The business journal for doctors in private practice
In this issue
How to hang onto staff Recruitment specialist Keith Hague says leadership is the key to staff retention P12
You'll miss out if you don't go green Jamie Foster spells out what sustainability means for private doctors P24
Prof Mark Whiteley on his clinic's resurgence n Page 14
Decrypting new ways of investing Dr Ben Holdsworth warns of the ten points you should remember about cryptocurrencies P34
GMC guidance change is labelled ‘confusing’
By Robin Stride
Independent practitioners are being exhorted to respond to GMC proposals which a defence body fears could have unintended consequences on doctors’ working lives.
The MDU’s concerns follow the launch of its ‘forensic’ analysis of the Council’s consultation proposing a shake-up of Good Medical Practice , reported by Independent Practitioner Today last month.
Defence experts have voiced strong reservations about the scale and nature of the proposed changes and believe some are unclear and fail to reflect the realities of medical practice.
Dr Caroline Fryar, the MDU’s director of medical services, said: ‘It is really important that all doctors read the consultation and envisage how they can see it working in practice. Ultimately, the guidance must work for doctors and we are keen to hear from members so we can ensure their views are heard.’
the profession if Good Medical Practice was updated every couple of years. But the MDU was struck by the scale and nature of the proposed changes. ‘Indeed, we feel that some of the proposed changes do not reflect the realities of medical practice.’
She appreciated the GMC had, however, committed to a meaningful consultation with doctors.
‘The GMC is clearly investing considerable resource in reaching out to the profession and other stakeholders to discuss their proposed changes – and a threemonth consultation period is a considerable one.
GMC chief executive Charlie Massey has described Good Medical Practice as the bedrock that helps guide ethical practice in a world of increasingly complex medicine.
Launching the consultation, he said: ‘This update is designed to reflect the type of fair, inclusive and compassionate workplaces we all want to see and that are good for doctors as well as for patients.
‘The guidance is one of the main tools used by the GMC in its fitness-to-practise processes. That’s why it is so important that this guidance – when finalised – is in the best possible shape. Every paragraph and every word of Good Medical Practice matters. That’s why we are being so forensic in our study of this new version’.
Dr Fryar said it would be too confusing and not in the interests of
Asked if she thought some proposals could lead to doctor confusion and result in them getting into trouble with the GMC, she replied: ‘There is a legitimate concern that some of the proposed changes lack clarity.
In association with
‘We believe the GMC will be receptive to constructive, considered and evidenced-based feedback. We always work collaboratively with the GMC to support the best interests of our members, and that’s the spirit in which we are approaching this crucial consultation.’
The draft updated Good Medical Practice runs to 16 pages and provides detailed guidance for doctors covering areas including ‘working with colleagues’, ‘working with patients’, ‘professional capabilities’ and ‘maintaining trust’.
‘There is a lot of evidence of the damage bad workplace cultures can do to patient safety and, ultimately, to the UK’s ability to retain the healthcare professionals it needs. Toxic cultures can also spread online, undermining public trust in the medical profession.
‘It is important our guidance reflects the reality of what doctors face and the cultures many are working in, and that it supports them to be able to do the best for their patients and for their colleagues.
‘We want this guidance to be relevant and helpful now and for years ahead and, to achieve that, we need to hear from those who will use it. That is what this consultation is all about.’
➱ continued on page 3
Dr Caroline Fryar, the MDU's director of medical practice
TELL US YOUR NEWS. Contact editorial director Robin Stride
ADVERTISE WITH US. To advertise in the digital journal, on our website or in our business and lifestyle directories, contact Andrew Schofield at Spot On Media. Phone: 0161 408 3912
Email: andrew@spotonmedia.co.uk
GET A SUBSCRIPTION DISCOUNT
£90 independent practitioners. £210 organisations. £90 GPs and practice managers (private & NHS).
Save £15 paying by direct debit: individuals £75 (organisations £180).
Delve into this digital edition of Independent Practitioner Today and you will find a wide range of experts writing on a vast variety of key issues for doctors in private practice.
Much of it is inspiring, so do not miss Prof Mark Whiteley’s moving story (page 14) of how his clinics have bounced back –with a new one just opening –following a horror time at Covid’s onset when the business was suffering and he was forced to sell his house.
If you are an entrepreneur with a story or wish to share how you have got your private practice back on the road again, then do get in touch.
In the wake of the pandemic our Troubleshooter Jane Braithwaite has some excellent advice to those doctors who are asking: ‘Now that my team have had a taste of home working, they all want to work from home more of the time.
‘How do I make this work?’ (page 22).
Selfpay issues are in the news as people face longer NHS waiting lists, so we are delighted to welcome Liz Heath, author of LaingBuisson’s latest report on UK self pay, reflecting on the market and whether optimism expressed by so many is founded on evidence of sustainable growth (page 20).
Of course, making sure you get paid is the problem for many independent practitioners and Simon Brignall of Medical Billing & Collection highlights ten more key areas for practices to examine as they seek to overcome these challenges (page 36).
But how do you get patients in the first place? Marketing expert Simon Marett has some advice (page 28).
We’ve run out of space to plug any more, so read on and enjoy benefiting from what our other 13 features this month have to offer.
GMC vague in its rulebook revamp Dr Caroline Fryar of the MDU examines the new version of the GMC’s Good Medical Practice and finds it ignores the everyday realities for doctors P18
Tap into the self-pay market
Following the latest LaingBuission report in self-pay, its author Liz Heath muses whether the optimism in the sector is founded on evidence P20
Be flexible if you want to keep staff Troubleshooter Jane Braithwaite answers a private doctor’s question about coping with staff who want to work from home P22
Getting your patients on board
How do you convert a visitor to your website to being a fully paid-up patient? Marketing expert Simon Marett has some suggestions P28
Listening can defuse gripes
While empathy is important when things go wrong, listening is the vital communication skill in these circumstances, says Kirsten Dyer P32
Getting your cash in Simon Brignall of Medical Billing and Collection brings to an end his series on 30 key areas for practices to overcome their billings woes P36
PLUS OUR REGULAR COLUMNS
Business Dilemmas: Duty of confidentiality exists after your patient dies
The MDU’s Dr Kathryn Leask answers a doctor’s query about giving a dead patient’s notes to a third party P44
Doctor on the Road: This SUV accelerates like a sports car
The electric BMW iX 50 Sports impresses our medical motoring correspondent Dr Tony Rimmer P46
Profits Focus: Groups fail to take off
The financial fortunes of anaesthetists come under the gaze of medical accountant Ray Stanbridge P49
Thousands of pension statements are wrong
NHS informs pension members of mistakes
By Edie Bourne
Nearly 3,000 NHS scheme members have been sent pension statements which are wrong.
The erroneous documents were dated between 20 April and 27 April but an investigation has been launched to see if the substantial mistake could span a greater date range.
The NHS Pension Agency has written to members who had received statements after 28 April to admit the error and to confirm they would be recalculating positions and issuing new statements.
Specialist financial planners Cavendish Medical has long warned about everyday occurrences of errors in the computergenerated pension statements.
Its technical director Patrick
Convey told Independent Practitioner Today : ‘Pension savings statements form the starting point of calculating a member’s position and whether they are likely to face an annual allowance charge.
‘However, we have seen many which are wrong – and sometimes the smallest mistake in the calculations can lead to very large problems.
‘These mistakes can be difficult to spot and can be easily missed by busy medical professionals or financial advisers not well versed in NHS nuances.
‘Every detail needs a thorough ‘sense check’ to ensure your own position is correct.
‘The figures will be used to calculate if an annual allowance charge will apply and mistakes can mean owing or being owed thousands of
GMC guidance ‘must reflect doctors’ lives’
The MDU’s Dr Caroline Fryar, writing in this issue of Independent Practitioner Today, notes many comments have been made about some of the new additions to Good Medical Practice – from displaying ‘kindness’ to obligations not to condone certain behaviour on social media and to have regard for global health when taking account of the resources available to treat patients. She argues: ‘Kindness, tackling abuse on social media, climate change – all of these issues matter profoundly and are of the utmost importance. However, Good Medical Practice is not a manifesto outlining the aspirations for the healthcare system – it is the principal document by which doctors
and their registration with the GMC is held to account.
‘Hence, the duties and responsibilities it places on the profession must reflect the realities of the healthcare system and the individual doctors within it. The guidance must be accessible, understandable and achievable for doctors.’
The GMC’s consultation on the draft updated Good Medical Practice runs until Wednesday 20 July. Find out more, including how to get involved, via this link.
MDU members are being encouraged to share their views by contacting at media@themdu.
com
See ‘GMC vague in its rulebook revamp’, page 18
pounds in wrongly calculated tax.’
The annual allowance limits the amount of tax free pension savings which can be accrued per year to £40,000.
For higher earners, the ‘tapered’ annual allowance applies which can be as low as £4,000.
Mr Convey continued: ‘Just last
month [in Independent Practitioner Today ] we warned that NHS Pension Scheme members made up a third of the total number of individuals exceeding the annual allowance in 201920 in the UK.
‘Doctors are already facing the harshest tax penalties and the most complex calculations on their pension – they must have figures they can rely on.
‘This area of pensions taxation is proving particularly distressing at present and doctors should not face these challenges alone while trying to do important medical work.
‘There is help available from NHS experts and a trained eye can spot errors on payslips and pension statements as well as conduct detailed modelling to plan the best options for your future.’
Carry tax loss forward to save in the long run
Practices have been warned to be cautious about using a 2021 Budget ruling allowing a oneyear carryback for trading losses to be extended to three years.
This meant businesses with losses during Covid19 could get money back for tax paid in that earlier threeyear period.
But accountants Humphrey and Co say with corporation tax rising to 25% from next April for profits over £250,000, doctors may benefit by carrying the loss forward.
A company’s loss making accounting period must end between 1 April 2020 and 31 March 2022 for the enhanced carry back – 202021 or 202122 for unincorporated businesses.
Bryan
It said the marginal rate was 26.5% for profits between £50,000 and £250,000 a year. So there was a trade off between a tax refund now and possible bigger future tax saving.
Partner Mike Bryan advised doctors to take professional advice. He said it was relevant for any sole trader or limited company that had made a loss.
‘If cash flow is the main issue now, carry it back. But if you can survive, then you may want to carry it forward, as you may get more tax relief next year due to impending tax increases.’
See ‘Setting yourself up as a company’, page 39
Patrick Convey of Cavendish Medical
Mike
AGM OF THE INDEPENDENT DOCTORS FEDERATION
IDF shows its caring side
Reports
by Robin Stride
New chief aims for inclusivity
The new president of the Independent Doctors Federation (IDF) has unveiled plans for the group to better serve private consultants and GPs who have suffered prejudice.
Dr Phil Batty said although the IDF was an inclusive organisation, he believed it could do better.
Giving his first speech in his new role, he told members at the group’s AGM: ‘We are sometimes prone to mistakes, leading some members to feel they do not “belong” in the IDF family or at particular events’.
He aims to tackle this by having representation from a dedicated diversity committee on the IDF’s executive.
Dr Batty, a consultant in sports and exercise medicine, said this was not for some political correctness gesture, but to consider members with particular needs, and was entirely consistent with the objects of the IDF’s articles of association.
He told the meeting in London: ‘We live in challenging times wrestling with social concerns, commonly termed “woke culture”. I have not had to overcome prejudice based on the colour of my skin, gender, sexual orientation, faith or disability.
‘I don’t know how that feels. None of us should feel dehumanised or ashamed of who we are. I pay tribute to those of you that have overcome and continue to fight prejudice. I could not practise or provide care to my patients without you.
‘And my life is richer because of you. I am proud to be your colleague and to serve as your president. I will continue to listen to your issues and hope that, by the end of my term, you can say that I was inclusive and that I spoke for
you. Indeed, I hope to hand this presidential medal to one of you in three years’ time.’
Dr Batty said the Oxford English Dictionary defined the word ‘woke’ as ‘being alert to injustice in society, especially racism’. He embraced a lot of ‘woke culture’, not because of ‘virtue signalling’, but because it was simply the right thing to do.
But he added that while he accepted that everyone needed to be held accountable, he deplored ‘the cruelty and viciousness of “cancel culture” and struggle with humourless militants’.
He said it was vital for the IDF to engage with new and younger GPs and consultants working in the independent sector for longterm sustainability and growth.
‘The independent sector is changing, with PMIs directing patient pathways, CMA [Competition and Markets Authority] directives and a newer employed model from providers. We need to continue constructive engagement and challenge many stakeholders.’
After the last couple of years, it was more important than ever to follow the timeless founding principles of the IDF ‘to support each other, have fun and grow together’.
Dr Batty announced the events team would be expanded and appealed for imaginative ideas for events where doctors could enjoy each other’s company and support one another.
QUALITY SERVICE: The federation’s specialist committee agreed to lobby insurers for better fees by demonstrating members’ excellent quality
Responsible Officer praised
IDF president Dr Phil Batty thanked the group’s Responsible Officer Dr Alex Harkins and her team who serve as a designated body for more 600 of its 1,450 members for revalidation.
Dr Batty called it a vital service for members from a wide range of practice and he reflected that it was rare but sad when members met a threshold to be referred to the GMC.
This was always in the strictest of confidence and difficult for the member – and Dr Harkins.
While the IDF would always fulfil its obligations, it would try to do this with ‘as much kindness as possible’, signposting members in difficulty to support.
Tributes for the former IDF boss
Tributes have been paid to private GP Dr Neil Haughton, who has left his post as president of the Independent Doctors Federation (IDF) after a threeyear term.
New president Dr Phil Batty told the group’s AGM he could not praise his predecessor enough for his work through incredibly difficult times.
‘It was not the fun gig he anticipated, but he leaves his term with the IDF in a much stronger and healthier position in spite of the pandemic.’
Founding member Dr Stuart Sanders told Dr Haughton: ‘Congratulations on a wonderful term as president. Considering that you have been president though diffi
Dr Phil Batty, IDF’s new president
cult times, you really have come up trumps.’
Despite the pandemic, his leadership was ‘a remarkable success’, with the IDF now more financially secure.
‘Ask for cut in indemnity fee’
Many consultants with falling incomes during the worst of Covid 19 missed out on a fee reduction from their medical defence bodies because they forgot to ask.
Dr Sean Preston, chairman of the IDF’s specialist committee, said a survey by the organisation found 25% of those questioned found access to their usual place of work was made more difficult because NHS patients were using beds and services for timecritical clinical care.
Writing in his annual report to the Federation’s journal IDF News, he reported: ‘Interestingly, most of those members did not contact their medical indemnity provider to discuss a fee reduction, but those who did were largely successful in doing so. If you don’t ask, you don’t get.’
PMIs lobbied to improve pay
The IDF’s specialist committee has agreed ‘almost unilaterally’ to lobby private medical insurers ‘for appropriate renumeration for timely, highquality care’.
Members have achieved some success after working in groups with insurers to help them describe excellence and quality.
Specialist committee chairman Dr Sean Preston told the AGM that
specialists should be rewarded for excellence in quality and also a good governance code.
Consultants’ representatives were able to describe what quality was and the insurers could follow – but it should not be the other way round.
He thanked Anne Coyne for her work over the year supporting members who had got into trouble with insurance companies. She had helped colleagues ‘negotiate difficult paths’.
Dr Preston described the pandemic as very tough for members in the specialists committee.
‘Some of us lost our jobs overnight, some of us lost our income overnight, some of us lost our place of work as patients came in from outside the private sector to have their essential operations investigations in there.’
Like him, some were redeployed and doctors were helped by the IDF to face the new digital world of Zoom.
Very quick negotiations were needed and he said he took his hat off to Bupa in particular because they were extremely good at explaining to their members how consultants were delivering a new online service.
The committee was very clear that remuneration had to be maintained throughout that time, and, as a result, ‘most but not all of the PMIs followed’.
But he added: ‘Surprisingly, quite a lot of the Vitality rewards had significantly dipped, so they had to have a slap on their wrist for their behaviour during the pandemic because they were not as good at remunerating our members for their Zoom calls. That now is getting slightly better, thankfully.’
The IDF is now represented on the Federation of Independent Practitioner Organisations (FIPO) by Mr Christian Barnick. Dr Glyn Towlerton, a consultant in spinal and pain medicine at Fortius Clinic, London, has taken over as the new chairman of the specialist committee, following completion of Dr Preston’s term.
PROMS are way to prove quality
The IDF is aiming to play a strong part in creating new patient reported outcome measures (PROMS).
Specialist committee chairman Dr Sean Preston said in his annual written report that they were an important factor in demonstrating high quality care, ‘but those we have are very few and far between’.
Private doctors should now rise to the opportunity emerging from patients being more willing to pay for their treatment, according to IDF president Dr Neil Haughton.
Demand has outstripped the ability of many independent GPs and consultants to keep up, he told the meeting.
He believed the IDF’s most significant achievement in recent times had been in surviving as a membership organisation during a global pandemic.
It had done its very best with ‘brilliant virtual education and social events’.
Private GP Dr Haughton thanked members of the IDF, which was founded on social networking, for their loyalty. He reported numbers joining had increased at the same rate they did in the years before Covid19.
‘I recently got an email from a member of two years expressing gratitude to the IDF and stating that in decades of membership of royal colleges and other organisations, they had received more support from the IDF than all the rest put together.’
Help offered to become ‘green’
Doctors have been exhorted to take simple measures in their medical practices to help reduce carbon emissions.
IDF GP committee chairman Dr Shaima Villait said in her annual written report that members were recently asked what they were doing in their workplace to help. She said the IDF would provide more support to members who wanted further information and advice on making their practices greener.
Dr Villait wrote: ‘We cannot wait for the pandemic to pass to rapidly reduce emissions. The 2015 Lancet Commission on Health and Climate Change called action on climate change the “greatest opportunity for public health in the 21st century”.’
The IDF has promised it will support members in their practice’s actions to combat climate change
Dr Neil Haughton: Congratulated for his wonderful term as president
Dr Shaima Villait, GP committee head
Vein clinic surges back from Covid
By a staff reporter
Leading vein clinic The Whiteley Clinic is expanding its services to patients on the south coast with the opening of a fourth clinic location.
The new Bournemouth venue, which opened last month, represent a huge boost for the business following a ‘torrid’ two years dealing with the pressures resulting from the pandemic (see Prof Mark Whiteley’s story on page 14).
It hosts a team of experienced venous specialists headed up by Dr David Beckett, an interventional radiologist with a special interest in minimally invasive vascular procedures.
He has over 20 years’ experience and has been part of The Whiteley Clinic team since 2010.
Joining him will be Judy Holdstock, chief vascular scientist at The Whiteley Clinic, who has been with the team since the clinic’s inception in 2003.
She has a specialist interest in the diagnosis of pelvic and ovarian
varicose veins and will lead the diagnostic ultrasound services.
Founded in Guildford by Prof Mark Whiteley, The Whiteley Clinic specialises in treating varicose veins and other related vein conditions, including thread veins, pelvic congestion syndrome (PCS) and phlebitis.
He was the first to introduce endovenous ‘keyhole’ surgery to the UK, performing the first radiofrequency ablation in 1999.
He developed The Whiteley Protocol, a pioneering approach to how vein health should be investigated and how the correct treatment or combination of treatments should be selected to give the optimal result in each individual patient.
The innovative method is used exclusively by the doctors and vascular scientists working or training at all four of The Whiteley Clinic’s locations, ensuring patients get the same standards of care, whichever consultant they see.
Prof Whiteley said: ‘We are very excited to be expanding our ser-
vices and opening-up a brand-new clinic on the south coast.
‘The Whiteley Clinic has already treated several patients from this region, who have travelled to see us at our other locations, so our hope is that the new Bournemouth clinic will allow us to reach even more patients in the area.’
Dr Beckett added: ‘I am very thrilled to be heading up such a wonderful team at the new Bournemouth clinic. Having been part of The Whiteley Clinic team for more than 12 years, I have seen first-hand how life-changing the pioneering treatments that we offer can be for patients.’
In Bournemouth, the clinic offers a full service for vein problems, including diagnosing and treating varicose veins, thread veins, venous eczema, haemosiderin, venous leg ulcers, phlebitis and DVT.
A diagnostic service for PCS, estimated to affect between 500,000 and 1.5m women in the UK, is also available. Treatments for PCS are performed at the specialist unit in Bond Street, London.
First novel reflux op performed
The UK’s first RefluxStopTM procedure has been performed at London’s independent charitable hospital King Edward VII’s.
Consultant gastrointestinal surgeon Mr Nicholas Boyle and his team are pioneering the minimally invasive technique which they say offers a solution to hundreds of thousands of people in the UK affected by gastro-oesophageal reflux disease.
Despite the proven benefits, just one in 100 patients are currently offered surgery.
Mr Boyle, founder of Reflux UK, said: ‘Reflux can be a complex condition and is best treated in the context of a specialist centre.
‘Establishing RefluxUK and the
Reflux Centre at King Edward VII’s provides the basis for more options, specialised solutions and better outcomes for a condition that can be incredibly debilitating to patients.
‘Our multidisciplinary team process is dedicated to treating the condition in the most effective way.
‘The addition of RefluxStopTM is an exciting development for patients, which will hopefully increase the number of patients eligible to undergo treatment which can transform their lives.’
Hospital chief executive Lindsey Condron called the new procedure a welcome step forward for improving the quality of life for those affected.
Unlike traditional fundoplication, RefluxStop does not compress the oesophagus. The hospital said in contrast the evidence is that most patients experience minimal swallowing difficulties following surgery or other potential sideeffects, including difficulties with belching or vomiting.
Performed as a keyhole operation, the procedure includes repair of a hiatus hernia when present and strengthening of the lower oesophageal valve (LOS) – failure of which is the primary cause of reflux.
A small silicone device is placed on the upper part of the stomach through minimally-invasive laparoscopic surgery and helps maintain the LOS in the correct
position, allowing it to work efficiently.
Patients are discharged the same day as their surgery, which limits the challenges with eating and swallowing during recovery, particularly for those with poor oesophageal motility.
Prof Mark Whiteley, clinic founder
Judy Holdstock, vascular scientist
Dr David Beckett, interventional radiologist
The Whiteley Clinic is based at Clinic @78, 78 Poole Road, Westbourne, Bournemouth, BH4 9DZ.
Surgeon Mr Nicholas Boyle, founder of Reflux UK
Doctor spurs relief effort for Ukraine
By Douglas Shepherd
A Ukrainian doctor practising in the UK has teamed up with his hospital operator to deliver over 110 tonnes of urgent medical supplies to hospitals across his homeland. His appeal has received a massive response from colleagues with more than £1.4m worth of medical supplies and funds donated by Circle Health Group’s 53 hospitals, staff and suppliers so far.
Dr Sergey Tadtayev, a consultant urological surgeon at Mount Alvernia Hospital, Guildford, and the Runnymede Hospital, Chertsey, Surrey, said: ‘My heart breaks for my fellow doctors back home who are fighting heroically to care for the sick and wounded – even as the bombs continue to fall.
‘Hospitals are struggling to get basic supplies because transport and manufacturing have been so badly disrupted, so I knew I had to do something to help.
‘Moving 100+ tonnes of medical supplies between hospitals sepa-
Compiled by Philip Housden
NHS preparing strategy for private patient units
NHS England and NHS Improvement Commercial are preparing a national strategy for Private Patient Development.
They have brought in Latchmore Associates to provide external strategic advice and support on how the NHS private patient offer in England could be optimised to generate the most efficient and effective return on investment. It is hoped the strategy will address the current regional variations across England and provide practical options, solutions and enablers to support private patient growth in trusts, which will include an assessment of investment opportunities.
The NHS Revenue and Finance Contracting Guidance for 2022-23 supports increasing private patient
rated by thousands of miles and several borders has been an incredible team effort, and I have been overwhelmed by the generosity of my colleagues at Circle Health Group.
‘They are moving heaven and earth to get help to those who really need it on the front line, and I am humbled by the solidarity and support for my homeland.’
Volunteer hauliers from the UK, Poland and Ukraine have made the journey since mid-March to deliver the urgent supplies to reach hospitals in Kyiv, Kharkiv, Mykoliav, Odessa and Lviv.
The latest delivery contained £185,000 of medical equipment loaded on 35 pallets, including five ventilators, an operating table, patient monitors, suction
tubing and chest drainage sets and sterile gowns.
The hospital’s medical director said: ‘We are sure that all the medical aid will help in the treatment of our patients during this terrible period. The support of people from Great Britain is now very valuable for Ukrainians. We will always remember this.’
Circle chief executive Paolo Pieri said: ‘It’s hard to know how to help in the face of such enormous suffering, but as a hospital operator and one of the UK’s largest employers we knew we could provide unique support for hospitals caring for the sick and injured.’ Those wishing to help should email sourcingteam@bmihealthcare.co.uk
revenues, currently estimated at around £600m, but now bouncing back from the Covid-affected total of £380m in 2020-21.
The total England private patient market is worth around £7b a year and NHSEI estimates the NHS share of this private patient market could be increased by up to £800m a year if best practice were to be shared to maximise opportunities based on the strengths and unique selling points of the NHS.
It is expected that the strategy and supporting plans will be available later this year.
Barts private unit to restore activity to pre-Covid levels
Following the recent opening of the £70m, 55-bed, three-theatre and 26-consulting room Nuffield Health at St Bartholomew’s Hospital last month (see page 30), the trust is aiming to optimise utilisation of spare and fallow capacity
without jeopardising the delivery of NHS services.
As I write, there is no ring-fenced or dedicated beds and clinical capacity for private patient care.
Two beds created from redundant space at the trust’s Newham Gateway Surgical Centre for private patient care have not been used for the intended purpose, due to the prioritisation of the recovery of NHS services, but will now be put into action.
The Gateway Surgical Centre, in the grounds of Newham Hospital, has 39 beds supporting day care and elective surgery from three operating theatres.
The two private care beds were created to make use of operating theatre down times and consultants’ own private time for potential private patient care.
A spokesperson said: ‘There are multiple resultant benefits to NHS services, as all the revenue goes to
the NHS services. Revenue from using theatre “down time” goes to contribute to the fixed costs. There are many NHS patients on the waiting lists who are capable and looking to pay for their care.
‘These patients are being treated in independent hospitals by consultants in their private time. Offering them the facility to treat the patients in an NHS hospital brings the much-needed funds into the NHS, takes the patient off the waiting list, and potentially frees up a slot for another NHS patient to receive care.’
The 2020-21 trust’s annual accounts reported that total private patient revenues were £1.56m, down 70% from £5.3m pre-Covid. This represents a decline from 0.36% to 0.1% of total trust income.
Philip Housden is a director of Housden Group
Dr Sergey Tadtayev (inset) and the first of many lorries setting off for the Ukraine with donated medical equipment
PPU WATCH
Mental health top of pay help claims
By Charles King
Doctors’ mental health problems have been highlighted by new figures showing these conditions accounted for the highest number of income protection claims last year.
Just over a quarter of claimers put mental health down as the primary factor behind their claim with the mutual Wesleyan Financial Services.
But hospital doctors and GPs recorded the highest number of mental health claims.
NEW HEAD FOR GMC
A consultant ophthalmologist has been appointed as the new chairwoman of the GMC.
Dame Carrie MacEwen, honorary professor at Dundee University, served as chair of the Academy of Medical Royal Colleges until 2020 and is past-president of the Royal College of Ophthalmologists.
She is only the second woman to hold the chair since the GMC was established 164 years ago.
Dame Carrie said: ‘This is a particularly challenging time for healthcare and I look forward to working collaboratively with partners across all four countries of the UK to support doctors to provide the best possible care for patients.’
GMC chief executive Charlie Massey said: ‘In particular, Carrie will play a vital role in driving forward our new strategy, which shifts the emphasis of our work from acting when things have gone wrong to continued support for all doctors in the delivery of the highest standards of care.’
As many as 39% of claims from hospital doctors were due to mental health issues and 38% of GPs also cited mental health as the primary reason for their claim.
Long hours and physically and emotionally exhausting workloads in the pandemic contributed to widespread burnout and a knockon impact on the mental health of a large number of health care professionals, the company said.
Alec Collie, its head of medical, said: ‘It is alarming that mental health tops the reasons for income
protection claims. Recent figures show that 58% of doctors are currently suffering from symptoms of depression, stress or anxiety and many are expected to leave their positions this year as a result of their mental health.’
Wesleyan said it had donated more than £100,000 to charities offering mental health support to doctors and dentists.
See www.wesleyan.co.uk/ news/2021/02/1-million-support-package and www.bmj. com/content/372/bmj.n22
Newmedica opens clinic in Worcester
Six consultant ophthalmologists have partnered to open a new eye health clinic and surgical centre.
Newmedica Worcester is run by a team of seven partners: operational director Josh Raden and specialists Mr Malcolm Woodcock, Mr Tarun Sharma, Mr Ranjit Nair, Mr Salman Mirza, Mr Thomas Jackson and Mr Matthew Edmunds.
The business, situated in Wainwright Road in the town’s Berkeley Business Park, expects to create 30 new jobs over the next 12 months.
Workers won’t talk emotions with employer
A survey of 8,000 UK adults has highlighted that two-thirds of respondents would not feel comfortable raising a mental or emotional well-being issue with their employer.
One-third are offered no physical or emotional well-being support at work, according to Nuffield Health’s 2022 Healthier Nation Index and they say mental health worsened in the last year.
Gosia Bowling, national lead for Emotional Wellbeing at the charity, said: ‘The pandemic has affected the mental health of many employees, so it’s more important than ever that employers find ways to create inclusive and connected workplace environments where people feel supported. Not only will this help productivity, but it will also boost happiness levels.’
New guidance on dealing with bad behaviour
Private doctors requiring advice to deal with bad behaviour from patients may find new guidance for NHS GP practices useful. It sets out the type of inappropriate or unacceptable behaviour that could lead to a warning, or removal from the practice list.
An updated version of NHS England’s Primary Medical Care Policy and Guidance Manual (PGM) includes a new chapter on the types of behaviour by patients that could lead to further action.
It is the latest venture from independent health provider Newmedica which has clinics across England.
Patients have free onsite parking with charging points for electric vehicles and there are good public transport links.
The clinic and surgical centre will provide private and NHS treatment for cataract surgery and aftercare, and will also offer YAG laser treatment. Additional services are planned for the coming months.
The Medical Defence Union has backed a call in the guidance for practices to review their policies on unacceptable patient behaviours to ‘explicitly’ include positions on not tolerating any form of discrimination or harassment.
Dr Ellie Mein, MDU medicolegal adviser, said: ‘It is never acceptable for healthcare professionals to be abused in the course of their work and this guidance will go some way to reassuring practice teams . . . of the situations when action should be taken.’
Intraoperative MRI treats first patient
By Leslie Berry
Delighted specialists at HCA’s The Wellington Hospital in London have used a new intraoperative magnetic resonance imaging (iMRI) scanner on its first patient.
The 3T Siemens scanner, integrated into the BrainLab digital operating theatre, allows a scan of a patient’s brain during surgery to give surgeons confidence they have achieved their treatment goal and reduced the need for the patient to have additional surgery in the early postoperative period.
Neurosurgeon Mr Ian Sabin, medical director of the London Gamma Knife Centre there, said: ‘The new iMRI scanner provides our patients with the gold standard of care.
‘With this technology, neurosurgery patients with brain tumours
Healthcode appoints new business boss
Online products and services company Healthcode has appointed Richard Aris to the new post of head of business development.
He will lead a team building long-term partnerships with doctors’ practices, hospitals and insurers to give them support and inform them of products and services aimed at helping them operate more efficiently.
Mr Aris said that in a previous private healthcare job he found businesses working ‘in quite an oldfashioned way’ compared to other sectors, particularly with administration of claims and remittances.
‘I always liked the idea of com-
‘Give patients more choice’
Record NHS waiting lists make it vital to give patients more choice and control of their care, according to the Independent Healthcare Providers Network (IHPN).
Mr Ian Sabin, consultant neurosurgeon at HCA’s The Wellington Hospital discussing a brain scan
will have the best possible chance of tumours being removed fully without the need for further surgery.’
Following the iMRI scan, if further surgery is needed, the surgeon can continue immediately, eliminating the need for patients to have a scan next day while conscious and reducing the risk of them having to undergo another operation.
Chief executive Mr Eric Reichle said the hospital’s investment in its neurosurgery centre further enabled its commitment to provide outstanding care for patients facing the most challenging neurological conditions.
Patients from across HCA’s private hospital and specialist centre network in the UK would have access to the best specialist support and care possible.
ing back and helping businesses to streamline their processes and this is Healthcode’s mission too, so it felt like the perfect match.’
He said the firm was developing exciting products which would support customers’ businesses and the industry as a whole.
His appointment is part of a transformation programme involving an overhaul of business systems and processes, as well as strategic recruitment to enable Healthcode to expand and operate effectively on a bigger scale.
Calling for concrete action to improve access to treatment, its chief executive David Hare said tackling the elective backlog was the public’s number-one priority
for the NHS and people wanted to see the Government delivering on its promises.
These included ‘significantly increasing the use of independent providers, and doing all it can to ensure that the additional National Insurance funding boost which is now in force delivers improved services for patients’.
Nuffield Hospital director doubles up by taking over nearby unit
A Nuffield Health hospital director has been given an additional job – doing the same role six miles away at another hospital in the group.
Justine Hillier’s new job is at Woking, Surrey, but she will also continue in her current post at the charity’s Guildford hospital.
Part of her remit is to identify shared ways of working across both hospitals.
She said: ‘By working together, we will be able to offer an even broader choice of diagnostic investigations and clinical services for people in local communities as well as providing greater opportunities for our staff to learn and develop.’
Ms Hillier, who joined the
Guildford hospital in 2015 as matron, added: ‘Having a nursing background has been invaluable in my transition to hospital director, as it has provided me with real insight into the delivery of safe, effective clinical care.’
Foreign docs without a lawyer suffer for it
Nearly two-in-five doctors (37%) who graduated overseas had no legal representation when facing a Medical Practitioners Tribunal Service (MPTS) hearing, according to figures obtained by the Medical Protection Society (MPS) covering 2018-21.
The figures, obtained through a Freedom of Information request, also showed overseas medical graduates without legal representation were more likely to receive a harsher sanction. 83% were either suspended or erased from the medical register, and only 8% received a ‘no impairment’ judgment.
In comparison, 55% of overseas
medical graduates with legal representation were either suspended or erased from the medical register, and 27% received a no impairment judgment.
A more lenient ‘warning’ was also a more common outcome for those overseas graduates with a lawyer present.
MPS president Prof Dame Jane Dacre said the GMC figures were a powerful reminder of how important it was for these doctors to ensure they had support with GMC investigations as soon as they started work. ‘I cannot imagine facing this process alone, without someone fighting my corner.’
Richard Aris
Justine Hillier
A look back through our journal’s archives of a decade ago reveals that although times change, some issues are not so new
A trawl through the archives: what made the news in 2012
Analysis of complaints due to fees
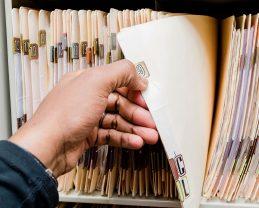
A defence body was launching a detailed analysis of complaints against independent practitioners after finding a high level of patient dissatisfaction over charges.
The MDU said over a quarter of 40 cases reported by private consultant members in a ‘snapshot review’ involved patients refusing to pay for their treatment or requesting a refund.
In around two-thirds of the cases, the doctor eventually agreed to waive fees or give a refund.
A spokesman for the union told Independent Practitioner Today: ‘While refunds and goodwill payments are a feature of complaints in independent practice, there is no guarantee that
this kind of goodwill gesture redress will settle a complaint or avoid a future negligence claim.
‘In addition, it may be a mistake to assume that a complainant is only interested in getting a refund.’
Huge pension disparity
Doctors who accepted a future NHS retirement age of 68 were being warned they would have to live for nearly another full century to match the pension benefits of those leaving their post in June 2012 at 60.
Dramatic new figures from financial advisers, released as BMA members prepared for industrial action over pension reforms, strongly challenged Government claims regarding the effect on consultants and GPs.
Reacting to the results of the association’s ballot on action, Health Secretary Andrew Lansley claimed: ‘Today’s newly qualified doctor who works to 65 will get the same pension as the average consultant retiring today would receive at 60 – the BMA has already accepted a pension age of 65. If doctors choose to work to 68, then they could expect to receive a larger pension of £68,000.’
But figures from specialist financial advisers Cavendish Medical suggested that although doctors might get a higher pension of £68,000 at 68, they would do well to equal benefits received by
their older colleagues retiring at 60 if they wanted to draw a lump sum of three times pension. It told Independent Practitioner Today that moving the normal retirement age back eight years to 68 had real implications for future senior consultants and GPs: ‘Simply put, by the age of 68, a doctor retiring at age 60 would have drawn £568,955 under the 1995 terms.
‘Those retiring at age 68 under the new Hutton terms would need to be alive and still drawing their pension at age 166 for the cumulative increase to exceed the benefits of colleagues who retired earlier.’
Call to ban surgery ads
The British Association of Aesthetic Plastic Surgeons was stepping up its pressure to win an outright ban on cosmetic surgery advertisement in public places such as billboards and public transport.
First clinic in UK for obese patients
Consultants set up what was billed as the UK’s first dedicated bariatric clinic. The Sudbury Clinic, in the grounds of BMI The Clementine Churchill Hospital, Harrow, north London, was designed and opened by weight loss surgery group Streamline Surgical.
Doctors start online GP service
Independent GPs set up what they called a revolutionary new concept – an online private general practice service.
GP At Home was the brainchild of private Harley Street GPs Dr Fiona Payne and Dr Justine Setchell (pictured above), who said they saw a need for people to be able to access medical advice and support quickly and conveniently.
Dr Payne said: ‘We are seeing demand for online service in all aspects of our lives, and access to GP services is no different – our pre-launch trials have shown a huge amount of interest.’
TELL US YOUR NEWS
How about making the news today? Independent Practitioner Today is always keen to hear from doctor entrepreneurs willing to share their stories in private practice – and from independent practitioners embarking on the journey.
Contact our editorial director Robin Stride at robin@ip-today. co.uk
Spending too much time on billing instead of patient care?
Let Medical Billing & Collection do the hard work for you.
With 30 years’ experience helping over 1,500 private consultants, groups, clinics and hospitals.
• Dedicated account manager
• Reduce bad debts to less than 0.5%
• Increase net income by up to 25%
• 24/7 online access to your data
• Faster payments through e-billing for insurers and patients.
Discover more at medbc.co.uk or 01494 763999
How to hang on to
With severe staffing shortages creating real dilemmas in private healthcare, recruitment specialist Keith Hague (below) explains why he believes great leadership is the cornerstone of staff retention
your staff
IN HEALTHCARE, the recruitment and retention of staff has become a serious challenge creating huge business dilemmas.
Suddenly we are faced with a European employment market that has greatly diminished since Brexit. Covid caused the lack of travel and isolation of staff who were once willing to become foot free.
The cheap supply of European healthcare staff is now a thing of the past and we have to get used to it. The tactics we tried in the past to retain staff cannot be relied upon because everyone is doing it.
Healthcare recruitment is not an isolated problem. Timpson, the well-known key-cutter and cobbler who have successfully hired reformed prisoners for 20 years,
now faces stiff competition from the likes of Greggs, Greene King, and even Pret a Manger.
Their chief executive James Timpson said that for years they took all the best people from prison and they were the only one doing this, now things are much harder as they fight the competition for scarce staff.
Jim Collins in his iconic leadership book Good to Great , selling over 3m copies since 2001, states that ‘people are not your most important asset, but the right people are.’
He is right, of course, but in today’s market do we really have the option of just appointing the right people or will anyone with the right qualification or experi -
ence suffice? The latter seems to be the case presently.
Both public and private sectors, of course, face the same challenging problems in healthcare, but here I want to concentrate on the private sector employment issues, and specifically on staff retention, because if you don’t have a retention problem you hardly need to recruit new people. So keeping staff has to be the first key challenge.
High turnover is the killer
In my early days as a healthcare chief executive both inside and outside the capital, turnover was manageable: around 3% to 4% outside and 9% to 10% inside.
However, a number of London chief executives have told me
I am always astounded by how chief executives want to sit in their offices all day, isolating themselves from the business on the grounds that they are so busy
recently that turnover can climb to 20% and when one fifth of your staff leave every year, that’s almost impossible to manage and it carries hefty recruitment costs that might in the event lead to nought.
In today’s tense staffing market the recruitment of good staff now relies more than ever upon the ability of one hospital to poach or steal good staff from its nearby competitor, offering huge uplifts in salary to do so.
But it doesn’t stop there. Hospitals are taking the view that stealing staff from the same hospital group is now an acceptable practice. One chief executive told me: ‘Who cares anyway, so long as we have the staff to service the next day’s shift.’
Yet this only saves the day, but does not sort out the problem in the longer term. This ‘I’m all right, Jack’ mentality is now common place as well as being a very expensive option.
One private hospital offered a £9,000 salary uplift to poach a topquality theatre nurse into their business.
Others faced with losing staff will suddenly offer that long-promised training course requested years ago plus a small top-up in salary for good measure. Again, it’s all about firefighting with no underpinning strategy.
The well tried ‘golden hello’, where staff are appointed on the promise of a lump sum of money on signing an employment contract, certainly gets people through the door.
And if you stay for three years, then along comes another lump sum just before Christmas, should you be asked to stay for another three years.
But how do the rest of the loyal staff, who have had no such offers, feel about that? From my experience, they become alienated and look to leave for a ‘golden hello’ themselves somewhere else – and why not? So we are back to where we started on that long circuitous journey that never ends.
It is not all about pay
Clearly, there are some good retention tactics that can work and your excellent HR director will tell you that staff development and training is a key to good retention, and this is true.
Yet it has to be well directed, with a long-term commitment given, and who gets the best devel-
The boss needs to be visible to walk the floors to listen to individuals’ concerns and always offer respect to the lower-paid echelons who can offer so much to any organisation
who can offer so much to any organisation.
Being genuine with people, being supportive and visible counts for a lot when it comes to retention.
Over the years, managers have persistently requested me to build bigger better new offices for them. But if you build offices for managers, they will sit in them all day. People want to see the boss and listen to their view.
Keith Hague’s warning of shortages was our front-page story last month
opment must not be down to who fills out the best form and who speaks the loudest.
Development programmes can, of course, be costly and they must be carefully managed and well directed. But they can work very effectively.
Numerous management papers have been written over the years which show that pay, while very important to staff, can be trumped by committing to a person’s longterm development prospects.
An opportunity to study for qualifications that allow a person to move to the next level in seniority can have very positive effects on retention.
Great leadership assists staff retention
Various tactics of retention have been tried over the many years I have been managing healthcare businesses, some good some not so, but one thing that has not really been explored is the link between staff retention and leadership.
When I speak to chief executives and other healthcare senior leaders, I am always astounded by how they want to sit in their offices all day, isolating themselves from the business on the grounds that they are so busy.
They believe that being a chief executive entitles them to acquire God-like status and have extreme importance. Most students of management will know that people don’t leave organisations, they leave the boss.
So the boss needs to be visible to walk the floors to listen to individuals’ concerns and always offer respect to the lower-paid echelons
HR directors believe it is a very modern concept to call themselves ‘people managers’, but when was the last time anyone saw a HR director walking the floors? I suggest that this is a rare event.
As head of the Wellington Hospital for many years, we had some incredible people. But probably the most important person was the guy from Brazil who delivered the laundry every day without fail. No fresh laundry, no business. It’s as simple as that.
Start listening to people; understand their problems. You may not be able to solve them, but just not talking for once and simply listening works enormously.
I have been mentoring a physician who is now a chief executive in the Gulf. He has learned the art of getting out of the office so much so that when his doctors want to see him, they don’t come to his office. He goes to see them – after their clinic list or between patients in the theatre rest room or in the local coffee shop. Same for staff. His door is never open because you don’t need to go to his office anymore; he goes into the nursing floors and departments to meet the people in their work setting.
He is admired by the organisation because he cares, and his new business into its second year is surpassing all targets. People want to work there.
I would maintain that the art of good caring management – being visible, taking time to listen to people and walking the floors to feel the temperature of the business – is the best antidote for poor staff retention. Staff rarely leave great bosses.
See ‘Be flexible if you want to retain staff’, page 22
Keith Hague is a director of Goddard and Hague, bespoke healthcare recruitment specialists
A PRIVATE CLINIC’S SUCCESS STORY
Proof that you can flourish after Covid
After a torrid two years, Prof Mark Whiteley’s clinic has gone from the depths of despair and through a consolidation process to emerge flourishing and expanding to new geographical areas. Here he reflects on the lessons learned since the first lockdown
PRE-COVID, MY FOCUS in run -
ning The Whiteley Clinic was to provide the best quality venous treatments possible. Any spare money was pumped back into research and development.
This was excellent for providing research-based high-quality patient care, publishing research papers and getting students through higher degrees, but left the business with no cash reserves. Before Covid I did not worry about this.
On the 23 March 2020, Prime Minister Boris Johnson announced
the national lockdown. One of the exemptions was medical facilities, but pressure from the media forced us to close our clinics (see www.dailymail.co.uk/femail/ article-8147079/Vein-doctor-starsdefies-government-advice.html).
Sudden closure
Indeed, many doctors found their private practices disappearing as network hospitals rented their beds to the NHS during this lockdown.
The sudden closure of our clinics, without any cash reserves,
could have been an utter disaster. Like most businesses, we applied for Covid loans, but apart from the furlough scheme, did not get any Government or bank help. With things looking pretty hopeless, I quickly sold my house to support the business and we had an offer in April and moved out in July. Fortunately, however, this turned out to be our lowest point. As the guidelines still excluded medical services from the lockdown, I phoned Public Health England to ask if we should have
The Clinic @78 in Bournemouth, which opened in May, is The Whiteley Clinic’s fourth location
Patients were getting desperate for assessment, as they were finding it very difficult to get medical advice from their GPs and A&E departments
MEMBERS OF THE CLINICAL TEAM
Dr David Beckett, an interventional radiologist with a specialist interest in minimally invasive vascular procedures
closed. Unfortunately, it would not give me a definitive answer.
Over the weeks, increasing numbers of patients were contacting us through our emergency phone number and website with infected ulcers, painful legs, swollen ankles and other concerns.
They were getting desperate for assessment, as they were finding it very difficult to get medical advice from their GPs and A&E departments.
At this time, I heard a Government minister interviewed on the BBC as saying that many businesses that had closed down had not needed to by the rules, and hence should not be supported financially!
This led us to explore how to reopen quickly and safely, providing a Covid-secure environment.
During April and May 2020, we worked towards providing a Covidsecure environment, with Cordell Health providing excellent advice and inspections.
Skeleton service
We had regular communications with the Care Quality Commission (CQC), informing it of what we were doing every step of the way. By taking these steps, we were able to set up a skeleton service in June 2020, ten weeks after the onset of the lockdown.
With regular staff testing, initially by PCR and then lateral flow tests, and imposing restrictions on our patients, which have since become routine for most medical clinics, we were soon back to fairly normal working.
Of course, there are still disruptions when a clinical member of staff tests positive for Covid, but we have now become used to these and try to build in some flexibility to keep our service as good as possible for patients.
On the business side, we had to take several emergency measures. We appointed a financial director who was very good in the shortterm at crisis management, and who negotiated with all our creditors to repay outstanding credit over 12 months.
We had discussions with all employees as to which jobs were essential, and which were nonessential and could be made redundant. Following these dis -
➱ continued on page 16
The free digital prescribing platform for all private prescribers.
CloudRx take care of the dispensing, payment and delivery of medicines direct to your patients, wherever in the country they may be, for more convenient access to their medicines.
TRANSFORMATIONAL
Order prescriptions at the touch of a button to support all consultations and add a whole new level of convenience for your patients.
SIMPLE, CONVENIENT AND SECURE
Simple and fast digital prescribing.
Legal paperless prescriptions, repeat prescriptions and controlled drugs.
Prescriber fees can be charged to the patient if requested.
INTEGRATED
Our API enables frictionless integration with healthcare brands & clinical software including Heydoc, MidexPRO, eClinic and YouClinic.
“We were struggling to keep up with the admin side of the prescriptions, not to mention storage for medication to cope with a huge increase in prescriptions. CloudRx immediately took away the strain. Since our partnership we have grown by more than 200% in size. We could not have done that without their support.”
– Dr Louise Newson, Newson Health
Sonographer Judy Holdstock, chief vascular scientist at the Whiteley Clinic
Prof Mark Whiteley, clinic founder
cussions, several of our staff were happy to undergo voluntary redundancy.
Naturally, there were a couple of staff who did not feel their jobs were redundant, but analysis persuaded them otherwise.
Finally, a review of all of our contracts highlighted several areas where money was not being spent wisely, or was frankly wasted, and these contracts were terminated.
By September 2020, our income had reached pre-pandemic levels, and with a much more efficient business structure, we started to have profitable months.
With the reduction of international travel for vein conferences, and by concentrating on the business itself, we ended up with an end-of-year profit higher than we had ever had before.
Now into our second year, and without the repeat of a lockdown and restart, our second year has shown even more business growth as well as increased profits.
Research department
Although we were able to keep on a basic level of research during lockdown, we have been able to grow our research department again, maintaining our position as innovators in the venous world.
The result of this is that despite Covid and the lockdowns, we are expanding the number of our clinics. We have just opened our fourth clinic in Bournemouth and are looking to open Whiteley Clinics elsewhere in the country.
As such, we are now looking to recruit more consultant surgeons or consultant interventional radiologists who wish to have a good private practice in venous disease, and we are employing more fulltime clinical vascular scientists (vascular technologists) to train in our protocols.
Comparing our experience of the pandemic with other doctors and healthcare providers has shown a variety of different experiences.
Many NHS consultants who have admitting rights to network private hospitals found themselves left ‘high and dry’ when those private hospitals rented their beds to the NHS during the pandemic.
We were fortunate that, by having our own ambulatory clinics,
How has your private practice got back on track after the easing of pandemic restrictions?
Share your story with Independent Practitioner
Today readers. Email robin@ ip-today.co.uk
INTERESTED? THEN GET IN TOUCH
Doctors who are interested in being part of this expanding network of clinics are welcome to contact Mark Whiteley directly for a confidential discussion in the first instance at mark@ thewhiteleyclinic.co.uk
Mark Whiteley and Judy Holdstock performing local anaesthetic endovenous surgery under ultrasound control
Operating at The Whiteley Clinic, Guildford, Surrey
Stressful times such as an unexpected pandemic go to show that to keep medical facilities open for patients, basic business principles need to be followed
we were in charge of our own facilities and so our consultants did not have these problems.
Several other clinics kept to the Government guidelines and did not close at all during the pandemic. Although these might have been held up as irresponsible early in the pandemic, history has now shown that this was the best thing to do and it was important to have kept medical clinics open, pro -
vided they had good Covid-secure protocols.
Although doctors often think that they are different from business people, and medicine is different from business, stressful times such as an unexpected pandemic go to show that to keep medical facilities open for patients, basic business principles need to be followed.
Increasing acceptance
Understandably, coming out of the pandemic, private health should be seeing a resurgence. There is rarely a week where the news does not feature the incredible NHS waiting lists and the lack of staff.
Moreover, the public continue to research their own health issues and there appears to be increasing acceptance of private healthcare. Data on 1,131 private hospitals and clinics by the business analysis company Plimsoll UK (Plimsoll.
co.uk) states that, in the last year, there has been a 6.6% growth in sales, but this is not fairly distributed over all private hospitals and clinics.
It quotes 176 (15.6%) are serial loss-makers and although the private health market is growing, 392 (34.7%) companies are in decline and 295 (26.1%) companies are in danger.
So, looking back over the pandemic, health has been the main focus of most news outlets over the last two years. The NHS has a huge backlog of patients on waiting lists and so opportunities for working in the private sector should be rosy.
However, business analysis shows that not all private hospitals and clinics are being successful, and hence not all doctors doing private practice are going to see the benefit of their labours.
The Whiteley Clinic has always aimed to be the premier vein clinic
in the UK, and potentially abroad, based on our research-led protocols and medium- to longterm results.
In practice, this means that patients are not only happy with their results in the short-term, but have the lowest chance of recurrence in the medium and long term.
This separates us from clinics that compete on price but fail to adopt the new approaches to venous diagnosis and treatment that attains these benefits.
With patients and other funders of healthcare becoming more sophisticated at checking outcomes, we believe that this approach will prove to be not only beneficial for patients but prove to be cost-effective in the medium to long term.
Prof Mark Whiteley’s clinics are at Guildford, London, Bristol and Bournemouth
GMC a bit vague in its rulebook revise
Following the launch of a consultation on a new version of Good Medical Practice, Dr Caroline Fryar (below) shares some initial reflections and asks whether the GMC guidance represents the realities of medical practice or, instead, the aspirations for what it should be
IT HAS been almost a decade since the last revision of Good Medical Practice
If you take just a moment to pause and reflect on all the developments and events that have taken place in UK healthcare since then, it is perhaps unsurprising that the GMC has decided to introduce a new version of this fundamental piece of guidance.
However, what is surprising, is the scale of the change the GMC is proposing in this new version.
Good Medical Practice is central to everything the GMC does. Indeed, it is one of the core tools used by the GMC in its fitness-to-practise processes, so every paragraph and every single word in the guidance document really does matter, as doctors will be judged against it.
A consultation on the new version of the guidance runs until 20 July. The MDU is forensically scrutinising all the changes and additions and will respond on behalf of our members.
In the first instance, here are some of our initial impressions.
This is a fundamental redraft of the guidance. Spread over four ‘domains’ – as before – but with three of the four now falling under new headings.
They are:
1 Working with colleagues – describing how professionals should treat each other and work together in the interests of patients and service improvement.
2 Working with patients –describing the different aspects of good doctor-patient relationships, particularly communication and shared decisionmaking as set out in the GMC’s more recent consent guidance.
3 Professional capabilities – an expanded section describing the range of capabilities that underpin safe, effective practice, including demonstrating leadership and reflective practice.
4 Maintaining trust –describing the conduct needed to maintain public confidence in the profession, with new duties concerning social media and dealing with sexual harassment.
Two central themes underpinning many of the changes and additions are a greater focus on the leadership expectations of all doctors as well as an increase in focus from the GMC on doctors using their professional judgement in a variety of situations.
In launching this new version of the guidance, the GMC is on record as saying that it believes all doctors are leaders.
This is a bold statement and may be challenging in practice. It is a statement that underpins a large number of the changes in the guidance – where the GMC has drawn heavily from Leadership and Management for Doctors and incorporated much of that into the new version of Good Medical Practice. However, when taken with an increase in focus on professional judgement, particularly with doctors’ obligations to maintain a good workplace culture, we have some concerns about the potential unintended consequences here.
These proposed additions are all linked to a fundamental question at the heart of this new version of Good Medical Practice: what the guidance is trying to be, and what it actually is
Is it clear what the GMC expects?
Let’s take paragraph 7 as an example. It states: ‘You should take action, or support others to take action, if you witness or are made aware of bullying, harassment or unfair discrimination.’
Now, quite rightly, the GMC does not want to be prescriptive about what kind of ‘action’ should be taken in these situations. So, what action would be sufficient?
Discriminatory comment
The GMC suggests it might be sufficient to simply ask the person on the receiving end of this treatment if they are OK; but is that really enough?
If everyone in a team meeting hears a discriminatory comment,
are all doctors present expected to be involved in taking action about that; what if the person subject to the treatment you witness specifically asks you not to take it any further?
These are just some of the open questions posed by these sorts of additions to the guidance, and underline why it is so important to attain maximum clarity from the GMC while not creating sweeping and burdensome duties on individual doctors.
Another example can be found at paragraph 22. It states: ‘You should treat patients with kindness, courtesy and respect.’
Focusing in this instance simply on the word ‘kindness’, doctors, of course, want to be kind to their patients – but what does it mean to be kind?
The GMC has said it is testing the word’s inclusion in Good Medical Practice , acknowledging that it means something different to different professionals. We also suggest it can mean something very different to different patients.
These proposed additions are all linked to a fundamental question at the heart of this new version of Good Medical Practice : what the guidance is trying to be, and what it actually is.
Aspiration or reality
There have already been many comments made about some of the new additions to Good Medical Practice – from the inclusion of that word ‘kindness’; to obligations not to condone certain behaviour on social media; to having regard for global health when taking account of the resources available to treat patients.
Kindness, tackling abuse on
We reported on the launch of the GMC’s consultation last month
social media, climate change – all of these issues matter profoundly and are of the utmost importance. However, Good Medical Practice is not a manifesto outlining the aspirations for the healthcare system: it is the principal document by which doctors and their registration with the GMC are held to account.
Hence, the duties and responsi-
bilities it places on the profession must reflect the realities of the healthcare system and the individual doctors within it. The guidance must be accessible, understandable and achievable for doctors.
Through guiding, supporting and defending our members in GMC matters, we have considerable experience of how Good Medical Practice is viewed by both doctors and the GMC itself.
We are thoroughly engaging with this consultation, as we want to ensure the guidance delivers for doctors, so they can deliver for patients.
This is a rare opportunity to actively shape a fundamental piece of guidance from the GMC. Independent practitioners can www.themdu.com/press-centre/ contact-the-press-office to share their views with the MDU.
Dr Caroline Fryar is the MDU’s director of medical services
Now open on weekends
Now open on weekends
Now open on weekends
NEW SESSIONS ARE AVAILABLE FOR INDEPENDENT PRIVATE PRACTICE ON WEEKENDS.
NEW SESSIONS ARE AVAILABLE FOR INDEPENDENT PRIVATE PRACTICE ON WEEKENDS.
NEW SESSIONS ARE AVAILABLE FOR INDEPENDENT PRIVATE PRACTICE ON WEEKENDS.
Fully CQC-registered clinic
Nursing support
Fully CQC-registered clinic
Fully CQC-registered clinic
Nursing support
Appontment-making
Nursing support
Secretarial support
Appontment-making
Appontment-making
Billing service
Secretarial support
Secretarial support
Billing service
In-house pharmacy
Billing service
In-house pharmacy
In-house pharmacy
We are a leading private outpatient clinic and we are inviting new applications for practising privileges for our extended opening hours on weekends.
We are a leading private outpatient clinic and we are inviting new applications for practising privileges for our extended opening hours on weekends.
We are a leading private outpatient clinic and we are inviting new applications for practising privileges for our extended opening hours on weekends.
Contact: david.briggs@londonmedical.co.uk 49 Marylebone High Street, London W1U 5HJ
Contact: david.briggs@londonmedical.co.uk 49 Marylebone High Street, London W1U 5HJ
Contact: david.briggs@londonmedical.co.uk 49 Marylebone High Street, London W1U 5HJ
londonmedical.co.uk
londonmedical.co.uk
londonmedical.co.uk
THE RISE IN SELF-PAY PATIENTS
Tap into the self-pay
Following the latest LaingBuisson report on self-pay, author Liz Heath (below) reflects on the private acute self-pay market and whether the optimism expressed by so many in the sector is founded on evidence of sustainable growth
THE EVER-GROWING scale of NHS waits has been cited by many as a reason for the surge in demand for private consultation and diagnostics.
In imaging, for example, some providers report increases of more than 50% in demand for self-pay MRI scanning.
And Spire Healthcare, in its halfyear statement for the period up to June 2021, reported 46.7% self-pay revenue growth compared with the same period in 2019. It could be argued that we are in the beginning of what should be a boom time for private acute and diagnostic providers – but what might be holding sustainable growth back?
The most commonly cited constraint on growth is capacity and resource, specifically staffing. This is an issue across the whole public and private health sector and one that does not have an easy solution.
Reluctance to enter
A newer factor, and possible barrier to growth, is for many consumers a reluctance to enter a world that, for some, has never been a part of their personal healthcare landscape.
This is something providers are aware of and messages of reassurance around quality of care, approachability and affordability are now frequently seen in multichannel promotion and consumer engagement.
LaingBuisson’s estimates of the self-pay market value in 2019 were around £1.1bn. As yet, full data on activity and revenues is not available for 2020-21, but estimates suggest a UK self-pay market value of between £780m to £850m.
As evidenced by Spire’s recent full year results for 2021, we should anticipate significant bounce-back through 2021and 2022.
This is not the case with cosmetic surgery. Despite some pent-up demand for cosmetic surgery in mid to late 2020 and into early 2021, there has not been a sustained surge in the same way as elective self-pay.
While people seem more willing and able to seek self-pay options
for elective treatment, they are not any more willing to pay for cosmetic surgery than they were prepandemic.
But we should also note that at the same time, demand for nonsurgical cosmetic treatments continues to grow.
Increase in interest
We are seeing definite signs that some areas of the UK not traditionally self-pay ‘hotspots’ are starting to change.
There has been an increase in interest in areas across northern and eastern England, Wales and Scotland as well as increased activity everywhere else, including the London and the South-east.
self-pay market
This suggests that either through choice – or a perceived lack of NHS choice – patients are actively seeking out self-pay options. These areas of recent growth also correspond with areas of lower private medical insurance (PMI) penetration.
We suggest that this lower PMI uptake may mean when a decision is made to opt for private treatment, it is less likely to be covered by insurance and thus self-pay becomes the only option.
In terms of specialty mix, those specialties and procedures driven by age-related conditions such as arthritis and cataracts continue to comprise the bulk of self-pay activity.
While the picture is complex, it is suggested that, for many older people, using disposable income or savings is a preferred option to preserve quality of life, particularly for those who have not been able to enjoy the type of lifestyle such as frequent holidays during the pandemic.
Cataract and joint replacement surgery also account for some of the largest volume waits for NHS treatment.
Connecting
with consumers
We know from research carried out by YouGov for the Private Healthcare Information Network (PHIN) that more people are considering private healthcare and that in the key self-pay demographic, the over 55s, this is much more pronounced.
But through the same research, costs of treatment were cited as a concern, as were provider reputation, outcomes and, for some, suspicions about the private sector.
However, common to this research and LaingBuisson’s own survey, the main factors influencing growth in demand for self-pay are access and waiting times for NHS diagnostics and treatment.
What the whole sector needs is to ensure its messages about private healthcare in general and self-pay in particular emphasise a welcoming approach, with reassurance about costs and affordability
The ability to spread the cost of treatment, often interest-free, is a key message for consumers that the sector should not be shy about.
It feels as though the whole sector is keen to embrace these new potential self-pay patients. But engaging proactively, ‘speaking the same language’ and connecting with consumers with simple, clear messages is going to be key to creating a thriving and sustainable self-pay market.
There are signs that this is beginning to happen, but undoubtedly more needs to be done to promote the benefits not just of self-pay but of the whole private acute sector.
Consultants returning PHIN research, published in March 2022, suggested that most, if not all, consultants had returned to private practice by the end of 2021.
Some specialties like orthopaedics were almost at pre-pandemic levels. All facets of the private healthcare landscape, including consultant availability, are vital to ensure that demand can be managed effectively and that access to treatment is swift and straightforward.
Are we right to be optimistic? 55.3% of respondents to a survey carried out by LaingBuisson felt the self-pay market would increase by 10-15% over the next three years.
This was up from 52% in 2020 and 45% in 2019. 29% believed the market would increase by 5-10% and just 7.9% believed it would remain static.
In the same survey, NHS waiting times and access to NHS services were overwhelming viewed as the main drivers for interest in selfpay.
As we have already seen, providers, analysts and other commentators are equally optimistic about the market. LaingBuisson is too.
We believe that the sector has the ability to harness the opportunity of growing demand for selfpay over the next three to five years when the prospects of NHS waiting times reducing significantly remain limited.
Many more people are also turning to paid-for healthcare as evidenced by the growth in demand for virtual GP services and diagnostics, for example.
How patients search for private information
It is also interesting to note that in our own research and that for PHIN, the way consumers are searching for information on private healthcare does appear to have permanently shifted.
As well as seeking information from peer groups and medical professionals, consumers are much more inclined to seek out online reviews, use Google or other review providers as well as the Care Quality Commission.
This presents a challenge for consultants and providers in ensuring their messages about safe care and affordability are visible and that they can evidence quality of care and outcomes in a way that supports informed consumer decision-making.
We cannot ignore the affordability of self-pay treatment either. Finance options have been offered by providers for many years, but the prominence of payment plans is much greater now.
On that note, it is really important to ensure that patients are able to quickly and easily engage with consultants, their secretaries or admin teams.
For many patients, their first touch-point in the private healthcare sector may be a call or email exchange and we need to ensure that not only are they given a swift and friendly welcome, but that we support them through a process that may be entirely new to them.
But what the whole sector needs is to ensure its messages about private healthcare in general and selfpay in particular emphasise a welcoming approach, with reassurance about costs and affordability.
And not least, clear and transparent information about the safety of care.
For more information on how to buy a copy of the LaingBuisson Selfpay Market Report 4th Edition, call: 020 7841 0045 or email: sales@laingbuisson. com
Be flexible if you want
Our troubleshooter Jane Braithwaite (right) answers independent practitioners’ frequently asked questions on business matters.
This month: Now that my team has had a taste of home working, they all want to work from home more of the time. How do I make this work?
want to retain staff
HOME WORKING is like Marmite; you either love it or hate it. Over the last few years, most people have had some experience of working from home and most people have strong views on the pros and cons.
The major pro for most people is the loss of a lengthy commute and the associated costs. This has given people back time to spend doing other activities that benefit them personally or they may have spent this extra time doing additional work that benefits their organisation.
As people have spent more time at home, many have developed increased anxiety about commuting and returning to the office and, as a result, they are actively looking for home-based roles.
There are obvious cons of home working too. It is especially difficult for more junior staff to receive the support they need in terms of day-to-day coaching and mentoring. On-the-job training plays a huge part in the ongoing development of individuals and this is much more difficult to achieve working remotely.
Isolation is also a big factor, and this is the major reason for some people not enjoying home working. This can be more of an issue for those living alone.
But home working during the Covid pandemic was a very different experience to working from home in more normal circumstances and isolation is generally less of an issue.
I have worked from home for many years and isolation has not been a factor prior to Covid, as there would be plenty of social interaction outside working hours. But during Covid, of course, this was not the case.
So I would encourage those who hated home working during the pandemic to keep an open mind as to how it might benefit them in the longer term.
In healthcare there are some roles that are well suited to home working, but there are many other roles where it is impossible to see how home working would work.
A lot of the roles within the supportive functions for healthcare practitioners, including administration, finance and marketing, can obviously be managed outside the office with the right investment in systems. But caring for patients has to be done within the clinic or hospital environment and it is hard to see how this will change significantly.
If your employees have enjoyed home working and are now reluctant to come back into your clinic, how can you address this?
Question your employees
In some industries, we have seen the introduction of various perks to attract employees back to the office including morning yoga classes, a daily supply of fresh fruit and areas dedicated to socialising with games such as table tennis and so on. These may be motivational for some employees, but I daresay not to the vast majority.
Before investing in possible solutions, a wise starting point is probably to ask your employees to describe why they feel reluctant to return to office working and ask them what actions you can take as their employer to address this.
Depending on the size of your organisation, this could be done in the form of an employee survey or through individual or team discussions. Once you understand the overall issues, it is easier to develop a plan to address and overcome the concerns.
In my experience, the desire to work from home is often driven by a need for greater flexibility over working hours. Many individuals have caring responsibilities either for young children or for parents. The time and associated cost spent commuting is another widely
The key to retaining employees may need to come from offering greater flexibility in terms of working hours, days and shift patterns
Hybrid approach
Video consultations have now become a well-accepted method of providing patient care, with both GPs and consultants communicating with their patients in this way regularly.
reported problem. What ever the reason for wanting greater flexibility, the outcome is usually the need to take a fresh look at working hours and how they can be changed to better suit the individual.
For some, it may be a shorter working day, finishing an hour earlier, and for others it might be changing to a three- or four-day working week.
Working remotely
As I mentioned earlier, there are some roles in healthcare that can be done remotely from home including customer/patient services, including all call answering, administration, finance, marketing and I am sure many others.
Employers should show a commitment to making home working a possibility for individuals in these roles or risk losing them to companies who will allow them to do so.
To enable this does require investment in systems and a review of processes and, most critically, a change of management style with the focus on outcomes and deliverables rather than presenteeism.
But what can we do for the individuals in roles that really do need to be based in the place of work whether it be a hospital, clinic or GP practice?
For nurses, doctors and many others in healthcare, the option to work from home is obviously very limited. But if we are openminded, we may be able to implement working practices that allow greater flexibility.
Clinics could be re-organised to take a hybrid approach, allowing a clinician to hold face-to-face clinics three days a week and hold video consultations on the remaining two days of the week and, of course, the video consultations could be made from anywhere, including home.
In roles where it really is not possible to introduce home working the key to retaining employees may need to come from offering greater flexibility in terms of working hours, days and shift patterns. This can be more complex to manage and an additional overhead on organising the day-to-day operations of the clinic, but a willingness to embrace flexibility by the employer will often generate a more flexible approach in the team who have a strong desire to make it work for them.
In summary, my recommendations are to fully understand why your employees are unhappy about returning to the office and develop a plan to address these concerns.
In terms of embracing flexibility, there are three main options: moving roles that can be moved to home-based working, introducing hybrid working, where possible, with a mix of office and home and finally looking for flexibility of hours and working patterns.
If you have any specific questions that you would like answered in coming editions, please do feel free to get in touch.
Jane Braithwaite is managing director of Designated Medical, which offers bespoke support across accountancy, marketing, medical PA, HR and recruitment
TRADING SUSTAINABLY
You’ll miss out if you don’t go green
Sustainability and ESG (environment, social, governance) in healthcare is increasingly in the spotlight. Jamie Foster spells out what it means for private hospitals, clinics and technology providers
ORGANISATIONS OPERATING in the healthcare sector are increasingly focused on sustainability as an essential part of their activities
These ‘green’ initiatives are often badged under the environment, social, governance (ESG) banner.
This focus stems from a number of angles: the moral imperative and wish to limit the damaging effect of operations on the wider environment and community, together with the opportunity to support those communities, and the continuing trend for both customers and governments to set compulsory sustainability related thresholds which suppliers must reach before being appointed.
With the UK Government having set a binding target to reach net zero emissions by 2050, the need to treat ESG as more than a tick-box exercise is increasingly apparent. And so it is a carrot-andstick approach, with many and varied angles of focus.
In this article, I look at what sustainability and ESG mean for private hospitals, clinics and technology providers, with a focus on the environmental aspect of ESG.
What is sustainability and ESG?
Many people use the terms ‘sustainability’ and ‘ESG’ interchangeably, and both are often used as shorthand for carbon reduction schemes or more generally green initiatives.
However, whereas sustainability is by definition a fairly vague concept, ESG is more clearly defined: environmental, social and governance. And, as a result, in many ways it is more helpful for companies to focus on ESG, since it can provide a framework for specific initiatives and criteria.
ESG is a huge area in its own right, and takes its starting point from the United Nations 17 Sustainable Development Goals, which range from the elimination of poverty, to clean sanitation, gender equality, climate action, sustainable cities and communities, and good health and wellbeing.
And so ESG can be seen as demonstrating a shift in emphasis from short-term profit maximisation as the primary objective of
ESG activity is increasingly a material factor influencing asset valuations, investment decisions and, consequently, access to capital
corporations towards a business model with positive societal impact covering three areas: ESG.
Securing investment and financing
Investment and financing are clearly important to support companies operating within the independent healthcare sector and more investors than ever are screening companies for ESG criteria when making investment decisions.
ESG activity is increasingly a material factor influencing asset valuations, investment decisions and, consequently, access to capital.
From a financing perspective, ‘green’ bonds and loans are available to fund environmentally focused projects, and sustainability linked loans incentivise borrowers to meet their sustainability commitments and reduce their environmental impact.
Likewise, other stakeholders –including employees and consumers – want to see firms considering these factors and shareholders are also demanding action.
As a result, healthcare companies are being required to respond, for example, through incorporation of sustainability linked financing into their business operations.
Net zero and the UK public sector
Achieving net carbon zero is becoming increasingly important from the perspective of governments and organisations alike worldwide.
In the UK, the NHS currently procures products from over 80,000 suppliers and, as such, is an essential customer for the independent sector. Its Greener NHS
programme commits it to two targets:
1. Reducing the NHS carbon footprint for emissions it controls directly to net zero by 2040, with an 80% reduction targeted between 2028 and 2032.
2. Reducing the NHS carbon footprint plus – that is for emissions which it does not control directly, but can influence – to net zero by 2045, with an 80% reduction targeted between 2036 and 2039.
How will the NHS meet these targets? The answer lies in the fact that 60% of the NHS carbon footprint is based within the NHS supply chain, which means that the NHS will need to use public procurement as leverage to effect change.
For example, recent UK public Procurement Policy Notes (PPNs) reference the need to consider ‘green’ concerns:
➲ PPN 06/20: Taking account of social value in the award of central government contracts, which is to be applied to the NHS from 2022;
➲ PPN 05/21: which mandates that contracting authorities should consider national priority outcomes including ‘tackling climate change and reducing waste’ in all their procurement activities; ➲ PPN 06/21: ‘Taking account of carbon reduction plans in the procurement of major government contracts’ mandates that, as a selection criteria, contracting authorities should require bidding suppliers to provide: i) A carbon reduction plan, using a defined template, confirming the supplier’s commitment to achieving net zero by 2050 in the UK; ii) Setting out the environmental management measures that they have in place and which will be in effect and utilised during the performance of the contract.
Building on this, the NHS has published a ‘Net Zero Supplier Roadmap’ which requires that, by the end of the decade, the NHS will no longer purchase from suppliers who do not meet or exceed its carbon zero commitments.
In view of these policy statements, the NHS, alongside wider government, is now affecting change through its supply chain contracts, which providers will need to be aware of when contract➱ continued on page 26
The ESG agenda needs focus now. It is tempting to think of it as a long-term issue, but actually it is a short-term one requiring decisions and actions without delay
INNOVATIONS IN HEALTHCARE PRODUCT, PATHWAY AND INFRASTRUCTURE
ing with government bodies and the NHS.
Independent providers are clearly taking the move to carbon zero onboard, with the Independent Healthcare Providers Network (IHPN) announcing an industrywide commitment for private healthcare providers to go beyond the NHS target to achieve net zero by 2035 – with a net zero supply chain by 2045.
Some members have committed beyond that ambitious target to achieve net zero by 2030.
Conclusions
The ESG agenda needs focus now. It is tempting to think of it as a long-term issue, but actually it is a short-term one requiring decisions and actions without delay.
Whether the imperative is moral, related to investment and financing or supplying to government and the NHS, businesses need to apply ESG to their wider decision-making and processes across all levels of the business and supply chain.
The good news, as demonstrated by the examples above, is that there are a multitude of ways in which these issues can be addressed and private hospitals, clinics and technology providers are already making the most of the many opportunities to do so.
Jamie Foster (below), a commercial lawyer with Hill Dickinson, specialises in the health and life sciences sector
Sustainability-related opportunities and challenges for the sector lie in innovating to create healthcare products and devices which are more environmentally friendly and designing healthcare pathways which enable the sector to reduce its contribution to carbon emissions.
From a social perspective, product and pathway innovations may also support healthcare systems to improve access to healthcare for less well-served communities.
In terms of products, there are many examples throughout healthcare services of items which continue to be used at great cost to the environment. The challenge is to eliminate these, while maintaining access to often life-changing treatments for patients.
A simple example is the metered dose asthma inhaler, the propellants in which create greenhouse gases accounting for 13% of the UK NHS carbon footprint.
Similarly damaging is the plastic used in throwaway devices which product innovators are currently working to eliminate.
The industrial process of remanufacturing, a step beyond simply recycling, is another innovation starting to take hold within the healthcare sector. This involves breaking down products or their components before restoring them to useful life and is an effective way of reducing waste and environmental impact.
Examples of healthcare devices which are being restored in this way include neonatal monitors and surgical tools including forceps, endoscopes and cytoscopes.
The challenge with this approach is guaranteeing the safety of the remanufactured devices, but if this can be achieved, this is a clear step to more sustainable use of such devices.
Before, and increasingly since, Covid, digital access to healthcare is being given greater priority.
Of course, digital healthcare solutions have grown exponentially during the pandemic. And they support sustainability initiatives in many ways, from reducing the need to travel to hospital centres, therefore effecting a reduction in carbon footprint, to increasing access to care and information for people regardless of their ability to engage in traditionally delivered services.
Examples include apps which help people to manage and treat a wide variety of conditions from diabetes to mental health, and physiotherapy.
And in terms of infrastructure, Community Diagnostic Centres, as well as supporting the Covid recovery plan, will take healthcare services closer to the communities that most need them.
Private sector clinic and hospital providers can also demonstrate their environmental commitments through infrastructure projects, powering their own premises using renewable sources, and partnering with public sector providers to help them do the same.
Do
Do
you specialise in
Do you specialise in treating varicose veins or venous conditions?
Do you specialise in treating varicose veins or venous conditions?
you specialise in treating varicose veins or venous conditions?
treating varicose veins or venous conditions?
Do you specialise in treating varicose veins or venous conditions?
We are looking for new consultants
Why join our award award-winning team?
We are looking for new consultants
We are looking for new consultants
We are looking for new consultants
We are looking for new consultants
Why join our award award-winning team?
Why join our award award-winning team?
Why join our award award-winning team?
Why join our award award-winning team?
Receive full training in The Whiteley Protocol
Receive full training in The Whiteley Protocol
Receive full training in The Whiteley Protocol
Receive full training in The Whiteley Protocol
Receive full training in The Whiteley Protocol
Ongoing support & training and Back-Office services will be provided
Ongoing support & training and Back-Office services will be provided
Ongoing support & training and Back-Office services will be provided
Ongoing support & training and Back-Office services will be provided
Ongoing support & training and Back-Office services will be provided
Become a member of The College of Phlebology
The Whiteley Clinic is expanding and we’re looking for full and part-time Surgeons and Interventional
The Whiteley Clinic is expanding and we’re looking for full and part-time Surgeons and Interventional Radiologists who want to specialise in treating varicose veins and other venous conditions.
The Whiteley Clinic is expanding and we’re looking for full and part-time Surgeons and Interventional Radiologists who want to specialise in treating varicose veins and other venous conditions.
The Whiteley Clinic is expanding and we’re looking for full and part-time Surgeons and Interventional Radiologists who want to specialise in treating varicose veins and other venous conditions.
Become a member of The College of Phlebology
The Whiteley Clinic is expanding and we’re looking for full and part-time Surgeons and Interventional Radiologists who want to specialise in treating varicose veins and other venous conditions.
Become a member of The College of Phlebology
Become a member of The College of Phlebology
Become a member of The College of Phlebology
Access to the Venous Registry
Access to the Venous Registry
Access to the Venous Registry
Access to the Venous Registry
Access to the Venous Registry
Excellent results and patient satisfaction
Excellent results and patient satisfaction
Excellent results and patient satisfaction
Excellent results and patient satisfaction
Excellent results and patient satisfaction
Radiologists who want to specialise in treating varicose veins and other venous conditions.
Positions available current clinic locations plus new locations to be announced.
Positions available current clinic locations plus new locations to be announced.
Positions available current clinic locations plus new locations to be announced.
Positions available current clinic locations plus new locations to be announced.
Positions available current clinic locations plus new locations to be announced.
Please contact us for more information at jobs@thewhiteleyclinic.co.uk
Please contact us for more information at jobs@thewhiteleyclinic.co.uk
Please contact us for more information at jobs@thewhiteleyclinic.co.uk
Please contact us for more information at jobs@thewhiteleyclinic.co.uk
Please contact us for more information at jobs@thewhiteleyclinic.co.uk
NHS Pensions & Annual Allowance Tax
Get ready in advance of April 2022 when the proposed changes to the NHS Pensions will allow you to reclaim some or all of any Annual Allowance tax you may have suffered in the past.
With our knowledge and in-house calculators, we will be able to predict in advance and check statements produced by NHS Pensions and Scottish Public Pensions Agency for accuracy for any refunds due.
For further information contact us at aa@semail.co.uk or telephone 01625 527351.
BOURNEMOUTH
BOURNEMOUTH
BOURNEMOUTH
BOURNEMOUTH
MARKETING YOURSELF
Getting new patients
Simon Marett (below) focuses on how independent practitioners can overcome the major challenge of converting a casual inquiry or first-time visitor to your website to being a fully paid-up patient
‘ONBOARDING’ IS a term now commonly used in business and healthcare circles and relates to the action or process of familiarising a new patient or customer with one’s products or services.
As we covered in April’s article, one of the biggest challenges a private clinic will face is finding or acquiring new patients, as it takes planning, time and often a little financial investment to attract them.
You may have decided to advertise in local newspapers or on social media or invest a little budget on Google Ads to build awareness of your practice and drive new visitors to your website.
Once a new patient or prospect has found you, how do you then ensure they proceed to the next stage to book and pay for an appointment?
A failure to take a close look at this onboarding stage of the patient journey can result in wasted effort and budget, as patients will just ‘bounce’ from your website and explore alternative options.
Overcoming the payment barrier
By far the biggest challenge that a clinic will encounter is the payment barrier and persuading a new patient to commit, book and pay for an appointment or consultation.
An initial consultation with a private consultant will often cost several hundred pounds, so how do you go about persuading a potential new patient that your clinic or healthcare service is right for them?
In the US and in other countries, it is common practice to pay for private healthcare, but consumer attitudes and behaviours in the UK are different because of the existence of the NHS. As a result, patients are not often used to nor comfortable with paying for private healthcare and require a great deal more convincing to move to the next stage.
Onboarding options
Marketing in private healthcare is becoming more sophisticated and complex, but the good news is that
healthcare practitioners have a good number of options and channels they can explore when onboarding new patients.
Every healthcare clinic is different and will operate in a field of healthcare where consumer behaviour will vary, so it is important to point out that there is no single perfect formula that can be applied across every practice.
Approaches and ideas need to be explored, tested and assessed to find the right blend that works for your clinic.
Here are some onboarding approaches to consider:
➲ Live chat
Browse through several healthcare websites and you will find various forms of ‘Live chat’ pop-ups.
From automated, pre-programmed chatbots to medical secretaries offering human real-time ‘chat’ functions, live chat can be a cost-effective way of engaging new visitors on your website to make an inquiry and for you to answer their questions.
patients on board
➲ Free ‘discovery’ calls
New patients will often want to find out more about a clinic or practitioner before committing to a paid consultation, so creating room in your diary for a series of short ‘discovery’ or introductory calls can be an effective way of onboarding new patients. These can be done by the doctor, but it is now common practice for a well-briefed practice manager or medical secretary to host these calls with a view to converting inquiries to paid consultations.
➲ Online symptoms checker
This can take time to plan and implement and will need a little help from a web development team, but can prove to be an excellent long-term investment.
Encouraging new visitors to complete a short survey relating to the symptoms they are experiencing can quickly highlight the options that are available to them and how you can help.
➲ Introductory webinars
The pandemic saw a huge surge in the number of healthcare webinars as patients moved online to have their questions answered. Organising a 30-minute monthly webinar for new patients can be a time- and cost-efficient way of giving new patients a chance to meet a practitioner and find out more about a clinic before committing.
➲ Free downloadable guides
Every healthcare website should include a useful overview for patients about symptoms, conditions and treatment options, but not everything needs to be freely available.
More in-depth guides or specific content can be for ‘registered’ visitors only and downloadable if patients provide an email address and sign-up to a newsletter or monthly update.
This gives your clinic the opportunity to contact them again in the future about your services and how you can help them.
As this hopefully demonstrates, there are a good range of options or approaches available to healthcare practitioners or clinics when it comes to onboarding new patients.
These may take a little time and effort to plan and implement, but once embedded into a clinic’s workflows and processes, they can prove to be a very effective way of converting new visitors or inquiries to paid patients by helping them along their journey.
As with any other aspect of healthcare marketing, it is often worth talking to a reputable marketing consultant or specialist for advice before you start. They will have tried and tested these approaches before and will be able to offer valuable advice and guidance that may save you time, effort and money by helping you avoid the pitfalls and common mistakes.
Ultimately, this will come down to generating a positive return on investment, ensuring that you’re tracking and analysing results and selecting the approach that works for your clinic or practice.
Next month, we will take a look at tracking the steps in a new patient’s journey and why making a good first impression is vital for any successful clinic.
Simon Marett is founder and director at Ellerton Marketing
GET A FREE BUSINESS ‘HEALTH CHECK’
Ellerton Marketing is providing a free 60-minute business ‘health check’ for Independent Practitioner Today readers and can help guide you through some of the key steps you should be thinking about when it comes to marketing your clinic and acquiring new patients.
Create
mPrescribe® app allows you to prescribe flexibly without a laptop, for same day or next day delivery to your patients nationwide
Secretary Supported
Administrator access reduces workload for practitioners. mPrescribe® facilitates patient entry, status monitoring and preparation of prescriptions for mobile authorisation.
Clinical Governance
Co-founded and co-owned by leading private clinicians, our secure and encrypted technology is compliant with all GPhC, GDPR and e-Prescribing regulations.
“Wonderful, seamless, easy to use service.” Dr Catrin Bevan, London General Practice
“Competitively priced.” Dr Sean White, Consultant in Pain Medicine
“Intuitive and secure.” Dr Tim Wigmore, Consultant Intensivist & Anaesthetist, Schoen Clinic
“Delivered the same day.... Outstanding!” Dr Elisa Astorri, Academic Physician Rheumatologist, Rheumatology
“Go the extra mile.” Dr John O’Donohue, Consultant Gastroenterologist
NUFFIELD HEALTH AT ST BARTHOLOMEW’S HOSPITAL
A peek at the City’s newest private unit
LONDON’S NEWEST private hospital, where over 200 consultants have practising privileges, has begun seeing patients – as reported on our website on 3 May.
It is the City Of London’s first independent hospital: the 55-bed Nuffield Health at St Bartholomew’s Hospital.
Nuffield Health has invested £70m into the project, built in collaboration with Barts Health NHS Trust which runs St Bartholomew’s Hospital.
The two organisations share many of the consultants, and surpluses generated from private patient activity will be invested back into NHS services.
Nuffield Health says consultants will benefit from the breadth of experts at the new hospital, with operating theatres featuring inbuilt live-streaming capabilities.
Live operations can be streamed to the hospital’s boardroom, providing training opportunities and clinical knowledge sharing.
Nuffield Health at St Bartholomew’s Hospital is split over two buildings and offers:
26 consultation rooms;
An oncology day unit – including access to Maggie’s at St Bartholomew’s Hospital;
Four advanced operating theatres;
Seven specialist intensive care beds;
Inpatient and outpatient physiotherapy services;
Free community programmes, including joint pain and Covid-19 recovery;
A full range of diagnostic services including an imaging suite and Siemens Magnetom Sola 1.5T MRI system with BioMatrix Technology;
Connection to the new Nuffield
Nuffield Health says consultants will benefit from the breadth of experts at the new hospital, with operating theatres featuring in-built live-streaming capabilities
The Nuffield hospital is situated in what was once the pathology wing and former residential staff quarters of St Bartholomew’s Hospital
Health Barbican Fitness and Wellbeing Centre’s state-of-theart gym floor, athletic zone, 25m swimming pool and spa facilities, dedicated prehab and rehab area and group exercise studios.
The on-site medical centre provides expert physiotherapy, emotional well-being services, private GP and a travel clinic.
The hospital says its cardiac care pathway includes cardiac rehabilitation, a unique feature in the independent sector.
It is operationally independent, with Nuffield Health leasing and renovating the former pathology and residential staff quarters buildings.
Jonathan Canham, business development director and interim hospital director, says: ‘Our new hospital – Nuffield Health’s 37th hospital in the UK – complements the internationally-leading cardiac care delivered at the neighbouring St Bartholomew’s Hospital.
‘Our private patients will have access to many leading consultants within cardiac, cancer, orthopaedics, and women’s healthcare.’
MEMBERS OF THE CLINICAL TEAM
Its cardiac care pathway includes cardiac rehabilitation, a unique feature in the independent sector
LEFT TO RIGHT, FROM TOP Dr Ajav Jain, cardiologist; Dr Patrick Wilson, gastroenterologist; Ms Laura Johnson, breast surgeon; Mr Paul Flora, vascular surgeon; Mr Kulvinder Lall, cardiothoracic surgeon; Mr Pasquale Giordano, colorectal surgeon.
MANAGERS
Jonathan Canham, interim hospital director; Anthony Fitzgerald, matron.
Left: The mamography unit Below and top: Two of the four operating theatres
While sensitivity and empathy are vital components of managing patient-clinician communication in a disclosure event, listening is the most important – and possibly the hardest skill – for navigating communication in these difficult circumstances.
Kirsten Dyer explains
Listening can defuse gripes
AS EXPERIENCED healthcare professionals, we understand the challenges of communication and the complexities associated with communicating to patients, their families and carers after care has gone wrong.
This is particularly true in situations where patients are vulnerable, seriously ill and they and their families are experiencing a stressful time.
When an adverse patient outcome has occurred, healthcare is increasingly offering an opportunity for transparent communications. This approach to communications, or open disclosure, may be applied as best practice or required by regulations such as the GMC’s duty of candour or National Quality Standards.
By communicating openly and honestly, we knowingly enter into challenging and difficult conversations that are often highly charged for all parties.
The needs of the patient and their families are paramount, yet we must not neglect our own needs and those of colleagues.
A supported and consistent approach can enable healthcare professionals to communicate effectively, openly and reduce any inclination to avoid a confrontational conversation.
No one wants to see a patient harmed or a family in distress. All of this responsibility for communication can feel like a tall order for doctors in stressful or complex situations.
Active listening
As Danielle Ofri described in the book What Patients Say, What Doctors Hear, a Swiss medical study in the early 2000s found that patients are often only given a brief space to tell their story.
The study showed patients speak for 12 seconds on average after a clinician asks: ‘What can I do for you today?’, before the clinician moves the conversation towards a diagnosis.1
This may be a result of workload pressures, yet the patient and their family may perceive they are not being heard.
What does all of this tell us about the art of listening in a busy healthcare environment?
As healthcare professionals, our
In the event of an adverse clinical outcome . . . patients and families both reported a strong need to hear from the person directly responsible for their care
natural inclination is to be fixers. Instinctively, we do listen but move on fast to inform and diagnose, sometimes before a patient has had the opportunity to finish telling us about their symptoms.
At Cognitive Institute, our many years of experience has taught us the power of listening is core to effective communications and is a learned skill. We help clinicians of all disciplines to learn about the benefits of listening.
We teach the value of ‘sitting in silence’ while still actively listening to a patient or a family member before progressing to problem solving and solution mode.
What really matters to patients and families?
In the event of an adverse clinical outcome, a prominent concern for healthcare providers and clinicians is often blame, and the fear of blame is then a likely barrier to truly hearing patients’ views. Yet, blame is often not the top priority for patients and their families.2
In a study by Moore, Bismark and Mello, many patients demonstrated satisfaction when listened to as opposed to being told what the clinicians wanted to share
with them. In the majority of cases, the most favourable outcomes for both parties were a result of transparent and compassionate patientclinician conversations and those where patients and families were treated with empathy in a non adversarial environment.
Importantly, patients and families both reported a strong need to hear from the person directly responsible for their care. The sample also found that, in difficult situations, offers of compensation and the presence of a division chief instead of the clinician were unwelcome with patients and families.
This underlines the importance of having the right people in the room during a disclosure event, and the positive influence this direct and personal engagement has on perceptions.
Nor is it surprising that small gestures can make a difference to families coping with medical injuries. Moore, Bismark and Mello’s work presents a range of communication based opportunities to improve outcomes after initial disclosure conversations.
These include making sure a patient’s preferred method of communication is used for all followup engagement, seeking feedback from them a few months down the track and making sure that patients are aware of any actions taken to improve safety.3
Facilitating full and frank incident investigations can be used to improve safety and quality and delivers benefits to patients by fostering openness and trust as part of the experience.
Benefits of an open culture
For independent healthcare providers, the benefits of an open culture are also multi faceted. The ongoing consequences of adverse events can be mitigated through continued dialogue and organisational learning.
Healthcare organisations are better able to manage the stress and consequences of an adverse event or complaint, while professional, ethical and moral obligations to truthfully disclose information about harmful incidents are also fulfilled.
Additionally, open disclosure may contribute to a safer health
system and enhance public trust in healthcare organisations.
These outcomes emerge from embedding better transparency and openness into healthcare, using the knowledge gained to help prevent recurrence of errors.
It is supported by the role that listening and effective communication play in strengthening relationships between a healthcare organisation and an individual in their care.4
Are we still scared of being sued?
While the case for authentic, open and transparent communication has continued to gain traction over the past 20 years and the sector’s approach has improved significantly, we still have some way to go before the bestpractice principles become a consistent, thoughtful and systemic part of our training and skills.
Ultimately, the fear of medicolegal litigation in the event of an error or failure of care remains a significant barrier to improving open and transparent communication with patients and their families.
The risk of legal action has many implications for both individual practitioners and employers when something goes wrong; potential reputational damage, the loss of employment and erosion of trust from patients, families and colleagues are just a few. Sometimes the implied threat is enough to stymie even the best open disclosure intentions or policies.
The benefits of prompt communication and resolution and shifting management of claims from defence to a patient safety focus are highlighted in a recent article by Sage, Boothman and Gallagher, in the context of addressing growing concerns about medical liability.
The article concludes that rather than waiting for complaints and lawsuits, a health system’s risk management approach must have a quick response system for address ing unfavourable patient outcomes.
The seizing of control over timing deals with persistent concerns about delayed claims from both risk managers and clinicians – and presumably patients. It also reduces financial uncertainty by promptly resolving most well
founded claims without legal action and shifting claims management from a ‘legal defensibility’ basis to a ‘patientsafety’ focus.
According to Wu, Huang, Stokes and Pronovost, when reporting the results of disclosing adverse events to patients and families, ‘it’s not what you say, it’s what they hear’. There is broad consensus that physicians and healthcare organisations should disclose adverse events, but it is largely understood that most practitioners need support to do so successfully.5
The clarion call is that while there remains genuine trepidation about open disclosure and legal implications, there is a huge opportunity for healthcare providers to focus investment and resources on improving outcomes and skills, with potential substantial payoff for culture, reputation and risk mitigation.
For information about MPS Partnerships’ transformational risk prevention programmes, including navigating adverse outcomes and duty of candour courses see www.mpspartnerships.org.
Kirsten Dyer (right) is senior clinical educator at Cognitive Institute and Medical Protection Society Partnerships
References
1. Ofri, D. (2017). What patients say, what doctors hear: what doctors say, what patients hear. Boston, Massachusetts: Beacon Press
2. Leape, LL (2006). Full Disclosure and Apology – An Idea Whose Time has Come. Physician Executive, 32(2).
3. Moore, J, Bismark, M and Mello, MM.(2017). Patients’ Experiences with Communication-and-Resolution Programs After Medical Injury. JAMA Internal Medicine, 177(11), p.1595.
4. Review: Implementation of the Australian Open Disclosure Framework. (2020). The Australian Commission on Safety and Quality in Health Care (safetyandquality.gov.au).
5. Wu, AW, Huang, I-Chan, Stokes, S. and Pronovost, PJ (2009). Disclosing Medical Errors to Patients: It’s Not What You Say, It’s What They Hear. Journal of General Internal Medicine, 24(9), pp.1012-17. Available at www. ncbi.nlm.nih.gov/pmc/articles/ PMC2726881/.
Decrypting new ways of investing
Stories around cryptocurrencies abound in the media. Dr Benjamin Holdsworth (left) warns of the ten points you should remember about digital assets
BLOCKCHAINS, WEB3, the metaverse, NFTs, cryptocurrencies, Bitcoin, Dogecoin, dApps and DAOs. These terms have surged into mainstream media from nowhere over a decade ago.
At the time of writing, the total value of crypto assets, if instantaneously and in a costless manner converted to US dollars, sits at around $2trillion. To provide some perspective, Microsoft’s total market capitalisation currently sits at around the same figure. Are crypto assets now too big to ignore?
Here we explore ten important points to remember if considering an allocation to digital assets.
1Complexity and perceived sophistication do not make something a good investment
An innovative product will not necessarily be revolutionary. There are many highly technical solutions in the digital assets space with exciting prospects, but without the benefit of hindsight it is impossible to know what technologies will become commonplace. For most, it is not necessary to gain an indepth understanding of
the mechanics and nuances of digital assets and blockchain technology.
Many people drive cars without a detailed knowledge of how the gearbox works or how the engine uses the fuel to generate power. It is, however, useful to understand some high level characteristics and considerations.
2
There are legitimate challenges to the future of many digital assets
A philosophical debate exists around what designates an asset’s ‘value’. What gives a verifiably ‘owned’ 600x600 digital image –which can be infinitely reproduced – worth?
Why is a bitcoin, with little use in daily life and not in physical form, valued at tens of thousands of dollars based simply on its verifiable scarcity? Why Bitcoin and not any of the other 10,000 or so cryptocurrencies?
How can widespread adoption get round the challenge of high transaction fees and slow transaction times? For example, Ethereum – another decentralised blockchain – can only process up to
around 30 transactions per second, while Visa claims capacity for over 65,000.
It is difficult to give firm answers to these questions, although they are valid challenges for these technologies to overcome to achieve mainstream adoption.
3 Beware fraudulent activity
Hacks and outright theft are real risks that exist in the space, with littletono route to compensation for investors.
Currently, there do appear to be some significantly vulnerable points – in the process of purchasing digital assets – whereby illicit activity occurs at a cost to investors. Examples of hacked wallets, stolen funds, corrupt exchanges and fake cryptocurrencies are frequent in financial media. These are unfortunate realities that exist.
4 Transaction costs are high
Owning digital assets directly can be costly. Transaction fees are high and liquidity could reasonably be an issue, particularly at the time of large market swings. There are lim
ited options to buy pooled investment products to gain exposure to digital assets and those that are available are expensive.
5 Much of the digital assets’ world is unregulated
A reasonable starting point as an investor is to first avoid any investment that is unregulated.
A lack of regulation gives rise to increased risks of criminal activity at a cost to the investor, and most likely an investment in which it is more difficult to know the true inherent risks.
Much of the digital assets’ world is unregulated. This may change in time, though the very nature of true decentralisation makes it difficult for a central regulator to engage in necessary oversight.
6 Environmental impact concerns are valid and material
Although the digital assets’ industry is broadly aware of the issue and has taken steps to improve the climate impact, it is still significant. The method of verification of bitcoin transactions is energy
The energy consumption of the bitcoin network in a single year could power all kettles in the UK for over 30 years
intensive, as miners compete for newly minted bitcoins by producing the most powerful processing units.
The Cambridge Bitcoin Electricity Consumption index provides some interesting comparisons, such as the fact that the estimated energy usage from mining bitcoins is comparable to the energy usage of countries such as Poland and comprises over 0.6% of global energy consumption. As another example, energy consumption of the bitcoin network in a single year could power all kettles in the UK for over 30 years.
7
There have been some great innovations
There is no doubt that there are some exciting and potentially disruptive innovations in the space. The challenge investors face is that, without the benefit of hindsight, it is impossible to know which innovations will prevail.
8
Many investors can benefit from indirect exposure to digital assets
By owning a diversified basket of securities, one can own the public companies that are developing, selling or implementing the new technology.
Investors calculate the expected future cash flows of firms – giving them a market value – and so owning these firms in a market weight gives investors the aggregate view of each company’s future.
9
Ownership of many digital assets comes with a highly volatile journey
Significant price swings are regular in the world of digital asset ownership.
In the past five years, the price of a bitcoin has seen daily movements of up to +26% and down to 39%. It’s a very bumpy ride.
10 Remember the tax consequences of ownership
Many investors are unaware of any potential tax liabilities that may arise due to ownership.
A nationwide survey in the US by Wakefield Research – commissioned by CoinTracker – found that just 3% of respondents correctly answered a list of questions relating to when crypto investors would be liable to pay tax. Proceeding without due caution can land investors in hot water.
Revolutionary technological advancement is a brilliant consequence of the capitalist system, and a key factor in economic growth.
The world of digital assets and blockchain technology is exciting and it would not be entirely surprising to see some of the innovations – many of which might not even exist today – become commonplace.
There is, however, a relatively deep technical knowledge required to understand digital assets, even at a basic level. This does not make them a simple investment, and any consideration about cryptocurrencies should be fully explored with the backing of solid financial advice.
Dr Benjamin Holdsworth is a director of Cavendish Medical, specialist financial planners helping consultants in private practice and the NHS
The content of this article is for information only and must not be considered as financial advice. Cavendish Medical recommends that you seek independent financial advice before making any financial decisions. Levels, bases of and reliefs from taxation may be subject to change and their value depends on the circumstances of the investor. The value of investments and the income from them can fluctuate and investors may get back less than the amount invested.
BOOK YOUR DEMO
Are you happy with your current software?
Maybe you're completely happy with the software you use to run your practice. Perhaps you have everything in one place, routine tasks are automated, and reporting is accurate and insightful. If so, stop reading now.
However, if you think the day to day running of your practice could be improved, we'd love the chance to demonstrate e-clinic to you.
The number one choice for private practice
Future-proof your practice and offer everything a modern patient expects:
> iPad compatibility
> Online booking & payments with fully integrated card processing
> Electronic consent & treatment forms
> Integrated drugs database & digital prescribing with direct delivery
> Fast & easy patient communications by email or text
Getting your cash in
As part of Medical Billing & Collection’s celebration of three decades in the sector, Simon Brignall (right) continues with a highlight of 30 key areas for practices to overcome their medical billing and collection challenges. Here are the all-important final ten…
INVOICING – THE WHO, THE HOW AND THE WHY
21
Private medical insurance companies
We covered in last month’s issue the coding complexity around insurance billing, so now it’s time to discuss the revenue cycle in relation to private medical insurance (PMI) billing.
Once an invoice has been correctly formulated and delivered to the insurance company following its agreed payment pathway, it then enters the PMI’s processing. Upon approval, a payment will be made to the practice under the terms of the policy and in line with the consultant’s terms with that insurer.
This could result in the invoice being paid in full, a partial payment or, in some rare circumstances, no payment at all.
These payments are mostly made to the practice via a BACS payment directly into the practice’s bank account or a cheque is sent. The insurance company will also send a remittance advice to notify the practice about the payment and this can include an
explanation when the total value of the invoice is not settled in full.
An invoice may not be settled in full for many reasons, but all of these require the practice to have adequate procedures to invoice and chase the patient for the balance. Failure to do so will mean that the practice will lose out on income or its cash flow will suffer.
Shortfalls are where the amount reimbursed under the policy does not cover the consultant’s fees in full;
An excess or co-payment means that the policy requires the patient to contribute towards the cost of treatment;
Some treatments are not covered under the terms of the policy;
Or the benefit may be exhausted.
This is why patients need to be made aware they are liable for any amount that is not reimbursed by their insurance provider.
The management of these outstanding balances in relation to insurance billing is an area most practices struggle with and is often the main reason consultants choose to engage our services.
22 Self-pay patients
As Independent Practitioner Today has reported, the selfpay area has grown considerably over the past ten years and is now either the largest or second largest area of revenue for many practices. The impact of the pandemic on NHS waiting lists has simply increased this trend.
The raising of self-pay invoices to patients should always be a priority, as these patients have the greatest risk of bad debts.
I also include in this category self-pay invoices raised for outstanding balances left over from the insurance billing we just discussed.
There are occasions when a practice should also consider requesting payment in advance, particularly when treating patients who do not reside in the UK, the invoice amount is considerable or where the practice undertakes a very large element of self-pay.
It is important that a practice has the full range of invoicing and payment options required to best service these patients. At Medical Billing & Collection (MBC) we
The raising of self-pay invoices to patients should always be a priority, as these patients have the greatest risk of bad debts
offer our clients a range of payment pathways and functionality including the ability to:
Invoice their patients electronically;
Collect payments on a 24/7 basis via our payment portal;
Settle all outstanding invoices at the same time;
Add a pay invoice button to their website;
Raise invoices and collect monies in advance, on the day and post treatment, depending on their specific needs.
23
Medico-legal work
In our experience, many consultants begin medico-legal work without ensuring they have adequate terms and conditions in place.
The longer revenue cycle for this work often means these practices carry higher aged debt.
This is important to realise because, when an invoice is raised, a tax liability is created which is why a robust chase process is vital to ensure cash flow is optimised.
Larger medico-legal practices are required to charge VAT and so the
situation is more challenging, as they have had to pay the tax to HMRC every quarter.
Your terms and conditions should cover all your fees in relation to this activity and all other associated costs for additional work, court time, travel costs and payment terms.
Your DNA (Did Not Attend) rules should be clear alongside your payment terms and any penalty clauses that may arise for late payment.
The most important step is to always make sure your fees and terms and conditions are accepted up front before taking on any case.
24 Embassy work
It is important to understand that embassy patients will often have complex conditions, and this is one of the main reasons why they travel to this country.
When you see the patients for their initial consultation, they may be accompanied by an interpreter, which means the consultation is likely to take longer than normal. So make sure you allow enough time in your schedule.
It is vital that you obtain a letter of guarantee (LOG) before you see a patient, because this will authorise treatment for the patient. Note that it must be in your name.
Without this key document, embassies will not process your invoice. Some embassies also require a copy of the medical report and all relevant documentation needs to be presented alongside your invoice.
Similarly, the medico-legal activity payments times in relation to this invoicing are longer, so it is important to ensure that the impact on a practice’s cash flow is taken into account.
25 Corporates
Many consultants take on activity that requires the invoicing of companies under standard 30-day terms. Often this may necessitate all activity for the month to be invoiced to the organisation on one invoice.
Examples of this would be:
C-level executives whose benefits packages include the provision of private GP cover or occupational health that is covered directly by the company;
Consultants who undertake
seminars and paid speaking events.
All of this activity needs to be invoiced in line with the preagreed contractual terms and chased accordingly.
IT’S TIME TO GET PAID
26 Payment reconciliation
This is an area which we continually see causes problems within a practice.
Often the practice is way behind with the reconciliation process or the remittances are not reconciled correctly against the invoices raised.
A regular complaint from consultants can be that they are unsure what the true picture of their outstanding debt is or whether an invoice has been paid or not.
Lack of access to accurate data at this key stage means it is impossible to have an effective chase process.
Each insurer should send a remittance to the practice when it makes payment. Payment is typically made electronically direct to the practice bank account.
The problem is that it is common for a practice to not receive a remittance or it can get mislaid and so unless the practice is chasing the insurer or reconciling the bank account on a regular basis, these invoices remain outstanding.
27 Outstanding balances
Reconciliation issues can cause further problems as any remittance which has been missed and hence not reconciled may result in a shortfall not being identified which, in turn, should have been invoiced to the patient. As a result, the practice cash flow suffers, leading to an increase in bad debts.
Even when the issue is finally discovered, invoicing patients months after the event is never a good thing, as it can lead to complaints from unhappy patients and often means that they are more reluctant to pay.
Often we face these issues when we chase the backlog of outstanding invoices for a practice. We reconcile all remittances the day they are received and any that are out-
standing are chased regularly with the insurance companies.
This ensures we remain on top of outstanding payments and that invoices in relation to shortfalls are raised to the patient in a timely fashion.
THE ART OF THE CHASE
28 Chasing aged debt
Without exception, we find this area gives most practices the biggest operational headache and is a task that is often deferred for a range of reasons.
Many practices find conversations that mix medicine and money challenging and often detract from the patient’s experience of their care.
In our experience, all invoices need to be routinely chased, including invoices sent to insurance companies. Reasons for a delay in the processing of invoices can be:
Non-receipt of the invoice due
to electronic data interchange (EDI) issues or postal problems;
Treatment that was not preauthorised;
Incorrect membership numbers or lapsed policy details provided by the patient.
For a robust chase process to be effective, it must be clearly defined and routinely applied. There needs to be clear understanding of who is responsible for this role so that there can be direct accountability for this is activity.
Once the chasing process has begun, it needs to be followed up on, otherwise the patient will think that you are not being serious. This will reflect on the professionalism of the practice and will give the patient permission to withhold or defer payment.
The process should allow for a mixture of communication methods used to contact the patient as well as the sending of formal letters. All this needs to be recorded on a complete log of any action taken.
Many practices find conversations that mix medicine and money challenging and often detract from the patient’s experience of their care
29 Debt decisions
Once all the avenues in the chasing process have been exhausted, the practice then needs to decide whether to send the patient to debt collection.
What you do will typically depend upon the patient, the circumstances involved in the treatment and the associated costs.
If you decide not to send the patient to the debt collectors, then the practice should consider writing the amount off as bad debt, as it is unlikely that the patient will choose to pay the outstanding amount in the future.
You may choose to consult your accountant, as they would know the individual circumstance of the practice and will be in the best position to offer the correct advice.
TIME TO PAY THE TAXMAN
30 HM Revenue and Customs
Finally, the practice needs to be able to raise financial reports from both a business and tax perspective.
Her Majesty’s Revenue and Customs (HMRC) takes the view that you are responsible for your own tax affairs and it does not consider ignorance or negligence a reasonable defence.
You should be able to run reports which show the number of invoices raised, payments received and outstanding invoices to ensure that all financial aspects of your practice are in order.
Historically, HMRC has looked upon the private medical sector as being a prime area where the financial procedures are not as robust as they should be. This has resulted in a higher percentage of investigations compared to other business sectors.
Our clients get 24/7 access to their data via our reporting dashboard. It has an array of reports to analyse the practice and our account managers are happy to field any request for tax information from their practice’s accountant.
Simon Brignall is director of business development at Medical Billing & Collection, which is celebrating 30 years of partnering with consultants in private practice
A PRIVATE PRACTICE – Our series for doctors embarking on the independent journey
Setting yourself up as a company
Since the introduction of pension-related tax charges, trading as a limited company has become the preferred trading option for most consultants in private practice.
A LIMITED COMPANY is primarily used as your trading structure for three main reasons:
➲ To limit your personal financial exposure. A company has limited liability which is contained within the entity thereby protecting the shareholders and directors.
Alec James (below) looks at the cycle of considering a company through to formation and cessation and highlights some key events where important decisions need to be made
➲ For financial flexibility. As the earnings from your private practice are moved from your personal tax return to a corporate tax return, you have flexibility to control your overall level of earnings, which can be beneficial to avoid or mitigate certain tax charges such as pension annual allowance charges.
➲ For potential tax efficiencies. Depending on the share structure, you may be able to use the company to reduce your overall tax liabilities. The savings and opportunities will, however, depend on your individual circum-
stances and you will therefore need to take professional advice.
For most consultants, the driving force behind the decision to use a limited company is usually a combination of all three.
Trading via a limited company requires a different thought process, particularly for those that have historically been selfemployed and have enjoyed a great deal of flexibility over access to the funds generated.
Separate entity
The key difference between selfemployment and being a limited company is that the income generated within a limited company is no longer yours; it is the company’s income, as it trades in its own right and is separate from you legally.
Decisions you make throughout the life of the company can often have an impact on the overall tax
efficiencies and it is important to seek the advice of a specialist medical accountant even at the very start.
Formation of the company
Once you have made the decision to trade via a limited company, you are presented with your first key decision – how will your company be structured?
A quick internet search will tell you that a company incorporation can cost as little as £10 if the forms are completed by yourself. This is sometimes referred to as an ‘Offthe-shelf company’.
It is not a good idea to form the company in this way, as key decisions around the share structure are made at this stage. Carrying out this stage yourself to save formation costs is usually a false economy, as almost inevitable changes to the structure will need ➱ continued on page 40
to be made later on, which is usually considerably more than the initial savings.
At the formation stage, you will need to decide who will be directors and shareholders of the firm. In private practice companies, it is common to be both a director and shareholder, but they are not mutually exclusive, allowing flexibility on who is involved in the business.
A director is an officer position within the company and is responsible for the day-to-day management of the company and for ensuring the annual reporting and legal requirements of the company are met. To remunerate them for their role, a director may receive a salary or benefits from the company such as an electric car.
Financial risk
Shareholders, on the other hand, stake an investment in the company – for small companies, this is usually £100 or less – and are therefore investors of the business and may have no day-to-day role within the business.
Because they have taken a financial risk of investing in the company, albeit a nominal amount, they are eligible to receive dividends from the company as a reward.
Dividends are the distributions made out of the company profits
Once your firm is up and running
ONCE TRADING, the four key documents which will need to be prepared annually for the company are:
Full accounts – for the directors and shareholders together with HM Revenue and Customs (HMRC);
Abridged accounts – a filleted version of the full accounts, which are filed on public record at Companies House;
Company corporation tax return;
Annual confirmation statement – a document detailing any changes in shareholdings during the year, again a public record.
Abridged accounts exclude the income and expenditure pages and any management information, leaving only the balance sheet and a few statutory disclosures being available to the public.
As limited companies are separate legal entities, the profits of the company are subject to corporation tax. This is currently 19% irrespective of profits, but this is increasing for companies earning more than £50,000 from 1 April 2023.
after corporation tax. Dividends are classified as investment income and are subject to lower income tax rates than earned income and also do not attract National Insurance contributions, often making them more favourable than a salary.
Once the company is formed, you will receive a Certificate of Incorporation – effectively the birth certificate of the company. You will need this to open a company bank account and also at various points in the firm’s life; for example, applying for finance.
When creating the bank account, it is extremely important the account is registered in the company name. Receipts from patients, insurers and solicitors should then be paid in the company bank account to avoid you receiving money personally that belongs to the company, which can create tax pitfalls.
In addition to the company current account, it is worth also opening a company savings account or, as some banks are now offering, have a current account with the ability to segregate monies. This will prove invaluable when saving for corporation tax.
You will also need to design a letterhead and invoice templates in the company and inform both the insurance companies and your indemnity provider that you will be trading via a limited company.
The accounts are drawn up to the company year-end. The company year-end is usually set by Companies House based on the date the company was incorporated.
Different year-end
Your company year-end does not need to follow the usual 5 April personal tax year-end. In fact, it is often advantageous to have a company with a year-end which does not follow the usual tax year, as this can be useful for tax planning.
The year-end can be changed and you may wish to consider this if, for example, your company is working in a group through another business structure such as a limited liability partnership (LLP) so that your company yearend moves in line with that of the LLP to aid accounting.
A company has nine months from the year-end to prepare the accounts and deliver a copy of the abridged accounts to Companies House. The accounts must follow a prescribed format, so you should seek the advice of a medical accountant to ensure you are not only in line with the requirements but are minimising the corporation tax payable.
The full accounts contain details of the income and expenditure of the company together with a balance sheet of the company. The balance sheet is a snapshot of the company worth as at the year-end date.
Following the new tax rates, the first £50,000 is taxed at 19%, with profits over £250,000 taxed at 25%, the earnings in between being taxed at an effective rate of tax of 26.5%.
Corporation tax is due to be paid nine months and one day after the company year end, irrespective of the year-end adopted. The corporation tax is calculated based on the profits in the full accounts. These profits are subject to adjustment for any non-allowable expenditure, but also provide tax relief on capital expenditure incurred during year, such as IT equipment, office furniture or electric vehicles.
Electric cars
Electric vehicles are currently extremely tax-efficient, with tax relief being available to the company whether purchased or leased. As a director, you will pay very minimal tax personally for having use of the car. Therefore, if you are considering a new electric vehicle, having it as a company car in your own business is likely to be the cheapest option.
Some companies may have additional reporting requirements if they have paid employees benefits in kind, such as electric cars, or are VAT-registered.
Most medical companies will not need to register for VAT, as the income generated is covered by the healthcare exemption. Those companies which provide procedures which are considered purely cosmetic or in relation to medico-legal work may need to consider VAT registration if income exceeds £85,000.
Electric vehicles are currently extremely tax-efficient
Winding your company up
AT SOME point in your career, you will find you no longer require your limited company; this is usually when you come to retire.
Few medics are able to sell their private practice at the end of their career and therefore the majority cease trading when they retire.
At this point, it is likely that there will be reserves left in the company.
Reserves are the post-corporation tax profits which have not been paid to the shareholders as dividends. The level of reserves at the end of the company’s life often dictates the winding-up procedure. If the reserves of the company are below £25,000, the company
can be wound up and removed from the Companies House register fairly simply by your accountant applying for the company to be struck off and corresponding with HMRC.
Before the strike-off, all the liabilities of the company must be settled. This includes any payments the company owes to HMRC, the directors and any other creditors such as your accountant. The remaining funds should then be paid to the shareholders.
For many medics, the reserves will be well in excess of £25,000, particularly if you have carried out any tax planning with your accountant. In these cases, the
Liquidation is simply the company realising its assets and paying the funds to the shareholders
company will need to be liquidated.
Liquidations are often reported in the press in a negative way, as we usually hear this word when a company is unable to meet its liabilities. However, the same terminology refers to a company that is solvent and being liquidated.
In fact, a liquidation is simply the company realising its assets and paying the funds to the shareholders. This could involve selling or transferring any assets the company has as well as collecting the final monies owed to the company.
A liquidation above £25,000 of reserves will need to involve a liquidator, which is a special type of accountant. Liquidations are often more tax-efficient than dividends because, providing certain key criteria are met, the final distributions from the company will be subject to capital gains tax rather than income tax.
This presents a tax-planning opportunity to work with a specialist medical accountant, as capital gains tax rates are lower than income tax rates.
Whatever stage you are at with you company, specialist medical accountancy advice is always invaluable to ensure that you are maximising your tax efficiencies both in the short and long term.
Next month: Understanding your payslip
Alec James is a partner at Sandison Easson & Co, specialist medical accountants
Free legal advice for Independent Practitioner Today readers
Independent Practitioner Today has joined forces with leading healthcare lawyers Hempsons to offer readers a free legal advice service.
We aim to help you navigate the ever more complex legal and regulatory issues involved in running and developing your private practice – and your lives.
Hempsons’ specialist lawyers have a long track-record of advising doctors – and an unrivalled understanding of the healthcare system as a whole.
Call Hempsons on 020 7839 0278 between 9am and 5pm Monday to Friday for your ten minutes of free legal advice.
Advice is available on: Business structures (including partnerships) Commercial contracts Disputes and litigation HR/employment
Premises
Regulatory requirements and investigations
The legal duties of maintaining a firm
Last month, we examined doctors’ duties as a company director and here Kirsty Odell and Georgina Hall (below) explain what you need to do once you have incorporated
MANY BUSINESSES are choosing to limit their liability by operating as corporate vehicles instead of as sole traders or partnerships.
One of the key benefits is the limited liability of a corporate entity’s members and the fact that it has its own legal identity.
While these, and others, provide some clear benefits to incorporation, there is the important element of administration that you need to be aware of. This is because the law requires you to ensure the administration of the company is properly recorded.
Below are some key requirements and the possible consequences of not meeting these reporting obligations.
Registered office address
A company must have a physical address in the UK and the name of
the company must be on display. The address will be publicly available online at Companies House.
Annual filings
The following must be submitted to Companies House by all companies, including dormant ones:
Confirmation Statement: records any changes to shareholders that have been made since the last statement – which must be not more than 12 months ago – and confirms that all other information held by Companies House is current and correct.
Annual Accounts: Unless exempt, every company must prepare accounts each financial year. Company accounts must be approved by the company directors before they are filed at Companies House. Annual accounts may be filed online or by post.
Filings driven by events
There are particular changes which may occur within a company that Companies House must be notified of;
For example, the appointment of a new director or the allotment of shares.
Most changes can be filed online at Companies House. You need to be aware that there is usually a deadline by which it has to be done.
By way of examples, Companies House must be notified of the following changes:
A change to the company’s registered office;
Allotment of shares;
Registration of charges;
Changes of directors;
Any change to the details of persons with significant control (PSCs).
Resolutions
Some company decisions must be taken by the shareholders rather than directors of the company.
The different decision-making options for the shareholders are set out below. The articles of association may provide whether certain decisions require an ordinary or a special resolution and there are specific decisions under company law that must be a special, rather than an ordinary, resolution:
☛ Ordinary resolutions – An ordinary resolution is passed when more than 50% of the votes made are in favour of the resolution. This type of resolution requires votes to be taken at a general meeting of shareholders, a board meeting of directors or by written resolution. Ordinary resolutions do not generally need to be filed at Companies House, and should be retained with the minutes of the meetings.
☛ Special resolutions – A special resolution is passed when 75% of shareholders’ votes are in favour of the resolution. This type of resolution is commonly used for decisions such as altering the articles of association, restructuring the company, reducing share capital and changes to the rights of shares. The need for a special resolution to make certain decisions may be required by law or stipulated within the articles of association. Special resolutions must be filed online or delivered to Companies House within 15 days of being passed.
☛ Written resolutions – These may be either ordinary or special resolutions and are passed in writing, rather than in person at a general meeting. Written resolutions can be proposed by a director or shareholder owning at least 5% of the voting rights in the company. Shareholders with more than one share may cast their votes differently with the shares, which is useful for a shareholder who is holding shares for others, like a partner holding shares on behalf of the partnership.
Statutory books
All companies must keep and maintain a set of statutory books, either electronically or in hard copy form. Companies are legally required to notify Companies House where the statutory books are kept, which is either the registered office or a ‘single alternative inspection location’. They must be kept up to date with any changes that take place. As a minimum, the statutory books must include the following registers:
Shareholders;
Allotments and transfers of shares;
Directors’ names;
Directors’ residential addresses;
Company secretary’s names and address;
PSCs;
Copies of shareholder resolutions passed and minutes of meetings.
Companies are obligated to record details of their beneficial ownership. This is known as the register of people with significant control
PSC Register
Companies are obligated to record details of their beneficial ownership. This is known as the register of people with significant control. This provides a level of transparency over who owns and controls the company. An officer of the company must identify the PSCs and record this on the companies own PSC register, and then provide this information to Companies House withing 14 days.
If this information changes later, the changes should be recorded in the same way. A PSC is someone who meets one or more of the following conditions:
Holds more than 25% of shares in the company;
Holds more than 25% of voting rights in the company;
Holds the right to appoint or remove the majority of the board of directors.
However, there may be people who do not meet this criteria but have a sufficient influence over
the company that they should be registered as PSCs. Generally, you do not have to register directors.
Filing at Companies House
Most of the filings can be made online to Companies House –either through the webfiling service or through a document upload facility. An authentication code is required for the majority of filings.
This a six-digit alphanumeric code. It is sent to the company’s registered office by Companies House following incorporation and it may be requested online.
What are the consequences of non-compliance?
If a company fails to file statutory information, there are specific offences under company law for each filing requirement. This is usually a fine for which the company and the directors may be liable. This includes failings to file the following:
Resolutions; Accounts;
Confirmation statement; Notice of appointments or changes in directors/secretaries; Allotment of shares.
Where the accounts and confirmation statements are late, and following relevant reminders, Companies House may seek action for a voluntary strike-off of the company if non-compliance continues.
It should also be noted that it is an offence to deliver misleading, false or deceptive documents to Companies House.
The company may wish to appoint formally a company secretary whose responsibility it is to ensure that these things are complied with. Some companies do instruct their solicitors or accountants to fulfil that role for them.
Whatever you decide, make certain your company administration is kept up to date.
For more information, either phone Kirsty Odell on 020 7484 7647 or email her at k.odell@ hempsons.co.uk or phone Justin Cumberlege on 020 7484 7575 or email him at j.cumberlege@hempsons.co.uk.
Kirsty Odell is an associate and Georgina Hall is a paralegal at specialist healthcare law firm Hempsons
BUSINESS DILEMMAS
Dilemma 1 Do I release dead patient’s notes?
QI am a private GP and, following the death of a patient, have been approached by the family requesting confidential information and records about the patient.
They have not stated why they require this information, so I am wary to share this, as I understand I have a duty of confidentiality to the patient even after death. What do I need to know?
AIt can be difficult to know what, when and to whom it is appropriate to disclose a deceased patient’s records. In paragraphs 134-138 of Confidentiality: good practice in handling patient information (2017), the GMC states that a practitioner’s duty of confidentiality continues after a patient has died.
Furthermore, the Access to Health Records Act 1990 in England, Scotland and Wales and the Access to Health Records (Northern Ireland) Order 1993 in Northern Ireland both give a deceased patient’s personal representative, and anyone who may have a claim arising out of the patient’s death, a right to make an application for the patient’s medical records.
However, this right of access is not automatically guaranteed and may be limited to information relevant to the possible claim when the applicant is not the personal representative.
Access should be limited or refused if one of the following conditions applies:
There is evidence the patient would not have expected the infor-
Duty exists after death
Dr Kathryn Leask (right) discusses how the duty of confidentiality applies even after a patient’s death
mation to be disclosed to the applicant;
The disclosure is likely to cause serious harm to anyone else;
It would also disclose information about a third party – other than a health professional involved in the care – who does not consent;
It would disclose information that is not relevant to any claim that may arise out of the patient’s death – if the applicant is not the personal representative;
It predates 1 November 1991 in England, Scotland and Wales, unless earlier records are required to understand subsequent entries.
Additionally, access must be refused to records containing a note, made at the patient’s request, stating they did not wish access to be given on an application under this legislation.
are requesting, why they require the medical records and for what purpose these will be used. Also ask them to confirm whether or not they are the personal representative of the deceased patient’s estate, preferably in writing. It should help you understand why the medical records are being sought, which ones may be relevant to the request and whether they can be disclosed.
3. You may want to seek the personal representative’s views on the application for disclosure; for example, in a will dispute case. If this is the case, you should ask the applicant/complainant if they are the personal representative of the patient’s estate – and if not, for the name and contact details of the personal representative, if known to them.
4. If the personal representative is known and the applicant/complainant is happy for them to be contacted, move to step 7.
5. If the applicant/complainant does not know the identity of the personal representative, proceed to step 8.
6. If the applicant/complainant objects to you making the personal representative aware of their application/complaint, you should ask for their reasons and explain that it may hinder your ability to respond to the request. Once the reasons are provided, move to step 8.
Unfortunately, this can be a complex and confusing process. It can sometimes be very difficult to discern what is being requested and why.
The GMC requirements and the national legislation can be distilled into a series of steps to follow when you receive a request for disclosure of the medical records.
These following steps are applicable when a third party asks for disclosure of medical records, and the practice is unsure about the nature of the request and/or identity of the third party.
1. You should make it clear to the applicant/complainant that while you have no wish to be obstructive, you must consider your duty of confidentiality to the patient, which is ongoing after death.
2. Ask the applicant/complainant to specify what information they
7. You should write to the personal representative, making them aware of the application/ complaint and seeking their views on the requested disclosure. If the personal representative opposes disclosure, ask them to explain their reasons so that you can take these into account when making your decision as to whether disclosure is appropriate.
8. Once you have all the necessary information from the applicant/ complainant and the personal representative, where appropriate, you should review it alongside the relevant parts of the patient’s records.
You should also form a view on whether the requested disclosure is: a) Required by the legislation or b) Reasonable under all the circumstances.
Dr Kathryn Leask is a medico-legal adviser at the Medical Defence Union
Fears about an old doctor
Dilemma 2
Should I report my colleague ?
QOver the last few months, I have become concerned about the standard of care that a senior colleague has provided to patients and that he is using management plans now considered outdated.
I am a relatively newly qualified consultant gastroenterologist who recently started working at a private clinic. Can you give me any advice on what should I do?
AThe safety of patients must come first at all times and this overrides any personal or professional loyalties if your colleague’s behaviour puts patients at risk as well as his own career and reputation.
In the first instance, it may be appropriate to talk to your colleague about your concerns and encourage him to seek help.
Be sympathetic but make it clear that you are concerned that patients are being put at risk and be clear that you will need to take action if the issue is not addressed. If you do not feel it is appropriate to discuss this directly with your colleague, you can report your concerns in line with the clinic’s procedure for raising issues. This would generally involve raising the matter with a senior manager in the department.
Keep a record
If you raise this verbally, keep a note of any discussions you have had, with whom and when. It is also advisable to follow up in writing and keep a record of correspondence so you can document the steps you have taken to raise your concern if necessary.
These actions are in line with the GMC’s guidance Raising and acting on concerns about patient safety (2012), which states that all doctors have a duty to act when they believe that patient safety is
Much soul-searching can take place in knowing what to do if you have concerns about a colleague. Dr Kathryn Leask gives her view
All doctors have a duty to act when they believe that patient safety is at risk or that patient care or dignity is being compromised
at risk or that patient care or dignity is being compromised. This duty overrides any personal or professional loyalties.
This guidance also explains that if the doctor is unable to put the matter right, then they should raise the concern with an appropriate person in their employing organisation.
The doctor does not need to wait for proof and can justify raising a concern if it is done honestly, on the basis of reasonable belief and via the appropriate channels, even if the doctor is mistaken.
While it may be difficult to raise concerns about a colleague’s health because of worries it could cause problems for them or make interactions uncomfortable, patient safety is paramount and if you feel a colleague’s health may put patient safety at risk, you should take steps to protect the patients.
Be reassured that reporting health concerns often means that a doctor is enabled to confront the issue and to access the help and support they need to practise safely in the future.
DOCTOR
ON THE ROAD: BMW iX 50 SPORT
This SUV accelerates like a sports car
An almost total lack of wind noise allied to a limousinesmooth ride makes any journey a completely relaxing experience
Our motoring correspondent Dr Tony Rimmer (right) considers the German car-maker’s latest offering as a real alternative to the Tesla Model X – with better build quality and better driving dynamics
BMW iX X-DRIVE 50 SPORT
Body: Five-seat SUV all-wheel drive
Engine: Dual electric motors. 2kWh battery
Maximum charge rate: 200kW DC
Power: 516bhp
Torque: 760Nm
Top speed: 125mph
Acceleration: 0-62mph in 4.6 seconds
Claimed range: 373miles
CO2 emissions: 0g/km
On-the-road price: £93,905
WE HAVE become used to progressive change in the technology used to aid our medical practice.
The quality of available scanning, for instance, has improved dramatically over the last decade and, for the future, we have robotic surgical techniques being developed to help over a wide range of specialties.
Keeping up to date with the speed of advancements can sometimes feel challenging.
It is a similar story regarding the electric car revolution. I have been very impressed with the latest releases from the big manufacturers, but it does not seem to take very long before a new model comes along to challenge the top spot as ‘best EV on sale’.
The latest contender comes in the form of a large SUV: the BMW iX.
BMW is no stranger to EV technology and it released the quirky i3 model in 2013. However, since that time, it has not launched another model on a dedicated ‘ground-up design’ all-electric platform.
The recent released iX3 SUV uses the chassis from the petrol X3 and the impressive i4 hatchback uses that from the 3-series. The brand is, of course, recognised for producing cars that are high-quality and, most importantly, good to drive.
Have they achieved this with the iX? I set out to find out with a long-range model, the iX 50.
There are two main power and battery options. The X-drive 40 has 332bhp, a 77kWh battery and a claimed range of 249 miles. The X-drive 50 has 516bhp, a huge 105 kWh battery and a claimed range of 373 miles.
You pay a significant extra £24k for the 50 model. Trim is Sport or M-Sport but both give compre -
hensive equipment as standard. There will be a performance M60 model available soon with a massive 619bhp to compete with the top Teslas, but it will come with a hefty starting price of £111k.
So, the first thing to mention about the iX is the elephant in the room – the divisive frontal appearance. A huge plastic kidney-grille dominates the look and, if nothing else, it gets the car noticed.
Although it reminds me of the 1960s’ Rover 3-litre, I quickly got used to it and indeed have warmed to it. It makes a design statement which I think all EVs should. The rest of the car has pretty standard SUV styling with some nice modern touches such as the slim lights front and rear.
The interior has a clean, fresh design. A large digital instrument and infotainment screen sweeps across the dashboard in front of the driver, but fortunately BMW has retained its excellent iDrive controller between the seats to control many functions.
Spacious feel
There is an airy, spacious feel about the cabin which extends to the rear, where passengers are treated to fantastic head- and legroom – a common feature among electric cars with a dedicated platform.
The boot is good but not as roomy as in the Audi e-tron, but at least there is room under the floor for the charging cables.
From behind the squared off steering wheel and seated in a commanding position, I set off to see if the iX drives like a BMW should. Well, this X-drive 50 model certainly has more than enough straight-line performance.
Acceleration is sportscar fast and completely linear, just an uninterrupted wave of power as one would expect from 516bhp fed through all four wheels.
However, like all electric cars, it is
how it corners with all that extra weight from the batteries that is its greatest challenge.
But the iX really does rather well. For a 2.5ton car, the body control is impressive and the steering is sharp and accurate, albeit without much feedback from the road surface.
Having said that, probably the most impressive aspect of how this BMW drives is the refinement. An almost total lack of wind noise allied to a limousine-smooth ride makes any journey a completely relaxing experience.
Passengers will appreciate this as much as the driver and long-distance travel is stress free for all. Indeed, despite this being an allelectric car, long distance travel is definitely possible – the claimed range of 373 miles from a full charge is a realistic 300 miles.
This makes the iX a serious single family car contender, although charging at home from a 7.4kW wall-box still takes 16hrs to charge from 0 to 100%.
Faster charging is available at dedicated fast-chargers on the road network, but these are still rare and it does become pricey.
In summary, the iX is an impressive piece of kit. As a demonstration of BMW’s commitment to future electric car development, it reassuringly retains the Munich brand’s DNA.
It would work well as a family SUV for any private practitioner who only needs one car. However, it is expensive, although the cheaper £69,905 X-drive 40 model does everything just as well if you can live with a reduced 200-mile real-world range.
Consider it as a real alternative to the Tesla Model X with better build quality and better driving dynamics.
Dr Tony Rimmer is a former NHS GP practising in Guildford, Surrey
BMW has retained its excellent iDrive controller between the seats to control many functions
LEGISLATING FOR SAFETY
Reform joins up care
David Hare (right) explains what the new Health and Care Act means for independent practitioners
AT THE end of April, the Health and Care Bill completed its passage through Parliament and will now establish some of the biggest reforms to how the healthcare system operates in almost a decade.
While the bill has largely gone under the radar during the last year due to Covid and the rising elective care backlogs, the new legislation contains a number of key reforms which will change the safety and quality landscape for independent providers and practitioners.
The most significant change in the now Health and Care Act is the abolition of clinical commissioning groups (CCGs) and the introduction of integrated care systems (ICSs) from 1 July,
This will bring together local providers who will have a much greater role in shaping local healthcare provision and commissioning new services.
As part of this change, regulation of healthcare services will also
move to what is described as a more ‘systems’ level.
While the Care Quality Commission (CQC) will continue to inspect individual services, the new Act includes a requirement for it to conduct reviews of ICSs.
The watchdog will look broadly across the system to see how integrated care boards – who will commission care – local authorities and providers of health, public health and adult social care services are working together.
Working in practice
While this makes sense in principle and should ensure that ICSs can be held accountable for the decisions they make that affect the quality and safety of care their local area, it throws up a huge range of issues around how it can work on a more practical level.
For example, what exactly will the CQC be assessing at ‘system level’?
If patient outcomes are poor in a particular area, to what extent can it be determined that this is down to an individual provider or the ‘system’ they work within?
And could this lead to duplication in assessments taking place across local areas?
Moreover, in assessing how well providers ‘work together’, how can it be demonstrated that more ‘collaborative’ working is actually making a difference to patient care on the ground?
There are not going to be any easy answers to this, and we will be continuing to engage with the CQC to ensure the needs of independent healthcare providers and those working in the sector are fully factored into this new way of working.
Share information
A more ‘integrated’ approach to regulation and inspection is also mirrored in the data world with the Health and Care Act setting out new powers for health or social
care bodies in England to share information.
The idea is that this will help ensure that data relating to all health services – including those delivered by independent sector providers – flows through the system in a standardised way so that it is always meaningful and easy to understand for any recipient or user.
In turn, it is hoped this will help improve the experience of patients who move between publicly and privately funded services; for example, such as individuals who receive their elective surgery in a private provider.
By encouraging the frictionless movement of information between providers, this will ultimately support timely and appropriate patient care decisions, something which IHPN has been calling on for some time.
David Hare is the chief executive of the Independent Healthcare Providers Network (IHPN)
A UNIFIED SAFETY INSPECTORATE
Another key change in the legislation is the transition of the Healthcare Safety Investigations Branch (HSIB) to the Health Services Safety Investigations Body (HSSIB).
This new body will have full operational independence from the Department for Health and Social Care, and will investigate qualifying incidents, with the powers to investigate and promote system learning.
Information gathered by the HSSIB during it investigations will also be subject to confidentiality protections through prohibition on disclosure, or ‘safe space’ protections, access to which can only be granted by the High Court – with an exemption for coroners.
And, critically, the remit of the HSSIB will encompass all healthcare, including that provided by the independent sector in England.
At the end of last year, HSIB published its inquiry into how the NHS and independent providers worked together during the pandemic –with some helpful recommendations on further strengthening relationships between the two sectors.
It is clear that, in its new manifestation, HSSIB will be an increasingly key player in the safety and quality improvement space.
Along with broader changes to the CQC’s regulatory approach, it is clear that the safety and quality landscape will be in a period of transition in the coming months and potentially years.
While these changes will take some time to bed in, IHPN will be working hard to ensure they enable independent providers and doctors to continue to deliver safe, high-quality care for millions of patients.
The care watchdog, the Care Quality Commission, will now oversee the commissioning of services and how all types of providers work together
Groups fail to take off. . .
... but incomes from private practice for anaesthetists have remained similar on average, according to latest figures. Ray Stanbridge reports
THERE IS currently a very wide range of incomes being earned by anaesthetists in private practice, as our table below, right, shows.
We reported last year in our 2019 figures that anaesthetists’ incomes were fairly stable between 2018-19 – and a similar pattern has emerged for 2019-20.
Gross incomes, on average, fell by £2,000 or 2%, going down from £101,000 to £99,000.
Costs of an average practice fell by £1,000 from £40,000 to £39,000. As a result, taxable profits dropped by £1,000 or 1.6% from £61,000 to £60,000.
As we have previously reported in this series, gross incomes tend to be markedly higher in London and the South-east than in the rest of the country, save where a local anaesthetist enjoys a quasimonopoly.
All in all, we have noticed little change in patterns from the previous year.
Readers should, of course, note that our survey covers a period prior to the Covid pandemic. We would expect 2021 gross income figures to be markedly different from 2020 figures for certain individuals.
Last year . . . we felt there would be a significant growth in groups. But that has not yet happened
Costs
Again there was, in total, little change in pattern from the previous year.
There appears to have been some reduction in staff costs, although this may be accounted for by some family tax planning rather than true market conduct.
Expenditure on use of home showed some increase, reflecting a rising trend among some anaesthetists to use home as their base office.
Accounting/legal costs showed a modest increase on average, primarily reflecting inflationary trends rather than any real change.
Other costs were mostly similar to the previous year.
What then of the future? We have noticed continuing growth in NHS-financed Choose and Book work.
Last year, we reported in Independent Practitioner Today that there had been changes in the composition of work for many anaesthetists and working in anaesthetic groups was increasingly common.
Back then, we anticipated some major change in the ways anaesthetists conducted their businesses, and we felt there would be
HOW ARE YOU DOING? Use
While our analysis should not be
a significant growth in groups. But that has not yet happened. This is partially because of the outbreak of the Covid pandemic in early 2020, which disrupted many underlying changes and trends in the sector. As we now know only too well, Covid has been a dominant factor over the past two years in the private medical sector.
seen as statistically significant, it does give a useful indication of what a typical anaesthetist earns and spends in private practice and the trends in the marketplace.
Criteria for acceptance in our survey have not changed. These are that a consultant anaesthetist:
Continues to work in the NHS and is not in full-time private practice;
Holds either an old-style or a new-style contract within the NHS;
Has been in private practice for at least five years;
Is seriously interested in pursuing private practice as a business;
Is earning at least £10,000 gross from private practice – previous criteria £5,000;
Trades either as a sole trader through a limited liability company or as a member of some other group.
Next month: Dermatologists and oncologists
Ray Stanbridge is a partner with accountancy, finance and tax advisory medical specialists, Stanbridge Associates
DON’T MISS OUR COMBINED JULY-AUGUST ISSUE
Coming in our July-August issue, published on 12 July.
With rocketing inflation, our troubleshooter Jane Braithwaite gives her response to doctor employers who are wondering how to handle the cost-of-living crisis for their staff
The self-pay scene in London: Following Liz Heath’s self-pay report in this issue, LaingBuisson’s Ted Townsend reveals what’s been going on –or not – in the City
A closer look at tracking the steps in a new patient’s journey and why making a good first impression is vital for any successful private healthcare business. Simon Marett of Ellerton Marketing has some excellent advice
Vicarious liability: A recent court case has thrown up legal implications which could prove costly for some independent practitioners. Elena Goodfellow, of Bevan Brittan, explains what it means and suggests action they can take
If you have NHS work, do you understand your pay slip? Sandison Easson accountant Richard Norbury warns that many don’t – and that can prove costly
Dr Sally Old, medico-legal adviser at the Medical Defence Union (MDU), discusses what to do if a patient wishes to make an advance decision to refuse medical treatment. Plus how to proceed when a patient does not want a chaperone present during an intimate examination.
INDEPENDENT PRACTITIONER TODAY
Published by The Independent Practitioner Ltd. Independent Practitioner Today is editorially independent and thanks Bupa for its assistance with distribution. Material is governed by copyright. No part of this publication may be reproduced, stored in a retrieval system or transmitted in any form without permission, unless for the purposes of reference and comment. Editorial layout is the copyright of the publishers. If you wish to use it for promotional purposes on websites or for reprints, we would be happy to discuss licensing the copyright to you.
In the first of a new three-part inquest series, Hempsons’ solicitors Thorrun Govind and James Down explain the inquest process and what happens if you are called to attend
’Live by performance, die by performance’. Investors do well to heed the common risk warning that ‘past performance is not a guide to future performance’, says Ben Holdsworth of Cavendish Medical Minor surgical procedures are usually straightforward, but practitioners should be aware of some common pitfalls. Dr Clare Devlin explains more
Dermatologists’ and oncologists’ income levels come under the spotlight in Ray Stanbridge’s Profits Focus
Bupa’s new quarterly Wellbeing index report
A medico-legal expert from the MDU presents the first of a new series looking at the revamp of the GMC’s fitness-to-practice guidance
The successful manager – a review of a new book providing ‘concrete, actionable solutions to help all managers, from the newly appointed to the seasoned professionals’
Our motoring correspondent Dr Tony Rimmer gives his verdict on the VW iD4
Plus all the latest news and our other regular writers from Medical Billing & Collection and the Independent Healthcare Providers Network
And don’t forget to check out our additional news updates every week online
ADVERTISERS: The deadline for booking adverts in our July-August issue is 24 June
Write to Independent Practitioner Today
7 Lindum Terrace, Lincoln LN2 5RP
CHANGING ADDRESS, EMAIL ADDRESS OR SUBSCRIPTION DETAILS?
Phone 01752 312140 or email karen@marketingcentre.co.uk
TELL US YOUR NEWS
Robin Stride, editorial director
Email: robin@ip-today.co.uk
Phone: 07909 997340 @robinstride
ADVERTISE WITH US
To advertise in the digital journal, on our website or in our business directory, contact advertising manager Andrew Schofield at Spot On Media. Phone: 0161 408 3912 Email: andrew@spotonmedia.co.uk
GET A SUBSCRIPTION DISCOUNT!
£90 independent practitioners.
£90 GPs and practice managers (private & NHS).
£210 organisations.
Save £15 paying by direct debit: individuals £75 (organisations £180). TO SUBSCRIBE
Email karen@marketingcentre.co.uk or phone 01752 312140
Publisher Gillian Nineham
Phone: 07767 353897.
Email: gillian.nineham@gmail.com
SAVE
£15 WITH DIRECT DEBIT!
Guarantee delivery of your next copy of Independent Practitioner Today. Take out a subscription and you will get full access to our news, features and previous issues on our website. See details on the left.