The business journal for doctors in private practice
In this issue
Hospital extends its reach
A picture tour of a new private clinic in London’s Cavendish Square P12
The nameplate is just the start of it
The most important things you need to do when starting out in private practice P22
Why we struggle to get risks in perspective when investing n See page 32
Medical indemnity at the press of a button
An enhancement to The Private Practice Register will streamline buying medical indemnity P24
Doctors are given more time to sort pension tax
By Robin Stride
Doctors who are asking the Government to pay their large tax bills caused by breaching annual pension savings limits in 2019-20 have been given more time to apply for help through the voluntary Scheme Pays system.
They have now been granted an extra eight months to sort out their applications.
The deadline, normally falling every 31 July, has been extended to 31 March 2022 to support those who are dealing with the impact of the Covid-19 pandemic.
When individuals elect to use Scheme Pays, the NHS Pension Scheme pays their annual allowance tax bill to HM Revenue and Customs (HMRC) on their behalf, with that member’s benefits in retirement being reduced accordingly.
The Government had previously agreed to pay the tax charge of clinicians in England and Wales who breached the annual allowance pensions savings limits for 2019-20 only – but those affected must apply for Scheme Pays to claim this offer.
Patrick Convey, technical direc-
In
association with
tor of specialist financial planners Cavendish Medical, explained: ‘This deadline extension is good news if you are struggling to complete the necessary forms in time.
‘However, one confusing element is that you will have already completed your 2019-20 tax return earlier this year. Hopefully, you told HMRC then that you intend to apply for Scheme Pays to settle any annual allowance charge and not opted to pay via self-assessment.
‘And even with the extension in place, I would encourage those that can to complete the forms as soon as possible so you do not forget to apply or run out of time.
‘It is also wise to get your figures double-checked – the McCloud judgment could mean that the numbers for the last few years need to be changed retrospectively.’
This judgment ruled that doctors affected by the deemed ‘age discrimination’ of moving to the 2015 NHS Pension Scheme have the right to make a ‘deferred choice’ of which remedy benefits to take.
Consequently, they can decide at the time of their retirement whether to accept the pension benefits from their previous 1995/2008 pension scheme or those from the
2015 scheme for the remedy period, which is from 1 April 2015 to 31 March 2022.
Mr Convey added: ‘Note that even when there is some good news for NHS scheme members like this Scheme Pays deadline extension, every change to the rules and regulations has the potential to make
the pension plan, and its calculations, ever more complex.
‘The best way to deal with this is to plan as far ahead as you can and seek help to check you are still on the right track when things do change.’
n See ‘Get tax relief for working at home’, page 4
Doctor set to save
£33,000
The extended deadline will generate wider knowledge of this topic and be a big bonus to those affected, according to the Association of Independent Specialist Medical Accountants (AISMA).
AISMA vice-chairman James Gransby said: ‘There are still clinicians who can benefit from this compensation who are unaware of its existence and so any effort to ensure everyone who can benefit knows that this exists is very welcome.
‘It also aligns the deadline to a second submission which is needed alongside the Scheme Pays Election form in order to benefit from the compensation mechanism. This is an important aspect not to be missed.
‘It is called a “2019/20 annual allowance charge compensation policy application form” and the next window of opportunity to submit this is between 2 August 2021 and 1 October 2021.’
He told Independent Practitioner Today: ‘A hospital consultant client of mine will benefit from this to the tune of over £33,000 and there will be much larger examples out there too.
‘We still recommend sending the Scheme Pays Election as soon as possible and not waiting until the extended deadline. This is because posthumous elections are not permitted and, sadly, there will always be cases where this becomes a factor.’
TELL US YOUR NEWS. Contact editorial director Robin Stride
Email: robin@ip-today.co.uk Phone: 07909 997340
@robinstride
ADVERTISE WITH US. To advertise in the journal or our website business and lifestyle directories, contact advertising manager Andrew Schofield at Spot On Media. Phone: 0161 408 3912
Email: andrew@spotonmedia.co.uk
GET A SUBSCRIPTION DISCOUNT
£90 independent practitioners. £210 organisations. £90 GPs and practice managers (private & NHS).
Save £15 paying by direct debit: individuals £75 (organisations £180).
Our series by Dr Clare Gerada, adapted from her excellent book Beneath The White Coat – doctors, their minds and mental health, has put the subject firmly under the spotlight in this journal for the last four issues.
As neurosurgeon Henry Marsh has commented, the volume is ‘full of the most profound insights into the difficulties that doctors face – but also as to how they can be helped.’ We recommend it to you.
The timing of our serialisation could not have been more topical with surveys of doctors from the BMA and others in recent months frequently revealing medics’ own concerns about health issues that have gathered pace as they toiled through the pandemic.
According to new Medical Defence Union (MDU) research, as many as 73% of medical members who responded to a survey stated they were stressed and/or anxious on a weekly basis. Sadly,
47% would not feel confident in raising a matter about their health and well-being.
They feel their stress and anxiety levels are worse now compared to the start of the pandemic and many continue to face huge concerns due to Covid-19.
Doctors should not feel they have to ‘just deal with it’, but, as the MDU says, it can be daunting to ask for help and reach out for support. If you are suffering, it is important to know you are not alone and we would encourage you, at the very least, to make the most of your support network right now.
This month’s instalment from Dr Gerada, ‘Doctors Treating Doctors’, can be found on page 42.
The pandemic has also affected many staff in private practice too, so do read Jane Braithwaite’s excellent ideas and advice about managing their mental health issues in the workplace, on page 18.
Your death rates are to be checked David Hare examines the implications for private healthcare providers of the roll-out of medical examiners, set up as a result of the Shipman Inquiry P10
Stop the negligence lawyers calling Clinical negligence claims notified by radiologists to the MDU are examined by Dr Shabbir Choudhury, who advises on how to manage risk P16
Nurture your staff’s mental health
The pandemic has taken a huge toll on healthcare workers, so Jane Braithwaite considers how to manage mental health issues in the workplace P18
Review your record-keeping
Simon Brignall advises consultants to ensure the important area of practice information reflects the needs of a modern private practice P26
A servant of two masters
Difficulties can arise when a clinician works both in the NHS and privately. Medical Protection’s Dr Heidi Mounsey offers some medico-legal guidance P31
Staff problems after lockdown
Doctor employers face ongoing staff management challenges as lockdown restrictions ease. Two lawyers highlight some areas needing consideration P34
PLUS OUR REGULAR COLUMNS
Accountant’s briefing: Do I buy a house through my business?
Ian Tongue answers this common question posed by doctors thinking of buying residential property P38
Doctor on the Road: Catch it if you can
Dr Tony Rimmer relishes his drive in the Porsche Cayman GTS, one of the last of its breed P41
Profits Focus: Profits not up to scratch
The financial performance of dermatologists and oncologists is revealed in our benchmarking series P48
Win overseas patients by appointing a Covid-19 guru
Doctors with a medical travel business are being recommended to appoint a ‘Covid-19 guru’ to help cut through the complexity and confusion of restrictions, quarantine, vaccination certificates and passports.
Takeover will ‘be good for doctors’
By Robin Stride
Medical tourism adviser Keith Pollard ( right ) says the concierge aspect of working for international patients is increasing important and clearly a source of competitive advantage.
Writing as editor in the International Medical Travel Journal, he warns that travel complexities for would-be patients from abroad could prove a big barrier to seeking UK treatment.
‘The rules and restrictions on international travel change on a daily basis. Your in-house Covid19 expert must be completely up to date not only with how these apply to your key source markets, but also how this impacts your potential patients and how you can support these patients to ensure that all aspects of their medical travel experience are worry-free,’ he says.
‘Creating competitive advantage in medical travel during and after this pandemic will be driven not just by treatment outcomes and cost. Building trust, removing “the fear of being stuck” – due to quarantine – and convincing the patient that you really understand the complexities of travel during Covid-19 will come to the fore.’
CONSULTANTS RUSH FOR PRIVATE CARE
Private practice is attracting such an ‘explosion of interest’ among consultants wanting to find out more that there is now a waiting list for the MDU’s latest virtual course.
See page 22
Consultants face an ‘exciting opportunity’ under plans for Spire hospitals to be bought by Ramsay Health in a £2.064bn deal.
Craig McNally, chief executive of the would-be buyers, claimed it would enable closer working with consultant partners and clinicians ‘to ensure further investment in clinical excellence in all our specialties’.
‘The transaction will also create the platform to address the growing patient demand for more convenient healthcare through increased investment in digital innovation and transformation.
‘We believe that the combined group will provide an exciting opportunity for Spire employees and consultant partners and look forward to welcoming them to Ramsay in due course.’
Spire chief executive Justin Ash said the deal, if allowed by the Competition and Markets Authority (CMA), would increase
choice to private and NHS patients and offer a platform where consultant partners could deliver ‘a positive difference to patients’.
The CMA may require a sale of some hospitals and/or clinics and is thought likely to require the two businesses to be held separately until its review is complete.
Together the two groups would have the largest number of outlets
in the £5.8m UK private hospital market. Ramsay UK works with over 3,000 consultants, runs 37 facilities, including three neurological rehabilitation centres and a mobile diagnostic scanning fleet, and is a leading independent provider to the NHS and a leader for electronic referrals from GPs.
Spire works with around 7,500 consultants and has 39 hospitals and eight clinics across England, Wales and Scotland.
Ramsay and Spire claim they would ‘lead the way on patient outcomes through bolstered partnerships with private health insurers, the NHS, consultant partners and associated clinical networks’.
Mr McNally said: ‘Ramsay will work closely with the Department of Health and Social Care to ensure all shared objectives are closely aligned and we stand ready to support the NHS in tackling the significant increase in waiting lists and the return of elective procedures in the UK.’
Defence cover quotes simplified
A new defence insurance policy gathers data for a quote from specialists’ profiles held in Healthcode’s Private Practice Register (The PPR).
According to Andy Foley, managing director of medical malpractice at global insurance broker Gallagher, its partnership with new company Doctors’ Indemnity will revolutionise the process for clinicians looking for insurance.
‘Previously, to get an accurate quote, clinicians would have to manually supply documentation to enable brokers and insurers to get a full understanding of their business and their insurance requirements,’ he said.
‘We are removing many of the obstacles clinicians faced and pro-
viding an automated and streamlined service. We work with a broad range of insurers, so clinicians using the service can be assured that they are getting access to a wide range of cover and policy options.’
Consultants’ PPR profile data held by the healthcare IT provider includes detailed practice information that feeds directly into the quote application.
Doctors’ Indemnity said this removed an administrative burden for consultants, ensured errors were avoided and gave insurers the confidence to allow them to price and quote accurately for each consultant’s practice.
Founder and director Lloyd Bowden said: ‘This is a game-chang-
ing new initiative that will raise the bar in the indemnity market while offering doctors and their patients optimum support, value and reassurance long into the future.’
Quotes can be obtained from multiple insurers to ensure competitive pricing and terms. Few private GPs have a PPR profile, so the firm said it would supply an electronic form for manual completion.
Doctors Indemnity said it works with Healthcode under a commercial relationship in providing information, with individual applicant’s permission only, to assist in completing doctors’ quotation requests.
See ‘Indemnity at the push of a button’, page 24
Craig McNally of Ramsay Health
Get tax relief for working at home
By Douglas Shepherd
Employed doctors in private practice, and staff employed by independent practitioners, may be able to benefit from tax relief claims for working from home due to coronavirus during 2021-22.
Over 550,000 employed workers have already claimed and are benefitting from the tax relief, according to HM Revenue and Customs (HMRC).
If employed workers were told to work at home by their employer because of coronavirus and, as a result, their household costs have increased, they are eligible to claim the ‘working from home’ tax relief.
HMRC said it was a ‘quick and easy’ procedure to claim via its online portal. It received more than three million claims for the tax relief for the 2020-21 tax year.
Myrtle Lloyd, HMRC’s director general for customer services, said: ‘Half a million people have already reduced their income tax this year by up to £125, by claiming tax relief on their working from home expenses.
‘We want everyone who’s eligible to benefit, so we’ve made it quick and easy to do online. Check if you’re eligible and apply at GOV.UK by searching ‘working from home tax relief.’
From 6 April 2020, the amount employers have been able to pay taxfree without employees having to provide evidence of an increased bill is up to £6 a week.
Employees who have not received the working from home expenses payment direct from their employer
More than 550,000 employed workers have
can apply to receive the tax relief from HMRC.
Eligible customers can claim tax relief based on the rate at which they pay tax. For example, if an employed worker pays the 20% basic rate of tax and claims tax relief on £6 a week, they would receive £1.20 a week in tax relief (20% of £6 a week) towards the cost of their household bills.
Higher-rate taxpayers would receive £2.40 a week – 40% of £6 a week. Over the course of the year, this could mean customers can reduce the tax they pay by £62.40 or £124.80 respectively.
Taxpayers can check if they are eligible via GOV.UK.
To claim for tax relief for working from home, employees can apply directly via GOV.UK for free.
Once their application has been approved, the online portal will adjust their tax code for the 202122 tax year. They will receive the tax relief directly through their salary until March 2022.
If employees were required to
for the
work from home last year but did not claim for the tax relief, they have not missed out.
HMRC said it would accept backdated claims for up to four years. They will receive a lump sum payment for any successful backdated claims.
A spokesman added: ‘Using an agent to apply for the working from home tax relief, and other similar schemes, could result in customers paying unnecessary fees or commission. Using the GOV.UK service is quick and free, and customers will receive 100% of the tax relief that is due. Agents will not be able to use the online portal to apply for the relief on a customer’s behalf.’
Since 6 April 2003, employers have been able to make tax-free payments to meet or re-imburse additional household costs to employees who work at home under homeworking arrangements.
Employees do not need to provide evidence to show their bills
TAX BREAK CAN BE BACKDATED
Tax preparation specialist David Redfern said: ‘Obviously, this past year has seen a widescale change in working patterns and it is refreshing to see HMRC loosen its rules to allow more employees to get help to cover their increased home expenses.’
For the current 2021-22 tax year, employees who work from home can claim a £312 allowance to cover additional costs such as heating, electricity and metered water due to more time spent at home.
Mr Redfern, of DSR Tax Refunds, added: ‘Employees who may be worried that they have been working from home since last March can take reassurance in the fact that tax refund claims can be backdated for four tax years, so if you have been working from home since the start of the pandemic, it isn’t too late to claim your allowance for the previous tax years covered.
‘This also includes any essential purchases you may have made at the start of the pandemic in order to kit out a workable home office. However you will only be able to claim for expenses which have not been reimbursed by your employer –tax relief is designed to ensure that you are not left out of pocket.’
Self-employed workers are not entitled to claim this tax allowance.
have increased unless they are applying for tax relief on costs above the £6 per week flat rate; then evidence of the increased costs may be required.
Employees will receive the tax relief that corresponds with the income tax rate that they pay. For example, it will differ in Scotland.
GMC to judge sick doctors under new rules
Proposals to reform the way regulators such as the GMC address concerns about doctors with health problems could penalise the most vulnerable medics, the MDU fears.
It is worried at Department of Health and Social Care plans to remove health as grounds for a fitness-to-practise investigation. Health would instead be dealt with
under ‘lack of competence’. The MDU’s Dr Matthew Lee said it was suggested the change would lead to a fairer and more proportionate system.
But it also risked undoing the many advances that have been made by the GMC in establishing sensitive and separate procedures for dealing with doctors in poor health.
already claimed
tax relief for working from home – and it can be backdated four years
HMRC sends out ‘worrying’ letters
By Charles King
Doctors are being warned of delays in payment of self-assessment tax refunds, and a threat to remove individuals from the self-assessment regime, unless ‘extensive and onerous’ information is provided to tax officials.
Accountants report a dramatic increase in letters from HM Revenue and Customs (HMRC) to clients demanding documents and information it calls ‘security procedures’ to ensure the ‘repayment amount claimed is correct’.
These security checks are ‘unusual and worrying’, according to Debbie Wilson, a tax expert and director at specialist medical accountants Hillier Hopkins, Watford. She said although HMRC states
in these letters that they are not an investigation into the self-assessment return itself, they could easily be misconstrued as one due to the threatening language used and implications if an individual fails to respond within 30 days.
‘Individuals face removal from the self-assessment regime and delays on receiving grants under the Self-Employment Income Support Scheme.
‘While we totally understand HMRC’s need to prevent fraudulent reclaims, individuals expecting a tax refund are being hit with the suggestion that their tax affairs are questionable and deliberately wrong.’
Taxpayers are asked to complete form R38, requiring extensive information, plus proof of identity and address.
Ms Wilson said HMRC had dismissed these letters as no more than a simple identity check. But she warned that its ‘aggressive and threatening nature’ would worry many taxpayers expecting a refund.
She added: ‘HMRC has confirmed that these letters are triggered when unspecified “risk indicators suggest that the customer or claim may not be legitimate”.
‘Despite the language used by HMRC, we would reassure individuals who receive such a letter not to panic or worry unduly. While it might sound like a tax investigation, it isn’t.
‘The letter shouldn’t, however, be ignored and you should ask your accountant or tax adviser for guidance on completing the required paperwork.’
HCA launches orthopaedic rehab service
An orthopaedic trauma rehabilitation programme at HCA’s London Bridge Hospital has opened in response to demand.
According to programme lead Mr Paul Culpan, a consultant trauma and orthopaedic surgeon, specialist care following a major trauma is currently very limited.
He said: ‘The new Orthopaedic Trauma Rehabilitation Programme will offer a solution to this problem and gives patients the best possible chance of rebuilding their health, and lives, after a major trauma.
‘This service offering is like nothing else available in London. Led by a team of people who are working with major trauma cases every day and using advanced technologies and therapies, our multidisciplinary approach will enable us to get the best out of each step of rehabilitation and recovery.’
Compiled by Philip Housden
London trust launches brand new mental health services
South London and Maudsley NHS Foundation Trust is launching a new private patients’ service.
Citing growing unmet demand for high-quality mental health provision, exacerbated by Covid19, the trust sees private market space for a specialist NHS player to provide additional choice for patients and payers.
The venture will initially offer an all-age general psychiatry outpatient service for common mental health problems.
Patients will be able to access a wide range of the Maudsley’s clinical academics, many of whom are at the forefront of research in their specialist area at the Institute of Psychiatry, Psychology and Neuroscience at King’s College London. Maudsley’s head of business development, Adam Pryce, said: ‘We see this venture as having
three prongs of benefit. The availability of a high-quality NHS PPU service is good for patient choice and offering a platform for consultants who wish to do private work helps with our medical recruitment and retention initiatives.
‘Obviously, there is also a commercial benefit that allows us to reinvest margins into local NHS services and infrastructure.’
The service, in Denmark Hill, south London, will also provide online consultations.
Launch is scheduled for September 2021. The trust’s income from private patients was stated as £124,000 out of more than £383m total patient-related incomes in the 2019-20 annual accounts, up from £108,000 the previous year.
Trust to put private fertility services out to tender
Responding to increasing competition, Leeds Teaching Hospitals NHS Trust (LTHT) aims to explore and test market opportunities to grow and sustain the inhouse PPU brand Leeds Fertility IVF service.
The last decade has seen an increasing trend nationally towards privately run fertility clinics, often in chains run by large commercial organisations.
In the south of England, almost all NHS and private fertility work is done in these private clinics. But in the north, it is common for large NHS teaching hospitals to run fertility clinics and for private clinics to set up in competition, doing private and NHS work.
A new competitor provider, abc ivf, recently opened in Leeds.
A trust briefing paper explains ‘there are no plans to change the service for patients, rather to maintain the current high quality and specialisation of services that are delivered. The decision to award a contract to a new provider is dependent on the quality of the bids submitted and the assessment LTHT makes of those bids.’
The trust report also says: ‘To mitigate the risk to the fertility services provided by Leeds Fertility, LTHT proposes to tender the Leeds Fertility IVF service for a contract period of ten years.’
The facility currently performs around 1,300 IVF/ICSI treatments and 700 frozen embryo transfers each year. In 2019-20, the trust reported total private patient revenues of £5.5m, up £628,000 and 12.8% from £4.9m the previous year.
Long-standing PPU manager retires
Sue Searle, general manager of Derby Private Health, University Hospitals of Derby and Burton NHS Foundation Trust, has retired after 26 years.
Starting out as a registered general nurse, she was hospital director at Derby’s Nuffield Health Hospital before developing the business case and operating model for the trust’s own dedicated private patients’ business.
Derby Private Health has gone from strength to strength in recent years, growing from revenues of £1.3m in 2013-14 to £5.1m in 2019-20.
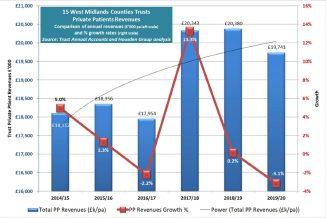
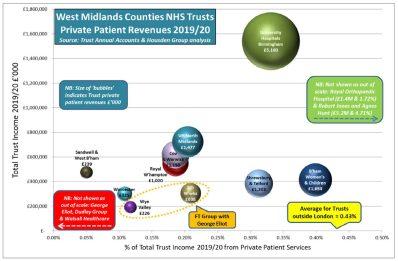
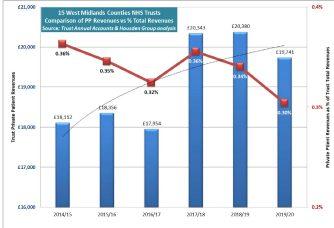
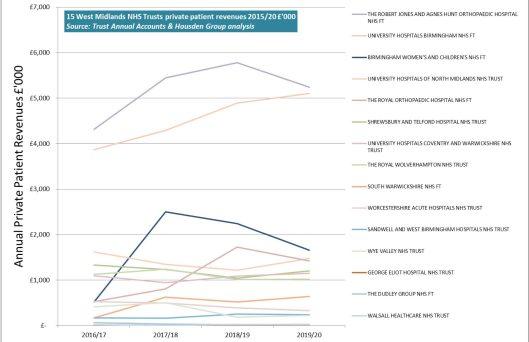
Philip Housden is a director of Housden Group. See his feature article on West Midlands PPUs on page 45
PPU WATCH
Covid's impact in figures
By Edie Bourne
Private Healthcare Information Network (PHIN) data on private activity in the UK confirms experiences of those private practitioners who saw a slow start to 2021.
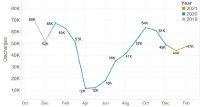
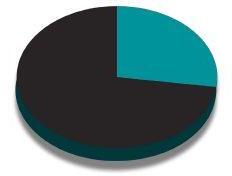
It said the number of people receiving privately funded acute treatment remained ‘fairly consistent’ from December 2020, with 44,000 episodes of care in January compared with 49,000 in December. February saw an increase in activity to 47,000 (Figure 1).
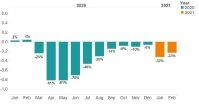
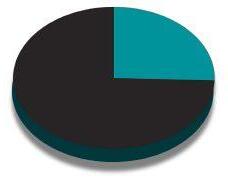
But January was down almost a third (32%) when compared to January 2020. February 2021 was 23% lower than the same month last year before the pandemic took hold in the UK (Figure 2).
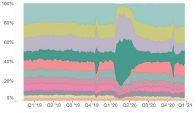
The specialty split shows few significant changes in market share in 2021. During March and April 2020, as the UK went into lockdown, medical oncology grew to a market share of 43% of all private activity.
The changes in market share were less dramatic at the beginning of 2021, with medical oncology growing 2% from 12% market share in December 2020 to 14% in February 2021 (Figure 3).
Schoen Clinic to develop new services
Developing relationships with consultants, GPs and private medical insurers is one of the targets of Schoen Clinic UK’s new group commercial director Mike Lord.
Previously commercial director at King Edward VII’s Hospital in London, he has taken up the new role just after the group won LaingBuisson’s 2020 Private Hospital Group of the Year award.
Mr Lord, who will work across orthopaedic and mental health, said: ‘I am passionate about enabling patients to access the best possible treatment and outcomes and I believe Schoen Clinic is firmly ahead of the curve in what it offers.
PHIN chief executive Dr Jon Fistein said: ‘While the signs at the end of last year pointed towards a potential recovery of private healthcare, the rise in hospital admissions of Covid-19 patients at the beginning of the year, along with the nationwide lockdown, seems to have led to a stagnation of private elective treatment.
‘As we start to open up, we may start to see the longer-term impact on NHS waiting lists and private care. We will continue to monitor this from the unique data we hold on private admissions across the UK.’
Admissions are counted as the number of hospital stays completed within the reporting period. Year-on-year change is calculated using only sites with confirmed volumes from 2019, 2020 and 2021 for each month.
While more hospital sites are submitting data, only those where a two-year comparison is possible have been included for year on year change. Estimates for 2020 and 2021 assume these sites are representative of the entire market, with confidence varying depending on number of submitting sites.
Mike Lord, commercial director of Schoen Clinic UK
‘With the ever-increasing importance of mental health services in the UK, I am particularly keen to ensure we continue to build on our proven capability in this area, through our offerings at Schoen Clinic York, Chelsea and Newbridge’.
He also aims to work with other new partners to further develop services at Schoen Clinic London, which opened in 2018.
Mr Lord previously held positions at Aviva Health UK and Nuffield Health. He replaces Dustin Reibe who is moving to head of clinical services for another healthcare provider.
Figure 1: Estimated count of private admissions (discharges) 2019-2021
Figure 2: Estimated change in activity by month compared to the previous year
Figure 3: Private activity by specialty as % total admissions
Clinics tie up to start lung testing service
A new one-stop lung health assessment service in London has been set up under a partnership between Queen Square Private Healthcare and Heart & Lung Health.
Led by a team of consultant cardiothoracic radiologists behind Heart & Lung Health, the new service uses low-dose CT scanning at the Queen Square Imaging Centre to detect subtle signs of early lung cancer in their earliest, most curable stage.
Jodee Cooper, chief executive of QS Enterprises, the charitable organisation operators of the Queen Square Imaging Centre, said: ‘While our focus has typically always been imaging for neuro
logical and neurosurgical conditions, owing to our co-location with the renowned National Hospital for Neurology and Neurosurgery, our facilities are well equipped to support all patients.
‘The expertise that the Heart & Lung Health team bring to this service has enabled us to develop an innovative service which will result in earlier lung cancer diagnosis and better outcomes for patients at high risk.’
A comprehensive lung health assessment, including a low-dose CT scan and consultation with a lung specialist, costs £699 with the Queen Square Imaging Centre.
HCA begins two new fertility clinics
Two new fertility outpatient clinics have been opened by Lister Fertility Clinic, part of HCA Healthcare UK.
They have been launched at the Beaconsfield Clinic in Buckinghamshire and HCA’s The Portland Hospital in central London in response to increased demand for fertility treatment.
The Lister Fertility Clinic has seen over 20,000 babies born since opening its doors in 1988 and performs approximately 2,400 fresh cycles of IVF each year.
A spokesperson said it is hoped that the new satellite clinics will make it easier for patients living across London and in areas outside of the capital, including Buckinghamshire and Oxfordshire, to access ‘world-leading services and the best medical minds in fertility’.
Services available include initial and follow-up fertility and gynaecology consultations, scans, ovulation induction, cycle monitoring, intrauterine insemination, frozen embryo transfer cycles and blood tests. Chelsea-based Lister Fertility Clinic remains the primary licensed centre for egg retrieval and embryo transfer.
At The Portland Hospital, the clinic will be led by consultant gynaecologist Mr Rehan Salim, who is joining after over 20 years’ experience in the NHS. He said: ‘There is growing demand for fertility services within central London and so the new outpatient clinic at The Portland Hospital offers a hugely exciting opportunity to reach a new pool of patients and further extend the expertise of Lister Fertility Clinic.’
Leading the Beaconsfield Clinic at the private GP practice Dr Now is consultant gynaecologist Mr Neale Watson. He said patients would find their fertility experience much easier as they would not have to travel so far for appointments and treatment.
Law change urged to support doctors
By a staff reporter
The ‘shameful’ disadvantage ethnic minority doctors still experience could be tackled by cutting red tape and giving greater autonomy to the GMC, according to its chief executive.
He said medical regulation reforms, currently being consulted on by the Department of Health and Social Care (DHSC), would give the council freedom to address discrimination and inequality within healthcare ‘laid so shockingly bare during the pandemic’.
The consultation, which runs until 16 June, proposes giving bodies like the GMC greater freedom over which cases to take forward, freeing up resources to drive improvements in culture, training and education.
Talking to health leaders at the Westminster Health Forum, Charlie Massey said: ‘The pandemic has showcased the deep pride we all hold in our health services. But it has exposed a shameful side too – that too many doctors from ethnic minorities continue to experience disadvantage.
‘This ranges from educational
attainment and career progression, to their likelihood of being referred to their regulator.’
Making long-awaited reforms would allow the GMC to focus on supporting and nurturing doctors, ‘rather than simply stepping in when things go wrong’.
The GMC chief said existing legal rigidity meant the emphasis of the GMC’s activities was in the wrong place, and he compared the current system to ‘using a hammer to crack a nut’.
‘We are required to fully assess every complaint we receive, even if it doesn’t raise serious fitness-topractise concerns and won’t meet
our legal thresholds. Reform will allow us to be much more focused in deciding which cases we investigate, and how we do it – ensuring fairer and faster outcomes.
‘It will also give us better options for concluding cases in a way that takes account of the needs of all parties. Defaulting to an adversarial panel hearing can be deeply stressful. Not only for the doctor but also for the complainant, especially for those who don’t want to give evidence in public.’
He added: ‘What we need is a more proportionate approach, where the course of action is determined by the case at hand, not legislative diktat.’
In 1983, the GMC dealt with less than one complaint a day; today it is roughly 10,000 a year.
But while medical practice has transformed over the years, the legislation governing the GMC is still stuck in the 1980s. Mr Massey said wholesale reform is needed.
‘Tinkering round the edges won’t cut it. What is required now is . . . a new model of regulation to meet 21st century needs. Galvanised by the pandemic, the chance for meaningful change is finally on the table.’
Sports service for children opens
A new paediatric sports medicine clinic has been opened by Cromwell Hospital.
Based in Kensington, the Children and Adolescent Sports Medicine Clinic is said to be the first of its kind to be set up on a Saturday in London, offering advice from a consultant and ongoing treatment the same day if required.
Hospital chief executive Philip Luce said: ‘Over the last year, many children have lost their fitness, become out of practice and not eased themselves back into com -
petitive sports, which has resulted in the need for this service.’
Children needing to be seen that day will be invited for an on-site outpatient consultation where they can be assessed, receive the necessary imaging and tests, and commence treatment that same day.
Prof Adrian Wilson, consultant orthopaedic and specialist knee surgeon at Cromwell Hospital, said: ‘With sports injuries, the faster it can be assessed and treated the better the outcome. We’ve seen many injuries left untreated,
which extends recovery time as well as being painful’.
The clinic is open from 8am till 6pm every Saturday except bank holiday weekends.
Charlie Massey, GMC chief executive
Prof Adrian Wilson, knee surgeon
A look back through our journal’s archives of a decade ago reveals that although times change, some issues are not so new
A trawl through the archives: what made the news in 2011
HMRC puts its foot down
Independent practitioners were facing an even tougher compliance regime as HM Revenue and Customs (HMRC) stepped up its campaign to boost ailing Treasury coffers.
After netting under 10% of the specialists who were expected to come forward under the previous year’s Tax Health Plan campaign, inspectors officially switched their attention to plumbers, offering a similar concessionary deal as the medical profession for confessing undeclared tax.
But doctors’ accountants were warned by advisers that their clients and GPs remained targets and could expect to come under more vigorous scrutiny when filing their 2010-11 business returns.
Tax expert Bob Trunchion told a meeting of the Association of Independent Specialist Medical Accountants that ‘a huge number’ of other accountants working for
doctors were letting their practitioner customers get away with ‘blue murder’.
He warned: ‘Dealing with HMRC has changed hugely in the last six months and is going to change hugely in the next six months.
‘If there is nothing to support what goes on a tax return, in future it won’t go in the tax return. It’s as simple as that.’
Doctors miss out on full value
Many independent practitioners were risking missing out on getting the best price for their practices on retirement because their accountants were not up to the intricate job of valuing them properly.
Medical accountants spent a day at a training seminar to ensure their doctor clients would make the most of their sale when they came to leave their jobs. US-based accountant and valuation expert
Mark Dietrich told Independent Practitioner Today: ‘Healthcare is a highly specialised industry and requires a unique skill set of the accountant to give the doctors the best advice.
‘If doctors are interested in selling their practice, they should seek out a medical accountant who is experienced in the valuation of practices.
‘And if they are interested in selling to another doctor, they should see someone with experience of medical transactions.’
Mileage test case starts
A consultant physician was set to be at the centre of an all-out assault by the medical profession to win recognition of independent practitioners’ mileage claims.
In a tax test case being prepared by accountants, he and his advisers were setting out why the taxman had, until then, been wrong to disallow him from claiming the cost of driving to the private hospital where he worked.
The case would argue for mileage claims to be allowed to the independent unit both from home and his NHS hospital.
If the doctor and his team were successful, then the case would have welcome implications for thousands of private doctors, who would then be able to argue for their claims to be allowed too.
Patients can compare prices online
From this month, patients were able to compare and book Harley Street’s leading doctors and services through the internet and their mobile devices, using a new website and mobile app.
HarleyStreet.com aimed to let private patients easily compare treatment options and prices, and book services and appointments from a database of around 5,000 London-based specialists, clinics and providers.
Patients track their care online
Consultant orthopaedic surgeons at Spire Bushey Hospital were the first in the private sector to trial an online patient-reported outcomes measures system, unveiled the previous month by Health Secretary Andrew Lansley.
A spot of publicity pays off
Business publicity hotted up for private skin specialists during Sun Awareness Week, promoted by the British Association of Dermatologists.
Consultant dermatologists at London’s Cadogan Clinic publicised the fact they would be available for advice, comment and mole checks – and received some useful press publicity as a result.
They were interviewed for national papers, magazines and a broadcast. A spokesman said: ‘It paid dividends for our ongoing PR activities.’
TELL US YOUR NEWS
Share your experience of what has and has not worked in your private practice. Even if it’s bad news, let us know and we can spread the word to stop others falling into the same pitfalls.. Contact editorial director Robin Stride at robin@ip-today.co.uk
Your death rates are about to be checked
National Medical Examiner Dr Alan Fletcher has published his first report, outlining progress and next steps in the roll-out of medical examiners. But with this new system set for a statutory footing in Government health service legislation, David Hare reports on the implications for independent healthcare providers treating millions of NHS and private patients
AS INDEPENDENT Practitioner
Today readers will be aware, implementation of medical examiners began in England and Wales in 2019 with the appointment of the National Medical Examiner and recruitment of national and regional teams.
Their introduction was one of the recommendations of the Shipman Inquiry and was designed to help make it easier to detect unusual patterns of deaths.
Indeed, a core part of the medical examiner role is to provide bereaved people with clear information about the cause of death, and an opportunity to raise any concerns they may have about the care and treatment provided to the deceased person.
Since 2019, medical examiner offices have now been established at 130 acute trusts in England –with five still to implement their plans – and at regional hubs in Wales.
Initially, they provided scrutiny of non-coronial deaths in acute care, with this remit being expanded in 2021 and 2022 to cover non-coronial deaths in other settings such as the community.
The first stage of rolling out this new system involved acute trusts in England and local health boards in Wales establishing medical examiner offices to certify all deaths within their own organisations.
Examiners’ increasing role
In the next phase, medical examiners offices are starting to review deaths in their geographic region but outside of their own organisations, including deaths in the independent sector.
Medical examiners’ offices are responsible for reaching agreement with other organisations to review their deaths and are being encouraged to work incrementally to increase the number of organisations they cover.
And in a bid to further improve safety and quality in the health system, their role is set to strengthen with the Government’s White Paper on NHS reform published earlier this year setting out the intention to make medical
examiners a statutory requirement so that all deaths not reviewed by a coroner are reviewed by a medical examiner, wherever they occur.
But what does this mean for the independent sector?
Chance to improve safety
Deaths in independent facilities are thankfully extremely low, but private providers should be prepared for increased scrutiny around any deaths in their organisation. There is an opportunity to further improve patient safety.
As part of the medical examiner’s role is to speak with bereaved families, healthcare providers may want to review how they communicate with families about a death and ensure their policies are con-
sistent with those of the medical examiners.
NHS England’s current message is that the independent sector does not need to take any formal action yet but should be ready to be contacted by the medical examiners’ office in their area.
It recommends each medical examiner’s office covers at least 3,000 deaths and that organisations with smaller numbers of deaths work with an existing office rather than establishing their own system.
A benefit of having medical examiners review the approximately 89% of deaths that do not go to the coroner is more accurate mortality statistics. This could change some care guidance and priorities.
As the Government’s forthcoming legislation on the NHS makes its way through Parliament, the Independent Healthcare Providers Network will be working with Parliamentarians across the Commons and the Lords to ensure independent providers are fully and explicitly recognised in the remit of medical examiners.
This is building on our work to ensure a truly ‘whole-systems approach’ to patient safety and guarantee our patients the best possible care.
David Hare is chief executive of the Independent Healthcare Providers Network (IHPN)
Medical examiners were recommended by the Shipman Inquiry and are designed to help make it easier to detect unusual patterns of deaths
Cancer hospital extends its reach
Private patient units (PPUs) are set for a healthy growth in the capital according to the boss of the new Royal Marsden Private Care facility in Cavendish Square, central London
THE ROYAL Marsden expanded its private care presence into the Harley Street area by officially opening a brand-new, researchled, diagnostic, outpatient and treatment facility last month.
Managing director Shams Maladwala told Independent Practitioner Today: ‘I think once we enter more of a recovery from the Covid-19 pandemic, the PPU segment – which had done very well pre-pandemic, with London PPUs accounting for around two-thirds of revenues across NHS PPUs – will continue to grow at a high rate.
‘By bringing more patients into London to be seen at Cavendish Square, we’re supporting the London healthcare community as a whole, as well as growing our share of the market.’
He believes research is a key differentiator for Royal Marsden Private Care because it means patients are able to access the latest and most innovative treatments.
‘Our integrated model means we can deliver the best quality and best safety governance, usually only seen in the NHS. This is great for the sponsors, private medical insurers or embassies because it means they can evidence the governance and evidence-based care we provide, as well as it being an efficient model.’
Exciting project
Prof Chris Nutting, consultant clinical oncologist and clinical director, added: ‘Patients will benefit from fast and direct access to consultants, specialising in a full range of cancer services and stateof-the-art diagnostic services, same-day scans and test results.
‘Cavendish Square is an exciting new project for us all and I’m look-
ing forward to working with colleagues alongside a new team who will be based at the centre as we all work towards the same shared goals to improve the lives of patients with cancer.
‘Expanding the reach of access to our Royal Marsden services in a new geographic area is a big milestone, especially having a presence in such a well-respected healthcare district in London.’
The hospital, which won the LaingBuisson Best Hospital Award in 2020 and is one of the few private hospitals to have been rated outstanding by the Care Quality Commission, is telling would-be referring doctors it offers worldclass expertise and outstanding facilities with multilingual guest relations staff to meet and assist patients and visitors in reception.
One-stop service
Patients can expect to have an appointment booked following their initial inquiry, with direct access to diagnostic services. A one-stop service means next day appointments and same-day scans can be offered, assessments and test results.
An onsite pathology department will conduct blood tests with rapid turnaround times and patients are promised fast and direct access to consultants, ‘confident that their treatment and care is based on the latest advances in oncology led by world-leading experts’.
Cavendish Square has also set up a new GP fast-track referral service giving direct booking into consultant clinics and same-day tests plus diagnostic and treatment plans.
Royal Marsden Private Care in Cavendish Square and its managing director Shams Maladwala
The seating areas in the main reception
Medical director Prof Chris Nutting with a patient
Senior diagnostic radiographer Ushma Neelakandan
Diagnostic radiographer Austine Nwachukwu
The medical day unit at Cavendish Square
The main reception area
Deputy Matron Farzana Baksh in the medical day unit
ACCOUNTANT’S CLINIC: THE BUILDING BLOCKS OF ACCOUNTANCY
to of top tips is for volatility and variables
Julia Burn continues with her A-Z of top tips. This month she turns to V
THERE DEFINITELY appears to be light at the end of a very long tunnel and, thankfully, the vaccine programme seems to be achieving the desired results and is allowing the country to re-open, albeit slowly and carefully.
There is still a level of uncertainty in the economy while things start to get back to normal and this will inevitably create volatility for independent practitioners’ business finances where it is not possible to return to normal immediately.
To try to stabilise through this volatile time, it will be necessary to identify fixed and variable costs to ensure the business is as efficient and flexible as possible to react and deal with the inevitable fluctuations that it may encounter.
Fixed costs for a business are those that will remain the same and continue to be incurred no matter what the level of income that the business generates. For example, premises rent and rates, wages for salaried staff on an annual salary, and subscriptions to professional bodies required for you to continue your trade that are generally an annual charge rather than being based on your level of income.
Other payments which are not fixed but required to be made at set time frames are things like PAYE, National Insurance and corpora-
tion tax, which will be dependent on the levels of salaries paid and profits generating.
Contrastingly, variable costs change with the volume of income the business generates. For example, specialist services that are required to be bought in, light and heat costs and general equipment required to service your clients.
Reviewing costs
Many independent practitioners’ businesses will be reviewing their cost base and looking at ways they can change the nature of some of their expenses from fixed to variable.
Businesses will be seeking to be more agile given the lessons of the pandemic and want to operate in a style which allows them to increase or decrease activity and costs at a moment’s notice.
It is likely that all our working lives will have changed with greater variability in working hours and practices.
Therefore, businesses need to harness the best elements of how people have worked during the pandemic to be able to be both relevant for employees and accessible to clients.
It appears unlikely we are simply going to go back to the way things were before, and ensuring businesses are agile and adaptable will be important to their success.
In a volatile economy, it is important to try and ensure that the majority of costs are variable rather than fixed
In a volatile economy, it is important to try and ensure that the majority of costs are variable rather than fixed, as that will enable the business to flex costs to match the level of income generated, therefore minimising financial exposure by only incurring those costs directly linked to the income.
Record-keeping
The importance of timely recordkeeping can not be underestimated. In a volatile economy, the most important factor will be the ability to react quickly to any changes.
To do this efficiently, records need to be updated on a live basis. It will also be essential to prepare a cash flow forecast which is flexed regularly to avoid unpleasant surprises.
Timing of cash flows will become ever more important,
especially with the assistance packages offered by the Government during the pandemic now becoming payable, including any taxes which may have previously been deferred also becoming due for payment.
Many accountants offer an outsourcing service where they will effectively run your company’s accounting function for you.
The service offered could include:
Maintaining the company’s book-keeping records;
Preparing monthly management accounts;
Preparing and updating cash flow forecasts for you.
These services will be more timeconsuming for you to fulfil in a volatile economy, so outsourcing them will enable you to focus more of your time doing what you do best, looking after your clients, safe in the knowledge that your finances are being kept up to date.
The outlook looks promising, though, and fingers crossed, the new normal will settle quickly, allowing you to regenerate and get back to levels of income previously achieved.
Julia Burn (right) is a director at Blick Rothenberg and part of the team that advises medical practitioners
CLINICAL NEGLIGENCE: RADIOLOGISTS
Stop the negligence lawyers from calling
Clinical negligence claims notified by MDU radiology members are examined here by Dr Shabbir Choudhury (right), who advises on how to manage risk
CONSULTANTS WORKING privately as radiologists who have been notified of a clinical negligence claim against them are often assisted by the MDU.
While claims are less frequently made against radiologists than consultants working in some surgical specialties, such as orthopaedics or cosmetic surgery, they remain relatively common and compensation can sometimes exceed a million pounds.
So managing known risks
linked to clinical negligence claims is important both to protect patients and to avoid claims being brought.
The analysis below is based on 200 recent claims brought against consultant radiologists working in the independent sector who were MDU members.
Nearly three-quarters of claims were successfully defended with compensation paid in only around a quarter of cases.
Of the cases that settled, the
majority were well in excess of £50,000.
However, this does not reflect the seriousness of the allegation but rather the cost of restoring the claimant to the position they would have been in had the negligence not occurred. But this figure does demonstrate the importance of having appropriate indemnity arrangements in place, as even lower-value claims can settle for costs that are beyond the means of most radiologists to pay.
REASONS FOR CLAIMS
1 Delayed or incorrect diagnosis
Eighty per cent of radiology clinical negligence claims related to a delayed diagnosis. A quarter of these cases involved a delayed diagnosis of cancer.
Other conditions commonly resulting in a claim being made were fractures and cauda equina syndrome.
Allegations usually centre on an abnormality not being detected,
but in some cases it was alleged that an abnormality was picked up but misinterpreted, leading to unnecessary or incorrect treatment.
2
Interventional radiology
Some claims involved a substantial interventional radiology element. Although interventional radiology is perceived to carry more risks, it is still far less commonly carried out than general radiology. It may also be that MDU members are more aware of the risk of interventional radiology and are justifiably cautious when undertaking complex procedures.
3
Medication issues
In a small number of cases,
the main allegation was about a medication issue such as allergic reactions or providing the wrong medication.
One claim involving the use of contrast in a child was settled for well over £100,000 with substan tial claimant’s legal costs.
4 Communication skills
A number of cases focused on the communication skills of the doctor, often when getting appro priate consent for a radiological procedure.
Dr Shabbir Choud hury (right) is medico-legal adviser and former sen ior medical claims handler at the Medical Defence Union
MANAGING RISKS
There are a number of actions radiologists can take, which, if managed appropriately, can help to reduce risks. These include:
☛ Ensure robust procedures are in place for communicating results to relevant parties to ensure appropriate and prompt follow-up and treatment.
☛ Consent should be obtained by an appropriate member of the team and, ideally, by the radiologist undertaking the procedure.
☛ Be aware of the GMC’s guidance on consent and other relevant guidelines such as those from NICE.
☛ Ensure the patient is aware of the risks, benefits and complications of the proposed procedure as well other therapeutic options. These should be carefully documented.
☛ Provide further information such as patient leaflets and information sheets which can help patient understanding. Remember that the use of these should be documented in the records.
☛ Consider the patient’s past medical history, medication history and allergies before administering pre-procedural medication and contrast media.
☛ Ensure appropriate hand-over to recovery staff for interventional procedures or those under sedation.
☛ Offer a chaperone to patients undergoing any intimate examinations – for example, pelvic ultrasound.
☛ Consider contacting the referring doctor if you find something unexpected or that needs urgent investigation.
☛ Have a system in place to verify the right site and patient undergoing treatment and to cross-check information provided against the referral.
☛ Ensure interruptions in the reporting room are kept to a minimum.
☛ If things go wrong, be open and honest with the patient by providing an explanation of what has happened and the likely shortand long-term effects of this. Say sorry and get advice from the MDU if you believe the incident triggers the organisation’s duty of candour requirements.
Our expert claims handlers and medico-legal advisers will defend claims whenever possible. They involve members in the conduct of their cases and will always seek your consent before settling a case.
While claims numbers have remained steady in recent years, the cost of claims has spiralled. This is not due to clinical standards but to a deteriorating legal environment which the MDU is campaigning to reform. You can see more at www.themdu.com/faircomp
A digital prescription platform to allow convenient prescribing from home
CloudRx is a digital prescription system that allows prescribers to create and send an electronic prescription to our fully licensed pharmacy for fast delivery direct to your patient. It can be used from home by doctors working away from their practices.
No cost to prescribers
Simple and quick prescription creation.
Legal paperless prescriptions, including repeat prescriptions and controlled drugs.
Patients receive text and email requesting secure payment. Alternatively, we can invoice the prescriber or clinic each month.
Prescriber Fees can be added if requested
Medicines are dispensed and dispatched by a variety of delivery options
Fully integrated into MidexPRO
Register for free by visiting cloudrx.co.uk
“We have worked with CloudRX to maintain a cold chain for the medication and direct delivery to patients at home.”
Dr Charlotte Norton, Medical Director of The Slimming Clinic, the UK’s largest chain of private doctor-led weight loss clinics
THE POWER OF PEOPLE
Nurture your staff’s mental well-being
Jane Braithwaite (right) considers how to manage mental health issues in the workplace
From the start of the Covid pandemic, we have been very aware of concerns relating to mental health and the increased number of people suffering from mental health problems.
This has largely been due to lockdown and the impact that has had, and we have heard how it has affected everybody, both young and old. More lately, we are hearing about the enormous toll on healthcare workers and some very concerning discussions relating to this.
AS PEOPLE who work in healthcare, we need to be very aware of the mental health issues employees – and we ourselves – may be experiencing.
It is important that we gain the best understanding so that as leaders, managers and role models, we can help and support our people – and to know what support is available for those who need it.
Before Covid, we knew mental health-related issues were the most common cause of long-term sickness in UK workplaces.
Surveys performed by the Chartered Institute of Personnel and Develop ment (CIPD) in 2019 reported that the impact of stress in particular had increased, with 37% of respondents saying that stressrelated absence had increased in the last year. They concluded: ‘Work-related stress, depression or anxiety accounts for 44% of workrelated ill health and 54% of working days lost in 2018-19.’
As well as sickness absence, poor mental health at work can lead to increased staff turnover, reduced engagement and high absenteeism.
Mental health problems affect around one-in-four people in in the UK in any given year.
As we recover from Covid, there is much evidence to suggest that the pandemic and measures taken to manage it, such as lockdown and social distancing, will have a significant impact upon the mental health of employees and the impact maybe felt for months or even years.
How will Covid-19 affect our mental health?
We do not yet know what the exact impacts of the pandemic on our mental health will be. People have been affected in different ways: many feeling isolated, others are fearful about catching the virus themselves and also anxious about their family and friends. Employees in healthcare have been working long hours with few rest periods in very difficult circumstances throughout the pandemic and have possibly not had the time or opportunity to reflect on their own well-being.
The workload in the healthcare sector is destined to remain high. As Covid numbers have decreased, many individuals have been
Employees in healthcare have been working long hours with few rest periods in very difficult circumstances throughout the pandemic and have possibly not had the time or opportunity to reflect on their own well-being
COMMUNICATE WITH EMPLOYEES
Circulate regular communications on well-being and mental health.
Arrange activities that encourage physical, mental, financial and social well-being
Raise awareness of mental health, working towards a culture where it is acceptable to talk about and seek support for poor mental health
Perform a workplace assessment in the form of a survey, allowing employees to respond anonymously, to gain a better understanding of the impact Covid has had and to gain insights into how your teams have been affected
Share information about mental health so that individuals are informed about symptoms. Sharing information about mental health can also enable employees to identify early signs in themselves and seek support
involved in the vaccine roll-out and are now facing the pressure of addressing long waiting lists of patients requiring non-Covid treatment.
This long-term stress has taken a toll and continues to do so. Our best defence against mental health is resilience, but, to maintain resilience, individuals need time to recuperate and this has not been possible in healthcare and is unlikely to be possible in the near future.
Mind, the mental health charity, reported that over half of adults and over two-thirds of young people said their mental health declined during lockdown. Young people and those with preexisting mental health conditions were particularly affected. The health impacts of lockdown include findings of fatigue, musculoskeletal conditions, poor work-life balance, reduced exercise and increased alcohol consumption. In relation to workplace mental health specifically, employees were reporting reduced motivation, loss of purpose, anxiety and isolation.
Evidence from previous quarantine situations also suggest that there are long-lasting effects on mental health.
Independent Practitioner Today is currently serialising parts of the book called Beneath the White Coat – Doctors, their minds and mental health, edited by Dr Clare Gerada, first published in 2020 (see page 42). In the book, the stress experienced by doctors is examined using supporting evidence and real-life case studies and offers practical steps for doctors to recover and thrive in their roles.
The book also demands policymakers, government and hospital
Provide access to resources that are available, including websites providing additional information, apps designed to enhance an individual’s well-being and phone support lines that operate to provide individual support.
SUPPORT YOUR MANAGERS
Brief managers on the potential mental health implications of Covid 19 and their specific roles and responsibilities in relation to supporting staff
Ensure all managers are aware of their responsibilities as an employer, especially their legal obligations
Define return-to-work programmes for those who have been furloughed or working from home and now returning to the office
If any roles are due to be made redundant, ensure managers have access to professional advisors to help them manage the redundancy process.
Provide managers with formal training on coaching techniques to enhance their ability to hold one-to-one discussion with their employees
Provide training for managers to help them identify the signs of poor mental health and well-being within their team
management ensure doctors are looked after and have access to the resources needed to ensure they remain healthy.
Working from home
Many people have been working from home during the pandemic and while most have found this to be more productive, still one-inthree people have found the opposite, according to research by MetLife UK.
Almost one-in-three (32%) workers admit that their productivity has declined as a result of the shift to home working. Of these employees, two in five (41%) believe that their mental wellbeing has impacted their productivity levels. The impact is understood to have been more apparent for younger groups aged below 30 and also older women aged 50 plus.
There is also a marked difference
between the statistics reported by employees and those reported by employers. Employers believe there has been a greater decline in productivity, with 56% of employers reporting that they perceive their employees’ personal wellbeing has impacted their productivity levels. This is significantly higher than the 32% of workers who reported their productivity has declined.
Productivity is absolutely key in any business, including healthcare, and therefore it follows that we should be concerned about our employees’ mental health and how this affects the productivity of our teams.
We need to do our best to understand the issues that our teams are facing and support them by implementing management strategies to reduce the impact in the workplace.
Understanding the issue
As mentioned previously, there seems to be a huge amount of information stating the enormity of the mental health problem caused by Covid, but there does not appear to be much research yet giving us useful data to understand the specifics of the issues and indeed how to address them.
One of the greatest challenges is that individuals are often unlikely to ask for help when they need it, and this is perhaps more extreme for those working in healthcare, who feel they should be able to manage their own well-being.
As managers and leaders, we need to work hard to encourage openness and make it easier and more comfortable for people to ask for help.
HR management
Most larger healthcare companies will have in-house HR departments providing expert support and who will be defining organisational strategies to help their managers and leaders deal with mental health issues in the workplace.
For smaller organisations, there is less support available and managers will need to address these issues themselves.
In an attempt to provide a useful guide, our HR managers have provided some input that I hope will be of value.
What is workplace mental health?
Obviously, healthcare professionals have a much greater awareness of mental health illness, but it is still useful to define what we are dealing with in relation to the workplace.
Mental health, like physical health, fluctuates over time and there are degrees of severity. Symptoms include struggling with low mood, anxiety and stress, and we know stress can contribute to other illnesses.
Conditions include depression, anxiety, phobias and bipolar, which tend to continue over a prolonged period.
As employers, one of our objectives should be to help individuals feel comfortable in talking about how they feel. In doing so, we must avoid attempting to diagnose and instead focus on discussing how the issues impact the
It is the employer’s duty to assess the risk of stress-related mental health issues arising from work and to take measures to control the risk
employer’s control; however, there are early actions that can be taken.
Supporting the mental health of employees in healthcare, many of whom continue to work under significantly increased pressure making them more vulnerable to stress and other mental health conditions, is vital and it is warranted to take a pro-active approach.
In a large organisation, the HR department may become involved to provide support and potentially the occupational health team, if needed.
employee’s work and their work life with a view to agreeing a plan to provide additional support.
A range of measures will need to be introduced and a good starting point for any manager developing their strategy is to understand our legal responsibilities as an employer.
These legal duties set the minimum requirements and must be adhered to, but there is a wealth of evidence arguing that employers who go above and beyond will benefit from improvements in employee engagement, reduced absence, reduction in staff turnover and improved organisational culture.
Employers have a duty to protect the health, safety and welfare of their employees, including mental health and well-being.
The UK Health and Safety Executive defines work-related stress as a reaction to excessive pressure or other type of demand placed on an individual at work. It is the employer’s duty to assess the risk of stress-related mental health issues arising from work and to take measures to control the risk.
Employees who have a mental health condition may be disabled and will therefore be protected from discrimination during employment as defined by the Equality Act 2010.
Employers are required to make reasonable adjustments for employees with disabilities, which may include amendments to working hours, location of work, changes to duties and the provision of additional equipment.
Prevention is always better than cure, but obviously in the case of mental health issues, prevention is not necessarily within the
Preventative measures largely relate to improving organisational culture by increased communication so that mental health issues can be more easily addressed and supporting managers by ensuring they are well informed, as they will play a pivotal role in the handling of any issues. (See box on previous page).
Providing support
Managers need to know the typical signs and symptoms of poor or declining mental health exhibited in the working environment.
These can include the following:
➤ Workaholic tendencies : Working long hours without breaks;
➤ Increased absence due to sickness;
➤ Any uncharacteristic behaviour: Emotional responses to situations which could include tearfulness or anger;
➤ Withdrawing from others on the team.
Any of these behaviours in isolation clearly do not imply that an individual has a mental health issue, but they do provide an opportunity for a manager to discuss well-being with an individual, which could prove to be valuable in preventing a potential issue.
When a manager holds a one-toone discussion with an individual, it is important they do not jump to any conclusions. Ideally, the conversation will start with an open discussion about how the employee is feeling, although we know that people are often reluctant to talk openly.
Within an organisation where mental health and well-being are discussed regularly, hopefully the employee will feel more able to be open and honest.
When an individual asks for help, it is important that help and support is made available in a timely manner.
In a smaller organisation, it may be relevant to seek advice from outside organisations and there are many suitable providers. Throughout any discussion of this nature, the manager must be non-judgemental. It is very clear that all people managers have a serious responsibility in their employees’ well-being, and they will also need to be supported and guided through this process.
Support available
The Chartered Institute of Personnel Directors provides a wealth of information on its website and while it is not specific to healthcare, it is a valuable resource for all managers dealing with HR issues. Specific to Covid, it is valuable to access the most up-to-date information and Cochrane produced a report, which was updated in January 2021, entitled ‘Supporting resilience and mental well-being in frontline healthcare professionals during and after a pandemic’.
The International Labour Organisation has also recently produced a report entitled ‘Protect the mental health of health and care workers in the Covid-19 pandemic’. Finally, the Academy of Medical Royal Colleges has a page on its website summarising all of the organisations available to provide support in relation to mental health matters for those working in the healthcare sector.
Over the coming months, we will have access to much more data regarding the long-term impacts of the Covid-19 pandemic. As leaders, we will need to learn and evolve to ensure we provide the best support possible so that we can continue to lead successful, high-performing companies and teams.
If you would like any further information in relation to this article, please do get in touch. I am always very happy to help and I am sure that my team of HR professionals will also be able to help with most workplace well-being questions.
Jane Braithwaite is managing director of Designated Medical
How do we collate the huge amount of data?
A new report from Elsevier outlines how Covid-19 could change research culture for the better by showing the need for co-ordinating data collection globally. Oli Cram reports
ELSEVIER’S ‘FUTURE of Research’ report provides insight into the impact of the Covid-19 on clinical trial data, highlighting how the lessons learnt from this global health crisis provide valuable learnings for the future.
The report summarises the key take-aways from a recent webinar series which cast a spotlight on three leading experts in the research community who explained how clinical research is adapting, innovating and transforming its operation to respond to Covid-19.
Despite the current pandemic being at the forefront of our minds, there are significant takeaways that resonate, not only for the present pandemic but also future health crises.
For example, how advanced technology and real-world data can be effectively used to expedite the route from evidence to practice by responding to evolving medical knowledge and recommended standards of care.
Standardising & harmonising the collection of data
The volume of health data is expected to grow dramatically in the years ahead. By digitising, collecting, collating and effectively using big data, healthcare organisations will be able to act faster.
Using data analytics in healthcare has the potential to improve outcomes; however, the report highlights that Covid-19 underscores the need for worldwide co-ordination to do this effectively.
The impact of the pandemic has led to greater collaboration,
As we look ahead, we must be prepared for future pandemics by establishing an efficient research response
increased confidence in findings and improved understanding between researchers.
By opening up data in a safe way, through international contributed datasets, we are finding ways to accelerate science faster than ever to effectively harness clinical information and support the delivery of knowledge driven care.
Ensuring continuity of care through global collaboration
Partnerships among researchers ensure that knowledge, skills and techniques are shared effectively and mutually benefit the participants.
In the current climate, the initiation of rapid, collaborative research was a vital element which facilitated the continuation of care for Covid-19 patients. Global partnerships enabled clinician-researchers to balance the challenges of delivering critical care to them alongside initiating research trials. Global research networks serve to increase research
involvement, to build research capacity and to develop a new and improved research culture.
Communicating research transparently
Over the past decade, there has been significant change in the media landscape with approximately a doubling in global scientific output every nine years, and 2020 has been no exception to the trend.
The scientific community’s response to Covid-19 has resulted in a large volume of research moving through the publication pipeline at extraordinary speed through the means of preprints, press releases and social media amp lification. Although the nature of this emergency warrants accelerated publishing, measures are required to safeguard the accuracy of scientific evidence.
As we look ahead, we must be prepared for future pandemics by establishing an efficient research response.
We need to develop a transparent and trusted system that clearly communicates what data is being collected and why, to effectively harness information to support the delivery of knowledge-driven care.
Global collaboration is an essential element that will allow clinician-researchers to effectively balance delivery of patient care while also channeling efforts to establish the required research trials to progress future evidencebased treatments.
It is vital that, going forward, we create a culture that promotes high-quality research by guaranteeing transparency and ethics.
To listen back to the Future of Research webinars or read the full summary report, please go to tinyurl.com/zedmet4b.
Oli Cram (right) is MACRO general manager at, Elsevier Clinical Solutions
SETTING UP A PRIVATE PRACTICE
The nameplate is just the start of it
New independent practitioners will want to avoid attracting unwanted attention from the GMC and other regulators. Mr Jerard Ross (right) looks at the most important considerations
THERE HAS been an explosion of interest in setting up in private practice, judging by the popularity of the MDU’s latest virtual course on the subject.
After the spring event rapidly sold out, there is now a waiting list for future dates which will be announced soon.
The course covers everything you need to know for your practice to thrive, including identifying your unique selling point, billing, marketing and accounting. But while it is important to get the business side right, you should not overlook your professional and ethical responsibilities.
Here are the MDU’s six medico-legal ‘must dos’ for anyone setting up in private practice:
1
Register with the relevant regulators
As a doctor in independent practice, you will almost certainly hold records for your patients. If that is the case, you will need to notify the Information Commissioner’s Office and be added to the register of data controllers (see point 5). Also, check whether you need to register with the Care Quality Commission (CQC), which monitors, inspects and regulates independent health and social care services, including private clinics, GPs and independent hospitals.
Failure to register with the CQC, when this is a requirement, can amount to a criminal offence, but this is a complex area. For example, if you will be consulting in a private hospital, it may not be necessary to register separately if the hospital is appropriately registered, is a responsible body and consultations are carried out under the organisation’s management and policies, including those relating to clinical governance, audit and complaints handling.
You may also be exempt if you are employed by the NHS alongside your private practice. However, this does not apply in all cases. Seek advice from your medical defence body about whether you need to register or visit the CQC website.
2
Ensure you have adequate indemnity NHS indemnity only applies to clinical negligence claims against NHS bodies and not your inde -
Take care when offering or providing private treatment to patients you have already seen on the NHS, so others do not misinterpret your actions pendent practice or private medico-legal work, so talk to your medical defence body about your indemnity requirements.
The GMC says: ‘If you carry out any private or independent practice, you must arrange adequate and appropriate insurance or indemnity. This applies even if the work is in addition to work you do for an NHS or health and social care body.’
You should also ensure that the healthcare professionals you employ, such as nurses, are suitably indemnified in their own right, where appropriate, and that you confirm their registration status.
Traditionally, claims for clinical negligence have been made against individual healthcare professionals. However, a claim may be made against a limited company, so consider whether you need to obtain a corporate policy.
3
Be up-front about fees
The GMC expects doctors to be honest and open in any financial dealings with patients, including the fees you set and any commercial arrangements and conflicts of interest.
It says: ‘You must tell patients about your fees, if possible before seeking their consent to treatment, including whether any part of the fee goes to another healthcare professional.’
Many practices and clinics chose to publish information about consultation fees on their practice website to assist patients.
The CQC requires registered providers to ‘give timely and accurate information about the cost of their care and treatment to people who use services’. Where a service user will be responsible for paying all or some of the costs of their care or treatment, the CQC says they must be given a statement specifying terms and conditions and
expected costs before treatment begins.
Finally, take care when offering or providing private treatment to patients you have already seen on the NHS, so others do not misinterpret your actions. Perceived conflicts of interest are a source of concern for patients, employers and the GMC.
4 Comply with advertising rules
When promoting your services, the GMC says ‘you must make sure the information you publish is factual and can be checked, and does not exploit patients’ vulnerability or lack of medical knowledge.’
Check your website and marketing material complies with the code published by the Committee of Advertising Practice (CAP). You may also need to consider the Medicines and Healthcare products Regulatory Agency’s guidance on the advertising of medicines: The Blue Guide.
If you are registered with the CQC, you need to apply for permission to use its logo and must abide by its terms and conditions. You will need informed, written consent before using patient testimonials or photographs.
When setting up your practice website, you must take reasonable steps to make it accessible to people with disabilities. The RNIB has a website accessibility scheme for businesses.
If you include links to other websites, state that you cannot guarantee that these sites are secure and you do not necessarily endorse their contents.
5 Protect patient data
Any doctor who holds patients’ medical records is required to register as a data controller and comply with the Data Protection Act 2018; for example, by publishing a privacy policy stating how patients’ information will be processed, protected and their data rights.
You can register and find specific guidance for healthcare organisations on the Information Commissioner’s Office (ICO) website.
In addition to keeping medical records safe and confidential, consider how long to retain records and who will handle them if you are no longer able to do so.
Although there are no guidelines for retention of clinical records in private practice, the GMC’s Confidentiality guidance [paragraph 130] states: ‘The UK health departments publish guidance on how long health records should be kept and how they should be disposed of. You should follow the guidance whether or not you work in the NHS.’
Remote consultations have become increasingly popular during the pandemic, but if you plan to offer this service or communicate with patients by email you must warn them that it may not be secure. Further guidance on remote consulting can be found on the GMC’s ethical hub.
6 Set up a complaints procedure
If you have practising privileges at an independent hospital, there will be an existing complaints procedure to follow, but you will need your own in-house complaints procedure if you see patients in other settings.
It makes sense to follow the principles in the Health Service Ombudsman’s guide to complaints handling and your policy should be clearly communicated to staff and patients.
Unlike complaints related to patients receiving NHS-funded care, there is no statutory framework for independent review of complaints from the independent sector.
Some independent healthcare organisations are members of the Independent Sector Complaints Adjudication Service, which publishes a Complaints Code of Practice for its members and offers an independent review service for cases where local resolution and complaints review within the organisation fails to resolve the complaint.
Registered independent practitioners are legally required to submit an annual summary of complaints to the CQC.
The Setting up in Private Practice course costs cost £149 for MDU members and £249 for non-members. To learn more, visit www.themdu.com/learnand-develop/course-listing/setting-up-in-private-practice
Mr Jerard Ross is a medico-legal adviser at the MDU
Indemnity at the push of a button
Medical indemnity cover is a regulatory requirement for doctors, but few relish gathering all the information when it comes to annual renewal or when looking for competitive quotes.
Fiona Booth (left) explores how an enhancement to Healthcode’s The Private Practice Register can streamline the process
‘Declare the past, diagnose the present, foretell the future.’ Hippocrates Healthcare is not without risk and practitioners deal in risk assessment every day. Getting the right medical indemnity cover for your specialty is not just about the cost or the financial risk, but also the stress or possible reputational implications of litigation from a dissatisfied patient.
Medical indemnity cover aims to protect the practitioner if they are accused of negligence, malpractice or a breach of clinical or professional care standards.
According to a leading insurer, 1 common medical indemnity claims include:
Misdiagnosis;
Failure to diagnose;
Surgical errors;
Incorrect treatment;
Prescription errors;
Failure to provide a clean environment;
Failing to adequately train doctors and other staff.
One of the many recommendations from The Paterson Inquiry was for the Government to look at reforming the regulation of indemnity products for healthcare professionals and introducing a nationwide ‘safety net’ to ensure patients are not left uncompensated.
While it is now over two years since the Department of Health and Social Care’s (DHSC) consultation on ‘appropriate clinical negligence cover’, there is, as I write, still no date for the muchanticipated Government response.
The outcome will affect the private sector, as the consultation was about indemnity cover for healthcare professionals who purchase their own indemnity cover, as they are not covered by existing or proposed statebacked schemes.
Current indemnity concerns
The consultation document highlighted concerns over the stability of the most popular forms of indemnity cover.
Currently, indemnity providers such as medical defence organisations (MDOs) provide cover for many healthcare professionals under discretionary indemnity arrangements, usually sold as subscription to a MDO.
The MDO model has served the private healthcare sector well for a
long time, but after Paterson and other high profile claims, many practitioners want certainty in these more litigious times, particularly if their MDO was unwilling or unable to settle a claim.
The Medical Practitioners Assurance Framework (MPAF) MPAF was launched in October 2019 by the Independent Healthcare Providers Network, also partly in response to the Paterson scandal. The MPAF has been adopted by all private hospital groups and is considered as evidence of good governance by the Care Quality Commission as a way of meeting its ‘Well Led’ key line of inquiry. Under MPAF, hospitals now need to have additional information in order to grant and oversee their practising privileges, including the requirement for practitioners to hold a valid certificate of adequate insurance cover or medical indemnity.
The latest enhancement to The Private Practice Register allows doctors to obtain a competitive insurance quote for mandatory medical indemnity cover using data from their profile
competitive insurance quote for mandatory medical indemnity cover using data from their profile.
This enhancement is designed to eliminate the need to repeatedly gather the relevant information and complete multiple application forms to obtain quotes.
In fact, by having an uptodate profile, practitioners will be able to save time and resources, and potentially money spent on adequate cover.
Limited, a Lloyds’ market medical indemnity broker. Both companies are authorised and regulated by the Financial Conduct Authority. Quotations via the PPR are available free of charge, with no obligation to buy.
At Healthcode, we are aligning The Private Practice Register (The PPR) with the MPAF to help practitioners and hospitals fulfil their obligations without having a huge administrative burden. The PPR already records both historical and current medical indemnity policy information, allowing practitioners to demonstrate the continuation of adequate cover.
The latest enhancement to The PPR allows doctors to obtain a
As almost all the required information is already held within The PPR, this data can now be used to obtain an online quotation at a click of a button, with no need to complete multiple forms. This proposal form will be prepopulated using data held within the PPR profile and can be amended, checked or supplemented by updating the relevant field in the profile.
The quotation will be fulfilled by Doctors’ Indemnity and Arthur J Gallagher Insurance Brokers
PATIENT CENTRED HEARING CARE
The PPR can help ease your admin burden by minimising duplication of effort and data. But it is still vital that practitioners understand the difference between discretionary and contractual indemnity and choose the most appropriate cover for their needs.
Medical indemnity is complex, but with an uptodate profile, at least the insurance quotation process can be less painful.
Fiona Booth is head of external affairs and stakeholder engagement at Healthcode
Exceptional audiological care starts with the right referral. At Pindrop Hearing, we understand each case as unique, and our team of expert Audiologists will work with your patients to find the right solution for them
• Specialists in Diagnostic Audiology including Paediatrics and Tinnitus rehabilitation
• Cutting edge on site facilities, including purpose built sound proof rooms and audiovestibular diagnostic services
• Comprehensive range of diagnostic tests including PTA, tympanometry and specialist tests including OAE's and VEMPS
•A wide range of hearing devices, not available on the NHS
• Outstanding aftercare and patient services
• Fully GDPR compliant
• Medico-Legal Audiology service including gold standard objective Audiological testing using Cortical AEP and ASSR
• Full COVID protection measures in all clinics alongside a dedicated online consultant portal
Make sure to review your record-keeping
Is the financial data about your private practice fit for purpose? Simon Brignall (right) advises consultants to ensure the important area of practice information reflects the needs of a modern private practice
IT IS important for all businesses to keep accurate financial records and ensure data published across a variety of platforms is accurate.
But for consultants working in private practice this can prove quite a challenge on top of the requirements to maintain clinical information about each patient’s treatment.
I have come across many private practices who experienced difficulties in this area resulting in:
Cash flow problems;
Lost income;
HM Revenue and Customs (HMRC) issues;
Unnecessary problems with patients.
Published private practice information
As private practice information is available to patients across a wide range of platforms, it is easy to lose track of all the sites where this data is stored. Keeping it up to date can prove challenging.
Consultants often have information about their practice included on the following:
➲ Bupa profile or other private medical insurer (PMI) referral platforms;
➲ Individual private practice website;
➲ Hospital and clinics sites where the consultant practises;
➲ Sites for groups – when applicable;
➲ Third-party review sites;
➲ The Private Healthcare Information Network (PHIN). It is important to check all this information is consistent and up to date across all these various sources.
The information available will be tailored to the site where it is being shown, but should include:
All the locations where you practice;
Contact information;
Pricing policy;
Payment terms and options.
A review of the practice’s data is often an ideal time to evaluate your pricing structure. It should consider the consultant’s experience, the demand for their services, the location and the consultant’s individual contractual relationships with each PMI. Lack of clarity around your pricing policy can lead to patient dissatisfaction and can also mean
invoices are raised incorrectly. Invoice errors can result in problems with both patients or insurance companies and income losses.
Ensuring your pricing is transparent means that the patients are aware of the costs up front and so disputes are less likely.
Patient registration forms
It is best practice to confirm with each patient the practice’s fee structure before treatment, while also making them aware of their responsibility for any liability should their insurance policy not cover the cost of treatment in full.
This simple step ensures that any ambiguity is removed and can be referred to during any dispute.
In the commercial world, companies have terms and conditions detailing how the business will conduct its activity with its clients, which forms a contract that can be referred to. In private healthcare, the patient registration form is typically where this area is covered. It is a good idea to ensure that the registration form includes wording covering patient liability.
We find most patients with medical insurance think all the treatment costs are covered, when in many cases there can be an outstanding balance that the patient will be required to pay.
Most patients’ private health insurance is provided through their employer and so they are unlikely to have examined the fine print of the policy. In many instances, the full cost of treatment is not covered in full for a variety of reasons.
Here are some of the main ones:
➤ The patient could have an excess or shortfall under the terms of the insurance policy;
➤ The patient has exceeded the benefit limit of the policy;
➤ The patient could have a policy with a co-pay clause requiring the patient to pay a percentage of each invoice.
Lack of clarity around your pricing policy can lead to patient dissatisfaction and can also mean invoices are raised incorrectly
Tax implications
Consultants trading as either sole traders or limited companies are required to provide accurate tax reporting either directly to HMRC or via their accountants.
HMRC is in the process of transitioning its Make Tax Digital initiative, which is currently scheduled to become mandatory in April 2023 for income tax and April 2026 for corporation tax.
The patient registration form should also inform the patient if the practice has any other commercial terms, such as for nonattendance, commonly referred to as DNA (Did Not Attend) clauses.
Timely invoicing
Patient registration forms are a good way to ensure the practice has all the relevant information to raise an invoice promptly.
This will include the following information:
Date of birth; Contact details; Insurance information.
All successful practices realise how important it is to obtain this information up front, removing the need to chase patients after treatment, which can be both problematic and time-consuming.
Missing data can lead to unnecessary delays, invoices being rejected by insurers and difficulties in chasing patients for payment. This often results in aged debt mounting up for the practice and can mean that the consultant is owed tens of thousands of pounds.
At Medical Billing and Collection, our procedures immediately highlight when data is missing, and steps are taken to resolve the problem as swiftly as possible either internally or with the practice/patient. As with most matters related to billing, the quicker you identify the problem, the more likely you are to resolve it.
This will require the submission of income data on a quarterly basis rather than the current system which allows this to be provided at the relevant accounting year-end.
HMRC says this will enable a more accurate projection of tax that is due, but considering the number of inquiries we have from consultants at their year-end, I think it is fair to assume many practices will find this difficult.
Tax inspectors often target private consultants due to a perception of deficiencies in their record-keeping. A request by a practice’s accountant to improve the quality of the financial information available can often be a reason a doctor is referred to us.
Every practice should be able to produce accurate reports that show the total invoices raised, payments received and its aged debt for a given tax period.
At Medical Billing and Collection, we supply all these reports directly to our client or their accountant and our clients can access this information via our reporting platform 24/7.
Summary
There is no time like the present to conduct a review of all of the data published about your practice and also the financial records that you keep.
It is important to see they are accurate and reflect the current situation; ensure you highlight any issues and then put steps in place to address these.
If all of this is just adding to your workload or you feel you would like to speak to an expert, then one simple solution might be to seek assistance from a medical billing company with years of experience in this area.
Simon Brignall is director of business development at Medical Billing and Collection
MARKETING AND BRANDING
Use the right type for the right type
Simon Marett and Michael Sullivan’s ‘Essential Guide to Design’ continues with a look into typography and the difference it can make to doctors’ branding, design and marketing
FONTS AND typefaces are often used interchangeably, but on a technical design level, there is a difference.
Typeface is a particular alphabet set and its corresponding accessories such as numerals and punctuation that share a common design. For example, Arial is a well-known typeface and the font is a specific set of glyphs within a typeface, such as Arial Bold or Light.
Not unlike colour that we covered last month, typography often gets neglected in design because of a lack of awareness and an understanding of the impact it can make to your healthcare practice.
Here are some key pointers to think about:
1 Know who your patients are
We have touched on this point before in previous articles, but it is important to re-emphasise it because it is one of the fundamental rules of marketing and design. Putting your personal opinions to one side and getting a good understanding of who your patients and potential customers are and what will appeal to them is a vital step in the process.
For example, you might really like the look of the Comic Sans typeface, but if you are opening a high-end women’s health clinic in west London, then this comic style typeface is not going to be a good or requisite fit for your pre-
mium practice and affluent audience.
You need to go back to the drawing board with your team or designer and look at a selection of typefaces that will work well and appeal to your audience.
Top Tip: Pick two or three typefaces that you think will work and then conduct a quick market survey with a handful of patients to get a steer on which they prefer. This is a good indicator of what might appeal to future patients and help your practice grow.
2
Use a framework for your typefaces
Once you have selected a handful of typefaces you think will work for your practice, the next step is to get a framework in place that will help
you decide what typefaces and fonts you use throughout your marketing and branding.
For private healthcare practices, consistency in branding is vital because you are operating in premium markets and precision of marketing execution is expected. A brand will be devalued if it is chopping and changing its typography and colour palette every month.
Remember, when you are using typography on your website or on a brochure or advert, there is often more than one typeface and font in play.
You will need to think about headlines, sub-headers, standfirsts, bullet points and body copy and when and where you might want to use bold, semi-bold, light or italics.
The Comic Sans typeface at the top may be your personal favourite, but is it in keeping with the image you want to project of a smart, professional practice?
Top Tip: It is often a good idea to select a unique, headline typeface that stands out and grabs people’s attention. The headline has two roles to play: to grab the attention of the reader and to communicate key information on the page, so using a font that stands out is important.
3
Serif and sans-serif fonts
You might have heard about serif and sans serif typefaces and you will experience them every day in newspapers and websites that you read.
Serif typefaces have semi-structural details or decorative flourishes on the ends of some of the strokes that make up letters and symbols.
Times New Roman and Courier are two common styles of serif fonts. Sans serif does not have these details or flourishes and common examples would be the Arial or Helvetica font.
So, which do you use for your healthcare practice? With thousands of typefaces available, there are no hard and fast rules and there has been a long-running debate in the design world about which is easier to read.
Sans serif is often viewed as being more modern but more difficult to read in body copy, while serif fonts can be viewed as oldfashioned.
Ultimately, it comes down to the individual practice brand, patients and personal preference. Whatever you decide, you will not want to change your guidelines frequently, so working with a recommended designer or agency is a good first step to get you up and running.
Top Tip: Ask your designer to create a short set of brand guidelines with some recommendations on blends of serif and sans serif typefaces that can work for your practice.
As a bare minimum, they should cover your logo, headlines and body copy and they should look consistent and work together as a family.
Serif typefaces have decorative flourishes on the ends of some of the strokes that make up letters and symbols, but sans serif does not have these details
4
Digital first, print second
Years ago, printed items such as brochures, business cards and flyers would have taken the lead on a clinic’s design and branding. Fast forward to 2021 and we live in a digital-first world where the majority of a patient’s experience with a healthcare practice is online and more likely on a mobile phone.
It is therefore vital to think about how typography is going to work on your core communication channels and touchpoints such as your website, emails and social media.
Your website is going to need to be easy to read, so breaking up large blocks of body copy into
You need to think about headlines, sub-headers, standfirst, bullet points and body copy when designing websites and brochures
digestible chunks of information with different colours and weights of type is a great starting point. Top Tip: Pulling out key statistics or testimonials into break-out boxes is a good tactic to employ to make a website easier to read. Try sampling different typefaces, weights and fonts to make the key information you want to communicate stand out.
As with colour, the world of typography and design is a complex one and there are some key points to consider when working on your healthcare practice brand.
Try involving your patients before making big design decisions to verify your preferences and test different typefaces, fonts, sizes and weightings to find a blend that works.
Consistent execution of logo, colour and typography over time are one of the keys to a successful healthcare brand and therefore a branding framework is always recommended.
You can do this yourself, but it is
often best to work with a recommended designer or marketing agency with a track record of doing this with other healthcare clients. They will have experience of working with typography before and will help you avoid pitfalls, expensive mistakes and save you time money and effort in the long run.
Next month we will be diving into the world of imagery and recommending some top tips for your marketing and branding.
Design
Simon Marett (below, left) is director of Ellerton Marketing, and Michael Sullivan (right) is creative director of Ellerton Marketing and Forty6
How we can better conduct the PROMS
Researcher Dr Michael Anderson (right) tells of his work on understanding the enablers and barriers that could improve the uptake of Patient Reported Outcome Measures (PROMs) in private healthcare
THE PRIVATE Healthcare Information Network (PHIN) has a huge role to play in improving transparency in private healthcare.
Publishing data on the sector is a strong enabler to protect patient safety as well as promote choice. One way in which PHIN is really pushing for this is through its ambitious Patient Reported Outcome Measures (PROMs) programme.
PROMS are the only standardised measure that produce outcomes from a patient perspective. There are several benefits in using them.
1
There is an intrinsic value in routinely using PROMS as they facilitate a shift towards providing more patientcentred care.
2 They can flag patients who do not experience as expected health gains post surgery, which can be investigated and additional support provided, if needed.
3 They can be useful from a comparative perspective. By identifying above or below average PROMs scores, hospitals and consultants can share best practice, and look into underlying factors driving below average performance.
PHIN’s ambition is to use PROMs nationally to inform patient choice.
It recently started reporting private hips and knees PROMs in 2019, which is a step towards achieving this. The programme should be widely acknowledged
and contributed to, but the completion rate for hips and knees PROMs to the network remains significantly below what is achieved in the NHS.
Key question
This formed the basis of my project’s key question: what are the enablers and barriers to improving PROMs uptake in the private healthcare sector?
To help answer this question, I will be focusing on behaviours and attitudes related to the collection, submission and use of PROMs data at eight different hospitals who work with PHIN.
I have selected a combination of hospitals which reflect both high and poor performance in collect
It has been eye-opening to begin to understand the real complexity of the processes and data that PHIN works with
quently and that consultants have access to the right insights from the data.
My project will have two main outcomes. Firstly, an overarching policy report for PHIN to use with consultants and hospitals to work through the barriers to collecting and using the data.
Secondly, a separate academic publication which will lean heavily on the questionnaire framework.
ing and submitting PROMs data to get a broad range of perspectives.
And I will be engaging with consultants and members of hospital staff at different levels, beginning with consultants, then speaking to nurses, administrators, managers and others.
Each interview will follow a set questionnaire covering 14 areas, from belief about capabilities and optimism, to reinforcements and social influences.
I have already begun the process of contacting these hospitals and interviewing consultants. It is too early for me to comment on the findings, but there are key areas I am looking at. These include:
Awareness – or lack thereof – of the PROMs programme among consultants and among staff at the hospitals;
Whether there is clear responsibility for collecting PROMs within hospitals;
To what degree data is used at site level; for example, whether staff are reviewing the data fre
I aim to complete this work by Autumn 2021, with potential for a presentation of some provisional findings this summer. However, this timeline is dependent on the level of engagement from the hospitals I will be working with.
It is exciting to be involved with this collaboration with PHIN, not least because the London School of Economics and Political Science, where I work, is the first academic institution the network has partnered with.
It has also been eyeopening to begin to understand the real complexity of the processes and data that PHIN works with.
I hope this work will also be of real benefit to patients and the wider private healthcare sector, as we look at developing strategies to maximise the value of PROMs data in understanding the impact of treatment on patients.
Dr Michael Anderson, a research officer at the LSE, is working with PHIN as a clinical fellow as part of a new partnership
ADVICE
Servant of two masters
Difficulties can arise when a clinician works both in the NHS and privately. Dr Heidi Mounsey (right) looks at a potential scenario and offers some guidance
IMAGINE YOU are a consultant general surgeon with both an NHS contract and practising privileges at the local private hospital.
The private hospital contacts you to say that a patient you operated on yesterday has become very unwell. The resident medical officer has reviewed the patient and considers an emergency return to theatre may be needed. You are asked to attend urgently.
However, you are contracted for NHS duties today and are just about to start your ward round. You have several complex patients who require consultant review. It is important to be aware of your obligations in a timetable clash like this.
The GMC’s Good Medical Practice states you must provide a good standard of practice and care. If you assess, diagnose or treat patients, you must promptly provide or arrange suitable advice, investigations or treatment where necessary and refer a patient to another practitioner when this serves the patient’s needs .
In managing this scenario, you must ensure the needs of both your private patient and your NHS patients are met. The document Terms and Conditions – Consultants (England) 2003 states that the consultant is responsible for ensuring that the provision of private professional services or fee paying services for other organisations does not result in detriment of NHS patients or services or diminish the public resources that are available for the NHS.1
This should be read in conjunction with A Code of Conduct for Private Practice which sets out that the provision of services for private patients should not prejudice the interest of NHS patients or disrupt NHS services. Except for the need
to provide emergency care, agreed NHS commitments should take precedence over private work.2
In this circumstance, you have been requested to attend to your private patient urgently, but you should also ensure your NHS patients are reviewed.
The options available to you may include:
Discussing the matter with your clinical lead to request that you are granted time to review your private patient and to seek cover for your NHS ward round;
Request that a colleague with practising privileges in the private hospital reviews your patient while you conduct your NHS ward round.
But it would be prudent to consider, prior to committing to both private and NHS work, how to prevent or mitigate this scenario by preemptively arranging for cover if this situation happened.
This could, for example, include reaching an agreement with another colleague who holds privileges in the same private hospital so that you cover each other’s private patients if an emergency
Except for the need to provide emergency care, agreed NHS commitments should take precedence over private work
arises; or arranging with NHS colleagues to cover your NHS duties were you to be urgently called away to the private hospital.
You should ensure your NHS lead approves any such crosscover arrangement and that you keep proof of the agreement.
It would also be prudent to ensure your contract or terms of engagement with your private patients makes clear that in the event of an urgent problem or emergency, another clinician would need to be involved if you are not available.
You may wish to consider whether it would be appropriate to request changes to your NHS job plan or to your scheduled times at the private hospital to minimise
any disruption that may be caused to your NHS work if a complication arose from a private procedure.
This might, for example, mean adjusting your timetable so you do not have NHS clinical commitments when it may be more likely that complications would occur in your private patients.
Failure to ensure all your patients, both NHS and private, receive the appropriate care may result in an adverse outcome for the patient, which may lead to a complaint or claim against you, or disciplinary and/or regulatory action.
Dr Heidi Mounsey is a medico-legal consultant at Medical Protection
It’s safe to go back in the water
Coconuts versus sharks! Dr Ben Holdsworth (right) on why we struggle to get risks in perspective
IF YOU have ever been fortunate enough to swim on Bondi Beach among the surfers, or in the chilly waters of Cape May – where the film Jaws was filmed – in the back of your mind may have lurked the thought that a large shark might just be out there looking for lunch. What was that shadow?
Yet most of us do not think twice about the risks of sitting under a coconut tree, which is far more likely to kill you from a falling coconut, as is the malaria-carrying mosquito that lands on bare flesh as the sun sets in paradise.
Nor did we consider the risk of a deep vein thrombosis from the long-haul flight we took to get there. We fixate on the shark.
Humans are irrational and find it hard to place risks in perspective, in part because they involve numbers – which many people hate –are influenced by fear or recent news and often depend on the way in which they are framed, to name just a few of the challenges.
We have a very clear recent example of our confusion with the extremely rare possible side-effects of some of the Covid-19 jabs.
Full of risks
Latest estimates suggest that the risk of dying from the vaccine due to blood clots is one in one million, which is similar to the chance of being murdered next month (nasty) or dying in a road accident on a 250-mile road trip.
Life is full of risks and those that we deem to be everyday consequences of modern life, we take, usually without batting an eyelid, such as: driving, using ladders, drinking alcohol, climbing mountains and walking through fields of cows – nearly 100 people were killed by cows between 2000 to 2020. Yet other exceptionally low risks we deem ‘too big’ to take.
It is similar with investing. Investors tend to worry about equity market crashes, perhaps not surprisingly, as equity markets can and have fallen by more than 50 % in the past.
Yet owners of equities should not be looking to sell them in the next few years but relying on fixed-income assets to meet liquidity needs.
In most cases, markets recover relatively quickly over, say, three to five years, sometimes more slowly.
With horizons well beyond these falls and recoveries, investors who stay the course should be rewarded – as they have been in the past –with strong returns above inflation.
The latter is the real risk to longterm investors. Avoiding equity market risk and putting money on deposit is actually the risky strategy in some instances.
Of course, large falls in values can occur from time to time and such a fall may coincide with when you need your money. If you might need your money back in the short term, or if you rely on it, taking risk may not be appropriate.
There are also those who prefer security and would not sleep well seeing large fluctuations in value. However, for those who can tolerate risk and who are investing over a reasonable length of time, investing can work well.
It is also important to note that some ‘individual’ company shares may not recover as we have seen with some of the firms disappearing from our high street. A diversified approach is critical, but the key point is that cash can carry its own risk.
Over the past ten years, those holding cash have lost around 1/5th or 20%, or £20 in every £100 of purchasing power, however you want to describe it. That is risky.
Managing risk in our lives is summed up well by Prof Dame Glynis Breakwell who wrote a book entitled The Psychology of Risk. ‘Risk surrounds and envelops us. Without understanding it, we risk everything and without capitalising on it, we gain nothing.’
Once we can get back to azure waters, brave the chance of sharks and stick with your equities. The risks will be worth it.
Dr Benjamin Holdsworth is a director of Cavendish Medical, specialist financial planners.
The content of this article is for information only and must not be considered as financial advice. Cavendish Medical always recommends that you seek independent financial advice before making any financial decisions. Levels, bases of and reliefs from taxation may be subject to change and their value depends on the individual circumstances of the investor. The value of investments and the income from them can fluctuate and investors may get back less than the amount invested.
Staff problems after lockdown
Managing holiday requests Holidays within the UK are now permitted and international leisure travel may be allowed to resume this summer.
Employers are likely to face an unusually large number of holiday requests for the spring and summer months, often with less notice than usual, since employees have not been able to book holidays in advance.
Doctor employers face ongoing staff management challenges as lockdown restrictions ease. Lucy Miles (right) and Isobel Davis (left) highlight some areas needing consideration
Employers are likely to face higher absence levels than usual as staff start to take more holiday than they might ordinarily
Many employees have avoided using their holiday entitlements so far this year due to the restrictions, which means that employers are likely to face higher absence levels than usual as staff start to take more holiday than they might ordinarily.
This could cause potential operational challenges for employers, who will need to balance business needs with holiday entitlements. It will be important to proactively manage holiday entitlements, where possible, and there are provisions within the Working Time Regulations 1998 which may assist employers where holiday requests need to be refused or where staff need to carry over more holiday than usual into the next holiday year.
Employers may also wish to encourage workers to liaise with each other, spread out their holidays evenly across the leave year when they can or alternatively request that employees take one or two longer blocks rather than several shorter periods if that is less disruptive.
Welcome those shielding back to the workplace safely Everyone who has been identified as clinically extremely vulnerable should now have been offered a Covid19 vaccine, and the Government is no longer advising that they do not attend the workplace, so it is anticipated that staff who have been shielding will start to return to work if they cannot work from home.
The first key step in being able to welcome back staff who have been shielding is a health and safety risk assessment.
All employers are required by law to carry out assessments to identify risks to their employees while at work and this is particularly important for vulnerable staff.
Risk assessments should not be
viewed as one off tasks but kept under review as Government guidance is adapted and changed, and employers should ensure that they keep clear and accurate records of their ongoing risk assessments.
The second crucial aspect is taking time to plan and consult with employees. ACAS, the arbitration service, suggests listening and talking to staff about their work and how risks will be managed. This should involve communicating what measures have been and will be taken to reduce the risks and ensure the workplace is Covidsecure.
Long-term remote working
Aside from the difficulties it has caused, the pandemic has also resulted in some positive outcomes including improved productivity, reduced congestion and better air quality.
For staff, advantages have included increased flexibility and
the saving of commuting time and costs. Many people would therefore like to retain the ability to work from home in the long term.
Employers are increasingly recognising that the general shift towards working more flexibly has benefits for businesses, including happier staff and costs savings from needing less office space – or even none.
Doctor employers should consult with staff about their views and consider all of the options and implications of the arrangements before implementing any significant or permanent changes to working practices.
Having done so, if you are proposing to make changes that alter employees’ terms and conditions of employment, you should consider amending the employment contract to avoid any future disputes. Ensure you have appropriate policies in place to govern the arrangements, such as a flexible
working/homeworking policy, health and safety policy, and data protection and information security policy.
Refusing to return or be vaccinated
If any employee refuses to attend the workplace for a health and safety reason and they are dismissed or subject to a detriment as a result, they could potentially bring certain claims in an Employment Tribunal, such as unfair dismissal and whistleblowing.
There are also real risks of a disability discrimination claim if the employee has a medical condition that could amount to a disability – and note, this can cover a wide range of medical conditions that are often not recognised as disabilities.
It is vital therefore that employers actively conduct and document risk assessments, manage issues sensitively and consistently,
and do all they reasonably can to implement adjustments before taking steps to insist employees return to the workplace.
Similarly, employers must be extremely cautious in managing issues which may arise in relation to employees having or not having the Covid19 vaccine.
There may be circumstances where it is legitimate to require staff to be vaccinated, but these will be relatively few and far between and dismissing an employee or subjecting them to a detriment for not being vaccinated could give rise to a whole host of potential legal claims.
If you experience difficulties with implementing returns to the workplace or managing staff issues arising in relation to the Covid19 vaccine, we can provide support and advice.
Lucy Miles is a partner and Isobel Davis a trainee solicitor at Hempsons
Free legal advice for Independent Practitioner Today readers
Independent Practitioner Today has joined forces with leading healthcare lawyers Hempsons to offer readers a free legal advice service.
We aim to help you navigate the ever more complex legal and regulatory issues involved in running and developing your private practice – and your lives.
Hempsons’ specialist lawyers have a long track-record of advising doctors – and an unrivalled understanding of the healthcare system as a whole.
Call Hempsons on 020 7839 0278 between 9am and 5pm Monday to Friday for your ten minutes’ of free legal advice.
Advice is available on:
Business structures (including partnerships)
Commercial contracts
Disputes and litigation
HR/employment
Premises
Regulatory requirements and investigations
An apology can defuse an error
Dr Ellie Mein (right) explains how to apologise to a patient following a prescription error
Dilemma 1 Do I say sorry for a scrip mistake?
QI am a private GP and a patient has written to say they believe I overprescribed their medication which subsequently caused them to be admitted to hospital.
The prescription was started by a consultant the patient had seen privately and the dosage error was made when I prescribed a repeat prescription.
Unfortunately, I had not received a letter from the consultant and I wasn’t able to get a hold of them to confirm the correct dosage, so I had to rely on the patient’s recollection.
Should I apologise for the error or would I be admitting legal liability for something that I feel wasn’t my fault?
ABy making a full and frank apology, you will not only reassure the patient but also reduce the likelihood of a complaint or claim in the future.
In addition, as the GMC outlines, you have an ethical duty to apologise if something has gone wrong, explain what happened and what steps will be taken to try to put things right.
Apologies can be provided in writing or in person, but as the patient has written to you, it would generally be appropriate to write back.
Remember that an apology is not an admission of liability in law. Although you may feel that
the error wasn’t your fault, it is acceptable to explain your viewpoint while still expressing that you are sorry.
An earnest and sincere apology, made in the first person, such as ‘I am sorry I prescribed a higher dose than you required’, may be all the patient wants to hear.
You can also explain why this happened: ‘As I had not received a letter from your consultant and was not able to contact them, we discussed your current dosage. I am sorry if I misunderstood what you told me.’
All organisations registered with the Care Quality Commission in England must also comply with the statutory duty of candour. While it applies to organisations rather than individual doctors, individuals still have an ethical and professional duty to be honest and open with patients when something goes wrong.
You can always offer a meeting to discuss matters and it can be helpful to advise how you will prevent such issues occurring in the future.
As discussed above, although an apology cannot prevent a complaint or a legal claim from arising, it is more likely to prevent it than a defensive response.
You should rest assured that apologising in this way does not mean you are accepting legal responsibility for what occurred and that a carefully considered genuine apology can prevent further issues down the line.
Dr Ellie Mein is a medico-legal adviser at the Medical Defence Union (MDU)
Problem with social media
The
downsides of posting on a private social media group are revealed here in a consultant’s question answered by Dr Sally Old (right)
Dilemma 2 How can I stop this recurring?
QI’m a consultant cardiologist who recently joined a private Facebook group following a conversation with a colleague who is also a member of the group. On the group, I and several other members discussed a treatment option and shared our experiences of patients who had undergone this treatment.
A few days later, I received a private message from a nurse, who was also a member of the Facebook group and consequently had seen the original post. The nurse explained that when she had seen the post, she knew that one of the patients I referred to was her aunt.
their own, the sum of published information online could be enough to identify a patient or someone close to them. You must not use publicly accessible social media to discuss individual patients or their care with those patients or anyone else.’
Consequently, there are a number of factors to consider when accessing closed social media groups and doctors need to be aware of the potential problems and risks when posting their thoughts online.
Firstly, it’s important to remember that these groups and forums can have hundreds of thousands of members. Often, this means that information is accessible to individuals outside the profession. To illustrate, there have been cases when people have used fake credentials to join private groups.
Another important factor to consider is the potential for someone within the group, to take a
The nurse was extremely angry that her aunt’s health had been discussed online. She has asked for a full, written apology and explanation to be sent to her aunt.
I am mortified and sincerely regret the distress his post had caused. How I can prevent this happening again?
ASocial media groups and forums can often be a useful platform to discuss the pressures of being a doctor and many are ‘closed’ forums, meaning that they allow discussion in a discreet ‘members only’ area.
In Doctors’ use of social media (2013), the GMC outlines the principles that doctors must adhere to when posting online.
In it, the GMC states: ‘Although individual pieces of information may not breach confidentiality on
screenshot of your post and publish it in another forum.
Comments can be taken out of context or misunderstood and it is easy to inadvertently cause offence. As a doctor, you need to consider whether you would be happy for a post to be shared with a wider audience and possibly with no reference to the original context in which it was made.
Social media plays an important role in engaging with the public and with other medical professionals in conservations around healthcare and by establishing national and international professional networks.
However, even when posting in a closed group, consider what the purpose of the post is and who may read it. If you are unsure, it may be best to alter your post or not to post the comment at all.
Dr Sally Old medico-legal adviser at the Medical MDU
Do I buy a house via my firm?
A common question for those with residential investment property or thinking of purchasing residential investment property is whether it should be owned personally or via a limited company.
Ian Tongue explores some of the considerations to make and provides a real-world example of a common scenario for consultants
IT IS reasonable for those who own residential investment property to feel like they have been squeezed with changes to the tax-deductibility of mortgage loan interest, increased stamp duty for second homes and changes to tax relief around expenses on repairs and renewals.
These changes have made people question whether personal ownership of rental property is a viable option. And with the significant amount of consultants trading through a company, it is natural to ask whether transferring or purchasing new property in the company is tax-efficient.
It is easy to look at the corporation tax rate of 19% and conclude that it must be tax-efficient, but to consider the position adequately you need to consider more factors, including the likely future sale of the property.
This article looks at the most common scenario for a consultant who is considering using their trading company to purchase residential property using rolled-up profits compared to using per-
sonal savings. Considerations for property trading companies and commercial premises are outside the scope of this article.
Personal ownership
When purchasing a property in addition to your main home, it is subject to the increased rate of stamp duty for second homes, which is a 3% surcharge on whichever rate is applicable based on the purchase price.
If the property is bought outright, the main tax-deductible costs will be letting fees, insurance and general running costs leading to a taxable profit upon which income tax is paid at your marginal rate of tax, for example, 40%.
Where a mortgage is in place, the loan interest is no longer taxdeductible in computing the profit from rental, but you are allowed to deduct 20% of the loan interest against the tax due. Effectively, the tax deduction available for mortgage interest is therefore limited to 20%, having previously been at your marginal rate of tax, as high as 45%.
Once the tax has been paid on the rental profit, any surplus funds are tax-paid disposable income for the individual.
If the property is sold, capital gains tax is paid at 28% for higherrate taxpayers and 18% for basicrate taxpayers on the gain after each owner has deducted any available capital gains tax annual allowances, currently £12,300. Therefore, for joint ownership with a spouse where no other capital gains are made in a tax year, the first £24,600 is exempt from capital gains tax.
Further reductions to the capital gain assessed may be available if you have lived in the property for a period of time.
Limited company purchase
When purchasing a property through a company, stamp duty is paid at prevailing rates and no beneficial rates apply.
Where a property is already owned personally, stamp duty would be payable to transfer the property to the limited company as though it was purchased from a third party. There may also be capital gains to pay on the transfer. As with personal ownership, most of the deductible costs will
Higher annual retained rental earnings for a company compared to disposal income for an individual can be quickly unwound by the level of capital gains tax payable down the line
rises in house prices if the thresholds remain static.
A ‘fair’ comparison
It can be difficult to make a fair comparison of the two ownership structures without knowing the timeline of ownership and prevailing tax rates for both individuals and companies.
We can, however, consider an example based on the current rules and tax rates which is reasonably reflective of a scenario that a consultant could face.
you have earned c£60,000 after tax over the ten-year ownership.
The limited company calculation is more complex as the profit on sale of the of property is taxed at corporation tax rates – with no annual exemption – and, following this, the retained profit from rental and the capital gain forms part of the retained profits of the company.
be similar, but any mortgage interest is allowable in full when calculating the profit from rental.
It should be noted that interest rates are often higher through a limited company than personally, but there can be a significant degree of variation in lending policies between banks and other financial institutions.
Once the tax has been paid on the rental profit, any surplus funds become retained earnings in the company.
For this profit to be extracted personally from a company that continues to trade, the profit will need to be distributed by way of a dividend and income tax paid at prevailing rates.
Where the company is ceasing, the retained funds can usually be extracted subject to more beneficial capital gains tax rates, provided that certain criteria is met.
High-value property
Where ‘high-value’ residential property is owned within a limited company, additional tax is payable which is known as an annual tax charge for enveloped dwellings. This was introduced around the time of the mortgage interest restriction came into force as a disincentive to own property within a limited company.
The threshold for this to apply is currently £500,000, which generates a tax charge of £3,700 per year and this increases in line with the property value. While many properties will not be of this level, the threshold level could change, bringing more properties under this charge.
The value of property for this charge is also reviewed periodically and therefore a property may attract the charge through general
The following are the assumptions for the calculations:
Property purchased for £150,000 – after the Covid stamp duty measures expire;
No mortgage required;
Joint ownership with a spouse and both higher-rate taxpayers;
Sold after ten years for £200,000;
Annual rental of £6,000 per year
– increasing by 2% a year;
Costs of £2,000 per year –increasing by 2% a year;
Tax-deductible repairs of £5,000 in year five and nine;
Corporation tax rates of 19% for the first two years and 25% thereafter in line with recent Budget announcements;
The company retains the profit made and these rolled-up funds are extracted along with the gain on the property at beneficial rates in year 10 (see below);
Selling fees are ignored.
Rental profit
Based on the above assumptions, under personal ownership the disposable income (profit after taxes paid) generated for a 40% taxpayer would be c£20,000 over the tenyear ownership period.
For a company where the profit is retained – that is to say, not paid out to the shareholders – the profit earned would be c£25,500.
Round one to the corporate ownership structure it would seem.
Capital gains tax
Where things quickly reverse is when you factor in the capital gains tax position.
Under personal ownership, the capital gain after acquisition costs in your pocket would be c£40,000. Add to this the disposable income above from rental activities and
The best-case scenario here is for a further 10% to be payable on the retained earnings at the point of liquidation which would leave c£56,000.
Therefore, based on the assumptions above, the company ownership route was c£4,000 worse than personal ownership.
This would be more significant if the funds could not be extracted favourably from the company in year 10; for example, they were treated as dividends rather than capital gains or capital gains tax rates increased.
Additionally, a spouse who is a basic-rate taxpayer would benefit from higher disposable income from rental profits under personal ownership and lower capital gains tax payable on the disposal.
There are likely to be certain scenarios where the company can work well, but often consultants are looking to invest in relatively low-value residential property using rolled-up funds in their company and so the balance between rental yield and anticipated capital growth is important.
As can be demonstrated in this simple and realistic example, higher annual retained rental earnings for a company compared to disposal income for an individual can be quickly unwound by the level of capital gains tax payable down the line.
It is important if you are considering investing in residential property via a limited company that you discuss matters with your accountant to ensure this is taxefficient for your circumstances.
Next month: Fighting fit for the boom in private work postCovid
Ian Tongue (right) is a partner with Sandison Easson accountants
DOCTOR ON THE ROAD: PORSCHE CAYMAN
This Cayman may be one of the last of its breed. If you can get one before it is too late, you won’t regret it, says Dr Tony Rimmer (left)
Catch it if you can
Porsche understands the needs of drivers who still want to experience the best of lightweight sports cars powered
There is a lot of luggage space in the front boot and under the rear hatch
SOME OF our most satisfying career moments happen when all our learning, experience and clinical acumen converge and we make correct decisions with the appropriate actions for the best outcome possible for the patient.
Like playing a musical instrument well, it is inordinately satisfying. It often happens without the influence of sophisticated high-tech investigations and tests. Somehow it makes us feel very fulfilled, joyful and human.
Driving used to be much like that. It was a visceral experience where our connection with the cars we drove was very raw and very direct.
Technological advances have brought us greater safety and greater convenience, but they have mostly blunted the involvement levels we have with the machines we drive.
The extra weight from batteries in the profusion of new hybrid and all-electric cars only compounds the issue.
Fortunately, we still have manufacturers like Porsche. Despite being at the forefront of electric car development – its Taycan is the most enjoyable EV to drive – it understands the needs of keen drivers who still want to experience the best of lightweight sports cars powered by efficient internal combustion engines before they disappear altogether. So welcome to the latest Cayman GTS 4.0
When the latest 718 model Cayman and Boxster appeared in 2017, Porsche swapped the naturally aspirated flat-six-cylinder engines with smaller 2.0 litre turbocharger units. The power and torque increased but the character
and lovely engine sounds almost disappeared.
Allied to Porsche’s albeit impressive automatic dual clutch PDK gearbox, the Cayman was still quick and handled brilliantly, but lacked any real soul. As a result, Porsche’s image and sales suffered.
There was a 4.0litre six-cylinder Cayman available, but it was the expensive and rare track-focused GT4 model. Without admitting it, Porsche has thankfully listened to its loyal followers and introduced the same 4.0 litre engine from the GT4 in a mainstream road-focused Cayman and called it the GTS.
Purposeful look
To satisfy keen purists like myself, it is also available with a six-speed manual gearbox which is great news. So, what is it like to drive?
The latest 718 Cayman is a goodlooking car. The updated styling still looks fresh and, particularly finished in the bright Python Green paint of my test car, has a sporty and purposeful look.
Narrower than the latest 911, it is a perfect size for our UK B-roads where many of our most interesting driving routes can be explored.
As I slipped behind the wheel and settled into the perfect driving position, all the familiar Porsche dials and controls were within easy reach. Not as up to date as the latest 911 or Taycan, they still give you all the information you need.
As soon as I turned the key, the sound of the brilliant six-cylinder engine brought a smile to my face. With 400bhp – only 20bhp down on the GT4 – this was going to be a fun drive.’
While gently getting into the groove, first impressions signal a
firm but comfortable and compliant ride. The gear lever has a short throw and the steering is nicely weighted and super-sharp.
As I picked up the pace, the GTS responded brilliantly. This is a thoroughbred sports car and is built to cover distances on our twisty roads swiftly and safely while giving the driver great satisfaction.
As good as it gets
Weighing less than 1.5 tons, the mid-engined Cayman shrugs off any changes of direction and so the handling and roadholding are as good as it gets in any car; Ferraris and McLarens included.
Without the added complication of turbochargers or superchargers, acceleration is linear, very strong and the engine loves to rev up to the red line. The manual gearbox is a joy; it may not be as lightningquick as the PDK box, but I prefer the greater control.
The brakes, in typical Porsche tradition, are impressively effective and fade-free. I had so much fun punting the GTS down my favourite roads, I just did not want to go home.
Despite all this performance, the Cayman also has a softer side to its
character. Although strictly a twoseater, there is a surprising amount of luggage space in the front boot and under the rear glass hatch. It is easy to drive in traffic and is quiet and refined on the motorway. You could easily live with the GTS as a daily driver and I would guarantee that you would arrive home after a long day in a better mood than when you left work.
Priced from £65,390, the GTS is about £20,000 less than the most basic 911, the Carrera. This makes it look like a bit of a bargain. Also, if you prefer open-air motoring, the mechanically identical Boxster GTS is only £2,000 more.
I think that as a relatively affordable example of a truly analogue sports car utilising all the modern developments of normally aspirated petrol power, the GTS is a tour de force.
With an increasing focus on electrification from all manufacturers, Porsche included, this Cayman may be one of the last of its breed. If you can get one before it is too late, you wont regret it.
Dr Tony Rimmer is a former NHS GP practising in Guildford, Surrey
PORSCHE 718 CAYMAN
gts
I had so much fun punting the GTS down my favourite roads, I just did not want to go home
Body: Two-seater coupé
Engine: 4.0litre six-cylinder
Power: 400bhp
Torque: 420Nm
Top speed: 182mph
Acceleration: 0-62 mph in 4.5 seconds
Economy: 27mpg combined cycle
CO2 emissions: 240g/km
On-the-road price: From £65,390
All the familiar Porsche dials and controls are within easy reach
DOCTORS AS PATIENTS
From professional to patient
With 58% of doctors now suffering from some form of anxiety or depression – and 46% saying their condition has worsened since last March – we are serialising sections of a new book edited by Dr Clare Gerada. This month: Doctors treating doctors
IT IS not just unwell doctors who find it hard to accept that they can be sick. Doctors who see and treat other doctors find it difficult as well.
Doctors often find it embarrassing to treat their own profession, and that they – the treating doctor – might be less qualified or knowledgeable than the sick one. Consulting with more senior individuals can be especially difficult given the rigid hierarchical practices that exist in medicine.
We have all been in this position and it is rarely comfortable, for either party. Having a discussion about the side-effects and mode of action of antidepressants might feel awkward with a professor of psychopharmacology.
However, what is important is to try and acknowledge and respect any additional expertise the sick doctor has, but always to allow them at the same time to be the vulnerable, ignorant and frightened patient needing simple explanations, reassurance and compassion.
When a doctor becomes a patient, consultations can be difficult, especially where mental health is concerned. In the first instance, both parties prefer ‘corridor conversations’: snippets of care outside the consulting room. Sitting outside the normal health system can have detrimental effects for the doctor, as unorthodox routes risks distorting the delivery of care. At the very least, the unwell doctor will not be part of the routine call-recall system and, as such, not followed up in the standard manner.
Tragic consquences
They might miss out on medication reviews or necessary tests. For others, it can have tragic consequences, as in the case of young psychiatrist Daksha Emson and her daughter. The boundaries with the health services she interacted with were so blurred that she missed out on many of the safetynetting systems designed to manage very sick individuals.
Following the birth of her first child, she developed severe postnatal psychosis and killed herself and her three-month-old baby, Freya. The subsequent inquiry into their deaths highlighted how Daksha’s treatment was different,
Doctors are trained to care for others, not each other. Even if a team member is seen to be struggling, rarely does someone pick this up or make inquiries
Independent Practitioner Today readers can save 20% on Routledge.com with discount code BWC21. Offer ends 31 August 2021. Order now: www.bit.ly/ Routledge_IPT
This has certainly been my experience. The implication being that the only role allowed is that of an ‘expert-patient’. This is a two-way collusion, as both parties have a vested interest in maintaining the status quo: that is, the denial of the wounded healer.
Over the years, there have been a number of personal accounts of doctors becoming patients and most of them illustrate how difficult it is for both sick doctor and treating doctor to deal with.
For example, this individual wrote about their experience of being ‘the unwilling occupant of a psychiatrist’s couch’. This doctor gives advice on how to ‘look after one of us’ (mentally ill doctors), much of which focuses on the importance of treating the sick doctor as a patient and not as someone in full control. 1 I would echo this advice.
All too often, mentally ill doctors are treated by trainers, employers and regulators as naughty schoolchildren or wrongdoers at having crossed the boundary from professional to patient.
Collusion of anonymity
just because she was a doctor and this was implicated in causing her to kill herself and her baby.
Her previous consultant, who had cared for her for many years, retired just before she became pregnant.
On his retirement, he transferred her back to the care of her GP, but, in his transfer letter, diminished the seriousness of her history, concentrating on her ‘good’ points, creating an unduly optimistic assessment of her health.
This despite Daksha, over the years, having been so unwell as to require long periods of inpatient care, some under compulsory admission. Daksha did not make her condition and previous history of illness known to her new psychiatrist; she hid this through worries that disclosure would negatively impact on her career.
Information was not passed between doctors involved in her care – GP and psychiatrist – in order to ‘respect’ her confidentiality. Information sharing was normal practice for other patients.
Once unwell, her psychiatrist did not place her on the Care Programme Approach, which
would have offered enhanced care, nor discuss her case with colleagues in the team meetings, again in the belief that he should maintain her confidentiality.
Finally, only informal arrangements were set up with a community psychiatric nurse, which were not adequate in the circumstances, but made in the belief that, as she was a psychiatrist, she would know what to do.
While singly none of these changes to normal practice contributed to her death, the accumulation of them did. Given the seriousness of her condition, she was excluded from the standard of care that would have been provided to any other, non-medically qualified patient with a similar illness and seriousness.
Treated differently
As Daksha illustrates, even once in the consulting room, the sick doctor is treated differently and often seen more as a colleague than a patient, sometimes even going as far as to suggest the sick doctor should treat or at the very least know how to manage themselves, even organise their own tests.
Doctors are trained to care for others, not each other. Even if a team member is seen to be struggling, rarely does someone pick this up or make inquiries. We lack a culture of mutual responsibility for each other, leading to a situation, described by the psychoanalyst Michael Balint, of a collusion of anonymity.
This typically was used to describe the collusion that occurs when ‘the patient is passed from one specialist to another with nobody taking responsibility for the whole person’.2
In the case of an unwell doctor at work, while everyone can see that something is wrong, and may even raise concerns with a colleague, no one wants to take any responsibility in the hope that someone else will deal with them or that the problem will disappear. I am not suggesting that we have a ‘duty of care’ for each other in the sense of needing to provide medical care. Rather that we have a duty of caring for each other as fellow professionals, all working hard towards a common aim of treating patients.
Many years ago, while training in psychiatry at the Maudsley Hospital, one of the psychiatric registrars jumped onto a dining table in the middle of the busy canteen.
At the top of his voice, he began a tirade about the corruption he had exposed in this hospital, how his consultant – an eminent professor – had tried to cover up a scandal involving the secret service and that only he (John) could save the world from the invasion that was around the corner.
Doctors paralysed
It was quite clear he was psychotic, yet no one seemed to know what to do. Here were dozens of psychiatrists with one of their own clearly in a distressed state and we were paralysed.
Eventually, a member of the kitchen staff gently coaxed him down from the table and took him by the hand to the psychiatric emergency clinic a short way down the corridor.
If this doctor, instead of a mental health problem, had had a physical emergency, he would have been overwhelmed with helping hands.
John, as I later learnt, had bipolar disorder. He had sought help from his GP in the previous week, who told him that, as a psychiatrist, he must know the best way to treat his condition or maybe he could ask a colleague for help.
Needless to say, he didn’t know how to access care, instead he became increasingly unwell, surrounded by his peers blind to his odd behaviour. Sadly, in my experience of working with mentally ill doctors, this scenario is not uncommon.
So good are doctors at not seeing distress in their own kind, they often describe the shock when the sick-doctor’s condition is subsequently brought to light.
Colleagues perform retrospective trawls through their memory to clues of the doctor’s problems; clues that they would have picked up on in their non-medical patients or colleagues.
The tell-tale signs of alcohol dependence – no one can fully disguise the stale smell of alcohol on the breath or clothes – or the sudden weight loss of someone not eating through depression, or
So good are doctors at not seeing distress in their own kind, they often describe the shock when the sick-doctor’s condition is subsequently brought to light
ening and distasteful aspect of illness can be projected into and contained (held) within health professionals, who, given their training and status, accept these projections demanded of them by society. If a doctor becomes unwell, how can they hold this pain?
less comfortable with and less trusting of unwell doctors, even to the point of seeking care elsewhere.5
even the small cuts of someone self-harming. The ‘bare below the elbow’ rule makes these cuts even more obvious.
It was only after the doctor’s condition has come to light that others admit ‘they thought something was up’ and illustrates how, both at the collective and individual level, doctors hold to the notion that they should not be ill.
Patients, the public and their views of sick doctors
Beyond the obvious of not wanting to wait longer for care, patients do not take kindly to doctors being unwell. This is because it breaks their – the public’s – belief that doctors are somehow immune from illness.
The sociologist Talcott Parsons described the ‘sick role’ in terms as having certain roles and responsibilities achieved through maintenance of a paternalistic stance and rigid boundaries between the roles of doctor and patient.
These roles act to maintain the tacit contract between patient and doctor; patients become unwell, not doctors. Both patient and doctors enter unconscious symbiotic processes.
The psychiatrist Thomas Main touched on this when he described the defensive interplay of projections between caregivers and patients and the ‘fantastic’ collusion that occurs between the two: ‘The helpful unconsciously require others to be helpless while the helpless will require others to be helpful. Staff and patients are thus inevitably to some extent creatures of each other.’3
In this process, the nasty, fright-
This theme of the collusion between doctor and patient forms the introduction by John Updike of the book The House of God: ‘We expect the world of doctors. Out of our own need, we revere them; we imagine that their training and expertise and saintly dedication have purged them of all the uncertainty, trepidation and disgust that we would feel in their position, seeing what they see and being asked to cure it.
‘Blood and vomit and pus do not revolt them; senility and dementia have no terror; it does not cause alarm for them to plunge into the slippery tangle of internal organs, or to handle the infected and contacts.’4
Of course, it makes sense that patients want their doctors to be well, as unwell physicians can impact on patient care.
A study of patients set out to determine how they, based on their own personal experience, perceived doctors’ health and its link to care. Three overarching themes emerged.
Patients’ views
Firstly, patients notice cues in their doctors that they interpret as signs of being well or unwell – the way doctors dressed, whether they looked tired, ran late, looked stressed, engaged in general dialogue with the patient and so on.
Secondly, patients formed views based on what they noticed, and these judgments directly influenced how they felt about their care.
Finally, patients made a direct link between doctor wellness and the care they received.
Unwell doctors were seen in a negative light by the patients in this study. For example, they were seen as less competent and more likely to make errors; less appropriate in their interactions, disorganised; and more likely to place added responsibilities on patients to limit their problem list.
Patients also described feeling
I have highlighted the difficulties other doctors have when asked to treat their own colleagues. Both the sick doctor and the treatingdoctor feel embarrassed and find it difficult to accept the change of role from professional to patient.
Nevertheless, it is important that we all accept when we need help. When doctors do seek help, they have remarkably good outcomes in terms of reduced distress, impairments, abstinence rates and overall improvements in their mental health.
This is why it is so important to encourage doctors to make that giant step – for them –from professional to patient. Maybe next time I am unwell, I will be open and honest enough to practise what I preach.
Next month: Sticking to the rules
Dr Clare Gerada (below) is medical director of the Practitioner Health Programme, London, and a former chairman of the RCGP
References:
1. McKall K. An insider’s guide to depression. BMJ 2001; 323(7319): 1011.
2. Balint E, Courtenay M, Elder A, Hull S, Julian P. The Doctor, the Patient and the Group: Balint Revisited. London and New York: Routledge, 1993.
3. Main T. Some psychodynamics of large groups. In: Kreeger L (ed). The Large Group. London: Constable, 1975, pp. 57-86.
4. Shen S. The House of God. London: Black Swan, 1985.
5. Lemaire J, Ewashina D, Polachek A, Dixit J, Yiu V. Understanding how patients perceive physician wellness and its links to patient care: A qualitative study. PLoS One, 2018 May 15; 13(5): e0196888.
PRIVATE PATIENT UNITS: THE WEST MIDLANDS
We continue our regional round-up of PPU progress with a review by Philip Housden (right) of the 15 NHS West Midlands acute trusts across the counties of Warwickshire, Worcestershire, Herefordshire, Shropshire, Staffordshire and the cities of the West Midlands conurbation
United front needed
THIS REVIEW is based on the information published in the Trust Annual Accounts for 2019-20, which was partially adversely impacted by the early months of the Covid pandemic.
For this group of trusts, the accounts show that total private patient revenues for the region fell by 3.1% in 2019-20, a drop of £639,000 to a total of £19.7m (see Figure 1 above).
This now represents 0.30% of these trusts’ total revenues, a slight drop from 0.34% the year before. This is below the combined national average outside of London of 0.43% (see bar chart overleaf, Figure 2).
Turning to the comparison of performance by trust (Figures 3 and 4 overleaf), the highest percentage of private revenues and proportion of total trust incomes in the region are delivered by the two specialist orthopaedic hospitals of the Royal Orthopaedic in Birmingham and Robert Jones and Agnes Hunt at Oswestry, Shropshire.
At Robert Jones and Agnes Hunt , the trust delivers services through RJAH Private Healthcare and its 16-bed private patient ward, The Ludlow Unit. The trust had
revenues of £5.2m in 2019-20, which was down 9.3% and £540,000 on the previous year.
This represents a regional high of 4.71% of total trust income – down from 5.56% in 2018-19 – and places the trust sixth outside London by percentage of turnover, but down from second in 2018-19.
The Ludlow Unit was turned into the hospital’s Covid ward at the beginning of the pandemic due to its individual side rooms with ensuite facilities, helping to safely isolate patients.
Dedicated private ward
The Royal Orthopaedic Hospital in Birmingham also has a dedicated private ward, the seven-bed Woodlands Suite. The trust’s private patient revenues fell by £301,000 and 17.4% in 2019-20 to reach £1.4m, which now represents 1.72% of turnover, down from 2.16% last year, but still a significant jump from 1.07% in 2017-18.
University Hospitals Birmingham’s private patient income for 2019-20 was £5.1m, up £213,000 and 4.4% on the £4.9m in 2018-19, the fourth consecutive year of growth.
This represents 0.33% of total
trust income, down from 0.35% of turnover the previous year. At present, the main contribution comes from The Mindelsohn Unit, a 12-bedded private ward, supporting a private radiotherapy service that includes the regional CyberKnife and a range of other specialist services.
However, the trust’s ambitious partnership development with HCA Healthcare UK to build a £100m specialist hospital facility offering both private and NHS capacity on the Queen Elizabeth Hospital Birmingham campus will change this significantly when it opens for patients in 2022.
New hospital
The eight-storey new hospital will include 50 private inpatient beds, 16 private day-case beds, four stateof-the-art operating theatres, modern outpatient services including consultation rooms and imaging suite and fully equipped day-case unit with outpatient chemotherapy and radiotherapy services.
The infrastructure investment will support complex surgical and medical procedures and treatments across cancer, cardiology, neurology, hepatobiliary, urology,
orthopaedics and stem cell transplantation.
This will give private patients access to a level of acute healthcare not currently available to the estimated 500,000 people in the region who have private health insurance or who want to self-pay for their care.
Across the city, Birmingham Women’s and Children’s Hospital presently offers private maternity and paediatric services. The private patient revenues of the trust were £1.64m in 2019-20, down £589,000 and 26% on the £2.24m achieved in 2018-19. This is 0.40% of total revenues, well down on the 0.58% achieved in the previous year.
University Hospitals of North Midlands in Stoke-on-Trent grew private patient revenues by £263,000 and 22% in 2019-20, to achieve 0.2% of total income. The trust at present only provides a limited range of private patient outpatient and ambulatory services, but this includes a specialist service through its MS (muscular sclerosis) Centre.
Shrewsbury and Telford’s revenues also grew last year, up 15.5%
and £161,000 to £1.2m, which is 0.31% of turnover. The trust’s Apley Clinic at The Princess Royal Hospital in Telford is an onsite private outpatients and diagnostic facility replacing their onsite tenbed private patient unit, Apley Ward, which the trust closed in 2015.
Another trust delivering growth in 2019-20 was University Hospitals of Coventry and Warwickshire which reported private patient revenues up 5.8% and £63,000 to £1.15m, which is 0.19% of trust total revenues. The trust has no in-house PPU but is understood to work closely with the onsite 52-bed BMI Meriden Hospital.
The Royal Wolverhampton Hospital’s private patient revenues also grew last year at a modest 1.0% and £10,000 to total £1.02m. The proportion of total trust income from private patients declined to 0.19%.
Research income
The trust has increased commercial income through the recently signed five-year Strategic Research Agreement with Sensyne Health plc to roll out clinical artificial intelligence research partnerships and received 0.9% of Sensyne’s issued share capital, £250,000 a year over the five-year term of the contract, for investment in research-related IT and royalties on revenue generated from the research.
South Warwickshire leads a Foundation Group of trusts including Wye Valley and George Eliot Hospitals. South Warwickshire delivers private healthcare services through a wholly-owned subsidiary company, SWFT Clinical Services, formed in 2011 and turned into a social enterprise in 2014.
That year, SWFT acquired The Stratford Clinic, formerly owned by Circle. From August 2019, The Grafton Suite became the new home for the ‘Stratford Clinic’, and it is now located in Stratford Hospital in a new dedicated suite with access to operating theatre sessions.
In 2019-20, South Warwickshire Trust’s private patient revenues increased by 23% and £120,000 to £638,000, which is 0.21% of turnover.
Elsewhere in the group, Wye Valley in Hereford also grew by
20% and £38,000 to £226,000 to reach 0.12% of turnover. However, George Eliot Hospital’s private patient revenues were again reported as £0.
Worcestershire Hospital’s most recent annual report and accounts do not set out private patient revenues, but in 2018-19 these were £389,000 and 0.1% of total trust incomes. The trust does not at present have any dedicated private patient beds or services.
Sandwell and West Birmingham Trust’s private patient incomes fell by 6% and £15,000 to £239,000 in 2019-20, only 0.05%
15 WEST MIDLANDS COUNTIES
NHS TRUSTS: Comparison of private patient revenues vs total revenues
Source: Trust annual accounts & Housden Group analysis
Figure 2
of total income. Elsewhere in the Black Country, Walsall and Dudley trusts deliver presently little revenues between them, reporting an aggregate of less than £50k a year.
The lion’s share of NHS trust private patient incomes in the West Midlands are delivered by Robert Jones and Agnes Hunt, the specialist orthopaedic hospital and University Hospital Birmingham.
It will be interesting to see how UHB’s income grows as it realises its partnership ambitions with HCA.
Of the rest, a significant number of trusts deliver around £1-2m in
revenues, despite several known to be under capacity constraints. This suggests it is unlikely that dedicated inpatient capacity for private patients will be brought forward by other trusts without partnership investment of the UHB-HCA type or perhaps other closer working arrangements will develop, hastened by the partnerships developed over the past year through the pandemic.
Next month: East Anglia
Philip Housden is managing director at Housden Group commercial healthcare consultancy
NHS Pensions & Annual Allowance Tax
Get ready in advance of April 2022 when the proposed changes to the NHS Pensions will allow you to reclaim some or all of any Annual Allowance tax you may have suffered in the past.
With our knowledge and in-house calculators, we will be able to predict in advance and check statements produced by NHS Pensions and Scottish Public Pensions Agency for accuracy for any refunds due.
For further information contact us at aa@semail.co.uk or telephone 01625 527351.
for private practitioners
PROFITS FOCUS: DERMATOLOGISTS
Profits not up to scratch
Falling profits have hit dermatologists, according to our latest benchmark survey. Ray Stanbridge reports
Back in 2017, we reported that dermatology and oncology were growth areas in the private medical sector. We also commented that, according to market analysts LaingBuisson, the private oncology market in London may be larger than the orthopaedic market.
It appears from our figures that there may have been some market correction in 2019, with both sectors reporting slight decreases in incomes and gross profits.
We have tried to report on a typical view of what the average consultant in private practice around the country is achieving. Our minimum income figure for inclusion are gross earnings of £10,000 and all those surveyed also have NHS jobs too.
We have commented, historically, that the ways in which consultants are changing how they practise maybe distorting income and costs trends. Consultants now trade through groups – both formal and informal – limited liability companies and limited-liability partnerships.
In some cases, consultants are now employed directly by hospitals and we are finding that this is a small but growing trend.
Most oncologists and dermatologists are now back to working full time following recent trends of declining Coronavirus incidents. We expect to see that consultants have found new methods of practice and that these will exhibit themselves in years to come.
OUR HEADLINE figure shows that gross private income for dermatologists fell on average by 6.7% from £163,000 to £152,000 between 2018 and 2019.
Costs fell by 2% from £56,000 to £54,000. As a result, pre-tax profits fell by 8.4% from £107,000 to £98,000.
Reasons for the changes
We did make a couple of technical adjustments, taking out of our survey a small number of extremely high-income earners. These would
have distorted what we are trying to achieve in depicting an average.
However, the main impact on reduced earnings was a reduction in self-pay rates. These have been growing for a number of years, but for some reason seem to have shown some decline, albeit small, in 2019.
Our view is that this is probably a temporary blip.
Costs remain much the same as in 2018. There was a small drop in use of medical supplies reflecting the fallen activity.
Secondly, there is a slight reduction in room hire costs for the same reason.
Use of home costs did show some increase. A number of dermatologists have created a virtual office at home and conduct most of their paperwork there rather than at clients or hospitals where they work.
Preliminary evidence suggests a
number of dermatologists continued to work during the Covid prohibitions. Given the easing of restrictions, many are now extremely busy.
Our view is that despite the 2019 blip and the effect of Covid in 2020, the future for dermatologists in private practice continues to be optimistic.
Future is bright despite this fall
OUR HEADLINE figures suggest that private oncologists’ gross incomes fell by 8.5% from £141,000 to £129,000 between 2018 and 2019.
Costs fell by 2.8% from £36,000 to £35,000. As a result, pre-tax profits fell by 10.4% from £105,000 to £94,000. This represents a similar pattern to that shown in our dermatologists’ survey.
We have had a look at why incomes appear to have fallen. Surprisingly, there does not appear to have been the growth in new patients as exhibited in previous years.
There seems also to have been a small growth in the number of oncologists in private practice thereby reducing market share to established players.
It appears there has been some pressure by insurers on fees and again, perhaps surprisingly, a small drop in self-pay.
In some cases, hospitals and clinics are getting the full benefit from tests and diagnostic fees. This was not necessarily the position historically. We need to undertake further work in these areas to understand more about the apparent drop in fees.
Oncologists’
costs
As with dermatologists, costs in 2019 were broadly similar to those in 2018.
Consulting room hire costs fell a little, reflecting the reduction in activity. Use of home costs, on the other hand, showed a slight increase. Again, as with dermatologists, many oncologists are increasingly doing their paperwork at home.
There was a slight reduction in motor and travel expenses, but these were not really significant. What, then, of the future? It appears that oncologists may have
been affected more by Covid lockdown than dermatologists, particularly in hospitals and clinics who were diverted away from dayto-day activity to service NHS Covid requirements.
However, early signs suggest that, as the pandemic restrictions ease, the market is starting to re-
HOW ARE YOU DOING? Use
invigorate rapidly and the future for oncologists in private practice remains bright.
Next time: General surgeons
Ray Stanbridge is a partner with accountancy, finance and tax advisory medical specialists, Stanbridge Associates
HOW DERMATOLOGISTS AND ONCOLOGISTS STACK UP
INCOME AND EXPENDITURE OF
Year ending 5 April. Figures rounded to nearest £1,000 (percentage is also rounded up)
Source: Stanbridge Associates Ltd.
Year ending 5 April. Figures rounded to nearest £1,000 (percentage is also rounded up)
Source: Stanbridge Associates Ltd.
THE PPR
(THE PRIVATE PRACTICE REGISTER)
Healthcode is the UK’s official medical bill clearing company and has provided secure and encrypted systems to healthcare professionals since 2000. Pre-pandemic we processed around 27,000 electronic medical bills to insurers daily.
What does The PPR mean for practitioners?
out and continuing, in private practice to maintain and market their practice profiles.
One centralised record to increase transparency
Easily keep up-to-date information in one central location and provide visibility to the organisations you have a relationship with.
Remain in control, build and maintain your profile
Once you have a PPR profile, you can build on it as your capabilities and/or qualifications expand, ensuring practice rights are easy to maintain.
The PPR is a solution that unites the sector. It is a secure online platform where practitioners can control their practice information and documents in one place, ensuring they are up to date and accurate. More than 24,000 practitioners now have a PPR profile, at zero cost, which provides a detailed picture of their clinical practice.
Alignment with the Medical Practitioners Assurance Framework (MPAF)
Ongoing development to support the requirements of the industry-adopted framework.
Fast-track your application for Private Medical Insurer recognition
Easy application for recognition with multiple insurers.
DON’T MISS OUR COMBINED JULY-AUGUST ISSUE
Coming in our July-August issue, published on 13 July.
Bouncing back for private practice business post-Covid. Accountant Ian Tongue has some useful tips and observations
Make sure your spending on publicity for your private practice work pays off. Our ‘Essential Guide to Design’ by Simon Marett and Michael Sullivan continues with advice on imagery: what is good and what is bad
Private practices for sale! Hempsons’ solicitor Kirsty Odell gives some excellent advice in ‘five steps to buying a private practice’ to help buyers prepare for the acquisition process. In our following issue, she will look at things from the perspective of the doctor who is selling
If you are practising in the ear, nose and throat specialty, then you wont want to miss our report on clinical negligence claims against ENT surgeons. Dr Gemma Taylor and Greta Barnes from the Medical Defence Union highlight what goes wrong and offer advice on managing risk
How technology can help you exceed patients’ expectations: Lengthening waiting lists for NHS treatment are a ‘push factor’ which should prompt more people to consider independent healthcare. But it is also important to consider the ‘pull factors’ that will lead them to your practice. Healthcode shows how technology can help you offer a high-quality level of service that will exceed the expectations of new patients and attract word-of mouth recommendations
Our Profits Focus benchmarking series by specialist medical accountant Ray Stanbridge puts the earnings of general surgeons in private practice under the microscope
INDEPENDENT PRACTITIONER
TODAY
The
Published by The Independent Practitioner Ltd. Independent Practitioner Today is editorially independent and thanks Bupa for its assistance with distribution. Material is governed by copyright. No part of this publication may be reproduced, stored in a retrieval system or transmitted in any form without permission, unless for the purposes of reference and comment. Editorial layout is the copyright of the publishers. If you wish to use it for promotional purposes on websites or for reprints, we would be happy to discuss licensing the copyright to you.
Medical Billing and Collection produces its roadmap for recovery
In the UK, there are now over 30 different sets of guidance for doctors to adhere to in areas relating to clinical, managerial, leadership, medico-legal, research, communication and other areas of their daily lives. In the last of her series, Dr Clare Gerada discusses what is expected of doctors, their professionalism and areas where they fail
With so many doctors telling surveys that they are considering leaving the NHS, Jane Braithwaite covers some ideas for those who are considering their career options – including a greater focus on private practice or looking at non-clinical jobs, such as joining a health tech firm
So when do you need to disclose a driving offence to the GMC? And what are the implications of conducting remote consultations abroad?
Dr Kathryn Leask, medico-legal adviser at the Medical Defence Union, answers more private consultants’ and GPs’ business dilemmas
If you work in a private patients unit in East Anglia, then don’t miss Philip Housden’s round-up of this region’s big, and not so big, successes
In our Accountant’s Clinic A-Z series, we arrive at the all important ‘W’ – for Working Capital
Our motoring correspondent Dr Tony Rimmer takes to the road in Audi’s e-tron
Plus some wise words for independent practitioners from specialist financial planners Cavendish Medical, the latest from the Independent Healthcare Providers Network and all the latest news and views
Don’t forget – you can find more news on our website throughout the month
ADVERTISERS: The deadline for booking adverts in our July-August issue is 25 June
Write to Independent Practitioner Today
7 Lindum Terrace, Lincoln LN2 5RP
CHANGING ADDRESS, EMAIL ADDRESS OR SUBSCRIPTION DETAILS?
Phone 01752 312140 or email karen@marketingcentre.co.uk
TELL US YOUR NEWS
Robin Stride, editorial director Email: robin@ip-today.co.uk Phone: 07909 997340 @robinstride
ADVERTISE WITH US
To advertise in the journal or our website business and lifestyle directories, contact advertising manager Andrew Schofield at Spot On Media. Phone: 0161 408 3912 Email: andrew@spotonmedia.co.uk
Follow Independent Practitioner Today on
GET A SUBSCRIPTION DISCOUNT!
£90 independent practitioners.
£90 GPs and practice managers (private & NHS).
£210 organisations.
Save £15 paying by direct debit: individuals £75 (organisations £180). TO SUBSCRIBE
Email karen@marketingcentre.co.uk or phone 01752 312140
Publisher Gillian Nineham Phone: 07767 353897.
Email: gillian.nineham@gmail.com
SAVE £15 WITH DIRECT DEBIT!
Guarantee delivery of your next copy of Independent Practitioner Today. Take out a subscription and you will get full access to our news, features and previous issues on our website. See details on the left.