The business journal for doctors in private practice
In this issue
If referrals start falling off
Our ‘Troubleshooters’ have some suggestions to help get numbers back up P14
The Jekyll and Hyde features of cash
The consequences of holding cash and not investing in capital markets P30
Look after women in the workplace
n See page 24 to find out what Bupa is doing
Private sector promotes women and safety
Supporting women in private healthcare is vital, says IHPN boss David Hare P36
A new era for insurance?
By Robin Stride
SEEKING YOUR ❶ OPINION
Doctors and patients are being invited to contribute to research for a major crusade by the Independent Doctors Federation (IDF) to address what it calls ‘restrictions on patient care’ by private medical insurers (PMIs).
The initiative aims to create ‘a path for improvement’ to ensure fair treatment of private doctors and avoid patient choice being compromised.
Organisers stress they want change through collaboration and are committed to working with all stakeholders to address concerns and improve patient experience.
Key issues identified by the campaign are listed as:
➲ ‘Limited treatment options: PMIs often dictate which treatments they cover and the associated reimbursement, potentially restricting doctors’ ability to pro-
vide the most appropriate care for their patients.
➲ ‘Reduced patient choice and derecognitions: Disagreements over fees can lead to derecognitions, where a doctor is no longer recognised by a PMI, limiting patient choice and potentially creating a two-tier healthcare system.
➲ ‘Lack of transparency and accountability: The current system lacks transparency around PMI fee structures and decision-making processes, raising concerns about fairness and patient well-being.
➲ ‘Stagnant PMI fees: PMI-assured fees have not kept pace with inflation, decreasing since the 1990s. This, coupled with rising practice costs and admin burdens, puts financial pressure on independent doctors, potentially impacting the quality of care provided.’
IDF specialist committee chairman Mr Andrew Roche said in the last decade he had seen private patients’ access to treatment being eroded with insurers increasingly
determining who they could see and sometimes what they could have done ‘based on absolutely no clinical reasoning’.
The consultant orthopaedic surgeon added: ‘The companies also threaten or indeed do remove doctors from their provider lists if doctors try to put their fees up, even in line with inflation. This then removes patient choice over which doctor they want to see.’
He called the IDF’s action long overdue and hoped it would achieve ‘a far more transparent, medically regulated system with patients able to choose whomever they wish to treat them and doctors able to be reimbursed equitably and fairly’.
IDF managing director Ken Mackness said: ‘We cannot ensure insurers will respond positively to the campaign. However, we are hoping to work together to find a solution to the current issues.’
The IDF emphasised its goal was not simply to raise consultants’
fees but to ensure patients receive the best possible care. It wants ‘fair and sustainable fee’ structures implemented with regular adjustments for inflation and rising practice costs; an independent body to oversee insurers’ policies/fees; and ‘clear and objective derecognition protocols including a fair appeals process managed by an independent body’ .
IDF president Dr Philip Batty stated that excellent care required doctors and patients working in partnership to explore evidencebased treatment options and continuity of care. ‘Our members and their patients report increasing restrictions, poor triage and frustration with PMIs. It is time to challenge systems that compromise excellence.’
n The doctors’ survey is open to all independent doctors in the UK. The Doctor Survey is at tinyurl.com/yr26fw2e and the Patient Survey is at tinyurl.com/ efbbtnx4.
Private doctors quizzed on workplace stress
SEEKING YOUR ❷ OPINION
Independent practitioners are taking part in major research to support their health and wellbeing in increasingly pressurised workplaces.
Our sponsors
Consultants and GPs in private practice are being asked to confidentially contribute to in-depth interviews designed to understand their work-related risks and strategies they use to address these.
The ‘Thrive at Work’ project, led
by Affinity Health at Work, is funded by the MPS Foundation, a global not-for-profit initiative which researches well-being of healthcare professionals, their teams and patient safety.
As many as 500 private practi -
tioners are due to participate in a survey based on the priorities identified in the interviews, measures of the work environment, plus health and self-related performance outcomes.
➱ continued on page 3
TELL US YOUR NEWS.
Contact editorial director Robin Stride (right)
Email: robin@ip-today.co.uk
How the Budget will affect you
Specialist medical accountant Alec James provides a summary of the key points from Jeremy Hunt’s latest address at the dispatch box P12
Phone: 07909 997340 @robinstride
ADVERTISE WITH US. To advertise in the digital journal, on our website or in our business and lifestyle directories, contact Andrew Schofield at Spot On Media. Phone: 0161 408 3912
Latest data from the Private Healthcare Information Network shows what was keeping independent consultants busy as self-pay admissions fell P18
What’s happening in aesthetics
Insights into aesthetic industry trends and practices have been revealed by over 300 practitioners who took part in an annual survery P21
The GMC has just updated its professional standards guidance in seven areas. The MDU’s Dr Sally Old looks at what has changed P16 NEWS
Indemnity doesn’t follow the patient
Dr Dawn McGuire of Medical Protection highlights two cases to demonstrate why it’s important to always have your own indemnity P28
OUR REGULAR COLUMNS
Business Dilemmas:
In the interests of a frail patient
Medico-legal advice on what to do if family members disagree about what is best for a very sick patient P42
Start a private practice:
Beware of triggering hidden taxes
Some decisions doctors make can cause a tax iability. Accountant Alec James on what to watch out for P44
Doctor on the Road:
Rugged EV, but no four-wheel drive
Want to go green in the urban jungle? Dr Tony Rimmer found the new electric Jeep a strong contender P48 www.independent-practitioner-today.co.uk
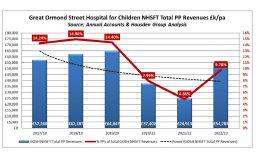
Imposing record in caring for kids
Our occasional PPU Focus series featuring private patient services within the NHS this month explores Great Ormond Street Hospital P32
Run your firm efficiently
Technology is transforming practice management. Derek Kelly unravels the impact of technology on operational processes in medical practice P34
New rules for holiday pay
What do the new Employment Rights Regulations mean for employers calculating annual leave allowances. Lawyer Rachel Levine explains P38
Doctors have just weeks for big pension decision
McCloud latest: Choice exercise launched for pension members
By Edie Bourne
Many doctors have been receiving letters from the NHS Pension Agency asking if they would like to change the decision they made about their pension when the 2015 scheme was first introduced.
This is being called ‘Choice 2 revocation’ and their decision must be made within a few weeks.
The original ‘Choice’ exercise gave all eligible members of the NHS Pension Scheme the option to move from the 1995 section into the 2008 section when it was introduced.
When the 2015 section was launched, ‘Choice 2’ gave mem -
bers who had remained in the 1995 section another opportunity to move.
As part of the McCloud remedy being implemented, members have now been given the option of revisiting their ‘Choice 2’ decision. This is because they may have moved believing the new sections offered more retirement flexibility – but now McCloud has given them further options anyway.
George Uglow, chartered financial planner at Cavendish Medical, told Independent Practitioner Today: ‘If you decided to move your 1995 section benefits to the 2008 section, you can now change your mind and move the benefits back.
‘Doctors have started to receive letters asking them to decide what they would like to do, but they only have until 20 May 2024 to notify the NHS Pensions Agency.’
This exercise has been launched as part of the McCloud remedy which aims to recompense NHS scheme members deemed to have suffered age discrimination when the 2015 pension scheme was introduced.
Those members now have the option to receive their original benefits from the 1995 or 2008 scheme for the seven years of the ‘remedy period’ – which runs from 2015 when the new pension scheme began to 2022.
Mr Uglow added: ‘If impacted by this choice, you need to consider whether you would have acted differently if you had been allowed to remain in the 1995 section.
‘For many, this chance to change their decision will be advantageous but that is not always the case.
‘Everyone’s circumstances are different so there are always things to consider – and not much time to deliberate the choice – so please ensure you are seeking the support of your financial adviser.’
Choice 2 revocation is not open to members who already moved their service as part of the original Choice exercise.
Survey to aid private doctors’ well-being
Questions for the survey will also consider awareness and acceptability of strategies and interventions to support workplace mental health.
Researchers aim to develop a range of resources and interventions, including downloadable guidance and two- to five-minute videos, to support clinicians in identifying work-related risks and taking preventative and supportive action.
Prof Jo Yarker, a psychologist and managing partner at research and consultancy organisation Affinity Health at Work, said: ‘Given the growing number of people using private healthcare due to long NHS waiting lists, private practitioners are under increased pressure and the need to support and protect their wellbeing has never been greater.
‘Research into the well-being of healthcare professionals is often
focused on the public sector and does not capture the nuances of working in the private sector – for example, running a profitable business, different governance structures and different patient demands when delivering a paidfor service.
‘Private settings are also typically smaller than their public counter-
parts and may have fewer support services available to clinicians.
‘Our project aims to identify aspects of the work environment that are considered most stressful, and target interventions and resources that help clinicians understand their personal workrelated risks and develop skills to manage these risks.
Research into the well-being of healthcare professionals is often focused on the public sector and does not capture the nuances of working in the private sector
PROF
JO YARKER
‘This will ultimately support their mental health and help healthcare professionals thrive in their work.’
Medical Protection Society (MPS)’s MPS Foundation has supported over 30 research projects worldwide since its 2022 formation.
To take part in the project, via an interview or survey, register your interest at www.affinityhealthatwork.com/current-studies/1759.
Psychologist Prof Jo Yarker
Doctor-centric group to open new outpost in Cambridge
By Robin Stride
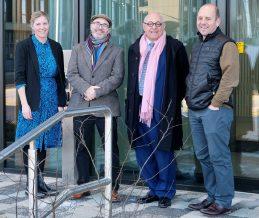
Private consultants and their partners have announced ambitious £55m plans to complete a ‘golden triangle’ of independent care facilities covering major university cities.
Welbeck Health Partners’ latest announcement is for a £25m centre to be opened in Cambridge next year as part of the group’s long-term strategy to operate regional day facilities across the UK.
This follows the unveiling of plans earlier this year to bring its brand to Oxford with a £30m development also due to come on stream in 2025.
Both are promising patients ‘an unrivalled healthcare experience’ and follow the success of the flagship OneWelbeck centre opened in London in 2019, which works with over 350 clinicians who see
more than 100,000 patients a year across a range of specialties.
Chief executive Andrew Chadwick-Jones said: ‘As one of the world’s leading locations for academic healthcare, selecting Cambridge for our newest practice was a natural fit for our model of partnering with world-class clinicians.
‘Geographically, Cambridge is close to our other centres in Oxford and London and completes the ‘golden triangle’ for us, meaning we can widen access to our services to more people across the south of England.’
Consultant urologist Mr Oliver Wiseman added: ‘I am thrilled to confirm we will be opening Welbeck Cambridge next year. We have ambitious plans to build a centre of excellence, delivering exceptional patient-centred care in a state-of-the-art facility.
‘Welbeck Health Partners oper-
(L-R) Katherine Friend, director, investment and asset management, Howard Group; Andrew Chadwick-Jones, chief executive Welbeck Health Partners; Peter Harper, chair Welbeck Health Partners; Mr Oliver Wiseman, consultant urologist, Welbeck Health Partners
ates in partnership with clinicians like me to harness their expertise and investment in the highestquality facilities for patients.
‘This means regional Welbeck centres like Welbeck Cambridge will be able to offer the most up-todate services and treatments based on the real wants and needs of local people. This approach helps us to better serve our patients and deliver an unrivalled standard of private healthcare.’
Welbeck has leased the new 32,000-square-foot Orion Building at property developer Howard Group’s Unity Campus and plans a range of medical services across more than 15 specialties, includ-
ing orthopaedics, heart health, digestive health, ENT, urology, gynecology and ophthalmology.
This is south of Cambridge city centre giving ‘excellent access from the M11 and ample parking’. Mr Chadwick-Jones called the site ‘a fantastic location’ due to the medical and scientific collaboration and innovation already happening on the Unity Campus.
‘We believe our commitment to delivering the highest standards of patient-centred care and cuttingedge technology and practices will help set us apart from other healthcare providers in Cambridge and have a positive impact on the local community.’
Welbeck’s Oxbridge plan part of its ethos
Welbeck Health Partners’ vision from the start has been to transform patient care through the use of new technologies to detect disease earlier and enable minimally invasive interventions, with the patient returning home the same day.
Consultants at Welbeck Oxford, in the north of the city, will offer 12 different specialties including heart and lung health, digestive health, ENT, endoscopy and neurology.
The success of OneWelbeck in London proved there was a growing demand for private healthcare that has a patient-centred
approach, according to chief executive Mr Andrew Chadwick-Jones.
He explained: ‘Oxford is a globally renowned hub for medical research and healthcare excellence.
‘We have been looking at expansion opportunities for some time and the quality of talent that already exists within the community of healthcare professionals in the city made it a desirable destination for us.
ner with the renowned Oxford medical professionals to improve the health provision in the local area, and develop Oxford as a health destination nationally and internationally.’
‘We have the ambition to part -
The group’s aim is to deliver the highest standards of patient care across the UK and internationally, which it believes starts with ‘partnering with world-class clinicians who truly understand the needs of their patients’.
Mr Chadwick-Jones said clinician partners invest and oversee the management and long-term strategy of the business. This allows them to make informed decisions on the services and infrastructure needed to best serve patients in their communities.
‘We believe our commitment to innovation, best practices and patient centered care will help set us apart in Oxford and we hope it will become the ‘go to’ private healthcare centre in the region, nationally and, in due course, internationally.’
Mr Andrew ChadwickJones
March of robots is shown in figures
By Douglas Shepherd
There is no turning back the march of the robots in private healthcare surgery, according to new figures from the Private Healthcare Information Network (PHIN).
These demonstrate what it calls ‘a dramatic rise’ in their number in the independent sector with a 928% increase between 2016 and 2022.
Across private healthcare providers and the NHS, there was a 341% combined increase and a record year is expected for 2024. Surgeons have performed nearly a quarter of a million (238,000) robot-assisted procedures over the
six-year period, with 49,000 in 2022 compared to 11,000 in 2016.
There were 48,000 roboticallyassisted procedures in the first three-quarters of 2023, the latest available data, so the UK is on track to register a record year when all the data is collected.
The number of robot-assisted procedures has risen every year since 2016 – except Covid-19affected 2020 – in both the NHS and independent sector.
PHIN said up to the end of 2022 nationally, robotic-assisted surgery was most used for prostate-related procedures at 43.7k. The next highest was for pelvic lymph nodes operations at 12.1k procedures.
In the same period, in the inde-
The London Clinic marks a private sector milestone
A patient with Parkinson’s disease has successfully undergone The London Clinic’s 100th deep brain stimulation (DBS). This milestone is a first in the UK private hospital sector.
Deep brain stimulation first appeared as a mainstream medical treatment in the 1980s and, since then, has been a developing area of research.
Lead neurogsurgeon Mr Erlick Pereira, who completed the operation nearly six years after he did the first surgery of its kind at the hospital, described DBS as a life-changing treatment for people
Mr Erlick Pereira (centre) and the DBS team at The London Clinic
with severe tremors, Parkinson’s disease and dystonia.
‘With a lot of degenerative diseases, there are no treatments available that can profoundly improve someone’s life immediately. The notion that, with neurosurgery, one’s function and quality of life can improve straight away is very satisfying, and exciting.’
DBS surgery involves implanting electrodes to the affected/damaged parts deep in the brain, which deliver high-frequency electrical current to address the abnormal movement patterns.
pendent sector, surgical procedures to restore the function of a joint were the most popular robotic-assisted procedure at 3.7k procedures.
Nuffield Health used robots the most (1.6k) for this type of procedure. HCA Healthcare UK carried out the largest volume of robotassisted procedures overall.
PHIN chief executive Dr Ian Gargan said: ‘Having robot assistance can aid accuracy with less invasive surgical approaches possible and we are seeing efficiencies with improved recovery rates, fewer complications and, therefore, opportunities to reduce waiting lists.
‘The robots are most often used
on the highest-volume procedures such as hip and knee replacements, so being able to use them to speed up procedures and reduce complications will help surgeons to conduct more of the types of operations most people are waiting for.
‘Looking at the trajectory in the growth of this type of surgery so far and knowing what is possible, we don’t see why there wouldn’t continue to be huge increases in the use of robotic assistants.’
Although robots are expensive, he believes private hospitals have the budgets to purchase them and ensure that as many patients as possible are treated as soon as possible.
‘I’ve recently been observing surgeons conducting robot-assisted procedures and, as an orthopaedic surgeon myself, I find the process fascinating and inspiring.
‘Overall, the surgical and economic benefits point toward greater use of robots imminently especially in orthopaedics and urology. As artificial intelligence develops, it can only further assist this valuable new technology.’
Surgeons and their teams at Nuffield Health Exeter Hospital have celebrated performing their 2,000th Mako robot-assisted surgical procedure.
The operation by orthopaedic surgeon Mr Jonathan Phillips was for knee replacement surgery.
He said: ‘It’s been an amazing journey over the last seven years to be a part of so many procedures and reach this milestone.
‘The opportunity to perform surgeries using the Mako robot is a
The surgical team at Nuffield’s Exeter hospital and surgeon Jonathan Phillips, centre, with their Mako robot
game-changer, improving the accuracy of hip and knee replacements. Our patients report better outcomes with faster recovery times, supporting their return to regular life.’
Mako uses a robotic-arm to remove damaged bone and cartilage and precisely position the new hip or knee implant. Surgeons create a bespoke 3D model using the robot’s software based on a patient’s anatomy from an in-depth CT scan.
Make it easier for users to feed back
By Agnes Rose
Independent practitioners wanting feedback from patients may need to give them more encouragement.
Private doctors are increasingly publishing patients’ views about their care on their websites and communications with customers – but it seems people are more likely to say what they think about commercial services and products than their health experiences.
More than half of people taking part in a survey (54%) said they found it easier to provide feedback about their experiences of commercial products and services such as hotels or meals, compared to providing feedback about health and social care.
Although over two-thirds (72%) of people said they felt health and social care services were a priority for them, only one in five said they
A quarter of patients think doctors would not listen to their feedback
had given feedback in the last two years.
When asked why they had not fed back about their experiences of care:
26% said they thought their feedback would not be listened to;
22% said they worried it would have a negative impact on their care:
21% said they did not want to cause a problem for the people caring for them.
People told the Care Quality
Commission (CQC) and health and care champion Healthwatch England (HWE) that sharing feedback about commercial products and services was less emotionally taxing (18%) and less personal (26%) than sharing about health experiences.
They felt feeding back commercially was often quicker and they had more available options to do so.
The research also found that many opted to confide in their family (15%) or a friend (14%) about a negative healthcare experience, but only 10% told the service directly.
The research came as part of a new Share for Better Care campaign launched by the CQC and HWE. They are working in collaboration with a variety of organisations including the Patients Association, Race Equality Foundation, National Dignity Council, Royal Association for Deaf people, National Voices, Challenging Behaviour Foundation, VoiceAbility and Disability Rights UK.
Although the campaign did not specifically ask about private patients’ experiences among the 2,000 people who took part, its backers say they aim to encourage everyone to give feedback on their experiences of care.
WHY HEALTH WATCHDOG AND CHARITIES SAY FEEDBACK IS IMPORTANT
Patients Association chief executive Rachel Power said: ‘We’d encourage patients and carers to share experiences of their care with the Care Quality Commission (CQC), whether those experiences have been good, middling or bad.’
She added: ‘Sharing poor experiences can provide essential warnings about a service where things might be going wrong, which would enable the CQC to take action. Good experiences offer insights into what a good service does.’
Jabeer Butt, chief executive of The Race Equality Foundation, said: ‘The research suggests that there are a number of reasons why people do not give feedback, but we would argue that at the core of all these reasons is trust.
‘If people trusted that they would be listened to, then they would feed back; similarly, if they trusted that they would not be disadvantaged, they would feed back.
‘We know trust is something that can be developed through clear communication, being transparent in the decision-making
process and putting people at the centre of how we organise and deliver support.
‘Our experience in working with people from Black, Asian and minoritised ethnic backgrounds is that trust is often the key to improving experiences of services. Hopefully, by developing trusting relationships, we will also do better in securing feedback from all.’
Jan Burns, chief executive of the National Dignity Council, said: ‘Feedback serves as a direct measure of the quality of care provided, offering insights into areas where improvements may be needed to ensure that all individuals receive care that respects their inherent dignity and fulfils their fundamental human right to being afforded kindness, respect and compassion.’
The CQC said in its most recent State of Care report that a combination of enduring difficulties linked to workforce retention and recruitment, poor capacity in services was restricting access and a challenging financial environment was risking unfair care developing into a ‘two-tier’ healthcare system.
This was forcing people into long waits for care unless they could pay for treatment sooner. The report also warned that this combination of challenges will further exacerbate existing heath inequalities and make people wait longer for care while their health deteriorates.
The research was conducted by One Poll in February 2024. It was a ‘representative national sample of 2,000 adults aged 18+ in England’. Share for Better Care runs until March 2025 and will have phases of activity over the next 12 months focusing on different audiences to increase awareness of the importance of feeding back about care experiences.
People are invited to share their care experiences at www.cqc.org.uk/give-feedbackon-care.
Deaf or hard of hearing and text relay: www.cqc.org.uk/contact-us/general-enquiries/ get-help-contacting-us-if-youre-deaf-or-hardhearing
Newmedica Leicester is a multimillion-pound eye clinic and surgical centre focused on supporting the NHS to help drive down waiting times.
The company is owned and led by four consultant ophthalmologists: Rishika Chaudhary, Rupal Morjaria, Li Jiang and Ricardo De Sousa Peixoto, alongside operations director Megan da Silva.
Clinical lead Mr Peixoto said: ‘We choose to use the highest-quality monofocal cataract replacement lenses for our NHS patients, reducing the likelihood of patients needing corrective treatment in the future.
‘This reduces costs for the NHS, allowing them to support other pressures and, most importantly, it means fewer patients going through the worry of avoidable treatment.’
Complaints by private patients rise by 13%
Private healthcare providers are experiencing a large rise in patients’ complaints about not managing their expectations and failing to communicate properly with them.
The Independent Sector Complaints Adjudication Service (ISCAS) has cited these types of gripes as key reasons behind a 13% increase in Stage 3 adjudication complaints for 2023-24 compared to 2022-23.
ISCAS’s complaints code Stage 3 adjudication gives dissatisfied complainants an independent review process with independent adjudication procedures.
During recent discussions between ISCAS, the Association of British Insurers and private health
PPU WATCH
Compiled by Philip Housden
Bath private hospital grows NHS patient capacity
Royal United Hospitals (RUH) Bath NHS Trust is investing in a £25m extension to its Sulis Hospital, which treats both NHS and private patients.
The new building, due for completion in late 2024, will create up to 100 new jobs and include two modular theatres, inpatient beds, seven extra day case pods and conversion of two existing theatres to laminar flow theatres.
Called the Sulis Elective Ortho-
Aesthetic doctors are bullish about future profits
Aesthetic practitioners have high hopes of a profitable year ahead, according to a major survey.
The economic climate may be tough but many respondents have revealed plans to expand their businesses.
insurance medical directors, Bupa reavealed invoicing complaints were rising and accounted for the highest percentage of overall monthly complaints.
Complaints about attitude have been the second highest complaint since last September, although reduced in January.
Alleged ineffective consultations and treatments had been on the decrease, but this year began to climb.
ISCAS reported that complaints about length of time to get an appointment remained steady, while complaints about cancelled or delayed appointments or treatments had the highest fluctuation range over six months of 4.6%.
And most say they are ‘fairly optimistic’ (51.6%) or ‘optimistic’ (36.3%) about their business prospects in 2024, with 80.1% saying they were on track to meet their objectives.
Accountants would, however, be horrified to know that as many as 48% of the more than 300 practitioners who took part admitted to having no business plan.
Of the 52% of people who had one, nearly three-quarters said it had changed from the previous year due to business growth, expansion, moving premises and increased economic benefits.
But others said they had changed their business plans due to moving direction, with a move towards
wellness being cited as one new avenue for business.
The Hamilton Fraser annual survey found around a quarter of respondents were relatively new to the aesthetic world, having been practising in it for less than three years.
Aesthetic practitioners motivations for doing this work included ‘giving people back their confidence’, ‘helping people feel better about themselves’ and ‘patient satisfaction’.
They cited growing market demand, diverse employment and entrepreneurial opportunities, and that having less stress than in the NHS had big attractions.
But some of the sector failed to meet up to expectations. They found they had too much competition from unqualified people, difficulty in getting enough clients, and not making enough money.
See the full report on page 21
paedic Centre, this will be an NHS elective surgery hub, serving patients from across the Southwest, delivering an additional 3,750 non-emergency, orthopaedic operations for NHS patients each year.
Around 60% of capacity will be used to carry out elective orthopaedic procedures that would otherwise be managed at the RUH’s main Combe Park site, with the remaining 40% available to support the wider region’s NHS elective recovery programme and future growth in demand from the ageing population.
Sulis Hospital director Simon Milner said: ‘This milestone enables us to continue offering exceptional healthcare to the wider community. Our agile approach means we can meet the growing demand for NHS healthcare while maintaining and growing our private practice.
‘Continuous investment in facilities and technology ensures high standards of patient-centred care.’
RUH acquired the former Circle Bath hospital in June 2021, with the objective of securing additional elective capacity for NHS patients in Bath and the South-west.
The acquisition has also enabled a significant rise in private patient revenues.
Trust private patient income before the acquisition was £585,000 – 0.2% of total trust income – and this has shot up to £16.1m, the 7th highest in England and highest outside London – 3.3% of total income, 6th highest in NHS.
Philip Housden (right) is director of Housden Group commercial healthcare consultancy
Mr Ricardo De Sousa Peixoto
Cancer care firm opens Surrey unit
By Douglas Shepherd
Cancer care provider GenesisCare has officially opened its new £30m centre in Guildford, Surrey – its 14th in the UK.
The centre and research hub, resulting from a partnership with the Royal Surrey NHS Foundation Trust, said it would provide patients with access to the latest treatment options for cancer, under the care of ‘top-class doctors and clinicians’.
Centre leader Jimmy Kwok announced: ‘We’ll be providing patients access to some of the most advanced diagnostic and radiotherapy treatments available and working closely with leading health professionals to deliver an outstanding personalised patient cancer care experience.’
Patients can access specialist services such as exercise medicine, a well-being programme and therapies including counselling, reflexology and acupuncture, delivered in partnership with the Penny Brohn UK charity.
Justin Hely, GenesisCare chief executive UK and Europe, said: ‘We’re delighted to be extending
Bupa recruits GenesisCare to expand its cancer units
Private cancer care provider GenesisCare has signed a new four-year agreement with Bupa which will see them working to expand radiotherapy and systemic therapy services for the insurer’s customers.
The new contract prioritises a range of initiatives including the further development and expansion of Bupa’s Cancer Specialist Centres network, set up in 2019 to help customers get a faster diagnosis and treatment at earlier stages.
Bupa’s specialist centres later expanded to include bowel and prostate cancer.
our partnership with Royal Surrey NHS Foundation Trust, a recognised centre of excellence for cancer.
‘Our new facility will offer innovative new treatments, novel therapies and clinical trials proven to deliver improved patient outcomes to cancer patients across the south-east of England.’
Louise Stead, chief executive of Royal Surrey NHS Foundation Trust, added: ‘We are very proud that our partnership with GenesisCare will provide private and eligible NHS patients access to new state-of-the-art treatment as we build on our position as one of the largest cancer centres in the UK.’
Bupa UK Insurance chief executive Alex Perry ( right ) said: ‘Cancer cases are on the rise in the UK. It’s estimated that by 2030, around 4m people will be living with the disease.
‘It’s vital that we continue innovating with our hospital partners to deliver life-changing improvements in cancer care through the further development of our Specialist Centres network.’
Plan to ape Singapore to ease GP shortage
Opportunities for private GP work in some areas could be frustrated under a think-tank’s blueprint to ease NHS pressures by allowing Singaporean doctors to prescribe medicines to British patients.
In a paper published by the Social Market Foundation, with a foreword from former health minister Lord Norman Warner, healthcare researcher Max Thilo identifies lessons for the UK’s healthcare system from Singapore’s ‘famously efficient and effective regime’.
As demand for GP services grows, he argues, the UK Government should consider liberalising pre -
scribing rights for Singaporean telemedicine providers and introducing Singaporean-style polyclinics in areas of England with poor access to primary care services.
Mr Thilo also calls for a shift from delivering acute services in hospitals to follow Singapore’s investment in polyclinics and lowcost telemedicine.
The polyclinics combine GP services with other healthcare offerings – such as diagnostic tests.
Singaporean polyclinics operate a ‘teamlet’ model, where patients with long-term conditions are cared for by a team comprising the
same doctor, two nurses and health co-ordinator.
Polyclinics have been explored in the past in the UK. Lord Darzi, a health minister in the Gordon Brown government, introduced polyclinics combining primary and some acute care. But the plans were abandoned in the early stages.
In his foreword, Lord Warner, health minister under Tony Blair, argues that the ‘time has come to revisit these ideas and draw on the experience of Singapore’.
Singapore-style polyclinics separate acute and chronic patients. This allows them to operate at
higher volumes. Doctors that cater for walk-in patients see 56 acute patients a day, during regular working hours. Polyclinics also drive down costs, it is said, by staffing the urgent care clinic with junior doctors.
Singaporean polyclinic doctors earn slightly more than the average English GP, but cost per appointment is lower in Singapore than in England.
The paper says Brits have increasingly been seeking out private care, as well as using international telemedicine apps to reach out to Singaporean GPs.
The purpose-built GenesisCare Surrey building was officially opened by (L-R) Justin Hely, GenesisCare chief executive UK and Europe; Dr Carla Perna, clinical oncologist and specialist adviser to the company, Jimmy Kwok, centre leader; the Royal Surrey NHS Foundation Trust’s chief executive Louise Stead and Joe Mills, the trust’s director of strategy
Infertility unit’s bid to help employees
By Olive Carterton
The world’s first IVF clinic, Bourn Hall, is joining forces with a charity’s Fertility in The Workplace (FiTW) initiative to help employers support staff experiencing fertility struggles.
Nearly eight out of ten (78%) people who have experienced fertility issues told Fertility Network UK they viewed fertility support or a fertility policy as very important when they were considering a new job or employer.
Clinic medical director and chief executive Dr Thanos Papathanasiou is confident Bourn Hall can help raise awareness of infertility and how it is treated.
He said while it was important for employers to make adjustments to support their staff, there was also a role for fertility clinics to be more supportive of people balancing treatment with work. Their help was needed so patients could keep ‘under the radar’ and not disclose their treatment if they wished.
Dr Thanos Papathanasiou
And he wants clinics to recognise the need for more flexible appointments and protocols to minimise the impact on a patient’s working day.
‘We talk to patients who don’t want to jeopardise their careers, so they are trying to make appointments and inject hormone medication in secret – all the while balancing a rollercoaster of emotions from hope to despair.
‘Additionally, some types of work can evoke emotional trig -
We talk to patients who don’t want to jeopardise their careers, so they are trying to make appointments and inject hormone medication in secret.
DR THANOS PAPATHANASIOU
more supportive working environment and retain staff.
‘If employers and managers are aware of what fertility treatments involve and what the outcomes can look like, they can better understand the associated stress and can create safe spaces for staff to talk in confidence.’
The FiTW initiative provides education and support packages to employers to help them develop pragmatic fertility policies that work for them and their staff, as well as providing effective signposting and well-being support.
It also offers one-to-one support to employees so they understand their workplace rights and how to approach their employer.
Until March 2025, due to Department of Health funding, these support packages are provided free of charge to small and medium enterprises across England.
gers. We see patients in professions such as teaching, midwifery and the police, where they work closely with children, often in distressing situations – and their managers have no knowledge of their personal trauma.’
FiTW co-ordinator Claire Heuclin said that flexibility to attend appointments and promoting greater understanding of what fertility treatment involves were two practical ways a fertility policy could help employers provide a
Fertility Network UK is also part of a Workplace Fertility Campaign Group convened by MP Nickie Aiken, who hosted a drop-in event for MPs at Westminster to raise awareness of the issues.
Dr Papathanasiou was there to provide insight into the clinical side of fertility treatments and Bourn Hall’s work with FiTW.
Ms Aiken is promoting a private members’ bill, Fertility Treatment (Employment Rights) Bill, which would give employees a legal right to take time off for fertility appointments.
Chance for doctors to air views on training
Doctors are being quizzed for the GMC’s annual medical training in the NHS survey with questions covering topics such as discriminatory behaviour, the quality of teaching, supervision and experience, and the impact of incivility and rudeness.
Consultants involved in NHS postgraduate medical training have until Thursday 2 May to take part in the study which last year attracted responses from 70,000 doctors across England, Northern Ireland, Scotland and Wales. Doctors are being urged to share, in confidence, their experience of workplace learning, support and supervision.
The GMC said this would pro -
vide an unparalleled picture of what is working well and what needs to be improved, enabling medical education bodies and employers to make sure that trainers and trainees are supported in their roles.
Answers to multiple-choice questions are published anonymously as aggregated totals. To further protect identity, results in departments with fewer than three responses are not reported.
Last year’s survey included questions on doctors’ experiences of discrimination for the first time. The results showed that most doctors in training said they worked in supportive environments.
But over a quarter said they had
experienced micro-aggressions, insults, stereotyping, negative comments or oppressive body language from colleagues.
Prof Colin Melville, the GMC’s medical director and director of education and standards, said: ‘This is an important opportunity for all trainees and trainers to tell us about their experiences. The
The GMC runs the national training survey every year to gain a picture of the experiences of doctors in training and of trainers
information they provide is key and goes a long way to ensuring the continued high quality of medical training in the UK.’
The survey is optimised for mobile phones and tablets and should take around 20 minutes to complete. There is also a shorter five-minute survey designed specifically for trainers.
Bourn Hall Clinic medical director
A look back through our journal’s archives of a decade ago reveals that although times change, some issues are not so new
A trawl through the archives: what made the news in 2014
Sell-off shock for HCA
Consultants, staff and management at HCA’s The Wellington and new £33m Platinum Medical Centre expressed indignation after the competition body gave the company a ‘Sophie’s Choice’ ultimatum.
In its long-awaited final report, the private healthcare market inquiry group ruled that HCA bosses should choose between sacrificing the London Bridge and Princess Grace hospitals or selling off the UK’s largest private hospital (The Wellington) plus its flagship diagnostic and outpatient centre instead.
The first two were already under threat of a forced sale by the Competition and Markets Authority (CMA) – formerly the
Competition Commission. But the sudden addition of the St John’s Wood hospitals came as a complete shock.
And that soon turned to disbelief when it was learned that BMI, the largest hospital group, had pulled off a great escape by not having to sell seven of its hospitals after all.
HCA vowed to fight the decision all the way through the courts, saying it was confident it would win.
It declared business as usual –including £120m of planned developments over the following two years, which would see London Bridge expand into London’s landmark building The Shard.
Company president and chief executive Michael Neeb fumed: ‘HCA legally acquired these hospitals, in the case of the London Bridge with explicit approval by the OFT, yet now after millions of pounds of investment, it is being forced to sell.
‘The CMA’s main allegation appears to be that HCA is too successful, too efficient, too innovative. It wants to punish HCA for that success.’
The future of Harley Street
Marketing experts were developing two new initiatives to promote the ‘Harley Street’ and the ‘London’ brand to overseas patients who would consider travelling for medical treatment. Ideas to promote London
aggressively as a world centre of private care were thrashed out at a summit on the future of Harley Street attended by many of the big players in private practice. It was hoped the initiative would help combat growing overseas competition around the world, which was hijacking thousands of potential patients who might otherwise have come to see consultants in the UK.
Tax officials get power to drain bank accounts
Doctor taxpayers’ bank accounts could be drained without prior notice under HM Revenue and Customs’ new power to recover unpaid tax unveiled in the Budget. Consultants and private GPs owing large amounts of tax would previously be chased by HMRC debt recovery officers and, if officials were unsuccessful, they
would then have to commence proceedings in court and obtain an order before being able to seize a taxpayers’ assets or cash.
But officials followed new policies similar to some payday lenders in reserving the right to drain bank accounts without warning.
Sale of goodwill is evaporating
Selling goodwill in medical practices was coming under the spotlight.
Tax inspectors had been arguing that goodwill for professionals, including doctors, did not exist, as it was entirely personal.
But this view was completely different to that held in many other developed areas of the world and particularly the US, where there was very active trading in medical practices, with sales of both free and personal goodwill.
• Contractual cover, not discretionary
• Private hospital recognised
• Protection after retirement included
• Cover for GMC matters
• In-house medico-legal support 24/7
• £10,000,000 limit as standard, more if required
• Zero excess option
• Reputation protection
• Medico-legal reports cover
• All specialties accommodated
• Trainee and NHS policies available
• Multiple policy/insurer schemes
• Company and Group
options
How the Budget will affect you
The Chancellor announced his Spring 2024 Budget, no doubt with one eye on the upcoming General Election. He did not announce any major policy changes, leading to speculation that there may be a further mini-Budget before voting day.
Time will tell if any significant tax changes are announced in the coming months, but Alec James meanwhile provides a summary of the key points from Jeremy Hunt’s latest address at the dispatch box
Tax rates and bands
As in in the last few Budgets, income tax rates and lower tax brackets remain unchanged for 2024-25.
The exception, of course, being that, from 6 April 2024, the additional rate of income tax now takes effect with earnings over £125,140 – previously £150,000. It had already been announced in the January 2024 Scottish Budget that the additional rate of tax would be increased from 45% to 48%.
The personal allowance, which was last increased from 6 April 2021, remains unchanged.
Many have seen that while there has been no increase in the tax rates, the freezing of the bands and personal allowances at a time when inflation has been running far higher than it has in the past means taxpayers are subsequently worse off.
National Insurance
Nearly all doctors will see a further 2% reduction in National Insurance contributions from 6 April 2024. Many of you will recall that a 2% reduction was announced at the end of last year and took effect from 6 January 2024.
For those whose primary source of income is from employments, from 6 April 2024 the main rate of Employee National Insurance contributions will be 8%.
For those whose primary source of income is from self-employed income, from 6 April 2024 the main rate of Class 4 National Insurance contributions will be 6%.
You may recall that changes to the Class 2 National Insurance limits had already been announced prior to the Budget.
With effect from 6 April 2024, while Class 2 National Insurance contributions exist, they will primarily be used to allow those with modest self-employed income to make voluntary contributions.
Therefore, most self-employed doctors will not need to make any Class 2 National Insurance contributions going forwards.
As with the tax brackets, the National Insurance brackets remain unchanged from 6 April 2024.
For most higher-rate taxpayers, the changes in National Insurance
The Budget can present some excellent planning opportunities, depending on your circumstances, and discussing your affairs with a specialist medical accountant could reap rewards
The sale of a residential property that is not your main place of residence is subject to capital gains tax (CGT).
In the Budget, it was announced that higher rate CGT on these gains will be reduced from 28% to 24% from 6 April 2024.
The other CGT rates remain unchanged. With mortgage interest rates rising, this may present an opportunity to sell buy-to-let properties, locking in lower rates of CGT and avoiding rising interest costs.
payers will be eligible to retain the benefit and those falling in between the two rates will taper at a slower rate.
Non-domiciled taxpayers
The rules for those considered as non-domiciled will change in April 2025 with new residence basis rules.
will result in an extra £1,300 in your ‘take home pay’ for 2024-25 compared to 2023-24.
VAT
Many doctors will have a form of income which is considered a taxable supply for VAT purposes. This includes sources such as medicolegal work.
In the Budget, it was announced that the VAT registration threshold would be increased from £85,000 to £90,000 with effect from 1 April 2024. The deregistration threshold has also been increased but to £88,000.
This marks the first increase in the VAT thresholds since April 2017.
Many doctors choose to limit their ‘VATable’ income sources to below the threshold to avoid the administrative burdens of being VAT-registered. The increase may allow for a little growth in this regard.
For those that do exceed the threshold for registering for VAT, there are various VAT schemes available that help reduce the administrative burdens.
These include ‘Flat rate’, ‘Cash basis’ and ‘Annual’ accounting. Discussions with a medical specialist accountant can help you identify if one of these schemes would work well for your business if you were required to register for VAT.
Properties
There were a number of changes announced in the Budget in relation to residential property ownership. These were announced in an attempt to alleviate the housing shortage, by making available more homes and increasing the terms of lets.
If you do choose to sell a buy-tolet property, it is important to remember HM Revenue and Custom’s (HMRC’s) strict reporting rules. Within 60 days of completion on the property sale, you must calculate and pay any CGT.
The Chancellor has abolished the reliefs and preferential treatment relating to furnished holiday lets with effect from April 2025 and Multiple Dwelling Relief for Stamp Duty Land Tax (SDLT) will be abolished from 1 June 2024, although, the relief may still be available for contracts exchanged before 6 March 2024.
These changes primarily relates to property that can be shown to be separate units. This applies to flats but also to high-value properties with two or more main entrances and separate living areas, such as annexes or ‘granny flats’.
Child Benefit
While not applicable to most senior doctors, those who are parttime or are registrars with children, the High Income Child Benefit Charge (HICBC) threshold has been increased.
Previously if the parent or highest-earning cohabiting parent had ‘adjusted income’ in excess of £50,000 and if either cohabiting parent was claiming Child Benefit, the higher earner was subject to HICBC.
This results in the individual paying a proportion of the claimed benefits back. Those whose threshold income was £60,000 or more were fully tapered, meaning all child benefits claimed had to be repaid with their self-assessment tax liability.
Thresholds will be increased from 6 April 2024 to £60,000 and £80,000 meaning many more tax-
New non-domiciled taxpayers arriving in the UK will still benefit for the first four years of 100% tax relief on foreign income and those existing non-domiciled tax payers will be transitioned to the new rules.
HMRC has described the new rules as a ‘modernised regime that is simpler and fairer’.
Annual allowance and lifetime allowance
While not announced in the Budget, various changes were announced last year in relation to pension savings annual allowance, increasing the annual allowance threshold from £40,000 to £60,000 and the aligning of the Consumer Price Index rates applied by NHS Pensions with those allowed by HMRC.
This will hopefully alleviate annual allowance tax charges for many doctors and allows for additional pension planning, particularly for those who work primarily in the private sector.
It was also announced that the lifetime allowance would be abolished by 5 April 2024 and replaced by the lump sum allowance. The lump sum allowance is currently £268,275 or 25% of any lifetime allowance protections you have in place.
With that in mind, within some of the publications that were published after the Budget was a deadline for claiming individual protection 2016 (IP2016). The deadline has been set as 5 April 2025.
The Budget can present some excellent planning opportunities, depending on your circumstances, and discussing your affairs with a specialist medical accountant could reap rewards.
Alec James (right) is a partner at Sandison Easson & Co, specialist medical accountants
TROUBLESHOOTERS
What to do if referrals
Independent Practitioner Today has called in private practice troubleshooters
Sue
O’Gorman
and Hannah Browning (right) to help doctors’ deal with the big questions affecting their business’s future
QI have been in private practice for several years, but the patient volumes have plateaued. I am willing to invest some time to review and understand my practice in more detail but don’t know where to start.
AAs a consultant, time is often in short supply. It is, therefore, even more important to understand what to look at within your practice to get the most out of your review.
Your practice should be looked at holistically, not just with a view to increasing the volumes of patients you see. There may be other aspects within your practice that are not working well and, by changing them, you could improve your experience or that of your patients.
Mystery shop
It is important to understand, in the first instance, if you are capturing every opportunity that is currently being generated. For some consultants this is a real quick win. Ask a friend or family member to call your practice at different points in the day – on a variety of days – and with the brief that they are looking to book an appointment but need some extra help to see if you are the right consultant.
1. Was the phone answered?
2. Was the secretary able to give relevant information about you and your practice?
3. Did they offer to book you an appointment?
4. How was the service; did it reflect how you would like to be portrayed?
Now do the same via email or a contact form on your website.
1. How long did the response take?
2. Did it provide all the info rmation that you would expect?
3. Was there an offer to book an appointment?
4. Did the response look and feel professional?
It is important to be impartial and critical when undertaking this process. The aim is to improve your practice and, by making some simple changes, it could have a big impact.
What
to do if your phone or emails are not being answered
Have a chat with your medical secretary to understand their workload and priorities and how these may vary from your expectations.
It might be that you can streamline or automate some of your practice functions that would enable your secretary to have more time to answer the phone.
Ultimately, the incoming inquiries to your practice are what will make it grow. This must be a priority and if your current secretarial service doesn’t support this, there are other options.
There are companies that are trained in taking healthcarerelated calls and make appointments. From a patient’s perspective, they are an extension to your practice.
The call team will work closely with your secretary to ensure streamlined flows of patients, giving you the reassurance that every inquiry is captured.
You have now established that your phone is being answered and are happy with the front-end patient experience. You can now look at extending the opportunities to grow referrals.
When was the last time you reviewed where your patients are coming from?
Your patient administration system should be able to create reports based on the referrer. This information will highlight which GPs, physios or surgeries refer to you most. Create a report that looks at the month-onmonth activity over a 12-month period. This will then show you which referrers have grown and those that have declined. If a surgery’s numbers have declined, then look at making contact with them or giving them a personal follow-up on a specific patient.
referrals start falling off
Ultimately, the incoming inquiries to your practice are what will make it grow. This must be a priority and if your current secretarial service doesn’t support this, there are other options
It may be that they have had staffing changes, and a reminder that you are available to answer queries is useful and relevant.
As well as looking at the referrer, reports should be generated to see which payer groups you see. This may highlight any issues with insurers or a particularly low result with self-pay may guide you towards a review of your fees.
How patients book with you is also relevant
Are they being generated through your website, via the hospital sales team or directly through your secretary?
Going to see the hospital sales team is always a good use of time. Offer to give a ten-minute overview of what you do and the types of patients you see.
This will help the team to be informed of your services and give them an opportunity for them to ask questions and to build your relationship with them.
You might have profiles on review websites, if you are paying for these services, so it is good to understand if they are generating referrals. Ensure you have the right processes in place to maximise the benefit from reviews.
Put in place processes that proactively ask patients to review your services and ensure that any post – positive or negative – gets a timely response.
Check any online profiles, this includes hospital websites and your Bupa profile.
Do you still hold all the posts and memberships?
Do you refer to any dates –‘Recently’, ‘in 2001’ and so on –that need updating or removing?
Is it clear the types of patients that you would like to see and what you specialise in?
Is there a photo that is good quality and recent?
Are all the contact details correct?
Try reading your profile from a patient’s perspective and ensure that you use language that is easily understood. Keeping your profile updated and fresh will help to attract patients.
Google a treatment or procedure that you offer and your location, and see how hard it is to find you.
For the consultants that come higher on a search result, what are they doing that you don’t?
Having a website is not a tickbox exercise. If you would like your website to generate referrals, then the site needs to be optimised and have new content added to it regularly.
Be clear with the marketing company – marketing is a specialist skill and one that should be outsourced – what your expectations are. They will be able to advise you on the best way to generate referrals and the cost.
Once you are making an investment, keep track of it each month to help monitor your return.
If you are not seeing the number of inquiries being generated after three to six months, then a new marketing strategy should be created. Taking control of this process will help you to understand your business better.
Protecting regular time within your diary to review and update your practice is an important routine to get into.
Each month, focus on a different area, but also remember to check that any amendments made previously are continuing to work and have a positive impact.
Sue O’Gorman is director of Medici Healthcare Consultancy.Website: www.medicihealthcareconsultancy. co.uk. Email: sue@medicihealthcareconsultancy.co.uk. Hannah Browning is director of Beyond Excellence Healthcare Consultancy. Website: www.beyondexcellenceconsultancy.co.uk. Email: info@ beyondexcellenceconsultancy.co.uk.
Brush up on guidance for expert witnesses
THE GMC’S new guidance on Providing witness statements or expert evidence as part of legal proceedings is a more wide-ranging version of Acting as a witness in legal proceedings (2013) and took effect on 30 January 2024.
The GMC’s intention is to explain the different ways that doctors can assist the justice system and to set out the relevant good practice principles.
At 18 pages, the new guidance is more detailed than its predecessor and while some content may be familiar to doctors who undertake medico-legal work, it’s a good idea to know what the regulator expects of professional and expert witnesses.
While this guidance does not specifically apply to non-statutory inquiries, such as an adverse incident investigation in your private hospital, the GMC still expects you to be guided by its general principles and repeats this point in paras 16-17. We also recommend seeking specific advice from your medical defence body in this situation.
Ten key principles (para 12)
The GMC has expanded on the general principles in its previous guidance. These apply to all doctors whatever their role in legal proceedings and are summarised below:
1 Act with ‘integrity, honesty and objectivity’.
expertise or direct knowledge. If required to answer, do so to the best of your ability and be clear about the limits of your knowledge.
8 Do not allow your relationships or opinions to affect your objectivity.
9 Manage conflicts of interest in line with the relevant GMC guidance and legal rules.
10 Reflect on learning points that arise from your participation in legal process.
Different roles
To supplement the new edition of Good Medical Practice, the GMC has also updated its professional standards guidance in seven areas. In this series, the MDU’s Sally Old (right) looks at what has changed. She starts with witness statements and expert evidence
Introduction (paras 3-7)
The GMC sets the scene by summarising that a doctor’s role in legal proceedings is to provide ‘factual, honest accounts of events and objective and impartial advice if giving an expert opinion on matters within their competence and experience’. It notes that the ‘quality and reliability’ of their evidence can make a significant difference to the outcome.
Defining
legal proceedings (paras 8-9)
While the GMC’s previous guidance focused on courts and tribunals, the new guidance has a broader scope. Besides civil claims, criminal cases and inquests/fatal accident inquiries, its definition of legal proceedings also includes:
Court applications for a legal ruling – for example, on patient capacity;
Tribunals including fitness-topractise hearings;
Statutory public inquiries with evidence-gathering powers;
Regulatory and investigatory bodies with evidence-gathering powers.
2
Take steps to understand the process, time-scales and your legal obligations including the handling of confidential information. The guidance includes a section with further resources from other organisations and relevant legislation, court rules and directions for all UK countries.
3
Respond promptly to requests, take practical steps to meet agreed deadlines and attend meetings and hearing when required.
4
Ensure evidence is ‘accurate and not misleading’ by taking reasonable steps to check and including all relevant information.
5 Use language and terminology that can be understood by someone without medical training, provided it is possible to do so without misleading, and explain terminology.
6 Stick to matters within the limits of your professional competence or where you have relevant knowledge and be clear about what is fact and what is opinion.
7
Explain and decline to comment on areas outside your
As before, the GMC guidance differentiates between being a witness of fact/professional witness and being an expert witness. In addition to the general principles above, it sets out the specific responsibilities for each when giving evidence.
Witness of fact/professional witness (paras 13-17)
This role is to help establish the facts in legal proceedings by providing a statement or oral evidence about your clinical findings and observations and decisions based on contemporaneous notes and clinical records as much as possible. If asked to comment on the actions of others, ‘this should be limited to matters which you have direct knowledge of’.
Expert witness (paras 18-34)
Expert witnesses use their specialist expertise and experience to give an impartial medical opinion on issues like the standard of care someone received or the patient’s condition and prognosis. It’s an attractive option for independent practitioners looking for another intellectual challenge or to boost their finances alongside their clinical work or after retirement. At the same time, expert wit -
nesses can find themselves under scrutiny.
In a previous MDU analysis of cases in which expert witness members sought our support, problems included complaints about the expert’s demeanour and attitude, the nature of their examination, that they had changed their view or that their report had contained inaccuracies.
The GMC covers the responsibilities of expert witnesses in some depth in the latest guidance, starting by emphasising the need for training to develop the necessary practical knowledge and competencies for the role, such as familiarity with relevant guidance, how to write an expert report that is fit for purpose and giving effective oral evidence.
It expects you to consider in each case whether you have the knowledge training and experience to assist the court.
We advise you to familiarise yourself with the new GMC guidance and seek advice from your defence body if you have any specific concerns.
OTHER HEADLINES IN THIS SECTION OF THE GUIDANCE ARE:
You have a duty to the court to be objective and impartial, which overrides any obligation to those who first instructed you.
Ask for clarification if your instructions are unclear so you can best assist the court. You should also check the position with the lawyer who instructed you if it’s not clear whether you have received all relevant evidence to form an opinion, including statements and reports from other parties.
If you are asked for an opinion on someone without being given the opportunity to consult with or examine them, you must explain the limits this puts on you and be able to justify your decision to proceed in this situation.
While the previous guidance refers to ‘a possible conflict of interest’, the GMC now says you must carefully consider whether there is any ‘potential or actual conflict of interest that may affect or call into question your ability to provide independent objective evidence’. You should tell the instructing lawyer about this without delay and only continue with their written assurance that this is acceptable.
You must be able to state the facts or assumptions on which your opinion is based; summarise the range of opinion on an issue and how you arrived at your view; and be clear if you don’t have enough information to reach a conclusion or your opinion is qualified.
Tell the instructing lawyer straight away if you change your view so they can inform others, including the court, if appropriate.
Respect the contributions of other experts and raise any concerns – for example, about their objectivity –with your instructing lawyer.
Make accurate notes when interviewing or examining parties in a case and seek advice from the instructing lawyer or your medical defence body if you identify a risk to their current health or safeguarding concerns.
Follow the GMC’s guidance on confidentiality and disclosure, including the requirements not to disclose anything covered by legal privilege. Seek advice from instructing lawyers or the court if you are concerned about pressure to make an inappropriate disclosure or believe information has been sent to you without patient consent.
You must have appropriate and adequate indemnity for expert witness work. Contact your medical defence body or indemnifier if you are unsure.
Diagnostic Audiology Including Paediatrics • Tinnitus Rehabilitation • Vestibular Testing • PTA & Tympanometry • Speech Audiometry • Speech In Noise Testing• Specialist Tests Including OAE, VEMP & ASSR • Ear Wax Removal • Independent Hearing Aid Provider
PRIVATE SECTOR MARKET DATA
The latest trends in private care activity
data from the Private Healthcare Information Network (PHIN) shows what was keeping independent consultants busy as self-pay admissions fell while insured admissions increased
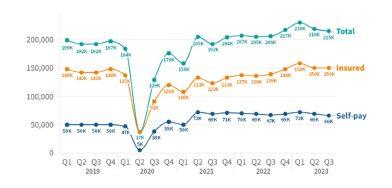
TRENDS IN the private healthcare sector identified by the national body tasked with pulling together the data show private admissions rose 4% across the UK by the end of quarter three in 2023 compared to the same period in 2022.
Self-pay admissions fell slightly to hit their lowest level since the pandemic, but private medical insurance admissions rose.
On course for record independent healthcare inpatient admissions in 2023
As predicted by a number of commentators and observers last year, PHIN’s figures confirm that the private sector is on course for a record year with more admissions than ever.
There were a total of 9,000 admissions, 4% higher than the same quarter in 2022, although the numbers have dropped in each quarter in 2023.
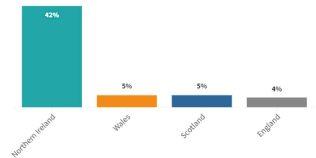
PHIN reports that the number of
admissions in Northern Ireland rose by 42%, the highest increase by far of any nation. Wales and Scotland were 5% up and England was 4%.
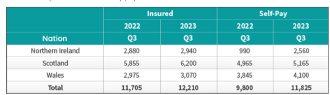
Private medical insurance
admissions remain high, but self-pay admission down to lowest levels post-pandemic
INSURED ADMISSIONS
The number of admissions paid for with private medical insurance stayed at the second highest level in PHIN records. There were 11,000 more insured admissions than in the same period in 2022 (8% increase).
Compared to Q3 2022, the number of admissions using private medical insurance rose in every English region except the Southwest, where they remained the same. They also rose in Scotland (+6%), Wales (+3%) and Northern Ireland (+2%).
The biggest rise in England came in the North-east (13%) and East Midlands (12%).
The largest rises by volume were in London (4,560) and the Southeast (1,775).
SELF-PAY ADMISSIONS
PHIN says: ‘Self-pay admissions were down by 1,000 (-1.5%) in Q3 2023 compared to Q3 in 2022. This is, in itself, only a small decline, but it means that selfpay admissions were at their lowest levels since before the pandemic.
‘Admissions financed by self-pay fell in every English region. The biggest percentage fall in England came in the South-west (10%) and London (-9%).
‘Those regions also had the largest fall by volume.
‘Self-pay continued to grow in the devolved nations: Northern Ireland (159%), Scotland (4%) and Wales (7%).’
PERCENTAGE CHANGE FOR ADMISSIONS FROM Q3 2022 TO Q3 2023
NorthernIreland
ADMISSIONS BY ENGLISH REGION BY PAYMENT METHOD
ADMISSIONS BY DEVOLVED NATION BY PAYMENT METHOD
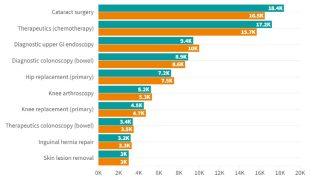
TOP TEN PROCEDURES
PHIN found the biggest increases by volume in admissions in the Top Ten procedures were for diagnostic upper GI endoscopies. These rose by 600 (6%). The next biggest volume increase was in hip replacement (primary) at 300 (4%).
Reports PHIN: ‘The biggest decrease was in cataract surgery which was down 1,900 (ten per cent). “Therapeutics – chemotherapy” also had reduced admissions, it was down 1,500 (8%). Patients require multiple admissions for
➱ continued on page 20
Cataract surgery
therapeutics (chemotherapy)
Diagnostic upper GI endsocopy
Diagnostoc colonoscopy (bowel)
Hip replacement (primary)
Knee arthroscopy
Knee replacement (primary)
Therapeutics colonoscopy (bowel)
Inguinal hernia repair
Skin lesion removal
TOP TEN PROCEDURES
Self-pay admissions were at their lowest levels since before the pandemic
chemotherapy and the number varies depending on their health and the type and stage of cancer.’
MARKET TRENDS
There was:
a 123% increase in peripheral nerve blocks;
a fall (-37%) in paravertebral blocks;
a 72% increase in diagnosticsblood test.
A trio of cosmetic surgeries – rhinoplasty (28%), breast enlargement (20%) and breast implants (19%) – were also down.
Since cosmetic surgery is nearly always paid for by self-paying patients, PHIN suggests the fall in these could be related to the fall in self-pay admissions.
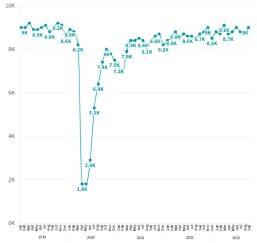
CONSULTANT NUMBERS
Active consultant numbers in private healthcare regularly fluctuate
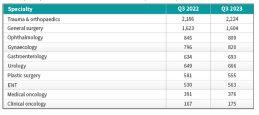
PHIN found the largest increase in active consultants in the Top Ten procedure groups was in gastroenterology, with an extra 59 consultants (9%)
Active consultants in private healthcare
Quarterly comparison of active consultants for the top ten PHIN specialties
and were down 240 (5%) from Q3 2022 to Q3 2023.
At the end of the quarter (September), there were 9,000 active consultants.
The data body found the largest increase in active consultants in the Top Ten procedure groups was in gastroenterology, with an extra 59 consultants (9%).
It says three procedures: Ophthalmology (-36), Plastic surgery (-26), Medical oncology (-15) shared the biggest decrease at 4%.
PATIENT DEMOGRAPHICS
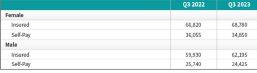
Volume of admissions by sex and payment method
There were more insured admissions and fewer self-paid admissions for both sexes compared to the same quarter in 2022.
The drop in self-pay was more pronounced for male admissions at 1,315 (-5%) compared to 1,205 (-3%) for females.
The growth in insured admissions for males was 2,265 (5%)
compared to 1,960 (3%) for females.
Volume of admissions by age
There was an increase in admissions in all age groups except for 20-24 and 70-74 (See graph below).
☛ All data described above taken from PHIN’s unique, national private dataset describing discharge activity (day case and inpatient).
This excludes activity outside of PHIN’s mandate from the Competition and Markets Authority, such as outpatient diagnostics and mental health.
PHIN said: ‘There is a time lag between collecting, validating and processing the data we receive from hospitals before we can publish it. This can be up to six months after treatment has been completed, to ensure a fair process and accurate data.
‘Activity numbers have been rounded to the nearest five, with percentage based on the unrounded figures.’
of admissions by sex and payment method
of admissions by age
Volume
Volume
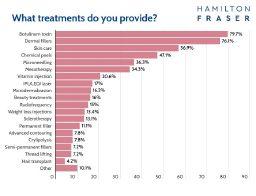
What’s happening in aesthetic medicine
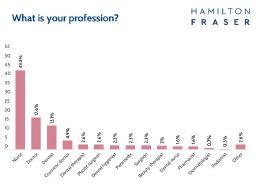
Insights into aesthetic industry trends and practices have been revealed by over 300 practitioners in the UK and Ireland who took part in an annual survey from cosmetic insurance services provider Hamilton Fraser
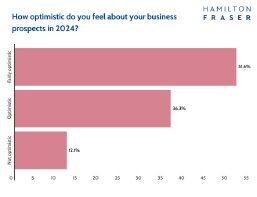
AESTHETIC PRACTITIONERS are displaying the cheery face of optimism for their businesses in the months ahead.
Findings of a survey revealed that despite the current economic climate, many have plans to expand their businesses and the majority feel ‘fairly optimistic’ (51.6%) or ‘optimistic’ (36.3%) about their business prospects in 2024. And eight in ten of them reckon they are on track to meet their objectives.
Perhaps surprisingly, only 52% admitted to having a business plan, but 70% of them said it had changed from the previous year due to business growth, expansion, moving premises and increased economic benefits.
The survey organisers comment that it is interesting to see that others said they had changed their business plans due to moving direction. A move towards wellness being was cited as one new avenue for business.
Evolving landscape
Eddie Hooker, founder and chief executive of Hamilton Fraser, explains the annual survey sheds light on the evolving landscape of aesthetics and serves as a compass for his company to ensure its services safeguard practitioners, their patients and the integrity of the care they provide.
‘Highlights of this year’s survey for me included the growing demand for regenerative procedures and preventative treatments, and we are committed to tailoring insurance solutions that align with these emerging trends,’ he says.
➱ continued on page 22
COMPLICATIONS AND COMPLAINTS
81% of poll participants said their patients had never experienced an infection following a treatment. 19% said this had happened once or twice, and only 0.3% admitted to infections occurring more than twice.
The majority had on more than one occasion said no to patients whom they deemed unsuitable for treatment. 31% had turned a patient away once or twice, and 25% had said no to treating unsuitable patients more than three times. Only 13.7% said they had never turned a patient away.
Did they ever regret treating a patient? The response was almost a 50/50 split, with 48% saying ‘yes’ and 52% saying ‘no’. Of those answering ‘yes’, the main reason given was that they felt the patient had unrealistic expectations of treatment.
Practitioners also stated body dysmorphia, patients wanting treatments for low costs, difficult or demanding patients and gut feelings as other reasons to say ‘no’.
91.5% routinely looked out for patients displaying any mental health problems, in particular, body dysmorphia, with questionnaires and screening during consultation being the main methods of analysis.
‘The insights into how practitioners are operating their businesses, their motivations and the industry dynamics at play also provide us with valuable insights to enhance our support for the aesthetic community, especially when it comes to our event, the Aesthetics Business Conference (ABC) – www.aestheticsbusinessconference.co.uk
‘We have a long history of working closely with the Joint Council for Cosmetic Practitioners (JCCP) and so I was pleased to see that the survey results reflected a commitment to patient safety, with 80.7% reporting no post-treatment infections and practitioners turning away unsuitable patients based on criteria like body dysmorphia and unrealistic expectations.’
He was also pleased to see that 91.5% of practitioners actively monitored for mental health issues – ‘emphasising our collective responsibility for holistic care’.
Findings of a survey revealed that despite the current economic climate, many have plans to expand their businesses and the majority feel ‘fairly optimistic’ (51.6%) or ‘optimistic’ (36.3%) about their business prospects in 2024
A large proportion of practitioners wait some years after qualifying before choosing to work in the sector. Many told the survey they still worked for the NHS (50.7%) or in other jobs and did aesthetics part-time, with 69.6% saying aesthetics was not their main source of income.
Flexible working hours
So why do they do it? Interest in non-surgical cosmetic treatments was cited as the main reason for moving into aesthetics, with 59.8% giving this as the top answer.
A new challenge and flexible working hours were the next big gest motivators, with 53.9% and 53.3% saying this was what drew them to the field.
Job satisfaction also came in high, with more than half (50.3%) stating this as their reason. Financial reasons were listed by 32%.
When asked if their motivations for joining the industry had been met, a third said ‘completely’ and just over half answered ‘mostly’. Reasons given for motivations having been met included: Entrepreneurial opportunities; Giving people back their confidence; Helping people feel better about themselves;
SURVEY HIGHLIGHTS:
87.9% said they were ‘fairly optimistic’ or ‘optimistic’ about their business prospects in 2024
69.6% said aesthetics was not their main source of income
Half of practitioners still worked for the NHS (50.7%)
Of those who had left the NHS, 24.8% would not consider returning due to a lack of work-life balance and flexibility, antisocial hours and stress
81.2% said their motivations for joining the industry had been ‘completely’ or ‘mostly’ met
The top trends are regenerative procedures, such as polynucleotides and exosomes, ‘prejuvenation’ preventative treatments for younger patients, new applications for RF microneedling and weight loss injections
Injectables were the most popular treatments offered with botulinum toxin and dermal fillers topping the poll
More than 85% had turned patients away if they felt they were unsuitable for treatment, citing body dysmorphia and unrealistic expectations as the top reasons
91.5% said they routinely looked out for patients displaying any mental health problems.
More than 85% of practitioners had turned patients away if they felt they were unsuitable for treatment, citing body dysmorphia and unrealistic expectations as the top reasons
AESTHETIC PRACTITIONERS: WHO ARE THEY?
Nurses made up the largest group of respondents (43.5%), followed by doctors/cosmetic doctors (22.5%), dentists (13.1%), dental therapists (2.6%) and plastic surgeons (2.6%). 74.8% were female and 24.8% were male.
They were fairly evenly spread geographically with the highest percentage (17%) based in London, then North-west (12%), South-east (11%), North-east (10%) and Yorkshire and The Humber (9.5%).
Just over a third of respondents owned their own premises, while 27.5% worked from a clinic within their home.
A further 20.9% practised from someone else’s clinic, while 16% operated from a beauty salon and 11.8% were mobile. 8.2% were based within a private hospital.
Three-quarters said they had completed an accredited prescribing course and registered their qualification with their regulatory body, while 12.4% said they worked alongside a qualified prescriber.
Most were in the 41-50 age group (26.8%), closely followed by those aged between 31-40 (26.1%) and those aged between 51-60 (18%). Those under 30 comprised 16.6%, and 12.4% were over 60.
Some respondents had been practising aesthetics for over 20 years (8.5%), with 22.2% practising for 10-20 years, 20.9% for six to ten years, and 19.9% for four to five years.
A fifth had been practising for one to three years and 6.5% for under one year.
New treatments coming onto the market;
Most practitioners worked solo, with 55.2% saying they worked alone. One in five worked alongside a nurse, while 5.9% worked with a doctor.
The same number said they worked with a plastic surgeon, and the same number again with a beauty therapist. 4.6% said they worked with a dentist.
Patient satisfaction;
Greater flexibility;
Too much competition by unqualified people; Being more difficult to get clients than expected;
Skincare ranked next, with 57% saying they offered it and 47% saying they performed chemical peels.
Microneedling was offered by 36.3%, with mesotherapy being named as a treatment by 34.3%.
for skincare solutions, followed by preventative ageing treatments. Treatments for menopause symptoms were an area where there was currently a lower demand but growing popularity.
Growing market demand;
Diverse employment opportunities;
Continuous learning and development;
Less stressful than their NHS job.
But some reasons the sector failed to meet expectations included:
Not making enough money to justify leaving the NHS;
The stress of keeping up with social media.
Seventeen per cent said they offered light-based device technology such as IPL, LED and laser, while 15% cited radiofrequency as being on their treatment menu. But as many as 61% said they didn’t use any technology at all in their clinic.
Treatment trends
It came as no surprise for Hamilton Fraser to find injectables came out top of the list of procedures. Eighty per cent of respondents naming botulinum toxin as a treatment they offered and 76.1% said they performed dermal fillers.
Weight loss injections were offered by 13.4% and body contouring procedures – including cryotherapy – by 15.6%.
Top choice of what is most commonly requested by patients was treatments to counter the signs of ageing.
There was also a high demand
The survey sponsors report: ‘In terms of trends, the greatest interest was in aesthetic regenerative procedures, with 64.1% stating this was an area they were interested in. ‘Prejuvenation’ – treating younger patients with preventative treatments – was also popular, with 58.2% of those who responded citing it as a top trend.
‘Practitioners were also excited about new applications for RF microneedling (43.1%) and weight loss injections (34.6%).’
Read the full results of the survey at www.hamiltonfraser.co. uk/content-hub/annualsurvey.
Look after women in the workplace
Women’s health is gaining the spotlight it deserves in recent years due to high-profile awareness campaigns on topics such as menopause and contraception. But while these steps have been critical in starting to break down taboos, there is still much more to be done, says Rita Trewartha RGN, head of clinical services at Bupa UK Insurance
AN EXTENSIVE survey by Bupa, in collaboration with research agency Censuswide, provides valuable insights into the day-today issues women face – and what steps can be taken to improve behaviours and attitudes.
The study, among 4,100 women and those assigned female at birth, is the latest in Bupa’s Wellbeing Index series.
Experiencing visible women’s symptoms in public Women’s health is often disproportionately stigmatised. Whether because of a medical condition or natural bodily functions, displaying visible symptoms of periods, pregnancy or menopause in public is still often met with distaste and a lack of understanding.
Bupa’s Wellbeing Index research found that 89% of respondents have experienced visible symptoms of health conditions or bodily functions specific to women in public at some point in the past. These included:
Sweating (76%);
Hot flushes (68%);
Leaking urine (58%);
Period blood leaking onto clothes (58%);
A breakout of spots or acne (58%);
Breast leaking, usually because of pregnancy or post-pregnancy (34%).
Other less obvious symptoms include heightened emotions –crying, angry outbursts – which were experienced by 69% of respondents, and severe pelvic or abdominal pain reported by 67%.
The impact on women’s well-being
The Bupa Wellbeing Index found that women experiencing visible symptoms needed to go to a public toilet (34%), had to abandon what they’re doing to go home early (34%) or rush to buy toiletries (20%) or new clothes (10%).
While these women’s health symptoms are entirely natural, many women have experienced judgement and intrusive comments as a result, causing shame and in some cases triggering poor mental health, such as anxiety and a fear of leaving their home.
Half of women who responded (56%) said that people around them
➱ continued on page 26
OUR ROLE AS HEALTHCARE PROVIDERS
The findings of this report highlight that a persistent stigma still exists despite the progress being made over time and there is clearly more work to be done.
The more we, as a society, foster a sense of openness around women’s health, the easier it will be to get to the root of a lot of related issues.
As healthcare providers, as well as employers, Bupa has a valuable role in normalising conversations about women’s health. We can support employers, educators and communities to become more inclusive. At Bupa, we are making a call to action.
We have pledged to:
Increase awareness of women’s health – Not just within Bupa, but across wider society. Through targeted campaigns, educational initiatives and open conversations, we aim to help everyone understand women’s health.
Create supportive workplaces – Recognising the pivotal role workplaces play, we commit to fostering environments where women feel supported in their health journeys.
This includes practical measures such as readily available sanitary products, along with training and resources available via Bupa’s Women’s Health Hub (www.bupa.co.uk/health-information/womens-health) to equip our workforce with the skills to address sensitive health topics.
Break the cycle of silence – Bupa encourages normalising the conversation in workplaces, schools and communities. We strive to let conversations about women’s health be as common as discussions about the weather – informed, encouraged and without judgement.
Empower through education – Knowledge is power and we commit to empowering our workforce, partners, schools and communities through comprehensive education on women’s health. By fostering an environment of understanding, we lay the groundwork for equality.
Will you join us? Societal progress in women’s health is long overdue. It is about levelling the playing field, so everyone thrives, without women having to take time out or leave the workplace completely to manage symptoms, which can also be detrimental.
Explore all chapters of the Bupa Wellbeing index at: www.bupa.co.uk/wellbeing-index
While most feel comfortable talking to a partner, friend or parent, respondents were more reluctant to talk about their health to a male manager at work
had commented on their visible symptoms. This led to them feeling embarrassed (50%) or self-conscious (46%), while others reported anxiety (38%), a negative impact on their mental health (14%) or feelings of depression (14%).
Two-thirds of women who experienced one of these symptoms (63%) reported at least one longterm consequence as a result. A third (33%) felt anxious about when it might happen again, while 12% cancelled social plans and 7% avoided the people present at the time.
Discomfort discussing women’s health
Past experiences and a lack of understanding about women’s health means many still feel uncomfortable talking about what is happening to them.
The Bupa Wellbeing Index found that over half of those surveyed (57%) feel that women’s health issues are still seen as taboo. As a result, a third (32%) of women feel generally uncomfortable when talking about their periods or menopause symptoms.
What is encouraging, though, is that many agree that progress has been made in tackling the taboo in recent years. The survey found that 45% of women agree that high-profile campaigns with celebrities and public figures raising awareness mean they feel more comfortable speaking about women’s health.
While most feel comfortable talking to a partner, friend or parent, respondents were more reluctant to talk about their health to a male manager at work – with 42% saying they wouldn’t feel comfortable.
This is compared with 30% who would feel reluctant to talk to a female manager.
CHANGING WORKPLACE ATTITUDES
Without proper understanding from managers or a workplace culture which encourages women to feel comfortable talking about their health, valuable talent is at risk of leaving the workforce.
The voices of all employees must be at the heart of any healthcare-related workplace initiatives or changes. So, what can be done to change this?
1
Educate
A quarter of women participating in the Bupa Wellbeing Index (24%) said they would welcome more open conversations, while 18% want mandatory training for managers.
This also feeds into the second most common request, which is for managers to show a better level of understanding over the reality of working – or not working – when you have a period, as cited by 34% of female workers.
Education around periods is vital to supporting colleagues. It is so important that we are educating everyone, not just those experiencing them. A great way to create an open culture is through internal campaigns, whether this is hosting external speakers, virtually or in person, or sharing personal stories from other people within the organisation.
It is about creating a culture which normalises conversations about periods, where everyone feels comfortable to talk about what they are experiencing and asks for support when they need it.
To give one real world example, Bupa offers a monthly support group set up for people who suffer with heavy and painful periods.
2
Provide access to menstrual products
On a practical level, over a third (36%) of women would welcome employers providing free sanitary products in workplaces.
Not only does this help employees who unexpectedly get their period, it signals that the business takes menstrual health seriously and is happy to support colleagues with the financial cost of periods.
It is important to make pads, tampons and other menstrual products available in a variety of locations, such as bathrooms, break rooms and vending machines.
3
Offer flexible working arrangements
The women participating in the Bupa Wellbeing Index felt that policy changes can play a role in driving change – whether that is days off for period health (30%), including period health in policies (26%) or providing access to services that support periods, such as GP appointments (19%).
If your workplace does not already have one and it is possible for you to introduce one, a flexible working policy is an effective step to support period health.
To give an example, it means that if a colleague has struggled to sleep due to night sweats, they can start work slightly later.
Even where roles can be done remotely, hybrid working patterns may also mean they feel pressured to come into the workplace, but make sure they know that if they are struggling with symptoms, they can work at home, where applicable.
Flexibility is key when it comes to supporting employees with periods if they do not want to take time off.
4 Offer support
Workplaces are doing more to support women’s health, and as more organisations step up to that challenge, it is essential that as well as offering flexible working hours and period products, they are providing access to services which can support with all of the symptoms.
At present, less than a fifth (18%) of women say the support offered for period health in their workplace is the best it could be.
Whether this is private GP services or employee assistance programmes (EAPs) to help with the mental health symptoms, having support and access to treatment mean that employees can stay well, remain in work and improve productivity. They are also less likely to leave an organisation if they feel it cares about their well-being.
Period
health in the workplace
In the workplace, periods can have a significant impact on well-being, comfort and productivity.
The effects are almost universal among women who have periods. Bupa’s Wellbeing Index data found that 94% have previously experienced disruptive symptoms.
Many women report regularly experiencing severe symptoms. Just under half (47%) of women suffer from severe period pain or cramps every month or most months, while a similar proportion (48%) regularly get headaches or migraines and nearly a third (31%) feel nauseous.
Despite this, 42% of women who experience symptoms have never called into work sick as a result. Even those who do call in sick due to their period don’t tell their employer the real reason why.
A third of women (34%) are too embarrassed to tell managers they need time off because of their period, saying they’re ill with something else, while 31% believe their manager wouldn’t understand.
Just 17% of women who have periods have taken time off and told their employer the real reason why – and the majority of this group (53%) only did so because their manager is a woman.
The most common reason why women don’t tell their employer when they take time out for period symptoms is because they worry their symptoms aren’t an acceptable reason to miss work (45%).
The impact of severe symptoms on work can be significant and women who experience them may find it difficult to concentrate, focus or be productive at work.
Those who end up working through period symptoms commonly reported feeling tired (41%), suffering with period pain (37%) or having to make frequent trips to the toilet due to heavy bleeding (30%).
As a result, they may have to take regular breaks, or change their working hours.
See page 36
Rita Trewartha (right) is head of clinical services at Bupa UK Insurance
Indemnity doesn’t follow the patient
There is a general belief that clinical indemnity follows the patient. In other words, doctors require their own indemnity or insurance if they treat a private patient, and state indemnity schemes apply when treating NHS patients.
But Dr Dawn McGuire (right) highlights two histopathology cases to demonstrate how this is not always the case and why it is important to ensure that your indemnity arrangements are adequate and appropriate
CASE SCENARIO 1
Mrs P had a skin biopsy and this was sent for histology report. She was an NHS patient and the procedure was carried out in an NHS hospital and processed in an NHS lab.
Due to the NHS backlog, the slides were sent to a private remote reporting company for more expeditious reporting. Dr A carried out the analysis and reporting of those slides.
Two years later, Mrs P brought a clinical negligence claim against the NHS trust for failure to diagnose basal cell carcinoma, alleging that the slides were erroneously reported as trichoepithelioma.
The trust initially accepted liability for the claim, but later requested substitution as a defendant, stating that the trust was not responsible for the private remote reporting company or Dr A’s acts or omission.
The contracts between the NHS
trust and the company, as well as Dr A’s employment or service provision contract, specified that Dr A would be required to hold his own indemnity in the event of a clinical negligence claim.
Dr A was therefore individually pursued as a defendant after court proceedings were served, much to his distress.
Dr A had read the contracts carefully. He was a member of the medical defence organisation I work for, Medical Protection, and had obtained the appropriate indemnity protection for the nature of the work he was undertaking.
He was provided with legal representation in a timely manner and averted a default judgment being served on him.
CASE SCENARIO 2
Mr S had a lump removed from his right upper arm privately. As the
private hospital did not have its own histopathology lab service, the excised samples were sent to an NHS hospital for processing and reporting under the service agreement through a commercial contract between the two hospitals.
Dr C was a consultant histopathologist employed by the NHS hospital and provided the histology report for Mr S’s lump, concluding it was a benign soft tissue tumour.
Eighteen months later, Mr S pursued a clinical negligence claim against the NHS hospital for incorrect reporting of the histopathology slides by Dr C, alleging that the lump was, in fact, a malignant sarcoma.
The claim was valued at £1.5m, as Mr S required amputation of his dominant arm.
The NHS trust initially refused to indemnify Dr C, as the patient was not an NHS patient of the hospital. Understandably, Dr C was very
Always check your contract(s) carefully and make sure you are clear on whether or not you need to arrange your own protection for clinical negligence claims
distressed and contacted us for advice.
We argued that the reporting formed part of Dr C’s NHS job plan and she was paid by her NHS employer for it. Dr C never had a separate contract or pay arrangement with the private hospital.
The NHS employer eventually agreed to accept full responsibility for this claim. Medical Protection continued to support Dr C with her professional report to her NHS
employer to assist with the defence of the claim.
Learning points
1
Due to waiting list initiatives, there are currently a myriad of agreements and contracts across the UK between independent healthcare providers and state commissioners. Do not assume each agreement or contract is the same.
2
Do not assume your medical defence organisation will be aware of what the various contracts stipulate and what indemnity you require.
Always check your contract(s) carefully and make sure you are clear on whether or not you need to arrange your own protection for clinical negligence claims.
3
If in doubt or you feel there is ambiguity, ask your employer for confirmation and
EXPERT TAX AND ACCOUNTANCY ADVICE YOU CAN TRUST
Sandison Easson is a firm of truly specialist medical accountants who provide personal and tailored advice to clients.
We act for medical professionals throughout all stages of their career with clients in almost every town in England, Scotland and Wales.
We cut through the complicated jargon and deliver practical, easy to understand advice. Call us today to organise your FREE no obligation consultation.
request they provide the confirmation in writing.
4
Always keep your contracts; you may need to revert to them many years from now. Negligence claims often surface years after you have stopped working.
5
If you have ascertained that statebacked indemnity will protect you against clinical negligence claims as part of a particular contract or agreement, remember a state scheme will not provide assistance with other medicolegal matters such as complaints, disciplinaries, regulatory investigations, inquests and criminal investigations.
Ensure you have membership with a medical defence organisation where you can request support with these issues.
Dr Dawn McGuire is a medico-legal consultant at Medical Protection
WE PROVIDE THE USUAL SERVICES YOU WOULD EXPECT FROM AN ACCOUNTANT SUCH AS PREPARATION OF YOUR ACCOUNTS AND TAX DECLARATIONS BUT OFFER SO MUCH MORE INCLUDING ADVICE ON:
• SETTING UP A NEW PRIVATE PRACTICE
• BUILDING AN EXISTING PRIVATE PRACTICE
• BUSINESS STRUCTURES TO PROTECT WEALTH
• BUSINESS STRUCTURES TO MAXIMISE TAX EFFICIENCY
• CLAIMING TAX REFUNDS INCLUDING OVERPAID ANNUAL ALLOWANCE TAX
• REMUNERATION PLANNING FOR YOU AND YOUR FAMILY
• UNDERSTAND ANNUAL ALLOWANCE TAX
• MAXIMISING LEGITIMATE EXPENSE CLAIMS
Jekyll and Hyde features of cash
Holding too much cash can be wealth destroying. George Uglow (below) warns of the consequences of not investing in capital markets
CASH IS the Dr Jekyll and Mr Hyde asset class of the investing world. It is good that Dr Jekyll moments for cash tend to come at times of market turmoil, such as in 2022, when bonds and equity markets both fell.
The opposite, evil Mr Hyde persona is cash’s terrible track record of maintaining or growing purchasing power over time for investors.
As an example, if we look at how cash performed during the Global Financial Crisis (2007-2009) and how it has performed since then compared to world (developed and emerging) equities, we can see it is a poor store of long-term value.
Over the whole period, 27% of its purchasing power was eroded, while ‘higher-risk’ equities’ purchasing power more than doubled, even when measured from the height of the market before the fall.
It can feel tempting to want to hold cash that pays a seemingly decent rate of interest, but the problem is that no one gives you a signal telling you when to get out of risky markets and into cash or when to get back into markets.
As John Bogle, founder of Vanguard Group and one of the ‘grandfathers’ of index investing, said: ‘The idea that a bell rings to signal when investors should get into or out of the stock market is simply not credible. After nearly 50 years in this business, I do not know of anybody who has done it successfully and consistently.
‘I don’t even know anybody who knows anybody who has done it
Trying to second-guess the market is a challenging sport with few winners. In the US, for example, over 90% of government bond funds failed to beat their market benchmarks over a ten-year period
Perhaps something also worth noting is that it is very difficult to second-guess where bond yields will be in the future. There is quite a bit of talk in the media that interest rates – being the Bank of England base rate – may come down in the next year.
That is in each central bank’s control. Bank deposit rates are generally set relative to this rate. Bond yields, on the other hand, are driven by the market’s aggregate view of the risks it perceives, which will already incorporate its own collective view on where the bank base rate will be in the future.
successfully and consistently. Yet market timing appears to be increasingly embraced by mutual fund investors and the professional managers of fund portfolios alike.’
In 2022, bonds and equities both fell, driven to a large extent by the rapid rise in inflation to double digits and the subsequent increase in both bank base rates –controlled by central banks – and bond yields – driven by the market’s need to be compensated for risks taken on. In this situation, some investors were tempted to retreat to cash.
After all, deposit holders could receive, say, 5% or so on their cash, so why bother with bonds or even investing in general?
Long-term premium
Answering the bond question, it should be remembered that, on average – as with placing a bank deposit – the longer you lend your money for, the higher the interest rate or yield in the case of bonds. For lending is what you are doing when you give the bank your money or buy a bond. So, for a long-term investor, this ‘term’ premium should provide a small higher expected long-term return.
In addition, often but not always at times of equity market crisis –2022 being a case in point – money tends to flood out of risky assets and into high-quality bonds, driving prices up.
In this case, investors receive both capital gains and yield. This provides a defensive element not available to those holding cash, who just receive the interest they are paid.
It is not the case that bond yields will fall just because the bank base rate is reduced, as that is already anticipated to some extent and reflected in bond prices today. No market timing bell there.
Trying to second-guess the market is a challenging sport with few winners. In the US, for example, over 90% of government bond funds failed to beat their market benchmarks over a ten-year period.
Data shows us that investing makes sense. As long as you take advice while maintaining sufficient liquidity and contingency funds, then there is no need to hold excess funds in cash reserves.
In terms of not investing at all, there is much evidence as to why long-term investors should avoid holding cash in lieu of investing.
If we look at the evidence since the start of 2023, an investor holding cash, which may have felt comfortable at the start of 2023, would have left valuable returns on the table.
George Uglow is a chartered financial planner with Cavendish Medical, specialist financial planners helping consultants in private practice and the NHS
The content of this article is for information only and must not be considered as financial advice. Cavendish Medical always recommends that you seek independent financial advice before making any financial decisions.
Levels, bases of and reliefs from taxation may be subject to change and their value depends on the individual circumstances of the investor. The value of investments and the income from them can fluctuate and investors may get back less than the amount invested.
GOSH, what an imposing in looking after very
Our occasional PPU Focus series featuring leading private patient services within the NHS this month explores Great Ormond Street Hospital International and Private Care. Philip Housden (below) reports
GREAT ORMOND Street Hospital’s (GOSH’s) dedicated International and Private Care service (I&PC) caters for UK self-pay and insured patients plus international patients from over 90 countries.
Treating over 5,000 patients every year, GOSH ensures a nurturing and family-centred experience across 75 private beds within three dedicated wards and specialist wards including intensive care units. It also has a dedicated outpatient department.
Private patient revenues at the trust have bounced back since Covid. The trust ranks third in England for both overall private revenues and percentage of trust income.
In 2022-23 the trust reported private patient income of £54.8m, up £24.9m (220%) on 2021-22. However, this is still some way short of the £64.8m achieved prepandemic when private patient
earnings represented over 14% of total trust income.
An equivalent for last year would be private patient income of in excess of £78m a year (see diagram below).
Being part of the NHS means that private patients also benefit directly from the trust’s infrastructure, research and education, as well as the multi-disciplinary approach to
treatment and care. These include up to 30 professionals: consultants, specialist nurses, radiologists, pathologists, allied health professionals and support services.
The ability to access the latest medical advancements, technologies and cutting-edge techniques means all patients receive the best possible treatment delivering excellent patient outcomes.
The private patient service includes dedicated referral, appointment, finance, interpreter and hospitality teams in London and an overseas referral office in the United Arab Emirates.
Leader in education
GOSH is a leader in educating paediatric specialist doctors, with the largest programme in Europe, and also offers Europe’s largest paediatric nurse education program.
It is committed to sharing best practice and knowledge with clinicians in the UK and around the world via its virtual learning environment, providing access to the
The entrance to London’s Great Ormond Street Hospital creates a colourful welcome to patients
imposing record very ill children
A PAEDIATRIC POWERHOUSE
Great Ormond Street Hospital for Children (GOSH) opened in central London in 1852 with just ten beds and has grown to be an international centre of excellence in paediatric care, championing education, research and innovation across 67 clinical specialties and subspecialties.
GOSH specialises in tertiary and quaternary care and has the largest cohort of super-specialist services of any hospital in the UK (20 specialties), which uniquely enables it to treat children suffering from rare, complex or multiple conditions ‘under one roof’.
Consistently ranked in the top ten best paediatric hospitals in the world by Newsweek and the best paediatric hospital in Europe, GOSH was acknowledged for its outstanding expertise in cardiac surgery, oncology and neurosurgery in 2024.
GOSH has now grown to accommodate 446 beds and, with the building of a new Children’s Cancer Centre, this will exceed 500 beds by 2028.
It also has extensive support infrastructure including: 15 theatres, five MRI machines –including an iMRI – CT scanner, three interventional radiology labs, endoscopy suite, cardiac catheterisation lab and procedure rooms.
GOSH is also globally recognised as the top paediatric centre for gene therapy in children and for its expertise in managing conjoined twins, treating cancer and leukaemia in children and performing epilepsy surgery.
Within the UK, GOSH is the largest paediatric centre for bone marrow transplants, paediatric intensive care, cardiac surgery, neurosurgery and renal services. same education and training as staff at GOSH.
Education is an enabler and, through its multi-year international partnerships in Africa, Europe and the Middle East, has been able to develop services, clinically support and provide education, training and consultancy to improve local specialist services in haematology, oncology, bone and marrow transplants, cardiac and intensive care. This is supplemented through
observerships, multi-year international fellowships and bespoke virtual clinical training webinar sessions.
Research prowess
In 2022-23 alone, there were over 900 active research studies with more than 2,200 participants at GOSH.
Research, in large part through the partnership with Univeristy College London Great Ormond Street Institute of Child Health
GOSH’s motto is “The child first and always”
(UCL GOS ICH), represents the largest concentration of paediatric research expertise in Europe. GOSH and UCL GOS ICH form a powerful research partnership that is only getting more impactful.
Medical research produced as a result of the partnership is cited three times more than the global average, according to a recent analysis.
This enables GOSH, working with its partners, to rapidly and robustly improve paediatric outcomes with cutting-edge treatments and therapies.
Chris Rockenbach, GOSH’s managing director of international and commercial, said: ‘Great Ormond Street Hospital has been delivering world-leading paediatric care, research and education for over 170 years.
‘The International and Private Care service remains committed to meeting the needs of the
patients we treat and through delivery of ambitious plans, we will be able to treat more children and make a positive impact on more lives.
‘These children are our future, and therefore it is important they are our sole focus providing confirmation of our motto “The child first and always”.’
Philip Housden is director of Housden Group commercial healthcare consultancy
Chris Rockenbach
Run your firm efficiently
As the healthcare industry strides boldly into the future, the convergence of technology and administrative processes has emerged as a transformative force. Derek Kelly (right) unravels the impact of technology on operational processes in medical practices
TRADITIONAL ADMINISTRATIVE
processes in doctors’ private medical practices often involve manual, time-consuming tasks. These lead to inefficiencies and challenges in maintaining seamless operations.
Managing appointments, handling patient records, submitting insurance claims, chasing payments and navigating regulatory requirements can become daunting tasks. And they divert valuable time and resources away from patient care.
But these conventional methods, while once considered standard, are proving to be increasingly inefficient in the face of the modern healthcare demands.
Billing errors, delayed reimbursement cycles and the complexity of managing diverse payer systems contribute to challenges that hinder the seamless functioning of medical practices.
TECHNOLOGICAL
INTEGRATION: Streamlining workflows for efficiency
The integration of technology heralds a new era of efficiency in healthcare administration. Advanced systems now automate repetitive tasks, streamline workflows and ensure that administrative processes are conducted with precision and speed.
From appointment scheduling and billing to managing patient records, technology facilitates a seamless approach, allowing medical practices to optimise their operational efficiency. Integrated systems ensure that data flows seamlessly across various facets of practice management, reducing redundancies and enhancing overall efficiency.
DATA
MANAGEMENT AND ANALYTICS: Informed decision-making for practices Modern healthcare practices are inundated with vast amounts of data. Technology-driven solutions not only aid efficient data management but also provide actionable insights through analytics. These empower healthcare administrators to make informed decisions, whether optimising resource allocation, identifying trends in patient demographics or enhancing practice performance. Real-time analytics offer a
Technology-driven solutions not only aid efficient data management but also provide actionable insights through analytics pro-active approach to identifying potential challenges and areas for improvement, contributing to a data-driven culture that strengthens the foundation of healthcare administration.
ENHANCED SECURITY AND COMPLIANCE: Safeguarding sensitive information
Security and compliance are paramount in healthcare administration. Modern technologies ensure the secure storage and transmission of sensitive patient information.
Robust encryption protocols, secure cloud storage and adherence to regulatory standards create a fortified environment that protects patient data from breaches while ensuring compliance with industry regulations.
INTEROPERABILITY: Creating a unified ecosystem for comprehensive management
The future of healthcare administration lies in the seamless integration of various systems in a medical practice. Interoperability ensures that administrative processes align cohesively with electronic health records, billing and other critical components. An integrated ecosystem not only minimises redundancy but also provides a comprehensive view of patient care. This approach enhances communication, reduces administrative burdens, and contributes to a more patientcentric administrative experience.
CHALLENGES AND CONSIDERATIONS: Navigating the path forward
The adoption of technology for operational excellence in healthcare administration is not without its challenges.
Implementing new systems may incur costs, require staff training and face potential resistance to change.
Successful navigation of this path involves strategic planning, comprehensive training programs and open communication channels.
But by emphasising the positive impact of technological integration on operational efficiency, healthcare practices can overcome resistance and pave the way for a more streamlined future.
A vision for tomorrow’s healthcare administration
As practices embrace technology for operational excellence, the
future of healthcare administration unfolds with promise and potential.
Beyond medical billing, these technological advancements reshape administrative processes, optimising workflows, enhancing data management and create a unified ecosystem that places patient care at the forefront.
I believe the road ahead involves a strategic blend of innovation, adaptation and a commitment to harnessing the full potential of technology.
In doing so, healthcare practices not only elevate their administrative capabilities, but also contribute to a healthcare ecosystem that is efficient, secure and dedicated to providing the best possible patient care in a rapidly evolving digital landscape.
Derek Kelly is marketing manager at Medserv, a company specialising in medical billing and collection
Free legal advice for Independent Practitioner Today readers
Independent Practitioner Today has joined forces with leading healthcare lawyers Hempsons to offer readers a free legal advice service.
We aim to help you navigate the ever more complex legal and regulatory issues involved in running and developing your private practice – and your lives.
Hempsons’ specialist lawyers have a long track-record of advising doctors – and an unrivalled understanding of the healthcare system as a whole.
Call Hempsons on 020 7839 0278 between 9am and 5pm Monday to Friday for your ten minutes of free legal advice.
Advice is available on:
Business structures (including partnerships) Commercial contracts Disputes and litigation
HR/employment Premises
Regulatory requirements and investigations
The sector promotes
Supporting women in private healthcare and encouraging their career development is vital, says Independent Healthcare Providers Network boss David Hare (right)
FOR LAST month’s annual International Women’s Day, especially within healthcare, it was incredibly important for us to celebrate the importance of women in our industry.
At the same time, we also recognised they are disproportionately under represented in leadership positions.
I
believe it is incumbent on all of
us to enable and support the women in our workplaces, who make up the bulk of the workforce of our industry
According to the World Health Organization, women account for 70% of the global healthcare sector and yet, at the executive level, women make up just 25% of healthcare leadership positions.
So I believe it is incumbent on all of us to enable and support the women in our workplaces, who make up the bulk of the workforce of our industry.
As part of International Woman’s Day, we platformed members of our Women Leaders in Independent Healthcare Network on our social media channels. They shared their experiences, perspectives, advice and things they would like to see improve.
promotes women and safety
We were pleased to see the positive reaction within the healthcare community to what they said, and the discourse it generated.
As part of the ongoing work of our Women Leaders in Independent Healthcare Network, we are holding a networking breakfast in late April.
There we will be having Helen Buckingham, director of strategy at the Nuffield Trust, and Alex Ryan, Acacium’s Group service development director, speak to attendees about their careers and what they have learned.
We were also extremely proud to see Danielle Henry, IHPN’s assistant director of policy and programmes, named to the Trade Association Forum’s Women in Trade Association (WiTA) Powerlist. This is the second iteration of the WiTA powerlist, which was created to champion the role of women in trade associations, celebrate their achievements and encourage the next generation of women into the association sector.
Showing off the sector’s
safety forte
We are only a few months into the year, but it already feels like so much has happened already and there’s plenty more on the horizon.
My Independent Healthcare Provider Network (IHPN) colleagues have been getting out and about in the past month.
They travelled to Liverpool for the opening of InHealth’s new community diagnostic centre (CDC) and also saw its patient referral centre in Rochdale and Alliance Medical’s CDC in Oldham.
These developments are great examples of how the independent sector can work very powerfully, especially in partnership with the NHS.
Our director of regulation, Dawn Hodgkins, hosted Prof Ted Baker and Rosie Benneyworth, the chair and interim chief executive of the Health Services Safety Investigations Body (HSSIB), to a day in London where they visited a number of our members.
They were able to see HCA Primary Care at the Shard, Bupa’s Cromwell Hospital, InHealth’s CDC in Fitzrovia and Nuffield Health at St Barth olomew’s Hospital.
All this was to help the HSSIB develop a better overview of systems risks, to highlight some of the innovative and fantastic work being done and gain a clearer understanding of the private healthcare landscape.
These visits come ahead of our annual patient safety conference in central London on 15 May where Rosie will be presenting along with Care Quality Commission (CQC) chief executive Ian Trenholm and the patient safety commissioner for England Dr Henrietta Hughes.
The conference has a focus this year on Culture of Caring: Listening, Leading and Learning.
It is a fantastic opportunity for senior clinical leaders, clinical governance leads and patient safety specialists to come together and learn more about how to create a culture of caring that supports safe care.
Big demand for private healthcare
We can already see the impacts that NHS waiting lists are having on the British people, through the release of PHIN’s quarterly data update.
The report shows strong continued demand for private healthcare, with large numbers of patients choosing to use the private sector to access healthcare.
It is also notable to see the numbers of insurance based admissions are still high, which insurers have also been reporting – with corporate insurance demand still strong.
There has been lots of discussion about the cost of inactivity to the economy, and we know that NHS waiting times are not only impacting people, but business is also concerned about the impact of these long delays on staff absence rates and productivity.
Our most recent research showed that a quarter of businesses are already offering private medical insurance to employees, and one in five are planning to introduce it within the next year, so businesses are being proactive in ensuring the wellbeing of their workforce.
We know from the research conducted in our Industry Barometer report that our members feel confident about the private care market, with 88% of them feeling positive or very positive about private medical insurance funded services, and 86% feeling positive or very positive about domestic selfpay services.
This, coupled with NHS waiting lists being such a driver of people choosing to go private, makes us think that the trend of increased demand for private healthcare looks set to continue strongly.
MPAF is adopted in Wales
We were delighted to be able to announce recently that, after nearly a year working closely with Welsh Government and Healthcare Inspectorate Wales (HIW), the Medical Practitioners Assurance Framework (MPAF) now has a letter of support from Welsh Government and Healthcare Inspectorate Wales.
This highlights that the use of the MPAF Wales will be seen as evidence of best practice during HIW inspections.
Obviously, this is very positive news for colleagues working in Wales, who admittedly are small in number.
But the wider point is that it is a further demonstration that the MPAF is still very much a yardstick and standard which is just as important and relevant today as it was when Sir Bruce Keogh launched it in October 2019 and when it was refreshed in 2022.
The MPAF contains key principles to strengthen and build upon the medical governance systems already in place in the sector and sets out expected practice in key areas.
In England, the CQC uses the framework’s principles in assessing how well led an independent service is, with the framework a requirement of the NHS’s 202223 Standard Contract which all independent sector providers of NHSfunded care must adhere to.
There is no question that as private healthcare continues to grow, so too will the expectations of patients and the scrutiny of the media and other stakeholders – all of which means that good clinical and medical governance will be under the spotlight like never before.
The IHPN’s Danielle Henry
New rules for holiday pay
What do the Government’s new Employment Rights Regulations mean for employers calculating annual leave allowances?
Rachel Levine (right) explains
EVERY INDEPENDENT healthcare provider who has employees or workers must be aware of the change to how holiday pay is calculated.
New regulations relating to holiday pay, and setting out changes to the Working Time Regulations, came into force on 1 January 2024. They contain some significant changes and aim to simplify or consolidate some of the processes for certain categories of workers. The Government has chosen to maintain many of the EU rules on holiday already in force, with a few changes and additions.
It is important that all employers are aware of the changes so that they can identify whether any of their employees or workers are likely to be affected.
1 When do the rules apply?
Although the regulations came into effect on 1 January 2024, they only begin to apply for an employer’s leave year beginning on or after 1 April 2024.
This means that for any independent healthcare provider business whose annual leave year runs from 1 January to 31 December, for example, the new rules will apply from 1 January 2025.
2
‘Irregular hours’ and ‘part-year’ workers
Before reviewing the changes themselves, it is important to understand some of the categories of workers that these regulations
➱ continued on page 40
apply to. For instance, ‘irregular hours’ and ‘part-year’ workers are defined in the regulations.
Irregular hours workers: These are workers where the number of paid hours that they work in each pay period is, under the terms of their contract, ‘wholly or mostly variable’.
This covers workers with an irregular number of hours, not workers who have irregular working patterns but a fixed number of hours. It might cover positions such as healthcare bank workers or specialist employees retained to meet irregular patient needs, with no consistent or guaranteed contractual hours.
Part-year workers: These are workers who are required to work only part of the year, with periods of at least a week where they are not required to work and for which they are not paid, such as seasonal workers covering private vaccina-
tion clinics or where the hours are adjusted to reflect reduced patient demand during certain months.
3
What are the main changes?
Holiday accrual for irregular hours and part-time workers.
The way in which irregular hours and part-year workers accrue annual leave is changing as a result of the new regulations.
This follows a Supreme Court ruling (Harpur Trust v Brazel), which caused significant difficulties for employers in calculating the holiday pay for these workers.
Under the new regulations, these workers will accrue annual leave entitlement for each pay period at the rate of 12.07% of the number of hours that they have worked during that pay period.
A ‘pay period’ is the period for which the worker is paid, such as monthly, weekly or fortnightly.
This means workers accruing holiday in this way will now build up holiday entitlement as they work, rather than being entitled to a full 5.6 weeks at the start of each holiday year regardless of what hours they work.
There is a maximum limit of accrued holiday in this way of 28 days per year, unless a higher limit is contractually agreed.
It will also be open to employers to provide these workers with more holiday than they have technically accrued, as long as – again – this is documented contractually.
Although there remains some ambiguity in relation to how or when these workers should be taking the accrued holiday – considering their types of contract – this provision is likely to be helpful for employers, particularly those who engage these types of workers on a large scale.
Rolled-up holiday pay
Rolled-up holiday pay is where an employer rolls up a payment of basic pay and holiday pay into one consolidated payment.
Although previously commonly used, this practice was ruled unlawful several years ago by the European Court of Justice in a case called Robinson-Steele, where the court commented that the use of the practice would risk discouraging workers to take leave.
These new regulations have reintroduced the provision of rolledup holiday pay for certain workers, provided that:
The worker is a part-year or irregular hours worker;
Holiday pay is calculated at 12.07% of all pay for work done; 12.07% is paid at the same time as the pay for the work done;
The holiday pay is itemised separately on the worker’s payslip. It will not be compulsory to pay
WHAT SHOULD EMPLOYERS DO?
There are a few steps that any independent healthcare provider business can take to ensure that they are prepared for when these regulations come into effect for them:
☛ Check you are properly accounting for overtime, commission and allowances in holiday pay when accruing leave under the new provisions.
☛ For irregular hours/partyear workers, check your systems are set up to calculate accrual of holiday accurately under the new provisions.
☛ For any workers that you want to use rolled-up holiday pay for, check that they meet the criteria for you to do so.
☛ Review your systems reminding workers to use their holiday entitlement and the rules on losing their unused holiday entitlement.
☛ Review your workplace policies to ensure that the new regulations are incorporated.
holiday in this way, but this reintroduction will be of benefit to any independent healthcare business which engages irregular hours workers due to the difficulties in calculating holiday through any other method.
Assuming that the worker is eligible to receive it, using rolled-up holiday pay allows employers to simply add a supplement onto an hourly rate of pay for work in order to satisfy their legal obligations –provided that the supplement is appropriately itemised on the payslip.
It should be noted, however, that there is still a responsibility on businesses to ensure that workers take their full statutory holiday (5.6 weeks).
This obligation remains regardless of whether that holiday time is paid as part of normal annual leave or has been paid via rolledup holiday pay.
If using rolled-up holiday pay, it means that the worker’s remaining holiday entitlement over and above what they have been paid via rolled-up holiday pay will be unpaid.
Using rolled-up holiday pay allows employers to simply add a supplement onto an hourly rate of pay for work in order to satisfy their legal obligations
Carrying leave forward
Under the new regulations, workers will continue to automatically be able to carry over four weeks of statutory leave, if the employer has not:
Recognised their right to paid annual leave;
Given them a reasonable opportunity to take leave or encourage them to do so;
Warned them of the risks of losing their annual leave entitlement at the end of the holiday year.
This is an important provision for employers to be aware of, as it highlights the risk of misclassifying someone as self-employed.
Should someone be wrongly classified as self-employed when, in fact, they satisfy the conditions of worker status, they will be entitled to statutory holiday, and any employer, relying on their selfemployed status, may fall foul of this provision.
Carried-over holiday under this provision cannot be carried forward beyond the end of the first full leave year where the employer has acknowledged the rights.
Other provisions for carrying over leave are also included in the regulations:
Where workers are unable to take annual leave due to family leave, they will be entitled to carry forward the full 5.6 weeks of statutory leave entitlement.
Where workers are unable to take annual leave due to being on sick leave, they will be entitled to carry forward the four weeks of EU statutory leave; however, the carried-over leave must be used within 18 months of the end of the holiday year in which the entitlement arose.
Rachel Levine is a solicitor at specialist healthcare law firm Hempsons. If you would like more information, please email Rachel at R.Levine@ hempsons.co.uk.
The free and integrated digital prescribing platform for all private prescribers.
CloudRx take care of the dispensing, payment and delivery of medicines direct to your patients, wherever in the country they may be, for more convenient access to their medicines.
TRANSFORMATIONAL
Order prescriptions at the touch of a button to add a whole new level of convenience for your patients.
SIMPLE, CONVENIENT AND SECURE
Simple and fast digital prescribing.
Legal paperless prescriptions, repeat prescriptions and controlled drugs.
Prescriber fees can be charged to the patient if required.
INTEGRATED
Our API enables frictionless integration with healthcare brands & clinical software including Semble, WriteUpp, MidexPRO, eClinic, Pabau and ClinicYou.
“We were struggling to keep up with the admin side of the prescriptions, not to mention storage for medication to cope with a huge increase in prescriptions. CloudRx immediately took away the strain. Since our partnership we have grown by more than 200% in size. We could not have achieved this seamless scalablity without them.”
– Dr Louise Newson, Newson Health
GP and MDU phone adviser Dr Rachel Sutcliffe responds to a request to discuss what to do if family members disagree about what is best for a patient
Dilemma 1 How can I settle siblings’ spat?
QI’m a private GP who has an older patient who recently moved into a nursing home following a stroke.
The patient is unable to speak or communicate, has a dense hemiplegia and is being fed via a percutaneous endoscopic gastrostomy (PEG). As such, the family and I agree that the patient lacks capacity to make decisions about their health and welfare, and that a care plan should be put in place to facilitate their care.
During the patient’s hospital admission, a DNACPR decision was agreed upon. Further to this, I believe it to be appropriate to prescribe antibiotic therapy for chest, skin or urine infections, but I don’t feel it is in the patient’s best interests to be admitted to hospital if they failed to respond to antibiotic therapy administered at home.
However, the patient’s daugh
In the interests of a frail patient
ter has told me that she disagrees with this view, saying that the patient has ‘no quality of life’ and is ‘being kept alive by the PEG’.
She feels this is cruel, not what the patient would have wished, and that they should be ‘allowed to die’.
The daughter has told both me and the care staff that she did not want the patient to have any active treatment, including antibiotics, and that she felt the PEG feed should be stopped.
The patient’s son, on the other hand, agrees with my approach and feels that the patient is comfortable and well cared for at the nursing home, but that the patient would not have wanted to be readmitted to hospital.
He wants the patient to have treatment to keep them comfortable – including antibiotics – at the nursing home.
I also understand that the siblings do not get along and that the two of them are unable to agree on how to proceed with their relative’s care.
I have a meeting next week with the care staff and the siblings and am not sure how to proceed. Can you advise?
AFirstly, it is positive that both siblings have agreed that the patient lacks capacity as defined by the Mental Capacity Act 2005.
If you have not done so already, it would be useful to document a capacity assessment and to check there was no advance decision or lasting power of attorney for health and welfare in place.
When this is confirmed, decisions about the patient’s medical care would then need to be made by you, as the decision-maker, in the patient’s best interests.
The patient’s daughter feels this is cruel, not what the patient would have wished, and that they should be ‘allowed to die’
The Mental Capacity Act Code of Practice (particularly paragraphs 5.63-5.69) may be helpful when considering how best to approach the meeting and family members who disagree about treatment. Ideally, as the decision-maker, it is your responsibility to determine the patient’s best interests and you would need to try and find a way of balancing the differing views and to decide between them. It might be possible to reach an agreement with the daughter at the meeting, but, if not, involving an advocate to act on the patient’s behalf could be considered. If the daughter disagrees with the final conclusions, it might be useful to arrange a more formal ‘best interests’ case conference. Ultimately, if all other attempts to resolve the dispute failed, the Court of Protection might need to decide on the patient’s best interests, but this would be unusual.
Flying in face of danger
Dilemma 2 Do I disclose her heart failure?
QI recently had an appointment with an older patient at my private general practice. During the appointment, she also asked for a twomonth supply of her medication as she was making ‘one last trip’ to visit her daughter in Spain.
I was quite concerned about the patient’s fitness to fly as she had recently developed severe symptomatic aortic stenosis, and a recent report from her private cardiologist had assessed her as having stage III heart failure using the NYHA functional classification system.
Having checked the UK Civil Aviation Authority (CAA) guidance, I shared with the patient that medical oxygen in flight is needed for those with class III heart failure and that the patient should disclose her diagnosis to the airline so that inflight oxygen could be arranged.
I also told the patient she could become seriously unwell and that her life could be at risk without oxygen.
The patient thanked me but said that she had no intention of
While other passengers might suffer inconvenience if a medical emergency occurred during the flight, GMC guidance would be supportive of a decision to maintain confidentiality. Paragraph 59 of the GMC’s confidentiality guidance states that doctors ‘should usually abide by a patient’s refusal to consent to disclosure, even if their decision leaves them (but no one else) at risk of death or serious harm.’ So what’s the way to tackle things if you feel it is
declaring her health problems to the airline because she was worried they would stop her travelling if she did and could not be persuaded even though I shared the CAA guidance with her.
I made detailed notes of the conversation, the advice given and that the patient had said she intended to board the flight without declaring her condition to the airline. However, I’m still quite concerned about the patient – is there anything else I can do?
AThe issue here is whether you could justify any disclosure about the patient to the airline in the absence of her consent.
This patient is an adult with capacity and has been appropriately informed of the risks to her health and life if she fails to disclose her medical history to the airline.
7467 8300
Beware of triggering
Warning! Some decisions doctors make can cause a tax liability that may unwittingly increase the amount you need to pay to HM Revenue and Customs. Accountant Alec James (right) reports
triggering hidden taxes
COMPANY CARS AND THE NHS FLEET SCHEME
Many doctors will have heard of company cars or the NHS fleet scheme. Both are very similar.
The difference is that company car costs are a deduction against your company profits, whereas the NHS fleet scheme costs are a deduction against your pensionable and taxable income from your NHS employment income.
To cover the personal use of the vehicles, the taxpayer with use of the vehicle is required to pay tax on the benefit-in-kind value of using the car.
This is calculated by taking the list price of the vehicle multiplied by a percentage which is based on the CO2 emissions of a vehicle and the fuel the vehicles use.
These schemes became popular when HM Revenue and Customs (HMRC) reduced the benefit-inkind rates on fully electric vehicles to 0% in April 2020. They are currently 2% of the list price of the car.
This results in very minimal tax being due on the benefit in kind but significant tax savings for the deduction of the costs of the car.
If you use the NHS fleet scheme, as I previously highlighted, this comes as a deduction against your pensionable income.
Depending on how long you have been contributing to the NHS Pension Scheme, when you return the vehicle at the end of the lease, this can cause growth in your legacy pension pots (1995/2008 schemes) that is in excess of the annual pension savings allowance.
The annual pension savings allowance is currently £60,000. If you have use of a company car provided from your personal company, there are a number of hidden tax liabilities that can arise if you do not take the correct steps. While not technically a tax liability, if the company car is not
purchased or leased in the company name, then the company cannot claim tax relief on costs of the vehicle or the associated running costs.
Therefore, these costs would be suffered by you personally rather than your company, thus losing the tax savings.
If you wish to use finance or a lease, these must also be in the company name.
Care must also be taken with your choice of car, as the tax treatment of a brand new electric car is different to a used one – including pre-registered vehicles – for the company.
Having a company car that is not fully electric, while tax deductible for the company, can lead to very significant personal tax liabilities for the employee using the car, because the benefit-in-kind percentage is much higher than an electric car.
If the company pays for petrol or diesel for company cars, it significantly increases the benefit-inkind charge, so it is usually best practice to pay for petrol and diesel personally.
It is always best to discuss any company cars or NHS fleet schemes cars with a specialist medical accountant prior to ordering.
PERSONAL USE OF COMPANY ASSETS
With inflation rates higher than they have been in the past, doctors with personal limited companies are often looking for ways of investing company funds rather than leaving funds in the company bank accounts.
Quite often this leads directors to consider investments such as high-value watches, jewellery, artwork or even classic vehicles.
While these investments are
allowable, provided they are in the company name, they are treated differently to other business costs. Instead of being deducted against your company profits, these costs form part of capital gains tax calculations when the asset is sold. It is important to remember that a limited company is a separate legal entity and therefore the assets purchased belong to the company and not you.
Any assets must not be used personally because they belong to your limited company, not you.
If you use a company asset personally, you will be liable to personal tax and your company would be liable to employers’ National Insurance contribution. In most cases, the liabilities are calculated using 20% of the value of the asset.
This value is based on when you first started to use the asset person-
If you have use of a company car, there are several hidden tax liabilities if you don’t take the correct steps
ally. This is particularly important if you make use of an appreciating asset.
It has been known that HMRC will review public photographs including social media to evidence that business assets are being used personally.
RESIDENTIAL PROPERTIES
Residential properties owned in a limited company have been another way doctors have tried to keep pace with inflation.
Again, while this is allowable, should you or a person connected to yourself use the property, you will be subject to a benefit-in-kind tax.
Companies that own high-value residential properties should take care that an annual tax is not chargeable. This applies to any property valued at more than £500,000 and the tax starts at £4,400 a year rising to £287,500 for properties worth more than £20m.
There are certain reliefs and exemptions available if the property is rented or actively marketed for rent, but you are still required to file an annual declaration.
You should also be aware that holding a large number of residential properties in the company is likely to mean that Business Asset Disposal Relief will not be availa-
ble when you wind the company up.
PRIVATE HEALTH COVER
A common benefit given to employees in the private sector across all industries is to provide a form of medical insurance or pay for treatment for an employee.
The arrangement works well for both employers and employees in that employers save tax on the payments made and the employee only pays tax on the cost of the policy.
Most private practice limited companies are family-owned businesses. While paying for private health insurance or costs are taxdeductible in your limited company, they will give rise to a tax charge to you personally and a employers National Insurance contribution for your company.
The net effect is that, after factoring in all the tax savings and charges, the overall tax savings are minimal and potentially adversely affected, but with the added administrative burden of operating a PAYE scheme and preparing P11d forms.
OVERDRAWN DIRECTORS LOAN ACCOUNT
Sometimes costs are inadvertently paid via a company that are deemed to be personal in nature.
week, which can be claimed in the absence of any other claim. However, there is a calculation that can be worked through to evidence a higher claim. This claim factors in the rooms in your home, the annual costs and the time spent working in the room.
Some doctors may try to formally rent a room from themselves to their business, effectively justifying 100% business use of a particular room in the household.
But care must be taken if considering this as a strategy of the business, as this can lead to a potential partial loss of principle private residence relief, which exempts any capital gains tax on the sale of your main place of residence. And it can also lead to the property being subject to business council tax rates. The rental income would also be subject to income tax for the owners of the property.
In such cases, the cost needs to be attributed to the particular director and potentially paid back to the company. This is known as a director’s loan.
Overdrawn directors loan accounts will be subject to a benefit-in-kind charge on the individual director’s tax return unless interest was charged – at the official HMRC rate or more – on the loan for the period of time it remained outstanding.
There is an exception to this rule, meaning that you do not have to charge interest or declare a benefit in kind for any loan up to the value of £10,000.
Regardless of the value of the loan, if it remains outstanding after nine months of the end of your corporation tax accounting period, then additional tax is payable known as Section 455 tax at 33.75%.
This tax can be reclaimed after you permanently repay the loan but it can take some time to recover from HMRC.
RENTING HOME AS OFFICE
Many doctors work from home, whether it being virtual appointments or administrative duties for their business. Claiming the use of home as office is an allowable cost. HMRC has a fixed rate of £6 per
Similar care should be taken if you chose to install a garden office in your home and pay for this via a limited company.
SELF-EMPLOYED ASSISTANTS
A lot of doctors will make use of self-employed assistants and secretaries. Sometimes these individuals may work on a self-employed basis or trade via a limited company.
HMRC pays attention to these arrangements, as they attract lower National Insurance rates and have the benefit of trading as a business rather than as employee. There are special rules in place called ‘Off Payroll Working’.
Various factors are taken into account when HMRC determines a status. These include how many businesses are invoiced, can the services be provided by a suitable replacement, if required, and can the work be refused.
Most of your practices will be treated as a ‘small business’. This means that it is up to the contractor to determine their own status. You should ensure that anybody who works regularly for you understands this and it may be a good idea to evidence that you have informed them you are a small business and tell them of their own responsibilities.
HMRC has a tool that can be used to help guide the status of a contractor which gives a result
If you use a residential property owned by your company, you will be subject to a benefit-in-kind tax
which can be used as evidence in the event of a HMRC inquiry.
It is also worth considering your own Off Payroll Working status if your business provides services to colleagues. This can be a complicated area and you should seek professional advice if you feel this applies to your business.
TAX-FREE CHILDCARE AND CHILD BENEFIT
When an individual has adjusted net income of more than £60,000 a year, HMRC starts to limit the amount of Child Benefit payment you or your partner are entitled to.
This is on a sliding scale such that when you reach £80,000 you will lose all of the Child Benefit and if this has been claimed, it will need to be repaid to HMRC.
In addition, many people make use of the free nursery hours and the HMRC tax-free childcare system. Access to these schemes is limited if your adjusted income is in excess of £100,000.
Breaching £100,000 means that parents are not eligible to use the Government Tax-Free Childcare scheme.
The £100,000 limit is also a cliff edge, so if your income exceeds the £100,000 threshold, the benefits claimed in the tax year are repayable to HMRC in full.
TAX ON PENSION GROWTH
The problems surrounding tax on excess pension growth (annual allowance tax) have been well documented and most medics are now at least aware of the issues.
If you have had a charge in the past, some individuals opted to use a ‘scheme pays election’.
A common mistake is that individuals use this option and declare it on their personal tax return but either do not submit a ‘scheme pays’ form to NHS Pensions or the form is rejected for some reason.
This means that HMRC never receives the funds from NHS Pensions and there remains an unpaid liability to the Treasury.
Often it can take years for HMRC to realise this is the case and, by the time it does, will charge interest and penalties for late payment.
Care must always be taken to ensure you do not have a hidden tax liability. Discussing your circumstances with a specialist medical accountant can ensure you are fully aware of any liabilities you may have.
Next month: What you need to know about working in other countries – Richard Norbury gives an update
a
Alec James is
partner at Sandison Easson & Co, specialist medical accountants
It has been known that HMRC will review public photographs including social media to evidence that business assets are being used personally
When an individual earns more than £60,000 HMRC starts to limit the amount of Child Benefit payment
DOCTOR ON THE ROAD: JEEP AVENGER
A rugged EV, but no four-wheel drive
Want to go green in the urban jungle? Dr Tony Rimmer (right) found this offering from an iconic marque a strong contender
It looks rugged and tough lower body panels give it a real off-road look
IF YOU were looking for a brand that represents ruggedness, some off-road ability and a touch of American character, you may well think of Jeep.
The Jeep started life in 1941 as the iconic small four-wheel-drive general purpose vehicle that was used by American troops all over the world during the Second World War.
You could say that it was the world’s first real 4x4, pre-dating the Land-Rover by seven years and started a trend that continues to this day. We all have images in our minds of heavily laden Jeeps tackling impossible looking terrain while looking tough and unstoppable.
Powerful brand
No amount of the manufacturer’s own advertising could create such a powerful brand image.
Unfortunately, in the post-war period, buyers wanted cheap family transport and the whole 4x4 movement had to wait another 20 years before becoming attractive.
Subsequently, Jeep had financial problems due to low sales numbers and the brand went through several ownerships.
In 2021, owners Fiat-Chrysler merged with Peugeot-Citroen to create Stellantis which is the fourth biggest global car producer behind Toyota, Volkswagen Group and the Hyundai Group.
Jeep has continued to produce cars with tough off-road appeal and, in the UK, offers four different classes of models of various sizes.
Like every other manufacturer, though, they have had to offer a pure electric option and in 2023
they launched the Avenger, a small crossover SUV.
I am old enough to remember the Hillman Avenger, but that is a different story. It is available in three trim levels: Longitude £34,800, Altitude £36,500 and the Summit £38,700, and it is this top model that I have been testing.
To keep costs down, the chassis and drivetrain is shared with other Stellantis EVs such as the Peugeot E-2008, Vauxhall Mokka E and the Citroen e-C4. A single 154bhp electric motor sends power to the front wheels fuelled by a reasonably sized 54kWh battery.
The body, however, is pure Jeep. It looks rugged and chunky with tough lower body panels giving it a real off-road look. Not that you would go looking for a steep muddy trail – there is no fourwheel drive here.
Ready for action
I have to say that, in the flesh, the Avenger looks the part: like a fullsized Tonka toy. It presents at its best in white or bright yellow to offset the contrasting black roof and cladding. With wheels at each corner, it looks ready for action.
Inside, the tough work-like theme continues with a body-coloured dashboard and the trim feels durable, if a bit scratchy. The driver has a large clear display in front with a large central infotainment screen offering all the usual amenities.
The front seats are comfortable and roomy, but the back seats are pretty cramped. This is a car that works OK with child seats or small adults, but would challenge a fully grown family of four. At least the
boot is of decent size and helped by the squared-off body design.
It is really on the road that the Avenger excels. Ironically, it is best suited to the urban jungle rather than the real jungle. Its compact dimensions, great visibility and instant electric get-up-and-go drivetrain make it a joy when nipping around town.
I can see it working really well as a second car to charge at home, zip to the supermarket, pick the kids up from school and have some fun while doing it. A real-world range of around 180 miles or so suits it well. The steering is direct and the ride is very compliant, less firm than many EVs.
So, Jeep has created a small electric urban runabout with a dose of character all of its own. The Avenger is a convincing small SUV, but suffers from the same stumbling block that has recently stalled the sales of all EVs: price.
The non-electric Avenger, which is coming to the UK imminently and powered by a 1.2litre engine with a manual gearbox, is –start-
ing at £23,600 – a full £11,000 cheaper than the cheapest electric version.
To those of us medics on a budget, particularly for a second car, that is significant. Still, I liked this electric version and the drivetrain suits its attributes. If you want to be green, give it some consideration.
Dr Tony Rimmer is a former GP practising in Guildford, Surrey
JEEP AVENGER summit
Body: Small five-door SUV
Engine: Single electric motor. 54kWh battery. Front-wheel drive Power: 154bhp
Torque: 260Nm
Top speed: 93mph
Acceleration: 0-62mph in 9.0 secs
Claimed range (WLTP): 245 miles CO2 emissions: 0g/km
On-the-road price: £38,700
The boot is of a decent size and helped by the squared-off body design
Inside, the work-like theme continues with a body-coloured dashboard
LOUD AND CLEAR?
Make sure you reach your target audience by advertising in Independent Practitioner Today
To discuss your requirements and for details of rates, contact Andrew Schofield at Spot On Media on 0161 408 3912 or email him at andrew@spotonmedia.co.uk
ADVERTISERS: The deadline for booking adverts in our May 2024 issue is 26 April
or for reprints, we would be happy to discuss licensing the copyright to you.
Published by The Independent Practitioner Ltd. Independent Practitioner Today is editorially independent.
Material is governed by copyright.
No part of this publication may be reproduced, stored in a retrieval system or transmitted in any form without permission, unless for the purposes of reference and comment. Editorial layout is the copyright of the publishers. If you wish to use it for promotional purposes on websites
WRITE TO Independent Practitioner Today 7 Lindum Terrace, Lincoln LN2 5RP
TELL US YOUR NEWS Robin Stride, editorial director Email: robin@ip-today.co.uk Phone: 07909 997340 @robinstride
ADVERTISE WITH US
To advertise in the digital journal, on our website or in our business directory, contact advertising manager Andrew Schofield at Spot On Media. Phone: 0161 408 3912 Email: andrew@spotonmedia.co.uk Follow Independent Practitioner Today on