The business journal for doctors in private practice
In this issue
Attributes of a good PA
Dawn Shrives provides the answer to the question ’What does a good PA look like?’ P14
Time to beef up IT security
Solicitor Aoife Ryan reports on what private doctors should do to bolster their cyber security to avoid ransomware attacks P18
A guide to bidding for NHS contracts
n See page 41
Brains that work outside the box
The different talents of neurodiverse staff can be an asset to business P21
Drive to boost London
By Robin Stride
A boom in overseas patient numbers is being forecast for private doctors in London under a new initiative to present the city as the ‘go to’ destination for independent healthcare.
Private hospital providers, collaborating on phase one of the project, have attracted support from the Department of Business and Trade and, if successful, then it could be widened to promote other areas of the UK.
One of the team involved told Independent Practitioner Today : ‘What we are intending to do is to put London on the medical tourism map in a much greater way than it ever has been before.
‘So the idea is we bring in a lot more international work into London in markets where we are not currently operating.’
Other past initiatives to increase the international patient footfall in London had proved disappointing. But Elizabeth Boultbee, head of global markets at the London Clinic, added that she was confident in the project’s success.
‘The difference in this is the providers and the chief executives have got together and said “we want to make this happen”. They have provided funding, the initial funding for the project manager.
‘And we haven’t been that protective about our knowledge. We
Elizabeth Boultbee
have been willing to share, we are willing to collaborate, which is what’s making the big difference. It is a new age of collaboration.
‘There are still lots of patients coming to London, but there are a lot more out there in markets that are relatively untapped and none of us have really any big presence in.’
The groundwork for the initiative involves bosses from the Cleveland Clinic, Cromwell Hospital, HCA, King Edward’s VII Hospital, the London Clinic and Phoenix Group, plus private providers in the NHS: Imperial and Chelsea and Westminster. Schoen has also taken part.
London is reckoned to be 15th by revenue in the league table of destinations for overseas patients. The aim is to bring it up to tenth within three years.
Project manager Michael Barker told this journal he believed inde
Our sponsors
What we are intending to do is to put London on the medical tourism map in a much greater way than it ever has been before
pendent practitioners would welcome the results because: ‘It will keep them busy with all sorts of interesting things to do.’
He gave further details of the venture, by what has been named the London International Healthcare Council (LIHC), at LaingBuisson’s Private Healthcare Summit 2023, calling it ‘a super exciting collaborative’ – with a special formula. His outline was well received.
‘The most important ingredient is not just about collaboration but getting Government support,’ he announced.
‘What we’ve been able to do over the last seven months is lobby the Department for Business and Trade. We have got them on side and they are willingly helping us now with a whole range of different connections into our choice markets that we think we want to engage in.
‘They are offering to help us with the marketing as well, creating an offer document…which they
would create around UK healthcare.
‘They have experience of exporting UK talent but very little of importing it in, so there is a good sense of synergy between the Department and providers.’
Mr Barker said the group had set out to be ‘very inclusive’ of providers and had contacted ‘masses’ of those operating in the London market.
Some decided not to join, but those who had were having a longterm strategic look at how they could start getting people around the table to really brand London and get patients coming there for treatment.
By the end of phase one, in September this year, providers are expected to have agreed minimum standards they will abide by. Phase two will see them beginning entering their first or second market of choice.
LIHC will act as an access platform with providers pitching for work from patients. Mr Barker said 97% of the work from international sources in the UK came to London, but the project was not limited to scaling the model up just there.
The group had started with ‘one or two’ markets, which he could not yet declare publicly, and at least three or four others were targeted to follow.
n See page 4 and page 6
TELL US YOUR NEWS. Contact editorial director Robin Stride
ADVERTISE WITH US. To advertise in the digital journal, on our website or in our business and lifestyle directories, contact Andrew Schofield at Spot On Media. Phone: 0161 408 3912
Email: andrew@spotonmedia.co.uk
GET A SUBSCRIPTION DISCOUNT
£90 independent practitioners. £210 organisations. £90 GPs and practice managers (private & NHS).
Save £15 paying by direct debit: individuals £75 (organisations £180).
Some very welcome good news could be on the horizon for independent practitioners practising in London.
The capital is not the magnet it once was for patients from overseas, but that could be about to change.
And if the background work of the recently formed London Inter national Healthcare Council (LIHC) is successful, then private doctors in other cities could later find the model benefits them too. What’s not to like!
As we enter our 16th year of publication at Independent Practitioner Today, we can recall various initiatives to tap the overseas market. None proved as effective in the long term as was hoped.
There was much talk from visionaries urging the private health market here to put more effort into marketing abroad. But it was not uncommon for
those who attended health travel fairs in other lands to find they were the only representatives from the UK.
This time, as reported in our page one story, it could be different. There is a lot of collaboration from leading healthcare providers in London to move the project forward.
They are paying the part-time salary of a manager for the initiative and – in a major coup –have successfully got the Department of Business and Trade involved.
It should be able to help open channels in targeted Middle East, Asian and African countries to help attract medical tourists here rather than around a dozen other markets that are more likely to get the business right now.
We wish LIHC every success and, like doctors who are wanting international patients, look forward to seeing progress.
Make your life simple
Derek Kelly of Medserv outlines the many benefits for doctors of having a total practice management solution for their private work P13
Why doctors seek medico-legal help
In the second of a two-part series, Dr Kathryn Leask reveals more reasons why consultants contact the Medical Defence Union for advice P16
Ensure you don’t fall behind Increased patient footfall benefits private practices, but many doctors face challenges as a result. Simon Brignall discusses what to do to solve them P24
Communicate to defuse gripes
Get armed for your response! Nicola Wheater of Ridouts law firm gives independent practitioners advice about responding to GMC complaints P28
Don’t get anchored down by bias
Dr Benjamin Holdsworth of Cavendish Medical underlines the importance of investors ignoring their biases and having a well-diversified portfolio P36
Ethical minefields of private practice
Dr Sophie Haroon of Medical Protection reflects on some medicolegal learning points from managing cases involving private practice P38
PLUS OUR REGULAR COLUMNS
Business Dilemmas: Non-accidental injury of a child
Dr Kathryn Leask answers a query from a private consultant caught up in a child protection case P44
Accountant’s tips: Why VAT should be on your radar
Alec James of accountants Sandison Easson gives advice on navigating the complexities of Value Added Tax P46
Doctor on the Road: VW bus has got a lot camper
Our motoring correspondent Dr Tony Rimmer is feeling cool and really buzzing after his latest road test P48
Pensions’ contribution levels to change again
Yet another survey to consider the impact of increasing salary thresholds
By Edie Bourne
The salary doctors can earn in their NHS jobs before increasing pension contributions is likely to rise following yet another health service pension consultation.
The latest two-week consultation, which concluded on 17 May, considered raising each of the contribution tier boundaries by around 5%.
This proposal is to cut the chance of members paying larger contributions, simply by increasing pay bands due to statutory raises.
As an example, the top NHS pension contribution rate of 13.5% is now paid by those earning £72,031.
But should the measures in the consultation be taken forward, the new salary band would be £75,633 before that rate applies.
Patrick Convey, technical director with specialist financial planners Cavendish Medical, told Independent Practitioner Today : ‘New contribution percentages were only adopted last October, so if this proposal is approved, it will be yet another change for mem -
bers to understand and plan around.
‘Following the earlier NHS consultation this year, which introduced substantial retirement flexibilities and the subsequent positive Budgetary changes, we may have hoped for a period of stability with regards to pensions.
‘However, it’s largely a positive move for those who may have been forced to increase pension contributions simply for receiving an inflationary pay rise.
‘And with defined-benefit schemes like the NHS, members are
contracted into making contributions – they cannot simply choose to pay less into the scheme because of other financial commitments.’
Mr Convey, talking as consultants were also voting on industrial action because of the significant real-term pay cuts over the last decade, agreed it was ‘a challenging time’ for many.
He said even the good news of the pensions tax lifetime allowance being abolished might not be enough to stem the tide of senior doctors leaving the medical profession.
Boosting ‘right to go private’ is welcomed
Private healthcare providers have welcomed Rishi Sunak’s bid to raise NHS patients’ awareness of their right to opt for independent doctor treatments.
Independent Healthcare Providers Network (IHPN) chief executive David Hare called the Prime Minister’s publicity campaign ‘good news’, while the Royal College of Surgeons of England said it backed short-term use of the private sector.
Mr Sunak’s plans to cut waiting lists would offer patients use of the NHS app to choose from NHS or independent providers.
He said: ‘Currently, just one-inten patients make a choice about where they receive care. We want to change that by helping the NHS to offer patients a real choice while also giving patients the information they need to decide.’
Mr Hare responded: ‘We know many patients want to be given a choice, as it can dramatically reduce their wait for NHS care. But too often patients are unclear that they have the right to choose a healthcare provider to deliver
their NHS care – whether an NHS organisation or an independent sector one – free at the point of use.
‘Delivering new ways for patients to use the NHS App to choose and progress their care is a very exciting development.’
‘It’s great to see this functionality and capability being rolled out. Millions of people downloaded the app during the pandemic, so using this technology will really help modernise how we access healthcare, putting control into
the hands of patients themselves.’
After consulting their GP, patients will be able to view information for up to five healthcare providers in the same region. They can then choose where they go for treatment using the NHS App or website.
Patients Association chief executive Rachel Power said: ‘We hope this announcement will make it easier for patients in England to use their long-established right to choose where they receive their care.
‘Work we’ve done shows patients’ awareness of choice is not high, nor are many offered choice regularly.
‘Earlier this year, our survey of patients’ experience of healthcare found around only one-in-six patients we questioned had been given the opportunity to choose where they had their hospital care.’
Royal College of Surgeons of England president Prof Neil Mortensen said the plan should speed up access to operations and help tackle the backlog.
But he warned the need to increase NHS surgical capacity remained. He said: ‘We support the use of the independent sector in the short term to help tackle the backlog, but it cannot be a permanent fix.
‘We need more operating theatres, as well as nursing and anaesthetic staff to support surgeons. NHS trusts must also ensure that training opportunities are still provided for surgical trainees when operations move to the independent sector.’
Prof Neil Mortensen, president of the Royal College of Surgeons of England
David Hare, chief executive of the Independent Healthcare Providers Network
PRIVATE HEALTHCARE SUMMIT 2023
Health therapies are on the rise
By Robin Stride
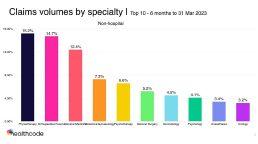
Evidence of the growing use of health therapies in the treatment of private patients has been revealed by IT solutions company Healthcode.
Among the top ten claims by specialty for treatments outside of hospital in the six months to 31 March 2023, three were performed by non-GMC registered practitioners.
The running order was:
Physiotherapy 15.2%;
Orthopaedics/trauma 14.7%;
General medicine 12.4%;
Obstetrics/gynaecology 7.3%,
Psychotherapy 6.6%;
General surgery 5.2%;
Dermatology 4.5%;
Psychology 4.1%;
Anaesthesia 3.4%;
Urology 3.2%.
According to the company’s head of external affairs, Fiona Booth, this illustrates the importance of health therapies, delivered outside a hospital setting, to help with issues like rehabilitation, muscular pain, mental health, diet and so on.
She told private healthcare bosses at LaingBuisson’s Independent Healthcare Summit: ‘Not all these services are available or readily accessible on the NHS, but they can transform the lives of patients – so to what extent do we want to promote this as an additional benefit? That’s a question for you to consider.’
Looking at claims volume originating from hospitals by specialty, it showed orthopaedics and trauma top – as usual – at 62,000 in March 2023, which was 24% higher than the same month in 2022.
Orthopaedic volumes slumped to just 12% of 2019 levels during the first lockdown, but Ms Booth said the specialty had now fully recuperated.
Growing demand for diagnostic procedures in private hospitals was evident with radiology coming second with 44,000 – a year on year rise of 21% – and pathology/haematology fourth with 26,000 – up 4% on the previous year.
Turning point
The former chief executive of the Association of Independent Healthcare Organisations (AIHO) said these figures needed to be seen in the context of a surge in these claims after lockdown restrictions were lifted in the summer of 2020.
‘We need to go right back to August 2020 to find the turning point. That month, there were just over 12,500 pathology/haematology claims, a year-on-year increase of 10%. By December 2020 there were more than 18,000 – a year on year increase of 56% and the num-
bers have continued to head north ever since.’
Other specialties were: physiotherapy 32,000, general surgery 26,000, obstetrics/gynaecology 21,000, oncology 18,000, urology 16,000, gastroenterology 15,000, and cardiology 14,000.
Ms Booth said diagnostic tests and imaging had become more sophisticated and their applications had grown, so Healthcode expected their role to grow.
The NHS was trying to increase its diagnostic capacity because it was struggling to meet the demand. 1.6m patients were waiting for a key diagnostic test at the end of February 2023 – up 94,000 from a year earlier.
She also highlighted a YouGov survey showing the median private healthcare spend in the last year was £500 – ‘which suggests
INVOICING SURGE
Healthcode is anticipating a record year for insured claims
It currently processes over 28,000 invoices a day, representing around £3.5bn.
It is reporting record volumes across the board for the first three months of 2023
In hospitals, it was 860,000 –10% higher than 2022
For non-hospitals –independent practitioners, their practices and clinics – it was 1.45m, up 25% on 2022, giving a total year-on-year rise of 21%
Hospital claims from every English, Scottish and Welsh region are trending above 2022
that patients were largely turning to providers for less expensive services such as diagnostic procedures to put their mind at rest’.
Ms Booth added: ‘Of course, it will be for private sector providers to consider whether they want to increase their own capacity with regard to diagnostic facilities, equipment and human resources.
‘However, it has certainly been interesting to read of late about a number of investments by providers in new outpatient and diagnostic centres.’
Waiting lists for NHS treatment were a ‘push factor’ for many people, prompting them to consider private healthcare. But it was equally important for providers to focus on the positive ‘pull factors’ that would attract patients and make it likely they would recommend the experience to friends and family.
‘Healthcare is about achieving the best outcome for patients, but, of course, private healthcare involves going the extra mile to exceed their expectations in terms of service efficiency, quality and value,’ she said.
Worry that sick doctors will be hit by GMC reform
By Douglas Shepherd
The MDU has renewed its plea for doctors’ fitness-to-practise procedures to continue to recognise health concerns as a special category.
Proposed legislation governing the way the GMC can pursue fitness-to-practise cases against physician associates and anaesthesia associates (PAs and AAs) forms a blueprint for the way doctors are regulated in future.
But the MDU fears current proposals mean the regulatory body’s ability to pursue fitness-to-practise action against a registrant under ‘health concerns’ will be removed.
Dr Michael Devlin, head of professional standards and liaison, said: ‘It is very disappointing that, despite strong support for the status quo from the MDU, medical royal colleges, trade unions and notably the GMC itself, the Government intends to remove the GMC’s ability to pursue fitness-to-practise action against a registrant under a distinct category of health concerns – something it is currently able to do.
‘Health concerns will instead be dealt with under the umbrella of “inability to provide care to a sufficient standard”. No rationale has been provided by the Government in its response to an earlier consul-
tation on why the GMC should lose this valuable fitness-to-practise mechanism.’
A recent MDU member survey found nine-in-ten healthcare professionals said they felt worn-out
Reforms restrict GMC’s options to act
The GMC has welcomed proposed Government legislation for regulating physician and anaesthesia associates (PAs and AAs), but fears some aspects will have ‘unintended consequences’.
Planned reforms will allow it more flexibility to adapt policies and procedures to meet the needs of doctors, patients and healthcare systems, but it says areas such as the grounds for fitness-to-practise action need a rethink.
The associates will in future be GMC-regulated and the reforms are set to be a template for regulating other healthcare professionals, including doctors.
According to the regulator, benefits include a simpler and streamlined regulatory framework, allowing faster resolution of fitness-to-practise cases, and faster and less adversarial processes.
There would also be an end to the ‘five-year rule’: the GMC cannot currently consider complaints about matters over five years old. The rule will not apply to AAs and PAs, and it is expected that, in future, it will not apply to doctors.
But the GMC says it wants some issues sorted before the proposals become law, including a plan to reduce the grounds on which fitness-to-practise action can be taken. There are currently six grounds, but the new law would cut that to just two: inability to provide care to a sufficient standard and misconduct.
The regulator argues that such a change, in particular dropping ‘adverse health’ as one of the grounds, risks unintended consequences, as it would have to look at a person’s current ability to provide care rather than focus on risk.
today’s patients and practitioners’.
‘There are issues to address and it is important the Government gets this right, but overall we welcome the proposals.
‘We are pleased to be another step closer to having a framework for regulating AAs and PAs, which will enhance their professional standing and the contribution they make to health services and patient care.
at the end of a working day and eight-in-ten felt burned-out.
Dr Devlin believes that, with the growing evidence of the health impacts of work pressures on doctors, the proposals should take account of this.
‘We urge the Government to reconsider these plans and to ensure reforms lead to a more compassionate system for those being investigated and, in particular, that health is retained as a standalone ground for impairment of fitness to practise.’
The MDU also asked the Government to prioritise delivering GMC reforms over doctor regulation.
Grilling fears put off expert witnesses
Medical expert witnesses who want to enhance their credibility have been advised about the importance of good preparation when giving evidence.
Lady Justice Simler told an Expert Witness Institute meeting they should also be careful not to step outside the bounds of expertise, nor express an opinion on legal issues.
It argues that such a move would undermine a compassionate approach to managing registrants’ health concerns and the practical effect could mean it having to wait for harm to have occurred before it was able to intervene.
GMC chief executive Charlie Massey said its work was governed by 40-year-old legislation and was ‘wildly misaligned to the needs of
‘The Government must continue to deliver on its commitment to prioritise this work. A more flexible and modern approach to regulation, so we can work “upstream” to prevent harm from occurring, will allow us to devote our energies to the work of highest priority –supporting clinicians to deliver first-class care for patients.’
The GMC’s response to the ‘Regulating anaesthesia associates and physician associates’ consultation is available online.
See ‘Communication key to defusing gripes’, page 28
She emphasised the importance of the expert witness role in legal cases, but highlighted difficulties securing experts across the country in a wide range of specialisms.
‘Renumeration and rates of pay are one factor … but another is fear of criticism from the courts; from counsel during cross examination; and criticism from those that they assess,’ she said.
She hoped greater awareness in the professions from which experts were drawn would attract more women and those from different and diverse backgrounds.
Dr Michael Devlin of the MDU
Charlie Massey
London’s market ‘under pressure’
By Douglas Shepherd
The big issue for private healthcare in London continues to be the fight for market share, according to a leading market commentator.
Ted Townsend said the increasing costs of employing or sharing revenue with consultants, plus staffing constraints, wage pressures and cost inflation, continued to impact the bottom line.
Revenue growth had returned to the market after a long period of drift, even pre-Covid, and with profit margins under pressure ‘it may be there will be some consolidation in the not-too-distant future.’
Mr Townsend, author of justreleased LaingBuisson’s Private Acute Healthcare Central London Market Report (9th edition), saw possible problems ahead for the NHS’s private patient units (PPUs) too.
He added: ‘PPU growth is not guaranteed, with some hospitals vulnerable to the loss of a few consultants or the transfer of specialities to other hospitals, as well as limited capacity – for example, access to ITU beds or theatres – or organisational cultures that are against doing private work.
‘At least some PPU hospitals are starting to operate more commer-
cially outside their hospital facility.’
The report says the Covid pandemic hit PPUs harder than the rest of the independent sector, with embassy patients not returning as quickly as expected, and some of the independent sector growth had likely come at their expense.
With new hospitals, such as Cleveland Clinic London, having come on stream in recent years and increasing the overall inpatient bed capacity by over 10%, competition for patients in this highly competitive market is described as ‘fierce’:
‘This now begs the question: is this the time for the independent sector to shine in London or will the pressures of rising costs hamper the sector’s growth in future years?’
The report looks at the state of the market after the peak of the Covid-19 pandemic, calendar 2021 being the latest period for which complete financial data is available.
‘Eye should be so lucky’ – ophthalmic surgeons open clinic
on former site of Kylie’s record label
Independent eye surgery provider OCL Vision is expanding its London operations with the opening of a new £2m clinic on Kensington High Street.
The clinic is set in the former London headquarters of Universal Music Group, record label to music superstars such as Kylie Minogue, Rihanna and Adele.
It will enable the company’s team of consultant surgeons, nurses and optometrists to treat up to 100 patients a day, matching the capacity of its flagship clinic on New Cavendish Street.
The clinic has two operating theatres, a dedicated laser surgery unit and seven consulting and diagnostic rooms.
Expansion into Kensington comes as OCL Vision, which opened its first clinic in 2018, sees demand for private eye care soar as the NHS wrestles with backlogs in ophthalmic operations such as cataract surgery.
Consultants Mr Ali Mearza, Mr Romesh Angunawela and Mr Mukhtar Bizrah will see laser patients and carry out cataract surgery, refractive lens exchange (RLE) and implantable contact lens surgery (ICL). Ms Sally Ameen will lead on glaucoma treatment, and vitreoretinal specialist Mr Chien Wong will treat retinal detachment and diabetic retinal disease.
The clinic will also house three dedicated optometrists and three technicians.
OCL Vision chief executive Paresh Patel said:
‘This opening represents our largest single investment in the company to date and is key to our growth strategy in the capital and beyond.
‘Our new Kensington clinic is equipped with some of the most sophisticated ophthalmic technology in the world and will be a vital addition to our successful facilities in Marylebone and Hertfordshire.
‘The strong growth that we have achieved since opening our doors four years ago is a testament to the vision, expertise and dedication of our team of over 13 consultant surgeons, as well as our commitment to providing wrap-around, personalised and patient-centred care.
‘We’ll be able to see up to an additional 100 patients a day at our Kensington clinic, doubling our capacity in central London and giving even more patients access to world-class treatment on their doorstep.’
Left to right: Mr Romesh Angunawela, OCL Vision founding partner; Mr Chien Wong, director and retina lead; Ms Susan Sarangapani, consultant ophthalmic surgeon; Mr Ali Mearza, director and founding partner; Mr Allon Barsam, founding partner; Mr Shahram Koshani, consultant ophthalmic surgeon
Ted Townsend, author of the LaingBuisson report
New members of ‘Harley St club’
Doctors in the Harley Street area have some new neighbours with the arrival of three more signings to The Howard de Walden Estate portfolio.
Cognacity, Orri and All Points North (APN) have all taken space in the Harley Street Medical Area (HSMA) as the landlords report occupier demand for prime healthcare space remains competitive.
Cognacity
Cognacity, a global expert in mental health and performance, is moving to larger premises in response to increased demand. It looks after individuals with a wide range of mental health problems, including depression, anxiety, stress, alcohol/drug-related problems and relationship issues, as well as delivering corporate mental health and performance programmes and executive coaching across a range of business and elite sport sectors.
The new clinic will be located at 22 Welbeck Street following ten years already spent on Harley Street. The new spaces configuration allows for 50% more clinical consulting rooms.
Dr Phil Hopley, its consultant psychiatrist and managing director, said: ‘We are delighted to have acquired new premises in the Harley Street Medical Area after ten years at 54 Harley Street.
‘Both our clients and the Cognacity team love the Marylebone area and are looking forward to remaining part of such an active community, developing opportunities to collaborate and network with our neighbours and fellow HSMA members.’
The
Orri Clinic
Orri, recently signed for 80-81 Wimpole Street, is a specialist treatment service for eating disorders, rated ‘Outstanding’ by the Care Quality Commission.
additional locations as well as a state-of-the art APN Connection app to support a lasting commitment to destigmatising mental healthcare and producing longterm results.
Dr Phil Hopley, consultant psychiatrist and managing director of Cognacity
It offers recovery-based, face-toface treatment programmes – both in person and online – following a stepped approach, so that treatment evolves with each individual as they progress in recovery.
Orri is taking a six-storey building, refurbished to offer purposebuilt, trauma-informed therapy spaces for both individual and group work and expects to open next month.
Chief executive and founder Kerrie Jones said: ‘Orri was founded to offer a new choice of outstanding and innovative treatment for eating disorder recovery.
It is for this reason that we were drawn to the Harley Street Medical Area and Howard de Walden for
their long-standing community of pioneering healthcare professionals who hold one another accountable to providing expert care.’
All Points North (APN) APN signed for space at 12 Upper Wimpole Street and opened last month.
A whole-person health company, it offers innovative treatment for the mind, body and soul across the full continuum of care. Its approach includes integrated, custom care plans and emerging, evidence-based treatments for onsite and outpatient services.
Since opening a flagship residence in Edward, Colorado, US, APN has expanded to include
Noah Nordheimer, founder and chief executive of APN, said: ‘When we first opened APN in the US, a large majority of our clients were flying in from the UK and surrounding countries throughout Europe and the Middle East – which demonstrates a need for more accessible mental health resources in that region of the world.
‘Harley Street is a hub for the UK’s behavioural health sector and we are pleased to call London our new home to build the bridge between APN, Europe and the Middle East and start helping a massively underserved market.’
Howard de Walden’s executive property director Julian Best added: ‘Demand for space across our healthcare portfolio remains strong and we currently have only two small suites available with some very exciting new healthcare projects underway and in the pipeline.
‘We remain focused on continuing to meet evolving occupier demand and work to ensure our buildings meet the high-quality standards that the Harley Street Medical Area is renowned for.
‘These latest signings reflect our continued strategic focus on medical and healthcare and, in particular, a response to the greater awareness of mental health to provide access to first-class specialist operators – sadly, a key issue that needs a concerted effort, as up to one-in-four adults are affected by a mental health issue.’
Julian Best, Howard de Walden’s executive property director
The reception area of APN’s new clinic in Upper Wimpole Street
100 up for private care’s trade body
By Olive Carterton
The Independent Healthcare Providers Network (IHPN) is celebrating a significant landmark after welcoming its 100th member.
Now it has its eyes on a new goal – to double the number of independent healthcare companies it represents.
Chief executive David Hare said the organisation was proud to have a more diverse membership than ever before.
These include providers of hospitals, community services, diagnostics, mobile operators, insourcing and primary care.
He said: ‘We have a huge variety of scale of members too – from FTSE-listed, to small specialist companies – all of whom are making a real difference, supporting or delivering high-quality patient care.’
Mr Hare believes one of IHPN’s strengths has been recognising and celebrating the needs and differences of members to provide appropriate support at both a sector-wide and very specific level.
‘I believe we’ve done a good job at adapting and welcoming members and recognising the need for particular support – or where smaller groups of members or interested parties can get benefit from talking together or sharing common goals.
‘I still believe passionately that we are definitely stronger united than divided.’
The IHPN has built up an active and well-established group of ophthalmology service providers, and a newer group for companies focusing on ‘insourcing’ – a different way of providing staffing solutions, supporting the NHS to deliver theatre lists in their own facilities.
Reflecting on members’ efforts and successes, Mr Hare said: ‘The things which stand out the most are the way that we and members have put so much time and effort into improving the sector’s quality and safety.
‘Over 90% of independent hospitals, and 91% of independent community health providers have
IHPN presses the case for private sector to cut waits
The Independent Healthcare Providers Network has expressed ‘huge concern’ at NHS performance figures showing the overall NHS waiting list has grown to a record high.
With 7.3m people now waiting for treatment, its policy and delivery director David Furness warned: ‘There’s a real risk that we get desensitised to the very high numbers we are seeing and forget that behind the figures are real people who are waiting too long for diagnosis and treatment.’
While there had been good progress on reducing the numbers of patients waiting more than 78
weeks, there was still much more to do, including ensuring every person on the waiting list could be seen and treated as quickly as possible.
Mr Furness added: ‘This includes making NHS patients aware of their legal right to choose the best provider for their NHS treatment, including the independent sector.
‘We hope that the Government’s much-needed elective recovery taskforce will focus on ways that more NHS patients can be made aware of their rights, to help them to get the treatment they need as quickly as possible and tackle other systemic issues so that more patients can be seen more quickly.’
“Good” or “Outstanding” overall ratings from the health and care regulator, the Care Quality Commission.
‘There is definitely more to do. But this is a strong indication that the general standards of care and patient safety in the private sector are higher than they have ever been.
‘Additionally, I think the support the sector gave to the NHS during the pandemic is also something we can collectively be hugely proud of.
‘Thousands of independent sector staff worked bravely and heroically alongside their NHS counterparts during a period of national crisis, and the response and co-ordination of a donation of one million items to Ukraine at the start of the war is another highlight.’
The 100th company to join IHPN is EndoCare Diagnostics, an independent provider delivering endoscope services in Manchester.
Jamie Marsh, its head of compliance and resilience, said: ‘As a young
Two medical schools get green light to award degrees
Two new medical schools have been given full approval by the General Medical Council, meaning they can award degrees to graduating students for the first time this year.
They are Anglia Ruskin University’s School of Medicine, in Chelmsford, Essex, and Aston Medical School, part of Aston University in Birmingham.
organisation, we were finding ourselves isolated and disconnected from national conversations and found it difficult to be kept up to date with any latest developments.
‘Since becoming a member, we’ve been very impressed with the service provided by the IHPN. We have received daily update briefings and been invited to a series of meetings both at a local and national footprint. I feel confident now that we have a sufficient support network of over 100 members we can connect into.’
Mr Hare added: ‘The future of the independent health sector looks bright. The sector is wellplaced to continue to grow and to play a leading role in the delivery of healthcare in the UK.
‘The IHPN is committed to supporting the sector’s growth, and to ensuring that the independent sector has a strong voice in the development of healthcare policy. Here’s to the next 100 members.’ See David Hare’s feature on page 34
Their medical graduates will be added to the medical register from this summer.
Dr Sanjiv Ahluwalia, head of the School of Medicine at Anglia Ruskin University, said: ‘One of our main aims is to ensure there are opportunities for people from all backgrounds to study medicine.
‘And we are proud to have a diverse student body that will serve the profession with distinction in the future.’
Prof Helen Cameron, dean of medical education at Aston Medical School, said: ‘Our focus on providing excellent education and support to a diverse range of students, including those from disadvantaged communities, has been at the heart of our mission since the school’s inception.’
David Hare, IHPN chief executive
New Bupa guide aids consultants
A new online guide from Bupa UK Insurance aims to help consultants get the most out of their partnership.
Developed in response to feedback from consultants, it is designed to answer the questions they ask most often.
Consultants told the insurer they wanted to know more about:
Marketing their private practice;
Clinical coding;
How to work effectively together.
The guide explains how consultants can promote themselves to Bupa patients, what patients expect of Bupa and consultants, and the policies and procedures that underpin the way the insurer and consultants work together. It also sets out invoicing options, how procedure codes are set in the
private sector and how to request new ones.
Bupa said the guide would be useful whether consultants were new to private practice or had been treating its customer patients for some time.
Mr Giles Davies, clinical director of breast surgery at the Cromwell
Nuffield takes action on
Nuffield Health’s teams across the UK are helping fight climate change by switching to lower carbon alternatives.
The healthcare charity group’s 37 hospitals across the UK have stopped using anaesthetic gas Desflurane and are using more Sevoflurane which has a much lower carbon footprint.
Dr Sumit Das, consultant paediatric anaesthetist at Nuffield Health Oxford Hospital and Oxford University NHS Foundation Trust, said: ‘Desflurane was originally introduced as an agent that promised a faster wake-up time. Systematic reviews show that patients wake up to three minutes faster with Desflurane compared to Sevoflurane.
‘However, no research paper has demonstrated that Desflurane leads to patients leaving recovery earlier. Given the significant negative impact of Desflurane on the climate, eradicating its use from Nuffield Health’s hospitals is a sig-
Hospital, said: ‘For newly appointed consultants in private practice, navigating Bupa recognition and running an efficient and digitalfirst practice can be daunting.
‘Many consultants do not know where to start. Having a guide to take them through the key steps makes the process much easier.
‘The sections on billing, the open referral network and platinum consultants are open and transparent conversations around the importance of high-quality care for Bupa insured patients.
‘This highlights how Bupa values high-quality care and makes it compelling for all consultants to strive to acquire platinum consultant status, which will enhance and grow their practice.’
Go to: www.bupa.co.uk/consultant-guide
climate change
nificant step towards reaching carbon net zero by 2040.’
Victoria Hadley, head of social impact and sustainability at Nuffield Health, said: ‘Our decision to stop using Desflurane across our hospitals will result in a reduction of just under 1,000 tonnes of carbon over the course of this year.
‘As part of our “Greener Surgery” strategy, we are also working hard to reduce our emissions associated with energy use, waste and single use items.’
Nuffield said it had set targets to reach carbon net zero by 2040, with a shorter-term goal of carbon net zero in its own operations by 2030.
The charity is prioritising the procurement of renewable-produced power and 100% of directly purchased electricity comes from natural renewable sources.
It is also investing in air handling units and upgrading building management systems to increase heating, ventilation and air conditioning energy efficiency across its 114 fitness and well-being centres.
Workers are more open to bosses on mental health
A new survey of 8,000 UK adults has highlighted an increase in mental health transparency in the workplace.
This year, 35% of UK employees said they had called in sick due to poor mental health – but gave another reason.
While this is a significant percentage, it is four percentage points lower than the findings from Nuffield Health’s 2022 report.
Only 29% feel comfortable enough to disclose to their employer if they need time off due to poor mental health.
Mental health prevention lead at Nuffield Health, Lisa Gunn, said: ‘As well as the day-to-day worries that come with our personal and working lives, employees have also had to deal with the impact of a global pandemic and now the ongoing cost-of-living crisis.
‘All these stressors combined can significantly affect the mental health of employees, so it’s more important than ever that businesses find ways to create open, transparent and connected workplace environments.’
She said that, in the past year, 48% said their work had negatively impacted their physical/ mental health, so it was imperative companies were equipped to recognise signs of mental distress, like anxiety, in others.
The research was conducted by Censuswide, among a sample of 8,000 nationally representative respondents across the UK. The data was collected between 17 February and 6 March 2023.
Dr Sumit Das and one of Nuffield Health’s theatres at Barts Hospital
A look back through our journal’s archives of a decade ago reveals that although times change, some issues are not so new
A trawl through the archives: what made the news in 2013
Pension problem due to a pay slip
Private consultants who also had NHS jobs were being urged to double-check their pay slips because they could be in for a five-figure pay-out.
But they were also being warned by financial advisers to seek advice because any salary backpayments could affect their future pensions.
Consultants were seeking salary rebates after discovering they were on the wrong pay threshold of their consultant contract.
Some had already received tens of thousands of pounds in backdated pay after financial experts discovered the problem during routine retirement planning.
Specialist financial planner Cavendish Medical told
Independent Practitioner Today it had uncovered a number of cases while checking the financial details of new clients.
In one case, it found a doctor had been on the wrong pay level for over four years, leading to an arrears payment of nearly £40,000.
The company’s technical director, Patrick Convey, warned: ‘Not only are the consultants affected missing out on their correct salaries, they could also face grave consequences with their pensions if nearing retirement.
‘When the mistake is rectified, the consultant could discover that his or her pension is more than projected, pushing them beyond the new lifetime allowance limit.’
App-solutely in charge
The UK’s first ever practice management app promised to transform independent practitioners’ lives by enabling them to efficiently manage their practices on the move.
ePractice App was developed for iPad and Android tablet computers by online practice management systems specialists Healthcode in response to demand from consultant customers.
The company said it was keen to reflect the changing way independent practitioners were wanting to access its online services.
With a pilot underway, Healthcode announced the app would be available free for existing customers.
A spokesman said: ‘We are
confident this will make life much easier for our customers, many of whom have their own consulting rooms, as well as practising privileges, in several hospitals and spend much of their time on the move between these locations.’
Op goes live on Twitter
A consultant orthopaedic surgeon’s operation was witnessed live by hundreds of people on Twitter after a private hospital decided to educate its followers about a relatively new procedure.
Viewers watched clips of the ‘Visionaire’ knee replacement done by Mr Tim Waters on a patient who was happy to talk about the operation and answer tweeters’ questions at Spire Bushey Hospital, Watford.
Self-pay prices published
The Association of Independent Healthcare Organisations –forerunner of the Independent Healthcare Providers Network –announced it was backing the publication of new pricing information for self-pay procedures on some private hospital websites.
A spokesperson said the approach represented significant progress towards the delivery of meaningful patient choice.
Being a private GP is ‘hard on pay’
As now, disgruntled NHS GPs were also thinking of going private a decade ago – but they were warned it was not a soft option.
A private GP in Harley Street told them at a BMA private practice conference that they could expect a big drop in income if they left the health service.
Dentists can’t use ‘Dr’
Dentists fell foul of the advertising watchdog for marketing themselves as doctors.
The Advertising Standards Authority told them not to use the word ‘Dr’ in their adverts unless they were medically qualified.
Alternatively, they should make clear that the title was being used as ‘a courtesy title’ and the practitioner did not hold a general medical qualification.
TELL US YOUR NEWS
How about making the news today? Independent Practitioner Today is always keen to hear from doctor entrepreneurs willing to share their stories in private practice – and from independent practitioners embarking on the journey.
Contact our editorial director Robin Stride at robin@ip-today. co.uk
Let experts manage the financial aspects of your private practice A service built on a solid foundation of dedicated account management to support you with your medical billing needs. The preferred choice for medical professionals
UK’s leading medical billing company for over 30 years
Trusted partner to more than 1,800 private consultants, groups, clinics and hospitals
Expertise in dedicated account management & 24/7 functionality
Proven track record in delivering outstanding service ensuring reduced bad debts and increased net income
Merger leads to a major private unit
Guy’s and St Thomas’ NHS Foundation Trust has been investing to grow private healthcare services post-merger with Royal Brompton and Harefield Hospitals. PPU expert Philip Housden reports on developments
In 2021, Royal Brompton and Harefield Hospitals’ merger with Guy’s and St Thomas’ NHS Foundation Trust formed one of the largest and strongest healthcare organisations in Europe.
The merger provided a once-ina-generation opportunity to combine leading specialist services and transform private patient care on a national and international stage through both Guy’s and St Thomas’ Private Healthcare and Royal Brompton and Harefield Hospitals Specialist Care.
Post-pandemic demand growth has led to the business investing in its facilities so that private patients can access an increased range of services located in central London.
Guy’s and St Thomas’ managing director of international and specialised services, David Shrimpton, explains: ‘Private patients benefit from the combined expertise provided by hospitals with greater access to our world-leading expert heart and lung care, the latest technology and innovations.’
Guy’s and St Thomas’ Private Healthcare enables private patients to access a unique combination of world-class complex medical services for adults and children.
Complex care specialties include cardiology, respiratory, thoracic and vascular surgery. The trust has the largest adult and children’s renal transplantation programme in Europe, as well as a comprehensive range of services in paediatrics, fertility, gynaecology, maternity, general surgery and medicine.
At St Thomas’ Hospital, private patients can access a range of facilities. Howard Ward is the private
adult inpatient ward, with nine bedrooms with ensuite facilities, with River Thames views opposite the Houses of Parliament, and the Westminster Maternity Suite has been offering private maternity services for over 25 years.
Private outpatient unit
The newly refurbished Westminster Bridge Consulting Rooms, open five days a week, provides a dedicated private outpatient facility of five consulting rooms, a range of specialist diagnostic services and a dedicated nursing team who undertake minor procedures.
At Evelina London Children’s Hospital, as one of only two specialist children’s hospitals in London, significant investment has been made with the opening of Sky Ward, a new cardiac and critical care unit, which offers private cubicles and a modern welcoming environment for children and families, with future plans including a new day surgery unit.
says: ‘we offer same-day appointments as well as a second opinion service so that patients don’t miss out on getting the care and treatment they need. We also have access to some of the most advanced diagnostic equipment and medical devices in the world.’
Harefield Hospital also boasts modern private inpatient and outpatient areas with diagnostic suites. Juniper Ward is the dedicated private inpatient ward, offering 16 modern rooms with en-suite bathrooms.
The Assisted Conception Unit at Guy’s Hospital is known worldwide as an innovator in fertility treatments. It is one of the leading providers of assisted conception techniques in the UK.
Three locations
Royal Brompton and Harefield Hospitals Specialist Care is based across three London locations. Private patients can choose to be treated at the Royal Brompton Hospital in Chelsea, Harefield Hospital in Middlesex or at the Wimpole Street dedicated outpatients and diagnostics facility in the Harley Street Medical Area (HSMA).
The Royal Brompton Consulting Rooms in the heart of Chelsea, provide private patient outpatients from the Old Fire Station, South Parade.
With six modern consulting rooms, the trust has expanded private patient services to include a range of outpatient diagnostic tests across cardiothoracic, cardiology and respiratory specialties, plus ECHO, ECG, phlebotomy and physiotherapy services.
On Royal Brompton Hospital’s private Sir Reginald Wilson Ward, dedicated staff care for cardiothoracic surgery patients, cardiology and respiratory patients in 28 spacious single-occupancy, ensuite rooms.
Additionally, and located at Royal Brompton Hospital, Sydney Street, the trust has also opened a new diagnostic imaging centre to provide easy access to the very latest in imaging technology for private patients all in one building.
General manager Fred Sendaula
‘We can arrange same-day or short-notice appointments with our respiratory and cardiac consultants. Our rapid diagnostics service offers MRI, echocardiography, CT, lung function and non-invasive tests,’ explains Gerri Hamer, general manager for private patients.
Central hub
Based in the Harley Street medical area, the recently expanded 77-79 Wimpole Street facility is Royal Brompton and Harefield Hospitals Specialist Care’s central hub, offering outpatient and diagnostic care for patients with heart and lung conditions.
Increasing demand has led to expansion at Wimpole Street into the neighbouring property. Zohreh Palmer, Wimpole Street general manager, explains: ‘It is significant that we have been able to expand our services to benefit our private patients. In doing so, we will be able to support the continued development of the wider trust, as all income generated through private patient activity is invested in our hospitals and our high-quality healthcare services.’
Private patient income at the new trust jumped to £50.6m in the last annual accounts for 2021-22. This is an increase of 67.5% over the combined £30.2m in the prior year, but still below the record combined £66.8m achieved prepandemic in 2019-20.
The trust is a clear second only to Royal Marsden in private patient earnings in the NHS. Guy’s and St Thomas’ private patient income represents 2.2% of total trust revenues; 11th highest of all trusts, but well below the 34% of Royal Marsden and 14.7% of Moorfields.
Philip Housden is director of Housden Group
Royal Brompton’s outpatients centre at 77 Wimpole Street
COMPUTERISED PRACTICE MANAGEMENT SYSTEMS
Make your life simple
Derek Kelly (below) looks at the benefits of a total practice management solution for your private work
PROVIDING HIGH-QUALITY
patient experiences continues to be the focus for private healthcare providers in 2023.
Managing a medical practice efficiently in today’s fast-paced and demanding healthcare industry is crucial to achieving this goal. As a result, more and more healthcare providers are turning to outsourced practice management systems to optimise operational workflows and enhance overall practice performance.
A robust practice management system offers healthcare providers and their secretaries a comprehensive solution for streamlining administrative tasks, enhancing patient communication, improving billing processes and ensuring regulatory compliance.
Enhanced efficiency and workflow optimisation
One primary advantage of a practice management system is its ability to streamline administrative tasks and optimise workflow processes.
Practice management software improves routine tasks such as appointment scheduling, patient registration and insurance verification, reducing the burden of paperwork on medical staff.
By eliminating manual processes and digitising patient records, these systems improve efficiency, reduce errors and allow medical professionals to spend more time with patients.
A well-implemented practice management system enhances patient experiences and can greatly improve patient satisfaction.
With features like online appointment scheduling, payment links and text reminders, patients can conveniently book appointments, receive notifications and even fill out forms prior to their visit, saving time and reducing waiting-room congestion.
Streamlined communication and collaboration
Practice management systems act as a centralised hub for communication and collaboration within a medical practice.
They allow healthcare providers, administrators and staff members to securely share patient information, exchange messages and collaborate on treatment plans.
Real-time updates and notifications ensure that everyone involved in a patient’s care is on the same page, fostering effective teamwork and co-ordination.
By leveraging these analytics, medical practices can identify areas for improvement, optimise resource allocation and make data-backed decisions to enhance overall practice efficiency.
Enhanced security and compliance
Protecting patient data is a top priority in healthcare, and practice management systems employ robust security measures to safeguard sensitive information and ensure compliance with industry regulations.
With encrypted data storage, role-based access controls and audit logs, software offers a secure environment for managing patient records and maintaining confidentiality.
This not only instils patient trust but also mitigates the risk of data breaches and associated legal consequences.
Integrated billing and revenue management
Integrated billing in a medical practice management system offers numerous benefits that streamline the billing process and boost the efficiency of practices.
Firstly, it eliminates the need for separate systems or manual processes by combining billing functionalities with other essential features, such as appointment scheduling and patient records.
This integration ensures that all relevant information is readily available, reducing errors and saving time. Additionally, integrated billing facilitates accurate and timely claims submission, leading to faster re-imbursement and improved cash flow. It also reduces the likelihood of coding errors and denials.
Moreover, it provides comprehensive reporting and analytics capabilities, allowing healthcare providers to track their billing performance, identify trends and make data-driven decisions to optimise revenue generation.
With integrated billing, medical practices can experience increased productivity, improved financial management and greater patient satisfaction.
Paper versus digital
Using a digital system instead of maintaining records in paper format offers several significant advantages. First and foremost, it improves efficiency by eliminat -
ing the need for manual paperwork and filing systems.
With a digital solution, healthcare providers can easily access patient information, medical histories and treatment plans with just a few clicks, saving time and reducing the risk of lost or misplaced records.
Electronic records are also more secure and confidential than paper files, as they can be protected with access controls. This ensures that sensitive patient data remains protected from unauthorised access or physical damage.
Digital systems can also enable seamless communication and collaboration among healthcare professionals, allowing for quick access to shared patient information and facilitating co-ordinated care.
Practice management system
Acquiring a practice management system is a prudent move that places medical practices in a leading position for providing efficient and patient-centric care. However, investing in such a system does not necessarily have to be a significant operational expense for your practice.
If you talk to us a Medserv, you will see how we can help you implement your new system so you can focus on growing your medical practice and providing high-quality patient care.
Derek Kelly is marketing manager at Medserv
Medserv supports its doctor customers from its HQ in Hayward’s Heath
MANAGING YOUR
The attributes of a good assistant
So you know why you need a personal assistant and now you are asking yourself ‘what should I look for in a PA?’ Dawn Shrives (below) provides the answer to the question ‘What does a good PA look like?’
I HAVE PUT together ten key points of the skills and qualities that we think make a good and successful personal assistant. It is a guide or check list, if you like, before engaging with a PA, so you will know what you need to look for when making that decision.
1 Excellent communication skills
A good PA needs to have strong communication skills. Please bear with me, there is a lot to say about this particular skill, which is why it is one of our ten qualities of a truly great assistant. Your PA will need to be able to interact easily with you and anyone in the practice/business at every level. They must be able to communicate effectively and efficiently with compassion, empathy and a focus on patient/client care. A PA should have awareness of the communication style required in any situation and adapt accordingly.
Knowing that a PA is conscientious and reliable allows you to hand over work and focus on your key tasks, confident in the knowledge that it will be done and done well
ing with unexpected challenges that do, and will, pop up.
4 Resourcefulness
A good PA must be resourceful; it is an instinctive ability that all great PAs need to have.
They must be able to find information and resources and deal with unexpected changes quickly and successfully.
7 Reliability
A good PA is reliable and a reliable PA is worth their weight in gold. Knowing that a PA is conscientious and reliable allows you to hand over work and focus on your key tasks, confident in the knowledge that it will be done and done well.
Diplomacy is ‘the art of dealing with people sensitively and tactfully’, and is a key skill in this category. It is the ability to communicate with people in a way that considers their feelings – and their potential reaction – and being able to find common ground with anyone and everyone. They need to have the ability to solve problems, work well under pressure with calmness and courtesy and be able to clearly pass on information and instructions with confidence.
They should be able to communicate both verbally and in writing, be confident and up to date with technology, and use it efficiently, especially in the world of remote and hybrid working.
2
Strong organisational skills
A good PA needs to be highly organised and will keep on track with important details and tasks. This is a must-have skill for an effective PA, and multitasking will be one of their superpowers. They should be able to juggle multiple tasks and deadlines without getting overwhelmed. They are very much detailed-oriented and will bring order to chaos; being organised and organising others is what they love to do. Fact!
3 Flexibility and adaptability
A good PA must be flexible and adaptable. They should be able to think on their feet and come up with quick and practical solutions when dealing with any last-minute changes.
Knowing and understanding your schedule and work pattern will help enable them to work efficiently and proactively when deal-
The must be able to make the impossible possible by anticipating and taking action using all available resources to hand, while maintaining a calm and positive attitude – like a swan, cool and calm on the surface.
5 Attention to detail
A good PA must and will pay attention to detail. They will care about the quality and presentation of the work they produce, the service they give and the image that is perceived.
A PA should be thorough in their work and double-check everything before sending it out and moving on. Attention to detail goes beyond proof-reading!
Quality is key in everything a PA does, and they will ensure that everything is professional and reflects your practice/business.
6 Initiative
A good PA needs to be able to show initiative, act quickly, confidently and not constantly wait for instructions.
They need to be able to handle tasks independently and proactively and not have to be told what to do for every task. Of course, this is once they have settled into the role; even the most super of all PAs need to know their way around first.
Being proactive and being able to pre-empt your needs is vital for a great PA, known in the trade as ‘supernatural anticipation’.
They need to be receptive to new opportunities to help improve processes and procedures and have the confidence to adopt new ways of working to support you and your objectives for your practice/business.
To help with speed and decisiveness, make sure they have all the information they need beforehand, so they can act quickly without having to wait for you to be available for clarity or permission.
8 Discretion and loyalty
A good PA must show discretion and professionalism at all times. They will know and understand the importance of confidentiality and know that they are privy to all kinds of personal and confidential information and matters.
Discretion is a fundamental must-have skill, coupled with trustworthiness and reliability, and should be demonstrated in all communications at all times.
9 Resilience
A good PA needs to be resilient. Situations change constantly and PAs are often faced with changing and challenging situations, relying on their self-confidence and resilience to bounce back from worst-case scenarios. And saving the best to last……
10
A good sense of humour
A good PA will have a good sense of humour. This, of course, is not a skill, but is probably the greatest asset any PA can have.
There is a lot of pressure for a PA to constantly operate at the highest level of business and so the ability to smile and laugh through the most challenging times, to crack a joke to help shift the focus when tension arises, is priceless, good for the soul and great for your abs!
So, there you have it. Great PAs possess a unique blend of a multitude of skills and talents, allowing them to take on virtually, in every sense of the word, any task that comes their way.
If you can find someone with all these qualities, you are on your way to finding an excellent PA who is practically perfect in every way – a real-life Mary Poppins of the remote/on-site office world.
Dawn Shrives is the director of Business Admin Services. Website: https://ds-bas.co.uk
MEDICO-LEGAL ADVICE
Why doctors seek medico-legal help
In the second of a two-part series, Dr Kathryn Leask (below) reveals more reasons why consultants contact the Medical Defence Union for advice
From our files, the most common reasons for consultants to contact us in relation to police investigations were allegations of inappropriate examination or sexual assault
Prosecution Service or by the patient’s defence team.
It is generally better for each clinician who has been directly involved in the patient’s care to provide a statement about their own role.
However, where a large number of clinical staff have been involved, it may be better for one person to take responsibility for the whole report and this will then often fall to the consultant.
Like other reports, it is important for these to be based on the clinical records, particularly if information can’t be obtained directly from other staff involved.
ADVICE REGARDING the GMC made up 9% of the recent consultant cases examined by the Medical Defence Union.
Regardless of the nature of the complaint or referral, it is always important to let your defence organisation know as soon as the GMC informs you of a concern about your fitness to practise.
It is important to establish the nature of the communication and whether this is a provisional inquiry, an investigation or an invitation to an interim orders tribunal hearing.
Doctors can be referred to the GMC by anyone, including patients, their carers, family or friends, employers, the police or the coroner.
The GMC will also follow up any self-referrals made by the doctor themselves. Where concerns have been raised that could be due to an illness such as drug or alcohol use disorder, the doctor is likely to be invited to attend health assessments.
It is important for careful thought and consideration to be given when responding to any GMC complaint and that the doctor engages in appropriate remediation and learning.
Professional witness
Being a professional witness made up 5% of cases. A professional witness provides a factual account of the care provided to the patient, as opposed to an expert who will be instructed to provide an opinion on a case.
Witness statements could be requested, for example, by the police to support the Crown
You could be asked to attend court to give oral evidence and while you would not need your own legal representative as a witness, contacting your defence organisation allows you to have support throughout the process.
And it ensures the statements you provide are well considered and fulfil the needs of the role.
Disciplinary proceedings
Another five per cent of consultants made contact about disciplinary proceedings.
Your defence organisation can be a source of great support if disciplinary proceedings are issued against you where clinical concerns have been raised about your performance or competence. Doctors find this process particularly stressful and difficult to navigate.
Certain procedures need to be followed and your defence organisation can ensure you are being treated fairly and help you to put your case forward and negotiate the best outcome for you.
Employment worries
Three per cent of consultants who contacted us sought advice about their employment situation.
While employment law advice falls outside our area of expertise, some members do contact us as a first port of call to get general advice and assistance in being signposted to the appropriate organisations who can help them – for example, where contractual issues arise between a doctor and their employer.
GMC witness
Two per cent of consultant cases related to being a GMC witness.
Being a witness in a GMC case, whether you are called by the GMC or by the doctor who is being investigated, should not raise any concerns about your own standing as a doctor. But, of course, it does understandably cause some anxiety.
When acting as a witness, in any forum, it is important to follow GMC guidance, ensuring reasonable steps are taken to check the information in a reference or testimonial is correct and relevant information is not deliberately left out.
It can be reassuring to have a medico-legal expert review testimonials written for GMC investigations.
Crime allegations
Although they are very rare and make up the least common reason for consultants (1%) to contact the MDU, criminal investigations do arise from doctors’ clinical practice. It is essential to have the appropriate support and representation from the outset.
From our files, the most common reasons for consultants to contact us in relation to police investigations were allegations of inappropriate examination or sexual assault.
This is generally related to intimate examinations. In some cases, the examination was one the doctor had not regarded as intimate, but the patient misunderstood the examination process.
These types of cases highlight the need for good communication and consent so patients fully understand why an examination is needed and what it examination entails.
The offer of a chaperone should be made for any intimate examination, in line with the GMC’s guidance.
The MDU has a dedicated team of lawyers who specialise in assisting doctors who face criminal allegations in relation to their clinical practice. They provide expert advice and support, accompanying doctors to interviews-undercaution, liaising with the police, and arranging representation in court.
Dr Kathryn Leask is a medico-legal adviser at the Medical Defence Union (MDU)
It’s time to beef up your IT security
The
high-profile ransomware attack on a major IT provider to the healthcare sector, Advanced, in August 2022 highlights a fast-growing risk to health care organisations – and independent consultants and GPs – and the need for greater focus on cyber security. Aoife Ryan (right) reports
BE WARNED – it is not just the NHS at risk from cyber-attacks.
The attack on IT provider Advanced last year affected a number of systems used by the independent health and care sector, including Carenotes and Crosscare.
And it had a severe impact both financially and in terms of clinical risk as access to medical notes were lost for a significant period of time.
Unfortunately, this attack was not a one-off and the healthcare sector globally appears to be one of the most targeted by cyber criminals.
The sector’s reliance on technology to create, store, manage and transmit sensitive patient data generates particular IT risks that threaten the operational resilience, performance and stability of the organisations that rely on it.
In response, both the US and EU are putting in place enhanced cyber security regulation requirements for businesses, including by requiring boards to take a proactive approach to managing cybersecurity risks rather than waiting to manage cyber incidents when they occur.
As I write, the UK is yet to clarify how it will implement the outcome of its consultation on proposals to improve the UK’s cyber resilience, although it has recently published a cyber security strategy for health and adult social care which sets out a plan to promote cyber resilience across the sector by 2030.
This does reference the wider independent health and care sector as well as the NHS. The Department for Science, Innovation and Technology’s cyber resilience policy defines cyber resilience as ‘the ability for organisations to prepare for, respond to and recover from cyber-attacks and security breaches’.
For health and social care, this means preventing, mitigating and recovering quickly from any cyber incident that may impact on the sector’s ability to provide continued care.
So what can you do?
In the UK, fewer that one-in-five businesses have a formal incident management plan for cyber security incidents, but have rather placed their focus on business con-
Unfortunately, this attack was not a one-off and the healthcare sector globally appears to be one of the most targeted by cyber criminals
tinuity. But surely prevention is better than cure?
It is often a lack of understanding and expertise which result in a business failing to put in place preventative measures, hoping that ‘it will never happen’ and ignoring the risk or relying on the purchase of cyber insurance.
However, the increasing regularity with which businesses are experiencing both phishing attacks and malware is surely evidence of the increasing need for active cyber defence (ACD).
There are a number of key basic elements which a business, including a healthcare business, should always have in place to mitigate cyber risk:
Technological protections
➲ All businesses should take regular back-ups, ideally daily, of their important business critical data to ensure they are recent and can be restored. If you can recover your data quickly, you are less likely to be impacted by a ransomware attack.
You should ensure back-ups are kept separate from your main system so they can’t be accessed if that system is compromised. Cloud storage may be the preferred option in this situation.
➲ An anti-virus software should be installed and, most importantly, kept up to date and measures put in place to ensure staff can only download apps from approved and reputable sources.
Staff access to systems should be controlled by two-factor authentication and staff should be advised that all IT equipment must be kept up to date with manufacturers’ software updates.
➱ continued on page 20
Strict controls should be put in place around the use of memory cards and USBs, as these can be a conduit for malware and viruses. There should always be a firewall in place between your network and external systems.
➲ As new technology is developed, it can be challenging to monitor and replace older technology as it becomes outdated and more vulnerable to cyber-attacks. Businesses need to keep ahead of outdated technology through maintenance and replacement.
➲ Finally, it is worth reviewing your organisation’s contracts with its IT suppliers to see what level of protection they are offering, both in terms of contractual protections such as ‘warranties’ designed to guarantee the cyber security of their products and what they commit to do if a cyber-attack does happen.
It can be difficult for smaller providers to negotiate effectively with large IT providers, but nevertheless these contractual issues are worth exploring.
Operational protections
➲ Training should be provided to staff to allow them to identify and avoid phishing attacks, at all levels of the business, recognising that certain areas are most vulnerable, including front of house and first point of contact.
Ensure staff are trained and signposted on how to deal with unusual requests and can identify what a phishing email may look like and how to report any suspicious activity.
Staff should be told that it is a responsibility of all individuals within the business and not just for the board or line managers.
➲ ‘Board level’ management of and engagement with risk in this area will nonetheless be key.
Bosses will need to ensure that they have meaningful information at a sufficient level of detail to allow them to properly assess the risks to their particular business. They will want to ensure that there is clarity as to exactly who is responsible for particular cyber security provisions and that risks and issues are reported up to them with sufficient regularity.
For example, are processes designed so that cyber risk is inte-
A cyber-attack places a business at risk of not only financial loss but also regulatory enforcement if significant failings are identified
BEWARE PAYING RANSOM DEMANDS
Another factor that businesses should be aware of is the UK authorities’ position on the payment of ransomware demands.
This is an increasingly contentious area and, while not necessarily unlawful, the payment of such demands can create risks and concerns in other areas.
Information Commissioner’s Officer and the National Cyber Security Centre Joint Guidance on ransomware makes clear their view, which, in summary, is that ‘paying ransoms to release locked data does not reduce the risk to individuals, is not an obligation under data protection law and is not considered as a reasonable step to safeguard data’.
There should not, therefore, be an expectation that cyber insurance which includes provision for such payments to be negotiated will necessarily assist in mitigating regulatory risk in this context, thus further reinforcing the maxim that prevention is better than the cure.
grated with business risk and the organisation has a holistic approach to risk management.
Staff need to be trained to identify and report risks and understand the importance of cyber security measures and what they mean for the organisation.
➲ Clear and visible management commitment to the issue will be a valuable tool in ensuring compliance with policies and procedures.
Within the relevant risk assessments, there should be clarity as to the potential motivations behind cyber attacks and likely targets within the organisation. Systems should be kept under review and tested by the IT to ensure defensive measures remain effective.
Because cyber attackers can often access email systems and impersonate senior management, all staff should be aware of procedures and protocols and be primed to identify and report unusual requests or instructions.
Easy reporting
Many organisations now have embedded tools which permit quick and easy reporting of suspicious emails to the IT team on a ‘one-click’ basis.
Staff should be able to report issues without fear of criticism or reprisals and sufficient resource should be allocated to maintain appropriate levels of compliance.
There are a number of obvious benefits to mitigating cyber risk, one of the key elements being to manage regulatory risk.
A cyber-attack places a business at risk of not only financial loss but also regulatory enforcement if significant failings are identified.
The General Data Protection Regulation (GDPR) and UKGDPR place parallel obligations upon businesses to ensure that data is processed securely by means of ‘appropriate technical and organisational measures’ taking into account the current state of available technology’.
There is no mandatory guidance to provide a framework for action, but rather the expectation that the risk will be assessed and appropriate control measures will be put in place to mitigate those risks.
Onus on business
This approach, often described as ‘outcomes-focused regulation’, places the onus upon business to prevent negative outcomes against a constantly shifting threat landscape.
Obvious parallels can be drawn with the analysis set out above, showing that sensible and proportionate measures which manage cyber risk serve equally to manage regulatory risk.
One effective step that can be taken is for organisations to engage with the National Cyber Security Centre’s (NCSC) Cyber Essentials programme, an ‘effective Government-backed scheme’ designed to protect organisations against a range of the most common cyber-attacks.
It gives the added assurance that the measures it recommends are supported by the most up-to-date threat assessment and government-backed intelligence, given the NCSC’s position as part of The Government Communications Headquarters (GCHQ).
In addition to the requirements imposed by GDPR/UKGDPR, a
business should take note, in assessing their regulatory risk, of the regulatory regime under Network Information Security Regulations (NIS).
At present, enforcement action under NIS has been limited. However, significant changes are planned by the UK government to both expand the remit of the legislation and to strengthen the UK’s cyber security provisions.
Increased enforcement These amendments, once in place, are likely to increase the scope and appetite for regulatory enforcement in this space.
Anecdotally, the NCSC has particular concerns around the security provisions of managed service providers, which will be brought within the scope of the revised regulations, and the potential for them to be used as a ‘back door’ into the businesses they provide services to.
Taken together, all of the above risk factors and mitigations will need to be on the radar of healthcare businesses, who should be proactively monitoring the risk environment and ensuring that sufficient resources are committed.
Senior management endorsement of the importance of these issues, cascaded down through the whole organisation, appropriate policies and procedures alongside education and training will be key. A successful risk management programme combined with employee engagement as the front line is the best line of defence.
Aoife Ryan is legal director at Hill Dickinson. Contact her at www.hilldickinson.com/people/aoife-ryan-0
EMPLOYING A NEURODIVERSE WORKFORCE
A brain that works outside the box
Neurodiversity can offer opportunities for different thinking and fresh ideas. To harness this potential, Dr Robin Clark argues we need to raise awareness of the condition and design the workplace so neurodiverse employees can thrive and make the most of their talents
WHERE A PERSON sits on the cognitive spectrum is unique to them. While most people think and act in a way that society perceives as the ‘norm’ (neurotypical), one-in-seven people in the UK are neurodivergent.1
Neurodiversity refers to alternative ways of thinking, behaving and processing information. It includes conditions such as dyslexia, autism, attention deficit hyperactivity disorder (ADHD), dyspraxia, dyscalculia and Tourette’s syndrome, and is sometimes seen as a challenge.
Following the Covid-19 pandemic, there was a lot of change to process in a short amount of time. A common reaction to change is stress, which can worsen anxiety and symptoms of neurodiverse conditions, such as ADHD.
During this time, many people also became aware that their brains were functioning and adapting in different ways to others. The pandemic acted as a ‘diagnostic tool’ for many un diagnosed neurodivergent individuals.
Our analysis of Google search data taken from January to December 2021, shows a 175% increase in searches for ‘neurodiverse meaning’ and 125% growth in people searching on
➱ continued on page 22
Google for ‘types of neurodiversity’. This shows there is a greater need for neurodiversity awareness.
Barriers
Research from The Institute of Leadership and Management 2 identifies some barriers that forward-thinking employers need to address.
Only one-in-four people would be comfortable recruiting and line-managing someone who is neurodivergent.
Barriers can also be found in specific neurodivergent traits too: 69% of diagnosed dyspraxics, 60% of diagnosed autistics and 53% of dyscalculics felt that colleagues behaved in ways that excluded them. In contrast, only 28% of neurotypicals believed this to be true.
Neurodiversity in the workplace
Our Google search data analysis also shows there has been a 120% increase in searches on ‘neurodiversity at work’, a 91% growth in Google searches for ‘ADHD workplace’, and an 86% rise in Google searches for ‘autism workplace’.
It seems that neurodiverse employees are turning to Google for advice and support.
However, with the right support, neurodivergent employees bring unique skills and talents to their role. Examples of skills neurodiverse individuals contribute to the workplace include:
Spotting trends;
Problem solving;
Creativity;
Data analysis;
Attention to detail;
Seeing things from a different perspective.
But many workplaces and working practices are not inclusive of neurodiverse ways of thinking. This can create barriers for neurodiverse employees, and it may lead to discrimination, pressure and underperformance.
As a manager, it is important to get to know each person in your team and understand how traditional workplaces might affect neurodivergent individuals. This will help you to support every employee to perform at their best.
And as a clinician, it is important to understand how these con-
It seems that neurodiverse employees are turning to Google for advice and support. However, with the right support, neurodivergent employees bring unique skills and talents to their role
ditions manifest to help support patients who may be struggling.
Support neurodiverse employees in the workplace
How much an employee’s neurodivergence impacts them at work is different for each individual.
However, as an employer, you can support your employees’ health and well-being by supporting their unique talents and understanding their needs.
1Get to know the individual
Try to get to know more about your team member’s neurodivergence, so you understand how you can best support them.
It’s important to remember that, even though there are some behaviours or characteristics that are common to neurodivergent conditions, these will vary from person to person, so always ask how you can best support each neurodiverse individual.
A personalised plan of action led by the neurodiverse individual can help them to feel supported in the workplace.
2 Provide supportive technology and equipment
Assistive technology and equipment may help some neurodivergent employees to carry out their role.
For example, some people with dyspraxia might experience difficulties with their motor co-ordination, which can make using office equipment like a keyboard, mouse or printer difficult.
Some things you can invest in that might help neurodivergent employees to feel more comfortable at work include:
Speech-to-text, text-to-speech or mind-mapping software;
Dictation tools;
A digital recorder;
A daily planner;
A screen overlay;
Dual-screens.
3
Communicate clearly
Some neurodivergent employees may communicate in different ways to neurotypical people.
For example, people with autism might not find it easy to read facial expressions or interpret your tone of voice and may take what you say literally.
They may not understand things like sarcasm or metaphors or how to filter out less important information.
So try to use direct language and say exactly what you mean. Ask specific questions, structure your instructions, avoid using jargon and allow enough time to process what you are saying.
It might also help to make sure you provide communications materials in a range of formats. For example, clearly documenting training materials and instructions in audio and visual formats may work better for someone with dyslexia than traditional written materials.
4
Assign work tasks appropriately
Try to think about the type of work, tasks and routines that will work best for the individual.
For example, some people with ADHD may find static or repetitive work challenging. So, they might work best in a diverse role, where they can take regular breaks and work flexible hours.
Or if your employee has dyslexia and has trouble with writing or numbers, you could re-assign tasks like spreadsheets and letter writing to other team members. Consider giving them jobs that play to their strengths instead.
Raising awareness and encouraging a greater understanding of neurodiversity in your practice can have benefits for both employees and employer
6
Be understanding
and empathetic
While it is important to be approachable and understanding so that your employees feel they can come and talk to you and ask for help if they need it, do not put any pressure on them to open up if they do not want to.
Make sure you arrange regular one-to-ones in a confidential space so you can check in and see how they are doing and whether you need to make any adjustments to their working practices.
Review these regularly to make sure they are working. But remember to always ask for the individual’s approval before making any adjustments.
It may also help to arrange coaching and mentoring for any personal development point they would like help with, such as timemanagement or organisation.
close their condition at work, as a manager, you can still raise awareness of neurodiversity while maintaining confidentiality. For example, try sharing useful resources and booklets via email or the company intranet.
Having a neurodiversity policy can also help to establish a framework for managers and employees to follow, reducing the risk of discrimination in the workplace.
8 Nurture good mental well-being
Mental health problems such as stress and anxiety are common in neurodivergent people. As a manager, try to remain empathetic and understanding of your neurodivergent employees, who are trying their best to navigate a neurotypical world.
As with all team members, make sure to monitor workload to stop anyone feeling overloaded, stressed or under pressure at work.
5
Consider the physical environment
Traditional workspaces are often designed with the needs of a neurotypical society in mind. But bright lighting, lots of noise and interruptions in a busy office may feel overstimulating for some neurodivergent employees.
Group work in a loud area may make it harder for some people to focus. If your employee finds this challenging, you could try:
Investing in adjustable lighting or desk lamps;
Using partitions and room dividers or providing a larger personal working space;
Providing standing desks;
Including clear instructions next to office equipment;
Allowing individuals to work from home;
Using pens, sticky notes, whiteboards, lockers and boxes to help with memory and organisation
It might also help to have specific quiet zones in your practice that are available for all employees to use when they need. This can help to create a supportive space while preventing neurodivergent individuals from feeling singled out.
If your employee needs support at work, try to remain patient and empathetic towards their feelings, as you would with any other employee.
Ensure the rest of your team have an awareness and understanding of neurodiversity to avoid any discrimination.
However, seek permission from the neurodivergent employee before disclosing any information, as they may prefer to keep this private.
7 Raise awareness of neurodiversity
Encouraging awareness of neurodiversity can help to educate everyone in your practice about the barriers neurodiverse employees face daily at work.
Education can also lead to greater equality and a more inclusive workplace.
Talking openly about neurodiversity and reducing the stigma surrounding it will help ensure neurodivergent employees are treated fairly.
It may also help neurodivergent employees to open up about any challenges they may be facing at work.
If your employee feels comfortable talking about their neurodivergence, they may wish to raise awareness themselves by delivering a coaching session to their colleagues.
But if they do not wish to dis -
Make small adjustments to make their working life easier and look out for their mental well-being. It might also help to hold oneto-ones more regularly, signpost neurodivergent individuals to your organisation’s mental health support services and ensure individuals have enough time to attend any appointments.
Conclusion
Raising awareness and encouraging a greater understanding of neurodiversity in your practice can have benefits for both employees and employer.
Creating an inclusive workplace where neurodiversity is celebrated and accepted can help you to recruit and retain a diverse and talented workforce. It can also help you to better understand and support your neurodivergent patients. Visit our Supporting neurodiversity in the workplace guide for more information: www.bupa. co.uk/~/media/Files/MMS/bins05299.
References
1. Equality, diversity, and inclusion, The University of Edinburgh, 2020
2. Workplace Neurodiversity: The Power Of Difference, The Institute of Leadership and Management, 2020
Dr Robin Clark (right) is medical director for Bupa Global and UK
Ensure you don’t fall
fall behind
Increased patient footfall is bringing big benefits to doctors’ private practices – but many face challenges as a result. Simon Brignall highlights the problems and discusses what you can do
THE RECOVERY from the pandemic has proved to be a boon to the private practice sector.
Many patients are turning to private healthcare due to the pressures on the NHS and much of this increased demand is coming from self-payers.
Older patients, many who had never interacted with the independent sector before, have chosen to dip into their life savings to fund treatments.
They have been more insulated from the recent financial pressures and at the same time have benefited from impressive increases in property prices over recent decades.
There are also greater quality-oflife expectations as bucket-list holidays to Machu Picchu replace trips to the bingo.
At my company, Civica Medical Billing and Collection, we have seen self-pay increase by more than 50% as a percentage of the invoices we have raised since 2019. And some practices has seen more than a 100% increase.
Privately insured patient activity has also remained strong. The combination of the ability to work from home and Government support meant we did not see the redundancies we have seen in previous downturns in sectors whose benefits include private healthcare.
All of this has meant we are seeing record invoicing from our consultants as they easily exceed their 2019 billing levels. This all sounds great so what is the problem?
Managing growth can be challenging and it is often when practice activity increases that problems arise.
Initially, these can be masked because everyone involved is busy just trying to manage patient demand. But it is not long before cracks start to appear.
Often consultants will suspect that, despite their increased work hours, the effort is not materialising in the practice cash flow.
For many, aged and bad debts are steadily increasing and some patients may even be complaining they have not received a bill at all.
Listed below are some of the issues we are seeing – and some solutions.
Medical secretary
The medical secretary is the bedrock of any successful practice, but they can quickly become overwhelmed when a practice sees increased activity.
Many secretaries work for more than one consultant and if they are experiencing the same increases in patient numbers across all the practices they manage, then problems can arise.
➱ continued on page 26
The free and integrated digital prescribing platform for all private prescribers.
CloudRx take care of the dispensing, payment and delivery of medicines direct to your patients, wherever in the country they may be, for more convenient access to their medicines.
TRANSFORMATIONAL
Order prescriptions at the touch of a button to add a whole new level of convenience for your patients.
SIMPLE, CONVENIENT AND SECURE
Simple and fast digital prescribing.
Legal paperless prescriptions, repeat prescriptions and controlled drugs.
Prescriber fees can be charged to the patient if required.
INTEGRATED
Our API enables frictionless integration with healthcare brands & clinical software including Semble, WriteUpp, MidexPRO, eClinic, Pabau and ClinicYou
“We were struggling to keep up with the admin side of the prescriptions, not to mention storage for medication to cope with a huge increase in prescriptions. CloudRx immediately took away the strain. Since our partnership we have grown by more than 200% in size. We could not have achieved this seamless scalablity without them.”
– Dr Louise Newson, Newson Health
Even if they manage to stay on top of the billing, tasks such as reconciliation and chasing are often set to one side and that leads to cash flow and bad debt trouble.
Medical secretaries are expected to wear many hats, including receptionist, personal assistant, sales ledger clerk, insurance guru, credit controller and debt collector.
This can be challenging and not many individuals have the combined skill set required to find the time to complete all these tasks perfectly.
Their tasks can be near impossible task for one person to cope with, especially as the practice expands.
We find that, once the practice reaches a certain size, the secretary is so busy dealing with the patients and the medical side of things that the billing and collection often gets neglected.
Many inquiries we receive are not from consultants but from medical secretaries who are feeling overwhelmed and require assistance. It is important to ensure your medical PA is on top of the increased activity and has all the support needed.
Outsourcing the medical billing and collection side of the practice to experts ensures practice finances are in good order. And there is the added benefit of the secretary enjoying more time to look after all the other elements of running the practice.
This often results in revenue increases as new patient inquiries are handled more efficiently. We ensure we form a strong partnership with the medical secretary, as we understand the differences in our separate roles and how we can effectively work as one team.
It is also good practice to split the medical and business side of things. The secretary’s conversations with patients are then focused on clinical needs and if the secretary leaves, then their replacement will be less stressful with minimal impact to the practice finances.
Invoicing delays
Raising prompt invoices is obviously important. But in very busy practices it is not uncommon for them to fall behind by weeks and even months.
That reflects badly on the practice, can negatively impact the patients’ view of their treatment and also means the cash flow suffers. The longer the delay in raising an invoice, the greater the risk it results in a bad debt.
Some medical insurance companies now have strict time limits, typically six months, in which they need to receive an invoice; otherwise they will not pay. Effectively, you could end up treating these patients for free.
Invoice promptly and you will also be aware of any issues and be able to improve your chances of satisfactory resolution.
To ensure good cash flow and minimise bad debts, as a good rule of thumb, the practice should set the goal of billing within 24 hours of any treatment.
Control your debt
The most common complaint I hear from practices who, even if they are on top of the billing, is around the reconciliation and chasing of outstanding payments.
This is often due to a mixture of shortfalls/excesses from insured patients, delays in payments from insurance companies and outstanding self-pay invoices.
Many practices reach out to us for this reason, often citing that the growth in demand has exacerbated this problem. We regularly speak to practices who have 20% or 30% of their annual income outstanding for this very reason, many with bad debt levels of 5% or more.
Practices often fall behind with the reconciliation process or have not reconciled remittances correctly.
Consultants regularly complain they do not have visibility on the practice finances, making them unsure about the true picture of their outstanding debt.
Lack of transparency at this key stage means it is impossible to have an effective chase process. Our clients, however, have access to up-to-date accurate data via a reporting dashboard.
Reconciliation
It is important that all payments received must be reconciled in a timely fashion. This includes selfpay patients who may be paying by card, bank transfer or cheque.
For insured patients, each insurer sends a remittance to the practice when it makes payment. In busy practices, this can be challenging because it is common for a remittance to be mislaid or not received.
So the invoices remain outstanding unless the practice is chasing the insurer or regularly reconciling their bank account.
That can lead to further problems from a shortfall being identified, which requires an invoice to the patient. Invoicing months after the event is never a good thing, as it can lead to complaints from unhappy patients and make them more reluctant to pay.
Chasing invoices
For a robust chase process to be effective, it must be clearly defined and routinely applied. There needs to be clear understanding who is responsible for this role so they are accountable.
Once it has begun, it needs following up or the patient may think you are not being serious
Many inquiries we receive are not from consultants but from medical secretaries who are feeling overwhelmed and require assistance. It is important to ensure your medical PA is on top of the increased activity and has all the support needed
and feel they have permission to withhold payment.
Chasing should allow for a mixture of communication methods to contact the patient as well as the sending of formal letters. All this need recording with a log of any action taken.
I’m pleased to say our robust reconciliation and chasing process ensures we have a bad debt rate of as low as 0.3% to 0.5%.
Simon Brignall (below) is director of business development at Civica Medical Billing and Collection
mPrescribe® app allows you to prescribe flexibly without a laptop, for delivery to your patients nationwide
Download the app and register online www.pharmacierge.com/register
Secretary Supported
GP and Consultant Reviews
Administrator access reduces workload for practitioners. mPrescribe® facilitates patient entry, status monitoring and preparation of prescriptions for mobile authorisation.
Clinical Governance
Co-founded and co-owned by leading private clinicians, our secure and encrypted technology is compliant with all GPhC, GDPR and e-Prescribing regulations.
“Wonderful, seamless, easy to use service.” Dr Catrin Bevan, London General Practice
“Intuitive and secure.” Dr Tim Wigmore, Consultant Anaesthetist and Intensivist
“Delivered the same day.... Outstanding!” Dr Elisa Astorri, Academic Physician Rheumatologist
“Go the extra mile.” Dr John O’Donohue, Consultant Gastroenterologist
“Consistent, efficient , friendly and responsive.” Dr Tim Ladbrooke, Courtfield Private Practice
Nicola Wheater gives independent practitioners advice about responding to GMC complaints
AS ALL doctors are aware, receiving a letter from the GMC can be a daunting experience.
But getting one confirming that a complaint has been raised against you by a patient and the regulator is now investigating it can be frightening.
While some doctors decide to bury their head in the sand and pretend nothing has changed, others are actively – and correctly – contacting their medical indemnifier to ascertain whether they can obtain assistance or are seeking independent legal advice at the first available opportunity.
You may ask why you should seek advice at such an early stage. The earlier a doctor does so, the
earlier he or she can start preparing their case and begin receiving legal advice specific to them.
All patient complaints should be treated seriously, especially those subject to GMC consideration, where there can be potential adverse repercussions for a doctor’s practice.
Failure to communicate
Even though patient complaints subject to GMC investigation may differ in complexity and severity, a common theme running through them is often a failure to effectively communicate with patients.
This not only impacts doctors but all allied healthcare professionals working at the coalface
and providing care to vulnerable patients.
While communication skills are a fundamental bedrock of being a doctor, each practitioner’s communication style is unique. Each patient’s perception of that doctor, and reaction to them and what they say, is ultimately subjective.
Thus, a direct, no-nonsensespeaking doctor who responds to a patient’s concerns may be regarded as showing a lack of compassion by the patient, while a doctor who continues to listen to a patient’s worries but repeats earlier advice given, may be perceived as dismissive of the patient’s concerns.
Other common examples of communication failures we have seen include a doctor allegedly being brusque with patients and a failure to obtain full consent before proceeding to examine a patient.
With the assistance of legal advice, they were able to effectively respond to the Rule 7 Letter
– see further detail below – and the case examiners determined that no further action was required.
As a direct result of all or any of the above, alongside any other potential failings alleged, the patient then submits a written complaint to the GMC, which is subsequently reviewed against the council’s threshold and accepted for investigation – where the threshold is met.
Good Medical Practice
Domain 3 of the GMC’s Good Medical Practice ( GMP ) covers ‘Communication, partnership and teamwork’ and specifically states in subsections 31-34 that doctors must:
Listen to patients, take account of their views and respond honestly to their questions;
Give patients the information they want or need to know in a way they can understand;
Be considerate to those close to the patient and be sensitive and responsive in giving them information and support;
Be readily accessible, when on duty, to patients and colleagues seeking information, advice or support.
Doctors must also ‘establish and maintain partnerships with patients’, and subsections 46-49 of GMP stipulates that this includes:
l Being polite and considerate;
l Treating patients as individuals and respecting their dignity and privacy;
l Treating patients fairly and with respect whatever their life choices and beliefs;
l Working in partnership with patients, sharing with them the information they will need to make decisions about their care, including their diagnosis and prognosis, the roles and responsibilities of the care team, how information is shared within that team and other relevant information should a patient be involved in teaching or research.
It is often the presence of communication allegations –among other clinical allegations – that result in a complaint being referred to a fitness-to-practise hearing
to make further inquiries or the imposition of a warning or undertakings as and where relevant.
Rule 7 response
At Ridouts, we have frequently seen communication allegations raised against healthcare professionals, including doctors, and find it is often the presence of communication allegations – among other clinical allegations – that result in a complaint being referred to an FTP hearing.
This is because case examiners, after the Rule 7 letter has been issued and responded to by the doctor, are unable to determine disputes of fact without supporting corroborative documentation.
Therefore, the only recourse available to them is to refer the complaint to an FTP hearing for full ventilation of the evidence.
Rule 7
Rule 7 of the GMC (Fitness to Practise) Rules Order of Council 2004 stipulates that the regulator will write to a doctor notifying them of allegations raising concern regarding their fitness to practise (FTP) and requesting written representations within 28 days from the date of the letter.
The GMC will also provide the doctor with a copy of the documents its relies on – for example, the patient complaint and supporting documents – and this is known as a ‘Rule 7 Letter’.
Case examiners
As doctors know, the case examiners are the gatekeepers of FTP complaints and their task is to determine how a complaint should be disposed of.
In doing so, they apply the following test, known as the ‘realistic prospect’ test, to complaints:
1) Is there a realistic prospect of the facts being found proven at an FTP hearing?
2) Is there a realistic prospect of impairment being found at an FTP hearing justifying action being taken by an FTP panel?
Where the case examiners response is affirmative to both, the case will be referred to an FTP hearing.
Where the response is in the negative, the case examiners will choose an alternative option. This can include taking no further action, adjournment of the matter
By doing this, the doctor is able to put forward submissions to case examiners, via their legal representative, that argue although there is a likelihood of the facts being found proven at an FTP hearing, current impairment is unlikely to be found and so an FTP referral hearing should not be made.
Support available
FTP investigations are naturally stressful for a doctor, but instructing an independent legal representative, or relying on a medical indemnifier, can provide the required level of support and reassurance as well as the necessary legal advice.
Therefore, where communication failings are alleged within the Rule 7 letter and are strongly refuted by the doctor, we have recommended our clients to provide an account to the case examiners setting out their version of events.
These have referenced and enclosed witness statements from any colleague who has overheard what was actually said.
This has provided the corroborative evidence required for the case examiners to close the case with no further action.
Further documentation that can assist the case examiners at this stage, and prevent them leaning in favor of referral to an FTP hearing, can include:
References from colleagues regarding communication style;
Testimonials from patients, where appropriate, and evidence of targeted communication and continuing professional development (CPD) undertaken.
Admission by doctor
There may be instances where a doctor admits their communication was sub-par.
Then we would recommend doctors submit evidence of remediation to the case examiners demonstrating this is not their usual practice, they have the necessary insight into their past failing/error and they have already remediated their communication technique and enclosed verifiable CPD to this effect.
However, not all doctors have access to support, so the GMC therefore set up the Doctor Support Service : phone 020 7383 6707 or email doctorsupportservice@bma.org.uk.
It is completely independent of the GMC and offers complimentary emotional and confidential support to doctors currently under an FTP investigation.
It can also provide a supporter to accompany a doctor to their FTP hearing for up to two days to provide them with the necessary emotional support.
Good communication skills are a fundamental part of being a doctor and conducting regular communication CPD, among other soft skills, will always stand a doctor in good stead, prove invaluable at any stage of an FTP investigation and improve day-to-day communication with patients.
Nicola Wheater (below) is a solicitor at Ridouts Professional Services Limited, a specialist law firm acting for health and social care providers, offering legal, operational and strategic on matters that could negatively impact their businesses
Inquisition by the GMC
Radical reform to GMC investigations are being urged following new research revealing significant numbers of private doctors are experiencing thoughts of suicide or quitting medicine due to their investigation.
As Independent Practitioner Today reported last month, three-in-four of 56 independent practitioners who took part said the process had a detrimental impact on their mental health, with 95% citing stress and anxiety.
A quarter considered leaving medicine, while a third reported experiencing suicidal thoughts during inquiries.
The figures were released by defence body Medical Protection Society (MPS) after it surveyed 197 doctors investigated by the regulator in the last five years. Of those, 56 were private practitioners: private only and private with some NHS.
Here is what they said (private practitioner results only).
1
Do you believe that the GMC investigation impacted on any of the following? (select all that apply)
2
Do you believe there was a detrimental impact on your mental health as a result of the investigation?
4
3 Which of the following did you seek help or support from to help with your mental health concerns?
all that apply)
Concern about what family/friends may think
Concern about what patients may think
Concern about what my employer may think
Concern about career implications
Attending meetings with or dealing with communications from MPS
Having to deal with communications from the GMC
Don’t know
5 Did you at any time during the investigation experience suicidal thoughts?
Yes
Don’t know
6 What, if anything, could the GMC have done differently to make the process less stressful? (select all that apply)
More frequent updates on how the investigation is progressing 29%
Less legalistic language in communications –27% Improvements in tone of communications
The process being completed more quickly
The process being less legalistic/adversarial –
What doctors said
‘I I did feel my life was not worth living after how much I had dedicated to being a doctor. To now have it all called in question and jeopardised was devastating.’
7 Who do you believe should offer more support when facing an investigation? (select all that apply)
8 How did the overall experience affect your future career plans? It made no impact on my career plans and I remained positive about the future
I learned from the experience and looked forward to continuing my career
‘Occasional thoughts that if I was no longer here, this would all go away.’
‘I was on antidepressants, but suicidal thoughts were impossible to keep out.’
‘From the first notification by the GMC of an investigation till after the tribunal, I had regular suicidal thoughts.’
‘Despite three years’ psychotherapy, I feel permanently damaged and half the person I once was: my confidence is gone, I am afraid of my own shadow.’
‘The only effect of the GMC investigation was to make me re-evaluate my relationship with medicine as a whole. I previously lived to work, but now I look forward to the time I leave the profession and can request voluntary erasure.’
‘Every day greeted me with a wave of despair. Every email ping made me jump.’
‘I contacted the GMC after the result of the
investigation happened. It said I had nothing to answer to – after about 18 months. They said that support was no longer covered. This actually was the time I needed support most, as I was so angry with what had happened.’
‘Even in the end, the tone of the outcome stated something along the lines of not enough evidence rather than innocent. It remains a feeling of “We are waiting to get you next time”.’
‘There is very little communication from GMC until the end of the investigation and, even then, there is no offer of support or understanding that their process may be quite detrimental to the well-being of the doctor.’
‘It took a lot of counselling to come to terms with this, even though no fault was found. The language in their comms is abysmal: “We didn’t get you this time, but we are watching you”.’
‘The letter made me feel guilty and that I was not good enough to be a doctor even before I had been listened to or investigated. Wish the process was more open-minded in its approach rather than starting with the premise that you are not fit to practise.’
‘In my case, the investigation was entirely unjustified – there was no wrongdoing or risk to patients and the complaint was very clearly malicious. Better triage of trivial, vexatious or malicious complaints would be an easy improvement for the GMC.’
‘What reassurance can I get that I will not be put through this nightmare repeatedly every time someone decides to consult Dr Google and disagree with my clinical judgements made in best interests?’
‘The GMC is, at present, acting as a wellmeaning but poorly informed vehicle for disappointed patients to vent their anger on a medical expert, since the complaint alone causes real damage even when groundless.’
‘The complaint against me was bizarre but was taken as gospel by the GMC. My career of
20 years and thousands of patient encounters felt reduced to, and threatened by, intense scrutiny of every second of a five- to ten-minute encounter.’
‘I have never been part of a more one-sided and biased process. It made me very keen to leave the profession and I now can’t wait to retire.’
‘I felt that the hearing was very adversarial. I felt like I was in a court of law being crossexamined by a barrister. I was tearful, remorseful and frightened.’
‘I cannot imagine how a doctor who is not legally represented would manage with such a difficult and aggressive process.’
‘Zero thought/consideration for the accused who, in the eyes of the GMC, are assumed
legally guilty until such time as they can legally extricate themselves. I’ve left medicine.’
‘Often I got no updates. One of the major blows was when I contacted the GMC, months after the preliminary inquiry started and expecting it would be concluded soon, only to be told that essentially nothing of substance had been done.’
‘I felt that I had no idea what was going on at points. My investigation ultimately took over one year before being closed. I would regard it as one of the most stressful years of my life. The tone of the investigation and the lack of human approach was notable.’
‘The case was closed without any action after two years, which I felt was far too long to investigate what emerged as a straightforward investigation.’
What needs to happen now
MPS recommends:
TONE OF COMMUNICATIONS
‘While the GMC has worked to improve the tone of its communications in recent years, this should be reviewed on an ongoing basis to make continual improvements.
‘The GMC should explain in the initial communication that it is required by law to review all complaints and allegations that a doctor’s fitness to practise may be impaired. This would offer some reassurance that the GMC is fulfilling its legal obligation, and not starting from a position that the doctor’s fitness to practise is impaired.
‘The GMC should review its communication with doctors when a case is closed with no action, to help doctors obtain closure. Members have reported that the GMC’s language can imply that they will always be looking over a doctor’s shoulder. After a long and stressful process, this can have a significant impact on mental well-being.
‘When the GMC closes a case with no action, they should provide guidance and reassurance to doctors regarding what circumstances a doctor would be expected to cite the investigation when completing an employment form’.
VEXATIOUS/MALICIOUS COMPLAINTS
‘The GMC should explore options to discourage complaints that clearly do not require regulatory action, including better communication to the public and profession on the threshold for a complaint.
‘In its initial communication with doctors, the GMC should include information, or a link to its policy for dealing with vexatious complaints.
‘The GMC should acknowledge any stress caused to doctors as a result of an investigation which is subsequently found to be based on a vexatious or spurious complaint and, where appropriate, offer an apology for the stress caused – reflecting its own guidance to doctors on duty of candour and an apology not being an admission of liability.’
PROCESS TOO ADVERSARIAL
‘The DHSC and the GMC should consider the role of mediation for some cases as part of the long overdue amendments to the Medical Act aimed at making the system of professional regulation less adversarial.’
INITIAL NOTIFICATION
‘While the GMC has worked to make improvements regarding the initial notification – including recently introducing an initial phone call following a pilot – this must be reviewed on an ongoing basis to make continual improvements.
‘The GMC should continue to take steps to ensure initial notifications do not land on a Friday when the doctor has more limited access to professional and well-being support.
‘The GMC should notify a doctor of the
outcome of an investigation a few days before their employer is notified.’
LENGTH OF PROCESS AND LACK OF UPDATES
‘The GMC should keep doctors fully informed when there are delays, to reduce the stress around time-frames and lack of communication.
‘The GMC should ensure investigators dealing with complaints at an early stage are suitably experienced in order to be able to close those cases not requiring further action swiftly.
‘The DHSC should prioritise legislation to amend the Medical Act ,which would enable the GMC to process complaints, and close those cases requiring no further action, more quickly.’
WELL-BEING SUPPORT
‘The GMC should ensure all communication and material for doctors facing a fitness-to-practise investigation includes details of how they can access mental wellbeing support that is available 24/7, not just Monday-Friday 9am–5pm.
‘MPS offers counselling to any members experiencing work-related stress or stress that they feel could impact their practice. However, there are registrants who may not have an medical defence organisation, so accessibility and awareness of the GMC support service is vital.’
Howzat for a milestone
As the Independent Healthcare Providers Network celebrates its 100th member joining, chief executive David Hare reflects on the growth and maturity of the independent healthcare sector in the UK which this membership organisation represents – its key moments, successes and challenges
David Hare, chief executive
Seema Kennedy, chairwoman
I REALISE THAT 100 is perhaps an arbitrary number to many, but as a lifelong cricket fan and batsman, there is a certain significance to reaching the magical three figures.
So, I hope readers will forgive me the indulgence of taking a moment to raise our bat and reflect on the organisation’s history, journey and, by extension, the wider successes and achievements of the independent health sector.
The Independent Healthcare Providers Network (IHPN) came into being in 2020 in its current guise as a stand-alone legal entity, but for two years prior to that we existed as IHPN, but within the NHS Confederation.
We were previously part of the NHS Partners Network, and those who’ve been around will probably also remember the Association of Independent Healthcare Organisations (AIHO) which closed at around that time.
In the run-up to 2020, we made the decision that it was best to
forge our own path independently – a situation which was further galvanised at the end of 2020 when we announced our first independent chairman, Lord Kamlesh Patel.
Kamlesh made a fantastic contribution to the organisation and the sector, and it was with sadness that we heard his decision to step down. But we’re delighted to have welcomed our first female chair, Seema Kennedy, and I am confident she will take us to even greater heights.
Today we have a team of 14, so we feel very much that we’re still a lean and agile set-up, and I have to say I’m indebted to them for their hard work. Kamlesh said as he stepped down that we ‘punch well above our weight’.
I would agree and my thanks are due to colleagues past and present who’ve got us to where we are. I’d also pay tribute to our members, whom it is a pleasure to represent.
In broad terms, the organisation has played a key role in advocating
for the interests of the independent sector and has been successful in securing a number of policy changes that have benefited independent providers.
A changing marketplace
In many ways, IHPN’s developments mirror those of the independent health sector itself. The sector has grown rapidly and now accounts for over 10% of all NHS bed days.
There were almost 2.25m acute patient journeys in 2022 and 3.5m scans and tests done by independent providers in the last year. Independent providers have also been successful in expanding into new markets, such as mental health, social care and community health – on the latter, 42% of NHS providers are from the independent sector.
We’ve also seen that diversification in our members – who now employ or contract more than 150,000 staff. We are very proud today to have a more diverse membership than ever before – whether that’s hospitals, community services, diagnostics, primary care, insourcing and mobile operators – the list goes on.
One of our strengths has been in adapting and welcoming members and recognising the need for particular support. Smaller groups of members, or interested parties, can get benefit from talking together or sharing common goals.
I still believe passionately in this and feel strongly that we are definitely more powerful united than divided.
Challenges and achievements
Nowhere has this power of collective working been more evident than in progressing vital work on quality and safety.
Everyone working in the sector will know that the Paterson scandal marked an important moment for everyone. It was, and still is, a
reminder of the need for constant vigilance, for robust governance and for us all to be uncompromising in the pursuit of excellence.
This means genuine engagement, sharing knowledge and best practice and recognising that this is not an area where collaboration, not competition is the best approach.
And it’s working. We were able to acknowledge another important milestone recently – over 90% of independent hospitals have ‘Good’ or ‘Outstanding’ overall ratings from the health and care regulator, the Care Quality Commission.
That’s up from 70% in 2018. This is a strong indication that the general standards of care and patient safety in the private sector are higher than they have ever been.
Another collective achievement I think we can take great pride in is how we supported the NHS during the pandemic. Independent hospitals played a key role in ensuring the continuation of vital NHS care during the pandemic with the delivery of over 3.3m NHS patient treatments.
One of our strengths has been in adapting and welcoming members and recognising the need for particular support. Smaller groups of members can get benefit from talking together or sharing common goals
hope will finally have reported by the time you read this – that we have come a long way.
The entire notion of a taskforce, set up directly by the Prime Minister, with the explicit purpose of finding ways to maximise the contribution of the independent sector in tackling NHS backlogs, would have seemed utterly fanciful not that long ago.
you hang around for long enough… However, this isn’t a time to be complacent. The current fair winds and following seas may be fleeting, but there are certainly opportunities to make lasting changes for the benefit of the sector and, most importantly, for patients.
Seeking feedback
Thousands of independent sector staff worked bravely and heroically alongside their NHS counterparts during a period of national crisis.
What was achieved collectively under the national contract undoubtedly saved lives and helped contain the post-pandemic backlog which the NHS and independent sectors are now working together to bring down.
Recovery progress
I reflected with colleagues recently following a meeting of the Government’s elective recovery taskforce – which I very much
Similarly, when I think about the polarised, shrill and often hysterical debate which usually surrounds private healthcare – it may just be a rose-tinted spectacle view – but I do detect a more positive, nuanced and pragmatic tone of debate than I have heard for some years about the future of healthcare and about the positive role of independent and private healthcare.
I had somewhat of an ‘Alice through the looking glass’ moment when I heard the reaction from Labour, effectively asking the Government ‘what took you so long?’ in respect of the taskforce, pointing back to Labour policies of the early 2000s to embrace the independent sector. I suppose if
Every year we ask our members for their considered, constructive views on how we’re doing, and it’s a matter of great pride that our members tell us really positive things about our impact, our support, our responsiveness and how we work on their behalf. That vote of confidence is great to hear.
The future of the independent health sector looks bright. The sector is well-placed to continue to grow and to play a leading role in the delivery of healthcare in the UK.
IHPN is committed to supporting the sector’s growth and to ensuring that the independent sector has a strong voice in the development of healthcare policy. Here’s to the next 100 members.
Annual Allowance Tax
Don’t get anchored
What biases do investors face when assessing their portfolio returns? Dr Benjamin Holdsworth underlines the importance of a well-diversified portfolio
BY AND LARGE , behavioural science suggests that human beings make lousy investors.
While we are excellent problem solvers, we suffer from a whole host of well documented biases that, on average, erode the investment returns on offer from markets.
Being aware of our biases is a useful exercise if we are to limit the impact that they have on our decision-making.
These biases are well known in investing and have specific names. For example, we should consider the issue of ‘anchoring’ – the tendency to be influenced by a particular reference point or ‘anchor’.
Overemphasising importance
There is also ‘recency bias’ which is overemphasising the importance of more recent experiences relative to older ones. Today’s capital markets are
anchored down by bias
While human beings are excellent problem solvers, we suffer from a whole host of well documented biases that, on average, erode the investment returns on offer from markets
extremely well integrated, costs are low and anyone with internet access can use the power of Google – or even perhaps ChatGPT? – to conduct their own research. However, historically investors have favoured companies listed in their home country as opposed to those abroad.
Partially, this was down to the additional cost, complexity and unfamiliarity of investing overseas, although these hurdles are relatively negligible nowadays. Even so, recent data tell us that ‘home bias’ – the extent to which the home country is weighted in a portfolio over and above its market weight – persists.
Perhaps anchoring to the performance of one’s domestic market is to be expected given the above.
Performed dismally
For UK investors, the FTSE 100 measures the performance of the largest 100 firms listed in the UK and is frequently quoted in newspapers and media outlets. For some time, the UK has performed dismally when compared to international (ex-UK) developed markets.
For example, the decade of the 2010s saw the FTSE 100 companies return 75% to investors while international equity markets delivered a staggering 255% in GBP terms.
Since the start of 2021, the roles have reversed with the FTSE 100 delivering 31% versus 16% from international markets. Recency bias is often witnessed in sports fans – perhaps betting on a team on a winning streak even though recent success might not indicate future play.
Similarly, if we look at shorter and longer period returns of the FTSE 100 and global developed equities, we can see how recency bias might work.
Recent data tell us that ‘home bias’ – the extent to which the home country is weighted in a portfolio over and above its market weight – persists
of almost not having any in terms of technology (1% vs 21% globally).
➲ This explains much of the recent performance differential above, where technology has struggled, energy stocks have flourished in the high-inflation environment, exacerbated by the Russian invasion of Ukraine.
➲ Over longer periods, technology stocks have dominated – Apple, Microsoft, Tesla and so on.
Over a 12-month period, the annual return might show that the UK has generally lagged global figures even when it has enjoyed a handful of periods of outperformance.
Yet if we look at ten-year timeframes, the viewpoint might be the opposite.
Getting swayed by recent performance, and perhaps anchoring to one’s domestic market, is best avoided.
Little sense
If we think more about risk rather than performance for a moment, there are also some very sensible reasons why having too many eggs in the 100 largest UK companies makes little sense from an investment portfolio perspective:
This is because:
➲ The FTSE 100 is highly concentrated with over 33% of the assets held in just the top ten companies – the likes of Shell, HSBC and AstraZeneca.
➲ The FTSE 100 is ‘overweight’ – holds more than the benchmark –to certain sectors such as energy (12% vs 5% globally) and underweight – holds less than the benchmark – to the point
➲ You have the potential to own shares in more than 10,000 companies across more than 50 countries. Diversifying across them all as a starting point makes good sense and should lead to a smoother investment journey. Be aware of the ‘anchor’ and make sure that you do not get overly influenced by what has just performed well. We cannot know which market will do well next, so we own all of them.
Dr Benjamin Holdsworth (right) is a director of Cavendish Medical, specialist financial planners helping consultants in private practice and the NHS
The content of this article is for information only and must not be considered as financial advice. Cavendish Medical always recommends that you seek independent financial advice before making any financial decisions. Levels, bases of and reliefs from taxation may be subject to change and their value depends on the individual circumstances of the investor. The value of investments and the income from them can fluctuate and investors may get back less than the amount invested.
ISSUES SPECIFIC TO PRIVATE PRACTICE
Ethical minefields of private practice
Always check, and double-check, contracts. The GMC requires you to have in place indemntiy/ insurance for the full scope of your practice
Dr
Sophie Haroon (below) reflects on some learning points from managing cases involving private practice
BOOK YOUR DEMO
DEMAND FOR private healthcare in the UK remains strong, spurred on by long waiting lists and patients turning to private healthcare through medical insurance or self-funding.
Private practice carries with it certain rights and responsibilities. The doctor-patient dynamic is also different.
Patients see themselves as customers; and the relationship can be more transactional, as fees are exchanged for clinical management.
Private patients can be some of the most challenging and demanding and when there is a mismatch between patient expectation and clinical management, complaints and claims in clinical negligence can arise.
1
Some patients seem able to view a claim quite dispassionately –rather like a claim on a house or car insurance policy. Taking this altogether, try not to take a complaint or claim to heart
have lost confidence and would not wish to consult you again. However, this is frequently not the case. Some patients seem able to view a claim quite dispassionately – rather like a claim on a house or car insurance policy. Taking this altogether, try not to take a complaint or claim to heart.
2 Bearing gifts
letters – and admittedly not just in private practice.
However, the point is that all patients are pleasant until it goes wrong. Whereas a ‘delightful’ NHS patient’s complaint or claim might fall to the NHS trust, it can feel quite personal when an individual clinician is pursued in their private capacity.
It is also reasonable to be circumspect about gifts from patients.
In the NHS, gifts are usually towards a team, but they can be more personal when delivered in the landscape of private healthcare.
The GMC provides useful advice on what clinicians must consider when accepting or declining such an offering from patients .
You might imagine that a patient, who has previously expressed dissatisfaction with the service they have received, would
The key is to think twice. Ensure acceptance does not affect, or appear to affect, your manage -
‘The charming patient’ ‘Thank you for referring this lovely lady/pleasant gentleman …’ is an opening line of many clinic ➱ continued on page 40
Are you happy with your current software?
Maybe you're completely happy with the software you use to run your practice. Perhaps you have everything in one place, routine tasks are automated, and reporting is accurate and insightful. If so, stop reading now.
However, if you think the day to day running of your practice could be improved, we'd love the chance to demonstrate e-clinic to you.
The number one choice for private practice
Future-proof your practice and offer everything a modern patient expects:
> iPad compatibility
> Online booking & payments with fully integrated card processing
> Electronic consent & treatment forms
> Integrated drugs database & digital prescribing with direct delivery
> Fast & easy patient communications by email or text
BOOK YOUR FREE 30 MINUTE DEMO Visit e-clinic.co.uk to find
&
ment of them or bring into question the trust of patients and the public in the medical profession.
3
What’s up with Whatsapp?
It is not uncommon for clinicians to share their personal or work mobile numbers with private patients.
On the surface, this may appear as an individualised service for the patient, allowing them to message and ask questions of their private clinicians any time, day or night.
However, there are downsides. Firstly, for the clinician, being at the beck and call of private patients is not synonymous with a good work-life balance.
Secondly, exchanges about clinical care over messaging apps such as Whatsapp are part of the clinical record. They should therefore be recorded in the patients’ records, not over a social medium.
If a complaint or claim arises, these trails are just as important to disclose. Also, their brevity, as is typical over this form of communication, can be easily misconstrued. My personal opinion is that Whatsapp is not an appropriate medium for patient communication.
We only have to read the news to see how seemingly private conversations on social media messaging platforms can become public. In medicine this also poses serious questions around confidentiality.
4 It’s not you, it’s me…
The doctor-patient relationship can sour even in private practice. But despite the more contractual nature of this relationship, extricating yourself from it is no simpler than it is in the NHS.
The GMC is clear that a complaint or a claim is not a valid reason for ending your professional relationship with a patient and indeed, could open yourself to criticism . Its guidance sets out helpful steps to follow before ending the relationship and what to do when a decision has been made to end it – importantly, how you must be able to justify reaching the end of the road.
Ultimately, the professional relationship should only be ended if there has been a complete breakdown in trust and you cannot provide good clinical care.
You must then also ensure you transfer your care to another individual, so the patient’s ongoing care is not compromised.
5
Co-operate with your medical defence organisation (MDO)
Just like you would expect your patients to co-operate with you when you advise them on their best clinical management, so too should you co-operate with your MDO when you receive a complaint or claim.
Letters from patients or solicitors may appear unmeritorious, but do not delay sending them to your MDO so they can assess the situation and take any necessary steps to protect your interests.
A delay or failing to co-operate with their advice could prejudice your position in the matter. There are always two sides of a story to tell. The patient/their solicitor have one side; give your MDO the time and opportunity to tell your side by liaising with them promptly.
6
‘It’s good to talk’ – keep your MDO updated
It is vital that you advise your MDO of the full scope of practice for the work you carry out and ensure other information about your membership is accurate and up to date, which includes information about income or volumes of work undertaken.
This will help to ensure your subscription is more tailored to you. If you do not have adequate
protection in place for the types and volume of work you undertake, this may affect your MDO’s ability to assist should a claim subsequently arise.
No one wants this to happen. Houses and cars have been sold by doctors to finance claims which otherwise could have been managed through an MDO.
7 Always check, and double-check, contracts
The GMC requires you to have in place indemnity/insurance for the full scope of your practice .
Procuring your own professional protection may sound obvious for work involving private patients, but it is also important to bear in mind that it may be required for NHS Waiting List Initiative work, where state indemnity does not cover this, and for seeing NHS patients through some private providers commissioned to deliver public care .
Importantly, check what it says in your contract regarding where indemnity lies for this type of work, clarify with your employer if needs be and if you need to provide your own indemnity/ insurance, obtain this before undertaking any such work.
8 All professional protection products are the same, aren’t they?
In short, no. There are ‘occurrence-based’ products which cover incidents occurring during the membership period, regardless of when the claim is made, and there are ‘claims made’ products which only protect against claims brought during the term of your membership period.
For the latter, this means that unless you secure ‘run-off cover’ when you leave the MDO, cease practice or retire, you have no protection in place if a claim later arises and the incident that gave rise to it was not reported within the terms of the policy.
There can be many personal reasons for choosing occurrencebased over claims-made or vice versa. It is important to understand the type of protection you have and when it may possibly cease. especially because claims can come out of the woodwork many years after the alleged incident.
Exchanges about clinical care over messaging apps such as Whatsapp are part of the clinical record. They should therefore be recorded in the patients’ records, not over a social medium
9 Indemnity/insurance covers everything bar the kitchen sink?
This is another no, I am afraid. Typically, you can request assistance with acts and/or omissions arising from the clinical care you provide to patients. Some incidents may arise in a clinical situation, but may not be related to direct clinical care.
This can be the case, for example, with data protection breaches. Be sure to consider where alternative arrangements are required, like an appropriate public liability insurance policy, or be prepared to seek and finance independent legal advice yourself in the event of such a claim arising.
10
The end of the road
Even private practice can become time-limited. Just as important as knowing the ins and outs of starting up is considering how to wind down.
Records are essential in helping to manage claims arising after you have retired, so they must not be prematurely disposed. The NHS has produced a detailed retention schedule based on the differing types of patient record . While there is no specific advice for private records, it is appropriate to follow the NHS Code of Practice, as the GMC requires records to be disposed of in line with the relevant data protection laws.
Dr Sophie Haroon is a medico-legal consultant at Medical Protection
A guide to bidding for NHS contracts
It may feel counter-intuitive, but independent practitioners wanting to grow their private practices should look at opportunities to secure contracts with the NHS. These are often time-limited and project-focused to help resolve issues. Robert McCartney (right) gives a legal view on preparing for procurement opportunities
AS OF January 2023, there was a backlog of 7.21m people waiting for treatment, up from 4.43m in February 2020. The NHS needs assistance to reduce this demand and it is willing to use the private sector.
Some of the most popular areas in recent years include the offering of insourcing services where teams of practitioners will dedicate weekends to visit hospitals and manage their surgical waiting lists.
Home visiting services have had a similar increase in popularity, especially where it assists with hospital discharges and reduces local GP burden.
Many independent practitioners
who run their own practices may find that their service is in a great position to either bid directly or to work as a collaborative to submit a joint submission.
The ability to offer a scalable solution is useful, but if your service is too small, consider contacting other larger entities and look for subcontracting arrangements.
The BMA has identified that many of the larger providers are on frameworks, but struggle to provide all areas, as they do not have the resources. Your service may be able to plug those gaps for them.
These can be great opportunities to grow your business or to provide
➱ continued on page 42
a sustainable revenue stream while your private revenue is increasing. However, you must be prepared to make the most of these opportunities, as they often have limited publicity and tight time-frames to respond to.
To assist with this, our lawyers have identified three stages in the procurement process and important steps to consider in each one.
Undertake an assessment of the opportunity
Submitting a bid takes a lot of time and resources. It is often a competitive tender and even when you are submitting to join a framework which may not have a limit on the number of successful applicants, there will be a tough assessment of your suitability.
Many people fall into the trap of preparing a bid without doing the assessment to ascertain whether it is worth doing in the first place.
This can at best result in lost time and effort and at worst may result in a contract being awarded that you cannot deliver or afford.
To avoid this, apply a decision process to the opportunity. We suggest the following two steps which can be undertaken with minimal time and resources. They will result in what is referred to as a ‘Go/No Go’ decision.
STEP ONE: STRATEGY AND VIABILITY
1 Is the opportunity aligned with your services and businesses? If not, will it be a significant departure or can you ensure delivery with minimal changes?
2 What would your service offering look like? Would you need additional support, premises, technology and are these resources available in the timeframe available?
3 Is the opportunity financially viable? This may be an initial assessment and should be returned to as the bid progresses and more accurate costs are identified, but no bid is worth proceeding with if it is going to be a strain on the business.
If the decision is to ‘Go’, then follow step two.
STEP TWO: ASSESS LIKELIHOOD OF SUCCESS
1 Who are the likely competitors?
2
Do you have a competitive advantage over the competition or any other unique selling points which improves your position in the competition?
3 Do you need partners?
These may be strategic – for example, support from a larger organisation which needs your expertise and brings with them experience in winning larger tenders.
Or they may be operational, such as other independent practitioners who can work together to provide a better service.
Can you be successful? Be honest with yourselves at this point.
If the decision at this stage is still to ‘Go’, it is time to turn to the detail of the tender and to commit the resources needed to make it the best submission you can.
Advance preparation
One of the benefits of the procurement system is that we already know that there are a core set of questions which must always be asked by commissioners.
This is called the Selection Questionnaire (SQ). More information on these requirements can be found here: www.hempsons. co.uk/news-articles/ppn-03-23-anew-standard-selection-questionnaire-from-1-april-2023/.
The NHS has some flexibility with regards to the questions, but if you are prepared to answer the questions relating to the following topics, it will significantly reduce the workload.
These can be sensitive subjects, but each question can result in an immediate fail for a bid, so it is essential that parties are honest and open from an early stage.
1
Confirm who is bidding. Are you a sole practitioner, a partnership, a limited company or some other legal entity?
It is important to be clear who is making the submission, as that entity will be the named party on any successful contract.
2
Is this bidder working on their own or are they part of a larger group?
Some common alternative examples are:
a) You are the lead contractor and will use other independent practitioner businesses as subcontractors;
b) You may be the lead contractor within a collaborative, pooling resources to improve the service offering;
c) You are a newly formed new joint venture owned by other organisations specifically to provide this service
3
Collate core information for your own entity and for all other partners to this bid.
This would include:
a) Full name, registered address, trading status, date of registration and company or charity registration number, if applicable;
b) Head office DUNS number –available from What is a D-U-N-S Number? (www.dnb.co.uk);
c) VAT number;
d) Details of the Persons of Significant Control, where appropriate and available on Companies House;
e) Details of any parent companies if your business or any of your
partners’ businesses are a subsidiary.
4
Collate compliance information with confirmation that none of the partners have concerns relating to the areas listed below.
Any declared breach will need to be reviewed and it should form part of your assessment as to whether you can continue working with the organisation.
a) Environmental, social, equality, human rights and professional misconduct issues;
b) Employment law obligations including Employment Tribunal outcomes;
c) Bankruptcy, insolvency or winding-up proceedings;
d) Details of any public contracts terminated for persistent deficiencies in performance;
e) Any involvement in this or other procurement opportunities during which concerns about their behaviour were raised.
5
Share financial performance information. Ideally, include two years of audited accounts, but if not possible, statements on turnover, profit and loss, cash flow and financial position.
You may wish to agree confidentiality clauses in relation to this. Some parties instruct accountants to review this information without a full disclosure to each other. This can be used to protect sensitive data from collaborators who may also be competitors.
Speak with insurance brokers to ensure that you and your collaboration, where applicable, can access suitable insurance, if not already in place.
6
Confirm that policies for the following topics are available:
a) Health and safety;
b) Human resources, including recruitment standards matching the NHS Employment Check Standards (www.nhsemployers. org/recruitment/employmentstandards-and-regulation);
c) Data protection, including examples of data protection impact assessments (DPIAs), data process-
Ensure that you fully understand the requirements and pay very close attention to the time-frames
STEP THREE: PREPARING YOUR RESPONSE
With the preparation completed, you can turn to the substantial questions which will be specific to the service being tendered for.
Ensure that you fully understand the requirements and pay very close attention to the timeframes.
ing agreements (DPAs) and information sharing agreements (ISAs); d) Safeguarding; e) Business continuity and disaster recovery plan.
7
Confirm that appropriate Care Quality Commission registration is in place where required.
Other questions will be asked at this stage, but the time requirement is significantly reduced if you have this information to hand before the bid document is published.
Commissioners may extend these if they decide it is appropriate, but there is almost never any leniency if you are late in submitting.
This is shown in the recent case of InHealth Intelligence Ltd v NHS England [2003]EWHC 352 (TCC) (www.hempsons.co.uk/news-articles/no-bid-no-chance/).
All bids will provide you with the opportunity to ask clarification questions and you should use this to resolve any uncertainties or difficulties with interpretation.
Most bids differ at this stage in the process. This reflects the nature of the services available.
For example, an insourcing solution will have very different requirements from an outsourced diagnostics service. The questions will therefore reflect these differences.
Hopefully, the time saved on preparing for the SQ questions will provide you and any partners you may have with the time needed to tackle the specific questions about service delivery models, staffing and to spend a significant proportion of your time ensuring your financial modelling is of a high standard.
These steps are an introduction to a very large topic and advice relating to bidding groups, joint ventures and procurement processes can be obtained from the Hempsons team.
Robert McCartney is an associate in the corporate and commercial healthcare team of the specialist healthcare firm Hempsons
Free legal advice for Independent Practitioner Today readers
Independent Practitioner Today has joined forces with leading healthcare lawyers Hempsons to offer readers a free legal advice service.
We aim to help you navigate the ever more complex legal and regulatory issues involved in running and developing your private practice – and your lives.
Hempsons’ specialist lawyers have a long track-record of advising doctors – and an unrivalled understanding of the healthcare system as a whole.
Call Hempsons on 020 7839 0278 between 9am and 5pm Monday to Friday for your ten minutes of free legal advice.
Advice is available on:
Business structures (including partnerships)
Commercial contracts
Disputes and litigation
HR/employment
Premises
Regulatory requirements and investigations
Michael Rourke
Tania Francis m.rourke@hempsons.co.uk t.francis@hempsons.co.uk
BUSINESS
Dilemma 1
What does this invitation mean?
QAs a consultant paediatrician specialising in respiratory medicine, I have been involved in the care of a child who is now suspected of having a non-accidental injury.
I examined the child during a routine follow-up appointment for their asthma.
Following this, I was contacted by the police to inform me that the father was arrested two days later in relation to unexplained bruising found on the child’s chest by a health visitor.
I provided a factual report stating that I had not noticed any bruising when I examined the child’s chest.
Now I have been contacted by the local authority in relation to a court hearing regarding the welfare of the child and I have been invited to intervene. I was unsure what this meant and whether it had any implications for me.
AWhere child protection proceedings are taking place and a healthcare professional receives documentation from a solicitor or a local authority inviting them to intervene, it suggests that allegations have been made against them with regards to how the child sustained the injury.
In this case, the father may have alleged that the injury to the child was caused when you examined
Non-accidental injury of a child
Dr Kathryn Leask (right) answers a consultant’s query about what to do if you are contacted by the local authority about a child protection case
You may need legal representation to protect your interests and represent you at the hearing
the child’s chest. As this could result in criminal liability for you, it is important that you contact your medical defence organisation as soon as possible.
You may need legal representation to protect your interests and represent you at the hearing.
It will be necessary for your legal representative to request full disclosure of documents being relied upon in court so that the exact nature of the allegations can be established and who the allegations have been made by.
This type of case emphasises the importance of good medical record-keeping.
In situations like this, the doctor would have had no reason to know that child protection concerns would be raised after their consultation with the child.
The notes will be vital with respect to providing evidence and the fact that there was no report of bruising, or other injury, during the examination and that no concerns were raised about the nature of the examination at the time.
When clinical photos show intimate images
Dilemma 2
What do I do with the pictures?
QI am a private paediatrician and regularly consult with a family over video, where appropriate.
On this occasion, the patient is a five-year-old girl. Her mother was concerned about skin lesions that had developed on the child’s thigh and emailed photographs of them to my practice with an e-consultation form, as she was unable to attend a face-to-face appointment.
The photographs are due to be uploaded by my administrative staff to the child’s record.
I have had a video consultation with the mother and child as well and found the photographs useful in reaching a diagnosis and being able to initiate treatment, as the lesions were difficult to see on video. The mother was aware these were to be added to the records and had agreed to this.
One of the photos included part of the child’s external genitalia, as one of the skin lesions was high up on the inner thigh.
A colleague has advised me that it is a criminal offence to keep images of children where intimate areas of the body are showing. Please could you advise as to what I should do with the images I have?
AYour colleague is correct in that receiving and storing intimate images of a child could constitute a criminal offence, if the image was regarded as indecent.
Where images are for the purposes of medical care and treatment, the defence of ‘legitimate reason’ could apply.
A paediatrician’s colleague advises that it is a criminal offence to keep certain photographs of a patient taken for medical purposes. So what should he do? Dr Kathryn Leask gives her response
A legitimate reason may arise where the photograph is clinically important to help reach a diagnosis. It may be important to store the photograph in the patient’s notes so that there is a record of the lesion and to show any progress in treatment.
It is important that the parent –or patient in the case of an older child or adult – is aware of the intention to store the image in the records and the reasons for this. Their consent should be documented.
Photographs should be sent to you securely and only those that are clinically necessary should be kept.
If there is more than one photograph and the image which shows the child’s genitalia is not needed for the purposes of having a record of the lesion, this should not be uploaded.
Once the photographs that are to be used have been uploaded to the records, the emailed images should be deleted.
Dr Kathryn Leask is a medico-legal adviser at the Medical Defence Union
A PRIVATE PRACTICE – Our series for doctors embarking on the independent journey
Why VAT should be on your radar
Value Added Tax is a levy applied to most products and services. It is a complex tax, but for many businesses it is part of the day-to-day finances. VAT is charged on invoices and recovered on certain costs incurred.
There are special provisions within the VAT legislation specific to medical services, but reviewing and evidencing that those exemptions apply is extremely important. Alec James (right) gives some wise advice
GENERALLY SPEAKING, VAT is not on the radar of many doctors. The reason is that there is an exemption which covers the majority of your work in the private sector.
There is detailed HM Revenue and Customs (HMRC) guidance regarding VAT for medics, referred to as VAT notice 701/57.
Fundamentally, where your income meets the following two requirements, the income is deemed to be exempt from VAT and therefore your business has no VAT obligations:
1
The services are within the profession in which you are registered to practice;
2
The primary purpose of the services is the protection, maintenance or restoration of the health of the person concerned.
As registered doctors providing medical care to patients, your private practice income would usually pass these two tests and therefore is exempt from VAT.
This means you are not required to charge the current VAT rate of 20% on your invoices.
Where an income stream does not meet the two requirements for VAT exemption, you need to consider your VAT position, because the income will be considered to be a ‘VAT-able supply’ – or ‘standard-rated’ as it is formally known.
Protection, maintenance or restoration of the health of a person concerned
This test has come under fire from HMRC in recent years, mainly aimed at cosmetic and aesthetic procedures.
Tax officials have argued that these medical procedures are not to restore a patient’s health, but instead are for purely cosmetic purposes.
There is a specific point within VAT notice 701/57 referring to cosmetic procedures. It reads: ‘Each case will need to be considered on its individual merits.
‘However, we will generally accept that cosmetic services are exempt where they’re undertaken as an element of a healthcare treatment programme. Where services are undertaken purely for cos -
metic reasons, they will be standard-rated.’
While this is in the guidance, it is not enough for the medic to simply make a decision that they believe their income to be exempt from VAT.
Instead, you should have evidence to support your stance. Unfortunately, this also has to be on a case-by-case basis.
It is hard to imagine that your patient records could potentially need to be reviewed by a HMRC official in the event of an inquiry. And while they cannot request to see the full patient notes, they can request to see an anonymised version to allow the inspector to review the VAT treatment of invoices raised to that patient.
It is therefore extremely important that you ensure your records include the reasons why the patient has come to see you, specifically the health condition that you are treating.
Your notes should make reference to factors that have led to the patient to seek your advice and services. This could be for a multi-
If you have a mixture of income streams, you should maintain detailed records of your invoices showing the amounts that are exempt from VAT and those that are taxable
tude of reasons and can include psychological factors.
For those patients that come to see you for purely cosmetic purposes, this would be a standardrated supply and you should monitor how much income is received on this basis to see if you need to register for VAT.
Other standard-rated income streams
There are other sources of income which do not meet the healthcare VAT exemption:
MEDICO-LEGAL WORK
Many of you will provide medicolegal reports. While these reports are linked to the protection, maintenance or restoration of a patient, this is not the primary purpose and therefore this income stream would not pass the healthcare exemption.
SPEAKER FEES
Speaker fees are another complex area where each presentation you give has to be considered individually.
Again, the VAT notice 701/57 has a specific point in relation to ‘Education services’. Lectures – be they one-off or a series – given as part of a medical training course or continuing professional development (CPD) and training sessions to first aiders, which are provided by a doctor in either a sole proprietor or partnership capacity, are exempt as a supply of private tuition under the education exemption.
Presentations aimed at promoting health are also considered to be exempt, as their principal purpose is to protect the health of the individuals attending.
However, presentations given to a non-medical audience on, for
when you receive the payment from your customer.
the latest medical developments are considered to be taxable.
Once again, the devil is in the detail and you should maintain evidence to support any invoices you raise in respect of speaker fees to show that the invoice is either exempt from VAT or is standardrated.
PRODUCT SALES
Some specialties have post-op products which you may sell to patients. These would generally be a standard-rated supply if they are sold individually.
If the product was included as part of your medical treatment, then it may then be covered by the healthcare exemption.
If you are unsure of the VAT status of an income stream, you should seek the advice of a specialist medical accountant.
Do I need to register for VAT?
Currently, the threshold for compulsory VAT registration is when your taxable income exceeds £85,000 on a rolling 12 monthly basis.
When considering this level, you only need to count the taxable or ‘VAT-able’ income of your business, not anything which would be exempt from VAT as detailed in VAT notice 701/57.
If you have a mixture of income streams, you should maintain detailed records of your invoices
showing the amounts that are exempt from VAT and those that are taxable.
This will prove invaluable when reviewing your position. Most book-keeping or invoices software systems will allow you to have various headings to allow you to quickly review this.
You are able to voluntarily register for VAT if your taxable income is below £85,000 and this can lead to some tax planning in certain circumstances.
It is worth noting that if all your income is covered by the healthcare exemption, then you are not able to register for VAT.
Having a VAT-registered business
If your business is VAT-registered, then you have certain obligations. Any invoices which you raise should include your business’s VAT registration number.
On invoices with taxable supplies, you should charge VAT. The invoice total should therefore be your fee plus the VAT charge.
The VAT is then collected from your customer and then forwarded to HMRC via your VAT return. When you pay that VAT over to HMRC is dependent on the type of accounting you do for VAT purposes.
Cash accounting vs standard/ invoice accounting
Cash accounting is where you only have to pay the VAT to HMRC
This is particularly beneficial if you do a lot of medico-legal work, as there can often be a period of time between you raising the invoice and your invoice being paid.
By using the cash accounting method, your business would not be adversely affected by paying VAT over to HMRC before you have received payment.
Alternatively, you can opt for the invoice or standard accounting method. This means that you incur VAT based on the date of the invoices rather than when the invoices are paid.
You are only able to use the cash accounting method if your taxable earnings are below £1.35m and therefore if the business’ taxable income is in excess of this, you will need to follow the standard method.
Generally speaking, VAT returns are required either quarterly or annually. The returns will declare all the VAT you need to pay over to HMRC.
But it’s not all doom and gloom
Being VAT-registered does have its benefits. If you are VAT-registered, you are able to reclaim VAT on costs incurred in respect of your business. This reduces the overall cost to your business.
If you have a business which has a mixture of taxable and exempt income streams, you may not be entitled to reclaim the full VAT on costs incurred. Instead, you cover a part of the VAT. This is based on the split of your income.
If you have a business which has both significant private practice and VAT-able income, it can sometimes be beneficial to hive off the VAT-able income into a separate business, be that on a selfemployed, partnership or limited company.
VAT is a complex area and with the added intricacies of the healthcare profession, the use of a specialist medical accountant or VAT expert to review your circumstances should be a part of your annual compliance.
Alec James is a partner at Sandison Easson & Co, specialist medical accountants
DOCTOR ON THE ROAD: VOLKSWAGEN ID BUZZ
The VW bus has got a lot camper
Feeling
cool and really buzzing.
That’s Independent Practitioner Today’s motoring correspondent Dr Tony Rimmer (right) after his latest road test
THE ELECTRIC car revolution is well and truly upon us. Hardly a week goes by without the release of yet another new EV from either an established brand or a manufacturer fresh to the scene.
Despite relatively high prices, the proportion of EVs to internal combustion engine cars is increasing month on month, albeit slowly.
Now that some supply issues made worse by the war in Ukraine are resolving, you will
notice there are more EVs on the roads near you.
The trouble is that the choice available can be bewildering and the vast majority of EVs are medium-sized SUVs which all have much the same practicalities and attributes.
Bit of personality
They all drive in much the same way and so we medics end up choosing on the basis of range and purchase price. There is obviously a place for
an EV that attracts us in a different way; something with character and a bit of personality. So welcome to the Volkswagen ID Buzz.
The classic VW bus has been around for decades and probably makes us think of trips to the coast in the sunshine, perhaps surfing when we get there.
Campervan versions have been immensely popular over the years and some of us may have been taken by our parents on exciting camping trips
inducing fond memories. You can’t help smiling when you see one of these old rear-engined VWs still on the road.
In the same way that the original bus was a development of the then current Beetle, the new ID Buzz shares the same MEB electric platform with its ID3, 4 and 5 siblings.
It shares the same 201bhp motor powering the rear wheels and uses the larger 77kWh battery. The styling is very van-like – there is a commercial van
variant – but takes many of the design elements of the classic bus to give it an unmistakable look.
The over-large VW badge on the front and the bonnet shaped to look like a smile bring back all the right memories.
It looks at its best with the optional two-tone paint with white on top and a bright colour such as yellow or orange below. However, this choice costs a hefty £2,790 extra.
Eco-friendly materials
Those cool design features continue on the inside too. Wide comfortable seats, numerous storage pockets and the use of contrasting eco-friendly materials create a light and airy passenger space.
The ID Buzz has five full-size seats and more than double the boot space of the ID4. The rear seats can slide to alter the available legroom and can recline to a decent degree too.
There will be a longer wheelbase version available at the end of the year that will have the option of seven seats and will probably form the base for camper variants.
The driver controls and infotainment system are lifted straight out of the other ID models, so unfortunately still suffer from the same heating and ventilation control frustrations on touch-sensitive slides.
However, all the positive elements remain, so the ID Buzz is an easy car to drive. It is made even easier by the van-like raised driver’s
position, tight turning circle and the abundance of glass to make manoeuvering in tight spaces a straightforward procedure.
Although it weighs 2.5 tonnes, the torquey 201bhp electric motor allows the Buzz to step off smartly and keep up with urban traffic without even trying.
Calm and smooth
The ride, even on the optional 21” wheels on my test car, was calm and smooth, but caught out occasionally by sharp ridges and potholes.
Body roll is minimal due to the low centre of gravity and the handling is predictable but not sporty.
This VW is at its best on the motorway where it lopes along at
70mph with ease and comfort. You are then only restricted by the range which is a realistic 200–220 miles; potentially frustrating on a long holiday haul.
With a £63,715 starting price, the ID Buzz is expensive even for an EV. However, there is nothing quite like it on the road and it will hold its value really well. It attracts positive comments wherever you go and it has a cheery character. It is a very practical and very roomy five-seater. Volkswagen should be congratulated on producing it and I am sure we will see some very interesting variants in due course.
Dr Toy Rimmer is a former NHS GP practising in Guildford, Surrey
The ID Buzz has five full-size seats and more than double the boot space of the ID4. The rear seats can slide to alter the available legroom and can recline to a decent degree too
VW ID BUZZ
Body: Five-seat SUV
Engine: Single electric motor, rear-wheel drive
Power: 204bhp
Torque: 255Nm
Top speed: 90mph
Acceleration: 0-62mph in 10.2 seconds
WLTP claimed range: 255 miles
CO2 emissions: 0g/km
On-the-road price: £63,715
WHAT’S COMING IN OUR COMBINED JULY-AUGUST ISSUE
Coming in our combined July-August issue, published on 11 July:
In our ‘Start A Private Practice’ series, specialist medical accountant Richard Norbury provides a useful round-up of the upcoming changes concerning tax
Patient feedback: People buying health insurance have high expectations of the care they should receive, so their feedback is valuable in helping insurers improve their service. Tricia Carley-White, head of clinical quality and governance at Bupa UK Insurance, explains
Week after week, cosmetic clinics and other ‘healthcare’ providers receive complaints about their advertising. Many are upheld by the Advertising Standards Authority. We find out where doctors, clinics and other are going wrong
Many consultants face a struggle with clinical documentation due to time constraints, while also needing to prioritise doctor-patient relationships. Outsourcing administrative tasks offers private practice consultants a practical solution to reduce the time they spend on their administration, explains Medserv’s Derek Kelly
Ophthalmologists see this! Claire Wratten, claims team manager, and Pete Renwick, lead claims handler at the Medical Defence Union, discuss the claims received from ophthalmology members
Dr Kathry Leask advises a consultant who requests help to respond to a request for information from an insurance provider. She also advises how to prepare for a meeting after an adverse incident
INDEPENDENT PRACTITIONER
TODAY
The business journal for doctors in private practice
Published by The Independent Practitioner Ltd. Independent Practitioner Today is editorially independent.
Material is governed by copyright.
No part of this publication may be reproduced, stored in a retrieval system or transmitted in any form without permission, unless for the purposes of reference and comment. Editorial layout is the copyright of the publishers. If you wish to use it for promotional purposes on websites or for reprints, we would be happy to discuss licensing the copyright to you.
Registered office: 7 Lindum Terrace, Lincoln LN2 5RP
A systematic approach to investing provides the best chance of experiencing a successful investing journey. Sticking to some key guiding principles – which are grounded in evidence and logic – gives investors a solid foundation on which to build a sensible investment solution, say specialist financial planners Cavendish Medical
Social media and its perils – who does the law protect, and how can you protect yourself? As an independent practitioner, you may have employees on social media and you need to be generally aware of the risks associated with it
After registering a service with the Care Quality Commission, the next interaction a provider is likely to have with the regulator is via an inspection. The end result of this is a published inspection report that may be accompanied by a Warning Notice, readable by the public, so all independent practitioners should be aware of their right to respond
The evolution of consent. Dr Emma Green, a medico-legal consultant at Medical Protection, discusses some defining cases that have led to the principles of consent and how they apply to current practice. The consent guidance can cause confusion or is grey
Musk be nice? Our motoring correspondent Dr Tony Rimmer gets behind the wheel of the Tesla Model Y
Our ‘Ten Years Ago’ feature underlines why it pays to check your payslips if you have an NHS job
Plus all the news, views and other regular features
ADVERTISERS: The deadline for booking adverts in our July-August issue is 23 June
Write to Independent Practitioner Today 7 Lindum Terrace, Lincoln LN2 5RP
CHANGING ADDRESS, EMAIL ADDRESS OR SUBSCRIPTION DETAILS?
Phone 01752 312140 or email karen@marketingcentre.co.uk
TELL US YOUR NEWS
Robin Stride, editorial director
Email: robin@ip-today.co.uk
Phone: 07909 997340 @robinstride
ADVERTISE WITH US
To advertise in the digital journal, on our website or in our business directory, contact advertising manager Andrew Schofield at Spot On Media. Phone: 0161 408 3912 Email: andrew@spotonmedia.co.uk
GET A SUBSCRIPTION DISCOUNT!
£90 independent practitioners. £90 GPs and practice managers (private & NHS).
£210 organisations.
Save £15 paying by direct debit: individuals £75 (organisations £180).
TO SUBSCRIBE
Email karen@marketingcentre.co.uk or phone 01752 312140