are companies that exist to provide every one of the functions listed above. This is the ultimate pick and mix of how to build your support service.
Keeping a core function with one provider then enhancing these with additional expertise can help you to individualise how your practice is run.
Sue O’Gorman is director of Medici Healthcare Consultancy. Website: www.medicihealthcareconsultancy. co.uk. Email: sue@medicihealthcareconsultancy.co.uk.
Hannah Browning is director of Beyond Excellence Healthcare Consultancy. Website: www.beyondexcellenceconsultancy.co.uk. Email: info@beyondexcellenceconsultancy. co.uk.
Do you know how to protect data?
Private healthcare organisations need to understand their data protection obligations and protect patients’ personal information. Rachel Clarke, of the Information Commissioner’s Office (ICO), shares practical advice
All staff should feel confident in handling people’s personal information safely and securely. It must be clear to staff about what records they are allowed to access
THE ICO’S ROLE AS A REGULATOR
As well as producing helpful guidance and taking action against individuals in the courts, we can also take enforcement action when organisations do not do enough to protect people’s personal information.
In the last year, we have acted against several healthcare organisations and shared the lessons all organisations can take from these incidents.
If we find evidence that medical records were accessed illegally by a member of staff, we can take action which includes prosecuting the person responsible in court
this does not mean you have the legal right to look at it for your own purposes. If we find evidence that medical records were accessed illegally by a member of staff, we can take action which includes prosecuting the person responsible in court.
For example, last year the ICO fined a medical secretary who accessed over 150 people’s records without a business reason to do so. We also fined a former 111 call centre adviser for illegally accessing the medical records of a child and his family.
TO PROVIDE vital services, all health organisations must process personal information. This can be anything from someone’s contact details to their medical records.
Anyone who processes personal information has a responsibility to protect it under data protection law. This includes keeping it secure, ensuring it is accurate and being transparent with people about how you plan to use it.
The health sector routinely handles sensitive information about the most intimate aspects of someone’s health, which is provided in confidence to trusted practitioners.
When accessing healthcare and other services, people need to trust that their medical information is in safe hands, only available to authorised staff and only used for a specified purpose.
As the UK’s data protection regulator, we want to remind private practitioners of the importance of prioritising data protection and ensuring all patients receive the privacy they are entitled to.
This is especially important in the wake of the recent data breach at the London Clinic where medical records were allegedly accessed unlawfully.
Our own data shows that over 1,500 incidents are reported by the health sector each year, ranging from cyber-attacks to human errors such as emailing personal information to the wrong person. By highlighting new guidance and practical steps below, we want to support all organisations, including private doctors, clinics and hospitals, to handle personal information responsibly and lawfully.
NHS Fife were reprimanded after an unauthorised person was able to enter a ward and access the personal information of 14 patients.
Similarly, NHS Lanarkshire received a reprimand following staff’s unauthorised use of WhatsApp to share patients’ personal data over the course of two years.
Any organisation that needs support to process or share personal information responsibly can find further guidance on our website: https://ico.org.uk/fororganisations/
Keeping patient data secure
Prioritising basic steps, such as staff training, double-checking records and restricting access can help to prevent personal data breaches before they happen, reducing the risk of harm for patients.
Healthcare organisations should ensure the following:
❶Staff are thoroughly trained
Organisations should ensure that all staff are properly trained so that they are aware of their organisation’s data protection obligations. Any data protection training should be role-specific, tailored and relevant to the tasks being completed.
All staff should feel confident in handling people’s personal information safely and securely. It must be clear to staff about what records they are allowed to access.
❷ Appropriate technical measures are in place
Appropriate security measures, such as passwords, multi-factor authentication and access controls, should be in place to ensure personal information can be seen only by people who need to use it.
❸ Any data sharing is compliant
There are situations where it may be necessary to share personal information about patients with third parties and you should have an appropriate system in place.
Our data-sharing code of practice provides guidance, alongside practical tools, to help organisations be confident they can share data within the law. It guides practitioners through the practical steps they need to take to share data while protecting people’s privacy.
❹ Staff are clear on the data breach reporting process
An organisation must report misuse of personal data to the ICO if there is a risk to people’s rights and freedoms, which is often the case with sensitive medical information.
This must be reported within 72 hours of becoming aware of the breach. If your organisation suffers a data breach because of a cyber-attack, you should report this to the ICO within 72 hours of becoming aware of it. The sooner you contact us with detailed information the better.
Accessing someone’s medical records without cause or consent can be a criminal offence. Working in private healthcare, your role may grant you access to other people’s personal information, but
Be transparent with people about their personal information
Under data protection law, people also have a right to know what is happening to their personal information. Patients must be informed about what information about them is being collected and understand the purposes for which this might be used.
Being transparent is essential to building public trust in health services. If people understand how and why their personal information is being used, they are likely to feel empowered to share their health information to both access your services and support other important initiatives such as medical research.
We have recently published new guidance to help heath organisations ensure they are being transparent with people about how their personal information is being used.
With this bespoke guidance, we want to improve their understanding of effective transparency, ensuring that they are clear, open and honest with everyone whose personal information is being used.
See https://ico.org.uk/fororganisations/uk-gdprguidance-and-resources/ data-protection-principles/ transparency-in-health-andsocial-care/
Rachel Clarke (right) is senior policy officer at the Information Commissioner’s Office (ICO)
Relations with patients
The GMC updated its supplementary standards guidance to complement the new edition of Good Medical Practice. In the second of its occasional series highlighting what has changed, the MDU’s Dr Catherine Wills (below) focuses on maintaining personal and professional boundaries
ESTABLISHING A GOOD rapport with patients and colleagues is a valuable skill for every independent practitioner, but it is important to act with professionalism.
The GMC’s new guidance on maintaining boundaries emphasises the need to maintain respectful relationships, defines unacceptable behaviour in more detail and sets out how doctors should respond, especially those in a leadership role.
It replaces two earlier documents: Maintaining a professional boundary between you and your patient and Sexual behaviour and your duty to report a colleague. Here are the main points.
Maintaining personal and professional boundaries
The GMC introduces the guidance with a reminder of the importance
of appropriate personal and professional boundaries in all areas of practice.
Not only must patients ‘be able to trust that medical professionals involved in their care will behave appropriately towards them during consultations’, but colleagues and staff must ‘feel safe and respected in their workplaces’ and ‘able to speak up when they experience or witness negative behaviours’.
Personal relationships with patients (par. 8-17)
The GMC explicitly forbids doctors from pursuing ‘a sexual or improper emotional relationship with a current patient’ or someone close to them, such as a family member. It is less definitive about former
patients, but says doctors must first consider all the factors that might make a relationship inappropriate. This includes how recently the professional relationship ended, whether you treated them over several years or for a single consultation, whether the patient was –or is – vulnerable because of their age or the nature of their condition and whether you would be –or could be seen to be – abusing your professional position.
Personal relationships with colleagues (par. 18-19)
The GMC considers consensual and reciprocated personal relationships between colleagues to be a private matter, although some hospitals or clinics might have their own Workplace Relationships Policy.
patients and colleagues
However, it continues that these relationships should not be allowed to have an adverse impact on clinical practice or team environments and the GMC also warns about the risks of power imbalances and situations where someone’s training or career might be affected.
Inappropriate sexual behaviours (par. 20-23)
The GMC says that all forms of sexual misconduct are unacceptable from the criminal (rape, sexual assault) to unacceptable sexual behaviour.
Paragraph 23 of the guidance gives examples including unwelcome touching, sexual gestures, leering, sexual banter, people asking intrusive questions or discussing their own sex life.
For the first time, the GMC provides guidance on what doctors should do if a patient behaves in a sexual way towards you
relevant information in line with GMC confidentiality guidance.
In the latest edition of Good Medical Practice , the GMC has been more explicit about the importance of positive workplace cultures and respect between colleagues.
The MDU always advises members not to ignore advances by patients, as it could be taken as encouragement.
Those in independent practice may or may not feel able to continue caring for a patient who has made an advance.
Other examples include sending sexually explicit messages or posts, displaying sexually graphic images, spreading sexual rumours, making promises in return for sexual favours, making sexual advances or ‘excessive or unwanted compliments on a person’s appearance’.
It says that all ‘can have devastating impacts on individual wellbeing, psychological safety, patient safety, and medical professionals’ careers’.
Later in the guidance (paragraph 34) it adds: ‘You must not act in a sexual way towards colleagues with the effect or purpose of causing offence, embarrassment, humiliation or distress’, which can include verbal or written comments and sharing images.
Reporting sexual behaviour towards patients (par. 24-28) and colleagues (par. 32-39)
If a patient tells you about – or you have other reason to believe there has been – a breach of sexual boundaries by a colleague, you must raise concerns promptly and support those affected.
When reporting concerns, you should usually respect patient confidentiality, but patient safety must come first, so there could be occasions when you need to breach patient confidentiality in the public interest.
If that happens, you must tell the patient, unless not safe or practical to do so, and disclose only
It echoes that message here, stressing that any doctor who becomes aware of inappropriate sexual behaviours in the workplace has a responsibility to take some action – for example, by offering support, challenging the behaviour or reporting the behaviour depending on the circumstances.
Those in a leadership or management role ‘must take active steps to create an environment where people can talk about concerns safely’.
Leaders/managers must act on concerns to make sure such unacceptable behaviours are adequately addressed, people are supported and concerns are dealt with or escalated promptly.
Speak to your medical defence organisation (MDO) if you are unsure about your responsibilities.
Sexual behaviour by patients (par. 10 and par. 29-31)
Around 15% of the 411 members who responded to a recent MDU survey were concerned that they had received an inappropriate gift from a patient or that the patient had an ulterior motive.
Some reported receiving cards and flowers on Valentine’s Day, while others had previously declined gifts of perfume and lingerie.
As our survey shows, it’s not uncommon for doctors to worry that a patient has developed an inappropriate attachment.
In this situation, the GMC says you should try and re-establish a professional boundary, but if this isn’t possible, you may need to end your professional relationship.
If you think it is possible to get the doctor-patient relationship back on track, politely explain that you need the relationship to return to a professional level, otherwise you will have to transfer their care to another doctor.
Keep a record of the conversation and follow it up in writing, as well as a log of all contact from the patient. If you are unsure about what to say or if the patient doesn’t seem to have heeded your request, seek advice from your MDO.
For the first time, the GMC provides guidance on what doctors should do if a patient behaves in a sexual way towards you.
If you feel safe to do so, it advises, tell the patient their behaviour is unacceptable and ask them to stop.
If they persist or you feel unsafe, ‘excuse yourself from the encounter and seek help’ as well as reporting the incident and seeking support if needed.
Annex: Good Medical Practice
After the main guidance, there’s an annex which signposts readers to the relevant section of Good Medical Practice covering colleagues, culture and safety (Domain 3).
We advise you to familiarise yourself with the new guidance and seek advice from your MDO if you have any specific concerns about professional boundaries or the behaviour of a colleague or patient.
See ‘Maintaining safety of staff and patients’, page 38
Dr Catherine Wills is the MDU’s deputy head of advisory services
Figuring the future
Figures in market analyst LaingBuisson’s Health Cover UK Market Report 19th edition signal a boom in work for thousands of doctors in private practice from patients with private medical insurance. Here we highlight some of the key findings for 2022
Private medical cover
including private health insurance – accounts for 80% of the total market value at £5.3 billion
£6.65 billion: the total health cover market value in the UK and up £385m on previous year
£461m: the value of health cash plans and reflecting rising demand after successive years of decline since 2018
£1,225: the average cost of private medical cover for subscribers in 2022. This market was valued at £5.3 billion, a 6% increase from 2021 levels or a 13.2% increase over five years
There is a long way to go before coverage reaches levels last seen across the UK population since the 2008 financial crash, but it is the first time there has been sustained growth in the sector for more than 15 years.’ Report author Tim Read, director of research and content at LaingBuisson
What’s ahead?
The report says: ‘With the national inflation rate steadily decreasing from record highs and wage growth remaining strong, any negative impacts associated with the wider economic environment on the individual may be easing.
‘While higher wage growth may limit the headroom of companies to invest in their broader employee benefits package, the competition for talent means that health cover remains a difficult benefit to remove from existing organisations and one that continues to be valued as a differentiator by potential new employees.’
6.1% up: the total health cover market in 2022. This is more than £385m on the year before
Company-paid PMI and self-insured made up a combined 64.1% of the total market size for private medical cover. £2,476m was company-paid and £933m came from self-insured schemes (healthcare trusts)
4.2m people were subscribed to medical cover schemes, with other people covered under the policies bringing the figure up to 7.3m
Covid drove a -2.2% drop in the market size 2020. But the value of health cover since then has grown much faster than historical norms.
Annual growth was 6.1% between 2020-2022, compared to 1.7% between 2008-2019
High inflation levels:
The Consumer Price Index was 7.9% in 2022 – stopped increases in the market value leading to an overall real-terms growth in the market
Four insurers
control over 90% of the private medical cover market: Bupa, AXA Health, Aviva and Vitality Health. Other ‘significant and noteworthy’ companies include Western Provident Association (WPA), The Exeter, Healix (which only manages self-insured companies), Westfield Health and National Friendly
The free and integrated digital prescribing platform for all private prescribers.
CloudRx take care of the dispensing, payment and delivery of medicines direct to your patients, wherever in the country they may be, for more convenient access to their medicines.
TRANSFORMATIONAL
Order prescriptions at the touch of a button to add a whole new level of convenience for your patients.
SIMPLE, CONVENIENT AND SECURE
Simple and fast digital prescribing. Legal paperless prescriptions, repeat prescriptions and controlled drugs. Prescriber fees can be charged to the patient if required.
INTEGRATED
Our API enables frictionless integration with healthcare brands & clinical software including Semble, WriteUpp, MidexPRO, eClinic, Pabau and ClinicYou
“We were struggling to keep up with the admin side of the prescriptions, not to mention storage for medication to cope with a huge increase in prescriptions. CloudRx immediately took away the strain. Since our partnership we have grown by more than 200% in size. We could not have achieved this seamless scalablity without them.”
– Dr Louise Newson, Newson Health
Paying by results becomes a reality
Patient-centred care has long been the goal of many healthcare systems. And now that many of the challenges of value-based healthcare can be overcome, this goal may be within reach for the private healthcare sector, says Dr Ravi Lukha (right), medical director at Bupa UK Insurance
HEALTH INSURERS in the UK mainly fund and deliver healthcare using a fee-for-service model, where providers are reimbursed for each service they give to patients. The advantages of this model are that there is a clear reimbursement structure, which has been in place for many years with established infrastructures such as claims processing to support it, and also offers patients flexibility in choosing treatment options.
But such traditional models of reimbursement can lead to misaligned incentives; for example, limiting the focus on patient outcomes and quality of care, discouraging preventive care and fragmenting care with lack of coordination among providers. In more extreme cases, it may also incentivise volume of care provided, leading to unnecessary tests or procedures, higher healthcare costs and poorer patient outcomes.
An alternative payment model is value-based healthcare, which aims to align incentives with a focus on optimising health outcomes that matter most to patients and the value of healthcare services provided.
The case for value-based healthcare
The Centre for Evidence-Based Medicine defines value-based healthcare as ‘the equitable, sus -
tainable and transparent use of the available resources to achieve better outcomes and experiences for every person’.1
Under value-based agreements, health insurers and providers align on reimbursement models to reward improvements in the health outcomes of patients, as well as the quality, equity and cost of care.
Therefore, value is defined as improved health outcomes – that matter most to patients – relative to the costs required to achieve them.
This provides an incentive to continually do better, which is in the patient’s best interest as well as the payer, as it evidences that money is well spent.
There are many advantages of a value-based healthcare model. Primarily, it puts the focus on quality of care provided and patient outcomes.
It also encourages greater coordination and collaboration among health insurers and providers. It can be used as an incentive to give greater priority to preventive care and improved use of healthcare resources can also offer the potential for cost savings. Therefore, it also has great potential for positive effects from an environmental sustainability
LEADING THE WAY
At Bupa, our ambition is ‘to be the world’s most customer-centric healthcare company’. This means a commitment to excellent customer experience, through great service and value, frictionless access and quality healthcare.
So as an organisation, we are very much aligned to the principles of value-based healthcare.
Cleveland Clinic has a 102-year history and experience through its not-for-profit model of employed, salaried consultants and implementation of value-based care with government and commercial health insurers in the US (Ohio and Florida) and in the United Arab Emirates.
Our relationship with Cleveland Clinic London began years before its 184-bed tertiary care hospital opening in 2022. Bupa leadership attended a week-long Value-Based Innovation Summit hosted in Cleveland, Ohio, in 2019 and this served as a roadmap for our collaborations.
Based on our team’s ideations and cross-team workshops from a clinical and commercial perspective on Cleveland Clinic London’s value-based care, we have agreed the first pilot value-based healthcare agreement of its kind.
It is for primary hip and knee surgeries, where insurance payment to Cleveland Clinic London will vary depending on efficiency, patient-reported outcomes and clinical outcomes data.
This agreement is designed to optimise the quality of patient care, with Bupa offering bonus payments to the hospital where it achieves agreed quality metrics and deducting payments where it does not. The pilot study includes Bupa Platinum consultants who practise at Cleveland Clinic London and work together in a multidisciplinary team-based approach. It will cover up to 100 primary hip and knee surgeries in the first year.
perspective, adding not just financial value but also social and environmental value.
Value-based healthcare is not a new concept; it has been part of healthcare system discussions for some time.
It has been implemented in many countries and healthcare systems around the world. But there are a number of challenges in its implementation in UK private healthcare.
Its disadvantages have largely been logistics-focused. For example, the complexity of designing and implementing value-based models, the dependence on effective health information technology and data sharing, and the challenges in measuring and reporting outcomes accurately.
Another key stumbling block has been the potential for financial risks that cannot be as readily predicted based on quality, efficiency and cost targets.
However, a number of factors are now enabling health systems to overcome these challenges and encouraging accelerated adoption.
Technology and data capabilities
Healthcare systems have aspired to deliver value-based healthcare for a long time, but it has proved challenging because it requires overcoming established practices and working across complex, siloed organisations.
The recent acceleration of digital technologies is helping healthcare systems to overcome these barriers. For example, these technologies enabled health outcomes to be used to remotely assess patients and provide remote care during the Covid-19 pandemic.
Providers no longer need to rely on crude customer risk stratification using information such as age and family history. Access to large health datasets is now opening the door to more accurate, personalised risk stratification and innovative funding models and will further improve resource allocation.
Patient expectations
Changing patient expectations will also be a significant driver of this trend. Consumers are becoming increasingly pro-active and
because reimbursement is linked to interventions that improve outcomes.
This removes the incentive for providers to charge for unnecessary or low-value activity, removing unnecessary interventions from the customer journey and meaning that valuable healthcare resources – including clinicians’ time – can be used more efficiently.
Health insurers can also be more transparent and assure their customer that they are offering them providers who deliver value as measured by quality and outcomes, rather than by costs.
Environmental issues
Healthcare systems are becoming increasingly aware of their responsibility towards the environment, driven by:
The significant effect that they themselves have on global carbon emissions;
The fact that healthcare systems are further burdened by the adverse health effects climate change has on population health; Healthcare professional advocacy and public awareness; Anticipated sustainability requirements in market.
engaged in their healthcare as demonstrated by findings from a recent survey of 300 participants across UK, Australia and Spain:2
This found that:
52% of respondents ‘agree’ or ‘completely agree’ with the statement: ‘I would like to use tests and tools at home that can help me to test for and diagnose conditions’; 48% of all respondents are interested or very interested in using a genetic test to understand their health risk.
As people become more informed about their healthcare choices, they will monitor their health and well-being, demand transparency about clinical quality and expect value for money.
Economic pressures
There is also a growing demand for value-based healthcare for economic reasons.
The Covid-19 pandemic intensified the pressure to understand healthcare spending from governments, employers and consumers.
A value-based healthcare model encourages the delivery of efficient, high-quality healthcare
Value-based healthcare can support in removing inefficiencies and waste in a system, as well as measuring the resources required to deliver any given healthcare intervention. This offers the opportunity to optimise health outcomes and reduce the environmental impact of clinical care.
Value-based healthcare represents a promising shift in healthcare delivery, focusing on patient outcomes, quality of care and efficient resource allocation.
While challenges exist, as health systems overcome logistical hurdles, value-based healthcare models may soon become a wider reality, offering better outcomes and experiences for the population.
References
1. Defining Value-based Healthcare in the NHS: The Centre for Evidence Based Medicine Report, May 2019.
2. A survey carried out by carried out by market research company Ipsos on behalf of Bupa, in January 2023. It included additional quotas for age, gender, self-reported health condition and private healthcare cover.
The Cleveland Clinic in London’s Grosvenor Place
A look back through our journal’s archives of a decade ago reveals that although times change, some issues are not so new
A trawl through the archives: what made the news in 2014
Bid to keep Ltd status for doctors
Consultants’ advisers were negotiating with HM Revenue and Customs (HMRC) over a tax disagreement which threatened specialists’ businesses with a potential ‘financial and legal nightmare’.
Tax inspectors operating the Government’s new anti-avoidance policy believed independent practitioners were reaping tax advantages by incorporating their businesses and, additionally, selling goodwill.
HMRC was convinced a professional was unable to incorporate their business activity via a limited company, a vehicle used by many professionals to offer their services.
But around 2,500 consultants in private practice were using this
trading vehicle, which accountants argued they were allowed to do under the corporation taxes acts.
HMRC believed these consultants were paying lower rates of tax at 20%, the rate of corporation tax on a company.
But accountants argued it appeared HMRC had forgotten that personal rates on investment income returns remained very high at 37.5% and any consultant shareholder withdrawing funds as profits would pay these rates because they were likely to be additional-rate taxpayers with taxable income over £150,000 a year.
Medical accountants were locked in talks with HMRC to address the apparent anomalies between tax officials’ views and what statute and their own guidance appeared to allow.
One warned: ‘If any doctors or other professionals who have incorporated were forced to revert to sole trader status, they would be thrown into a financial and legal nightmare.’
HCA fights order to sell hospitals
HCA launched the first phase of its fight to prevent forced sales of some of its leading hospitals in London.
It formally lodged an appeal against the Competition and Markets Authority (CMA) ruling on divestment after being issued with a ‘Sophie’s Choice’ ultimatum.
HCA bosses were told they had to choose between sacrificing the London Bridge and Princess Grace hospitals or selling off the UK’s largest private hospital – The Wellington – and its nearby flagship diagnostic and outpatient unit The Platinum Medical Centre.
Beware the tax sting in tail of merit awards
Consultants were warned of a hefty financial sting in the tail arising from a long-awaited but delayed announcement of the 2013 round of clinical excellence awards (CEAs).
Senior doctors’ awards, which would be backdated to April 2013, had been delayed following a report from the Doctors and Dentists Review Body recommending extensive changes ‘so that they better recognise current excellence’.
The amount of awards had fallen considerably in recent years, with the number of national awards halved to around 300 since 2010.
Consultants were eligible to receive national or local CEAs ranging up to £75,000 a year.
But Simon Bruce, of specialist financial advisers Cavendish Medical, warned senior doctors to be aware of the consequences that receiving an award could have on their pension.
He said: ‘Consultants who gain a CEA can discover their
achievement proves to be a substantial tax burden.
‘Those receiving significant annual increases such as a CEA could be a target for the muchreduced pension annual allowance rate, resulting in a large tax bill. And doctors need to remember that the onus is on the individual to tell HM Revenue and Customs if they are liable for a tax charge.’
BMI card offers 0%
op loans for patients
A card from hospital group BMI allowed patients to spread the cost of treatment with 12 months’ interest-free credit when treated at the group’s hospitals.
GMC looks into doctors’ claims that it’s unfair
The GMC commissioned research to look at the consistency and fairness of its investigations into doctors and the outcomes.
It ordered the work after stark differences emerged between the perceptions of white and of black and minority ethnic doctors about the way complaints were handled.
What we can learn if it all goes wrong
The learnings from general surgery claims in private practice are shared here by Dr Sarah Townley (right)
OUR MEDICO-LEGAL teams support private practitioners with a range of potential issues arising from professional practice – from complaints through to inquests and, of course, clinical negligence claims.
But our preferred approach at Medical Protection is to proactively assist members in helping them to reduce their risk while doing their day-to-day roles and, as part of this, we regularly review and share themes and learnings from a range of past claims.
My report here looks into clinical negligence claims experienced by general surgery consultants working in private practice in the UK over a ten-year period (2010-20), excluding any bariatric procedures.
These several hundred claims vary enormously in their complexity, but also in terms of cost,
with some claims being valued at over £1m.
Most claims have a variety of underlying allegations including surgical technique, diagnosis, pre/ post-operative care, consent and medical treatment.
Although surgical technique appears as the dominant allegation, most claims involve a mix of many of the themes, and consent in particular can often be a crucial factor in the decision whether to defend or settle a claim.
Surgical technique
The commonest outcomes due to alleged inadequate surgical technique were bowel perforation, bile leak, nerve injury and poor cosmetic outcome.
Often cited as a contribution to these injuries was an alleged failure to correctly identify the rele-
vant anatomical structures, particularly in laparoscopic cholecystectomies.
After these injuries, concerns were often raised that the injury was not identified during the operation and hence a significant delay in treatment occurred. The choice of operation/approach was also questioned in several claims, particularly when more conservative options were available.
Diagnosis
Many claims centered around an alleged delay in diagnosis, particularly in relation to cancer diagnoses. Often this was due to a perceived delay in undertaking appropriate imaging, failure to consider alternative diagnoses or failure to involve a multidisciplinary team or appropriate specialists.
In some very high-value claims, the critical error originated from a simple administrative omission such as failing to organise a followup appointment, with potentially life-changing results.
Pre- and postoperative care
Criticism of pre-operative care mainly arose from the alleged failure of the clinician to consider the risks and implications of the patient’s previous medical history, and commonly their risk of thrombo-embolism.
These often led to further allegations involving the failure to discuss alternative treatment options or delaying treatment.
For postoperative care, allegations often involved the failure to identify deterioration in the patient condition – for example, deteriorating renal function, increased analgesia use, signs of
MINIMISE YOUR RISK OF A CLAIM
1 Review your consent discussion and documentation. Ensure that a patient is aware of the risks, benefits and complications of the procedure, but also any alternative or subsequent treatment option. Consider how the consent process may need to be tailored to that individual depending on any comorbidities, medical or social history and allow sufficient time for the patient to consider their options. Ensure you are up to date on the latest GMC guidance regarding consent.
2 Consider the use of supporting information such as patient information leaflets or online guides to ensure full patient understanding at a time that is convenient to them. Use of these should also be documented in the records and regularly reviewed to ensure they are still fit for purpose.
3
Be alert to the possibility of adjacent organ injury peri-operatively and have a low threshold for early review or to involve specialist colleagues at an early juncture.
4
You may be a very experienced surgeon, but it is always beneficial to continually evaluate your procedural skills or competency, perhaps through data or observation by a colleague. Alternatively, you may want to consider observing other colleagues to refresh your skills and knowledge or consider alternative techniques.
5 Ensure you undertake a thorough, consistent and documented pre-assessment of the patient, involving any specialist colleagues as needed to support your clinical reasoning.
6
Document a clear postoperative plan of when and how you should be contacted should any complications arise, how often observations should be undertaken, when other specialties should be involved, if required, and have a clear procedure for ensuring all test results are reviewed.
Main allegation in general surgery – Claims by %
sepsis – resulting in delay in further imaging and subsequent treatment. Failure to diagnose postoperative DVT/PE also featured prominently.
Consent
As we see in many clinical negligence claims, consent allegations centred around two themes: risks and alternative treatment options. Many of the claims related to alleged failure to advise of specific risks such as bowel injury, nerve injury and inadequate cosmetic outcome. Increasingly, however, allegations in relation to consent are extending to failure to advise
of alternative treatment options, particularly a conservative/nonsurgical approach.
The recent case of McCulloch v Forth Valley Health Board (2023) brought this area into focus and clarified that a doctor should inform a patient about reasonable alternative treatment options by applying the Bolam professional practice test.
A doctor should not simply inform a patient about the treatment option that the doctor themselves prefers.
Dr Sarah Townley is deputy medical director at Medical Protection
CASE STUDY
Patient A was referred by their GP to Mr B, a consultant general surgeon, with recurrent abdominal pain.
The patient was a 50-year-old obese female who had experienced recurrent bouts of biliary colic and acute cholecystitis. Recent ultrasound demonstrated a dilated gallbladder containing multiple large mobile calculi.
Mr B saw her in his clinic at the private hospital and explained the findings of the recent ultrasound. He discussed the possibility of undertaking a laparoscopic cholecystectomy and drew diagrams to explain the procedure and anatomy involved.
A week later, Patient A was admitted to hospital for her procedure. Pre-operatively Mr B visited the patient, discussed the risks again with her and she signed the consent form.
The form outlined that the procedure was a laparoscopic cholecystectomy with a 5% possibility of conversion to an open procedure.
It also referenced diagrams that were drawn in clinic to explain the risks, but did not specifically list the risks apart from bleeding and infection.
The operation was carried out the following day without any apparent difficulties. Mr B documented that the ‘critical view’ was obtained following initial dissection and the cystic duct and artery were clearly identified. The gallbladder was removed and because the operative field appeared dry, no drain was required.
Patient A was reviewed postoperatively on several occasions by Mr B and discharged two days later following satisfactory observations. Histology confirmed a gallbladder containing numerous stones and an appearance consistent with cholecystitis.
Unfortunately, Patient A was
re-admitted two days later with jaundice and dark urine. Her abdomen was soft and non-tender; however, her liver function tests were abnormal. Following 24 hours of observation, Mr B made a provisional diagnosis of gravel in the common bile duct and elected to undertake an ultrasound the following day.
This demonstrated two calculi in the proximal common duct and dilated intra-hepatic ducts. On this basis, Mr B felt the most likely cause of the jaundice was obstruction of the common duct by stones.
He referred her for an ERCP, which occurred five days later and she was found by Mr B’s colleague to have a normal bile duct up to a specific level where four clips were found to completely occlude the duct.
It was found impossible to pass contrast or a guide wire past the obstruction. The following day Patient A was taken for a laparotomy by Mr B to explore the common bile duct obstruction, remove the clip and repair the bile duct. She made a slow and steady recovery and was discharged home eight days later.
A claim was brought against Mr B for failure to clearly outline the risks of a bile leak and increased risks of a surgical procedure in a patient with obesity, failure to correctly identify the critical anatomy during the operation and failure to refer to a specialist hepatobiliary surgeon for the bile duct repair.
Following the involvement of a clinical expert to assess the merits of the allegations, the claim was settled on Mr B’s behalf.
He reflected following the process and acknowledged that he would now have a lower threshold for converting to an open procedure if struggling to identify critical anatomy and would ensure more detailed documentation of the consent process in future.
Derek Kelly (right) explores their impact on revenue cycle management for private healthcare providers, highlighting how it drives informed decisionmaking, identifies revenue opportunities and elevates overall financial performance BILLING AND COLLECTION
Data analytics can bring in the cash
Data analytics can drive informed decision-making, identify revenue opportunities and enhance overall financial performance in doctors’ medical billing operations.
EFFECTIVE REVENUE cycle management is essential for financial stability and operational excellence in healthcare.
While medical billing traditionally focuses on claims submission and reimbursement, integrating data analytics offers new insights and avenues for improvement in private practice.
Understanding the impact of data analytics
Data analytics provide valuable insights from the wealth of billing and financial data available to healthcare providers.
And by using analytics tools and techniques, providers can better understand their revenue cycles, identify trends and make datadriven decisions to improve efficiency and financial outcomes.
Whether it is identifying underperforming revenue streams, optimising reimbursement processes, or mitigating revenue leakage, data analytics can give you a solid foundation for informed decisionmaking at every stage of the revenue cycle.
Identifying revenue opportunities
One of the most significant benefits of data analytics in revenue cycle management is its ability to uncover untapped revenue opportunities.
By analysing billing and financial data, consultant providers and their teams can identify areas for potential improvement. This might include aspects such as reducing denials and rejections, improving coding accuracy and streamlining claims processing workflows.
Data analytics also enables proactive identification of revenue cycle bottlenecks and inefficiencies, and this allows doctors and their practices to fix the problem and optimise revenue capture and accelerate cash flow.
Analytics can also be helpful in forecasting revenue trends, anticipating cash flow fluctuations and pro-actively addressing potential revenue risks.
Ultimately, providers can then allocate resources more effectively, prioritise revenue-generating
activities and adapt their revenue cycle strategies to meet evolving trends and regulatory requirements.
Realising the potential with reporting systems
Medical billing companies like Medserv offer a comprehensive reporting system that give consultants greater understanding of their revenue cycles and, when they act on this, it helps them make improvements.
These reporting systems allow medical professionals to gain greater understanding of their financial performance, identify revenue opportunities and make informed decisions to drive the growth of their medical practice.
Harness the power of the reporting systems available and you can streamline a variety of processes, optimise revenue capture and achieve greater financial success.
Benefits of data-driven awareness
Data-driven insights enable providers to allocate resources more
effectively, prioritise revenue-generating activities and adapt revenue cycle strategies to meet the changing market and regulatory requirements.
By forecasting revenue trends and prudently addressing potential risks, you can achieve greater financial success.
With systems like our live reporting system, doctors can unlock the full potential of their revenue cycle management efforts, driving practice growth and financial success.
Empowering providers, empowering patients
The impact of data analytics in revenue cycle management extends far beyond balance sheets and profit margins.
And it is not just about improving financial performance. Data provides the power to help you better understand the needs of your patients and anticipate challenges.
Derek Kelly is marketing manager at Medserv
Diagnostic Audiology Including Paediatrics • Tinnitus Rehabilitation • Vestibular Testing • PTA & Tympanometry • Speech Audiometry • Speech In Noise Testing• Specialist Tests Including OAE, VEMP & ASSR • Ear Wax Removal • Independent Hearing Aid Provider
Fertility patients hate making a fuss
Patient complaints-handling expert Sally Taber (below) outlines what fertility doctors treating private patients should be aware of
IT HAS been acknowledged by the Competition and Markets Authority (CMA) that fertility patients can be reluctant to complain.
One reason applicable to many patients purchasing fertility treatment is that it tends to be a uniquely private experience.
They feel that there is no understood ‘norm’ in relation to how someone should be treated or what they reasonably expect from a clinic.
Let me draw your attention to the fact that the CMA issued guidance for fertility clinics as long ago as June 2021 and this sets out the competition watchdog’s views on how consumer law applies to clinics in the fertility sector.
It covers:
Information provision – what information clinics should provide to prospective patients and existing patients and when;
Commercial practices – what
clinics should do to ensure that their commercial practices are fair, in particular to ensure that their commercial practices meet the objective standard of professional diligence;
Contract terms – what clinics should do to ensure that their terms are fair;
Complaints handling – what clinics should do to ensure that their complaints handling processes are accessible, clear and fair.
Contact me
As director of the Independent Sector Complaints Adjudication Service (ISCAS), I would welcome contact from fertility units that hopefully may wish to follow the good practices advocated above.
You can contact me at sally.taber@ iscas.org.uk.
The CMA has also published a report setting out the findings from the latest patient research it
The competition watchdog has signposted the Independent Sector Complaints Adjudication Service as one of the options the complaint can be escalated to
commissioned which looks at how self funding IVF patients choose between clinics and treatment options.
This also includes a chapter on patients’ willingness to raise a concern or complaint with clinics, which is obviously of interest to us at the Independent Sector Complaints Adjudication Service . It has signposted ISCAS as one of
the options the complaint can be escalated to.
The others are the Human Fertilisation and Embryology Authority (HFEA) and the professional regulators such as the GMC.
In a report in September 2022, the CMA made this recommendation to the HFEA:
‘We recommend the HFEA encourages all licensed clinics to join an independent Alternative Dispute Resolution (ADR) scheme, just as the Care Quality Comission does. We further recommend that the HFEA considers whether membership of an ADR scheme could be incorporated into their Code of Practice.’
More information about the CMA’s work, copies of the reports, a press notice and the open letter to the sector can be found from the Government website at www. gov.uk/cmacases/selffundedivfconsumerlawguidance.
My patient was desperate. Having tried lifestyle changes and other treatment options for his debilitating hyperhidrosis and blushing, he wanted a sympathectomy.
Two years after the surgery I received a letter that set my heart racing. It was from the patient’s solicitors, requesting a copy of his medical records. Chronic compensatory sweating had led to severe depression, and he deeply regretted the operation.
Medical Protection were immediately there for me. My medicolegal consultant concluded that I’d undertaken a thorough consent process, and was in a strong position to defend an allegation of negligence. The patient’s solicitors agreed, and thankfully no further action was taken.
This has reaffirmed two things for me: the importance of a detailed consent discussion and the support I get from Medical Protection. They know exactly what to do and always have a plan for doing it. As well as helping with legal advice, they offer risk reduction courses to prevent problems happening. I’ve always known I needed protection. Now I fully appreciate the value of everything my membership gives me.
Celebrating becoming sweet 16
June is our birthday month and we are celebrating 16 years of bringing consultants and GPs in private practice news, advice and tips to ease their business journey.
A big thank-you to all our sponsors, advertisers and readers for all your support that has contributed to our successful growth. Here we present a look back at just some of the important issues we’ve brought to you on the way.
Editor Robin Stride
Inflation’s perfect storm
➽ July 2022: Economic pressures combined with insurers ‘delisting’ tactics put pressure on consultants
EXPERT TAX AND ACCOUNTANCY ADVICE YOU CAN TRUST
Sandison Easson is a firm of truly specialist medical accountants who provide personal and tailored advice to clients.
We act for medical professionals throughout all stages of their career with clients in almost every town in England, Scotland and Wales.
We cut through the complicated jargon and deliver practical, easy to understand advice. Call us today to organise your FREE no obligation consultation.
➽ May 2024: Analysts LaingBuisson report much faster market growth in insurance than historic norms
WE PROVIDE THE USUAL SERVICES YOU WOULD EXPECT FROM AN ACCOUNTANT SUCH AS PREPARATION OF YOUR ACCOUNTS AND TAX DECLARATIONS BUT OFFER SO MUCH MORE INCLUDING ADVICE ON:
• SETTING UP A NEW PRIVATE PRACTICE
• BUILDING AN EXISTING PRIVATE PRACTICE
• BUSINESS STRUCTURES TO PROTECT WEALTH
• BUSINESS STRUCTURES TO MAXIMISE TAX EFFICIENCY
• CLAIMING TAX REFUNDS INCLUDING OVERPAID ANNUAL ALLOWANCE TAX
• REMUNERATION PLANNING FOR YOU AND YOUR FAMILY
• UNDERSTAND ANNUAL ALLOWANCE TAX
• MAXIMISING LEGITIMATE EXPENSE CLAIMS
Looking to the future is always a bit hazy
Do recent returns give investors FOMO – fear of missing out? Samuel Kirton shows why investors should gain comfort by holding a broad market exposure
If one were to be influenced by the recent returns of the US market and allocate more assets to it, one would risk having all of their investment eggs in one basket
MOST INVESTORS are aware that, in the past few years, the US market has delivered above-average returns, compared to many other markets.
There has also been quite a lot written in the media lately pointing out that just a handful of stocks have driven most of its returns.
As the old saying goes, investing is simple but not easy.
It is simple to look back at market data today and wish that we had, for example, owned more US equities and less UK and emerging market equities over the past ten years, given their annualised returns of around 14.5%, 5.0% and 6.5%, respectively.
Yet that would be to succumb to ‘recency bias’, where one is influenced largely by what has just happened and extrapolating this into the future.
The difficult part is knowing, instead, that you need to build and own a robust portfolio for the future that will work for you across a potentially wide range of unknown market events and outcomes.
Eggs in one basket
If one were to be influenced by the recent returns of the US market and allocate more assets to it, one would risk having all of their investment eggs in one basket.
As it is, the US already represents around 62% of global market capitalisation across developed and emerging markets.
Students of market history will also recall that the US market suffered what has become known as the ‘lost decade’ in the 2000s where the market went sideways over a ten-year period.
If we look at data from various developed markets from 20042023, it is evident that there was no discernible year-on-year pattern that an investor can take advantage of.
Interestingly, the US stock market has not been the best performer in any of the past 20 years.
The best performing market was, in fact, Denmark, which delivered an annualised return of almost 16%, which compares to 11% for the US and 9.4% for developed markets as a whole.
And the Danish market has been
driven largely by one stock – Novo Nordisk, which is 60% of the market!
The reality is that markets work pretty well at incorporating information into prices, and trying to beat the market – through either market timing or stock picking – is a tough game, with very few winners.
Simply making your investment bed out of exposure to a diversified market and lying in it over time makes a huge amount of sense in the absence of market timing signals and an ability to foresee the future.
‘Since the future cannot be predicted, it is impossible to specify in advance what the best asset allocation will be. Rather, our job is to find an allocation that will do reasonably well over a wide range of circumstances.’
William Bernstein, author of The Intelligent Asset Allocator
Samuel Kirton (above) is a financial planner with Cavendish Medical, specialist financial planners helping consultants in private practice and the NHS
The content of this article is for information only and must not be considered as financial advice. Cavendish Medical always recommends that you seek independent financial advice before making any financial decisions.
Levels, bases of and reliefs from taxation may be subject to change and their value depends on the individual circumstances of the investor. The value of investments and the income from them can fluctuate and investors may get back less than the amount invested.
Death is going through change
The Medical Examiners (England) Regulations 2024 come into force this autumn on 9 September and are relevant in private medical practice. Lawyer Liz Hackett (right) guides you through the changes
THERE HAVE been many calls for a review and changes to the death certification system in England and Wales. It has remained largely unchanged for over 50 years.
In its third report, the Shipman Inquiry – led by Dame Janet Smith – concluded that the current one was not only confusing, but that it failed to provide adequate safeguards.
Calls for changes were renewed by:
The Francis Inquiry into fail-
ings in care at Mid Staffordshire NHS Foundation Trust between 2004 and 2009;
The investigation into the management, delivery and outcomes of care provided by the maternity and neonatal services at the University Hospitals of Morecambe Bay NHS Foundation Trust between 2004 and 2013.
Acute trusts in England and local health boards in Wales were asked by NHS England and NHS Wales Shared Services
Partnership in 2019 to set up medical examiner offices on a non-statutory basis for the purpose of reviewing their own organisations’ certification of deaths.
While not currently mandatory, it has become standard practice across England and Wales for deaths in hospital to be scrutinised by a medical examiner.
Those deaths that the medical examiner believes may not have been natural or where a
culpable human failing may have contributed to death are referred by them to the coroner.
In addition to the Medical Examiners Regulations, two other regulations will be introduced:
1
The Medial Certificate of Cause of Death (MCCD) Regulations 2024;
2 The National Medical Examiner (Additional Functions) Regulations 2024.
As part of the Department of Health’s Death Certification Reforms, from 9 September 2024 a new statutory medical examiner system is being introduced across England and Wales.
To a large degree, the new system will look like it does now. But there will be a mandatory requirement for all deaths that are not investigated by a coroner to be subject to review by medical examiners.
Under the leadership of Dr Alan Fletcher, the National Medical Examiner for England and Wales, senior medical doctors with varying specialties form teams of medical examiners contracted by acute trusts – and some specialist trusts – and health boards.
These teams are supported by medical examiner officers and appropriate training is provided to medical examiners in the clinical and legal elements of death certification.
Medical examiners and their officers will be funded annually by the National Medical Examiner’s Officer with one full-time equivalent examiner for approximately 3,000 deaths.
The role of examiners is to:
Review the medical records and any supporting diagnostic information;
Agree the proposed medical cause of death and accuracy of the MCCD with the completing doctor;
Discuss the cause of death with the bereaved and establish any concerns or questions they may have;
Act as medical resource for the coroner;
Identify those cases for further review under local mortality and governance arrangements.
As all deaths that are outside of the coronial process will now be examined by medical examiners, all healthcare providers in England and Wales, including GP practices and independent healthcare providers, must ensure they have:
Systems in place to inform medical examiners of deaths requiring independent scrutiny;
Share records of deceased patients with medical examiners in a timely manner. Regional medical examiners will support these processes.
The Notification of Deaths Regulations 2019 – subject to minor amendment – will remain in force and attending practitioners should continue to notify deaths that meet the criteria to the coroner.
In non-coronial cases the process is therefore:
1
The ‘attending practitioner’ to propose the cause of death for the MCCD;
2
The attending practitioner must send the MCCD to the medical examiner;
3 The medical examiner will scrutinise MCCD, consider the records and decide whether to refer the death to the coroner;
4 If the death is not referred to the coroner, the medical examiner will add their signature to the new MCCD and submit it to the registrar;
5
If the registrar has any queries, these will be directed to the medical examiner.
There is a change to who can propose the medical cause of death for the MCCD.
The requirement that the MCCD be completed by an attending med-
ical practitioner who has seen the deceased during their last illness –or if not seen in the 28 days prior to their death, refer to the coroner –has been removed and a medical practitioner will be an attending practitioner if they have attended the deceased in their lifetime.
This represents a simplification of the current rules, aiming to improve efficiency, mortality data and reduce the number of deaths being referred to the coroner.
There will be additional changes to the MCCD documentation to support the collection of data.
It is hoped that the changes to death certification through the medical examiner system and increased independent scrutiny of all deaths will provide better safeguards for the bereaved and wider public and be a means of improving learning from deaths.
They will also ensure that appropriate cases are referred to the coroner.
Liz Hackett is a partner at specialist healthcare law firm Hempsons. If you would like more information, please email L.Hackett@hempsons.co.uk.
Free legal advice for Independent Practitioner Today readers
Independent Practitioner Today has joined forces with leading healthcare lawyers Hempsons to offer readers a free legal advice service.
We aim to help you navigate the ever more complex legal and regulatory issues involved in running and developing your private practice – and your lives.
Hempsons’ specialist lawyers have a long track-record of advising doctors – and an unrivalled understanding of the healthcare system as a whole.
Call Hempsons on 020 7839 0278 between 9am and 5pm Monday to Friday for your ten minutes of free legal advice.
Advice is available on: Business structures (including partnerships)
Commercial contracts
Disputes and litigation HR/employment
Premises
Regulatory requirements and investigations
Maintaining safety of
It has been a busy period for healthcare regulation. David Hare, head of the Independent Healthcare Providers Network (IHPN), gives a heads-up on just some of the recent developments that independent practitioners need to know about
58,000 staff reported unwarranted sexual approaches from patients or other members of the public last year, which equates to one in 12 NHS workers
of staff and patients
ENSURING THE safety and dignity of healthcare staff should be the top priority of all healthcare providers, and NHS England’s recently published letter outlining the findings from the NHS Staff Survey regarding sexual safety was sobering reading.
Overall, 58,000 staff reported unwarranted sexual approaches from patients or other members of the public last year, which equates to one in every 12 NHS workers. These findings highlight the prevalence of the problem and re affirmed the importance of empowering healthcare colleagues who have experienced or witnessed these crimes to speak up, report and call out this behaviour – wherever they work in the health system.
While over half of IHPN members have signed up to the NHS’s Sexual Safety in Healthcare Charter, which is designed to tackle this abuse, we want to see all independent providers becoming signatories.
We strongly encourage those who have not signed up to do so as soon as possible.
This is a real priority for IHPN and we are also making an effort to support our members and those working in the sector on this, including with a campaign group. The group is called Surviving in Scrubs and was set up by two doctors to raise awareness of and put an end to sexism, sexual harassment and sexual assault in healthcare – to ensure our members are best placed to tackle this issue.
Do we really aid those who speak up?
As Independent Practitioner Today readers will, of course, be aware, healthcare providers and professionals have a fundamental responsibility to be open and honest with patients under their care, particularly in the rare cases when things go wrong.
There has long been a professional ‘duty of candour’ which is regulated by the GMC and other professional regulators and which applies to individual practitioners.
However, since 2015, all health and social care providers have a statutory obligation around ‘duty of candour’.
They must be open and honest with patients and their families when something goes wrong that appears to have caused, or could lead to, moderate harm or worse in the future – known as a ‘notifiable safety incident’.
This was introduced in light of the Mid Staffs scandal where it became clear that a lack of an open and transparent culture and an ability for staff to be candid around when things go wrong was a key contributor to patient harm.
Since then, the Care Quality Commission has been assessing providers’ commitment to duty of candour as part of its inspection regime.
understand the duty and whether providers have adequate systems and senior level accountability for monitoring the duty which can support organisational learning.
Here at the Independent Healthcare Providers Network (IHPN) we welcome this review; it is something we have long been calling for.
In particular, there are currently two parts to the duty of candour regulations – one for NHS providers and one for all other organisations – something we feel is not in line with a ‘whole systems’ approach to safety and quality.
Likewise, many new patient safety initiatives have been put in place since duty of candour was introduced in 2015 – most recently ‘Learning from Patient Safety Events’ – and ensuring all these programmes align and help rather than hinder providers fostering open, transparent cultures will be key.
Getting ready for medical examiners
The Department of Health and Social Care (DHSC) also recently announced the first major reforms to the death certification system in England and Wales in over 50 years. (See our ‘Keep It Legal’ feature on page 36).
Ensuring all these programmes align and help rather than hinder providers fostering open, transparent cultures will be key
We want to see all independent providers becoming signatories to the NHS’s Sexual Safety in Healthcare Charter
But the Department of Health and Social Care (DHSC) is now undertaking a review to understand to what extent the duty of candour is honoured, monitored and enforced by providers.
This includes how well staff
While a medical examiner system has been implemented across the countries since 2019, the Government has confirmed that this system will now be put on a statutory footing.
This means that all deaths in any health setting, including the inde
pendent sector, that are not investigated by a coroner will be reviewed by a medical examiner. And all healthcare providers will be required to share records of deceased patients with medical examiner offices.
This is something IHPN has been working with NHS England for some time on, and will provide real benefits in ensuring both NHS and independent providers can better support bereaved people and drive further improvements in patient safety.
IHPN has been working closely with the National Medical Examiner, Dr Alan Fletcher, to ensure the sector and those working in it are well prepared for the changes.
We are pleased many of our members are already making early connections with medical examiner offices to help staff understand the new regulations.
David Hare (right) is chief executive of the Independent Healthcare Providers Network (IHPN)
BUSINESS DILEMMAS
Dr
Kathryn Leask (below) explains how to respond to a request for information from the police
Dilemma 1 Must I hand over my patient data?
QI am a private GP who has recently received a court order from the police in relation to one of my patients.
I have been asked to provide the police with a copy of the patient’s medical records, particularly sections that relate to the patient’s mental health.
The police have stated that this is in conjunction with a serious crime. However, I’ve not obtained the consent of the patient. Should I comply with the patient’s request?
ADisclosing patient information without consent can only be justified in limited circumstances.
Even if a request is from the police, your legal and ethical duties of confidentiality still apply. However, paragraph 17 the GMC’s
The police ask about my patient
confidentiality guidance states that ‘You must disclose information if it is required by statute or if ordered to by a judge or presiding officer of the court’.
Be aware, that often a court will not ordinarily order the disclosure of medical records where criminal proceedings have not yet begun.
Furthermore, paragraphs 90-95 of the confidentiality guidance explains that doctors should only disclose the information that is required by the court and that you should object if attempts are made to compel you to disclose information that appears to you to be irrelevant.
Also, if the information requested includes details that may put someone at risk of harm, then it is imperative that the judge is informed.
You also have a duty to tell the patient whose information is being requested what information you will disclose unless this is not practicable, or it would undermine the purpose of the disclosure, or you feel that doing so
Even if a request is from the police, your legal and ethical duties of confidentiality still apply might put yourself or others at risk of serious harm.
There are other examples in which you would be legally required to disclose information to the police. For examples:
The Road Traffic Act 1988 allows the police, under certain circumstances, to require information from anyone, which may lead to the identification of a driver alleged to have committed a road traffic offence. It is an offence to fail to comply.
Under the Terrorism Act 2000 it is an offence not to disclose as soon as reasonably practicable information which you believe
might be of ‘material assistance’ in preventing an act of terrorism or in apprehending a person who has committed, has prepared or has instigated an act of terrorism.
If you discover an act of female genital mutilation (FGM) which appears to have been carried out on a girl under the age of 18 in England and Wales.
Additionally, the GMC also says you ‘must participate in procedures set up to protect the public from violent and sex offenders, such as multi-agency public protection arrangements (MAPPA) in England, Wales and Scotland and public protection arrangements in Northern Ireland (PPANI)’.
Finally, seek advice from your medical defence organisation if you have any questions or concerns when potentially disclosing information to the police. We also recommend that you seek advice before acting on a court order, to ensure it is valid.
Dr Kathryn Leask is a medico-legal adviser at the Medical Defence Union
When journalists call
tacted by a journalist a daunting experience.
If a journalist contacts you, remember to stay calm and politely ask them to leave their name, contact details and the name of the organisation they work for, stating that you will respond to them later.
Most journalists will be happy with this and it allows you time to gather your thoughts and prepare a response.
Dilemma 2
Should I speak to this reporter?
QI’m a private consultant medical oncologist who has been contacted by a journalist at a national newspaper asking for a comment in response to claims made by the family of a recently deceased patient into the quality and appropriateness of treatment their relative received. What should I do?
AThe increase in press articles about alleged medical wrongdoings can make being con-
If relevant, you may also wish to discuss this with your colleagues if you are in a practice or private hospital.
In Confidentiality: responding to criticism in the media , the GMC states that ‘you must not put information you have learned in confidence about a patient in the public domain without that patient’s explicit consent. You should usually limit your public response to an explanation of your legal and professional duty of confidentiality’.
While it may be tempting to respond, medical professionals must always consider the duty of confidentiality to a patient regardless of whether a patient or their loved-ones make any comments in either traditional or on social media.
The GMC supports this when it says: ‘Disputes between patients and doctors conducted in public can also prolong or intensify conflict and may undermine public confidence in the profession.’
It is always best to say as little as possible. The more you say, the more chance there is for it to be interpreted negatively.
Consequently, a short, yet appropriate response is: ‘Due to patient confidentiality, I am unable to comment on this matter.’
Ideally, and if possible, it is preferable to put this response in an email to the journalist, as it ensures you and, where appropriate your colleagues, have a written record which can be referred to if needed.
Sending a response via email also prevents a journalist asking for a comment ‘off the record’.
This is to be avoided, as there is nothing to prevent a journalist from using this information. It is good practice to assume that anything said to a journalist will be used and never to say anything that deviates from the planned response.
Usually, press interest in a story will be short-lived, only lasting for a day or two. Despite its short lifespan, attention from the media can be stressful for you.
As such, it is wise to contact your medico-defence organisation whose press office will be able to advise you further.
How you can hit top profits
Many independent practitioners have soldiered on with their business even when it is not really paying them very well to do so.
So how do you ensure your practice is profitable?
Specialist medical accountant Alec James (right) gives his top ten tips – in no particular order of importance – for maximising your rewards
1
Trading structure
A key decision that needs to be made in relation to your private practice is the trading structure your business adopts.
The most popular choices adopted are:
Sole trader – or self-employed;
Limited company;
Partnership;
Limited liability partnership or LLP.
The business structure adopted can offer tax efficiencies and levels of liability protection. The trading structure adopted is not set in stone and you may move from one
structure to another; for example from sole trader to a limited company.
This could be for several reasons such as growth in your private practice, change in legislation or a change in personal circumstances.
Long-term financial goals should be considered when choosing the business structure. Discussing this with a specialist accountant who is au fait with nuances of private practices is essential.
2
Review your fees
One of the biggest factors that affects the profitability of your
practice is the fee income generated.
It goes without saying that the insurance market makes up a large proportion of the private medical sector and registration with the insurers is an integral part of starting in private practice.
The insurers have tariff rates for procedures. Negotiating fees higher than the tariff rates can be very difficult.
However, the rates are reviewed and ensuring that you are invoicing for the correct procedure and associated rate helps maximise your profits.
The self-pay market is a little different, as the fees you charge do not need to be approved by an insurer.
Reviewing these fees regularly is essential.
You should factor in inflation as well as personal aspects such as your expertise and knowledge.
It can be tempting to ‘sense check’ your fees with colleagues; but you must be very careful not to infringe any Competition and Markets Authority rules.
Penalties can be issued on businesses where uncompetitive practices have been taking place.
3
Monitor your finances
Monitoring the finances of your business is very important. There is a popular business saying: ‘Revenue is vanity, profit is sanity, cash is king’.
A key strength of a successful business is ensuring that you are paid for the work you do. Working with insurers means you will always be paid in arrears, but for self-pay it is usual to take payment prior to any appointments. This helps to minimise the risk of not being paid.
As a business, you must keep accurate business records for the event of a HM Revenue and Customs (HMRC) inquiry. But these records can also help ensure you regularly chase outstanding invoices to ensure payment.
There are various software solutions for both the clinical aspect of your business and book-keeping software which allows you to monitor the practice profits.
4
First impressions count
Once you are established, the first – and generally one of the most important – appointments you generally make would be for a secretary. As the first person a potential patient will speak to, your business requires the services of a high-quality secretary.
Secretaries for the private medical sector work differently to NHS secretaries. In addition to managing clinics, they will often be responsible for the billing and chasing of payments for your business.
Ensuring you allow for plenty of time for your secretary to perform these duties helps maximise the recovery of fees.
You will need to ascertain whether the secretary is an employee of your business or provides services to your business and is self-employed.
It is common for the secretary to be self-employed, but some prefer the security and lower hassle of being employed. This is not a choice, instead it is a status based on the agreement of terms between you and the secretary. It is always a good idea to discuss this with your accountant.
5 Marketing
If you are aiming to grow your private practice, you may
wish to look at your marketing requirements. Depending on your specialty, the costs can be significant.
These days, as a minimum, consultants working privately would be expected to have a high-quality website and social media platforms. You may also consider using a marketing agency, advertising in the media or using Google Adwords.
Using these services can help grow your business significantly, but they can be very expensive. You should ensure that you monitor your campaigns. A simple question of how a patient found you helps you monitor your campaigns, allowing you to spend more wisely.
6 Time management
As your practice grows, you will become time poor. At this time, you may wish to consider outsourcing some of the administrative duties of your business to other professionals such as billing companies or accountants.
While this comes at a cost to your business, it allows you to focus your attention on seeing patients, generating additional income.
7 Consider your costs
In an article about business profitability, it would be difficult not to talk about reviewing your business costs and while you should review them, don’t dismiss the long-term impact for shortterm gains.
A good example is defence cover, which is generally one of the largest costs of a private practice. Yes, you may be able to obtain a cheaper deal, but compare the terms of the policy – for example, run-off cover or excess payments payable in the event of a claim.
A successful private practice will generally be working with highquality advisers who attract a higher cost but provide pro-active services to the business.
8 Make use of technology
Since Covid, electronic communications such a Microsoft Teams and Zoom have become more prominent in our professional lives.
Making use of these systems can allow you to be more available and
The tips set out here are not an exhaustive list but they cover key areas for you to consider when looking to maximise your practice profits and continue to grow your business
potentially allowing your business to grow with minimal costs and time requirements.
9 Diversify your income streams
Another way to help improve the practice profitability is by diversifying the income sources. Depending on your specialty, this could include medico-legal fees or reporting fees – for example, with radiology.
These sources of income generally have low overheads associated and can be done outside of normal operating times, making them more flexible.
Private medical treatments generally fall outside the scope of VAT with the key exception of purely cosmetic procedures. However, some types of income, such as medico-legal fees, are potentially subject to VAT.
The threshold for registering for VAT is £90,000 a year. This only applies to the ‘VAT-able’ income rather than the total income of the business, which gives a scope to generate a good additional source of income without the administrative burden of registering for VAT.
10 Tax efficiencies
While technically not a cost to your business, one of the largest outlays you or your company will make each year is your tax payments to HMRC.
With the tax payments calculations based on the profits of your business, it is therefore important to ensure you obtain the tax relief you are entitled and pay the right amount of tax.
If you have a limited company, there can be tax-efficient benefits that the company can provide for you and your family such as the use of an electric car, staff entertaining or trivial benefits.
Making use of these schemes can help maximise your ‘take home’ pay from your business.
You may also be able to involve your family within the business, particularly spouses in a different tax bracket to yourself. Discussing these options with an accountant who specialises in the medical sector would be wise.
Alec James is a partner at Sandison Easson & Co, specialist medical accountants
DOCTOR ON THE ROAD: VW TIGUAN
VW’s glad tidings of comfort and joy
Volkswagen’s latest Tiguan offering is a great all-rounder for the ‘family’ doctor, reports Dr Tony Rimmer (right)
A central console knob can select a number of pre-determined ambient audio and lighting settings. They are called Lounge, Energetic, Joy, Minimal and Me
ONCE CAR-MAKERS find something that works well, they refine it over time. They develop a model that hits the mark and its success can be measured by public popularity and high sales figures.
One such model that VW got right, apart from the Golf, is the Tiguan. This medium-sized SUV was first launched in 2007 and its underpinnings were straight from the Golf Mark 5, current at that time.
Seventeen years and seven million cars later, we now have the third-generation Tiguan, which sits on an updated platform borrowed from other current VW products that allows a much wider variance of powertrain and suspension settings.
Of particular note is a plug-in hybrid version that has a 148bhp electric motor and a 20kWh battery that allows up to 60 miles of silent, non-polluting travel if fully charged.
Allied to a 1.5litre petrol engine, this would seem to give the best of both worlds, allowing pure EV
There is a welcome return to some tactile physical controls instead of everything having to be accessed via the touchscreen
tion. This has, I think successfully, given the new Tiguan more kerb appeal particularly at the rear.
Re-designed external lights help the situation and it is noteworthy that VW’s excellent LED Matrix headlight system is available as an option.
Step inside and the improvements to the interior are obvious.
Volkswagen has been criticised over recent years for a reduction in the perceived quality of the interior trim of most of their cars, but this Tiguan seems to have made a positive move in the right direction.
Volkswagen way. The controls are direct and positive, the engine has a sprightly feel and the DSG gearbox shifts smoothly and effortlessly.
Handling is pretty well controlled, but this is not a keen drivers car. A bit too much body roll and a surprisingly unsettled ride takes the edge off a swift drive along one of my favourite B-roads. It is fine as a motorway cruiser –wind and road noise are adequately suppressed albeit not to premium-class levels.
local journeys and the petrol engine for long trips.
As usual, this would only make sense if you have a wall charger fitted at home. Also, the extra few thousand pounds in price that the plug-in model commands may be hard to justify.
Although, surprisingly, VW still offers a 2.0litre diesel-powered Tiguan, the best and most sensible version for most medic families will be the mild-hybrid 150bhp 1.5litre model.
There is no plug-in facility, but a 48-volt system provides an 18bhp power boost and instant torque when moving off.
There are five trim levels to choose from and my test car was an Elegance model, which has all the important options included and feels a little more up-market.
Although the new Tiguan starts at £34,075, this version costs £39,290.
So, first impressions. The somewhat boxy styling of the previous two versions has been softened and rounded for this Mark 3 itera-
Softer-feel plastics and a larger 12.9-inch infotainment screen help; as does a welcome return to some tactile physical controls instead of everything having to be accessed via the touchscreen.
‘Driver experience switch’
This is the first Volkswagen to offer its new ‘driver experience switch’. This is a central console knob that can select a number of pre-determined audio and ambient lighting settings depending on your mood.
They are called Lounge, Energetic, Joy, Minimal and Me. I am still undecided as to whether these really add to the driving and passenger experience or if they are just, well, a gimmick.
The driving position is good, the front seats are comfortable and rear-seat passengers are treated rather well too. Plenty of headroom and knee room means that a family of five can journey in comfort.
The hatchback opens a boot space that is one of the biggest in this class of car, so the need for a roof-box on family holidays is reduced significantly.
Out on the road, the new Tiguan thankfully drives in a typical
So, the latest Tiguan continues where the previous Mark 2 left off. It is a great all-rounder for any family. It is well made, has a good brand image, is versatile and is reasonable value.
There is still a lot of life left in the internal combustion engine car, particularly using mild-hybrid technology as in this version of the Tiguan. A real-world 40mpg and the absence of any range anxiety is not to be ignored.
Dr Tony Rimmer is a former NHS GP practising in Guildford, Surrey
The boot is one of the biggest in this class of car
CHECK OUT OUR BUSINESS DIRECTORY
Independent Practitioner Today features an online advertising directory to complement our journal and website.
Split into ‘business’ and ‘lifestyle’ directories, they list the services private doctors need to run their practices or spend their well-earned money on.
ADVERTISERS: The deadline for booking adverts in our July-August issue is 28 June
or for reprints, we would be happy to discuss licensing the copyright to you.
Published by The Independent Practitioner Ltd. Independent Practitioner Today is editorially independent.
Material is governed by copyright.
No part of this publication may be reproduced, stored in a retrieval system or transmitted in any form without permission, unless for the purposes of reference and comment. Editorial layout is the copyright of the publishers. If you wish to use it for promotional purposes on websites
WRITE TO Independent Practitioner Today 7 Lindum Terrace, Lincoln LN2 5RP
TELL US YOUR NEWS Robin Stride, editorial director Email: robin@ip-today.co.uk Phone: 07909 997340 @robinstride
ADVERTISE WITH US
To advertise in the digital journal, on our website or in our business directory, contact advertising manager Andrew Schofield at Spot On Media. Phone: 0161 408 3912 Email: andrew@spotonmedia.co.uk Follow Independent Practitioner Today on