The business journal for doctors in private practice
In this issue
Rules for prescribing drugs remotely
In this issue
Back down to earth like meteorites
Markets go down and up! Dr Benjamin Holdsworth looks at the lessons that investors can learn from the last year
n See page 36
The most important language to master Clinical codes are undergoing a revamp to make life easier for doctors. Healthcode’s Jess Donelan has the low-down P22
Self-pay set to flourish
By Robin Stride
A 10-15% rise in self-pay volumes is being predicted in a major study from market analysts.
It says the pandemic has given the private healthcare sector a boost due to the suspension of all but very urgent NHS elective treatment coupled with higher wait times.
This has led to ‘a surge in inquiries for self-pay treatment with private consultants, clinics and hospitals’, according to LaingBuisson.
It reports rising interest particularly in orthopaedics, ophthalmology, gastroenterology, gynaecology, and urology – but adds that the challenge will be to convert interest to business.
The third edition of LaingBuisson’s Private Healthcare Self-Pay UK Market Report notes that treatment remains affordable and accessible for many although continuing restrictions mean it is hard to satisfy demand.
But it suggests that with the over55s being the main demographic for self-pay and limited opportunity to spend on leisure, holidays and eating out, they might spend more short-term on health and well-being.
LaingBuisson says self-pay growth
The MDU’s Dr Kathryn Leask discusses the impact of the GMC’s new guidelines P32 In association with
has been seen in specialty-specific services, including vein clinics, imaging clinics, ophthalmology providers and day surgery-only clinics – and some of these out-compete full-service hospitals on cost.
At the same time, finance options are becoming more popular because patients can spread the cost of treatment. Covid-19 has also led to the rapid digitisation of services across all sectors of healthcare.
The research finds no reason to believe the popularity of online consultations will decline and notes that private GPs’ online services were already growing in popularity before the pandemic.
Report author Liz Heath said: ‘Self-pay continues to show real and evidenced growth. While there are indications of an increased interest in private medical insurance, both from companies and individuals, in the wake of the pandemic, growth from insured patients is expected to remain static or slow for the foreseeable future.
‘Conversely, confidence in selfpay is high, with 52% of those surveyed expecting that this market will grow by 10-15% over the next three years – up from 45% in 2019 –and no one thinking the market will decrease.
‘We will, of course, have to wait to
When the boot is on the other foot
Why doctors with mental health problems are bad at being patients P52
see how the market normalises after the pandemic and its related restrictions lift. While the NHS has faced challenges in restarting elective treatment, self-pay is looking attractive even if currently wait times are longer than usual and we may anticipate that even once the NHS fully resumes elective treatment,
A CAPITAL INVESTMENT:
A world-leading cancer hospital has opened up a research-led diagnostic outpatient and treatment centre in central London. Read all about it on page 7
the private healthcare wait times will also reduce.
‘The question is whether people, having discovered that paying directly for medical care is an option, continue to call on it, whether for a virtual private GP appointment or more complex surgery.’
continued on page 6
MAIN TRENDS HIGHLIGHTED IN REPORT
n Self-pay market growth seen by all hospital groups
n Providers predict pent-up demand will increase self-pay demand in 2021 and beyond
n Bias towards growth among providers the South-east and London
n More transparent pricing across independent providers – but anomalies in published pricing
n Improved consumer-centric approach to self-payers
n Growth in interest in private healthcare, including private medical insurance
n NHS waiting times directly influencing self-pay demand
n Continued ‘mix and match’ approach to ‘paid’ healthcare, with patients choosing to suit their needs, such as accessing online private GP services of diagnostics
n Growth among well established NHS PPUs Source:
LaingBuisson
TELL US YOUR NEWS. Contact editorial director Robin Stride
The prospects of seeing improved income for consultants and private hospitals from self-pay in the wake of the easing of pandemic restrictions will be welcomed by thousands of specialists.
After the financial difficulties experienced by doctors in private practice during the height of the pandemic, there are hopes of a return to normal flows of non-insured patients plus a little bit – or even a lot – more.
A jigsaw of factors are now in play. Yes, some people have managed to save more during the pandemic’s lockdowns and may be more inclined to spend it on treatments. Cosmetic procedures to boost morale already show a resurgence.
But this could, for now, be countered by a continued reluctance to use public transport and wariness about spending savings just in case they join the ranks of the unemployed. Things are, however, looking a little rosier as our front-page story testifies.
A 10-15% rise in self-pay volumes is being predicted in a major study from market analysts LaingBuisson. It reports a private healthcare sector boost due to longer waiting times and the suspension of NHS elective treatments.
This has led to ‘a surge in inquiries for self-pay treatment with private consultants, clinics and hospitals’, according to LaingBuisson.
Increased interest is being seen, for instance, in orthopaedics, ophthalmology, gastroenterology, gynaecology and urology – but it, of course, recognises that the challenge will be to convert interest to business.
Self-pay market growth, however, is being reported by all hospital groups and there must be useful lessons for consultants to consider from the encouraging self-pay results achieved since Easter by The London Clinic, which has transformed its offering (see page 6).
PLUS
Patients willing to pay
Liz Heath, author of LaingBuisson’s latest report into the UK self-pay market, shares some insights and considers key issues for consultants P16
Getting the best out of your team
All private doctors want a highperforming team. Jane Braithwaite has some interesting ideas to help you do this in your daily work P18
How to mess up a social media stunt
Independent practitioners sometimes turn to social media stunts to create publicity for their practice. But beware, as they can spectacularly back-fire P26
Reasons patients sue their urologist MDU medico-legal adviser Dr Shabbir Choudhury analyses clinical negligence claims affecting urologists and provides advice on managing risk P28
You need to be colour co-ordinated Strike the bright note! Advice on how to use colour in your branding and marketing, and how to avoid the colour clangers that can ruin your design P30
You’re all in it together
Lawyer Lisa Davison explains how ‘declarations of trusts’ are useful tools for private doctors to protect valuable property investments P38
OUR REGULAR COLUMNS
Doctor on the Road: The Golf is closing with the innovators
If you’re ready to go electric, Dr Tony Rimmer recommends you give the VW ID.3 a test drive P44
Survive a private practice: Avoid a pension tax shock
Accountant Ian Tongue cuts through the jargon to help you understand pension tax issues P50
Profits Focus: Big changes on the horizon
Our unique benchmarking survey reveals big changes appear to be on the way for anaesthetists P55
Doctors retain too much cash in firm
By Edie Bourne
Private practices are being warned there could be a costly price resulting from their policies to store cash.
Many doctors could be storing too much cash in their business accounts and could see the value eroded by inflation, according to specialist financial planners Cavendish Medical.
Doctors with limited companies will often choose to retain their profits in the practice rather than draw dividends from excess funds which would be subject to their
personal rate of income tax – often at the level of an additional rate taxpayer.
Their aim is that when the practice is liquidated at retirement, the business may qualify for Entrepreneurs Relief, which reduces the capital gains tax (CGT) payable to just 10%.
But Patrick Convey, technical director at Cavendish Medical, explained why this could be a problem.
He said: ‘This strategy can be effective for some doctors who would prefer to pay a reduced rate of CGT rather than a substantial
IDF supports members through Covid struggle
Private doctors’ representatives have highlighted some major issues facing independent practitioners as they deal with the Covid-19 fallout in the months and years ahead.
And the importance of looking after their own health and mental well-being is stressed in the Independent Doctors Federation’s annual journal IDF News. Its GP committee chairman Dr Di Louden encourages members to use the organisation’s psychiatry scheme if they are experiencing difficulties.
This service is provided by some of the group’s psychiatrists who offer clinical appointments to members, with the first appointment partially sponsored by an IDF corporate member.
She reports that with the growth of telemedicine, consultations take place by phone or video with face-toface only when clinically necessary.
IDF specialist committee chairman Dr Sean Preston says relations with private medical insurers were invaluable as consultants’ income
streams dropped and priorities changed.
Bupa was ‘particularly helpful’ in using its patient portal to highlight which doctors were open for business, specifically those able to see patients virtually.
He supported many members who were hard hit as private hospitals were stripped of equipment and contracted out to the NHS.
While things have improved significantly, IDF president Dr Neil Haughton tells members of his concerns at the difficulty in supporting patients when referral networks and hospitals no longer functioned in the same way.
He writes: ‘. . . I worry about the medical diagnoses that have been delayed over this year, both in private and NHS medicine.’
The journal’s surgeon editor Mr Greg Williams reflects that while missing face-to-face interaction at medical meetings, the delivery of educational content was uncompromised. He wonders if doctors will fully return to globetrotting in order to attend conferences.
rate of income tax on their earnings. However, many are keeping significant sums in their business.
‘Business accounts will be paying very little interest and the value of the cash will not be keeping pace with inflation. Put simply, your money today will have less purchasing power than in a year’s time.’
The problem first surfaced during a seminar the company ran for doctor clients early in March.
Mr Convey told Independent Practitioner Today: ‘In addition, the rate of Entrepreneurs Relief is not guaranteed in the future nor do we
Health cover ‘needs to be holistic’, says AMII chief
A more integrated approach to the private medical insurance offering in a post-pandemic environment is being called for by the new executive chairman of the Association of Medical Insurers and Intermediaries.
David Middleton said: ‘Mental health and well-being are top of most of our clients’ objectives. I am currently a trustee of a mental health charity that supports athletes and I have been staggered by the amount of young people seeking help particularly in the last 12 months.
‘Yet, as an industry in both healthcare and risk, we are still
know which limit will be applicable.
‘The lifetime limit of Entrepreneurs Relief has already been reduced from £10m to £1m. We also do not know what could happen to the rules surrounding CGT.
‘There are alternative options; for example, it is possible for the business to invest in a corporate investment account with the aim of generating a return which at least matches inflation in the medium term.’
Cavendish Medical is advising doctors that, as with all important financial decisions, the merit of this strategy must be carefully considered and is dependent on many key factors – there is never a one-size-fits-all option.
Mr Convey added: ‘And, of course, money that is invested may fall in value as well as rise. However, keeping too much cash in zero-interest accounts for several years could be particularly ineffective.’
David Middleton, new AMII boss
very much working in silos and are still product driven. We really need to work more closely, as physical, financial, mental and social wellbeing cannot and should not be treated separately.’
He told the group’s AGM that insurers had responded well during Covid-19 with a willingness to help and support intermediaries and the end customer, with telemedicine and additional support services.
And he commended insurers for pledging to not profit from the pandemic. Some had already made appropriate premium refunds to clients.
Share your experience of what has and has not worked in your private practice. Even if it’s bad news, let us know and we can spread the word to prevent other independent practitioners falling into the same pitfalls. Contact editorial director Robin Stride at robin@ip-today.co.uk
HOW COVID HIT DOCTORS’ PAY
29% report a decrease in earnings, reasons included:
Covid-19 ‘wiped out private practice’
Fewer hours worked during Covid due to burnout and stress
No access to hospital theatres
Loss of waiting list initiatives
Lockdown: inability to do non-essential profitable work
Increased tax and contributions
Prolonged absence due to sick days and self-isolation
Other Medscape research has suggested many doctors are considering changing jobs or type of practice due to burnout, which could have affected income
Drop in pay spurs docs to seek more private work
By Robin Stride
Significant numbers of doctors say they plan to take on more private practice to boost their earnings after suffering big pay losses due to Covid-19.
Income dropped for 29% of doctors taking part in a major pay survey of those working in private practice and the NHS – and 27% reported they now aim to do more private work.
Referral delays, restrictions on private practice, and time-consuming infection control measures are among reasons cited for lower incomes.
Women doctors were disproportionally affected with a greater fall in pay compared to their male counterparts, according to the survey of over 1,000 doctors by a health information service. They reported 30% lower pay than their male counterparts.
Over 60% of doctors felt underrewarded for their work, according to the Medscape UK Doctors’ Salary and Satisfaction Survey 2021.
New Nuffield hospital at Barts appoints its director of nursing
Nuffield Health’s 32nd hospital in the UK – and first in London – has reached a milestone by appointing its ‘matron’ and director of nursing.
Anthony Fitzgerald will lead nursing care across cardiology, cardiac surgery, oncology and orthopaedics, the key clinical specialties at the new Nuffield Health at St Bartholomew’s Hospital, the City of London’s only independent hospital which opens in the autumn.
Facilities include 55 individual en-suite rooms, four advanced digital operating theatres, seven specialist intensive care beds and 28 consultation rooms
He called his role that of a very ‘traditional matron’, adding: ‘Our aim is to use our unique connected healthcare approach to offer our patients a complete pathway.
has worked for Optegra Eye Health Care and the Harley Street Clinic. He said: ‘Our ability to provide connected healthcare services and the fact that Nuffield Health is a charity enables us to attract the best nurses and clinicians in London.
Doctors across specialties were included in the survey, with 73% working in the NHS, 23% operating in both the NHS and private sector, and 4% in the private sector only.
Twenty-nine per cent were considering leaving the UK to practise abroad, more commonly considered by the under-45s (45%) than over-45s (20%).
The survey, conducted between 10 November 2020 to 16 February 2021, suggests the gender earnings gap increased during the pandemic, with female doctors reporting a 10% reduction in earnings on average, which accounted for double that reported by male doctors.
The average earnings gap between GPs and specialists also widened.
GPs reported an average drop of £12,000 compared with specialists, who reported an average decrease of £9,000.
A third of doctors reported a rise in earnings with enhanced private practice due to NHS shutdowns among common reasons cited.
‘For example, a patient could be referred by a Nuffield Health GP, receive treatment at our new hospital and then choose to receive rehabilitation at any at any one of our 113 fitness and well-being centre across the UK, including 21 within London.’
Mr Fitzgerald was previously chief nurse at Schoen Clinic and
‘We want our nurses to come from a range of backgrounds, from the NHS and the independent sector, and to be passionate about delivering excellence to our patients. Our nurses and clinicians will have more time with patients, have opportunities to develop their careers and a good work-life balance.’.
PHIN steps up drive to get doctors to publish fees
Specialists can expect more contact with the Private Healthcare Information Network (PHIN) following limited communications while so many addressed the pandemic.
They will be asked to check they are searchable on a revamped website for the organisation, where more patients will look for private healthcare services.
Patients have requested details of the services offered by consultants, the locations they provide care and information about treatment costs starting at a consultation.
PHIN’s consultant relationship manager Anne Coyne said it wanted to encourage all independent practitioner consultants to showcase in front of those considering private treatment.
‘We are always here to help consultants to create and improve their profiles and ensure that information about their fees is up to date.
‘We will also be reminding consultants who have yet to submit fee information that they have a legal obligation to do so.’
Anthony Fitzgerald
Anne Coyne
Private care ‘Oscars’ held online
Doctors, their teams and their hospitals are celebrating following the announcement of the winners at the LaingBuisson Awards 2020 last month, which had been greatly delayed due to the pandemic.
Hundreds of sector-leading organisations gathered at a virtual event to reflect on the past year and shine a spotlight on the amazing work executed during the midst of a global pandemic.
The awards ceremony was attended by hundreds of key decision-makers, chief executives and industry experts, where they celebrated their team, colleagues and associates in the field.
The 15th LaingBuisson Awards
recognised 32 winners across seven categories: Social Care, Clinical Services, Innovators & Leaders, Investors & Finance, Property, Advisers and, most recently added, Outstanding Response to Covid.
Winners of the 2020 award included the following:
Outstanding Response to Covid in Healthcare Award:
The Montefiore Hospital, part of Spire Healthcare.
‘An independent hospital that was ahead of the curve in terms of offering support to the NHS and its patients and which adopted and integrated new technology quickly and effectively to facilitate the safe treatment of patients.’
Hospital Award: The Royal Marsden – Royal Marsden Private Care.
‘Highly differentiated offer providing excellent outcomes for patients and great support and development for colleagues.’
Hospital Group Award: Schoen Clinic UK
‘Significant innovation, and investment, into the delivery of mental health services. The patient-recorded outcome measures (PROMS) platform sounds very interesting as well.’
Public Private Partnership Award: Cromwell Hospital and The Royal Marsden –Royal Marsden Private Care.
A star of adaptation
The Montefiore Hospital’s Outstanding Response to Covid in Healthcare Award recognised its early response to the crisis while ensuring its cancer patients continued to receive care throughout the pandemic.
Director of clinical services
Lynette Awdry said: ‘When we opened our doors in 2012, little did we know we would be supporting our NHS colleagues during a global pandemic eight years later.’
The accolade was given to the hospital in Hove, East Sussex, because it demonstrated ‘a strong culture delivering better care, excellent communication, early responses, adapting to and overcoming challenges during the pandemic including the turn-around of a challenging situation in healthcare’.
The Montefiore’s response to the Covid-19 outbreak and Government lockdown restrictions was ahead of its competitors in the region.
were created to enable clinicians to stay on site if required.
Based on the proposal, the trust assigned The Montefiore to be a regional hub for clinically urgent surgery. The trust’s leads came to view the hospital, so they could then inform their patients.
By 15 April, The Montefiore was running theatre lists and a Covid swabbing and pre-op test service for NHS time-critical patients. It was the first independent hospital in the region to do surgery of any volume.
‘Great initiative between charitable, public and private sector to ensure access to cancer treatments while freeing up acute beds to manage the Covid-19 pandemic.’
Nursing Practice Award: The London Breast Institute –Princess Grace Hospital.
‘An exceptional example of true innovation based on an understanding of patients’ needs.’
Innovation in Care Award: The Good Care Group
‘Good use of innovation and technology to support its underlying care and people business.’
Entry to the 2021 awards has now opened.
Schoen shines in mental health care
Schoen Clinic UK’s award for the 2020 Private Hospital Group of the Year celebrates ‘excellence in the provision of acute or mental health services with a focus on innovation and differentiation as a result of an individual hospital initiative or investment’.
Managing director Andy Davey said: ‘To win this award at the best of times is an accolade, but to do so in reflection of such a challenging year for the whole healthcare profession, is a staggering achievement.’
Simultaneously, the hospital completed a detailed assessment of its own resources and skill set and, by the Easter weekend 2020, had made a proposal to Brighton and Sussex University Hospitals NHS Trust – recently renamed University Hospitals Sussex – to become a ‘green’ oncology Covid NHS hub.
The geography of the entire hospital was redesigned with designated zones – red, amber, green – for patients on different pathways to keep them safe.
The hospital ward was one such protected zone and on-call beds
In early March last year, before any national directive, the hospital’s management team had already decided to stop elective surgery, focusing only on timecritical procedures, such as cancer, and had informed all affected patients.
The hospital quickly adapted to digital technology to communicate with patients, GPs, consultants and staff. Zoom was used to host GP information events, patient physiotherapy classes and cancer support groups, daily staff meetings, to communicate with other private hospitals and weekly meetings with the trust.
At the same time, it continued to provide care for its cancer patients, including practical and emotional support such as launching a home delivery service for chemotherapy drugs, and making regular contact with chemotherapy patients via Zoom or phone to see how they were coping.
Schoen Clinic UK currently comprises four facilities:
Schoen Clinic Day Centre for Mental Health Chelsea – treating anxiety, mood and eating disorders;
Schoen Clinic Newbridge –treating children and young people with eating disorders;
Schoen Clinic York – treating adults with eating disorders.
The group’s ethos is to use the best consultants and deliver ‘highquality, specialised care with a relentless focus on clinical outcome excellence’.
The Spire Montefiore Hospital in Hove, East Sussex
LAINGBUISSON AWARDS
Boost self-pay by patient approach
By Robin Stride
A London independent hospital is reporting a 25% increase in the number of patients asking for details of self-pay pricing.
The London Clinic told Independent Practitioner Today it has seen a 5.6% rise in the number of patients coming through the door in the first four months of 2021 for pay-ityourself treatments.
Both figures are comparisons to 2019 rather last year when Covid19 sparked a large drop in activity.
Inpatient day case admissions are up 40% on last year and outpatient episodes up 122%.
The figures are reported as the charitable hospital sees encouraging results from a move last month to try and meet market needs and offer increased support for consultants and patients at the same time.
Business development manager Georgina Bishop said the hospital decided to expand its self-pay offering and heavily invested in setting up a new department that is prepared to give patients time as they talk things through. ‘If it takes 15 minutes, it takes 15 minutes – it is not a call centre environment.’
The hospital trebled its number of self-pay advisers so there is now a six-strong team managing inquiries from people who represent just some of the massive
backlog of pent-up demand. Consultants need support to help manage that too.
She said: ‘We focused on what the market needs. Patients are distressed, concerned about their health care and are having a lot of concerns about seeing their GP.
‘Rather than focus on targets and numbers, we talked about the service we wanted to offer – that was just as important to us. For me, it was more about being able to offer what I tend to think of as ‘a safe place to land’ for patients, a place where they can be listened to, take time and for us to understand their needs.
view of the self-pay market, but I don’t share that. I think in the next couple of years that’s going to escalate quickly. But I’m not sure I can put a number on that.’
Travel restrictions have so far hampered a resumption of international business. but self-payers have been coming from far afield in the UK, some from many hundreds of miles.
Miss Bishop said consultants understood inclusive pricing packages were now what many patients were looking for. ‘We have a range of all-inclusive packages so you know how much you are going to pay; they are really popular.
Montefiore’s chief charts route back after Covid
‘We wanted to be that team that would signpost people to the right services and consultant and see that they understand how it all works.’
Miss Bishop said one of the most important aspects of service is the ability to support patients whatever their needs – all in one place.
While The London Clinic’s selfpay efforts, which are helped by zero-interest-rate packages available through an outside lender, already show encouraging results, she thinks the non-insurance side of the market will flourish much more.
‘There was quite a pessimistic
‘There have been a notable number of inquiries for gastro/intestinal procedures and bariatric surgery – the pounds have gone on during lockdown. ENT and ophthalmology is strong, plus cosmetic and reconstructive, and rhinoplasty.’
One of the first things consultants want to do when they start a new practice at the hospital is sign up for these packages, she said.
‘I think everybody is very happy to be back doing private work and being able to support those patients. Consultants are happy to be back seeing the support we are giving them.’
The new managing director of the Montefiore Hospital in Hove has announced the management team will be looking for ways to enhance the services on offer. Rachel Dixon said her first priorities will be to ensure the patient journey is as safe as possible while re-adjusting the hospital rated ‘outstanding’ by the Care Quality Commission back to its normal workload post-Covid.
She added: ‘This is a modern hospital with a top-class diagnostic suite and an awardwinning dedicated oncology unit which provides specialist care across Sussex. And it has an excellent reputation for highclass patient experience with exceptional clinical outcomes for patients.’
Simplify your offering to get more patients
Continued from page 1
According to Richard Gregory, a leading commentator on self-pay, there are several factors clouding potential self-pay growth.
Writing in this month’s Independent Practitioner Today, he says doctors will be flat-out trying to clear the NHS backlog, but the same doctors will be needed to do likewise for insured patients and who will be asked to carry out self-pay work.
Trusts could push back against doctors trying to see patients privately and much of what happens will be outside of hospital and consultants’ control.
Self-pay growth has slowed over the last three years and LaingBuisson has consistently revised downwards its forecasts despite the growing and ageing waiting list.
Mr Gregory adds: ‘My belief is that this is a direct result of the
industry’s relative failure to adapt its offering quickly enough to respond to retail consumers. In short, it is a supply-side weakness.
‘Private operators have enjoyed double-digit growth in inquiries, which has not translated into similar growth rates in revenue and activity. Much work is still needed to be done in the key areas of pricing transparency and simplicity; of the promotion of payment options;
of proposition clarity; of onboarding from initial inquiry; and of meeting customer expectations around service levels.’
He advises consultants who get most of their self-pay work from private operators or directly through their own marketing to work on these critical supply-side factors to convert more of the excess pent-up demand into real self-pay growth. See pages 9 and 16
Georgina Bishop
PPU WATCH
Royal Marsden opens large private unit in central London
By Philip Housden
The Royal Marsden has expanded its private care presence in London by officially opening a new research-led diagnostic outpatient and treatment facility in Cavendish Square.
Its new facility between Oxford Street and Harley Street offers world leading standards of cancer care to patients in a calm, modern and reassuring environment.
Housed within an Edwardian listed building, it is a dedicated and comprehensive cancer diagnostic and treatment centre and part of The Royal Marsden’s Private Care service provision.
The venue offers patients fast and direct access to the hospital’s world-leading diagnostic and research-active consultants specialising in a full range of cancers.
It houses a diagnostic imaging suite offering MRI, CT, X-ray, ultra-
sound and mammography, plus other clinical specialties, including genetics, plastic surgery and reconstruction and pain management.
A one-stop diagnostic service will be offered at the centre, where patients can expect to have an appointment booked following their initial inquiry, direct access to diagnostic services, same-day scans and test results.
The centre is also home to a minor procedure suite and a medical day unit with treatment bays.
These are promised to provide the highest level of patient-focused care for UK and overseas patients who are receiving some of the most advanced cancer treatments.
Cavendish Square will initially see both private and NHS patients, ensuring that all those with suspected cancer receive quick access to diagnostic tests.
It will also contribute to the financial sustainability of The
Royal Marsden, ensuring all patients benefit as part of the integrated partnership between the tust’s NHS and private services.
This model means revenue generated from Private Care is reinvested back into the NHS trust, ensuring that all patients can be offered the highest standards of cancer treatment and care.
Prof Chris Nutting, consultant clinical oncologist and clinical director of The Royal Marsden Private Care at Cavendish Square, said: ‘The Royal Marsden sees and treats 60,000 NHS and private patients every year and Cavendish Square is an exciting new development that will allow our multidisciplinary teams to offer world-class standards of cancer care to even more patients, diagnosing cancers faster with a targeted and personalised approach.’
Managing director Shams Maladwala said: ‘Improving patient
access to better and more rapid diagnostics is a priority at The Royal Marsden, and Cavendish Square is part of a broader strategy to diagnose cancer faster and earlier.
‘Thanks to our integrated model, patients seeking the very best private cancer treatment can do so safe in the knowledge that it is backed by the strictest safety standards and governance usually only seen in the NHS.
‘Further investment in the trust’s NHS services from Private Care revenue provides the best of both worlds for both patients and clinicians, supporting The Royal Marsden in continuing to be worldwide leaders in the field of cancer diagnosis, treatment, care, research and education.’
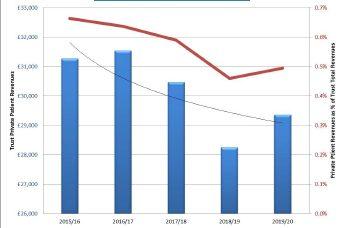
Royal Marsden has by far the highest private patient revenues in the NHS, with growth of £11.3m and 9.3% to reach £132.6m in 2019-20 – 20% of the NHS total.
New mega-trust creates opportunities
Royal Brompton and Harefield hospitals has merged with Guy’s and St Thomas’ to become one of the largest and strongest healthcare organisations in Europe. Both trusts feature in the top ten NHS trusts for private patient income, with combined revenues of £67m in 2019-20.
The merger is already paying dividends, as the Brompton’s private diagnostics and outpatients centre at 77 Wimpole Street has
been opened up to Guy’s and St Thomas’ consultants.
Wimpole Street offers consulting rooms and imaging including MRI, CT, PET-CT, non-invasive cardiology and more.
Talking about the merger, Kim Foord-Paton, head of private patients, said: ‘We’re excited to work with colleagues from Royal Brompton and Harefield Hospitals (RB&HH) and build on our collective excellence in patient care.
‘With RB&HH now part of the Guy’s and St Thomas’ family, there’s a great opportunity to share our facilities and resources, starting with utilising RB&HH’s Wimpole Street outpatient and diagnostic facility, which offers state-of-the-art equipment and a modern, welcoming environment for consultants and private patients.’
David Shrimpton, managing director of RB&HH Specialist Care
added: ‘We are all very excited to be part of Guy’s and St Thomas’ NHS Foundation Trust and have no doubt it will bring many opportunities to deliver even better heart and lung care to our private patients by accessing our new integrated healthcare services.’
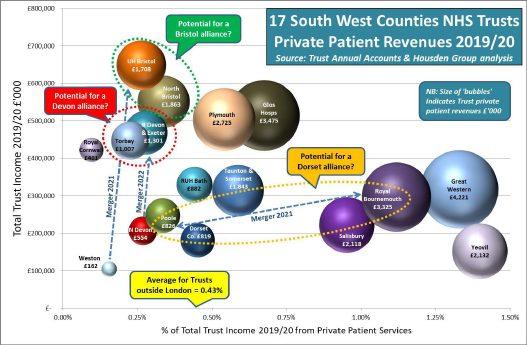
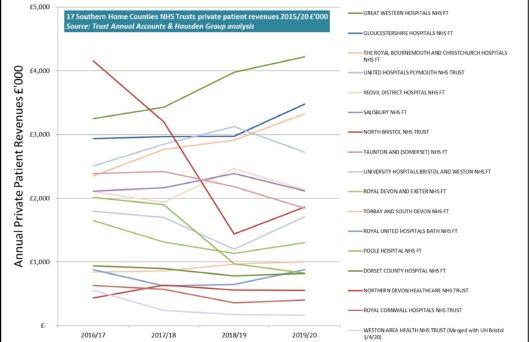
Philip Housden is a director of Housden Group. See his feature article on PPUs in the South-west region on page 47
Shams Maladwala, managing director of the Cavendish Square facility
Have a say on training
By a staff reporter
Doctors are being urged by the GMC to have their say on how the pandemic has affected their workplace learning.
Senior doctors who act as trainers, plus tens of thousands of doctors in training – including in private hospitals – are being asked to take part in the regulator’s National Training Survey (NTS), making it the UK’s largest annual insight into workplace education and training.
Orthopods are braced to care for post-Covid sports injuries
Consultant orthopaedic surgeons are bracing themselves for a surge of sports injuries as people get back to tennis and golf as the pandemic eases.
According to the medical director at Orthopaedic Specialists, people are at an increased risk of potential serious upper-limb injuries.
Mr Ali Noorani, consultant orthopaedic and trauma surgeon for shoulders, elbows and upper limbs, predicts that serious injuries will not result from falling or breaking bones.
People will suffer instead because sports players’ bodies are no longer used to the intense sharp movements required after a year of sedentary home-working, which has stopped the need for those movements.
He said: ‘It is great to get back to sport, but even those who have maintained their fitness throughout lockdown will not be prepared for the sort of movement competitive sport requires.’
Mr Noorani said three different groups of people were at risk of injury in competitive sport:
Celebratory sports participants – A large group of people who are not normally active at all
Prof Colin Melville, the council’s medical director and director of education and standards, said:
‘The pandemic continues to have a huge impact on all aspects of healthcare. The NTS will help us understand the extent of that impact on training. The responses will influence our work with others to help make sure training recovers as we move on from this extraordinary time.
‘But to do so effectively, we need to have input from as many doctors as possible: trainers as well as
but will mark the end of lockdown by expressing their freedom and liberation engaging in sporting activities once courts and courses all re-open.
Temporarily inactive – Lots of people who usually would be actively playing sport throughout the year but have done not much activity at all through lockdown.
These people have potentially had a year out from their chosen sport.
Active – A third group has been active during lockdown, engaging in home exercise regimes such as interactive treadmills, running and work-outs. However, even though this group is keeping fit, they are not playing competitive or active sports and are therefore at risk of injury caused by ballistic movement.
The lockdown has already impacted upper-limb injuries over the last year. Mr Noorani reports a significant rise in cycling injuries as people took to the roads in increased numbers.
trainees from all parts of the UK and from across different specialties and workplaces. Every voice counts. The more voices we hear from, the more we can do to improve the places where doctors train and to improve the training they receive.’
This year’s NTS is open until 18 May. The 2020 survey was scaled down due to the pandemic, but the last full NTS in 2019 was completed by more than 75,000 doctors, including around 95% of trainees.
Questions, tailored to trainers
and trainees, cover areas including:
Workloads and burn-out;
Time available to deliver or receive training;
Access to break rooms and study spaces;
Incivility and rudeness in the workplace;
The pandemic’s impact.
The GMC said responses would provide an unparalleled picture of healthcare training environments across all four UK countries and help ensure trainers and young doctors were properly supported.
Eye surgeons target lockdown’s legacy
A year of working from home has enabled six million commuters to save £145 a month on average, enough to pay for life-changing surgery and be free of glasses and contact lenses, according to a group of consultant ophthalmic surgeons.
In a poll of 2,000 workers, OCL Vision eye clinics – formerly Ophthalmic Consultants of London – found that 39% feel their eyes are suffering from the increased screen time, with eye strain emerging as a common problem.
It said the ongoing cost and hassle of wearing contacts or glasses prompted almost two-thirds of people with vision problems to say they would like to be rid of them for good.
OCL Vision consultant laser surgeon Mr Allon Barsam said: ‘Our research reveals that nearly twothirds of glasses and contact lens wearers want to be rid of them, so it’s exciting to think that so many now have the option to turn a pretty grim year into a positive legacy: permanently better eyesight.’
The company said laser surgery typically costs around £2,000 per eye, but with a range of finance options available,it has launched an interactive tool to help people decide if the sums add up for them.
By inputting what they spend on glasses or contacts, users ‘can see at a glance if it’s worth making the leap to laser – and correcting their eyesight for good’, it said.
Consultant ophthalmic
surgeon
Mr Ali Noorani, medical director at Orthopaedic Specialists
Mr Allon Barsam of OCL Vision
WAITING LISTS AND SELF-PAY
Some words of caution about self-pay growth
Are independent practitioners facing a surge of self-pay patients as a result of Covid-19 causing NHS waiting lists to soar? Richard Gregory says the private sector has a lot of
work to do to cash in on any boom
ALL PRIVATE operators will tell you that the number-one driver of self-pay growth is the collective market forces at play in the NHS –politics, capacity, commissioning and demand management.
But, first and foremost, it is the size and nature of the waiting lists for elective surgery.
It therefore stands to reason, post-Covid and as the country gets back on its feet, that there will be huge pent-up demand for self-pay, leading to a healthy revenue growth for hospitals and consultants, doesn’t it?
I don’t think it is as simple as that. True, there is pent-up demand for ‘healthcare’, but how much of this is demand for selfpay? I am not sure. Nor is LaingBuisson. At its last Private Acute Healthcare Conference in October 2020, it predicted that self-pay would not recover to 2019 levels before 2022.
Let’s explore the market dynam-
RICHARD GREGORY,
Leading commentator on self-pay and runs his own healthcare consulting business
ics at play currently and see what consultants and private operators can do to encourage more people, willing and able, into paying for their own healthcare.
Firstly, what external factors are at play, which are influencing my caution?
1
Although the correlation between growth in self-pay and waiting lists is fairly strong statistically – self-pay grows as waiting lists grow – it doesn’t feel that actual self-pay penetration into waiting lists is that high.
Since 2016, one million people have been added to the waiting list, representing growth of almost 30%. The number of people waiting more than 18 weeks has risen from 300,000 to 1.4m, which is growth of over 460%.
According to LaingBuisson, in the same period self-pay has risen from £943m to £1.16bn, a growth rate of 23%. This 23% increase represents approximately 72,000
more patients for self-pay in a period of time where one million have joined the waiting list and over one million more are waiting over 18 weeks. Unspectacular.
2
Doctors will be flat-out trying to clear the NHS backlog, but it is the same doctors who will be needed to do likewise for patients with medical insurance and who will be called upon to carry out self-pay work. A huge capacity dilemma and juggling act.
3 Will more trusts push back against doctors trying to see patients privately while the NHS remains in such a challenging situation, as NHSE and senior clinical leaders did in London in January? The political situation is on a knife-edge of sensitivity.
4 People are fearful of their jobs going forward, not to mention the many who already find themselves out of work. The unemployment rate sits at 5.1%, the highest since 2015, and 2021 shows the biggest annual rise since the financial crash
There are, however, some other more favourable factors, which could offset these to some extent:
Rising consumer confidence among the higher earners and those with savings, who collectively dominate self-pay customer demographics;
House prices are expected to rise by around 4% this year now that the stamp duty holiday has been extended;
The NHS will struggle to get any sort of hold on the waiting lists within the next five years. Government is not yet pledging the level of investment, which would be needed.
Covid imposes severe restrictions on the way healthcare is delivered; the extra resources needed are not there to deliver the
work and the existing workforce is exhausted.
This is the complex and unpredictable landscape ahead, much of which is out of hospital and consultants’ control.
But I will go back to the performance of self-pay over the last five years, which has not been as stellar as many commentators have been predicting or expecting each year.
Growth slowed
Indeed, self-pay growth has slowed over the last three years and LaingBuisson has consistently revised downwards its forecasts despite the growing and ageing waiting list.
My belief is that this is a direct result of the industry’s relative failure to adapt its offering quickly enough to respond to retail consumers. In short, it is a supply-side weakness.
Private operators have enjoyed double-digit growth in inquiries, which has not translated into similar growth rates in revenue and activity.
Much work is still needed to be done in the key areas of pricing transparency and simplicity; of the promotion of payment options; of proposition clarity; of onboarding from initial inquiry; and of meeting customer expectations around service levels.
If you are a consultant or consultant group who gets most of their self-pay work from private operators or directly through your own marketing, the message is the same.
Work on these critical supplyside factors, which are totally within your control, to convert more of the excess pent-up demand into real self-pay growth.
See LaingBuisson’s self-pay report, page 16
A look back through our journal’s archives of a decade ago reveals that although times change, some issues are not so new
A trawl through the archives: what made the news in 2011
Self-pay income boost
The chairman of the BMA’s private practice committee was forecasting a change of fortunes for independent practitioners as patients paid for their own private treatments to escape NHS financial restrictions.
Mr Derek Machin said only 15% of consultants had increased their private profits over the previous year.
But he went on to assure doctors: ‘There is an inevitability over the next decade that private practice will increase.’
He told 170 consultants and GPs at the association’s annual private practice conference that preliminary findings of the BMA’s latest survey showed private earnings were frozen for 40% of specialists in the previous year and dropped for 45% of them.
Mr Machin claimed the health service was facing ‘a slow attrition’ which would intensify. He said the situation was so bad in some areas that some consultants were rethinking decisions to stay purely salaried.
A gynaecologist at the meeting explained he was at the event because he had changed his mind about never doing private practice.
He explained: ‘I am getting tired of turning people away because I don’t do private work. But the primary care trust is broke.’
GPs unaware what private sector offers
Private specialists faced a huge challenge to educate GPs about their services to maximise new business potential.
92% of GPs expected to refer patients privately in the next 12 months, four in ten were seeing a rise in patients asking about privately funded treatment, and nearly a third aimed to make more private referrals.
But findings of a Spire Healthcare survey of more than 500 GPs also revealed many specialists risked missing out on referrals because family doctors were unaware of how good they were and what they could do.
Spire clinical director Dr J. J. de Gorter said: ‘Established ideas about private healthcare are preventing patients from receiving full information and the ability to make informed choices.’
NHS pension woes could mean more private rivals
Increased numbers of doctors could join the hunt for more private work as a result of concerns about the NHS Pension Scheme, we reported.
The BMA was warning the Government that many doctors might retire early from the health service due to predicted further rises in pension contributions.
It reported it had seen Government Actuarial Department figures showing contributions could almost double by 2015.
Those paying 7.5% or 8.5% of salary could, it was predicted, pay double within four years.
Every doctor to suffer a tax probe
Established and would-be private consultants and GPs were warned they could expect to suffer some sort of tax inquiry during their career.
Martin Murray, a partner at accountants Sandison Easson and Co, warned that HM Revenue and Customs was coming down harder on doctors.
He suggested they paid for the ‘well worth it’ protection of one of the insurance policies offered by
most accountants ‘for around £200-£300’.
The average time for a tax aspect inquiry to be completed into doctors’ affairs was 18 months to two years.
Present incorrect
Gifts to doctors such as mugs, diaries and stationery were banned under an updated code from the Association of the British Pharmaceutical Industry.
2% dip in NHS’s private patient income
Recessionary pressures, and what was known as the private patient cap, led to a 2% drop in NHS income from treating patients in private patient units.
According to market analysts Laing & Buisson, total private patient income of NHS trusts was £430m in 2009-10, down from £439m the previous year.
TELL US YOUR NEWS
Share your experience of what has and has not worked in your private practice. Even if it’s bad news, let us know and we can spread the word to stop others falling into the same pitfalls.. Contact editorial director Robin Stride at robin@ip-today.co.uk
We’re part of a whole
What does the Government’s response to the Paterson Inquiry mean for doctors working in independent sector? David Hare (right) reports
AT THE end of March, the Government published its longawaited update on its response to the former Bishop of Norwich’s inquiry into jailed surgeon Ian Paterson (see our website news story, 23 March).
The Government’s statement focused on work around five of the inquiry’s recommendations, notably patient information, patient consent, multidisciplinary teams, patient recall and ongoing care. Its work on responding to the Paterson Inquiry is still ongoing, and a full response to the Bishop’s report is expected by the end of the year. But what does this interim update mean for independent healthcare providers and those working in the sector?
The Covid-19 pandemic has, of course, dominated the work of the healthcare system in the past year and it was welcome to see the Government acknowledge the ‘critical role that the independent sector has played in supporting the NHS’ over the last year.
In this light, therefore, it made clear the importance of improving safety and governance across both the NHS and the independent sector and the need for any recommendations to be implemented across the entire healthcare landscape – an important principle we at the Independent Healthcare Providers Network (IHPN) have been advocating for some time.
A key thread throughout the Rt Revd Graham James’s inquiry was the importance of all healthcare organisations directly providing clear and simple information to patients around all aspects of their care to give them full confidence in the quality of treatment they are receiving.
As part of this, the Government supported the inquiry’s recom -
mendation to have consultants write to patients, rather than GPs, and suggests that guidance published by the Academy of Medical Colleges could be incorporated into the requirements of the NHS Standard Contract.
As the recommendation specifically states that both consultants in the NHS and independent sector should adopt this practice, the inquiry’s report indicates that there should also be requirements for consultants undertaking nonNHS commissioned work to write directly to patients.
Period of reflection
Linked to this, the Government also recommended there should be a short period introduced into the process of patients giving consent for surgical procedures, to allow them time to reflect on their diagnosis and treatment options, with the GMC monitoring this as part of Good Medical Practice
The Government’s update on the Paterson inquiry also focused on multidisciplinary team (MDT) working and calls for the Care Quality Commission (CQC) to assure itself that all hospital providers are complying effectively with up-to-date national guidance on MDT meetings.
The Government made clear the importance of improving safety and governance across both the NHS and the independent sector
UK-wide medical device information system;
2
Establishing a Patient Safety Commissioner for England with responsibility for medicines and medical devices;
3
Extending the remit of the Health Service Safety Investigation Branch to independent providers.
As part of this, it is suggested that the CQC will work to make questions about MDTs mandatory in its assessments.
This is an area of treatment planning which IHPN’s Medical Practitioners Assurance Framework (MPAF) highlights, making clear that independent providers should formalise arrangements for multidisciplinary team-working, including:
How relevant clinical data is transferred;
How the teams are reviewed;
Outcomes audited.
Further recommendations from the Government relate to the work that both University Hospitals Birmingham NHS Trust and Spire Healthcare have done to contact all of Paterson’s patients and review their care, as well as providing support and follow-up care as needed.
Medical device information
In addition to responding to these five recommendations, the Government also used its statement to highlight three pieces of legislation it is implementing to support patient safety:
1
Amending the Medicines and Medical Devices Bill to create a power to establish a
Each of the actions specifically mentions and involves the independent sector, reflecting the importance of having a ‘wholesystems’ approach that promotes patient safety across the entire healthcare landscape in the UK, rather than being siloed between the NHS and independent sector.
Core role
So what to make of this update from the Government?
Of course, there is much progress to be made to ensure the highest possible levels of patient safety in the long term – not least the need to drive forward the data agenda to better capture both consultant scope of practice and clinical outcomes across the health system.
However, the broad thrust of the Government’s response, that the independent sector plays a core role in healthcare provision and as such a ‘whole systems’ approach to patient safety and clinical governance is needed, is undoubtedly the right one.
We will continue to work with all stakeholders to ensure the full response to the former Bishop’s inquiry supports those working in the independent sector to deliver the safest and highest quality care to patients that they deserve.
David Hare is chief executive of the Independent Healthcare Providers Network
ACCOUNTANT’S CLINIC: THE BUILDING BLOCKS OF ACCOUNTANCY
Julia Burn (right) continues with her A-Z of top tips. This month she turns to the letter U
is for Unlocking to of top tips
Operational and financial matters to consider as lockdown eases and the last elements of support that you can claim come to an end
THANKFULLY, LOCKDOWN restrictions are continuing to ease and life can gradually get back to some form of normality as this process continues.
This month, I concentrate on the operational and financial aspects which will affect businesses as the country begins the gradual process of ‘unlocking’.
Operational factors
Many businesses, including private medical practices, have had to close their doors during the pandemic, either fully or partially.
It is going to take time for people to get their heads around returning
to some form of normality and it is anticipated that this will be a gradual process and many businesses will not return to working full time in their usual place of work.
Operational factors to consider will include getting buildings ready for re-opening where they have had to close. This will inevitably incur additional costs of deep cleaning and redesigning workplaces to incorporate any social distancing measures that are likely to stay in place in some form for an indeterminable period of time.
Another consideration will involve managing staff who maintain an element of working from
home to ensure that the right level of staff are on site at the right times to ensure the business runs smoothly.
Covid self-testing
Businesses will also need to consider processes to put in place for staff to carry out self-testing for Covid, where this is considered appropriate; agreeing how often tests need to be performed, how they are recorded and monitored. Many people have delayed taking annual leave due to the travel restrictions in place and this could cause additional pressures for businesses as the country begins to
unlock and staff want to take time off. Managing staff to ensure that everyone does not decide to take annual leave at the same time could be quite a task.
Another consideration which has become a hot topic among businesses and the country in general is mental well-being.
Ensuring that businesses have provision in place to support their staff, some of whom will have had to shield or may be nervous about returning to a normal way of life, will be a major onus. This support needs to encompass those who have suffered difficulties with loneliness and felt isolated due to
THE SELF-PAY MARKET
Patients willing to pay
Liz
Heath (right), author of LaingBuisson’s
latest report into the UK self-pay market, shares some insights and considers key issues for consultants
THE SELF-PAY market is doing well despite economic uncertainty created by Covid-19 and Brexit.
With NHS elective surgery restricted and few opportunities to spend on discretionary items such as holidays and leisure, many people are discovering that paying for treatment is affordable and accessible.
The LaingBuisson report reveals a sense of optimism about the future of self-pay. A ‘pent-up demand’ is driving interest and there appears to be a direct correlation between the well-publicised waiting lists for NHS elective procedures and diagnostics and inquiries about self-pay.
This relationship has not always been easy to determine in the past, but delayed access to NHS services now seems to be the primary driver. The scale of growth is difficult to estimate, as there are still capacity issues impacting the ability of many private sector providers.
These will ease through 2021 and early 2022 when we will be able to assess whether opportunity has translated into activity. Interest in private medical insurance products has also grown in recent months.
As expected, there is some regionality to the self-pay market. London and the South-east’s higher-density population and greater prosperity continues to drive market growth. However, research by Private Healthcare UK showed that, compared to 2019, visits to its website from all UK regions were significantly up in 2020.
This suggests that interest in private healthcare overall has jumped noticeably in the past year. Providers are reporting heightened interest in self-pay in traditionally lower-volume regions such as northern England.
Sustained growth
The cycle of growth in self-pay treatment tends to follow the UK economic cycle. However, the recent sustained growth in the self-pay sector appears to be better than might have been expected given the economic challenges around Covid-19 and Brexit.
Recent data on the increase in personal savings among some segments of the population may also indicate that decisions about discretionary spending – such as that on private healthcare – may become easier for some.
Around 59% of respondents to LaingBuisson’s survey believed the main growth in self-pay is likely to come from the over-55 age groups. This is a slight reduction on 2019 although, given the various demographic drivers, still puts the over55s in the core growth group for self-pay, and mirrors feedback from other sources.
Twenty-one per cent of respondents felt there was potential growth in the 35-44 age group, higher than for the 45-54 age group. This may reflect the rapid
adoption of technology and willingness to embrace digitisation around self-pay services such as GP consultations and diagnostics in a younger demographic.
As a barometer of general interest in private healthcare and specifically the cost of private treatment, Google Trends shows that interest has not diminished in the UK and aside from a dip in spring and early summer 2020, the general trajectory and relative search interest has been sustained and has shown some peaks towards late 2020.
This may relate to corresponding news coverage about record NHS waiting times and may also correspond to increased promotion of private medical insurance and a range of private healthcare services during late 2020 and early 2021.
Is confidence justified?
In 2019, an estimated 21% of independent acute medical hospital revenue was derived from self-paying patients residing in the UK, equivalent to £1,117m. Self-pay spending at independent hospitals continues to show growth.
LaingBuisson estimates tend to be more cautious than some others, but even considering slight dips in some years, the overall trajectory remains positive and providers are optimistic about prospects.
Over the five-year period between 2014 and 2018 inclusive, private self-pay growth averaged 7.4% annually in real terms,
REASONS TO BE CHEERFUL
Market confidence is high.
Over 50% of survey respondents expect the UK self-pay market to grow by 10-15% in the next three years
With access to elective NHS treatments restricted, patients are discovering self-funded private healthcare is both affordable and accessible –opening the market to a new audience
Finance options are increasingly popular and provide another key driver for growth
reflecting a period of high private demand for many acute medical treatments. Strong self-pay business continues to underpin profitability for hospitals and clinics. This contrasts to demand for cosmetic surgery self-pay, which has shown little or no growth over the same period.
Recently, we have seen an upswing in interest in self-pay spending in the Midlands and the North. This is supported by recent data from Healthcode, the online solutions provider for private healthcare. It showed a surge in billed insured activity in the West Midlands at the end of 2020 and a return to pre-Covid levels in most other areas, including – encouragingly – London.
Of note was also an increase in activity in areas such as the Northeast and South-west. By and large, most providers have experienced good growth in self-pay recently. Some, such as Nuffield Health, have outperformed the market for several years.
The report costs £895 for a single user printed hard copy or £2,238 for a multi-user digital PDF plus printed hard copy. Details at www.laingbuisson.com
Understanding how potential patients seek information
AN IMPORTANT change in the way potential patients seek information is emerging. Social media and rapid availability of information play an important part and perhaps the role of the GP may be declining.
Through analysis of Google Trends, we noted that there were subtle differences in the way searches occur. For example, for some procedures, there were more searches related to price than cost. Understanding the tone and language used by potential patients and matching that in communication, whatever the medium, is becoming much more important.
Decreasing length of stay and an increase in outpatient/ambulatory procedures means that the cost of self-pay treatment may be considered more affordable than previously.
Certainly, when other factors such as long NHS waits come into play, more patients are clearly considering funding their own treatment. The wide availability of finance plans to spread the cost is also a positive factor.
Affordability was cited as a key factor in engaging with potential patients and the ability to easily illustrate how to spread the cost of treatment appears to be a successful tactic. The ability to fix and guarantee the price is an important consumer consideration.
Ophthalmology is a specialty where the costs of accessing private treatment are relatively lower than 20 years ago and competition in this sector has ensured prices remain accessible.
Restrictive NHS funding criteria continue to have an impact in driving growth in private ophthalmology. The presence of many specialist ophthalmology providers has also ensured a more commercial approach.
There is greater transparency of information available on quality, and provider groups are working to
further develop publicly available quality and outcome measures.
It is not clear yet how much the public has engaged with this, although LaingBuisson’s survey suggested growing impact from the Private Healthcare Inform ation Network’s work. We also noted consultants increasingly provide information on their own outcomes via their personal websites. Consultants can be more proactive in supporting patient decision-making. Visibility and greater discussion of outcomes and quality measures are important.
For most patients who choose the self-pay option at their local hospital, price is not the key determinant – even if the same procedure is available at a much lower price elsewhere.
Rather it is an overall perception of value for money from the consumer perspective, which may include ‘soft’ and ‘hard’ quality indicators.
The challenge for providers –and consultants – may be to try and distil some of these positive factors into promotional and media messages as well as personal interactions and consultations.
Room for improvement
We continue to be of the view that consumers are not being as well served by the systems and processes around self-pay inquiries.
Navigating through online information, online chat or using a helpline needs to be easy and stress-free, especially given that they may be seeking help while worrying about their medical condition.
Unfamiliarity with private healthcare is common and so potential patients need strong, supportive guidance. If affordability is a key consumer concern, then guide prices for procedures and consultant fees need to be easily accessible and transparent. Consumer expectations have been heightened by the concept of
TIME TO FOCUS ON THE CONSULTANT’S ROLE
The shift to collaborative and group working presents many opportunities for consultants and providers, not least the ability to engage proactively with providers to design and deliver self-pay pathways.
Many consultants are establishing a strong online and digital presence which can have a role in influencing patient choice. The ability to leverage ‘consultant power’ collaboratively and productively offers many mutual benefits.
We have seen how Covid-19 has amplified demand for self-pay. This has come with challenges, not least releasing capacity to meet that demand while, for some providers, juggling the requirement to provide NHS capacity.
Issues around theatre scheduling and capacity have been evident, but perhaps these needed addressing anyway. Certainly, providers told us that the pandemic had provided an opportunity for them to re-evaluate many aspects of their service delivery and specifically the patient journey for self-pay patients – including customer experience and better capacity planning.
Providers told us they had renewed focus on the consultant-provider relationship during 2020 – a critical factor in optimising future opportunities.
Bupa reported that traffic to its Consultant Finder service increased significantly during 2020. In early 2020, it reported around 70,000 visits per week. This had increased to 110,000 by early 2021.
Therefore, it is vital for providers and consultants to ensure all information provided to third parties is timely and accurate so inquiries can be properly dealt with.
‘on demand’ for many everyday services, and private healthcare is no different.
Online no longer means sitting at a desktop computer and access is 24/7 from virtually anywhere.
LaingBuisson’s random mystery shopping for common self-pay procedures found provider responses mainly satisfactory, but not always timely. The live chat function offered by one provider worked well.
Demographic shift
The UK population’s growth rate in mid-2017 and mid-2018, at 0.6%, was slower than any year since mid-2004. In 1998, around one in six people were 65 years and over (15.9%); this increased to one in every five people in 2018 (18.3%) and is projected to reach around one in every four people (24.2%) by 2038.
These headline data from the Office for National Statistics are important in shaping the self-pay market. The ‘baby boomer’ generation is widely acknowledged to have more disposable income due to generous pensions and the ability to invest in leisure and other activities related to quality of life.
If the NHS cannot offer them timely treatment, then they may increasingly look to the private sector.
Department for Work and Pensions (DWP) data in 2018 showed pensioners had higher annual incomes than 20 years previously. Significantly, 67% received money from private pensions, a 5% rise from 1998.
In 2019, the proportion receiving income from private pensions had grown again to 69%. The DWP reported that the percentage of pensioners in the top half of the overall population income distribution in 2017-18 was 49%. In 1994-95 this was 38%. Pensioner couples in the South-east have the highest pensioner income, 14% higher than the UK average.
The potential to deliver sustained self-pay growth requires a collaborative approach from all involved in the design, delivery, and financing of the self-pay market.
If we have learnt anything from the past year, it is that the old rules and restraints can torn up. New relationships, strategies and focus will be required to realise the opportunities this market offers.
Getting the best out of your team
All independent practitioners want a high-performing team – Jane Braithwaite (below) has some interesting ideas to help you do this in your daily work
AS LEADERS , we want to lead high-performing teams and, as team members, we want to be working as part of them.
Working in a great team is an absolute pleasure and has an enormous impact over how we feel about our work and the company we are employed by.
Of course, the opposite is also true and working in a dysfunctional team is deeply negative and has a huge impact on performance. It can be enough to encourage individuals to leave and pursue other options.
So how do we establish a great team, how do we lead one and how do we play our part in contributing to the success of the team?
Let’s start by exploring some examples of great teams. The sporting world is a good place to begin. Anybody who is loyal to a particular team or club will know all too well the highs and lows associated with team performance.
When a team is failing, the manager often gets put under enormous pressure and the result can be a swift departure, as experienced by Chelsea and Tottenham Hotspur FCs’ head coaches Frank Lampard and José Mourinho this season.
Many of us have recently enjoyed the Six Nations rugby championship and each team taking part has been analysed by professionals, the media and all of us at home watching. Each team has its own characteristics, with Wales being admired for their grit and determination while England was heavily criticised for a lack of discipline.
Back in 2003 when the England ruby team won the Rugby World Cup, the team was led by Sir Clive Woodward, who helpfully shares his winning strategy.
Woodward says that ‘great teams are made up of great individuals’ and he focuses on creating a winning culture and claims a formula for creating ‘champion individuals’.
Woodward lists four key criteria to create a winning team: Talent – individual talent; Teachability – ‘It’s often the most experienced person who is unteachable’; Pressure – the warrior spirit; Will – commitment to win.
Working in a great team is an absolute pleasure and has an enormous impact over how we feel about our work and the company we are employed by
In his 2003 team, Woodward describes having five champions and ten warriors, and he highlights the importance of coaching on two levels: for individuals and for the team together.
Woodward’s approach was clearly successful and he continues to support sporting organisations but also offers coaching and consultancy to business executives.
Significant improvement
Another team strategy brought to our attention is the ‘aggregation of marginal or incremental gains’. The strategy works on the premise that if we can improve every aspect of a team’s performance by 1%, the overall result will be a significant improvement.
This approach was highly publicised following the success of the British cycling team in 2008 and 2012 and although its achievements are being questioned, the strategy is still popular in the business environment.
One of my personal favourite sporting strategies that has been embraced by business is described in the book Will it make the boat go faster? as described by Ben HuntDavis in which he documents how his team adopted this strategy and subsequently won the gold medal in the rowing eight at the 2000 Olympics in Sydney.
I like this, as it is simple and can be used to immediately ensure everyone on the team is on the same page.
In business, we might use this strategy to achieve a project within tight time-scales or to focus on a particular aspect of our service – for example: ‘Does it make the patient experience better?’ or ‘Does it make the treatment safe?’ It’s a great way to ensure focus and gain momentum to achieve shortand medium-term goals.
These examples of sporting successes in team performance provide plenty of interesting learning opportunities that can be adapted for business and we may pick up ideas from numerous sources as we create our own leadership and team management strategies.
Each of us can use best practice to influence our leadership style, but, ultimately, our approach will be unique to us and our personalities.
As we build our own style, it is important to break down the aspects of teamwork and ensure we consider each aspect to build a good all-encompassing approach. Reflecting back to the wise words of Sir Clive Woodward, we can consider the four elements of team success that he bases his approach on.
1. Talent
To create the greatest team, we want to have the greatest leader and the most talented individuals. While this might be realistic for Chelsea FC, most of us are restrained by factors such as money, availability of talent, and geography.
In the real world, what we really need to aim for is the most talented individuals available to us and ensuring that each individual delivers to the best of their ability.
A team also requires a group of people with differing but complementary talents.
In a healthcare setting, our teams potentially comprise doctors, nurses, administrative support and business managers, all of whom have very different skills and have been educated differently.
All these individuals must find a way to work together to the benefit of the patient. As well as having differing skills, a team will also be home to lots of different personality types and character types.
Some people are eternal optimists, always anticipating the best possible outcome and seem oblivious to any potential barriers. Others will be the complete opposite, preferring to plan for the worst-case scenario so that all bases are covered and prepared for. When two people of opposite types such as these come together, they can either create a perfectly ➱ p20
balanced partnership or they can find it impossible to work together and hit a brick wall.
Another potential conflict can arise when one person is an ideas person and another is a detailed planner. The detailed plan that is essential to one person can be viewed as a barrier to progress and a time-wasting activity to the person who has the great idea and wants to get on with delivering it.
Again, a balance of these two styles is ideal, but how do we bring different personalities such as these together to work collaboratively?
In last month’s article, I talked about leaders needing to develop self-awareness and to understand their natural style. I suggested using psychometric profiling tools such as Myers Briggs and C-me profiling and, again, these tools are equally relevant to individuals working together as a team.
Once an individual understands their own style and also the natural style of others on their team, they can learn the right way to communicate and work with one another to achieve success.
The ‘ideas person’ learns that by listening to the detailed-oriented individual, their idea has a far greater chance of success as a result of the detailed plan that will
be developed ensuring that every outcome is prepared for.
2. Teachability
An ability and willingness to learn is an important attribute for all team members.
Too often, we associate this with more junior team members, but actually it is relevant to even the most senior members of a team and Woodward is quite right when he states: ‘It’s often the most experienced person who is unteachable’.
To work well as a team, every individual needs to be prepared to adapt their ways of working for the good of the team. The well-known management phrase: ‘It’s my way or the highway’ might feel powerful, but what if there is a better way?
3. Pressure
When Woodward says pressure, what he really means is the ability to perform under pressure and he believes the only way to ensure an individual and therefore the team can succeed under pressure is to practice by exposing the team to pressure regularly.
He uses role play requiring the team to work through every eventuality to ensure they know exactly what to do in each situa -
tion. This easily relates to complex surgical procedures and can also be adapted to the business environment – for example, the launch of a new service, clinic or company.
Personally, I would also argue that all teams must think about how to recover from being under pressure and build resilience. It is clearly not possible for any individual or team to perform under constant pressure.
We need to build in mechanisms for recognising long periods of extreme pressure and have plans to relieve it and allow recovery.
This may involve adjusting holiday allowance, time off in lieu or activities within the working day to allow for recuperation, but they must be built in. This will be the topic for my next article.
4. Will
A team needs to be driven by an agreed goal or objective and to share a joint motivation to succeed and achieve the goal. This is why the strategy of ‘Will it make the boat go faster?’ is so effective, as it aligns the whole team to one clear, simple goal.
If a team has one or more members who doubt the goal is achievable, then this will have a draining impact on the team’s morale and
The only way to ensure an individual and therefore the team can succeed under pressure is to practice by exposing the team to pressure regularly
reduce each person’s motivation to succeed.
Summary
It is said that ‘teamwork makes the dream work’ and we all agree wholeheartedly, but achieving the dream requires an investment of effort on a consistent basis.
The most talented individuals might be individually amazing, but unless they can work together as a team, their talents can be wasted.
Humans are tribal and evolved working together in teams, intrinsically knowing it makes them more effective and ultimately our lives more enjoyable.
In recent months, we have seen an increasing number of reports of the effects of Covid on mental health and this is particularly apparent within the health care community.
Next month, I explore the information we are being presented with and start to identify ways we can help to address and alleviate these issues.
If you would like to share your comments regarding leadership or discuss support for you and your team, please get in touch.
Jane Braithwaite is managing director of Designated Medical
WORLD-RENOWNED CANCER HOSPITAL EXPANDS
Research-led cancer care in central London
The Royal Marsden Private Care has opened a new diagnostic and treatment centre in Cavendish Square
THE ROYAL Marsden has expanded its Private Care presence in London by opening a brand-new, research-led, diagnostic, outpatient and treatment facility in Cavendish Square.
Located in the heart of the capital’s world-renowned and respected healthcare district between Oxford Street and Harley Street, housed in an Edwardian listed building, the new facility offers CQC-rated ‘Outstanding’ standards of cancer care to patients in a calm, modern and reassuring environment.
Cavendish Square will offer patients fast and direct access to The Royal Marsden’s world-leading diagnostic and research active consultants specialising in a full range of cancer services.
Cavendish Square will initially see both private care and NHS patients, ensuring that all patients with suspected cancer receive quick access to diagnostic tests.
The centre will also contribute
to the financial sustainability of The Royal Marsden, ensuring all patients benefit as part of the unique, integrated partnership between The Royal Marsden’s NHS and Private Care services.
Prof Chris Nutting, consultant clinical oncologist and clinical director of The Royal Marsden Private Care at Cavendish Square,
SERVICES AND FACILITIES AT CAVENDISH SQUARE
➲ Fully comprehensive cancer diagnostic and treatment centre with fast and direct access to research-led diagnostic experts covering all main tumour groups and clinical specialties
➲ Same-day and next-day appointments with world- leading consultants in surgery, medical oncology, clinical oncology, haematology and genetics
➲ One-stop diagnostic appointments
➲ State-of-the-art full diagnostic imaging suite offering CT, MRI, CT, X-ray, mammography, ultrasound, nasoendoscopy and colposcopy
➲ Medical Day Unit with 12 chemotherapy chairs in bespoke treatment bays, which will provide the highest level of patientfocused care for UK and overseas patients who are receiving some of the most advanced cancer treatments
➲ Seven outpatient consulting rooms
➲ Onsite pathology with rapid blood test turnaround times
➲ Minor procedure suite
➲ Onsite pharmacy
said: ‘The Royal Marsden sees and treats 60,000 NHS and private patients every year and Cavendish Square is an exciting new development that will allow our multidisciplinary teams to offer world-class standards of cancer care to even more patients, diagnosing cancers faster with a targeted and personalised approach.’
Shams Maladwala, managing director of The Royal Marsden Private Care, said: ‘Improving
patient access to better and more rapid diagnostics is a priority at The Royal Marsden, and Caven dish Square is part of a broader strategy to diagnose cancer faster and earlier.
‘Thanks to our integrated model, patients seeking the very best private cancer treatment can do so safe in the knowledge that it is backed by the strictest safety standards and governance usually only seen in the NHS.
‘Further investment in the trust’s NHS services from Private Care revenue provides the best of both worlds for both patients and clinicians, supporting The Royal Marsden in continuing to be worldwide leaders in the field of cancer diagnosis, treatment, care, research and education.’
At Cavendish Square, you and your patients will benefit from The Royal Marsden’s new GP fast-track referral service, which includes:
Additional capacity for private patient appointments;
Fast access for your patients;
Direct booking into consultant clinics;
Same-day tests plus diagnostic and treatment plans;
Feedback on patients’ consultation and treatment pathway;
Dedicated contact centre for rapid appointment bookings.
Referring your private patients to Cavendish Square is quick and easy. Get in touch with our Private Care Contact Centre on 020 4502 3873 or at privatepatients@rmh.nhs.uk. www.royalmarsden.nhs.uk/ private-care
Prof Chris Nutting, Clinical Director of The Royal Marsden Private Care at Cavendish Square, outside the new diagnostic and treatment facility
Shams Maladwala, managing director at Cavendish Square
The most important language to master
Clinical codes are commonly used by independent practices for billing as well as recording clinical events, but making sense of all those letters and numbers can feel like trying to master a foreign language.
Healthcode coding analyst Jess Donelan (right) offers practical advice and looks at the wider potential of coding in the sector. He also explains how Healthcode is using its expertise to make the world of codes accessible for all
Few independent practitioners have the resources to employ professional clinical coders, but Healthcode’s expertise in this area can help you bridge the gap
UNLESS YOU are a techie, you are unlikely to spend much time thinking about codes and yet the truth is that they underpin our daily lives.
In our age of technology, all our digital information is recorded in alphanumeric codes so it can be easily processed by organisations, from HM Revenue and Customs to membership organisations and retailers.
This is particularly relevant to the healthcare sector where it is necessary to collect masses of information about patients, morbidity and treatments to track the progress of disease and make timely and informed decisions about matters such as resource allocation.
Clinical coding allows this vital data to be recorded in a standard format so it can be analysed in seconds by computer and shared with other healthcare providers.
In the independent healthcare sector, clinical coding has not been embraced as it has in the NHS, but this is changing.
Here are the main types of clinical codes you are likely to come across as an independent practitioner, and their uses:
➥ Diagnosis codes
First produced by the World Health Organisation (WHO) in 1949, the Inter national Classification of Disease (ICD) provides common alphanumeric codes for hundreds of thousands of pathogens and health problems such as antimicrobial resistance.
Member states, including the UK, are currently using ICD-10, but this is due to be replaced by ICD-11 in January 2022.
Some independent hospitals in the UK record patient diagnoses using ICD-10, but many still use
version of its predecessor code, ICD-9.
➥ Procedure codes
In the independent sector, invasive procedures and surgical interventions, including biopsies, hysterectomies or hernia repairs, are recorded for billing using the Clinical Coding and Schedule Development Group (CCSD) codes. There are approximately 3,000 CCSD codes.
NHS hospitals code interventions and surgical procedures using OPCS-4 – the latest version of the Office of Population Censuses and Surveys’ Classification of Surgical Operations and Procedures.
➥ Industry Standard Codes
Healthcode developed this coding system so independent providers could record and charge private medical insurers (PMIs) for the
large numbers of services which are not covered by CCSD. There are approximately 28,000 codes covering services such as pathology, radiology and prosthetics.
➥ Code for success
The world of clinical coding tends to be highly specialised, which is why the NHS and some larger private hospital groups employ trained and qualified clinical coding teams to code patient records for hospital episode statistics. Few independent practitioners have the resources to employ professional clinical coders, but Healthcode’s expertise in this area can help you bridge the gap. Here are three areas where we are making clinical codes more understandable and accessible to our customers so they can operate more efficiently.
a
Healthcode is collating CCSD codes into groups for The Private Practice Register so that they are more readily understood by those without coding training
Support with billing
When billing PMIs, practitioners must use the correct procedure or service charge code and description.
Different insurers have their own schedule of procedures and fees, which means that a charge and procedure that is valid for one PMI might not be accepted by another.
Along with missing/incorrect patient information, a coding error is one of the most common reasons for an electronic bill to be rejected when Healthcode’s Clearing Service automatically checks the bill against the relevant PMI rules.
Practitioners are understandably frustrated when this happens, but it is important to stress this is not because Healthcode itself has rejected the code or code combination but because it is not accepted by that PMI.
From Healthcode’s perspective, we want to help you ensure your bills are validated first time and enter the PMI’s payment cycle without delay.
To maximise your chances of success, we recommend the following:
1
Check the PMI’s website for its schedule of procedures and fees. For example, Aviva, Axa Health, Bupa and VitalityHealth.
2
Check with the PMI at the pre-authorisation stage if you are unsure about which code applies in order to minimise the chance of rejection when you come to bill.
3
Contact Healthcode’s expert coding team if you are struggling with rejected codes, pre-authorisations and other coding queries.
We can explain what codes you can and cannot bill for and ,where necessary, we can liaise directly with PMIs to address problems and help ensure pre-authorised codes are accepted by the Clearing Service. Email us direct at coding@ healthcode.co.uk
4
If you are using Healthcode’s billing software, you can simply select the correct code from the dropdown menu which learns the codes you use most frequently for that PMI.
New codes are data esperanto
INDEPENDENT HOSPITALS are required to submit information on admitted patient spells to the Private Healthcare Information Network (PHIN) which publishes performance measures about hospitals and consultants.
PHIN requires hospitals to use the same ICD-10 diagnoses and OPCS-4 procedures codes that are used in the NHS, but as noted above, independent hospitals generally use ICD-9 and CCSD codes.
To help hospitals meet their obligations, Healthcode has developed clinical coding tools that feature clever dual coding technology.
This enables providers to code diagnoses or procedures in the recognised format for billing and then translate, where possible, these into the equivalent ICD-10 and OPCS codes for submission to PHIN.
Simplifying procedure codes
Healthcode’s current coding project is perhaps its most ambitious and driven by the need to record practitioners’ scope of practice in a clear and accessible way on The Private Practice Register (The PPR).
Scope of practice data is needed by practitioners for appraisal and revalidation purposes, but it is also required by hospitals so they can manage consultants’ practising privileges in line with the Medical Practitioner’s Assurance Framework (MPAF).
Our Clearing Service technology enables us to capture partial scope of practice data in the form of the CCSD procedure codes used
on validated hospital bills where the consultant is identified as the controlling specialist.
However, it is important that this data is presented on The PPR in an accessible format so it can be readily understood by someone with no coding training – practitioners themselves and hospital staff with governance responsibilities.
To achieve this, Healthcode is reviewing its master list of CCSD procedure codes and collating these into groups with a plain language description.
To date, we have categorised 2,000 CCSD codes into 600 unambiguous procedure groups.
For example, the procedure group ‘repair of hernia – abdominal wall’ includes 30 CCSD codes such as ‘primary repair of inguinal hernia’ (CCSD code T2000) and ‘laparoscopic repair of recurrent inguinal hernia – bilateral (CCSD code T2112). See table on page 23 for examples.
The purpose of this mammoth exercise is to make codes accessible for more people.
Users will be able to see a simple definition for the procedure group under a practitioner’s scope of practice and then expand it to see the specific CCSD codes and procedures they have performed at qualifying hospital and clinic sites over a rolling 12-month period.
We are also encouraging doctors to give us their feedback as we roll out the scope of practice capability on the PPR by specialty over the next few months to ensure the procedure groups and descriptions are clear and correct.
The purpose of this mammoth exercise is to make codes accessible for more people
COVID AND CODES
The pandemic has again demonstrated the purpose and importance of clinical codes in healthcare.
It is notable that the WHO wasted little time in providing emergency codes for diagnoses of Covid to help epidemiologists study the outbreak and it has since issued more codes to document post-Covid conditions and immunisation.
Clinical coding seems esoteric, but it represents the most efficient format for providers to collect and share masses of data with other organisations such as the Private Healthcare Information Network and the NHS.
From developing service charge codes for billing to coding tools and our new procedure groups, Healthcode has taken the lead in developing applications for clinical codes so that the independent healthcare sector can use them effectively. Its ultimate objective is to democratise clinical codes so we can all access and benefit from this important resource.
Independent Practitioner Today now features an online advertising directory to complement our journal and website.
Split into ‘business’ and ‘lifestyle’ directories, they list the services independent practitioners need to run their practices or spend their well-earned money on.
How to get a social media stunt to fail
Independent practitioners, especially in the aesthetics world, sometimes turn to social media stunts to create publicity for what they and their practice can do for patients. But are they worth the reputational risk? PR expert Nikki Milovanovic considers the ups and downs – and shows how not to do it
A COLLEAGUE ONCE shared a prospective client’s request: ‘I’d like one of those viral videos, please.’
My reaction made us both glad I’d not been in that meeting, as there’s insufficient Botox on the planet to provide me with a poker face.
Social media virality is increasingly thrown about as a buzzword, but, like that client, many misinterpret the concept, which may seem to skew positive or evoke the ALS Challenge, which saw hundreds of thousands of people raise awareness to the motor neurone disease.
Virality is neutral and it is a gamble: how – or if – media generates attention depends as much on the content as it does on the audience.
While the creator has control
over content, it gets tricky, since posts are designed to reach the widest possible audience and therefore delivery of the message is not restricted solely to the receptive. When this happens, the creator can lose control of their content as it is repurposed.
Rock-solid strategy
Stunts can yield tremendous success and may even become news stories themselves – like the time I April Fooled the UK aesthetics sector to raise awareness about hideous ‘plastic surgery’ simulation apps geared toward children. When PR, social media and the stars align like that, it can be absolute magic, but they require a rocksolid strategy that considers the ‘what ifs’.
In the real world, one might be
more inclined to tune out messages that don’t appeal, but digital stunts are far more likely to come under scrutiny, becoming exponentially amplified and loaded with sentiment as they are shared among audiences.
Let’s propose that the final result of a stunt breaks down like this:
20% loved it;
45% hated it – and aren’t afraid to tell the world;
20% are staying quiet – AKA ‘watching with popcorn’;
15% missed it – but will find out if there’s a ‘train wreck’.
Even that 20% positive gain with a 20% ‘neutral’ response can’t justify the spend, and it certainly doesn’t offset the cost of reputation damage.
While, at one time or another, we’ve all put effort into something
only to have it turn out with a less of a ‘bang’ than we’d hoped, the risk with stunts is that they backfire into a horrific implosion. And, as the saying goes, the internet is forever.
By contrast, with the right strategy, the risk can pay off hugely; for example, when I created a campaign that first raised eyebrows – the natural way – for a multinational implant manufacturer.
Positive results
It subsequently resulted in eminent plastic surgeons around the world participating in a challenge that showcased the product, and led hundreds of surgeons to engage with their sales team. This stunt generated positive results internationally for over two
years and cost the client a fraction of their marketing budget.
Now, when I strongly urge you to have a social media expert at your side when negotiating the wild world of stunts, I can hear and understand a bristle of ‘Well, you would say that, wouldn’t you?’
Fair enough, but if you knew how much more business is gained in helping clinics pick up the pieces after a mis-step versus through encouragement of expert assistance, you might reflect differently.
Successful business owners know their clientele’s interests, likes and dislikes, but are they invariably best-placed to determine how other audiences may interpret their efforts?
In my experience, those adamant the answer is ‘yes’ are least likely to recognise when it is not the case, due to cognitive bias.
Less desirable meaning
While a desired audience may have the shared understanding vital to appreciate your effort, others may interpret or infer a drastically different, less desirable meaning.
Additionally, efforts typically must contend with the deliberate misconstruing of message by competitors and others with the intent to hamper – or outright sabotage –a campaign and whether such action achieves a small-scale disadvantage, or worse.
Several days of scandal and serious reputation damage, even viewing the fallout from afar, can leave business owners skittish about the return on investment on creative strategies.
Now, if, for some reason, it is your desire to go forth and have a stunt backfire spectacularly, I will not question why. Instead, I will only advise the following six surefire steps to help you reach your own goal:
1 Ensure your message only resonates with your target demographic – whether that’s ‘those with a sense of humour’ or ‘those who would actually undergo this treatment’.
Bonus fail points if it only resonates with your peer group.
2 Whenever possible, use stereotyping – history has demonstrated this is never problematic.
Use your judgement, ignore ‘naysayers’. Crucial if you want your effort to fail while reaching a whole community, especially if you otherwise have no connection to said community.
3
If you really want to fail in the aesthetics sphere, why not exploit psychologically vul nerable people?
Capitalising on emotionally fraught experiences like divorce or bereavement are certain to capture that negative attention you crave.
4 If there’s one thing women love more than encounter ing the male gaze, it’s catering to it. So fail with oomph by honing in on how they can/should exist in the world.
5 Everyone loves a fail with a ‘gotcha’ moment – so shove a camera and mic at a stranger during a global pandemic to teach them about facial ageing.
Bonus 100m fail points if the cost of proposed treatment is 30% or more than the cost of producing the stunt.
6
If you want to fail with maximum impact, piggyback your stunt on a controversial topic getting a lot of news coverage, then fail hard by innovating an aesthetics-adjacent hashtag.
Such ingenuity will definitely be an asset for crazy-gluing your professional reputation back together.
For everyone else who does not want to risk reputation, I offer this: no matter how certain you are that your creative idea will result in positive attention, bring it to a trusted social media expert – one who crucially has experience executing stunts within the aesthetic sector and beyond.
Nikki Milovanovic (below) is the founder and managing director of Sophisticated Comms, a London based agency specialising in creative strategy, social media and public rela tions for the lifestyle, beauty, health and wellness sectors
A digital prescription platform to allow convenient prescribing from home
CloudRx is a digital prescription system that allows prescribers to create and send an electronic prescription to our fully licensed pharmacy for fast delivery direct to your patient. It can be used from home by doctors working away from their practices.
No cost to prescribers
Simple and quick prescription creation.
Legal paperless prescriptions, including repeat prescriptions and controlled drugs.
Patients receive text and email requesting secure payment. Alternatively, we can invoice the prescriber or clinic each month.
Prescriber Fees can be added if requested
Medicines are dispensed and dispatched by a variety of delivery options
Fully integrated into MidexPRO
Register for free by visiting cloudrx.co.uk
“We have worked with CloudRX to maintain a cold chain for the medication and direct delivery to patients at home.”
Dr Charlotte Norton, Medical Director of The Slimming Clinic, the UK’s largest chain of private doctor-led weight loss clinics
The reasons patients sue their urologist
THIS ANALYSIS of urology claims looks at clinical negligence claims arising out of our urology members’ private practice.
I examine the trends observed over a recent ten-year period, the reasons for litigation and risk factors that might reduce the chance of a claim being made in future.
Over the decade, the frequency of claim notifications initially rose to a peak in 2015, but has slowly reduced since then. More than 75% of claims opened in the period have been successfully defended and closed with no payment of compensation or claimant costs.
Almost half of the settled claims cost the MDU over £100k each to settle. But remember that the level of compensation paid in clinical negligence claims bears little or no relation to the seriousness of the allegations, but reflects the cost of restoring the claimant to a position they would have been in had the negligence not occurred. However, this does demonstrate the need for urologists to have appropriate indemnity arrangements in place, as even lower-value claims can settle for damages and costs that are beyond the means of most members to pay.
What are the reasons for claims involving urologists?
➲ Poor outcome/ complications after surgery
The single largest reason for urology claims is due to allegations concerning unintended consequences of surgery.
The commonest of these, in order of occurrence, were:
Infection;
Renal damage;
Incontinence and erectile dysfunction;
Bladder or bowel perforation;
Retained foreign bodies.
Dr Shabbir Choudhury (below) medico-legal adviser and former senior medical claims handler at the Medical Defence Union, analyses clinical negligence claims affecting urologists and provides advice on managing risk
➲ Delayed diagnosis of cancer
The second largest reason for urology claims was an allegation of delayed diagnosis and that, had certain investigations or actions been carried out, the patient would have been diagnosed with cancer sooner, which would allow for either an effective cure or would have improved prognosis.
➲ Failure to obtain consent
The third most common reason for claims were allegations around the consent procedure and whether
If things go wrong, be open and honest with the patient and provide an explanation of what has happened the surgeon had adequately explained the risk of the procedure.
It was alleged that this had an impact on whether the patient would have chosen not to undergo the treatment or may have done so at a later time.
Managing risks
Claims involving urologists often focus on a few key areas, such as the surgical technique being inadequate, investigations not being performed early enough or a lack of communication skills, which resulted in inadequate consent being taken.
However, there are ways to reduce risk and, in turn, the likelihood of a claim, which include:
➤ Ensure robust procedures are in place for communicating results to the relevant parties to ensure appropriate and prompt follow-up and treatment.
➤ Be aware of the GMC’s guid -
ance on consent and other relevant guidance such as those of NICE.
➤ Consent should be obtained by an appropriate member of the team and, ideally, by the urologist undertaking the procedure.
➤ Ensure that the patient is aware of the risks, benefits and complications of the procedure as well as other therapeutic options.
Discuss these options in a way the patient can understand, avoiding medical jargon wherever possible. Document this carefully.
➤ Supporting information such as patient leaflets and information sheets can help patient understanding.
The use of these should be documented in the records.
➤ Check that the patient understands the procedure you propose to undertake and is aware of the possible complications.
➤ If things go wrong, be open and honest with the patient and provide an explanation of what has happened and the likely short- and long-term effects of this.
Say sorry and get advice from your medical defence organisation if you believe the incident triggers your ‘duty of candour’ requirement.
➤ If there is a time lag between consent being obtained and the procedure being carried out, it is important to ensure that the patient still consents to the appropriate procedure and it is still appropriate.
NHS Pensions & Annual Allowance Tax
Get ready in advance of April 2022 when the proposed changes to the NHS Pensions will allow you to reclaim some or all of any Annual Allowance tax you may have suffered in the past.
With our knowledge and in-house calculators, we will be able to predict in advance and check statements produced by NHS Pensions and Scottish Public Pensions Agency for accuracy for any refunds due.
For further information contact us at aa@semail.co.uk or telephone 01625 527351.
➤ The surgeon carrying out the procedure needs to ensure that he or she is adequately trained and experienced in undertaking it.
➤ Ensure that good records are kept throughout and procedures audited for both outcomes and complications.
➤ Offer a chaperone to patients undergoing any intimate examinations.
➤ Have a system in place to verify the right site and patient undergoing treatment and to cross-check information provided against the referral.
It can be very distressing to find out a patient is bringing a claim against you.
The MDU understands how stressful this is and will defend claims whenever possible.
It is also campaigning to reform the legal environment surrounding compensation payments.
To learn more, visit www. themdu.com/faircomp
MARKETING & BRANDING
Strike the bright note! Simon Marett and Michael Sullivan show how to use colour in your design, branding and marketing
Why you need to be
IN OUR first two articles, we covered the dos and don’ts of logo and website design. As you will have hopefully learnt from the articles, successful branding is more than just a logo.
It is about the whole package of logo, imagery, typography and also colour. This month, we look at how to use colour effectively in your branding, design and marketing.
Colour is an area of marketing that is often overlooked, but, like imagery, it is an area that requires close attention, because it can help you connect with your audiences on a deeper, emotional level and draw a potential customer or patient towards a particular brand or practice.
When it comes to the world of healthcare, the use of blues and white are ubiquitous because of their association with medicine, health, cleanliness and doctors.
The challenge for any healthcare practice using a similar set of col-
ours in its branding is how you can differentiate yourself and stand out from the competition.
Here are some key points for you to consider:
1
Use brand guidelines to achieve consistency
Consistency in branding is important if you want your healthcare practice to grow and be successful. This means that your execution across your marketing will all need to look and feel the same.
Where this creates problems is when you are working with multiple suppliers, printers and partners or you have different members of your team responsible for marketing tasks such as email marketing, your website or social media.
Brand guidelines are one of the first things we recommend to our client. Set down in a short document, they will act as a rule-book for you, your partners and employees to follow when it comes to
working with your brand and covers everything from typefaces in emails to the colours to use in your printed material.
Not only will it save you valuable time by making you more efficient, but it will also save you money by helping you avoid branding errors and expensive marketing mistakes.
TOP TIP: If you do not have them in place already, ask your designer to create a short set of brand guidelines immediately.
As a bare minimum, they should cover use of your logo, typefaces to use for headlines, body copy and the colours to use with your marketing and brand.
2 Beware text on dark backgrounds
We covered this briefly in our website article in March’s issue, but striking a good balance between space, imagery and text can really make the difference whether you
are building a website or creating a new brochure for your clinic.
One of the most common mistakes we come across is where large amounts of text are placed on a dark background.
Using a dark background colour can help a website or brochure look sleek and sophisticated, but if you then place a lot of copy on top, it can make it difficult to read and can be a major turn-off for readers.
TOP TIP: If you are insisting upon using a dark colour in your design and brand, use copy sparingly or speak to a professional designer about creating templates that enable you to work with the colour.
3 Less is more
We speak to many healthcare practitioners who want a new website and have a strong idea about the colours they want to use because they have already designed the logo.
Successful branding is all about consistency and repeating the same logo, messaging, typography and imagery repeatedly so that it is recognised
The good and bad use of colour: these two different versions of a brochure demonstrate how it is much easier to read text on a lighter background
colour co-ordinated
Bright red and orange might look great on your logo and business card, but that does not necessarily mean that everything on your website needs to be in those colours.
The majority of our clients are private practices who are providing a premium service to their patients and customers. Be mindful that overusing strong colours may devalue your premium brand because the design may end up looking cheap, amateur and overpowering.
TOP TIP: If strong colours are what you want, go ahead, but discuss with your designer how these colours can be used subtly and sparingly to achieve that premium look and feel you are after.
Also, ask your designer to create a primary and secondary colour palette in your brand guidelines to help break up these strong colours.
4
Think twice when using orange and purple
When I started my career in marketing over 20 years ago, once of my first lessons I learned from the printer I worked with was to try and avoid using orange and purple in printed material.
This is because these two colours are considered to be the hardest to match in print. This is because they have specified contrasts that if they are slightly off, can be very noticeable.
Successful branding is all about consistency and repeating the same logo, messaging, typography and imagery repeatedly so that it is recognised.
The same rule applies with colour and this is why printing with orange and purple can be difficult. The orange can turn lighter or darker or more red, yellow and green, so several printed items may look noticeably different to the eye.
TOP TIP : If you are planning to use a lot of printed material in your practice for signage, brochures and reading material, consider avoiding the heavy use of purple or orange and select a different colour instead.
To conclude....
As you will see, there is more to using colour and successful branding than first meets the eye.
We always recommend taking the time to consider the colours you want to use across your brand and marketing, because they may be linked to your healthcare practice for a long period of time.
A starting point for any healthcare practice – whether you’re just starting out or you’ve been established for years – is brand guidelines.
Any good designer or marketing professional will have worked with brand guidelines in the past and will be able to demonstrate how
they can work for your individual practice’s needs. These are a quick and inexpensive way of creating brand consistency and will help you avoid costly branding mistakes in the future.
Next month, we will take a closer look at typography and the use of different use of fonts in marketing and branding.
Simon Marett (below, left) and Michael Sullivan (right) are managing director and creative director of Ellerton Marketing Ltd, a specialist strategic marketing consultancy for independent healthcare practitioners
Rules for prescribing
The GMC’s updated prescribing guidance and its impact on independent doctors is discussed by
medico-legal adviser Dr Kathryn Leask
THE GMC’s updated prescribing guidance Good practice in prescribing and managing medicines and devices – effective from 5 April –places more emphasis on remote prescribing and consent.
Throughout the pandemic, more and more consultations have been held remotely and while there will inevitably be patients who need to be seen face to face, remote consultations are very likely to continue.
The guidance makes clear that it applies to all prescribing regardless of the setting. Where remote consultations are used, prescribing must be compatible with the guidance and you need to have the appropriate knowledge and skills to use the technology required for your role.
While the guidance does not distinguish between NHS and private prescriptions, there are some areas which may particularly impact those working in private practice.
Firstly, there is more emphasis on establishing a dialogue with patients. Not only does this allow you to obtain the information you need to prescribe safely, the dialogue should provide an opportunity for the patient to ask questions to help them decide whether or not to have the care or treatment you are offering.
Questionnaire issue
The guidance specifically mentions the need to raise concerns if you are prescribing remotely based on a questionnaire, which provides no opportunity for a twoway dialogue with the patient. You should take a proportionate approach when obtaining a patient’s consent to prescribe. Verbal consent is generally adequate providing the patient has been given all the information they need to make a decision and has had the opportunity to ask questions.
There may, however, be occasions when a patient’s signature is required; for example, to comply with a Medicines and Healthcare products Regulatory Agency drug safety alert about a medicine with serious side-effects.
As with all treatments, it is important to ensure the patient has capacity to make decisions about their care. Assessing capacity is a core clinical skill and you should be able to draw reasonable conclusions about your patient’s capacity during the dialogue you have with them.
During a remote consultation, you will need to consider whether you should physically examine the patient.
Some forms of examination and assessment can take place during a video consultation. However, this won’t be adequate in all cases and the need for a physical examination should be considered to ensure prescribing is done safely.
Additionally, you need to consider whether you have all the information you need to prescribe safely. As a private clinician, you may not have access to the patient’s clinical records and may not be in a position to verify the information you are given.
Patient’s permission
If you are not the patient’s regular prescriber, you should ask for the patient’s permission to contact their GP or other treating doctors to obtain or confirm relevant information. If the patient refuses, you must be able to justify your decision to prescribe.
In doing so, you have to consider any medication the patient is obtaining from other sources, such as the internet.
As well as obtaining information you need to prescribe safely, you should obtain the patient’s consent to allow you to share information with their GP.
prescribing drugs remotely
If you do not have access to a patient’s medical records, you must not prescribe controlled drugs or medicines that could be open to abuse, overuse or misuse
If the patient refuses, you should explain the risks associated with not sharing information to other potential prescribers and those involved in their care.
This discussion and any decisions you make should be documented in the records. If you decide that you are not able to prescribe safely, you should provide the patient with other options and alternative services.
Under pressure
During a remote consultation, you should also consider whether the patient is able to talk to you freely. In some situations, you will need to consider whether they are being put under pressure by others who may be present with them or who may be in the room but not visible to you.
Furthermore, in some instances, a patient will ask for treatment which you don’t believe is clinically appropriate for them. You
should discuss this with the patient so that you can understand their reasons and expectations.
If, after discussion, you do not believe the treatment is appropriate, you should not prescribe it and explore other options that may be available. This may include offering the patient a second opinion.
The GMC’s guidance also makes specific reference to controlled drugs and other medicines where additional safeguards are needed.
The GMC advises that if you do not have access to a patient’s medical records, you must not prescribe controlled drugs or medicines that could be open to abuse, overuse or misuse.
This includes where there is a risk of addiction and the need for monitoring is important. The exception to this is when there is no other person with access to the patient’s records available and pre-
scribing is necessary to avoid a serious deterioration in the patient’s health or it is necessary to avoid serious harm.
Limited quantity
It may also be necessary to prescribe to ensure continuity of treatment where a patient is unexpectedly unable to access medication for a limited time. If such a situation arises, you should provide a limited quantity to allow treatment to continue until the patient is able to access suitable care from a professional with access to their records.
You will also need to consider whether the patient is also obtaining medication from other sources.
Some private clinicians may be consulting remotely with patients abroad. It is important to consider how the patient’s condition will be monitored and whether there are any differences in the licensed
name of the medication and the recommend dose.
It is also important to ensure you have the appropriate insurance or indemnity in place to cover your practice in another country and also whether you need to be registered with the regulatory authority where the patient is based. If the service provider you work for is based outside the UK, you need to be aware that there may not be established local mechanisms to provide effective systems of regulation and this may have an impact on patient safety.
Learn more at: www.themdu.com/guidance-andadvice/latest-updates-and-advice/whatyou-need-to-know-about-the-gmcsnew-guidance-on-prescribing
Dr Kathryn Leask (right) is medicolegal adviser at the Medical Defence Union
BILLING AND COLLECTION
Ensure you benefit from the recovery
Simon Brignall discusses the lessons every practice can learn from the rollercoaster impact of the pandemic
MANAGING Covid-19’s impact has defined our professional and personal lives over the past year, and independent practitioners will be dealing with its ramifications for some time.
It is noticeable that each successive lockdown had less impact on our client doctors’ incomes than the last and there has been strong demand for Medical Billing and Collection’s services as restrictions relax.
There are two areas that every practice can review to ensure they are best positioned to benefit from the recovery.
1 Self-pay
Plenty of articles have detailed the fall in patients accessing care across all specialties from cardiology to cancer.
Recent reports suggest NHS waiting lists could rise from under five million now to anywhere
from six to ten million patients this year.
Headlines about record waiting lists have always translated into a large demand for private healthcare from patients unprepared to wait.
The major trend of the last decade was the growth of the self-pay market and we fully expect this sector will continue to form a significant portion of the recovery supported by this demand.
Managing self-pay
Considering the self-pay sector’s importance, it is vital to ensure these patients are dealt with correctly from both a billing and collection perspective.
Urgency is often lacking regarding the billing of self-pay patients and, more importantly, the collecting of outstanding money.
This frequently means a large amount of outstanding debt –either chased intermittently or not chased at all – resulting in debts that quickly mount up to significant sums of money.
Typically, we see a lack of robust procedures in place to deal with these patients and the provision of a simple-to-use payment facility. It is important that your practice has systems in place to deal with the various types of self-pay patients you are likely to come across.
UK self-pay
For UK self-pay patients, you need to have a published price list or to have notified the patient of their fee in advance.
It is good working practice to also confirm both the methods of payments available as well as
For UK selfpay patients, you need to have a published price list or to have notified the patient of their fee in advance
when payment is due, so patients will not only know to expect an invoice but also understand how they are to pay.
Medical Billing and Collection (MBC) offers a variety of methods tailored to a practice’s needs.
These are:
E-billing of patients after their treatment by email, which includes a link to our payment portal enabling the patient to pay 24/7;
E-billing and collection of payment ahead of their treatment;
Collection by the practice on the day via our client self-pay portal.
When you are invoicing patients post-treatment, you will need to put in place a robust chasing process where the patient is contacted for payment after an agreed period and ensure this is routinely followed until collection.
Failure to implement and adhere to a chase policy is the most common reason why debt levels increase and can lead to cash flow difficulties.
Overseas patients
If you are going to see a patient who is not a UK resident, it is even
IMPORTANCE OF REVIEWING YOUR FEES
It is always important for practices to regularly review their fees.
Understandably, the past year’s events mean a fee review was not high on priority lists, but if you have not done this for some time, it is worthwhile. Many consultants find this a stressful exercise, so it gets deferred.
Consultants need to decide whether they will adhere to each private medical insurance company’s price schedule for procedures and, if they do, they must know the price list for each one. Each has its own specific price for every code provided by the Clinical Coding and Schedule Development group (CCSD).
Fees for an individual procedure can vary by as much as 100%, so its important to ensure you have the current correct tariff.
Consultation fee rates also need to be decided. Sometimes the contract that the consultant has signed with the insurer will dictate what they are required to charge for both the CCSD codes and the consultation fees.
The review should include the self-pay sector for both consultations and procedures. This is an area where you have complete autonomy to set a fee that reflects both the demand for your services and your experience.
Get this wrong and you can miss out on patients because the pricing is too high. Even worse, you can lose thousands of pounds due to pricing being too low.
Our experience is that consultants typically do not get this right because they have either not done enough research when initially setting their pricing or, more commonly, they have not reviewed their pricing regularly, if at all. In many cases, it can be years since their pricing was last reviewed and updated.
Taking time to review these two key areas of your practice will ensure that, after a rollercoaster year, you are able to benefit from the increased demand for your services. The simplest and often best way of doing this, of course, is to contact a medical billing company with years of expertise in this area. Then you can focus on patient care.
more important to make sure your fees and method of payment are made clear. Once the patient leaves the country, it is extremely difficult to ensure these invoices are paid.
When we deal with overseas patients, it is generally standard practice to collect money in advance.
Where a payment is collected by the hospital, we raise an invoice to the hospital for doctors’ fees.
It is important to follow up with the hospital’s finance department to ensure these payments are made to the practice because these can easily get delayed or missed.
2 Insurance shortfalls
Even the most efficient practices find chasing insurance shortfalls and excesses challenging. Often these invoices make up a significant proportion of their outstanding debts.
This is because most patients do not review the terms of their insurance policy and assume all costs will be met by their insurer.
So when they receive an invoice for an outstanding balance not covered by their insurance company, it can quite often come as a shock to them.
Ignore invoice
We find many patients ignore the invoice, thinking that it is either a copy of what has been sent to the insurer or that their insurance company is liable.
This is why it is important to follow up with the patient directly and explain why they have received an invoice.
A large part of our work is liaison between the insurer and the patient to ensure it is clear who owes the money.
Some patients contest this with their insurer, believing the company is liable, so it is important to tackle issues quickly to minimise delays.
Once the patient accepts the money is owed by them, then the outstanding balances needs chasing.
Simon Brignall (right) is director of business development at Medical Billing and Collection
When we deal with overseas patients, it is generally standard practice to collect money in advance
LONG-TERM INVESTMENT STRATEGIES
Markets go down and up!
Dr Benjamin Holdsworth looks at the lessons to be learned from the last year
AS AN investor, one is always learning. Our perception of investing is guided by our experience.
Those old enough to have been investing in the 1970s will retain uncomfortable memories of rampant inflation and the impact that had on cash, bonds and the general travails of life when prices spiral upwards.
Others who lived through the birth of the internet and the boom and subsequent bust of the ‘dot.com era’ of the late 1990s and early 2000s, may also be living through a sense of déjà vu.
For most investors, interest rates have been on a steady longterm decline, making mortgages cheaper and supporting bond and equity prices. In the past 12 months, we have been reminded of some useful lessons that can –hopefully – make us all better investors.
Several key lessons stand out :
1 Markets go down as well as up I n the decade following the global financial crisis, investors were treated to a long and almost uninterrupted run of rising
equity, bond and property markets. It seemed as if everything always went up.
The first quarter of 2020 reminded us that this is not always the case. Some equity markets fell in excess of one third of their value. It could have been much worse.
A useful rule of thumb is that the equity content of a portfolio could easily fall by 50%, as it has in the past on several occasions. Equity investors get rewarded for taking on this uncertainty and pain, eventually.
2 Short-term pain does not become long-term pain unless you sell Those who need their money in under a year should not own any equities at all.
In reality, most investors have very long-term horizons; after all, if you are 60 you should be planning to be invested for at least another 40 years.
Yet it is a sad fact that some investors panic and sell out when markets nosedive, even though they do not need their money that year or probably for many years.
Broad global markets have recouped all of their losses – and more – since the start of 2020 to the start of March 2021. Bailing out of a long-term strategy can be costly.
Most investors who need to withdraw money from their portfolios own high-quality bonds that they can sell to meet expenses, leaving their equities intact.
3
High-yielding bonds have equity-like characteristics
During painful sell-offs, investors need to be able to rely on their bonds to help ease the pain. Unfortunately, high-quality bonds – that is to say, bonds from the most credit-worthy issuers –pay low yields.
Yet, high-yielding bonds –from lower-quality corporate and emerging market borrowers – are not the solution, as they act far more like equities, just when you do not want them to.
Sticking with high-quality bonds is an insurance policy. Owning the right level of insurance coverage is important.
Back down to earth like
meteorites
4
Fads, trends and social media tips are dangerous to your wealth
In the past few months, we have seen extraordinary share price rises of many growth-oriented companies, particularly in the US. For example, Tesla’s stock price rose from US$121 a year ago to a high of $883 on 25 January 2021.
Social media pumping of stocks like GameStop and the ‘enthusiasm’ of online retail investors pushed some stocks ‘to the moon’. Yet most turned out – or will turn out – to be meteor-
ites falling back to earth. Tesla’s stock price has fallen by around a third since then.
Owning stocks is for the long run. Owning them for shortterm gains is gambling with costly consequences for most. Let others take the losses. Remember that owning a diversified portfolio means that you already own many of tomorrow’s winners. Be happy with that.
5 Inflation may not be dead
We have been living for some time in a relatively benign infla-
tion environment. Yet, the huge levels of government stimulus and consequent growth of the money supply, not least the US$1.9 trillion – that is to say, $1,900,000,000,000 – package in the US, risk fanning inflation. Inflation is a form of unlegislated, invidious taxation.
6
Bonds do not always go up
I nflation – or the fear of inflation – is bad for bonds. Bond yields that incorporate the market’s view on future inflation have risen of late as a consequence, pushing bond prices down. Bond yields have been falling for around 40 years to historic lows, so this is new to many investors.
Owning shorter-dated bonds helps lessen the pain and investors benefit more quickly from the rise in yields.
7 Gold is not a good short-term hedge of inflation
The salaries of comparably ranked army officers from Roman times to today – a mere 2,000 years – are almost identical in gold terms , which means the price of gold has kept up with inflation. But just as we are potentially experiencing a rise in inflation, gold prices have been slumping from above £2,050 per ounce in August 2020 to below £1,700 per ounce today.
In fact, gold’s inflation-busting myth relates to the 1970s when inflation was rampant and gold prices rose dramatically. Correlation does not imply causation.
and gloom, but there is light at the end of the tunnel.
These lessons lead us to some obvious conclusions about portfolios. We should own a sensible balance between bonds and equities and understand that owning high-quality bonds is an expensive, but necessary insurance policy for most and allows us to meet our nearer-term liabilities.
We should also own a globallydiversified equity portfolio. A few US technology stocks cannot continue to out-run markets for ever. Keep the faith in your long-term portfolio strategy and turn your eyes away from market temptations.
Building wealth from investing is a long, boring process interspersed with years like the one we have just had. We survived what the markets threw at us and will survive whatever comes our way again.
Dr Benjamin Holdsworth (right) is director of Cavendish Medical, specialist financial planners helping consultants in private practice and the NHS
The content of this article is for information only and must not be considered as financial advice. Cavendish Medical always recommends that you seek independent financial advice before making any financial decisions.
Owning stocks is for the long run. Owning them for short-term gains is gambling with costly consequences for most
8 It is always darkest before dawn
The last 12-month period has seen some tough times for everyone, both in terms of our personal lives and in the markets. It is always easy to see the doom
Levels, bases of and reliefs from taxation may be subject to change and their value depends on the individual circumstances of the investor. The value of investments and the income from them can fluctuate and investors may get back less than the amount invested.
You’re all in it together
A Declaration of Trust is a useful tool for independent practitioners to protect valuable property investments and exposure to unforeseen liabilities.
Lisa Davison explains how they are especially important now with pressures on the healthcare sector sparking more professional disputes
With the uncertain economic climate and pressures faced by healthcare professionals, it is more important than ever for practitioners to protect individual property investments
And doctors should ensure that their existing structure is robust enough to sustain long-term demands on private practices.
What is a Declaration of Trust?
A Declaration of Trust is a legally binding agreement which sets out the arrangements governing any jointly owned or leased premises.
It states:
Each owner’s share in the premises;
How income and expenses of the premises are shared;
The procedure and timetable for purchasing a retired or deceased partner’s share of the premises;
The basis of determining the value of the premises;
What happens if there is negative equity in the premises;
Property owners’ rights and obligations in respect of the premises pre- and post-retirement, including loans.
When Is a Declaration of Trust required?
Private practitioners will usually need a base in which to provide their services, whether this be a room in a private clinic as an individual or standalone purposebuilt premises for the practice.
Such occupation may be documented by way of:
Licence – if occupation is shared with other users or access times are limited;
Lease – which may be of whole or part of a building;
Freehold or long leasehold investment – where premises are purchased often with other partners and often with bank or other third party funding.
However property is held, there may be significant investments and/or liabilities involved –whether this be rent or licence fee payable under a lease or licence arrangement or mortgage payments payable on investment property.
To share or limit those liabilities, practitioners often join together to pool resources and cost.
A Declaration of Trust should be
A well thought out and comprehensive Declaration of Trust not only is vital to protect individual investments, but is also a tool to minimise the risk of disputes going forwards
ensuring that the intentions relating to the premises are not lost, which ultimately protects the investment of the property owners.
Declaration of Trust and lease liabilities
As mentioned above, a Declaration of Trust may also be applicable to leasehold premises. Like freehold property, a lease may only have a maximum of four names on the legal title.
There may, however, be more than four partners in the practice or four property owners.
Technically speaking, those individuals named on the lease are those individuals on the hook for the liabilities under the lease.
there is a risk that a retiring partner could remain liable to the landlord under the lease; for example, under an authorised guarantee agreement (AGA). An AGA is essentially a form of guarantee which may be required from the landlord on an assignment of the Lease.
As an extra layer of protection, the Declaration of Trust should further state that a retiring partner should be fully indemnified by the ongoing partners of the practice –as they are the parties with control of the funds and day-to-day management of the practice.
Added benefit
considered in any property arrangement where more than one practitioner or property owner is involved.
Co-ownership of property creates a trust in land and unless otherwise documented, each co-owner has an equal beneficial share in the premises.
Rebutting this presumption is therefore particularly important when individual partners’ investments in the premises are different.
Practitioners generally document and regulate their business with a formal partnership or limited liability partnership (LLP) agreement.
Separate agreement
However, it is best practice to also enter into a separate Declaration of Trust between the property owners.
This is because when new individuals join the practice, there is a risk that the change is not dealt with correctly, which could potentially create an agreement at will.
When an agreement at will is created, the provisions of any formal partnership or LLP agreement no longer applies and any provisions within that agreement protecting the valuable property interests are therefore no longer enforceable.
Under an agreement at will, all partners of the practice have the prospect of claiming a share, even if they have not paid for it and that includes a share in the practice.
A separate Declaration of Trust survives a change of practitioners,
Liabilities are often expressed to be ‘joint and several’, meaning each individual named on the lease is potentially exposed to the entire liabilities due under the lease – this could include all rental payments, any service charge payments and dilapidations.
This clearly would not be the intention of the individual partners and is cause for concern for any partner, not least a partner who has since retired and left the practice.
This can be addressed by all partners entering into a separate Declaration of Trust, which declares not only that all partners have an equal right to occupy the premises but also makes it clear that the obligations arising under the lease are to be shared by all the partners – whether equal or not –not just those whose names appear on the face of it.
Upon retirement of a partner,
With the pressures facing professional partnerships in the healthcare sector, we have seen a dramatic increase in the number of professional disputes.
A well thought out and comprehensive Declaration of Trust not only is vital to protect individual investments, but is also a tool to minimise the risk of disputes going forwards.
Used correctly, a Declaration of Trust provides the added benefits of allowing flexible funding options through unequal or thirdparty investments, enabling flexibility in terms of property ownership outside of the practice and provides a clear distinction of liabilities as part of succession planning and retirement of partners.
Lisa Davison (pictured right) is real estate partner at law company
Hempsons
THE LAW ON CONSENT
You must tell them about alternatives
Following a rise in claims alleging clinicians failed to explain possible alternative treatment, Dr Emma Green looks at the case law surrounding therapeutic options, GMC guidance on consent and how these impact on information provided to patients
HIGH-PROFILE CASES on consent, most notably Montgomery vs Lanarkshire (2015) and Chester vs Afshar (2014), have brought the consent process into considerable focus.
However, there has recently been an increasing number of claims alleging failure to explain alternative treatment options, including the option of no treatment.
Case law
Consent has been debated in courts since Bolam vs Friern Hospital Management Committee (1957) and has moved forward considerably from a paternalistic, doctor-centred process, towards a
patient-focused consent process.
The case of Montgomery vs Lanarkshire Health Board (2015) was pivotal in changing how consent is viewed by the courts and highlighted the importance of material risk from a patient perspective.
It highlighted the importance of a failure to discuss the treatment option of caesarean section in a patient where shoulder dystocia was a foreseeable risk in a person with diabetes, but where the risk of serious harm – including hypoxic brain injury – was considered to be negligible due to a 0.1% risk and so was not discussed.
This was despite the fact that Mrs
Montgomery had concerns over the baby’s size but had not asked about the specific complications.
The court accepted that if she had been told about the risk of dystocia, she would have chosen to have a caesarean.
Her appeal was successful, and the judgment held that the assessment of whether consent was adequate in a clinical negligence claim would not be assessed by the Bolam test.
Instead, doctors must provide information about all material risks; they must disclose any risk to which a reasonable person in the patient’s position would attach significance.
Alternative options were highlighted some years earlier in the case of Birch vs UCL NHS Foundation Trust (2008), a case referenced in the Montgomery verdict, but with which few clinicians may be familiar.
In this case, Mrs Birch, a type 1 diabetic, was admitted to hospital with blurred vision, headache and nausea and vomiting.
The consultant neurologist felt, due to the atypical presentation for a vascular cause of her painful, pupil-sparing 3rd nerve palsy, that an MRI scan should be done to exclude aneurysm or cavernous sinus pathology.
Due to lack of availability of an
MRI scan at the admitting centre, Mrs Birch was transferred and the receiving neurosurgical team felt angiography was required. She subsequently underwent catheter angiogram and suffered a dense hemiplegia.
Despite having consented for a 1% risk of stroke associated with the angiography, Mrs Birch made a successful claim. The judge found that the decision to undertake angiography was not negligent, but the failure to discuss alternative options, including an MRI scan, was a breach of duty.
The more recent case of Bayley vs George Eliot NHS Hospital Trust (2017) clarified that reasonable treatment depends on the patient, their treatment and prognosis, but, more importantly, that a reasonable treatment must be accepted practice and more than ‘experimental’ and which would work for the condition in question.
GMC position and medicolegal advice on consent Medical Protection has provided guidance on consent in line with the GMC guidance on Decision Making and Consent 1
A key principle is that respect for patients’ autonomy is expressed in consent law. To impose care or treatment on people without respecting their wishes and right to self-determination is not only unethical, but illegal.
For consent to be valid:
➲ The patient must be competent – mental capacity is decision-specific. Assessment of a person’s capacity should be based on his/her ability to understand, retain and weigh in the balance the information relevant to a particular decision. The person must also be able to communicate the decision.
➲ The patient must have sufficient information to make a choice – without adequate information, patients are unable to make decisions about their treatment.
Patients should be given time to ask questions. The GMC and the courts expect patients to be given all information material to their decision, with the proviso that it would not cause the patient serious harm.
This is the key point in consent, and the alternative treatment
NEW CONSENT RULES IN SUMMARY
Consent needs to consider not only the risks involved in the proposed treatment, but, in order to be valid, should discuss other options for the patient, including doing nothing.
Patients should be aware of the risks associated with alternate options and if a practitioner is unable to offer an option, appropriate offer of referral should be made.
The scope of reasonable alternative treatment options can be summarised below:
Alternative treatment option must be within knowledge of reasonably competent clinician;
Alternative treatment must be accepted practice;
Alternative treatment should be appropriate and not just a ‘possible treatment’.
While this may not be routine practice for all clinicians, the legal and ethical position on consent is clear that options should be discussed routinely, unless considered to be detrimental to a patient – therapeutic exception – or in emergency situations.
options not being discussed would be considered as insufficient information.
➲ The patient must be able to give their consent freely –pressuring patients into consenting to treatment invalidates the consent.
As of 9 November 2020, the GMC guidance on consent has been updated.2
It remains clear that doctors should provide information about ‘options for treating or managing the condition, including the option not to treat’ (paragraph 10c) and inform patients of the risks associated with each of these options, including the option of doing nothing (paragraph 10e).
The guidance also re-iterates that they should not rely on assumptions about the information a patient might want or need, the factors a patient might consider significant or the importance a patient might attach to different outcomes.
What does this mean in practice?
Historically, consent was often a single process, undertaken at the bedside or as a brief discussion in clinic.
But to be valid, unless there is therapeutic exception, it should be considered now as a journey where patients are given sufficient information and have a time period of opportunity to consider their options.
Often clinicians express concern that patients should not be over-
loaded with information or will not read leaflets or information provided.
However, unless it is specifically stated by a patient and documented that they do not wish for further information, it should not be presumed.
It is recognised that consent forms often lack specific areas to record discussion about alternative treatment options, hence it is sometimes omitted or not documented.
In other clinical scenarios, doctors only discuss those treatments which they themselves perform when other alternatives may be suitable for a patient.
In clinical negligence law, on the basis of Montgomery, it would be difficult to defend this practice.
Medical records can be used to record discussions and patient information leaflets can also be used to outline other treatment options, provided they are kept regularly updated to reflect changing practice.
Where a patient information leaflet is given, this should be made clear in the records or on the consent form. Claims have been successfully defended where a copy of the information given has been included in the patient record.
When claims arise further down the line, it may be difficult to obtain a copy of the exact information that was given to a patient.
Alternative therapeutic options are available in all clinical scenarios of consent, as doing nothing is always an option for a patient.
Consent should be considered now as a journey where patients are given sufficient information and have a time period of opportunity to consider their options
Even when the decision is not considered to be in the patient’s best interest, provided they have capacity, this does not mean the consent is not valid.
Clinicians should not presume a patient is aware of the option of doing nothing, nor presume that their attendance in seeking a therapeutic solution is indicative that this must be the only outcome for them.
If a clinician is unable to provide a specific alternative option either through skill set or clinical restrictions, this does not mean a patient should not be made aware of that option, providing it is reasonable for the clinician to be aware of the procedure.
If necessary, referral to an alternative clinician or centre may be required to ensure the patient is consenting to the treatment option they want.
If possible, patients should be informed of the available avenues to return should they have further questions regarding the proposed treatment.
References:
1. GMC: Consent: patients and doctors making decisions together; 2008
2. GMC: Guidance on professional standards and ethics for doctors; Decision making and consent; (came into effect on 9 November 2020)
Dr Emma Green (right) is a medicolegal consultant at Medical Protection
Asked to be a witness
Dilemma 1 What’s the job of expert witness?
QI’m a consultant haematologist who has been approached to be an expert witness in an upcoming court case.
neuroradiology, neurosurgery, haematology, neonatology and genetics.
A number of factors were noted to act as a disincentive to doctors from going into expert work and included court processes, lack of support and training and perceived criticism by lawyers, the judiciary and the press.
A response to a doctor’s inquiry gives Dr Kathryn Leask (right) the chance to explain the extensive role of the doctor as an expert witness in court
NOW OPEN ON SATURDAYS
Please can you give me more information as to what this role entails and how it differs from being a professional witness?
ADoctors can be asked to provide a witness statement for the police or the court following an interaction with a patient.
This may, for example, relate to an assessment of a patient who has been the victim of an alleged assault or where a doctor has reviewed a child where a non-accidental injury is suspected.
Where you have been involved in the patient’s care, any witness statement you are asked to provide should be on the basis that you are acting as a professional witness or witness of fact, as opposed to an expert.
However, this may not always be clear cut. It is important to understand the distinction between the role of a professional witness and that of an expert to ensure that you do not become involved in a case where you inadvertently put yourself forward as expert, for example, for the Crown Prosecution Service.
A report1 published in October 2020 by a working group on medical experts in the Family Courts, established by The President of the Family Division, noted that there is a paucity of medical expert witnesses willing to participate in Family Court cases involving children.
The working group found that the main shortage areas for medical expert witnesses were in child psychiatry, paediatrics, radiology,
A particular problem for doctors was also about the inflexibility in being scheduled as a witness. It was also acknowledged that engaging in expert witness work and providing reports was timeconsuming, requiring meticulous scrutiny of medical records and investigation results, including radiological imaging and, potentially, examination of the patient.
This paucity in the availability of experts, particularly for Family Court cases, may result in the need for the police, or other parties, to approach doctors more informally where an expert opinion is needed. If you are asked to provide information to the police, particularly about a patient you may not have seen or been directly involved in the care of, it is important to make it clear at the outset what your role is.
Clear distinction
If the police contact you, asking for an opinion about a patient you are not familiar with, you may find yourself being referred to as an expert and being summoned to give evidence in court on that basis. There is a clear distinction between the two roles.2 The role of a professional witness is to provide a factual account of the assessment of the patient and not an opinion as to how the injury occurred, other than to report what you have been told by the patient or the person accompanying them.
It is important to make it clear in your witness statement that any reference to the mechanism of injury relates to what you have been told rather than being based on your opinion or assessment. If you are not in the positon to give a prognosis or comment on how an injury has impacted on a patient’s life, you should decline to do so.
It is important to be mindful of the GMC’s guidance3 on acting as a witness in legal proceedings, which places a particular empha-
sis on recognising and working within the limits of your competence and making sure that any reports you write are not misleading and do not deliberately leave out relevant information.
An expert witness’ role4 involves assisting the court on specialist or technical matters which are within the witness’ expertise.
As an expert, you should have had the opportunity to consider all the available evidence before forming an opinion.
An expert will not normally have been involved in the direct care of the patient before the legal proceedings start, although may need to physically assess the patient once they do become involved in the case.
Specialist training
To act as an expert, a doctor would be expected to have sufficient experience as a specialist and would normally have at least ten to 15 years’ experience in that subject.
An expert needs to have knowledge of the court processes and procedures and it would generally be expected that they have had some specialist training in the role of an expert witness as well as having the appropriate indemnity.
To address concerns doctors have about engaging in medical expert work, particularly in relation to the lack of training and support, the medical royal colleges and professional bodies have been encouraged to create resources, including those online, to support expert witness work and raise awareness of the training that is available from other sources, such as the Academy of Experts 5 and the Expert Witness Institute.6
Dr Kathryn Leask is a medico-legal adviser at the Medical Defence Union
1. The President of the Family Division Working Group on Medical Experts in the Family Courts, Final Report (October 2020)
Police want a consultant psychiatrist to disclose medical records. But does she have to? Dr Kathryn Leask gives her response
Dilemma 2
Must I hand over patient’s notes?
QI am a private consultant psychiatrist and have been contacted by the police who have requested a copy of a patient’s medical records to assist them in investigating a crime.
They are hoping there will be information in the medical record that will help the Crown Prosec ution Service make a charging decision.
Although the police say he may have committed a serious crime, he is not currently a risk to the public and has capacity.
I understand that the patient, on the advice of his solicitor, has refused to provide his consent to allow the disclosure of his medical records.
The police officer has presented me with a production order, signed by a judge, which orders the disclosure. I assume I must comply with this order?
AIt is not unusual for requests to be made by the police for the medical records of patients to help with a criminal investigation.
If the patient is not an immediate threat to the public and they have capacity, their consent should be sought by the police before information is disclosed.
Where consent is refused or where the patient lacks capacity but you cannot justify disclosure in the patient’s or the public interest, the police may, under certain circumstances, obtain a court order. Court orders, however appropriate they seem, need to be viewed with caution.
Before a person has been charged with a criminal offence, medical records are referred to as excluded material. This means, before a charge has been made, the
police have no right of access to records even with a court order.
After a patient has been charged, the police can apply to the court for medical records to be disclosed. If the judge agrees, they can make a production order.
So it is important to be aware of the circumstances when the police can rely on a production order, as these are sometimes agreed by a judge under situations when they should not have been. It is important to seek advice early from your medical defence organisation.
In this case, it is important to establish whether the patient has
been charged and, if not, the production order will not have been legally granted. This does not mean that the order can be ignored.
While bringing this to the attention of the police will hopefully dissuade them from utilising the order to secure the medical records, it does still need to be discharged. This can be done by the police or, if appropriate, your medical defence provider.
Where you receive a court order, even if this does seem to be lawful and valid, it is a good idea to contact your representative there before relying on the order.
DOCTOR ON THE ROAD: VW ID.3
The Golf is closing with the innovators
If you are ready to take the electric plunge, then Dr Tony Rimmer (right) recommends you give this offering from Volkswagen a test drive
IS NOW the right time to buy into a new technology?
We medics will have asked ourselves this question many times over many years about many different aspects of our work.
As first adopters, we must take a risk. We may be stuck with quickly outdated and expensive equipment or we may hit the first wave of an emerging revolutionary market and reap the benefits of being a trailblazer.
With motoring, the electrification of all our cars is the biggest and most dramatic change since the dawn of the internal combustion vehicle in 1885 and the arrival of Karl Benz’s tricycle.
There have been some false starts over the years and many of us may remember the electric milk-floats that delivered bottled milk when we were young; the technology has been around for decades.
It has taken the increased awareness of CO2-induced global warm-
The ID.3 has been designed from the ground up using all the technical know-how and experience that VW can throw at it
ing and the negative effects of poor air quality in urban environments to nudge us into embracing and developing the technology.
David vs Goliath
The car industry, you could argue, has been slow to change. It took a Silicon Valley upstart, Elon Musk with Tesla, to act as David while the established global car makers watched on as Goliath. However, now the giants have awoken and are starting to release
their own electric cars after several years of development and spending billions of pounds. It is of great significance then, that we are now able to buy the first all-electric car from the biggest of all manufacturers, the VW Group.
It is the ID.3 and it has been designed from the ground up using all the technical know-how and experience that VW can throw at it. So what is it like and is it a breakthrough product that we medics really need to take note of?
I have been driving the £35,880 1st Edition model of the ID.3, which is the only version available at the moment. It has lots of standard equipment, a 201bhp electric motor and a 62kWh battery which gives a claimed maximum range of 260 miles.
Main competitor
There will be other variants available in due course, some with different-sized batteries too. It can ➱ p46
Free legal advice for Independent Practitioner Today readers
Independent Practitioner Today has joined forces with leading healthcare lawyers Hempsons to offer readers a free legal advice service.
We aim to help you navigate the ever more complex legal and regulatory issues involved in running and developing your private practice – and your lives.
Hempsons’ specialist lawyers have a long track-record of advising doctors – and an unrivalled understanding of the healthcare system as a whole.
Call Hempsons on 020 7839 0278 between 9am and 5pm Monday to Friday for your ten minutes’ of free legal advice.
Advice is available on:
Business structures (including partnerships)
Commercial contracts
Disputes and litigation
HR/employment
Premises
Regulatory requirements and investigations
Rourke
take up to 100kw DC charging at a plug-in station and can charge up fully overnight at home from a 7.2kW or 11kW unit. Its main competitor in the market is the wellestablished £36,395 Nisssan Leaf e+ Tecca.
In the flesh, the ID.3 looks smart and modern: not too futuristic like the BMW i3 and not too plain like the Leaf. It suits bright colours and on its standard 19-inch alloy wheels looks almost sporty.
Futuristic theme
Step inside and the futuristic theme continues. The digital dash and touchscreen is clear and easy to use – not as intuitive as in the Polestar 2, but better, in my view, than the truly minimalist approach of the Tesla Model 3.
So, first impressions are positive. Continuing the evidence that VW has spent a lot of time making this a suitable alternative to the estab-
lished internal-combustion Golf is that the interior space and packaging is on a par with the older design.
The boot is just as big and there is even more room in the back seats for three passengers – the benefit comes from a longer wheelbase and a flat floor above the batteries.
Behind the wheel, I quickly got comfortable and I like the slightly raised driving position. However, the seats lack adequate lateral support for my liking. The ID.3 takes off from rest swiftly in typical electric car fashion and what becomes quickly apparent is the excellent smooth ride.
Despite our rough roads and the large alloy wheels, it really is impressive. The steering is sharp and with the instant electric surge available, it makes negotiating urban traffic stress-free and even fun.
VOLKSWAGEN ID.3 1st EDITION
Body: Five-seat hatchback, front-wheel drive
Engine: One electric motor and one lithium-ion battery
Power: 201bhp
Torque: 310Nm
Top speed: 99mph
Acceleration: 0-62mph in 7.3seconds
Claimed range: 260 miles
Realistic range: Around 200 miles
CO2 emissions: 0g/km
On-the-road price: £35,880
Out on the motorway, the Volkswagen continues to impress. Wind noise is notably suppressed so cruising at 70mph becomes limousine-like, as there is no engine noise and the ride remains smooth.
Limitations of
battery
It is only on twisting A and B roads that the limitations of the batteryladen chassis become apparent. Despite a low centre of gravity, you cannot cheat physics, so cornering is perfectly fine but not sporty.
Also, I would prefer the regenerative braking to have a more powerful setting – there are two available but neither gives a true one-pedal-driving ability. To give VW its due, this is a deliberate ploy so as not to put off buyers new to electric cars.
So, is the ID3 a gamechanger? Well, it is a really good all-electric car which I would highly recom-
mend. The real-world range of this version is around 200 miles. If you wait for the 77kWh battery version you will get a more useful and real 270 mile range. It will be more expensive, though. As a rule of thumb, you can calculate the real-world range of an electric car by multiplying the battery size in kWh by 3 to 3.5 miles/kWh. Manufacturers will always quote a range based on a super-ideal 4m/kWh.
You could always wait for the next VW products to use the same chassis and batteries; the VW ID4 or Skoda’s Enyaq SUV which will be better value.
Any medic who feels ready to take the electric plunge has an ever-increasing choice of excellent cars and that can only be a good thing.
Dr Tony Rimmer is a former NHS GP practising in Guildford, Surrey
There is even more room in the back seats for three passengers than in the Golf
The digital dashboard is clear and easy to use – and better than the minimalist Tesla Model 3
PRIVATE PATIENT UNITS: THE SOUTH-WEST
Our monthly look at private patient units by Philip Housden turns its attention to the private services in the 17 – soon to be 14 – NHS trusts delivering acute care services to the south-west counties of Dorset, Devon, Cornwall, Wiltshire, Somerset and Gloucestershire
Figure 1
United front needed
THIS REVIEW is based on the information published in the Trust Annual Accounts for 2019-20, which was partially adversely impacted by the early months of the Covid pandemic.
The annual accounts for this group of trusts shows that regional total private patient revenues grew by £1.1m to £29.4m (up 3.9%) after a fall of £2.2m from £28.25m in 2018-19.
This now represents 0.49% of these trusts’ total revenues, up from 0.46% last year, but well short of the 0.78% achieved in 2018-19. The combined national average outside of London is 0.43%.
Great Western Trust in Swindon continues to lead the region, delivering revenues of £4.2m, up £246,000 and 6.2% on 2018-19 and 1.33% of total trust incomes. The trust operates a 20-bed dedicated PPU, branded Shalbourne Private Health Care.
Gloucestershire Hospitals grew £504,000 and 17% to £3.5m revenues in 2019-20. The trust offers
limited bed access at Cheltenham General, but has no dedicated inpatient capacity for private patients on the Gloucester Royal site.
The trust continues to search for a balanced solution for delivering dedicated private inpatient capacity. The Cheltenham General site in particular has strong potential, which would be delivered if the 15-bed Knightsbridge Ward was still fully available for private patients.
Gloucester is not as strong a catchment, but the Royal Infirmary has the surgical infrastructure providing the high-quality patient safety back-up clinicians most value.
Move forward
Royal Bournemouth has moved forward in the past year with revenues up £412,000 and 14.1% to a five-year high of £3.3m. This was achieved after opening additional capacity above the five original dedicated private beds within the Bournemouth Private Clinic.
The trust also hosts a cardiology
joint venture with Regent’s Park Healthcare called the Dorset Heart Clinic, and has plans to extend inpatient bed capacity.
Bournemouth and Poole trusts have now completed a merger to form University Hospitals Dorset from April 2021. It is to be expected that the experienced private patient leadership at Royal Bournemouth can now revitalise the service at Poole and the steep decline in private patient revenues on that site.
These were down a further £147,000 and 15% in 2019-20 and over £1m down in two years since the ending of the ring-fencing of Poole Hospital’s Cornelia Suite, a dedicated six-bed PPU opened in 2013.
Figure 2 (overleaf) suggests the potential for a county-wide approach, given that Dorset County in Dorchester is keen to develop private patient services, as it relatively underperforms Bournemouth’s 1.12% of total revenues, achieving £819,000 reve -
nues and a 4.6% increase in 2019-20 at 0.45% of total revenues. At Plymouth, the trust fell back £398,000 and 12.7% in 2019-20 to total private patient revenues of £2.7m – 0.54% of turnover. The trust has historically ring-fenced capacity in The Meavy Clinic.
As the trust provides a wide range of specialist regional services, the trust catchment for complex activity is a market opportunity which may drive further growth.
Additional opportunities
Salisbury has declined £272,000 –a fall of 11.4% – in 2019-20 at 0.95% of total trust incomes. The trust has four dedicated beds in the Clarendon Suite, which is small by PPU standards, and addition revenues from diagnostic and other earnings.
The trust’s plans for a new day case unit and other campus developments may raise additional opportunities in the future.
Yeovil is a trust with a track
record of successful commercial developments and provides private patient inpatient services through the 14-bed Kingston Wing.
Private patient incomes fell £332,000 last year to £2.1m, but the trust still enjoys the highest percentage of trust revenues in the South-west, now at 1.4% of turnover, a drop from 1.61% in 2018-19.
Nearby Taunton also fell back £332,000 (15.5%) last year and, like several trusts, reversed gains from the previous year. The trust provides services including the 12-bed Parkside Unit PPU at Musgrove Park Hospital.
Diagnostic centre
The merger from April 2020 to create Taunton and Somerset NHS Foundation Trust provides opportunities for growth of private provision into community services as does the recently agreed partnership with Rutherford Diagnostics Ltd to create an off-campus diagnostics centre delivering CT, MRI and ultrasound scans and X-rays to meet growing demand for NHS diagnostic services.
North Bristol NHS Trust is the largest trust in the south-west of England, providing hospital and community healthcare to Bristol, south Gloucestershire and north Somerset. Southmead Hospital is the specialist regional centre for a number of services including neurosurgery, renal medicine, plas -
tics, orthopaedics and major trauma.
As recently as 2016-17, North Bristol was the highest-earning trust by revenues in the region and a recent period of decline was arrested last year with growth of £424,000 to £1.8m – but still only 0.34% of turnover.
The redevelopment of the new Brunel building at Southmead Hospital Bristol, where 75% of the 800-beds are single rooms, offers an opportunity to deliver private patient inpatient services alongside NHS care.
Across the city, private patient revenue at University Hospitals 17 South-west
Bristol grew £507,000 and 42.2% last year to £1.7m, reversing the steeply decline in 2018/19. Again, the trust does not have a dedicated private patient unit.
The trust has merged with Weston from April 2020, where Weston’s 12-bed Waterside Suite delivers a local private patient service and income for that trust of £162,000, a fall of 6.4% and £11,000 in 2019-20.
Service gap
Even though neither of the two large trusts in Bristol currently provides dedicated private patient service and the city and catchment is well provided for by independent hospitals, there is still a gap for delivery of complex and specialist services.
This may be an opportunity for cross-city working between them and a new city-wide approach with the trusts jointly developing a stronger private practice ‘chain’ together.
Royal United Hospitals Bath operates in one of the most competitive private hospital markets outside of London.
The trust is growing private patient revenues, but from a low base of 0.44% of total incomes, increasing by 36.7% and £237,000 to £882,000 in 2019-20.
However, the relative affluence and size of the drive-time catchment means that there remains local market potential. It is understood that, because of this potential, the trust is considering a review of options for further growth in private patient services.
In Devon, the Royal Devon and Exeter did have plans to invest in dedicated new capacity for some time, but the work programme, announced in 2019, for an investment of £1.8m to open a new 12-bed PPU inpatient ward was delayed and perhaps will not be open until at least 2022.
Trust revenues grew 14.4% and £164,000 to £1.3m in 2019-20, still only 0.28% of total income. The trust will merge with Northern Devon from April 2022, where private patient revenues held steady at £554,000 – a fall of £6,000 and 1.1% – at 0.27% of total incomes. Although the trust had a PPU, this capacity has been used for
NHS activity for some years. Despite local consultant support, the market seems too small and geographically isolated to achieve a new service on its own and so the forthcoming merger may provide a boost with the support of the dedicated manager and team from Royal Devon and Exeter.
Weak competition
Along the coast, Torbay and South Devon has enjoyed six years of growth, with an increase of £38,000 and 3.9% last year to a new high of £1m. The trust faces relatively weak local independent sector competition and therefore also has opportunities for growth. Perhaps this could be accelerated through an alliance with their neighbours in Exeter?
Across the Tamar, Royal Cornwall reversed four years of decline last year with growth of 11.1% and £40,000 revenues in 2019-20 to reach £401,000.
This is still only 0.1% of total trust incomes, the lowest private patient earnings of the trust in the region. It is not known whether the trust plans to develop a local
private patient service, but Ramsay’s Duchy Hospital is situated close to the trust’s main site at Truro and is therefore in a good position to provide a convenient local service to consultants.
Looking to the future postCovid, the ageing population, increasing patient safety agenda and rising restrictions on NHS access and lengthening waiting times, means that there remain opportunities for all the southwest trusts to consider the benefits of growing private patient services.
The region is the home of the most active regional group of NHS PPU managers and this supportive network provides a strong base for developing future co-operation, alliances and even city- and county-wide networks/groups/ chains of NHS PPUs to exploit these market opportunities.
Perhaps such partnerships could now start to develop in Dorset, Bristol and Devon?
Next month: West Midlands
Philip Housden is managing director of Housden Group commercial healthcare consultancy
Figure 3
A PRIVATE PRACTICE
– Our series for doctors embarking on the independent journey
Avoid a pension tax
Understanding pensions tax issues are a source of many a doctor’s headache. Ian Tongue cuts through the jargon and gives some smart tips
BEING PRUDENT and saving for your retirement has historically been rewarded with tax relief, but, in more recent times, those with final salary-type pension schemes have been faced with worries over receiving a large tax bill.
Changes to the NHS Pension Scheme have been significant, so understanding your position and planning are the key to avoiding pension tax shocks.
The issue
Think of the issue as twofold involving the analogy of a bucket.
The rate at which you are filling the bucket is the pension annual allowance. If you fill the bucket too quickly, you get an annual allowance tax charge which is assessed every year as part of your self-assessment tax return.
Think of the lifetime allowance charge as the capacity of the bucket, which, when reached, prompts a lifetime allowance charge when you come to retire.
It is really important to note that the lifetime allowance is not a maximum figure that your pension can be, but a level at which the rate of increase of pension benefits can reduce due to a tax charge being incurred on the element of pension over the capacity of the bucket.
Working with an accountant and independent financial adviser who understands your NHS pension is crucial to your understanding of the pension, as the rules around this are complex and not easy to research yourself.
Definitely do not make decisions based on what others have done, as this can often be incorrect for your circumstances.
Annual allowance
When you hear of colleagues having a tax charge on their pension, it is more than likely going to be an annual allowance charge, as these are calculated and included on your personal tax return annually. These charges can either be paid with any other tax due for that year or the pension scheme can pay the tax due with what is called a ‘scheme pays’ election.
A ‘scheme pays’ election is a behind-the-scenes loan that incurs interest and when you come to retire, you lose some of your pension based on how much you owe.
Working with an accountant and independent financial adviser who understands your NHS pension is crucial to your understanding of the pension, as the rules around this are complex and not easy to research yourself
Pay increments;
An inflationary pay rise;
A national merit award;
Other pensionable roles.
Having a combination of these factors can be the perfect storm for a significant tax liability and therefore having an accountant that can explain your circumstances and help you plan is the best way to mitigate or avoid annual allowance tax charges altogether.
The tax payable is automatically deducted from your pension which applies for life. Often the reduction in the pension is modest, as the pension forgone would have been taxed at 40%.
McCloud remedy
Following the Hutton report in 2011, new pension schemes were proposed across the public sector to move away from schemes based on final salary to being career earnings-based.
For many, the ‘scheme pays’ option is the choice made due to cash flow constraints, but for those who are able to pay the tax, do not assume that the ‘scheme pays’ route should be avoided. Speak with your accountant and adviser to understand your position before making a decision.
The introduction of annual allowance tapering from 2016-17 was the tipping point for most consultants and GPs to have exposure to pension tax charges. Instead of receiving a £40,000 allowance each year, it could be as low as £10,000 depending on earnings and pension growth combined once the earnings threshold of £110,000 is exceeded.
Concession too late
Compounding the problem was NHS Pensions’ reluctance to allow the ‘scheme pays’ facility where a member was tapered. Thankfully, NHS Pensions made concessions later on, but not until many had suffered significant tax charges and some even left the scheme directly as a result.
As things stand, the landscape has improved because the earnings threshold for annual allowance tapering is now £200,000, so you would need to have combined earnings and pension growth of £312,000 to hit the lowest available annual allowance which is now just £4,000.
For most, there are tax planning opportunities to ensure that you preserve all of your £40,000 allowance each year. Having a medical accountant should ensure that you are best placed here.
With a £40,000 allowance and the ability to look back three years to utilise any unused relief, most will be able to avoid tax charges, but certain key factors will always be a risk:
Compensation scheme
In the run-up to the general election in 2019, many doctors were unable to carry out waiting list work without being hurt financially by the annual allowance tapering mechanism and this finally became the catalyst for change.
Changing tax legislation is a long process, so, as an interim measure, the Government announced a compensation scheme. This means any annual allowance charge for 2019-20 would effectively be compensated using a legally binding arrangement between the employing trust, NHS Pensions and the Government.
Most people are eligible for this, but notable exceptions are those working in Scotland and those who do not carry out clinical work.
There is a process to apply for the compensation scheme which requires a ‘scheme pays’ election for 2019-20 to be submitted first. The scheme pays election deadline for 2019-20 is 31 July 2021, so do not delay if you have an annual allowance charge for that year.
At the time of writing, the compensation scheme can be applied for up to 31 March 2022, so there is less pressure for that, but it is probably best to deal with both at the same time.
Lifetime allowance charge
The lifetime allowance charge is applied at retirement and NHS Pensions will carry out the necessary calculations. Some will have pension protection from when the limits reduced and it is important that you have details of this when preparing your paperwork.
Where the lifetime allowance is exceeded, a tax charge on the excess is applied at 25% if taken as income.
The way in which these were forced onto members was based on age and, following a legal challenge, this was deemed to be illegal by the courts due to age discrimination. The ‘fix’ for this is what is known as the McCloud remedy.
The McCloud remedy has many elements to it, but is basically giving members a choice for the period 1 April 2015 to 31 March 2022 whether they want to be in the 2015 scheme or go back to their legacy scheme, usually the 1995 scheme. From 1 April 2022, every NHS Pension Scheme member will be in the 2015 scheme.
The implications of this in the context of this article are that previous calculations of pension annual allowance will need to be revised and the value of a member’s pension will be different depending on which scheme is adopted.
Your actual choice will be made at retirement, so, for most, this is not an immediate consideration but many will want to know their position in advance.
Pension annual allowance charges have been particularly punitive over recent years and have acted as a disincentive to work.
Thankfully, the landscape is now fairer for most members, with reduced exposure to annual allowance charges and more pension options. It is refreshing to be writing at last about positive changes to pensions.
Next month: Is owning residential property in a company taxefficient?
Ian Tongue (right) is a partner with Sandison Easson accountants
DOCTORS AS PATIENTS
When the boot is on the other foot
With 58% of doctors now suffering from some form of anxiety or depression – and 46% saying their condition has worsened since last March – we are serialising sections of a new book edited by Dr Clare Gerada (right). This month: Doctors as patients
IT IS often said that doctors make the worst patients.
Systemic barriers to accessing care as well as cultural and individual factors play their part in keeping doctors away from the consulting room and relying on self-care or ‘corridor consultations’ instead.
Maybe our reluctance to seek help is that we are all too familiar with what it means to be sick, to have vulnerabilities and relinquish authority and trust to another and we recoil against this. I certainly prefer to manage my own health problems.
If I seek help, which I have had to, then it is with a feeling of shame and embarrassment that I am taking up the precious time of another.
I have had mental health problems; no one can go through nearly four decades of caring without some of the emotional impact of our patients sticking to us, and everyone, even the most robust, is not immune from the pain of significant life events.
But when my depression hit me, when I too became sad, felt worthless, hopeless and even had thoughts of suicide, I found it difficult to seek the help of another doctor, of going to my own GP, someone I knew professionally.
I worried she might consider me unworthy and incompetent to care for patients or force me to refer myself to ‘the authorities’.
Irrational concerns
I did seek help, but by-passed all ‘standard’ routes, instead, using a pseudonym, I contacted a psychologist privately.
The anonymity did not last long. As with the patients in my service who also try to hide behind their mother’s maiden name, my email address gave away my real identity.
My concerns are shared by many doctors; irrational concerns in the main, but real, nevertheless. Maybe it is because I am older, with my ‘stiff upper lip’ mentality more ingrained than in the younger, more enlightened generation that I have found it so hard to seek care.
Or maybe, as with most doctors I meet, becoming a patient means relinquishing our identity of the powerful, knowledgeable, invinci-
Doctors average less than three days’ sickness per year, while in the general population the figure is eight days and for nurses it is 15
of depression, 14% in the last year. Yet, despite these high levels of mental illness – and a knowledge of mental health services given their specialties – they would not seek care, rather prefer to suffer in silence.
Reasons given, in order of responses, were:
Not wanting to let their colleagues down; Loss of confidentiality; Fear of letting patients down; Worries about their career.
ble professional and this step is difficult.
In 2008, against a growing concern of suicide among doctors, the report Mental Health and Ill Health in Doctors was published. It discussed a range of issues relevant to this professional group, including stigma, secrecy and shame.
It said these three factors contribute to doctors failing to take on the sick role and instead work when unwell. Doctors average less than three days’ sickness per year, while in the general population the figure is eight days and for nurses it is 15.
A paper two years later, called Invisible Patients looked at the barriers to doctors seeking help and the subsequent risks to both patients and doctors due to this failure to seek timely care.
Alternative paths
That doctors are reluctant to present themselves to services for mental health problems is demonstrated by the findings of a number of surveys.
For example, one study published in 2009, found only 13% of doctors would seek help through professional routes.
The majority would choose, as I did, alternative paths such as selfmedication or informal help from friends or family.
Most, when asked why, said they feared their career would be jeopardised if they approached a colleague.
A survey sent to all GPs and psychiatrists in Devon and Cornwall found nearly one-half reported that they had suffered an episode
Surprisingly, the group most reluctant to seek care for mental health problems are psychiatrists, with one study reporting nearly 90% would be averse to consulting with another mental health professional.
Terrible crime
Fear is often at the root of why doctors do not seek care. For some of my own patients, this has been so great that it is as if they are trying to conceal a terrible crime. They tell no one, not even those closest to them, how they are feeling.
Others have consulted doctors in the private sector under the mistaken belief that this will buy them anonymity.
In my experience, what doctors worry about most about falls into two main categories. The first is around loss of confidentiality, with others being told about their mental health problems without their consent.
The second is that, by disclosing mental illness, it will mean they will be referred to the regulator or sanctioned. Both of these have some basis in reality. Medicine is a small world and it does not take long for two doctors who have never met each other to find they have mutual friends or colleagues in common.
Many doctors also live in the same area they work in – as I do. Their local hospital is often the one in which they work or their neighbouring practices are within the same clinical network as their own practice.
Others have relationships with doctors, are related to them or, as with me, are married to one, making our social networks among the profession even more entangled. This makes it very difficult to con-
sult with someone with no personal or professional ties to you or your family.
At a pinch, this might be acceptable if the reason for needing a consultation is not sensitive. However, if it is for a mental illness or a personal problem, it can be difficult for medical professionals to discuss it with friends or colleagues.
Perhaps the most extreme example I can remember of the inability to obtain a confidential space was a psychiatrist who, having attended his own GP for help with depression, found a few weeks later at his referral management multidisciplinary team meeting that he had been referred to his own team.
Breach of confidentiality
The fear of breach of confidentiality also relates to one’s personal issues being relayed beyond the privacy of the consulting room to others in their wider educational, professional or employment circles. To be blunt, doctors do not trust the system to keep their problems confidential.
This is especially the case once a mental illness has been disclosed in the workplace – for example, to a training supervisor – when it is not uncommon to have other individuals, each claiming ‘a need to know’, also told about the doctor’s illness. These can include appraisers, trainers, medical directors, senior managers and human resources and secretarial staff.
I once counted 17 individuals being told about a doctor who had recently been diagnosed with attention deficit disorder, all assuming they had a right to know. Even when a doctor is offered confidentiality at their place of work, this rarely happens.
Each staff member tells another ‘in good faith’ and with the assurance ‘I am only telling you in strict confidence but I think you should know; please don’t pass on… but… Dr XYZ is off sick with…’. This then gets passed onto another member of staff, even those who have no direct involvement, and another, with the message slightly altered each time as in the children’s game Chinese whispers. In the end, the doctor’s problem might as well be posted on the world-wide web for all to see.
A psychiatrist, having attended his own GP for help with depression, found a few weeks later at his referral management multidisciplinary team meeting that he had been referred to his own team
It is patients, on the other side of the consulting room, who become unwell, not doctors.
The American neurosurgeon, Paul Kalanithi, has written about his personal experience of being unwell in When Breath Becomes Air, published posthumously. He developed a brain tumour. His narrative illustrates how difficult it is for doctors to take on the patient role.
doing, reduce their fear of seeking help.
Still, however, the ‘system’ is predicated on the assumption that a doctor with mental illness is dangerous and needs monitoring and even restrictions placed on their practice. This is as far from the truth and is the same as assuming that any doctor with cancer needs the same restrictions.
Sadly, in my experience, colleagues derive vicarious gratification from the drama that a sick doctor brings to the boredom of their everyday working life, especially if their illness is related to addiction.
There is also the issue that once disclosed and placed on work records, it is impossible to remove and the diagnosis is carried forward for evermore into any new posts. The doctor then has to face with each move of a job – which can be every six months for doctors in training – having to go over their past illness and be interrogated as whether they are fit to practise.
This is not, I hasten to add, just for serious mental illnesses, but for problems such as past history of depression, an eating disorder, dyspraxia or indeed any diagnosis that the doctor has placed on their record.
The second major concern for doctors is that of being referred to the regulator. This is a largely unfounded fear, as very few doctors with mental illness are investigated by the GMC and fewer still receive sanctions. However, this does not prevent the anxiety.
Aside from worries around admitting to mental health problems, there is also the real concern of not being treated with compassion when they are unwell and wanting care.
Becoming a patient
Given the ‘rules’ of medicine, it should be clearer why we find it so difficult to become patients. Crossing that invisible divide between health professional and patient is a fundamental challenge to our personal and professional identity.
He wrote: ‘Why was I so authoritative in a surgeon’s coat, but so meek in a patient’s gown?’ The answer to his question is because as the complete object, the ‘doctor’, we create an aura of invincibility around ourselves.
Becoming unwell is challenging, even in the short term, as, with this, comes the loss of the trappings of power, knowledge, status and authority defined by our group norms.
The behaviour of ‘working nevertheless’ and giving a façade of coping, not just to colleagues and patients but also to ourselves, is hard wired into the medical culture. Doctors who take time off are not viewed favourably by those who have to pick up the work left by their absence.
Sympathy fatigue
This creates the norm that illness equates with weakness, and doctors should be strong and healthy and cope themselves with illness and stress. Colleagues who are absent due to illness tend to create ‘sympathy fatigue’ and blame rather than compassion and understanding.
When doctors do get into a consulting room, they tend to act differently, as they visibly try to regain control of their medical identity, by, for example, ‘talking shop’ or underplaying their symptoms.
Sick doctors are different to other patients. They present late, and then with diagnoses rather than saying what is wrong with them. They minimise their symptoms, such as deliberately scoring lower on alcohol screening questionnaires or masking the true extent of their negative thinking.
But the tide is turning and once services can offer confidentiality, containment and skill in managing their problems, doctors are willing to present to care and, in so
Of course, unwell doctors, just as those who might have an acute physical illness or broken leg, will need time to recover and recuperate and, on return to work, they might need reasonable adjustments to be made.
But my experience of over 10,000 mentally ill doctors is that the overwhelming majority pose no risk at all to their patients and where they might pose a risk, this can be identified ahead by the medical team and measures put in place to reduce this it.
Next month: Doctors treating doctors
Dr Clare Gerada is medical director of the Practitioner Health Programme, London, and a former chairman of the RCGP
Independent Practitioner Today readers can save 20% on Routledge.com with discount code BWC21. Offer ends 31 August 2021. Order now: www.bit.ly/ Routledge_IPT
Big changes on horizon
Big changes in the way many anaesthetists work are tipped to be on the way. Ray Stanbridge reports on the findings in his latest benchmark survey
OUR ANALYSIS suggests that consultant anaesthetists have enjoyed a fairly stable income in 2019 with remarkably similar figures to 2018. But, as discussed below, we believe that there are major changes ahead, which potentially will change how many anaesthetists will work in future.
The average anaesthetist’s gross income from part-time private practice rose from £97,000 in 2018 to £101,000 in 2019 – a 4% increase. Clearly, there is a bias for those who work in the greater London region.
But costs have also gone up by about £4,000 a year, jumping from
£36,000 to £40,000 or by about 11%.
As a result, taxable profits have remained constant at £61,000 for the year.
What then are the reasons for these changes?
Home costs increase In 2018-19, there seems to have been some growth in private sector activity as opposed to Choose and Book work, which remains the preferred choice of many. This is despite ongoing pressure on anaesthetists’ fees from insurers.
There has been some increase on the incidence of home costs,
where consultants increasingly do their administration. Hopefully, they have arranged their affairs to avoid the risk of a capital gains tax charge when they come to sell their homes.
Given an increase in use of home, it is perhaps not surprising to see that office costs have risen.
There has been some growth in courses and conference costs. These courses are often conducted at attractive venues. We would expect this expenditure to reduce significantly in ensuing years as the effects of the Covid pandemic come into financial accounts.
Apart from these changes, we have seen little else has changed cost wise.
What then of the future?
Fundamental changes
Consultant anaesthetists have probably experienced a more difficult time in 2019-20 and 2020-21 with the impact of Covid-19. However, we believe that there are early signs that more fundamental changes may be afoot.
An increasing number of hospitals are looking at the pros and cons of employing their anaesthetists on a full or part-time basis.
For a number, this could be highly attractive – there are some cost savings to be made, as these
are met by hospitals rather than out of the consultant’s own pocket. There is also the potential for additional security.
However, for some, the tax burden will be higher and this may not be an attractive option for ‘high flying’ anaesthetists with large private practices.
Attractive deals
It is also a fact that some hospital groups are offering attractive deals to some anaesthetic consultants to become employed. We would expect a sizeable minority to take up some of these attractive options in future years.
As a result, we would expect to see a very different structure of the anaesthetic profession in future, perhaps with the younger consultants taking up an employment option while older specialists consolidate into groups. Solitary high flyers will still always expect to do well.
These are interesting times for anaesthetists and we will keep a close eye on what is going on. Our criteria for inclusion in the survey this year has changed so that the minimum income doubles to £10,000.
Anaesthetists tend to earn more when working within a group,
Year ending 5 April. Figures
particularly where they have developed a strong brand structure.
Where a local anaesthetist has a monopoly or quasi monopoly in a local given area, his or her income maybe higher than shown in our survey.
In effecting year-on-year com -
parisons, we are also aware of the impact of Choose and Book work on some consultants’ activity, the trading methodology they choose and the impact of groups.
The full criteria for acceptance in our survey remain as before. These are that those surveyed:
Continue to work in the NHS and not be in full-time private practice;
Hold either an old-style or a new-style contract within the NHS;
Must have been in private practice for at least five years;
Must be seriously interested in pursuing private practice as a business;
Have been earning at least £10,000 a year from private practice;
Trade either as a sole trader, through a limited liability company or a limited liability partnership or as a member of some other group.
Although our sample should not be regarded as statistically significant, we believe it does give a useful benchmark guide to this specialty’s income, expenses and profits.
We note that there are large regional variations in income with occasional outliers.
Next month: Oncologists and dermatologists
Ray Stanbridge is a partner with accountancy, finance and tax advisory medical specialists, Stanbridge Associates
HOW ARE YOU DOING?
Use
benchmarks to compare your financial performance with others
THE CLEARING SERVICE
ACCURATE, EFFICIENT, SECURE AND COST-EFFECTIVE ALTERNATIVE TO TRADITIONAL PAPER INVOICING.
Healthcode is the UK’s official medical bill clearing company and has provided secure and encrypted systems to healthcare professionals since 2000. Pre-pandemic we processed around 27,000 electronic medical bills to insurers daily.
What is the Clearing Service? Benefits of the Clearing Service
The Clearing Service is the process whereby Healthcode accepts invoices from providers, validates them for completeness and correctness and then forwards them securely to the relevant PMI. Sometimes referred to as ‘claims scrubbing’, the process entails checking for correct use of codes, formats and prevents time-consuming and costly processing errors that could delay the reimbursement process.
How it works
Convenient and efficient
You can submit invoices to all the major PMIs from one platform.
Minimise human errors, invoice queries and rejections
Validated invoices automatically sent to the correct recipient.
Better cash flow and forecasting
Validated invoices enter the insurer payment cycle quicker with confirmation of receipt.
Protect sensitive data
A secure, encrypted system which protects both your and your patient information.
Expert technical support
Our customer services team are here to support you and answer any queries you may have.
Coming in our May issue, published on 8 June.
Doctors treating doctors: It is not just unwell doctors who find it hard to accept that they can be sick, doctors who see and treat other doctors find it difficult and embarrassing as well. Dr Clare Gerada continues our series adapted from her book Beneath The White Coat –Doctors, Their Minds and Mental Health
Getting a clear picture of radiology claims: Dr Shabbir Choudhury, medico-legal adviser at the MDU, analyses clinical negligence claims notified by radiology members and advises on how to manage risk
In recent months, we have seen an increasing number of reports of the effects of Covid on mental health, particularly apparent within the healthcare community. Jane Braithwaite identifies ways independent practitioners can help to alleviate these issues in their staff
Lots of independent practitioners do it, but is owning residential property in a firm tax-efficient? Accountant Ian Tongue gives his views
In response to demand for information about setting up in private practice, the MDU’s Dr Jerard Ross looks at the most important considerations for new independent practitioners to avoid attracting unwanted attention from the GMC and other regulators
Our motoring correspondent Dr Tony Rimmer says the Porsche Cayman 4.0 GTS is surely just what the doctor ordered
Elsevier’s Future of Research report provides insight into the impact of the Covid-19 on clinical trial data, highlighting how the lessons learnt from this global health crisis provide valuable learnings for the future
INDEPENDENT PRACTITIONER
TODAY
The
Published by The Independent Practitioner Ltd. Independent Practitioner Today is editorially independent and thanks Bupa for its assistance with distribution. Material is governed by copyright. No part of this publication may be reproduced, stored in a retrieval system or transmitted in any form without permission, unless for the purposes of reference and comment. Editorial layout is the copyright of the publishers. If you wish to use it for promotional purposes on websites or for reprints, we would be happy to discuss licensing the copyright to you.
Branding in your practice – Simon Marett and Michael Sullivan’s series to help you close the gap between good and bad has some important advice on imagery
Profits Focus puts the earnings of dermatologists and oncologists under the microscope
Some difficult scenarios can sometimes arise when a clinician works both in the NHS and privately. Dr Heidi Mounsey, medico-legal consultant at Medical Protection, offers some guidance
Medical indemnity cover is vital for practitioners, but few relish gathering all the information when it comes to annual renewal or when looking for competitive quotes. Healthcode’s Fiona Booth explores how an enhancement to The Private Practice Register streamlines the process
We take a peek at Royal Marsden Private Care’s new facility in Cavendish Square
Researcher Dr Michael Anderson, clinical adviser to the Private Healthcare Information Network, tells how we could improve the uptake of Patient Reported Outcome Measures in private healthcare
If you work in one of the West Midlands PPUs, then don’t miss Philip Housden’s analysis of their financial performance
How to apologise to a patient following a prescription error and advice on the downsides of posting on a private social media group are covered in our Business Dilemmas series
Plus all the other regular features, latest news and view
Don’t forget – you can find more news on our website throughout the month
ADVERTISERS: The deadline for booking adverts in our June issue is 21 May
Write to Independent Practitioner Today 7 Lindum Terrace, Lincoln LN2 5RP
CHANGING ADDRESS, EMAIL ADDRESS OR SUBSCRIPTION DETAILS? Phone 01752 312140 or email karen@marketingcentre.co.uk
TELL US YOUR NEWS
Robin Stride, editorial director Email: robin@ip-today.co.uk Phone: 07909 997340 @robinstride
ADVERTISE WITH US
To advertise in the journal or our website business and lifestyle directories, contact advertising manager Andrew Schofield at Spot On Media. Phone: 0161 408 3912 Email: andrew@spotonmedia.co.uk
GET A SUBSCRIPTION DISCOUNT!
£90 independent practitioners.
£90 GPs and practice managers (private & NHS).
£210 organisations.
Save £15 paying by direct debit: individuals £75 (organisations £180).
TO SUBSCRIBE
Email karen@marketingcentre.co.uk or phone 01752 312140
Publisher Gillian Nineham Phone: 07767 353897.
Email: gillian.nineham@gmail.com
Guarantee delivery of your next copy of Independent Practitioner Today. Take out a subscription and you will get full access to our news, features and previous issues on our website. See details on the left.