Talking centre stage Forum theatre is proving useful in helping private doctors improve their communication skills P12
The business journal for doctors in private practice
Expert advice
Our marketing guru Dev Lall gives tips to help make you an expert at being an expert P26
Picturing a way to make big savings
How a Harley St chambers saved £55k by developing its own picture archive and communication system. n See page 18
Move into court work
Our new series shows you everything you need to know to become an expert witness P28
Doctors’ tax shocker
By Robin Stride
Hundreds of independent practitioners will be forced to make hefty shock payments to HM Revenue and Customs (HMRC) after coming unstuck while trying to limit their tax bills.
Many now face having to hand over six-figure tax sums they thought they had escaped by entering tax avoidance schemes.
Courts will ultimately decide the legality of these vehicles, but meanwhile tax inspectors are using new powers to demand millions of pounds worth of taxes from high earners who have put money into them.
The Accelerated Tax Payments (ATPs) measures are affecting private consultants and GPs, NHS GPs, and dentists.
Tax expert Vanessa Sanders of Stanbridge Associates said: ‘Frighteningly now, under initial measures introduced in July 2014, HMRC is able to issue ATP notices to tax scheme users demanding the tax to be paid in advance of any court decisions.’
Accountants say a high-earning doctor who ‘typically’ put £200,000 offshore could expect to pay HMRC £140,000 in income tax and national insurance plus 100% penalties and then interest.
Mrs Sanders told Independent Practitioner Today : ‘For someone having to pay up, then a bill of
In association with
£280,000 is not uncommon. Then there could be court costs to defend an action which could be £25,000-£100,000. A total pay-out could be two-and-a-half times the initial investment.’
Other doctors will have to pay much more. Some have put all their profits, totalling £500,000 in one year, into tax avoidance schemes.
Mrs Sanders said: ‘This will be a massive shock to many doctors. Some are in disbelief at the amount they might have to pay.
‘But, in my many years of experience, if you live in the UK, you have to pay tax in the UK and accept that and be efficient. No amount of tax planning makes it magically disappear.
‘We have warned against these schemes, but clearly some doctors have gone ahead and done it anyway’.
From considering the latest rounds of tax returns, she estimates around 3.5% of hospital consultants have been persuaded to enter into avoidance unwittingly, believing it to be legal and moral. Evidence of tax avoidance includes some offshore trusts and personal management companies.
She is worried that some promoters of avoidance may tell doctors they have counsel’s opinion that these ideas are not schemes but efficiencies and are perfectly in accordance with the legislation.
Former tax inspector Mrs
and only one tends to win. The case is not decided until tested.
‘Some firms may even use the famous 1929 quote from Privy Counsellor Lord Clyde, serving time as Lord Advocate and Lord
SPANNING THE DIVIDE
An architect’s impression depicts how a dazzling new walkway will link buildings at HCA’s Portland Hospital in London. See full story on page 7
moral or other, so as to arrange his legal relations to his business or to his property as to enable the Inland Revenue to put the largest possible shovel into his stores.
➱
you just wouldn’t credit it how your practice could be affected by big differences in credit agency ratings P10
surgeons’ mission faces a hard graft a charity aims to twin every plastic surgery unit with one in a developing country P16 going mobile
Some exciting quality improvements that mobile apps can offer your practice P20 expert advice
our marketing guru gives his tips to make you an expert at being an expert P26 remote control
With doctors increasingly ‘seeing’ patients remotely, we offer medico-legal advice P36
The peaks of investment how to go about turning your dreams of an alpine holiday home into reality P38
It’s economy for the stupid
Spring is sprung and, according to private healthcare analysts LaingBuisson, there is reason to be optimistic that the independent sector is emerging slowly from what has been a long winter for many doctors (see p5).
With more money around, you might hope to see growth in the market, but the British Association of Plastic, Reconstructive and Aesthetic Surgeons (BAPRAS) – see page 7 – has come up with some chilling research that could be mirrored in some other specialties.
Over half of the patients in its study of 6,314 people said keeping costs down was a major
consideration when they chose a clinic or surgeon.
Sadly, a lot of the two million people considering or already committing to beauty surgery in the next year will therefore be tempted by apparently cheaper and better deals abroad.
A quarter don’t even check surgeons’ credentials. BAPRAS president Mr Nigel Mercer warns that many people spend more time choosing an electrician.
So doesn’t it make you wonder just how useful the results of the Competition and Markets Authority’s drive for more transparency on fees and outcomes will be to doctors and patients?
Tell us your news Editorial director Robin Stride at robin@ip-today.co.uk
Phone: 07909 997340 @robinstride
To adverTise Contact advertising manager Margaret Floate at margifloate@btinternet.com Phone: 01483 824094
To subscribe lisa@marketingcentre.co.uk Phone 01752 312140
Publisher: Gillian Nineham at gill@ip-today.co.uk Phone: 07767 353897
Head of design: Jonathan Anstee chief sub-editor: Vincent Dawe 12,000 circulation figures verified by the Audit Bureau of Circulations
Beef up your pension pot to stem cuts
by leslie berry
Senior doctors could miss out on substantial pension saving tax breaks unless they take action to beef up their retirement pots.
Financial advisers fear higher rate tax relief could be abolished – leaving private consultants and GPs with many thousands of pounds less in their nest egg than they anticipated.
Speculation has been mounting into whether higher rate pension tax relief will be abolished after the general election following Pensions Minister Steve Webb’s announcement that he would like to introduce a flat rate of tax relief for pension savings at just 33%.
All pension savers are entitled to tax relief on their contributions which is currently paid at their highest rate of income tax – 40 or 45% for most senior doctors.
When they retire, they pay tax on withdrawals which could be just 20% depending on their personal circumstances.
Patrick Convey, technical director of specialist financial planners Cavendish Medical, warned: ‘While this is a subject often debated before election cam
➱ continued from front page
‘‘The Inland Revenue is not slow – and quite rightly – to take every advantage which is open to it under the taxing statutes for the purpose of depleting the taxpayer’s pocket. And the taxpayer is, in like manner, entitled to be astute to prevent, so far as he honestly
paigns, these latest proposals carry more weight than previously and have been building for some time.
‘Note that NHS doctors currently pay their NHS Pension contributions through gross pay, so receive full tax relief – up to 45% – at source. This will therefore be a considerable change if the proposals go ahead.
‘It is up to the individual to ensure they are making the most of current tax relief opportunities before any detrimental amendments are introduced.’
Mr Webb has long championed a flat rate of tax relief on pensions. He said: ‘I would be very surprised if the next government leaves [higher rate tax relief] alone. They will be looking for money … any chancellor will have to look at this pool of money. I’ve found the idea being increasingly well received, both within and beyond the party.’
His announcement indicates a possible Lib Dem policy on pensions in their election manifesto. Labour has already promised to cut pension tax relief for those earning £150,000 from 45% to 20%.
can, the depletion of his means by the Inland Revenue’’.’
She advised doctors with one of these schemes to contact their promoter for reassurance and keep in regular contact.
Next month: Ten things a promotor may not tell you about Accelerated Tax Payments
Tell us your sTory
share your experience of what has and has not worked in your private practice. even if it’s bad news, let us know and we can spread the word to prevent other independent practitioners falling into the same pitfalls. contact editorial director robin stride at robin@ip-today.co.uk
E-billing on the up
by a staff reporter
A huge growth in the number of private doctors submitting electronic invoices is being reported by private healthcare online solutions company Healthcode.
It is believed last year’s 76% rise – nearly three times the rate in the previous 12 months – has been fuelled by new independent practitioners (NIPS) embracing ebilling and established practices reacting to greater competition by exploring more efficient ways to operate.
Last year, Healthcode revealed that more than 3,700 doctors had
launched a private practice in the previous three years (Independent Practitioner Today, March 2014).
Independent practices are fast catching up with hospitals who were early adopters of e billing with the company. Consultants’ invoices now represent 32% of the total submitted, compared with 22% in 2013 and 12% in 2010.
Total e bill volumes rose nearly 20% last year.
Healthcode managing director Peter Connor said: ‘I’m delighted that independent practitioners are making the leap forward from paper invoices because automating this timeconsuming process
has significant advantages, especially for new businesses.
‘Not only can practices reduce administrative costs but they can also improve their cash flow, as electronic invoices are usually settled faster.’
October 2014 was the most active month for independent practitioners and hospitals, with more than 375,000 bills submitted.
Healthcode said e billing from hospitals grew 5% last year after a slight contraction the previous 12 months. This could reflect an increase in activity levels and provided ‘a reason for optimism’.
royal opening for new fertility clinic
HrH The duchess of cornwall officially opened The Poundbury Fertility clinic at King edward vii’s Hospital in london. it will offer patients a balance of conventional medicine alongside complementary therapies.
led by fertility specialist mr michael dooley, the team includes mr alfred cutner, specialising in advanced laparoscopic gynaecological surgery and mr davor Jurkovic, a leading expert in diagnostic ultrasound scanning.
Hospital chief executive andrew robertson said the unit aimed to be ‘london’s premier fertility centre’. gynaecologist mr michael savvas is leading a new menopause service launched at the clinic last month.
Patients say doctors give satisfaction
As many as 98% of patients are satisfied with the overall experience provided by their doctor, a survey found.
An analysis based on 50,000 interviews by medical revalidation firm Equiniti 360 Clinical covered private and NHS experience, but gave no separate figures for the independent sector.
Founder Jo Parker Swift said: ‘Patients across the UK are hugely positive about their relationships with their doctors.’
Duty to tell if you suspect terrorist act
Doctors have been warned by the MDU of their legal duty to disclose information about patients which might prevent a terrorist act.
Although doctors have a duty of confidentiality, they are legally obliged to tell police if they become aware of information about a patient which they think might be relevant in preventing terrorism.
Independent practitioners are advised to take defence body advice if considering disclosing information.
Free aid to make your own mobile app
Independent Practitioner Today readers are being offered a free 12step guide to writing a mobile app brief for the healthcare industry.
Digital healthcare agency Integrated Change’s 21 page document aims to guide healthcare organisations considering developing a mobile application through the ‘often undervalued’ step of writing the initial brief.
Mobile applications are being increasingly adopted in healthcare to improve services, efficiency, solve problems and meet business goals.
But the firm’s development director Scott Hague said simply launching an app was no guarantee it would be successful nor meet endusers’ needs and expectations.
He said: ‘Developing a mobile application can be a complex task and it’s often a significant investment. If the foundations aren’t correctly set from the beginning, the process can prove unnecessarily costly and timeconsuming.
‘All too often, healthcare organisations forget some of the fundamentals in the planning stages of developing a healthcare app and it’s these omissions that can turn up later in the process and cause problems.
‘Healthcare organisations can save time and money when developing an app by creating a solid brief that every stakeholder can contribute to and shape.’
The Integrated Change guide, from scott@
integratedchange.net, aims to ensure an app:
Has clear objectives;
Meets the audience’s needs;
Is available on the right platform at the right time;
Adheres to any relevant regulation;
Is simple to use;
Is well supported;
Provides data about user interaction that can be used to enhance and improve it later.
What app are you developing for your business and patients? Make sure everyone knows – tell Independent Practitioner Today: by emailing robin@ip-today.co.uk
see page 20
Poundbury consultants Mr Michael Savvas, Mr Alfred Cutner and Mr Michael Dooley with HRH The Duchess of Cornwall
Sports health unit to attract the best
By Leslie Berry
Top sports doctors will be based at a new sports health and science research facility operated by HCA at premier league football champions Manchester City’s Etihad Campus.
The Manchester Institute of Health and Performance (MIHP), the first of its kind in the UK, will be a multidisciplinary diagnostic, education, research and development facility next to the recently opened City Football Academy. It is the result of five years of planning and research by a partnership made up of Manchester City Council, City Football Group and Sport England.
HCA said MIHP will deliver programmes for the local community as well as for elite athletes and will be supported by a team of specialised doctors, sports injury specialists, nurses, physiotherapists and healthcare researchers.
The centre has been designed to deepen collaboration across sports disciplines, enhance physical performance and provide continued sport development programmes for elite athletes and the sports science and health practitioners who support them.
New cancer centre to open in Kent in November
A new Cancer Partners UK diagnostic and treatment centre opening in Kent in November is ‘great news’ for patients, according to consultant clinical oncologist Dr Russell Burcombe.
The centre in King’s Hill, west of Maidstone, will focus on deliver-
Top teams will collaborate with and benefit from MIHP, including Manchester City Football Club, Manchester City Women’s Football Club, British Cycling, GB Disability Swimming and GB Taekwondo – part of an evergrowing group of elite athletes based in East Manchester.
The English Institute of Sport, which provides services to Manchester’s elite athletes, will operate there and other athletes performing at their sports’ highest level will benefit from the cutting-edge research and diagnostic capability of the centre.
MIHP, due to open in early 2016, will also have ‘a clear public
ing early diagnosis and rapid access to treatment for patients with breast, urological and gynaecological conditions.
Asia rivals UK for health tourism
South-east Asia continues to witness a medical tourism boom as governments promote affordable healthcare for visitors, according to an analyst with research firm GlobalData.
Jennifer Ryan said medical tourism, once the preserve of affluent patients, was now a burgeoning industry and big source of revenue.
She said: ‘Numerous websites exist to help patients plan their trips, with information on everything from hospital and hotel stays to restaurant and sight-seeing recommendations, as patients can enjoy a relaxing post-treatment vacation without having to travel any further.’
Malaysia saw over 670,000 patients from abroad in 2012 and predicted this to rise 14.9%.
health agenda’, helping to investigate health and fitness within the general population.
Director Dr Stephen McGregor said it would be a facility for all, aiming to improve people’s wellbeing and lifestyle whatever their sporting levels.
HCA JointVentures chief executive Sarah Fisher said: ‘MIHP is unique and will bring tremendous benefits to the community in East Manchester as well as professional and amateur sports people.’
HCA aims to announce details of more private healthcare initiatives in the North-west over the coming months.
Bid to get health tourists to the UK
Doctors and those with medical tourism business interests are meeting for a summit on 15/16 April at London’s Royal Garden Hotel in Kensington aimed at stimulating the industry’s long-term development. Details at http://summit. imtj.com/book-place.
Organiser Keith Pollard said many were seeking a way to deliver sustainable growth. ‘The philosophy of “if we build it, they will come” has meant that, in some destinations, the supply of healthcare facilities has outstripped the expectations of demand.’
HCA expands medical centre at Sevenoaks
A £1.4m refurbishment and expansion at HCA’s Sevenoaks Medical Centre will bring a host of new services – and make life easier for consultants.
Manager Mikaela Saunders announced a wide range of new services including cardiology, dietetics, ENT, and a one-stop breast clinic.
The orthopaedic and sports medicine services will be expanded with a new gym, avail-
able to patients from other specialties.
A new diagnostic equipment and imaging service will allow patients to be assessed with results on the same day, removing the need for patients to travel to London. And there will be a new picture archiving and communication System (PACS) so any consultant at another HCA unit will have instant access to scans.
An artist’s impression of the new sports research unit in Manchester
Private sector recovery
By a staff reporter
Private healthcare has been given a positive diagnosis in the latest LaingBuisson research into the sector.
The healthcare consultancy’s figures show that revenues generated by independent sector providers in the 12 health and care market segments it monitors as part of its annual Healthcare Market Review exercise stood at £44.3bn in 2013-14 (£40.5bn in 2012-13).
shifted since the Coalition Government came to power, comparing 2014 – or the latest available year – with 2009 as the last full year of the former Labour administration.
Despite continuing rough terrain for independent sector involvement in the UK health and care sectors, growth in these markets outstripped the previous year.
Growth was positive in each of the major market slices which LaingBuisson has reported on in the past year, apart from homecare which saw a small drop.
The main growth driver throughout has been outsourcing of publicly-paid services and, to a lesser extent, a resurgence of privately-paid healthcare as Britain emerges from the recession.
With a general election fast approaching in May, LaingBuisson looked at how markets have
The weighted average share of healthcare markets – totalling more than £100bn a year – which is outsourced from the NHS to independent sector providers for profit and not-forprofit combined rose from 4.8% in 2009 to 7.0% in 2014.
In contrast, the privatepay share of healthcare markets dropped from 5.9% in 2009 to 4.8% in 2014.
LaingBuisson said this was driven by the recession as private demand proved vulnerable to drops in disposable income; for example, in medical insurance, privately-paid elective surgery and private dentistry.
Chief executive and report author William Laing said the sector was ‘on the cusp of a period of renewed opportunities for independent healthcare providers’ as general economic health slowly improved.
Despite ongoing political arguments over the role of private providers in delivering NHS services,
UK IndEPEndEnT HEALTHCArE MArKET VALUE By SUB-SECTOr, UK 2014
Health/Care market
* LaingBuisson figures remain as last year – new research will be available from September 2015. ** of which private GPs earn £550m
and the high-profile breakdown of the Circle/Hinchingbrooke contract, prospects looked ‘reasonably positive’.
These were driven by a broad direction of change towards pluralism in public healthcare markets, stronger self-pay demand
Investment in private care soars, but barriers remain
Private investment into the UK healthcare sector is soaring – with transaction volumes exceeding £4.5bn in 2014, according to research by commercial property and real estate services adviser CBRE.
Director David Batchelor claimed that far more could be done, with £20bn of capital looking for opportunities to invest in the healthcare sector if barriers to investors were removed. He said: ‘It is critical that more progress is made to realise invest-
ment opportunities across the public and independent sectors.
The healthcare sector has experienced years of under-investment and the NHS is creaking under the pressures now being placed upon it due to trends such as an ageing population.
‘A new wave of investment is critical to ensuring the private health sector can evolve to meet the needs of the population, and lessons of the past need to be learnt about how the public sector can engage in a sustainable long-term
manner with the private sector.’
According to CBRE analysis, overseas investors remained the most active in 2014, involved in more than £1.76bn of transactions.
But domestic investors are returning to the market, contributing more than £800m.
This return to UK healthcare was led by institutions Legal & General and M&G and specialist investors Assura and Target Healthcare REIT, who between them invested more than £560m last year.
and a surge in overseas demand for UK based – primarily London – hospitals.
LaingBuisson’s Healthcare Market Review, 27th edition, sponsored by GVA Health Property Advisers, £765. Phone: 020 7923 5396
Protection (PMP) has extended its offering to surgeons after teaming up with Berkshire Hathaway International Insurance Ltd.
Chief executive Juliet Bentley claimed customers would be offered more flexible, longer-lasting coverage at 30-40% below the cost of less comprehensive schemes.
PMP said its policies prevented insurers unilaterally settling a claim without reasonable consent. ‘A traditional UK mal practice policy restricts this right, giving the insurance firm an ability to settle without recourse to an objecting surgeon.’
report author William Laing
Beware fake equipment
By Robin Stride
Independent practitioners are being warned to beware of attempts to pass off counterfeit personal protective equipment (PPE) as the real thing.
PPE fraud is now a major problem in many industries and the healthcare sector is being urged to be vigilant in order to prevent imitation products finding their way into medical practices and hospitals.
One supplier told Independent
Practitioner Today it had seen a rise in the number of counterfeit and inferior PPE products in the UK and believes the healthcare sector is an ‘obvious industry’ for counterfeiters to expand into.
Lee Wright, marketing director at Slingsby, said: ‘Over the last couple of years, it’s been well publicised that cheap, substandard, and even counterfeit PPE is finding its way into the UK.
‘Many of the examples we have seen are very poor quality and fail to offer any real protection, as well
MEDIcAL SEcREtARY PIcKS uP AwARD
as being non-compliant with safety standards. Some products even come with falsified certifications.
‘A lot of inferior products are targeted at the construction industry and include high-visibility clothing, gloves and goggles that fail to meet minimum safety requirements, but as more employers become aware of the problem, the counterfeiters are being forced to expand into other industries.’
At the moment, manufacturers
Dr Rowland Illing, director at Leading Interventional Oncology Network (LION) in Devonshire Street, London, successfully nominated his secretary Manju Sharma for a gong at the British Society of Medical Secretaries and Administrators’ (BSMSA) Private Medical Secretary of the Year awards. She was runner-up, but illness prevented her appearing in the awards picture published in our December/January issue.
Also in the picture are Kathy Perkins of the BSMSA and Kingsley Hollis of the sponsors, management software company Helix Health.
Elderly rejuvenating
Private consultant surgeons are reporting a surge in the number of people aged over 65 having cosmetic surgery in the UK.
Nuffield Health’s first plastic surgery insight survey from 31 hospitals reveals 64% of surgeons reported a rise in older people seeking surgery.
The hospital group’s patient figures paint the same picture, with patients aged over 65 up by 49% in 2014 from 2007.
Eight-two per cent of the surgeons reported more men seeking cosmetic surgery in the form of nose jobs, eyelid lifts and ‘man boob’ removal.
Ninety-five per cent saw a rise in the number of previously overweight or obese patients looking
for surgery after dramatic weight loss.
Mr Ian Whitworth, consultant plastic surgeon at Nuffield Health Bournemouth, said: ‘I’m now seeing many more people in their 60s, 70s and even their 80s seeking plastic surgery, as they not only want to remain fit and healthy into their old age but they want to look well too.
‘I think this trend will continue as this is an expanding age-group.’
Fifteen years ago, surgery on men was ‘very rare’, but now they make up 10-15% of his patients.
Consultants were asked about penis extensions, buttock implants and even a forked tongue. But most patients wanted a natural look.
All surgeons agreed a key motivator for most patients was the desire to improve self-confidence.
wHAt cOSMEtIc SuRgEONS fOuND
95% expect an increase in male patients
82% expect to see more elderly people
Most thought plastic surgery would increasingly become the norm – many view it as the norm already in most parts of the uK
Becoming more commonplace: face transplants, light-weight breast implants and mid face lifts
are solely responsible for checking products comply with performance standards, he said. But a new draft EU PPE directive would close a loophole that enables companies to sell substandard products without being accountable for their quality.
Under the proposals, retailers and distributors of these products would be responsible for ensuring products they sell met required safety standards, which Slingsby believes would help to eradicate counterfeit PPE.
Consultants talk to team with wireless headsets
Consultant physicians and clinical team members at HCA’s London Bridge Hospital are using wireless headsets to improve clinical communications between them.
Quail Digital devices are proving useful in the electrophysiology (EP) labs, where pacemakers, defibrillators, bi-ventricular and resynchronisation therapy devices are also implanted.
The system provides hands-free communications between the treatment lab and monitoring room, which are separated by insulated partitions and glass.
It runs on a high-quality 1.881.90 GHz frequency band, allowing multiple systems to be used in the same area without risk of interference with other medical equipment.
Electrophysiology specialist Neill Townshend said: ‘Excellent audio quality means that all clinicians have a clear understanding of progress within the lab, which significantly boosts performance and safety.
‘The technology has been a worthwhile investment and its use in our EP labs is proving highly beneficial.’
From left: Dr Rowland Illing, Manju Sharma, Kathy Perkins and Kingsley Hollis
Mr Nigel Mercer (right) and the plastic surgeons’ new logo for their campaign to get patients to choose their surgeons with care
range of free guides from some of the UK’s most experienced plastic surgeons.
BAPRAS said many patients did not know that any doctor can say they are a cosmetic surgeon.
By Edie Bourne
Surgeons and clinics are being urged to display their backing for a national initiative aimed at encouraging patients to think more carefully about cosmetic surgery treatments and whom they ask to do it.
They are being asked to ‘proudly display’ a British Association of Plastic, Reconstructive and Aesthetic Surgeons (BAPRAS) campaign logo on their website to show patients they want to help them make safe, informed decisions.
The body wants them to get in touch to discuss how they can intensify the campaign – which has had a big media profile in
recent weeks – and to ensure they are able to follow its professional guidelines.
According to BAPRAS president and consultant plastic surgeon Mr Nigel Mercer, thousands of people are putting themselves at serious risk by rushing in to major procedures recklessly, without consideration for their own safety. He said many people spent more time choosing an electrician than they do a surgeon.
BAPRAS found a quarter of all people having cosmetic surgery in the UK (24%) do not check their surgeon’s credentials, a fifth (21%) are unaware of the risks associated with the procedure and a further fifth (22%) are not even
clear on the potential outcomes of their procedure before going ahead.
With over two million people in the UK considering or already committing to cosmetic surgery in the next year, BAPRAS warned that many may experience longterm damage unless they take a considered and safe approach.
It found 59% of patients undertaking surgery less than two weeks after their first consultation are actually less confident about their appearance afterwards.
The campaign, Think Over Before You Make Over, aims to help anyone considering surgery to ensure the decision is the right one for them, and includes a
Bid to boost safe cosmetic surgery Bridge to enlarge hospital
HCA’s London’s Portland Hospital for Women and Children is to build a stunning new bridge linking it to an adjacent building that will allow it to double the size of its specialist children’s hospital. The iconic bridge will initially enable the opening of three new paediatric floors at 215 Great Portland Street, providing 20 new inpatient beds to make a total of 80 dedicated private paediatric beds. The hospital already has two existing outpatient floors in this building.
This £20m expansion will also provide more extensive paediatric rehabilitation facilities, including therapy suites and the first UK robot-assisted Lokomat walking
therapy system for children with cerebral palsy.
The Portland is the UK’s largest provider of private paediatric care and last year its unique team of 120 senior consultant paediatric subspecialists handled over 50,000 paediatric outpatient appointments.
Chief executive Janene Madden said the expansion was driven by increasing UK and international demand: ‘We are delighted to have been granted planning permission for our link bridge. It marks a milestone in the history of The Portland which is the only private hospital of its kind in the UK.
‘This expansion will help to further enhance London’s growing
reputation as a world-class centre of excellence for complex medicine.’
She said increasing demand for private paediatric care was outstripping the demand for adults. Over the last four years, paediatric patients had risen 80%. ‘We were in danger of running out of space.’
Women’s services will be expanded too. The Portland treats all paediatric medical conditions except cancer and cardiac cases, which are referred to nearby sister hospital The Harley Street Clinic.
It has the most modern diagnostic, treatment and surgical facilities supported by a paediatric intensive care and neonatology unit for babies and children up to the age of 16. Its neonatal and
It advises patients to choose surgery based on professional skills, but says half of all cosmetic surgery patients say keeping costs down is a major consideration. Twenty-seven per cent are unaware if any aftercare is available should something go wrong.
BAPRAS said: ‘These problems are frequently associated with patients travelling overseas for cosmetic surgery, but are also widespread among patients in the UK.’
It found 51% of patients felt marketing from clinics made them more likely to consider a treatment than they would have otherwise.
BAPRAS is working with the Royal College of Surgeons’ Cosmetic Surgery Interspecialty Committee (CSIC) to advance recommendations that will ensure all cosmetic surgeons, whether from a plastic surgery background or not, can prove high standards of training in the areas they are practising.
But as these recommendations are not yet in place, it is telling the public to use the GMC Specialist Register as the safest approach to choosing a surgeon.
paediatric specialists carry out the most complex surgical procedures and, uniquely, The Portland has its own specialist neuro-rehabilitation unit.
The new bridge was designed by William Matthews, the project lead for Renzo Piano who designed The Shard at London Bridge.
AccoUnTAnT’s clinic
Make sure expenses don’t get expensive
Don’t cut corners with your expense claims – you could end up paying a lot more if you don’t make acceptable submissions to the the taxman. Susan Hutter (right) gives a timely reminder for the new tax year
One Of the benefits of running your own business or being a sole trader is that you can reduce some of your tax bill by claiming certain business expenses.
However, remember this is not a meal ticket to spend freely and claim personal expenses too.
As you can imagine, HM Revenue and Customs (HMRC) is very wise to any untoward activity and has the right to investigate if it feels your claim does not ‘add up’.
Motor expenses
The HMRC takes a particularly dim view of business owners that estimate their motor expenses. It is not currently acceptable to claim motor expenses from your home to place of work.
You can, however, claim motor expenses from a private hospital to another separate office.
The easiest and accepted way to claim is by calculating your vehicle mileage – you are allowed 45p a mile for the first 10,000 business miles and thereafter 25p a mile.
You should also be prepared to keep a detailed log of your business mileage and the reason for your business journeys.
This way, the HMRC is more likely to accept the claim if you do find you have to drive between two conferences in one week from Lands end to John O’Groats.
Subscriptions to journals and all training can be claimed against tax
other travelling expenses
Lots of consultants in private practice will find themselves travelling to training events and conferences both in the UK and abroad.
The good news is that all business-related expenses, including travel, accommodation and sustenance are tax-deductible. But, if you take a spouse, then you cannot claim expenses for them.
Should you wish to combine a business trip with a holiday, then you must be reasonable about where the division starts. Let us say you are away for ten days, and five days are business-related ones, then you will be allowed expenses for this period.
Use of home as an office
Many doctors use a room in their home to write reports and do other administrative work. As long as this room is used for business, you can claim the proportion of the room as part of the overall home and factor in items such as mortgage interest and utility bills.
But note that if the room is not used exclusively for business, then the claim should be reduced.
clothing
You cannot claim for a designer suit or dress, even if you like looking smart for work. But, you can claim for any protective clothing.
salaries
If your spouse or children work for you on a regular/semi-regular basis – such as performing bookkeeping or IT maintenance – then you are allowed to claim for their salaries.
However, be sure that the salary you pay them is commensurate with the level and hours of work they perform. Paying your spouse £20K for dropping off the accounts once a year will not be viewed as acceptable by the HMRC.
Miscellaneous
finally, there are still many items you can claim legitimately –expenses are not always a draconian affair.
Items such as computers and other IT-related expenses for the business, journals and other subscriptions, professional indemnity cover and all training can be submitted against tax.
Remember to keep all receipts as welll as all you back-up documentation.
As with all business accounts, you should keep all the records for at least six years, although best practice is seven to be on the safe side.
Susan Hutter is a specialist accountant for the medical profession at Shelley Stock Hutter LLP
You just would not
An investigation has highlighted huge disparities in UK credit agencies’ ratings which, warn accountants, is hampering growth for Britain’s small and medium-sized enterprises. Could your business be affected? Leslie Berry reports
HundrEdS of thousands of uK businesses daily rely on credit rating agencies to secure sufficient credit ratings and limits that will allow them to finance and grow their business.
Getting the correct limit or rating in this economic environment is crucial, as companies have to prove their viability to investors, suppliers and the banks.
Many businesses also rely heavily on credit ratings to decide whether and on what scale to transact business with other companies.
But a recent investigation carried out by accountants and business advisers Shelley Stock Hutter (SSH) showed up widely different credit ratings and credit limits recommended for the same businesses.
The firm, which carried out an analysis of 100 private companies’ credit reports in december 2014,
found dun and Bradstreet (d&B), Experian and Creditsafe recommend vastly different credit limits for the same businesses.
And the difference between the highest and lowest average rating of the three agencies for the 100 companies was 150%.
dramatic differences
The latest investigation follows on from previous research carried out by the accountants on the same 100 firms during november 2011.
Excerpts from the d ecember 2014 investigation include:
Company 1 had three credit limits which ranged from £1.5m to £4.9m;
Company 76 ranged from 0 to £18k with a rating of 4/100 to 83/100;
Company 6: the limits between 2011 and 2014 by two agencies were reduced, while one increased
creditometer
WHat can affect your Business rating?
changes in accounting reference date
changes in officers of the company
moving registered office
the level of net assets on the balance sheet
the number of finance providers, statutory arrears and county court judgments
theirs dramatically despite all relying on the same information.
Bobby Lane, a partner at SSH who oversaw both investigations, comments: ‘Three years on and still there is no change.
‘We raised a warning signal back
in november 2011 and had hoped that the credit rating agencies would work together to provide greater transparency and put an end to these inconsistent credit ratings.
‘The latest findings clearly show that hundreds of thousands – and possibly millions of businesses –are still at risk of what continues to be the credit rating lottery.
‘Every government has continually referred to u K small to medium-sized enterprises (SME) as the lifeblood of the economy; however, these huge variations can seriously jeopardise their ability to trade.
‘on the one hand, an incorrect rating will affect their ability to gain credit from suppliers and raise finance.
‘In addition, it could deter companies from growing by avoiding trading or offering terms to pot-
credit it
ential customers that are creditworthy. If a business trades with a customer on the basis of an incorrect rating and it goes wrong, there could be potentially catastrophic consequences.
different methods
‘Many small businesses are unaware that credit agencies use different methods to decide on ratings and limits. But it is not all their fault. The calculations are based on publicly available information such as abbreviated accounts, which give little information.
‘The more information that is available in the public domain, the more information there is to make an assessment. So to improve their chances of a correct rating, businesses should not be afraid to provide more detailed information.’ His firm, which has a portfolio
of private doctor clients, is urging any SME concerned about its credit rating to approach credit agencies with explanations of the issues affecting their business and the trends in their numbers.
Then, it says, the credit agencies can gain a much better under standing of the position of their business and give a fairer result.
SSH believes businesses must also be aware of the lottery and assess the effect on their business of the relationship and use these limits and ratings as part of a more detailed ‘due diligence’ exercise on their customers.
Mr Lane argues that credit agen cies must be prepared to show how they arrive at their recom mendations and he wants to see guidelines drawn up to show the factors that could affect a busi ness’s rating.
impLications of inconsistent ratings
ssH partner Bobby Lane (right) told independent practitioner today: ‘the results of our research have serious implications for businesses and professionals across all sectors.
‘for those practitioners who extend credit to corporate clients or patients, relying solely on a credit rating or limit provided by one of the agencies could have significant and possible catastrophic implications should that rating or limit be incorrect.
‘furthermore, it could restrict a practice from taking on new patients.
‘of more concern is the ratings or limits being supplied by agencies on practices. most wrongly assume that this will have no effect on them.
‘if you are looking to expand, refinance or lease new equipment, then a bank will be obtaining a limit or rating on your practice. if they go to an agency that has given you a bad limit, you may well be declined the finance needed to grow the practice.
‘also, your suppliers from medical suppliers to your landlord may well obtain a limit or rating on your practice before extending you credit. if they get a bad result, they could well refuse to provide any credit terms. this will have huge implications for the cash flow of the practice.
‘the key is to ensure you know what the agencies are saying about your practice. Do your research.
‘if you do not like what you see, then do something about it and approach the relevant agency with more information to enable them to provide the correct result that will help you to not only manage the practice’s finance but potentially unblock any barriers to financing its growth.’
Talking centre
Forum theatre is proving a useful tool to help independent practitioners improve their communication skills. Actor
Richard Matthews shows how
Doctors who are effective communicators will always have a head start in independent practice: from winning the confidence of patients and colleagues, to asserting themselves with colleagues when required.
At the same time, poor communication is such a common factor in complaints and workplace disputes that practice owners are effectively sabotaging their business if they do not prioritise interpersonal skills when recruiting or promoting front-line staff.
But it is not just about hiring smooth talkers.
Even the most articulate employees can struggle in a confrontation with an angry or distressed patient, perhaps because the other person’s reaction is unexpected.
And, occasionally, practitioners’ body language and tone of voice let them down.
In short, it is one thing to know the principles of effective communication but applying them in
It is one thing to know the principles of effective communication but applying them in reallife situations can be more challenging
real-life situations can be more challenging.
Rehearsal time
the best communication training therefore includes opportunities for participants to put what they have learned to the test. traditionally, this has been done through role-play exercises. this approach has much to recommend it – it is quite straightforward, quick to organise and participants can receive useful feedback from their peers. But it does have some drawbacks. role-plays can make people feel cripplingly self-conscious and they rarely feel realistic to observers because those taking part know each other and are familiar to the audience. this means the learning points can be missed.
But here I want to look at another interactive training technique which engages participants through their imagination.
Unlike role-plays, forum theatre brings scenarios to life by using
professional actors to perform, challenge audiences and facilitate audience participation.
Forum theatre brings scenarios to life by using professional actors to perform, challenge audiences and facilitate audience participation
From conducting an employee’s performance review to giving bad news to a patient, the technique can be used to explore, in a more credible way, a range of sensitive situations that might arise in independent practice.
scene setting
Forum theatre is not new. It emerged in the 70s and 80s from the work of renowned Brazilian theatre director, Augusto Boal. Boal was a political figure who sought to break down social barriers by encouraging audiences to get actively involved with his productions.
In a 1997 article about his work,1 Boal explained his philosophy: ‘ we aren’t content, any of us, to be just actors and spectators we also want to write our own scripts for every scene we are involved in. we are in charge of the wardrobe… we are also the
directors who stage our own actions.’
And he recalled how he and his colleagues devised Forum theatre in Peru as part of a literacy programme: ‘It was here we first came up with a play in which the main character didn’t know what he was supposed to do or else made wrong or unsuitable decisions. so I asked the audience what they would have done instead.’
Forum theatre has caught on as a way to engage new audiences with the dramatic arts, but the interactive format has also become popular with businesses as a learning and development tool for staff. Indeed, type the words ‘forum theatre’ and ‘business’ into Google’s search engine and you will get over 40m results.
the next act
In recent years, the healthcare sector has also begun to appreciate the potential of forum theatre. Notably, the technique has been used on a number of occasions by the GMc, both as an educational tool for healthcare professionals and to spark debate.
In 2008, for example, the GMc collaborated with the r oyal National theatre, Alzheimer’s society and other patient groups in a series of forum theatre events around the country. t hese were intended to generate discussion with patients in the early stages of dementia, and with carers and doctors about how best to reach treatment decisions. this process was used to inform the GM c ’s 2008 Consent Guidance 2 the council’s Learning Disabilities website3 currently features a specially commissioned play about a patient with Down’s syndrome, and the problems that she
faces when trying to access appropriate healthcare.
t his play was performed in a UK tour of forum theatre events during 2010 to an invited audience of doctors, people with learning disabilities and their carers. Each performance was followed by a discussion exploring how a change in the doctor’s behaviour could affect the outcome, and audience members were encouraged to step onto the stage.
And, in 2013, the GM c commissioned a forum theatre element to its Welcome to UK Practice
Pilots, 4 an induction programme for doctors new to UK practice about the ethical and professional standards they were expected to meet.
In this instance, the plays about dementia and domestic violence covered ‘the themes of teamwork, communication, consent, respect for patients and ensuring equal access to care’.
Forum theatre techniques are also being used to train the doctors and healthcare professionals of tomorrow.
For example, a presentation on the use of forum theatre at s outhampton University was included in an Educating for Excellent care workshop5 organised by the c ouncil of Deans of ➱ p14
health in 2014, which showcased examples of innovation in health higher education.
stage directions
My company, Pitch to Perfection, has been providing forum theatre training for corporate clients for the last two-and-a-half years, alongside my acting work.
In the last year, we have been working with Dr Mike r oddis ( right ), of MJ r oddis Associates, to deliver sessions in healthcare settings, usually as part of a more extensive professional development course. the process usually works like this:
Verbal briefing – Mike and I discuss the type of organisation and its communication needs.
Draft scenario and script – I work up a short scenario in collaboration with Mike and review this with the client. In most cases, there will be a script for the actors to work with, but sometimes the session is wholly improvised. the most important requirement is that the scene will be familiar to practice employees; for example, explaining to a patient that a procedure has not gone to plan.
Casting – to keep costs to a minimum, the cast is very small. I tend to use actors that I know well and have some experience of the process because they need to be able to adjust to performing in different environments and relate to people in different professions. It is also important the actors can listen, involve the audience and respond to suggestions – this is not the place for ‘method-actor’ debates about character motivation.
Staging – t he simplicity of forum theatre is part of its attraction. Very little preparation is required; the action takes place at clients’ workplaces and the actors do not need a real stage – just a table and chairs, at most. t he audience can be as small as four or as large as the space allows. the most important thing is their willingness to get involved.
The simplicity of forum theatre is part of its attraction. Very little preparation is required
Performance(s) – Before the action begins, I will set the scene for the audience and explain that their role is to watch what happens and think about what the lead character does well in terms of his/her communication and the mistakes he or she makes. the scene is played once so everyone can form an opinion about what happens and why.
Audience participation – once the scene has been performed, we encourage the audience to get involved, point out mistakes and suggest ways the outcome might be improved with a different approach, sometimes working in groups to devise the alternative dialogue for a critical moment. s ome audience members are prepared to take on the role of the protagonist themselves to demonstrate how it should be done. An important element of audience participation is analysing what the character says, as well as non-verbal communication such as the way the character makes their entrance, facial expressions, tone of voice and other nuances. It is also essential that the actors in the scene are asked how they have been made to feel, both the original version of the scene, and in the subsequent versions changed by the audience (see below).
this helps raise the audience’s awareness of the effect that different approaches to communication can have.
Encore – these suggestions are used when the scenes are replayed to see how a change of approach can influence the outcome and which is most effective.
we might replay the scene two or three times, depending on the level of participation. By the end of the session – which typically lasts up to 1.5 hours – the audience and actors have usually reached a consensus about the most appropriate and effective way to communicate in that scenario.
Feedback – As with any training, we always ask people to complete evaluation forms following forum theatre sessions. to date, I’ve been delighted by the enthusiastic response from participants.
Forum theatre draws the audience in and helps them focus on the unfolding drama and their response to it
Epilogue
the use of professional actors and realistic situations is key to the potential of forum theatre as a useful and cost-effective training technique in independent healthcare. As its creator intended, it is a process which breaks down barriers and promotes better understanding.
Forum theatre draws the audience in and helps them focus on the unfolding drama and their response to it – rather than worrying whether they are making a fool of themselves in front of their boss. But it also means participants can be challenged by people with a different perspective, rather than fall back on lazy assumptions; for example, a patient is being difficult or unreasonable if they do not accept what the doctor is telling them. today’s independent practitioners appreciate the importance of communication within a successful practice. Forum theatre is a very powerful tool to demonstrate what this means in reality.
References
1. The theatre of the oppressed, Augusto Boal, The Unesco Courier, November 1997. http://unesdoc.unesco.org/ images/0010/001095/109538eo.pdf
2. Work of the Standards and Ethics Committee 2006-2007, GMC Council paper, 5 December 2007. www.gmc-uk. org/10___Work_of_the_Standards_ and_Ethics_Committee_2006_2007. pdf_25399368.pdf
4. Welcome to UK Practice piloting, paper for GMC’s Strategy and Policy Board, 16 May 2013. www.gmc-uk.org/07___ Welcome_to_UK_Practice_piloting. pdf_56266425.pdf
5. Educating for Excellent Care workshop, Council of Deans of Health, 19 February 2014. www.councilofdeans.org.uk/ 2014/02/educating-for-excellent-careworkshop-27-january-2014/
Richard Matthews (right) worked in the corporate world before becoming a professional actor and forum theatre practitioner. His company, Pitch to Perfection, provides forum theatre sessions for MJ Roddis Associates
is continuously updated based on the latest medical research to bring you current evidence-based recommendations.
Our unparalleled team of physicians and editors places new research in the context of the existing body of medical knowledge using their professional expertise and first-hand clinical experience.
This combination of Evidence & Experience is invaluable in crafting point-of-care recommendations trusted by more than 850,000 clinicians worldwide.
To learn more or to subscribe risk-free, visit learn.uptodate.com/EXPERIENCE or call +1-800-998-6374 | +1-781-392-2000.
TRAining sURgEons AbRoAd
Surgeons’ mission faces a hard graft
A life-saving charity has been officially launched with the mission to twin every British plastic surgery unit with one in a developing country. Tingy Simoes reports
Set up by consultant plastic surgeon Miss Barbara Jemec, BFIRSt – the British Foundation for International Reconstructive Surgery and training (www.bfirst.org.uk) – has already sent uK surgeons to Cambodia.
It is planning to work with other countries such as Myanmar and Bangladesh to deliver training and surgical skills to local medics, ensuring that everyone has access to expert surgical care. With deformities and traumatic injuries often resulting in social exclusion, poverty and destitution, BFIRSt not only trains surgeons on location, but also ensures that the training has practical longevity and is tailored according to the resources available. this means that each country will have a unique package that best fits their needs and available resources.
t he charity, launched at the British Association of p lastic, Reconstruc tive and Aesthetic Surgeons’ (BApRAS) Winter Scientific Meeting at the Royal College of Surgeons of england, recognises that the benefits of such a drive are mutual, with uKbased surgeons also learning valuable skills while at the location.
Londonbased plastic and reconstructive surgeon Mr Greg O’toole was supported by BFIRS t on a recent trip to Cambodia.
He says: ‘BFIRSt supported my trip to the Children’s Surgical Centre in p hnom p enh, which offers free care to Cambodians. We treated many patients with injury
to the brachial plexus – the spaghetti junction of nerves in the neck that supply the arm and hand.
‘ t hese injuries are often the result of a moped accident, as the rider lands awkwardly and stretches the nerves beyond breaking point. Operations included nerve grafts and tendon transfer procedures.’
severe burns
Mr O’toole added: ‘We also saw several children with severe burns. Much of life in rural communities has not changed in centuries, with reliance on fire for food and warmth.’
‘toddlers are drawn to the flames with inevitable consequences; their hands grasp red hot embers, which melt fingers together and all are then lost in a ball of scar.
‘ to be able to use their hands again gives these vulnerable children the chance to return to their lives and their schools and one day to plough the fields, harvest the rice and support families of their own.’
t he training means that local clinicians become equipped to treat a wide range of conditions, such as cleft lip and palate, lifealtering burns, congenital deformities and injuries, which may otherwise result in abandonment in the case of babies and children, or marginalisation and loss of work in the case of adults.
Ranging from simple surgical techniques to more complex procedures, training will give surgeons the skills that are taken for
granted in First World countries. the educational programme is handson, facetoface tutoring in the local environment, treating reconstructive problems using local resources.
BFIRSt’s training packages also incorporate training for surgeons’ staff, such as nurses and therapists, enabling the medical and surgical team to provide holistic care for all patients. the charity is currently training a number of surgeons abroad, including three in Cambodia.
Chairman of BFIRSt Miss Jemec says: ‘BFIRSt equips surgeons with an array of key skills, allowing them to offer lifesaving – and livelihoodsaving – care. the vision for BFIRSt is to provide surgeons in developing countries the skill set they require to continue using the techniques they have learned via our tailored training packages.
‘Our longterm vision is to have
most of the u K plastic surgery units twinned with a unit abroad, forging long term friendships, collaboration and support. BFIRS t ’s mission is to release some of the world’s most vulnerable adults and children from the poverty, destitution and marginalisation caused by deformity, disability and disfigurement.
‘We are incredibly proud to being on the road to achieving this with the official launch of our charity.’
In three trips to Cambodia alone, BFIRSt surgeons working alongside local teams treated over 45 hand surgery cases including burns and trauma, congenital deformities, tumours and snake bites.
Greg O’toole adds: ‘During my time in Cambodia with BFirst, I was also able to treat children with birth defects such as microtia – being born without one or both ears.
Amazing initiative
‘the expertise for this type of surgery was unavailable in p hnom p enh and so my visit was also a good opportunity to teach the principles of the techniques involved to local surgeons.
‘I feel privileged to have been able to offer help and training. BFIRS t is an amazing initiative which has, and will continue to, save the lives of many.’
BFIRSt has also funded fellowships, which involve surgeons from resourcepoor countries visiting uK plastic surgery centres, where they are taught relevant surgical skills.
Plastic and hand surgeon Miss barbara Jemec, who works at The Wellington Hospital, london
One such surgeon is Dr Rashedul Islam, who came to the u K in 2013 through BFIRS t. Dr Islam, a plastic surgeon from Bangladesh, stayed for six weeks to train.
the skills he learned while on location were not limited to surgical techniques. He also took away with him knowledge of the daytoday running of a uKbased surgical unit.
Dr Islam says: ‘I am very thankful for the opportunity BFIRSt has given me, which allowed me to visit a plastic surgery unit in the u K and have a closer view as to how the system works.
‘I was very impressed with the unit, the consultant and staff. thanks to the amazing training I received, since returning to Bangladesh I have been able to carry out more operations and procedures than before, which have benefited many patients. I would like to thank all those
involved in the process right from the beginning. I am so grateful for having been given this unique, and very positive, experience.’
Unable to walk
British surgeons have already operated on many injured or disfigured people around the world in similar missions to BFIRS t ’s, such as treating a twoyearold in rural Ghana who had suffered burns to his leg, resulting in scar tissue so severe that he became progressively unable to walk.
Visiting u K plastic surgeons were able to release the scar tissue, giving him the ability to walk again, also training the local team in this technique.
In uganda, the whole of a teen’s scalp had been burnt off, meaning his skull was visible and exposed.
using an operating microscope, muscle from his back was detached and placed on his skull.
AbouT bFIRST
ReconSTRucTIng lIveS. RebuIldIng FuTuReS.
bFIRST is a uK registered charity which trains surgeons working in the poorest countries in the world to enable them to undertake reconstructive plastic surgery, releasing children and adults from the state of poverty and destitution associated with disability and deformity.
The vision is of a world in which reconstructive plastic surgeons, hospital and nursing staff and related professionals in poorer countries receive the necessary training and supplies to enable them to perform reconstructive surgery and rehabilitate patients.
bFIRST was established to bring the fantastic, individual efforts of many surgeons together into a coherent whole. This unified approach enables them to attract diverse funding for new initiatives to meet the enormous unmet needs of this often forgotten group of patients.
british Foundation for International Reconstructive Surgery and Training www.bfirst.org.uk
He was the first patient in the unit – and probably the entire country – to undergo microsurgery.
BFIRS t relies on donations to continue with its mission.
Suggested amounts range from just £40, which can pay for gloves,
antiseptic cleaning solution and dressings for 15 patients, to £850, which can pay for a week’s plastic surgery training for a local doctor.
Donations can be made on the BFIRST website at https:// mydonate.bt.com/charities/bfirst
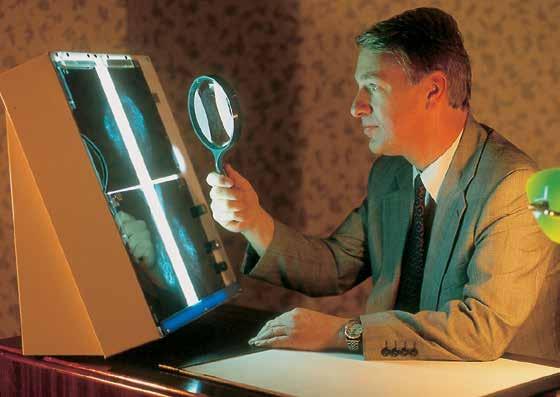
Picturing a way to make big savings
Consultants at 108 Medical Chambers, Harley Street, have saved themselves £55k by developing their own upgrade of a picture archive and communication system (PACS) in house. Hamish Millar shares how they did it
108 Medical chaMbers is an independent diagnostic and imaging centre within the heart of harley street.
as with most independent centres, we found the cost was historically a restriction to gaining access to hospital Pacs systems. Patients often also wanted their films in hard copy to show other doctors who did not have access to digital readers – although all had access to a lightbox.
but, as time went by, it became more complex, and costly, to set up the various imaging devices to talk to printers.
We found the reduced supply of
Xray film and increasing use of cdrOMs being brought to clinic by patients from other centres, meant that we had to explore new ways of producing and storing our own data.
cloud solution
We knew we needed a solution to be able to consolidate our studies both for internal purposes and increasingly for external access and reporting by our doctors or others. s o we looked at a Pacs ‘cloud’ solution.
This seemed to fulfil quite a lot of our needs – especially regarding external access, as all the data is
stored on external computers linked through the internet.
b ut it soon became apparent that the large number and size of the studies meant the costs of this started to increase incrementally. a different solution was required.
We met with a number of established Pacs providers, but they were still wanting us to pay in excess of sixfigure sums – including unrecoverable VaT – plus significant annual licensing fees. if this was to be our only option, then so be it, we thought. but, to explore further, we put a small team together including our director of radiology dr William
Teh, consultant surgeon and medical advisory committee chairman Mr s imon Marsh, head radiographer sally bucklitsch and our i T network management company 247it ltd, which had managed our network for many years.
Amalgamating archives research and networking identified a wellrespected and affordable open source Pacs solution called c lear c anvas. i t is used extensively in canada. Our i T company worked with all the relevant people internally and set up a demonstration which we all played with and liked.
Traditional method: radiologists and surgeons place the X-ray films on a lightbox to examine mammographies
247it also enabled connectivity to all our existing equipment and came up with a strategy to amalgamate all our existing archive studies from the past two years.
h appily, within two months, we had a facility available to all the consultants on their desktop.
i t allowed them to see all the imaging for a patient both historically and across the range of imaging that we offer, from mammography to ultrasound and original computed radiography Xray imaging.
We are also able to take studies from patients off cd s that were taken elsewhere and import them directly into Pacs, so the consultants are able to see these instantly.
Large saving
a nd we can also export any imaging from a patient that we have done, of any type, directly to a cd so they can take it away if they require.
We are enjoying a large cost and administrative saving, although film is still used occasionally when patients are going to certain theatres, for example.
The reporting doctors and consultants are also able to access images remotely because part of the P acs system includes a webbased retrieval and viewing facility.
We are lucky enough to be in a geographical area with a highspeed fibre connection. This means access to the entire system, including archives, is available to external consultants.
The system was specified to cater for the next three years’ worth of imaging requirements as well as the two years of archive –more than 16T b of storage on some impressive highspeed network attached storage (N as ) devices using raid (redundant array of independent disks), a way of storing the same data in different places on multiple hard disks. a rchiving and back up facilities have been added to make it robust.
There is also the potential to transfer studies to other systems, although we have not really used this aspect yet.
The icing on the cake was that our i T company managed to source some reasonably priced Ultra 4k 28” monitors. These are high enough resolution to use as review and diagnostic screens and they cost us a fraction of the price for conventional diagnostic viewing equipment.
so what did it cost? at £45,000 it is less than half the price of many quoted systems, and that included all the work of transferring the systems and consolidation of all the imaging.
The solution has worked brilliantly for us.
For more information, email Hamish Millar at hamish@ 108harleystreet.co.uk or Adrian Hutchin at adrian@24-7-it.co.uk if you would like to discuss this as a solution to your PACS requirements
Hamish Millar is managing director at 108 Medical Chambers, Harley St
Premium Medical Protection provide bespoke Medical Professional indemnity insurance and aims to achieve up to 30% premium reduction..... and provide unique and comprehensive cover including:
Consent to Settle
Inde nite Run O into retirement
(Subject to Terms & Conditions)
Up to £10m liability
AA+ rated insurer
(Source: Standard & Poor’s ratings 2013)
Clyde & Co lawyers, Medical Malpractice specialists
* Subject to acceptance
The computer system’s monitors allow doctors to view all types of scans
Is mobile technology benefiting your private hospital or practice and its patients as much as it should? Scott Hague outlines some exciting possibilities that could improve quality for all
Going mobile
The modern-day smartphone is as powerful as some of the computers that graced our homes in the not-too-distant past. and the common perception that ‘everyone has one’ isn’t too far from being accurate.
a ccording to Google’s ‘ o ur m obile Planet’, in 2011, 30% of the UK population owned a smartphone. By 2012, it was 51%. In 2013, that reached 62%.
Kantar data put that number at 71% in 2014 and went a step further to forecast that well over 80% of the UK population will have a smartphone by the end of this year.
We overtook the US for smartphone penetration over two years ago.
The UK population has accepted and embraced mobile technology and, more to the point, adopts a very future-thinking approach to it.
There’s no resistance when a new phone with smarter functionality comes out. you only have to look at the queues outside a pple stores up and down the country on device launch day to see that.
Far from resisting mobile device progress, the British public yearns for it. a nd the rate at which
progress is happening in mobiles is phenomenal. In some sectors, three-quarters of all traffic to a website comes from a smartphone or tablet device. and it is growing. yet, in spite of this, the healthcare sector has not taken advantage of the technology in the same way as, say, the retail sector has.
nhs lagging behind
It is perhaps unsurprising that the nhS is, at present, failing to keep up with its patients. a study we conducted at Integrated Change found that the nhS experienced a 118% increase in mobile traffic to its websites over a 12-month period.
yet fewer than half of these sites are optimised for the mobile user. despite these figures, we have dealt with teams within the nhS who have some creative, innovative ideas using mobile technology that would indeed offer patient benefits.
h owever, turning them into a reality can be, at times, hindered
by the nature of the public sector.
But the private sector is also, in many ways, missing the opportunity to use mobile technology to enhance the experience for the patient and to increase operating efficiency as well.
In this and an article next month, I intend to elaborate on some of the potential opportunities for private healthcare starting here with some example uses for mobile apps and moving on in the second part to discuss mobile web opportunities.
Mobile apps and your patients
nobody knows your patients like you do. you know their demographics, healthcare challenges and motivators in depth.
But our experience suggests that some private healthcare providers have something of a blind spot when it comes to understanding their patients from a digital perspective.
This means understanding:
What devices they have;
DOSAGE REQUIRED
What they use them for;
Where they use them and why.
healthcare providers can make accessing information more straightforward by adopting mobile technology.
o ur d ecember 2014 study included interviews with 100 private orthopaedic patients aged between 15 and 65. almost half of the patients we interviewed stated they would like to make, amend and cancel appointments using a mobile app.
not only is this something that would be highly efficient for the patient, but it is one potential use that could offer clear administrative efficiencies for the hospitals as well.
I am by no means medically trained. But over the years, I have worked with a number of healthcare providers and believe mobile technologies could alleviate some of the challenges and frustrations that exist.
ExAMplEs oF soME oThER
poTEnTiAl UsEs oF Apps inpatient care
By loaning your patients iPads or other tablet devices, you could feasibly:
enable patients to access entertainment (TV and radio apps already exist).
develop an app to allow your patients to:
❍ order their meals;
❍ Be reminded about medication they should be taking;
❍ Complete questionnaires and authorisation documents relevant to the stage they are at during care;
❍ Pay for their care;
❍ access information relating to their stay in the hospital, such as upcoming milestones or visits from the consultant;
❍ Get them to tell you their comfort levels – such as pain or nausea.
Sign up to avoid miSSing an iSSue
Dear Reader,
Subscribing to Independent Practitioner Today is the only way you can be sure you will see every issue. Don’t risk missing out. Our personal subscription for doctors and managers is only £85 a year and £200 for organisations. But you can cut this to just £70 and £175 respectively if you pay by direct debit.
So take advantage of this offer now for our unique business magazine dedicated to supporting you in your private practice. We’re confident your subscription will repay itself many times over!
Editorial director
Doctors, please give GMC No. (See rates listed above)
Please debit my Mastercard/Visa/ Amex/Diners Card No
Expiry
indicates this item must be filled
Instructions to your Bank or Building Society to pay Direct Debits
Society
Banks and Building Societies may not accept direct debit instructions for some types of account Signature(s)
Name and full address of your bank/Building Society Banks and Building Societies may not accept Direct Debit instructions for some types of account To: The Manager
post your application (no postage required – UK only) to: independent practitioner today Subscriptions department, FreepoSt, po Box 36, plymouth, pL1 1Br
subscribe online at www.independent-practitioner-today.co.uk if you
Provide patients with access to Facetime, Skype and other video communication applications to assist them in keeping in touch with friends and family. you could even link up the consultant to provide the patient with remote advice or care (see feature on page 36).
a nd consider the possibilities for outpatient care too. you could be connected to patients once they are released from hospital and enable them to access information about their aftercare, to supply information to doctors and nurses and make follow-up appointments.
And for hospital medical staff
develop an app that allows a ward manager to:
❍ r eceive notifications about test results for patients;
❍ receive feedback on patient satisfaction on the level of care –while the patient is still there and there’s something that can be done about it;
❍ Complete ward rounds without paper.
It is not just the patients and medical professionals who can benefit. administrative efficiencies can by achieved by streamlining estate management, managing staff training and supplying staff with rotas.
or you could provide a one-stop employee app that gives workers tube and train times, updates on the business, connects them to affiliated third-party companies, displays their benefits or holidays remaining and so much more. all can be achieved through mobile technology.
That is just today. With wearable technology just getting started and a big launch in the form of apple Watch due soon, integrating mobiles could become even less invasive in the very near future.
Think about monitoring patients once they have left care, helping them through rehab, setting them goals and enabling two-way communication between their physio or physician. The possibilities are endless.
integrating mobile in private healthcare
of course, it is easy for me to say all this is possible. But implemen-
tation of such ideas is not an easy task. So where do you, as a private healthcare provider, even start? my own experience of providing mobile consultancy, and then development and implementation in a private healthcare setting, has taught me that the most effective approach includes these steps:
1
Talk to your staff across all departments and find out what their frustrations and challenges are.
What is taking them longer than it should? What makes their day more difficult? how do they think their job could be made more efficient and how do they think your hospital or clinic could provide a better environment or better care for its patients? Survey staff and assess the responses in detail.
2
Talk to your patients. Find out what you can do to improve things from their perspective. Take the opportunity to get to know them digitally. Which devices do they use regularly? What do they do on those devices? What would they like to be able to do or access in relation to their care on their devices? Why not place a tablet device with a simple survey installed,
place it in waiting rooms and prompt patients for their views or suggestions? It does not have to be complex.
From this, identify a number of problems you would like to solve through mobile technology. Get to truly know what the problems are inside out.
3
Speak to IT! Find out what is feasible with your existing systems and where the challenges of adopting mobile might lie. IT should not lead the project. But their buy-in and experience will be essential, as with all other stakeholders, in ensuring any project or change can be implemented efficiently.
4
Get a complete project spec together. Consider which platforms you would want to develop any mobile apps on. Consider how patients will access the apps.
Will you loan them devices or will they access on their own? If it is the latter, you need to research your patients and find out what devices they are using. you will need to work closely with IT or your mobile project developer here, ensuring you have a tight brief and clear idea of how the project will go.
5 Keep on developing and improving. When you launch your first version of it, you have the opportunity to get feedback and improve on the feedback. a nd it’s key to be flexible enough to be prepared to make future alterations and changes based on new technologies and shifts in the mobile space.
6
Track usage. Use analytics to track what patients and staff are doing on your app, how they’re interacting and so on. This data could be incredibly valuable in ensuring your use of mobile stays ahead of your patient and staff expectations mobile is far from new. But the pace of change remains remarkable and the adoption figures are astounding.
By getting to understand your staff and patients’ challenges, by starting small and testing and by really getting to grips with what your organisation’s biggest problems are, mobile can become the vehicle to power the solution.
Scott Hague (below) is development director and owner of Integrated Change, a digital healthcare agency which develop mobile apps, medical websites and online marketing strategies specifically for healthcare
A sURgEon on A mission
Generous inventor
He has an eye for business and a business for eyes, but Mr Bobby Qureshi (pictured, right) wants to use the proceeds from the sale of an exciting new technology to fund the world’s biggest campaign to save eyesight. Leslie
Berry reports
With regular appearances in the world’s media launching some of the most advanced, ‘space-age’ technologies, it is hard to deny that harley Street eye surgeon Mr Bobby Qureshi has an ‘eye’ for business.
Most recently, he made international headlines through joining forces with an award-winning Spanish physicist to utilise hubble telescope technology. the resulting development has been hailed as the most significant breakthrough in the treatment of the major cause of blindness in those aged over 55 in the Western world: the debilitating disease age-related macular degeneration (aMD). globally, over 13m cataract procedures are performed each year on patients who, he says, are suitable for an implant that can help alleviate their symptoms from aMD.
The iolAMD implant and an illustration showing its position in the eye after surgery
t his is growing at almost 4% annually and there are no currently accepted surgical solutions. Previous attempts at a solution required extensive incisions of up to 11mm carrying significant risks and have not been widely adopted.
Mr Qureshi and optical physicist Prof Pablo artal’s ‘revolutionary’ implant iol a MD (www. iol a MD.com) is not just able to successfully treat millions of sufferers, but also light up the eyes of investors and financial markets internationally with potential returns put at circa $2.5bn.
game-changing technology according to rob hill, chief executive of l ondon e ye h ospital Pharma, the innovation company which has brought iol a MD to market, there are very few recent precedents for a game-changing technology like this in the world of ophthalmic surgery.
he says: ‘One of the most recent was intralase, which brought to market a new way of cutting flaps in la S i K surgery. i ntra l ase sold for $808m in 2007, based on sales
of only $131m. We are confident that with the reasonable unit price, the simplicity of the procedure and the size of the market, iol a MD will be making not just eye health but financial history.’
the new patented technology is expected to help millions of sufferers in the early and middle stages of dry a MD, for whom until now there has never been an accepted treatment.
Dry a MD affects nine times more people than wet a MD. i n dry a MD, there is a build-up of waste products in the retina which support the cells that give us vision.
But wet a MD involves breakages in the retina as some blood vessels grow abnormally.
lucentis, the injection used to treat wet a MD, is worth over $2.4bn annually to its owners Novartis. Wet a MD, however, only affects 10% of the world’s sufferers, leaving the market wide open to the new iolaMD implant.
t he tiny iol a MD implant, which has regulatory approval and is based on an approach by NaSa to tackle fuzzy images from the h ubble telescope, can be inserted in just two minutes via a tiny incision (3mm) by any competent eye surgeon trained in cataract surgery. t he training required is minimal.
another great benefit is that it can be done at the same time as cataract surgery, as 50% of the 23m annual cataract patients already suffer a degree of aMD.
simple solution
the lens is effective in the treatment of dry aMD, established wet forms of aMD and other macular disease, including diabetic maculopathy caused by diabetes.
Mr Qureshi’s objective had been to find a simple and cost-effective solution to the ever-growing problem of age-related blindness. he approached Prof artal – the first-ever european winner of the
prestigious e dward h l and award for scientific contributions to the advancement of visual optics – with his quest.
Mr Qureshi, who is the london eye hospital Pharma’s chief medical officer, says: ‘ t he idea just made common sense to me as an eye surgeon. i perform cataract operations day in, day out, but had been frustrated by not being able to successfully treat my aMD patients.
‘Now at the same time as i perform routine cataract surgery, i can implant iolaMD and reduce the visual compromises caused by aMD.’
Numerous clinical studies are ongoing to verify the success of the hundreds of patients that Mr Qureshi has already treated at the london eye hospital. additionally, there are many academic centres around the world who have independently verified these findings.
the current one-off cost of the iol a MD surgery to patients is around £6,000 per eye, which is equivalent to the annual cost of injections for wet aMD.
l ondon e ye h ospital Pharma said it hopes to make iol a MD accessible to patients on the NhS and through insurers.
Mr Qureshi says: ‘i’m just concerned about saving eyesight. this technology isn’t just a step forward, it’s a giant leap towards restoring vision to millions of people around the world.
Biggest campaign
‘i want to use all of the resources we have, including the proceeds from the sale of this exciting new technology, to fund the world’s biggest campaign to save eyesight.
LonDon EyE HospiTAL pHArMA
London Eye Hospital pharma was formed to bring innovative ideas to the wider ophthalmic market. As well as having access to the latest technology via its own eye hospital, it wanted to be intimately involved in developing cutting-edge products and technologies.
it says that, by developing its own ideas, it can drive the science of ophthalmology forward and ultimately help more people.
sation aimed at the eradication of this condition is www.londoneyehospitaltrust.org.
iolaMD was launched at one of the world’s leading eye surgery congresses, e uropean Society of Cataract & r efractive Surgeons last September at the excel exhibition centre in l ondon (www. escrs.org).
‘Our pledge is to rectify that once and for all and any revenue created by iolaMD is sure to be a part of this promise to deliver.’
Mr Qureshi’s charitable organi-
‘Millions of children around the world go blind unnecessarily due to entirely preventable conditions such as trachoma – and i see it as my mission to eradicate this disease.
t he l ondon e ye h ospital and its team already have a long list of successful launches including: the Symfony lens, which could spell the end of both distance and reading glasses for some patients; t he l ight a djustable l ens, which is the most technologically advanced implant now available, with the capacity to be altered after surgery to optimise vision; Pioneering use of the teneo laser, which is used to treat nearand far-sightedness, astigmatism (misshaped cornea or lens) and presbyopia (age-related far-sightedness).
mARkETing yoURsElF
Expert advice
So you think you’re an expert? This month, surgeon Dev Lall (right) gives his tips to help make you an expert at being an expert
It is perfectly possible to self-create expert status in the minds of the public. In short, it can be manufactured
If there’s one thing everybody likes, it’s an expert. Which is entirely understandable, because expert status implies both quality and, to a lesser extent, exclusivity. the Oxford Dictionary defines an expert as ‘a person who is very knowledgeable about or skilful in a particular area’.
As a consumer, no matter what you need doing, be it gardening, cleaning, having your car serviced or your knee replaced, you would naturally like it to be done by an expert.
And, as consultants, we would all, of course, like to be considered an expert in our fields.
Why is expert status a good thing?
Clearly, being an expert is highly desirable. It implies respect, authority, power and prestige. It makes you an opinion leader and creates demand for your opinions on a variety of topics. It makes you sought-after professionally by both colleagues and patients, Nhs and private.
It increases your likelihood of being interviewed and seen in the press, which is good for the practice and good for the ego. It makes you not only visible but, more importantly, pre-eminent.
And it means you can command higher fees for your private work.
I’m sure all of us would agree these are good things. But as you read this, you have probably already recognised a problem. Because while we might all agree with the above, we also all know of many experts – people with national or even international academic standing – who, outside academia, experience none of the advantages that I have mentioned above.
their private practice does not reflect their expertise in the field. Why is this?
Well, there are two sides to expert status. the first, of course, is the opinion of your peers and this is, in turn, largely supported by objective evidence – publications, on-going research studies and so on.
the other side of the coin is the opinion of the public. And when it comes to public opinion about your abilities and status, the criteria for expert status are quite dif-
ferent to that required by your peers. And, most importantly, public opinion is almost entirely subjective.
Why the oxford Dictionary is wrong
When it comes to public opinion, both your peers and the Oxford Dictionary are wrong. e xpert status has little to do with your abilities.
As with the truth in politics, when it comes to expert status in the minds of the public, it’s all about perception. And virtually synonymous with expert status in the mind of the public is visibility and celebrity.
Understandably, this is not something that sits well with bona fide experts, those with an academic or clinical pedigree –and indeed with the majority of the profession, I think.
Yet, there is an even nastier surprise for genuine experts, one that explains why there are so many doctors who are invisible and have poorly-performing private practices.
Because it is perfectly possible to self-create expert status in the minds of the public. In short, it can be manufactured.
How to create expert status
Now, this is not intended as any kind of ethical discussion. It is a given that, clinically, you need to act within the bounds of your own professional competence, that you treat/refer as appropriate, that you do not misrepresent yourself or your abilities, and that you behave honestly.
What it is about is creating a public persona synonymous with expertise, so you can reap the benefits.
Creating expert status in the minds of the public is extraordinarily easy. In fact, it is an inevitable by-product of effective promotion and marketing of yourself and your practice.
t here are many factors that imply expertise, and some of the main ones are as follows:
Being seen in the press
Being in the press clearly implies expert status. In a very real sense, you are being publicly endorsed by the media outlet concerned. It is proclaiming you to be someone
with an opinion worth listening to. Ipso facto, you an expert. the amazing thing is that being in the press does something else too – it confers celebrity status on you as well. And in a celebrityobsessed culture, this is no bad thing at all.
Type and frequency of media exposure
In terms of potency, television is most powerful, followed by radio and newspaper exposure when it comes to creating the ‘expert’ persona. On the other hand, frequency of exposure is also important, and the more often you are seen, the better.
Being a celebrity
If there’s one thing that Joe and Julie Public just love, it’s celebrity. Just look at how people on the trashiest and most inconsequential of t V programmes are perceived by the public.
t here are many examples of people considered to be both celebrities and experts mainly because they have a lot of exposure on tV:
Mr Motivator (fitness);
Alan titchmarsh (gardening);
Jamie Oliver (cooking);
trinny and suzannah (fashion);
Various tV GPs (medicine).
All of these have a high media profile and so are considered experts for that reason alone. Celebrity status is simply a byproduct of media presence.
Declaring yourself to be an expert
One very simple way to become an expert is simply by claiming expert status. While, in the eyes of your colleagues, you might be a perfectly competent but very ordinary eNt surgeon, by claiming to expertise wherever possible – in the press, on your website, in interviews and so on – that is exactly how you will be perceived. And perception, as we’ve already seen, is all.
Charging higher fees high prices in and of themselves speak of expertise. It would, after all, be very odd if you were an expert yet charged ‘the going rate’ for what you do.
I have no idea if any of the tV GPs see patients privately, but if
so, their patients would not only expect to be charged a premium but would gladly pay it. Would you expect to pay anything other than a premium price to have Jamie Oliver cook for you, or Alan titchmarsh do your gardening?
Accessibility
Celebrities and experts are harder to get to than non-experts. You can infer and bolster the impression of expertise by making it more difficult for people to reach you. No one, after all, waits in line to see the guru at the bottom of the mountain.
Association
Celebrity and glamour rub off. And celebrity and glamour in the eye of the public are closely related to expertise. so, if possible, be seen with the rich and famous and have photos of yourself with them on your website and elsewhere.
Is it relevant to your ability to treat haemorrhoids? No. Is it worthwhile doing? Absolutely.
social proof
Personal recommendation from friends and colleagues is very powerful. A close second is testimonials from the public speaking of how well you looked after them. s o use them liberally on your website and in all your literature, wherever you can.
Presentation
People expect scientists to look and behave in certain ways; a bit crazy like Doc Brown in Back to the Future. And while they don’t expect or want their doctor to be ‘off the wall’, they do expect him or her to exhibit professionalism, be welldressed and well-spoken. s o to best fit the role of expert, dress up rather than down and posh up the language.
Being a published author few things speak of expertise like the writing of a book. And while we all have research publications to our name, this doesn’t really cut it.
You’ll find A Patient’s Guide to Living with XYZ is far more supportive of your claim to expertise. Yet, in my opinion, it can be
incredibly easy to write and selfpublish a book.
You don’t need special expertise beyond a thorough knowledge of your subject, but you do need an ability to talk about it in layman’s terms.
Quality of your website
As with the way you dress and speak, people will expect your website to convey quality and professionalism.
It should both openly state your expertise as well as imply it by being a high-quality design, written well and with as much social proof in the form of testimonials, evidence of publicity (‘As seen on Channel 4’ and so on) as possible.
Wealth
Wealth is inextricably associated with expert status and celebrity. While consultants will never be poor, it is important to always convey the impression of affluence, if not wealth.
this includes the way you speak and dress, but also your environment – your consulting rooms. If the carpet is worn and the place looks like it needs a lick of paint, that does not support the image of success – and experts are expected to be successful.
in summary
the benefits to your private practice of being seen as an expert are many, and the amazing thing is that it is a natural – in fact, inevitable – consequence of effective marketing.
Not only is expert status good for the private practice, it is great for the ego and can be a lot of fun. You don’t have to have been appointed as a consultant for many years, work in a subspecialty or have doctorates to your name. You don’t have to ‘do your time’ and wait to be anointed as an expert by your colleagues and peers.
It’s self-created. self-engineered. simply walk the walk and talk the talk. In other words, fake it till you make it.
How to be an medico-legal expert: turn to page 28
Mr Dev Lall is an upper-GI surgeon and runs a specialist private practice consultancy. He can be found at www.PrivatePracticeExpert.co.uk
So you want to be an expert witness?
Being an expert witness is an attractive proposition for increasing numbers of independent practitioners and can bring handsome rewards. Some like the kudos, others see it as a natural progression of their career, some do it for the money and a few do it for altruistic reasons.
In this Independent Practitioner Today serialisation of his brilliant new book, Michael R. Young sets out some basics for getting started and gives some useful tips. We are also offering readers a discount to buy the whole book, The Effective and Efficient Clinical Negligence Witness: see page 30
As an expert, you will be taken out of the relatively cosy clinical environment in which you are master, into a seemingly hostile world
The OxfOrd english dictionary defines an expert as ‘a person who has great knowledge or skill in a particular area’.
Of course, any aspiring expert witness must be an expert in his or her chosen clinical specialty, but to be a successful expert witness, you will also need to develop five key skills; namely, the ability to:
Write clear, concise, grammatically correct and accurately spelt prose;
r ead large quantities of text quickly, accurately and critically;
Classify evidence precisely and assess its value and reliability;
Argue logically, consistently and skeptically;
Marshal various sorts of evidence to support a logical argument.
These are not necessarily the skills you were taught at medical or dental school, but they are essential skills for the expert. An expert is, by the very nature of the job, also a professional writer.
There are many definitions of ‘expert witness’, but the key elements are that:
They are believed to have knowledge beyond that of the average person in their profession;
Others, either officially or legally, rely upon their specialist opinion;
They testify on matters that they have not seen or heard at first hand.
A layperson can only give evidence based on fact, whereas expert evidence is opinion based.
The medical or dental expert working in clinical negligence will be expected to carry out the following tasks:
examine patients (the claimant);
Provide lawyers with written reports;
Answer questions put to him or her in writing by lawyers;
Answer verbal questions put to him or her by lawyers;
Attend case conferences and meetings;
Attend at court for trials.
There are no defined qualifications for being an expert witness, but people should not seriously consider putting themselves forward for the role unless they have a relevant postgraduate clinical qualification.
Conversely, having a string of letters after your name won’t necessarily make you an excellent expert.
Your duty is ultimately to help the court. An expert witness is not a hired gun
Technical expertise does not automatically qualify someone to be an expert witness: very different skills and competencies are also required. As well as possessing the necessary clinical qualifications, you will also need years of clinical experience under your belt.
By the time I was seriously involved in expert witness work, I had between ten and 12 years’ clinical experience behind me. I had at different times been a clinical teacher of restorative dentistry and of children’s dentistry, and I had a postgraduate dental degree. This combination of experience and qualifications gave me the self-belief to become an expert.
Hostile world
As an expert, you will be taken out of the relatively cosy clinical environment in which you are master, into a seemingly hostile world in which non-clinicians – solicitors, barristers and judges – put endless questions to you, challenging you to provide them with certainties.
The legal profession is not like medicine or dentistry: lawyers have been trained to extract information from documents, to ask closed questions and, above all, to win their argument no matter which side they are on.
An excellent solicitor or barrister will be able to present a good argument from both sides. Lawyers will question you about the general and the particular, the empirical and the theoretical, the objective and the subjective.
If you are going to survive as an expert you will have to be objec-
tive and be prepared to draw out favourable as well as unfavourable aspects of a case.
You must also never venture beyond your own expertise, and you must be honest in your opinions and be prepared to admit when you do not know something.
Your duty is ultimately to help the court, and this duty overrides any obligation to the person from whom you have received instructions or by whom you are paid. An expert witness is not a hired gun.
Once you’ve pinpointed the problem or problems with the care or treatment, the lawyers will want to know why it was wrong, how it went wrong, and could it have been predicted or prevented. In fact, they will want the answer to almost every question you can think of.
I came up with this little rhyme that to me sums up the clinical negligence expert’s relationship with the lawyers: I thought I knew the answers to how and what and when; That was until the lawyers asked me the same again.
If nothing you have read so far has put you off becoming an expert witness, then the next step is to undertake an honest appraisal of your personal qualities.
expert witness work is no place for the arrogant, opinionated bully. It demands a very clear head, an even temper and the ability to listen to and respect other people’s opinions.
It is a role that is intellectually demanding. If you hated writing ➱ p30
essays as an undergraduate or if you are more at home with a scalpel or a drill than piles of papers, then expert work is probably not for you.
Your work as an expert is also too important to be tagged on the end of a busy working day, but when is the best time to work?
I preferred to read case notes in the afternoon, but writing is much more demanding. I’m a morning person, so I like to rise early and get straight on with writing. Once I start making too many typographical errors, I know it is time to call it a day. I never write if I am tired or if I am not in the mood. discover your best time.
An accident of chance
Becoming an expert witness may be a conscious decision or you might fall into it almost by accident as I did.
One of my patients, a clerk of chambers, asked me one day if I could help out one of his firms of solicitors. The solicitors wanted a report for one of their clients, who was claiming damages for a fall the client had suffered.
I agreed to help. I’d never done anything like this before. I wrote the report. The claim was settled. I was paid, although probably not as much as all my time and effort was worth.
More work started to come my way: insurance claims, and dental negligence cases. This was the start of my role as an expert witness. The insurance claims were relatively easy to advise on, but the negligence cases required a whole new set of skills.
d ifferent people become an expert witness for different reasons. Some like the kudos, others see it as a natural progression of their career, some do it for the money and a few do it for altruistic reasons. What is your motivation?
If you would like to read what a few doctors have to say about their reasons for becoming an expert witness, then I can suggest an article written by helen Jaques, ‘Being an e xpert Witness’, published in BMJ Careers in May 2011 (available at: http://careers.bmj. com/careers/advice/view-article. html?id=20003042).
Whatever the reason, your first
steps along your new career path are important and require the same degree of professionalism and dedication that you give to your main career.
You will have to run your clinical career alongside your expert work – expert work is not something you can pick up in retirement. Once you cease work as a clinician, your usefulness as an expert rapidly diminishes.
Time management
Before you even begin to look for work or accept your first instructions, determine how and when you are actually going to fit it into what is probably already a very busy working life.
As I have said, your role as an expert is too important and exacting to be relegated to the end of a busy working day.
each case is different in terms of complexity, and hence the amount of time you are going to have to spend on each one varies enormously. however, on average, each case is going to take up not less than ten hours of your time. If you are a good expert, word will soon get round and you could suddenly find yourself with several cases on the go at any one time.
You will find it hard to say no to
sPecIAl offeR! BuY The Book And sAve £20
The book costs £60, but Independent Practitioner Today has secured discount of a third off for readers, so you pay only £40. listen to the audio content which accompanies the book at this website: www.otmoorpublishing. com/audio. for more information and to order, email stephen.bonner@otmoorpublishing.com, quoting reference ‘Young/IPT’.
new work. You are under no obligation to accept or complete a set number of cases per year, unless you have become a provisional member of one of the expert witness organisations and are trying to move up to full membership. Be careful you don’t take on too much work.
expert work is not something you can pick up in retirement. once you cease work as a clinician, your usefulness as an expert rapidly diminishes
You will need to set aside time during the day or at weekends when you are guaranteed not to be disturbed. I suggest you start off with at least one half-day a fortnight, which you will need to increase as your caseload increases. e ven if you don’t have sufficient expert work to keep you occupied for this half day, you can always use the time to look for work. f rom the outset, you will need to adopt the habits of an organisational saint.
control access to files
Case files must be kept apart from your day-to-day files and records. You must also carefully control who has access to this confidential information. I would definitely keep the case files away from others with whom you work.
I found expert work to be very different from anything I had ever done in dentistry. however, having a BA stood me in good stead. As a classics and history graduate, and an amateur archaeologist, I was used to ‘interrogating’ documentary evidence, both primary and secondary, all too aware of the limits of oral history, and used to interpreting material remains.
But expert work still presented me with new challenges. I was on a steep learning curve, but once I realised that the law is very different to dentistry and that they are indeed two very different intellectual disciplines, I was OK.
As useful as my training as a historian was, at the back of my mind was something I’d read in Julian Barnes’s novel The Sense of an Ending, that ‘history is that certainty produced at the point where the imperfections of memory meet the inadequacies of documentation’. I leave you to draw your own conclusion.
Adapted from The Effective andEfficientClinicalNegligence Expert Witness, by Michael R. Young, price £60 from Otmoor Publishing
Celebrating our 22nd year in Business
www.medbc.co.uk
Come and join the hundreds of other consultants who use MBC and experience the following benefits:
• Bad debts of less than 0.5%
• Increase in net income by up to 25%
• Freedom for the consultant and secretary to focus on the medical side of the practice
• 24/7 online access to both your financial and practice management data
• Having a service tailored to your needs with your own Account Manager
• Our fees are only charged on the money that we collect for the practice and NOT on what we invoice which means we share the same objectives
Special offer:
To celebrate our 22nd year in business we are for a limited period of time offering all new clients an introductory discount of 20%*
Further information:
MBC – More than just a billing company
Please visit www.medbc.co.uk for more detailed information or phone 01494 763999 and speak to Garry Chapman to establish how we may assist your practice.
*Terms and conditions apply
Super-annuation
Some big pension changes affecting independent practitioners and their private pensions are about to kick in. Patrick Convey (below) explains the opportunities ahead for doctors
IN AprIl, savers in the UK will see the biggest changes to pensions in decades. Unusually for the industry in recent years, there is actually good news.
Many column inches have already been printed regarding savers’ future rights to take as much as they want, when they want, from their private pension pots in the form of cash lump sums.
But these so-called pension freedoms have arrived very quickly, causing some degree of confusion and an industry which is not quite ready to embrace the revolution.
Even the regulatory body, the Financial Conduct Authority (FCA), has announced it is introducing fairly last-minute additional protections for savers.
ahead
What do the changes actually mean?
Senior doctors aged over 55 – and crucially, their spouses – will no longer need to buy an annuity to provide income until they die.
Savers will not be limited to a once-only chance to take a single tax-free lump sum. Instead, you will have complete access to your pension savings – subject to your marginal rate of income tax in that year – effectively dipping in as you need to.
It is this key area which has generated those ‘freedom’-related headlines. After many years of retirees being locked into poor annuity rates, the news provides some welcome relief.
In practice, however, this is likely to be of greater benefit to the spouses of doctors where pen-
sion funding has been made from partnership earnings or limited company profits and where their rate of income tax is likely to be much lower in retirement than their higher-earning partner.
Flexible drawdown
Medical professionals are likely to ease themselves into full retirement over a number of years. For this reason, many consider ‘income drawdown’ which lets you draw an income from your pension pot while leaving the remainder invested. You choose how much lump sum or income to take and where the fund will be invested. Not only will you keep control of your capital, you will have increased flexibility should economic or personal circumstances change.
As savers access more of their pensions, the amount of extra tax collected by HM r evenue and Customs is expected to rise from £320m in 2015-16 to £1.2bn in 2018-19.
Before drawing any funds from your private pension, bear in mind the impact it may have on your annual allowance.
Savers who choose to draw down more than their tax-free lump sum of 25% from a private pension may see their annual allowance limit cut from the standard £40,000 to £10,000 per year once it is crystallised. Their annual allowance will then remain at that level for life.
This could cause extra confusion for those monitoring annual savings limits in more than one pension.
Recycling your pension?
Critics have argued that the new freedoms could allow savers to ‘recycle’ their tax-free allowance, whereby an individual boosts their pension savings by taking their tax-free cash and, as a result, increases their payments into a pension plan to gain further tax relief.
In response, the Government has proposed to limit the amount of pensions tax-free cash that can be ‘recycled’ at just £7,500 per year – a figure of £10,000 was originally anticipated.
Doctors can now choose to pass their private pots on to loved ones tax-free, as pensions do not form part of a person’s estate for inheritance tax purposes
While Australians are generally credited with having greater pension provisions than the British, those ‘down-under’ were quick to realise that their high life expectancy – the world’s fourth longest – would need substantial funding. For research has shown that a quarter of Australians with superannuation funds at age 55 were found to have depleted those funds by age 70.
An alternative is ‘phased retirement’ where your pension savings are split into segments, giving you control of which segments you want to turn into an income and when – useful if you don’t want to retire completely. Your cash flow can then be shaped to reflect your circumstances at that time; for example, less income at the start if still working part-time. If you die, the balance of the fund segments not yet accessed can be passed on to loved ones outside of your estate.
Tax implications
One key consideration when taking your pension is tax. Making large withdrawals will lead to substantial income tax payments, so you may need to consider staging them carefully.
Again, this is likely to impact spouses more than senior medical professionals, who may no longer be funding pensions due to lifetime allowance restrictions.
Passing on pensions
To add to the good news, the Chancellor announced that the harsh death tax due on private pensions will be abolished from April.
Doctors can now choose to pass their private pots on to loved ones tax-free, as pensions do not form part of a person’s estate for inheritance tax purposes.
Currently, pension pots are taxed at up to 55% on death once a person has started to take income or taken tax-free cash.
But, in the future, when someone older than 75 dies, their heirs will pay income tax at the marginal rate and no tax charge will apply if aged under 75 – subject to
them having available lifetime allowance remaining.
Whereas, previously, independent practitioners may have stripped funds out of their personal pension or self-invested pension in retirement, this new move will make it much more attractive to keep pension funds invested and to pass these on to family members in the future.
The new rules will only apply to those who have their pension funds invested in income drawdown rather than in annuities, but it is still a very attractive option for higher-rate taxpayers.
A higher-rate tax-paying doctor could contribute to a private pension, enjoy tax relief on the sum and then leave it tax-free to loved ones if they die before 75. If they die after 75, it could be subject to only 20% tax if withdrawn by a basic rate taxpayer – a very useful inheritance tool, depending on an individual’s circumstances.
Maintaining your lifestyle
Your retirement might last two or three decades and few of us relish the thought of downgrading from our current standard of living. The onus is therefore on you and your adviser to ensure that you do not exhaust your funds before time.
Much has been made about the danger of pensioners going on a l amborghini-buying spree once the pension freedoms come into play. In reality, those who have worked hard and saved throughout their careers are unlikely to throw caution to the wind in later life.
Evidence from Australia, however, where retirees have had greater access to pensions for some years, shows that with independence comes responsibility.
However, the far bigger problem for the majority of their older population was actually a failure to draw on their pensions.
A recent report showed that, faced with the risk of outliving their assets, savers were choosing to live more frugally in retirement.
This fear of consumption was not only leading to less-enriched lives but was impacting the Australian economy as a whole. Navigating their own financial futures was proving so challenging that many were drifting back to the relative safety of annuitytype products despite the poor returns.
opportunities knock pensions are still the main tool for creating long-term financial security. After countless negative changes in recent years, these latest enhancements are to be embraced.
With careful planning, as well as providing tax benefits on contributions and a flexible income in retirement, pensions can now be used to pass on assets to future generations as part of an overall investment strategy.
Patrick Convey is technical director of Cavendish Medical, specialist financial planners helping senior consultants in private practice and the NHS.
The content of this article is for information only and must not be considered as financial advice. Cavendish Medical always recommends that you seek independent financial advice before making any financial decisions. Levels, bases of and reliefs from taxation may be subject to change and their value depends on the individual circumstances of the investor. The value of investments and the income from them can fluctuate and investors may get back less than the amount invested.
AdvicE on billing
Charges against doctors
the new financial year is coming and there are important billing issues to address for many practices. In the first of two articles, Garry Chapman (below) sets out the key areas to put right
It looks like the year ahead is going to be another one of change for all independent practitioners across the entire spectrum of the market.
taking this into account, it is the perfect time to take stock of the way that the medical billing and collection process works within the practice.
I have highlighted what I consider to be the main billing issues to address with five covered in this article and the remainder in next month’s issue of Independent Practitioner Today. infrastructure there are still a lot of consultants working in private practice who operate their billing process either manually or on a word processing and spreadsheet platform. to make matters worse, these
software programmes are typically being run on laptops, notebooks or PCs that are never backed-up.
this means that if the device is either lost or the software becomes corrupt, then the finances of the consultant are put at risk from both a monetary and tax perspective.
o ne of the first issues that a consultant should address is to ensure that they set up the running of their private practice on a sound basis with the correct infrastructure.
t his would involve having a robust auditable system in place to facilitate the financial elements of the practice, including the ability to raise invoices, reconcile payments and the facility to chase the outstanding invoices in an efficient way by phone and letter.
there should also be a system in place to collect payments from self-pay patients. the best system would involve having the ability to collect money by a debit or credit card, which means that the practice would have to operate a credit card pin and chip system.
Terms and conditions
Another area which is very rarely addressed correctly within a private practice is to have the terms and conditions written down and presented to the patient prior to any treatment taking place. this would typically take place in a patient registration form and cover areas such as pricing, shortfalls and any payment terms
applicable, including where the consultation is not attended. It is important for the consultant not to forget that although they are treating the patient medically in the same way as they do in the NHs, the key difference is that it is being done privately and therefore the patient should be liable for any costs irrespective of what insurance policy they hold. If the terms and conditions are clear, then it helps both the practice and the patient.
Pricing
this is an area which we find to be the one that gives most consultants the biggest headache. the reason for this is that it is a
doctors
An area very rarely addressed correctly is to have the terms and conditions written down and presented to the patient prior to any treatment taking place
changes for the codes that they use within their own specialty.
t hese changes can occur on a monthly basis. New ones to get to grips with can either be replacement codes, brand new ones or a change of description involving the use of multiple codes billed together.
very difficult area both within the insurance market as well as the self-pay sector.
the consultant has to decide if they are going to adhere to each price schedule of the insurance firm. All insurers have their own specific prices for each CCsD code and these can differ by up to 100%.
o n top of this, they have to decide what rate they are going to charge for their consultation fees. In some cases, the contract the consultant has signed with the insurer will dictate what they can charge for both the CCsD codes and the consultation fees.
Where the contract does not do so, they need to decide what to charge, and this also includes the self-pay sector for both consultations and CCsD codes.
If the consultant gets this wrong, it can lead to being incorrectly priced within the market and therefore a loss of patients because the pricing is too high or to the loss of thousands of pounds due to the pricing being too low. our experience is that consultants typically do not charge correctly. this is because they have either not done enough research when setting the pricing in the first place or they have not reviewed the pricing on a regular basis.
ccSd
once the consultant has decided on the pricing policy for the practice, they will need to make sure they keep abreast of all the CCsD
All of the above can also have an impact on what can be charged dependent upon each insurer. In our experience, ignorance in this area can often lead to undercharging for procedures carried out within the practice.
Speed
o nce all of the above has been addressed, then the practice needs to raise the invoices promptly.
Unfortunately, in our experience, it is not uncommon for the practice to be many weeks behind in raising invoices.
this is typically due to the pressure of other work within the practice or where the consultant has not got around to doing it themselves.
Well, this really should be classified as a criminal offence, as it actually puts the practice at risk particularly from a cash flow perspective. t he longer time left before the invoice is raised also increases the risk of having bad debts.
the practice should set the goal of billing within 24 hours of any treatment carried out, which will ensure good cash flow and help minimise bad debts.
Next month: In my next article, I will cover the remaining five billing issues to address. In the meantime, you can either start on addressing the billing issues highlighted above within your practice or you can contact a professional medical billing and collection company to assist you in solving these issues.
Garry Chapman is managing director at Medical Billing and Collection
PROBLEMS WITH THE TAX MAN?
HMRC tax investigations and disputes create difficult and stressful times.
As an award winning firm of tax experts, our highly experienced partners specialise in resolving problems relating to tax investigations and disputes with HMRC.
To find out, in confidence, how we can help call 0800 734 3333.
‘Here to help. Not to judge.’
Remote
control
With
independent practitioners increasingly ‘seeing’ their patients remotely, Dr Richenda Tisdale (right) gives some useful medico-legal advice
I grew up in a rural part of england and can vividly remember my father’s weekends on call as the local gp
One weekend in four would be spent driving round the Cornish countryside from one house-call to the next, bleeper in hand. If a call came in while he was driving, he had to look for a phone box to ring home to my mother who would have taken the details from the answering service.
Sometimes, my brother and I would go with him, and even now I could tell you the location of every phone box within 30 miles.
In one generation, we have moved on, through the first mobile phones, to a time when video conversations have become commonplace.
remote doctor-patient consultations are not a new concept. p hone consultations have been widely used, particularly in primary care, to triage, assess and manage patients, for some time.
‘Telemedicine’, with video links between doctors, has also been in use for many years, although largely on a clinician-to-clinician basis for educational purposes and to share specialist knowledge
with generalists working in remote regions.
The widespread availability of mobile video technology such as Skype and Facetime has prompted some doctors to consider whether this could replace or be a useful adjunct to face-to-face consultations in certain situations.
Doctors working both within the NHS and the independent sector are regularly providing services via phone, email, text message and video link. In a time of increasing demand on medical services and high patient expectation, looking to technology to optimise efficiency and patient satisfaction is entirely understandable.
Advantages for all side
There may be advantages for patients who have difficulty attending a consultation, particularly those with mobility problems, full-time workers or patients who need to arrange childcare. A phone or video chat can be a convenient alternative to attending a gp. This may also be true for patients in remote areas who wish to seek a specialist opinion without travelling long distances. For doctors, too, there can be
advantages. A video call may offer certain benefits over a phone conversation in that it may be possible to glean more information by seeing the patient on screen rather than simply by speaking to them – for example, some signs such as rashes may be visible.
But the gold-standard consultation remains an assessment in person and there are potential pitfalls to any remote consultation.
Pitfalls of remote consulting
First, there are limitations of what can be achieved during the consultation and the patient should be reminded of this when arranging an appointment.
Indeed, triage is important also to ensure the appropriateness of a virtual consultation. w hile a video consultation may allow for a full history to be taken, options for examination are limited to a visual inspection dependent on picture resolution and lighting.
You may be able to observe some clinical measurements such as respiratory rate; however, there is currently no option to check other observations such as heart rate or to undertake a full examination.
Video consultations may therefore be more appropriate for some situations than others; for example, where there is no need to physically examine the patient.
Before making any management plan on the basis of a remote consultation, a doctor should assure themselves that their assessment of the patient is adequate for this purpose.
The technological limitations of the consultation in terms of the quality and stability of the connection are also factors which could frustrate an attempt to have a meaningful consultation via video.
Some groups of patients may find it difficult to access or use technology for these purposes, and it is important to consider alternatives for these groups. Doctors should be mindful of the need to ensure that there are sufficient face-to-face appointments available for these patients.
Patient privacy and consent
If the examination requires a patient to partially undress, this raises the issue of privacy and the usual considerations surrounding intimate examinations.
A doctor should consider whether it is appropriate to conduct such an examination over a video link at all.
In all cases, consent should be sought, an explanation provided as to why visualisation of the relevant area is necessary and the patient given the opportunity to undress in privacy as they would during any other consultation.
If a clinician suspects that a faceto-face consultation is necessary in any event – for example, if a patient presents with a breast lump – it would be advisable to ask the patient to make an appointment in person rather than requiring them to undress during a video consultation if this is not going to alter the management plan.
Making recordings of patients
There is also the matter of whether the consultations are recorded or stored either as part of the clinical record or for training and clinical governance purposes.
If still images or any part of the consultation is to be recorded, then care must be given as to how and where they are stored.
The gMC has issued guidance entitled Making and using visual and audio recordings of patients , which applies to images of patients made using any recording device.
It makes clear that patient consent should be sought to make a recording and that if this is to be disclosed for a secondary purpose, such as teaching, training or assessment, that you have the patient’s specific consent to do so. The gMC also requires that there are secure arrangements for storing recordings.
It is important to consider the security of virtual consultations, and it may be wise to seek specialist advice to ensure that the system used is fit for purpose and that the consultation cannot be ‘hacked’ or accessed by other parties.
safe prescribing
In its guidance Good practice in prescribing and managing medicines and devices, the g MC includes a section specifically relating to remote prescribing via phone, videolink or online.
remote prescribing is accepted, provided that the prescriber can satisfy themselves that they have
undertaken an adequate assessment of the patient in order to be able to prescribe safely.
This includes ensuring that the prescriber has sufficient knowledge of the patient’s health and history, and gives consideration to the limitations of the remote assessment and the potential need for a physical examination. patients might not know all of their relevant medical information and may not be forthcoming with all of it in any event, and so a doctor may feel more confident prescribing remotely for a patient who is well known to him or her, rather than on an ad hoc basis.
As with any consultation, it is important to keep detailed clinical records. when making a note following a video consultation, it may be helpful to include the nature of the consultation, clear documentation of the history, management plan and ‘safetynetting’ advice on what steps the
patient should take in the event that their condition worsens or does not improve.
It would also be helpful to make a comment on the technical quality of the video consultation itself.
If a doctor proposes to offer video consultations, they should inform their medical defence organisation to discuss this potential adjustment in their working practice.
Video consultations may play a role in medical assessment. But it is worth bearing in mind that they may not be suitable for all patients nor all conditions.
If in any doubt as to whether a video consultation has been sufficient for the purpose, it may be worth advising a prompt face-toface review of the patient.
Dr Richenda Tisdale is a medico-legal adviser at the Medical Protection Society
invEsTing in pRopERTy AbRoAd
Last month’s article on the most popular French ski resorts to buy property whetted many readers’ appetites – so here’s how to go about turning your dreams into reality. Dylan Mitchell reports
The peaks of investment
Both real estate and mortgages in France are highly regulated.
t his makes it one of the most secure property markets in the world and one of the reasons that it has long been a popular place for investment and second homes.
t hat said, arranging a French mortgage and buying a property can still seem like a minefield to the uninitiated. to help, here are some key points to consider.
Whether you are looking for a holiday home, an investment or a combination of the two, in the French alps you have a couple of options.
Holiday home/buy to let throughout the alps, there are a wide range of chalets and apartments available for all budgets.
t he most famous resorts of Val d’Isere, Courchevel and so on offer luxurious properties for €1m to €5m.
More affordable properties are also available in less well known resorts.
Should you want to receive an income from these properties, local management agents will be able to maintain and manage the rentals for you. typically you would expect to pay a management fee of 25% plus costs such as cleaners, taxes and insurance.
French leasebacks
t his is a form of buy to let that was created by the French government in the 60s. essentially, you would purchase a chalet or apartment and then lease it back to a hotel group in return for a guaranteed rental income.
a s part of the government incentive, investors receive a 20% Vat rebate off the purchase price and owners can deduct 4% a year for depreciation against income. t his, when combined with a mortgage repayment, will virtu-
ally eliminate French income tax for the first 20 years.
leasebacks offer the advantage of a hands-off property investment, with tax incentives, that owners can use for up to six months a year.
although there is a lot of protection for buyers investing into French property, investors would be advised to only lease their properties to large, established hotel groups.
What about the summer? often buyers are so focused on getting a ski property that they overlook the summer months.
When the snow melts away, it reveals a beautiful lush green mountain range dotted with picturesque alpine villages. there are festivals throughout the summer and the weather is fantastic with long, hot, sunny days, making it an ideal destination with a wide range of activities such as hiking, cycling,
mountain biking, canoeing, white water rafting, paragliding, horse riding, golf and many more. When looking at property in the a lps, consider what options are available in the summer, which will allow you to make use of your property all year round and will most likely make a better long-term investment.
What are you looking for?
three of the most important criteria to keep in mind are capital appreciation, cash flow and personal use.
Capital appreciation
By investing into areas that are up and coming or are undergoing rejuvenation projects, you will be able to benefit from the natural upturn in real estate prices. at the moment, among others, areas in the alps to watch include Courchevel, Chatel and SainteFoy-tarentaise.
What about the summer?
Often buyers are so focused on getting a ski property that they overlook the summer months
Cash flow
When looking for a property that will provide you with a return, there are a couple of things to consider.
Firstly, the rental income that the property generates should ideally cover your mortgage repayments and any other costs, which would make it ‘cash flow positive’.
If you are also going to use the property, then another consideration should be how much you are saving each year on family holidays, which could be considerable if you have children.
personal use
ensure that your property has the facilities that you will want. For example, if you’re looking for a ski property, ensure that it has ski lockers, is close to the lifts and within easy walking distance to the shops and restaurants.
If you are looking for a property that you can use all year round, then also make sure you are within a real village or town where people live all year round and which has easy access to lots of summer activities.
Mortgages
French banks will calculate affordability of one-third of your income before tax. For example, you earn £60,000 a year, which means that the bank will accept that £20,000 a year can be used to pay for the rent or mortgage on your main residence plus the cost of the new mortgage on the property in France.
t his is a very simple example and some banks are more flexible in their criteria, but this will give you a good estimate.
loan to value (ltV) is the percentage of the purchase price that you can borrow. Non-residents can currently borrow up to 85% of the purchase price, which means that you would need to contribute a 15% deposit plus the legal fees paid to the notaire.
t he banks will also charge an arrangement fee of 1%, but this is often capped for larger mortgages.
a ll French banks require life insurance and the policy will need to be issued before the mortgage starts.
the interest rates, lending criteria and types of products vary ➱ p40
...cuts into lost fees!
“MidexPro thinks like a doctor, not a computer exper t”
All you need to run your private practice including document management, diary, clinical data, even test ordering and lab reports from TDL.
From paper billing (incl VAT) to electronic billing (EDI) to management of bulk purchase contracts.
Grow seamlessly from a small solo practice through to a large group practice, remote access network system
MidexPro is the cost effective practice management system with support second to none.
Free download of the full working package (30 day limited) from www.midexpro.com or call for a CD.
Try it for yourself with no sales pressure.
“MidexPro has revolutionised our lives; it is just so easy”
greatly from one bank to another. It really is worthwhile seeking advice from a French mortgage adviser before starting the process of buying a property.
The notaire
Unlike in the UK where each party appoints their own solicitor to represent them, in France a notaire is appointed to handle the property transaction for both the buyer and seller. this is because the notaire does not represent each party, but instead acts on behalf of France.
the notaire’s primary responsibility is to make sure that all matters relating to the purchase are legally correct, which ensures that the buyer is protected under French law. t he notaire’s role includes everything from ensuring the title deeds are properly compiled, through to checking that the property has the necessary planning and permissions.
When paying a deposit, ensure that this is held by the notaire instead of the estate agent. also, if possible, ask for an english- speaking notaire to be appointed.
purchase agreements
A new concept providing real benefits to patients
• Weight-bearing scans and variable patient positioning enables a more precise diagnosis
• Truly open system is a solution for claustrophobic patients without compromise in image quality
If you are buying a new property from a developer, then you will sign a ‘reservation agreement’. If it’s an existing property, then you will sign a compromis de vente
You should receive an english version of the contract or ask the notaire to explain it to you in detail.
t hese agreements tend to be standard and will allow you a seven-day cooling off period after signing, which gives you the option to change your mind and withdraw from the purchase.
t he notaire will then refund your deposit. You also have 30 days to arrange a mortgage, although it is worth asking for this to be extended to 60 days, as it can take this long to arrange a mortgage in France.
Foreign exchange
the British Pound is currently at a six-year high against the e uro, making this an opportune time to buy property in France.
h owever, you can save even more money by using the services of a Foreign exchange Dealer.
t heir services are available to anyone, not just the ultrawealthy, and they will typically save you 3% to 5% on the exchange rates offered by the high street banks, which makes a big difference when you are considering buying a property.
Taxes
France has double tax treaties with all members of the e U, including the UK. t his ensures that if you pay any tax in France, that tax is deducted against any tax liability in the UK, if any. o wners of French property should be aware of income tax, capital gains tax, taxe foncier, taxe d’habitation and wealth tax. t his can seem like a lot to cope with, but the French tax regime is clear and well regulated, making it fairly simple to organise.
You can also simply appoint a French accountant to deal with this process on your behalf.
Property in the French a lps comes in a variety of shapes, sizes and to suit all budgets. If skiing back to your own chalet or apartment at the end of an exhilarating day on the slopes is your dream, then maybe now is the time to make that dream come true?
Dylan Mitchell is director of French Leaseback.com
THE pRivATE MEdiCAL
sECRETARy/pA
oF yEAR AWARd 2015
The British Society of Medical Secretaries and Administrators seek nominations for this prestigious award to recognise and reward an innovative medical secretary, personal assistant or administrator working within an independent clinical environment who demonstrates an outstanding performance over and above the standard expected in their role.
The BSMSA and BSMSA Training are again sponsoring this award, together with Helix Health and Howard de Walden Estates (Medical Area). Nominations can be made by doctors, managers or colleagues. We hope that you will support the award and nominate a deserving winner.
Private Medical Secretary of the Year Award in 2015 (PMSYA-15)
The Winner will receive £500, Second Place £250 and Third £50 Closing date for entries is 30 June. Short-listed nominees will be invited for interview in September. The award will be presented to the winners in October 2015.
If you would like a nomination form or any further information, please contact kathy.perkins@bsmsa.org.uk
ArE YOu A NEW INDEPENDENT PrACTITIONEr?
Independent Practitioner Today is your vital resource! To see previous editions, as well as getting full access to all articles on our website, sign up today to become a subscriber.
Subscriptions cost only £70 if you use direct debit for our annual ten issues a year – and you will then have access to a library of useful articles to help you, going back to our launch in June 2008. You will find many of the answers to the questions you are asking are just waiting to be read!
Take Control
Harley Street has, for much of its history, been more than just a street name. Like Downing Street, Savile Row and Fleet Street, it has become a synonym for an entire sector: a widely understood shorthand for high quality private medical services, dispensed from beautiful period buildings in the heart of London.
of your private practice billing
As the freehold owner of the majority of the area’s buildings, the Howard de Walden Estate has helped shape Harley Street’s fortunes since the first doctors began arriving in the area in the late 19th century. For many decades, this was the most renowned and in-demand medical area in the world. But as international competition increases, history and reputation alone will not be enough to sustain that position. Over the past few years, we at the Estate have been working hard to put into action a clear strategy designed to enhance the Harley Street Medical Area’s global reputation.
In this, we have learnt some valuable lessons from the Estate’s successful overhaul of the Marylebone Village retail area. The first is the importance of supporting a small number of ‘anchor’ institutions which help set the tone—in the case of the high street, it was Waitrose and the Conran Shop; in the Harley Street Medical Area it is the hospitals. Over the past decade we have worked closely with The London Clinic and HCA to provide significant quantities of additional accommodation, including The London Clinic’s 70,000 sq ft Cancer Centre on Marylebone Road, and we are currently in discussions with King Edward VII over opportunities for expansion.
The Estate has also learnt the value of creating a balanced community of tenants, consistent in quality but diverse in function. When a shop becomes available in Marylebone Village, we actively seek out retailers who will improve the overall offering. We are now applying this thinking to the Harley Street Medical Area, with a small group of external consultants advising us on which areas of specialism are currently missing and who the most respected operators are. Gone are the days when a refurbished medical property will simply be thrown out to the open market; instead we search the world for the right specialists.
At Medser v we specialise in providing the highest standards of private prac tice billing ser vices for hundreds of hospital consultants throughout the UK and Ireland.
- Online access to all your billing information - Extremely cost- effective - Charges are based on revenue collected
An example of this policy in action is the redevelopment of 11 Harley Street, now home to Isokinetic, an internationally recognised sports rehabilitation specialist. We were extremely keen for Isokinetic to choose Marylebone as the location for its first facility outside of Italy, so worked closely with the clinic to provide the necessary accommodation. The result is the presence on Harley Street of a highly regarded new tenant in a genuinely world class facility. Other similarly welcome new arrivals include the Royal Brompton Hospital and a state of the art eye clinic. To attract the right tenants we need to provide the highest possible standard of accommodation. One of the attractions of Harley Street is the aesthetic value of the period buildings, but the area’s historic fabric is the source of some major challenges. Providing modern medical
To subscribe, use the form on page 22, phone 01752 312140, email lisa@marketingcentre.co.uk or go to our website at www.independent-practitioner-today.co.uk
Open and honest
A
strong doctorpatient relationship is dependent on both parties being open and honest with each other. Dr Philip Zack (below) discusses two clinical scenarios where this principle is put to the test
Dilemma 1
Do I have duty of candour here?
QYesterday, I operated on a middle-aged man with an inguinal hernia.
The following morning, the patient complained of discomfort in his abdomen and, on examination, the site of the operation was bruised and painful.
Further investigations revealed an uncontrolled bleeding point in the wound and he will need another procedure to stop the bleeding.
Of course, I will apologise to the patient and explain what has gone wrong, but I’ve heard about a new legal duty of candour and wonder if this applies?
AAs you know, you have an existing professional duty of candour which is set out by the GMC in paragraph 55 of Good Medical Practice (2013) and this should be your priority.
This states: ‘You must be open and honest with patients if things go wrong. If a patient under your care has suffered harm or distress, you should:
Put matters right, if that is possible;
Offer an apology;
Explain fully and promptly what has happened and the likely short-term and long-term effects.’
A statutory duty of candour, which became law in November last year, now applies in NHS hospitals and it is due to be introduced to other Care Quality Commission providers, including private hospitals in England, in April 2015.
The duty applies to the organisation where you have practising privileges rather than to you, the individual doctor.
Once the statutory duty of candour applies, you should co-operate with the hospital’s internal reporting policies and procedures and help it meet the obligations set out in the relevant regulations.1
These include notifying the manager responsible for duty of candour arrangements.
He or she will decide whether an incident reaches the threshold for notification under the statutory duty.
This decision may not be straightforward because a notifiable patient safety incident has a specific statutory meaning: it applies to incidents where a patient suffered – or could have suffered – unintended harm that results in death, severe harm,
moderate harm or prolonged psychological harm.
In this scenario, your ethical duty to tell the patient that something has gone wrong will apply.
Should a similar incident happen after 1 April 2015, the statutory duty of candour would almost certainly apply, as it fulfils the criteria for moderate harm because it includes an unplanned return to surgery and a prolonged episode of care.
You may already have experience of how the reporting procedures might work in the private sector if you have seen them in operation in the NHS.
It may be useful to talk to the relevant hospital manager to clarify what the specific requirements of your hospital will be in due course and what will be expected of you as the senior clinician caring for the patient.
Dilemma 2
What if patient won’t open up?
QA man in his 50s and his wife have come to see me together. The wife is clearly worried about her husband’s memory, explaining that she pestered him into coming to see me ‘under protest’ because he kept losing his keys and missing appointments.
I assessed the patient and carried out a mini mental state examination, which made me think there was something wrong. However, the patient, doesn’t want to discuss it and refuses to take the matter any further. What should I do?
AThis is a difficult situation and it is advisable to ask the patient’s wife if she will leave so
you can talk to the patient alone. This will give you the opportunity to explain to him why you think a referral to a memory clinic is appropriate in his case and address the reasons for his reluctance. You can also find out what, if anything, he wants you to tell his wife.
In this situation, the GMC 2 advises you to explain to the patient why it is important that he understands the options available to him and try to find out why he doesn’t want to know more about his recent memory lapses.
For example, it is possible he may reveal that he fears a diagnosis of early-onset dementia because nothing can be done to help him.
If this is the case, you could reassure him that support is available, as well as treatments that might slow the progress of the condition.
However, if you cannot per -
suade the patient to agree to a more detailed investigation, you must respect his wishes. Even then, it is still important to leave the door open so make it clear he can change his mind at any time.
Even if the patient insists he doesn’t want any further information, it is likely his wife will take a different view, but you will need the patient’s consent to discuss his condition further with her.
The GMC’s confidentiality guidance3 says you should ‘establish with the patient what information they want you to share, who with, and in what circumstances’.
Again, if the patient doesn’t want his wife to know, you are obliged to respect his wishes, although you could encourage the couple to discuss the matter together.
Make sure you keep a record of the consultation and the outcome of your discussion with the
patient, including his wishes about disclosing information to his wife.
This will be a useful reminder if he returns at a later date and could be important if you are later asked to justify your approach.
References
1. Regulation 20 of The Health and Social Care Act 2008 (Regulated Activities) Regulations 2014. www.legislation.gov. uk/ukdsi/2014/9780111117613/contents
2. Paragraphs 13-17, Consent guidance: Patients and doctors making decisions together, GMC, 2008. www.gmc-uk.org/ guidance/ethical_guidance/consent_ guidance_reasons_for_not_sharing_ information.asp?WT.mc_id= SMTWAZW2141101
Dr Philip Zack is a medico-legal adviser at the Medical Defence Union
An independent firm offering one to one meetings anywhere in the UK giving advice and help with:
• how to start in private practice
• how to maximise private practice income
• ways to reduce tax payments
• setting up in Chambers/Groups
• limited companies and LLP’s
• financial planning
• record keeping
• computer software
• tax and financial advice re: car purchases
• pensions: NHS, personal and employee schemes
• purchase of consulting rooms and surgeries
• inheritance tax and capital gains tax planning
• VAT
For more information please contact us by: Wilmslow
Phone: 01625 527351
Fax: 01625 539315
Harley Street
Phone: 020 7307 8759
Fax: 01625 539315
Email: info@sandisoneasson.co.uk
Website: www.sandisoneasson.co.uk
STARTiNg A pRivATE pRAcTicE
Look out for these
1
Not taking advice
One of the best sources of advice are your fellow colleagues. If you are starting out, remember that they were all in your shoes at some point and the vast majority will be helpful, provided you don’t step on their toes too much.
Many of the private hospitals put on new consultant seminars where a collection of speakers guide you through their experiences. I often speak at such events and find that the different subject matters discussed are invaluable to those starting out.
2
Not understanding your tax position
Despite what HM Revenue and Customs’ (HMRC) slogans say, many consultants do find tax matters taxing.
Most consultants will not have had any financial training and, with your salary taxed at source, things should generally have worked themselves out over the years. However, engaging in private work requires a thorough understanding of the tax system to avoid getting caught out later on.
With the 31 January deadline recently passed, the most frustrating conversations are with those who submitted their records at the eleventh hour and have not made adequate provision for the tax.
In almost all cases, this can be avoided by taking the time to understand what you need to be doing and apply it from the start. Tax returns can usually be completed within a month or two of the 5 April tax year ending, so don’t put it off; send the information to your accountant at the earliest opportunity. This will give
Whether you are starting out or a more established private doctor, there are a number of pitfalls in your way that should be avoided. While not exhaustive and in no particular order, these mistakes highlighted here represent some of the more common problem areas seen by accountant Ian Tongue
you the maximum time to ensure that you have enough put aside for tax and are exploiting any tax planning opportunities available.
Meet with your accountant regularly, as it can often take a few meetings for certain concepts to be reinforced.
3
The three ‘A’s Availability, affability and ability are the keys to success in your private practice. Ability should be a given, but ignoring the other two will ensure that your private work is not as successful as it could be.
Be realistic on your available time to ensure that you do not spread yourself too thinly. It can be difficult to find that work-life balance and most doctors find a more gradual increase in workload helps to discover that point.
4 Trying to do everything yourself
Trying to save money by doing everything yourself may seem like a good idea, but it is a false economy if it prevents you from performing your work. The opportunity cost of tying up your time on matters that can be dealt with by others can be significant.
Often spouses can get involved in certain aspects of the private practice and this can also be taxefficient depending on their financial circumstances.
5
Failing to monitor the quality of your secretary
Having an efficient secretary is another key factor to a successful private practice. Most doctors with larger practices put a great deal of faith in their secretaries and many would put this near the top of the
HOLiDAY viLLA TO LET
list of key factors for ensuring a successful private practice.
Many secretaries provide more than secretarial work and manage the debts and, crucially, ensure you get paid for the work you perform. Monitor their work to ensure that you are getting the best from them and if you find yourself in a position where things are not working as planned, you should seek alternative services.
6
Not investing in iT
Investing in your business is a key rule for any business owner. Failure to do so can lead to inefficiencies holding back your business. One of the key tools that has a significant benefit is your IT infrastructure and in particular the use of bespoke practice management software.
Most providers offer a trial and your secretary may be familiar with a certain product. The market leaders offer web-based access to your records, and consultants I speak with say that the investment pays off in no time at all and makes your life easier.
7 Not keeping your business under continuous review
The NHS is a dynamic environment and the amount of private work available is clearly linked. For those not keeping their ear to the ground, they could find their work drying up or taken away with external providers tendering for NHS work.
This is where being part of a group can help, as you can pool ideas and have more strength in numbers.
8
Not getting the timing right
Looking back and thinking ‘I should have done XYZ before now’ is usually a key sign that you have not undertaken a financial plan of action. Many clients come to see me to discuss the milestone events that require changes to business structure and it is best to know these from the outset so you can take advantage of circumstances at the earliest opportunity. The business itself should have a plan from the start and be reviewed periodically. You should always remember the saying that ‘failing to plan is planning to fail’.
9
Following the herd
When first entering into private practice, looking at what your colleagues are doing that works is a great starting point. But some markets are saturated, thus making it harder to grow your practice and penetrate the market.
With the onset of digital media, those that do not keep ahead of the game may find themselves losing out. Make sure that you are using digital media and understand where to advertise your practice particularly in the highly competitive markets. Nowadays, a good website by itself is not usually enough.
10
The ‘too good to be true’ tax scheme
I think it is fair to say that everyone wants to pay less tax. Sadly, there are many consultants out there who are lured into investing into tax schemes and planning that simply don’t work.
They expect the professionals selling such products to be just that and honest about the risks, but in many cases people are caught out.
Usually, there are substantial fees payable up front and they almost inevitably result in a tax inquiry which can take years to resolve, during which time interest is accruing if the scheme is unsuccessful.
HMRC certainly has the bit between its teeth regarding tax avoidance and has new sweeping measures to target what it sees as artificial arrangements. This new ‘General Anti-Abuse Rule’ (GAAR) will, no doubt, catch out a number of planning arrangements and, with the powers to name and shame taxpayers, there could be unwelcome publicity.
If a tax avoidance scheme seems too good to true, then it probably is.
Doing your best to avoid pitfalls will inevitably ensure that you are best placed to run a successful and profitable private practice. Don’t just sit back and let your business meander; take control, nurture it and it will pay off with success.
Ian Tongue (right) is a partner with accountants Sandison Easson and Co
Beautiful family-friendly villa in unspoilt region of Tuscany, italy, with stunning lake/mountain views and fenced pool. Sleeps 10/12. plenty of toys, outdoor pizza oven, spa treatments, babysitter and cook available. Weekly rentals and family cooking/yoga breaks. phone: 0778 557 1292. www.holiday-villa-in-tuscany.com
AFFORDABLE pROvENcE
Le Luc, var. Home from home, 4 bedrooms, 2 bathrooms, modern fitted kitchen. pool. Boules court. Attractive garden. Stunning views. 45 minutes to St Tropez. Between Nice and Aix-en-provence. Sleeps 6/7. Website: www.irelandinfrance.co.uk. phone: 01372 379381. Mob: 07789 766040. Email: angela.ireland60@btinternet.com
LET DOCTORS TAKE CARE OF YOUR HOLIDAY LETS
Now you can rent out your holiday home to another doctor. Advertise it in Independent Practitioner Today, where it will be seen by 12,000 of your colleagues – many of whom are looking to rent a high-end property in a nice location for a well-earned break.
Get in touch with our advertising manager Margaret Floate, who will arrange to have your property nicely displayed. Email: margifloate@btinternet.com Phone: 01483 824094
docToR on ThE RoAd: inFiniTi q50
To Infiniti . . .
Excuse me going on about the Infiniti 50, says our motoring correspondent Dr Tony Rimmer (below), but it does give more and more than you might expect for your money
ANy MeDICAl business trying to break into an established market needs to have a solid and competitive business plan.
It has to offer something above and beyond established services from rival organisations. Reputations are then built over time on a proven track record.
The process sounds simple, but is fraught with potential setbacks and, in some cases, can fail completely.
It is no different in the car market and the most profitable sector is also the most cut-throat: the premium executive segment. The well-known players, mostly e uropean makes, jostle for position on a constant basis and take any potential external competition very seriously.
The Japanese makers have been trying to get a slice of this lucrative market for some years now. However, the one you are likely to think of first – Toyota’s premium
brand l exus – has only just scratched the surface.
l ess well-known but also launched in the same year, 1989, is Nissan’s premium brand, Infiniti. Our doctor colleagues in America are well aware of it, but it is only now that Nissan is pushing for a greater market share in the more challenging european arena.
Targeting the big-hitters
So what model does Infiniti offer that would appeal to discerning private medical practitioners such as us? Well, with the Q50, the brand has gone straight for the jugular and aimed at the midsized premium saloons such as the Audi A4, Mercedes C-class and the market leading BMW 3-series.
The biggest seller will be the £28,000 2.2litre diesel-engined version which borrows its powerplant from Mercedes.
But my test car was the hybrid petrol/electric flagship model,
It is the first car in the world to be sold with Direct Adaptive Steering using electronic steer-by-wire technology
which also benefits from fourwheel drive and costs £42,000. There is also a £34,125 four-cylinder 2.0litre petrol turbo model.
As ever, in this premium sector, styling and external looks are hugely important to attract buyers and there is no doubt that Infiniti have done a good job here.
The external styling is smart and sophisticated, if slightly anonymous. Non-car people will recognise an executive car, but will be hard-pushed to identify the make.
Infiniti really needs to work on
and beyond
a distinctive brand DNA. Its German rivals are instantly recognisable.
Step inside and those medics who like high tech are going to love the large dual-screen central touch-sensitive control monitors.
A superb satnav display sits above a general control panel that can operate everything from the stereo to the dynamic driving options.
Interior quality is right up there with BMW and all passengers will feel pampered. There is plenty of room too. The rear legroom is equal to the Audi A4 and better than the Mercedes C-class.
Steer by wire
So the Infiniti does well for showroom appeal, but what about road manners? Well, the Q50 is the first car in the world to be sold with Direct Adaptive Steering using electronic steer-by-wire technology.
That means that there is no physical connection between the steering wheel and the steering rack. This is to eliminate distracting vibrations from road surfaces and get rid of mechanical losses in the system giving faster response.
It is a great idea and I am sure there is a great future in potential ‘tuning’ of steering control, but in reality it can be a bit off-putting. By removing road feel, there is a lack of connection that separates man and machine to a degree that feels too artificial for the keen driver. The same cannot be said for the performance of the Hybrid model.
A 300bhp 3.5litre V6 petrol engine combined with a 60bhp electric motor makes this a real sports saloon. The four-wheel drive, like Audi’s Quattro system, means that traction is never challenged and this Infiniti is swift enough to embarrass many sports cars.
Handling is reasonable although not thrilling, but the ride is excellent. This is a car for the motorway rather than ‘A’ roads. e conomy for such a powerful car is impressive and the hybrid system delivers 41.5mpg with 139g/km CO 2 emissions. The 170bhp 2.2litre diesel gives 63mpg with 115g/km CO2 emisions. The 211bhp 2.0litre turbo petrol model returns 43.5mpg
Value for money
So what does Infiniti offer as a new player in this highly competitive market? Well, like lexus, you get a lot of car for your money.
To buy a e uropean rival with similar equipment to the standard features on the Q50 would cost you several thousand pounds more.
Value for money is the key and any successful private medical practitioner will know just how important this can be.
New and more exciting Infiniti models are on the way, so my advice is to resist brand snobbery and keep an eye on this important Japanese brand over the next few years.
Dr Rimmer is a GP practising in Guildford, Surrey
InfInITI q50 S Hybrid AwD
Body: four-door, five-seater saloon
Engine: 3.5 litre V6 petrol/ electric motor
Power: 364bhp
Torque: 403lb/ft
Top speed: 155mph
Acceleration: 0-60mph in 5.4 secs
Claimed economy: (Combined) 41.5mpg
CO2 emissions: 139g/km
On-the-road price: £41,630
PRoFiTs FocUs: RAdiologisTs
DO yOU FIND OUR PROFITS FOCUS SeRIeS USeFUL?
Please let us know if it helps you or not. and if it doesn’t, what other data would you like to see presented?
email robin@ip-today.co.uk
Radiologists’ contrasts
A big income drop has hit many radiologists, finds Ray Stanbridge in our latest benchmarking series. Additional material from Martin Murray
Our fOrecast when we looked at radiologists’ earnings a year ago in Independent Practitioner Today was that the market for radiology services would become more liberalised following the anticipated report of the c ompetition and Markets authority (cMa).
We also anticipated there would be a further widening of income ranges for consultant radiologists. Well, our predictions have partially, but not wholly, come true.
Our headline figures are that consultant radiologists’ gross private practice incomes fell by a dis-
appointing 11.2% from £107,000 in 2012 to £95,000 in 2013. c osts remained constant at £27,000. as a result, taxable profits dropped by £12,000 from £80,000 to £68,000. Margins fell from 74.8% to 71.6%.
We have, first of all, to make the now familiar warnings. It has, in recent years, become increasingly difficult to prepare a representative and statistically accurate comparison of trends of radiologists’ private practice incomes and costs. this has been the result of the trend for incorporation among aveRage INCOMe aND eXPeNDITURe OF a CONSULTaNT
some consultants, the growth of groups and the decision by some to invest in hardware.
In addition, others have become virtual employees of private hospitals. t his has affected their income and cost structures.
changed market so the market structure for radiologists is now very different to what it was when we commenced our survey work.
as in previous years, our income survey is restricted to those consultant radiologists who are not in full-time private practice. to qualify for our survey they must:
Have had at least five years experience in the private sector;
earn at least £5,000 a year gross from private practice;
Be seriously interested in private practice as a business. t his condition effectively excludes most small earners who look to their practices merely to meet school fees or holiday costs;
Hold either an old-style NH s maximum part-time contract or a new contract;
Work either as a sole trader through a formal or informal or limited liability partnership or group or a limited liability firm.
Having made all the caveats, there was a fall in average
incomes. t his was probably the effect of reduced fees from both insurers and private hospitals, since many consultant radiologists reported similar levels of activity to previous years.
We have, however, continued to see a widening of income ranges. there are some very large radiology practices working in the uK and these have been growing rapidly over the past few years. In this respect, our forecasts have proved to be reasonably accurate. t here have been some movements on costs. firstly, our analysis shows that there has been a very small decline in costs of medical supplies and/or assistants.
We cannot see any particular reason for this, save that more radiologists are probably being paid by private hospitals who themselves meet these costs.
s taff costs have shown a very small increase. this is commonly payments to family members for secretarial or billing services. the rise in such remuneration costs has broadly mirrored the national rise in personal allowances.
Motor and travel costs have shown some increase. t his is reflected largely by the fact that some consultants are enjoying more exotic cPD training.
Year ending 5 April. Figures rounded to nearest £1,000 (percentage is also rounded up)
Source: Stanbridge Associates Ltd. Additional information: Sandison Easson and Co
We anticipate continuing growth in larger practices and therefore a continuing widening of income ranges
Finally, there has been a small growth in accounting/legal fees. For many, such fees have shown little changes, but there has been some rise. Divorce costs for some radiologists will have had an effect on average figures.
Watchdog remedies
Our analysis shows that other costs in operating a practice have generally been similar. However, there is an ongoing trend that margins are falling as cost rises exceed income rises, despite yearto-year variations. What then of the future? We have now had the CMA remedies
for those who are entrepreneurs, we would expect to see some substantial income growth in interventional radiology fees
and this may have the effect of putting pressure on some radiologists who have their own clinics and have entered into financial arrangements with private hospitals. Insurers have also intensified their efforts to put pressure on fees.
We therefore expect to see in future three phenomena:
Firstly, average incomes and margins will continue to show a small, but noticeable decline in both monetary and real terms.
Secondly, we anticipate continuing growth in larger practices and therefore a continuing widening of income ranges.
Thirdly, for those who are entrepreneurs, we would expect to see some substantial income growth in interventional radiology fees as this becomes more commonplace.
The caveat here is that some opportunities are, in fact, taken up by private hospitals rather than radiologists investing in their own equipment.
In this respect, the decisions and rulings of the CMA may, in the long term, serve to frustrate innovation and to actually reduce competition. Time will tell.
next month: Urologists
Ray Stanbridge runs an accountancy, finance and tax advisory service specialising in the medical profession. Martin Murray is a partner at Sandison Easson & Co, specialist medical accountants
Anaesthetists
years ending 5 april
Source: Stanbridge Associates Ltd
what’s coMing in our april edition
Make sure you don’t miss our next issue, published on 23 April. Only subscribers to the journal are guaranteed to receive every copy and we don’t think anybody who is serious about continuing private practice in the future, when there is so much happening that will affect them, can afford to miss any issue.
Coming up next month:
Mastering the aesthetics business: Pam Underdown writes the first of a new series to help medical professionals decide if entering the medical aesthetic/cosmetic marketplace is right for them and, if so, the key areas they need to focus on and the mistakes to avoid
Cavendish Medical advises on what private consultants and GPs should be thinking about in this new tax year
Are you as upwardly mobile as you thought? Doctors and private hospitals and clinics are losing business because they are not understanding the mobile-using patient, warns Scott Hague
Countdown to the general election – accountant Susan Hutter gives some financial tips to act on before the big vote
Social media is evolving more than ever from a marketing tool to a business strategy for private practice. Catherine Harriss reports on the changes and their possible impacts, while surgeon Dev Lall examines the unexpected power of LinkedIn
Profits Focus examines the profits, income and expenses of urologists
Our motoring correspondent Dr Tony Rimmer is impressed with Volvo’s XC60
EDITORIAL INqUIRIES
Garry Chapman of Medical Billing and Collection advises on the operational aspects to sort out to ensure you get paid for all your hard work – something many fail to achieve
Business Dilemmas: Dr Nicola Lennard of the MDU answers two readers whose websites have thrown up unexpected difficulties
Conflict in teams can be extremely unpleasant, affecting morale and performance and can exert a financial toll on a practice. Professional mediator Mike Hill explains how the mediation process can help resolve workplace disputes or personality clashes. He also highlights the challenges for independent practices that are considering this step.
New pension rules mean doctors could use the money in their pension to invest in property in the UK and overseas. Dylan Mitchell investigates
Starting a private practice: How to handle a tax investigation if you are targeted
More in our new series on becoming a clinical negligence expert witness
ADVERTISERS: The deadline for booking advertising for our April issue falls on 27 March
Published by The Independent Practitioner Ltd. Independent Practitioner Today is editorially independent and thanks Bupa for its assistance with distribution.
Printed by The Magazine Printing Co. Material is governed by copyright. No part of this publication may be reproduced, stored in a retrieval system or transmitted in any form without permission, unless for the purposes of reference and comment. Editorial layout is the copyright of the publishers. If you wish to use it for promotional purposes on websites or for reprints, we would be happy to discuss licensing the copyright to you.
£85 GPs and practice managers (private & NHS). £200 organisations.
But if you pay by direct debit, individuals pay only £70, and organisations £175
Call Proact Ltd on 01752 312140
Email: lisa@marketingcentre.co.uk
Robin Stride, editorial director @robinstride
GUARANTEE yOUR COPy
To guarantee your copy of Independent Practitioner Today by taking out a subscription (at the rates shown on the left), phone 01752 312140 or send off a subscription form on page 22 or email lisa@marketingcentre.co.uk or go to the ‘About’ page of our website www.independent-practitioner-today.co.uk
If you pay by direct debit, individuals pay only £70 for a subscription. Just fill in the form on page 22 and send it to the Freepost address shown at the bottom of the form. BACK ISSUES: £12.50 including post & packaging
Phone 01752 312140 or Email lisa@marketingcentre.co.uk
The professional’s choice for practice management
Client management and financial control is the lifeblood of any enterprise. The latest Healthcode online ePractice management tool is the professional’s choice for practice management, giving you the control you need wherever you are. Our ePractice management solution meets the needs of a range of healthcare providers, from independent practitioners to large enterprise organisations. Our different service levels mean that ePractice will grow with your practice.
Take Direct Control
Access your patient details, appointments, bills and financial status from anywhere, any time.
What the professional’s say...
Protect Your Practice
The diary management feature on ePractice manager means I can focus on treating patients, while my PA is able to coordinate my appointments remotely.
Mr Barlow-Kearsley, Founder, Total Footcare Solutions
Long Term Partner
We use Healthcode’s ePractice manager system for all our invoicing, which streamlines everything for us. Roughly 75% of our invoices are submitted electronically, payments are now made much more quickly, which is good for the cash-flow.
John Morgan, Accounts Director, Jenny Morgan Secretariat
Call us today to arrange a demo and to discuss your requirements on 01784 263 150 quoting: IPT. For further information visit: www.healthcode.co.uk/ipt