16-pages of contacts to help boost your private practice
No secrets online
What can doctor employers do to maintain confidentiality in the social media age? P20
pRimaTe paTienT
‘i’d go ape if i felt normal – now get yer hands off me!’ Whatever star patient Bornean orangutan Vicky, aged 31, was really thinking during her latest ‘primate practice’ encounter, she was overjoyed with the results of the op courtesy of consultants from nuffield Health, The Grosvenor Hospital, Chester.
Turn to page 26 to see her winning smile after meeting up with enT surgeon mr Jawed Tahery, anaesthetist Dr paul Jamieson and their specialist team
Reform fuels pay gap
By Robin Stride
A widening income gap is emerging between the highest and lowestearning independent practitioner consultants in the wake of the Competition and Markets Authority’s (CMA’s) rulings affecting how they conduct their business. There has been a surge in the number of top-income consultants, but the outlook for many others is proving bleaker and – ironically – more specialists are now quitting the competitive market arena to take on extra NHS work or private hospital salaried posts.
Consultants at a conference heard there was now a ‘big growth’
in £500k+ incomes, while more specialists earning only £15,000£20,000 a year were starting to pack up their private practices.
They were now having to typically pay £50-£55 an hour as a result of the CMA’s order restricting or banning incentive schemes and doctors’ benefits from private hospitals.
In a ‘state of the nation’ report, accountant Ray Stanbridge said hospitals were charging £15-£25 an hour for room hire and consultants were paying from £15 an hour for secretaries. They were charged £30 an hour for the best secretaries and the average was £22.
He observed: ‘People are saying enough is enough and they cannot be bothered.’
Mr Stanbridge warned the BMA private practice conference that some of the results of the CMA’s measures might not be what it expected and could be anticompetitive rather than pro-competitive.
With consultants’ joint venture equity participation alongside private hospital operators restricted to 5% ownership by individual referring doctors, some were maintaining their investments but had stopped referring.
He also warned that, in some cases, hospitals were trying to
‘shaft doctors’ to sell their shares cheaply. Some consultants were winding down their clinics.
Mr Stanbridge told the conference at BMA House in London that costs for individual consultants would rise.
And he predicted that although many specialists might see little practical effect, the outcomes of the CMA’s measures would include:
Reduced profitability in private practices;
More hospital control;
Less consultant innovation;
Fewer consultants entering private practice.
☞ Turn to page 7
Preparing to call it a day our resident accountant advises on using the recent pension freedoms to save P10
Find your marketing niche our marketing guru dev Lall reveals how to pitch yourself when starting out P16
want to rocket your profits? these tips from an accountant will help you boost your private practice P30
How we cut out the middle man a doctor duo has set up a private practice directory website akin to airbnb P40 a drive on drugs a medico-legal expert answers doctors’ questions on new drug-drive laws P42
avoid the pain when buying in spain advice on tackling the processes of buying your dream holiday property in Spain P46
Ensure your numbers tally
We publish for the first time in this issue an example of the new ‘information dashboard’ that private doctors will be getting familiar with in the future following the Competition and Markets Authority inquiry.
Take a look at p25 to get an idea of how your work might be displayed in future, showing activity, demographics and length of stay profiles benchmarked against sector averages.
It includes a breakdown of activity across hospitals, time and funding types: a level of detail from the recently established Private Healthcare Information Network (PHIN) that
approaches the hugely detailed match activity analysis published for each Premier League footballer after every game.
The first consultant to see one about himself appears to have welcomed it. But how about you? Do let us know.
PHIN says it will continue working with consultants it has an established dialogue with to refine the data’s content and format and see what support you need before rolling it out.
We’d recommend if you are among the others, then make known to PHIN any comments or concerns you may have while you still can.
Tell us your news Editorial director Robin Stride at robin@ip-today.co.uk
Phone: 07909 997340 @robinstride
To adverTise Contact advertising manager Margaret Floate at margifloate@btinternet.com Phone: 01483 824094
To subscribe lisa@marketingcentre.co.uk Phone 01752 312140
Publisher: Gillian Nineham at gill@ip-today.co.uk Phone: 07767 353897
Head of design: Jonathan Anstee chief sub-editor: Vincent Dawe 12,450 circulation figures verified by the Audit Bureau of Circulations
Rich face cuts to allowances for pensions
by leslie berry
Senior doctors could see their pension contributions limited in the wake of last month’s general election result.
The Conservatives’ manifesto declared that those earning over £150,000 will be limited as to how much they can contribute to their retirement pots.
For every £1 of earnings over £150,000, the annual allowance would reduce by 50p so that those earning £210,000 and above would have an allowance of just £10,000 rather than the current £40,000.
Doctors’ advisers are awaiting further details expected to be announced at the ‘emergency’ Budget on 8 July.
But Simon Bruce, managing director of specialist financial planners Cavendish Medical, warned: ‘Consultants should be mindful of any NHS pay rises received through increments,
new management positions, clinical excellence awards or by any other means.
‘Excess pension saving could result in an annual allowance tax charge of up to 50% without careful planning.’
The preelection proposal to cut the Lifetime Allowance – the total amount which can be saved into your pension free of tax – to £1m from April 2016 will now go ahead.
Details of a new corresponding pension protection scheme have not yet been announced by HM Revenue and Customs.
The new Government pledged to introduce a new Family Home Allowance to increase the inheritance tax threshold to £1m for couples where a family home is included.
One welcome outcome of the election for many doctors living in London and the Southeast is that the proposed mansion tax is no longer on the cards.
Turn to page 6
Private doctors to get more
help to prepare for CQC inspections
Independent practitioners are to get more help to enable them to deal with Care Quality Commission (CQC) requirements
Following a successful teachin on the new fundamental standards, run by the Independent Doctors Federation (IDF) last month, it plans to organise similar events.
IDF independent CQC adviser Martha Walker said: ‘Feedback from the meeting was very positive with delegates saying they found the evening very practical and helpful.
‘They enjoyed the opportunity to discuss the various issues arising with colleagues.’
Her presentation looked at the new format for inspection, the director’s role, duty of candour, how to assess evidence and the doctor’s role in the whole process.
A workshop generated a lively Q&A session as doctors worked through practical examples of the sort of questions they will face on an actual inspection.
martha walker, adviser on cQc issues
Growth of multiple sites
by a staff reporter
Most independent practitioners practise from multiple locations, with 55% seeing patients at more than one treatment site.
Thirteen per cent divide their time between more than four different locations, according to a study of more than 7,000 users of Healthcode, the online practice management and billing systems specialist.
And just over one per cent practised at more than eight sites.
The company said analysis of its ePractice users highlighted the
challenge for today’s practitioners, who need to manage their business and treat their patients across several sites.
Of the 85 different specialties and subspecialties included, the vast majority of psychiatrists practised from just one site. The most likely to be multi site practices were pain management specialists (80%), oral surgeons (71%) and plastic surgeons (70%).
Half of pain management practitioners treated patients from more than five locations. This reflected the varied nature of the work in hospitals and outpatient clinics,
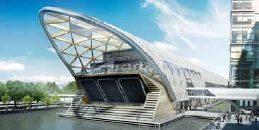
‘suPerclinic’ For suPer sTaTion
a £2.9m bupa ‘superclinic’ is to open this august on the ground floor of the new canary wharf crossrail Place development in london. it aims to be a ‘one-stop shop’, designed to help people struggling to keep up with their healthcare management due to busy lifestyles. services will include health assessments, gP appointments, dental, physiotherapy and sports physician, travel vaccinations, and evening and weekend appointments. The 8,000 square-foot Health and dental centre will house eight dental surgeries and 17 consultation rooms to offer professionals a single base for their healthcare needs.
the range of conditions where pain management now plays an important part and the importance of local access for patients with debilitating illnesses.
Other specialties where around 10% of practices had five or more treatment sites were ENT, paediatrics, immunology and anaesthetics.
Healthcode managing director Peter Connor said: ‘We know many independent practitioners clock up many miles during the course of a working week, so they can be available for their patients.
‘However, multi site practice can present a challenge when it comes to managing the daytoday business tasks such as invoicing, keeping track of patient appointments and cash flow.
‘Software packages which can only be accessed from one or two office computers are clearly a less flexible option in this situation than a secure online practice management system which enables practitioners to stay in control from any computer with an internet connection.’
PMI sellers to promote consumer confidence
The new chairman of the Association of Medical Insurers and Intermediaries (AMII) says a key aim of the trade body will be to promote consumer confidence in the health and wellbeing sector.
Stuart Scullion claimed recent constitutional changes which enabled corporate membership would help the trade group present a stronger voice on industry issues.
He said: ‘The health and wellbeing landscape is changing. We are determined to uphold a code of ethics and conduct, showing
our ability to selfregulate in the interests of the consumer.
‘We aim to promote consumer confidence in the health and wellbeing sector by raising professional standards and through the demonstration of the value of independent advice.’
Mr Scullion said technology would play an ever increasing role in the way the industry developed and evolved among the ‘iPad generation’.
He hoped to see the NHS and private sector working much more closely together.
Bowel scopes top treatment league
Gastrointestinal endoscopies and biopsies were the most common procedures carried out on insured patients in UK private hospitals last year.
Private hospitals billed for more than 827,000 procedures on admitted patients in 2014, including more than 70,800 diagnostic colonoscopies and gastroscopies.
According to Healthcode, investigations were increasingly carried out during the same
patient visit to minimise inconvenience and distress.
Company boss Peter Connor said: ‘We have long championed the use of accurate coding procedures because they enable hospitals and insurers to analyse demand and allocate resources appropriately.
‘But, in this instance, it allows us to demonstrate the important contribution made by the private sector to the diagnosis and treatment of cancer and other diseases in the UK.’
definition
% of total procedures
1. diagnostic colonoscopy (includes forceps biopsy of colon and ileum) 4%
2. diagnostic oesophago-gastro-duodenoscopy (includes including forceps biopsy urease test and dye spray) 3.6%
3. one or two injections +/- aspiration, into joint(s), cyst, bursa or soft tissue, with image guidance 3.6% 4. diagnostic endoscopic examination of bladder, including any biopsy 2.5%
5. arthroscopic operation on knee 2.5%
ToP Five Procedure codes invoiced by PrivaTe HosPiTals in 2014
Peter connor
HCA sell-off ruling review
By Edie Bourne
A three-month wait is expected before the Competition and Markets Authority (CMA) announces provisional findings on whether HCA should be forced to sell some of its London hospitals.
Initially, HCA was told it must sell either The Well ington and The Platinum Medical Centre or London Bridge and Princess Grace hospitals.
However, last December, the CMA admitted its case against the hospital group had been flawed. Accordingly, the Competition Appeal Tribunal (CAT) quashed part of the CMA’s final report relating to the healthcare market in central London and remitted it back to the CMA to reconsider and reach a new decision.
CAT ruled then that the remittal could be carried out by the inquiry
Essex cancer centre takes shape
Building has begun on a new Cancer Care Centre at Springfield Hospital, Chelmsford, Essex. Ramsay Healthcare announced the £16m development through partnership with specialist radiotherapy provider, GenesisCare, earlier this year. The £16m expansion programme includes therapy and chemotherapy, a sixth operating theatre and additional inpatient, day patient and outpatient facilities. It also includes a radiotherapy cancer centre at its Ramsay sister hospital, Rivers in Sawbridgeworth, Hertfordshire. Local consultant oncologists are involved in the development, due to open later this year. A spokesman said the hospital was in confidential discussions with consultants on a number of issues. Hospital general manager David Hewitt said: ‘We are very excited to be able to combine the expertise of Ramsay, GenesisCare and local cancer specialists to provide mid-Essex with comprehensive cancer care including radiotherapy – a long-awaited service for our patients.’
Nuffield Health has bought two more health and fitness clubs – The CityPoint Club, Moorgate, and Market Sports, Shoreditch – as part of its strategy to create a national network of well-being centres.
Spokesman Dr Andrew Jones said: ‘These acquisitions comple-
ment our current offering in London, enabling us to support more local people with our unique integrated health and well-being proposition.’
Nuffield Health now operates 77 consumer gyms and 208 corporate fitness and well-being sites.
team that carried out the original investigation. HCA challenged the use of the same group that initially ordered the divestments before the issue was referred back on appeal and it also appealed on two other grounds related to costs from its appeal to the CAT.
But the appeal court dismissed the challenge on all three grounds.
An HCA International spokes-
man said: ‘We look forward to re-affirming our case against the CMA’s findings ahead of its next round of analysis.’
The CAT has also dismissed two other appeals relating to the private healthcare investigation, one by AXA PPP ( Independent Practitioner Today, April 2015) and the other by the Federation of Independent Practitioner Organisations (May 2015).
Major expansion for King Edward VII unit
More consultants are to be invited to practise at King Edward VII Hospital, Marylebone, as a result of plans to open eight new ‘centres of excellence’ over the next two years.
These include women and men’s health, primary care, orthopaedics and pain management.
Chief executive Andrew Robertson said a major refurbishment following a £30m donation from The Michael Uren Foundation would include a new outpatient building,
more operating theatres, a day surgery unit and consulting rooms.
The women’s centre – one of the first to be developed – will include fertility treatment, a breast centre and a menopause service and will house an IVF laboratory and a DEXA scan for osteoporosis.
New head appointments at the hospital in recent weeks include Sue O’Gorman – marketing and business development; Marcus Whiteley – operations; and Juliet Moss – fundraising.
Insured patients want to use apps to access care
Six-in-ten people (58%) believe their health management would be easier if they could access more healthcare services digitally.
Over a third (36%) told the Bupa survey they thought it would help to get access to more engaging tools such as apps to help them stay healthy.
But only 16% of respondents said they currently use digital healthcare services, although twothirds regularly use them to manage other areas of their lives such as banking.
Forty-two per cent spent five hours a month or more managing and maintaining their health and well-being and 19% over 15 hours.
Bupa UK managing director Richard Bowden said: ‘Understand ably, people’s needs are changing and they want different things from healthcare. That is why, over the next three years, we will be investing heavily in our products and services to ensure they meet our customers’ needs and help to tackle the UK’s biggest healthcare challenges.’
Bupa said it would be improving connectivity and developing online and digital services to help people access health information. Its Bupa Boost, launched earlier this year, is designed to support employers in improving the wellbeing of their workforce.
An artist’s impression of the Cancer Centre at Chelmsford
A towering achievement
A team from The London Orthopaedic Clinic (TLOC) has cycled from Crystal Palace to Paris in aid of Help for Heroes.
Led by Dr Deane Halfpenny, they pedaled nearly 500k with the aim of raising awareness of the important work the charity does, plus £10,000 to give its work a boost.
TLOC managing director
Kathryn Bryant said: ‘Help for Heroes has estimated that out of 220,560 individuals deployed to Afghanistan and Iraq between 2001 and 2014, up to 75,000 servicemen and women and their families may need their support in the future. We feel passionate about supporting this charity.’ www.justgiving.com/londonorthopaedic
RCGP recognition
Dr Susan Horsewood-Lee, of Chelsea, is the first female private GP to have been awarded an RCGP fellowship under the college’s nomination system launched in 2010.
GP defence sub warning
NHS GPs have been warned they will need to pay higher defence subscriptions if they start seeing private patients.
Defence body the MDDUS said members were required to ensure they were in the correct membership category and paying the appropriate subscription associated with their work.
The warning was addressed to members taking on private GP sessions or treating non-NHS patients other than ad hoc private patients within their predominantly NHS GP list.
The MDDUS said that higher rates might apply for those GPs
who work in the following areas:
Forensic/police physician (FME) work;
Attendance at sporting events where remuneration is received, including treatment of athletes and players;
Private travel clinic or a private walk-in centre;
Occupational health physician work;
Cosmetic surgery procedures.
The number of NHS GPs contemplating private practice continues to rise, with their specialty for the first time outnumbering consultants at this year’s BMA private practice conference.
Bupa spreads its physio net
By Robin Stride
Bupa has reported its new physiotherapy network launched this month has so far attracted 85% of those on its previous scheme to apply, with the majority being offered a fees uplift.
A spokeswoman said applications were still coming through and it was hoped to open the network up to other physiotherapists who were not on the previous scheme.
It was hoped to open the network up to other physiotherapists who were not on the previous scheme. The network offers access to over 3,500 physiotherapy facilities.
Bupa said: ‘It will deliver good value for customers because all therapists are fee-assured and won’t send patients unexpected bills.
‘Customers will also benefit because all network practices have met Bupa’s quality criteria, customer service standards and agreed to fees for two years.’
Bupa UK’s director of health and benefits management, Alex Perry, said: ‘People tell us that cost is one
of the main barriers that stops them using private healthcare. Our new network is another example of how we are securing long-term agreements with doctors, hospitals and therapists to give customers access to highquality, good value healthcare.’
He said the insurer wanted to work with other hospital groups in a similar way as with Spire, which last November agreed fixed prices for six years until April 2021.
The physiotherapy network will continue supporting Bupa’s selfreferral service, which provides customers with direct access to a physiotherapist via a phone helpline without a GP referral.
Bupa said this meant people could get quick access to advice and treatment when they needed it.
The insurer reported corporate sector growth with an increase in employers extending private healthcare to more, and in some instances, all employees. It said this was a direct result of agreements with some hospitals which ensured prices for treating Bupa customers would not rise in 2015.
Simplyhealth sells PMI arm
Simplyhealth has agreed to sell its private medical insurance business to AXA PPP, subject to regulatory authority clearance.
Doctors have been told the company believes scale will become increasingly important to be successful in the long term and it thinks its health insurance wing
will have a better long-term future as part of a group with a larger PMI business.
Its focus now will be on helping customers with their everyday health needs through funding, delivery and guidance. Simplyhealth said business would be as usual until it received approval.
Bid to boost teaching and research skill
Every doctor a scientist and a scholar is the title of a new BMA publication which calls for lifelong training and development of research and teaching skills for all doctors.
Produced by the association’s medical academic staff committee, it cautions against research and teaching being seen as the preserve of a small group of doc-
tors, when it should be viewed as central to the job of all doctors.
The group’s co-chairman Dr Peter Dangerfield said: ‘It’s vital for the continued improvement of
patient care that all doctors are encouraged and supported to develop their scientific and research skills and expertise throughout their career.
L-R: Olivia Cummins, marketing and PR lead; Dr Deane Halfpenny, musculoskeletal pain physician; Kathryn Bryant, managing director of TLOC
Election fall-out:
What needs to be done
So what is the future for independent practitioners and private healthcare following the election of the new Conservative Government? Here are a selection of views given to Independent Practitioner Today
Andrew Robertson, chief executive, King Edward VII Hospital:
‘Now that a clear majority Government has been established that has a mandate to make meaningful changes in healthcare across the UK, I am hopeful that, over the next five years, we will see more collaboration between private healthcare and the NHS, which I believe will ultimately be in the interests of patients.’
Keith Pollard, chief executive at Intuition Communication Ltd:
‘The private healthcare industry breathed a deep sigh of relief when the election went their way.
‘It could have been very different. Labour’s antiprivatisation mantra is off the agenda. The private sector will continue to support an ailing NHS, and may start to record some decent growth. A return of tax allowances on private insurance might even be on the cards.’
Fiona Booth, chief executive of the Association of Independent Healthcare Organisations (AIHO):
‘The election of a Conservative majority Government suggests continuity in terms of healthcare policy over the next Parliament.
‘We’d anticipate NHS England and the ideas set out in the NHS’s Five Year Forward View , such as new models of care and further decentralisation, being strengthened by the election outcome.
‘The independent healthcare sector understands the pressures facing the NHS. The pre election debate focused on funding, but talk
of the larger efficiencies and savings that are also needed over the next five years hardly featured at all.
‘At the same time, patients also want greater access to highquality care. The independent sector can make a vital contribution to this significant task in terms of providing additional capacity and expertise that reduces pressure on the NHS, as well as providing alternative options for patients.
‘In addition, the independent sector is also a firstrate innovator in management and clinical care – R&D that ultimately benefits all types of patients. It is important that this key role is also understood across the health sector, including Government and MPs in the new Parliament.
‘AIHO will be working hard at achieving that goal and ensuring that independent hospitals are seen as an essential complement to the NHS.’
Matt James, chief executive, Private Healthcare Information Network (PHIN):
‘From PHIN’s perspective, the key benefit of the election result is that we are operating in a relatively known environment with the hope of stability among our members and among critical stakeholder organisations such as the Competition and Markets Authority, Care Quality Commission and Health and Social Care Information Centre.
‘Private healthcare is on a clear track toward better information for patients and it would have been a shame if that had been delayed by political uncertainty or major changes.’
James Gransby, partner, MHA MacIntyre Hudson, accountants:
‘One thing that came with the election result is the sense that there should at least be some stability and clarity as to the direction of travel.
‘This would have been one of the challenges of a coalition government.
‘It will be interesting to see how the “tax lock” promises made on taxation will play out over this parliament – namely, no increases in income tax rates, no increases in VAT, nor an extension of its scope, and no increase in National Insurance nor an increase in its ceiling above the higher rate threshold.
‘The Chancellor will have to be more imaginative than in the past to achieve his taxation revenue aims and we will see what his stance is after his first Budget announcement.
‘A period of stability around pension taxation would be welcome from accountants and financial advisers alike. This has become a particularly tumultuous subject over the last decade.’
Brian O’Connor, Independent Doctors Federation’s specialists’ committee chairman:
‘The stability of a majority Conservative government may well lead to a more mature approach to the delivery of healthcare.
‘Grownup conversations need to be had to tackle the challenges ahead. The independent sector is ideally placed to complement the NHS and deliver some of the targets of health and social care.’
Let’s stem big rise in compLaints against doctors tackling the rising cost of clinical negligence claims against doctors should be a top priority for the new administration, according to defence body the medical protection society (mps). concerned that legal costs can dwarf compensation payments, it proposes a fixed-costs regime for small value claims should be introduced to redress the balance. in a recent case relating to delayed diagnosis of skin cancer, damages of £30,000 for the patient were agreed within five months, yet legal costs were claimed to the sum of £60,000. these costs were eventually settled at £42,000.
medical director dr rob Hendry said: ‘tough decisions about healthcare funding are made every day and the costs of clinical negligence should not be seen as separate or unconnected from this.
‘Quite simply, more money being set aside to cover the cost of clinical negligence claims, particularly in the nHs, means that front-line services will have less funding available to them. Ultimately, the patient will suffer as a result.
‘We need to have a debate about whether the cost of clinical negligence claims is affordable for society. our analysis of claims shows that gps are more likely to be sued now than ever before and it is not unusual for claimants’ lawyers’ costs to exceed the damages awarded to claimants in lower-value clinical negligence claims.’
the mps said it would also like the focus of the new government to be ‘on removing the culture of fear in healthcare’ and ‘creating a collaborative, open, learning environment where healthcare professionals are encouraged to want to be accountable’.
it added: ‘While safeguarding the public must be a priority, regulation is not always the best way of achieving this and could lead to healthcare professionals practising defensively, taking the focus away from the best interests of the patient.’
Costly CMA legacy
By Robin Stride
Consultants’ profit margins in private practice are falling and they can expect their costs to rise still further as a result of the Competition and Markets Authority (CMA) inquiry ‘remedies’.
Two factors identified by accountants for this are rising labour costs and higher spending on marketing and managing the practice.
In a ‘state of the nation’ address to would be and existing independent practitioners, specialist medical accountant Ray Stanbridge revealed how profit margins had fallen year on year for hundreds of consultants:
Orthopaedics had dropped from 73% in 2011 to 69.9% in 2012 and 67.8% in 2013;
Ophthalmologists had seen a fall from 65.4% to 56.5% and then 56.4% in the same years;
For gynaecologists, profit margins had slimmed from 59.8% to 57% and then 52.8%, while urologists were down from 67.2% in 2011 to 64.1% in 2013.
Mr Stanbridge, of Stanbridge Associates, said consultants’ fees as a percentage of the market were also falling. Meanwhile, the hospitals’ percentage had risen for 20 years and showed signs of continuing this trend.
But, despite these pressures, he gave some good news, saying the private practice market was growing and consultants overall were ‘doing well’.
Selfpay income was starting to
finaL impact of cma RULingS
Reduced profitability of private practices
more hospital control
Less consultant innovation
more consultants will not enter into private practice
BUt: for many, little practical effect
HoW doctoRS can SUcceed in financiaL teRmS
ensure your availability, affability and ability, in that order
Start earning young
avoid confrontation with insurers
avoid the gmc, hospital managers and the taxman
carefully choose your area of location and discipline
Keep up to date
avoid divorce or affairs
consultants’ fees as a percentage of the market are falling. meanwhile, the hospitals’ percentage has risen for 20 years and shows signs of continuing this trend
increase again and instead of going to insurers, some people were putting aside money every month in case they needed it for treatment.
He told consultants at a BMA private practice conference that oncologists and dermatologists were seeing higher incomes while cardiologists’ earnings were also starting to rise.
According to his figures, there were 15,000 ‘active consultants’ in the market and their average fee income is £110,000. Their major payer is – the NHS.
tHe cma RULingS on pRivate pRactice
any new incentive scheme linked to referrals is prohibited
any existing scheme to be terminated by 6 april 2015
Joint venture equity participation restricted to 5% ownership by referring consultants
more openness about fees and outcomes
note: these prohibitions apply to deals with ‘hospital operators’
tHiS WiLL ReSULt in:
immediate cma impact on private practice
Some measures may be anti-competitive rather than pro-competitive
costs for individual consultants will rise
Some consultants will ‘wind up’ their clinics
appoint a good financial adviser, solicitor and accountant
Those doctors in one of the 200 consultants’ groups – which he said were proving increasingly popular with patients – were earning an average of 15% more (something regularly reported in our Profits Focus series – Ed). Young consultants were earning more than what accountants had historically predicted, but older ones were often seeing a decline in income.
Money was going to newer consultants, due to the action of private medical insurers, but Mr Stanbridge told the meeting other specialists were benefiting from ‘doing deals’ with insurance firms.
otHeR Significant maRKet featUReS
more junior consultants electing not to go into private practice
growth in groups
money going from established specialists to newer consultants
Range of private practice incomes widening
increased regional variation –m25 is the place to be
more professionalism evident
more ‘performance’ data being produced
Source: Stanbridge Associates
Whether you are organising an industry-leading conference, holding a regular training day or looking to fill a job vacancy, independent practitioner today is the place to reach your target audience.
To discuss all your advertising requirements and find out what we can do to help you, contact our advertising manager margaret floate phone: 01483 824094
Helping to keep your patients safe
The role of the medical regulator inevitably needs to change to ensure we continue to protect patients while also supporting doctors working in increasingly diverse environments.
When I took up the role of chairman of the GMC at the start of this year, I knew it would undoubtedly be a challenge as well as a great honour. There is a great deal I want to achieve and I look forward to leading the organisation as it continues to strive for improvement.
In the past 40 years, I have had many roles: medical student, doctor in training, consultant, dean of a medical school, director of an NhS trust, president of a royal college, chairman of the Academy of Medical r oyal Colleges, and I
As a practising doctor, I am very much aware that most doctors only associate the GMc with our fitnessto-practise process
new concept providing real benefits to patients
• Weight-bearing scans and variable patient positioning enables a more precise diagnosis
• Truly open system is a solution for claustrophobic patients without compromise in image quality
have also served on the GMC’s Council.
I am all too aware that, over the course of this time, medicine has become a more demanding career than ever. Doctors are facing unprecedented pressures and the independent sector places its own unique stresses on doctors, who often combine NhS careers with private sector commitments.
During my time as chairman of the GMC, I plan to continue in regular clinical practice to make sure I remain in touch with the realities that doctors face every day, so I will continue seeing emergencies in A&e and teaching undergraduates and doctors in training on the wards.
Dreaded letter
As a practising doctor, I am very much aware that most doctors only associate the GMC with our fitness-to-practise process. I can sympathise with this and I understand the impact it can have on doctors.
During my career, I have twice been investigated in relation to child protection work, so I have first-hand experience of what it feels like to receive the dreaded letter and the inevitable stress that it causes.
But fitness to practise is only one part of the GMC’s responsibilities. We are primarily here to
protect patients and we achieve this through oversight of all stages of medical education and training, setting professional standards and making sure the doctors on our register are competent and fit to treat patients.
o ver the last decade, we have made huge changes across all our areas of work to help improve standards of medical practice and better protect patients.
Reaching out
A really important part of this is reaching out to the profession and we are doing this more than ever before. Creating a culture in which safe, compassionate care can flourish, and where doctors feel empowered to raise concerns whatever the stage of their career, is not something that professional regulation can achieve alone.
our regional liaison service in england and our offices in Northern Ireland, Scotland and Wales allow us to listen to and understand the needs of doctors across the UK.
o ur staff hold meetings to explain and discuss the work we do, so we are in the best position to meet doctors’ needs through a range of different initiatives across all four countries.
We also foster conversations among doctors right across the
By professor terence stephenson chairman, GMc
UK about what more we can do to help make medical practice more open, safe and compassionate.
At this year’s GMC conference, it was encouraging to listen to such spirited and thoughtful discussion, as well see the comments from doctors across the UK on social media.
This year, we are also hosting a series of events across the UK to explore some of the key challenges relating to medical professionalism, so we can hear directly from front-line clinicians about their experiences.
Key priorities
But we know there is more we can do to improve and, at the GMC conference, I outlined our four key priorities to help create a more open, safe and compassionate culture in the medical profession:
1 explore the idea of a national licensing exam, to reassure the public that all new doctors practising in the UK are of a comparable standard, and to raise the standard of The Professional and l inguistic Assessments Board (PlAB) exam to ensure all international medical graduates are safe to practise in the UK.
2 Make our guidance more relevant and useful in clinical practice and find new ways to support doctors faced with difficult ethical and professional decisions.
3 Further develop our medical register to make it more transparent and useful for patients, doctors and employers.
4 Speed up our fitness-to-practise procedures, reduce the stress of our investigations and better support doctors who have their fitness to practise called into question.
These changes cannot be achieved overnight, but I am determined that we deliver on our priorities to help all doctors provide safe and compassionate care to their patients and empower them to create a more open and transparent culture in wards and practices across the UK.
If we deliver on our reforms, my hope would be that when doctors are asked ‘What does the GMC do for you?’ they reply: ‘The GMC helps me to keep my patients safe’. n
opinion
I have first-hand experience of what it feels like to receive the dreaded letter and the inevitable stress that it causes
ACCOUNTANT’S CLINIC: pENSIONS
Preparing to call it a day
Whatever your stage of life, it has never been as important as it is now to take action about your pension.
To benefit from the changes introduced from 6 April 2015 and enjoy a comfortable retirement – especially if you plan to retire early – you need to have saved enough to make this a reality. The tax breaks available on pension contributions, and also ISA savings, act as a clear incentive to save as much as you can comfortably afford. Susan Hutter provides some useful guidance
In the March 2014 Budget, the Chancellor announced far-reaching changes to pensions which will affect nearly all consultants.
From 6 April 2015, those who have a private pension plan – a money purchase plan, not the nh S Superannuation Scheme –have carte blanche over what can be withdrawn.
Up until 5 April 2015, the rules were quite strict and inflexible. You could draw a maximum amount of 25% tax-free from the fund and the rest could either purchase an annuity or be drawn down, but with restrictions so that the drawdown would more or less resemble an annuity.
But that all changed on 6 April, as, from that date, you can draw what you like and you do not have to buy an annuity. now 25% of what you draw is tax-free and the rest is taxed at your marginal rate of tax. t his offers a huge amount of flexibility.
But it is obviously sensible only to draw what you need and avoid paying higher-rate tax unless you have to. Remember that while it is in the pension scheme, the fund grows tax-free.
As soon as it is withdrawn and invested outside of the pension scheme, all the income will be subject to tax – although there is more flexibility over the range of investments available.
Furthermore, it is important to find out from your pension provider what the cost will be of taking advantage of the new rules. It may be that your pension provider will not offer the flexibility you require and, if this is the case, you may need to look into transferring your pension to an alternative provider.
Many Independent Practitioner
Today readers will also be aware that, from 6 April this year, what is known as the ‘lifetime allowance’ was decreased from £1.25m to £1m. Prior to 6 April 2014, it had been £1.5m.
Anything above this will attract an extra tax charge. You are able to make an election to protect the lifetime allowance at original rates, depending on the value of your pension.
I strongly advise doctors to take advice in this connection as soon as possible because the elections are subject to time constraints.
For those consultants who have benefits from the nh S Pension Scheme, the legislation is more complicated, as the two do interact and are impacted by the new rules.
In these circumstances, it is advisable to go to a specialist who is used to dealing with the nh S Pension Scheme.
t he above is relatively good news for those specialists who have a substantial pension pot. But I have seen many cases where consultants who, having left the nhS Pension Scheme some years ago, do not have adequate funds put aside for retirement.
So what should they be doing now?
the simple answer is save as much as possible into a private pension scheme, as this is the best vehicle for tax mitigation.
Up to £40,000 a year can be paid into a private scheme, and if the previous three years’ allowances have not been used, you can dip into those allowances as well.
Contributions into a private pension plan attract tax relief at your marginal rate of tax.
t herefore, if you are a 45% taxpayer and pay £10,000 into a pension plan, the effective cost will be £5,500.
the fund itself grows free of tax, and, on retirement, 25% of the benefits can be drawn tax-free. And you can start drawing from the fund from age 55 onwards.
Spouses
For those doctors who have breached the lifetime allowance, you can look at paying into a pension plan for your spouse.
You can do this if your spouse is employed in your practice. this can either be through a sole trader business or a limited company.
As employer, you can set up a pension plan for your spouse and pay contributions into it. t he contributions will be deductible from your profit for tax purposes.
In this way, you can start building up a second ‘pension pot’ that will not fall foul of the lifetime allowance.
Unlike a salary, you will not have to pay employers’ national Insurance on the contributions into the plan. therefore, this is a tax-efficient method of saving.
Susan Hutter (right) is a partner at Shelley Stock Hutter and a specialist accountant for the healthcare industry
‘NiSa’ WaY TO SaVE
it is also a good idea to look at individual Savings accounts (iSas). Many doctors miss out here.
although the payment into an iSa is not taxdeductible, the fund itself grows tax-free.
The maximum investment is £15,240 a year per person.
But, from 6 april, the rules were improved as the Chancellor introduced a ‘withdraw and replace’ clause.
Up until 6 april, if you withdrew money from an iSa, you could not replace it without eating into your annual maximum allowance.
However, from 6 april onwards, you can. For example, if have an iSa with £10,000 in it and withdraw £5,000 in august 2015, you can replace that £5,000 prior to 5 april 2016 and in addition pay £15,240 into your iSa
So if you have exhausted your pension savings, the next port of call is definitely an iSa
apart from anything else, an iSa is a far more flexible form of saving than a pension, as the monies can be withdrawn at any time, meaning you do not have to wait until the age of 55.
as with pensions, it is important to find out from your iSa provider the costs of ‘withdrawing and replacing’. With a cash iSa, there may be zero costs, but with a stocks and shares iSa there are likely to be some costs attached to these transactions.
More choice means more opportunity, but this also comes with more responsibility. it is very important to make the right decisions for your financial future and it is therefore vital that professional advice is taken at each step.
Put yourself in their position
The patient’s decision to come to you is a complex journey. In the third of her major series for Independent Practitioner Today, Pam Underdown explains how to understand the buying process that a potential patient goes through to find you –from the research and comparisons through to what makes them ultimately go ahead with their treatment
We have so much information available that it means choosing and buying isn’t easier, but more complex than ever before
You’re noT just a new aesthetic business owner; you’re a consumer, too.
Have you ever thought about how you have changed the way you buy things today, compared to ten or 20 years ago?
Back then, you probably searched through the Yellow Pages, asked a friend, saw an advert in the local press or perhaps even sent off a stamped addressed envelope for more information.
What about today?
Consider the last time you needed a new car or a restaurant for a night out. Did you:
Search on Google to see which options you had?
Ask for a recommendation on Facebook?
Check reviews on Google+ or TripAdvisor?
‘Like’ or follow a business that you were considering?
u se your mobile phone to search for a phone number while out and about?
The chances are that you did some or all of these – which shows just how big an impact the web, social media and mobile devices have on the way we buy today.
Before the internet, consumers had limited ways to discover a new business, so the decision journey was quite straightforward. But now, nearly every step takes place online.
This shift online has made it much harder for businesses to
reach potential customers because we as consumers are all bombarded with so many messages that we often ignore them.
In addition to this, we have so much information available that it means choosing and buying isn’t easier, but more complex than ever before – with pages of listings, directories, blogs, videos, reviews, social media and websites to sort through and decide or ignore and delete.
So, what is the impact on your new aesthetic business? Today, the average consumer uses more than ten sources of information to make a purchase decision, up from just five sources in 2010 (Google, 2012).
Turning these highly educated consumers into paying patients is more complex than it used to be. In fact, it requires you to be in the right place at the right time in order to give prospective patients the information and the confidence they need to make the decision to contact you instead of a competitor.
You will need to take the time to really understand the buying journey and decision process your patients will embark upon in order to find you, research you, compare you to competitors and ultimately choose you.
Sometimes, it’s not easy to think like a patient and put yourself in their shoes, simply because the majority of aesthetic profes
marketing ‘mUsts’
make sure all your online and offline marketing:
1 Creates awareness and makes a good impression when people visit your website, and in reviews and social media profiles
2 increases the likelihood that your business will be seen when people search for your treatments or services
3 ensures you stand out from your competition
4 reminds those who aren’t ready to buy yet about your business, so you are at the forefront of their mind when they are ready to get in touch
5 Catches their attention and holds their interest so they learn more about you, then contact you
6 engages and entertains them so they share it with their friends
sionals have never been a full paying patient before.
Your prospective patients are online searching for your treatments and services and socialising on the social networks. You need to be everywhere your prospects are, so they can find you, learn more about you and ultimately choose you.
consider this:
Your prospective patients are using the web and mobile devices to instantly research a treatment, product or service anywhere, anytime.
Your prospective patients are forming powerful and quick impressions of your business after seeing pictures, videos, posts and reviews.
Some of your patients will instantly share their experiences with hundreds, even thousands, of others.
There is a huge amount of information available online that enables consumers to make more informed decisions on what to buy and who to buy from.
But at the same time, it creates a whole lot of work and additional marketing expense for business owners like you that are trying to reach them.
Think about your own experiences. I have sometimes taken days to choose a hotel for a weekend away, hours reading reviews and looking at photos, simply because I was overwhelmed with the choice and had ‘paralysis by analysis’.
First of all, you need to define your ideal patient, then identify how they buy your treatments or services and ensure all of your marketing communications are focused on the benefits and the results. It’s all about ‘what’s in it for them’ and not all about you.
Then, in order to reach prospective patients at the right time, you need to create a strong web presence that influences them at every stage along their decision making journey.
You need to provide both helpful content, that you build, and engaging advertising, that you buy, across the many places your prospective patients will be ‘hanging out’.
And, to pull it all together, you need a robust website with fresh
What they look for
the prospective patient is doing a cost-benefit analysis in their heads to decide if what you are offering them is worth the time, money and effort and if the benefits will outweigh the risk. are you offering both great results and great value? you need to help them see and feel what you offer is more than worth it. the aesthetic patient is always asking themselves: ‘is the price worth the time, money, effort or can i get the same result for less elsewhere?’
to attract and keep them, you must show them why they should choose you over your competitors.
What do you do better than anyone else? What do you offer that no one else does? it is very hard in the early days of your new business to establish those unique differentiators, so if they aren’t obvious to you now, then you do need to work out how you can differentiate yourself from your competition in a way that matters to your patients. more about that next month.
for now, in order to attract your ideal patients, you must really understand the needs of your patients and the outcome of their experience: both from a tangible and intangible perspective. for example, the tangible results you provide mean that lines are softened and complexions are more radiant.
however, it is the intangible results they provide to your patients that really matter and make the difference: improved confidence, self-esteem and an inner glow.
remember, your patients aren’t buying what you do – the science, the technique, nor the new equipment you’re using; they are buying the results, the benefits and the feelings – in other words, the outcome.
gmC seeks yoUr vieW
Doctors have until 1 september to respond to a gmC consultation on plans to make cosmetic procedures safer. to take part, either answer the questions online on its website, email cosmeticpracticeproject@gmc-uk.org or write to: standards and ethics team, gmC, regents Place, 350 euston road, london, nW1 3Jn the gmC is calling on cosmetic doctors to allow patients time to think before agreeing to go ahead with treatment.
i have sometimes taken days to choose a hotel for a weekend away, simply because i was overwhelmed by choice and had ‘paralysis by analysis’
content that helps you get listed on the first page of Google, creates a great first impression with visitors and compels them to contact you.
So you should engage the right web design and development professional experienced in the aesthetics field, who can set you up with a comprehensive web presence to make sure that you are in all of the places that your prospective patients are searching, surfing and socialising.
This involves claiming key sites on the web such as Google + and Yell, buying targeted advertising such as Facebook Ads and Google
Ad Words, and creating a steady stream of fresh, authentic and engaging content – using written and video blogs, articles and also devising and answering frequentlyasked questions.
ensure that all of your marketing communications do really ‘talk’ to your prospective patients in a way that appeals to their needs, emotions and desires. Then make sure that all of your online and offline marketing does the six things outlined in the box on page 13.
Multiple marketing tactics
As patients are influenced emotionally and logically all the way through their journey to buy, this means that you can’t just market to them at the beginning and expect to win their business. It is your job to use multiple online and offline marketing tactics throughout every stage of their journey to help them discover, contact and choose you.
All of your marketing efforts must address your patients’ emotional motivators for wanting enhancement, but also equip them with the logical reasons why you are the perfect choice, so they can easily relay that back to their family and friends if they are challenged.
Since consumers buy based on emotion followed by logical justification (buyers’ remorse), it is your job to remind them in subtle ways that you are more qualified, more experienced and more skilled than others.
The decisionmaking process is a vast subject. However, here are some basics to consider:
Decisions are quickly reached by emotion and then justified with logic;
People base their decisions on prejudices, habits and past experience much more than on their knowledge;
It takes a split second to make a buying decision, but getting ready to make that decision can take a long time.
Next month: How to create a simple and useable marketing and business plan that you can use as your success blueprint for your first year of business
Pam Underdown (left) is chief executive at Aesthetic Business Transformation
83 WIMPOLE STREET IS A NEW DEVELOPMENT BEHIND A RETAINED FAÇADE TO PROVIDE APPROX, 7945 SQ FT / 738 SQ M OF MODERN, OPEN PLAN ACCOMMODATION.
AMENITIES
AIR CONDITIONING
NEW DEVELOPMENT
8 PERSON PASSENGER LIFT, DDA COMPLIANT COURTYARD (LG)
Michael Watt 020 7747 3142 mwatt@matthews-goodman.co.uk
7290 0970
MARYLEBONE LONDON W1
Find your marketing
It can often be difficult for independent practitioners to know where to start in marketing their private practice.
Surgeon Mr
Dev
Lall covers some of the basics for taking that first scary step
It can feel a bit scary the first time you promote yourself and your practice.
and although the fear is entirely in your head, that makes it none the less real. You still feel uncomfortable.
It all boils down to that muchoverused phrase ‘getting out of your comfort zone’. Most of us are quite happy if we are left to get on with the job of caring for patients and simply waiting for them to turn up in our clinics – n HS or private.
What people often overlook is that the nHS is a giant machine designed to deliver patients to you as well as providing the means for you to treat them. to succeed privately, you not only have to create the machine to care for your patients, but you also have to create the machine to deliver patients to your practice.
marketing niche
t his is seldom recognised and even more rarely spoken about.
Practical campaign planning
OK, so in this series we’ve talked about some of the many ways of marketing your private practice, but how do we actually get started? the first step is to decide which condition(s) you want to treat. the temptation is always to keep it wide open – ‘any orthopaedic problem’ or ‘any general surgical problem’ – but this is a big mistake, for two reasons. Firstly, clinical governance issues. It is tricky both morally and medico-legally to justify treating a patient with a condition privately that you do not treat regularly either privately or on the nHS. this should go without saying.
Secondly, you market yourself and your practice by reaching out to potential patients with conditions you treat by appealing to them as the only sensible choice to treat that condition. You do this by crafting a message that addresses their concerns and anxieties about their symptoms/signs/ diagnosis.
It is impossible to do this effectively with a campaign that does not focus on one condition or symptom only.
So, for example, the concerns of a patient with rectal bleeding would be quite different to the concerns of a patient with a lump in the groin. Yet, as a general surgeon, you might well treat both colorectal diseases as well as perform hernia surgery.
Weigh up the factors When choosing
Which patients to target these include:
1
2
What are the financial rewards? is it financially worthwhile to target a given condition?
What conditions do you enjoy treating? Yes, most of us are in private practice to earn supplemental income – but if it’s not enjoyable, it will rapidly make your life miserable.
3 What conditions take least effort to treat? if you’ve got to call in to the hospital twice a day and liaise with intensivists while a patient recovers from surgery in the itu, then that is clearly far more onerous than a patient with a similar hospital stay but remains on a regular ward – or goes home the same day.
4 What is the lifetime value of each patient? Which clinical conditions earn you the greatest income over the duration of your care of the patient, from initial outpatient appointment to final discharge? Do the sums, don’t rely on assumptions – you might be surprised at the answer.
5
What is the incidence/prevalence of the condition? You might be the world’s top expert at treating insulinomas, you might love treating patients with the condition and it might be incredibly financially rewarding privately, but if there are only five cases a year diagnosed in the uK, then seeking these patients out isn’t necessarily going to be the greatest idea.
6 how are you going to find people with that condition? some conditions have very vague or non-specific symptoms. others such as ‘tiredness’ encompass a vast number of possible causes. how will you find the patients you’re after?
PROBLEMS WITH THE TAX MAN?
HMRC tax investigations and disputes create difficult and stressful times.
As an award winning firm of tax experts, our highly experienced partners specialise in resolving problems relating to tax investigations and disputes with HMRC.
To find out, in confidence, how we can help call 0800 734 3333.
‘Here to help. Not to judge.’
So, for that reason, you need different messages to appeal to each of them and encourage them to consult with you.
Choosing
your target condition
So how do we choose which condition to go for?
this almost sounds like a nonquestion, because, of course, we all have conditions we’re quite happy to treat and I’m sure every consultant reading this will have maybe half-a-dozen conditions in mind already.
Yet it bears thinking about in more detail, because while we want as many people as possible to benefit from our care, the underlying reason we’re in private practice in the first place is to make money.
Why else would you work in your spare time?
So you need to weigh up various factors when choosing which
You need to target a condition or symptom cluster that is ‘an inch wide but a mile deep’
patients to target in your campaign (see panel on page 17).
In the end, it boils down to this: you need to target a condition or symptom cluster that is ‘an inch wide but a mile deep’.
t hat is to say, it should be tightly focused – lump in groin, pain in hip, rectal bleeding and so on, but there must be enough people out there with those symptoms within the ‘catchment area’ of your practice to make it worthwhile looking for them – in other words, marketing to them.
Targeting patients
So you’ve decided the condition/ symptom you want to focus on; the next question is how are you going to find those patients?
t here are a myriad ways of doing this, but it is worth asking yourself a few questions which will help inform your decision (see box to the right)
Sometimes the only way to
use clinical stories as much as possible, too, to get the message across in your advertising
reach out to the patients you want is through mass advertising, but if you ponder long enough, you can often find a way of reaching the patients you want through more targeted efforts as set out in the box on the right. t his is, of course, far from an exhaustive list.
Connecting
and converting
Once you know your target condi tion and where to find them, you need to consider how to turn them into patients. and the key to achieving this is communica tion.
We’ve talked about persuasive communication in the past, but one element that we didn’t cover is mirroring.
You will probably be aware of the subject of body language, and how numerous unspoken ges tures, postures and mannerisms contribute to an unspoken mes sage of liking or disliking, for example.
An independent firm offering one to one meetings anywhere in the UK giving advice and help with:
• how to start in private practice
• how to maximise private practice income
• ways to reduce tax payments
• setting up in Chambers/Groups
• limited companies and LLP’s
• financial planning
• record keeping
• computer software
• tax and financial advice re: car purchases
• pensions: NHS, personal and employee schemes
• purchase of consulting rooms and surgeries
• inheritance tax and capital gains tax planning
• VAT
For more information please contact us by:
Wilmslow
Phone: 01625 527351
Fax: 01625 539315
Harley Street
Phone: 020 7307 8759
Fax: 01625 539315
Email: info@sandisoneasson.co.uk
Website: www.sandisoneasson.co.uk
Questions to asK YourseLf
1 is anyone out there searching for help with the condition you’re targeting? if so, ‘pay-per-click’ online advertising might be a viable option.
2 is it possible to demographically target these people? in which case, facebook might work in your favour.
3 Do people with these conditions/symptoms band together in some way, such as a self-help
One of those that contributes to liking is using similar – if not the same – words and phrases back at the person you are having a conversation with.
t his same principle applies in promoting yourself and your practice to people you would like to treat as patients. and the great ‘in’ that you have here is that
You need to know if your marketing efforts have been worthwhile, which means you
Tracking
Many advertising and promotional efforts require money. But all promotional efforts require time –even search engine optimisation. t his means there is always a ‘cost’ to advertising. But you need to know if your marketing efforts have been worthwhile, which means you need to track every -
There aren’t any secrets online
Social media has transformed the way we do business and share information, sometimes with people we barely know. So in a medical environment, what are the risks of using social media and how can doctors who are employers ensure their staff use it safely? Julie Price reports of your private practice billing At Medser v we specialise in providing
Take Control
Social media has completely changed the way people communicate with each other, particularly in the workplace.
as of 31 december 2014, 890m people logged onto Facebook daily and more than a third of the UK population were visiting the website every day.1
Twitter only launched in 2006 but has already grown to include 230m users who create around 500m tweets every day. linkedin also has more than 259m users in more than 200 countries and territories.2
The prevalence of social media means it is hardly surprising that employees use sites like Facebook or Twitter at work, for keeping up to date with friends and followers or posting about their own lives.
i n any commercial environment, employers must realise the importance of regulating the way their staff use social media both in and out of work. New manpower data reveals: ‘75% of employers say their organisations do not
have a formal policy regarding the use of social networking sites at work.’3
i n healthcare, there are undoubted benefits to using social media for both staff working in primary and secondary care, and for patients.
c linicians can use it as a platform to network effectively and share knowledge, while patients can use it to gain information about healthcare services and issues. However, there are risks.
promoting your practice
Social media channels can offer new opportunities to communicate with patients. many of these channels also represent effective outlets to promote healthcare, share health advice and communicate practice information and events such as closures or even a c are Quality c ommission inspection. They also present many new challenges for healthcare professionals. Patient confidentiality is a key issue – the very public nature of social media means doctors must take care to avoid unintentional disclosures.
a doctor’s professionalism and reputation could also be affected when communicating via social media, as any comments made relating to patients, colleagues or employers can be viewed by a wider audience.
a lthough many online accounts provide privacy settings for users, there is still little control over the potential reach a seemingly innocent comment may have.
To combat these potential issues, the G mc ’s Doctors’ use of social media (2013) guidelines states6 that ‘standards expected of doctors do not change simply because they are communicating through social media rather than face to face or through other traditional media’. NHS e mployers’ guide for new starters advises the following test: ‘When using social media, remember if you wouldn’t say it aloud in the canteen, don’t post it online.’7
clinical staff
Social media sites can blur the boundary between an individual’s public and professional life. many inappropriate posts, related to
a good Policy
clinic and practice staff should bear in mind that any content they post on social media should not:
interfere with their work commitments
contain libellous, defamatory, bullying or harassing content
contain breaches of copyright and data protection
contain material of an illegal, sexual or offensive nature
include confidential information about practice patients, ex-patients, staff and other practices and healthcare organisations
Bring the practice or profession into disrepute nor compromise the practice’s reputation
personal comments and activity outside of clinical practice, have landed healthcare professionals in trouble.
doctors should not only restrict their posts, but also bear in mind that anything they do post could call into question their fitness to practise.
The Gmc states in Confidentiality (october 2009): ‘You should not share identifiable information about patients where you can be overheard, for example, in a public place or an internet chat forum.’4
Furthermore, the G mc ’s Good Medical Practice, Para 69, cautions: ‘You should remember when using social media that communications intended for friends or family may become more widely available.’5
it is wholly inappropriate for a doctor or member of staff to post any comments about a patient on
• Initial data capture of archived patient files, including ongoing processing of live files/data
• Reduction in labour costs and time associated with manual paper filing
• Consultants have remote access to patient data when and wherever they need it
• Complies with the national initiatives
suBscRiBe By diRect
Dear Reader,
Subscribing to Independent Practitioner Today is the only way you can be sure you will see every issue. Don’t risk missing out. Our personal subscription for doctors and managers is only £85 a year and £200 for organisations. But you can cut this to just £70 and £175 respectively if you pay by direct debit.
So take advantage of this offer now for our unique business journal dedicated to supporting you in your private practice. We’re confident your subscription will repay itself many times over!
Editorial director
enclose a cheque for £ ........... made payable to the
* indicates this item must be filled in Doctors, please give GMC No. (See rates listed above)
i would like to pay by direct debit (please complete all details in box below). Don’t forget, it’s £15 cheaper to pay by direct
Instructions to your Bank or Building Society to pay Direct Debits
Name and full address of your bank/Building Society
To: The Manager
Society
Banks and Building Societies may not accept direct debit instructions for some types of account Signature(s)
No. (Do not complete)
Instruction to pay your Bank or Building Society Please pay The Independent Practitioner Limited Direct Debits from the account detailed in this Instruction subject to safeguards assured by the Direct Debit Guarantee. I understand that this Instruction may remain with The Independent Practitioner Limited, and if so,
Banks and Building Societies may not accept Direct Debit instructions for some types of account
post your application (no postage required – uK only) to: independent practitioner today Subscriptions department, FreepoSt, po Box 36, plymouth, pL1 1Br
Direct Debits Name and full address of your bank/Building Society Banks and Building Societies may not accept Direct Debit instructions for some types of account To: The Manager Bank/Building Society Address Postcode Ref. No. (Do not complete)
subscribe online at www.independent-practitioner-today.co.uk if you
change, The Independent Practitioner Limited will notify you 10 working days in advance of your account being debited or as otherwise agreed.
If an error is made by The Independent Practitioner Limited or your Bank or Building Society, you are guaranteed a full and immediate refund from your branch of the amount paid.
You can cancel a Direct Debit at any time, by writing to your Bank or Building Society. Please also send a copy of your letter to us.
such sites and at the m edical Protection Society ( m PS) we would expect that the G mc would take an extremely strict line about this, especially if the patient is identifiable.
if the practice discovers that a patient has posted a negative comment on a site, they should contact mPS so that we can advise as to how the matter may be resolved.
i n addition, such sites often have a quick means by which abusive comments can be reported –for example, via a ‘report post’ link – so the social media network may also take action against anyone posting outside of its rules.
The m PS view is that doctors and their practice staff should be cautious when posting on social media sites, for example Facebook, and should avoid adding patients as friends.
consider this scenario:
m iss H, a practice receptionist, had a particularly difficult day at work. She had found one of the patients very demanding.
That evening, at home, she discussed her working day with friends on Facebook, who were all aware of the practice she works at, and discussed her difficult patient.
a mutual friend of the patient was able to identify her from the comments and made a complaint and forwarded the posts to the practice manager.
The next day, miss H was called into a meeting with her practice manager and the doctors and the matter was investigated. i n the circumstances, the practice and the doctors could find themselves facing a claim for breach of confidentiality.
miss H did not believe that she had done anything wrong, as the comments had been posted online in her own time, however she was severely reprimanded.
The practice manager realised that, although there was a confidentiality agreement, the practice did not have a policy on the use of social media.
What policy should a private practice have in place?
everyone working in hospitals or general practice, whether private or NHS – or other healthcare set
tings – must understand the rules of confidentiality.
all information about patients is confidential; from the most sensitive diagnosis to having even visited the clinic or surgery or, in general practice, even being registered there.
Staff should regularly receive training on the importance of maintaining patient confidentiality.
The practice should ensure that all staff receive and sign a copy of the confidentiality agreement. This should include a clause regarding the use of social networking sites and respecting patient confidentiality as well as maintaining a professional persona. They should also consider having an iT policy.
a s part of a wider internet/ social networking policy, employers may want to include references or clauses informing staff how to use social media effectively and sensibly both in the workplace and during personal use.
i t is important that staff are aware that when it comes to using social media, they are representing the practice at all times.
Risk assessments
mPS experience suggests the need for many doctors to re visit the confidentiality subject.
e ach year, m PS undertakes c linical Risk Self a ssessments (cRSas) of general practices, both private and NHS. The c RS a is a systematic approach to identifying risks and developing practical solutions to ensure quality of practice and preventing harm to patients.
over the past nine years, it has conducted more than 1,300 cRSas in general practice.
The data collected analysing the results of more than 100 c RS a s conducted during 2014 reveals that 94% of practices visited had risks associated with confidentiality, with five main risks being identified (see table above, right).
There will continue to be an increase in the use of social media, so it is fundamentally important that all staff working in any private practice understand the importance of maintaining patient and staff confidentiality. i t is very easy to post a com
are able to overhear conversations
of
ment, but it is more difficult to take it down afterwards – if somebody retweets a disparaging comment or shares a negative post, you lose control of the content.
Remember that conversations via social media are not private –millions of people may be listening in.
Julie Price is head of risk management and education consultancy at the Medical Protection Society
References
1. Zephoria (2015). The Top 20 Valuable Facebook Statistics – Updated February 2015. https://zephoria.com/top-15-valuable-facebook-statistics/
2. Linklaters (2014) Social media and the law: A handbook for UK companies January 2014. www.linklaters.com/pdfs/ mkt/london/tmt-social-media-report.pdf
3. Manpower (2010). Social Networks vs. Management? Harness the Power of Social Media. https://candidate.manpower. com/wps/wcm/connect/fe3bdf004322b07ea89cee4f3871948a/ Social+networks.pdf?MOD=AJPERES
5. GMC (2013): Good Medical Practice (April 2013). www.gmc-uk.org/guidance/ good_medical_practice/20463.asp
6. GMC (2013), Doctors’ use of social media. www.gmc-uk.org/guidance/ethical_guidance/21186.asp
7. NHS Employers (2014), Quick guide for new starters, New to the NHS? Your Guide to Using Social Media in the NHS. www. nhsemployers.org/~/media/Employers/ Publications/NOVEMBER%20Your%20 guide%20to%20using%20social%20 media%20in%20the%20NHS.pdf
Preparing for the data revolution
Now it is all systems go on implementing the Competition and Market Authority’s information remedies. Matt James reports on progress at the Private Healthcare Information Network
It Is time to update you on recent progress toward implementing the Competition and Market Authority’s (CMA’s) ‘information remedies’ to bring about better information for patients in a way that supports hospitals and consultants.
With the CMA’s order in force from 1 April 2015, there has been a lot of activity happening in all quarters of the private healthcare industry.
the Private Healthcare Information Network (PHIN) took up its official role as the CMA’s independent information organisation at the start of the month.
We marked the occasion with a rather special board meeting where the four directors who have been in post since October 2013 were joined by four new nonexecutive directors who are independent of any stakeholder group.
they bring great experience and capability to our board and we hope they will give particular confidence to consultants.
the first is Dr Gerard Panting, who will be known to many of you from his 20 years at the Medical Protection society.
Qualified both as a doctor and a lawyer, Gerard was nominated by the Federation of Independent Practitioner Organisations (FIPO) on behalf of the associations representing consultants.
FIPO’s own board includes rep
resentatives of the BMA, Independent Doctors Federation (IDF), Federation of s urgical s pecialty Associations (F ss A) and major specialty associations.
Next of the new non execs is Prof s ir Norman Williams, who will be known to many Independent Practitioner Today readers as a recent past president of the Royal College of s urgeons of England, and as a leading surgeon in the field of bowel disorders.
Also familiar to specialists will be Prof sir Cyril Chantler, a retired paediatric nephrologist who recently stepped down as chairman of the UCL Partners Academic Health science Network.
And the final non executive director is Prof Nancy Devlin of the Office of Health Economics, one of the country’s leading academic authorities on health outcomes measurement.
they join our existing directors, Fiona Booth – who sits on our board as the nomination of Association of Independent Healthcare Organisations (AIHO), the representative body for hospitals, and Don Grocott, representing the Private Patients’ Forum.
Add ition ally, there are PHIN’s chairman Dr Andrew VallanceOwen and myself. to round out the nominations from sections of the industry in accordance with the CMA’s order, we are now seeking a nomination from the private medical insurers.
An anonymised ‘information dashboard’ of statistics gathered on a real surgeon, showing the format that other consultants will face in the future
the other body with the right to nominate directors to PHIN’s board is the CMA itself. We have appointed their candidates Jayne scott and Michael Hutchings.
Collectively, the job of these directors will be to ensure PHIN operates effectively and fairly, achieving the purposes set out for it by both its members and the CMA on behalf of patients.
Working with all parties
At the same time, it must respect and work closely with all parts of the private healthcare industry.
We have also agreed that FIPO will be our conduit to the professional associations, ensuring that we coordinate as we reach out to consultants of all specialties.
And we will also work through the hospital operators, and are receiving very helpful co operation from the GMC.
It is a huge task to reach out to
over 12,500 consultants in private practice to enable them to access, check and use their data.
But I am pleased to report a small, but important, first step on that journey, as we recently shared an ‘information dashboard’ with a consultant for the first time.
this showed his private practice across two hospitals, with simple measures such as:
Distribution of activity;
Demographics and ‘length of stay’ profiles benchmarked against sector averages;
Breakdown of activity across hospitals;
time and funding types.
An anonymised version is illustrated above.
to be honest, we expected a barrage of questions and data issues, and were very pleasantly surprised with a reaction that can be summed up as: ‘ t hanks very
Dr Gerard Panting, nominated by the Federation of Independent Practitioner Organisations
Dr Andrew Vallance-Owen, PHIN’s chairman
much: this is very helpful for appraisal. see you next year’. For the next few weeks, we will continue to work with consultants with whom we have an established dialogue to refine the content and format of the information and establish what support is needed, before rolling out gradually across hospitals and specialties.
Don Grocott, representing the Private Patients’ Forum
Fiona Booth, nominated by the Association of Independent Healthcare Organisations
I am afraid you will have to wait for the clinical metrics and NHsfunded activity, though.
t hose statistics will follow in due course.
For now, we want to get lines of communication and access established, and hopefully give consultants data that will be of value.
Fast movers
In other news on statistics:
AVIVA HAs become the first private medical insurer to begin referring patients to PHIN’s website in its marketing and service materials, as required in the CMA’s order.
We had not expected insurers to move so quickly, but the company was very keen to get on with it and show support for improved information.
Aspen Healthcare, meanwhile, has become the first provider to go live with a new PROMs platform for private patients.
From April, it has been collecting PROMs questionnaires covering primary hip and knee replacements. It is using the same Oxford scores as used by the NHs and National Joint Registry, and groin hernias using the patient outcome measure EQ 5D, again as per the NHs
For cataracts, the Catquest measure emerged as the preferred tool for this very highvolume private procedure from our discussions with hospitals, insurers and professional associations last year.
It is great to see providers moving forward so positively.
Tracking re-admissions
PHIN has completed preliminary analysis of a pilot data linkage exercise on readmissions.
t his is to test the process for improving the measurement of transfers, readmissions and mortalities where patients are treated in a private hospital and transferred or re admitted post discharge to an NHs hospital.
to do that, we have to follow the patient and look for linked NHs records within a defined time period (2830 days).
A cohort of 436,000 patients’ records from 2012 were matched to their associated HEs records by the Health and social Care Information Centre, with the results analysed for us by Northgate.
the whole process was achieved with neither PHIN nor It systems supplier Northgate ever having access to personal data, maintaining high standards of confidentiality and information governance. Results were unsurprising but helpful. While the majority of readmissions – around twothirds –come back into the originating private hospital, the majority of mortalities following transfer or readmission occurred in NHs units. the numbers may, however, be lower than is often touted by the sector’s critics.
this pilot exercise will not support scrutiny at a detailed level – by hospital/consultant/ procedure –but it has, in our view, shown a
compelling case for seeking permission to persist with such data linkage on a routine basis to improve the accuracy of these indicators.
It is worth remembering that, hitherto, the originating private hospital and responsible consultant would often simply be unaware of a later re admission or death of one of their patients, unless they were made aware by the relevant NHs hospital.
I hope that we can share further details of that pilot exercise once it has been fully written up and reviewed.
And I also look forward to the point at which the Cosmetic surgery Interspecialty Committee of the Royal College of surgeons of England, established to take forward the recommendations of sir Bruce Keogh’s review following the PIP breast implant scandal, is able to share its work more publicly.
PHIN has been closely involved in and very impressed by the committee, chaired by steve Cannon, and in particular the Clinical Quality and Outcomes group, chaired by Mr Michael Cadier, president of BAAPs they are doing important work that will contribute significantly to the safety of cosmetic patients. that is it for now. We will keep you up to date and look forward to working with you directly.
Matt James is chief executive at PHIN
Private doctors perform ENT op on ‘jungle VIP’
YOU CAN get almost any type of patient turning up in private practice these days – as consultant ENt surgeon Mr Jawed tahery and anaesthetist Dr Paul Jamieson know only too well.
Happily, their Bornean orangutan patient, Vicky, aged 31, is all smiles again after successfully undergoing double surgery for the first time in UK history.
she had two operations to alleviate severe congestion caused by chronic sinusitis and air sacculitis.
Consultant EN t surgeon Mr Jawed tahery from Nuffield Health, the Grosvenor Hospital in Chester, carried out functional endoscopic sinus surgery and zoo vets Karen Archer and Andrew Moore performed marsupialisation of the air sac.
t hey were joined by Dr Jamieson, staff nurse Virginia Kayembe from Nuffield Health, and a team of specialist primate keepers from Blackpool Zoo as well as other human and animal medical specialists.
It is the second time Vicky has had surgical treatment for her problems. Her first operation was carried out in April last year at
Chester Zoo, where Blackpool Zoo’s orangutans were housed temporarily while their new £1m home was being built.
But this is the first time the two procedures have been done simultaneously.
Both were successful and Vicky rejoined daughters s ummer and Cherie, and male of the group, Ramon, less than 24 hours after the operation. s he is now being closely monitored by keepers.
similar anatomies
Mr tahery, who carried out Vicky’s first functional endoscopic sinus surgery in 2014, said: ‘As an ear, nose and throat surgeon, I have carried out this procedure many times, but it is very rare to get the opportunity to operate on an animal.
‘the anatomy of an orangutan and a human are similar, but the orangutan doesn’t have frontal and ethmoid sinuses and their bones are much harder.
‘the aim of the operation was to restore drainage in the sinuses and increase ventilation of the nasal cavity and I am delighted with the results.’
The surgical team at The Grosvenor Hospital, Chester, swings into action
op ApE
➱ continued from page 25
GOING APe
Back among friends! All smiles again after the op.
Consultants and all the staff worked as a gesture of good will – no fees
Insurance and indemnity was all covered by the zoo in advance
Vicky’s favourite food: yogurt
Her characteristics: highly intelligent and bossy
That smile: photographed thousands of times
Bornean orangutans: becoming critically endangered in the wild due to deforestation and hunting
Veterinary surgeon Ms Archer, from Oakhill Veterinary Centre in Preston, said: ‘ t he teamwork between top human and animal medical specialists in this case was the key to its success.’
Colleague Mr Moore added: ‘Air sacculitis is a common condition in orangutans and this type of surgery goes a long way to help alleviate symptoms and limits the risk of potentially life threatening complications that may occur without such treatment.
‘It has been an absolute pleasure to work with a whole host of professionals and field leaders.’
Blackpool Zoo animal manager Peter Dillingham has worked with
Vicky since she was born there. He described her as ‘very special to everyone here’.
‘ s he has had these two conditions for many years and it has been fantastic to work with such esteemed medical experts to make this procedure a reality. Less than 24 hours after the surgery, she was back in with the rest of the orangutans and is recovering well.’
wHAT ABOuT yOu?
what’s the strangest operation you ever carried out privately?
email: robin@ip-today.co.uk
Vet nurse Sara Jones tends to her unusual patient
Mr Jawed Tahery, eNT surgeon
Case to alter practice
Why should a Scottish obstetric case affect what everyone does in private practice and the NHS? Lawyer Bertie Leigh explains
The days when independent practitioners could assume their indemnifiers would permit them to remain in benefit and unlimited practice have long since departed.
high-risk practitioners may find the benefits of membership are withdrawn – and buying indemnity elsewhere is challenging. Without it, the GMC will not permit doctors to practise.
This means that medical practitioners, particularly surgeons, must take enormous care to avoid being sued.
In a recent case, a Mrs Montgomery recovered damages not because her doctor was negligent in treating her, but because she was not counselled about the advantages of an alternative sort of therapy.
she was not offered an elective caesarean section even though her short stature and diabetic status meant she was at increased risk of shoulder dystocia. The case turned not on whether it was negligent not to offer her a caesarean section, but on the failure to respect her autonomy by counselling her on the alternatives to a normal delivery.
The traditional model of consent to treatment has been interpreted as meaning doctors had to counsel a patient about any positive intervention they proposed and to obtain consent to a specific procedure. The duty to counsel about the alternatives available has often been overlooked and unrecorded. Nobody signs a consent form to a non-invasive therapy.
It is not a bad starting point to suppose a court will work on the rule of thumb that what is not written down probably did not happen. doctors will struggle to persuade the court, often years after the event, that they dis -
readers
independent Practitioner Today has teamed up with leading healthcare lawyers hempsons to offer readers a free legal advice service.
For details, see the advert on the page opposite Free LegaL advice For
cussed matters with patients that they have failed to record in the clinical notes.
s ome cases change the whole pattern of clinical negligence litigation in ways that are not intended by the courts at the time.
The traditional Bolam Test recognised the multiplicity of medical opinion and said that a doctor would not be negligent if he had acted in accordance with a responsible body of opinion.
changing role of the expert
This meant in practice that an expert witness was simply required to demonstrate there was a recognised school of thought that would have acted as the defendant had acted.
In the 1990s, the role of the expert was transformed when the house of Lords said that for the school of thought to be responsible, it had to stand up to analysis.
This requires the expert not only to describe the intellectual landscape, but to then defend the school of thought in question. so having initially been a dispassionate witness who was there to describe the range of opinion, the expert became an advocate for the school of thought he was there to defend.
Montgomery v Lanark will be just as far-reaching. a doctor who is counselling a patient before a procedure cannot discharge the duty imposed by the law by getting the patient’s signature on a consent form recording the risk in question. The law now demands
that the patient be counselled in a way that will enable them to handle the information effectively and to take their own decision.
This means that the timing of the counselling, the time given to the process and the means used to convey the information will all come under close scrutiny.
The doctor is required not only to place all the information about the procedure and the alternatives before the patient that a reasonable patient is likely to want to know, but also to take cognisance of any particular features of an individual patient of which they are aware.
If you know that a given patient has a particular interest in some aspect of a case, then you must respond to that particular interest constructively. you must also counsel them.
implications for doctors
a ll of this has implications for physicians as well as surgeons. Where a GP refers a patient for an angioplasty, the cardiologists will have a duty to counsel patients about the full range of options available to treat ischaemic heart disease, including purely medical therapies and bypass grafts.
spinal surgeons will have a duty to advise about physiotherapy, osteopathy and epidural blockade when offering spinal surgery.
Less obviously, osteopaths, physiotherapists and anaesthetists are likely to find that they have a duty to explain the potential advantages of surgery, even
though these are not therapies that they offer themselves.
h owever, it is not only the range of options that have to be dealt with in counselling patients in this new era; it is also the time that is devoted to the process.
The Montgomery case reflects a profound secular change in the relationship between the doctor and the patient. We now expect our doctors to be teachers and guides, as well as advising upon and performing procedures.
The doctor’s role is to empower the patient and guide them towards a longer and healthier life. Those who fail to advise us to stop smoking or to moderate our drinking will fail to discharge their obligations.
so much is conventional thinking today. But it is far from conventional for doctors to make adequate records of their discussion of other treatment modalities that they do not offer and do not think is appropriate for this patient.
In Montgomery, while the law may have just caught up with what good doctors were doing already, it has also raised the bar and will encourage even the best to reconsider their practice.
We may expect to see far more use of decision aids in which doctors encourage patients to access medical materials on the internet. a nd we may anticipate that a greater proportion of most medical interviews will be diverted towards counselling the patient rather than taking a history or performing an examination.
The Brave New World continues to evolve.
Bertie Leigh is senior partner at Hempsons solicitors, chairman of NCEPOD – the Clinical Disputes Forum – and president of the Society for Ethics in Law and Medicine
Free legal advice for Independent Practitioner Today readers
Independent Practitioner Today has joined forces with leading niche healthcare lawyers Hempsons to offer readers a free legal advice service.
We aim to help you navigate the ever more complex legal and regulatory issues involved in running and developing your private practice – and your lives.
Hempsons’ specialist lawyers have a long track-record of advising doctors – and an unrivalled understanding of the healthcare system as a whole.
Call Hempsons on 020 7839 0278 between 9am and 5pm Monday to Friday for your ten minutes’ of free legal advice.
Advice is available on:
Business structures – Ian Hempseed
Commercial contracts – Faisal Dhalla
Competition – Lindsay Draffan
Disputes – Hilary King
HR/employment – Fiona McLellan
Premises – Lynne Abbess
Essentially Medical has been organising free, consultant-led medical education meetings for GPs in their surgeries for the past ten years. Using consultants from NHS hospitals local to the GP practices, they have arranged more than 1,500 meetings around London, Middlesex and Hertfordshire, and are soon to launch their service in SE London and Kent.
Refreshments are sponsored by pharmaceutical companies and each attendee receives a Certificate of Participation.
Dr Martin Harris, a North-West London GP, said: ‘This service allows us to keep updating our skills and knowledge in the comfort of our own practice.’
Mr Daryll Baker, Head of Vascular Services at the Royal Free Hospital, said: ‘I’ve been involved with Essentially Medical since its early days. It’s a superb, informal way of helping GPs and consultants put names to faces rather than rely on listings in a handbook.’
For details, contact Evelyn Diamond by phoning 01923 850225 or 07929 633108 or email info@essentiallymedical.co.uk
An AccoUnTAnT’s AdvicE
Want to rocket your
Whether you are an experienced private practitioner, or just starting out, James Gransby’s tips will help you boost your private practice income
Building your reputation and working hard are the key ingredients to a successful private practice. But there is no magic wand.
As a specialist medical accountant, i see every financial aspect of my clients’ private practices and, by observation and inquiry, i would like to share with you the things i see which can help you boost your practice income.
1
Be organised
This pervades the rest of the advice below and so is worth mentioning from the outset.
Whether it is chasing patients for payment or arranging your diary, being organised is fundamental.
Some tasks are able to be delegated; for example, a good secretary will organise your appointments, can keep your accounts in order and ensure important deadlines are not missed.
This not only frees up your time to see more patients, but also helps to ensure your practice runs efficiently and therefore more profitably.
There is also software available which can help with organisation, linking your diary to billing through to accounts.
Travel time is unproductive and so should generally be kept to a minimum. i s there a more local private hospital that you could
work at, perhaps one that has just opened?
Being available to see patients is also of paramount importance, as reputation and ability are only valuable if your patients can see you when they need to.
Encouraging a phone follow-up review as opposed to a face-toface meeting is a method that some of my clients adopt, when the possibility to do so presents itself.
Perhaps technology can play a part here, as with consultations via video link.
Actions:
Check you are delegating enough.
is your software fit for purpose?
Can you work more efficiently by cutting travel time or making better use of technology?
2 Be in the know
if you are fortunate enough to have colleagues who have been successful in building a strong private practice and do not mind sharing their secrets with you, then you are already ahead of the game.
For some, this is a taboo subject, akin to asking someone their earnings. i f you have advice to give someone, then they will be more willing to give you something in return.
By being connected and asking around, you may be the first to
your profits?
...cuts into lost fees!
“MidexPro thinks like a doctor, not a computer exper t”
All you need to run your private practice including document management, diary, clinical data, even test ordering and lab reports from TDL.
From paper billing (incl VAT) to electronic billing (EDI) to management of bulk purchase contracts.
know if a colleague is looking to give up their private practice, leaving space for someone to fill their shoes.
AcTions:
Consider whether you are communicating enough with your peers.
Are any colleagues thinking about giving up their private practice?
3
Be tax-efficient
There will always be tax to pay, but needlessly paying more than needed to Her Majesty’s revenue and Customs is not sensible.
it is fair to say that middle- and high-income earners have been a key target for tax hikes in the last five years, whether it is:
The loss of Child Benefit – for those earning over £50,000 since January 2013;
The loss of tax-free personal allowance and an effective 60% tax band – for those earning between £100,000 and £120,000 since April 2010;
The Additional rate tax band, currently 45% but previously 50% – for those earning over £150k, introduced in April 2010.
Corporate tax rates have been falling over the same period to encourage corporate growth and discourage an exodus of trade by companies to lower corporate taxpaying countries.
correct structure
Choosing the correct structure for your private practice is extremely important. Company tax rates at 20% are more favourable than personal tax rates for many, even when factoring in the personal tax on extraction of profits from the company.
Even at private fee levels as low as £20,000 it is possible in some circumstances to save tax in excess of the additional costs of running the company.
An example is where an individual is subject to the effective 60% tax rate where private fee income when added to nHS salary takes total taxable income over £100,000 and either not all income is used for personal expenditure or where a spouse can be involved.
involving your spouse in your business where there is the opportunity to do so may also reap rewards in the form of lower overall tax for the family unit.
This is especially true where the spouse pays tax in a lower marginal tax band or has the availability of unused personal allowances. other spousal tax planning is then possible, such as making spouse pension contributions.
Simple, yet overlooked steps, such as claiming for all expenses, should take place. Examples include the use of a personal ➱ p32
Grow seamlessly from a small solo practice through to a large group practice, remote access network system
MidexPro is the cost effective practice management system with support second to none.
Free download of the full working package (30 day limited) from www.midexpro.com or call for a CD.
Try it for yourself with no sales pressure.
“MidexPro has revolutionised our lives; it is just so easy”
mobile phone for business and charges for using your home as an office.
yet i often encounter inertia from doctors. For example, someone who was told some time ago that a limited company would not save them any tax has stayed a sole trader despite other factors having changed.
Factors such as an increase in income, marital changes and a changing tax landscape all beg the question of whether the current business structure is the most efficient.
if their accountant has not been proactive in looking after their interests and having the conversation about business structures, then unnecessary tax may have been paid
AcTions:
review your business structure.
Ensure all allowable expenses are being claimed.
4 Be front of mind to referrers referrals may come from gPs, colleagues or former patients, to name a few, and it makes their job easier when recommending patients to you if they can find you easily.
Private hospitals are generally good at helping you with this. Whether it be evenings organised for you to network with g Ps, creating an online profile for you summarising your credentials and specialisms or including you in their brochures and circulars, all of this helps to raise your profile and visibility to referrers.
There are actions you can take yourself to bolster this, including creating your own website, the cost of doing so being tax-deductible. The local press, whether newspaper or radio, may be interested in hearing what you have to say and so raising your profile.
AcTions:
Check you are optimising the exposure that private hospitals can give.
Ensure your website is up and running and current.
5 collaboration
i am increasingly meeting with groups of individuals having come together as a collective unit or asking for advice in doing so.
While this is not something
Limited liability partnerships (LLPs) can be flexible in terms of tax and also provide a valuable degree of legal protection should adverse events occur within the LLP
new, it is definitely worth looking into, as the tried and tested benefits of building a brand, increasing appointment availability to patients coupled with the economies of scale of cost-sharing – for instance, a secretary – can also be expanded into tax efficiencies within the correct structure. l imited liability partnerships (llPs) can be flexible in terms of tax and also provide a valuable degree of legal protection should adverse events occur within the llP.
AcTions:
instigate new or revisit old conversations with colleagues regarding pooling resources if this might be beneficial.
6 Maximise the fee you charge
i recognise that, for certain work, there is often a barrier in the form of fee levels being dictated by the private health insurers. This leaves increasing the volume of patients seen as the only apparent way to boost income.
i f not all income comes from this source, then there is scope to set fees at different levels. The underlying market forces of supply and demand come into play and it is those with superior reputations or a rare specialty who can command the premium prices. do not be complacent with setting and reviewing your fees; ensure they are regularly revisited and set at an appropriate level for the work in question.
AcTions:
review your fee levels.
Create a diary note to benchmark your fees against current trends at least annually.
7 shop around for your medical indemnity cover
Just recently, i have seen some of my clients experience rising premiums, especially when crossing into higher income tiers.
Premiums are set based on income levels – with a deduction allowed for costs, often capped at a percentage of income. Thus, it is important to know how your insurer calculates your premium, as you may be able to get the same level of cover from an alternative provider at a lower cost.
Also ensure when submitting your annual figures that credit is given for any work that is indemnified already; for example, nHS Choose and Book work, if applicable.
Fundamentally, though, always ensure that the cover is adequate for the work you are performing.
AcTions:
obtain quotes from alternative medical indemnity insurers.
Ensure credit is given for indemnified work.
8
search out alternative income streams
Many of my clients have multiple income streams, such as writing medico-legal reports alongside the more mainstream work.
As medico-legal work may be able to be performed from home, then it could present a middle ground in your work-life balance and add some flexibility.
if your work is in an area where there is a lot of competition from other practitioners, or if there is otherwise not enough work to go round, then it could be worthwhile considering branching out into a subspecialty in which you have an interest or perhaps even consider an alternative location.
i f you do decide to sign up to work at a new location, then once you are given the necessary privileges, you must then work out how to get the most from your time there.
you should weigh up how long you plan to spend there each week and the fee to charge.
AcTions:
investigate the opportunity to earn income from other sources or locations.
Leaving the NHS can be a valid option and has certainly worked for some of my clients in boosting their income
9
ditch your nHs job oK, this is not appropriate for all, but for the right individual with the opportunities and mindset to do so, leaving the nHS can be a valid option and has certainly worked for some of my clients in boosting their income.
This obviously comes with risks around job and income security, together with the fact that it also forfeits ongoing membership of the nHS Pension Scheme.
Being business-like becomes key here, as you would be relying totally on your skill at winning new work to keep the income coming in.
AcTions:
Consider whether this could this be right for you.
10 Think ahead to the future and reflect on where you are now
i saw a surgeon recently to review how he could run his private prac-
Looking to the future is a very important part of building a sustainable private practice
tice more tax-efficiently. He had spent the previous evening giving a talk to an audience of gPs.
Two evenings in a row where he could have seen private patients were instead spent attempting to secure future work streams and ensuring that he keeps more of the money he earns after the work is performed.
looking to the future is a very important part of building a sustainable private practice. Ensuring that work coming through is of the quality and type that you desire needs clear communication to your referrers of the type of work you are looking for.
Boosting your income is not just about seeing more patients. Benefits can come from taking the time to work on your business rather than just being routinely in it.
James Gransby (left) is a partner at MHA MacIntyre Hudson
An easy to use software system, which fully supports the clinician and office staff and makes the whole process of running a busy Practice a lot easier.
Call now for a chat and ask about a free, no obligation demonstration of our comprehensive system that has been designed to save your Practice time and money.
Curing doctors’ money malaise
Consultants are facing a multitude of problems when it comes to medical billing and collection. Independent Practitioner Today asked billing expert Garry Chapman (right) to keep a ‘warts and all’ diary of the issues he encounters in a typical working week. Here is his report
It is an early start to the week for me with a trip to the south coast for a 7.30am meeting with an orthopaedic surgeon and his secretary.
He had been referred to me by several of our clients who work in the same specialty and geographical location.
The surgeon explains that, as the practice has expanded, they have struggled to cope with the workload and the debt had continued to grow. They were also having problems dealing with the private medical insurers on their complex operations.
I explain how we could assist the practice on all aspects including taking over the process of liaising with the insurers for their complex operations which would allow the secretary to have the time to carry out all her other important tasks. I leave at 9am with all the paperwork signed, so that we can start working for them at the end of the month.
In the late morning, I arrive at our office where I have a management meeting with our general manager and his management team to review the previous week’s operation and discuss any key issues that have arisen since.
Today, the major talking point is the letters being sent out by both Bupa and AXA PPP to consultants in the UK regarding reducing consultation fees and procedure code fees.
After agreeing a way forward, we send out a broadcast message to all our clients instructing them to contact us before responding – should they receive a letter – so that we can explain what the financial implications are to their practice and what options they have available.
I then have an internal hand-over meeting with the account manager who is going to be working with the new practice that signed up this morning, so they can have everything set up ready.
I leave the office mid-afternoon to go to one of the major private hospitals to have a review meeting with a client.
We review his pricing structure which has not changed for many years and he decides to leave the prices where they are.
I then present him with his billing reports which show him that since he has been with us, he has billed over £1.3m and we have written off only £743.
Needless to say, he is extremely happy with our service and continues to recommend us to his colleagues. I head for home – it’s time for responding to the emails.
In London all day today. The first meeting is with an anaesthetist who called me last week.
I meet him at 9.30am. He explains he has been doing his own billing for 20 years but has reached the point where he is finding it very difficult to keep abreast of all the changes taking place on the insurers’ pricing structures and chasing the ever-increasing shortfalls that patients have to pay.
He states that he was recommended to MBC by a colleague and after looking at the testimonials on our website, he recognised a number of his colleagues using our services.
I explained how we work and that our service is tailored to the needs of the individual consultant, which he was very happy with. He decides to go ahead and start using our services straight away.
It’s been a good start to the week with two new consultants joining us. I pick up a voicemail message from a surgeon expressing an interest in our services, as he had been recommended to us by his anaesthetist.The week just got better.
My remaining meetings today are review meetings with some of my existing clients. The first is with one of our physicians and is relatively quick, as she is pushed for time because she has an emergency.
We agree to monitor her practice closely over the next few weeks, as she has just changed secretary so wants to make sure her clinic information is still coming to us regularly.
My second meeting is with one of our surgeons who is thinking about
reducing her NHS practice and growing her private practice. We discuss what her timetable is in doing this and work through some options for her to consider before making a final decision.
I agree to provide a report which breaks down where her patients are coming from and to introduce her to a company that could build her a website if she choses to take up that option.
Before I start the last meeting of the day, I finally connect with the surgeon who left a message earlier in the day. We agree a date for next week to meet and discuss his requirements in further detail.
My final meeting of the day does not happen, as upon arriving at the hospital, I am informed that the consultant has been delayed in theatre and will re-arrange for a future date. I head home to respond to my emails received today.
WEDNESDAY
Another early start as I head off for a golf day. I am very happy to receive the invitation, as there will be a lot of consultants attending, so it should be a good chance to network. I speak with a number of people who may well be in touch, so it is worthwhile attending, but – alas – my golf is poor. Considering I am a high handicapper, that’s no surprise.
I head home after lunch to change into a suit and tie, as I am presenting at an event in the evening for consultants who are new to private practice.
The seminar is due to start at 6.30pm, but we eventually begin at 7pm
UK Top 20 accountants specialising in the healthcare sector
• National firm of the Year 2013
AISMA member (Maidstone and Leicester offices)
• 12 offices including London City
• Tax Structures for Hospital Consultants - dispelling myths
• Surgeon groups and consortia
GP Practices including mergers and federations
• Solvent liquidations (for companies at the end of their lives)
For more information please contact: South East
James Gransby FCA
E: james.gransby@mhllp.co.uk
T: +44 (0)1622 754033
M: +44 (0)7712321899
East Midlands
Robert Nelson DChA FCA
E: robert.nelson@mhllp.co.uk
T: +44 (0)1162 894289
M: +44 (0)7814009160
General email: healthcare@mhllp.co.uk www.macintyrehudson.co.uk
due to some late arrivals. There are five other presenters and all aspects of running a private practice are covered from billing and collection, marketing, website design, software through to accountants’ services and tax advice.
All the presentations are well received and everyone comments on how useful the evening has been. The majority of doctors attending are either just starting out or have been in private practice for between one and two years.
I leave the event at 9pm and head home with several people stating they want to meet in the near future. So a good end to a long day.
THURSDAY
In the office today with various internal meetings. The bank manager is coming to see me for our annual meeting and I am meeting with our software company to review some functionality changes we are considering to enhance our service.
I also have several second interviews lined up, as we are recruiting for more account managers to handle the growth we are experiencing.
All the meetings go well and I sign off on the software development work and the bank manager leaves after giving us a glowing tribute.
We have agreed terms with two of the candidates and they can both start in a month’s time, so it has been an excellent day. I leave the office at 4pm to attend a dinner at the Royal Society of Medicine in London. It is attended by 11 others: a mixture of consultants, GPs and people from other companies who work in the private healthcare space.
After a delicious meal and excellent company with some lively debate about the insurance sector, I head home at 10pm.
FRIDAY
It’s an early again, as I have a meeting in Manchester with a dermatologist who found Medical Billing and Collection on the internet and then spent some time looking at our website. He was sufficiently impressed to want to have a meeting. I arrive at 10.30am, 30 minutes early, as there was no problems with the traffic. For a change, the M6 is fine. Fortunately, the consultant is able to see me early and he explains he has several issues regarding his billing and collection. These include having a large backlog of outstanding invoices amounting to over £100,000.
His wife has been doing the billing, but is finding it harder and harder to cope with as the practice grows and she is also looking after the children at the same time.
I explain how we can help him collect his backlog and also how we could work with him in the future. He is particularly impressed with the fact that we only charge on what we collect and not what we invoice.
He says he will talk it over with his wife and come back to me next week. I thank him for his time and leave Manchester at 11.30am hoping I will have the same fortune with the traffic on the way home.
No such luck. I’m back working through admin in the early evening when the dermatologist I met earlier today rings to say his wife is very happy and relieved to hand over the billing. He wants us to start as soon as possible.
After a busy and successful week, it’s time for a cold glass of something nice.
Garry Chapman is managing director at Medical Billing and Collection
Uniting both the Surgical and Non-Surgical Communities
Over 200 world renowned exhibitors
4,000 high level medical healthcare professionals
Over 100 expert faculty
FREE World-class speakers with CPD certified content
FREE conference programme, workshop theatres and live demonstrations
“I believe it is important to use this opportunity to bring together board members, doctors, nurses, managers, pharmacists and all those who are seeking to deliver improved safety outcomes for their patients” DrMikeDurkin,NHSEngland Network with peers. Learn from experts. Implement
• Extensive case study-driven seminar content, delivered by world class speakers & influencers
• Learn how to improve patient safety standards and quality from the experts
• Practical solutions & best practise you can put into action from industry leaders and organisations
• Choose from over 40 hours of CPD
• Get practical advice from over 100 product & service providers
To register and find out more please visit www.ccr-expo.com For more information visit www.patientfirstuk.com Education grants are being distributed from May. For more information email d.earl@closerstillmedia.com
Get yourself noticed
In the fourth part of his series on becoming a clinical negligence expert witness, Michael R. Young covers how to find work, write an expert CV and gives tips to help you encourage solicitors to keep coming back to you
A number of national expert witness organisations maintain expert databases of specialists and, as a first step, you should get your name onto at least one of these lists.
Joining one, such as the expert Witness Institute, TA e or the Society of e xpert Witnesses, is important, as they are often the first place solicitors look when they want to find an expert to help them with a particular case. These organisations usually have a vetting procedure, so you must prove to them that you are competent as an expert witness. m embership gives credence to your commitment.
for their fee, they help you find work, but there are practical reasons for joining too:
They have a helpline, so you’ll have a readily accessible source of information and support;
They often offer discounted professional indemnity for members;
m ost run training courses on various aspects of the work and for different experience levels;
Some will offer mentoring;
Their websites, newsletters and journals are an easily accessible source of essential, up-to-date information;
They can provide you with report templates and terms of business: useful to get you started;
Some have arrangements with hotels and can offer accommodation discounts.
I suggest you look at all of the organisations, compare what they offer, and decide which one you would prefer to join.
Marketing yourself
If you are not prepared to tell potential customers who you are and what you have to offer, then you are going to struggle to find work.
Having your name on a database and/or completing hours of training as an expert witness is no guarantee of work. r emember that although you may be well known in your clinical field, to the legal profession you are an unknown.
To get your career off the ground, you are going to have to be very proactive and that requires a marketing plan. You should at the very least think about the key or unique features that will make you stand out from other experts.
everything you are going to do as an expert should be done with the utmost attention to detail and with precision. my advice is simple: Aim to be the best!
Next month: How to manage your time and your cases
the book costs £60, but independent practitioner today has secured discount of a third off for readers, so you pay only £40. listen to the audio content which accompanies the book at this website: www.otmoorpublishing.com/audio. for more information and to order, email stephen.bonner@ otmoorpublishing.com, quoting reference ‘Young/ipt’.
WRiting an effective cv
Your cv is a vital marketing tool in your search for work. Remember, your cv is a brief account of your career; it should be no more than two sides of a4.
it should be targeted to the specific role of an expert
it should be carefully and clearly laid out, logically ordered and easy to read
it must be informative yet concise
the content, spelling and grammar must be accurate. focus on those aspects of your careers that will paint a very positive picture of you as a potential expert witness. it will be attached to every report you write, so keep it updated and periodically freshen it up.
there is no ‘one best way’ to construct your cv it is your document and can be structured as you wish within a basic framework. You will have to show you can:
Read large quantities of text quickly, accurately and critically
classify evidence precisely and assess its value and reliability
argue logically consistently and sceptically
Marshal various sorts of evidence to support a logical argument
Adapted from The Effective and Efficient Clinical Negligence Expert Witness, by Michael R. Young, price £60, from Otmoor Publishing special offeR! BuY the Book and save £20
Celebrating our 22nd year in Business
www.medbc.co.uk
ome and join the hundreds of other consultants who use MBC and experience the following benefits:
• Bad debts of less than 0.5%
Come and join the hundreds of other consultants who use MBC and experience the following benefits:
• Increase in net income by up to 25%
• Bad debts of less than 0.5%
• Increase in net income by up to 25%
• Freedom for the consultant and secretary to focus on the medical side of the practice
• Having a service tailored to your needs with your own Account Manager
• Having a service tailored to your needs with your own Account Manager
• Our fees are only charged on the money that we collect for the practice and NOT on what we invoice which means we share the same objectives
• 24/7 online access to both your financial and practice management data
• Freedom for the consultant and secretary to focus on the medical side of the practice
• 24/7 online access to both your financial and practice management data
• Our fees are only charged on the money that we collect for the practice and NOT on what we invoice which means we share the same objectives
Special offer:
Special offer:
To celebrate our 22nd year in business we are for a limited period of time offering all new clients an introductory discount of 20%*
Further information:
To celebrate our 22nd year in business we are for a limited period of time offering all new clients an introductory discount of 20%*
Further information:
MBC – More than just a billing company
MBC – More than just a billing company
Please visit www.medbc.co.uk for more detailed information or phone 01494 763999 and speak to Garry Chapman to establish how we may assist your practice.
*Terms and conditions apply
Please visit www.medbc.co.uk for more detailed information or phone 01494 763999 and speak to Garry Chapman to establish how we may assist your practice.
How we cut out
Consultant
psychiatrist Dr Mahnaz Hashmi explains how letting an apartment through Airbnb led her and husband Dr Barry Lambert, a consultant paediatric anaesthetist, to
set up a private healthcare business that emphasises the personal relationship between practitioner and patient
Building up private practice in healthcare can be a frustrating experience.
You do the work, but it can take ages to get paid. There are so many steps: usually the hospital bills the patient; you may have to bill the insurer, the hospital or the patient; your payment gets delayed and you cycle through endless variations on the theme.
l ike any business, sometimes you have to chase up the payment. That’s difficult when you’re an individual healthcare practitioner, because you’re often so busy working that you don’t have the time. There’s also a sense of frustration because you feel that patients aren’t getting the best deal either.
But one day, my husband Barry and i realised that we’d felt this frustration before.
We own an apartment, which we had been hiring out through a lettings agency. The experience was getting increasingly difficult. We had very little control, the agency took huge fees and the apartment was still empty much of the time. Then we came across Airbnb.
it was a totally different experience. We loved the website, which is full of gorgeous pictures of quirky houses around the world.
Even more, we loved feeling empowered and running our own business. Airbnb made the process much more personal and we felt comfortable about the people using our apartment because we had been in touch with them ourselves.
That’s when we had the idea: why wouldn’t this person-to-person contact work for private healthcare? it would put the clinician-patient relationship back at the heart of care. Medstars was born.
supporting patients, helping regulated practitioners Medstars provides a website where patients can find, book and pay for appointments with private practitioners. Our initial plan was to launch in london and the West Midlands, but we’ve had so much interest from elsewhere in the country that we’re now signing up practitioners nationwide.
All the health practitioners on the site are registered with a statutory regulator, with powers delegated by the p rofessional Standards Authority. We felt that the regulation was really important, because this has sometimes been a problem in the private sector.
patients often don’t understand the difference between regulated and unregulated practitioners, and what this means for their treatment. Some have been caught
out by poor care from people who aren’t all they claimed to be.
With Medstars, patients can be confident that everyone on the site meets a certain level of qualification and evidence of continuing professional development. practitioners can be comfortable that their professional reputation will be upheld.
Medstars is free to sign up, for both practitioners and patients. practitioners build their own profiles on the site, highlighting their experience, skills and interests, to help patients find the right specialist for them.
They can choose which of their services to offer, from initial consultation to surgical procedures. The advantage is that patients pay up-front.
i n due course, we’ll also have articles and videos to help patients choose the right practi-
Stars of the show: (left to right) Dr Mahnaz Hashmi, Mr William Van Niekerk and Dr Barry Lambert
the middle men
tioner, whether that’s a doctor, optician, dentist or chiropractor. After all, it’s frustrating for both you and the patient to have to refer someone on because you don’t have quite the right expertise to help.
Finding the right practitioner may be even more important for expats and people coming from abroad. in recent years, increasing numbers of people have arrived from overseas for a holiday, but wanting private healthcare as well.
These people have plenty of money, but they often don’t have time to wait for an appointment. instead, they need to know that they’re booked with the right healthcare practitioner. Medstars will provide a reliable resource to find and book an appointment before travelling.
When a patient books and pays for an appointment, we deduct 7% of the consultation or treatment fee. This is released to the practitioner within a week of the completed consultation, to build trust among patients and increase practitioners’ cash flow. Once you’ve had five bookings confirmed and paid, so that you’re confident that the site is working for you, there is also an annual membership fee starting at £99.
Rewarding good service
p atients who have booked through Medstars can leave feedback on the practitioner they have seen. Medstars will reward good reviews by moving you up the rankings.
it will also reward good support to customers, such as responding quickly to direct messages from patients. it’s all about putting the practitioner-patient relationship back at the heart of healthcare, where it should be.
i’ve seen huge changes in both the n HS and private healthcare since i qualified. But whether you’re working in the nHS or privately, sometimes you’re concentrating so hard on the business and management aspects that you struggle to maintain personal contact with your patients. Medstars will help private healthcare practitioners to resolve that dilemma. instead of worrying about your website or social media profile, we’ll handle that side of things with our experienced digital marketing and tech experts, and you can concentrate on your patients. You don’t even need to have a secretary if you don’t want one.
getting started
Barry and i are both doctors, but we decided that Medstars needed a broader professional ‘reach’, beyond our own specialties.
Barry knew William van niekerk from Birmingham Children’s Hospital where they work together treating children with significant burn injuries. William ‘got it’ instantly and was really interested in what we wanted to achieve. He has an extensive private practice, and he immediately grasped the potential.
Yolandé, William’s wife, is our finance director. She is a chartered accountant, has worked for grant Thornton, Mazars and K p M g , and additionally has expertise in taxation and corporate finance, so we’re really lucky to have her on board.
We started the company with our own cash. We deliberately chose not to go to banks, because we wanted to test ourselves against the criteria used by organisations focused on assessing start-ups.
For additional financial support we approached Eu and government-funded organisation with a broad remit to encourage entrepreneurship in the uK.
Since then, we have won the prestigious 2014 Science Capital i nnovative Healthcare Business p lan Award, which was hugely encouraging. The next step is to look for investment to grow the business.
p erhaps one of the most challenging aspects was designing our website. However, through strong working partnerships with our designers and developers, we have achieve our ambitions.
The look of our website was very important to us. Traditionally, medical sites can be a bit dreary. There are pictures of people with stethoscopes or there are pictures of flowers.
We didn’t want that. Our model was Airbnb, after all, and the look and feel of that website makes it a pleasure to visit. We wanted people to feel the same about Medstars.
We love Jan Bowman’s work, and have one of her pictures at home. She’s based both in
Birmingham and in london, just like Medstars, so it seemed to fit.
We commissioned her to produce the art for our website. She loved the idea of Medstars and she loved the challenge of creating ‘medical art’ without using traditional imagery. We’re absolutely thrilled with the look of the site now.
plans and challenges
Although it feels like we have achieved much, we know that the next few months will be hard work.
Firstly, and most importantly, we need to encourage more healthcare practitioners to sign up, so that there are plenty of choices for patients.
So please go and have a look at www.medstars.co.uk and sign up for free to see what it can do for you . We have started our social medial and digital marketing campaign and you can follow us on Facebook and Twitter at @medstarsuK.
Finally, we need to ensure that Medstars delivers on its promise, for patients and for practitioners.
A drive on
drugs
Independent practitioners have been raising a number of issues following the new drug-driving legislation. Dr Nicola Lennard (left) responds
Dilemma 1 Will law change affect scrips?
QI am a consultant psychiatrist and I have heard there is a new offence of drug-driving which includes prescription drugs like benzodiazepines.
I wonder if you think that I should alter my prescribing hab-
its for these medications as a result?
AYou are right that there is a new offence of drug-driving, which came into force in March 2015. The new law means it is illegal to drive with more than a specified amount of some controlled drugs in the blood.
This should not affect the way you prescribe the medications in question, however, as it is antici-
pated that patients taking therapeutic doses of prescribed medication should not be over the specified limit for the drugs.
There are two groups of medications covered by the new offence – licensed medications and recreational drugs.
Common recreational drugs include cannabis, cocaine, MDMA, LSD, ketamine, heroin/ diamorphine metabolite and methylamphetamine. The limits
for these have been set at a low level.
The second group are mainly licensed medications, for which higher limits are acceptable in the bloodstream. They include benzodiazepines (clonazepam, oxazepam, diazepam, lorazepam, temazepam), methadone and morphine. Amphetamine may be added to the regulations at a later date.
It is worth remembering that it remains the responsibility of the driver to consider whether their ability to drive is, or may be, impaired and, if in doubt, to refrain from driving.
However, you may be asked by patients about the impact of their medications on their ability to drive and whether they might be prosecuted if stopped and investigated by the police.
Some patients may also ask you for written confirmation that they are prescribed a medication, to keep with them in case they are stopped.
When prescribing, you are responsible for providing appropriate advice to the patient about the potential risk for a medication to impair their ability to drive. For example, you will already be advising patients about the risks and side-effects of medications, such as drowsiness.
The last government issued guidance for healthcare professionals to help them explain the new law to patients taking these medicines.1
At the MDU, we advise that you clearly document advice you give to patients about their medications. This is in line with GMC advice requiring doctors to keep accurate and contemporaneous records which should include ‘the information given to patients’ ( Good Medical Practice , 2013, Paragraph 21.c).
You may wish to take particular care to record the advice about driving while taking medication, including any written advice, and other factors which may impact on the patient’s fitness to drive, such as drinking alcohol.
Dilemma 2
Patient wants a medical defence
QI’m a chronic pain physician and a patient whom I have been prescribing morphine to has asked for a ‘medical defence’, as he was stopped by the police while driving and he was apparently found to be over the limit for the drug in a blood test. What should I do?
sional’s advice can then be properly used in such circumstances as a basis for the patient’s statutory “medical defence”.’
If providing a report for the patient, you should bear in mind your duty of confidentiality and disclose only the minimum amount of information necessary for the purpose.
Relevant information might include: the dose prescribed and advice you provided to the patient – for example, about any risk of drowsiness while taking the medication or the need to refrain from driving for a specific period: for example, post-operatively.
If you think that the patient is taking more of their medication than is being prescribed – for example, because he is requesting repeat prescriptions too frequently – then it would be advisable to discuss the issue of fitness to drive with the patient, ensur-
AIf the police suspect that a driver’s fitness to drive may be impaired due to drugs, they can stop and screen them at the roadside for the presence of drugs in their saliva.
If the test is positive, then the driver may face blood tests which would identify whether their blood level of the drug is above the new legal limit.
According to Government guidance, your patient can raise a medical defence if:
‘The drug was lawfully prescribed, supplied or purchased over the counter for medical or dental purposes; and
The drug was taken in accordance with advice given by the person who prescribed or supplied the drug, and in accordance with any accompanying written instructions – so far as the latter are consistent with any advice of the prescriber.’1
The Government advice states that when considering a medical defence, the advice from a prescriber ‘can be considered, including patient-specific advice following assessment of the particular prescribing needs for that individual patient.
‘This advice can sometimes differ from the general instructions in the medicine’s information leaflet. That healthcare profes -
ing this discussion is carefully documented.
It was already an offence to drive while impaired by drugs and the police may still prosecute a person under section 4 of the Road Traffic Act 1988 for driving while impaired through drugs, for which there is no medical defence.
If you provide patients with an information leaflet about medications or particular treatments, you may want to update these to reflect the new drug-driving legislation. The government guidance provides a list of points to consider when doing this.
Dr Nicola Lennard is a medico-legal adviser at the Medical Defence Union
Crosscare - providing private practices with efficient paperless working
Crosscare is a proven clinical system used within private practices and specialist clinics in and around Harley Street and across the UK.
Alongside the standard clinical record keeping and prescribing systems, Crosscare’s appointments, reporting and integrated accounting modules make the tracking of workload, invoices and revenues simple and user friendly.
We understand that each practice works in their own unique way, so being a fully customisable system, Crosscare can be easily tailored to fit your individual needs.
For further information on how our Crosscare solution can help your practice call us now on 01233 722670 or visit www.advancedcomputersoftware.com/ahc
ChARiTy AppEAl
Teaching the teachers
Many independent practitioners take time out from busy workloads to give back to communities here and abroad. In this month’s Independent Practitioner Today, Simon Bruce announces the launch of a charity appeal to help doctors who train doctors
Trauma is an increasingly significant cause of death and disability throughout the world. The World Health Organisation estimates that around five million people die each year from serious injury, the vast majority in the developing world.
The Primary Trauma Care Foundation (PTCF) is a small uK charity formed in 1996 which aims to reduce the number of deaths from trauma or serious injury by providing training for frontline staff in over 60 countries around the world.
in doing so, not only are local doctors given vital knowledge of how to cope with trauma cases with basic equipment but they can then go on to train other health professionals in the area. a ll PTCF courses are provided free to trainees in the developing world. The cost of coordinating these courses is met by generous donations.
For that reason, we are delighted to launch the Cavendish medical 10th a nniversary Charity Challenge. To celebrate our company’s tenth birthday, a team from Cavendish will be tackling the infamous ‘Three Peaks Challenge’, climbing the highest three peaks of England, s cotland and Wales all within 24 hours to raise funds for Primary Trauma Care.
From 1921 June 2015, our team of eight were due to climb s nowdon in Wales (1,085m), s cafell Pike in England (978m) and Ben Nevis, in s cotland (1,344m). To keep to the strict time limit, we needed to reach the summit of Ben Nevis in five hours, scafell Pike in four hours
and snowdon in four hours, with around ten hours of driving in between.
The aim was to travel to Fort William in scotland on Friday 19 June, ready to climb our first mountain, Ben Nevis, next day. Then we were off to scafell Pike that night, before finishing with s nowdon on the s unday morning. The total walking distance is estimated at 42 kilometres (26 miles) with a total ascent of 9,800 feet (3,000m).
We are proud to have PTCF patron and past president of the r oyal College of s urgeons of England s ir Terence English as one of our wellwishers.
Why primary trauma care?
The outstanding work of Primary Trauma Care Foundation was recommended to Cavendish medical by client Dr Jeanne Frossard, an anaesthetist at university College London Hospitals who has volunteered to teach the PTC course many times.
Jeanne said: ‘The PTC course is an amazing, sustainable trauma management course that can be adapted to low income settings where trauma management is very poor due to lack of infrastructure and training.
‘it is run by volunteer trainers who give their time and skill for free, but it desperately needs
funds to move forward, update and improve.
‘my first course as a PTC instructor was in 2005 in rwanda. since then, i have helped set up courses in Gaza, West Bank, Jordan, Lebanon, iraq, rwanda, Namibia, malawi, madagascar and China.
‘i have found it so rewarding after five days leaving about 40 trained people, 12 of which are instructors with the skills and confidence to teach trauma management in their countries and start a cascade.
‘Trauma is one of the biggest killers in the developing world. There is now a PTC community in over 60 countries and 12 language translations.
Above: Anaesthetist Dr Jeanne Frossard with her trauma course students in Rwanda. Top right: Dr Said Kilindimo, an emergency medicine resident at Muhimbili Hospital, Dar es Salaam, Tanzania, teaches on another course
‘We regularly get reports from natural disaster and conflict areas telling us how PTC has helped. The training has given the chance for doctors and nurses to give the patient the best possible outcome with limited resources.
‘Please get behind the Cavendish m edical Charity Chal lenge and support this very worthy cause. The PTC worldwide network offers proven, adaptable training using local resources to reduce mortality and morbidity in these countries.’
Donations that make a difference although training typically starts in the capital city, in the best hospitals and with respected and experienced doctors, PTCF’s vision is that it spreads as far as possible into the more remote areas and becomes locally sustainable. This is why participants train with minimum equipment and
facilities, and are encouraged to find solutions to local problems. The trainees are usually health professionals who deal with trauma management in difficult situations.
Cavendish medical opened for business in 2005 with a small number of medical clients looking for specialist help with their financial affairs. Today we help over 450 medical families live life to the full, safe in the knowledge that their future financial security has been assured.
We are delighted to be able to do something worthwhile to support medical professions in other countries and to help them save more lives in their own communities. We are confident that the work of Primary Trauma Care will keep us motivated during this sleepdeprived test of endurance.
To donate to the Cavendish medical 10th anniversary Charity Challenge, please visit www.
Prof Sir Terence English, past-president, Royal College of Surgeons of England: ‘Courses in Primary Trauma Care (PTC) were the brainchild of Douglas Wilkinson, a consultant anaesthetist in Oxford, who adapted the expensive and technically demanding Advanced Trauma Life Support course (ATLS) for application in developing countries.
‘The two-day PTCF course trains doctors how to assess and then manage seriously injured patients at the time of their injury, when it is essential to do the right thing if the patient is to survive.
‘My involvement with the foundation started 12 years ago when a colleague and I took the course to Peshawar in north-west Pakistan. It soon became international and by now has been delivered in more than 60 countries by volunteers who have been trained in the course locally.
The PTCF’s courses have saved – and continue to save – countless lives worldwide and it is a charity well worth supporting.’
cavendishmedical.com or https:// secure.thebiggive.org.uk/projects/ view/22860.
For more information about the Primary Trauma Care Foundation, please visit www.primarytraumacare.org.
Simon Bruce (right) is managing director of Cavendish Medical, specialist financial planners helping senior consultants in private practice and the NHS
InvEsTIng In pRopERTy AbRoAD
Avoid pain when buying in Spain
With Spain’s fantastic climate, food, wine and lifestyle, it’s hardly surprising that it is the number one holiday destination for Britons and also for holiday homes. Following last month’s article about where to buy for investment or a holiday home, Dylan Mitchell looks at the process of buying property in Spain and turning that dream into a reality
The buying process
First things first: you will need an NIE number (numero de identificacion de extranjeros), which is a Spanish tax number.
This is similar to the National Insurance number in the UK. You will need an NIE number before you can sign to buy a property with the notaire, but also if you’re planning to work or start a business in Spain.
It is possible to apply for an NIE number yourself at a police station, but there are law firms that can apply on your behalf for a reasonable fee, which will save you a day of queues and paperwork.
When buying an existing property, you start by making an offer and negotiating the price.
Once everyone has agreed on a price, the lawyer will perform the necessary checks on the property – owner’s details, boundary lines – and draw up a sales agreement.
When your lawyer has confirmed that everything is as it should be, then you will sign the agreement and pay a deposit; typically 10%. This is the point of no return.
If you decide to pull out, you could lose your deposit and if the seller decides to pull out, then he must pay you twice your deposit as compensation. You now have four to 12 weeks to arrange a mortgage, insurance and open a bank account.
You will then meet with the notary and sign the deeds and take possession of the property.
It is prudent to have the property surveyed – although this is not common practice in Spain.
You can contact Spanish-based members of the Royal Institute of Chartered Surveyors via the website www.rics.org/es/
Debts
and encumbrances
In Spain, unlike the UK, debts stay with the property. If the previous owner has any unpaid bills or property taxes after you’ve completed on the purchase, then you could be responsible for repaying those bills.
This is especially an issue if the seller is not a Spanish resident, as
it is very difficult to pursue them overseas.
So it is therefore important to get confirmation that all utility bills and taxes have been paid in full.
Spain is well known for the practice of under-declaring the sale price and paying a portion of the price in cash. This is done so
port de soller, Mallorca
that the seller can pay less capital gains tax.
However, this is not only illegal, but it also means that when you come to sell the property, you will pay more capital gains tax, because you declared a lower purchase price.
If you are buying an off-plan property from a developer, it’s important to ensure that the company you’re dealing with actually exists and the person who is signing on behalf of the developers has the authority to do so.
For this information, check the Mercantile Registry, where the company ought to be registered. You can go to any Mercantile Registry office or use the www. registradores.org website to get information about the company’s registration, officers, attorneys-infact and bylaws.
Reservation agreement
When you have chosen the apartment or villa that you want to purchase, you will sign a reservation agreement that will include all the details of the property, including the price.
The property will then be taken off the market for a limited period of time, usually 30 days, which allows you the time to arrange a mortgage and for your lawyer to complete the required legal checks.
Once everything is in place, you will sign the sales agreement (escritura de compraventa) and you, or the bank providing your mortgage, will start making stage payments to the developer until construction is finished.
After signing the sales agreement for an existing property, or after making all the stage payments and construction has finished on an off-plan property, you will also need to ensure that the property is correctly registered on the property register and all fees are settled.
Note that it can take several months for your property to be registered and for you to receive the title deeds.
Arranging mortgages
There are two main strategies people use to arrange a mortgage to buy property in Spain.
One is to release equity from a property that you already own in
in spain, debts stay with the property. if the previous owner has any unpaid bills or property taxes, then you could be responsible for repaying those bills
Taxes anD buying fees
as a rule, you should assume that your costs and taxes will equate to between 12% to 15% of the property purchase price.
Legal fees are usually between €1,000 to €2,500.
iVa is the spanish equivalent of VaT and is charged on the purchase of off-plan property at 10% – plus stamp duty of 1%.
stamp duty is 6% to 7% depending on the region and is charged on the purchase price of an existing property.
notary fees range from 0.5% to 1%.
Property registration fees are approximately 1%.
if the property is located within an estate or complex, there will be maintenance charges for looking after the buildings, grounds and swimming pool.
iT is aLso iMPorTanT To be aware of The Taxes ThaT you wiLL be resPonsibLe for afTer buying The ProPerTy:
Personal taxes for non-residents on income earned in spain, such as rental income or interest on savings, is charged at a flat rate of 24%. for non-resident property owners who don’t rent their properties, there is an assumed level of income, based on the premise that you have derived a benefit from owning the property, which should be taxed.
Capital gains tax will be levied on any gain made on the property at the point of selling.
wealth tax is levied on assets within spain that are above a certain threshold.
Local property tax (impuesto sobre bienes inmuebles) is similar to council tax in the uK and provides funds for the local municipality.
the UK. This can be quicker, but the Spanish property will be in a different currency to the mortgage, which could work for you or against you.
Also, if you rent the property in Spain, a Spanish mortgage would be an expense against the income tax on the rent.
The other option is, of course, to apply for a mortgage with a Spanish bank. Typically, you can expect to borrow 60% to 70% of the value of the property with terms of up to 30 years or age 80.
As you can see, buying property in Spain is very different to the UK, and it’s important to seek legal advice from a qualified professional.
However, it’s really just a case of becoming familiar with a different system. Once you have bought the property and you are sitting on your warm terrace, looking at a beautiful view, eating tapas … it will all be worth it.
Dylan
Mitchell is director of Spain4Property.com
The Association of Independent Specialist Medical Accountants is a national network of firms advising over 3,000 medical practices across the UK. For some of the best advice available on accounting, taxation and pensions, visit our website and find your nearest AISMA accountant. www.aisma.org.uk or call Liz Densley on 01424 730345
DocToR on ThE RoAD: AUDi TT
Audi and welcome
At last – the latest Audi TT is fun to drive. It’s a head-turner and a practical car for everyday use, says Independent Practitioner Today’s motoring correspondent Dr Tony Rimmer
If your private practice captures an above-average share of the available market, then you are obviously doing something right.
And if you capture twice as much as your nearest competitor, then you must be doing something very special.
This usually happens as a result of lots of hard work and many hours spent raising clinical standards and quality. Sometimes, however, success cannot be foreseen and your popularity booms due to unpredictable factors.
This is exactly what happened to Audi in 1998 when it launched the original TT.
Its modern sleek design hid a very humble Volkswagen Golf chassis and engine under the skin, but the car-buying public went mad for it.
Design icon
Audi couldn’t keep up with production and a long waiting list developed. This only intensified the demand and when production caught up, the TT outsold its nearest rival by two to one.
It has remained in this position ever since and, apart from the styling, there is no logical explanation for this. But car-makers cannot stand still, however much
The TT has certainly had a successful update, with sharper lines and a more aggressive frontal aspect
a design icon they have stumbled upon.
The TT entered a second generation in 2006, lost 95kg in weight and had a mild face-lift.
Now, in 2015, we have the third generation. Another 50kg has been lost, there is a new adaptive chassis and the engines have more power. Styling has been evolutionary rather that revolutionary. Like BMW’s MINI, why spoil a good thing?
There are three engines available and various drive-train and gearbox options. There are two main trim levels: Sport and S-line.
The entry model has a 182bhp
The LCD replaces the usual dials with electronic versions which change size depending on what other information you want to present
2.0 litre turbo-diesel engine married to a manual six-speed gearbox and front-wheel drive. Quattro is not available with the diesel engine.
Next is the 227bhp 2.0-litre petrol T f Si four-cylinder turbo engine as used in the Golf GTI and this is available either as twowheel drive of Quattro.
Also available is the seven-speed dual-clutch S-tronic gearbox; Audi’s version of VW’s DSG box. And at the top of the range is the 307bhp TTS using a tuned version of the 2.0-litre petrol engine and Quattro drive.
Style appeal
As I’ve outlined, the TT has always appealed for its style, not its driving prowess. It could never really be described as a sports car and was always hampered by the fourdoor saloon Volkswagen underpinnings.
But the new car now sits on VW’s latest and advanced MQB platform. This has transformed the Golf Mk 7and the latest Audi A3. Does it improve the TT? I have been driving a 2.0 T f Si Quattro S-line S-tronic to find out.
Well, first impressions are surprisingly positive, because many of my colleagues asked about the test car when they had previously ignored much more sporty and expensive machinery in the car park.
The TT has certainly had a successful update, with sharper lines and a more aggressive frontal aspect. The S-line package includes LED headlights and a neat touch are the ‘sweeping’ indicators that flow from the centre outwards.
With the S-line you also get
large 19-inch wheels that look great but do nothing for the ride. Stick to 18-inch wheels if you can.
The TT has always appealed for its style, not its driving prowess
As we spend the vast majority of our time with our cars on the inside looking out, the interior environment is probably more important than the styling. This is where Audi always does well.
Advanced features
No other car-maker produces such consistent high quality when it comes to interior layout and materials. Not only that, the TT has some special new and advanced features.
Standard on all models is the high-resolution LCD 12.3-inch ‘virtual cockpit’ display situated directly in front of the driver.
The LCD replaces the usual dials with electronic versions which change size depending on what other information you want to present.
Just like the latest medical scanning equipment, it makes everything else before it seem old-fashioned and outdated. Audi is showing us the future.
Although the TT is a two-door
AuDi TT 2.0 TFSi Quattro S-line S-tronic
Body: Two plus two coupé hatchback
Engine: 2.0 litre four-cylinder
petrol turbo
Power: 277bhp
Torque: 350Nm
Top speed: 150mph
Acceleration: 0-60mph in 6.6 secs
Claimed range: up to 47.9mpg
On-the-road price: £35,335
This Audi is not only a supremely stylish coupé but also a very practical car for everyday use
coupé, it has hatchback practicality. The boot is large and becomes a lot bigger and remains flat if you fold the occasional rear seats.
The rear seats themselves are only big enough for children or small adults for very short distances. This Audi is not only a supremely stylish coupé but also a very practical car for everyday use.
But how does it drive? Well, the new Audi is a revelation. Gone is the feeling of driving a saloon car wearing a stylish suit; the TT now drives like a sports car.
It is not as good as a Porsche Cayman or Boxster, but it can give the BMW Z4 and Toyota GT86 a run for their money.
The steering has real feel and the chassis works in a really planted sort of way, particularly along twisty roads. The Golf GTI engine gives plenty of power and, with Quattro grip, can be applied effectively in all weathers.
The S-tronic gearbox works smoothly and is less clunky at low speeds than earlier versions of DSG. The new car is fun to drive and this could not have been said, in all honesty, about its predecessors.
Audi seem to go from strength to strength and the new TT will appeal to a lot of my medical colleagues.
Choose your model carefully and you will enjoy an advanced and stylish sports coupé that is easy to live with and turns a few heads.
Dr Tony Rimmer (right) is a GP practising in Guildford, Surrey
Flying under the radar
Keeping under HM Revenue and Customs’ radar is always a good idea and running your business effectively and taking professional advice is the key way of doing this. However, people do get caught out from time to time with things they had not envisaged or did not think were important.
Ian Tongue examines the common areas that can be overlooked and which can lead you to being caught out by the taxman
Record-keeping
HMRC now H as the power to fine businesses which it feels have kept inadequate accounting records.
It does not explicitly state what ‘adequate’ is, but it can be broadly inter preted as a record-keeping system that is complete and accurate and kept up to date on a timely basis.
Your accountant should advise you on your accounting system if failings are apparent. But the best option is to set things up properly from the outset and therefore take advice in this area before trading.
There are numerous electronic accounting packages on the market which act as a practice management and billing system. Provided these are used correctly, then they form the basis of a robust accounting system.
Quality and scope of work by accountants
w hen it comes to accountancy services, you generally get what you pay for. If you shop on price, you are likely to get less time spent on your affairs and a reduced level of work.
Unlike doctors, the accountancy profession is largely unregulated and, unfortunately, anyone can call themselves an accountant.
Engag ing an accountant who is regulated by a professional body such as The Institute of Chartered accountants in England and wales (IC a E w ) ensures the quality of work produced should be of a high standard and the accountant is answerable for their advice.
one of the key areas for those trading as sole traders that can lead to being caught out is only producing an ‘income and expenditure’ account rather than a full set of accounts, which includes a balance sheet.
a balance sheet is a snapshot
of the assets and liabilities of the business at the financial year and to produce it, everything has to be reconciled.
In plain speak, this means that instead of taking your income figure from a spreadsheet or other records in isolation, there has been a check performed to the physical income received into the bank account and the amounts owing to the business are in line with the movements during the year.
Introduction
If a balance sheet is produced, it allows the accountant to include this on your tax return and HMRC should gain comfort from the fact that the business has produced one, which, in turn, should reduce your risk of an inquiry.
Welcome to the BVRLA – I’m delighted that you’ve decided to join the trade association that provides a face for the vehicle rental and leasing industry, communicating its messages to customers, the media and government. The BVRLA’s corporate identity, particularly its logo, forms part of that message.
So why not turn to the experts in the field to help you find the vehicle that suits your needs?
anthony K associates are vehicle leasing brokers specialising in providing vehicle contracts for doctors and all associated professions in the medical sector.
The BVRLA has three categories of membership, each with a logo that members are entitled to use (and, in some situations, are obliged to use). Appropriate use of our logo tells your customers, your suppliers, and the rest of the world that you adhere to the high standards that come with BVRLA membership.
testimonials from our very many happy customers are proof of our attention to customer service and our practised ability to help clients get the vehicle they want quickly and easily.
This brief guide explains how we expect our logos to be displayed – and how they should not be displayed. These are not hard-and-fast rules, and we sometimes depart from them ourselves, but we do expect our members to respect them and to gain our prior approval before using our logo in any way other than described here.
Expense claims
HMRC does not release selection criteria for inquiries, but expenses that look unusually high either in quantum or as a proportion of income are always fair game for a question or two from the taxman.
If you need a copy of our logo, for use on your printed marketing material, or to go on a page of your website, please contact our communications team, who will be happy to send you an EPS or JPEG version appropriate for your purposes.
If you have any queries about use of the BVRLA logo that are not addressed in this guide, they will also be able to help
The first important aspect is to ensure that your expenditure claims are reasonable and can be supported under inquiry. There have been a few contentious issues concerning medics of late; for example, motor and travel claims and it is important that your accountant is aware of the current state of play.
Gerry Keaney Chief executive, BVRLA
Typical sensitive areas:
salary to spouse (or generally), particularly if no PaYE scheme is maintained;
Using home as an office;
Motor and travel;
Legal and professional fees.
The second aspect is disclosure on the tax return itself. There are sections within the tax return itself that can be used to add additional information.
overseas income/gains
The medical profession in the UK is very diverse with doctors from all over the world working here. Changes in recent years to counter tax avoidance have thrown a much wider net over worldwide income and this can certainly be an area where people get caught out.
the BVRLA Logo
For UK tax residents who were born here – and therefore domiciled here – you are assessed on your worldwide income.
This does not differentiate on country or province and therefore any interest you receive on a swiss bank account, for example, must be disclosed in the same way as a UK-based bank.
This has caught a lot of people out who thought that they were safe having money ‘offshore’, and transitional arrangements for many of these jurisdictions have been agreed to allow people to ‘own up’, so to speak.
For those that are tax resident in the UK but were not born here –and therefore most likely domiciled elsewhere – the rules are complex. Different rules exist depending on the length of time you have been in the UK and the nature and size of income/gain.
It is extremely important that you make your accountant aware of your worldwide position, as HMRC is unsympathetic to taxpayers forgetting about their property empire abroad.
operating a pAyE scheme Consultants often get confused on what they can pay staff and what their obligations are in relation to running a payroll.
Failure to operate a P a YE scheme, when required, can attract significant financial penalties and therefore it is important you understand your obligations if you are employing anyone.
Payments in excess of £485 a month – from 6 april 2015 – to an individual require a PaYE scheme to be opened and administered. a dditionally, employers have obligations under the Government’s new measures to provide workplace pensions for employees. This is known as auto-enrolment and can be onerous for employers. This subject was covered in more detail in the november 2014 edition of Independent Practitioner Today, page 48-49
pension Annual Allowance Statements
n ew legislation came into force for the 2011-12 tax year limiting the amount of tax relief available on superannuation (pension) contributions. This level was reduced to £50,000, but since 6
hmrc is unsympathetic to taxpayers forgetting about their property empire abroad
april 2014 has further reduced to £40,000 a year.
For most people not contributing to a public sector pension, it is straightforward, as they can simply add up the contributions made into their pension.
However, for those who are members of the n H s Pension scheme, the calculation is based upon the increase in pension benefits (accrual) in the year.
Therefore, a significant pay increment or clinical excellence award is likely to result in you exceeding the annual level.
In many cases, if you have exceeded the annual allowance level, the excess can be extinguished by utilising any unused relief from the previous three years.
However, the timing of receipt of statements from nHs Pensions has been sporadic, primarily due to them not receiving timely information from the various nHs bodies that employ people.
Your accountant should be looking at this for you each year and forewarning you if there could be an issue. If this is not on your accountant’s radar, then go elsewhere.
pension protection since the Government’s pension simplification measures on 6 april 2006, known as ‘ a -Day’, it has subsequently tinkered with lifetime pension values and annual contribution amounts to pension schemes.
a t each point of tightening things up, HMRC has offered pension protection. These are Primary, Enhanced and Fixed Protection (2012 and 2014).
There are strict rules for the
certain work that consultants commonly carry out is not regarded as medical and is regarded as ‘standard rated’ for vAT
retention of such pension protection and recent changes to bring in a new n H s Pension s cheme (the 2015 scheme) will result in many needing to withdraw their pension protection.
Failure to do so can attract significant penalties potentially running into thousands of pounds. If you have any form of pension protection, it is vital that you discuss matters with your financial adviser as soon as possible.
vAT
VaT is part of everyone’s daily life and we pay it over on much of our daily expenditure. For most consultants, however, their private practice is comprised mainly of medical work which is ‘exempt’ from VaT and therefore not a consideration for the private practice business.
But certain work that consultants commonly carry out is not regarded as medical and is regarded as ‘standard rated’ for VaT.
The most common is medicolegal work. But purely cosmetic procedures are also affected and this is a minefield and is subject to ongoing attention from HMRC. It is vital that your accounting system allows you to separate out different sources of income.
For those carrying out ‘standard-rated’ work, it is important that they are able to track their rolling 12-month income on a monthly basis. This is because compulsory VaT registration is required if you exceed the VaT registration threshold – £81,000 at the time of writing – on a 12-month rolling basis.
Failure to register on time can result in significant penalties and, more importantly, the income you received following the date you should have registered from is deemed to have the Va T included and therefore financial loss can occur.
Having a good relationship with your accountant and keeping him or her informed in all aspects of your financial affairs is the key to ensuring that the above risks are managed in your individual circumstances.
next month: A payroll scheme explained
Ian Tongue (left) is a partner with accountants Sandison Easson and Co
do you FInd our proFITs Focus serIes useFul? please let us know if it helps you or not. And if it doesn’t, what other data would you like to see presented? email robin@ip-today.co.uk
Healthy future in the air
Future
income trends for anaesthetists
look optimistic following the return of a majority Conservative Government in last month’s general election, reports ray stanbridge. Additional
material from martin murray
a s w E have stated in previous Profits Focus reports, it is becoming increasingly difficult to accurately report on trends of consultant anaesthetists’ private practice incomes.
a naesthetists, as with other consultants, have taken to incorporating their practices. o thers have joined formal and informal groups. Yet others have chosen to do n H s work through taking additional PaYE sessions.
as we also reported last year –Independent Practitioner Today,
June 2014 – yet other types of anaesthetists have established new sources of income, such as pain management clinics. all of these factors has led to increasing problems in trying to compare like with like.
Difficult market
In addition to the structural changes going on in the organisation of anaesthetists’ practice, 2013 was a difficult market.
The private medical sector was still depressed and the industry
AverAge Income And eXpendITure oF A consulTAnT AnAesTheTIsT wITh An esTAblIshed prIvATe prAcTIce
Win for group practices
By Robin Stride
Private anaesthetists have welcomed an appeal judgment upholding a Competition and Markets Authority (CMA) finding that forming and operating an anaesthetic group does not lead to adverse effects on competition.
Anaesthetists
was subject to downward pressure on fees from insurers.
Year ending 5 April. Figures rounded to nearest £1,000 (percentage is also rounded up)
Source: Stanbridge Associates Ltd. Additional information: Sandison Easson and Co
The Association of Anaesthetists of Great Britain and Ireland (AAGBI) supported the original CMA ruling in April 2014 which was part of the authority’s private healthcare investigation. AXA PPP subsequently challenged that before the Competition Appeal Tribunal (CAT) last January, but last month heard that it had lost on all three grounds. Dr Paul Barker, chairman of the AAGBI Independent Practice Com mittee, told Independent Practitioner Today: ‘Patient safety is
and postoperatively further improve safety and quality of care.’ He said the AAGBI, which represents 10,800 anaesthetists, welcomed any opportunity to improve safety and quality of care, as these were priorities for patients and members. AAGBI engaged with every stage of the inquiry, submitted evidence
also, it faced the attack by aXa PPP against the Competition and Markets a uthority (CM a ) decision that anaesthetist groups were not anti-competitive.
working through groups and offering their patients an effective and cost-efficient service.
leniently and the public is unprotected. Changes to the Medical Act approved by Parliament will also enable reforms to the way complaints about doctors are handled. Tribunals, run by the Medical Practitioners Tribunal Service (MPTS) operating separately from the GMC, will now be
For many groups, the recent decision in favour of the CMa will come as a relief for many anaesthetists, particularly for those who are
Despite the adverse market situation, we are pleased to report that consultant anaesthetists’ average gross fees rose by about 2.7% between 2012 and 2013, from £72,000 to £74,000.
Costs rose, on average, by about
who our AnAesTheTIsTs Are
In this survey, our anaesthetists:
Help in marketing for aesthetic practices
continue to work in the nhs and are not in full-time private practice
hold either an old-style or a new-style contract with the nhs
have been in private practice for at least five years
Are seriously interested in pursuing private practice as a business
have generated gross income of at least £5,000 for the year under review – ending 5 April 2013
may or may not have incorporated the business and/or be a member of a formal or informal group
4.3% from £23,000 to £24,000. as a result, taxable profit, on average, increased by about 2% from £49,000 to £50,000. surprisingly, gross margins fell slightly from 68.1% in 2012 to 67.6% in 2013.
These results are strong and perhaps reflect the critical role of anaesthetists in the private health sector.
costs constant
Insured activity seems to have been stable, but there has been growth in nHs Choose and Book work and also, in certain areas, in self-pay work. Trends here are not
strong, but sufficient to trigger a small income growth.
By and large, costs have been relatively constant. There was a modest increase in average staff costs from £10,000 to £11,000.
a s previously reported, this largely represents payments to spouses reflecting the growth in the personal allowance during the years of the coalition government. There seems to have been a slight reduction in general office costs for many anaesthetists, for reasons that do not appear to be obvious.
The only other cost increase was that of courses and conferences. It looks as if some anaesthetists, fol-
lowing a period of austerity, have decided to reserve their attendances at more exotic overseas training destinations.
w hat then of the future? a s noted above, the recent decision of the Competition a ppeal Tribunal supporting the CMa can only help stimulate the growth of groups.
we would expect insurers to change tack and seek to negotiate with groups. These are likely to become an increasingly strong feature in the market. Empirically, membership of groups is likely –all other things being equal – to stimulate income.
with the return of a majority Conservative Government, we also expect to see some stimulus in the private medical market.
For these two reasons, we are reasonably optimistic as to the future income trends for anaesthetists at least over the next five years.
w hether or not they will achieve their stated objectives of parity with surgeons over this period is, however, still problematic in our view.
next month: general surgeons
Ray Stanbridge runs an accountancy, finance and tax advisory service specialising in the medical profession. Martin Murray is a partner at Sandison Easson and Co, specialist medical accountants
what’S coMing in our julY-auguSt edition
make sure you don’t miss our next issue, published on 23 July. only subscribers to the journal are guaranteed to receive every copy and we don’t think anybody who is serious about continuing private practice in the future, when there is so much happening that will affect them, can afford to miss any issue.
coming up next month:
don’t miss Tingy simoes’s first instalment of her brilliant new series ‘cutting It Fine’. There is a misconception among surgeons of what it is the press are there for and what their needs are. understanding the media’s objectives and ‘marrying’ those with a need for education and promotion is integral to the success of the relationship with them.
Are you happy being a ‘business singleton’ or are you keen to build up your practice and start employing others? depending on your plans and business acumen, there are a number of options for growth
ophthalmic surgeon mr Ahmed el-Amir describes his experiences and the thinking behind his decision to start up a new multidisciplinary eye clinic in harley street
get the most out of your transcription service
The only way your marketing can work is if it stands out. surgeon dev lall has some tips, while in our ‘breaking Into The Aesthetics business’ series, pam underdown shows why you need a marketing plan
edITorIAl InQuIrIes
‘doctor on the road’ columnist dr Tony rimmer reviews the porsche cayenne
Ian Tongue’s ‘starting A private practice’ series looks at what you need to know about a payroll scheme if you are employing staff
Accountant ray stanbridge’s ten rules to avoid the taxman
Try our summer crossword. It is designed to help you improve your medical billing and collection requirements
business dilemmas: dr nicola lennard answers your concerns about risk management and consent
what now for doctors’ finances under the conservatives? cavendish
medical’s simon bruce reports
common mistakes independent practitioners make with managing their clinical waste
A lawyer casts an eye on the impact on doctors of the competition and markets Authority’s private healthcare market investigation order
Tips to help clinical negligence expert witnesses manage their cases and time
profits Focus looks at the earnings figures for general surgeons
AdverTIsers: The deadline for booking advertising for our July-August issue falls on 26 June
Robin Stride, editorial director
Email: robin@ip-today.co.uk
Tel: 07909 997340
AdverTIsIng InQuIrIes
Margaret Floate, advertising manager
published by The Independent Practitioner Ltd. Independent Practitioner
Today is editorially independent and thanks Bupa for its assistance with distribution. printed by pepper communications ltd Material is governed by copyright. No part of this publication may be reproduced, stored in a retrieval system or transmitted in any form without permission, unless for the purposes of reference and comment. Editorial layout is the copyright of the publishers. If you wish to use it for promotional purposes on websites or for reprints, we would be happy to discuss licensing the copyright to you.
£85 GPs and practice managers (private & NHS). £200 organisations.
But if you pay by direct debit, individuals pay only £70, and organisations £175
Call Proact Ltd on 01752 312140
Email: lisa@marketingcentre.co.uk
IPT
guArAnTee your copy
To guarantee your copy of Independent practitioner Today by taking out a subscription (at the rates shown on the left), phone 01752 312140 or send off a subscription form on page 22 or email lisa@marketingcentre.co.uk or go to the ‘About’ page of our website www.independent-practitioner-today.co.uk
If you pay by direct debit, individuals pay only £70 for a subscription. Just fill in the form on page 22 and send it to the Freepost address shown at the bottom of the form.
bAck Issues: £12.50 including post & packaging chAngIng Address or subscrIpTIon deTAIls?
phone 01752 312140 or email lisa@marketingcentre.co.uk
The professional’s choice for practice management
Client management and financial control is the lifeblood of any enterprise. The latest Healthcode online ePractice management tool is the professional’s choice for practice management, giving you the control you need wherever you are. Our ePractice management solution meets the needs of a range of healthcare providers, from independent practitioners to large enterprise organisations. Our different service levels means that ePractice will grow with your practice.
Take Direct Control
Access your patient details, appointments, bills and financial status from anywhere, any time.
What the professional’s say...
Protect Your Practice
The diary management feature on ePractice manager means I can focus on treating patients, while my PA is able to coordinate my appointments remotely.
Mr Barlow-Kearsley, Founder, Total Footcare Solutions
Long Term Partner
I’m delighted to say that we have never looked back. The system is really intuitive which has made it quick and easy to learn and yet it provides all the functionality we need. Most importantly, our consultants tell us it is working well for them too.
Catherine Goodsell, PA to the Hospital Director, Spire Sussex Hospital
Call us today to arrange a demo and to discuss your requirements on 01784 263 150 quoting: IPT. For further information visit: www.healthcode.co.uk/ipt