The business journal for doctors in private practice
Encounters with the meeja A marketing expert shares her tips on getting vital media exposure for doctors P16
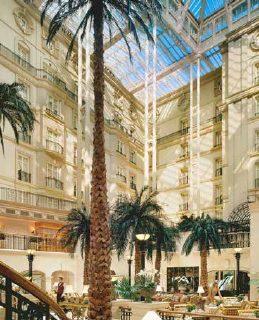
A lesson in hospitality
Seeing behind the scenes at a leading hotel is complementing cancer care P26
By Robin Stride
Independent practitioners are being urged to urgently review if they are competing fairly over fees following the first case of a consultants’ group breaking competition law.
The Consultant Eye Surgeons Partnership (CESP) Ltd, representing interests of 37 limited liability partnerships (LLPs) and their 200 consultant members, was fined £382,000 by the Competition and Markets Authority (CMA) last August after admitting liability for a number of infringements (Independent Practitioner Today, September 2015).
But the CMA believes many consultants may remain unaware how
competition law can affect the way they work. Now it says it wants to help doctors’ businesses ensure they avoid making the same errors. Ultimately, it suggests doctors take legal advice over any concerns that the way they operate could risk breaking competition law.
CMA’s senior director for antitrust enforcement, Ann Pope, stressed it was important for private consultants to ask themselves who their competitors were. She agreed it might seem an odd question when patient care was the primary focus. But she said competition played a vital role in ensuring self-pay and insured patients benefited from a well-functioning market – lower prices, more choice and better quality.
Mrs Pope warned consultants working as part of a group to check they were not discussing or sharing information that could land them in trouble:
‘If you and your fellow group members work as part of an LLP or limited company and only apply your services via this intermediary, then you are part of one economic unit and any discussions you have internally about fees would not be a competition issue.
‘The situation becomes more complicated if you also work as a sole trader outside the group, as well as being a member of a group, as decisions made internally within the group could then be used to influence your commercial conduct as a sole trader – such as
Pay and pensions are the two biggest questions we are asked about – so get Monday 22 February in your 2016 diary right now! For Independent Practitioner Today is teaming up with the Royal Society of Medicine (RSM) to present a seminar called ‘Your fees, your pension – your future: how doing nothing is not an option’. There will be talks from top speakers Ray Stanbridge, of Stanbridge Associates specialist medical accountants, and Simon Bruce of
Cavendish Medical, plus plenty of opportunity to ask questions.
The free event at the RSM in Wimpole Street, London, begins with 7pm registration for a 7.30pm start and ends at 8.30pm with a one-hour drinks reception and chance to mix with Harley Street area colleagues.
In April 2016, private doctors will see a host of regulatory changes which could impact on their finances – a lower lifetime allowance pension limit, a cut to high earners’ annual allowance rates and higher
taxes on company profit dividends.
The Chancellor’s consultation on pensions tax relief could also mean significant changes.
As ever when storm clouds gather, your main priority should be to check the status of your own finances. Does your wealth need protecting? Do you have a plan for the future? This is the ideal time to review your current situation and ensure your long-term security.
Major changes are also forecast for private practice in the next five
P46
the fees that you may charge for specific procedures.’
Choices about fees or whether a group intended to accept an insurer’s or facility’s package price should be made independently and not as a result of discussion with other consultant groups. CESP said it had paid the fine in full, noted the CMA’s comments and taken appropriate action.
In our next issue, Mrs Pope will explore the case in more detail. n Independent Practitioner Today readers can get ten minutes of free legal advice from niche healthcare lawyers Hempsons by phone on 020 7839 0278, 9am5pm Monday to Friday. n See feature on page 34 and the CMA’s latest plans on page 50
Are you fixing prices? Opportunity to sort out your finances
years such as a rise in self-pay patients, declining insurance business, group growth, salaried consultants and re-imbursement increasingly linked to economics. Ray Stanbridge will review trends and show how to adapt to take advantage of new opportunities and avoid potential hazards. This exclusive event is for Independent Practitioner Today readers, RSM members and invited guests. Apply for registration at www.rsm.ac.uk/feespensions2016.
emulate a theme park experience
How to create a compelling experience for aesthetic patients and see profits soar P12
where stressed doctors can go for help a medico-legal expert says doctors can get help without fear of job repercussions P20
get rid of those hang-ups are you losing custom through bad phone manners? it’s time to ring the change P23
spies in the room
What to do when faced with patients who covertly record consultations with you P32
our
cover: a mounting headache for many a top lawyer’s personal view on the medical indemnity arena P34 is it buy-to-let or buy toilet?
a look at the myths behind the headlines of investing in buy-to-let properties P42
Pension rights for same-sex unions ‘unfair’
by leslie berry
Same-sex marriage doctors could find their pension benefits are worse than heterosexual couples following a failed Court of Appeal hearing.
Survivors’ pension benefits are currently only payable on death on NHS service accrued after the 2005 Civil Partnership Act.
This status was challenged by John Walker, aged 62, who retired in 2003 before civil partnerships came in. He claimed it was unlawful for his husband to not get a full spousal pension if he dies.
Convey said: ‘This is yet another example of the substantial complexity surrounding pensions and is a really important status to be aware of.
‘Doctors in this position must consider what steps they need to take to ensure their loved ones can maintain their current lifestyle upon the event of their death.’
There is already considerable discrepancy in the way surviving male and female partners of 1995 NHS Pension Scheme members receive benefits.
Good ideas not to be mist
One of our staff set off through the fog, and well before dawn, to go climbing earlier this month. We thought he would have to call it off, but as he got to the car park below the mountain, the visibility dramatically improved.
By the time dawn broke, he was on the peak in a different world, enjoying a clear blue sky as the sun shone on a sea of silver cloud covering the less adventurous below.
Sunny inspiration and new ideas are often nearer than people think when the business mist descends.
You just have to set out on
Phone: 07909 997340 @robinstride
what might initially appear to be a pointless journey.
Take the specialist oncology centre (page 26) that dared to be different and ventured behind the scenes at a five-star London hotel. Now it uses the good practice it saw to complement cancer care for its patients.
Or you could look ‘over the fence’ at what private doctors in the aesthetic world are doing to create a compelling patient experience (see page 12).
Inviting the press to meet you may be another unusual direction. But as we report on page 5, it is already paying off for some consultants.
Tell us your news Editorial director Robin Stride at robin@ip-today.co.uk
To adverTise Contact advertising manager Margaret Floate at margifloate@btinternet.com Phone: 01483 824094
To subscribe lisa@marketingcentre.co.uk Phone 01752 312140
Publisher: Gillian Nineham at gill@ip-today.co.uk Phone: 07767 353897
Head of design: Jonathan Anstee chief sub-editor: Vincent Dawe 12,450 circulation figures verified by the Audit Bureau of Circulations ediTorial commenT
Mr Walker retired from a limited company with an annual £85,000 final salary pension after 23 years. He took on a civil partnership in 2006 and married when the law allowed.
According to specialist financial planners Cavendish Medical, if he was married to a woman, she would collect £41,000 p.a. after his death. But as he retired before laws banning discrimination on sexual orientation grounds came into force, his husband would only receive a few hundred pounds a year.
Technical director Patrick
Members’ widows can get half their spouse’s pension paid for life. But widowers get only half their partner’s pension based on actual NHS service after 6 April 1988.
Mr Convey added: ‘It seems implausible this situation is in place, but several legal challenges have been brought against the current status and all have failed.
‘As many as two-thirds of occupational pension schemes choose to pay exactly the same survivor benefits to spouses, civil partners, unmarried partners and unmarried same-sex couples on a voluntary basis. Unfortunately, the NHS is not one of them.’
Healthcode boosts IT system to protect against hackers
Healthcode is upgrading its IT systems to ensure data it processes for consultants and hospitals remains secure from loss and cyber-attacks.
The specialist in online billing and practice management systems has invested in a dedicated IT infrastructure from managed IT services provider Claranet.
Healthcode boss Peter Connor said: ‘A huge volume of financial and patient data goes through our systems – for example, we process
18,000 bills from consultants and hospitals daily. Given the highly confidential nature of this data, our customers rightly expect us to protect them from reputational damage by meeting the highest security standards.
‘Our new system is resilient against data breaches with an inbuilt disaster recovery system. We can reassure doctors their data stays entirely in the UK, in line with established data protection principles.’
Looking for eye surgeons
by robin stride
More than 40 consultant ophthalmologists have been granted practising privileges so far at the new Optegra Eye Hospital, London –and others are on the way.
Hospital director Amy Richardson told Independent Practitioner Today the facility was actively seeking more.
She said: ‘The majority are signed up under our “partnership model” and agree to charge within our fee structure in return for a share of patients generated by Optegra’s marketing.
‘We also have surgeons using our facilities, both surgical and outpatient, on a facility fee basis who do not benefit from Optegra patients.’
The Queen Anne Street, W1, unit was officially ‘launched’ at a Guy Fawkes’s night reception on the 42nd floor of the Leadenhall Building. Doors of the six-floor building in two adjacent houses open to patients on 14 December.
The £13m investment offers a full laser suite, medical ophthalmology rooms, theatres and a 11-bed ward.
Equipment includes ReLEx SMILE: a bladeless, flapless, minimally invasive alternative to laser surgery.
Bosses said consultants would treat ‘the A to Z of eye health care’ including stem cell transplants.
Innovative services include a telemedicine service for community optometrists wanting advice
Medical help app omits private GPs
Private GPs will miss out on the chance to increase income from patients seeking medical help using a new app.
The company behind GP Surgery App said it would only use NHS GPs, who will be paid undisclosed sums for their time –whether or not they get calls.
Punter Southall Health & Protection’s app is billed as ‘a unique, reliable and affordable around-the-clock telephone GP facility’. Employers pay around £1 per employee a month.
The firm said NHS GP services were under extreme pressure and many people faced a long wait for an appointment, resulting in health concerns for employers, unnecessary sickness absence, and extra visits to consultants.
Its Med24 Service provides guar-
Tell us your sTory
anteed phone access to GPs 24/7, 365 days a year. There is an e-consultation facility and the option of private prescriptions delivered directly to home or work, plus specialist referrals.
Users can access a library of medically validated fact sheets, including 1,100 health conditions, treatments, travel advice and immunisation, plus a facility to store their own medical information and a symptom checker tool.
Executive director Jan Lawson said: ‘We are particularly pleased to have developed a service for our clients with real breadth and depth at a fraction of the cost of other heavily marketed services.’
The service is provided in conjunction with Medical Solutions UK Ltd, which has taken on more than 50 NHS GPs.
share your experience of what has and has not worked in your private practice. even if it’s bad news, let us know and we can spread the word to prevent other independent practitioners falling into the same pitfalls. contact editorial director robin stride at robin@ip-today.co.uk
on optical coherence tomography (OCT) images, and a Low Vision Clinic offering a vision loss counselling service to support those whose conditions are untreatable and ensure they can maximise their remaining vision with innovative, practical solutions.
Patients have their own dedicated spaces for the duration of their stay, both pre- and postoperatively.
Managing director Rory Passmore said the opening marked a key development for the business.
‘Dedicated specialist eye hospitals can deliver an unsurpassed level of treatment, as we invest in leading surgeons and an unprecedented volume of diagnostic and surgical equipment,’ he said.
US clinic holds its fire on large London unit
Plans for a 200,000 square-foot building in London’s Grosvenor Place leased to the Cleveland Clinic are expected to be made clear shortly.
As we went to press, the US hospital provider said it was ‘studying our options’ for the property.
Mr Hasan Jouni, Cleveland Clinic’s international relations program manager, told Independent Practitioner Today there had been no decision on whether it would be a medical facility.
He said: ‘We’ve acquired the place but we’ve not made any plans or finalised any plans as to what to do with it.’
Independent Practitioner Today reported plans a year ago for private doctors to be given practising privileges in a palatial £600m international hospital in the city.
Asked if the Cleveland Clinic had a message for independent practitioners, Mr Jouni replied ‘not at the moment’.
Inspecting private doctors
More than 40 Independent Doctors Federation (IDF) members met a top health watchdog in the runup to last month’s deadline for comments on the consultation about how they are to be inspected. They had a ‘relaxed and constructive discussion’ with Care Quality Commission (CQC) deputy chief inspector for primary care, Prof Ursula Gallagher, submitted a corporate
response and were told IDF involvement was welcome.
10% cQc fee rise sHock for PrivaTe docTors www.independentpractitioner-today.co.uk
IDF regulation committee chairman Dr James MacKay told her the federation was keen to continue its relationship with the CQC in working to promote excellence in the independent sector. There have been regular inspection procedure workshops between the two bodies in the last 18 months.
The optegra eye Hospital in Queen anne street is to open next month
British Association of Aesthetic Plastic Surgeons’ annual scientific meeting
By a staff reporter
Worried plastic surgeons have launched a rescue operation to encourage the next generation of independent practitioners in their specialty.
The British Association of Aesthetic Plastic Surgeons (BAAPS) announced it will take up the mantle of responsibility for training with a groundbreaking new programme.
This will be run alongside colleagues in other plastic surgery societies and the National Institute of Aesthetic Research ‘for the development of the profession, but, most importantly of all, for patient safety’.
Trainees wanting to develop ‘a wellrounded career in aesthetics’ will be offered a series of fully funded threemonth fellowships under the aegis of some of the UK’s top exponents.
The initiative was unveiled at the Annual Scientific Meeting of BAAPS amid reports of a rapid
Boost to train surgeons Marketing rules are ‘still flouted’
Studies unveiled at the conference show Government recommendations emerging from the recent Keogh review continue to be shamelessly flouted by the industry, BAAPS warned.
Research by medical students
Sohaib Rufa and Chris Davis revealed that while there have been some improvements in cosmetic surgery marketing in the last two years, the guidelines determined by the review continue to be pointedly ignored, mostly by the larger commercial chains.
Their study, examining the top 50 providers of cosmetic surgery (as listed by Google), showed that:
14% of consultations still don’t take place with the operating surgeon but a salesperson or intermediary. This is worse than in 2013,
drop in NHS funding for cosmetic surgery and vanishing training opportunities for the upcoming generation of surgeons.
A study presented by trainee member Mr Reza Nassab revealed that since the advent of Clinical Com missioning Groups (CCGs):
There has been a 14% fall in provision for breast augmentation, with tighter restrictions;
Only 22% of CCGs offer breast lifts – but again with tight restrictions;
conditions such as facial palsy or congenital deformities.
BAAPS president Mr Michael Cadier said it was a wellknown adage that it took 10,000 hours training to truly master a craft and in bygone NHS days this was entirely possible for aesthetic plastic surgery.
A good percentage of CCGs still offer eyelid surgery, but this is entirely for visual obstruction and not for aesthetic purposes;
79% of CCGs still offer nose surgery, but these are only offered for airway obstruction, trauma or congenital defects;
CCGs approve funding for a third less facelift surgery than their forerunners – primary care trusts –once did and purely for significant
But with the advent of the European Working Time Directive and a rise in medicolegal worries –which means trainees don’t get as much of a chance to perform surgical procedures under supervision due to litigation fears – they were lucky to get 3,000 hours before they were consultants.
He said: ‘While they will have plenty of exposure to reconstructive treatment for burns, trauma and other medical conditions such as tumours, it does mean there’s a whole new generation of consultants going into private practice offering procedures such as facelifts and breast aug
mentation having had virtually no contact with these types of ops during their time on the NHS.
‘It is high time that we stop relying on the health service to prepare them for the private sector – why, indeed, should public funding go towards this arena?’
Paid for by the BAAPS with support from the British Association of Plastic, Reconstructive and Aesthetic Surgeons (BAPRAS), the fellowships offer handson practice, mentorship, access to specialist expertise and how to deal with complications – everything they need to know to become competent aesthetic plastic surgeons with a wide range.
National Institute of Aesthetic Research chief executive Brendan Eley, who is collaborating on the programme, said: ‘Not only will trainees be able to access the expertise and guidance of top surgeons in busy private units, but fellows will be further rewarded for undertaking quality research and audits.’
where 90% did take place with the surgeon;
40% offered free consultations;
16% offered promotional deals, such as ‘bridal packages’, incentives to have more surgery or ‘refer a friend’ – half of which were timelinked (such as ‘book by Friday’);
Only 60% stipulated the recommended 14day coolingoff period.
Their research found that noncompliant providers were typically chain companies rather than independent individuals or small group practices.
Consultant plastic surgeon and BAPRAS president Mr Nigel Mercer said: ‘While the private sector is wide in scope, it is clear that some of the more “conveyorbelt”style commercial entities are simply not an appropriate environment
for young surgeons to be exposed to a wide variety of complex procedures and to learn how to deal with complications.
‘Starting out in private practice can be a lonely stage professionally, without having the added pressure of delivering high volumes of patients in a stack ’em high manner. Moreover, as this research shows, many of these companies continue to market in an unethical manner.
‘Credentialing will soon be implemented, but this is simply the most basic level for a clinician to be able to legally practise. We want to develop experienced surgeons operating at the gold standard and this is what these fellowships [see story above] are designed to provide. The public deserves no less.’
Put yourself forward to host trainee
Experienced BAAPS/BAPRAS surgeons can apply to host trainees. The ‘fellow’ will be attached to a group of consultants (at least two) who have a high volume of work, otherwise three or more to ensure a wide range of exposure.
Trainees will be expected to perform 40 halfday operating sessions, 20 half day outpatient sessions and a half day for audit and research and provide logbooks. Participating units are expected to expose the fellow to minimum numbers of breast (20), truncal (10), facial and periorbital (20), botulinum toxin (10) cases, among others such as nasal, ear and dermal filler injections.
Michael Cadier, BAAPs president
Tie-ups with insurers will help doctors ‘in long run’
Insurers’ joint ventures have been welcomed by the Association of Medical Insurers and Intermediaries (AMII) as good for the market.
Executive committee member Claire Ginnelly said a purchasing alliance between Aviva Health and VitalityHealth should mean lower claims costs and more affordable premiums for customers.
She said: ‘Cost is still a major issue in this market place and it is for the benefit of all if we can get some growth.
‘The hospitals and consultants might have a different view, as their income may well be reduced by the coming together of these two organisations, but the cost of claims is something which needs to be tackled if we are to see premiums affordable to more people in the future.
‘We have seen a similar situation with Benenden and Bupa when they entered into their new contractual relationship in October. This has given Benenden customers access to more facilities and consultants while at the same time being able to contain costs.’
The managing director of Premier Choice Healthcare added that AMII was striving to get insurers working together on issues affecting the whole industry. Working together to encourage growth was a key objective.
She added: ‘Moves like this should be welcomed by the industry. Also, it is encouraging to see providers working together in this way.’
Specialists bridge gap with the press
By Robin Stride
Consultants enjoyed a more unusual approach to marketing when they were invited to ‘meet the press’ for a drink and a chat.
Journalists representing a wide range of trade and national press turned up for the event organised by HCA’s London Bridge Hospital.
An HCA spokesman said: ‘We had 17 members of the press attend, many of whom contacted us after the event to say how much they enjoyed it and how beneficial it would be in relation to upcoming features.
‘Consultants also responded positively to this event, as they felt it was informative and enabled them to engage with media in a relaxed setting.’
Consultant orthopaedic surgeon Mr Ian McDermott told Independent Practitioner Today that the evening, held in a private bar, was an excellent opportunity to meet a wide variety of different journalists from various organisations. These ranged from websites offering lifestyle advice to the over 50s to newspapers such as The Mail on Sunday and specialist journals.
He said: ‘This event was great fun and a really positive PR opportunity for myself, for our practice – London Sports Orthopaedics –and for London Bridge Hospital itself.
‘I’ve never been to a PR event quite like this, and this simply
shows how the management team at London Bridge Hospital really are incredibly switchedon and why they’re so successful.’
Specialists said they found the journalists interesting to speak to and keen to hear of the latest medical and surgical advances in their specialist fields.
Doctors left with several people’s cards, and with requests from a number of journalists to contact them with details of new advances and interesting patient stories.
Journalists departed with a variety of highquality publications including one outlining the hospital’s history and a ‘press book’ featuring biographies, photos and special interests of the consultants they met.
London Bridge Hospital chief
executive John Reay said the event was designed to provide an exclusive insight into some of its worldclass consultants and clinical specialists.
Welcoming the press he said: ‘We look forward to working with you, by assisting on any editorial needs through expert comment and guidance on a range of health stories and issues.
‘Our specialists have significantly contributed to their field, and are dedicated in educating, informing and raising awareness about latest treatments and developments.’
The hospital and its PR company, Spreckley, said they were delighted with how well the event went and were ‘extremely keen’ to replicate this in the future.
Big rise in submitting bills electronically
E
billing by independent practitioner rose by 81% in JanuaryJune 2015 compared with the same period last year, according to the official clearing company for medical bills to private medical insurers.
Healthcode said this reflected a 64% rise this year in ebilling by consultants.
Ebilling in the private healthcare sector saw another landmark last March when over 425,000 bills were processed and cleared, the first time the monthly total exceeded 400,000.
Healthcode boss Peter Connor said: ‘The upwards trend shows private doctors are fast recognising the business benefits of billing electronically, especially for their cash flow.
‘Because ebills are validated on submission, they are less likely to be queried and can be settled faster. Users receive instant confirmation that a bill has been received by the insurer or if there is a problem they need to correct.’
The London Bridge Hospital (centre), soon to be expanding into The Shard
John Reay, London Bridge Hospital CEO
‘Talk more with your accountant’
By Robin Stride
Consultants have been advised to ensure they have an interactive relationship with their accountant and not just leave things to chance.
Specialist medical accountant
Vanessa Sanders told members of the London Consultants Association that some specialists just used advisers to fill in and send off their tax return.
But they needed to keep their advisers up to date and have conversations with them.
Mrs Sanders, of Stanbridge Associates, said doctors should ensure their accountant was earning the ‘taxdeductible’ fee paid to them. Problems doctors never knew they even had could then be solved.
She also gave some useful ‘avoid the taxman’ tips at the meeting, held shortly after a court case where a consultant was fined £200,000 and given a suspended two year jail sentence after admitting stealing £409,611 by failing to declare any taxable income from private practice.
Her tips included:
Keep all receipts and invoices for expenses;
Submit all tax returns online and in time;
Keep records for four years;
Use diaries as underlying records;
Use a logical invoicing system;
Define debtors at yearend;
Have a policy for bad debt recovery;
Saying sorry is best way to defuse a complaint
A sincere apology when things go wrong can help prevent patient complaints escalating, a medical defence organisation advises.
Match up pay in slips, insurer notices and invoice numbers;
Keep a car mileage log;
Have a business bank account.
HMRC fines of up to 100% of the tax loss, plus penalties and naming and shaming lay in wait for doctors falling foul of the rules, she warned. Late filing would mean a £100 fine plus £10 a day until filed. For late payment of tax, 5% of the outstanding balance was due every six months, with interest being charged at 4%. Company fines were even more stringent and could include prosecution.
Performance data is a help, not threat, consultants told
The LCA event lined up a number of speakers to examine ‘the changing financial and regulatory landscape of private practice’.
Association chairman Mr Neil Tolley said he could not remember a time when there were so many issues affecting consultants’ professional lives.
One big issue for many is the performance data to be published by the new Private Healthcare Information Network (PHIN). Its chief executive Matt James told consultants the body was not a regulator; it was ‘here to help’ and wanted them and hospitals to do well from what it published.
He displayed a dummy ‘Consultant Practice Overview’ printout showing an example of activity
(see Independent Practitioner Today, June 2015) and assured doctors they would be able to see, check and approve data prepublication through ‘a secure information portal’ from early 2016.
Hospitals needed to be ready to collect data by 1 January 2016 and this is required by next September, with publication due by April 2017.
Mr James said PHIN would work with the hospitals, GMC and others to give every consultant the opportunity to comply.
itioner Organisations’ (FIPO) clinical outcomes advisory group and also specialty and professional associations to ensure the collection, analysis and publication of data was appropriate, fair and robust for each specialty.
Mr Neil Tolley, LCA chairman
It was also working with the Federation of Independent Pract
Some consultants, however, expressed concerns during a question and answer session; with Oxford cardiothoracic surgeon Prof Stephen Westaby saying there had to be a level playing field if data was published – ‘and we all know that you can never have a level playing field’.
According to a recent report, an inadequate apology was the most common reason hospital complaints in England were referred to the Parliamentary and Health Service Ombudsman, accounting for 34% of all complaints investigated in 201415.
The MDDUS said receiving a complaint from a patient was the single most common reason doctors asked it for advice. Types of complaints include patients being unhappy with a delay in diagnosis or treatment, prescribing errors and poor communication.
MDDUS medical adviser Dr Greg Dollman said many of these complaints could be dealt with by way of an apology and an honest and direct explanation.
He said: ‘Sorry might seem like the hardest word, but there are times when a doctor should apologise to a patient. Many doctors might be reluctant to apologise, but saying sorry is not an admission of guilt or liability in any potential litigation and is not a sign of weakness. In fact, at times it is the right thing to do and a genuine apology may be all that a patient wants.
‘It can be stressful for doctors receiving complaints about the care they provide, but they should avoid acting defensively. An open and honest approach can help resolve complaints at the earliest possible stage.’
He said even where a doctor believed no mistake was made, it was still possible to adopt a conciliatory tone and express regret that the patient was dissatisfied.
The GMC’s Good Medical Practice states: ‘Patients who complain about the care or treatment they have received have a right to expect a prompt, open, constructive and honest response including an explanation and, if appropriate, an apology.’
LoNdoN coNSuLtaNtS aSSociatioN mEEtiNg
Vanessa Sanders
Glowing praise for private PAs
By Edie Bourne
The British Society of Medical Secretaries and Administrators
(BSMSA) private medical secretary/PA 2015 award has been won by David Lawrence of HCA’s The Portland Hospital, London.
Gynaecologists Prof Sarah Creighton and Mr Alfred Cutner nominated him for completely transforming their private practice over the last two years.
They said the PA’s office management and administrative skills had moved them into the 21st century and brought huge benefits for them and the women they look after.
Highly commended as joint runners up in the awards sponsored by DGL Practice Manager, and Howard de Walden (Harley Street Medical Area) were Peter Hinton of The Priory Hospital, Roehampton, and Alexis Coward of HCA’s Harley Street Clinic Diagnostic Centre.
Kathy Perkins, of the awards committee, said: ‘During our inter views in London, we also interviewed NHS secretaries/PAs for their sector award. What came through very clearly was the difference between the people working in the private sector and those working in the NHS.
‘Put simply, working in a private practice for a medical secretary/PA – a ‘private practice manager’ – is akin to running a business with all the ramifications that entails.
‘They have to know, in addition
to excellent general office management skills, financial accounting, liaising with private health insurers – or directly with the patient – detailed knowledge about the speciality of their consultant/s and the ramifications if surgery is also involved. Marketing the practice and HR management are other facets not faced by the NHS nominees’.
She described Mr Lawrence as an excellent example of how the traditional role of a medical secretary has changed over the years from being mainly a femaledominated post to that which is now seen as a highly professional position.
‘His selfconfidence and attitude to his job while managing a practice which is dominated by female patients was noteworthy and helped him to gain the winning title.’
Runnerup Miss Coward recently compiled a new system for managing patients with implanted devices who require regular follow up, many of them using remote transmissions with wireless 3G monitors from home.
Mrs Perkins said: ‘Backed up by a superb spreadsheet, this system means there is a clear pathway for all device patients to be monitored appropriately. This is so important, as many of these devices have been implanted for serious lifethreatening arrhythmias. She shows diligence, commitment and initiative to the practice.’
Other runnerup Mr Hinton literally started from scratch, with no previous clerical or typing skills. Over the past couple of years, he transformed himself and the practice and is now running a paperless office.
Doctors told to be aware of duties to report FGM
Private GPs and consultants are being urged to be aware of their professional obligations relating to reporting and treating victims of female genital mutilation (FGM).
Home Office guidelines make reporting cases in patients under 18 years to the police mandatory.
The defence body Medical Protection warned that failure to appropriately report a case might result in proceedings being launched against them.
Medical director Dr Rob Hendry said: ‘If the child has capacity, doctors should try to obtain their consent before disclosing information to the police, unless this puts them or others at risk of harm or may jeopardise an investigation.
‘If consent is withheld or the child lacks capacity, the doctor must still report to the authorities. Girls considered to be at risk of FGM should be referred to the appropriate local children services or Multi Agency Safeguarding Hub.’
Doctors with concerns about their obligations should contact their defence body.
Care staff have more sick days
Healthcare workers have taken an average 25 sick days in the last five years compared to 15 days by staff in 25 industries surveyed by insurance company There.
Nearly half blamed the cause on overwork and 37.5% cited catching something from a patient.
Surgeons worried about NHS bed shortages
Four in five surgeons have expressed extreme concern about NHS bed availability, with nine in ten stating this has an adverse impact on waiting times.
According to findings from the British Health Report 2015, com
missioned by Your Legal Friend, 77% of medical professionals believe pressure on bed availability leads to an increased waiting time, strain on resources (74%) and patient dissatisfaction (72%).
The report found a huge dispar
ity over how long patients spend in hospitals after an operation.
Topping the table was the East of England, with patients spending on average eight days in hospital, followed by the South west (seven) and the Midlands (six).
Those in London spend just four days in hospital after surgery and those in the North west, Northeast and Northern Ireland just three days. This compares to the fiveday national average stay in hospital following an operation.
Winning combination: (L-R) Alexis Coward, Kingsley Hollis of sponsors DGL Practice Manager, David Lawrence (winner) and Peter Hinton
Avoid public rows with colleagues
In prIvate practice, there is perhaps more of a need to show professionalism and to be supportive of colleagues for the benefit of the patient.
Care must be taken to avoid overt criticism of colleagues and of any treatment provided by them and expressed directly to a patient.
Criticism reduces the confidence of patients in the profession as a whole and can cause unnecessary stress for the colleague who is the recipient. It is best to avoid getting drawn into making criticisms of another doctor, no matter how much a patient may pressurise you.
patients should be advised that any worries should be raised, in the first instance, with the doctor concerned, who is, after all, the person best placed to comment because only that doctor is in possession of all the facts.
You can comment objectively on what you find on examination, but not on what might or might not have been the case when you were not present.
Many criticisms made by clinicians are because they feel that they have a duty to offer their views on treatment provided elsewhere, whenever a patient seeks their professional opinion and advice.
Critical opinions may be given with the best of intentions, but without knowing all the relevant facts – including what problems were faced by the previous doctor at the time – they can be uninformed and possibly irresponsible. they will usually be judgmental rather than objective and factual.
Defamation
Defamation is defined as the publication of a false statement that lowers the reputation of a person in the eyes of right-thinking members of society. For such a statement to be actionable as being defamatory, it has to meet certain legal requirements. the defamatory statement usually has to be voiced and brought to the attention of others, have no lawful justification or be made with the object of discrediting the
By ms Beryl De souza
Plastic surgeon, associate tutor at Imperial College and honorary secretary of the medical Women’s Federation
person concerned or exposing him to hatred, contempt or ridicule.
professional rivalries
a relationship breakdown between professional colleagues brings with it an additional complication in that patients and members of staff can become drawn into the conflict.
professional rivalry is usually a trigger and the anger experienced in such disputes can sometimes result in inappropriate comments being made about a professional colleague.
these remarks are often made to patients, members of staff or colleagues. In many cases, the clear intention is to undermine or discredit the other person involved.
p rofessional life creates many instances where colleagues are competing for jobs, for representative appointments or positions of responsibility in medical associations, colleges and councils.
Competitiveness and fierce ambition can verge upon ruthlessness and professional jealousies can have unfortunate consequences.
past differences between professional colleagues can come to the surface when it comes to appointments and personality clashes can get in the way, so there is an
Difficult situations are caused by a breakdown in the relationship between professional colleagues. But these can be avoided through scrupulous adherence to basic ethical principles
immediate care to those in the wider community.
If you see or hear something that leads you to believe that patients could be placed at risk or the quality of their care compromised by the actions or performance of a colleague, then you have an ethical duty to take reasonable and appropriate steps. this would mean raising concerns with the colleague directly as a means of finding out more. Your colleague might need support and to ignore your ability to offer such support would be unethical. Medical associations and medical defence organisations can be useful sources of advice in these circumstances.
It is unwise to act upon ‘hearsay’ rumours about a professional colleague or to jump to conclusions without trying to find out both sides of the story.
essential need to adhere to good medical practice.
extreme care should be taken to separate facts from personal opinions and recognise situations where you might be biased, especially if you stand to gain personally from expressing a particular view.
try to keep any comments objective and proportional to the context in which your views are being sought.
It is unworthy and unethical to deliberately disseminate adverse information about a professional colleague, even if true, if the purpose of doing so is vexatious or self-serving.
In this context, it is wrong to abuse your position of authority as a referee by giving a biased reference that can affect the progress of your colleague. and, of course, it is also wrong to use an authoritative position – be it on a college, association or society – to give your own views about an individual that can affect the role of the individual in their workplace.
Raising concerns
a s part of your professional responsibility, your first duty is to the patient, and this extends beyond patients under your
Dealing with a problem yourself at a lower level, however difficult and awkward at the time, can prevent it from escalating. alternatively, you may have to report your concerns to other colleagues or a higher authority. It is best to take advice as to how best to manage the situation. the way in which concerns are raised has an important ethical dimension. It is not difficult to distinguish a genuine concern to protect patients while trying to support a professional colleague from a vexatious attempt to cause problems for a colleague.
Difficult situations are caused by a breakdown in the relationship between professional colleagues. But these can be avoided through scrupulous adherence to basic ethical principles.
Where conflicts do arise, every effort should be made to contain them in a manner which maintains the continuity and quality of patient care and avoids placing patients at risk.
It is really important to maintain public confidence in the profession and avoid bringing the medical profession into disrepute. treat professional colleagues as you would wish to be treated yourself. n
For an introductory discussion, please call Peter Goddard on +44 (0)203 356 9699 or mobile +44 (0)780 314 4954 www.worldwidehealthcare.co.uk For the last 18 years, we have been helping healthcare organisations manage and transform their operations, both in the UK and abroad.
We exist to help independent practitioners start, transform and grow their practices and businesses. We help to plan and develop medical facilities and to market healthcare services using all available communications channels and technologies. While you concentrate on caring for patients, we aim to take away the burden of managing your practice or business.
We build unique teams for every situation and change that team as your needs change and, uniquely, we have experts who can deal with crises who are available 24x7. We combine clinical expertise with commercial sense; we see the full picture and we provide support when and where it’s needed most.
We work with both public and private sector healthcare providers, and we have an enviable track record in operations management, clinical advice, consultancy and development.
ACCOUNTANT’S CLINIC: TAx RETURNS
Many happy returns
Susan Hutter (right) provides some tips on speeding up and smoothing out the process of filing your tax return
Few private consultants and Gps enjoy the process of gathering information for their tax returns and accounts preparation. But, the longer one leaves the process, the worse it gets. For those who file tax returns after the deadline date, there are some nasty fines and penalties levied by HM revenue and Customs.
Filing dates
the tax return for 2014-15, covering the year to 5 april 2015, has to be filed by 31 January 2016. i f not, a late filing penalty of £100 will be levied and if the return is more than three months late, taxpayers are charged £10 for each day. Beyond this, the fines only get worse.
Document gathering
During and after the end of the tax year, most independent practitioners will receive a number of documents that are required for their personal tax return preparation, for example:
✎ a Form p 60 for their NHS appointment, if they are a consultant. this is a summary of salary and tax deducted;
✎ For those that trade as a limited company, a p 60 from that company;
✎ Dividend vouchers, such as from their own company or shareholdings in quoted companies;
✎ Bank and building society certificates of interest received. it is a good idea to use the previous year’s tax return as a check list and, as and when the documents come in, tick them off. remember to update the checklist for any changes since the previous tax year; for example, new
bank or building society accounts.
Not all banks and building societies send interest certificates automatically and therefore will need to be contacted in order to request the interest details.
it goes without saying that all documentation received throughout the tax year should be filed in sensible order so that you can lay your hands on it easily when requested by your accountant.
Practice accounts
Doctors who have a private practice income as self-employed will need to gather together all details of income and expenditure in this connection.
instead of waiting until the end of the tax year, it is a better idea to write up the practice’s books and records on a regular basis, at least quarterly and preferably monthly.
t he practice accountant will need to know the following information about ‘cut-off’:
Monies owed to the practice at the end of the financial year regarding work carried out during
the year, whether or not it was invoiced in the year;
Details of any bad debts: for instance, where a patient or insurance company is unlikely to pay;
Details of any practice expenditure incurred but not paid for by the end of the tax year.
i t is advisable to prepare the above information as soon as possible after the year-end date, as it becomes increasingly difficult to deal with this after a long time lapse.
the more orderly the presentation of the records to your accountant, the less costly it will be in fee terms, but also your accountant will be able to turn around the work far more efficiently and quickly than if you just provide them with the source documentation.
Consultants who trade as a limited company will need to ensure that the practice accountant has full information regarding dividends and salary drawn from the company in the tax year. this may not be the same as the
As soul destroying as the task is, organisation is the key to success and the sooner you deal with matters after the end of the tax year, the better
company’s year-end date. Once again, it is advisable to keep the company’s books and records up to date on a regular basis so that it is quite easy for you to obtain this information.
it is worth discussing the whole procedure with your accountant, as they will be able to advise you on the most streamlined way of presenting the information to them and when they will require it.
Most accountants are generally quiet during the summer months and therefore would be able to provide a quick turnaround if you get the information to them during that time.
Usually accountants prefer it if everything is sent at once. However, for doctors with practice accounts, ask your accountants if they want that information first. then work on investment and other income so that this can be provided to the accountant hot on the heels of the accounts information.
as soul destroying as the task is, organisation is the key to success and the sooner you deal with matters after the end of the tax year, the better.
Susan Hutter is a partner at specialist medical accountants Shelley Stock Hutter
is continuously updated based on the latest medical research to bring you current evidence-based recommendations.
Our unparalleled team of physicians and editors places new research in the context of the existing body of medical knowledge using their professional expertise and first-hand clinical experience.
This combination of Evidence & Experience is invaluable in crafting point-of-care recommendations trusted by more than one million clinicians worldwide.
Plus, you may earn RCGP CPD learning credits while researching topics in UpToDate.
Emulate a theme park experience. . .
. . . but don’t be a Mickey Mouse outfit. In the seventh of her essential series for doctors in the aesthetics world, Pam Underdown reveals how to create a compelling patient experience – and watch your profits grow overnight
DiD you know: The No.1 reason patients will leave your clinic is not because of a bad result? it will be because of ‘perceived indifference’; meaning they didn’t feel valued, so they don’t feel compelled to return.
So the key is to make sure your patients feel special, valued and appreciated by creating a compelling patient experience. The more special they feel being around you, your staff and your clinic, the more likely they are to pay, stay and refer.
So, how do you create a compelling patient experience? We already know that today’s aesthetic patient is a fickle consumer. The patient who wants cosmetic procedures is engulfed in emotions.
They are uncomfortable about a physical aspect they want rejuvenated, enhanced or removed and that leads to vulnerability. They are most likely confused about what to do and who should do it. When they call your clinic and visit you in person, they expect a good patient experience every time.
Have you ever been in a restaurant where you could feel the cohesiveness? i t felt like a welloiled machine. Almost like a play where everyone was on their mark and every step was running smoothly.
Theme park effect
What about the most famous theme parks in the world? isn’t it amazing that nearly everyone who attends a Disney theme park comes away with a good feeling about the visit? Many will wait in a queue for an hour in the heat and humidity yet feel that they have had a good experience or certainly got their money’s worth. There is, indeed, magic in the Magic Kingdom. That magic can be transferred to the clinic of medicine and the delivery of medical aesthetic services and procedures.
Wouldn’t it be a nice goal or objective that everyone that left your clinic would have the same feeling of a positive experience as when they leave a Disney theme park?
Many of the Disney methods of motivating employees and satisfying the guests are not Mickey Mouse. They are great for the good for the guests, the employ-
ees, their families and the entire community.
Why not do the same for your own clinic? Let’s look at some of the similarities between the aesthetics marketplace and a Disney theme park.
The common denominator is that both organisations have paying ‘guests’. These guests expect to pay large entrance fees and therefore have high expectations of the service and the outcome of their experience.
How any business can live up to the expectations of their ‘guests’ will determine their satisfaction, their image in the marketplace and, ultimately, their overall business success.
Magic moments
Disney has recognised that there are critical ‘magic moments’ or ‘moments of truth’ where the guests have contact with the employees and the ‘Disney mystique’. Disney has made an effort to clearly identify these magic moments.
The Disney organisation estimates that there are an average of 74 contacts per day between a single guest and the employees on the front line. These are contacts where Disney has an opportunity to create a positive impression on the guest and to make sure his experience is a favourable one. Disney definitely understands that you seldom get a second chance to make a good first impression.
in the aesthetics marketplace a similar attitude as Disney’s should be adopted towards patients (guests).
When the ‘magic moments of truth’ are identified, you can anticipate that the patients will leave with their expectations having been met. When you place a priority of managing the ‘magic moments’, you can expect to exceed the patient’s expectations. i t is then that the patients will have a positive feeling about the delivery of their procedure and the aesthetics market in general.
Study the magic moments where the ‘guest’ has contact and passes judgement on your business. Do this regularly, with a fresh perspective each ➱ p14
time. Make sure you ‘mystery shop’ your own clinic regularly. you are in the business of providing cosmetic treatments. But you are also in the first impression business and you have to create positive impressions. Start with your reception area, treatment rooms and bathrooms as well your desk and office.
Make sure every area reflects your attention to detail and your ability to be organised and efficient.
show appreciation
What do you do to show your patients that you appreciate them? After all, there are probably several other medical aesthetic businesses in your town or city who do what you do.
Do you show the patients who choose to have their procedures with you that you value and appreciate their business? Feeling appreciated is an experience that is universally meaningful.
you could invite special patients to experience a Special offer Day earlier than the general public or you could have an invitation-only event one evening and give ViPs an additional X per cent discount. o r you could gift-wrap their retail purchases or periodically give them for free that favourite face cream they often buy. Always make sure that you let them know that you are extending this exclusive offer to them because they are a valued patient and you want to show them that you appreciate them.
Focus on attentiveness to ensure you and your team become ‘masters of detail’. your team are your eyes and ears, so train them to notice and when it is appropriate to act on even the smallest pieces of information they observe or discover about a patient. if you know it’s their birthday, make sure you send a personalised birthday card – and voucher, if
possible – but also extend birthday wishes in person when you see them.
And if a staff member overhears a conversation in which one of your patients mentions they either like or dislike something, remember that within minutes, anyone who might come into contact with that patient knows about it. So make sure they only say good things about your business and the service they received.
Recognition is essential
Greeting your patient by name is a very meaningful and treasured detail that adds greatly to the way they experience doing business with you.
your receptionist should make sure she knows just who will be walking in the door next, and immediately greet them with eye contact and their name. There is nothing more flattering and there is nothing that makes someone
feel more special than receiving a warm, friendly greeting by name when walking into a place of business.
Whenever i speak to aesthetic professionals, they inevitably tell me ‘ i just want to make my patients happy’. Then i ask them what they are doing to make them happy.
i’m told they give them a good result, their staff phone them to follow up to find out how their results are and they send out email newsletters and special offers periodically. And that’s about it.
But let me ask you this: Would you ask a member of your team to phone your partner/spouse to ask them how they are today? you wouldn’t? Why not? Because it’s impersonal.
you have a relationship with your spouse and you need to keep in touch personally. The same thing is true for your high-spend
You have a relationship with your spouse and you need to keep in touch personally. The same thing is true for your high-spend patients
patients. i f you want them to return and refer, they have to feel cared for and cared about.
i f you go the extra mile, that alone builds mountains of patient loyalty because they’ll remember and tell their friends how caring you are.
Little things
Anyone can do the big things right; it’s the little things that differentiate one business from another and that influence patients to choose one over the other.
o ften, small-business owners cut out the little details when times get tough, and this is a big mistake.
next issue: how to convert your website visitors into paying patients
Attentiveness and recognition cost nothing, nor do personalisation and consideration. it is often the little details that patients recall even more than the product they purchased or the service they received.
Little details that patients
notice and that makes them feel good about not only making the purchase, but making the purchase from you, is a significant part of the overall patient experience. Remember your own personal experiences and how they made you feel – good or bad. your aesthetic patients need more compelling reasons to invest in aesthetics, so, now more than ever, give them those reasons.
Educate them on little things they can do right now to look fantastic. Motivate them to act now with a special offer and a tight expiration date.
Encourage them to refer their friends so they too, can look fabulous. A compelling patient experience means more engaged patients, spending more money more frequently and bringing their friends.
Pam Underdown (left) is chief executive at Aesthetic Business Transformations
An independent firm offering one to one meetings anywhere in the UK giving advice and help with:
• how to start in private practice
• how to maximise private practice income
• ways to reduce tax payments
• setting up in Chambers/Groups
• limited companies and LLP’s
• financial planning
• record keeping
• computer software
• tax and financial advice re: car purchases
• pensions: NHS, personal and employee schemes
• purchase of consulting rooms and surgeries
• inheritance tax and capital gains tax planning
• VAT
For more information please contact us by: Wilmslow
Phone: 01625 527351
Fax: 01625 539315
Harley Street
Phone: 020 7307 8759
Fax: 01625 539315
Email: info@sandisoneasson.co.uk
Website: www.sandisoneasson.co.uk
Close encounters with the meeja
Doctor in the (broadcasting) house fixer Tingy Simoes (right) shares the good, bad and the ugly of trying to help private doctors get valuable media exposure
One O f my most memorable days – despite the therapy required to try and forget it –involved some interviews I set up with a plastic surgeon. f amed for his common-sense pronouncements, I chanced putting him in front of a newspaper journalist to explore the latest aesthetic trends. When asked about a brand of jeans that claimed to eliminate cellulite, he rolled his eyes and groaned ‘God, why don’t women just go to the gym?’
While I was busy breathing into a paper bag, the reporter then asked about a supposed trend in toe-reshaping for women who desired svelte feet that fit into strappy ‘Sex and the City’ heels. ‘I thought that trend died out in China a thousand years ago,’ he snapped.
Outspoken, in some measure, can be good, as there’s definitely too much spin out there. I realise this observation, coming from a PR, may appear paradoxical, but no-nonsense can be refreshing to journalists used to the polished question-dodging typical of politicians. While the above example is an extreme, many will appreciate the plastic surgeon’s full and frank ripostes.
Hyper-specialised healthcare
While on the subject of foot-binding (well, orthopaedic) woes, when my recent story about Morton’s n euroma ( Independent Practitioner Today , September 2015, page 38) hit the press, I was asked by a BBC Radio 4 programme for experts to comment on the disorder.
Unfortunately, the main author of the research was abroad, so I spent a traumatising afternoon trying to locate a trauma and orthopaedics specialist willing to participate.
When they say healthcare is becoming hyper-specialised, they aren’t kidding. My first possible candidate sniffed ‘I don’t do feet’; for the following spokesperson only knees would do; the next just concentrated on the left elbow; another mainly dealt with the second knuckle of the ring finger . . . you get the idea.
I finally located one who didn’t turn his nose up at the subject –but he didn’t agree with the research. In desperation, I gave Radio 4 a couple of phone numbers and started planning how to fake my own death.
Yet it’s not unreasonable to stick to what you know. You wouldn’t have a cardiologist talking about hip replacements, just like you wouldn’t have an en T talking about boob jobs. But maybe, with all the hoopla around credentialing, we also need media ‘badging’?
Avoid arrogance
Due to another story appearing in the news one morning, I was forced to work my way through more than a dozen hand surgeons (That sounds wrong, but you get my drift).
One after the other I rang. One after the other demanded precisely the exact same thing: ‘Whom else did you ask?’ I’d rattle off a list of names, and one after the other they jeered: ‘Ha! Those people know nothing. I am the only person who is qualified to comment on this. However, I am currently on holiday – please inform the media I’m back next Tuesday.’
‘I’ll make sure to tell them,’ I mumbled, rolling my eyes so hard I nearly fell off my chair. In my time in healthcare PR (close to 20 years), I’ve dealt with every stereotype: the harried GP, the cuddly paediatrician, the rugby-playing orthopod, the well-
turned-out plastic surgeon. These are all easy typecasts and, as such, can be cheap pigeonholes. However, academic research has shown that medical and surgical disciplines do have at least some specific characteristics. Whether they wildly differ from the general population is still unclear. According to PubMed – my Google – the consensus seems to be that both surgeons and physicians tend to score at similar degrees of openness and low levels of neuroticism (ahem). Surgeons score higher in competitiveness (no, really?) and extroversion; physicians higher in agreeableness.
Media-friendly specialties
Yet do these supposed features hold true in private practice? My exposure as a publicist dealing with clinicians over the last two decades has at least allowed me to garner plenty of fodder in one area: how they deal with the media.
So when faced with journalists, do our medics resemble the cantankerous Lancelot Spratt or the caring Dr finlay? Hugh Laurie’s misanthropic House or Martin Clunes’s vascular surgeon-turnedGP Doc Martin? George Clooney’s Dr Ross in ER (a girl can dream) or the coldly ambitious cardio trainee Cristina Yang of Grey’s Anatomy?
The recent #ILookLikeASurgeon campaign made waves on Twitter (check it out in the BMJ if you’ve been living under a rock), demonstrating it’s impossible to encompass what any clinical specialty is ‘meant’ to be or look like.
However, I can, with confidence gathered from experience, posit the theory that the vast majority of clinicians – with few exceptions like the handful of smoothtalkin’ celeb docs we see on the telly – are unused to the requirements and frankly unglamorous realities of dealing with the press .
The intrusion of media interest into the sacrosanctity of consulting and operating rooms is a relatively new phenomenon. Some of it is to be expected in a post-Staffordshire/PIP breast implant/outcome publishing controversy world, but the relationship between private practitioners and mainstream journalists is still in its toddler years.
When it works, it’s a heavenly union: journalists, and by extension the public, need you. They need illumination, explanation, opinion in this fast-paced and confusing – sometimes conflicting – world of health news.
• Completely open scanner that is well tolerated by claustrophobic patients
• Weight-bearing scans for spine and joints enable a more precise diagnosis
• Patients who are large or cannot lie down can be accommodated
The quirks of this bumbling courtship (both have so much to gain from each other, you see) offer fertile ground for either damaging or hilarious gaffes, which is also the reason I probably need to be on beta-blockers.
You as clinicians and the media have a beautiful gift to offer each other and that is to demystify science, promote safety and standards, educate people and make the profession look good, even if it’s just to The Sun readers – all three million of ’em.
If nothing else, I know now where to go when I next work on a story about the second knuckle of the ring finger – only of the right hand, mind.
Tingy Simoes is owner/managing director of Wavelength Marketing Communications (www.wavelengthgroup.com) and author of the firstever PR manual for doctors and surgeons: How to Cut it in the Media by CRC Press.
➥ Next issue: How to choose a PR agency or decide exactly what kind of support is needed, with practical tips and examples on finding the right mix. For more information go online at: www.mri-london.com or call 020 7370 6003 Medserena Upright MRI Centre 114a Cromwell Road, Kensington, London, SW7 4ES
Where stressed doctors
Working in medicine is demanding. With patient expectations on the rise, heavy workloads and the fear of attracting a complaint or clinical negligence claim, it is not surprising that it is impacting on some doctors’ mental well-being. Dr Pallavi Bradshaw examines the issues
Consider the following scenario: a patient presents with low mood, disturbed sleep and poor appetite.
in this case, you would have no hesitation in making the appropriate diagnosis and assessment of the patient’s mental health.
You would also direct them to the help they need with the appropriate urgency. so why can it be so difficult for some doctors to recognise this within themselves or their colleagues?
According to a recent Medical Protection survey, 75% of doctors admitted that they had suffered from stress as part of their job, while 49% had anxiety, and 32% had experienced depression.1
these figures are worrying, but what is more concerning is that 40% of doctors who had experience of mental health issues did not discuss them with anyone. Perhaps unsurprisingly, doctors can find it difficult to play the patient role.
there is such pressure on medics to be resilient and, coupled with a fear of being perceived as unable to cope, this can lead to them being in denial about the fact they may be suffering.
t he stigma associated with mental health issues often means doctors fail to seek help at the early stage of their symptoms occurring.
We reported on the Medical Protection survey of doctors in September
Another factor that may prevent doctors from opening up about mental health issues is the impact they believe their illness may have on their career.
Informing the Gmc
While 91% of doctors who responded to the Medical Protection survey would speak to their GP if they had a significant mental health issue, 55% would not feel at all confident about informing the GMC.
d octors have a professional obligation to consider the impact
their health could have on the care they provide patients, but it is important for doctors to know that, firstly, there is no requirement to inform the GMC that they have mental health issues and, secondly, if they do inform them, it will not automatically put their careers at risk.
Given that doctors might be hesitant to come forward and speak to others about their problems, how can they receive the help they need?
to begin with, colleagues can look out for one another.
Colleagues may be the first to pick up on signs of others not coping or being subdued. By providing support to those who may be vulnerable and offering them a chance to discuss their issues, colleagues can play an important role in assisting doctors who are in difficulty.
i n addition, our experience shows that because many doctors fail to identify the signs in themselves or are worried about admitting them, it can be beneficial for a colleague to raise their concerns with the medical practitioner in question.
Realising too late
i n many cases, our experience also shows that doctors tend to realise very late on in their illness that they need help, by which point it may have had an effect on their working life.
if doctors present at a late stage, they often need more than just time off from work to recuperate and they may then also come to the attention of the regulator. While the GMC process is meant to be supportive to the doctor, it can lead to a deterioration in the doctor’s mental health as highlighted in a study carried out by the GMC.2
i would urge any doctor concerned about their mental health to seek advice and support. t he
doctors can go for help
earlier help is sought, the better for both the doctor and their patients. We must challenge the remaining stigma attached to mental health and accept that there may be times when doctors are unable to manage the emotional stresses of clinical practice, which are often coupled with a poor worklife balance. d enying symptoms or hoping that they will pass is likely to be counterproductive and may lead to serious problems with employers – such as suspension or dismissal – and with the GMC and for patient care.
t here is clearly a role for colleagues to play where a doctor may lack insight and while it may be a difficult conversation to have, we owe an obligation to our fellow doctors and to patient safety to make sure we are all healthy and fit to practise.
counselling services
if doctors need emotional or clinical treatment, they can use dedicated counselling services such as the d octors for d octors service from the BMA or the nhs Practitioner h ealth Programme.
Medical Protection also offers a counselling service to its members if they are experiencing stress because of a medicolegal problem.
Prevention is always better than cure and while we may always be fighting against an ever increasing workload and patient demand, as a private practitioner you may have some control over the business of clinics and lists.
i t is also important to ensure that while you may work in relative isolation, you have colleagues with whom you can discuss any concerns or a GP whom you trust.
References
1. Medical Protection conducted a survey of members across all medical specialties, including general medicine, surgical specialties and anaesthetics, to find out their personal experiences of mental health issues. The survey ran from 18 June to 3 July 2015 and received 631 responses. 2. www.gmc-uk.org/Internal_review_ into_suicide_in_FTP_processes.pdf _59088696.pdf
Dr Pallavi Bradshaw (right) is a senior medico-legal adviser at Medical Protection t: 01992 676162 www. ppmsoftware.com/ppm e: tomhunt@ppmsoftware.com
An easy to use software system, which fully supports the clinician and office staff and makes the whole process of running a busy Practice a lot easier.
Call now for a chat and ask about a free, no obligation demonstration of our comprehensive system that has been designed to save your Practice time and money.
SUBSCRIBE BY DIRECT DEBIT AND SAVE £15
Dear Reader,
Subscribing to Independent Practitioner Today is the only way you can be sure you will see every issue. Don’t risk missing out. Our personal subscription for doctors and managers is only £85 a year and £200 for organisations. But you can cut this to just £70 and £175 respectively if you pay by direct debit.
So take advantage of this offer now for our unique business journal dedicated to supporting you in your private practice. We’re confident your subscription will repay itself many times over!
Editorial director
APPLICATION FOR SUBSCRIPTION
I encose a cheque made payable to The Independent Practitioner Ltd Please debit my Mastercard/Visa/
it’s £15 cheaper to pay by direct debit; £25 less for organisations.
Instructions to your Bank or Building Society to pay Direct Debits
Name and full address of your bank/Building Society Banks and Building Societies may not accept Direct Debit instructions for some types of account
(No
at www.independent-practitioner-today.co.uk
refund from your branch of the amount paid. You can cancel a Direct Debit at any time, by
and
IMPORTANCE OF PHONE MANNERS
Get rid of those hang-ups
Your secretary is the most important person in your practice after you, says surgeon Mr Dev Lall. So do you need to ring the changes?
IF THERE’S one thing every business owner seems to complain about, it is problems with staff: hiring, firing and especially managing them.
We’ve all had experience working in units with staff problems, and it is always miserable. People that don’t work well together, are lazy or simply not very good at their jobs makes for stress all round.
Conversely, of course, the right person in the right job makes your practice not only work smoothly and efficiently but also enjoyable, for both you and your patients.
In private practice, the most common person a consultant will employ is a private secretary/personal assistant (PA), and the person that is most commonly selected for the job is the NHS secretary. But I believe this is a big mistake.
The varied role of a PA Secretaries/PAs have very varied roles. They are almost always expected to answer calls from patients on the phone and by email, type clinic letters, file cor-
respondence, deal with calls and referrals from other clinicians, file and retrieve notes and manage your diary.
Often they are also expected to deal with invoicing and chasing up unpaid bills too, as well as a multitude of other tasks.
They are critically important to the smooth running or otherwise of your practice. Yet they are often hired with little or no thought.
The problem is that while all the tasks that a PA has to do matter, they are not of equal importance. And the most important task they have is the one that is frequently handled the worst.
That task is answering the phone. It may sound trivial, but think about it: when a private patient wants to book an appointment, what do they do? They pick up the phone.
If you are not a full-timer in private practice, then remind yourself about what you see when you walk past the open door of the secretary pool in your NHS hospital.
Often what you see is maybe four or five women bustling ➱ p24
about, chatting to each other, on the phone, being asked to do something by a junior doctor, dealing with referrals from doctors from other specialties, typing letters, filing clinic letters and so on.
Phones unanswered
It is busy and often noisy. Frequently, one or other secretary is away from her desk – getting notes, in the bathroom, at the photocopier, lunch break, cigarette break, on a day off. There is almost constantly one or more phones ringing in the background unanswered.
How often have your rung your secretary and not had the phone answered? How often have you left a message on the answer machine? And how long does it take for her to call you back? And how often have you got the answer machine and not bothered to leave a message, preferring to call back later?
How many times have NHS patients complained to you about the difficulty they had getting through to your NHS secretary?
Yes, this is the NHS. But if you ask your NHS secretary to be your private secretary, it is also what your private patients experience too.
The fact is that whenever any one of us rings an organisation of any sort, we expect it to be answered promptly and politely by someone who can help us with our query.
And, of course, when it comes to private patients, they are often much more demanding than NHS patients. This is understandably so because we are selling a pre -
mium service: access to us and our expertise. Personally.
And we specifically tell patients they won’t experience the queues, delays and other ‘hassles’ they perceive to be the lot of the NHS patient.
Annoyed patients
So what happens when a private patient rings and doesn’t get through to your secretary or leaves a message that is unanswered for X amount of time?
They get annoyed.
That’s bad enough, because you want to provide a top-class service and you haven’t done so. But worse still, if they have had a less than fantastic experience of your practice, they’re less likely to recommend you to their friends and family.
Worse still, if a new patient phones to make an appointment and is confronted by an unanswered phone, they are unlikely to leave a message. They are far more likely to hang up and ring a competitor colleague for an appointment instead.
And this is even before considering issues of politeness, education, phone manners and so on
The problem is that many NHS secretaries generally see answering the phone as an utter pain and distraction from getting their ‘real work’ done
by your secretary, which can cause a patient ringing in to want to go elsewhere. Think back to how you felt the last time you spoke to a rude or off-hand GP receptionist or shop salesperson.
Difficult circumstances
The problem is that many NHS secretaries generally see answering the phone as an utter pain and distraction from getting their ‘real work’ done.
Before talking about possible solutions, I want to make clear that the vast majority of secretaries – whether NHS or private – are doing the best they can in often difficult circumstances.
So I’d say do not employ your NHS secretary as your private secretary without a great deal of thought if you expect him/her to take calls from private patients. No matter how good and efficient they are, they won’t be able to prioritise answering your private patient inquiries. But this does not necessarily mean they can’t be employed to deal with other aspects of your private workload. This is, of course, most relevant if you’re just starting out in private practice, but not much help if you already have a private secretary. What then?
If your secretary is great at his/ her job, you should consider employing someone specifically to answer the phone and reply to patient emails.
This would free your initial secretary to spend more of her time doing what she does well. It would also allow you to select someone better suited to the task of dealing with patients on the phone. You would select that person for politeness, intelligence and manner, and train them to:
Answer the phone ideally within three rings;
Reply to calls with a script set by you;
Specify how often she should check for email queries and in that they should be replied to within two hours – or whatever;
When to escalate calls to you.
The point is that the new employee would be selected because he/she was better suited to this aspect of the job.
If your current private secretary isn’t particularly good at any aspect of her job, then you need to consider letting her go and starting again. Again, think long and hard before taking on an NHS secretary whom you also expect to do your private work.
The PA’s job is not an easy one. It is often thankless, has duties that vary day to day and they have to put up with cranky patients and cranky consultants, both of whom want XYZ done right away. Yet, despite this, they do the best they can.
It is my belief that the most important aspect of a secretary’s
I don’t like answer machines. You don’t like answer machines. And your private patients don’t like answer machines either
job is dealing with patients: specifically picking up the phone whenever it rings, replying to emails promptly and making sure that as few people as possible ever talk to the answering machine –and those few get their calls returned immediately.
Vital jobs
And because these few jobs are so critically important, they should be made the only tasks of a single person. That person should never be your NHS secretary – they simply don’t have the time to do it.
The filing, typing and everything else should be handled by someone else – your NHS secretary might be just the person.
One of the very first steps to growing your private practice is to fill the ‘holes in your bucket’ – in other words, plug the holes where you are letting income slip through your fingers.
One of the easiest ways to do this is to make sure your phone is answered each and every time, to make sure no inquiry from a private patient is missed.
I don’t like answer machines. You don’t like answer machines. And your private patients don’t like answer machines either.
Next issue: The ‘Holy Grail’ of private practice –continuity income
Mr Dev Lall (left) is an upper-GI surgeon and runs a specialist private practice consultancy. He can be found at www.PrivatePractice Expert.co.uk
A lesson in hospitality
Five-star service as standard – how seeing behind the scenes at a leading London hotel is complementing cancer care. Lucy Reynolds reports
into the five-star Landmark London hotel and you will immediately be struck by its distinctive style and ambience – the elegance of its furnishings, the deluxe facilities and the welcome that greets you.
n ot much propinquity to a cancer treatment clinic, you might think. But think again.
Leaders in oncology Care (LoC) is a specialist oncology centre, devoted to delivering innovative cancer treatments and exceptional patient care. And it saw in the Landmark Hotel a model of design and service it could emulate to help patients.
Visitors to the clinic often comment that it does not feel like a hospital at all. With its plumpcushioned couches and golden drapes, it is more like a luxury hotel. But the similarities don’t end with interior design and this is not a story of style over substance.
For the clinic runs very similarly to a hotel, too, with cancer patients being booked into the
treatment suite as they would be booked into a hotel room and drugs being made to order on site, much as a room service order for food is placed to a hotel’s kitchen. these similarities immediately struck designers who had been commissioned by L o C’s chief executive Guy Reynolds to enhance patient and staff experience at the clinic.
The user perspective the team at Uscreates specialise in applying design thinking to health and well-being services, and are always looking for new ways to understand the user’s perspective.
Co-founding director Zoë Stanton explains: ‘We had the idea of taking a group of L o C employees behind the scenes at a high-end hotel to explore the similarities and see what happens in the background to create a fivestar guest experience.
‘And it was a fantastic exercise – we had the chief executive ➱ p28
Step
The Leaders in Oncology Care treatment suite and front entrance in Harley Street
there, clinicians, nurses, treatment suite co-ordinators, receptionists – the whole team; and you could see ideas like light bulbs going off from the second we stepped through the door.’
Having shadowed LoC patients and staff for the preceding fortnight, the designers had already worked with the clinic’s team to identify three areas to trial rapid improvements:
1
2
Scheduling appointments;
Streamlining communications through reception;
3 Further optimising pharmacy services.
So, on arriving at the hotel, the LoC group was divided into these three ‘task teams’. each one was met by a Landmark London employee, and guided to whichever part of the hotel best reflected what the LoC team did at the clinic.
scheduling
appointments
the ‘scheduling’ group was met by the hotel’s event sales manager, Leah Rose-Davis. LoC’s head of clinical services Marcella o ’Brien says: ‘We were shown how the hotel’s bookings team use telephone guidelines for all of their conversations with guests –all of the staff follow these guide-
lines so that guests get the same information every time and any team member can carry out this conversation.’
What also captured the group’s imagination was the way in which guests’ stays were logged onto the system, to anticipate check-in and check-out times.
Ms Rose-Davis explains: ‘We capture as much information about a stay as possible, so we know that, if a guest is here for business and has a 7am flight, they are likely to check out early, allowing the room to be made up for the next arrival.
‘ o r if a guest is staying for a birthday break, they’ll probably take a slower pace, so we assume a later check-out for that room. By predicting how long guests might stay, we’re able to manage our rooms very efficiently.’
t he team was struck by this approach. Ms o’Brien recalls: ‘We were immediately thinking of how we could do things in the clinic. After we’d seen how the booking team worked, the ‘scheduling’ group came back together for a brainstorm and came up with lots of ideas.’
Several of these underwent rapid testing at the clinic in subsequent weeks and have now been adopted.
taking the idea of using ‘scripts’ from the booking team, the LoC has developed its own script. this enables treatment suite co-ordinators – who manage patient flow through the chemotherapy suite – to phone patients the day before they receive Herceptin treatment to check they are oK and still able to attend their appointment.
this means that patients receive clear information in advance of treatment, without a clinician having to run through these checks on the day of the appointment.
saving clinicians time the estimated saving of clinician time is one hour per treatment.
With the clinic running 1,364 Herceptin cycles a year (2014 data), this amounts to a saving of two days a week of patient time in the chair and one nursing shift a week freed up for other patient care.
Following their time with the hotel bookings team, the scheduling group also identified that they did not currently capture data on patient time in treatment.
LoC’s head of business intelligence Steve Rumbles says: ‘We wanted to know how long patients were spending in the treatment chair, so that we could baseline this to measure improvements and so that we could schedule
bookings more accurately – like hotel rooms.’
t wo approaches were rapid tested for a week. t he first involved sticking a piece of paper to the wall and asking nurses to log when patients arrived for and left treatment.
After a week, the piece of paper was pretty empty, so the prototype was deemed unsuccessful. t he second prototype involved treatment suite co-ordinators logging patient arrival and departure times on the M o SA i Q patient information management system. one week into the trial, 40% of patient episodes had been logged accurately, compared to 0% previously, and this data is now being comprehensively collected as standard to build a clear picture of patient treatment times and support accurate appointment scheduling.
Welcoming guests t he ‘reception’ task group was collected by the hotel’s guest experience manager Gautier Colin and taken to the check-in desk.
there they were walked through the whole journey for each customer and shown the customer relationship management system used to log this.
The interior of the Leaders in Oncology Care clinic and its chief executive Guy Reynolds (inset)
Luxury lessons: the north
He told them: ‘Whenever a guest checks in or phones to make a reservation, we capture detailed information, including a photo, so that we can build a guest profile. t his means that we know their likes and dislikes
‘But the photo-bank also means that all of our team, from porters and cleaners through to managers, can greet each guest by their first name when they see them.’
L o C receptionist George Crispin recalls: ‘this was another revelation. Cancer treatment is extremely stressful, and feeling that you’re with people who know you well makes a huge difference.
‘We thought: “Wouldn’t it be amazing if our clinic reception and the treatment suite could identify patients when they arrived, and greet them by first name from the reception area?”.’
And exactly this approach is now underway at the clinic. After interviewing 72 patients to see if they would be happy to build a staff and patient photo-bank, over 90% said ‘yes’, so work is now in train to photograph patients on arrival.
it is hoped the resulting photobank will enable a culture of familiarity to grow, meaning that patients and their families feel
supported and cared for as indi viduals.
t he ‘reception’ team has also put forward a business case for introducing an electronic switch board akin to that at t he Land mark London.
this will handle the huge num ber of calls currently processed by reception staff daily, ensuring that phone calls are always dealt with promptly and streamed to the right place, while freeing up valuable time for receptionists to interact face to face with patients without being interrupted by the phone.
t he switchboard will save an estimated 2.5 hours a day of receptionist time (625 hours a year) to re-invest in patient care.
pharmacy improvements
the pharmacy group was guided by food and beverage training manager Anna napora to one of the hotel’s restaurants.
Here she explained how the hotel deals with numerous food orders among multiple restau rants.
She talked the group through the electronic system, and the preparation and communication processes, which enable the right food to arrive with the right ➱ p30
north reception area at The Landmark Hotel
guests at the right time – while still remaining hot.
L o C clinical marketing manager nicole elliott says: ‘We have a pharmacy on site at 95 Harley Street, where each patient’s treatment is individually prepared according to their needs. it’s just like having a restaurant, really –the pharmacy has to make lots of different prescriptions from scratch, for lots of different patients.
‘From the time a nurse places an order, pharmacy has 45 minutes to turn it around. it has to get the right drug to the right patient in time, just like room service.’
the impact of seeing the hotel kitchen in operation had a remarkable effect. After a tour and presentation from Anna, the LoC group thrust themselves into a brainstorm about possible ways to streamline the drug-making process in the clinic.
Again, a rapid testing of these ideas was carried out in the following weeks, and two of the ideas inspired by the hotel have led to permanent changes.
For a top hotel kitchen to run like clockwork, a lot of preparation work is undertaken in advance. For instance, potato
chips are hand cut in the morning to enable them to be cooked quickly on demand.
Using the same principle, the LoC pharmacy has now started to pre-make the drug paclitaxel the night before a patient’s visit to the clinic.
pre-prepared drugs
this is ideal for pre-fabrication, as the dosage a patient receives tends not to change from week to week once treatment commences. pre-fabrication of the treatment means that, as soon as the patient arrives, the drugs are ready to go.
t he initiative is working well with a noticeable difference in turnaround time, reduced phone calls between nurses and pharmacy to check on drug development and minimal wastage due to the predictable dosage throughout treatment.
Based on these strong results, the pharmacy is now pre-making all treatments, where possible. t he only treatments which are not currently being pre-made are those involving very high-cost drugs or those which are based on current body weight and require the patient to be weighed before the drug is manufactured.
t he pharmacy team has also used the idea of the kitchen’s electronic order tracking system to enhance communication across the team.
i t already used an electronic dashboard to monitor drug manufacture against the 45-minute window, but the nursing team did not have sight of this information so had to phone the pharmacy to check on progress.
to address this, a shared dashboard has now been trialed, which gives nurses access to the pharmacy dashboard so they can monitor drugs as they are being prepared.
this has reduced the number of phone calls to the pharmacist,
meaning fewer interruptions and less stress. And it has created better teamwork by giving nurses a clearer understanding of the timings of chemotherapy manufacture.
Further enhancements to the prototype are now underway to replace the excel spreadsheet format with a more ‘real time’ tracking system, and ensure the dashboard is located somewhere that is convenient for nurses to monitor – just as the Landmark London’s waiting staff can see the progress of a food order while they are serving tables.
Some of the most powerful principles from this work have been related to design – service design,
Quality treatment: the hotel’s stunning courtyard – the Winter Garden
rather than interior design. this is not about opulent bowls of fruit or lavish curtains, but about the key principles of people-focused design solutions.
Leaders in oncology care
L o C is a specialist cancer treatment centre set up by four leading consultants in 2005 devoted to delivering innovative cancer treatments, exceptional patient care and a unique, individual patient experience.
A spokesman told Independent Practitioner Today: ‘At the heart of how we operate is a belief in treating people in a very personal way, with consideration and respect taking into account particular circumstances of their lives.
‘Supporting the whole patient has been a distinguishing feature of LoC and we strive to ensure continual patient support before, during and beyond cancer treatment.
‘ e xcellence is standard at the
LoC, but we’re always striving for perfection. to support our mission to be the very best, we engaged Uscreates to listen to our staff and patients, to identify areas where we might improve; and to jointly create solutions to:
Achieve best of class in patient experience;
Foster a first-rate working environment for staff;
Deliver the most efficient services possible.
‘A six-step process was undertaken, centred around the principle of ‘rapid results’, where prototypes are tried and tested quickly in situ before being developed into full interventions:
1
Listening, shadowing, learning – talking to people, observing practice and reviewing information;
2 Behind-the-scenes workshop in the Landmark London
hotel – looking for service similarities and innovative improvement ideas;
3
Designing prototype improvements – three ‘task force’ teams looking for quick wins in: Streamlining L o C’s reception process;
Scheduling appointments more smartly;
o ptimising communications with the on-site pharmacy.
4
Rapid testing of prototypes in situ – to quickly see which ideas would or would not work;
5
Selecting prototypes to run with – planning implementation for the long term, with chief executive endorsement and support for change;
6
Monitoring what is working and how we are excelling –regular impact and evaluation
reports, with designated leads for each initiative.
‘this work has led to significant transformation on the ground.’
The Landmark London hotel t he five-star Landmark London ranks among the finest of the capital’s leading luxury hotels.
A spokesman said: ‘our luxury hotel combines classic British elegance and grandeur with the deluxe facilities required by today’s discerning travellers, such as hotel conference rooms, fantastic restaurants and bars, and a luxurious spa andhealth club with a 15 metre swimming pool and a gymnasium.
‘We continually strive to ensure that we not only meet our guests’ expectations, but that we exceed them. We take pride in offering the highest level of service to ensure that we continue to be one of the leading five-star hotels in London.’
Spies in the room
The idea of a patient secretly recording a consultation is likely to leave a practitioner feeling shocked, uncomfortable or even threatened. However, it may come as a surprise to some doctors that the law offers little or no protection from patients covertly recording consultations. Dr Mary Peddie (right) reports
The I n CR e ASI n G use of smartphones and other devices makes it easier for patients wishing to make an audio – or in some cases a video – recording of a medical appointment with their doctor.
We have encountered calls from distressed members who have dis-
covered a consultation had been covertly recorded by the patient.
While it may be unsettling to discover that a patient has secretly recorded your conversation, the reality is that there is no legal provision to stop them from doing so.
The situation in the private sec-
tor is no different from nhS practice and private doctors who find themselves in this situation should avoid defensive or kneejerk reactions and simply accept that the prospect of covert recording by a patient is a product of the digital age.
MDDUS has received a growing number of calls on the subject and many of these are from doctors who are either aware of a patient covertly recording their conversation or, in some instances, simply suspect that they have been recorded.
Recent examples of calls we received include:
Patients who have covertly recorded numerous consultations;
Patients who have secretly recorded a discussion with practice staff at reception;
Doctors who have approached a patient they suspect of recording a consultation, only for the patient to deny doing so – despite it being a patient’s right to record the consultation;
Doctors wanting to know if they can refuse a patient’s request to record the consultation;
Doctors who have threatened to remove patients who have covertly recorded a consultation.
Patients’ right to record
Some doctors are surprised to hear that patients are within their rights to record a consultation. For patients do not need a doctor’s consent to record the consultation, as information in a recording does not specifically attract the protection of section 36 of the Data Protection Act.
This says: ‘Personal data processed by an individual only for the purposes of that individual’s personal family or household affairs (including recreational purposes) are exempt from data protection principles.’
This only applies if the personal data is used for domestic purposes – the private use of the patient. n one of the data protection principles apply to covert recording of a doctor’s appointment, nor do any of the rights which the DPA gives to data subjects, including the right to be notified that such recording is taking place.
Despite it being legal, practitioners may believe that recording consultations is intrusive, shows a lack of trust and is damaging to the doctor/patient relationship.
h owever, patients not only have the right to record a consultation, but they can then use the information obtained as they choose, provided they stay within the domestic/recreational scope.
A doctor’s initial thought may be that the patient will try to use the recording to challenge them and, while this may be the case in some instances, it is our experience that the majority of record-
Facts anD tiPs
Doctors should avoid defensive or knee-jerk reactions upon discovering covert recordings
Knowing the consultation is being recorded should not impact on delivery of care
Patients have the right to record a consultation and don’t need the doctor’s permission
Patients can use the information from the recording as they wish
Discuss reasons for recording consultation with the patient
Practitioners acting professionally have nothing to fear from a recording
there will be occasions when a dissatisfied patient uses a recording to pursue a complaint or claim, as – even if obtained covertly – recordings can be admissible evidence in court
ings support the actions of the doctor and confirm that they acted in an appropriate manner, both personally and clinically.
Of course, there will be occasions when a dissatisfied patient uses a recording to pursue a complaint or claim, as – even if obtained covertly – recordings can be admissible evidence in court.
Common courtesy
In an ideal world, patients would not feel the need to covertly record a consultation and would be open about it. however, doctors should not necessarily feel threatened when they become aware of a recording.
Sometimes a patient may inform the doctor of their intentions as a common courtesy. This scenario would enable the doctor and patient to discuss the patient’s reasons for wanting to record the consultation.
Indeed, a recording may be helpful in avoiding misunderstandings. We are all aware that patients often do not understand a doctor’s best attempts at explanations in layman’s terms. It is worth considering whether there may be a genuine and positive reason for the patient recording the appointment in the first instance.
Doctors should discuss these
reasons, as the patient may not feel confident of remembering or fully understanding complex instructions from their doctor or they may wish to share the information with their family to help them reach a decision on treatment options.
Knowing that a consultation is being recorded should not have any impact on how doctors deliver care. Practitioners acting professionally should have nothing to fear from an audio or video recording, covert or otherwise.
But this will be no substitute for keeping clear, comprehensive and accurate written records of consultations, which will help protect them if the patient attempts to use the recording to support a complaint.
Turning the tables
So what about turning the tables and recording patient consultations?
GMC guidance Making and using visual and audio recordings of patients is clear on the responsibilities of doctors wishing to record patient consultations for any reason.
Consent must be obtained and any recording must be treated with the same level of confidentiality as a written record.
The guidance states: ‘You must get the patient’s consent to make a recording that forms part of the investigation or treatment of a condition, or contributes to the patient’s care. You should explain to the patients why a recording would assist their care, what form the recording will take and that it will be stored securely.’
The only caveat to this is where covert recoding is deemed necessary for child protection issues. For example, where there are grounds to suspect that a child is being harmed by a patient or carer.
In such cases, it would be advisable to seek advice from your defence body prior to any recording being made. This is because covert recordings will fall within the scope of the Regulation of Investigatory Powers Act 2000 and, in most circumstances, should be carried out by the police with an appropriate warrant.
Dr Mary Peddie is a medical adviser for MDDUS
Cover: a mounting headache
Lawyer Bertie
Leigh describes the way in which the increasingly complex world of indemnity insurance contains problems that, he argues, may threaten the stability of many independent practitioners’
state of mind
There can be few more frightening events in the professional life of a doctor than to receive a letter from a solicitor proposing to bring an action for compensation from a patient alleging negligence.
The recipient should know that this probably heralds the start of an arduous form of mid-career audit. If things go badly, there may be public humiliation ahead.
This claim could be followed by a complaint to the GMc that may end the doctor’s career. The days have long past when substandard clinical practice was assumed to be something that would be sorted out, often behind closed doors, between the patient’s lawyers and those acting for the doctor’s indemnifiers.
One thing that the recipient of such a letter is unlikely to worry about is whether this letter poses a threat to his or her own financial well-being. a n indemnified doctor feels comfort in his insur-
ance cover and is not likely to think that an adverse judgment against him will require him to put the house on the market and take the children out of private schools.
Huge liabilities
Indeed, in the nh S, that is still the case. There is no likelihood that the indemnifier, the nh S Litigation a uthority ( nh SL a ), will not indemnify the trust that employs the doctor and it is vanishingly rare for a single case of
The tail of the NHS Litigation Authority’s future liabilities is supposed to be £26bn
negligence to threaten the doctor’s future employment, unless it is through the agency of the GMc h owever, the days have long past when other indemnifiers have treated individual claims as part of life’s rich tapestry.
The scale of modern claims is now extraordinary. The tail of nh SL a future liabilities is supposed to be £26bn. If it were shared among the 200,000 doctors, it would come to more than £130,000 for each.
headache for many
If we allow that obstetricians have 20 times the average exposure, you can see that each of them would need to have provided well over £2m for their own liabilities.
The old system in which the medical profession managed the problem through a pay-as-you-go mutual fund could not have survived the modern inflation in damages for obstetric cases, in which we have seen a recent case attract an award of £14.5m.
Indeed, in 1990 when the then government took over all the hospital liabilities, the total sum that it accepted from the MDU in respect of its historical tale of liabilities, including those future claims that had been incurred but not reported, amounted to about the same as was awarded in this case this year of James robshaw v. Lincoln c ounty h ospital – the 12-year-old boy left catastrophically disabled by being starved of oxygen during his birth.
Profoundly disturbing
There have been a number of results of this process of adjustment that are profoundly disturbing for practitioners.
First and foremost, any doctor in private practice or general practice who is the victim of a very large award will have to justify his continued membership of the medical defence organisation. It is not unknown for practitioners to see their subscriptions doubled to figures in excess of £250,000. It is routine for their continued membership to be scrutinised by a committee and for some of them to be asked to take their business elsewhere. Finding another indemnifier may not be easy on the basis of an adverse record. e ven those who are brave enough to ‘go bare’ are not free to do so. a failure to hold appropriate indemnity sufficient to protect your patients is a breach of the GMc’s guidance in
Any doctor who is the victim of a very large award will have to justify his continued membership of the medical defence organisation
Good Medical Practice and so means that the doctor may be found guilty of serious professional misconduct simply by continuing to practise.
One of the reasons why conventional cover with the medical defence organisations is so expensive is because it is based on occurrences during the period rather than claims made.
If you are a member of the MDU, the MPS or the MDDUS on a conventional basis, then any event that happens during the period of benefit will be covered by them, even if the claim is made 20 or 30 years hence.
Unviable system
By then, damages may have inflated ten-fold as they have since 1990. It is a daunting prospect that the equivalent of this year’s case of r obshaw, which attracted £14.5m, might in 2040 attract an award of £140m.
Given that there is in reality no limitation law to protect practitioners and their indemnifiers in cases of significant brain damage, such a threat is not purely theoretical and unless something is done to control the level of damages awarded, the present system simply will not be viable.
Many doctors are quitting the defence organisations in favour of lower-price cover from insurance companies that pay damages on a claims-made basis.
It is much easier to write such insurance because if you are only covering the practitioner in respect of claims made during the next 12 months, you have a pretty clear idea of what the upper limit of damages is likely to be. no one has ever been awarded more than £14.5m and the average cerebral palsy baby award is still only about £6m. Take away obstetrics and the reality is that very few awards get more than £1m and the insurance can be
Many doctors are quitting the defence organisations in favour of lower-price cover from insurance companies that pay damages on a claims-made basis
written on a catastrophe basis –that is on the assumption that such events will be very rare.
By contrast, no one is in a position to advise the insurers about the upper limit of their exposure in a single case when they are writing occurrence-based business in which they will be liable for a claim whenever it is made in the future.
Old-style policies undercut as a result, it is not unknown to see claims-made policies written at a level that undercuts occurrence-based cover by a third.
Further savings can be made if they do not include the legal expenses insurance that medical defence organisations provide to protect the practitioner in the case of a GM c complaint. a nd there may be other respects in which benefits that medical defence organisation (MDO) members take for granted are not replicated by the insurers. a t a third of the price, many doctors think it is attractive.
Sometimes the policies come with a promise that the doctor will be given run-off cover, which means that the insurers will agree to pick up claims made in the future as if the policy had always been the equivalent of an occurrence-based policy.
Often the insurers say that they will provide that run-off cover for nothing as the MDOs will, if the practitioner remains in benefit until retirement.
Others say that they will allow the practitioner who wants to retire prematurely, or to transfer to another provider, to purchase the same benefit if they will pay two or three years’ premiums all at once.
The trouble with both such promises of run-off cover is that they depend upon the practitioner remaining being able to
pay the premiums quoted in the final years.
If the doctor has an adverse claims record, there is no limit to the extent to which the insurer is entitled to increase the premium. a s a result, it may become impossible for the doctor to be able to afford to remain in benefit with that indemnifier until their retirement or they may be unable to afford to pay the premium quoted in the final three years. This is not an attractive position.
Voided insurance policies even worse than this, when doctors chop and change between indemnifiers, they have to make declarations about every circumstance. If they fail to mention a threatened claim when they transfer their liability to a new indemnifier, they may find the whole policy is voided.
This can happen when they fail to mention distant events. One of my clients was surprised to find cover that he thought had been
secure was voided because when he transferred his indemnity to a new indemnifier three years earlier, he had failed to mention an event which had happened 12 years before that.
This distant event had not resulted in any claim being made against him. It was a GMc case. e ven worse than that, many claims-made policies will only cover the practitioner in respect of claims that are made during that year and reported to the insurer. If the claim is not reported to the indemnifier in the same year in which the claim is made, then the practitioner may find that the claim is disowned, that they are ‘going bare’ and they have to explain themselves to the GMc.
There must be a temptation not to trouble the insurer for fear that next year’s premium will be increased. Problems arise when doctors receive letters that they do not recognise as claims, merely complaints that they think they can answer completely themselves.
Sometimes it may seem as if the doctor has two lots of cover. If a doctor transfers to a claims-made policy on 1 January 2014 and then gets a claim in respect of an event that happened in 2012 when he had occurrence-based insurance, you might suppose that he would be indemnified by both organisations and he need not worry.
dangers of transferring h owever, it does not work like that. The MDO may say that if the doctor has transferred to a claimsmade policy so that he has bought another indemnifier on risk, their obligation to indemnify is terminated.
They, no doubt, rely upon the fact that the claims-made policy is much cheaper than theirs. however, if the new indemnifier disowns the claim because it was not mentioned in the application when they think it should have been, the practitioner who thought that he was indemnified in two different ways may find he
is out in the cold without any cover at all.
c learly, it is a nasty world out there in which a letter before action may threaten the doctor’s ability to continue to practise and may also result in the unwelcome discovery that the indemnifier thinks their obligation to look after the doctor has ended.
This is all a sad change from the way it used to be. My grandfather bought life membership from the MPS when he qualified in 1919 for £50 and never gave the problem another thought until he stopped operating at the age of 82. autre temps, autre mores, no doubt; but more to the point, autre monnai as well.
Bertie Leigh (right) is a consultant at Hempsons solicitors. His views are his own and should not be attributed to any of his clients or associates
Free legal advice for independent Practitioner Today readers IPT
independent Practitioner Today has joined forces with leading niche healthcare lawyers Hempsons to offer readers a free legal advice service.
We aim to help you navigate the ever more complex legal and regulatory issues involved in running and developing your private practice – and your lives.
Hempsons’ specialist lawyers have a long track-record of advising doctors – and an unrivalled understanding of the healthcare system as a whole.
call Hempsons on 020 7839 0278 between 9am and 5pm monday to Friday for your ten minutes’ of free legal advice.
Advice is available on: Business structures: commercial contracts: ian Hempseed Faisal dhalla competition: disputes: lindsay draffan Hilary King
Are patients turning on to your website – or are you turning them off? Joel Calliste shows what factors you need to get right
a weBSITe ShOULD be viewed as the online window to a business.
r egardless of business sector, target audiences have a set of expectations against which they will judge credibility and make decisions.
as websites are a key influencer in the decision-making process, it’s important to not only determine what best to include but also what to leave out.
➲ NeArLy A THird of peopLe BeTweeN 25 ANd 45 expeCT To Be ABLe To view A weBSiTe oN A MoBiLe deviCe (28.12%)
In a survey by my company, current and prospective private patients were asked what they felt the biggest turn-offs were for them when viewing a private medical practitioner website.
The lack of information to explain treatments came top in the list of the biggest turn-offs across the board (see box, top right). This is a fundamental issue,
especially when it’s ultimately the information on the business.
e ven when a prospective patient visits a website following a recommendation, reassurance is required that the practitioner they have found is the right one for them and that the treatment is the right course of action. Those doctors who already guide website visitors will be reaping the benefits.
➲ THe geNerAL LooK
ANd feeL of A weBSiTe BeiNg ouT-dATed iS THe SeCoNd BiggeST TurNoff (23.47%)
Men (12.1%) are more likely to be turned off if a website can’t be viewed via a mobile phone or tablet than women (7.5%), and when analysing results according to the type of care sought, 33% of general surgery patients are negatively influenced if the website is both outdated and not mobile-responsive.
There are many private practi-
Keeping a website fresh, up to date and professional reflects well on the attention to detail a private doctor will pay to their patients
BiggeST weBSiTe TurN-offs
Lack of information to explain treatments
general look and feel being outdated
Not able to view the website on a mobile phone or tablet
Lack of guidance about cost/price of plans
old-fashioned images
Talking in the third person/corporate language
Adverts
Lack of verifiable/scientific, peer-reviewed, citations
Selling the practice rather than giving a balanced view on procedures
Slogans
tioners who have invested in a website. Unfortunately, many of them did so years ago and haven’t had the time to update it since.
The website design and quality of images can often be all it takes to build the perception of being outdated. and if it can’t be viewed on a mobile device and includes old information – such as a halfhearted attempt at a blog or an event last attended in 2008 – then a negative impression can all add up.
➲ 45.2% of privATe pATieNTS Are NegATiveLy iNfLueNCed By THe LACK of iNforMATioN AvAiLABLe To expLAiN TreATMeNTS
Ultimately, keeping a website fresh, up to date and professional reflects well on the attention to detail a private doctor will pay to their patients.
Joel Calliste (right) is co founder of Smart Medical Web
Common billing qUEsTions
So where is my money?
Independent practitioners were warned in Independent Practitioner Today last month to be on the alert for fraudsters targeting their practice finances. But, at the same time, some need to beware they don’t defraud themselves. Here, Gary Nials (right) answers related questions he says he is repeatedly asked by consultants – even those who have been in private practice for some time
so where is my money?
This is a question most often asked around the time the tax bill is due.
Invariably, the question is asked because the consultant has never reconciled their bank account.
Most private medical insurers pay by bank transfer directly into a consultant’s bank account. They also send a remittance advice showing which invoices have been paid and which have not.
It is incredibly important that you reconcile your bank account and this is done regularly to ensure you understand what is going into your account.
Likewise, often consultants take money out and eventually lose track of outgoings. Without reconciling your bank account, you could be defrauding yourself because you have no idea as to what is in your bank.
My advice is to set aside time each week to reconcile your bank account and understand what is going on.
Remittance from insurers should be reconciled against your invoices as soon as they are received.
What should i be charging for this?
Usually, this is simple to answer if the consultant is registered with Bupa or AXA and has agreed to bill to their respective fee schedules.
You have no choice and have to abide by their fee schedule for the procedure codes and you will have agreed your consultation fees as part of signing up.
Without reconciling your bank account, you could be defrauding yourself because you have no idea as to what is in your bank
For other private medical insurers, they either publish a fee schedule or the stock answer from their provider service team is ‘what the consultant considers is fair and reasonable’.
This gives you a bit more freedom and most people abide by the insurer’s procedure fee schedule but vary their consultation fee. Setting self-pay fees is similar to how any other service business would set their prices. It depends on your location and the competition in your specialty. Investigation and market research is the key here to determining pricing. Also a lot will depend on the time and resources you put into the procedure. If the procedure is for an embassy patient, you may
Setting selfpay fees is similar to how any other service business would set their prices. It depends on your location and the competition in your specialty
want to include a price increase for the length of time taken, as it will typically take longer due to the involvement of an interpreter. Research is the key to setting your prices.
Why can’t i bill those two procedures together?
Private medical insurers have limited what procedures can be billed together when invoicing for an operation.
They consider some procedures are part and parcel of other procedures or is so frequently performed that it is in effect part and parcel.
They are trying to avoid component parts of a single procedure being itemised out and billed as if they were separate or additional procedures. This practice is known as unbundling and considered fraudulent.
So what can be billed with what? Two places to look would be the insurer’s website and their fee schedules. Or you could use the Clinical Coding and Schedule Development Group website at www.ccsd.org.uk.
It is important that you do stay up to date with any unacceptable combinations and pay attention when invoicing any insurer.
Why do embassies take so long to pay?
The embassies are always busy and the major ones in particular. It is not unusual for them to have a backlog of invoices waiting to be paid.
money?
To shorten the payment time for embassies, always send the correct paperwork with the invoice and chase constantly
Reasons for this vary, but ultimately it is down to the sheer volume of paperwork that they have to deal with.
If you are not chasing on a regular basis for your payments, you will find they take a long time to pay.
With all the paperwork they have, it is likely that your invoice has slowly moved to the bottom of a very big pile.
Another reason for delay is not sending a ‘letter of guarantee’ or, in the case of some embassies, not sending a medical report.
Not sending these vital documents with the invoice always delays payment and you will not be told that you have missed these documents unless you chase.
So to shorten the payment time for embassies, always send the correct paperwork with the invoice and chase constantly.
should i bill patients for any shortfall or waive the fees?
Generally speaking, if the patient’s private medical insurer is not covering all the costs, most consultants would still charge them for the shortfall.
The reasoning is that the consultant is not responsible for what the insurers will contribute. However, if you have an agreement with the insurer not to ‘shortfall’ patients, then you should have invoiced according to the fee schedule in the first place. That way, the shortfall would not have occurred.
This is one of those areas which becomes a personal decision based upon who the patient is to you and how many times that you have seen them. Where you have agreed to bill to private medical insurer guidelines, you cannot charge patients a shortfall.
Gary Nials is the managing director of Medical Billing and Collection
Crosscare - providing private practices with efficient paperless working
Crosscare is a proven clinical system used within private practices and specialist clinics in and around Harley Street and across the UK.
Alongside the standard clinical record keeping and prescribing systems, Crosscare’s appointments, reporting and integrated accounting modules make the tracking of workload, invoices and revenues simple and user friendly.
We understand that each practice works in their own unique way, so being a fully customisable system, Crosscare can be easily tailored to fit your individual needs.
For further information on how our Crosscare solution can help your practice call us now on 01233 722670 or visit www.advancedcomputersoftware.com/ahc
bREAkiNg iNTo mEdico-lEgAl woRk
Take note: tables make best sense
Our medico-legal work series continues with advice from Michael R. Young on making your notes
speCial offeR! buY the book anD save £20 the book costs £60, but independent practitioner today has secured discount of a third off for readers, so you pay only £40. listen to the audio content which accompanies the book at this website: www.otmoorpublishing.com/audio. for more information and to order, email stephen.bonner@ otmoorpublishing.com, quoting reference ‘Young/ipt’.
exaMple of a siMple table to use
Date page patient’s Radiographs, number records models, special tests etc
1/1/2015 15/2/2015 16/2/2015
Cases obviously vary in their complexity, but even for the simplest ones you have to start the preparatory phase of writing a report by reading through the records.
you should begin by reading all of the records once, but without making any notes.
Number the pages if the solicitor has not already done this. Numbering the pages helps you quickly locate information later after you have made your notes. you should then read the records again, but this time paying very close attention to the text. i never used a highlighter because highlighted text is very distracting when you later read the records through again.
i suggest the following method when making notes:
✍ a nnotate in the margins in pencil as you read, but be aware that this too may make subsequent readings difficult. Make more extensive notes on a separate sheet of paper or in a notebook.
✍ Note everything that is relevant:
❍ Chronology;
❍ any treatment that was carried out, why it was done and the outcome;
❍ any care that was given, why it was given and the outcome;
❍ a ny advice that was given, why it was given and whether or not it was followed;
❍ anything that stands out as having not been done.
✍ The doctor’s version of events may be at odds with the patient’s and you need to draw this out without giving one side primacy over the other.
you must never omit information just because you think it would favour the other side’s case if you include it. your report must be balanced and objective and so must the evidence you uncover.
Resist the temptation to start writing the report as soon as you receive the records. as in an exam, time spent planning the answer is never wasted
✍ Medical records are notorious for their incomprehensibility. if you are unsure what an entry means or if there could be more than one interpretation, then make a note.
The other side in the case will try to emphasise the version that best suits their argument – you should have already spotted the various interpretations. as well as making notes in sentence and paragraph form, it might help to set everything out in a table.
Tabulating information is sometimes the only way to compare and contrast the various versions of events. Things that at first may not be obvious sometimes begin to stand out.
Resist the temptation to start writing the report as soon as you receive the records. as in an exam, time spent planning the answer is never wasted.
Read the records, make some notes, and then leave it for a few days while you mull things over. only when you fully understand the background, complexity and what you are being asked to do should you move on to the next stage – that is, writing the report.
Next issue: The macrostructure of a report
adapted from The Effective and Efficient Clinical Negligence Expert Witness , by Michael R. young, price £60 from otmoor Publishing
patient’s Defendant’s other Comments witness statement info statement
PROBLEMS WITH THE TAX MAN?
HMRC tax investigations and disputes create difficult and stressful times.
As an award winning firm of tax experts, our highly experienced partners specialise in resolving problems relating to tax investigations and disputes with HMRC.
To find out, in confidence, how we can help call 0800 734 3333.
‘Here to help. Not to judge.’
Is it buy-to-let or buy toilet?
Are buy-to-let properties a suitable investment for you? A lot of doctors think they are. Simon Bruce (right) examines the myth behind the headlines
‘You can’t go wrong with property’. a phrase we often hear accompanied by an example of substantial house price rises over a 30-year period.
But is the buy-to-let market the best investment choice for senior doctors?
t he pension freedoms which came into force earlier this year were quickly followed by a raft of media stories suggesting to savers that they should use some of their retirement cash to put down a deposit on a property in the ‘lucrative’ buy-to-let market.
‘Experts’ predicted a boom in the number of older landlords and yet another marketing term was coined: ‘granlords’.
Banks and building societies moved swiftly to capitalise on the trend with nationwide amending its lending criteria to offer new
mortgages to people up to age 70, with a maximum term of 35 years.
t he chirpy headlines did not last long. the recent move by the chancellor to improve first-time buyers’ chances of getting on to the property ladder by curbing landlords’ profits has made some rental homeowners question the return on their investment.
By april 2020, the tax relief that private landlords receive on their mortgage interest payments will be cut from 40% or 45% to 20%. this tax increase, which was completely unexpected by the property industry, will be phased in from 2017.
Higher-rate taxpayers who own buy-to-let properties with large mortgages will pay significantly more tax than before. Research shows that some could see the new tax levels pushing them into a loss situation – particularly if the Bank of England raises the base rate of interest.
Let us look at a property worth £100,000 with an 85% loan-tovalue mortgage and a mortgage interest rate of 5%. under the new measures, a higher-rate taxpayer would lose £100 per year.
Full impact
If the rate increases by just 0.5% or 1%, the landlord could face a loss of several hundred pounds. n ow consider that the average rental property is worth many times more than this and the full impact of these new tax changes becomes evident.
Even before this bold change, buy-to-let yields were not what they once were. Some 15 to 20 years ago, landlords might have enjoyed rental yields of around 15% and house values which jumped substantially with inflation.
today those yields might be more like 5% or 6% and much lower in London. then take into consideration the managing agent’s fees, maintenance and insurance and the returns look much less.
a recent uK study showed that one-in-eight landlords fail to consider additional costs when calculating the profitability of their property portfolio. t he survey results suggested more than half do not factor in repair costs or void periods when tenants move out.
For those at the decumulation stage – unwinding assets to provide a retirement income stream to enjoy in later life –buy-to-let can be a poor choice
With everything included, the total average cost of a buy-to-let property, including letting agent fees, maintenance, repairs, marketing fees and mortgage interest, amounted to £8,359 a year and, in the South-east, these costs could be much higher.
u nlike owner-occupier mortgages, those no longer in full-time employment face little difficulty in securing mortgages on buy-tolet properties, as providers will lend based on speculative rental yields rather than personal income levels.
High entry costs
However, entry costs for investors remain high – most lenders may insist on minimum deposits of 20%, with the best rates available reserved for those with deposits of 40% or above.
t here is no doubt that many have made good money from buy-to-let investments in the last few decades, which has, as a consequence, attracted many followers into property as an investment strategy.
It is easy to see why buy-to-lets feel like an attractive option – our television channels are full of property programmes, our weekend papers urge us to consider them as a pension alternative. We firmly believe we understand property much more than intangible items like stocks and shares.
We all have experience of managing a mortgage, so even taking on high levels of debt does not feel as risky as with other investments.
But becoming a landlord is akin to starting a very high leveraged business – with all the associated costs, tax and risks that go with such an enterprise.
a nd all businesses face chal -
lenging times. Houses are no different; every landlord will have a troublesome tenant story.
While, for many, retirement is a chance to kick back and relax or take on new pursuits, few will relish the inevitable late-night phone call regarding an errant washing machine or emergency leak.
a nd if you have bought in an area far away from your own home in order to maximise profitability on cheaper houses, your maintenance issues, even with an agent, become even more challenging.
poor choice
Lettings agents report that they are now helping more widows in their 80s who now face the logistics of a buy-to-let property alone.
For those at the decumulation stage – unwinding assets to provide a retirement income stream to enjoy in later life – buy-to-let can be a poor choice. It is a timeconsuming business, not a quick road to riches, as one is faced with a further 20 years ahead of finance repayments.
Property is ‘illiquid’ – slow to convert to cash should the need arise, with high transaction costs. this makes it a better ‘accumulation’ asset for those with time to build up their wealth over several decades, giving the property time to appreciate in value.
If you are about to embark on a happy, stress-free retirement, consider carefully the best use of your assets and whether you have the time, energy and funds available to launch what is essentially a personal business venture.
Simon Bruce is managing director of Cavendish Medical, specialist financial planners helping senior consultants in private practice and the NHS
The content of this article is for information only and must not be considered as financial advice. Cavendish Medical always recommends that you seek independent financial advice before making any financial decisions.
Levels, bases of and reliefs from taxation may be subject to change and their value depends on the individual circumstances of the investor. The value of investments and the income from them can fluctuate and investors may get back less than the amount invested.
When relatives start to intrude
Dr Bev Ward, MDU medico-legal adviser, looks at dilemmas you might face when dealing with patients’ relatives
Dilemma 1 Should I honour secrecy appeal?
QI’m an orthopaedic surgeon and recently performed an arthroscopy on a 60-year-old man. While the patient was still coming round from surgery, the patient’s wife took me to one side and said that she didn’t want me to pass on any information about her husband’s condition to his son.
She said they had had a difficult relationship for years and he really didn’t want his son to know anything about his treatment.
I understand from a colleague that the son rang earlier to ask about how his father was recovering. What should I tell him?
AAnyone who has had a sick relative knows how worrying it can be. It’s understandable that family members will want to know about the care being provided to their relative and feel they have a right to be kept informed.
However, you have a duty of confidentiality to all patients and no information should usually be disclosed to any third party, including relatives, without the express consent of the patient.
You need to establish with the patient, when he has recovered from the surgery and has capacity, what information he wants you to share, with whom and in what circumstances.
The GMC provides detailed guidance about sharing information with a patient’s partner, carers relatives or friends. This is particularly important where a
patient has fluctuating or diminished capacity or is likely to lose capacity, even if this will be temporary.
It is important not to assume that the patient is happy to have information freely disclosed to their relatives, including their spouse and children, if you haven’t established this with the patient.
The MDU has seen complaints from relatives about breaches of confidentiality when the clinician had assumed that information could be shared.
In the meantime, you should explain to the wife that you will need to speak to the patient to establish with whom he would like information shared when he has recovered from the surgery.
Dilemma 2
Do I ignore plea not to tell
Qfamily?
I’m a consultant geneticist and a patient who has been diagnosed with a BRCA gene has refused to let me tell her estranged family about the risk to them.
Can I pass on the information without the patient’s consent?
AIn the first instance, you should do all you can to encourage the patient to discuss this with their family. Does the patient understand the potential risks to her family if the information is not passed on?
Would she prefer you to tell relatives if the relationship with them is difficult? If you cannot persuade the patient to inform her family or let you do so, you will need to decide whether it is appropriate to disclose information without consent, to protect others from a risk of serious harm. The GMC provides detailed guidance about public interest disclosures, so seek advice from your medical defence organisation if you are unsure how to proceed. If you decide that it is in the public interest to pass on the information to the relatives, you should tell the patient that you are planning to do so and document your discussions in the records.
Dilemma 3
Must I heed view of her daughter?
QI am a private GP and one of my patients suffers from dementia and is in a care
their behalf or has been appointed to represent them.
Under the Mental Capacity Act, a patient can appoint a person known as Lasting Powers of Attorney (LPA) to have powers to make decisions on their behalf about financial matters or healthcare.
It is important that you ask to see the document, as the powers granted vary. Most LPAs only cover financial and property affairs, and these can be activated while the patient still has capacity.
Some LPAs cover health and welfare, but these can only operate if the patient lacks capacity. In addition, the LPA must be registered with the Office of the Public Guardian (OPG) in order to be effective, and stamped by the office on each page.
If there is any doubt, an application can be made to the OPG to search the register and check the LPA is registered.
Personal welfare LPAs can be general – covering all aspects of personal welfare – or specific, and you should check the terms of the LPA to ensure the attorney has the power to deal with the healthcare issue in question.
An LPA cannot grant the power to an attorney to demand specific forms of treatment that you do not believe are necessary or appropriate for the patient. Attorneys can only make decisions that are in the patient’s best interests.
While you should consider the views of the patient’s daughter, you are not obliged to follow her instructions if you do not think doing so would be in the patient’s best interest. If in doubt, check with your medical defence organisation.
Dr Bev Ward (right) is a medico- legal adviser at the MDU
home. She recently suffered from a chest infection and was briefly admitted to hospital and then discharged. However, the patient’s daughter thinks she is too poorly to be back in the care home and should be re-admitted to hospital.
She explained that she has a lasting power of attorney which means she can take healthcare decisions on her mother’s behalf. Do I need to follow her instructions?
AThe treatment of patients who lack capacity is governed by the Mental Capacity Act 2005 in England and Wales, and the Adults with Incapacity (Scotland) Act 2005. Relatives and carers are often closely involved, and naturally wish to be kept informed about the patient’s health.
You are obliged to act in the best interests of a patient who lacks capacity to make decisions about their care.
When determining the patient’s best interests, you must consider the views of anyone the patient asks you to consult, the people close to the patient – which might include family members, carers or friends, anyone who has legal authority to make a decision on
doCToR on ThE RoAd: mclAREn 650S SpidER
Who needs drugs?
the
Very few prescribable drugs could produce the same sense of euphoria in a petrol-headed medic as the elation felt by our tester Dr Tony Rimmer (above, right) when he was handed the keys of this incredible supercar
There IS nothing like aiming for the stars. Independent practitioners all know of a rival medical provider who seems to be doing rather well by offering a particularly exclusive service.
Why not compete yourself?
Initial thoughts may be negative. h ow could you possibly go up against an established organisation who seems to have cornered that particular end of the market so effectively?
Well, nothing ventured, nothing gained.
In the world of cars, this is exactly what McLaren did about eight years ago under the guiding eye of founder and chief executive ron Dennis.
he noted that there was serious money to be made in the lucrative supercar market. Formula One rivals Ferrari were making sub -
stantial profits from road cars whose sales benefited from their racing link. McLaren has a fantastic Grand Prix racing heritage too, so why not join the party?
After a brief but successful toedipping in 1992 when they produced just 100 world-beating FI models, it was nearly 20 years before McLaren built another sports car. In 2011, it revealed the MP4 12C to the world.
Teething problems
This mid-engined supercar may have had an awkward name but was packed with cutting-edge technology and features. Unfortunately, teething problems spoilt initial reports from the motoring press. Three years and many improvements later, the 12C was replaced by the current 650S.
Although few of us will ever be able to afford a new supercar, naturally I felt it was important to report to my medical colleagues just what these cars are really like to drive.
Are they just dream machines? Are they all show but disappointing in reality? Can they possibly be worth their vast expense?
Well, I was lucky enough to be offered the loan of a brand new 650S Spider by McLaren and I spent a couple of days getting under the skin of this top-notch sportscar.
As I approached the futuristic McLaren Technical Centre in Woking, Surrey, to collect the car, I wondered how best to assess their latest supercar. A trip south to visit Goodwood Motor Circuit seemed appropriate.
The space-age building in
On
open road, the 650s is a rocket-ship on four wheels
Woking where they make the 650S is where they build and develop their Formula One cars as well. Any surgical colleague would feel right at home there. The spotless surfaces and bright lighting could be straight out of a modern operating theatre – and attention to detail is second to none.
Then, there it was. In the covered forecourt, glinting in the sunshine, was the metallic red 650S test car. It looked stunning. Powered by a twin turbo 3.8litre V8 engine producing 641bhp, the McLaren can accelerate to 60 mph in 3.0 seconds, 100mph in 5.7 seconds and has a top speed of 207 mph.
Sense of euphoria
After a full explanation of the various controls, I was handed the keys and tried to act casually as I cruised away from McLaren’s headquarters and contemplated the next 48 hours with open roads ahead of me.
Very few prescribable drugs could produce the same sense of euphoria in a petrol-headed medic. As I acclimatised myself behind the wheel, two things struck me. Firstly, this is a very easy car to drive and cruising through town is a piece of cake.
The seven-speed double-clutch gearbox shifts unobtrusively and the ride is surprisingly good if ‘Normal’ mode is selected from the variable chassis settings.
The cabin is fully lined with leather and carbon fibre and (top, left) the retractable hardtop folds away in only 17 seconds at the press of a button
The second thing is how much positive attention the car attracts.
Looking around the cabin, it is fully lined with a combination of leather and carbon fibre and the quality is second to none.
I found the driving position to be absolutely perfect and the sports seats are really comfortable. Pressing a console button folded the retractable hardtop away in only 17 seconds.
Compressing organs
On the open road, the 650S is a rocket-ship on four wheels.
I’ve driven a few fast cars over the years, but this McLaren is truly
super-quick. The acceleration is enough to compress your internal organs like nothing else and the brakes are equally impressive.
huge carbon-ceramic discs bite hard and excess speed is shed as quickly as it builds up. however, this is no straight-line dragster. handling is razor-sharp and the car shrinks around you as it tackles challenging twisty roads without drawing breath.
The engine feels unburstable and the wonderful sound it makes is enjoyed even more with the Spider roof lowered.
In ‘Sport’ mode, the chassis tightens up and gearchanges, controlled by the steering column paddles, are instantaneous.
There is an even more aggressive ‘Track’ mode which you would not use unless you were on a racing circuit. This McLaren can be a racing car one minute and a comfortable sports car the next.
This hugely impressive car is the ‘thinking man’s’ Ferrari or Lamborghini. Not as extrovert, but equally capable, the McLaren brand has filled the shoes of ageing Aston Martin and given us a truly modern British sports car that beats anything else the world can offer.
Any of you doctor colleagues who get the chance to drive one, never mind own one, will be very lucky indeed.
Dr Tony Rimmer is a GP practising in Guildford, Surrey
Remain in retirement
Doctors will have seen many changes to their pension following the Hutton report. The Government compounded these with a fundamental shake-up of the taxation aspects. These affect the size of a doctor’s pension as well as how much can be saved each year. Ian Tongue explains the changes and how they may affect you
The huTTon reporT in March 2011 was 215 pages long and looked at the funding of public sector pensions. Its impact can be easily summarised as ‘pay more, work longer and potentially get less’.
We have recently seen the 2015 nh S p ension Scheme implemented, which is the last of the major changes that have been in the pipeline for the health service. retirement linked to state pension age and pensions based on a career average all reinforce the h utton conclusions and affect younger consultants.
running alongside the hutton report was the Government review of the tax relief available on pensions.
Significant pension reform took place from 6 April 2006, known as ‘A’ Day, when the Government capped how much you have in your pension pot to £1.5m, and this rose to £1.8m by 2010-11.
At the same time, the amount that could be saved increased to £255,000 a year. This was all to encourage saving for pensions. These were happy days, which didn’t last for long.
For then the recession hit and a series of fundamental changes were brought about, as they pushed the right buttons politically.
What followed was largely a series of stealth taxes to arrive at the position today.
What is the position today?
This is complex and depends on a whole host of factors including:
Age;
Length of service;
Superannuable earnings;
Total earnings;
nhS scheme you are in (1995, 2008 or 2015);
private pensions;
Tax rate.
It is not surprising that many
consultants and Gps are confused with the changes and the impact on them.
The headline figures for the 2015-16 year are that you can save £40,000 a year into a pension and have a lifetime ‘pot’ from all pension sources of £1.25m.
A particularly nasty announcement in the recent Budget was to reduce the annual allowance to a minimum of £10,000 on a sliding scale between earnings of £150,000 and £210,000.
This is similar to the loss of personal tax allowances and is expected to impact upon a substantial number of consultants carrying out private work. This applies from 6 April 2016 and planning may be required to ensure you are best placed going into the 2016-17 tax year.
The overall pot value or ‘lifetime allowance’ is to be further reduced to £1m from 6 April 2016.
What is the Annual Allowance?
The Annual Allowance is a limit set by hM revenue and Customs (hMrC) and is currently £40,000 for the 2015-16 tax year. The deemed pension input or increase is quite simply an arithmetically formula that bears no relationship to actual true pension contribution or growth within the nhS pension Scheme.
For example
Let us look at the scenario facing an nhS consultant with 25 years’ service under the 1995 scheme with superannuable earnings of £85,000 for 2013-14 and £90,000 for 2014-15 combined with 1% inflation.
Pension at the beginning of the year: 24/80 x £85,000 = £25,500
Allowing for 1% inflation, this increases to £25,755.
anthony K associates are vehicle leasing brokers specialising in providing vehicle contracts for doctors and all associated professions in the medical sector.
The BVRLA has three categories of membership, each with a logo that members are entitled to use (and, in some situations, are obliged to use). Appropriate use of our logo tells your customers, your suppliers, and the rest of the world that you adhere to the high standards that come with BVRLA membership.
testimonials from our very many happy customers are proof of our attention to customer service and our practised ability to help clients get the vehicle they want quickly and easily.
This brief guide explains how we expect our logos to be displayed – and how they should not be displayed. These are not hard-and-fast rules, and we sometimes depart from them ourselves, but we do expect our members to respect them and to gain our prior approval before using our logo in any way
If you need a copy of our logo, for use on your printed marketing material, or to go on a page of your website, please contact our communications team, who will be happy to send you an EPS or JPEG version appropriate for your purposes. If you have any queries about use of the BVRLA logo that are not addressed in this guide, they will also be able to help Chief executive, BVRLA
Using the BVRLA Logo
Watchdog renews squeeze
The long-running fight for
the future of some leading private hospitals in the capital goes on. Robin Stride reports
S WIFT re S pon S e S are being demanded to the latest Competition and Markets Authority (CMA) private healthcare report this month, which claims lack of price competition harms customers in London.
Interested parties must adhere to a 3 December deadline for written views on a 215-page document, plus other papers, arguing the case for and against what would be a massive shake-up for hCA hospitals in the capital.
The provider has already been threatened with having to sell either The Wellington and p latinum Medical Centre, or The London Bridge hospital and The princess Grace hospital.
After an h CA appeal, the Competition Appeal Tribunal (CAT) set aside part of the CMA’s
➱ continued from page 49
Pension at the end of the year:
25/80 x £90,000 = £28,125
Therefore, the increase in pension from one year to the next is £2,370 (£28,125-£25,755).
hMrC has provided a formula to notionally value this increase and this is by a multiplication factor of 16 plus lump sum increase, which results in a multiplication factor of 19 under the 1995 scheme.
Therefore, in this example, the deemed pension contribution is £45,030. Actual contributions would have been in the region of £12,000 pre-tax.
As the number of years of service increase, so does the pension accrual. Should the above increase in pay have happened with 30 years’ experience and, say, from £120,000 to £125,000, the notional increase in pension for tax purposes would be £55,860.
p ay increments and clinical
findings last January and returned the issue to the watchdog – which has now issued its provisional findings report.
It found ‘a competition problem’ still needed addressing. It said h CA’s ‘large market share, combined with high barriers to entry and expansion in central London, result in h CA facing weak competitive constraints and this leads to hCA charging higher prices to private medical insurers than would be expected in a wellfunctioning market’.
Expansion ban
As well as divestment of one or more hospitals, hCA now faces two other possibilities – being forced to rent out facilities at one or more of its hospitals and a ban on more central London expansion.
excellence awards are the key triggers for exceeding the limit, but other factors can be significant such as:
promotion;
Back pay;
Added years or additional benefits;
Mental health officer status;
Multiple superannuable salaried posts;
Divorce and pension-sharing arrangements;
errors in payroll information.
Clearly, for those with combined earnings more than £210,000 from 6 April 2016, you will be hit hard, as the limit of £10,000 only equates to a pension accrual of £526 for those in the 1995 scheme, which will be easy to reach.
For those that have exceeded the limit, more often than not you will have unused relief from the prior three years where you did not reach the limit in order to extin-
The CMA’s roger Witcomb said: ‘We will now consult widely and listen carefully to all responses to our provisional findings and potential remedies before we publish our final report.’
response hearings are due next month, parties’ submissions in February 2016 and a final report and decision in March.
An h CA spokesman said: ‘We note the new and alternative remedies in the CMA’s provisional
guish any tax charge. however, as time goes on for those with tapered annual allowances, the unused relief will be lost.
How do i get a statement of deemed pension benefits?
If you have exceeded the annual allowance in a particular tax year, you should automatically receive a statement from nhS pensions. The emphasis here is on the word ‘should’, as this is not always the case.
nhS pensions is under an obligation to provide you with a statement only if they have received the information to carry out the calculations. They used to issue provisional statements based on estimated figures, but this stopped in 2014 due to the number of queries raised.
An ‘Annual Allowance statement’ can be obtained from nhS p ensions in Fleetwood, Lancashire, by writing to them about
findings. Since this process began, over three years ago, London’s private healthcare market has continued to grow and diversify.
‘ r ecent investments by the Cleveland Clinic and VpS in large new facilities and Spire’s plans for a new central London hospital by 2018 are yet further signs that London offers an open, accessible and competitive market.’
According to Alex perry, general manager, Bupa uK Customer, the
whether you have exceeded the limit or not. It is a straightforward process and I recommend to all consultants that they obtain one. As of now, all consultants should be able to obtain a statement in relation to 2014-15. It will also disclose the figures for 2011-12, 2012-13 and 2013-14.
i have exceeded the limit, what next?
Assuming that you do not have enough unused relief to extinguish the excess, you will incur a tax charge. This is payable at your marginal rate of tax, usually 40% or 45% at current rates. Therefore, an additional-rate taxpayer exceeding the limit by £10,000 would have to pay £4,500 in tax. The tapering of the annual allowance from £40,000 to £10,000 therefore could result in an additional tax charge of £13,500. This is a tax planning opportunity and should be dis -
Future fears: The Wellington Hospital, St John’s Wood, London
squeeze on HCA to sell units
report was good news for the insurer’s customers ‘who have been paying for the lack of competition among hospitals in central London’.
h e said divestments by h CA were needed to fix this, adding: ‘In fact, the CMA needs to go further than they are currently suggesting and we hope to see stronger solutions on the table as the process continues.
‘The private health insurance
cussed with an accountant who understands this fully.
If the tax charge is less than £2,000, you will have to pay this under self-assessment. For anything over £2,000, you can either pay the tax or opt for the pension scheme to pay it.
If the latter, a ‘scheme pays’ election is essentially a loan and the combined value of the capital and rolled-up interest is deducted from your pension at the end, thus reducing your annual pension.
For those electing for the scheme to pay, there is a strict time-scale. You must elect by 31 July of the following year to which the charge relates. For example, for the 2013-14 tax year, the deadline was 31 July 2015.
lifetime Allowance
The Lifetime Allowance keeps falling and is scheduled to reduce from the current £1.25m to £1m from 6 April 2016. £1m sounds a
market is not growing and we need action to deliver better value, quality and transparency for customers, to make private healthcare more affordable for more people.’
Higher prices
According to the provisional findings report, a revised insured pricing analysis (I pA) demonstrates that h CA, on average, charges higher prices than its closest competitor, The London Clinic (TLC),
lot of money to the average person, but for an nh S consultant under the 1995 pension scheme, this is a pension of £43,478 which is easily achievable in an average nhS consultant’s career.
As with the annual allowance, tax charges arise for exceeding the limit, but a different formula is applied here. The charge is 25% of the excess over the lifetime allowance at the time that benefits are crystalised.
The impact of exceeding the allowance can be modest when viewed on a annual basis, as any tax charge is taken over 20 years from the annual pension.
For example, exceeding the allowance by £100,000 will cost you £750 per year for a 40% taxpayer or £63 per month.
Pension protection
Since ‘A-Day’, there have been so many forms of protection that you would be forgiven in think-
for treatments they both provide.
But it admits ‘. . . we can no longer conclude on the size of this price difference, as we cannot rule out the possibility that our I pA may not fully account for differences in patient complexity between hCA and TLC’.
The CMA states, however, it does not believe that differences in patient complexity ‘are likely to be the major driver of the price difference that we observe’.
It adds that it has recently become aware of future large-scale entry into London by hospital operators VpS and the Cleveland Clinic (see page 3).
If this happens, it says ‘this would be likely to significantly increase the level of competitive constraint on hCA. however, at this stage, we do not have sufficient evidence to determine if and when their entry is likely to take place and the timeframe over which these facilities may start to exert any competitive constraint on hCA.
‘Most importantly, we have not seen any evidence to suggest that
ing these changes are sponsored by a contraceptive manufacturer! primary, enhanced, Fixed 2012 and 2014 and now individual protection exist. Some are standalone, but others can be held in conjunction with each other.
The forms of pension protection that are most appropriate will depend on your individual circumstances and some forms of protection need to be revoked as your circumstances change. You must seek professional advice to ensure that your position is reviewed based on your individual circumstances.
The perfect storm
Certain consultants can find themselves in the perfect storm of tax changes hitting them concurrently. These include loss of personal allowances, 45% tax, annual allowance and lifetime allowance charges. Due to the complexities and interaction of these variables,
the threat of such entry has placed any significant constraint on hCA to date.’
Market analysts LaingBuisson puts London private hospital market growth at around nine per cent annually since 2006.
Advanced oncotherapy is developing a proton beam therapy centre as part of a joint venture with Circle health for the treatment of cancer on harley Street, due to be completed by the end of 2016.
As well as numerous new entrants and expansions in the market recently, plans include a new surgical centre from Fortius Group.
Bupa Cromwell opened a new paediatric walk-in centre as part of its hospital redevelopment programme in April 2014 and has upgraded its facilities, recently adding an angiography suite, a CT scanner and two MrI scanners.
Meanwhile, nhS private patient unit capacity and revenue growth has reportedly outstripped independent hospital operator growth since 2011.
bespoke advice is essential to ensure that your individual position is considered fully.
What can i do?
Minimising the impact of the changes can be a challenge and there is no ‘one size fits all’ approach. Specialist medical accountants are formulating mitigation strategies for clients and the value of engaging a specialist accountant has increased significantly. p ension changes can be confusing, so seeking professional advice relating to your personal circumstances is essential to reduce the negative impact on you.
next month: A look at best practice for accounting systems
Ian Tongue (left) is a partner with accountants Sandison Easson & Co
Under threat: Princess Grace Hospital in London’s Nottingham Place
Guilty of charges?
Lack of clarity about specialists’ and hospital fees is the biggest financial complaint issue brought to the attention of the private sector’s adjudication service. Disa young (right) has some tips to help steer clear of trouble
p rivate patients’ complaints about financial matters form a fair chunk of the gripes handled by the i ndependent s ector c omplaints a djudication s ervice (iscas).
Just under 10% of all complaints received by iscas in 2014 related to:
Fees;
Fees administration;
Billing.
Financial complaints are a growing area and the implementation of the c ompetition and Markets authority (cMa) private healthcare Market investigation Order is likely to have a further impact on this.
t he main financial issue that patients complained to iscas about was a lack of transparency around consultant and hospital fees.
should the cMa order be implemented as currently proposed, consultants will be required to be transparent about their fees by 2017.
t he p rivate h ealthcare i nformation n etwork ( phin ) is currently working with the relevant organisations on how this can be achieved.
iscas also receives a sizable number of complaints from patients who did not understand that various tests or scans recommended by the consultant following the initial consultation would be added to their bill.
t hese patients had assumed that additional tests and scans were included in the initial cost quoted.
Linked to this are situations where patients claim not to have been informed by the consultant
that they would be charged separately by the hospital.
insurance coverage complaints are common, where patients have not taken on board that the responsibility for checking their insurance coverage and limits lies with themselves and not with the consultant.
an awkward type of complaint to address is that from patients who deem that the treatment they have received has not been successful or achieved the outcome they were after and therefore do not feel that they should have to pay for it.
iscas is also receiving a growing number of complaints about the ‘aggressive’ approach taken by debt collection agencies employed by hospitals and consultants.
Principles of agreeing fees
the BMa’s private practice committee has produced guidance to highlight the key principles of good billing practice in the independent sector.
it is available to BMa members at www.bma.org.uk. t he document is currently being updated in light of the implementation of the c M a p rivate h ealthcare Market investigation Order.
ISCaS is receiving a growing number of complaints about the ‘aggressive’ approach taken by debt collection agencies employed by hospitals and consultants
The Independent Sector Complaints adjudication Service (ISCaS) is the recognised complaints management framework for independent healthcare providers.
ISCaS provides independent adjudication on clinical and non-clinical complaints made by privately-funded patients.
ants should advise patients to check the re-imbursement levels that will be available for their procedure.
pMi may cover the cost of the private treatment in full or in part. Where the treatment is covered in part, the patient should be told that they are responsible for paying the difference between the consultant’s fee and the pMi reimbursement.
Principles are as follows:
c onsultants should inform patients of the likely fee that will be charged for their private medical procedure in advance of their treatment. t he scope of the fee should be explained in full, including all the planned elements of the expected treatment process.
the iscas view is that while consultants must explain to patients that there will be a separate hospital fee covering the hospital’s services, as a general principle, consultants are best advised not to quote what hospital fees are lest they quote these incorrectly.
We think the best approach is to direct the patient to where they can find out the information from the hospital.
Where patients hold private medical insurance (pMi), consult-
it is advisable that consultants send patients a letter outlining the responsibility of payment of fees before their treatment. the BMa guidance provides a template. i n the independent hospitals context, patients do not always appreciate the subtleties of the practising privileges relationship between consultants and independent hospitals; they generally understand consultants to be employees of the hospital. While this distinction is significant in terms of financial arrangements, it is sensible to work in partnership with the hospital on explaining fees and responding to complaints about fees.
For more information about ISCAS, see www.iscas.org.uk
Disa Young is senior adviser at ISCAS
In association with
PRoFiTs FocUs: oRThoPAEdic sURgEons
DO yOU FIND OUR PROFITS FOCUS SeRIeS USeFUL?
Please let us know if it helps you or not. and if it doesn’t, what other data would you like to see presented? email robin@ip-today.co.uk
A growing public profile
Escalating costs have bitten hard into orthopaedic surgeons’ profits, finds Ray Stanbridge in our exclusive benchmarking series. Thanks goodness then for Choose and Book. Additional material from Martin Murray
OrthOpaedic surgeOns continue to be the star financial performers of the private medical sector, as they have been for many years.
Our figures show that between 2013 and 2014, gross incomes increased by 3.4% from £174,000 to £180,000.
But costs showed a much larger increase, going up by 12.5% from £56,000 on average to £63,000.
a s a result, net taxable profit has fallen very slightly by 0.8% from £118,000 to £117,000.
Our surveys are a representative sample of the performance of some typical private practices around the country. they are not statistically significant and it is increasingly difficult to compile them and to present any meaningful comparisons due to a number of factors.
t hese include the changing nature in which consultants practise legally, the growth of groups, the altering mixture of practice with an increasing nhs choose and Book component and the
impact of tax and employment changes.
the good news is that incomes have continued to show some growth. t his is primarily the result of additional self-pay work – particularly in the London/M25 region – but, more significantly, additional nhs choose and Book work.
Becoming employees
nhs expenditure now exceeds 30% of the spend in the private sector. For some orthopaedic consultants, nhs c hoose and Book work accounts for in excess of 70% of their total income.
surely, as Independent Practitioner Today reported last month, some consultants will become employees of private hospitals in due course?
Meanwhile, we are seeing a continuing squeeze from insurers on fees. in some cases, they are being very aggressive in their handling of consultants.
inevitably, costs have shown a rise in a number of areas. s taff expenses continue to increase. Our figures are an average of ‘family’ and ‘professional’ staff. there is an upward trend, driven particularly by the ever increasing personal allowance.
home use has increased. since the historic samadian tax case ruling in 2013, reported regularly in this journal, a number of clients now use their homes as a ‘business base’ and claim appropriate costs accordingly. this factor may also account for some growth in office costs.
WhO OUR ORThOPaeDIC SURgeONS aRe
For the purposes of this study, note that our orthopaedic surgeons sample is restricted to those who:
earn at least £5,000 a year gross from private practice
have had at least five years private practice experience
are seriously interested in private practice as a business
hold either an old-style or a new-style NhS contract
May or may not work through a group, a limited liability partnership or a limited liability company
Year ending 5
c ar costs have shown an increase, though not all of the costs after the s amadian car tax court case are tax-deductible.
there has been a slight increase in accountancy/legal costs in the year.
sadly, orthopaedic consultants are at a higher risk than some of their colleagues when it comes to divorce.
While any divorce legal fees are excluded from our analysis – as they are deemed to be a capital item – there is an increasing
amount of accounting work required where these unfortunate events happen.
‘Other costs’ continue to grow, particularly in the area of marketing and public relations.
as we have previously reported, there is a good response to professional marketing and websites, particularly in the self-pay market.
continuing trends
Overall, our analysis of orthopaedic surgeons performance between 2013 and 2014 shows a
‘steady as she goes’ picture. What then of the future?
there are major changes ongoing, but our preliminary 2015 figures suggest that this trend may continue.
Fees are likely to increase, particularly if choose and Book work continues.
c osts will rise – particularly with respect to room hire costs following the implementation of the c ompetition and Markets authority report findings in april 2015.
p erhaps the one cost that has not risen last year was indemnity cover. More consultants are looking away from the traditional providers and this is having a short-term cost restraint impact. Whether or not there is a longerterm hidden impact, time will tell.
For the time being, we anticipate a continuance of the ‘steady as she goes’ experience – though this does mask a significant number of structural changes going on in the market.
next month: ophthalmologists
Ray Stanbridge runs an accountancy, finance and tax advisory service specialising in the medical profession. Martin Murray is a partner at Sandison Easson and Co, specialist medical accountants
what’S coming in oUr december-janUarY iSSUe
Make sure you don’t miss our next issue, published on 7 January 2016. Only subscribers to the journal are guaranteed to receive every copy and we don’t think anybody who is serious about continuing private practice in the future, when there is so much happening that will affect them, can afford to miss any issue.
Coming up next month:
are you competing fairly? Many consultants are thought to be unaware of how competition law can affect the way they work. ann Pope, senior director for anti-trust enforcement at the Competition and Markets authority, explains why it is important to understand the rules
Regardless of the size of your business, it is vital you do not neglect back-office procedures. Susan hutter gives some top tips to ensure you are doing everything to maximise productivity
Consultant ophthalmic surgeon Mr Larry Benjamin tells about the skills and knowledge private doctors can bring to a medical charity, both in the field and on the board
Prepare for your website revolution 1: growth of social media and instant access has put private patients far more in control of decisions that may have traditionally relied on expert recommendation alone.
Smart Medical Web picks out three areas to focus on as a priority
Prepare for your website revolution 2: The secrets of website conversion. Pamela Underdown continues her aesthetics series by revealing how to convert your website visitors into paying patients
Doctors in trouble: how the Royal Medical Benevolent Fund is helping doctors in difficulty
eDITORIaL INqUIRIeS
Sports stars and you. Following a football club doctor’s high-profile back-page publicity, Dr Rachel Birch of Medical Protection examines what to consider if you are asked to be a team doctor
Why you don’t need PR. Clinicians are bombarded with choice of marketing, PR, web design, social media, business development, search engine optimisation and pay-per-click agencies in a way that’s never happened before. Tingy Simoes has some timely advice
any practice considering embassy work needs a vigorous process in place to chase payments. Medical Billing and Collection’s gary Nials has some useful tips
Surgeon Mr Dev Lall believes there is a lot you can do to improve your profits by thinking ‘continuity income’
Starting a private practice: Ian Tongue takes a look at accounting systems
Medico-legal work – tips for the macrostructure of a report
‘Inter-generational planning’ – how to make the most of the financial assets of the whole family
aDveRTISeRS: The deadline for booking advertising for our December-January issue falls on 27 November
Robin Stride, editorial director
Email: robin@ip-today.co.uk
Tel: 07909 997340
aDveRTISINg INqUIRIeS
Margaret Floate, advertising manager
Email: margifloate@btinternet.com
Published by The Independent Practitioner Ltd. Independent Practitioner
Today is editorially independent and thanks Bupa for its assistance with distribution.
Printed by Pepper Communications Ltd
Material is governed by copyright. No part of this publication may be reproduced, stored in a retrieval system or transmitted in any form without permission, unless for the purposes of reference and comment. Editorial layout is the copyright of the publishers. If you wish to use it for promotional purposes on websites or for reprints, we would be happy to discuss licensing the copyright to you.
Registered office: 7 Lindum Terrace, Lincoln LN2 5RP
Write to Independent Practitioner Today PO Box 198, Cranleigh GU6 9BB
Tel: 01483 824094
Publisher Gillian Nineham Tel: 07767 353897.
Email: gill@ip-today.co.uk
SUBSCRIPTIONS
£85 independent practitioners.
£85 GPs and practice managers (private & NHS). £200 organisations. But if you pay by direct debit, individuals pay only £70, and organisations £175 Call Proact Ltd on 01752 312140
Email: lisa@marketingcentre.co.uk
gUaRaNTee yOUR COPy
To guarantee your copy of Independent Practitioner Today by taking out a subscription (at the rates shown on the left), phone 01752 312140 or send off a subscription form on page 22 or email lisa@marketingcentre.co.uk or go to the ‘about’ page of our website www.independent-practitioner-today.co.uk
If you pay by direct debit, individuals pay only £70 for a subscription. Just fill in the form on page 22 and send it to the Freepost address shown at the bottom of the form.
BaCk ISSUeS: £12.50 including post & packaging ChaNgINg aDDReSS OR SUBSCRIPTION DeTaILS?
Phone 01752 312140 or email lisa@marketingcentre.co.uk
Robin Stride, editorial director @robinstride
circulation figures verified by the Audit Bureau of Circulations
The business journal for doctors in private practice