Three features to help you keep your business data safe, starting on P14
The business journal for doctors in private practice
Where do you find the cash?
Advice on how doctors can fund their property investment deals P28
Don’t be an HMRC target Specialist medical accountant Ian Tongue shows how you can reduce your risk of a probe by the taxman P40
Tougher vetting for private consultants
By Robin Stride
Consultants face a practising privileges shake-up under private hospital plans to strengthen clinical governance and bring a more standardised approach to working arrangements.
An Independent Healthcare Providers Network (IHPN) initiative starting in England also envisages more proactive and two-way information sharing between private providers and the NHS via Responsible Officers (ROs).
The Medical Practitioners Assurance Framework (MPAF) forms part of the sector’s response to the Bishop of Norwich’s inquiry due soon into issues around the rogue surgeon Ian Paterson case.
Principles in the document, which sets out 23 ‘responsibilities’ for practitioners, reinforce expected practice in key areas. These include clinical governance structures, patient safety, clinical quality, continuous improvement, whole practice appraisal and raising and responding to staff and patients’ concerns.
Former NHS England national medical director Sir Bruce Keogh,
who headed the work, said the vast majority of independent care was of high quality and was underpinned by robust safety and medical governance processes.
But more could and should be done to ensure clinicians and independent providers worked together to perform to the highest possible standards.
Federation of Independent Practitioner Organisations chairman Mr Richard Packard believed MPAF would enable a more co-ordinated approach to improve communication at all levels about a consultant’s practice and should help timely identification of any problems to allow early rectification.
He said: ‘The MPAF makes some sensible recommendations relating to the responsibilities of consult -
Key aspects of consultants’ practising privileges will be standardised –such as approval requirements for them to use new procedures and treatments
ants in relation to their practising privileges, which FIPO is pleased to support. This is a dynamic document which will evolve over time and should lead to greater assurance for patients.’
An IHPN practising privileges template document will update the Independent Healthcare Advisory Services guidance. Key aspects of practising privileges, such as how and when they will be reviewed, scope of practice and approval requirements for consultants to use new procedures and treatments, will be standardised.
The framework follows a Care Quality Commission (CQC) report last year revealing 41% of private hospitals required improvement and 1% were inadequate for safety. Thirty per cent required improve-
ment and 3% were inadequate for being well led.
Private hospitals have given MPAF widespread support. Heidi Smoult, CQC’s lead for independent health, called it an important step forward in bringing stronger medical governance across the independent sector.
She added: ‘While sign-up to the framework is not mandatory nor something CQC has the power to enforce, where providers can demonstrate effective and robust implementation of its principles, this will be considered as evidence of good governance and will inform the judgement we make about how well-led services being provided by that organisation are.’
BMA private practice committee chairman Dr Shree Datta called the framework a helpful stepping-stone to improve consistency and boost confidence in all independent healthcare settings. She said everyone should work towards a unified platform to centralise all information for doctors and patients. The framework will be reviewed next year to keep principles aligned to changes in best practice.
➱ continued on page 4
TELL US YOUR NEWS Contact editorial director Robin Stride
Are they who they say they are?
A look at how criminals attempt to obtain funds fraudulently by targeting medical practices using phishing and vishing techniques P18
ADVERTISE WITH US Contact advertising manager Margaret Floate at margifloate@btinternet.com Phone: 01483 824094
GET A SUBSCRIPTION DISCOUNT
£90 independent practitioners.
£90 GPs and practice managers (private & NHS). £210 organisations.
Save £15 paying by direct debit: individuals £75 (organisations £180).
TO SUBSCRIBE – USE SUBSCRIPTION FORM ON PAGE 23
Or email karen@marketingcentre.co.uk Or phone 01752 312140. Or go to the ‘Subscribe’ page of our website www.independent-practitioner-today.co.uk
Chief sub-editor: Vincent Dawe
Head of design: Jonathan Anstee
Publisher: Gillian Nineham at gill@ip-today.co.uk Phone: 07767 353897
EDITORIAL COMMENT
Safety boost or box-ticking?
So the promised ‘Consultant Oversight Framework’ we have been waiting for is finally with us some six months later than originally expected and now called the Medical Practitioners Assurance Framework (MPAF) [See stories page 1 and 4].
All being well, its existence will have been notified by now to most specialists via their organisations and work will be going on among the interested parties to fill in the gaps and produce template documents to be used in independent hospitals across England – and later in the other home countries too.
With 28 pages to digest and 23 ‘medical practitioners’ responsibilities’ to consider, there could be much to think about and put into operation. Some, such as ‘to comply with the GMC’s Good Medical Practice’, will be taken as read.
But perhaps others could be more of a challenge in some
circumstances, such as ‘to work collaboratively with all staff and support all colleagues in being able to speak up if they have any concerns about patient safety in the setting in which they work.’
As Sir Bruce Keogh has said, the MPAF ‘fires a starting gun for a series of discussions and deliberations to improve care and confidence in the private sector’.
Will this gun be welcome by all? We have been told some consultants will see it negatively; viewing it as more timeconsuming paperwork and change they had no input into.
David Hare of The Independent Healthcare Providers Network argues it should make life easier and streamline existing requirements by bringing together a lot of what people are, or should be, doing anyway.
Let us know what happens near you.
Checks in the post
The perils of closed social media forums. Medico-legal expert Dr Sally Old discusses the pitfalls of posting on private social media groups P20
The fateful days of my last patient
Surgeon Mr David Sellu, convicted for gross negligence manslaughter of a private patient – but overturned on appeal – continues his story P24
Sharing outcomes
A pilot is being set up to examine how the independent sector can participate in the National Clinical Audits Programme. David Hare reports P32
Poor practice data will cost you a lot
Are your financial records really up to date? Simon Brignall warns that many consultants need to check to ensure the paperwork meets their needs P34
Never too old to think long term
How far ahead should you be looking? Dr Benjamin Holdsworth looks at a prudent investment horizon, whatever your age P36
PLUS OUR REGULAR COLUMNS
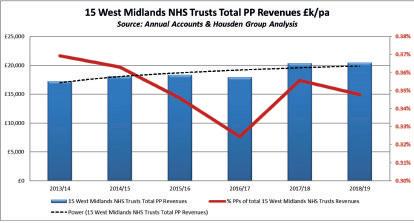
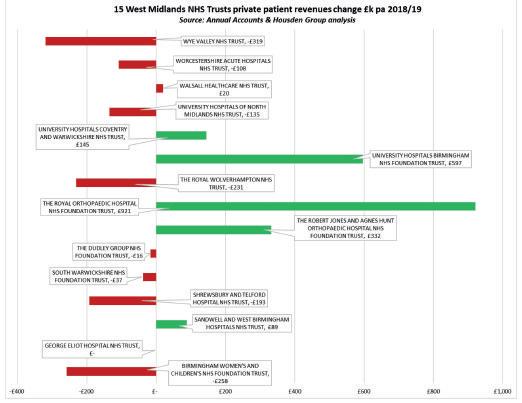
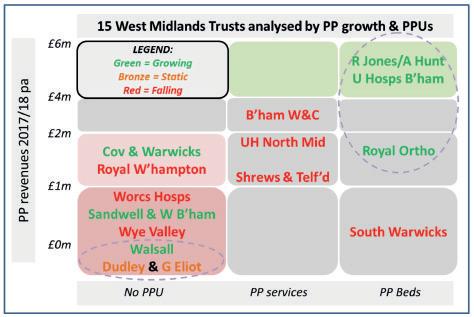
Private Patient Units: Orthopaedic units show how to do it
Our monthly look at the fortunes of PPUs in different regions turns its focus on the West Midlands P43
Doctor on the Road: Stylish evolution of the people carrier
Keen-driving ‘family doctors’ will find this seven-seater equal to the class leaders P46
Profits Focus: Orthopods still cutting it
Our unique benchmarking series looks at the financial fortunes of orthopaedic surgeons P48
Pension tax haul soars
By Edie Bourne
Doctors are among thousands of pension savers generating record payments to the taxman by breaching strict yearly limits.
HM Revenue and Customs (HMRC) revenue from ‘annual allowance’ breaches hit £812m in 2017-18, a rise of at least 40% on £517m in 2016-17. The figure was £143m in 2015-16.
Some 26,550 pension savers reported a breach of the annual allowance rate – up by a staggering 11,000% in a decade. Ten years ago, just 230 people triggered the extra tax charge. The average extra tax bill is now £30,584 per person.
The annual allowance limits the amount of tax-free pension savings which can be accrued each year. As well as the standard allowance, which has fallen from a peak of £255,000 in 2011 to just £40,000, a ‘tapered’ annual allowance was introduced in 2016.
This cuts the limit down further on a sliding scale to as little as £10,000 for those with an ‘adjusted income’ – taxable income plus pension savings – of more than £150,000 a year. But the first test is whether the individual earns more than £100,000 from all sources – known as the ‘threshold income’.
The Government consultation closed this month on proposals to make pension saving more flexible as record numbers of doctors continued to cut their NHS hours or considered early retirement to avoid large-scale tax hits.
Tax yields from taxpayers break-
ing the lifetime allowance, which governs tax-free pension savings, overall topped £185m in 2017-18, up from £102m in 2016-17 and £66m in 2015-16. The lifetime allowance has been cut from £1.8m in 2012 to just £1.055m now.
Patrick Convey, director of specialist financial planners Caven dish Medical, said: ‘These substantial figures show the extent of the problem that doctors are facing. The harsh savings limits continue to trap NHS scheme members who are diligently saving for retirement, but, unlike other professionals, are tied into making fixed contributions to their pensions.
‘The proposals to introduce more flexibility in pension saving could go some way to easing doctors’ significant tax concerns, but the new measures will still add extra layers of complexity to the already needlessly complicated pension issue.
‘Whatever the outcome of the
consultation, you should look at your own tax position very carefully, and as soon as you can, to avoid generating extra cash for the taxman.
Cavendish Medical’s Dr Benjamin Holdsworth advised doctors to use a specialist medical accountant who understands the NHS pension and is proactive to allow forward planning.
He told a London Consultants
Association meeting it was important for them to understand their own personal tax position and have some idea of all tax liabilities for each year ahead.
Doing things early would help: Tax returns early in the light of current pension tax complexities to ‘give your accountant a chance’; Obtaining information early from NHS Pensions. It could take 12 weeks for annual allowance statement requests to arrive.
And he advised doctors to check annual allowance information carefully, as there were ‘very frequent errors’ involving backdated payments, variability in pensionable pay and moving from fulltime to part-time or vice versa.
Dr Holdsworth recommended taking paid specialist pension advice before making any decisions around the scheme, such as stopping added years or opting out.
See AISMA on pensions, page 7 ‘You’re never too old to think long-term’, page 36
Only radical reform can cure the current pension crisis, says BMA
Doctors’ pensions tax nightmare will only be cured by fundamental tax reform, the BMA has warned in its response to the Government’s proposed NHS Pension Scheme flexibilities.
It said it could only back a temporary fix if employers paying, say, only 20% of their usual contribution into a doctor’s pension paid the remaining 80% back to the clinician as part of their salary.
Without compulsory recycling, any flexibilities represented a realterm pay cut.
The BMA warned the only solution was scrapping the annual and tapered annual allowance. Its pensions committee chairman Dr Paul Youngs said: ‘Doctors are trapped in a dilemma between wanting to care for patients and not wanting to end up financially worse off.’
Support for inspections for private GPs
Private GPs are to be supported under a new partnership between the Independent Doctors Federation (IDF) and the Royal College of General Practitioners (RCGP) Development Service. They will assist practices deemed ‘inadequate’ by the Care Quality Commission (CQC) using a team
of experienced primary care professionals.
The team will interview all the staff, look at all protocols, policies, training and governance, and make recommendations that IDF president Dr Neil Haughton believes should allow the practice to turn around its CQC rating.
He told Independent Practitioner Today : ‘These are our businesses, which we have built up over many years, nurturing our patients’ needs, and to have that challenged can be incredibly stressful and financially disastrous, which is why investing in this joint venture would be money well spent.’
IDF president Dr Neil Haughton
Patrick Convey: ‘Figures show the extent of the problems doctors face’
Benjamin Holdsworth: Told doctors to act early to plan for pension tax
Tighter vetting to aid patient safety
The group representing private care providers said the assurance framework was a boon for patients.
David Hare, boss of the Independent Healthcare Providers Network said it would give confidence to patients that independent healthcare providers were committed to delivering the safest possible care.
MPAF’s expectations include consistency in recruitment processes of directly employed consultants, ongoing performance management, appraisal and review.
Consultants are required to submit data about the quality of their performance to relevant national registries available to the sector and to the Private Healthcare Information Network (PHIN).
Providers will want assurance
that doctors are participating in quality improvement activities on application for, or review of, practising privileges.
Practitioners would have to share as a minimum their summary appraisal outcomes and personal development plan to inform a practising privileges review. If this failed to give enough information to enable a decision, then they would have to provide additional relevant information from the whole practice appraisal.
The MPAF says bigger hospital groups should appoint a clinician as a national lead for clinical governance and consider appointing local or regional lead consultants to support them.
It wants relevant governance information about doctors’ performance, including activity data,
HOW PRACTISING PRIVILEGES WILL BE REGULATED
Dataset to be considered in an annual or biennial review of practising privileges includes:
Agreed scope of practice review and compliance, including discussion about required volumes for surgical activity and/or ensure practice is sufficient to maintain competency
Clinical audit review, clinical metrics or clinical outcomes data derived from the organisation’s clinical governance systems
Relevant registry data where appropriate; for example, National Joint Registry data for orthopaedics
Adverse events and outcomes review
Investigated complaints and outcomes
Concerns, investigations or changes to: i) practice in other hospitals where the doctor works; ii) recognition from an insurer/commissioner.
Concerns relating to a doctor’s work, such as situational awareness and coping with stress
Consideration of professional behaviour, including patient as first concern, commitment to quality/safety, collaborative team-working, openness/transparency, fairness, honesty, integrity, insight into strengths/ weaknesses, commitment to reflection and learning in line with GMC guidance
shared quickly, possibly using a new standard sector wide template, plus clarity on how the unit’s medical advisory committee or similar body works and fits into the overall clinical governance structure.
Health lawyers Browne Jacobson said the MPAF provided welcome clarity on what expected practice is and an excellent opportunity for organisations to review their systems and processes. It was ‘a much needed part of the toolkit for Responsible Officers and independent healthcare organisations.’
Sir Bruce was supported by an expert advisory group including representatives from royal colleges, the CQC, GMC, NHS England & Improvement, the Department of Health and Social Care, the Patients Association and HCA.
Dataset to be considered on application for practising privileges includes:
Standard dataset and ID check: proof of identity including recent photograph, basic demographic/identity information, work permit if necessary, Disclosure and Barring Service and Information Commissioner’s Office registration, evidence of compliance with relevant mandatory training and Hep B/Hep C/HIV status, CV and references, designated body and RO
Satisfactory evidence of conduct in previous employment
Current registration with the GMC, entry on the specialist register and other appropriate professional registrations
Valid certificate of adequate defence cover to an appropriate level
All locations where a doctor holds practising privileges or works
Evidence of participation in annual whole practice appraisal, including sharing of appraisal summaries and personal development plans as a minimum and relevant information from whole practice appraisals if insufficient. Providers should consider a mandatory requirement of at least one whole practice appraisal before approving practising privileges applications
Description of scope of practice, including surgeon’s procedure codes, procedures done, volume of work in each area of practice and registries where outcome data is shared
Evidence of participation in quality improvement activities
Immediacy of availability of attendance, such as minimum availability/travel distance requirements and requirement to have back-up for known non-availability appropriate to level of care being delivered
Cheaper defence
Adrian Stevenson, chief executive officer at Independent Care, said: ‘One of the benefits should be that medical malpractice underwriters will be able to price their premiums more competitively on the basis that the framework will manage risks more consistently and effectively and increase the volume of members covered by an industrywide policy. Some of the savings could be passed onto consultants and to the operators.’
The effect on PPUs
Independent Practitioner Today’s private patient unit columnist Philip Housden said the patient safety agenda would lead to NHS trusts and independent hospitals working more transparently on clinical governance. Consultants could be expected to encourage their NHS trusts to develop PPU capacity ‘to ensure most complex patients are treated in the safest environment, which in most health economies is going to be the NHS hospital campus’.
Transparent data
MPAF could capitalise on a Healthcode initiative to improve information accuracy and transparency.
The company’s Fiona Booth, who headed the IHPN’s precursor, said: ‘Healthcode has developed The Private Practice Register (PPR) as a central source of reliable information about independent practitioners which is held on a single, secure platform that connects private medical insurers, practitioners and hospitals.
‘It now has more than 16,000 practitioner profiles, includes a wealth of information about their private and NHS practice and is being rolled out to hospitals to help them keep track of their consultant populations.
‘The MPAF builds on current processes within the independent sector and we hope the IHPN will make the most of available technology. The PPR offers strong foundations on which we can build better lines of communication, improved governance and quality assurance which is in the interests of stakeholders and patients.’
➱ continued from front page
Cromwell
joins Bupa’s breast
cancer nexus
Bupa has extended its network of specialist centres for breast cancer to include Bupa Cromwell Hospital, London.
The centres offer Bupa UK Insurance customers an appointment with a consultant within two working days of calling its Cancer Direct Access service and all initial diagnostic tests are completed in one appointment.
Londoners are less likely than national average to identify eight common signs of breast cancer, research has found. Difficulties accessing services coupled with lack of awareness mean women are delaying seeking medical help.
Other specialist centres are at Harley Street Clinic, Marylebone; The Lister Hospital, Chelsea; The London Bridge Hospital; The Wellington Hospital, St John’s Wood; The Wilmslow Hospital, Cheshire, where treatment is delivered at The Christie Private Care, part of HCA Healthcare UK.
Surgeons now have a new trade union
A new union, the Confederation of British Surgery, is ‘the first and only trade union to be recognised under UK law to protect the welfare of surgeons, including the extended team and their families’.
It said it aims to represent all surgeons, regardless of surgical speciality or affiliation, and negotiates on their behalf the terms and conditions of service, contracts of employment, litigation and insurance.
President Mr John MacFie said surgeons needed better representation. The CBS wanted to share best practice and expertise across all specialties and faster resolution of complaints and fair recompense to patients who have been harmed. It will work with The Federation of Surgical Speciality Associations, which represents and coordinates the views, aims and policies of surgeons in the UK and Ireland.
Psychiatry support for private docs
By Robin Stride
Private consultant and GP mem
bers of the Independent Doctors Federation (IDF) are being offered mental health assistance from a new psychiatry support network.
Twenty private psychiatrists within the membership have agreed to help and provide consultations, some at reduced rates.
Fees are being subsidised by prescription medicine delivery company Phamacierge.
IDF president Dr Neil Haughton said the initiative was a response to the fact that pressures on doctors were rising and many independent practitioners found it difficult to access really confidential mental health support.
They were also ‘not good’ at recognising personal mental health issues.
He said: ‘The pressure of being in private practice is you are on your own, you are independent and if you are not good enough, your business fails. Patient expectations are higher, too, so you have to up your game.’
Pharmacierge cofounder Edward Ungar, told Independent Practitioner Today: ‘Working with private practices across the UK to reduce clinician stress and workload when managing private prescriptions, our core values are to promote health and wellbeing.
‘We are aligned with the IDF in recognising that clinicians’ own mental health is of paramount importance when offering exceptional levels of care to their patients.’
The IDF move was planned before our story last month announcing independent practitioners will have access to their own ‘wellbeing guardians’ in private surgeries, clinics and hospitals under plans being promoted
Awards launch at PPUs’ annual get-together
Private Patient Unit (PPU) representatives will be at their sixth annual Private Patient Service Development conference on Thursday 12 March 2020, at Governors Hall, St Thomas’ Hospital, London.
by the Medical Protection Society. Similar posts are being developed in the NHS.
The BMA has called for more mental health support after a report found only half of doctors were aware of any services to help them with physical and mental health problems at their workplace. One in five respondents said no support services were provided.
A new BMA study last month, ‘Mental Health and the Medical Profession’, said as there was often little or no support in the workplace, many doctors faced long periods of sick leave because of mental illness or, in the most severe cases, resigned, retired or retrained.
The association has launched a Mental Wellbeing Charter calling for more to be done to improve awareness and support for doctors’ mental health and welfare.
The BMA believes 80% of doctors are at substantial risk of burnout and 40% are experiencing symptoms of depression, anxiety, burnout, stress or a mental health condition.
The networking event supports the continuing positive development of private patient services across the NHS and shares best practice.
An innovation for 2020 is the introduction of achievement awards to recognise excellence in the sector for growth, patient experience and quality and professional service excellence.
Case studies will be led by PPU leaders, and sessions with medical insurers, PHIN and NHSE. A wide range of service suppliers to the sector are expected, along with dozens of trusts.
Details at www.sbkhealthcare. co.uk/home/title/2412/nhsconference/nhs private patient servicedevelopment2020/
Poor scores for disability units
Fourteen independent mental health hospitals that admit people with a learning disability and/or autism have been rated inadequate and put into special measures in the last year.
The Care Quality Commission said two of these services had since improved, three had closed and one service was still registered but was closed to new admissions with no people resident.
Make sure the private healthcare industry knows who you are, where you are and what you do. Tell us your story. Contact editorial director Robin Stride at robin@ip-today.co.uk or phone him on 07909 997340
ENTREPRENEUR DOCTORS
Private doctors find it hard to know where to go to get mental health support, according to the IDF
Key to growth in private practice is marketing
By Robin Stride
Consultants are achieving up to a 35% growth in patients in London as a result of using marketing.
Independent Practitioner Today columnist Jane Braithwaite told a London Consultants Association (LCA) seminar that the surge came as a result of work her business services company Designated Medical had been doing with doctors. She advised specialists that with 80% of patients now researching their doctor in advance, they should not underestimate the value of marketing consultants’ practices. For those using social media, she recommended LinkedIn as ‘the one to go for’ above Twitter, Facebook, Instagram, YouTube and Pinterest.
Other speakers at the event, called ‘So you think you want to be a private consultant?’, painted a less upbeat picture of life in private practice.
Ophthalmologist Mr Richard Packard, chairman of the Federation of Independent Practitioner Organisations, gave a detailed synopsis of big changes in the market over the last 25 years, which he argued had empowered insurers.
At least, he quipped, all the private medical insurers still wanted the consultant provider to be a doctor.
He advised anyone considering being a private consultant to seek advice from their accountant or other professional about the options of being a sole trader, in a limited liability partnership, set -
ting up a limited company or being employed. There were pros and cons for each.
His summary of the challenges for consultants now was:
Developing and keeping a reputation based on more than price;
Having clinical decisions made by private medical insurers for referral and management purposes;
The theat of increasing overheads from indemnity insurance, staff costs and rentals;
Continuity of private practice particularly as a young consultant outside the M25;
The Private Healthcare Information Network (PHIN), outcome data accuracy and ownership of this;
PHIN and how the Competition
and Markets Authority fee remedy is published and patients are informed;
GDPR – which could stand for Giving Data on Patients Recklessly leading to a big fine – and the ability to communicate clinical information.
Coming soon, he forecasted, was:
Managed care with restricted access for patients to the consultant and hospital of their choice;
Clinical decisions made by insurers based on cost not quality despite PHIN data;
Control of fee-setting across the board, so no real competition;
Greater scrutiny of practising privileges and scope of practice with enhanced governance after the Paterson inquiry, for greater assurance for patients.
PREDICTIONS OF WHAT PRIVATE PRACTITIONERS OF THE FUTURE COULD FACE
1. THERE MAY BE CONDITIONS ATTACHED
Having ≥2 years as a consultant in good standing
≥2 years unsupervised private practice (≥2 x 3-hour sessions a week)
Holding practising privileges ≥ one hospital
√ £10m insurance cover per occurrence
Expected to ‘understand key features of private healthcare’
Billing within published fee maxima for new and follow-up patients
Not allowed to bill fees greater than allowed by other private medical insurers
Must bill electronically, abiding by insurer’s invoicing and coding rules
Registration with Healthcode and Private Patient Register
2. SOME POSITIVE ASPECTS
Increase in self-pay patients as the NHS struggles to deliver on waiting times where package prices compete
New methods of consultant engagement – employment by hospitals (Cleveland and Schoen clinics)
In some specialties, there are opportunities not covered by private medical insurance policies, such as cosmetic surgery or refractive eye surgery
Chronic illnesses will not be covered by insurers, but many patients prefer continuity of care after initial contact
Source: FIPO chairman Mr Richard Packard
Expert outlines cure to problem of surging defence costs
Dr Christine Tomkins, chief executive at the Medical Defence Union (MDU), said the drivers of claims were far removed from the clinical coal face.
Two years ago, the union had 110 claims from consultant members who had never had a claim in 20 years of membership. Last year, the figure was 89 claims.
Appealing for a reform of the tort system, she criticised the Personal Injury Discount Rate (PIDR), used
to work out compensation awards for future care and loss of earnings.
Currently set at -0.25% since last August, this meant that a claim settled in 2014 for £4.82m for a negligent management of child with sepsis would now cost £8.04m. A tetraplegia case following spinal surgery, settled in 2012 for £9.2m, would now be £15.5m.
Dr Tomkins stressed these valuations did not take account of claims inflation of around 10% for
many years. High-value claims were doubling in value every seven years.
She said claims could be made many years after an incident although there was a three-year limit from the date of knowledge.
The MDU’s longest consultant claim was notified 38 years after the incident.
And 45 consultant claims notified between 2017-2019 had incident dates from 1980 and 2010.
Dr Tomkins said the discount rate should reflect the way damages were invested. Personal injury defendants should be allowed to buy health and social care from public providers and the same care needed to be available to all patients with the same condition. There should be an ultimate limitation period and a limit on recoverable future loss of earnings; for example, three times the national average salary a year.
LONDON
Call centre eliminates human error
A visiting doctor service has developed ‘the first fully-functioning virtual call centre for doctors’.
Doctorcall’s system aims to better integrate services around the needs of patients while eliminating human error and delay.
It replaces call handlers, finetunes communication and means patients and clients can place calls directly into the system, while being able to view important information including ETAs, tracking doctors and also real-time medical reports.
Patients can see what help is available before logging their case. The technology is designed to learn from every case it manages and the firm says it has already successfully handled more than 10,000 cases.
Founder Dr Charles Levinson said: ‘Our aim was to take human error and delay out of the equation and to use experience to enhance performance so we could model the behaviour of the best call handlers to optimise case management.’
Doctorcall said its system delivers the potential for better and more cost-effective care, with results so far proving transformative – allowing cases to be handled more efficiently than before and delivering significant savings for their clients.
It can remember detailed specific instructions for thousands of clients and patients.
Self-payers can now be e-billed
By Leslie Berry
Independent practitioners will be able to send invoices to patients and receive their payments online through a new link-up between online platform companies Healthcode and Patient Zone.
They can test the service using a short pilot study combining the former’s e-billing tool with a secure billing and payment portal for patients developed by the latter.
The aim is to help them improve cash flow, giving practices a faster and more efficient way to bill selffunded patients and private medical insurance shortfalls and assist patients.
Practices in the pilot will be able
to create a patient e-bill on Healthcode’s ePractice system and send it to Patient Zone where patients can access the bill and pay by credit or debit card.
Practitioners won’t have to set up a merchant account for these transactions, as the processing fee is included in the fee from Patient Zone, whose platform is encrypted and meets the Payment Card Industry (PCI) data security standards.
Healthcode managing director Peter Connor said: ‘When we surveyed customers last year, e-billing and payments for patients were at the top of their wish list, so I’m delighted to be working with Patient Zone to make this a reality.
‘Once the pilot has been completed, I’m confident that it will become an essential service for ePractice users who want a fast, simple and secure way to manage these transactions.
‘Healthcode’s collaboration with Patient Zone is also proof of the value of interoperable technology which enables ePractice to connect seamlessly with the Patient Zone platform.’
Patient Zone charges 2.5% plus VAT of the total bill for the service. Boss Richard Shawyer added: ‘As self-pay continues to grow, we can improve the patients’ experience by giving them access to a secure online portal where they can pay and then focus on their recovery.’
AISMA hits out over pensions
Proposed NHS Pension Scheme flexibilities are unworkable and discriminatory, says the Association of Independent Specialist Medical Accountants (AISMA).
It labelled the proposals uninformed tinkering with the regulations and urged for a complete rethink of pensions tax legislation.
Oncology centre hailed for support of
The psychology and well-being team at The Christie Private Care, part of HCA Healthcare UK, has been awarded an ‘outstanding team of the year 2019’ accolade.
Zenith Global Health Awards recognised its support group, the well-being space cancer survivorship programme, free to all patients and families.
Patients identified the need for it, saying there was a gap in care
patients
after medical treatment and subsequently they felt lost, isolated and anxious.
They describe how the programme in Manchester helps them move from just ‘existing’ between hospital appointments to ‘living’ their life again.
The programme includes groups for men, women, people with metastatic secondary cancer, partners and loved ones.
Vice-chairman Deborah Wood, healthcare services partner at MHA Moore and Smalley, said the proposals made it no easier for doctors to understand their pension position.
Deciding on a reasonable percentage of pay to pension to avoid a tax charge represented ‘a game of
Atlantic
storms fail to stop sailing surgeon
Harley Street consultant plastic surgeon Mr David Gateley, featured in our September issue, completed his Clipper Round the World Race, arriving in Punta del Este, Uruguay, in mid-October.
Sailing over 5,000 nautical miles from Portugal, the crew weathered extremes of conditions from the lull of the doldrums to Storm Lorenzo. He was raising money for Unicef UK and Child Action Nepal.
chance for all doctors’. Ms Wood said doctors would welcome a simplified system that cut their fees for accountancy, tax and pensions advice.
This could be achieved by implementing Office of Tax Simplification advice to scrap the annual allowance cap on pensions.
David Gately: Reached Uruguay in the Clipper Round the World Yacht Race
Action needed to cure BMA sexism
By a staff reporter
More women doctors should be included on BMA committees under a quota basis to better reflect the percentages of men and women in each branch of practice, a QC has recommended.
Women across the organisation should also get together in a women’s group to support and mentor each other, the senior barrister says.
These are among a string of recommendations from QC Daphne Romney, who was called in to investigate after women GPs complained of sexism and sexual harassment in the organisation.
She found ‘a large number’ of doctors and staff who felt undervalued, ignored and patronised because they were women due to an ‘old boys’ club’ culture ‘that lingers on without proper challenge, which treats women as of less importance and ability’.
Ms Romney said problems arose across the BMA and called for all its committee members, which would include those in its private practice committee, to undergo specially designed training in diversity, equality, anti-bullying, activebystander and collegiate working.
She continued: ‘These courses should not be online courses, where full attention is not always required. To mend the BMA, active
participation, commitment and learning is required.
‘There will, of course, be those who think that they do not need it. Many of those are likely to be the people who need it most. The training should concentrate in particular on the impact that words and actions have on others, and the importance of respecting colleagues.’
Her inquiry found unacceptable behaviour including shouting, demeaning women, sexual harassment and bullying. ‘Some of this may be generational, but that does not make it any less offensive,’ she said.
The BMA has apologised after publishing the independent report into sexism in the association and vowed it was committed to reform.
Council chairman Dr Chaand Nagpaul said: ‘I am truly appalled to learn that members and staff have been subjected to sexism and sexual harassment and the behaviours described in this report. These behaviours have no place within the BMA.
‘I am deeply sorry to those who have been affected and I thank all those individuals who came forward to contribute to the review – I recognise their strength and courage in speaking out.
‘The report makes for difficult reading. I am determined that we
learn from it and, most importantly, that we make the necessary changes to ensure we become a truly inclusive association by implementing the recommendations.’
BMA policy-making body chairman Dr Helena McKeown said: ‘I want the BMA to be an organisation that, as a doctor and as a woman, I am proud to be a part of and those who follow me will also be proud. This is a springboard for change and that change has already begun.’
The BMA said it had introduced measures to promote equality and tackle discriminatory behaviour, including:
➲ An independent and external 24-hour support line, so that any BMA member or member of staff experiencing sexism or any discriminatory behaviour can speak to someone in confidence;
➲ An independent complaints investigation process carried out by an experienced external firm so that members and staff can be assured of impartiality;
➲ ‘Equality Matters’ , a programme which provides learning for all BMA members and staff on equality, diversity and inclusion;
➲ The initial development of bespoke face-to-face training for all members in elected roles and for chairmen of committees on inclusive leadership.
Doubling of students is needed to fill empty posts
Physicians’ royal colleges in England and Scotland want medical school places doubled after finding huge gaps in NHS consultant provision caused partially by the pensions tax problem.
Royal College of Physicians of London’s president, Prof Andrew Goddard, urged the Government to do more to retain doctors. A census of 8,656 physicians found the Midlands had 161 vacancies, London 62 and the North 85.
Orthopaedic surgeons boost profits by 6% by containing costs
Orthopaedic surgeons in private practice achieved an average profit increase of nearly 6%, according to Independent Practitioner Today’s latest benchmarking survey.
Gross incomes rose by around 1.6% between 2017 and 2018, going up from £190,000 to £193,000, medical accountants Stanbridge Associates revealed.
Orthopaedic surgeons managed their costs well and these fell by about 5.7% on average, dropping from £69,000 to £65,000.
See page 48
Harley St cannabis centre gets green light
Harley Street’s new cannabis treatment centre, Sapphire Medical Clinic, ( Independent Practitioner Today, September 2019) has got the green light from the Care Quality Commission. It becomes the first to receive official approval from the regulator to operate.
Managing director and academic lead Dr Mikael Sodergren said: ‘We can now be the lifeline for GPs who are not permitted to prescribe
themselves but who think their patients could benefit from medical cannabis.
‘From today, those GPs can be sure that their patients are able to be treated in the UK by world-class experts in their conditions, who understand cannabis as a medicine and how it interacts with other treatments that patients might be on.
‘For patients who have too long been denied access to cannabis-
based products as part of the conventional treatment pathway, this decision could be life-changing.’
Medical director Dr Michael Platt said the firm would set up a registry of patient response and efficacy. He said this would help build an evidence base crucial for more widespread prescribing.
Sapphire Medical Clinics will operate on GP referral basis via its website.
Dr Mikael Sodergren of Sapphire
VIRTUAL EXHIBITION
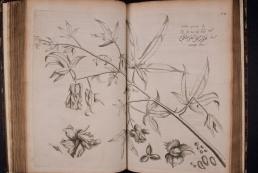
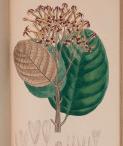
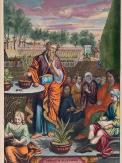
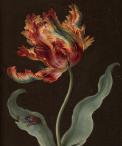
Rare texts go online
The Royal College of Surgeons of England’s library has launched its first ever digital exhibition. We preview some of the rare and striking images from its archives
THE COLLEGE’S exhibition, entitled ‘Medicinae Plantae: healing plants through time’, highlights the important role of herbalism in medical education from the late 15th up to the 19th century.
The tradition of studying and using plants for their healing properties was once at the core of medical education.
Plants were used from root to flower and the process of finding, preparing and determining the correct dosage to administer for differing ailments were all explored in print.
Available on the RCS website, the exhibition draws together images and explanatory information on some of the most beautiful, classic and unusual books in its library’s collection.
Forty works are included in the exhibition, ranging from Schöffer’s Herbarius Latinus , published in 1484, to Esenbeck’s Planta Medicinales, published in 1833.
Rupert Williams, Royal College of Surgeons’ director of library and archives, said: ‘Our exhibition represents just a fraction of the fascinating special collections that make up the RCS’s archives and we want as many people as possible to be able to access them.’
Horti Medici Amstelodamensis by Johannes Commelin
An Illustration of the Sexual System of Linnaeus by John Miller
John Hunter’s Watercolour Floral Paintings
Icones Plantarium by Joseph Jacob Plenck
Planta Medicinales by Nees von Esenbeck
Herbarius Latinus by Peter Schöffer
Hortus Malabaricus by Hendrik van Rheede, Amsterdam 1678-1693
Horti Medici Amstelodamensis by Johannes Commelin
Plantae Selectae by Christoph Trew
A look back through our journal’s archives of ten years ago reveals that although times change, some issues are not so new
A trawl through the archives: what made the news in 2009
Profits rise by 10%
Specialists with a private practice beat the recession and the falling self-pay market the previous year with a 10% profits rise.
Figures from Laing’s Healthcare Market Review 2009-10 estimated 20,000 independent practitioners in medical and surgical specialties averaged £78,000 gross and £55,000 after expenses, compared to £71,250 and £50,000 the previous year.
Accountants said the doubledigit increase reflected lower costs and high-fee NHS business farmed out to the private sector.
Independent hospital support –no longer allowed following the 2014 Competition and Markets Authority order – was said to be helping consultants cut room costs by up to £4,000 a year. Specialists were also earning fees under profit-share arrangements.
We reported that estimates for 2008 showed the NHS’s proportion
of funding for independent acute medical/surgical inpatient, day case and outpatients more than doubled in four years to 23.1%.
Self-pay dropped again, from 16% to 13.3%, overseas patients also fell and private medical insurance was similar at 61.3%.
Private medical insurance edged higher, covering 10.4% of the UK population by the end of 2008.
50% tax rate looms
Medical accountants reported a surge of anxious consultants making contact for advice on setting up companies to escape a 50% tax band being introduced the following year.
Tax specialist Vanessa Sanders of Stanbridge Associates said: ‘Most people earning over £100k are doing it or seriously considering it. They are converting into companies to defer tax increases and give them greater flexibility in tax planning.
‘The 50% tax rate is really hitting people and making them think what they can do. The average consultant will have to pay £5k-£8k more next year than this year even on the same income.’
Harley Street TV
Broadcasting by internet television channel HarleyStreetTV.com began with a series of short films for patients on breast cancer.
Be wary of your website
Specialists were missing out on getting more private patients because their websites were so bad.
Medical marketing expert Darren Clare agreed with findings from Spire Healthcare that patients were increasingly using the internet to find surgeons and travel a long way for treatment. He said there were hundreds of badly designed websites that had been set up for doctors by a brother-in-law or a surgeon and they were worse than useless because they were badly designed and written.
Said Mr Clare: ‘Websites have to be congruent with the professional service doctors are offering. But a lot look like DIY jobs and, in our view, that’s worse than having no website at all. Doctors are not gaining the business they should get.’
Patients are prepared to travel
Surgeons with a private practice in some of the more remote areas of the UK could potentially attract patients from far outside their locality, a new survey suggested. It found distance was no object these days for many patients who were looking for a ‘skilled surgeon’.
As many as 42% of patients
would travel as far as necessary to get the surgeon they wanted, according to the study by eDigital-Research.
RO scheme criticised
Health department plans for doctors’ Responsible Officers (ROs) under revalidation were slammed by the Independent Healthcare Advisory Services (IHAS).
The IHAS said draft regulations and guidance on the RO’s role were ‘complicated and confusing’ and would place an unprecedented additional burden on independentsector medical directors.
Doctors are tax probe targets
The recession was making private doctors increasingly likely to be targeted for a tax inquiry, a former tax inspector warned.
Andrew Fenton said HM Revenue and Customs (HMRC) wanted to plug a massive shortfall in tax receipts.
SUBSCRIBE TODAY
Don’t miss out on what we report and advise in the future. Sign up for a £75 subscription today –consultants, GPs and practice managers can save £15 with a direct debit.
See page 22
Refer your patient and you will receive the radiologist’s report in as little as 2 working days.
If your patient is claustrophobic or bariatric, refer them to our Open MRI scanner in London for a same day appointment from £399.
It’s easy to book your patients online, but if you want to chat first, we are available 24/7:
info@mriplus.co.uk 0208 103 4089
www.mriplus.co.uk
ACCOUNTANT’S CLINIC: THE BUILDING BLOCKS OF ACCOUNTANCY
This month, we get to ‘E’ in our A-Z guide of essential matters that consultants and GPs need to consider to run their private practices efficiently. Susan Hutter reports
to of is for Expenses top tips
DOCTORS’ EXPENSES have been regarded much more strictly in recent years by HM Revenue and Customs (HMRC).
Most practitioners, sensibly, decided to cut back on the amount of the claims, particularly concerning the ‘old chestnuts’: motor expenses and the claim for use of home as office.
When HMRC started to investigate motor expenses in more detail, it led to a well-known case that became the subject of a tax tribunal hearing.
The consultant concerned claimed that his typical weekly journeys supported a 65% business mileage claim, whereas HMRC disputed this and proposed only 6%. The case concluded with a figure somewhere in between.
However, it is a stark message to all consultants and GPs about how much they could claim in 2019 and beyond.
It is worth stressing that travel between your surgery and your home is not tax-deductible. And what if your home is your office?
In nearly all cases, HMRC will not allow travel from your home to
your place of work, even if you do use your home as an office.
Usually, it will only allow mileage between private hospitals/surgeries if you work from more than one.
Additionally, one can also claim mileage for travelling to courses and conferences for business purposes.
Be careful
Do be careful – if your claim is challenged by HMRC, it has the right to go back for six years and adjust the figures, which would end up meaning additional money for you to pay back. I recommend everyone keeps a mileage log of all business mileage so they never have to worry if questioned.
As far as use of home as office is concerned, this has always been a confusing area. If you have a room in your home that you use exclusively for work, then the expenses attached to that room would be tax-deductible.
This includes all relevant bills, such as lighting, heating and cleaning. The bills should be apportioned based on the square
footage of the room that is used compared to the rest of the home.
If, however, the room is used for other purposes, so it is not exclusively for business, the claim would have to be reduced further.
In all cases, it is imperative to keep accurate records of the expenditure that you are claiming and also back up calculations on how you arrived at the claim.
However, there is also good news on expenses. Over recent years, successive governments have tried to encourage business investment in research and development by offering generous tax breaks to those businesses who carry out such work.
Research and development (R&D) tax relief is given in the form of tax credit to consultants and GPs who trade via a limited company.
Unfortunately, the relief is not available to unincorporated businesses and therefore those practitioners who are going to be spending material sums in this area may wish to consider incorporation if they do not trade as a limited company at the moment.
To obtain this special tax relief, the expenditure must be on a project which seeks to ‘achieve an advance in overall knowledge or capability in a field of science or technology through the resolution of scientific or technological uncertainty’.
Tax credit
If you are lost in the jargon of the explanation, I recommend you take specialist advice before deciding whether to spend the money. If you meet the criteria, for every £100 spent on the R&D, your company can claim an additional £130 of deduction against profit.
This is what is known as the R&D tax credit. For example, if your company spends £100,000 on qualifying R&D, not only will it receive tax relief on that £100,000, it will receive tax relief on a further £130,000, a total of £230,000. This results in a corporation tax saving of 19% or £43,700, so it is well worth exploring. There are several expenses that can be included on the R&D tax credit claim, including relevant salaries for directors and employees.
is also for Enterprise Investment Scheme
OFTEN SPECIAL projects – including research and development –will require funding.
Funding may also be required if you are considering expanding your practice (see ‘Expansion’ below).
For whatever reason, if you require a cash injection from third parties, you could incentivise them due to the tax breaks available under the Enterprise Investment Scheme (EIS). Once again, this is only relevant for practices that trade as limited companies.
There is an additional relief for new businesses, which works in a similar way, known as Seed Enterprise Investment Scheme (SEIS). These reliefs are available to shareholders with less than a 30% holding, including shares owned by connected parties.
If a company is a qualifying trading company, and most medical practices are, then any capital investment into new shares will achieve 30% tax relief under EIS and 50% under SEIS.
Where an investor pays £20,000 for their shares, the tax relief would therefore be £6,000 and £10,000 respectively. The maximum investment in a tax year is £1m for EIS and £100,000 for SEIS.
SEIS is more generous, but the rules are stricter.
EIS is available to businesses that have been trading for at least four years but less than seven years, and SEIS for businesses that have been trading for less than two years.
Providing all conditions are met, and the shares are held for three years or more on the sale of the shares, there is no capital gains tax liability.
And there would be no clawback on the original income tax relief. There are also potential capital gains tax savings on making the initial investments. This is by way of deferment of capital gains tax in the case of EIS or cancellation of capital gains tax in the case of SEIS.
is also for Expansion
MANY INDEPENDENT practitioners will have heard of ‘centres of excellence’ which have been growing in popularity in the medical profession for quite a few years now.
Put simply, several consultants in the same or complementary disciplines form a group, either formally or informally, in one location to provide a centre of excellence in a speciality.
The individual consultants do not have to form a joint legal struc-
ture. If they wish, they can remain separate, either trading as limited companies or sole traders.
However, in many cases, the consultants have formed partnerships, limited liability partnerships or limited companies in which they are the shareholders and directors.
The limited company structure has tax advantages, particularly for those who are going to invest in research and development expenditure, and also those who wish to
Successive governments have tried to encourage business investment in research and development by offering generous tax breaks to those businesses who carry out such work
raise capital from third parties. These advantages are explained under the expenses claim and EIS sections above.
When considering expansion, keep a level head, as it is vital that businesses do not start to ‘overtrade’. This means that the top line expands too quickly for the structure to cope.
Delivery of services is compromised and then the business will often fail. Therefore, planning the expansion sensibly is vital. In these circumstances, it is worth taking the advice of the practice accountant.
An advantage of expansion is that it assists with succession planning. An issue that faces consultants and GPs planning their retirement is finding someone to take over their practice when they would ideally like to take things a little easier. Centres of excellence provide an ideal opportunity for a consultant with, say, five or six years left to practise to wind down in an organised manner.
In all cases, I recommend that professional advice is taken.
Susan Hutter (right) is a partner at Blick Rothenberg and part of the team that advises medical practitioners
When considering expansion, keep a level head, as it is vital that businesses do not start to ‘overtrade’
DATA?
The EU General Data Protection Regulation (GDPR), in place for over a year now, has raised the bar for data protection compliance for private practices.
Jane Braithwaite and Karen Heaton (below, left and right) start a six-part series on what GDPR compliance means for your practice management by examining a range of topics that independent practitioners and their managers need to get on top of
Are you doing enough to shield your
LET’S START with why it is important to establish a data privacy and security awareness culture in your practice. To do that, it is worth outlining some of the core intentions from the EU’s General Data Protect Regulation (GDPR).
Legally obliged
Did you know that data protection compliance covers both data security and data privacy? Many organisations understand security – whether this is the physical or digital security of their practice data.
However, we find that data privacy is not well-understood and it is this aspect of the regulations which require a greater understanding.
So, data security alone is not enough for compliance with GDPR. You need to ensure data privacy is not compromised.
Data privacy
There are many aspects to consider with data privacy. Fundamentally, your practice must continually understand and record:
What data you have;
Why you have it;
Where it came from;
What you do with it;
How long do you keep it;
Where it is stored;
Who has access to it;
Whether there is an appropriate lawful basis for using it.
So, from a practice management perspective, some operational rigour is needed to ensure only data you need is stored and used and that you are not storing it for longer than you need it.
And you must ensure you have a legal basis for all the data you use and only process it in relation to the services you offer and not for any other reason.
For example, if you have consultation notes for a patient who then chooses not to take up your services, you would not be able to store their notes for the next ten years in case they changed their minds.
A more reasonable time period would need to be applied to this scenario and certainly one the potential patient is made aware of. How would you make them aware of this? It would need to be outlined in the privacy notice. Compliance with data privacy
also involves ensuring your practice can continually comply with the GDPR rights of individuals whose data you hold.
These rights include:
Access to data;
Information about the data held;
Deletion and correction of data, restrictions on the processing of data;
Data transfers to another party;
Restrictions on automatic profiling of data.
Does your practice have staff who are trained and understand what to do if a patient or member of staff asks about their rights?
Are there operational procedures and IT systems in place to be able to respond to data requests?
Or what about being able to demonstrate to a regulator or the GMC that the practice is compliant with GDPR?
Fines for non-compliance can be significant at a time when data risks are increasing
For private practices, data protection risks are high because of the sensitive personal data being processed, including information on children.
Hefty fines
This is problematic for your practice because the Information Commissioner’s Office (ICO) has shown in recent months that it is not afraid to exercise its power to issue a hefty fine to those who are not compliant with GDPR.
The level of fines from regulators is based on a combination of factors. So it will look for evidence of how the practice complies with the regulations in order to assess penalties or other enforcement actions. Building a culture of data privacy and security into your business operations allows you to demonstrate this.
For example, a medical centre in London left sensitive patient data in an empty building in July 2015 and received a penalty of £35,000 which was levied under the previous Data Protection Act 1998. This could have been higher under the current GDPR.
The ICO investigation found that the data was left from July 2015 to February 2017 during which time access to the building was granted to other organisa
Cloud-Based Electronic Patient Records and Patient Portal
• Integrated Electronic Patient Record (EPR) and Clinic Management
• Comprehensive documentation of patient encounters
• Data analytics to deepen your understanding of your patients
• Streamlined workflows improve the provider and patient experience
tions. Emails to the medical centre about the unsecured data had not been actioned.
All enforcement actions by the ICO are published on its website, so it is not just the cost of any penalty which private practices need to consider, but the reputational damage from publication of the actions.
Practices face increased regulatory risks at a time when cyber attacks are increasing and becoming ever more sophisticated.
As a practice, you cannot be expected to invest your time and money into keeping up to date on the phishing and malware techniques that cybercriminals are using (see page 18).
But you can create a culture of awareness with your staff and use market-leading cyber security tools to ensure you limit these risks.
If you have an effective cyber security software in place, it is likely that an attack will get through by dint of human error. So, staff training must be effective and done regularly.
From a data breach perspective, it is not a case of ‘if’, but more likely ‘when’ it will happen. What you do to protect that data before and after the breach, how you manage the breach response, what you learn from it and what you can prove that you have put into action as a result of the breach will make a difference to how damaging the breach is and how the ICO responds.
The same applies to Subject Access Requests. Patients and employees will make these requests and it is essential the
Anyone could be the cause of a data breach. It could be the person who leaves patient information on the photocopier or the staff member who staples the wrong piece of paper to the back of the bundle
practice responds according to the regulations.
These can be extremely timeconsuming with tight 30-day deadlines, so we will discuss tips for streamlining these later in our series.
The benefits of building a security awareness culture
By creating a data privacy and security awareness culture in your practice, you can begin to reduce the costs and potential damage from data-related incidents.
Benefits for patients:
Your staff will demonstrate that they understand and respect the protection of patient personal data. This provides comfort to patients – one of many factors patients look for when choosing a medical practice.
Benefits for staff:
They gain additional knowledge, skills and the freedom to act and
The Accountancy Solutions
A dedicated accountancy firm established for over a decade, we understand the individual needs of medical professionals and work closely with them to develop a personal plan. You are never just a number to us, and we pride ourselves on our bespoke services that make us stand out from the crowd. Contact us for free advice and no-obligation quote.
take decisions based on the practice management culture which has been built.
They become ambassadors for good data protection procedures and can quickly train new staff members as well as identify and suggest continual improvements. There is ownership and buy-in.
Benefits for the practice:
It could mean the difference between having a breach and protecting your practice from one. This protects your reputation, avoids costly fines and the regulator’s attention while also streamlining practice management operations.
Building the culture does not have to be complex or difficult. In this series we will provide information on the top priorities you can adopt for your data protection regime, if you have not already done so.
We bring you up to date with the latest ICO guidance on cookies and what your responsibilities are for compliance.
However, when security awareness and data privacy are treated as a tick-box exercise to be done once a year at best to comply with regulations, then you are increasing your risk of non-compliance with the regulations, including a data breach. Why? Because data protection is not at the centre of regular operational procedures for the practice.
How do you ensure your staff have data privacy at the front of their minds when doing their jobs? Simply make it part of their working culture.
Making the commitment
Falling foul of the regulations can be easily done. Anyone could be the cause of a data breach. It could be the person who leaves patient information on the photocopier or the staff member who staples the wrong piece of paper to the back of the bundle.
It can be as simple as having a busy Friday afternoon, when an email pops in at 4.50pm telling you to take action because your password needs renewing on that website you use regularly. You don’t stop to check the veracity of the email or the hyperlink.
Poor handling of Subject Access Requests could result in com -
plaints to the regulator. Given the high-risk data private practices must process, the regulator may decide to investigate your data protection compliance.
Ignorance of the regulations is not an excuse; it is essential to keep your staff up to date, informed and empowered.
It takes time to change a workplace culture, but it is not difficult. It is not achieved in a halfhour meeting explaining a new operating procedure, but it can be built into the daily routine of the practice.
It also needs to be implemented by the entire practice – from top down and bottom up. This requires commitment, not necessarily additional costs.
You and your staff are incredibly busy running the practice, so by embedding a privacy and security culture into the practice, it becomes part of what they do and how they protect your patients, the practice and themselves.
Help and support can be obtained from external data protection consultancies offering guidance on building a data privacy and security culture or providing the services of outsourced data protection officer. The task does not have to be daunting or expensive and often results in better management of your practice. In our next article, we continue on our compliance journey and look at the top five priorities for building data privacy and security awareness into your practice and why you need them.
Jane Braithwaite is managing director of Designated Medical, which offers business services for private consultants, including medical secretary support, book-keeping and digital marketing.
Karen Heaton is the founder of Data Protection 4 Business, which offers consultancy services to design and implement GDPR-compliant solutions as well as online training, outsourced data protection officers and specialised software technology to support data protection.
Together, Designated Medical and Data Protection 4 Business offer consultancy services and support to help private practices and clinics design and embed a data protection compliance culture into their organisations
New Year, New Solution
Make your life easier by using one of the UK’s leading virtual practice management system.
DGL Practice Manager simplifies your processes and workflows allowing you to manage all areas of the practice or clinic from one location, including:
Appointment Scheduling
Clinical Procedures
Electronic Patient Records
Patient Correspondence
Financial Accounting Reporting
DGL Practice Manager offers a cloud-based, safe and secure solution. It saves time and increases efficiencies by helping clinicians and administrative staff run a paperless practice or clinic.
Contact us today for more information:
Web: www.dglpm.co.uk
Email: dglsales@clanwilliamhealth.com
Phone: 01280 824 600
DGL Practice Manager is very user-friendly and provides us with everything we need including a feature-rich accounts package. I have absolutely no hesitation in recommending the system and find all the staff very helpful and pleasant.
Joanne Murray-Brown. Secretary to Mr Sarangi, Orthopaedic Surgeon.
Are they really who they say they are?
Vin Pandha continues her popular series with a look at how criminals attempt to obtain funds fraudulently by targeting surgeries and medical practices using phishing and vishing techniques
PHISHING
Phishing is the fraudulent attempt to obtain sensitive information such as usernames, passwords and credit card details by disguising oneself as a trustworthy entity in an electronic communication.
The most common form of phishing is via email. Typically, it will appear to have come from a known or trusted organisation such as the bank or a government department and will show a sender’s email address which looks identical or extremely similar to the genuine organisation.
When the origin of a fake electronic communication is hidden and the sending information is made to look like it has originated from a genuine source, it is known as ‘spoofing’. Fraudsters can easily and cheaply obtain software which allows them to spoof email addresses.
In its most basic form, a phishing email is not personalised towards a specific victim and is usually sent to large numbers of people at the same time, hoping that a percentage of them will take the bait by clicking on a link or opening an attachment contained within the email.
We are all likely to have received some kind of phishing email either at work or personally, as such a large volume of these emails are sent every day. An example is an email purporting to be from the tax office promising you a tax refund if you click on the link contained within the email. Something that seems too good to be true often is.
Spear phishing
Another form of phishing, ‘spear phishing’, can be far more effective for fraudsters. This type of attack involves an email which is sent to a target victim. It includes information tailored to them specifically and is therefore more likely to result in them being tricked into thinking it’s genuine.
If an email addresses someone personally and includes factually true information about them or their work, it is more likely to appear genuine and be acted upon.
SMiShing is another form of phishing and as the emphasis on SMS suggests, is an attack delivered by SMS text message.
Similar to email, the message
If an email addresses someone personally and includes factually true information about them or their work, it is more likely to appear genuine and be acted upon
TOP TIPS TO ENABLE YOUR PRACTICE TO GUARD AGAINST PHISHING AND VISHING
1
Never provide online banking passwords or online payment authorisation codes on the phone or in response to an email or text message. A genuine bank employee will never ask you to divulge these.
2
The bank will never ask you to move funds to a ‘safe’ account. If you receive a call asking for you to take this action, hang up immediately and contact your known contact at the bank.
will be ‘spoofed’ so that it appears to have come from a genuine sender and it will encourage the recipient to divulge sensitive information such as passwords or to click on a malicious link.
The message has a link to a phone number to call where an automated voice asks you to state passwords or other confidential information.
In other cases, the text message appears to come from your bank with some requirement for urgent action and a link contained within which directs you to a site that you think is secure. The fraudsters are hoping to catch you off guard: to act now and think later.
Phishing attacks can result in fraudsters stealing funds from your surgery or practice if a member of staff believes that an email or text is genuine and they enter online banking passwords or transaction authorisation codes into a reply message or into a website that is linked from the email or text.
In some cases, by clicking on the link or attachment contained within the phishing email, the user may unwittingly download malicious software (malware) onto their device, which can enable the fraudsters to steal information and may lead to a largerscale fraud or cyberattack later.
VISHING
Vishing is short for voice phishing and is a form of criminal phone fraud, using social engineering over the phone system to gain access to private personal and financial information for the purpose of financial reward. (See my article last month on this manipulation technique).
As with emails and text messages, when fraudsters make a scam phone call, they usually use ‘spoofing’ software.
This enables them to make the
3
4
Never input online banking passwords or online payment authorisation codes after following a hyperlink in an email or text.
Ensure you log into your genuine online banking service by entering the correct web address in your browser bar and look out for the padlock symbol to ensure you are on a secure site.
5
Do not click on links within other emails or texts or open email attachments unless you know who sent the message and you can be sure it is genuine.
6
Do not give out sensitive or internal-only information via phone, email or text without verifying the identity of the person asking for that information. If necessary, call them back using a number you know to be correct.
7
Ensure all computers are protected by high-quality antivirus software and run frequent scans. Always ensure software updates are actioned promptly and keep firewalls switched on.
8
Train employees on how to spot and prevent phishing and vishing attacks and conduct regular checks or tests to ensure that they are following correct procedures.
number which appears on a potential victim’s incoming caller display show the genuine or trusted number for the organisation they are pretending to be. When the fraudster claims to be a genuine caller and points out the correct incoming caller number should be displaying, a victim is often drawn in.
Another approach a fraudster may take when making a vishing phone call is to use information they know about the medical practice to convince an employee that they are a genuine caller.
For example, details of a supplier, a name from their accounts department and how much the practice last paid them could lead to the belief that it is the genuine supplier on the phone.
In recent vishing scams, fraudsters have tricked their victims into thinking that their bank account is under attack and then go on to provide instructions on how they can move their money into a ‘safe account’ to prevent any loss from occurring.
This socalled safe account is, of course, controlled by the fraudsters and unsuspecting victims who think they are being helped unfortunately lose their funds.
Like phishing attacks, a vishing phone call can result in fraudsters stealing funds from your surgery or practice if you reveal online banking passwords and transaction authorisation codes to a caller you believe to be from the bank.
Follow our top tips to protect your practice from falling victim to this type of scam.
Vin Pandha (below) is commercial fraud manager at Lloyds Banking Group
Checks in
The perils of closed social media forums. Dr Sally Old (below) discusses the pitfalls of posting on private social media groups
SOCIAL MEDIA groups and forums can often be a useful platform to discuss the pressures of being a doctor; for example, sharing best practice, voicing frustrations or asking questions to colleagues.
There are numerous forums which are ‘closed’, meaning that they allow discussion in a discreet ‘members only’ area. However, are such forums a safe place when there is the potential for comments posted on such groups to be leaked onto the wider internet?
In Doctors’ use of social media (2013), the GMC outlines the principles that doctors must adhere to when posting online. In it, the GMC states:
‘Although individual pieces of information may not breach confidentiality on their own, the sum of published information online could be enough to identify a patient or someone close to them. You must not use publicly accessible social media to discuss individual patients or their care with those patients or anyone else.’
Private social media groups may seem secure, but it is important to remember that these forums can have hundreds of thousands of members.
Often, this means that information is accessible to individuals outside the profession. To illus -
trate, there have been cases when people have used fake credentials to join private groups. Another important factor to consider is the potential for someone within the group to take a screenshot of your post and publish it in another forum.
Out of context
Comments can be taken out of context or misunderstood and it is easy to inadvertently cause offence. As a doctor, you need to consider whether you would be happy for a post to be shared with a wider audience and possibly with no reference to the original context in which it was made. Social media plays an important role in engaging with the public and with other medical profes -
the post
sionals in conversations around healthcare and by establishing national and international professional networks.
However, doctors need to be aware of the potential problems and risks when posting their thoughts online.
The MDU’s advice is that prior to posting, even in a closed group, consider what the purpose of the post is and who may read it.
Could it potentially identify an individual and what could be the repercussions if the post was reproduced elsewhere? If you are unsure, it may be best to alter your post or not to post the comment at all.
Dr Sally Old is a medico-legal adviser at the Medical Defence Union
SALUTARY LESSON
A consultant recently joined a private Facebook group to participate in a discussion about a patient who had recently undergone an operation. The consultant and several other members of the group then played ‘top trumps’ as they shared their experiences of patients who had undergone similar treatment.
A few days later, the consultant got a private message from a nurse, who was also a member of the Facebook group and consequently had seen the original post. The nurse explained that when she had seen the post, she knew that they were referring to her mother.
The nurse was extremely angry that her mother’s health had been mocked online. She demanded a written apology and explanation to be sent to her mother with the threat of a GMC referral if she remained dissatisfied.
The MDU member was given advice on how to approach this complaint and after a written response and a meeting with the patient and her daughter, no further action was taken.
The daughter was able to explain to the consultant in person how unprofessional and disrespectful she had found his post, particularly at a time when her family had received bad news. The consultant appreciated this and sincerely regretted the distress his post had caused.
SUBSCRIBE TODAY TO GET EVERY ISSUE IN 2020 AND READ US ONLINE
Dear Reader,
Subscribing to Independent Practitioner Today is the only way you can be sure you will see every issue and have the option of reading us online using our special page-turnable edition. Don’t risk missing out. Our personal subscription for doctors and managers is only £90 a year and £210 for organisations. But you can cut this to just £75 and £180 respectively if you pay by direct debit.
So take advantage of this offer now for our unique business journal dedicated to supporting you in your private practice. We’re confident your subscription will repay itself many times over!
Editorial director
APPLICATION FOR SUBSCRIPTION
Instructions to your Bank or Building Society to pay Direct Debits
Name and full address of your bank/Building Society
To: The Manager Bank/Building Society Address Postcode Ref. No.
Banks and Building Societies may not accept Direct Debit instructions for some types of account
send a copy of your letter to us.
ON TRIAL FOR MANSLAUGHTER
The fateful days of my last patient
Surgeon Mr David Sellu, (below) convicted for gross negligence
manslaughter of a patient – overturned on appeal after a 30-month prison sentence – continues his story from last month
11 February 2010: Ealing Hospital, 7.45am to 6.15pm. The Clementine Churchill Hospital, 7pm to 10.40pm, then home I thought I had an ordinary day ahead. But I was about to learn that an ability to relate past occurrences with precision could make the difference between a credible defence and a prison sentence in a court of law.
My encounters with patients were carefully documented, so I have been able to consult my notes to help me construct what happened on that fateful day.
I spent the previous one performing two successful major cancer operations. I saw the patients in the ITU and then called their relatives to announce progress.
8.30am. Next, it was the multidisciplinary team meeting (MDTM) followed by a busy outpatient clinic lasting until lunchtime. 12.20pm. I quickly lunched in my office and finished dictating letters.
1.10pm. On the wards to see four ill patients – there was not enough time for a full ward round. Then, at 1.30pm, an endoscopy list until five, plus another visit to the ITU and wards.
6.20pm. I packed my bags for the Clementine Churchill Hospital, the private hospital in Harrow, about seven miles away. An even
ing clinic was booked from seven to nine.
My wife Catherine was still awake when I got home after 10pm. She too had been through a busy day as matron in charge of the A&E department where I practised.
She prepared me a late dinner and I stayed up to update my records, dictate GP letters and obtain notes for next day.
Looking back, as I would do over the coming months and years, I would discover that I’d seen two patients in the ITU in the morning and discussed 15 patients at the MDTM. Twentyone patients consulted me in the clinic at Ealing up to lunchtime. I visited six more in the ward. In the afternoon, I did six endoscopic examinations.
At the Clementine, I saw on the ward three patients and five in the clinic. About halfway through that clinic, I was asked by an orthopaedic consultant colleague Mr John
Hollingdale to see a patient complaining of abdominal pain five days after an elective knee replacement.
It was Mr Hughes, my last patient, whom I saw just after 9pm, who was to change everything. The 66 year old retired builder from Co. Armagh, Northern Ireland, was evidently tall, stocky and had been classified as obese.
I shook his hands gently. ‘My name is David Sellu and I am a consultant general and bowel surgeon.’ His eyes lit up. I said why I was there.
He seemed relieved and said he tried to explain to staff about his pain but they did not understand him nor could he understand what they said to him. He had to ring Mr Hollingdale’s secretary to ask him to come.
I summarised what I knew and asked him to fill in any details I may have missed. He was a little breathless and had to pause between sentences.
Perforated bowel
He had woken at about 5am that morning with pain in his lower tummy. ‘I have never had this type of pain before. It got a little worse and then eased for several hours, but it has started again.’
After examining him, I washed my hands and left to look at the
abdominal, chest Xray and blood test results from earlier that day. Twenty minutes later, I returned and said I suspected he might have a puncture in a part of his bowel. ‘Is that serious, doctor?’ He sat up as he spoke.
‘I don’t know at this stage,’ I said as I held his hand gently. ‘I will arrange for you to have an intravenous drip because I don’t want you to have anything more to eat or drink, to rest your bowel. Also, you are a bit dry and you need fluids to make up the amount you are missing.’
I could sense relief that, after a long day, at last something was being done for him. I continued: ‘I will ask the nurses to give you strong painkiller injections tonight. I will get the resident doctor to do some more tests and I will get him to prescribe some further medicines for you. I will arrange for you to have a CT scan first thing tomorrow.’
I explained what this was and how it would give us more information to decide what to do next. I informed him that some bowel perforations were more effectively managed by doing a major abdominal operation, but some could be treated in the Xray department by the radiologist inserting a tube into the abdominal cavity with a local anaesthetic under Xray guidance. We would know what treatment
was appropriate when the CT was done. For now, he agreed with me that his overall general condition was satisfactory. I informed him that the preliminary tests showed nothing alarming and it was safe to wait until the morning.
I wrote the word ‘Urgent’ at the top of the CT scan request form and handed it to the nurse in charge, explaining I wanted the test done first thing in the morning.
Same day: home, about 11pm I phoned the hospital several times to inquire about anaesthetists, in case I needed to operate on Mr Hughes the next day. The hospital had no rota of anaesthetists; something that would be alluded to later in the course of this case.
NHS hospitals had anaesthetists on stand by 24 hours a day, but only some private hospitals did. Anaesthetists were difficult to find for an emergency and major abdominal operation, a specialised procedure.
I also spoke to the resident hospital doctor, who told me the tests I requested were normal. I instructed him to give the patient antibiotics. It transpired later that he did not do the tests, even though I had documented the request in the patient’s notes and confirmed this with verbal instructions. I was falsely assured the tests were normal when, in fact, they
had not been carried out. The antibiotics were not prescribed either; that the antibiotics failed to reach the patient would, as it turned out, be blamed on me.
Next day, Friday 12 February 2010: Home, about 6.30am
The nurse looking after Mr Hughes through the night rang to give an update. At one point, his urine output had dropped, probably because he was still short of fluid.
She had informed the same resident doctor who was looking after him the previous day and he had asked for the intravenous fluid volume to be increased.
She did this, and the urine output in subsequent hours returned to acceptable levels. Overall, she assured me, the patient’s condition had otherwise remained stable.
It would later be noted that the same resident doctor had worked for seven days, looking after more than a hundred patients, with only short breaks for sleep and refreshment. Such practices, it appears, were common in private hospitals.
Friday 12 February 2010: The Clementine Churchill Hospital, about 9.30am
I had other patients and three prebooked sessions: one endoscopy list in the morning, another in the early afternoon and a clinic in the evening. I briefly visited Mr
Hughes and confirmed his condition had indeed remained stable save for the problems described earlier by the nurse.
The prosecution would not believe that I made this visit, as I did not write it in the notes and the nurse who was looking after him that morning was busy with other patients in single rooms on the ward.
Mr Hughes had not yet had the CT scan I’d hoped would have been done by 9am, so I rang the imaging department to try to expedite it. It was occupied with elective scans and did not take kindly to interruptions, even for emergency tests.
Same day: The endoscopy unit, Clementine Churchill Hospital, 10am
I performed one endoscopy test for which I gave the sedative myself. I finished at 10.45am and saw patients on other wards in the hospital. Mr Hughes’s CT scan was still not done.
I drove home to collect some records and, on my way back, received a phone call saying Mr Hughes’s CT scan was done and showed a perforation of his large bowel. From the description given, it was clear the only way to deal with this was to perform a major operation to remove the perforated section of his bowel.
I was falsely assured the tests were normal when, in fact, they had not been carried out
Same day: Car park, Clementine Churchill Hospital, 1.47pm I rang the theatre to inquire when there would be a free slot to perform an emergency operation. The definition of emergency is often confused and the jury grappled with this issue during my trial.
Mr Hughes’s condition did not require an immediate operation. However, if a free theatre was available and I had an anaesthetist, I would have cancelled other engagements and operated.
The time of the phone call was on my mobile phone records, which were to form an important part of the documents used by the prosecution.
I was told the next available slot without invoking a breakthrough procedure would be about 7pm. I did not invoke a breakthrough procedure, as I had no anaesthetist.
By chance, that afternoon at 2pm, I was performing another endoscopy examination on a patient who wanted to be fully anaesthetised.
The anaesthetist I booked was not going to be available to help me operate on Mr Hughes due to other engagements later that day and, of course, no theatre was yet available.
She kindly helped me find an anaesthetist due at 6pm for what was described as a short gynaecological procedure expected to last about an hour.
This meant that by about 7pm that day, I would have a free theatre and an anaesthetist. It took a considerable amount of time and numerous phone calls by my anaesthetist and me to find someone willing to assist.
I was often asked during subsequent investigations why I had not transferred Mr Hughes to the NHS hospital, where it was assumed the operation would be done faster.
To consider such a referral, this meant finding a hospital with a surgeon free to operate, an appropriate intensive care unit and a free bed to follow. Just putting a patient in an ambulance and sending them to the nearest hospital would be irresponsible and dangerous.
It is not unknown for patients to be operated on 24 or more hours
I was often asked during subsequent investigations why I had not transferred Mr Hughes to the NHS hospital
after arrival in a new location. We already had an ITU bed for Mr Hughes, so it was a matter of waiting hopefully until a theatre was empty.
On my way from the car park to the hospital, I met the radiologist who performed and reported the scans and he confirmed the patient indeed had a perforation of his large bowel; he had sent a detailed report to the ward. I went to see Mr Hughes to update him.
Same day: Blenheim Suite, Clementine Churchill Hospital, 4pm
I had a careful look at his CT scan report before I saw him in his room. He was still in pain but had been receiving intravenous injections of morphine, with reasonable effect. He said he was unwell but, overall, his condition remained stable.
I explained what the CT scan had revealed and he listened attentively. I told him about the condition, explained the potential for a bowel rupture and its possible effects, and said I believed his knee operation six days earlier had nothing to do with the perforation.
I said an operation was the only option we had and related the course of planned action. I drew another diagram of the tummy and the bowel, and informed him about a temporary colostomy.
I explained the operation’s benefits and potential complications, but Mr Hughes made it clear he did not need too much detail and he was willing to sign his consent form.
Same day: Consulting rooms, Clementine Churchill Hospital, 5-7pm and after
The anaesthetist confirmed in a phone call when I discussed the proposed operation that he would be in the hospital at 6pm and would call for the patient to be taken to theatre as soon as the other operation was over.
I saw four or five patients. In between them, I phoned to inquire about Mr Hughes and I was reassured his condition remained unchanged.
Just after 7 pm, I was informed of a problem. The gynaecologist needed the help of another consultant, which meant a delay, but
I said an operation was the only option we had and related the course of planned action
the anaesthetist was unable to come and talk to me about it.
I went back to the consulting rooms and returned 45 minutes later. Now I insisted on talking to the anaesthetist.
He explained the matter was out of his hands but he would send for Mr Hughes as soon as the operation was over.
I had no choice. I tried to phone other anaesthetists but, as expected on a Friday evening, no one was available.
Same day: Theatre, Clementine Churchill Hospital, 10pm to 4am the following day
Mr Hughes arrived nearly three hours after schedule.
I was about to start the operation when the anaesthetist asked me to stop. The patient’s condition had suddenly deteriorated; his blood pressure had dropped and his pulse rate had risen, both significantly.
The senior anaesthetist arrived quickly, helped improve the patient’s condition and gave the goahead to start the operation.
1am
This was already a difficult operation, but I encountered more bleeding than expected. I noted one cause: Mr Hughes had cirrhosis of his liver.
My part of the operation took three hours and the patient was in theatre for nearly six.
Saturday 13 February 2010: ITU, Clementine Churchill Hospital, 2pm
In the ITU, he was kept unconscious and a machine breathed for him. Medications were given to support his heart and kidneys, which were failing.
It was still early to predict his chances of recovery, but they were not good. I left him in the hands of the ITU staff.
☛ Adapted from Did He Save Lives?
A Surgeon’s Story, £9.99, Sweetcroft Publishing, ISBN 9781912892327 from Amazon. His story continues here next issue
Sunday 14 February 2010: Ealing Hospital, about 4pm My mobile phone rang at about 4pm and I was told the bad news. ‘Mr Hughes died at 15.38. I have spoken to the relatives and I will issue a death certificate.’
Thus began a series of investigations that were to last nearly eight years.
INVESTING IN PROPERTY
Where do you find the cash?
Money, money, money –
Dr
Lafina
Diamandis shows how doctors
can fund their property investment deals
NOT HAVING enough money to invest in property is a common obstacle for people starting out.
Most developers who have used up their own funds find money from elsewhere, which enables them to continue doing business and building new housing developments.
These sources of money could fund the deposit or the rest of the purchase, the refurbishment, legal fees or any other property cost:
Personal savings
You may be able to invest these in a property with or without mortgage finance. This may be through buying or controlling a property through lease options or rent to rent.
Equity release
If you’re already a homeowner and your property value has risen, you may be able to release equity through a mortgage or remortgaging, rather than obtaining it by selling your property.
Using your pension to invest in property
It’s also possible to invest in commercial property using a selfinvested personal pension (SIPP).
But take financial advice, as there are specific criteria and you should certainly have educated yourself in property investment before taking any risks with your pension funds.
Many people have realised that the returns they can make from property are far greater than the returns they can make from their pension.
Inheritance
If you’re due an inheritance at a certain time, you can inquire whether your inheritance could be released to you early. But consider any inheritance tax due on the funds inherited, if applicable.
Family and friends
When entrepreneurs look for seed funding to get their project or busi-
ness to the next level, commonly the first source of funding they turn to is family and friends.
Although some people might lend out of the goodness of their hearts and because they trust and believe in you, why not make it worthwhile for them and offer them a good rate of interest or a share of the profits in return for the loan?
Note that the interest earned on loans is subject to income tax at the lender’s personal income tax rate.
This source of funding isn’t without its difficulties. Borrowing money from family and friends can cause tension, stress and, worse still, ruin relationships –particularly if things go wrong – so consider this funding source carefully and make sure your deal is legally watertight.
Mortgage finance for doctors
Most investors use mortgage finance to finance their investments, as it is the best way to leverage their cash. Due to current low interest rates, it’s also a cheap way of financing deals without using up all your own cash.
For example, if you use £100,000 cash to buy one house worth £100,000, your cash flow and capital appreciation are limited. If you use the same £100,000 to buy four £100,000 houses with a £25,000 mortgage on each, you can benefit from a greater cash flow and capital appreciation over a period of time. For first-time buyers, the loan amount will primarily be based on your income and expenditure, so it can be important to look at a provider or speak with a broker who understands our profession and how you’re paid.
Some lenders will let doctors borrow more than normal.
Options are reduced for firsttime buyers on a buy-to-let (BTL) basis, as a lot of lenders left this market after the 2008 recession, but more and more providers are moving back into this sector.
A lender’s approach to locum doctors varies depending on how you are set up. If you operate as a sole trader or via a limited company, they will usually want to see at least a year’s accounts or personal tax returns. For a sole trader, they would look at your net profit and, for a limited company, typically it is your salary and dividends.
Keep copies of any payslips and P60s to show a track record of regular work. The key is having clear proof of your income and satisfying the underwriter that it is sustainable.
For doctors buying a second property as an investment, the deposit requirement is larger for mortgages for BTL or houses in multiple occupation (HMO), with the minimum amount being 15%, subject to the rental calculation fitting.
Interest-only borrowing is more readily available for BTL – which is great for those looking to keep the monthly payments down to generate a cash flow from the rent.
A misconception about HMOs is that you need to have a track record of letting properties previously, as there are specialist lenders who can lend to first-time landlords looking to buy a HMO as their first property investment. But the deposit requirement in this instance increases to a minimum of 20%.
Bridging loans
These can be a useful but expensive way to fund properties. Bridging finance is sometimes used by investors to complete on properties they want to refurbish and later refinance using a conventional mortgage to release the cash invested in the deal plus some profits. It is also used in emergencies.
Access to bridging finance is faster than applying for a mortgage and the endless paperwork that can entail. The main drawback with bridging finance is the high cost: typically 1% per month plus considerable entry/exit fees. But the price is falling thanks to increased competition.
Joint venture finance
Another investor who puts up the funds in return for your knowledge, time or other assets you bring to the deal. A joint venture (JV) involves sharing the risks as well as the rewards and should only be carried out with a high net worth or sophisticated investor in accordance with the Financial Conduct Authority’s (FCA) guidance.
I am not FCA-approved nor a financial adviser, so please ensure that you get financial advice from a qualified person before proceeding with a JV.
Whether you are the person running the project or investing the funds, you should never feel pressured into investing in a deal or discussing investment opportunities without completing the basic compliance. If someone is not willing to do things properly from the very beginning, imagine what might happen later down the line. Finding the right business partner can take time and the process of getting into a financial relationship with someone should not be rushed.
Peer-to-peer loans
Here, investors lend to people or businesses who repay the cash plus interest accrued over the term of the loan. This is desirable for investors who want to earn a good return on cash that may otherwise be sitting in the bank.
There are now peer-to-peer lending platforms dedicated to arranging loans between investors and property developers. One, Blend Network, offers opportunities for lenders to invest anything from £1,000 upwards and earn up to 15% return a year secured against property.
Crowdfunding
Crowdfunding has burst onto the property scene in recent years with a variety of platforms available through which anyone can invest in property for a good return or raise funds for their projects. Like peer-to-peer lending, the great thing about these platforms is that they make it possible for anyone to invest as little as £50 in a deal and, provided that the project is successful, reap the rewards of investing in property ‘hands-free’. It is possible to crowdfund the equity, where investors are share-
The project was so popular that 28 speedy investors overfunded it in just seven minutes, raising almost £93,000
PROJECT COSTS: STATION ROAD, SEVENOAKS
Purchase price
Purchase costs (includes conveyancing, SDLT and professional fees)
Development cost (includes professional fees and interest on debt)
Selling cost
Gross development value of six flats
£437,500
£56,550
£373,054
£16,600
£216,296
FUNDING REQUIRED FOR THE PROJECT Total equity investment £240,000 Total debt required £650,000
holders in the business and can earn a percentage of the profits, or to crowdfund the debt part of the funding required, where investors generally earn a fixed return on the funds borrowed.
From the property developer’s perspective, they get their deal analysed by the platform – which often requires a project to meet minimum criteria – and they can access a wider group of potential investors and ensure they are FCA-compliant.
The platform takes care of the legal side with regards to having multiple investors on board and ensures that they are eligible to invest.
I have always wanted to find a way to help doctors to profit from property investments without requiring huge lump sums to get started. When I found out about crowdfunding, it seemed like the perfect way to help people like doctors get involved in projects normally only available to professional investors.
In May 2018, I decided to offer the medical community the opportunity to co-invest with myself and my business partner doctor-developer John Friis in a commercial to residential conversion project: the Station Road Project in Sevenoaks, Kent. The box above is a summary of our project finances.
We aimed to raise £80,000 and offered our investors a projected return of 20% on their funds. The project was so popular that 28 speedy investors over-funded it in just seven minutes, raising almost £93,000.
We are converting a 2,700ft 2 commercial property, currently used as an office block, into six residential apartments which we will sell.
We are really delighted to be sharing our process, skills and experience with our investors and hope that by learning while they earn, they can also develop the knowledge and confidence to do their own projects in the future.
We funded our project through the Simple Crowdfunding platform and you can take a look at our Station Road crowdfunding project on the website below and, if interested, register your interest for our next project at www.simplecrowdfunding.co.uk/property/ detail/1098.
The pitfalls of crowdfunding? For me there are very few. An important consideration is that most platforms will charge quite a high fee on the debt or equity raised, so you need to include this extra fee in your deal costs and analysis.
If you are not able to raise the cash required, it can have a negative impact, as people may lose confidence in the developer or the project without good reason. If you end up not raising the cash required to complete the deal, it can create an assumption about the developer or the deal and potentially damage your reputation.
Crowdfunding also looks easier than it is and a crowdfunding campaign requires careful and timely planning.
Next issue: Property management and landlord essentials
Dr Lafina Diamandis is co-founder of Eurekadoc, a start-up helping doctors to realise their full potential through diverse medical education and careers curation and is passionate about helping doctors to become financially independent through property even with limited time, funds or experience
CREATING A GREAT CONSUMER EXPERIENCE: DESIGNING FOR THE SENSES
Mood is altered by sound,
Nick Butcher and Dr Nick Hayward continue their series by discussing the power of our senses and how we can use these to create a positive visitor experience in private clinics
LET’S START with our olfactory sense, as this is said to be one of the most powerful in affecting our feelings of well-being.
Our sense of smell is strongly linked to our memory centre –thus smells can affect our emotions and even recover lost memories. Research at Toronto University has shown that memories triggered by smells tend to be clearer, more intense and more emotional.1
Pleasant smells have long been associated with better performance, concentration and relaxation. Essential oils have been in use for thousands of years to aid a variety of health matters. Cinnamon, lavender and sandalwood for stress relief. Jasmine, patchouli and rose for easing anger.
A report from the University of Maryland states ‘there is now scientific evidence to suggest that aromatherapy with lavender may slow the activity of the nervous system, improve sleep quality and lift the mood of people with sleep disorders’. 2
Research has even shown that athletes who inhaled peppermint fragrance ran faster trial times than when running without using
peppermint first.3 Children have also performed better in exams when exposed to the smell of fresh strawberries.
While humans have only five million receptor cells in our noses – a dog has 200 million – we are still able to detect between 10,000 and 10 billion different odours. People can distinguish between the bad smell of danger and good healthy scents, and so our minds react to these accordingly.
We encounter many environments that have not had any consideration given to the powerful influence of smells. Yet how many of us remember that ‘back to school’ feeling when we smell newly varnished hall floors? Or experience the stomach-churning whiff of overused and under-ventilated shopping centre toilets?
Negative association
Many patients and visitors often refer to the ‘smell of hospitals’ and this is largely a negative association. That chemical smell of clinical environments can quickly trigger healthcare fears, anxieties, memories of difficult life events and even memories of the death of a close friend or relative.
At the recently renovated public welfare facilities at Kent’s Bluewater shopping centre ( pictured below) , we designed the baby changing counters to incorporate air extraction from the used nappy bins. The public was so appreciative that ‘likes’ on the Bluewater
Facebook page jumped 100-fold as mums expressed their gratitude at solving the pong problem.
Interestingly, pleasant aromas also affect how we spend our money. Well documented research has shown that shoppers found identical shoes more attractive when in a room with a nice smell; they also valued them at higher prices.
A Las Vegas casino found that slot machines which had a nice smell sprayed around them generated 50% more gambled money. This illustrates that patients and staff in clinical settings may be more likely to engage with their surroundings and take up services if we can optimise the air around them.
Fortunately, injecting pleasant and hopefully subliminal aromas into spaces is now very easy and cost-effective. It is possible to develop your own branded aroma which can become an important tool in helping to create the intended positive and consistent healthcare experiences.
Effect of sound
Sound is an equally important factor in creating a great visitor and patient experience.
We all know of the harmful effects of unwanted and prolonged loud noise. But what about the less obvious sounds that subtly eat into our subconscious?
A squeaking door hinge, a rattling fan or a low-level drone of medical equipment can all impact our physiology and emotions, particularly if the sound is continuous or repetitive.
Sounds above 60 decibels have been proven to have cardiovascular effects such as higher pulse rates, higher blood pressure, increased cholesterol levels, and can even cause irregular heartbeats.4
A study carried out by Barregard at the University of Gothenburg, Sweden, in 2009 found that men
who lived next to a major highway and train line for more than ten years were three times more likely to have high blood pressure than those that were not exposed to such noise pollution.
Of course, the opposite to noise pollution also applies. Most of us find natural sounds, such as waves breaking gently on a shoreline, relaxing. Interestingly, waves break at around 12 cycles a minute, which is the same respiratory frequency for most of us during our sleep.
Birdsong helps us feel safe and secure, which is thought to be a throwback to our ancestry as a lack of birdsong meant danger in ancient rural settings. These sounds can be successfully added to environments to help patients, staff and visitors feel relaxed, calm and well.
Ill-considered ‘sound casting’ Today, music seems to fill our lives from every direction. From cars, shops and a multitude of devices delivering whatever, wherever and whenever we want it.
But simply pumping out sound in the hope that everyone will approve just doesn’t quite work. We all have different needs and preferences within shared environments.
Our shopping centre clients’ surveys have shown that, generally, 60% of people disagree with the type of music being played. This, coupled with often poorquality speakers, means that illconsidered ‘sound casting’ can be far more negative than positive within user experiences.
Well-constructed, generative soundscapes can be created using new technologies where an everchanging music score specific to the time of day can deliver ‘on brand’. Such relevant visitor/ patient audio touchpoints really do add a positive sensory experience. An example of how relevance affects us subconsciously is where
sound, smell and touch
a well-known supermarket did an experiment where they played either German or French music in the wine aisle on alternate days. The corresponding country wine sales increased dramatically on the days when the associated music was played.5
Fundamental influence
A third sensory experience is touch. By this, we mean the sensations and feelings generated by interacting with the different materials, finishes and textures
that surround us. Touch is the first sense that we acquire as babies, illustrating its fundamental influence on our sense of wellness.
Let’s consider flooring as an example. The differences in the walking experience between a carpet and a hard floor are substantial. But comparisons between a wood floor feel and a vinyl surface feel can be less clearly made. Similarly, a hard but beautiful marble floor would generate a different temperature and feel to those of a basic concrete floor.
Both are hard, but the perceived quality has a large part to play in our emotional response as well. When designing with such materials, our choices can be driven by cost, by suitability, by colour and tone and by style. All influence our choice, but it is also important to consider how they physically feel and how this makes us feel too.
A 2010 study by Ackerman revealed that the physical qualities of objects people touched – their hardness or softness, heaviness or lightness, roughness or smoothness – tilted people’s judgements toward those same abstract qualities.
Sitting in a hard wooden chair, for example, seemed to make people more rigid in a negotiation, or that holding a warm pack helped mitigate feelings of loneliness. What Ackerman also explains is that if these notions become conscious, then the mind will overrule the feelings.
In summary, multisensory exposures can connect us with our deep personal experiences, often subconsciously, and help us form an understanding and opinion of the space we are in. Using scents, sounds and materials sensitively
to deliver feelings of wellness, quality, cleanliness, professionalism and openness is a wise approach when designing healthcare settings.
3. Instant effects of peppermint essential oil on the physiological parameters and exercise performance by Abbas Meamarbashi in Avicenna Journal of Phytomedicine
Nick Butcher is creative director of branding and design agency Beyond London and Dr Nick Hayward an academic clinician in Southampton
Feelings can be influenced by different materials, finishes and textures that surround us. Sound can also be used to create a great visitor experience
DRIVE TO IMPROVE SAFETY
Sharing outcomes
Plaudits
for audit
– a pilot project is being set up to examine how the independent sector can participate in the National Clinical Audits Programme. David Hare (below) reports
KNOW YOUR COPS FROM YOUR POPS AND NODS
➫ National Clinical Audit and Patient Outcomes Programme (NCAPOP)
➫ National Audit of Breast Cancer in Older Patients (NABCOP)
➫ Effectiveness Key Line of Enquiry (KLOE)
➫ Independent Healthcare Providers Network (IHPN)
HAVING COMPARABLE,
reliable information about the performance of clinical services is a key tool in supporting quality assurance and quality improvement in healthcare, with national clinical audits playing a vital role in the patient safety agenda.
Historically, independent healthcare providers have been unable to fully contribute to most clinical audits.
But significant work is being done in this area to break down the barriers and ensure the independent sector can help play a role in driving up standards across the health system.
Independent providers are able to contribute to a small number of audits, such as the National Joint Registry. But a number of key barriers have prevented them from submitting data and information to other programmes within the scope of the National Clinical Audit and Patient Outcomes Programme (NCAPOP). This is commissioned and managed by Healthcare Quality Improvement Partnership (HQIP).
As part of the Independent Healthcare Providers Network’s (IHPN’s) programme of work to improve safety and transparency in the sector, we have been working closely with HQIP on involving independent providers in the NCAPOP.
Submitting to audits
These discussions culminated in two workshops last year where IHPN and its members committed to further transparency on performance and patient safety and to submitting to various audits and registries.
Following these workshops, subsequent work has taken place with HQIP, Public Health England and the relevant royal colleges.
We are pleased to have been able to announce that this year, a pilot is being launched to explore how
to overcome the barriers and obstacles to independent healthcare providers in England being included in future national clinical audits.
This pilot project will focus on procedures relating to breast cancer in older people and cataract surgery, with the pilot anticipated to be completed in summer 2020.
These audits – The National Ophthalmology Audit (NOD) and the National Audit of Breast Cancer in Older Patients (NABCOP) – were selected because of their relevance for the sector and the extent to which it is possible to explore the broad range of issues likely to arise with other audits.
The NOD, for example, is a highvolume audit, whereas NABCOP presents challenges exploring connected data across multiple interactions over time, with requirements for extracting information from the national cancer registries.
Key objectives
The key objectives of the pilot are therefore to explore and define the practical, technical, information governance and financial challenges of supporting the participation of independent sector providers in NCAPOP.
By piloting participation in two national clinical audits, IHPN will work with HQIP to identify and present solutions for allowing the wider involvement of the independent sector in NCAPOP.
We strongly believe that with independent acute providers treating over a million patients every year, involving the sector in the
national programme will have huge benefits in enabling a more comprehensive and reliable picture of the quality of care in the English health system.
And it will also send an important signal to regulatory and policy stakeholders that the sector is fully committed to the quality and transparency agenda.
This is particularly the case with the Care Quality Commission which draws on NCAPOP audit data to inform its regulatory inspections, notably the Effectiveness Key Line of Enquiry (KLOE).
Moreover, information collected through the audit can be used as part of the appraisal and revalidation process for doctors, particularly for audits providing consultantlevel data. The GMC has highlighted expectations of participation in relevant national clinical audits in its guidance materials.
Of course, no one can deny that significant work and resources will be needed to participate in the pilot study, given that clinical audits will require the sector to collect and submit data for hundreds of thousands of patients.
But in helping to play our role in improving healthcare’s quality and transparency overall and allowing patients to be better informed on decisions about their care, our involvement in clinical audits will bring huge benefits to the patients that the sector serves.
David Hare is chief executive of the Independent Healthcare Providers Network
Poor practice data will cost you a lot
Are your financial records really up to date? Simon Brignall warns that many consultants need to check to ensure the paperwork meets your current needs
CONSULTANTS MUST wear many hats these days to run a successful modern private practice.
Managing the various aspects can prove to be ever more challenging and I often find they have difficulty in ensuring all their financial and pricing records are current.
At the heart of medical finance
As director of business development at Medical Billing and Collection, I have seen many practices experience a wide variety of difficulties in these areas.
And that can lead to:
Issues around cash flow;
Losses of income;
Problems with the taxman.
Let’s take a look at some of the most common issues:
Practice information
Nowadays, consultants need to provide information about their practice across a wide range of sources. The need for this data to be readily available to patients across a variety of platforms means it is very easy to lose track of where this data is stored.
Most consultants have a Bupa profile as well as having a biography page on the websites of each of the hospital and clinic locations where they practice.
Some specialists choose to use
third-party portals to find patients as well as promoting their services through their own website. There is also the requirement to supply information about the practice, including fees, to the Private Healthcare Information Network (PHIN).
It is important to check that all this information is consistent and up to date across these various sources.
You should include:
All the locations where you can be seen;
Your contact information;
Pricing policy;
Payment options.
This review process should also be an ideal opportunity to revisit your pricing structure.
Your pricing structure needs to be clear to your patients and to the person whose task it is within the practice to raise the billing. In our experience, lack of clarity around your pricing policy can lead to patient dissatisfaction.
It can also mean that invoices are raised incorrectly, resulting in problems with insurance companies and even losses of income. Transparency around pricing ensures your patients are aware of the costs they will incur from the start and so disputes are less likely.
Patient registration forms
It is good practice to confirm with your patients your pricing policy before treatment starts.
You should also make them aware of their responsibility for any liability to avoid any ambiguity should their insurance policy not cover all the treatment costs.
For pricing in a commercial environment, the terms and conditions describe how the company will conduct its business with its clients and typically form part of a commercial contract.
In private healthcare, and particularly for consultants, the patient registration form is typically where this area is covered. It is a good idea that your registration form includes wording stating that the patient is liable for any costs incurred as a result of not being covered by their insurer.
In our experience, when a patient has private health insurance, many of them immediately think that all the costs of the treatment are covered. But, of course, in many cases there can be an addi-
A practice should be able to produce accurate reports that show the total invoices raised, payments received and their aged debt for a given tax period
tional cost element that the patient will be required to pay.
Most patients have private health insurance through their employers and, as such, most of them are unaware of the small print of their own policies, which may leave them with an outstanding balance.
This can be for many reasons and the main ones are:
They could have an excess or shortfall under the terms of the insurance policy;
They could have exceeded the benefit limit of the policy;
They could have a policy which is called co-share, where they are required to pay a percentage of each invoice.
The patient registration form should also inform the patient if the practice has any other commercial terms, such as charging for DNA (Did Not Attend) consultations or where they have not been cancelled within set time limits.
Raising an invoice
Patient registration forms also allow the practice to obtain all the relevant patient information to ensure an invoice can be raised promptly.
This will include a patient’s date of birth, contact details and insurance information, when applicable. These days, it should always cover mobile number and email address, so you have the best chance of contacting the patient if they have a shortfall to pay.
All successful practices realise how important it is to obtain all this information up front to negate the need to chase patients after treatment, which can be both problematic and time-consuming. Missing data can cause invoices to be rejected by insurers, delays in invoicing and lead to difficulties in chasing patients for payment. This
can all result in a practice’s aged debt mounting up and often means that a consultant ends up being owed tens of thousands of pounds.
At Medical Billing and Collection, our billing procedures immediately highlight when this important data is missing. We then seek to resolve the problem either through internal investigation, when possible, or by notifying the practice immediately what information we require.
As with most matters related to billing, the quicker you identify the problem the more likely you are to resolve it.
Paying tax
Nobody enjoys paying the taxman, but quite often this can be made even more onerous because of difficulties in providing accurate financial information to your accountant.
HM Revenue and Customs (HMRC) is in the process of transitioning towards quarterly reporting as part of its Make Tax Digital initiative which is currently scheduled to become mandatory in April 2020.
This will require the submission of income data on a quarterly basis rather than the current system allowing this to be done at the accounting year-end.
HMRC says this will enable more accurate projection of tax due. But considering the number of inquiries we have from consultants when their tax is due, I think it is fair to assume that many will find this challenging without having the appropriate data to hand at the touch of a button.
It is well known that HMRC targets private consultants, as there is a perception that their recordkeeping is not always as thorough as they would like. Tax investigations are far from enjoyable, as anyone who has had to go through this process will attest.
A request by your accountant to improve the quality of the financial information you provide them can be one of the most common reasons a doctor reaches out to us.
A practice should be able to produce accurate reports that show the total invoices raised, payments received and their aged debt for a given tax period. At Medical Billing and Collection, we can supply all these reports directly to our client or their accountant, which gives our consultants peace of mind.
I would suggest there is no time like the present to review all the financial records you keep for your practice.
Check to see that they are up to date and meet your current needs; highlight any areas of concern and then put steps in place to address these.
If all of this is just adding to your workload or you feel you would like to speak to an expert, then one simple solution might be to seek assistance from a professional medical billing company.
See ‘Don’t be an HMRC target’, page 40
Simon Brignall (pictured right) is director of business development at Medical Billing and Collection
You’re never too old to think long term
How far ahead should you be looking?
Dr Benjamin Holdsworth (below) looks at a prudent investment horizon, whatever your age
MANY INVESTORS nearing retire-
ment – or already in it – question taking a ‘long-term’ approach and whether they should still be investing in the stock market.
When it comes to ‘systematic’ investing – capturing specific market risks in a disciplined and rulesbased manner – a further question might also be: ‘Should I still own value and small cap stocks, as their excess returns, relative to the market, can take some time to come through?’
The investing lifecycle
If we step back and think about the life cycle of investing, it starts with the accumulation phase where
investors build assets in an investment portfolio, sacrificing today’s consumption for tomorrow’s retirement income.
Horizons tend to be long, not least because you cannot take assets and income from most pension plans until you are 55. Prior to the pension freedoms, delivered by the former Chancellor George Osborne in 2015, most people were obliged to use their pension pots to buy an annuity.
This, in effect, meant that an individual in the accumulation phase had to think about managing a shortening horizon as retirement approached – often by moving out of equities and into
bonds. Equities are shares in a company whereas bonds are certificates bought from the government or a company that guarantee to pay back the holder with interest. Equities therefore carry greater risk but also offer the opportunity for greater reward.
Investment horizon
For many investors today, while the accumulation of assets stops when employment income stops as they approach retirement at, say, 60, their investment horizon may well still be around 40 years, if they intend to take an income from the portfolio over their retirement.
Even at 80, when investors may begin to ask themselves the question ‘how long is long-term?’, they should still consider 20 years to be a sensible horizon.
After all, according to the Office for National Statistics, today, an 80-year-old woman has an average life expectancy of 90, a one-in-four chance of reaching 94 and a onein-ten chance of getting to 98.
Mr Osborne’s pension freedoms have also made pensions an extremely efficient means of legally avoiding inheritance tax, as they can be passed on tax-free to any family member – or anyone else, for that matter.
As such, for some investors, their true investment horizon may not simply be their own longevity but that of children and even grandchildren.
What does historical data tell us about how long ‘long’ is?
A pot of assets held in an investment portfolio in retirement may serve a number of purposes:
Providing a secure and relatively stable level of retirement income;
Supplementing income from another source; for example, defined benefit and state pensions;
Supplying funds to be used, perhaps, to help younger family members or to support philanthropic causes.
It is impossible to model all investment scenarios, but it is possible to look at the return outcomes of different investment horizons and different allocations between equities, bonds and cash. If we look at data going back to 1926, we can see that:
☛ As an investor in equities, you have around a one-infour to a one-in-three chance that you will suffer a loss in any one year. Yet, at a ten-year horizon, a 60% equity/40% bond ‘balanced’ portfolio has a better than onein-20 chance.
☛ For long-term investors, cash is an extremely dangerous asset class, particularly when viewed after the effects on inflation, as it should be.
It is worth noting that, over the ten years since the credit crisis, those placing their assets in UK cash have lost over 20% of their purchasing power.
☛ In periods of market downturn, portfolios ‘tilted’ towards value and smaller company stocks tend to fall less sharply than portfolios that are not tilted when considered over the longer term.
Note that a portfolio ‘tilt’ is simply an investment strategy that overweighs a particular investment style; for example, tilting to small cap stocks.
This helps answer the question whether an investor who is 80 should still include value and smaller company stocks in any equity allocation they hold. They probably should.
☛ Investors with horizons longer than ten years – even those simply seeking to maintain purchasing power – should own a meaningful level of equities in their portfolio.
☛ Cash and bonds alone are unsuitable for most longerterm investors.
What constitutes the right balance between equities and bonds will depend on an investor’s individual circumstances, not least their experience of investing, their human capital outstanding, their tolerance for losses in the pursuit of favourable gains, their financial capacity for suffering losses and their need to generate returns in the first place.
Finding this balance can be challenging, but academic research suggests that equities should play a material role in most longer-term investor portfolios and that ‘long term’ in investment should be defined as ten to 15 years minimum.
Dr Benjamin Holdsworth is director of Cavendish Medical, specialist financial planners helping consultants in private practice and the NHS
The content of this article is for information only and must not be considered as financial advice. Cavendish Medical always recommends that you seek independent financial advice before making any financial decisions. Levels, bases of and reliefs from taxation may be subject to change and their value depends on the individual circumstances of the investor. The value of investments and the income from them can fluctuate and investors may get back less than the amount invested.
PROBLEMS WITH THE TAX MAN?
HMRC tax investigations and disputes create difficult and stressful times.
As an award winning firm of tax experts, our highly experienced partners specialise in resolving problems relating to tax investigations and disputes with HMRC.
To find out, in confidence, how we can help call 0800 734 3333.
‘Here to help. Not to judge.’
BUSINESS DILEMMAS
A claim needs testing
A surgeon fears a solicitor’s letter means that he will have to go to court and give evidence at a trial. Dr Shabbir Choudhury (below) responds
PRIVILEGES NOW AVAILABLE
Dilemma 1 Does this mean I will go to court?
QI am a surgeon in independent practice and I have just received a letter of claim from a firm of solicitors acting for a patient in his 40s whom I saw almost three years ago.
The patient unfortunately went on to be diagnosed with bowel cancer and I have not been involved in the care since he was referred to the oncology team.
I am very concerned that this means I will have to go to court and give evidence at trial. Is this the case?
AIt’s very unlikely you will have to go to court, as very few cases ever go to trial.
The majority of claims the Medical Defence Union (MDU) sees do not result in compensation being paid because the patient had not been negligently harmed.
This was the case for 83% of medical claims we closed in 2017. Out of the remaining cases, the majority are resolved by us without going to court. If cases are one of the few that reaches a trial, defence organisations will be able to advise and support you.
It is important you tell your defence representatives straight away about the solicitor’s letter. There are many steps involved in investigating a claim, which I summarise below.
A letter of claim lists allegations made against you and other possible defendants. It is part of the preaction protocol for the resolution of clinical disputes.
This process allows solicitors to bring a claim for clinical negli -
gence without necessarily going through the courts. The courts do not have the ability to deal with every medical claim and therefore they expect most to be either successfully defended or settled without the need for a trial.
To succeed in a clinical negligence claim, the patient’s solicitors need to prove that you breached your duty of care to the patient and that this resulted in harm – known as causation.
Instructed experts will comment on what a reasonable doctor in your position should have done –known as the Bolam test – and on causation.
For a competent adult patient, the claim can be brought up to three years from the date of the patient’s knowledge that something went wrong.
We usually have only four months to form a response after receiving a letter of claim. This is only a short window of time, especially as we need to thoroughly investigate the allegations and may need to instruct independent medical experts as well.
After investigating, you will be involved in the decision about whether to defend the case or if, in the view of expert evidence, it would be advisable to settle the claim.
If the patient’s solicitors refuse to accept the defence of the case, court proceedings are usually issued.
However, bear in mind that even after court proceedings have been issued, most cases in our experience are resolved well before the claim needs to go to court. And only when both sides firmly believe they are in the right will a case go to trial.
Dr Shabbir Choudhury is a senior medical claims handler at the MDU
A disquieting missive
For doctors, it is one of the most worrying questions they ever ask: ‘Am I being sued?’ Dr Shabbir Choudhury answers a private consultant’s fears after opening a ‘letter of notification’
Dilemma 2
Does this mean I am being sued?
QI am an ENT surgeon in independent practice and I’ve received a letter of notification from a solicitor about a young patient who recently consulted me about a pinnaplasty.
The solicitors already have the patient’s records, which were sent by the hospital, and the letter suggests the patient’s father is unhappy about the operation.
Does this mean I am being sued? And what action do I need to take?
AA letter of notification is an intermediate stage between the request for a patient’s records and a formal letter of claim.
It informs you that the claimant’s solicitors’ initial investigations suggest the patient may have a claim against you. They may have received provisional expert evidence or simply conducted their own review of the records to arrive at this conclusion.
A letter of notification is a recent development in the clinical negligence world.
It differs from a letter of claim, which lists more formal allega -
tions about a breach of duty of care and how this has harmed the patient. Although the letter of notification does not have to list allegations, it should notify you that a claim may be forthcoming.
This might seem alarming, but it provides you and your defence body with an opportunity to investigate the care provided to the patient.
While this is not a formal claim for compensation, it is important to take this seriously and inform your defence body as soon as possible.
Doing so will allow it to contact the claimant’s solicitors on your behalf and initiate investigations.
Following this, you can discuss whether to provide a response to the letter of notification.
Although a formal response does not have to be provided, if it is clear that the claim should be defended, it may be advantageous to do so.
Alternatively, it may become apparent that an early settlement offer should be made, which can resolve the case promptly and minimise the distress caused by the legal process.
Although litigation is common and there are few doctors who will not encounter a claim or a potential claim at some point in their career, bear in mind that in the vast majority of cases, claims are resolved without the medical practitioner having to attend a court trial.
Upright
• Completely open scanner that is well tolerated by claustrophobic patients
• Weight-bearing scans for spine and joints enable a more precise diagnosis
• Patients who are large or cannot lie down can be accommodated
more information go online at: www.trulyopenmri.com or call: 020 7370 6003 0161 434 8039
A PRIVATE PRACTICE – Our series for doctors embarking on the independent journey
target Don’t be an HMRC
Reduce your risk of a probe by the taxman.
Ian Tongue (left) shows how
ONE OF the most stressful aspects of running your own business and having to submit tax returns annually is the dreaded HM Revenue and Customs (HMRC) tax inquiry.
In the career of an independent practitioner, there is a good chance that you will be subject to one, so understanding the key risk factors to reduce the danger of this is important, as these inquiries can be expensive even with a clean bill of financial health.
What is an enquiry?
The income tax system for individuals and the corporation tax system for companies are based around self-assessment. This means that HMRC receives a series of figures only and no supporting paperwork is usually sent.
HMRC does not reveal the exact method of selection for inquiries but one of the first aspects is for their algorithms to look at
expenses to see if they look in proportion to other businesses.
Additionally, HMRC is receiving more and more information electronically and therefore already has information on its systems to compare your tax return entries to others. Omission of information already on its systems is usually an automatic inquiry, unless trivial.
The most common type of inquiry is known as an ‘aspect’ inquiry and this type is targeted at one or a small number of aspects of your tax return.
Substantial bill
In this type of inquiry, it is normal for the focus to just be on the area raised. A full inquiry is more involved and often requires the taxpayer/business to submit all the source accounting records. It inevitably results in a lot of questions and a substantial bill to deal with the inquiry.
CALCULATE YOUR NHS ANNUAL ALLOWANCE
It is important to note that it is very unlikely that the fees paid to deal with your annual tax affairs will cover a subsequent HMRC inquiry on the figures.
Therefore, most accountants will offer an insurance policy to shield you against the cost. In this situation, you should not face any costs to deal with the inquiry, but if tax, penalties and interest is due, the insurance is unlikely to cover this.
These polices will also not usually cover any tax avoidance schemes or aggressive tax plan -
ning, but separate policies may be available for those.
We are in a transition period of HMRC upgrading its systems to what it calls ‘Making Tax Digital’ or MTD. This new system will result in its receiving information quarterly and it believes this will increase tax revenues from more accurate disclosure of financial information.
For those with a suitably qualified accountant, this is unlikely and those more cynical of the change believe HMRC will eventu-
ally change the payment system under self-assessment to more frequent payments than the present one.
It has become more and more important to engage the services of a specialist medical accountant who can advise on your position and often mitigate or extinguish your exposure to annual allowance charges.
Being subjected to an HMRC inquiry can be very stressful, but the key thing is to avoid opening up yourself to risk by ensuring that you
COMMON AREAS FOR A TAX INQUIRY
While not exhaustive, the most common areas for inquiry for a consultant are:
Omission of savings income or capital gains
Omission of foreign income
Motor and travel claims
Conferences and meetings
Professional subscriptions
Employment status of secretary
High-income child benefit charge
Ad hoc PAYE income
Pension Annual allowance charges
OMISSION OF SAVINGS INCOME OR CAPITAL GAINS
It can be easy to forget to supply this information to your accountant or assume the amounts are immaterial, but this is one area that HMRC does receive information from the banks and other financial institutions and therefore it is important that you send everything to your accountant.
If you have an investment portfolio, it is important to supply your accountant with the relevant tax information, as the portfolio may incur income or capital gains without realising.
OMISSION OF FOREIGN EARNINGS
With the increasing number of doctors working in the UK from overseas and HMRC having information shared by its foreign counterparts, this has become a relatively common area for inquiry.
There have been several amnesties and disclosure facilities for those who may have not realised that their foreign income needed to be revealed, but now these have largely finished, HMRC will, no doubt, crack down on those who have not disclosed their income.
If you have come to the UK from overseas, your obligation to disclose your foreign income will depend on your circumstances and the amounts involved, so it is important that you discuss matters with your accountant to ensure that you are disclosing all necessary items on your UK tax return.
MOTOR AND TRAVEL CLAIMS
This was the hot topic many years ago and with the principles established in the ‘Samadian’ tax case from 2013, mileage claims have significantly reduced as the scope or ‘business travel’ became defined. Therefore, if you have a higher than normal business use of your vehicle, you will be increasing your risk of an inquiry. Always maintain a periodic mileage log that is representative of your normal pattern to support any mileage claim.
CONFERENCES AND MEETINGS
This can be an area of challenge, as many specialist courses are held abroad and therefore become a significant cost within the accounts.
These expense claims are usually easy to defend if the trip was solely for business purposes, but care should be taken with the amount to claim if there is a duality of purpose; for example, a holiday is tagged on or you travel with family.
PROFESSIONAL SUBSCRIPTIONS
Depending on your specialty and type of work undertaken, your indemnity insurance and professional subscriptions may be your largest expense within your accounts.
As this is not common across other professions, this can lead to HMRC asking questions. It is important that you supply your accountant with the correct details of your expenses and the periods covered in order that an accurate amount can be claimed within your private practice.
EMPLOYMENT STATUS OF SECRETARY
It is important to note that it is not a choice for a secretary or person working for you to decide between being an employee or selfemployed. It is a fact determined by comparing the worker’s employment situation against HMRC’s check list.
supply your accountant with all the information they ask you for. Keeping good accounting records is very important and is a requirement, so make sure your systems are robust and ensure that you disclose all your financial circumstances to your accountant even if you think something may not be relevant.
Next issue: New year – time for a financial review of your private practice
A challenge of employment status would look at many factors and, on the balance of indicators, would suggest a status.
As a minimum, you would expect there to be a contract in place and, if self-employed, this should be a contract for services. Discuss your circumstances with your accountant to ensure that you are not at risk here.
HIGH-INCOME CHILD BENEFIT CHARGE
For those earning more than £50,000 a year where you or your spouse are still receiving child benefit, you may have to repay the child benefit in full or in part via your tax return. It can be easy to overlook an amount being paid into perhaps a separate account or direct to your spouse. HMRC’s systems can link the payment of child benefit and the income of the household and therefore it is important that you inform your accountant if you are still receiving child benefit.
AD HOC PAYE INCOME
It is relatively common for consultants to carry out short-term or ad doc work, such as university teaching, and often these payments are made under PAYE using a separate employment reference to your main employment.
As HMRC will receive an end-of-year report from all employers disclosing your earnings, it is important that you supply the end-of-year P60 for all sources or a P45 if you have ceased the employment during the year.
PENSION ANNUAL ALLOWANCE CHARGES
Much has been written about the unfair and onerous pension annual allowance charge. HMRC is now starting to target doctors to check their annual allowance position.
This area is most probably the biggest risk of an unexpected tax charge for a doctor due to the complexity of the rules and lack of timely information being available from NHS Pensions to meet the tax deadlines.
Ian Tongue is a partner with Sandison Easson Accountants
PRIVATE PATIENT UNITS
Orthopaedic units show how to do it
Our monthly analysis of private patient revenue growth moves to the West Midlands’ 15 NHS acute trusts across the counties of Warwickshire, Worcestershire, Herefordshire, Shropshire, Staffordshire. Philip Housden (right) reports
ALL THE figures in this article are from recently published 2018-19 trust accounts. They show that total private patient revenues for the region grew slightly by 0.5% in 2018-19, up £107,000 to £20.45m (see Figure 1 on the right).
This now represents 0.34% of these trusts’ total revenues, a slight drop from 0.36% the year before and below the combined national average outside London of 0.5%.
These trusts vary significantly by turnover, private patient revenues, growth and range of facilities (see Figure 2 overleaf).
In the city of Birmingham, there has been substantial consolidation of providers. University Hospitals Birmingham’s private patient income for 2018-19 was £4.89m at 0.35% of turnover, up £600,000 (14%) from the previous year.
The main contribution came from The Mindelsohn Unit, a private radiotherapy service incorporating the regional cyber knife and 12-bed private patient ward.
But the trust’s ambitious partnership development with HCA Healthcare UK to build a £100m specialist hospital offering both NHS capacity and 66 private beds on the Queen Elizabeth Hospital Birmingham campus will change this significantly when it opens in 2022.
Across the city, Birmingham Women’s & Children’s Hospital presently offers private maternity and paediatric services. The private patient revenues of the trust
were £2.24m last year, down 10.3% and £258,000 on 2017-18.
The region has two specialist orthopaedic hospitals in the Royal Orthopaedic in Birmingham and Robert Jones and Agnes Hunt at Oswestry. Both have dedicated private beds and are enjoying growth.
Orthopaedic units
In the city, the Royal Orthopaedic Hospital increased revenues through the seven-bed Woodlands Suite by 114% and £921,000 to reach £1.7m. This now represents 2.16% of turnover, a significant jump from 1.07% in 2017-18.
Robert Jones and Agnes Hunt delivers services through RJAH
Private Healthcare and the 16-bed ward in the Ludlow Unit. The trust’s PPU achieved growth of 6.1% and £332,000 last year, which now represent a regional high of 5.56% of total trust income and places the trust second outside London by percentage of turnover. Another trust delivering growth was University Hospitals of Coventry and Warwickshire, which reported private patient revenues up 15.4% from £942,000 to £1.09m – now 0.19% of total revenues. The trust has no in-house PPU but is understood to work closely with the onsite 52-bed BMI Meriden Hospital.
By contrast, there were several
large West Midlands trusts where private patient incomes fell last year.
Social enterprise
South Warwickshire leads a foundation group of trusts including Wye Valley and George Eliot Hospitals. It delivers private healthcare services through a wholly-owned subsidiary company, SWFT Clinical Services, formed in 2011 and turned into a social enterprise in 2014. That year SWFT acquired The Stratford Clinic, formerly owned by Circle. In 2016, the trust commenced private fertility services ➱ p44
Figure 1
and opened 15 predominantly amenity beds in the Beauchamp Suite at Warwick Hospital.
In 2018-19, South Warwick’s revenues declined by 5.9% to £586,000 – 0.21% of turnover –while Wye Valley in Hereford also fell by 63% and £319,000 to only £188,000 and 0.11% of turnover. George Eliot Hospital’s revenues were again zero or close to it.
University Hospitals of North Midlands presently provides only a limited range of private patient outpatient and ambulatory services, but this includes a specialist service through its Muscular Sclerosis Centre.
Total revenues were £1.2m in 2018-19, down 10% and £135,000 on the previous year. The Royal Stoke campus has received funding for an additional three wards and 84 beds to help with significant demand pressures.
As the market is a relatively
strong one for private healthcare, this could also enable the trust to enter the inpatient private care market, particularly to support those most complex patients who cannot be supported in the local independent hospitals.
Declining trend
Shrewsbury and Telford’s revenues also fell last year, down 15.6% and £193,000 to £1.04m, which is 0.31% of turnover. The trust’s Apley Clinic in Shrewsbury is an private outpatients and diagnostic facility. These figures continue the trust’s long term declining trend from £2.3m and 0.83% in 2012-13, when the trust made use of a tenbed private patient ward.
Worcestershire Hospitals also reported a decline, with income down 22% from £497,000 to £389,000 in 2018-19. The trust does not have any dedicated private patient beds or services.
Royal Wolverhampton private patient revenues dropped last year too, a fall of 18.6% and £231k. The proportion of total trust income from private patient declined to 0.21% from 0.27%.
The trust provides a range of regional services which could be expected to lead to higher-complexity private activity shifting to the trust. It has over the past two years become a leading provider of GP services in the city, but has not yet led to a stimulus of demand by utilising this link to engage with GPs and their patients to ask them to use their medical insurance.
City-country split
Elsewhere in the ‘Black Country’, Walsall and Dudley trusts deliver presently very little revenues between them, reporting an aggregate of less than £50,000 a year. Meanwhile, Sandwell enjoyed an increase from £165,000 to
£254,000 (54%), though this still represents only 0.06% of turnover.
West Midlands trusts’ private patient performance presently splits between two groups. The strongest returns are in the city of Birmingham trusts and the two specialist orthopaedic trusts.
Of the rest, most of these are relatively ‘stuck’ below £2m revenues, with several known to be under capacity constraints. For these, the decline may well be due to bed and other capacity challenges.
But the absence of private patient capability in all these trusts most likely results in the costs for many insured patients falling back on the NHS for most complex treatments. Perhaps smaller ‘entry-level’ private patient units could be part of future capacity and winter planning.
Next month: Yorkshire
Philip Housden is a director of Housden Group
Having served healthcare professionals since its inception in 1993, Tax-Link, chartered tax advisers and accountants in Wimbledon, has built a wealth of knowledge and experience in dealing with taxation issues faced by doctors in private practice. Our focus is on tax planning and compliance.
l Tax structuring to suit personal circumstances (LLP, limited companies)
l Solvent liquidations
l Consultant groups and consortia
l Assessment of pension contributions in light of tapering annual allowances
l Ad hoc assistance with HMRC investigations and reviews.
DOCTOR ON THE ROAD: SEAT TARRACO
Stylish evolution of the people-carrier
The handling has a sharpness to it that is almost sporty and fits SEAT’s advertised youthful brand image
Z
Keen-driving ‘family’ doctors will find this sevenseater – with foldaway seats –equal to the class leaders, says Dr Tony Rimmer
IT WOULD be naïve for any independent practitioner to believe that local competition can be ignored when striving for a successful private practice.
Both individually and organisationally, we need to be aware of what is happening around us and we should be able to respond swiftly and effectively to minimise any threat to our business.
Ideally, we should be ahead of the game, but sometimes we may find ourselves following rivals. If this is the case, then we must make sure that our offerings are at least equal to or better than those of our competitors.
Spanish brand SEAT found itself in this position as it was
trying to expand its successful range of SUVs to include a seven-seat model. Ahead of it were Peugeot, with its stylish 5008, and sister brand Skoda with the Kodiaq (Independent Practitioner Today, May 2019). It has have now launched the Tarraco.
Replacing people-carriers
Seven-seat SUVs are a natural market progression to replace the people-carriers of old, like the SEAT Alhambra, that were always popular with buyers with expanding families.
As many of us know, as soon as you have more than two children, the space needed in the regular family transport to accommodate all the associ -
ated paraphernalia seems to increase exponentially.
With the children growing, the benefit of an extra couple of seats in the back of the car becomes very useful for trips with their friends or other family members. But this is usually just an occasional need.
And that is why the Tarraco, just like its earlier-mentioned competitors, has rearmost seats that fold completely away to provide a flat floor and very large luggage area.
The SEAT is based on the same MQB chassis as many other VW group products including Skoda Kodiaq and even the VW Golf.
Engines are also shared
throughout the brands and the Tarraco is available with a 1.5 litre petrol engine and a 2.0 litre diesel engine with various power outputs. Most models have frontwheel drive and a manual gearbox, but four-wheel drive and a DSG automatic box is available on the top models.
There are four trim levels to choose from: SE, SE Technology, Xcellence and Xcellence Lux, and all models get digital dials and an eight-inch infotainment touch screen.
Stylish pose
Apple Car-Play and Android Auto are useful standard features. My test car was an SE Technology model with the 2.0 litre TDI diesel engine, front-wheel drive and the manual gearbox. This, at £31,055, represents a sensible and good value model to go for.
First impressions, as ever, count for a lot and the Tarraco strikes a stylish pose at the kerbside. Like other models in SEAT’s range, it looks sharp and up to date. I think
that it looks better than the Kodiaq on the road.
The interior has a similar flavour: functional with a twist of Spanish flare. The seats are comfortable and the trim quality, although not Audi level, is good.
The middle row rear-seat passengers have lots of headroom and legroom and the whole seat can slide forwards and backwards too.
The two rearmost seats are quite difficult to access and they are really only suitable for children and young teenagers, but that is the same situation for the Tarraco’s competitors. Luggage space is enormous if the rear seats are folded and not as bad as you would think when they are in use.
Sharp handling
Out on the road, the SEAT continues to differentiate itself from rivals. The steering is precise and the gearbox is slick. The handling has a sharpness to it that is almost sporty and fits SEAT’s advertised youthful brand image.
The 148bhp diesel engine is
driver
SEAT TARRACO SE TECHNOLOGY
2.0 tdi 150ps manual
Body: Seven-seat SUV
Engine: 2.0 litre four-cylinder turbo-diesel
Power: 148bhp
Torque: 340Nm
Top speed: 126mph
Acceleration: 0-62mph in 9.8 seconds
Claimed economy: 44.1–47.9mpg (WLTP combined)
CO2 emissions: 129g/km
On-the-road price: £31,055
powerful enough, reasonably quiet and the broad spread of torque is welcome.
The ride, even on the bigger 18-inch alloy wheels of the SE Technology model, is firm but comfortable over most road surfaces. Also, wind and road noise seems particularly well suppressed.
So, SEAT may have entered this seven-seat market late, but the Tarraco equals the class leaders and
feels the most engaging for the keen driver.
It is a well-equipped, comfortable and dynamic family SUV. It will appeal to many of you practitioners who like your cars to have a bit of driving verve and you will welcome the family-friendly nature of the packaging.
Dr Tony Rimmer is a former NHS GP practising in Guildford, Surrey
SEAT may have entered this seven-seat market late, but the Tarraco equals the class leaders and feels the most engaging for the keen
Orthopods still cutting it
Orthopaedic surgeons continue to be on average the highest earners in private practice, as Ray Stanbridge’s latest analysis demonstrates
THEY’VE DONE very well! Gross incomes increased by about 1.6% between 2017 and 2018, rising from £190,000 to £193,000.
Costs fell by about 5.7% on average, dropping from £69,000 to £65,000. As a result, taxable profits rose by about 5.5% from £121,000 to £128,000.
Orthopaedic surgeons are still at the top of the tree in the independent practitioner income stakes.
We are aware of ongoing fee pressures by insurers on orthopaedic surgeons and this primarily accounts for the modest growth
in gross fees. There was some growth in self-pay, but this market seems to have grown quicker according to the latest figures we have for 2018-19, the year after our survey.
Biggest factors
The two biggest factors in the improvements in performance between 2017 and 2018 have been the fall in staff/room costs and in insurance/indemnity costs.
Following implementation of the Competition and Markets Authority (CMA) findings, hospitals have had to charge ‘market
rates’ to orthopaedic surgeons for room hire and other services.
As a result, consulting room hire costs have risen, but secretarial costs have fallen, as consultants have taken advantage of hospital offers.
Perhaps the most interesting change is in the apparent fall in indemnity/insurance costs.
New providers were very active in the marketplace in 2017-18 offering, at first sight, some very attractive deals.
We have yet to observe if adequate retrospective cover is appropriate, so the jury is still out as to whether savings are real and sustainable. Certainly in 2017-18, savings did occur.
Home base
Most of the other costs showed little change over the year, with the exception of ‘use of home’ costs.
Following the famous Samadian tax case judgment, many consultants have established a genuine ‘business base’ at home.
What then of the future?
As mentioned above, there has been growth in the self-pay market in 2018-19 and we would expect orthopaedic surgeons to have taken full benefit of this.
And we would expect them to retain their pre-eminence in terms
The two biggest factors in the improvements in performance between 2017 and 2018 have been the fall in staff/room costs and in insurance/indemnity costs
of income among consultants over the next few years
Last November, when I wrote about this specialty, I said: ‘The private orthopaedic market is changing very rapidly. There is, for example, considerable interest by insurers in looking at new orthopaedic pathways, with less stays in hospital.’ This still seems to be the case.
Groups growing
Meanwhile, staff pay has risen significantly, at the expense of insured patients.
Groups are developing ever more rapidly in the orthopaedic sector.
In addition, some consultants may have chosen to incorporate
Year ending 5 April. Figures rounded to nearest £1,000 (percentage
The Healthcare Property Company (HPC) has developed, financed and project managed healthcare buildings for almost 25 years, from primary care to specialist clinics and laboratories.
Contact us to find out how we can help with your bespoke requirements.
and a number have entered into salaried employment arrangements with employers such as the Schoen Clinic, London, which has been well-covered in Independent Practitioner Today
All this variety makes it increasingly difficult to fairly record yearon-year changes. But this survey still aims to be a reflection of what a typical orthopaedic surgeon in the UK earns and spends in his
practice rather than be a statistically significant survey.
Obviously, there is a bias towards London and the South-east, as this is the largest market. This is a reflected in our regional figures to some extent.
Criteria for entering into our survey means that consultants have to satisfy a number of conditions. They must:
Each have earned at least £5,000 a year gross from private practice. (We will be increasing this in future, as we have used this level for some years now);
Have at least five years’ private practice experience;
Be seriously interested in the business of private practice;
Have either an old-style or newstyle NHS contract;
May or may not have worked through a group or through a limited liability company.
Next month: Ophthalmologists
Ray Stanbridge is a partner with accountancy, finance and tax advisory medical specialists, Stanbridge Associates
HOW ARE YOU DOING?
Years ending 5 April
HAVE A 20-20 VISION FOR YOUR PRACTICE!
Subscribing for just £75 direct debit to Independent Practitioner Today – and it’s tax deductible! – will keep you abreast of all the big private practice changes affecting you in 2020 and help the business side of your practice to stay ahead of the curve. See subscription information below. Coming in our December-January issue, published on 2 January:
Start the new year with a financial review of your practice. A top specialist medical accountant suggests what you should look at
Market research reveals near-static growth in the cosmetic surgery sector pitted against a buoyant market for non-surgical interventions such as Botox and injectable fillers. Analyst Liz Heath gives the details
The new Medical Practitioners Assurance Framework for the independent sector and a recent employment tribunal case illustrate that whistle-blowing does not just affect employed doctors. Lawyer Paul Spencer reports
Impersonation fraudsters are targeting practices by tricking staff into making payments to fraudulent accounts. Lloyd’s Banking Group’s Vin Pandha continues her series to help you fight cyber fraud.
A new initiative for private GPs aims to help those struggling with Care Quality Commission inspections. The Independent Doctors Federation’s Dr Neil Haughton gives the details
With myths about the General Data Protection Regulation circulating on the internet, it can be time-consuming to determine what you need to do to be compliant. Jane Braithwaite and Karen Heaton give advice
INDEPENDENT PRACTITIONER
The
TELL US YOUR NEWS
Robin Stride, editorial director
Email: robin@ip-today.co.uk
@robinstride Circulation figures verified by the Audit Bureau of Circulations
Phone: 07909 997340
Published by The Independent Practitioner Ltd. Independent Practitioner Today is editorially independent and thanks Bupa for its assistance with distribution. Printed by Pepper Communications Ltd Material is governed by copyright. No part of this publication may be reproduced, stored in a retrieval system or transmitted in any form without permission, unless for the purposes of reference and comment. Editorial layout is the copyright of the publishers. If you wish to use it for promotional purposes on websites or for reprints, we would be happy to discuss licensing the copyright to you.
Registered office: 7 Lindum Terrace, Lincoln LN2 5RP
Write to Independent Practitioner Today PO Box 198, Cranleigh GU6 9BB
Property investing for doctors: Dr Lafina Diamandis shows the property management and landlord essentials
In Accountant’s Clinic’s A-Z of business terms you need to know, Susan Hutter reaches the ‘F’s: for Filing deadlines, Finance team, Financial records, Forecasting and employing people in your Family
Surgeon Mr David Sellu continues his life-changing story that saw him wrongly imprisoned after a patient’s death
Doctors’ business dilemmas are answered. Am I indemnified for this type of work and how can I ensure I have consent for the continuing treatment of a child in the absence of parental responsibility?
If you have got a private practice in Yorkshire, then don’t miss Philip Housden’s analysis of private patient units in the region
How patients’ wishes can be respected when the patient is no longer able to communicate their preferences is explained by Dr Ellie Mein
Cavendish Medical’s Dr Benjamin Holdsworth on why inheritance planning is about more than just tax. Talking about inheritance and acting sooner is your first step to help your offspring
The second-generation Range Rover Evoque grabs the premium SUV top spot for our reviewer Dr Tony Rimmer
Our unique benchmarking series, Profits Focus, turns its focus on ophthalmologists income, expenses, profits and trends
ADVERTISERS: The deadline for booking adverts in our Dec-Jan issue is 2 December
ADVERTISE WITH US
Margaret Floate, advertising manager Email: margifloate@btinternet.com Phone: 01483 824094
GET A SUBSCRIPTION DISCOUNT!
£90 independent practitioners. £90 GPs and practice managers (private & NHS). £210 organisations. Save £15 paying by direct debit: individuals £75 (organisations £180).
TO SUBSCRIBE – USE SUBSCRIPTION FORM ON PAGE 23 or EMAIL: karen@marketingcentre.co.uk or phone 01752 312140 or go to the ‘Subscribe’ page of our website www. independent-practitioner-today.co.uk
Publisher Gillian Nineham
Phone: 07767 353897. Email: gill@ip-today.co.uk
SAVE £15 WITH DIRECT DEBIT!
Guarantee delivery of your next copy of Independent Practitioner Today. Take out a subscription and you will get full access to our news, features and previous issues on our website. See details on the left.
BACK ISSUES: £12.50 including post & packaging
Phone 01752 312140 or Email karen@marketingcentre.co.uk
Giving voice to the private sector
INDEPENDENT PRACTITIONER
Thanks to Healthcode for helping us to reduce the use of plastic
The new president of the Independent Doctors Federation, private GP Dr Neil Haughton, reveals his plans and hopes for the organisation in the years ahead n See page 18
business journal for doctors in private practice
Make access to self-pay easy
The private healthcare sector needs to do much more to make it easier for patients to access. And clearing up price confusion would be a good place to start, argues Keith Pollard n See page 21
What are you doing to attract patients
ADDRESS LABEL
Jane Braithwaite shows you how to choose the right marketing strategy to attract new patients and grow your practice
n See page 26
If undelivered, please return to: The Marketing Centre, 12 Mary Seacole Road, The Millfields, Plymouth, PL1 3JY
What are you doing sector
Integrated online solutions on one platform built to give customers time efficiency, compliance, robust data security and ability to connect seamlessly
Your financial and practice management on one secure platform
Improve:
• cash flow
• operational efficiency
Peace of mind knowing:
• your data is held securely and backed up
• your data is hosted in the UK
• no additional back office costs
A cost-effective integrated toolkit on one platform that:
• is scalable
return to: The Marketing Centre, 12 Mary Seacole Road, The Millfields, Plymouth, PL1 3JY
• includes key tools to manage both your financial and administrative tasks and processes
• allows you to manage your practice bookings for one or multiple locations
• maintains and manages your patient records and their associated transactions
• gives you the ability to communicate securely with other organisations such as hospitals and insurers
For more information and a demo of the system: ( 01784 263 150