The business journal for doctors in private practice
In this issue
Price-fixing detectives are on your case
Advice on how to avoid breaching anti-cartel laws P16
Harness people power
Jane Braithwaite begins a new series on managing people, exploring employment models and leadership styles P22
In this issue
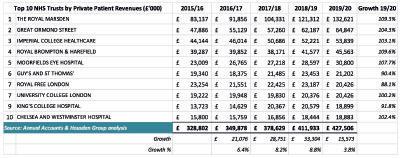
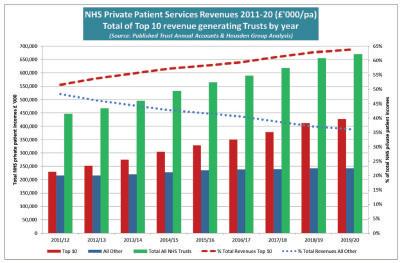
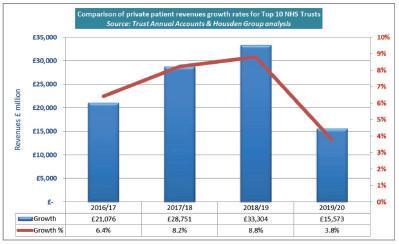
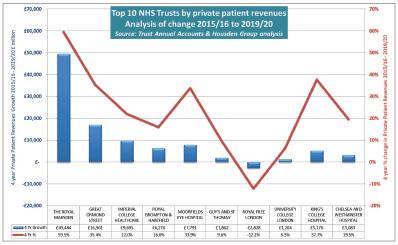
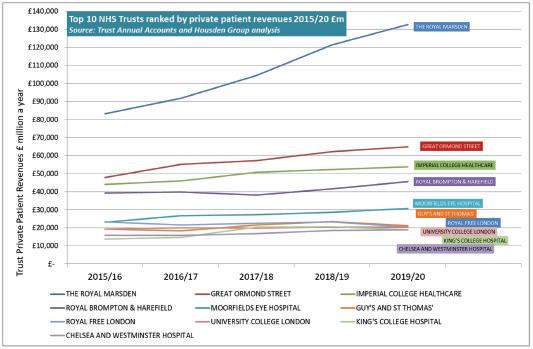
The top ten PPUs
The published accounts for 2019-20 show that all of the top-earning private patient units are in London n p44
A new dawn in my fight for justice
Surgeon David Sellu gains his release from prison after getting his conviction for manslaughter overturned P30
Take a fiscal check-up
By Robin Stride
Independent practitioners who also work in the NHS are being urged to take a pensions and tax health check-up as they contemplate their future in 2021 and beyond.
This time of year makes many doctors question their desire to keep working, according to specialist medical financial advisers.
Patrick Convey, technical director at Cavendish Medical, reports this is particularly so right now, as they face the usual winter crisis and extra challenges dealing with the ongoing pandemic.
He told Independent Practitioner Today : ‘After such a momentous period in history and the significant burden of harsh tax limits in recent years, many consultants we speak to are keen to explore other routes – whether that is reducing NHS commitments in favour of private work or retiring early.
‘The key to making successful lifestyle changes is planning ahead and ensuring you have conducted extensive financial modelling to verify the best course of action.’
With 2021 stretching in front of them, he believes many consultants and GPs in private practice should check their own pension and tax position as soon as they can.
Mr Convey said: ‘Are the figures in their personal pensions state -
ment just received from the NHS Pensions Agency correct?
‘Have they applied to Scheme Pays to ensure the Government pays their 2019-20 pension tax charge?
‘We have yet to see the outcome of the “pensions flexibility” consultation from 2019, but we would hope to see the results of the 2020 consultation into the 2015 Pension Scheme age discrimination this year. There could be important decisions ahead for the busy consultant.
‘As always, we would counsel accepting some professional help to check where you are now and to find the best route ahead.’
He doubted a pay rise, signalled in Chancellor Rishi Sunak’s November Spending Review, would be enough to ease a likely workforce crisis.
The level of increase has not been specified, leading to many consultants questioning if the rise will be higher than inflation, said Mr Convey.
Mr Sunak had told MPs: ‘Taking account of the pay review bodies’ advice, we will provide a pay rise to over a million nurses, doctors and others working in the NHS.’
Mr Convey said with the public sector otherwise forced to accept a ‘pause’ in their pay increases, it seemed the Government was attempting to address the enormous commitment of the health service workforce.
‘However, there is little confidence among our clients that the increase will be substantial given that the decision has been deferred until 2021. Also, the Chancellor stated that the review bodies’
advice would be taken into account – but this has been ignored in the past.’
Medical accountants Stanbridge Associates’ partner Vanessa Sanders advised: ‘Plan for how much you will need and work backwards from a broad base and over a number of years. This means considering how you trade in private practice and how to draw income earned.
‘Consider what are your financial needs and how best to approach meeting these. This could be through increased hours in the NHS or through private work.’
Patrick Convey Vanessa Sanders ➱ continued on page 7
This time of year makes many doctors question their desire to keep working
TELL US YOUR NEWS. Contact editorial director Robin Stride
Agility is key to surviving the crisis
How can consultants plan strategically for their practice while adapting quickly as the pandemic unfolds? A hospital’s clinical director gives his views P14
ADVERTISE WITH US. To advertise in the journal or our website business and lifestyle directories, contact Andrew Schofield at Spot On Media. Email: andrew@spotonmedia.co.uk
Phone: 0161 408 3912
GET A SUBSCRIPTION DISCOUNT
£90 independent practitioners. £210 organisations. £90 GPs and practice managers (private & NHS).
Save £15 paying by direct debit: individuals £75 (organisations £180).
TO SUBSCRIBE
Email karen@marketingcentre.co.uk Or phone 01752 312140.
Chief sub-editor: Vincent Dawe
Head of design: Jonathan Anstee
Publisher: Gillian Nineham
Email: gillian.nineham@gmail.com
Phone: 07767 353897
EDITORIAL
COMMENT
Prophet warning for 2021
In our issue only 12 months ago, we dreamed up a promotional catchphrase on the new year we were entering.
The need to have ‘20-20 vision’ to run a successful private practice and get ahead for the decade in front was a play on words which inevitably also occurred to other media scribes too.
We wrote in this column about much uncertainty ahead for thousands of consultants and GPs in private practice.
And in innocence of what was to come, we somewhat prophetically warned: ‘Doctors and their working environments will be affected on many fronts under the new Tory Government . . . we expect a host of changes in coming months and our expert writers will be seeking to help . . .’
Well, we all know what happened next and before the winter waned. Even the most visionary could not have foreseen it.
Private hospitals were soon requisitioned by the NHS and
the unthinkable was happening, with many independent consultants and GPs joining a global fight for physical and business survival.
Work dried up for many, doctors on zero incomes needed Government ‘bounce back’ loans, consultants announced retirement was their only option and at one point even the Federation of Independent Practitioner Organisations (FIPO) was asking ‘Can private practice survive?’
But survive it has, and although there is still a long way to go, its practitioners have been resilient and widely adapted to new ways of working as they struggle to stay afloat during the Covid-19 crisis.
Much more good and bad is inevitably on its way and the need to maintain a visionary outlook if you are staying in private practice is even greater now than we could ever have anticipated last year.
When patients fall between 2 stools
Poor communication between doctors when handing over patients is a known medico-legal risk. Dr Sarah Coope shows how to avoid gaps P25
You must give them all the gen New GMC guidance on consent is intended to support doctors in having a meaningful discussion with patients. The MDU summarises key points P28
Charting these stormy waters
Simon Brignall provides ten simple medical billing rules to help you chart your practice through the current difficult economic climate P36
Interest rates fall below freezing
Cash is not a sensible long-term option when interest rates head into negative territory. So ensure your longer-term assets are sensibly invested P38
Renting property is now less daunting
The Royal Institution of Chartered Surveyors has updated is code for leasing business premises, which makes negotiating leases simpler P40
PLUS OUR REGULAR COLUMNS
Start a private practice: Better pension news
Accountant Ian Tongue examines the good news surrounding pensions’ tax-free allowances P48
Doctor on the Road: Nice motor comes with a big charge
Your decision to buy an electric car like this Hyundai Kona has to be ecological, not financial P50
Profits Focus: A good eye for earnings
Ophthalmologists come under the spotlight of our unique benchmarking series on specialists’ finances P52
Surge predicted in private insurance
By Robin Stride
Hopes are high in the insurance industry for a 2021 surge in the number of potential patients covered for private medical treatment.
Private health insurers and the independent professionals who advise corporate and individual buyers have been told by their trade organisation to gear up to sell.
Stuart Scullion, chairman of the Association of Independent Medical Insurers and Intermed iaries (AMII), told them: ‘New business inquiries are buoyant. We need to convert them into customers.’
Speaking at the body’s 2020 Health and Wellbeing Summit, he said: ‘Moving forward, each of us has a real responsibility to define to consumers and policyholders, how, by maintaining their cover, value continues to be delivered –not least in the protection of their underwriting.
‘Let’s not hear any more of that silly nonsense “I’m going to cancel my policy because I can’t have treatment in a private hospital”.
‘With more than 140,000 people still waiting for routine treatment after 12 months and an all-time high backlog of more than 4.3m,
there has never been a better time to extol the virtues of health and protection insurances.’
Mr Scullion praised health insurers and health cash plan providers for the ‘magnificent’ way they had supported clients and intermediaries during Covid-19.
He cited a combination of waiving pandemic exclusions under their general terms and conditions, enhancing NHS cash benefits for Covid patients, and offering a combination of payment holidays and options.
The AMII helped its insurance company members, and others, develop their plans during the pandemic, but believes there was unjust criticism that it took too long.
Mr Scullion told the Zoom meeting, attended by over 230 delegates: ‘There is much to be said for the old adage “Do it once and do it right”.’
Reflecting on the last nine months, he said: ‘The building of the Nightingale hospital facilities and the commandeering of private hospital beds to deliver routine treatment ensured the NHS had adequate emergency capability to cope with a huge explosion of
Covid-19 related hospitalisations in the Spring.
‘But the knock-on effect was to put unwelcome pressure on private hospitals, consultants and health insurers as, for a short time, private treatment all but ground to a halt.
‘The Financial Conduct Authority gave us clear instructions around the need to ensure our products and services continue to deliver value, including an outline of how “value” should be considered.
‘Overnight, “value” had to be delivered by another means. Insurers embraced the need for regular communication to support clients and intermediaries through the challenges faced as a result of Covid-19; not least in terms of home working, provision of digital GP services, including online consultations and mental health support as we all came to terms with the impact of lockdown.’
At the peak of the first lockdown, the AMII orchestrated an industrywide initiative for the digital transfer of personal data and underwriting in the small and mediumsized enterprises and corporate markets. It is hoped to extend this to consumers and an update is due in early 2021.
A BAD ‘OWN GOAL’
AMII chairman Stuart Scullion hit out at business interruption insurance underwriters who refused to meet claims during the pandemic from small business owners like doctors and dentists.
He said insurance generally tended to get a bad press but the sector needed to make sure it did not contribute to that by scoring own goals.
But underwriters had done the insurance industry ‘no favours’ over the past few months.
Mr Scullion complained: ‘This is despite a High Court ruling on the test case brought by the Financial Conduct Authority, which said that most businesses with this insurance should be entitled to compensation after being shut down by the Government in March.
‘The case is at the Supreme Court as we speak so watch this space.’
Anxiety over shortfall in anaesthetists
Surgeons have expressed fears of a worrying shortage of consultant anaesthetists in private practice as the winter presses on. Their concerns were aired in front of Health Select Committee chairman Jeremy Hunt during a digital meeting of The London Consultants’ Association (LCA).
Former Health Secretary Mr Hunt was present to give his views on how, despite the pandemic, quality and safety in healthcare can be improved.
An LCA spokesperson told Independent Practitioner Today: ‘There is clearly a fear we are not going to have enough anaesthetists to go
TELL US YOUR STORY
Share your experience of what has and has not worked in your private practice. Even if it’s bad news, let us know and we can spread the word to prevent other independent practitioners falling into the same pitfalls. Contact editorial director Robin Stride at robin@ip-today.co.uk
round. The worry is if they are needed for Covid care and are pulled from helping to deal with all the elective surgery backlog.’
Mr Hunt, whose cross-party Commons’ committee holds the Government to account for policy, spending and administration, was said to have contributed to a ‘refreshingly honest and open discussion’.
He was emphatic about the need for a robust workforce plan to resource future care and gratefully acknowledged the welcome role played by private doctors and independent hospitals in support-
ing the NHS during the pandemic. The LCA reported a lively question and answer session moderated by its chairman, Dr Mark Vanderpump.
Stuart Scullion, head of the AMII
Jeremy Hunt MP
Beware surge in tax rebate scams
By Edie Bourne
Beware of scammers! That’s the New Year message from HM Revenue and Customs (HMRC ) to all those doctor self-assessment taxpayers still completing their returns for the 31 January 2021 deadline.
Fraudsters are using calls, emails or texts to contact customers. In the last year, tax officials responded to over 846,000 referrals of suspicious contact and reported over 15,500 malicious web pages to internet service providers to be taken down. Almost 500,000 of the referrals offered bogus tax rebates.
Many scams target customers to inform them of a fake ‘tax rebate’ or ‘tax refund’ they are due. The imposters use language intended to convince them to hand over personal information, including bank details, to claim the ‘refund’. Criminals use this information to access customers’ bank accounts, trick them into paying fictitious tax bills or sell on their personal information to other criminals.
‘We know that criminals take advantage of the self-assessment deadline to panic customers into sharing their personal or financial details and even paying bogus “tax due”.’
Pauline Smith, head of Action Fraud, said: ‘It’s important to remember if you’re contacted out the blue by someone purporting to be from HMRC asking for your personal or financial details, or offering you a tax rebate, grant or refund, this could be a scam.
‘Do not respond; hang up the phone and take care not to click on any links in unexpected emails or text messages. You should contact
HMRC directly using a phone number you’ve used before to check whether the communication you have received is genuine.
‘If you’ve been the victim of fraud, contact your bank immediately and please report it to Action Fraud online at actionfraud.police. uk or by calling 0300 123 2040.’
Customers can report suspicious activity to HMRC at phishing@ hmrc.gov.uk and texts to 60599. They can also report phone scams online on GOV.UK.
It could be a scam if it is unexpected, offers a refund, tax rebate or grant, asks for personal information like bank details, is threatening or tells you to transfer money.
Private practice ran ‘illegally’
A private general practice provider was ordered to pay nearly £13,000 after admitting it had run its service illegally.
Tudor Medical Matters Ltd, which operates a surgery in Rawtenstall, Lancashire, was fined £8,000 at Blackpool Magistrates’ Court. The company was also ordered to pay £4,962.55 costs, following a prosecution brought by the Care Quality Commission (CQC).
At an earlier previous hearing, Tudor Medical Matters pleaded guilty to providing regulated activities, including diagnostic screening and treatment, without CQC registration – a criminal offence
under section 10 of the Health and Social Care Act 2008.
The prosecution was brought after CQC inspectors visited the company’s premises on 24 October 2018, prompted by concerns raised by a pharmacist about a potentially inappropriate dose of medication prescribed by a GP at the practice. At that time, a GP surgery was not registered at this location.
Inspectors found price lists for services and patient records showing the company was offering numerous regulated activities –including consultations, blood tests and scan referrals.
In an interview with inspectors,
a representative of Tudor Medical Matters admitted providing regulated activities without registration since early 2017.
Following the CQC’s intervention, the company applied for registration but continued to break the law by providing regulated services before its application was approved on 17 October 2019.
Joyce Frederick, CQC’s deputy chief inspector of registration, said: ‘It is unacceptable that Tudor Medical Matters broke the law and risked people’s safety by operating without the benefit of CQC registration, so I welcome its guilty plea in this case.’
Consultants will be contacted in the first quarter of 2021 with an update from Healthcode on its plans to implement charges for its Clearing Service.
As previously reported on our website, the company said these would be delayed following the national lockdown and the affect this uncertainty was having on the industry.
A spokesperson said: ‘Rest assured, we’ll give you plenty of advance notice before these new charges are introduced.’
Planned charges are £6.99 per month to subscribe to the Clearing Service for electronic medical bills and a transaction fee of 25p per cleared invoice.
Eye hospital group Optegra has set its sights on an ‘ambitious growth strategy’ under new ownership. H2 Equity Partners (H2) has exchanged contracts to acquire the company, which has 23 eye hospitals in the UK, Czech Republic and Poland. Completion of the acquisition is expected early in 2021.
Optegra chief executive Dr Peter Byloos said: ‘We have been keen to support our consultant surgeons and all clinical teams with improved pathways as well as new virtual consultations, which have both really aligned our work.
‘As we enter this new phase with H2, we will continue to involve our clinicians both at board level in terms of governance and strategy, as well as decisions on a dayto-day basis’.
HMRC’s Karl Khan said:
Dr Peter Byloos, Optegra CEO
Scams inform victims of a fake ‘tax rebate’ or a ‘tax refund’ they are due
Help for doctors facing hearings
By Olive Carterton
A new ‘buddy’ support network launched by the MDU aims to help doctors trying to deal with the stress of a medico-legal investigation.
Members will be supported by volunteers among their peers who have themselves been through a GMC investigation or a claim.
MDU head of advisory services
Dr Caroline Fryar said: ‘So far, both the peers and the members who
Learning to steer clear of breaking cartel laws
London Consultants Association (LCA) members were given a ‘competition surgery’ by leading competition law barrister Prof Suzanne Rab.
She gave a detailed exposition of the complexities of competition law and how it applies to individual consultants and their business arrangements.
The LCA said consultants at the meeting were now well prepared to present challenging and informed questions to the Competition and Markets Auth ority (CMA) at a follow-up discussion.
A spokesperson said: ‘The LCA hopes that these expert sessions will ensure consultants do not unknowingly fall foul of the complexities and intricacies of competition law.
‘In addition, it will enable consultants to challenge other areas where seemingly anti-competitive practices are being introduced.’
Competition rules in private practice – what you need to know: CMA director Louise Banér gives advice on page 16
have been involved have found the experience positive.’
The purpose of the contact is not to discuss case specifics but to offer doctors the chance to question and get advice from a ‘buddy’ who has been through similar tough times.
One ‘buddy’ doctor recalled: ‘When I was facing the stress of a fitness-to-practise investigation, this service would have been enormously helpful.
‘It would have been wonderful to
speak to somebody who had been in the same boat and who understood what I was feeling and why. Whether they need a one-off session or ongoing support, someone to talk to or just someone to listen, I’m going to be here for them.’
The doctor added: ‘I had no immediate friends or colleagues who had been through a GMC investigation, but, of course, you always read the horror stories and expect something ghastly to hap-
Colonoscopy uses AI to detect polyps
The London Clinic reports it is the first UK hospital to employ GI Genius, a revolutionary device using artificial intelligence (AI) to enhance colonoscopy quality.
Produced by global medical device company Medtronic, the module is the first system to use AI to detect colorectal polyps.
It acts as a second observer during colonoscopies, helping to assist doctors by identifying lesions and small mucosal abnor-
pen. My sleep was disturbed. My days were disturbed. I was probably a complete nightmare to live with.
‘My MDU adviser was someone I could cling to and she proved to be an absolute rock. She reassured me that if I had a problem, they would deal with it and that I should try to focus on looking after myself.’
Buddies will draw on their own experiences to provide personal support, guidance, reassurance and hope.
Doctors’ Covid experiences to be collected
malities that may signal cancer.
Consultant gastroenterologist Dr Rehan Haidry said: ‘The system represents an important advancement in technology and is a crucial step in the fight against colorectal cancer, supporting both patients and doctors.
‘The technology is incredibly powerful and is proven to be extremely precise in identifying lesions in the colonic mucosa that can be difficult to detect.’
The Royal College of Physicians of Edinburgh has launched a Covid19 digital archive to document doctors’ and other healthcare workers’ experiences living and working through the pandemic.
This ongoing archiving project includes a range of insightful materials such as diaries, photographs and interviews, providing a record of the professional and personal impact of the pandemic on healthcare workers.
The archive aims to be useful for historical research and contains stories from doctors treating Covid-19 patients on the front line, highlighting the myriad of challenges they have faced.
The exhaustion, the frustrations, the determination and the hope all come through as healthcare workers document their experiences of dealing with Covid-19.
Topics include treating Covid-19 patients, accessing personal protective equipment (PPE), the health and well-being of healthcare workers, changing work routines, treating non-Covid patients, the public response to the pandemic through the eyes of doctors, and the views of doctors on lockdown.
Dr Rehan Haidry (above) and the GI Genius equipment in action (left)
Dr Caroline Fryar
WE LOVE OUR ROBO-OPS
OPERATING MACHINE IS A CENTURY ‘STRYKER’ AT WIMBLEDON HOSPITAL
Surgeons have celebrated completing 100 operations using robot technology at Aspen’s Parkside Private Hospital, Wimbledon.
They have used a Stryker Mako robotic arm to help carry out joint replacement surgery, allowing patients to return to active life quicker than more traditional surgery.
First used at the hospital in 2019, it works by using CT scans to generate an exact model of the patient’s knee or hip.
That information is then fed back through the Mako robot, allowing the surgeon to determine how much bone to remove to improve the accuracy and precision of the procedure. If the robotic cutting tool passes
over an area of the joint that does not need removing, it shuts off automatically, not starting again until it reaches parts mapped out for removal.
Orthopaedic surgeon Mr Giles Heilpern, who conducted the 100th operation and did the first robotic operation at Parkside in 2019, called the machine ‘fantastic’.
He said: ‘Results to date have exceeded expectation. Patients report less pain and better early function after surgery and go on to achieve excellent long-term outcomes.
‘I am proud to be involved with this innovative technology and genuinely see it as a game-changer in knee replacements.’
Consultant orthopaedic surgeon Mr Jonathan Miles alongside the Mako Robotic Arm
Wellington begins robotic ortho ops
By Robin Stride
HCA’s The Wellington Hospital has launched its new Mako Robotic Arm to patients.
The first operations using the system, a total knee and a total hip replacement, were performed by consultant orthopaedic surgeon Mr Jonathan Miles.
He will work alongside a team of senior orthopaedic consultants in using the system, which combines three key components:
3D CT-based planning;
Haptic technology for accurate cutting;
Data analytics – to provide patients with a minimally-invasive surgical option for their full or partial knee or hip replacement.
The Mako SmartRobotics system can help surgeons perform complex hip and knee surgery where patients feel less pain, have quicker recovery, gain better motion and
function and, over time, have fewer revisions than standard hip and knee replacements.
Mr Miles said: ‘We’re thrilled to be introducing a Mako Robotic Arm to the orthopaedics offering at The Wellington Hospital, providing patients with a gold standard surgical option.
‘Using the high-level measurement and pre-operative planning offered by the Mako, we will be able to find and fit the optimum joint dimensions, angles and ligament tension for each patient’s implant.
‘This level of precision means we can minimise post-operative pain and bleeding, shorten recovery times and even extend the lifecycle of the joint with a decreased need for revision surgeries.’
HCA Healthcare UK also offers procedures with the Mako robotic arm at The Princess Grace Hospital and The Lister Hospital, both in London.
Robot gynae procedures come to London Bridge
A new Robotic Gynaecology Service at London Bridge Hospital offers improved accuracy, lower infection rates, plus shorter length of stay and recovery periods.
Three ‘robotic’ consultants – Mr Simon Butler-Manuel, Mr Anil Tailor and Mr Jayanta Chatterjee –say they are delighted to lead the service catering for a wide variety of conditions.
HCA said over the last 11 years the trio had performed over 1,400 gynae-robotic operations in the country’s highest-volume centre at The Royal Surrey NHS Foundation Trust, Guildford, with a conversion rate to an open procedure of under 1% – significantly less than laparoscopic surgery rates.
The London Bridge facility opens as many women face longer NHS waits for routine surgery for benign gynaecological conditions, such as troublesome fibroids, endometriosis and period problems, which are seen to be less urgent despite often debilitating pain.
It said key benefits to patients undergoing minimally invasive,
robotic-assisted procedures – with systems such as Intuitive’s da Vinci robot – will include shorter length of stay, lower risk of infection, less scarring, less blood loss and pain, lower conversion to open rates than laparoscopic and faster recovery times.
Mr Tailor said: ‘Medical attitudes towards robotic surgery in the field of gynaecology desperately need to change. Robotic hysterectomies are extremely predictable and reliable, with the lowest rate of complications encountered compared with laparoscopic surgery.
‘Approximately 90% of benign hysterectomy surgeries could be approached minimally invasively; however, approximately 60% are still needlessly performed through an open bikini-line incision.
‘Furthermore, more than 80% of hysterectomies for womb cancers should be amenable to keyhole surgery even despite the fact that a large proportion of these patients are hugely overweight. In this group of patients with obesity, robotic surgery is especially beneficial.’
(From left)
Mr Anil Tailor, Mr Jayanta Chatterjee and Mr Simon Butler-Manuel
Lure patients by remote sevices
By Leslie Berry
Private GPs may be able to attract more male patients by promoting the availability of their remote services, a study suggests.
According to a survey of 1,000 male NHS patients, 82% said they fear seeing a healthcare professional in person and would much prefer a remote consultation option.
They told health management and appointment booking app myGP this includes via a phone consultation (40%), an instant messaging service (30%), a video consultation (21%) or an artificial health bot to avoid all human interaction (19%).
Nearly 80% claim the pandemic has made them more mindful of their health.
PPU WATCH
Compiled by Philip Housden
PHIN charging trusts despite big drop in PPU activity
NHS trust private patient managers are urged to contact the Private Healthcare Information Network (PHIN) regarding payment of fees for 2020-21.
PHIN is raising invoices based on last year’s activity despite the impact of Covid-19. As has been reported in Independent Practitioner Today, since March this year virtually all PPU capacity has been redirected in support of NHS services throughout the pandemic.
Income levels are expected to be around 75% down on last year as a result.
PHIN charges fees to private providers based on past trading performance and is therefore charging trusts now based on 2019-20 levels.
PHIN has offered the following: ‘We appreciate that these are challenging times for all healthcare providers and we have been work-
myGP medical adviser Dr Tom York, said: ‘Being a digital native GP, I value the ease of access and efficiency that remote consultations offer, and now knowing that 82% of males are even more likely to seek medical advice or reassurance when they can do so remotely, I feel even more confident in offering them.’
App founder Tobias Alpsten said:
ing with the NHS, Independent Healthcare Providers Network and the Competition and Markets Authority (CMA) on the Covid-19 response and are aware of the situation on the ground with many hospitals.
‘In line with the CMA Order, our subscription fees ... are based on 2019 activity. However, we realise that this doesn’t align with the actual activity on the ground for many providers at the moment and we can offer extended payment terms should they be required.
‘While we were not actively chasing data submissions, the CMA has confirmed the obligations under the Order remain for all private providers and consultants.’
Provider for Isle of Man PPU to be appointed early 2021
The unit at Noble’s Hospital was closed at the start of 2019 and private services suspended for up to 18 months while a review of services took place.
‘In the last 12 months, we have seen a 22% increase in males downloading the myGP app to access medical advice and support, and we saw a definite spike at the beginning of the pandemic.
‘With digital access comes increased choice – some patients will opt for full anonymity, and be happy to be helped by an informed health bot, and some will opt for a video consultation with a GP, which can remove the awkwardness of being in the same room.
‘Allowing patients to request and book an appointment with a few clicks on a smartphone makes a big difference too. Not having to find a private place to speak to a receptionist can mean the difference between seeking advice or not, for some patients – it certainly does for me.’
The island’s Department of Health and Social Care (DHSC) was almost ready to tender for an external provider in the new private unit at the hospital when the Covid-19 pandemic struck.
During the crisis, the unit was turned into an operational unit for patients who were Covid-19 positive, but in the summer it was converted back to its original purpose.
Health Minister David Ashford confirmed that work on setting up the PPU was resumed in August and the first phase of redevelopment started in October providing private outpatient services, preoperative assessment and diagnostics work and limited overnight stays in November.
The minister said a specification for the ‘procurement of a service by a provider external to DHSC’ had been developed and a competitive tendering process would then follow with the aim of awarding a contract within this financial year.
Philip Housden is a director of Housden Group (see page 42)
REASONS FOR FORGOING MEDICAL ADVICE
A key reason men put off seeking medical advice preCovid was lack of flexible appointment times (55%) around their office working hours; an issue temporarily removed as people work at home.
The third biggest barrier to men seeking medical advice is embarrassment.
The study revealed the top ten health issues that men are most embarrassed to seek medical advice about:
Sex-related genital complaints – 41%
Non sex-related genital complaints – 21%
Rectum – anything that needs a stool sample/internal examination – 17%
Mental health – 13%
Urine infections – 9%
Bad breath – 8%
Gas / wind – 6%
Snoring – 6%
Weight issues – 5%
Bodily odours – 5%
What to include in your check-up
➱ continued from front page
Accountant Vanessa Sanders said key issues to consider include:
Taking earlier retirement due to proposed Capital Gains Tax changes suggested by the Office of Tax Simplification;
Acting now if you have reasonable company reserves and are soon retiring from private practice. Tax rises are inevitable and ownermanaged small/medium firms are under Government scrutiny;
If your business life is far from over, but you have reserves under a company umbrella because you do not pay a commercial level of dividend to shareholders, you may need to consider implementing a strategy and looking at investment plans with your advisers;
Ensure advisers work together to provide holistic advice rather than looking at specific issues;
Think how you will maintain school fees.
By Olive Carterton
Independent practitioners, among a number of professionals who may have sold a second home during 2019-20, are being reminded to declare it on their self-assessment tax return.
They have until 31 January 2021 to declare any profit made from selling a UK residential property, which was not their main home, during the 2019-20 financial year, and pay the capital gains tax (CGT) due.
Since 6 April 2020, there have been changes to how customers declare and pay CGT.
UK residents who dispose of a UK residential property that is not their main home and make a capital gain where there is tax to pay, should use the online service to inform HM Revenue and Customs (HMRC) and pay the tax due within 30 days of completion.
Non-UK residents disposing of UK land and property should also use the HMRC online service,
Tell the tax office if you have sold a second home Improve workplace culture to aid retention
Poor working environments are a major factor why doctors leave the NHS, GMC chairwoman Dame Clare Marx has warned.
She told bosses at a ‘Leaders in Healthcare’ conference to use the pandemic as a chance to improve workplace cultures – or risk failing to retain their workforce and threatening patient safety.
Orthopaedic surgeon Dame Clare said doctors’ workplace experiences were crucial in many deciding to leave the profession, and why those who had left were often reluctant to come back.
Renal Services (UK) Ltd, the second largest independent provider of dialysis in the UK, will be delivering services at the new 184-bed Cleveland Clinic London.
It will also provide renal nurses for four dialysis rooms at the eight-storey 33 Grosvenor Place hospital.
Hospital chief executive Dr Brian Donley said: ‘We are excited to be bringing Cleveland Clinic’s patient-focused model of care to the UK. And with a superb trackrecord in safety and quality, Renal Services will deliver the highest quality care to our patients requiring dialysis when the hospital opens in early 2022.’
Renal Services operates 19 satellite units partnering with several NHS trusts across England and Wales. regardless of whether there is a gain or not.
The new rules affect landlords or property developers selling on part of their residential property portfolio or UK residents who sell a residential property that is not their primary home.
HMRC’s Karl Khan said: ‘The 2019-20 tax year is the last year UK residents will be required to pay CGT for the sale of properties as part of the self-assessment process and we want to make sure they are aware of the new requirements.
‘We’re making it easier for customers to pay any tax that is owed. UK residents, including property developers and landlords, should now use the online service to make any CGT declarations immediately after selling a residential property.’
Taxpayers will still be required to inform HMRC of CGT liabilities on their 2020-21 self-assessment tax return, but any payments already paid will not count towards their annual tax return bill.
New research, due to be fully published soon, found over 35% of doctors said dissatisfaction with their working environment was a reason for leaving.
Twenty-five per cent said it was a reason why they did not want to return.
‘The environments in which doctors work – the support they receive, the way they communicate with those around them, the ability they have to influence outcomes – have a material impact. Compassionate culture matters,’ she told the meeting.
Psychiatrist Dr Ed Burns (right), of The Priory Group, told an Association of Medical Insurers and Intermed iaries meeting that employer support for staff mental well-being will be fundamental as a result of Covid-19.
Dr Burns said: ‘We really need to focus on supporting the physical needs for people with mental health conditions due to Covid. The longer things have gone on, I’ve seen a surge in mental health issues.’
GMC chairwoman Dame Clare Marx
The Cleveland Hospital building
Beauty ops experience ‘Zoom boom’ due to virus Diagnostic unit to open in Somerset
By Douglas Shepherd
Cosmetic surgeons are facing a ‘Zoom boom’ in business during 2021 – as a direct result of the pandemic.
With millions of people only meeting via video conferences during Covid-19, many have had a prolonged daily update of their features on a screen – and are less impressed than they used to be at what they see.
Patients dissatisfied with their looks have been turning to the cosmetic market as a result and operators are reporting a sharp upturn in inquiries and procedures.
According to the author of a new report on the cosmetic market, anecdotal tales about people polishing their appearances due to more videoconferencing is reflected in the data.
Liz Heath said: ‘It looks as though cosmetic surgery and the non-surgical cosmetic treatment market will be among the few not to have experienced long-term adverse effects because of the pandemic.’
She points out that cosmetic treatments have lost their stigma over the past decade or so as people have been willing to discuss them openly on social media.
Less expensive non-surgical procedures have made them more accessible to a wider range of people.
Talking at the launch of her second edition of the LaingBuisson Cosmetic Surgery UK Market Report, she reported that many people now saw an operation as part of
their usual beauty and well-being regime.
Ms Heath said: ‘Meanwhile, the pandemic has put many of us “on camera” regularly for the first time in our lives.
‘Maybe we should therefore not be surprised that there has been a surge in demand for cosmetic treatments, even if their discretionary nature would make them appear to be a prime candidate for removal from personal budgets, given the current economic uncertainty.’
Most cosmetic surgery is discretionary spend and is typically sensitive to fragility in the economic cycle, but market analysts LaingBuisson say it has remained robust during the pandemic.
In line with demand patterns in recent years, there has been a surge in inquiries for non-invasive cosmetic procedures.
Surgical treatments declined by 10% to August 2020, although this can in part be explained by all inpatient facilities and their staff
being dedicated to the pandemic response from 24 March 2020.
The British Association of Aesthetic Plastic Surgeons has reported that members have seen a 60-70% increase in virtual consultations during the pandemic.
Also, aside from a dip in April, Google trends show that interest in cosmetic surgery is now more or less at pre-pandemic levels.
The report also covers the prepandemic market as it was in 2019. It shows a cosmetic surgery market worth around £286m in 2018 and projections based on this data show that the market had dipped to £271m by 2019.
In contrast, the non-surgical market is believed to be valued at around £3bn. This segment is the main volume driver of growth, offering ease of accessibility and faster recovery than surgical procedures.
LaingBuisson said there was a trend for people who go down the non-surgical route to ultimately turn to surgery as non-surgical interventions failed to offer the desired results or they mixed and matched surgical and non-surgical options.
‘This means those providers who offer both surgical and non-surgical procedures are most likely to benefit from the growing interest in cosmetic treatments, which has resulted from their normalisation across all socio-economic and demographic groups.’
Among surgical procedures, the most popular continue to be breast enhancement and body contouring, though rising prices for these procedures is dampening growth.
The expanding diagnostics market is to have five new entries from Rutherford Diagnostics, which is building its first centre in Taunton, Somerset.
Opening later in 2021, its offering will include computed tomography, MRI, ultrasound and X-ray.
The company, a subsidiary of Rutherford Health, has also agreed a partnership with Somerset NHS Foundation Trust which will see the centre providing its services to the trust for ten years. This will also be available to private patients in the South-west.
Dr Steven Powell, chief diagnostics officer, said: ‘Diagnostics centres such as ours are all the more important now given the impact of Covid-19 on testing and screening for various diseases.’
David Shannon, of the NHS trust, said: ‘It will mean that many of our patients will be able to receive their diagnostic tests at another modern facility away from the excellent unit at Musgrove Park Hospital.
‘We have also agreed with Rutherford Diagnostics that there will be exciting opportunities for our colleagues to work at the new centre while maintaining their employment with us.’
Innovation is seen as important for business recovery by 86% of small firms in health-related sectors.
But despite this, almost half say cost is the main barrier for them when it comes to pursuing innovative activity, according to research from R&D specialists GovGrant.
Chief executive Luke Hamm said the Government needed to do more to incentivise UK businesses to innovate and build back better.
‘For the health sector in particular, innovation is at the forefront of the response to Covid-19 that will help drive recovery from the pandemic and we can’t afford for cost to be such a big part of the reason for why it’s not happening.’
Statistics in the LaingBuisson Cosmetic Surgery Market Report confirm the anecdotal trend
Report author Liz Heath
A look back through our journal’s archives of a decade ago reveals that although times change, some issues are not so new
A trawl through the archives: what made the news in 2011
GPs should ask patients about PMI
BMI Healthcare increased pressure on GPs to routinely check patients’ private medical insurance status by saying the NHS could potentially save over £285m a year if they did.
Research for hospital groups found most GPs did not even ask.
Hopes of a prosperous New Year
Independent practitioners were told they would face exciting new business opportunities in the coming year despite reports of a decline in private medical insurance and self-pay patients.
According to one expert, it was a ‘fantastic time’ to enter the sector and specialist could be ‘very optimistic’ about private prospects.
Barrister Stephen Collier, then general counsel at BMI Healthcare, told doctors at a conference that although consultants had seen some decline in private activity, he was confident that there would be a turn-around in the next 12 months.
He said private practice’s biggest driver would be the economy, particularly £20bn of budget cuts planned for the NHS.
Big rush to quit NHS to go private
A 200% increase was reported in the number of senior doctors looking to take 24-hour retirement from the NHS and do more private work.
Consultants were particularly concerned about the reduced £50,000 annual pension savings allowance being introduced in three months’ time and the lower lifetime allowance of £1.5m from April 2012.
The next few months provided a short window of opportunity to exit the NHS with accrued pension benefits mostly intact and bypass harsh tax rates of 50 to 55%.
Independent financial planner Simon Bruce, of Cavendish Medical, said: ‘With the new annual allowance alone expected to raise £4bn in tax for the Treasury, some consultants are rightly looking at every possible
way to safeguard their NHS and personal pensions from further attack.
‘It is clear that the Government intends to pursue those it perceives as possessing the broadest shoulders and, without action, the consequences are lower pensions with reduced sums.’
Private doctors believed their numbers could also be swelled by specialists leaving the health service if NHS Employers successfully got the pay Review Body to dump the consultants’ £400m clinical excellence award scheme.
Private bosses lobby MPs
The chief executive of a new group representing the UK’s big five private hospital groups told MPs the sector looked forward to seeing how a new Health Bill would promote healthcare competition.
Richard Jones said the private medical services market was ‘vigorously competitive’ and this brought benefits to patients, as it stimulated innovation, customer focus and value for money.
Speaking at the official launch of the H5 Private Hospitals Alliance at a House of Commons’ reception, he said independent hospitals wanted the Bill to create a fair, competitive framework for the private sector and foundation trusts to attract patients on a level playing field that regarded innovation and quality.
Mr Jones said the group would make the case for the UK to take full advantage of its private hospital sector as an essential complement to the NHS.
Check you’re not overpaid
Independent practitioners who also received NHS salaries were advised to regularly check their pay slips – in case they were being paid too much.
We warned that overpayments did eventually get spotted by NHS trusts and it was then that consultants could be thrown into a tax nightmare.
According to the Hospital Consultants and Specialists Association, some members had been overpaid by more than £50,000. It warned: ‘You may not be surprised to learn that trusts fight hard to recover this money.’
TELL US YOUR NEWS
Share your experience of what has and has not worked in your private practice. Even if it’s bad news, let us know and we can spread the word to prevent other independent practitioners falling into the same pitfalls. Contact editorial director Robin Stride at robin@ip-today.co.uk
Richard Jones, of the H5 Private Hospitals Alliance
ACCOUNTANT’S CLINIC: THE BUILDING BLOCKS OF ACCOUNTANCY
to of top tips
is for quick thinking
Julia Burn continues with her A–Z of top tips. This month she turns to ‘Q’
IN THIS ever-evolving world we live in, it is important for businesses to stay up to date with current changes and have the ability to adapt to new ways. This will inevitably require a vast amount of quick thinking.
Not only are we dealing with the fallout from the Covid-19 pandemic and the effect that various lockdowns have had on businesses, but also changes that will come into place as a result of Brexit.
The Covid-19 support measures are constantly changing – as Independent Practitioner Today has regularly shown with the news updates on its website – making it difficult to plan conventionally. Businesses need to plan but also be agile to react to this changing economic landscape
Not all of the fallout will be negative for private medical practitioners. Due to the NHS having to divert many of its services to cope with the Covid-19 pandemic, the subsequent delays in routine appointments and procedures mean more patients will inevitably turn to private practices to speed up the process once lockdowns and restrictions ease.
Practices will therefore need to adapt to facilitate a potential new influx of clients.
Day-to-day business needs
Keeping on top of accounting and finance records will be an even more important task than usual to ensure that any issues arising are dealt with quickly and ensuring that they do not affect the smooth running of the practice.
Many accountants offer outsourcing solutions, which provide a back-office function keeping your financial records up to date on a regular basis, leaving you the time and resources to concentrate on the day-to-day running of the practice.
Maintaining up-to-date information allows quick decisions to be made to keep costs controlled and cut as and when necessary.
And maintaining cash flow forecasts will give a reliable way to make sure that any pinch points are identified quickly so they can be dealt with appropriately.
Unless you are working as an employee, tax on income from private practice is usually paid by you twice a year under the self-assess-
ment regime. Tax is paid in equal instalments, which are estimated based on your previous year’s liability, by 31 July and then the balance by 31 January.
Actual tax due for the year is calculated based on your actual liability for the tax year, any additional amounts are then due by 31 January, together with your tax return.
Due to the Coronavirus pandemic, the Government initially allowed the taxpayers to defer their 31 July 2020 payments on account for the 2019-20 tax year to 31 January 2021. This has now been extended further and your 31 January 2021 tax bill can now be paid over 12 months, by 31 January 2022 – as long as it’s below £30,000.
However, deferring your payment will mean that your January 2022 tax bill may be higher than usual. If you have funds available to pay any deferred payments by 31 January 2021, you may wish to consider doing so to help your January 2022 cash flow.
If your tax returns and tax payments are late, penalties and late payment interest will be due, so
you must ensure that your affairs are kept up to date.
Government support for businesses
The Government has provided various measures to support businesses during the pandemic, including the furlough scheme, the bounce-back loan, the business interruption loan scheme and ability to arrange deferment of HM Revenue and Customs liabilities.
The furlough scheme has evolved during this time and there also have been extensions to the original schemes.
It is important to keep up to date with any changes in these schemes if they are being utilised to ensure your business is abiding by current regulations and obtaining the best support available.
It would be a good idea to keep in regular contact with your accountant, who will be up to date on all of the changes.
Adapting to change
As I write, we have now been through our second lockdown and are continuing to be affected by local tier restrictions, which means we are constantly needing to adapt our way of life as well as our businesses.
Working from home looks like it will become the way forward. This may affect footfall into practices and it may mean that more appointments are held online rather than face to face.
So it will be necessary to ensure the relevant technology is in place to deliver the services in a secure way and ensuring all elements of data protection are complied with.
As well as adapting to changes resulting from the pandemic, there may also be changes due to Brexit. The UK officially left the EU as a member on 31 January 2020. On 1 February 2020, a transitional phase commenced during which EU laws, membership of the single market and customs union, EU trade policy and ongoing budgetary commitments continue to apply to the UK.
The UK Government has replaced the existing arrangements with effect from 1 January 2021 with a UK-EU free trade agreement. The EU’s single market rules created a trading bloc and customs union with its member states to guarantee free movement of goods, services, people and capital among EU member states.
The practice will need to understand how these changes affect them and adapt to them quickly to ensure that they remain compliant.
The best way to do this will be to keep in regular contact with your accountant who will be up to date on all of the changes.
The future
Due to the uncertainties created by the pandemic and Brexit it is inevitable that some working practices will need to change.
One thing we can be certain of is that we now know that we are able to adapt quickly to change and that private practices will continue to deliver the excellent service that their clients are used to receiving albeit in a slightly different format.
Julia Burn is a senior manager at Blick Rothenberg and part of the team that advises medical practitioners
ADAPTING TO THE PANDEMIC
Agility is the key to surviving the crisis
As the profession faces ongoing challenges over winter, how can consultants plan strategically for their practice while adapting quickly as the situation unfolds?
Mr Alan Farthing, director of clinical strategy at King Edward VII’s Hospital (pictured right), gives Independent Practitioner Today his views
WHEN A GLOBAL pandemic such as Covid-19 arrives, there are no rules or previous randomised trials. There is no textbook to refer to nor tutorials from a respected senior figure.
The situation is unique and the medical profession with its associated support teams is at the head.
Clinicians are well versed in the art of making rapid and meaningful decisions. An intraoperative change of plan may occasionally make the difference between life
and death and will frequently increase or decrease the risk of complications.
Clear and logical thinking on those occasions will determine the quality of care that patients receive.
Decisive thinking
Despite the uncertainties of the pandemic, the same clinical principles still exist, whereby clear, logical and decisive thinking will make all the difference to a
patient’s outcome – and a consultant’s practice.
‘Good things come to those who wait, but only what is left over from those who hustle’, said Abraham Lincoln.
This was certainly the case back in March. King Edward VII’s Hospital is an independent hospital in central London and we were able to be agile, responsive, decisive and able to hustle when Covid struck.
Consultants working across pri-
The clear, logical and agile thinking that makes a clinician good at managing one patient is also necessary when delivering healthcare to large groups of patients
vate and NHS practices are uniquely positioned to see what services were needed in this situation. We were able to act, stepping up to support the emergency response and providing priority care to patients according to need.
We did not wait to be told what was required, but simply got on with the job.
The first plan on how we could play a role in this national crisis was put forward on Thursday morning; that plan was activated at 7pm on the Friday and at 9am on the Monday – the day the contract with the NHS commenced – there were NHS patients anaesthetised in every theatre commencing their urgent cancer treatment.
As the needs changed over the coming weeks with the sector being centrally organised, the hospital changed again to provide care for patients with urgent benign conditions.
Moving forwards, the private sector will need to provide care for more self-funding patients.
The number of people waiting more than a year for their NHS treatment has risen from 400 to 32,000 in London alone over these last few months and some will
choose to use private healthcare facilities rather than wait.
Harnessing technology
Many aspects of life have been fastforwarded by years in this crisis. Changes that were due to be trialled have already become the standard and practices that were thinking about the future have rapidly progressed.
Greater utilisation of telemedicine, for example, has been a great success both in terms of Covid-safety, but also in terms of convenience for patients and time efficiency for clinicians.
Working with a partner who similarly embraces new technology to adapt to the current situation should also be a key consideration for those looking to expand their services.
Collaboration is the future
A time of national crisis has taught us that we are better working together than as individuals and that adaptable and forward-thinking organisations, where actions speak louder than words, will thrive.
Perhaps more than ever, it has emphasised that the clear, logical and agile thinking that makes a clinician good at managing one patient is also necessary when delivering healthcare to large groups of patients.
As a consultant, a major component in both being able to plan strategically and adapt quickly is by establishing a collaborative relationship with a private healthcare provider.
One that treats doctors as individuals, not numbers, that encourages and listens to consultants’ feedback and adapts as their practices adapt – improving their own professional development and the care they can offer patients.
We all hope that 2020 will not be repeated and that the lessons learned from this crisis will help us be more resilient as a society. Similarly, those of us who are charged with providing good healthcare have learned that working together within those agile, decisive and responsive organisations will find their services are required more than ever before.
As usual, those providing the highest quality of care will be most in demand.
A digital prescription platform to allow convenient prescribing from home
CloudRx is a digital prescription system that allows prescribers to create and send an electronic prescription to our fully licensed pharmacy for fast delivery direct to your patient. It can be used from home by doctors working away from their practices.
No cost to prescribers
Simple and quick prescription creation.
Legal paperless prescriptions, including repeat prescriptions and controlled drugs.
Patients receive text and email requesting secure payment. Alternatively, we can invoice the prescriber or clinic each month.
Prescriber Fees can be added if requested
Medicines are dispensed and dispatched by a variety of delivery options
Fully integrated into Midex Pro
“We have worked with CloudRX to maintain a cold chain for the medication and direct delivery to patients at home.”
Mr Alan Farthing
Dr Charlotte Norton, Medical Director of The Slimming Clinic, the UK’s largest chain of private doctor-led weight loss clinics
Price-fixing detectives are on your case
Louise Banér (below), director of the Competition and Markets Authority, gives advice to readers on how to avoid breaching anticartel rules
How we
FAIR COMPETITION is a fundamental component of a healthy and successful economy. When businesses agree to avoid competing with each other, they undermine this, with harmful consequences for consumers.
In the case of private medical healthcare, this may mean patients paying more and having less choice.
Earlier this year, I led an investigation into price fixing in the private ophthalmology sector. This resulted in the Competition and Markets Authority (CMA) imposing a fine of £1.2m on a private hospital group for facilitating a price-fixing arrangement for self-pay ophthalmology consultation fees, as well as fining six consultants involved.
This case is not the only instance where the CMA has taken action in the private medical healthcare sector.
In 2015, we imposed a fine of c£380,000 on Consultant Eye Surgeons Partnership (CESP) Ltd, which broke competition law by agreeing prices, recommending its members refuse to accept lower fees from an insurer and facilitating the sharing of confidential business intentions, including on future pricing, between members.
Just prior to this, in 2014, we also published the final report of our market investigation into private healthcare, which included recommendations on pricing transparency that are now being implemented by the Private Healthcare Information Network.
The private healthcare sector is therefore firmly on the CMA’s radar and the purpose of this article is to help private practitioners learn from our previous investigations and avoid making similar mistakes.
A key message is that competition law and the rules that govern businesses apply equally to you, as private practitioners, as they do to large corporations.
Yet we know from research with a broad range of businesses across the country that awareness and understanding of competition law remains low.
Only 57% of those we polled know that it is illegal to fix prices and 41% don’t know that
attending a meeting where rivals agree prices is illegal.
Over half (59%) don’t know that agreeing to split up markets and share customers with competitors is illegal.
This lack of understanding of competition rules is worrying. Not knowing that a business practice is illegal is no excuse for wrongdoing and the consequences of getting caught are serious (see box on the right).
I and colleagues at the CMA believe that the majority of private practitioners want, above all, to do the right thing for their patients and to comply with the law. The good news is that we have advice and information to help you.
Below I set out some key points that can act as a guide.
Re-cap on competition rules – what you need to know
➲ It is illegal to fix prices or to exchange or share confidential and commercially sensitive pricing information, such as future pricing intentions, with competing service providers such as independent consultants in private practice or between private healthcare groups.
➲ It is illegal to facilitate price-fixing agreements between consultants in private practice by suggesting or allowing an arrangement where competing service providers co-ordinate or agree to fix prices for their patients.
➲ Equally, it is illegal to facilitate the exchange or sharing of confidential and commercially sensitive pricing information, such as future pricing intentions, between competing independent consultants in private practice.
➲ It is illegal to agree to divide or share markets –such as particular places – or customers between competitors.
➲ It doesn’t matter if not all your competitors are involved; all it takes to set up an illegal agreement or arrangement is at least two competitors and one or more emails or a meeting.
➲ Price-fixing covers more than agreeing to raise prices. You will still be breaking the law if your prices stay the
THE SANCTIONS
If you are caught instigating, participating in or facilitating anti-competitive practices you could face fines of up to 10% of your annual global turnover. Company directors could be banned from acting as a director for up to 15 years. In the most serious criminal cases, individuals could face prison.
same and you have agreed with one or more of your competitors not to lower them.
➲ You can find out what prices are charged by your competitors where this information is publicly available, but you must not discuss with rivals their future prices or pricing intentions.
➲ If you are approached to join an illegal arrangement, reject the approach immediately and unequivocally, seek legal advice and report the incident to the CMA.
Be clear on who your competitors are
Your competitors are typically other private medical practitioners and private clinics and hospitals who offer services that patients and commissioners of care would consider substitutes for the services you offer – such as for the same procedure and in the same geographic market. The exception is where two or more medical practitioners form a business – for example, a group such as a limited liability partnership – and do all their private work exclusively for that business.
Subject to certain conditions, and provided you cease your activities as a sole trader, you and your business partners are likely to be viewed as a single economic unit – known in competition law as a ‘single undertaking’ – rather than as competing businesses.
If you work for such a group, then your competitors are those medical practitioners, competing groups and private clinics who offer services that are substitutes for the services your group offers.
Agreeing fees in a group
If your group is acting as one undertaking, then an agreement about fees charged by that group is not considered an agreement between competitors. It is an internal management decision only.
Groups and their members may wish to take specialist legal advice on whether the group constitutes a single economic unit and therefore one undertaking for competition law purposes.
Agreeing fees in a group when also working outside the group
If you also work outside the group as a sole trader, then you do not form a single undertaking with the group.
This means that you may be directly competing with the group and/or its members if they also work outside the group as sole traders.
If you work both within and out-
side a group, then consider establishing clear rules on who is allowed to receive the group’s pricing information which relates to offering similar services to customers in the same geographic market.
For example, you could change the type of membership to limit the exchange of competitively sensitive information and the co-ordination of commercial response by competitors.
Whatever structure is chosen, to be compliant it will need to avoid the exchange of commercially sensitive information between competitors.
Circumstances which do not pose a risk to competition law
Competition law does not prevent you from adapting yourself intelligently to the existing or anticipated conduct of your competitors, which may include charging the
same fees as other professionals in your field.
The law does prohibit, as I have explained above, any direct or indirect contact by which a private medical practitioner may influence the commercial conduct of competitors, such as the prices they will charge.
It is important to note that there are many circumstances where private medical practitioners can co-operate and exchange information with their competitors to achieve positive outcomes for patients.
These could include the joint purchasing of services, educational activities or exchanging information for the purpose of improving services to patients, such as offering new and additional services and extending opening hours. For more detail on this, see our specific advice: Private medical professionals: information on competition law.
What to do if you think you may have broken the law
However, if you find yourself in a situation where you think the law may have been broken, there are significant benefits to coming forward and being one of the first to report the illegality – provided you fully co-operate with a CMA investigation. This can include avoiding being fined.
Even after an investigation has started, you can still benefit from reduced fines through our leniency programme.
Individuals may also be eligible for immunity from prosecution and director disqualification if they come forward independently and co-operate with us.
If you think you could be at risk of breaking the law, always seek independent legal advice.
For more information on how best to spot and report anti-competitive practices, visit: gov.uk/ cheating-or-competing.
Some light for 2021
David Hare (right) casts a look back at 2020 and is optimistic for independent practitioners in the year ahead
AS WE embarked on the new decade, with a new Government and the UK’s departure from the EU confirmed in law, 2020 was set to usher in a new period of stability for the health sector.
And, for independent providers, it would be an opportunity for further progress on the quality and safety agendas, with the longawaited publication of the Bishop of Norwich’s inquiry into rogue surgeon Ian Paterson due for release and significant work in train around NHS legislation and the promotion of the UK as a destination for international patient activity.
However, the Coronavirus pandemic changed everything. Representing the biggest challenge to the health system in its history, the pandemic has had an enormous impact on everything and everybody, shaking the kaleidoscope and causing challenges very few of us could have foreseen as 2020 was ushered in, not least for the livelihoods of many independent doctors working in the UK.
Key positives
For all the challenges, however, there are some key positives from 2020 that will put the entire healthcare system in better stead as we move past the pandemic and, as 2021 begins, it feels appropriate to stay positive.
Firstly, the pandemic has demonstrated just what can be achieved when all parts of the health system works together and that it is in the interests of the NHS and the nation as a whole to have a strong independent health sector in the UK.
Almost two million operations, scans, consultations and chemotherapy sessions have been delivered under the historic partnership
2020 wallplanner
between the NHS and independent hospitals.
The sector and its workforce have played an essential role in ensuring vital treatment, notably cancer care, could continue during the pandemic.
And with NHS waiting timings rising at an exponential rate, the full might of the independent health sector and its workforce is going to be needed not only in supporting the NHS in getting waiting lists down, but also treating the many more people who will be looking to privately fund their healthcare in a bid to access faster treatment.
The past year has also shed some necessary light on how the NHS and independent health sector work together and what more can be done to improve joint working. Indeed, 2020 saw the resolution of one of the key issues the health system has been grappling with for a number of years – how to ensure that independent healthcare providers are able to play their part in training the next generation of medical professionals.
With whole NHS teams coming across to deliver care in independent facilities, the need to host and support junior doctors in the sector transformed from a worthy ambition to a real necessity.
New training opportunities
Following a landmark agreement with NHS England and Health Education England, junior doctors will now benefit from fantastic new training opportunities in independent providers.
This will allow them to experience and contribute to the highquality care the sector delivers to patients, along with the teamwork, management and the broader culture of healthcare in independent hospitals, embedding this in the sector for years to come.
Indeed, there is now a real understanding from Government and healthcare bodies that they must look at the healthcare workforce in the round, and not just those in the NHS.
Earlier on in 2020, the Independent Healthcare Providers Network
worked with the Government to successfully ensure that those working in the independent health sector would benefit from the Home Office’s visa extension for healthcare workers, with parity of access to PPE, testing and other support a key tenet of the contract between the NHS and independent providers.
Of course, with the prospect of a vaccine becoming more real for more people every day, life will indeed once more get back to some kind of ‘normal’.
And while 2020 might have been a year that some consultants working in the sector would wish to forget, the ‘whole systems’ response to the Covid pandemic and the key role the sector has played will not be forgotten by the NHS, Government, regulators, and other key bodies.
That bodes well for a constructive, productive 2021 for the sector and its workforce.
David Hare is chief executive of the Independent Healthcare Providers Network
The danger of too much showing off
Social media is, by nature, social – and like any social gathering, there are not only rules dictating acceptable conduct, but also ‘unwritten rules’ that encourage success. Nikki Milovanovic (right) focuses on two classic faux pas in online self-promotion
WE’VE ALL had the real-life encounters with those tiresome individuals who drone on about their experiences, expertise and achievements – mostly because they never stop talking.
But how many of us genuinely want to listen to, or engage with, those who speak exclusively about themselves?
These individuals may appear to have an entourage, but I’d argue their audiences are comprised of four distinct groups:
Those who care;
Those who don’t;
Those who joined because they saw a large group of people;
Those wondering how they got stuck listening – and how they can extricate themselves.
While it’s universally agreed that such boorish behaviour in our social lives is intolerable – or, at least, unlikely to win you any friends or repeat invites – somehow, this knowledge has failed to translate to social media.
This is largely because it’s widely thought that the tools to success are right at everyone’s fingertips, making expertise seem just a few clicks away; and because the whole point seems to be ‘getting your brand out there’.
In my experience, it’s wise to focus on generating engaging promotional content to help your private health clinic or service get the attention they deserve, organically, and for the right reasons.
Silence can be golden
This may be controversial, but sometimes not talking about yourself can better establish rapport with a quality audience who genuinely cares what you have to say.
The UK aesthetic sector is a wonderful, diverse, dedicated community comprised of highly intelligent, brilliant innovators. But with great innovation comes the great responsibility to recognise that a significant percentage of our ideas might not be as great as we think.
This news may come as a shock to some, but I promise it is 100% evidence-based: one perfect example of creativity and innovation going completely haywire is the clinic which enthusiastically approached me, as it wanted to roll out its highly questionable concept of portraying injectable treatments as fast food – complete with a £99 menu. #TrueStory.
These medics strongly felt the low price point would serve to undercut competition, and the imagery would be a fun, creative way to disrupt the norm and help them stand out from the crowd.
Reputational damage
As they excitedly envisioned syringes of ketchup and mustard injecting volume into a 100% allbeef patty, I knew I was dealing with a serious case of ‘aesthetic yikes’ with strong potential to cause long-lasting damage to their professional reputations, as well as to the brand. The internet never forgets.
Ultimately, the clinic agreed I had a point in saying this was perhaps not one of their greatest hits, but even then, the looming spectre of BotoxBurgergate continued to haunt us problematically.
When trying to build anything – whether that’s a brand on social media or a new technique of working – it’s essential that we are open to receiving valuable, pragmatic and real-world feedback.
Unfortunately, since these aesthetics experts had been so invested in their ‘amazing’ idea, justified criticism came across as hampering creativity. Instead, they should have seen this criticism as allowing them to more accurately assess that they’d spent hours trudging into uncharted territory – that was unexplored for good reason – and that they should have brought the concept to the social media expert first. #TopTip.
I’m loath to ever give the cosmetic cowboys anything resembling credit, but if they’ve taught us anything, it’s that just because someone has the tools to do something, doesn’t mean they should.
While a poor social media strategy isn’t likely to land anyone in A&E, it can certainly do a lot of harm to a practice’s potential, as well as be costly and time-consuming to reverse.
Off-putting promotion
It is essential for clinics on social media to demonstrate their relevance while striving to deliver balanced content, because, as we all know, constant self-promotion is off-putting; and desperation, much like a condiment-filled syringe, is never attractive.
I previously postulated that four distinct audiences surround realworld egomaniacs, but like most social behaviours, these become expanded and amplified online.
For aesthetic clinics, they can include rival clinics in sock puppet attire, bots and, of course, the second-best friend of the virtually vainglorious: fake followers. These audiences are useless – and sometimes harmful.
More than ever before, real audiences are hyperaware of the banquet of choice laid out in front of them and savvy aesthetic practitioners know not all social media efforts are equal.
Moreover, the savviest practitioners don’t waste their valuable time trying to master the minutiae of #SoMe. They hire an expert to brainstorm and execute proven strategies and continue doing what they do best: providing excellence in aesthetic treatment to happy patients, who want to spread the word about their fantastic results.
Nikki Milovanovic is the founder and managing director of Sophisticated Comms, a London-based agency specialising in creative strategy, social media and public relations for the lifestyle, beauty, health and wellness
sectors While a poor social media strategy isn’t likely to land anyone in A&E, it can certainly do a lot of harm to a practice’s potential, as well as be costly and time-consuming to reverse
MidexPRO
One touch e-Billing
y 24/7 online Cloud access on Mac OS and Windows
y Go paperless by typing and importing documents
y Encrypted software to ISO270001 standards & DSP Toolkit compliant
y Outstanding UK support via email, phone and live chat
y Card payment facility with Hero Health y Dispense & dispatch prescriptions to patients for next day delivery using CloudRX
THE POWER OF PEOPLE
Jane Braithwaite explores the broad subject of managing people and teams, covering topics such as our responsibility as employers, leadership styles, different employment models and well-being.
In this issue, she recommends the three ‘C’s – clarity, communication and care – for improving the power of your people and managing your team through this difficult period
power Harness people
IT IS the people within them that make companies and businesses work, and this is especially true in healthcare.
Despite huge advances in technology, including the automation of many administrative processes such as the incorporation of robotic surgery and the use of artificial intelligence in diagnosis, it is still fundamental in all healthcare businesses to have the right people, with the right skills and attitude in the right roles.
There are very few examples of services or businesses where one person can do everything and, in most cases, it takes a team effort.
If you are a surgeon, for example, there may be moments where you feel you are alone, but caring for your patients is a communal effort and requires the commitment and dedication of a group of people with varied skill sets working together.
A well performing team is a joy and being part of such a team is fulfilling on many levels: the sense
of achievement and belonging, the feeling of being respected and of making a valued personal contribution.
But for every high-performing team, there is an opposite, less successful example. Most of us have experienced at least one team in our career that is verging on dysfunctional.
Prior to the Covid-19 pandemic, we were already aware that, in the UK, people were feeling under pressure and struggling to maintain a healthy work-life balance.
Of greatest concern in this current climate is the increased pressure that people are experiencing in both their personal and professional lives. Everyone is attempting to handle the uncertainty of Covid, coping with the lack of control, worries about their health, finances and the health of their friends, families and colleagues.
Relying on adrenaline
In a crisis, we rely on adrenaline to help us perform and, in most cases, the crisis is short-lived and this short-term solution is appropriate. To continue to rely on adrenaline on a long-term basis is potentially damaging and we expect this to cause numerous longer-term issues.
In the early days and weeks of the pandemic, business owners, including those in private healthcare, focused on survival. What do we need to do to get through this? At the time, there was a sense that this would last for weeks rather than months.
The Government announced measures to support employers in the form of the job retention scheme alongside various loans and grants, to support us in achieving the goal of survival.
Many individuals were furloughed from their positions and some continue to be furloughed at the time of writing due to a further extension of the policy.
While being furloughed may sound like a pretty good deal, many have suffered with increased stress due to job insecurity and anxieties related to financial and career impacts.
In the worst-case scenarios, we have seen an increasing number of people being made redundant and there is an expectation this will continue as the Government
One unanticipated symptom of furlough is a tension between work colleagues where those who have continued to work perceive their furloughed colleagues to have had the easy option, leading to an underlying resentment
schemes eventually come to an end.
For those individuals who have worked throughout the pandemic, we are seeing signs of burn-out.
However, one unanticipated symptom of furlough is a tension between work colleagues where those who have continued to work perceive their furloughed colleagues to have had the easy option, leading to an underlying resentment.
Many of us have been adapting to working from home either on a part-time or full-time basis and this brings about a new set of challenges.
Initially, it was the logistical issues of home-working that focused our attention. Setting up secure IT systems, adapting to working in a paperless manner, talking to one another via Zoom and so on.
As the weeks and months have passed, our focus has shifted to the reality of working remotely longterm, managing teams of remote workers and ensuring everyone remains motivated and productive.
Bringing staff back
Clinics and offices have faced the challenge of bringing their employees back in a Covid-safe manner and adapting the physical environment to ensure it is safe and compliant.
Space limitations have reduced the number of people who can physically be in the workplace on any particular day, leaving members of staff continuing to work at home on a part- or full-time basis.
Some people have been reluctant to return to the office, either because they love working from
home or they are scared to come back, particularly if their commute involves public transport.
The current crisis looks set to continue for some time and, as leaders and managers in healthcare, we need to take action to address these issues and support the people that make up our teams so that they continue to be high performing.
With that in mind, how do we create high-performing teams in this current climate? It is a challenge!
In this Independent Practitioner Today series entitled ‘The power of people’, we will explore the broad subject of managing people and teams, covering topics such as our responsibility as employers, leadership styles, different employment models and well-being.
This month, my initial recommendations for improving the power of your people and managing your team through this difficult period are clarity, communication and care.
Clarity
Clarity helps to alleviate a lack of control and improving clarity may help many people to deal with the current environment.
Many of us may feel that we need to regroup and rebuild, and we are faced with the challenge of doing this in difficult circumstances, as the immediate future is not totally clear to us.
In times of uncertainty like this, it is often valuable to go back to basics and consider the way in which we manage people, to review our responsibilities as employers and improve our policies and processes from a people perspective.
We adapted our workplaces very quickly to allow our organisations to continue to operate and survive the crisis.
Our teams accepted this and changed quickly too, but, in our haste, we may have lost some clarity regarding roles and responsibilities.
We need to reconnect with our teams to understand how the changes have affected them, how they are feeling about these changes, what is working well now and what needs addressing.
Ensuring that everybody has clarity on their individual respon-
Good leaders communicate with their teams, both individually and together, on a regular basis. If in doubt, over-communicate
sibilities and how their role impacts on others within the team will enhance both individual and team performance.
A positive way to do this is to review each team member’s objectives so they have absolute clarity of what is expected of them in the short term, the next month and quarter.
Communication
Good leaders communicate with their teams, both individually and together, on a regular basis. If in doubt, over-communicate.
In a time of crisis, we all need reassurance, and communication is vital to provide this reassurance. Ensuring everyone is aware of the current situation and what changes are happening is important, even at times when we are not entirely sure ourselves.
Many people are interacting less with work colleagues as well as in their personal lives and this can lead to feelings of isolation.
If your team is working remotely, communication is even more important. You can communicate in a variety of ways including emails, video and phone calls.
Not all communication needs to be formal and you may want to recreate the office atmosphere by agreeing a regular, perhaps weekly, opportunity for a general chit chat over a cup of tea.
Care
Caring for our teams and providing additional support will pay dividends in the short and long term.
The topic of mental health is being discussed more openly than ever and appropriately so, given the number of individuals in the UK who are suffering from some form of mental health problem.
Again, we were aware that this was a big issue prior to Covid, but this has exacerbated the situation in a big way.
Absence from work due to mental health has increased over the last few years, which has led to mental health becoming a boardroom discussion, as it impacts on the productivity of an organisation.
As employers, we have a ‘duty of care’ and a responsibility to do all we reasonably can to support our employees’ health, safety and well-being.
If a member of our team has a mental health issue, we need to talk to them to determine what support they might need. If an employee feels they are well supported, the issue is less likely to build up, which results in less time off, improved morale and greater loyalty.
Creating a culture where mental health can be talked about as openly as physical health will allow individuals to raise their concerns and worries before they become significant.
You could consider running an employee survey, asking specific questions relating to well-being and mental health and collecting responses in an anonymous way to give you a true picture of how your team are feeling.
Having one-to-one discussions
with each employee allows an opportunity for personal issues to be raised and discussed in a safe environment.
Consider creating a mental health or well-being champion for your organisation or making mental health training available.
Leaders who address well-being and mental health will allow their team to succeed and will also benefit from greater loyalty on a longterm basis.
Next month we will be exploring the topic of flexible working, remote working and home working. We will cover how to manage a remote team, the technology that enables efficient remote working and how to ensure you reap the benefits of a flexible working policy.
Many of you will have concerns about how to ensure people work well together, particularly in terms of creativity, and how to recruit new team members and ensure they feel part of the existing team.
This is a topic very dear to my heart, as everyone in my company has been based at home, working flexibly, since I started the business back in 2013.
Clearly, I am a big fan of flexible working, but I will talk openly and honestly about the pros and cons and how to avoid some of the pitfalls.
I will also address the question I am most asked by those who are sceptical about home working which is ‘How do I know my team are working when they are at home?’
Jane Braithwaite is managing director of Designated Medical, which offers business services for private consultants, including medical secretary support, bookkeeping and digital marketing
Reduce the risks of patients falling betwe en two stools
Patients travel across bridges when they move from the care of one professional to another. Communication between clinicians forms the structure of these handover bridges and is a known point of medico-legal risk. Dr Sarah Coope (right) looks at the gaps in information, misunderstandings and assumptions that can increase the risk of errors, conflict and complaints
WE CANNOT have complete control over our patients’ illness and disease progression or the way they respond to interventions.
But we can take steps to ensure there is a strong bridge of communication to support effective continuity of care for the patient, give protection against adverse events and reduce medico-legal risk.
Imagine you are between appointments in your busy private clinic on a Friday afternoon and your colleague rings you..
She asks you if you mind covering for her this weekend, as she needs to go and visit her elderly mother who has had a fall; she has performed a routine operation on a private inpatient earlier that day and says everything is fine.
How do you respond? Most of us
would agree to do this, knowing that these arrangements often need to be reciprocated. However, how strong is that bridge as the patient moves across to your care and responsibility, albeit temporarily?
More questions
No doubt, you would usually ask more questions before ending the call. You would seek to find out more about the patient’s background, to assess whether there is any likely risk of complication and establish what the plan is for his discharge.
You would likely check that your colleague has documented this conversation with you in the patient’s records for medico-legal reasons, but also so that ward staff
know that you have agreed to be contacted if necessary.
However, would you make a note yourself of the patient’s details, history and current status so that you have this information available to remind you, now that you have taken over responsibility?
Frayed cables
For much of the time, despite any weakness in the communication bridge at the point of transition, these situations pass uneventfully. The patient recovers with no complications. You are not called by the ward and your colleague takes over their care again on Monday. However, there are inevitably occasions when this is not the case. You accept a handover from a colleague, either a cover arrangement
such as this or agree to give a second opinion, arrange an admission or transfer of your patient, and then things go wrong as they move between care providers.
Sometimes this is due to complications arising that you could not have foreseen, but other times analysis of adverse outcomes indicates that communication failure between colleagues around the time of the handover is frequently the root cause.1,2
For example, a significant underlying condition is not mentioned, a drug is missed off their transfer sheet or a key abnormal observation or result isn’t alluded to. And not having this information may lead to poor decision-making or suboptimal management.
If the communication bridge has weak structure and gaps, the care of the patient can easily fall through.
Often several health professionals are involved in a typical patient’s care journey, from the GP to consultant specialist, radiologist, theatre and ward staff, pharmacist, physiotherapist and back to the GP.
The more people who are involved, the more bridges the patient is crossing and the greater the chance of there being miscommunication and errors.
Many conversations about patient care with our colleagues
take place over the phone rather than in-person. Remote communication can exacerbate the risks further, primarily due to a lack of visual and non-verbal information in the interaction.
The oft-stated phrase ‘words make up only 7% of your message’ resonates here. Aside from the content of your spoken words, the other 93% of the communication comes from the style of delivery.
This includes the speaker’s body language, tone of voice and attitude which all convey crucial meaning; however, much of this is missing on the phone.
And what is said is therefore
‘SBAR’ CHECK-LIST
S – SITUATION
Identify yourself and the site/unit you are calling from
Identify the patient by name and the reason for your communication
Describe your concern.
B – BACKGROUND
Give the patient’s reason for admission
Explain significant medical history
Inform the receiver of the information of the patient’s background, admitting diagnosis, date of admission, prior procedures, current medications, allergies, pertinent laboratory results and other relevant diagnostic results.
A – ASSESSMENT
Vital signs
Trajectory of the patient’s condition
Clinical impressions, concerns.
You need to think critically when informing the receiver of your assessment of the situation. This means you have considered the possible underlying reason for your patient’s condition. Not only have you reviewed your findings from your assessment but you have also consolidated these with other objective indicators, such as laboratory results.
R– RECOMMENDATION
That is, what would you like to happen by the end of the conversation. Any advice that is given on the phone needs to be repeated back to ensure accuracy.
Explain what you need – be specific about request and time-frame
Make suggestions
Clarify expectations. Have clear agenda/request/ purpose – include concerns/fear about what’s likely to happen.
more open to misinterpretation. So particularly for complex cases, discussing the patient over a video call might be a less risky option to consider if face to face isn’t possible.
Common causes of gaps
What stops us from transmitting key information when referring a patient or ensuring that we have received all the facts we need to know when accepting a handover remotely?
What jeopardises the strength in these telecommunication bridges, that can affect safe transition of patient care?
There are, in fact, a range of factors
Remote communication can exacerbate the risks further, primarily due to a lack of visual and non-verbal information in the interaction
consciously strengthening the factors that you can address.
Those factors affecting the quality of the information obtained include:
Inadequate preparation before the call;
Lack of relevant facts about the patient’s situation, current status or background;
Missing detail about the care received so far;
Unclear message, agenda or request;
Lack of confidentiality or privacy when taking the call;
Not building a positive connection or rapport;
Ignoring verbal cues;
Abrupt or dismissive manner;
Interrupting or talking over;
Assumptions about a colleague’s level of knowledge and skill;
Not clarifying areas that are ambiguous;
Not speaking up or challenging potentially suboptimal decisions.
Strengthening the transition conversation
All the above potential weak links are important. However, the key thing to focus on is ensuring that adequate, relevant information is included in a handover.
A framework can be helpful to have in the forefront of your mind, to aid preparation before making a call or during accepting a patient.
You may already be familiar with the SBAR model 3 widely used in clinical settings although initially developed by Dr Michael Leonard for the US military to assist with safe communication on nuclear submarines.
At Medical Protection, we have
also developed another model for safe transfer of patient care which we teach in our Mastering Professional Interactions workshop (see box on the left)
So, how strong are your remote interactions with colleagues in these situations? Next time you pick up the phone to accept or make a patient handover, remember the bridge analogy and aim to build a safe, solid structure into your communication.
By reflecting on this, and making changes to the way that you present or receive vital information about a patient, you can fill in the gaps, strengthen the connection, increase the chance of a smooth transition of care and mitigate the associated medico-legal risk.
Overcoming risky remote interactions with colleagues, forms part of Medical Protection’s new fourpart series of webinars on telemedicine. Medical Protection members can find out more about these webinars via our e-learning platform prism.medicalprotection.org.
References:
1. Joint Commission on Accreditation of Healthcare Organizations. The Joint Commission guide to improving staff communication. Oakbrook Terrace, IL: Joint Commission Resources; 2005
2. Beckman H.B., Markakis et al. ‘The doctor-patient relationship and malpractice: Lessons from plaintiff depositions’. Archives of Internal Medicine 1994; 154: 1365-70
3. Improvement.nhs.uk. SBAR communication tool
Dr Sarah Coope is senior medical educator at Medical Protection
affecting either the quality of the interaction or of the information.
Those affecting the quality of the interaction include:
Barriers in access to, availability and approachability of colleagues;
Unstable connection and signal if using a mobile device;
High level of external interruptions, distractions and time pressure;
Existing dysfunctional relationships and lack of trust;
Reluctance to take responsibility. These are not always easy to eliminate or resolve, but it is helpful to be aware of them and compensate, where possible, by
At the heart of medical finance
You must give them all the information
The GMC guidance entitled ‘Decision-making and consent’ came into effect from 9 November and is intended to support doctors in having a meaningful discussion with their patients. The MDU’s Dr Kathryn Leask (right) summarises the essential points for independent practitioners
THE GMC’s new consent guidance replaces ‘Consent: patients and doctors making decisions together’ – but it does not represent a radical departure. The need to involve patients in decisions about their own care and treatment remains at the heart of good practice.
However, the latest guidance reflects changes to case law, notably the judgment in the Montgomery case (see ‘Doctors must now tell patients of all relevant risks’, Independent Practitioner Today, April 2015).
Consequently, there is even greater focus on understanding the concerns and priorities of individual patients, discussing the benefits and harms of treatment options, and answering their specific questions.
Consent forms can be helpful ‘but filling in a consent form isn’t a substitute for a meaningful dialogue tailored to the individual patient’s needs’.
The GMC also hopes that its new guidance will be easier for doctors to apply in everyday practice. It notes that ‘obtaining a patient’s consent needn’t always be a formal, time-consuming process’ (paragraph 6) and the emphasis should be ‘on the quality of ongoing dialogue between patient and doctor’.
Principles of consent
The GMC begins by setting out seven principles of decision-making and consent:
1
All patients have the right to be involved in decisions about their treatment and care and be supported to make informed decisions if they are able.
2
Decision-making is an ongoing process focused on meaningful dialogue: the exchange of relevant information specific to the individual patient.
3 All patients have the right to be listened to and to be given the information they need to make a decision and the time and support they need to understand it.
4
Doctors must try to find out what matters to patients so they can share relevant information about the benefits and harms of proposed options and reasonable alternatives, including the option to take no action.
The guidance says you must explain your reasons for recommending an option for treatment or care and share information about reasonable alternatives, including the option to take no action
although you should still explain what you are going to do and why.
Dialogue with patients
The largest section of the new consent guidance (paragraphs 8-49) considers how to have a meaningful dialogue with individual patients. The purpose of this is to:
Help the patient understand their role in the decision-making process and their right to choose whether or not to have treatment or care;
5
Doctors must start from the presumption that all adult patients have capacity to make decisions about their treatment and care. A patient can only be judged to lack capacity to make a specific decision at a specific time, and only after assessment in line with legal requirements.
6 The choice of treatment or care for patients who lack capacity must be of overall benefit to them, and decisions should be made in consultation with those who are close to them or advocating for them.
7 Patients whose right to consent is affected by law should be supported to be involved in the decision-making process, and to exercise choice if possible.
A proportionate approach
The guidance applies to every health and care decision made with every patient, whether the interaction takes place face to face or remotely.
It includes decisions about innovative treatments and decisions about mental health, but not consent to disclosure of information – covered in the GMC’s confidentiality guidance.
At the same time, the GMC accepts the need for a proportionate approach. It acknowledges that not every paragraph will be relevant at all times and doctors will need to apply their judgement in individual circumstances, such as in an emergency.
It also says that, for most healthcare decisions, you can rely on verbal or even non-verbal consent, rather than obtaining a signature; however, you should make sure this is recorded in the notes.
For example, paragraph 7 states this might be reasonable ‘for some quick, minimally or non-invasive interventions’ like examinations,
Ensure the patient has the opportunity to consider relevant information that might influence their choice;
Try to reach a shared understanding of their expectations and limits of available options.
Paragraph 10 outlines the information that you should usually provide to a patient about their diagnosis and options – which echoes previous consent guidance.
Paragraph 13 provides other examples of information that might be relevant, including reference to innovative treatments, bills the patient may have to pay, conflicts of interests you may have and the patient’s right to seek a second opinion.
The GMC reminds doctors that you ‘should be aware of how your own preferences might influence the advice you give and the language you use’ (paragraph 11).
It says you must explain your reasons for recommending an option for treatment or care and share information about reasonable alternatives, including the option to take no action. Patients must not be pressurised to accept your advice.
There may be circumstances in which you cannot share all relevant information immediately –such as where you are awaiting test results – but the GMC says in this situation you should tell the patient there is more to discuss and ensure arrangements are made to share the information as soon as it is appropriate.
Information should not be withheld at the request of someone close to the patient or because you are concerned the patient might become upset. Legal advice should be sought if you are considering withholding information for any reason (paragraphs 14 and 15).
The GMC emphasises that
meaningful dialogue requires an exchange of information which includes finding out what matters to the patient.
This means listening to the patient, encouraging them to ask questions and exploring with them their wishes and fears and what activities are important to their quality of life and their expectations. In particular, you should find out what risks an individual patient would and would not be prepared to take to achieve a desired outcome (paragraphs 16-20).
Tailoring discussions
Paragraph 22 and 23 set out what information you should usually include when discussing benefits and harms of different treatment options. It recommends you tailor discussions to individual patients and be guided by what is important to them personally.
With any medical treatment there will always be an element of uncertainty. While answering patients’ questions as fully as possible, you ‘must be clear about the limits of your knowledge’ and explain if you are unable to answer a question with certainty (paragraphs 25 and 26).
The guidance says you should be alert to signs that patients may need extra support during consent discussions and suggests ways to achieve this, including accommodating their wishes to record the discussion or involve someone else in discussions; sharing information in their preferred format and giving them time to consider their decision, before and afterwards (paragraphs 27 and 28).
In the next issue I will look at other sections of the guidance relevant for private practitioners.
Dr Leask is a medico-legal adviser with the MDU
IMPRISONED FOR MANSLAUGHTER
A new dawn in my fight for justice
Surgeon Mr David Sellu (right), convicted for gross negligence manslaughter of a private patient – overturned on appeal after a 30-month prison sentence – finishes his serialised story with events following his release from jail
I CAME OUT of prison in February 2015, but was not allowed to travel abroad until May 2016, the end of my sentence.
For a 30-month prison sentence, I had served half, or 15 months, behind bars and would do the remainder out in the community on licence.
Travel was nevertheless permitted to other destinations in the country with prior arrangement with the approval of my probation officer.
I was required to see my probation officer once a month and was obliged to inform him every time I left home if I was
going to stay the night elsewhere. This served as a constant reminder that I was still a prisoner.
If I infringed these conditions, I would be arrested and returned to prison. My wife Catherine and I decided to go to Hayling Island for one night during the summer of 2015 and she did the booking online.
My usual probation officer was away at the time, but he had informed me that he did not want me to seek permission to go away but merely to inform him where I was going, for the record.
He had warned me during our
previous meeting that he would be taking time off to go on holiday but would pass my case to his deputy. I rang the deputy on the morning of our proposed departure and was subjected to intense interrogation.
What was my full name? What was the crime I was serving time for? Where was I going? How were we going to get there? What were the precise address and the phone number of the hotel we were going to stay in? Did we have any connections there? What were the precise day, date and time I would be returning home? And much more.
My appeal process
While I was in prison, a group of my friends teamed up with my family and started a long appeal process to have my conviction overturned.
It was felt that I had been unfairly targeted for prosecution in such a complex case and been convicted by a jury who did not understand what they were deliberating on.
Moreover, those so-called experts who had given evidence against me did not understand their remit: their duty was to be objective and judge me on the evidence against the standards of practice prevailing at the
time the alleged offence took place.
As my defence barrister at the Medical Practitioners Tribunal Service (MPTS), Mr Ian Stern QC, pointed out at the later hearing, it was not about what the expert would have done or what theoretically the ideal management would have been, but what a reasonable group of surgeons would have done in the circumstances, given the state of knowledge, the prevalent practice at the time and the resources available to them.
The Empey report, which featured prominently in this case, failed utterly to disclose systemic errors on the part of the hospital. At the time of preparing the appeal against my conviction, we applied for and obtained documents and emails that had been exchanged between the investigators leading this inquiry.
The clinical specialist interrogator sent one telling email to his colleague. It read:
‘Dear Mike,
‘. . . It looks like the problem is systemic, in that DS (David Sellu) answers confirm he has difficulty getting anaesthetists …
‘. . . The challenge is to know whether the problem is systemic i.e. within CCH (Clementine Churchill Hospital) or just with DS. I suspect the latter and we have no real knowledge of the former’ [my emphasis].
Leave to appeal
My friends were not alone in fighting my case. While the press had been hostile towards me prior to this point, some papers began to express doubts about the prosecution of my case once they became aware of some of the facts in this patient’s management.
We continued to fight the case and in December 2015 three judges headed by Lady Justice Heather Hallett granted me leave to appeal my conviction. The appeal was heard in the Royal Courts of Justice before the President of the Queen’s Bench Division, Sir Brian Leveson and Lord Justice Irwin and Mr Justice Globe.
On 15 November 2016, my conviction was quashed. In passing judgment, the judges were critical of the prosecuting barrister, the prosecution experts and the trial judge in the conduct of my trial.
In passing judgment, the [appeal] judges were critical of the prosecuting barrister, the prosecution experts and the trial judge in the conduct of my trial
As I have mentioned previously, the jury in my trial had told the judge that they did not understand what they were deliberating on, but the judge had failed to give adequate guidance on which to reach a judgment. This is what the appeal judges had to say:
‘In the circumstances, we do not believe that Mr Sellu had the benefit of sufficiently detailed directions to the jury in relation to the concept of gross negligence contained within the offence of gross negligence manslaughter.’
[Neutral Citation Number: (2016) EWCA Crim 1716].
Travesty of justice
This travesty had taken place in the Old Bailey, the highest criminal court in the land.
The Crown Prosecution Service (CPS) were given the opportunity to decide whether they wished to retry me, but they wrote the next day to say that they did not.
There were several reasons given in newspaper reports for why the CPS had not conducted a retrial: this case was no longer in the public interest; the family wanted to draw a line under this matter and wanted it closed; ‘Mr Sellu has already served his sentence’.
One sacred tenet in English law is that one is innocent until proved guilty in a court of law. I was therefore cleared of the manslaughter of Mr Hughes and it was obviously a relief to know that I was no longer seen a killer.
As far as I know, there are only two reasons why the CPS prosecutes cases: it is in the public interest and there is a realistic prospect of a conviction.
I do not recognise any of the other justifications quoted by the papers, particularly the last one about my serving my sentence. Surprisingly, this was repeated by
a senior lawyer from the CPS at a meeting I spoke at the Royal Society of Medicine in 2017.
To say that I had served my sentence is a statement that implies that somehow I had been punished for something I had done wrong. I had served a sentence, not my sentence.
No apology
The CPS did not want to rerun this case because there was now no possibility that they would win, but they were not prepared to admit this. I received no apology and no compensation for wrongful imprisonment.
Moreover, the CPS did not retract any of the caustic comments they had been so quick to make shortly after my conviction and imprisonment, nor did they issue any clarification that I am aware of that I was now an innocent person.
Doctors were being urged to
issue apologies when things went wrong, to exercise what was referred to as ‘the duty of candour’. It appears that when the CPS made mistakes, they exempted themselves from this duty.
This was not the end of the matter, however. I was summoned by the MPTS to an Interim Order Tribunal at the beginning of February 2017 at which they would look at my GMC registration in the light of the quashing of my conviction.
It was noteworthy that from the time I was charged with manslaughter and perjury in 2012 to this point, I had been suspended from the register and was therefore not permitted to practise my profession.
My solicitor wrote to warn me to expect a difficult time ahead because the expert report into my
Upright Positional
• Completely open scanner that is well tolerated by claustrophobic patients
• Weight-bearing scans for spine and joints enable a more precise diagnosis
• Patients who are large or cannot lie down can be accommodated
For more information go online at: www.trulyopenmri.com or call: 020 7370 6003 0161 434 8039
handling of the deceased patient’s case was very damning.
The meeting lasted one day and after arguments by the GMC barrister and counter-arguments by mine, the tribunal restored me on the register but with stringent conditions.
In effect, I could start working again as a surgeon but only under close supervision, with a long list of the things I was not allowed to do unless my supervisor was in the room with me.
I returned to work, initially at St George’s Hospital in London and later at St Mark’s Hospital as an honorary consultant surgeon. It was strange going in for clinical work again after a break of nearly five years.
Some things never changed: the outpatient clinics, for example, were as busy and chaotic as they were when I last worked and most people were just as pleasant. Doctors, nurses and other healthcare staff worked equally hard trying to get increasing numbers of patients through theatre with dwindling resources.
Frustrating technology
On the other hand, technology had moved forward significantly, and was now more frustrating and pervasive.
There was so much reliance on computers that hospitals were completely paralysed when, as happened shortly after I returned to practice, the IT systems failed in several hospitals in the country, following a malicious virus attack.
Manual laboratory and radiology requests were now almost completely replaced by electronic ones and, in many cases, the results were now also shared digitally. In my discipline of colorectal surgery, the proportion of patients having laparoscopic or keyhole surgery for abdominal problems had increased.
Multidisciplinary teams (MDTs) had all but replaced the individual as the decision-maker. MDTs lasted about two hours before busy clinics back in 2012, but now they took up the whole morning.
I got the feeling that doctors were afraid to take clinical actions until they had discussed their case in an MDT, expecting perhaps that others would share the blame for any complications that occurred.
There were 11 charges and these were systemically found not proved by the panel
There was now evidence of defensive practice, in which doctors were always looking over their shoulders in case they made mistakes and did tests and operations more to cover their own backs than for the benefit of the patients.
I was told that this was because of the ever-present threat of complaints, litigation and referrals to the GMC. Such defensive practices were sometimes harmful to patients and wasted resources.
But I was grateful to all the doctors and administrators who welcomed me back to doing something I had always enjoyed – surgical practice.
Unreliable witness
As expected, the GMC decided to take my case to the MPTS for a Fitness to Practise hearing. I was finally able to sit in the same room as the GMC expert and, for all the criticisms of me, he came across as out of touch and was deemed an unreliable witness by the panel. There were 11 charges and these were systemically found not proved by the panel. A long list of witnesses were called, some of whom were interviewed by video link and phone.
Two witnesses who were involved with the care of the patient who died had moved abroad: one to Singapore and the other to Portugal. They gave their evidence by video.
In the end, I was exonerated of all blame in the management of Mr Hughes and my name restored to the medical register with all conditions removed.
Behind bars, I had missed birthdays and anniversaries and, importantly, my son’s graduation from the University of Manchester after six years of hard work. During my trial, James had been in the middle of preparing for his final examinations.
Some days he would come to court all day, go back to Manchester in the evening and to lectures the next day. I was worried that this would impact adversely on his performance, but I was relieved and proud that he qualified as a doctor in the summer of 2014. He came to see me when I came home on temporary leave from prison in August 2014 and asked to talk to Catherine and me.
We were a close-knit family and I always encouraged our children to come to us with their problems. But we also allowed them to make decisions regarding the courses they wanted to do at university and the jobs they wanted to pursue.
Source of pride
James had chosen to read medicine and it was a source of pride for me to know that he had put Manchester, my old medical school, as first choice.
Now I was home, James had something to tell me. His voice faltered at first, but he went on to explain what was on his mind. ‘Mum, Dad, I do not want to pursue a career in medicine. I want to get out,’ he said.
He was looking at Catherine and then fixed his gaze nervously on me. He did not wait for a reaction, but went on to say that he had seen how humiliated I’d been during the course of the investigation and particularly the trial.
In his words, I had given my entire professional life to the practice of medicine and, as he now reminded me, I’d made sacrifices, which included missing out on birthday celebrations, sports days, and nativity plays. Yet, because of a single incident, my previous track record and my contribution to society in general had amounted to zero when it came to mitigating my sentence.
If this was what he could expect from the profession, then he was not prepared to start his foundation hospital training.
Adapted from Did He Save Lives?
A Surgeon’s Story, £9.99, Sweetcroft Publishing ISBN 9781912892327 from Amazon
Catherine looked at me to say something, which I now did. I reminded James that as a 24-yearold, he had spent six years in medical school, equivalent to a quarter of his life and much of the whole of his adult life. He had invested a huge amount of time and effort to his studies and he was going to be encumbered with over £80,000 of debt in the form of a student loan. But he had made up his mind and nothing we said would change that. He later went into business and never again set foot in a hospital to work. For our part, we had no choice but to respect his decision. Medicine had lost another doctor, and we were convinced that James would have made an excellent doctor.
Much more than a bill clearing house
From invoice clearing to The Private Practice Register, Healthcode has been in the vanguard of a technology revolution in the independent healthcare sector for two decades. But while its online solutions are widely used to automate time-consuming administrative tasks, how much do you know about the company behind them? Peter Connor gives the low-down
1
Healthcode marked its 20th anniversary in 2020 Healthcode was established in 2000 with an urgent mission – create an invoice clearing service for healthcare providers who send electronic bills to private medical insurers. The company later launched its Clearing Service, which now processes invoices worth around £3.3bn each year. But it has not stopped there. Over the last 20 years, the com -
pany has continued to apply its energy and expertise to develop new online services that help healthcare organisations connect and operate more efficiently.
In 2020, Healthcode was recognised at the annual HealthInvestor Awards which celebrate excellence in the private healthcare sector, winning IT innovator of the year and being short-listed in the technology provider of the year category.
2 Most private providers use Healthcode’s Clearing Service to submit electronic bills for validation Before Healthcode developed its Clearing Service, most providers printed and posted invoices to insurers, an inefficient and timeconsuming process which could lead to lengthy delays in payment if the bill did not meet the insurer’s rules or in the event of query. Now around 60% of practition-
Around 60% of practitioners and 98% of hospitals generate electronic bills using the specialist software of their choice and then submit them online through Healthcode’s Clearing Service
ers and 98% of hospitals generate electronic bills using the specialist software of their choice and then submit them online through Healthcode’s Clearing Service. Each invoice is then automatically validated against the specific rules set by the private medical insurer (PMI). The information checked includes:
➲ Invoice number and date; ➲ Provider details, name, number
or professional number, specialty and billing address;
➲ Patient’s full name, birth date, address, insurance company/paying organisation, policy number (in the correct format), diagnosis and description where applicable, lead consultant;
➲ Treatment type, date, service delivered, procedure code and description where applicable, fee;
In the event of an error, the system tells practitioners exactly what is missing or incorrect, allowing them to correct the invoice and resubmit.
A status display shows when an invoice has been successfully validated and received by the PMI.
3
In 2019, Healthcode’s Clearing Service checked and processed 28,000 invoices daily
The volume of electronic bills processed and validated by the Clearing Service has risen every year since it was launched.
In 2004, it was just under 2m a year; by 2012 it was more than 3m, but it had rocketed to over 7m by 2019.
Initially, this growth was driven by hospitals, but in 2018 the number of bills from non-hospital providers – including independent practitioners – overtook those from hospitals.
The Clearing Service has helped make electronic billing standard practice across the sector which benefits providers as much as PMIs on the following grounds:
Cost – electronic billing entails a fraction of the printing, postage and manpower costs associated with paper billing;
Security – all data is encrypted;
Efficiency – bills can be submitted to the leading PMIs from one online platform
Cash flow – validated electronic bills enter the insurer payment cycle quicker and can be paid as soon as one week after submission.
4
The Invoice Clearing Service is one of a range of online solutions developed by Healthcode for independent practitioners
While Healthcode is associated with electronic billing, its technical expertise means it has also become a leading provider of
Healthcode’s development team’s current project is a centralised electronic booking application that will transform patients’ access to private healthcare
tain accuracy and be accessible to organisations that needed to know.
More than 20,000 practitioners now use The PPR to control their profile and connect to the major insurers and more than 300 hospital providers.
It provides an efficient way to ensure these stakeholders can access details of their current practice, such as contact information, NHS and private practice information, medical secretary details, publications, bank details, medical indemnity certification, insurer recognition details and fitness-topractise information.
This makes it easier to maintain insurer recognition, hospital practising privileges and get paid.
8
All Healthcode’s solutions are designed to be interoperable Healthcode believes technology should not create barriers but instead make it easier for organisations and practitioners to connect and share information efficiently and securely. Its developers therefore aim to ensure solutions are compatible with the systems used by key stakeholders in the healthcare sector.
Take the Clearing Service, for example. All the leading insurers are able to accept invoices submitted this way: AXA Health, Aviva, Bupa, Bupa Global, Cigna Healthcare, Healix, VitalityHealth and WPA.
online solutions for independent practitioners, including:
ePractice Electronic billing and payment tracking software;
ePractice Practice management software ;
Secure messaging;
Clinical coding tools;
The Private Practice Register (The PPR).
5
Healthcode operates independently of private medical insurers
Healthcode is jointly owned by Aviva, AXA Health, Bupa, Nuffield Health and VitalityHealth.
It operates independently of its shareholders and therefore does not make decisions based on the requirements of the UK private insurance market. Share holders do not have access to data held or processed by Healthcode.
6
The Private Practice Register (The PPR) is the first central information resource to connect practitioners, hospitals and private medical insurers
The PPR was first released in 2016 to fast-track the process of applying for private medical insurers’ recognition.
The idea was for independent practitioners to have a secure online platform to store all the relevant practice information and supporting documents so it would be far quicker and easier to main-
Practitioners who join The PPR are also showing their support for appropriate information-sharing across the private health sector, which is a prerequisite for safe, high-quality care.
7 Healthcode meets stringent information security standards to protect confidential data
To safeguard the enormous quantities of sensitive financial and patient data it processes for independent practitioners, hospitals, NHS private patient units and insurers, Healthcode uses a range of stringent data protection measures:
➥ Systems are secured in accordance with internet banking conventions, using 2048-bit certificates for full end-to-end encryption.
➥ Its infrastructure is in the UK and is of enterprise quality, designed to contain no single point of failure.
➥ Healthcode takes a back-up copy of the data regularly, which is securely stored.
➥ Users must have their own login ID and password and are prompted to change their password every 90 days. Accounts are locked if they are not accessed for 90 days.
➥ Its Information Security Manage ment System complies with the requirements of ISO/IEC 27001:2013 and we have maintained this accreditation since achieving it in 2009. We are also certified by the Governmentbacked Cyber Essentials scheme.
And at the front end, the service is open to practitioners who use Healthcode’s own ePractice software and those using common third-party practice management software such as DGL or Lumeon. Over the years, the company has consistently promoted the value of collaboration within the sector, from the development of common industry standards in areas like billing and data, to sectorwide projects like The PPR.
9
Healthcode is developing a centralised e-booking service to transform access to private healthcare
The PPR is Healthcode’s most ambitious project to date and continues to evolve in response to the needs of the industry.
However, the company has no intention of standing still. Inspired by the computer reservation websites in the travel and hospitality industries, its development team’s current project is a centralised electronic booking application that will transform patients’ access to private healthcare.
Peter Connor (below) is managing director of Healthcode
BILLING AND COLLECTION ADVICE
stormy waters Charting these
Simon Brignall provides ten simple medical billing rules to help you chart your practice through the current difficult economic climate
THE PAST year has proven to be extremely challenging to all of us in the independent healthcare sector and when the economic climate is as unpredictable as right now, it is important to ensure your practice is best positioned to navigate through it.
Cash flow, outstanding debt, revenue optimisation and staffing have all thrown up a range of difficulties to independent practitioners during 2020 and it looks like 2021 will be no different.
With this is mind, I thought it would be beneficial to outline some simple rules for your practice that are good to follow in normal circumstances – but are especially important to put in place as we start 2021.
1
Make sure your work is invoiced as soon as possible.
It seems obvious, but time and time again practices fail to ensure this takes place – and that leads to a range of issues.
Some major insurers now enforce time limits for submitting invoices and if you miss the deadline, they will not pay.
Delays in invoicing means that problems are not highlighted in a timely fashion and can also be indicative of poor service to patients and a major contributor to their dissatisfaction.
Knowledge of any shortfall is delayed and patients assume the invoice has been settled, resulting in an unnecessary bone of contention.
Late invoicing of patients can
also lead the patient to think that you are not serious about wanting payment.
2 Ensure your practice has a robust process for chasing outstanding invoices on a consistent and continual basis until they are paid in full.
Failures in this important area mean continued high levels of bad debt and means that received income is well below the activity of the consultant. Almost every practice that joins Medical Billing and Collection has an outstanding invoice backlog going back many years.
Debt levels are typically more than 20% of turnover and I have seen some over the past year that were 50-100% of annual turnover.
But, on average, consultant customers average debts of under 0.5% after signing up with us.
3
Make yourself aware of any bad payers so you can decide if you want to continue seeing them while they have outstanding invoices.
Continuing to see patients that are running up bad debts means you will end up regularly throwing money away. Having visibility around this key area means you can take steps to police this more effectively.
When we take on a practice’s backlog of outstanding invoices, there are often patients who have built up debt over years, yet the practice continued to see them despite never being paid.
4
Review the way your work is being billed to ensure that you are compliant with the rules and regulations communicated monthly from the Clinical Coding and Schedule Development group (CCSD). Keep abreast of the CCSD’s monthly changes and establish if they affect your specialty and, as such, impact your income. Practices commonly make billing errors through being unaware of these changes. Remember to review what rules each private medical insurer adopts, because each can choose their own variants.
5 Regularly review your procedure fees.
This is important if you bill to insurance guidelines, because
these constantly change and these changes are not often communicated clearly.
You could be charging less than you could or more than you should. Practices still make wrong assumptions, leading to issues with insurance companies or revenue losses.
6
See that your price structure/policy is clear and that your patients are made aware of it before commencing treatment. A clearly defined, well documented and communicated patient registration form is vital in the modern practice. It will ensure no room for ambiguity when it comes to settlement. Transparency of fee and payment terms is of paramount importance
Transparency of fee and payment terms is of paramount importance and is also a key requirement of the Competition and Markets Authority
and is also a key requirement of the Competition and Markets Authority (see page 15).
7
Ensure you have access to key management information on your practice to allow you to make informed decisions. This vital area is often overlooked. Losses can easily follow if access to accurate information is limited.
All practices should know where patients are being referred from, which insurers they are dealing with, how much income is derived from self-pay and the most common procedure codes that are carried out.
Consultants should know financially what is happening within their practice. This means having access to reports showing the revenue that was generated each month, the income that was received and what is happening with outstanding invoices.
Without access to accurate realtime data, it is difficult to understand which direction your practice is going. This means it can be very easy to come to the wrong conclusions and make illinformed decisions.
We provide access to our online reporting platform, which gives our clients 24/7 visibility to this information to assist them in running their practice.
8 Make sure you spend as much time as possible focusing on your core skill set – treating and looking after the patient. Running a private practice is not easy and many tasks do not fall naturally into a consultant’s skill set.
If you and your secretary focus on the medical side of the practice, this will, in turn, make you more money, because you are focused
on what you do best rather than spending time on tasks that can be easily delegated.
Take stock and consider what elements of your practice could be outsourced – this will enable you to generate more revenue.
9
Ensure you have a robust secure IT infrastructure in place to deal with your practice’s administration.
This can be a common weakness in many practices and is often only highlighted after it is too late.
Enjoy the peace of mind that comes from ensuring your business is on a secure platform and that your data is safe.
A wide range of options can facilitate this that are not difficult to implement and will ensure the practice data is secure.
10
Consider if you should join thousands of other doctors who have outsourced this crucial element.
For most consultants, the billing and collection is exceedingly difficult to manage and when done incorrectly it often results in consistent financial losses.
Outsourcing could be the best decision you make this year with many benefits. Our fees are calculated against received income, which means that our costs are correlated to the cash flow of your practice.
This is especially beneficial when your income stream is less predictable.
Outsourcing to a billing company means that its capacity is on tap to ensure that this key role is effectively managed without service interruptions due to issues around access to staff.
Simon Brignall is director of business development at Medical Billing and Collection
Interest rates fall below freezing
Dr Benjamin Holdsworth (below) shows why your cash is not a sensible long-term option. So ensure your longer-term assets are sensibly invested
TODAY, GOVERNMENT bond yields and bank deposit rates sit very substantially – and uncomfortably – below where they were five and ten years ago, in negative after-inflation terms and more or less zero before inflation terms.
In March 2020, the UK Government issued its first negativeyielding gilt, borrowing £3.8bn at -0.003% for a three-year maturity. The negative yield means investors who hold the debt to maturity will get back less than they paid.
On a retail basis, falling yields are evidenced in the NS&I products on offer from the UK Government. The days of indexlinked certificates at inflation as measured by Retail Price Index + 1% seem like nirvana.
The recent slashing of rates across the board on NS&I products leaves savers struggling to cover the erosion of their cash by inflation.
Negative interest rates
The Bank of England – alongside other central banks – has hinted that negative interest rates remain in its arsenal of tools to help the economy. Denmark has already seen home loan offers at a negative interest rate, meaning that mortgage borrowers pay back less than they borrow!
One can perhaps see why the ‘Old Lady of Threadneedle Street’ – the nickname for the Bank of England since a cartoon published in 1797 – sees this as a useful stimulant in helping firms and consumers to have the confidence to borrow.
Note:
However, if commercial banks are charged for placing deposits with the Bank of England, then, in all likelihood, they will pass these costs onto retail depositors.
In effect, negative interest rates represent a transfer from savers to borrowers. There would also appear to be limitations to negative rates, as banks and individuals might well decide to hold bank notes instead at no cost if negative interest rates persist.
A possible solution
One possible solution is to run a system of dual interest rates.
Specifically, this could be targeted at one rate for bank lending – for example, 1% – and one for bank deposits, such as +0. 5%.
Various terms and conditions could be applied, such as directing the type of lending the banks could do with this facility.
It has even been suggested that this could be used to drive a new ‘green deal’ where money would be available to companies focused on sustainability.
Borrowers’ net income would rise, as would the benefits of greater economic stimulus through lending to companies to invest in projects. At the very least, this is an interesting concept.
The one thing that is certain is that it will be extremely hard to
preserve the purchasing power of cash in the coming months and possibly years.
Having enough cash to meet emergency liquidity needs is important, but make sure that any longer longer-term assets are sensibly invested.
Dr Benjamin Holdsworth is director of Cavendish Medical, specialist financial planners helping consultants in private practice and the NHS
The content of this article is for information only and must not be considered as financial advice. Cavendish Medical always recommends that you seek independent financial advice before making any financial decisions.
Levels, bases of and reliefs from taxation may be subject to change and their value depends on the individual circumstances of the investor. The value of investments and the income from them can fluctuate and investors may get back less than the amount invested.
CALCULATE YOUR NHS ANNUAL ALLOWANCE
Renting property is now less daunting
Independent practitioners need to be aware of The Royal Institution of Chartered Surveyors’ updated Code for Leasing Business Premises, effective from 1 September 2020, on negotiating leases whether as a landlord or as a tenant. Myles Evans (right) explains
THE OBJECTIVE of the Code for Leasing Business Premises is to improve the quality and fairness of negotiations on lease terms.
The code is also intended to promote the issue of comprehensive ‘heads of terms’, which should in turn make the legal drafting process more efficient.
Heads of terms are the commercial terms of the lease agreed in principle between the parties and the code includes a useful template to follow.
The template also functions as a
useful check list and road map to orient the uninitiated towards the issues they should be thinking about ahead of negotiations.
The code will be relevant to current and prospective landlords, tenants and agents involved in negotiating heads of terms and leases.
A 2007 iteration of the code was a fair attempt to summarise broad principles and provide guidelines and ‘tips’ for negotiations.
The big difference between the old and the new is that the 2020 code now includes mandatory
requirements which are compulsory for members of the Royal Institution of Chartered Surveyors.
Mandatory requirements
Examples of some of the mandatory requirements are as follows:
Lease negotiations must be approached in a constructive and collaborative manner.
An unrepresented party must be advised about the existence of the code and its supplemental guide and must be recommended to obtain professional advice.
This has the obvious benefit of ensuring that negotiations can be efficiently done, but also ensures that no one party can immediately bamboozle the other with legalese and industry know-how.
A comprehensive set of minimum requirements for heads of terms – see the code for detail.
Negotiations should aim to produce letting terms that achieve a fair balance between the parties having regard to their respective commercial interests.
In addition to mandatory require-
ments, the code also includes provisions indicating – but not mandating – good practice. These include not only matters to be covered by the parties and their agents when negotiating heads of terms, but also by the parties and their legal advisers in the negotiation of the lease itself.
Break options
One issue of particular note for prospective tenants is in relation to tenant break options – that is to say, a tenant’s right to bring the lease to an end at a specified point before the end of the lease term.
The code states that, unless agreed in the heads of terms, the tenant’s break option should only be conditional on the tenant paying all basic rent up to the date of the break, giving up occupation and leaving no subtenants or other occupiers behind.
This is useful, as the conditions attaching to a tenant’s break are
The 2020 code goes some way towards creating a level playing field from the outset of negotiations, at which stage parties are often unrepresented
often subject to extensive negotiation and can cause real problems later if not properly considered at the outset.
The 2020 code is generally far more comprehensive than the 2007 code and is aimed at assisting those that might not find leases relevant to their daily practice.
For example, the 2007 code has a very basic introduction to lease negotiations, providing some terminology for the uninitiated on who a landlord is or a tenant.
It even explains what ‘heads of terms’ are, so that parties can understand the basics.
However, what the 2020 code adds is detail to ensure that even a party that is new to lease negotiation, and even property transactions as a whole, could use the 2020 code as a complete guide without the need to refer to a plethora of other documentation.
Level playing field
The 2020 code goes some way towards creating a level playing field from the outset of negotiations, at which stage parties are often unrepresented.
Those without experience in the world of leases and property more generally can look to the code for guidance and gain a broad understanding of the issues that need to be considered.
The code should not be substituted for seeking professional advice – from a surveyor and solici-
tor as required – and the code makes it clear that both parties should be encouraged to obtain advice from property professionals. Where the 2007 code had tips for the reader and felt more of a ‘try to do it this way’ approach, the 2020 code reads more formally than the 2007 code, given the introduction of mandatory requirements.
It is a welcome addition to the industry and should, at the very least, assist prospective landlords and tenants who are less than familiar with lease negotiations.
The full 2020 code can be found at www.rics.org/uk/upholdingprofessional-standards/sectorstandards/real-estate/code-for-leasingbusiness-premises-1st-edition. For further information or for property-related inquiries, please email me at m.evans@hempsons.co.uk.
Myles Evans is a senior solicitor at Hempsons
Free legal advice for Independent Practitioner Today readers
Independent Practitioner Today has joined forces with leading healthcare lawyers Hempsons to offer readers a free legal advice service.
We aim to help you navigate the ever more complex legal and regulatory issues involved in running and developing your private practice – and your lives.
Hempsons’ specialist lawyers have a long track-record of advising doctors – and an unrivalled understanding of the healthcare system as a whole.
Call Hempsons on 020 7839 0278 between 9am and 5pm Monday to Friday for your ten minutes’ of free legal advice.
Advice is available on:
Business structures (including partnerships)
Commercial contracts
Disputes and litigation
HR/employment
Premises
Regulatory requirements and investigations
Michael Rourke
Tania Francis m.rourke@hempsons.co.uk t.francis@hempsons.co.uk
Blackout and a driving ban
NOW OPEN ON SATURDAYS
Fully CQC-registered clinic
Appontment-making
Billing service
Nursing support
Secretarial support
In-house pharmacy
We are a leading private outpatient clinic and we are inviting new applications for practising privileges for our extended opening hours on Saturdays.
A consultant asks for advice after giving a patient bad news about his fitness to drive. Dr Sissy Frank (right) gives her response
as he had earlier given the same account to his GP and only suddenly changed after you had advised him not to drive.
Dilemma 1 What do I do if he alters his story?
QA 55-year-old male patient attended my private cardiology clinic for investigation, as he had a blackout the previous week when getting dressed for work. The patient was seen by his GP and obtained a referral to see me.
When he saw me, the patient was clear he had experienced no symptoms before losing consciousness and that this had never happened before. As there was no obvious cause, I arranged some investigations.
Following DVLA guidance, I also told him he would need to refrain from driving for the time being and report the blackout to the DVLA.
Before he left the clinic, the patient asked to see me again and said that he had now remembered slipping and knocking his head in the shower shortly before the blackout. He wanted to know if this could be the reason for his loss of consciousness and if that meant he was safe to drive.
I don’t know whether to believe him because he had given the previous version of events to his GP as well and had only changed his story after I raised the issue of driving. Should I change my advice?
AAs the patient had given a consistent account of events to both you and the GP prior to providing a different history, you were justified in following the DVLA’s guidance (Assessing fitness to drive: a guide for medical professionals).
The GMC’s guidance, Confidentiality: patients’ fitness to drive and reporting concerns to the DVLA or DVA, is clear that drivers are legally responsible for telling the DVLA or DVA (Northern Ireland) about any condition or treatment that might affect their safety behind the wheel.
The DVLA/DVA is legally responsible for determining if drivers are medically unfit to drive.
Your role as a doctor is to inform patients if they have a condition that could impair their fitness to drive and explain their legal duty.
The DVLA also expects doctors to remind patients that it may affect their insurance cover if they choose to ignore medical advice. If you are now uncertain about the patient’s ability to drive safely, it may help to discuss the case with a DVLA medical adviser in confidence. Contact details for the DVLA and DVA can be found in the DVLA’s guidance for medical professionals.
Ultimately, you have a duty to protect the health of your patient and the wider public. The tests you have arranged should help rule out a medical condition that makes it unsafe for the patient to drive, so you may conclude that it makes sense to continue with these.
You will need to explain this to your patient and reiterate your advice not to drive in the meanwhile. If your patient is unhappy about this, you could suggest he seek a second opinion. However, he should still not drive in the meantime.
If you cannot persuade him not to drive or discover that he is driving against your advice, you should warn the patient that you are obliged to report this. Disclosures to the DVLA/DVA should only include relevant medical information and you will need to inform the patient in writing afterwards that you have done so. Hopefully, this will not be necessary, but matters related to driving can be emotive, so keep detailed notes of the discussions with the patient so you can explain your approach in the event of a problem.
Dr Sissy Frank is a medico legal adviser with the MDU New sessions are available for independent private practice on Saturdays.
It would be difficult to disregard that version of events, particularly
Keeping patient notes
A consultant’s imminent retirement raises the question of retention of private records. Dr Kathryn Leask (right) gives her response
Dilemma 2
How long should I retain notes?
QI am a consultant cardiologist and have a small private practice which I am due to retire from in six months’ time. I have handed over my active private patients to other colleagues, with the patients’ consent.
How long do I need to retain the records for of those patients whom I have now discharged?
AAs a private consultant, if you are responsible for holding patient records, you should be registered as a Data Controller with the Office of the Information Commissioner.
In terms of retention of clinical records, ideally they should be retained for as long as possible or at least for the minimum periods recommended in national guidance or required by statute.
There is no definitive guidance relating to the retention of private clinical records, as the regulations which did cover this – schedule 3 of The Private and Voluntary Health Care (England) Regulations 2001 – are no longer in force.
The GMC advises doctors that, in relation to the retention of medical records, they should follow the UK health departments’ guidance, whether or not they work within the NHS.
Therefore, it would be appropriate to follow the Information Governance Alliance’s Records Management Code of Practice for Health and Social Care 2016. Different retention periods apply to different types of record and these are set out in Appendix 3 of the guidance.
The recommended retention periods contained in the guidance are the minimum period for which records should be retained.
For patients where an adverse incident or a complaint is known about, it might be appropriate for records to be retained for longer than the minimum periods in the guidance.
It is worth remembering that a clinical negligence claim can arise many years after the initial event and a patient has a period of three years by which to raise a claim once they become aware of a problem.
While there are advantages of retaining records from a medicolegal point of view, this needs to be balanced by the requirements of the Data Protection Legislation, which says you should not retain records for longer than necessary.
When the time comes to dispose of the records, you should ensure that this is carried out using appropriate methods; for example, by crosscut shredding, by incineration or by using a commercial company holding the necessary accreditations.
Should any records remain in your possession at the time of your death, the executor of your estate might need to seek further advice on how best to store or dispose of these.
Dr Kathryn Leask is a medicolegal adviser with the MDU
PRIVATE PATIENT UNITS
Capital still stays top of PPU league
Philip Housden begins the round-up of the PPU market, based on the published 2019-20 annual accounts with the top ten performing trusts. They are all in central London
LONDON IS the engine of growth not only for the private patient market in England but it is also the core effort within the NHS when it comes to private patient services and incomes.
Central London trusts have delivered the lion’s share of revenues for the NHS PPU sector for many years, and these trends have continued, if not accelerated, in the last financial year.
Revenues for the top ten trusts climbed to a new record of £427.5m in 2019-20. This is an increase of £15.6m (See Figure 1 on the right).
The top ten now deliver 63.8% of total NHS revenues, up from 62.9% the previous year.
Over the past decade from 201112, collective growth of 86% has enabled this proportion to increase from 51.6% (See Figure 2 on the opposite page).
In fact, the clear and consistent long-term trend has been for the aggregation of NHS private patient earnings within the top ten.
1 8
Figure
Central London trusts have delivered the lion’s share of revenues for the NHS PPU sector for many years, and these trends have continued, if not accelerated, in the last financial year
During that time, overall private patient revenues delivered by the 140 or so other NHS acute trusts in the rest of London and across England has remained broadly static, increasing by only 12.5%.
Significant movements
This headline masks significant movements by region and by trust and these trends and themes will be explored in future articles.
The annual growth rate last year was 3.8%, which is well down on the average of 6-9% achieved in the most recent three years (see Figure 3 on the right).
Aggregate growth for this group of trusts has been 30% since 201516. The year’s deflated growth rate can largely be explained by the adverse impact of Covid-19, which required trusts across the UK to close private patient capacity and re-direct it to NHS services during March and largely to continue to do so since then.
1The Royal Marsden continues to be number one. The trust grew revenues 9.3% and £11.3m to £132.6 m in 2019-20 and is up £49.4m (59.5%) over the past four years (See Figures 4 & 5 overleaf).
This is now 19.8% of the total NHS private patient revenues and 33.6% of the trust’s total patientrelated income – the largest proportion in the NHS by far.
The trust continues to plan expansion and will be opening a new facility in Cavendish Square in the spring of 2021.
Based in the heart of London’s healthcare district, just behind Oxford Street, Private Care at Cavendish Square will be a comprehensive cancer centre covering
all of the main cancer pathways and a convenient location for patients visiting London from around the UK and further afield.
The trust says Cavendish Square will offer patients fast and direct access to world-leading diagnostic experts in cancer and state-of-theart diagnostic technology in a modern environment.
2
Great Ormond Street Hospital for Children (GOSH) is number 2.
The trust increased private patient revenues by £2.65m and
4.3% to reach £64.8m and is also second for private patient revenues as a percentage of total income, with this being 14.4% in 2019-20.
GOSH treats children from around the world and to support patient referrals from the Gulf region the trust has a regional office in Dubai Healthcare City.
The trust’s international patient focus has meant GOSH private patient incomes have been disproportionately adversely affected by the pandemic restrictions on travel to and from the UK in 2020.
3
In third spot is Imperial College Healthcare, where private patient revenues increased in 2019-20 to £53.8m, up £1.6m and 3.1% on the previous year.
Delivering care from across five locations around west London, the trust has an international reputation for private maternity care at both the Lindo Wing of St Mary’s Hospital and at Queen Charlotte’s and Chelsea Hospital. Imperial is the only NHS trust with more than 100 dedicated private patient beds.
Figure 2
Figure 3
4
Royal Brompton and Harefield is number four by turnover and also number four by proportion of income, with 11.4% of total revenues achieved through private patient services.
In 2019-20, growth was 9.6% and £4m to reach £45.6m. This was the highest growth rate across the Top 10. The trust provides inpatient services from Chelsea and Harefield sites as well as an outpatients and diagnostic centre for private patients at 77 Wimpole Street in the Harley Street area.
The merger with Guy’s and St Thomas’ from February 2021 will deliver a combined private patient income of around £67m a year, perhaps enabling the new trust to leapfrog GOSH and Imperial into second place in the NHS top ten.
5
At five is Moorfields, which achieved growth of 7.7% and £2.2m to rise to total private patient revenues of £30.8m in 2019-20.
Growth has been achieved through service development – for example, self-pay laser eye surgery – and the addition of new capacity, raising the number of patient rooms from 23 to 27.
The trust reports that, at the end of 2020, private patient activity has returned to pre-Covid levels, supported by the development of telemedicine services which has enabled it to remain in touch with international patient demand.
Looking ahead, the Moorfields trust is considering expansion of its private consulting room presence in central London and is designing additional private patient capacity within the new hospital planned for the St Pancras Hospital site in King’s Cross, Camden, which may open in around five years’ time.
6
Guy’s and St Thomas’, in sixth place, experienced a 9.6% fall in private patient revenues in 2019-20, dropping back to £21.2m from £23.45m in 2018-19.
A significant part of service provision is the collaboration with HCA to deliver private cancer care at the Guy’s site.
The trust’s Private Patient Services adapted to support the response to Covid-19, but it is understood that private patient services have now resumed with
healthy interest from new consultants joining private practice. It is accepting international patients where appropriate safety guidance is met and offering virtual consultations where specialist expertise is required.
Looking forwards, Guy’s and St Thomas’ Private Healthcare has an ambitious growth strategy including plans to expand its current facility.
The forthcoming merger with Royal Brompton and Harefield Hospitals is the opportunity to build a strong partnership that delivers an exceptional cardiovascular care offer for private patients from the UK and internationally.
7Royal Free – joint seventh with UCL, see below – also saw an adverse impact from Covid19 in the latter part of 2019-20, which meant the trust ended the year with income of £20.4m, down 11.9% and £2.8m on the previous year’s total of £23.2m.
The general lack of progress over the past few years is illustrated by the graphic comparing growth rates across the top ten (Figure 5), where Royal Free is the only top ten trust to have declined in private patient revenues during the last four years, with a drop of minus 12.2%.
This is understood to be due to the connected challenges of constrained access to overcommitted
Figure 4
Guy’s Cancer Centre with the Shard behind the Guy’s Hospital Tower
facilities shared with the NHS, such as ITU and theatres and variable international demand and delivery.
With real progress on returning to private patient activity not expected until the new financial year, the challenge for Royal Free will be how the trust fits its PPU into some likely substantial reconfiguration of services that comes out of the Covid experience.
However, the trust’s off-maincampus facility at Hadley Wood in High Barnet continues to do well and has more than doubled business from pre-Covid times with hopes for potential growth still to come.
8
University College London’s private patient income being static in 2019-20, the trust moved up from ninth to joint seventh place in the top ten as revenues increased by 0.2% and £50,000 to £20.4m.
UCL’s private patient services are presently based across eight specialist sites in and around Bloomsbury, central London, and
offer a wide range of private services, including neurology and neurosurgery, fertility, maternity, teenage cancers and ear nose and throat treatment.
The trust can be expected to receive a boost to private patient incomes from April 2021 worth over £3m a year when it takes control of Mount Vernon Cancer Centre at Northwood from East and North Hertfordshire.
9 In ninth place, King’s College Hospital’s private patient revenues declined by £1.7m (8.2%) in 2019-20 to £18.9m.
All the trust’s 21 beds in the private inpatient unit, The Guthrie Wing, were reallocated as a Covid assessment area supporting the emergency department in March and this explains the headline fall in what was otherwise a steady year.
However, in the current financial year, the trust has not yet recommenced private patient activity but is committed to do so, starting with some ambulatory day surgery patients out of hours,
planned to start before the end of 2020.
Looking further ahead, the trust has strategic plans to at least double private patient capacity to 45-60 beds and is exploring options for either redevelopment of the present building or relocation on site. The projected timeline to open these is at least two to three years away.
10
Finally, at number ten in the NHS is Chelsea and Westminster Hospital, which grew private patient revenues 2.4% last year (£439,000) to £18.9m.
Looking ahead, the trust is aiming to deliver a more ‘focused’ private patient proposition that replicates the trust’s reputation as a centre of excellence for women’s and children’s services.
The West Middlesex site now offers a satellite IVF fertility service as an extension of the highly regarded IVF service offered at Chelsea and Westminster, in addition to private cardiac services.
These top ten trusts were achieving an increasing share of the cen-
tral London private patient market until Covid-19 forced a closure and redirection of most of their dedicated capacity.
The recent NHS PPU Barometer ( Independent Practitioner Today , November) demonstrated how the impact of the pandemic is expected to lead to a reduction in excess of 50% of the 2019-20 incomes in 2020-21.
Many of the top ten report a gradual return to offering capacity for private patients, but until international travel restrictions are lifted, private patient revenues cannot be expected to return to pre-pandemic levels for some time. Next month: The rising stars
Philip Housden (below) is a director of Housden Group
Figure 5
Better pension news
Over the last few years, there have been many articles written about the tax charges around pensions and usually these have been delivering bad news. The last 12 months have been tough for everyone, but at least there has been plenty of good news on the pensions front, reports Ian Tongue
Pension annual allowance
After many years of having to navigate around pension tax charges and tapering of the annual allowance, it still surprises me how many new clients come to us from accountants who have little or no idea about it.
Even worse is the client who thought they would save money and prepare their own tax return and ignore the tapering.
The pension annual allowance is still £40,000 a year, but the big change is that the earnings level where the reduction or tapering of this allowance starts has increased from £110,000 to £200,000.
This applies from the 6 April
2020 and is a welcome change. This new threshold provides greater scope to take planning steps to retain the full allowance.
A sting in the tail on this is that the previous minimum annual allowance that you could have was £10,000, but this has now been reduced to £4,000, which effectively prevents higher earners from having much tax relief on their pension savings.
Pension tapering
The original threshold for pension annual allowance tapering of £110,000 resulted in significant amounts of doctors incurring an annual allowance charge.
While waiting list work within the NHS was not additional superannuable income, the effect of having higher earnings was often the catalyst for incurring a tax charge. This became a disincentive to work and the waiting lists started to climb.
With an increase of the tapering threshold to £200,000, it has resulted in a significant amount of doctors no longer facing annual allowance tapering.
And for those with earnings above this sum, due to carrying out private work, tax planning opportunities exist to retain your full allowance.
For those still affected by annual allowance tapering, the calculation is the same as before, whereby you add earnings and pension savings together to determine how much of your allowance is retained.
However, instead of the minimum allowance being £10,000 this is now just £4,000. So if you are in this position, it is important to discuss your options with an
The good news is that, for many, the risk of paying tax for breaching the annual allowance has reduced significantly pension
accountant who understands the NHS Pension Scheme.
Pension growth
When comparing your annual allowance to your pension savings, it is important to understand that the NHS Pension Scheme is a special type of pension scheme.
Most pension schemes are investment funds and the value could go up or down. In this scenario, how much you contribute into the scheme is your pension savings.
The NHS Pension Schemes are different, as what you put in is your contribution to be a member of the scheme and what you get out is based on a formula.
For the 1995 and 2008 schemes, this is based on length of service and earnings, although the calculations differ. For the 2015 Pension Scheme, your career average earnings are used to determine pension benefits.
For those doctors who were moved into the 2015 on or after 1 April 2015, your current earnings are relevant for both your 2015 pension growth calculations and for your calculations under the 1995 and 2008 schemes.
Depending on which scheme you are a member of, your annual pension growth can be hugely different.
Factors such as pay increments and changes in roles can have a significant impact on the calculations and therefore before making any changes to your role, it is always a good idea, again, to discuss the impact with your accountant.
Paying annual allowance charges
Where a tax charge is incurred, you have the option of paying this through self-assessment or asking
the pension scheme to pay the charge, which is known as a ‘scheme pays’ election.
Paying through self-assessment gets the charge out of the way, but it does have the effect of increasing payments on account and therefore the tax may be more than you are expecting.
This can, of course, be reviewed if the payments on account would be too high for the following year.
Using the ‘scheme pays’ facility is effectively a loan arrangement behind the scenes, but instead of this being repaid or deducted against your pension in one amount, there is a formula to determine how much of your eventual pension you will lose.
The loan carries variable interest at a percentage above inflation with the interest rate currently at 2.4%, but it has been as high as 3% above inflation.
Again, as part of the measures to try and get doctors performing waiting list work, there is a special arrangement for 2019-20 in relation to using the ‘scheme pays’ facility.
While the system itself is identical to earlier years, there is a ‘promise’ to make good the effect of using the facility for the 2019-20 year only.
The exact mechanics of this has not been seen yet, but there is an overriding principle that members using the facility for 2019-20 will not be financially disadvantaged, so it is seen as good news.
The BMA has frequently-asked questions and further information regarding this facility on its website for those unsure of whether to take this option.
Pension lifetime allowance
There has been no change to the lifetime allowance, which is how big your pension can be before triggering a separate tax charge.
Often the level is viewed as a ceiling. This is not the case, but it is fair to say that the value-formoney calculation of additional pension growth is reduced once you start incurring lifetime allowance charges.
The current level lifetime allowance level is £1.073m, so speak to your independent financial adviser to understand your position.
Pension reform
To complicate matters, consultation ended in October to allow members of the 2015 NHS Pension scheme a choice to roll back into the 1995/2008 pension scheme for the period 1 April 2015–31 March 2022.
From 1 April 2022, it is proposed that everyone who is a member of the NHS Pension Scheme will be in the 2015 pension scheme or equivalent.
This is generally seen as particularly good news, but the impact on each member needs to be considered independently.
At the time of writing, the final document has not been issued, but it is proposed to allow members to elect early for this treatment or wait until retirement and select the best option.
Hopefully, there will be options here for those who do want to secure this treatment, but whether a decision is made before or at retirement, if the outcome is to go back into your legacy scheme, then all of the pension growth calculations will need to be revised.
This could mean that tax has been suffered or could mean that tax is payable. The consultation proposes an unlimited period for the taxpayer to go back and recover tax, but only a four-year window for HM Revenue and Customs.
It remains to be seen what the full options will be, but one thing for certain is that you will need a specialist medical accountant and independent financial adviser to guide you through this process.
Pensions have been a sore point for many years, with governments making many changes to public sector pensions.
The good news is that, for many, the risk of paying tax for breaching an annual allowance has reduced significantly and pension reform is on its way to give members some welcome options regarding their NHS pension.
Next month: Getting financially fit for Spring
Ian Tongue (right) is a partner with Sandison Easson specialist medical accountants
DOCTOR ON THE ROAD: HYUNDAI KONA ELECTRIC
Nice motor comes with a big charge
Your decision to buy a car like this has to be an ecological and environmental one, not about saving money, says our motoring correspondent Dr Tony Rimmer (right)
Sharing its drivetrain with the KIA eNiro and KIA Soul, the Kona is a smart-looking small SUV and is available with two battery sizes; 39kWh and 64kWh
ELECTRIFICATION IS just starting to have an influence on the carpurchasing thoughts of many doctors, and the choice is getting bigger all the time.
With the proliferation of new electric cars reaching the market over the last 12 months, things can only get better for the consumer.
Crucially, purchase cost will decrease and electric range will increase.
First adopters have had to have deep pockets, as the earliest electric cars on the market such as the Tesla Model S, the Jaguar iPace and Audi’s E-Tron are all expensive upper-premium vehicles.
What about everyday cars and small SUVs to appeal to more buyers at reasonable cost?
Well, Nissan has the Leaf and most recently Volkswagen has revealed the new ID 3, but it is the South Korean manufacturers KIA and Hyundai who offer well engineered, well equipped electric cars at reasonable prices.
One of the first cheaper cars to make electric motoring truly feasible was the Hyundai Kona Electric, launched in 2018. I have been testing the latest mildly updated version.
Sharing its drivetrain with the KIA eNiro and KIA Soul, the Kona is a smart-looking small SUV and is available with two battery sizes; 39kWh and 64kWh.
The claimed range for each is up to 155 miles and an impressive 300 miles respectively. You pay an extra £4,000 for the bigger battery,
but it does have almost twice the range.
My test car had the bigger 64KWh battery and was the midspecification £36,150 Premium model.
Great features include Apple/ Android connectivity, a 10.25inch touchscreen, all-round parking sensors and rear camera, a leather steering wheel and adaptive cruise control.
The interior is a functional and comfortable place to be. The plastics are good quality and there is plenty of room for four people, possibly five.
The hatchback boot is reasonably spacious at 332 litres and has useful underfloor space to stow the charging cables.
Effortless acceleration
With an electric motor that has a 201bhp output, this Kona is no slouch. Acceleration, although not as stunningly quick as a Tesla Model 3, is swift and effortless.
The huge torque range of the motor gives it the feel of driving a big three-litre six-cylinder petrol engine – without the noise.
However, all electric cars are heavy because of their batteries and the Kona is no exception.
At 1.7 tonnes, it feels its weight round corners, but the ride benefits, as most irregularities get smoothed over by the supple suspension.
The steering is direct and the handling is safe but fairly nondescript. It is not sporty like the MINI Electric (see November’s
issue). The regenerative braking can be altered in three steps of strength.
On its most powerful setting, this means driving almost without touching the brake pedal, but it does take some practice to use it smoothly. Nonetheless, you do preserve the battery level and extend the range in this mode, so it is worth persevering.
Easy charging
Charging is easy with a charging port in the front grille. I found it really convenient to charge up at the local Waitrose while shopping for an hour or two.
Now that many charging posts accept phone Apps or even contactless payments, it has become much easier to find a charging site within easy reach.
As usual though, it is better to charge regularly at home where a 7kWh wall-charging outlet will charge the Kona from empty to full in 9 hours and 35 minutes, i.e. overnight.
Buying an electric car is a deliberate and expensive decision. The Kona is also available in petrol form and self-charging Hybrid form and remember that a 1.0 litre petrol model in identical Premium trim will only cost you £23,250 – a massive saving of £13,000.
That will pay for many years of petrol, so your decision has to be an ecological and environmental one, not one for saving money.
The Kona Electric is an impressive electric car with an impressive driving range. In the real world, a regular 250 miles should be possible. If you are ready to go down the electric route and it suites your lifestyle, then it is definitely worth a look.
However, competitors in this sector are coming along thick and fast. KIA’s models are worth a look as is the Peugeot e-2008 and Mazda’s MX-30.
Dr Tony Rimmer is a former NHS GP practising in Guildford, Surrey
HYUNDAI KONA ELECTRIC
64kwh premium
Acceleration, although not as stunningly quick as a Tesla Model 3, is swift and effortless
Body: Five seat hatchback SUV
Engine: Single electric motor. Front-wheel drive
Power: 201bhp
Torque: 395Nm
Top speed: 93mph
Acceleration: 0-62 mph in 8.5 secs
Claimed range (WLTP): 300 miles
CO2 emissions: 0g/km
On-the-road price: £36,150
The Kona can be fully charged at home in 9 hours 35 minutes
A good eye for earnings
The highest-earning consultants in this specialty have recorded a £60k+ profit rise compared to last year – but the average is a very different story. Ray Stanbridge reports
A FEW OPHTHALMOLOGISTS appear to have had an outstanding year in 2018-19 – but this was not typical of the sector as a whole.
Our headline figures show that average gross incomes rose by 6% in 2018-19, going up from £139,000 to £148,000.
Their costs went up by 6.5%, rising from £61,000 to £65,000 and, as a result, taxable profits have risen by 5% from £78,000 to £83,000.
Margins have remained constant at about 56%.
What then are the reasons for changes between 2018 and 2019? Average income continues to rise, in some cases by significant amounts.
Self-pay growth
This is primarily the result of a growth in self-pay and, where contracts are awarded, in the continued growth of Choose and Book work – albeit at lower margins.
This is a particularly important but volatile source of income for many consultants.
AVERAGE INCOME AND EXPENDITURE OF A CONSULTANT OPHTHALMOLOGIST
Groups are developing in the orthopaedic sector and these generally generate higher income for their members than singletons are able to achieve
Costs have, by and large, grown with inflation.
Staff expenses have shown some increase, reflecting to an extent the growth in personal allowances – where family members are employed – and upward market pressure on secretarial costs, par ticularly in London where exter nal employees are recruited.
There has been a modest growth in room hire fees and professional indemnity costs, largely reflecting the growth in activity.
Marketing costs
Other costs have remained broadly the same, except for ‘other’. The drop here reflects a fall primarily in marketing costs.
By 2018 most consultant oph thalmologists who wished to invest in websites and basic mar keting material had already done so.
From what we can see, ophthal mologists in private practice have continued to enjoy growth in the year to March 2020.
But extremely limited data to date suggests that many private practice incomes collapsed for a few months from March-April 2020 as Covid-19 took hold and the first lockdown began. All of this will be reported in future issues.
In this Profits Focus, we have amended our criteria for entry to our survey from the figure of £5,000 minimum earnings in the private sector to £10,000.
Consultants included in our sur vey are those who:
Expertly different Protection as unique as you are
With the world’s largest medicolegal team and the greatest reserves of any defence organisation, we’re here to protect both your finances and reputation.
Medical Protection membership benefits include:
• Discretionary support that has the flexibility to ask, ‘How can we help?’
• Support in GMC investigations and representation at hearings
• The right to request assistance with criminal investigations
• Access to a free counselling service as part of your membership for stress or anxiety that you feel could impact your practice
• Free access to the Croner advice line which provides support with tax and VAT, company law and health and safety support
Are not in full-time private prac tice;
HOW ARE YOU DOING?
Have spent at least five years in private practice;
Are seriously interested in private practice as a business;
Earn at least £10,000 a year in the private sector;
May or may not have been a member of a group or have incor porated.
Collecting consistent and fair comparisons on a year-to-year basis has become more difficult because ophthalmology consult ants now trade in a variety of ways; for example, through limited lia bility partnerships or limited lia bility companies, both of which complicate the collection of com parable data.
Our survey is not statistically sig nificant but aims to try to measure, in an increasingly complex situation, what is happening to consultants in the ophthalmology market in the UK.
Next time: Gynaecologists
Ray Stanbridge is a partner with accountancy, finance and tax advisory medical specialists, Stanbridge Associates Limited
Years ending 5 April
Source: Stanbridge Associates Ltd
Innovative industry online solutions at the heart of the healthcare community
By industry for industry, Healthcode are the experts in information technology focussing solely on solutions for the healthcare sector. Trusted by leading hospitals, independent practitioners and insurers to deliver high quality, secure, cost effective IT systems that connect key stakeholders to seamlessly enable transparency within the sector and enhance patient safety.
• Circa 20k clinician accounts
• Over 300 private hospitals
• All major private medical insurers
• Process and clear an average of 28k bills daily worth £3bn
22k practitioner accounts £3.3bn
The team at Independent Practitioner Today wish to thank our loyal readers, sponsors, advertisers and editorial contributors for all their support in the year just passed and send you every good wish for 2021. Coming in our February issue, published on 9 February 2021:
Technology should help and not hinder your business. Healthcode explains how to get the best from a practice management system
Setting up a healthcare business in England and Wales? What do you need to know for it to be legal? Kirsty Odell gives guidance on the legal considerations that you need to think about
Our second in The Power Of People series by Jane Braithwaite explores the topic of flexible working, remote working and home working. She will cover how to manage a remote team, the technology that enables efficient remote working and how to ensure you reap the benefits of a flexible working policy
Common hazards employees face while working from home and tips on how to prevent them. While many are enjoying the benefits of avoiding tedious commutes, a better work-life balance and more autonomy over their working day, remote working poses dangers to employees’ physical health that may be unexpected or go unnoticed.
Beth Husted offers some tips for doctor employers and employees to consider while working from home
Update on the GMC’s new consent guidance: In the second of a two articles, MDU medico-legal adviser Dr Kathryn Leask continues to discuss factors in the guidance that are of particular importance for private practitioners
INDEPENDENT PRACTITIONER
TODAY
Published by The Independent Practitioner Ltd. Independent Practitioner Today is editorially independent and thanks Bupa for its assistance with distribution.
Material is governed by copyright. No part of this publication may be reproduced, stored in a retrieval system or transmitted in any form without permission, unless for the purposes of reference and comment. Editorial layout is the copyright of the publishers. If you wish to use it for promotional purposes on websites or for reprints, we would be happy to discuss licensing the copyright to you.
In Business Dilemmas, MDU medico-legal adviser Dr Kathryn Leask explores the implications of the Access to Health Records Act 1990 for a private gastroenterologist, and Dr Sissy Frank discusses raising concerns about a colleague’s behaviour
How not to buy into your own hype. Tingy Simoes shares some useful insights
Get your business financially fit for the Spring. Medical accountant Ian Tongue suggests an action plan
Private patient units: which NHS trusts are the rising stars right now. Philip Housden reports on the fast-growing ones
Our A-Z of accountancy issues for independent practitioners arrives at the one everyone wants to know about: ‘R’ for remuneration
Profits Focus reports on the latest figures for gynaecologists in private practice
Medical Billing and Collection’s Simon Brignall gives advice to help ensure all your hard work gets paid for
Topical tips from specialist financial planners Cavendish Medical
Plus all the latest news and views
Don’t forget to catch up with more news affecting independent practitioners and their business on the home, news and feature pages of our website: www.independent-practitioner-today.co.uk
ADVERTISERS: The deadline for booking adverts in our February 2021 issue is 22 January
Write to Independent Practitioner Today 7 Lindum Terrace, Lincoln LN2 5RP
CHANGING ADDRESS, EMAIL ADDRESS OR SUBSCRIPTION DETAILS?
Phone 01752 312140 or email karen@marketingcentre.co.uk
TELL US YOUR NEWS
Robin Stride, editorial director
Email: robin@ip-today.co.uk
GET A SUBSCRIPTION DISCOUNT!
£90 independent practitioners.
£90 GPs and practice managers (private & NHS).
£210 organisations.
Save £15 paying by direct debit: individuals £75 (organisations £180).
TO SUBSCRIBE
Email karen@marketingcentre.co.uk or phone 01752 312140
Publisher Gillian Nineham
Phone: 07767 353897.
Email: gillian.nineham@gmail.com
Phone: 07909 997340 @robinstride
ADVERTISE WITH US
To advertise in the journal or our website business and lifestyle directories, contact Andrew Schofield at Spot On Media Email: andrew@spotonmedia.co.uk Phone: 0161 408 3912
SAVE £15 WITH DIRECT DEBIT!
Guarantee delivery of your next copy of Independent Practitioner Today. Take out a subscription and you will get full access to our news, features and previous issues on our website. See details on the left.
BACK ISSUES: £12.50 including post & packaging
The business journal for doctors in private practice