The business journal for doctors in private practice
More than a pretty face
How to prepare a marketing plan for setting up a practice in aesthetic medicine P10
Brainstorming time
Doctors aiming to get into business got a helping hand at a special event P23
Ethical rules of the road
Readers’ questions about patients’ issues with the DVLA are tackled by an expert P36
Enter the ‘fees for all’ era
By Robin Stride
A landmark judgment from the Competition Appeal Tribunal (CAT) paves the way for all consultants’ fees to be compulsorily published.
Prices – and performance – will be shown alongside those of private hospitals they work from on a website databank run by the Private Healthcare Information Network (PHIN).
Fee data is tipped to go live following the failure of an appeal by the Federation of Independent Practitioners Organisations (FIPO) against rulings arising from the Competition and Markets Authority’s long running inquiry into alleged curbs in competition in private healthcare. The CAT dismissed FIPO’s appeal on all seven grounds of its challenge.
PHIN boss Matt James responded: ‘We’re glad this decision clears the way for the publication of fee information alongside quality measures so that consumers have the full picture.’
He told Independent Practitioner Today: ‘Consumers considering private healthcare want to find the best treatment and to know how much it will cost. If they’re insured, they want to know that their insurance covers the treatment they’re looking for with the consultant they want to see.
‘That’s pretty simple. What is
more complicated is making sure the publication of information represents all parties and options fairly, and that’s what PHIN will be working on, with FIPO and others, over the next couple of years.’
FIPO said it was ‘disappointed’ with CAT’s two to one majority judgment backing the CMA’s view that private medical insurers’ power had no adverse effect on competition. It would pursue ‘all options available’.
Barrister Mr Aidan Robertson said FIPO could take the case further with permission from appeal authorities, but he told doctors at the BMA private practice committee conference it would have to show an error of law in the judgment and he saw no prospect of the case reopening.
In a lengthy statement available on our website, FIPO welcomed a strong dissenting opinion from the tribunal’s non lawyer member, economist Dermot Glynn.
FIPO agreed with his conclusions ‘that because there is no real price competition between consultants vis à vis the policyholders, the imposition of a fee information remedy on consultants (the remedy adopted by the CMA) cannot do anything to improve the competitive outcome.
‘Indeed, FIPO agrees that providing this information may well facilitate tacit collusion, encouraging
We’re glad this decision clears the way for the publication of fee information alongside quality measures so that consumers have the full picture
Matt James, PHIN chief executive
smaller private medical insurers to follow the Bupa or AXA PPP benefit schedules, leading to further loss of competition between consultants.’
FIPO had also challenged the CMA’s view that there was an adverse effect on competition arising from the lack of independent publicly available performance and fee information on consultants.
The CMA said this should be remedied by requiring healthcare operators and consultants to publish information about specialists’ fees and other aspects of their practice –the ‘Information Remedy’.
FIPO challenged the CMA’s ‘Private Medical Insurers’ Decision’ on six grounds and the ‘Information Remedy’ on one issue.
There was no ruling on costs.
The Independent Doctors Federation (IDF) was also disappointed at the ‘complex judgment’. Spokesman consultant physician Dr Brian
O’Connor said:
‘The dissenting opinion given by Dermot Glynn was highly critical of the CMA. Indeed, his reasons for dissenting reflects the view of the IDF.
‘We have always said that fee capping and prevention of flexible pricing restricts patients’ choice, leading to an adverse effect on competition. Patients are not necessarily directed to the best available consultant.’
He said the IDF, which sits on FIPO’s board, would be commenting more fully on behalf of members. n Turn to page 8 for the decisions on the seven grounds of appeal. For more on this story, see our website. Turn to page 5 for more on PHIN’s databank
design tricks to perk up your practice an architect shows what to do to brighten up your clinic without costing a lot P14
The best way to reach your goal tips from our resident marketing guru on managing time spent on promotion P20
dealing with dr google
What to do with the cyberchondriacs who come in with print-outs from the web P26
ensure patients know your terms How to stay ahead of the competition authorities by publishing your fees P32
The sun shines on spanish properties Spanish real estate is a good investment now. But where are the hotspots? P34
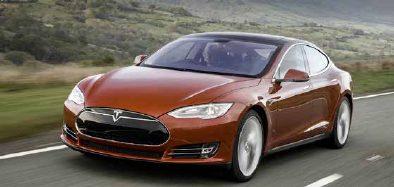
a bright spark
it’s electrifying! our motoring writer gets a buzz from the tesla Model S P41
ediTorial commenT
Leaving no leaf unturned
At Independent Practitioner Today we’ve been expanding the resources available to new and established private doctors.
And a lot of it is free because we are committed to helping you build up your practice and to cut through the hassle for you where we can.
Many thanks to all of you who have complimented us on our new website at www.independent-practitioner-today. co.uk. One of the features being enjoyed by subscribers, and doctors who have been signing up to receive two initial issues free online, is our online turnable edition.
This is a handy option format for the increasing number of readers who want to access us on an electronic format.
Why not make use of our free Tax Guide 2015 , released last month? This is also page-turnable on the website, and this month’s free offering, from James Gransby, is now available too: Your Company Life Cycle –how to use your company efficiently during the stages of its life
Also this month, we welcome top legal firm Hempsons to our fold. We’ve negotiated a cracking deal for readers: free legal advice from their team of experts. See the story on this page.
Tell us your news Editorial director Robin Stride at robin@ip-today.co.uk
Phone: 07909 997340 @robinstride
To adverTise Contact advertising manager Margaret Floate at margifloate@btinternet.com Phone: 01483 824094
To subscribe lisa@marketingcentre.co.uk Phone 01752 312140
Publisher: Gillian Nineham at gill@ip-today.co.uk Phone: 07767 353897
Head of design: Jonathan Anstee chief sub-editor: Vincent Dawe 12,450 circulation figures verified by the Audit Bureau of Circulations
Doctors fazed by errant NHS pension letter
by leslie berry
Senior doctors have been unduly worried over their retirement plans after mistakenly receiving NHS Pensions Agency letters about the new NHS 2015 pension scheme.
Many have subsequently discovered they are not actually impacted by the new pension scheme, which came into force in April.
Financial planners at specialists Cavendish Medical have reported a rise in the number of doctors contacting them for advice about the scheme called ‘2015 NHSPS’.
No longer based on final salary, the new scheme is based on Career Average Revalued Earnings (CARE) and has a much later normal retirement age.
Cavendish managing director Simon Bruce said: ‘In March and April, we received a high number of calls from senior doctors who had received information leaflets about the new pension scheme in their payslips.
‘Others had been confused after receiving letters regarding the Choice 2 exercise. But when we looked into their individual situa-
tions, many were actually exempt from transferring to the new pension scheme and had no reason to be receiving misleading communication.’
Approximately 75% of existing NHS employees and all new employees will join 2015 NHSPS – but Cavendish Medical told Independent Practitioner Today that the majority of senior doctors aged 50 or over will be exempt. Doctors born after 1962 could be affected and will move to the new scheme for their future service only.
Individuals born before this date will either be exempted altogether and remain members of the 1995 or 2008 pensions or will be subject to ‘tapering protection’.
They will still join 2015 NHSPS, but their joining date will be delayed, depending on how close to their normal pension age they were on 1 April 2012.
The Choice 2 exercise gave eligible members of the 1995 section the opportunity to reconsider their choice made back in 2009, not to move to the 2008 pension scheme.
IPT and Hempsons launch free legal advice line for readers
Independent Practitioner Today is delighted to join forces with leading niche healthcare lawyers
Hempsons to offer readers a free legal advice service.
It aims to help you navigate the ever more complex legal and regulatory issues involved in running and developing your private practice – and your lives.
Hempsons’ specialist lawyers have a long track-record of advising doctors and an unrivalled
understanding of the healthcare system as a whole.
Call Hempsons on 020 7839 0278 between 9am and 5pm Monday to Friday for ten minutes’ free legal advice.
Advice is available on: business structures, Ian Hempseed; commercial contracts, Faisal Dhalla; competition, Lindsay Draffon; disputes, Hilary King; HR/employment, Fiona McLellan; premises, Lynne Abbess.
Fight to stop salary jobs
by robin stride
A private doctors’ leader has urged consultants to know the dangers they face if they sign up for independent hospital salaried posts.
Dr Brian O’Connor, specialists’ committee chairman of the Independent Doctors Federation (IDF), said some hospitals’ senior management believed employment contracts would abolish the administrative burden for doctors and benefit them and their patients.
But the IDF disagreed and believed the NHS job plan model would not transfer well into the private model of personalised consultant-delivered care.
He warned: ‘Ultimately, a system of salaried consultants in private hospitals would diminish if not abolish the influence of doctors, whose independence would be sacrificed in the interests of their
employer, which may be at variance with best clinical practice.’
Dr O’Connor told the IDF’s annual meeting that the traditional fee-per-item model of delivering healthcare would, however, need revising and the profession might need to look at different ways of delivering healthcare.
He said the private practice landscape had changed dramatically in the last year and consultants faced major threats to their independence – to the likely detriment of patient care.
The IDF policy was to engage rather than confront insurers and in the last year it had a ‘constructive dialogue’ at talks with them.
But he complained that some insurers ignored ‘the three guiding principles of independent practice’ – the freedom of the GP and patient to choose their consultant, the primacy of the GMC and royal colleges to confer specialist recog-
nition and the specialists’ right to set their own professional fees.
Dr O’Connor said: ‘Open referral continues, the threat of derecognition remains and fee capping has persisted. It seems to be more prevalent outside of London and younger consultants, appointed since 2010 are more affected.
‘We will continue to talk to the private medical insurers (PMIs) in a constructive way and to argue that limiting the potential fee earning of consultants is damaging private practice in the long term, not because consultants want to line their pockets, but because consultants want to deliver high-quality care.
‘This cannot be achieved at the bargain-basement fee reimbursement levels now being imposed by the major PMIs. If this persists, private practice will disintegrate particularly outside of the major centres.’
He said the IDF also needed to have a voice into the Private Healthcare Information Network. Specialists were concerned that, without their involvement, the outcome data required would be influenced by the hospital providers and the PMIs but not by the doctors.
Aspen buys big stake in cancer centre
Independent hospital group Aspen Healthcare has acquired 50% of the ownership of Nova Healthcare, the specialist private patient cancer facility of the Leeds Cancer Centre Nova specialises in the care and treatment for patients that have been diagnosed with cancer, blood disorders and neurological diseases.
Aspen said the facility was a successful example of an independ-
ent sector healthcare provider working in co-operation with prominent local NHS consultants and the Leeds Teaching Hospitals NHS Trust to see private patients.
Services are provided at the Leeds Cancer Centre at St James’s University Hospital.
Aspen’s chief executive Des Shiels said: ‘This partnership presents a unique opportunity to support the NHS trust while at the same time supporting clinicians in
their private practice in order to deliver excellent and advanced clinical care.’
He said the group would grow and develop private patient services at Nova Healthcare.
Nova’s founder and director Ron Gilden said Aspen’s experience of running high-quality surgical and inpatient facilities would be instrumental to expansion plans to develop new services in partnership with consultants and the trust.
Doctor fined for hiding private earnings
A consultant has been fined £230,000 for failing to declare £1.4m private practice income. He also received four concurrent, two-year jail sentences, suspended for three years at Belfast Crown Court.
Dr Francis Gerard D’Arcy, aged 73, of Malone Road, Belfast, had pleaded guilty to four charges at an earlier hearing.
The partially retired ear, nose and throat specialist, who evaded £700,000 in tax, was given the opportunity to fully disclose his income, but he failed to do so.
In March 2013, he was interviewed by HM Revenue and Customs’ officers and admitted to supressing his £1.4m income, earned in private practice.
HMRC received a payment of
£736,542.14 in March 2014 in relation to the income tax and VAT owed by Dr D’Arcy for the period 2008-12.
He pleaded guilty to four counts of being knowingly concerned in the cheating of the public revenue contrary to Common Law when he appeared at Belfast Crown Court on 5 March 2015. He was sentenced there on 23 April.
His company was formerly a wholly owned subsidiary of Health care Technologies International (HTI), which has also developed a large NHS centre in Belfast in Northern Ireland and private centres in London and Wimbledon.
In partnership with Guy’s and St Thomas’ NHS Foundation Trust, HTI is developing a satellite cancer centre at Queen Mary Hospital, Sidcup, Kent.
share your experience of what has and has not worked in your private practice. even if it’s bad news, let us know and we can spread the word to prevent other independent practitioners falling into the same pitfalls. contact editorial director robin stride at robin@ip-today.co.uk or phone him on 07909 997340
dr brian o’connor of the idF
IDF wants private GPs as inspectors
By Robin Stride
Private GPs are pressing the Care Quality Commission (CQC) to supply private GPs to inspect them – not NHS doctors.
This is because their representatives are less than impressed so far with the treatment they have had from the inspection body.
The Independent Doctors Federation’s (IDF) GP committee chairman said there had been a number of consultation meetings about new inspection protocols, which should be more tailored to the service being inspected.
Newly appointed Dr Neil Haughton told the IDF’s AGM
that the premise and promise was that ‘expert’ inspectors, such as GPs, practice nurses and pharmacists, would be used.
The IDF had argued that inspectors should therefore be from, or at least understand, private practice rather than judge private GPs in the same way as their NHS colleagues.
Dr Haughton, of the Notting Hill Practice, told members: ‘We are committed to providing as much information as they need and have put in considerable hours of effort, but we remain to be convinced that they are listening effectively.
Certainly, the last meeting we had was very unsatisfactory.’
He added: ‘I have invited the senior national GP inspector to my own practice to see how we work and stress the differences that needs to be taken into account and he is due to visit in the next couple of months.
‘It does seem we are speaking different languages sometimes, but we can hope – we should not be their default whipping horse.’
The IDF is holding a workshop on the new CQC inspection format at The King’s Fund on 28 May.
‘Stock up on meningitis jab’
Consider stocking up while you can. That’s the IDF’s message about the new meningitis B vaccine to private GPs.
GP committee chairman Dr Neil Haughton, who succeeds Dr Fiona Payne, said private GPs were the first in the UK to provide the vac-
Botox scrips need patient to be seen
Doctors who prescribe Botox and other injectable cosmetics remotely are being reminded they must first examine the patient in person or put their registration at risk.
Defence body MDDUS said it still regularly receives calls from members regarding remote prescribing, particularly prescribing and administering of Botox.
Medical adviser Dr Naeem Nazem said: ‘Before prescribing Botox or
cine and advise the manufacturer about marketing it. But he warned: ‘Now that the Government has finally decided on a national vaccination programme, I fear that our supply will be restricted.’
He asked those having problems with supply to let the IDF know.
other injectable cosmetics, doctors must have a face-to-face consultation with the patient to establish their medical history and reasons for wanting the treatment.
‘Doctors must not use telephone, Skype or any other form of video-link to assess a patient in order to prescribe Botox, Dysport, Vistabel or other injectable cosmetic medicines.’
Earlier this year, a leading cosmetic doctor was suspended for 12 months after acting ‘dishonestly’ and encouraging nurses to obtain Botox illegally. A BBC investigation in 2012 exposed the doctor’s misconduct and the GMC tightened up its guidance on the prescribing of injectable cosmetics.
Joint event with royal college
A joint Royal College of General Practitioners/IDF symposium is being planned for later this year.
IDF members without the MRCGP have been reminded they can get this as an extension of revalidation rather than examination.
Training guides
The IDF plans mandatory training guidelines and courses to help GP members obtain training in basic life support, care of vulnerable adults and child protection. A pilot course is due this summer.
Membership tally It’s good to talk
Recent IDF meetings with private medical insurers, especially Bupa, were ‘constructive’, according to IDF chairman Dr Peter King-Lewis. He said: ‘There are other organisations who don’t believe in this way forward, but we believe we can make a difference.’
IDF chairman Dr Peter King-Lewis reported membership of 1,146 doctors, with 38% outside London. Twenty-eight per cent were in the under-50s group The Indees.
To pastures new Appraisal
The IDF will move soon to new premises to make way for redevelopment at its 126 Harley St address by landlords Howard de Walden.
service
564 doctors have had appraisals from IDF appraisers in the year ending 31 March 2015. 83% of respondents found the process useful for professional development.
New neglect law fear
More doctors could face police investigations following the launch of a new criminal offence of wilful neglect or ill-treatment.
According to Dr Michael Devlin of the Medical Defence Union, the new law is likely to lead to more police investigations if there is any question that a doctor may have wilfully neglected or illtreated a patient through something they did or neglected to do.
The defence body believes there would need to be a significant or serious departure from acceptable standards for there to be an offence and the Department of Health has
said the new offence is not designed to penalise doctors who make genuine accidents or errors. But Dr Devlin said doctors would be wondering what they can do to avoid such a stressful investigation.
He advised: ‘It is vital that they tell patients if there is a significant delay in their treatment or diagnosis. Clinicians should explain to patients why the delay has happened, what they are doing to try to speed things up, as well as ensuring the patient understands the need to get urgent advice if their condition worsens.’
iNdEpENdENt doctorS’ FEdEratioN (idF) aNNual gENEral mEEtiNg
Dr Neil Haughton
GPs to reap data benefit
By Leslie Berry
A new national databank of information about private consultants’ work, fees and outcomes is tipped to attract a huge GP following.
The data, being compiled by the Private Healthcare Information Network (PHIN) following instructions from the Competition and Markets Authority (CMA), is set to be fully available to patients by 2017.
But PHIN’s boss has revealed the body thinks GPs will become key users of its website’s performance intelligence and said it aimed to be a useful tool for them too.
Chief executive Matt James told Independent Practitioner Today: ‘It’s a service for patients, but GPs will inevitably find it of value. For GPs the reality is they have quite limited information about private healthcare services and providers in their area and almost no information outside their area when specialist referrals need to be made.
‘They tend to know a number of consultants personally, but don’t have data and information. GPs
are likely to be the people who look at our website most frequently if they want to better understand the private healthcare option.’
PHIN expects to produce GP-specific information after 2017.
Mr James admitted some consultants saw the PHIN development as a threat. He said: ‘There are many who are deeply nervous about it – and many deeply keen on it.
‘Last month, we shared data with our very first private consultant and we expected all sorts of concerns. But the message we got back was “Thanks very much – it’s very useful for appraisal and revalidation. I look forward to hearing from you next year’’.’
Earlier, he outlined databank progress to around 130 attendees at the AGM of the Association of Medical Insurance Intermediaries (AMII).
He emphasised that PHIN would seek consultants’ approval before publishing information and would work with them directly.
Mr James said his body now had
Upright MRI welcomed
A new Upright MRI Centre in Edg baston, Birmingham, has reported ‘a fantastic response’ to the development from healthcare professionals.
Medical director Dr David Grant said: ‘The upright open scanner is designed to provide weight-bearing and positional imaging for patients in a non-claustrophobic
environment. During the scan, patients can see the radiographer at all times, are able to watch TV or a DVD and can simply walk out once the scan is complete.’
Research by United Open MRI, the company behind the centre, found 22% of adults in the UK who have had a conventional MRI did not like being in a confined space.
MacMillan backs HCA unit
London Bridge Hospital is the first HCA hospital to gain the MacMillan accreditation, a mark of the oncology department’s consistently high standards in care, support, services and facilities.
The Macmillan Quality Environment Mark (MQEM) takes into account design and use of space,
the user’s ‘journey’ and voice, and service experience.
Ratings can vary between 1 (poor) and 5 (excellent). London Bridge Hospital achieved an average of four across all sections.
Oncology services are set to move to a new cancer treatment centre in October 2016.
11 PeRfORMANCe MeASUReS wILL Be AvAILABLe ON tHe PHIN weBSIte By 2017
data from 195 independent hospitals across 12 providers. This would rise to 320 hospitals from 130 providers as it added private patient units, cosmetic hospitals and the remaining independents.
The CMA requires PHIN to publish 11 performance measures for private hospitals and consultants by April 2017. All private hospitals must submit detailed data and
Candour law now applies to all doctors
All doctors working in independent practice in England are now covered by the statutory duty of candour introduced for NHS bodies last November.
Dr Michael Devlin, of the MDU, said independent practitioners now had a legal obligation to tell a patient or their representative if a notifiable patient safety incident occurs, provide a full explanation of what happened and offer an apology.
He added: ‘While the duty applies to organisations rather than individuals, CQC guidance makes it clear that all staff must co-operate in order to ensure that the duty is met.’
this will be directly comparable and compatible with NHS data. He said letters from private medical insurers must direct patients to PHIN when a policy is taken out or renewed and at preauthorisation.
Letters from consultants before outpatients and before admission must also direct patients to the network.
Aid for insomnia
A new website for The Sleep Centre at London Bridge Hospital aims to give up-to-date information about the different types of sleep disorders, tips for better sleep and the special services available. Go to www.londonbridgesleepcentre.co.uk.
Charitable staff
Staff celebrated the first birthday of KIMS Hospital, Maidstone, by raising £2,598 for the British Heart Foundation. Most of the cash came from 355 people at the Kent hospital who exchanged a free heart health check for a fiver.
Highgate’s high
Aspen’s Highgate Private Hospital, north London, has opened its first medical admissions unit.
Around 200 doctors and representatives from hospitals, clinics and associated companies worldwide visited Kensington’s Royal Garden Hotel, London, to share ideas and information on medical tourism. Robin Stride reports
Look the part if you want publicity
Consultants who want to build a reputation in the press and online have been advised to make sure they ‘look the part’ in their publicity material.
Media training expert Steve Bustin said: ‘It you want people to know you are a surgeon, then look like a surgeon. Most of them end up looking like an accountant.’
He advised specialists to invest ‘a couple of hundred quid’ for half a day with a professional photographer to ensure they got the job done properly.
Photos of the doctor could then be sent to media outlets who were covering stories about their patients’ treatments. In most cases, newspapers and magazines were unlikely to send a photographer to take a picture of the doctor.
ConfEREnCE QUoTES:
‘Transparency is the word that repeats itself again and again at this conference.’
Ilana Geva, international branding expert
Ignorance of EU law stops travelling for treatment
A medical tourism academic has blasted ‘outstanding ignorance’ in the UK of an EU directive allowing patients to get their state health service to pay for faster treatment in other member states.
Dr David Botterill, senior research fellow at Oxford Brookes University, said: ‘I have no confidence it’s offered in any way as a treatment option.’
Speaking of his and his wife’s experiences in trying to take up
Mr Bustin said investing in communications was a small outlay compared to the value of publicity it could generate: ‘A piece in Independent Practitioner Today, The Sun or The Telegraph could be worth thousands to a practice.’
Talking to the conference earlier, he warned that doctors would not like to hear it but the lay media was far more interested in their patients than them.
Journalists wanted stories about their readers, what had happened to them and pictures of them.
He said there were very few consumer-friendly photos they could use that depicted medical travel and there was a reluctance to publish detailed pictures of operations.
So doctors wanting to promote a pioneering technique or treat -
‘We need to be transparent about what costs cover.’
Dr Sharon Kleefield, PhD, Harvard Medical School, US
‘Article 56’ in the NHS, he said his GP had never heard of it.
And he claimed ‘the system’ was astounded and offended that anybody would choose to be treated anywhere else.
He said the couple were made to feel like they were subversives and undermining ‘this wonderful institution of the NHS’.
Dr Botterill questioned whether there was not a degree of ‘economic self-interest and protection of private income’ in the system.
The couple successfully got the NHS to pay a hospital in Ghent , Belgium, for the hip replacement needed.
During an open session of the meeting, a consultant in the audience suggested he should share his experience with the GMC.
ment in the media would do best to think about the human interest angle and use case studies, because people were much more likely to react to what patients said about their experience.
They should also be prepared to find that the resulting press features carried another view, perhaps from one of their competitors.
Former BBC journalist Mr Bustin, who is now chief executive at Medical Media Training, said he received a lot of press releases saying ‘this is the best technique’.
But he advised doctors and clinics who were claiming this sort of thing to make sure it really was. They needed to be able to prove it and show it was safe.
Journalists would ask for data and before-and-after photographs,
particularly in the cosmetic sector. So it was worth having a contract with patients who would be willing to take part in media work. Case studies could be used to highlight the great experience people had and their excellent results.
Mr Bustin highlighted what he saw as the difference between advertising and editorial: ‘An advert says “Hey, look at me; I’m great!” Editorial says “Hey, don’t these people look great!’’
He told the audience it was the industry’s job to try and change negative reporting and put a positive spin on things. They should try and connect with journalists; for example, through Twitter. ‘If you have a good story, tell the world. The media appetite is there.’
‘It’s about word of mouse rather than word of mouth in our category.’
Peter Nash, strategic manager, Tourism Ireland
‘An educated consumer is our best patient.’
Film-maker Suzanne Garber, producer, ‘GAUZE: A Thinly Veiled Look at International Healthcare’
A satellite abroad
Medical tourism has given consultants from the UK some unexpected job opportunities abroad while working in an NHS capacity.
One of them is ophthalmologist
Dr Chris Canning, whose work at Moorfields Eye Hospital includes being director of international development and developing the London hospital’s brand overseas.
He spent six years in Dubai, United Arab Emirates, building and running the first NHS clinical facility to be established abroad.
So what is an NHS hospital doing building a satellite abroad?
He told the conference that although revenue was a factor, profit was not the central motive.
Other pluses involved reputation, research and displaying corporate social responsibility. The service was set up a decade ago for people wanting high-quality treatment they could afford to pay for.
Dr Canning said key learning points for consultants to glean from his experience was to know the market. His team did not and expected 70% of the patients they would be treating would be UK expatriates.
But, for his specialty, it turned out the bulk of the business was from older local people rather than younger patients who were in Dubai to work.
HCA flies the flag for UK in travel awards
HCA’s Wellington Hospital, London, flew the flag for Britain when its acute neurological rehabilitation unit was voted the only host country winner at the Medical Travel Awards 2015.
It topped the Specialist International Patient Centre category at the event, run by the website International Medical Travel Journal (IMTJ).
The Wellington Hospital’s facility is the largest private unit in the UK with 56 dedicated rooms for patients requiring complex inpatient rehabilitation.
The judges’ citation read: ‘The hospital is internationally renowned and admits the highest volume of overseas and UK patients across the HCA International group. The rehabilitation unit is internationally recognised for its excellence and promotes a true “team approach” to care.
‘International patient volumes have grown year on year and now outnumber UK patients three to one. The Wellington Hospital took the overarching strategic aim for 2014 to deliver excellent care
to more patients from overseas by selecting the rehabilitation unit to drive this forward.
‘A variety of initiatives were deployed to achieve outcomes: increase in international patients, achieving CARF Accreditation and excellent patient satisfaction results.’
The awards celebrate innovation and excellence in the medical travel, medical tourism and health tourism industry.
Winners took their gongs from comedian and media doctor Dr Phil Hammond at an evening dinner during the IMTJ Medical Travel Summit 2015.
Highly commended in the International Hospital of the Year category was BMI Healthcare. Judges said eyebrows were raised when it set an ambitious target to raise international patient numbers by 50% in 2014.
The citation read: ‘Thanks to a clear understanding of the market, continuous consultation with partners, patients and clients, innovative, multi-level improvements were quickly implemented.
As a result, 2,265 international patients were treated in 2014 – up 126% over 2013.
‘Referrers and patients are deeply satisfied with the service, with countless examples of positive client feedback and patient satisfaction scores in excess of 90%.’
Judging panel chairman and IMTJ managing editor Keith Pollard said the awards celebrated the best providers in the industry and aimed to encourage others to strive to match them.
He went on: ‘The judges wanted to reward innovation and excellence, highlight best practice and celebrate those who are leading the way in the industry and delivering successful outcomes for patients.
‘All our winners exemplify the way the medical tourism industry should be run: professional, offering exceptional patient care and providing the best possible medical outcomes. I’m already looking forward to next year’s awards in the hope that other clinics and companies will have raised their game to match or even better this year’s winners.’
THE 2015 WInnERS
Medical Travel Destination of the Year: Malaysia
International Hospital of the Year: Bumrungrad International Hospital, Bangkok, Thailand
International Cosmetic Surgery Clinic of the Year: Beverly Wilshire Medical Centre, Kuala Lumpur, Malaysia
Specialist International Patient Centre of the Year: Wellington Hospital, acute neurological rehabilitation unit, London
International Dental Clinic of the Year: Imperial Dental Specialist Centre, Kuala Lumpur, Malaysia
Medical Spa of the Year: Cocoon Medical Spa, Bali, Indonesia
Marketing Initiative of the Year: Apollo Health City, Hyderabad, India
Excellence in Customer Service: Gleneagles Kuala Lumpur, Malaysia
Best Quality Initiative: Imperial Dental Specialist Centre, Malaysia
Medical Travel Agency of the Year: france Surgery, Toulouse, france
International Infertility Clinic of the Year: Memorial Sisli Hospital ART and Genetics Centre, Istanbul, Turkey
Medical Travel Website of the Year: Ramsay Sime Darby Health Care, Malaysia
Sanjiv Malik Lifetime Award: Josef Woodman, Patients Beyond Borders
imtj mEdical travEl Summit 2015
Why specialists lost competition appeal
The failure of the Federation of Independent Practitioner Organisations’ (FIPO) appeal to the Competition Appeal Tribunal (see page one) has been greeted with disappointment from the appellant, the Independent Doctors Federation and the BMA’s private practice committee.
Here is a quick run-down of the arguments and rulings, prepared as an summary by the Registry of the Competition Appeals Tribunal
1FIPO claimed the ‘PMI decision’ was based on the factually erroneous or irrational finding that consumer choice was not restricted by the insurers’ practice of directing policyholders to consultants whose fees were within the insurers’ caps.
The tribunal, by majority, dismissed this challenge on the basis that the Competition and Market Authority (CMA) had well in mind that the practical availability for policyholders (who did not hold open referral policies) of payment of topup fees could be substantially constrained by reason of the restrictions on the freedom of action of consultants.
2
FIPO argued that the PMI decision was based on the finding that consultants could compete below the fee caps, such finding being unsupported by probative evidence.
Therefore, FIPO argued that this finding was irrational and/or
amounted to a fundamental error of fact.
FIPO also contended that the PMI decision was procedurally unfair, as that finding had not been put to it. For the reasons set out in the judgment, the tribunal, by majority, dismissed both the rationality and procedural challenge under this ground.
The CMA had made a detailed study of the relevant market and was well placed to assess what scope there could be for competition between consultants on price and quality.
Based on this evidence, it was entitled to conclude that there was a real prospect of consultants being able to compete on price even below the cap.
As to the procedural challenge, the CMA had set out the relevant Theories of Harm in its Statement of Issues. Thus it was obvious that if FIPO wished to present a case that, for example, reimbursement rates were so low as to preclude any competition between consultants below those rates, it should do so.
Moreover, the CMA’s position was made clear in subsequent documents provided to FIPO, and FIPO made representations on several occasions. Therefore, the tribunal concluded that the CMA satisfied its obligation to consult fairly pursuant to section 169 of the Act and the general requirements of fairness in public law.
3-4
FIPO submitted that the PMI decision was reached on the basis of a factually erroneous finding that the buyer power of the insurers had not resulted in a reduction in the overall number of consultants in private practice, when, in fact, the numbers had reduced.
6
FIPO also argued that the CMA irrationally failed to conduct any investigation into whether the number of consultants was likely to fall significantly in the future.
The tribunal unanimously dismissed both of these grounds and concluded that the CMA’s assessment was both rational and lawful. The CMA had conducted a careful analysis of what had been happening in relation to consultant numbers generally and in private practice; and it also addressed what was likely to happen in the future.
5
FIPO contended that the PMI decision was based on the unevidenced finding that the fee constraints imposed by PMIs would benefit customers in so far as premiums would be reduced for policyholders.
For the reasons set out in the judgment, the tribunal unanimously concluded that the CMA’s reasoning, albeit thin, was clearly rational.
FIPO claimed that the PMI decision was based on the unevidenced assumption that it was in the interests of the insurers to ensure that there were highquality consultants in private practice.
As explained in the judgment, the tribunal, by majority, rejected this ground of challenge. The CMA’s assessment was based on straightforward reasoning, which could not be said to be irrational, and was also supported by evidence.
7
FIPO contended that the Information Remedy was not an effective remedy.
However, it conceded at the hearing that this challenge could not succeed unless the tribunal was persuaded that the PMI decision was unlawful.
As the tribunal dismissed, by majority, FIPO’s application for review in connection with the CMA’s PMI decision, this ground of challenge was dismissed, by majority, as well.
Don’t compromise on your practice management software...
...Join our community of over 6000 DGL Practice Manager users to be assured you are using the most advanced practice management system in the UK.
I can 100% recommend DGL Practice Manager to anyone wishing to set up a private practice...my job has been simplified enormously by the sophistication of the software.
Liz Edwards LLB, Consultant Private Practice Manager, Nuffield Hospital,
Cambridge
Contact us today to arrange a free, no obligation demonstration of our software. Quote IPT15 and receive a FREE 30-DAY TRIAL copy of DGL Practice Manager.
It takes more than
In the second of her new series, Pam Underdown injects some solid advice into how you should prepare a marketing plan for setting up a private practice in aesthetic medicine
Congratulations on your decision to move into the exciting world of medical aesthetics. as we discussed last month, the antiageing market is booming – not only are more consumers using these services than ever before, but more healthcare professionals are entering the field, which means more patients, but much more competition. so first things first . . . what about you? Why have you really decided to establish a new aesthetics business? What type of business do you want to build? Perhaps a ‘lifestyle business’ earning additional income on top of your day job? o r perhaps you want to build the most successful clinics in your area and become known for being
than a pretty face
one of the top practitioners in the uK, working hard to build a business that is profitable, sustainable and will give you the freedom you desire? one that can be sold on or retired from in the future?
Whatever your goals and dreams for your business, you will need to answer many questions to help you form the basis of your business and marketing plans.
Good business plan
Your plans do not need to be on a War And Peace scale; they just need to be working documents that will help you to promote and run your new business effectively. t hey will keep you on track, helping you to measure and improve as you go and ensuring you don’t wait until your
year-end – please don’t! – to see if you have reached your financial targets and business objectives.
a good business plan needs to address a variety of important topics, including:
Budgets;
Profit and loss (P&l) analysis;
Product line evaluation;
Marketing strategies;
time-scales;
Competitive analysis;
routes to market;
technology assessments – to name but a few.
Ensure you know the direct costs, indirect costs and overheads that are associated with your new business and keep a close eye on each.
You also need a clear understanding of your target market and your competition. What do they already offer? are there any gaps that you could fill? Whom do you want to attract? are you aiming at the younger clientele who are perhaps modelling themselves on the glamorous ‘C-list celebrities’ or are you going for the more mature clientele, who have the disposable income but are more discerning?
Deep connections
You will also need to consider what your ideal patient will want from you. remember, they are not just buying ‘wrinkle reduction’; you are often dealing with high emotions and deeper reasons for wanting cosmetic enhancement.
You need to take the time to understand what really motivates them to become a patient, so you can start to build a deep connection with them.
and the questions keep coming:
Which product and service offerings are most needed in your area?
Which will be most profitable to deliver?
What equipment will you need?
How do you choose which supplier(s) to use?
should you buy or lease equipment now or wait until you have mastered injectables?
Do you have sufficient insurance?
Which training provider are you going to use?
➱ p12
How are you going to find enough models to practise on to build your confidence and experience?
a nd perhaps the most important question of all is: do you know which marketing efforts it will take to get a steady stream of your ideal patients through your door, once you have exhausted your list of friends and family? a nd how will you keep the patients coming back?
You must also have a clear understanding of the online and offline marketing strategies you plan to use, an ample budget and last, but certainly not least, a commitment to stay the course and succeed, no matter what.
Where is your business going to be this time next year? What will it look like? What are each one of your patients’ worth? What are they worth in the first month, year and lifetime value? i s one more valuable than another based on what they buy, what they don’t buy, what aftercare they require? How long will they stay?
Master the market the key is to master the marketing and understand it before you decide to outsource or delegate it to a third party.
this is essential, even when you know you won’t be carrying out the day-to-day actions yourself. You must take the time to really understand exactly what the marketer is doing with your money.
Every skill is learnable, so take the necessary time now to truly understand marketing, learn how to articulate what you want and then outsource or delegate the day-to-day ‘doing’ of it to someone who clearly understands your vision, your needs and your expectations. trust me, it will be worth it in the long run.
Make sure you stand out by offering a special something that defines you and your business and sets you apart from the crowd: What is your unique offering (usP)? is there something that sets you apart, something that will attract prospective patients?
Find it and capitalise on it. i f not, you may wish to reconsider your move into aesthetics, as there are many providers who don’t offer anything unique and are simply peddling commodities.
One of the greatest pitfalls is trying to be
everything to everybody. When you offer too many choices, you ultimately just confuse the patient while reducing your potential profitability
a sk yourself: ‘Why should patients choose me instead of Dr X?’ one of the greatest pitfalls of any business – and especially in aesthetics – is trying to be everything to everybody. When you offer too many choices, you ultimately just confuse the patient while reducing your potential profitability.
Creating a service menu that offers competitive – but not too cheap – prices is essential. But your ultimate goal is to create a solid concept of who you are and what your aesthetics business is: something that maintains your integrity while being marketable.
Take a step back if you want to be really successful, take a step back, look at the marketplace and ask how you can positively disrupt it. You can disrupt by price, by innovating and charging more (like a pple), by using technology, by sheer quality of service or by becoming a master of marketing.
internal marketing starts with making sure your clinic has an ambience that is inviting, comfortable and is a representation of you. too many clinics feel just that – clinical. ( s ee architect nicholas Jamieson’s ten ways to make your practice more welcoming on page 14).
l ike a doctor’s waiting room. t he best ones manage to find a balance between a clinical feel –after all, you are offering medical treatments – but one that encourages your patients to relax, return and refer.
Being new to the industry, you will need to offer something that will entice patients away from elsewhere. it all starts with a compelling and unique experience, one that makes your patients feel listened to, valued and special, one they will remember, one that gives results and value for money. remember, people will forget what you said or did, but they will never forget how you made them feel. Minimise or avoid ‘traditional advertising’. You are not an established brand yet, so concentrate your marketing efforts and budget on ‘laser-focused’ marketing, rather than the ‘spray and pray’ approach.
t hink about it. traditional advertising methods are likely to
If you want to be really successful, take a step back, look at the marketplace and ask how you can positively disrupt it
be the most expensive part of any marketing budget, so anyone considering this should research very carefully, before they decide on, or get talked into, anything. i know many new businesses who waste money on radio, print advertising in local papers and magazines and even billboards and it still amazes me to this day. l et’s face it, if any aesthetic patient happens to actually see or hear the advert at the time it is placed, are you really going to convert them if they are happy with their current practitioner? if it was you, would an advert on the radio or a billboard with a pretty face convince you to stop and take a chance on someone new? Probably not. as an industry consultant, not a day goes by when i don’t see a business owner making questionable decisions about their marketing spend, often replacing the essential 20-30% of revenue that should be used to promote and market their business in favour of fancy clinic décor or the latest new equipment.
Many fall for the latest shiny object after hearing a sales rep talk about a brand new product, service or marketing gimmick.
Plan on earning success the hard way, one patient at a time, and follow tried and tested marketing methods to build a long-term, sustainable and profitable business. Join us next month as i explain the buying journey – emotional and logical – that a potential patient goes through in order to find a practitioner. How potential clients start their research and make comparisons, through to what makes them ultimately pick up the phone and then go ahead with their treatment.
Pam Underdown (pictured below) is chief executive at Aesthetic Business Transformations
Celebrating our 22nd year in Business
www.medbc.co.uk
Come and join the hundreds of other consultants who use MBC and experience the following benefits:
• Bad debts of less than 0.5%
• Increase in net income by up to 25%
• Freedom for the consultant and secretary to focus on the medical side of the practice
• 24/7 online access to both your financial and practice management data
• Having a service tailored to your needs with your own Account Manager
• Our fees are only charged on the money that we collect for the practice and NOT on what we invoice which means we share the same objectives
Special offer:
To celebrate our 22nd year in business we are for a limited period of time offering all new clients an introductory discount of 20%*
Further information:
MBC – More than just a billing company
Please visit www.medbc.co.uk for more detailed information or phone 01494 763999 and speak to Garry Chapman to establish how we may assist your practice.
*Terms and conditions apply
Design tricks to perk
Even if you don’t own your premises or have the budget for a new build or a conversion, there is still a lot you can do to make your practice a nicer place to be. Architect Nicholas Jamieson (right) shows how
As we all know, patients visiting their doctor are anxious about something – otherwise they would not be there.
It is also generally recognised that the environment patients find themselves in can play a major role in their well-being.
Patients visiting your practice want to feel calm and reassured –and the design of the internal environment, if carefully considered, can play an enormous role. we have all seen those television programmes that show drab and unattractive interiors being dramatically changed – within days and at a cost less than most builders would charge for hiring a Portaloo.
Although a worthwhile makeover of your medical practice is unlikely to be quite as painless, it is surprising what can be achieved while carrying out even a modest extension or refurbishment project.
Here are ten things that really can make a difference – just by being thought about properly, and without adding any more to the construction budget.
Slate flooring in the entrance hall and oak in the reception leads patients naturally through the building
A warm, welcoming reception area – but make sure patients talking to receptionists can’t be overheard
perk up your clinic
1
Let there be light, naturally
It is surprising how, with a little ingenuity, natural light can be brought into spaces set deep within buildings.
Light makes such a difference –even if it is no more than a shaft of light from a hidden source, a view of the clouds scudding by through a rooflight or just a perceptible change in light levels as the sun comes out.
2
don’t be LEd astray
Although the technology is improving, most LeD (light-emitting diode) lights continue to give off a harsh, cold light and the bulbs cost a fortune.
Contrary to popular belief, it is still possible to use halogen lights, which provide a warm comforting light – without upsetting the building control officer or destroying the environment.
There are even fittings available that will allow halogen bulbs to be replaced with LeD bulbs, once the technology has caught up.
3 Make your reception and administration staff love you
The key to their hearts is storage, storage and more storage. They love it.
Design it to suit their specific needs and provide plenty of it. Clever design can create lots of useful storage from all those nooks and crannies that you did not even realise were there.
Also provide lots of places properly designed for the pinning-up of notices. Do all of the above for yourself too.
Having thereby de-cluttered, your patients will enjoy being in a calm, controlled environment.
Paint warmer colours in reception areas, and cooler colours where patients are examined
Natural light and a different feel to consulting and examination areas make this space interesting yet reassuring
4
At your service
You do not need to pepper your walls and ceilings with access panels. Neither do you need a horrible buro-landschafttype, gridded ceiling.
surprisingly, a lot of access panels are used only when services are initially commissioned and are never used again.
Better to leave a hole in the ceiling until commissioning is completed, then permanently seal it up.
Of course, some access panels are needed, but with a little effort it is always possible to find ways of incorporating them into the design so that they are either completely hidden or so well camouflaged that they are effectively invisible.
5 don’t be a one-trick pony
Do two tricks at once: create an environment that is warm and
Do two tricks at once: create an environment that is warm and welcoming but which also shows you are providing a high standard of modern clinical practice
welcoming, but which also shows you are providing a high standard of modern clinical practice.
How do you do it? The secret is to treat rooms, or parts of rooms, differently. Lay oak flooring in waiting areas and rubber in consulting rooms.
Fit veneered or painted joinery in one end of consulting rooms, where your desk is, and laminate in the other, next to the couch.
Paint warmer colours in reception areas, and cooler colours where patients are examined.
6
Furniture removals
Yes, get rid of that tatty old desk, and ugly office chair.
Of course, you are attached to them, and keeping them saves money, but your patients would rather you had something more cheerful.
The good news is there is a vast range of affordable modern furniture available.
The bad news is that, if you listen to the sales reps, you will probably end up with something that, at best, does not suit the design of your practice and, at worst, is just plain ugly.
Unless you know your Finn Juhl from your ernest Race, you should probably take the advice of a professional designer, preferably the one who designed your interiors. whatever you do, do not delegate furniture selection to the project manager.
7 Art counsel
There are many good sources of things to hang on the walls: websites that sell beautiful posters or fine art prints, local dealers or perhaps a nearby art school.
The problem is not getting the art, but getting the right art. everyone thinks they know what they like, but, as with furniture, unless you have a collector’s eye, you should consider taking advice.
w hat do you buy? w ill it engage your patients’ imagination? where should it be hung? How high? s hould the frames align with any particular architectural features? w hat type of frame?
Discuss it with your architect or designer.
8
An ear for an eye what you hear is as important as what you see, so do not forget acoustics. Ideally, your patients should be able to speak to the receptionist without feeling they are being overheard – which is not always easy to achieve.
It may be necessary to create some background sound: running water, music or, more pragmatically, an electronic noise-masking system.
9 sign language
Ideally, the architectural design, by means of spatial arrangement, use of materials, and lighting, should lead your patients naturally to their destination, without over-reliance upon signage.
s ignage should be clear, neat and well designed – and really must suit the design of everything else. This means your sign designer and architect need to work closely together. Avoid inyour-face logos and brash colours.
10 Remember: one size does not fit all s ome architects and designers specialise in clinical buildings. s adly, many of them prefer to churn out a standard product which, although reliable and ticks all the compliance boxes, does not address the unique requirements of individual practitioners and their patients.
If extending or refurbishing, try to use an architect that will reexamine your needs from scratch, and be prepared for them to come up with something unexpected.
It need not cost more, and will give you something you and your patients love.
Following the above advice should lead to a practice that is fresh and appealing – not only to patients but also to you and your staff. Laurence Llewelyn-Bowen, eat your heart out!
Nicholas Jamieson is a director at Barbara Weiss Architects, London
Got a new private practice or developing your old one?
Tell independent Practitioner Today your good news. Contact robin@ip-today.co.uk
...cuts into lost fees!
“MidexPro thinks like a doctor, not a computer exper t”
All you need to run your private practice including document management, diary, clinical data, even test ordering and lab reports from TDL.
From paper billing (incl. VAT) to electronic billing (EDI) to management of bulk purchase contracts.
Grow seamlessly from a small solo practice through to a large group practice, remote access network system.
MidexPro is the cost effective practice management system with support second to none.
Free download of the full working package (30 day limited) from www.midexpro.com or call for a CD.
Try it for yourself with no sales pressure.
“MidexPro has revolutionised our lives; it is just so easy”
Take a weather check
Are you doing enough to maximise the profitability and performance of your business? Susan Hutter (right) takes a look at current best practice issues, what has changed over the past few years and what you can do to springclean your business
Cash flow and late payers
Most private medical insurers continue to have a 60-day payment plan in place, sometimes longer, so do make sure you take control of all the details that your practice sends through to the insurer.
This way, you can be sure that the insurance company has no administrative reason to delay payment.
However, be aware there are still shortfalls where the insurance company rates are lower than the rates charged to patients, and the patients, for whatever reason, do not pay the shortfall.
Dealing with large organisations/embassies
I have noticed that many of my clients find it extremely difficult to get paid on a timely basis, and sometimes at all, from certain embassies and larger corporates.
I realise that consultants do not wish to turn away business from such sources, as it can be extremely profitable. However, there is no point in doing the work if you are not going to get paid within a reasonable time period.
When dealing with any large organisation, it is sensible to ensure that you understand the ‘chain of command’: who you should be sending the paperwork to and exactly the details that will be required.
There may be more than one person in the organisation that you will have to deal with. Your staff should be au fait with the procedures so that they can ensure that the original invoices and sup-
porting paperwork go to the right department at the outset.
Subsequently, they will need to follow up. The best advice is to both call and email.
At the start of a relationship with an organisation, it is a good idea to have a meeting with the relevant personnel so that names can be matched with faces. That always makes things easier when you are trying to chase debts.
Staff skills
Never underestimate the importance of good record-keeping practices. Do ensure staff have all the necessary skills and training. It will pay dividends, as information will be collated on a more timely and accurate basis and costs can be kept in check.
Your practice software provider may provide inhouse or onsite training, and/or your accountant may be willing to assist.
Centres of excellence
A development that is now coming to the fore is the building of ‘centres of excellence’. This is where consultants are joining together with others in the same and complementary, areas as themselves to produce a ‘one-stop shop’ for their specialty. It is too early to say whether the days of the ‘lone consultant’ are numbered, but those participating in these centres are finding that they can also take part in alternative profit streams that were not open to them before; for example, scans, implants and imaging.
Never underestimate the importance of good record-keeping practices. Do ensure staff have all the necessary skills and training
This is especially true if they are founder ‘members’ and in at the outset.
As far as patients are concerned, the offer of one location for everything, with the exception of the hospital stay, is very attractive.
For a young consultant who has recently set up in private practice, joining a centre of excellence is often a kick start to their private career.
It does not mean that you cannot work within the NHS as well; in fact, in most cases, it is a definite advantage. It is certainly something worth looking at.
Susan Hutter is a specialist accountant for the medical profession and a partner at Shelley Stock Hutter
An easy to use software system, which fully supports the clinician and office staff and makes the whole process of running a busy Practice a lot easier. Call now for a chat and ask about a free, no obligation demonstration of our comprehensive system that has been designed to save your Practice time and money.
We are all so busy, busy, busy that it becomes a huge challenge to actually ‘get stuff done’. Surgeon Mr Dev Lall (right) shares what time management tips work for him – and urges colleagues to adopt a ‘pay yourself first’ strategy
One questi O n i ’m regularly asked when working one on one with clients to grow their private practices is this: ‘How can i get all this stuff done?’
After all, we all put a stack of hours into our n H s careers followed by a significant time commitment to our private practices. t hen there is time spent with our families and time sleeping. Once you do the maths and factor all that in, there is precious little to allocate to marketing and growing our private practices. And that means the time you have available to achieve your goals – the reason you work so hard in the first place – is really quite limited.
t his makes strategy critically important. s o how do you get stuff done?
What follows is my personal answer, based upon my own experiences and information i have picked up from high-achieving friends. i t is also based in large part on a book by Brian P. Moran and Michael Lennington entitled The 12-week Year
Get beyond the fluffy and airyfairy stuff and there is information there that can make a dramatic difference to your productivity.
Those problem resolutions
How often do we find that we set a goal at the beginning of the year
then promptly forget about it? then suddenly it is October and realisation dawns about how little time is left. At which point, we either rush and cram to get as much done as possible or, more often perhaps, we give up and promise ourselves that next year will be different. At which point, the cycle too often begins again.
Too much time is a problem
A year is a long time and hard to relate to. Perhaps the problem, paradoxically, is that we are giving ourselves too much time.
And that means we need to think on a smaller time-scale. For various reasons, 12 weeks is a good starting point, not least
because it is not only easier to visualise and relate to than a year, but also has a sense of immediacy of action attached to it. it is far harder to be complacent about a deadline 12 weeks away than one 52 weeks away, after all. But before how we choose how to spend the time we have, we need a direction. And that requires . . .
Step 1: A vision
t his is basically a compelling mental image of the life you want to lead in, say, three years’ time. it has to be personal and important to you.
s o, for example, you may say that you want to be earning ‘X’ amount of money each year from
reach your goal
your private practice or perhaps you may want to cut your n H s sessions by 50% without dropping your income.
t he ‘what’ does not matter so much as the fact that the vision has real meaning to you and has a concrete end-point. this is your ‘why’ – your reason for working privately in the first place.
Step 2: Planning
OK, so you know where you want to be in three years’ time. so how do you get there?
You need to break down the big vision into individual steps, each of which takes you materially and measurably closer to where you want to be. these ‘mini goals’ or waypoints serve as markers of your progress, and you aim to perform each of them over a 12-week period.
Planning is critical to achieving the end goal, because it is your blueprint to achieving your vision – to taking you from where you are now to where you want to be.
You know that if you complete the steps, you will achieve your end goal – your vision. so if you want to cut your n H s commitment by 50% in three years’ time, for example, you know the income you will need to make up from your private clinical or medico-legal practice to allow that to happen.
By dividing that by 12 (12 blocks of 12 weeks each) you know how much extra income you need to earn each block to be able to cut your sessions by 50% in three years’ time.
Step 3: Process control
A plan alone is not enough: you need to create weekly plans for achieving each of those 12-week waypoints. You need defined steps to execute, and process control is simply executing the steps
you need to complete to reach your 12-week goal.
this is the ‘how to’ of achieving the vision you created for your life three years down the line.
Step 4: Score-keeping this is measuring where we are in relation to our 12-week plan. What have we done and what have we yet to do to complete that 12-week segment?
i t sounds dull, but serves as a constant reminder of our progress. And because anything measured improves, it has the wonderful side-effect of motivating us to stick to our plan and to keep implementing.
Remember, though: actions have consequences – results. And while we can control our actions, we cannot always control our results. if we could, every surgeon would have zero mortality and morbidity rates and none of us would ever get complaints.
And this is true of our marketing efforts: we cannot guarantee the success of any particular marketing effort we make. Yet we know that marketing your private practice works.
it generates a steady stream of income and new patients for you. e ven if you cannot predict the success of any individual strategy or campaign, you know that as long as you do the marketing, the income will follow. You will get nearer to your desired income. in other words, actions are our lead indicators whereas results are our lag indicators. And since we do not have full control over our results, the only sensible thing to measure are our lead indicators –our actions.
i n practical terms, this means you need to measure your execution of the necessary marketing steps you take and assess the results you get further down the
line, say, at the end of each 12-week period. At this point, you can decide if you need to change your marketing approach or not.
Step 5: Time use
We all know that work expands to fill the time available to do it. if you have a certain number of tasks to do before catching an early afternoon flight that day, you can be sure you will get everything done somehow. Conversely, if you have a full day to accomplish the same tasks, you always seem to finish the work at the end of the day.
The essence of time management
A useful approach is simply to cut down on the time we allow ourselves to get stuff done, to prevent ourselves frittering time away. secondly, we need to focus on doing the things that only we can do, and delegating or deleting everything else.
thirdly, we need to employ the 80:20 principle so we work only on those tasks critical to achieving our 12-month goals. And finally, i recommend time-blocking: a strategy i call ‘paying yourself first’.
The ‘paying yourself first’ strategy
quite simply, this means that no matter what is going on each day, week or month, you allocate a certain amount of inviolable time to working strategically; time you spend working to make your three-year vision a reality. And the reason i call it ‘paying yourself first’ is because no matter what else is going on, i do this at the beginning of each day before i do anything else. i find that if you leave it to the end of the day, you are tired and it is just too easy to put it off to another time.
The power of the process
One of the wonderful things about this overall approach is that it not only forces you to think about what you really want out of life but also to make a plan to achieve that vision. it also serves as a wake-up call for you to recognise the passage of time and to prove that if you are ever actually going to achieve your vision, you are going to have to get a move on.
s omething else to consider, though, is this: if you execute your plan to achieve your vision with 85% reliability, you will almost certainly achieve your vision at the end of three years. And yet … if you complete your plan in a quarter of the time, you will also reach your vision in a quarter of the time. the time is going to pass anyway: how are you going to spend it?
Final thoughts
As i said earlier, this is my personal answer to getting stuff done. i t is not the only answer. there are other approaches, some of which may work better than mine. in the end, you have to find a solution that works for you.
Yet, what is abundantly clear is that to achieve your vision, whether in private practice or otherwise, it is not going to happen on its own.
Waiting for it to happen by magic is no solution at all. Like a ship or an aircraft, you have to take charge and steer your life in the direction you wish it to go. in other words, you have to take ownership.
Mr Dev Lall is an upper-GI surgeon and runs a specialist private practice consultancy. He can be found online at www.PrivatePracticeExpert.co.uk
sign up To avoiD Missing an issuE
Dear Reader,
Subscribing to Independent Practitioner Today is the only way you can be sure you will see every issue. Don’t risk missing out. Our personal subscription for doctors and managers is only £85 a year and £200 for organisations. But you can cut this to just £70 and £175 respectively if you pay by direct debit.
So take advantage of this offer now for our unique business magazine dedicated to supporting you in your private practice. We’re confident your subscription will repay itself many times over!
Editorial director
rates listed above) post your application (no postage required – UK only) to: independent practitioner today Subscriptions department, FreepoSt, po Box 36, plymouth, pL1 1Br
for
I encose a cheque made payable to The Independent Practitioner Ltd
Please debit my Mastercard/Visa/ Amex/Diners Card No Expiry Date Security No ***
Instructions to your Bank or Building Society to pay Direct Debits
Name and full address of your bank/Building Society Banks and Building Societies may not accept Direct Debit instructions for some types of account To: The Manager
Instructions to your Bank or Building Society to pay Direct Debits Name and full address of your bank/Building Society Banks and
at www.independent-practitioner-today.co.uk if
Brainstormingly successful
Doctors aiming to get into business in the private sector were given a helping hand at a special event organised to give them advice from some very different independent practitioner entrepreneurs. Dr Charlie Easmon (right) reports
ThE four organisErs wErE:
Dr Charlie Easmon – www. yourexcellenthealth.co.uk
Dr abeyna Jones – trainee in occupational health and co-founder of www. medicfootprints.org
Dr Evgenia galinskaya –former doctor and now a career coach for doctors with www. otheroptionsforDoctors.com
sara sabin – accountant and Dr Jones’s business partner in www.medicfootprints.org
The day was supported, among others, by:
a photographer ex-doctor who is now an investor
Dr avi Mehra of www. doctorpreneurs.com
Medical student James gupta who has sold one business already to addison Lee (Jump in) and now has www.mycqs.com.
Our first Enterprising Doctors Day seminar turned out to be a great success with 27 people (26 doctors and one dentist) giving up their saturday to come along. s omeone even flew in from Denmark.
We met at a business start-up venue called Made simple (www. madesimplegroup.com), which had excellent facilities and gave us all information on their support services for new businesses. these include company incorporation and a London registered office address.
the aims of the day were to help doctors who were thinking of going into business and to advise them of the ‘dos’ and the pitfalls.
the day started with brief introductions and by the time all our guests had told their story, i really
wished we had a Health Minister or a head of NHs human resources in attendance, because we had heard far too many stories of disillusioned doctors who were seeking a way out.
Prof Mark Whiteley (www. whiteleyclinic.com), who has built up a £4m+ turnover private practice in vascular surgery and aesthetics, explained his life and entrepreneurial journey from being wrongly labelled a ‘dumb’ child prior to realisation that he was dyslexic.
His rugby skills as well as his academic application got him through medical school. Mark confirmed that hard work, personal sacrifice and commitment are required for success.
He explained that you need to decide if you are a ‘lifestyle business’ or an ‘exit’ business and advised us all never to confuse the two.
Dr Amanda Penny shared how she found her true love as a creative maker of fantastic cakes and pastry. s he has worked with Michelin-starred chef r aymond Blanc, among others, and now runs a successful, high-quality business – www.amandapennycakes.com
suppressed creativity
Amanda’s journey included finding her true self and then applying herself hard to learn her craft.
she explained some of the pros and cons of working from home with young children with normal demands while trying to have a professional business call.
And she reminded us that many doctors are creative, but for many this creativity is suppressed.
Dr Abeyna Jones, co-founder of www.medicfootprints.com, talked about the importance of diversity of thought and personnel required in all organisations.
s he reminded us that to get ahead in business, it is important to be social and that the average doctor lacks skills in self-promotion.
And she emphasised how important it is to realise your strengths and weaknesses before you embark on any enterprise. to be a successful entrepreneurial doctor, you must know yourself, know your product, know your market and know your niche.
To be a successful entrepreneurial doctor, you must know yourself, know your product, know your market and know your niche
Dr Jones summed up that:
1 Diversity in leadership is essential for success and profitability in business. Diverse companies have a competitive edge over companies with nondiverse leadership. Her recommended read is Why Diversity Matters by McKinsey & Company. 2 Companies lacking diversity in leadership lose their competitive edge.
3 u nconscious bias is a huge determining factor towards inequalities in the workplace. Accountant Sara Sabin outlined the basics of cash flow, profit and loss and balance sheets and the importance of finding the right experts to help you from the start and throughout your journey. she does consulting work with very wealthy private clients and can help provide a guide on how to write a business plan.
As a non-medic, she contributed to the event hugely because she had a fresh and objective perspective on the world outside of medicine.
Dr Evgenia Galinskaya shared her secrets of effective career development and explained why it is important to learn about self before any professional transitions. As a certified professional coach, she helps doctors create greater clarity and focus when they are planning their careers or entrepreneurial venture. the delegates had an opportunity to discover their work values through a hands-on exercise with special cards. to conclude the workshop, Evgenia lead a ‘master-
EnTErprisE sTarTs young or oLD
it was great to have a mixture of doctors in attendance – from medical students to senior consultants to gps. attendees included the very recently retired who were looking to do something else.
Many of our delegates commented on how it was great to meet likeminded people and to have the opportunity to network. it is a recurring theme when you speak to doctors that they can sometimes feel that they are isolated in their feelings of wanting to do something else, especially as they do not want to waste years and years of taking exams and rigorous training.
Bringing together in one room a group of people who share the same ethos can go a long way to alleviating these negative assumptions. no time is ever really wasted; our skills can always be used as a stepping stone.
There is a Linkedin forum for those interested in our next steps for entrepreneurial doctors: ☞ www.medicfootprints.org/blog/workshop-enterprising-doctors
mind’ session. i n small groups, the delegates had a chance to brainstorm their business ideas and to crowd-source solutions to their current career and business challenges.
satisfaction of aiding doctors s he explained her journey from disillusioned dermatologist to now doing something she really loves and the satisfaction of helping doctors find what they really want to do with their lives.
A random chance to hear a professional coach was her inspiration and led some years later to her new path.
for my talk, i spoke on entrepreneurial myths and gave the audience my story of success, failure and then rise again, which i wrote about in Independent Practitioner Today in March last year.
i told of what i had learnt about having the right people in the right place at the right time and i quoted the old adage ‘hire slowly, fire quickly’.
My recommendations included medical accountancy experts such
as Independent Practitioner Today columnist ray stanbridge (www. stanbridgeassociates.com) and marketing expert books such as Guerilla Marketing by Jay Levinson.
After all, failure is common. Nine out of ten businesses fail in the first five years. However, ‘fail fast and learn’ is one of my tips.
Do not give up, learn to com partmentalise concerns, keep learning, keep connected, seek mentors and read biographies and autobiographies.
i also urged delegates to accept that you do not have to have an original idea but better execution – as recommended by the great business author ram Charan.
And i emphasised two other things: a growth curve may be too fast or too slow and it is important to always be able to get access to cash early before you need it.
Dr Charlie Easmon is president of The International Association of Physicians for the Overseas Services (www.shoreland.com/iapos) and medical director of Your Excellent Health Service, Harley Street
Dealing with ‘Dr Google’
The
cyberchondriacs are increasingly appearing in private practice and the NHS. Dr Greg Dollman (right) downloads some advice
How s H ould private doctors react to patients who turn up for their appointment armed with printed notes or information on their smartphone or health app?
The growing role of the internet in society today means that such a scenario is becoming more common. Indeed, many private patients may be more likely than others to access medical information on their own health prior to an appointment.
However, instead of feeling threatened or dismissing the increasing number of patients who self-diagnose on the internet before attending appointments, independent practitioners should work together with these webwise patients.
A recent survey by the Astellas
Innovation debate revealed that three-quarters of doctors had noticed a marked increase in the number of patients ‘self-diagnosing’ from the internet over the last year, while 21% had seen an increase in patients presenting with data generated from health apps and smart devices.
increase in worried well
Furthermore, 82% said they had concerns that a mass of data and readings from healthcare devices and apps will make people unnecessarily worried about their health and 88% agreed it would lead to an increase in the worried well wanting appointments.
Interestingly, while 73% said they were always happy to discuss data that patients bring in regard-
ing their health concerns, only one-in-four doctors agreed that the data would help them in identifying patients’ undiagnosed health issues more quickly.
It may be tempting to label them cyberchondriacs or the worried well, but the reality is that some patients who are anxious about their health use the internet to diagnose themselves with everything from brain tumours to exotic infectious diseases.
It is perhaps inevitable that some patients will attempt to selfdiagnose using information obtained online via their smartphone, tablet or app. This latest study revealed that a third of patients do so before booking their appointment.
It can be a fine balancing act for
independent practitioners when faced with patients who, prior to their scheduled appointment, have already sought a ‘second opinion’ via their health app or a google search.
losing control
doctors may feel concerned over losing control of the consultation and time that should be used to examine the patient may instead be spent looking through their findings.
s ome practitioners may feel anxious, intimidated or even threatened by web-wise patients arriving at their practice armed with a dossier of medical information. It can be disconcerting to have a patient showing you information from their health app or
Top Tips
Don’t dismiss web-wise patients
patients should be encouraged to show an interest in their own health
Carefully consider any information presented by the patient
Work in partnership with patients
Don’t feel pressurised into treatment or prescribing unfamiliar drugs
turning up with print-outs of their symptoms, complete with their own diagnosis.
while internet information can be inaccurate or misleading, patients should be encouraged to take an interest in and be responsible for their own health and, by working together with the doctor, they can gain a better understanding of any condition or symptoms they have.
doctors should listen to what every patient has to say and this includes carefully considering information presented to them by the patient. working in partnership with the patient involves sharing decision-making, where possible, and respecting their views.
Helpful opportunity
It is unlikely that doctors will have every diagnosis at their fingertips and they should welcome a patient’s considered and subjective review of their own symptoms and circumstances. They should see it as both an occasion to build on the doctor-patient partnership as well as a helpful opportunity for continuing their own professional development.
As with all medical consultations, a doctor should acknowledge the information provided by a colleague or patient, using this as a starting point for their own attentive and personalised review.
There is a risk that patients who self-diagnose will have unrealistic expectations and may want their doctor to provide a certain course of treatment based on their findings online. Mddus has encountered some cases where patients have requested unlicensed or specialist medicines from their doctors as a result of their own internet research.
Going to a private practitioner does not entitle patients to ask the doctor to work outside of their competence or provide treatment based on their own research on the web.
GMC guidance Good Medical
Practice states: ‘Prescribe drugs or treatment only when you have adequate knowledge of the patient’s health and are satisfied that the drugs or treatment serve the patient’s needs.’
Practitioners should not feel pressurised into prescribing unfamiliar drugs. Each prescriber takes responsibility for the prescription they issue. doctors must be prepared to explain any actions and are reminded of their professional duty to work within the field of their own knowledge and expertise.
w here agreement cannot be reached, doctors need to respect a patient’s autonomy and right to decide, even if they disagree. we have had cases where the relationship between doctor and patient has broken down due to a disagreement of treatment.
doctors are entitled not to provide treatment requested by a patient that they do not believe is in their best interests.
In these situations, doctors must explain their reasons to the patient as is detailed in the GMC’s Consent: patients and doctors making decisions together: ‘If a patient asks for a treatment that the doctor considers would not be of overall benefit to them, the doctor should discuss the issues with the patient and explore the reasons for the request.
‘If, after discussion, the doctor still considers that the treatment would not be of overall benefit to the patient, they do not have to provide the treatment. But they should explain their reasons to the patient and explain another other options that are available, including the option to seek a second opinion.’
However, a shared decision, complete with a full and frank discussion of risks and benefits, is more likely to ensure a positive patient experience and outcome.
Dr Greg Dollman is a medical adviser for UK-wide medical defence organisation MDDUS
Upright Positional MRI
A new concept providing real benefits to patients
• Weight-bearing scans and variable patient positioning enables a more precise diagnosis
• Truly open system is a solution for claustrophobic patients without compromise in image quality
How much do you think
In this Independent Practitioner Today serialisation of his brilliant new book, Michael R. Young this month looks at pricing and setting your fees
Take Control
of your private practice billing
At Medser v we specialise in providing the highest standards of private prac tice billing ser vices for hundreds of hospital consultants throughout the UK and Ireland
- Online access to all your billing information
- Extremely cost- effective
- Charges are based on revenue collected
- Tax deductible
- Comprehensive repor ting
- Completely conndential
think you’re worth?
Setting your fees is a personal matter and is about you asking yourself ‘How much am i worth?’
it is a paradox that the professions often talk of their earning capacity as being so much per hour rather than so many thousands a year.
i would stick to charging by the hour. t he hour is a nice unit to work in and it is something to which solicitors are attuned.
However, daily (or half-day) rates may be applicable if, for example, you have to attend a case conference or attend court. the expert organisations will be able to offer advice and help with setting your fees.
Having said that, sometimes you will not be able to set your own fees for a case. the solicitors, who will have been told by the funding insurance company, will tell you how much you are going to be paid.
t his is all on the back of the Jackson reforms and predetermined costs. Before the publication of the Jackson report, whenever an expert was asked by a solicitor to give an estimate of his or her costs for, say, writing a report, the expert would come up with a figure, which hopefully the solicitor would agree to pay. not now!
Set your fees too low and you may find yourself inundated with work but not reaping the financial rewards your expertise deserves
A delicate balance
A word of caution. if you set your fees too high, you risk pricing yourself out of the market. Set them too low and you may find yourself inundated with work but not reaping the financial rewards your expertise deserves.
i would speak to some solicitors before you actually set your fees, and ask them how much they pay for expert services. Some experts tend to have a set fee for a report irrespective of how long it actually take them to write.
it is more professional and honest to cost out each report individ-
You will need to maintain very accurate time records of all the work you do
ually and to stress to the solicitors that you will only invoice them for the actual time taken.
you will need to maintain very accurate time records of all the work you do. Be generous with your initial estimate and then, when you invoice the solicitors for less than your original quote, they will feel as if you have given them real value for money. that is not being dishonest. i t is about creating the right impression. if you are registered for VAt, you ➱ p30
will have to charge this on top of your fees, of course. review your fees annually and only increase them in line with what you think the market will stand. Ask solicitors what they think is a reasonable fee.
Screening reports
occasionally, you might be asked to provide a report – often a screening report – for a low fee, either because the case is privately funded and the potential claimant wants to test the water before committing him or herself to a larger financial obligation, or because the solicitors want to know upfront whether they have more than a 50% chance of winning the case.
Whether you accept this work depends on which firm is asking. if it is one for whom you undertake a lot of work, then you should, for the sake of maintaining goodwill, agree to it.
Free legal advice for independent Practitioner Today readers
independent Practitioner Today has joined forces with leading niche healthcare lawyers Hempsons to offer readers a free legal advice service.
iPt
We aim to help you navigate the ever more complex legal and regulatory issues involved in running and developing your private practice – and your lives.
Hempsons’ specialist lawyers have a long track-record of advising doctors – and an unrivalled understanding of the healthcare system as a whole.
call Hempsons on 020 7839 0278 between 9am and 5pm monday to Friday for your ten minutes’ of free legal advice.
Advice is available on: business structures – ian Hempseed commercial contracts – Faisal dhalla competition – lindsay draffon disputes – Hilary king HR/employment – Fiona mclellan Premises – lynne Abbess
You will have to accept that for a proportion of your time you will not earn any money at all
in the early part of your career, you may want to take on this type of work fairly often to give yourself much-needed experience. i f you prove yourself to be a capable expert, then more work will follow, hopefully of the more lucrative kind.
i n the end, how much you receive for a specific piece of work or service depends on negotiation between you and those who are paying.
it is a sobering thought that you will not be paid for every minute you spend on a case. you will have to accept that for a proportion of your time you will not earn any money at all.
Estimating fees
At first, i was not very good at estimating my fees. the first report i ever did took me a very long time, and the fee i charged probably equated to the minimum wage. As you become more experienced, you will have a better idea about how long things are going to take you.
Adapted from The Effective and Efficient Clinical Negligence Expert Witness, by Michael R. Young, price £60 from Otmoor Publishing n ext month: Top tips on finding work, writing your cV and marketing yourself
you also have to decide whether or not you want to earn at the same rate as you do from your main job. i was happy to work for less because the money i was earning from my expert work was not needed to support my business. one or two solicitors have told me that they expect their experts to charge low fees because they (the experts) don’t have any significant overheads or costs associated with this work. i’m not sure i agree with their reasoning. if you happen to have severely underestimated your fees for a particular case, you can always ask for more. But it is unlikely the solicitor will agree to pay you more unless you’ve been an excellent expert and have produced an excellent report.
Special offeR! BuY the Book and Save £20
the book costs £60, but independent practitioner today has secured discount of a third off for readers, so you pay only £40.
listen to the audio content which accompanies the book at this website: www.otmoorpublishing. com/audio.
for more information and to order, email stephen.bonner@otmoorpublishing.com, quoting reference ‘Young/ipt’.
Help with gripes
How do you treat your complaints? disa Young (right) outlines the work of an organisation that can help independent practitioners
Com P l A int S HA ndling in healthcare is under intense regulatory scrutiny. High-profile public inquiries and complaints reviews have led the Care Quality Commission (CQC) to position complaints prominently within its new approach to regulation. o ver the past 14 years, the i ndependent Healthcare Sector Complaints Adjudication Service ( i SCAS) has established itself as the recognised complaints management framework for the independent healthcare sector.
i t has broad recognition and support from the systems regulators across the u K and has an operating protocol with the CQC and Healthcare i nspectorate Wales – and is working towards one with Healthcare i mprovement Scotland. t he regulators recognise the importance of signposting the public to iSCAS.
i SCAS independent adjudication affords those complainants from member hospitals and clinics an independent review process for complaints that cannot be resolved locally.
if you are are not a member of i SCAS, where do you direct patients whose complaints you cannot resolve?
in the new regulatory landscape in england, the CQC is seeking to use the intelligence from complaints to better understand the quality of care and to examine how well practitioners handle complaints to encourage improvement in their services.
i SCAS is adapting to this and extending its services to support members in meeting these requirements.
the CQC will require that practitioners demonstrate that ‘complaints [are] appropriately investigated and appropriate action taken in response’. i nspectors will examine how practitioners utilise feedback from complaints to bring about quality improvement in their services.
Sharing best practice
recognising this, iSCAS now facilitates the sharing of best practice in complaints handling through the medium of a members-only e-newsletter.
it has also begun a programme of training seminars promoting learning from complaints. A recent seminar focused on conducting an effective complaints investigation in the initial stages of a complaint.
iSCAS has an extensive repository of information about independent sector complaints. other
over the past 14 years, the independent healthcare Sector complaints adjudication Service has established itself as the recognised complaints management framework for the independent healthcare sector
doctors Federation and resident medical officers services; and drug and alcohol rehabilitation clinics. the iSCAS Complaints Code of Practice sets out the standards that i SCAS members agree to meet when handling privatelyfunded patient complaints about their services.
learning points covered in the seminars included:
t he need for accurate and detailed record-keeping;
t he importance of thorough consent processes;
managing patient expectations in terms of outcomes, especially in the cosmetic surgery arena;
Presenting accurate profiles of clinicians.
A consideration for the future is whether and how anonymised complaints data across the independent healthcare sector might be published to further improve the quality of services and complaints handling.
what is iScAS?
iSCAS is a voluntary membership scheme that represents the vast majority of all independent healthcare providers across the uK. the three largest member categories are: acute hospitals (56%); specialist cosmetic providers (18%); and specialist ‘other’ clinics – neuro-rehabilitation, diagnostics, pregnancy services (16%). the remainder of the membership comprises mental health hospitals; the i ndependent
An independent review of complaints about nHS-funded treatment in an iSCAS member hospital is provided by the Parliamentary and Health Service ombudsman or equivalent ombudsman in the devolved countries.
iSCAS independent adjudicators conduct a desk-top review of complaints and employ the services of clinical experts where required. they considered 40 complaints cases in 2014 and 151 heads of complaint within those cases. the service is free for complainants to use and is funded by the membership. the average cost of an adjudication case in 2014 was £2,412.
independent adjudicators have the ability to award a goodwill payment to complainants in recognition of inconvenience and distress and in 2014 the average size of such a payment was £479. t he three largest categories of heads of complaint adjudicated on were: complaints handling (20%), nursing care (19%) and consultant care (17%).
For more information about iSCAS, visit our website at: www. iscas.org.uk
The ISCAS Annual Report 2014 is available at www.iscas.org.uk/ iscas-annual-report
Disa Young is senior adviser at ISCAS
Ensure patients know your terms
With the Competition and Markets Authority pushing for greater transparency over consultants’ fees, and hospitals publishing more information about specialists who use their facilities, Garry Chapman (right) says it’s time to ‘get ahead of the curve’
As regulAr readers of Independent Practitioner Today will be aware, the Private Healthcare Information Network (PHIN) has now been appointed by the Competition and Markets Authority (CMA) to run a consumer-based website providing data on both hospitals and consultants. (see also lead news story on page 5).
This will enable patients to have more information and allow many of them to make their own choices about treatment.
At the same time, the CMA has been pushing for greater transparency in fees by consultants, while hospitals are publishing more information about them.
so, while all these changes are taking place in the market, we would recommend getting ahead of the curve by implementing a process for your own data on both pricing and performance.
For pricing in a commercial environment, the ‘terms and conditions’ describe how the company will conduct its business with its clients and typically form part of a commercial contract. In private healthcare, and particularly for consultants, we are talking about the patient registration form.
It has always been our advice for each practice to use a patient reg-
istration form to notify patients about how they charge. This, in turn, leads to fewer fee problems with them later on.
Where possible, we recommend that a practice has a set of words which describe how the transaction between the patient and the practice will work in relation to its pricing and the payment of any treatment provided.
In light of the CMA report, the practice may also want to consider having the consultant’s biography as part of this document, including any statistics on performance and any work that they have published.
This wording can be printed on the headed paper of the practice and handed to the patient or it can be emailed to new patients when they book an initial consultation.
Make the patient aware
The important thing is that the patient is made aware of the information before treatment starts in order to avoid any ambiguity.
In our experience, when a patient has private health insurance, many of them immediately think that all the costs of the treatment are covered, when, in reality, there is in most cases a cost element that the patient has to pay.
it has always been our advice for each practice to use a patient registration form to notify patients about how they charge. this, in turn, leads to fewer fee problems with them later on
for consultations that patients do not attend where they have not been cancelled in advance or cancelled at the last minute. These ,of course, are often referred to as DNAs (Did Not Attends).
Another area which often needs clarity is if the practice charges for items that are typically not covered by the insurance companies. These can be items such as writing prescriptions or consultations carried out by phone.
A template to use
The vast majority of patients have health insurance through their companies, so most of them are unaware of the small print of their own policies, which typically leave them with a shortfall.
This can be for many reasons and the main ones are:
They could have an excess on the insurance policy for the first part of the treatment;
They could have exceeded the benefit limit of the policy;
They could have a policy which is called co-share, where they have to pay a percentage of each invoice.
The patient registration form should also inform the patient if the practice has any other commercial terms, such as charging
All of the above need to be incorporated into a patient registration form as well as any other commercial considerations particular to the specific practice – such as charging for domiciliary visits. If the practice has a website, I would also suggest that the wording published on it matches your patient registration form so that the message is consistent across all forms of media.
There are too many variables across the sector to cover all of them in this article. However, I have provided an example on the right, which you could use as a template and then adapt to your particular practice.
Garry Chapman is managing director at Medical Billing and Collection
Use this form as a template and then adapt the wording for your practice:
Patient reGistration form
Patients CoVereD BY meDiCaL insUranCe
this is a private appointment and the patient’s insurance provider will be contacted for payment. should the insurance provider not cover the full cost of the treatment, then the patient will be responsible for settling any outstanding amount.
it is the patient’s responsibility to obtain authorisation prior to any treatment. the consultant will submit claims relating to the treatment direct to the insurance provider.
seLf-PaYinG Patients
this is a private appointment and the patient is responsible for all charges, so payment may be requested in advance, if full costs are known, or immediately after any treatment.
fee sCHeDULe
the consultant’s fee schedule is typically met by the insurance providers. However, as there are so many different policies in existence, it is the patient’s responsibility to establish if their own policy will cover both the treatment and the costs of the treatment and identify if they will incur any shortfall. or
the consultant’s fee schedule is not always covered in full by the insurance companies, as the consultant has his/her own price schedule.
as there are so many different policies in existence, it is the patient’s responsibility to establish if their own policy will cover both the treatment and the costs of the treatment and identify if they will incur any shortfall.
We can provide quotations upon request for any treatment.
PLease note
if the patient fails to attend an appointment without providing notification of at least 48 hours by phone or email between monday and friday 9am-5pm, then they will be charged a cancellation fee of XX% of the consultation/procedure fee.
the consultant’s fees are completely separate to the invoices the patient may receive from the hospital for tests or procedures carried out.
the consultant’s fees for the following items are not typically covered under the insurance policies:
• Home visits
£xx
• Phone consultations £xx
• Prescription charges £xx
The sun shines on
Spanish real estate … is now a good time to buy? And, if so, where should you look? Dylan Mitchell finds out
Since 2007, the Spanish property market has been one of the worst hit by the global recession, with reports of prices in some areas falling by 50% to 70%. So where are the best opportunities for an investment?
i n the past, the main reasons people have looked to either move to Spain or to buy a holiday home are for better weather, a less stressful way of life, beautiful beaches, fantastic golf courses and great food and wine. i t’s worth remembering that all those things have not changed.
What has changed is that property prices in many areas have plummeted and mortgage interest rates are at an all-time low. This means that the villa or apartment that you always wanted has now become the most affordable in a generation and it’s an incredible opportunity for investors.
So where should you buy? This will depend on the type of property you want to buy and how you want to use it.
if you are looking for an investment property to let on a long-
term basis, then the major cities of Madrid and Barcelona, where people work and need permanent accommodation, would be good places to look.
But if you are looking to invest into vacation properties, then on the coast, near a good golf course would be ideal. Obviously, if you would like to emigrate to Spain or buy a holiday home for your family holidays, your own personal preference is what really matters.
Is Spain a good place to invest?
Yes. For a number of reasons:
Property prices are the lowest in a generation, which means that they can’t go much lower, but there is massive potential for capital growth over the next ten years.
Mortgage interest rates are the lowest ever. This makes buying a property much more affordable, will allow you to buy larger properties than you would have been able to afford previously and will allow you to repay the mortgage much quicker than the normal 20-25 years.
San Sebastián on Spain’s northern coast
on Spanish property
Quantative easing (Qe). This is when the central banks increase the money supply in a country. When this happens the excess money has to go somewhere, and it ends up in assets like the stock market and property market.
The UK and US have been doing Qe for a few years now and that is one of the reasons that both countries’ property markets and stock markets are performing so well.
The e uropean c entral Bank started a Q e programme in January this year, which means that money is only starting to reach the property markets.
UK Pensions. in April, the UK pension legislation changed to allow you to withdraw all the money in your pension. While this might not be right for everyone, it’s estimated that over £5bn will be withdrawn.
Some of that money will be reinvested into the property markets in the UK and overseas. As Spain and France are the two top destinations for Britons to buy property, it’s likely that both countries’ real estate markets will receive a boost.
WhERE ARE SpAIn’S hoTSpoTS FoR InvESTmEnT pRopERTy?
San Sebastián
Set on Spain’s northern coast, only 20km from the French border, in the Basque country.
Of the seven three-star Michelin restaurants in Spain, three are in San Sebastián, which also boasts Spain’s most expensive real estate. Although most visitors choose the Mediterranean coast, the Atlantic coast is rustic and incredibly beautiful. Worth a visit.
madrid and Barcelona if you would prefer a typical buyto-let investment for a long-term let, then the financial centre of Madrid or the major coastal city of Barcelona would be good places to look.
in Spain, tenants are highly protected, so it’s advisable to protect yourself with landlord insurance, which is readily available and will maintain your rental income for a period of time, if your tenant stops paying.
Balearic Islands
Mallorca, ibiza and Menorca combine to be one of e urope’s most popular holiday destinations.
Due to demand, property prices in these beautiful Mediterranean islands have hardly fallen at all during the recession and, as demand begins to pick up again, are expected to rise even more.
it is possible to buy a two-bedroom apartment in Mallorca for €150,000, but the city of Palma will cost considerably more.
i biza and Mallorca will offer high weekly rents, but it’s a seasonal market, so an investment property could sit empty for large parts of the year.
Property on mainland Spain will offer more year-round rental opportunities.
Costa Blanca
Set along more than 200km of beautiful coastline in Alicante, c osta Blanca is one of the most popular destinations in Spain for holidays and second homes.
The southern part of c osta Blanca offers a lot of opportunities for investors, with lots of golf estates offering villas and apartments. The warm climate allows golf estates to attract visitors all year round: in the peak seasons for family holidays and in the low seasons for golf competitions and business conventions.
i n the north, there are fewer estates and less development in general. Planning restrictions were a lot stricter in this part. With fewer apartments and more luxury villas, the average property price tends to be higher than in the south.
The ‘Tren de la costa’ is a new train service that will transform the c osta Blanca’s rail network. c onnecting Alicante- e lche airport throughout the province, it will make travel easier and faster. This can only have a positive impact on real estate prices.
Costa del Sol
The ‘Sunshine coast’ of Andalusia in the south of Spain is famous for
some of the best golf courses in europe, combined with fantastic beaches and an all-year-round warm-to-hot climate.
These golf estates are popular destinations for holidaymakers and offer ideal villas and apartments for investors. Marbella is home to the rich and famous; very much the place to be seen in the summer.
Canary Islands
These volcanic islands in the Atlantic are very popular with holidaymakers all year round. in fact, more than 12 million people visit the islands each year.
The islands are busy in the summer and winter, as they are the UK’s closest destination for winter sun.
This wrap-around season means that the most popular islands of Tenerife, Fuerteventura, Gran canaria and Lanzarote would be good locations for vacation rental apartments or villas.
Whether it’s a golf resort, seaside town, bustling major city or quiet hill top village, you’ll find it in Spain, and priced to sell.
Dylan Mitchell is director of property investment firm FrenchLeaseback.com
Doctors’ questions about patients’ issues with the DVLA are tackled here by Dr Nicola
Ethical rules of the road
Dilemma 1 Bus driver does not want to stop
QI am currently treating a patient with a newly diagnosed abdominal aortic aneurysm. The aneurysm is 6.5cm in diameter.
The patient works as a bus driver and says he does not want to inform his employers in case they make him stop driving. What should I do?
AThere are a number of medical conditions included on a list published by the Driver and Vehicle Licensing Agency (DVLA) which may indicate that a patient is unfit to drive. Abdominal aortic aneurysms are one condition on this list (www.gov.uk/government/organisations/driver-andvehicle-licensing-agency).
As your patient is a bus driver, this means he is a group D licenceholder and is therefore subject to more stringent medical standards than other licence-holders, such as those who drive a car or motor cycle, who are categorised as category A and B (www.gov.uk/olddriving-licence-categories).
This reflects the higher risk that
category D drivers may pose to themselves and the wider public.
The DVLA should be notified of any aneurysm of 6cm or more in diameter. However, category D drivers will be disqualified from driving if they have an aneurysm of 5.5cm or more.
This means that if a category D driver has an aneurysm of 5.5cm or more, they must inform the DVLA and should not drive again. Category A or B drivers may be permitted to continue to drive until the aneurysm reaches 6.5cm in size.
Any driver will be allowed to resume driving once a satisfactory surgical repair has taken place. It is the licence-holder’s duty to notify the DVLA of any medical condition which may affect their ability to drive and it is an offence if they do not alert the DVLA of any such condition.
You should inform your patient that his aneurysm may affect his ability to drive and that he has a legal duty to inform the DVLA of his condition.
If the patient does not seem convinced of the importance of informing the DVLA or refuses to accept that he can no longer drive, you may wish to suggest that he obtains a second opinion. However, you must inform him
that, in the meantime, he should not drive.
You may find it useful to have an information leaflet to hand to give to patients in order to complement the verbal advice. You should document in the patient’s medical record what information and advice was given to the patient at the time of diagnosis.
Dilemma 2
Should I report him to the DVLA?
QI advised my patient of his duty to report his medical condition to the DVLA and that he must not drive and arranged for him to return for a CT scan and a review in two weeks’ time. When he returned, it became clear that he was still driving and had not informed the DVLA or his employer.
What should I do? Should I break confidentiality and inform the DVLA?
ABreaking patient confidentiality is something which most doctors find very difficult. In general, it is not something that a doctor will consider doing. However, there are some cir -
cumstances where it is, in fact, required. The GMC is clear that you should contact the DVLA immediately if you discover that a patient is continuing to drive against your advice.
Before you contact the DVLA, the GMC advises that every effort should be made to persuade the patient to stop driving voluntarily.
If you do feel it is necessary to contact the DVLA, you should attempt to inform the patient that you are planning to do so and the reasons why.
It is important that you only disclose the minimum information necessary to the DVLA and do not disclose the patient’s full medical records.
Once you have made the disclosure, you should inform the patient in writing of what information you have disclosed and a note should be made in the patient’s records setting out your actions and explaining your reasons behind your decision to disclose, as you may be asked to justify your actions if the patient makes a complaint.
Dr Nicola Lennard (right) is a medico-legal adviser at the MDU
Avoid
Don’t go over the pension pot limit
Don’t ignore the ‘£1m pension’ news. Patrick Convey explains why your own finances could be caught by new limits and what to do to prepare for the big change in the months ahead
Given the near constant amendments to pensions in the last few years and the fact that the most drastic changes to the industry in recent history took place from last month, it would have been feasible to expect that pensions could have been left out of this year’s Budget.
Unfortunately, the rumours of a cut to the lifetime allowance had been circling for some time.
From April 2016, the lifetime allowance – the maximum amount which can be saved into a pension tax free – will be reduced to £1m.
now, you would be forgiven for not paying much attention to the lifetime allowance change.
Pensions are not always very
interesting and are, of course, far too complicated. i t is easy to switch off from what is happening here and now.
But make no mistake; if you are a senior doctor paying into the nhS Pension, then this cut could have a very real impact on your retirement savings.
t he sums involved may seem too substantial to be of relevance.
But long-standing members of final salary schemes will be caught by the new threshold.
if you are tied into making contributions into the nhS Pension and have served the organisation for many years, there is a very real danger that your pension will easily reach the £1m mark.
For years, our politicians have
been telling us to save for our future, to be prepared to fund our own retirements.
Yet, unbelievably, far from under-saving, we now have a situation where many hard-working doctors are over-saving into their pensions and will face harsh tax penalties because of it.
What is the lifetime allowance?
the lifetime allowance (LtA) was only introduced around nine years ago, but has been altered many times since.
it started at £1.5m, was increased to £1.8m in a fleeting moment of generosity before being cut to £1.5m in 2012. i n 2014, it was reduced further to just £1.25m.
Above this limit, you will incur punitive tax rates of up to 55% on any benefits taken.
You might believe these sums are of little significance, as you have not put £1m into your pension, but the LtA is not a limit on contributions over a lifetime; the threshold refers to how much your pension might be worth when you finally retire.
hM Revenue and Customs calculates the value of a final salary pension pot as 20 times the annual pension plus any lump sum you take.
t he Chancellor has declared that the lifetime allowance limit will remain at £1m until 2018, before increasing in line with inflation every year thereafter.
But despite this promise, more people will be trapped in future. instead, it would be reasonable to expect the lifetime allowance to be increased with the same ‘triple-lock’ guarantee applied to the state pension. i t rises by the higher of inflation (as measured by the Consumer Price i ndex), average earnings or a minimum of 2.5%.
in addition, there is no guarantee this pledge to protect the lifetime allowance will be upheld. three years is a very long time in politics and guarantees are often expensive for the state to maintain in the long run.
Why is the change important to you?
As an example, a consultant with an nh S pensionable salary of £100,000 with somewhere between 30 to 35 years’ service within the pension scheme by age 60 will reach £1m in their pension pot.
A salary of £88,000 with 40
years’ service will also hit the pension ceiling.
t hese figures do not take into account salary increases from clinical excellence awards nor oncall payments nor any private pensions that may be in force alongside the nhS pension.
And yet doctors have long realised that private pensions are a necessary supplement, as the nhS pension alone will not provide for a luxurious retirement.
While it obviously presents a good foundation, a £1m pension pot will offer an annual income of around £43,500 – taking into account the lump sum payment – a figure much lower than the average consultant’s salary.
have you considered how your lifestyle might have to change in retirement if you are not properly prepared financially?
Consider as well that there might be financial commitments such as dependents at university or in long-term care or personal projects that you hope to enjoy.
What can be done to avoid 55% tax?
Yo U W i LL need to check your own position carefully.
Start by getting an up-to-date valuation of all your pension plans before calculating the forecasted value at your planned time of retirement.
Seek expert help. For the majority of busy medical professionals these calculations are an onerous task with a high risk of mistakes for the untrained eye.
Your options to mitigate any tax due will depend largely on your age, how long until retirement and whether you wish to keep accruing benefits.
t here is one year left to make arrangements before the new limit applies, so taking action sooner rather than later is crucial in terms of planning.
i n our experience, getting the necessary information from the nhS Pensions Agency and other pension providers can prove challenging and certainly time-consuming.
i f you are near to the limit
PROBLEMS WITH THE TAX MAN?
already, you will need to keep a close eye on the value of your pension. i deally, you will want to achieve a final pension pot as close as possible to the lifetime cap without exceeding it.
pension protection plans
You may be in a position to apply for the Government’s pension protection plan, i ndividual Protection 2014 ( i P14), if the value of your pension rights exceeds £1.25m.
t he scheme will allow you to protect your current pension fund value up to £1.5m. importantly, you will still be able to accrue benefits through both the nh S and private pension schemes without losing the protection.
this is a key area to get right.
Many new clients seek our help having previously been poorly advised in the area of pension protection. often their former advisers do not consider the importance of different protection products or
HMRC tax investigations and disputes create difficult and stressful times.
As an award winning firm of tax experts, our highly experienced partners specialise in resolving problems relating to tax investigations and disputes with HMRC.
To find out, in confidence, how we can help call 0800 734 3333.
‘Here to help. Not to judge.’
do not wish to advise on the complex nhS Pension.
Applications for iP14 are now open and will remain so until August 2017. i ndividuals who already hold previous protection schemes such as Fixed or enhanced Protection can also apply.
t he Government may also launch new pension protection schemes as a sweetener following this latest allowance cut, but no official guidance has yet been given at the time of writing.
opting out of saving
Some savers may choose to opt out of further pension savings in order to avoid tax penalties, but this is an option for a limited few and requires careful consideration.
For most, paying tax – even sizeable duties – still presents a more favourable option than losing the valuable benefits that are accrued. if you are already aged over 55,
you may consider taking money out of your pension earlier than anticipated. i f the withdrawn funds achieve any growth, it will not be tested against the lifetime allowance again until you reach the age of 75.
Last year, the Chancellor announced that the harsh 55% death tax due on private pensions will be abolished from April 2015.
Many doctors may now choose to pass their private pots on to loved ones tax-free, as pensions do not form part of a person’s estate for inheritance tax purposes.
Although this could prove a useful inheritance tool to help future generations, individuals should be particularly wary of the complexities now surrounding both pension contributions and pension withdrawals.
You should also make full use of the newly increased iSA allowance – now at £15,240 for the tax year ahead.
For most, paying tax –even sizeable duties – still presents a more favourable option than losing the valuable benefits that are accrued
Do not forget that this cap applies to all members of the family and can present a useful savings vehicle.
As an example, if a doctor and his/her spouse invested around £30,000 a year every year for the next 15 years and achieved a 3% real return after charges and inflation, the final fund will be worth over £650,000. From this, under current legislation, tax-free withdrawals can be taken without restriction to supplement the nhS Pension.
doing nothing is not an option
t he state offers tax relief to encourage us to save ‘enough’ for our retirement so that we do not become a burden in later life, but only to a certain degree.
But this latest move suggests the last Government would rather we did not save any more than is required for a fairly simple existence. And a cut to higher-rate tax relief on pensions has already been proposed as part of the preelection speculation.
Whatever your own personal situation, doing nothing could cost you tens of thousands of pounds. You have limited time available to take important decisions, so the sooner you can start the process the better.
Remember that despite the apparent dissuasion, the need to finance your retirement remains – particularly if you want to live life to the full. the political tinkering merely means finding a better way to fund those plans of yours.
Patrick Convey (left) is technical director of Cavendish Medical, specialist financial planners helping senior consultants in private practice and the NHS
The content of this article is for information only and must not be considered as financial advice. Cavendish Medical always recommends that you seek independent financial advice before making any financial decisions.
Levels, bases of and reliefs from taxation may be subject to change and their value depends on the individual circumstances of the investor. The value of investments and the income from them can fluctuate and investors may get back less than the amount invested.
A bright spark
It’s electrifying! Independent Practitioner Today’s motoring correspondent dr tony rimmer gets a buzz from the Tesla Model S
Our medical education and training structures have a strong peer-learning element. Our successful and experienced colleagues provide an invaluable guide for all doctors during their career development.
as independent medical practitioners, we run our own businesses and would do well to look at what features have made some well-known business people effective and prosperous.
One such entrepreneurial icon
is the co-founder of PayPal, elon musk. This 43-year-old americanc anadian has made his many millions in tech industries.
a qualified engineer, he sold his shares in PayPal to eBay in 2002 and became a three-figure millionaire overnight. Since then, he has been able to indulge and invest in several futuristic tech-based companies that include Solarcity, which is the second-largest producer of solar power systems in america.
His passion for reducing our global c O 2 output was also directed to our motoring habits and he established his all-electricpowered car brand Tesla about ten years ago.
Force to be reckoned with
The first model was a sports car based on a l otus platform and, although interesting, had significant limitations, particularly with the vehicle’s range. it was only with the launch of
the premium hatchback model S in 2012 that Tesla has become a force to be reckoned with. First released in its uS home market, it is now available in right-hand drive on the uK market.
i have been lucky enough to spend a week living with this ground-breaking car just to see what it’s really like and whether it fits the bill for the environmentally conscious private medical practitioner.
Introduction
being all-electric, the tesla s has a big boot at the front and a large hatchback at the rear
teslA model s
body: Five-seat hatchback (seven-seat option)
engine: one or two electric motors
Power: 380bhp
(691bhp in performance model)
torque: 600nm
top speed: 125mph
Acceleration: 0-60mph in 5.5 secs
Welcome to the BVRLA – I’m delighted that you’ve decided to join the trade association that provides a face for the vehicle rental and leasing industry, communicating its messages to customers, the media and government. The BVRLA’s corporate identity, particularly its logo, forms part of that message.
the enormous 17-inch touchscreen is constantly connected to the internet via 3g
Claimed range: up to 310 miles on-the-road price: £54,955 to £73,755
The BVRLA has three categories of membership, each with a logo that members are entitled to use (and, in some situations, are obliged to use). Appropriate use of our logo tells your customers, your suppliers, and the rest of the world that you adhere to the high standards that come with BVRLA membership.
the Model S is the size of a BMW 5 series and, being all-electric, has a big boot at the front and a large hatchback at the rear. impressively, tesla offers the option of two rearfacing seats in the back which turn it into a true seven-seater.
lovely touches
e xterior looks are rather bland, but there are some lovely touches. the stylish door handles lie flush with the bodywork but extend gracefully when you unlock the car.
Although the styling is nothing special, the technology under the skin certainly is. A powerful 380bhp electric motor between the rear wheels has a single moving part: the rotor.
Petrol and diesel engines have hundreds of moving parts. there is the option of an all-wheel-drive Model S which has smaller elec-
thing else i have ever driven. Use a gentle right foot and progress is smooth, effortless and will get you more miles from a full charge.
This brief guide explains how we expect our logos to be displayed – and how they should not be displayed. These are not hard-and-fast rules, and we sometimes depart from them ourselves, but we do expect our members to respect them and to gain our prior approval before using our logo in any way other than described here.
If you need a copy of our logo, for use on your printed marketing material, or to go on a page of your website, please contact our communications team, who will be happy to send you an EPS or JPEG version appropriate for your purposes.
If you have any queries about use of the BVRLA logo that are not addressed in this guide, they will also be able to help
talking of charge and range, tesla quotes a maximum range of 310 miles and i reckon a realworld 250 miles is achievable. this is impressive and not unlike a tankful of fuel in a normal car. to charge, you can plug the car in overnight using a special home-fitted charging point to get up to 68 miles per hour of charge. tesla is investing massively in a nationwide network of supercharging stations.
Gerry Keaney Chief executive, BVRLA
tric motors; one at the rear and one between the front wheels (both 190 bhp).
the top performance model has a 470bhp motor at the rear and a 221bhp motor at the front. n o wonder it has an ‘insane mode’ on the driving option list. A 0-60mph time of 3.2 seconds is in Lamborghini territory.
Step inside and the first thing that strikes you in a dramatic way is the enormous 17-inch central touchscreen. Constantly connected to the internet via 3G, the screen controls all major functions and makes every other car you have driven before positively prehistoric.
the Google earth-based satnav has all the functionality that you are used to on your home PC and feels very futuristic in a car. the general interior, leather seats and trim are of premium quality,
although perhaps not up to Audi standards.
Because the tesla is all electric, there is no central drive tunnel, which means lots of space for legs and feet, most noticeable for rearseat passengers.
My test car was the rear-drive version and when i drove off for the first time, two things immediately struck me: the total absence of engine noise and the phenomenal take-off from rest.
Astonishing acceleration electric motors deliver maximum torque from rest and this translates to a feeling of being propelled by a massive iron fist in a velvet glove. h andling is more American than UK-biased, but the air suspension is impressive over our rough roads.
the instant throttle response is highly addictive and unlike any-
these are free and exclusive to tesla owners and can charge at a massive 170 miles per half-hour. During my time with the car, i never had a single episode of range anxiety and drove a few hundred miles in total.
the tesla is a taste of the future and a futuristic technological masterpiece. t he car’s driving software is even updated automatically while you sleep via the 3G network.
i was besotted by its combination of power and smoothness with the certain smugness that comes from knowing that you are adding nothing to pollution levels as you drive.
Future models such as the soonto-be-released Model X SUv are going to be even better. if you are the type of independent practitioner who likes to be at the cutting edge and enjoys taking risks, you are likely to have a very successful practice and you will love the tesla.
Dr Rimmer is a GP practising in Guildford, Surrey
Using the BVRLA Logo
so why not turn to the experts in the field to help you find the vehicle that suits your needs?
anthony K associates are vehicle leasing brokers specialising in providing vehicle contracts for doctors and all associated professions in the medical sector. testimonials from our very many happy customers are proof of our attention to customer service and our practised ability to help clients get the vehicle
Make
the
most from your
meeting with your accountant. Ian Tongue suggests some of the more common areas to discuss
Meetings of like minds
There is no hard and fast rule about how often you should meet with your accountant.
But it should be frequent enough to ensure that you are on the right path financially and you understand the tax and financial aspects of running your practice.
Understanding the tax system
With limited or no financial training, it is understandable that running a business is daunting and the concepts can be difficult to understand.
i find that clients are often apologetic when they say they would like to go over something that we have discussed previously. But don’t be.
Your accountant should be happy to discuss matters as many times as it takes and in a clear and concise manner.
Like doctors, your accountant needs to have a certain ‘bedside manner’ and if they are not looking after you in this way, go elsewhere.
When you are in the early years, keep regular contact with your
Like doctors, your accountant needs a certain ‘bedside manner’
accountant, as this is the crucial time for things to be set up properly from the start– particular with saving for tax.
Getting behind with tax can be very distressing and takes a long time to recover from and therefore it is essential you highlight any areas of uncertainty and discuss them.
Update your accountant on your personal circumstances
A meeting is a great opportunity to update you accountant on your circumstances.
Your accountant should be made aware of:
Any new family members;
Marriage situation;
inheritance;
Your current outlook for the future.
it is surprising what a difference not informing your accountant about these can make.
For example, the new rules around the receipt of child benefit can catch you out, as more often than not it needs to be stopped or repaid due to you not being eligible. With the payments-onaccount system for self-assessment applying to child benefit, it can be an unexpected surprise if you are not prepared.
informing your accountant of any changes in your spouse’s circumstances is extremely important. if they are earning less than previously, even if relatively temporary, it can often mean that tax planning opportunities exist.
Update them on your work
position
Updating your accountant on your current N hs and private practice level is vital when you are considering the trading structure and profit extraction from the company.
it is common for accountants to only hear of changes in Nhs commitment after the event because consultants have not thought this to be relevant to the main business. As this income is taxed before the private practice, any changes can have a significant impact on the level of tax paid on your independent work.
Additionally, any increase to your level of superannuable Nhs pay will have an impact on the level of pension contribution made in any one year. it is important to remember that for the purposes of this calculation, your actual contributions into the Nhs scheme are disregarded and the increase in your pension accrual is notionally valued.
Therefore, a significant increment, clinical excellence award or payments into personal pensions can result in you exceeding the annual allowance which is currently £40,000 a year. it is important that you keep your accountant informed of all changes and intentions in this area.
1
2
3
4
5
Confirm if anything needs to be brought to the meeting – for example, accounting/tax records
Provide update on your personal circumstances –for example, marriage, divorce, birth and so on
Provide update on current and known future changes to NHS position
Provide update and forecast of private practice position
Confirm that current trading structure is most appropriate for circumstances and discuss any available tax planning opportunities
6 Discuss any areas of uncertainty – for example, tax system, accounting concepts
7 Confirm dates and amounts of next tax payments and dates for information submission to accountant
8 Obtain feedback on latest accounts and information supplied – for example, record-keeping
9 Update on retirement planning, if appropriate
10
Provide accountant with any feedback on their service
Discuss the composition of your private practice income, particularly if you are carrying out medico-legal work, as you may need to be VAT-registered.
Discuss your record-keeping h M r evenue and Customs now has powers to fine businesses that do not keep adequate accounting records. Doctors often ask for feedback on their systems and it is usually easier to explain such concepts at a meeting rather than in a letter or email.
A meeting can also be a good opportunity to discuss electronic accounting packages and their merits over more basic systems. Many consultants can function perfectly well for a period without a bespoke practice management package, but the vast majority i speak with who have taken the plunge have not looked back once that decision to invest has been made.
h aving an accountant that is familiar with these packages is an obvious benefit.
Meeting up to discuss matters re-inforces the relationship between you and your professional adviser
Discuss your employees if you are employing a secretary or spouse, then it is important that you discuss your obligations under the new pensions legislation for ‘auto-enrolment’.
Depending on the level of salary paid to the employee, you will have differing obligations and may need to operate a pension scheme as well as a payroll. if you are employing anyone, it is important that you have this discussion at your next meeting.
no substitute for talking
With the digital age we live in, it is now easier than ever to communicate. Many matters can be dealt with through email, but i always say to clients that there is no substitute for a meeting.
receiving an email with lots of detailed questions may seem the easiest way to cover matters, but often it can take several responses to and fro to resolve issues and explain matters that it would have been easier to meet up to discuss things.
Appointments do not always have to be face to face and if you are struggling to arrange a meeting face to face, arrange a phone appointment or video call. You will certainly get more advice and content than asking a series of questions by email.
Reinforce the relationship
Meeting up to discuss matters reinforces the relationship between you and your professional adviser. it can take a while to have total confidence in a third party to deal with such important matters, which is why they need to build that relationship and demonstrate their expertise.
Meeting up should ensure that you gain that confidence and should be the building blocks for a long-term engagement.
Your meeting is an integral part of having a professional adviser engaged. ensuring that you have regular contact and keeping them updated ensures that opportunities are exploited and potential problems are averted.
next month: how to avoid the long arm of hm Revenue and customs
Ian Tongue (left) is a partner with accountants Sandison Easson and Co
Join us to put boot into leg ulcers
A new charity is calling for more founder members from among Independent Practitioner Today readers. Prof Mark Whiteley explains
Leg u L cers are an increasing problem in the community, with estimates of one-in-500 people being affected in the uK.
Traditionally, leg ulcers have been a long-term chronic problem that are treated with dressings and compression, often resulting in a temporary healing. unfortunately, unless this compression is continued, the recurrence rates are very high.
Increasing interest in venous disease over the last two decades has resulted in the understanding that most venous leg ulcers can now be cured with superficial venous treatments – such as endovenous laser or foam sclerotherapy – and some by deep venous treatments such as stenting.
research from edinburgh several years ago showed the cost of curing a venous leg ulcer surgically is approximately the same as one year of dressings and bandaging. e vidence for curing leg ulcers using simple endovenous techniques has resulted in the National Institute of Health and clinical excellence publishing a recommendation in July 2013 ( cg 168) that anyone who has had a leg ulcer for two weeks or more should be referred to a vascular service. However, this is clearly not happening. so the Leg ulcer charity has been founded with the following aims:
1 Empowerment of patients, their families and carers to understand that their leg ulcers may be curable and to help them ask for the correct investigations and treatment.
2
Research: the Leg u lcer charity is already sponsoring
Do you organise conferences, training days or meetings?
Then advertise them with us
a PhD student to look at the consequences of having a leg ulcer to the patient and the people around them.
3
Professional education and development: educational days for doctors and nurses involved in the treatment of patients with leg ulcers.
4
Assistance to patients with leg ulcers : finally, our ultimate aim will be to raise enough money to be able to provide assistance to patients with leg ulcers who are curable but who are unable to find a cure local to themselves.
We have recently had coverage in the Daily Express and have an increasingly prominent internet profile.
Now the charity is looking for doctors or nurses who wish to become involved as founding members and get involved with spreading the word, educational days and fundraising.
Founding members are asked to donate £1,000 as a one-off contribution and then an annual subscription of £250 to assist the charity to achieve its aims. These donations can be gift-Aided.
For more information, please email info@legulcercharity.org or go to the website www.legulcercharity.org.
Prof Mark Whiteley is a consultant vascular surgeon at the Whiteley Clinic, Guildford, and executive chairman of the Leg Ulcer Charity. Other trustees are Bryn Edwards, a chartered accountant; Ian Clapp, now retired after a career working for Investment Banks in the City; and Mr Barrie Price, consultant vascular surgeon
Whether you are organising an industry-leading conference, holding a regular training day or looking to fill a job vacancy, Independent Practitioner Today is the place to reach your target audience.
To discuss all your advertising requirements and find out what we can do to help you, contact our advertising manager
Margaret Floate
Phone: 01483 824094
Email: margifloate@btinternet.com
Network with peers. Learn from experts. Implement change. PATIENT SAFETY. PATIENT FIRST
“I believe it is important to use this opportunity to bring together board members, doctors, nurses, managers, pharmacists and all those who are seeking to deliver improved safety outcomes for their patients”
DrMikeDurkin,NHSEngland
standards and quality from the experts
• Practical solutions & best practise you can put into action from industry leaders and organisations
• Choose from over 40 hours of CPD
• Get practical advice from over 100 product & service providers
Uniting both the Surgical and Non-Surgical Communities
Over 200 world renowned exhibitors
4,000 high level medical healthcare professionals
Over 100 expert faculty
FREE World-class speakers with CPD certified content
FREE conference programme, workshop theatres and live demonstrations
To register and find out more please visit www.ccr-expo.com
@ccr_expo #CCR2015 www.facebook.com/ccrexpo1
Big disparity in income
Independent Practitioner Today’s unique income and expenses benchmarking series gives its second full-year analysis of the two newest specialties covered in this series. Ray Stanbridge reports, with additional material by Martin Murray
An increAsingly wide disparity in earnings is evident between those consultant dermatologists and oncologists who are serious about developing their practices and those who consider private practice work as essentially parttime.
As with other specialists, both have looked to incorporation and to groupings as a means of developing their practices and, for many, the growth of choose and Book work has had an important influence on incomes.
Our figures, while not statistically significant, reflect a trend of earnings and expenditure of consultants in private practice, but
note a number of caveats regarding our criteria for selecting consultants for this survey.
consultants must:
Have had at least five years’ experience in the private sector;
Have earned at least £5,000 a year gross in the private sector in the year to 5 April 2013;
Be interested in pursuing private practice as a business;
Hold, or have held, an old-style n H s maximum part-time contract or a ‘new’ contract;
Work either as a sole trader, through a limited liability partnership or group, or through the medium of a limited liability company.
RaNge OF gROSS INCOMe By RegION
Income 2012
DeRMaTOLOgISTS’ BIg
Skin doctors pick up NHS’s shavings
Dermatologists have bounced back from the previous year’s profits drop with a double-digit increase
Our H e A dline figures show that average gross incomes have risen by 11% in 2012 to 2013, going up from £109,000 to £121,000.
costs rose too – by nearly 12% between the two years – increasing from £34,000 to £38,000.
As a result, taxable profits went up by 11% from £75,000 to £83,000. Margins have remained fairly constant at about 68%. it seems that fee increases have arisen from two main sources.
Firstly, dermatologists are undertaking an increasing amount of c hoose and Book patients, and work that effectively has been ‘ditched’ by the nHs.
secondly, there does seem to be an increasing self-pay market from the ‘worried well’ who are looking, for example, for mole checks. it seems that dermatologists have benefited significantly from massive publicity in this area.
Our survey shows that there has been a modest increase in costs of medical supplies and assistants, although we can find no particular explanation for this.
s taff costs have risen slightly. There does seem to be, as we have reported for other specialties, a correlation between average salary costs and increases in the personal allowance.
Obviously, professional secretarial costs are generally significantly higher than for employing family members and our averages do distort significant differences. s urprisingly, consulting room hire costs seem to have shown a slight drift downwards. We would
expect this to reverse – and we have no explanation as to why it has happened – as the full effect of c ompetition and Markets Authority measures introduced in October 2014 come to bear fruit. These ban private hospitals offering subsidised perks.
There has been some increase in motor and travel costs – primarily we believe, as consultants attended more exotic conferences.
marketing savvy
Finally, there has been a growth in ‘other’ costs, on average from £4,000 to £5,000. This is essentially expenditure on marketing support.
d ermatologists are becoming increasingly marketing savvy and they are showing they realise that expenditure on marketing does generally reap rewards.
Our view in our 2014 survey was that the progression for dermatologists’ net incomes in private practice was good. This has been proven by our findings here.
Many dermatologists have to work harder to achieve the same results. But the market is growing and notwithstanding many of the industry problems – particularly dealing with insurers – we expect this trend to continue.
aveRage INCOMe aND eXPeNDITURe OF a CONSULTaNT DeRMaTOLOgIST WITH aN eSTaBLISHeD PRIvaTe PRaCTICe
How ARE YoU Doing?
Use
to compare your financial performance with others
Year ending 5 April. Figures rounded to nearest
rounded up)
Source: Stanbridge Associates Ltd. Additional information: Sandison Easson and Co
Urologists
Radiologists
gynaecologists
orthopaedic
EnT
Anaesthetists
years ending 5 april
Source: Stanbridge Associates Ltd
➱ Oncologists, p50
Competition hits profits
OncOlOgists’ private practice gross incomes went up by 1.7% from £114,000 to £116,000 between 2012 and 2013 – a much smaller rate of increase than their dermatology colleagues experienced.
c osts, however, showed an increase of about 9%, from £33,000 on average to £36,000. a s a result, taxable profits dropped by about 1.2% from £81,000 to £80,000. Margins have fallen from £81,000 to £80,000.
We anticipated in our May 2014 Independent Practitioner Today survey that income would rise. a ctual increases have been less than we anticipated.
We are aware that some oncologists have had difficulties with insurers, but this is not enough to explain our figures.
i t may be that there are more young oncologists entering the market and some business is being directed from older, more established clinicians to newly appointed ones. Our data is, however, not extensive enough to prove or disprove this hypothesis.
staff costs have increased from £12,000 to £13,000. this is almost certainly for the reasons described above.
t here has been a small rise in costs of subscriptions/professional indemnity, but this is probably due to timing issues rather than substantial increases in real terms.
as with dermatologists, we see that oncologists seem to be starting to enjoy more exotic travel in
pursuit of their requirements for continuing professional development.
it is perhaps interesting to note that we have not observed any real increase in marketing expenditure by consultants – included in ‘other’ costs – between 2012 and 2013. t his differentiates them from their dermatology colleagues. We would have expected to see some growth in costs. t he picture, overall looks a steady one. latest figures suggest that this trend will continue. We would expect over time to see a further income growth for oncologists in private practice, linked, for no other reason from the ageing of the population and the increased prevalence of cancer as we grow older.
Of course, as we went to press, there were uncertainties as to what will happen in the n H s depending on which party wins the election. But, in the long term, our view of income trends still remains fairly positive. next month: Anaesthetists
Year ending 5 April. Figures rounded to nearest £1,000 (percentage is also rounded up)
Source: Stanbridge Associates Ltd. Additional information: Sandison Easson and Co
Ray Stanbridge runs an accountancy, finance and tax advisory service specialising in the medical profession. Martin Murray is a partner at Sandison Easson and Co, specialist medical accountants
whAt’S coMing in oUr JUne edition
Make sure you don’t miss our next issue, published on 25 June. Only subscribers to the journal are guaranteed to receive every copy and we don’t think anybody who is serious about continuing private practice in the future, can afford to miss any issue when there is so much happening that will affect them.
10 ways to boost your private practice income. accountant James gransby reveals what is behind the successful businesses of many high earners
an update from the Private Healthcare Information Network on implementing the Competition and Markets authority’s ‘information remedies’ in the sector
Reports from the BMa’s annual private practice conference
Watch out for the nasties – things that can trip up the DIy investor
In a special message to readers, new gMC chairman Prof Terence Stephenson sets out four priorities ‘to help create a more open, safe and compassionate culture in the medical profession’
Breaking Into The aesthetics Business. Pam Underdown continues her detailed and informative series with a study of why people really buy
a working week in the life of a medical billing and collection boss. a lot of consultants could learn a lot to benefit their private practice from the ‘patients’ garry Chapman meets
eDITORIaL INqUIRIeS
Whatever your age, it has never been more important to take action about your pension, says accountant Susan Hutter
are you new to private practice? Then you will need to know how to avoid the long arm of HM Revenue and Customs. In our ‘Starting a Private Practice’ series, accountant Ian Tongue reveals the key areas where people get caught out
Surgeon Mr Dev Lall says, to succeed in private practice, you have to create the machine to deliver patients to you
How to find work as a clinical negligence expert witness, writing an expert Cv, and tips to encourage solicitors to keep coming back to you
Dr Nicola Lennard of the MDU looks at the implications for private doctors of new drug-driving legislation affecting their patients
Confidentiality and social media – Julie Price of the MPS spells out some key areas to consider in the modern private practice
Our ‘Doctor on the Road’, Dr Tony Rimmer, shows why he thinks the new audi TT will appeal to a lot of his colleagues
Profits Focus looks at the earnings of anaesthetists
Plus all the latest news and views affecting your private practice
aDveRTISeRS: The deadline for booking advertising for our June issue falls on 29 May
Robin Stride, editorial director
Email: robin@ip-today.co.uk
Tel: 07909 997340
aDveRTISINg INqUIRIeS
Margaret Floate, advertising manager
Published by The Independent Practitioner Ltd. Independent Practitioner
Today is editorially independent and thanks Bupa for its assistance with distribution.
Printed by Pepper Communications Ltd Material is governed by copyright. No part of this publication may be reproduced, stored in a retrieval system or transmitted in any form without permission, unless for the purposes of reference and comment. Editorial layout is the copyright of the publishers. If you wish to use it for promotional purposes on websites or for reprints, we would be happy to discuss licensing the copyright to you.
£85 GPs and practice managers (private & NHS). £200 organisations.
But if you pay by direct debit, individuals pay only £70, and organisations £175 Call Proact Ltd on 01752 312140
Email: lisa@marketingcentre.co.uk
Robin Stride, editorial director @robinstride
gUaRaNTee yOUR COPy
To guarantee your copy of Independent Practitioner Today by taking out a subscription (at the rates shown on the left), phone 01752 312140 or send off a subscription form on page 22 or email lisa@marketingcentre.co.uk or go to the ‘about’ page of our website www.independent-practitioner-today.co.uk
If you pay by direct debit, individuals pay only £70 for a subscription. Just fill in the form on page 22 and send it to the Freepost address shown at the bottom of the form.
BaCk ISSUeS: £12.50 including post & packaging CHaNgINg aDDReSS OR SUBSCRIPTION DeTaILS?
Phone 01752 312140 or email lisa@marketingcentre.co.uk
The professional’s choice for practice management
Client management and financial control is the lifeblood of any enterprise. The latest Healthcode online ePractice management tool is the professional’s choice for practice management, giving you the control you need wherever you are. Our ePractice management solution meets the needs of a range of healthcare providers, from independent practitioners to large enterprise organisations. Our different service levels mean that ePractice will grow with your practice.
Take Direct Control
Access your patient details, appointments, bills and financial status from anywhere, any time.
What the professional’s say...
Protect Your Practice
The diary management feature on ePractice manager means I can focus on treating patients, while my PA is able to coordinate my appointments remotely.
Mr Barlow-Kearsley, Founder, Total Footcare Solutions
Long Term Partner
We use Healthcode’s ePractice manager system for all our invoicing, which streamlines everything for us. Roughly 75% of our invoices are submitted electronically, payments are now made much more quickly, which is good for the cash-flow.
John Morgan, Accounts Director, Jenny Morgan Secretariat
Call us today to arrange a demo and to discuss your requirements on 01784 263 150 quoting: IPT. For further information visit: www.healthcode.co.uk/ipt