The business journal for doctors in private practice
In this issue
How to ensure you’re paid
Some advice on invoicing in the latest of our practice management series P14
A cure for errors?
A doctor entrepreneur outlines his plan to end costly, over-long alleged negligence cases P25
Budget’s tax freeze on health cover is hailed
By Robin Stride
The private healthcare industry sighed with relief after its strong pre-Budget lobbying helped stave off a further rise in insurance premium tax on medical cover.
Now it will step up its campaign to get the Government to consider the wider implications of generating revenue from taxing health insurance – and to commit to making it totally tax-exempt.
Fears of a damaging rise from 12% to 20% were rife as it was revealed that the tax on health insurance had cost the NHS millions of pound.
Association of Medical Insurers and Intermediaries (AMII) chairman Stuart Scullion highlighted new research by Bupa and economics consultancy Cebr showing previous hikes in the tax had driven thousands of people to cancel or downgrade their health cover, costing the NHS £126m a year.
He said a relieved AMII was now urging the Government to make healthcare spend exempt from this tax like other zero-rated insurance such as life or critical illness.
‘The Government should be encouraging the purchase of pri-
vate medical insurance as a means of reducing the strain on an already overstretched NHS, not pushing thousands of people back onto it.’
Welcoming the freeze, Bupa Insurance chief executive Alex Perry said at 12% the tax was still too high. And when businesses or individuals cancelled health insurance, they were solely reliant on the NHS, putting it under more pressure.
‘We believe health insurance should be zero-rated like life or critical illness insurance. As an industry, we need to highlight the negative impact this tax has on people choosing to do the right thing by insuring their health and continue to campaign for fairer tax treatment of health insurance.’
Private healthcare strategy expert Ted Townsend warned that private hospitals and clinicians would still be pressured by insurer claim and pathway management policies although ‘it could have got worse’.
Doctors and their advisers also breathed a sigh of relief after the Chancellor avoided raising the pension tax take, freezing pensions’ tax relief and leaving the annual allowance unchanged.
But Andrew Pow, of the Association of Independent Special ist
Medical Accountants, said there was no respite for NHS consultants with earnings of £110,000 and over, who remain locked into potentially paying punitive annual allowance tax charges.
Specialist financial planners
Cavendish Medical’s Dr Benjamin Holdsworth reported doctors were breathing a sigh of relief. The lifetime allowance will rise from £1,030,000 to £1,055,000 for 2019-20.
A further boost to independent doctors was not scrapping entrepreneurs’ relief, as speculated. But qualifying conditions are stricter.
If a doctor sells part of or all their
offer the Gamma Knife Icon fractionated radiosurgery to treat both private and NHS patients.
n See story next issue
business, capital gains tax drops to 10% from the standard 20% if they have owned it over a year. This qualifying period extends to two years from April 2019.
But an immediate restriction means shareholders must have at least a 5% stake in their company’s profits and net assets to be eligible.
Dr Holdsworth advised: ‘Many doctors build up successful, profitable businesses and should plan their exit strategy carefully. Entrepreneur’s relief can be useful, but early planning of all your available options is important.’
n Accountant’s analysis, page 13
OPENING NIGHT: Baroness Karren Brady opened The London Gamma Knife Centre accompanied by its medical director Mr Ian Sabin and Jane Whitney Smith, deputy chief executive at the Wellington Hospital, which is the first London centre to
In this issue
answers to financial questions
accountant Susan Hutter responds to more of the most frequent questions she has been receiving lately from private doctors P12
a-Z of getting the money in nvoicing and collecting the money pose huge problems for many practices, so an expert presents an a-Z of billing to help guide you to a more successful outcome P18
High-tech outfit investing in itself
With the London clinic being a charity, we asked its chief executive al russell how that effects the way it operates and where all the money goes P30
editorial comment
It’s an iniquitous policy
Private healthcare sector lobbying from the Association of Medical Insurers and Intermediaries (AMII) – and many others – has paid off, with no further rises in the rate of insurance premium tax on medical insurance policies; and for that we can all be thankful.
But let’s not get too carried away with the Budget’s good news (page one). The rate of this damaging tax has almost doubled in the last three years, going up from 6.5% to 12%. And the threat of a no deal Brexit could yet see it rise again.
Had it done so – and a 20% rate to bring it in line with VAT was widely predicted – then this issue of Independent Practitioner Today would have carried a very different front page.
According to one poll, as many as one in three private medical insurance policyholders were ready to think about
cancelling their policy if their premium went up.
The same percentage of people would consider taking out insurance if costs were lower. So we wish the AMII – made up mainly of the people who sell these policies to individuals and companies – every success in its renewed efforts to make the Government see sense.
There is a very impressive case to remove the premium tax from private medical insurance and cash plans altogether.
As the AMII says, the tax has a greater impact on people who have the most need to keep their health insurance, such as older individuals with riskier health profiles who pay higher premiums.
It is these people who are being forced back into using NHS services as the cost of health cover becomes beyond their reach.
Finding your way to a safe lease doctors and managers entering practice lease negotiations know it is a complex journey. Lawyer bryn morgan gives some helpful tips and warns of the traps P34
take gripes seriously
Sally taber of the independent Healthcare Sector complaints adjudication Service discusses how to improve systems to support good handling of complaints P38
How the nHS was organised
So how did we get here? independent practitioner today looks back on the history of the nHS in the second of a series adapted from a new book by dr ellen Welch P40
Start a Private Practice: what to beware of if a vat-man nears accountant ian tongue looks at the area where doctors need to be vat-registered P48 doctor on the road: things are looking up motoring correspondent dr tony rimmer is exited to be driving a dynamic small car – the vW Up! P50
Profits Focus: Heads just above water our unique benchmarking series looks at the financial fortunes of orthopaedic surgeons P52
tell US yoUr newS Editorial director Robin Stride at robin@ip-today.co.uk Phone: 07909 997340 @robinstride to advertiSe Contact advertising manager Margaret Floate at margifloate@btinternet.com Phone: 01483 824094
SUbScriPtion rateS
£90 independent practitioners. £90 GPs and practice managers (private & NHS). £210 organisations. Save £15 paying by direct debit: individuals £75 (organisations £180). to SUbScribe – USe SUbScriPtion Form on Page 24 or email: lisa@marketingcentre.co.uk Or phone 01752 312140 Or go to the ‘Subscribe’ page of our website www.independent-practitioner-today.co.uk chief sub-editor: Vincent Dawe Head of design: Jonathan Anstee Publisher: Gillian Nineham at gill@ip-today.co.uk Phone: 07767 353897
Don’t fall into tax trap by breaching pension limit
by edie bourne
Retirement saving doctors are urged this month to check they are not over rewarding the taxman.
Independent practitioners are among individuals generating record payments to the taxman by breaching strict yearly limits.
New figures show HM Revenue and Customs’ (HMRC) income from annual allowance breaches rose from £143m to £517m in 201617.
Some 16,590 pension savers reported a breach of the annual
Discussion of consent is hindered by workload
Heavy workloads are undermining doctorpatient relationships by eroding the time they have together to discuss treatment and care, the GMC has warned.
The warning came as the regulator launched a consultation on the draft of its updated consent guidance.
This responds to doctors’ feedback and aims to help them work most effectively with patients to make decisions about their care.
GMC education director Prof Colin Melville said: ‘In the ten years since we first published guidance on consent, much has changed.
‘Patients have more access to medical information outside the consulting room and rightfully expect to discuss options with their doctors before important decisions are made about their care.’
The draft guidance, including surveys for doctors and patients, are available on its website. Consultation ends on 23 January.
allowance rate of £40,000 through their tax returns, compared to 5,430 the previous year.
The annual allowance limits the amount of taxfree pension savings which can be accrued each year. As well as the standard allowance, down from a £255,000 peak in 2011 to just £40,000, a new ‘tapered’ annual allowance was introduced in 2016.
This reduces the limit down further on a sliding scale to as little as £10,000 for those earning over £150,000 a year.
It has also been revealed that the tax yield from taxpayers
breaking the lifetime allowance, which governs tax free pension savings overall, reached £102m in 201617, up from £66m the year before. The lifetime allowance has been cut from £1.8m in 2012 to just £1.03m now.
Dr Benjamin Holdsworth, director of specialist financial planners Cavendish Medical, warned that rather than encouraging individuals to save for retirement, doctors and other higher earners were being penalised by everreducing limits.
‘In fact, since the socalled ‘pension simplification’ in 2006, total
annual allowance tax charges have netted HMRC over £1,200m and lifetime allowance breaches have generated a revenue of £335m.
‘As the annual and lifetime allowances are bringing in substantial income for the Treasury, we are likely to see further cuts to pensions savings limits in the future.
‘The only way to avoid walking blindly into tax traps is to look very carefully at your own situation and plan what can be done to mitigate needless charges well in advance.’
Premium tax causes health cover to fall for second year
Rocketing insurance premium tax is a key reason why the UK medical cover market showed flat growth for the second year running, with only four million policies taken up, according to analysts.
LaingBuisson said the market has been ‘onerously burdened’ by steep rises in the tax resulting in more lapses.
Health Cover Market Report author and economist Philip Blackburn called demand for private medical cover ‘stagnant’.
He said: ‘Driving this has been the high cost of taking out standard cover, exacerbated by the recent sharp increase in tax burden from insurance premium tax.’
LaingBuisson found:
Downtrading and higher ex cesses have featured to keep insurance affordable;
A trend towards family coverage;
A fall in claims’ value;
New business generated by joiner discount offers and incentives;
Interest generated by higher NHS waiting lists and rationing;
More access to private GP services and mental health counselling for employees, as many insurance and cash plan policies now offer these services as standard;
Growth in cash plans and dental cover.
It believes more potential lies in innovation.
Its report said: ‘There is a growing focus on supporting employee well being through physical and mental health prevention, and key issues for employers include reducing sickness rates and improving productivity.
faced by corporate buyers and also appeals to individuals.’
Mr Blackburn said new products supported by technology apps were likely to be popular, as they enabled fast, convenient and ongoing access to primary care.
‘Certainly, innovation is centred on corporate well being, as greater physical and mental healthcare prevention is intended to deliver pay offs long term through a healthier workforce for clients.’
The high cost of standard private medical insurance meant growth of fully comprehensive corporate healthcare packages was a challenge for insurers, he said.
‘Consequently, repositioning the offering of the health insurer as a “health and wellbeing provider” creates a differentiator which answers questions being
Big premium rises would see more individuals exit to fully rely on the NHS or use savings to selfpay.
LaingBuisson Health Cover Market report, 15th edition
Robin Stride reports from LaingBuisson’s big event at the Royal Society of Medicine, bringing together operators, insurers, associated companies and clinicians
A Bupa and HCA Healthcare UK partnership announced at the conference will give patients fast access for breast cancer care at specialist centres in London and Manchester.
In a first for a UK health insurer and hospital provider, patients from next January will be able to see a consultant within two working days of contacting the insurer, with all initial diagnostic tests completed in one appointment.
Any needed treatment will be given within 31 days of calling Bupa – under half the time set out in national targets.
A multidisciplinary team will provide personalised treatment plans including access to genetic testing and advanced genomics.
Patients will have support from Bupa’s oncology specialist support team and HCA clinical nurse specialists, plus psychological sup -
port services for themselves and their family before during and after treatment.
Research shows that over 90% of women diagnosed with breast cancer at the earliest stage survive for at least five years compared to around 15% diagnosed with the most advanced stage of disease.
The hospital group’s president and chief executive Mike Neeb said HCA was proud to work in partnership with Bupa.
‘Our shared aim is ensuring that we provide patients with the highest quality care and experience possible and through this first-in-kind initiative, patients will be able to get answers on their cancer symptoms without delay or the need for multiple pre-authorisations.
‘For patients that need treatment, they will have immediate access to specialist cancer care led
by our multidisciplinary teams of consultants from some of the UK’s largest teaching hospitals.
‘This provides the combined expertise, experience and understanding of a whole team of clinicians in specialist and subspecialist areas of cancer treatment.’
Bupa Insurance UK chief executive Alex Perry said the partnership aimed to provide the best cancer treatment in the UK.
Around 11,000 customers were impacted by breast cancer each year and for cancer diagnosis and treatment, every day counted.
‘Early cancer detection can have a significant impact on someone’s chance of survival and reduce their need for complex and invasive treatment.
‘Waiting to find out whether symptoms are cancerous is very stressful; we want our customers
to get the all-clear or a diagnosis and access to treatment as soon as possible.’
Patients can also receive ongoing support from Bupa’s cancer nurses and advisers, who develop individual action plans, including lifestyle advice to support secondary prevention and staying healthy.
Specialist centres must meet an ‘outstanding’ or ‘good’ Care Quality Commission rating. They are:
The Harley Street Clinic, Marylebone, London (outstanding);
The Lister Hospital, Chelsea (outstanding);
The London Bridge Hospital, London Bridge (outstanding);
The Wellington Hospital, St John’s Wood, London (good);
The Wilmslow Hospital, Cheshire – treatment delivered at The Christie Private Care, part of HCA Healthcare UK (outstanding).
Cancer tie-up a UK first Spire points route to success
A hospital group boss laid out his prescription for what the private healthcare market must do to boost its revenues during challenging times.
Justin Ash, chief executive of Spire Healthcare, said: ‘I’m optimistic about the future – as long as we change things.’
➲ self-pay
He called for the market to be more consumer-focused and establish a clear, alternative proposition for patients who cannot or will not wait for treatment.
This meant ensuring the private sector was ‘open for business’ and could be easily accessed.
Patients should be able to see transparent payment plans with a variety of payment options.
And providers needed to create
an increased awareness of the selfpay option so that it was seen as normal, he said.
➲ Private medical insurers
Mr Ash called on them to be more innovative to make insurance more affordable and accessible, particularly for small companies and individuals.
They needed to campaign against proposed insurance tax rises, which were bad for patients, and drive the quality agenda.
He said they needed to recognise the importance and associated cost of quality, and recognise the hospitals’ role as ‘quality providers and guardians of consultant performance’.
➲ The nHs
Mr Ash said the NHS needed to adapt too. Waiting list pressure
could not be alleviated without private hospitals’ support and the health service needed to recognise the role the independent sector played ‘as true partners to the NHS’. Partners needed stability and consistency and the idea that the
independent sector was an illegitimate partner had to end.
The health service should be allocating work based on quality rather than cost and commit to doing what was right for the patient. Patients should get timely choice of access to quality care providers.
Quoting from a poll of 2,000 people last April, he said access and quality issues underpinned patients’ motivation to use private hospitals.
Nearly a quarter of the population were currently willing to consider going private and 49% were open to self-pay.
He told the meeting that Spire was determined to get 100% of its hospitals rated by the CQC as good or outstanding by 2022.
The private healthcare industry is in a fight for its survival as it faces its most difficult point ‘arguably in living memory’.
If it is to survive and grow it must recognise that its old proposition and ways of working just won’t do, according to the boss of Bupa Insurance UK.
Chief executive Alex Perry called on delegates at the LaingBuisson Private Acute Healthcare Conference 2018 in London to back a fundamentally different proposition and offer a service that is about more than just quicker treatment access.
He warned: ‘Independent healthcare will only survive and thrive in this country when it can demonstrate that it provides the highest quality care you can get, anywhere – for you, for your family and for your colleagues.
‘It is only when we offer the best care and the best service that we can deliver a real change in our fortunes.
‘It is only when we can prove that we offer this that we will get
Change is vital, says Bupa boss
the ground-swell of support and demand that we need to grow.’
Speaking before the Budget, he said the sector faced an increasingly hostile fiscal environment. Rocketing insurance premium tax was hitting the market and when added to benefit-in-kind taxes and to National Insurance, employers and employees between them faced an effective tax rate on health insurance premiums of between 49% and 72%.
Mr Perry said the industry also faced:
A political climate as challenging as it has been in many years, with hostility in some quarters to the role of independent healthcare in the wider health system.
The Brexit effect, with nurses and other clinical staff from the EU increasingly difficult to recruit and a risk of the City – ‘a key sector for us all’ – moving jobs overseas.
Less NHS work hitting hospital revenues and profits and hurting the sector’s ability to invest;
Developments like the Paterson
inquiry and the Care Quality Commission’s critical report on the independent sector (Independent Practitioner Today, May 2018) meaning quality and safety was under unprecedented scrutiny and criticism.
Mr Perry said nobody in independent healthcare could feel comfortable listening to last month’s BBC Radio 4’s File on 4 report, entitled Paying the Price –Private Hospitals
This highlighted that the Care Quality Commission had said four in ten private hospitals needed to improve safety, outcomes in private hospitals were a ‘dark field’ – not subject to the same reporting requirements as the NHS – and that the sector did not know as much about outcomes as the NHS.
He continued: ‘We cannot leave ourselves open to these charges; we just won’t survive in today’s world if we do.
‘We have to be able to demonstrate clearly, objectively and convincingly that you are better
off being treated in the independent sector – that it is a better experience with better outcomes. Otherwise who’s going to pay money to do this?’
Mr Perry said the Private Health care Information Network’s (PHIN’s) work on data and transparency should be accelerated ‘so that we can compare ourselves like for like with the wider healthcare system and demonstrate that we deliver better outcomes’.
And there needed to be more progress on data sharing to identify where care was not good enough and to be able to demonstrate those areas where private healthcare delivered excellence.
There had been good engagement with PHIN from consultants, but the hospital picture was mixed. The whole industry needed to step up, he concluded.
Next month: Quality doesn’t just apply to providers – insurers need to up their game as well See more from the conference on page 6
Figures indicate a tough time ahead
Revenue growth funded by selfpay – up at 10.2% last year – is predicted to grow less over the next three years.
Conference director Ted Townsend said Brexit was a concern for potential patients, so they were deferring economic decisions.
He painted a somewhat bleak picture in forecasts for private medical insurance and private
healthcare earnings from the NHS and overseas.
Many in the audience of hospital operators and others in the industry shared his predictions, although 40% felt his self-pay forecast was too pessimistic. However, 16% at the conference thought he was too optimistic.
Mr Townsend said the market was being hit by a fall in interna-
tional private funding due to more competition abroad and potential patients struggling to get visas to come to the UK.
Nominal data for London’s private acute market growth forecasts pointed to an ‘unheard of’ 7% drop last year.
He predicted much overcapacity would push prices down, especially in the capital.
Alex Perry, chief executive of Bupa
Conference director Ted Townsend
Clinic relaxes its ‘salary only’ plan
Consultants who get jobs at the under-construction 200-bed Cleveland Clinic in London will be able to continue working in the NHS.
The hospital has championed the cause for bringing a US-style of salaried service for consultants in the capital.
But it has now made it clear that its specialists could have salaried posts in both the independent sector and the health service.
And other doctors could work there even without being salaried.
It told Independent Practitioner Today: ‘Cleveland Clinic London will offer a mixed model of employment. Some of our doctors will be fully employed by the hospital, but we will encourage them to continue their practice in the NHS should they choose to do so.
‘Cleveland Clinic will also offer
doctors the opportunity to apply for practising privileges at 33 Grosvenor Place.’
A year ago, we reported remarks from its then chief operating officer Mr Keith Hague who told LaingBuisson’s Private Acute Healthcare conference that doctors’ expressions of interest in working on a salaried basis at the hospital had gone through the four-figure mark.
He expected around 50 employed
doctor staff would be in place during the initial stages, although Independent Doctors Federation (IDF) president-elect Dr Neil Haughton – at the same meeting –warned that private doctors liked being self-employed, adding: ‘I wonder where you are going to get all the doctors from.’
Surgeon Mr Brian Donley, appointed Cleveland’s chief executive earlier this year, told this year’s LaingBuisson conference:
‘We would expect and encourage our clinicians to continue to work
IDF president Dr Brian O’Connor responded that he now believed a salaried service ‘may actually be the way to go for doctors in the independent sector’. Andreas Ludowig, executive director of the new Schoen Clinic London, told the meeting that most of its consultants would be employees there and also in the NHS.
He said the unit favoured independent salaried doctors because it wanted ‘all the players on our team’, adding ‘I hear from insurers that more are going that way’.
Insurers urged to scrap small print
Private medical insurers need to continue improving products or services and enable easier access to the right care.
They should also scrap some of the still-too-common ‘small print mentality’, the conference heard.
Bupa Insurance chief executive Alex Perry said his company had taken steps forward; for example, by introducing its ‘Cancer Promise’.
This guaranteed customers no financial nor time limits placed on their cancer care and gave access to all appropriate cancer drugs and treatments and dedicated support.
He said the insurer’s Cancer Direct Access, introduced a year ago, was the most comprehensive
self-referral cancer service in the UK. Patients did not need a GP referral if worried about cancer symptoms, they just called Bupa.
And last April’s launch of Business Mental Health Advantage was another example. It gave the most extensive mental health cover available to UK businesses ‘covering all mental illness with none of the usual restrictions you get for chronic conditions or ongoing treatment’.
Mr Perry signalled that other developments were on the way.
He told the conference it used to be said that someone who experienced good customer service would tell two people about it, while those with bad customer experience would tell ten.
But social media had blown this out of the water, enabling bad service reports to be shared with thousands.
Bupa was now inviting a random sample of customers to rate their experiences through the online review platform TrustPilot. ‘We’re already seeing real benefits and I’m proud that we now have a four-star rating and a TrustScore of eight out of ten, leading the way among UK health insurers.’
Its experience with TrustPilot had also demonstrated that customers did not distinguish between the insurer and the provider. ‘Many of the comments we get, both good and bad, are to some extent about providers – the hospital they were treated in or
the consultant who cared for them.’
All parts of our sector needed to deliver a five-star experience if customers were going to trust, stay, pay and recommend it.
Mr Perry said Bupa was determined to do what it could to drive new standards for quality and it would increasingly guide patients to where there was demonstrated good quality and away from areas where it was poor or uncertain.
He urged all parties to continue working together to control costs. ‘There is more we can all do to improve our own processes to help bring down costs and improve affordability and we must remain committed to delivering those improvements.’
Surgeon Mr Brian Donley, the Cleveland Clinic’s chief executive
in the NHS.’
Cleveland Clinic aims to open its hospital in Grosvenor Place in ‘early 2021’
Complaints in PPUs now have a remedy
NHS PPUs are required to have an independent review stage for complaint management. Sally Taber reports
If you are an NHS or private consultant working in a health service private patient unit (PPU) under practising privileges, then there is something you should know.
What you may not realise is that, if a private patient complaint involves you, then the NHS system of resolving complaints does not apply in the NHS PPU where you work if it is treating private patients. That means it becomes your responsibility to resolve, under para 61 of the GMC Code of Practice.
Regardless of opinions on the matter, resolution then becomes a time-consuming and critical issue that can only distract from the proper business of running your clinical practice.
Often a complaint may be about matters outside your consultant’s purview: nursing, patient care pathway, hotel services and so on.
The Department of Health last year changed the rules to permit NHS PPUs to subscribe to the Independent Healthcare Sector Complaints Adjudication Service
(ISCAS). This body is the answer for NHS PPUs to their present predicament of being unable to resolve difficult complaints by independent review.
There is nothing so unsatisfactory as a complaint left unresolved – unhappy patient, unhappy provider, lessons unlearned.
This is often the situation in NHS PPUs. A percentage of the 527 complainants who contacted ISCAS last year were from PPUs – and ISCAS could do nothing about them.
NHS PPU patients are unable to resort to the Parliamentary and Health Service Ombudsman nor, until 2017, could they resort to the long-established ISCAS.
From early 2018, it has become possible for PPUs to offer their consultants a way to meet their obligations and avoid falling into the bureaucratic morass that is involved in resolving a difficult complaint.
Three highly respected PPUs now subscribe to ISCAS: Imperial Private Healthcare, the Sefton Suite in Liverpool and the Royal
this represents fell back slightly from 1.12% to 1.09%.
More are in the pipeline – but it needs to be many more.
Joining involves the PPU management subscribing to ISCAS and agreeing to abide by the ISCAS Code three-stage process (see www.iscas.org.uk). Subscriptions are reasonable; for example, £675 a year per PPU for a privatelyfunded turnover up to £5m.
What ISCAS brings new for PPUs is final adjudication by an independent adjudicator to give a result binding on both patient and provider. This meets requirements for the Care Quality Commission in England and for Health Improvement Scotland, as well as in Wales and Northern Ireland.
Under the ISCAS Code, patients and the PPU agree beforehand that the outcome of the inde-
performance will be shared in forthcoming issues.
Any adjudicated goodwill payments to patients relate to the inconvenience suffered. Eighty per cent of complaints in 2017-18 attracted goodwill payments averaging £813 – 12% involved calling in expert clinical advice.
The patient pays nothing. The PPU pays the independent adjudicator’s fees after a complaint completes adjudication.
Complaints are a fact of life in medicine. Dealing with them effectively safeguards reputations and makes for happy patients. Many PPUs still fail with this. There is a remedy and that is subscribing to ISCAS.
‘Take gripes seriously’, page 38
Sally
Taber is director of ISCAS
Private Healthcare Information Network (PHIN).
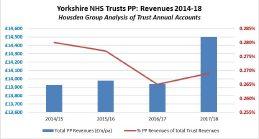
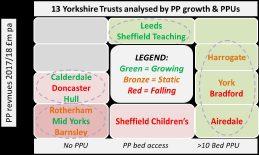
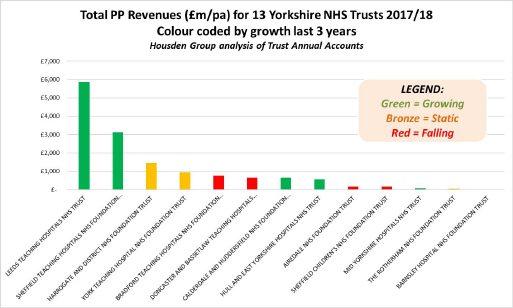
Compiled by Philip Housden
PPUs break £600m revenues for the first time NHS trust annual accounts for 2017-18 show it was another record year for the sector.
Preliminary analysis by Housden Group finds that total revenues were £619m, up £31m (5.3%) on the 2016-17 total of £588m.
Overall, the proportion of total NHS patient activity revenues that
Regional breakdowns highlight that effectively all of this growth was delivered by the London region trusts, which aggregated £402m – up £31m year on year –of which Royal Marsden contributed £104m, holding on to first position.
London’s total share of the NHS PPU ‘market’ rose from 63% to 65%.
A much more detailed analysis of the regional and trust by trust
PPU national event
A development day for NHS PPUs will take place on 19 March 2019, hosted by Royal Derby Hospital.
It provides the opportunity to meet the managers of a range of successful units and learn from real-life case studies, including a tour of Derby Private Health, the onsite in-house PPU.
The main healthcare insurers will also be presenting, as will the
Up-to-date insight into how the dynamic NHS PPU sector is changing will be provided by Housden Group.
Further details and booking at www.sbk-healthcare.co.uk/home/ title/2367/nhsconference/nhsprivate-patient-servicedevelopment/#agenda.
Philip Housden is a director of Housden Group. Read his feature article on page 42
App to thwart bullying over NHS job plans
By a staff reporter
A new app is coming to the aid of consultants who have criticised bullying related to their NHS job planning meetings.
Dr Diary, from the BMA, aims to help them track the work they do and plan their jobs better. Specialists enter work activity data into a calendar to build up a picture of how much they are working and a resulting report can be downloaded, shared or printed in preparation for job planning meetings.
The app comes after a BMA survey found nearly a quarter of consultants had experienced job plan-related bullying.
Half of them said they had a negative experience in their last job planning meeting ( Indepen dent Practitioner Today, September 2018)
The association said the app cuts down on the hours doctors spend meticulously recording how they spend time at work, whether that be with patients, teaching or professional development, and is a simple solution for doctors to prepare for their job planning review with confidence.
It should also make it easier to negotiate a positive change to
Dr Robert Harwood: Said the BMA app would give doctors confidence
their work schedules and push back against increasing workloads.
Excited BMA consultants committee chairman Dr Robert Harwood said: ‘I know that so many of our members will find it incredibly useful. Job planning is supposed to be a chance for doctors and employers to agree duties, responsibilities and objectives for the coming year, but our members have reported having negative experiences.’
‘Dr Diary will help level the playing field for consultants and associate specialists and give them a sense of confidence ahead of the job planning process.’
Diagnostic centre for Liverpool’s research hub
A diagnostics centre is to be built in Liverpool’s £1bn Paddington Village development by Rutherford Diagnostics, a Proton Partners International subsidiary. It will be opposite the Royal College of Physicians’ new northern headquarters and next to the Rutherford Cancer Centre North West, one of a network offering high-energy proton beam therapy to cancer patients.
Proton boss Mike Moran said: ‘This centre aspires to be a leader in the prediction, prevention and earliest possible detection of disease, as well as being equipped to conduct the most complex of diagnostic tests across a wide range of conditions.’
Rutherford Diagnostics will work alongside private healthcare organisations and NHS foundation trusts.
City mayor Joe Anderson said
the project was a boost for plans to create a world-leading medical research and innovation hub.
Aidan Kehoe, chief executive of the Royal Liverpool & Broadgreen Hospitals NHS Trust, said: ‘It is our unique type of public-private partnership that will be critical in enabling Liverpool’s Knowledge Quarter to become a centre of excellence in the provision of health and cancer care.
‘Our vision has always been to develop the Liverpool Biocampus to attract pioneering academics, clinicians and businesses that will ultimately benefit the people of Liverpool through improved health outcomes and economic growth in the city.’ Technologies that Rutherford Diagnostics will provide include CT, PET-CT, MRI, ultrasound, endoscopy, genomics and personalised screening.
Training in ‘system failure’ for GMC sleuths
GMC plans to give case examiners and clinical experts ‘human factors’* training have been welcomed by a doctors’ defence body.
The council will also draw on human factors experts to better understand system failures when investigating doctors.
Dr Caroline Fryar, of the Medical Defence Union (MDU), said recent high-profile cases of doctors prosecuted for gross negligence man-
slaughter had demonstrated they could be held individually accountable for tragic incidents where system errors also played a part.
She said: ‘Doctors are often required to make decisions and take action or decide to take no action in circumstances over which they have no control and are far from ideal.
‘For example, they may be short-
staffed and trying to do the job of two or more colleagues while juggling the care of seriously ill patients.
‘We are glad that the GMC is recognising and taking into account the fact that doctors are often put in a position where they are unable to control their environment and circumstances but must carry on and treat patients as best as they can.’
* The GMC describes human factors as ‘a social science which studies and attempts to optimise the interactions of humans, technology and the environment at work.
‘It is a standard tool of safety investigation and improvement in several industries such as civil aviation, nuclear power and military planning which seek to balance high risk and high reliability.’
New rules to cut January tax bill for high earners
By Linda-Rose Ward
Rule changes around pension annual allowance tax charges will bring welcome relief to doctors in England and Wales facing unprecedented tax bills in January 2019.
Higher-earning doctors can now elect for the NHS Pension Scheme to pay over the tax on the full annual allowance charge instead of having to find significant amounts of cash themselves from their own funds.
For the 2016-17 tax year, pension scheme members could only ask the body to pay the tax on the excess over the standard £40,000 annual allowance.
However, some higher-earning doctors have their annual allowance tapered down to £10,000,
which meant their tax bills were significantly higher than in previous years (see example below).
The Department of Health and Social Care has instructed that, for 2017-18, the NHS Pension Scheme should pay over all the tax on the excess over the tapered allowance. The Scottish pension scheme has already adopted this rule change.
The change follows lobbying from the Association of Independent Specialist Medical Accountants (AISMA) and other bodies.
AISMA representative David Walker, a tax adviser at accountancy firm MHA Moore and Smalley, said: ‘The change in the rules will alleviate the immediate cash flow worries of doctors facing many thousands of pounds in extra tax charges.’
He explained: ‘Doctors who elect for the scheme to pay the tax should understand that there will be a larger reduction in final benefits paid by the pension scheme.
‘This will need to be factored into any decision the doctor makes about whether to elect for
HOW IT WORKS
the whole amount of tax to be paid by the scheme.
‘Advice should be sought from a suitably qualified financial adviser who has specialist knowledge of the NHS Pension Scheme.’
➮ A previous version of this story appeared on our website
In 2016-17, a doctor with pension benefit growth of £60,000 and a fully tapered allowance of £10,000 – and no unused allowances available from earlier years – could ask the pension scheme to pay the tax on the £20,000 above the standard £40,000.
But he or she would have to pay the tax through their self-assessment on the balance of £30,000 above their tapered allowance of £10,000.
For a 45% tax-payer, this amounted to a further £13,500 in their January 2018 payment, plus payments on account for the following year.
In 2017-18, a doctor in the same situation can now ask the scheme to pay the tax on the whole excess of £50,000.
Good news slows growing pension tax grab
It is so refreshing for doctors to receive some good news from the Government about their finances, writes Patrick Convey (right), technical director of specialist financial planners Cavendish Medical Scheme Pays – where the pension scheme pays any tax charges resulting from the annual allowance on your behalf in return for reduced pension benefits in the future –will also now apply to tax charges which arise from the new tapered annual allowance.
doctors facing successive annual tax bills through self-assessment.
More doctors than before are breaching the annual allowance because the new taper means that some can only enjoy yearly pension ‘growth’ of £10,000. This figure is easily achieved with NHS pension growth before considering any contributions to private pensions.
payments can escalate quickly and the future consumer price index inflation rate is unknown.
You will also need all the necessary information to hand before the application deadline, which is normally 31 July each year.
This move will be welcomed by
More doctors will now be able to apply for Scheme Pays – there can even be tax advantages to reducing your eventual future benefits. But be mindful that the interest
There are also some alternative options: some personal pension schemes will allow you to pay the annual allowance charge from personal pension funds, which can be tax-efficient and will protect your NHS pension.
Before making any decisions, you should request your annual statement from the NHS Pensions
Agency if you have not already received it.
The agency is obliged to send statements to those breaching the annual allowance, but not to those exceeding the tapered annual allowance – make sure you don’t fall between the gap.
Last year, the Treasury had a record tax haul of £517m from savers breaching the annual allowance – up from £143 the previous year. Without expert help, many doctors unwittingly fall into a tax trap and yet with careful planning ahead of time, other routes are available.
Botches from foreign beauty ops ‘set to rise’
Plastic surgeons expect a high influx of patients arriving with complications at the beginning of 2019 after going abroad for new year aesthetic procedures.
Consultant plastic surgeon and outgoing British Association of Aesthetic Plastic Surgeons (BAAPS) president Mr Simon Withey has warned the public: ‘People are experiencing a rude awakening when they arrive back on British
shores, many disappointed, and some desperately ill.
‘Surgery is simply not something you can return at the January sales, and it should never be tied to seasonal discounts and incentives.’
He said a vulnerable group of patients were openly being targeted through social media and the internet to travel abroad for cheaper cosmetic surgery – and this trend was likely to rise.
A trawl through the archives: what made the news in 2008
A look back through our journal’s archives of ten years ago reveals that although times change, some issues are not so new
Self-pay is first victim
The recession was rife this time ten years ago and independent practitioners were warned they could not expect their earnings to escape the economic downturn.
New figures showed the average private income the previous year for an estimated 20,000 specialists fell from £71,500 gross to £71,250. After expenses, they earned only around £50,000 before tax.
Earnings from self-pay patients dropped for the first time in some years – down from 17.5% of independent medical/surgical hospital revenue in 2006 to 16% in 2007.
According to Laing’s Healthcare Market Review 2008-09, the drop resulted from the faltering economic climate and more NHS waiting list cuts.
Economist William Laing told Independent Practitioner Today: ‘The main feature of the review is that self-pay is down – it is being hit by the economic climate.
‘Private consultants are not immune from the downturn – but they are more immune than others.’
He warned: ‘Self-pay will go down a little bit more – it is an inevitable feature of the current recession.’
We told you this would happen
Our Profits Focus feature – as so often has happened over the last decade – proved prophetic for orthopaedic surgeons.
Accountants said they expected to see more marketing in this specialty, a growth of well-run groups and to see them ‘add value’ to their members.
‘For example, we expect to see the development over the next few years of group professional indemnity insurance schemes, offering discounts,’ they said.
Our writers also predicted that orthopaedic surgeons would increasingly use accounting data and analysis to demonstrate their real value in a market where insurers were driving costs down through a range of means.
Don’t trust the trust
Consultants in private practice were being warned to ensure they got their payment terms agreed before they took on NHS work.
Accountants issued the advice after a gynaecologist complained at a London Consultants Association meeting that one trust owed money going back eight months for operations carried out to help it meet its 18-week referral to treatment target.
The surgeon, who claimed to be owed for 18 procedures, said: ‘It’s not just me – many of the consultants have been complaining they haven’t been paid.’
Take an easy wind down to retirement
Be aware right from the outset how you might wind down your practice, advised accountant Martin Murray.
He said for consultants involved in preparing medico-legal reports, for example, the winding down of this side of the private practice could take a long time, as repeat requests from solicitors and other interested parties might be received several months later on the same patient.
‘Tax is a big issue and, for the unwary and unprepared consultant, can come as a shock.
‘Basically, depending on the financial year-end of the private practice and when cessation occurs, it can in some circumstances meant that tax is still payable for nearly a year after the private practice has ended.’
Mr Murray, of Sandison Easson & Co, said consultants approaching retirement should not ignore buying equipment, as accelerated capital allowances were available and although adjustments had to be made for tax purposes on these items after the cessation of the practice, they could still be beneficial.
SubScribe today
don’t miss out on what we report and advise in the future. Sign up for a £75 subscription today –consultants, GPs and practice managers can save £15 with a direct debit. See page 24
Rethink
Independent practitioner investors were advised to quit their common habit of collecting financial products and go for a much more targeted investment strategy in future.
A financial adviser said they should urgently review their investment and pension plans because it was not too late to limit market turmoil damage to financial portfolios.
Payments By Results and tariffs might lead to a universal fee-forservice system for independent practitioners taking on NHS work, a healthcare market expert claimed.
He told doctors at a London Consultants Association meeting that clinicians organising themselves in groups rather than operating as individuals could help prevent such downward pressure on fees as hospitals and commissioners adopted these payment models.
Michael Green, chief executive of Trust Health Ltd, predicted limited liability partnerships (LLPs) or chambers would become more common as the UK healthcare market changed.
William Laing
Sharing OutcOmE data
Our data journey must begin with a first step
There may be problems with healthcare data. . . but it is the future, says Prof Antony Narula
As doc T ors know, there are inherent issues with many healthcare data schemes.
The difficulty is, when there are high-profile cases of poor care, there is a tendency to over-legislate. In trying to legislate for individual cases, you can often come up with a huge bureaucracy with limited benefit.
If you look at the publication of annual performance data from the NHs, it has been fraught with problems. In the first year, some vascular surgeons were pilloried in the national media for activity which had been wrongly attributed to them. It was a shambles.
There are also problems with what can be meaningfully measured using data. There is a trap here in social sciences known as the McNamara fallacy, named after r obert McNamara, the U s secretary of defence in the 1960s.
As he pointed out, you can’t measure what’s important, so you measure what you can, and that becomes important.
s urgery is often the starting point for measurement, because surgery fits into neat and identifiable units of activity.
But in a specialty like mine –ENT – the conversion to surgery rate is only 8-15%, meaning that much of our activity simply isn’t subject to measurement.
It could take two to four years to really get the data right; but, if you don’t start somewhere, then you aren’t going to get anywhere
was re-admitted? I don’t know, but they would certainly want to know to try to improve outcomes. of course, data on private care is starting to dramatically improve. Within orthopaedics there is the GIrFT programme, which brings together whole practice activity.
The Private Healthcare Information Network (PHIN) requires hospitals to collect data on private healthcare using the same standards and definition used by the NHs, and PHIN will publish performance measures for hospitals and consultants on a public website.
Validation process
The most common indicator of quality and safety of surgery is mortality. While mortalities must always be reported and investigated, the likelihood of mortalities is so low that any rate is likely to not be statistically viable.
genuine concerns
I understand the hesitation towards the increasing number of healthcare data initiatives. There are genuine concerns around process and implementation, but there is also real potential with robust healthcare data to better understand and improve care.
In my time as president of ENT UK, I was involved in a number of data initiatives: some more successful than others. Where the research question was clearly articulated and the process robust, data gave unique and important insights.
A bugbear of mine while the president of ENT-UK was paediat-
rics. Why should someone work with children in the private sector when they don’t in the NHs?
Having the actual evidence of someone’s experience and the procedures they undertake across their practice is crucial. Where the private sector and NH s have famously not worked together, a seamless approach to data collection across NHs and private practice has to be the way forward.
A seamless approach will also bring new insights with re-admissions. When I was working at st Mary’s Hospital, I remember a case of a patient who had come in after a severe post-operative bleed. This followed a tonsillectomy – in a local independent hospital – that ruptured while recovering at home.
We all hear anecdotal stories of this happening, but do we know how common this is? And more importantly – did the independent hospital ever know the patient
As part of this process, PHIN has been encouraging consultants to review their practice data and validate it for publication. While I have experienced issues with accessing its platform, and there were inaccuracies within the data, I’m encouraged there is validation. I want to have confidence in my data, so having the chance to review it is right – even if the system can be frustrating. some consultants will be sceptical about the data, but we are in the 21st century. When I was appointed in 1989, if you referred a patient, everyone would look at you as if to say: ‘What’s wrong; are you scared or are you not properly trained?’
In one generation that has changed completely and now it’s considered good practice to refer people on. Today we have to accept that data transparency is the way forward for healthcare. There will inevitably be issues within the data and this could take two to four years to really get the data right; but the fact is, if you don’t start somewhere, then you aren’t going to get anywhere.
PROF ANTONy NARULA, Consultant ENT surgeon, who concentrates on private practice following early retirement from NHS in 2014
Answers to difficult financial questions
In this month’s column, Susan Hutter (right) responds to more of the most frequent questions she has been receiving lately from private doctors
Qi trade as a limited company and i have had an offer from someone to buy my practice. What should i be aware of from a tax point of view?
If poss I ble , sell your shares directly to the purchaser as opposed to the company selling its assets – including goodwill – to the purchaser.
If you sell your shares, as long as your company is a trading company – that is to say, not top heavy with investment assets –you will get entrepreneurs Relief on the profit on sale of the shares, which means the effective rate of capital gains tax is only 10%.
If you do not qualify for entrepreneurs Relief, the rate of capital gains tax is 20% – which is still lower than income tax rates.
The downside of a company selling their assets is that the money will go into the company. The company will have to pay corporation tax on the gain, which is at 19%.
Then, in order to get cash out of the company, one would have to liquidate the company, which in itself is expensive.
The rate of capital gains tax on the distribution will be 10% or 20% depending on whether you get entrepreneurs Relief. If you do not formally liquidate the company and take the cash out as a dividend, you will have to pay the income tax rate.
Q i have just received an email from HM Revenue and customs about a refund. What should i do?
s o RRy T o say this, but this is a scam. HM Revenue and Customs (HMRC) will never send notifications about tax refunds via email.
As a rule of thumb, HMRC will
only enter into email correspondence with a taxpayer or their accountant with prior agreement. If you receive such an email without such agreement, then under no circumstances visit the website in the email nor open any attachments and do not disclose any information. Report the incident to your IT provider or an IT consultant, as they may need to strengthen your firewalls.
If it happens again – even after the firewall has been strengthened – do not even open the email, as this could implant a virus in your computer.
Qi’ve heard about Making Tax Digital in the press. What is it and how will it affect me?
MAkIng TAx Digital (MTD) is a part of the government’s plans to make it easier for you to get your tax right and keep on top of your affairs.
o nce the MTD regime is in place, details of your income and expenditure will be transmitted to HMRC in ‘real time’ and so they will need to be recorded as and when received/incurred. This may, in turn, remove the obligation to submit the annual tax returns for some of you.
MTD will allow you to monitor your tax affairs or check your tax position throughout the tax year and not only when your tax return is completed. MTD will allow HMRC to collect certain information directly from third parties – so you will not need to notify them of income such as employment, bank interest –which will make the tax compliance easier.
MTD is likely to commence in April 2020 or later.
Susan Hutter is a partner at Blick Rothenberg and part of the team that advises medical practitioners
THe cHancellor HaS Been good To privaTe docTorS
The Budget was favourable for most independent practitioners, writes Susan Hutter
Personal allowances and higher-rate tax bracket
The Chancellor, after saying he had frozen personal allowances and the higher-rate tax threshold, decided to raise them from 6 April 2019. Personal allowances: from £11,850 to £12,500; Higher-rate tax threshold: from £46,350 to £50,000.
Most doctors have above £100,000 total income: the figure where personal allowances are depleted. But those with a lower-earning spouse can transfer income-earning assets to them to decrease the marginal rate of tax for the ‘family’.
Those employing spouses in the practice, as long as the work carried out is commensurate with the remuneration, can look at increasing the salary to take advantage of the changes.
Property lettings
For specialists selling an investment property that has been their principal private residence but then subsequently let, £40,000 of any gain is tax-free.
But, from April 2020, this will only apply where the property owner is in shared occupancy with the tenant.
The final period exemption will be reduced from 18 months to nine months. Although this will increase the capital gains tax burden on sale, many feared the final period exemption would be abolished completely.
Research and Development (R&D) tax credits
Many doctors have achieved useful tax reliefs, and sometimes a tax refund, because they carry out qualifying R&D work within their company. The tax refund occurs where the tax credit was more than the corporation tax due.
But, from 1 April 2020, the tax credit for lossmaking companies will be restricted to three times the company’s total PAYE and National Insurance liabilities for the year. This will hit those who have outsourced the R&D work to non-employees.
savings tax
The band of savings income subject to the nil per cent band will be kept at its current level of £5,000.
Similarly, the ISA annual subscription stays at £20,000. Those who have not used their allowance should pay for the 2018-19 tax year by 5 April 2019.
stamp Duty land Tax and First Time Buyers’ Relief
The Chancellor is extending First Time Buyers’ Relief so that all qualifying shared ownership property purchasers can benefit. Qualifying properties are those costing up to £500,000 and the relief means buyers will not have to pay stamp duty on the purchase.
Those with kids needing help from the bank of mum and dad should bear this in mind if their children wish to buy a property with a friend.
Annual investment Allowance (AiA)
There is a temporary rise in the AIA, from £200,000 to £1m. This is qualifying capital expenditure for trading businesses and could interest those refurbishing a surgery or kitting out a new one from scratch.
The capital expenditure can be written off in the accounts in the year it is spent and will be available for two years from 1 January 2019.
More appointments Brilliant service
Billing And collEcTion
How to ensure you get paid
Invoicing and credit control is a time-consuming task in private practice, but it is essential for obvious reasons. Yet it is the area of practice management that is most often overlooked.
Jane
Braithwaite
reports
Many doctors and medical secretaries are highly focused on patient care, as they should be of course, and therefore billing and collecting the money becomes the lowest priority.
It is not natural for a doctor to switch conversation with a patient from their symptoms and care plan to payment.
Likewise, a medical secretary has often chosen to work in the field of healthcare due to a desire to care for patients and is less comfortable handling the billing side.
Private consultants can sometimes struggle with the
contrast between private practice and working for the nHs
It can be difficult to feel comfortable charging for your medical services after years of n H s work, which is ‘free’ to patients.
Robust credit control
But managing payments and debts is crucial for any business and you will not thrive or grow as a private consultant without a robust credit control strategy from the outset.
In a bigger clinic or hospital, there is often a department that handles invoicing and
billing. this team will often be more aligned with the finance team and this makes total sense. But in a smaller practice, billing must be handled by the secretarial team.
It is well reported in the business world that cash flow is king, especially in the first years of a new business. this is just as true for a consultant working in the private world as it is for a clinic or hospital. delays in receiving payment can put a great deal of strain on cash flow in a private medical practice and we need to ensure this is avoided.
Using good systems will help alleviate and automate much of the process relating to invoicing and collection. It is also key to define good processes and ensure the system is set up to support these processes.
Most private clinics will be invoicing both insurance companies and self-pay patients. They may also be invoicing embassies and legal companies.
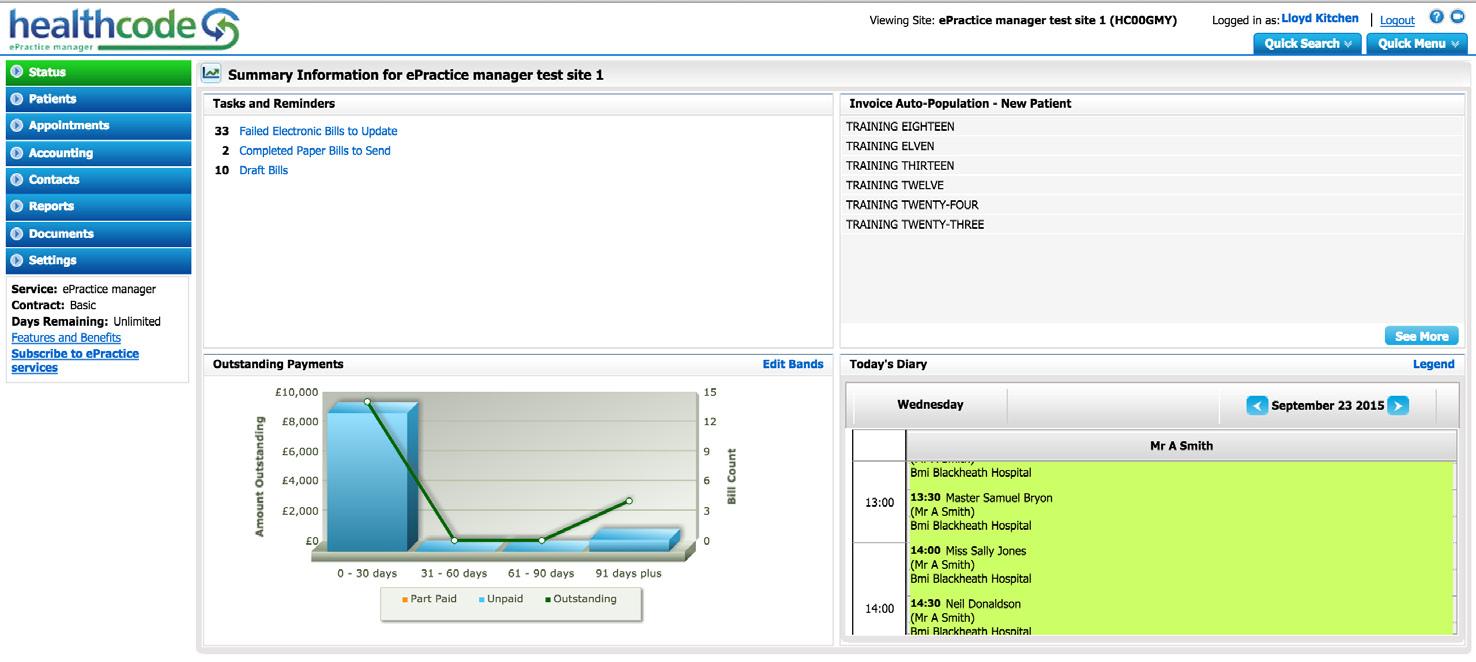
You may already have a practice management software system in place, which could also handle billings, reminders and management accounts.
This could also make it much easier to comply with increasing requests from insurers to send billing information electronically using electronic data interchange.
Submitting invoices electronically will also speed up payment settlement, which should greatly help with credit control.
Electronic billing
The use of technology is imperative, particularly for invoicing insurance companies.
A good practice management system will link to Healthcode and allow electronic billing. All private doctors should be using this technology, as it ensures that insurance invoices are dealt with very quickly and smoothly.
A good practice management system will also ensure that invoicing self-pay patients is simple and easy.
Invoice templates can be created with pick lists of the most commonly used items. Invoices can be sent to patients via email ➱ p16
or by post, if preferred, but I would use email as widely as possible to reduce costs and eliminate delays.
Shortfalls from insurance payments will need to be dealt with in the same way as self-pay patients. It seems that many aged debts are due to lack of transparency over insurance shortfalls.
Patients simply are not aware that their insurance will not cover the entire cost of the consultation, treatment or procedure. This could be remedied by improving communications with patients.
It might mean incorporating a short discussion about payment in the consultation itself, reworking the written information given to patients afterwards or even following up appointments with a short email to clarify information.
If you are sending invoices to embassies and law firms for medico-legal work, these will be created in the same way as for selfpay patients, but a greater focus on chasing for payment will be needed, as these invoices often take much longer to be paid.
My advice would be to attempt to build relationships with key contacts within the organisation to smooth the way.
Reconciliation
The next step in the invoicing process is to reconcile payments received against the invoices issued. If you are using electronic billing for insurance patients, this process will be easier for you.
Insurance companies will regularly send you remittance advice notes that need to be checked against the invoices on the system. If self-pay patients are paying by credit card, the payments should be marked as paid on the day payment is made. There is nothing worse than chasing a patient for payment when they have already paid.
Bankers’ Automated Clearing Services (BACS) payments will need to be reconciled with bank statements and that is a harder task than it sounds.
Encourage patients to quote their invoice number when making a payment to ease the process. Payments should be reconciled regularly so that you have an accurate picture of your current debt. I would suggest that a reconciliation is done at least weekly. At the end of each month, a
report of current debt should be produced and reviewed by key members of the team to identify and address issues early and therefore avoid that debt growing into a mountain of unpaid dues.
credit control process
Each practice needs to define their credit control process. An invoice sent to an insurance company or self-pay patient may be paid promptly, but quite often this is not the case and the debt will need to be chased.
There will always be patients who do not pay on time and standard protocols to collect payment owed will need to be followed.
A robust monitoring system must be in place so that you can keep track of reminders sent. This can be managed within your practice management system.
A good practice management system will allow you to set up a process for chasing debt, but you will need to define the parameters. You can set up standard template letters to be sent after certain periods of time.
The time allowed may differ depending on your practice. You may feel that patients should be allowed a month to pay before receiving their first reminder.
This might be the case in a practice where you are seeing the patients regularly and have every confidence that they will pay at their next appointment. In another practice, you may want the reminder to be sent seven days after the initial invoice.
You can set up a series of reminder letters to be sent by email to patients chasing their payment.
These letter templates must be created and while the first might be a very gentle reminder, the third reminder needs to be a little sterner.
Eventually, someone will need to pick up the phone to chase payment and that is not a task liked by most. If a patient is ignoring your letters, then a phone call may be just what is needed to prompt payment.
Again, you need to decide at what stage this occurs. Do you wait one month or three months before taking such a step? What feels right in your practice?
Are your invoices eAsy to Action?
is your invoice template clear and easy to understand? is vital information prominently displayed, such as fees and expected payment dates? is it clear how to make a payment by bacs or credit card?
Would trAining help?
if you are handling credit control in-house, could your medical secretary benefit from some further training to assist with the financial aspects of the role?
systems And processes
Are you using the systems to enable the process? have you defined your credit control processes?
code it right
incorrect procedure coding is one of the main reasons why invoices are not paid by insurers. make this a focus for your practice to save time and money.
mind the shortfAll
insurance shortfalls are a common reason why invoices aren’t paid on time. let your patients know if there will be a shortfall between your fee and the cost the insurer will fund.
remind your Busy pAtients
to
pAy send reminders within a reasonably short period of time. this is a way to both manage relationships and increase the likelihood that invoices will be paid in a timely manner.
reconciliAtion
ensure you are reconciling payments each week, including insurance payments and BAcs payments.
deBt report
produce a monthly debt report and assess how this is increasing/ decreasing month on month. if it’s increasing, review and refine your credit control processes. ideally, all debts should be less than 90 days. Anything above 90 days is an issue that needs addressing.
debt collection
Thankfully, most patients do pay what is owed, but there will be a small percentage who ignore emails, letters and phone calls.
You need to be clear on how you will handle this. Are you happy to accept a certain percentage of non-payment and simply write this off? Or do you want to take this further and involve a debt collection agency. Obviously, this is a last resort, but one you will need to consider.
Whether you are running a large hospital or a small clinic, you have a choice whether to handle invoicing and credit management in-house or to outsource.
in-house billing and collection
Many consultants choose to handle credit control themselves when they first start out in private practice, in partnership with their medical secretary. This can be a workable solution while the practice builds, and needs to be scalable once the practice becomes busier.
You may need to employ additional members of staff to manage the workload. You may employ a medical secretary and a billing specialist who are able to work closely together but have defined roles. As always, effective and clear procedures need to be in place from the very start.
It is imperative that administrative and financial processes are reviewed regularly and documented to avoid key person dependency. You do not want to find yourself in a situation where someone is sick and no one else knows how the systems and processes work.
There are a number of accountants who specialise in the private medical sector who could help with reviewing and recording your clinic procedures. And while this may seem expensive, it may turn out out to be a cost which repays the investment many times over.
Consultants and their secretaries often find chasing debts to be an uncomfortable task and not one that fits easily with the medical ethos.
You will need to ensure that you and your team stay informed about technological advances so that you and your patients can benefit from them.
the primary advantage to outsourcing billing and collection is that consultants can spend more time concentrating on developing the medical side of the business
On the positive side, handling invoicing in-house means that you have complete control and can feel comfortable that every communication with your patients is made by a member of your team.
outsourcing invoicing
Many consultants move their entire invoicing work to an external company, which will send invoices, liaise with insurers and chase payments.
Most of these companies charge a percentage fee for the invoices they process and collect on behalf of your practice.
They can also chase aged debts and provide a variety of management reports such as insurance breakdowns and bank reconciliation information.
Some firms have their own custom software for this, while others integrate with industry-standard practice management software.
The primary advantage to
outsourcing billing and collection is that consultants can spend more time concentrating on developing the medical side of the business.
The downside is the additional cost, although this should be weighed against the potential savings outsourcing may provide. Consultants should also consider whether relationships with patients could be negatively impacted by moving invoicing to an external company. As always, communicating regularly with patients may help offset any problems.
Following the tips provided in this article may hopefully mean fewer debts are left to chase.
see the a-Z of billing, page 18
Jane Braithwaite is the managing director of Designated Medical, which offers business services for private consultants, including medical secretary support, book-keeping and digital marketing
EXPERT ADVICE YOU CAN TRUST
ADVICE YOU CAN TRUST
EXPERT ADVICE YOU CAN TRUST
Since starting in the mid 1970’s Sandison Easson has continued to grow and is one of the largest independent medical specialist accountants in the UK.
Since starting in the mid 1970’s Sandison Easson has continued to grow and is one of the largest independent medical specialist accountants in the UK.
Since starting in the mid 1970’s Sandison Easson has continued to grow and is one of the largest independent medical specialist accountants in the UK.
Sandison Easson acts for medical professionals throughout all stages of their career and has clients in almost every town in England, Scotland and Wales.
Sandison Easson acts for medical professionals throughout all stages of their career and has clients in almost every town in England, Scotland and Wales.
Sandison Easson acts for medical professionals throughout all stages of their career and has clients in almost every town in England, Scotland and Wales.
We provide the usual services you would expect from an accountant such as preparation of your accounts and tax declarations but offer so much more including advice on:
We provide the usual services you would expect from an accountant such as preparation of your accounts and tax declarations but offer so much more including advice on:
We provide the usual services you would expect from an accountant such as preparation of your accounts and tax declarations but offer so much more including advice on:
• Setting up in Private Practice
• Setting up in Private Practice
• Setting up in Private Practice
• Developing your Private Practice
• Developing your Private Practice
• Developing your Private Practice
• Tapering of the Annual Allowance
• Tapering of the Annual Allowance
• Tapering of the Annual Allowance
• Lifetime Allowance planning
• Lifetime Allowance planning
• Lifetime Allowance planning
• Personal Allowance planning
• Personal Allowance planning
• Personal Allowance planning
SPECIALIST MEDICAL ACCOUNTANTS T 01625 527 351
SPECIALIST MEDICAL ACCOUNTANTS
• Reviewing your PAYE Coding Notices SPECIALIST MEDICAL ACCOUNTANTS
• Expenses that you can claim and those you cannot
• Expenses that you can claim and those you cannot
• Expenses that you can claim and those you cannot
• Minimising your tax bills
• Minimising your tax bills
• Minimising your tax bills
• Reviewing your PAYE Coding Notices
• Reviewing your PAYE Coding Notices
T 01625 527 351
T 01625 527 351 E info@sandisoneasson.co.uk
www.sandisoneasson.co.uk
E info@sandisoneasson.co.uk W www.sandisoneasson.co.uk
A Rex Buildings, Wilmslow, Cheshire, SK9 1HY
BUILDING FOR SUCCESS
A-Z of getting the money in
Invoicing and collecting the money pose huge problems for many doctors building their practices and they are often owed many thousands of pounds before they ask for help. Findlay Fyfe presents an A-Z of billing to guide you to success
Ais for audit trail . Do you have a clear policy for communication and interaction with payment companies and patients to ensure you are tackling your practices invoices efficiently?
B is for benchmark . When taking on a new practice –and typically yearly thereafter –our experts at Medical Billing and Collection (MBC) will carry out a benchmark on the practice professional fees to show where there may be scope for review.
C is for the Clinical Coding and Schedule Development group (CCSD). Make sure your practice is up to date with new codes, unbundling and charging changes to codes. These are updated monthly. Failure to keep this updated could run the risk of your practice being deregistered by many private medical insurers.
D is for Did Not Attend (DNA) or, more importantly, deciding what the practice should charge patients who do not turn up for the consultation. Additionally, you need to ensure that any potential charge is clearly detailed in the terms and conditions.
A new histopathology partnership
Creating a better patient journey
Cellular Pathology Services has been providing specialist histopathology services UK wide since 2007. Our laboratory is CQC registered, ISO 15189:2012 accredited and trainingapproved by the IBMS.
Our streamlined processes, consultant led reporting and secure electronic dispatching of results (90% of histology cases reported within 72hrs), will enable your practice to expedite the patient journey, reduce administrative burden and reinvest the saved time elsewhere.
Bespoke services model
The delivery of our histopathology service is adapted to match the exact requirements of each and every practice. Our account management team makes sure that the transition from your existing histopathology provider to CPS is a seamless and stress free process; taking the pressure of your team whilst maintaining a continuous service and improved service to your patients.
I receive an efficient, professional and very rapid turnaround from CPS which is great for patients in terms of getting results back. They add value to my private practice with no delay for specialist histology reports. The quality of the work is excellent and I know that if there is ever a problem, I will get a phone call for clinical pathological correlation. The team at CPS are very friendly and are
very quick to answer the phone. CPS also sets up the MDT AND provides a brilliant Mohs service. Dr Dev Shah, Consultant Dermatologist & Mohs Surgeon
An extension of your team
Our specialist client services team will deal with all of your enquiries, supporting your practice, consultants and their secretaries. From ordering consumables to arranging a courier pickup, organising MDTs and liaising with our consultant pathologists; we become an extension of your team.
You’re never on your own. Our consultant pathologists are available around the clock for clinical pathological discussions and will attend MDTs personally when and if required. Our helpful and knowledgeable client services team are at hand 9am to 6pm, Monday to Friday with a dedicated out-of-hours service for any urgent requests or access to results.
I have been in Independent Practice, as a Consultant Urological Surgeon, since 2011. I have used CPS exclusively for all my histopathology. The service is excellent and timely. Clear reports with images are produced and are now available through their online service. Drs El-Jabour & Mitra are always available for telephone discussions and attend MDTs as required. Altogether an excellent service that I recommend to all my consultant colleagues. Mr George Fowlis, Consultant Urological Surgeon
Only a phone call away
We prefer to work as a close and long term partner and collaborator, helping our clients to provide a world-class standard of care for every patient.
If you are looking to conduct a review of your current histopathology partner or are actively looking for a new provider that structures their service specifically around your practice, then call our team today on 01923 233299.
E is for embassies. If you chose to see embassy patients, be aware of the new lower pricing structures that embassies will now accept and understand that payment may take some time.
This may mean you pay tax on the invoice before you have been paid. In addition, only see patients with a letter of guarantee (LOG), otherwise the embassy will not pay that invoice.
• Completely open scanner that is well tolerated by claustrophobic patients
• Weight-bearing scans for spine and joints enable a more precise diagnosis
• Patients who are large or cannot lie down can be accommodated
Fis for fees and understanding what each private medical insurer will pay for each CCSD code. Payment rates will vary for each insurer and the differences can be as much as 100%.
Ensure your practice is aware of what it can be charging to ensure you are maximising your revenue.
I is for incorporated. Since the last round of income tax increases, a high proportion of consultants have gone from being self-employed to making their practice a limited company in order to be more tax-efficient.
J is for January , which is the best time to review the practice’s commercial side. Review any decisions that need to be taken on key commercial aspects such as fees, debts and internal procedures so they can be implemented before the start of the new tax year.
Gis for the EU’s General Data Protection Regulation (GDPR). There are a lot of mixed messages regarding GDPR legislation and how to comply. Be clear about what your requirement is as a practice and be sure any third party you work with is also compliant.
K is for knowledge. In private practice, it is important to have a keen commercial perspective. It is rare to find this among independent practitioners, so if it is not available, then outsourcing those key areas to obtain the required level of expertise should be seriously considered.
His for Her Majesty’s Revenue and Customs Make sure that billing for the practice is auditable and organised so that figures can be easily generated for the tax returns.
This will save time and give a sense of comfort should the taxman ever wish to come and inspect your practice; then the figures will be clear and easy to read.
L is for limited liability partnerships (LLPs), which is an alternative to incorporation when forming a group of consultants who are going to work together and trade as one entity. Being bigger can have billing
advantages – but bigger billing and collection problems if that part of the business is not functioning properly.
Pis for private medical insurer. Ensure you are billing the correct fees to each insurer. Ensure that you renegotiate agreements when you can.
Mis for medical billing and collection . This should always be one of the main priorities within a practice.
If the practice is too busy to correctly chase and address invoices, then it needs to consider outsourcing this vital area.
This should ensure that the bad debts are kept at less than 0.5% and that the codes are billed at the correct rate, leaving the practice to focus solely on the medical side.
Qis for quote. Ensure when the practice charges outside of the private medical insurer fee schedule, or does complex work, that the patient is fully informed of all the costs so that they can liaise with their insurer to understand what it will cover and what the shortfall will be.
You may need to supply supporting information to a private medical insurer.
Nis for new consultants entering private practice. With the reduced re-imbursement levels available to new consultants from insurers, it is doubly important that they ensure billing and collection is quick, accurate and efficient.
When starting up in private practice, you should not be worried about any potential cash flow issues. But this becomes more prevalent as the practice and the overheads grow.
Ris for registration form This should be part of any new patient process within the practice. It details all the patient demographics, including mobile number and email address as well as their insurance policy details. It should also have disclaimers if you are using a third-party company or wish to contact patients after treatment in a marketing campaign. Stay on the right side of the GDPR legislation.
Ois for overseas patients and understanding that if the practice decides to see these patients, then they need to consider how to collect the money from them.
Typically, the best way of operating is to get paid up front in advance of any treatment.
S is for self pay . This is the fastest-growing sector and has risen to a third of my compa➱ p22
BILLING FIGURES
ny’s billing totals over the past few years. Now it is typically the largest or second largest part of most practices.
It is important to set the fees at the right level to ensure both a good market share but also to ensure the best rates are paid.
W is for website. To take full advantage of the growing self-pay sector, every consultant should have a website. To ensure ongoing traffic, keep it relevant and keep it up to date.
Tis for terms and conditions
Make sure your practice’s costs are transparent and that the patient is made aware of all known costs and potential liabilities. Should this be on the back of your registration form?
X is for Xmas, when I reckon all consultants should take a well-earned break from private practice, if possible. It is the only time of the year when even the patients do not want to be seen unless it’s absolutely necessary. And it’s a time to recharge the batteries and look forward to the New Year.
35% of a practice’s billing is, on average, to self-pay patients
45% is billed to the private medical insurers
20% is billed to other companies
5% of a consultant’s turnover is typically written off
0.5% – less than this figure is what Medical Billing and Collection writes off for its clients
Uis for undercharging , which – unfortunately from our experience – is happening in most practices.
This occurs for a number of reasons and typically has been going on for a number of years. We find it is usually due to a lack of knowledge or understanding of the commercial market and how the insurers calculate their fee schedules.
Y is for you. And you need to take a business view along with your clinical view. This is where a third-party company can help add value to your practice and, of course, to make sure that the billing and collection side of your business is tied down and firmly under control.
V is for voicemail. Any practice should consider having an ‘overflow service’ where any calls coming into the practice out of normal operating hours are answered by an external source. This will help you from losing potential revenue.
Z is for Zzzzzzzzz. Sleep easy. This is the sound that the independent practitioner makes while lying back sleeping soundly knowing that the practice’s billing and collection is under control, there is no bad debt and the tax aspects of the business are under control.
Findlay Fyfe (right) is the managing director of Medical Billing and Collection
Are informal business links placing your future at risk?
Practitioners establishing loose tie-ups with other medical professionals could miss out on potential benefits – and leave themselves vulnerable. Peter Anderson reports
PRACTITIONERS joining forces as informal associates are being alerted to the benefits of creating more structured partnerships and companies – and of the potential risks that their looser working arrangements can present.
Evidence suggests that a growing number of individuals in the medical profession have been reaching out to industry colleagues in order to create more flexible working – for example by being able to share workloads at busy periods or ensure cover during holidays or illness.
But, according to insurance specialist Medical Risk Services Limited (MRSL), this can mean practitioners are missing out on considerable financial benefits that are available to more structured groups and businesses. It could also mean individual doctors and medical personnel are unwittingly caught out if one of their “casual” business colleagues runs into difficulty, for example through legal action from a disgruntled patient.
Roger Houston, MRSL’s cofounder, explained: ‘Medical professionals are typically aware of the potential legal implications of action being taken against a member of their team or direct staff.
‘This so-called vicarious liability also extends between practitioners working within the same company or group, but can be mitigated against by taking out group-wide insurance that covers the entire business.’
He added: ‘However, the legal liability could also pass from one
practitioner to another in a much more informal working arrangement but – because the individuals are operating independently – they’re often missing out on the potential benefits available from specialist entity-wide indemnity products.
‘As one potential client recently reflected, it means practitioners operating in an informal grouping are experiencing all the risks of being part of a wider business, but none of the protections.’
MRSL, a key provider of insurance, advice and services to medical practitioners, has been working since 2004 to help doctors and medical businesses mitigate and manage their risks and reduce their indemnity costs.
Group-wide benefits
As the company points out, those working as part of a formal business or partnership are also able to work together in securing group-wide employers’ liability cover, insurance against disciplinary matters or potential data breaches, and cover for potential employee disputes.
Further advantages can come, according to MRSL, when doctors set up a group and also transfer their cover from a medical defence organisation to the commercial insurance sector. These can include issues surrounding increasing causation defences and statute of limitation.
The business also highlights that potential issues are not merely faced by doctors, but also by their nursing staffs and support teams, as well as external
operators such as administrators and accountants.
In the key area of cover for entities versus that for individual practitioners, MRSL can advise on run-off cover in addition to the very significant issues surrounding vicarious liability.
According to Mr Houston: ‘The insurance and financial implications of working as an individual, a recognised company or an informal unit can be potentially huge. It’s vital that practitioners are aware of all the specific legal requirements and opportunities – and that they can therefore capitalise on what’s available.’
Clear processes in place
The processes of forming a company are only too clear to Stanbridge Associates, a leading specialist accountancy firm. The business has been providing financial and tax advice and services to medical professionals for more than two decades.
Director Vanessa Sanders said: ‘Setting up a limited company is
relatively easy to do but many directors of small entities fail to understand they are operating a business which is separate to them as individuals.
‘There is a risk of HMRC – and possibly others such as the courts – being able to look through the protection of the limited liability and say the person was acting as a sole trader. This means taxes can be applied to the person rather than the company at higher rates. It also means the limited liability in the event of claims may be subject to scrutiny.’
She said many newly formed companies failed to appreciate they had regulations to which they must adhere, such as employers’ liability insurance, or that they needed to inform their professional indemnity insurer when they operated as a limited company.
For further information on MRSL and its services, please phone 0203 058 3733, email enquiries@mrslenterprise.com or visit www.mrslenterprise.com
Dear Reader,
SUBSCRIBE TODAY TO GET EVERY ISSUE – AND READ US ONLINE
Subscribing to Independent Practitioner Today is the only way you can be sure you will see every issue and have the option of reading us online using our special page-turnable edition. Don’t risk missing out. Our personal subscription for doctors and managers is only £90 a year and £210 for organisations. But you can cut this to just £75 and £180 respectively if you pay by direct debit. So take advantage of this offer now for our unique business journal dedicated to supporting you in your private practice. We’re confident your subscription will repay itself many times over!
Editorial director
APPLICATION FOR SUBSCRIPTION
Private practitioner* r r Organisation*
Please debit my Mastercard/Visa/Amex/Diners Card No
I encose a cheque made payable to The Independent Practitioner Ltd Please debit my Mastercard/Visa/
Expiry date *Security No†
† Last 3 digits on signature strip
I would like to pay by direct debit (please complete all details in box below). Don’t forget, it’s £15 cheaper to pay by direct debit; £30
Instructions to your Bank or Building Society to pay Direct Debits Name and full address of your bank/Building Society
of
your application (No postage required – UK only) to: Independent Practitioner Today Subscriptions Department, FREEPOST, PO Box 36, Plymouth, PL1 1BR
to:
and Building Societies may not accept Direct Debit instructions
Or subscribe online at www.independent-practitioner-today.co.uk if
a Direct Debit at any time, by writing to your Bank or Building Society. Please also send a copy of your letter to us.
A cure for errors?
SPIRALLING MEDICAL negligence costs are perhaps the greatest threat to the future of the NHS.
Over the last three years, there has been a threefold increase in pay-outs to patients who believe they have suffered as a result of medical negligence.
Patients seek and deserve four things:
1. An apology; 2. An explanation; 3. Compensation; 4. Rapid resolution of their claim. If the NHS and the private medical sector are to fulfil their obligations to patients and pursue the ‘Duty of Candour’ that is a requirement for all who work in the NHS – and by inference in the private sector too – there can be no discussion about or disagreement with these four fundamental objectives.
The same principles apply to the private medical sector. Under the present system, these aims are not met. All too often, patients who believe that their treatment has caused them an injury face a Doctor expert witnesses and patients are hugely frustrated with the
Managers, doctors, nurses and all healthcare workers are required to hold true to these fundamentals.
brick wall at the hospital where they have been treated.
Their initial attempt to be given an explanation and to understand what went wrong is met with a system that discourages openness. In frustration, patients seek advice from lawyers, who promote themselves as champions of patients’ rights.
The ironic result is that the initial decision whether or not a patient has suffered an injury as a result of negligence is made by lawyers and not by medical or nursing professionals.
Distortion of facts
Having made the decision that there has been negligence, lawyers will endeavour to ‘win’ the case. This leads to distortion of the clinical facts.
Doctors are trained to evaluate all the evidence and make a decision based on that. Lawyers are trained to look at all the evidence
and to discard that which does not fit their case.
This starts a protracted, stressful and costly ‘patient journey’. The outcome of cases is settled by an adversarial legal approach that often does not reflect the clinical picture.
In the most recent report from NHS Resolution (NHSR), the headline figures in the financial overview reveal that the total paid out in compensation and costs has risen from £1.7bn in 2016-17 to £2.2bn in 2017-18. More than £400m of this was due to the change in the Personal Injury Discount Rate (PIDR) over which NHSR has no control.
NHSR chairman Ian Dilks wrote:
‘At current prices, the annual “cost of harm” is now circa £7-£8bn, roughly double the figure prior to 2016-17.’
At the top of the list of priorities must be the injured patient. However, there are other stake-
All too often, patients who believe that their treatment has caused them an injury face a brick wall at the hospital where they have been treated
holders apart from the injured patient.
The enormous increase in the cost of funding medical negligence claims is reducing the amount of money available for patient care. The costs are funded by each trust paying to the NHSR a sum that is in the region of 2% of their total budget.
Wider implications
This has a negative impact on the care of many NHS patients. Although compensation must be paid to those who deserve it, there are wider implications that must be identified and acknowledged.
In 2017-18, there were 10,673 new clinical negligence claims made in the NHS. This figure must be seen in the context of some 20m ‘episodes’ of care. No compensation is paid in one third of the claims investigated.
The stress for the patients and for the doctors involved is enor-
Having served healthcare professionals since its inception in 1993, TaxLink, chartered tax advisers and accountants in Wimbledon, has built a wealth of knowledge and experience in dealing with taxation issues faced by doctors in private practice. Our focus is on tax planning and compliance.
l Tax structuring to suit personal circumstances (LLP, limited companies)
l Solvent liquidations
l Consultant groups and consortia
l Assessment of pension contributions in light of tapering annual allowances
l Ad hoc assistance with HMRC investigations and reviews.
mous. The threat of litigation leads to defensive and risk-averse medicine, both of which are expensive and result in poor practice.
There is a panel of solicitors that receives instructions from the NHSR and who ask experts for what is described as a ‘short report’. There is no NHSR definition of such a report; each firm of solicitors has its own definition and decides what fee to offer.
The initial request for a short report frequently includes that the report need not be Part 35 compliant. These are the Civil Procedure Rules that are the regulations set out by the Ministry of Justice to which experts and assessors must conform when writing reports. This does not mean the report will not be disclosed.
But the fee offered is derisory and does not allow the expert to write a report that does justice to both the claimant and the defendant.
Once the case has been taken over by lawyers, the best opportunity for successful mediation has been lost. There is no incentive for lawyers to pursue resolution by mediation
To write a report that involves giving an opinion on the potential negligence of a medical colleague is among the very greatest professional responsibilities.
It is a travesty if such a responsibility is not undertaken with the same thoroughness as if the instruction had been for a Part 35 compliant report to the court.
Slow uptake
Mediation is a strategy supported by the NHSR. So far, the uptake has been slow. Of 16,338 claims that were settled in the last 12 months, 189 were settled by mediation.
The drawback to the current mediation initiative is that the two fundamental prerequisites to mediation are not met. The two sides must agree that mediation is the way forward. Mediation must be seen to be independent.
Mediation will only be likely to be successful if introduced at the very earliest stage of the ‘patient
journey’. Once the case has been taken over by lawyers, the best opportunity for successful mediation has been lost. There is no incentive for lawyers to pursue resolution by mediation. There is a very strong financial disincentive. Independent Medical Negligence Resolution (IMNR) has been set up to contribute to changing the way in which medical negligence claims are handled and to address the concerns listed above.
Injured patients, chief executives of both private and public hospitals, malpractice insurance companies, medical negligence solicitors and indeed NHSR can all access IMNR directly.
IMNR will work with all those who want to avoid a lengthy, expensive, stressful and confrontational approach by first exploring the possibility of alternative dispute resolution.
At a meeting with Helen
IMNR is intending to contribute to a streamlining of the medical negligence system that will be to the benefit of all
Vernon, the chief executive of NHSR, I explained that IMNR would wish to work with them, as we shared the intention of offering rapid resolution.
We will work with any agency that shares our belief that, at the beginning of any complaint, every effort must be made to pursue one or other means of alternative dispute resolution.
In the public or private sector, patients who feel that they have been injured can approach IMNR directly. Their clinical situation will be assessed by medical expert witnesses who are acknowledged leaders in their field.
The higher the quality of the report, the less contentious the outcome, the less room there is for lawyers to pick holes and the less chance there is that a case will end up in court and the quicker their case will be resolved.
➲ Experts are required to block off dates months and even years ahead of a trial window that has been reserved for a court case, when we know full well that there is less than a 1% chance of the case coming to court.
➲ The outcome of cases is settled by an adversarial legal approach that does not reflect the clinical picture.
➲ Many solicitors and the agencies that t hey use are very slow to settle fee notes.
Frustrations avoided
We reported on the launch of Independent Medical Negligence Resolution last month www.macintyrehudson.co.uk
Chartered Accountants, Tax & Business Advisers specialising in the Healthcare Sector
• Tax structures for Hospital Consultants
• Surgeon groups and consortia
• GP practices, including mergers and federations
• Solvent liquidations
Contact James Gransby Partner & Head of Healthcare
E: james.gransby@mhllp.co.uk
T: 03330 100221
Increasing stress
The posturing that is part and parcel of the adversarial legal system means that although cases are settled out of court, this may not be until close to a trial date that has been set months or even years in advance.
This adds to the delay, increasing the stress for both claimant and defendant and increasing costs, solicitors’ costs, counsels’ costs, medical witness costs and court costs.
The agencies that many solicitors use add further costs without contributing added value.
For those who write expert witness reports, there are many frustrations:
➲ Documents are often poorly presented. Photocopying, pagination and indexing are inaccurate or absent.
➲ The agencies that many solicitors use are inefficient and contribute to further delays, adding to costs but not value.
➲ After months of previous silence, expert witnesses are often required to respond at short notice to revise a report, to respond to Part 35 questions or to provide a joint report.
➲ Not uncommonly, experts are not informed when a case has been settled and the outcome of the case is not revealed. Experts are deprived of an important feedback on their report.
There will be many advantages for medical expert witnesses when instructions come through IMNR. The frustrations identified above will be avoided. The expert will know that they are contributing to improved care of the injured patient, helping to resolve claims rapidly and thereby reducing stress for claimants and for the doctors involved.
The higher the quality of the report, the less contentious the outcome and the less room there is for lawyers to pick holes and the less chance there is that a case will end up in court.
In an article published in The Daily Telegraph in February 2018, Niall Dickson, chief executive of the NHS Confederation, wrote: ‘Calling for a comprehensive package of legal reform of anything in the current political and parliamentary logjam may seem a lost cause, but there will come a time when parliamentarians can think of something other than Brexit, and we need to lay the ground now.’
In the meantime, IMNR is intending to contribute to a streamlining of the medical negligence system that will be to the benefit of all.
If you are an experienced medical expert witness and would like to know more, email me at director@imnr.org.uk
Mr Hugh Whitfield (right) is a consultant urological surgeon at King Edward VII Ho s pital, Devon shire St, London, and a medical expert witness and the founder of IMNR
High-tech business investing in itself
With The London Clinic being a charity, we asked its chief executive
Al Russell (below) where all the money goes
DURING MY first year as chief executive of The London Clinic, it has surprised me how few people realise we are a charity.
Charitable status has been fundamental to who we are as a hospital since 1935 and will continue to be in years to come.
Our purpose as a charity is to re-invest our surplus profit to advance healthcare and support research and education.
This, in turn, must benefit not only our patients and their families, but also the wider medical community.
To achieve this, we have to run a great hospital and a great business. We are hospital, a business and a charity.
Investing our income
We are governed by the chairman and board of trustees and they delegate the day-to-day management of the hospital to myself and the executive board of directors.
While we have no need to impress profit-driven shareholders, we do have a responsibility as a charity to grow our surplus profit so we can re-invest this back into the hospital to fulfil our charitable purpose.
While it’s true that we do not pay any tax on our surplus, it’s also true that we cannot benefit from any off-setting tax allowances on capital investment, which is what we use the profits for.
Our investment decisions are made against additional nonfinancial criteria:
Delivering exceptional patient care ;
Clinical innovation in technology and treatments;
Advancing healthcare knowledge and medical research.
Highly rated
We collect monthly patient feedback and measure trends closely. One of the questions that we ask is whether a patient would recommend The London Clinic to their friends or their family.
Throughout 2017 and 2018, we consistently scored in the high 90s percentage for the answer to
this question. Trust and faith in our nursing staff also scores consistently in the high 90s.
One of our largest insurers rated us as a top hospital performer in greater London for both patient experience and for having the lowest number of patient complaints.
Our high nurse-to-patient ratios, 32 clinical nurse specialists and 24/7 resident medical officer cover in specialist disease areas provide dedicated inpatient and outpatient expertise to consultants, patients and families. The quality of our nursing is a source of great pride within the organisation.
p32
Free care for patients
Palliative care for cancer is not re-imbursed by insurers, so we deliver these services at no cost to patients in the Duchess of Devonshire Wing. Helping and supporting patients through this incredibly difficult time is fundamental to our charitable ethos and ‘caring’ value.
The Care Quality Commission rated our complementary palliative care service as ‘outstanding’ and we are very proud of the work we do for these and all of our patients. In 2017, more than 90 patients and their families benefited from this service.
For many people diagnosed from blood cancer, a stem cell transplant is often the only chance of a cure. We are the only private hospital in the UK to offer bone marrow and peripheral stem cell collection, supported by our on-site pathology and dedicated stem cell laboratory, accredited by JACIE and UKAS.
We have worked with Anthony Nolan, the UK’s largest blood cancer charity, for over 17 years to provide bone marrow and peripheral stem cell collection services. We also provide stem cell collection and laboratory services to British Bone Marrow Registry, DKMS and a major NHS trust.
In 2017, around 730 stem cell and bone marrow collections were performed by The London Clinic, benefiting patients across the world. We are largest stem cell collection point in Europe and we run this service in a fantastic partnership led by The London Haematology Group.
Complementary therapy
The London Clinic also offers complementary counselling sessions free of charge to our cancer patients and their families.
Each session is tailored to each individual, drawing upon a range of therapeutic techniques, including mindfulness-based cognitive therapy, solution-focused therapy and relaxation in order to promote positive coping with cancer.
Our hospital offers complementary therapy services, such as reflexology and spiritual healing, to help patients with their transition back to their lives outside the hospital. In 2017, we supported 107 patients with our complementary therapies and counselling services.
The Duchess of Devonshire Wing, where all of our cancer care is provided, recently won the award of International Cancer Centre of the Year at this year’s IMTJ Medical Travel Awards.
The Duchess of Devonshire Wing, where all of our cancer care is provided, recently won the award of International Cancer Centre of the Year at this year’s IMTJ Medical Travel Awards
ABOVE: The
Competing against other international hospitals, winning the International Cancer Centre of the Year category is pleasing to win because cancer centres must show evidence of the numbers and type of patients treated, quality and range of services and patient satisfaction feedback.
Patients receive an exclusive cancer care pathway from diagnosis through to outpatient support.
Clinical innovation
There are many examples of clinical innovation, but I’ll share some of the most recent ones.
This year, Mr Dinesh Nathwani,
consultant orthopaedic surgeon, introduced a new service utilising a cutting-edge Navio robot with sophisticated computer navigation, revolutionising knee replacement surgery.
The device uses 3D infra-red technology that aids the surgeon to minimise the amount of bone removed from the knee, ensuring the artificial joint is more accurately placed to suit the patient’s anatomy.
This aims to improve the longevity and comfort of the implant as well as reducing the overall time the patient spends in the hospital, thus further minimising the risk of post-operative complications.
We were also proud to treat our first patient with Parkinson’s disease using deep brain stimulation (DBS). This is a procedure in which stimulating electrodes are placed into the deep structures of the brain.
This is led by Mr Erlick Pereira, consultant neurosurgeon and spinal surgeon. For the procedure, electrodes are connected to an implanted pulse generator which is battery powered.
Selected patients with treatment-resistant movement disorders such as Parkinson’s disease, tremor and dystonia can benefit.
There are nursing stations outside every room in the ICU, so patients can be monitored and cared for without being disturbed
new Siemens Magnetom Vida 3T MRI scanner is lowered in through the roof of the Duchess of Devonshire Wing in July
Successful DBS allows a decrease in medication or makes a medication regimen more tolerable in these disorders.
There are gains in movement and control. The intervention is used for carefully selected patients, in accordance with clinical eligibility criteria, who cannot be adequately controlled with drugs or whose drugs have severe side-effects.
Intensive care
We opened our intensive care unit (ICU) in November 2016, which provides advanced, safe care (level two and three) to our patients and support to our surgeons performing complex surgery.
The decision in 2012 to build a new ICU was influenced by the vision to provide clinical excellence for our consultants and the desire to provide more privacy and dignity for patients.
Building it in a busy hospital in
central London was challenging and we are delighted by the highquality outcome.
The ICU has natural light and ensuite wet rooms with hoist access from beds in all 13 individual patient rooms and a sophisticated airflow system throughout the unit for infection control.
There are nursing stations outside every room, so patients can be monitored and cared for without being disturbed.
And our rooms have ‘smart glass’ technology which can switch from transparent to opaque with the press of a button – giving privacy to patients and their visitors.
We are the first UK hospital to invest in the newest Siemens 3T MRI scanning technology that offers exceptional quality imaging, supporting specialty areas such as orthopaedics, oncology, urology and neurology.
Our MRI facilities have been
designed with patient comfort in mind as we want them to feel at ease during their scan. This opened in mid-September. These are examples of new procedures and facilities that we decide to invest in with an approach that is not a typical ‘return on investment’ equation. Our charitable purpose is often the decisive factor in our decision.
Advancing healthcare knowledge and research
Our Advanced Therapies Centre (ATC) manages phase I-IV clinical trials for new medicines and special access programmes for unlicensed medicines. We currently have two open oncology clinical trials and five in the pipeline.
We provide research governance, clinical trial management and quality assurance and facilities collaboration with seven NHS hospitals, universities and charities. Examples of where we have
ADVERTORIAL: MEDICAL RISK SERVICES LIMITED
supported our consultants include Target R for breast cancer and RADIOCYST for pancreatic cysts.
Our investment in staff and wider healthcare community is a major priority. Our clinical nurse specialist team provides mentoring and advice for student nurses from City University who are starting their careers.
Our radiotherapy and radiology departments support students from City University throughout their training.
We also invest heavily to develop our own clinical and non-clinical teams, with a substantial training programme ranging from professional development courses to leadership diploma qualifications for our managers that are accredited by the Chartered Management Institute.
We will continue to work hard to deliver excellence, increase our surplus profit and invest in our charitable purpose.
Pelican support fits the bill
MEDICAL RISK Services Limited (MRSL) has extended its support for good causes by announcing a year-long tie-up with the Pelican Cancer Foundation charity.
MRSL, a leading provider of insurance, advice and services to medical practitioners, will offer practical and specialist help to the charity, will help promote its work and will seek fundraising opportunities.
The initiative will also see MRSL donate part of its commission from any medical indemnity or insurance product placed with it by a medical business during the 12 months.
MRSL director Chris Cloke Browne said: ‘We’re absolutely delighted to offer our support to Pelican for the next year. The charity has been working tirelessly for more than a quarter of a century, making a huge difference to those people affected by cancer.’
Created to support pioneering
colorectal surgical work, Pelican focuses its efforts and resources on improving precision surgery for cancer of the bowel, liver, bladder and prostate.
The charity leads research into pelvic cancer surgery and treatment, while also delivering professional courses for surgeons and cancer teams, in order to
develop and communicate latest procedures.
It aims to discover the most effective treatment for each individual patient, refining treatment options to achieve the best outcomes for patients’ survival and quality of life.
Tim Lockwood, community and corporate fundraiser with
Pelican, said: ‘We are very excited and thrilled that MRSL will be partnering with us over the next year in helping make a difference by innovating precision surgery for patients with below-the-belt cancers.’
Fundraising initiatives
MRSL’s support for Pelican comes on the heels of a range of fundraising initiatives, for organisations including Crohn’s & Colitis UK and Basingstoke-based St Michael’s Hospice. It has also supported Challengers, which runs community-based projects for children and young people with disabilities.
More details on Pelican Cancer Foundation are available by visiting www.pelicancancer.org or phoning 01256 314746.
For further information on MRSL and its services, please contact 0203 058 3733, email enquiries@mrslenterprise.com or visit www.mrslenterprise.com
Pelican’s Tim Lockwood (left) with MRSL director Chris Cloke Browne
KEEP IT LEGAL: RENTAL AGREEMENTS
Finding your way to a safe lease
Doctors and managers entering practice lease negotiations know it is a complex journey. Bryn Morgan gives some really useful tips to help and warns of the traps
IF YOU have a private practice, you will know that the location, quality and cost of your premises are of fundamental importance to the ongoing success of the business.
Your practice may even be synonymous with its location, and maintaining that presence
could be crucial to the goodwill of the business and its sale value.
If you do not own your practice premises, the chances are that you have or are looking to take a lease, which will typically be for a fixed term at a market rent.
Either your practice may be
starting out and looking to enter its first lease or the end of your lease term may be approaching and you are looking to renew or perhaps relocate. In either case, what are the key issues you should be considering when starting lease negotiations?
The truth is that agreeing lease terms is highly complex and professional assistance should always be sought. But we will consider here some of the common tips and traps to look out for when negotiating with your landlord and planning for the future of your practice.
1
Length of term
It goes without saying that the duration of the lease should be carefully aligned with the current and anticipated future requirements of your practice.
Clearly, the longer the lease, the more security you will have and the easier it is to justify initial fitout costs and improvements. However, this should also be balanced against the increased commitment and liability under a lengthier term such as rent and repair costs, which will inevitably mount up over time.
Your surveyor should explain to you how the length of the lease impacts on rental and other commercial terms, but it is important to appreciate that the term length always has valuation consequences.
For instance, a landlord holding the premises as an investment is more likely to agree a lower rent in return for a longer term, particularly if your financial covenant is strong.
If you are a smaller private practice, it may be tempting to seek a lease expiry date which ties in with the retirement plans of the practice’s key principal(s).
However, the lease being close to expiry at the time of the retirement(s) may damage the prospects of selling the practice as a going concern. In a worst-case scenario, this could leave the retired principal(s) not only with the cost of winding up the business but perhaps of greater significance, with a reduced or even zero value of the goodwill of the business.
2
Security of tenure
Tenants who occupy premises in England and Wales for business purposes benefit from security of tenure under the Landlord and Tenant Act 1954, unless they have agreed otherwise with the landlord.
This protection means that when the lease expires, the tenant will have statutory rights to renew unless the landlord is able to obtain possession under certain statutory grounds – for example, if the landlord wishes to redevelop the premises or to occupy them for his own purposes.
If the landlord can recover possession under any of the grounds listed, he may have to pay statu-
tory compensation to the tenant – although this is not likely to provide very much, as it is based upon the rateable value of the premises.
You should check whether the lease you are being offered either has this protection or alternatively excludes it.
A landlord may wish to exclude the 1954 Act to make it easier to obtain possession when the lease ends or – even if willing to renew the lease – to place it in a stronger negotiating position.
In other cases, the landlord may have no alternative other than to exclude the lease from the Act; for example, where this is a requirement of his own lease in circumstances where you are taking a sublease.
Either way, you should consider this point carefully, particularly in a case where the location of the premises is crucial to the establishment and ongoing success of your business for the long term.
3 Options and pre-emption rights
If the premises are key to your long-term vision for the practice, it may be worth considering whether you can negotiate within the lease an option and/or preemption agreement with the landlord.
An option can give you the right to call on the landlord to sell his interest in the premises to you, usually at market value.
A right of pre-emption would require the landlord to offer to sell the premises to you before he can sell it to a third party.
4
Means of exiting the lease
Of course, there may be circumstances in which the practice or its principals would want to exit liability from the lease before the term expires. The extent to which this is possible will depend on the terms of the lease.
In particular, it is important to ensure that the alienation provisions allow for the assignment and sub-letting of the premises subject to acceptable conditions.
On an assignment of a lease, an outgoing tenant may be required to guarantee the performance of the lease by the new tenant, ➱ p36
PROBLEMS WITH THE TAX MAN?
HMRC tax investigations and disputes create difficult and stressful times. As an award winning firm of tax experts, our highly experienced partners specialise in resolving problems relating to tax investigations and disputes with HMRC.
3333.
‘Here to help. Not to judge.’
although it is possible that exceptions may be agreed – for instance, where the lease is being assigned to other partners in your practice on a retirement and the tenant covenant remains strong.
Under a sub-letting, you can pass on some of the liability under the lease to your sub-tenant. This may, for instance, be helpful if you have spare rooms in the premises which you could rent out to offset your own rent.
However, so far as your relationship with your landlord is concerned, you would remain liable for all of the tenant obligations under your own lease.
It may also be possible to agree break options allowing you to end your lease before the expiry of the term. It is important to check that any proposed tenant break option is not subject to onerous conditions which could prevent it from being freely exercised.
You should also be aware that the inclusion of a tenant break option is likely to lead to the landlord seeking a higher rent. It should be kept in mind that
exercising a break option is very much the nuclear option, which not only would require the practice to vacate but would also likely bring forward any terminal dilapidations’ costs arising under the repair obligations in the lease.
5 Repairs and service charges
When considering lease repairing obligations, the first question to ask is whether the terms are FRI (full repairing and insuring) or IRI (internal repairing and insuring).
An FRI lease will make the tenant fully responsible for the costs of repairs to the premises. If the FRI lease is of the whole of a building, then the tenant will often be responsible for undertaking the maintenance themselves – and this is likely to include everything from the internal plasterwork to the exterior and structural parts, including the roof and the foundations.
A common mistake is for a tenant to believe they have no FRI liability if the lease makes them personally responsible for carry-
ing out internal maintenance only.
However, a lease which imposes a service charge on the tenant which includes the repair costs of the structure and exterior – notwithstanding the works are the responsibility of the landlord – is also an FRI lease. This may well be relevant in the case of a lease of only part of a building.
A tenant under an IRI lease is likely to pay a higher market rent to its landlord than under a FRI lease of the same premises, as the landlord is effectively carrying the risk of the premises’ maintenance.
Whether the lease is FRI or IRI, you should consider whether your repairing obligations should be limited by reference to a ‘schedule of condition’ which documents any existing wants of repair for which you do not want to be responsible.
Depending on bargaining positions, it may also be possible to agree a service charge cap to limit your exposure to higher-thananticipated service charges.
6
Succession planning for partnerships
If you operate your business through a partnership, careful succession planning is always an essential requirement and even more so where there are lease liabilities.
If done well and tied in with well negotiated lease alienation provisions, then there is no reason why arrangements should not work for both retiring and new partners.
ment of the lease and to indemnify the outgoing partner against future lease liability;
D. A reserve fund is built up over the life of the lease against the costs of future repair, decorating and any reinstatement costs.
This should provide for a sensible balance between the interests of the senior and junior partners in a practice. A senior partner will want to ensure he or she can retire without having to worry about future liability under the lease.
On the other hand, a junior partner should be aware of the ‘last man standing’ risk and would be advised to ensure a reserve fund is in place to fund future liabilities.
Stamp Duty Land Tax
The adage that the only things certain in life are death and taxes is unfortunately largely true in the context of the Stamp Duty Land Tax (SDLT) tax payable by a tenant taking or renewing a lease.
The amount of SDLT increases in proportion to both the length of the lease and the level of rent and should be checked early in any lease negotiations. It may also be worth considering whether the terms could be more tax-efficient; for example, in some cases it may be beneficial to opt for a shorter initial term with a tenant right to renew rather than opting for a longer term coupled with a tenant break option.
Professional team
Anaesthesia, Critical Care & Pain
Dermatology • General Practice
Plastic Surgery • Radiology
Trauma & Orthopaedics
Hands-on workshops
Multidisciplinary lectures
Satellite and joint sessions
Bedside ultrasound course
Contribution from allied specialities
Keynote lectures by invited speakers
As part of good succession planning, best practice advice is always to ensure that when entering a new lease, the practice puts in place an updated form of partnership deed and declaration of trust to ensure that:
A. All partners in the practice legally enjoy the benefit of, but share the burden of, the lease. And, as a maximum of four partners can be named on a lease, this is particularly important for larger practices;
B. All decisions relating to the lease are subject to the usual partnership decision-making protocols;
C. Contractual arrangements are in place to deal with the retirement or death of a partner. Typically, the continuing partners may agree to accept an assign -
Every lease negotiation carries with it legal, valuation, building condition and taxation considerations and risks.
It is therefore not only important to seek professional input from experts in these fields, but also to ensure your advisers understand the significance of the healthcare environment in which you operate your business and the issues which are specific to it.
Bryn Morgan (below) is a solicitor at healthcare law firm Hempsons. He advises healthcare practitioners and providers on property transactions and their partnership and business arrangements
Take gripes seriously
A shocking 80% of complaints in the private healthcare sector are about bad handling of patient concerns, we revealed last month. Sally Taber (right), of the Independent Healthcare Sector Complaints
Adjudication Service (ISCAS), discusses improving systems and processes to support good handling of complaints
GOOD COMPLAINTS management is an integral part of good governance and quality management, as I wrote in my September 2017 Independent Practitioner Today article ‘Getting to Grips with Complaints’.
I remarked that if patients have concerns, we must listen to them and find a way to satisfy them if that is possible.
In doing this, we get to see ourselves as patients see us, and that is sometimes very enlightening.
And it is not easy to do that if it is your own work or your hospital or clinic that is being criticised.
A level head and cool approach is needed if a patient’s concerns are to be addressed empathetically and we are to gain valuable lessons to apply to the future care we give.
The tried-and-tested ISCAS Complaints Code of Practice is the helpful tool of choice used by 95% of independent healthcare providers to evaluate complaints and to draw out the learning points they may contain.
The code is not to be used just by doctors, because almost invariably the substance of the complaints adjudicated through the agency of ISCAS touch upon multiple aspects of the patient’s pathway through the clinic or hospital.
Our Annual Report1 bands the heads of complaints into five categories:
Clinicians will be concerned to know that 23% of complainants carp about clinical outcomes.
Poorly understood
Fifty-two per cent complain about consultants/medical care. One lesson learned under this head of complaint is that doctors’ reports received by patients are often poorly understood.
Recent guidance from the Academy of Medical Royal Col leges, entitled Please, write to me. Writing outpatient clinic letters to patients, 2 is valuable.
At ISCAS, the impartial Adjudication Of Complaint reports – written by expert adjudicators, often with benefit of clinical advice –go to the chief executive of the hospital or group where the complaint originated, and we would expect them to be shared with any clinician mentioned in them.
If, as a clinician, you are mentioned, then the adjudication should be part of your revalidation portfolio.
The stand-out finding in our 2017 report is that complaints about complaints handling have rocketed from 22% mentions by complainants in January 2015, to
Our report last month revealed the extent of complaints mishandling
fitness-to-practise findings and the effects of clinical revalidation, good standards are perhaps driving out bad.
The third improvement is to help providers test the quality of their handling of complaints.
ISCAS has developed a template to support self-assessment of compliance with the ISCAS Complaints Code of Practice and, from 2019, will make its use compulsory.
If it proves non-compliance with the code, providers must provide an action plan to achieve compliance.
Finally, sharing lessons learned. ISCAS does this by means of position statements derived from the themes identified in the independent adjudications.
The position statement on complaints management and practising privileges makes clear to all subscribers that independent health providers are to give a
single response to a complaint and that it is not acceptable for consultants with practising privileges to write separate responses to complainants.
The position statement on complaints management on fees requires that providers be transparent about fees charged to service users, including those charged by individuals granted practising privileges – although this has, of course, just been overtaken by the mandate from the Competition and Markets Authority requiring this to happen next year.
Currently under consideration is the governance around second opinions.
We outlined ISCAS’s code of practice in our September issue last year
The position statement on complaints management on fees requires that providers be transparent about fees charged to service users
The first improvement is more and better training based on the collated outcomes of recent complaints. ISCAS provides annual training to its subscribing organisations, who are encouraged to cascade their knowledge and skills throughout their teams and into their operating protocols.
Over 70 attended this year. Consultants in a private hospital or clinic who are faced with a complaint will expect to rely upon skilled assistance under the practising privileges arrangements.
80% mentions by complainants in March 2018.
Assuming that the healthcare given to private patients remains generally of the same competence, there could be a number of reasons for this result.
Perhaps there is a greater awareness of the routes to make a complaint now that the ISCAS code is widely publicised in independent hospitals and clinics. Or there could be a systemic problem that needs to be addressed.
Taking the latter to be probable, ISCAS has sought to improve systems and processes to support good handling of complaints in the independent sector.
Sharing knowledge
The second is sharing knowledge of issues raised by complainants. The statutory regulators, such as the Care Quality Commis sion (CQC) and GMC, recognise ISCAS adjudications in the independent sector.
All share information through a formal system of anonymised exchanges of summary information about complaints and their outcomes. Common problem areas are found, clusters of inadequacy sighted and trends identified.
Taken together with the professional regulators’ exchanges of
TRACING OUR ROOTS
How the NHS was organised
So how did we get here? Independent Practitioner Today looks back on the history of the National Health Service in the second of a series adapted from a new book by Dr Ellen Welch (right)
THE NHS was planned as a threetier service, with the Minister of Health overseeing it at the top, and three tiers which could interact with each other to suit the needs of the patient to include:
Hospitals – Both the municipal and voluntary hospitals were nationalised and organised into 14 regional groups or hospital boards.
Primary care – GPs, dentists, pharmacists and opticians all remained as selfemployed professionals, contracted by local executive councils to provide services to the NHS so that the patient did not have to pay directly.
Local authority services – Community services, such as the provision of midwifery and health visiting services, school medical services, ambulance services, immunisation and public health, remained the responsibility of the local authorities.
The
birth of the NHS
On 5 July 1948, medical care in the UK became free, for all people including foreigners living temporarily in Britain. Overnight, Health Minister Aneurin Bevan was in charge of 2,688 hospitals in the UK, describing the new NHS as ‘the most civilised step any country has ever taken’.
In spite of the bickering, almost
everyone was prepared to make the NHS work. ‘The war made us realise that we were all neighbours’.
Additional resources for the new NHS were negligible. The same number of doctors and nurses went to work in the same hospitals on 5 July in the same way they had the day before, but what had changed was improved accessibility for patients and a more equitable distribution of existing services.
The Times commented that the masses had joined the middle classes. Demand for the NHS exceeded all predictions. During planning, the predicted annual cost was £170m.
In its first full year of operation, costs exceeded £305m. One million pounds was budgeted for opticians, but, within a year, 5.25m spectacle prescriptions had produced a bill amounting to £32m.
Similarly with prescriptions – in 1947, doctors issued 7m prescriptions each month, which rose to 19m per month by 1951.
Commentators in the BMJ in 1949 predicted the rate of NHS expenditure would lead to national ruin.
They reasoned that the predicted NHS budgets planned for before its initiation had ignored the effects of the aging population and the figures were based on
a false conception of health –meaning that before the NHS, people were cured of simpler and cheaper diseases but fell victim to more complex and more expensive diseases – for which the NHS was now footing the bill.
In 1950, Prime Minister Clement Atlee promoted Hugh Gaitskell to be Chancellor of the Exchequer. To balance the budget, he proposed savings of £13m annually by imposing charges for dentures and spectacles provided by the NHS.
Both Nye Bevan and Harold Wilson resigned from government the very next day in protest. The Conservative government went on to introduce charges for prescriptions of one shilling (5p) in 1952.
Apart from a period between 1965 and 1968, prescription charges in England have continued ever since. Today, prescriptions cost £8.80 per item and provide an estimated £450m revenue for the NHS annually.
A system of exemptions for prescription charges is in place, including those on low incomes, pensioners and students, pregnant women and people with long-term medical conditions, meaning that, on average, 90% of all NHS prescriptions are dispensed free of charge.
There are growing concerns about wastage of medications prescribed for free, which in 2009 was estimated in the region of £150m of avoidable waste.
GPs and their changing relationship with consultants
Before 1948, GPs worked as independent traders treating people who had the money to pay them, often from a consulting room in their own home.
In 1911, GPs were contracted by local insurance committees administering Lloyd George’s National Insurance Scheme, to provide general medical services, and were paid a capitation fee for every patient registered with them.
At the inception of the NHS, this independent contractor status was clung to, from a fear of becoming a salaried employee of the state, but this independence was deceptive.
GPs continued to be free to
organise their own practices, but the work they did for the NHS was controlled by a tightly defined contract.
They received a capitation fee for each patient registered with them, and their expenses were averaged and included in this payment per patient.
No money could pass between patient and doctor – with few exceptions such as payment for a private medical certificate. The NHS Act of 1946 had planned for health centres to be a main feature of primary care.
They envisaged clinics aimed at health promotion made up of GPs, dentists and local health authority clinics, funded by the public purse, but this programme was aborted before it even started.
Prior to the NHS, a few GPs had made a handsome living by treating wealthy private patients, but the majority were poorly paid, so the NHS provided them with security.
Overwhelmed by demand
Lord Beveridge had predicted that the initial jump in demand for GPs’ services would eventually fall once people became accustomed to the system, but this never happened and GPs were overwhelmed
Newspaper adverts explained to people how to use their new National Health Service
with demands from patients who had previously avoided seeking care for financial reasons.
Within a month, 90% of the population had registered with a GP. Each GP was personally responsible for the care of their patients 24 hours a day, seven days a week, 365 days a year, meaning single-handed doctors could be on call around the clock with no respite.
GPs were assigned as the gatekeepers for the NHS, transferring the decision to go for hospital treatment from the patient to the doctor.
A patients' guide produced by the Ministry of Health in 1948 declared that the GP would ‘arrange for the patient every kind of specialist care he is himself unable to give. Except in emergency, hospital and specialists would not normally accept a patient for advice or treatment unless he has been sent by his family doctor’.
This suited hospital consultants, who felt protected from ‘trivial’ cases.
The government also enjoyed increased cost-effectiveness, while the GPs themselves enjoyed the continuing responsibility for ‘their’ patients.
This changed the relationship between GPs and consultants, who had previously relied on GP referral as a source of private income.
Now they had plenty of NHS patients to keep them busy, few consultants made a substantial income privately and no longer had financial reasons to be grateful to GPs.
In the current debates about NHS privatisation, the statement frequently pops up that ‘GPs are private providers’. NHS GPs may be run as private businesses, but they differ from private GP practices in that they do not compete for patients or for profit. They work to NHS contracts, follow NHS guidelines, and see NHS patients.
☛ Adapted from The NHS At 70 – A Living History, by Dr Ellen Welch, a cruise ship doctor and GP in West London. £12.99 from www.pen-and-sword.co.uk
PRIVATE PATIENT UNITS
A mixed bag – but still an opportunity
In our latest tour of NHS private patient units (PPUs), Philip Housden (right) analyses private patient revenue growth for 13 NHS acute trusts across the county of Yorkshire
FOR THIS group of trusts, the accounts show that total private patient revenues increased in 201718 after a period of stagnation.*
Total revenues are estimated at £14.5m in 2017-18, up approximately 4% from £13.9m in 201617 (Figure 1).
This level of income represents a stable 0.27% of these trusts’ total revenues. This remains below the combined national average outside of London of 0.5%.
These 13 acute trusts vary significantly by private patient revenues (Figure 2 on opposite page). For the following analysis, the trusts have been grouped together, where relevant, according to whether or not they have a dedicated private patient unit or not and present turnover (Figure 3).
Top earner
The region’s top earner is Leeds Teaching Hospital Trust at £5.85m, up £264k year on year (4.7%) and £1.1m in last two years.
This places the trust in the top ten earning trusts outside of London and represents 0.57% of trust revenues. The trust achieves the majority of these earnings through a partnership with Nova Healthcare located within St James’s Institute of Oncology in the Leeds Cancer Centre in Bexley Wing.
Nova is part of Aspen Healthcare, recently purchased by NMC from Tenet ( Independent Practi
tioner Today, September 2018). The service offers the full range of cancer treatment including radiotherapy, gamma knife and robotic surgery and chemotherapy.
There is also access to private beds within the Bexley Wing for patients requiring inpatient admission.
Sheffield Teaching Trust has no specific private patient services,
but instead offers a range of treatments privately across its five hospitals.
Incomes have grown in the last two years, but longer-term review shows these overall to have remained between £2.9m to £3.1m for the past several years, this holding steady at 0.35% of turnover.
Also in Sheffield is the specialist
Children’s Hospital Trust, one of only four such trusts in the NHS – the others being Great Ormond Street, Birmingham Children’s and Alder Hey in Liverpool. The trust most recently reported private patient revenues of £165k, only 0.1% of turnover, and is understood to be considering a strategic market review of the opportunities to develop private patient services to meet both UK and overseas demand.
Hot spots
Harrogate and York, by contrast, both have private patient units and are located in relative hot spots for private medical insurance take-up. Harrogate’s ten-bed Harlow Suite is branded the Harrogate Harlow Private Healthcare Service and has achieved £1.4m revenues in 2017-18, up nearly £200k on the previous year, making up for an equivalent fall last year.
Harrogate achieves 0.72% of trust turnover as private income, the highest in the region and, together with Leeds, are the only two in Yorkshire ahead of the outof-London national average.
York Hospitals Trust offers private patient services at York, Bridlington and also at Scarborough. These are for a range of surgical, ambulatory and diagnostic services.
The group service is not separately branded. Revenues have remained around £1m for several
Figure 1
Figure 3
years, but the 2017-18 total is not yet published. However, this does represent a gently declining proportion of total incomes, down from 0.25% four years ago to an estimated 0.19% today.
Range of services
Bradford also has a PPU, recently investing in refurbishing the 12bedded The York Suite located on Level 4 of the Duke of York Wing at the Bradford Royal Infirmary. This offers a range of medical care and surgical interventions from out-patient consultations, diagnostic scanning, minor day-case treatments, to complex surgery.
The trust reported a disappointing 14% drop in private patient incomes from £894k to £768k in the 2017-18 annual accounts. This continues the long-term decline in the proportion of overall trust incomes from private patients which stood at nearly 0.5% seven years ago but is now down to 0.22%.
Airedale Hospital similarly has a PPU, with Ward 19 having 11 bedrooms and two private consulting rooms. As with Bradford, the unit delivers a relatively low and declining contribution to overall trust finances. Last year, the trust reported only £166k private
patient revenues, only 0.11% of the total.
Of the remaining trusts, these can be split into two groups, none of which have a dedicated private patient ward.
The first comprises Doncaster, Calderdale and Hull, each of which has private patient revenues of over £500k a year. The latter two achieved significant growth of over £150k in the year, each being >35% up on 2016-17 and also representing growth in real terms, as the proportion of total trust incomes it represents also improved. Note that Doncaster’s accounts do not show up the separate private patient revenues.
The second and final group has very little private patient incomes to report. Mid Yorkshire, Rotherham and Barnsley together reported under £100k private patient revenues in 2016-17, each being less than 0.03% of turnover.
Significant revenues
NHS trusts in Yorkshire offer a mixed bag, with growth within the major teaching hospitals and significant revenues where there is a private patient ward.
There is no single correlation between PPU beds and success, however, as some trusts have a sig-
nificant proportion of their earnings unrelated to patient admission and are so not dependent on a PPU – with fertility services being one such example – and others find that private patient beds have been utilised for winter pressures. Across the region, there remain several trusts with the likely opportunity to develop new private patient services and facilities – perhaps linking up with neighbouring trusts already providing a successful service?
Even the trusts that operate within the most challenging socioeconomic catchments still provide
an infrastructure that the local independent sector cannot match and so closer working arrangements with these operators, mainly around complex treatments requiring 24/7 infrastructure, remains an income opportunity.
* The figures used here are predominantly from the recently published 201718 annual accounts. However, four trusts have not yet published private patient revenues at the time of writing and so previous year accounts have been used. Next month: North-west
Philip Housden is a director of Housden Group
Is there a right time to jump?
IT COMES as no surprise that recent BMJ figures show a steep rise in the number of doctors retiring early.
Medical colleagues at the top of the profession tell us that medicine has changed beyond recognition – not always for the better.
The happy tales of technological breakthroughs and unprecedented advances in healthcare cannot counter the increasing red tape, rising debt and constant attacks
on salaries, pensions and taxation that doctors face.
In the office, we have witnessed a steady increase in clients choosing to retire ahead of time – keen to enjoy their hard-earned wealth at the optimum moment. If part of the NHS pension’s 1995 section, doctors can take retirement from as early as 50 in exchange for reduced benefits.
However, not many choose to quit medicine completely over -
night. The preferred option is either a steady reduction of hours while retaining some level of medical practice (wind down) or reduced responsibility or workload (step down). Others are opting to ‘retire and return’.
Popular option
Should I stay or should I go? Dr Benjamin Holdsworth on why more doctors are choosing to leave medicine early
Clinical excellence awards are lost upon retirement, but the pension benefits received can be higher, so many find they are better off financially.
Taking this option will cap the value of your pension pot and could provide a welcome escape
The latter has proved popular because doctors can decrease their professional commitments yet maintain their financial earnings by claiming pension benefits while working. Although their base salary may be reduced, doctors will save on pension contributions.
route from the lifetime allowance tax-free pensions savings cap of £1m, a figure easily exceeded by the pension of many senior doctors.
Note that breaching the limit will trigger a tax charge of up to 55% on the excess savings.
To qualify, you must effectively resign from your NHS contract of employment and take a 24-hour break in service.
You will stop paying pension contributions and access your taxfree lump sum plus a regular pension payment. You can return to work on a new contract, but for the first month, must not work more than 16 hours per week. After that period, you can choose to return to either full- or parttime employment without any restriction on hours.
Consultants remaining on the 1995 pension scheme and aged 60 or over can access the lump sum without penalty, while those who have moved to the 2008 scheme must wait until they are aged over 65.
You can often negotiate a more flexible working contract and can lose less favourable parts such as reducing the level of programmed activitities undertaken or dropping on-call commitments.
Deciding factor
For many, the ability to access a tax-free lump sum at a time when they or their dependents most need it can be a deciding factor.
Although the nation is living longer, most of us will need considerably more income aged 60 –possibly paying for children’s further education or care for elderly – than at age 80. And it is better to achieve that elusive work-life balance while still fit enough to enjoy it.
You would need to ensure that your NHS trust is likely to want to take you back. If you are returning after a break in service, you are effectively ‘cheaper’ because there are no pension contributions to pay, but any clash with current management will void this advantage.
On the other side of the deal, your new contract is only likely to be on a one-year renewable basis, which could lead to less career security as well as a perceived change of status. By giving up a
long-term contract, you could lose some of your rights should you be made redundant in the future.
There is also the loss of valuable death-in-service payments – worth twice the relevant pensionable salary – and ill-health benefits, both of which are more likely to be useful to those nearing retirement age.
It is a win for the NHS too. By offering this agreement, it is able to retain some of the talent pool of senior doctors who bring vital skills and experience to the service as well as their ability to train younger generations.
What retirement age is right for you?
Clients tell us you will know when the time is right to step back or step down, but detailed financial modelling makes the decisionmaking process much clearer and will point to the very best time economically, all things considered.
There can be many issues to factor in to the discussion: an exit strategy for your private practice, the tax due on your accrued pensions savings, the needs of any dependents and the potential to receive a lump-sum payment from your benefits.
In every case, weighing up your own options ahead of time allows for a more successful transition from full-time practice to retirement in whatever guise is relevant to you.
The content of this article is for information only and must not be considered as financial advice. Cavendish Medical always recommends that you seek independent financial advice before making any financial decisions. Levels, bases of and reliefs from taxation may be subject to change and their value depends on the individual circumstances of the investor. The value of investments and the income from them can fluctuate and investors may get back less than the amount invested.
Dr Benjamin Holdsworth (right) is a doctor and director of Cavendish Med ical, specialist financial planners helping consultants in private practice and the NHS
Try Before you Buy…
Investing in a Practice Management System is a huge commitment. That’s why we offer you a FREE 30 day trial to see if our software is right tor you.
The Cost Effective, Secure & Private Practice Management System.
Support is FREE throughout your trial via telephone, online chat or email.
Thinking of moving from your current Practice Management supplier?
• Access anytime, 24/7, on any device
Changing your software may seem daunting and time consuming, but it doesn’t need to be.
• Data backed up in ‘real time’ on the Microsoft Azure Platform
• Clear, user friendly interface
• Go Paperless by typing & importing documents
Talk to our Support team today on 0330 999 3399 and ask how moving to MidexPro can give you a more cost-effective alternative and hear how we can minimise the impact to your practice whilst you move.
One Touch eBilling
•
• Advanced analytical Practice Data available
• Encrypted software to IS027001 standards with Optional 2-Factor Authentication
•
Outstanding UK support via Email, Phone & Live Chat
For a FREE 30 day trial of the system, Please call 0330 999 3399 or email support@midexpro.com
E: support@midexpro.com
T: 0330 999 3399
W: midexpro.com
Teenager avoids taking medicine
Dr Nicola Lennard (right) explores the issues surrounding a teenage patient who is nonco-operative
Dilemma 1
She doesn’t want to tell her mother
QA 14-year-old girl has been attending my private diabetes clinic for some years. I have become concerned that she has been deliberately avoiding her insulin injections, as her HbA1C level is elevated and she has lost several kilos in weight.
Her mother used to supervise her medication, but the patient was reluctant to involve her and confided they had been arguing a lot recently. Can I ignore the patient’s wishes?
AIf your patient is unable to trust you not to disclose information without her consent, it may deter her from seeking your help in future, which could be detrimental to her health.
But, at the same time, you also need to consider the damage that could result from failing to adhere to her insulin regimen and whether your patient fully understands the risks she is taking.
Make another attempt to advise the patient about the risk of lifethreatening diabetic complications such as diabetic ketoacidosis and discuss the reasons why she might not be taking her medication.
If this problem coincides with the patient taking responsibility for her own injections, it is worth exploring whether she need additional medical support or if there are any alternative modes of treatment that she might find easier to administer such as an insulin pump.
The patient’s behaviour could indicate the onset of an eating disorder, so you could also suggest that she sees a counsellor.
If the patient is unwilling to
engage with you and refuses consent to involve her parents, you need to consider whether you would be justified in making a disclosure to her parents against her wishes.
In 0-18 years: Guidance for all Doctors, 1 the GMC says that you can disclose information about a patient without consent if required by law; if there is an overriding public interest which outweighs their right to confidentiality; or if this is in the best interests of a young person who does not have the maturity or understanding to make a decision about disclosure.
In this case, sharing information with the girl’s parents may be necessary because her behaviour puts her at risk of serious harm, while it is likely to be in her interests to receive more understanding and support from her parents. However, it is also advisable to consider whether her reluctance is a sign of other potential problems.
If you decide to disclose information to the girl’s parents, you should usually still tell her of your intention, unless that would undermine the purpose of the disclosure or put her at increased risk. In these circumstances, the GMC says disclosures should be made promptly and you should record your discussions and reasons. If you decide that disclosure is not justified, you should record your reasons for not disclosing.
Reference
1. Paragraphs 42-52, 0-18 years: Guidance for all Doctors, GMC; updated 8 April 2018. www.gmc-uk. org/ethical-guidance/ethical-guidancefor-doctors/0-18-years/principles-ofconfidentiality
Dr Nicola Lennard is a medico-legal adviser at the MDU
Dr Beverley Ward explains how to respond to inappropriate advances from a patient
If they get too friendly
Dilemma 2
How can I stop her pestering?
QI am a consultant who has recently treated a patient for an ankle injury. After this, I started to receive several inappropriate messages, via social media, inviting me to meet for drinks and dinner.
I have ignored all messages and am hoping that a colleague will see the patient for future appointments.
But is there anything else that I can do to prevent the patient contacting me further?
AThe increasing prevalence of social media means that doctors are more accessible to patients than ever before.
Advances can range from receiving unwanted letters and gifts to texts or social media messages and unfortunately, these can quickly escalate.
For example, in 2016, there was the case of Dr Eleanor Aston who was subject to seven years of harassment from her stalker who was a former patient.
It is always vital to maintain professional boundaries in your relationships with your patients. If you have reason to believe that a patient wants a personal relationship with you, tell them as
soon as possible that your relationship with them must remain professional.
Block the patient and do not respond directly to any texts or social media messages they send.
Inappropriate behaviour
Make it clear to them that their behaviour is inappropriate and must stop. If you feel threatened or are in danger, you should consider reporting the patient to the police.
Make colleagues aware of the situation and if your professional relationship with the patient has broken down, transfer the care of the patient to a colleague.
You should explain the reason to the patient, and it’s also important to keep a log of all messages and to get support from your medical defence organisation.
But if you continue to care for the patient, it is worthwhile to use a chaperone for all consultations.
There are some steps you can take to try to avoid receiving unwanted attention from patients.
For example, accepting gifts from patients can be misconstrued, so consider very carefully whether it may be better to politely refuse a gift.
Do not use personal email addresses or mobile numbers for work purposes. Withhold your phone number if you must use it to contact a patient and review your social media privacy settings.
Dr Beverley Ward is a medicolegal adviser at the MDU
A PRIVATE PRACTICE: VALUE-ADDED TAX
What to beware of if a VAT-man nears
We are all used to paying VAT on many of our dayto-day purchases, but for private practices it is the exception rather than the norm to be VAT-registered. This is in contrast to the vast majority of private businesses outside of the medical profession which are VAT-registered.
Ian Tongue explores the more common situations where VAT registration may be required and highlights some grey areas where you need to be prepared
THE LAW requires you to register and charge VAT on your income where your ‘taxable supplies’ exceed £85,000 a year on a 12-month rolling basis.
Taxable supplies is a term within the legislation that covers a huge range of goods and services and basically means that VAT must be charged if you are supplying enough of it.
Also within the legislation are special exemptions to charging VAT and the most notable one for doctors is in relation to the provision of medical services by a health professional, which is regarded as an exempt supply for VAT purposes.
No matter how much exempt work is performed by the health professional, VAT registration is not required and is not charged. It is this exemption for medical work within the VAT legislation that results in most private practices not needing to register for VAT.
What is exempt medical work?
To be regarded as exempt, the work needs to satisfy two conditions:
1
The services are within the profession in which you are registered to practise.
2
The primary purpose of the services is the protection, maintenance or restoration of the health of the person concerned.
The first condition is usually a given, but the second condition can be subject to some debate for certain work, in particular cosmetic or aesthetic work.
The clear majority of work undertaken in relation to a known medical condition is going to be exempt from VAT.
Work undertaken for purely cosmetic or aesthetic purposes is not medical and would be regarded as a taxable supply within your private practice. If you are undertaking work such as this, if your income level reaches £85,000 or more per year, you must register for VAT and charge VAT at 20% on your work. It is important to note that the £85,000 limit is on a 12-month rolling basis and therefore you are required to look at this each and every month rather than at your financial year-end.
The most common type of work performed by a doctor that is subject to VAT is medico-legal report writing
Medico-legal reports
The most common type of work performed by a doctor that is subject to VAT is medico-legal report writing. It is common within such reports to assess a patient’s condition and possibly make recommendations for treatment.
However, the key factor to consider is that the principal reason for completing the report is for a third party to make a decision –for example, a court – rather than for the protection, maintenance or restoration of the health of the person concerned.
Where you are carrying out more than the compulsory VAT registration limit – currently £85,000 – of this type of work, you must register for VAT and account to HM Revenue and Customs (HMRC).
What does VAT registration mean?
Being VAT-registered results in you becoming a collector of tax for HMRC. You apply VAT to your prices, currently at 20%, and pay this over to HMRC periodically after deducting any VAT that you can recover on your costs.
Claiming back VAT on costs is about the only benefit of being VAT-registered and, for most, this would not be a reason to register for VAT voluntarily – that is to say, for those with taxable earnings less than £85,000. The additional hassle and admin normally would outweigh the savings from being VAT-registered.
When registered, you are required to submit a VAT return to HMRC that details how much you owe them, which is then paid over. Schemes exist to make this process easier, but expect to have
a visit periodically from HMRC to ensure you are collecting their money correctly.
Schemes to make life easier
As a VAT-registered business, you can apply for certain VAT schemes to make accounting for VAT less of a burden.
There are different criteria for each scheme, which your accountant can discuss, but a brief description of the common ones are as follows:
Annual accounting scheme
– Complete one VAT return per year and make estimated payments.
Cash accounting scheme –only pay over the VAT when you get paid yourself.
Flat-rate scheme – pay over a set amount of VAT based on your business sector.
These schemes are not mutually exclusive, so it is normal to look at using a combination of the schemes available.
Cosmetic and aesthetic work
VAT was a big issue among aesthetic practitioners coming to various stands at their annual conference and show, CCR Expo, at Olympia last month.
The VAT guidance notices in issue indicate that work carried out for purely cosmetic or aesthetic purposes is not medical and should be treated as a taxable supply – that is to say, VAT payable on the service.
This area has been a hot topic for years and, to date, no definitive tax case exists to provide practical and useful guidance for identifying when a procedure is purely cosmetic or aesthetic.
There have been tax inquiries taking place behind the scenes, but none of these have reached the level required to be tax law and used as a reference.
Down to the doctor
An EU case a few years ago was expected to provide significant guidance in this area, but, unfortunately, fell short of expectations. It did, however, reiterate that a procedure needs to be purely cosmetic or aesthetic to be standard rated – that is to say, no element of medical treatment.
As things stand, it is down to the individual doctor to determine whether the work undertaken satisfies the criteria to be regarded as an exempt medical supply.
If the exemption cannot be supported, the work will be a taxable supply for VAT purposes.
It is important that within your
medical notes you record on a case by case basis your assessment of whether a medical condition is being treated where a procedure is cosmetic or aesthetic.
This should include both physical and psychological aspects. While HMRC cannot see the notes itself under a general inquiry, officials can ask for an anonymised sample, so it is important that you keep adequate records to support the VAT status.
When it comes to which procedures are regarded as cosmetic, ask yourself the general question of whether the lay person would think they are and ensure that you pay more attention to the documentation that may be required for the taxman.
VAT is a complex tax, but, for many, it will never be an issue to worry about within their private practice.
For those undertaking reportwriting or work that could be regarded as purely cosmetic or aesthetic, it is important that you understand your obligations.
Liaising with your accountant will ensure that you are best placed to avoid a costly mistake in this area.
Next month: A guide to the self-assessment tax system
Ian Tongue (right) is a partner with Sandison Easson accountants
DOCTOR ON THE ROAD: VOLKSWAGEN UP!
Things are looking
If you are looking for a new small car that is great around town but practical and fun, then this VW ticks all the boxes and provides the perfect antidote to the hard work of running a busy medical practice, says Dr Tony Rimmer (left)
SOMETIMES, RETURNING to basics can have the greatest benefit to ongoing advancement. Working as independent practitioners, revisiting the essential elements of good clinical practice can boost professional and client satisfaction.
When systems and practices have worked well in the past, it is worth examining the reasons behind those successes to try and replicate them.
In the world of cars, manufacturers are constantly studying all elements of their best-selling vehicles to see if they can replicate the positive attributes in newer models. A good example is the success, over the years, of the hot hatchback.
All of us who enjoy cars that give us a bit more satisfaction than just simply travelling in an anodyne manner from A to B, will have a soft spot for hot hatches. Volkswagen, the company that gave us the market’s first GTI model in 1975, have most recently turned their attention to their little city car, the Up!
Extra power
By turbocharging the 1.0-litre three-cylinder engine found in lower models, they have squeezed out an extra 23bhp to give 115bhp in total. This is about the same power as the original Golf GTI Mk1 in a car that weighs about the same as its iconic predecessor. As a result, their performance figures are almost identical.
Externally, the famous GTI insignia are all there. Double stripes down each side and red trim strips are complemented by special alloy wheels.
The interior gets tartan trim and a thicker steering wheel together with a GTI gearknob. Airconditioning and heated seats are standard on the GTI, but sat-nav is only available as an app, ‘Maps + More’, which has to be downloaded onto your smartphone which can sit in an integrated dock.
The standard car comes with three doors, but for an extra £400 the five-door model provides extra versatility.
Ever since ‘dieselgate’, VW has been keen to promote its green credentials and the Up! GTI is one of the first of its cars to launch with a petrol particulate filter.
The styling is effective in disguising the boxy proportions and looks grown-up and smart
RIGHT: This small pocket rocket revels in tackling fast A and B roads. The steering is direct, the brakes are strong and the chassis stays flat around the tightest turns
This reduces particulate emissions by up to 95%.
The Up! has been around since 2011 and has spawned identical sister models: SEAT’s Mii and Skoda’s Citigo. It has long been regarded in the motoring world as being one of the best city cars. It has superb packaging and is great value compared to most rivals. The styling is effective in disguising the boxy proportions and looks grown-up and smart.
Clear instruments
My test car was finished in white with a contrasting black roof, which suits its character perfectly. The interior is typically Volkswagen, which means clear instruments and solid functional switchgear.
The standard sports seats are firm but comfortable and, being a city car, all-round visibility is excellent. Rear space is pretty good for such a small car with enough room for two adults and the boot is surprisingly large with a deep floor.
As there is no integral infotainment screen, controls for the radio and what-have-you are fairly basic, but work well enough. I did not get a chance to use VW’s own satnav software, but the smartphone dock is perfectly situated centrally
The interior gets tartan trim and a thicker steering wheel together with a GTI gear knob. Airconditioning and heated seats are standard on the GTI
above the main dashboard, so using Google Maps is really easy to use as an alternative.
So, enough about the design and controls. It is a GTI, after all; so how does it drive? Well, the first thing you notice on start-up is the sporty exhaust note.
This has immediate appeal even before you turn a wheel and, although some of the noise is artificially enhanced via the audio speakers, it will impress any petrolhead.
Take-off is swift rather than super-fast, but the six-speed gearbox snicks easily between ratios, so the engine is always on the boil. Aided by its compact dimensions, the Up! can dart in and out of traffic like a dodgem.
Great fun
The steering is direct, the brakes are strong and the chassis stays flat around even the tightest of turns. I was also relieved to find that as I left the urban traffic behind and headed for open roads, the GTI did not feel out of its depth. In fact, this small pocket rocket revels in tackling fast A and B roads. It accelerates strongly, hugs the road and does it all at a speed that avoids the risk of losing your licence. It is just great fun to drive and I found myself extending
every journey just to enjoy the experience.
It holds its own even on motorway trips. It may be a bit noisy but never feels underpowered.
I think that Volkswagen has really nailed it with the Up! GTI. If you are looking for a new small car that is great around town but practical and fun, then it ticks all the boxes.
As an antidote to the hard work of running a busy medical practice, I cannot think of a cheaper way to blow the cobwebs away.
Dr Tony Rimmer is a former NHS GP practising in Guildford, Surrey
VOLKSWAGEN UP! GTI 1.0 LITRE TSI
Body: Four-seat hatchback. Front-wheel drive
Engine: 1.0 litre three-cylinder turbo petrol
Power: 115bhp
Torque: 200Nm
Top speed: 122mph
Acceleration: 0-60mph in 8.7 secs
Claimed economy: Combined 58.9mpg
CO2 emissions: 110g/km
On-the-road price: £14,455
All you need to know about accountancy for private practitioners
Heads just above water
Our latest income benchmarking survey finds orthopaedic surgeons up against a lot of new challenges. But Ray Stanbridge says they are still increasing their incomes despite rising expenses – and things look good for the year ahead
THE PRIVATE orthopaedic market is changing very rapidly.
There is, for example, considerable interest by insurers in looking at new orthopaedic pathways, with less stays in hospital.
Meanwhile, staff pay has risen significantly, largely at the expense of insured patients.
And groups are developing ever more rapidly in the orthopaedic sector.
On top of that, many consultants have chosen to incorporate and, more recently, some are looking at an employment option.
This is the preferred model of new hospital players to the market, such as the Schoen Clinic London and the Cleveland Clinic, still in construction.
But other established hospital groups are also looking at this option too.
So, with all these changes, it is becoming tougher to illustrate clear trends in orthopaedic surgeons’ income and costs. But here is what I deduce:
Despite everything, the average gross income from private practice for orthopaedic surgeons
AVERAGE INCOME AND EXPENDITURE OF A CONSULTANT ORTHOPAEDIC
increased by 4.3% from £182,000 to £190,000 between 2106 and 2017.
The trouble for them was that costs increased by 9.5% from £63,000 to £69,000 on average. As a result, their pre-tax profits grew by just 1.7%, going up from £119,000 to £121,000.
Income has continued to grow steadily, although, as we reported in the November 2017 issue of Independent Practitioner Today , many orthopaedic surgeons are getting less pay for the same work. They know the result well: they are having to work harder to stand still.
For many consultants, NHS Choose and Book work continues to be important. We have noticed a continued growth in self-pay and, for those in London, a small decline in embassy referred work.
Expenses
Staff costs and consultant room hire costs have shown relatively large increases between 2016 and 2017.
Much of this goes back to the controversial April 2015 ruling of the Competition and Markets Authority requiring hospitals to charge for room hire and secretarial services at full market value.
Many orthopaedic surgeons are getting less pay for the same work. They know the result well: they are having to work harder to stand still
In addition, for those consultants who employ family members, salaries have risen in many cases in line with the growth of the personal allowances.
We have noticed some stability in the ‘average’ professional indemnity/insurance costs. There has been a move by some consultants to the new providers, who have been advertising in Independent Practitioner Today, and we have seen a good number of cases where surgeons have achieved significant reductions in premiums.
On average, consultants who use their homes as a business base have charged a little more for such facilities than is historically the case and these are reflected in the table on the left.
There was some slight fall in bad
Year ending 5 April. Figures rounded to nearest £1,000 (percentage is also rounded up)
Source: Stanbridge Associates Ltd.
Healthcare 2019, the ideal event for you.
Future Healthcare 2019 is the UK’s leading healthcare Exhibition and Conference taking place at Olympia London from 18 to 19 March 2019. The event will provide a unique gathering of global healthcare buyers and leaders across government, associations and industry.
Future Healthcare 2019 will connect you with global VIP Buyers, Senior Procurement Officers, Governments, and Distributors across the public and private sector. It will present you with a vital opportunity to demonstrate your products, services and capabilities to the senior decision-making audience who will attend.
Can your business afford to miss this unique opportunity?
Dawn Barclay-Ross, Event Director +44 (0) 203 740 4666 dawn@futurehealthcareuk.com
debts, evidently as a result of more consultants using medical billing and collection companies. The use of the phone has also reduced, although we can find no clear reason for these observations.
‘Other’ costs continue to be pri-
marily marketing-based. There was little change.
What then of the future? Orthopaedic surgeons continue to hold the position as the highest earning consultants, on average.
We see no reason for this to ORTHOPAEDIC SURGEONS’ PROFITS ROSE DESPITE A BIG RISE IN EXPENSES
change, at least in the short term. For a number of cases, there is less Choose and Book work than there has been historically, but this seems to have been replaced by more self-pay work.
We forecast that it will be a case of ‘steady as she goes’ with no material changes in income and expenditure between 2017 and 2018.
Note that the consultants who continue to be in our benchmarking survey must still satisfy a number of pre-conditions. These surgeons must:
Each have earned at least £5,000 a year gross from private practice;
Have at least five years’ private practice experience;
Be seriously interested in the business of private practice;
Have an old-style or new-style NHS contract;
May or may not have worked through a group or through a limited liability company.
Next time: Ophthalmologists
Ray Stanbridge is a partner with accountancy, finance and tax advisory medical specialists, Stanbridge Associates
HOW ARE YOU DOING?
Use
WHAT’S COMING IN OUR DECEMBER-JANUARY ISSUE
Make sure you don’t miss our next issue, published on 3 January 2019. You may not receive every issue if you have not yet subscribed to the journal. Don’t risk missing out on vital topics we tackle next time:
Tackling the disease of error in healthcare – risks and opportunities in the private healthcare sector
Our trio of writers – two doctors and a pilot – are co-founders of a business on a mission to improve patient outcomes by helping healthcare professionals understand why errors occur. A major new series for Independent Practitioner Today gives a startling insight into attitudes and aims to inspire you with a wealth of practical patient safety solutions
The most successful independent practitioners ‘work smart’ and have been able to steal back time so they can focus more on patients and developing their practice. Kingsley Hollis suggests five areas for suitable treatment
A guide to self-assessment for tax – plus . . .
We answer two questions doctors ask this time of year: ‘I am going to be filing my tax return – could you advise me what the taxman will accept as legitimate expenses against my practice income?’ and ‘I don’t have enough money to pay my tax bill. What is your advice?’
Watch out for the rolling contract: terms and conditions apply but many doctors get caught out, warns Hempsons solicitor Michael Rourke
A chaperone should always be offered where any intimate examination is proposed, even if the doctor and patient are of the same sex, says Dr Gabrielle Pendlebury of the MPS
INDEPENDENT PRACTITIONER
TODAY
Published by The Independent Practitioner Ltd. Independent Practitioner Today is editorially independent and thanks Bupa for its assistance with distribution. Printed by Pepper Communications Ltd Material is governed by copyright. No part of this publication may be reproduced, stored in a retrieval system or transmitted in any form without permission, unless for the purposes of reference and comment. Editorial layout is the copyright of the publishers. If you wish to use it for promotional purposes on websites or for reprints, we would be happy to discuss licensing the copyright to you.
Registered office: 7 Lindum Terrace, Lincoln LN2 5RP
Write to Independent Practitioner Today PO Box 198, Cranleigh GU6 9BB
EDITORIAL INQUIRIES
Robin Stride, editorial director
Email: robin@ip-today.co.uk Phone: 07909 997340
@robinstride
Go on, you know you want to! Ten ways to create a great impression – some great advice from Stephanie Vaughan-Jones of Moneypenny to give you a five-star rating
What should you be asking your financial planner? Dr Benjamin Holdsworth on how to ensure you have the right help in place
Ophthalmologists’ earnings come under the microscope in our latest Profits Focus benchmarking survey
If you work in a PPU in the North-west, then you wont want to miss Philip Housden’s latest report on the finances of units in the region
Business Dilemmas: A surgeon is called to give evidence as an interested party after a patient dies and a mother asks a doctor to alter her child’s surname name. The MDU’s Ellie Mein has the answers
Money-saving tips for doctors new to private practice – and a lot of established practitioners would benefit from following the advice
Tracing our roots – more on the big moments over the last 70 years that got us to where we are today
Doctor On The Road’s Dr Tony Rimmer tests out the DS7 Crossback
Ten Years Ago – new plans for Harley Street
ADVERTISERS: The deadline for booking adverts in our joint December-January issue is 7 December
ADVERTISING INQUIRIES
Margaret Floate, advertising manager Email: margifloate@btinternet.com Phone: 01483 824094
SUBSCRIPTION RATES
£90 independent practitioners. £90 GPs and practice managers (private & NHS). £210 organisations. Save £15 paying by direct debit: individuals £75 (organisations £180).
TO SUBSCRIBE – USE SUBSCRIPTION FORM ON PAGE 24 or EMAIL: lisa@marketingcentre.co.uk or phone 01752 312140 or go to the ‘Subscribe’ page of our website www. independent-practitioner-today.co.uk
Guarantee delivery of your next copy of Independent Practitioner Today. Take out a subscription and you will get full access to our news, features and previous issues on our website. See details on the left.
BACK ISSUES: £12.50 including post & packaging CHANGING ADDRESS OR SUBSCRIPTION DETAILS?
Phone 01752 312140 or Email lisa@marketingcentre.co.uk
Circulation figures verified by the Audit Bureau of Circulations
The business journal for doctors in private practice
Electronic Billing
Remove printing, posting and admin costs
Payment Tracking
Ensure you have been paid for the bills you submit
Financial Reporting
Keep track of your practices’ performance
Complimentary App
Free Apple and Android app available
Appointments and Diary
Manage your schedule and send appointment letters
Membership Enquiry
Real-time online checks for patient membership number
Pre-populated Invoices
Which contain the information you require to submit bills
Shortfall Reminders and Letters
Automated prompts to keep you on top of any shortfalls