An accountant advises on the most common business howlers that trip practices up P18
The business journal for doctors in private practice
How crises cause brain block Our series on eliminating human error looks at how best to manage crises P34
Salaried consultant jobs in private practice have their critics, but four specialists tell us why they enjoy their new employed status n See page 26
Beware the pension tax taper A financial adviser and an accountant give their views on tackling the flaming tax headache P48
Courts are after you!
By Robin Stride
A recruitment drive is underway to find consultants and GPs who want to increase their private incomes by taking on legal work.
They are needed for often lucrative employment in writing reports and giving court evidence as expert medical witnesses.
A shortage of doctors taking on these roles was highlighted at a BMA medico-legal conference where some of the 110 specialists indicated they charged £400+ an hour for the work.
Negligence barrister Dr Simon Fox QC, who generally instructs in cases exceeding £1m in value, told attendees to ‘spread the word’
about doctor shortages in this field.
He described medical expert witness duties as ‘interesting and well paid’.
However, consultants and GPs at the meeting revealed a huge discrepancy in the fees they charge for their expertise. Of 110 present, a show of hands found most doctors charged £250 an hour or under, while others were getting £300£350 and beyond. The survey was stopped before it revealed how much the highest earner was paid.
BMA medico-legal committee chairman Dr Jan Wise ran the ‘hands-up’ study in response to a doctor’s question about how much a ‘reasonable’ fee would be.
He suggested that doctors should
factor in everything that might be relevant, such as their NHS equivalent rate, holidays and pension. They should keep a real record, like solicitors, of the time they spent on medical expert witness work.
Dr Wise said their fee should be much closer to those in the audience who were at the higher end, adding: ‘We are probably all undercharging’.
In the light of new evidence, some doctors are now reviewing their fees.
Dr Wise told Independent Practitioner Today later that the dearth of experts had a range of contributing factors. ‘While the intellectual rigour and the adversarial atmosphere of the court appeals to some, the
ability of a barrister – a compelling narrator, orally articulate – deters many doctors from engaging in expert witness work.
‘As the trained Rottweilers of our legal system, they are supremely able to persuade the listener to accept the righteousness of their cause.’
He said the deterrents to becoming an expert witness seemed ‘nigh on insurmountable’.
These included lawyer intimidation, an employment regime where adjusting job plans to accommodate the work or time to give evidence was a Sisyphean task – as well as the detriment to existing patient care – and the impact of vexatious complaints to a regulator.
➱ continued on page 3
KAT’S GOT THE CREAM
Former GP Dr Anahita Mansouri, consultant gynaecologist Miss Poonam Pradhan, consultant plastic surgeon Mrs Chien C. Kat and aesthetic nurse specialist Natasha Rankin have got together to launch a new ‘super-clinic’ for patients in and around Birmingham.
Mrs Kat said: ‘Most of our aesthetic clients are female and many feel comfortable with having a consultation with a woman because they feel we understand their needs.’ n See story on page 5
TELL US YOUR NEWS Contact editorial director Robin Stride
Current cover doesn’t work
What is the future of indemnity cover for doctors? David Hare sets out the healthcare providers’ view on what now should happen P14
TO ADVERTISE Contact advertising manager Margaret Floate at margifloate@btinternet.com Phone: 01483 824094
SUBSCRIPTION RATES
£90 independent practitioners.
£90 GPs and practice managers (private & NHS). £210 organisations.
Save £15 paying by direct debit: individuals £75 (organisations £180).
TO SUBSCRIBE – USE SUBSCRIPTION FORM ON PAGE 23 or EMAIL: lisa@marketingcentre.co.uk Or phone 01752 312140. Or go to the ‘Subscribe’ page of our website www.independent-practitioner-today.co.uk
Chief sub-editor: Vincent Dawe
Head of design: Jonathan Anstee
Publisher: Gillian Nineham at gill@ip-today.co.uk Phone: 07767 353897
EDITORIAL COMMENT
Great need to smarten up
What we would like to be the ideal perception of private healthcare takes a bashing when we get a national report that unearths widespread failings at the sharp end.
Our story (see page 11), on the Care Quality Commission (CQC) report – The state of care in independent doctor and clinic services providing primary medical care –shows there is much to be done before the sector gets the overwhelming praise it would like.
The document, available on the regulation authority’s website, is worth a good read for independent practitioners and their staff. Safety was inspectors’ biggest concern. They criticised nearly half of the private consulting doctor services analysed – 32 out of 66 first inspection reports.
But it does not contain all bad news and there are examples of what the CQC considers is good practice, as well as the bad.
A guide to take you to the top
Starting a new series exploring the roles of marketing strategies, social media, email marketing and using analytics to know and grow your audience P20
Get clear on transparency
Anne Coyne of the Private Healthcare Information Network reveals how her team has helped consultants submit fee data to its website about to go live P32
How to make your team thrive
Successful independent practices display five important features. An expert in computerised practice management systems reveals these ingredients P38
Fight bad debt by using these forces
Some stressed doctors whose practices and clinics figured in the report are unhappy with the results because they think the watchdog is punitive and they disagree with the outcome.
The introduction of ratings from this month will surely lead to wider controversy for those down the lower end.
But what the public thinks now about independent doctors and clinics should concern us all.
Even before the report’s findings, a CQC survey found some respondents felt their care was no better than on the NHS. The main difference was appointment availability.
And of those who had not used a private doctor, 47% said if they did, they would still want to see an NHS service afterwards for a second opinion.
There is a big PR job to be done to show, at their best, what independent consultants, GPs and their clinics can offer.
With consultants’ fees being published by PHIN, now is the perfect time to take stock of the way your practice’s medical billing and collection is working P40
For the record
Record-keeping is an issue widely discussed but one that doctors regularly get wrong. Solicitor Amie Roadnight has five suggestions to help P42
PLUS OUR REGULAR COLUMNS
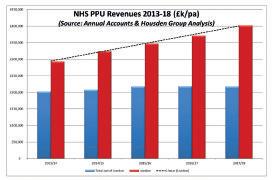
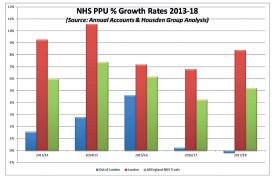
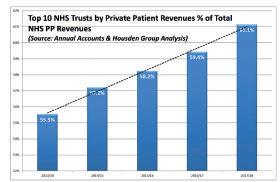
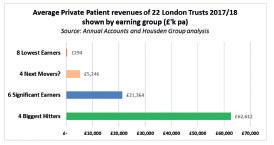
Private Patient Units series: Capital feat for London’s PPUs
Philip Housden’s analysis of accounts shows private units in London’s hospitals continue their surge in growth P51
Doctor on the Road: A hybrid in more ways than one
Motoring correspondent Dr Tony Rimmer takes a spin in a five-seat sports car with environmental credentials P54
Profits Focus: Keeping a steady flow
Our unique benchmarking series looks at the financial fortunes of urologists P56
Don’t quit the NHS pension
By Edie Bourne
Doctors breaking tax-relief ceilings on pension savings should think twice about leaving the NHS pension scheme, warn specialist medical financial advisers.
HM Revenue and Customs (HMRC) has revealed that the amount of money raised from those exceeding the ‘lifetime allowance’ has surged by nearly 2,000% over the past decade. Tax revenue has increased from £5m in 2006-07 to £102m in 2016-17.
The lifetime allowance restricts total tax-free pensions savings to £1,055,000 from April 2019. In 2011-12, the allowance stood at £1.8m and was cut to just £1m in 2016-17. It now rises with inflation each year.
Doctors breaching the allowance may be subject to tax charges of up to 55% on any excess savings – and more medical professionals than ever before are being caught by the lower threshold.
As the BMA and medical colleges lobby the Government to end the misery for doctors affected by strict pension savings limits, many doctors are choosing to quit the NHS Pension Scheme altogether.
But Patrick Convey, technical director of Cavendish Medical, explained why that may be a mistake.
He said: ‘Doctors have witnessed
unprecedented levels of changes to their pensions and tax in recent years. With a defined-benefit pension scheme such as the NHS, members are tied into making regular contributions, so when a savings limit is looming, they are unable to avoid breaching the threshold, whereas higher earners in the private sector can reduce pension payments accordingly.
‘More clients are considering early retirement, reducing their hours or leaving the pension scheme. However, opting out of the NHS scheme is not a decision which should be taken without detailed financial modelling which can pinpoint whether this is the best move for you.
‘Despite the issues with the NHS scheme, it provides a high level of security and substantial benefits such as death in service and illhealth support which can’t be provided through private pensions.
‘Even when considering tax charges, the pension and ancillary benefits can be much higher.
‘Before making a major decision, you should ensure that you have taken account of every nuance of the pension scheme and fully considered all options for reducing tax liabilities where possible.’
Pension protection schemes are available to restore previous lifetime allowance thresholds if savers meet the application criteria.
Medico-legal tasks help clinical work
➱ continued from front page
According to Sir Martin Spencer, chairman of the Expert Witness Institute (EWI), doctors should take on expert work with a view to improving their own practice.
He said: ‘Medico-legal work gives doctors a perspective on the work of others in their field: they see how others practise, the mistakes they make, the judgements that have to be made. Medico-legal experts, in informing the court of appropriate practice, need to update their own knowledge, for example by revisiting and reminding themselves of NICE guidelines.
‘In considering questions of cau-
sation, they may need to review relevant studies/papers and give the court a view on the balance of probability. All this is stimulating and interesting. The work is wellpaid, rewarding, invigorating and intellectually challenging.’
EWI governor Amanda Stevens said: ‘The lack of available experts in some specialist areas can cause delays in bringing cases to court. It is a sad fact that in children’s brain injury cases, experts such as paediatric neurologists and neonatologists are in such short supply solicitors can wait up to a year to secure their services.’
See conference report, page 6 What should an independent practitioner take into account in arriving at a reasonable fee to charge for an hourly rate? Doctors and accountants – let’s hear what you would advise. Contact robin@ip-today.co.uk
Harley Street’s global reach
A new online service enables Harley Street specialists’ expertise to be shared with patients around the globe.
People can book a video consultation on HarleyStreet.com website or request a second opinion from London’s leading surgeons and physicians.
Users of the LaingBuisson service, provided in partnership with Trustedoctor, select their preferred specialist and then securely upload their medical records, images and scans to a secure online environment.
Doctors accept the request and schedule a response within 72 hours. Fees are set at the same rate as the doctor’s usual initial consultation rate – typically £200-£300 in the Harley Street area.
LaingBuisson’s Keith Pollard said: ‘Until now, it’s not been easy for patients to consult with these specialists from afar. The new service enables a patient anywhere in the world to access their knowledge and expertise. It puts the best of London’s private healthcare at their fingertips, on their PC or their mobile device.’
BMA slates ministers for ‘unfair’ pension tax
A consultants’ leader has hit out at pension tax rules which are hitting some specialists with tax bills of tens of thousands of pounds.
Dr Gary Wannan, acting chairman of the BMA consultants committee, said: ‘It just simply cannot be right that these unfair and pernicious regulations are landing hard-working doctors with exorbitant tax bills for simply doing their jobs to the best of their abilities.’
He told the consultants’ annual conference that when many seniors became doctors, they thought if they continued paying into their pension pots they would receive a fair pension in recognition.
But then annual and lifetime tax allowances came along and they were repaid ‘with unexpected and unavoidable tax bills in the tens of thousands of pounds’.
Dr Wannan said this was often
simply for covering a colleague’s absence or helping in a time of high service demand. Doctors were being penalised for caring too much.
‘Our recent survey of consultants in England showed that 60% of consultants, from over 4,000 survey responses, intend to retire at or before the age of 60. An additional one-third plan to reduce their work commitment or have already done so. In both cases, chief among the
causes were annual and lifetime allowance regulations.’
The BMA consultants’ committee had repeatedly advised the Government that more would retire early if no action was taken.
His committee wrote to the Chancellor and Health Secretary and in January asking them to urgently look at repealing these taxes for public sector workers. But Dr Wannan claimed they had failed to listen.
The HarleyStreet.com website
Private doctor services slated by care watchdog
By Olive Carterton
Private GPs, consultants and independent specialist clinics have come under fire from Care Quality Commission (CQC) inspectors for the variable quality of care being provided.
Safety is the biggest concern highlighted in a new report from the watchdog which, while identifying some good practice, criticised nearly half of the private consulting doctor services analysed – 32 out of 66 first inspection reports.
Slimming clinics –16 out of 38 first inspection reports analysed –were also failing to provide safe care in accordance with the relevant regulations.
Most providers improved upon re-inspection, but there were concerns across independent primary care services about the safety and efficacy of prescribing.
Fears were also raised about poor record-keeping and clinicians not communicating their activity with the patient’s GP. The CQC said this was often linked to limited functionality and interconnectivity of IT systems.
Its wide-ranging report looks at the quality of care being provided by private GPs, GMC-registered clinicians who provide consultations and/or treatments, travel clinics, slimming clinics, circumcision clinics, allergy clinics.
According to the CQC’s Ursula Gallagher, deputy chief inspector of general practice and lead for independent providers, some providers displayed a limited awareness of their responsibilities – not just to their patients but to the wider healthcare system.
She hoped the report would help providers identify what they now needed to do and where they might focus their efforts.
‘Everyone providing these types of services has a legal responsibil-
ity to offer safe, high-quality care that not only meets the needs of the people using it, but also meets the legal requirements that exist to protect patients,’ she said.
‘Where this isn’t the case and we see risks to patient safety, we will not, and have not, hesitated to stop providers from operating.’
Nearly a quarter of slimming clinics – nine of 38 first inspection reports analysed – were not meeting the regulations for effective care, with some found to be treating people with medicines not recommended by the National Institute for Health and Care Excellence (NICE) or the Royal College of Physicians.
Inspectors found examples of appetite suppressants being prescribed to patients with a body mass index lower than that recommended, or to patients with high blood pressure.
Re-inspections of slimming clinics showed providers had addressed concerns and applied learning both from inspections of their own services and those of other providers.
But not all services improved sufficiently and one had its registration to operate removed.
Concerns were also found around safeguarding in other types of providers, such as circumcision clinics. While these services had systems to obtain consent from both adults with parental responsibility in place, they had not always obtained written consent from both parents before a procedure, or only asked for consent from both parents when the provider suspected a possible dispute.
Independent services are inspected against the same criteria as all other healthcare providers but only from this month will they receive a quality rating.
The State of Care in Independent Doctor and Clinic Services Providing Primary Medical Care
SAFETY IS THE CQC’s WATCHWORD
By Martha Walker
There has been mixed reaction to the way these CQC inspections were carried out.
Some doctors are satisfied and some found it stressful but fair. But many consider them punitive.
The regulators will, no doubt, find themselves again at odds with some of the doctors they inspected with their analysis.
Results of the CQC’s 18-month programme of compliance inspections for independent doctors was published just days before the introduction this month of ratings for the independent sector.
Based on a sample of 104 inspections, it found many independent providers were responding well to their patient’s requirements and delivering services tailored to specific needs.
The report mirrors the individual clinic inspections under the five themes: safe, effective, caring, responsive and well led, and covers a wide range of independent providers including GPs, consultants and doctors providing individual services.
Safety is the regulator’s biggest concern, as nearly half the providers were not giving safe care in line with CQC regulations.
Areas that CQC inspectors highlighted as needing improvement included prescribing processes and medicines management, consent, record-keeping and clinical governance.
A quarter of the first 38 slimming clinics inspected were considered as not providing effective care.
On re-inspection, there was improvement in many clinics – but beware. Clearly, the CQC will not hesitate to take more enforcement action if it thinks patient safety is at risk.
See next month’s Independent Practitioner Today for a full analysis
Martha Walker (right) is an independent CQC adviser at cqcconsultancy.co.uk
‘Super-clinic’ launches
By Douglas Shepherd
A team of medical women are working across specialties for a newly launched ‘super-clinic’ called Kat & Co Aesthetics.
Headed by consultant plastic surgeon Mrs Chien C. Kat, the service is housed in a four-storey property in Edgbaston, Birmingham, where she is supported by a specialist gynaecologist, aesthetic doctor and aesthetic nurse.
Mrs Kat said: ‘My philosophy, which is shared by the team, is that
we don’t just provide surgical treatment, because not everyone needs it.
‘People have different needs in different phases of their lives. By providing the full spectrum of therapies and treatments, from non-surgical to surgical, we can cater to younger patients who want to keep on top of their maintenance and more mature patients who need more of a nip and tuck.
‘Our holistic approach means we can provide what is best for the patient, from basic skin care to
complex surgical procedures. Our patients love to come to a place where they can see a team of dedicated professionals who work cohesively together and who are committed to being the best in their field.’
Dr Ana Mansouri, a former GP, has joined the team and offers a range of aesthetic procedures. She has a specialist interest in dietetics and provides nutritional and weight management advice.
The clinic now has the services of consultant gynaecologist Miss
Poonam Pradhan. She said her work was a good complement to the aesthetic services and meant women could come to discuss any issue, from urinary problems to menopause and period pains to post-birth complications.
Mrs Kat’s husband, Dr Haw Kat, is the clinic’s laser specialist, while consultant dermatologist Dr Camilio Diaz offers follicular unit transplants and follicular unit extraction, and aesthetic nurse specialist Natasha Rankin makes up the team.
Up to 150 consultants and their patients are due to enjoy improved facilities following a £30m private hospital redevelopment.
The private charity-owned New Victoria Hospital in Kingston upon Thames is celebrating its 60th anniversary with the opening this month of a new main entrance and reception, leading into a new outpatient suite with increased capacity.
It includes 12 consulting rooms, a cardiac diagnostic room, five treatment rooms including for colposcopy, audiology and phlebotomy.
This completes the construction of The Victoria Foundation Wing, which opened in 2016, housing four theatres, a 14-bed day surgery unit and a CT scanner.
David Marshall has been appointed chief executive, bringing international experience, having worked in Australia, the Middle East and South Africa. He was CEO at the Hospital of St John and St Elizabeth in London for six years. He succeeds Graham Ball, who becomes the hospital’s executive chairman.
Mr Marshall said: ‘Our patients will continue to receive the quality of care we have always provided, but this will now be in a five-star environment.
Eye
‘Our staff have continued to work in difficult circumstances during all the building work and now they will be able to do their jobs in a more comfortable environment in purpose-built facilities.’
Mr Marshall has previously run his own business providing management consultancy services to the healthcare sector and he worked as executive director of BMI’s Clementine Churchill Hospital in Harrow, north London.
Hospital owners, The Victoria Foundation charity, helps finance patients’ care and supports young people destined to become the future generations of doctors by ensuring they are not prevented from doing so through lack of finances.
Consultant founders of a new clinic say they aim to take personalised eye care to a new level of professionalism and provide a model for collaborative working among the UK’s top eye surgeons.
The three eye surgeons have teamed up to launch a new clinic, Ophthalmic Consultants of London (OCL), specialising in laser and lens vision correction surgery.
The private clinic has been set up by NHS consultant surgeons Mr Ali Mearza, Mr Allon Barsam and Mr Romesh Angunawela, all specialists in laser eye surgery, cataract and lens replacement surgery and corneal transplantation.
Treatment is performed at the clinic in New Cavendish Street and satellite locations across the capital, and in Hertfordshire, with all treatments delivered by one of the three founding surgeons.
OCL will provide a wide range of eye-related surgical procedures including cataract surgery, LASIK
Founding directors and ophthalmic surgeons (from left) Mr Ali Mearza, Mr Romesh Angunawela, Mrs Juliet Hicks, chief operating officer, and Mr Allon Barsam
for an opportunity A revamp helps unit celebrate its 60th
and LASEK laser eye surgery, refractive lens exchange surgery as well as other types of vision correction surgical techniques.
The three founding partners hold part-time NHS consultant positions at Moorfields, Imperial College Healthcare and Luton and Dunstable UCL.
They said they were the only clinic in London to offer the Z8 LDV Femtosecond laser and the Schwind Amaris 1050RS excimer laser for laser vision correction.
Mr Mearza, who is also clinical director of ophthalmology and lead consultant ophthalmic surgeon at London’s Imperial College Healthcare NHS Trust, said: ‘OCL has been conceived and designed to ensure excellence throughout the patient journey, from the initial consultation to treatment and aftercare. That’s why we have invested in the latest innovative technology, with a combination of equipment unique to the clinic.’
New hospital head David Marshall
Avoid courting disaster
More than 100 consultants and GPs attended this year’s BMA Expert Witness Conference in London. Reports by Robin Stride
A mini survival guide for doctors writing medico-legal reports was given by a barrister and mediator.
Simon Robinson, of Five Paper Chambers, said the hallmarks were to be clear, direct, honest and trustworthy.
Doctors should write for the intelligent lay person, explaining any technical key terms and they should address the points in the letter of instruction or guidance and highlight any additional relevant information.
Good reports should also specify the documentation used, such as GP medical records. They should refer to any relevant guidance, set out a clear chronological summary of facts and show a clear objective opinion.
Doctors were warned to avoid making derogatory comments about a patient or healthcare providers or professionals.
Mr Robinson said if a medical expert’s opinion was that someone fell below the standards to be expected, then they should explain why.
Authors should set out their qualifications and experience, address conflicts of interest, include a statement of truth and acknowledge the duty to the court.
Doctors should know what the legal definitions were and if they believed the letter of guidance was unclear, they should ask the solicitors or the court for clarification.
Mr Robinson spelled out seven ‘don’ts’ (see box on right).
He advised would-be experts to make sure they had turned off their phones before giving court evidence – or they might risk the whole court hearing their embarrassing ring tone.
Witnesses needed to ensure they answered the question they were asked and avoid being tempted to go beyond their competence.
And when writing the report? Avoid ‘double-justifying’ the text of the presentation. It is easier to read by justifying only on the left.
Explanation avoids litigation
People are, in fact, very reluctant to sue doctors, according to doctor and barrister Dr Simon Fox.
He said, in his experience, most were driven to it by a lack of an explanation or an apology on a background of a serious adverse outcome, including death.
Dr Fox said if an early explanation and apology had been given, then, over the last quarter of a century, this would have avoided most of his clients from litigating.
Talking of judges, he told doctors they would be amazed at the ignorance of some of them. Experts should not assume their judge had any understanding of medicine.
Cautionary tales
Some doctors have made a spectacular mess of their duties and liabilities as an expert witness.
In one personal injury claim case, two doctors were criticised by the judge and their reports were disregarded. One doctor was judged to be a family friend of the claimant and the other was facing a GMC investigation.
Another case went awry due to a medical expert lying over his experience. He also referred to a text book to back his evidence, aware that a later edition had removed that particular text. When challenged, he claimed the earlier edition ‘suited the occasion’.
These were among cautionary tales told by Michael Horne QC, a barrister at Serjeants’ Inn Chambers.
He amazed his audience with
SEVEN DON’Ts
1 Don’t be partisan; your duty is to the court, not the parties
2 Don’t be argumentative, but stand your ground appropriately if you feel confident in your professional opinion
3 Don’t make assumptions
4 Don’t be afraid to change your mind
5 Don’t be afraid to agree points with the other side’s expert
6 Don’t try to argue the law with lawyers
7 Don’t go beyond your competence
tales of cases going wrong. In another hearing, it turned out that two doctors failed to declare they had worked closely together before and had collaborated on a research paper.
Another expert witness appeared not to understand the anatomy nor the basics of managing the condition she was meant to be expert.
Shear arrogance was the undoing of another witness, whose stance throughout was said to be that he was right and everybody else was wrong.
Next month: 20 quick tips to help you survive the witness box as a medical expert witness, given by Augustus Ullstein QC
Welsh proton beam centre starts work
The first NHS Wales cancer patient to receive proton beam therapy has started treatment at the private Rutherford Cancer Centre South Wales in Newport.
Prof Roger Taylor, senior clinical advisor and consultant clinical oncologist at the centre, said: ‘The
availability of proton beam therapy at a local clinic is an important step forward in cancer care in the UK and we are pleased to be able to provide treatment for this young man.
‘While proton therapy is not a panacea for all types of cancer, we
have seen where it can be beneficial in treating a range of tumours. Working with the NHS in Wales means that adult patients have an option to be treated closer to home.’
The Rutherford Cancer Centre Thames Valley, in Reading, and the
Rutherford Cancer Centre North East, in Bedlington, Northumberland, will open proton beam therapy suites ‘within a few months’.
A centre in Liverpool – the Rutherford Cancer Centre North West – is currently under construction.
Compiled by Philip Housden
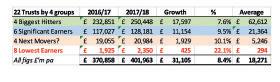
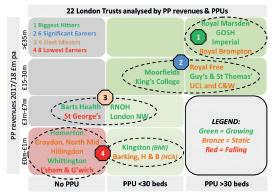
PPUs – a big opportunity to increase doctors’ fee growth
I have been urging my colleagues in PPUs to seize the £bn-a-year opportunity that private patients now present to the NHS – and the wider ‘win-win-win’ this delivers.
My message was – and is – that PPU growth is a win not only for NHS trusts and their patients, but also to consultants in fee growth.
I told the national Private Patient Services Conference 2019 that, looking more widely, the potential renaissance in NHS PPU provision was now a route for insurers to develop their product offer to their existing and new members.
It is my belief that expanded geographical access and depth and range of service could finally stimulate the stagnant insurance takeup rates.
Trusts from across the NHS attended the annual PPU gathering, hosted by Derby Private Health.
Delegates enjoyed seeing the high-quality private patient facilities at Royal Derby Hospital and heard of investment plans for dedicated theatre capacity to enable expansion.
They learned from the sharing of some successful PPU case studies from Derby, Nash Basildon and the Royal National Orthopaedic Hospital (RNOH).
Each provided practical insights on how to make PPUs successful by fully aligning them within their parent NHS trust.
Attenders received updates on the impact on the growing sector from agents of the Comp etition and Markets Authority and the Private Healthcare Informa tion Network and there was a positive dialogue with senior representatives of the four main insurers.
The event concluded with a summary of the key sector trends driving growth, principally patient safety and self-pay patient access and choice.
New private care facilities open at the RNOH
As a centre of excellence, RNOH has long offered patients the expertise of world-leading consultants, providing pioneering services in musculoskeletal care. Now the
trust’s PPU facilities have expanded from 18 to 28 inpatient beds with a ward moving into the top floor of the new Stanmore Wing.
The trust reported revenues of £6.7m in 2017-18 and the investment provides further impetus to the trend for NHS trusts to take increasing private patient market share from London private units.
RNOH’s chief executive Rob Hurd said the new facilities brought together already worldleading orthopaedic services with the facilities to match.
‘Expert multidisciplinary teams are co-located and working closely with some of the most motivated staff and highly-rated orthopaedic services, research and teaching in the NHS. Surplus private care income is reinvested in enhancing the hospital’s services for all patients and staff,’ Mr Hurd said.
BMI to sell hospital to NHS
In a boost to the NHS PPU sector, BMI Healthcare has announced the sale of BMI South Cheshire Private Hospital to the local trust.
The deal will see Mid Cheshire Hospitals NHS Foundation Trust take over the running of the hospital and continue to offer and
Learn how to avoid social media traps
Independent practitioners can brush up on social media using a new e-learning course to help them use social media ethically and effectively – and avoid careerdamaging pitfalls.
The MDU resource, open to both members and non-members, includes fictional scenarios based on common queries and concerns received from members, including:
Marketing yourself and your practice effectively and ethically using social media;
Patient confidentiality hazards associated with online media and how to avoid them;
Maintaining professional boundaries with patients;
Understanding when and how to respond to online criticism.
develop services for private patients. The private hospital is located at Crewe’s Leighton Hospital.
Mark Oldham, the trust’s finance director, said: ‘The acquisition is great news. Private patients will continue to benefit from the excellent facilities at South Cheshire Private Hospital, while being able to access a wider range of services and facilities at Leighton Hospital.
‘All patients will benefit from the additional funding that the private hospital will bring, as it will be reinvested locally into both private and NHS services.’
Mid Cheshire Trust reported private patient revenues of £1.5m at 0.7% of turnover in 2017-18, and ranked 50th out of 151 non-London NHS trusts.
This is a sign of the increasing pressure on provincial independent hospitals, as BMI Healthcare has also decided to close Somerfield Hospital in Kent and Fernbrae Hospital, Dundee. In addition, BMI Coombe Wing at Kingston Hospital transfers to in-house trust control from this month.
Philip Housden is a director of Housden Group. See his feature article on London PPUs on page 51
The union’s Dr Caroline Fryar said: ‘Social media can be a positive platform for medical professionals; however, it is important to take a careful approach and avoid mistakes, such as inappropriate comments or photos, which can damage your reputation and career.
‘The MDU’s new social media e-learning course helps to equip medical professionals with the knowledge to promote themselves and their practice ethically on social media; to understand the reputational risks associated with social media and considers howyou can respond appropriately to online complaints.’
To complete the social media e-learning course, visit www. themdu.com/learn-and-develop/ social-media-e-learning.
New £100m
HCA hospital
Consultants in a wide range of specialties will be practising at a new £100m hospital in Birmingham from 2022. It will be equipped to provide ‘some of the most complex surgical and medical procedures’. See more details on this story, and a picture, on page 47
The Royal National Orthopaedic Hospital’s new Stanmore Wing
RECRUITING PRACTICE STAFF
Cutting staff salaries is just false economy
SOURCING, RECRUITING and retaining staff is not an easy task these days.
It takes time to find decent staff and even more time to train them, only to receive their notice to quit six months later.
The financial burden this has is one that we hear about regularly from our clients.
A successful practice cannot run efficiently without a strong team providing not just the back office but also adhering to compliance and, even more importantly, providing excellent customer/patient service.
Ideally as a doctor running a busy practice or working in a busy hospital, you want your support team to stay for as long as possible.
Patients undoubtedly appreciate building a relationship with, for example, the practice manager or medical secretary, as they are the initial point of contact, taking their details, booking them in, even having to discuss initial sensitive reasons for seeing a specialist.
It can be the difference between a patient returning, if necessary,
BY JO MARKS, Director, Artemis Medical Recruitment
or not, thus impacting again on the financial aspect of a successful clinic.
become apparent in sourcing nonclinical support staff to our clients running private clinics and in the bigger private hospitals, that try ing to cut costs on salaries has had a detrimental effect in many ways.
staff initially, as the best staff can expect and request a specific start ing point.
Cleveland Clinic to open precursor satellite
Consultants will be seeing their first patients for the new Cleveland Clinic London next autumn.
Its first outpatient centre will be at 24 Portland Place, Marylebone, which it has leased from landlords The Howard de Walden Estate.
Chief executive Dr Brian Donley said outpatient services were expected to be ready there from Autumn 2020, ahead of the hospital’s opening ‘in early 2021’.
to go to the centre for diagnostic services and to see private GPs.
Simon Baynham, executive property director at The Howard de Walden Estate, said: ‘London is uniquely placed as a centre of global medical excellence and Cleveland Clinic London will be a hugely important addition to the
Dr Brian Donley
medical provision in The Harley Street medical area.’
Cleveland Clinic London at 33 Grosvenor Place is a short distance from the outpatient unit.
The hospital has signed an agreement for a 20-year lease of the six-floor 28,000ft 2
Portland Place building, which is currently used for office space.
The eight-storey new hospital is
a 324,000ft building and is cur rently under construction.
It will have 185 inpatient beds, eight operating rooms, an imaging suite, endoscopy and catheterisa tion labs, day case rooms for sur gery and a neurological suite with rehabilitation.
The facility will offer specialty services focusing on general sur gery, cardiology, orthopaedics and neurology.
Treat newly diagnosed non transplant eligible multiple myeloma patients with Darzalex® for a deep and meaningful response1
GIVES THEM THE TIME THEY NEED¹
60%
Estimated¶ progression free survival rate at 30 months vs 28% VMP (primary endpoint)¹
A TREATMENT THEY CAN RESPOND TO¹
91%
Overall response rate vs. 74% VMP (secondary endpoint§, p<0.001)3
A TREATMENT THEY CAN STAY WITH¹
7%
Treatment discontinuation rates due to adverse events vs 10% VMP*¹
DARZALEX® has approval in combination with VELCADE® (bortezomib), melphalan and prednisone (DVMP) and was studied in a phase 3 trial of 706 patients with a median follow up of 27.8 months.¹
DVMP is indicated for the treatment of adult patients with newly diagnosed multiple myeloma who are ineligible for autologous stem cell transplants.2
Please refer to the Summary of Product Characteristics (SmPCs) for further indications.
¶ Kaplan-Meir Estimate.
§ Secondary endpoints were overall response rate and the rates of very good partial response or better (comprising very good partial, complete, and stringent complete responses), complete response or better (comprising complete and stringent complete responses), negative status for minimal residual disease (at a threshold of 1 tumour cell per 105 white cells) and overall survival. Other end points were safety, side-effect profile, time to response and duration of response.¹
*The most common adverse events ( ≥20% of patients) with DVMP of any grade included neutropenia (50%), thrombocytopenia (49%), peripheral sensory neuropathy (28%), anaemia (28%), upper respiratory tract infection (26%), diarrhoea (24%), pyrexia (23%), and nausea (21%).3 27.7% of DVMP patients experienced an infusion-related reaction with the majority occurring at the 1st infusion.3 All drugs have associated risks and benefits, please refer to individual SmPCs for further information. VMP; Velcade®, melphalan and prednisone.
Prescribing information and adverse event reporting can be found on the reverse.
PHGB/DAR/1018/0014
Date of preparation: January 2019
DARZALEX®
ACTIVE INGREDIENT(S): Daratumumab
Please refer to Summary of Product Characteristics (SmPC) before prescribing.
INDICATION(S): Newly diagnosed multiple myeloma: In combination with bortezomib, melphalan and prednisone in adults, ineligible for autologous stem cell transplant. Relapsed/Refractory multiple myeloma: Monotherapy for adults whose prior therapy included a proteasome inhibitor and an immunomodulatory agent and who have demonstrated disease progression on last therapy. In combination with lenalidomide/dexamethasone or bortezomib/dexamethasone in adults who have received ≥ one prior therapy.
DOSAGE & ADMINISTRATION: Administration by healthcare professional where resuscitation facilities available.
Dilute with sodium chloride 0.9% solution for injection and administer by intravenous infusion using incremental escalation of infusion rate only if previous infusion well-tolerated.
Adults: Newly diagnosed multiple myeloma: Combination with bortezomib, melphalan and prednisone (6 week cycle): 16 mg/kg body weight weekly for 6 weeks followed by every 3 weeks up to Week 54, then every 4 weeks from Week 55, until disease progression. Relapsed/Refractory multiple myeloma: Monotherapy and combination with lenalidomide (4 week cycle): 16 mg/kg body weight weekly for 8 weeks followed by every 2 weeks up to Week 24, then every 4 weeks from Week 25. Combination with bortezomib (3 week cycle): 16 mg/kg body weight weekly for 9 weeks followed by every 3 weeks up to Week 24, then every 4 weeks from Week 25. First prescribed dose: prescribed 16 mg/kg dose at Week 1 may be split over two consecutive days i.e. 8 mg/kg on Day 1 and Day 2 respectively Refer to SmPC for further details.
Recommended concomitant medications for management of infusion-related reactions (IRRs): To reduce risk, administer pre-infusion medications to all patients 1-3 hours prior to every infusion: i.e. corticosteroid (monotherapy: methylprednisolone (or equivalent) iv then iv or oral following second infusion; combination: dexamethasone (or equivalent) iv then iv or oral from second infusion) plus oral antipyretics and oral or intravenous antihistamine. If dexamethasone given on infusion day, do not take IRRs, administer post-infusion oral corticosteroid: monotherapy e.g. methylprednisolone on each of two days following all infusions; combination: methylprednisolone the day after infusion, but may not be needed if dexamethasone or prednisone continued. Consider short/long acting bronchodilators and inhaled corticosteroids in patients with history of chronic obstructive pulmonary disorder Any grade/ severity IRRs, interrupt Darzalex immediately and manage symptoms. Re-starting Darzalex: reduce infusion rate (refer to SmPC); Grade 4 IRRs (or third occurrence of Grade 3) – per manently discontinue. No dose reductions of DARZALEX recommended. For haematological toxicity, dose delay may be required to allow recovery of blood cell counts. Consider anti viral prophylaxis for prevention of herpes zoster virus reactivation. Children: No data available. Elderly/Renal impairment/Hepatic impairment: No dose adjustments.
CONTRAINDICATIONS: Hypersensitivity to active substance or excipients.
SPECIAL WARNINGS & PRECAUTIONS: IRRs: Symptoms predominantly include nasal congestion, cough, throat irritation, chills, vomiting and nausea; can cause serious IRRs including anaphylactic reactions. Monitor for IRRs throughout the infusion. For any Grade of IRR, continue monitoring post-infusion until Dosage and Administration). Institute medical management/supportive treatment as needed. If an anaphylactic reaction or life threatening (Grade 4) IRR occurs, initiate appropriate emergency resuscitation immediately and discontinue Darzalex immediately and per manently. Neutropenia/ Thrombocytopenia: Darzalex may increase neutropenia and thrombocytopenia induced by background therapy; monitor for infections & periodic complete blood cell counts (refer to relevant SmPCs); consider supportive care. Indirect Antiglobulin Test (Indirect Coombs Test): Binds to CD38; may mask detection of antibodies to minor antigens; ABO and Rh blood typing not impacted. Inter ference may occur up to 6 months post-treatment. Type and screen patients prior to starting daratumumab; consider phenotyping; red blood cell genotyping not affected by daratumumab. Infor m blood transfusion centres when appropriate. If emergency transfusion required, give non-cross-matched ABO/RhD-compatible RBCs. Contains sodium.
VELCADE® 3.5 mg POWDER FOR SOLUTION FOR INJECTION PRESCRIBING INFORMATION
ACTIVE INGREDIENT: Bortezomib
Please refer to Summary of Product Characteristics (SmPC) before prescribing
NDICATIONS: Adults only. Monotherapy or with pegylated liposomal doxorubicin or dexamethasone: progressive multiple myeloma in patients who have had at least 1 prior therapy and already undergone/are not suitable for haematopoietic stem cell transplant. With melphalan & prednisone: for previously untreated multiple myeloma in patients not eligible for high-dose chemotherapy with haematopoietic stem cell transplant. With dexamethasone, or with dexamethasone and thalidomide: for induction treatment of previously untreated multiple myeloma in patients eligible for high-dose chemotherapy with haematopoietic stem cell transplant. With rituximab, cyclophosphamide, doxorubicin and prednisone: for previously untreated mantle cell lymphoma (MCL) in patients unsuitable for haematopoietic stem cell transplantation.
DOSAGE & ADMINISTRATION: Adults and Elderly: Administer as 3-5 second IV bolus or SC in thighs/ abdomen. At least 72 hours between consecutive doses. Recommended dose 1.3mg/m2 body sur face
Treatment of progressive multiple myeloma (after at least 1 prior therapy) VELCADE treatment cycle: twice weekly for 2 weeks in 21-days treatment cycle. Two cycles of VELCADE remission should receive total of 8 cycles.
Monotherapy: as above. Combination with pegylated liposomal doxorubicin: 30 mg/m² pegylated liposomal doxorubicin (1h IV infusion) on day 4 of VELCADE treatment cycle. Combination with dexamethasone: 20 mg oral dexamethasone on days 1, 2, 4, 5, 8, 9, 11, and 12 of VELCADE treatment cycle.
Previously untreated multiple myeloma patients not eligible for haematopoietic stem cell transplant
Combination with oral melphalan (9mg/m2) and prednisone (60mg/m2): 9 x 6-weeks treatment cycles.
Combination with oral dexamethasone (40mg): 4 x 21-days treatment cycles.
Combination with oral dexamethasone (40mg) and thalidomide (50mg): 4 x 28-days treatment cycles.
At least partial responders: 2 additional cycles. For other medicinal products, see appropriate SmPCs. Previously untreated mantle cell lymphoma not suitable for haematopoietic stem cell transplantation
Combination therapy with rituximab, cyclophosphamide, doxorubicin and prednisone (VcRCAP): 6 - 8 x 21-days treatment cycles. (For other medicinal products, see appropriate SmPCs.)
Children: no recommendation on posology can be made; refer to SmPC for current available data. Hepatic Impairment: mild - no dose adjustment; moderate or severe - start on reduced dose of 0.7 mg/ mg/m2 or reduction to 0.5 mg/m2 based on tolerability. Renal Impairment: See precautions.
CONTRAINDICATIONS: Hypersensitivity to active substance, boron or any excipients. Acute diffuse
SPECIAL WARNINGS & PRECAUTIONS: Do not administer intrathecally. Monitor complete blood counts; consider platelet transfusion. GI toxicity very common; monitor closely. In MCL, transient neutropenia reported between cycles; monitor for signs/symptoms of infection, treat promptly; consider prophylactic granulocyte colony stimulating factors if delayed cycles. Herpes zoster virus reactivation: anti-viral prophylaxis recommended. Screen for Hepatitis B Virus reactivation/infection when rituximab combination; consider antiviral prophylaxis (see SmPC for rituximab). Very rarely John Cunningham virus infection resulting in Progressive Multifocal Leukoencephalopathy (PML) and death; monitor regularly for PML symptoms, discontinue if diagnosed. Peripheral neuropathy common; requires to SC route. Special care if risk factors for seizures. Caution when history of syncope with medicinal products linked with hypotension, or dehydration due to recurrent diarr hoea/vomiting. Discontinue treatment if Posterior Reversible Encephalopathy Syndrome (PRES) occurs. Development/exacerbation of congestive heart failure/QT prolongation; monitor closely if cardiac risk factors. Renal impair ment
(ARDS); baseline chest radiograph recommended. If new/worsening pulmonary symptoms per for m
Immunocomplex-mediated reactions e.g. serum sickness, polyarthritis with rash, proliferative glomerulonephritis: discontinue if severe. Bortezomib exposure increased in moderate/severe hepatic impair ment; reduce doses, closely monitor Patients with high pre-treatment tumour burden at risk of tumour lysis syndrome; monitor closely. Concomitant CYP3A4-inhibitors: monitor closely. Caution with CYP3A4 or CYP2C19 substrates.
SIDE EFFECTS: Very common: IRRs, pneumonia, upper respiratory tract infection, anaemia, neutropenia, thrombocytopenia, lymphopenia, peripheral sensory neuropathy, headache, hypertension, cough, dyspnoea, nausea, diarr hoea, vomiting, muscle spasms, fatigue, pyrexia, peripheral oedema. Common: Other side effects: anaphylactic reaction (rare). Refer to SmPC for other side effects.
PREGNANCY: Effective contraception during and for 3 months after treatment in women of child-
LACTATION: Not known if daratumumab is excreted into breast milk.
INTERACTIONS: No studies per for med. Not anticipated to alter drug-metabolising enzymes. Daratumumab binds to CD38 on RBCs and inter feres with compatibility testing (including antibody screening and cross matching). Inter ference mitigation methods include treating reagent RBCs with dithiothreitol (DTT) to disrupt daratumumab binding or other locally validated methods. However Kell-negative units should be supplied after ruling out/identifying alloantibodies using DTT-treated RBCs. Alternatively, consider phenotyping or genotyping. Daratumumab detected on serum protein to facilitate deter mination of a complete response in patients with persistent very good partial response. Refer to SmPC for full details of interactions.
Adverse events should be reported. ▼ This medicinal product is subject to additional monitoring and it is therefore important to report any suspected adverse events related to this medicinal product. Reporting forms and information can be found at www.mhra.gov.uk/ yellowcard or search for MHRA Yellow Card in the Google Play or Apple App Store. Adverse events should also be reported to Janssen-Cilag Limited on 01494 567447 or at dsafety@its. jnj.com.
MCL: sepsis (inc septic shock), Herpes virus infection, bacterial infections, hypersensitivity, diabetes and right ventricular), myocardial ischaemia, ventricular dysfunction, hiccups, gastritis, oral ulceration, der matitis, musculoskeletal pain, urinary tract infection, injection site reaction, hyperbilirubinaemia, protein analyses abnor mal, weight increased.
Other side effects include: tumour lysis syndrome, pulmonary hypertension, pancytopenia, anaphylactic shock/reaction, hearing impaired (up to and inc deafness), cardiovascular disorder (inc cardiogenic shock), pulmonary embolism, acute respiratory distress syndrome, colitis (inc clostridium
Multiple Myeloma: cardiac failure, Posterior Reversible Encephalopathy Syndrome, acute diffuse meningoencephalitis herpetic, Epstein-Barr virus infection, neoplasm malignant, leukaemia plasmacytic, mycosis fungoides, neoplasm benign, lymphadenopathy, febrile neutropenia, thrombocytopenic purpura, hypersensitivity, type III immune complex mediated reaction, Cushing’s syndrome, mental disorder suicidal ideation, psychotic disorder haemorr hage intracranial, peripheral sensory motor neuropathy, encephalopathy, neurotoxicity, cerebral haemorr hage, seizure disorders, paralysis, coma, eye haemorr hage, optic neuropathy, different degrees of visual impair ment, cardiac tamponade, torsade de pointes, angina unstable, cardiac valve disorders, sinus arrest, cerebrovascular accident, deep vein thrombosis, thrombophlebitis, phlebitis, vasculitis, peripheral embolism, pulmonary alveolar haemorr hage, bronchospasm, wheezing, respiratory failure, apnoea, haemoptysis, respiratory alkalosis, throat tightness, pancreatitis, haematemesis, gastro-intestinal obstruction, enteritis, megacolon, peritonitis, gastrointestinal ulceration & per foration, hepatotoxicity, hepatitis, cholestatis, hepatic haemorr hage, acute febrile neutrophilic der matosis, toxic skin eruption, toxic epider mal necrolysis, StevensJohnson syndrome, purpura, erythema multifor me, myopathies, r habdomyolysis, renal failure, urinary retention, oliguria, death, multi-organ failure, ECG abnor mality. MCL: hepatitis B infection, bronchopneumonia, autonomic nervous system imbalance, vertigo, pneumonitis, pulmonary oedema (inc acute). Refer to SmPC for other side effects.
PREGNANCY: No clinical data available for bortezomib. Thalidomide contraindicated during pregnancy and in women of childbearing potential unless all conditions of thalidomide pregnancy prevention programme met. Male and female patients of childbearing potential must use effective contraceptive measures during treatment and for 3 months following.
LACTATION: Not recommended.
INTERACTIONS: Closely monitor when bortezomib is combined with potent CYP3A4-inhibitors (e.g. ketoconazole, ritonavir). Concomitant use of bortezomib with strong CYP3A4 inducers (e.g. rifampicin, carbamazepine, phenytoin, phenobarbital and St. John’s Wort) not recommended. Hypo/ hyperglycaemia reported in diabetic patients receiving oral hypoglycaemics.
FURTHER INFORMATION IS AVAILABLE FROM: Janssen-Cilag Limited, 50-100 Holmers Far m Way, High Wycombe, Buckinghamshire, HP12 4EG, UK.
Prescribing infor mation last revised: January 2016
Adverse events should be reported.
Reporting forms and information can be found at www.mhra.gov.uk/yellowcard. Adverse events should also be reported to Janssen-Cilag Limited on 01494 567447.
Dimopoulous et al. Daratumumab, Bortezomib, Melphalan
Private ambulance services criticised
By Leslie Berry
Alarm bells are ringing over the state of independent ambulance services, following a Care Quality Commission (CQC) investigation. Now the inspection watchdog is calling on private ambulance operators and the wider system to do more to ensure patients’ safety. It expressed continuing concern about the overall standard of care across the independent ambulance sector. Although it saw evidence of good practice and improvements made by some operators, worries remain about how safely and effectively others are caring for patients.
A CQC report analysing findings from a comprehensive inspection programme of independent ambulance services in England reveals that the quality and safety of services varies greatly.
Inspectors found vehicles given no regular servicing, missing or faulty equipment – including paediatric apparatus for transporting children in emergencies – and an absence of regular equipment checks.
Many providers offered either no or very limited staff training. The CQC said: ‘This was particularly apparent in relation to emergency driver response training to ensure the skills required to transport a patient using blue lights or sirens, training to equip staff to recognise and escalate safeguarding concerns and to effectively support patients with mental health needs.’
Checks to ensure that staff had the appropriate employment references, Disclosure and Barring Service certificates, and driving
licence categories – for example, to operate heavier vehicles – were enforced inconsistently.
Medicine management standards were extremely variable. Some services had robust policies to support the safe administration of medication, but others showed a lack of understanding, especially around controlled drugs and the need for their safe administration and secure storage. Some services did not have the required Home Office licence for the procurement and storage of controlled drugs.
The CQC is urging those who commission independent ambulances to ensure they make safety and quality a priority – and take guidance from its quality ratings awarded to independent ambulance services.
Sally Taber, director of the Ind ependent Healthcare Sector Complaints Adjudication Service, welcomed the ‘long overdue’ report.
She said it highlighted the need to learn through experience about how to improve service and safety.
Ms Taber said ISCAS had offered to help install the tried and tested independent sector complaints process, which would help operators meet CQC recommendations on learning from complaints and concerns. She was in continued discussions with two independent ambulance trade organisations about this.
THE WATCHDOG’S PLEA FOR ACTION
Ellen Armistead, CQC’s deputy chief inspector of hospitals and lead for ambulance services, said: ‘We have found and highlighted pockets of good practice in individual services, with compassionate one-to-one care from ambulance staff, and evidence of improvements in some services when we have been back to re-inspect.
‘But we remain concerned about the overall standard of care across the independent ambulance sector.
‘Providers have a responsibility to ensure that people within their care receive appropriate treatment, that the vehicles used to transport patients are fitted with the right equipment, that staff are appropriately trained and supported to carry out their roles, risks and incidents are reported and addressed, and that medicines are stored securely. This was not the case in many of the services we inspected.
‘It is wholly unacceptable for people using these services to be put at risk and where we have identified concerns, we have held those providers to account by making clear where improvements must be made –using our enforcement powers where needed to protect people.
‘Those who deliver and commission care must learn from the services that are getting it right so that people are protected from risk and can have confidence in the quality of care they receive from independent ambulance services across the country.’
Private units offer to cut waiting lists
The private hospitals’ and clinics’ trade body has appealed to the NHS to make more use of the independent sector to help cut waiting times.
David Hare, chief executive of the Independent Healthcare Providers Network, said it was vital that significant spare capacity in pri
vate units was utilised by local NHS areas to ensure patients were treated as quickly as possible, including through exercising their right to choose the best care provider for them.
He was reacting to a National Audit Office report on NHS waiting times for elective and cancer treatment.
Mr Hare said this demonstrated once again the desperate lack of elective capacity in the NHS which forced patients to wait ever longer for vital treatment such as hip replacements and cataracts.
Added Mr Hare: ‘It’s now been almost three years since the NHS last met its target to treat 92% of
elective patients within 18 weeks and the NAO is absolutely right in calling for NHS England and Improvement to urgently set out how the health service will address this declining performance and ensure the right incentives are in place to ensure patients get speedier access to care.’
Sally Taber, complaints service boss
A
A trawl through the archives: what made the news in 2009
Pay rise revealed
Nearly one-in-five doctors with a private practice had seen their income rise the previous year, according to a BMA private practice committee survey.
If found 17% of private doctors increased earnings, 43% stayed the same and 40% suffered a decrease.
Average income was said to be £65,533 (£49,050 net) among the 715 usable responders to a survey sent randomly to 3,000 members.
Shorter NHS waiting times were the main factor affecting income.
Twenty-three per cent earned under £10,000, but 17% got more than £100,000, 5% over £200,000 and 2% £300,000 plus. But the BMA published no data on doctors earning far more.
Keep your nose clean
Consultants were given advice on staying off the management radar if they wanted to keep a presence in the NHS and run a private practice at the same time.
Former consultant chemical pathologist and then director of Healthcare Performance Ltd, Dr Mike Roddis, produced the following ‘survival check-list’:
Get your job plan agreed;
Get your appraisal signed off;
Keep your portfolio up to date including your continuing medical education;
Do your supporting programmed activities (SPAs);
Pay attention to personal conduct and behaviour issues;
Do not renege on your clinical sessions;
Abide by NHS trust policies
Attend regular NHS meetings for multidisciplinary teams and directorate affairs;
Keep to the rules on leave;
Attend to time management;
Comply with the NHS rules on private practice;
Co-operate with the NHS on complaints and incident investigations.
Super group takes off
We announced the first ‘supergroup’ launch to raise the profile of consultants and market them overseas.
Doctors paid £5,000 for clinical memberships of the Harley Street Alliance, and signed up to ten
Project executive Tam McDonald said he saw half of the 260 clinics in the area as potential members. ‘At a time of recession when there is any worry at all about what the UK has to sell to other countries, it is time to shout out the benefits of our world-class healthcare sector,’ Mr McDonald said.
One alliance member said: ‘We were impressed by the focus on patient care and the desire to re-establish Harley Street as a band representing clinical excellence. We felt alliance membership would also permit greater marketing exposure at a lesser cost than could be gained individually.’
Taxman’s new probing powers
Doctors’ businesses were warned to be alert to new HM Revenue and Customs information and inspection powers from this month.
These covered PAYE, VAT, income and other taxes and gave the tax inspectors powers to visit businesses to inspect the premises, assets and records and request information and documents.
A spokesman said: ‘This new approach to compliance checks will improve HMRC’s ability to ensure that the right tax is paid at the right time.’
No time like the present
Young specialists aiming to pursue private practice were warned it would be ‘the kiss of death’ to delay their plans.
Independent Practitioner Today columnist and accountant Martin Murray said if they put off private work for six months until after settling into their consultant posts, they would miss out on referrals. He told a conference run by the Medical Protection Society and the Hospital Consultants and Specialists Association that the recession was making some private doctors suffer. But others said their businesses were booming.
Mr Murray, of Sandison Easson and Co, advised doctors to:
Beware white lies if you ask consultants how much they charge. One advised a young colleague there was ‘no money at all’ in a certain procedure. But it was the only operation he did.
Save for your tax bill. One consultant failed to and had to go to an insolvency practitioner.
Establish your own private practice independently of a group. Then if you fall out you won’t have to start again.
SUBSCRIBE TODAY
Don’t miss out on what we report and advise in the future. Sign up for a £75 subscription today –consultants, GPs and practice managers can save £15 with a direct debit.
See page 24
MEDICAL INDEMNITY REFORMS
Medical indemnity –what you should know
If you’re working in the medical sector, you must read this, writes Kevin McCluskie
THE GOVERNMENT is concerned that private patients are being seen by consultants who are supported by an unregulated indemnity based on ‘discretionary cover’ as offered by the medical defence organisations (MDOs).
Any claim could be refused without consultant recourse, leaving both the consultant and the patient exposed to financial loss.
The Government wants to review this and has issued a consultation paper on Appropriate Clinical Negligence Cover for those who practise in the independent private health sector.
The paper seeks views of two options:
1. Leave arrangements as they are;
2. Introduce legislation to ensure that consultants in independent private practice hold appropriate cover that is subject to appropriate supervision by a regulator.
Currently in the UK, the regulators in question are the Financial Conduct Authority (FCA) or the Prud ential Regulation Authority (PRA).
The Government has clearly signalled that its preference is option two.
This means that ‘discretionary indemnity’, which is currently offered by the MDOs, could become a thing of the past.
This is because:
MDOs that offer ‘discretionary cover’ have no legal obligation to pay any valid claims;
MDOs have no legal requirement to ensure that they have adequate funds to pay claims;
MDOs have no legal require -
ment to declare their financial position;
MDOs are not bound by FCA rules to treat customers fairly.
What is the alternative?
Currently, the alternative is the insurance market, which has been active in this area for many years.
Why conventional insurance?
The cover that the insurance companies offer is not discretionary; it is guaranteed within the policy and enforced by law.
Insurers are regulated by the FCA and the PRA, and this gives greater all-round financial security and claims funds are regulated and guaranteed by law.
Insurers offer stable pricing which is cost-effective based on individual circumstances.
Insurance offers wide cover, designed for 21st century risk threats.
Besides clinical negligence and GMC investigations, an insurance bundle of cover could offer such things as defence of reputation,
cyber liability, tax investigations and more.
Insurance policies are flexible contracts and are tailored to fit consultants’ personal circumstances.
For instance, excesses can be chosen to reduce costs, limited companies can be included and retroactive dates to pick up historical claims and run-off cover to offer indemnity after retirement are now standard.
What action should I be taking?
Check your current indemnity policy to establish whether you only have ‘discretionary cover’ and then decide if that’s a risk you are prepared to continue to take.
If not, then you need to look at the alternatives and act sooner rather than later.
Currently, there are several insurers who can underwrite medical indemnity insurance.
If the Government takes decisive action, it is expected demand will outstrip supply by a considerable margin while the market adjusts to the new rules.
Check your current indemnity policy to establish whether you only have ‘discretionary cover’ and then decide if that’s a risk you are prepared to continue to take
We have experience of this when the Solicitors Mutual Fund failed in 2000 and solicitors had to buy insurance – many being unable to obtain it.
How do I do this?
Contact Medical Broking Company; we have vast experience in this sector and are regulated by the Financial Conduct Authority.
We have to offer impartial professional advice by law regarding which policy is right for your circumstances.
Visit https://medbc.co.uk/medical-indemnity for more information, where you can fill out an inquiry form and we will get back to you. Alternatively, get in touch by phone on 01494 387800 and talk to us. Or email us at medmal@ medbc.co.uk.
Get the facts and explore your options.
Kevin McCluskie is the managing director of Medical Broking Company with extensive experience in this sector and can be reached using the above contact details
THE BATTLE FOR YOUR DEFENCE
Current cover doesn’t work
What is the future of indemnity cover for doctors?
David Hare (right) sets out the healthcare providers’ view on what now should happen
MEDICAL INDEMNITY of clinicians has undoubtedly risen up the healthcare agenda over the last few years, with a clear case for reform emerging.
Most notably, the Paterson case –where breast surgeon Ian Paterson convinced patients to undergo unnecessary surgery – brought to light a number of key issues around indemnity cover for consultants working in the independent sector.
This includes issues around:
Where the liability sits when clinicians operate in both the NHS and independent sector;
When there are multiple indemnifiers;
The current gaps in protection under the discretionary model of cover.
With this area ripe for reform, the Government published a consultation late last year on what indemnity cover for healthcare professionals should look like for those who are not covered by any existing or proposed state-backed scheme. The Government has been committed to launching a state-backed scheme, largely to help stem rising clinical negligence costs.
comprehensive insurance indemnity cover that works for the benefit of patients.
Indeed, the principle behind any new scheme must be that patients should always be compensated when things have gone wrong and they have been harmed. Nothing less will do.
Quite rightly, the Department of Health and Social Care (DHSC) also recognises that healthcare professionals are disadvantaged by a discretionary model of indemnity cover.
Unaware of cover
Medical defence organisations (MDOs) do not have to disclose their full financial position, meaning that healthcare professionals may be unaware of the extent of their financial cover.
Furthermore, because MDOs are not subject to regulation on financial conduct and fair treatment, healthcare professionals can be left at risk of unfair treatment.
The IHPN believes that compulsory, affordable and comprehensive insurance is the way forward for giving doctors indemnity cover
As the representative body for independent healthcare providers, the Independent Healthcare Providers Network (IHPN) welcomed the opportunity to contribute to this consultation, which closed at the end of February.
For us, we are clear that the starting point when looking at reform must be the introduction of fully
IHPN’s key priority for any new legislative/regulatory change is therefore that the current discretionary model of indemnity cover for healthcare professionals in the independent sector should cease, with compensating payments made to private patients in all cases even where negligence or criminal intent has been established.
But we, of course, understand that while this principle may be a simple one, the development of a new system will be a far more com-
plex challenge and needs to be carefully considered. It is essential that potential market instability and an increase in costs are militated against.
Having looked closely at the approaches taken in other sectors, we believe that compulsory, affordable and comprehensive insurance would be one practical solution to ensure that all healthcare professionals hold appropriate clinical negligence cover.
This has worked well in the legal sector where, in September 2000, the Solicitors’ Indemnity Fund ceased to provide indemnity to solicitor practices in England and Wales.
The solicitors’ profession and its regulator took the opportunity at the outset to define the minimum cover that should be accepted, covering a range of areas; for instance, minimum limits of indemnity, minimum run-off periods and cover to be included for ‘deliberate
We must avoid a situation, therefore, where the discretionary model of cover is simply replaced by an insurance system with significant exclusions and limits
acts’. In September 2000, the Fund stood at some £240m.
When commercial insurance was introduced, this pushed the premium pot down to around £150m, although it recovered to around £180m the following year.
Seventeen years after the mutual was folded, the premium pot is at about the same level as it was in the fund’s last year.
Insurance would not, of course, be a panacea, however, and it is critical to bear in mind that insurers do not insure against criminal
acts. Therefore, in instances such as the recent Ian Paterson case, an insurer would not necessarily have taken a different approach to the one taken in relation to Paterson.
We must avoid a situation, therefore, where the discretionary model of cover is simply replaced by an insurance system with significant exclusions and limits.
Safety net
One way to overcome this would be to introduce a mechanism such as an industry-wide risk pool, which would help ensure patients subjected to criminal acts by healthcare professionals receive adequate compensation.
The DHSC has shown real leadership in the area, working together with IHPN and other key stakeholders, and we believe there’s a real opportunity to make longterm change to the indemnity landscape to ensure that private patients are afforded the same legal
and financial protections as NHS patients.
But while the ultimate purpose of this policy change is, of course, to strengthen patient compensation, we are clear that this can only be achieved if doctors across the independent health sector are fully engaged in this work.
We have therefore called for a comprehensive education campaign for independent healthcare professionals during any transition period so that they are aware of the new requirements placed upon them as well as any limits and exclusions of their cover.
We look forward to working with healthcare professionals as this policy agenda moves forward and ensuring that doctors are not treated unfairly or left unaware of their level of cover.
David Hare is chief executive of the Independent Healthcare Providers Network (IHPN)
CHARITY FUNDRAISER
Going to the end of the earth
‘Dr Mike on a Bike’ is cycling round the world to raise funds for a charity helping doctors. The Royal Medical Benevolent Fund’s Joe Meredith (right) reports
A BRIGHTON-BASED junior doctor is taking on a 19,000-mile round-the-world cycle trip, turning an eight-month career break into an extreme challenge in support of medical colleagues under pressure.
Dr Michael Nally, AKA ‘Dr Mike on a Bike’, plans to ride through 22 countries as he circumnavigates the globe to raise money for charities the Royal Medical Benevolent Fund (RMBF) and Mind.
The 26-year-old aims to raise £20,000 for the charities while spotlighting the pressure that doctors face at work, and the high incidence of mental health issues in the profession.
The suicide rate among doctors is double that of the general population and this sobering statistic was a key reason he decided to take on this gruelling challenge in support of his colleagues.
Dr Nally said: ‘When I was a foundation doctor, my friend told me about his colleague, also a junior doctor, who sadly took their own life. For me, this raised a lot of questions about what was happening in the system for doctors to feel that low.
‘I then read about Sophie Spooner, a paediatric trainee who tragically took her own life after experiencing mental health problems. Her mother explained that Sophie had struggled to find a
mental health service that would have understood her problem in the context of being a doctor and that if she’d had the right help, she would still be here. The story had a profound effect on me.
‘My goal is to raise money and awareness for the increasing numbers of doctors under stress and pressure. There are so many positives to being a doctor and being the person people turn to when they need mending.
‘I want people to know that sometimes doctors need mending too and if just one doctor can get some help as a result of me cycling round the world, it will be worth it.’
Dr Nally set off in February from Buckingham Palace for the first leg of the trip which took him through Europe to Istanbul.
Cycling 80 to 110 miles a day, he will go on to navigate the Indian coast, through Myanmar and Malaysia on to Australia and New Zealand. After crossing the Pacific Ocean, he will cover around 4,500 miles across the US and Canada, before returning to London via Portugal, Spain and France.
Two close friends, Charlie and Will, are set to cycle alongside him for the later stages and provide vital moral support as the journey nears its close.
Supporters can track Mike’s progress through his Facebook, Twitter and Instagram updates,
and can donate to help him reach his fundraising goal at www. virginmoneygiving.com/drmikeonabike .
Steve Crone, chief executive of the RMBF, said: ‘It’s a real pleasure to meet a young doctor with so much passion for his chosen profession and such a determination to make things better for his colleagues.
‘By taking on this challenge for the RMBF and Mind, Dr Mike will help us make a real difference to the lives of doctors under pressure.
‘We are extremely grateful for his efforts and excited to be a part of his journey – we can only imagine the stories that he’ll be collecting along the trip.’
Working in both Brighton and Worthing Hospitals, Mike always felt well supported. Dr George Findlay, chief medical officer and deputy chief executive of Brighton and Sussex University Hospitals NHS Trust and Western Sussex Hospitals NHS Trust, said: ‘This is an amazing challenge, raising awareness for a very important cause. Mike has a real passion for our profession and for supporting his colleagues – some of whom will be joining him at stages along his route.
‘Being a doctor is uniquely rewarding, but also uniquely challenging and it is vital that our colleagues can receive the support they need, when they need it.’
Hello from Istanbul and thanks for reading my story. I’m now eight countries into my journey and really appreciating all of the messages of support so far! I think if there’s one thing I’d love readers to know, it’s that we have a charity which is behind us as doctors. The RMBF supports UK-registered doctors at all stages in their careers. If I can help just one fellow doctor by supporting the RMBF and Mind UK, then it will make all of the 19,000 miles worth it!
DR MIKE NALLY SAYS:
‘The most important thing for you to know about me is that I am in no way a professional athlete. Coming in at 6ft 5ins, weighing more than 100kg and having a lifelong weakness for all things sugar and dough have put paid to any flourishing sporting career. Having said that, I enjoy a game of rugby and have spent plenty of time in the saddle over the years.
‘This challenge will allow me to continue my love affair with cycling and at the same time raise awareness for an issue that I feel very strongly about. I was shocked when I learnt that doctors are twice as likely to commit suicide compared with the general population.
‘Year on year, the number of doctors struggling with anxiety, depression and burnout is growing with little in the way of support on offer. It’s my firm belief that, without healthy doctors, you simply cannot have healthy patients.’
DONATE AND FOLLOW DR MIKE ON A BIKE
Donate: www.virginmoneygiving.com/drmikeonabike
Website: www.drmikeonabike.com/
Facebook: www.facebook.com/drmikeonabike
Twitter: twitter.com/Drmikeonabike
Instagram: www.instagram.com/drmikeonabike/
The Royal Medical Benevolent Fund is the UK charity for doctors, medical students and their families.
It provides vital financial help to doctors facing hardship as a result of illness, injury, bereavement or disability.
Most of the doctors it helps are under the age of 40 – often those who have not yet had the chance to build up a financial safety net.
It also works with the BMA to provide DocHealth, which offers confidential psychotherapeutic support for all doctors.
Mind provides advice and support to empower anyone experiencing a mental health problem. It campaigns to improve services, raise awareness and promote understanding of mental health issues.
Upright Positional
• Completely open scanner that is well tolerated by claustrophobic patients
• Weight-bearing scans for spine and joints enable a more precise diagnosis
• Patients who are large or cannot lie down can be accommodated
For more information go online at: www.trulyopenmri.com or call: 020 7370 6003 0161 434 8039
Many doctors with busy private practices, especially those who also have an NHS practice, sometimes allow the management of their finances and their practice to take a back seat and, inevitably, mistakes occur as a result.
Susan Hutter gives her advice on how to avoid some of the most common business howlers that trip practices up
HOWLER 1
Getting in an accounting year’s mix-up
Whether consultants or GPs trade as a limited company, a partnership or sole trader, practice accounts have to be prepared on what is known as ‘the accruals’ basis as opposed to a ‘cash’ basis.
What this means is that the practice accounts have to show all revenue for work done by the practice in the financial year whether or not received.
Often one could be owed at least four weeks’ fees at any one point in time and as long as the debt is collectable, it does need to be included. If not, income should reflect the revenue earned and if a bad debt occurs, it should be shown separately under practice expenses.
Similarly, as far as expenses are concerned, if they have been incurred by the practice year-end, whether or not they are paid after the year-end, they still have to be included in the practice accounts. Confusion about this causes issues when the practice accountant attempts to prepare the yearend accounts.
Often the doctor/practice manager does not send the information to the accountants until quite a long time after the year-end. If they have not recorded the correct cut-off information regarding revenue and expenses, it is extremely difficult to unpick the situation at the time the accounts are prepared.
It is recommended that GPs, consultants and their practice managers make a note of receivables and payables a few days after the practice year-end so that this information can be supplied to the practice accountants.
HOWLER 2
Carrying on seeing patients who owe the practice money
This is not only a pitfall fallen into by the medical profession; many other small businesses behave in the same way.
They become so concerned about their patients/clients that they carry on servicing them despite the fact that the bill for the previous appointment/treatment remains unpaid.
There may be good reasons for late payment – and we all know
that many working in the profession do not wish to let their patients down for obvious reasons.
However, although it may be unsavoury for consultants and GPs to ask their self-paying patients directly to pay old debts, their PAs could do this on their behalf and therefore a procedure should be put in place to cover this issue.
HOWLER 3
Falling behind with bookkeeping and record-keeping
Many medical practitioners only attempt to write up their books and records – or get someone else to do it – once a year for the purpose of preparing year-end accounts and tax returns.
This results in a scramble to get everything done on time. It also results in inaccurate records being provided. It is advisable to write up the books and records on a regular basis: monthly or quarterly.
Apart from everything else, this would highlight financial issues as they arise as opposed to waiting for a year or more when it is often too late to do something about them.
HOWLER 4
Using untrained book-keepers
Many of those in the profession have efficient and able PAs. However, unless the PAs are trained book-keepers, it is a mistake to think that they can do the book-keeping for the practice without any training.
Most accountants will provide some training and/or direct assistance with book-keeping.
If your PA has time and the ability, it is worth availing yourself of training for them so that they understand what they are doing when dealing with the book-keeping of the practice. If not, then consider getting a part-time bookkeeper to cover this work.
HOWLER 5
Not putting employees on the payroll
Many consultants and GPs think they can treat their PA and other employees as ‘self-employed’.
This could lead to problems for your business, as HM Revenue and Customs (HMRC), in most cases, will regard that person as an employee who should be dealt
Although it may be unsavoury for doctors to ask their selfpaying patients directly to pay old debts, their PAs could do this on their behalf
with under Pay As You Earn (PAYE) within a formal payroll structure.
If you do not do this, and pay your staff gross, assuming that they will prepare their own tax returns under self-assessment, you are making a grave error. If there is an inspection by HMRC – and they do make inspections from time to time – they will pick this up immediately.
The consequences are that if the person whom the consultant/GP has regarded as self-employed is actually an employee, their pay going back six years will be grossed up for tax and employer’s National Insurance, which can almost double the bill.
There will also be interest and penalties to pay.
Even if the person concerned has accounted for income tax themselves and if HMRC agrees to deduct this from the final bill, there will still be a large balance to pay.
As always, it is best to get expert guidance before deciding whether someone can work as ‘selfemployed’.
Susan Hutter (below) is a partner at Blick Rothenberg and part of the team that advises medical practitioners
Unless the PAs are trained book-keepers, it is a mistake to think that they can do the bookkeeping for the practice without any training
NEW SERIES: PRIVATE PRACTICE GROWTH GUIDE
The Private Practice Growth Guide is designed to give independent practitioners the knowledge and tools they need to develop their private practice.
Whether you are an experienced independent practitioner or are new to private practice, this series by Jane Braithwaite (left) will serve as a helpful guide to the exciting, and sometimes confusing, world of healthcare marketing.
Across the six-article series, we will explore the roles of marketing strategies, social media, content marketing, email marketing and using analytics to know and grow your audience. But first we start with the basics…
guide take to the
A guide to take you the top
WELCOME TO Medical Marketing 101: how to start, grow and scale your practice
Take a seat and pay attention, because this short course in healthcare marketing will provide a glossary and understanding of terms and themes we will build on across the series.
By the end of this article, you will know your ABCs from your B2Cs, gain an awareness of digital and traditional marketing practices and understand the importance of targeting the right audience for your product and services.
And if you have experience in this field already, you will find it a helpful refresher.
So, what is marketing?
Marketing can be described simply as getting your name out to the right people in order to sell your product or service.
Easy enough, right? And whether your practice uses social media, networking events, email marketing or a combination of methods, the ultimate aim remains the same: becoming the person people think of when they need what you provide.
Marketing within private healthcare is a relatively recent phenomenon in the UK and is certainly behind other major sectors in terms of investment and established practices.
However, as the sector grows in scale and competition, larger numbers of healthcare practices are employing full-time marketing managers or resourcing their practices with external marketing support.
Entering private practice
You may be used to seeing dozens of patients in a single NHS clinic with barely a moment to think and now you’re twiddling your thumbs in an expensive private facility while your outgoings pile up.
Don’t panic. It takes time to build up a reputation, and understanding this early on will help you make and meet realistic targets and budgets.
Marketing is a long-term effort and you will need to be consistent in your level of engagement and commitment. Sporadic periods of activity won’t help you to expand your network and audience, so you will need to set aside dedicated time for marketing, whether you manage it yourself or resource outside help for your practice.
For the more experienced independent practitioner, take note of Coca-Cola, which, despite being the leading name in the soft drinks industry for decades, still invests millions of pounds a year in marketing.
Complacency can kill a brand and it’s important to continue to invest your time and resources into effective marketing, whether your clinic is empty or booking months in advance.
Understanding your product
This is not the time for modesty, but you do need to be very honest with yourself. You are the product and the service you offer needs to stand out from the crowd if you want to market yourself effectively.
A great marketing campaign may attract new patients in the short term, but in order to retain patients
➱ p22
and grow your practice, the patient experience needs to be exceptional from initial inquiry to discharge.
Sometimes you will need to step into the shoes of your consumer. Try calling or emailing your office on occasion to see that communications are being answered promptly.
Try to find a specific piece of information on your website. Was it easy? Did you find it? If not, your patients won’t have found it either.
Above all, be clear about your expectations with your support team and be open to suggestions. If it benefits the patient experience, it will grow your practice over time.
There are many options available to independent practitioners to resource your practice and improve internal efficiency and this should be a priority before you seek to expand your practice.
Have a unique selling point (USP)
Your USP is what sets you apart from the competition. It may be an uncommon treatment or surgical technique you are trained in, an area of research you were involved with or being available out of hours, but you need to offer something more than the person listed above you on Google. Be thoughtful and creative when establishing your USP, but ensure you can deliver whatever it is you promise. Your USP may change over time – you can’t be the winter sports injury guru all year round – or it may not prove to be as unique as you thought. Keep thinking and establish your niche.
How do I get my name out there?
There are a number of established methods to build a private practice, but you need to have established your product and audience first.
Broadly speaking, your target audience will be split between prospective patients (the consumer) and your referrers (the business) and how you engage with each group needs to be tailored to them. Your product is you, and you will need to be honest with yourself in identifying your own strengths and weaknesses in order to market yourself effectively.
Each patient that enters your practice is a potential brand ambassador with their own network of family, friends and colleagues, as well as an extended network of social media followers
and allied health practitioners, such as physiotherapists and osteopaths.
Engaging with your referrers will take many shapes and forms, such as providing education for continuing professional development or specialist training, offering joint consultations and attending multidisciplinary team meetings or simply getting together for a coffee – or something stronger.
We will take a deeper look at some B2B strategies that will grow your network and increase your brand and reputation next month.
I don’t use social media, why should my practice?
B2C marketing
B2C (Business to Consumer) marketing within healthcare is how you get your name across to prospective patients and will largely be shaped by your field of expertise.
For example, an orthopaedic surgeon may provide tips for athletes to avoid the common sports injuries they see in their practice.
A dermatologist might instead share pictures for spotting the signs of a cancerous mole. In both examples, the B2C strategy is the same and is the most commonly used B2C strategy within the sector: promoting wellness over illness.
It may seem counterproductive for a healthcare professional to attract consumers by telling the patient how to avoid the problem, but doing so helps foster a sense of trust and responsibility so that patients will be more inclined to seek their services when required.
This is just one of many tried and tested B2C strategies that will be explored in more detail in the next article of our series.
B2B marketing
B2B (Business to Business) marketing is how you engage with your referrers and other associated enterprises.
If you provide a supra-specialist service, then your referrers may be limited. However, for the majority of readers, your referrers will include GPs, embassies, insurance providers, healthcare concierges
ent and responsible healthcare sector.
If you claim that a high percentage of your patients would recommend you, be prepared to show that data.
Each patient that enters your practice is a potential brand ambassador with their own network of family, friends and colleagues, as well as an extended network of social media followers.
Social media provides your practice with a platform to reach millions of people, audience figures previously reserved for prohibitively expensive TV and billboard advertising, at a fraction of the cost.
An active audience awaits, but the true challenge then is determining what to say and show about your practice in a way that will engage the audience and help them to remember your name when they need your service.
A great marketer will curate content for your practice that can be shared across digital platforms in a consistent fashion, but if you are doing this yourself, then establish a routine for your online posts.
Over time, your audience will know when to look out for new content and will keep coming back for more. Remember, it is much better to regularly post once a week than to post five things in a day and have nothing to say tomorrow.
If you are not an active social media user, why not create a personal profile so you can learn the ropes before going live with your practice? You might feel initially self-conscious, but once you learn to have fun with your posts, great content will naturally follow.
Outcomes and feedback
In whatever way you choose to market your practice, you will need outcome data and patient feedback to demonstrate that your product really works.
As King Charles II famously said: ‘97% of statistics are made up on the spot’, but this simply won’t fly within the increasingly transpar-
A patient may thank your PA for an excellent level of service without ever thinking to leave a review or comment for your digital platforms, so your support staff need to understand the necessity of inviting, obtaining and publishing written feedback.
Peer reviews and recommendations are becoming more common within private practice, but if you don’t share praise for your hardworking colleagues, don’t expect to receive anything back. You should have no reluctance in publicly endorsing the colleagues you work with regularly in your private practice – they are an extension of the service you provide.
You should now have an understanding of the essentials of medical marketing and will have a lot of ideas about how to effectively market your product. Note your ideas and see how you can develop them over the course of the next month.
Ensure you have a crystal-clear understanding of what your product is and who the target audience will be before you invest in any marketing activity and remember that consistency is key. Why not set aside an hour or two this week to focus on the basics and build on this as each week progresses.
Great marketing comes from the initial strategy as much as the final execution and you should take as much time as it needs to plan your marketing efforts, whether that be for the month, the quarter or the year.
Next month, we’ll explore some tried and tested medical marketing strategies as well as some exciting trends we anticipate in 2019
Jane Braithwaite is the managing director of Designated Medical, which offers business services for private consultants, including medical secretary support, book-keeping and digital marketing
SUBSCRIBE TODAY TO GET OUR TEN ISSUES A YEAR – AND READ US ONLINE
Dear Reader,
Subscribing to Independent Practitioner Today is the only way you can be sure you will see every issue and have the option of reading us online using our special page-turnable edition. Don’t risk missing out. Our personal subscription for doctors and managers is only £90 a year and £210 for organisations. But you can cut this to just £75 and £180 respectively if you pay by direct debit.
So take advantage of this offer now for our unique business journal dedicated to supporting you in your private practice. We’re confident your subscription will repay itself many times over!
Editorial director
APPLICATION FOR SUBSCRIPTION
Instructions to your Bank or Building Society to pay Direct Debits
Name and full address of your bank/Building Society
To: The Manager Bank/Building Society Address Postcode Ref. No.
Banks and Building Societies may not accept Direct Debit instructions for some types of account
a copy of your letter to us.
THE SALARIED PRIVATE DOCTOR
The salaried consultant model in private practice is now with us – and more are set to go this route in future.
Here, four orthopaedic surgeons employed by the new Schoen Clinic London – Mr Rohit Shetty, Mr Giuseppe Sforza, Mr Adrian Carlos and Mr Alexander Montgomery – talk frankly to Independent Practitioner Today about the attraction of employed status
Employed can spell freedom
QHow long were you, or have you been, a consultant in the NHS?
Mr Shetty
I joined the NHS as a consultant orthopaedic and spinal surgeon in January 2010. My initial appointment was split between Whittington Hea lth, London, and The National Hospital for Neuro logy and Neurosurgery, Queen Square, part of University College London Hospitals. I did this for six years before moving to work full time at the Whittington Health.
Mr Sforza Eight years.
Mr Carlos I have been an NHS consultant for eight years.
Mr Montgomery I have been a consultant in the NHS for about seven years.
Q
What is your NHS status now – are you resigned or do you still run some NHS sessions? If so, how many? If you are resigned from the NHS, when did you do so?
Mr Shetty
I am a consultant orthopaedic and spinal surgeon at the Whittington Hospital in North Central London.
Mr Sforza
I moved to full private practice at the beginning of 2015. Until August 2016, I held an honorary contract with an NHS hospital but have
since stopped any clinical activity in NHS hospitals. I do treat a limited number of patients outside of London, through the NHS, under the Choose and Book auspices.
Mr Carlos I am still an NHS consultant.
Mr Montgomery I am clinical lead of spinal surgery for the Royal London Hospital (Barts Health). We are the busiest spinal trauma unit in Europe and serve a population of 3m people for elective surgery.
QWhat is your previous private experience?
Mr Shetty
My previous private practice was at Queen Square private consulting rooms, Wellington Hospital, Highgate Private Hospital and BMI Garden Hospital, Hendon, London.
Mr Sforza
I have worked in several private hospitals in Italy and the UK. In the UK, I have worked with hospitals of the following groups: HCA, Ramsay Healthcare, Spire, BMI, Aspen, Circle.
Mr Carlos
I have worked as an independent practitioner in Manchester and joined a private group in London prior to joining Schoen Clinic.
Mr Montgomery
Prior to Schoen clinic, I was mainly based in the City, but did have a clinic once a week in the West End as well.
Mr Rohit Shetty
Mr Giuseppe Sforza
Mr Adrian Carlos
Mr Alexander Montgomery
QAre you working elsewhere in private practice?
Mr Shetty
I am exclusive to Schoen Clinic London since the opening in August 2018.
Mr Sforza
Yes, when I’m not in London, I still work in Reading in three different hospitals: Berkshire Independent Hospital, Spire Dunedin Hospital, Circle Reading Hospital.
Mr Carlos
Not since joining Schoen Clinic London.
Mr Montgomery
All my private practice is based at Schoen Clinic London.
QSo what is the attraction of working at Schoen as an employee?
Mr Shetty
I enjoy working for the NHS, as I feel I am constantly being challenged and it helps me develop and grow more professionally and personally.
Previously, I missed that in the independent private sector. However, Schoen Clinic London has given me the opportunity to do this as part of the multidisciplinary approach.
vulnerable as an individual. Also, they look after the administrative side of things giving me more time to focus on patient care.
Mr Sforza
There is a strong and close relationship with colleagues, managers and Schoen employees. Working in a team with several orthopaedic colleagues allows me to discuss cases in depth with other upper-limb surgeons and pick new, interesting ideas and approaches from other orthopaedic colleagues who specialise in other joints.
Crossover between colleagues is the norm and it is much safer for patients.
The management has been brilliant in helping me keep my activity as a teacher and speaker in orthopaedic meetings.
I am very grateful for the opportunity they are giving me to continue to work in this field without stopping my participation in specialty meetings and courses.
Marketing is often expensive and time-consuming for a private consultant. However, at Schoen Clinic London, there is an exceptional hard-working team that reaches out to patients and finds new market opportunities that would be inaccessible for single players.
ing issues like bad debt and shortfalls and facilitating systems like online booking that is the future in private medical practice.
Mr Carlos
You can concentrate on the clinical aspect of work: helping, caring for and treating patients. This is the area of work I enjoy; I trained hard for many years and I know how to do well.
The non-clinical aspects of private practice are expertly managed for you. As an employee, you are professionally indemnified, receive a pension should you want it and you have the financial stability a regular salary provides.
Mr Montgomery
There are many attractions; some are clinical and some practical. On a clinical level, there is definitely a difference working in a team of people who are employed under the same roof.
You are a genuine team like it is in the NHS. We have processes and governance structures in place like you would in the NHS.
as a whole makes more sense for the future with premiums going up and surgeons under ever more scrutiny.
On a personal level, I would rather be employed and have the tax come out of my account every month than work out the increasingly complicated tax returns at the end of the year.
QHow does working at Schoen differ from your previous private practice experience?
Mr Shetty
Personally, I feel very much part of a family which is providing high-quality patient care. Every aspect is focused around the patient.
The practice is very transparent as we measure patient outcomes, something I believe is a new concept in private care in the UK.
Mr Sforza
There is a very close relationship between colleagues, and everybody is willing to solve possible problems and improve the system. The fact that the hospital focuses only on orthopaedics means we all work in the same direction and it is very easy to share common experiences.
The management and secretarial team understand and support our practice extremely well and it is very easy to create cross-referrals or work together on the same patients where another expert pair of hands is needed.
Mr Carlos
I previously worked at several clinics in different areas of the City and operated at two different hospitals. At Schoen, I can consolidate the work into a single-site practice.
Schoen Clinic London has outstanding facilities including outpatient services, a complete radiology unit – providing X-rays, CT scans, MRI, ultrasound and interventional capabilities – inpatient care in impressive ensuite, catered rooms and state-of-the-art operating theatres, all under one roof.
Lastly, the hospital deals with all the financial aspects within private healthcare insurance, resolv-
The multidisciplinary teams are rigorous and you can use the varying skills of your colleagues to help manage the patients when needed. The Schoen Clinic Group’s record on data and outcome collection were a big draw to come here.
On a practical level, having your indemnity covered by the hospital
This creates a better experience for patients and can shorten the treatment period, providing an
I feel more supported and less ➱ p28
opportunity to employ a ‘onestop’ clinic for some conditions.
The managerial, administrative and marketing aspects of a practice are not something I have been specifically trained to do. However, these are dealt with by experts in order for you to concentrate on the clinical side of work.
Mr Montgomery
We are very much a team under one roof and that is the biggest difference.
The hospital itself is surprisingly large with seven storeys, but it’s very much a family atmosphere in the building, which makes it a nice environment to work in.
QIs it more fulfilling, professionaly? What do you enjoy about it?
Mr Shetty
I enjoy the weekly multidisciplinary team spinal meetings. My colleagues, on occasions, challenge the decision-making process of each other and it allows us to give the patient a collective opinion even though they are under the care of an individual consultant.
There is good evidence that this improves patient confidence and outcomes.
Mr Sforza
Professionally, you find yourself surrounded by some of the most capable and skilful surgeons in the UK. Being part of that makes me proud and pushes me to keep up with new techniques and learn new skills.
Mr Carlos
It is fulfilling, I feel my time is used more efficiently, I know every aspect of patient care is under expert hands. I worry less about the non-clinical side of the work and, because of this, it leads to a better work-life balance.
I feel the hospital is clinicianled, the specialists are well supported and there is a strong feeling and common aim of everyone doing the best for the patients.
Mr Montgomery
Yes, it is more fulfilling – for the reasons given above. Working as a team makes it more fulfilling and also knowing that our outcomes are being collected allowing us to keep improving our practice.
QMuch has been said of the good teamwork element at Schoen. How would you say working in a multidisciplinary team impacts the way you work?
Mr Shetty
The multidisciplinary team process, joint consultant operating cases and second opinions do have a significant impact on patient experience and outcomes.
We are an exclusive orthopaedic hospital and interdisciplinary referrals mean that most of the conditions can be managed inhouse. This means that the patient does not have to travel to different hospitals and the care is provided under one roof. From the insurance point of view, it certainly drives down cost while providing top quality care.
Mr Sforza
The multidisciplinary team meetings are a great opportunity to discuss and learn about interesting cases with different surgeons, radiologists, sports medicine experts and musculoskeletal physios. The impact we would like to obtain with this kind of clinical teamwork is an accurate, prompt and comprehensive diagnosis as well as a plan to follow up with other clinicians, speeding up treatment and recovery for our patients.
Working side by side with intensivists in the ward and in the postoperative care unit makes you feel more comfortable about your patient’s safety and gives peace of mind that they are in very capable hands outside theatre.
Being able to reduce the amount of stress and time for the patient to go back to their own life is the target that we should have always in mind. In my experience, working in a multidisciplinary team is the most rapid and effective way to find a successful solution.
Mr Carlos
This is an important reason of why I joined Schoen Clinic London. The hospital specialises in spinal and orthopaedic care and is focused on care for these patients. Everyone in the hospital is dedicated to care for this group of patients and conditions.
This is unique for a hospital. Schoen Clinic London has a strong ethos of working as a team, not only within a subspecialty group but in multiple disciplines. We regularly discuss cases in MDT meetings, and everyone continues to learn and improve. This will benefit all patients.
As an employee, it negates the idea of ‘sole ownership’ and I have shared patients with complex problems with other colleagues in order to get the best for the patient.
This includes being seen in clinic by several specialists at the same time or operating as a specialist team on the same patient.
Mr Montgomery
Decisions in spinal surgery are seldom straight-forward and often have a number of options. Working in an environment where you can come to a consensus and seek the professional opinion from colleagues can only be good for patient care.
QAre you confident publicity of the Private Healthcare Information Network (PHIN) will back up the claimed ‘high quality’ outcomes for Schoen in UK?
Mr Shetty
The numbers and the outcome will speak for itself.
Mr Sforza
I hope so, especially when the collection of patient-reported outcome measures (PROMS) and other questionnaires will be enclosed in the full evaluation.
Mr Carlos
Yes. The ‘high-quality’ outcome measures are an important aspect of Schoen Clinic London’s practice. They aim to prove that patients are receiving the best care in the hospital. It may take a year to accumulate enough data to robustly prove this.
Mr Montgomery
Yes, I think once the hospital is fully settled into its processes and has optimised its pathways, I have no doubt it will show very good data, outcome collection and quality with it.
QIt has been said that the country has lost the ability to innovate. Can you/will you be able to innovate more now? How is the wheel being re-invented at Schoen?
Mr Shetty
My NHS hospital has been recently selected as one of the UK centres by AO Spine Europe for a hospitalbased spinal simulated course. I have already spoken to AO Spine Europe about conducting a similar course at Schoen Clinic London.
They are excited about the idea of bringing in state-of-the-art training and innovation to a private sector hospital in the UK, as this has never been done before.
It’s both challenging and exciting times. We are also in the process of getting a robotic arm for pedicle screw placement.
Mr Sforza
Innovation comes from a culture of support and co-operation between different disciplines in a specific field.
Research, support in collecting data, continuous attention to detail, together with pursuit of efficiency and adoption of best techniques, might raise the bar and allow us to obtain better results and lead to innovation in our working environment.
Mr Carlos
It is easier to innovate at Schoen Clinic London; the teamwork approach makes it easier to identify areas needing improvement and innovation and to then find a solution. There is a strong positive attitude towards improvement and change from management and the employed staff.
➱ p30
Mr Montgomery
A lot of time is spent by private surgeons in the UK merely running their private practice with all the different aspects and hurdles that come with running your own business.
I already feel, after four months, that I have a lot more time for clinical care and improving my clinical practice.
The Schoen family are committed to an environment where we can achieve the best standards and so naturally, innovation will be easier to achieve.
QDid you ever feel isolated in private practice? If so, has that changed now?
Mr Shetty
Totally isolated at times. Governance for complex cases was an issue, but now I feel confident and comfortable with the teamwork process at Schoen Clinic. I know that help and advice is available to me and my patients 24/7 if required.
Mr Sforza
Yes, this was a common problem, and the reason why I have created several groups in different hospitals where I have worked. Now I do not experience this feeling anymore thanks to the group of colleagues I work with.
Mr Carlos
It can be isolating in private practice, particularly if you set up solely on your own. Personally, I feel less isolated in a group and even more supported as an employed consultant.
Mr Montgomery
I was part of a group before but with only one other spine surgeon, so the change is quite palpable with ten other colleagues now.
Q Is there anything you miss about the NHS?
Mr Carlos
I am still in the NHS. However, in general, an independent private practitioner will see patients by themselves and sometimes even solely run the practice. This can feel ‘lonely’ and differs
from the NHS, which is multidisciplinary, and you work as a team. However, fortunately, the teamwork approach has been maintained at Schoen Clinic London.
QIf the future is bright and the future is ‘orange’ (Schoen’s logo), how does that look in five years’ time at Schoen?
Mr Shetty
I would say in five years’ time the Schoen model would have declared itself as the most effective way to deliver modern and highquality care to patients through a multidisciplinary team approach.
Mr Sforza
I see a hospital that in the future will continue to go from strength to strength, with an increasing approval from the public and health insurers that will change the equilibrium of private healthcare in central London and possibly even throughout the country.
Mr Carlos
The hospital should be established and showing excellent outcome measures, which should reassure patients they will receive best care.
I assume that the group will expand and build new centres throughout London and the UK. They will continue to attract and employ the best specialists.
Mr Montgomery
I would expect to have outcome collection and data showing our quality is unmatched elsewhere in the private world – both as individuals and as a hospital.
QWhat has been the reaction of your old colleagues to you taking employment privately?
Mr Shetty
Some of my colleagues felt that working in a salaried model would mean losing your identity as an individual consultant.
I was apprehensive too, but the last few months has proved us wrong. Schoen allows us to practise individually and supports us to grow and develop our practice in a safe and caring environment.
Mr Sforza
Most of them were worried for me and didn’t like the idea of having exclusivity in an open market like London, where freedom of movement seems the best way to reach full capacity of work in private practice.
Instead, some have immediately picked up on the idea and like the new opportunities that are now opening in London. I suspect that there will be an increase of this new hospital model in the future.
Mr Carlos
A mixture of reactions, particularly as it’s a new model that has not been used yet in private care.
There had been anxiety that it will remove clinician autonomy, but this has not been the case at all. I would say quite the opposite and the clinicians have been supported to do what they do best.
Mr Montgomery
A lot of people are sceptical about change. A lot of people felt the model would not work and some that the hospital could not afford
it. So far, that talk seems very farfetched. The Schoen family has opened a new hospital every year for the last 20 years, so are very experienced in opening new hospitals.
QDo you know many other consultants who have or would like to take the employment route?
Mr Shetty
I have several of my colleagues who would love to join our organisation.
Mr Sforza
A few and mostly for good reasons; for example, they want to leave the NHS, they want to move parttime or work in a team.
Mr Carlos
There have been increasing numbers of consultants who have approached me and are interested in the employed model of work.
Mr Montgomery
Yes, there seem to be a lot that are interested.
QAre there any other benefits about being employed privately by Schoen?
Mr Shetty
It’s possibly in one of the best locations in Central London and Marylebone.
Mr Sforza
Professional indemnity is a costly and worrisome topic between private consultants. New regulations and heavy fines in the cyber sector can also make life difficult, so having an employer that takes care of these aspects and that has a stronger power to negotiate our policies reduces stress and paperwork for all of us.
Mr Carlos
Another positive aspect of being an employee is devolvement of good clinical care from potential personal financial incentives. I am content to know that my patients cannot perceive any financial incentives on my part when I make recommendations in their management in regard to any intervention I may offer them.
CONSULTANTS’
Better get clear on
Independent Practitioner Today talked with Anne Coyne (right), consultant relationship manager for the Private Healthcare Information Network, about how her team has been helping 14,000 private healthcare consultants submit fee data in the lead-up to this month’s start of fees going live on its website
Always on the go?
SINCE EARLY January, the Private Healthcare Information Network (PHIN) has been asking consultants to provide it with information about the fees they charge to their private self-pay patients.
Consultants must provide this information as a requirement of Article 22 of the Competition and Markets Auth ority (CMA) order, which followed a long-running inquiry into private healthcare.
According to Ms Coyne, the team has been encouraged by the number of consultants coming forward so far and this shows doctors’ commitment to make healthcare costs more transparent and easier to understand.
She said over 3,000 consultants had submitted some fee information and the aim was to publish this on the PHIN portal by the end of this month.
The fee information required at this point are for:
The fees charged to self-pay patients for initial consultations;
Follow-up consultations;
Those procedures consultants perform routinely.
PHIN is asking consultants to provide their fees for procedures that they perform, as indicated by the hospitals. Consultants can also provide information about clinics and consulting rooms where they see patients.
Said Ms Coyne: ‘Submitting the data in this way ensures that each consultant validates their own fee data. While on the PHIN portal, consultants have the opportunity to review their practice reports, notify hospitals of any data changes that need to be made, review and approve their performance measures and create a profile about their practice.
‘We are pleased that several consultants have told us that the process to submit fees is very straightforward and it’s easy to complete.’
Package pricing
For those who have raised concerns, she and her colleague Ellie say they have endeavoured to reassure and give support.
‘Some consultants have raised concerns regarding package pricing and the process for submitting this information,’ reports Ms Coyne. ‘Many consultants have package price arrangements in place with hospitals that incorporate their fees as well as hospital costs and we also require these prices. Where these arrangements are in place, we have asked hospitals to provide this information.’
While there is currently no legal requirement on hospitals to provide this information to PHIN, it has been asked of them in order to
‘support a commitment to transparency of costs for patients’.
Ms Coyne says she encourages consultants to work with their hospitals to make that information available to PHIN. It is important to note that PHIN asks consultants to provide an indicative fee for their services even if a package price is in place.
‘Our ambition is to have package prices available when fee information appears on our website in April, but that has a number of dependencies, such as hospitals providing their packaged prices.’
If consultants want to know more about the fee submission process, there are several ways PHIN says it can help.
There is an online guide for consultants that provides step-by-step information to logging onto the PHIN consultant portal and submitting fees.
✆ There is a phone service available to consultants Monday to Friday to contact the PHIN consultant team on 0203 143 3177 where they can either seek advice over the phone or leave a message for one of the team members to come back to them.
There is also the option to contact PHIN by email at consultants@phin.org.uk.
Ms Coyne says: ‘Ellie and I try to respond to queries and messages as
Providing first class medical consulting and therapy rooms at prime locations in Central London and Liverpool
London www.tenharleystreet.co.uk 020 7467 8300
quickly as possible, but sometimes we need to do some further work to ensure we can give a full and complete answer. We hope that consultants will understand that we cannot provide an immediate reply.’
The fees publication requirement from the CMA applies to all consultants working in private healthcare, so PHIN says it will be working to ensure that all of them can submit their fee information on its consultant portal.
This includes the submission of fee information for those consultants who may only see patients in outpatient units as well as consulting rooms.
In the coming months, PHIN will be working with hospitals to promote the collection of feedback from patients so that they can provide consultants with patient satisfaction information.
PHIN is progressing its work on publishing patient-reported outcome measures (PROMs) data, but Ms Coyle said it will talk with consultants and representative bodies on their approach to this before it happens.
Consultants are being asked to provide their fee information using the secure PHIN Consultant Portal. The online guide for consultants, and the secure portal, can be accessed at https://portal.phin. org.uk/Consultants.
Liverpool www.eightyeightrodneystreet.co.uk 0151 709 7066
Advertisers in Independent Practitioner
Today are attracted by our ability to reach 14,000 doctors with a private practice and their managers/administrators every month in print and online. Let your advert be seen 24 hours a day, every day of the year when you advertise with us.
Margaret Floate at margifloate@btinternet.com or phone her on 01483 824094
TACKLING THE DISEASE OF ERROR IN HEALTHCARE
How crises cause brain
Our trio of writers – two doctors and an airline pilot – are co-founders of a business on a mission to improve patient outcomes by helping healthcare professionals understand why errors occur.
Analysis of a number of high-profile medical errors has demonstrated poor crisis management. In their fourth and last article in the series, John Reynard, Tim Kane and Peter Stevenson discuss the Elaine Bromiley case as a classic example of poor crisis management, and analyse it according to High Reliability Organisation (HRO) principles, focusing especially on our psychological response to a crisis
Time passes very quickly when one is concentrating intently, as any surgeon can tell you during a long operation. When one looks at the clock, an hour can have passed in a what seems like a fleeting moment
brain block
AN ANALYSIS of a large number of aviation disasters revealed that crises were not infrequently managed badly, even by highly experienced air crew.
The aviation industry realised that a systematic approach to crisis management had to be developed which involved training before the event and developing systems of managing a crisis in a better way once one had unfolded.
Aviation has led the way in practising common crises in a simulator – an environment where pilots can test their response to a crisis and then, critically, can practise in safety to get better at handling it.
The ergonomics – people’s efficiency in their working environment – of crisis management have been addressed by a number of industries.
Everyone will have experienced the unpleasant sensation caused by the surge of adrenaline rush, which, in turn, causes a rise in pulse and blood pressure. Less well known and understood is the cognitive response to a crisis, a response which can impair effective management of what is happening.
Forgetting important steps
The cognitive response to a crisis is described by some HROs, particularly in the US, as ‘tachypsychia’. The components of tachypsychia include:
Omitting vital actions and forgetting important steps;
Auditory exclusion – failing to hear verbal input from colleagues and equipment alarms;
Loss of time awareness;
Memory lapses;
Loss of situation awareness and fixation – too much focus on the wrong thing;
Communication failures;
Problems using the emergency equipment because of impaired motor skills and hand-eye co-ordination;
‘Visual exclusion’: tunnel vision. Our psychology evolved to deal with predators – essentially lions and bears. It did not evolve to deal with an airway crisis because such problems only became relevant after the administration of the first anaesthetic in 1846 at the Massachusetts General Hospital. Before then, there had been no need to understand or develop a better psychological response.
When faced with a predator, as a general rule, the best response is to turn, run or climb the nearest available tall tree: the so-called flight response. The fight response was an alternative but usually riskier strategy.
The response is automatic. No mental reasoning is required. An awareness of time and of what is going on in the peripheral visual field are not important and focusing on what other people might be saying is generally of little importance. Tachypsychia in such a situation is helpful and its evolution allowed us to succeed in evading predators.
Programmed to respond
Our psychological response to a crisis in an operating theatre derives from the same physiological system underlying the flight or fight response just described. In evolutionary terms, we are programmed to respond in the same way.
The problem with that same response in the example of the airway crisis is that these various components combine to impair our cognition during such crisis and hamper our ability to acquire information and analyse that information. Our ability to reason in an airway crisis is critical to its effectiveness management.
If we think this all sounds a bit theoretical and irrelevant to crisis analysis and management, then think again. Let us consider the case of Elaine Bromiley, a fit woman in her 30s undergoing an elective and minor ENT procedure from which she should have made a complete recovery [Bromiley 2015].
The experience of the team on the day could not have been better. The lead anaesthetist had over ten years’ experience at consultant level and was described by anaesthetic colleagues as diligent.
A second anaesthetist who attended the crisis had difficult airways skills. The consultant ENT surgeon had 30 years’ experience at consultant level. No team of doctors was better placed to insert a surgical airway.
Why then, faced with the crisis of ‘can’t intubate, can’t ventilate’, the correct management of which is a surgical airway, did they con➱ p36
tinue with attempts to intubate Elaine? Any of them could have easily done a cricothyroidotomy or tracheostomy.
Even more remarkable, at least on first ‘analysis’, is that the nurses knew exactly what needed to be done – they prepared the tracheostomy equipment – but the doctors appeared not to listen to them.
Things went from bad to worse. Elaine’s oxygen saturations remained critically low for most of the crisis and she died a few days later – having been brain dead within the first 30 minutes – after never regaining consciousness.
When analysed according to HRO principles of accident causation, this is a classic case of three doctors experiencing the negative effects of tachypsychia on cognitive function.
All three doctors experienced loss of time awareness. They all had auditory exclusion – it wasn’t that they didn’t listen to the nurses, but
rather that they didn’t hear the nurses.
They all lost awareness of the situation, thinking it was not as serious as it really was and became fixated on a single task – namely continued attempts at intubation. They had all developed ‘mind-lock’.
Loss of time awareness
All three doctors experienced loss of time awareness thinking they had only been trying to intubate Elaine for a few minutes, rather than 20 minutes.
The high level of mental concentration required to analyse and manage a complex problem slows down our mental metronome. Time passes very quickly when one is concentrating intently, as any surgeon can tell you during a long operation. When one looks at the clock, an hour can have passed in a what seems like a fleeting moment.
Mind-lock has been seen in many mismanaged crises in avia-
tion and the nuclear power industry. It was a major component of the Three Mile Island nuclear disaster in 1979.
Roger Green, a leading aviation human factors expert in the 1980s, said that his analysis of aircraft accidents revealed many cases where pilots carried on with a flawed course of action while the aircraft’s warning systems were ‘screaming at them that they had got it wrong’ [BBC TV Horizon documentary 1986].
The experience of mind-lock was eloquently described by another anaesthetist’s experience of an airway crisis – unrecognised oesophageal intubation – in the following way: ‘By that stage I had got myself into a mind-set I could not break’.
Once we understand the basic concept of tachypsychia and appreciate its impact on our cognition, a more sophisticated 21st century approach to crisis management can be developed.
Having served healthcare professionals since its inception in 1993, Tax-Link, chartered tax advisers and accountants in Wimbledon, has built a wealth of knowledge and experience in dealing with taxation issues faced by doctors in private practice. Our focus is on tax planning and compliance.
l Tax structuring to suit personal circumstances (LLP, limited companies)
l Solvent liquidations
l Consultant groups and consortia
l Assessment of pension contributions in light of tapering annual allowances
l Ad hoc assistance with HMRC investigations and reviews.
The high level of mental concentration required to analyse and manage a complex problem slows down our mental metronome
Crucial to effective crisis management is the allocation of an individual to record time. This individual can be the team leader who calls out time every minute while directing the other team members.
Critically, that leader remains hands-off so he or she maintains an overview of the situation and does not become focused on technical tasks – intubation, a tracheostomy. The approach to trauma management, much of which can aptly be
described as crisis management, adopted by the British and US armies at Camp Bastion is a good example of the hands-off approach to team leadership.
Speaking-up protocols
To allow individuals to speak up in a crisis when they have noticed something that concerns them, or simply to allow juniors to input their observations into crisis management, HROs have developed ‘stepped’ speaking-up protocols.
The Probe, Alert, Challenge, and Emergency system (PACE) is used globally by aircrew to express concern. ‘I need some clarity here’ is the opening phrase for the probe step.
‘I am uncomfortable about this’ is a phrase for the alert step. ‘You must listen’ is the opening phrase for the challenge. In 30 years of commercial airline flying by one of us, he has never had to advance beyond ‘I am uncomfortable about
this’ – those words have great meaning.
Healthcare has a long way to go to improve crisis management and to allow juniors to speak up when concerned. But as with all of the concepts discussed in these four articles, much can be learnt by adopting techniques which are used by HROs.
John Reynard, Tim Kane, and Peter Stevenson are co-founders of Practical Patient Safety Solutions.
Peter Stevenson has been an airline pilot and human factors instructor for over 30 years. He flies Airbus A330 airliners on inter continental routes for a major UK airline.
Tim Kane is a consultant trauma and orthopaedic surgeon at Spire Portsmouth Hospital and the city’s Queen Alexandra Hospital.
John Reynard is a consultant urological surgeon and honorary senior lecturer in the Nuffield Department of Surgical Sciences at the University of Oxford. He is an honorary consultant urologist to The National Spinal Injuries Centre at Stoke Mandeville Hospital. He holds a masters degree in Medical Law and Ethics.
References
Bromiley M. The husband’s story: from tragedy to learning and action. BMJ Quality and Safety, 13 May 2015. BBC TV Horizon programme: TheWrong Stuff, 1986.
Further reading
W.B. Runciman, A.F. Merry. Crises in clinical care: an approach to management, Qual Saf Health Care 2005;14: 156-1635
How to make your team
Successful independent practices display five important features. Kingsley Hollis (below) reveals these five ingredients you should emulate
I MEET A LOT of specialists who are just starting in private practice and I’m always impressed to see their dedication and professional skill.
But while everyone I meet is in their element with patients and clinical work, many are very nervous about the commercial side of practice ownership.
At the same time, there are many examples of practices which have been able to combine excellent patient care with a strong business focus and they have some common traits which could benefit us all. And here’s what they are:
1
They understand the importance of cash flow
Put simply, a negative cash flow position means the practice is bringing in less money than it has spent and is likely to run short of working capital.
The problem is famously summed up by Mr Micawber in Dickens’s David Copperfield: ‘Annual income twenty pounds, annual expenditure nineteen [pounds] nineteen [shillings] and six [pence], result: happiness. Annual income twenty pounds, annual expenditure twenty pounds nought and six, result: misery.’
There are a number of ways to boost cash flow. An obvious one is to keep expenses to a minimum, but that is often easier said than done.
A more unethical tactic is to hold onto your cash as long as possible by extending credit terms and paying late, but it is also a sure-fire way to alienate suppliers.
One of the best ways to achieve a healthy cash flow is to focus on bringing more money in by invoicing promptly. To this end, sending
bills electronically is a sensible move. Electronic clearing systems such as Healthcode’s validate invoices as they are submitted to ensure they include all the information required by the individual private medical insurer and are ready for payment.
Of course, it is just as important to keep track of the payments you have received to ensure that outstanding invoices or shortfalls can be identified and chased up.
Every practice should have a system to reconcile receipts against invoices which is why we made it a feature of Healthcode’s practice management solution. See Accountant’s Clinic on page 18 for more tips on improving cash flow.
2 Teamwork
Good teamwork is obviously vital for all healthcare profession-
als in a clinical setting, but extends to your administrative staff too.
Whether you are a single-handed practitioner with support from a family member or you have a large multi-site practice, all your staff need to be able to communicate effectively with patients, each other and with you.
An informed and responsive receptionist and secretary/practice manager are key to a positive experience for patients, particularly when making an appointment or answering a query about fees.
Ensuring staff receive basic training in communications and complaints handling is a good idea, while regular appraisals and staff meetings will help everyone to feel engaged with their work and able to give their best.
You can also help by ensuring your team is not left in the lurch. A
team thrive
shared practice diary will mean your team knows your whereabouts in an emergency.
It is also worth considering an electronic appointment system which enables staff to get a realtime view of appointment slots for a specific day and book something there and then, without the need to check your availability.
3
Informed decisionmaking
It is only possible to make smart decisions if you have an accurate picture of how your practice is operating.
For example, what services/procedures have generated the most income in the previous year; what proportion of ‘did not attends’ have you experienced; how many outstanding invoices do you have?
It is possible to generate business reports the old-fashioned way by cross-checking files and drawing up spreadsheets, but by the time this is done, the information could be out of date.
Happily, the technology exists to get an instant view of how your practice is doing and create more in-depth reports on a whole range of metrics.
Healthcode provides more than 20 financial reports in its practice management system, covering important areas such as debt analysis, activity summaries and payment reconciliation. All can be exported to other software so they can be anonymised and shared, if required.
4 Meeting patient expectations
Knowing what your customer wants is a golden rule in any business. In general, we know that private patients value good-quality, compassionate care, clinical expertise and minimal waiting times.
On the other hand, how do you know whether your practice is hitting the mark? Obviously, you can keep track of complaints and
online feedback, but many more people will take their custom elsewhere rather than actually make a complaint.
In my experience, practices who actively seek patients’ feedback, through short surveys, suggestion boxes or the ‘friends and family test’ are best placed to understand and meet their needs and expectations.
5 Being adaptable
The health sector – both public and private – is often characterised as being quite set in its ways. However, the last few years have presented some significant challenges, from new rules surrounding information transparency to the EU’s General Data Protection Regulation (GDPR).
It feels like change is in the air for private practice, with the growth in self-funded patients and the move to services like online booking.
For Healthcode’s part, we want to help practitioners utilise technology so they can streamline their practice processes and ensure they are not left behind.
Just as the best doctors are able to adapt to rapid changes in a patient’s condition, the most effective business leaders are open to new information and ready to modify their approach in response to changing circumstances.
The right mindset can make the difference between success and stagnation.
Over the years, I have had the pleasure of seeing many independent practices take off and achieve their potential and I’m always proud if I have been able to help in some way.
While every practice is different, I think the underlying principles of success are universal.
Next month: Early adopter vs ‘wait and see’
Kingsley Hollis is head of business development (ePractice) at Healthcode
PROBLEMS WITH THE TAX MAN?
HMRC tax investigations and disputes create difficult and stressful times.
As an award winning firm of tax experts, our highly experienced partners specialise in resolving problems relating to tax investigations and disputes with HMRC.
To find out, in confidence, how we can help call 0800 734 3333.
‘Here to help. Not to judge.’
GETTING THE MONEY IN
With consultants’ fee levels very much in the news now that they are being published by the Private Healthcare Information Network, Garry Chapman suggests it is the perfect time to take stock of the way your practice’s medical billing and collection is working. He identifies 11 billing issues to address in private practices. Last month, he dealt with the first five and here tackles the remaining six
Fight bad debt using these forces
THE ISSUES addressed in my points to five last month revolved around setting up the practice in order to carry out the process smoothly and efficiently.
Now it is time to attack the oper ational aspects of the medical bill ing and collection process.
1 INVOICING
My last article covered the reasons why you need to bill promptly. But I am constantly surprised to see that this golden rule is not always followed and it is not uncommon to find a practice running many weeks or months behind in raising the invoices. Before sending the invoice out to
tain all the correct information, which can cause cash-flow issues.
Insurers
Raising invoices to the private medical insurance companies still needs to be done quickly so that there is the best chance of it being settled in full.
If there is a delay in sending the invoice, you run the risk of the pol icy benefit limits being exceeded by other consultants’ claims, which means that the amount becomes the liability of the patient, which creates more administration work
fall, it can be sent to the patient for payment much quicker.
2 SELF-PAY
On top of this, some insurers have time constraints on when you can send the invoice.
Over the past few years, there has been a major push by insurers to send invoices electronically. This is a major benefit to them, but there is also a huge benefit to the practice, as it means that the invoice should be assessed and paid quicker due to less human involvement.
As Independent Practitioner Today has reported, this area has grown considerably over the past few years and is now either the biggest or second biggest area of revenue and it continues to grow. So raising the invoice directly to the patient should be the priority of the practice, as this area is the biggest risk of bad debts.
Under this heading, I also include invoices raised for shortfalls caused by the terms of the
by forces
remittance to the practice when it sends the money, which is typically done electronically direct to the practice bank account.
But, in practice, the remittance does not always arrive at the practice, so unless the practice is chasing the insurer or reconciling the bank account on a regular basis, the invoices remain outstanding.
When this happens, it can then lead to further problems. The remittance which has been missed and not reconciled can have shortfalls identified on it which should have been sent to the patient. If it is not sent, you have got more bad
Trying to send invoices to patients months after the event is never a good thing, as it can lead to complaints from unhappy patients or bad debts; either way is not good.
At Medical Billing and Collection, we know about the above problems because, when we chase a backlog of outstanding invoices for a practice, we encounter these issues all the time.
The way to rectify this is to make sure that remittances are reconciled the same day that they are received and then to regularly chase the missing ones from the insurers.
This will ensure you keep on top of outstanding invoices and know at the earliest opportunity if you must invoice a shortfall to the patient.
CHASING
otherwise the patient will think that you are not being serious –and that will just lead to even more bad debt.
The process should consist of contacting the patient as well as sending letters and all of this should be recorded so that you keep a log of any action taken.
5 DEBT DECISIONS
Once all the avenues in the chasing process have been exhausted, the practice then needs to decide to either send the patient to debt collectors for them to continue chasing with the potential of eventually taking legal action to collect the debt.
What you do will typically depend upon the patient, the circumstances involved in the treatment and the associated costs.
If you decide not to send the patient to the debt collectors, then the practice should consider writing the amount off as bad debt. It is unlikely that the patient will choose to pay the outstanding amount for some random reason in the future.
Before taking this final action, the accountant should be consulted, as they would know the individual circumstance of the practice and be in the best position to offer the correct advice.
6 TAX REPORTS
HM Revenue and Customs (HMRC) takes the view that you are responsible for your own tax affairs and it does not consider ignorance or negligence as any reasonable defence.
You should be running reports on invoices raised, payments received and outstanding invoices on a monthly basis to ensure that all financial aspects of your practice are in order.
If not, then you have the information in a timely manner in order to take any action needed to keep your practice on track and avoid any cash-flow issues and to minimise bad debts.
Unfortunately, the HMRC looks upon the medical arena as being a prime area where the financial affairs are not as robust as they should be.
This leads to a higher percentage of investigations compared to other areas of business.
Most people underestimate the important area of medical billing and collection. I can assure you that it is not easy and it is getting harder and harder to do it internally.
Once all the above has been addressed, the practice then needs to be able to raise financial reports from both a business and tax perspective. This is even more important with the start this month of Making Tax Digital for VATregistered practices.
If you decide to continue to carry out this process internally, then I urge you to act to ensure it is done correctly, otherwise it is something that you may regret later. If you do not want to invest the time and effort to do this internally, then you should consider outsourcing this crucial area to a medical billing and collection company and let the professionals do this for you.
Garry Chapman is executive chairman of Medical Billing and Collection insurance policy, such as patient excesses, benefit limits or co-
There are times when a practice should also consider requesting payment in advance, particularly when seeing patients who do not reside in the UK or where there is a very large element of self-pay.
3 RECONCILIATION
This is another area which we continually see causes problems within a practice; often the practice is way behind with the reconciliation process or the remittances are not reconciled correctly against the invoices raised.
Each insurer should send a
This is the area we find to be the one that gives most practices the biggest operational problem. Few practices find it easy to deal with the patient on both a medical and financial level, as it can lead to many issues on both sides.
In our experience, every invoice potentially needs chasing, including invoices sent to the insurers.
Reasons for a delay in processing the invoice can be the:
Invoice does not reach them if it is posted;
Patient has not got the treatment pre-authorised;
Patient has given you the wrong membership number.
The practice must decide what process it is going to introduce and who is going to be responsible for carrying that out.
Once the chasing process has begun, it needs to be followed,
CHENIES MEWS
IMAGING CENTRE
SPECIALIST MRI IN THE HEART OF LONDON
• Advanced Cardiac MRI
• 3T Neuro MRI
• MRI for patients with cardiac pacemakers
T: 0203 887 0566
E: referrals@cheniesmews.com
W: www.cheniesmews.com
Record-keeping is an issue widely discussed, the subject of much advice and guidance, but doctors regularly get it wrong. Amie Roadnight has five suggestions to help
For the record
IT IS important that records are accurate, not only to ensure safe and appropriate patient care, but also as a safeguard for you if things go wrong.
After all, your records are – or should be – a first-hand, contemporaneous account of your appointment with the patient and therefore, arguably, the most reliable source of evidence as to what happened.
The following five points are some suggestions you might want to consider for your records:
1
Doctors, like lawyers, are known for their appallingly bad handwriting. But luckily, it is common now for a practitioner to keep electronic typed records using a computer.
If you make handwritten records, ensure they are legible, so that you and others are able to read what you have written – or follow up with a full typed summary/letter. If you are using computerised records, ensure that there are no typographical errors which may cause your note to hold an entirely different meaning to the note you were intending to make.
2
Record your discussions with a patient, the options you have provided them and the risks and benefits of each.
Unfortunately, in the increasingly litigious world we find ourselves in, too many times we see allegations being made against a doctor about the failure to inform the patient of all the treatment
options, or to warn of possible side-effects or complications.
A patient cannot be expected to remember everything that has been discussed at their appointment with you. With so much information to take in, it is understandable that they may forget parts of the discussion.
As well as making a contemporaneous record confirming your discussions with the patient, including treatment options and the risks and benefits for each, it is therefore a good idea to follow that up with a letter to the patient summarising your discussions.
That may seem very time-consuming, but you may find that you can use precedents or enclose standardised advice leaflets, and use the letter to tailor these to the
patient’s own individual circumstances.
This will ensure that in the case of dispute, you have a record of what you told your patient.
This will, of course, only be helpful if you have actually discussed and recorded all the relevant options, risks and benefits –including the option of doing nothing. This applies to medical treatment as well as surgical treatment.
3
You should always date and sign your notes. Ensuring your notes are contemporaneous is vitally important.
The GMC makes it clear that your notes should be made at the time of the consultation or as soon as possible thereafter.
You should not disguise any change you make to a record.
Sometimes there may be a legitimate reason to go back into the record at a later date and add something to your note. However, it is only acceptable to do this if you make it clear that the note you are adding is not contemporaneous and you date and sign the addition or amendment.
Seeking to amend your records without making it clear that you are doing so can lead to allegations of dishonesty by the GMC and as you would expect such allegations, if found proven, can result in severe adverse outcomes.
4Avoid offensive language in your notes. The patient can request their medical records at any time. The last thing they will expect to see in their medical records is a flippant remark or a rude comment about themselves. This could lead to a GMC referral
Seeking to amend your records without making it clear that you are doing so can lead to allegations of dishonesty by the GMC
and result in unwelcome publicity about your lack of professionalism, which could harm your reputation. Stick to the facts and focus on the treatment.
5Finally, ensure that everything you dictate and any investigations you request are checked by you. Remember, X-rays, test results and correspondence with a patient or their GP form part of the patient’s clinical records.
You need to satisfy yourself that a letter being sent out in your name accurately reflects what you have dictated, and that you have reviewed the results of any investigations you have requested.
Any errors occurring as a result of you not checking letters or the results of investigations could result in harm to the patient and a claim against you or a referral to the GMC.
Good records take time and you
If you ever find yourself being hauled before the GMC or on the receiving end of a clinical negligence claim, you will be relieved to have made such comprehensive notes
may feel, quite legitimately, that you simply do not have time to ensure every detail is recorded.
But if you ever find yourself being hauled before the GMC or on the receiving end of a clinical negligence claim, you will be relieved to have made such comprehensive notes.
And I can assure you that you will then save time when meeting with your solicitor to work out what you said to the patient at each appointment, not to mention the fact that you will be better able to defend your actions.
These simple steps could go a long way to covering your ‘proverbial’ if you ever did find yourself before the GMC or at the other end of a claim.
Amie Roadnight (right) is a solicitor at Hempsons
Free legal advice for Independent Practitioner Today readers
Independent Practitioner Today has joined forces with leading healthcare lawyers Hempsons to offer readers a free legal advice service.
We aim to help you navigate the ever more complex legal and regulatory issues involved in running and developing your private practice – and your lives.
Hempsons’ specialist lawyers have a long track-record of advising doctors – and an unrivalled understanding of the healthcare system as a whole.
Call Hempsons on 020 7839 0278 between 9am and 5pm Monday to Friday for your ten minutes’ of free legal advice.
Advice is available on:
Business structures (including partnerships)
Commercial contracts
Disputes and litigation
HR/employment
Premises
Regulatory requirements and investigations
TRACING OUR ROOTS
Where we are today in private healthcare owes much to the development of the NHS. Dr Ellen Welch (right) presents more of the key milestones down its 70 years
NHS in a new with same
2000s
THE NEW millennium brings further NHS reshuffling and financial crises. New Labour’s victory in 1997 brought The NHS Plan in 2000, which promised to rebuild the NHS for the 21st century.
There is an influx of migrants, particularly from the EU, and retired Brits also emigrate to sunnier climes in their thousands, prompting the government to say that the NHS should not be free for those who do not live in the UK.
Smoking is banned in public places in 2007 and smartphones and social media become commonplace by the end of the decade. The NHS tries to keep up by introducing the National Programme for IT, aiming for a paperless NHS.
Its ultimate failure is deemed to be a result of an underestimation of the scale of the project, combined with a top-down management approach – centralised authority making decisions on behalf of local organisations, with a lack of adequate engagement with the people actually using it.
2000 The NHS Plan sets out a strategy to increase staffing, hospital beds and decrease waiting times. This is formalised by the 2001 Health and Social Care Act.
A new model of financing is agreed called the Private Finance Initiative (PFI) , which involves using private-sector money instead of public money.
Loans are taken from private companies with high interest rates – some over 70% – to build new hospitals and clinics, which the NHS is required to pay off like a mortgage over the following decades.
These schemes are poorly negotiated by civil servants against
opportunistic financiers, resulting in huge debts for NHS trusts.
A report from the Centre for Health and the Public Interest in 2017 showed that companies running PFI contracts between 2010 and 2015 to build and run NHS hospitals and services made pre-tax profits of £831m from the NHS – money which has been taken away from patient care and is often more than it cost to build the hospitals in the first place. Over the next five years, £1bn of taxpayers’ funds will go towards paying for PFIs.
NHS Walk-in Centres open to deal with minor illnesses and injuries, offering round-the-clock access. They are nurse-led, available to everyone without needing an appointment or needing to register.
2001 Bristol Heart Scandal report published. During the 1990s, high mortality rates were found among babies undergoing cardiac surgery at the Bristol Royal Infirmary. The inquiry revealed a lax approach to safety, with a lack of leadership, teamwork and staff shortages, which ultimately led to the development of regulatory bodies.
The Commission for Healthcare Improvement is created as directed by the Health Act of 1999. This is the first organisation to formally assess the performance of NHS hospitals – now known as the Care Quality Commission or CQC.
The National Patient Safety Agency is set up – now part of NHS Improvement – to drive improved patient care, prompted by reports such as the DoH’s report An Organisation with a Memory, which suggested that, every year, 28,000 written complaints are made
new century problems
about aspects of clinical treatment in NHS hospitals; that hospitalacquired infections cost the NHS £1bn and that more than £400m is paid by the NHS annually to settle clinical negligence claims.
9-11 Terrorist Attack on the World Trade Centre in New York.
2002 NHS Reorganisations.
Based on the White Paper Shifting the Balance of Power , 95 health authorities are abolished and partly replaced by primary care trusts (PCTs), which are set up as administrative bodies responsible for commissioning healthcare, and 28 strategic health authorities, which are to provide regional management for the NHS and oversee the PCTs. The PCTs are given responsibility for 80% of the health budget.
The Nursing and Midwifery Council (NMC) is founded to regulate nurses and midwives and set educational standards, replacing the UKCC.
National Programme for IT (NPfIT)is launched with the idea of creating a paperless NHS, with an integrated IT system throughout the entire NHS – 30,000 GPs and 300 hospitals.
An agency called NHS Connecting for Health was formed in 2005 to deliver this project; replacing what was before it: the NHS Information Authority.
The motivation for the ambitious project came from Cabinet level, but the delivery did not translate into reality. Hit by technical problems and contractual wrangling, the £11bn scheme was scrapped in 2011 and labelled a fiasco.
The Health and Social Care Information Centre (HSCIC) was created as a special health auth -
ority and took over parts of the NPfIT in 2013 when NHS Connecting for Health ceased to exist. It was rebranded as the catchier NHS Digital in 2016. NHS Digital now runs the Spine service in England – a central, secure system for patient data.
The Wanless Report , commissioned by the Treasury to look at healthcare spending and future trends, concluded that future NHS spending would rise, mainly due to patients demanding more choice and higher-quality services.
2003 NHS Reorganisation
The Health and Social Care (Community Standards) Act is passed, allowing for the establishment of foundation trusts and new GP contracts.
This act introduced ‘Alternative Provider Medical Services’ or APMS contracts, which allowed non-NHS providers to be commissioned by the PCTs to deliver care.
NHS foundation trusts are established as part of the government’s plan to continue the internal market. There are set up as a ‘halfway house’ between the public and private sectors to try to make healthcare more efficient.
Foundation status aims to give trust managers financial and managerial freedom from the Department of Health, by allowing them to borrow money privately, without prior approval from the Treasury, and invest this money as they see fit in local services.
Monitor is established to regulate NHS foundation trusts in terms of quality and finances. It became part of NHS Improvement in 2016.
Independent Sector Treatment Centres (ISTCs) are first opened. These focus on providing routine elective treatments, such as cataract surgery, for NHS patients by the private sector as part of the 2000 NHS Plan to reduce NHS waiting lists, promising greater efficiency and patient choice.
They promised more than they delivered. Unable to employ NHS staff at the outset, they were staffed by overseas doctors, whose quality of training and familiarity with the NHS was questioned.
They negatively impacted the training of junior doctors, who previously learned by doing the ‘straightforward’ procedures the ISTCs took on. The finances were also problematic, in that they were paid whether they reached the required targets or not.
They were not regulated in the same way as the NHS, and data could not be collected on their productivity in the same way as in the NHS due to commercial sensitivity and poor data collection.
2004 New GP contracts are renegotiated, resulting in more autonomy for practices regarding the range of services they provide and a focus on performancerelated pay for reaching standards set out in the Quality and Outcomes Framework (QOF). Stronger regulatory mechanisms are introduced for GPs including annual appraisals and a requirement to register with the CQC.
GPs traditionally carried out evening house calls and emergency night visits providing continuity to their patients. The new contracts allowed GPs to opt out of this – virtually all did –passing responsibility for out of hours care to the PCTs.
Private companies, such as Harmoni, Serco and Virgin, stepped in to take this role costing more than £392m in 2005.
Hospital consultants’ contracts are also renegotiated, aiming to increase the direct amount of time they spend with patients.
Four-hour targets are introduced into emergency departments to reduce waiting times. The NHS Plan in 2000 stated that, by 2004, no one should be waiting for more
than four hours in the emergency department from arrival to admission, transfer or discharge, and financial incentives to meet these targets were introduced. Government funding was invested in recruiting new emergency department nurses and increasing consultant numbers.
Facebook launched
2006 NHS Bowel Screening programme is launched, offering home faecal occult blood testing, detecting an estimated 3,000 cancers each year.
2007 Smoking is banned in restaurants, pubs and public places in England. A year after this, there is a significant decline in hospital admissions for heart attacks, asthma and lung infections.
2008 HPV (Human papilloma virus) vaccination programme is launched to help prevent cervical cancer.
The Darzi Review – High Quality Care for All is published, led by Lord Ara Darzi, a colorectal surgeon and health minister. A year-long review of the NHS is carried out, engaging 65,000 healthcare staff, patients and the public to discuss visions for the future of the NHS and to examine barriers to delivering these visions.
Global financial crisis
2009 The NHS Abdominal Aortic Aneurysm (AAA) screening programme is launched for men.
☛ Adapted from The NHS At 70 – A Living History, by Dr Ellen Welch, a cruise ship doctor and GP in West London. £12.99 from www.pen-and-sword.co.uk
SPECIAL OFFER!
Independent Practitioner Today readers can get 25% off 'The NHS at 70', plus free UK p&p.
Quote NHS70 at www. pen-and-sword.co.uk
BUSINESS DILEMMAS
Patient raises money for a bogus disease
What should a doctor do when a patient is found to be seeking donations for treatment – for a condition she doesn’t have? Dr Kathryn Leask (left) advises
Dilemma
Do I report this plea for funds?
QI recently carried out a laparoscopic ovarian cystec tomy on a postmenopausal patient because
there was concern the cyst could be cancerous.
The patient was extremely fearful about this possibility and decided to pay for private treatment because she wanted to have the procedure quickly.
Fortunately, the cyst turned out to be benign, but now one of my colleagues has alerted me to a
fundraising page set up by the patient to seek donations for ongoing private treatment, which gives the impression that she has ovarian cancer.
What should I do?
AIt is possible that the patient is still very anxious about her prognosis, so your first move should be to contact her and check that she understands that her cyst was not cancerous.
The GMC 1 expects you to ‘give patients the information they want or need to know in a way they can understand’ and says you should make arrangements, where possible, to meet patients’ language and communication needs.
One approach might be to tell the patient that one of your colleagues has drawn the fundraising page to your attention and you want to reassure her that she does not have ovarian cancer in case she is worrying unnecessarily.
This could also be an opportunity to discuss the patient’s mental health and whether she would benefit from further support.
Bearing in mind that the patient may not be in a position to pay for private treatment, you could also seek her consent to write to her GP about the situation and recommend that she is referred for some form of counselling, if necessary.
Another possibility is that patient has simply not found the opportunity to update her fundraising page since she received news that the cyst was benign.
If this is the case, it would certainly be worth drawing this to her attention, as her actions could be regarded as misleading and
even fraudulent. It is likely that, when prompted, the patient will update the page or take it down.
In the unlikely event that the patient refuses to take down the page, you will need to decide whether you would be justified in reporting your concerns. However, this would necessarily involve disclosing confidential details of the patient’s medical history when her consent is unlikely to be forthcoming.
The GMC’s latest Confidentiality guidance2 says that such disclosures can be made in the public interest if the benefits to an individual or to society of the disclosure outweigh the patient’s and the public interest in keeping the information confidential.
However, this would usually be in situations where disclosure is necessary ‘for the prevention, detection or prosecution of serious crime, especially crimes against the person’ such as domestic violence.
Fraud is not thought to meet the public interest threshold, but the GMC advises you to seek specific advice ‘from a Caldicott or data guardian or similar expert adviser who is not directly connected with the use for which disclosure is being considered’.
It says that, where possible, this should be done without revealing the identity of the patient.
References
1. Paragraph 32, Good Medical Practice, GMC, 2013.
2. Paragraph 63-70, Confidentiality: good practice in handling patient information, GMC, 2017.
Dr Kathryn Leask is a MDU medico-legal adviser
Birmingham to get new 138-bed private hospital
CONSTRUCTION WORK has begun on a new £100m private hospital in Birmingham, which will provide extra capacity for NHS patients as well as serving private patients.
The 138-bed specialist unit is being built on the Queen Elizabeth Hospital Birmingham campus for a partnership between HCA Healthcare UK and University Hospitals Birmingham NHS Trust Foundation Trust.
The capital is provided by M&G Investments with investment from HCA UK.
The hospital will include a radiotherapy unit and up-to-date operating theatres. It will be equipped with the latest technology to provide some of the most complex procedures and treatments across cancer, cardiology, neurology, hepatobiliary, urology, orthopaedics and stem cell transplantation.
This will give patients access to a level of acute private healthcare not currently available to the 500,000 people in the region who have private health insurance or who want to self-pay for their care.
Claire Smith, chief executive of HCA UK Joint Ventures, said: ‘We know that many patients in the region have to travel for acute private care and we are looking forward to being able to provide these services locally.’
M&G has acquired a long leasehold interest in the site and will finance the construction of the hospital, which is being developed by specialist healthcare property company Prime, with HCA UK entering into a long-term underlease with M&G upon building completion. The 14,728m2 facility is being built by VINCI Construction UK.
Shailendra Shah, head of UK long income investment at M&G Real Estate, said: ‘By financing this construction through long-term leases, which track any rises in inflation, it has been possible to attract pension funds and others to the sector. This
approach brings benefits to healthcare providers, patients and retirement savers through sustainable long-term returns generated for pension funds.’
Will Bilbrough, development director at Prime, said: ‘Selecting M&G and VINCI, achieving financial closure and seeing construction start is the culmination of two-and-a-half years of partnership working between HCA UK, UHB and Prime to develop proposals for this state-of-the-art hospital and we are looking forward to seeing our vision become a reality.’
Prime secured planning permission for the eight-storey building in April 2018 and financial closure was achieved in February 2019, moving the project forward into the construction phase which is expected to be completed in 2022.
M&G Secured Lease Income Fund generates long-term inflation-linked cash flows by investing in ‘income strips’ – a real estate transaction whereby the property interest reverts to the other contracted party for a nominal sum following a long lease term.
The fund has provided capital to universities, local authorities and the corporate sector and has a portfolio including committed developments of £732m. But this is the fund’s first transaction in the healthcare sector.
An artist’s impression of the new £100m hospital on the Queen Elizabeth Hospital Birmingham campus
DEALING WITH PENSION TAX
Beware the annual allowance A financial planner’s view
Will you join the thousands caught out by the ‘taper’? Dr Benjamin Holdsworth (right) sets out the essential steps needed to check your pension’s tax position
MORE AND more doctors are triggering substantial tax bills because of harsh pension savings regulations, which are difficult to understand and easy to get very wrong.
In January, a Freedom of Information Act request to HM Revenue and Customs revealed that the average tax bill individuals faced for breaching yearly pension contribution limits in 2016 17 was £29,635, with some obviously paying much more.
In total, a record tax haul of £517m was added to Treasury accounts from pension tax breaches that year – when the new limits were first applied.
Many of those getting caught out are senior doctors with decades of NHS service, tied into making contributions to the pension scheme.
The annual restriction on the amount you can contribute to your pension free of tax is known as the ‘annual allowance’.
New rules decrease the standard annual allowance of £40,000 to as
low as £10,000 a year for doctors with a ‘threshold income’ of more than £110,000 – this is known as a ‘tapered annual allowance’.
Excess pensions savings above the allowance will generate a tax bill charged at your marginal rate of income tax.
Extremely complicated
But the ‘taper’ adds another level of complexity to the already challenging allowance. There are several major factors to consider – you will not know your level of income for the year until the end of it and, more importantly, you will not know what your pension input will be, because these are calculated retrospectively.
This means you may only find out if you are on course to breach the allowance long after you were able to mitigate the situation.
It is important to check where you stand for the current year as soon as possible. Here we propose some key steps you should take:
You may only find out if you are on course to breach the annual allowance long after you were able to mitigate the situation
Step 2 Calculate your approximate threshold income for the current/forthcoming year
Step 1 Check previous years
Have the payroll figures been submitted correctly in your previous calculations?
Have you had any backdated pay?
Have you received your increments correctly?
Have you reduced your sessions in the middle of a year?
We often see payslips which contain small errors leading to big differences in your pay and subsequent pension inputs.
To establish if you will be subject to the tapered annual allowance, you must first calculate your ‘threshold income’, which is your income from all sources. You should include your NHS income and adhoc NHS work, as well as private practice earnings, dividends from investments and buytolet property income. If your threshold income is likely to be more than £110,000, you will need to check your ‘adjusted income’ to ascertain whether the tapered allowance will apply. ‘Adjusted income’ is your threshold income plus your pension input for the year.
Step 3 Establish whether your private practice is structured efficiently
It may be possible to reduce your threshold income by amending the structure of your private prac
tice. There are multiple options: sole trader, partnership or limited company. It is important that you take advice from a specialist medical accountant in this area.
While your pension position is not necessarily the main driver, it is now very important that your accountant considers it. This is likely to require a ‘multidisciplinary approach’ with a pension specialist and your accountant.
If you have a company, what level of dividend are you planning on taking? Ideally, dividends should be planned rather than ‘allocated’.
Step 4 Assess your likely NHS pension input for the year
Calculating pension contributions for a definedbenefit scheme such as the NHS is difficult. It is not based on the amount that you and your employer have paid into your NHS pension but on the deemed ‘growth’ in the year.
A
Ultimately, you should start a tax year with an idea of the tax bill potentially coming your way as accurately as possible
Your pension input will not be the same as the previous year and it is important this has been accurately modelled. You will need to be mindful of pay rises or clinical exellence awards (CEAs), which will increase pensionable pay and therefore your pension input. Ultimately, you should start a tax year with an idea of the tax bill potentially coming your way as accurately as possible.
PRIVATE PRACTICE
Step 5 Estimate your approximate tax bill and how you intend to pay it
There are multiple options for paying a tax charge for breaching an annual allowance: via selfassessment, through the NHS Scheme Pays option or utilising your personal pension pot.
With NHS Scheme Pays, the pension scheme pays the tax charge on your behalf in return for reduced pension benefits in the future and will charge interest each year until retirement.
There can be tax advantages with this option, but you should be mindful that the interest payments can escalate quickly and the future inflation rate is unknown. However, you should have some idea of the reduction to the benefits to enable you to make the right decision.
You will also need all the necessary information to hand before the application deadline, which is normally 31 July each year.
You could also use a personal pension to pay the tax charge –this is typically the best option of the three. However, it is essential you receive the right advice in this area.
Dr Benjamin Holdsworth is director of Cavendish Medical, specialist financial planners helping consultants in private practice and the NHS
The content of this article is for information only and must not be considered as financial advice. Cavendish Medical always recommends that you seek independent financial advice before making any financial decisions.
Levels, bases of and reliefs from taxation may be subject to change and their value depends on the individual circumstances of the investor. The value of investments and the income from them can fluctuate and investors may get back less than the amount invested.
– Our series for doctors considering the independent journey
Beware the annual allowance
An accountant’s view
Independent practitioners have endured three years of the punitive annual allowance tapering measures. These have caused significant angst and disbelief at some huge tax charges arising from having allowance-busting pension savings. Ian Tongue (right) recaps on the issues and suggests ways to help mitigate the tax
The annual allowance
The Government sought to restrict tax relief on pension contributions, primarily to recognise that most people cannot afford to pay up to £255,000 into a pension and get tax relief of £127,500, as the additional rate of income tax was 50% in 201011.
So, for the 201112 tax year, the annual allowance limit dropped to
£50,000 and then to £40,000 from 201415.
These limits should have ensured most independent practitioners escaped annual allowance charges in most years.
But from 2016 17 onwards, annual allowance ‘tapering’ was introduced and many consultants had their allowance cut to just £10,000.
As a result, many consultants will experience an annual allowance charge year after year, particularly those in the new NHS 2015 pension scheme and/or in receipt of a merit award or other increase to superannuable pay.
Pension savings
It is easy to look at pension contributions deducted against an NHS
salary and conclude you have no problem with excessive pension saving. But the nature of the NHS Pension Schemes means actual contributions are disregarded and the growth in your pension is substituted instead.
So, a consultant with £90,000 pensionable pay would make contributions of 13.5%, which is
£12,150 before tax relief, £7,290 after tax for a 40% taxpayer.
As a comparison, excluding inflation factors, £90,000 of superannuable income within the 2015 NHS Pension Scheme would result in £26,667 of growth at the time of writing. It is proposed to increase this figure.
Your pension growth is based on the pension scheme rules and the accrual of pension is different between the 1995, 2008 and 2015 pension schemes.
For those active members who were not within ten years of retirement in April 2015, you will be in more than one scheme. Inflation also comes into play and can significantly affect the figures due to factors used by HMRC and NHS Pensions being one year out of sync.
It is a complicated calculation, so
it is essential to get specialist advice or you could sleepwalk into a big tax charge.
How bad is it?
For some consultants, the tax charge is eyewatering. This is usually in response to an event that step changes their eventual pension, particularly those with significant service in the 1995 scheme. A negative in response to a positive is one way to view it, but it hardly makes the pill easier to swallow.
A national merit award, local clinical excellence award (before April 2018) or pay increment are the usual triggers for high pension growth, but taking on additional superannuable roles can have the same effect.
Temporary superannuable roles can come with a tax charge that
does not translate to a step change in the pension, so consider your position carefully.
Some trusts now offer temporary additional posts as nonsuperannuable, which is helpful to not spike pension growth but can still affect annual allowance tapering.
In the runup to the 31 January 2019 deadline, I had a significant number of new clients doing no private work. But due to their NHS earnings and pension growth, they had significant annual allowance charges. Don’t assume annual allowance charges are for those with large private practices.
A lot of misleading information regarding the relationship between earnings and takehome pay can result in a doctor acting without obtaining considered advice.
For example, I have seen graphs plotting income against takehome pay where all the income is superannuable. But most consultants reach a ceiling level of superannuable pay which makes the figures materially different.
Scheme pays option
Once any annual allowance charge is known, the next stage is to work out how on earth you are going to pay it. Thankfully, NHS Pensions softened its position for the 2017 18 tax year allowing members to pay any tax amount due from excess pension saving.
Previously, members had to pay up to £13,500 in tax through selfassessment, with the balance paid by the scheme.
The ‘scheme pays’ option is effectively an interestbearing loan with a current interest rate of 2.8% above inflation annually. Upon retirement, the loan is recovered by reference to a recovery factor determined by NHS Pensions.
If you are in a position to choose to pay the tax or take the ‘scheme pays’ option, talk to your financial adviser, as the outcome will affect your pension on retirement.
sion scheme number with the pensions regulator.
This is relevant, as members were forced into the ‘new’ scheme and this affected public sector workers generally following on from a report on public sector pensions by Lord Hutton.
The judiciary and fire service are currently in a legal battle arguing that forcing members into a new pension scheme with a different retirement age was discriminatory and illegal.
It is unclear at the time of writing whether this challenge will be successful, but no doubt if it was, it would significantly affect members’ pensions and annual allowance calculations.
What can be done?
This is where having a medical specialist accountant can really pay dividends.
Commonly, the most effective measures reduce overall income to preserve or reinstate your annual allowance. Where this is not possible, consideration to cut superannuable income or the composition of income can be made.
It may be time to consider if continued scheme membership is deriving enough benefits. Or if you are close to retirement to consider the timing. Taking an independent financial adviser’s advice is essential.
Some consultants are trying to limit the time they spend in the scheme by leaving and rejoining periodically. This method works to reduce pension growth, but should only be considered if the reduction to your pension on retirement is fully understood. It remains to be seen whether the NHS trusts or NHS Pensions reject this ‘hokey cokey’ approach in the longer term.
The effect of annual allowance tapering cannot be played down, but with the right advice, the hit can often be significantly mitigated.
Don’t assume annual allowance charges are for those with large private practices
But they don’t have a crystal ball, so without knowing how long you will live, don’t expect a particularly concrete answer.
Recent developments – 2015 NHS pension scheme
Unlike the 2008 pension scheme, the 2015 one is completely new, carrying a different registered pen
Whatever your private practice size, it is essential to consider your position to avoid an unexpected tax charge.
Next month: Taxing your houses
Ian Tongue is a partner with Sandison Easson specialist medical accountants
PRIVATE PATIENT UNITS
Our analysis of England’s NHS trust private patient earnings by region has completed its ten-region cycle, so Philip Housden returns to the capital for updated data from the latest published trust annual accounts, and market news
Capital feat for London’s PPUs
THE LONG TERM trend for London to be the engine of growth for the whole NHS PPU sector has continued, if not accelerated, over the past year.
Revenues for 22 trusts within greater London climbed to £402m, up 8.4% from £371m in 2016 17. The extent to which growth continues to be skewed between London and the rest of England is shown in figures 1 and 2 overleaf. London now represents 65% of total revenues, an increase from 59% over five years. During that time, overall private patient revenues outside London have remained static, albeit that there
have been significant movements by region and by trust: themes to be explored in future articles.
The concentration of private patient activity within the largest ten trusts has continued, reaching 61% in 201718 (Figure 3, overleaf). All these toptenearning trusts are in London.
They have driven the market as much as responded to it. In recent years, their private patient services have become largely synonymous with the overall NHS trust brand.
As market analysts LaingBuisson have recently stated, earnings have largely grown from overseas patients attracted to the highest
quality infrastructure that the super specialised London NHS trust tertiary centres provide.
Last year’s analysis proposed the division of the 22 acute trusts in Greater London into four distinct groups, split by private patient revenue growth and by percentage of overall trust patient incomes (Figures 4, 5 and 6 on page 53).
This grouping was useful and has again been used to highlight trends:
1
The big four of Royal Marsden, Great Ormond Street, Royal Brompton and Imperial, each with earnings of £35m a year or more, enjoying significant year on year
growth and with private patients now accounting for between 11% and 33% of overall incomes and an average of £62m a year each.
2
The next six significant earners of Moorfields, Royal Free, Guy’s and St Thomas’, King’s College, UCL and Chelsea and Westminster. This group’s earnings are growing at nearly 10% a year and are presently between £27m and £16m a year.
3
The Royal National Orthopaedic Hospital, St George’s, Bart’s and London North West are
➱ p52
An analysis of their accounts shows London trusts’ PPUs continue to surge ahead of the rest of the country
four trusts that comprise a potential group of next movers, each with significant infrastructure on which to grow their present earnings which range from £3.5m to £6.7m a year.
4The final group is made up of the eight lowest earners, for whom private patients account for not more than £850k a year and 0.3% of trust revenues, significantly below the London average of 3.4%.
The Big Four have expressed ambitions to invest to grow further and so this trend is expected to continue. Royal Marsden achieved its stated ambition of exceeding £100m a year from private patients, growing more than 50% in the past three years and the closest trust in England to a fully mixed public private model of care.
It is understood that the growth trend has continued into 201819, with an outturn around £115m likely, representing another annual increase of 10% and a private patient income level that will then be 34% of total trust patient income.
Great Ormond Street has cultivated the international market and continued to grow strongly and the 2017 18 growth of £2m revenues is set to rise significantly into 2018 19 accounts when an outturn of £62m may be achieved, roughly an 8% increase.
Royal Brompton invested in both a diagnostic and outpatient centre in Wimpole Street and improved facilities at Harefield to support the expansion for the private market. The trust is also active in the Middle East market.
Reported revenues, however, remain flat at £38m in 201718.
Imperial enjoyed a significant annual increase in revenue of 10% (£4.5m) in 201718 to over £50m for the first time, although this momentum does not seem to have been fully carried forward into 201819.
Significant earners
The next group of significant earners are similarly following a strategy of investing to grow.
Moorfields is arguably already among the biggest hitters, with £27.2m revenues in 2017 18. Of
The Big Four have expressed ambitions to invest to grow further and so this trend is expected to continue
this, around half is now achieved through Dubai in the United Arab Emirates (UAE). The trust is investing around £3m capital in a private patient theatre and admission suite facilities.
The Royal Free’s investment in a new facility at Hadley Wood, Barnet, which extends capacity and referral catchment, is part of an ambitious growth plan. Private patient revenues grew £874k (4%) to £22.4m in 2017 18, but is reported as behind planned levels of contribution for 2018 19 in recent board reports.
Guy’s and St Thomas’ £100m integrated partnership cancer centre with HCA on the Guy’s campus is expected to deliver a further boost to revenues growth in 201819 that improved by more than £3m in 201718 to £21.5m.
King’s College has facilities in Camberwell and Orpington in south London and has expanded its private patient services through a footprint overseas, in the UAE’s capital Abu Dhabi, to cater for international demand.
The trust achieved revenues of £20.4m in 2017 18, a significant rise of 39%. UCL’s revenues remained flat at £19.8m.
Chelsea and Westminster has plans for growth on the West Middlesex campus and increased revenues by more than £1m to nearly £17m in 201819.
Figure 1
Figure 2
Figure 3
The third group is made up of four trusts with ambitions to grow private patient activity. These trusts have perhaps relatively under-performed when benchmarked alongside other central London trusts, but are taking steps to be the next movers
St George’s has still not yet moved forward with long standing plans to invest in a PPU and private patient revenues declined by £1.1m (25%) to £3.5m in 201718.
By contrast, London North West enjoyed growth of 18% to £5.1m in 201718 and the trust is considering investing in additional capacity at St Mark’s, Harrow.
Missing out
Finally, a word about the eight other trusts presently missing out on this growth – depicted in thebottom left of figure 6, below right).
Each are physically located further away from central London and cannot therefore enjoy the same access to the international patient market, but it is striking that they are performing less well than a high number of similarlysized trusts outside the capital.
Ambitions to grow
The third group is made up of four trusts with ambitions to grow private patient activity. These trusts have perhaps relatively underperformed when benchmarked alongside other central London trusts, but are taking steps to be the next movers. They averaged over 10% growth in 2017 18 to aggregate over £21m.
Bart’s Health grew 53% – nearly £2m – in the 12 months to end of March 2018, achieved by a thorough review of present tariffs leading to renegotiated prices with major insurers and a drive to capture and charge for all activity.
Further mediumterm growth is expected now that Barts will have access to the partnership private patient facility being built by Nuffield Health in former surgeons’ accommodation and pathology buildings.
The Royal National Orthopaedic Hospital at Stanmore has already made a move and invested in growth. An expansion from 18 to 28 beds has been made possible by moving the PPU into the new Stanmore Wing that opened in December 2018.
A brand refresh and the new capacity gives optimism that the trust will make a jump from the present revenues of £6.8m a year that grew 5% last year.
Of the eight, there are two that have worked in partnership with independent healthcare providers and both have chosen to end these arrangements.
Kingston Hospital has tendered for the management of its Coombe Wing PPU, having ended a long term contract with BMI, with the new arrangements to commence from April 2019.
Barking, Havering and Redbridge’s partnership with HCA at Queen’s ended in early 2018, and the trust is reviewing options for a replacement arrangement that brings control and earnings back inhouse.
The remaining six trusts aggregate only £1.6m between them and these all remain opportunities for further private patient investment and growth.
Next month: the southern home counties
Philip Housden (below) is a director of Housden Group www.housdengroup.co.uk
Figure 4
Figure 5
Figure 6
DOCTOR ON THE ROAD: PORSCHE PANAMERA 4 E-HYBRID SPORT
A hybrid in more ways
For independent practitioners who want some of the urban benefits of electric motoring but still enjoy sporty driving on the open road, this car could possibly be the answer. Our motoring correspondent Dr Tony Rimmer (left) reports
ways than one
BRAND ASSOCIATION is something that independent practitioners should perhaps take more notice of.
If your clinic has close ties with renowned centres of academic research and learning, then you should tell your clients. They will be impressed and more likely to use your services.
For example, Porsche – known for success on the race-track – uses its new five-door Panamera as the Doctor’s car at 911 Carrera Cup events. Public exposure and association like this is priceless and is helping the company sell its saloon models alongside its pure sports cars.
Porsche’s first official foray into the premium saloon marketplace was in 2009 with the launch of the original Panamera. Production of this large premium sports hatch was quite a risk from a company with an unimpeachable history of making sports cars like the Boxster and the iconic 911.
But the Panamera had a problem; its styling was not appealing. In trying to follow 911 design cues, the rounded bodywork failed to translate when applied to a large five-door hatchback.
Much-needed facelift
However, on the road, the car was a great drive. Engine choices ranged from a 3.0 litre six-cylinder petrol unit up to a range-topping 4.8 litre turbo with a 3.0 litre diesel for those wanting better economy.
In 2013, a much-needed facelift improved the external appearance to some degree and, looking toward the future, a plug-in Hybrid model, the E-Hybrid, was released featuring a 330bhp petrol V6 with a 95bhp electric motor.
All-electric range was about 30 miles in ideal conditions. In 2017, the current second generation Panamera was introduced and with it, the option of a sports-estate body shell, the Sport Turismo.
For those of you practitioners
who want some of the urban benefits of electric motoring but still enjoy sporty driving, and the sound of a powerful V6 petrol engine on the open road, this car could possibly be the answer.
The 2.9 litre twin-turbo V6 engine produces 330bhp, is linked to a 136bhp electric motor and drives all four wheels through an eight-speed dual clutch gearbox. Air suspension is standard, as are different damping modes via the Porsche Active Suspension Management; Comfort, Sport and Sport+.
This new generation Panamera, particularly in Sport Turismo form, is now a smart and good-looking car. The front and rear LED light clusters together with the elongated roof line give this five-door hatch/estate a really purposeful and sporty appearance. A wide stance and big alloy wheels complete the picture.
Redesigned interior
If the new external styling is a pleasant surprise, then the completely redesigned interior is a revelation. Gone is the multitude of separate function buttons.
They are replaced by touch-sensitive controls on a completely smooth surface that extends up to a huge and really clear infotainment/ sat-nav screen. The driver sits in a sports seat with a perfect driving position; the rev-counter directly in front, as is Porsche tradition. Although Porsche claims that the Sport Turismo is a five seater, the middle rear seat passenger needs to be slim and lithe to be comfortable. The other rear passengers have plenty of room, just as in any executive saloon. The extended boot means that access and space is not dissimilar to the sibling Macan SUV model. My dog certainly had no complaints. You sit low in the Panamera and this, together with the high-quality Porsche ambience, makes you feel secure and confident. Moving off from rest in all-electric mode is
PORSCHE PANAMERA 4
e-hybrid sport turismo
Body: Five-seat hatchback/estate
Engine: 2.0 litre V6 turbo-petrol & 100kW electric motor
Power: 330bhp (petrol) & 136bhp (electric)
Torgue: 700Nm combined
Top speed: 170mph
Acceleration: 0-62mph in 4.6 seconds
Claimed economy: Combined 113mpg
CO2 emissions: 56g/km
On the road price: £83,288
not dissimilar to a Tesla; acceleration is brisk and silent.
Although you might not get as far as the claimed 31 miles maximum in electric-only mode, you can certainly do lots of urban motoring safe in the knowledge that you are doing your bit to save the planet – in a Porsche.
However, once you hit the open road, it is too much of a temptation not to allow the V6 engine to come alive. Indeed, the batteries will need a top-up anyway. The transfer from electric to petrol power is seamless and the excellent gearbox ensures a smooth transition.
But you are driving a Porsche, so you expect a spirited, sporty drive when you want it. No problem, just select Sport+ and the full potential power of a combined 466bhp is at your disposal.
The multitude of separate function buttons are replaced by touch-sensitive controls on a completely smooth surface that extends up to a huge infotainment/ sat-nav screen
Handling is really sharp considering this is a heavy car. It carries an extra 310kg of electric motor and batteries compared to the nonhybrid version. The standard air suspension has a brilliant range of abilities. The ride is really smooth in Comfort mode but tightens up really nicely in the Sport modes.
So the new Panamera can wear the Porsche badge with pride. As a comparison, a Tesla Model S can be fast in a straight line but it is not a driver’s car.
If you fancy a high-quality sports saloon that is both practical, eco-friendly and delivers a thrill when you want it to, take a closer look at this latest offering from Stuttgart.
Dr Tony Rimmer is a former NHS GP practising in Guildford, Surrey
All you need to know about accountancy for private practitioners
Keeping a steady flow
A
below-inflation profits rise has hit specialists in our latest benchmarking survey, reports Ray Stanbridge, but like many others they are enjoying a growth in self-pay
THE TREND confronting consultant urologists who have an NHS practice as well as a private one has continued.
While there has been income growth for many, costs have risen significantly.
As a result, profits have shown modest growth and margins have remained constant.
Our latest benchmark figures for this specialty show that, for the average urologist in private practice, gross incomes increased by 2% between 2016 and 2017 from £141,000 to £144,000.
Costs have risen by about 1.8% from £53,000 to £54,000.
As a result, taxable profits have increased by only 2.2%, from £88,000 to £90,000; slightly below the rate of inflation.
Less pressure
As reported in Independent Practitioner Today in 2018, there is a significant growth in self-pay patients for many urologists. This trend, nationally, has continued too.
There does, however, seem to have been less pressure from insur-
AVERAGE INCOME AND EXPENDITURE OF A CONSULTANT UROLOGIST WITH AN ESTABLISHED PRIVATE PRACTICE
ers on urologists’ fees over this period. They seem to have diverted their attention to dermatologists and cardiologists!
I have identified some modest changes in costs. Surprisingly, there has been a slight fall in the spend on medical supplies and assistants. The implication is that several urologists are using fewer assistants to help them than historically.
Staff costs have shown a small increase. For urologists this primarily reflects, in 2017, market trends and secretarial salaries rather than growth in personal allowances.
Reputable alternative
Expenditure
One of the interesting observations in our analysis is that industry defence costs seem to have shown a slight fall. There are a few reputable alternatives to the traditional medical defence organisation providers and they offer a competitive product at a lower price.
There is also evidence that an increasing number of urologists are ‘shopping around’ for a better deal. There seems to be some point when we would expect traditional defence bodies to respond to this market trend, which is happening in several disciplines.
One of the interesting observations in our analysis is that industry defence costs seem to have shown a slight fall
Travel costs seems to have shown a small increase. This represents, for many, costs of travel to attend professional conferences abroad.
Accounting/legal costs have also shown a modest increase. Again, this possibly represents market rate increases in fees rather than any greater use of professional services by most urologists – those divorcing being the exception.
Marketing costs
Finally, ‘other’ costs seem to have shown a small decrease. For many this represents costs of marketing/ websites.
Those who have considered websites have possibly acquired and paid for them, so this trend is probably to be expected, as consultants move into a ‘mainte -
Year ending 5 April. Figures rounded
EXPERT ADVICE YOU CAN TRUST
EXPERT ADVICE YOU CAN TRUST
EXPERT ADVICE YOU CAN TRUST
Since starting in the mid 1970’s Sandison Easson has continued to grow and is one of the largest independent medical specialist accountants in the UK.
Since starting in the mid 1970’s Sandison Easson has continued to grow and is one of the largest independent medical specialist accountants in the UK.
Since starting in the mid 1970’s Sandison Easson has continued to grow and is one of the largest independent medical specialist accountants in the UK.
Sandison Easson acts for medical professionals throughout all stages of their career and has clients in almost every town in England, Scotland and Wales.
Sandison Easson acts for medical professionals throughout all stages of their career and has clients in almost every town in England, Scotland and Wales.
Sandison Easson acts for medical professionals throughout all stages of their career and has clients in almost every town in England, Scotland and Wales.
We provide the usual services you would expect from an accountant such as preparation of your accounts and tax declarations but offer so much more including advice on:
We provide the usual services you would expect from an accountant such as preparation of your accounts and tax declarations but offer so much more including advice on:
We provide the usual services you would expect from an accountant such as preparation of your accounts and tax declarations but offer so much more including advice on:
• Setting up in Private Practice
• Setting up in Private Practice
• Setting up in Private Practice
• Developing your Private Practice
• Developing your Private Practice
• Developing your Private Practice
• Tapering of the Annual Allowance
• Tapering of the Annual Allowance
• Tapering of the Annual Allowance
• Lifetime Allowance planning
• Lifetime Allowance planning
• Lifetime Allowance planning
• Personal Allowance planning
• Personal Allowance planning
• Personal Allowance planning
SPECIALIST
SPECIALIST
MEDICAL ACCOUNTANTS
MEDICAL ACCOUNTANTS
SPECIALIST MEDICAL ACCOUNTANTS
• Expenses that you can claim and those you cannot
• Expenses that you can claim and those you cannot
• Expenses that you can claim and those you cannot
• Minimising your tax bills
• Minimising your tax bills
• Minimising your tax bills
• Reviewing your PAYE Coding Notices
• Reviewing your PAYE Coding Notices
• Reviewing your PAYE Coding Notices
T 01625 527 351
T 01625 527 351
E info@sandisoneasson.co.uk W www.sandisoneasson.co.uk
E info@sandisoneasson.co.uk W www.sandisoneasson.co.uk
T 01625 527 351 E info@sandisoneasson.co.uk W www.sandisoneasson.co.uk
A Rex Buildings, Wilmslow, Cheshire, SK9 1HY
A Rex Buildings, Wilmslow, Cheshire, SK9 1HY
Also at 1 Harley Street, London, W1G 9QD
Also at 1 Harley Street, London, W1G 9QD
A Rex Buildings, Wilmslow, Cheshire, SK9 1HY Also at 1 Harley Street, London, W1G 9QD
nance’ mode for their marketing and business development work.
Our view is that current trends are likely to continue through 2018 and 2019. There continues to be increasing interest in groups.
Over the next ten years, we would expect consultant urolo -
gists to be a member of a group, to work through locum agencies or be employed by private hospitals.
As I stated last year, an increasing number of urologists are likely to join groups. Others have chosen to incorporate. Yet others have decided, primarily in the country,
to specialise in ‘Choose and Book’ work, where there are fewer costs.
Apart from uncertainty facing ‘Choose and Book’ work at present, the other comments are still relevant.
Note that our sample of urologists is restricted to those who:
Have either an old-style or a new-style NHS contract;
Have been in practice for at least five years;
Have been earning at least £5,000 a year from private practice;
May be trading as a sole practitioner or as a member of a group;
May or may not have incorporated;
Will continue to do at least some NHS work, meaning that they are not in full-time private practice.
Our sample may not be statistically significant, but it does aim to represent an average picture of what is going on in the market place.
Next month: Anaesthetists
Ray Stanbridge is a partner with accountancy, finance and tax advisory medical specialists, Stanbridge Associates Ltd
HOW ARE YOU DOING?
Years ending 5 April
WHAT’S COMING IN OUR MAY ISSUE...
Make sure you don’t miss our next issue, published on 23 May. You may not receive every issue if you have not yet subscribed to the journal. Don’t risk missing out on vital topics we tackle next time:
Engagement with the consumer is something private healthcare providers really need to get right. There’s a vast untapped market out there of middle-income consumers who can’t afford health insurance and don’t access private healthcare – they don’t understand it and they think they can’t afford it. Don’t miss Keith Pollard’s detailed look at the self-pay market.
Five top ways to free up cash flow in your practice – our Accountant’s Clinic author Susan Hutter knows exactly what to do
The new president of the Independent Doctors Federation, private GP Dr Neil Haughton (right), spells out his aims for the body and its members over the next three years
Reports from the annual private practice committee conference of the BMA
With the CQC now starting to rate independent doctors, Martha Walker analyses its criteria for giving you Outstanding, Good, Requires Improvement or Inadequate ratings and looks closer at the watchdog’s concerns about private GP, consultant and clinic safety
PLUS Following the CQC’s shock report on the state of private ambulance services – Sally Taber of the Independent Healthcare Sector Complaints Adjudication Service gives us a check-list of what you should expect from your ambulance company
INDEPENDENT PRACTITIONER
EDITORIAL INQUIRIES
Robin Stride, editorial director
Email: robin@ip-today.co.uk
Phone: 07909 997340
Published by The Independent Practitioner Ltd. Independent Practitioner Today is editorially independent and thanks Bupa for its assistance with distribution.
Printed by Pepper Communications Ltd Material is governed by copyright. No part of this publication may be reproduced, stored in a retrieval system or transmitted in any form without permission, unless for the purposes of reference and comment. Editorial layout is the copyright of the publishers. If you wish to use it for promotional purposes on websites or for reprints, we would be happy to discuss licensing the copyright to you.
Registered office: 7 Lindum Terrace, Lincoln LN2 5RP Write to
Practitioner Today PO Box 198, Cranleigh GU6 9BB
Called to give evidence? Tips to help you survive the witness box
En route to success – or already there? Seven good reasons why you should get cracking now on that will or updating the one you have
Choosing the right marketing strategy to attract new patients and grow your practice. Jane Braithwaite of Medical Marketing takes a deeper look at how to analyse your strengths and weaknesses to help you develop your marketing plan and choose the best strategy
Markets are meant to fall, says Cavendish Medical’s Dr Benjamin Holdsworth, but can you keep the falls in perspective?
A cardiologist tells how his finances were rejuvenated after the busyness of work got in the way of his billing
In our series on the ups and downs of private patient units, Philip Housden visits the southern counties
Ray Stanbridge’s unique benchmarking series, Profits Focus, finds anaesthetists’ incomes have been swallowed up by rising expenses
Tricky situation: an MDU adviser responds to a private GP’s request for help after a patient who tests positive for a mutation says she does not want this information shared with other family members. How does he inform them of the possible risks facing them?
Our motoring correspondent Dr Tony Rimmer goes out and about with the Skoda Kodiaq
Start A Private Practice: taxing your houses
ADVERTISERS: The deadline for booking adverts in our May issue is 26 April
ADVERTISING INQUIRIES
Margaret Floate, advertising manager Email: margifloate@btinternet.com Phone: 01483 824094
SUBSCRIPTION RATES
£90 independent practitioners. £90 GPs and practice managers (private & NHS). £210 organisations. Save £15 paying by direct debit: individuals £75 (organisations £180).
TO SUBSCRIBE – USE SUBSCRIPTION FORM ON PAGE 25 or EMAIL: lisa@marketingcentre.co.uk or phone 01752 312140 or go to the ‘Subscribe’ page of our website www. independent-practitioner-today.co.uk
£15 WITH DIRECT DEBIT! Guarantee delivery of your next copy of Independent Practitioner Today. Take out a subscription and you will get full access to our news, features and previous issues on our website. See details on the left.
ISSUES: £12.50 including post & packaging
Electronic Billing
Remove printing, posting and admin costs
Payment Tracking
Ensure you have been paid for the bills you submit
Financial Reporting
Keep track of your practices’ performance
Complimentary App
Free Apple and Android app available
Appointments and Diary
Manage your schedule and send appointment letters
Membership Enquiry
Real-time online checks for patient membership number
Pre-populated Invoices
Which contain the information you require to submit bills
Shortfall Reminders and Letters
Automated prompts to keep you on top of any shortfalls