The business journal for doctors in private practice
Breathe in ... and relax
A look at how we use coping strategies for stress and whether they work P18
What do patients think of you?
Dealing with patient testimonials in private practice P28
Racing towards tax-efficient cars
A look at the current position for those buying a car regarded as tax-efficient P50
Salary option ‘surging’
By Robin Stride
Doctors’ expressions of interest in working on a salaried basis in a new flagship private hospital has gone through the four-figure mark, its chief operating officer has revealed.
Mr Keith Hague said London’s Cleveland Clinic, due to open in two-and-a-half years’ time with an initial 200 beds (29 ITU), had sparked interest from ‘thousands’.
His remarks came in response to a challenge from a representative of the Independent Doctors Federation (IDF), whose members have voiced opposition in recent months to a private salaried service model.
IDF president-elect Dr Neil Haughton, chairman of the group’s GP Committee, warned him that private doctors liked being self-employed, adding: ‘I wonder where you are going to get all the doctors from?’
Mr Hague replied that as well as consultants, there was interest from young doctors and from physicians overseas.
He expected around 50 employed doctor staff would be in place during the initial stages, working alongside more than 300 ‘credentialed’ staff, and they would be on a one-year rolling contract after five years.
The credentialed staff were needed because it would be impos-
sible to start with a fully employed model.
He told LaingBuisson’s Private Acute Healthcare Conference that the $1bn+ hospital project at 33 Grosvenor Place, Belgravia, currently under construction, marked ‘a big cultural change in the UK’.
Mr Hague, the former chief executive at HCA’s The Wellington Hospital, said the Cleveland Clinic would have 395,000 square feet available for medical use and would be consultant-led.
If it made a profit in the first ten years, then the management would be pleased. The project was about patients, not making money.
He said the clinic was trying to build a healthcare campus in the area, involving the use of other buildings, and later it was hoped to build peripheral referral sites.
It is planned to have an ‘institute’ consultant leadership structure headed by a president who will be a doctor, not a manager. Under this doctor comes a chief of staff and then there will be eight institutes, each with a chairman, nurse and accountancy support.
The institutes are heart and vascular, digestive disease, neurosciences, orthopaedics, surgical subspecialties, general medicine, critical care and anaesthesia, and hospital services. The key consultant leadership is due to be appointed in quarter one of 2018.
Mr Hague argued that the salary
model was fulfilling a need among consultants he knew who were saying private practice was not for them due to rising cost issues.
He cited problem areas as the level of re-imbursements offered by insurers and defence and secretarial costs.
A main outpatient centre will
be five minutes’ walk away, with a third building for 350 office staff nearby.
Cleveland Clinic’s main campus in the US, where it owns and runs ten full-service regional hospitals and 18 family health services, has 50 buildings on 166 acres in the centre of Cleveland, Ohio.
➱ continued on page 3
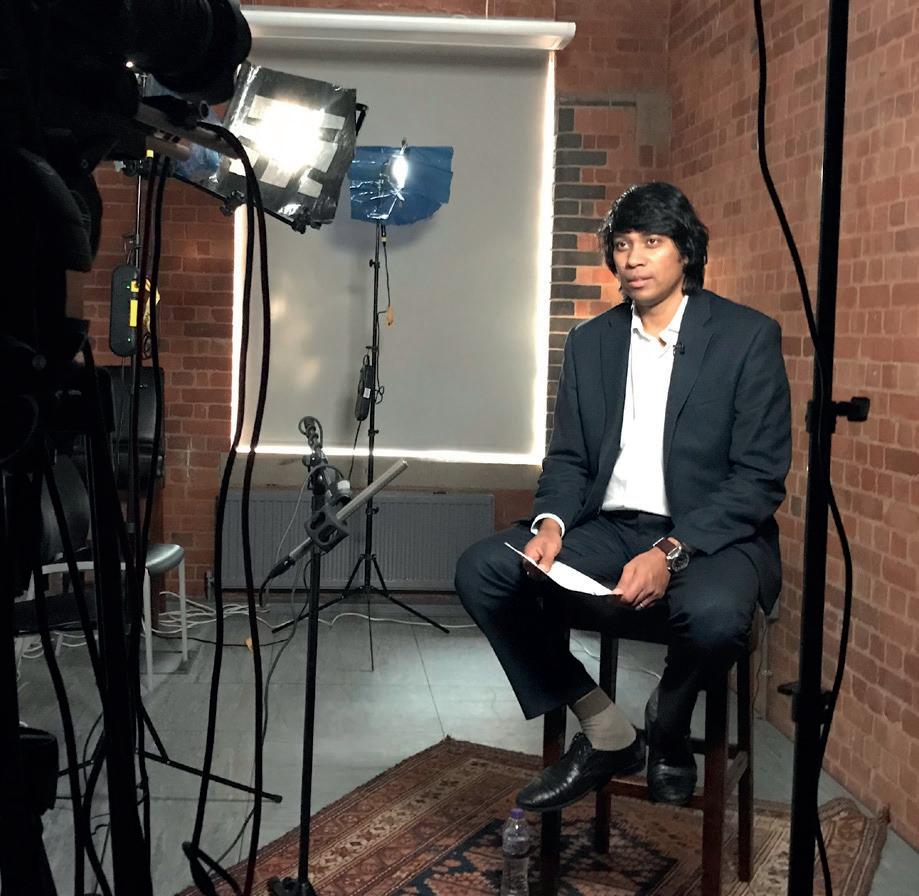
Pictured at an exhibition
The Royal College of Physicians is celebrating women who have made an impact on medicine. Find out how by turning to page 36
Surgeon with brainwaves an enterprising surgeon has a successful sideline in designing instruments P14
How to convert phone callers advice on treating your phone callers with courtesy to win them over as patients P22
Keeping up with google
Why failing to implement Google updates risks your website being overlooked P32
Plan to curb rise in indemnity fees the mdU calls for a change to the way compensation payments are awarded P34
don’t let them take your licence away a lawyer and doctor advises on revalidation and how to stay licensed to practice P40
guard your pension
Financial planners cavendish medical show how to avoid excess tax on pensions P44
editorial comment
Ratings war to break out
Get ready. The ratings war is on its way in private practice.
Independent doctors who are registered to provide medical services with the Care Quality Commission (CQC) are to be rated alongside independent hospitals and NHS colleagues.
Sometime soon, the CQC will issue another consultation document and this will be about the methodology of rating.
Private doctors affected are bound to be nervous for their business because there are just four categories: Outstanding, Good, Requires Improvement and Inadequate. But hopefully it will be a chance to shine.
Stephen Rippon, head of policy relating to CQC at the Department of Health (DoH), discussed the ratings at an Independent Doctors Federation meeting, and members broadly accepted the proposal.
Eventually, we expect the CQC will become even busier in the private healthcare sector because it looks like the DoH wants it to rate most services provided by independent medical providers – although notable exceptions appear to include dentists.
As we went to press, no date had yet been given for the launch of ratings, but we’ll help you prepare.
tell US yoUr newS Editorial director Robin Stride at robin@ip-today.co.uk Phone: 07909 997340 @robinstride
to advertiSe Contact advertising manager Margaret Floate at margifloate@btinternet.com Phone: 01483 824094 to SUBScriBe lisa@marketingcentre.co.uk Phone 01752 312140
Publisher: Gillian Nineham at gill@ip-today.co.uk Phone: 07767 353897
Head of design: Jonathan Anstee chief sub-editor: Vincent Dawe Circulation figures verified by the Audit Bureau of Circulations
Act to avoid a shock tax bill
By edie Bourne
Doctors are again being urged to urgently request any missing pension statement from NHS Pensions to try and prevent unexpected tax bills of many thousands of pounds.
Specialist medical financial advisers Cavendish Medical warned that a case backlog at the authority had caused 16week delays and could mean doctors face harsh tax penalties without realising the full extent of their situation.
Financial planner Dr Benjamin Holdsworth said some doctors relied on the agency issuing annual letters detailing their pension contributions for the preceding tax year.
But this only happened automatically if the doctor had ‘deemed growth’ in their pension pot of over £40,000 – the annual allowance limit.
He said: ‘There is a new tapered annual allowance, which means senior doctors earning over £150,000 from all sources, which includes their pension growth, face a significantly lower limit of just £10,000 a year.
‘NHS Pensions will not send letters warning these individuals that they are about to breach their reduced annual allowance, meaning they will pay tax on the excess at their marginal rate of tax. This is now affecting the majority of consultants above the age of 45, and sometimes earlier.’
‘We have been advising doctors reading Independent Practitioner Today to request a statement from NHS Pensions for some months now. Sadly, we’re hearing that the agency is quoting some 16 weeks to send doctors the information they require to check their position – a situation which is completely unacceptable.
‘By this time, a doctor’s tax submission will have been filed without the full detail of pension saving and no clear picture of how much tax is owed.
‘This opens the doctor up to significant penalties from HMRC, on top of the original tax, as well as potentially losing the option to pay the tax charge from the NHS pension scheme, which in itself can be very costly.
‘We are seeing clients on an almost daily basis needing to find £13,500 to meet additional tax charges – and often much higher.’
Dr Holdsworth said it was easy for busy doctors to let complex matters slide, but this was one situation where not acting fast could cause a ‘substantial headache and a hefty tax bill’.
As we went to press, NHS Pensions announced it had no backlog of Annual Allowance statement requests for 201617.
A spokesman said it could only calculate the pension input amount (pension growth) and issue pension savings statements for members if it had received annual membership and pensionable pay updates from employing authorities.
He continued: ‘This means that, for the 2016 17 tax year statements, members’ records were required to be updated by the employing authority to 31 March 2017 by 6 July 2017. This will apply to NHS consultants undertaking private work .
‘We have sent out 35,000 statements to those exceeding the Standard Annual Allowance where we had all of the information to calculate the pension growth.
‘If members have not received a 2016 17 statement, they can request one from us as long as we have the relevant membership information from their employing authority. We will issue them with a statement within 90 days, in line with the requirements of the Finance Act 2004.
‘Anyone who hasn’t received one by now and requires one should either contact us through our helpline 0300 3301 346 or via nhsbsa.annualallowance@nhs.net.’
NHS GPs may get defence fees cut, but private work not covered
New Government plans may rescue NHS GPs in England from rocketing defence premiums – but private doctors still face a big financial hit.
Meanwhile, the established defence bodies continue to campaign for a legal reform package to tackle the root of the issue – soaring litigation costs – and strike a balance between reasonable but also affordable compensation.
Simon Kayll, chief executive at the Medical Protection Society, said it recognised independent practitioners’ concern about the rising cost of clinical negligence.
He added: ‘The impact on consultants has been dependent on the amount of private work they do and their specialty.
‘The discount rate change [used to calculate long term injury awards] will have less of an impact for specialties where there is a lower risk of receiving a claim that includes future care costs or loss of earnings.’
Details of the state backed scheme for GPs are still awaited, but it will not cover them for nonNHS work, representation at inquests, GMC hearings, disciplinary investigations and advice and support.
See ‘Defence body’s bid to curb indemnity fees’, page 34
Brexit snuffs out insurance revival
By charles King
Rocketing insurance premium tax and fears over Brexit have come as a double whammy for hopes of a private medical insurance revival.
Latest figures showing static demand last year brought a warning from a leading healthcare economist for the independent sector to expect no big turnaround until there is a marked increase in business confidence.
Market analysts
LaingBuisson latest Health Cover market report shows 2.2% contraction in individualpaid policies to 928,000, a similar fall as posted in the previous three years, now covering 1.47m people (2.2% of population).
There was only a 0.6% growth in corporate medical cover policies, which reached 3.09m and covered 5.42m lives (8.3% of population).
ance premium tax in November 2015, pushing up cover prices.’
LaingBuisson said latest results followed a buoyant 2015 when two large corporates extended medical cover to their entire employee population, providing a significant boost, and the first significant growth since years of decline after the recession of the late 2000s.
Meanwhile demand for private healthcare from self payers is growing 10% annually.
Report author Philip Blackburn said: ‘The uncertain economic landscape triggered by Brexit snuffed out the whiff of optimism from corporate private medical cover growth in 2015, and future significant growth is likely to need a solid upturn in business confidence from corporate Britain.
many on the NHS and a steady increase in average NHS waiting, overall demand for private medical cover from individuals continues to decline.
‘This is largely attributed to the high price of medical cover, and consistent premium increases well above inflation.
‘The challenge insurers’ face to turn this around was dealt a heavy blow when HM Treasury doubled insurance premium tax – from 6% to 12% between November 2015 and June 2017 – leading to sharp upward pressure on premiums for insurance customers and a significant tax burden going forward. A slowdown in household spending in 2017 also doesn’t help.’
It said: ‘The UK market for private medical cover, worth £4.83bn, flatlined in 2016 with 4.02m policies covering 6.89m lives, some 10.5% of the population.
‘Defining events for demand during the year were the UK’s Brexit decision, which created economic and business uncertainty, and a sharp rise in insur
‘Nevertheless, private medical cover is highly valued by employees, and employers are increasingly committed to workplace benefits and services which support employee health and wellbeing. And quick access to healthcare services, which private cover offers, is the vital cornerstone.
‘Despite very high waits for
Cash plan policies reached 2.52m, covering 3.43m people, some 5.2% of the UK population in 2016. Employer demand rose strongly as the number of company paid cash plan policies reached a record 1.01m (up 11.8%), while health cash plans funded by individuals (employeepaid and personalpaid) continued to shrink, down 6.8% to be 1.51m.
Mr Blackburn added: ‘As a lowcost cover option, health cash plans continue to be very popular with employers, as the number of employer funded policies has almost doubled in the space of five years.’
Salaried doctors ‘confer advantage’
➱ continued from front page
Kevin Sears, executive director of Cleveland Clinic’s market and network services, said there was an appetite for competition in the marketplace, the group had a deep commitment to transparency of outcomes, and would bring value to London.
Its length of stay for knee replacements had fallen from 3.4
days in 2013 to 2.4 days in 2015.
Salaried consultants will provide a ‘competitive advantage’, according to the executive director of a German hospital group opening up in London next Spring.
Mr Andreas Ludowig said he had spent a lot of time recruiting consultants in central London for the 39 bed Schoen Clinic London, at 66 Wigmore Street.
It will focus on ‘worldclass’ spinal care and orthopaedics for adults.
He told the conference a salaried service was not for all but some advantages included no need to travel around London for work and administration and billing taken care of by the employer.
Mr Ludowig said specialists often felt they had nobody to talk
to when doing private practice under the employment model but the consultants due to work for Schoen were ‘looking forward to working together in a team with peers’.
They would have a contract with indefinite length and everything else that applied to a proper salaried contract in any other type of job.
Priory Group opens up in Harley Street
By Charles King
The Priory Group has opened a new clinic, The Priory Wellbeing Centre, at 41 Harley Street following a £300,000 investment.
It offers access to therapists, psychiatrists, psychologists and other healthcare professionals, with flexible consulting hours: Monday to Friday 8am to 8.30pm.
The Harley Street centre has close links with and clinical support from Priory Hospitals in north London, Roehampton, Woking, Chelmsford and Hayes Grove, Kent, enabling people to access additional or more intensive support if required.
Dr Hayley van Zwanenberg, associate medical director and clinical director of Priory Group’s Wellbeing Centres, said: ‘Priory’s Wellbeing Centres have proven incredibly popular across the UK
and it feels timely and appropriate that we should bring our expertise to a second central London location, synonymous with highquality and specialist healthcare.’
Consultant psychiatrist Dr Kathryn Hollins, a UK expert in parent and child mental health, said: ‘Specialist psychological treatments will be available in our new parenthood, pregnancy and family life service.
‘There is greater understanding of the importance of emotional well-being during pregnancy and the early years of childhood development and family life. More people are choosing to invest in their families’ health and happiness and we want to support them.’
The centre will offer psychological support and treatment for individuals and couples trying for a baby – including through fertility treatment and adoption – as
Andrew Hynard, chief executive of landlords The Howard de Walden Estate, said: ‘The Priory will add enormous value to the Harley Street area’s offering. Its specialists have a long and trusted track record of helping people affected by mental health issues and addiction.
‘This new clinic in the Harley Street Medical Area is central to our overall vision for the area, which is to attract the brightest talent in medicine and to deliver the very best patient care.’
well as treatment for moderate antenatal and postnatal depression and anxiety.
Priory Healthcare, part of the Priory Group, has nearly 100 registered healthcare locations, comprising both hospitals and clinics.
Mental health support for employers
Software ranks clinics’ billing performance against others
Hospitals can see how their e-billing performance ranks against others using a new innovation from Healthcode, the UK’s official clearing organisation for private medical bills.
The Performance Dashboard reveals data about an individual hospital’s electronic billing: the percentage of invoices sent electronically and that pass validation first time, and the average number of days to submit an e-bill.
Users can view two charts for each category showing their organisation’s performance over the previous 30 and 90 days. Each chart’s colour – red, amber or green – indicates if it is doing well or if there is potential cause for concern.
Each hospital gets industry averages for each performance indicator and its industry rank. The data enables organisations to properly evaluate billing operation efficiency and pinpoint areas for improvement. Healthcode plans to extend this to hospital groups.
The pack also covers serious illness such as schizophrenia, bipolar and personality disorders.
College president Prof Wendy
The Royal College of Psychiatrists has produced a special pack of mental health information for employers and employees covering the most common range of conditions such as depression, anxiety and sleeping problems. There is also aids on seasonal affective disorder, obsessive compulsive disorder, post-natal depression and mental health in pregnancy, self-harm and eating disorders.
Burn said: ‘It makes sense for businesses to look after the mental health of their employees.
‘It can make a real difference if they have the right information to hand, if they can say to an employee experiencing a mental health issue: “We understand”.’
Managing director Peter Connor said: ‘We wanted to provide useful performance metrics for hospitals which help their business maximise cash flow, and we hope the element of healthy competition which comes from seeing their industry rank will inspire them to increase their billing productivity and accuracy to benefit the whole private health sector.’
Heart centre PPU taken over by trust
NHS private patient hospital services at The Essex Cardiothoracic Centre (CTC), formerly managed by Ramsay Health Care and called the Orwell Suite, have been brought in-house.
The change brings Basildon and Thurrock University Hospitals in line with most other NHS trusts,
who manage private patient units (PPUs) themselves and use the financial surplus to support services.
Now called Nash Basildon, it opened after refurbishment and expects to expand the range of procedures offered.
Spokesman Tom Abell said:
‘Having a PPU within a specialist centre like the CTC also offers patients the peace of mind of having easy access to specialist theatres and critical care facilities, if needed, which is only available in a limited number of private hospitals.’
A working group including consultant representatives concluded
that the trust would benefit from bringing private patient management in-house.
PPU adviser Philip Housden, of Housden Group, said it was planned to extend the new branding – Nash Private Healthcare – to Southend and Broomfield Hospital sites.
Dr Hayley van Zwanenberg
College campaign to stop bullying
By Olive Carterton
The Royal College of Surgeons of Edinburgh has reinforced its continued commitment to eradicate bullying in healthcare by launching a new campaign.
Its initiative, ‘Let’s Remove It’, aims to encourage healthcare professionals to speak up and stamp out this behaviour.
The college is also campaigning for the GMC to introduce compulsory training on bullying, including medical education (CPD) credits for all foundation year doctors.
And it is arguing for individuals who bully and undermine to have their training responsibilities removed.
The college has developed:
A new digital resource full of factual and legal information, with links to literature, case studies and e-learning tools. The hub provides support for people who are being bullied and strategies so surgeons are able to reflect on their own behaviour to make sure that they are not part of the problem;
Posters and presentations for all hospitals;
A performance workshop ‘How to survive and thrive as a surgeon’, which will include work on team behaviour and how to build and
support successful, effective teams.
RCSEd president and consultant general and colorectal surgeon
Prof Michael Lavelle-Jones said:
‘The sentencing of surgeon Ian Paterson has once again raised the issue of bullying and undermining in healthcare and highlighted the terrible consequences that this behaviour can have for patients.
‘The college has a zero tolerance approach to bullying, undermining and harassment and categorically condemns this in all circumstances. But we want to do more. We want to change the culture of healthcare to ensure that this kind of behaviour becomes so unacceptable it can no longer go on.
‘We want to offer support to those who have been bullied, and to get people to reflect on their own behaviour and take owner -
ship of the fact that this is everyone’s problem.
‘As professionals, we have a duty to protect our patients from damaging and unnecessary treatments and, as professionals, we have a right to be protected from being bullied and undermined.’
In the first UK study of its kind, published in its journal The Surgeon, the college revealed onein-six trainees suffer from posttraumatic stress disorder (PTSD).
Quoting research, it said in the NHS, aspiring surgeons were three times more likely to be victims of bullying than anyone else.
Study authors said symptoms of insomnia, anger, poor concentration, hyper-vigilance and exaggerated startle had implications for patient safety, as did ‘the endemic culture’ of bullying in surgery.
Doctors’ data portal about to launch
The Private Healthcare Information Network (PHIN) was this month due to launch its new online portal to enable consultants to review their clinical private and NHS practice data for the first time. It aims to publish data on private specialists from mid-2018, starting with procedure numbers, average length of stay and profile information. Data can be validated through ‘a secure’ online portal.
PHIN said it was working with royal colleges, professional associ-
ations and hospitals to promote engagement.
Royal College of Surgeons’ president Prof Derek Alderson encouraged surgeons to support the development and work to improve it as it matured.
He said: ‘There have been a large number of initiatives in the NHS to improve patient safety. Yet the same focus from Government and healthcare leaders has not happened in the private sector. The recent abhorrent case of Ian
Website with videos to help beauty doctors with training
A subscription-based website, e-MASTR.com, has been developed to boost education among aesthetic practitioners.
Clinicians are supported with more than 120 high-definition videos ‘throughout all areas of aesthetic practice’, including consultation processes.
The videos present a wide range of patient types: young and old, male and female, mothers and daughters, identical twins, those with few or many treatment indications and people of different ethnicities.
Developer Dr Tapan Patel, medical director of PHI Clinic at 102 Harley Street, said: ‘Our new platform has been specifically created to complement existing training through workshops, journals and conferences, and the beautifullyshot videos create a fresh, engaging and memorable way of learning.
‘A key aspect of e-MASTR is that it’s all online, accessible anywhere. The idea is for practitioners to dip in and out, allowing them to fit in training around their busy clinic schedule.’
Paterson served as a reminder that this sector needs as much focus on safety as the NHS.’
PHIN said consultants’ data and information would only be published if doctors were confident it was complete, accurate and gave a fair view of their practice.
It asked all consultants in private healthcare to login, check and work with their hospitals to ensure data was complete and correct. Go to portal.phin.org.uk/ Consultants.
Expo to promote yourself abroad
Future Healthcare, the international healthcare exhibition and conference on 13-14 March 2018, at Olympia London, has partnered with Healthcare UK, which aims to help providers in the private and public sector to do more business overseas.
Organisers say they expect over 4,000 attendees from 65 countries with exhibitors from 25.
Dr Tapan Patel
The RCSEd’s campaign poster and college president Prof Michael Lavelle-Jones
LaingBuisson private acute heaLthcare conference
GPs ‘block access to private care’
By Robin Stride
Patients are having a hard time getting referred to a private consultant of their choice because some GP ‘gatekeepers’ only want to point them in the direction of the NHS.
Dissatisfaction at barriers to real patient choice surfaced at the LaingBuisson Private Acute Healthcare Conference in London as speakers spoke of the private consultant route being resisted by the patients’ GPs – and even blocked.
Fiona Booth, chief executive of the Association of Independent Healthcare Organisations (AIHO), said GPs were sometimes reluctant to offer the independent sector as an option as a result of ‘misguided loyalty’ – regardless of the patients’ funding model.
She added: ‘I have experienced this myself in my own endeavour to obtain a referral.’
Independent Doctors Federation GP Committee chairman Dr Neil Haughton agreed that some NHS GPs gave their patient ‘a hard time’ for wanting to go private. He cited the case of one GP who was ‘openly rude about it’.
Patients also had problems in securing referrals to private doctors in London due to the high number of locum GPs, he said.
While he was ‘well aware’ that NHS GPs had lost their contact with secondary care doctors, he said it should not take that much investi-
gation for them to find out who the best person might be for the patient.
Ms Booth said it needed to be known that patients who were referred to the independent sector could get seen quicker and at the same NHS tariff price, reducing waiting times and repeat visits.
If it were not for those patients harnessing healthcare outside of the NHS, pressure on the NHS would be even greater.
But misguided loyalty was not always the case and often it was as simple as being able to give GPs the right facts and figures and a script so they could feel more confident about talking about the independent sector and see it as a healthcare partner.
She told the conference: ‘Some GPs reported to me that they felt awkward about talking about financing or payment of healthcare and didn’t want to bring paying for healthcare or finance into the consultation.
‘Others said it would be helpful if they had information to hand that they could give to patients.’
Ms Booth said the NHS constitution enshrined the right for patients to make choices about receiving NHS-commissioned services – and the choice ‘to go independent’ was at the centre of this decision.
Recent AIHO research (Independent Practitioner Today, July-August 2017) showed that the two least satisfactory aspects of a patient’s
experience when receiving independent healthcare was firstly to do with the information they received to enable their choice and, secondly, the referral process.
Most people said their GP’s recommendation guided their choice of provider and they only rated the quality of this information two out of ten.
Ms Booth said recent surveys had shown that the number of patients being offered choice over where they were treated had reduced. And for those patients who went down a private treatment route, fewer than a quarter had the option raised by their GP
‘We know GPs are often the gateway to patients choosing an independent provider, regardless of their funding model. And we know patients want clear, accessible information. So, the conclusion is quite simple – as a sector, we need to work with GPs to improve the information they provide and many AIHO members are doing just that.’
AIHO members all worked with primary care providers and were using education, awareness-raising and myth-busting to develop and enhance their relationships with GPs with a view to increasing referrals, whether these were NHS funded, private medical insurance or self- pay.
‘Sometimes it is just simply a case of making GPs aware of the
benefits of using the independent sector. GPs want speedy access to secondary care – which will often also reduce GP surgery repeat visits; they want to be able to put faces to known and trusted consultants and, in the case of NHSfunded patients at the same NHS tariff price, giving greater choice to patients,’ Ms Booth added. Another avenue to improve private referrals was working with clinical commissioning groups and other organisations who influence GPs, creating awareness of the sector’s role and contribution, she said.
She expected the Private Healthcare Information Network to play a big part there, enabling GPs to gather their own information about specific hospitals and consultants, and directing patients to its website too – offering them the chance to make an informed choice.
Dr Howard Freeman, clinical director of the NHS Partners Network, said it was working with the NHS to produce answers to ‘frequently-asked questions’ from NHS professionals on choosing the private sector for elective care.
One reason why GPs were not offering patients a choice was because they did not know they could refer outside the local provider. Public education was the key to this, he said.
Watchdog reports on visits to private units
The Care Quality Commission (CQC) had inspected 197 acute independent hospitals by 31 July 2017, according to CQC figures given to the conference by its head of quality inspection, Carolyn Jenkinson.
7% were rated as outstanding, 71% were good, 27 ‘required improvement’ and 2% were inadequate.
Ms Jenkinson said common themes from independent healthcare inspections included:
The quality of leadership, man-
agement and governance – an important influence in driving improvement in the quality of care;
Services needed to be more responsive to individual’s needs, such as those for people with dementia;
Learning from incidents and the
quality of incident investigation; Infection, prevention & control; Children’s services and safeguarding.
She promised ‘a more targeted, responsive and collaborative approach in future’.
Fiona Booth, AIHO chief executive
private acute heaLthcare conference
Private sector ‘too timid’
A think tank boss hit out at the private sector for having too quiet a voice in politics.
Reform director Andrew Haldenby warned delegates at the meeting – who represented a wide sphere of movers and shakers within the industry – that it was ‘extremely risky’ to rely on tacit support of the Government.
While the Conservatives maintained ‘radio silence’ on the private sector, the Labour Party was making the case against the private sector, he said.
It had said it would reverse NHS privatisation, ensure excess private profits were not made out of the NHS at the expense of patient
care and increase the tax on private medical insurance premiums.
He told the meeting that politicians and officials were extremely sensitive to campaigns and ‘the other side’ campaigned every day.
Mr Haldenby advised them to campaign, not just lobby, and to:
Make their case as enthusiastically as the defence firms;
Base their campaign on the facts of what they did and the benefits of it – provide information;
Hold one big event per quarter with some supporting literature;
Take advert space above the escalator at Westminster tube –‘Why is it always BAE?’
He said the public was on the
private sector’s side – but people needed to hear from them.
His message was backed by Steve Gray, chief executive of Nuffield Health, who said many people were unaware of what the private sector did. Everyone needed to speak together with one voice to provide the answer and also say why and how well they did it.
Some 43% of Care Quality Commission inspection ratings for non-specialist acute hospitals were ‘good’ or ‘outstanding’, compared to 71% for the independent sector. Private hospitals had to get their figures to 100% ‘outstanding’ and share best practice to help achieve that.
Group eyes up repeat after successful training event
Consultant feedback from an industry education day run by eye group Optegra was so positive that the company will run another event in the Spring.
Seventy consultants attended the meeting and there is an open invitation for other Independent Practitioner Today readers to join in the next continuing professional development (CPD) event.
Gloria McCall, business development director for Optegra Eye Health Care, said: ‘This event was a great opportunity to bring a number of our consultants together, as well as welcoming consultants and fellows from other medical establishments.
‘A good day was had by all, with positive feedback that it was very beneficial to their day-to-day working life as consultants and that it provided a lot of information across many areas of ophthalmology.
‘The attendees hoped this was the first of many. We are looking to host another consultant event
in early spring and invite anyone who would be interested to join us to get in touch.’
Readers wanting to go should email her at Gloria.mccall@optegra.com.
The first CPD event, ‘Today’s Business, Tomorrow’s Technology’, in London, offered something for all consultants across ophthalmology specialties, including:
Mr Richard Packard, of Arnott Eye Associates, with an overview of Optegra’s collaboration working to improve outcomes with the European Society of Cataract and Refractive Surgeons;
Mr Robert Morris, consultant ophthalmic surgeon, on keeping up to date with the changing face of CPD and how to manage it in working life using mobile apps;
Mr Mark Ashley, a lawyer, on the best ways to manage risk in patient management and how best to keep trouble-free;
Mr Richard Heighton, of insurance brokerage Lucas Fettes and Partners, on indemnity changes
Mr Guz Gazzard, consultant ophthalmic surgeon at Moorfields Hospital, with an overview of what is available in glaucoma stent surgery, with the pros and cons of all devices on the market;
Andrew Haldenby: Said the public was on the private sector’s side, but people needed to hear from it
Mr Robert Morris: talked about managing cpd using apps
Fixing poor beauty ops is on the rise
A British Association of Aesthetic Plastic Surgeons (BAAPS) member survey has revealed 80% of them have recently experienced an exponential rise in requests for ‘revisional’ work – fixing botched procedures.
A poll of BAAPS’ 230 members found eight in ten have witnessed an alarming increase in patients’ requests to correct failed cosmetic procedures in the last five years.
Some surgeons said a third of their own practice’s work was just fixing other people’s mistakes.
Others said they declined to treat these cases because the problems were often unsolvable.
Surgeons identified the reasons for the revisions as falling into three main culprits:
40% cited patients being incorrectly selected for the initial surgery. They had been medically or psychologically unsuitable for a particular procedure, yet it was performed nevertheless;
30% stated the original procedure had been clearly carried out by someone with dangerously inadequate training;
30% were left to pick up the pieces from cheap deals abroad.
Survey results were announced at the BAAPS’ Annual Scientific Meeting, held at the Clinical Cosmetic and Reconstructive Expo at London’s Kensington Olympia.
Consultant plastic surgeon and BAAPS president Mr Simon Withey, whose own practice saw
as much as 40% revisional work last year, said: ‘Patient selection is one of the most key issues to consider when considering who is appropriate for a procedure.
‘I have seen many people who were clearly not appropriate for surgery – ranging from unrealistic expectations, to the more extreme body dysmorphia, contraindicated medications, smokers, pre-existing medical conditions which should have ruled them out. And yet, unscrupulous practitioners have endangered their health entirely for profit.
‘There is currently – perhaps unsurprisingly, in these turbulent times – a measure of financial uncertainty in the UK. Thus, affordability is one of the biggest drivers in the rise of cosmetic medical tourism deals offering allinclusive package holidays and the promise of a high-quality service at heavily discounted rates.
‘But these promotions conveniently gloss over the increased risk of complications post-surgery due
Survey findingS
Lack of regulation leading to ‘cowboy’ proliferation
Criteria for patient selection ignored by untrained practitioners
uK patients seduced by cheap offers abroad, leaving nHS to pick up the tab when something goes wrong
to travel, less robust regulations and credentialing, as well as a lack of consistent follow-up.
‘This has directly led to an increase in the number of reported cases of people returning to the UK with serious complications after receiving cosmetic surgery abroad. Consequently, many patients are being treated in the NHS for complications.’
He said one study presented at the conference in one hospital alone pinpointed the average cost of each patient at £13,500 each, on average – a total of over £282,000 just for 21 patients.
Consultant plastic surgeon and BAAPS council member Miss Mary O’Brien, who oversees the training committee at the association, said training properly to become a plastic surgeon took many years –a minimum of about 16.
Consultant plastic surgeon and BAAPS president-elect Mr Paul
Harris said: ‘Cosmetic surgery has seen a major change in the way providers communicate with prospective patients, much of this is now internet based and not regulated. Indeed, many studies presented at our meeting have highlighted the unethical ways cosmetic surgery is marketed, including via social media.
‘Interestingly, by analysing search engine data, another study showed that the UK has more interest in aesthetic treatments than even our counterparts in the US. The British population’s interest in procedures such as non-surgicals and liposuction wildly outweighs America’s.
‘This stresses even more the importance of events such as our annual meeting, a shared platform seeing professionals from all over the world presenting on the latest advances with an ethical approach towards patient safety.’
Scrapping of NHS pay cap welcomed
Doctors with an NHS contract have welcomed the Government’s confirmation of the scrapping of the pay cap in the health service.
Danny Mortimer, chief executive of NHS Employers, said it was
helpful to receive Health Secretary Jeremy Hunt’s confirmation of an end to the ceiling, which echoed the messages to the pay review bodies from the Treasury.
NHS Employers was awaiting
further details in the 22 November Budget as we went to press – and through the deliberations of the pay review bodies.
Mr Mortimer warned: ‘The NHS is clear, however, that additional investment is needed to support pay awards above the present pay cap.
‘We are also clear that alongside action we are taking locally, national support is needed in other areas to improve supply and retention.’
Mr Paul Harris: Said studies show unethical way surgery is marketed
Miss Mary O’Brien: Training to be a cosmetic surgeon takes 16 years
By Leslie Berry
A new ‘live chat’ service from outsourced communications provider Moneypenny enables private doctors’ customers to instantly converse with a real person using texting software as an alternative to a phone call.
The service is available 24/7 on either a fully outsourced basis or to take over when clinics’ own staff become too busy.
Company managing director Joanna Swash said the service gave
The taxman warns about sites looking like HMRC
Doctors and their accountants are being warned to watch out for ‘costly and deceptive’ websites when searching for HM Revenue and Customs (HMRC).
When someone searches online for the tax authority’s phone numbers or digital services, they can be directed to other websites and some of these promote premium rate, non-HMRC numbers as a means of reaching the department.
These are, in fact, call forwarding services which connect callers to HMRC, but at a hefty price, despite HMRC’s own 0300 numbers being free or charged at the national landline rate.
In other cases, sites charge for forwarding information to HMRC which can be provided free of charge through the GOV.UK website.
HMRC said it had averted more than a million visits to deceptive
Service allows patients to chat
customers another route to communicate with businesses, as not everyone always wanted to call.
‘It is also excellent for customer service and will increase the number of inquiries generated for our clients. Moneypenny is a great example of this, as we recently launched Live Chat on Moneypenny.com and it has already increased our inquiries by 30%.’
The firm already answers calls for private healthcare providers of all sizes across the UK, either on an overflow or fully outsourced basis.
websites, including those promoting misleading and costly helpline numbers.
Tax officials say too often this is an attempt to mislead customers and gain business at their expense, without making clear the service is not affiliated with HMRC.
Since January, HMRC’s cyber security team has taken control of more than 75 of these dubious sites by challenging their ownership.
Any members of the public trying to access these sites will now be redirected to HMRC’s GOV.UK pages, which provide HMRC’s genuine contact numbers as well as advice on how to spot these misleading sites.
HMRC’s customer services director Angela MacDonald, said: ‘HMRC takes the abuse of its brand very seriously. Attempts to dupe customers in this way won’t be tolerated and we will always act to protect the public from malicious or misleading websites.’
Other types of scams are also being targeted by HMRC. It has requested the removal of over 20,000 malicious websites in the last year. Information on how to spot these scams is published on the HMRC website.
The company said it expected interest in its Live Chat service from clinics to significantly increase in the upcoming months.
Stephanie Vaughan-Jones, channel manager at Moneypenny, said: ‘Delivering excellent service is an ongoing priority for healthcare practices, and increasingly conversations with our healthcare clients involve how they can capture more inquiries.
‘Healthcare providers know all too well that to stay ahead of the competition, they must offer a
customer service platform people want to use, one of convenience and handled by professional and friendly people.’
Bid to ditch label ‘junior doctors’
Consultants will no longer work with ‘junior doctors’ if campaigners get their way.
Consideration is being given to changing the job title following a campaign by academics in the Oxford Health Alliance backed by England’s Chief Medical Officer Dame Sally Davies.
The term ‘junior doctor’ is said to be detrimental to self-esteem and misunderstood by the public.
Doctors’ leaders welcoming the campaign include Prof Derek Bell, president of the Royal College of Physicians of Edinburgh, and Dr Katherine Walesby, chairman of the college’s trainees and members’ committee.
The college has long supported proposals to change the term ‘jun-
ior doctor’ to something that more adequately reflects their experience and training, they said.
They added: ‘Doctors in training are fully-qualified doctors often with many years of experience after graduation.
‘It is essential that this group of doctors are recognised for their contribution to the NHS and the vital role that they play in healthcare teams across the country. Changing their title would also provide more clarity to patients.
‘Doctors in training are the future of medicine and their wellbeing and morale are important not just at an individual level but as a reflection of a functioning, sustainable and valued workforce that makes up the NHS.’
TeLL uS yOur STOry
Share your experience of what has and has not worked in your private practice. even if it’s bad news, let us know and we can spread the word to prevent other independent practitioners falling into the same pitfalls. Contact editorial director robin Stride at robin@ip-today.co.uk or phone him on 07909 997340
Stephanie vaughan-Jones
GMC ConsUlTATion
What should we be teaching trainees?
Doctors are being asked for their feedback to the GMC to help shape the future skills of graduates
The GMC h AS launched a consultation on the knowledge, skills and professional behaviours needed by newly-qualified doctors in order to help shape the future development of undergraduate medical education.
Its Outcomes for graduates – what doctors must know and be able to do by the time they graduate from medical school – has been updated to better reflect modern medical education and practice.
Doctors will be expected to have an understanding of areas such as population health and managing the care of patients with multiple diseases, complex areas of practice such as consent, confidentiality and safeguarding, and an appreciation of the needs of patients from diverse backgrounds.
There are also new outcomes stressing the importance of doctors’ personal well-being, helping them to incorporate self-care into their personal and professional lives.
Outcomes proposed for inclusion in medical school curricula emphasise the importance of new doctors:
Working in partnership with patients, families and carers;
Raising and acting on issues of patient safety;
Understanding their responsibility to safeguard vulnerable patients.
shifts in medicine
Dr Colin Melville, the GMC’s director of education and standards, says: ‘Medical schools play a unique role in the development of the UK’s medical profession.
We want to help them make sure their curricula continue to produce newly-qualified doctors who can respond confidently to any pressures and challenges they may face from their first day of practice.
‘The outcomes are forwardlooking, to equip the doctors of tomorrow with the knowledge and skills they need to engage with emerging areas of healthcare such as genomics and population health.
‘Some of the outcomes we propose also reflect the shifts we have seen in medicine in recent years –such as the need for doctors to work more collaboratively with patients to plan their care, which
is likely to involve treatment for a range of complex and related conditions.’
The GMC believes the outcomes it sets bring a measure of consistency to undergraduate medical education, although medical schools have the freedom to design and deliver their own curricula for students.
Common threshold
Its Outcomes for graduates will also be integral to the future development of its Medical Licensing Assessment (MLA), which would provide assurance that doctors working in the UK have met a common threshold.
The GMC held a consultation on its MLA proposals earlier this year.
A consultation report published by the council indicated broad support for the concept of the assessment, as well as some concerns about its implementation.
It is currently considering responses to the consultation, and will announce next steps later this year.
The OuTcOmes fOr graduaTes prOvides:
a guide for students on what they need to learn
a basis for medical schools to develop their curricula
a framework for the gmc to regulate medical schools against
a guide for employers and those designing postgraduate training on what newly qualified doctors can be expected to know and do
Dr Melville added that it was now a critical time for reforms across medical education, at both undergraduate and postgraduate level.
‘Our work on developing the MLA is continuing, but it is vital that the UK educates, trains and assesses our future doctors in a way that helps them meet the demands of a healthcare environment that is changing rapidly.’
The GMC’s review of existing outcomes for graduates has received input from all four UK countries, including educators, doctors in training and lay people, and also representatives of the Medical Schools Council along with experts in law, diversity and communication, and doctors with both primary and secondary care backgrounds.
The consultation runs until 10 January 2018.
To read the proposed updated Outcomes for graduates and to give feedback as part of the consultation, go to www.gmc-uk.org/education/31336.asp.
THE FIRST 9-VALENT HUMAN PAPILLOMAVIRUS (HPV) VACCINE
GARDASIL® 9 contains 9 HPV types that account for 89% of HPV-related anogenital cancers and 90% of genital warts in Europe.1,2*
* Cervical, vulval, vaginal and anal cancers caused by oncogenic HPV types 16, 18, 31, 33, 45, 52 & 58 genital warts caused by HPV types 6 & 11. Not all cases of anogenital cancer are caused by HPV. The HPV prevalence is: ~100% in cervical cancer; ~88% in anal cancer; ~19% in vulval cancer; ~71% vaginal cancer.2
GARDASIL® 9 is indicated for active immunisation of individuals from the age of 9 years against premalignant lesions and cancers affecting the cervix, vulva, vagina and anus caused by vaccine HPV types and genital warts caused by speci c HPV types. The indication is based on data in males and females aged 9-26 years.
GARDASIL® 9 is not the vaccine offered in the national immunisation programme. The use of HPV vaccines should be in accordance with of cial recommendations.
For information on ef cacy rates and safety considerations, refer to the Summary of Product Characteristics available on the eMC website.
To order please contact AAH on 0844 561 8899.
GARDASIL ® 9 ▼
Human Papillomavirus 9 valent Vaccine (Recombinant, adsorbed))
PRESCRIBING INFORMATION
Refer to Summary of Product Characteristics before prescribing
Adverse events should be reported. Reporting forms and information can be found at www.mhra.gov.uk/yellowcard. Adverse events should also be reported to MSD (Tel: 01992 467272).
PRESENTATION Gardasil 9 is supplied as a single dose pre- lled syringe containing 0.5 millilitre of suspension. Each dose of vaccine contains highly puri ed virus-like particles (VLPs) of the major capsid L1 protein of Human Papillomavirus (HPV). These are type 6 (30 mg), type 11 (40 mg), type 16 (60 mg), type 18 (40 mg), type 31 (20 mg), type 33 (20 mg), type 45 (20 mg), type 52 (20 mg) and type 58 (20 mg). USES Gardasil 9 is a vaccine for use from the age of 9 years for the prevention of premalignant lesions and cancers affecting the cervix, vulva, vagina and anus caused by vaccine HPVtypes and genital warts (condyloma acuminata) caused by speci c HPV types. The indication is based on the demonstration of ef cacy of Gardasil 9 in males and females 16 to 26 years of age and on the demonstration of immunogenicity of Gardasil 9 in children and adolescents aged 9 to 15 years. The use of Gardasil 9 should be in accordance with of cial recommendations. DOSAGE AND ADMINISTRATION Individuals 9 to and including 14 years of age at time of rst injection: Gardasil 9 can be administered according to a 2-dose schedule. The second dose should be administered between 5 and 13 months after the rst dose. If the second vaccine dose is administered earlier than 5 months after the rst dose, a third dose should always be administered. Gardasil 9 can be administered according to a 3-dose (0, 2, 6 months) schedule. The second dose should be administered at least one month after the rst dose and the third dose should be administered at least 3 months after the second dose. All three doses should be given within a 1-year period. Individuals 15 years of age and older at time of rst injection: Gardasil 9 should be administered according to a 3-dose (0, 2, 6 months) schedule. The second dose should be administered at least one month after the rst dose and the third dose should be administered at least 3 months after the second dose. All three doses should be given within a 1-year period. It is recommended that individuals who receive a rst dose of Gardasil 9 complete the vaccination course with Gardasil 9. The need for a booster dose has not been established. Studies using a mixed regimen (interchangeability) of HPV vaccines were not performed for Gardasil 9. Subjects previously vaccinated with a 3-dose regimen of quadrivalent HPV types 6, 11, 16, and 18 vaccine (Gardasil or Silgard), hereafter
referred to as qHPV vaccine, may receive 3 doses of Gardasil 9. The use of Gardasil 9 should be in accordance with of cial recommendations. Paediatric population (children <9 years of age): The safety and ef cacy of Gardasil 9 in children below 9 years of age have not been established. No data are available. Population ≥ 27 years of age: The safety and ef cacy of Gardasil 9 in individuals 27 years of age and older have not been studied. The vaccine should be administered by intramuscular injection. The preferred site is the deltoid area of the upper arm or in the higher anterolateral area of the thigh. Gardasil 9 must not be injected intravascularly, subcutaneously or intradermally. The vaccine should not be mixed in the same syringe with any other vaccines and solution. CONTRAINDICATIONS Hypersensitivity to any component of the vaccine including active substances and/or excipients. Individuals with hypersensitivity after previous administration of Gardasil 9 or Gardasil /Silgard should not receive Gardasil 9. PRECAUTIONS The decision to vaccinate an individual should take into account the risk for previous HPV exposure and potential bene t from vaccination. As with all injectable vaccines, appropriate medical treatment and supervision should always be readily available in case of rare anaphylactic reactions following the administration of the vaccine. The vaccine should be given with caution to individuals with thrombocytopaenia or any coagulation disorder because bleeding may occur following an intramuscular administration in these individuals. Syncope (fainting), sometimes associated with falling, can occur following, or even before, any vaccination, especially in adolescents as a psychogenic response to the needle injection. This can be accompanied by several neurological signs such as transient visual disturbance, paraesthesia, and tonic-clonic limb movements during recovery. Therefore, vaccinees should be observed for approximately 15 minutes after vaccination. It is important that procedures are in place to avoid injury from fainting. Vaccination should be postponed in individuals suffering from an acute severe febrile illness. However, the presence of a minor infection, such as a mild upper respiratory tract infection or lowgrade fever, is not a contraindication for immunisation. As with any vaccine, vaccination with Gardasil 9 may not result in protection in all vaccine recipients. Gardasil 9 will only protect against diseases that are caused by HPV types targeted by the vaccine. Therefore, appropriate precautions against sexually transmitted diseases should continue to be used. The vaccine is for prophylactic use only and has no effect on active HPV infections or established clinical disease. The vaccine has not been shown to have a therapeutic effect and is not indicated for treatment of cervical, vulvar, vaginal and anal cancer, high-grade cervical, vulvar, vaginal and anal dysplastic lesions or genital warts. It is also not intended to prevent progression of other established HPV-related lesions. Gardasil 9 does not prevent lesions due to a vaccine HPV type in
9-VALENT HPV PROTECTION
individuals infected with that HPV type at the time of vaccination. Vaccination is not a substitute for routine cervical screening. There are no data on the use of Gardasil 9 in individuals with impaired immune responsiveness. Safety and immunogenicity of a qHPV vaccine have been assessed in individuals aged from 7 to 12 years who are known to be infected with human immunode ciency virus (HIV). Individuals with impaired immune responsiveness, due to either the use of potent immunosuppressive therapy, a genetic defect, Human Immunode ciency Virus (HIV) infection, or other causes, may not respond to Gardasil 9. Long-term follow-up studies are currently ongoing to determine the duration of protection. There are no safety, immunogenicity or ef cacy data to support interchangeability of Gardasil 9 with bivalent or quadrivalent HPV vaccines. Pregnancy, lactation and fertility: There are insuf cient data to recommend use of Gardasil 9 during pregnancy, therefore vaccination should be postponed until after completion of pregnancy. The vaccine can be given to breastfeeding women. No human data on the effect of Gardasil 9 on fertility are available. SIDE EFFECTS Refer to Summary of Product Characteristics for complete information on side-effects. Very common side effects include: erythema, pain and swelling at the injection site and headache. Common side effects include: pruritus and bruising at the injection site, dizziness, nausea, pyrexia and fatigue. The post-marketing safety experience with qHPV vaccine is relevant to Gardasil 9 since the vaccines contain L1 HPV proteins of 4 of the same HPV types. The following adverse experiences have been spontaneously reported during post-approval use of qHPV vaccine and may also be seen in post-marketing experience with Gardasil 9: urticaria, bronchospasm, idiopathic thrombocytopenic purpura, acute disseminated encephalomyelitis, Guillain-Barré Syndrome and hypersensitivity reactions, including anaphylactic/ anaphylactoid reactions. PACKAGE QUANTITIES AND BASIC NHS
COST Single pack containing one 0.5 millilitre dose pre- lled syringe with two separate needles: £105.00 per dose Marketing
References: 1. GARDASIL® 9 SmPC, 2017. 2. Hartwig S et al
Estimation of the epidemiological burden of HPV‐related anogenital cancers, precancerous lesions, and genital warts in women and men in Europe: potential additional bene t of a nine‐valent second generation HPV vaccine compared to rst generation HPV vaccines. Papillomavirus Res 2015; 1:90–100.
Date of preparation: October 2017 VACC-1231710-0006
Despite what some might believe, the taxman isn’t some villainous character looking to see medical businesses and doctor entrepreneurs fail.
On the contrary, HMRC wants the taxpayer to succeed and, wherever possible and appropriate, receive tax relief on anything promoting business activity generally, as well as on innovation and investment.
Susan Hutter (below) discusses different ways the taxman can help or give back to you and your business
Bright ideas can pay off
Research
and Development Tax Credit
You can only get this relief if you practise as a limited company. R&D tax credits are tax relief for qualifying R&D expenditure –which is 230% of the qualifying expenditure. So, if you spend £100,000 on inventions, you will get tax relief on £230,000.
Even if your company is not paying corporation tax, because it is loss-making, you can still get a tax refund, albeit at a lower rate, which is 14.5%.
Be sure that is something innovative and new, as the HM Revenue and Customs (HMRC) will scrutinise if unsure. Take expert advice.
Enterprise Investment Scheme (EIS) and Seed Enterprise Investment Scheme (SEIS)
This is a relief for people investing in a company. When it is a startup, the first £150,000 raised can be raised under the SEIS whereby the taxpayer gets 50% tax relief of the investment.
Thereafter, EIS relief is available and the taxpayer gets 30% tax relief on the investment. The maximum holding is 30%. As long as you hold your shares for three years or more, there is no capital gains tax on sale.
The beauty of this scheme is that you can pre-clear this with HMRC and present them with a business plan. If HMRC rejects this, it will tell you why and it gives you a chance to tweak the business plan and re-apply.
Time to pay
Let’s say you not have put enough money aside to pay income or corporation tax or PAYE for employees.
While tax officials expect you to make a reserve, they tend to be understanding about the predicament and give you longer to pay –as long as you have a good reason.
What I have found lately is the taxpayer has a better chance of getting a ‘Time to pay’ deal if he or she deals direct with HMRC to
plead their own case, rather than using their agent/accountant.
Generally, HMRC will expect to be paid within six months of the due. Also, it usually will only allow time to pay if you have not get any other tax outstanding –personal or corporate – and you haven’t been late before.
Annual Investment Allowance (AIA)
This is an allowance given to prac tices who spend money on mov able plant and machinery – for example, scanning equipment or computers.
For qualifying expenditure of up to £200,000, you can claim the total purchase price as tax deduc tion against your profit in the year of purchase.
This is only for equipment you are purchasing and not renting. Also, this does not include cars.
Susan Hutter is a specialist medical accountant and partner at Shelley Stock Hutter
HM Revenue and Customs wants the entrepreneur doctor to succeed, not fail
Entrepreneurial
neurosurgeon Mr Richard Ashpole (above) has a successful sideline in designing surgical instruments
In AddITIon to my usual duties as a consultant neurosurgeon at Queen’s Medical Centre, nottingham (QMC), I have a longstanding and entirely amateur interest in designing and developing neurosurgical instruments and other ‘bits of kit’.
My first foray into this field was as a junior registrar when I designed, and had made, a set of instruments to assemble all manner of ventriculo-peritoneal shunt systems by a non-touch technique. These were patented, and then manufactured and distributed in conjunction with a UK company.
In 2010, as a consultant, I designed a prototype for a new set of instrumentation to more accurately and safely insert a relatively new type of artificial cervical disc. The design rights were bought by the disc’s parent company and I
Surgeon with brainwaves
was taken on to develop it and bring it successfully to market.
These instruments are now used ubiquitously for this disc, and with the money from this project I took the plunge and set up my company, neurodesign.
Training simulator
one of my main current projects is the design and development of a neurosurgical training simulator. With the increasing limitations on junior doctors’ hours and the consequent reduction in surgical exposure, simulation training will have an increasing role.
Until recently, there was no neurosurgical simulator; the specialty having lagged behind many others in this respect. So I set about trying to design one.
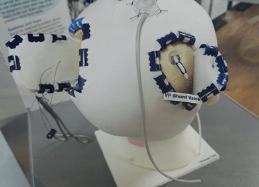
The ‘Realistic operative Workstation for Educating neurosurgical
Apprentices’ (Rowena) is a threepart brain surgery simulator based on, and named after, my daughter Rowena.
It consists of a plastic head and neck with realistic skull base anatomy, which forms the permanent base of the device. o nto this is fixed a ‘cranial top’ consisting of the skull, underlying dura and overlying scalp; fixed together in a way that these important surgical planes dissect apart in a realistic manner.
Initial development of this consisted of persuading a British company to indulge me with my idea and then trying out a number of plastic hemispheres of different properties to find a format that cut and drilled like real bone.
These were then covered in a variety of plastics in order to mimic the scalp and dura and, on
many occasions after work, both I and my children would try out various mock craniotomies on these, which were clamped to a workmate in the kitchen.
Having found a formula that worked, a cranial vault was made and simply affixed to a basic plastic face that the company had ‘knocking around’. Thus was born the first prototype.
Positive response
The response to a few test procedures was reassuringly positive and we decided that a new, definitive head and neck was required. My collaborator dismissed any idea of using my own ‘ugly mug’ and my daughter, Rowena, kindly volunteered.
After a day of mould-making, the Rowena acronym was com -
posed, somewhat tongue in cheek, in the car home – and seems to have stuck.
Following some experimental training courses, there was a significant demand for a realistic brain with ventricles, which would enormously increase the number of procedures that could be taught.
This was similarly developed via a number of ‘plastic footballs’ before the final version was produced with full ventricular anatomy. This was one of the longest stages of development, as we had to find a plastic that was firm enough to maintain its shape and yet would cleave in the same way as a real brain.
Practise techniques
Using this simulator, trainees can practise all the basic and some of the more complex neurosurgical procedures; starting with positioning the head in a three-point headrest, working through burr holes and basic flaps, ventricular access and drains, intracranial pressure monitors, right up to complex flaps across the midline and some posterior fossa approaches.
The ventricular system enables it to be used to teach neuroendoscopy and, as it is CT and MR compatible, it can be used with the image guidance systems which are becoming an increasing part of modern neurosurgery.
Mock haematomata, tumours and fractures have also been used, and we already have a paediatric version with fontanelles and open sutures.
The cranial top is essentially a consumable and, once drilled and sawed to destruction, is inexpensively replaced, while the brain has a significantly longer lifespan.
Since 2012, we have run a total of nine simulator courses at QMC, each over two days with eight delegates, so more than 70 trainees have been through this one course. others have been set up in Sheffield, Glasgow, London, the Royal College of Surgeons and the Man chester n eurosurgical Boot Camp, which all new trainees must now attend.
Simulators have been sold to Australia, Russia and, this summer, we ran our first workshops in Europe: in nijmegen, Holland.
Most recently, it is being used to help develop a robotic surgery system, for which there may also be training needs and, to date, over 200 simulator heads, brains and tops have been sold.
n eurodesign also has several other ongoing projects. one is an anchoring device for cerebrospinal fluid drains, which solves the near universal problem of these fine tubes being pulled, or falling, out of place, thus necessitating another operation with all the morbidity and costs that entails.
This design has been registered with the World Intellectual Property o rganisation. It has been patient-tested and CE (European conformity)-marked and is being licensed to a commercial manufacturer.
Another design is for a new intraoperative neurosurgical instrument for which global patents have been applied and which is being developed in conjunction with a major instrument company. Finally, there is an electronic diagnostic device, currently at the second prototype stage, and also an adjunct to tumour surgery, neither of which are yet in the public domain.
‘Hobby business’
In its seven years of existence, n eurodesign has taken three products to market, with three more in various stages of development and a commensurate intellectual property portfolio. It has also won three design and innovation awards.
What we used to refer to as ‘dad’s hobby business’ is becoming a bit more involved, although still based on a workbench at home in the back of my laundry.
Interestingly, I now find I am going to meetings as a trade stand rather than as a delegate and giving talks on entrepreneurship and innovation rather than just my last 100 operations, which is quite a change and much more fun.
o ver that time, the learning curve has been steep at times, with a panoply of new skills required including:
Setting up and running a firm;
Registering and maintaining various types of intellectual property;
negotiating manufacturing and licensing agreements;
(Left) A simulated subdural haematoma in the ‘Rowena’ simulator
Craniotomy using the Rowena simulator
(Below) The Rowena simulator used to demonstrate different neurosurgical procedures
CE marking;
Making prototypes;
Constructing design files.
Intellectual property alone is a massive field with a whole variety of different rights, registrations and protections. Some, such as basic copyright, are free. Some, such as various types of design registration, inexpensive; and others, such as patents, very expensive and complex.
While there are intellectual property and licensing lawyers to assist with this – and these people are some of the most helpful you will encounter – they don’t come free of charge.
n egotiating licensing agreements for manufacture and sale is another area where, as a mere doctor, one can feel very ignorant and under-equipped.
You have to learn to appreciate the different approaches and negotiating stances of various different companies and nationalities.
one of the most important skills has been to try and develop an idea as far as possible, including at least a rudimentary design file and, if possible, a prototype. This is absolutely crucial in gaining access to the appropriate decisionmaker when approaching a potential collaborator to get backing for the idea.
It is an immensely rewarding experience utilising, as it does, one’s medical skills, but in a totally different way and completely outwith the aegis of the nHS.
There is something uniquely satisfying about using equipment you have designed yourself and taken, quite literally, from the kitchen table to the operating table.
With a little knowledge, a willingness to learn – not least from your many mistakes – and a bit of tenacity, the process is actually a little easier than one might initially imagine.
(Above) Three pictures of Discocerv cervical arthroplasty instruments designed by Mr Ashpole and (below) his company’s logo
Breathe in . . . and relax
Consultant psychologist Dr Michael Sinclair invites you to explore the ways that you may usually respond to your own stress experience and to take a pragmatic approach in considering whether these ‘coping strategies’ are working well for you, or not coping wiTh bURn-oUT
some of the very real stressors that come with working as a medical consultant I highlighted in last’s month’s article. Unfortunately, many doctors don’t own up to feeling stressed or, worse still, that they aren’t coping too well. This is understandable; however, this is also a real problem. Attempting to hide and suppress our stress is likely to exacerbate it.
Research from an arm of psychology called contextual behavioural science, shows us that engaging in behaviour that functions as a means of experiential avoidance is likely to lead to more suffering in life.
In this article, I invite you to explore the ways you may usually respond to your own stress experience and to take a pragmatic approach in considering whether these coping strategies are working or not.
stressful situations, whether at work or at home in our relation
Stressful situations, whether at work or at home in our relationships, will invariably trigger our fight or flight response
ships, will invariably trigger our fight or flight response.
In this protective state of high alert, our minds will produce a plethora of interpretations and assumptions about our stressful circumstances, in the form of judging, evaluating, criticising ourselves or others, perhaps regretting what has happened and/or worrying about the terrible things that might go wrong.
Avoidance strategy
All this thinking serves an experiential avoidance function; it’s our super charged problem solving mind trying its best to protect us from any nasty eventualities and even more stress.
It’s therefore all too easy to get caught up in these compelling products of our mind. We tend to become singleminded, persisting in our attempts to suppress, eliminate and control away any stress and associated emotional pain,
like failure, not being good enough, the rejection that comes with others’ disapproval of us and all the underlying vulnerability of this.
Along with worrying and/or beating ourselves up to avoid more distress, we might do this in any number of other ways, too, such as:
Drinking alcohol or taking drugs to feel less stressed;
Avoiding certain meetings or people to feel less anxious;
Working longer and harder even when unwell to avoid the guilt of letting others down;
Not seeking help or self prescribing to avoid the shame, embarrassment and sense of failure that will come with disclosing to another professional that you may not be coping so well.
Perhaps you have tried some of these strategies or maybe others that also function to eradicate
stress and avoid these painful and unwanted experiences.
This is usually not a good idea. But don’t take my word for it. How does all this work for you? If the strategies you use to avoid your stress work just fine, keep doing them; I’m not here to mess with anything that is working for you.
However, I would encourage you to take a pragmatic approach and ask yourself three questions about each of the ‘coping’ strategies that you use:
1 How effective is this strategy in helping me feel better in the short term? A: Probably, or you wouldn’t persist in doing it.
2 How effective is it in helping me feel better in the long term? A: Usually not; it’s unlikely to eradicate stress ultimately, because that is impossible and probably makes it worse.
3 How effective is it in moving me closer towards being the kind of doctor/colleague/partner/ parent I want to be? or, living the life I truly want? A: Probably not so effective, in both cases.
what we try to resist often persists
Your experience may tell you – as it often does for most of us – that this struggle of trying to eradicate and control stress often proves to be a futile endeavour and, what’s more, it usually makes the stress even more intense.
If you worry and beat yourself up to avoid the worst happening and to improve your performance, you are likely to feel less confident, become anxious and agitated and therefore ineffective on the job.
If you use alcohol and/or drugs to avoid your stress, you might become more stressed around your health or relationships and perhaps have difficulty sleeping, which stresses you out even more.
If you avoid certain places or people to not feel anxious, you’re likely to become more anxious about missing out on important relationships, learning opportunities and career development. Working harder and longer hours to avoid the guilt of letting others down might result in becoming tired and exhausted and having to take time off from work and then an even greater sense of guilt to deal with.
If you use alcohol and/or drugs to avoid your stress, you might become more stressed around your health or relationships and perhaps have difficulty sleeping, which stresses you out even more
selfprescribing medication and delaying seeking professional help to avoid the embarrassment and shame of not coping may result in feeling increasingly overwhelmed, further psychological problems and a greater sense of failure.
We seem to forget that stress and these associated emotions such as failure and shame are a condition of life and not a problem to be solved.
While we remain stuck in the loop of struggling with our unwanted emotions, our ability to fully attend to the present moment is diminished.
Consequently, we fail to take in new information about the circumstances around us and lose sight of what is important and what we might otherwise really care about.
Altogether, we become behaviourally ineffective, as our range of coping responses becomes limited and restricted as we focus on eliminating the threat (our stress) as we see it.
Consequently, we fail to adapt in a fluid manner and in a more meaningful way to the demands of any stressful situation we may find ourselves in. In other words, we become stuck in our ways and psychologically rigid.
so, what can you do?
If the ways that you are responding to your stress are not working out too well for you, would you then be willing to consider some alternative ways of responding to it when it shows up?
You probably know of and have tried all the common stress man
agement techniques before, such as keeping active and taking regular exercise, eating well and ensuring you get adequate rest and sleep, relaxation, positive thinking, distraction, challenging yourself with new hobbies, working smarter rather than longer or harder. You have probably given this kind of advice to patients yourself.
These strategies really can work and can be extremely helpful in certain contexts and certain times. Do them if they work for you.
I’m not knocking these techniques at all and you should add them to your toolkit for stress management. If you don’t know them, take a look online or read any stress management selfhelp book to refresh. However, what do we do when they don’t work?
We seem to forget that stress and these associated emotions such as failure and shame are a condition of life and not a problem to be solved
I’m interested in sharing and getting you to try something new. over the next two articles, I will highlight a number of interesting and effective alternatives which are not necessarily focused on the eradication of stress, but more to do with changing our response to it and to be used alongside, and in the presence of stress.
When we ‘open up’ to stress, and lessen our pre occupation with trying to eradicate it, we may find that life becomes fuller and that, paradoxically, stress becomes less of a problem.
Dr Michael Sinclair (below) is a consultant counselling psychologist. He is the clinical director of City Psychology Group in London, with clinics in Liverpool Street, Harley Street and Canary Wharf. He is the author of a range of selfhelp books, including Mindfulness for Busy People, Working with Mindfulness, The Little ACT Workbook, The Little CBT Workbook, and Fear and SelfLoathing in the City
He provides effective, evidencebased psychological interventions to individuals of all ages, couples and families experiencing a range of psychological problems such as stress, anxiety and depression and adjustment to physical health conditions. He provides training to medical and other health practitioners, consultation to a growing number of corporate occupational health departments and delivers psychological interventions to large firms to improve employees’ health and performance
oUTsEc TRAnscRipTion sERvicEs
Shhh! Do you want to know a secret?
There is a solution to the struggle of finding experienced and reliable typists in the medical sector. Use the services of an army of committed home-workers
exAsPeRATeD PRACTICe managers are increasingly under pressure to find committed and reliable secretarial staff, who are as rare as the proverbial ‘hens’ teeth. stress is increasing with job roles comprising accounts, patient and insurance company billing, credit control, governance, health and safety, HR, complaints, reception duties, clinic and procedures bookings, patient liaison and appointments.
And let’s not forget the monumental task of both managing the consultants and ensuring typing reflects the practice’s reputation for efficiency and timecritical referral letters – often needed within hours of a client’s appointment. s o why is it getting more and more difficult to recruit quality staff? The answer is twofold: practices are increasingly pressured to squeeze costs and, in doing so, find their staff are leaving in droves, choosing instead the enviable alternative of ‘working from home’.
These savvy, intelligent and highly experienced secretaries have embraced technology and have chosen to leave the pressures of taskdriven, pushedtothelimit employers for independent selfemployment within the comfort of their home. No commute and, better still, no travel expenses.
it’s a no-brainer
And here is the secret as to why they do it – they can earn as much per hour sitting in the comfort of their own home as they did after deductions in the stressful office environment. It’s a bit of a nobrainer, so this phenomena is increasing, like the lack of goodquality staff, day by day. so how can we encourage them to come back to the workplace?
The answer: you can’t. But, by the use of technology, you will have topquality secretaries at your disposal day on day. It’s simple, costeffective and can be used as and when required.
Besides costsavings, increased efficiency, topquality dedicated sectorspecific secretaries, no worries about sickness or holiday absence, what is there not to like?
A stress free answer: join the increasing number of private practices using the services of outsec, a British medical trans cription company established in 2002.
stephanie Carmichael, medical head of department, explains: ‘I myself worked in both private and the NHs for over 25 years. I experienced, as management, the stress of reaching targets, booking patients, maintaining staffing levels and getting the typing done.
‘After all, recruitment was limited to the employment possibilities within the local vicinity. There would always be one or two exceptionally reliable secretaries and others that were there because there was no other option.
My vision
‘Inevitably, there was sickness leave, unexpected simultaneous noshows, unending recruitment issues – headaches on a regular basis. I worked out what was happening in the industry and approached outsec, as I could see the vision of a first rate, secure and fast turnaround typing service dedicated to the medical sector.
‘In addition, knowing the importance of IT security, information governance and patient data security, I have set up o ut s ec’s medical department to mirror the typing requirements of private and national health practitioners in the 21st century.
‘A word to the wise, though –not every medical transcription company complies with these areas of knowledge and security,
for no other reason than they do not know, since they have not worked within both sectors.
‘mistakes have been made in the past, but do not be hoodwinked by canny providers; it is crucial in our industry to talk with people who know your industry intimately.
‘We are not trying to replace the all important secretary; we are enhancing the service that your practice provides for your patients through an unrivalled typing service, whereby we work with the practice.
‘We do not simply have typists; we have experienced, dedicated and committed transcriptionists, who, like myself, have been there and done that!
‘An added bonus: with upward of 100 CVs received a week, we are in the enviable position of being able to “cherrypick” our transcriptionists. Can you say the same?
‘Bright times are ahead and now practice managers can have it all. A partnership with o ut s ec will comprise of all benefit, no stress and, above all, substantial saving on your time.
‘frantic calls to a temp agency will be a thing of the past. so too will be asking secretaries to work through their lunch hour or stay late to get the typing done, or stepping in yourself to ensure the practice’s reputation is intact – all will be taken care of by our partnership. What’s more, the costeffectiveness will enable you to ask for a raise!
‘It’s simple, it’s easy and I suggest you give me a call. Remember, I have been in your position, so I know what I am talking about.’
☛ Phone: 01366 348088. Website: www.outsec.co.uk
•
How to convert
I would be very surprised to hear of any private practices that would not like to convert every person who called with a new inquiry into a patient on their books.
No practice will have a 100% success record with new patient inquiries over the line.
while callers sometimes simply change their minds, often it’s the practice itself which gets in the way of converting callers into patients.
Phone call-handling should be treated in much the same way as the reception area and even the website. It should aim to present a
professional, high-quality and caring image every time a patient steps foot in the clinic or visits the website.
o ne could argue that the website and reception area are easier to get right than a phone call, as they give a visual representation of the practice.
Presenting the practice over the phone is a greater skill but important to get right to increase patient numbers.
Who is representing the practice?
It doesn’t matter how many patients a clinic has on its books, if
convert callers
the staff members handling the calls are not skilled in transforming call inquiries into patients, they could be losing these opportunities at the very first conversation.
e very inquiry is precious to a practice and should be treated as thus. For prospective patients, those first impressions – and the way they are handled – are absolutely vital for them to make a decision as to whether or not they become your patient.
when a potential patient walks into the clinic, they should be treated like a VIP, and the same goes for those who ring with inquiries. o ften this requires a change in practice mindset.
If you had a million-pound patient, you wouldn’t think about letting anyone but the best treat them.
So putting anyone other than the very best at handling calls on the phone demeans the value of these inquiries.
Be a proactive call-handler
If you follow the key principles of good call-handling – you’re listening, being professional and polite, efficient and reassuring – it will engage the caller and they will be more receptive to what you can offer them.
It’s at this point that many practices lose the potential patient by ‘iffing’ away the conversation. A practice doesn’t want the caller to go away and think about whether or not to give them their business, but to be absolutely convinced during the call itself.
one way of achieving this is by using proactive language when speaking with the caller. Instead of saying ‘if we were to treat you’, say ‘when we see you’ and ‘when we treat you’ and so on.
This positive, affirming language goes a long way to persuading a caller that the practice they have inquired with not only wants their business but will start working with them right away.
That the practice is so confident and reassuring, there is no decision left to be made.
Create meaningful connections
Get customer service right and you will leave the competition behind. There may always be another practice a person can become a patient of, but that practice won’t be able to replicate your stellar customer service.
That personal connection a patient has with their practice is created during the vital first moments of communication.
The trick is to remember that you are speaking to a real person and aim to establish a relationship that can be nurtured and built on in the future. Take a personal interest in the caller.
If they complain about a medical issue, sympathise with them and tell them you’re sorry they’re feeling that way.
If they are calling because they are unhappy with their current practice or have been mistreated in the past, imagine yourself in their position; an understanding ear and reassuring tone would be exactly what you would look for. be natural during these conversations. No one wants to talk to someone reading from a script, especially when it comes to discussing health matters.
And here is the time to demonstrate how respected the caller would be as a patient. e stablish how they like to be addressed, their correct title, the best means of contacting them and when, and remain patient with them at all times.
This behaviour is noticed more than you think.
Stephanie Vaughan-Jones (right) is channel manager at phone answering specialist firm Moneypenny
PROBLEMS WITH THE TAX MAN?
HMRC tax investigations and disputes create difficult and stressful times.
As an award winning firm of tax experts, our highly experienced partners specialise in resolving problems relating to tax investigations and disputes with HMRC.
To find out, in confidence, how we can help call 0800 734 3333.
‘Here to help. Not to judge.’
Dear Reader,
subscribe ToDay To geT every issue anD reaD us onLine
Subscribing to Independent Practitioner Today is the only way you can be sure you will see every issue and have the option of reading us online using our special page-turnable edition. Don’t risk missing out. Our personal subscription for doctors and managers is only £90 a year and £210 for organisations. But you can cut this to just £75 and £180 respectively if you pay by direct debit. So take advantage of this offer now for our unique business journal dedicated to supporting you in your private practice. We’re confident your subscription will repay itself many times over!
Editorial director
Doctors, please give GMC No. (See rates listed above)
r * indicates this item must be filled
I encose a cheque made payable to The Independent Practitioner Ltd
Please debit my Mastercard/Visa/ Amex/Diners
Instructions to your Bank or Building Society to pay Direct Debits
Name and full address of your bank/Building Society
Society
Name(s) of account holders
sort code
No
banks and building Societies may not accept direct debit instructions for some types of account
Banks and Building Societies may not accept Direct Debit instructions for some types of account To: The Manager
post your application (no postage required – UK only) to: independent practitioner today Subscriptions department, FreepoSt, po box 36, plymouth, pL1 1br
Please post to: Proact Ltd Subscriptions Dept., 12 Mary Seacole Road, The Millfields, PLYMOUTH PL1 3JY Or email to: jackie@marketingcentre.co.uk Or
phone: 01752 312140 Fax: 01752 313162 email: lisa@marketingcentre.co.uk or subscribe online at www.independent-practitioner-today.co.uk if you want to pay by card
payment dates change, The Independent Practitioner Limited will notify you 10 working days in advance of your account being debited or as otherwise agreed.
If an error is made by The Independent Practitioner Limited or your Bank or Building Society, you are guaranteed a full and immediate refund from your branch of the amount paid.
You can cancel a Direct Debit at any time, by writing to your
ApplicATion FoR SUbScRipTion
SETTing TARgETS
So you have a history of setting goals for yourself. Surgeon Dev Lall believes it’s important to maintain that momentum throughout your career to maintain job and personal satisfaction
Always another summit to climb
The T emp TaT ion during our training is to view the consultant post as the ultimate prize: the end goal.
While that is entirely understandable, it is only after you have been in post for several years that you realise the consultant job is merely a waypoint: a stepping stone to something else.
The trouble, in in my experience, is that many people have no idea what that ‘something else’ could be.
o ne next step is private practice, of course, but a few years down the line, one can find oneself dissatisfied. is there nothing more to do except work until retirement?
Finding the next step
if you’ve wandered around a bookshop recently, you will probably have noticed there are a lot of business books out there. There have also been vast numbers of books on self-improvement published lately, which seems to be a malady we have caught from the US where this kind of thing is big business.
Flick through any of these books and you will see that one of the things they all stress is the importance of goal-setting.
The logic goes: if you don’t have a destination, how can you possibly get there? and how will you even know that you’re there?
But, in my opinion, there’s a
deeper reason for goal-setting, and although one man’s experience hardly counts as gold-standard evidence, it is a useful starting point for discussion.
What i see among so many consultants is a certain aimlessness, a feeling of being slightly adrift. perhaps this isn’t so surprising: we fought so hard as juniors to progress onto the next step of our training that once we reach the lofty level of consultant that –unless academia is your goal –well, what then?
The solution, i believe, is to set new goals. You have achieved what you thought was the ultimate prize – a consultant job – so now perhaps it’s time to reach for a new goal.
i would define a goal as a major, long-term objective in your life. Typical examples include:
☛ ‘i want to earn £1m a year privately’;
☛ ‘i want to be able to retire by the age of 55’;
☛ ‘ i want to earn enough through my private practice so that i can reduce my nh S sessions/leave the nhS completely’;
☛ ‘ i want to be able to sell my private practice when i retire’;
☛ ‘i want to be able to afford to sail around the world’.
The acronym S ma RT is often used; namely that goals should be:
Specific;
measurable;
attainable;
Realistic;
Time-limited.
You’ve probably heard that before, so i don’t propose to go over that in any detail here.
But, to that, i would add the obvious: that goals are always personal to the individual; and add the not-so-obvious: that they do
What i see among so many consultants is a certain aimlessness, a feeling of being slightly adrift
not have to be professional or revolve around your private practice per se.
The problem, as the american self-help expert earl nightingale identified, is that people can be divided into two types: Goal People and River People
Goal People have clear objectives and focus upon obtaining them, one by one. They have a clear roadmap in their minds as to how to achieve their goal and relentlessly pursue it.
River People don’t take this approach at all. They are happiest when doing the thing they love and do not live by any kind of structured plan towards an overarching end point. They merely move from one thing they enjoy to the next.
i n other words, Goal People attain pleasure from getting closer to their objective – and ultimately reaching it – whereas River People get their pleasure from the journey, not the destination.
The truth is, of course, that we’re all of us a combination of these traits. We might take a goaloriented approach in our professional lives and a river approach in our personal lives, for example.
Two types of goal are particularly relevant to us. o ne simply states ‘ i want to make lots of money’. The other is ‘ i want to make enough money to do (some-
thing)’. i n both cases, learning how to grow your private practice is critical.
goal-setting and private practice
oK, so you’ve got a specific goal in mind. You’ve decided when you want to achieve it by. a nd although it might be a big ‘ask’, you believe it is attainable.
The next step is to clearly identify where you are in relation to that goal to see how far away you are from it. it’s a good idea to plot both these points on a timeline which is the amount of time you’ve set yourself to get there.
Then break it down into waypoints – objectives – along the way. The idea is that achieving each of these gets you closer to your goal. it also serves as encouragement that you’re making progress when things inevitably get difficult.
Some of these steps will need to be accomplished in sequence; for others, the order of completion will not matter. For example, you might be currently earning £100,000 a year and want to increase that to £200,000 in two years’ time. That means your goal is to double your monthly income from £8,334 to £16,667.
Strategies vs tactics
i believe the way you increase your private income is through marketing yourself and your practice.
You might decide you want more G p referrals, or you want more people to come via online sources, or you want to create a higher personal profile – celebrity, in other words – and have people find you as a result of that. each of these is an individual strategy.
Tactics on the other hand refer
to the individual steps that comprise the strategy. So if your strategy was to increase Gp referrals, you might hold regular Gp meetings every six weeks or so on various topics, visit certain practices every few months, offer to hold outlying clinics at practices, publish a regular newsletter for Gps, or set up a direct access hotline where the Gp could call your secretary and expect a reply from you personally within the hour.
Goals are important because they eliminate the aimlessness so many people have after becoming consultants. a nd even though many of us are by inclination river people rather than goal people, the goals we set need not be professional nor financially motivated.
n ot everyone is financially driven and wants to earn many hundreds of thousands of pounds or more through private practice just because they can.
Your goal could be travelling the world, retiring early, that holiday home in Tuscany or whatever.
But the wonderful thing is that because we as doctors have an alternative income stream available to us through private practice, we can generate the income we need to allow us to do what really matters to us in our lives.
This includes: spending more time with the family, the holiday home we visit half a dozen times a year or the taking-a-year-out-travelling-the-world stuff.
a successful private practice can be an end in itself. But, for many of us, it is merely the means to the end.
Dev Lall is a surgeon who runs a specialist private practice consultancy www.privatepracticeexpert.co.uk
PATiEnT TEsTiMoniAls
What do patients think of you?
The power of the patient testimonial presents a growing challenge for doctors in private practice. Jane Braithwaite (below) shows how to keep up to speed with this phenomenon, the best way to deal with a bad review and how this can be managed so your practice gets the best out of these sites
It’s a famIlIar situation: you need a particular service but don’t know where to start. Hotel recommendations, restaurant reviews, a good electrician…
Our first point of call is usually a preferred search engine, followed by a thorough read of the reviews of countless service providers.
Word of mouth still plays a part in identifying and eventually choosing a service, but sites such as t rip a dvisor, Glassdoor and Checkatrade have all become go-to places
for people looking for a glimpse at what they can expect before committing to a purchase or organising a service. the situation is no different when it comes to private healthcare. a recent survey conducted by software advice found that around 80% of patients use online reviews when searching for doctors. the situation is no different when it comes to identifying medical and healthcare services. a recent survey by Brightlocal found that 84% of those questioned valued an
online review as much as a word-ofmouth review, and that medical and healthcare professionals are the third most searched-for services –with restaurants and hotels at numbers one and two respectively.
s ites such as Doctify and top Doctors offer patients a platform both to share experiences and to find out more about the services on offer.
for consumers, these sites can be a goldmine of information, but for physicians there can be a risk: the bad patient review.
How can doctors keep up to speed with this phenomenon, what is the
best way to deal with a bad patient review and how can this be managed so your practice gets the best out of these sites?
Maintain confidentiality
Before considering how to deal with online patient reviews, it is worth remembering that these interactions need to be treated the same way as a face-to-face clinic appointment – confidentially. Patient review sites could be described as a recent phenomenon and can be used to feed into social media. a s a result, they have the potential to reach out to huge num-
bers of people – and unidentified people, at that.
With this in mind, one of the most important things to keep in mind when managing or responding to patient reviews is confidentiality.
Doctors are still obliged to maintain confidentiality, even if a patient has taken the decision to publically discuss their experience with you.
By responding directly to reviews, you could run the risk of publically disclosing that the reviewer is, in fact, your patient – something ➱ p30
which you may not have consent to do.
t he G m C’s guidance on Good Medical Practice reminds doctors of this and advises that, when communicating publically, patient confidentiality must be maintained. this extends to social media. ( s ee ‘ t here aren’t any secrets online’, IPT June 2015). studies around this subject have shown there is a lot of uncertainty around the legal implications of interacting with patients via social media. so it may be worthwhile considering a response strategy that takes any discussions offline to a more confidential setting, such as in clinic or over the phone. this way, you will certainly not be accused of a breach of privacy.
Response strategies
response strategies to unfavourable online patient reviews could be similar to strategies that deal with complaints received in a more traditional fashion through contacting your office directly. all practices should have a strategy in place to deal with disappointed or disgruntled patients, and this should always involve a swift initial response – even if more investigation is required to determine the circumstances that led to the complaint or bad review being made.
t he patient’s records should then be reviewed, along with any correspondence such as emails. a full review of the situation means that you will be better placed to respond confidently and appropriately to the complaint at hand.
Managing expectations
Of course, the best policy is to identify potential problems and deal with them before they reach a point where distress and disappointment has taken someone to the point of leaving a bad patient review.
Work closely with your staff, and make sure they know to alert you to any comments that – if left unchecked – could develop into a more serious complaint. for example, has a patient commented to your secretary that they always seem to be waiting an unacceptable amount of time to be seen in clinic? Has the patient had to chase the office for information they have been promised?
In cases such as these, use a personal touch – acknowledge the patient’s disappointment and explain why this happened. Honesty is appreciated and respected, and will hopefully contribute to a more open patientdoctor relationship in the future.
Manage your online presence
If you have a practice website, management of your online presence could be expanded to include monitoring patient review sites and liaising with the teams who run them to ensure that you are making the most of the services they offer.
s ites such as top Doctor also have a reputation to maintain; they pride themselves on connecting with only the very best, using a recommendation system to ensure they only take on respected professionals, so it is in the interests of both parties to make sure that the relationship is fruitful.
some sites also offer marketing services, supporting doctors with P r activities and social media activity. It is therefore extremely worthwhile connecting with these teams to find out more about how they can help grow your practice.
t hese sites can also help to improve patient’s initial opinion of your practice; some offer 24-hour online access to clinic appointments, meaning patients don’t have to wait for office hours to book in. this speedy, easy way to book appointments can’t help but give a potential patient a great first impression.
Constructive criticism – a blessing in disguise so are patient reviews something to be scared of? this is debatable.
While it is not pleasant to know that a patient is dissatisfied with your services, and there is always a chance that a critical comment may put some people off, it is worth remembering that all reviews – both good and bad – will contribute to you having a much better understanding of how your practice is performing.
Without knowing what you are doing wrong, how can it ever be put right?
Jane Braithwaite is managing director of Designated Medical
Top Tips for managing paTienT reviews
regularly request testimonials from satisfied patients. obtain consent to use these pieces on your own website – with the option of being anonymous – and gradually add this content over time. This will help to keep your website fresh
Use feedback forms. monitoring patient satisfaction in this way will enable you to keep track of any trends and make changes to your practice based on this feedback
Utilise in-house marketing teams at review websites. each service offers more than just a review service, so it is useful to reach out to the relevant teams to see how you can make the most of these services, such as direct appointment booking and advice on how to make the most of your site profile
manage expectations. raising expectations can often result in disappointment; be honest and realistic; your patient will respect this, and your relationship will benefit
manage your online presence. Utilise your practice manager or medical secretary; as the voice of your practice, they may be able to identify patients who would be willing to contribute a glowing review and can co-ordinate your online/social media activity to include these testimonials
Consider filming testimonials. some patients may be willing to contribute to a short film that you can embed in your website. By combining this with written reviews and testimonials, you will appeal to the different ways people engage with online information
Deal with bad reviews appropriately. Don’t ignore it, don’t overreact, don’t lash out. Have a response strategy in place and involve your practice staff in this. This might include offering the patient a free consultation or phone consultation to discuss their concerns. above all, be sincere and treat the patient with respect – even if you feel their complaint is unreasonable
Utilise your social media channels. if you receive a good review, spread the word and share it with your network
Connect with your patients. identify patients who you think may be willing to share their story and ask them formally – using the right tone: personal, showing gratitude and appreciation for their comments – to contribute a testimonial
Use reviews that demonstrate the breadth of your experience. if you offer different types of treatment, try to engage patients from different treatment areas to contribute reviews. The same applies for one-off, rare treatments. if you are a specialist in a particular procedure that is not commonly carried out, a good patient testimonial can act as a beacon to anyone searching for information on these rare treatments
at margifloate@btinternet.com
Keeping up with
Make it your business to be visible to potential patients
Doctors who fail to implement new Google updates for their websites face being overlooked, warns Geoff Meakin (right)
Over the past 18 months, Google has been overhauling its local search results experience, including the map listings that regularly appear when searching for local services.
these developments represent a big change in the search engine giant’s approach to local searches.
research by Google and Oxera shows that around 80% of people now use the internet to find local information. Businesses with complete local listings are twice as likely to gain customer trust and 38% more likely to attract visits to a physical address.
these factors, coupled with the
ever-increasing use of mobile devices and voice search – with devices such as Amazon e cho –have made local search a priority for the company.
to keep pace with this, Google is creating a seamless service that allows patients or consumers to search for local information, book consultations and plan their journey without ever needing to visit or contact the practitioner or even visit their website.
this change will be facilitated through Google’s ‘My Business’ Listing and Google Maps for Android.
there is now far less incentive for searchers to click through to individual websites and search for the information they need there when they can immediately gain that information on the search engine results page itself.
r ecent research supports this, showing that up to 34% of all searches do not result in a click through to any website at all.
In addition, up to 70% of user actions – such as phoning, getting directions or filling in a contact form – now take place via Google itself compared to 25% that visit a website to achieve the same actions.
Independent practitioners will therefore be putting themselves
at risk of being overlooked by searchers in favour of competitors if they fail to create and maintain a Google My Business listing.
booking consultations
At present, Google is trialling direct online bookings for the spa, beauty and aviation sectors, which, if successful, are highly likely to be rolled out to the healthcare sector.
Online booking for fitness classes was originally trialled in the US in December 2016. t his later rolled out to the entire US in March, with users being able to pay online using Google Wallet. Currently, bookings can only be taken if vendors are registered with a third-party service. however, given the weight of evidence above, it is hard to imagine that the same feature will not be rolled out to other, more litigious, industries such as healthcare once they have ironed out any issues.
Text
messages
Users will soon be able to contact the Google My Business listings directly via SMS text messaging. t he mobile phone has now become an integral part of our lives and the ability to use SMS text is a clear extension of this.
Google My Business allows clin-
There is now far less incentive for searchers to click through to individual websites and search for the information they need there
ics to register and verify a mobile phone number to their practice. When viewing your clinic details on the Google results page, patients will then be able to tap on the ‘text’ button to immediately open the chosen text service installed on their phone.
texting is often seen as a good alternative to phoning when a patient does not have to time to wait on hold, makes contact outside of office hours or when a phone call would not be discreet enough – for example, during work time when other colleagues or staff may be listening.
there are potential pitfalls with this technology for private clinicians. Doctors and administrative staff must be careful when responding to texts to ensure that the phone is registered to that patient and that any texts sent do not contain sensitive personal information. Patients, too, should be reminded not to send confidential information.
Clinics that opt to use this technology should also ensure that they are able to respond quickly, as their average response time will be displayed. A slow response time may well outweigh the benefits of using the feature.
google post
In a bid to rival twitter, a Google Posts feature has been introduced allowing practitioners to share real time updates complete with eye-catching pictures and relevant ‘Calls to Action’ such as learn more, buy, reserve, sign up or attend an event.
It is not difficult to see how this tool could be employed by clinicians to encourage visitors to learn more about their procedures and accreditations, reserve a consultation or sign up for ongoing marketing such as an email newsletter or blog.
Again, these posts will be displayed within the search results
themselves and will be made available via Google My Business.
Videos
Clinics can now upload short 30second videos to their listing in Google Maps, which, again, will be displayed directly in the search results page. this can be done by signing up for free to become a ‘Google Local Guide’ or by hiring one.
Practices with impressive stateof-the-art facilities or new equipment for imaging and diagnostics should consider showcasing these to promote their services.
Alternatively, if your clinic already has a promotional video, 30 seconds of this can be uploaded instead.
this highlights the importance for clinics to actively monitor their My Business page and their online reputation more generally. t he new ability for disgruntled patients to upload videos directly to your business listing in real time is one that should not be overlooked.
Additional information
Medical practices can now add information to their Google maps listing which allows patients and visitors to plan their consultations in advance. this can include details such as wheelchair access, parking information and WiFi availability. Simple measures such
How we reported on Google’s changes in last month’s issue
as these can make a patient experience a lot easier with very little effort.
Answering questions
Users can now ask questions directly to the search engine and practices can respond to these via the search results page itself. this provides a good opportunity for clinics to promote their benefits by answering questions such as ‘ h ow soon will I get an appointment?’, ‘how long will my consultation be?’, ‘What services
do you offer?’ and ‘how do I pay?’ Doing so will free up clinic staff from having to answer such questions, as well as providing the information directly from search results without users ever having to visit the page.
t his service can be added via local searches on the popular Google Chrome app.
All the above factors are now leading many online marketers to advise businesses to view Google My Business listings as a possible replacement of their website’s homepage.
For the medical industry, this is not yet the case, but there is a clear movement towards providing users as much useful data as quickly and directly as possible.
In September 2016, Google made it possible to allow multiple users to manage a Google My Business listing. this means you can now delegate the management of this service to a medical secretary or agency that deals in search engine optimisation.
In an industry where rapid treatment is the main impetus for service users, it would be naive to overlook the potential threats and opportunities these changes present to the consultation and treatment process.
Geoff Meakin is a digital marketing consultant and owner of SERP Health LLP
Defence body’s bid to curb indemnity fees
An unexpected decision to change the formula for calculating personal injury compensation payments has had damaging consequences for the cost of indemnity. Dr Christine Tomkins (right), MDU chief executive, explains the impact on the profession and patients
When the former Lord Chancellor, Liz truss, announced she was cutting the discount rate for legal compensation payments to a historic low from 20 March 2017, she exacerbated a problem which was already reaching crisis point. the decision to cut the rate to minus 0.75% significantly increased the size of compensation awards overnight.
For those unfamiliar with the term, the discount rate is the interest rate used to calculate the size of lumpsum compensation payments in personal injury claims and is supposed to reflect the return claimants would expect to get from investing their money. t he lower the discount rate, the more that defendants have to pay in compensation.
claims doubling
Many higher value cases more than doubled in size. For example, an MDU case in which a patient had tetraplegia following spinal surgery and 45 years’ life expectancy could receive a compensation payment of £9.2m under the previous discount rate and £17.4m under the new rate.
In one nhS cerebral palsy case in which a settlement was agreed at £10.4m just before the discount rate was changed, the judge told the two sides to reconsider in the light of the change in the rules. A £10.4m settlement became a £25.3m settlement.
As the MDU has repeatedly
Independent Practitioner Today has reported widely on the problem of indemnity fee costs
warned, such disproportionately high levels of compensation not only diverts cash from the health service provision, it also drives up the cost of indemnity with profound consequences for patient care and individual doctors.
impact on spinal surgeons and obstetricians
t he deteriorating medico legal climate means we have been forced to take some tough decisions in the interests of all our members.
As a not for profit mutual organisation, we have a responsibility to ensure there is enough money in the mutual fund to meet future claims and legal expenses – as well as other essential member services such as representation at the GMC. Claims inflation, rising at 10% a
year for several years, has long been the greatest pressure on that fund.
After reviewing the indemnity risk for the limited number of MDU members undertaking private spinal surgery, we regretfully concluded that subscriptions would have had to be set at a level which would no longer be affordable for them.
As a result, it was impossible for us to continue to provide indemnity to spinal surgeons (Independent Practitioner Today , July/ August 2017, page 8) beyond their current membership year, meaning we notified them of the need to obtain indemnity or insurance elsewhere if they intended to continue with private spinal surgery.
We are also making important changes to our benefits of membership for doctors in private obstetric practice ( Independent Practitioner Today, October 2017, page 3).
At the end of their membership year, these consultants will need to request a quote for ongoing indemnity, which will be offered on an annual ‘claims made’ rather than the MDU’s traditional occurrence basis.
this means the member will be able to request assistance for incidents notified during that membership year and will need to keep renewing membership to notify claims in future.
to keep reporting claims after leaving the MDU or retiring, members will need to purchase
extended reporting rights after that period – also known as runoff.
the MDU is no longer indemnifying new obstetricians in private practice. We are also not indemnifying existing obstetricians in private practice who may wish to switch from other medical defence organisations.
Unsustainable costs
t hese changes are further evidence that the cost of the clinical negligence system is unsustainable. t his is not the fault of doctors: clinical standards remain demonstrably high.
the fact is that claim numbers and costs are outside the control of doctors and the discount rate change is a prime example.
Added to that, the legal environment promotes litigation over resolving concerns in other ways and stimulates increasing numbers of claims.
One piece of good news is that the Government has recently signalled a change of heart on this issue, partly in response to widespread criticism from motor insurers – who warned of a steep rise in premiums – as well as pressure from the MDU.
Its latest proposals, if enacted, would change the way the discount rate is set and extend expertise available to the Lord Chancellor by creating an independent expert panel. It is suggested this may bring the rate up
to between 0% and 1% from its current level of 0.75%.1 however, the proposed changes will take time to implement and won’t address the long term underlying problem of medical claims inflation.
More radical measures are needed, a point recognised by the national Audit Office’s report2 into clinical negligence claims, which concluded that the Government needs to take a stronger approach to curb clinical negligence costs.
t he MDU is currently campaigning for a package of legal measures that will make the claims system more proportionate and sustainable. these are to:
➥ Repeal outdated clinical negligence law
Section 2(4) of the Law Reform (Personal Injuries) Act 1948, requires all personal injury defendants to disregard the availability of nhS care when paying compensation.
Patients who have been injured while receiving nh S treatment must be compensated on the basis they will receive private treatment for life.
t his 1948 law should be changed so that defendants could compensate patients by paying the nhS and local authorities to provide damaged patients with appropriately designed public health and care packages.
➥ introduce fixed legal
costs
In lowervalue claims, many lawyers receive more in costs than their negligently damaged clients receive in compensation.
Recommendations by Lord Justice Jackson 3 to establish a working party to examine fixing costs for clinical negligence claims valued at up to £25,000 do not go far enough. there should be mandatory fixed limits on legal fees in medical negligence claims valued at up to £250,000.
➥ cap compensation for loss of future earnings
two patients with similar injuries and care needs can currently receive vastly different levels of clinical negligence damages, because one was a higher earner. A cap on future earnings compensation would ensure compensation is awarded on a more equitable basis.
Patients harmed as a result of
medical negligence should be properly and fairly compensated, but the current system benefits no one. We must move to a fairer way of doing things to prevent many dedicated clinicians being forced out of independent practice. You can show your support via the MDU’s Fair Compensation campaign. Find more details on our website at www.themdu.com/ faircomp
References
1. Annual Report and Accounts 2016-17, NHS Resolution, 13 July 2017 http://resolution.nhs.uk/annual-reportand-accounts-201617/
2. Managing the costs of clinical negligence in trusts, National Audit Office, 7 September 2017. www.nao.org.uk/ report/managing-the-costs-of-clinicalnegligence-in-trusts/
3. Review of civil litigation costs, Lord Justice Jackson, 31 July 2017. www.judiciary.gov.uk/publications/review-of-civillitigation-costs-supplemental-reportfixed-recoverable-costs/
‘womEn in mEdicinE’ ExhibiTion
Inspiring others
The Royal College of Physicians has brought together the leading medical bodies in the UK and Republic of Ireland to profile 52 of the most influential clinicians from the past and present in an exhibition at its London headquarters.
The timing of Women in Medicine is significant, as 2017 is the centenary of the Medical Women’s Federation, and also the first time in history that the majority of the world-renowned medical royal colleges have been led by women
‘Women in medicine: a celebration’ is a free exhibition of specially commissioned photographic portraits honouring contemporary and historical women in medicine.
i t showcases a number of today’s leading female clinicians, pictured with the women from the history of medicine who have inspired them.
the exhibition is the result of a project, co-ordinated by the royal c ollege of Physicians, that brings together the leading medical bodies in the UK and ireland. each institution has nominated a modern-day doctor to represent their specialism or area of practice, who in turn pays tribute to a remarkable woman who went before them.
among the historical women featured are internationally acclaimed individuals such as e lizabeth Garrett anderson, britain’s first formally qualified and recognised female doctor; d ame Sheila Sherlock, the prime mover in the establishment of liver disease as a
ern hospice movement. the present day is represented by past and current presidents of the royal colleges of physicians, surgeons, general practitioners, obstetricians and gynaecologists, pathologists and paediatrics, and child health.
if you want to visit...
the exhibition runs from 3 october to 19 January 2018
opening times at 11 st andrews Pl, Regent’s Park, London nw1 4LE: Monday-friday only, 9am-5pm (last entry 4.30pm). opening times can vary. Please check the visiting page on the RCP website for closure days
Email history@rcplondon.ac.uk or phone 020 3075 1543
women in Medicine tours: take a special exhibition tour and join a walk on the history of women in medicine with the college’s guiding partners Discover Medical London
they are joined by new photographs of many other pre-eminent female figures from medical fields as diverse as academic publishing and public health, radiology, ophthalmology, education and anaesthesia.
d r Johnny b oylan, exhibition co-ordinator and national medical director’s clinical fellow, explained: ‘all of the women featured in this exhibition are true inspirations.
‘From the earliest pioneers, who overcame prejudice and the seemingly endless barriers placed in their way to gain entry to the profession, to the brilliant clinicians who now lead not only their fields, but many of the world’s most renowned medical organisations.
‘We hope that this exhibition, and the wider project of which it is part, will bring these women in medicine, and the positive impact they have made, to the widest possible audience, inspiring generations to come.’
rcP president Prof Jane dacre said: ‘not only has it marked the centenary of the medical Women’s Federation, an organisation that has done more than any other to promote and support female clinicians over the past 100 years, but it also saw a moment, the first in history, when a majority of the medical royal colleges were led by women.
‘the stories of these remarkable women and their outstanding achievements, opening up access to medicine for others and improving, sometimes revolutionising, healthcare for all, not only deserve to be told but demand to be saluted.
Women in medicine: a celebration
Prof Clare Marx with exhibition organiser
Dr Johnny Boyland and photographer John Case
anderson
Member of the court of assistants, ociety of apothecaries,
‘Elizabeth Garrett anderson is the original inspiration to women working in the medical professions. he not only became the first female doctor, but opened the door for thousands of others.’
iona Caldicott
Past president, Royal College of Psychiatrists, haped by her early experiences as a medical officer in London asylums, Helen Boyle went on to revolutionise mental healthcare, at the forefront of introducing early treatment.’
Dr Judy Evans
Honorary secretary, Royal College of surgeons of Edinburgh
‘Gertrude Herzfeld was a true trailblazer for women in surgery, a beloved and charismatic figure in the story of medicine in scotland.’
Professor Dame Parveen Kumar
President, Medical women’s federation
‘Jane walker was vocal in the fight for professional parity at a time when women doctors were very much in the minority. she combined her campaigning with being a true clinical pioneer.’
Professor Jane Dacre
President, Royal College of Physicians, ‘sheila sherlock was a true medical pioneer and innovator. Her talent, dedication and leadership were the driving force behind countless medical advances.’
Dr Ruth Brown
Past vice-president, Royal College of Emergency Medicine
‘the courage and vision of sheila Christian and her tireless energy in promoting high standards of emergency care are a vital part of the foundation of our specialty in the uK.’
Professor Dame anna Dominiczak nominated by the Royal College of Physicians and surgeons of Glasgow
‘Marion Gilchrist opened the eyes of many women to the opportunities a changing world could offer them and, through her work, saved the sight of many Glaswegians.’
Dr suzy Lishman
President, Royal College of Pathologists ‘i haven’t had to face the discrimination that Dorothy Russell dealt with, thanks to her and the other women who fought to become doctors and paved the way for future generations of women.’
Professor Carrie MacEwen
President, Royal College of ophthalmologists
‘ida Mann was a brilliant researcher, clinician and leader, who clearly saw the influence of social factors on disease. she has been an inspiration for decades and generations to come.’
Professor angela thomas
Director of heritage, Royal College of Physicians of Edinburgh
‘Ella Pringle was a committed clinician with a clear social conscience and keen eye for how to organise and improve services for patients, particularly mothers and children.’
Professor Jenny Higham
Chair, Medical schools Council
‘Marie stopes was a pioneer of the 20th century in the field of birth control. she released women from the endless treadmill of producing children, giving them time to order their own lives.’
Professor Eilis McGovern
Past-president, Royal College of surgeons in ireland
‘Emily winifred Dickson paved a path for women surgeons in ireland. never put off by barriers placed in her way, she became the first female surgical fellow in Great Britain and ireland.’
Dr Ramani Moonesinghe
Director Health services Research Centre, Royal College of anaesthetists
‘Kitty Lloyd-williams led a life of outstanding contribution.a highly respected clinician, she will be remembered for her transformational leadership of the London school of Medicine for women.’
Professor neena Modi
President, Royal College of Paediatrics & Child Health
‘June Lloyd was a brilliant paediatrician, determined advocate for children’s health and instrumental in the establishment of the Royal College of Paediatrics and Child Health.’
Miss Clare Marx
Past-president, Royal College of surgeons
‘Eleanor Davies-Colley made her way as the first woman in a man’s world, devoting her life to the service of her patients and the practice of the art of surgery.’
Professor Lesley Regan
President, Royal College of obstetricians and Gynaecologists
‘Hilda Lloyd was a woman ahead of her time. the obstetric “flying squads” she established provided emergency care to mothers and babies who might otherwise well have died.’
Professor Joanna wardlaw fellow, Royal College of Radiologists
‘Marie Curie was a supremely intelligent, motivated, hardworking, yet humble scientist, whose groundbreaking scientific discoveries transformed medicine.’
Dr fiona Godlee
Editor in chief, the BMJ
‘the redoubtable sophia Jex-Blake was a powerful voice calling for women’s admission to universities and the medical profession. all of us working in these fields owe a debt to her.’
Dr asha Kasliwal
President, faculty of sexual and Reproductive Healthcare
‘anandibai Joshi opened the gates for many young women in india. she dared to dream and had the courage to pursue an education, demonstrating that there are no glass ceilings.’
Professor wendy Reid
national medical director, Health Education England
‘Louisa aldrich-Blake was, quite simply, a powerhouse. the first woman in Britain to gain a specialist qualification in surgery, she practised at the highest level, innovating as she did so.’
Professor sheona MacLeod
Chair, Conference of Postgraduate Medical Deans
‘vicky osgood was passionate about professional education and putting the patient at the centre of everything we, as clinicians, do. she is a greatly missed force for good.’
Professor Dame Margaret whitehead nominated by the faculty of Public Health ‘Rosemary Rue was undeterred by prejudice against her as a medic, both married and a mother. overcoming discrimination, and many other difficulties, she became an inspirational medical leader.’
Professor Mary Horgan
President, Royal College of Physicians of ireland
‘Dorothy stopford Price pioneered BCG vaccination in ireland in the 1930s. Her work was pivotal in ending the irish tuberculosis epidemic in the mid20th century, saving the lives of thousands’
Dr anna Batchelor
Past dean, faculty of intensive Care Medicine
‘Gillian Hanson had the vision to realise that intensive care needed to be staffed by highly trained specialists, requiring skills from physicians as well as anaesthetists.’
Professor Helen stokes-Lampard
Chair of council, Royal College of General Practitioners
‘Mollie McBride was a wise, courageous and pragmatic woman whose energy and desire to make changes to benefit the whole nHs are as relevant today as when she was embarking on her career.’
Dr flic Gabbay
Co-founder, faculty of Pharmaceutical Medicine
‘Cicely saunders was a woman with a real passion for making a difference; she let nothing stand in the way of fulfilling her belief that hospice care was essential for the dying.’
FOR MOST doctors, appraisals and revalidation are straightforward.
If you are employed by an NHS trust – even if you also have a private practice – that trust is likely to be your ‘designated body’ (DB) and you will have a Responsible Officer (RO), often the medical director of your employing trust.
If you are a GP in England on the Performers List, your DB will be NHS England and your RO will be based in your local area team.
Purely private doctors have a number of other options for their DB, including the private hospital where they work or have practising privileges, the Independent Doctors Federation and some of the royal college faculties.
However, there are doctors who have trouble identifying a DB and RO, perhaps because their practice is unusual in some way. This can lead to difficulties.
It is open to doctors in this situation to find a ‘suitable person’ –someone who has been approved by the GMC and who can make a revalidation recommendation to the GMC about you.
The GMC publishes a list of suitable persons (SPs) on its website. It is well worth exploring this option if you do not have a DB and RO, as your SP will be able to assess your fitness to practise in your chosen field, which may be unusual or very niche.
Final option
If you do not have a DB/RO or an SP, the final option is to submit an annual revalidation return to the GMC to include evidence about your practice and your annual appraisal, which can be done by an independent provider of medical appraisals.
In addition, you will need to take an exam every five years. This assessment is provided by the GMC, and there is a fee, which is currently £1,100.
There are 12 different assessments and you would need to choose the assessment most relevant to your area of practice.
That is where the difficulty often lies. Almost by definition, someone who does not have a DB/RO or an SP tends not to fit into a neat category or work in one of the more mainstream specialties.
That may make it difficult for
if you fail the assessment, the GMC will take steps to withdraw your licence to practise and it will be stressful, time-consuming and expensive to appeal that decision
in response to its notice, you will have the right to appeal that decision – on the papers or at an oral hearing. There is a 28-day time limit to lodge that appeal.
There are often good grounds for challenging a decision by the GMC to withdraw a doctor’s license – it may be that the doctor has been unable to engage with revalidation because of illness or other mitigating circumstances.
in a nuTshell
Revalidation is the process by which doctors are required to demonstrate that they are up to date and fit to practise.
Doctors must revalidate every five years, and, in order to do so, they must have annual appraisals based on the GMC’s guidance, Good Medical Practice.
you to pass the GMC’s assessment in one of the 12 areas it offers.
These are: anaesthetics, emergency medicine, general practice, histopathology, medicine, obstetrics and gynaecology, ophthalmology, paediatrics, psychiatry, radiology, surgery, and a foundation paper for doctors who do not practice in a specialty area.
If you fail the assessment, the GMC will take steps to withdraw your licence to practise and it will be stressful, time-consuming and expensive to appeal that decision.
If you are having difficulty finding a DB/RO, you may therefore want to explore the possibly of finding an SP, rather than submitting to the GMC’s revalidation return and assessment system.
Recinding your licence
Whatever option you choose, if your RO or SP makes a recommendation to the GMC that you should not be revalidated (a notification of non-engagement), you will face the prospect of the GMC taking steps to withdraw your licence to practise.
The first step is that the GMC will send you a notice of its intention to withdraw your licence, and if you want to challenge this, you must respond within 28 days and provide it with as much additional evidence as possible. The notice will tell you what is required.
It is essential that you do so within the time limit. You may be able to persuade the GMC to defer its decision and give you more time or even to change its decision and revalidate you.
The alternative is to accept withdrawal of your licence to practise, without which you cannot work as a doctor in the UK. If the GMC decides to withdraw your licence, even after you have provided additional information
False sense of security
Or it may be that they have done what was required but not provided the necessary information or presented it clearly enough.
Sometimes, doctors are lulled into a false sense of security because they pass their annual appraisals, but they are not in fact doing all that they need to do to enable their RO to recommend revalidation.
If that is the case, the RO – or someone else on their behalf –should contact the doctor and let them know that there is a problem. You should be proactive and ensure that, before your revalidation date, you contact your RO if you have not heard from them, and ensure that they are happy with the information you have provided.
Make sure that the GMC has your up-to-date contact details. It will send you a formal notice four months before your revalidation date and this will serve as a useful reminder to you.
We hope you sail through your five-yearly revalidations without difficulty. But if you should ever need any legal assistance, specialist lawyers such as the team at Hempsons will be able to help.
Tania Francis is a solicitor and a partner at specialist healthcare law firm Hempsons. She is also a qualified doctor – who has relinquished her licence to practise!
Tania advises doctors, dentists and other healthcare practitioners and providers. She specialises in regulatory law and clinical negligence and healthcare-related contractual disputes, including cases where there are related criminal proceedings
Billing And collEcTion
The art of the
With costs continuing to rise –think medical indemnity – and private fees generally under continuing pressure, few practices have the luxury of being able to let invoices go unpaid for any great length of time before the painful consequence is felt.
so it is essential that any private practice has robust procedures in place with respect to raising invoices and ensuring that they are systematically chased. Discipline and routine are key ingredients to achieving this.
Failure to chase debts could mean that you are working for free or have issues both around cash flow as well with h M Revenue and customs. Remember – tax is due on invoices being raised and sent, not on money being received.
in light of this, i have a quick
Having a stopstart approach to billing and collection generally proves ineffective. Findlay Fyfe says it is picking up the phone and creating momentum in chasing invoices that gets results
question. h ow soon does your practice manage to process and send invoices after treatment? is it hours, days, weeks or even months in some cases?
i deally, your practice will be sending out the invoice the same day as treatment or the day after; certainly within 24 hours. Remember, the quicker the invoice is raised, the better the chance it will be paid in a timely fashion.
often the secretary, who will be responsible for sending the invoice and chasing it up through to collection, will have many other things to do throughout the day, such as dealing with patients, writing letters, answering emails and/or the phone, being an agony aunt or marketing.
Struggle with billing
Even if you are big enough to have an accounts department, unless you have fit for purpose software and long serving staff who are familiar with the practice’s systems (see our earlier Independent Practitioner Today article on Key Person Dependency, November 2016, page 21), you can easily struggle with the billing and collection process.
i ncreasingly, private medical insurers only take invoices by electronic data interchange (EDi), such as h ealthcode or Bupa online; Vitality being the latest one to adopt this approach exclusively.
t he process of submission for each insurer needs to be understood as well as its individual pricing and coding rules.
i f data is entered incorrectly, which includes patient details, this electronic process generates error messages that need to be actioned.
Another key ingredient therefore to any collection process is
chase
We continue to be surprised how practices fail to prioritise getting paid for work carried out
actioning problems and quickly. it is all too easy in a busy practice to set aside billing and collection issues.
We continue to be surprised how practices fail to prioritise getting paid for work carried out. Don’t get me wrong: some do, but still many do not.
dipping in and out
Dipping in and out of this vital part of any practice just does not work. For embassy and medicolegal work, you might only need to chase every few months, knowing payments will take longer. however, with selfpay and private medical insurance work constituting the backbone to most private practices in the UK, payments should be made within weeks and, at the most, a month or two of treatment. i f not, you should be asking why.
Picking up the phone and calling a patient or the payer is a fun
damental part of the process to getting your bills paid.
i f nothing else, it ensures the invoice has been received and allows any queries to be raised early on.
With private medical insurance policies, there are increasing amounts of copayments as well as the standard excesses, which are often discovered by the practice only once the private medical insurance remittance advice and/ or payment has been received. Again, the sooner the patient is made aware a payment is due for their treatment, the better.
lack of resources
the problem is many practices do not have the resources or spare time to do this. As a result, practices are having to wait much longer than they should to get paid and, in extreme cases, have to write off money because they have either fallen foul of private
medical insurance rules – six months in some cases – or simply given up on chasing money owed.
Email and the post are not nearly as effective as the phone. Key to this, as mentioned earlier, is momentum – which means sending invoices and making phone calls, multiple times if needs be, to get a response and, in effect, get paid.
Now, i understand that the first priority for the consultant or GP is the care of the patient and this should always be the case.
But unless the practice takes a long hard look at the way it functions in terms of the billing and collection process, it may not survive in private practice to treat the patients.
Findlay Fyfe (right) is managing director of Medical Billing and Collection
The Focus oF every pracTice musT be on:
making sure that invoices are raised and sent quickly
ensuring that every procedure is billed correctly
routinely chase invoices in a disciplined fashion
monitor and respond to eDi error messages
reconciling remittances against invoices
chasing any excesses or shortfalls/balance payments
making phone calls rather than just using email or post
Free legal advice for independent Practitioner Today readers iPt
independent Practitioner Today has joined forces with leading niche healthcare lawyers Hempsons to offer readers a free legal advice service.
We aim to help you navigate the ever more complex legal and regulatory issues involved in running and developing your private practice – and your lives.
Hempsons’ specialist lawyers have a long track-record of advising doctors – and an unrivalled understanding of the healthcare system as a whole.
call Hempsons on 020 7839 0278 between 9am and 5pm monday to Friday for your ten minutes’ of free legal advice.
Advice is available on:
Business structures: commercial contracts: ian Hempseed Faisal dhalla
The Treasury is clawing extra tax from your pension savings. Cavendish Medical financial planners’ Patrick Convey (left) shows how to avoid excess tax payments
According to g overnment figures, the treasury has increased by 80% in the last year the tax it collected from savers breaching the lifetime allowance. over the last five years, the tax revenue has tripled.
Yet there are still many doctors who will walk blindly into the lifetime allowance tax trap without taking some simple steps to mitigate their tax liabilities.
t he lifetime allowance (LtA) limits the total amount which can be paid into a pension while benefitting from tax relief. in 20152016, HM revenue and customs (HMrc) gained £36m from individuals exceeding the allowance –the year when it was reduced to just £1m, catching many savers unaware.
Above the £1m threshold, you will incur punitive tax rates of up to 55% on anything taken as a lump sum and 25% on top of your marginal rate of income tax if taken as income.
You might believe these sums are of little significance, as you have not paid £1m into your pension. But the LtA is not a limit on contributions over a lifetime; the threshold refers to how much your pension might be worth when you finally retire.
the nHS pension is based upon your length of service and your pensionable salary. As these increase over time, this will make a substantial difference to the final value of your pension pot.
Could you be affected?
Every senior doctor is likely to breach the new allowance due to
the very nature of how the pension scheme works.
As an example, a consultant in the 1995 section of the scheme with an nHS pensionable salary of £100,000 with 35 years’ service within the pension scheme by age 60 will reach £1m in their pension pot. A salary of £88,000 with 40 years’ service will also hit the pension ceiling.
the top basic pay grade on the consultant contract is now over £103,000, so most consultants will reach a pensionable salary that is much higher than the examples above, once on-call responsibilities, clinical excellence awards and other pensionable elements are taken in to account.
if individuals also have private pensions, this could push them further over the lifetime allowance.
Many doctors view private pensions as a necessary supplement.
While the nHS pension obviously presents a good foundation, a £1m pension pot will offer an annual income of around £43k – a figure much lower than the average consultant’s salary. Have you considered how your life might have to change in retirement if you are not properly prepared financially?
c onsider as well that there might be financial commitments such as dependents at university or in long-term care or personal projects that you hope to enjoy.
What can you do?
there are a range of government protection schemes which can help savers restore the value of
than ever – but with careful planning you can reduce your tax liabilities considerably
their pension against lifetime allowance changes.
Unfortunately, the pension protections available are nearly as complicated as the pension schemes themselves, so it is a very difficult area for the busy professional to get right. We see many new clients who have received incorrect pension protection advice.
o ne such scheme, i ndividual Protection 2016 (iP2016), is now open for applications for those that had pension savings in excess of £1m as at 5 April 2016. You should seek help to determine if this is the correct protection for your pot.
i n recent years, we have seen products such as iSAs being used
alongside pensions to save for retirement.
What about the annual allowance?
As well as the lifetime allowance, there is an annual allowance which limits the amount of tax-relievable pension contributions you can make each year to £40,000. For members of the n HS scheme, pension growth rather than actual contributions are measured. You should be wary of any n HS pay rises received through increments, new management positions or clinical excellence awards. Pension ‘growth’ in excess of this £40,000 figure will be taxed at up to 45%. But there is a new ‘tapered’
Negotiating your pension savings is more complex
annual allowance for those with adjusted income earnings over £150,000 which reduces this figure further, down to as low as £10,000 for high-achieving doctors.
remember that it is your total income which will be tested –including any dividends, rental income, bonuses, benefits in kind and the growth in your pension, not just your contributions. this is a highly complex calculation for a busy professional with several income streams.
t he n HS Pensions Agency is currently issuing letters notifying those who have ‘saved’ more than the annual allowance cap for the last tax year.
HM rc bases calculations for pensions’ contributions on the deemed growth of the pension in the year, so the figures used bear little resemblance to the amount you have actually paid into your pot. c heck the sums carefully –many have been wrong.
However, the letters will only be sent to those likely to breach the £40,000 figure – not those who may breach the new tapered annual allowance. if your pension ‘grows’ by more than £10,000 in a year, you may still exceed the annual allowance limit but may not be made aware.
What are your options?
You should request your own annual allowance pensions’ statement as soon as possible. t he nHS is not the fastest at responding to requests. You will need to allow time for all calculations to be checked before your tax return can be filed.
the annual allowance is a much more complex area than the lifetime allowance with many more variables, so getting expert help is important. if you breach your allowance in any one year, you are allowed to carry forward any unused allow-
ances from the three previous tax years. if there is still a breach, the excess is added to your income for the tax year and taxed at your marginal rate of income tax.
You then have the option to pay the tax bill – which could be tens of thousands of pounds – or elect for the n HS pension scheme to pay some or all under the ‘Scheme Pays’ rules.
You will accrue interest on the amount paid at the rate of 3% each year plus the relevant consumer Price index rate of inflation.
t he amount you owe will be converted into a reduction of pension and lump sum benefits upon retirement, but there can be tax advantages in doing this.
negotiating your pension savings is more complex than ever –but with careful planning you can reduce your tax liabilities considerably.
taking some time to make informed choices now can make a
vast difference to your future lifestyle.
Patrick Convey is technical director of Cavendish Medical, specialist financial planners helping consultants in private practice and the NHS
The content of this article is for information only and must not be considered as financial advice. Cavendish Medical always recommends that you seek independent financial advice before making any financial decisions.
Levels, bases of and reliefs from taxation may be subject to change and their value depends on the individual circumstances of the investor. The value of investments and the income from them can fluctuate and investors may get back less than the amount invested. Cavendish Medical Ltd. is regulated by the Financial Conduct Authority to provide independent financial advice to individuals and businesses.
For more information, please visit www.cavendishmedical.com
EXPERT ADVICE YOU CAN TRUST
EXPERT ADVICE YOU CAN TRUST
EXPERT ADVICE YOU CAN TRUST
Since starting in the mid 1970’s Sandison Easson has continued to grow and is one of the largest independent medical specialist accountants in the UK.
Since starting in the mid 1970’s Sandison Easson has continued to grow and is one of the largest independent medical specialist accountants in the UK.
Since starting in the mid 1970’s Sandison Easson has continued to grow and is one of the largest independent medical specialist accountants in the UK.
Sandison Easson acts for medical professionals throughout all stages of their career and has clients in almost every town in England, Scotland and Wales.
Sandison Easson acts for medical professionals throughout all stages of their career and has clients in almost every town in England, Scotland and Wales.
Sandison Easson acts for medical professionals throughout all stages of their career and has clients in almost every town in England, Scotland and Wales.
We provide the usual services you would expect from an accountant such as preparation of your accounts and tax declarations but offer so much more including advice on:
We provide the usual services you would expect from an accountant such as preparation of your accounts and tax declarations but offer so much more including advice on:
We provide the usual services you would expect from an accountant such as preparation of your accounts and tax declarations but offer so much more including advice on:
• Setting up in Private Practice
• Setting up in Private Practice
• Setting up in Private Practice
• Developing your Private Practice
• Developing your Private Practice
• Developing your Private Practice
• Tapering of the Annual Allowance
• Tapering of the Annual Allowance
• Tapering of the Annual Allowance
• Lifetime Allowance planning
• Lifetime Allowance planning
• Lifetime Allowance planning
• Personal Allowance planning
• Personal Allowance planning
• Personal Allowance planning
SPECIALIST MEDICAL ACCOUNTANTS T 01625 527 351
SPECIALIST MEDICAL ACCOUNTANTS
• Reviewing your PAYE Coding Notices SPECIALIST MEDICAL ACCOUNTANTS
• Expenses that you can claim and those you cannot
• Expenses that you can claim and those you cannot
• Expenses that you can claim and those you cannot
• Minimising your tax bills
• Minimising your tax bills
• Minimising your tax bills
• Reviewing your PAYE Coding Notices
• Reviewing your PAYE Coding Notices
T 01625 527 351 E info@sandisoneasson.co.uk W www.sandisoneasson.co.uk
www.sandisoneasson.co.uk
Rex Buildings, Wilmslow, Cheshire, SK9 1HY
is bitter pill to swallow GMC letter
Dr Edward Farnan dispenses a medicolegal response to a doctor who selfprescribed and was shopped by the chemist
Dilemma 1
What do I about this GMC letter?
QI have recently received a worrying letter from the GMC explaining that my local pharmacist had written to it expressing concerns about a prescription I had written for myself for diclofenac 25mg and diazepam 2mg.
I had been prescribed diclofenac a few weeks before by my GP when I had had severe back pain.
The pain continued but I was unable to make a follow-up appointment, consequently, I had written a private prescription on a blank piece of paper, and added the low dose benzodiazepine for short-term use as a muscle relaxant to help me cope with a long flight.
I am surprised that the pharmacist had dispensed the prescription without expressing any concern to me, but had then decided to write to the GMC.
What should I do?
AI would advise contacting your medical defence organisation, who can help you draft a response to the GMC.
Also, bear in mind that it is normal practice for the GMC to write to a doctor’s employer (if you have one) to ask if they have any
other concerns about the employee’s performance or conduct.
The GMC’s core ethical guidance states that doctors should not, in general, treat themselves or people to whom they are close. Specifically, paragraph 16 of Good Medical Practice (2013) states that you must ‘wherever possible, avoid providing medical care for yourself or anyone with whom you have a close personal relationship’.
Further guidance is available in Good Practice in Prescribing and Managing Medicines and Devices (2013) which says ‘you must not prescribe a controlled medicine for yourself or someone close to you unless no other person with the legal right is available to… prescribe without a delay which would put your, or the patient’s, life or health at risk’.
It would also be wise to review and reflect on the GMC’s prescribing guidance which includes the difficulties associated with making objective decisions about one’s own health and undertake further learning to update your knowledge of safe prescribing –for example, supplementary reading and/or participating in an online course).
This may help to reassure the GMC that this was an isolated incident, and one which is unlikely to be repeated.
Dr Edward Farnan is a medico-legal adviser at the MDU
Discussing dementia
Dr Oliver Lord (right), medico-legal adviser at the MDU, looks at sharing information with a patient’s family members
Dilemma 2
How do I react to husband’s plea?
QI am a private GP and am currently treating an elderly woman who has recently been diagnosed with Alzheimer’s disease.
The patient’s husband has requested a meeting with me because he would like to know what he can expect regarding his wife’s prognosis.
He does not want his wife to attend this meeting, as he thinks it will upset her. However, I
believe she should attend as she has capacity. What should I do?
AAccording to the GMC’s Confidentiality guidance,
‘you should not refuse to listen to the views or concerns of those close to the patient on the grounds of confidentiality. The information they give you might be helpful in your care of the patient’ (paragraph 39).
However, a private meeting without your patient may be viewed as a breach of trust.
It is vital that the patient is involved as much as possible in discussions about their diagnosis and treatment plan, especially if they
have the capacity to understand. Consequently, it would make sense to talk to her now about what information she is happy for you to share with her husband.
Early discussions about what information a patient wishes to share and with whom they wish to share it is ‘particularly important if the patient has fluctuating or diminished capacity or is likely to lose capacity, even temporarily’ (paragraph 36).
It may be a good idea to discuss with the patient whether she wishes to give her husband or another person a Lasting Power of
Attorney so that you can share relevant information with them when the patient loses capacity.
A meeting with the patient’s husband, without the patient being present, may be beneficial to listen to his concerns and provide general information about the course and treatment of the disease.
But if you decide to do this, remember not to inadvertently disclose personal information without the patient’s consent and make clear that you might need to tell the patient about the conversation, ‘if it has influenced your assessment and treatment’ (paragraph 40).
Renault has upped its game with this smart, comfortable and practical family SUV, says Independent Practitioner Today
motoring correspondent Dr Tony Rimmer (right)
The all-new Koleos completes Renault’s crossover range above the Captur and Kadjar DocToR
Beauty in the beast
A view of future services and facilities on offer is the basis for all regular business plan updates and any independent practitioner will recognise this format.
for a proactive and expanding practice, an idea of how the business should look in one year and five years is a key strategic tool.
Motor manufacturers all have long-term plans. They may have to be revised with changes in technology, political ideology, law and market forces, but there is always a view of the future to work towards.
The recent trend towards SUvtype cars instead of hatchbacks and estates has resulted in all manufacturers featuring them in their model line-up. The larger manufacturers will have a full range of such vehicles.
Such a manufacturer is Renault and the all-new Koleos completes its crossover range above the Captur and Kadjar.
it is built on the Renault-Nissan common platform also used for the Scenic and espace models. it is a volvo XC60/Audi Q5-sized car that claims to have executiveclass features without premium pricing. However, it is not available with seven seats. only two engines are available, both turbo-diesels. Surprisingly, given the current anti-diesel publicity, no petrol variant is offered.
The 1.6litre four-cylinder version produces 130bhp with 320Nm of torque and the 2.0litre four-cylinder version produces 175bhp with 380Nm.
Panoramic sun roof
The 1.6litre engine can only be specified with two-wheel drive and a six-speed manual gearbox. The 2.0litre version has fourwheel drive with a continuously variable transmission (X-Tronic) automatic gearbox option. There are two trim levels avail-
able for both engines: Dynamic S Nav and Signature Nav. Both trims feature as standard equipment an opening panoramic sunroof, rear camera and parking sensors and Apple CarPlay and Android Auto. They also get active emergency braking system, blind spot warning, traffic sign recognition and hill start assist.
The Signature Nav adds an 8.7inch touchscreen, a powered Automatic Tailgate and Nappa leather.
Drives predictably
All the cars available for testing at the UK launch i attended were top-of-the-range Signature Nav dCi 175 4wD Auto X-Tronic models, so we were unable to drive the 1.6litre version with a manual gearbox. However, this flagship model is likely to be the one with greatest appeal to us medics.
o n-the-road price starts at £27,500 and rises to £34,200 for the range-topping model as tested.
This new Renault drives predictably for a car of this type. The Koleos, particularly aided by its automatic gearbox, is a piece of cake to drive. There is adequate performance from the 2.0litre engine and the steering is light for town manoeuvring.
interestingly, constantly variable automatic transmissions have come a long way since original
versions were spoiled by their habit of holding on to very high engine revs for ages when accelerating.
The X-tronic system behaves more like a multi-ratio automatic and the driver can choose a sevenspeed sequential mode to benefit from engine braking.
The ride is firm but smooth and the handling, when driving along twisty A or B roads, feels safe and secure without too much body roll. This is not a car to satisfy the keen driver, but that is not its aim either.
The cabin of this top model is certainly a pleasant place to be and aided by the leather seats and large A4 format touch-screen. The driver’s seat has electric adjustability and all the familiar Renault controls fall comfortably to hand. The fascia and door trim materials, however, fail to lift the interior into the executive territory occupied by more expensive rivals.
Huge boot
You cannot complain about interior space, though. Sitting in the back seats behind ‘my six-foot self’ was a position with plenty of headroom and legroom and three adults could easily fit across the rear bench.
The lack of a seven-seat option may well put off some of you family buyers, but Renault encour -
RenAUlT KoleoS SignATURe nav dCi 175 4wD x-TRoniC
engine: 2.0 litre turbo-diesel
Transmission: Continuously variable automatic
Power: 175bhp
Torque: 380nm
Acceleration: 0-62mph in 9.5 secs
Top speed: 125mph
Fuel economy: Combined 47.9mpg
Co2: 156g/km
Benefit-in-kind (company car tax) band: 33%
insurance group: 23e
on-the-road price: £34,200
The cabin of this top model is a pleasant place to be, aided by the leather seats and large A4 format touch-screen
ages you to look at the Scenic range instead. The long wheelbase helps luggage space and the boot is huge with a handy removable floor-panel positioned at the same height as the sill to form a flat floor.
The Koleos is a smart, comfortable and practical family SUV that does everything it is designed to do in a functional way
Renault claims 47.9mpg on the combined cycle for this top model, which is about average for the class and probably translates into 35-40mpg in the real world.
The Koleos is a smart, comfortable and practical family SUv that does everything it is designed to do in a functional way.
it is safe, has up-to-date equipment and in-car technology and represents good value when compared to similarly specified premium competitors.
Renault has really upped its game and this new car feels well made and solid. Just don’t expect the driving experience to light up any fires for the keen motorist.
Dr Tony Rimmer is a former NHS GP practising in Guildford, Surrey
Racing towards tax-efficient cars
Ian Tongue looks at the current position for those considering buying a car regarded as tax-efficient by the motor trade
With the Government recently announcing a ban on the sale of new petrol and diesel cars from 2040, it has naturally raised more interest in electric and ultra-lowemission vehicles.
A visit to the car dealer may leave you confused with the terminology and perhaps the seemingly too-good-to-be-true tax savings.
What is tax-efficient?
t here are different scales of tax efficiency, but, on the whole, people generally refer to tax-efficient cars as those attracting the 100% first year allowance – ultra-lowemissions or zero-emission cars.
For the tax year 2017-18, this is any vehicle with emissions with 75g/km or less, which usually means a fully electric or hybrid vehicle.
The
first year allowance
By some, this is seen as the holy grail of tax relief: you buy a car and are allowed to deduct this against your taxable profits in year one. Brilliant, but…
t he first year allowance is an acceleration of tax relief rather than necessarily giving you some-
thing more than you may have had anyway. i n particular, the mechanics of accounting for vehicles are different whether you are self-employed or trading as a limited company.
Additionally, leasing a car does not attract a first year allowance, as you are renting the car.
Self-employed
i f you are self-employed and using a private car for business, it can still qualify for the first year allowance if the vehicle has emissions of 75g/km or less.
h owever, the tax relief is restricted for business use only.
Let’s take an £80,000 electric sports car and compare the position to a gas-guzzler of the same cost with 50% business use.
For the electric car, this is an immediate deduction against your income tax liability in the year of acquisition. the car is purchased for £80,000 but you claim 50% of the cost at your marginal tax rate of, say, 45%. t his is an £18,000 reduction to your income tax liability. Brilliant.
For the gas-guzzler car, the tax relief in the year of acquisition is
only 8% and that is restricted for business use. this equates to only £2,880 tax saved. Not so good. At this point, the salesmen of low-emission cars want you to feel like the taxman has gifted you a decent proportion of your vehicle and get you to sign on the dotted line. But what happens in subsequent years?
Let’s roll things on to year four when the car is sold for £25,000. the electric car has all of its tax relief in year one and so received no further allowances in years two or three. in year four, the car is disposed of and, because it is a privately-owned vehicle, a balancing charge arises on the £25,000 residual value.
i n the year of disposal, you therefore pay additional income tax of £5,625 to dispose of the car, assuming tax rates remain stable. the overall tax saved is therefore £12,375 (£18,000 - £5,625).
For the gas-guzzler, it only received 8% allowances (restricted to 50% business use) in years one, two and three, and therefore has a ‘tax value’ of £62,295 in year four against a residual value of £25,000. i n year four, you can claim a
NHS fleeT ScHeme
The NHS fleet scheme is available to most NHS employees and can appear attractive. The same ‘benefit in kind’ calculations apply, so low-emission cars keep the cost down.
But, in choosing an NHS fleet car, you have three main areas of cost to consider:
The salary sacrificed and resulting loss of net pay;
The benefit in kind;
Potential loss of pension, particularly those in the 2015 pension scheme.
The key thing is to work out the total cost to see if this compares favourably to private ownership and that will depend on the car and your own circumstances.
balancing allowance of £8,391. Add this to the allowances given in years one, two and three, and you’ve guessed it, the tax relief is £12,375.
As you can see, you go from thinking the first year allowance is brilliant in year one to a position where you pay some of that tax relief back to dispose of your car!
For the self-employed, the first year allowance is merely a timing difference. if you want an electric car, buy one; if you want a gas guzzler car, buy one. Don’t let the tax tail wag the dog!
Company car
this is where it gets more complicated. i f you were an employee negotiating with your employer and you were given a low-emission company car as part of your package, it would no doubt be beneficial.
however, what about those that own the company and therefore are restricting their disposal income – through lower divi -
dends or salary – by buying a car through your company?
the same rules apply in terms of qualifying for the first year allowance as highlighted above, but as the vehicle is not privately owned, the rules are different in relation to the disposal charge or allowance. i n simple terms, the negative factor of paying back the tax relief on the disposal where you have claimed the first year allowance applies, but the big balancing allowance doesn’t and the car continues to get drip-fed tax relief for a long time after disposal. eventually, you will end up in the same position as the sole trader scenario, but this will be less beneficial from a cash flow perspective.
Another fundamental difference with a company car is that you are also required to pay additional income tax personally on the ‘benefit in kind’ of being given a vehicle.
the benefit in kind is effectively like a notional salary and is calculated by reference to original list
➱ p52
price and emissions for modern vehicles.
Classic cars have different rules. So, in this type of trading structure, the gas-guzzler becomes a huge tax charge for the privilege of being given this as a company car.
to put this in context, the electric car in the example above would attract an 8% benefit in kind rate for 201718, costing £2,880 a year in personal income tax for a 45% taxpayer, in contrast to the gasguzzler, which would be a 37% charge against list price, amounting to £13,320 in income tax each year the car is provided. therefore, it usually makes little
sense to have a medium- to highemission car as a company car in your own business.
Additionally, you need to consider that the company pays National insurance on the benefit in kind in a similar way to how it would if the benefit in kind was additional salary.
however, when you look at cars qualifying for the first year allowance, it can be tax-efficient, particularly as the ‘benefit in kind’ rate is set to fall to just 2% in 2020-21 –a cost of just £720 a year in the above example for an £80,000 car.
As with many decisions such as this, your own circumstances will determine whether you will save money overall when compared to extracting the money from your company and buying it personally.
i f you are considering a company car, it is important that your accountant calculates the true cost for you in advance of your commitment to buy.
The future
Clearly there is an irreversible drive to cut pollution and emissions that will lead to widespread electric vehicle ownership, particularly as these vehicles improve and range make them practical.
But what then?
t he i nstitute of Fiscal Studies has predicted a huge slump in fuel excise duty and vehicle tax as we adopt electric vehicles, and that was before the announcement to stop the sales of new diesel and petrol vehicles in 2040.
the current benefit in kind for a fully electric vehicle is 8% and this is scheduled to rise every year until 2019-20 until it reaches 16% and then it drops all the way down to 2% for 2020-21. No information has been provided past that date.
Clearly, if there is a funding black hole, this rate will be reviewed. But who knows whether it will remain low to fur-
ther encourage electric ownership, for a period of time at least.
Buying a car is a very personal thing and i always encourage clients to not chase the tax relief and buy the car that is most suitable for their needs, whether it be a people carrier, electric or a petrol/ diesel sports car for all that hard work.
Whichever you choose, your trading structure will have a fundamental impact on whether it makes sense to have this as a company car. involve your accountant in any vehicle considerations to ensure that, whatever you choose, you get the maximum tax relief available.
Next month: Avoiding the long arm of the taxman
Ian Tongue (right) is a partner with Sandison Easson chartered accountants
Less pay for same work
In this issue of Independent Practitioner Today, we are at the start of a new cycle of reporting on consultants’ earnings and incomes – with the very first results coming in from the changes as a result of the controversial Competition and Markets Authority report into private healthcare. Ray Stanbridge reports
Our he ADL i N e figures suggest that orthopaedic consultants’ average gross earnings have fallen by about 1.6% between 2015 and 2016 from £185,000 to £182,000. Costs, however, have shown a fall of about 3% between the two years. As a result, taxable profits have only fallen by about 0.8%, from £120,000 to £119,000. What then are the reasons for these changes? there is the effect in the marketplace of the open
referral system and also the increasing amount of lower-value ‘Choose and Book’ work undertaken by many surgeons, particularly outside of London.
paid less
Some consultants have experienced a growth in self-pay, but the impact of open referral and ‘Choose and Book’ fees has been enough to tip the averages.
Needless to say, many consult-
aveRage INcOme aND eXPeNDITURe Of a cONSUlTaNT ORTHOPaeDIc SURgeON WITH aN
many consultants are doing the same amount of work as previously – although being paid a little less for it
Expenditure
ants are doing the same amount of work as previously – although being paid a little less for it.
t here has been a slight fall in staff costs for reasons we cannot explain – although senior secretaries in one or two large practices in our sample have retired.
t his is perhaps a surprising observation given the impact of the Competition and Markets Authority (CMA) rulings.
t he CMA’s rulings have impacted on room hire costs, which have shown some rise. We expect further increases in 201617.
there has been a modest fall in the average cost of defence cover, which may come as a surprise to readers. But there is now an increasing market available for consultants to choose their provider.
For those with a lower claims rate, and possibly prepared to take risks with lower retrospective cover, there are savings to be made.
An increasingly number of consultants have been ‘shopping around’ for better deals.
Future costs
there seems to have been a slight fall in office costs, although phone costs have risen slightly. But this is probably the impact of ‘rounding’ on our figures rather than anything significant.
‘Other’ costs seem to have fallen slightly – most consultants already have their websites in real terms, so we would expect costs to fall slightly.
For the future, i would expect to see higher secretary and room hire costs as a result of the full effect of the CMA changes becoming apparent.
Year ending 5 April. Figures rounded to nearest
Source: Stanbridge Associates Ltd.
And i also predict more pressure on fees where patients have medical cover. Nonetheless, i would expect orthopaedic surgeons to retain pre-eminence as the top earners in the medical sector on average.
i ncome differentials of those
consultants who are in groups will rise over and above those who continue as a sole trader.
there are a number of warnings and caveats about the survey to be aware of. this is not a statistically valid set of results – rather it is a reflection of the financial perfor-
mance of typical orthopaedic surgeons in private practice.
Changes in the market place are making a year-to-year comparison increasingly difficult. t hese changes include the growth of consultant groups, the impact of incorporation on costs and the rising number of younger consultants now subject to the open referral system of cost control, utilised by a number of insurers.
Alongside the structural changes, consultants who are part of our sample survey have to satisfy the following tests.
these surgeons:
earn at least £5,000 a year gross from private practice;
Must have had at least five years’ private practice experience;
Are seriously interested in private practice business;
Are either on the old-style or new-style NhS contract;
May or may not work through a group or a limited liability company.
Next time: ophthalmologists
Ray Stanbridge is a partner with accountancy, finance and tax advisory
Associates Ltd
ending 5 april
ORTHOPaeDIc SURgeONS’
what’S coming in oUr december-JanUarY iSSUe
make sure you don’t miss our next issue, published on 4 January 2018. you may not receive every issue if you have not yet subscribed to the journal. Don’t risk missing out on vital topics we tackle next time, including:
The Budget – a review of the main Budget changes, how they affect independent practitioners and what you should do
How to deal with a negative online review
2017: the year that was. a round-up of the big news affecting independent practitioners
If you haven’t prepared the information for your 2016-17 tax year, you need to get your skates on, as the filing date is 31 January 2018.
Susan Hutter gives some top tips about submitting a tidy tax return
coping with independent practitioner burn-out. Try these alternatives for coping with stress. consultant counselling psychologist Dr michael Sinclair shares five effective strategies
medical professionals’ legal and ethical duties to patients who may be experiencing domestic violence
executive information for private doctors. Jane Braithwaite shows how to analyse your business and make changes based on practice data
your brain could stop you being a good investor! cavendish medical’s Dr Benjamin Holdsworth shows why behavioural finance should be important to you
Taking up medical billing and collection? findlay fyfe answers independent practitioners’ common questions
eDITORIal INqUIRIeS
Preparing for retirement from private practice: we look at the rules and practicalities a retiring doctor may need to consider
PPUs – 2018-19 will see a big increase in their growth, predicts Philip Housden. So how can you be part of it?
for many independent practitioners there is a clear angst that Hm Revenue and customs may come calling with an unexpected tax bill or inquiry. We explore some common areas of risk and the steps that can be taken to minimise an inspector’s call
Just don’t risk it! lawyers are coming across doctors who are taking a big risk by having no indemnity cover
Doctor On The Road looks at one car that should definitely fit in the consultants’ car park
Profits focus casts an eye on the latest earnings of ophthalmologists
PlUS all the latest news and views
aDveRTISeRS: The deadline for booking advertising for our December-January issue falls on 1 December
Robin Stride, editorial director
Email: robin@ip-today.co.uk
Tel: 07909 997340
aDveRTISINg INqUIRIeS
Published by The Independent Practitioner Ltd. Independent Practitioner Today is editorially independent and thanks Bupa for its assistance with distribution.
Printed by Pepper communications ltd
Material is governed by copyright. No part of this publication may be reproduced, stored in a retrieval system or transmitted in any form without permission, unless for the purposes of reference and comment. Editorial layout is the copyright of the publishers. If you wish to use it for promotional purposes on websites or for reprints, we would be happy to discuss licensing the copyright to you.
£90 GPs and practice managers (private & NHS). £210 organisations.
But if you pay by direct debit, individuals pay only £75, and organisations £180 Call Proact Ltd on 01752 312140
Email: lisa@marketingcentre.co.uk
Save £15
WITH DIRecT DeBIT!
guarantee you get the next copy of Independent Practitioner Today. Take out a subscription (at the rates shown on the left) by phoning 01752 312140 or by sending off a subscription form on page 24 or by emailing us at lisa@independent-practitioner-today.co.uk. Or go to the ‘Subscribe’ page of our website www.independent-practitioner-today.co.uk
If you subscribe by direct debit, individuals pay only £75. Just fill in the form on page 24 and send it to the freepost address shown at the bottom of the form.
BacK ISSUeS: £12.50 including post & packaging cHaNgINg aDDReSS OR SUBScRIPTION DeTaIlS?
Phone 01752 312140 or email lisa@marketingcentre.co.uk