The business journal for doctors in private practice
In this issue
The window to private doctors
What independent practitioners need to know about the Private Healthcare Information Network P12
What drives patients to adhere to advice?
A look at the work of Bupa’s behavioural insights team P14
Doctors who are investors in a unique unit reveal why they got involved n Page 28
Get off to a good start in 2022
Complaints code to give doctors a say
By Robin Stride
A revised code of practice for complaints management in private practice gives independent consultants more say during investigations into patients’ grievances.
The Independent Sector Complaints Adjudication Service (ISCAS) revamp, effective for new cases notified from January 2022, aims to promote a just and learning culture where complaints are positively welcomed.
With complaints in the private sector heading for record levels this financial year, the organisation says complaints need to be investigated thoroughly and fairly – with independent services giving patients fair and accountable responses.
ISCAS director Sally Taber told Independent Practitioner Today : ‘What we’ve found is organisations don’t always take comments from all staff on a particular matter of complaint, including consultants, so we want to ensure we get comments from all involved in the complaints.
‘Frequently, one of the criticisms is that the consultant should have
written a statement as well. Our hope is organisations will take on board that it is not just their own staff but consultants with practising privileges, and physios, for example, as well.
‘Handling a complaint takes time and that’s why they have to get it right in the first place.’
Covid19 has, in many cases, led to delays in processing complaints documentation due to staff sickness, furlough, isolation and working from home. It has been a
frustrating time for adjudicators, Ms Taber said.
The vast majority of providers are ISCAS subscribers and from last April to November received 200 heads of complaint: complaints handling 52, consultant medical care 40, clinical and nonmedical/ nursing 21, finance (mostly billing problems) 21, discharge 20, accommodation 19, consent 14, and administration 13.
Ms Taber said: ‘Learning from complaints and making note of how complaints are handled are important. There are still a lot of consultants working in consortia/ groups who haven’t taken notice of ISCAS because they don’t subscribe.
‘But to have the satisfaction of an external review stage for the patients they treat is very important otherwise they are operating a closed culture which can be a breeding ground for patients’ concerns.’
Complaints about nonsubscribers to ISCAS emerge when their dissatisfied patients approach the body for help only to find their provider has not signed up to the code so the complaint cannot be taken further.
1Jane Braithwaite shows how to give your business a fresh start with a strategic plan P24 In association with
Its new streamlined code, replacing a sevenstage process with four used in the NHS by the Parliamentary and Healthcare Services Ombudsman, is as follows:
Promoting a just and learning culture
‘Seeing complaints as an opportunity to develop and improve services and people, acknowledging when mistakes occur or things go wrong and being held accountable for them, learning from complaints, and acting on lessons learned’.
Ms Taber said: ‘The biggest issues we have are still consultant complaints and handling. Often the complaints are around cosmetic surgery outcomes. Doctors have often not seen complaints as an opportunity to learn from how they have done things.
‘We are going to be breaking down the categories that we analyse so we can have some more details. If the organisation is not using the complaint code correctly, then there is a learning culture for them to develop to pass on to consultants.’
➱ continued on page 4
ISCAS’s new code of practice
TELL US YOUR NEWS. Contact editorial director Robin Stride
ADVERTISE WITH US. To advertise in the journal or our website business and lifestyle directories, contact advertising manager
Andrew Schofield at Spot On Media. Phone: 0161 408 3912
Email: andrew@spotonmedia.co.uk
GET A SUBSCRIPTION DISCOUNT
£90 independent practitioners. £210 organisations. £90 GPs and practice managers (private & NHS).
Save £15 paying by direct debit: individuals £75 (organisations £180).
TO SUBSCRIBE
Email karen@marketingcentre.co.uk
Or phone 01752 312140.
Chief sub-editor: Vincent Dawe
Head of design: Jonathan Anstee
Publisher: Gillian Nineham
Email: gillian.nineham@gmail.com
Phone: 07767 353897
Follow Independent Practitioner Today on
EDITORIAL COMMENT
Prepare yourself for 2022
Doctors, private hospitals and related organisations were awaiting the Government’s full response to the Paterson Report recommendations as we put the finishing touches to this issue of Independent Practitioner Today
By now, you will have, no doubt, caught up with its reaction and feedback from interested parties in our online news reports.
The test of the recommendations, designed to improve patient safety, were always going to be whether the Government and regulators acted on them.
It is nearly two years now since the inquiry team, led by the former Bishop of Norwich the Rt Revd Graham James, produced its report, so we have had a long wait. Progress now is probably unlikely to be as swift as many would like.
But what cannot wait long in 2022 is the need for many practices to address a range of issues
that will boost their businesses in the months ahead.
Now is an opportunity to take stock and review strategies and objectives submerged by the Covid onslaught. Jane Braithwaite shows how to give your business a fresh start, on page 22.
New Year’s resolutions for your business really could boost your income, writes Medical Billing and Collection’s Simon Brignall on page 24, and he gives ten for starters.
A review of procedure fees is particularly important, as you could be over- or under-charging due to making incorrect assumptions, leading to issues with insurance companies or lost revenue.
And how about finally properly sorting out the practice invoice system to ensure bills go out quickly and are studiously chased? If your debt levels are over 20% of turnover, you need professional help.
React in haste and repent at leisure
Medico-legal expert Dr Bobby Nicholas discusses how best to handle any negative view you may receive from patients on comparison websites P18
Co-operation is critical
Lyca Health chairwoman Prema Subaskaran says it is vital we build a lasting partnership between the public and private healthcare sectors P20
Psychiatric claims under scrutiny
Clinical negligence claims involving psychiatrists are analysed by the MDU’s Dr Shabbir Choudhury, who offers useful tips on managing risks P22
Don’t come a cropper when investing
Past performance is no indicator of future outcomes. Dr Ben Holdsworth reveals why controlling structure and risk is more important P34
Should I incorporate?
Lawyer Justin Cumberlege, a partner in Hempsons’ healthcare team, explains what should be considered when forming a corporate entity P36
I posted records to wrong patient
A private GP’s mistake leads to a breach of confidential data. Dr Ellie Mein of the MDU advises on how to respond to in this situation P38
PLUS OUR REGULAR COLUMNS
Doctor on the Road: Enjoy the last of a dying breed
Dr Tony Rimmer revels in the petrol power of the Alfa Romeo Quadrifoglio before elecricity takes over P40
Starting a private practice: The figures have me in a spin
Ian Tongue looks at the key points of your annual accounts and shows how to interpret them P42
Profits Focus: Coming through Covid
Our benchmark survey reveals how ophthalmologists are inching back after being hit by the pandemic P49
Get advice to navigate the pension labyrinth
By Edie Bourne
Independent practitioners currently aged 59 or older who are still working and are part of the NHS Pension Scheme will face the biggest impact when all members are moved to the 2015 Pension in April 2022.
When members were first moved to the 2015 scheme following a review by Lord Hutton, those within ten years of retirement age on 1 April 2012 were ‘protected’ and allowed to remain in their current 1995 scheme.
But, in 2020, in what has become known as the McCloud judgment, a court ruling said this action was discriminatory
The remedy to this judgment is that everyone who was forced to move to the new scheme can now choose to take advantage of the benefits from their former scheme for a set time from 2015 to 2022. These benefits are likely to be much more valuable. In addition, to reset everyone’s position, all remaining public sector workers will now be moved to the 2015 scheme in April.
Patrick Convey, technical director at specialist financial planners Cavendish Medical, warned that while this arrangement has been known for some time, many doctors were still unaware that they will effectively lose the protection they were given back in 2015 in just a few months’ time.
‘If you were born before April 1962, you will stop accruing your previous pension which is based on final salary and length of service in April 2022.
‘You will not be able to draw the newly accrued benefits from age 60. Instead, your new NHS pension will be based on an average salary, with benefits available to you at state pension age, so most likely, at age 67.
‘You will still retain a final salary link in your old scheme. This means that if your salary goes up a band, this will increase your benefits in that part of your pension.
‘For many people, though, moving to the new scheme could be detrimental and may have an impact on lifetime and annual allowance positions, as you will
have two inputs per year instead of one.
‘The NHS pension is now so complex and particularly challenging for busy doctors to manage. This January will be the first time those subject to the harshest tapered annual allowance of just £4,000 will be navigating their 2020-21 tax returns.
‘At the same time, there is an ongoing consultation to reduce contributions, but the official regulations of the McCloud remedy have not yet been released. Many scheme members could be unpicking the last seven years of tax returns in line with the new benefits they will receive.’
He added: ‘I cannot say it
Not checking your own position thoroughly at this time could be a very costly mistake
strongly enough, but if you do not have expert help to guide you through this maze, you should seek assistance as soon as possible. Not checking your own position thoroughly at this time could be a very costly mistake.’
Last October, the Government declared that individuals receiving extra benefits as part of the McCloud remedy would not be subjected to additional tax charges.
The McCloud remedy legislation is not due until October 2023 and the Government consultation into pension contributions is due to end in January, with new input tiers expected to be in place by April 2022.
Help for enforcing compulsory jabs for staff
Doctors who employ staff have been promised support from the Independent Healthcare Providers Network (IHPN), as they implement Government requirements for Covid-19 vaccinations for employees from 1 April.
These will be mandatory for all healthcare workers who have ‘direct face-to-face contact’ with patients, including non-clinical staff such as receptionists and cleaners.
Writing for Independent Practitioner Today – in the features section of this issue – the IHPN’s director of regulation says the organisation will support providers and practitioners to ensure the
sector is fully prepared to implement mandatory vaccines.
Dawn Hodgkins assures doctors the network is working to ensure that guidance is fully applicable to the independent sector and provides a clear and usable framework.
This will include consideration of staff groups included in the policy as well as clarity over medical and other exemptions.
She adds: ‘Acknowledging the diversity of the independent healthcare sector, a particular focus of this work will be to influence policy development so that any guidance is also appropriate for non-hospital-based services.
‘This includes independent practitioners delivering primary and community care where there may be further complexities in implementing the policy.’
IHPN aims to help share good practice among independent providers and practitioners and the wider health system around increasing vaccine uptake among
staff and resolving operational issues relating to the policy.
‘This will help ensure the sector is as fully prepared as possible ahead of 3 February, which is the last date that a member of staff can have their first vaccination ahead of a 1 April implementation date,’ she says.
☛ Solicitors Hempsons have advised employers to note that doctors’ professional obligations in the GMC’s Good Medical Practice include: ‘You should be immunised against common serious communicable diseases (unless otherwise contraindicated).’
See ‘Getting ready for mandatory jabs’, page 45
PATRICK CONVEY (left)
What’s in the revised code on complaints
2
Welcoming complaints in a positive way
‘Actively seeking and welcoming feedback, acting on concerns and complaints, recognising complaints as a positive way to improve services, encouraging and empowering staff to resolve concerns quickly to the satisfaction of all parties’.
Ms Taber said adjudications should be regarded as a way of improving rather doing nothing in response. One hospital group responded to a ‘nasty complaint’ this winter with a team meeting to see what could be learned, which was ‘great’.
3 Being thorough and fair
‘Conducting a thorough, fair and objective investigation without bias or discrimination, obtaining comments from all staff involved in complaints – including consultants with practising privileges, keeping complainants updated with progress and giving an open and honest answer to complaints.’
4 Giving fair and accountable responses
‘Explaining what has happened and whether any mistakes occurred, explaining whether complaints have or have not been upheld, giving clear reasons for decisions, identifying any learning from complaints and explaining actions that have been taken to improve services’.
ISCAS subscribers will receive a self-assessment tool to ensure they have taken all possible learning from complaints.
Sally Taber, director of the Independent Sector Complaints Adjudication Service
Anaesthetists at a click of a button
By Douglas Shepherd
Surgeons who need an anaesthetist with the correct skill sets, admitting rights and availability are being linked up via a doctordesigned app.
The Alloc8tor software, used to allocate 150 anaesthetists to thousands of surgical lists in 15 southof-England hospitals over the last four years, is now being rolled out across central London’s private healthcare sector.
Its designers say location and subspecialty filters ensure anaesthetists are only invited to lists relevant to them – ‘so gone are the days of being inundated with offers of work you would never do’.
Operating lists needing an anaesthetist are created by an administrator, normally an anaesthetic or surgical secretary, who can also include the Clinical Coding and Schedule Development Group (CCSD) codes and insurers.
Anaesthetists can then see the insured fees for cases on the list. Three-hundred surgeons are represented on the platform.
Administrators can select which anaesthetists to invite, based on the skill sets groups the anaesthetists have put themselves into or they can select private groups of their preferred anaesthetists that they control entry into.
Automated emails/SMS and inapp alerts are then sent to all interested parties, such as anaesthetists,
surgeons and theatre managers, at all stages of the allocation process, thus keeping everyone informed.
Anaesthetists answer with a Yes/ No/Maybe via the app and lists are either auto-allocated to the first positive responder or can be allocated by the administrator.
On allocation to an anaesthetist, the list disappears from everyone else’s app and drops into the ‘allocated’ section for the relevant anaesthetist.
Alloc8tor is free to join for anaesthetists and the basic functionality will remain free with optional premium features to be introduced in 2022.
The company aims to centralise the multitude of WhatsApp groups currently used so that, at any time, the anaesthetist has one place to visit to see work availability across the private hospitals in London that they work in.
Secretaries have easy access to a multitude of anaesthetists, who all have appropriate skills and admitting rights, and can see the up-todate responses.
Alloc8tor Ltd director, consultant anaesthetist Dr Harry Akerman, who co-founded the company with his friend Mike Crompton, said: ‘We are very
excited by the opportunity of extending Alloc8tor’s functionality and we believe that there is a lot that we can bring to the anaesthetic market in London.
‘Outside of London, the market dynamics are very variable. We welcome discussion with groups of anaesthetists and would consider these opportunities on a case-by-case basis.’
He told Independent Practitioner Today: ‘In London, Alloc8tor is free for anaesthetists and the core basic package always will be. We plan to introduce premium features in 2022 for the anaesthetists for which we would charge a subscription.
‘After the initial launch period, we will be charging for the administrative users – those advertising the work: hospitals, surgical secretaries – £15 per month plus VAT. In the future, we will be offering additional services and features that will be optional add-ons to the basic platform for all users.’
He said the company looked forward to growing and digitising many more time-consuming oldfashioned processes that took a lot of effort.
One orthopaedic secretary in London said the app had transformed the process of booking anaesthetists for her practice.
A user-friendly interface, clear colour coding, quick response times and live updates had saved much time and effort and she no longer needed to send out repetitive emails or messages to try and source anaesthetic cover for ad-hoc cases.
Alloc8tor’s early days were focused on delivering a well-supported service to anaesthetic groups, but the break of the Covid pandemic gave time and the opportunity to further develop the platform so it is now a dedicated iOS and Android application – seen as critical to its success in the London market.
Alloc8tor Ltd director and anaesthetist Dr Harry Akerman
The Alloc8tor works on both iOS and Android computer platforms
➱ continued from front page
Software to identify and fix payment shortfalls
Private hospitals are being promised an efficient way to identify and collect shortfalls and patients’ online payments using an automated service from a Healthcode partnership.
Codes were created by the company after analysing 15,500 shortfall messages contained in insurer remittances received in a 30-day period. These enable it to automatically scan electronic insurer remittances to see if there is a patient liable shortfall.
The system creates a shortfall invoice with the payer’s details and hospital specific branding and messaging when this happens.
Online platform patientzone then issues a collection notice with a unique link via email or text message which can be used to access its website and pay the balance due.
When the money is collected, it sends a receipt to the payer and notifies Healthcode, which provides an electronic remittance to the hospital so the transaction can be closed.
Healthcode said the service enabled hospitals to provide a convenient and secure online payment facility to patients and other payers without setting up a merchant account or paying credit card processing fees.
patientzone charges 2.5% +VAT commission when the bill is paid and deposits the money in the hospital’s account each week.
Hospitals can also set up branded automatic payment reminders at their preferred intervals at a cost of 10p +VAT for electronic reminders and 55p for paper reminders. Payers are not charged to use the patientzone platform.
Richard Shawyer, patientzone’s managing director, said: ‘This is an easy win for private hospitals who want patients to have a convenient and safe way to settle their account and create a positive impression.’
Free lessons for billing software
By Olive Carterton
Independent practitioners can now get free online tutorials to make the most of the tools and features available on Healthcode’s innovative software.
The Healthcode Academy is bringing them personalised oneto-one training for ePractice and The Private Practice Register (The PPR) with product specialists.
Training aims to ensure customers are fully aware of the company’s software capabilities so they can get the best return on their investment.
The academy provides a modular training programme so customers can build up their skills and confidence with each session.
Initially, there are three modules covering electronic billing and collections in ePractice and four modules focusing on The PPR,
Independent cancer unit gets latest robotic gear
The Christie Private Care has acquired the advanced robotic integrated surgical system, the da Vinci Xi, bringing a level of minimally invasive complex cancer surgery to private patients unavailable elsewhere in the Manchester area.
Urological and robotic surgeon Mr Aziz Gulamhusein said: ‘The da Vinci Xi is the latest robotic platform and this enhanced technology means, as surgeons, we can gain different visual perspectives and reach different angles, allowing us to operate with greater precision than ever before.
‘This investment means we are now able to offer more patients
Healthcode’s online directory of practitioners.
Each free tutorial uses the customer’s own Healthcode account to make it as familiar and relevant as possible, enabling them to test their understanding and practise what they have learnt in a real-world situation, from creating an electronic bill to maintaining their PPR profile.
tech companies to develop solutions that push the boundaries, but new technology can be daunting and the real test is whether it helps improve people’s lives.
Personalised tutorials last between 30 minutes and one hour and are available to anyone with a Healthcode user ID and password.
Customers can register online at www.healthcode.co.uk/lp/healthcode-academy where they will be able to book a convenient slot.
They will receive a certificate and a useful training manual on completion of each module.
Healthcode managing director Peter Connor said: ‘It’s exciting for
‘The idea of the academy is to ensure that Healthcode customers have the support they need to familiarise themselves with the capabilities of the system and make the most of its tools and features in their own practice.’
Ahmed Khan, service delivery manager ePractice, has been overseeing the academy launch and believes it will transform the way customers use their accounts.
He said: ‘By giving them the chance to explore ePractice and The PPR with the support of our product specialists, customers will quickly build their understanding, skills and confidence.’
access to timely robotic surgical treatment, provided by expert and highly skilled clinical teams, helping to provide excellent outcomes with rapid recovery.’
The hospital said that, unlike other systems, firefly fluorescence imaging was built into the robot to give surgeons real-time visualisation and assessment of vessels, bile
ducts and tissue perfusion – allowing them to operate more easily across multiple quadrants of the body and giving them better access during complex procedures.
The da Vinci Xi is the latest addition to the newly installed £7.8m operating theatres at The Christie Private Care’s, part of HCA Healthcare UK.
Mr Aziz Gulamhusein and Mr Jeremy Oates (back, right) with their team
Healthcode’s Peter Connor
Celebrating the inspiring
Nearly 1,000 guests celebrated the best in private health and social care at the ‘medical oscars’ – the 16th LaingBuisson Awards.
Held in the spectacular ballroom of the London’s Park Plaza Westminster Bridge, the event was hosted by comedian Tom Allen, who entertained before handing out gongs with the hosts’ nonexecutive director Stephen Dorrell.
This was the first in person awards celebration for two years and finalists were chosen by an independent panel of judges from a record 490 nominations.
LaingBuisson founder and exec
Circle Health recognised as top hospital group . . . again
Circle Health Group has again been named as the UK’s leading private hospital group – this time at the annual LaingBussion awards.
The accolade, presented during a glitzy evening celebrating private healthcare, came in recognition of the group’s excellence in the delivery of care, in addition to innovation and transformation in challenging circumstances.
This is the second high profile healthcare award it has won since acquiring BMI Healthcare two years ago.
The first came at the annual Health Investor Awards where it was awarded ‘Private Hospital Group of the Year’ in response to the extraordinary contribution clinical teams made at the height of the pandemic.
Judges at the LaingBussion event noted that Circle Health Group stood out in its delivery of acute health services and focus on technological inno vation.
They also recognised the work of its teams during Covid19 when its
utive chairman William Laing said the awards offered providers and advisers the opportunity to recognise and celebrate the most inspiring and innovative work in the independent sector.
He added: ‘The nominations were hugely impressive and included many deserving projects, organisations and professionals who are dedicated to tremendous health and care causes, and I know that the judges’ decisions were not easy ones. We are delighted with the awards’ continued success and congratulate all our finalists and winners.’
David Anderson, commercial director at Circle, with Nicky Green of category sponsors Capsticks
50 hospitals gave urgent care to more than 700,000 NHS patients.
The group, which has stated it is committed to being the leading private hospital group for technology and digital innovation, invested £100m in facilities last year.
It said these were all factors that judges noted as having set it apart from other finalists.
Mr Paul Manning, its chief medical officer, said: ‘The investment we have made into our facilities and services has made a tangible difference to the quality of services we deliver across a range of specialties.
‘Winning awards like this not only shows that we are doing the right thing, but it also inspires us to keep pushing to deliver the best patient outcomes and to become the most attractive private hospital group for consultants to do their private practice with.’
THE WINNERS – AND JUDGES’ COMMENTS
THE 31 WINNERS INCLUDED:
HOSPITAL: sponsored and presented by Ben Heaver, commercial director, Streets Heaver Healthcare Computing
Schoen Clinic Newbridge
‘An impressive submission demonstrating innovation in its approach to eating disorders.’
LARGE RESIDENTIAL CARE: sponsored by HPC Healthcare Property Consultants
Care UK
‘Outstanding ratings are very hard to achieve and this demonstrates that their commitment to quality and their ability to deliver what the regulator is looking for is second to none.’
HOSPITAL GROUP: sponsored and presented by Ian Cooper, partner, Capsticks
Circle Health Group
‘Really impressive on the innovation front, both in terms of introducing rehab to the UK and the Spanish partnership. UK acute care is well in need of revolutionising; glad you are on that journey.’
MANAGEMENT EXCELLENCE: sponsored and presented by Chris Howe, national account manager, Apetito
King Edward VII’s Hospital
‘Really good to read this submission which really demonstrated management and values and diversification.’
LENDER:
Shawbrook Bank
‘An experienced leading healthcare team able to make rapid decisions to respond to customer needs alongside strong commitment through various stakeholder support initiatives.’
PRIMARY CARE AND DIAGNOSTICS: sponsored and presented by Dasos Kirtsides and Christos Christodoulou, Shawbrook Bank
Limbic
‘Incredibly impressive innovation which enables faster access to a critical service – very impressive.’
INNOVATION IN HEALTH TECH:
Check4Cancer
‘I really value this nomination, as there are so many unnecessary early deaths from cancer which will only rise because of lockdown. Early detection can only saves lives.’
HEALTHCARE OUTCOMES: sponsored and presented by Chris Kenny, MDDUS
Ramsay Health Care UK
‘Excellent statement – We are not afraid to challenge the status quo to find better ways and the ‘no blink approach’.
EXCELLENCE IN TRAINING:
Cromwell Hospital
‘Equality and diversity is at the very heart of this submission which is of paramount importance to ensure all needs are met with parity.’
NURSING PRACTICE: sponsored and presented by Fahim Modak, Zentar Healthcare
King Edward VII’s Hospital
‘Excellent example of working with the British Society of Gynaecological Endoscopy and the use of a clinical nurse specialist.’
Cromwell Hospital’s Respect, Equality, Diversity and Inclusion (REDI) Network won the Excellence in Training Award.
Influenced by movements such as Black Lives Matter, over the last year REDI has transformed its equality and diversity committee. As a result, it has grown from a handful of dedicated volunteers to a strong network with a clearly governed and defined committee and structure.
Double success for King Edward VII’s unit
King Edward VII’s Hospital scooped two categories at the Awards: Nursing Practice and Management Excellence.
The former recognises providers who have delivered improvements and innovation to nursing and patient management.
This achievement was demonstrated by a partnership with the British Society of Gynaecological Endoscopy to streamline patient
Globally and nationally, inequality in healthcare remains a significant issue and the REDI team is focusing its efforts to address this, putting new practices in place to make sure that the hospital’s patients and colleagues feel seen, heard, respected and welcomed. For example, the team is developing an Allyship programme to help colleagues grow and support their diverse range of patients.
By wearing an Allyship badge, patients can feel more confident disclosing personal information, and take comfort knowing their care can be specifically tailored to their needs.
The London hospital is also broadening its use of inclusive language, with consultants using gender neutral pronouns when discussing matters such as prostate cancer.
A Cromwell Hospital spokesman
Cromwell triumphs for giving patients respect
said: ‘I’m incredibly proud of how much the team has achieved in the last year; from marking culturally important events and festivals, to educating our people on important issues in the diversity space.
‘Their dedication to making important changes has helped our people and patients feel able to bring their whole selves to the Cromwell Hospital, and this award is testament to their hard work.’
journeys for endometriosis treatment.
The award recognised the hospital’s commitment to wider social projects too.
King Edward VII’s Hospital’s Veterans’ Pain Management Programme has catered to 450 members of the armed forces, managing health conditions and improving quality of life for serving and exservice personnel and their families.
The Management Excellence category, recognising exceptional clinical or patient outcomes, financial results or employee engagement, was made in response to the hospital’s colorectal robotics service and lymphatic microsurgical approach to breast cancer.
Chief executive Lindsey Condron said: ‘We are extremely proud that our achievements were recognised by LaingBuisson, which included
our support of the NHS in the response to the Covid 19 pandemic, as well as the team’s agility and innovation in establishing and delivering new clinical services.
‘By using the latest technologies and working collaboratively and innovatively, we’ve been able to demonstrate our clinical excellence and deliver the best outcomes for our patients.’
More awards ➱ p8
Cromwell Hospital’s REDI team pictured with LaingBuisson non-executive
director Stephen Dorrell (left) & master of ceremonies, comedian Tom Allen (right)
Pictured right: King Edward VII’s management team
Schoen makes it three in a row
Schoen Clinic Newbridge proudly picked up the award for the 2021 Hospital of the Year at the annual LaingBuisson Awards.
The group’s latest accolade follows taking the 2019 Hospital of The Year award for Schoen Clinic’s orthopaedic and spinal hospital in London and Private Hospital Group of the year in 2020.
Awards this year were the biggest ever with finalists chosen from 490 nominations.
The Hospital of the Year award honours ‘excellence in the provision of acute or mental health services with a focus on innovation and differentiation as a result of an
individual hospital initiative or investment’.
UK managing director Andy Davey said: ‘To win an award three years in a row is truly outstanding for our group and Schoen Clinic Newbridge deserve this recognition for the amazing work they do helping children and young people with eating disorders.
‘They are heavily involved in clinical research and consistently strive for the best possible clinical outcome for the patients they care for.’
Hospital director Natalie Maley said: ‘I’m so proud that we’ve been recognised for excelling in our field
and, for this, we have our colleagues to thank.
‘Their dedication and enthusiasm for our patients, to each other and to our hospital – is what stands us apart. It is a privilege to work with such an engaged and committed group of colleagues.’
Schoen Clinic UK currently comprises four facilities:
Schoen Clinic Orthopaedic and Spinal Hospital London;
Schoen Clinic Day Centre for Mental Health Chelsea, treating anxiety, mood and eating disorders;
Schoen Clinic Newbridge, treating children and young people with eating disorders;
Schoen Clinic York, treating adults with eating disorders.
The Group says it aims to find ‘the very best consultants and medical colleagues’ and observes ‘a relentless focus on clinical outcome excellence’.
(ABOVE) Rachel Matthews, director of Schoen’s mental health services (in red dress), and Newbridge Clinic’s director Natalie Maley
Ramsay receives plaudits for speaking up for safety
Ramsay Health Care UK won the LaingBuisson Healthcare Outcomes Award, recognising it for excellence in the delivery of better healthcare outcomes.
Judges were particularly impressed with the rollout of its Speaking Up for Safety programme which promotes a strong culture of professional accountability and freedom to raise safety issues.
The company sees this as an important part of its continuous improvement agenda to deliver safe care for its patients.
Ramsay medical director Mr Charles Ranaboldo, a consultant vascular surgeon, and and Viv Heckford, national director for clinical services, collected the award.
She said: ‘I am absolutely delighted that Ramsay has received this prestigious award and I am very proud that the hard work of all our teams has been recognised.
‘Ramsay is committed to address behaviours that undermine a culture of safety and to ensuring that all our patients receive the safest and most reliable patient care.’
Members of the Schoen Clinic Newbridge with the Hospital of the Year Award
Ramsay’s director for clinical services, Viv Heckford, and the firm’s medical director Mr Charles Ranaboldo after being presented with the award by MDDUS chief executive Chris Kenny (left), who sponsored the category
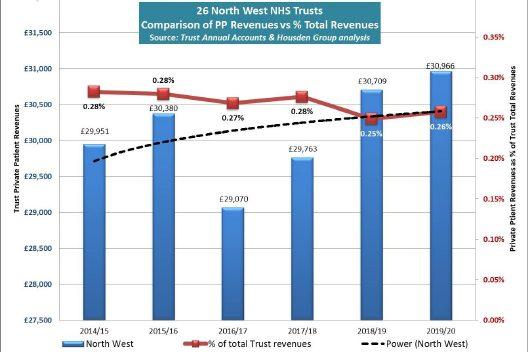
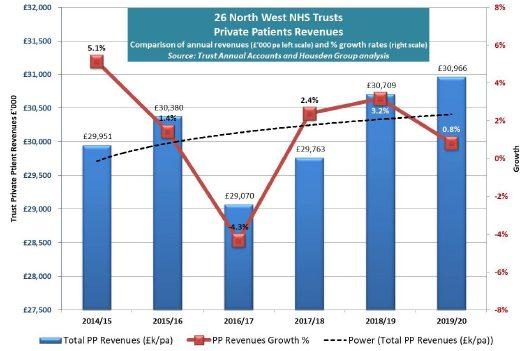
Covid harm costs NHS trusts £295m
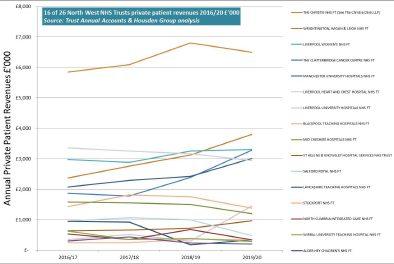
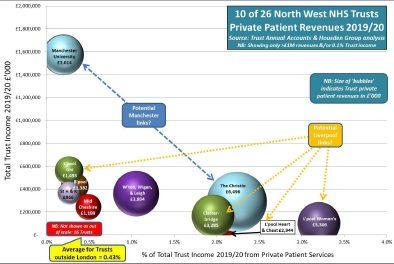
Compiled by Philip Housden
With all but one of 141 acute NHS trusts in England having now published their annual reports and accounts for 2020 21, the key headlines relating to the impact of Covid on private patient incomes are now clearer:
☛ Total revenues were £380m, down 44% and £295m on 201920, and so represents a fall in income to the NHS of approximately £25m a month.
☛ Highest individual trust income was once again The Royal Marsden with £102.3m. This was down £30.3m, but at 22.9% the yearonyear reduction was much less than the sector average.
☛ For the first time for many years, not all of the top ten revenue generating trusts were from London. Cambridge University Hospitals, with £7.8m income achieved eighth place and Oxford University Hospitals, at £6.7m, was in ninth.
This, in turn meant, that UCL dropped from sixth to 12th with incomes of £5.9m, down £15.9m and 73%.
Private eye group sees its
numbers
nearly double
Royal Free also fell and is now the 18th highest income trust, down from eighth in 201920, with revenues of £3.6m, a fall of 82% and £16.8m on last year.
☛ All London trusts together declined by 43% and the average for all out of London trusts’ incomes was a fall of 46%.
☛ Regionally, the declines ranged from a low of 32% in the Northwest to 56% in both Yorkshire and the East Midlands.
☛ Interestingly, there was no marked difference between the
average reduction of 44% for the 53 trusts with designated private patient beds and the 43% fall for the 88 trusts without designated beds. A more indepth analysis of the full picture, region by region, will be shared in a future issue of Independent Practitioner Today
The trust whose annual report remains outstanding as I write is University Hospitals of Leicester.
Philip Housden is a director of Housden Group. See his feature article on PPUs in the North-west on page 46
(From left to right) Mr Ali Mearza, Mr Romesh Angunawela, Mr Shahram Kashani, Ms Susan Sarangapani, Dr Allon Barsam and Mr Chien Wong
Patient numbers seen by consultants at the doctorowned private OCL Vision clinic have risen 92% and operations are up 84% in a year.
Three years after launch, the London-only consultantowned, comprehensive eye care facility has trebled its staff and the number of consultant surgeons to nine. The clinic’s specialists had 3,600 new patient consultations in the year to November 2021, up from
just under 1,900, and did 2,700 surgical procedures. Founding partner Dr Allon Barsam said: ‘We set up OCL Vision to provide the highest level of specialised private eye care in the UK.
‘We’re delighted with the growth of our business. This reflects a growing trust in our services from our patients, other consultant eye surgeons, GPs and our referring optometrists.’
Moorfields opens private West End unit
The London Claremont Clinic on New Cavendish Street, Marylebone, in the heart of London’s medical district, is now part of Moorfields Private, the private patient division of Moorfields Eye Hospital NHS Foundation Trust.
It is an outpatient facility with eight consulting rooms, diagnostics and minor treatment rooms, and replaces the trust’s Upper Wimpole Street site.
Andrew Robertson, director of private care, explains: ‘This has been an exciting opportunity for Moorfields Private. As a worldrenowned centre of excellence for ophthalmic care, we are delighted to have extended our services and capacity in the heart of London’s clinical district, providing patients with more choice when accessing private services, consultants and treatment.
‘It strengthens our position as one of the country’s leading providers of private eye care and will enable us to re invest more back into Moorfields Eye Hospital’s NHS services.’
In 202021, Moorfields reported private patient revenues of £24.3m, £6.5m and 21% down on 201920, but beating the London and Englandwide average.
The trust now has the fourth highest grossing NHS private patient service, up from fifth place.
Mr Maghizh Anandan has been appointed as a consultant eye surgeon at Optegra Eye Hospital Birmingham, joining from the Royal Derby Hospital. He will lead refractive surgery including laser vision correction, lens replacement and private cataract surgery.
The Royal Marsden’s private unit in London’s Cavendish Square
Avoid being taken in by scammers, warns HMRC
By Leslie Berry
Doctors are among professionals being warned they could be targeted by tax scams in the run-up to the 31 January self-assessment deadline.
HM Revenue and Customs (HMRC) is reminding them to be on their guard after 800,000 tax-related scams were reported in the last year.
Fraudsters use self-assessment to try and steal money or personal information from unsuspecting individuals. Tax officials have received 360,000 bogus tax rebate referrals in the last year alone.
Customers may expect to hear from HMRC at this time of year and more than four million have in the last few weeks been issued with guidance and support, prompting them to think about how they intend to pay their tax bill and to seek support if they are unable to pay in full by 31 January.
But the department is also warning customers not to be taken in by malicious emails, phone calls or texts, thinking that these are genuine HMRC communications referring to their tax return.
HMRC’s director general for cus-
TAKE PROTECTION – FOLLOW THESE TIPS
If a phone call, text or email is unexpected, do not give out private information or reply to it, and do not download attachments or click on links before first checking on GOV.UK that the contact is genuine
Do not trust caller ID on phones. Numbers can be spoofed
It is OK to reject, refuse or ignore any requests – only criminals will try to rush or panic you
Search ‘scams’ on GOV.UK for information on how to recognise genuine HMRC contact and how to avoid and report scams
Forward suspicious texts claiming to be from HMRC to 60599 and emails to phishing@hmrc.gov.uk. Report tax scam phone calls on GOV.
UK
Contact your bank immediately if you think you have fallen victim to a scam, and report it to Action Fraud. In Scotland, contact the police on 101
tomer services, Myrtle Lloyd, advised: ‘Never let yourself be rushed. If someone contacts you saying they’re from HMRC, wanting you to urgently transfer money or give personal information, be on your guard.
‘HMRC will also never ring up threatening arrest. Only criminals do that. Swindles come in many forms. Some threaten immediate arrest for tax evasion, others offer a tax rebate.
‘Contacts like these should set alarm bells ringing, so if you are in any doubt whether the email,
phone call or text is genuine, you can check the ‘HMRC scams’ advice on GOV.UK and find out how to report them to us.’
Criminals use emails, phone calls and text messages to try and dupe individuals, and often mimic Government messages to make them appear authentic in the hope that victims are tricked into handing over money or personal or financial information.
Customers can report suspicious phone calls using a form on GOV. UK; customers can also forward suspicious emails claiming to be
from HMRC to phishing@hmrc. gov.uk and texts to 60599.
HMRC has a dedicated team working on cyber and phone crimes. They use innovative technologies to prevent malicious communications from ever reaching the customer. Since 2017, these technical controls have prevented 500 million emails from reaching HMRC’s customers.
More recently, new controls have prevented 90% of the most convincing SMS messages from reaching the public and controls have been applied to prevent spoofing of most HMRC helpline numbers.
HMRC is also reminding selfassessment customers to doublecheck websites and online forms before using them to complete their 2020-21 tax return. People can be taken in by misleading websites designed to make them pay for help in submitting tax returns or charging to connect them to HMRC phone lines.
Customers who are in any doubt about whether a website is genuine should visit GOV.UK for more information about self-assessment and use the free signposted tax return forms.
Care firm gets huge fine for not registering with CQC
An independent ambulance service who provided services without being registered with the Care Quality Commission (CQC) has been fined £4,000 – the maximum amount allowed in law.
The care watchdog issued a fixed penalty notice to Medicar Euro-
pean, based at Ascot Barn, Ashford, in Kent. Inspectors found the provider transported 28 patients between 24 July 2020 to 7 August 2020 despite not being registered.
It is an offence under the Health and Social Care Act 2008 to carry
out a regulated activity – in this case, provide the activity of transport services, triage and medical advice provided remotely – without being registered.
Emma Boger, CQC’s head of registration, said: ‘This is first time we have taken this action against an
independent ambulance provider and I hope it sends a clear message to others that where we find providers operating outside of the law, we will always use our enforcement powers to protect people and hold them to account to stop poor and illegal practice.’
A look back through our journal’s archives of a decade ago reveals that although times change, some issues are not so new
A trawl through the archives: what made the news in 2012
Self-pay shoppers
Private consultants were being urged to launch their own ‘January sales’ drive at GPs to try and tap into what we called ‘a new breed of self-pay shopper’.
The marketing advice came after a quarter of GPs in a survey reported a rise in the number of patients asking about private healthcare or self-pay in the previous six months.
Scores of private hospitals had also seen a welcome rise in noninsured patients.
One hospital group’s clinical director recommended consultants adopted five New Year resolutions to boost self-pay referrals:
1. Meet with GPs face to face –either at an evening hosted by their private hospital or by travelling to meet the doctor and their team at the surgery. Keep them up to date with clinical practice developments.
2. Call GPs to let them know how their patients had fared after surgery. This only took ‘two minutes per patient’ at the end of the session and GPs would value the personal touch.
3. Work with your private hospital to ensure GPs are kept up to date about your services and how these differ from those available through the local primary care trust.
4. Work with hospitals to demonstrate the quality of your clinical outcomes and patient experience.
5. Encourage GPs to invite those with insurance to exercise their opportunity to use it.
Merit awards hit by tax hike on pensions
Consultants were shocked to find their hard-earned clinical excellence awards could be eroded by a 50% tax hit.
Cuts in the maximum tax-free contributions they could make to private and NHS pensions meant they would be taxed on half of anything they annually invested above £50,000.
Until the previous April, tax only kicked in above £255,000 a year. Specialist financial planners Cavendish Medical warned doctors it was imperative to find out their total annual contributions across both NHS and private pensions, as the onus was on the individual to tell HM Revenue and Customs if they were liable for the charge.
Rise in spot checks on clinics
Independent practitioners were facing an increased likelihood of an unannounced watchdog inspection in 2012 from the Care Quality Commission (CQC).
Practice managers in the Harley Street area were already reporting a rise in unexpected visits.
A CQC inspector told a Practice Managers Forum meeting that most inspections were now unannounced.
Doctors quit early
A sharp rise in the number of consultants taking voluntary early retirement in 2011 reflected growing dissatisfaction about changes underway in the NHS, the BMA said.
According to a BMJ Careers report, the proportion of senior doctors taking voluntary early retirement before the age of 60 leapt by 72.4%, from 98 doctors in 2010 to 169 in 2011.
The BMA Consultants Committee cited NHS pension changes as one reason why many consultants were opting to go at the earliest opportunity.
Other factors included NHS reforms and work intensity, partly due to a drop in junior doctors’ availability following new working time restrictions.
Taxman plays tough
Doctors were shocked to receive letters from tax officials erroneously claiming they had not filed their tax returns.
The Association of Independent Specialist Medical Accountants reported a number of doctors were sent letters from HM Revenue and Customs (HMRC) saying their tax returns had not been sent in.
But tax offices later admitted these were sent out in error.
The mix-ups followed HMRC letters to 2,500 doctors and dentists claiming it knew their tax affairs were not up to date.
Law on jobs to be eased
Doctor employers and their managers will have to swot up on a new raft of employment laws under Government proposals.
Business Secretary Vince Cable wants bosses to have a simpler and quicker way of dismissing staff.
TELL US YOUR NEWS
Share your experience of what has and has not worked in your private practice. Even if it’s bad news, let us know and we can spread the word to stop others falling into the same pitfalls.
Contact editorial director Robin Stride at robin@ip-today.co.uk
THE PRIVATE HEALTHCARE INFORMATION NETWORK
The window to private doctors
Independent Practitioner Today asked Anne Coyne, (right), consultant relationship manager at the Private Healthcare Information Network (PHIN), what were the top six things consultants
needed to know about the organisation
1
Private healthcare is seeing strong signs of recovery
As has been widely reported from PHIN’s data, we are seeing strong signs of recovery post-pandemic within the private healthcare sector, not only across England but across the whole of the UK.
This is particularly evident for self-pay, which has seen a jump of 30% from the second quarter of 2019 to the same quarter in 2021.
Much of this has been driven by a rise in hip and knee replacement surgery and cataract surgery – all of which are now more commonly paid for through self-pay.
2
We have a new patient facing website
PHIN launched a new-look website this summer and has seen traffic from patients grow steadily ever since. We now have more than 20,000 unique visitors trawling more than 70,000 pages each month.
The design of the website is based on what patients told us would be helpful to them and is based around consultant profiles.
Patients can now search for consultants by name, specialty or location and are given supporting information about common procedures.
Since we launched, more than 2,000 patients have contacted a consultant or their secretary through our website, and that number continues to grow.
The PHIN website not only plays a unique role in providing independent information to patients about hospitals and consultants, but it also offers consultants an opportunity to promote their practice to patients.
Patients continue to tell us that they are more likely to look at a profile that provides information about:
A consultant’s training; Their specialty and subspecialty interests;
The procedures that they perform;
When the profile includes a photograph of the consultant. We encourage consultants who have yet to create a profile about themselves and their practice to log onto the PHIN Portal and do so. This will help patients access the information that they need.
3
Patient satisfaction –independent feedback from patients
PHIN’s market research confirms that feedback from other patients who have received treatment or care from a consultant will influence their treatment decisions. As such, we recently started publishing our independently collected patient feedback scores for individual consultants.
Working with hospital doctors, we use a standard set of questions and responses to generate two measures of patient feedback on our website: patient satisfaction and patient experience.
The measure is published when PHIN has received 30 or more complete feedback responses and is wholly independent. Any comments provided by patients are available to the hospitals submitting the feedback on the portal –these are not published on PHIN’s website.
4
We co-design with consultants –particularly our portal We made some changes to the PHIN portal last year and wanted to test how well these changes have been received.
At a recent review, we listened to the feedback of consultants – both what we heard directly as we go out and attend meetings, but also through a series of structured interviews.
This is just a single stage of an ongoing process to design our systems in collaboration with consultants so that we respond to their needs.
There are legal obligations on consultants for engaging with PHIN, but it should also be a benefit and a positive experience – we know that your time is precious. The portal is here to support consultants to create profiles and submit fee information but also to review the episode data that has
At Xyla Elective Care, we provide NHS-funded care both in acute hospitals and in the community These services are designed to support new and evolving care delivery models to ensure patients can be seen virtually where appropriate as well as the usual face-to-face delivery options
Our purpose is to further the seamless integration of highquality care between primary and secondary institutions for the benefit of patients To achieve this purpose we recognise that we cannot do business as usual not only in the way we serve our clients, but the people we recruit into operational roles as well as those who join our frontline clinical teams
As part of the Acacium Group, we benefit from the infrastructure of a large, successful organisation with over 20 years of experience as the largest provider of workforce solutions to the healthcare sector in the UK and Europe
Career opportunities
been submitted to PHIN from private hospitals.
We recommend that consultants take time to review this information in their Practice Report on the portal and use the ‘data issue process’ to notify hospitals of any queries on the data submitted
5
Fulfilling
legal obligations
We are there to support consultants and add benefits, but there are also legal obligations – specifically around transparency of costs and fees.
More than 8,000 consultants have approved their fees for publication so far, allowing us to publish these for the benefit of patients and increase transparency.
We contact all consultants who fall under these legal obligations directly using their GMC registered email address. If you receive an email from PHIN, please read it and take appropriate action.
6
We have just published more safety measures
In early December, we published a further set of safety measures. These will include unplanned re-admission, mortalities, unplanned transfers, serious injuries and returns to theatre.
Understanding the sensitivities and complexities involved in publishing this type of information, we will be publishing by hospital sites only.
We continue to work closely with the royal colleges and specialty associations, as well as with private hospitals, the Competition and Mar kets Authority (CMA) and others as we develop our strategy over the next five years to publish all of the required measures and bring greater value to patients.
And we will always consult widely to ensure there should be no surprises when we publish new information.
To meet the growing demand for our surgical and outpatient services Xyla Elective Care is recruiting experienced Consultants interested in joining our team to work alongside dedicated colleagues in a supportive environment and within an organisation with a reputation of having robust clinical governance and strong organisational structures We have job opportunities for this role in various locations across the UK
We are now hiring:
ENT Consultants
General Surgeons
Urologist
Ophthalmologist
Gynaecologist
Benefits
“If you have the right work experience this is an excellent opportunity You must be fully trained and currently practising in the same field within the NHS There is a strong culture of teamwork and putting the patients first ” Tosin Ajala Gynaecologist at Xyla elective Care
Our clinician workforce undergoes a robust recruitment process and thorough competency review, so you can be assured that you will work for the best clinical teams
We are committed to innovate patient pathways – you will be given the opportunity to deliver patient care in new and exciting ways
We have a reputation for having robust clinical governance, so you can be assured that you will not be exposed to unmitigated clinical risks
We regularly ask for your feedback to allow us to tailor work to suit your needs
Detailed operations manuals ensure you are adequately prepared to support each contract
How to join our team
Are you still thinking about it? Find out more about Xyla Elective Care and make the smart career choice to expand your experience
What drives patients to adhere to advice
Many healthcare challenges today are social or behavioural in nature rather than purely medical. Understanding how people behave in the real world, rather than how we want them to behave, is key to designing effective healthcare interventions.
Dr Caroline Wood (right), head of behavioural insights and research at Bupa, explains how behavioural insights benefit healthcare
BEHAVIOURAL INSIGHTS are used to understand how humans make choices, applying thinking from diverse fields including psychology, sociology, behavioural economics and anthropology. Research from these areas shows that, as humans, we are irrational thinkers and often behave in ways that are counterintuitive and not always in our best interests. This has big implications for healthcare.
For example, patients can make poor lifestyle choices that negatively impact their overall quality of life or health outcomes – such as smoking, poor diet, lack of exercise – or fail to stick to medication regimens or recommended treatment pathways.
Understanding the science of why people do what they do can help us to deliver better healthcare and enable us to design more effective products and services
that work alongside human psychology.
Incorporating behavioural insights into your practice
We know many diseases can be preventable if patients follow optimal health behaviours.
Clinicians play an important role in influencing patients’ health behaviours and advising them about how they can make healthier choices.
Each patient interaction is an opportunity to deliver a brief behavioural intervention to provide advice and motivate patients to make meaningful behaviour changes.
These touchpoints are important in preventing disease and controlling the burden of noncommunicable diseases on society.
In the UK, this approach to tackling preventable diseases is what’s called ‘making every contact count’ (Health Education England/Public Health England: www.makingeverycontactcount. co.uk).
Having an awareness of what behavioural insight is and how it can support patient care is rapidly becoming a differentiator in the clinician’s toolkit.
The ability to understand patient motivations and identify barriers in current behaviour enables clinicians to tailor the support they provide more closely to patients and deliver a more personalised, efficient standard of healthcare.
What a behavioural insights team does
Perhaps the most high-profile behavioural insights team or, ‘nudge unit’ as they are now popularly known, was the team established by David Cameron’s UK government in 2010.
Since then, many organisations have established their own behavioural insights teams, and have demonstrated how behavioural insights can have a big impact on public health and healthcare systems through making simple changes.
For example, increasing organ donor consent rates by 38% through changing how consent was framed on a sign-up webpage or reducing the number of missed
At Bupa UK, we are on a journey to embed behavioural insights in our products and services, with the aim of supporting our customers and our people to make better choices and lasting lifestyle changes
This approach means you end up wasting time, money and other resources trying to find the solution.
By taking a behavioural science approach, we first understand why people aren’t behaving as expected before trying to change their behaviour.
hospital appointments by 25% through simply sending patients timely reminders by text message.
At Bupa UK, we are on a journey to embed behavioural insights in our products and services, with the aim of supporting our customers and our people to make better choices and lasting lifestyle changes.
Our behavioural insights team is made up of individuals with a range of backgrounds, including behavioural economics, psychology and public health.
Our evidence-based, interdisciplinary approach enables us to create simple and targeted interventions to improve health and well-being.
We use this interdisciplinary expertise to understand a range of health-related challenges and create simple and targeted interventions to bring about change.
We offer insight to a wide range of challenges including how to increase participation in health and well-being initiatives and improve adherence to health programmes through to how to optimise people’s engagement with health information.
When people aren’t behaving in the way that we expect them to, the tendency is to dive straight into solution mode and try lots of approaches to change their behaviour.
Some of these might work, some might work well for a while and then lose their impact, some might not work at all.
The problem with using this ‘kitchen sink’ approach is that there is no roadmap to help you choose your next strategy or help you understand why what you tried didn’t work.
This provides us with a theorybased ‘roadmap’ to help guide our design of a solution. Having this guide means we can bring about change more quickly, streamline our costs and resources, and increase confidence that the solution will directly address the behaviour and barrier unique to the context.
Supporting our patients
We know that our residents living in Bupa care homes are particularly susceptible to the flu virus, with two-thirds of outbreaks during the winter originating in care homes.
To help keep both our residents and people safe and well, it is imperative that our people receive the flu jab.
We interviewed our people working in care homes and reviewed existing literature on flu vaccination to find out the main barriers to uptake.
We discovered these included common misperceptions, such as the vaccine not being necessary or causing flu itself, which we were then able to address through targeted communications to dispel flu myths and make it easier for people to get their vaccine.
Making these small changes led to an 11% increase in flu vaccine uptake among our staff.
Enhancing our clinical practice
Antimicrobial resistance is a top global public health threat facing humanity. 1 In light of this, we have worked closely with our Bupa UK pharmaceutical managers to reduce antibiotic prescribing where prescription of certain drugs was not always necessary.
Drawing on insights from similar effective interventions 2 designed by the UK behavioural insights team, we sent a behaviourally informed letter to consultants to clearly communicate national guidelines and make it
really simple to understand what was required of them.
Following the intervention, spend on unnecessary prescriptions fell and one hospital group introduced an automated process in its prescribing systems, meaning that the change was maintained over time.
Upskilling our clinicians
We have also developed two bespoke, interactive training programmes for our front-line clinicians: one for health advisers in our clinics and another targeted at dentists across our global practices.
These provide them with the tools to embed principles from behavioural insights into their practice to enhance the interactions they have with patients.
Bupa’s health assessments offer a fantastic opportunity for customers to identify and address their own health risks.
However, the hardest part is often knowing how to best support and motivate customers to make the necessary changes after their health assessment, like increasing physical activity or adopting a healthier diet.
Knowing how to approach customer conversations like these and what to say at which point enables our health advisers to better support our customers to adopt a healthier lifestyle.
Working closely with our health advisers and consulting regularly with academic experts at University College London, we have developed bite-size learning videos, interactive quizzes and inpractice examples structured around a framework we call the Bupa 3Bs: behaviour, barriers and behaviour change techniques.
➲
B1 – Behaviour: It’s important to first identify what behaviour you want to target for change or to support your patient to change.
Not having a clear target in mind, selecting a change that doesn’t sufficiently motivate or appeal to your patient or trying to make too many changes at once can jeopardise chances of success.
➲
B2 – Barriers: Taking the time to explore existing barriers to change as well as things that may
facilitate the desired behaviour can help you more closely tailor the support you provide.
The COM-B model is a simple framework which can help you identify barriers from patient conversations. The model proposes that for behaviour change to happen, patients must have the:
Capability – the know-how, ability;
Opportunity – resources such as time, a supportive network around them;
Motivation – the drive to change, wants and needs.
If one or more of these is missing, then this may prevent change from happening and is where your support would be best focused.
➲ B3 – Behaviour change techniques (BCTs) : BCTs are the ‘ingredients’ of a patient conversation about change and can include techniques such as helping them set a goal, providing information about any consequences if they chose not to make changes, as well as showing them in person how to do the behaviour.
In the training, we introduce trainees to twelve of the most commonly used, evidence-based BCTs that can be built into patient conversations to build motivation to change, plan and set goals, as well as to support patients to maintain that change. For a full list of techniques, go to www.sbm.org/ UserFiles/file/Michie-etal2013 BCTV193techniquesAddlFile Taxonomy.pdf.
The twelve techniques are:
1. Goal setting;
2. Action planning; 3. Feedback on behaviour; 4. Social support; 5. Restructuring the environment; 6. Commitment; 7. Self-monitoring; 8. Instructions on how to perform behaviour; 9. Information about health consequences; 10. Problem solving; 11. Rewards; 12. Credible source, e.g. communications from a respected person.
ALTHOUGH SOMETIMES difficult to conceptualise a ‘typical’ patient appointment, there are some common features that most patient-clinician interactions will share.
Here’s how you could implement the 3Bs into your own practice:
Before the appointment
Reviewing the patient’s history and medical notes may help you identify any areas to prioritise for change or to explore further with your patient during their time with you.
Gathering insights and selecting a target behaviour
➤ Welcoming your patient into the clinic room and engaging them in conversation provides an opportunity to build rapport and establish strong relationships.
Not only does developing a good rapport encourage patients to be open with you, it also builds patient confidence and motivation for behaviour change.
This first part of the appointment is key, as it gives you a great opportunity to find out more about your patient’s lifestyle, including anything that may influence their readiness and motivation for change.
➤ Assessing their health status follows, finding out more about their health behaviour and any problems they might be having. This is where you bring in B1 (behaviour) and B2 (barriers) of the 3Bs.
It’s where you identify an appropriate target behaviour, consider whether there are any barriers to change and start to discuss goals with the patient.
➤ Having assessed your patient, you will likely already have a good idea about what they need to do – that is to say, their target behaviour – to improve their health. This is the perfect time to find out whether the target behaviour you have in mind would also be a good ‘fit’ for your patient
Exploring barriers
➤ When talking with your patient, listen to see if they mention anything that could be a barrier for change.
Keeping the simple idea of the COM-B model in your mind as they are speaking can help you identify whether it’s a capability, opportunity or motivation issue and where to focus.
Setting goals and providing ongoing support
➤ Building effective behaviour change techniques (B3) into your conversation can help you take your patient from thinking about change, through to setting goals and onto maintaining change after their appointment.
End of the appointment
➤ The end of the appointment typically involves confirming next steps and any goals before bringing the appointment to a close. The final step in the process is to update the patient records as you usually would.
DEALING WITH BAD ONLINE REVIEWS
React in haste and you’ll repent at leisure
The increasing use of social media and prevalence of online review or comparison sites has provided patients with various platforms to comment on the care or treatment they have received at a private clinic. We like to see positive comments from patients, but negative comments can be challenging. Dr Bobby Nicholas (right) discusses how best to handle these
FEEDBACK IN general can be useful in helping a doctor make improvements to the service they provide.
But receiving negative comments can be challenging and even more so if unfair criticism has been published online in view of colleagues, patients and friends. And it can also be particularly frustrating if it is felt that there is no right of reply.
The language used on social media and review sites can often be emotive and confrontational and is not what we usually expect in the course of spoken dialogue. This, together with limited safeguards to prevent patients from making unpleasant or factually inaccurate posts, makes it understandable that private practitioners are concerned.
We at Medical Protection are often asked to provide support and advice for private doctors who feel they are being unfairly portrayed in online comments.
How a doctor responds to negative feedback can be an important factor in whether matters escalate. Some types of comments may warrant reporting to the website, although this does not prevent the person from simply posting the comments elsewhere.
Doctors sometimes feel that negative feedback amounts to defamation. However, taking legal action over a comment needs to be
considered very carefully, as this can risk inviting more attention and publicity around the comments or issue.
When receiving such negative feedback, it is tempting to defend one’s reputation by engaging in a war of words with the patient via social media or website.
Duty of confidentiality
But doctors need to be mindful of their duty of confidentiality when responding to feedback on public forums.
When writing in haste, in particular, it is possible that comments may inadvertently breach doctor-patient confidentiality. It can also be tempting to become defensive and respond by saying that many other patients are happy with the service provided, or to try and provide a more balanced picture through evidencing positive feedback.
Becoming aggressive or defensive is, however, generally an unhelpful approach, as it can often lead to more confrontation. Attempting to evidence positive comments or feedback may also backfire and instead engage other patients who were unhappy with some aspect of the service they received.
Doctors and clinic staff need to be ready to deal with online criticism and should use it as an opportunity to demonstrate they take concerns seriously and want to improve the care they provide patients.
A good response will reflect well on the practice and will help to counterbalance the negative remarks that have been made.
Doctors need to be mindful of their duty of confidentiality when responding to feedback on public forums
CHECK OUT OUR BUSINESS DIRECTORY
Independent Practitioner Today features an online advertising directory to complement our journal and website.
For example, an effective response would express genuine disappointment that the patient did not have a positive experience and offer the opportunity to discuss the concerns in more detail offline.
By resolving the complaint, the person posting the negative comments may choose to remove the comments themselves.
Bear in mind that if you think a comment is unreasonable or unfair, others may see it that way too. Informal patients’ surveys in the US found that 65% of patients tended to ignore negative reviews that seemed unreasonable or exaggerated.
Similar US surveys found that almost one-in-five patients will disregard a negative review if the provider has responded in a thoughtful manner.
A calm and professional response will come across well to others who may read comments and is the best way to try to resolve the patient’s concerns.
Dr Bobby Nicholas is a medico-legal adviser at Medical Protection
FIVE STEPS TO DEAL WITH NEGATIVE REVIEWS
1 Although a prompt response is important, try to make sure the reply is calm, measured and not written in haste
2
3
4
Thank the patient for his/her comments, acknowledge concerns he/ she has raised and apologise, if appropriate
Explain that you take all concerns very seriously and that you will investigate the matter further
Invite the patient to contact you directly, giving him/her specific contact details to arrange a phone call or meeting. Consider using your complaints procedure to resolve any expressions of dissatisfaction
5
Bear in mind your duty of confidentiality and do not disclose any personal information about the patient or their treatment
Contact your medical defence provider for further advice if you are unsure of how to proceed upon receiving a negative online comment
Split into ‘business’ and ‘lifestyle’ directories, they list the services private doctors need to run their practices or spend their well-earned money on.
THE LESSONS OF COVID
The public and private healthcare sectors have built mutually beneficial relationships over the last 22 months. But Lyca Health chairperson Prema Subaskaran (below) says it is vital we build what will be a lasting partnership after Covid-19
Co-operation is critical
NO PUBLIC service sector has been more adversely affected by the Covid-19 pandemic than healthcare.
As we find ourselves approaching the second anniversary of the pandemic, it is important for us to pause to reflect on the outstanding work of the public and independent sector professionals who came together to tackle a once in a generation crisis.
No single public health crisis has placed a greater strain on the healthcare systems of every country in the world in modern history.
According to the World Health Organization, by November 2021 more than 248m people worldwide had contracted Covid-19 and 5m had died of the virus. Yet, despite these figures, a large proportion of the population has become desensitised to its devas-
tating effects that we must now learn to live with.
In the UK, the NHS was – at the time of writing – reporting nearly 10m Covid-19 cases. This is the fourth highest in the world. Unsurprisingly, public health services reached maximum capacity some time ago, resulting in lengthy waiting times and delayed care, with many areas seeing ambulances queueing outside A&E departments for hours waiting for patients to be admitted.
Record waits
The number of people waiting for hospital treatment in England have been at record highs and tens of thousands are having to wait for over a year. Operations have been cancelled, sometimes at very short notice, as the NHS continues to grapple with the crisis.
As we look to the future in terms of how we ease this burden and ensure that the worsening clinical, operational, legal and staffing challenges can be better managed, it will be important for the NHS to work more closely with private health providers.
We have seen the public and private sectors form mutually beneficial relationships over the past 22 months and, consequently, relationships and perceptions have changed.
This welcome shift presents a long-term opportunity for the independent sector and the NHS to continue to work together.
We have already seen the benefits of greater collaboration during the pandemic, so how do we ensure there is a sustainable partnership between the two sectors in the future?
greater investment. For example, the system has been overstretched and at maximum capacity.
Technology could be the answer
tors to monitor recovery and intervene where necessary to reduce the chance of re-admissions.
It is one of my ambitions at LycaHealth to make such connectivity a reality – to pool readings from devices in the cloud that are then reviewed by trained physicians, with key information provided back to patients via a dedicated portal that may be accessed with ease via smartphones or other devices.
When it comes to healthcare, the public and independent sectors are ultimately working towards the same end goal – providing patients with a clear, complete and uncluttered pathway from diagnostics to treatment.
Yet, given the current landscape the healthcare sector is operating in, achieving this has been a challenge.
Every path to a positive patient outcome begins with a correct and timely diagnosis, but outdated processes undermined by human and system errors can cause healthcare providers to fall at this very first hurdle.
This systemic challenge means that all too often it is not possible to pull information on medical history or that delays in data sharing or misunderstandings in communication mean that critical information can reach the desired party far too late.
Many healthcare bodies have improved their practices drastically in recent times to combat these challenges, introducing new technologies that can deliver improved process efficiencies and reduce human error.
This is where I believe that the healthcare industry needs to make
In situations like this, it’s important we implement technologies and tools that can help to get the system more organised and better integrate and balance considerations of patient symptoms, history, demeanour and environmental factors. In doing so, we can reduce the amount of manual labour on the physician.
Transforming aftercare
At LycaHealth, we strongly advocate that healthcare practitioners should also focus on providing long-term aftercare for those patients who need it.
Given the strains placed on healthcare systems, something of a revolving door has been established as the norm, where practitioners must get patients in, treated and out quickly to try to manage the ever-growing numbers.
Today, when a patient leaves the doctor’s practice or hospital, they are given a treatment plan or discharge instructions, but there is no guarantee that they will follow that plan or call their physician if they encounter problems.
This is where we believe that smart sensors can help. With cutting-edge devices such as wearables and smart scales, patients are never alone after leaving hospital, staying connected to allow doc -
New, cutting-edge facilities
There are many ways in which technologies can deliver benefits to healthcare systems and practitioners, from improved efficiency and a reduced strain, to more accurate and optimal patient outcomes.
A great example of this is our work at KIMS Hospital in Maidstone, Kent. KIMS Hospital is already one of the largest private hospitals in south-east England, and we are working with them to bring high-quality, accessible health services to local communities in the UK.
Over the coming years, we will be investing in upgrading KIMS’s hospital technology and facilities for existing and future enhanced services, including supporting the growth of cancer care, treatment and recovery facilities.
As part of our commitment to cutting-edge facilities and innovation, we have also launched two new state-of-the-art health centres in the UK: the Canary Wharf Breast Centre and The Orpington Breast Centre.
Both centres have been equipped with the latest imaging and diagnostic technology including 3D imaging tomosynthesis capabili -
ties providing a more advanced and detailed imaging technique. Combined with the world-class practitioners who operate there, the use of such technologies ensures there is no need to wait for lengthy referrals and access to treatment, with rapid diagnostic times allowing results to be processed in as little as 24 hours.
Collectively improving patient outcomes
Despite these undoubted successes, there is still work to be done if current challenges are to be overcome. New technology should underpin this whole process. There is significant opportunity to become smarter about the way in which we use artificial intelligence and machine learning with data sets to improve the quality of clinical care. But how do we get there? And how do we ensure that cutting-edge healthcare can be accessible to all?
Collaboration and partnership is key. The surge in global healthcare demand should not simply be a burden on public health organisations such as the NHS.
The pandemic has laid the foundations for greater collaboration between public and independent enterprises, be it addressing greater demand, swapping vital knowledge or sharing experiences, approaches and expertise to drive collective improvement that saves lives.
We have reached a pivotal moment in global healthcare. Neither sector can go it alone.
Entities of all shapes and sizes must continue working together, to put the patient first, address their needs and improve outcomes for all. Never have health partnerships been more important.
CLINICAL NEGLIGENCE: PSYCHIATRISTS
Psychiatric claims under the spotlight
Clinical negligence claims involving psychiatrists are analysed here by Dr Shabbir Choudhury, who offers some useful tips on managing common risks
A number of claims focused on allegations that there was a failure to recognise a patient was at risk of suicide or self-harm
THE MDU supports psychiatrist members with issues ranging from regulatory investigations, service complaints, performance concerns, inquests and tricky medicolegal or ethical scenarios.
We also support members working in private practice who find themselves facing a clinical negligence claim and this article focusses on those cases.
In claims settled on behalf of the MDU’s members working in psychiatry over a recent ten-year period, we successfully defended more than 90% of cases.
WHAT ARE THE REASONS FOR CLAIMS INVOLVING PSYCHIATRISTS?
Risk of self-harm or suicide
A number of claims focused on allegations that there was a failure to recognise a patient was at risk of suicide or self-harm or that the patient was inadequately managed, often following multiple consultations.
There may be a great number of factors which lead a patient to take their own life, so it can be difficult for a claimant to prove causation. That is to say, for a claim to be successful, the claimant would have to demonstrate that, but for the alleged negligent act by the doctor, the patient would not have committed suicide.
Deprivation of liberty
In a number of cases, it was alleged the patient had been inappropriately detained in hospital for treatment. Only one such case was settled in the review period, but it highlights the importance of ensuring all appropriate alternatives are considered.
However, when there is no reasonable alternative to detention, it’s important to ensure there is appropriate input from all involved parties and that the reasons and discussions are thoroughly documented.
This is a complex area of the law and it is always worth getting medico-legal advice if there is any doubt about detaining a patient.
Addiction
A handful of cases involved patients with an alcohol or drug addiction. These claims tend to have long histories with many doctors involved and, therefore,
establishing where accountability lies can be very difficult.
It is always important to ensure all clinicians involved in a patient’s care communicate thoroughly with each other and agree who takes responsibility for each aspect of care.
Other reasons for claims included:
The treatment of bipolar disorder;
Medication errors;
An incorrect psychiatric diagnosis being made;
Breach of confidentiality.
Managing risks
Claims involving psychiatrists are very diverse. However, there are some common risk factors, which, if managed appropriately, can help to reduce risks.
These include:
☛ Ensuring that where there is a significant risk of suicide or selfharm, both the patient and the medication prescribed are appropriately reviewed. Be aware of and follow appropriate guidelines.
☛ Being prepared to refer patients for specialist treatment when necessary. This is in line with GMC requirements to ‘recognise and work within the limits of your competence’ (paragraph 14, Good Medical Practice). You should ensure that you have the appropriate qualifications, skills and experience for the care you provide.
☛ Being aware of the current available guidance on the prescription of antidepressants, including the BNF and NICE.
☛ Having a system in place to review patients on long-term medication.
☛ Getting expert advice from your medical defence body if there is any doubt about whether a patient’s detention is appropriate and lawful.
☛ Clearly documenting your discussions with patients and family members.
If things go wrong, be open and honest with the patient by providing an explanation of what has happened and the likely shortand long-term effects of this.
Say sorry and get advice from the MDU if you believe the incident triggers the organisation’s duty of candour requirements. (See last month’s ‘Your duty to own up’.)
It can be very troubling to find out a patient is bringing a claim against you. If you face a claim, you can be assured that the MDU understands how stressful this is and the importance of mounting a robust defence of your position.
While claims numbers have remained steady in recent years, the cost have spiralled. This is not due to clinical standards but to a deteriorating legal environment which the MDU is campaigning to reform. You can see more at www. themdu.com/faircomp.
Dr Shabbir
Choudhury (right) is a medico-legal adviser and former senior medical claims handler at the Medical Defence Union (MDU)
Get off to a good start in 2022
FROM A STRATEGIC perspective, I take time to review and plan every quarter. I make the most of the ‘back to school’ feeling in September and at the start of the new year, which is an obvious time to reflect on everything in life including business.
April and July are the two other times during the year when I pause to review progress and make plans for the coming quarter.
Over the last two years, with the changing environment caused by the impact of Covid, my strategic planning has become less proactive, and my focus has been on managing the ups and downs caused by the Covid crisis.
But performing in ‘crisis’ mode
for such a long time is not healthy for us in either our personal lives or for the success of our businesses. So the start of 2022 is a more significant opportunity than it might normally have been for all of us to take stock and set our agenda for the coming year.
My strategic planning will involve reviewing my previous plans and assessing what has been successful, what we have achieved and identifying the areas where we made less progress than hoped.
To be honest, due to the challenges of the last two years, there are a few objectives that I set for my business that were purposely parked and I am sure I am not alone.
Due to a lack of time to focus on the more proactive side of growing the business and to allow time for the day-to-day management of the effects of Covid some activities needed to be taken off the agenda in the short term.
The start of 2022 will provide a great opportunity to decide whether the time is right to reset those objectives and restart progress.
I am also an addict of business plans and notebooks, and I have used most of the widely known business plans/journals.
Currently, my favourite is the Clever Fox Planner Pro, which I highly recommend for anyone like me who enjoys structure and handwriting out plans. Clever Fox allows you to set your strategic plan and then manage it on a dayto-day basis.
The new year is also a good time to check that business basics are being managed well. No business, clinic or practice can succeed and grow if the basics are not well organised.
Most importantly, good processes and systems ensure that the business runs smoothly and that patients, clients and employees are happy.
Conversely, poor processes lead to a drain on management time with time spent addressing issues and firefighting reducing time available for patient care and more strategic activity.
Over the last two years, it is possible that many of us have taken less time to review the basic operations of our businesses and this is a good time to check and act, if needed.
In my experience, there are a number of areas that may have been overlooked in private medical practice and I have highlighted some of these below in an attempt to help.
Patient experience
Are you capturing and reviewing feedback from your patients? This is an activity that may have been lost in recent months and it is worth re-establishing good processes; firstly, asking your patients for feedback and regularly reviewing matters with your team.
Over the last few months, patient expectations may have changed and it is important to ensure that your practice delivers against its current requirements to maintain an excellent reputation.
Employee satisfaction
The challenge of surviving the Covid pandemic has affected everyone to a greater or lesser extent and, in private healthcare, employees have been under increased pressure to deal with changes in their working environment.
Now is a good time to assess how your employees are feeling and to ensure that their well-being is being prioritised by you as an employer. An employee survey is a good way to gain feedback in an anonymous way to allow you to get a realistic picture of the challenges your team is facing.
The information gathered can be used by you and your senior team to develop an action plan to address any issues and ensure that your team know their well-being is a top priority for you.
Pricing
Most businesses review their pricing on an annual basis to ensure they are competitive but also in line with inflation and the cost of running their business.
In private healthcare, the insurance companies restrict the ability to make significant changes, but it is important to review self-pay pricing and also review the costs of delivering the services you offer.
If the insurance rates have remained unchanged but costs of equipment or medical supplies have increased, then it is important to make efforts to try to reduce costs in some way to ensure profitability.
Marketing
Is your marketing in line with your objectives and how well is it delivering against your objectives? Now would be a good time to re-assess your marketing activities and ensure they are delivering the results you are aiming for.
Are all of your marketing and communication materials consistent in their look and feel?
Is your website working well from a technical perspective and is it compliant in terms of cookie policies and privacy? Are you communicating regularly with your patients and referrers via a newsletter and/or via social media?
Regulatory matters
Working in private healthcare requires adherence to numerous legal and regulatory regimes including the GMC and the Care Quality Commission. The new year is a good time to check that everything is updated, and you are adhering to the latest requirements.
One good example is the Private Healthcare Information Network (PHIN), which has made some changes and launched a new website recently. All doctors need to ensure they have completed their profile on the new PHIN site.
Invoicing and credit control
In my experience, invoicing and credit control is the most overlooked aspect of running a successful private healthcare practice.
It is not unusual for me to meet a doctor who has recently discovered that invoices have not been sent to patients or their insurance companies. It is even more common to hear that a significant amount of aged debt has accumulated as a result of a non-existent credit control function.
I always suggest a monthly check of invoices raised and of aged debt to make sure your credit control processes are working and if this hasn’t been done for a while, then this is a good process to establish for the new year.
If you need any assistance with your fresh start in 2022, please feel free to get in touch. But, for now, I wish you a Happy New Year.
Jane Braithwaite is managing director of Designated Medical, which offers flexible, experienced support for all your private practice needs
BILLING AND COLLECTION
Matters you need to fix in the coming year
New Year’s resolutions for your business really could boost your income in 2022. Simon Brignall suggests ten for independent practitioners to consider
WHERE IT ALL STARTED
GOOD INTENTIONS come in many guises. It could be to lose weight, stop drinking or to do more exercise. As we commence 2022, it is time to make our new year’s resolutions; but where did this custom begin?
It is said that the ancient Babylonians were the first people to make new year’s resolutions, over 4,000 years ago. They were also the first to conduct recorded new year celebrations although for them the year began in mid-March as this was when the crops were planted. Most sources state that the practice of making moral promises at the beginning of our calendar year dates back to the Roman times. Romans worshipped the god Janus, who had two faces, allowing him to look forwards and backwards at the same time. One face would reflect on past events and the other face would look forward into the future. Romans used the image of this deity of transitions and changes on
the first month of their calendars, which is why the name January is derived from him. In the year 153bc, the Roman senate fixed the start of the calendar new year at the first of January.
The tradition has been around for millennia, so there must be some benefit in having your own New Year resolutions. And so why not for your business?
As it is the time of good intentions, why not take this opportunity to review the way you operate the financial aspects of your practice? Implementing these resolutions really could make a significant impact to your profit line, and even if you only adhere to a few of them over the next 12 months, you will still see the difference they make.
Outlined on the opposite page are my suggestions for you to consider including as part of your financial New Year’s resolutions.
1
I will review the way my work is being billed to ensure I am compliant with the rules and regulations communicated monthly from the Clinical Coding and Schedule Development group (CCSD). Keep abreast of the CCSD’s monthly changes and establish whether they affect your specialty and possibly your income.
Practices commonly make billing errors as a result of being unaware of the changes. It is good practice to establish what rules each insurer adopts, because they can choose their own variants.
2
I will ensure I regularly review my procedure fees.
This is important if you bill to insurance guidelines, as the rates constantly change and are not often communicated clearly. You may be charging less than you could or more than you should. Practices still make incorrect assumptions, leading to issues with insurance companies or lost revenue.
3
I will make sure my work is invoiced as soon as possible.
Some major insurers now enforce time limits for submitting invoices and if you miss the deadline, they will not pay.
Late invoices can be an indicator to patients of poor service and a major contributor to their dissatisfaction. They can also often lead to bad debts.
Delays in informing patients that there is still a shortfall to pay means that they assume that their invoice has been settled – resulting in a bone of contention when they are asked to pay.
Invoices sent late to patients can also be ignored, as they think you are not serious about wanting payment.
4
I will make sure that my price structure/policy is clear and that my patients are made aware of it before commencing treatment.
A clearly defined and well documented price structure that is communicated as part of a patient’s registration form is vital in the modern practice.
This will ensure there is no room for ambiguity when it comes to settlement, as it can include a clause outlining their obligation should their insurance company not settle their invoice in full.
Fee and payment terms transparency is of paramount importance and it is also a key requirement of the Competition and Markets Authority (CMA) and Private Healthcare Information Network.
5
I will ensure my practice has a robust process for chasing outstanding invoices on a consistent and continual basis until they are fully paid.
Failures in this important area mean continued high levels of bad debt. Almost every practice that joins Medical Billing and Collection (MBC) has an outstanding invoice backlog, with some going back years.
Debt levels are typically over 20% of turnover and sometimes have reached between 50-100% of annual turnover.
On average, we achieve bad debts of less than 0.5%, which is a significant improvement on their current arrangements.
6
I will make myself aware of any patients that don’t pay so I can decide if I want to continue seeing them while they have outstanding invoices. If you do not have a procedure for problem payers, you will end up regularly throwing money away. Visibility around this key area means you can take steps to police this more effectively.
When we take on a backlog of outstanding invoices, there are often patients who have built up debt over years. Practices continued to see them despite never being paid.
7
I will ensure I have key management information on my practice to allow me to make informed decisions for the future. This vital area is often overlooked and can mean that the wrong assumptions are made.
All practices should have information that shows where their
patients are referred from, the volume of patients seen for each insurer and how much of their income comprises of self-pay and other patient payment types such as embassy and medico-legal.
Consultants should have a good understanding of the practice’s finances. This means they know what is happening to the revenue that is generated each month, similarly for payments received and information about outstanding invoices.
Without access to real-time accurate data, it is difficult to understand which direction your practice is going, and it is very easy to come to the wrong conclusions.
At MBC, we provide our clients with access to a market leading dashboard and reporting tool that can provide access to all the above information and more on a 24/7 basis.
8 I will make sure I spend as much time as possible focusing on my core skill set – treating and looking after the patient. Running a private practice is not easy and many tasks do not fall naturally into a consultant’s skill set.
If you and your secretary are able to focus on the medical side of the practice, this will, in turn, make you more money, because you are focused on what you do best rather than spending time on tasks that can be easily delegated.
Take stock and consider what elements of your practice could be outsourced, enabling you to generate more revenue.
9
I will ensure I have a robust secure IT infrastructure in place to deal with my practice’s administration.
This can be a common weakness in many practices and is often only highlighted when it’s too late.
Enjoy the peace of mind that you get from knowing that your business is on a secure platform and that your data cannot be lost. There is an increasingly wide range of options available to you to facilitate this, so it should not be difficult to implement and you can always ask your colleagues for recommendations.
10
I will consider whether I should join thousands of other doctors who have outsourced this crucial element to a professional billing company.
For most consultants, the billing and collection side of their practice is very difficult to manage and when done wrongly it often results in consistent financial losses and frustrations.
Outsourcing could be the best and simplest resolution you make this year to resolve all the issues I have highlighted and guarantee your practice is future-proofed against what lies ahead.
Simon Brignall (right) is director of business development at Medical Billing and Collection
PROFILE OF AN INNOVATIVE PRIVATE CLINIC
OneWelbeck, founded in Marylebone, London, by over 100 specialist investors, is one of the country’s largest facilities for diagnostics, therapies and minimally invasive surgery. Some of its leading consultants tell Independent Practitioner Today all about the big attraction of being involved They are:
Prof Jane Setterfield, consultant dermatologist and oral medicine specialist, chairwoman of OneWelbeck Skin Health & Allergy
A unit where much the
Prof Guri Sandhu, consultant laryngologist and head and neck surgeon, chairman of OneWelbeck Ear Nose & Throat
Dr Natasha Beach, sports and musculoskeletal medicine consultant, OneWelbeck Orthopaedics
How long have you worked at OneWelbeck and what attracted you to having your private practice there?
Prof Dame Lesley Regan, consultant obstetrician and gynaecologist, chairwoman of OneWelbeck Women’s Health
Prof Setterfield: I have worked at OneWelbeck for eight months. I was attracted to practice there for several reasons, But, fundamentally, I loved the concept of being able to select a team of dermatologists, allergists and surgeons who are all highly regarded and experienced and whom I knew and trusted to
where doctors are the equal partners
provide excellent patient care across the whole field of skin health.
Prof Sandhu: The Ear, Nose and Throat Clinic at OneWelbeck has been running since the beginning of 2021. The attraction was the ‘shared ownership and shared profit’ model.
The consultants have shared in all the decision-making with respect to the clinic infrastructure and the number and nature of support staff.
Dr Beach: I started at OneWelbeck Orthopaedics when it first opened in spring 2020. I like the fact that it is consultantlead, meaning that the doctors working here are heavily involved in the decisions made within the clinic. The facilities are also fantastic for the patients.
I was attracted by the idea of having high-quality services for all aspects of women’s health located in the same place.
The location and the layout of the sixth floor is very attractive and welcoming. The women’s health services are located on the sixth floor and breast screening services are co-located with gynaecology.
pregnancy, menopause, urogynaecology, gynae cancers screening and treatment and so on.
My dream was that instead of women having to attend three to four different appointments to go through simple services to keep them fit and healthy, that they could access them all in the same place and at the same time.
How does working at OneWelbeck differ from your previous private practice experience?
Prof Setterfield: The facility is modern with a spacious feel. There is a relaxed yet efficient environment that ensures patients have a good experience throughout.
The entire team is carefully selected, and each is looked after so that staff are happy in their work and are able to provide the best care for patients.
Prof Sandhu: The main difference is that this is a clinical partnership. Our group’s ‘mission statement’ was to bring together clinicians who were world leaders in their fields or the ‘rising stars’ of the future and colleagues you would be happy to have as friends.
There was also the promise of a high-tech clinic within a luxurious environment, which has been delivered beyond expectations.
Dr Beach: Here I have the flexibility to see patients outside of my normal clinic hours, meaning we can offer flexibility to our patients.
Gynaecology is not just a single specialty: it includes many different areas of specialist expertise, contraception, menstrual period problems, cervical screening, early
Prof Dame Regan: As I mentioned before, having all women’s health services in one place makes a huge difference.
Prof Dame Regan: I started working at OneWelbeck in January 2021, bringing my gynaecology clinic over from St Mary’s Hospital and the London Wing. ➱ p30
Also, the different floors at OneWelbeck house many other specialties that so many of my female patients would also like to access; for example, digestive health, heart health, hormone and skin health.
I love the idea that I can ring up colleagues on another floor specialising in other areas of medicine and get excellent advice for my ladies.
It also works the other way round: I often receive calls or texts from other floors asking ‘who is the best person to send this lady who has xxx problem to for advice?’.
The investors model means that it encourages collaboration instead of competition.
It is good for my practice if the women you send to see me get the best advice.
And if I decide that I am not the best person to give it to them, then it is in my best interests to refer them on to someone who has more expertise in that area of women’s health.
Is it more fulfilling professionally?
Prof Setterfield: Yes, every aspect of our dermatology service has been carefully planned to ensure a streamlined highly professional service.
Prof Sandhu: Being a ‘shareholder’, you have a feeling of ownership and, as a result, you are all invested in the success of the clinic. You have a say in nearly all decisions. Any growth or success is yours to celebrate.
Dr Beach: Yes, I love working here, and I know that my patients always have a positive experience which, in turn, makes my job that much more satisfying.
Prof Dame Regan: Definitely, because at the end of a clinic I really feel that the patients have had a pleasant experience, received firstrate advice and may even have undergone a procedure during their visit – a real one stop shop.
Everyone is incentivised to get the best services for their patients rather than competing to see everyone themselves. Fees for scans and blood tests go into the communal pot
We have, to date, 22 of the top London dermatologists, plastic surgeons and allergists in London. This is unrivalled and singles us out as the leading private dermatology clinic. We are centrally located and so are accessible to much of London
Prof Sandhu: I walk into the clinic and there is a relaxed environment and you are clearly walking into a medical facility that belongs in the 21st century.
What do you particularly enjoy about it?
Prof Setterfield: As the lead clinician, I have particularly enjoyed planning a bespoke dermatology clinic with the very best facility, the most modern equipment, including a unique 3D artificial intelligence-equipped mole-mapping service and, most importantly, inviting some of the best dermatologists in London to join the group.
The staff are polite and welcoming and there is very much a ‘can do’ work ethic. You know that you have had a hand in creating this.
Dr Beach: Having consultants from other specialties around –such as pain management, radiology and rheumatology – and others – so that we can bounce ideas off each other.
Prof Dame Regan: Friendly staff, lovely surroundings, proximity to other experts, diagnostics and imaging facilities.
The waiting area and coffee bar serving the allergy, ENT and dermatology departments
How does the business model enable innovation?
Prof Setterfield: As partners in the organisation, we are able to influence any decision regarding our service, provide evidence for new innovation and ensure that we remain the leading dermatology centre in London.
Prof Sandhu: The consultants are basically equal owners in the clinics. This means that we have equal responsibility for all expenditure and earnings. The partnership can come up with ideas and innovations and propose them at one of the regular meetings with management. Neither side is financially motivated to push wasteful ideas. To date, nothing that we have proposed has been rejected, but sometimes we have been advised about the practical difficulties of a proposal and provided alternative solutions.
Dr Beach: Having a financial stake in the business means that we are key decision-makers, so we get to
influence what happens in the centre, and particularly the treatments we offer.
This means we can be at the forefront of medical innovation and ensure our patients can access the latest technology.
Prof Dame Regan: Everyone is incentivised to get the best services for their patients rather than competing to see everyone themselves. Fees for scans and blood tests go into the communal pot.
OneWelbeck promotes the aim of ‘empowered doctors’. How does this work in practice?
Prof Setterfield: By being in a partnership, the doctors can ensure that every aspect of our service is optimised and kept up to date. We have been able to invite the colleagues that we know provide excellent care both in the NHS and private sector and many of us are also highly academic leaders in our respective fields.
The free digital prescribing platform for all private prescribers.
CloudRx take care of the dispensing, payment and delivery of medicines direct to your patients, wherever in the country they may be, for more convenient access to their medicines.
TRANSFORMATIONAL
Order prescriptions at the touch of a button to support all consultations and add a whole new level of convenience for your patients.
SIMPLE, CONVENIENT AND SECURE
Simple and fast digital prescribing.
Legal paperless prescriptions, repeat prescriptions and controlled drugs.
Prescriber fees can be charged to the patient if requested.
INTEGRATED
Our API enables frictionless integration with healthcare brands & clinical software including Heydoc, MidexPRO, eClinic and YouClinic.
“We were struggling to keep up with the admin side of the prescriptions, not to mention storage for medication to cope with a huge increase in prescriptions. CloudRx immediately took away the strain. Since our partnership we have grown by more than 200% in size. We could not have done that without their support.”
– Dr Louise Newson, Newson Health
The reception at the orthopaedic centre (above) and stunning roof terrace (below)
Prof Sandhu: I do feel empowered at OneWelbeck. I have a say in the running of my medical practice and, as a group, we can agree the direction and growth of the clinic for the benefit of patients.
As a novel model of decisionmaking, when we started, we had concerns that we would be dictated to as in many other private clinics. This has never happened.
Dr Beach: Personally, I am a member of the commercial team which helps decide the direction that we want the clinic floor to go to.
Rather than simply being told about what is happening with our commercial strategy, I can influence how our budget is spent on areas such as marketing and events. This wouldn’t happen in a standardly operated practice.
Prof Dame Regan: It is great to be able to reach out to other specialties and ask for advice and recommendations about which doctor or treatment would be best.
I often receive queries from other specialties at OneWelbeck and I may say ‘I can happily see your lady’ or I might say ‘I think the best person to see her will be Dr X’ and give them the contact details.
What is the ‘new model of excellence’ you aim to provide to referrers and patients?
Prof Setterfield: The new model of excellence ensures that patients are looked after by the best person for their specific problem. Initial triaging of referrals as well as cross referrals between consultants is standard practice.
As we have ensured that the full range of expertise is available, patients should feel confident that they are being looked after by the right person.
Prof Sandhu: By any measure, within OneWelbeck ENT, we have doctors and allied health professionals who are leaders in their respective areas of interest, most of them internationally respected.
The partnership will aim to direct patients to the doctor best qualified to manage their condition.
Patients will be seen in a comfortable and friendly environment using equipment that provides the highest standards for investigations and treatments.
The clinic will always be competitive with its fees for both selfpayers and insured patients.
Rather than simply being told about what is happening with our commercial strategy, I can influence how our budget is spent
Dr Beach: Quite often within the world of sports medicine, a patient will need to travel to different locations to see various specialists and for scans and X-rays.
With the OneWelbeck model, we streamline the number of appointments a patient needs, minimising stress and enabling them to see the specialists they need as quickly as possible, which speeds up the recovery journey.
Prof Dame Regan: Women’s health has never been given the prioritisation it needs and women have been disadvantaged by the bureaucracy of our NHS and private health services for decades.
This is an opportunity to really offer women the services and the maintenance care they need to remain fit, healthy and productive throughout their life course.
In the past, we have tended to wait for women to develop a problem and then try to treat it. That is not good medicine and it is also more expensive. When we do better for women, everyone benefits and we can provide better care for less money.
Did you ever feel isolated in previous private practice? If so, has that changed now?
Prof Setterfield: Yes, this was one of the limitations of private practice elsewhere compared with working in a team as for example in the NHS.
At OneWelbeck, we have the benefit of working within a great team but with the advantage of having developed a highly efficient and innovative centre. We would all be happy for any of us to look after our families and friends
Prof Sandhu: As a ‘sole operator’, you do sometimes feel isolated in private practice.
Working in a partnership with friendly and talented colleagues removes any such isolation. There is always someone with whom to have a friendly chat or exchange ideas.
Another view of the waiting area for the allergy, ENT and dermatology departments
Don’t come a cropper with investments
WHEN BUILDING an investment portfolio at Cavendish, we employ a focus based on risk rather than on performance. Taking on sensible risks should be rewarded appropriately.
We concentrate on the things we can control: portfolio structure – for example, country and sector exposures, stock concentrations, product costs and avoiding exposure to specific risks such as counterparty or leverage.
We accept that there are things we cannot control such as shortterm portfolio performance as a result of movements in equity markets due to the never-ending release of new information.
Many investors will try, and generally fail, to control this either by themselves or by selecting fund managers they believe can do so. For most, this outcome-focused approach to investing is not where success lies.
An important part of the process
Past performance alone is no indicator of future outcomes.
Dr Benjamin Holdsworth (right) reveals why controlling structure and risk is more important
when building your portfolios is searching, or ‘screening’, for potentially suitable products to capture market returns.
We review a universe of tens of thousands of possibly suitable products to get down to one solution to capture specific market exposures in the portfolio. This is no mean feat and requires a comprehensive and rigorous process.
Taking a major part of our portfolios such as developed equities as an example, we look to find investments that can capture the returns of these markets and do so effectively through time.
Screening process
Our screening process considers a wide array of datapoints, none of which measure performance, to filter down to the solution we use in our portfolios. To focus on fund longevity – thus mitigating the risk of the fund closing – we look for funds of a sufficient size and age.
Our screening process considers a wide array of datapoints, none of which measure performance, to filter down to the solution we use in our portfolios
To ensure the solution holds an exposure to the developed equity market, we look through the fund to see where the underlying stocks are listed and verify this matches the structure of the market we are looking to capture.
We screen out investments with higher charges, those with insufficient diversification and those lacking in transparency.
The result of this risk-focused, rather than outcome-focused, approach is that we are left with a
high-quality short list of ‘on watch’ investments.
Manager’s philosopy
For the final step in the selection process, we consider the fund manager’s philosophy and approach, as well as any data that sets the investment apart on this competitive watch list.
When reviewing the competitors that make up the watch list, we see that their past performance is in fact strong relative to other participants in the industry.
Despite not screening on performance, and instead focusing on process, we end up with a list of investments that have performed strongly because of their sound structure, placing them predominantly in the top quartile of all managers in the same category, particularly over the longer term.
What is more, this entire process is repeated at least annually. In this way, investors can have every con-
NHS Pensions & Annual Allowance Tax
Get ready in advance of April 2022 when the proposed changes to the NHS Pensions will allow you to reclaim some or all of any Annual Allowance tax you may have suffered in the past.
With our knowledge and in-house calculators, we will be able to predict in advance and check statements produced by NHS Pensions and Scottish Public Pensions Agency for accuracy for any refunds due.
For further information contact us at aa@semail.co.uk or telephone 01625 527351.
fidence that their portfolio comprises high-quality investment products as a result of a screening process which is not outcomefocused, but risk-focused. This gives the investor every opportunity to achieve strong outcomes going forward.
Dr Benjamin Holdsworth is a director of Cavendish Medical, specialist financial planners helping consultants in private practice and the NHS
The content of this article is for information only and must not be considered as financial advice. Cavendish Medical always recommends that you seek independent financial advice before making any financial decisions.
Levels, bases of and reliefs from taxation may be subject to change and their value depends on the individual circumstances of the investor. The value of investments and the income from them can fluctuate and investors may get back less than the amount invested.
Should I incorporate?
SHOULD YOU incorporate your business? The answer is: liability.
Simply put, if you are not trading in a corporate entity you are going to be personally liable for any uninsured losses.
If you are a sole trader or a traditional unincorporated general partnership, your house and all your other personal assets are exposed to be taken if a large claim is successfully made against you in connection with your business and the business has insufficient resources to meet the liability.
When you are trading as an incorporated body, your liability is limited to the value of the business.
There is also an additional benefit with a corporate entity; it has its own legal personality, so it enters contracts in its own name, whereas if you carry on your business as a sole trader or partnership, it is you – and each one of the partners – who enter the contracts.
While your individual clinical work may be covered by unlimited insurance cover, other risks are not usually, and that includes claims by employees, landlords or other contractors, which may either be uninsured or insured but subject to limits on the cover.
If you incorporate the business effectively, such claims would be brought against the corporate entity rather than against you individually – although you would still remain personally liable for clinical claims – and so you would shelter your hard built-up wealth.
This remains a prime motivator for incorporating as claims get higher and the willingness to sue greater.
There are two primary forms of incorporation: the company and the limited liability partnership (LLP).
The tax treatment of the different forms of corporate entity is the remit of your accountants and tax advisers, but, aside from tax considerations, it is worth considering the model which is preferrable for
Accountants have had their say on these pages, now
lawyer Justin Cumberlege, (left) a partner in Hempsons’ healthcare team, explains what should be considered when forming a corporate entity
you when considering the functions you want the structure to achieve.
First, if you are a sole trader, you may form a company, but an LLP requires two members, as it is a form of partnership, albeit with its own distinct corporate personality.
Members’ agreement
If you start with two partners, and your partner leaves, you have a sixmonth window of opportunity to find another partner, otherwise the benefit of being an LLP is lost.
As a company, by default, you will have model articles of association imposed if you do not write your own.
An LLP does not have a members’ agreement under statute, and the risk of not having one is great, because there will be no evidence
as to what you have agreed for profit-sharing, capital investment in the business, how decisions are made, exit provisions and the other terms and conditions typically found in a partnership agreement.
If you are going to have different ownership rights and returns between members, a company is usually the preferred option, because, with a company, you are able to vary the shareholding of members and, with it, the weight of their voting, the amount they receive in dividends and the interest in the capital in the company.
While it is possible to replicate something similar with an LLP, it is not as straightforward as utilising a company share structure.
The extraction of profits from an LLP is relatively easy, as they are
attributed to the partners. With a company, you may leave the profits in the company for future investment or to pay out at a later date.
Tax burden reduced
Losses may be off-set against future profits, which helps reduce the tax burden for companies, so if you are starting up a business, this may be attractive.
You may expel members of a company, although it is more complicated to remove a shareholder than a member of an LLP, provided you have an LLP agreement which provides for the expulsion of a member, normally by simply passing a resolution. Shares in a company can only be dealt with in specific ways as set out in the Companies Act 2006.
If you do decide to incorporate, you create a separate legal person and therefore none of your existing registrations or contracts will be valid unless you take the appropriate action to either transfer them or make new arrangements in the name of the company or LLP.
You will have to register the new entity with the Care Quality Commission as a provider of healthcare services, as well as register with the Information Commissioner’s Office.
Insurance cover
Insurance cover will need to be taken out by the new entity and cover for medical negligence, as the corporate may be sued as well as the individual clinician in such circumstances.
All the contracts of the business will need to be assigned or novated over to the new entity. Some contracts may be deemed to be terminated in such circumstances and a
penalty incurred for early termination, so you must check them beforehand.
Other contracts may have a ‘change of control’ provision, meaning the other party is able to terminate the contract if the ownership of your corporate entity changes. Sometimes there is a threshold of, say 25%, but in a small company that might easily happen.
Staff will be transferred automatically upon the business transferring in accordance with the Transfer of Undertakings (Protection of Employment) Regulations. But it is important that you follow the statutory procedure, otherwise staff may be entitled to compensation.
If you have a lease of premises, the landlord will have to agree to the assignment of the lease to the new entity in most cases. If you own the premises personally, then you should either put a lease in
place permitting the corporate entity to occupy it so that you are able to claim all the expenses off the business or sell the property to the corporate entity.
Personal guarantees
Landlords and some other contractors may require personal guarantees from the members of the LLP or directors of the company, so, in these cases, having limited liability through the corporate entity will have been circumvented and therefore lost.
Do not forget to set up a new bank account for the business in the name of the new corporate entity. The bank may require personal guarantees from you as well.
Once up and running, it is important to comply with the statutory requirements of a corporate entity, particularly the filing of accounts and other changes that occur, such as changes of directors, and a compliance state-
ment must be filed every year. While they are not usually particularly onerous, it is important to comply with the requirements.
There are significant differences between companies and LLPs, so it is important from the outset to decide which one you want to form and to be clear about the reasons why and the advantages it would bring in carrying out the functions of the business.
Discuss this with your lawyers and accountants – probably together – to determine which would be the most favourable for you and the others running the business with you.
Disclaimer: This article is for information purposes only and should not be relied on as legal advice. Neither the authors nor Hempsons will be liable for losses arising from reliance on the information in this article. The article is based on the law of England and there might be variations in other jurisdictions.
Free legal advice for Independent Practitioner Today readers
Independent Practitioner Today has joined forces with leading healthcare lawyers Hempsons to offer readers a free legal advice service.
We aim to help you navigate the ever more complex legal and regulatory issues involved in running and developing your private practice – and your lives.
Hempsons’ specialist lawyers have a long track-record of advising doctors – and an unrivalled understanding of the healthcare system as a whole.
Call Hempsons on 020 7839 0278 between 9am and 5pm Monday to Friday for your ten minutes of free legal advice.
Advice is available on:
Business structures (including partnerships)
Commercial contracts
Disputes and litigation
HR/employment
Premises
Regulatory requirements and investigations
Michael Rourke Tania Francis m.rourke@hempsons.co.uk
BUSINESS
Oops! A private GP’s mistake leads to a breach of confidential data, something which can result in a massive fine. Dr Ellie Mein (below) advises on how to respond in this situation
I posted records to wrong patient
Dilemma 1 What should I do after data error?
QI’m a private GP who recently emailed a letter intended for one patient to another with a similar name.
While this was an accident, the letter – which a patient had requested for ongoing custody proceedings – outlined mental health history, medication history and details relating to drug and alcohol misuse.
I was then contacted by the second patient who was shocked to receive a letter containing such sensitive details, realising that it did not relate to her.
I apologised to the second patient for this data breach, have ensured that the letter was deleted and have also rung the patient who was the subject of the letter to explain what had happened. What else should I do?
AA personal data breach is defined as ‘a breach of security leading to the accidental or unlawful destruction, loss, alteration, unauthorised disclosure of,
or access to, personal data transmitted, stored or otherwise processed.’
Under data protection law, practices are responsible for patient data and legally obliged to store it securely and protect it from unauthorised or unlawful processing.
Relatively common
Data security incidents are relatively common within healthcare settings. The most recent data security incident trends published by the Information Commissioner’s Office (ICO), show that between April 2021 to June 2021 there were 607 data security incidents in the health sector, up from 420 the previous quarter.
The ease and speed in which data can be shared, along with the current surge in clinical administration being experienced, may partly be behind the increase in data loss incidents.
According to the ICO, the commonest reasons for data to fall into the wrong hands were that it was lost or stolen from an insecure location (112 incidents) or sent to the incorrect recipient – 67 by email and 56 by post or fax.
In 73 incidents, there was unauthorised access to the system – 65 non-cyber and eight via cyber
methods. In 19 cases, there was verbal disclosure. In eight cases, failing to use bcc (‘blind carbon copy’) in an email meant email addresses were visible to all recipients.
As you have discovered, such breaches are distressing for the patients involved, but they also have wider implications such as reputational damage and potentially a significant financial penalty.
Higher risk
The General Data Protection Regulation (GDPR) states that you should inform the data subject if a breach is likely to result in a high risk to their rights and freedoms, such as if the data refers to a person’s health. This is a higher level of risk than under the ICO notification procedures.
An accidental disclosure of patient records or sensitive medical information is likely to be of high risk to the rights and freedoms of patients, requiring you to inform the data subject.
This is because of the significant impact on those affected due to the sensitivity of the data and the potential for confidential medical details to become known to others.
Failure to notify a breach appropriately can result in an administrative fine which could be up to €10m or 2% of your global turnover.
Consequently, make sure all your staff are aware of what constitutes a data breach, and that it is not just loss of personal data. Have robust procedures in place to detect, investigate and report breaches.
Finally, contact your medical defence organisation for further advice and support on dealing with a data breach.
Dr Ellie Mein is medico-legal adviser at the Medical Defence Union
Just when you can and cannot provide a fit note for a patient is often a source of confusion. Dr Kathryn Leask (below) answers a private GP’s query
Dilemma 2
Can I backdate their fit note?
QI am a private GP and have seen and assessed a patient recently. He’d had a minor operation on his hand three weeks previously but wasn’t given a fit note by the hospital.
The patient has asked me to provide a fit note. I was happy to provide this from the date of my assessment, but the patient has asked me to backdate this, as he had been off work for three weeks before he saw me.
I explained that I wasn’t able to do this; however, the patient says I can use the assessment from the hospital. Can I issue a fit note in these circumstances?
AThe Department of Work and Pensions has provided specific guidance on the issuing of fit notes, which may be helpful to discuss with your patient.
The section entitled ‘When can I backdate a Statement of Fitness for Work?’ is most relevant to your situation. The guidance states that a backdated certificate can only be provided if it is based on a previous assessment.
This would be, for example, a face-to-face or phone consulta -
Rules on issuing patients’ fit notes
tion. Although a report from another doctor or registered healthcare professional can be considered, the fit note cannot be backdated from the date of your assessment.
While you would not be able to issue a fit note, you could offer to provide a letter to the appropriate person to confirm the patient’s clinical history.
This should be a factual account of the care provided to the patient and you should make it clear at which point you were and were not involved in the patient’s care and what assessments you did personally. You should ensure you have appropriate evidence to justify the information you are providing.
The other option would be for the patient to contact the hospital where the operation was performed to see whether the consultant whose care the patient was under would be prepared to provide a backdated certificate, as presumably this wasn’t issued at the time of his discharge or follow-up outpatient review.
The consultant may be happy to do so, given that they would have formally assessed the patient and can base any certificate on this.
Dr Kathryn Leask is a medico-legal adviser at the Medical Defence Union
DOCTOR ON THE ROAD: ALFA ROMEO GIULIA QUADRIFOGLIO
Enjoy the last of a dying breed
If you love driving, then this may be one of the last chances to indulge in very special petrol-powered enjoyment before we are all engulfed by the very worthy electric revolution, says Dr Tony Rimmer (left)
spoilers that keep the car’s potential hidden from non-enthusiasts. The four-leaf clover badging on the front wings is a particularly neat touch.
It is a good-looking car. The cabin and boot are as practical as in lesser models, which means it could easily function as a daily driver for a family of four.
WHAT’S IN a name? If an address in Harley Street is mentioned, we automatically think of high-quality private medicine.
Car makers work very hard to create brand names that evoke a strong sense of the values they aspire to in the minds of buyers. It takes decades to build up this reputation and a long history, often with motor sport involved, is the key to success. One such company is Alfa Romeo.
First established in 1910, it had a racing team that was successfully run by Enzo Ferrari before he set up his own titular company. Over the years, drivers have bought Alfa Romeos to enjoy a sporty drive and reflect on the rich heritage.
Sporty image
Now, despite making saloon cars and SUVs, the company needs to keep this sporty image and one way to do it is to produce a halo model.
BMW has its M cars, Audi has its RS models and Alfa has its special Quadrifoglio (four-leaf clover) models.
Its Giulia four-door saloon has recently been updated after a successful four years since launch and the Quadrifoglio model has benefited too.
To find out whether it competes with the similarly-sized and equally powerful BMW M3 saloon, I have been assessing this rather exceptional Alfa.
The Giulia’s styling still looks fresh after four years and, in Quadrifoglio form, is adorned by some obvious but subtle vents and
Sweetly balanced
An updated infotainment screen works well but, apart from the lovely leather steering wheel and seats, the interior build quality is not quite up to the level of German competitors.
The sweetly balanced 2.9litre V6 engine produces a truly awesome 503bhp and drives the back wheels with the aid of a very necessary electronic traction control. Adjustable dampers allow the superbly tuned suspension to transfer all this power to the tarmac.
Performance is electrifying. The 0-62mph sprint in 3.9 seconds is accompanied by a glorious soundtrack from the sports exhaust – music to the ears of petrolheads and a total contrast to the silent acceleration that defines all electric cars.
Driving this Alfa Romeo on the open road is an absolute delight for anyone who appreciates and enjoys a properly sorted and capable sports saloon.
Unencumbered by the significant weight of batteries in electric cars, it feels nimble and light on its feet. The steering is particularly impressive with just the right amount of feedback and sensitivity to allow accurate placement through any set of challenging bends.
An eight-speed automatic box shifts swiftly and works really well in manual mode via the steeringwheel paddles.
The power delivery is, as you would expect, instantly accessible and huge. This is a brutally quick
Apart from the lovely leather steering wheel and seats, the interior build quality is not quite up to the level of German competitors
car and devours A and B roads in equal measure. Keen drivers will only be able to explore the Quadrifoglio’s limits on a racetrack.
Despite this massive performance potential, this Giulia has a softer side too. The ride, although firm, is comfortable and passengers will be perfectly happy on a long motorway trip. Allow the gearbox to change up early in Comfort mode and even the noise levels are subdued.
So, are there any downsides to this impressive breadth of abilities? Well, the Quadrifoglio is not cheap; the starting price is £68,995, which is almost twice as much as the Giulia 2.0 Turbo.
Running costs will be high, too, with a real-world fuel consumption of no more than 20mpg if you explore the performance potential. Does it give the M3 a run for its money? I have driven the latest M3 Competition with identical power and four-wheel drive and although it is an impressive car, just as fast and better built, it lacks the addictive drama of the Alfa.
If you are a medic who loves driving, the Giulia Quadrifoglio may be one of the last chances to indulge in very special petrol-powered enjoyment before we are all engulfed by the very worthy electric revolution.
Dr Tony Rimmer is a former NHS GP practising in Guildford, Surrey
ALFA ROMEO GIULIA QUADRIFOGLIO
Body: Four-door saloon Engine: 2.9litre V6 turbo petrol Power: 503bhp
Torque: 600Nm
Top speed: 191mph
Acceleration: 0-60mph in 3.9 secs
WLTP combined mpg: 27.2mpg
CO2 emissions: 235g/km
On-the-road price: £68,995
The 0-62mph sprint in 3.9 seconds is accompanied by a glorious soundtrack from the sports exhaust
A PRIVATE PRACTICE – Our series for doctors embarking on the independent journey
The figures have. . .
. . . got me in a spin
Every year, you should receive a set of accounts from your accountant that summarise the financial activity of your practice. For many, the figures can be a challenge to understand, so Ian Tongue (left) looks at the key points of your annual accounts and some useful pointers on how to interpret them
THE BASICS
Accounts or financial statements normally comprise of a profit and loss account and a balance sheet and both are prepared up to a financial year/period end.
The profit and loss account can also be referred to as an income and expenditure account and both are often interchangeably used, although subtly different. These are a summary of the income and expenses of the practice, which then result in a profit or loss for the business.
The balance sheet is a snapshot of the assets and liabilities of the business as at the financial yearend date and, for most private practices, can be regarded as the net worth of the business.
The way in which your accountant prepares the figures is governed by accounting standards as well as tax legislation and often these can be different – i.e. the
accounting treatment differs to the tax treatment. This is the reason why often your taxable profit from your private practice is different to your accounting profit.
The financial year-end is normally the end of a month and, for ease, many businesses use the tax or fiscal year-end to prepare their figures up to.
There can be cash flow advantages to not having a financial year-end the same as the tax yearend and your accountant should explain the pros and cons of adopting this.
One very important part of accounting standards and principles is what is known as the accruals basis. In simple terms, this means that you disclose your income on the basis of when you earn money and not when you are paid.
When it comes to expenses under the accruals basis, you claim costs on the basis of being incurred
rather than paid. For smaller private practices with earnings below the VAT registration limit – currently £85,000 per year – a receipts basis is possible, but generally it works out best to go with the accruals basis from the start to avoid having to transition from one basis to the other later on.
PROFITS AND LOSS ACCOUNT
When it comes to reviewing the profit and loss account, you should be presented with the current year figures and the previous year, assuming this is not the first period of trade for the business.
Comparing the costs year on year and considering whether they are in line with your expectations is a key analytical tool. Many costs will increase as your fee income increases, but others are largely fixed and are not as variable based on fee income.
It is common for consultants to pay for expenses outside of their business bank account and it is very important that you make your accountant aware of these costs so that they can be included within the profit and loss account, otherwise you will not get tax relief on these costs and will overpay your taxes.
BALANCE SHEET
It is always advisable to prepare a balance sheet as part of your accounts. To do this, your accountant needs to have your bank statements and other source documents.
Preparing a balance sheet ensures that you have a reconciled bank account and the fees declared are accurate taking into account a review of the fees raised and income received.
It costs more for your accountant to prepare this statement, but it provides you with comfort that when you sign your tax return off as complete and accurate, work has been undertaken behind the scenes to support this statement. It is a false economy to ask your accountant to prepare only the profit and loss account and presenting just these figures is likely to raise your chances of an inquiry by HM Revenue and Customs.
ACCOUNTING
A common scenario is for a consultant to look at the accounting profit in their accounts and try and find the same figure on their tax return. It can be the same figure but more commonly the figures are different.
This arises due to the tax treatment of an expense being different to the accounting treatment. The most common example is in relation to buying assets to be used in your business such as medical or office equipment.
For accounting purposes, you spread the cost of these assets and this is known as your depreciation charge. But for tax purposes, you can actually deduct the cost in year one.
In fact, at the moment, there are enhanced allowances whereby you can claim more than the cost to encourage businesses to invest. In this situation, the taxable profit will be lower in the year that you bought assets and potentially higher in subsequent years as you had all of the tax relief up front.
In addition to the above, the other most common areas where the accounting and taxation treatment differ are legal fees and entertaining costs. These expenses can be incurred by the business, but tax relief may be restricted or not available.
It is a false economy to ask your accountant to prepare only the profit and loss account and presenting just these figures is likely to raise your chances of an inquiry by HM Revenue and Customs
Creditors represent expenditure and liabilities that are not paid as at the date the accounts are drawn up.
A private practice would not normally have large creditors, but it is important that you look at this figure and understand how much your business owes, which will assist with cash flow and budgeting.
DEBTORS
One of the most important numbers to look at are your debtors, which is a figure shown as a current asset within the balance sheet.
The debtors figure represents all monies owed to you at the date that the accounts were drawn up to.
Debtors are assets, but the push should always be to collect these debts and turn them into cash within the bank account.
Clinical private practices should not really have more than six to eight weeks of income outstanding. So if your private practice has more than that, question why this is the case, as you may have old debts or perhaps part payments against fees and both situations require investigation.
Medico-legal work can often take a long time to be paid and, for those starting out, the terms of payment can be rather onerous.
When entering into such work, you need to factor the longer payment terms into the rates charged and ensure that when you submit your accounting records to your accountant you include any outstanding debts from earlier years.
It is important that you regularly chase your outstanding debts and usually your secretary undertakes this on a regular basis.
We are all used to paying VAT on large amounts of our own spending and, outside of private medicine, most businesses have to account for VAT as part of running their business.
For clinical private practices, it is unlikely that you would have to register for VAT, as the vast majority of work undertaken is exempt from VAT.
The main type of work that is sensitive to VAT is medico-legal or purely cosmetic work.
If your business is VATregistered, it is important to understand how this is accounted for within your accounts, as the income figure is excluding VAT, as are many of the expenses, no doubt. But debtors, for example, would include VAT.
It is important that, if you are VAT-registered, you have a greater understanding of the financial figures and your accounting systems are extremely robust.
In conclusion, you will receive accounts every year from your accountant and therefore to get the most from them you should take the time to understand the key components and how to interpret them.
You should always receive some written commentary on the figures presented, but it is always best to meet with your accountant to discuss the figures, which should improve your understanding of the figures presented.
Next time: Planning for the new tax year
Ian Tongue is a partner with Sandison Easson accountants
NEW COVID LEGISLATION
Getting ready for mandatory jabs
Dawn Hodgkins (below) discusses what doctors need to know about mandatory Covid vaccines
IT IS, incredibly, coming up for two years since coronavirus hit our shores.
And as a sign that the virus will likely be with us for some time, the Government has confirmed that, from 1 April 2022, Covid-19 vaccinations will be mandatory for all healthcare workers who have ‘direct face-to-face contact’ with patients, including non-clinical staff such as receptionists, porters and cleaners.
While vaccines to protect against Hepatitis B have long been strongly recommended for healthcare practitioners, this is the first time that a vaccination will become a legal requirement.
And with over 150,000 people working in the independent healthcare sector, we at the Independent Healthcare Providers Network (IHPN) will be supporting providers and practitioners in the coming months to ensure the sector is fully prepared to implement mandatory vaccines.
Earlier this year, the Office for National Statistics reported that more than 400 healthcare workers in England have died as a result of Covid within 28 days of a positive Covid test and, globally, the pandemic is thought to have taken the
lives of 180,000 people working in healthcare.
Vaccines have been proven to play an absolutely critical role in both protecting patients and staff, as well as reducing the risk of Covid-19 transmission. And to that end, we firmly support the principle of the Government’s recently announced proposals to make Covid-19 vaccination a condition of deployment in the healthcare sector.
Practical concerns
The devil is, of course, always in the detail and there are a number of practical concerns that we are working on closely with the Department of Health and Social Care (DHSC) and NHS England to ensure the successful implementation of the policy.
As part of NHS England’s Vaccine as a Condition Of Deployment (VCOD) Phase 2 Working Group –as well as working directly with DHSC ministers and civil servants – the IHPN is therefore working to ensure that guidance is fully applicable to the independent sector and provides a clear and usable framework for those working in it.
This will include consideration of staff groups included in the pol-
care sector also raises significant human resource and legal issues.
IHPN will urge the Government to provide clarity about the alignment between the legal requirement to be vaccinated and current employment law, and what steps will be taken to mitigate employers’ exposure to legal challenges arising from enforcing this policy.
We will also be working with the Care Quality Commission on how it will assess compliance with the mandatory vaccination policy, as well as its assessment of staffing levels if the numbers of available staff to provide care are reduced and cannot be replaced due to their vaccination status.
IHPN will also work to ensure that there is accurate data about vaccination rates among independent healthcare staff.
This will support the DHSC in carrying out its full impact assessment of the introduction of VCOD, and also help practitioners fully understand the position in their own organisations so that they can take appropriate action.
icy as well as clarity over medical and other exemptions.
For example:
Whether or not members of staff who deal with immune-suppressed patients should be prioritised in recognition of the particular vulnerabilities of that group;
The potential impacts on certain groups, including BAME staff who may be more likely to refuse the vaccine on religious or cultural grounds;
Young women who are concerned that the vaccine could affect fertility or be dangerous during pregnancy – despite evidence showing vaccines are safe in these circumstances.
Acknowledging diversity
Acknowledging the diversity of the independent healthcare sector, a particular focus of this work will be to influence policy development so that any guidance is also appropriate for non-hospital-based services.
This includes independent practitioners delivering primary and community care where there may be further complexities in implementing the policy.
Making Covid vaccines a condition of deployment in the health-
IHPN will be helping share good practice among independent providers and practitioners and the wider health system around increasing vaccine uptake among staff and resolving operational issues relating to the policy.
This will help ensure the sector is as fully prepared as possible ahead of 3 February which is the last date that a member of staff can have their first vaccination ahead of a 1 April implementation date. Implementing mandatory Covid vaccines is undoubtedly one of the biggest current issues facing healthcare providers and practitioners. We do not doubt the significant impact it will have at a time when the health system is already under immense pressure.
But doctors should be reassured that supporting providers in the coming months to ensure they can comply with the new regulations is an absolute priority for us. We want to help minimise any potential disruption to workforce supply and ensure that you can continue to deliver care for the millions of patients who rely on the sector every year.
Dawn Hodgkins is director of regulation at the Independent Healthcare Providers Network
Investing pays off
Our regional review of private performance in the NHS continues as Philip Housden analyses private patient revenue growth for 26 NHS acute trusts across the North West region covering the conurbations of Greater Manchester and Liverpool, and counties of Cheshire, Lancashire and Cumbria
AT THE time of writing, only 13 of the 26 trusts had published their 2020-21 Annual Report and Accounts and so this review is still based on the information published in the Trust Annual Accounts for 2019-20, a year partially adversely impacted by the early months of the Covid pandemic.
One trust, East Lancashire Hospitals, did not publish its pri-
vate patient income within its financial statements supporting the annual accounts, so a judgement estimate has been made regarding private patient incomes for that trust.
For this regional group of trusts, the accounts show that total private patient revenues increased in 2019-20 by 0.8%, a decrease on previous year growth of 3.2%.
Total revenues are stated as
£31.0m in 2018-19, up £257,000 from £30.7m in 2018-19 (Figures 1 and 2). This level of income represents a small decline from 0.34% to 0.32% of these trusts total patientrelated activity revenues. This remains below the combined national average outside of London of 0.43%.
The year-on-year private patient revenues performance of these 26 acute trusts varied significantly
(Figures 3 and 4). The following commentary analyses the trusts with the top ten private patient revenues, which are those over £1m and/or greater than 0.1% of total trust incomes.
The regional top earner remains The Christie Hospital at £6.5m, down £307,000 year on year (-4.5%). The trust remains well in the top ten-earning trusts outside of London by revenue.
Figure 1
This is now 2.06% of the trust’s revenues, down from 2.4% the previous year. These earnings principally come from the trust’s longterm partnership with HCA Healthcare, which was agreed in 2009 and are 2.23% of total trust revenues, down from 2.85% the year before.
Branded The Christie Private Clinic, this provides a dedicated outpatient suite and day care unit, oncology wards with 34 beds and a haematology transplant unit.
The joint venture itself, The Christie Clinic LLP, reported a 10% jump in revenue to £43.5m as patient admissions and outpatient visits to the specialist oncology provider continue to climb.
New high
Second by revenues is Wrightington, Wigan and Leigh, where the JCW Private Patients wing has delivered increasing private patient revenues for the last three years and in 2019-20 these reached a new high of £3.8m.
This was an increase of £681,000
on the prior year, up 21.8%, and 1.05% of total trust revenues. The JCW Wing has outpatient consultation rooms and 16 en-suite bedrooms.
Third highest in the North-west is Liverpool Women’s Hospital , which has dedicated private patient facilities and reported growth of £53,000 to climb to £3.3m (up 1.6%).
The trust’s PPU, The Catharine Suite, opened in 2009 and is located on the Crown Street site, supporting a range of private gynaecology and cosmetic surgery procedures plus a range of nonsurgical cosmetic procedures. The Catharine Suite comprises two consultation rooms and a treatment room, as well as seven single en-suite rooms.
Fourth is The Clatterbridge Cancer Centre , which in June 2021 opened a new private patient facility, Clatterbridge Private Clinic, to meet demand from the trust’s catchment across Cheshire, Merseyside and beyond.
The clinic is based inside The
The regional top earner remains The Christie Hospital at £6.5m, down £307,000 year on year (-4.5%). The trust remains well in the top ten-earning trusts outside of London by revenue
In 2019-20, the trust’s private patient revenues were £3.3m, up 37.3% and £893,000 from £2.4m the year before. That is 1.95% of total trust revenues, a new high. Fifth highest is Manchester University Hospitals which does not have a dedicated inpatient service for trust private patients.
Clatterbridge Cancer Centre’s new 11-storey specialist cancer hospital, which opened in June 2020.
Innovative treatments
Based in the heart of Liverpool’s Knowledge Quarter, the clinic offers inpatient and outpatient care, a rapid diagnostic service and a range of servicces including radiotherapy, chemotherapy, immunotherapy and other targeted drug therapies, as well as innovative treatments such as Papillon Therapy – a specialist form of radiotherapy for rectal cancers.
However, it is the Private Patient Centre at the Manchester Royal Eye Hospital that delivers the majority of trust earnings, with paediatrics and to a lesser extent dental also contributing. The trust achieves a relatively modest 0.19% of turnover at £3.0m, but this was up 28.1% and £600,000 from 0.11% and £2.4m revenues the year before.
The Private Patient Centre at the Manchester Royal Eye Hospital has a series of dedicated private consulting rooms and en-suite inpatient rooms.
In sixth place, Liverpool Heart and Chest Hospital, revenues fell back for the third year in a row, this time by 7.5% and £228,000 to
Figure 2
£2.94m. The trust’s private patients are principally delivered through the six-bed Maple Suite and represent 2.03% of total trust revenues, down from 2.31% in 2018-19 and well down on the high of 3.27% in 2014-15.
Across the city, in seventh, is Liverpool University Hospitals, formed from the merger of Aintree University Hospital with Royal Liverpool and Broadgreen from 1 October 2019, mid-way through the 2019-20 financial year.
The new trust’s private patient revenues in 2019-20 were £1,455,000, down 12.3% and £205,000 from a combined £1,660,000 in 2018-19. This is 1.35% of the new trust’s total income.
The combined trust has access to the 19 bed Sefton Suite at Aintree, which has a theatre, access to intensive care units, physiotherapy facilities and specialist nurses, and outpatient consulting rooms and diagnostic imaging facilities at Kenilworth Road Diagnostic Centre.
In eighth, Blackpool Teaching Hospitals does have a small dedicated inpatient facility for private patients. Earnings from Victoria Hospital’s six-bed Lancashire Suite were £1.38m last year, down by 21.3% and £374,000 from £1.75m in 2018-19. This is now 0.33% of total trust revenues.
Purchase completed
Ninth by revenues is Mid Cheshire Hospital in Macclesfield. The trust completed the purchase from BMI of the South Cheshire Hospital at Crewe, located on the Leighton Hospital NHS campus, in February 2020.
This provided the trust with additional two operating theatres and 32 beds, and post-Covid expectations are that this could lead to a significant increase on the £1.2m revenues achieved in 2019-20. That figure was £308,000 and 20.4% down on the previous year and a drop from 0.66% to 0.49% of total revenues.
Concluding the North-west’s top ten trusts is St Helen’s and Knowsley , where the trust increased revenues by 34% and £246,000 last year to £966,000 –the eighth consecutive year of growth, now reaching 0.26% of total trust revenues.
Of the remaining trusts, none have a dedicated inpatient PPU, although Salford Royal offers services for private day-case and ambulatory services from The Salford Clinic and delivered £483,000 revenues, a 51.8% fall.
The 26 trusts across this large region deliver very different private patient performance. Unsurprisingly, the minority of
trusts that have invested in dedicated inpatient capacity have achieved the best returns.
Post-Covid, perhaps neighbouring trusts, particularly those within the two major cities of Liverpool and Manchester, could pool their expertise and resources in order to drive revenues and brand presence in the biggest markets.
Further, these centres of excel -
lence might consider supporting some of the other trusts across the North-west to modernise and professionalise the delivery of their private patient services, or in several cases, start up a new service.
Next time: The North-east
Philip Housden is managing director of Housden Group commercial healthcare consultancy
Figure 3
Figure 4
Coming through Covid
Consultant ophthalmologists recorded only a small income growth as practices headed for last year’s Covid disruption. Ray Stanbridge reports
PRIVATE PRACTICE incomes
began to collapse for many specialties in the run-up to the first lockdown and beyond, but ophthalmologists were not significantly hit by Coronavirus in the year to 31 March 2020.
Our headline figures show that, on average, gross income rose by 4%, going up from £148,000 in 2018-19 to £154,000 in 2019-20. Costs rose by an average of 6%, increasing from £65,000 to £69,000. As a result, taxable profits went up by 2%, from £83,000 to £85,000. Margins fell slightly from 56% to 55.2%.
What then are the reasons for the changes in 2019-20?
We have seen continued growth in self-pay and significant amounts of Choose and Book work have been generated by some consultants within the year. But the results are expected to be significantly different for 2020-21.
Market rates
Expenses have generally shown a small increase in the year. Staff costs have risen where consultants have endeavoured to pay market rates for the secretarial and administrative support or have been
Early sight of accounts coming through suggests that incomes have been growing strongly in 2021-22 as Covid restrictions have been relaxed
charged market rates for these services from their private hospitals and clinics.
Consulting room hire charges have increased slightly, reflecting small changes in usage or costs increases imposed in line with the 2014 Competition and Markets Authority rulings.
Increasing number of consultants are now using their homes as a base and, as a result, cost charges have increased. This trend also continued strongly into 2020-21, when online consultations from home became quite common.
Other costs remain broadly similar to 2019 levels, although some have shown small inflationary increases.
Slight recovery
What then of the future? As we know, for the first few months of the 2020-21 financial year many independent practitioners’ incomes collapsed. Business recovered slightly from the second half of 2021. Early sight of accounts coming through suggests that incomes have been growing strongly in 2021-22 as Covid restrictions have been relaxed.
Although our survey is not statistically significant, it does try to measure – in an increasingly difficult marketplace – what is actually
happening to the financial side of a consultant ophthalmologist’s business in the UK.
With the changing structure of doctors’ businesses, it is increasing
difficulty to collect consistent and fair comparisons on a year-to-year basis. Ophthalmology consultants now trade in a variety of ways; for example, through limited liability
partnerships or companies, both of which create difficulties in the collection of consistent data.
For some ophthalmologists, Choose and Book work – at lower real margins – are a very important source of income.
Our survey has been conducted on the same basis as in previous years, but the initial gross income for inclusion in the survey has increased from £5,000 to £10,000 a year.
Consultants included in our survey in addition include those who:
Are not in full time private practice;
Have spent at least five years in private practice;
Are showing serious interest in doing private practice as a business;
May or may have been a member of a group or have incorporated.
Next time: Gynaecologists
Ray Stanbridge is a partner with accountancy, finance and tax advisory medical specialists, Stanbridge Associates Limited
Coming in our February issue, published on 8 February.
Answering independent practitioners’ business problems – Jane Braithwaite turns troubleshooter in response to some difficult scenarios experienced by private doctors
It is not far away now, so are you planning for the new tax year? You should be. Accountant Ian Tongue gives some topical advice to help you on your way
Dr Kathryn Leask, medico-legal adviser at the MDU, discusses what to do if a patient becomes abusive; while her colleague Dr Sally Old answers a male private GP’s inquiry about a young teenager who needs a breast examination but does not want a chaperone
If you work in a private patient unit in the North-east, then don’t miss Philip Housden’s round up of the region’s financial successes and disappointments
Keep it legal: Litigation can be stressful, time-consuming and expensive. In the first of a series of articles about the employment tribunal process, Hempsons’ solicitor Julia Gray explains the key stages and how to avoid common pitfalls experienced by employers
Gynaecologists’ income, expenses and profits go under the financial microscope in Ray Stanbridge’s benchmarking series Profits Focus
Private patient information on anti-microbial resistance. As Bupa launches a patient video on the subject, one of its writers talks about the scale of the problem, the impact of Covid-19, the future, and shares some pointers on how clinicians can discuss the issue with their patients.
Latest information from the Independent Healthcare Providers Network – which is bringing out a new version of its Medical Practitioners Assurance Framework in 2022
INDEPENDENT PRACTITIONER
TODAY
Published by The Independent Practitioner Ltd. Independent Practitioner Today is editorially independent and thanks Bupa for its assistance with distribution. Material is governed by copyright. No part of this publication may be reproduced, stored in a retrieval system or transmitted in any form without permission, unless for the purposes of reference and comment. Editorial layout is the copyright of the publishers. If you wish to use it for promotional purposes on websites or for reprints, we would be happy to discuss licensing the copyright to you.
We are all prone to FOMO (fear of missing out) when we look back at stellar stock and fund performance. A Cavendish Medical expert notes that the average investor would have done just as well owning a US index tracker fund over the same period. The tortoise wins the long-term race!
Our motoring correspondent Dr Tony Rimmer gets behind the wheel of a new version of the famous muscle car, the Ford Mustang Mach-E
How private practitioners can sustain physical and mental well-being and help the team perform at its best in these tough times. Tips from Dr Stephen Priestley, senior medical educator for Medical Protection’s Risk Prevention and Cognitive Institute
‘Our award for management excellence in private healthcare’. King Edward VII’s Hospital, London, gives the detail behind its achievement
Medical Billing and Collection’s Simon Brignall gives advice to help the business side of your practice run smoothly
Ten Years Ago – doctors with a private practice were being advised to think hard about how they could protect their business from collateral damage in the wake of the Poly Implant Prothese (PIP) scandal
And don’t forget to check out our additional news updates every week online
ADVERTISERS: The deadline for booking adverts in our February 2022 issue is 21 January
Write to Independent Practitioner Today 7 Lindum Terrace, Lincoln LN2 5RP
CHANGING ADDRESS, EMAIL ADDRESS OR SUBSCRIPTION DETAILS?
Phone 01752 312140 or email karen@marketingcentre.co.uk
TELL US YOUR NEWS
Robin Stride, editorial director Email: robin@ip-today.co.uk Phone: 07909 997340 @robinstride
ADVERTISE WITH US
To advertise in the journal or our website business and lifestyle directories, contact advertising manager Andrew Schofield at Spot On Media. Phone: 0161 408 3912 Email: andrew@spotonmedia.co.uk
GET A SUBSCRIPTION DISCOUNT!
£90 independent practitioners.
£90 GPs and practice managers (private & NHS).
£210 organisations.
Save £15 paying by direct debit: individuals £75 (organisations £180). TO SUBSCRIBE
Email karen@marketingcentre.co.uk or phone 01752 312140
Publisher Gillian Nineham Phone: 07767 353897.
Email: gillian.nineham@gmail.com
SAVE £15 WITH DIRECT DEBIT!
Guarantee delivery of your next copy of Independent Practitioner Today. Take out a subscription and you will get full access to our news, features and previous issues on our website. See details on the left.