The business journal for doctors in private practice
In this issue
Are you visible to patients?
Marketing expert Catherine Harriss reveals how patients find you online P16
Self-referral diagnostic testing is on the rise Hugh Risebrow explains the findings of LaingBuisson’s UK diagnostics market report P22
Analysis of the Budget
n See page 12
Weather the storm; don’t predict it
Benjamin Holdsworth on how to avoid predicting the unpredictable when investing P38
CMA reins in openness
By Robin Stride
Consultants have welcomed a pledge to limit the amount of information to be made freely available about their private patient outcomes.
Their response follows a new report from the Private Healthcare Information Network (PHIN) saying that, for specialists, publication into the public domain of measures beyond volume, length of stay, patient feedback and links to registries is not currently recommended.
PHIN explained that other measures – required by the Competition and Markets Authority’s (CMA’s) private healthcare ‘transparency’ order of 2014 – were ‘not yet appropriate for use as publicly available comparators; for example, because the quality and power of the data limits valid, statistical comparison’.
In a document, supported by the CMA, PHIN said it would continue to keep these issues under review in consultation with stakeholders.
The Federation of Independent Practitioner Organisations (FIPO) said it was pleased the CMA had accepted PHIN’s recommendations to limit the publication of consultant-level metrics until more valid information can be made available.
It added: ‘FIPO has long argued that outcome metrics derived from
In
association with
hospital episode statistics are not a suitable vehicle to differentiate clinical performance.
‘Realistically, patient choice of consultant is limited anyway, as it is only self-pay patients who are not constrained when choosing their consultant.’
In a 42-page assessment of what is needed to complete the CMA’s demands, known as ‘Private Healthcare Order Article 21’, PHIN recommended: ‘Information on all the Article 21 measures on consultant and hospital practice should be published on the restricted-access part of the PHIN website (the portal), so consultants and hospitals can use the information to monitor and improve performance.
‘Ultimately, this will benefit patients and consumers by improving the availability of data and transparency across the sector.
‘It will also enable hospitals and consultants to benchmark their performance against their peers –for example, to support their own clinical governance and quality improvement initiatives – and is a necessary step towards any wider publication.’
PHIN said publication in the public domain for the hospitallevel metrics was essentially complete.
But it needed to look at ways to improve compliance, including data presentation, coverage/participation and data quality. It also aims to
adopt some minor, technical enhancements to specific measures.
It said it should publish nationally aggregated data about procedures, with the ability for this to be broken down to show how outcomes may vary for different patient groups.
PHIN chairwoman Jayne Scott said the document marked ‘a significant milestone’ in the delivery of the CMA’s Order, as it set out the data that could be ‘meaningfully’ published for each remaining measure.
‘This means publishing data that is understandable by both patients and clinicians so that it can inform patient choice, facilitate shared decision-making or allow statistically valid comparisons between healthcare providers.
‘We remain committed to the principle of publishing data for use by patients but, as set out in detail in this document, this will be contingent on factors such as the quality, and statistical power, of the inbound data.
‘I am grateful to everyone who has been involved in this process which will continue our acceleration of activities and the improvements in patient care that should result.’
PHIN will work with the Patients’ Association and other patient research organisations to help it present information ‘in ways that are most meaningful and helpful’.
There is a 2026 deadline for publishing the CMA’s demands for information on various performance measures covering surgical procedures carried out in private hospitals.
PHIN said the report built on its ‘Roadmap and delivery plan 20222026 for the Private Healthcare Market Investigation Order 2014’, issued last year, and followed consultation with the private healthcare sector. This included private doctors’ representatives.
n https://www.phin.org.uk/ news/phin-publishes-evidencedbased-assessment-to-acceleratecompletion-of-cma-order ➤ See FIPO’s policy-shaping evidence to PHIN on page 5 and also on our website
Jayne Scott, PHIN chairwoman
TELL US YOUR NEWS. Contact editorial director Robin Stride
ADVERTISE WITH US. To advertise in the digital journal, on our website or in our business and lifestyle directories, contact Andrew Schofield at Spot On Media. Phone: 0161 408 3912
Email: andrew@spotonmedia.co.uk
GET A SUBSCRIPTION DISCOUNT
£90 independent practitioners. £210 organisations. £90 GPs and practice managers (private & NHS).
Save £15 paying by direct debit: individuals £75 (organisations £180).
TO SUBSCRIBE
Email karen@marketingcentre.co.uk
Or phone 01752 312140
Chief sub-editor: Vincent Dawe
Head of design: Jonathan Anstee
Publisher: Gillian Nineham
Email: gillian.nineham@gmail.com
Phone: 07767 353897
Follow Independent Practitioner Today on
EDITORIAL COMMENT
Pension tax may be back
It took a former Health Secretary to at last come up with what senior doctors and their representatives have been calling for over many years.
Chancellor Jeremy Hunt’s Spring Budget last month sprung a big surprise for financial commentators, consultants and GPs.
His pension rule changes, effective from 6 April 2023, went further than many dreamed of by scrapping the dreaded lifetime allowance of £1,073,100 completely – 17 years after its introduction.
The best that most had hoped for was to push up the cut-off point.
At the same time, the annual allowance was raised by 50% –from £40,000 to £60,000. That has been welcomed, although there is still a limit, which might mildly annoy the highest paid.
Just how much these changes will provide an incentive for doc-
tors to stay in their NHS jobs remains to be seen.
Help has come too late for those doctors who have already retired and were hit by lifetime allowance tax charges.
Doctors will be wise now to take professional advice on a raft of rules and complexities affecting their pensions – plus other developments in the pipeline –before deciding what is best to do next.
There is also the question of how long the Budget’s measures will be in force. What if Labour comes to power?
There must be a General Election by 23 January 2025 and the opposition has signalled it will be only too ready to bring back tax hits on pension limits.
Next month, one of our regular columnists will provide a closer look at the pension and retirement changes that impact you. Meanwhile, check out page 12 for an accountant’s analysis.
Ten ways to make you tax-efficient
As we start the new tax year, accountant Julia Burn gives ten top accountancy things to consider for your private practice business P14
The value of mentoring
Independent practitioners are often isolated from their peers. Dr Caroline Obsorne-White of Medical Protection shows the usefulness of a mentor P19
Behind the scenes of GMC helpline
We talked to those taking helpline calls about the impact it has had in giving clinicians a way to speak up, often in the most sensitive scenarios P24
Keep a track of your records
Dr Kathryn Leask gives advice on how long you should retain your patients’ medical records and explains how to dispose of them responsibly P26
Caring for embassy patients
With London starting to see increased demand from embassy patients, Simon Brignall discusses some essential billing and collection matters in their care P28
Watch how you hire advisers
Solicitor Robert McCartney has a warning to everyone who works as or who uses freelance workers –including ‘independent’ doctors P40
PLUS OUR REGULAR COLUMNS
Business Dilemmas: When a patient wants to change their name
Dr Kathryn Leask responds to private doctors’ queries in the latest of our medico-legal series P42
Accountant’s tips:
Get in your accountant’s good books
Alec James of accountants Sandison Easson shows how to keep financial documentation neat and simple P44
Doctor on the Road: There’s a hole in this Polo
Can the VW Polo GTI match the ultimate thrills offered by its big brother – the Golf – and its competitors? P46
Retirement flexibilities in the NHS confirmed
Partial retirement options opened up to help stop workforce exodus
By Edie Bourne
Doctors will be able to retire from the NHS, take pension benefits and then rejoin the pension scheme under officially confirmed new rules.
They will also be able to partially retire while retaining their current job role.
The outcome of the Department of Health and Social Care’s (DHSC’s) consultation into NHS retirement flexibilities was published last month after eight weeks of consideration.
As well as improving retirement options for doctors, the plans include changes to the pension valuation method which can lead to additional tax payments.
From April, doctors can retire, draw their NHS Pension benefits and rejoin the 2015 scheme to accrue further benefits – to be known as ‘retire and rejoin’.
There is no set limit to the pension benefits which can be accrued, as long as the member is under 75.
The previous 16-hour maximum working limit for the first month after ‘retirement’ has also been removed, but a minimum 24-hour break is required before re-joining.
From October this year, doctors can also take partial retirement
while keeping their job role and current terms and conditions. This will allow members of the 1995 section to enjoy the same facility as those in the 2008 section and 2015 scheme.
The new plans give those age 55 and over the choice to take up to 100% of their pension benefits.
Patrick Convey, technical director at specialist financial planners Cavendish Medical, said: ‘The con-
sultation outcome has provided many positive steps – something we’re not used to seeing for doctors pensions in recent years.
‘Along with the Budget news reducing pensions’ tax limits, there may be more options to discuss for those planning retirement.
‘We are also pleased that those who would like to continue working are able to do this while accessing their benefits.
IMPORTANT ADVICE FOR DOCTORS NOW – TAKE ADVICE!
Patrick Convey (right), technical director at specialist financial planners Cavendish Medical, issued the following message to Independent Practitioner Today readers:
‘With these NHS developments and new pensions tax savings limits announced in the Budget, it’s important that doctors have full discussions with their adviser to assess if their own plans should be updated.
‘Last month, the second consultation for the McCloud remedy was also launched to discern how the Government plans to implement the Remedy, which is due to be in place by October.
‘There are therefore many elements to consider now as part of a full retirement plan.’
The McCloud Remedy ‘Part 2’ consultation will last for 12 weeks and finish on 6 June 2023.
‘However, there are nuances to consider. Those wishing to apply for the partial retirement opportunity must agree to reduce their pensionable pay by at least 10%. This may prove particularly challenging for consultants who work a set number of programmed activities.
‘We await further guidance from the DHSC on how this might work in practice, but it could involve an agreement between the employer and consultant to make some PAs non-pensionable, for example.’
One of the other key outcomes from the consultation is a revision to the way pension growth is valued.
From the 2022-23 tax year onwards, the date that the 2015 pension scheme is revalued each year will be moved.
On 1 April each year, the 2015 pension is revalued to keep in line with the cost of living, using the Consumer Price Index rate from the previous year plus an additional 1.5%.
This date will now move to the 6 April each year to remove an anomaly which generates skewed pension growth and subsequently, larger pension tax payments.
See an accountant’s Budget report on page 12 and other coverage on our website news section
Budget dashes hope of medical cover boost
Hopes of incentives to boost the number of private medical insurance customers were dashed in the Spring Budget.
The Association of Medical Insurers and Intermediaries (AMII) reacted with disappointment at the lack of tax breaks for getting cover. It argued that tax relief on
Insurance Premium Tax would encourage health cover uptake, support a healthier population and incentivise employers to look after staff health, ultimately helping more to stay in work.
AMII executive chairman Dave Middleton said: ‘It is disappointing that the Chancellor has simultaneously raised corporation tax – from
18 to 25% – while refraining from introducing tax relief for the private medical insurance industry.’
With the NHS under such pressure, he added that the Government had missed the chance to take positive steps to encourage growth in the private medical insurance market.
‘While we welcome the £400m
of funding for mental health and musculoskeletal support, I would urge the Chancellor to go further and review the announcements made in the Budget to offer some much-needed respite for the private health and well-being sector.’ Tax relief on private cover premiums were also called for by the Confederation of British Industry
Takeover unites two MSK clinics
By Edie Bourne
Fortius Clinic, the UK’s largest single orthopaedic musculoskeletal group, has agreed to acquire Schoen Clinic London.
The acquisition is billed to create ‘a unique centre of excellence in orthopaedics and sports medicine in the capital’.
Fortius Clinic chief executive Jim McAvoy hailed the deal as a significant step forward for the company, allowing it to expand its range of services and offer a more comprehensive service to patients.
‘It complements our existing Fortius facilities, providing us with the extra capacity, options, and flexibility to support our consultants and patients at a dedicated centre of excellence in the heart of London.
‘We are excited to welcome Schoen Clinic London’s consultants, clinical teams and colleagues to the Fortius Clinic family, and we look forward to delivering world class care to even more patients as we strive to become Europe’s trusted partner in orthopaedics and sports medicine.’
All Schoen Clinic London members of staff, which included doctors on an employed contract, will be transferred across to Fortius Clinic. It is envisaged patient care will continue as normal throughout the transition period and beyond.
Fortius Clinic is part of Affidea
Group, the largest European medical provider operating over 330 clinics and leading outpatient and diagnostic centres, as well as centres of excellence in a variety of specialties for more than 12m patients every year.
Affidea’s chief executive and chairman Guy Blomfield said: ‘The combination of the Fortius and Schoen Clinic London clinical teams is compelling and will provide the London market with an unparalleled orthopaedic centre of excellence.
‘The UK, as with many European health systems, is underprovided for in this important category of care, and this combination will be the reference point to further develop higher acuity capacity across our European footprint.
‘While Affidea is Europe’s largest diagnostic and out of hospital care provider, it also has a significant number of single specialty hospital facilities in cancer care and orthopaedics. Our strategy to selectively add complementary centres of excellence for our patients is an important driver of service growth for the group.’
Schoen Clinic Group chief executive Dr Mate Ivancic said: ‘Our UK vision for the future is to significantly grow our footprint and capabilities in mental health treatment areas, as there is an unprecedented demand for mental health treatments in the UK.’
Completion of the Schoen Clinic London acquisition by Fortius Clinic is subject to limited regulatory approvals.
Strikes hit big healthcare meeting
One of private healthcare’s biggest annual events – themed as ‘Navigating the Future Together’ –had to be postponed due to fears that most attendees and speakers would not be able to find their way there.
LaingBuisson’s 10th Private Healthcare Summit, at Westminster’s QEII Centre, fell victim to a
planned tube strike and was called off with just over a week to go.
The educational and networking event planned to stimulate the private healthcare sector ‘to look forward, not back, and consider how providers, payers and patients will interact in a changing world of healthcare’.
Conference speakers from vari
ous countries were due to tackle some key issues facing the sector, including economic turmoil and the impact on healthcare, cost containment, recruitment and retention, the meaning of ‘valuebased healthcare’ and developing a digital community.
The new date for the event is Wednesday 17 May.
Private care trade body appoints new chair
The Independent Healthcare Providers Network’s (IHPN’s) new chairwoman is former Tory MP and Government minister Seema Kennedy, replacing Lord Kamlesh Patel of Bradford.
Under Theresa May’s premiership, she was Immigration Minister and Public Health Minister, and previously Parliamentary Private Secretary to the Prime Minister between 2017 and 2019, responsible for relations between MPs and Downing Street during the Brexit negotiations.
While MP for South Ribble in Lancashire, she cochaired the Jo Cox Loneliness Commission and earlier worked as a lawyer in the City with involvement on projects including the Emirates Stadium and St Bart’s Hospital. She said: ‘Healthcare professionals in the independent sector have played a vital role in recent years. They’ve supported the health of the nation through the pandemic, and now, often working in partnership with the NHS, are leading the way during a challenging period of recovery.
‘I will play my part to ensure our members and their staff continue to play an essential role in tackling care backlogs and that NHS and private patients are able to access timely, high quality care.’
IHPN chief executive David Hare said: ‘She has a wealth of experience in the commercial and political worlds and a real understanding of the challenges and opportunities which face the sector and our members.’
Former minister Seema Kennedy
The reception of Schoen Clinic in London’s Wigmore Street and the front of the Fortius Clinic in Marylebone (inset)
Brain clinic wins quality mark ‘first’ for research
By Douglas Shepherd
A pioneering private mind and brain clinic has become the first network of clinical trial sites to achieve the best practice Global Clinical Site Assessment Standard (GCSA).
Re:Cognition Health’s commercial clinical research operating processes went through a rigorous evidence based assessment to achieve all seven quality modules. The consultant founded company has eight centres in the UK and the US for international trials of disease modifying and new symptomatic drugs for Alzheimer’s disease and other neurological conditions.
It achieved the GCSA quality standard in key business areas: workforce quality accreditation (WQA), patient engagement, feasibility, study start up and initiation, study management and
closedown, R&D business strategy and governance.
The GCSA highlights high performing sites and provides an independent assessment and report on the quality, efficiency and effectiveness of current operational processes. It is part of IAOCR, the international accrediting organisation for clinical research.
Clinical operations director
Vicky Eyre said Re:Cognition Health wanted to ensure it was providing the best quality service to patients, their families, sponsors and clients, while also developing our team.
‘Through the GCSA accreditation process, we have been able to demonstrate best practices and processes. We are very proud of our fantastic team and we are
delighted that their hard work has been recognised with this accreditation.’
The GCSA gold standard has been ratified by a global advisory board of industry experts from a broad range of global and UK organisations and leads to a distinctive, internationally recognised quality mark.
This evidences that participating sites are operating to the highest global standards and builds confidence for patients, clinical trial sponsors and clinical research organisations.
Dr Conor ClerkinOliver, principal investigator at the company’s Birmingham centre, said: ‘In terms of the impact the accreditation process has had so far, we have seen that it is really useful to get an outside view from an independent organisation, receiving good, clear, structured feedback to streamline and improve processes.’
FIPO reacts to CMA’s easing of rules
The Federation of Independent Practitioner Organisations (FIPO) has welcomed the Private Healthcare Information Network’s (PHIN’s) recommendations to limit the publication of consultant level metrics until more valid information can be made available. (See page 1).
It gave the following responses to earlier proposals below:
Recommendation: Publication should initially focus on information related to admitted privately-funded care only.
Whole practice information is a worthy aim. However, the nature of NHS patient episode attribution and the manner in which NHSfunded care in the private sector is provided is at variance with the exclusively consultantled practice for privately funded patients. For that reason, we endorse PHIN’s
reticence in pursuing this at the moment.
FIPO supports this recommendation.
Recommendation: Information for all measures should be published in the PHIN portal for hospitals and consultants as a first step, as increasing transparency and openness in the sector is an important mechanism for addressing the AEC (Adverse Effects on Competition).
FIPO has repeatedly stated that the metrics as defined by the Competition and Markets Authority (CMA) are not necessarily indicators of consultant quality and valid comparisons based on these data are not possible.
FIPO is pleased that PHIN recognises the lack of statistical robust
ness and their limited value to patients.
However, restricted access to these metrics can reasonably allow their use as a governance tool to drive improvement. FIPO has always believed that metrics should be used to drive improvements and not for judgement.
FIPO supports this recommendation.
Recommendation: Information should be published to show information about procedures at a national level, as this will help inform consumer/patient choice.
FIPO believes that publication of national procedure volumes, with the added benefit of patient segmentation, will be useful for systemlevel resource allocation. FIPO would be wary of its use by private
sector stakeholders with a vested interest and does not believe that it would inform patient choice of private provider.
FIPO gives limited support for this recommendation.
Recommendation: There should be an increased focus on publishing information about compliance with the CMA’s Order.
FIPO knows that many consultants have tried unsuccessfully to engage with this process for a number of reasons. We believe that compliance with the order should be transparent at a hospital provider level. This would allow consultants to see which providers are able to support their efforts to engage.
FIPO gives limited support for this recommendation.
➲ See full response on our website
Dr Conor Clerkin-Oliver
Vicky Eyre, clinical operations director
Poor op practice harms surgeons
By Olive Carterton
Surgeons are facing early retirement and even spinal operations due to poor selfcare while in operating theatres, a study has found.
It highlighted a lack of awareness surrounding musculoskeletal disorders in surgical staff, caused by poor posture in the operating room – and the impact on the personal lives of surgeons and hospital departments.
The study – A Multi Centre Review of Musculoskeletal Disorders in Surgical Staff – was presented by junior doctor Rohan Bassi at the British Association of Plastic, Reconstructive and Aesthetic Surgeons (BAPRAS) annual conference.
BAPRAS president and consultant plastic surgeon Ms Ruth Waters said: ‘The presentation highlighted the importance of looking after surgeon and surgical staff well being in the operating theatre.
‘It’s imperative that these issues are raised and addressed to preserve the health and wellbeing of our surgical workforce, ensuring they are able to perform their vital duties without being hindered by preventable MSK conditions.’
The presentation drew information from an audit at Buckinghamshire Hospitals NHS Trust, where MSK disorders accounted for 727 absence days over just one year.
Discomfort was most commonly felt only an hour into an operation and one in seven surgeons outlined concerns about the impact of the pain upon their concentration and performance.
Recurring suggestions from victims included:
Installing ergonomic seats for surgeons;
Improving the placement of patients and tables;
Providing advice on posture and relaxation;
Having hospital authorities
offer physiotherapy and exercises to surgeons and surgical staff.
Study author Dr Bassi is calling for a raising of awareness and targeted training programmes to mitigate the risk of musculoskeletal conditions, work absences and early retirements.
He said: ‘The extended duration of some procedures, which can last upwards of seven hours, and the requirement to maintain physically taxing positions can result in substantial strain to the neck, shoulders, upper and lower back.
‘There have been documented cases of surgeons being forced into early retirement due to preventa
KEY FINDINGS
ble musculoskeletal disorders, as well as one surgeon having to undergo a spinal fusion surgery.’
One aspect of the study, devel
oped in consultation with consultant plastic surgeon Mr Daniel Markeson, centred on evaluating the efficacy of raising awareness about the negative impacts of poor posture.
Information posters included illustrations of recommended exercises designed to counteract these effects and a physiotherapist’s tips presented at an academic and well being day were well received by surgeons.
Dr Bassi added: ‘Implementing practices, such as engaging in brief stretching sessions every hour and monitoring the posture of surgical team members during procedures, can promote a culture of accountability within the surgical environment.
‘To raise awareness of the importance of addressing musculoskeletal health in surgery, it is crucial to provide relevant education and training to surgical staff during dedicated wellness sessions and academic halfdays.
‘Proactively addressing the issue can help prevent the occurrence of an MSK disorder epidemic among surgical personnel.’
The most common time to feel discomfort was at 60 minutes, with the average being 93 minutes
Only 3% of surgeons reported having had previous stretching/ exercise training
The four most common areas for discomfort were: lower back (42%), neck (41%), shoulders (35%) and upper back (32%)
The study revealed notable correlations between contiguous body regions, suggesting that discomfort in one region is almost invariably associated with discomfort in a neighbouring area
13% reported impact on stamina
14% reported impact on concentration and performance
25% reported impact on quality of life
34% reported impact on general posture
Results from 102 participants
Private GPs urged to question watchdog criticism
Independent GPs are being advised by a leading lawyer to be ready to challenge the Care Quality Commission (CQC) over clinical criticism.
His warning came after his firm noted an increase in aggressive critical findings by inspectors leading to poor ratings.
Paul Ridout, managing director of law firm Ridouts in London, told Independent Practitioner Today: ‘We have observed CQC describing medical treatment and prescribing decisions as “unsafe” or “requires improvement”.
‘Often the inspectors do not have clinical qualification and/or experience and, even where they do, that experience may not be current.
‘There can be a range of appropriate treatment options. Differences within themselves do not suggest a lack of safety. Even an outlier may be completely acceptable in the particular patient presentation.’
He warned that the CQC rarely discussed before coming to judgement and relied heavily on its reading of notes, which did not give a complete picture.
Mr Ridout added: ‘A finding of unsafe practice can have very serious and farreaching implications beyond the CQC report itself.
‘Independent practitioners are more vulnerable than those with NHS or employer support. Always take the time and effort to justify your clinical decisions.
‘Remember that there are only ten working days to challenge from receipt of the draft report. Always ensure that your clinical notes are detailed and support your decisionmaking.’
Ms Ruth Waters, BAPRAS president
Solicitor Paul Ridout
Private units improve their watchdog rating
By Douglas Shepherd
Nine out of ten independent hospitals have – for the first time –achieved the top two ‘good’ or ‘outstanding’ overall ratings from the Care Quality Commission (CQC).
Analysis by the Independent Healthcare Providers Network (IHPN) has shown that 91% of acute independent, nonspecialist hospitals have now been assessed as being in the top two categories overall for quality of care.
Reaching the milestone of more than 90% being rated ‘good’ or ‘outstanding’ – a rise from 70% in 2018 – is seen as an important marker for the sector and a demonstration of a strong commitment to continuous improvement around safety and quality.
The other CQC ratings are ‘inadequate’ and ‘requires improvement’.
Dawn Hodgkins, IHPN director of regulation, said: ‘Despite the huge challenges presented by the pandemic and ongoing health system recovery, this demonstrates the commitment of clinicians and leaders across the independent
sector to deliver the very best quality of care and the safest services.
‘I’ve been really encouraged by the improvements I’ve seen in the culture of many providers, where there’s been a better focus on creating an open, learning environment where improvement is actively sought, with greater openness and honesty.’
She said a good indication of this were the increasing numbers of providers’ Freedom To Speak Up (FTSU) Guardians, now numbering nearly 230.
IHPN medical director Dr Howard Freeman said: ‘One of the key ways we have seen improvements is through better clinical governance. We now have better systematic, written standards and frameworks and that is now showing up in providers’ CQC ratings which is incredibly pleasing.’
The Medical Practitioners Assurance Framework (MPAF), launched in 2019 and refreshed late last year, is seen as having made important contributions to safety improvements.
Led by former National NHS Medical Director, Sir Bruce Keogh, the MPAF contains key principles
to strengthen and build on medical governance systems already in place in the sector. It sets out expected practice in a number of key areas, which providers are expected to adhere to.
Dr Freeman added: ‘The embedding of the MPAF has been a great step forward. It’s also been very positive to see how the GMC and CQC have recognised and endorsed the MPAF.
‘It has informed how the CQC assesses how “well led” independent services are, and it’s a requirement of the NHS standard contract too.’
IHPN chief executive David Hare said the 91% achievement was a strong indication that the general standards of care and patient safety in the private sector were higher than they had ever been.
‘Achieving this level of consistent high performance is really encouraging. It’s a good indication that patients can really trust the quality of care in the independent sector.
‘But we know providers are committed to maintaining and improving these already high standards, so the journey doesn’t stop here.
See page 38
GPs ‘to go same way as dentists’ and become private
A surge in private GP numbers is being predicted following Government imposition of their NHS contract effective this month. The development has brought howls of protest with GP leaders warning extra workload and lack of practice investment will lead to an exodus of more doctors from the health service and longer patient waits.
Healthcare commentator Roy Lilley responded with a warning that NHS GPs would go the same way as dentists after having their cage rattled while being busier than ever.
Writing in his daily blog on nhsmanagers.net, he said: ‘The haruspex in me is saying: GPs won’t give up being GPs, but they are very likely to give up the NHS and become private GPs.
‘Internet searches for “private GP” are up 151% in England. Most leading health insurers now have access to roundtheclock “virtual GP” services. They are quick, cheap to set up and popular.
‘Expect the Waitrose middle classes to be prepared to take money out of their purse to have the convenience and reassurance of having a GP in their pocket.’
Calling the imposed contract in England seemingly crass and cackhanded, he criticised the imposition ahead of the publication of the Delivery Plan for Recovering Access to Primary Care.
‘As we don’t know what’s in the recovery plan, quite how we can contract for the year that will deliver most of it, seems baseaboutface to me.’
Mr Lilley reported that, at January 2023, there were the equivalent of 2,078 fewer fully qualified, full time NHS GPs and 2,224 more patients compared to eight years ago.
Dawn Hodgkins, IHPN director of regulation
Commentator Roy Lilley has chaired health authorities and NHS hospitals
Howard Freeman, medical director of the IHPN
Teamwork core to new private unit
By Agnes Rose
HCA Healthcare UK’s new multispecialty private hospital, opening in Birmingham this autumn, has announced the appointment of its medical director.
Behind the driving seat at The Harborne Hospital is Mr Simon Radley, who has more than 37 years’ experience in the healthcare industry, specialising in general and colorectal surgery.
He has played a key role in introducing new surgical protocols and techniques to the University Hosp ital Birmingham and was instrumental in setting up the Birmingham Bowel Clinic, the first private centre of excellence for managing bowel conditions in the West Midlands.
In his new role, he will be responsible for providing medical leadership, supporting the consultant body and – along with the leadership team – ‘creating a progressive and inclusive culture within the hospital’.
Mr Radley said The Harborne Hospital would offer comprehensive and specialist care across multiple disciplines.
‘Throughout my career, collaborating with the best clinicians to deliver patients the best treatment and care has always been paramount to me. This is an approach which I intend to carry through to my role as medical director at The Harborne Hospital.’
Claire Smith, chief executive of Joint Ventures at HCA, said:
‘Simon’s extensive experience with launching new clinics, techniques and protocols, alongside his leadership and business background, will support our commitment to having exceptional people, delivering exceptional care.
‘Simon was trained in Birmingham and has continued to work in the region for the majority of his career, so we can think of no one better to lead and manage the hospital’s highly qualified workforce.’
HCA said he would work with
London Bridge Hospital opens GP clinic
A new walk-in GP centre has been opened by HCA’s London Bridge Hospital.
It offers immediate access to GP-led medical care for professionals working in The City, as well as commuters and tourists who need a quick appointment.
Fifteen-minute face-to-face GP appointments for anyone aged 18+ cost £80.
Located opposite London Bridge station at 29 Tooley Street, the facility offers patients same-day access to GPs, without the need to book an appointment.
HCA said patients could walk in or call ahead and a private clinician would be available to see them on the same day ‘with no waits or delays’.
The centre, on the London Bridge Hospital campus, gives access to facilities including imaging, outpatients and diagnostics, as well as a broad population of specialist consultants if needed. It can also support private referrals into London Bridge Hospital through HCA UK’s 24/7 Acute Admissions Service
HCA Healthcare UK reports a significant increase in
demand for primary care services since 2019, most notably across:
Health screenings (25%);
Occupational health appointments (28%);
Specialist referrals (62%).
London Bridge Hospital boss Janene Madden said:
‘Our patients can see a private GP on the same day or at a time that suits, giving them greater control of when they can access care, as well as peace of mind.’
chief nursing officer Claire Hubbard ‘to actively promote a culture of quality, improvement and learning within its workforce’.
Mr Radley’s training began at Birmingham University Medical School and he continued surgical training in general surgery in the West Midlands, before completing specialist colorectal surgical training at St Marks Hospital in London.
He took up a post as senior lecturer and honorary consultant surgeon in colorectal surgery at Birmingham University and the Queen Elizabeth Hospital, becoming a consultant colorectal surgeon at University Hospital Birmingham in 2002.
More recently he has become increasingly involved in introducing new consultants to private practice with an emphasis on building teams and partnerships, encouraging collegiate working within the independent sector.
Cleveland Clinic opens cancer centre in United Arab Emirates
Cleveland Clinic has opened a new cancer facility at its Abu Dhabi hospital in the United Arab Emirates.
It said the 205,000 square foot unit, the Fatima bint Mubarak Center, would help eliminate the need for patients to travel abroad for their treatment and care. Cancer is the third most common cause of death in the UAE and the primary reason patients travel out of the region for care.
Simon Radley, appointed medical director of Harborne Hospital
An artist’s impression of HCA’s Harborne Hospital in Birmingham, located on the Queen Elizabeth Hospital Birmingham campus
Venous registry hits milestone
By Olive Carterton
A consultant’s initiative of a web database to collect and store information about patients with venous disease has reached a significant milestone with the enrolment of its 3,000th patient.
The registry was established by the College of Phlebology, a professional organisation dedicated to advancing the field of venous medicine.
The College of Phlebology Venous Registry collects data related to the diagnosis and treatment of venous disease, including patient demographics, medical history, imaging studies, treatments received and patient outcomes.
Data is collected from participating healthcare providers and used for research to improve understanding of venous disease and identify best practices for its diagnosis and treatment.
The registry also includes patient-reported outcomes (PROMs) including quality-of-life measures and recurrence, collected automatically from patients at six months, one year and then annually thereafter.
Reaching this milestone is a significant achievement for the College of Phlebology and demonstrates a growing interest and participation in the registry among healthcare providers and researchers.
The registry has already yielded important insights into the diag-
nosis and treatment of venous disease. As registry patient numbers continue to grow, it is expected to become an even more valuable resource for clinicians and researchers.
College founder Prof Mark Whiteley, of the Whiteley Clinic, is the main participating healthcare provider in the registry. He believes the database is an invaluable tool to help doctors better understand the venous disease and improve patient care.
He told Independent Practitioner Today : ‘By collecting data from a large number of patients, we are able to identify trends and best practices that can help us provide more effective treatments and better outcomes for our patients.’
Doctor participants can download their own statistics with a
comparison to other members of the registry. They can use this data for their own revalidation and to ensure their results fall within the normal outcomes for venous treatments.
Patients can also be reassured that if they choose doctors who are part of the College of Phlebology Venous Registry, then their results will be monitored and checked for acceptable outcomes.
The college is encouraging more healthcare providers to participate in the registry and so continue the momentum and growth of the database.
As the registry continues to expand, it is expected to have an even greater impact on the diagnosis and treatment of venous disease and ultimately improve patient care.
New IT boosts eye groups’ appointments
Specialist surgeon-owned clinics in eye care group OCL Vision expect to benefit from faster scheduling of appointments and other features following the company’s implementation of new software. Their private eye care facilities in London and Hertfordshire are
Private sector hails Budget assistance for occupational health service
The private hospitals’ trade body has welcomed announcements in the Budget of plans to make more occupational health services available to the UK’s workforce.
An occupational health subsidy pilot for small businesses will be widened with more funding as the Government seeks to encourage employees to get help while they are still in a job.
A consultation is expected to propose a requirement for employers to provide occupational health services.
David Hare, chief executive of the Independent Healthcare Providers Net work, said the Budget announcements highlighting the importance of occupational health services were encouraging.
With businesses concerned about ever-increasing absence rates and NHS waiting times currently so high, he thought it was good to stimulate employers to provide and develop occupational health so employees could access the right support to keeping them fit and well.
Mr Hare added: ‘Several of our members already provide vital support to businesses and organisations. This includes services like screenings, health assessments, physiotherapy, nursing, emotional and mental health support, risk assessments or creating ergonomic work environments.
OCL Vision chief executive Paresh
Patel said clinics were currently rolling out the system.
installing Streets Heaver’s EHR and PAS system, Compucare 8, to bring improvements in the way clinical data, patient records and administrative tasks are managed. The software includes a range of features such as electronic patient records, appointment scheduling, billing and invoicing.
Paresh Patel
‘Responsive, high-quality occupational health services can be vital preventative measures or lead to earlier interventions and diagnoses.
‘All of this can reduce time away from work, as well as the physical and mental stress for everyone concerned. Creating more opportunity for people to benefit from these kinds of services at work can only be a good thing.’
IHPN’s David Hare
A look back through our journal’s archives of a decade ago reveals that although times change, some issues are not so new
A trawl through the archives: what made the news in 2013
Another rise in pension contribution
Private doctors paying into an NHS pension were feeling the pinch after being hit by the second contribution hike in 13 months.
Some saw deductions of up to 13.3% of their pay at a time when they were hurting from Chancellor George Osborne’s one-year extension of an NHS salary pay freeze.
The Department of Health implemented the first of its annual pension rises in April 2012, when the average consultant’s contribution rose from 8.5% to 9.9%.
In this second wave, for consultants with pensionable NHS salary of up to £110,000, the increase in contributions was from 9.9% to 12.3%.
For those with NHS salaries of over £110,000, the increase was from 10.9% to 13.3%.
We reported that doctors faced further contributions rises, up to a maximum of 14.5% for highest earners, in 2014-15.
Specialist financial planners
Cavendish Medical said doctors had felt another blow due to the Budget’s extension of the 1% pay rise cap for public sector works for an extra year to 2015-16.
Managing director Simon Bruce said: ‘The current pay rise at 1% is less than half of the CPI inflation rate of 2.7%, meaning an effectual pay cut. And even at this level, this rise is still large enough to negate “fixed protection” for those active members signed up to it.
Patients call for doctors’ prices in advance
Nearly one-in-ten patients interviewed in an independent ICM poll of private medical insurers’ customers said doctors should inform them of the consultation cost and likely cost of any subsequent treatments before an initial appointment.
84% thought specialists should ensure they were aware of outcome data for their treatment and the consultant’s success rate.
87% expected insurers to pursue value for money on their behalf, three-quarters thought some doctors charged too much, and 76% believed insurers should use medical evidence to help prevent their customers from going through unnecessary and ineffective treatments.
Patients ask GP about self-pay
Two-in-five NHS GPs reported a rise in the number of patients asking about self-pay treatment.
A ComRes survey for Spire Healthcare found half of the 1,000 GPs interviewed thought the private sector offered good value for money for patients seeking self-pay treatment or using their private medical insurance.
Software allows faster bill payment
Consultants and providers were being promised faster payment with new ‘intelligent validation’ technology from healthcare online solutions firm Healthcode.
The technology checked the policy-holder information on the bill submitted by the provider against that on the insurer’s own database and recognised any discrepancies.
Bupa, the first medical insurer to take up the procedure, said the secure solution would help smooth out the small number of errors encountered in the electronic billing process – which would benefit consultants, providers and its members.
One hospital group producing more than 3,000 bills daily said the service allowed the patient information to be 100% correct
before it reached the insurer ‘and we are more likely to be re-imbursed more efficiently’.
Revalidation boosts IDF membership
Scores of private doctors signed up to strengthen the voice of the Independent Doctors Federation. Much of the 26% membership rise resulted from doctors joining for appraisal and revalidation, using the organisation’s designated body status.
Medical tourists quit
Private doctors were warned they risked losing out on a medical tourism boom because they were not harnessing marketing opportunities.
The International Medical Travel Journal warned the UK ‘continues to sit back on its laurels’ when it comes to the medical travel sector.
TELL US YOUR NEWS
How about making the news today? Independent Practitioner Today is always keen to hear from doctor entrepreneurs willing to share their stories in private practice – and from independent practitioners embarking on the journey.
Contact our editorial director Robin Stride at robin@ip-today. co.uk
Financial year end stressing you out?
Make your end of the year less taxing with Civica Medical Billing and Collection
Let Civica Medical Billing and Collection provide you with support while you focus on your practice.
Using Civica Medical Billing and Collection you can:
• Reduce bad debts to less than 0.5%
• Increase net income by up to 25%
• Your own dedicated account manager
• Get timely, accurate, easy-to-read financial reports
• 24/7 online access to your data
• Faster payments through e-billing for insurers and patients
BUDGET ANALYSIS
What will Chancellor Jeremy Hunt’s Spring Budget mean for you? Richard Norbury (right) highlights the main areas affecting Independent Practitioner Today readers and suggests some action points
What came out of this red box?
FOR DOCTORS , the announcements on pension legislation is likely to be welcome news, although the changes will not remove the issues of annual allowance tax for all.
But the higher annual allowance level will help many doctors reduce or extinguish their annual allowance tax liabilities.
Lifetime allowance
The Government announced that, from the 6 April 2023, the Lifetime Allowance (LTA) charge would be removed and that in 2024 it would be abolished altogether.
Many of you may have different forms of lifetime allowance tax protection and although the LTA tax no longer applies, there is a limit on the maximum tax-free lump sum that can be taken, which from 6 April 2023 is £268,275 –25% of the current LTA.
Currently, if the tax-free lump sum is exceeded, the excess is taxed at 55%, but from 6 April 2023 onwards, the excess will now be taxed at an individual’s marginal rate of tax.
For those of you that are considering partial retirement and pensionable return under the new rules, you should consider that the LTA may well be resurrected in the future by a Labour administration.
Annual allowance
The annual allowance limit is set to increase from £40,000 to £60,000 from 6 April 2023.
This is good news, but the issue of tapering of the annual allowance may still arise.
Be mindful that tapering – only to be applicable if taxable income exceeds £200,000 – can still reduce the £60,000 annual allowance. The lowest tapered value increases from £4,000 to £10,000.
In addition, if your 1995/2008 pension scheme grows by less than inflation, the new rules will allow an offset against the 2015 scheme growth.
Corporation tax
It had been announced last year that corporation tax would increase from 19% to 25% from 1 April 2023. Companies with profits between £50,001 and £250,000 will have their rates apportioned such that the overall rate is lower and companies with profits of up
to £50,000 will continue to pay 19% tax.
For investment companies, corporation tax is 25% irrespective of the level of profits.
In scenarios where company accounting year-ends are not 31 March and profits exceed £50,000, an apportioned tax rate will be applicable.
Childcare working parents
This has been extended to children from nine months to school age, but this will be delayed until April 2024 and then there will be a staged implementation.
The ‘cliff edge’ threshold of £100,000 still applies, meaning any parent having adjusted net income over this amount results in ineligibility for the scheme. Tax planning opportunities exist and should be discussed with an accountant.
Capital allowances
From 1 April 2023 to 31 March 2026, full expensing has been introduced. Basically, this allows companies to write off eligible capital expenses immediately against profits.
For special rate expenditure, which does not qualify for full expensing, a 50% first-year allowance can be claimed instead. Capital allowances can be claimed on the balance of expenditure in subsequent accounting periods.
Although this only applies to
limited companies, self-employed individuals and partnerships continue to have a similar type of relief known as the Annual Investment Allowance.
Share dividends
Previously, it was announced that the tax-free dividend allowance from 6 April 2023 will drop from £2,000 to £1,000 and in the following tax year to £500.
The Government increased the individual tax on dividends when the National Insurance rates increased by 1.25% due to the ‘health and social care levy’ and has decided to keep the rates of 8.75% for a basic-rate taxpayer, 33.75% for a higher-rate taxpayer and 39.35% for an additional-rate taxpayer.
Tax thresholds
Announced last year, the threshold at which the 45% rate of tax applies drops from £150,000 to £125,140. This is also the threshold where individuals will now pay the 39.35% tax rate on dividends.
Capital gains tax
The capital gains exemption threshold was previously set at £12,300, meaning any capital gains above this amount in a particular tax year were subject to tax.
From 6 April 2023, this threshold has been reduced to £6,000 and the plans are for this to be
The annual allowance limit is set to increase from £40,000 to £60,000 from 6 April 2023. This is good news, but the issue of tapering of the annual allowance may still arise
☛ Detailed news on the Budget, and reaction to it, are featured in the news section of our website
halved from 6 April 2024, meaning only £3,000 of gains are exempt from tax after this date.
Change of basis of taxation
Although not officially part of the Budget, sole practitioners or partnerships with non-31 March or 5 April year-ends will undergo a transition in the tax year 2023-24, whereby the ‘current year basis of assessment’ will be changed to a fiscal year basis.
The financial year-end of accounts can still be retained, if so desired, but adjustments made to tax profits on a fiscal year basis.
If the change in taxation increases tax as a consequence, then provisions are in place to allow this additional amount to be paid over five tax years.
The additional tax would have always been payable arising on retirement from a partnership or cessation of private practice, but at least now there is the welcome opportunity to spread it over five years.
Given the significant changes, it is an opportune time to review your affairs and trading structure with a specialist medical accountant to ensure your current trading structure is still the right strategy for your private practice going forward.
Richard Norbury is a partner with Sandison Easson specialist medical accountants
Childcare payments will be payable to children from 9 months to school age
Ten ways to ensure you are more tax-efficient
As we start a new tax year, Julia Burn (right) gives ten top accountancy things to consider for your private practice business
to you x-efficient
1 Capital/fixed asset expenditure
With the super deduction and 100% first-year capital allowances available, it may be worthwhile spending money on capital equipment needed by the business before the accounting year-end rather than after it in order to bring forward the available tax relief.
For qualifying assets, the level of capital allowances available basically means that the cost incurred can be fully deducted – or in some cases enhanced – from the company profits before corporation tax is charged, therefore reducing the amount of tax payable.
2 Remuneration
For owner-managed businesses, it is essential that you have a discussion with your accountant to ascertain the most tax-efficient way to remunerate yourself. These discussions should at least be had before the end of the tax year – 5 April each year – and also before the end of the business’s accounting year, if that is different.
If you are a director and shareholder in the business, it may be worthwhile taking a mixture of salary and dividends to make use of all available tax allowances and to benefit from the differences in tax rates.
Based on your total income, your accountant will be able to review the most tax-efficient way for you and the business to pay you your remuneration.
3
Long-term contracts/ work in progress
Contracts and treatment plans that span an accounting year-end need to be considered.
If a patient is receiving a longterm treatment, a discussion with your accountant should be had to understand when the income for that treatment should be recognised for accounting purposes, as it is unlikely to match when the invoices are actually raised. The income recognition also affects the timing of any tax liability.
4 Cash flow forecasts
Understanding your business’s cash-flow forecast and being able to anticipate when
pinch points could occur is always an essential part of the management process.
This is even more important currently due to the nature of the economy and the requirement to have a tight handle on your company cash flow and to understand when funds are likely to flow both in and out.
Understanding the company’s debtor recoverability – that is to say, when customers pay and whether different types of customers, such as the self-payers and the insured, have different payment terms – plays a big part in building cash flow forecasts.
It is also important to understand whether there are cash restraints affecting the business that require a thorough review of costs to identify potential areas for cost-cutting.
5 Tax liabilities
It is important to understand the timing of all tax liabilities, whether they relate to the business or you personally.
There is a distinction between the tax liability due dates for limited companies and businesses that are sole traders or partnerships. Limited companies have to pay corporation tax nine months after the end of their accounting year – which is different for each company.
Sole traders and partnerships have to pay income tax and this is due on 31 January following the tax year (5 April) and they may also have to make a payment on 31 July if they are subject to payments on account.
Other tax payment dates to also be aware of are PAYE, National Insurance and VAT, where applicable. It is useful to diarise these to ensure there are no unwelcome surprises.
6 Growth plans
Review growth plans and understand the resource requirements that this will require.
Will you need to employ more staff to achieve the growth plan, how much will this cost, how will this be funded and will there be any other ancillary costs – for example, will the business need more space?
What other additional costs may there be? When considering fund-
ing for the business, will new investors be required or will bank funding be needed?
7 Succession planning
It is important to consider the company’s succession planning route.
When you retire, you may want to sell the business or there may be someone internally that will step into your shoes and continue the practice.
Whichever exit strategy you choose, you will need to discuss with your accountant to ensure that the strategy achieves the most tax-efficient route for you.
It is also important to understand early on what the potential tax consequences of a sale may be and to plan for this well in advance.
8 Properties
Does the business own any properties? Are these being fully utilised? If – as many businesses have done as a result of Covid –there is an element of hybrid working, is there available space that could be sub-let?
9 Accounting records
It is important to have accurate, timely accounting records to enable the business to run as efficiently as possible while you concentrate on your clients/patients. Are you using the best software for your business? Is the booking and invoicing function fully integrated with the accounting package?
Is there anything that could be done to streamline the process and make real-time information available?
10 Group practices
Where the practice is part of a group and there are any functions that can be centralised, consider ways to share costs. Are the different branches set up in the most tax-efficient way?
In summary, there are many factors for a business to consider regarding their finances and these are not just concentrating on the year-end accounts and tax prepared once a year.
Julia Burn is a director at accountants Blick Rothenberg and part of the team that advises medical practitioners
HOW PATIENTS FIND YOU
Patients are taking their health into their own hands as far as they can by increasingly looking online.
Catherine Harriss explains there is now an obligation for private doctors to provide the information they need… if they really want to increase their practice
Are you visible to patients?
PATIENTS ARE looking for you online. And negative perceived changes in our NHS mean more people are doing it.
Patients are no longer waiting; instead they are seeking out their own information – either learning more about their condition or seeking answers to their health issues.
In early 2020, it was calculated that 7% of Google’s daily searches were health-related. That’s around one billion every day.
Whatever information is available to them, they will use. Unfortunately for them, this can be incorrect as well as correct.
Why are people searching online?
Eighty-four per cent of people want to solve their own problems using search engines.
As 92% of the global search market is dominated by Google, then this means that, for the purposes of this article, I am only going to talk about Google.
In 2021, the terms relating to Coronavirus took three of the top five Google searches.
Yes, we were still in the midst of a pandemic, but people were taking it upon themselves to find the answers to their questions online. We know that GP surgeries were overwhelmed and so another source of information was sought.
In the same year, 56% of web searches took place on smartphones.
This indicates to me that people are using their phones more and more to find immediate answers and solutions to their problems. People spend nearly four hours of their day on their smartphones.
We also know that, in 2019, seven out of ten internet users in the US would look up customer reviews on their phones while in a shop when approaching an employee.
Who is searching online?
In brief, most people are searching online and the trend is only going to increase. By the year 2025, it is predicted that 95% of people will have a smartphone.
In 2021, 88% of adults owned one, with 96% in the 16- to 24-year-old age group, but 78% aged 55 and above.
➱ continued on page 18
The free digital prescribing platform for all private prescribers.
CloudRx take care of the dispensing, payment and delivery of medicines direct to your patients, wherever in the country they may be, for more convenient access to their medicines.
TRANSFORMATIONAL
Order prescriptions at the touch of a button to support all consultations and add a whole new level of convenience for your patients.
SIMPLE, CONVENIENT AND SECURE
Simple and fast digital prescribing.
Legal paperless prescriptions, repeat prescriptions and controlled drugs.
Prescriber fees can be charged to the patient if requested.
INTEGRATED
Our API enables frictionless integration with healthcare brands & clinical software including Heydoc, MidexPRO, eClinic and YouClinic.
“We were struggling to keep up with the admin side of the prescriptions, not to mention storage for medication to cope with a huge increase in prescriptions. CloudRx immediately took away the strain. Since our partnership we have grown by more than 200% in size. We could not have done that without their support.”
– Dr Louise Newson, Newson Health
How are people searching online?
In the main, people are using what are known as ‘long-tailed’ keywords to find the answers to their specific problems. 92% of searches are for search terms that have four or more words, thus the name ‘long tail’.
For example, you may be a chest physician and one of your main symptoms for disease is the presence of a cough.
While you might think that the term ‘persistent cough’ would be an obvious search term, a user might search for ‘cough that won’t go away’. In fact, 3.5k people in the UK search this term every month.
Another 1.1k of searches then search for ‘I have a cough that won’t go away but I am not sick’.
So, as a chest physician, you want to help someone with a persistent cough because it could be a symptom of many ailments. By responding to a potential patient’s needs directly, you are more likely to engage a possible patient and also educate them correctly.
From experience, ranking high up on Google for the search term ‘persistent cough’ is going to be far more difficult than ‘I have a cough that won’t go away but I am not sick’.
If you can answer this, then there is a greater chance that your target audience will read your article and then move further around your website and hopefully make contact.
Focusing down, when a user does land on a website, 30% of users will do a more detailed search using the search bar. So, if your content is lacking, users will move to another site.
When a user finds the information they need via a search function on a website, then they are more likely to book or buy. In essence, the user experience needs to be easy and straightforward.
This behaviour means that if the information you provide is not available or is written in a way that is not easily understood, then you have lost a possible patient.
Where are they searching online?
Google, Youtube and Facebook, predominantly.
In the UK, 71% of British people
consider Google to be more relevant1 than other search engines. Youtube’s use has grown by 40% since 2014 with more than 500 hours of video being uploaded every minute.
Facebook has 3bn active monthly active users. In the UK, around 66% of the total UK population are Facebook users.
In context, Google receives 40,000 search queries per second. In the UK, 3.2m people every day use YouTube to learn about fitness or health and 46% of all searches looking for local information.
After talking to friends and relatives and seeking their opinions, the next step is to conduct an online search, look at the reviews and think about the location.
I have heard this thought process happen day after day through the thousands of conversations I have had with patients and it remains irrefutable.
This is the logical progression and very rarely, it seems, is the GP mentioned. Patients are taking their own health into their own hands as far as they can and so there is an obligation to provide information that they need . . . if you want to increase your practice.
Doctors’ YouTube channels Recently, in October 2022, YouTube launched health product features 2 in the US. This means that for licensed healthcare professionals in the US, there will be the opportunity to make their YouTube channels eligible for talking about health-related issues and, subsequently, providing credible and trusted information.
There is no doubt that it is only a matter of time before this becomes an option for UK health professionals too.
With so many users of Facebook in the UK, it is not surprising that many seek out medical information there. For many, Facebook is a virtual support group where patients learn from patient leaders. Using the search bar, Facebook becomes a search engine of its own, but researchers at Health Feedback3 found that seven out of ten articles that were shared contained misleading or false information.
In fact, it removed more than 20m posts that related to misinformation about Covid. Through the
WHAT ARE PEOPLE SEARCHING FOR?
According to Trial Facts,4 almost 100% of internet users aged between 18 and 49 seek health-related information online:
66% have looked online for information about a specific disease or medical problem
55% have looked online for information about a certain medical treatment or procedure
47% have looked online for information about doctors or other health professionals
45% have looked online for information about prescription or overthe-counter medications
35% have looked online for information about alternative treatments or medicines
20% have looked online for information about experimental treatments or medicines
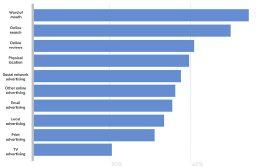
HOW PEOPLE GET HEALTH INFORMATION
support groups I have helped to manage on Facebook, it is clear that one of the major roles of such groups is to clarify the truth and to support individuals to get the healthcare they need from the right people.
Time to be a creator
It really is time to be a creator of content and let others be consumers. Having spent years connecting patients to the right medical help, to help a patient directly so that they feel you are communicating directly with them is never more so important.
Create content via articles that seek to answer your ideal patient’s queries. By implementing this approach and then sharing on your clinic’s social media, you will quickly build up your authenticity, trust and approachability.
All these are major qualities of a clinic that engages patient’s
online. More importantly, you will be contributing correct information to the internet, helping many others in the process.
Catherine Harriss (right) is founder of MultiWorks Marketing.
Website: https:// attractdreamcustomers.com
From: Google’s Impact in the UK 2020
The value of mentoring
Private practitioners work in busy, challenging environments and are often isolated from their peers. Dr Caroline Osborne-White (right) discusses the value of a mentor in stimulating reflection and sharing concerns
MENTORING CAN be described as a protected relationship that supports learning and experimentation, and helps individuals develop their potential.
A mentoring relationship is one where both mentor and mentee recognise the need for personal development. Successful mentoring is based upon trust and confidentiality.
It gives a doctor the opportunity to reflect on their experiences, both good and bad, and look to what they want for the future.
It is important to have someone in your professional life who respects, challenges and supports you in your career. This person can also support you in a demanding environment or in becoming an effective leader even as you reach the later stages of your career.
Many medical organisations, including the BMA, support mentoring for doctors, as it can reduce the risk of adverse events and bring problems to the fore at an early stage, reducing the risk of major and escalating difficulties. The GMC also encourages mentoring.
Benefits of a mentor
You may already have a ‘business mentor’ but having a mentor to help with the clinical and ‘soft’ skills can be just as valuable.
Private practice, especially in small or singled-handed clinics, can mean a restricted approach to problem solving, where the risk of not keeping up to date with the necessary knowledge and skills can be higher.
Significant research has been undertaken into the value of mentoring in the UK over the years, including by the Department of Health and the Doctors Forum. Articles have also been published in medical journals. They conclude that practitioners involved in mentoring report their experiences very positively.
Mentors can increase their mentee’s confidence, job satisfaction and sense of collegiality, facilitate a renewed focus on aims and objectives, improve working relationships, enhance problem solving and help reduce the risk of complaints.
Mentoring can provide support and assistance in developing strategies for dealing with specific ➱ continued on page 20
issues. These issues can vary widely from looking into ideas for small changes to dealing with serious professional and interpersonal relationships.
Many of the strategies practitioners adopt through discussion with their mentor can be lifechanging. These strategies can be used in resolving a major crisis in their professional life, making major changes in ways of thinking and acting or considering significant changes in direction.
The Doctor’s Forum found that practitioners who had a mentor really valued the time dedicated to them for reflection, with someone they trusted actively listening and challenging their thinking, but not problem solving on their behalf.
This allowed them to work through their problems in absolute confidence, within the ethical framework accepted by all doctors.
Barriers to mentoring
There are a number of reasons why practitioners may not wish to engage in a mentoring scheme.
These may include a lack of perceived need, time constraints or a misunderstanding of what is involved. It is also worth remembering that you can seek a different mentor should you wish to.
Taking on the role of a mentor is personally satisfying as you are contributing to the development of a fellow doctor, while refining your existing skill set
What could mentoring involve?
In the UK, mentoring is not a homogenous, standard product; there are considerable variations in how it is perceived and practised.
There are different mentoring models – most characterised by the flow of help in a single direction.However, co-mentoring is also an option where the emphasis is on mutual support and an open dialogue between two autonomous practitioners.
One of the key ingredients in many mentoring arrangements is the skill of ‘active listening’, a technique that assists those who are speaking, helping them to explore their thoughts and experience at their own pace without interruption and without the listener giving advice.
TIPS FOR MAKING THE MOST OF MENTORING
Reflect on your long-term goals
Learn and accept feedback
Practise good communication
Practise high standards of professionalism
Consider a periodic mentor check-up
There are many mentoring programmes across the country offering different types of mentoring schemes. You can contact your royal college or local deanery to find out more.
Revalidation
Revalidation is a vital part of the profession, and engaging with reflective practice will assist in appraisals and continuing professional development. It can help you to gather evidence of your achievements and lessons learned on an ongoing basis.
Being a mentor
The benefits of having a mentor are well recognised; however, there is much value to be gained from mentoring someone else.
Taking on the role of a mentor is personally satisfying as you are contributing to the development of a fellow doctor, while refining your existing skill set.
It can be used as an opportunity
to review and validate what you know and what you have accomplished. Teaching another doctor helps you to remember all that you have learned – and have the satisfaction of being able to pass it on.
You may even learn from your mentee. Often your mentee will be younger than you and they may have knowledge you do not have or look at a task in a different way. They can help you to enhance your people-development skills and you may even learn more about yourself.
Going forward
The evidence is clear that all practitioners can benefit from mentoring, whether in the capacity of a mentee or a mentor.
Practitioners often act as mentors to less experienced colleagues during times of transition, but mentorship should extend further than this and be incorporated at all stages of a medical career.
CASE STUDY: HOW MENTORING HELPED A DOCTOR
Dr A was a paediatrician who had been working as a consultant for four years. She had been involved in a sad case of domestic abuse involving several children.
One child had suffered extensive injuries and nearly died. The child’s parents were charged in the criminal courts and Dr A had to give evidence in the trial.
The trial was very stressful and Dr A received verbal abuse outside court from friends and family of the parents. Dr A found this very traumatic and had to take time off work to recover.
Dr A returned to work, but felt that work was much more stressful now than before. She questioned every decision that she made and was very anxious about facing another situation involving non-accidental injury of a child.
She received a complaint from another family about a very minor understanding and she had the full support of her colleagues in responding to the complaint.
However, she recognised that she had found dealing with the complaint more stressful than any similar situation in the past.
Dr A discussed how she was feeling with clinical director, Dr B, also a consultant paediatrician. Dr B had faced a similar experience a few years previously, where he had been involved in an adverse incident that had changed his way of thinking and made work more stressful.
Dr B had successful mentoring and recommended this mentor.
The mentor, Dr C, was a professor of paediatrics, and an experienced mentor. Dr A approached Dr C, and Dr C agreed to be Dr A’s mentor.
Dr A was then able to discuss her experience with Dr C, and Dr C gave Dr A time to explore what had changed as a result of the case of nonaccidental injury. They were also able to explore what Dr A thought would be beneficial to her.
Over time, they discussed that Dr A’s main concern had been about giving evidence in court and how stressful that had been, and Dr A was able to conclude that she was fearful of having to go to court again.
Dr A felt that time to undertake continuing professional development in this area, including about appearing as a witness and preparing for court, would help.
They also established that it would be helpful for Dr A to go and observe some court cases so that she could experience different scenarios as an observer rather than a witness. The aim was for this to make her more confident should she be called to court again.
Dr C remained Dr A’s mentor for several years, with decreasing contact as Dr A’s confidence and self-esteem returned. Over time, Dr A realised that she had a lot to offer as a mentor herself and started the process of training to become a mentor to support others.
Dr Caroline Osborne-White is a medico-legal adviser for Medical Protection
Download the app and register online www.pharmacierge.com/register
mPrescribe® app allows you to prescribe flexibly without a laptop, for delivery to your patients nationwide
Secretary Supported
GP and Consultant Reviews
Administrator access reduces workload for practitioners. mPrescribe® facilitates patient entry, status monitoring and preparation of prescriptions for mobile authorisation.
Clinical Governance
Co-founded and co-owned by leading private clinicians, our secure and encrypted technology is compliant with all GPhC, GDPR and e-Prescribing regulations.
“Wonderful, seamless, easy to use service.” Dr Catrin Bevan, London General Practice
“Intuitive and secure.” Dr Tim Wigmore, Consultant Anaesthetist and Intensivist
“Delivered the same day.... Outstanding!” Dr Elisa Astorri, Academic Physician Rheumatologist
“Go the extra mile.” Dr John O’Donohue, Consultant Gastroenterologist
“Consistent, efficient , friendly and responsive.” Dr Tim Ladbrooke, Courtfield Private Practice
Self-referral diagnostic testing is on the rise
LaingBuisson has recently published the second edition of the UK diagnostics report which provides detailed analyses of the £8.5bn spent in the UK on imaging and laboratory diagnostics. Hugh Risebrow (left) reports
CONSULTANTS IN private practice will typically refer 7080% of patients they see for at least one diagnostic test.
Most radiologists and histopathologists will have income from reporting private cases and or NHS backlog cases. There are a number of facts and trends which may interest those in private practice.
Independent healthcare only accounts for 3% of pathology tests and 5% of images, as many patients have diagnostics within the NHS and elective treatment uses less diagnostics.
Private diagnostics accounts for over 15% of market value due to the much higher prices charged to medical insurance and private patients than incurred in the NHS.
There are cases where private patients can access more sophisticated diagnostics, especially genetic testing related to determining the optimum cancer treatment, where the NHS is far behind many European social health insurance funds.
Low rates
By contrast, since the last LaingBuisson Diagnostics UK Market Report three years ago, private medical insurers have anecdotally become more willing to fund tests which will, for example, avoid unnecessary chemotherapy.
The overall rate of MRI and CT scans and the number of radiologists and pathologists in the UK per capita is well below the OECD average.
The UK has the second lowest combined number of radiology/ histology consultants per 100K, and about half the median figure. CT and MRI scans are at c60% and 80% of the OECD respectively.
Interestingly, the utilisation of scans and expensive tests such as genomics in private care is much more in line with affluent countries.
The UK model of private diagnostics, especially outside London, typically involves consultants referring patients to the imaging and pathology services provided by the private hospital where they are undertaking the clinic.
UK consultants do not receive any financial benefit from this.
Hugh Risebrow is the author of the Laingbuisson Diagnostics UK Market Report
This is very different to the model often found on the Continent, where many imaging centres and some labs – even after private equityowned groups rolling these up – are owned by radiologists and pathologists and pay the referring consultants for their clinical input to the test.
Manpower shortage
The UK has reversed the trend in training radiologists, but demand still outstrips supply. Histopathology training places continue to go unfilled.
There is a large demand for reporting of backlog NHS histology and radiology. One key difference, with the low level of digitisation in NHS histology, is
that while a growing amount of backlog radiology and nighttime urgent scans can be reported overseas, very limited amounts of histology are being reported offshore. The typical amount paid to radiologists and histologists for private patient cases – £60£80 for an MRI, CT or simple histology case – is four to five times the amount typically paid for NHS backlog work. While private medical insurers have driven down fees to consultants for procedures and outpatient appointments, particularly as most are now ‘fee assured’, radiologists and histologists have been relatively immune from this, possibly because the hospital charges the insurer for a reported case and the hospital usually pays the consultant.
More recently, we are hearing about a growth in self-referred MRI and CT scans, dubbed by one provider a ‘reassurogram’
It will be interesting to see when and whether these rates are cut –less likely while there is such a shortage of consultants.
New technologies
The report looks at new technology. There has been a huge flow of private equity funds into articicial intelligence (AI), but little of this is yet impacting diagnosis. There is some use of AI in streamlining the reporting of prostate and breast biopsies.
Technologies to use AI as one of the reporters for mammograms appear close to clinical use after several years of being used to support audit. The NHS focus seems to be to use these as cost saving.
Private providers are more likely to use them to improve outcomes while retaining the use of consultants. The impact over the next three to five years is likely to be limited, but longer term it will be interesting to see how AI will support consultants.
The latest LaingBuisson Diagnostics UK Market Report looks at the short term impact of Covid. Private investigations and procedures declined dramatically during Covid as bed capacity was initially purchased for Covid patients and the Covid guidelines reduced capacity.
Changed behaviour
Meanwhile, private labs saw their revenues more than treble and their profits grow by a factor of more than ten on the back of Covid testing, with no benefit to independent practitioners.
Covid does seem to have significantly changed consumer/ patient behaviours. We are all much more used to being tested and to sampling ourselves.
Many people have become much more aware of their health
and are more interested in measurements of health and taking control of their own health.
We are also much more used to Teams meetings and hence more willing to accept virtual consultations.
Combining these factors with difficulty accessing GP appointments, we are seeing a growth in consumers purchasing diagnostic tests without a medical referral.
Typical examples are wellman/ wellwoman tests as a general health check, allergy tests or patients buying PSA, thyroid function, vitamin D or other tests to monitor issues of specific concern, especially where NHS funding is limited.
There are a number of providers of these tests who either offer a postal service (Medichecks and Thriva) or access to phlebotomist (Randox and London Medical Laboratories) or both.
Self-referred MRIs
More recently, we are hearing about a growth in self referred MRI and CT scans, dubbed by one provider a ‘reassurogram’.
While this may be good for the diagnostic companies, the ethics of testing without symptoms, medical history or medical referral need examining.
We also need to consider the potential impact of patients concerned about a result slightly outside of a reference range.
Direct to consumer testing, excluding Covid tests, without medical referral still only accounts for 5% by value of the market – <1% by volume due to much higher prices – but appears to be finally growing after a lot of false starts.
Diagnostics UK Market Report – 2nd Edition – LaingBuisson
Hugh Risebrow is the chief executive of healthcare consultancy Latchmore Associates, who specialise in strategic and commercial advice to private and NHS providers.
He is the non-executive chairman of Spencer Private Hospitals, a nonexecutive director of Digital Pathology Partners, who provide histology reporting services to the NHS, and sits on the UK advisory board of Citadel, who provide laboratory and radiology software. He was previously chief executive of Synlab UK and commercial director at Guy’s & St Thomas’ NHS Foundation Trust
Behind the scenes of the GMC helpline
It has been just over ten years since the launch of the GMC’s confidential helpline, an anonymous route for doctors and health professionals to discuss or raise a safety concern.
Independent Practitioner Today talked to those taking the calls about the impact it has had in giving clinicians and their colleagues a way to speak up, often in the most complex and sensitive scenarios
CONFIDENTIAL HELPLINE IS OPEN TO ALL SECTORS OF HEALTHCARE
‘Thousands of patients use the private sector every year in the UK and, as with all of healthcare, safety is a top priority. Our confidential helpline is a source of support open to health professionals across all sectors.
‘If you have a safety concern you want to discuss, get in touch.’
CHARLIE MASSEY, GMC CHIEF EXECUTIVE
SINCE ITS launch in December 2012, nearly 5,000 calls have been made to the GMC helpline.
Dayo Harland and Peter Landray have worked in the contact centre for five years, beginning as contact centre advisers.
Both are now senior advisers and split their time between calls, emails and webchat, answering general inquiries as well as calls to the confidential helpline.
WHAT IS THE PURPOSE OF THE HELPLINE?
Dayo: It’s a confidential way for doctors to address things that may be going on in work or even just things they want to discuss or sound out.
It’s also for other health professionals if they have a concern about a doctor and patient safety. If you decide to raise a concern, we’ll support you to do so.
We also signpost callers to other organisations that people may want to reach out to.
The BMA has a lot of support for doctors on things like well-being and mental health.
Sometimes the issues are wider than an individual case where a doctor’s fitness to practise is not the issue, or not the only issue, so we can advise on the next steps for that, as well as looking into the concern where we can.
HOW DOES A HELPLINE CALL DIFFER FROM YOUR AVERAGE CALL INTO THE CONTACT CENTRE?
Peter: Because of the anonymity, there’s much more pressure to gather information. We’re making sure that if a concern needs to be investigated, we have as much detail as possible.
The calls can also be a lot longer, often more than an hour to cover everything.
Because calls are often anonymous, once that call ends it could be the last time you speak to that person.
DO YOU RECEIVE CALLS FROM THE PRIVATE SECTOR AS WELL AS THE NHS?
Dayo: We do; from doctors themselves and also colleagues who want to discuss the conduct of those they work with.
Recently, I spoke to a caller with a concern around inaccurate medical notes and follow-up care.
Peter: Every concern raised is treated in the same way – from your initial phone call right through to the triage and investigation stages.
WHAT ARE THE CHALLENGES OF CALLERS WISHING TO REMAIN ANONYMOUS?
Peter: If we miss out one key piece of information, we’ve no way of going back to a caller to find out more or request things like further evidence.
It’s understandable that people might be daunted by it and how raising a concern might reflect on them, so we try to support that however we can
Peter: Someone calling might never have spoken to anyone about the issue before and just want to speak to somebody who understands why they’re concerned and help them do something about it.
WHAT KIND OF ISSUES OR CONCERNS DO YOU TYPICALLY HANDLE?
Peter: We do have less serious calls that come through – we recently received a call to the helpline from a patient who was not very happy that their doctor had retired, which I’m sure was flattering for the doctor in question, but not something the confidential helpline is designed for.
Dayo: An option we let people know about is to make a temporary email account to keep up to date with how a concern progresses and be contactable while still remaining anonymous.
It’s understandable that people might be daunted by it and how raising a concern might reflect on them, so we try to support that however we can.
We get a lot of calls where someone is calling on behalf of a colleague they’re concerned about or just to see what the process might be for another person.
The last call I took was a person concerned that their colleague was being taken advantage of professionally by a superior and often undermined.
That’s a complicated situation for those involved, so we need to work around that sensitively.
HOW DO YOU HELP CALLERS TO FEEL MORE COMFORTABLE SPEAKING TO YOU?
Dayo: The main thing is to let people speak. I’m not there to make any decisions or judgements; I’m there to listen and take information down when there is a safety concern and let them know of support available to them.
All information could be relevant, depending on how a concern progresses, so we’re exploring all avenues to build a picture to pass on to the investigating team. My view is that if it is important to the caller, it’s important to the GMC.
But there are some very serious ones too. I took a call not that long ago which raised a concern involving the death of a patient. That’s when it really hits home how important these avenues are.
WHAT HAPPENS TO A CONCERN AFTER CONTACTING THE CONFIDENTIAL HELPLINE?
Dayo: All calls we receive go to the GMC’s Fitness to Practise investigations team, who then triage them and if a serious or repeated concern is found, it will be investigated further.
WHAT WOULD YOU SAY TO THOSE THINKING OF CONTACTING THE CONFIDENTIAL HELPLINE?
Peter: Recently on a call, a person told me ‘If I don’t do it now, I might not do it at all’, so there’s a sense of duty there for a lot of people, but we understand it’s also nerve-wracking.
I would just reassure anyone thinking of calling that they are going to be heard and going to be taken seriously.
It’ll be a friendly voice that they come through to. We’re here to support you and trained to do so sensitively. For some people, it’s enough to have the conversation, but if there is an issue that needs to be acted upon, we’ll take it forward.
If you are a doctor or health professional and would like to use the confidential helpline, you can find out more on this page of the GMC website: www.gmc-uk.org/ concerns.
Keep a track of your records
How long you should retain your patient’s medical records is a frequently raised issue by independent practitioners. Dr Kathryn Leask gives advice and explains how to dispose of them responsibly
Mental health records, including psychology records, are retained for 20 years after cessation of treatment or ten years after death;
Obstetrics, maternity, antenatal and postnatal records are to be retained for 25 years after care has ceased, but as they are also considered to be part of the child’s record, the longer retention period should be considered;
Records used in evidence in pub lic inquiries must not be destroyed until guidance is issued by the rel evant inquiry;
Complaints records must be kept separately from the patient file and retained for ten years from the closure of the complaint or any related processes such as liti gation.
The MDU regularly receives requests for assistance many years after the event in question and an absence of records can make it much harder to mount an
RECORDS HAVE a number of important functions, from supporting clinical decision-making and continuity of care to providing evidence of what happened in the event of a complaint or claim. But how do you decide when they have served their purpose and what should you do when that time comes?
Retention periods
There is no specific statutory provision covering the retention of private medical records. However, the GMC says: ‘The UK health departments publish guidance on how long health records should be kept and how they should be disposed of. You should follow the guidance, even if you do not work in the NHS.’
The most recent is the Records Management Code of Practice published in 2021 by NHSX covering NHS and social care records. It sets out the minimum retention periods for many key types of medical records, including:
Adult health records are usually retained for eight years;
Children’s records are retained until 25th birthday, or 26th if the patient was 17 when treatment ended;
GP records for deceased patients are usually retained for ten years after death;
GP records for patients who have deregistered and the reason is unknown are still to be retained for 100 years. This is under review;
The code is a live document that is subject to amendments, so it makes sense to check the latest version on the NHS website rather than relying on a downloaded PDF version.
Practitioners in other parts of the UK should follow the Scottish Government Records Management Code of Practice for Health and Social Care (Scotland) 2020, the Welsh Records Management Code of Practice for Health and Social Care 2022 and the Good Management, Good Records –Disposal Schedule in Northern Ireland.
Bear in mind that the recommended retention periods are the minimum. It might be appropriate for records to be retained for longer if you are aware of an adverse incident or a complaint, so it is a good idea to review records before consigning them to the ‘destruction pile’.
The MDU regularly receives requests for assistance many years after the event in question and an absence of records can make it much harder to mount an effective defence against allegations.
At the same time, you should balance these medico-legal considerations against the requirements of the Data Protection Act 1998, which says you should not retain records for longer than necessary. If in doubt, seek advice from your medical defence organisation.
Secure storage
You might decide to archive paper records that are no longer in daily use until they are no longer needed. If so, they must be stored
KEEPING TRACK
Independent practitioners have a responsibility to look after their patient’s medical records, but records management outside the NHS can be challenging, so be ready to seek expert advice.
Above all, it is important to keep track of all the records held by your practice so you can check when they were created, their minimum retention date, date of review and their whereabouts/date of destruction.
securely, protected from damp, and accessible should it be necessary to respond to a complaint or claim. It is important to keep a record of archived material and review it at regular intervals so it isn’t forgotten.
Be careful about storing records off-site: some self-storage may not be sufficiently secure or dampproof and it could be difficult to find and retrieve a record if they have been stacked on shelves and not properly labelled.
Confidential record management companies may be a better option, but you should ensure they comply with data protection law and meet industry standards (ISO 27001:2013 – Information Security Management Systems).
Disposal
If you are satisfied that records can be destroyed, this should be carried out in such a way that protects patient confidentiality and in accordance with national and local waste disposal requirements.
Paper records
Documents which include identifiable patient information should be destroyed by cross-cut shredding or incineration. Do not simply throw out records with domestic waste, as they could later be found on landfill.
If you are outsourcing the destruction of records, use a licensed confidential waste disposal company and have a suitable written agreement with them.
This should acknowledge the
records’ confidential nature and confirm the company will take all reasonable steps to protect that confidentiality. NHSX signposts organisations to guidance on information destruction which is available from the British Security Industry Association (BSIA).
Computer-held records
We recommend that you talk to an IT professional about permanently destroying electronic records, as these may be difficult to delete entirely from a hard drive.
As above, be sure the company concerned is reputable and follows data protection law. The NHSX recommends checking providers are on the ISO Register. It also points users to the Information Commissioner’s Office guidance on deleting personal data, which covers putting information beyond use if it cannot be fully deleted.
Dr Kathryn Leask (right) is a medicolegal adviser with the Medical Defence Union (MDU)
It’s a diplomatic mission caring for embassy patients
With London starting to see increased demand from embassy patients, Simon Brignall discusses some essential billing and collection matters you need to be aware of when looking after these patients
IT IS key for any business to have a mixture of revenue streams to create a portfolio effect that lessens the impact of shifts in demand –and the private healthcare sector is no different.
There are many patient groups outside of the traditional private medical insurance and self-pay sector where a consultant can operate and generate additional revenue and, in London, treating embassy patients is one such option.
The patient mix of private practices in central London often differs to those practices located around the UK, as practices outside of the capital may include NHS patients being treated in private hospitals.
Many central London-based practices capitalise on the benefits of medical tourism, which can appear in the form of international self-pay patients or patients whose treatment is funded by
other countries via their diplomatic mission.
The ‘black swan’ nature of the pandemic and its impact on international travel meant that these patients have been in short supply. The demand from international patients accessing healthcare in the UK saw a significant reduction because the impact of lockdowns and travel restrictions were suffered by overseas patients wanting to come to the UK for treatment.
Signs of recovery
But recent data from market analysts LaingBuisson suggests that this market is showing signs of recovery from the lows of 2020.
There is an expectation that embassy patient activity through central London-based independent hospitals in 2023 will finally surpass 2019 levels by 10%.
So let’s explore embassy work and what you need to know from a ➱ continued on page 30
billing and collection perspective if you are thinking of including this sector as part of your patient mix.
There are more than 50 embassies within London; however, most of the patients come from the big four, which are Kuwait Health, Kuwait Military, United Arab Emirates Medical and Qatar. Here are some important things you need to be aware of should you decide to treat this important patient category.
Complex cases
The patients that you will be sent by the embassies often have complex conditions and this is one of the main reasons why they travel to this country.
These can include patients whose previous procedures/treatments were unsuccessful or require revisional surgeries.
Allow enough time
When you see the patients for their consultation, they will normally be accompanied by an interpreter.
Before you treat an embassy patient, it is crucial for you to obtain a Letter of Guarantee
This, in combination with the probability of the patient presenting with a complex case, means that the consultation is likely to take longer than normal and so you will need to allow more time in your clinic diary.
Do you have all the necessary documentation?
Before you treat an embassy patient, it is crucial for you to obtain a Letter of Guarantee –referred to as LOG.
The LOG will authorise treatment for the patient and it is important for it to be issued in your name.
This is a precursor to raising an invoice to an embassy, because, without this vital document, it is unlikely your invoice will be paid.
Impact
on your cash flow
Probably the most important point to consider about taking on embassy activity is that payment often can take a long time.
The impact this can have on a practice’s cash flow should be
Probably the most important point to consider about taking on embassy activity is that payment often can take a long time
understood and may limit the amount of this type of activity you do when compared to other patient groups with faster payment cycles.
Embassy
guide
As many consultants start seeing embassy patients without having given due consideration to all the points I highlighted above, I thought it would be useful to produce a simple check list to assist you (see box below).
As you can see from this article, it is crucial for you to get your practice prepared correctly, preferably before you start treating patients.
Failure to do so could mean that you end up seeing a lot of patients where you end up waiting a long time for payment – or worse, not get paid.
Simon Brignall (right) is director of business development at Civica Medical Billing and Collection
A USEFUL CHECK LIST FOR EMBASSY WORK
LETTER OF GUARANTEE
It is vital that a letter of guarantee (LOG) is obtained before any treatment is carried out.
This document will vary slightly depending upon the embassy it is issued by. It will typically specify the patient’s demographic details along with the appointment date(s) and the reason for the treatment as well as specifying the consultant and the location.
Always check that the dates specified in the LOG cover the treatment dates on the invoice, as this can often be a reason an invoice is rejected.
There is normally a set of terms and conditions covering the LOG and you must always submit this document in conjunction with your invoice to the embassy in a timely manner to ensure the best possible chance of receiving payment.
Some embassies also require a medical report along with the invoice and LOG. If this process is not followed correctly, then you run a much greater risk of treating patients without getting paid.
ANAESTHETISTS
Anaesthetists will require a LOG in their own name, not the name of the surgeon carrying out the operation.
CHARGE APPROPRIATELY
Your treatment fees need careful consideration before you start to see patients, as your patient may require a mixture of inpatient and outpatient consultations, inpatient care, procedures and occasionally intensive care.
Procedure pricing should also consider the level of complexity, especially when it is beyond the scope of what is described by the Clinical Coding and Schedule Development group (CCSD) schedule.
Your fees may also want to reflect the impact of some of the other issues I have discussed that arise when treating this patient group.
Whatever your decision, it is important that this is communicated clearly to the relevant embassy to avoid any misunderstanding or disputes about payment.
DELAYED PAYMENT CYCLE
Be prepared for the extended duration of the embassies’ payment cycles and allow for this within your practice’s cash flow.
There are taxation impacts to consider, as you may find yourself paying tax to HM Revenue and Customs (HMRC) on invoices that have still not been paid. This could have a devastating effect on your cash flow if you have not planned accordingly.
CHASING
Make sure you have a robust system in place to chase for payment and that it is routinely followed to ensure your money is collected.
The embassies are always busy, particularly the big four, and it is not uncommon for them to have a sizeable backlog of invoices waiting to be paid.
It is vital to keep a record of when and how your invoices were sent to the relevant embassy and copies of all supplementary documentation provided in case they get misplaced.
It is important to monitor your outstanding debt and should you continue to have issues collecting payment with a particular embassy, then you need to think long and hard about taking on other cases from them until the problem is addressed.
Chasing outstanding money on a continual basis is the hardest part of this whole process, because most practices are not geared up for this.
It is both time-consuming and requires a specific skill set. It is rare to find a practice which has the time to chase these invoices on a continual basis and maintain adequate records to support this.
How to improve your appointment booking
Private clinics can grow their business by streamlining appointment booking and filling unbooked appointment slots. Tim Morris (right) offers three ideas
1Use live chat technology to schedule appointments there and then
Installing live chat technology onto your website is a great way to convert browsing people into inquiries and prompt them into booking appointments with your practice.
When done properly, trained operators will be on hand to help field clients’ questions about services on offer. Previously, independent health practitioners had to wait for clients to phone or fill in online forms.
Nowadays, you can reach your customers at the source with a trained, proactive live-chat operator to message your vistors to your website and massively boost their engagement with your business. Using live chat also enables you to take preliminary information about the client ahead of time, asking specific questions to better prepare for appointments, reassure them if needed and book introductory meetings.
If your client wants further information, your web-chat operator can book them in for a call or consultation with one of the clinicians at your practice. This means your website visitor has now become a fully engaged potential new client.
2
Offer a 24/7 omnichannel appointment booking experience
Appointment booking has changed significantly over the past decade with clients now
wanting to reach businesses on the channel of their choice at a time to suit them.
Ensuring your practice has multiple channels for interacting with customers and booking appointments outside of traditional 9 to 5 working hours is now a necessity in 2023.
Increase sales
By offering the opportunity to book an appointment on all your channels – live chat, social media, website, over the phone or visiting your clinic – you can improve your business’s interaction and increase sales by capturing your customers at the peak of their interest.
Not only does giving your clients access to your practice across all touchpoints help capture more appointments, but I believe it will also help to exceed their expectations.
Why? Because they have an easy way to interact with you on their terms – whenever and wherever it is convenient for them. No more frustrations for them having to
Ensuring your practice has multiple channels for interacting with customers and booking appointments outside of traditional 9 to 5 working hours is now a necessity in 2023
wait until morning to ring your reception or only being able to call at certain times to get something scheduled.
With this seamless blend of online and offline channels, your customers can schedule appointments as they please and get the tailored experiences they crave.
3 Save time and generate leads through outsourcing
Anyone who owns a clinic understands that time is money. Often –especially as an independent
practitioner – your focus needs to be on the business-critical activities rather than administration.
So, to perfect your appointment booking services, I suggest outsourcing your communications to a team of trained experts with access to your diary.
Then, in response to customer inquiries, appointments can be scheduled on your behalf, eliminating the time wasted playing phone ping-pong with customers.
Another benefit to outsourcing appointment booking is that your client benefits from an immediate sense of satisfaction having achieved their desired level of commitment from you, first time. Outsourcing diary management, reception and customer service also allows you to turn what would once have been a missed call or opportunity into a confirmed appointment, which massively benefits lead conversion.
Tim Morris is managing director of customer communications specialist, Cymphony
In 2021, the World Health Organization declared climate change the biggest health threat to humanity. Dr Robin Clark (right), medical director for Bupa Global and UK, explains how, as a leading healthcare company, Bupa is determined to be at the forefront of the sector in addressing this
Climate change represents a devastating threat to human health, with the acute and chronic impacts also carrying a significant financial cost
Cromwell Hospital has become the first private hospital in the UK to trial an innovative medical device which captures and recycles waste anaesthetic gases, preventing them from polluting the atmosphere
Bupa IS COMMITTED to helping people live longer, healthier, happier lives and making a better world. Making a better world means playing our full part in addressing the climate emergency.
We know that people’s health is inextricably linked to the health of the planet. That’s why we have made a commitment to get to net zero by 2040, including across our supply chain and across all the countries we operate in – one of the most ambitious targets any healthcare organisation has set, underpinned by rigorous sciencebased targets.
Climate change represents a devastating threat to human health, with the acute and chronic impacts also carrying a significant financial cost. Mitigating the health and economic impacts of climate
change requires action from government, businesses, charities and all parts of society. In the course of treating patients, the healthcare sector is itself a cause of pollution from greenhouse gases and other pollutants.
Tackling emissions
According to NHS Carbon Footprint Plus figures, the health and social care system in England alone accounts for approximately 5% of the country’s national greenhouse gas emissions. The true figure will be higher when emissions from the private sector are factored in too.
The biggest impacts on the NHS carbon footprint come from its supply chain; for example, pharmaceuticals and medical equipment, followed by building energy, anaesthetic
gases and travel of staff, patients and visitors.1
Tackling emissions related to energy will deliver significant gains. However, there are other steps we can take now to move the dial in the right direction; for example, by reconsidering our procurement choices.
While single-use disposable devices have become popular in an effort to reduce hospitalacquired infections, their environmental impact is longer than their lifecycle.
Bupa is investing in and delivering innovation that helps make healthcare more sustainable through our ecoDisruptive programme to find and support sustainable, scalable start-ups and innovative solutions that will improve people’s health and the health of the planet.
And we are putting this into
action at the Cromwell Hospital, in London. Here are some of the ways we are doing that.
Recycling anaesthetic gases
About 95% of the anaesthetic used during surgery is exhaled by patients and released into the atmosphere as waste. This equates to 97,000 tonnes of carbon dioxide equivalent (CO2e) each year in the UK alone.2
Cromwell Hospital has become the first private hospital in the UK to trial an innovative medical device which captures and recycles waste anaesthetic gases, preventing them from polluting the atmosphere.
The trial was made possible through Bupa’s eco-Disruptive programme, which sees employees partner with sustainability start-ups to tackle environmental challenges.
The SID-Dock, developed by SageTech Medical, can capture 99.9% of waste anaesthetic agents (sevoflurane, isoflurane, desflurane) through actively controlled adsorption onto a re-usable capture canister. The captured waste is then recovered and recycled for future reuse.
It fits easily and safely into hospital operating theatres, without having to make changes to any existing equipment.
When the cannisters are full, SageTech Medical collects them from the hospital and takes them to their processing facility where the captured anaesthetic is purified and recycled back into pharmaceuticals, ready to be used again by hospitals.
This unique circular economy solution not only reduces direct emissions but means the volume of virgin drug that needs to be manufactured is also significantly reduced, conserving natural resources and reducing the associated emissions.
Fitting effortlessly
Cromwell Hospital has been trialling the SID-Dock for over six weeks now, as I write, and the team say that one of its biggest attributes is how effortlessly it fits into the hospital’s systems in theatre. Space is a commodity and they were initially concerned about how it would integrate with the equipment already there.
However, the footprint of the SID-Dock is very small; it fits in next to the anaesthetic machines without causing any disruption.
Another surprise was how quiet the machine is. This is very important, as loud machinery noises can disrupt surgeons. The SID-Dock makes minimal noise when in use. It does need a power source, but it has low energy consumption.
As my colleague Mehnuhlik Lynch, anaesthetic team leader at Cromwell Hospital, said: ‘Clinicians are becoming more and more aware about the impact their clinical practice is having on the environment.
‘Using SageTech’s solution, we can help reduce the carbon footprint of anaesthesia and give patients a greener choice for their healthcare. We’re really excited to be trialling this ground-breaking technology at Cromwell Hospital.’
Scrubs made from recycled plastic waste
Each year, 14m tonnes of plastic waste is dumped in our oceans. It destroys marine life by causing physical suffocation as well as constantly leaching chemicals and colouring agents.
And when it breaks down into microplastics, it causes devastating effects on reefs, water temperatures and lifecycles of aquatic animals.
Instead of using crude oil to make new plastic, Upcycled Medical turns existing marine litter (waste plastic) into upcycled clothing, including the scrubs that healthcare professionals at Cromwell Hospital have been wearing in theatres since the end of 2021 and in ITU since autumn 2022.
This helps to bring down the amount of plastic that goes into our oceans and ensures that there is no need to create new plastics in future, saving our fuel sources too.
Upcycled Medical, which was another participant in Bupa’s ecoDisruptive programme, treats waste salvaged from the oceans –including PET plastic, glass, metal and rubber – then turns it into pellets which are then bound into yarn.
This yarn is used to create medical clothing which is comfortable, durable and can be worn over long periods of time. Approximately seven to nine bottles that would have gone to landfill go into the making of every piece of medical clothing.
Re-usable anaesthetic equipment trays
It is important to realise the impact of using plastics in healthcare. Most single-use plastic items are considered as clinical waste post-use, so they can’t be recycled. Instead they must go into clinical waste, which is ultimately incinerated.
The team at Cromwell Hospital felt strongly that we should all be considering switching to smarter ways of using plastics to reduce carbon impact. That is why they began looking into trays that can be re-used and decontaminated safely so as not to pose an infection control risk.
The re-usable plastic trays from Henley Medical Supplies are very durable and have received positive feedback from the teams using them.
They use different colour trays to reduce cross contamination and as an additional safety measure when handling medications, with emergency drugs placed on a yellow tray.
This makes them easy for clinicians to spot them when needed. Other general anaesthetic drugs are put on green trays.
After use, the trays can be disinfected with cleaning wipes or put through an autoclave for sterilisation if needed.
By switching to re-usable trays, Cromwell Hospital has not only saved over 9,000 single-use trays from being incinerated each year, it has also reduced its costs by £4,000 per year.
Bupa’s Cromwell Hospital in South Kensington, London, is pioneering many green initiatives. Mehnuhlik Lynch (below) is the anaesthetic team leader trialling the recycling of anaesthetic gasses
Laryngoscope handles
Previously, Cromwell Hospital used metal single-use laryngoscope handles that contain lithium iron batteries. These handles were used once in line with the manufacturer’s instructions, which meant that they had to be discarded in clinical waste for incineration.
In February 2023, the team switched to metal re-usable laryngoscope handles from Timesco, which can be cleaned with disinfectant wipes or sterilised in an autoclave.
The handles, which are covered by a five-year guarantee, are compatible with rechargeable batteries instead of single-use ones and can be autoclaved up to 4,000 times. This cuts our environmental impact by saving 1,900 single-use handles with lithium batteries from being incinerated every year. And it has also saved the hospital a projected £6,000 per year that can be re-invested into patient care.
As Cromwell has shown, it is easy to take simple steps and make careful procurement choices to positively impact the environment. We want to be a catalyst for change, sharing best practice and working with our partners across the healthcare sector to accelerate reaching Net Zero.
References
1. Delivering a ‘Net Zero’ National Health Service, NHS, July 2022
2. The carbon footprint of general anaesthetics: A case study in the UK. Hu, X, et al. Resources, Conservation and Recycling 2021; Volume 167
BOOK YOUR DEMO
Are you happy with your current software?
Maybe you're completely happy with the software you use to run your practice. Perhaps you have everything in one place, routine tasks are automated, and reporting is accurate and insightful. If so, stop reading now.
However, if you think the day to day running of your practice could be improved, we'd love the chance to demonstrate e-clinic to you.
The number one choice for private practice
Future-proof your practice and offer everything a modern patient expects:
> iPad compatibility
> Online booking & payments with fully integrated card processing
> Electronic consent & treatment forms
> Integrated drugs database & digital prescribing with direct delivery
> Fast & easy patient communications by email or text
BOOK YOUR FREE 30 MINUTE DEMO Visit e-clinic.co.uk to find out more & book a demo
SAFETY AND QUALITY
Figures prove that we’re improving
New figures reveal an important milestone achievement for independent sector healthcare quality and safety. David Hare (below) reports
Independent Practitioner Today readers will be more familiar than most with the significant emphasis, prioritisation and progress which has been made in recent years in ensuring that safe, high-quality care is embedded throughout the independent healthcare sector. The private sector in the UK has always maintained very high standards of safety and of quality of care, underpinned by a robust regulatory regime.
But in recent times, and particularly in the aftermath of the Paterson saga, it was right and appropriate that we all took the opportunity to ask ourselves what more we could do to ensure that every stone was unturned to deliver the most robust governance and the highest possible commitment to outstanding patient care.
Recent analysis we at the Independent Healthcare Providers Network (IHPN) have conducted shows that, while there is undoubtedly still work to do, the picture is more encouraging than ever.
Our most recent research demonstrates that for the first time, nine out of ten independent hospitals have ‘good’ or ‘outstanding’ overall ratings from the health and care watchdog, the Care Quality Commission (CQC).
Nine out of ten independent hospitals have ‘good’ or ‘outstanding’ overall ratings from the Care Quality Commission
Ninety-one per cent of acute independent, non-specialist hospitals, who deliver a wide range of services to both NHS and private patients – including orthopaedics, oncology, ophthalmology, gynaecology, gastroenterology, dermatology and general surgery – have now been assessed as being in the top two categories overall for quality of care.
Reaching this milestone is an important marker for the sector.
In 2018, the figure was 70%, so this shows a not insignificant positive change. And it is a clear demonstration of the sector’s strong commitment to continuous improvement around safety and quality.
We think it is a strong indication that the general standards of care and patient safety in the private sector are higher than they have ever been.
I discussed this recently with two of my senior clinical director
There has been a better focus on creating an open, learning environment where improvement is actively sought, with greater openness and honesty
colleagues, Dr Howard Freeman (IHPN medical director) and Dawn Hodgkins (director of regulation, formerly a senior nurse), to get their views on where they felt the sector was and what was still to do. They reflected positively on the improvements they had seen in the culture of many independent and private providers.
There has been a better focus on creating an open, learning environment where improvement is actively sought, with greater openness and honesty – reflected
by the fact that there are now nearly 230 Freedom to Speak Up Guardians operating across the sector.
Another highlight they cited is the improvements we have seen which come through improved clinical governance. We now have better systematic, written standards and frameworks and that is in no small part driving these improved ratings.
Readers will be familiar, of course, with the Medical Practitioners Assurance Framework (MPAF), launched in 2019 and refreshed at the end of 2022, which I have written about before in this journal.
The embedding of the MPAF has been a great step forward. It has also been very positive to see how the GMC and CQC have recognised and endorsed the MPAF. It has informed how the CQC assesses how ‘well led’ independent services are and it
is a requirement of the NHS standard contract too.
So, where next? It is very encouraging that our sector is achieving this level of consistent high performance. And I think it is a good indication that patients can really trust the quality of care in the independent sector.
But we should all consider this just a step on the journey and redouble our existing efforts to maintain and improve these already high standards. So the journey does not stop here.
There is still more to do to work collaboratively and closely as a system, including with the NHS and with the key regulatory and professional standards agencies to make sure we are doing everything we can to deliver world-leading safety and quality of care to patients.
David Hare is chief executive of the IHPN
Free legal advice for Independent Practitioner Today readers
Independent Practitioner Today has joined forces with leading healthcare lawyers Hempsons to offer readers a free legal advice service.
We aim to help you navigate the ever more complex legal and regulatory issues involved in running and developing your private practice – and your lives.
Hempsons’ specialist lawyers have a long track-record of advising doctors – and an unrivalled understanding of the healthcare system as a whole.
Call Hempsons on 020 7839 0278 between 9am and 5pm Monday to Friday for your ten minutes of free legal advice.
Advice is available on:
Business structures (including partnerships)
Commercial contracts
Disputes and litigation
HR/employment
Premises Regulatory requirements and investigations
Are investment forecasts valid? Dr Benjamin Holdsworth on how to avoid predicting the unpredictable
Weather the storm – don’t predict it
Data covering each sector of the global developed equity markets in the last decade shows us the randomness of performance
EACH YEAR , investors face a barrage of commentary and speculation from the financial press about which stock, sector or country is set to do well in the coming months.
The quotes below are taken from articles published by well-known media outlets in recent weeks and demonstrate that 2023 is no different:
‘2023 could be a very good year for renewables’ FORBES ADVISOR
‘US stocks have long dominated investor allocations, but it may be time to consider selectively owning emerging markets (EM) stocks’ MORGAN STANLEY
‘We see energy sector earnings easing from historically elevated levels yet holding up amid tight energy supply. Higher interest rates bode well for bank profitability. We like healthcare, given appealing valuations and likely cash flow resilience during downturns’ BLACKROCK
‘Materials – especially metals – look even better than energy at the start of 2023, based on supportive valuations and this industry group’s past performance in periods of weaker manufacturing data’ FIDELITY
Predictions and forecasts are all well and good, but investors would be wise to tread carefully before positioning their portfolio to benefit from narratives like the above.
Many convince themselves that they have spotted a pattern in past returns or that somehow the past can be used to navigate an uncertain future. They are likely mistaken.
As Warren Buffet eloquently puts it: ‘Forecasts usually tell us more about the forecaster than of the future.’
Data covering each sector of the global developed equity markets in the last decade shows us the randomness of performance.
For example, in 2014 and 2015, healthcare came out on top while energy stocks were rock bottom. However, in 2016 the roles reversed, with energy delivering a 40% premium over and above healthcare stocks.
Abrupt halt
Another topical example is that of technology. For the first nine years of the last decade, the tech sector beat the overall developed market every single year and came in the top three, two-thirds of the time.
Last year, the streak came to an abrupt halt as technology fared relatively poorly.
The energy sector, on the other hand, reaped the benefits of the surging post-pandemic demand for oil and gas, exacerbated by supply shocks caused by Russia’s invasion of Ukraine.
The temptation to chop and change is strong. Over the last four years, a portfolio invested in a technology index fund at the start of 2019 and switched to an energy one in 2021 would have enjoyed outstanding average returns of around 46% per year.
While this would have been superb, it represents a classic case of investing using the rear view mirror. Hindsight is bliss.
The challenge that all investors face is that forecasting investment returns based on the information we have today is a highly challenging game to win consistently over the long term.
Unexpected shocks
If markets work, then prices effectively reflect an equilibrium position between the views of buyers and sellers and their expectations for the future.
Unexpected shocks, such as pandemics, wars, financial crises and political turbulence are quickly factored into expectations, and prices adjust accordingly. Very few individuals possess
Many investors convince themselves that they have spotted a pattern in past returns or that somehow the past can be used to navigate an uncertain future. They are likely mistaken
the skill – or fortune – to anticipate such events and reposition their portfolio appropriately.
Evidence from data and research firm Morningstar’s database of global developed equities managers confirms this.
Of the 5,269 active funds available at the start of 2013, 3,242 (62%) failed to survive the period, 1,841 (35%) survived the period but were beaten by the broad developed market, and a mere 186 (4%) survived the period and outperformed.
Take it from the late, great John Bogle:‘We deceive ourselves when we believe that past stock market return patterns provide the bounds by which we can predict the future.’
Dr Benjamin Holdsworth (right) is a director of Cavendish Medical, specialist financial planners helping consultants in private practice and the NHS
The content of this article is for information only and must not be considered as financial advice. Cavendish Medical always recommends that you seek independent financial advice before making any financial decisions.
Levels, bases of and reliefs from taxation may be subject to change and their value depends on the individual circumstances of the investor. The value of investments and the income from them can fluctuate and investors may get back less than the amount invested.
Watch how you hire
Solicitor Robert McCartney (right) has a warning to everyone who works as or who uses freelance workers – including ‘independent’ doctors
HM REVENUE and Customs (HMRC) is currently making a loud and very public statement about the role of freelancers through its prosecutions of television personalities including Gary Lineker, Lorraine Kelly, Kaye Adams and Eamonn Holmes.
Get it wrong and there may be a large amount of additional National Insurance to pay.
To date, the tax department has lost two, won one and, in the case against Gary Lineker, the game is still in play.
This is a warning to everyone who works as and who uses free -
lance workers and independent consultants, be they other doctors, businessmen or tradesmen. Healthcare businesses often bring in people who are ‘selfemployed’, but in fact work solely for the same person, do regular hours every week and cannot substitute someone else if they are away.
Are these people really self-employed?
If you are engaging people in this way, are you confident that the arrangements you have in place are suitable and could withstand
have is to enter a contract for services from the individual.
advisers
scrutiny by HMRC and/or employment tribunals?
It is not just an issue about tax, but also the employment rights of the person doing work for you.
Why use independent workers in specialist advisory roles and freelance workers?
Many businesses will hire in others to help manage specific projects and tasks. These people are a great resource for bringing in expertise which may not exist within the employed team. Some common examples within the health sector are advisers on quality and governance, project managers, restructure support, book-keepers and additional clinicians.
Why could this be a problem?
This method of accessing additional support is recognised as an important part of the economy. But it can be abused.
HMRC is concerned about tax avoidance, and using these structures for less informed, often young and junior staff has been deemed exploitative.
Significant fines and employment liabilities could arise for the business inappropriately using these structures.
What questions should you ask to determine if an individual is independent?
This list has been produced to help any private doctor’s business considering, or currently using, independent workers. It will help them decide if they are engaging an employee or a truly independent person.
1 Is the individual responsible for how and when they work?
This is easier to evidence with senior roles and subject experts who are being used to deliver outcomes. The greater the level of
control you have over them, the more likely that they will be deemed an employee.
There may be some inevitable limitations on this due to the nature of the role required.
Opening hours, security requirements, industry standard practices and defined methodologies to deliver the outcomes may be further considerations which may limit how and when someone works, but not to the extent that they deprive them of independent status.
2
Do they work through their own company or are they an individual?
Many individuals establish personal service companies (PSCs) to act as an intermediary between themselves and the client business.
The authorities will look beyond this to the actual relationship, as demonstrated with the celebrities mentioned above, but it is a useful indicator.
Evidence that the PSC has other contracts, possibly additional employees and understands the liabilities they are adopting will be relevant.
3 Does the individual provide a defined service?
Employees will work in accordance with their job description and specification. Although these should be well defined, in reality it is known that their roles often evolve and change in response to meet the demands of their team and the employer. It is rare for these to be strictly limited.
Independent workers should be instructed to provide specific services. These are normally defined in a service specification with the focus being upon the delivery of detailed objectives.
There is rarely variation to this and, if there is, this should be clearly documented.
Is the individual responsible for how and when they work? The greater the level of control you have over them, the more likely that they will be deemed an employee
4 Can they send someone else to do the work?
This is often referred to as substitution arrangements and it is easier for some to do than others.
Many independent medical consultants work alone and do not have access to alternatives. However, the focus would be on whether they have the legal right to send an alternative.
In addition to helping to assess the legality of the structure, including provisions of this nature will help with business continuity. It should give you assurance that the work will be completed even if the person becomes unavailable.
5 Can the individual work for other clients?
This is another question which goes to one of the core issues of whether there are too many restrictions on a person to be deemed independent.
A reasonable approach may be applied here to restrict working for competitors and ensuring confidentiality.
6 Would HMRC consider the individual to be an employee for tax purposes?
Use the tool produced by HMRC found at www.gov.uk/guidance/ check-employment-status-for-tax to get an initial view. The tests relating to taxation and employment statuses do differ.
How do you reduce the risk?
Once you are confident there are good answers to the above points – because they can answer ‘yes’ or they can clearly explain why they may be unable to answer in the affirmative – the best security you
This is not conclusive, because what you actually do and what is written could be very different and HMRC will test that.
The person providing the required service would normally provide the contract, but in some cases it could be produced by the person requiring the service.
This is more probable following a competitive bidding or quotation process which included the terms and specifications that will need to be delivered.
When reviewing or producing a suitable contract, consider the following issues.
1. Whom are you contracting with? Is it a company or a person?
2. Is the contract for a defined and limited term or is it dependent on specific deliverables?
3. Have you checked any necessary compliance obligations on the contractor and are these detailed in the contract?
4. Do the specifications reflect the requirements of the business?
5. Are payment arrangements appropriately detailed? How will fees be calculated, when will invoices be raised and will there be any offset or clawback arrangements?
6. How will you manage disputes and issues when they arise?
7. Is there a substitution clause?
8. How is intellectual property to be managed and who owns any products, services, documents or the like produced during the period of engagement?
9. How is liability managed? Are there indemnities and does the consultant have suitable insurance or indemnity cover.
These do not need to be excessively complicated contracts, but it is important to ensure that they give you the protections you need.
Get an accountant’s and/or lawyer’s advice to review any relationships of this nature you currently have or may be considering.
Having a suitable contract to protect the parties is paramount. And it will give everyone confidence if HMRC starts making inquiries, provided you have been complying with the terms of the agreement.
Robert McCartney is an associate at Hempsons solicitors
What do you do if a patient decides to change their name by deed poll? Dr Kathryn Leask (below) answers a private GP’s question Dilemma 1 Can I accept this deed poll paper?
A patient wants to alter their name
Government website www.gov. uk/change-name-deed-poll/ make-an-adult-deed-poll.
QI am a private GP and have been asked by a patient to change the name on their records.
They have provided me with a copy of ‘Deed of Change Name (Deed Poll)’ document, which they have made themself. Is there any other action I need to take and can I accept this document in order to change the name on their records?
AAny person over the age of 16 who has capacity can make their own deed poll and wording is available at the
The deed poll should be witnessed, but there is no stipulation on who can act as a witness. Some organisations, such as a bank, may need an ‘enrolled’ deed poll.
Public record
Those over 18 years can enrol a deed poll with the King’s Bench Division of the Royal Courts of Justice so that their new name is on public record.
It is for individual organisations to decide whether they require an enrolled deed poll as proof of a name change.
For those under the age of 18, an unenrolled deed poll can be made using a specialist deed poll agency or a solicitor or they can apply for
an enrolled deed poll from the courts.
Those who are 16 and 17 can make their own unenrolled deed poll; however, if they need an enrolled deed poll, the young person will either need agreement from everyone with parental responsibility or a court order.
Where an enrolled deed poll is used, the new name will usually appear on public record in The Gazette.
It is for your practice to decide, therefore, whether your procedure for changing a patient’s name requires an enrolled deed poll or whether an unenrolled deed poll is acceptable.
Dr Kathryn Leask is a medico-legal adviser at the Medical Defence Union (MDU)
Trapped in parents’ fight about vaccines
Vaccinating a child leads to a disagreement between the parents – and the doctor is the piggy in the middle. Dr Kathryn Leask (right) advises on what to do
Dilemma 2
Can one parent give OK for jab?
QI am a private paediatrician and am due to give a patient their pre-school boosters.
The child’s mother has provided her consent for the vaccinations to go ahead.
However, I have received a letter from the child’s father objecting to the vaccinations and saying he does not provide his consent.
My understanding is that I only need consent from one parent to provide treatment but wasn’t sure whether this also applied to vaccinations.
AWhile consent from one person with parental responsibility is usually sufficient (section 2[7] of the Children Act 1989), there are some situations where having consent from all those with parental responsibility is recommended.
This can include non-therapeutic procedures such as circumcisions for religious reasons and immunisations.
The Green Book states that if one parent agrees but another disagrees, the immunisation should not be carried out until both parents can agree or there is a specific
court approval that the immunisation is in the child’s best interests.
It may be helpful to speak to both parents, particularly the father, to establish what their concerns are to see if you can resolve these.
Discussing the potential risks as compared to the potential benefits of the vaccine may help to reassure the parents as to what is in the child’s best interests.
Particular concerns
This will give you an opportunity to establish whether the father has any particular concerns which you would not otherwise be aware of.
If, after discussion, the father agrees to the vaccination, this should be documented in the notes, and it may be prudent to obtain written consent.
If the parents continue to disagree, either can make an application to the court under section 8 of the Children Act 1989 for a special issue order. It will be for the court to decide on how the issue should be resolved.
If you felt the child was particularly vulnerable if left unvaccinated while the parents decided on the course of action, it may be appropriate to discuss this with your local child safeguarding lead to see whether a court order in favour of vaccination can be obtained.
If you were to do this, you should keep the parents informed.
LET US HELP YOU GROW YOUR PRIVATE PRACTICE AT WEEKENDS
LONDON MEDICAL, the award-winning outpatient clinic in the Harley Street Medical Area is expanding its weekend opening hours. We are inviting applications for practicing privileges.
We can offer you:
Fully CQC-registered clinic
Nursing support
Appontment-making
Secretarial support
Billing service
In-house pharmacy
For more details
Contact: david.briggs@londonmedical.co.uk
49 Marylebone High Street, London W1U 5HJ
Get in good books of your accountant
A pet hate of medical accountants is being handed a carrier bag full of haphazard paperwork and loose receipts. Alec James shows how to keep the documentation simple
EVERY TAXPAYER needs to keep records to support the entries made on their tax return. How those records are kept and how long you need to retain the records for is dependent on your tax affairs.
In the event of a HM Revenue and Customs’ (HMRC) inquiry, you can be charged penalties if you do not keep accurate, complete and readable records.
Accurate record-keeping ensures you are compliant with your tax office and that you pay the right amount of tax.
Records can either be kept physically or electronically and many book-keeping software providers now allow you to store electronic versions of records within their program.
If you keep your records electronically, you do not need to keep a physical copy, but you should ensure the data is backed up and kept secure.
Here is a review of the financial records you need to retain and the minimum time you need to keep them.
Personal tax return records
Many doctors will need to complete a tax return due to their taxable earnings being in excess of £100,000, even if they do not have any untaxed income such as selfemployment, dividend or rental income.
You should retain records to support all the entries on your return. This would include P60s, P45s,
P11ds and evidence of expense claims such as professional subscriptions.
These records should be held for a minimum of 22 months after the end of the tax year. As the 2022-23 tax year ends on the 5 April 2023, those records will need to be retained until at least 31 January 2025.
Business records
Many Independent Practitioner Today readers will have additional sources of income, whether it is private practice, medico-legal or speaker fees. It may be that you receive this income as a sole trader, a partnership or via a separate legal entity such as a limited company or limited liability partnership (LLP).
Whether you are self-employed or trade via a limited company, it may be beneficial to open a separate savings account to save for tax
Whatever your trading status, HMRC deems these sources of income to be a business and the records you need to keep and the retention policies are different to those for your personal tax return. You should ensure your business records are kept separate from your personal account records. There are lots of different types of records you will need to keep as a business.
Businesses need to be able to maintain the following records:
Summaries of income;
Summaries of business expenditure and purchases;
Money extracted from the business account;
Mileage records. Generally speaking, these records need to be held for a minimum of six years from the end of the financial year-end.
Bank accounts
A limited company, LLP or partnership would usually hold their own bank accounts because the funds belong to the business until they are paid to you. Depending on the business structure, amounts paid to you could be a taxable income stream.
If you are trading on a selfemployed basis, while the income is your own, it is best practice to have a separate bank account for these earnings. This will assist you both in terms of being compliant with HMRC, but also to allow you to ensure you are receiving all the monies you are due.
Whatever your business structure, all business income should be paid into the business account. Business expenditure can be paid from your business bank account. These would be the directly attributable costs that you need to spend to manage your business. Whether you are self-employed or trade via a limited company, it may be beneficial to open a sepa-
rate savings account to save for tax, whether this is personal or corporation tax. The amount to save should be discussed with an accountant.
Income and expenditure
Your business needs to keep a record of invoices raised and amounts received. Depending on the level of income you receive, this could be a simple spreadsheet or cashbook detailing the invoice number, amount and the date of the invoice.
You should then record the amount received and the date the monies are received. You should also keep copies of all the invoices you have raised within a financial year.
This will allow you or your secretary to ensure all invoices are paid. A similar record of expenditure should also be maintained. Again, evidence to support all the costs incurred should be held with the exception of those that are of a trivial amount.
As your business grows, you may find that a spreadsheet or cashbook is no longer sufficient for your needs and you may look at other solutions.
Primarily, there are three options:
Using practice management software;
Using a billing company;
Using book-keeping software.
There are practice management software providers which are specific to doctors. These are designed to store your patient records, including notes, letters and photographs as well as offering a solution for billing your patients or their insurer.
Having these detailed records all in one place will operate your practice efficiently and will allow you or your secretary to easily identify and subsequently chase any outstanding fees.
As these products are not accountancy based, while there is quite often an option for making entries in relation to costs incurred by your business, the system won’t be as detailed as book-keeping software.
Billing companies will often use their own software to maintain the invoices and provide you with regular reports. The advantage here is that this takes away the
administrative burden from you in respect of billing and chasing outstanding debts.
A billing company would be more expensive than maintaining the records yourself – but it often means that, as a business, you recover more of your fees.
Book-keeping software is generally not specific to the medical professional and so the invoicing function may not be as detailed as many doctors require.
These types of solutions will give a full accounting product which includes a reconciliation of your business bank accounts and will allow you to record all your costs, ensuring you get the maximum tax relief available.
Optimum results
There are advantages and disadvantages with any of the solutions and sometimes, depending on the size of your business, a combination of using practice management software/billing company together with book-keeping software will give the most optimum results.
Many of the practice management software providers will have links between book-keeping software providers to allow importing of data, therefore reducing duplications of work.
There are certain requirements that your invoices must follow, particularly if you trade as a limited company. Discussions with an accountant regarding the invoicing process can prove very beneficial.
Wherever possible, you should pay for expenses from your business account, but there may be occasions when you incur a cost on behalf of your business. If you do, you should ensure the costs are recorded.
Many doctors’ businesses won’t need to register for VAT due to the healthcare exemption. However if you are VAT-registered, any of this tax reclaimed would need to be evidenced with supporting documentation.
Mileage
Many consultants will use their personal vehicles for business purposes. To obtain tax relief on business use of a vehicle, a detailed mileage log should be kept of any business journeys.
Generally speaking, journeys between home and a single place of work are not an allowable expense.
PAYE schemes
If you operate a PAYE scheme, you will need to retain the employee financial records for three years after the end of the tax year. This would include details of what you have paid your employees and the reports submitted to HMRC.
From a HR perspective, there may be non-financial records you need to hold – but do ensure you remain compliant with data protection regulations.
Making Tax Digital
For those who are registered for VAT, Making Tax Digital (MTD) has been in place since April 2019. For all other businesses, most information regarding a taxpayer’s affairs is submitted annually to HMRC via a self-assessment tax return.
MTD will move this to more regular reporting. The new measures effectively mean all businesses will need to use a digital accounting system with a direct link to submit the information to HMRC.
The plans were to introduce this reporting from April 2023; however, this has once again been delayed. HMRC now plans to start rolling out MTD from April 2026.
MTD may have been delayed, but many doctors have seen the benefits that digital accounting systems have in relation helping maintain records. If you are not currently using a digital system, it may be worth considering reviewing the systems you have to ensure the records you keep are sufficient.
A conversation with a medical specialist accountant can be extremely beneficial in finding the right solution for you.
Next month: Top tips for succeeding in private practice
Alec James (below) is a partner at Sandison Easson & Co, specialist medical accountants
DOCTOR ON THE ROAD: VOLKSWAGEN POLO GTI
There’s
The VW Polo GTI has grown to the same size of some previous versions of the sporty Golf –favourite among many doctors. But can it match the ultimate thrills offered by competitors? Our motoring correspondent Dr Tony Rimmer (left) finds out
WE MEDICS tend to be levelheaded, pragmatic and appreciative of good design. In our work, we are much happier working with high-quality kit that is more likely to get the job done safely and efficiently.
This tends to produce better outcomes for our patients. It is also more professionally satisfying to operate equipment and systems that work with predictable reliability.
It is no wonder, then, that when it comes to choosing a new car, we gravitate towards the higher-quality premium brands.
For many years, the go-to car maker for many medics was Volkswagen. Its products were practical with solid build quality and no-nonsense Germanic design.
Grown in size
If you were a bit of a petrol head, you could choose the Golf GTI, the ultimate car to cover all needs ranging from high practicality to excellent driving dynamics.
The current Golf GTI Mark 8 remains a great car, but has grown in size and price. What many of us are looking for is a sporty hatch -
a hole in this Polo
back that costs less, works comfortably as a daily drive or as a second car to have some fun in but remains useful and practical.
So what about the Volkswagen Polo? They do a GTI version and it is the perfect size – the same as the old Golf Mark 4.
I have been testing the latest Polo GTI, last updated in 2021 to include better tech and some mild bodywork tweaks.
It is powered by the 2.0litre turbo petrol engine that we know well from the Golf and produces a healthy 204bhp linked to a sevenspeed direct-shift gearbox (DSG) dual clutch transmission.
No manual gearbox
Unfortunately, for a sporty car, you cannot get a manual transmission and this, in my view, marks against it as a true driver’s car. Both its closest competitors – the Ford Fiesta ST and the Hyundai i20N benefit from manual shifts.
You cannot complain about the interior though. Every Polo has high-quality furnishings and these are supplemented in the GTI by some very comfortable sports seats and a lovely leather steering wheel.
The driving position is perfect and there is reasonable room in the back for two adults or three children to sit without feeling constricted.
Boot space is impressive, so this hot hatch can really function as a useful family runabout too. All the latest tech is on hand including Apple CarPlay and Android Auto.
Something lacking
Out on the road, this GTI feels solid and planted. The ride is, not unexpectedly, firm but not uncomfortable.
Performance is strong as one would expect and the Polo is the perfect size to tackle our relatively narrow roads, so it can be driven with great gusto on any crosscountry trip.
The steering is pretty sharp and there is minimal body roll, but I found that swift driving revealed something lacking in the driving experience. It was difficult to focus on why this was.
All the elements are there to produce a car that is just as sporty and just as quick as its Golf GTi brother, but it just is not as rewarding or as much fun for the keen driver.
Both the Fiesta ST and the i20N are more enjoyable and entertaining to drive. The lack of a manual gearbox may have something to do with it, but a Golf GTI with the same DSG box and almost the same engine is better.
If you drive in a more relaxed manner, the Polo starts to show its real strengths. It is a quiet and comfortable companion on long trips, whereas its competitors would be noisier and more frenetic.
Fuel consumption is impressive, too, with an overall 40mpg being realistic and I even saw 45mpg on a round trip to Shropshire.
So, the latest Polo model is a
I found that swift driving revealed something lacking in the driving experience
well-made quality product that is roomy, comfortable, well equipped and refined.
But, unfortunately, the GTI is a bit of a mixed bag. It looks smart and sporty and you cannot complain about the extra performance on tap.
As long as you do not expect the ultimate thrills that competitors offer, you will not be disappointed. Perhaps the more cultured and mature character will be more appealing to us level-headed medics.
Dr Tony Rimmer is a former NHS GP practising in Guildford, Surrey
VOLKSWAGEN POLO GTI 2.0 TSI
Body: Five-seat hatchback, front-wheel drive
Engine: 2.0 litre four-cylinder turbo petrol
Power: 204bhp
Torque: 320Nm
Top speed: 149mph
Acceleration: 0-62mph in 6.5 seconds
Claimed economy: Combined 41.5mpg
CO2 emissions: 154g/km
On-the-road price: £28,540
The driving position is perfect and there is reasonable room in the back for two adults or three children to sit without feeling constricted
HERE’S WHAT’S COMING IN OUR MAY ISSUE
Coming in our May issue, published on 9 May:
Top tips for succeeding in private practice. This is part of our long-running series from Sandison Easson specialist medical accountants aimed at consultants who are starting the independent practitioner journey – but we know a lot of you ‘old hands’ are eager to check out their advice too
Hempsons’ solicitor and qualified doctor Tania Francis look at some important lessons to be learned from recent GMC decisions in fitness-to-practise decisions
Efforts to publish more about you and your practice are ramping up. The Private Healthcare Information Network explains more about what the organisation’s new evidenced-based assessment of the Competition and Markets Authority’s Order requirements mean for consultants
So, what are your consultant colleagues asking their defence body for advice about? In the first of a two-part series, Dr Kathryn Leask, medico-legal adviser at the Medical Defence Union, has the answers
Neurodiversity – what does it mean within the workplace? Solicitor Lee-Anne Crossman of Hill Dickinson considers how to create a more inclusive workforce and encourage a celebration of different minds
An online directory of more than 100,000 UK consultants and GPs has become an invaluable resource for those working in and allied to the healthcare industry. SpecialistInfo’s chief executive and consultant ENT surgeon Ms Olivia Whiteside tells its story
Tackling the nursing shortage in the UK: Robert Landor of Trinity Healthcare reveals how his company is working to resolve this worrying issue
INDEPENDENT PRACTITIONER
Published by The Independent Practitioner Ltd. Independent Practitioner Today is editorially independent.
Material is governed by copyright.
No part of this publication may be reproduced, stored in a retrieval system or transmitted in any form without permission, unless for the purposes of reference and comment. Editorial layout is the copyright of the publishers. If you wish to use it for promotional purposes on websites or for reprints, we would be happy to discuss licensing the copyright to you.
Registered office: 7 Lindum Terrace, Lincoln LN2 5RP
Could expert witness work be a role for you? As efforts are made to try and encourage more women doctors to take on this work, Dr Rebecca Whiticar discusses her role as an expert witness, the rewards, the skills needed, how you get involved, and how it will benefit you
Private patient units are a potential £1bn opportunity for the NHS, argues Hugh Risebrow head of specialist healthcare advisory company Latchmore Healthcare Associates LLP, which has advised 16 trusts and NHS England on aspects of private patient strategy.
Our Business Dilemmas series continues as Dr Kathryn Leask, medicolegal adviser at the Medical Defence Union, discusses what to do if you are issued a Community Resolution Order. And she responds to a request from a retiring orthopaedic surgeon: how do I dispose of a skeleton I’ve had since medical school and used for teaching purposes?
Independent Practitioner Today motoring correspondent Tony Rimmer reviews the KIA Nero EV. Will it be a thumbs up or a thumbs down?
Specialist financial advisers Cavendish Medical delve into the detail of the pension and retirement changes that impact you
Simon Brignall of Civica Medical Billing and Collection will answer the question ‘Is it time to outsource?’
Plus all the latest news and views
Would you like your private practice featured in Independent Practitioner Today? Contact robin@ip-today.co.uk
And don’t forget to check out our additional news updates every week online
ADVERTISERS: The deadline for booking adverts in our May issue is 21 April
Write to Independent Practitioner Today 7 Lindum Terrace, Lincoln LN2 5RP
CHANGING ADDRESS, EMAIL ADDRESS OR SUBSCRIPTION DETAILS?
Phone 01752 312140 or email karen@marketingcentre.co.uk
TELL US YOUR NEWS
Robin Stride, editorial director Email: robin@ip-today.co.uk Phone: 07909 997340 @robinstride
ADVERTISE WITH US
To advertise in the digital journal, on our website or in our business directory, contact advertising manager Andrew Schofield at Spot On Media. Phone: 0161 408 3912 Email: andrew@spotonmedia.co.uk
GET A SUBSCRIPTION DISCOUNT!
£90 independent practitioners. £90 GPs and practice managers (private & NHS).
£210 organisations.
Save £15 paying by direct debit: individuals £75 (organisations £180).
TO SUBSCRIBE
Email karen@marketingcentre.co.uk or phone 01752 312140