Mr Ian Mackay of the Independent Doctors Federation gives an update on revalidation P16
The business journal for doctors in private practice
You can’t afford to ignore social media
Should you Tweet, Share or Like? Jane Braithwaite advises on modern healthcare marketing P20
Stop your defence fees rocketing Dr Gabrielle Pendlebury highlights the ten big issues influencing what private doctors pay for their indemnity P26
You and the NHS pension 5 porkies to be aware of
Porky 1: Senior doctors should quit the NHS Pension Scheme
Porky 2: I should retire from the NHS rather than face tax bills
Porky 3: The NHS Pension Scheme is no longer worth paying into
n Don’t miss our myth-exploding article on page 36
Porky 4: Opting for the pension scheme to pay my annual allowance tax charge is the best choice for me
Porky 5: I can probably go it alone
TELL US YOUR NEWS Contact editorial director Robin Stride
Get the most out of your accountant
Susan Hutter begins a new series – an A-Z guide of essential matters that GPs and consultants need to consider to run their private practices efficiently P14
ADVERTISE WITH US Contact advertising manager Margaret Floate at margifloate@btinternet.com Phone: 01483 824094
GET A SUBSCRIPTION DISCOUNT
£90 independent practitioners.
£90 GPs and practice managers (private & NHS).
£210 organisations.
Save £15 paying by direct debit: individuals £75 (organisations £180).
TO SUBSCRIBE – USE SUBSCRIPTION FORM ON PAGE 25
Or email karen@marketingcentre.co.uk Or phone 01752 312140. Or go to the ‘Subscribe’ page of our website www.independent-practitioner-today.co.uk
Chief sub-editor: Vincent Dawe
Head of design: Jonathan Anstee
Circulation figures verified by the Audit Bureau of Circulations
Publisher: Gillian Nineham at gill@ip-today.co.uk Phone: 07767 353897
EDITORIAL COMMENT
Tackling your big issues
Independent practitioners are facing a huge range of big issues right now and these are reflected in this month’s pages, where we have got together a team of experts in their fields to give advice and opinion.
Top of the concerns for increasing numbers of consultants and GPs is the pension tax issue which is causing wider anxiety as each month goes by.
As this editorial was being written, news came through of every consultant in one NHS department taking the drastic step of informing hospital bosses that the tax charges meant they could no longer give overtime support, as they were severely penalised for working longer.
Rumours of some sort of solution, allowing a degree of flexibility to ease the pension tax problem, were circulating as we went to press.
But with ministers otherwise occupied in a Conservative
Party leadership battle and in Brexit, it appeared no quick fix was about to be unveiled.
In this issue, specialist financial advisers Cavendish Medical tackle the most prevalent misunderstandings surrounding doctors’ NHS pensions (page 36) – a useful clarification of some important facts about the taper on the allowance for pension tax, which we hope will help dispel a few myths.
Other big subjects not to be missed this month include:
An update on revalidation from the Independent Doctors Federation’s Responsible Officer (page 16);
Ten factors that affect how much you pay for your medical defence organisation subscription (page 26);
A look at how the ‘Montgomery’ case on informed consent has changed the landscape for medical practitioners five years on (page 40).
The lonely path to keeping up to date
Difficulties encountered by doctors on the revalidation road include confusion and conflicting advice. Two experts guide you through the maze P18
The tests for tech
Whether a technophile or a technophobe, you should consider these five big issues before deciding whether to invest in new technology P32
A week in the life of a bill chaser
With rising numbers of private doctors seeking help to recover fees, we asked Simon Brignall to keep a diary about the issues he deals with for clients P34
Pension tax porkies
More senior doctors are triggering harsh tax bills because of pension tax. But rash decision are unwise and there are five porkies to watch out for P36
See things from the patient’s view
The Montgomery Case five years on: Lawyer Niloo Bozorgi reflects on how the landscape surrounding informed consents has changed for doctors P40
PLUS OUR REGULAR COLUMNS
Start a private practice: Don’t pay too much tax on your gear
Accountant Ian Tongue looks at how to get the maximum tax relief on your capital expenditure P46
Doctor on the Road:
Raising the bar with this stylish saloon
Into a world where plain SUVs seem to dominate, Peugeot unleashes the refreshingly different ‘508’ P48
Profits Focus:
Playing out of their skin
Our unique benchmarking series looks at the financial fortunes of both dermatologists and oncologists P52
Don’t give up your pension safeguard
By Edie Bourne
Thousands of pension savers have unwittingly cancelled the protection they had put in place to guard against tax charges on their lifetime savings.
HM Revenue and Customs (HMRC) has revealed that more than 12,000 individuals have lost one of the different types of ‘lifetime allowance’ protections in the last 12 years.
The lifetime allowance limits the amount which can be saved into a pension freeoftax overall. It currently stands at £1.055m but has been as high as £1.8m in 201112.
Each time the Government has reduced the allowance, it has launched pension protection schemes to allow savers to preserve their previous savings allowance so long as certain criteria are met.
Unfortunately, one of these criteria for those with a certain type of safeguard known as ‘Fixed Protection’ is ceasing all contributions to the pension or the protection becomes void.
Dr Benjamin Holdsworth, director of specialist financial planners Cavendish Medical said there were a range of Government protection schemes which can help savers restore the value of their pension against lifetime allowance changes.
Dr
Benjamin Holdsworth,
director of financial planners Cavendish Medical
He told Independent Practitioner Today : ‘Unfortunately, the pension protections available are nearly as complicated as the pension schemes themselves, so it is a very difficult area for the busy professional to get right. We see many new clients who have previously received incorrect pension protection advice.
‘Every middle to senior doctor is likely to breach the lifetime allowance due to the very nature of making pension contributions into the NHS scheme over a number of decades.
‘However, with careful planning and a complete examination of their financial position, their tax liabilities could be minimised,’ The HMRC figures also stated that
nearly two thirds of the lifetime allowance breaches recorded were due to the introduction of pension autoenrolment.
Dr Holdsworth continued: ‘By failing to opt out of their pension scheme or by being re enrolled accidentally, some savers will have unknowingly breached the conditions of their “fixed” pension protection. The result could be a very large tax bill.
‘The issues doctors are facing in terms of the tax implications of their pensions are needlessly complex and particularly punitive.
‘While Government ministers are currently meeting to discuss ways to improve the situation and reduce the impact on the NHS workforce, doctors should do everything they can to ensure they are not walking blindly into tax charges which could be avoided.’
The pension protection schemes savers may already have in place include Enhanced Protection, Primary Protection, Fixed Protection 2012, Fixed Protection 2014 and Individual Protection 2014.
A further scheme, Individual Protection 2016, is still open for applications for savers who had pension savings in excess of £1m as at 5 April 2016.
Fixed Protection 2016 is also available for those with no pension input after 5 April 2016.
IDF shows its services to doctors out of London
The Independent Doctors Federation (IDF) is continuing its bid to increase private doctor membership outside London.
Its latest ‘roadshow’ visited Birmingham and showcased the organisation’s benefits and services to 40 independent practitioners.
The event was hosted by the Calthorpe Estates, the developers behind the creation of the Edgbaston Medical Quarter, home to over 550 medical companies, 180 medical organisations, 44 GP clinics/routine care facilities and 80 specialist care centres and hospitals.
An IDF spokesperson said: ‘The centres of private practice outside of London have many similar but also many different challenges in establishing and growing independent medical practice.’
Regional ambassadors Prof Robert Scott and Dr Andrew Leahy are points of contact for local members.
sure the private healthcare industry knows who you are, where you are and what you do.
Time with NHS GP to move nearer private ones
Consultation times for GPs in the NHS will move closer to those in private practice in the next decade, according to predictions from the RCGP.
It forecasts 15minute consultation times for GPs in the NHS, instead of ten minutes – only half the time many private GPs spend with their patients.
Private GP Dr Neil Haughton, president of the Independent
Doctors Federation, commented: ‘30 minutes is our standard consultation and patients welcome the opportunity to explain their symptoms in full.
‘It gives me enough time to evaluate often complex and multiple problems in a safe manner. Any increase in NHS consultation time is welcome, of
course, but where are the extra GPs going to come from?’
The RCGP’s Fit for the Future vision of what general practice in the health service will look like in 2030 also foresees networks of practices and an end to GPs working in isolation.
These will evolve into ‘well being hubs’ with expanded
teams offering a wider range of both clinical and nonclinical services.
Access will increasingly be via digital and video channels and the GP patient record will become a personalised ‘data dashboard’, accessible by healthcare professionals nationwide.
So how do you see private general practice in 2030? Let us know: Email robin@iptoday.co.uk.
Dr Neil Haughton
Fee obscurity is shown in survey
By Robin Stride
A new survey backs up calls in Independent Practitioner Today for clearer information on fees in private hospitals.
According to the Private Healthcare Information Network (PHIN), private healthcare prices are becoming more transparent but more progress is needed.
Its criticism came after it commissioned an informal secret shopper exercise* and frequently found several exchanges with hospitals and consultants’ medical secretaries were needed to discover if the fees quoted were all inclusive or subject to other charges.
Patients of consultants who did not offer a package price had the greatest difficulty.
PHIN has now produced a guide (see box) and video along with a check list of key things self pay patients can ask when considering treatment options and costs.
And it believes information published on its website this Spring will help patients compare medical fees before seeking treatment, including a comparative tool for regional price differences.
PHIN’s website shows information about the typical fees charged by over 4,500 consultants for initial consultations, treatment, and follow up consultations for the most common elective procedures performed privately in the UK.
Unsurprisingly, for initial and follow up consultations – and many procedures –there is a premium to pay for treatment in London. Cataract surgery, the most common private procedure, is most expensive in the South west, according to the data submitted to PHIN.
Doctors Federation specialists committee chairman, said: ‘Greater transparency in consultants’ fees can only be of benefit to the selfpaying public, but these are only a fraction of the total cost to the patient.
PHIN boss Matt James said the private healthcare sector should do more to ensure that terms, conditions and price were constructed with the patient in mind: ‘This is understandably very complex, and will take time to work through, but is the right thing to do for patients.
‘Patients should know that they have legal rights to have fees set out in advance, so they can better compare their options before committing to a particular consultant.’
Dr Sean Preston, Independent
‘It’s pleasing to hear that PHIN’s work continues, as hospital charges and unforeseen complications can also lead to unpleasant surprises for patients.’
Adam Land, of the Competition and Markets Authority (CMA) said: ‘Consult ants’ fees need to be clear and accessible if people are to make informed choices. That is why the CMA appointed PHIN to collect and publish information on consultants’ pricing.’
*An independent researcher asked five private healthcare providers how much it might cost to have three of the most common procedures in the private healthcare sector – cataract operations, knee ligament reconstruction and breast augmentation. Five healthcare providers were given identical scenarios and were asked for fees.
RECOMMENDATIONS FOR TREATING SELF-PAYERS
To ensure greater transparency of fees for self-pay patients, PHIN recommends:
1
All 15,000+ consultants in the UK who offer private treatment publish their fees on its website in order to meet their current legal obligations.
Consultants should already be giving patients comprehensive written quotes for fees prior to consultations, diagnostic tests or treatment – as required by the Competition and Markets Authority.
2
All private hospitals likewise publish their prices to ensure that patients get a complete, transparent and fair picture of costs when choosing a provider. PHIN already enables hospitals to publish prices for common procedures, and some hospitals have begun to publish their inclusive package prices.
3 The private healthcare sector should work more together to ensure that patients can get a guide price for the full expected price of treatment and that prices, terms and conditions can be easily compared. These can then be published by PHIN.
It said: ‘Despite improved transparency on price, patients may still struggle to compare terms and conditions between providers – for example, whether diagnostic, physio or follow-ups are included in a quoted price.’
CHECK LIST FOR PATIENTS
Have you checked your consultant’s profile on PHIN’s website?
On their profile, you will be able to see how many of a procedure they have performed in the last year, their typical fees and whether they treat patients under a package price. You can also compare their fees with the typical fees charged in your region.
Has your consultant outlined the fee for the initial consultation and diagnostic tests? Your consultant is required by law to outline the price for the initial consultation in writing before you attend. If any diagnostic tests are required during your initial consultation, your consultant should outline these costs during the appointment.
Has your consultant outlined their fees for your treatment? Your consultant is required by law to outline their total expected fee for all diagnostic tests and treatment in writing following the initial consultation. If they have not done this, you should let the hospital know and ask for a letter that sets out the fees clearly.
Have you checked the terms and conditions to see what is and is not included in the price you have been quoted?
The features covered in the price you have been quoted will differ by hospital and consultant. This is true for a package price or pay-perservice price. You should check with both the consultant and hospital what is included in the price, along with any additional costs you may be liable to pay.
Matt James, PHIN’s chief executive
Dr Sean Preston of the IDF
Patients who are insured ‘will cause the most problem’
Publishing private healthcare fee data is a significant step in achieving better information for selfpay patients, according to the Federation of Independent Practitioner Organisations (FIPO).
It said it fully supported consultations and treatment fee transparency and was keen to ensure any information provided to patients was robust and accurate.
FIPO also backed a PHIN warning about medical fees being ‘just one part of the total price of private healthcare’.
It said fee disclosure for selfpay patients was ‘a relatively straightforward business’, but argued this was not so for the 75% of patients with private medical insurance.
A FIPO statement complained that the vast majority of consultants no longer set their own fees because these were dictated by insurers –making redundant any competition by price.
‘Many more senior and experienced consultants have either had their recognition removed by the insurers or are not recommended at the point of preauthorisation, as they may be more expensive.
‘This inhibits patient choice and interferes with the CMA’s aim of encouraging greater competition.’
It said patients were less interested in fee rates and more interested in a consultant’s level of expertise and experience.
‘FIPO has always been concerned that a strong personal relationship between doctor and patient should remain sacrosanct. Medical ethics and professionalism must not be overshadowed by an overwhelming emphasis on cost, especially when real freedom of choice may be constrained; for example, by conditions imposed by insurers.
‘Patients are not consumers in the classic business sense. The complexities of healthcare extend beyond cost alone and FIPO believes that patients should fully understand the implications of their choice and its possible impact on achieving the best possible personal outcome.’
Hospitals slow in giving safety data
By Robin Stride
Consultants have voiced frustra
tion to the Private Healthcare Information Network (PHIN) over the failure of some independent hospitals to send in completed activity data for publishing.
As we went to press, as many as 483 hospitals had not submitted sufficiently complete and valid data for the network to publish a robust view of their adverse events for patients. Of these, 228 hospitals had made ‘little or no progress’.
PHIN chairman Dr Andrew VallanceOwen said: ‘Over the last year, we have seen noticeable improvements in the quality of data we have received from hospitals and we
are pleased that there is now a critical mass of hospitals for which we can begin publishing the first adverse events and health improvement measures. It is our priority to make this available to patients on our website this autumn.
‘However, it has taken a frustratingly long time to reach this point. There are still too many hospitals that are not providing reassurance over the quality of services that they deliver to patients.
‘Complete, valid and accurate information is crucial for helping patients make informed choices about their care. Where this transparency is not available, patients should rightly raise questions about the care provided.’
The Competition and Markets
Healthcode recruits top practice manager
The founder and former chairman of the Harley Street area’s Practice Managers’ Forum has taken on a new role as product marketing manager for healthcare technology specialists Healthcode.
Desné Marston will focus on the company’s ePractice services, which enable independent practices to control their financial transactions and practice tasks from one secure online platform.
She brings more than 20 years’ experience of practice management systems to her new role, most recently overseeing all aspects of practice administration at the Harley Street ENT Clinic in London, including billing through Healthcode’s billing service.
Mrs Marston said it was an exciting time to join Healthcode, because there were so many developments in the pipeline with the
potential to transform the business of private practice.
‘I’m delighted to have the opportunity to contribute to the process and help make the system the best it can be for customers so they can ensure their practices reach their potential,’ she added.
Kingsley Hollis, head of business development (ePractice), said her appointment would help ensure the company had the right blend of technical expertise and practical industry experience.
Mrs Marston has worked for single handed practitioners, clinics and in a private hospital setting. The Practice Managers’ Forum attracted over 300 members from the private sector and the NHS.
Healthcode said she was providing a practice manager’s insight into how practices operate and would be involved with product
Authority (CMA) requires all private healthcare providers in the UK to provide comprehensive data on activity, safety and care outcomes to PHIN.
PHIN now publishes the number of procedures undertaken and other basic measures for 382 hospitals providing an estimated 96% of private healthcare activity. Eightynine hospitals have submitted sufficiently complete and detailed data to support the publication of the first adverse events – patient safety – measures.
In addition, 68 hospitals have submitted sufficient data to support the publication of the first measures of health improvement, known as Patient Reported Outcome Measures or PROMs.
development from initial concept to marketplace. She is meeting existing and prospective customers to find out what they want from a practice management system.
Desné Marston, former Practice Managers’ Forum chief in London
Surgeon starts new clinic in Crystal Palace
General surgeon and aesthetic doctor Mayoni Gooneratne has opened a new wellness clinic in Crystal Palace, London. It complements her first outlet in Lewisham which was commended for best new clinic at the Aesthetics Awards 2017. Her clinics offer ‘skinfit, bodyfit and mindfit’ services: ‘We know that looking good is only part of the picture: feeling good is an essential part of achieving that glow!’
New
recruit for London eye group
Ophthalmic surgeon Ms Sally Ameen, who specialises in cataract surgery and glaucoma treatment, has joined Ophthalmic Consultants of London (OCL) as a salaried associate. Operating also at London’s Imperial College Healthcare NHS Trust, she joins the three founding directors surgeons Mr Ali Mearza, Mr Allon Barsam and Mr Romesh Angunawela; all specialists in laser eye surgery, cataract and lens replacement surgery and corneal transplantation.
Mayo and Oxford link to launch in capital
Four salaried specialists have been appointed by ‘Mayo Clinic Healthcare in partnership with Oxford University Clinic’ to form the core medical team at its new preventative healthcare facility due to open this summer.
Committed to delivering ‘a unique approach to patient-centred care’, the clinic will offer premium screening and diagnostic services at 15 Portland Place, London, in the first example of a
new partnership between the two world-leading names.
The four specialists are:
Dr Robert Orford, preventative medicine specialist and former director of the executive healthcare programme at Mayo Clinic;
Dr Kevin C. Fleming, consultant at Mayo Clinic and expert in stressrelated conditions;
Dr Sihame Benmira, specialist in general and emergency medicine;
GP Dr Sandeep Kapur.
Leading orthopod moves his practice to Bupa unit
Orthopaedic surgeon Mr Simon Moyes will move his Capital Orthopaedics and Sports Medicine practice to Bupa Cromwell Hospital.
He said: ‘The hospital has the most advanced diagnostic and treatment technologies in the UK and I will be able to offer my patients the hospital’s unique patient pathway, where they will able to be seen, imaged and reviewed all in one appointment and under one roof.
‘The operating theatres, facilities and nursing care at the hospital have a fantastic reputation, which will complement my orthopaedic and sports
medicine offering.’ Mr Moyes will also see patients at Basinghall Clinic, the hospital’s outpatient centre in the City of London.
Hospital director Philip Luce said: ‘We are already a centre of excellence in orthopaedics and his expertise will enhance this to provide our patients with a first class service, something which we are constantly striving to provide.’
Mr Moyes, who pioneered keyhole surgery use in shoulders and ankles, specialises in knee, shoulder, foot and ankle disorders.
Medical director Dr Stephen Cassivi said the clinic will provide an exclusive diagnostic and screening service for individuals and corporate clients seeking to take a proactive approach to their health.
‘With a focus on tailored, personalised care, a dedicated clinician will co-ordinate all aspects of the service to ensure the experience is delivered seamlessly and provides peace of mind to clients with busy lives.’
(From left) Dr Kevin C. Fleming, Dr Sandeep Kapur, Dr Robert Orford, Dr Stephen Cassivi and Dr Sihame Benmira
Innovations guide to stop mavericks
By a staff reporter
Entrepreneurial surgeons have been given new guidance with updated thinking on the development and implementation of surgical innovations such as robot-assisted surgery and new operating techniques.
The Royal College of Surgeons of England (RCS) says a strong framework is needed for developing surgical innovations to ensure patient safety, as well as the patients’ best interests, always come first. It has previously called for national guidelines on the introduction of new procedures and technologies and indicated it is ready to work with the Department of Health and Social Care and the GMC in developing these.
This followed an inquiry by the Newcastle coroner Karen Dilks into the tragic death of a 69-year-old man, Stephen Pettitt, who suffered multiple organ failure after robotassisted heart valve surgery.
The RCS has since written to her
Firms try to fight stress
Businesses are trying to combat the stress associated with today’s non-stop lifestyle by promoting more well-being behaviours such as leaving on time (40%), using flexitime (35%), having regular breaks (33%) and working from home (31%).
But only two-thirds of those in leadership roles say they feel these initiatives apply to them too, according to a survey.
The latest business barometer research from Close Brothers Invoice Finance found nearly a fifth (19%) of senior decision-makers saying that well-being practices do not apply to them, while 13% said they were only partially relevant.
to outline the training and consent requirements in relation to the introduction of new surgical techniques.
New technologies and techniques have huge potential to improve patient care, the college believes, from developments in three-dimensional printing, artificial intelligence, robotics and nanotechnology to advances in regenerative medicine and the ability to grow organs and tissues in the laboratory.
But it says that as exciting as this is, there are significant risks in allowing innovation to occur in the absence of a clear guiding principle.
RCS council member Mr Peter
Lamont helped develop the new guidance entitled ‘Surgical innovation, new techniques and technologies’.
He said: ‘As our Commission on the Future of Surgery recently found, surgery is set to be transformed for millions of patients by a new wave of technologies. These technologies are expected to affect every type of surgery, including the way it is provided and the way we train surgeons.
‘Historically, though, the development of new surgical techniques have often taken place in the absence of the rigour associated with the development of new medicines or devices.
‘It is absolutely vital that surgical
THE GUIDANCE SETS OUT:
☛ The clinical governance and oversight needed to introduce innovations principles for how training should be undertaken
☛ What the patient consent requirements are
☛ How conflicts of interest should be managed
☛ How new techniques should be translated into wider practice
☛ The need for measuring long-term outcomes
innovation places both patient safety and the best interests of the patients at the core. The introduction of new technologies or techniques in surgery has no place for the maverick surgeon who proceeds without appropriate peer review or training.
‘Surgeons by nature are innovators and we hope that these guidelines will help them bring their new ideas forward in a way that most benefits patient care.’
The new RCS guidance highlights the challenges commonly faced by surgeon innovators and signposts sources of assistance. It is also directed at medical and clinical directors charged with providing oversight of surgical activity.
London Clinic’s endoscopy team win GI accreditation
Consultants and staff at the London Clinic’s endoscopy team are celebrating after achieving sought-after JAG accreditation from the Royal College of Physicians.
The initials stand for the college’s Joint Advisory Group on gastrointestinal (GI) endoscopy and reflect a patient-experience, quality and workforce-focused scheme based on the principle of independent assessment against recognised standards.
Delighted lead consultant Dr Rehan Haidry expressed pride in his team: ‘The assessors highlight
the safe, quality care within a patient-centred environment, cohesive teamwork and learning culture in their report.’
Medical director Mr Satya Bhattacharya said the JAG accreditation, developed for all UK independent and NHS endoscopy services, recognised consultants’ clinical excellence.
Around 550 endoscopy units in the UK are engaged with JAG; about 180 are private but less than a third are accredited. Increasingly, insurers are realising that their patients benefit from being looked after in JAG-accredited units.
Lead consultant Dr Rehan Haidry
Third proton beam centre opens
A step change in the UK’s proton beam therapy capability has been signalled with the opening of a cancer centre in Northumberland.
Just over a year ago, there were no facilities operational and no alternative but to send patients to the US or Europe for costly and disruptive treatment.
But the arrival of three Rutherford proton beam therapy centres, in Wales, Berkshire and now at Bomarsund, Northumberland – plus an NHS facility in Manchester – means a transformed landscape for advanced cancer care.
The first prospective cohort of patients at the Rutherford Cancer Centre North East are already undergoing assessment for proton beam therapy.
Proton beam therapy is a type of radiotherapy delivering heavily charged protons in a more targeted manner to reduce damage to peripheral tissue and organs. It can also help reduce unwelcome sideeffects.
Mike Moran, chief executive of the centres’ operators, Proton Partners International, said: ‘The opening of the proton beam therapy suite at our Northeast centre is an exciting milestone in the development of high energy proton beam facilities in this country.
‘Historically, the UK has lagged behind leading countries in the
provision of this form of cancer treatment, but now a complementary mix of private and public facilities are offering patients access to the most advanced technology that can enhance patient outcomes.’
Chris Land, the new centre’s manager, said the opening was a landmark moment in the development of cancer care in the
Northeast and a significant step in transforming the way certain types of cancer were treated.
‘While proton beam therapy is not a panacea, it has been proven to be particularly effective in the treatment of hardtoreach tumours and children, as it reduces damage to surrounding healthy tissue.’
The Rutherford Cancer Centre North East has launched a partnership with the cancer charity Fighting Against All Cancers (FACT).
Charity founder Joanne Smith said: ‘The arrival of highenergy proton beam therapy is an exciting development for the region. Given that the Northeast has the highest rate of cancer incidence in England, new advances in the provision of stateoftheart cancer care to patients in the region is very welcome.
‘We are delighted to have partnered with the Rutherford to ensure patients receive a supportive, professional and holistic experience during a challenging time.’
Taxman warns of rise in scams using cash baits
By Leslie Berry
Taxpayers have been warned to continue to beware of phishing scams allegedly eminating from HM Revenue and Customs (HMRC). Despite continued action and warnings, cases continue to rise, with criminals using increasingly sophisticated methods to target the unwary.
They use landlines, emails, text messages and social media to distribute bogus HMRC information and it is increasingly difficult to know which forms of HMRC contact you can trust.
Bogus refund texts and emails are the most common ‘phishing’ method used, often containing
links to fake HMRC websites or malicious software designed to damage your computer or smartphone.
Tax-preparation specialist David Redfern said: ‘I’m sure most people can recognise how appealing it is when you receive a text or email claiming that you are owed money, often sums over £1,000, and it is tempting to click on the link to claim the refund.
‘However, these emails and texts are never genuine. HMRC does not communicate with taxpayers in that method – they usually communicate via letter. And any emails from HMRC deliberately don’t contain any links for the very reason that they don’t want taxpayers
to get caught out by phishing scams.
‘Bogus links are usually intended to harvest your financial information, such as bank account details or card details. HMRC will never ask you for your card details to issue you with a refund. Similarly, never open attachments to emails.
‘The best way to deal with these texts or emails is to report them to HMRC and then delete them.’
HMRC recommends that all phishing texts and scams are emailed to phishing@hmrc.gsi. gov.uk, even if it seems like a familiar scam that you have seen before.
Inspectors say recent scams have involved direct messages sent to
social media users, again offering a tax refund as bait.
Mr Redfern, managing director of DSR Tax Claims Ltd, said although HMRC had a number of Twitter accounts to provide a customer support option and distribute information regarding UK tax, it did not use them to contact individual taxpayers nor to gather any form of personal information.
‘HMRC will never use a social media account to inform you about your personal or business taxes, whether it is to inform you of a tax refund or request your personal or financial information. These messages should be treated as other HMRC phishing scams to be reported and then deleted.’
Manager Chris Land with FACT founder Joanne Smith at the Bomarsund centre
Cut NHS waits with private units’ help
By Douglas Shepherd
The private hospitals trade body has urged NHS bosses to come up with a firm strategy involving independent units to bring down rocketing waiting times.
As many as 4.23m people were waiting to start planned, consultant-led hospital treatment in the first quarter of 2019 – 10% more than the same period last year.
The NHS England performance figures, showing the NHS failed to meet its target to stabilise waiting lists for elective treatment, were described as ‘shocking’ by the BMA.
David Hare, chief executive of the Independent Healthcare Providers Network (IHPN), said the NHS last year made a clear commitment to keep waiting lists for routine care stable and to halve the number of people waiting more than 52 weeks for treatment.
The number of people waiting over 52 weeks had halved but he said the figures showed the health service had fallen far short of stabilising the waiting list. Over 380,000 more people are now on it.
He said: ‘While we welcome the recent NHS Long Term Plan com -
mitments to increase the amount of planned surgery delivered year on year, including through making use of independent sector capacity, what we now need from NHS England is a clear delivery plan on how to get waiting times down.
‘This must include utilising the spare capacity available in the independent sector and communicating much more effectively the legal rights that patients have to choose the best provider for them.’
More than 240,000 additional people were now waiting for much-needed treatment – ‘equivalent to the population of Brighton’.
There were 491,102 patients waiting longer than 18 weeks for planned treatment in March 2018 and 21,956 operations were cancelled at the last minute during January-March 2019.
The IHPN’s call is echoed by doctors’ groups. Prof Derek Alderson, president of the Royal College of Surgeons, said: ‘It’s hard to see the waiting list decreasing in any significant way without a clear plan.
‘That is why the RCS is calling for a five-year plan – with a commitment to increase hospital beds – to
nated capacity of 32 beds on the old campus.
properly deal with the backlog of patients waiting for treatment.’
BMA council chairman Dr Chaand Nagpaul called the performance figures ‘shocking’ and among the worst released by NHS England.
He said that, despite the Government’s ambition for the health service outlined in its NHS Long Term Plan, the stark reality for both doctors and patients was a system in deep crisis.
‘With over 304,000 patients waiting more than four hours in major emergency departments –an increase of 38% since last year–and with the number of trolley waits of over four hours rising by 39% since last April, patients are suffering.
‘The figures for cancer care are equally worrying; the numbers of patients seen by a specialist within two weeks of an urgent GP referral and the numbers treated within two months have both fallen.’
Dr Nagpaul urged the Government to act to avoid widescale last-minute cancellations of operations. He said it should set a target for the reduction of the cancellation of operations and a plan for how this target would be achieved.
Majority don’t fear being operated on by a robot
Changing attitudes to healthcare delivery are reflected in a new survey showing that 56% of Europeans would undergo surgery with ‘Dr Robot’.
A similar percentage would be happy to receive treatment from their GP via webcam.
These are two key findings of the STADA Health Report 2019.
The report also shows that 80% of Europeans would take a gene test and 38% would be willing to get a biosensor implant.
Overall, men are more open to medical trends and new health technologies than women
Around 2,000 people each from Belgium, France, Germany, Italy, Poland, Russia, Serbia, Spain and the UK, aged between 18 and 99, took part in the survey.
Compiled by Philip Housden
Royal Papworth relocates its private patient unit
The new Royal Papworth Hospital located on the Cambridge Biomedical Campus is now open for patients.
Costing £200m, the facility houses five operating theatres, five cardiac catheterisation labs, extensive diagnostic modalities and over 300 beds.
The trust has 12 independent beds, retaining the Varrier-Jones Ward name for private patients. This is an apparent significant reduction on the previous desig -
However, it is to be anticipated that the apparent shortfall will be made up from flexible use of other inpatient, ambulatory and diagnostic capacity.
The unit has been open for patients since the beginning of last month (May).
Royal Papworth is the second highest private patient revenue earner outside London with private patient income in 2017-18 of £8.15m.
This total was down £834,000 on the £8.98m achieved in 2016-17 and represents a small decline from 6.63% to 6.07% of total trust incomes.
As the UK’s largest cardiothoracic hospital, Papworth has a distinctive edge and focus ensuring that the brand can stand out sufficiently to support private patient local, regional and international demand.
Alder Hey to develop international private patients
Alder Hey Children’s Hospital, Liverpool – one of Europe’s busiest children’s hospitals – is planning private patients expansion.
The new hospital opened in 2015 and has enabled growth in private patient earnings, climbing from £90k in 2015-16 to reach revenues of £434k in 2017-18.
However, this still represents
only 0.19% of total revenues – well below the out-of-London average of all NHS trusts of 0.5%.
In contrast, London’s Great Ormond Street Hospital is second only to Royal Marsden as the highest earning NHS trust at 14.2%.
The trust has strategic aims to be a global centre of excellence and has recently appointed Pioneer Healthcare as preferred partner to expand and enhance the private patient offering at Alder Hey. The partnership is expected to go live from September 2019.
Philip Housden is a director of Housden Group. See his feature article on southern home counties PPUs on page 42
PPU WATCH
would recommend UpToDate to a colleague
trust UpToDate as a point-of-care clinical information resource
say UpToDate improves the quality of care they provide
A look back through our journal’s archives of ten years ago reveals that although times change, some issues are not so new
A trawl through the archives: what made the news in 2009
Expenses probe alert
A tax inspection crackdown on doctors with a private practice meant their expense claims were facing even greater scrutiny than those of MPs.
Independent practitioners were warned they were ahead of entertainers and professional footballers in 2009 as target No.1 for HM Revenue and Customs.
The alert came from a former tax inspector at an Independent Practitioner Today seminar entitled ’20 ways to save tax’.
Sole practitioners and medical groups were often at risk of a costly and time-consuming tax inquiry because their records were so ‘terrible’, claimed Vanessa Sanders, of Stanbridge Associates specialist medical accountants.
She highlighted several problem areas for doctors including car claims, lack of records, using NHS secretaries and using a personal account instead of a business.
Merit award threat
Consultants claimed they had been warned their future clinical excellence awards would be at risk if they worked for NHS-funded alternative providers.
Evidence to a Co-operation and Competition Panel inquiry, from the Hospital Consultants and Specialists Association (HCSA) alleged some doctors were being threatened with being ‘named and shamed’ to their trust board.
They were given ‘less than thinly veiled threats’ that any applications for awards would be unlikely to be favourably regarded.
The HCSA said it had first-hand knowledge of some trust chief executives actively trying to persuade NHS consultants to boycott other providers.
Doctors were told this would amount to a conflict of interest and damage their employer’s business interest.
But the TUC-affiliated union said competition from a plurality of providers entering the NHS market was an inevitable result of Government policy.
Cosmetic surgeons can sell PMI
Cosmetic surgeons could now sell patients insurance at a profit to pay for corrective procedures for putting right complications.
A scheme was available to practitioner members of the British Association of Aesthetic Plastic Surgeons or from the British Association of Plastic, Reconstructive and Aesthetic Surgeons, at £225 per patient.
Private units publish data
Private hospital work for consultants was tipped to rise following publication of new benchmark figures enabling patients to compare independentsector providers with one another and the NHS.
The Hellenic Project, we reported, would collect and compare anonymous clinical and non-clinical information about patients from hospital groups and from submissions to third-party agencies such as the Care Quality Commission.
Advice on poor payers
Consultants and GPs who worked as expert witnesses were told they were entitled to hang onto their work until they had been fully paid.
The BMA medico-legal committee said if doctor expert witnesses had not received payments for their reports, they might want to think of keeping them until the money was received, subject to a specific defence body advice.
Coding
‘can’t cope’
Consultants expressed growing dissatisfaction at the inability of the procedure coding system to cope with their current business. They complained at a London Consultants’ Association meeting that some codes made no sense, while others that were needed did not appear to exist.
One surgeon said: ‘We have several procedures that don’t have a code. The trouble is, medicine is moving too fast for the codes to catch up.’
Revalidation imminent
Private GP Dr Jack Edmonds, chairman of the then Independent Doctors Forum, warned that revalidation was coming and showed readers how to be prepared.
He wrote: ‘Like author John Bunyan’s hero in the classic Pilgrim’s Progress, this is the first step on a long road with many an obstacle and distraction on our way to the Celestial City.’
SUBSCRIBE TODAY
Don’t miss out on what we report and advise in the future. Sign up for a £75 subscription today –consultants, GPs and practice managers can save £15 with a direct debit.
See page 24
ACCOUNTANT’S CLINIC: THE BUILDING BLOCKS OF ACCOUNTANCY
Get the most out of your accountant
Susan Hutter (below) gives her first article in a new A-Z guide of essential matters that consultants and GPs need to consider in order to run their private practices efficiently
‘A’ IS FOR accountants, and what you should be looking for in the accountant you choose to act for your practice.
The key issues to consider are: It is helpful if the accountant acts for others in the medical profession as well as yourself, as they will be familiar with and a specialist in a wide range of relevant financial and tax issues affecting your profession.
Do make sure your accountant has the back-up of a firm with the capacity to cope and to ensure that there is
always someone there for you to talk to.
It goes without saying that you should be able to directly contact the partner in charge of your case.
However, if possible, make sure you are given one or two other contacts – depending on the size of the firm – who will have the knowhow on your business and are often dealing with the accounts preparation and tax issues.
Do check whether your accountant has in-house book-keeping capability. You may process your own records
or use your personal assistant (PA) to do so.
However, if your accountant can do these tasks for a reasonable fee and take over the responsibility, it may be worth considering this.
I know from many dealings with the profession that this is the least favourite part of the running a business!
Alternatively, it may be that you just need cover from time to time when your PA/in-house bookkeeper is on leave or you are temporarily without a book-keeper. It is also useful for your in-house
book-keeper/PA to have someone they can ask about day-to-day issues on the book-keeping side.
Depending on how you trade, there are different compliance rules that you must adhere to. A limited company/LLP being the most ‘compliance heavy’, and sole trader/ partnership being less so. Nevertheless, even with these structures, there are still quite a few hoops to go through. This should be borne in mind when reflecting on the fees being charged by your accountant.
The advice is to always get a fee quote in advance. It is sensible to obtain multiple quotes. Remember that it is possible that someone quoting to take over your job will offer a lower fee than you are currently paying, then, after say a year or two increase it.
So you need to tackle this, particularly if the quote is substantially lower than your current fees.
‘A’ is also for administration Generally, this is the least favourite part of the job for busy consultants and GPs. But if you do not get your back-office in order, problems are likely to arise which will take a lot longer to solve than if you had tackled them at the time as opposed to leaving things to fester.
These days, most consultants and GPs have a personal assistant who can deal with most of the admin work, but you do need to check that this is being done. The key areas are:
Doing the work and sending the invoices out is one aspect, but someone must be on top of the debt collection process
Practice records: It is sensible that these are kept up to date at least on a monthly basis. Leaving everything until the year-end accounts information is requested by the practice accountant is never a good idea.
Prompt invoicing is vital.
The sooner you get your invoices out to the insurance companies or the patient, where applicable, the sooner you are going to get paid.
Some consultants ensure that
their back-office staff provide the invoice to the patient at the time of the consultation.
Others shy away from this, but, either way, the invoice should be dispatched as soon as possible after the treatment.
Debt collection: Many consultants and GPs forget that cash is king. Doing the work and sending the invoices out is one aspect, but someone must be on top of the debt collection process.
This should be looked at in the middle of the month as well as month end. If you have a plethora of invoices, it may be worth looking at having a debt collection agency in to assist you. There are a number who specialise in supporting the medical profession on such matters.
Do ensure that the cash flow is managed. No busi-
ness can survive without a reasonable cash flow. At its basic level, one must ensure that there is money available to pay debts as they fall due.
One of the bugbears for consultants and GPs is payment of their tax bills, whether corporation tax for those who trade as a company or income tax for the others. Even consultants and GPs who do not trade as a company will also have an income tax liability.
If you are unsure as to the dates and amounts of these tax bills, ask your accountant for regular summaries of the amounts of tax due and the due dates and ensure that you put money aside on a monthly basis to pay the tax.
Similar comments apply to all large and regular cash outflows.
Susan Hutter is a partner at Blick Rothenberg Accountants and part of the team that advises medical practitioners
Getting good patient feedback – but for some specialties it’s harder than others
Up to date on revalidation?
Mr Ian Mackay, Responsible Officer for the Independent Doctors Federation, gives Independent Practitioner Today readers an update on revalidation following Sir Keith Pearson’s review
IN JANUARY 2017, the GMC published Sir Keith Pearson’s independent review of revalidation entitled Taking revalidation forward In response to this, a Revalidation Oversight Group was established with representation from many groups including the independent sector.
The conclusions of this group were encapsulated in a November 2018 report entitled ‘Taking revalidation forward: Working with others to improve revalidation’. This aims to help doctors understand what is, and what is not, required for revalidation, to improve the appraisal experience and to reduce the burden for doctors.
One of Sir Keith’s big concerns related to patient feedback and his recommendation was: ‘The GMC should work with stakeholders to identify a range of measures by which to track the impact of revalidation on patient care and safety over time.’
While the majority of the recommendations have now been reviewed, recommendations regarding patient feedback have been delayed for further review.
The ease with which patient feedback can be achieved depends very much on the doctor’s scope of work. While GPs may be able to obtain this from sufficient patients in a short space of time, others –including doctors whose sole scope of work is Section 12 assess
ments – will find it considerably more challenging.
Some doctors undertaking medicolegal work may also find it difficult to obtain feedback from patients and may have concerns about whether it is appropriate to be seeking feedback at all from patients/clients.
The alternative view is that if their work involves consulting with and examining their clients, this is no different to any other clinician and this concurs with the current requirement.
Respond more frequently
Patients may prefer to respond more frequently and by other means rather than by completing a form, which may not cover their concerns or be appropriate for the doctor’s scope of work.
There is a suggestion that Responsible Officers (ROs) should be more flexible in agreeing to alternative methods for collecting information or indeed the type of information that is collected. However, flexibility may lead to a lack of consistency within a designated body or indeed from one organisation to another.
The GMC is doing work to understand how:
It would be possible to make it easier for patients to provide feedback;
To make the feedback more meaningful for doctors;
To do so without increasing the burden.
If you have concerns or helpful ideas on patient feedback, the GMC would welcome your views and you should ensure that you respond to the GMC survey ( Independent Practitioner Today , May 2019) taking place from 30 April to the 23 July 2019.
In the meantime, the GMC provides a significant amount of useful information on the Revalidation Resources section of its website.
Here, among other things, you will find an increased number of case studies for doctors covering a wide variety of scenarios which may help you better understand how you might meet this important requirement.
Sir Keith Pearson’s report highlighted the importance of making the requirements for revalidation clearer.
Too much time
Some doctors were of the opinion that they were spending too much time collecting supporting information and the GMC has now introduced new overarching principles regarding the supporting information doctors should collect, namely ‘quality not quantity’ and ‘proportionality’.
For those with any doubts about what is required for appraisal and revalidation, it is well worth looking at the GMC document called Guidance on Supporting information for appraisal and revalidation , which can be downloaded easily from the Revalidation Resources section of the GMC website.
Confusion regarding the difference between the GMC’s requirements and those of an employer, royal college or contracting organisation is not unusual.
The GMC has now made the distinction between what is required for revalidation and local requirements clearer and has emphasised that failure to meet local requirements – for example, completion of health and safety training –should not influence a doctor’s revalidation recommendation.
As a part of the Revalidation Oversight Group’s work, the Independent Doctors Federation (IDF) undertook an audit tracking
the impact of revalid ation on 500 doctors connected to the federation.
One positive conclusion from this is that ‘appraisal appears to be flagging concerns that warrant further action, enabling the RO to step in and ensure that the necessary governance measures are put in place to ensure a doctor remains up to date and fit to practise, ultimately leading to improved patient safety’.
A copy of the full audit report is available from the ‘News’ section of the IDF website: www. idf.uk.net.
Working part-time
It is not unusual for some doctors working in the independent sector, particularly after semiretirement, to work parttime and therefore to undertake a low volume of clinical work.
This can present a challenge as to whether they are doing enough work to remain up to date and fit to practise.
The Royal College of General Practitioners (RCGP) together with a group of Responsible Officers, sessional doctors and the BMA, has developed a structured reflective template entitled ‘Supporting doctors who undertake a low volume of NHS general practice clinical work’.
Although intended for GPs working in the NHS, it can equally be adapted to other doctors working less than 40 clinical sessions a year, allowing them to demonstrate that safeguards are in place for them to practise safely and to give the necessary confidence that they are providing a good quality of care.
Lastly, doctors should ask themselves: do I need to hold a licence to practise?
The GMC has created a ‘licensing resource hub’, which provides advice to guide doctors regarding whether they need to continue to hold a licence.
This includes advice resulting from common inquiries and there are also several case studies to help this area to be understood more clearly.
See more guidance on revalidation, page 18
Cloud-Based Electronic Patient Records and Patient Portal
eClinicalWorks is a leader among independent, ambulatory practices, covering primary care and more than 50 specialities.
• Integrated Electronic Patient Record (EPR) and Clinic Management
• Comprehensive documentation of patient encounters
• Data analytics to deepen your understanding of your patients
• Streamlined workflows improve the provider and patient experience
Call to arrange a demo to see how we can help meet your needs!
Stuart Tebbutt
07891 217313
The lonely trail to keep up to date
Difficulties encountered by independent practitioners in the pathway to revalidation include confusion, inaccurate information, conflicting advice and time constraints. Kate Lewis and Darren Wiggins (right) guide you through the maze
THE REVALIDATION pathway for independent practitioners can seem a lonely and daunting prospect to tread.
You are largely responsible for your own direction and supervision that is consistent with your licence to practise. You will not normally be connected to a ‘designated body’.
A designated body is an organisation that provides regular appraisals, clinical governance and support with revalidation for its employees.
It is responsible for ensuring that all its doctors are up to date and fit to practise and can meet the requirements of revalidation. For this purpose, it must appoint a Responsible Officer (RO) to support the process.
The designated body is also responsible for reporting figures on a quarterly basis to NHS England.
It is also responsible for implementing a full suite of policies and procedures to embed quality assurance throughout the appraisal and
revalidation process and clinical governance systems. Appraisals are required yearly as part of the revalidation process.
Failing to engage with the appraisal process will most certainly cause problems and damage your ability to undergo revalidation.
The demands upon self employed independent practitioners are different from those working in paid employment and pose various challenges in terms of maintaining professional standards, ethics and competence.
If you are not connected to a designated body?
The GMC provides a tool on its website to assist you to find a connection.
If you do not have a designated body, the process for revalidation via the GMC can be laborious in terms of having to complete an appraisal, an annual return and an assessment so that it is assured that you are fit to practise.
You must ensure your appraiser
complies with the GMC and NHS England criteria and requirements. To satisfy yourself that they do, you should ask to view a copy of their training certificate, which should be renewed every three years with annual refresher updates and regular peer review and network meetings.
The appraiser must hold GMC registration with a licence to practise and have a prescribed connection to a designated body or suitable person.
They also must have, within the last 12 months, performed at least five appraisals before carrying out your appraisal. Without this information, how can you assure the quality of your appraisal or make sure that you are receiving a good service?
The GMC will want a report on your appraisal, fully completed, signed and dated by your appraiser as part of your annual return.
As part of its verification process it may contact the appraiser to ensure all the information and conditions have been met.
Revalidation without an RO or suitable person
Revalidation is normally recommended by your RO to the GMC. Without a responsible officer or suitable person, the GMC will ask you to take an assessment, usually within the year that you are due to revalidate.
You must book your assessment within the timeframe it gives you and take the assessment on the date you have booked and meet the required standard in the assessment. The assessment is designed to test minimum competence.
Failure to book the assessment in time to meet the revalidation requirements, or not meeting the required standard, may result in the process of your licence to practise withdrawal by the GMC.
The revalidation assessment is a multiplechoice exam of 120 questions, lasting two hours. There are 12 of these assessments based on the respective royal colleges’ core curriculums and you will be required to choose the assessment that matches your specialty area
the closest. There is a fee currently of £1,127 and the assessment takes place in Manchester.
What else is involved in the revalidation process?
Multisource feedback;
Statistical analysis report;
Selfassessment;
Concerns;
Compliments;
Deferral;
Casebased discussions;
Significant events;
Reflection;
Continuing professional development;
Administration.
You need to balance your responsibilities to comply with the appraisal and revalidation process with your duty of care and responsibilities to your patients. Of course, remaining up to date and fit to practise forms an enormous part of that duty of care. Appraisal should not be seen as a
burden or a punishment, but as a positive, supportive and encouraging you to improve and maintain quality patient care provision.
Appraisal is the opportunity to reflect with your qualified appraiser and discuss your development, goals and aspirations. It is not a pass or fail matter.
Your appraiser’s role is to facilitate your development and help you to maintain a portfolio of documentation that supports your evidence of fitness to practise.
Appraisers are not there to make a decision about your revalidation recommendation. Their purpose is to summarise comprehensively your evidence to present to the RO and show that you comply with the revalidation requirements.
Your RO is the person who has the statutory responsibility to make the revalidation recommendation to the GMC and only he or she can decide if your revalidation date should be deferred.
APPRAISERS: THEIR ROLE AND OBLIGATIONS
Medical appraiser have an important professional role. They must:
Be trained in the appropriate skills and knowledge of medical appraisal
Understand the context, scope and nature of work that you do
Undertake continuing professional development as an appraiser and attend peer networking sessions
Be formally accountable to a Responsible Officer
Be free of conflict of interest or bias to perform your appraisal
Be subject to ongoing review of appraisal outputs as part of a quality assurance programme
Be subject to regular feedback
Do not despair
There is a plethora of help available on the GMC website and other organisations such as the royal colleges and independent providers, who are available to provide support, guidance and advice. It does not have to be a seemingly impenetrable road to navigate.
The key to successful appraisal and revalidation is clear under
standing of what exactly is required of you and how you can manage the process as part of your daily routine so that it does not become burdensome and stressful for you.
Kate Lewis and Darren Wiggins work for ACI Training and Consultancy Ltd, specialists in revalidation and appraisal services
EXPERT ADVICE YOU CAN TRUST
EXPERT ADVICE YOU CAN TRUST
EXPERT ADVICE YOU CAN TRUST
Since starting in the mid 1970’s Sandison Easson has continued to grow and is one of the largest independent medical specialist accountants in the UK.
Since starting in the mid 1970’s Sandison Easson has continued to grow and is one of the largest independent medical specialist accountants in the UK.
Since starting in the mid 1970’s Sandison Easson has continued to grow and is one of the largest independent medical specialist accountants in the UK.
Sandison Easson acts for medical professionals throughout all stages of their career and has clients in almost every town in England, Scotland and Wales.
Sandison Easson acts for medical professionals throughout all stages of their career and has clients in almost every town in England, Scotland and Wales.
Sandison Easson acts for medical professionals throughout all stages of their career and has clients in almost every town in England, Scotland and Wales.
We provide the usual services you would expect from an accountant such as preparation of your accounts and tax declarations but offer so much more including advice on:
We provide the usual services you would expect from an accountant such as preparation of your accounts and tax declarations but offer so much more including advice on:
We provide the usual services you would expect from an accountant such as preparation of your accounts and tax declarations but offer so much more including advice on:
• Setting up in Private Practice
• Setting up in Private Practice
• Setting up in Private Practice
• Developing your Private Practice
• Developing your Private Practice
• Developing your Private Practice
• Tapering of the Annual Allowance
• Tapering of the Annual Allowance
• Tapering of the Annual Allowance
• Lifetime Allowance planning
• Lifetime Allowance planning
• Lifetime Allowance planning
• Personal Allowance planning
• Personal Allowance planning
• Personal Allowance planning
• Expenses that you can claim and those you cannot
• Expenses that you can claim and those you cannot
• Reviewing your PAYE Coding Notices SPECIALIST
• Expenses that you can claim and those you cannot
• Minimising your tax bills
• Minimising your tax bills
• Minimising your tax bills
• Reviewing your PAYE Coding Notices
• Reviewing your PAYE Coding Notices
T 01625 527
T 01625 527 351 E info@sandisoneasson.co.uk W www.sandisoneasson.co.uk
PRIVATE PRACTICE GROWTH GUIDE: GOING ONLINE
You can’t afford to ignore social media
The Private Practice Growth Guide is designed to give independent practitioners the knowledge and tools they need to develop their private practice.
Whether you are an experienced private consultant or GP, or are new to private practice, this series by Jane Braithwaite will serve as a helpful guide to the exciting, and sometimes confusing, world of healthcare marketing.
This month, in the third article of the series: Should I Tweet, Share or Like – and how will it affect my practice?
IN MY LAST article, I discussed the importance of choosing and implementing a marketing strategy in order to identify a key audience and subsequently grow your practice.
This month, I explore the role of social media within healthcare marketing with some eye-opening statistics, tips for building a website for your practice, and a guide to the various social media platforms you may consider adopting.
But if you think a tweet is only a sound a bird makes, then fear not! Our jargon-free guide aims to make the digital realm approachable and understandable, whatever your level of experience.
Does your practice need to be online?
For many private practitioners, patient referrals stem from wordof-mouth recommendations; either from previous patients or other practitioners within a larger network.
You may have earned a reputation as being a specialist who is available in a pinch, perhaps you are well known for your charming bedside manner or maybe your admin team is renowned for its efficiency.
If this sounds like you, then you may be thinking that there is no added benefit to taking your practice online.
After all, why go to the expense of managing a website and social media account when you already have a name out there? Will a patient really choose a competitor because their practice is online?
Well, yes. A recent survey of 1,700 adults undertaken by doctor. com found that four out of five respondents used the internet to make a healthcare-related search last year.
And, crucially, three out of five survey respondents would choose one healthcare provider over another based on the strength of their online presence – measured on the availability of relevant,
accurate and compelling information.
It is not just the younger generation who are searching online either; more than 76% of respondents over the age of 60 reported to have searched for a healthcare provider online.
So, having your name out there is great and will get patients looking in a certain direction, but if they can’t find you online, they may instead choose a competitor whose practice is.
Getting
online
You may be sold on the virtues of getting your practice online and raising your visibility to untold thousands of potential patients, but where do you begin?
A website should be your first investment in building your online presence and should be viewed as a digital shop-front for your service. A good website will be attractive, easy to use and full of helpful information for every stage of the patient journey.
Your contact and pricing information, practice hours and locations should also be prominent. If you already have a good website, you may wish to use the following section as a check list to ensure you’re covering the vital areas.
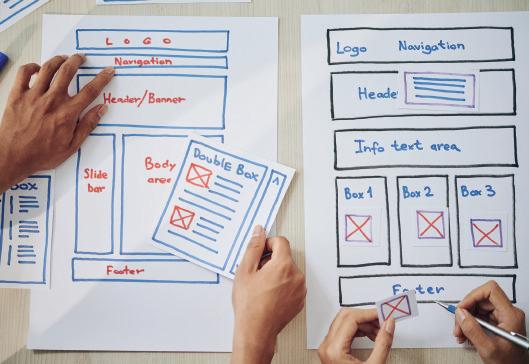
Creating a website
If you are building a website for the first time, there are many low-cost options available to do it yourself or you may wish to resource this to a dedicated team or individual. In any case, you should first seek to identify as many questions that you anticipate your patients may have and, at the very least, you must ensure your website provides answers to the following key questions we have identified:
Is this the right specialist for me and my problem?
How will they fix my problem?
Are they nearby?
When is the soonest they can see me?
How much will it cost?
Will my insurer cover this?
What do other patients say about them?
By focusing your website around these basic and common questions, you will be better placed to ensure that the content you display is relevant to your patients. You can use the above questions to inform a basic site map of how your website should look and function, before even turning on your computer.
Your basic site map might look like this:
Homepage
This is your digital shop-front and needs to send a clear image of who you are and what you do. Your homepage should contain links to further information across the rest of the website and is your central hub.
About
me/us
This is your chance to tell the public at large a little bit about yourself and what you do.
Remember, this is not a profes-
sional CV, but a chance to convey your personality and your professional interests in a brief summary. You can always add a link to your CV for the more discerning patient. A recent photograph of yourself is also a must.
Conditions
If I have a problem, I want to know that you can ‘fix it’ and the best way to demonstrate this is with a concise list of the conditions you treat.
Remember to tailor the content to your audience and consider when and where is appropriate to use laymen’s terms.
Treatments
Assuming you can fix my problem, I want to know how you intend to do it. If a range of treatment options are available, then the pros and cons, cost and availability of each treatment should be clearly listed.
Consider listing these in order of least to most invasive, as many
patients are fearful of surgical intervention and will avoid it at all costs.
Fees/insurers
You should provide a robust fee schedule of all treatment options you offer in your practice, as well as providing a list of insurers you are recognised with.
Transparency with your fees is not only a regulatory requirement, it will reduce the number of speculative inquiries from patients seeking free treatment. If you are involved in a self-pay package scheme, then ensure you include this as well as links to any additional information.
Testimonials
Patient reviews are becoming increasingly important to the ways in which we choose our healthcare providers.
Services like Doctify help to streamline the process of obtaining and sharing feedback on your website, but it’s essential that your
admin team takes a proactive approach to obtaining reviews.
Contact us
Ensure that you provide clear contact information for each of the practice locations you work at, including your hours of admin cover, to manage expectations of any speculative inquiries.
Once you have the basic information, you can add additional content over time to make the site even more helpful for your patients. The basics will help potential patients find and choose you and your services, but consider also adding information for existing patients, such as information leaflets for preand post-treatment care.
It takes a large investment of time to create your own website and write the content, but it doesn’t have to all be done at once. If you struggle, consider resourcing your website development and ongoing management to a specialist team.
Use the check list in the article below to help you create a basic site map of how your website should look, even before you switch on your computer
Increasing numbers of patients are using social media as a deciding factor when choosing a healthcare provider
THE ROLE OF VARIOUS SOCIAL MEDIA WITHIN HEALTHCARE MARKETING
The advent of private healthcare and social media is a relatively recent phenomenon and continues to divide opinion among the medical community.
It was not so long ago that the BMJ actively sought to discourage healthcare practitioners from promoting their practices on social media, and many of the original fears that led to this decision are still prevalent today, such as a perception that it would be damaging to the professional boundaries that exist between patients and doctors.
Some medics are just not fans of social media, in any capacity, and may think of it as a platform for showing off and seeking attention. Regardless of these views, social media is here and it is here to stay.
And, if it continues to affect the status quo of how patients seek out healthcare practitioners, then the onus is on us to move with the times.
Increasing numbers of patients are using social media as a deciding factor when choosing a healthcare provider and, in order to grow your practice, you need to have a strong online presence.
Let us first look at the major social media platforms; what separates them from one another and how we can use them to our advantage within private practice.
Facebook
Events and groups are Facebook’s speciality and there are several local and national groups that recommend healthcare providers to other users, such as Mumsnet and Highgate Mums –definitely one for the north London practitioners to engage with.
It is well worth checking to see what users may be saying about your practice and how you are perceived online.
Twitter
With its limited word count per post – or ‘tweet’ in the common vernacular – Twitter is a great platform for short updates about your services. Trying to fill next week’s clinic? Consider sending short posts that detail your availability and then provide a contact number to book an appointment today. Tweets stack up in a users’ news feed, so post regularly each day to ensure your message is top of the list.
Instagram
Among the most visual social media platform, Instagram is full of photographs, drawings and videos from a range of businesses and individuals.
It uses a system of hashtags (#) to help users find content relevant to them. We recommend using five to nine hashtags per post such as: #london #medical #treatment.
This is a great platform for aesthetic clinicians but, with a little imagination and creativity, anyone can create an exciting image to capture the public’s attention and raise brand awareness for your practice.
LinkedIn
A powerful networking tool to help you link with peers, referrers and other members of the professional community.
LinkedIn should be used for engaging on a professional and intellectual level, and successful users regularly post and comment on articles and news stories related to their work.
Although classified as a social media platform, this is not Facebook and your posts and comments should always be respectful and professional – so no smiley faces, emojis or swearing, please.
Building a strong online presence for your practice may include adopting all of these platforms or just one. Whatever you decide, make the most of the platform(s) you use and remember that consistency is key.
Create engaging content first and steadily release it online at a scheduled day and time. Better to post once a week, every week, then to send five posts in a day and run out of content.
Consider also the audience whenever you post and time it accordingly; for example, 8am on a Monday would be a good way to reach the blurry eyed commuters. Avoid posting on Friday afternoons, as most mobile phone activity at this time will be reserved for finding the nearest pub!
So the digital world may be considered a new frontier for private practice and, if you abstain from adopting an online presence, you may be losing ground to more forward-thinking competitors.
It can be intimidating to start, particularly if you do not use social media in a personal capacity, but there are several resources out there to help you. Whatever you do, be consistent in your efforts and gradually build your online presence over time.
Next month, I will help you build on your social media knowledge as we explore ‘content marketing’ and look at what it is and why you need it.
Jane Braithwaite (right) is the managing director of Designated Medical, which offers business services for private consultants, including medical secretary support, book-keeping and digital marketing
The digital world may be considered a new frontier for private practice and, if you abstain from adopting an online presence, you may be losing ground to more forward-thinking competitors
Is the revalidation and appraisal process giving you a headache?
The MLU can help you.
We are specialists in administering appraisals and revalidation and can help to simplify and streamline the process for you and save you money at the same time.
How do we do this? Our dedicated administration team will support and guide you through the process by:
➢ Reducing existing costs by supporting you in the process of finding a designated body;
➢ By administering your appraisals;
➢ Appointing an experienced Responsible Officer and a select team of medical, qualified appraisers;
➢ Providing a robust system of clinical governance in line with regulatory requirements.
We can also help private practices/clinics/hospitals to become a designated body. The process is simple and we provide cost-effective solutions which include policies and procedures and quality audits for each designated body.
SPECIAL OFFER – £15 direct debit saving
TO RECEIVE OUR TEN ISSUES A YEAR
Dear Reader,
Subscribing to Independent Practitioner Today is the only way you can be sure you will see every issue and have the option of reading us online using our special page-turnable edition. Don’t risk missing out. Our personal subscription for doctors and managers is only £90 a year and £210 for organisations. But you can cut this to just £75 and £180 respectively if you pay by direct debit.
So take advantage of this offer now for our unique business journal dedicated to supporting you in your private practice. We’re confident your subscription will repay itself many times over!
Editorial director
APPLICATION FOR SUBSCRIPTION
Instructions to your Bank or Building Society to pay Direct Debits
Name and full address of your bank/Building Society
To: The Manager Bank/Building Society Address Postcode Ref. No.
Banks and Building Societies may not accept Direct Debit instructions for some types of account
a copy of your letter to us.
THE COSTS OF INDEMNITY
Stop your defence
Various factors help decide what private doctors pay for their indemnity subscription fee.
Dr Gabrielle Pendlebury highlights ten of the biggest issues
MANY DIFFERENT components make up a member’s subscription rate to a medical defence organisation (MDO) and each of these are assessed annually.
A change in any of those pricing factors can have a positive or negative impact on what doctors pay.
Most of the subscription is based upon the risks for the area of practice, including the number and size of claims for the types of work a health professional does and the estimated costs of any future assistance.
MDOs also look at the general costs of providing member benefits, such as medico-legal advice and support, and they estimate how much those costs could rise in future years.
This is to ensure they have enough money in the mutual fund to meet the likely needs of the members now and in the future.
1‘If it’s not written down, it did not happen’
Medical notes should not be treated as an infallible guide to the treatment provided. But recordkeeping failures, such as minimal or inadequate entries, mean that a person reading the notes cannot
work out what has happened at a previous consultation.
This can lead to the presumption that a certain event, such as taking blood pressure, did not happen, even if it did.
Good record-keeping can often stop claims at the outset and easily resolve complaints. Or, when things have veered off course, give a clear indication where things went wrong, allowing for targeted remediation to improve practice.
But recent case law shows that insufficiently detailed notes are not an adequate defence. For example, it is preferable to note which specific features were absent rather than recording ‘no red flags’.
2
Avoid
complaints by matching your expectations
Do not be pressurised into providing treatment you do not think is in the patient’s best interests.
Patients may have unrealistic expectations of what can be achieved from medical intervention, which may lead to an unhappy patient and a complaint or claim.
If you are concerned a patient has not appreciated the limitations of treatment, it is important to document the discussions in as much detail as possible within the medical record.
It may be helpful to suggest that they return with family members for further discussions. You may also want to offer them a second opinion.
3 Keeping up to date and revalidation
GMC guidance says ‘you must keep your professional knowledge and skills up to date’. The ruling body also expects you to regularly take part in activities that maintain and develop your competence and performance, and to be famil-
iar with guidelines and developments that affect your work.
It can be challenging to show evidence of this at yearly appraisals, particularly for doctors who work solely in private practice, who may have fewer opportunities for taking part in continuing professional development (CPD), audit and peer feedback.
Identifying and addressing this early is key to a smooth appraisal and revalidation process. Most MDOs offer a range of courses, often free to members, and these provide CPD on areas that are essential to good practice.
4 Communication and confidentiality
Clear communication between professionals is an essential part of minimising risk. Some patients may require shared-care arrangements, especially in relation to prescribing. It is good practice to keep those with overall responsibility for the patient’s care informed, such as the patient’s GP, provided your patient does not object.
If a patient will not allow you to contact their GP, then you are responsible for their care until their treatment and any aftercare is completed.
You may wish to decide whether such refusal would enable you to proceed safely or whether referral to another clinician would be more appropriate in the circumstances.
The rules of confidentiality are no different in private practice and you must be careful of any inadvertent breaches; for example, by reception staff in waiting areas.
5 Financial conflicts of interest and promoting your services
Allegations of clinicians accepting referral fees have recently been widely publicised. You must not
fees rocketing
You must not allow any financial or commercial interests to affect the way you prescribe for, treat or refer patients
allow any financial or commercial interests to affect the way you prescribe for, treat or refer patients.
The GMC says ‘you must be honest in financial and commercial dealings with patients, employers, insurers and other organisations or individuals’.
Transparency is essential to protect your professional welfare. It is important not to ask for or to accept any inducement that may affect, or be seen to affect, the way you prescribe for, treat or refer patients.
Giving a clear description of your fees, prior to seeking your
patient’s consent to treatment, can reduce misunderstandings and prevent conflict at a later date. Ensuring formal approval for use of NHS facilities for seeing private practice will prevent contractual challenges.
Avoid NHS clashes
The BMA advises that ancillary NHS staff cannot be used for free, and NHS secretaries or receptionists should not be asked to work privately without payment. Be sure not to undertake private practice at times when you have NHS ➱ p28
commitments or when you are signed off as unfit to work.
If you choose to advertise your services, the GMC says you must make sure the information you publish is factual and can be checked, and does not exploit patients’ vulnerability or lack of medical knowledge.
You should not make unjustifiable claims about the quality of service you provide and should not hand out business cards to your NHS patients.
6
Legal requirements
Different jurisdictions impose different regulatory and legal duties on doctors. Hence it is important to ensure you are aware and compliant with the requirements of the jurisdiction in which the patient is located.
This may require you to verify the location of a patient whom you are not consulting face to face.
Documentation and storage of
You should not make unjustifiable claims about the quality of service you provide and should not hand out business cards to your NHS patients
information relating to private patients should be comparable to that provided in the NHS. The EU’s General Data Protection regulation (GDPR) applies to all individuals and organisations that have day-to-day responsibilities for data protection.
All doctors should consider, therefore, how the GDPR impacts on their practice. Doctors who carry out private practice are required to register with the Information Commissioner.
You should also check whether you are required to register with the Care Quality Commission (CQC), which regulates the independent healthcare sector in England. A failure to register may result in a fine or referral to the GMC.
7 Duty of candour
There is a professional duty to be open and honest with patients when things go wrong.
An early response to complaints, providing a full explanation and apology, where appropriate, can often diffuse tension and resolve the matter.
Although the statutory ‘duty of candour’ applies to organisations, as the treating doctor, the responsibility of informing the patient may fall to you.
8 Informed consent
The Montgomery v Lanarkshire case of March 2015 drew fresh attention to informed consent.
The doctor has a duty to disclose the information and material risks that the patient, or a reasonable person in the patient’s position, would likely regard as significant. It is therefore important to consider what would be relevant to the individual patient when taking consent for treatment and not just take a blanket approach to consent.
9
Prescribing
Good Medical Practice says that ‘you must recognise and work within the limits of your competence and that you must keep your knowledge and skills up to date. ‘You must maintain and develop the knowledge and skills in pharmacology and therapeutics, as well as prescribing and medicines management, relevant to your role and prescribing practice.’
Patients can often place pressure on clinicians to comply with requests without understanding the complexity of this area.
This is particularly so in the context of treating unregistered patients for whom you do not have full records and whom you might be assessing remotely by phone or Skype. Particular caution is warranted when facing requests to prescribe drugs with addictive potential.
Being cognisant with the relevant guidance can aid decision-
making and prevent the risk of falling foul of inappropriate requests. A review of your practice in light of the above issues will protect your professional welfare and hopefully avert anxiety around these areas.
Should questions arise, your MDO can clarify any points and consider your practice with you, in relation to these issues.
10
Indemnity
The GMC emphasises that the obligation is on doctors to ensure their indemnity arrangements are adequate and appropriate for the risks and nature of their whole scope of clinical practice. This includes ensuring you are indemnified to practise in the country in which the patient is located.
Hence it is important to verify the location of a patient with whom you are undertaking a telemedicine consultation.
The obligation is on doctors to ensure their indemnity arrangements are adequate and appropriate for the risks and nature of their whole scope of clinical practice
The GMC advises doctors to speak to their MDO or insurance provider about their indemnity ‘and the extent to which they will be able to meet the legal requirement to have appropriate cover’.
Regularly updating your indemnifier about the changes in your scope of practice can avoid inadvertent presumptions about your indemnity and ensure that you are fully protected.
This will also help to ensure you are paying the right price.
Dr Gabrielle Pendlebury is a medicolegal consultant at Medical Protection
DRIVE TO IMPROVE SAFETY
Both sectors need to share care data
Patient safety, highlighted in a major report from the Royal College of Surgeons of England last month, remains high on the agenda at the Independent Healthcare Providers Network. David Hare (right) explains why data sharing is vital
BACK IN 2015, former Health Secretary Jeremy Hunt declared it his mission to make the NHS ‘the safest healthcare system in the world’.
Since then, there has undoubtedly been an increase in momentum around ensuring that patient safety is the top priority for all
healthcare providers, including those in the independent sector.
And despite the change at the top of the Department of Health and Social Care with the arrival of Matt Hancock as Health Secretary last year, patient safety issues continue to make the press on an almost daily basis.
Indeed, the latest story to hit the news on this was a recent report from the Royal College of Surgeons of England (RCS) called ‘Recommendations for assuring standards in the independent sector’.
This looks at what can be done to better align data collection and safety standards between the NHS
and independent sector and learn lessons from the Ian Paterson case. At the heart of the RCS’s report is the acknowledgement that there has been significant progress made on this agenda in recent years. This includes a wide-ranging programme of work that the Independent Healthcare Providers
Having served healthcare professionals since its inception in 1993, Tax-Link, chartered tax advisers and accountants in Wimbledon, has built a wealth of knowledge and experience in dealing with taxation issues faced by doctors in private practice. Our focus is on tax planning and compliance.
l Tax structuring to suit personal circumstances (LLP, limited companies)
l Solvent liquidations
l Consultant groups and consortia
l Assessment of pension contributions in light of tapering annual allowances
l Ad hoc assistance with HMRC investigations and reviews. For more information and tax-efficient advice, please:
Phone: 020 8540 1920 Email: rakesh@tax-link.com Address: The Long Lodge, 265-269 Kingston
Our front page in May revealed the college’s plan for greater scrutiny
Network (IHPN) has been doing to bring independent-sector providers together to understand what more needs to be done by providers, regulators and other key health bodies to ensure that patients can be confident of the care they receive, regardless of where they receive it.
Patient outcomes
A key part of this is the importance of collecting and publishing data on patient outcomes. And the report rightly highlights the work IHPN has been doing with the RCS and the Health Quality Improvement Partnership (HQIP) to review which existing national clinical audits the independent sector can contribute to and the barriers that need to be overcome.
While the independent sector currently contributes data to the National Joint Registry, it has, to date, not been enabled to contribute to the majority of national clinical audits that collect data on care outcomes, including cancer audits, despite the fact that many independent providers regularly offer cancer treatment.
The RCS has made clear that any obstacles to the sector’s participation should be identified and overcome by the relevant bodies.
Equally, while the Care Quality Commission’s (CQC’s) report last year into independent acute hospitals found that the vast majority of sites were delivering safe care for patients, the RCS rightly echoes the commission’s call for greater consistency around clinical governance procedures.
The care watchdog says this will
enable more effective monitoring of consultants’ work and ensure patients are treated safely.
This is one of IHPN’s key priorities and we are grateful for the RCS’s support for the development of our ‘Consultant Oversight Framework’ for independent hospitals, which is being led by former NHS national medical director Sir Bruce Keogh.
The framework aims to outline a set of key principles to help improve the consistency of clinical governance around medical practitioners across the sector and to raise the overall bar in medical leadership.
Indeed, as we know, the flow of consultants working in both the NHS and independent health sector is considerable and ensuring appropriate oversight and the monitoring of their whole clinical practice is vital to the safety agenda.
We therefore welcomed the RCS report’s backing for IHPN’s call for a single dataset or repository about a consultant’s whole clinical practice to be available to the independent and/or NHS hospitals where they work.
As reported in last month’s Independent Practitioner Today, this would include information about a consultant’s:
Practising privileges;
Indemnity cover;
Scope of practice;
Identity of Responsible Officer;
Appraisal status.
And it would ensure that concerns about a doctors’ conduct or performance are quickly identified and shared with the relevant bodies so that appropriate action can be taken promptly.
Much of the media coverage of the RCS’s report was around what independent hospitals need to do to increase the amount of safety data being made available.
But the report also makes clear that it is the responsibility of the entire healthcare sector, with the support of the clinical profession, to do more to minimise the risk of a future Paterson.
That means stronger oversight and protection for patients, regardless of whether they have their care delivered in the NHS or the independent sector.
David Hare is chief executive of the Independent Healthcare Providers Network
The tests for tech
Whether you are a technophile or technophobe, Kingsley Hollis says you should consider these five big issues before deciding whether to invest in new technology
THOSE PEOPLE who will queue all night for the launch of the latest must-have gadget have a name –‘early adopters’.
And they are loved by technology giants because they are willing – and wealthy enough – to try innovative products and spread the word.
The term comes from a 1962 book called Diffusion of Innovations1 by Everett M Rogers, a US sociologist who was interested in how ideas are spread until they reach critical mass.
According to him, people can be divided into five groups depending on how long they take to adopt new technology:
Innovators;
Early adopters;
Early majority;
Late majority;
Laggards – these are the ones
CHENIES MEWS
IMAGING CENTRE
SPECIALIST MRI IN THE HEART OF LONDON
• Advanced Cardiac MRI
• 3T Neuro MRI
• MRI for patients with cardiac pacemakers
T: 0203 887 0566
E: referrals@cheniesmews.com
W: www.cheniesmews.com
who are the most reluctant to abandon tradition.
How does this apply to independent practice?
I meet many consultants who are enthusiastic about the potential of new technology and like to keep their finger on the pulse.
But others are only concerned with having a tried and tested system they can depend on.
It would not be right to push practices towards new technology for the sake of it, as my job is to help practitioners find the right solution for them.
However, I advise every practice in this position to consider the following:
1The financial outlay Practices need to decide whether they are willing to com-
mit the resources to a new system, but this shouldn’t be a blank cheque.
As a case study of what can go wrong, it is hard to beat The National Programme for IT, an abandoned project to upgrade NHS computer systems, which was thought to have cost more than £12bn over ten years.
You need to understand the true cost of any new technology so you can determine whether it is affordable. For example, will you need to factor in upgrade costs or ongoing expenses like back-up and technical support?
2 Efficiency
Technology that makes it quicker and easier to carry out essential administrative tasks could quickly pay for itself by boosting productivity.
From Henry Ford’s assembly line to Amazon’s supply chain management, technology driven innovations made a dramatic difference to the performance of those companies.
The downside of being the first to try new technology is that you are more likely to have to deal with early bugs and system glitches which are fixed for later users.
Early adopters often relish engaging with tech companies in this way if it means they can influence future developments, but this is not for everyone. Technology should not disrupt your practice; it should support it.
3
The cost of doing nothing
There is also a price to pay for clinging onto outdated technology, sometimes referred to as a laggard penalty.
In February, the Government announced it was phasing out the non-emergency use of pagers by the end of 2021. The NHS currently pays £6.6m a year for these 1990s relics and that is without considering their impact on operational efficiency.
Whether it is lost revenue, poor cash flow or disgruntled staff, you need to consider the financial implications of sticking with the status quo.
4
What are your competitors doing?
In every business, it makes sense to keep an eye on your competitors or there is a risk they will steal a march on you.
Customers’ expectations are constantly evolving and there are countless examples of companies that lost ground because their products or services were perceived as old-fashioned or out of touch.
Big names are not immune either – look at what happened to Nokia or Kodak: two giants who fell into decline because they failed to innovate at the same pace as their rivals.
5 Your staff
In some cases, practitioners are persuaded to adopt new technology by employees who are fed up with time-consuming administrative tasks and know there is a better way.
It certainly makes sense to ask new recruits about their experience of technology in other practices, as this might be transferrable to your own situation.
Bear in mind that some staff may be more adaptable than others. If someone’s computer skills are limited to what they need to get the job done, you should think carefully about how to implement any new technology and how easy it is to use.
On the other hand, if staff feel that you are not interested in investing in something to help them work more productively, they might be tempted to look for a new employer.
As with every technology company, my company Healthcode is constantly developing innovative online products and services which help practices operate effectively.
We are always delighted when our customers are enthusiastic about new solutions and functionality and we certainly welcome user feedback, as it helps us learn and improve.
But whether someone is a technophile or a technophobe, I have found the best approach to building a positive working relationship with customers has echoes of the clinical consent process.
In other words, technology providers need to listen to doctors, discuss their options and give them all the information they need to make their own decision.
Reference
Technology that makes it quicker and easier to carry out essential administrative tasks could quickly pay for itself by boosting productivity
1. Diffusion of Innovations, Everett M Rogers. First published 1962; 5th Edition, 16 August 2003, Simon and Schuster. www.simonandschuster.co.uk/ books/Diffusion-of-Innovations-5thEdition/Everett-M-Rogers/ 9780743222099
Kingsley Hollis (below) is head of business development (ePractice) at Healthcode
PROBLEMS WITH THE TAX MAN?
HMRC tax investigations and disputes create difficult and stressful times.
As an award winning firm of tax experts, our highly experienced partners specialise in resolving problems relating to tax investigations and disputes with HMRC.
To find out, in confidence, how we can help call 0800 734 3333.
‘Here
BILLING AND COLLECTION
A week in the life
With increasing numbers of private doctors seeking help to recover fees and prevent future shortfalls, Independent Practitioner Today asked Simon Brignall to keep a diary about the variety of issues he deals with for consultant clients
MONDAY
An early start to the week and the familiar sight of traffic congestion on the M25, but I still make my 8am appointment.
provider and the various payment arrangements at the locations they work at means that things can get out of hand very quickly.
He explains that since his practice secretary retired a few years back, he has had a series of secretaries and is concerned that the billing and chasing has gone awry. His
I am meeting with a cardiologist who has a common billing problem. He has been referred by a colleague who uses us.
last secretary was often off sick before finally resigning.
The final straw was when his new secretary realised the billing had not been raised for several months.
It is obvious the lack of continuity has cost the practice. Most importantly, I let him know that we can help. He is clearly relieved and asks me to meet his new secretary to discuss how she will be sending us the data for the unraised billing and the outstanding invoices.
I leave at 9.30am with all the paperwork signed, so we can get to work as soon as possible.
Back at our office late morning, I have a hand-over meeting with the account manager who will be taking the practice through our ‘Intensive Care’ process.
It is important that I detail all the issues raised at the meeting so procedures can be put in place to address them.
As we are close to the deadlines to submit invoicing with some of the insurers, the practice needs to ensure that this data is prioritised so that the consultant does not lose out on this income.
TUESDAY
Today I am presenting to a group of urologists who have been given a recommendation about our services by another group we partner with.
Groups have all the same issues that we see with individual consultants, but they are often amplified due to the amount of work.
The requirement to manage different pricing schedules for each
I take the time to establish the structure of the group, and how they currently operate, so that I can tailor my presentation to show the most effective way we could work with them.
The group currently has seven consultants and expects to grow to ten over the next few months. This means they will soon outgrow their current administration arrangements.
The fact we only charge a fee against what we collect – so our costs are correlated against received income – is well received.
The group’s lead consultant informs me that the binary nature of decisions around staffing have been difficult, as the group has expanded. They will let me know their decision by the end of the week and I am hopeful.
WEDNESDAY
I am in London all day today and my first meeting is at 8.30am with an ENT surgeon who called me last week.
The consultant explains that his wife has been doing his billing for 15 years but has finally had enough.
She is finding it very difficult to keep abreast of all the changes taking place: from updates to private medical insurance fees for procedures to the requirement by some insurers to raise invoices electronically.
The raising and chasing of invoices in relation to shortfalls is definitely not something she relishes.
The often-touted complaint that patients would not do this in a restaurant or hotel is aired. If I had £10 for every time I heard this complaint, I would be a wealthy man!
I explain how we operate and
of a bill chaser
do and is very common with consultants who manage foreign selfpay patients.
that our service is tailored to the needs of the individual consultant. He decides to start using our services straight away.
I think his wife will be very happy to pass this responsibility to us. It’s been a good start to the week with two new consultants joining us.
My remaining meetings today are with existing clients. I have a review meeting with a physician whose practice is ready to come out of our intensive care process. When she joined, she had concerns about how easy it would be get information to us from her practice management system and there was also more than £75k in aged debt that had been steadily increasing.
The meeting went well, as she confirmed that her secretary was finding the transfer of the detailed clinic list surprisingly easy and I was able to update her that we had managed to collect 87% of her bad debt at this early stage.
I head off in a positive mood.
My next meeting was with of one of our surgeons who has a large successful practice. This is an unexpectedly long meeting, as his next patient had cancelled and now he wants to go into the fine detail of the practice.
I had brought a couple of reports with me, but we ended up accessing his data using his log-on to our reporting tool to obtain additional reporting.
We looked at the frequency and value of his most common procedures with self-pay patients, as he wanted to review his fees.
He mentions that he felt that his GP referrals had declined and so I show him a year-on-year comparison of his referrals.
We found that one GP had dropped off quite considerably and he indicated that he would call them to check to see if there had been any issues.
It is very important to monitor and maintain these important
The range of people at the event was a good mix of established consultants, clinic practice managers and new consultants and I find the evening to be productive with some promising leads.
FRIDAY
I have a train to catch to Liverpool to a meeting with an ophthalmologist. When I spoke to him initially, it was clear his problem was a backlog of outstanding invoices.
drivers of a private practice and I know he will address this.
We review his self-pay pricing and he asks for the agreed fee increases to start from the beginning of next month.
THURSDAY
Tonight, I am presenting at an event at the King’s Fund in London called ‘How to improve your private practice’.
There are a range of presenters covering all aspects of running a private practice including billing and collection, marketing, social media, website design, software, accounts and tax planning.
There is a Q&A session at the end and I find myself being called on to answer many questions around billing, such as ‘how far we can go back when chasing outstanding invoices?’ to ‘can we collect money up front?’.
I let them know we can legally go back six years and collecting money up front is something we
In our meeting, the consultant elaborated that he was embarrassed to say he was owed at least £150k. I assured him that we have consultants come to us with even higher amounts.
In fact, we have had individual consultants who are owed as much as £400k and some clinics have had amounts close to a £1m.
I explained how we could help him collect his backlog and also how we could work with him moving forward. He is particularly impressed with the fact that we only charge on what we collect and not what we invoice.
I add that, as we share common goals, this means this problem will become a thing of the past. He was happy to proceed and so completed our induction forms there and then.
I head back to Liverpool Lime Street Station in time to make my train back to London. Good news as I am checking my emails on the train; there is one from the group that I presented to on Monday, which says they wish to go ahead. I agree a meeting next week to finalise the paperwork.
Simon Brignall (right) is director of business development at Medical Billing and Collection
EXPLODING THE MYTHS OF PENSION TAX
Pension tax
More senior doctors are triggering harsh tax bills because of pensions tax. However, rash decisions are unwise, warns Hugh Davies, and there are five porkies to watch out for
WE HAVE reported many times in Independent PractitionerToday in recent months that more senior doctors than ever before are facing substantial tax bills because of stricter rules regarding pensions tax.
Since the socalled ‘pension simplification’ in 2006, total tax charges from breaching the annual allowance have netted HM Revenue and
Customs over £1.2bn and lifetime allowance breaches have generated a revenue of £335m.
As you are aware, the yearly restriction on the amount you can contribute to your pension freeoftax is known as the ‘annual allowance’.
New rules decrease the standard annual allowance of £40,000 to as low as £10,000 a year for doctors
with a ‘threshold income’ of more than £110,000 – this is known as a ‘tapered annual allowance’. Excess pensions savings above the allowance will generate a tax bill charged at your marginal rate of income tax.
Caught in net
As the tax relievable pensions savings limits are now lower, the net is catching
more and more doctors who are tied into making contributions into the NHS Pension Scheme. Workers with private pensions, on the other hand, can simply adjust their pension contributions to fall below the cap – albeit with a smaller pension as a result. News of the problem has been gathering momentum, with not only the BMA calling for Government action,
➱ p38
but now mainstream media addressing how the tax is impacting the NHS workforce.
According to a recent Financial Times investigation, the tapered annual allowance is ‘fuelling an NHS staffing crisis as large number of senior staff are routinely turning down extra shifts through fear of being landed with punitive bills’.
In April, the Government ruled out changing pensions tax legislation following an official Parliamentary review raised by MP Paul Masterson ( Independent Practitioner Today, May 2019).
He shared concerns about the impact the taper was having on consultants and other doctors, with many choosing to reduce their hours or retire early. He said he believed there was a ‘serious potential knockon effect of very senior doctors turning down hours or taking early retirement’.
This culmination of factors has led many consultants to question whether they should be changing their work patterns, taking early retirement or quitting the NHS pension scheme altogether.
In recent weeks, we have counselled several clients who had become concerned by the mounting confusion among their peers and colleagues about what action to take.
With this in mind, we believe it is useful to clarify some important facts about the taper and to dispel a few myths:
PORKY 1:
Senior doctors should quit the NHS Pension Scheme
More medics are opting out of the NHS Pension Scheme, according to official figures. A total of 245,561 people opted out of the NHS Pension Scheme between 2015 and 2017, with 102,755 opting out
in 2016 alone – the year in which the taper was introduced – a 78% increase from the previous year.
The age group with the highest number of NHS Pension Scheme leavers in that time were the 46 to 55year olds, with a 94% increase in 2016.
However, despite the challenges with the NHS scheme, for the vast majority of members, there are too many advantages to ignore.
Lose benefits
The pension is Governmentbacked and indexlinked in retirement and also provides benefits for a surviving spouse. If you opt out, you will also lose other benefits such as death in service and may also face reduced ill health retirement options.
In truth, opting out of the NHS scheme is a financially sound move for only a limited number of individuals.
Before making any decision to leave, we would advise looking at detailed financial modelling, which could help to pinpoint whether it is the best move for you and, if so, the optimal time to leave.
PORKY 2: I should retire from the NHS rather than face tax bills
Many doctors are having to deal with complex pension tax positions that are factoring into their retirement decisions.
We have found that few clients wish to stop clinical work altogether, with many preferring to continue in their careers in some capacity, if the opportunities exist for them to do so.
Often, it is possible to navigate a path between remaining in practice and the tax challenges this may cause.
One often overlooked point is
In truth, opting out of the NHS scheme is a financially sound move for only a limited number of individuals
that by paying some annual allowance tax charges, however undesired at the time, the scheme member will reduce their eventual total pensions savings and be less likely to breach the lifetime allowance later on.
PORKY 3: The NHS pension scheme is no longer worth paying into
New clients will often ask me if the NHS Pension Scheme still represents good value for money.
It looks very different to ten years ago and in ten or 20 years’ time – when current 2015 scheme members are retiring – it will most
likely look very different again. Nonetheless, the value of the scheme largely depends on how long you live.
If you retire at 60 and live for another three decades, then the scheme has been worthwhile. If you pass away the day after you retire, you will not have reaped the same rewards, although your spouse may continue to enjoy the benefits.
Of course, the future is unknown and, statistically, you will live to enjoy a long retirement.
The NHS scheme still represents the best value pension you can buy and a private equivalent simply does not exist.
PORKY 4: Opting for the pension scheme to pay my annual allowance tax charge is the best choice for me
There are multiple options for paying an annual allowance tax charge: via self assessment, through the NHS Scheme Pays option or utilising your personal pension pot.
With NHS Scheme Pays, the pension scheme pays the tax charge on your behalf in return for reduced pension benefits in the future and will charge interest each year until retirement.
There can be tax advantages with this option, but you should be mindful that the interest payments can escalate quickly and the future inflation rate is unknown. However, you should have some idea of the reduction to the benefits to enable you to make the right decision. You will also need all the necessary information to hand before the application deadline, which is normally 31 July each year.
You could also use a personal pension to pay the tax charge; this is typically the best option of the
three. However, it is essential you receive the right advice in this area.
PORKY 5: I can probably go it alone
The calculations required for the tapered annual allowance are extremely complicated, even for financial planners not used to dealing with the nuances of the NHS remuneration and pension package.
Every year we conduct ‘rescue missions’ of new clients who had chosen not to seek advice initially or who had been poorly advised because the professional who helped them did not fully understand the complex income streams of their medical client.
One major issue that we are seeing time and again are incorrect pay levels for NHS staff.
Significant problems
When we scrutinise pay slips, we often discover that a consultant has not been paid the correct pay level – sometimes for several years – and therefore not only are they owed substantial back pay, but their tax position has been incorrect, causing significant problems.
There are many important factors to consider when looking at your financial situation in relation to the tapered annual allowance. Please do not underestimate how complex the issue is, but remem
ber that all problems are surmountable with careful analysis. Ensure you have all the financial facts to hand and spend some time talking to people with experience in this area so that you are able to make wellconsidered decisions.
Hugh Davies (left) is a senior financial planner at Cavendish Medical, specialist financial planners helping consultants in private practice and the NHS
The content of this article is for information only and must not be considered as financial advice. Cavendish Medical always recommends that you seek independent financial advice before making any financial decisions. Levels, bases of and reliefs from taxation may be subject to change and their value depends on the individual circumstances of the investor. The value of investments and the income from them can fluctuate and investors may get back less than the amount invested.
Free legal advice for Independent Practitioner Today readers
Independent Practitioner Today has joined forces with leading healthcare lawyers Hempsons to offer readers a free legal advice service.
We aim to help you navigate the ever more complex legal and regulatory issues involved in running and developing your private practice – and your lives.
Hempsons’ specialist lawyers have a long track-record of advising doctors – and an unrivalled understanding of the healthcare system as a whole.
Call Hempsons on 020 7839 0278 between 9am and 5pm Monday to Friday for your ten minutes’ of free legal advice.
Advice is available on: Business structures (including partnerships) Commercial contracts
Disputes and litigation
HR/employment
Premises
Regulatory requirements and investigations
Michael Rourke Tania Francis m.rourke@hempsons.co.uk t.francis@hempsons.co.uk
See things from the patient’s view
Montgomery five years on: Niloo Bozorgi reflects on how the consent landscape has changed for doctors
IN 2015 , the Supreme Court handed down judgment in the case of Montgomery v Lanarkshire HA [2015] and effectively changed the understood legal definition of informed consent.
The doctor who is counselling a patient before a procedure or course of treatment is now judged on whether they discharged duties imposed on them professionally and by the law.
Judgment is made not by reference to what information a reasonable doctor would have imparted, but rather by reference to whether a reasonable patient has been provided with all information material to their agreement to such treatment.
This advice must deal with all the realistic alternatives open to the patient, including those the doctor is not able or willing to perform.
The move was welcomed by many as bringing the legal duties of medical practitioners in line with long-held regulatory professional standards.
But others feared that the newly defined legal obligation encouraged a defensive style of medical practice that shifted the focus from helping the patient to protecting the doctor.
Duties of the doctor
Five years on, the full implications of this case are undoubtedly yet to be seen. However, the handful of cases that have so far tested the principles laid down in Montgomery have fine-tuned the legal duties of the doctors and the expectations of the patient.
Medical practitioners have long been cautioned that, as a rule of thumb, the court will be likely to find that what is not recorded in a patient’s notes or subsequent clinic letters probably did not happen.
Courts will be sceptical of witness testimony, often provided years after the event, that a doctor discussed matters with their patient which they then failed to record in the notes.
The principle has been reiterated yet again in a recent case, where the court found a surgeon to have breached their duties towards a patient – regardless of their skill in the operating theatre – as they were a poor communicator of risks.
This conclusion was reached on
the basis that although in his witness statement the surgeon stated that he would have mentioned certain risks that he failed to record – because it was his usual practice to do so – he failed to mention those very same risks when he gave evidence in chief about the risks of the operation.
A situation like this can best be avoided if the contemporaneous records match what the surgeon’s usual practice is said to have been.
In the very same case, a signed consent form quoting paralysis as a risk was deemed not to constitute informed consent because the patient was said to have been rushed into signing the form without appreciating the full implications of the risks.
The patient needs to understand the incidence or the frequency of the risk as well as the likely severity on the facts of their own case.
Risk-benefit analysis
Another recent case was settled out of court because it was anticipated that the claimant’s factual evidence would have been found more reliable than that of the treating surgeon, who was alleged to have failed to provide a riskbenefit analysis of the different available treatment options.
Providing such risk-benefit analysis is an integral part of a medical practitioner’s duty. This is complicated by the fact that before their surgical ordeal, many patients have little interest in hearing about the risks they must take and many doctors recognise and respect an obligation to protect them from the fear associated with such disagreeable realities.
When things go well – as they do for most patients – the patients are grateful. In the minority of cases, when things go wrong, the attitudes change dramatically and patients become obsessively interested in the details they failed to absorb through inattention.
The courts are only called upon to be the arbiters of whether doctors have discharged their professional duties towards a patient in the minority of cases where things have gone wrong.
It is as though they view matters through the wrong end of a telescope: the doctor may have a waiting room of 20 patients, 19 of whom may be expected to do very
well, yet the court only judges what should have been said on the basis of the 20th case who suffered the 5% risk.
In that context, it can be difficult to remember that a doctor’s role is not to overload their patient with information that they have no interest in hearing.
Most patients do not want to hear about all the adverse risks and benefits, let alone those associated with all the other possible available private treatment options in the UK and abroad.
And most doctors do not have time in the typical outpatient clinic to provide such a discourse, still less to make a detailed note of what has been said.
The reality is that both doctor and patient need to ensure that the discussion of relevant information is held in a way to enable the patient to use it meaningfully.
Montgomery has reflected a secular change in expectations that doctors will provide patients with some additional information as was already spelled out in guidance from the GMC.
We now must organise medical services so that this duty can be discharged. Patients must be persuaded to work harder to absorb information – the autonomous empowered patient cannot be a soft option.
And we must not lose sight of a doctor’s role as a guide and counsellor as to why a treatment may ultimately be in a patient’s best interest despite all the inherent risks.
Independent practitioners do have several advantages. They can organise their own clinics so that
they have enough time to explain things to their patients.
They are often able to control the environment, providing a place where their patients will feel comfortable and able to take time to read written material and visual aids that their doctor can provide.
But because private doctors control their own work situations, they also must be more self-disciplined. They must be careful to resist the temptations to take short cuts when making notes.
Nor must they be more informal. It is not so long since consent forms were regarded as an unnecessary intrusion in a relationship where the private patient could be trusted not to allege that they had not fully consented to a procedure.
Above all, private doctors must be able to rebut the allegation most memorably articulated by George Bernard Shaw in his preface to Doctors Dilemmas that a certain treatment was recommended because the doctor had an interest in being paid to perform it.
Niloo Bozorgi (below) is a trainee solicitor at Hempsons. She works in the healthcare litigation department running her own caseload under supervised by senior solicitor Bertie Leigh
Companies and doctors are increasingly discovering the
PRIVATE PATIENT UNITS
Feeling the force of tough competition
Our analysis of England’s NHS trust private patient earnings by region continues with a look at progress in the northern Home Counties. Philip Housden reports
THIS MONTH , we continue our second annual round of reviewing the NHS PPU sector across all regions of England with a focus on the eight NHS trusts delivering acute care services to the northern home counties of Oxfordshire, Berkshire, Buckinghamshire, Bedfordshire and Hertfordshire.
Figures from the published 201718 annual accounts for this group of trusts, published in autumn 2018, shows that total private patient revenues fell by £1.45m (6.9%) to £19.7m (Figure 1).
This represents 0.66% – down from 0.77% – of these trusts’ total revenues. The combined national average outside of London is 0.5%.
The top trust in this group by both overall earnings and per centage of turnover remains Oxford University Hospitals. Oxford has developed local success through utilising specialty capacity across their four main hospital sites.
The trust’s private patient revenues fell by £794,000 and 9.2% in 2017-18 to £7.8m. Despite this fall, Oxford hospitals are still ranked 13th highest private patient earners within the NHS and third outside London.
In 2017, it announced a partnership with the Mayo Clinic to open an outpatient and ambulatory London base, although the date of this summer’s opening is not yet clear.
Royal Berkshire’s private patient revenues also fell back in 2017-18 by £517,000 (23%), mainly due to
accounting treatment rather than underlying activity.
The trust operates in a crowded local independent hospital market and concentrates on complex surgery and niche services that the local competitors cannot provide, but remains as yet without designated private patient beds.
It has reconsidered updating previous plans to open PPU inpatient capacity, but these have not yet been approved.
Branded clinic
Bedford Hospital has produced private patient revenues growth in real terms annually since 2011-12, growing last year by £41,000 (2.8%) to £1.48m.
The trust reports further growth in 2018-19 with a forecast close to
£1.8m. All this is achieved through the capture of diagnostic and lowvolume specialty activity through their branded outpatient offer, the Bridges Clinic.
This offers a range of medical specialties, including endoscopy, cosmetic procedures, diagnostic imaging and physiotherapy.
Luton and Dunstable is in merger talks with Bedford and does have an inpatient PPU, the Cobham Clinic, with 13 beds. The trust fell back by 3.9% last year to £2.07m, and is just under 0.8% of turnover.
Buckinghamshire Healthcare delivers a limited range of private patient services from both the High Wycombe and Stoke Mandeville sites.
Expansion plans
East and North Hertfordshire Hospitals offer a range of private outpatients, day case and a small range of inpatient services across the Lister Hospital in Stevenage, Mount Vernon in Northwood and the new QEII Hospital, Welwyn. The earnings of the trust remained flat at just under £3.5m in 2017-18, just under 1.0% of total revenues. The trust also has a co-
At Wycombe Hospital, the trust has worked with the on-campus BMI Shelburne Hospital. It remains to be seen whether this arrangement will change given the ongoing review of BMI’s estate. In 2017-18, the trust’s private patient revenues were £2.35m, up 0.9% on the previous year and representing 0.61% of total revenues.
Figure 1
located BMI hospital, Bishop’s Wood, on the Mount Vernon site. It is investing in private patient expansion and has recently advertised for a business manager to drive growth.
The West Hertfordshire Trust Hospitals in Watford, St Alban’s and Hemel Hempstead sit in an attractive market for private patients, but, as a result, they face competition from Spire Hospitals at Bushey, near Watford, and Harpenden and a range of other providers.
The financial impact has been an ongoing decline, with a drop of £105,000 to only £303,000 revenues in 2017-18 representing a new low of 0.1% of turnover.
In early 2019, the trust launched a physiotherapy service for private patients at the West Hertfordshire Therapy Unit in Abbots Langley, which will provide specialist treatment including women’s health,
muscular treatments and care for sports injuries.
Milton Keynes similarly has not yet invested into the PPU market. Earnings are stuck at £0.5m turnover, dropping by 4.5% and £23,000 last year to a new low of 0.25% of total trust revenues.
However, the potential to break into the attractive growing market has re-opened due to the cancelling of Spire’s ambitions to open a private hospital in the city.
Attractive market
The northern home counties remain an attractive market for private patients, but as they are also a key market for the independent hospital provider groups, competition is strong.
Present trust earnings have recently slipped back and this is both a function of that competition – local and from London – but
also a function of the lack of investment in capacity and capability by NHS trusts in recent years. Opportunities remain to develop new private patient services in this area, as the underlying demand factors are expected to remain strong. In particular, the ageing population, increasing patient safety
agenda and the limits on range of services delivered by private hospitals are all driving complex insured activity into NHS trust sites throughout the country.
Next month: East Anglia Philip Housden is a director of Housden Group
Figure 3
Figure 2
The stress from a claim
A surgeon suffers huge emotional distress when a claim is received more than two years after an operation. Dr Ellie Mein gives some sound advice on how to respond
Dilemma 1 How can I cope with this claim?
QUpright Positional MRI
• Completely open scanner that is well tolerated by claustrophobic patients
• Weight-bearing scans for spine and joints enable a more precise diagnosis
• Patients who are large or cannot lie down can be accommodated
I am a consultant orthopaedic surgeon who has a patient with a history of dislocations of his left shoulder.
Following a diagnostic arthroscopy and a CT arthrogram of the joint, I discussed the options available to the patient. These included not having surgery and risk further dislocations or to undergo a Latarjet procedure, advising the patient that this would require an overnight stay.
The patient chose to have surgery but, against my advice, discharged himself later the same day.
Some days later, the patient required surgical exploration of his wound to evacuate a haematoma that had developed after the initial procedure. Twelve weeks after the surgery, he was diagnosed as having sustained a rupture of the left long head of biceps tendon.
The patient has now brought a claim against me, more than two years after the surgery. They have alleged that during the operation, I failed to inspect the operative field sufficiently and
that an arterial blood vessel was actively bleeding.
This claim has caused a great deal of emotional distress and I’m very concerned on how this will impact upon my professional reputation.
What should I do?
AUnfortunately, the expectations of patients are ever increasing and so it is important to know how best to respond to a claim made against you.
First, it is important not to respond directly to any allegations against you or to contact the patient directly to refute what has been written. Doing so can make the claim more difficult to manage.
Your defence body can guide you throughout the process and it is vital that you involve them as soon as possible. This is because the civil litigation process runs to a strict schedule: there are 40 days to respond to a letter requesting clinical records and four months to respond in full to a letter of claim.
At the MDU, we ask members to send us all the correspondence from the patient’s solicitor, a signed note formally instructing them, contact details, the patient’s records and a factual report of your involvement with the patient and details of any other clinicians involved.
If a case proceeds to the next
stage where you receive a letter of claim – and many cases don’t – we might also decide to seek advice from an independent medical expert.
Next, remember not to make any comment about the case on either social media or to a journalist. To do this runs the risk of breaching patient confidentiality and will attract more negative attention to the case.
If you are approached, explain that you are unable to provide a comment due to patient confidentiality; this applies even if the claimant has publically discussed the case.
Depending on the outcome, you may want to make a brief statement at the end of a case, but your defence body can advise you on this when the time comes.
It is wise to leave the day-to-day management of the claim to your defence body, although you should respond as soon as possible to any requests for information from your claims handler or solicitor.
As the civil litigation process can move quite slowly, it can be months or even years before action is taken. Even after formal proceedings have begun, it is not unusual for claims to be discontinued, particularly after expert reports have been obtained and exchanged.
It is very unlikely that a claim will proceed to a trial, but for the few cases that do, your medical defence body can provide you with legal representation and help you to prepare.
Lastly, it is only normal to feel angry or upset, but a claim is not an indictment of you or your practice.
Consider how many patients you have successfully treated in your professional career. This is not cancelled out because you have received a claim.
Dr Ellie Mein (below) is a medicolegal adviser with the MDU
Involving the coroner
A
patient’s death sparks a quandary for her doctor. Dr Ellie Mein responds
Dilemma 2
I can’t sign this death certificate
QA patient of mine, a woman in her 50s, has died. She had only been my patient for the last six months and I saw her on a single occasion three months before her death.
I was aware from her notes of a problem with alcohol abuse and her relatives now tell me that she was neglecting herself. In short, I do not know whether I can sign the death certificate.
Should I ask the coroner’s permission?
AThe coroner is unable to give you authority to sign a death certificate. The doctor attending the deceased patient in their last illness is required by statute to complete a death certificate, giving the cause of death to the best of their knowledge and belief.
If you feel you are without the knowledge and belief to complete the certificate, then it can be completed to show that the death has been reported to the coroner.
You may wish to prevent a delay by reporting a death informally to the coroner and seek reassurance to issue a death certificate.
But after receiving this reassurance, the doctor should not initial the certificate to indicate the coroner has been informed. If it is initialled, the death cannot be registered without the coroner’s authority, which produces the very delay the doctor sought to avoid.
You are not legally obliged to report a death to the coroner, but you should if there is any doubt or suspicion about the cause of death.
You should also be aware of the circumstances in which a case has to be referred to the coroner, which includes deaths which may be due to an accident, suicide, violence or neglect, deaths in, or shortly after, release from prison
or police custody, deaths during, or shortly after, an operation or anaesthetic or cases where the cause of death is unknown or uncertain.
Additionally, some coroners require notification of all deaths which occurred within 24 hours of admission to hospital.
In Scotland, all sudden, suspicious, accidental, unexpected and unexplained deaths are investigated by the procurator fiscal, rather than a coroner’s office.
Section 1 of the Fatal Accidents and Sudden Deaths Inquiry (Scotland) Act 1976 states that the procurator fiscal may hold a public
inquiry before a sheriff into any death which is sudden, suspicious or unexplained or gives rise to serious public concern.
Doctors can be ordered to give evidence and answer any questions put to them at the inquiry, although no witness is obliged to answer questions which could result in an incriminating answer.
Subsequently, the sheriff issues a final report which includes details of the time, place and cause of death, any reasonable precautions which could have prevented the death and defects in any system that contributed to the death and any other relevant facts.
CONSULTING ROOMS AVAILABLE
l Modern clinic over 3 floors open Monday – Friday
l CQC-registered
l Multi-specialty outpatient services
l State-of-the-art ophthalmic equipment and lasers
l Diagnostic Endocrine & Cardiac procedures
l Mini theatre for Dermatology & Ophthalmology
l Pharmacy
A PRIVATE PRACTICE – Our series for doctors considering the independent journey
Don’t pay too much
Some things you buy for your business will not be deducted in full against income in the year of purchase. This is generally known as capital expenditure.
Many consultants and private GPs have medical equipment, office equipment and possibly premises, and these types of expenditures are given special treatment for both accounting and tax.
Ian Tongue (right) takes a simple look at the concepts and steps to ensure you are obtaining the maximum tax relief on these costs
CAPITAL Vs REVENUE EXPENDITURE
Costs that are one-off in connection with trading activity are generally deducted against the income they relate to.
Typical examples of this are room rental, secretarial fees and defence cover, although the latter may be spread over a different period to your accounting or financial year end.
Capital expenditure, on the other hand, will typically generate economic benefits over a number of years and so your accountants will include these as capital expenditure and charge the profit and loss account with a proportion of the expenditure each year.
This is known as a depreciation policy and the rates of depreciation will vary depending on the classification of the asset in question.
So if, for example, you bought a new computer for £1,000 and your depreciation policy was over four years – 25% per year – a £250 expense would be shown in the financial accounts each year until the asset is written down to nil.
Other depreciation policies may apply a percentage against the value brought forward rather than writing off over a fixed period.
It is important to note that depreciation in the context of
accounting is not expected to represent loss in market value and is a tool to spread the cost of an asset over its expected useful life.
CAPITAL ALLOWANCES
Capital allowances can be viewed as the tax form of depreciation. Therefore, the calculated capital allowances for a period are deducted from profits after the accounting depreciation has been added back to profits.
This system exists to help control the amount of available tax relief on capital expenditure, as an accounting depreciation policy would, no doubt, be manipulated if it was a tax-deductible expense.
The above may imply that capital allowances are not as much as the depreciation charge, but for a smaller or medium-sized business which is investing less than a large business, special allowances are available that provide you with all of the tax relief up front.
This special allowance is known as the annual investment allowance or AIA and has varied over the last seven years or so from £25,000 to the current £1m mark per year for qualifying expenditure.
So this means that the vast majority of equipment and fixtures purchased by a consultant or GP in private practice will be given
For a smaller or medium-sized business which is investing less than a large business, special allowances are available that provide you with all of the tax relief up front
PREMISES
Many consultants have purchased premises or have taken long-term leases followed by incurring substantial capital expenditure in relation to the conversion to medical premises.
This type of expenditure will be a mixture of classifications for capital allowance purposes, and correctly analysing them for claiming capital allowances will ensure that you gain the maximum tax relief on the costs incurred.
100% tax relief in the year of purchase.
Going back to the earlier example of a computer purchase, it results in £1,000 being deducted against profits in the year of purchase.
For any assets that are not covered by the annual investment allowance, the standard headline capital allowance rates for most assets is 18% per year but can be as low as 6% per year. This is calculated on a reducing balance basis rather than the percentage against the original purchase cost.
Other special rates or enhanced capital allowances exist for special expenditure and these could well be relevant in the construction or refurbishment of a building with energy-saving or environment plant and machinery.
The use of specialist surveyors who analyse the costs and prepare a report maximising the capital allowance claim is usually very beneficial. Your accountant is likely to work with one or more of these companies, so if you are in this position, ask them for recommendation.
Capital allowances can be a complex area, but the basics are quite straightforward.
Before planning any capital purchases, ensure you discuss matters with your accountant and they can advise on your specific circumstances.
Next month: The pros and cons of tax-efficient investments
Ian Tongue is a partner with Sandison Easson accountants
tax on your gear
THE BRAKE ON CARS IS EASING
Cars are often a topic of conversation I have with doctors who are considering buying a vehicle through their private practice or perhaps through salary sacrifice under the NHS fleet scheme.
Historically, few practical cars satisfied the criteria for special tax treatment. But, over the last few years, a number of mainstream models have appeared that are attractive to own and many can be used as an everyday vehicle.
There is a special rate for cars emitting less than 50g/km, which, like the annual investment allowance mentioned in the main story, allows the business to deduct the cost in full in the year of purchase.
But here are a few words of warning:
1
SELF-EMPLOYED BUSINESSES – the amount of capital allowances is restricted to the business use percentage and, upon subsequent resale, you will pay back some of the tax relief enjoyed in year one.
2 LIMITED COMPANY BUSINESSES – the user of the vehicle will have a ‘benefit in kind’ and tax is payable based on list price and emissions using a percentage method per year. The ‘benefit in kind’ percentage is due to fall from 16% in 2019-20 to just 2% in 2020-21 for certain fully electric vehicles.
Whether this actually happens and, if so, for how long, remains to be seen. But, on paper, this makes fully electric vehicles or ultra-lowemission petrol hybrids with good range very attractive indeed. Additionally, as with the selfemployed, some tax may be repaid on subsequent resale.
3
NHS SALARY SACRIFICE – the ‘benefit in kind’ rates mentioned above apply to having a car through the NHS fleet scheme, so ultra-low-emission cars fare best.
Often, the effective monthly cost can be attractive and it can help those with annual allowance charge issues.
DOCTOR ON THE ROAD: PEUGEOT 508
Raising the bar with
The sleek and low body looks purposeful with great design features are both ends. It is a car to give you a warm glow every time you glance at it
In a world where plain-looking SUVs seem to dominate the family car market, Dr Tony Rimmer finds it refreshingly enjoyable to drive a new entry into the medium saloon/ hatchback market
THERE HAVE been many changes in medical practice over the years and new procedures, activities and services we doctors offer may be partially influenced by vogues and fashions in the sphere of scientific advancement.
However, once they are established as normal practice, they lose the appeal of individuality.
In the world of cars, consider the ubiquitousness of the SUV as the now normal choice for family transport.
Not so long ago, we all drove around in saloon cars, hatchbacks or estates. Currently, these body styles make up a really small proportion of new car sales. Peugeot means to challenge this with its all-new 508 model.
This French manufacturer has a long history of producing some excellent family cars. The 404 model of the 1960s was a favourite both in France and in many African territories, where it earned a reputation for ruggedness and reliability.
The subsequent 504 model of the 1970s prolonged this theme and, indeed, as I witnessed on a
recent trip to Senegal, continues to provide study transport for many in difficult conditions.
The 504 was also a success in the UK – my own father owned two –and competed very successfully with homegrown British Leyland products which lacked the modern sophistication of design and solid build quality.
Market declined
It was only in the 1980s and 1990s with the advent of modern hatchbacks like the VW Golf that the
market for family saloons declined.
Move into the 2000s and beyond and we now live in a world where all family cars seem to be plainlooking SUVs. It is refreshing to see a new entry into the medium saloon/hatchback market.
A lower and sleeker body shape allows the stylists and designers free rein and, in the case of the new Peugeot 508, to create a good-looking car.
So can Peugeot tempt us out of our SUVs? Will a more conven -
this stylish saloon
A lower and sleeker body shape allows the stylists and designers free rein and, in the case of the new Peugeot 508, to create a good-looking car
tional but more attractive car do all the things that we expect of family transport? To find out, I have been driving the 508 and my test car was a GT-line model with a four-cylinder 1.6 litre turbo-petrol engine producing 180bhp.
There are three main trim levels; Allure, GT-line and GT but all models have an extensive equipment list as standard. There is a baseline Active model, but it is only available with the 130bhp 1.5 litre diesel engine, which may have great economy but feels a little underpowered in a car of this size.
A 2.0 litre diesel is available with either 160 or 174bhp, but these are ➱ p50
Innovative property developers
The Healthcare Property Company (HPC) has developed, financed and project managed healthcare buildings for almost 25 years, from primary care to specialist clinics and laboratories.
You view the main instrument panel above the steering wheel rather than through it
The infotainment screen has useful piano key-like shortcut buttons
only suitable if you do big mileages. Top of the range is a 225bhp version of the 1.6 litre turbo-petrol unit, but this is a bit pricey and not as fast and sporty as it seems to promise.
Warm glow
If first impressions and showroom appeal are reflected in sales, then Peugeot has a winner on its hands with the new 508.
The sleek and low body looks purposeful with great design features at both ends. It is a car to give you a warm glow every time you glance at it parked on your drive. That is not something you could say about any SUV that I can think of, including Peugeot’s own smart 3008 and 5008 models.
Step inside and the stylish design continues. The i-Cockpit design, which is now a Peugeot trademark, means that you view the main instrument panel above the steering wheel rather than through it.
This is a real ‘Marmite’ feature; some drivers will love it, but some just won’t get on with it. I like it myself, but think that it works more effectively in their more upright SUV models than in the 508.
A large and clear central infotainment screen is easy to use and sports some useful piano key-like shortcut buttons that work really well.
Front seat room and comfort is luxurious and there is plenty of room in the back for growing children.
But if you carry passengers of six feet tall or more, they will complain of limited rear headroom and you won’t get three of them across the whole bench. The hatchback boot is easy to access but of average size.
Great
appeal
Out on the road, the 508 has great appeal. You sit closer to the road than in any SUV and the wellsorted suspension allows for fun behind the wheel.
The steering wheel itself is quite small and this accentuates the sporty character. The ride is comfortable but can be caught out by sudden jolts if you hit a pothole.
It is fantastic for smooth motorway cruising, though. The 180bhp petrol engine is quiet and has plenty of power. The eight-speed automatic gearbox makes the most of it in all situations.
I really liked the 508. As an alternative to the usual SUV offerings, it is like a breath of fresh air. For those of you who like to be a bit different, appreciate a good-looking car but like practicality, too, it really is worth taking a test drive.
Dr Tony Rimmer (right) is a former NHS GP practising in Guildford, Surrey
I really liked the 508. As an alternative to the usual SUV offerings, it is like a breath of fresh air
PEUGEOT 508 1.6L pure-tech
180 gt-Line
Body: Five-door hatchback. Front-wheel drive
Engine: 1.6 litre four-cylinder turbo-petrol
Power: 180bhp
Torgue: 50Nm
Top speed: 143mph
Acceleration: 0-62mph in 7.9 seconds
Claimed economy: Combined: 40.2mpg
CO2 emissions: 125g/km
On the road price: £31,645
If first impressions are reflected in sales, Peugeot has a winner on its hands
All you need to know about accountancy for private practitioners
PROFITS FOCUS: DERMATOLOGISTS
Playing out of their skin
Ray Stanbridge reported in 2017 how dermatology – and oncology, opposite – are growth areas in the private medical sector. How right he was
OUR FIGURES suggest that on average dermatology private practice gross incomes have risen by 7.5% from £134,000 to £144,000 between 2016 and 2017.
Costs have risen by about 10.4% over the year. As a result, pre-tax profits have risen by 5.5% from £86,000 to £91,000.
This is a very credible performance at a time when some insurers have been quite determined in their treatment of dermatologists with their desire to reduce their fees.
The key to growth in income appears to be in self-pay, as reported elsewhere. Rising growth in costs of private medical insurance premiums, the impact of rising insurance premium tax and the relative attraction of ISAs as a nest-egg to use for an operation has caused the fundamental shift in payment patterns.
Costs have shown some noticeable changes in the year. Staff costs have shown a fall. An increasing
number of consultant dermatologists are now applying for management services or off-site typing, and this is having an effect on direct costs.
On the other hand, consulting room charges, which may include increasing costs to consultants, are often provided with fully managed services.
Shopping around
Surprisingly, indemnity/insurance premium costs seem to have shown some small fall. It may be –although this has not been obvious to us – that dermatologists have been shopping around the open market and securing marginally cheaper premiums.
Doctors’ use of their home has increased, primarily as a result of an increase in hospital fees. This, of course, follows Competition and Markets Authority rulings and the decision in the 2014 Samadian tax case allowing the use of a secondary business base.
There has been a small increase in motor and travel expenses, bad debts – although dermatologists are generally good in this respect –and accounting/legal fees. Finally, ‘other costs’ have shown a small fall. It seems that dermatologists have been attending less expensive conferences and cutting back a little on their marketing expenses.
Our initial view of 2019 is that dermatologists generally seem to be continuing a growth trend in net incomes – apart from those who have seriously fallen out with insurers.
Ray Stanbridge is a partner with accountancy, finance and tax advisory medical specialists, Stanbridge Associates
DERMATOLOGISTS’ COSTS RISE FAILED TO DENT
A grand outcome
SOME REPORTS in central London suggests that the market for oncology services is greater than for orthopaedic services.
Our headline figure suggests that private practice oncologists have increased their gross incomes by £5,000 a year, from £138,000 to £143,000 between 2016 and 2017. That is a rise of about 3.6%.
Costs have shown a small fall of about 6.2% from £44,000 to £41,000 over the year. As a result, average taxable incomes have increased by 8.5% from £94,000 to £102,000 – a very good performance.
Our view is that while oncology fees have not yet been tackled heavily by insurers – and doubtless they will – the main growth has been in self-pay, as with dermatologists. This is particularly where treatment costs are fairly short-term.
Surprisingly, staff costs have stabilised at about £16,000 average. Some oncologists paid their secretaries directly rather than through a clinic or hospital-managed model.
Even so, oncologists seem to have negotiated well with respect to room charges, and clinic costs have shown little change.
Professional defence subscriptions have been shown to be stable and, again, some oncologists have been playing the market.
Other costs have remained broadly the same with, if anything, slightly downward pressures. Changes have not been as obvious as with dermatologists, on average.
The market still seems to be looking strong for oncologists; their incomes are affected by the inflow of traffic from abroad for treatment and this is variable.
Currently, the market is growing. Short-term political influences do have an effect. We would expect to see more consolidation in the market over the next few years with principal growth of new groups and hospital-controlled teams.
Nevertheless, the future for oncology private practice, based
OUR CRITERIA FOR SELECTING CONSULTANTS FOR THE SURVEY ARE THAT THEY MUST:
Have at least five years’ experience of the private sector
Have earned at least £5,000 gross in the private sector for the year starting 5 April 2017
Have or have held an old-style NHS maximum or part-time contract
Be seriously interested in conducting private practice business
Work either as a sole trader through a limited
partnership or group or through the medium of a limited
on the early results of 2018 figures, still look to be very promising.
As regular readers know, our analysis represents a typical view of what the average consultant in private practice around the country is achieving.
The ways consultants are changing their practice is distorting income trends. No longer does the
HOW ARE YOU DOING?
Use these benchmarks to compare your financial performance with others
role of individual consultant practice predominate.
Consultants now trade through groups (formal and informal), limited liability companies and in some cases are now employed. All these factors have and will have an effect on financial results. Next time: General surgeons
company ➱ Tables and graphs, p54
Ophthalmologists
Orthopaedic surgeons
Cardiologists
General surgeons
Years ending 5 April
Source: Stanbridge Associates Ltd
HOW DERMATOLOGISTS AND ONCOLOGISTS STACK UP
INCOME AND EXPENDITURE OF A
Year ending 5 April. Figures rounded to nearest £1,000 (percentage is also rounded up)
Source: Stanbridge Associates Ltd.
Year ending 5 April. Figures rounded to nearest £1,000 (percentage is also rounded up)
Source: Stanbridge Associates Ltd.
BE SURE TO SEE OUR JULY-AUGUST ISSUE...
Make sure you don’t miss our next issue, published on 25 July. You may not receive every issue if you have not yet subscribed to the journal. Don’t risk missing out on vital topics we tackle next time:
Create a great user experience in your private practice! The first in our new series tackles branding – is yours really working for you?
Your Top Ten guide to billing
Independent practitioners and their investments. Why a ‘set-and-forget’ approach is never just that. Cavendish Medical’s Dr Benjamin Holdsworth on the behind-the-scenes work your adviser should be doing
A doctor asks for advice after a former patient he admits he is attracted to invites him out for a coffee. Dr Kathryn Leask, MDU medico-legal adviser, explores the ethics of a potential relationship in our Business Dilemmas series. Plus, a private consultant who aims to retire later this year is advised what to do with his patients’ records
Keep it Legal – The attitude towards litigants in person: an end to latitude? Niloo Bozorgi explores the additional challenges of defending a claim when the patient is not legally represented and hopes that the courts may be becoming a little less lenient towards such litigants
Content marketing: what it is and why you need it. Don’t miss Jane Braithwaite’s latest wisdom in our Private Practice Growth Guide
INDEPENDENT PRACTITIONER
TODAY
Circulations
Published by The Independent Practitioner Ltd. Independent Practitioner Today is editorially independent and thanks Bupa for its assistance with distribution.
Printed by Pepper Communications Ltd Material is governed by copyright. No part of this publication may be reproduced, stored in a retrieval system or transmitted in any form without permission, unless for the purposes of reference and comment. Editorial layout is the copyright of the publishers. If you wish to use it for promotional purposes on websites or for reprints, we would be happy to discuss licensing the copyright to you.
Registered office: 7 Lindum Terrace, Lincoln LN2 5RP
Write to Independent Practitioner Today PO Box 198, Cranleigh GU6 9BB
TELL US YOUR NEWS
Robin Stride, editorial director
Email:
robin@ip-today.co.uk
Phone: 07909 997340
@robinstride
ADVERTISE WITH US
The second in our series of A-Z business terms you need to know turns to ‘B’ – for book-keeping, buying a business and buying into a business and breaking up
Profits Focus: Ray Stanbridge turns the financial spotlight on general surgeons’ incomes, expenses and profits
Start a private practice – the pros and cons of tax-efficient investments
Healthcode’s ‘technology in practice’ series looks at turning information into your biggest asset
Risky business: Dr Gabrielle Pendlebury of Medical Protection advises on how best to manage things when a patient does not want to know the risks
Private patient units – what’s going on in East Anglia
Beaming at the Beamer? Doctor On The Road’s Dr Tony Rimmer drives the BMW 8 series coupé
Ten Years Ago – a decade back, there were fears revalidation plans would jeopardise the future of private doctors’ practices, while doctors’ companies were warned they risked costly claims, as they only had cover for clinical liabilities
Plus all the latest news and views
ADVERTISERS: The deadline for booking adverts in our July-August issue is 28 June
Margaret Floate, advertising manager Email: margifloate@btinternet.com Phone: 01483 824094
GET A SUBSCRIPTION DISCOUNT!
£90 independent practitioners.
£90 GPs and practice managers (private & NHS). £210 organisations. Save £15 paying by direct debit: individuals £75 (organisations £180).
TO SUBSCRIBE – USE SUBSCRIPTION FORM ON PAGE 25 or EMAIL: karen@marketingcentre.co.uk or phone 01752 312140 or go to the ‘Subscribe’ page of our website www. independent-practitioner-today.co.uk
Guarantee delivery of your next copy of Independent Practitioner Today. Take out a subscription and you will get full access to our news, features and previous issues on our website. See details on the left.